
Effects of adjustable gastric banding on gastroesophageal reflux and esophageal motility: a...
96
LAPAROSCOPIC ADJUSTABLE GASTRIC BANDING Effect on gastroesophageal reflux, esophageal motility and gastric function Justin de Jong
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Effects of adjustable gastric banding on gastroesophageal reflux and esophageal motility: a...

LAPAROSCOPIC ADJUSTABLE
GASTRIC BANDING
Effect on gastroesophageal reflux,
esophageal motility and gastric function
Justin de Jong

Printing of this thesis was financially supported by
AllerganAstraZeneca BVSt. Antonius Ziekenhuis NieuwegeinJohnson & Johnson (Ethicon Endosurgery)
Laparoscopic adjustable gastric banding: Effect on gastroesophageal reflux, esophageal motility and gastric functionDe Jong, Justus ReinierThesis, University Utrecht, with a summary in Dutch
ISBN: 978-90-39350874Printed by: SENZ Grafische Media, WoerdenCover: LES TOURISTES by Elisabeth Buffoli 1989, Paris© J.R. de Jong, Utrecht 2009

LAPAROSCOPIC ADJUSTABLE
GASTRIC BANDING
Effect on gastroesophageal reflux,esophageal motility and gastric function
Laparoscopische maagbandplaatsing Invloed op gastro-oesofageale reflux, oesofagusmotiliteit en maagfunctie (met een samenvatting in het Nederlands)
PROEFSCHRIFTter verkrijging van de graad van doctor aan
de Universiteit Utrecht op gezag van de rector magnificus,
prof. dr. J.C. Stoof, ingevolge het besluit van
het college voor promoties in het openbaar te verdedigen
op donderdag 11 juni 2009 des ochtends te 10.30 uur
door
Justus Reinier de Jong
geboren op 9 januari 1970
te Kockengen

Promotoren: Prof. dr. A.J.P.M. SmoutProf. dr. H.G. Gooszen
Co-promotoren: Dr. B. van RamshorstDr. R. Timmer

Voor mijn ouders, Scheltine, Joep, Guido en Maartje

CONTENTS
Chapter 1 General introduction and outline of the thesis 7
Chapter 2 The influence of laparoscopic adjustable gastric banding on gastroesophageal reflux 15
Chapter 3 The influence of laparoscopic adjustable gastric banding on esophageal motility 27
Chapter 4 Weight loss after laparoscopic adjustable gastric banding is not caused by altered gastric emptying 39
Chapter 5 Esophageal dilatation after laparoscopic adjustable gastric banding 47
Chapter 6 Sustained weight loss two years after laparoscopic adjustable gastric banding for morbid obesity 59
Chapter 7 The influence of laparoscopic adjustable gastric banding on gastroesophageal reflux and esophageal motility. A systematic review 69
Chapter 8 Summary, conclusions, and future perspectives 83
Chapter 9 Samenvatting in het Nederlands 89
Dankwoord 94
Curriculum Vitae 96
Beoordelingscommissie 96

Chapter 1
GENERAL INTRODUCTION AND OUTLINE OF THE THESIS
“Corpulence is not only a disease itself, but the harbinger of others” (Hippocrates)

OBESITYObesity has increased markedly since 1980 and has reached epidemic proportions worldwide.The problems of overweight and obesity have achieved global recognition only during the past 10years, in contrast to underweight, malnutrition, and infectious diseases, which used to be the moredominant public health issues.Among adults overweight is defined as a body mass index of 25 or greater, obesity is defined as abody mass index of 30 or greater. Among children and adolescents, overweight is defined as abody mass index for age at or above the 95th percentile of a specified reference population. In theUSA in 2003–2004, 32.9% of adults 20–74 years old were obese and more than 17% ofteenagers (age 12–19y) were overweight1.The prevalence of obesity in the Netherlands has also increased in recent years. According to selfreported data overweight (obesity) prevalence in adult males increased from 37% (4%) in 1981 to51% (10%) in 2004, and in adult females from 30% (6%) in 1981 to 42% (12%) in 2004,according to self-reported data. In boys and girls, obesity prevalence doubled from 1980 to 1997,and again from 1997 to 2002–2004 a two- to threefold increase was seen for almost all ages.According to the most recent data, overweight (obesity) prevalence figures range, depending onage, from 9.2% to 17.3% (2.5–4.3%) in boys, and from 14.6% to 24.6% (2.3–6.5%) in girls2.The increasing prevalence of obesity is a public health threat as it is related to chronic morbiditiesand disabilities such as diabetes mellitus, cardiovascular disease, nonalcoholic fatty liver diseaseand gastroesophageal reflux disease. Obesity is also associated with a modestly increased risk ofall-cause mortality1.
OBESITY AND GASTROESOPHAGEAL REFLUX
Historical overviewAlready in the early seventies it was stated that excessive fat stores impair health with themechanical burden on the abdomen being the most important factor, resulting in a predispositionfor gastroesophageal reflux3. At the time, medical textbooks recommended body weight reduc-tion as a first step in the treatment of gastroesophageal refluxin the obese patient, although thesestatements were not supported by objective data4.The first studies on factors influencing gastroesophageal reflux in obese patients predominantlyused manometry and were carried out in the 80s. The study groups consisted mainly of patientsseeking surgery for their overweight.The results of these studies were controversial and reported no difference5 6 in LES pressures ordecreased LES pressures7 8 in obese subjects when compared with non-obese subjects. An increased gastroesophageal pressure gradient or increased gastric pressure in obese personswas found in many studies9 6 10 11 and the gradient was reported to decrease after weight loss6 11.Other overweight-associated abnormalities proposed were prolonged esophageal transit time10,an increase in transient relaxations of the LES12 and the presence of a hiatal hernia13.All forementioned studies did not use a reflux symptom score and often used data from otherresearch groups as a reference for normal values.
The first studies in which prolonged pH recordings were used, also yielded discrepant findingsconcerning the relationship between obesity and gastroesophageal reflux.In 1994, Schmitt et al. were the first to report a significant effect of weight loss brought about bydiet and a fitness program on heartburn and total reflux time as measured by 24-hour pH record-ing14.
8

In 1995, a study in morbidly obese patients the prevalence of reflux symptoms and total refluxtime were found not to be different from the general population15. In contrast, Rigaud described arelationship between the number of reflux episodes in 3 hours of pH monitoring and increase inwaist/hip ratio, BMI and energy or fat intake16. Kjellin et al. found no influence of weight loss(10kg) in slightly obese patients (BMI 31.4) on reflux symptoms, total reflux time and LES pres-sure17. The difference with earlier reports is possibly caused by the limited weight loss in the slight-ly obese patients. Mathus-Vliegen et al reported a normal total reflux time in 17 morbidly obesepatients. Weight loss and gastric distension by an intragastric balloon did not change the severityof gastroesophageal reflux18.
With the increasing attention for morbid obesity and its epidemic growth an increasing number ofstudies on the relationship between obesity and gastroesophageal reflux have been publishedsince 1999. With these studies the evidence for the existence of a positive relationship betweengastroesophageal reflux and obesity has accumulated.In a retrospective analysis in 1389 patients excessive body weight was identified as a significantindependent risk factor for hiatal hernia and excessive body weight was also significantly associatedwith esophagitis19. In a study evaluating 30 patients presenting for bariatric surgery, those withpathological reflux showed significantly higher body mass indices than those with physiologicalreflux. The same pattern was found for reflux symptoms20. In a study in 61 morbidly obesepatients who were evaluated for bariatric surgery 39.3% of the patients had heartburn and/orregurgitation and 49% had an abnormal DeMeester score during pH recording21. In a group of345 morbidly obese patients reflux symptoms were reported by 35.8% and an increasedDeMeester score was found in 51.7% of the patients. Overall in 73% of the cases there was anabnormal pH monitoring. In 52.6% of the patients an hiatal hernia and in 31.4% reflux esophagi-tis was found during endoscopy. Esophagitis was associated with increased weight22.
Recently, studies using esophageal impedance monitoring and high-resolution manometry con-tributed to a better understanding of the relation between gastroesophageal reflux and obesity23 24.In a study in 22 obese and 22 non-obese patients with gastroesophageal reflux, motility abnor-malities were found to be more frequent and more severe in obese subjects23. Using high-resolu-tion manometry Pandolfino et al. showed that obese subjects are more likely to have gastroe-sophageal junction disruption, hiatus hernia and an increased intragastric pressure and gastroe-sophageal pressure gradient24, supporting the more than 20 years old theory9. Wu and co-workersshowed that obesity is associated with an increased incidence of transient LES relaxations andincreased acid reflux during the postprandial period in subjects without GERD. They stated thatabnormal postprandial LES function may be an early event in the pathogenesis of obesity-relatedGERD25.
From 2000 to 2008, many population-based studies on the relationship between obesity and gas-troesophageal reflux were performed in Europe and the USA. The majority of these studies report-ed a clear relationship of obesity with gastroesophageal reflux symptoms26-38.In a population-based study including 1000 participants, reflux symptoms were found to be inde-pendently associated with BMI and upper endoscopy findings were more prevalent in obese per-sons35. In contrast, a study in 1000 patients in the Netherlands who were referred for endoscopy-could not demonstrate a significant relationship between obesity and reflux symptoms39.Finally, there is accumulating data that obesity is associated with Barrett’s esophagus and adeno-carcinoma40-43. A meta-analysis published in 2005 points at an increased risk for GERD symptoms,erosive esophagitis or esophageal adenocarcinoma in subjects with overweight or obesity44.
9

OBESITY SURGERY There is growing consensus that bariatric surgery is the only treatment that results in long-termsustained weight loss in individuals who have severe obesity and are at the risk for obesity-relatedmortality and co-morbidity45-47.The number of bariatric surgery procedures has increased significantly over the past fewdecades48-51. In the United States the number of bariatric surgical procedures increased from13,386 in 1998 to 121,055 in 2004, constituting an 800% increase52. The rise in number of pro-cedures carried out worldwide has increased from 40,000 to 146,301 procedures between 1998and 200353.The first bariatric procedure (jejunoileal bypass) was performed in the early 1950s. The last decadeshave shown an evolution in operative gastrointestinal interventions including malabsorptive, mal-absorptive/restrictive, restrictive and neither malabsorptive nor restrictive procedures. Prostheticswere introduced with the vertical banded gastroplasty ring or band in the early 1980s, theadjustable gastric band in the late 1980s, and the gastric pacing electrode in the late 1990s.Laparoscopy entered the field in the 1990s and dominates bariatric surgery by the 21st century45 54.
LAPAROSCOPIC ADJUSTABLE GASTRIC BANDINGIn 1978, in the USA, Wilkinson and Peloso were the first to place a nonadjustable band, consistingof 2-cm wide Marlex mesh, around the upper part of a patient’s stomach during open surgery55.In 1982, Kolle, in Norway, also described the placement of a nonadjustable gastric band duringopen surgery56. In 1983, Molina and Oria reported a comparable procedure, described as gastricsegmentation, using a nonadjustable Dacron graft to encircle the upper stomach, resulting in asmaller pouch57. In the early nineties, Näslund, in Sweden, also performed gastric banding usingMarlex mesh bands58 and Frydenburg, in Australia, initiated gastric banding with a 1.5-cm-widesilicone band reinforced with a layer of mesh59. None of these early gastric banding procedureswas successful. The problem of creating a standard stoma diameter with the fixed-size non-adjustable gastric bands caused high failure rates. Complications were numerous, the most com-mon of which were “slipping” -in which the stomach prolapsed anteriorly and posteriorly upwardthrough the band-, band erosions and intractable vomiting and gastroesophageal reflux.Moreover, with time, the surgically created pouch gradually dilated, causing unsatisfactory weightloss.
An important modification of the proximal gastric banding technique was accomplished by theAustrian surgeons Szinicz and Schnapka, who performed experiments in which they encircled theupper stomach of rabbits with a ring of silicone elastomer60. The ring contained a balloon on itsinner surface, attached to a subcutaneous port. The volume of the band balloon could be adjustedby adding or removing saline via the port. In 1985, the Swedish investigators Hallberg and Forsellfirst described what is now known as the Swedish Adjustable Gastric Band ([SAGB] Ethicon Endo-Surgery, Inc., Cincinnati, OH)61. In the same period, Kuzmak and coworkers reported the clinicaluse of an inflatable Silastic band, later known as the Lap-Band (Allergan Inc., Irvine, CA)62. Boththe SAGB and the Lap-Band are connected to a subcutaneous port through which fluid can beadded or removed to adjust the gastric stomal size.Laparoscopic insertion of the band was the next step. In 1993, Broadbent et al., in Australia, andCatona et al., in Italy, were the first to implant nonadjustable gastric bands laparoscopically63 64. In1995, Belachew et al., working in Belgium, using laparoscopic techniques to place an adjustablegastric band65. In 1995, several investigators presented early results of laparoscopic adjustablegastric banding. By this time, both the Lap-Band and the SAGB were available for use in mostparts of the world.
10

As gastric banding gained popularity, the bands created by Forsell and Kuzmak underwent severalmodifications. Kuzmak’s band, now available as the Lap-Band, was accepted for use in Europe inthe mid 1990s and received approval from the U.S. Food and Drug Administration (FDA) in 2001.Forsell’s SAGB has been available in Sweden for the treatment of morbid obesity since 1987, wascommercially marketed in Europe since 1996, and was approved for use in the U.S. in late 2007 asthe Realize Band (Ethicon Endo-Surgery, Inc.)66.
In the late 1990s it was reported that laparoscopic adjustable gastric banding resulted in adecrease of gastroesophageal reflux symptoms67-69. However, these studies were lacking objectivemeasurements (pH recording and esophageal manometry). These prompted our prospective stud-ies in morbidly obese patients who were candidates for laparoscopic adjustable gastric banding inthe St Antonius Hospital in Nieuwegein.
AIM OF THIS THESISThe aim of the studies desribed in this thesis was to assess the outcome of adjustable gastric band-ing and to evaluate the effects of laparoscopic adjustable gastric banding on gastroesophagealreflux and esophageal and gastric function. Chapter 2 describes a study that focused on the influence of laparoscopic adjustable gastric band-ing on gastroesophageal reflux.The effect of laparoscopic adjustable gastric banding on the lower esophageal sphincter andesophageal motility is reported in Chapter 3.The role of gastric emptying on weight loss after laparoscopic adjustable gastric banding isdescribed in Chapter 4.Chapter 5 describes the effect of a study in which the influence of laparoscopic adjustable gastricbanding on esophageal dilatation was evaluated.A retrospective analysis concerning the effects of laparoscopic adjustable gastric banding on
weight loss in a consecutive series of 411 patients is described in Chapter 6.Chapter 7 is a systematic review of all reports on the effects of adjustable gastric banding on gas-troesophageal reflux.
The specific questions to be answered in this thesis were:• Does laparoscopic adjustable gastric banding affect gastroesophageal reflux?• Does laparoscopic adjustable gastric banding affect esophageal motility?• Is there a change in gastric emptying after laparoscopic adjustable gastric banding and, if so,
does this contribute to the weight loss?• Does laparoscopic adjustable gastric banding cause esophageal dilatation?• Do all morbidly obese subjects benefit from adjustable gastric banding?
REFERENCES1. Ogden CL, Yanovski SZ, Carroll MD,Flegal KM. The epidemiology of obesity. Gastroenterology 2007;
132:2087-1022. Schokker DF, Visscher TL, Nooyens AC, van Baak MA, Seidell JC. Prevalence of overweight and obesity in
the Netherlands. Obes Rev 2007; 8:101-83. Mann GV. The influence of obesity on health. N Engl J Med 1974; 291:178-854. Chernow B, Castell DO. Diet and heartburn. JAMA 1979; 241:2307-85. O’Brien TF, Stroop EM. Lower esopageal sphincter pressure and esophageal function in obese humans. J
Clin Gastroenterol 1980; 2:145-86. Backman L, Granstrom L, Lindahl J et al. Manometric studies of lower esophageal sphincter in extreme
obesity. Acta Chir Scand 1983; 149:193-7
11

7. Feldshon SD, Villar HV, Paplanus SH et al. Evaluation of cardioesophageal reflux after gastric partitioning..Am J Gastroenterol 1983; 78:679 (abstract)
8. Hagen J, Deitel M, Khanna RK. Ilves R. Gastroesophageal reflux in the massively obese. Int Surg 1987;72:1-3
9. Wren SF, DaCosta LR, Beck IT. Gastroesophageal pressure gradients and lower esophageal sphincter pres-sures in severely obese patients. Gastroenterology 1982; 82:1129
10. Mercer CD, Rue C, Hanelin L, Hill LD. Effect of obesity on esophageal transit. Am J Surg 1987; 149:177-8111. Orlando RC, Kinard HB. Effect of morbid obesity on lower esophageal sphincter pressure.
Gastroenterology 1987; 76:1212 (abstract)12. Freidin N, Ren J, Sluss J, McCallum RW. The effect of a large meal and graded intragastric distension on
transient LES relaxation frequency in normals. Gastroenterology 1988; 95:866 (abstract)13. Stene-Larsen G, Weberg R, Froyshov Lsrsen I, Bjortuft O, Hoel B, Berstad A. Relationship of overweight to
hiatus hernia and reflux oesophagitis. Scand J Gastroenterol 1988; 23:427-3214. Schmitt CM, Brazer SR, Hamilton MA. The effect of a diet & fitness program on gastroesophageal reflux.
Am J Gastroenterol 1994; 89:1626 (abstract)15. Lundell L, Ruth M, Sanberg N, Bove-Nielsen M. Does massive obesity promote abnormal gastroe-
sophageal reflux? Dig Dis Sci 1995; 40:1632-516. Rigaud D, Merrouche M, Le Moel G, Vatier J, Paycha F, Cadiot G, Naoui N, Mignon M. Factors of gastroe-
sophageal acid reflux in severe obesity. Gastroenterol Clin Biol 1995; 19:818-2517. Kjellin A, Ramel S, Rossner S, Thor K. Gastroesophageal reflux in obese patients is not reduced by weight
reduction. Scand J Gastroenterol 1996; 31: 1047-5118. Mathus-Vliegen LMH, Tytgat GNJ. Twenty-four-hour pH measurements in morbid obesity: effects of mas-
sive overweight, weight loss and gastric distension. Eur J Gastroenterol Hepatol 1996; 8:635-4019. Wilson LJ, Ma W, Hirschowitz I. Association of obesity with hiatal hernia and esophagitis. Am J
Gastroenterol 1999; 94:2840-420. Fisher BL, Pennathur A, Mutnick JL, Little AG. Obesity correlates with gastroesophageal reflux. Dig Dis Sci
1999; 44:2290-421. Hong D, Khajanchee YS, Pereira N, Lockhart B, Patterson EJ, Swanstrom LL. Manometric abnormalities
and gastroesophageal reflux disease in the morbidly obese. Obes Surg 2004; 14:744-922. Suter M, Dorta G, Giusti V, Calmes JM. Gastro-esophageal reflux and esophageal motility disorders in
morbidly obese patients. Obes Surg 2004; 14:959-6623. Quiroga E, Cuenca-Abente F, Flum D, Dellinger EP, OElschlager BK. Impaired esophageal function in mor-
bidly obese patients with gastroesophageal reflux disease: evaluation with multichannel intraluminalimpedance. Surg Endosc 2006; 20:739-43
24. Pandolfino JE, El-Serag HB, Zhang Q, et al. Obesity: a challenge to esophagogastric junction integrity.Gastroenterology 2006; 130639-49
25. Wu JCY, Mui LM, Cheung CMY, Chan Y, Sung JJY. Obesity is associated with increased transient loweresophageal sphincter relaxation. Gastroenterology 2007; 132:883-889
26. Lagergren J, Bergstrom R, Nyren O. No relation between body mass and gastro-oesophageal reflux symp-toms in a Swedish population based study. Gut 2000; 47: 26-29
27. Locke GR III, Talley NJ, Fett SL, Zinsmeister AR, Melton III LJ. Risk factors associated with symptoms ofgastroesophageal reflux. Am J Med 1999; 106:642-9
28. Ruhl CE, Everhart JE. Overweight, but not high dietary fat intake, increases risk of gastroesphageal refluxdisease hospitalization:NHANES I Epidemiologic follow up study. Ann Epidemiol 1999:424-35
29. Murray L, Johnston B, Lane A et al. Relationship between body-mass and gastro-esophageal reflux symp-toms: The Bristol Helicobacter Project. Int J Epidemiol 2003; 32:645-50
30. Nilsson M, Johnsen R, Ye W, Hveem K, Lagergren J. Obesity and estrogen as risk factors for gastroe-sophageal reflux symptoms. JAMA 2003; 290:66-72
31. Nandurkar S, Locke GR III, Fett S et al. Relationship between body mass index, diet, excercise and gastroe-sophageal reflux symptoms in a community. Aliment Pharmacol Ther 2004; 20:497-505
32. Talley NJ, Quan C, Jones MP, et al. The association of upper and lower gastrointestinal tract symptomswith body mass index in an Australian cohort. Neurogastroenterol Motil 2004; 16:413-9
12

33. Diaz-Rubio M, Moreno-Elola-Olaso C, Rey E, Locke GR III, Rodriguez-Artalejo F Symptoms of gastroe-sophageal reflux: Prevalence , severity, duration and associated factors in a Spanish population. AlimentPharmacol Ther 2004; 19:95-105
34. El-Serag HB, Graham DY, Satia JA, Rabeneck L. Obesity is an independent risk factor for GERD symptomsand erosive esophagitis. Am J Gastroenterol 2005; 100:1243-50
35. Aro P, Ronkainen J, Talley NJ, Storskrubb T, Bolling-Sterneveld E, Agreus L. Body mass index and chronicunexplained gastrointestinal symptoms: an adult endoscopic population based study. Gut 2005; 54:1377-83
36. Jacobson BC, Somers SC, Fuchs CS, et al. Body-mass index and symptoms of gastroesophageal reflux inwomen. N Engl J Med 2006; 354:2340-8
37. Corley DA, Kubo A, Zhao W. Abdominal obesity, ethnicity and gastroesophageal reflux symptoms. Gut2007; 56:756-62
38. El Serag HB, Ergun GA, Pandolfino J, et al. Obesity increases oesophageal acid exposure. Gut 2007;56:756-62
39. Van Oijen MGH, Josemanders DFGM, Laheij RJF, Van Rossum LGM, Tan ACITL, Jansen JBMJ.Gastrointestinal disorders and symptoms: does body mass index matter? Neth J Med 2006; 64:45-9
40. Freeman HJ. Risk of gastrointestinal malignancies and mechanisms of cancer development with obesityand its treatment. Best Pract Res Clin Gastroenterol 2004; 18:1167-75
41. Stein DJ, El-Serag HB, Kuczynski J et al. The association of body mass index with barrett’s esophagus.Aliment Pharmacol Ther 2005; 22:1005-10
42. El-Serag HB, Kvapil P, Hacken-Bitar J, et al. Abdominal obesity and the risk of barrett’s esophagus. Am JGastroenterol 2005; 100:2151-6
43. Edelstein ZR, Farrow DC, Bronner MP, et al. Central adiposity and risk of barrett’s esophagus.Gastroenterology 2007133:403-11
44. Hampel H, Abraham NS, El-Serag HB. Meta-analysis: Obesity and the risk for gastroesophageal reflux dis-ease and its complications. Ann Intern Med 2005; 143:199-211
45. Buchwald H. The future of bariatric surgery. Obes Surg 2005; 15:598–60546. Maggard MA, Sugarman LR, Suttorp M, Maglione M., Sugerman HJ, Livingston EH, Nguyen NT, Li Z,
Mojica WA, Hilton L, Rhodes S, Morton SC, Shekelle PG. Meta-analysis: surgical treatment of obesity. AnnIntern Med 2005; 142:547–559
47. Sugerman HJ, Kral JG. Evidence-based medicine reports on obesity surgery: a critique. Int J Obes 2005;29:735–745
48. Davis MM, Slish K, Chao C, Cabana MD. National trends in bariatric surgery, 1996–2002. Arch Surg 2006;141:71–74
49. Steinbrook R. Surgery for severe obesity. N Engl J Med 2004; 350:1075–107950. Santry HP, Gillen DL, Lauderdale DS. Trends in bariatric surgical procedures. JAMA 2005; 294:1909–191751. Trus TL, Pope GD, Finlayson SRG. National trends in utilization and outcomes of bariatric surgery. Surg
Endosc 2005; 19:616–62052. Zhao Y, Encinosa W. Agency for Healthcare Research and Quality AHRQ Bariatric Surgery Utilization and
Outcomes in 1998 and 2004. Statistical Brief #23. January 200753. Buchwald H, Williams SE. Bariatric surgery worldwide 2003. Obes Surg 2004; 14:1157–116454. Elder KA, Wolfe BM. Bariatric Surgery: A Review of Procedures and Outcomes Gastroenterology 2007;
132:2253-227155. Wilkinson LH, Peloso OA. Gastric (reservoir) reduction for morbid obesity. Arch Surg 1981; 116:602–556. Kolle K. Gastric banding [abstract]. OMGI 7th Congress, Stockholm.1982; 145:3757. Molina M, Oria HE. Gastric segmentation: a new, safe, effective, simple, readily revised and fully reversible
surgical procedure for the correction of morbid obesity [abstract 15]. In: 6th Bariatric Surgery Colloquium;Iowa City, IA: June 2-3, 1983
58. Näslund E, Granström L, Stockeld D, Backman L. Marlex mesh gastric banding: a 7-12 year follow-up.Obes Surg 1994; 4:269 –73
59. Frydenberg HB. Modification of gastric banding, using a fundal suture. Obes Surg 1991; 1:315–760. Szinicz G, Mueller L, Erhard W, et al. “Reversible gastric banding” in surgical treatment of morbid
obestiy0results of animal experiments. Res Exp Med (Berl) 1989; 189:55– 60
13

61. Hallberg D. Forsell O. Ballongband vid behandling av massiv överwikt. Svinsk Kirurgi 1985; 344:106–862. Kuzmak LI. Silicone gastric banding: a simple and effective operation for morbid obesity. Contemp Surg
1986; 28:13–863. Broadbent R, Tracy M, Harrington P. Laparoscopic gastric banding:a preliminary report. Obes Surg 1993;
3:63–764. Catona A, Gossenberg M, La Manna A. Laparoscopic gastric banding:preliminary series. Obes Surg 1993;
3:207–965. Belachew M, Legrand M, Vincinti V, Deffechereux T, Jourdan JL, Monami B, Jacquet N. Laparoscopic
placement of adjustable silicone gastric band in the treatment of morbid obesity: how to do it. Obes Surg1995; 5:66–70
66. Steffen R. The history and role of gastric banding. Surg Obes Relat Dis 2008; 4:S7–S1367. Niville E, Vankeirsbilck J, Dams A. Laparoscopic esophagogastric banding: a preliminary experience. Obes
Surg 1998; 39-4368. Angrisani L, Iovino P, Lorenzo M et al. Treatment of morbid obesity and gastroesophageal reflux with
hiatal hernia by Lap-Band. Obes Surg 1998; 8:39-4369. Dixon JB, O’Brien PE. Gastroesophageal reflux in obesity: the effect of Lap-Band placement. Obes Surg
1999; 9:527-31
14

Chapter 2
THE INFLUENCE OF LAPAROSCOPIC ADJUSTABLE
GASTRIC BANDING ON GASTROOESOPHAGEAL REFLUX
JR de Jong1, B van Ramshorst1, R Timmer2, HG Gooszen3, AJPM Smout4
Departments of Surgery1 and Gastroenterology2, St Antonius Hospital Nieuwegein,
Departments of Surgery3 and Gastroenterology4, University Medical Center, Utrecht, The Netherlands
Obes Surg 2004; 14:399-406

