Incidence of gastroesophageal reflux disease and positive maxillary antral cultures in children with...
16
Accepted Manuscript Title: Incidence of Gastroesophageal Reflux Disease & Positive Maxillary Antral Cultures in Children with Symptoms of Chronic Rhinosinusitis Author: Javan Nation Michael Kaufman Meredith Allen Anthony Sheyn James Coticchia PII: S0165-5876(13)00544-2 DOI: http://dx.doi.org/doi:10.1016/j.ijporl.2013.10.057 Reference: PEDOT 6869 To appear in: International Journal of Pediatric Otorhinolaryngology Received date: 5-8-2013 Revised date: 14-10-2013 Accepted date: 15-10-2013 Please cite this article as: J. Nation, M. Kaufman, M. Allen, A. Sheyn, J. Coticchia, Incidence of Gastroesophageal Reflux Disease & Positive Maxillary Antral Cultures in Children with Symptoms of Chronic Rhinosinusitis, International Journal of Pediatric Otorhinolaryngology (2013), http://dx.doi.org/10.1016/j.ijporl.2013.10.057 This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Incidence of gastroesophageal reflux disease and positive maxillary antral cultures in children with...

Accepted Manuscript
Title: Incidence of Gastroesophageal Reflux Disease &Positive Maxillary Antral Cultures in Children withSymptoms of Chronic Rhinosinusitis
Author: Javan Nation Michael Kaufman Meredith AllenAnthony Sheyn James Coticchia
PII: S0165-5876(13)00544-2DOI: http://dx.doi.org/doi:10.1016/j.ijporl.2013.10.057Reference: PEDOT 6869
To appear in: International Journal of Pediatric Otorhinolaryngology
Received date: 5-8-2013Revised date: 14-10-2013Accepted date: 15-10-2013
Please cite this article as: J. Nation, M. Kaufman, M. Allen, A. Sheyn, J. Coticchia,Incidence of Gastroesophageal Reflux Disease & Positive Maxillary Antral Cultures inChildren with Symptoms of Chronic Rhinosinusitis, International Journal of PediatricOtorhinolaryngology (2013), http://dx.doi.org/10.1016/j.ijporl.2013.10.057
This is a PDF file of an unedited manuscript that has been accepted for publication.As a service to our customers we are providing this early version of the manuscript.The manuscript will undergo copyediting, typesetting, and review of the resulting proofbefore it is published in its final form. Please note that during the production processerrors may be discovered which could affect the content, and all legal disclaimers thatapply to the journal pertain.
Page 1 of 15
Accep
ted
Man
uscr
ipt
Incidence of Gastroesophageal Reflux Disease & Positive Maxillary Antral Cultures in Children with Symptoms of
Chronic Rhinosinusitis
Javan Nation M.D., Michael Kaufman B.S., Meredith Allen, Anthony Sheyn M.D., James Coticchia M.D.
Author Affiliations: Wayne State University Department of Otolaryngology-Head and Neck Surgery (Drs Nation, Sheyn, and Coticchia) Wayne State University School of Medicine (Mr Kaufman) University of Florida (Ms Allen)
Corresponding Author: Javan Nation 4201 St. Antoine 5E-UHC Detroit, MI 48201 [email protected]
Cell: 951.897.2125 No conflicts of interest to disclose for any of the authors
*Title Page

Page 2 of 15
Accep
ted
Man
uscr
ipt
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
Incidence of Gastroesophageal Reflux Disease & Positive Maxillary Antral Cultures in Children with Symptoms of
Chronic Rhinosinusitis Javan Nation M.D., Michael Kaufman B.S., Meredith Allen, Anthony Sheyn M.D., James
Coticchia M.D. Author Affiliations: Wayne State University Department of Otolaryngology-Head and Neck Surgery (Drs Nation, Sheyn, and Coticchia) Wayne State University School of Medicine (Mr Kaufman) University of Florida (Ms Allen) Corresponding Author: Javan Nation 4201 St. Antoine 5E-UHC Detroit, MI 48201 [email protected] Cell: 951.897.2125 No conflicts of interest to disclose
*Manuscript

Page 3 of 15
Accep
ted
Man
uscr
ipt
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
Abstract Objective: Studies have shown that gastroesophageal reflux disease occurs more frequently than expected in children with chronic rhinosinusitis. The objective of this study is to further understand the relationship of pediatric chronic rhinosinusitis and gastroesophageal reflux disease in children with symptoms of rhinorrhea, nasal congestion, and chronic cough. Methods: A retrospective chart review of 63 children, ages 6 months to 10 years old with rhinorrhea, nasal congestion, and chronic cough. The patients underwent maxillary cultures, adenoidectomy, and distal third esophageal biopsies. Children with esophageal biopsies showing esophagitis were classified as positive for gastroesophageal reflux disease, and maxillary antral swabs growing a high density of bacteria were classified as positive for chronic rhinosinusitis. Results: Six months to 5 years old children (n=43), 6 (14%) had simultaneous positive maxillary antral cultures and positive esophageal biopsies, 11 (26%) had positive esophageal biopsies alone, 23 (53%) had positive maxillary antral cultures alone, and 3 (7%) had neither. Six to 10 years old children (n=20), 9 (45%) had simultaneous positive maxillary antral cultures and positive esophageal biopsies, 1 (5%) patient had positive esophageal biopsies alone, 3 (15%) patients had positive maxillary antral cultures alone, and 7 (35%) patients had neither. Twenty-seven (42%) of the patients from the whole study had gastroesophageal reflux positive biopsies. The younger children were statistically likely to have chronic rhinosinusitis and gastroesophageal reflux disease independently of each other (p=0.0002). A direct group comparison found the younger group to have independent chronic rhinosinusitis and gastroesophageal reflux disease and the older group to have simultaneous chronic rhinosinusitis and gastroesophageal reflux disease (p=0.0006). Conclusion: In children with the presenting symptoms of rhinorrhea, nasal congestion, and chronic cough, younger children tend to have either chronic rhinosinusitis or gastroesophageal reflux disease, whereas older children tend to have a more complicated etiology of chronic rhinosinusitis and gastroesophageal reflux disease or other. In all of these patients gastroesophageal reflux disease plays an important role, as over 40% of all patients had gastroesophageal positive biopsies.
Page 4 of 15
Accep
ted
Man
uscr
ipt
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
Introduction Chronic rhinosinusitis (CRS) has a severe impact on the health related quality of life in the pediatric population and is a challenging disease for physicians to treat [1]. Studies have demonstrated that gastroesophageal reflux disease (GERD) occurs more frequently than expected in patients with CRS [2]. The signs and symptoms of pediatric sinusitis include chronic cough, rhinorrhea, nasal congestion, and post nasal drip. Some common pediatric symptoms of GERD include nasopharyngeal inflammation and secretions, sore throat, chronic cough, recurrent pneumonia, and chronic and/or recurrent middle ear infections [3-5]. The similarity in nasal symptoms of discharge and congestion from nasal inflammation makes an accurate diagnosis of GERD and/or CRS challenging. CRS is one of the most common diseases in the pediatric population [6], and the diagnosis is made primarily clinically. Practice guidelines have been issued by the American Academy of Pediatrics [7], however the pathogenesis and management of this disease continues to be relatively undetermined [8]. Sinus aspiration with recovery of bacteria in high density (≥104 colony-forming units/mL) from the paranasal sinuses remains the gold standard for the diagnosis of acute or chronic bacterial sinusitis [9]. CRS in children has multiple etiologies including viral and bacterial upper airway infections, allergies, GERD, smoking irritants, cystic fibrosis, immunodeficiency, mucociliary disorders, and nasal and sinus anatomical abnormalities [10-12]. The bacteriology of CRS includes the 3 main pathogens associated with acute disease: Streptococcus pneumoniae, Haemophilus influenza, and Moraxella catarrhalis. Chronic sinusitis also includes Staphylococcus aureus, Pseudomonas, anaerobic bacteria, and fungi. Studies have shown that the role of bacterial infection as a primary cause of chronic infection has not been defined and that noninfectious factors such as GERD, allergy, etc., may play more of a role in the chronic inflammation of the paranasal sinuses [13, 14]. It is estimated that 5 –13% of viral upper respiratory infections are complicated by secondary bacterial sinusitis [15], 5–10% of which do not respond to conventional antimicrobial therapy [16]. Studies have found that children in the 1-5 year old age group are found to respond more frequently to a single course of antibiotics, compared to the older children in the 4-7 year-old group that tend to have more chronic symptoms [17]. Most healthy infants have occasional regurgitation known as physiologic reflux. Nelson reported an incidence of gastroesophageal reflux (GER) in up to 60% of infants aged 6 months, which declined to 5% at the end of the first year of life [18]. GER at this age is due mainly to lower esophageal sphincter immaturity and a predominantly liquid diet. Reflux fades by 1 year of age as solids are introduced into the diet and the lower esophageal sphincter matures [19]. Persistent and bothersome gastroesophageal reflux in children resulting in secondary conditions such as respiratory symptoms, apnea, and failure to thrive; is considered pathologic and thus termed GERD. In children, GERD is associated with an increased risk of sinusitis, asthma, laryngitis, and bronchiectasis [20]. Studies have shown that 10%
