A single-blind, partial crossover clinical trial of the effects of inhaled fluticasone propionate...
12
VOLUME 63, No. 5, MAY 2002 A Single-Blind, Partial Crossover Clinical Trial of the Effects of Inhaled Fluticasone Propionate and Nedocromil Sodium on Airway Hyperresponsiveness to Methacholine Alessandro Vatrella, MD,’ Cirolamo Pelaia, MD,’ Roberto Parrella, MD,’ Loredana M. Lembo, MD,3 Rosa D. Crembiale, MD,’ Matte0 Sofia, MD,’ and Serafino A. Marsico, MD3 ‘Department of Clinical and Experimental Medicine, University of Naples “Federico II, u Naples, *Department of Experimental and Clinical Medicine, University “Magna Crcecia” of Catanzaro, Catanzaro, and 3Department of Cardiothoracic and Respiratory Sciences, 2nd University of Naples, Naples, Italy ABSTRACT Background: Airway inflammation plays a central role in the pathogenesis of asthma, even in the mildest forms and at the earliest stages. Therapeutic strategies now aim to relieve bronchoconstriction as well as focus primarily on controlling the underlying inflammatory process. Clinical trials of children and adults with asthma have demonstrated that inhaled corticosteroids and cro- mones (such as nedocromil sodium [NS]) improve symptoms and lung func- tion, as well as decrease nonspecific bronchial hyperresponsiveness. Objective: The aim of this study was to compare the effects of various anti- inflammatory therapeutic regimens using inhaled fluticasone propionate (FP) and/or NS on airway hyperresponsiveness to methacholine. Methods: Patients with mild, persistent asthma, who tested positive to a Dermatophagoides pteronyssinus skin prick test, were randomly assigned to 1 of 4 treatment groups: (1) FP for 16 weeks; (2) FP for 8 weeks, followed by NS for 8 weeks; (3) NS for 8 weeks, followed by FP for 8 weeks; or (4) NS for 16 weeks. Each patient was evaluated every 4 weeks. Results: Thirty-two patients with asthma (16 men and 16 women; age range, 18-48 years) were included in the study; 8 patients were randomly assigned to each of the 4 treatment groups. During treatment with FP alone, the provocative dose of methacholine required to induce a 20% decrease in forced expiratory volume in 1 second (PD& was significantly higher than that recorded during treatment with NS alone (P < 0.05 at weeks 12 and 16). However, both drugs induced progressive increases in PD,, versus baseline values throughout the study. Moreover, when FP was administered as the second drug (after NS), a Accepted for publication April 3, 2002. Printed in the USA. Reproduction in whole or part is not permitted. 0011-393x/02/$1 9.00 316
Transcript of A single-blind, partial crossover clinical trial of the effects of inhaled fluticasone propionate...

VOLUME 63, No. 5, MAY 2002
A Single-Blind, Partial Crossover Clinical Trial of the Effects of Inhaled Fluticasone Propionate and Nedocromil Sodium on Airway Hyperresponsiveness to Methacholine Alessandro Vatrella, MD,’ Cirolamo Pelaia, MD,’ Roberto Parrella, MD,’ Loredana M. Lembo, MD,3 Rosa D. Crembiale, MD,’ Matte0 Sofia, MD,’ and Serafino A. Marsico, MD3
‘Department of Clinical and Experimental Medicine, University of Naples “Federico II, u Naples, *Department of Experimental and Clinical Medicine, University “Magna Crcecia” of Catanzaro, Catanzaro, and 3Department of Cardiothoracic and Respiratory Sciences, 2nd University of Naples, Naples, Italy
ABSTRACT Background: Airway inflammation plays a central role in the pathogenesis
of asthma, even in the mildest forms and at the earliest stages. Therapeutic strategies now aim to relieve bronchoconstriction as well as focus primarily on controlling the underlying inflammatory process. Clinical trials of children and adults with asthma have demonstrated that inhaled corticosteroids and cro- mones (such as nedocromil sodium [NS]) improve symptoms and lung func- tion, as well as decrease nonspecific bronchial hyperresponsiveness.
