The Impact of Acute Oral Sodium Propionate Supplementation ...

International Journal of Pediatric Otorhinolaryngology 78 (2014) 1393–1399
The use of large volume low pressure nasal saline with fluticasonepropionate for the treatment of pediatric acute rhinosinusitis
Selahattin Tugrul a, Remzi Dogan b,*, Eren Sabri Baki a, Aysenur Meric a, Orhan Ozturan a
aBezmialem Vakif University, Faculty of Medicine, Department of Otorhinolaryngology, Fatih, Istanbul, TurkeybBayrampasa State Hospital, Department of Otorhinolaryngology, Bayrampasa, Istanbul, Turkey
A R T I C L E I N F O
Article history:Received 13 February 2014Received in revised form 31 May 2014Accepted 5 June 2014Available online 16 June 2014
A B S T R A C T
Objectives: Fluticasone propionate and nasal saline irrigation have been used in the treatment ofsinonasal diseases for a long time. Our study investigates the effect of the combination of large volumelow pressure nasal saline irrigation and fluticasone propionate for the treatment of pediatric acuterhinosinusitis.Methods: Ninety-one pediatric patients with acute rhinosinusitis were included in our study. The patientswere randomized into two groups. The first group (n = 45) was treated with standard therapy(antibiotherapy + nasal decongestant) for 2 weeks, the second group was treated with the large volumelow pressure nasal saline + fluticasone propionate combination for 3 weeks. The clinical scores, radiologicevaluations (X-ray Waters view), peak nasal inspiratory flow (PNIF) measurements, total symptom scoresand hematologic parameters (WBC, CRP, ESR) of the patients were evaluated and compared.Results: There were no significant differences in between the two groups regarding age, gender, heightand weight. Even though the clinical scores of Group 2 improved more rapidly, there were no significantdifferences in between groups regarding clinical scores by the 21st day. There were no significantdifferences in post treatment radiologic evaluations (Waters graphy). Both groups had significantimprovement of their post treatment PNIF values, yet the improvement was more marked in Group 2than in Group 1. The rhinorrhea, nasal congestion, throat itching and cough symptoms improved morerapidly in Group 2 than in Group 1. Post-treatment nose itching and sneezing symptoms weresignificantly less in Group 2. The values of hematologic parameters were significantly reduced at the endof the 3rd week in both groups.Conclusions: Our study is a first in investigating the combined use of large volume low pressure nasalsaline and fluticasone propionate in acute pediatric rhinosinusitis, and the results reveal that thecombination therapy was effective. Low pressure large volume nasal saline + fluticasone propionatecombination can be employed as a new line of therapy for the treatment of pediatric acute rhinosinusitis,either by itself or combined with standard therapy.
ã 2014 Elsevier Ireland Ltd. All rights reserved.
Contents lists available at ScienceDirect
International Journal of Pediatric Otorhinolaryngology
journal homepage: www.elsevier .com/ locate / i jpor l
1. Introduction
Rhinosinusitis is an inflammation of the nasal cavity and theparanasal sinus mucosae which can be destructive to regional bonystructures in advanced cases, spreading to neighboring tissues.Acute bacterial rhinosinusitis (ABR) is the infection of paranasalsinuses, seen commonly 7–10 days after worsening of thesymptoms of an upper respiratory tract infection (URTI), andcontinues for less than 30 days [1]. ABR constitutes 5–10% of allcomplications following pediatric URTI [2].
* Corresponding author. Tel.: +90 505 7915844; fax: +90 212 544 35 94.E-mail address: [email protected] (R. Dogan).
http://dx.doi.org/10.1016/j.ijporl.2014.06.0060165-5876/ã 2014 Elsevier Ireland Ltd. All rights reserved.
Symptoms of ABR consist of coughing (increased at nights),rhinorrhea, nasal obstruction, open mouth breathing, hyponasalspeech and snoring [3]. Facial pain and headache are usually seenin children older than 8 years, or in subacute and chronic forms ofthe disease [4]. Especially in children, ABR can rapidly becomplicated, spreading to the orbital or intracranial tissues, eitherby direct invasion of neighboring tissues or through thebloodstream [5,6]. Presently, the prevalence of rhinosinusitisand the relevant economic costs keep escalating [7].
Today the treatment of ABR consists of systemic therapies(antibiotherapy, corticosteroids, antihistamines), topical therapies(nasal corticosteroids, saline irrigation, nasal decongestants, nasalantihistamines) and various combinations of those therapies. Inthe USA, ABR is one of the most common indications for antibiotic

Table 1Clinical severity scoring points.a
Symptom or sign Points
Abnormal nasal or postnasal dischargeMinimal 1Severe 2
Nasal congestion 1Cough 2Malodorous breath 1Facial tenderness 3Erythematous nasal mucosa 1Fever
<385 �C 1�385 �C 2
Headache (retro-orbital)Severe 3Mild 1
a Score: <8 = mild; �8 = severe.
1394 S. Tugrul et al. / International Journal of Pediatric Otorhinolaryngology 78 (2014) 1393–1399
use [8]. Studies indicate that despite the frequent use of antibiotics,no significant differences in recovery rates were observed betweenthe groups treated with antibiotics and those given the placebo[9,10]. Hence, today the use of topical drugs in pediatric ABR casesis on the rise. Although topical therapy (saline irrigation, nasaldecongestants, steroids, antihistamines and fungucides) use iscurrently increasing, data confirming the effectiveness of suchtherapies is still relatively scant in medical literature, other thanthat for topical steroids [11]. However, it was reported that largevolume low pressure nasal irrigation solutions, since they canreach every point of the nasal cavity in large volumes, do decreasepostoperative obstruction and edema, thus increasing recoveryrates [12]. Those solutions can safely be used in pediatric agegroups, with good patient compliance [13]. Our study comparedstandard therapy (antibiotherapy + nasal decongestant) with acombination of large volume low pressure nasal saline irrigation(LVLP-NSI) + fluticasone propionate (FP) therapy, using clinical,symptomatic, radiologic and hematologic parameters.
