
Interaction Between Chemokines and Oxidative Stress: Possible Pathogenic Role in Acute Coronary...
7
Interaction Between Chemokines and Oxidative Stress: Possible Pathogenic Role in Acute Coronary Syndromes Pål Aukrust, MD, PHD,*² Rolf K. Berge, PHD,‡ Thor Ueland, BS,§ Ellinor Aaser, MD,\ Jan Kristian Damås, MD,²\ Lisbeth Wikeby, RN,²\ Anne Brunsvig, BS,\ Fredrik Mu ¨ller, MD, PHD,*² Kolbjørn Forfang, MD, PHD,\ Stig S. Frøland, MD, PHD,*² Lars Gullestad, MD, PHD\ Oslo and Bergen, Norway OBJECTIVES We sought to study the relationships between chemokines and oxidative stress in acute coronary syndrome. BACKGROUND In view of existing knowledge on the participation of leukocytes and oxidative stress in the pathogenesis of acute coronary syndrome, we hypothesized that chemokines may play a role in recruiting and activating leukocytes in this disorder. METHODS The levels of chemokines and oxidative stress were studied in 38 patients with stable and 38 with unstable angina and in 20 controls. In separate in vitro experiments the effect of chemokines on reactive oxygen species in monocytes and the effect of antioxidants on chemokine levels in these cells were also studied. RESULTS 1) Angina patients had raised serum levels of chemokines in both cross-sectional and longitudinal testing, with particularly high levels of interleukin (IL)-8, monocyte chemoat- tractant protein (MCP)-1 and macrophage inflammatory peptide (MIP)-1-alpha in unstable disease. 2) T cells, and particularly monocytes, seem to contribute to the raised IL-8, MCP-1 and MIP-1-alpha levels in unstable angina. 3) Concomitantly, and significantly correlated with MCP-1 and IL-8 levels, stable and particularly unstable angina patients had decreased plasma levels of antioxidants and increased lipid peroxidation, suggesting enhanced oxidative stress. 4) Monocyte chemoattractant protein-1 enhanced the generation of O 2 2 in monocytes from unstable angina patients, and the antioxidant glutathione-monoethyl ester suppressed the production of IL-8 and MCP-1 in these cells. CONCLUSIONS Our findings suggest an interaction between chemokines and oxidative stress in unstable angina. This interaction may represent a vicious circle involved in the pathogenesis of acute coronary syndromes. (J Am Coll Cardiol 2001;37:485–91) © 2001 by the American College of Cardiology Increasing evidence supports the involvement of inflamma- tion in atherogenesis and in the pathogenesis of acute coronary syndrome. Thus, activated monocytes, T cells and granulocytes have been demonstrated in patients with un- stable angina (1,2), and extensive infiltration of blood- derived macrophages and T cells into the vessel wall is seen in the active stages of atherosclerosis (3). Chemokines are a family of inflammatory cytokines characterized by their ability to cause directed migration of leukocytes, and raised levels are found in several inflammatory disorders (4). There is also some evidence suggesting that chemokines, e.g., interleukin (IL)-8 and monocyte chemoattractant protein 1 (MCP-1), may play a role in the pathogenesis of athero- sclerosis (5,6). In addition to being potent chemoattractants, several other leukocyte responses such as enzyme secretion and induction of reactive oxygen species (ROS) have been observed in vitro after chemokine stimulation (4,7). Some of these responses may clearly be relevant to the development of coronary artery disease (CAD). In particular, enhanced oxidative stress has been implicated in the pathogenesis of CAD and in the triggering of unstable angina (8). In view of the existing knowledge on the association of leukocyte activation and oxidative stress with atherosclerosis and acute coronary syndrome, we hypothesized that chemokines may play an important role in recruiting and activating leuko- cytes and in enhancing oxidative stress in these disorders. In the present study we investigated this hypothesis by differ- ent experimental approaches in stable and unstable angina patients. METHODS Patients and controls. Between January and June 1998 patients undergoing diagnostic coronary angiography in the coronary care unit at our hospital were consecutively regis- tered. Among those fulfilling the criteria of unstable angina (see following text), 38 patients were selected randomly for participation in the study (Table 1). All patients with unstable angina had experienced ischemic chest pain at rest within the proceeding 48 h, with no evidence of myocardial From the *Section of Clinical Immunology and Infectious Diseases; ²Research Institute for Internal Medicine; §Section of Endocrinology, Medical Department, \Department of Cardiology; Rikshospitalet, Oslo; ‡Department of Clinical Biology, Division of Clinical Biochemistry, Haukeland Hospital, Bergen, Norway. This work was supported by the Norwegian Council of Cardiovascular Disease, the Research Council of Norway, Anders Jahre’s Foundation and Medinnova Foundation, Oslo, Norway. Manuscript received May 8, 2000; revised manuscript received August 21, 2000, accepted October 2, 2000. Journal of the American College of Cardiology Vol. 37, No. 2, 2001 © 2001 by the American College of Cardiology ISSN 0735-1097/01/$20.00 Published by Elsevier Science Inc. PII S0735-1097(00)01110-4
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Interaction Between Chemokines and Oxidative Stress: Possible Pathogenic Role in Acute Coronary...

