
Chemokines in Respiratory Viral Infections: Focus on Their Diagnostic and Therapeutic Potential
Upload
northwesternCategory
view
1download
0
Evaluation of the presence of B-cell attractant chemokines inchronic rhinosinusitis
Monica Patadia, M.D.1, Julian Dixon, M.D.1, David Conley, M.D.1, Rakesh Chandra, M.D.1,Anju Peters, M.D.2, Lydia A. Suh, B.S.2, Atsushi Kato, Ph.D.1,2, Roderick Carter, B.S.2,Kathleen Harris, B.S.2, Leslie Grammer, M.D.2, Robert Kern, M.D.1, and Robert Schleimer,Ph.D.21Department of Otolaryngology, Northwestern University Feinberg School of Medicine, Chicago,Illinois2Division of Allergy and Immunology, Department of Medicine, Northwestern University FeinbergSchool of Medicine, Chicago, Illinois
AbstractBackground—B-cell responses may play a role in the pathogenesis of nasal polyposis via localIgA and IgE production and activation of eosinophils and mast cells. B-cell attracting chemokinesmay therefore have relevance in the pathogenesis of chronic rhinosinusitis with nasal polyps(CRSwNPs)
Methods—Polyp and inferior turbinate tissues were obtained from CRSwNPs, CRS without NPs(CRSsNPs), and control patients; ELISA and reverse-transcription polymerase chain reaction wereused to detect levels of protein and mRNA for selected B-cell chemokines (B-cell attractingchemokine 1 [CXCL13/BCA-1/BLC]), thymus expressed chemokine (CCL25/TECK), mucosae-associated epithelial chemokine (CCL28/MEC), stromal cell–derived factor-1alpha (CXCL12/SDF-1alpha), and selected chemokine receptor genes (CXCR4, CXCR5, and CXCR7).
Results—BCA-1 and SDF-1alpha protein levels were significantly increased in polyp tissuecompared with turbinate tissue from CRSsNP patients and controls (p < 0.05 and p < 0.01,respectively). Differences in TECK and MEC were not significant. For mRNA, expression ofBCA-1 was significantly up-regulated in polyp tissue and levels correlated with CD20 mRNAexpression. Additionally, significant up-regulation of mRNA for the SDF-1alpha receptorsCXCR7 and CXCR4 was detected in polyps, while there was a trend for up-regulation of theBCA-1 receptor CXCR5.
Conclusion—Elevated levels of the BCA-1 and SDF-1alpha and their receptors may account foran increased presence of B cells and their products, contributing to eosinophilic inflammation inpatients with CRSwNP.
KeywordsB-cell recruitment; CCL25/TECK; CCL28/MEC; chemokines; chronic rhinosinusitis; CXCL12/SDF-1alpha; CXCL13/BCA-1; nasal polyposis
Copyright © 2010, OceanSide Publications, Inc., U.S.A.
Address correspondence and reprint requests to Monica O. Patadia, M.D., Department of Otolaryngology, Northwestern University,767 North St. Clair, Suite 1325, Chicago, IL 60611, [email protected] Patadia, M.D., and Julian Dixon, M.D., contributed equally to this work
NIH Public AccessAuthor ManuscriptAm J Rhinol Allergy. Author manuscript; available in PMC 2012 April 24.
Published in final edited form as:Am J Rhinol Allergy. 2010 ; 24(1): 11–16. doi:10.2500/ajra.2010.24.3386.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Chronic rhinosinusitis (CRS) is a common clinical syndrome characterized by persistent,symptomatic mucosal inflammation. Subjective and objective criteria have been establishedto define CRS, but the etiology and pathogenesis remain incompletely understood.1,2 CRS iscommonly subdivided into two types, CRS with nasal polyps (CRSwNPs) and CRS withoutNPs (CRSsNPs), as determined by endoscopic and radiographic evaluations. In westerncountries, CRSwNP is typically characterized by a skewed TH2 pattern of inflammation anda marked tissue eosinophilia.3,4 Eotaxins and IL-5 have been implicated in the induction ofthis mucosal eosinophilia in CRSwNP patients because these factors are significantlyelevated in polyp tissue compared with CRSsNP tissue or sinonasal tissue from healthysubjects.5,6 Although these reports account for the accumulation and persistence ofeosinophils in polyp tissue, they do not address the triggers for eosinophil degranulation orthe accumulation of other inflammatory cell types, which are presumably also significantfactors in the pathophysiology of CRSwNPs.