Objective: The aim of this study was to compare the effects of various anti- inflammatory therapeutic regimens using inhaled fluticasone propionate (FP) and/or NS on airway hyperresponsiveness to methacholine.
Methods: Patients with mild, persistent asthma, who tested positive to a Dermatophagoides pteronyssinus skin prick test, were randomly assigned to 1 of 4 treatment groups: (1) FP for 16 weeks; (2) FP for 8 weeks, followed by NS for 8 weeks; (3) NS for 8 weeks, followed by FP for 8 weeks; or (4) NS for 16 weeks. Each patient was evaluated every 4 weeks.
Results: Thirty-two patients with asthma (16 men and 16 women; age range, 18-48 years) were included in the study; 8 patients were randomly assigned to each of the 4 treatment groups. During treatment with FP alone, the provocative dose of methacholine required to induce a 20% decrease in forced expiratory volume in 1 second (PD& was significantly higher than that recorded during treatment with NS alone (P < 0.05 at weeks 12 and 16). However, both drugs induced progressive increases in PD,, versus baseline values throughout the study. Moreover, when FP was administered as the second drug (after NS), a
Accepted for publication April 3, 2002. Printed in the USA. Reproduction in whole or part is not permitted. 0011-393x/02/$1 9.00
316

A. VatreNa et al.
further increase in PD,, compared with the values at week 8 occurred at both week 12 (P < 0.01) and week 16 (P < 0.001). In contrast, when NS was adminis- tered after 8 weeks of treatment with FP, methacholine PDzO decreased signifi- cantly compared with week 8 (P < 0.001 and P < 0.01 at weeks 12 and 16, respectively).
Conclusions: Our results suggest that, in this limited population of asthmatic patients who were treated for 16 weeks, FP was effective in increasing the PD,, and that NS exerted an effective, progressive protective action against bron- chial hyperresponsiveness to methacholine, thereby partially limiting the nega- tive consequences of FP withdrawal on airway inflammation.
Key words: fluticasone, nedocromil, airway hyperresponsiveness. (Cur-r Ther Res Clin Exp. 2002;63:316-327)
INTRODUCTION Because airway inflammation is known to play a central role in the pathogen- esis of asthma, even in the mildest forms and at the earliest stages,’ therapeutic strategies now aim not only at relieving bronchoconstriction but focus primar- ily on controlling the underlying inflammatory process. Inhaled glucocorticoids are widely used for the treatment of asthma when its severity causes shortness of breath during the day and frequent awakenings during the night, thus inter- fering with quality of life and requiring long-term use of beta,-adrenergic ago- nists more than once daily.’ However, long-term corticosteroid treatment may produce systemic and/or local side effects, such as dysphonia and oral candi- diasis.3 Systemic effects of inhaled corticosteroids depend on both the drug fraction reaching the intrapulmonary airways, where it is almost completely absorbed into the systemic circulation, and the amount of drug deposited in the oropharynx (-80% to 90%) where it is swallowed and then absorbed into the circulation from the gastrointestinal tract.4 Although systemic side effects are rare, they may include suppression of hypothalamic-pituitary-adrenal axis and reduced prepubertal growth.3 Moreover, further information is needed about the possible negative effects of inhaled glucocorticoids in patients with dis- eases such as diabetes, osteoporosis, and hypertension, conditions that are considered relative contraindications to the use of these drugs.