ABSTRACTBackground: Laparoscopic adjustable gastric banding (LAGB) influences gastroesophageal reflux.Methods: 26 patients undergoing gastric banding were assessed by a questionnaire for symp-tom analysis, 24-hour pH monitoring, endoscopy and barium swallows, preoperatively, at 6weeks and at 6 months after operation.Results: Gastric banding had minimal effect on heartburn scores but regurgitation and belch-ing scores increased significantly during follow-up. Use of acid-reducing drugs was decreasedsignificantly at 6 weeks and increased significantly at 6 months. Pathological reflux was pres-ent in 13 of the 26 patients preoperatively. At 6 months pathological reflux was found in only6 of these 13 patients, but 4 of the 13 patients with preoperative normal reflux patterns haddeveloped pathological reflux.Six months after the operation esophagitis had disappeared in 6 patients and was increased in9 patients.In 9 patients a pouch was found at 6 months. Pouch formation was significantly correlated withthe presence of pathological reflux, esophagitis and the use of acid-reducing medication.Preoperative presence of a hiatal hernia did not influence pouch formation or pathological reflux.Conclusion: LAGB decreases gastroesophageal reflux if there is no pouch formation duringfollow-up.
INTRODUCTIONThe prevalence of morbid obesity, defined as a body mass index (BMI) > 40 kg/m2, is increasingdramatically in the Western world, leading to rising annual healthcare costs due to obesity-associ-ated morbidity and mortality1- 3. Surgery has been shown to be the most effective treatment inselected patients to establish a long-term weight reduction, improve the quality of life and controlor cure co-morbidity4- 6. In recent years laparoscopic adjustable gastric banding (LAGB) was intro-duced as a minimally invasive restrictive operation, and excellent results as to safety and efficacyare reported7. Although many reports include evaluation of procedure-related complications, rela-tively little is known about the effect of LAGB on the lower esophageal sphincter (LES) physiologyand gastroesophageal reflux (GER). Some studies suggest an increase in GER after banding,whereas others report a decrease or no effect of banding on GER8-13. The influences of band posi-tion and volume on GER have remained unstudied.In this prospective study we evaluated the influence of LABG on LES physiology and GER in rela-tion to the role of surgical technique, pouch development and pre-existent hiatal hernia.
MATERIALS AND METHODSFrom July 1998 to March 2000, 76 consecutive morbidly obese patients underwent a LAGB proce-dure with the Lap-Band® System (Inamed, Santa Barbara, CA). Inclusion criteria were BMI � 40kg/m2, or BMI > 35 with serious co-morbidity. All patients were thoroughly screened beforesurgery by a specialist panel consisting of an internist, dietician, psychologist and bariatric surgeon.Twenty-six patients out of this group (23 female and 3 male) with a mean age 41.3 (SD ± 6.4)years and mean BMI of 47.0 (SD ± 1.2) agreed to enrole in the study protocol. Written informedconsent was obtained from each patient. The study was approved by the Medical EthicsCommittee of St. Antonius hospital.
Surgical procedureAll operations were performed by one surgeon (BvR) with a large experience in laparoscopic pro-cedures. The operation was performed according to the technique described by Belachew7 and co-
16

workers with the modification that the retrogastric tunnel was created high at the stomach, fromthe lesser curvature at or near the gastroesophageal junction to the angle of His at the greater cur-vature without the formation of a gastric pouch proximal to the band. To prevent band migrationthe gastric fundus was sutured to the proximal stomach over the anterior aspect of the band with3 or 4 non-absorbable seromuscular sutures. The reservoir through which the band could beinflated to adjust stomal diameter was placed on the rectus sheath just below the xiphoid process.Postoperatively, all patients used a liquid diet for 4 weeks. At 6 weeks, the first stoma adjustmentwas carried out by filling the band with 2 ml of saline. Patients were followed at regular intervals,and further stoma adjustments were made according to each patient’s individual need, dependingon the degree of weight loss.
Upper GI endoscopyUpper GI endoscopy was performed before surgery and at 6 months postoperatively. Esophagitiswas classified according to the classification of Savary-Miller. A hiatal hernia was diagnosed if theproximal border of the gastric folds started � 2 cm proximal to the diaphragmatic impression.Barrett’s esophagus was defined as a columnar segment extending � 2 cm from the proximal bor-der of the gastric folds, which contained intestinal metaplasia on histological examination.
Pouch formationA barium swallow was performed on the first postoperative day and at 6 months after the opera-tion, to assess the position of the band in relation to the LES. A pouch was diagnosed if gastricfolds or a part of the stomach was seen proximal to the band. To quantify the pouch size, a ratiowas calculated between the maximum diameter of the pouch and the maximum diameter of theband. The pouch size was judged to be large if the ratio was � 1.
Symptom assessmentTo assess reflux and other upper GI symptoms the patients completed a questionnaire preopera-tively, at 6 weeks and at 6 months follow-up. The questionnaire included questions about heart-burn (at day- and nighttime), regurgitation, nausea and excessive belching. The intensity at whichthese symptoms occurred in the week before examination was scored using an ascending scalefrom 0 to 4 (0 = no symptoms, 1 = symptoms on 1 or 2 days, 2 = symptoms on 3 or 4 days, 3 =symptoms on 5 or 6 days and 4 = daily symptoms). The use of proton pump inhibitors (PPI), H2-receptor antagonists (H2-RA), antacids and prokinetic drugs, alcohol intake (units/week) andsmoking habits (number of cigarettes/day) were recorded.
24-hour pH recordingAn ambulatory esophageal 24-hour pH measurement was performed pre-operatively, at 6 weeksand at 6 months. Acid-reducing medication was discontinued at least 5 days prior to examination.After an overnight fast, the glass pH electrode (Mettler-Toledo, Switzerland) was placed 5 cmabove the proximal border of the LES, which was determined by stationary pull-through manom-etry. The catheter was connected to a portable data logger (MMS, Enschede, The Netherlands).Patients were given a diary card to record drinks and meals taken during the study period. At theend of the 24-hour period, the data were downloaded to a personal computer and further ana-lyzed using commercially available software (MMS, Enschede, The Netherlands). The analyzedparameters included the percentage of time with an esophageal pH < 4 (total, upright andsupine), the number of reflux episodes, the number of reflux episodes > 5 minutes and the dura-tion of the longest reflux episode. Gastroesophageal reflux was considered pathological when thepercentage of time with oesophageal pH < 4 was 4.2 % or more.
17

StatisticsData were statistically analyzed by a SPSS 8.0 package. A p-value < 0.05 was considered significant.The Mann-Whitney U test was used to compare continuous variables between unrelated groups,and the Wilcoxon Signed Ranks test was used for repeated measurements in the same patients. ThePearson correlationcoefficient was used to asses any relationship between the different variables.The Bonferroni correction was used to adjust the significance levels in multiple comparisons.
Figure 1. Grading of esophagitis according to Savary-Miller, before and 6 months after the operation
RESULTSThe BMI (mean ± SEM) of the patients decreased from 47 ± 1.2 to 42.4 ± 1.0 at 6 weeks and to36.7± 1.0 at 6 months (p < 0.01 for all intervals). The patients in the study group were compara-ble to the total group of patients operated upon in the study period with regards to age, and BMIat operation and at follow-up.
Upper GI endoscopyPreoperatively, all patients underwent endoscopy. At 6 months 3 patients refused to undergo a secondendoscopy. Figure 1 shows the esophagitis grading preoperatively and at 6 months follow-up. Beforeoperation, esophagitis was found in 16 out of 26 patients (61.5%). Esophagitis was grade I in 10patients (38.5 %) and grade II in 6 patients (23.1 %). In one patient, Barrett metaplasia was foundwithout esophagitis. A hiatal hernia (type I) was observed in 18 patients (69.2%). Preoperatively,reflux esophagitis was significantly more frequent in patients with a hiatal hernia (p = 0.033).At 6 months esophagitis was found in 16 patients (69.5%). In 6 patients (26%), the esophagitishad disappeared, and in eight patients (35%) it was unchanged. In 9 patients (39%) theesophagitis had increased or was diagnosed for the first time. Reflux esophagitis was graded gradeI in 8 patients (34.8%), grade II in 5 patients (21.7%) and grade III in 1 patient (4.3%).In 6 of the 9 patients with an increase in esophagitis a large pouch (ratio � 1) was diagnosed at 6months after the operation.
Pouch developmentAt 6 months a large pouch was found in 9 patients. In one patient, a smaller pouch was diag-nosed. The mean pouch / band ratio was 1.3, with a range from 0.8 to 1.75. Five of the patients
18
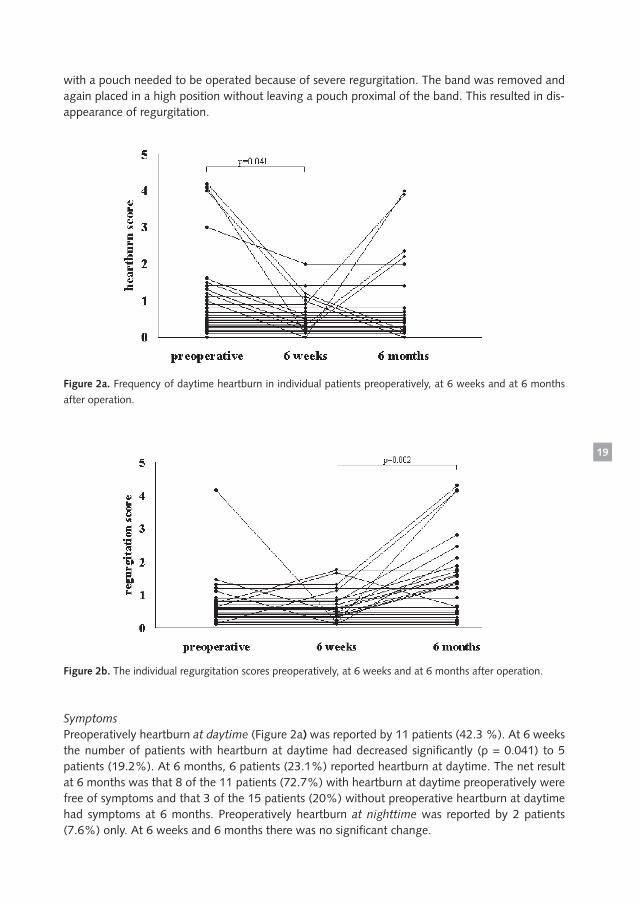
with a pouch needed to be operated because of severe regurgitation. The band was removed andagain placed in a high position without leaving a pouch proximal of the band. This resulted in dis-appearance of regurgitation.
Figure 2a. Frequency of daytime heartburn in individual patients preoperatively, at 6 weeks and at 6 months
after operation.
Figure 2b. The individual regurgitation scores preoperatively, at 6 weeks and at 6 months after operation.
SymptomsPreoperatively heartburn at daytime (Figure 2a) was reported by 11 patients (42.3 %). At 6 weeksthe number of patients with heartburn at daytime had decreased significantly (p = 0.041) to 5patients (19.2%). At 6 months, 6 patients (23.1%) reported heartburn at daytime. The net resultat 6 months was that 8 of the 11 patients (72.7%) with heartburn at daytime preoperatively werefree of symptoms and that 3 of the 15 patients (20%) without preoperative heartburn at daytimehad symptoms at 6 months. Preoperatively heartburn at nighttime was reported by 2 patients(7.6%) only. At 6 weeks and 6 months there was no significant change.
19

Excessive belching was found preoperatively in 7 patients (26.7%); in 3 patients (11.5%), exces-sive belching occurred every day. At 6 weeks there was a significant increase (p = 0.015) to 14patients (53.8%), and 8 of these patients (30.8%) reported daily belching. At 6 months there wasno further increase of belching.Nausea was reported by 2 patients (7.7%) preoperatively; by 4 patients (15.4%) at 6 weeks andby 5 patients (19.2%) at 6 months. At 6 months, there was a significant difference (p = 0.043)compared with the preoperative situation.As shown in Figure 2b, the number of patients with regurgitation increased from 2 patients(7.7%) preoperatively to 4 patients (15.4%) at 6 weeks (not significant) and a significant increaseto 14 patients (53.8%) at 6 months (p = 0.002). There were no statistically significant differences in symptom scores, at any point in time, betweenpatients with a hiatal hernia preoperatively (n = 18) and those without (n = 8).Before operation acid-reducing medication was used by 10 patients (38.5%). Three patients(11.5%) used an H2-RA daily and 2 patients (7.7%) used a PPI daily. At 6 weeks only one patientneeded to use an H2-RA (p = 0.007). At 6 months there was a significant increase in the use ofacid-reducing medication to 19.2 % of the patients (p = 0.041). Four patients (15.4%) used a PPIand one patient (3.8%) used an H2-RA. All of these five patients had developed a pouch.Preoperatively, 5 patients smoked cigarettes (5-20, median 15) and 2 patients used alcohol(3U/day). During follow up, this did not change.
Figure 3. Percentage of time with esophageal pH < 4 for the individual patients.
pH monitoringAnalysis of pH recordings for the total patiënt group (Table 1) preoperatively and at 6 weeksrevealed a decrease in number of reflux episodes for total, upright and supine position, but afterBonferroni correction for multiple comparisons, only the decrease in supine reflux episodesremained statistically significant. Other reflux variables such as the percentage of total reflux timedid not change. At 6 months there were no significant differences in reflux variables comparedwith the pre-operative state.Analysis of the pH recordings for the individual patients showed that before operation 13 of the26 patients had pathological reflux. At 6 weeks, 10 of these 13 patients (76.9%) showed normalreflux patterns, and 3 patients had persistent pathological reflux. Three patients of the initially
20

reflux-positive group without reflux at 6 weeks (33.3%) again showed pathological reflux at 6months. At 6 months, 46.2% of the patients with preoperative pathological reflux showed adecrease in esophageal acid exposure.Twelve patients out of 13 without preoperative pathological reflux had normal reflux patterns at 6weeks. One patient with pathological reflux at 6 weeks showed a normal reflux pattern at 6months. At 6 months, 4 of the 11 patients (36.4%) without pathological reflux at 6 weeks showeda pathological reflux pattern. Thus, 30.1% of the patients without pathological reflux preopera-tively had a pathological reflux pattern at 6 months (Figure 3).The presence of a pouch was foundto be a major determinant for the presence of pathological reflux. As shown in Figure 4 and Table2, the 9 patients with a pouch at 6 months had significantly higher esophageal acid exposure val-ues than the patients without a pouch.
Table 1. Reflux parameters preoperatively, at 6 weeks and at 6 months after the operation.
p-valuespreoperative 6 weeks 6 months pre- 6wk pre-
6wk 6mnth 6mnth
total reflux time (%) 5.2 (0.7) 3.8 (1.1) 7.1 (1.7) NS NS NSupright reflux time (%) 6.9 (0.8) 5.3 (1.5) 6.5 (1.5) NS NS NSsupine reflux time (%) 2.3 (0.8) 0.9 (0.4) 7.5 (2.4) NS 0.013* NSreflux episodes (n) 38.6 (4.0) 23.5 (4.7) 39 (9.8) 0.013* NS NSupright reflux episodes (n) 35.3 (3.4) 22.5 (4.5) 32.9 (8.8) 0.023* NS NSsupine reflux episodes (n) 3.2 (0.7) 1 (0.3) 6.2 (2.1) 0.004 0.022* NSreflux episodes > 5min (n) 2.4 (0.5) 1.8 (0.8) 3.6 (0.9) NS NS NSupright reflux episodes > 5min (n) 1.8 (0.3) 1.7 (0.8) 1.7 (0.4) NS NS NSsupine reflux episode > 5min (n) 0.6 (0.2) 0.1 (0.1) 1.9 (0.7) NS 0.018* NSlongest reflux episode upright (min) 7.8 (0.8) 8.4 (2.2) 12.3 (3.2) NS NS NSlongest reflux episode supine (min) 5.5 (1.7) 3.6 (1.8) 16.7 (5.2) NS 0.015* 0.05*
Data given as mean ± SEM, NS = not significant), *= not significant after Bonferroni correction (n = 26).
Figure 4. Mean percentage of time with esophageal pH < 4 depicted for patients with or without a pouch at 6months follow-up.
21

CorrelationsAt 6 months the presence of a pouch was associated with esophagitis (r = 0.505, p = 0.017), useof acid-reducing medication (r = 0.427, p = 0.033), number of reflux periods in supine position (r= 0.427, p = 0.048) and total reflux time (r = 0.698, p < 0.001).Analysis of the relationship between pouch and reflux symptoms yielded a significant correlationonly for day-time heartburn (r = 0.528, p = 0.007) and belching (0.472, p = 0.048).There was no significant relationship between pouch formation and the preoperative existence ofa hiatal hernia. A correlation between pouch size with grade of filling of the band (mean 2.38 ±0.07 ml) and percentage of time with esophageal pH < 4 or reflux symptoms could not be found.Smoking or the use of alcohol showed no correlation with reflux esophagitis, reflux symptoms andesophageal acid time preoperatively and during follow-up.
Table 2. Reflux parameters at 6 months
Pouch + Pouch – p(n = 9) (n = 17)
reflux episodes (n) 72.9 (17.7) 15.4 (6.5) 0.002upright reflux episodes (n) 58.6 (16.8) 14.8 (6.4) 0.009*supine reflux episodes (n) 14.3 (4.0) 0.68 (0.5) < 0.001reflux episodes > 5min (n) 7.5 (1.5) 1.0 (0.2) < 0.001upright reflux episodes > 5min (n) 2.8 (0.7) 0.93 (0.2) 0.006*supine reflux episode > 5min (n) 4.7 (1.4) 0.06 (0.06) < 0.001longest reflux episode upright (min) 19.0 (7.4) 7.28 (1.3) NSlongest reflux episode supine (min) 40 (9.0) 1.1 (0.7) < 0.001
Data given as mean ± SEM, NS = not significant), * = not significant after Bonferroni correction (n = 26).
Comparison of patients with or without a pouch at 6 months after operation.
DISCUSSIONThis prospective follow-up study describes the influence of the Lap-Band® on the loweresophageal sphincter (LES) physiology and gastroesophageal reflux (GER). Considerable inter-indi-vidual differences in the course of symptoms and objective parameters of GER were found, as weobserved patients who developed, lost and kept reflux symptoms, pathological reflux and refluxesophagitis at different follow-up intervals. Three important general observations were made:Firstly, the unfilled Lap-Band, when placed in a high esophago-gastric position is an effective anti-reflux device in obese patients. A significant decrease was shown in pathological reflux recordingsat 6 weeks follow-up. Secondly, a clear relationship was found between pouch formation duringfollow-up and reflux symptoms, pathological reflux, reflux esophagitis and the use of acid-reduc-ing drugs. Thirdly, the presence of a hiatal hernia showed no effect on the postoperative GER pat-tern.The influence of obesity and the influence of weight loss on GER are somewhat controversial butshould be kept in mind for a correct interpretation of our results. Several reports supporting a neg-ative effect of obesity14-17 and a positive effect of weight loss18 are available, but reports whichsuggest no influence can be found as well19. Most treatment regimens for GERD therefore includebody weight reduction. In our study all patients lost weight, but in some reflux increased while inothers reflux decreased during follow-up. The anti-reflux effect of the band was appreciated by
22

our patients immediately following surgery when no significant weight reduction had beenachieved yet. Moreover no correlation between weight loss and reflux was found.In the literature a positive effect of the adjustable band on GER has been suggested, but mainly onclinical observations10 20. However, until now only a few objective measurements were reported.Anderson21 found a decrease in symptoms and reflux esophagitis after placement of an adjustableband. Angrisani22 found total disappearance of pathological reflux and reflux symptoms in 11patients after adjustable gastric banding and repair of a hiatal hernia. Dixon et al.12, in a retrospec-tive analysis, found total resolution of reflux symptoms in 75% of the patients, improvement in 15%, no change in 6% and aggravation in 4%. They suggested the pouch as determining factor butdid not perform regular upper GI series. In the only prospective study employing the Swedishband (i.e. another type of silicone adjustable gastric band) Weiss et al.23 reported pathologicalreflux in 34.9% of the 43 patients preoperatively and postoperative resolution of GER in all at sixmonth follow-up.Increased GER following gastric banding has been reported by many, in some studies even leadingto discontinuation of the banding method8 9 12 24 25. Westling24 found an enormous increase inreflux esophagitis from 15 % to 56 % at two years follow-up. Morino25 even found esophagitis in60% after LAGB.In the studies published thus far it has remained unclear which factors determine whether GERand esophagitis increase or decrease after adjustable gastric banding. Is it the follow-up time, fill-ing grade of the band, position of the band or the preoperative presence of a hiatal hernia?Our results are in accordance with the findings of Ovrebo and coworkers8 who in a series of 15patients who underwent a non-adjustable Dacron gastric banding (without hiatal hernia repair),found an increase in heartburn and regurgitation, from 14 and 13% to 63 and 69% respectively.The total reflux time increased from 6.4% to 30.9%, which was found to be mainly because of anincrease in supine reflux. It should be noted that Ovrebo et al. performed non-adjustable gastricbanding procedures with the intentional formation of a pouch. In contrast, Lundell9 et al. did notfind an effect of non-adjustable gastric banding on symptoms and reflux. It is unclear from thestudies of Ovrebo and Lundell whether there were individual patients in whom esophageal acidexposure and symptoms improved.The anti-reflux effect of a proximally placed gastric band is likely to be caused by an augmentationof the LES by creating a longer intraabdominal pressure zone or by pulling the stomach more inthe abdomen in the presence of a hiatal hernia. These mechanisms are similar to those provided bythe Angelchik prosthesis12 23 26. In case of a pouch the band is not able to support the LES, andprobably creates an anatomical situation comparable with hiatal hernia, favoring reflux27.The presence of a hiatal hernia is considered by some authors as a contraindication againstLASGB28, but Angrisani11 reported the simultaneous succesful treatment of obesity and hiatal her-nia by band placement and closing the hiatus. The significance of a concomittant hiatal hernia inpouch development is unclear and in our study no significant relationship was found.Our study shows that pouch formation is a crucial determining factor in the occurrence of GER inpatients following LAGB. Development of a pouch was observed only after filling the band. Theeffect of pouch formation on GER stresses the importance of a meticulous surgical technique, inorder to avoid pouch enlargement and fundus slippage through the band, which are reported tooccur in up to 18%29.Contrary to the former technique of gastric banding with the intentional formation of a 25-30 mlpouch proximal to the band, a ‘virtually-no-pouch’ procedure is presently advocated with place-ment of the band at or near the gastro-esophageal junction by means of the so-called pars flaccidatechnique30. High placement of the band avoids tunnelling of the band through the omental bursabut instead firmly anchors the band posteriorly in the fibrous tissues at the gastroesophageal junc-
23

tion. In combination with a number of anterior gastro-gastric sutures over the band a firm anteriorand posterior fixation is realized which prevents pouch enlargement and band migration. Despitehigher placement of the band, we and others observed pouch formation at 6 months, in somecases requiring surgical correction31. The most probable cause is inaccurate placement of the band.It is as yet unknown whether or not such high position of the band will lead to dilatation of theesophagus. A few reports are available in literature in which esophageal dilatation was seen in upto 71% of the patients with concomitant esophageal motility disorders23 32. The role of these dis-orders in gastroesophageal reflux needs to be investigated further.In our series, the grade of esophagitis increased in 39.1 % of the patients during 6 months follow-up; in most cases a pouch was diagnosed. In our series one case of Barrett’s esophagus was foundpreoperatively with an unchanged aspect at 6 months follow-up. Naslund33 found at 9 years fol-low-up after non-adjustable gastric banding the development of a Barrett’s esophagus in 4.3 % ofthe patients without clear symptomatology and despite the use of acid-reducing drugs. Theobserved increase of esophagitis in our study and the fact that obesity and gastroesophagealreflux are risk factors for the development af adenocarcinoma of the esophagus34 35, make endo-scopic follow-up after (non)-adjustable gastric banding mandatory at present.In summary, our study has shown positive and negative effects of adjustable gastric banding ongastro-esophageal reflux. Band placement at the gastroesophageal junction has a strong antirefluxeffect which can be maintained at follow-up if pouch development or enlargement can be avoid-ed. If a pouch develops by herniation of the proximal stomach through the band, an increase inpathological reflux, reflux symptoms and reflux esophagitis will be found. Long term follow-upafter LAGB is absolutely necessary to evaluate the balance between positive effects such as weightloss and an antireflux effect, and negative effects such as development or deterioration of refluxdisease.
REFERENCES1. Seidell JC, Deerenberg I. Obesity in Europe; prevalence and consequences for use of medical care.
Pharmacoeconomics 1994; 5 (Suppl. 1):38-442. Colditz GA. Economic costs of severe obesity. In: Gastrointestinal surgery for severe obesity.NIH Consensus
Development Conference, National Institutes of Health, Bethesda, Maryland 1991:24-303. Martin LF, Tan TL, Horn JR, et al. Comparison of the costs associated with medical and surgical treatment
of obesity. Surgery 1995; 118:599-6074. Brolin RE. NIH Consensus Development Panel: Gastrointestinal surgery for severe obesity. Nutrition 1996;
12:403-4045. Naslund I, Agren G. Is obesity surgery worthwile? Obes Surg 1999; 9:3266. Kral JG. The role of surgery in obesity management. Int J Risk Safety Med 1995; 7:111-1207. Belachew M, Legrand M, Vincent V, et al. Laparoscopic adjustable gastric banding. World J Surg 1998;
22:955-9638. Ovrebo KK, Hattlebak JG, Viste A, et al. Gastroesophageal reflux in morbidly obese patients treated with
gastric banding or vertical banded gastroplasty. Ann Surg 1998; 228:51-589. Lundell L, Ruth M, Olbe L. Vertical banded gastroplasty or gastric banding for morbid obesity: effects on
gastroesophageal reflux Eur J Surg 1997; 163:525-53110. Niville E, Vankeirsbilck J, Dams A. Laparoscopic esophagogastric banding: a preliminary experience. Obes
Surg 1998; 8:39-4311. Angrisani L, Iovino P, Lorenzo M, et al. Treatment of morbid obesity and gastroesophageal reflux with
hiatal hernia by Lap-Band. Obes Surg 1999; 9:396-39812. Dixon JB, O’Brien PE. Gastroesophageal reflux in obesity: the effect of Lap-band placement. Obes Surg
1999; 9:527-53113. Forsell P, Hallerback B, Glise H, et al. Complications following Swedish adjustable gastric banding: a long
term follow-up. Obes Surg 1999; 9:11-16
24