Recent reports suggest that B-cell accumulation, local B-cell class switch recombination,and local immunoglobulin production may be of great importance to mucosal inflammatorydiseases in the lower and upper airway as well. B-cell and plasma cell numbers as well asIgE and IgA concentrations have been reported to be increased in polypoid sinonasalmucosal tissue from patients with CRSwNPs when compared with controls orCRSsNPs.4,7–9 Furthermore, it is well established that mucosal B cells undergo class switchrecombination to express IgA, and that IgA can serve as a trigger for eosinophildegranulation by binding to surface receptors present on these cells. These findings suggesta possible link between local B cells, IgA, and eosinophilic degranulation in CRSwNPs.9
The mechanisms by which B cells accumulate in the sinonasal mucosa may therefore havesignificance in the pathogenesis of nasal polyposis. B-cell–activating factor of the TNFfamily (BAFF) has been identified to play an important role in B-cell survival, proliferation,and maturation, and levels of BAFF are significantly elevated in nasal polyp tissuecompared with control tissues.9,10 Although local production of BAFF, and other factorssuch as IL-6, may expand or maintain the B cells that migrate to sinus tissue, very littleinformation is available as to how B cells and their precursors are initially attracted to nasaltissue in patients with CRS.
Chemokines are a family of small cytokines 8–10 kDa in size that induce chemotaxis ofmotile cells including B cells. Elevated levels of various chemokines in nasal polyp tissue(e.g., the C-C chemokine RANTES) are already believed to promote local chemotaxis of Tcells and eosinophils in CRSwNPs.11–13 The current study assessed levels of four B cellattracting chemokines in nasal polyp and control tissues: B-cell attracting chemokine 1(CXCL13/BCA-1/BLC), thymus expressed chemokine (CCL25/TECK), mucosae-associatedepithelial chemokine (CCL28/MEC), and stromal cell–derived factor 1α (CXCL12/SDF-1α). Each of these chemokines has been shown to recruit B cells or IgA+ plasmablastsin studies in mice and humans.14–16 Chemokine levels were measured by ELISA of tissuehomogenates. In a second set of experiments, quantitative real-time polymerase chainreaction (PCR) was performed on cDNA from additional sinus tissue samples to detect thepresence of mRNA for selected chemokine and chemokine receptor genes. The presentinvestigation is an extension of an earlier preliminary report.17
MATERIALS AND METHODSStudy Design
BCA-1, TECK, MEC, and SDF-1α were assayed and levels in polyp samples fromCRSwNP patients and inferior turbinate samples from CRSwNP patients, CRSsNP patients,and normal controls were compared. Concentrations of each chemokine in tissuehomogenates were determined using ELISA. A panel of additional tissue specimens was
Patadia et al. Page 2
Am J Rhinol Allergy. Author manuscript; available in PMC 2012 April 24.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

evaluated by real-time PCR using specific primers to quantify mRNA levels of relevantchemokine receptor genes, as well as BCA-1 and CD20.
Subjects and SpecimensSubjects with CRSwNPs or CRSsNPs or controls with no evidence of CRS were invited toparticipate in the study. Each patient gave informed consent, and the study was approved bythe Institutional Review Board at Northwestern University. The diagnosis of CRSwNPs orCRSsNPs in this study was based on clinical criteria defined by a recent expert consensuspanel and confirmed by office endoscopy and computed tomography (CT) imaging.1 AllCRS patients undergoing endoscopic sinus surgery had previously failed adequate trials ofmaximal medical therapy including prolonged antibiotic regimens, nasal steroid sprays, oralsteroids, saline irrigations, and decongestants.
The population was limited to otherwise healthy adults between the ages of 18 and 70 years.Subjects taking anticoagulants, who have received an organ transplant, who have taken oralcorticosteroids or antibiotics within the previous 2 weeks, or who have a confoundingconcomitant disease such as sarcoidosis or immunodeficiency were excluded from the study.Additional exclusion criteria included patients with antrochoanal polyps, cystic fibrosis,allergic fungal sinusitis, or unilateral nasal polyps.
All tissue samples were obtained during planned endoscopic sinus surgery in patients withCRS. Control sinonasal tissue was obtained from patients without evidence of CRS, rhinitis,or asthma (normal patients) undergoing nasal and sinus surgery for noninflammatory diseasesuch as septoplasty, rhinoplasty, fracture repair, or pituitary tumor surgery. The studysamples for ELISA included CRSwNP polyp tissue (n = 17), CRSwNP inferior turbinate (n= 6), CRSsNP inferior turbinate (n = 8), and normal inferior turbinate (n = 6). Seven patientswere diagnosed with allergic rhinitis by positive skin testing (three patients with CRSsNPsand four patients with CRSwNPs). Nine of the patients were noted to be on intranasalsteroids at the time of specimen collection (three patients with CRSsNPs and six patientswith CRSwNPs). Two patients were on antihistamines at the time of specimen collection,both of whom had CRSwNPs. Tissue samples included for analysis of mRNA were from aseparate group of subjects and consisted of polyp tissue taken from CRSwNPs (n = 15),inferior turbinate tissue from CRSwNPs (n = 12), inferior turbinate tissue from patients withCRSsNPs (n = 9), and inferior turbinate tissue from normal controls (n = 12). Five patientswere diagnosed with allergic rhinitis by positive skin testing (one patient with CRSsNPs andfour patients with CRSwNPs). Fifteen patients were noted to be on intranasal steroids at thetime of specimen collection (3 patients with CRSsNPs and 12 patients with CRSwNPs).Data regarding antihistamine use were not available in this subset.