2. Material and method
2.1. Study design
The study was conducted during February 2012 and May 2013,after acquiring the permission of the local Ethics Committee of ouruniversity. It was a prospective, randomized and controlled study,including 105 pediatric patients with acute rhinosinusitis.
Criteria for inclusion were:
1. URTI not resolving in 10 days or worsening, continuation of allor most of the initial symptoms for 10 days
2. Purulent discharge from the middle meatus, observed duringendoscopic nasal examination
3. Abnormal findings (air-fluid level in the maxillary sinus,mucosal thickening) in the X-ray Waters view.
Criteria for exclusion were:
1. A diagnosis of allergic rhinitis.2. Antibiotic therapy (for ABR) for a duration of 2 weeks before
admission to the study group.3. Previous nasal surgery.4. Presence of adenoids.5. Presence of immune deficiency, cystic fibrosis, upper respira-
tory tract anomalies.6. No pathologic findings in endoscopic nasal examination and
on the X-ray Waters view.7. Presence of sinusitis complications (orbital or intracranial
spread).8. Antibiotic therapy for any other indications.
One hundred and five patients, aged 5–18 years, complyingwith the above criteria were included in the study. The allocationsequence was generated by the nurse (who was not included in thestudy). Participants, investigators, and physicians were blinded togroup assignment.
Group 1 (n = 53): Standard therapy was conducted withamoxicillin/clavulanate (90 mg/kg/day amoxicillin + 6.4 mg/kg/day clavulanate) for 14 days, twice a day, and 2 puffs ofxylometazoline hydrochloride per nostril twice daily for 5 days.
Group 2 (n = 52): Therapy was conducted with large volume lowpressure nasal irrigation solution (Abfen Sinüs Rinse kit 25 �120mL) + Fluticasone propionate (Flixonase nasal drops, 28 containers,GSK). The study designed that in Group 2 takes fluticasone for 3weeks, 1 nasule within 120 mL SF lavaged twice a day. This dose,400 mg of FP, diluated in SF. FP previously used in a study 400 mg a
day for 8 weeks [14]. Warm drinking water (120 mL) was pouredinto the plastic application bottle, and one pack of Sinus Rinse kitand one container of Flixonase nasal drops solution were added tothe water. After shaking the bottle thoroughly, the solution wasapplied to both nasal cavities. A nurse was assigned for teachingthe children and their families how to use the kit. During theteaching session, preparation and application of the kit wasexplained in detail, and practiced.
2.2. Evaluation methods
After their physical examination, all patients were randomlyassigned to two groups, according to the allocation sequence wasgenerated by the nurse (who was not included in the study). Theirclinical scores, radiologic findings (X-ray Waters view), peak nasalinspiratory flow (PNIF) measurements, total symptom scores (TSS)and the hematologic parameters (WBC, CRP, ESR) were evaluatedblinded.
2.3. Clinical scores
For assessing the severity of the clinical status, the clinicalseverity scoring system defined by Wald was employed [15]. Nasalor postnasal discharge, nasal congestion, coughing, malodorousbreath, periorbital swelling, facial tenderness, erythematous nasalmucosa, fever and headache were evaluated according to thescoring system, (Table 1). While a score under 8 indicated a milderclinic, a score of 8 or more indicated a severe clinical condition. Thescoring was calculated at the beginning of the study, and wasrepeated at the 7th, 14th and 21st days for both groups.
2.4. Radiologic evaluation
Patients in both groups had pre-treatment and post-treatment21st day X-ray Waters view taken for evaluating their maxillarysinuses [16]. The maxillary sinus at the X-ray Waters view wasbroken up to 32 different regions, and each region was given ascore, as 1: opaque (pathologic), or 0: lucent (normal). The totalscore for the 32 regions were calculated for each sinus, the averageof the left and right maxillary sinus scores was taken as the finalscore, and the results were compared.
2.5. Peak nasal inspiratory flowmetry (PNIF)
Peak nasal inspiratory flowmetry (PNIF) (L/min., Clement ClarkInternational, Essex, UK) is an objective method for assessing (theseverity of) nasal obstruction, and also for evaluating the responseto therapy [17–19]. The test is performed with a mask placed over

Fig. 1. Number of patients and drop-outs in the groups during the follow-up period.
Table 2Mean clinical scores of the groups (Mean � SD).
Groups Basal 7th day 14th day 21th day
Group 1 12.92 � 2.71 11.78 � 1.53 7.07 � 1.49a* 6.54 � 1.27Group 2 13.23 � 1.41 7.86 � 0.95a** 6.85 � 1.19 5.77 � 1.25Student's tindependent
p > 0.05 p < 0.05 p > 0.05 p > 0.05
a: repetead Anova and Bonforoni tests were used.a*Significant difference between basal and 14th day scores in Group 1 (p < 0.05).a**Significant difference between basal and 7th day scores in Group 2 (p < 0.05).
S. Tugrul et al. / International Journal of Pediatric Otorhinolaryngology 78 (2014) 1393–1399 1395
the face of the patient while the patient takes a deep breath fromthe nose, mouth closed. The test is repeated 3 times, and theaverage of those 3 measurements is calculated. PNIF wasperformed at the beginning of the study, and was repeated onday 21. Children who could not perform the initial test wereexcluded from the study.