Page 5 of 15
Accep
ted
Man
uscr
ipt
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
of infants suffer from GERD, and that up to 25% of asymptomatic children have GERD with 8% having nasopharyngeal reflux [21, 22]. The “gold standard” for the diagnosis of GERD is the 24-hour pH probe [23], and the double electrode pH probe with distal esophageal plus pharyngeal or proximal esophageal electrodes is considered the “gold standard” for diagnosis of nasopharyngeal reflux and the extraesophageal manifestations of GERD [3]. Esophageal biopsy showing histologic esophagitis is a rapid, safe and effective diagnostic test for GERD that can be done during rigid esophagoscopy [24]. Laryngopharyngeal reflux (LPR) is defined as the extraesophageal reflux of gastric contents into the larynx and hypopharynx and when the reflux reaches the nasopharynx it is termed nasopharyngeal reflux (NPR). LPR is considered a distinct entity from GERD, as patients with LPR do not have the complaints of heartburn or other esophagitis symptoms [25]. LPR is commonly associated with hoarseness, dysphagia, globus sensation, and chronic throat clearing [26, 27]. The reflux of gastric contents into the pharynx is also associated with the nasal symptoms, and it has been demonstrated that NPR plays a role in refractory sinusitis [28]. Wise et al. provided evidence using pH probe testing, that patients with pathological NPR and LPR have the increased symptom of postnasal drip [29].
Both CRS and GERD are common diseases affecting patients, however studies demonstrate that GERD occurs more frequently than expected in patients with CRS [2]. The objective of this study was to further explore the relationship of CRS and GERD by studying the incidence of simultaneous or independent CRS and GERD, using maxillary antral cultures and esophageal biopsies as presumptive diagnostic tests, in children with symptoms of nasal rhinorrhea, congestion, and chronic cough.
Methods The study was designed as a retrospective chart review of the medical records of 63 children ages 6 months to 10 years old at Wayne State University who presented to clinic with symptoms of nasal congestion, rhinorrhea, and cough lasting longer than 12 weeks, refractory to first line antimicrobial therapy. Approval from the institutional review board at Wayne State University was obtained before proceeding with the retrospective chart review. The following information was acquired: age, sex, presenting signs and symptoms, duration of symptoms, concurrent surgical procedures performed, maxillary sinus culture, and esophageal biopsy results. The procedures took place from September 2010 to September 2011. The patients had been taken to the operating room to undergo adenoidectomy, bronchoscopy, esophagoscopy with biopsy, and nasal endoscopy with culture and biopsy of the osteomeatal complex. The osteomeatal complex was carefully swabbed in order to prevent contamination. During esophagoscopy a note was made of any signs of mucosal ulcerations, mucosal cobble stoning, or esophagitis. Biopsies were taken of the distal one third of the esophagus and sent for histologic assessment of esophagitis or other abnormalities.

Page 6 of 15
Accep
ted
Man
uscr
ipt
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
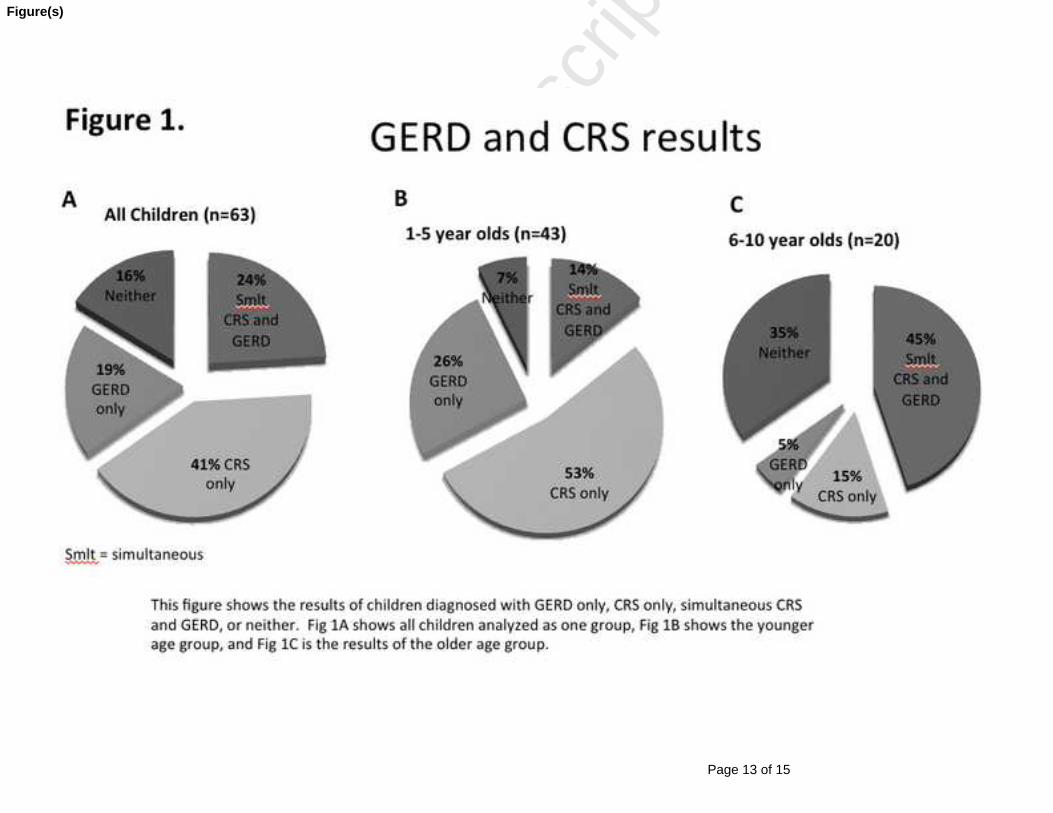
The children were divided into two separate age groups for the purpose of analysis, the younger group was 6 months to 5 years old, and the older group was 6 to 10 years old. Forty-three of the patients were in the younger group, and twenty patients were in the older group. Children with an esophageal biopsy showing esophagitis were classified as positive for GERD, and nasal swabs growing a high density of bacteria were classified as positive for CRS. Results Twenty-seven of the 63 children had esophageal biopsies that were positive for esophagitis. Eighteen (66%) children were in the 6-month to 5-year-old age group, and 9 (34%) were in the 6-10 year old age group. When analyzing all the patients as one group (n=63), 15 (24%) patients were found to have simultaneous positive maxillary antral cultures and positive esophageal biopsies, 12 (19%) patients had positive esophageal biopsies alone, 26 (41%) patients had positive maxillary antral cultures alone, and 10 (16%) patients had neither (Fig. 1A). When analyzing the patients in two separate age groups, some interesting differences were found. In the younger age group (n=43), 6 (14%) patients were found to have simultaneous positive maxillary antral cultures and positive esophageal biopsies, 11 (26%) patients had positive esophageal biopsies alone, 23 (53%) patients had positive maxillary antral cultures alone, and 3 (7%) patients had neither (Fig 1B). In the older age group (n=20), 9 (45%) patients were found to have simultaneous positive maxillary antral cultures and positive esophageal biopsies, 1 (5%) patient had positive esophageal biopsies alone, 3 (15%) patients had positive maxillary antral cultures alone, and 7 (35%) patients had neither (Fig. 1C). An analysis of the younger age group alone revealed that in patients with an esophageal biopsy positive for esophagitis, 61% had a negative maxillary antral culture, and 39% had a positive maxillary antral culture. Of the children with a negative esophageal biopsy, 92% had a positive antral culture and only 8% had a negative culture (Fig. 2). In other words, the 6-month to 5-year-old children were statistically likely to have positive maxillary antral cultures and positive esophageal biopsies independently of each other (Two tailed Fisher Exact Test p=0.0002). When comparing the two age groups, it was statistically significant for the younger group to have independent positive maxillary antral cultures and positive esophageal biopsies and the older group to have simultaneous positive maxillary antral cultures and positive esophageal biopsies (Two tailed Fisher Exact Test p=0.0006). Twenty-seven of the 63 (42%) of the patients studied had biopsy proven GERD. This prevalence of GERD was consistent when analyzing the two age groups separately, with the younger age group having 41% GERD prevalence, and the older group having 45% GERD prevalence (Fig. 3). Twenty-eight of the 43 patients in the younger group had positive sinus cultures with 43% S. pneumonia, 28% H. Influenza, 11% M. catarrhalis, 7% S. aureus, and
Page 7 of 15
Accep
ted
Man
uscr
ipt
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
11% methicillin resistant S. aureus. Eleven of the 20 patients in the older group had positive sinus cultures with 9% S. pneumonia, 0% H. Influenza, 46% M. catarrhalis, 36% S. aureus, and 9% methicillin resistant S. aureus (Table 1). Discussion The symptomatic etiologies between the two age groups of children are shown to be different. The younger children in this study were found to have the symptoms of nasal congestion, nasal drainage, and cough secondary to either CRS only, or GERD only, while 14% were found to suffer from these diseases simultaneously. In comparison, the older children tended to either suffer from both CRS and GERD simultaneously, or have these symptoms from a different etiology all together. Thirty-five percent of the older children with nasal congestion, nasal drainage, and cough had neither positive cultures nor positive esophageal biopsies, suggesting that their symptoms are from other etiologies such as allergies, smoking irritants, nasal sinus anatomical abnormalities, bacterial biofilms, or other. This is consistent with studies demonstrating that 1-5 year old children are found to respond more frequently to a single course of antibiotics, compared to the older children in the 4-7 year-old group that tend to have more chronic symptoms [17]. In our study, 53% of the younger children had CRS only, which would be more likely to respond to a simple course of oral antibiotics, whereas the older children tended to have a multifactorial etiology, which would not respond to a simple course of antibiotics. The connection between GERD and CRS was first proposed by Holmes et al in the 1950’s, however a clear understanding of the pathophysiology is still lacking [30]. Different mechanisms have been proposed to explain the affects that reflux may have on the paranasal sinus mucosa. One theory is the mechanism of the direct effect of refluxate on paranasal mucosa from LPR causing an inflammatory response. The entity of LPR playing a role in sinus symptoms by refluxate into the nasopharynx has been demonstrated by the use of 24-hour pH probe studies, and a higher number of NPR events below pH 4 and pH 5 are associated with refractory CRS [28], as well as the finding of pepsin in the nasal aspirates of children suffering from LPR [31]. However, this theory of direct NPR has been challenged by other studies. Wong et al. demonstrated that nasopharyngeal reflux is a rare event and only 2 episodes of 809-reflux events recorded were found to reach the nasopharynx [32]. Despite the contrasting literature, a link between CRS and GERD seems to exist, and is supported by studies that show proton-pump inhibitor treatment improving CRS symptoms [33-35]. Another mechanism to help explain this link is the “gastronasal reflex”, which was demonstrated in a study by Wong et al. The study showed a tendency for an increase in nasal mucus production, nasal symptom scores and, to a lesser extent, nasal inspiratory peak flow after esophageal stimulation with both normal saline and hydrochloric acid. Their results support the possibility that a neural reflex exists between the esophagus and the paranasal sinuses via the vagus nerve [36].