14. Wilson LJ, Ma W, Hirschowitz BI. Association of obesity with hiatal hernia and esophagitis. Am JGastroenterol 1999; 94:840-844
15. Stene Larsen G, Weberg R, Froyshov I. Relationship of overweight to hiatus hernia and reflux esophagitis.Scand J Gastroenterol 1988; 23:427-432
16. Hagen J, Deitel M, Khanna RK, et al. Gastroesophageal reflux in the massively obese. Int Surg 1987; 72:1-317. Fisher BL, Pennathur AA, Mutnick JL. Obesity correlates with gastroesophageal reflux. Dig Dis Sci 1999;
44:2290-229418. Fraser Moodie CA, Norton B, Gornall C. Weight loss has an independent beneficial effect on symptoms of
gastroesophageal reflux in patients who are overweight. Scand J Gastroenterol 1999; 34:337-34019. Kjellin A, Ramel S, Rossner S. Gastroesophageal reflux in obese patients is not reduced by weight reduc-
tion. Scand J Gastroenterol 1996; 31:1047-105120. O’Brien P, Brown WA, Smith A. Prospective study of laparoscopically placed adjustable gastric band in the
treatment of morbid obesity. Br J Surg 1999; 85:113-11821. Anderson P. Endoscopic and histological evaluation of the Lap-band at 12 months. Obes Surg 1999; 9:330
(abstract)22. Angrisani L, Paola I, Santoro T. The use of Lap-band for simultaneous treatment of obesity and gastroe-
sophageal reflux disease with or without hiatal hernia. Obes Surg 2000; 10:139 (abstract)23. Weiss HG, Nehoda H, Labeck B, et al. Treatment of morbid obesity with laparoscopic adjustable gastric
banding affects esophageal motility. Am J Surg 2000; 180:479-48224. Westling A, Bjurling K, Ohrvall M. Silicone adjustable gastric banding: disappointing results. Obes Surg
1998; 8:467-47425. Morino M, Toppino M, Garrone C. Disappointing long term results of laparoscopic adjustable gastric
banding. Br J Surg 1997; 84:868-926. Bonavina L, DeMeester T, Mason R, et al. Mechanical effect of the Angelchik prosthesis on the competency
of the gastric cardia: pathophysiologic implications and surgical perspectives. Dis Esoph 1997; 10:115-11827. Kahrilas PJ. Anatomy and physiology of the gastroesophageal junction. Gastroenterol Clin N Am 1997;
26:467-48528. Greenstein RJ, Nissan A, Jaffin B. Esophageal anatomy and function in laparoscopic gastric restrictive
bariatric surgery: implications for patient selection. Obes Surg 1998; 8:199-20629. Zimmermann JM, Blanc M, Mashoyan P, et al. Preliminary study concerning a single institution’s experi-
ence with 1410 cases of adjustable gastric banding performed from July 1995 to April 2001. Obes Surg2001; 11:520 (abstract)
30. Catona A, La Manna L, Forsell P. Swedish adjustable gastric band: laparoscopic technique and preliminaryresults. Obes Surg 2000; 10:15-21
31. Niville E, Dams A. Late pouch dilation after laparoscopic adjustable gastric and esophagogastric banding:Incidence, treatment and outcome. Obes Surg 1999; 9:381-384
32. DeMaria EJ, Sugarman HJ, Meador JG, et al. High failure rate after laparoscopic adjustable silicone gastricbanding for treatment of morbid obesity. Ann Surg 2001; 233:809-818
33. Naslund I, Stockeld D, Granstrom L. Six cases of Barrett’s esophagus after gastric surgery for massive obe-sity: an extended case report. Obes Surg 1996; 6:155-158
34. Lagergren J, Bergstrom R, Lindgren A. Symptomatic gastroesophageal reflux as risk factor for esophagealadenocarcinoma. N Eng J Med 1999; 340:825-831
35. Snook KL, Ritchie JD. Carcinoma of esophagus after adjustable gastric banding. Obes Surg 2003; 13:800-2
25


Chapter 3
EFFECT OF LAPAROSCOPIC
GASTRIC BANDING ON ESOPHAGEAL MOTILITY
JR de Jong*, B van Ramshorst**, R.Timmer***, HG Gooszen*, AJPM Smout****
Department of Surgery, University Medical Center, Utrecht*, Department of Surgery, St Antonius Hospital**, Nieuwegein, Department of Gastroenterology,
St Antonius Hospital, Nieuwegein***, Department of Gastroenterology, University Medical Center, Utrecht****, The Netherlands
Obes Surg 2006; 16:52-8

ABSTRACTBackground: Alterations in esophageal motility may occur after placement of an adjustablegastric band, as treatment for morbid obesity, near the gastroesophageal junction. It causesan outlet obstruction especially during follow up after the band is filled.Methods: 29 morbidly obese patients underwent conventional manometry preoperatively, sixweeks postoperatively, before and after filling the band, and at six months postoperatively. Aquestionnaire was used to assess upper gastrointestinal symptoms during follow-up.Results: After band placement, there was a significant increase in lower esophageal sphincter(LES) end-expiratory pressure at 6 weeks with an empty band: 1.3 (0.9-1.9) kPa (median(interquartile range) (p = 0.003), 6 weeks with a filled band: 2.1 (1.5-2.8) kPa (p = 0.0001)and at six months: 1.5 (1.3-1.9) kPa (p = 0.001), compared to the preoperative pressure: 0.8(0.6-1.3) kPa. Also after band placement, the high pressure zone length increased (preop 5.0(4.3-6.0) cm vs 6 weeks 6.0 (5.0-6.5) cm. (p = 0.003). The propagation of peristaltic contrac-tions was not significantly altered after band placement.Heartburn decreased 6 weeks postoperatively (p = 0.04) but increased at 6 months.Heartburn at 6 months was correlated with pouch formation (0.667; p < 0.01).Conclusion: Adjustable gastric band placement causes an increase in LES pressure and lengthof the high pressure zone. It decreases reflux symptoms in the short term, but this effectappears not to be related with an effect on LES pressure or length. Pouch formation increasesreflux symptoms without having any relationship to LES pressure and length. Band placementin the short-term does not disturb propagation of esophageal contractions.
INTRODUCTIONLaparoscopic adjustable gastric banding (LAGB) has been increasingly used to treat morbid obesi-ty. Several short- and long-term complications have been described, such as gastric herniation orslippage, band erosion, port-site infection, gastric perforation and esophageal dilatation. Little isknown about the function of the lower esophageal sphincter (LES) and the esophageal body afterband placement. Because the gastric band is placed near the gastroesophageal junction, an effectof the band on the LES and/or on esophageal motility may be expected. Morbidly obese patients who were selected for bariatric surgery have shown a prevalence ofasymptomatic esophageal motility disorders in 61%1. Band placement has been found to cause anincrease in LES resting pressure2,3 and an impairment of LES relaxation leading to esophagealdilatation and an increase in defective contractions, not associated with an increase in dysphagia2.In contrast, Iovino et al.3 reported an increase in LES pressure, LES length and dysphagia afterband placement, but found no difference in LES relaxation, peristaltic contractions and amplitudeof peristaltic contraction. LES insufficiency preoperatively was related to esophageal dilatation andesophageal dysmotility after band placement 4. It has also been reported that esophageal dys-motilty was associated with pouch dilatation4,5. We hypothesized that LAGB causes increase in LES length and pressure and that LES pressureincreases after filling the band, leading to an increase in dysphagia and ultimately an increase inamplitude of esophageal contractions. Therefore, a prospective follow-up study was performed tostudy the influence of band placement and filling of the band on LES and esophageal motility andesophageal symptoms.
PATIENT AND METHODSBetween July 1998 and March 2000, 76 consecutive morbidly obese patients underwent a LAGBprocedure with the 10-cm Lap-Band® system (Inamed, Santa Barbara, CA, USA). Inclusion criteria
28

for this operation were a BMI > 40, or a BMI between 35 and 40 with serious co-morbidity (pul-monary, cardiovascular, musculoskeletal or endocrine disorders). All patients were thoroughlyscreened before surgery by an experienced panel consisting of an internist, a dietician, a psycholo-gist and a bariatric surgeon. Twenty-nine patients out of this group, 26 female and three male,with a mean age of 41.3 (SD ±6.4) years and a mean BMI of 46.1 (SD ±4.8) agreed to participatein the study. Written informed consent was obtained from each patient. The study was approvedby the Medical Ethics Committee of the St. Antonius Hospital.
SurgeryAll operations were performed by one experienced laparoscopic surgeon (BvR), using the perigas-tric technique described by Belachew and co-workers6. To prevent band migration the gastric fun-dus was sutured to the proximal stomach over the anterior aspect of the band with three or fournon-absorbable seromuscular sutures. The reservoir through which the band could be inflated toadjust the stomal diameter was placed on the rectus sheath just below the xiphoid process.Postoperatively, all patients took a liquid diet for 4 weeks. At 6 weeks the first stoma adjustmentwas carried out by filling the band with 2 ml of saline. Patients were followed at regular intervalsand further stoma adjustments were made, depending on the degree of weight loss. At 6 months,the mean filling volume of the band was 2.4 ml(1.8-3.2).
Symptom assessmentTo assess upper GI symptoms the patients completed a questionnaire preoperatively, at 6 weeks(before filling of the band) and at 6 months follow-up. The questionnaire included questionsabout heartburn (at day- and nighttime), regurgitation, nausea , belching and dysphagia. Theintensity at which these symptoms occurred in the week prior to examination was scored using anascending scale from 0 to 4 (0 = no symptoms, 1 = symptoms on one or two days, 2 = symptomson three or four days, 3 = symptoms on five or six days and 4 = daily symptoms).
ManometryA conventional manometry was carried out before operation, 6 weeks (before and after filling of theband) and 6 months after operation, using a water-perfused (0.5ml/min) three- lumen catheter withthe side holes 5 cm apart and oriented in three different directions. The patients were measured in asupine position. Drugs with a possible effect on esophageal motility were discontinued at least fivedays prior to examination. A stationary pull through maneuver was done during which the catheterwas withdrawn in steps of 1 cm. End-expiratory LES pressure (endexpiratory gastric pressure subtract-ed from actual endexpiratory pressure recording in LES channel) was measured as the mean of valuesfrom the three recording orifices. Normal range for endexpiratory LES pressure in our laboratory is0.5-3.4 kPa. The total length of the high-pressure zone at the esophagogastric junction was meas-ured. Thereafter, the catheter was positioned with the distal orifice 5 cm above the proximal border ofthe LES, and the response of the esophageal body to 10 wet swallows (5 ml of tap water at roomtemperature) was evaluated. The esophageal contractions were categorized in peristaltic, non-trans-mitted and simultaneous. The peak amplitude of the ten swallow-induced contractions was calculat-ed for each of the three measured levels. The duration of the contractions was measured from thebeginning of the upstroke to the end of the downstroke. The propagation velocity of the contractionwaves was calculated from peak-to-peak intervals between peristaltic waves at adjacent side holes. When a “ramp”(pressure elevation caused by the water bolus) was present7, the ramp pressure(endexpiratory esophageal pressure subtracted from maximum ramp pressure) was determined foreach recording level (proximal, mid and distal). The LES nadir pressure7 was measured for each ofthe LES relaxations induced by the wet swallows. A nadir pressure < 1.1 kPa (8 mmHg) was con-sidered complete8.
29

Pouch formationA barium study of the esophagus was performed on the first postoperative day and at 6 monthsafter operation in order to assess the position of the band in relation to the LES. A pouch was diag-nosed if gastric folds or a part of the stomach were seen proximal to the band. In order to quanti-fy the pouch size, a ratio was calculated between the maximum diameter of the pouch and themaximum diameter of the band. The pouch size was judged to be large if the ratio was � 1.
StatisticsThe data were statistically analyzed by using a SPSS 9.0 package. A p-value < 0.05 was consideredto be significant. The Mann-Whitney U test was used to compare continuous variables betweenunrelated groups, and the Wilcoxon Signed Ranks test was used for repeated measurements in thesame patients. The Spearman’s rank correlation test was used to assess relationship between thedifferent variables. Bonferroni correction was done for multiple comparisons.
Figure 1. Grading of esophagitis according to Savary-Miller, before and 6 months after the operation.
RESULTSWeight lossPreoperatively Body Mass Index (BMI) was 46.1 ±4.8 kg/m2 (mean ±SD). At 6 weeks there was asignificant decrease to 42.1 ±4.6 kg/m2, and at 6 months a significant decrease to 36.7 ±4.4)kg/m2 was found (p < 0.001).
Symptom assessmentPreoperatively heartburn at daytime was reported by 11 patients (37.9%). At 6 weeks, the num-ber of patients with heartburn at daytime had decreased to five patients (17.2%) (p = 0.041). At 6months, 6 patients (20.6%) reported heartburn at daytime; 8 of the 11 patients (72.7%) who hadheartburn at daytime preoperatively were free of symptoms, and 3 of the 15 patients (20%) with-out preoperative heartburn at daytime had symptoms at six months. Preoperatively heartburn atnight-time was reported by 2 patients (6.9%) only. At 6 weeks and 6 months, there was no signif-icant change. The number of patients with regurgitation increased from 2 patients (6.9%) preoperatively to 4patients (13.8.%) at 6 weeks (not significant) and to 14 patients (48.3%) at 6 months (p = 0.002).Dysphagia increased significantly during follow up (Figure 1), both from preoperatively to 6 weeks
30
dysp
hagi
a sc
ore

(p = 0.0001) and from 6 weeks to 6 months (p = 0.002). At 6 weeks 44.8% of the patients experi-enced dysphagia only once or twice a week, and only 6.9% had dysphagia every day. At 6 months37.9% of the patients showed dysphagia once or twice a week and 13.8% had dysphagia every day. There were no statistically significant differences in symptom scores at any point in time, betweenpatients with a hiatal hernia preoperatively (n = 19) and those without (n = 10)
Figure 2. End-expiratory LES pressure (kPa) in the individual patients during follow-up.
LES pressureThere was a small but statistically significant increase in LES pressure 6 weeks after operation(empty band) compared to the preoperative pressures. Filling of the band resulted in a pro-nounced further increase. At 6 months, there was a significant decrease compared to six weeksafter operation, but there was still a significant difference compared to the preoperative pressures.(Table 1, Figure 2).
High pressure zone lengthThe length of the high-pressure zone at the esophagogastric junction showed a significantincrease after positioning of the band. This increase persisted throughout the 6 month follow-up.(Table 1, Figure 3). Two distinct high pressure zones (one caused by the band and one by theLES ), were seen in only one patient, who had a large pouch at 6 months postoperatively.
LES nadir pressureBoth placement and filling of the band caused a significant rise in LES nadir pressure (Table 1,Figure 4). There was no significant difference between 6 weeks and 6 months postoperatively.Preoperatively, LES relaxation was complete in all patients before band insufflation. After bandinsufflations, 4 patients had an incomplete LES relaxation.
Ramp pressureThe ramp pressure phenomenon was observed more often after gastric banding, and bandingincreased the amplitude of the ramp pressure. Filling of the band had little or no effect on ramppressure (Table1).
31
LES
pres
sure
(kP
a)

32
Tabl
e 1.
Man
omet
ry p
aram
eter
s fo
r th
e di
ffer
ent
inte
rval
s
preo
pera
tive
6 w
eeks
6 w
eeks
6 m
onth
spr
eope
rati
ve6
wee
ks e
mpt
ypr
eope
rati
vevs
6 w
eeks
empt
yfi
lled
empt
yvs
6 w
eeks
fill
edvs
6 m
onth
s
LES
ende
xp. p
ress
ure
(kPa
)0.
8 (0
.6-1
.3)
1.3
(0.9
-1.9
)2.
1 (1
.5-2
.8)
1.5
(1.3
-1.9
)0.
003
0.00
010.
001
high
-pre
ssur
e zo
ne le
ngth
9cm
)5.
0 (4
.3-6
.0)
6.0
(5.0
-6.5
)6.
0 (5
.7-7
.0)
6.0
(5.5
-6.4
)0.
003
0.03
*0.
01*
rela
xatio
n (%
)10
0 (1
00-1
00)
72.7
(60
-88.
8)66
.8 (
50.9
-82.
4)57
.9 (
48.6
-75.
4)0.
001
ns0.
0001
resi
dual
rel
axat
ion
pres
sure
(kP
a)0
(0-0
)0.
3 (0
.2-0
.4)
0.7
(0.4
-0.9
)0.
65 (
0.3-
0.8)
0.00
010.
0001
0.00
01
% o
f sw
allo
ws
wit
h ra
mp
pres
sure
prox
imal
10 (
0-45
)50
(10
-80)
40 (
12.5
-80)
50 (
20-9
0)0.
007
ns0.
003
Mid
0 (0
-30)
40 (
20-6
5)50
(30
-70)
55 (
7.5-
90)
0.00
01ns
0.00
1D
ista
l30
(0-
60)
60 (
50-8
5)80
(70
-100
)80
(62
.5-1
00)
0.00
010.
02*
0.00
01
ram
p pr
essu
re (
kPa)
prox
imal
1.7
(0-2
.9)
2.3
(1.6
-2.6
)2.
4 (1
.8-2
.7)
2.6
(1.9
-3.0
)ns
ns0.
01*
Mid
0 (0
-2.8
)2.
6 (1
.7-2
.7)
2.6
(2.4
-2.9
)2.
5 (1
.2-2
.9)
0.00
8ns
0.00
4D
ista
l2.
9 (0
-3.2
)3.
2 (2
.7-3
.8)
3.0
(2.5
-3.9
)2.
9 (2
.8-3
.3)
0.03
*ns
ns
prop
agat
ion
(%)
peris
talti
c90
(90
-100
)10
0 (8
5-10
0)10
0 (1
00-1
00)
100
(80-
100)
ns0.
02*
nssi
mul
tane
ous
10 (
0-10
)0
(0-1
5)0
0 (0
-20)
ns0.
03*
nsno
n-tr
ansm
itted
00
00
nsns
nsre
trog
rad
00
00
nsns
ns

33
Preo
pera
tive
6 w
eeks
6 w
eeks
6mon
ths
Preo
pera
tive
6 w
eeks
em
pty
Preo
pera
tive
empt
yfi
lled
vs 6
wee
ksem
pty
vs 6
wee
ks f
illed
vs 6
mon
ths
ampl
itud
e pe
rist
alti
c co
ntra
ctio
n (k
Pa)
prox
imal
6.9
(5.3
-9.6
)7.
1 (5
.5-8
.5)
9.1
(5.4
-10.
2)6.
3 (4
.4-1
0.8)
ns0.
03*
nsM
id12
.0 (
8.9-
15.4
)11
.8 (
7.6-
17)
11.2
(6.
7-14
.8)
12.1
(7.
5-17
.9)
nsns
nsD
ista
l11
.5 (
7.6-
17.5
)14
.0 (
8.0-
15.7
)12
.1 (
7.4-
18.6
)13
.6 (
8.9-
18.6
)ns
nsns
dura
tion
con
trac
tion
(s)
prox
imal
3.4
(2.7
-3.8
)3.
5 (2
.9-4
.0)
3.6
(3.2
-4.3
)3.
5 (3
.0-4
.1)
nsns
0.03
*M
id3.
5 (3
.3-4
.4)
3.9
(3.5
-4.5
)3.
9 (3
.4-4
.3)
4.1
(3.4
-4.3
)ns
nsns
Dis
tal
3.8
(3.1
-4.4
)4.
1 (3
.3-4
.5)
3.8
(3.5
-4.6
)4.
2 (3
.4-4
.5)
nsns
0.04
*
velo
city
(cm
/s)
prox
-mid
4.2
(2.5
-5.5
)2.
6 (2
.0-4
.2)
3.1
(2.4
-5.7
)4.
2 (2
.3-5
.2)
0.03
*ns
nsm
id-d
ista
l4.
4 (3
.8-5
.3)
3.8
(3.5
-5.7
)3.
7 (2
.8-4
.5)
4.1
(3.5
-5.0
)ns
0.03
*ns
Valu
es e
xpre
ssed
in m
edia
n (in
terq
uart
ile r
ange
); n
s =
not
sig
nific
ant;
* =
not
sig
nific
ant
afte
r Bo
nfer
roni
cor
rect
ion

PeristalsisPeak amplitudes of the esophageal contractions at the different levels were not affected by place-ment of the band only. Likewise, the durations of esophageal contractions remained unaltered.Propagation velocity decreased from the proximal to the mid part of the esophagus preoperative-ly compared to 6 weeks. There was also a decrease for the mid part to the distal part of the esoph-agus at six weeks after filling of the band (Table 1).
Figure 3. Length of the lower esophageal high-pressure zone (cm) in the individual patients.
Pouch developmentAt 6 months, a large pouch was found in 9 patients. In 1 patient, a smaller pouch was diagnosed.The mean pouch / band ratio was 1.3, with a range from 0.8 to 1.75. Five of the patients with apouch needed to be operated because of severe regurgitation. The band was removed andreplaced in a higher position to leave a minimal pouch proximal to the band. This resulted in reso-lution of regurgitation.
Figure 4. LES nadir pressures (kPa) during follow-up in the individual patients.
34
leng
th o
f hi
gh-p
ress
ure
zone
(cm
)le
ngth
of
high
-pre
ssur
e zo
ne (
cm)

Correlations Dysphagia at 6 weeks postoperatively was positively correlated with pyrosis at day-time (0.476; p= 0.009) and belching (0.539; p = 0.003) and was negatively correlated with the percentage ofLES relaxation (-0.414; p = 0.04). There was no relationship between dysphagia and ramp pres-sure and between dysphagia and LES pressure.At 6 months a relationship was found between the presence of a pouch and heartburn at day- andnight-time (0.745; p < 0.01 and 0.496; p = 0.01) and regurgitation (0.397; p = 0.04).At 6 weeks postoperatively, the LES pressure was positively correlated with the distal esophagealcontraction amplitude and distal ramp pressure (0.467; p = 0.01 and 0.547; p = 0.005).At 6 weeks and 6 months postoperatively, the relaxation nadir pressure showed a positive relation-ship with the distal contraction amplitude (0.612; p = 0.001 and 0.550; p = 0.008).
DISCUSSIONIn this study we examined morbidly obese subjects who underwent placement of an adjustablegastric band near or at the gastroesophageal junction.After band placement there was a significant decrease in reflux symptoms. However, a significantrelationship between LES pressure, length, hiatal hernia and reflux symptoms could not be demon-strated. This may reflect the fact that the principal mechanism of reflux is transient loweresophageal sphincter relaxation (TLESR)9. Triggers of transient relaxation are gastric distension,right lateral decubitus posture and meals high in fat10. The manometric technique used in thisstudy did not allow recording of TLESRs. After placement of the band the patients had a liquid dietfor the first 6 weeks and after filling the band at 6 weeks, most of them were unable to eat largemeals. These changes in eating behaviour may reduce the trigger for TLESRs and are a possibleexplanation for the decrease in reflux symptoms11. The formation of a pouch seemed to play a rolein the postoperative increase of reflux symptoms. It is tempting to speculate the pouch functionslike a hiatal hernia with stasis of acid material which can reflux to the esophagus. We found signif-icant effects of band placement on LES characteristics, i.e. an increased sphincter pressure andlength and a decreased relaxation. In contrast, no significant effect on esophageal body motilitywas found. In previous manometric studies performed in morbidly obese persons, LES pressures varying from11.3 + 3.8 to 27.2 + 2.1 mmHg have been found12-18. In all but one case12 no difference with anon-obese control group was found. The LES pressures found preoperatively in this study (0.2-2.1kPa, 1.5-15.8 mmHg) seem to be somewhat lower than those reported in the literature, but thismay be due to differences in measurement technique. Our patients were comparable to literaturein the sense that most patients showed a LES pressure that was within the limits of normal for ourlaboratory.The effect of adjustable gastric band placement on LES pressure and esophageal motility has beeninvestigated in two studies2,3. Weiss et al2, using the Swedish band, found a significant postopera-tive increase of LES resting pressure and an impairment of LES relaxation. The number ofesophageal contractions with defective propagation increased significantly. In contrast we found atendency towards more effective peristaltic propagations after placement of the Lap-Band®.Iovino and coworkers2 found no difference in preoperative LES length, contraction amplitudes orduration between patients and control subjects and between patients with normal and withabnormal esophageal acid exposure. In their study postoperative manometry, performed in only11 of the 43 patients, showed a higher mean LES pressure and an increased LES length and waveduration of esophageal contractions. No differences were found in LES relaxation, percentage ofperistaltic waves and wave amplitude.In the 1970s Angelchick19 introduced a silicone prosthesis for the treatment of gastroesophageal
35

reflux. The device was placed around the distal esophagus. The adjustable gastric band is placedslightly more distal than the Angelchick prosthesis but otherwise seems comparable to it. In astudy of the Angelchick prosthesis in primates a significant increase in LES pressure and LES lengthwas found20. The authors supposed that the effect was caused by a so called posterior padding ofthe gastroesophageal junction, which resulted in changes in the length-tension relationship of theLES and an increased LES pressure. Bonavina et al21 found an increase in LES competence byapplying the Angelchick prosthesis. They supposed the prosthesis prevented unfolding of the LESwhen challenged by intragastric pressure.The decrease of LES pressure we found at six months (Table 1, Figure 2) may be a sign of adapta-tion or weakening of the smooth muscle, because in none of the patients fluid was removed outof the band.After placement and filling of the band, there was a significant increase in ramp pressure. Mittal etal found a relationship between ramp pressure and dysphagia22, but like Mathew et al7 we did notobserve such a relationship.In conclusion, this case-control study shows that in morbidly obese patients, preoperativeesophageal and LES motor function are not markedly abnormal. Adjustable band placement caus-es an increase in LES pressure and high pressure zone length. Placement of the band decreasesreflux symptoms but this effect does not appear to be related to an effect on LES pressure orlength. Pouch formation increases reflux symptoms, without having any relationship to LES pres-sure or length. Band placement does not disturb propagation of esophageal contractions.Further studies are needed to determine whether the anti-reflux properties of the band are causedby a decrease of transient relaxations, by a change in eating pattern, or by other mechanisms.
REFERENCES1. Jaffin BW, Knoepflmacher P, Greenstein R. High prevalence of asymptomatic esophageal motility disorders
among morbidly obese patients. Obes Surg 1999; 9:390-52. Weiss HG, Nehoda H, Labeck B et al. Treatment of morbid obesity with laparoscopic adjustable gastric
banding affects esophageal motility. Am J Surg 2001; 180:479-4823. Iovino P, Angrisani L, Tremolaterra F et al. Abnormal esophageal acid exposure is common in morbidly obese
patients and improves after a successful Lap-band system implantation. Surg Endosc 2002; 16:1631-54. Wiesner W, Hauser M, Schob et al.Pseudo-achalasia following laparoscopically placed adjustable gastric
bandiing. Obes Surg 2001; 11:513-85. Greenstein RJ, Nissan A, Jaffin B. Esophageal anatomy and function in laparoscopic gastric restrictive
bariatric surgery: implications for patient selection. Obes Surg 1998; 8:199-2066.Belachew M, Legrand M, Vincent V, et al. Laparoscopic adjustable gastric banding. World J Surg 1998;
22:955-9637. Mathew G, Watson DI, Myers JC et al. Oesophageal motility before and after laparoscopic Nissen fundo-
plication. Br J Surg 1997; 84:1465-14698. Castell DO, Castell JA Esophageal motilty testing. 2nd edition p. 87, Appleton & Lange, Norwalk,
Connecticut 19949. Dent J, Dodds WJ, Friedman RH et al. Mechanism of gastroesophageal reflux in recumbent asymptomatic
human subjects. J Clin Invest 1980; 65:256-6710. Mittal RK, Balaban DH. The esophagogastric junction. N Eng J Med 1997; 336:924-93211. Hatlebakk, Castell DO,. Obesity and gastroesophageal reflux. Motility 1998; 42:4-612. Angrisani L, Iovino P, Lorenzo M et al. Treatment of morbid obesity and gastroesophageal reflux with
hiatal hernia by Lap-Band. Obes Surg 1999; 9:396-39813. O ‘Brien TF, Stroop EM. Lower esophageal sphincter pressure and esophageal function in obese humans. J
Clin Gastroenterol 1980; 2:145-14814. Backman L, Granstrom L, Lindahl J et al. Manometric studies of lower esophageal sphincter in extreme
obesity. Acta Chir Scand 1983; 149:193-197
36