2.6. Total symptom score (TSS)
Sinusitis symptoms were evaluated by the 4-step grading scale,as defined in relevant literature [16]. 0 (none): no symptoms; 1(mild): symptom present but not troublesome; 2(moderate):symptom sometimes troublesome; 3(severe): symptom usuallytroublesome. The study evaluated the nasal, non-nasal and generalsymptoms, and graded them in 4-steps. Patients over 6 years filledin their own symptom scores, while family members helped theyounger patients fill in theirs. The scoring was recorded every day,day and night, by the patient or a family member, beginning fromthe start of the study, continuing to day 21. Weekly average scoreswere calculated and the results were compared.
2.7. Hematologic parameters
Blood samples were taken at the start of the studyand on the 21stday following treatment: WBC, CRP and ESR values were compared.
3. Statistics
Statistical analysis was carried out using the Statistical Packagefor the Social Sciences version 13.0 software for Windows (SPSSInc., Chicago, Illinois, USA). All quantitative variables wereestimated using measures of central location (i.e. mean andmedian) and measures of dispersion (i.e. standard deviation (SD)).Data normality was checked using the Kolmogorov–Smirnov testsof normality. Studen’s t independent test was used for comparingbetween group variable data. Leven test was used for equality ofvariances. Repeated Anova test was used for within groupvariability analysis. In comparing time series analyses of thegroups, Bonforonti test was employed. Chi-square test was used forcomparing qualitative data of the groups. Pearson correlationanalysis was used for comparing correlation of the evaluationmethods of the groups. A value of p < 0.05 was accepted asstatistically significant.
4. Results
One hundred and five acute rhinosinusitis patients whocomplied to the inclusion and exclusion criteria (Group 1:n = 53, Group 2: n = 52) were included in our study. Two patients
in Group 1 were excluded from the study for not showing up at the1st week follow-up appointment, and 3 more were excluded fordiscontinuing their therapy regimen on the 8th day (Fig. 1). Threepatients in Group 2 were excluded from the study for not showingup at the 1st week follow-up, 2 more were excluded for notrecording their symptoms scores regularly, and one more patientwas excluded because of discontinuing therapy on day 15 (Fig. 1).Due to those drop-outs, Group 1 was reduced to 45 patients, Group2 to 46 patients, and statistical analyses were performedaccordingly.
All of the children included in the study have not fever butcough,headache and nasal symptoms were presented. We don’tsupport saline irrigation over antibiotics even in the presence offever and acute otitis in children. Any side effects with antibioticsor steroids had to leave the study did not observed.
There was no significant difference between the ages andgenders of the 2 groups: Group 1: 11.9 � 3.52 years (27 male/18female); Group 2: 13.2 � 4.03 years (24 male/22 female) (p > 0.05).
There was also no significant difference between the weightand height of the children: Group 1: 36.24 � 8.61 kg.,146.23 � 10.85cm.; Group 2: 38.07 � 11.24 kg., 151.37 � 13.07 cm. (p > 0,05).
4.1. Clinical scores
There was no significant difference between the mean pre-treatment clinical scores of the groups (p > 0.05). There was asignificant difference between the clinical scores of Groups 1 and 2on the the 7th day after treatment (p < 0.05). On day 7, the clinicalscores of Group 2 have improved more. On the 14th and 21st daysafter treatment, no significant differences were observed betweenthe groups regarding their clinical scores, and both groups wereseen to have improved likewise (p < 0.05)(Table 2) (Fig. 2).
4.2. Radiologic evaluation
Pre-treatment X-ray Waters view scoring revealed no signifi-cant difference between the two groups (p = 0.341) (Table 3).Likewise, there was no significant difference between the groups in
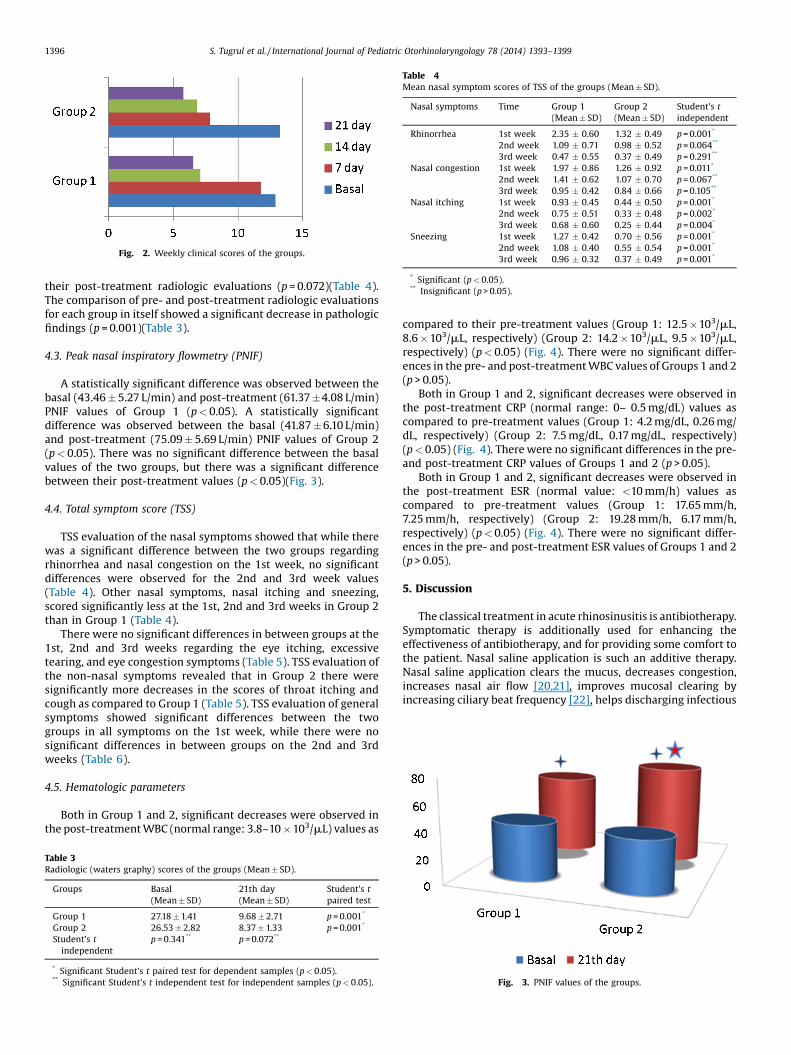
Fig. 2. Weekly clinical scores of the groups.