Page 8 of 15
Accep
ted
Man
uscr
ipt
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
All of the children in this study suffered from the same nasal symptoms, despite not all having the same disease etiology. Nineteen percent of all the children were found to have GERD only, suggesting that GERD plays a role in nasal symptoms. Forty-five percent of the older children were found to have simultaneous GERD and CRS, also suggesting that GERD potentially plays a role in the development of CRS in older children. However, a limitation of this study is that it cannot provide direct evidence of a GERD mechanism responsible for nasal symptoms or the development of CRS. Many studies have demonstrated the role paranasal and nasopharyngeal biofilms play in chronic rhinosinusitis. Bacterial biofilms are sessile communities of interacting bacteria attached to a surface and encased in a hydrated matrix rather than living in a motile “planktonic” or free-floating state [37]. In the planktonic state, bacteria can produce a host response setting off the acute infection cascade resulting in fevers, inflammation, and leukocyte stimulation. Standard antibiotic therapy can only eliminate the planktonic cells, leaving the sessile forms to propagate within the biofilm and to continue to disseminate when the therapy is terminated. The exopolysaccharides matrix protects from phagocytosis and other host defense mechanisms due to lack of accessibility by immunoglobulins and complement. These features make biofilm bacteria tricky to culture using standard techniques, problematic to eradicate with antimicrobial therapy, and permits for the development of effective and widespread antimicrobial resistance. In this study, a negative culture result does not necessarily rule out the possibility of a bacterial infection as the disease causing bacteria are potentially encased in biofilm. An explanation for the decreased cultures in the older age group could be that the older children have had more recurrent infections and opportunities for biofilms to be established. A study by Criddle et al. demonstrated that clinical resolution of symptom’s were achieved in 96% of children with rhinorrhea, nasal congestion and obstruction, and chronic cough using adenoidectomy plus long term dual antimicrobial therapy [38]. The difference in etiology between the two groups is important when considering treatment. When treating younger patients, a single modality therapy of either antibiotics or reflux medications is more likely to be adequate. The older children according to this study are more likely to need either multimodality therapy of antibiotics and reflux medications, long-term antimicrobial therapy to eradicate biofilms, or further workup looking for a different etiology. The two groups had differences in bacterial culture results, as 71% of the younger children grew either S. pneumonia or H. influenza, and 82% of the older children grew either M. catarrhalis or S. aureus. The most apparent finding among the patient cohort and similarity between the two age groups is that over 40% of all the patients suffered from GERD. Close to half of the patients presenting to clinic with rhinorrhea, nasal congestion, and chronic cough have an associated GERD diagnosis. GERD prophylaxis in these patients to assess for improvement in symptoms before further workup would be a reasonable
Page 9 of 15
Accep
ted
Man
uscr
ipt
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
therapeutic option. Conclusion In conclusion, symptoms of nasal congestion, nasal drainage, and cough are common symptoms in children. CRS and GERD are very common diseases found in children, however the incidence of simultaneous or independent disease in children belonging to the 6-month to 5-year-old age group is different compared to children in the 6-10 year old age group. Children in the younger age group were more likely to have independent CRS or GERD, while the older children were more likely to have these diseases simultaneously. Over 40% of patients with these presenting symptoms suffer from underlying GERD. This is important when considering the etiology of nasal symptoms and effective therapy. References [1] J.M. Cunningham, E.J. Chiu, J.M. Landgraf, R.E. Gliklich, The health impact of
chronic recurrent rhinosinusitis in children, Arch. Otolaryngol. Head Neck Surg. 126 (2000) 1363-1368.