15. Fisher BL, Pennathur A, Mutnick JL et al. Obesity correlates with gastroesophageal reflux. Dig Dis Sci1999; 44:2290-4
16. Mercer CD, Wren SF, DaCosta LR et al. Gastroesophageal pressure gradients and lower esophagealsphincter pressures in severely obese patients. Gastroenterology. 1982; 82:1129 (abstract)
17. Orlando RC, Kinard HB. Effect of morbid obesity on lower esophageal sphincter pressure (LESP).Gastroenterology 1979; 76:1212 (abstract)
18. Hagen J, Deitel M, Khanna RK et al. Gastroesophageal reflux in the massively obese. Int Surg 1987; 72:1-319. Angelchick JP, Cohen R. A new surgical procedure for the treatment of gastroesophageal reflux and hiatal
hernia. Surg Gyn Obstet 1979; 148:246-24820. Benjamin SB, Knuff TK, Fink M et al. The Angelchik prosthesis. Effects on the lower esophageal sphincter
in primates. Ann Surg 1983; 197: 63-67 21. Bonavina L, DeMeester T, Mason R et al. Mechanical effect of the Angelchik prosthesis on the competency
of the gastric cardia: pathophysiologic implications and surgical perspectives. Dis Esoph 1997; 10:115-11822. Mittal RV, Ren J, McCallum RW et al. Modulation of feline esophageal contractions by bolus volume and
outflow obstruction. Am J Physiol 1990; 258:G208-15
37


Chapter 4
WEIGHT LOSS AFTER LAPAROSCOPIC
ADJUSTABLE GASTRIC BANDING IS NOT CAUSED
BY ALTERED GASTRIC EMPTYING
JR de Jong1, B van Ramshorst2, HG Gooszen3, AJPM Smout4, MMC Tiel-Van Buul5
1. Dept. of Surgery, University Medical Center, Maastricht2. Dept. of Surgery , St Antonius Hospital, Nieuwegein3. Dept. of Surgery, University Medical Center, Utrecht
4. Dept. of Gastroenterology, University Medical Center, Utrecht5. Dept. of Nuclear Medicine, St Antonius Hospital, Nieuwegein
Obes Surg 2009; 19:287-292

ABSTRACTBackground: In order to know the role of gastric emptying in the mechanism of weight lossand early satiety after a restrictive surgical procedure for treatment of morbid obesity, a con-secutive series of patients were scintigraphically investigated before and after laparoscopicadjustable gastric banding.Methods: Sixteen patients undergoing laparoscopic adjustable gastric banding underwentpreoperatively and at six months postoperatively, a gastric emptying study (solid meal, singleisotope). Esophageal retention time, lag phase, peak activity time, gastric emptying rate, fun-dus emptying rate, and weight loss were recorded. Upper GI symptom assessment was carriedout by using a standardized questionnaire. Gastric emptying parameters were correlated withthe upper GI symptoms.Results: Gastric band placement showed no significant influence on postoperative gastricemptying rate [median % (interquartile range): 42 (23.3-59) preoperatively vs 38 (31-71)postoperatively and fundus emptying rate: 59 (37-91) preoperatively vs 70 (53-89) postoper-atively]; however, an increase in early satiety was found. Neither gastric emptying rate norfundus emptying rate showed a relation with early satiety or weight loss. Furthermore, nocorrelation was found between early satiety and lag phase, esophageal retention time, start ofactivity, and peak activity time in proximal stomach. Conclusion: Laparoscopic adjustable gastric banding seems not to affect gastric emptying.Neither a relation between postoperative gastric emptying rate and weight loss nor betweenearly satiety and weight loss was found. Therefore, it is unlikely that gastric emptying plays arole in the mechanism of weight loss following laparoscopic adjustable gastric banding.
INTRODUCTIONNowadays laparoscopic adjustable gastric banding is one of the most frequent surgical options fortreatment of morbid obesity. By creating a very small gastric reservoir of the proximal stomach with anarrow opening to the distal part of the stomach, gastric banding is a so-called restrictive procedure.It results in a reduced oral intake by causing dysphagia, fullness and early satiety leading to weightloss. However, the exact mechanism of early satiety and weight loss after such restrictive proce-dures remains unclear.Retention of solid food in the gastric pouch with slowing of gastric emptying rate after gastroplas-ty has been proposed as an important factor in the mechanism of early satiety and weight loss [1-5]. However, others reported early satiety and weight loss after gastroplasty but did not find a sig-nificant retention in the gastric pouch or a decreased gastric emptying rate [6-8]. Further evidencefor the existence of a relation between early satiety, weight loss and a change in gastric emptyingrate was found in patients with functional dyspepsia [9] and in an experiment in which glucagon-like-peptide was administered to obese subjects [10]. Recently amylin, a pancreatic hormone, wasfound to play a role in early satiety, weight loss and to slow gastric emptying [11].Based on the aforementioned studies, we hypothesized that gastric emptying might also play arole in early satiety and weight loss after gastric banding. Therefore, a prospective case controlstudy was performed to study the influence of laparoscopic adjustable gastric banding on gastricemptying, weight loss and gastrointestinal symptoms.
MATERIALS AND METHODSA consecutive series of 16 patients, 12 women and 4 men operated in the St. Antonius Hospitalwere included in the study. Their mean age was 40.5 years ( range 29-57). Their mean body massindex (BMI) was 47.8 (standard error of mean (SEM) 1.7) kg/m2. Patients with diabetes were
40

excluded. All patients gave written informed consent. The study protocol was approved by theEthical Review Committee of the St. Antonius Hospital, Nieuwegein.One postoperative emptying study could not be carried out because of pregnancy.
SURGERYAll operations were performed by one experienced laparoscopic surgeon. The operation was per-formed according to the technique described by Belachew et al [12] in which the band was placednear the gastroesophageal junction leaving a minimal pouch proximal to the band. To preventband migration, the gastric fundus was sutured to the proximal stomach over the anterior aspectof the band with three or four non-absorbable seromuscular sutures. The reservoir through whichthe band could be inflated to adjust the stomal diameter was placed on the rectus sheath justbelow the xiphoid process. Postoperatively all patients used a liquid diet for 4 weeks. At 6 weeksthe first stoma adjustment was carried out by filling the band with 2 ml of saline. Patients were fol-lowed at regular intervals, and further stoma adjustments were made according to each patient’sindividual need, depending on the degree of weight loss. At 6 months the mean filling grade ofthe band was 2.0 ml (range 1.8-2.4).
GASTRIC EMPTYING SCINTIGRAPHYGastric emptying studies using a single isotope technique [13] were performed after an overnightfast (during which the patients also refrained from smoking), before and at 6 months after laparo-scopic adjustable gastric banding. In order to reduce the intraindividual variability in gastric empty-ing, all medication, including proton pump inhibitors and prokinetic drugs, was stopped at least 3days prior to the study. The solid component of the meal (pancake; 350-400 kcal; 63% carbohy-drate, 18% protein, 19% fat) was labeled with 12 MBq Tc-99m sulphur colloid. Patients were askedto eat the pancake within 5 minutes. If this was not possible the ingestion stopped after 5 minutes.The weight and duration of the ingested meal were noted. Immediately after start of the inges-tion, scintigraphic anterior dynamic images (1 min/frame) were acquired with the patient in halfsitting position over a 90-minute period using a SMV DST-Xli gamma camera connected to a ded-icated computer. After the dynamic study, a static lateral image of 120 seconds was obtainedimmediately after drinking of 15 ml Tc-99m sulfur colloid labeled water.
ANALYSIS OF SCINTIGRAPHIC GASTRIC EMPTYINGData were analysed using dedicated software (NUD HERMES, Sweden, program made by J.J.J.Born and J.Habraken, Amsterdam, The Netherlands) and were corrected for subject movement,tissue attenuation and radioactive decay. Attenuation correction was performed using a lateralcorrection method [14]. In the corrected images, regions of interest were drawn for the esopha-gus, total stomach, the proximal stomach and the intestine to calculate the gastric emptying rateand intragastric transport.The time interval between meal ingestion and the first radioactivity in the duodenum (lag phase),the post-lag emptying rate (% of the ingested meal/hour), the time of arrival of activity in theproximal stomach (min), the time of complete clearance of activity from the distal esophagus afteringestion of the meal (min), the time at which there was first peak activity in the proximal stomach(min) and the emptying rate of the proximal to the distal stomach (%/hour) were parameters ofinterest. Scintigraphic parameters of patients with a gastric emptying rate > 25%/hour were comparedwith those of patients with a gastric emptying rate < 25%/hour which was arbitrarily consideredas delayed. The emptying curves of the proximal stomach were considered normal if the fundusemptying rate was > 60 %/hr.
41

SYMPTOM ASSESSMENTTo assess upper GI symptoms, patients completed a questionnaire preoperatively and at 6 monthsfollow-up. The questionnaire included questions about heartburn (at day- and nighttime), regurgi-tation, nausea, vomiting, belching, dysphagia and early satiety. The intensity at which these symp-toms occurred in the week prior to examination was scored using an ascending scale from 0 to 4(0 = no symptoms, 1 = symptoms on 1 or 2 days, 2 = symptoms on 3 or 4 days, 3 = symptoms on5 or 6 days and 4 = daily symptoms).The scores were correlated with the gastric emptying parameters.
STATISTICAL ANALYSISData were statistically analyzed by using a SPSS 12.0 package. A p-value < 0.05 was considered tobe significant. The Mann-Whitney U test was used to compare continuous variables betweengroups, and the Wilcoxon Signed Ranks test was used for repeated measurements in the samepatients. Correlation between pre- and postoperative symptoms and gastric emptying were calcu-lated, using the Spearman’s rank correlation test for each group. Data will be presented as medianand interquartile range, unless stated otherwise. Bonferroni correction was applied for multiplecomparisons.
RESULTS
WEIGHT LOSSThere was a significant weight loss for the whole group from a mean BMI of 47.8 (SEM 1.6) to41.7 (SEM 2.1) kg/m2 (p = 0.001). A relation between preoperative BMI, postoperative BMI, andweight loss with any of the gastric emptying parameters was not found.
SYMPTOMSPreoperatively, heartburn was the only symptom reported (two of the 16 patients). Postopera-tively, vomiting once or twice per week was found in five of the 16 patients and one patient vom-ited daily. Dysphagia was reported by 13 of the 16 postoperative patients. Dysphagia occurredonce a week in five patients and everyday in three patients. Early satiety was experienced by 11 ofthe 16 postoperative patients; in all cases, this symptom occurred daily. Statistically, neither gastric emptying rate nor fundus emptying rate showed a relation with earlysatiety, dysphagia or weight loss. Furthermore, no correlation was found between early satietyand lag time, esophageal retention time, start of activity and peak activity time in the proximalstomach.
Table 1Emptying parameters for the whole group of patients (n = 16)
preoperative postoperative p-value
Lag phase (min) 15.5 (9-27.7) 18 (4-30) NSGastric emptying rate (%/hr) 42 (23.3-59) 38 (31-71) NSGlobal maximum (min) 18 (10.5-25.5) 22 (8-30) NSStart fundus activity (min) 1 (1-1) 2 (1-3) 0.01*Fundus maximum (min) 6.5 (5-17) 10 (7-19) NSFundus emptying rate (%/hr) 59 (37-91) 70 (53-89) NSRetention distal esophagus (min) 0 (0-3.8) 10 (3-28) 0.009*
42

Table 2Emptying parameters for the group of patients with gastric emptying preoperatively > 25%/hr (n = 11)
preoperative postoperative p-value
Lag phase (min) 14 (9-28) 19.5 (6.3-34.8) NSGastric emptying rate (%/hr) 53 (42-81) 58.5 (30-104.3) NSGlobal maximum (min) 21 (10-26) 22.5 (14-31) NSStart fundus activity (min) 1 (1-1) 2.5 (1-6.5) 0.02*Fundus maximum (min) 5 (5-20) 10 (6.8-21.8) NSFundus emptying rate (%/hr) 75 (48-107) 79 (53.5-110.5) NSRetention distal esophagus (min) 0 (0-5) 13.5 (2.3-33.8) NS
Table 3Emptying parameters for the group of patients with preoperative gastric emptying < 25%/hr (n = 5)
preoperative postoperative p-value
Lag phase (min) 23 (7-39.5) 18 (3-33.5) NSGastric emptying rate (%/hr) 20 (17.5-23.5) 38 (31.5-49.5) 0.04*Global maximum (min) 15 (11-34.5) 14 (7-37.5) NSStart fundus activity (min) 1 (1-2) 1 (1-13) NSFundus maximum (min) 7 (5.5-27) 7 (6.5-30.5) NSFundus emptying rate (%/hr) 34 (28.5-59) 65 (49-79.5) NSRetention distal esophagus (min) 0 (0-12.5) 3 (1.5-32.5) NS
Data given as median (interquartile range)NS not significant * p value not significant after Bonferroni correction
GASTRIC EMPTYINGPreoperatively, the mean amount of ingested pancake was 100.3 g (range, 76-100 g). Only threepatients were not able to eat the total pancake within 5 min. Postoperatively the mean amount ofingested pancake was 83.7 g (range 28.4-114 g). Eight patients had to stop their meal at 5 min.There was no significant difference between the ingested amount of pancake pre- and postopera-tively (p = 0.069).Pre- and postoperatively, no correlation between the amount of ingested pancake and the rate ofgastric emptying was found. Postoperatively only a correlation was found between the amount ofingested pancake and the lag phase (-0.588, p = 0.02).When the preoperative and postoperative gastric emptying variables for the total group ofpatients were compared (Table 1) differences were found for the start of filling of the proximalstomach (p = 0.01) and the duration of activity remaining in the distal esophagus (p = 0.009). Theformer differences lost statistical difference after Bonferroni correction. Neither gastric emptyingnor fundic emptying were altered significantly by band placement.(Figures 1 and 2, Table1)When divided in a group of patients with a preoperative gastric emptying rate of > 25%/h (Table2) and a group with a preoperative gastric emptying rate < 25%/h (Table 3), no significant effectof band placement on any of the scintigraphic parameters was found.
43

Figure 1. Gastric emptying rate for individuals preoperatively and 6 months postoperatively.
Preoperatively, five of the 16 (31.3%) patients had a gastric emptying rate < 25%. In four of thefive patients, there was also a fundic emptying rate < 60%. Postoperatively, all five patientsshowed a gastric emptying rate > 25%.Preoperatively, eight of 16 patients (50%) had a fundus emptying rate < 60%/hr. Postoperatively,in six of the eight patients the fundus emptying rates increased (Figure 2). In one patient the fun-dus emptying rate decreased. In four of the six patients, the increase in fundus emptying rate alsoresulted in an increase in gastric emptying rate to > 25%/hr.
Figure 2. Gastric emptying rate for individuals preoperatively and 6 months postoperatively.
DISCUSSIONIn the literature, controversial reports are found concerning the gastric emptying rate in morbidlyobese people. Some authors claim that there is no difference in gastric emptying rate comparingwith a matched control group of non-obese subjects [14,15], while others found a high emptyingrate in obese subjects [16,17]. There are also reports of a delayed gastric emptying rate [18,19]like we found in about one-third of our patients preoperatively. The results of some of these stud-ies may be influenced by not performing attenuation correction or Compton scatter [16] and onlyusing a posterior camera [15].
44

In this study, in 16 morbidly obese patients, no major effect of laparoscopic gastric banding ongastric emptying was found. Therefore it is felt to be unlikely that the significant increase in vom-iting and early satiety, after band placement is caused by an effect of the band on gastric empty-ing. The fact that no clear relationship was found between gastric emptying variables and earlysatiety and weight loss lends further support to this conclusion. It is likely that the effect of the sur-gical procedure is related to limitation in the size of the meal accompanied by early satiety causedby a decrease in accommodation of the fundus [20]. This is in agreement with two reports on theeffects of vertical gastroplasty on gastric emptying [20-21].Some studies proposed a delayed gastric emptying with prolonged satiety as an additional mecha-nism for weight loss [4,10]. Villar et al. [4] found a delayed gastric emptying in patients after gas-troplasty but not in patients with a gastric bypass. Naslund et al. [5] observed delayed emptyingafter gastroplasty and after gastric bypass. Horowitz et al. [22] found a delay in emptying for solidfood after gastric bypass surgery. However, in neither of these studies, a relation between the delayin gastric emptying and weight loss could be demonstrated. We also cannot confirm the existenceof a relationship between BMI and gastric emptying as reported by others [18,19,23].Early satiety that is often found after Nissen fundoplication [24-26] and partial fundoplication[27,28] is thought to be caused by delayed gastric emptying [29], while others [26] state thatearly satiety finds its origin in the alterations, which occur after fundoplication resulting inenhancement of gastric emptying. Gastric band placement also leads to structural changes of theproximal stomach, in particular when a fundic wrap is used to fix the band. These changes mayalter the postprandial accommodation of the proximal stomach and may stimulate emptying ofthe fundus to the distal stomach, thereby resulting in accelerated gastric emptying. However, inour study no relationship was found between the delayed fundus- emptying rate, accelerated fun-dus-emptying rate, and weight loss.It is imaginable that during the placement of the band the nerve of Latarjet can be damaged,which possibly leads to changes in gastric function. Such damage of the vagal nerve may con-tribute to weight loss after bariatric surgery because it is accompanied by reduced sensations ofhunger [30], and it decreases the intake of liquids [3]. We did not test the vagus function and weonly used a solid meal. Therefore, our study does not provide additional information on the contri-bution of vagal dysfunction to weight loss after gastric band placement.In conclusion: Laparoscopic adjustable gastric banding does not affect gastric emptying. Further-more, there was a relationship neither between postoperative gastric emptying rate and weightloss nor between the symptoms dysphagia, vomiting, early satiety and weight loss. It is thereforefelt to be unlikely that gastric emptying plays a role in the mechanism of weight loss followinglaparoscopic adjustable gastric banding.
REFERENCES1. Horowitz M, Collins PJ, Chatterton BE, et al. Gastric emptying after gastroplasty for morbid obesity. Br J
Surg 1984; 71:435-72. Gannon MX, Pears DJ, Chandler ST, et al. The effect of gastric partitioning on gastric emptying in morbid-
ly obese patients. Br J Surg 1985; 72:952-43. Kral JG, Gortz L, Hermansson G, et al. Gastroplasty for obesity:long term weight loss improved by vagoto-
my.World J Surg 1993; 17:75-94. Villar HV, Wangenteen SL, Burks TF, et al. Mechanism of satiety and gastric emptying after gastric parti-
tioning and bypass. Surgery 1981; 90:229-365. Naslund I, Beckman KW. Gastric emptying rate after gastric bypass and gastroplasty. Scand J Gastroenterol
1987; 22:193-2016. Andersen T, Pedersen BH, Henriksen JH, et al. Pouch emptying of solid foods after gastroplasty for morbid
obesity. Scand J Gastroenterol 1985; 20:1175-9
45

7. Mistiaen W, Vaneerdeweg W, Blockx P, et al. Gastric emptying rate measurement after vertical bandedgastroplasty. Obes Surg 2000; 10:245-9
8. Vezina WC, Grace DM, Chamberlain MJ, et al. Gastric emptying before and after transverse gastroplastyfor morbid obesity. Clin Nucl Med 1986; 11:308-12
9. Fischler B, Tack J, De Gucht V, et al. Heterogenity of symptom pattern, psychosocial factors, and patho-physiological mechanisms in severe functional dyspepsia. Gastroenterology. 2003; 124:903-10. 10.Naslund E, King N, Mansten S, et al. Prandial subcutaneous injections of glucagon-like peptide-1 causeweight loss in obese human subjects. Br J Nutr 2004; 91:439-46.
11. Reda TK, Geliebter A, Pi-Sunyer FX. Amylin, food intake and obesity. Obes Res 2002; 10:1087-912. Belachew M, Belva PH, Desaive C. Long-term results of laparoscopic adjustabe gastric banding for the
treatment of morbid obesity. Obes Surg 2002; 564-813. Collins PJ, Horowitz M, Cook DJ, et al. Gastric emptying in normal subjects a reproducibltechnique using a
single scintillation camera and computer system. Gut 1983; 24:1117-2514. Ziesmann HA, Fahey FH, Atkins FB, et al. Standardization and quantification of radionuclide solid gastric-
emptying studies. J Nucl Med 2004; 45:760-415. Hutson WR, Wald A, Obesity and weight reduction do not influence gastric emptying and antral motility.
Am J Gastroenterol 1993; 88:1405-916. Wright RA, Krinsky S, Fleeman C, et al. Gastric emptying and obesity. Gastroenterology 1983; 84:747-5117. Tosetti C, Corinaldesi R, Stanghellini V, et al. Gastric emptying of solids in morbid obesity. Int J Obes 1996;
20:200-518. Maddox A, Horowitz M, Wishart J, et al. Gastric and oesophageal emptying in in obesity. Scand J
Gastroenterol 1989; 24:593-819. Horowitz M, Collins PJ, Cook DJ, et al. Abnormalities of gastric emptying in obese patients. Int J Obes
1983; 7:415-2120. Christian PE, Datz FL, Moore JG. Gastric emptying studies in the morbidly obese before and after gastro-
plasty. J Nucl Med 1986; 27:1686-9021. Behrns KE, Soper NJ, Sarr MG, et al. Anatomic, motor and clinical assessment of vertical banded gastro-
plasty. Gastroenterology 1989; 97: 91-722. Horowitz M, Cook DJ, Collins PJ, et al. Measurements of gastric emptying after gastric bypas surgery using
radionuclides. Br J Surg 1982; 69:655-723. Brogna A, Ferrara R, Bucceri AM, et al. Gastric emptying rates of solid food in relation to body mass index:
an ultrasonographic and scintigraphic study. Eur J Radiol 1998; 27:258-6324. Vu MK, Straathof JW, Arndt JW, et al. Motor and sensory function of the proximal stomach in reflux dis-
ease and after laparoscopic Nissen fundoplication. Am J Gastroenterol 1999; 94:1481-8925. Swanstrom L, Wayne R. Spectrum of gastrointestinal symptoms after laparoscopic fundoplication. Am J
Surg 1994; 167:538-4126. Bais JE, Samsom M, Boudesteijn EAJ, et al.The impact of delayed gastric emptying on the outcome of
antireflux surgery. Ann Surg 2001; 234:139-4627. Lindeboom MYA, Vu MK,Ringers J, et al. Function of the proximal stomach after partial versus complete
laparoscopic fundoplication. Am J Gastroenterol 2003; 98: 284-9028. Karim SS. Comparison of total vs partial fundoplication in the management of gastroesophageal disease.
Am J Surg 1997; 173: 375-829. Lundell LR, Myers JC, Jamieson GG. Delayed gastric emptying and its relationship to symptoms of gas
bloat after antireflux surgery. Eur J Surg 1994; 160:161-630. Mordes JP, el Lozy M, Herrera MG, et al. Effects of vagotomy with and without pyloroplasty on weight
and food intake in rats. Am J Physiol 1979; 236:61-6
46

Chapter 5
ESOPHAGEAL DILATATION AFTER
LAPAROSCOPIC ADJUSTABLE GASTRIC BANDING
JR de Jong1, C Tiethof2, B van Ramshorst3, HG Gooszen1, AJPM Smout3
1. Dept. of Surgery, University Medical Center, Utrecht2. Dept. of Radiology, St Antonius Hospital, Nieuwegein
3. Dept. of Surgery , St Antonius Hospital, Nieuwegein4. Dept. of Gastroenterology, University Medical Center, Utrecht
Accepted Surg Endosc

ABSTRACTBackground: The occurrence of esophageal dilatation after laparoscopic adjustable gastricbanding (LASGB) was not yet investigated systematically.Methods: Forty-five patients after LASGB were assessed for the development of esophagealdilatation by standardised barium swallow studies carried out after the operation and after amean follow-up period of 39.3 months. The diameter of the esophagus postoperatively andduring follow-up was calculated in millimeters (mm) by using the known diameter of the gas-tric band. An increase in diameter > 130% compared to the postoperative diameter was con-sidered as dilatation. Symptoms were assessed by a questionnaire. In 11 patients with dilata-tion the band was emptied and a barium swallow performed in order to assess whether thedilatation was reversible.Results: A significant increase in the esophageal diameter (median (InterQuartileRange) wasfound comparing the early postoperative and follow-up data: 16.3 (14-18.7) mm vs. 20.7(18.1-26.8)mm (p < 0.01). In 25 of the 45 patients (55.6%) the dilatation percentageexceeded 130%. In 7 of the 11 patients the dilatation after emptying of the band still exceed-ed 130%. The increase of esophageal diameter was significantly correlated with the durationof follow-up, with regurgitation, heartburn during nighttime, and slow esophageal clearance.Conclusion: Laparoscopic adjustable gastric banding causes esophageal dilatation in abouthalf of the patients. This dilatation is correlated with symptoms and is partly reversible afteremptying of the band. The clinical relevance of the dilatation is unclear.
INTRODUCTION Laparoscopic adjustable silicone gastric banding (LASGB) is an established operation in the treat-ment of morbid obesity. Several complications after LASGB have been described such as pouchdilatation, problems with the access port (infection and dislocation) and gastric erosion. However,it took more than ten years before a critical article was published which advised against laparo-scopic adjustable gastric banding because of the high failure rate and the high incidence ofesophageal dilatation (71%) accompanied by poor weight loss1. In the same year Peternac et al2
reported an incidence of esophageal dilatation of 60% after adjustable gastric banding, with ahigh ratio of esophageal exhaustion and impaired weight loss during long term follow-up.Until then esophageal dilatation had occasionally been reported but not mentioned as a complica-tion. Placement of the band near the gastroesophageal junction in order to prevent the problem ofpouch dilatation3 was found to decrease LES relaxation and to promote esophageal stasis anddilatation4. Wiesner et al.5 found a relation between esophageal dilatation, poor weight loss andpreoperative insufficiency of the LES.More recent literature, with larger series of patients, reported commonly low percentages ofesophageal dilatation6-10. Dilatation of the esophagus was in most cases the result of a small stomasize by overfilling the band but was reversible by removal of fluid out of the band.In order to assess the incidence and impact of esophageal dilatation after LASGB we Performed astudy in which we analysed a cohort of patients for the development of esophageal dilatation. Wetried to quantify dilatation and also assessed the relationship between esophageal dilatation andduration of follow-up, weight loss, filling of the band, symptoms, and possible reversal of thedilatation after emptying the gastric band.
MATERIALS AND METHODSForty-five out of 180 patients who underwent a LASGB procedure (Lap Band®, 9.75cm, InamedHealth, Santa Barbara, California) between January 1996 and August 1999 agreed to participate
48

in the study for assessment of esophageal dilatation in February 2001.The patients were randomly chosen and asked by phone to participate in the study. The group ofparticipating patients was representative for the overall group (Table 1). In December 2007 thegroup of patients was again reviewed with special focus on weight loss and incidents.Written informed consent was obtained from each patient. The study was approved by theMedical Ethics Committee of the St Antonius Hospital.Outcomes were calculated for the whole group of patients and also for subgroups of patients whowere operated in.1996 (n = 11), 1997 (n = 12), 1998 (n = 11) and 1999 (n = 11).
Table 1Comparison of study group with overall group
Study group (n = 45) Overall group (n = 180)
BMI preoperative 45.1 (4.1) 45.3 (5.2)
BMI 2001 34.8 (6.2) 35.1 (7.1)
%EBL 2001 51.2 50.3
BMI 2007 35.4 (6.1) 36.0 (6.4)
%EBL 2007 48.3 46
Male (%) 4 (8.9) 23 (13)
Female (%) 41 (91.1) 154 (87)
Age (range) 36.7 (22-52) 38 (17-60)
BMI in mean (Standard Deviation).%EBL = percent of excess BMI loss compared to preoperative BMI
Diagnostic studiesThe patients were analyzed by repeated standardised barium swallow studies immediately afterthe operation and after a mean postoperative follow-up period of 39.4 (range19-64) months. Thebarium studies were independently analysed by two authors (JdJ, CT) and the different outcomeswere discussed. Patients were asked to drink the barium continuously till the cup was empty.Clearance of the esophagus was judged radiographically and was considered delayed when mostbarium stayed, for at least 30 seconds, proximal to the band after finishing drinking.The diameter of the esophagus (proximal to the esophageal ampulla) postoperatively and duringfollow-up was calculated in millimeters (mm) by using the known diameter of the gastric band. Anincrease in diameter > 130%, compared to the postoperative diameter, was considered as dilata-tion1,11.In 11 patients of the group with esophageal dilatation > 130% (n = 25) the band was totally emp-tied after the barium follow-up study in order to assess the reversibility of the esophageal dilata-tion. One hour after emptying a second barium study was performed after which the band wasfilled with the original volume.
49