Table 4Mean nasal symptom scores of TSS of the groups (Mean � SD).
Nasal symptoms Time Group 1(Mean � SD)
Group 2(Mean � SD)
Student's tindependent
Rhinorrhea 1st week 2.35 � 0.60 1.32 � 0.49 p = 0.001*
2nd week 1.09 � 0.71 0.98 � 0.52 p = 0.064**
3rd week 0.47 � 0.55 0.37 � 0.49 p = 0.291**
Nasal congestion 1st week 1.97 � 0.86 1.26 � 0.92 p = 0.011*
2nd week 1.41 � 0.62 1.07 � 0.70 p = 0.067**
3rd week 0.95 � 0.42 0.84 � 0.66 p = 0.105**
Nasal itching 1st week 0.93 � 0.45 0.44 � 0.50 p = 0.001*
2nd week 0.75 � 0.51 0.33 � 0.48 p = 0.002*
3rd week 0.68 � 0.60 0.25 � 0.44 p = 0.004*
Sneezing 1st week 1.27 � 0.42 0.70 � 0.56 p = 0.001*
2nd week 1.08 � 0.40 0.55 � 0.54 p = 0.001*
3rd week 0.96 � 0.32 0.37 � 0.49 p = 0.001*
* Significant (p < 0.05).** Insignificant (p > 0.05).
1396 S. Tugrul et al. / International Journal of Pediatric Otorhinolaryngology 78 (2014) 1393–1399
their post-treatment radiologic evaluations (p = 0.072)(Table 4).The comparison of pre- and post-treatment radiologic evaluationsfor each group in itself showed a significant decrease in pathologicfindings (p = 0.001)(Table 3).
4.3. Peak nasal inspiratory flowmetry (PNIF)
A statistically significant difference was observed between thebasal (43.46 � 5.27 L/min) and post-treatment (61.37 �4.08 L/min)PNIF values of Group 1 (p < 0.05). A statistically significantdifference was observed between the basal (41.87 � 6.10 L/min)and post-treatment (75.09 � 5.69 L/min) PNIF values of Group 2(p < 0.05). There was no significant difference between the basalvalues of the two groups, but there was a significant differencebetween their post-treatment values (p < 0.05)(Fig. 3).
4.4. Total symptom score (TSS)
TSS evaluation of the nasal symptoms showed that while therewas a significant difference between the two groups regardingrhinorrhea and nasal congestion on the 1st week, no significantdifferences were observed for the 2nd and 3rd week values(Table 4). Other nasal symptoms, nasal itching and sneezing,scored significantly less at the 1st, 2nd and 3rd weeks in Group 2than in Group 1 (Table 4).
There were no significant differences in between groups at the1st, 2nd and 3rd weeks regarding the eye itching, excessivetearing, and eye congestion symptoms (Table 5). TSS evaluation ofthe non-nasal symptoms revealed that in Group 2 there weresignificantly more decreases in the scores of throat itching andcough as compared to Group 1 (Table 5). TSS evaluation of generalsymptoms showed significant differences between the twogroups in all symptoms on the 1st week, while there were nosignificant differences in between groups on the 2nd and 3rdweeks (Table 6).
4.5. Hematologic parameters
Both in Group 1 and 2, significant decreases were observed inthe post-treatment WBC (normal range: 3.8–10 � 103/mL) values as
Table 3Radiologic (waters graphy) scores of the groups (Mean � SD).
Groups Basal(Mean � SD)
21th day(Mean � SD)
Student’s tpaired test
Group 1 27.18 � 1.41 9.68 � 2.71 p = 0.001*
Group 2 26.53 � 2.82 8.37 � 1.33 p = 0.001*
Student’s tindependent
p = 0.341** p = 0.072**
* Significant Student’s t paired test for dependent samples (p < 0.05).** Significant Student’s t independent test for independent samples (p < 0.05).
compared to their pre-treatment values (Group 1: 12.5 �103/mL,8.6 � 103/mL, respectively) (Group 2: 14.2 �103/mL, 9.5 �103/mL,respectively) (p < 0.05) (Fig. 4). There were no significant differ-ences in the pre- and post-treatment WBC values of Groups 1 and 2(p > 0.05).
Both in Group 1 and 2, significant decreases were observed inthe post-treatment CRP (normal range: 0– 0.5 mg/dL) values ascompared to pre-treatment values (Group 1: 4.2 mg/dL, 0.26 mg/dL, respectively) (Group 2: 7.5 mg/dL, 0.17 mg/dL, respectively)(p < 0.05) (Fig. 4). There were no significant differences in the pre-and post-treatment CRP values of Groups 1 and 2 (p > 0.05).
Both in Group 1 and 2, significant decreases were observed inthe post-treatment ESR (normal value: <10 mm/h) values ascompared to pre-treatment values (Group 1: 17.65 mm/h,7.25 mm/h, respectively) (Group 2: 19.28 mm/h, 6.17 mm/h,respectively) (p < 0.05) (Fig. 4). There were no significant differ-ences in the pre- and post-treatment ESR values of Groups 1 and 2(p > 0.05).
5. Discussion
The classical treatment in acute rhinosinusitis is antibiotherapy.Symptomatic therapy is additionally used for enhancing theeffectiveness of antibiotherapy, and for providing some comfort tothe patient. Nasal saline application is such an additive therapy.Nasal saline application clears the mucus, decreases congestion,increases nasal air flow [20,21], improves mucosal clearing byincreasing ciliary beat frequency [22], helps discharging infectious
Fig. 3. PNIF values of the groups.