Interaction Between Chemokinesand Oxidative Stress: PossiblePathogenic Role in Acute Coronary SyndromesPål Aukrust, MD, PHD,*† Rolf K. Berge, PHD,‡ Thor Ueland, BS,§ Ellinor Aaser, MD,\Jan Kristian Damås, MD,†\ Lisbeth Wikeby, RN,†\ Anne Brunsvig, BS,\ Fredrik Muller, MD, PHD,*†Kolbjørn Forfang, MD, PHD,\ Stig S. Frøland, MD, PHD,*† Lars Gullestad, MD, PHD\
Oslo and Bergen, Norway
OBJECTIVES We sought to study the relationships between chemokines and oxidative stress in acutecoronary syndrome.
BACKGROUND In view of existing knowledge on the participation of leukocytes and oxidative stress in thepathogenesis of acute coronary syndrome, we hypothesized that chemokines may play a rolein recruiting and activating leukocytes in this disorder.
METHODS The levels of chemokines and oxidative stress were studied in 38 patients with stable and 38with unstable angina and in 20 controls. In separate in vitro experiments the effect ofchemokines on reactive oxygen species in monocytes and the effect of antioxidants onchemokine levels in these cells were also studied.
RESULTS 1) Angina patients had raised serum levels of chemokines in both cross-sectional andlongitudinal testing, with particularly high levels of interleukin (IL)-8, monocyte chemoat-tractant protein (MCP)-1 and macrophage inflammatory peptide (MIP)-1-alpha in unstabledisease. 2) T cells, and particularly monocytes, seem to contribute to the raised IL-8, MCP-1and MIP-1-alpha levels in unstable angina. 3) Concomitantly, and significantly correlatedwith MCP-1 and IL-8 levels, stable and particularly unstable angina patients had decreasedplasma levels of antioxidants and increased lipid peroxidation, suggesting enhanced oxidativestress. 4) Monocyte chemoattractant protein-1 enhanced the generation of O2
2 in monocytesfrom unstable angina patients, and the antioxidant glutathione-monoethyl ester suppressedthe production of IL-8 and MCP-1 in these cells.
CONCLUSIONS Our findings suggest an interaction between chemokines and oxidative stress in unstableangina. This interaction may represent a vicious circle involved in the pathogenesis of acutecoronary syndromes. (J Am Coll Cardiol 2001;37:485–91) © 2001 by the American Collegeof Cardiology
Increasing evidence supports the involvement of inflamma-tion in atherogenesis and in the pathogenesis of acutecoronary syndrome. Thus, activated monocytes, T cells andgranulocytes have been demonstrated in patients with un-stable angina (1,2), and extensive infiltration of blood-derived macrophages and T cells into the vessel wall is seenin the active stages of atherosclerosis (3). Chemokines are afamily of inflammatory cytokines characterized by theirability to cause directed migration of leukocytes, and raisedlevels are found in several inflammatory disorders (4). Thereis also some evidence suggesting that chemokines, e.g.,interleukin (IL)-8 and monocyte chemoattractant protein 1(MCP-1), may play a role in the pathogenesis of athero-sclerosis (5,6). In addition to being potent chemoattractants,several other leukocyte responses such as enzyme secretionand induction of reactive oxygen species (ROS) have been
observed in vitro after chemokine stimulation (4,7). Some ofthese responses may clearly be relevant to the developmentof coronary artery disease (CAD). In particular, enhancedoxidative stress has been implicated in the pathogenesis ofCAD and in the triggering of unstable angina (8). In viewof the existing knowledge on the association of leukocyteactivation and oxidative stress with atherosclerosis and acutecoronary syndrome, we hypothesized that chemokines mayplay an important role in recruiting and activating leuko-cytes and in enhancing oxidative stress in these disorders. Inthe present study we investigated this hypothesis by differ-ent experimental approaches in stable and unstable anginapatients.