[2] D.W. Chambers, W.E. Davis, P.R. Cook, G.J. Nishioka, D.T. Rudman. Long-term outcome analysis of functional endoscopic sinus surgery: correlation of symptoms with endoscopic examination findings and potential prognostic variables, Laryngoscope 107 (1997) 504-510.
[3] P. Contencin, P. Narcy, Nasopharyngeal pH monitoring in infants and children with chronic rhinopharyngitis, Int. J. Pediatr. Otorhinolaryngol. 22 (1991) 249-256.
[4] C.D. Phipps, W.E. Wood, W.S. Gibson, W.J. Cochran. Gastroesophageal reflux contributing to chronic sinus disease in children: a prospective analysis, Arch. Otolaryngol. Head Neck Surg. 126 (2000) 831-836.
[5] M. Velepic, V. Rozmanic, M. Velepic, M. Bonifacic, Gastroesophageal reflux, allergy and chronic tubotympanal disorders in children. Int. J. Pediatr. Otorhinolaryngol. 55 (2000) 187-190.
[6] R.Lusk, Pediatric chronic rhinosinusitis, Curr. Opin. Otolaryn. Head Neck Surg. 14 (2006) 393-396.
[7] J.P. Ioannidis, J. Lau, Technical report: evidence for the diagnosis and treatment of acute uncomplicated sinusitis in children: a systematic overview, Pediatrics 108 (2001) E57.
[8] R.W. Steele, Clin Pediatr (Phila) 44 (2005) 465-471. [9] Clinical practice guideline: management of sinusitis, Pediatrics 108 (2001)
798-808. [10] Brook I. Bacteriology of acute and chronic ethmoid sinusitis. J. Clin. Microbiol.
43 (2005) 3479-3480. [11] B.T. Costa Carvalho, A.T. Nagao, C. Arslanian, M.M. Carneiro Sampaio, C.K.
Naspitz, R.U. Sorensen, et al. Immunological evaluation of allergic

Page 10 of 15
Accep
ted
Man
uscr
ipt
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
respiratory children with recurrent sinusitis, Pediatr. Allergy Immunol. 16 (2005) 534-538.
[12] S. Haruna, K. Sawada, T. Nakajima, H. Moriyama Relationship between pediatric sinusitis and middle turbinate pneumatization--ethmoidal sinus pyocele thought to be caused by middle turbinate pneumatization, Int. J. Pediatr. Otorhinolaryngol. 69 (2005) 375-379.
[13] J.M. Gwaltney Jr., Acute community-acquired sinusitis. Clin. Infect. Dis. 23 (1996) 1209-1223; quiz 1224-1205.
[14] E.R. Wald, Chronic sinusitis in children, J. Pediatr. 127 (1995) 339-347. [15] M.A. Sande, J.M. Gwaltney, Acute community-acquired bacterial sinusitis:
continuing challenges and current management, Clin. Infect. Dis. 39 (2004) Suppl 3: S151-158.
[16] J.M. Gwaltney Jr., W.M. Scheld, M.A. Sande, A. Sydnor, The microbial etiology and antimicrobial therapy of adults with acute community-acquired sinusitis: a fifteen-year experience at the University of Virginia and review of other selected studies, J. Allergy Clin. Immunol. 90 (1992) 457-461.
[17] K.H. Chan, C.P. Winslow, M.J. Levin, M.J. Abzug, J.E. Shira, A.H. Liu, et al. Clinical practice guidelines for the management of chronic sinusitis in children, Otolaryngol. Head Neck Surg. 120 (1999) 328-334.