Specimen Preparation and AssayPreparation of Polyp/Sinus Tissue Extracts—Sinonasal surgical tissue samples weretreated and proteins were extracted as described previously.9 Briefly, 100 mg of polyp orinferior turbinate tissue was suspended in 1 mL of PBS-Tween in the presence of a cocktailof protease inhibitors (Sigma Chemical Co., St. Louis, MO) added at a 1:100 dilution. Thesamples were then homogenized for ~1 minute on ice at 24,000 rpm with an Ultra-TurraxT8 Homogenizer (IKA Works, Inc., Wilmington, NC). The tissue suspension was allowed tosettle for 30 minutes on ice. The suspensions were then centrifuged at 4000 rpm for 20minutes at 4°C. The supernatants were collected and stored at −80°C until analysis. Theprotein concentrations for the extracts were determined by the Bradford method using aBIORAD protein assay kit (Bio-Rad, Hercules, CA).
Patadia et al. Page 3
Am J Rhinol Allergy. Author manuscript; available in PMC 2012 April 24.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

ELISA—Before ELISA analysis, samples were thawed at room temperature and vortexed toensure a well-mixed sample. Chemokines were assayed using commercially available assaykits (R&D, Minneapolis, MN). The color intensity was measured using MicroPlate ReaderSoftware applied to the sandwich enzyme immunoassay technique. Concentrations ofchemokines in the tissue homogenate were normalized to the concentration of total protein.The minimum detectable concentration was 1.64 pg/mL for human BCA-1, 16 pg/mL forSDF-1α, and 62.5 pg/mL for TECK and MEC.
Real-Time PCR—Total RNA from sinus tissue was extracted using QIAzol (Qiagen,Valencia, CA) and was cleaned and treated with DNase I using RNeasy (Qiagen) accordingto the manufacturer’s instructions. Quality of total RNA from sinus tissue was assessed witha 2100 Bioanalyzer (Agilent Technologies, Santa Clara, CA) using a RNA 6000 NanoLabChip (Agilent Technologies). Single-strand cDNA was synthesized with SuperScript IIreverse transcriptase (Invitrogen, Carlsbad, CA) and random primers. Semiquantitative real-time reverse-transcription (RT) PCR was performed with a TaqMan method using anApplied Biosystems 7500 Sequence Detection System (Applied Biosystems, Foster City,CA) as described previously. Primer and probe sets for five genes, CXCR4 (sense, 5′-CTGAGAAGCATGACGGACAAGTA-3′; antisense, 5′-CAGAAGGGAAGCGTGATGACA-3′; FAM/black hole quencher 1 [BHQ1] labeledprobe, 5′-CTGTCAGTGGCCGACCTCCTCT-3′), CXCR7 (sense, 5′-CAACCTCTTCGGCAGCATTT-3′; antisense,5′GGGTGTTGGTGAAGTAGGTGATG-3′; FAM/BHQ1 labeled probe, 5′-TGCATGAGCGTGGACCGCTACCT-3′), CXCR5 (sense, 5′-CTGGCGCAGGAGCAGTCT-3′; antisense, 5′-CCACGGTGAGCCCTTAGGA-3′; FAM/BHQ1 labeled probe, 5′-TCCCAGTGTCCCCTTTTATTGCTGCTTT-3′), BCA-1 (sense,5′-GGACTCAGAGCTCAAGTCTGAACTC-3′; antisense, 5′-CAGCAGCATGAGAAGCAGAGA-3′; FAM/BHQ1 labeled probe, 5′-TCCAGACAGAATGAAGTTCATCTCGA-3′), and CD20 (sense, 5′-CACTCTTCAGGAGGATGTCTTCACT-3′; antisense, 5′-TCTGGACAGCCCCCAAAGT-3′; FAM/MGB labeled probe; 5′-TCTTCATGAGGGAATCTA-3′) were synthesized by Applied Biosystems or IntegratedDNA Technologies (Coralville, IA). A primer and probe set for β-glucuronidase (human β-glucuronidase endogenous control, part number 4326320) was purchased from AppliedBiosystems. To determine the exact copy number of the target genes, quantified aliquots ofpurified PCR fragments of the target genes were serially diluted and used as standards ineach experiment. Aliquots of cDNA equivalent to 10 ng of total RNA were used for real-time PCR. The mRNA expression levels were normalized to the median expression of thehousekeeping gene, β-glucuronidase.