METHODS
Patients and controls. Between January and June 1998patients undergoing diagnostic coronary angiography in thecoronary care unit at our hospital were consecutively regis-tered. Among those fulfilling the criteria of unstable angina(see following text), 38 patients were selected randomly forparticipation in the study (Table 1). All patients withunstable angina had experienced ischemic chest pain at restwithin the proceeding 48 h, with no evidence of myocardial
From the *Section of Clinical Immunology and Infectious Diseases; †ResearchInstitute for Internal Medicine; §Section of Endocrinology, Medical Department,\Department of Cardiology; Rikshospitalet, Oslo; ‡Department of Clinical Biology,Division of Clinical Biochemistry, Haukeland Hospital, Bergen, Norway. This workwas supported by the Norwegian Council of Cardiovascular Disease, the ResearchCouncil of Norway, Anders Jahre’s Foundation and Medinnova Foundation, Oslo,Norway.
Manuscript received May 8, 2000; revised manuscript received August 21, 2000,accepted October 2, 2000.
Journal of the American College of Cardiology Vol. 37, No. 2, 2001© 2001 by the American College of Cardiology ISSN 0735-1097/01/$20.00Published by Elsevier Science Inc. PII S0735-1097(00)01110-4

necrosis by enzymatic criteria. Transient ST-T segmentdepression and/or T-wave inversion were present in allcases. For comparison, 38 patients with stable angina wererandomly selected among those attending the Departmentof Cardiology at our hospital in the same period fordiagnostic coronary angiography (Table 1). All these pa-tients had stable effort angina of .6 months duration and apositive exercise test. Exclusion criteria included myocardialinfarction within the previous month, ECG abnormalitiesinvalidating ST-segment analyses, thrombolytic therapy theprevious month, body temperature .38.0°C or the occur-rence of inflammatory disease likely to be associated withacute-phase response (e.g., infections, malignancies orautoimmune disorders). Controls in the study were 20gender- and age-matched healthy blood donors (15 malesand five females, age 53 6 15 years). Blood collection andisolation of monocytes and T (CD31) cells for the study wasperformed as previously described (9,10). Informed consent
for participation in the study was obtained from all individ-uals.Superoxide anion (O2
2) assay. Monocytes (3 3 105/ml;200 ml/well) were cultured in 96-well trays (Costar, Cam-bridge, Massachusetts) in RPMI 1640 with L-glutamine(Gibco, Paisley, United Kingdom) supplemented with 10%fetal calf serum (Myoclone, Gibco) either alone or withdifferent concentrations of MCP-1, IL-8 or macrophageinflammatory peptide 1-alpha (MIP-1-alpha), all fromR&D Systems, Minneapolis, Minnesota. After 20 h, O2
2
generation in monocytes was measured by the superoxidedismutase-inhibitable reduction of cytochrome c as previ-ously described (10).Chemokine production in vitro. CD31T cells (106cells/ml) and monocytes (3 3 105cells/ml) were incubated in96-well trays (200 ml/well, Costar) in medium alone (RPMI1640 with 2 mmol/l L-glutamine and 25 mmol/L HEPESbuffer; Gibco, supplemented with 10% fetal calf serum) orwith stimulants: CD31 T cells: anti-CD3 monoclonalantibodies (final concentration 1.2 ng/ml; clone SpvT3b) (9)combined with anti-CD28 monoclonal antibodies (finalconcentration 50 ng/ml; clone 15E8 (402); CLB, Amster-dam, Netherlands) and cross-linking immunomagneticbeads (9); monocytes: lipopolysaccharide (LPS) from E. coliO26:B6 (final concentration 10 ng/ml, Sigma). In someexperiments different concentrations of glutathione-monoethyl ester (Bachem, Bubendorf, Switzerland) wereadded to cultures before stimulation. Cell-free supernatantswere harvested after 48 h and stored at 280°C.Measurements of chemokines. Levels of RANTES,MCP-1, MIP-1-alpha, IL-8, ENA-78 and GRO-alphawere determined by enzyme immunoassays (R&D Sys-tems).
