
Anti-inflammatory Effect from Indomethacin Nanoparticles Inhaled by Male Mice

78
Indian Journal of Medical Sciences, Vol. 67, No. 3 and 4, March and April 2013
EFFECT OF INHALED FLUTICASONE AND SALMETEROL ON TRACHEAL RESPONSIVENESS AND LUNG INFLAMMATION:
INFLUENCE OF ADMINISTRATION TIME AND ALLERGEN‑FREE PERIOD
MOHAMMAD REZA KHAZDAIR, MOHAMMAD HOSSEIN BOSKABADY, ABBAS TABATABAEE1, MAHMOUD HOSSEINI, MAHDI ABBASNEJAD2
ABSTRACT
BACKGROUND: The effect of inhaled fluticasone propionate (FP) and salmeterol (SM) on tracheal responsiveness (TR) to methacholine and lung pathology of sensitized guinea pig was examined. MATERIALS AND METHODS: Six groups of guinea pigs (n = 7) were sensitized to ovalbumin (OA). Three groups were subjected to inhaled FP and SM, one group during (A), one group after sensitization (for 18 days, B) and other group during sensitization but with 18‑days delay before measurements (C). Other three groups were treated with placebo. RESULTS: The TR to methacholine and tracheal muscle contractility were significantly higher than those of control group (P < 0.001 for all cases). The lungs of placebo groups showed variable pathological changes (nonsignificant to P < 0.001) compared to control group. TR, intra‑alveolar and interabronchoal hemorrhagie (P < 0.001 in only group A) in treated groups with FP and SM were significantly decreased compared to placebo groups. The improvement in all variables in treatment groups A and C were more pronounced than group B. CONCLUSION: These results showed a protective effect of FP and SM on tracheal responsiveness and lung pathology during sensitization which was more effective than after sensitization.
Key words: Asthma, fluticasone propionate, lung pathology, salmeterol, tracheal responsiveness
ORIGINAL ARTICLE
Applied Physiology Research Centre and Department of Physiology, School of Medicine, Mashhad University of Medical Sciences, Mashhad, 1Department of Pathology, Ghaem Medical Centre, Mashhad University of Medical Sciences, Mashhad,2Department of Biology, Faculty of Seines, Kerman University of shahid bahonar, Kerman, Iran
Address for correspondence: Dr. Mohammad Hossein Boskabady, Department of Physiology, School of Medicine, Mashhad University of Medical Science, Mashhad‑9177948564, Iran. E‑mail: [email protected]
INTRODUCTION
Asthma is a chronic inflammatory disorder of the airway,[1] characterized by airway
Access this article onlineQuick Response Code: Website:
www.indianjmedsci.org
DOI:10.4103/0019-5359.121121PMID:
*****************************
[Downloaded free from http://www.indianjmedsci.org on Wednesday, January 22, 2014, IP: 95.38.81.151] || Click here to download free Android application for thisjournal

79FLUTICASONE + SALMETEROL, ADMINISTRATION TIME, LUNG PATHOLOGY AND ASTHMA
Indian Journal of Medical Sciences, Vol. 67, No. 3 and 4, March and April 2013
hyper‑responsiveness (AHR).[2] In fact asthma is a two‑component disease characterized by airway inflammation[3] and smooth muscle dysfunction.[4] The most effective treatment, therefore, is a drug which targets both components of the disease.
Adding of long acting β‑agonists (LABA) leads to greater improvement in treatment of asthma than increasing the dose of inhaled corticosteroid (ICS).[5‑10] Several in vitro and in vivo animal studies also indicated that LABA could also suppress inflammatory process.[11‑15] The combination of salmeterol (SM) and fluticasone propionate (FP) enhances aspects of allergen‑induced airway remodeling[16] and is able to control peripheral blood T‑cell activation in asthmatic patients more efficiently.[17] There are evidences in favor of bidirectional interaction between β‑agonists and steroids on various pathophysiological aspects of asthma.[18,19]
In this study, the effect of an inhaled corticosteroid, FP and LABA, SM, on tracheal responsiveness to methacholine and lung pathology, during and after sensitization of guinea pigs was investigated.