Table 5Mean non-nasal symptom scores of TSS of the groups (Mean � SD).
Non-nasal symptoms Time Group 1(Mean � SD)
Group 2(Mean � SD)
Student's tindependent
Eye itching 1st week 0.54 � 0.53 0.43 � 0.66 p = 0.450**
2nd week 0.47 � 0.61 0.38 � 0.57 p = 0.328**
3rd week 0.41 � 0.39 0.31 � 0.45 p = 0.396**
Tearing 1st week 0.14 � 0.23 0.13 � 0.16 p = 0.248**
2nd week 0.10 � 0.19 0.18 � 0.21 p = 0.401**
3rd week 0.12 � 0.15 0.11 � 0.20 p = 0.624**
Eye congestion 1st week 0.07 � 0.34 0.08 � 0.18 p = 0.574**
2nd week 0.09 � 0.29 0.17 � 0.19 p = 0.382**
3rd week 0.12 � 0.36 0.15 � 0.31 p = 0.214**
Throat itching 1st week 0.62 � 0.65 0.27 � 0.45 p = 0.019*
2nd week 0.55 � 0.53 0.26 � 0.41 p = 0.034*
3rd week 0.48 � 0.50 0.20 � 0.437 p = 0.004*
Cough 1st week 1.92 � 0.78 1.13 � 0.48 p = 0.001*
2nd week 1.51 � 0.95 0.95 � 0.38 p = 0.013*
3rd week 1.24 � 0.68 0.77 � 0.42 p = 0.004*
* Significant (p < 0.05).** Insignificant (p > 0.05).
S. Tugrul et al. / International Journal of Pediatric Otorhinolaryngology 78 (2014) 1393–1399 1397
material from the sinuses, and decreases cough due to post-nasaldischarge [23]. Research has shown that nasal saline application,due to its aforementioned effects, is efficient as an auxiliarytreatment in the pediatric age group for allergic rhinitis, and acuteand chronic rhinosinusitis [21,22,24,25].
Today, intranasal corticosteroids are favored in the treatment ofrhinitis and rhinosinusitis. The 2009 Cochrane report recommendsthe use of intranasal corticosteroids for the treatment of acuterhinosinusitis, either by themselves or together with antibiother-apy [26]. Intranasal corticosteroids act by inhibiting cytokinerelease and reducing the number of inflammatory cells. Thus theydecrease the inflammation of nasal mucosa [27].
Large volume low pressure nasal saline irrigation has beenshown to be more efficient than small volume high pressuresaline irrigation which used to be the classical application insinonasal infections, and its use keeps increasing. In our study weaimed to investigate the application of large volume low pressuresaline and fluticasone propionate together, for nasal irrigation inpediatric acute rhinosinusitis patients. Thus, we could combinethe beneficial effects of nasal saline irrigation with a nasalcorticosteroid which, given in a large volume solution, wouldreach to more points of the nasal mucosa. To investigate theeffectiveness of such a combination, a group of pediatric patientswere treated with the classical therapy regimen (systemicantibiotherapy and nasal decongestant), and another group wastreated with large volume low pressure nasal saline together withfluticasone propionate.
Clinical improvement started at the 1st week in Group 2patients, and at the second week in Group 1 (Fig. 2, Table 2). At theend of the 3rd week, significant clinical improvement wasobserved in both groups (Fig. 2, Table 2). Various studies reported
Table 6Mean general symptom scores of TSS of the groups (Mean � SD).
General symptoms Time Group(Mean
Sleep quality 1st week 1.48 �2nd week 1.03 �3rd week 0.76 �
Daytime sleep 1st week 1.35 �2nd week 0.97 �3rd week 0.83 �
Activity 1st week 0.68 �2nd week 0.36 �3rd week 0.26 �
* Significant (p < 0.05).** Insignificant (p > 0.05).
that intranasal corticosteroids assisted antibiotics in the improve-ment of clinical symptoms in acute rhinosinusitis [28,29]. A recentstudy concluded that the sole use of mometasone furoate nasalspray in acute rhinosinusitis helped improve clinical symptoms[30]. The Cochrane Report of 2010 suggests the use of salineirrigation in acute rhinosinusitis either by itself or as an adjunct toantibiotherapy [31]. Data from 2 separate randomized, clinicaltrials showed no significant differences in the recovery rates ofpatients with acute rhinosinusitis who received placebo comparedwith antibiotics [32,33]. The application method we have used inour study allows both the saline and the corticosteroid to reach thenasal mucosa and the sinuses locally and in high concentrations.We have combined the two methods approved by medicalliterature, considering the combination may provide a moreeffective treatment, and may bring forward a more rapid clinicalimprovement.
Although today the radiologic evaluation of rhinosinusitis inadults depends on computed tomography (CT) images, in thepediatric age group CT imaging is employed mostly when surgeryis considered, or when a complication is suspected [34,35]. In ourstudy, because of both the high cost and the radiation risk of the CT,we preferred to use the Waters graphy for radiologic evaluation inconfirming clinical findings. In both of our study groups, there wasa significant improvement in the radiologic findings (X-ray Watersview) of post-treatment images as compared to pre-treatmentimages (p < 0.05)(Table 3). Nasal saline irrigation clears exudativematerial in the sinuses and decreases edema [20,23]. Fluticasonepropionate inhibits the cytokines which trigger the formation ofinflammatory cells, thus inhibiting exudation, edema and inflam-matory cells [36]. The treatment method we have employed allowslarger volumes of nasal saline and corticosteroid to enter the
1 � SD)
Group 2(Mean � SD)
Student's tindependent
0.57 1.12 � 0.77 p = 0.016*
0.49 0.89 � 0.67 p = 0.379**
0.58 0.65 � 0.51 p = 0.418**
0.74 0.86 � 0.40 p = 0.024*
0.56 0.75 � 0.42 p = 0.437**
0.65 0.77 � 0.61 p = 0.532**
0.31 0.42 � 0.47 p = 0.024*
0.25 0.32 � 0.34 p = 0.417**
0.20 0.21 � 0.35 p = 0.426**

Fig. 4. Comparison of pre- and post-treatment (values of) hematologic parameters of the groups.