To avoid the use of corticosteroids, other anti-inflammatory drugs (eg, leu- kotriene modifiers and cromones5) are sometimes used for asthma treatment. Cromones include disodium cromoglycate and nedocromil sodium (NS), a so- dium salt of pyranoquinoline tricyclic dicarboxylic acid, whose antiallergic and anti-inflammatory properties have been demonstrated both in vitro and in vivo.6T7 NS inhibits both early- and late-phase asthmatic responses induced by allergen challenge,8 and it can prevent bronchoconstriction induced by exer- cise,g310 inhaled sulfur dioxide,” cold air,‘* distilled water,13’14 substance P,15 and adenosine.16 Furthermore, NS appears to reduce airway hyperresponsive-
317

CURRENT THERAPEUTIC RESEARCH@
ness to inhaled histamine17 and methacholine. *‘J’ Another positive feature of NS is its nearly complete lack of significant side effects.”
Clinical trials involving adults and children with asthma have demonstrated that inhaled corticosteroids and NS improve symptoms and lung function, and decrease nonspecific bronchial hyperresponsiveness.387v21.22 Comparison of the therapeutic properties of NS and inhaled glucocorticoids (eg, beclomethasone dipropionate and budesonide) suggests that glucocorticoids possess greater antiasthma activity than N?x*~,*~
To further investigate whether patients with mild, persistent asthma may reduce their use of inhaled steroids by receiving an alternative form of treat- ment, we compared the effects of fluticasone propionate (FP) (200 pg daily) and NS (8 mg daily) on airway hyperresponsiveness to methacholine. The low dos- age of FP was chosen because a recent review25 of clinical studies showed that 50 to 250 pg of this drug, given twice daily for 4 to 24 weeks, effectively con- trolled mild to moderate asthma in adolescents and adults.
The aim of our study was to compare the effects of different therapeutic regimens using FP and/or NS on nonspecific bronchial hyperresponsiveness, which is a reliable marker of airway inflammation.
PATIENTS AND METHODS
Patients Patients with mild, persistent asthma were recruited for the study from the outpatient department (Table l). The study protocol was approved by the eth- ics committee of “V. Monaldi” University Hospital, Naples, Italy. Informed writ- ten consent was obtained from each patient entering the study.
Patients were included in the study if they met the following criteria: (1) presence of mild persistent asthma according to National Heart, Lung, and Blood Institute/World Health Organization standards*; (2) prechallenge forced expiratory volume in 1 second (FEV,) 280% of the predicted value; (3) increase in FEV, 215% in response to 200 pg of inhaled salbutamol; (4) presence of bronchial hyperresponsiveness, with a provocative dose of inhaled methacho- line causing a 20% fall in FEV, from prechallenge values (PD20) 900 pg; and (5) atopy, with a positive skin test reaction only to house dust mites, and high total and mite-specific immunoglobulin E serum levels.
Patients were excluded from the study if they had used corticosteroids, cromones, theophylline, leukotriene modifiers, or antihistamines within 8 weeks of entering the study, or if they had an upper respiratory tract infection.
Study Design The study was carried out according to a randomized, partial crossover, single- blind design. After a 2-week washout period, patients were randomly divided into 4 groups; 2 groups received FP (50 pg/puff, 2 puffs twice daily) and 2 received NS (2 mg/puff, 2 puffs twice daily) from a metered dose inhaler (MDI).
318

A. VoWello et al,
Table 1. Patient characteristics by treatment group.