MATERIALS AND METHODS
Animal sensitization and animal groupsSensitization of animals to (OA) was performed using the method previously described.[20‑22] Briefly, guinea pigs were sensitized to 10 mg OA (Sigma Chemical Ltd, UK) and 100 mg Al(OH)3 dissolved in 1 ml saline i.p. One week later the same dose was repeated as a booster dose. From day 17th, the animals were exposed to an aerosolized OA solution 4% for 18 ± 1 days, 4 mins each day.
The aerosol was administered in a closed chamber, dimensions 30 × 20 × 20 cm. Control animals were treated similarly but saline was used instead of OA solution. The study was approved by the ethical committee of the Mashhad University of Medical Sciences.
Seven different groups of guinea pigs (n = 7 or each group) were as follows [Figure 1]:• Control group (group C): Receiving Al(OH)3
alone dissolved in 1 ml normal saline and inhaled saline aerosol instead of OA
• Treatment and placebo groups A: Treated with 250 µg inhaled FP twice/day + 100 µg inhaled SM twice/day or placebo (composition; CFC‑free propellant HFA as4a; 1 ,1 ,1 ,2 ‑Te t ra f luoroe thane) (GlaxoSmithKline Research Triangle, NC) during sensitization period for 18 days
• Treatment and placebo groups B: Treated with FP + SM or placebo after sensitization period for 18 days
• Treatment and placebo groups C: Treated with FP + SM or placebo during sensitization period, evaluated with 18‑days delay.
Aerosol FP and placebo was administered using ordinary canister through a modified spacer as previously described.[23]
Tissue preparationsGuinea pigs were sacrificed and trachea was removed. Each trachea was cut into 10 rings (each containing 2‑3 cartilaginous rings). All the rings were then cut open opposite the tracheal is muscle, and sutured together to form a tracheal chain.[24]
Tissue was then suspended in a 10‑ml organ bath (Schuler organ bath type 809,
[Downloaded free from http://www.indianjmedsci.org on Wednesday, January 22, 2014, IP: 95.38.81.151] || Click here to download free Android application for thisjournal

80 INDIAN JOURNAL OF MEDICAL SCIENCES
Indian Journal of Medical Sciences, Vol. 67, No. 3 and 4, March and April 2013
March‑Hugstetten, Germany) containing Krebs‑Henseliet solution of the following composition (mM): NaCl 120, NaHCO3 25, MgSO4 0.5, KH2PO4 1.2, KCl 4.72, CaCl2 2.5 and dextrose 11. The Krebs solution was maintained at 37oC and gassed with 95% O2 and 5% CO2. Tissue was suspended under isotonic tension of 1 g and allowed to equilibrate for at least 1 h while it was washed with Krebs solution every 15 mins.
Responses were measured using vernier control type 850 N sensor with sensitivity range: 0‑20 g and resolution: 0.2 mm/turn
(Hugo‑Sachs Elektronik, Germany) and amplified with amplifier (ML/118 quadribridge amp, March‑Hugstetten, Germany) and recorded on powerlab (ML‑750, 4 channel recorder, March‑Hugstetten).
Assessment of tracheal response to methacholineIn each exper iment a cumulat ive log concentration‑response curves of methacholine hydrochloride (Sigma Chemical Ltd., U.K.) were obtained. Consecutive concentrations (including 10−7‑10−2 M) were added every 2 mins and the contraction due to each concentration was
Figure 1: Description of control, three placebo and three treated sensitized groups. FP + SM: Fluticasone propionate (250 µg) and salmeterol (100 µg), OA: Ovalbumin, NS normal saline
[Downloaded free from http://www.indianjmedsci.org on Wednesday, January 22, 2014, IP: 95.38.81.151] || Click here to download free Android application for thisjournal

81FLUTICASONE + SALMETEROL, ADMINISTRATION TIME, LUNG PATHOLOGY AND ASTHMA
Indian Journal of Medical Sciences, Vol. 67, No. 3 and 4, March and April 2013
recorded at the end of 2 mins. The percentage of contraction of the tracheal smooth muscle due to each concentration of methacholine in proportion to the maximum contraction obtained by its final concentration (plateau) was plotted against log concentration of methacholine. The effective concentration of methacholine, causing 50% of maximum response (EC50) was measured. Tracheal muscle contractility obtained by 100‑µM methacholine was converted to gram, according to calibration of transducer.