Abbreviations and AcronymsCAD 5 coronary artery diseaseENA-78 5 epithelial neutrophil-activating
peptide-78GRO-alpha 5 growth-regulated oncogene alphaIL-8 5 interleukin-8LPS 5 lipopolysaccharideMCP-1 5 monocyte chemoattractant protein 1MIP-1-alpha 5 macrophage inflammatory peptide
1-alphaO2
2 5 superoxide anionRANTES 5 regulated on activation normally T cell
expressed and secretedROS 5 reactive oxygen species
Table 1. Characteristics of the Study Group
StableAngina
(n 5 38)
UnstableAngina
(n 5 38) p Value
Age (yrs) 59 6 11 58 6 12 0.600Gender (males/females) 31/7 29/9 0.576Smokers (%) 21 47 0.030Medication (%)
Calcium antagonist 15 22 0.422Aspirin 91 89 0.752HMG CoA reductase inhibitors 74 53 0.075Beta blockers 88 97 0.147Long-acting nitrates 41 50 0.462Infusion of nitroglycerin 0 17 0.013Warfarin 12 14 0.792
Numbers of affected coronaryarteries (%)
0.132
1 44 312 35 263 21 43
Total cholesterol (mmol/l) 4.8 6 0.9 4.9 6 1.0 0.870HDL cholesterol (mmol/l) 1.1 6 0.3 0.9 6 0.3 0.031Triglycerides (mmol/l) 1.8 6 1.1 1.8 6 0.9 0.927
Data are given as mean 6 SD.HDL 5 high density lipoprotein; HMG CoA 5 hepatic hydroxymethylglutaryl coenzyme A.
486 Aukrust et al. JACC Vol. 37, No. 2, 2001Enhanced Chemokine Levels in Unstable Angina February 2001:485–91

Parameters of oxidative stress and vitamin levels inplasma. Concentrations of vitamin C, vitamin E and beta-carotene were measured by high-performance liquid chro-matography (11). Total (free and esterified) 8-isoprostane(8-iso Prostaglandin F2a) in plasma were analyzed byenzyme immunoassay (Cayman Chemical, Ann Arbor,Michigan). Sample purification and recovery analyses wereperformed according to the purification protocol providedby the manufacturer.Statistical analysis. When comparing three groups, one-way ANOVA was followed by Scheffe’s post hoc test forstatistical significance. The chemokine data were not nor-mally distributed and were subjected to logarithmic trans-formation before the ANOVA analysis was performed. Forcomparisons within the same individuals over time, theWilcoxon matched pairs test was used. P-values are consid-ered significant when ,0.05.