[18] S.P. Nelson, E.H. Chen, G.M. Syniar, K.K. Christoffel. Prevalence of symptoms of gastroesophageal reflux during infancy, Arch. Pediatr. Adolesc. Med. 151 (1997) 569-572.
[19] J.J. Barron, H. Tan, J. Spalding, A.W. Bakst, J. Singer Proton pump inhibitor utilization patterns in infants. J. Pediatr. Gastroenterol. Nutr. 45 (2007) 421-427.
[20] H.B. El-Serag, M. Gilger, M. Kuebeler, L. Rabeneck. Extraesophageal associations of gastroesophageal reflux disease in children without neurologic defects. Gastroenterology 121 (2001)1294-1299.
[21] B. Keles, K. Ozturk, H. Arbag, E. Gunel, B. Ozer, Frequency of pharyngeal reflux in children with adenoid hyperplasia, Int. J. Pediatr. Otorhinolaryngol. 69 (2005) 1103-1107.
[22] Y. Vandenplas, L. Sacre-Smits, Continuous 24-hour esophageal pH monitoring in 285 asymptomatic infants 0-15 months old, J. Pediatr. Gastroenterol. Nutr. 6 (1987) 220-224.
[23] G.O. Andze, M.L. Brandt, D. St Vil, A.L. Bensoussan, H. Blanchard, Diagnosis and treatment of gastroesophageal reflux in 500 children with respiratory symptoms: the value of pH monitoring, J. Pediatr. Surg. 26 (1991) 295-299.
[24] R.F. Yellon, J. Coticchia, S. Dixit, Esophageal biopsy for the diagnosis of gastroesophageal reflux-associated otolaryngologic problems in children, Am. J. Med. 108 (2000) Suppl 4a: 131S-138S.
[25] J.A. Koufman, J.E. Aviv, R.R. Casiano, G.Y. Shaw, Laryngopharyngeal reflux: position statement of the committee on speech, voice, and swallowing disorders of the American Academy of Otolaryngology-Head and Neck Surgery, Otolaryngol. Head Neck Surg. 127 (2002) 32-35.
[26] C.N. Ford, Evaluation and management of laryngopharyngeal reflux, JAMA 294 (2005) 1534-1540.
Page 11 of 15
Accep
ted
Man
uscr
ipt
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
[27] J.A. Koufman, The otolaryngologic manifestations of gastroesophageal reflux disease (GERD): a clinical investigation of 225 patients using ambulatory 24-hour pH monitoring and an experimental investigation of the role of acid and pepsin in the development of laryngeal injury, Laryngoscope 101 (1991) 1-78.
[28] J.M. DelGaudio, Direct nasopharyngeal reflux of gastric acid is a contributing factor in refractory chronic rhinosinusitis, Laryngoscope; 115 (2005) 946-957.
[29] S.K. Wise, J.C. Wise, J.M. DelGaudio, Association of nasopharyngeal and laryngopharyngeal reflux with postnasal drip symptomatology in patients with and without rhinosinusitis, Am. J. Rhinol. 20 (2006) 283-289.
[30] T.H. Holmes, S. Wolf, H.G. Wolff, The Nose: An Experimental Study of Reactions Within the Nose in Human Subjects During Various Life Experiences. City: Charles C. Thomas, 1950.
[31] T.A. Loehrl, T.L Samuels, D.M Poetker, R.J. Toohill, J.H. Blumin, N. Johnston, The role of extraesophageal reflux in medically and surgically refractory rhinosinusitis, Laryngoscope 122 (2012) 1425-1430.
[32] I.W. Wong, T.I. Omari, J.C. Myers, G. Rees, S.B. Nair, G.G. Jamieson, P.J. Wormald, Nasopharyngeal pH monitoring in chronic sinusitis patients using a novel four channel probe, Laryngoscope 114 (2004) 1582-1585.
[33] J. K. DiBaise, B.F. Olusola, J.V. Huerter, E.M. Quigley, Role of GERD in chronic resistant sinusitis: a prospective, open label, pilot trial, Am. J. Gastroenterol. 97 (2002) 843-850.
[34] S.R. Megale, A.B. Scanavini, E.C. Andrade, M.I. Fernandes, W.T. Anselmo-Lima Gastroesophageal reflux disease: its importance in ear, nose, and throat practice, Int. J. Pediatr. Otorhinolaryngol. 70 (2006) 81-88.
[35] R.L. Pincus, H.H. Kim, S. Silvers, S. Gold, A study of the link between gastric reflux and chronic sinusitis in adults, Ear Nose Throat J. 85 (2006)174-178.