Pathological evaluationThe lungs with the remaining trachea were removed and placed into the buffered formalin 10% (37%, Merck, Germany). Seven days later, tissues were dried by its passage through ethanol 70‑100% and cleared by passage through xylol. The paraffin block of the tissues were prepared and the specimens were cut in 4‑µm slices and were stained with Hematoxylin‑eosin (H and E). The tissues were then evaluated blinded under a light microscope. The pathological changes in the lung were scored as follows: No pathological changes = 0; patchy changes + = 1; patchy changes ++ = 2; local changes = 3; severe changes (in the most parts of the lung) = 4.
StatisticsThe percent improvement in each treatment group was calculated in cases, the treatment data was greater than corresponding placebo as [(TreatmentA1‑PlaceboA1)/PlaceboA1] X 100). In cases, the treatment data was lower than corresponding placebo, the improvement was calculated by [(PlaceboA1‑TreatmentA1)/TreatmentA1] X 100).
All data were quoted as mean ± SEM. The data of three placebo groups were compared
with treated guinea pigs using unpaired “t” test. The comparison of data between three treatment groups, three placebo groups and six groups of animals treated with the FP and SM and placebo with control animals were done using one way analysis of variance (ANOVA) with Tukey‑Kramer post test. Significance was accepted at P < 0.05. All statistical analysis was performed using Instate software.
RESULTS
HistologyThe pathological changes in the lung of sensitized groups were included: Intra‑alveolar hemorrhage, intrabronchial hemorrhage, increasing interstitial tissue, and macrophages [Figure 2]. Pathological changes in all three placebo groups were significantly greater than control group except increasing interstitial tissue and macrophages in placebo groups B and C (P < 0.05‑<0.001) [Table 1, Figure 3].
Treatment wi th FP and SM improved intra‑alveolar, intrabronchial hemorrhage interstitial tissue, and macrophages which were statistically significant only for group A (P < 0.001 for both cases) [Figure 3a‑c]. Improvement of all pathological changes in group B was significantly less than those of groups A and C which was statistically significant for intra‑alveolar and intrabronchial hemorrhage between groups B and A (P < 0.05 for both cases) [Table 2].
Tracheal response and contractility to methacholineConcentration response curves to methacholine in all placebo groups showed left ward shift
[Downloaded free from http://www.indianjmedsci.org on Wednesday, January 22, 2014, IP: 95.38.81.151] || Click here to download free Android application for thisjournal

82 INDIAN JOURNAL OF MEDICAL SCIENCES
Indian Journal of Medical Sciences, Vol. 67, No. 3 and 4, March and April 2013
compared to the curve of control group. However, the curves of all treated groups were shifted to the right compared to corresponding placebo groups [Figure 4].
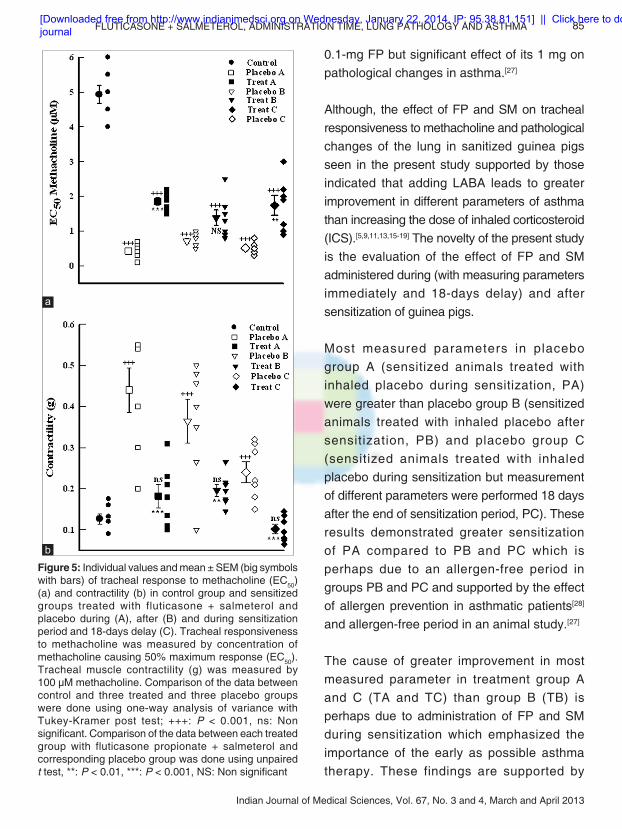
The mean values of EC50 and contractility response of tracheal chains to 100‑µM methacholine in all placebo groups (A, B, and C) were significantly lower than control group
Figure 2: A sample of photographs of lung specimens in control group, placebo group A (Pa), placebo group B (Pb), placebo group C (Pc), treatment group A (Ta), treatment group B (Tb), and treatment group C (Tc). Intra‑alveolar hemorrhagie, intrabronchial hemorrhagie, increasing interstitial tissue and macrophages are evident in three placebo group photographs. Intra‑alveolar and intrabronchial hemorrhagie was significantly reduced in treatment groups (magnification 10 × 10)