Immunohistochemistry—The CD20 antibody used is a mouse monoclonal tissue culturesupernatant, CD20 Ab-1 Clone L26 (Thermo Fisher Scientific, Fremont, CA). Three-micrometer sections of formalin-fixed, paraffin-embedded tissue from CRSwNP patientswere incubated with CD20 antibody at a dilution of 1:250 overnight, for 16–20 hours, at4°C. After rinsing, biotinylated horse anti-mouse secondary antibody (Vector Laboratories,Burlingame, CA) was used for 1 hour at room temperature, at a dilution of 1:500. After asecond rinsing, sections were incubated with avidin-peroxidase complex (Vectastain EliteABC Kit; Vector Laboratories) for 1 hour at room temperature. After a third rinsing,sections were incubated with diaminobenzidine chromogen (Invitrogen, South SanFrancisco, CA) for 10 minutes. Counterstaining with Gill modified hematoxylin (EMDChemicals, Durmstadt, Germany) was done for 5–10 seconds. Sections were dehydrated,cleared, and mounted, and photographs were then taken using a MicroFire AR digital
Patadia et al. Page 4
Am J Rhinol Allergy. Author manuscript; available in PMC 2012 April 24.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

microscope camera (Optronics, Goleta, CA). Supernatant, clone L26, was run at a dilutionof 1:250.
Data AnalysisComparisons between groups were made using the Mann-Whitney U test on Prism Version4 (GraphPad Software, Inc., La Jolla, CA). A value of p < 0.05 was considered significant.Correlations were assessed using the Spearman’s rank correlation. A value of p < 0.05 wasconsidered significant. Use of nasal steroids or presence of positive skin testing was notsignificantly associated with alterations of either ELISA or RT-PCR findings (not shown).
RESULTSEnzyme-Linked Immunosorbent Assay
Extracts from a total of 37 sinonasal surgical samples were processed for ELISA, which wasperformed for each of the four chemokines studied. The patients’ ages ranged from 25 to 74years, with a mean age of 43 ± 12 years, with 11 total female patients and 26 male patients(Table 1). SDF-1α was prominently expressed in polyp tissue as shown in Fig. 1 A. SDF-1αwas never detected in extracts of inferior turbinate tissues from CRSsNP patients andcontrols. This difference in expression between CRSwNP samples and turbinate samplesfrom normal and CRSsNPs and CRSwNPs was statistically significant with values of p =0.01 or less for each comparison. As shown in Fig. 1 B, levels of expression of BCA-1 weredramatically increased in polyp tissue compared with turbinate tissue from CRSwNPpatients, CRSs-NPs, and controls. Compared with normal tissue, levels of BCA-1 wereelevated over 20-fold. Statistical evaluation indicated that polyp tissue manifestedsignificantly higher levels of BCA-1 compared with turbinate tissue from control andCRSsNP patients (p < 0.05 in each case) but not turbinate tissue from CRSwNP patients (p= 0.08). TECK expression displayed considerable variability and there were no significantdifferences between groups regarding levels of this chemokine (Fig. 1 C). Levels of MECexpression also displayed variability and were significantly lower in inferior turbinate tissuefrom CRSsNP patients (Fig. 1 D). This finding was recently confirmed in a microarray studyof CRS (not shown).
Real-Time PCRExtracts from a total of 48 sinonasal surgical samples were processed for quantitative real-time PCR for receptors for SDF-1α (CXCR4 and CXCR7) and BCA-1 (CXCR5), as well asBCA-1 itself. The patients’ ages ranged from 20 to 77 years, with a mean age of 39 ± 9years, with 18 total female patients and 30 male patients (Table 1). Levels of mRNA forCD20 were also assayed from polyp tissue. Significantly increased levels of CXCR4 (Fig. 2A) and CXCR7 (Fig. 2 B) mRNA were shown in polyp tissue when compared with tissuesamples from controls and CRSsNP patients, as well as turbinate tissue from CRSwNPpatients (p < 0.02 for all associations). Levels of CXCR5 mRNA exhibited a trend towardincreased expression in polyp tissue, but this did not reach significance (Fig. 2 C). Levels ofBCA-1 mRNA, however, were elevated in polyp tissue when compared with tissue samplesfrom controls and CRSsNP patients (p < 0.05 for both; Fig. 3 A). Furthermore, BCA-1mRNA levels were found to positively correlate with mRNA levels of its receptor CXCR5 (r= 0.56 and p < 0.0001; Fig. 3 B), as well as mRNA levels of the B-cell marker CD20 (r =0.64 and p < 0.0001; Fig. 3 C).