RESULTS
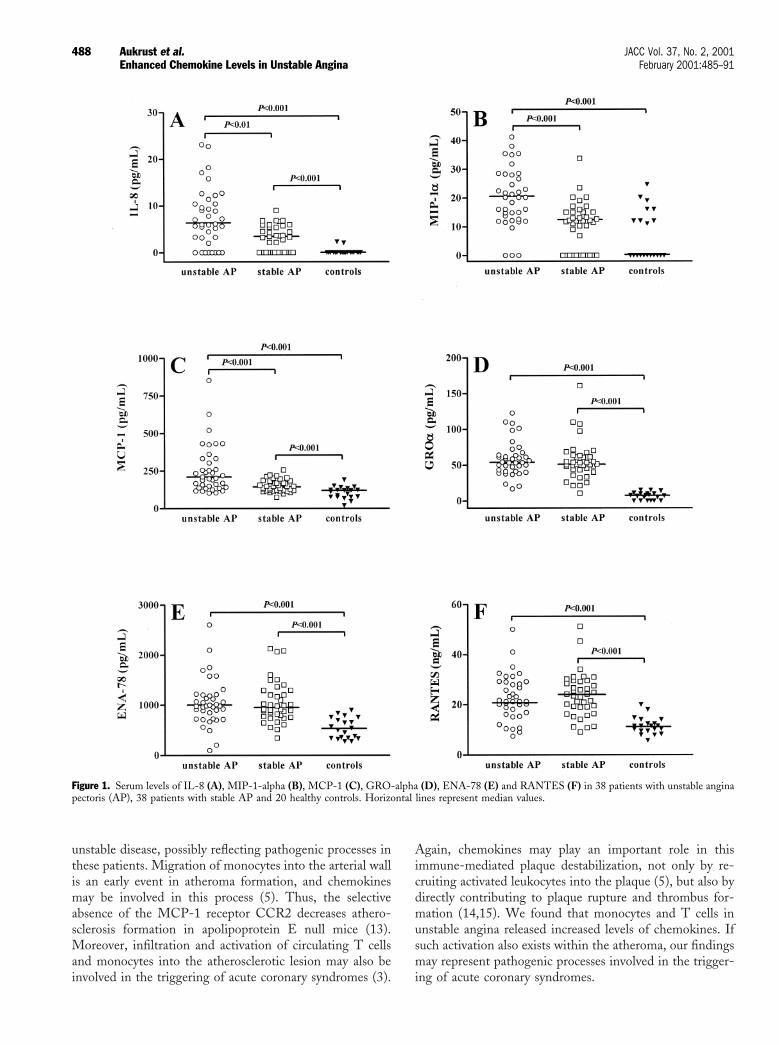
Serum levels of chemokines in angina patients. Levels ofall measured chemokines were elevated in both unstable andstable angina patients comparing healthy controls (Fig. 1).Although there were no significant differences in RANTES,ENA-78 or GRO-alpha levels between stable and unstableangina, particularly high IL-8, MCP-1 and MIP-1-alphalevels were found in unstable disease (Fig. 1). In ten patientswith unstable angina, blood samples were also availablebefore the patients developed an unstable disease (mediantime between blood samplings: 12 [range 4 to 20] weeks).Concomitant with the progression from stable to unstableangina, there was a significant rise in IL-8, MCP-1 andMIP-1-alpha (p , 0.005), but not in levels of the otherthree chemokines (data not shown).Release of chemokines from monocytes and T cells inperipheral blood. To possibly define the cellular sources ofIL-8, MCP-1 and MIP-1-alpha in unstable angina, spon-taneous and stimulated release of these chemokines from Tcells and monocytes were measured in five patients withstable angina, five with unstable angina and five controls.Monocytes in unstable angina released increased levels ofIL-8, MIP-1-alpha and MCP-1 both spontaneously andafter LPS stimulation, comparing cells in stable anginapatients (p , 0.05) and controls (p , 0.01). Furthermore,anti-CD3/anti-CD28 stimulated T cells from patients withunstable disease released higher levels of MIP-1-alphacomparing the two other groups of individuals (p , 0.05).Chemokine levels in relation to oxidative stress. We firstanalyzed plasma levels of 8-isoprostane, a sensitive markerof lipid peroxidation (12), and the antioxidant vitaminsbeta-carotene, vitamin C and vitamin E in 40 anginapatients (20 with stable and 20 with unstable disease) andten controls. Angina patients had raised 8-isoprostaneconcentrations compared with controls, with particularlyhigh levels in unstable disease (Fig. 2). Furthermore, vita-min C, vitamin E and beta-carotene levels in unstable
angina were significantly decreased compared with bothstable angina patients and controls (Fig. 2). In unstableangina, IL-8 and MCP-1 were positively correlated with8-isoprostane (r 5 0.71, p , 0.001; r 5 0.65, p , 0.005)and negatively correlated with vitamin E (r 5 20.61, p ,0.01; r 5 20.69, p , 0.001) and beta-carotene levels (r 520.57, p , 0.01; r 5 20.50, p , 0.05), IL-8 and MCP-1,respectively.The effect of chemokines on oxidative stress and viceversa. By additional experiments we further examined therelationship between oxidative stress and chemokines in sevenpatients with stable angina, seven with unstable angina andseven controls. Several significant findings were revealed. First,spontaneous and zymosan-stimulated O2
2generation wasmarkedly enhanced in monocytes from unstable, but not fromstable angina patients, compared with controls (Fig. 3). Sec-ond, MCP-1, but not IL-8 or MIP-1-alpha, markedly en-hanced zymosan-stimulated O2
2generation in monocytesfrom both patients and controls, with particularly enhancingeffect in those with unstable disease, when added to cellcultures at the start of the culture period (Fig. 3A). Finally,MCP-1, but not IL-8 or MIP-1-alpha, also directly inducedO2
2generation in a dose-dependent manner in both patientsand controls, with particularly enhancing effect in unstableangina, when added to monocytes after 20 h of culture inmedium alone (Fig. 4C).