[Downloaded free from http://www.indianjmedsci.org on Wednesday, January 22, 2014, IP: 95.38.81.151] || Click here to download free Android application for thisjournal

83FLUTICASONE + SALMETEROL, ADMINISTRATION TIME, LUNG PATHOLOGY AND ASTHMA
Indian Journal of Medical Sciences, Vol. 67, No. 3 and 4, March and April 2013
(P < 0.001 for all cases), [Table 3, Figure 5a and b]. The contractility responses in treatment groups A, B, and C (P < 0.001 for groups A and C and P < 0.01 for groups B) but mean values of EC50 in treatment groups A and C were significantly and that of group B nonsignificantly improved compared to corresponding placebo groups (P < 0.001 for group A and P < 0.01 for group C), [Figure 5a and b]. Improvement of tracheal responsiveness to methacholine (EC50) and tracheal contractility response to 100‑µM methacholine in treatment protocol B was nonsignificantly lower than that of treatment group A and C [Table 2].
DISCUSSION
The results showed increased tracheal
response to methacholine and histological changes of the lung in sensitized compared to control animals which were similar to the results of the previous studies.[21,25,26]
It is well known that the most effective treatment of asthma is one which targets both components (airway inf lammation and smooth muscle dysfunction) of the disease. Therefore, in this study, FP and SM was administered during, after and during sensitization with 18‑days delay in measurements.
The effects of FP and SM treatment on pathological changes of lung in the present study are supported by a previous study indicating the absence of measurable effect of
Table 1: The mean±SEM values of intra‑alveolar hemorrhagie, intrabronchial hemorhhagie, increasing interstitial tissue and macrophages in control group and sensitized groups treated (T) with fluticasone+salmeterol and placebo (P) during (A), after (B) and during with 18‑days delay in measurements (C) and statistical differences between three placebo and treatment groupsParameters C PA PB PC TA TB TC Intra‑alveolar hemorrhagie 0.00±0.00 2.00±0.21 2.28±0.28 2.00±0.30 0.28±0.18 1.71±0.35 + 1±0.37Intrabronchial hemorrhagie 0.14±0.14 3.14±0.26 2.57±0.29 3.0±0.30 1.28±0.18 2±0.37 2.71±0.35*Increasing interstitial tissue and mac
0.00±0.00 1.00±0.30 0.85±0.34 0.57±0.29 2.14±0.34 1.57±0.42 1.71±0.35
The pathological changes in the lung of sensitized group were included: Intra‑alveolar hemorrhagie, intrabronchial hemorhhagie, increasing interstitial tissue and macrophages which were scored as follows: No pathological changes=0, patchy changes +=1, patchy changes ++=2, local changes=3, severe changes (in the most parts of the lung)=4. Comparison of the data between control and three treated and three placebo groups were done using one way analysis of variance with Tukey‑Kramer post test. Statistical significance for the difference between the data of group A vs group B: +, P<0.05
Table 2: Differences in improvement of tracheal responses to methacholine and pathological changes in three treatment groups A, B, and CParameters TA TB TC