Symptom assessmentSymptoms at follow-up were assessed by a questionnaire which was given on the same day as thebarium study was performed. The questionnaire included questions about heartburn (both day-and nighttime), regurgitation and dysphagia. The intensity at which the symptoms occurred in theweek prior to examination was scored using an ascending scale from 0 to 4 (0 = no symptoms, 1 =symptoms on 1 or 2 days, 2 = symptoms on 3 or 4 days, 3 = symptoms on 5 or 6 days and 4 =daily symptoms).
StatisticsThe data were statistically analyzed by using a SPSS 12.0 package. A p-value < 0.05 was consid-ered to be significant. The Mann-Whitney U test was used to compare continuous variablesbetween unrelated groups, and the Wilcoxon Signed Ranks test was used for repeated measure-ments on the same patients. The Spearman’s rank correlation test was used to assess any relation-ship between the different variables.
SurgeryAll operations were performed by one surgeon (BvR). The operation was performed according tothe perigastric technique, with the modification of a very small gastric pouch proximal to theband9. Postoperatively the band was left empty. All patients used a liquid diet for 4 weeks. At 6weeks adjustments were made in the outpatient clinic if there was no weight loss. Two ml of salinewas given followed by a glass of water to assure there was no outlet obstruction. The patientswere followed at intervals of three months during the first year postoperatively and every sixmonths for the next years, or earlier if there was a problem. The patients were seen by a surgeonand a nurse practicioner. Further stoma adjustments were made according to each patient’s indi-vidual needs, depending on the degree of weight loss and feeling of satiety.
RESULTSA significant increase in the esophageal diameter was found comparing the early postoperativeand follow-up data of the total group (p < 0.01) (Table 2). In 25 of the 45 patients (55.6%) thedilatation percentage exceeded 130%. Twelve of the 45 patients (26.7%) showed delayed claer-ance of esophagus. Ten of these patients had a dilatation factor > 130% (83.3%).There was no difference in the postoperative diameter between the cohorts operated on in 1996,1997, 1998 and 1999. The diameters of the esophagus measured in 2001 showed differencesbetween the cohorts. The largest median diameter was found for the group operated on in 1996(Figure 1).The symptoms of the patients in the different cohorts and for the total group are listed in Table 2a.There was no significant difference between the different groups for incidence and intensity ofregurgitation, heartburn and dysphagia.After initial significant weight loss found in 2001 no further weight loss was found in 2007 (Table2). Eight of the 45 patients (17.8 %) had their gastric band removed and underwent a gastricbypass. These patients initially had succesfull weight loss after the banding procedure but showedsignificant weight gain on the long term (Table 2).Emptying of the band (Figure 2), carried out in 11 patients with a dilatation of more than 130%,resulted in a decrease of the dilatation. However in 7 of the 11 patients (63.6%) the dilatationpercentage after emptying still exceeded 130% compared to the postoperative diameter.In the total group of patients the increase of esophageal diameter correlated significantly withduration of follow-up after primary surgery (0.465, p = 0.002), regurgitation during nighttime(0.581, p < 0.001, heartburn during daytime (0.368, p = 0.02), heartburn during nighttime (0.59,
50

p = 0.001), dysphagia (0.322, p = 0.046) and delayed esophageal clearance (0.550, p = 0.001).The grade of filling of the band and pouch dilatation was not correlated with esophageal dilata-tion.
Figure 1. Diameters of the esophagus postoperative and at follow-up for the different cohorts
DISCUSSIONIn this study, esophageal dilation was observed in a proportion of our patients who underwentLASGB. The dilatation appeared to be partly reversible after one hour by decreasing the volume ofthe band. The dilatation tended to increase during follow-up after the operation.The conventionel placement of a Lap Band was the perigastric method. Later, a more proximal gas-tric band placement with a smaller pouch was advocated to prevent pouch dilatation and gastricprolaps/slippage (esophagogastric banding and pars flaccida method)3,8. It is imaginable that in allgastric banding procedures but certainly these with a small pouch, the distal esophagus sometimeswill function as a reservoir for solid food especially when the band is filled during follow-up. Thisfact possibly contributes to the development of esophageal dilatation postoperatively.There is little evidence that different techniques of band placement influence esophageal dilata-tion. Weiss et al.4 found a high incidence of esophageal dilatation after esophagogastric banding3
compared to classical gastric banding.Previously, esophageal dilatation found in barium studies have been reported in literature, with anincidence ranging from 0.5% to 77.9 %4-18 (Table 3). A few reports mention esophageal dilatationas one of the reasons to reoperate after LASGB (1.8 to 4.1 % of the reoperations)10,13,14. However,it is unclear in most reports whether all patients had barium follow-up studies and how esophagealdilatation was defined. Therefore, it is difficult to compare these differences in outcome.
51

52
Tabl
e 2.
Para
met
ers
of t
he d
iffer
ent
coho
rts
and
of t
he t
otal
gro
up o
f pa
tient
s
Coh
ort
1996
1997
1998
1999
tota
l gro
up
BMI p
reop
(kg
/m2 )
45 (
42.5
-46.
1)44
.6 (
42.9
-47.
7)44
.3 (
43-4
9)43
(40
-51)
44.4
(42
.5-4
7.7)
BMI 2
001
35.3
(31
.6-3
8.4)
32.9
(30
-44.
8)32
.4 (
31.2
-36.
2)34
.1 (
29.2
-40)
33.7
(30
.8-3
8.7)
BMI 2
007
34.5
(30
.8-4
1.3)
33.8
(30
.3-3
9.1)
35.1
(33
.6-4
0.7)
34.7
(31
.7-3
8.7)
34.7
(31
.6-3
9.3)
band
vol
ume
2001
(m
l)3.
4 (2
.8-4
.0)
2.5
(2.0
-3.4
)3
(2.4
-3.4
)3.
0 (1
.8-4
.0)
3.2
(2.2
-3.6
)
band
vol
ume
2007
(ml)
4.4
(3.4
-4.6
)3.
0 (2
.3-3
.4)
3.2
(2.9
-3.7
)2.
8 (2
.6-3
.8)
3.2
(2.6
-3.8
)
esop
h. d
iam
eter
pos
top
(mm
)15
.1 (
13.6
-18.
7)17
.9 (
15.7
-21.
7)16
.3 (
14.1
-18.
2)15
.5 (
13.2
-18.
7)16
.3 (
14-1
8.7)
esop
h. d
iam
eter
200
1 (m
m)
28.4
(18
.5-3
1.9)
#22
.8 (
19.8
-31.
2)20
.2 (
18.1
-24.
6)18
.0 (
16.3
-20.
1)#
20.7
(18
.1-2
6.8)
dila
tatio
n (%
)17
0 (1
24.8
-189
.5)*
129.
2 (9
7.3-
156)
136.
6 (1
14.5
-152
.6)*
110.
4 (1
03-1
55.5
)*13
6.1
(107
.5-1
62.2
)
follo
w-u
p 20
01 (
mon
ths)
60 (
51-6
4)42
.5 (
41-4
7)32
(29
-35)
24 (
23-2
5)40
(26
.5-4
9)
% E
BL 2
001
47.7
49.8
58.5
49.3
51.3
% E
BL 2
007
52.6
50.3
4244
.847
.4
n =
11
n =
12
n =
11
n =
11
n =
45
rein
terv
entio
ns p
osto
p-20
01sl
ippa
ge n
= 4
slip
page
n =
3sl
ippa
ge n
= 3
slip
page
n =
1sl
ippa
ge n
= 1
1po
rt n
= 2
port
n =
1po
rt n
= 1
port
n =
4
rein
terv
entio
ns 2
001-
2007
gast
ric b
ypas
s n
= 3
gast
ric b
ypas
s n
= 2
gast
ric b
ypas
s n
= 1
gast
ric b
ypas
s n
= 2
gast
ric b
ypas
s n
= 8
slip
page
n =
4po
rt n
= 1
slip
page
n =
4sl
ippa
ge n
= 2
port
n =
1

Figure 2. The change of the esophageal diameter after deflation of the gastric band
Table 3Symptoms reported by patients in the week prior to the barium study at follow-up.
Heartburn daytime nighttime
Intensity 0 1 2 3 4 0 1 2 3 4
1996 (n = 11) 7 2 1 0 1 6 1 2 1 1
1997 (n = 12) 6 3 1 0 2 8 4 0 0 0
1998 (n = 11) 8 2 0 0 1 10 1 0 0 0
1999 (n = 11) 6 4 0 0 1 8 1 1 0 1
Regurgitation daytime nighttime
Intensity 0 1 2 3 4 0 1 2 3 4
1996 (n = 11) 7 4 0 0 0 7 0 4 0 0
1997 (n = 12) 10 1 0 1 0 10 1 1 0 0
1998 (n = 11) 10 1 0 0 0 10 1 0 0 0
1999 (n = 11) 8 2 0 0 1 9 1 0 0 1
53
diam
eter
of
esop
hagu
s (m
m)

Dysphagia
Intensity 0 1 2 3 4
1996 (n = 11) 3 6 1 1 0
1997 (n = 12) 5 5 2 0 0
1998 (n = 11) 3 4 1 1 2
1999 (n = 11) 5 4 1 0 1
Data in numbers of patients.0 = no symptoms, 1 = 1or 2 days, 3 = 3 or 4 days, 4 = every day
The problem in quantifying esophageal dilatation is that there is no standard measurement foresophageal dilatation by contrast esophagography11. Another problem is the definition of normalor pathologic dilatation.Dargent proposed a system for analysing and discriminating different stages of esophageal dilata-tion. He reported esophageal dilatation as a common finding following gastric banding but irre-versible esophageal dilatation was rare10. However he did not support his proposal with clear data.The question is whether the different stages of dilatation are clear and reproducible because radio-logical interpretations can be considered subjective11.Fielding et al. found, in his series of 1234 patients, esophageal dilatation in one patient after longterm follow-up examinations which were performed on only 34 patients8. Neither a definition norcriteria to diagnose dilatation were reported. It is also unclear whether these 34 patients were rep-resentative for the overall group of patients.Lew and co-workers found an increase in esophageal diameter of 4 mm after 6 months andanother 4 mm after 12 months. However, the percentage of patients without dilatation was notgiven19.Milone et al. reported esophageal dilatation after one year in 14% of their patients. They used adiameter of 35 mm as a cutoff point for dilatation20. Using this reference point we would haveonly two patients ( 4.4% instead of 55.6%) with esophageal dilatation. This fact shows the diffi-culty of interpreting the reported percentages of dilatation by using different definitions ofesophageal dilatation.We did not perform esophagography preoperatively therefore we were only able to compare thebarium studies taken 24 hour postoperatively with the follow-up studies.There is no evidence in literature that the gastric banding procedure itself has a negative or posi-tive influence on the esophageal diameter seen in a barium swallow study. But it is imaginable thata band, placed more or less tightly around the stomach, causes a relative outlet obstruction, result-ing in more stretching of the esophagus. Therefore our postoperative esophageal diameter couldbe already increased, compared to the preoperative diameter. Despite these considerations anincrease of diameter during follow-up was found.The study of DeMaria and co-workers1 was the first recorded study which focused on esophagealdilatation after laparoscopic adjustable gastric banding. They found a dilatation of the esophagusin 71% (18 of 25 patients) which was accompanied by lower weight loss. They found dilatationonly in patients with a follow–up of at least one year. However, this study was one in the so called
54

trial-A in order to get FDA approval for use of the Lap Band in the US. In this study the poorresults were possibly caused by the learning curve and adjustment policy.If esophageal dilatation occurs, the strategy is to empty the band temporarily, which will result in adecrease in esophageal diameter with a better passage of food, but also in weight gain. Slowlyrefilling is advocated8 but return of dilatation is not excluded.Esophageal dilatation related to follow-up duration was also reported by others16.
Table 4Percentages of esophageal dilatation reported in literature.
Author year n (total) dilatation (%) FU
Westling 1998 22 (77) 17 24
Forsell 1999 2 (326) 0.6 28
Niville 1999 7 (9) 77.8 11
Weiss 2000 12 (43) 27.9 6
DeMaria 2001 18 (25) 71 21
Peternac 2001 31 (68) 45.8 12
Weiss # 2002 5 (28) 27.7 23
10 (24) 71.4 24
Ceelen 2003 7 (625) 1.1 20*
Weiner 2003 24 (984) 2.4 56*
Chevallier 2004 5 (1000) 0.5 NA
Gutschow 2005 6 (20) 30 56*
Fielding 2005 1 (34) 2.9 67
Dargent 2005 505 (1232) 41 NA
Klaus # 2006 18 (52) 34.6 33
20 (112) 17.9 33
Milone 2008 17 (121) 14 12
FU = mean follow-up in months, * = median, n = number of patientsNA = not available, # = groups created by author for study purposes
55

Wiesner et al.5 found a relation between esophageal dilatation, poor weight loss and preoperativeinsufficiency of the LES. Klaus et al reported that dilatation was related to poor esophageal motili-ty17. However reports about the long-term effects of esophageal dilatation on esophageal motilityare lacking and also the role of altered motility in the development of esophageal dilatation isunclear.Assessment of esophageal dilatation after emptying the band was reported in four studies1,4,17,21.In all these studies a decrease of the dilatation was observed, but details were not provided. Theeffect of emptying the band in our study was not followed for more than one hour and it is possi-ble that further decrease of diameter would have occurred if we had waited longer before repeat-ing the barium study.It is also possible that, in the long term, esophageal dilatation may further increase with the risk fordecompensation of the esophagus like in achalasia.We only studied 45 out of 180 patients. This relatively small group of patients seems representa-tive for the total group of patients, but it is possible we over- or underestimate the percentage ofdilatation. Our method to quantify esophageal dilatation was similar to the method of DeMaria etal.1 but is not evidence based.More systematic studies with larger group of patients are needed to definitively answer the ques-tion whether esophageal dilatation is a real problem and which is the best way to quantifyesophageal dilatation. In conclusion: There is evidence of the development of esophageal dilatation after laparoscopicadjustable gastric banding. Esophageal dilatation seems related to time after surgery and insuffla-tion of the band. Dilatation is (partly) reversible after emptying the band. Long-term, perhapseven life-long follow-up is needed in order to assess if further widening and loss of function of theesophagus will take place.
REFERENCES1. DeMaria EJ, Sugarman HJ, Meador JG, Doty JM, Kellum LM, Wolfe L, Szucs RA, Turner MA (2001) High
failure rate after laparoscopic adjustable silicone gastric banding for treatment of morbid obesity. Ann Surg233:809-18
2. Peternac D, Hauser R, Weber M, Schob O (2001) The effects of laparoscopic adjustable gastric banding onthe proximal pouch and the esophagus. Obes Surg 11:76-86
3. Niville E, Dams A. Late pouch dilatation after laparoscopic adjustable gastric and esophagogastric banding:Incidence, treatment and outcome (1999) Obes Surg 9:381-384
4. Weiss HG, Nehoda H, Labeck B, Peer-Kuehberger MD, Oberwalder M, Aigner F, Wetscher GJ (2002)Adjustable gastric and esophagogastric banding: a randomized trial. Obes Surg 12:573-8
5. Wiesner W, Hauser M, Schob O, Weber M, Hauser RS (2001) Pseudo-achalasia following laparoscopicallyplaced adjustable gastric banding. Obes Surg 11:513-8
6. WeinerR, Blanco-Engert R, Weiner S, Matkowitz R, Schaefer L, Pomhoff I (2003) Outcome after laparo-scopic adjustable gastric banding - 8 years experience. Obes Surg 13:427-434
7. Chevallier JM, Zinzindohoue F, Douard R, Blanche JP, Berta JL, Altman JJ, Cugnenc PH (2004)Complications after laparoscopic adjustable gastric banding for morbid obesity:experience with 1,000patients over 7 years. Obes Surg 14:407-14
8. Fielding GA, Duncombe JE (2005) Clinical and radiological follow-up of laparoscopic adjustable gastricbands, 1998 and 2000: a comparison of two techniques. Obes Surg 15:634-40
9. Belachew M, Belva PH, Desaive C (2002) Long-term results of laparoscopic adjustabe gastric banding forthe treatment of morbid obesity. Obes Surg 564-568
10. Dargent J (2005) Esophageal dilatation after laparoscopic adjustable gastric banding: definition and strate-gy. Obes Surg 15:843-848
11. DeMaria E (2003) Laparoscopic adjustable silicone gastric banding:complications. J Laparoendoscop AdvSurg Techn 13:271-277
56

12. Weiss HG, Nehoda H, Labeck B, Peer-Kühberger MD, Klingler P, Gadenstätter M, Aigner F, Wetscher GJ(2000). Treatment of morbid obesity with laparoscopic adjustable gastric banding affects esophagealmotility. Am J Surg 180:479-82
13. Gustavsson S, Westling A (2002) Laparoscopic adjustable gastric banding: complications and side effectsresponsible for the poor long-term outcome. Semin Laparoscopic Surg 9:115-24
14. Weiss HG, Kirchmayr W, Klaus A, Bonatti H, Mühlmann G, Nehoda H, Himpens J, Aigner F (2004) Surgicalrevision after failure of laparoscopic adjustable gastric banding. Br J Surg 91:235-41
15. Forsell P, Hallerback B, Gilse H, Hellers G (1999) Complications following swedish adjustable gastric band-ing: a long term follow-up. Obes Surg 9:11-16
16. Gutschow CA, Collet P, Prenzel K, Holscher AH, Schneider PM (2005) Long-term results and gastroe-sophageal reflux in a series of laparoscopic adjustable gastric banding. J Gastrointest Surg 9:941-948
17. Klaus A, Gruber I, Wetscher G, Nehoda H,Aigner F, Peer R, Margreiter R, Weiss H (2006) Prevalentesophageal body motility disorders underlie aggravation of GERD symptoms in morbidly obese patientsfollowing adjustable gastric banding. Arch Surg 141:247-251
18. Ceelen W, Walder J, Cardon A, Van Renterghem K, Hesse U, El Malt M, Pattyn P (2003) Surgical treat-ment of severe obesity with a low-pressure adjustable gastric band: experimental data and clinical resultsin 625 patients. Ann Surg 237:10-16
19. Lew JI, Daud A, DiGorgi MF, Olivero-Rivera L, Davis DG, Bessler M (2006) Preoperative esophagealmanometry and outcome of laparoscopic adjustable silicone gastric banding. Surg Endosc 20:1242-47
20. Milone L, Daud A, Durak E, Olovero-Rivero L, Schrope B, Inabnet WB, Davis D, Bessler M (2008)Esophageal dilatation after laparoscopic adjustable gastric banding. Surg Endosc 22:1482-86
21. Spivak H, Hewitt MF, Onn A, Halff EE (2005) Weight loss and improvement of obesity-related illness in500 U.S. patients following laparoscopic adjustable gastric banding procedure. Am J Surg 189:27-32
57


Chapter 6
SUSTAINED WEIGHT LOSS 2 YEARS AFTER
LAPAROSCOPIC ADJUSTABLE GASTRIC BANDING
FOR MORBID OBESITY
W.W. te Riele, J.R. de Jong*, J.M. Vogten, M.J. Wiezer, P.H.Th.J. Slee#, B. van Ramshorst
Departments of Surgery and Internal Medicine#, Sint Antonius Hospital Nieuwegein, the Netherlands
Department of Pediatric Surgery*,Wilhelmina Children’s Hospital,Utrecht, the Netherlands
Ned Tijdschr Geneeskd 2007; 151:1130-5

ABSTRACTObjective: To analyse the results of the laparoscopic adjustable gastric banding (LAGB) proce-dure for morbid obesity.Design: Retrospective, descriptive.Methods: From November 1, 1995 to May 31, 2005, laparoscopic adjustable banding surgerywas performed in St. Antonius Hospital, Nieuwegein, the Netherlands, in 411 patients.Inclusion criteria were BMI > or = 40 kg/m(2) or BMI > 35 kg/m(2) and severe comorbiditywith > 3 attempts at weight loss in the past. Selection, inclusion and follow-up were per-formed in a specialised, multidisciplinary setting. Height, weight, and complications wereprospectively recorded. In 1995-2000 the perigastric surgical procedure was used and in2000-2005 the pars-flaccida method.Results: The study group consisted of 350 (85%) women and 61 (I5%) men with a medianage of 38 years (range 17-60). Out of these 411 patients, the median weight was 133.4 kg,the median overweight, 69.6 kg and the median BMI 46.3 kg/m2. Two years after surgery,data was known for 267 patients where 206 (77%) had a weight loss > 30%, and 7 patients(3%) a weight gain. The median BMI difference was then -10.2 kg/m2 (range +4.7—26.4).The median loss of overweight was 46.3% (+10.00—97.8). The weight loss remained stablein the following years. The most commonly seen complications were fundus slippage (13%)and port-a-cath related complications (7%). These occurred more often in patients who hadhad the perigastric method surgery than in the parsflaccida surgical method.Conclusion: Three quarters of the patients with morbid obesity who received laparoscopic gas-tric banding surgery had achieved and sustained weight loss at 2 years following surgery. Thepars-flaccida method resulted in fewer complications than the perigastric surgical method.
INTRODUCTIONObesity is a increasing threat to public health. Approximately half of all Dutch people have over-weight (defined as body mass index (BMI) � 25 kg/m2). Severe overweight or obesity (BMI � 30kg/m2) has a prevalence of approximately 10% for men and 11% for women and shows a risingtrend over time (National Compass Public Health 2005; www.rivm.nl)1. The prevalence of over-weight children has doubled in recent decades to about 10%2.Obesity is associated with an increased mortality risk (relative risk (RR): 1.8 and 2.5 with a BMI of 35and 40 kg/m2, respectively) and severe co-morbidity. This includes cardiovascular disease, diabetesmellitus type 2, dyslipidemia, symptomatic cholelithiasis, gastroesophageal reflux, sleep-apnoe syn-drome, osteoarthritis and low backpain3-6. These co-morbidities may lead to a reduced quality of life3.The treatment of patients with morbid obesity (BMI � 40 kg/m2) focuses primarily on reducing co-morbidity. A weight reduction of 10% already results in a significant decrease in co-morbidity7, 8.Because of the limited results of conservative therapy, an increasing attention to bariatric surgery(i.e. the surgical treatment of patients with morbid obesity) has been reported9, 10. Bariatric surgeryhas been proven effective for decreasing body weight on long term, thereby reducing risk factorsand co-morbidity with improving the quality of life11, 12. Patients with a BMI � 40 kg / m2 or BMI� 35 kg / m2 with serious co-morbidities, with � 3 attempts to lose weight through dietarychanges and drug therapy are eligible for bariatric surgery6.13.A frequently used procedure in laparoscopic bariatric surgery is the placement of a gastric band.The initial experience with this surgery was reported in 199114. A Dutch study of 30 patients witha short follow-up of 10 months was already published in 1994 in this journal15. In 1995 thelaparoscopic gastric banding procedure was introduced in our hospital. We describe the results of411 patients who underwent a laparoscopic gastric banding procedure in a period of 10 years.
60

METHODS
Patients All patients in the St. Antonius Hospital in Nieuwegein, in the period from November 1995 till May2005, who underwent a gastric band placement were included in the study. The patients wereselected by a multidisciplinary team (internist, psychologist, dietician and surgeon) on the basis ofinternational guidelines for surgical treatment of morbid obesity6. These patients fulfilled the inclu-sion criteria of a BMI � 40 kg/m2 or BMI � 35 kg/m2, serious co-morbidities and � 3 priorattempts to weight reduction through dietary changes and drug therapy. The main exclusion crite-ria were portal hypertension and severe psychiatric co-morbidity.
Figure 1. Silicone gastric band which is placed near the the gastroesophageal junction. The inside of the bandconsists of a balloon, which is connected to a tube and a subcutaneously located port-a-cath system. By fillingor emptying the balloon, the nurse-practitioner adjust the diameter of the balloon in the outpatient clinic.
SurgeryThe silicone gastric band is placed laparoscopically near the the gastroesophageal junction.Because the band is on the inside equipped with a balloon, which is connected to a tube and asubcutaneous located port-a-cath system, it is possible to adjust the band diameter by filling oremptying the balloon.(Figure 1). During the study period two different gastric bands with similarmechanism of action were used16.The first 210 banding procedures were carried out by the peri-gastric technique, the last 201 according to the pars-flaccida technique17. All interventions wereperformed by one surgeon (BvR).
Follow-up and data collectionBody weight data and complications were recorded in a prospective database. Postoperatively,during the first year, all patients were seen every 3 months in the outpatient clinic. Thereafter theywere monitored every 6 months.
Outcome Measures The percentage of successfully treated patients was calculated based on the number of patientswith a postoperative follow-up � 2 years. Successful obesity treatment was defined as a excessweight loss > 30%. We also looked at complications that occurred < and � 30 days after surgery.
61

Statistical analysis The overweight and weight loss were calculated using the ideal body weight according to thelength-weight tables of the Metropolitan Life Insurance Company18. Statistical differencesbetween pre-and postoperative weight were calculated using the Mann-Whitney U test.The group of patients was further divided for subgroup-analysis using the baseline BMI (cate-gories: 35-39.9, 40-44.9, 50-54.9, and � 55 kg/m2).
RESULTS
Study PopulationIn the study period a laparoscopic gastric banding procedure was carried out in 411 patients. Thepatient characteristics are listed in Table 1. The median stay in hospital of the patients was 2 days(range: 1-10).
Table 1. Preoperative data of 411 patients in whom a laparoscopic gastric band was placed, St. AntoniusHospital, Nieuwegein, 1995 /’05
number of women (%) 350 (85)
median age in years (range) 38 (17-60)
median weight in kg (range) 133.4 (88.4-230.0)
median excess weight in kg (range) 69.6 (32.1-113.4)
median BMI in kg/m2 (range) 46.3 (36.2-84.3)
number of patients with BMI in kg/m2 (%)
35-39.9 39 (9)
40-44.9 156 (38)
45-49.9 112 (27)
50-54.9 57 (14)
> 55 47 (11)
Follow-upFifty-two of the 411 patients (13%) did not complete follow-up: in the period 1995-199941/210 patients (20%) were lost from follow-up, in the period 2000-2005 8/201 patients (4 %).Three patients died due to a non-surgery related cause (2 with a malignancy and 1 by suicide).The median follow-up time of the other 359 patients was 39 months (range 3-108). There were267 patients with a follow-up time � 2 years. Out of this group, 26 patients (10%) were lostfrom follow-up.
62