When the antioxidant glutathione-monoethyl ester wasadded to monocyte cultures, there was a dose-dependentreduction in LPS-stimulated release of IL-8 and MCP-1,but not MIP-1-alpha, in both patients and controls, with aparticularly suppressive effect in unstable angina (Fig. 4Aand B). In stable and particularly in unstable angina such areduction was also found in the spontaneous release of thesechemokines (Fig. 4C and D). Glutathione-monoethyl esteralso suppressed MCP-1, but not MIP-1-alpha levels, instimulated T cells in both patients and controls (data notshown).
DISCUSSION
The present study shows that raised levels of several che-mokines characterize angina patients, particularly those withunstable disease. Concomitantly, and significantly corre-lated with raised MCP-1 and IL-8 levels, stable andparticularly unstable angina patients had decreased plasmalevels of antioxidants and increased lipid peroxidation,suggesting enhanced oxidative stress in these patients.Finally, MCP-1 was found to enhance ROS generation inmonocytes from unstable angina patients and the antioxi-dant glutathione-monoethyl ester reduced the production ofIL-8 and MCP-1 in these cells, suggesting an interactionbetween chemokines and oxidative stress in unstable angina.Enhanced levels of CXC- and CC-chemokines in unsta-ble angina. We demonstrate that angina patients haveraised levels of both CC and CXC-chemokines with par-ticularly high IL-8, MCP-1 and MIP-1-alpha levels in
487JACC Vol. 37, No. 2, 2001 Aukrust et al.February 2001:485–91 Enhanced Chemokine Levels in Unstable Angina
unstable disease, possibly reflecting pathogenic processes inthese patients. Migration of monocytes into the arterial wallis an early event in atheroma formation, and chemokinesmay be involved in this process (5). Thus, the selectiveabsence of the MCP-1 receptor CCR2 decreases athero-sclerosis formation in apolipoprotein E null mice (13).Moreover, infiltration and activation of circulating T cellsand monocytes into the atherosclerotic lesion may also beinvolved in the triggering of acute coronary syndromes (3).
Again, chemokines may play an important role in thisimmune-mediated plaque destabilization, not only by re-cruiting activated leukocytes into the plaque (5), but also bydirectly contributing to plaque rupture and thrombus for-mation (14,15). We found that monocytes and T cells inunstable angina released increased levels of chemokines. Ifsuch activation also exists within the atheroma, our findingsmay represent pathogenic processes involved in the trigger-ing of acute coronary syndromes.
Figure 1. Serum levels of IL-8 (A), MIP-1-alpha (B), MCP-1 (C), GRO-alpha (D), ENA-78 (E) and RANTES (F) in 38 patients with unstable anginapectoris (AP), 38 patients with stable AP and 20 healthy controls. Horizontal lines represent median values.
488 Aukrust et al. JACC Vol. 37, No. 2, 2001Enhanced Chemokine Levels in Unstable Angina February 2001:485–91

MCP-1 enhances ROS generation from monocytes inunstable angina. We found markedly decreased levels ofseveral antioxidants in angina patients, with particularly lowlevels in unstable disease. This decrease in unstable angina wasaccompanied by increased lipid peroxidation and enhancedROS generation in monocytes, suggesting enhanced oxidative
stress in these patients. Although several factors may mediateenhanced ROS generation in unstable angina (e.g., oxidizedLDL, hypoxia/reoxygenation) (8), our results suggest thatchemokines and particularly MCP-1 may be involved. Severalcytokines may prime phagocytes for enhanced ROS generation(9), but only certain chemokines may directly induce ROS
Figure 2. Plasma levels of 8-isoprostane (A), beta-carotene (B), vitamin C (C) and vitamin E (D) in 20 patients with unstable angina pectoris (AP), 20patients with stable AP and 10 healthy controls. Horizontal lines represent median values.