EC50 481.85±171.88 138.66±47.02 459.71±246.86Contractility (mg) 184.14±63.07 102.42±18.30 167.85±49.99Intra‑alveolar hemorrhagie 171.42±18.44 58.33±20.66 + 150±32.73Intrabronchial hemorrhagie 171.42±35.95 40.42±13.04 + 85.71±35.90Interstitial tissue and mac 107.14±27.66 57.14±36.88 135.71±32.20Values are quoted as mean±SEM. Percent improvements were achieved as follows: In cases, the treatment data was greater than corresponding placebo, the data obtained in treatment group minus the data obtained in corresponding placebo group divided by the data obtained in the same placebo group, multiplied 100 (e.g., [(TreatmentA1‑PlaceboA1)/ PlaceboA1]100). In cases, the treatment data was lower than corresponding placebo, the data obtained in placebo group minus the data obtained in corresponding treatment group divided by the data obtained in the same treatment group, multiplied 100 (e.g., [(PlaceboA1‑TreatmentA1)/ TreatmentA1]100). Comparison of the data between three treatment groups was done using unpaired t test, Statistical significance for the difference between the data of group A vs group B: +, P<0.05
[Downloaded free from http://www.indianjmedsci.org on Wednesday, January 22, 2014, IP: 95.38.81.151] || Click here to download free Android application for thisjournal

84 INDIAN JOURNAL OF MEDICAL SCIENCES
Indian Journal of Medical Sciences, Vol. 67, No. 3 and 4, March and April 2013
Figure 3: Mean ± SEM of score of the interalveolar hemorrhage (a), intrabronchial hemorrhage (b), interstitial tissue and macrophage (c), in control group and sensitized groups treated (T) with fluticasone + salmeterol and placebo during (A), after (B) and during sensitization period and 18‑days delay (C). Comparison of the data between control and three treated groups with fluticasone propionate + salmeterol and three placebo groups were done using one way analysis of variance with Tukey‑Kramer post‑test, +: P < 0.05, +++: P < 0.001, ns: Non significant. Comparison of the data between each treated group with fluticasone propionate and salmeterol corresponding placebo group was done using unpaired t test, ***: P < 0.001, NS: Non significant
c
b
a
Figure 4: Cumulative log concentration‑response curves of methacholine induced contraction of isolated trachea in control group and groups treated with fluticasone + salmeterol and placebo during (a), after (b) and during sensitization period and 18‑days delay (c). Concentration response curves to methacholine in three placebo groups showed left ward shift compared to the curve of control group. However, the curves of three treated groups were shifted to the right compared to corresponding placebo groups
c
b
a
[Downloaded free from http://www.indianjmedsci.org on Wednesday, January 22, 2014, IP: 95.38.81.151] || Click here to download free Android application for thisjournal
85FLUTICASONE + SALMETEROL, ADMINISTRATION TIME, LUNG PATHOLOGY AND ASTHMA
Indian Journal of Medical Sciences, Vol. 67, No. 3 and 4, March and April 2013
0.1‑mg FP but significant effect of its 1 mg on pathological changes in asthma.[27]
Although, the effect of FP and SM on tracheal responsiveness to methacholine and pathological changes of the lung in sanitized guinea pigs seen in the present study supported by those indicated that adding LABA leads to greater improvement in different parameters of asthma than increasing the dose of inhaled corticosteroid (ICS).[5,9,11,13,15‑19] The novelty of the present study is the evaluation of the effect of FP and SM administered during (with measuring parameters immediately and 18‑days delay) and after sensitization of guinea pigs.