1398 S. Tugrul et al. / International Journal of Pediatric Otorhinolaryngology 78 (2014) 1393–1399
maxillary sinuses; we believe that may be the reason underlyingradiologic improvement without the use of antibiotherapy.
One of the most important factors that effect the quality of lifein acute rhinosinusitis is the decrease of nasal air flow due toedema and inflammation. In both of our study groups, post-treatment PNIF values were significantly increased as compared topre-treatment values. However, on day 21, the PNIF values of Group2 were significantly higher than those of Group 1 (p < 0.05)(Fig. 3).We think that increase to be due to the large volume low pressuresaline + fluticasone propionate therapy applied in Group 2. Variousstudies indicated that both nasal saline and nasal corticosteroidshave increased the PNIF values [16,17,37,38]. Our study implies thatthe combined effect of those treatments resulted in a higherincrease in the PNIF values, and our results are compatible withrelevant literature.
Rhinorrhea and nasal congestion are the two main symptomsencountered in acute rhinosinusitis. Rhinorrhea and nasalcongestion symptoms have improved more rapidly in Group 2than in the group treated with standard therapy (Table 4). Variousstudies indicate that the use of nasal corticosteroid in acuterhinosinusitis significantly reduces nasal congestion [30,39,40].Studies recommend the use of nasal saline irrigation in acuterhinosinusitis since it reduces rhinorrhea and nasal congestion[16,20,23]. Large volume low pressure nasal saline was found to bemore efficient in reducing post-op nasal congestion than highpressure small volume nasal saline [12]. Our study implies that themixture we have used in our study reduced both rhinorrhea andnasal congestion more rapidly because of its combined effect, andour results are compatible with relevant literature.
Fluticasone propionate use is an effective method for reducingthe allergic symptoms of nasal itching and sneezing [41]. Likewisein our study nasal itching and sneezing of the children with acuterhinosinusitis decreased significantly in Group 2 than in Group 1(Table 4).
One of the main reasons for sore throat and cough during acuterhinosinusitis is post-nasal discharge. It is known that nasal salinesolutions inhibit nasal edema and prevent post-nasal discharge,thus alleviating the sore throat and cough symptoms [16,23,42].The findings of our study are compatible with literature since sorethroat and cough complaints decreased significantly in Group 2 ascompared to Group 1 (Table 5).
General symptoms such as sleep disturbances and daily activityimproved more rapidly in Group 2 than in Group 1 (Table 6). Wethink that because the solution used for Group 2 could reach everypoint of the nasal cavity in high concentrations, it created a more
rapid improvement than that seen with systemic therapy. Thisfinding also supports the effectiveness of the combined therapy.
The most important mechanism in the development of acuterhinosinusitis is superinfection by bacteria after a viral infection[11]. Acute bacterial rhinosinusitis may be a self limited diseasethat resolves in about 4 weeks. This time period varies according tothe species of infecting bacteria [43]. When the disease is not selflimiting, acute rhinosinusitis can advance to subacute and chronicforms. Therefore, antibiotherapy is recommended in acutepediatric rhinosinusitis [43]. Antibiotic use for pediatric acuterhinosinusitis is one of the most common indications forantibiotherapy in the USA [8]. WBC, CRP and ESR values assistthe decision to initiate antibiotherapy, and also for the follow-up ofpatients. In our study there were no significant differencesregarding the pre- and post-op hematologic parameters (WBC,CRP, ESR) in between the two group (Fig. 4). Some studies reportedthat there was no significant difference between antibiotherapyand placebo in the treatment of acute rhinosinusitis [9,10]. Thecombination therapy used in our study may be used as analternative to antibiotherapy.
Antibiotherapy and nasal decongestants used in acuterhinosinusitis may not be well tolerated by the patients due tovarious side effects. Antibiotherapy, especially in the pediatric agegroup, may cause gastrointestinal side effects which sometimesmay hinder the continuation of therapy. Due to the risk of rhinitismedicamentosa, nasal decongestants have to be discontinuedafter 5 days, and this short time period is not sufficient to provideadequate symptomatic relief. The large volume low pressurenasal saline and fluticasone propionate mixture used in our studydoes not have such side effects. Since fluticasone propionate isdiluted in the large volume solution and applied to the nasalcavity with a low pressure, potential side effects which may beseen when employed by itself (epistaxis, sore throat, dryness inthe nose, nasal burning) [44,45] are not encountered in thiscombination therapy.
As mentioned previously spray and drop forms of FP are safelyused in children. A study showed that the systemic bioavailabilityfrom intranasally administered FP is very low, with the dropsformulation (0.06%) producing an approximately eight-fold lowerestimated bioavailability compared with Fluticasone propionatenasal spray (FPANS) (0.51%). Compared with other intranasallyadministered corticosteroids FP appears to have low systemicbioavailability (FPANS (0.51%) and FP nasal drops (0.06%) comparedwith triamcinolone acetonide 44%, beclomethasone dipropionate44% and budesonide 31%. Nasal drops are cleared more quickly

S. Tugrul et al. / International Journal of Pediatric Otorhinolaryngology 78 (2014) 1393–1399 1399
from the nose than nasal spray, and this supports that nasal dropshave a very low systemic bioavailability [46].