Figure 2. Excess weight loss in 260 of the 267 patients who underwent a gastric banding procedure 2 yearsbefore. In 7 patients (3%) the weight increased (not shown)
Number (%) of patients excess weight loss (%) % of patients
7(3) 0-9.9
14 (5) 10-19.9
33 (12) 20-29.9
37 (14) 30-39.9
54 (20) 40-49.9
55 (21) 50-59.9
30 (11) 60-69.9
16 (6) 70-79.9
8 (3) 80-89.9
6 (2) 90-100
Excess weight lossOf the 267 patients with follow-up data of � 2 years in 206 (77%) a decrease in overweight �30% was found (Figure 2). In 7 (3%) patients the weight increased. The median BMI reduction 2 years after laparoscopic gastric banding BMI was 10.2 points (Table2). The median excess weight loss was 46.3% (see Table 2). The decrease was almost stable dur-ing the following years (Figure 3). In the subgroups with a lower preoperative BMI, the percentageexcess weight loss after gastric banding was higher than in the groups with a higher baseline valueof BMI (see Table 2).
ComplicationsIn 19 of the 411 patients (5%) a conversion to an open procedure was performed due to a hyper-trophic liver lobe, bleeding or complex anatomy.Early complications were wound infections, gastric perforation and laceration of the liver (Table 3). Late complications were herniation of the fundus through the band, problems related to the port-a-cathsystem (leakage, infection and dislocation) and gastric erosion. Fundus herniation was seenmore often after the perigastric than after the pars flaccida technique (see Table 3). The complica-tions did not affect the final weight loss (data not shown).No thromboembolic complications were found during follow-up. The surgically related mortalityrate was zero.In 90 of the 411 patients (22%) a reoperation was carried out ( fundus herniation (n = 55), revi-sion of the port-a-cath system (n = 30) and removal of the gastric band (n = 5).
63

Table 2. Decrease of overweight in 267 patients, 2 years after laparoscopic gastric banding 1995-2005, St.
Antonius Hospital, Nieuwegein
Total (n = 267) Women (n = 228) Men (n = 39)
Preoperative
Median BMI (kg/m2) 44.9 44.5 46.4
Range 36.1-69.1 36.1-69.1 36.2-60.1
Median difference between pre- and postoperative
BMI (kg/m2) -10.2 -10.3 -9.8Range +4.7- -26.4* +4.7- -26.4 -1.5- -22.2
Excess weight loss (%) -46.3 -45.4 -46.2
Range +10.0- -97.8 +10- -97.8 -9.4—80.4
Preoperative
Subgroup classified according to BMI 35-39.9 40-44.9 45-49.9 50-54.9 > 55
Number of patients (n) 25 102 70 38 32
Median BMI (kg/m2) 38.7 42.2 47.1 51.1 58.6
Range 36.1-39.9 40.0-44.8 45.0-49.7 50.1-54.9 55.3-69.1
Median difference between pre- and postoperative
BMI (kg/m2) 8.9 9.3 11.1 13.6 14.3
Excess weight loss (%) 54 46 43 45 38
DISCUSSIONIn contrast to our neighboring countries, in our country there is only little experience in the surgi-cal treatment of obesity. Our report includes the first long-term results of laparoscopic gastricbanding in the Netherlands and shows a statistically significant and sustainable reduction of �30% overweight in 77% of the patients with a follow-up duration � 2 years. The reported medi-an BMI decrease of 10.2 points and the median excess weight loss of 46.3% correspond with theresults reported in the literature11,19-21. Buchwald et al. found in a meta-analysis, a mean decreasein BMI of 10.4 points and an excess weight loss of 47.5%22.
64

Figure 3. Course of weight loss for 411 patients after laparoscopic gastric banding expressed as (a) BMI and(b) percentage of overweight lost. In 7 of the 267 patients (3%), the weight increased. N = number of patientsinvolved
The advantages of the laparoscopic placement of the gastric band are the minimally invasive char-acter of surgery and the rapid clinical recovery. A randomized study in our department alreadyshowed that surgery is safe and cost effective and is possible as day care surgery23. Other advan-tages are the possibility of calibration of the band with a controlled food intake and finally, thereversibility of the operation. If there is insufficient effect of the band or insufficient adherence ofthe patient, the band can be removed leaving the integrity of the gastrointestinal tract undis-turbed.After switching to the pars flaccida technique by placing the band just below the gastro-oesophageal junction the rate of herniation decreased significantl24.Other complications were mainly related to the port-a-cath reservoir and were treated in the out-patient clinic or day care surgery. The complications did not affect the final weight loss. In the literature, long-term results are often expressed as patients in follow-up.
65
med
ian
BM
I (kg
/m2 )
exce
ss w
eigh
t lo
ss (
%)

Table 3. Number (%) of patients with a complication after laparoscopic adjustable gastric banding, St.Antonius Hospital, Nieuwegein, 1995-2005
Perigastric method Pars flaccida method Total1995-2000 (n = 210) 2000-2005 (n = 201) 1995-2005 (n = 411)*
< 30 days postoperative
Wound infection 3 3 6 (1.5
Gastric perforation 2 1 3 (0.7)
Liver laceration 1 0 1 (0.2
> 30 days postoperative
Herniation of the fundus† 50 5 55 (13)
Port-a-cath problems‡ 18 12 30 (7)
Gastric erosion 1 0 1 (0.2)
* of 52 of the 411 patients incomplete follow-up data were available. In the remaining 359 patients, themedian follow-up time was 39 months (range: 3-108).
† The median time to occurrence of a fundus herniation was 20 months (range: 1-87). ‡ The median time to occurrence of a port-a-cath problem was 25 months (range: 4-82).
Shen et al. showed a clear relationhip between an adequate follow-up and weight loss in patientsafter laparoscopic gastric banding25. During the follow-up we lost 13% of the patients, the major-ity in the early period of the study. After the appointment of a nurse-practitioner, this loss wasminimized and a follow-up percentage of 96 was achieved.Usually, a decrease in body weight > 30% is considered as a measure of successful obesity treat-ment26.The maximum weight loss in the majority of patients from has been achieved 1.5 to 2 years post-operatively. In our study 77% of the patients with a follow-up time � 2 years showed an excessweight loss � 30% (see Figure 2). If we consider the patients lost after 2 years as failures (n = 26of 206), the success rate decreased to 67% (180/267).The success of the surgical treatment of morbid obesity should not only be measured in terms ofweight loss, but also expressed in decrease of co-morbidity and increase in quality of life. In previ-ous studies, we already reported a statistically significant improvement in the quality of life afterlaparoscopic gastric banding12,27. The effect of surgery on the co-morbidities in this group havenot been analyzed till now. However, it is known from the literature that a weight loss of 10% isalready associated with a significant reduction of comorbidity7,8. Buchwald et al. showed in ameta-analysis a significant decrease of diabetes mellitus, hyperlipidemia, hypertension and sleepapnoe syndrome after bariatric surgery22.In the analysis of the subgroups, classified according to BMI at the start of the study, we found agreater effect of treatment for patients with lower baseline BMI (excess weight loss 54%) com-
66

pared to patients with a higher value (excess weight loss 38% ). The indication for bariatric sur-gery in patients with a BMI � 50 is still the subject of discussion28.In contrast with the practice in Europe and Australia, the preferred surgical procedure in theUnited States is the laparoscopic gastric bypass procedure. This operation results in a greaterweight loss within a shorter time and gives a higher percentage of successfully treated patientsthan the gastric banding procedure. However, the price is a significantly increased morbidity andmortality29.Randomized comparative studies of the results of the gastric bypass procedure and laparoscopicgastric banding are lacking so far, but would respond to the question which operation is the bestfor patients with (severe) morbid obesity.
CONCLUSIONThree quarters of the patients with morbid obesity who received laparoscopic gastric banding sur-gery had achieved and sustained weight loss at 2 years following surgery. The pars-flaccidamethod resulted in fewer complications than the perigastric surgical method.
REFERENCES1. Visscher TL, Kromhout D, Seidell JC. Long-term and recent time trends in the prevalence of obesity among
dutch men and women. Int J Obes Relat Metab Disord. 2002; 26:1218-24.2. Hirasing RA, Fredriks AM, Buuren S van, Verloove-Vanhorick SP, Wit JM. Toegenomen prevalentie van
overgewicht en obesitas bij Nederlandse kinderen en signalering daarvan aan de hand van internationalenormen en nieuwe referentiediagrammen. Ned Tijdschr Geneesk 2001; 145:1303-8.
3. Fauci AS, Braunwald E, Isselbacher KJ, Wilson JD, Martin JB, et al. Harrison’s Principles of internal medi-cine. 14e editie. McGraw Hill. New York 1998. pp 454-62.
4. Calle EE, Rodriguez C, Walker-Thurmond K, Thun MJ. Overweight, obesity, and mortality from cancer in aprospectively studied cohort of U.S. adults. N Engl J Med. 2003; 348:1625-38.
5. Mokdad AH, Ford ES, Bowman BA, Dietz WH, Vinicor F, Bales VS, et al. Prevalence of obesity, diabetes,and obesity-related health risk factors, 2001. JAMA 2003; 289:76-9.
6. Clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults—the evidence report. National Institutes of Health. Obes Res 1998; 6 Suppl 2:51S-209S.
7. Lean ME, Powrie JK, Anderson AS, Garthwaite PH. Obesity, weight loss and prognosis in type 2 diabetes.Diabet Med 1990; 7:228-33.
8. Lavie CJ, Milani RV. Effects of cardiac rehabilitation, exercise training, and weight reduction on exercisecapacity, coronary risk factors, behavioral characteristics, and quality of life in obese coronary patients. AmJ Cardiol. 1997; 79(4):397-401.
9. Goodrick GK, Foreyt JP. Why treatments for obesity don’t last. J Am Diet Assoc. 1991; 91(10):1243-7.10. Maggard MA, Shugarman LR, Suttorp M, Maglione M, Sugarman HJ, Livingston EH, et al. Meta-analysis:
surgical treatment of obesity. Ann Intern Med.2005; 142(7):547-59.11. Sjostrom L, Lindroos AK, Peltonen M, Torgerson J, Bouchard C, et al.Lifestyle, diabetes, and cardiovascular
risk factors 10 years after bariatric surgery. N Engl J Med. 2004; 351(26):2683-93.12. Larsen JK, Geenen R, Ramshorst B van, Brand N, Wit P de, Stroebe W, et al. Psychosocial functioning
before and after laparoscopic adjustable gastric banding: a cross-sectional study. Obes Surg 2003;13(4):629-36.
13. Zelissen PM, Mathus-Vliegen EM. Behandeling van overgewicht en obesitas bij volwassenen: voorstelvoor een richtlijn. Ned Tijdschr Geneesk 2004; 148(42):2060-6.
14. Kuzmak LI. A review of seven years’ experience with silicone gastric banding. Obes Surg 1991; 1(4):403-8.15. Eerten PV van, Tuinebreijer WE, Breederveld RS, Kreis RW, Hunfeld MA, Groot GH de. Bariatrische
chirurgie met een variabele maagband voor morbide obesitas: eerste 30 patiënten in Nederland. NedTijdschr Geneeskd 1994; 138(15):762-6.
16. Fried M, Miller K, Kormanova K. Literature review of comparative studies of complications with swedishband and lap-band. Obes Surg 2004; 14(2):256-60.
67

17. Belachew M, Zimmermann JM. Evolution of a paradigm for laparoscopic adjustable gastric banding. Am JSurg 2002; 184(6B):21S-5S.
18. Robinett-Weiss N, Hixson ML, Keir B, Sieberg J. The Metropolitan height-weight tables: perspectives foruse. J Am Diet Assoc 1984; 84(12):1480-1.
19. Ceelen W, Walder J, Cardon A, Renterghem K van, Hesse U, El Malt M, et al. Surgical treatment of severeobesity with a low-pressure adjustable gastric band: experimental data and clinical results in 625 patients.Ann Surg 2003; 237(1):10-6.
20. Zinzindohoue F, Chevallier JM, Douard R, Elian N, Ferraz JM, Blanche JP, et al. Laparoscopic gastric band-ing: a minimally invasive surgical treatment for morbid obesity: prospective study of 500 consecutivepatients. Ann Surg 2003; 237(1):1-9.
21. Angrisani L, Di Lorenzo N, Favretti F, Furbetta F, Iuppa A, Doldi SB, et al. The Italian Group for LAP-BAND:predictive value of initial body mass index for weight loss after 5 years of follow-up. Surg Endosc 2004;18(10):1524-7.
22. Buchwald H, Avidor Y, Braunwald E, Jensen MD, Pories W, Fahrbach L et al. Bariatric surgery. A systematicreview and meta-analysis. JAMA 2004; 292(14):1724-37.
23. Wasowicz DK, Bliemer B, Boom FA, de Zwaan NM, Ramshorst B van. Laparoscopic Adjustable GastricBanding: outpatient procedure versus overnight stay, a randomized study. Obes Surg. 2003; 13:ASBAAbstracts P47.
24. O’Brien PE, Dixon JB, Laurie C, Anderson M. A Prospective Randomized Trial of Placement of theLaparoscopic Adjustable Gastric Band: Comparison of the Perigastric and Pars Flaccida Pathways. ObesSurg 2005; 15(6):820-6.
25. Shen R, Dugay G, Rajaram K, Cabrera I, Siegel N, Ren CJ. Impact of patient follow-up on weight loss afterbariatric surgery. Obes Surg 2004; 14:514-19.
26. Favretti F, Cadiere GB, Segato G, Busetto L, Loffredo A, Vertruyen M, et al. Bariatric analysis and reportingoutcome system (BAROS) applied to laparoscopic gastric banding patients. Obes Surg 1998; 8(5):500-4.
27. Schok M, Geenen R, Antwerpen T van, de Wit P, Brand N, Ramshorst B van. Quality of life after laparo-scopic adjustable gastric banding for severe obesity; postoperative and retrospective preoperative evalua-tions. Obes Surg 2000; 10:502-08.
28. Parikh MS, Shen R, Weiner M, Siegel N, Ren CJ. Laparoscopic Bariatric Surgery in Super-Obese Patients(BMI > 50) Is Safe and Effective: a Review of 332 Patients. Obes Surg 2005; 15(6):858-63.
29. Angrisani L, Lorenzo M, Borrelli V. Laparoscopic adjustable gastric banding versus Roux-en-Y gastricbypass: 5-year results of a prospective randomized trial. Surg Obes Relat Dis. 2007; 2 :127-32.

Chapter 7
EFFECTS OF ADJUSTABLE GASTRIC BANDING
ON GASTROESOPHAGEAL REFLUX AND
ESOPHAGEAL MOTILITY. A SYSTEMATIC REVIEW
J.R .de Jong1, M.G.H. Besselink2,3, B van Ramshorst2, H.G.Gooszen3, A.J.P.M. Smout4
1. Dept. of Pediatric Surgery, Academic Medical Center, Amsterdam2. Dept. of Surgery, St Antonius Hospital, Nieuwegein
3. Dept. of Surgery, University Medical Center, Utrecht4. Dept. of Gastroenterology, University Medical Center, Utrecht
Submitted

ABSTRACTBackground: Controversial opinions exists concerning the effect of laparoscopic adjustablegastric banding on gastroesophageal reflux. We aimed to review the effect of gastric bandingon gastroesophageal reflux and esophageal motility.Methods: MEDLINE and EMBASE databases were searched for relevant studies on patientsundergoing adjustable gastric banding. Outcome measures were: reflux symptoms, medica-tion use, esophagitis, pathological reflux measured by pH recording, LES (lower esophagealsphincter) function and esophageal peristalsis. Data are expressed as: mean (range).Results: Seventeen studies were identified with a total of 1839 patients. The prevalence ofreflux symptoms decreased postoperatively from 32.2% (16-48.4) to 9.1% (0-26.9) andmedication use from 27.5% ( 16-38.5) to 9.5% (3.1-19.2). Newly developed reflux symp-toms were found in 15% (6.1-20) of the patients. The percentage of esophagitis decreasedpostoperatively from 33.3% (19.4-61.6) to 27% (2.3-60.8). Newly developed esophagitiswas observed in 22.9% (0-38.4). Pathological reflux was found in 55.8% (34.9-77.4) preop-eratively and postoperatively in 29.4% (0-41.7) of the patients. LES pressures increased from12.9 mmHg (6-22) to 16.9 mmHg (11.3-21.4). LES relaxation decreased from 100% to79.7% (58-86). The percentage of dysmotility increased from 3.5% (0-10) to12.6% (0-25).Conclusion: Adjustable gastric banding has anti-reflux properties resulting in resolution orimprovement of reflux symptoms, normalized pH monitoring results and a decrease ofesophagitis. However, worsening or newly developed reflux symptoms and esophagitis arefound in a subset of patients during longer follow-up. Pouch dilatation, filling of the band anddisordered esophageal motility are possible causative factors. Adjustable gastric bandingincreases LES pressure, but decreases LES relaxation and is associated with an increase in dis-turbed esophageal peristalsis.
INTRODUCTIONObesity is considered an important risk factor for gastroesophageal reflux and esophagitis (1-4).There are also studies however, in which no relation between obesity and reflux was found (5,6).Although it is reasonable to assume that weight loss will result in decrease of reflux and weightreduction is often recommended as a first line conservative treatment, there is a lack of literaturesupporting this recommendation (7). Even an increase of reflux after weight loss has been reported(8). During the last decades several operations have been developed to treat morbid obesity withgood long-term weight loss (9). The surgical procedures can be divided into (a) restrictive proce-dures in which the stomach is partitioned by staple lines, mesh or band, (b) procedures that inducemalabsorption and (c) procedures in which combinations of the aforementioned techniques areused. In the classical restrictive procedures (non-adjustable gastric banding, vertical banded gastro-plasty, horizontal gastroplasty) the stomal size between the partitioned stomach could not beadjusted after the completion of the procedure. The most popular restrictive procedure nowadaysis the adjustable silicone gastric banding in which the stomal size can be modified postoperatively. It is well known from the past that the classical restrictive procedures led to an increase in refluxsymptoms and esophagitis which led to abolition of these procedures in many centers for obesitysurgery (10-14). This may be caused by the fact that in all cases a proximal gastric pouch is creat-ed with a relatively narrow stoma which is likely to lead to increased resistance to flow and toincreased gastroesophageal reflux.Controversial opinions exist about the effect of adjustable gastric banding on gastroesophagealreflux and esophageal motility (15-20). We aimed to review all published reports about the effectsof adjustable gastric banding on gastroeesophageal reflux and esophageal motility.
70

71
Tabl
e 1
Dem
ogra
phy
of p
atie
nts
in in
clud
ed s
tudi
es w
ith in
dica
tion
of r
elev
ance
for
the
diff
eren
t su
bjec
ts o
f th
e re
view
.
Sex
ratio
Ref
eren
ceYe
arC
ount
ryIn
clus
ion
F M
Age
BM
I pre
opB
MI p
osto
pFU
NST
Rel
evan
ce
Niv
ille41
§19
98Be
lgiu
m19
94-1
997
9333
37 (
NR
)†42
.3 (
NR
)†N
RN
R12
6PG
EG
1D
ixon
2319
99A
ustr
alia
1996
-199
845
3
39 (
23-5
8)*
45 (
7)†
NR
2448
PG1,
2A
nder
son34
2000
Aus
tral
iaN
RN
RN
RN
RN
R24
60PG
3W
eiss
1520
00A
ustr
ia19
98-1
999
36
739
(19
-63)
*42
.5 (
39.3
-47.
3)*
33.1
(29
.4-3
7.3)
*6
43PG
1,3,
4,5
Wei
ss29
2001
Aus
tria
1998
-199
940
7
36 (
32-4
3.5)
¥43
.5 (
40.8
-47.
5)¥
33.5
(29.
6-37
.2)¥
9
47PF
1,5
Wei
ss27
§20
02A
ustr
ia19
98-1
998
244
40 (
18-6
2)42
.5 (
39.3
-47.
3)*
25.1
(22
.4-3
6.3)
*24
52PF
EG
1K
oren
kov35
2002
Ger
man
y19
97-2
000
246
38 (
25-5
4)*
46.4
(5.
4)$
NR
2232
PG1,
5D
e Jo
ng19
2004
Net
herla
nds
1998
-200
023
3
41.3
(6.
4)†
47 (
1.2)
#36
.7 (
1.0)
#6
26PG
1,2,
3,4
Frig
g3820
04Sw
itzer
land
1996
-200
223
362
41(1
8-67
)‡45
(31
-75)
‡35
(22
-52)
‡44
295
PG P
F1
Sute
r1720
05Sw
itzer
land
1999
-200
237
6
39 (
25-5
9)‡
42.2
(34
.4-5
3.2)
‡33
.8 (
NR
)10
43PG
PF
1,3,
4,5
Spiv
ak38
2005
USA
2000
-200
3N
R42
(18
-63)
‡45
.2 (
35-6
1)‡
35.1
(N
R)
2016
3PG
PF
1,2
Ahr
oni43
2005
USA
2002
-200
316
134
43.8
(19
-70)
‡45
.8 (
7.7)
†32
.3 (
7.0)
†12
149
PF1,
2G
utsc
how
1620
05G
erm
any
1997
-200
327
437
(20
-61)
‡46
.5 (
38.3
-59.
8)‡
35 (
7.8)
†59
,331
PG1
Kla
us28
2006
Aus
tria
1996
-200
249
988
39 (
8.8)
†46
.7 (
9.8)
†28
.2 (
5.1)
†33
587
PF1
Lew
37§
2006
USA
2001
-200
358
1945
(8.
3)†
47.9
(4.
5)†
NR
1277
PF1
Tolo
nen20
2006
Finl
and
2003
-200
426
544
(11
)†46
(5.
5)†
38.4
(6.
5)†
1931
PF1,
2,3,
4,5
De
Jong
1820
06N
ethe
rland
s19
98-2
000
263
41.3
(6.
4)†
46.1
(4.
8)†
36.7
(4.
4)†
629
PG5
NR
= n
ot r
epor
ted;
N =
num
ber
of p
atie
nts;
FU
= f
ollo
w-u
p tim
e in
mon
ths,
ST
= s
urgi
cal t
echn
ique
:PF
= p
ars
flacc
ida,
PG =
per
igas
tric
, EG
= e
soph
agog
astr
ic V
alue
s ar
e m
edia
n (r
ange
)*, m
ean
(SD
)†, m
ean
(ran
ge)‡
, mea
n (S
EM)#
, med
ian
(SD
)$, m
edia
n (in
terq
uart
ile r
ange
)¥1
= r
eflu
x sy
mpt
oms,
2 =
med
icat
ion
use,
3 =
eso
phag
itis,
4 =
pH
mon
itorin
g, 5
= m
anom
etry
§ =
aut
hors
cre
ated
tw
o gr
oups
, mea
n re
sults
of
both
gro
ups
are
give
n

METHODSThe MEDLINE and EMBASE databases were searched for studies published since 1990 untilDecember 31, 2006. The following keywords and combinations were used: gastric banding,reflux, gastroesophageal reflux, reflux symptoms, motility, esophagitis, endoscopy, manometry,pH monitoring. Also the abstracts of major meetings concerning surgical treatment of morbidobesity, ASBS (American Society for Bariatric Surgery), IFSO (International Federation for theSurgery of Obesity) and Australia and New Zealand Society of Obesity Surgeons, werescreened. Reference lists of all selected articles that included information about adjustable gas-tric banding and reflux were reviewed for other relevant articles. Studies were excluded whenthey involved non-adults, were written in another language than English or concerned animalexperiments.The following selection criteria were used for inclusion in this study: (a) study design: prospective, (b)reflux symptoms: only studies with pre- and postoperative reports of reflux symptoms (heartburn andregurgitation), (c) medication use: studies with pre- and postoperative results, (d) pH recordings:studies with pre- and postoperative recordings with the results reported as total reflux time orDeMeester score, (e) manometry: studies with pre- and postoperative recordings, (e) esophagitis:studies with pre-and postoperative esophagogastroduodenoscopy reporting the grade of esophagitis. Only studies in which postoperative results were reported in more than 75% of the patients wereincluded.Articles were retrieved and reviewed by two authors (JRdJ and BvR). All differences were discussedamong the reviewers. Characteristics of studies involved in the systematic review are given in Table 1.
Our study questions were:1) Does adjustable gastric banding diminish reflux symptoms and decrease use of antacid med-
ication?2) Is there a decrease in pathological reflux measured by pH monitoring after adjustable gastric
banding?3) Does adjustable gastric banding decrease esophagitis?4) Is there a change in esophageal motility after adjustable gastric banding?
RESULTS
Reflux symptoms and use of medicationOf 21 detected studies, five studies were excluded because of retrospective data collection (21),restriction to patients who had a crural repair (22), reporting on the same group of patientstwice (23,24), impossibility to retrieve percentages by use of a cumulative scoring system (25)or identification of patients with reflux disease on the basis of use of proton pump inhibitors(26).Fifteen studies were available for the assessment of reflux symptoms. Eleven of these studies,reported reflux symptoms in general. Three studies discriminated between heartburn and regurgi-tation (16,19,27). Only five studies analyzed the use of medication (Table 2).As shown in Table 2 the preoperative incidence of reflux symptoms varied from 16% to 57%.A decrease in reflux symptoms and use of antacids after adjustable gastric banding was found inall studies. Only one study reported an increase in heartburn (16). However an increase in regurgi-tation after gastric banding was found in three studies with a mean follow-up of 29 months (range6-59.3 ) (15,16,19). Newly developed reflux symptoms after gastric banding in patients withoutprior symptoms were found in 6 to 50 % of patients (Table 3).
72

Table 2. The effect of adjustable gastric banding on reflux symptoms and the use of medication
Reference N Reflux symptoms Heartburn Regurgitation Medication FUpreop postop preop postop preop postop preop postop
Niville 40 25 10 NR
86 31.4 0 NR
Dixon 274 16 4.4 16 3.1 24
Weiss 43 27.9 2.3 6
Weiss 47 29.8 8.5 9
Weiss 28 33.1 11.1 27.7 0 23
24 42.9 14.3 21.4 35.7 24
Korenkov 30 18.8 9.3 22
De Jong 26 42.3 26.9 42.3 23.1 7.7 53.8 38.5 19.2 6
Frigg 295 57 11.4 44
Spivak 163 29.4 3.6 29.4 3.6 20
Ahroni 149 50.3 18.1 8.7 12
Suter 43 28.8 17.7 10
Gutschow 31 19.4 33.3 0 33.3 59
Klaus 587 27.9 8.9 33
Lew 77 29 14.3 12
39 8 12
Tolonen 31 48.4 6.1 35.5 12.9 19
N = number of patients; NR = not reported; FU = follow up in monthsReflux symtoms, heartburn, regurgitation and medication: % of patients
73

Table 3. Evolution of reflux symptoms (%) following laparoscopic adjustable gastric banding.
Reference resolution improvement worsening newly developed
Ahroni 81.3 10.6
Lew 92
100
Frigg 79 11 6.1
Suter 84.6 18.7
Gutschow 84 13.9*
50 #
De Jong 72.7 20 *
46 #
Klaus 68.3 31.7
Korenkov 10 7 12.5
Spivak 72.9 14.6
Tolonen 86.6 18.8
* = heartburn, # = regurgitation
pH monitoringOf 9 studies, 4 were excluded because: follow-up studies were only performed in a subset of thepreoperative population (25,27), follow-up was reported in < 75 % of the patients (16,25) orbecause postoperative reflux parameters were missing (28).Four studies in which pH monitoring was performed before and after adjustable gastric bandingwere included (Table 5). One author published two studies that fulfilled the inclusion criteria but(15,29) only the study with special interest in gastroesophageal reflux was included (15).The interval between the pre- and post-operative pH recordings varied from 6 to 19 months.A decrease in the percentage of patients with pathological reflux was found in all studies.However the mean total reflux time (especially reflux in supine position) increased in two studies(17,19). In these studies there were several patients with severe reflux postoperatively who con-tributed to the increase in mean time.Two studies reported the development of pathological reflux in 14.3% (20) and 30.1% (19) ofpatients postoperatively who did not have pathological reflux preoperatively.
74