Most measured parameters in placebo group A (sensitized animals treated with inhaled placebo during sensitization, PA) were greater than placebo group B (sensitized animals treated with inhaled placebo after sensitization, PB) and placebo group C (sensitized animals treated with inhaled placebo during sensitization but measurement of different parameters were performed 18 days after the end of sensitization period, PC). These results demonstrated greater sensitization of PA compared to PB and PC which is perhaps due to an allergen‑free period in groups PB and PC and supported by the effect of allergen prevention in asthmatic patients[28] and allergen‑free period in an animal study.[27]
The cause of greater improvement in most measured parameter in treatment group A and C (TA and TC) than group B (TB) is perhaps due to administration of FP and SM during sensitization which emphasized the importance of the early as possible asthma therapy. These findings are supported by
Figure 5: Individual values and mean ± SEM (big symbols with bars) of tracheal response to methacholine (EC50) (a) and contractility (b) in control group and sensitized groups treated with fluticasone + salmeterol and placebo during (A), after (B) and during sensitization period and 18‑days delay (C). Tracheal responsiveness to methacholine was measured by concentration of methacholine causing 50% maximum response (EC50). Tracheal muscle contractility (g) was measured by 100 µM methacholine. Comparison of the data between control and three treated and three placebo groups were done using one‑way analysis of variance with Tukey‑Kramer post test; +++: P < 0.001, ns: Non significant. Comparison of the data between each treated group with fluticasone propionate + salmeterol and corresponding placebo group was done using unpaired t test, **: P < 0.01, ***: P < 0.001, NS: Non significant
b
a
[Downloaded free from http://www.indianjmedsci.org on Wednesday, January 22, 2014, IP: 95.38.81.151] || Click here to download free Android application for thisjournal

86 INDIAN JOURNAL OF MEDICAL SCIENCES
Indian Journal of Medical Sciences, Vol. 67, No. 3 and 4, March and April 2013
a permanent loss of pulmonary function or even induce remission in some patients in early treatment of airway inflammation.[29] The cause of less improvement of some parameters in group TC compared to TA is perhaps a nontreated period of 18 days in this group which emphasizes the importance of continues treatment in asthmatic patients. The other important findings of the present study is incomplete prevention of tracheal responsiveness and lung pathological changes in treated sensitized guinea pigs with FP and SM neither during nor after sensitization.
The effect of FP alone administered during or after sensitization was examined in our previous study.[30] In fact the present study is the next step of our previous study aimed to investigate; (1) Is the combination of FP and SM different with FP alone? and (2) Is an allergen‑free period in animals treated during sensitization affect the results? Comparison of the results of two studies showed that treatment of sensitized guinea pigs with combination of FP + SM during sensitization lead to more improvement in most variables compared to animals treated with only FP. There was no significant difference in tracheal responsiveness to methacholine, between two drugs treated after sensitization. Therefore, the results of both studies showed that treatment
during sensitization is more effective than after sensitization. In addition, the results of the present study showed that treatment of sensitized animals with FP and SM is more effective than FP alone especially in group treated during sensitization. The cause of greater improvement in some parameter in animals treated with FP alone after sensitization is not clear to us.
In conclusion, these results showed that treatment with an inhaled corticosteroid, FP plus an inhaled LABA, SM on tracheal respons iveness to methachol ine and pathological changes of the lung during sensitization (development of inflammation and pathological changes) was more effective than after sensitization (establishment of inflammation and pathological changes). Therefore, the results emphasized that asthma therapy should begin as soon as possible early of development of inflammation in the airways of asthmatic patients. The importance of an allergen‑free environment in the treatment of asthma disease is also indicated.
ACKNOWLEDGMENTS
This study was financially supported by the Research Council of Mashhad University of Medical Sciences, Mashhad, Iran. This paper is a part of a M.Sc. thesis.
Table 3: The mean±SEM values of tracheal responsiveness to methacholine and tracheal contractility in control group and sensitized groups treated (T) with fluticasone+salmeterol and placebo (P) during (A), after (B) and during sensitization period with 18‑days delay in measurements (C) and statistical differences between three placebo and treatment groupsParameters C PA PB PC TA TB Tc
EC50 (µmol) 4.92±0.25 0.42±0.07 0.71±0.07 + 0.51±0.05 1.85±0.09 1.38±0.22 1.74±0.28Contractility (g) 0.12±0.01 0.44±0.05 0.36±0.05 0.24±0.03* 0.182±0.02 0.196±0.01 0.102±0.01*Tracheal responsiveness to methacholine was measured by concentration of methacholine causing 50% maximum response (EC50). Comparison of the data between three treated and three placebo groups were done using one way analysis of variance with Tukey‑Kramer post test. Statistical significance for the difference between the data of group A vs group B: +, P<0.05, Statistical significance for the difference between the data of group A vs group B and C: *, P<0.5, Statistical significance for the difference between the data of group B vs group C: P<0.01
[Downloaded free from http://www.indianjmedsci.org on Wednesday, January 22, 2014, IP: 95.38.81.151] || Click here to download free Android application for thisjournal
87FLUTICASONE + SALMETEROL, ADMINISTRATION TIME, LUNG PATHOLOGY AND ASTHMA
Indian Journal of Medical Sciences, Vol. 67, No. 3 and 4, March and April 2013
REFERENCES
1. Busse W, Banks‑Schlegel SP, Larson GL. Childhood versus adult‑onset asthma. Am J Respir Crit Care Med 1995;151:1635‑9.