The large volume low pressure nasal saline irrigation apparatuswe have used in our study is quite easy to employ. It was reportedthat its use in the pediatric age group was convenient and was welltolerated [12]. While there is no difference between the classical(high pressure small volume) and the large volume low pressurenasal saline apparatuses regarding the convenience of application,the low pressure apparatus was found to be more effective inrelieving symptoms [13]. In our study, the low pressure apparatuswas used in the pediatric age group without any problems.
The limitation of our study is the lack of a placebo group. Thestrengths of our study are: presenting a new method for the firsttime in medical literature, use of clear inclusion and exclusioncriteria in patient selection, a low patient drop-out rate, and theinclusion of supportive tests (radiography, PNIF, hematologictests).
Our study indicates that the combination of large volume lowpressure saline and fluticasone propionate, when used together fornasal irrigation, is an effective treatment method for pediatricacute rhinosinusitis.
6. Conclusion
Our study is a first in medical literature in using a large volumelow pressure nasal saline and fluticasone propionate mixture fornasal irrigation, and the results indicate the efficiency of such acombination in pediatric acute rhinosinusitis. The treatmentemployed in our study can be applied as a therapy method inpediatric acute rhinosinusitis, either alone or as an adjunct toantibiotherapy, and placebo-controlled randomized additionaltrials with this method are needed to confirm our findings.
References
[1] American Academy of Pediatrics Subcommittee on Management of SinusitisCommittee on Quality Improvement, Clinical practice guideline: managementof sinusitis, Pediatrics 108 (2001) 798–808.
[2] K. Revai, L.A. Dobbs, S. Nair, et al., Incidence of acute otitis media and sinusitiscomplicating upper respiratory tract infection: the effect of age, Pediatrics 119(6) (2007) 1408–1412.
[3] K.A. Kronemer, W.H. McAlister, Sinusitis and its imaging in the pediatricpopulation, Pediatr. Radiol. 27 (1997) 837–846.
[4] S.F. Dowell, B. Schwartz, W.R. Phillips, Appropriate use of antibiotics for URIs inchildren. Part I. Otitis media and acute sinusitis. The Pediatric URI ConsensusTeam, Am. Fam. Physician 58 (1998) 1113–1118.
[5] S. Esposito, S. Bosis, M. Bellasio, et al., From clinical practice to guidelines:howto recognize rhinosinusitis in children, Pediatr. Allergy Immunol. 18(2007) 48–50.
[6] S. Esposito, N. Principi, Rhinosinusitis managementin pediatrics: an overview,Int. J. Immunopathol. Pharmacol. 23 (2010) 53–55.
[7] C. Bachert, K. Hormann, R. Mosges, et al., An update on the diagnosis andtreatment of sinusitis and nasalpolyposis, Allergy 58 (2003) 176–191.
[8] M.J. Smith, Evidence for the diagnosis and treatment of acute uncomplicatedsinusitis in children: asystematic review, Pediatrics 132 (1) (2013) 284–296.
[9] W. Stalman, G.A. van Essen, Y. van der Graaf, et al., The end of antibiotictreatment in adults with acute sinusitis-like complaints in generalpractice? Aplacebo-controlled double-blind randomized doxycyclinetrial, Br. J. Gen. Pract.47 (1997) 794–799.
[10] F.L. Van Buchem, J.A. Knottnerus, V.J. Schrijnemaekers, et al., Primary-care-based randomised placebo-controlled trial of antibiotic treatment in acutemaxillary sinusitis, Lancet 349 (1997) 683–687.
[11] F. Mori, A. Fiocchi, S. Barni, et al., Management of acute rhinosinusitis, Pediatr.Allergy Immunol. 22 (2012) 27–31.
[12] R.J. Salib, S. Talpallikar, S. Uppal, et al., Prospective randomised single-blindedclinical trial comparing the efficacy and tolerability of the nasal douchingproducts SterimarTM and Sinus RinseTM following functional endoscopic sinussurgery, Clin. Otolaryngol. 38 (4) (2013) 297–305.
[13] J.S. Jeffe, B. Bhushan, J.W. Schroeder Jr., Nasal saline irrigation in children: astudy of compliance and tolerance, Int. J. Pediatr. Otorhinolaryngol. 76 (3)(2012) 409–413.
[14] H. Demirhan, F. Aksoy, O. Ozturan, et al., Medical treatment of adenoidhypertrophy with “fluticasone propionate nasal drops”, Int. J. Pediatr.Otorhinolaryngol. 74 (7) (2010) 773–776.
[15] E.R. Wald, D. Chiponis, J. Ledesmamedina, Comparative effectiveness ofamoxicillinand amoxicillin-clavulanate potassium inacute para-nasal sinusinfections in children:a double-blind, placebo-controlledtrial, Pediatrics 77 (6)(1986) 795–800.
[16] Y.H. Wang, C.P. Yang, M.S. Ku, et al., Efficacy of nasal irrigation in the treatmentof acute sinusitis in children, Int. J. Pediatr. Otorhinolaryngol. 73 (12) (2009)1696–1701.
[17] C. Ahlstrom Emanuelson, M. Anderson, et al., Effects of topical formoterolalone and in combination with budesonide in a pollen season model of allergicrhinitis, Respir. Med. 101 (6) (2007) 1106–1112.
[18] D. Can, R. Tanac, E. Demir, et al., Is the usage of intranasal glucocorticosteroidsalone in allergic rhinitis sufficient? Allergy Asthma Proc. 27 (2006) 248–253.
[19] M.I. Barnes, J.H. Ward, T.C. Fardon, et al., Effects of levocetirizine as add-ontherapy to fluticazone in seasonal allergic rhinitis, Clin. Exp. Allergy 36 (2006)676–684.
[20] L.T. Tomooka, C. Murphy, T.M. Davidson, Clinical study and literature review ofnasal irrigation, Laryngoscope 110 (7) (2000) 1189–1193.