Figure 3. MCP-1 and production of reactive oxygen species in monocytes from seven patients with unstable angina pectoris (AP), seven patients with stableAP and seven healthy controls. (A) The effect of different concentrations of MCP-1 on zymosan-stimulated O2
2 generation when added to cell culturesat the start of the culture period (20 hours before zymosan stimulation). (B) The effect of different concentrations of MCP-1 on O2
2 generation when addedto monocytes after 20 h of culture in medium alone. *p , 0.05 and **p , 0.01 versus no addition of MCP-1. Data are given as mean 6 SEM. Note: bothunstimulated and zymosan-stimulated O2
2 generation after 20 h of culture in medium alone (MCP-1 5 0 ng/ml) were significantly raised in unstableangina patients comparing both those with stable disease and healthy controls (p , 0.01).
489JACC Vol. 37, No. 2, 2001 Aukrust et al.February 2001:485–91 Enhanced Chemokine Levels in Unstable Angina

generation as demonstrated for MCP-1 in the present study,with particularly enhancing effects in monocytes in unstableangina.Antioxidants impair the release of chemokines frommonocytes in unstable angina. Whereas MCP-1 en-hanced ROS generation in monocytes from unstable anginapatients, glutathione-monoethyl ester markedly suppressedMCP-1 and IL-8 production in these cells. Several studieshave demonstrated that oxidative stress may activate thetranscription factor NF-kappa-B in various cell types (16).Notably, NF-kappa-B, which recently was found to beactivated in leukocytes from unstable angina patients (17), isinvolved in the induction of IL-8 and MCP-1 in both Tcells and monocytes (18,19). Thus, if similar mechanismsalso operate in vivo within an atherosclerotic lesion, theinteraction between chemokines and oxidative stress mayrepresent a pathogenic loop in unstable angina.Interaction between chemokines and oxidative stress—possible pathogenic role in plaque rupture. Unstableangina patients had raised levels of chemokines and oxida-tive stress compared with stable angina patients, and as forspontaneous and MCP-1 induced O2
2 production, therewas no overlap between the two patient groups. Thesefindings may be of interest. Thus, enhanced ROS genera-tion within the atherosclerotic plaque may promote apopto-
sis and enhance the activity of matrix degrading enzymeswithin the atherosclerotic lesion, potentially promotingplaque destabilization (20). Also, although moderatelyraised chemokine levels may play a role in the developmentof stable angina, more marked chemokine activation inpatients with a pre-existing atherosclerotic plaque, particu-larly when combined with enhanced oxidative stress, maycontribute to the promotion of plaque rupture.Conclusions. The interaction between chemokines andoxidative stress in angina patients may represent pathogenicmechanisms. Though it may not necessarily be the initialevent, this “pathogenic loop” may contribute to the progres-sion of atherosclerosis in these patients. Even more impor-tantly, this vicious circle seems to be particularly activated inunstable disease, and such interaction between chemokinesand oxidation may represent pathogenic processes involvedin the triggering of acute coronary syndromes.
Reprint requests and correspondence: Dr. Pål Aukrust, Section ofClinical Immunology and Infectious Diseases, Medical Department,Rikshospitalet, Sognsvannsveien 20, N-0027 Oslo, Norway. E-mail:pal.aukrust@rikshospitalet.
Figure 4. The effect of different concentrations of glutathione-monoethyl ester on the release of MCP-1 (A and C) and IL-8 (B and D) in LPS-stimulated(A and B) and unstimulated (C and D) monocytes from seven patients with unstable angina pectoris (AP), seven patients with stable AP and seven healthycontrols. Cells were cultured for 48 h. *p , 0.05 and **p , 0.01 versus no addition of glutathione-monoethyl ester.
490 Aukrust et al. JACC Vol. 37, No. 2, 2001Enhanced Chemokine Levels in Unstable Angina February 2001:485–91

REFERENCES
1. Serneri GGN, Prisco D, Martini F, et al. Acute T-cell activation isdetectable in unstable angina. Circulation 1997;95:1806–12.