2. Padrid P, Snook S, Finucane T, Shiue P, Cozzi P, Solway J, et al. Persistent airway hyperresponsiveness and histologic alterations after chronic antigen challenge in cats. Am J Respir Crit Care Med 1995;151:184‑93.
3. Kelly C, Ward C, Stenton CS, Bird G, Hendrick DJ, Walters EH. Number and activity of inflammatory cells in bronchoalveolar lavage fluid in asthma, and their relation to airway responsiveness. Thorax 1998;43:684‑92.
4. Johnson M. Combination therapy for asthma: Complementary effects of long‑acting ß2‑agonists and corticosteroids. Curr Allergy Clin Immunol 2002;15:16‑22.
5. Jarjour NN, Wilson SJ, Koenig SM, Laviolette M, Moore WC, Davis WB, et al . Control of airway inflammation maintained at a lower steroid dose with 100/50 microg of fluticasone propionate/salmeterol. J Allergy Clin Immunol 2006;118:44‑52.
6. Kips JC, O’Connor BJ, Inman MD, Svensson K, Pauwels RA, O’Byrne PM. A long‑term study of the anti‑inflammatory effect of low‑dose budesonide plus formoterol versus high‑dose budesonide in asthma. Am J Respir Crit Care Med 2000;161(Pt 1):996‑1001.
7. Matz J, Emmett A, Rickard K, Kalberg C. Addition of salmeterol to low‑dose fluticasone versus higher‑dose fluticasone: An analysis of asthma exacerbations. J Allergy Clin Immunol 2001;107:783‑9.
8. Olivieri D, Chetta A, Del Donno M, Bertorelli G, Casalini A, Pesci A, et al. Effect of short‑term treatment with low‑dose inhaled fluticasone propionate on airway inflammation and remodeling in mild asthma: A placebo‑controlled study. Am J Respir Crit Care Med 1997;155:1864‑71.
9. Shrewsbury S, Pyke S, Britton M. Meta‑analysis
of increased dose of inhaled steroid or addition of salmeterol in symptomatic asthma (MIASMA). BMJ 2000;320:1368‑73.
10. Sont JK, Willems LN, Bel EH, van Krieken JH, Vandenbroucke JP, Sterk PJ. Clinical control and histopathologic outcome of asthma when using airway hyperresponsiveness as an additional guide to long‑term treatment. The AMPUL study group. Am J Respir Crit Care Med 1999;159(Pt 1):1043‑51.
11. Boulet LP, Chakir J, Milot J, Boutet M, Laviolette M. Effect of salmeterol on allergen‑induced airway inflammation in mild allergic asthma. Clin Exp Allergy 2001;31:430‑7.
12. Hallsworth MP, Twort CH, Lee TH, Hirst SJ. β2‑Adrenoceptor agonists inhibit release of eosinophil‑activating cytokines from human airway smooth muscle cells. Br J Pharmacol 2001;132:729‑41.
13. Roberts JA, Bradding P, Britten KM, Walls AF, Wilson S, Gratziou C, et al. The long‑acting β2‑agonist salmeterol xinafoate: Effects on airway inflammation in asthma. Eur Respir J 1999;14:275‑82.
14. Sarir H, Mortaz E, Karimi K, Johnson M, Nijkamp FP, Folkerts G. Combination of fluticasone propionate and salmeterol potentiates the suppression of cigarette smoke‑induced IL‑8 production by macrophages. Eur J Pharmacol 2007;571:55‑61.
15. Singam R, Jena PK, Behera S, Hellermann GR, Lockey RF, Ledford D, et al. Combined fluticasone propionate and salmeterol reduces RSV infection more effectively than either of them alone in allergen‑sensitized mice. Virol J 2006;3:32.
16. Vanacker NJ, Palmans E, Pauwels RA, Kips JC. Effect of combining salmeterol and fluticasone on the progression of airway remodeling. Am J Respir Crit Care Med 2002;166:1128‑34.