DISCUSSIONThe goal of this study was to determine the presence of B-cell chemoattractant chemokinesthat may contribute to the accumulation of B lymphocytes and plasma cells observed in
Patadia et al. Page 5
Am J Rhinol Allergy. Author manuscript; available in PMC 2012 April 24.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

sinonasal tissues of patients with CRS. We performed ELISA assays on detergent extracts oftissue taken from patients and controls during sinus surgery to evaluate expression of fourchemokines known to recruit B cells based on studies in mice and humans. The results fromthe study show that SDF-1α and BCA-1, but not TECK or MEC, were elevated in nasalpolyp tissue and thus may play a role in B-cell recruitment to nasal polyp tissue. Follow-upexamination of mRNA levels revealed that receptors for SDF-1α (CXCR4 and CXCR7) andBCA-1 (CXCR5) were also up-regulated in polyp tissue, further implicating a role for thesechemokines in CRSwNPs. At last, the present report also shows a positive correlationbetween BCA-1 mRNA and B-cell populations in polyp tissue, as reflected by CD20mRNA.
A specific role for the observed elevations of SDF-1α in the development of nasal polyposisis uncertain at present, but this chemokine activates migration through CXCR4 and is knownto contribute to B-cell trafficking. Other investigators have observed CXCR4 mRNA to besignificantly elevated in the nasal tissue of symptomatic allergic rhinitis patients whencompared with normal subjects.18 A bradykinin challenge was also noted to significantlyincrease CXCR4 mRNA levels in nasal tissue of mild allergic rhinitis patients whencompared with normal subjects.18 The present data complement the aforementionedobservations by showing significant elevations of both CXCR4 mRNA and the CXCR4ligand SDF-1α in polyp tissue samples. Moreover, mRNA of a recently established alternatereceptor for SDF-1α, CXCR7, was also significantly elevated in polyp tissue samples.SDF-1α is also a potent and effective factor for the recruitment of stem cells and is thoughtto play a role in tissue regenerative responses.19 The present observation of elevatedSDF-1α may therefore also reflect an ongoing regenerative response.
BCA-1 is mainly produced by reticular cells, such as follicular dendritic cells. Others havealso recently suggested a potential role for this chemokine in CRS using microarrayanalysis. These authors observed greater than a fivefold up-regulation of BCA-1 geneexpression in sinus mucosa of children with CRS compared with controls, supporting thepresent findings that increased BCA-1 protein levels were evident in polyp tissue.20 Thischemokine has been reported to attract CXCR5+ cells to B-cell follicles in lymphoid tissues.Naive B cells are known to be CXCR5+ and migrate to lymph nodes mainly via modifiedhigh endothelial venules, which present BCA-1 juxtaposed to, or inside of, the lymphoidfollicle. These naive B cells are next attracted to the mantle zone where BCA-1 is releasedfrom dendritic elements such as the follicular dendritic cell tips. During embryogenesis,CXCL13 plays a key role in the recruitment of lymphoid tissue inducer cells, which initiatethe formation and organization of lymphoid organs, such as lymph nodes and Peyer’spatches. BCA-1 and CXCR5 are expressed in normal human gut–associated lymphoid tissuestructures, both in the ileum and colon, as well as in irregular lymphoid aggregates ofinflammatory bowel disease lesions. It has also been found that the induction of BCA-1expression is one of the strongest correlates for the development of ectopic lymphoidfollicles in rheumatoid joints. The overexpression of BCA-1 at ectopic sites, such as thepancreas, is sufficient to drive the development of ectopic lymphoid follicles with B cells,follicular dendritic cells, and high endothelial venules.21
Another recent study has noted that inducible bronchus-associated lymphoid tissue, which ismost prevalent in patients with pulmonary complications of autoimmune diseases such asrheumatoid arthritis and Sjogren’s syndrome, consists of numerous B-cell folliclescontaining germinal centers and follicular dendritic cells. Interestingly, expression oflymphoid-organizing chemokines, such as BCA-1, and also BAFF, correlated with anincreased number and structural complexity of inducible bronchus-associated lymphoidtissue areas in the lung.22 Although there are no formal reports of the formation of isolatedlymphoid follicles in CRS, we and others have observed foci of lymphoid neogenesis to be
Patadia et al. Page 6
Am J Rhinol Allergy. Author manuscript; available in PMC 2012 April 24.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

present in polyp tissue in the patients with CRSwNPs (Fig. 4); thus it is possible that onerole of BCA-1 is to recruit and capture B cells that are attracted to the sinuses in isolatedfollicles. It is interesting to note that specialized B helper T cells that reside in follicles andare important in their formation are also attracted by BCA-1 and migrate via the actions ofCXCR5.23
Because B-cell production of IgA and IgE in nasal polyp tissue may play a role in localinflammation, chemokines that attract B cells may have significant relevance to thepathogenesis of CRSwNPs.4,7 Taken together, the present data suggest that SDF-1α andBCA-1 may play roles in the recruitment and retention of B cells in the tissues of patientswith CRSwNPs. Additionally, our previous data have revealed that IgA levels were three- tosixfold higher in polyp extracts than in tissue extracts from other groups, further implicatinga significant role for B cells in the pathogenesis of CRSwNPs.4 Investigations are underwayto elucidate whether these chemokines recruit progenitor cells that then differentiate,proliferate, and reside in the tissue or recruit mature cells to sites of the inflammation in thesinuses and upper airways. Additional studies will attempt to correlate expression of B-cellchemokines with lymphoid follicular development and antibody production in polyp tissue.