Table 4. Effect of adjustable gastric banding on esophagitis as detected by endoscopy
Reference Anderson Weiss De Jong Suter TolonenYear 2000 2000 2004 2005 2006
Number of patients preop 60 43 26 43 31
postop 60 43 23 36 25
Esophagitis (%) preop 40 23.3 61.6 22.2 19.4
Grade 1 32 23.3* 38.5 22.2* 19.4*
2 4 23.1
3 0 0 0 0 0
4 0 0 0 0 0
5 4 0 0 0 0
Esophagitis (%) postop 28 2.3 60.8 36.1 8
Grade (%) 1 24 2.3* 34.8 36.1* 8*
2 4 21.7
3 0 0 4.3 0 0
4 0 0 0 0 0
5 0 0 0 0 0
Follow-up (months) 24 6 6 9.6 19
Alterations in esophagitis (%) resolved NR 90 37.5 62.5 NR
unchanged NR 10 50 37.5 NR
worsened NR 0 12.5 0 NR
newly developed NR 0 30.4 38.4 NR
NR = not reported, * = reported grade 1 and 2 together
EsophagitisOf 14 potentially relevant studies nine studies were excluded because of having less than 75% follow-up endoscopy (16,27,30), examining only pre- or postoperative patients (29,31-33), giving no per-centages of esophagitis (28) or excluding patients without postoperative endoscopy (27). Five studieswere included (Table 4 ), four of which were full text articles (15,17,19,20)) and one abstract (34).
75

Table 5. The influence of adjustable gastric banding on reflux measured by pH recording
Reference Weiss Suter de Jong TolonenNumber of patients
preop 43 43 26 31
postop 43 36 26 24
De Meester score
preop 10.7 (5.3-15)‡ 17.04 38.5 (24.9)†
postop 2.9 (0.9-5.6)‡ 18.47 18.6 (20.4)†
% pathologic reflux
preop 34.9 61 50 77.4
postop 0 41.7 38.4 37.5
% total time pH < 4
preop 4.58$ 5.2 (0.7)* 9.5 (6.2)†
postop 4.84$ 7.1 (1.7)* 3.5 (3.7)†
Supine reflux %
preop 2.07$ 2.3 (0.8)*
postop 5.03$ 7.5 (2.4)*
Upright reflux %
preop 6.16$ 6.9 (0.8)*
postop 4.47$ 6.5 (1.5)*
Reflux episodes
preop 74.6$ 38.6 (4.0)* 44.6 (23.7)†
postop 53.1$ 39 (9.8)* 22.9 (17.1)†
Follow up (months) 6 9.6 6 19
Values are: mean (SEM) *, mean (SD)†, median (range)‡, mean$
76

Preoperatively, esophagitis was found in up to 60 % of patients, mainly grade 1 and 2 accordingto Savary Miller. (Table 4 )A decrease in esophagitis after adjustable gastric banding varying from 4.6 to 21 percent wasfound in four studies. Only Suter et al. found an increase of esophagitis in 13.9% of their patientsduring 9.6 month follow-up (17). No single study demonstrated a statistically significant increasein the grade of esophagitis after adjustable gastric banding.Three studies reported the alterations in esophagitis per patient (15,17,19). Adjustable gastricbanding resulted in healing of the esophagitis in 37.5 to 90 % of patients. New onset esophagitisin patients without esophagitis preoperatively was observed at follow-up endoscopy in up to38.4% (range 30.4-38.4) of the patients after adjustable gastric banding.
Esophageal motilityOf 10 studies identified, 4 were excluded because of incomplete follow-up (25,29), not providingdata on manometry (16), or only measuring a subset of patients with reflux symptoms (28). Sixstudies were appropriate for analysing results of esophageal manometry preoperatively and post-operatively (Table 6).As shown in table 6, impaired esophageal peristalsis after band placement was found by fourauthors (15,17,20,27). One study could not confirm a negative influence of adjustable gastricbanding on esophageal motility (18).All but one studies found an increase of the LES pressure after adjustable gastric banding. In moststudies, gastric banding was found to lead to decreased LES relaxation. In two studies the lengthof the LES ( or high pressure zone length) was increased by the procedure (18,35).
DISCUSSIONThis review demonstrates mainly positive effects of adjustable gastric banding on gastroe-sophageal reflux resulting in a decrease in reflux symptoms, reduced use of antacid medication,a decreased prevalence of esophagitis and a lower percentage of patients with pathologicalreflux.The antireflux effect of the band is likely to be caused by an augmentation of the LES by creatinga longer intraabdominal pressure zone or by pulling the the stomach more in the abdomen in thepresence of a hiatal hernia (19).These mechanisms are similar to those previously reported follow-ing placement of the Angelchick prosthesis for gastroesophageal reflux disease (36)
REFLUX SYMPTOMSThe positive influence of band placement on reflux symptoms was reported to occur immediatelyafter the operation or within 6 weeks , prior to any major weight loss, suggesting an effect of theband itself (19,23,37,38). Beside the positive effect of adjustable gastric banding, worsened ornewly developed reflux symptoms in patients were reported postoperatively (16,17,19,20,28,35,39). It has been proposed that longer follow-up time after operation with progressive filling of thegastric band and pouch dilatation are responsible for the development of new or worsened refluxsymptoms (16,17,19).Some authors suggested a relation between postoperative reflux symptoms and pouch dilatation(19,38,40). More evidence for the role of pouch size and reflux symptoms was reported by Nivilleand co-workers who compared esophagogastric band placement (i.e. around the distal esopha-gus, leaving almost no pouch) and conventional adjustable gastric banding (41). In that study acomplete resolution of gastroesophageal reflux symptoms following esophagogastric banding wasfound and the decrease of reflux symptoms was smaller in the group of patients with the conven-tional gastric banding procedure (larger pouch).
77

78
Tabl
e 6.
Influ
ence
of
lapa
rosc
opic
adj
usta
ble
gast
ric b
andi
ng in
the
low
er e
soph
agea
l sph
inct
er a
nd e
soph
agea
l mot
ility
Ref
eren
ceW
eiss
Wei
ssK
oren
kov
Sute
rD
e Jo
ngTo
lone
nN
umbe
r of
pat
ient
spr
eop
4347
3043
2931
post
op43
4730
4029
25
LES
pres
sure
(m
mH
g)pr
eop
10.9
(8-
15.6
)†10
.7 (
7.8-
13.5
)†12
.1 (
4.8)
*16
.2 (
0.9)
‡6
(4.5
-9.4
)†22
.0 (
9.1)
*po
stop
21 (
11-2
6)†
18 (
14.9
-27.
5)†
13.3
(4.
8)*
16.7
(1.
8)‡
11.3
(9.
8-14
.3)†
21.4
(9.
2)*
Dys
mot
ility
(%
)pr
eop
0 (0
-20)
†0
(0-1
0)†
NR
4,6
10 (
0-10
)†3,
2po
stop
20 (
7.5-
43)†
25 (
12.5
-37.
5)N
R10
,20
(0-2
0)†
8
LES
rela
xatio
n (%
)pr
eop
100
(100
-100
)†10
0 (1
00-1
00)
100
(0)*
NR
100
(100
-100
)†N
Rpo
stop
86 (
65-1
00)†
75 (
52-7
7)10
0 (0
)*N
R58
(48
.6-7
5.4)
†N
R
LES
leng
th (
cm)
preo
pN
RN
R3.
9 (0
.7)*
NR
5.0
(4.3
-6.0
)†N
Rpo
stop
NR
NR
4.2
(0.5
)*N
R6.
0 (5
.5-6
.4)†
NR
Follo
w-u
p (m
onth
s)6
8,9
229,
66
19
NR
= n
ot r
epor
ted
Valu
es a
re :
mea
n(SD
)*, m
ean
(SEM
)‡, m
edia
n (in
terq
uart
ile r
ange
)†

An increase in regurgitation was found by several authors during follow-up (16,19,27). Weiss andcoworkers observed an increase in regurgitation in the group of patients treated by esophagogas-tric band placement which resulted in stasis of food in the esophagus (27). De Jong and Gutschowdescribed the progressive filling of the band with stasis in the pouch and /or esophagus as a factorthat promotes regurgitation (16,19).Apart from the role of the pouch and the filling grade of the band, it is unclear why in somepatients reflux symptoms develop during follow-up whereas in others they do not.
pH monitoringThe studies in which pH recording was carried out showed a clear decrease in patients with apathological reflux.It appears that the likelihood of increased esophageal acid exposure increases with increasingintervals after adjustable gastric banding. De Jong and coworkers found a decrease in reflux timeat 6 weeks postoperatively, before filling of the band, but an increase at 6 months (19). Weiss andco-workers initially described normal esophageal acid exposure in all patients postoperatively butin later studies carried out by this group an increase in reflux was found after a follow- up of 33months (15,28). This worsening was associated with poor esophageal motility preoperatively.The increase in supine reflux reported by Suter and De Jong supports the theory of stasis of foodas discussed by analysing the reflux symptoms (17,19).In line with the observed effects of adjustable gastric banding on reflux symptoms and esophagi-tis, pH studies have shown that in some patients without reflux disease preoperatively the opera-tion induces reflux disease, whereas in other patients pre-existing reflux disease is improved orcured by the procedure (19,20). Other (not included) studies found also newly developed patho-logical reflux in 23% and 54.5% (16,28).
ESOPHAGITISIn general a positive effect of gastric banding on esophagitis was reported. Only the study of Suter etal found an increase in reflux esophagitis, however not statistically significant. Newly developedesophagitis (17,18) resembled the pattern found in the analysis of reflux symptoms. The postoperativeincidence of esophagitis could even be higher because not all patients had a follow-up endoscopy. Esophagitis after gastric banding was also found to be related to the presence of pouch dilatation(18,25,40). However, others did not find such relationship (17).
ESOPHAGEAL MOTILITYThe studies using esophageal manometry revealed an overall increase in LES pressure, with adecrease in LES relaxation in nearly all studies. An increase in percentage of dysmotility wasreported by most authors (15,17,20). Others found no increase in dysmotility (18,42). The reasonfor these differences are not clear but the position of the band may play a role because impairedperistalsis was found more frequently after esophagogastric banding (placement of the band atthe gastroesophageal junction) (27).Klaus and coworkers (also from the Weiss group) found an association between an increase indefective propagation of esophageal contractions after band placement and more severe refluxproblems postoperatively (28).Whereas a clear relationship between low LES pressure and abnormal esophageal acid exposurewas found by some (25), others did not support this finding (17)
In this study we systematically reviewed the influence of adjustable gastric banding on gastroe-sophageal reflux and esophageal motility. The studies used in this review were prospective but
79

non-randomised studies. Therefore the evidence is not very strong. The different follow-up peri-ods, different techniques of band placement and the relatively small numbers of patients partici-pating in pH monitoring, endoscopy, and manometry studies are important factors which shouldbe kept in mind interpreting the outcome of this review.Future research should focus on the mechanisms in which gastric banding influences gastroe-sophageal reflux and which factors induce newly developed reflux in subjects without reflux pre-operatively.Conclusions: Adjustable gastric banding has anti-reflux properties especially on the short term.However, worsening or newly developed reflux symptoms are found in a subset of patients duringlonger follow-up. Adjustable gastric banding increases LES pressure and length, but decreases LESrelaxation and is associated with an increase in disturbed esophageal peristalsis.
REFERENCES 1. Hampel H, Neena SA, El-Serag HB. Meta-analysis: Obesity and the risk for gastroesophageal reflux disease
and its complications. Ann Int Med 2005; 143:199-2112. El-Serag HB, Graham DY, Satia JA, et al. Obesity is an independent risk factor for GERD symptoms and
erosive esophagitis. Am J Gastroenterol 2005; 100:1243-503. Wilson LJ, Wenzhou M, Hirschowitz BI. Association of obestity with hiatal hernia and esophagitis. Am J
Gastroenterol 1999; 94:2840-444. Suter M, Dorta G, Giusti V, et al. Gastro-esophageal reflux and esophageal motility disorders in morbidly
obese patients. Obes Surg 2004; 14:959-665. Lundell L, Ruth M, Olbe L. Vertical banded gastroplasty or gastric banding for morbid obesity: effects on
gastro-oesophageal reflux. Eur J Surg 1997; 163:525-316. Lagergren J, Bergstrom R, Nyren O. No relation between body mass and gastrooesophageal reflux symp-
toms in a Swedish population based study. Gut 2000; 47:26-97. Kjellin A, Ramel S, Rossner S. Gastroesophageal reflux in obese patients is not reduced by weight reduc-
tion. Scand J Gastroenterol 1996; 31:1047-518. Mathus Vliegen EM, Tytgat GN. Gastro-oesophageal reflux in obese subjects: influence of overweight,
weight loss and chronic gastric balloon distension. Scand J Gastroenterol. 2002; 11:1246-52.9. Brolin RE. NIH Consensus Development Panel: Gastrointestinal surgery for severe obesity. Nutrition 1996;
12:403-410. Ovrebo KK, Hatlebakk JG, Viste A, et al. Gastroesophagel reflux in morbidly obese patients treated with
gastric banding or vertical banded gastroplasty. Ann Surg 1998; 228:51-811. Naslund E, Stockeld D, Granstrom L, et al. Six cases of Barrett’s esophagus after gastric restrictive surgery
for massive obesity: an extended case report. Obes Surg 1996; 6:155-812. Downie JRF. Ulcerating oesophagitis as a late complication of gastroplasty. Obes Surg 1991; 1:108
(abstract)13. Balsiger BM, Murr MM, Mai J, et al. Gastroesophageal reflux after intact vertical banded gastroplasty cor-
rection by conversion to Roux-en-Y gastric bypass. J Gastrointest Surg 2000; 4:276-8114. Fisher BL. Erosive esophagitis following horizontal gastroplasty for morbid obesity: Treatment by gastric
bypass Obes Surg 1994; 4:370-515. Weiss HG, Nehoda H, Labeck B, et al. Treatment of morbid obesity with laparoscopic adjustable gastric
banding affects esophageal motility. Am J Surg 2000; 180:479-8216. Gutschow CA, Collet P, Prenzel K, et al. Long-term results and gastroesophageal reflux in a series of
laparoscopic adjustable gastric banding. J Gastrointest Surg 2005; 9:941-817. Suter M, Dorta G, Giusti V, et al. Gastric banding interferes with esophageal motility and gastroesophageal
reflux. Arch Surg 2005; 140:639-4318. De Jong JR, Van Ramshorst B, Timmer R, et al. Effect of laparoscopic gastric banding on esophageal motil-
ity. Obes Surg 2006; 16:52-819. De Jong JR, Van Ramshorst B, Timmer R, et al. The influence of laparoscopic adjustable gastric banding on
gastroesophageal reflux. Obes Surg 2004; 14:399-406
80

20. Tolonen P, Victorzon M, Niemi R, et al. Does gastric banding for morbid obesity reduce or increase gas-troesophageal reflux? Obes Surg 2006; 16:1469-74
21. Angrisani L, Iovino P, Lorenzo M, et al. Treatment of morbid obesity and gastroesophageal reflux withhiatal hernia by Lap-Band. Obes Surg 1999; 9:396-8
22. Dolan K, Finch R, Fielding G. Laparoscopic gastric banding and crural repair in the obese patients with ahiatal hernia. Obes Surg 2003; 13:772-5
23. Dixon JB, O’Brien PE. Gastroesophageal reflux in obesity: the effect of Lap-Band placement. Obes Surg1999; 9:527-31
24. O’Brien PE, Dixon JB, Brown W, et al. The laparoscopic adjustable gastric band (Lap-Band): a prospectivestudy of medium-term effects on weight, health and quality of life. Obes Surg 2002; 12:652-60
25. Iovino P, Angrisani L, Tremolaterra F, et al. Abnormal esophageal acid exposure is common in morbidlyobese patients and improves after a successful Lap-band system implantation. Surg Endosc 2002; 16:1631-5
26. Himpens J, Dapri G, Cadiere GB. A prospective randomised study between laparoscopic gastric bandingand laparosocpic isolated sleeve gastrectomy. Results after 1 and 3 years. Obes Surg 2006; 16:1450-6
27. Weiss HG, Nehoda H, Labeck B, et al. Adjustable gastric and esophagogastric banding: a randomized clin-ical trial. Obes Surg 2002; 12:573-8
28. Klaus A, Gruber I, Wetscher G, et al. Prevalent esophageal body motility disorders underlie aggravation ofGERD symptoms in morbidly obese patients following adjustable gastric banding. Arch Surg 2006;141:247-51
29. Weiss H, Labeck B, Klocker J, et al. Effects of adjustable gastric banding on altered gut neuropeptide levelsin morbidly obese patients. Obes Surg 2001; 11:735-9
30. Restuccia A, Elmore U, Perrotta N, et al. Endoscopic assessment in patients undergone laparoscopic gastricbanding. Obes Surg 1998; 8:398 (abstract)
31. Frigg A, Peterli R, Zynamon A, et al. Radiologic and endoscopic evaluation for laparoscopic adjustable gas-tric banding: preoperative and follow-up. Obes Surg. 2001; 11:594-9
32. Westling A, Bjurling K, Ohrvall M, et al. Silicone adjustable gastric banding: disappointing results. ObesSurg 1998; 8:467-74
33. Victorzon M, Tolonen P. Intermediate results following laparoscopic adjustable gastric banding for morbidobesity. Dig Surg 2002; 19:354-8
34. Anderson P. Endoscopic and histological evaluation of the Lap-Band at 12 months. Obes Surg 1999; 9:330(abstract)
35. Korenkov M, Kohler L, Yucel N, et al. Esophageal motility and reflux symptoms before and after bariatricsurgery. Obes Surg 2002; 12:72-6
36. Bonavina L, DeMeester T, Mason R, et al. Mechanical effect of the Angelchik prosthesis on the competen-cy of the gastric cardia: pathophysiologic implications and surgical perspectives. Dis Esoph 1997; 10:115-8
37. Lew JI, Daud A, DiGorgi MF, et al. Preoperative esophageal manometry and outcome of laparoscopicadjustable silicone gastric banding. Surg Endosc 2006; 20:1242-7
38. Spivak H, Hewitt MF, et al. Weight loss and improvement of obesity-related illness in 500 U.S. patients fol-lowing laparoscopic adjustable gastric banding procedure. Am J Surg 2005; 189:27-32
39. Frigg A, Peterli R, Peters T, et al. Reduction in co-morbidities 4 years after laparoscopic adjustable gastricbanding. Obes Surg 2004; 14:216-23
40. Forsell P, Hallerback B, Gilse H, et al. Complications following swedish adjustable gastric banding: a longterm follow-up. Obes Surg 1999; 9:11-6
41. Niville E, Vankeirsbilck J, Dams A, et al. Laparoscopic adjustable esophagogastric banding: a preliminaryexperience. Obes Surg. 1998 Feb; 8(1):39-43.
42. O’Brien PE, Dixon JB. Lap-band: outcomes and results. J. Laparoendosc Adv Surg Tech A 2003:13:265-7043. Ahroni JH, Montgomery KF, Watkins BM. Laparoscopic adjustable gastric banding: weight loss, co-mor-
bidities, medication usage and quality of life at one year. Obes Surg 2005; 15:641-7
81


Chapter 8
SUMMARY, CONCLUSIONS AND FUTURE PERSPECTIVES

In Chapter 1 a general introduction was given about the epidemiology of obesity, the relationshipbetween obesity and gastroesophageal reflux and laparoscopic adjustable gastric banding. Obesity has increased markedly since 1980 and has gained epidemic proportions worldwide.The increasing prevalence of obesity is a threat for the public health as it is related to severalchronic morbidities and disabilities. Bariatric surgery is the only treatment option for individuals who have clinically severe obesity andare at the high risk for obesity-related mortality and co-morbidity.The number of bariatric surgery procedures has increased significantly over the past few decades.Nowadays one of the most performed surgical procedures for treatment of morbid obesity is thelaparoscopic adjustable silicone gastric banding (LASGB).In the late 1990s it was reported that laparoscopic adjustable gastric and esophagogastric bandingresulted in a decrease or resolution of gastroesophageal reflux symptoms. However, these studieswere lacking objective measurements like pH recording and esophageal manometry. In order toget more insight in the effect of laparoscopic adjustable gastric banding on gastroesesophagealreflux we started our studies in morbidly obese patients who were candidates for laparoscopicadjustable gastric banding in the St Antonius Hospital in Nieuwegein. The results of these studiesare described in this thesis.
In Chapter 2 we studied the effect of LASGB on gastroesophageal reflux. Twenty-six patientsundergoing gastric banding were assessed by a questionnaire for symptom analysis, 24-hour pHmonitoring, endoscopy and barium swallows, preoperatively, at 6 weeks and at 6 months afteroperation. Gastric banding had minimal effect on heartburn scores but regurgitation and belchingscores increased significantly during follow-up. Use of acid-reducing drugs was decreased signifi-cantly at 6 weeks and increased significantly at 6 months. Pathological reflux was present in 13 ofthe 26 patients preoperatively. At 6 months pathological reflux was found in only 6 of these 13patients, but 4 of the 13 patients with preoperatively normal reflux patterns had developed patho-logical reflux. Six months after the operation esophagitis had disappeared in 6 patients and was increased in 9patients. In 9 patients a pouch dilatation was found at 6 months. Pouch dilatation was significant-ly correlated with the presence of pathological reflux, esophagitis and the use of acid-reducingmedication. Pre-operative presence of a hiatal hernia did not influence pouch dilatation or patho-logical reflux.It was concluded that LASGB decreases gastroesophageal reflux if there is no pouch formationduring follow-up.
Alterations in esophageal motility may occur after placement of an adjustable gastric band nearthe gastroesophageal junction. The band may cause obstruction especially during follow-up afterthe band is filled.
In Chapter 3 we studied the effect of LASGB on esophageal motility and lower esophageal sphinc-ter functioning. Twenty-nine morbidly obese patients underwent conventional manometry preoperatively, sixweeks postoperatively before and after filling the band and at six months postoperatively. A ques-tionnaire was used to assess upper gastrointestinal symptoms during follow-up.After band placement, there was a significant increase in lower esophageal sphincter (LES) endex-piratory pressure at six weeks with an empty band: 1.3 (0.9-1.9) kPa (median(interquartile range)(p = 0.003), six weeks with a filled band: 2.1 (1.5-2.8) kPa (p = 0.0001) and at six months: 1.5(1.3-1.9) kPa (p = 0.001) after band placement compared to the preoperative pressure: 0.8 (0.6-
84

1.3) kPa . The length of the high-pressure zone also increased after band placement (preop 5.0(4.3-6.0)cm vs six weeks 6.0 (5.0-6.5) cm (p = 0.003). The propagation of peristaltic contractionswas not significantly altered after band placement.Heartburn decreased six weeks postoperatively (p = 0.04) but increased at six months. Heartburnat six months was correlated with pouch formation (0.667; p < 0.01). We concluded that adjustable gastric band placement causes an increase in LES pressure and high-pressure zone length. It decreases reflux symptoms on the short term but this effect appears not tobe related with an effect on LES pressure or length. Pouch formation increases reflux symptomswithout having any relationship with LES pressure and length. Band placement on the short termdoes not disturb propagation of esophageal contractions.
In Chapter 4 the role of gastric emptying in the mechanism of weight loss and early satiety was stud-ied in a consecutive series of patients who were scintigraphically investigated before and after LASGB.Sixteen patients undergoing LASGB underwent a gastric emptying study (solid meal, single iso-tope) preoperatively and at six months postoperatively. Esophageal retention time, lag phase,peak activity time, gastric emptying rate, fundus emptying rate and weight loss were recorded.Upper gastrointestinal (GI) symptom assessment was carried out by use of a standardized ques-tionnaire. Gastric emptying parameters were correlated with the upper GI symptoms.Gastric band placement showed no significant influence on postoperative gastric emptying rateand fundus emptying rate, however an increase in early satiety was found. Neither gastric empty-ing rate nor fundus emptying rate showed a relation with early satiety or weight loss. Also no cor-relation was found between early satiety and lag phase, esophageal retention time, start of activi-ty and peak activity time in the proximal stomach. It was concluded that LASGB does not affect gastric emptying. Neither a relation between postop-erative gastric emptying rate and weight loss, nor between early satiety and weight loss wasfound. Therefore, it is unlikely that gastric emptying plays a role in the mechanism of weight lossfollowing LASGB.
In Chapter 5 the occurrence of esophageal dilatation after LASGB was investigated. Forty-fivepatients after LASGB were assessed for the development of esophageal dilatation by standardisedbarium swallow studies carried out after the operation and after a mean follow-up period of 39.3months. The diameter of the esophagus postoperatively and during follow-up was calculated inmillimeters by using the known diameter of the gastric band. An increase in diameter > 130%compared to the postoperative diameter was considered as dilatation. Symptoms were assessed bya questionnaire. In 11 patients with dilatation the band was emptied and a barium swallow per-formed in order to assess whether the dilatation was reversible. A significant increase in the esophageal diameter (median (interquartile range) was found compar-ing the early postoperative and follow-up data: 16.3 (14-18.7) mm vs. 20.7 (18.1-26.8)mm (p <0.01). In 25 of the 45 patients (55.6%) the dilatation percentage exceeded 130%. In 7 of the 11patients the dilatation after emptying of the band still exceeded 130%. The increase ofesophageal diameter was significantly correlated with the duration of follow-up, with regurgita-tion, heartburn during nighttime, and slow esophageal clearance.It was concluded that LASGB causes esophageal dilatation in about half of the patients. Thisdilatation is correlated with symptoms and is partly reversible after emptying of the band. The clin-ical relevance of the dilatation is unclear.
In Chapter 6 we retrospectively analysed the results of the LASGB procedure for morbid obesity in411 patients. Height, weight, and complications were prospectively recorded. The study group
85

consisted of 350 (85%) women and 61 (I5%) men with a median age of 38 years (range 17-60).In these 411 patients, the median weight was 133.4 kg, the median overweight 69.6 kg and themedian BMI 46.3 kg/m2. Two years after surgery, data was available for 267 patients 206 (77%)of whom had a weight loss > 30%, and 7 patients (3%) a weight gain. The median BMI differencewas then -10.2 kg/m2 (range +4.7—26.4). The median loss of overweight was 46.3% (+10.00—97.8). The weight loss remained stable in the following years. The most commonly seen complica-tions were fundus slippage (13%) and port-related complications (7%). It was concluded thatthree quarters of the patients with morbid obesity who received LASGB surgery had achieved andsustained weight loss at 2 years following surgery.
Controversial opinions exist concerning the effect of gastric banding on gastroesophageal reflux.In Chapter 7 we performed a systematic review on the the effect of LASGB on gastroesophagealreflux and esophageal motility. MEDLINE and EMBASE databases were searched for relevant stud-ies on patients undergoing adjustable gastric banding. Outcome measures were: reflux symptoms,medication use, esophagitis, pathological reflux measured by pH recording, LES (lower esophagealsphincter) function and esophageal peristalsis. Data were expressed as mean (range). Seventeen studies were identified with a total of 1839 patients. The prevalence of reflux symp-toms decreased postoperatively from 32.2% (16-48.4) to 9.1% ( 0-26.9) and medication usefrom 27.5% ( 16-38.5) to 9.5% (3.1-19.2). Newly developed reflux symptoms were found in15% (6.1-20) of the patients. The percentage of esophagitis decreased postoperatively from33.3% (19.4-61.6) to 27% (2.3-60.8). Newly developed esophagitis was observed in 22.9% (0-38.4). Pathological reflux was found 55.8% (34.9-77.4) preoperatively and postoperatively in29.4% (0-41.7). LES pressures increased from 12.9 mmHg (6-22) to 16.9 mmHg (11.3-21.4). LESrelaxation decreased from 100% to 79.7% (58-86). The percentage of dysmotility increased from3.5% (0-10) to12.6% (0-25).It was concluded that LASGB has anti-reflux properties resulting in resolution or improvement ofreflux symptoms, normalized pH monitoring results and a decrease of esophagitis. However, wors-ening or newly developed reflux symptoms and esophagitis are found in a subset of patients dur-ing longer follow-up. Pouch dilatation, filling of the band and disordered esophageal motility arepossible causative factors. Adjustable gastric banding increases LES pressure, but decreases LESrelaxation and is associated with an increase in disturbed esophageal peristalsis.
ANSWERS TO STUDY QUESTIONS OF THIS THESIS
Chapter 2Does laparoscopic adjustable gastric banding affect gastroesophageal reflux?Adjustable gastric banding decreases gastroesophageal reflux, but in a small subset of patients anincrease in gastroesophageal reflux will develop.
Chapter 3Does laparoscopic adjustable gastric banding affect esophageal motility?Adjustable gastric band placement causes an increase in LES pressure and high-pressure zonelength. Band placement on the short term does not disturb propagation of esophageal contractions.
Chapter 4Is there a change in gastric emptying after laparoscopic adjustable gastric banding and, if so, does this contribute to the weight loss?
86