17. Pace E, Gagliardo R, Melis M, La Grutta S, Ferraro M, Siena L, et al. Synergistic effects of fluticasone propionate and salmeterol on
[Downloaded free from http://www.indianjmedsci.org on Wednesday, January 22, 2014, IP: 95.38.81.151] || Click here to download free Android application for thisjournal

88 INDIAN JOURNAL OF MEDICAL SCIENCES
Indian Journal of Medical Sciences, Vol. 67, No. 3 and 4, March and April 2013
in vitro T‑cell activation and apoptosis in asthma. J Allergy Clin Immunol 2004;114:1216‑23.
18. Anderson GP. Interactions between corticosteroids and beta‑adrenergic agonists in asthma disease induction, progression, and exacerbation. Am J Respir Crit Care Med 2000;161:S188‑96.
19. Giannini D, Bacci E, Dente FL, Di Franco A, Vagaggini B, Testi R, et al. Inhaled beclomethasone dipropionate reverts tolerance to the protective effect of salmeterol on allergen challenge. Chest 1999;115:629‑34.
20. Boskabady MH, Kiani S, Aslani MR. Tracheal responsiveness to both isoprenaline and beta‑adrenoreceptor blockade by propranolol in cigarette smoke exposed and sensitized guinea pigs. Respirology 2006;11:572‑8.
21. Boskabady MH, Kiani S. The effect of exposure of guinea pigs to cigarette smoke and their sensit ization with ovalbumin in tracheal responsiveness to histamine and histamine (H1) receptor blockade by chlorpheniramine. Pathophysiology 2007;14:97‑104.
22. McCaig D. Comparison of autonomic responses in the trachea isolated from normal and albumin‑sensitive guinea‑pig. Br J Phamacol 1987;92:809‑16.
23. Sorkness RL, Remus JL, Rosenthal LA. Systemic and pulmonary effects of fluticasone administered through a metered‑dose inhaler in rats. J Allergy Clin Immunol 2004;14:1027‑32.
24. Boskabady MH, Aslani MR. Relaxant effect of Crocus sativus (saffron) on guinea‑pig tracheal
chains and its possible mechanisms. J Pharm Pharmacol 2006;58:1385‑90.
25. Blyth DI, Pedrick MS, Savage TJ, Hessel EM, Fattah D. Lung inflammation and epithelial changes in a murine model of atopic asthma. Am J Respir Cell Mol Biol 1996;14:425‑38.
26. Fujitani Y, Trifilieff A. In vivo and in vitro effects of SAR 943, a rapamycin analogue, on airway inflammation and remodeling. Am J Respir Crit Care Med 2003;167:193‑8.
27. Vanacker NJ, Palmans E, Kips JC, Pauwels RA. Fluticasone inhibits but does not reverse allergen‑induced structural airway changes. Am J Respir Crit Care Med 2001;163:674‑9.
28. Woodcock A, Custovic A. Allergen avoidance: Does it work? Br Med Bull 2000;56:1071‑86.
29. Juniper EF, Kline PA, Vanzieleghem MA, Ramsdale EH, O’Byrne P, Hargreave FE. Effect of long‑term treatment with inhaled corticosteroids on airway hyperresponsiveness and clinical asthma in non steroid‑dependent asthmatics. Am Rev Respir Dis 1990;142:832‑6.
30. Boskabady MH, Eslamizade MJ, Tabatabaei A, Nemati H, Mansouri F. Effect of inhaled fluticasone on lung inflammation administered during and after guinea pig sensitization. Arch Bronconeumol 2010;46:215‑22.
How to cite this article: Khazdair MR, Boskabady MH, Tabatabaee A, Hosseini M, Abbasnejad M. Effect of inhaled fluticasone and salmeterol on tracheal responsiveness and lung inflammation: Influence of administration time and allergen‑free period. Indian J Med Sci 2013;67:78‑88.Source of Support: Nil. Conflict of Interest: None declared.
[Downloaded free from http://www.indianjmedsci.org on Wednesday, January 22, 2014, IP: 95.38.81.151] || Click here to download free Android application for thisjournal
Copyright © 2022 FDOKUMEN




