AcknowledgmentsSupport for the conduct of the study and preparation of the article was provided by an American Rhinologic SocietyCORE Grant, grants R01 HL068546, R01 HL078860, and R01 AI072570, from the National Institutes of Healthand the Ernest S. Bazley Trust
REFERENCES1. Fokkens W, Lund V, Mullol J. European position paper on rhinosinusitis and nasal polyps group.
European Position Paper on Rhinosinusitis and Nasal Polyps. Rhinol Suppl. 2007; 20:1–136.[PubMed: 17844873]
2. Kern RC, Conley DB, Walsh W, et al. Perspectives on the etiology of chronic rhinosinusitis: Animmune barrier hypothesis. Am J Rhinol. 2008; 22:549–559. [PubMed: 18786300]
3. Zhang N, Van Zele T, Perez-Novo C, et al. Different types of T-effector cells orchestrate mucosalinflammation in chronic sinus disease. J Allergy Clin Immunol. 2008; 122:961–968. [PubMed:18804271]
4. Van Zele T, Clayes S, Gavaert P, et al. Differentiation of chronic sinus diseases by measurement ofinflammatory mediators. Allergy. 2006; 61:1280–1289. [PubMed: 17002703]
5. Olze H, Forster U, Zuberbier T, et al. Eosinphilic nasal polyps are a rich source of eotaxin, eotaxin-2and eotaxin-3. Rhinology. 2006; 44:145–150. [PubMed: 16792175]
6. Bachert C, Wagenmann M, Hauser U, et al. IL-5 synthesis is upregulated in human nasal polyptissue. J Allergy Clin Immunol. 1997; 99:837–842. [PubMed: 9215253]
7. Polzehl D, Moeller P, Riechelmann H, et al. Distinct features of chronic rhinosinusitis with andwithout nasal polyps. Allergy. 2006; 61:1275–1279. [PubMed: 17002702]
8. Van Zele T, Holtappels G, Cauwenberge P, Bachert C. Local immunoglobulin production in nasalpolyposis is modulated by superantigens. Clin Exp Allergy. 2007; 37:1840–1847. [PubMed:17941912]
9. Kato A, Peters A, Suh L, et al. Evidence of a role for B cell-activating factor of the TNF family inthe pathogenesis of chronic rhinosinusitis with nasal polyps. J Allergy Clin Immunol. 2008;121:1385–1392. [PubMed: 18410958]
10. Schneider P, MacKay F, Steiner V, et al. BAFF, a novel ligand of the tumor necrosis factor family,stimulates B cell growth. J Exp Med. 1999; 189:1747–1756. [PubMed: 10359578]
11. Bachert C, Gevaert P, Holtappels G, et al. Nasal polyposis: From cytokines to growth. Am JRhinol. 2000; 14:279–290. [PubMed: 11068652]
Patadia et al. Page 7
Am J Rhinol Allergy. Author manuscript; available in PMC 2012 April 24.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
12. Beck LA, Stellato C, Beall LD, et al. Detection of the chemokine RANTES and endothelialadhesion molecules in nasal polyps. J Allergy Clin Immunol. 1996; 98:766–780. [PubMed:8876553]
13. Hamilos DL, Leung DY, Huston DP, et al. GM-CSF, IL-5 and RANTES immunoreactivity andmRNA expression in chronic hyperplastic sinusitis with nasal polyposis (NP). Clin Exp Allergy.1998; 28:1145–1152. [PubMed: 9761019]
14. Feng N, Jaimes MC, Lazarus NH, et al. Redundant role of chemokines CCL25/TECK and CCL28/MEC in IgA+ plasmablast recruitment to the intestinal lamina propria after rotavirus infection. JImmunol. 2006; 176:5749–5759. [PubMed: 16670280]
15. Lazarus NH, Kunkel EJ, Johnston B, et al. A common mucosal chemokine (mucosae-associatedepithelial chemokine/CCL28) selectively attracts IgA plasmablasts. J Immunol. 2003; 1703799-3305.