2. Mazzone A, De Servi S, Ricevuti G, et al. Increased expression ofneutrophil and monocyte adhesion molecules in unstable coronaryartery disease. Circulation 1993;88:358–63.
3. Entmann ML, Ballantyne CM. Inflammation and acute coronarysyndromes. Circulation 1993;88:800–3.
4. Baggiolini M, Dewald B, Moser B. Interleukin-8 and related chemo-tactic cytokines: CXC and CC chemokines. Adv Immunol 1994;55:97–179.
5. Reape TJ, Groot PH. Chemokines and atherosclerosis. Atherosclero-sis 1999;147:213–25.
6. Nelken L, Coughlin S, Gordon D, Wilkox J. Monocyte chemoattrac-tant protein-1 in human atheromatous plaques. J Clin Invest 1991;88:1121–7.
7. Rollins BJ, Walz A, Baggiolini M. Recombinant human MCP-1/JEinduces chemotaxis, calcium flux, and the respiratory burst in humanmonocytes. Blood 1991;78:1112–6.
8. Maxwell SRJ, Lip GYH. Free redicals and antioxidants in cardiovas-cular disease. Br J Clin Pharmacol 1997;44:307–17.
9. Aukrust P, Muller F, Ueland T, et al. Enhanced levels of soluble andmembrane-bound CD40 ligand in patients with unstable angina—possible reflection of T lymphocyte and platelet involvement in thepathogenesis of acute coronary syndromes. Circulation 1999;100:614–20.
10. Aukrust P, Ueland T, Muller F, et al. Elevated circulating levels ofC-C chemokines in patients with congestive heart failure. Circulation1998;97:1136–43.
11. Aukrust P, Berge RK, Muller F, Ueland PM, Svardal AM, FrølandSS. Elevated plasma levels of reduced homocysteine in commonvariable immunodeficiency—a marker of enhanced oxidative stress.Eur J Clin Invest 1997;27:723–30.
12. Voutilainen S, Morrow JD, Roberts LJ, et al. Enhanced in vivo lipidperoxidation at elevated plasma total homocysteine levels. ArteriosclerThromb Vasc Biol 1999;19:1263–6.
13. Dawson TC, Kuziel WA, Osahar TA, Maeda N. Absence of CCchemokine receptor-2 reduces atherosclerosis in apolipoproteinE-deficient mice. Atherosclerosis 1999;143:205–11.
14. Moreau M, Brocheriou I, Petit L, Ninio E, Chapman MJ, Rouis M.Interleukin-8 mediates downregulation of tissue inhibitor ofmetalloproteinase-1 expression in cholesterol-loaded human macro-phages: relevance to stability of atherosclerotic plaque. Circulation1999;99:420–6.
15. Schecter AD, Rollins BJ, Zhang YJ, et al. Tissue factor is induced bymonocyte chemoattractant protein-1 in human aortic smooth muscleand THP-1 cells. J Biol Chem 1997;272:28568–73.
16. Li N, Karin M. Is NF-kB the sensor of oxidative stress? FASEB J1999;13:1137–43.
17. Ritchie ME. Nuclear factor-kB is selectively and markedly activated inhumans with unstable angina pectoris. Circulation 1998;98:1707–13.
18. DeForge LE, Preston AM, Takeuchi E, Kenney J, Boxer LA, RemickDG. Regulation of interleukin 8 gene expression by oxidant stress.J Biol Chem 1993;268:25568–76.
19. Lee JS, Kahlon SS, Culbreth R, Cooper AD Jr. Modulation ofmonocyte chemokine production and nuclear factor kappa B activity byoxidants. J Interferon Cytokine Res 1999;19:761–7.
20. Davies MJ. Reactive oxygen species, metalloproteinases and plaquestability. Circulation 1998;97:2382–3.
491JACC Vol. 37, No. 2, 2001 Aukrust et al.February 2001:485–91 Enhanced Chemokine Levels in Unstable Angina









![Syndromes drépanocytaires atypiques : à propos de deux cas [Atypical sickle cell syndromes: A report on two cases]](https://static.fdokumen.com/doc/165x107/6319e3d265e4a6af371005c0/syndromes-drepanocytaires-atypiques-a-propos-de-deux-cas-atypical-sickle-cell.jpg)