Patient No. Sex AgeW Height(cm) FEV, (% pred) PD,, @g)
FP+ FP 1 2 3 4 5 6 7 8
Mean +SD
FP+NS 9
10 11 12 13 14 15 16 Mean +SD
NS+FP 17 18 19 20 21 22 23 24 Mean+SD
NS+NS 25 26 27 28 29 30 31 32 Mean+SD
F F F F M M F M
F M F M M F F M
M M M M F F F M
F F F M F M M M
22 151 80 56 25 158 84 70 31 165 93 215 23 165 91 330 20 185 86 70 26 173 83 235 24 167 90 90 30 175 87 120
25.1 + 3.8 167.4 + 10.5 86.8 -I- 4.4 148.3 + 100.0
33 166 94 135 18 158 92 350 31 160 97 90 21 173 81 55 22 161 86 80 26 172 84 110 30 168 96 280 28 175 88 100
26.1 + 5.3 166.6 + 6.5 89.8 + 5.9 150.0 + 106.1
24 183 93 70 23 178 91 100 18 164 84 70 27 172 81 190 28 165 92 160 25 167 90 150 27 170 84 45 24 180 92 215
24.5 + 3.2 172.4 + 7.2 88.4 + 4.6 125.0 + 62.4
24 166 87 350 48 158 84 85 18 160 95 180 24 173 86 30 34 161 90 110 32 172 94 250 30 168 89 145 26 175 83 75
29.5 + 9.1 166.6 + 6.5 88.5 + 4.4 153.1 + 104.7
FEV, = forced expiratory volume in 1 second; PD,, = the provocative dose of methacholine required to induce a 20% decrease in FEV,; FP + FP = fluticasone propionate (FP) for 16 weeks; F = female; M = male; FP + NS = FP for 8 weeks, followed by nedocromil sodium (NS) for 8 weeks; NS + FP = NS for 8 weeks, followed by FP for 8 weeks; NS + NS = NS for 16 weeks.
319

CURRENT THERAPEUTIC RESEARCH@
Group assignment was not stratified by any selected variable, and randomiza- tion was casual. Although the study was initially planned as a double-blind trial, it was later converted to a single-blind design because some patients experi- enced a bitter taste when inhaling NS, a known side effect of this drug.
After 8 weeks of active therapy, 1 FP group and 1 NS group were randomly selected to switch to the other treatment (ie, FP to NS or NS to FP), while the other 2 groups continued the same treatment (Figure 1). This second treatment period also lasted 8 weeks. Thus, at the end of the study, the patients had been assigned to 1 of 4 treatment regimens: (1) FP for 16 weeks; (2) FP for 8 weeks, followed by NS for 8 weeks; (3) NS for 8 weeks, followed by FP for 8 weeks; and (4) NS for 16 weeks.
During the trial, patients were allowed to inhale salbutamol from an MD1 as rescue medication; no other antiasthma drug was permitted. Compliance was assessed on the basis of symptom monitoring and the need for rescue medi- cation. Adverse events were assessed on a clinical basis, thus checking for dysphonia/hoarseness, oral candidiasis, and cough.
Pulmonary Function and Methacholine Challenge At the end of the 2-week washout period, and after 4, 8, 12, and 16 weeks of active treatment, pulmonary function and methacholine responsiveness were assessed. Salbutamol and study medications were withheld for at least 12 hours before performing the tests. FEV,, which was obtained with a Spirostar FG-90 (Werner Gut AG, Basel, Switzerland), was used as a measure of bronchial cali- ber; the best of 3 consecutive measurements was chosen. Methacholine was administered by a metered nebulizer dosimeter (MB3, Mefar, Brescia, Italy) connected to a mouthpiece and activated by patient inspiratory maneuver. Two solutions of lyophilic methacholine (0.2% and 1%) (Lofarma, Milan, Italy) were freshly prepared from powder preparations by dilution in distilled wa- ter. The dosimeter was activated for 0.6 second to provide an output of
NS NS 1
I I I 2 Weeks 8 Weeks 8 Weeks
Figure 1. Study design. FP = fluticasone propionate; NS = nedocromil sodium.
320

A. Vatrella et al.
9.9 f 0.25 pg/puff. After baseline measurements of FEV,, phosphate buffer was inhaled (5 breaths), followed by cumulative doses of methacholine (from 20 to 2400 ug). FEV, was measured 1 minute after phosphate buffer inhalation, and all subsequent changes in FEV, were compared with the postbuffer value. Inhalations were performed while the nose was clipped and consisted of a slow submaximal inspiratory maneuver starting at functional residual capacity. The test was discontinued if FEV, dropped >20% or if the highest dose of metha- choline was reached. Dose-response curves were constructed by plotting the logarithmic value of the dose against the percent decrement in FEV,. PD,, was calculated by linear interpolation between the last 2 points.