16. Barone F, Bombardieri M, Rosado MM, et al. CXCL13, CCL21, and CXCL12 expression insalivary glands of patients with Sjogren’s syndrome and MALT lymphoma: Association withreactive and malignant areas of lymphoid organization. J Immunol. 2008; 180:5130–5151.[PubMed: 18354239]
17. Patadia, M.; Conley, D.; Chandra, R., et al. Mechanisms of B cell recruitment in chronicrhinosinusitis with nasal polyposis (CRSwNP). Oral Presentation at the 54th American RhinologicSociety Annual Scientific Meeting; September 20, 2008; Chicago, IL.
18. Eddleston J, Christiansen SC, Zuraw BL. Functional expression of the C-X-C chemokine receptorCXCR4 by human bronchial epithelial cells: Regulation by proinflammatory mediators. JImmunol. 2002; 169:6445–6451. [PubMed: 12444153]
19. Gomperts BN, Belperio JA, Rao PN, et al. Circulating progenitor epithelial cells traffic viaCXCR4/CXCL12 in response to airway injury. J Immunol. 2006; 176:1916–1927. [PubMed:16424223]
20. Wu X, Ghimbovschi S, Aujla PK, et al. Expression profiling of inflammatory mediators inpediatric sinus mucosa. Arch Otolaryngol Head Neck Surg. 2009; 135:65–72. [PubMed:19153309]
21. Moreno J, Hartson L, Navarro C, et al. Inducible bronchus-associated lymphoid tissue (iBALT) inpatients with pulmonary complications of rheumatoid arthritis. J Clin Invest. 2006; 116:3183–3192. [PubMed: 17143328]
22. Moyron-Quiroz JE, Rangel-Moreno J, Kusser K, et al. Role of inducible bronchus associatedlymphoid tissue (iBALT) in respiratory immunity. Nat Med. 2004; 10:927–934. [PubMed:15311275]
23. Ansel KM, McHeyzer-Williams LJ, Ngo VN, et al. In vivo-activated CD4 T cells upregulate CXCchemokine receptor 5 and reprogram their response to lymphoid chemokines. J Exp Med. 1999;190:1123–1134. [PubMed: 10523610]
Patadia et al. Page 8
Am J Rhinol Allergy. Author manuscript; available in PMC 2012 April 24.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 1.The concentration of (A) SDF-1α, (B) BCA-1, (C) TECK, and (D) MEC in tissuehomogenates of inferior turbinate and polyp samples was measured using ELISA.Concentration was normalized to the concentration of total protein. Levels of both SDF-1αand BCA-1 were significantly different between CRSwNP polyp tissue and samples fromCRSsNP as well as normals. Normal IT = inferior turbinate tissue from control patients;CRSsNP IT = inferior turbinate tissue from chronic rhinosinusitis without nasal polyppatients; CRSwNP IT = inferior turbinate tissue from chronic rhinosinusitis with nasal polyppatients; CRSwNP polyp = polyp tissue from chronic rhinosinusitis with nasal polyppatients; SDF = stromal cell–derived factor; BCA = B-cell attracting chemokines; TECK =thymus expressed chemokine; MEC = mucosae-associated epithelial chemokine.
Patadia et al. Page 9
Am J Rhinol Allergy. Author manuscript; available in PMC 2012 April 24.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 2.Total RNA was extracted from polyps and from turbinate tissue in patients with CRSwNPs,CRSsNPs, and CRS-free controls and was analyzed by RT-PCR. (A) CXCR4 and (B)CXCR7 mRNA levels were significantly elevated in polyps compared with all other tissuetypes. (C) CXCR5 mRNA levels were also elevated in polyp tissue but this was notstatistically significant. CRSwNPs = chronic rhinosinusitis with nasal polyps; CRSsNPs =chronic rhinosinusitis without nasal polyps; RT-PCR = reverse-transcription polymerasechain reaction.
Patadia et al. Page 10
Am J Rhinol Allergy. Author manuscript; available in PMC 2012 April 24.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 3.Levels of BCA-1, CD20, and CXCR5 mRNA were analyzed by RT-PCR in the indicatedsamples; (A) BCA-1 mRNA levels were significantly elevated in polyps compared withtissue from CRSsNP patients and normal controls. BCA-1 mRNA levels also positivelycorrelated with mRNA levels for (B) CXCR5 and (C) CD20, and both of these associationswere statistically significant. BCA = B-cell attracting chemokines; RT-PCR = reverse-transcription polymerase chain reaction; CRSsNPs = chronic rhinosinusitis without nasalpolyps.