[21] J.W. Georgitis, Nasal hyperthermia and simple irrigation for perennial rhinitis:changes in inflammatory mediators, Chest 106 (1994) 1487–1492.
[22] A.R. Talbot, T.M. Herr, D.S. Parsons, Mucociliary clearance and bufferedhypertonic saline solution, Laryngoscope 107 (4) (1997) 500–503.
[23] M.Kaliner,Medicalmanagementofsinusitis,Am.J.Med.Sci.316(1)(1998)21–28.[24] R. Zeiger, M. Shatz, Chronic rhinitis: a practical approach to diagnosis and
treatment, II: treatment, Immunol. Allergy Pract. 4 (3) (1982) 26.[25] W. Garavello, M. Romagnoli, L. Sordo, et al., Hypersaline nasal irrigation in
children with symptomatic seasonal allergicrhinitis: a randomized study,Pediatr. Allergy Immunol . 14 (2003) 140–143.
[26] A. Zalmanovici, J. Yaphe, Intranasal steroids for acute sinusitis, CochraneDatabase Syst. Rev. 7 (4) (2009) CD005149.
[27] H. Derendorf, E.O. Meltzer, Molecular and clinical pharmacology of intranasalcorticosteroids: clinical and therapeutic implications, Allergy 63 (10) (2008)1292–1300.
[28] I.B. Barlan, E. Erkan, M. Bakir, et al., Intranasal budesonide spray as an adjunctto oral antibiotic therapy for acute sinusitis in children, Ann. Allergy AsthmaImmunol. 78 (1997) 598–601.
[29] R.J. Dolor, D.L. Witsell, A.S. Hellkamp, et al., Comparison of cefuroxime with orwithout intranasal fluticasone for the treatment of rhinosinusitis. The CAFFSTrial: a randomized controlled trial, JAMA 286 (2001) 3097–3105.
[30] E.O. Meltzer, D. Gates, C. Bachert, Mometasone furoate nasal spray increasesthe number of minimal- symptom days in patients with acuterhinosinusitis,Ann. Allergy Asthma Immunol. 108 (4) (2012) 275–279.
[31] J.C. Kassel, D. King, G.K. Spurling, Saline nasal irrigation for acute upperrespiratory tract infections, Cochrane Database Syst. Rev. 17 (3) (2010)CD006821.
[32] W. Stalman, G.A. van Essen, Y. van der Graaf, et al., The end of antibiotictreatment in adults with acute sinusitis-like complaints in general practice? aplacebo-controlled double-blind randomized doxycycline trial, Br. J. Gen.Pract. 47 (1997) 794–799.
[33] F.L. Van Buchem, J.A. Knottnerus, V.J. Schrijnemaekers, et al., Primary-care-based randomised placebo-controlled trial of antibiotic treatment in acutemaxillary sinusitis, Lancet 349 (1997) 683–687.
[34] S. Esposito, N. Principi, Italian Society of Pediatrics, et al., Acute and subacuterhinosinusitis in children: guidelines to diagnosis and treatment, J. Chemother.20 (2008) 147–157.
[35] N. Principi, S. Esposito, New insights into pediatric rhinosinusitis, Pediatr.Allergy Immunol. 18 (2007) 7–9.
[36] A. Parikh, G.K. Scadding, Y. Darby, et al., Topical corticosteroids in chronicrhinosinusitis: a randomized, double-blind, placebo- controlled trial usingfluticasone propionate aqueous nasal spray, Rhinology 39 (2) (2001) 75–79.
[37] I. Vlckova, P. Navrátil, R. Kana, et al., Effective treatment of mild-to-moderatenasal polyposi with fluticasone delivered by a novel device, Rhinology 47 (4)(2009) 419–426.
[38] F.S. Hansen, P.G. Djupesland, W.J. Fokkens, Preliminary efficacy of fluticasonedelivered by a novel device in recalcitrant chronic rhinosinusitis, Rhinology 48(3) (2010) 292–299.
[39] E. Meltzer, H. Orgel, J. Backhaus, et al., Intranasal flunisolide spray as an adjunctto oral antibiotic therapy for sinusitis, J. All. Clin. Immunol. 92 (1993) 812–823.
[40] A.S. Nayak, G.A. Settipane, A. Pedinoff, et al., Effective dose range ofmometasone furoate nasal spray in the treatment of acute rhinosinusitis,Ann. Allergy Asthma Immunol. 89 (3) (2002) 271–278.
[41] W. Wu, R.D. Walters, G.A. Nadeau, An integrated analysis of the efficacy offluticasone furoate nasal spray versus placebo on the nasal symptoms ofperennial allergic rhinitis, Allergy Asthma Proc. 34 (3) (2013) 283–291.
[42] Y.H. Wang, M.S. Ku, H.L. Sun, et al., Efficacy of nasal irrigation in the treatmentof acute sinusitis in atopic children, J. Microbiol. Immunol. Infect. 30 (2012)1182–1684.
[43] E.R. Wald, Beginning antibiotics for acuterhinosinusitis and choosing the righttreatment, Clin. Rev. Allergy Immunol. 30 (2006) 143–152.
[44] P. Demoly, Safety of intranasal corticosteroids in acute rhinosinusitis, Am. J.Otolaryngol. 29 (2008) 403–413.
[45] M. Zitt, T. Kosoglou, J. Hubbell, Mometasone furoate nasal spray: a review ofsafety and systemic effects, Drug Saf. 30 (2007) 317–326.
[46] P.T. Daley-Yates, R.C. Baker, Systemic bioavailability of fluticasone propionateadministered as nasal drops and aqueous nasal spray formulations, Br. J. Clin.Pharmacol. 51 (2001) 103–105.
Copyright © 2022 FDOKUMEN