[36] I.W. Wong, G. Rees, L. Greiff, J.C. Myers, G.G. Jamieson, P.J. Wormald, Gastroesophageal reflux disease and chronic sinusitis: in search of an esophageal-nasal reflex, Am. J. Rhinol. Allergy 24 (2010) 255-259.
[37] R.M. Donlan, J.W. Costerton, Biofilms: survival mechanisms of clinically relevant microorganisms, Clin. Microbiol. Rev. 15 (2002) 167-193.
[38] M.W. Criddle, A. Stinson, M. Savliwala, J. Coticchia, Pediatric chronic rhinosinusitis: a retrospective review, Am. J. Otolaryngol. 29 (2008) 372-378.
Page 12 of 15
Accep
ted
Man
uscr
ipt
Table 1. Sinus Cxs
S. Pneumonia
H. Influenza
M. Catarrhalis
S. Aureus
MRSA
6m-5y (%)
43 28 11 7 11
6y-10y (%)
9 0 46 36 9
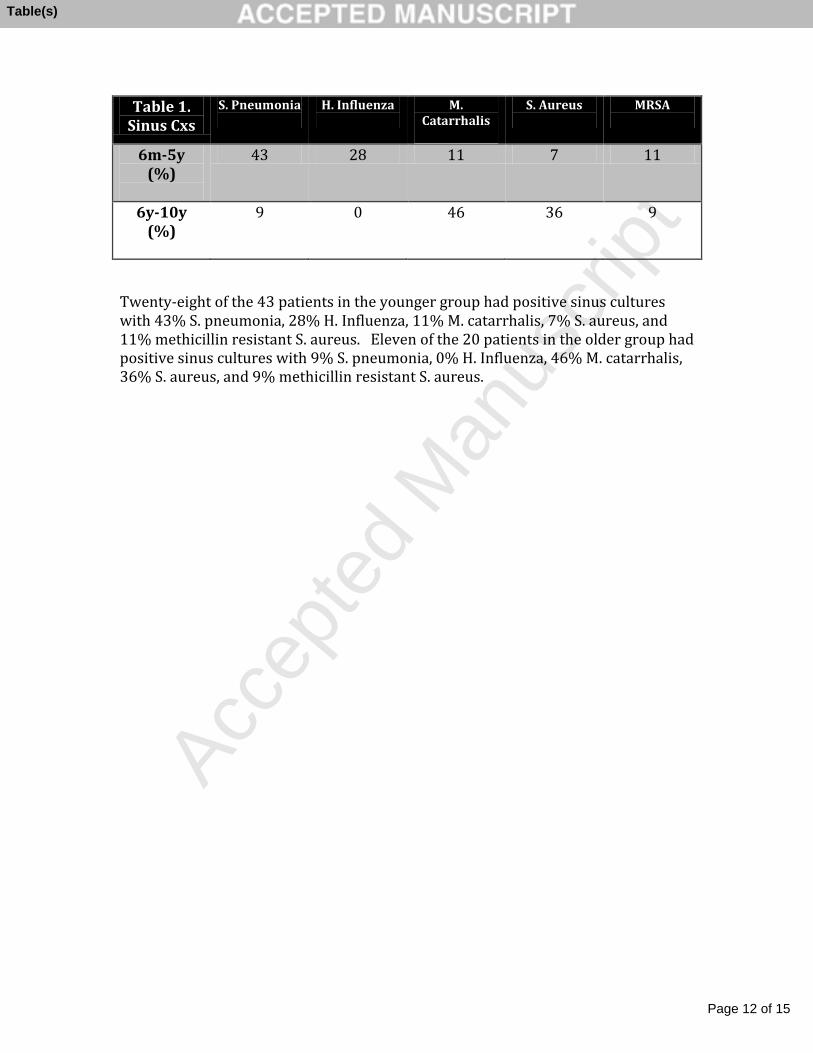
Twenty-eight of the 43 patients in the younger group had positive sinus cultures with 43% S. pneumonia, 28% H. Influenza, 11% M. catarrhalis, 7% S. aureus, and 11% methicillin resistant S. aureus. Eleven of the 20 patients in the older group had positive sinus cultures with 9% S. pneumonia, 0% H. Influenza, 46% M. catarrhalis, 36% S. aureus, and 9% methicillin resistant S. aureus.
Table(s)
Page 13 of 15
Accep
ted
Man
uscr
ipt
Figure(s)

Page 14 of 15
Accep
ted
Man
uscr
ipt
Figure(s)

Page 15 of 15
Accep
ted
Man
uscr
ipt
Figure(s)