Patadia et al. Page 11
Am J Rhinol Allergy. Author manuscript; available in PMC 2012 April 24.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
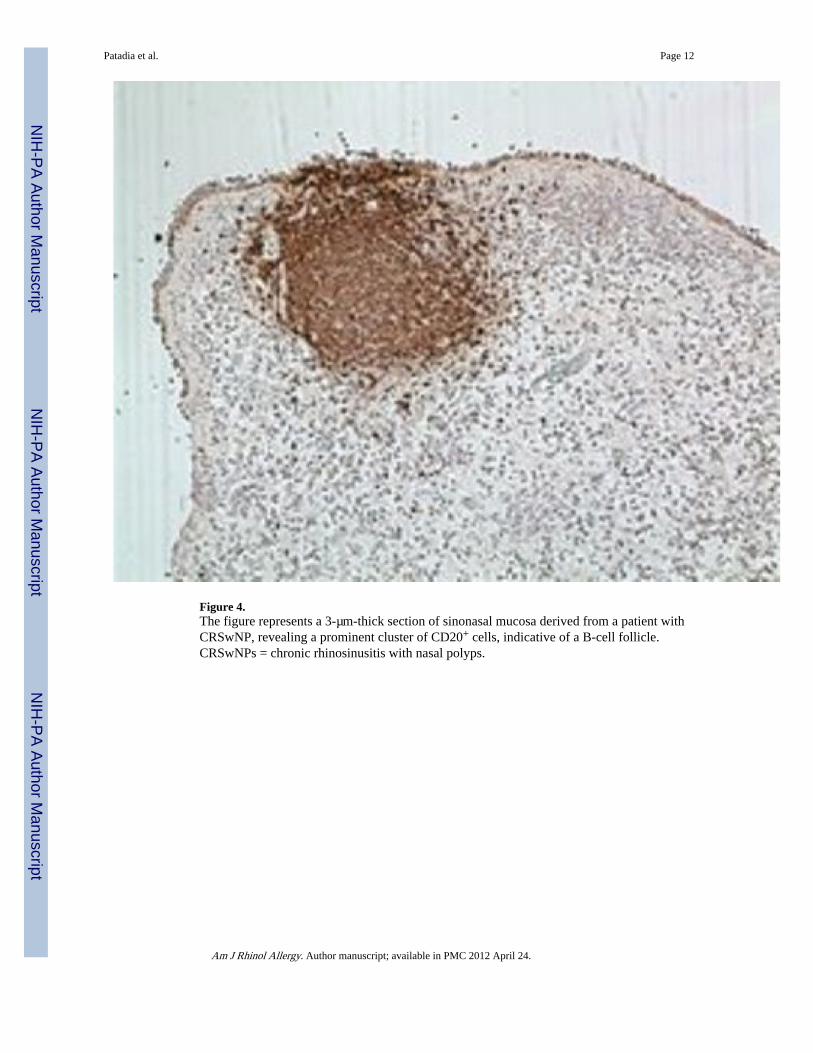
Figure 4.The figure represents a 3-µm-thick section of sinonasal mucosa derived from a patient withCRSwNP, revealing a prominent cluster of CD20+ cells, indicative of a B-cell follicle.CRSwNPs = chronic rhinosinusitis with nasal polyps.
Patadia et al. Page 12
Am J Rhinol Allergy. Author manuscript; available in PMC 2012 April 24.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Patadia et al. Page 13
Table 1
Subject characteristics
Sample Type ELISA Studies RT-PCR Studies
Age Median (range; yr) Gender Age Median (range; yr) Gender
Normal IT 38 (31–59) 1 female, 5 males 36 (20–77) 2 females, 10 males
CRSsNP IT 44 (25–64) 5 females, 3 males 34 (27–55) 6 females, 6 males
CRSwNP IT 32 (27–54) 2 females, 4 males 44 (28–69) 5 females, 4 males
CRSwNP polyp 44 (28–74) 3 females, 14 males 44 (28–74) 5 females, 10 males
IT = inferior turbinate; CRSsNP = chronic rhinosinusitis without nasal polyp; CRSwNP = chronic rhinosinusitis with nasal polyp; RT-PCR =reverse-transcription polymerase chain reaction‥
Am J Rhinol Allergy. Author manuscript; available in PMC 2012 April 24.
Copyright © 2022 FDOKUMEN




