Gastric band placement has no significant effect on postoperative gastric emptying rate and fun-dus emptying rate. Neither gastric emptying rate nor fundus emptying rate showed a relation withearly satiety or weight loss.
Chapter 5Does laparoscopic adjustable gastric banding cause esophageal dilatation?LASGB causes esophageal dilatation in about half of the patients. This dilatation is correlated withsymptoms and length of follow-up and is partly reversible after emptying of the band.
Chapter 6Do all morbidly obese subjects benefit from adjustable gastric banding?Three quarters of the patients with morbid obesity who underwent laparoscopic gastric bandingsurgery has sustained weight loss at two years following surgery. In subjects with a BMI > 50LAGB seems to be less effective than in those with a BMI < 50.
FUTURE PERSPECTIVESAs identified in chapters 2 and 3, gastric banding influences gastroesophageal reflux. The exactmechanism in which gastric banding decreases and sometimes increases gastroesophageal reflux isunclear and should be elucidated. The role of transient relaxations of the lower esophageal sphincter, pre-existent esophageal motil-ity disorders and weight loss on gastroesophageal reflux postoperatively is not fully understood.Intra-esophageal impedance monitoring, high-resolution manometry and 3-D ultrasound of theLES probably provides more insight in the (patho)-physiology of gastroesophageal reflux afterLASGB.
In chapter 4 an increase in early satiety was found after LASGB, but a relation with gastric empty-ing was not demonstrated. The mechanism of early satiety after adjustable gastric banding isimportant and needs to be unravelled because it is one of the keys in the success of bariatric surgi-cal operations. Alterations of the proximal stomach after gastric band placement by using a fundicwrap to fix the band may play a role by increasing early satiety. Barostat studies possibly will helpto identify changes in postprandial accommodation of the proximal stomach and explain theoccurrence of early satiety.
As identified in chapter 5 LASGB causes esophageal dilatation. However, the definition of esophagealdilatation is unclear and should be further determined and quantified. Long term studies in largegroups of patients, in which barium swallows and manometry are performed, are needed, in order toconfirm or exclude that decompensation of the esophagus will occur on the long term.
In chapter 6 we reported that in three quarters of the patients with morbid obesity who receivedLASGB, sustained weight loss is achieved at two years following surgery. Patients with extremeobesity (BMI > 50) seems to have less effect of the banding procedure than patients with a BMI <50. A prospective randomized study is warranted to conclude if it is better for patients withextreme obesity to undergo a gastric bypass procedure instead of a gastric banding procedure.
87


Chapter 9
SAMENVATTING, CONCLUSIES EN
TOEKOMSTPERSPECTIEVEN

In hoofdstuk 1 wordt een algemene inleiding gegeven over de epidemiologie van overgewicht, derelatie tussen overgewicht en gastro-oesofageale reflux en laparoscopische maagbandplaatsing. Het aantal mensen met overgewicht is enorm toegenomen sinds 1980 en heeft wereldwijd epi-demische vormen aangenomen. De toenemende prevalentie van overgewicht is een bedreiging voor de volksgezondheid omdatovergewicht is gerelateerd aan verschillende chronische ziektes en handicaps. Bariatrische chirurgie is de enige effectieve behandeling voor individuën met ernstig overgewicht.Het aantal operaties voor overgewicht is sterk toegenomen in de afgelopen decennia. Op ditmoment is de laparoscopische maagbandplaatsing een van de meest uitgevoerde operaties.Eind 90er jaren werd in de literatuur gemeld dat laparoscopische maagbandplaatsing een afname vangastro-oesophageale refluxklachten gaf. Echter, in deze studies ontbraken objectieve metingen zoalspH-meting en manometrie. Om meer inzicht in het effect van laparoscopische maagbandplaatsing opgastro-oesophageale reflux te krijgen werd gestart met onderzoek bij patienten met ziekelijkovergewicht die in aanmerking kwamen voor laparoscopische maagbandplaatsing in het St AntoniusZiekenhuis te Nieuwegein. De resultaten van deze studies zijn beschreven in dit proefschrift.
In hoofdstuk 2 werd het effect van laparoscopische maagbandplaatsing op gastro-oesofagealereflux bestudeerd. Zesentwintig patiënten die een maagbandplaatsing kregen werden bestudeerdmet behulp van: een vragenlijst voor symptoom analyse, 24-uurs pH-meting, oesofagogastroduo-denoscopie en oesophagus-passagefoto’s. De onderzoeken werden preoperatief, 6 weken en 6maanden na de operatie uitgevoerd. Maagbandplaatsing had een gering effect op zuurbranden,maar regurgitatie nam aanzienlijk toe tijdens het vervolgonderzoek. Het gebruik van zuurrem-mende middelen was 6 weken na de operatie aanzienlijk gedaald maar vertoonde 6 maanden nade operatie een duidelijke stijging. Pathologische reflux was aanwezig bij 13 van de 26 patiëntenvoor de operatie. Zes maanden na de operatie werd pathologische reflux bij slechts 6 van deze 13patiënten gemeten, maar 4 van de 13 patiënten met een normaal preoperatief refluxpatroonbleken na 6 maanden pathologische reflux te hebben ontwikkeld. Zes maanden na de operatie was de oesophagitis verdwenen bij 6 patiënten maar toegenomen bij9 patiënten. Bij 9 patiënten werd 6 maanden na de operatie een pouchvergroting vastgesteld.Pouchvergroting was significant gecorreleerd met de aanwezigheid van pathologische reflux,oesofagitis en het gebruik van zuurremmende medicatie. Pre-operatieve aanwezigheid van eenhiatus hernia had geen invloed op de pouchvergroting of pathologische reflux. De conclusie was dat laparoscopische maagbandplaatsing gastro-oesofageale reflux vermindertmits er geen pouchvergroting optreedt na de operatie.
Veranderingen in de oesofagusmotiliteit zouden kunnen optreden na plaatsing van een maagbandin de buurt van de overgang van oesophagus naar maag doordat er een obstructie wordtveroorzaakt, met name als de maagband wordt opgeblazen.
In hoofdstuk 3 onderzochten we het effect van de maagband op de oesofagusmotiliteit en onder-ste oesofagussfincter. Bij 29 patiënten met ziekelijk overgewicht werd vóór de maagbandplaatsing,zes weken na de operatie (vóór en na het vullen van de band) en zes maanden na de operatie, eenmanometrie verricht. Een vragenlijst werd gebruikt om de gastro-intestinale symptomen te scoren. Na plaatsing van de maagband was er een significante toename in de druk van de ondersteoesofagussfincter. Preoperatief was de druk: 0,8 (0,6-1,3) kPa (mediaan (interquartile range). Nazes weken met een lege band was de druk 1,3 (0.9-1.9) kPa (p = 0,003), na zes weken met eengevulde band was de druk 2,1 (1.5-2.8) kPa (p = 0,0001) en na zes maanden was de druk 1,5(1.3-1.9) kPa (p = 0,001). Ook de lengte van de hogedrukzone was toegenomen na band- plaats-
90

ing (preop 5.0 (4.3-6.0) cm vs zes weken 6.0 (5.0-6.5) cm. (p = 0,003). Het aantal peristaltischecontracties was niet significant gewijzigd na plaatsing van de band. Zuurbranden werd minder gezien zes weken na de operatie (p = 0,04), maar nam weer toe bij zesmaanden. Zuurbranden na 6 maanden was gecorreleerd met pouchvergroting (0,667; p < 0,01). Geconcludeerd werd dat maagbandplaatsing zorgt voor een toename in de druk van de ondersteoesofagussfincter en een langere hogedrukzone bewerkstelligt. Maagbandplaatsing vermindertrefluxsymptomen op de korte termijn maar dit lijkt niet te zijn gecorreleerd met druk of lengte vande onderste oesofagussfincter. Pouchvorming veroorzaakt een toename van reflux-symptomen,zonder dat er een relatie is met druk en lengte van de onderste oesofagussfincter. Maagbandplaatsing verstoort de oesfagusperistaltiek niet, althans niet op korte termijn.
In hoofdstuk 4 werd de rol van de maagontlediging bij gewichtsverlies en vroege verzadigingonderzocht in een opeenvolgende reeks van patiënten. Zestien patiënten ondergingen preoper-atief en zes maanden na maagbandplaatsing een maagontledigingsonderzoek (vast voedsel, enkelisotoop). Oesofagus-retentietijd, ”lag phase”, tijd tot maximum aktiviteit, maagontledigingssnel-heid, fundusontledigingssnelheid en gewichtsverlies werden gemeten. Symptoomanalyse werduitgevoerd met behulp van een gestandaardiseerde vragenlijst. Maagontledigingsparameters wer-den gecorreleerd met de symptomen.Maagbandplaatsing bleek geen significante invloed te hebben op de postoperatieve maag-en fundu-sontledigingssnelheid. Wel werd een significante toename van vroege verzadiging gerapporteerd. Desnelheid van maag-en fundusontlediging bleken geen relatie te hebben met het optreden van vroegeverzadiging of gewichtsverlies. Ook werd er geen relatie gevonden tussen vroege verzadiging met lagphase, oesofagusretentietijd, start van de activiteit en de maximale activiteit in proximale maag. Geconcludeerd werd dat maagbandplaasting geen significante invloed heeft op maagontledig-ingssnelheid. Daarom is het onwaarschijnlijk dat de snelheid van maaglediging een rol speelt bijhet mechanisme van gewichtsverlies na maagbandplaatsing.
In hoofdstuk 5 werd bij 45 patiënten het optreden van oesofagusdilatatie na maagbandplaatsingonderzocht met behulp van gestandaardiseerde slikfoto’s. De vervolgslikfoto’s werden gemiddeld 39,3maanden na de eerste slikfoto gemaakt. De diameter van de slokdarm werd gemeten in millimeterswaarbij de bekende vaste diameter van de maagband werd gebruikt als referentiepunt. Een toenamevan de diameter van 130% ten opzichte van de diameter net na de operatie werd beschouwd als slok-darmverwijding. Symptomen werden beoordeeld door middel van een vragenlijst. Bij 11 patiënten met een verwijding van de slokdarm werd de maagband geleegd waarna opnieuween slikfoto werd gemaakt met het doel te beoordelen of de slokdarmverwijding omkeerbaar was. Voor de hele groep werd er een significante stijging van de oesofagus diameter (mediaan(interquartile range) gevonden wanneer de slikfoto’s direkt na de operatie werden vergelekn metde latere slikfoto’s: 16,3 (14-18,7) mm versus 20,7 (18,1-26,8) mm (p < 0,01). Bij 25 van de 45patiënten (55,6%) was er sprake van dilatatie-percentage > 130%. In 7 van de 11 patiënten bleekdat er na het legen van de band nog steeds sprake was van een diameter- toename van > 130%.De toename van de oesofagusdiameter was significant gecorreleerd met duur van de follow-up,regurgitatie, nachtelijk zuurbranden, en vertraagde oesofagus- lediging. De conclusie was dat maagbandplaatsing oesofagusdilatatie veroorzaakt bij ongeveer de helft vande patiënten. Deze verwijding is gecorreleerd met symptomen en is gedeeltelijk reversibel na hetlegen van de band. De klinische relevantie van de slokdarmverwijding is onduidelijk.
In hoofdstuk 6 werden bij 411 patienten retrospectief de resultaten van laparoscopische maag-bandplaatsing beoordeeld. Van deze 411 patiënten was het mediane gewicht 133,4 kg, het medi-
91

ane overgewicht 69,6 kg en de mediane BMI 46,3 kg/m2. Van 267 patiënten waren gegevensbekend 2 jaar na de operatie. Twee jaar na de operatie hadden 206 patiënten (77%) eenovergewichtsverlies > 30% en 7 patiënten (3%) een gewichtstoename. De mediane afname vanhet overgewicht was 46,3% (+10,0-–97,8). Het gewichtsverlies was in de jaren erna stabiel. Demeest frequente complicaties waren fundusherniatie (13%) en problemen met de “port” (7%).Deze deden zich vaker voor bij de perigastrische methode dan bij de pars-flaccidatechniek.Geconcludeerd werd dat na laparoscopische maagbandplaatsing wegens morbide obesitas bijdriekwart van de patiënten een duurzaam gewichtsverlies bereikt wordt. De pars-flaccidatechniekgaat met minder complicaties gepaard dan de perigastrische methode.
In de literatuur vindt men verdeelde meningen betreffende de invloed van maagbandplaatsing opgastro-oesofageale reflux. In hoofdstuk 7 beschreven wij een systematische review over het effectvan maagbandplaatsing op gastro-oesofageale reflux en oesofagus motiliteit. MEDLINE enEMBASE databases werden doorzocht voor relevante studies over maagbandplaatsing en gastro-oesofageale reflux. Punten van onderzoek waren: refluxsymptomen, medicatie gebruik,oesophagitis, pathologische reflux gemeten met 24-uurs pH-metingen, onderste oesofagussfinc-terfunctie en oesofagusperistaltiek. Gegevens werden uitgedrukt als gemiddelden (range). Zeventien studies met een totaal van 1.839 patiënten voldeden aan de selectiecriteria. Deprevalentie van reflux-symptomen na de operatie daalde van 32,2% (16-48.4) tot 9,1% (0-26,9)en medicatiegebruik van 27,5% (16-38.5) tot 9,5% (3,1-19,2). Nieuw ontwikkelde reflux-symp-tomen werden gemeld door 15% (6.1-20) van de patiënten. Het percentage oesofagitis postoper-atief daalde van 33,3% (19.4-61.6) tot 27% (2.3-60.8). Nieuw ontwikkelde oesophagitis werdwaargenomen bij 22,9% (0-38,4) van de patienten. Pathologische reflux werd gevonden bij55,8% (34.9-77.4) voor- en na de operatie bij 29,4% (0-41,7) van de patienten. De druk in deonderste oesophagussfincter nam toe van 12,9 mmHg (6-22) tot 16,9 mmHg (11.3-21.4). Hetrelaxatie-percentage van de onderste oesofagussfincter daalde van 100% naar 79,7% (58-86).Het percentage dysmotiliteit steeg van 3,5% (0-10) to12.6% (0-25). De conclusie was dat maagbandplaatsing kan leiden tot het verdwijnen of verminderen vanrefluxsymptomen, het normaliseren van pH-metingen en een afname van oesophagitis. Echter,gedurende langere follow-up werden ook verslechtering of nieuw ontwikkelde refluxsymptomenen oesofagitis gevonden in een subgroep van patiënten. Hierbij zijn pouch-vergroting, het vullenvan de band en verstoorde oesofagusmotiliteit mogelijke oorzakelijke factoren.Maagbandplaatsing verhoogt de druk in de onderste oesofagussfincter vermindert de mogelijkheidtot sfincterrelaxatie en wordt geassocieerd met een toename van gestoorde oesofagusperistaltiek.
STUDIEVRAGEN EN ANTWOORDEN OP DEZE VRAGEN
Hoofdstuk 2 Beinvloedt laparoscopische maagbandplaatsing gastro-oesofageale reflux?Laparoscopische maagbandplaatsing vermindert gastro-oesofageale reflux als er geen pouch-ver-groting ontstaat. Echter, in een kleine groep patienten ontstaat gastro-oesofageale reflux.
Hoofdstuk 3 Heeft laparoscopische maagbandplaatsing invloed op de oesofagusmotiliteit? Maagbandplaatsing zorgt voor een toename in de druk van de onderste oesofagussfincter en vooreen langere hogedrukzone. Bandplaatsing verstoort op de korte termijn de oesofagus- peristaltiekniet.
92

Hoofdstuk 4 Verandert de maagontlediging na laparoscopische maagbandplaatsing en draagt dit bij aan hetgewichtsverlies? Maagbandplaatsing bleek geen significante invloed op de postoperatieve maag-en fundus-ontledigingssnelheid te hebben. Zowel maag- als fundusontledigingssnelheid bleken geen relatiete hebben met het optreden van vroege verzadiging of gewichtsverlies.
Hoofdstuk 5 Veroorzaakt laparoscopische maagbandplaatsing oesofagusverwijding?Maagbandplaatsing veroorzaakt bij ongeveer de helft van de patienten een oesofagus-verwijding.Deze verwijding is gecorreleerd met symptomen en is gedeeltelijk reversibel na het legen van demaagband.
Hoofdstuk 6 Hebben alle patienten met ziekelijk overgewicht baat bij een maagbandplaatsing?Driekwart van de patiënten met ziekelijk overgewicht die een maagband geplaatst krijgen, hebbeneen blijvend gewichtsverlies 2 jaar na de operatie. Mensen met een BMI > 50 lijken minder baat tehebben bij een maagband dan mensen met een BMI < 50.
TOEKOMSTIG ONDERZOEKZoals beschreven in de hoofdstukken 2 en 3, beïnvloedt maagbandplaatsing gastro-oesofagealereflux. Het exacte mechanisme waardoor de maagband zorgt voor afname en soms voor toenamevan gastro-oesofageale reflux is onduidelijk. De rol hierbij van transiente relaxaties van de onder-ste oesofagussfincter, pre-existente oesofagusmotiliteitstoornissen en gewichtsverlies is nogonvoldoende onderzocht. Impedantiemeting, hoge-resolutie manometrie en 3-D echografie vande onderste oesofagussfincter zouden meer inzicht kunnen geven in de (patho)fysiologie van gas-tro-oesofageale reflux na maagbandplaatsing.
In hoofdstuk 4 bleek dat maagbandplaatsing gepaard gaat met toename van gevoelens van vroegeverzadiging tijdens de maaltijd, maar een relatie met de maagontlediging werd niet aangetoond.Het mechanisme van vroegtijdige verzadiging is belangrijk en dient te worden ontrafeld daar het desleutel tot succes is van de chirurgische behandeling van overgewicht. Veranderingen van de proxi-male maag na maagbandplaatsing waarbij een deel van de fundus wordt gebruikt om de band teborgen zouden een rol kunnen spelen bij het ontstaan van vroege verzadiging. Barostatstudieszouden een rol kunnen spelen bij het meten van veranderingen van de proximale maag.
In hoofdstuk 5 werd beschreven dat maagbandplaatsing oesofagusdilatatie kan veroorzaken. Dedefinitie van oesofagusdilatatie en klinische relevantie is onduidelijk en moet worden vastgesteld.Lange termijn studies bij een groot aantal patiënten, waarbij slikfoto’s en manometrie wordengebruikt, zijn nodig om te bevestigen of er op de lange termijn er decompensatie van de oesofa-gus optreedt.
In hoofdstuk 6 hebben wij gemeld dat bij driekwart van de patiënten met morbide obesitas dieeen laparoscopische maagband kregen er een blijvend gewichtsverlies is opgetreden 2 jaar na deoperatie. Patiënten met extreem overgewicht (BMI > 50) leken minder effect te hebben van demaagband dan patiënten met een BMI < 50. Een prospectieve gerandomiseerde studie is nodigom vast te stellen of het beter is voor patiënten met extreem overgewicht om een gastric-bypass-procedure te ondergaan in plaats van een maagbandprocedure.
93

DANKWOORD
Een dankwoord voor velen aan het einde van een lang promotietraject is zeker op zijn plaats. Iedereen heeft veel geduld moeten hebben. Maar nu is het dan zover. Onderzoek doen, de opleiding tot chirurg volgen, en dan ook nog trouwen en vader worden, wassoms wat veel van het goede. Meer dan tachtig procent van mijn proefschrift is geschreven na elfuur ’s avonds.Een proefschrift schrijven is daarom, naast een wetenschappelijke uitdaging, ook zeker een proevevan doorzettingsvermogen. Velen hebben hun steentje bijgedragen maar uiteindelijk moet je hetwel zelf doen. Een aantal mensen wil ik in het bijzonder noemen.
Prof. Smout, beste André, zeer veel dank voor al je bemoeienissen. Je bent de grote motorgeweest achter de diverse manuscripten. Uiteindelijk is het toch afgekomen. Als ik weer eens eendip had en met je sprak zag ik het altijd weer zitten. Een historisch moment is aangebroken, zoalsje pas schreef. Je humor en verbazingwekkende vermogen teksten te herordenen en boven hetniveau van het Wim Kok Engels uit te tillen verdienen veel waardering. Na een indringende mailvan jou eind vorig jaar bleek ik toch wel snel te kunnen werken…
Prof. Gooszen, beste Hein, als niet geboren wetenschapper ben ik, mede dankzij jouw opmerkin-gen bij de diverse manuscripten en je tip om Marc Besselink eens te raadplegen betreffende desystematic review, er uiteindelijk in geslaagd een boekje af te leveren.
Dr. Timmer, beste Robin, jij stond aan de basis van dit proefschrift. Van jou heb ik geleerd hoe jeeen manometrie en pH-metrie moet verrichten en interpreteren. De liefde voor de gastro-enterologie is hierna niet meer overgegaan. Ook als kinderchirurg ligt mijn interesse bij kinderenmet stoornissen van het maag- darmstelsel.
Dr B. van Ramshorst, beste Bert, het is zover. Ook jij bent vanaf het begin bij dit proefschriftbetrokken geweest. Je enorme werklust en werktempo heeft je tot een van de bekendste baria-trisch chirurgen in Nederland gemaakt. Ik denk nog met plezier terug aan al die mooie congressenop mooie plaatsen waar we gebivakkeerd hebben. Ik hoop dat je rode oor rechts na al die ver-halen van mij op de terugweg uit Salzburg weer zijn normale kleur heeft gekregen.
Afdeling Endoscopie in het St Antonius Ziekenhuis, dank voor de gastvrijheid die ik mocht ervarentijdens het uitvoeren van mijn metingen.
Afdeling Radiologie, Cas Tiethof en Ruud de Graaf, inmiddels ook oud- Antonianen. Dank voorjullie bijdrage en tijd bij het uitvoeren van de dilatatiestudie.
Afdeling Nucleaire Geneeskunde, Dr. Monique van Buul, bedankt voor je geduld om mij iets teleren over maagontlediging. Dank ook aan de laboranten, in het bijzonder Marielle Otten, die elkekeer weer mijn patiënten moest inplannen.
Wouter te Riele, medeonderzoeker, dank voor je inspanning betreffende het resultatenartikel.Succes met het afronden van je eigen boekje.
94

Het hele proefschrift was niets geworden zonder de patiënten die hebben meegewerkt aan dediverse studies. Misschien denken ze nog wel eens aan die dokter De Jong die weer belde vooreven een meting met die slangetjes door de neus. Niet één keer, maar wel vijf of soms zes keer.
Brigitte Bliemer, nurse practicioner, bedankt voor het bijhouden van de database en het af en toeaanleveren van gegevens. De beoordelingscommissie, Prof. Ter Braak, Prof. Akkermans, Prof. Kon, Prof. Van der Graaf enProf. Greve. wil ik bedanken voor het beoordelen van mijn manuscript.
Ik hoef niemand te bedanken voor het geven van extra vrije tijd voor onderzoek, want studie-verlof heb ik nooit gekregen.
Paranimfen Rob en Wouter, oud-huisgenoten, het doet me deugd jullie als paranimfen aan mijnzijde te hebben. Ik hoop dat onze vriendschap nog zeer lang mag blijven bestaan.
Lieve Scheltine, je wilde me graag helpen. Ik wilde dat ik wat van je scherpe analytische geest had,dan was het boekje vast eerder klaar geweest.
Lieve Joep, Guido en Maartje, eindelijk heeft papa zijn boekje af en dat ondanks jullie…A
Tot slot citeer ik een gedeelte uit het eerste boek van de Confessiones van Augustinus waarin ietsgezegd wordt over mijn inspiratiebron:
Magnus es, domine, et laudabilis valde (…)inquietum est cor nostrum donec requiescat in te.
Groot zijt Gij, Heer, en alle lof waardig (…)onrustig is ons hart totdat het rust vindt in U.
95

CURRICULUM VITAEJustus Reinier (Justin) de Jong werd op 9 januari 1970 geboren in Kockengen. In 1988 haalde hijzijn VWO diploma op het Van Lodenstein College te Amersfoort. Aansluitend studeerde hijGeneeskunde in Utrecht waar hij in 1996 zijn artsenbul ontving. Hierna werkte hij als AGNIOChirurgie in het St Elizabeth Ziekenhuis te Amersfoort en het St Antonius Ziekenhuis teNieuwegein. In januari 1999 startte hij met de opleiding Heelkunde in het St Antonius Ziekenhuiste Nieuwegein (opleider dr. P.M.N.Y.H. Go). In deze tijd werd het onderzoek gestart dat geleidheeft tot dit proefschrift. Vanaf 2002 tot 2005 werd de opleiding Heelkunde vervolgd in hetAcademisch Ziekenhuis te Utrecht (Opleider Prof. dr. I.H.M. Borel Rinkes). De vervolgopleiding totkinderchirurg vond plaats in het Wilhelmina Kinderziekenhuis te Utrecht (opleiders Prof. dr.N.M.A. Bax en dr. D.C. van der Zee) en in het Kinderchirurgisch Centrum te Amsterdam (Opleiderprof. dr. H.A. Heij). Na een jaar in Utrecht en Maastricht te hebben gewerkt als kinderchirurg isJustin sinds 2009 opgenomen in de staf van het Kinderchirurgisch Centrum te Amsterdam. Justinwoont in Linschoten en is getrouwd met Scheltine Suur. Samen hebben zij drie kinderen: Joep,Guido en Maartje.
BEOORDELINGSCOMMISSIE
Prof. dr. L.M.A. AkkermansAfdeling Experimentele Heelkunde, Universitair Medisch Centrum, Utrecht
Prof. dr. M. KonAfdeling Plastische en Reconstructieve Chirurgie, Universitair Medisch Centrum, Utrecht
Prof. dr. E.W.M.T. ter BraakAfdeling Interne Geneeskunde, Universitair Medisch Centrum, Utrecht
Prof. dr. Y. van der GraafJulius Centrum voor Gezondheidswetenschappen en Eerstelijns Geneeskunde, Universitair MedischCentrum, Utrecht
Prof. dr. J.W. Greve Universitair Medisch Centrum, Maastricht, Atrium Medisch Centrum Heerlen
96




