Statistical Analysis The Student t test for paired data was used to analyze changes within groups; differences among groups were analyzed using l-way analysis of variance and Student t test for unpaired observations. P < 0.05 was considered statistically significant.
RESULTS Thirty-two patients with asthma (16 men and 16 women; age range, 18-48 years) who were allergic to house dust mites were included in the study (Table l). All enrolled patients completed the study. Baseline methacholine PD,, values were not significantly different among the various groups.
All treatments increased methacholine PD,, compared with baseline values at each measurement point+ 8, 12, and 16 weeks (Table If). Patients who received FP alone had larger changes in PD,, than those who received NS alone. In fact, mean PD,, values recorded after treatment with FP were always higher than those recorded after NS (Figure 2) with significant differences detectable at weeks 12 and 16 (P < 0.05). Treatments with either FP or NS induced pro- gressive improvements throughout the study in the pharmacologic effects of these drugs, with significant differences still occurring at week 12 compared with week 8 PD,, values (P < 0.001 for the FP group and P < 0.05 for the NS
group). When administered after NS, FP elicited a further decrease in airway hyper-
responsiveness to methacholine (Figure 2) with PD,, being significantly increased compared with week 8 at both week 12 (P < 0.01) and week 16 (P < 0.001). In contrast, when administered after FP, NS produced a signifi- cant decrease in methacholine PD,, values at week 12 (P < 0.001) and week 16 (P < 0.01) compared with values at week 8 (Figure 2).
No clinically relevant adverse events were reported during the trial.
DISCUSSION Because bronchial hyperresponsiveness appears to be closely related to airway inflammation, thereby largely responsible for the functional and clinical mani-
321
CURRENT THERAPEUTIC RESEARCH@
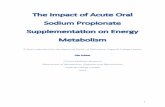
Table II. After-treatment values (pg)ofthe provocative dose of methacholine required to induce a 20% decrease in forced expiratoryvolume in 1 second.
Week No.
Patient No. Baseline 4 8 12 16
FP+ FP 1 2 3 4 5 6 7 8
Mean+SD
FP+NS 9 10 11 12 13 14 15 16 Mean + SD
NS+FP 17 18 19 20 21 22 23 24 Mean + SD
NS+NS 25 26 27 28 29 30 31 32 Mean+ SD
56 153 185 243 295 70 290 400 440 500
215 420 480 560 580 330 550 560 600 710 70 290 350 480 520
235 465 525 610 630 90 240 335 420 505
120 235 275 315 360 148.3 + 100.0 330.4 + 134.4 388.8 + 128.3 458.5 +132.3 512.5 + 135.3
135 520 600 420 400 350 550 800 650 700 90 240 260 120 150 55 190 200 175 180 80 650 700 600 550
110 240 280 210 230 280 690 860 735 670 100 265 380 285 275
150.0 + 106.1 481.1 +205.1 510.0+261.6 399.4 + 237.1 394.4 + 220.6
70 175 300 450 600 100 95 120 180 180 70 180 175 200 300
190 280 280 470 460 160 150 180 235 355 150 180 165 240 280 45 85 110 220 290
215 300 340 485 450 125.0 + 62.4 180.6 + 77.1 208.8 + 86.3 310.0 + 132.8 364.4 + 132.5
350 505 580 650 720 85 160 150 235 260 180 190 200 190 210 30 50 200 220 300
110 70 100 110 100 250 325 350 480 560 145 160 180 180 205 75 110 145 200 185
153.1 +104.7 196.3 + 150.9 238.1 + 156.4 283.1 +183.6 317.5 +211.6
FP + FP = fluticasone propionate (FP) for 16 weeks; FP + NS = FP for 8 weeks, followed by nedocromil sodium (NS) for 8 weeks; NS + FP = NS for 8 weeks, followed by FP for 8 weeks; NS + NS = NS for 16 weeks.
322

A. Vatrella et al.
4 Fluticasone pro ionate -o- Nedocromil so d? wm
600 ,
Baseline I I I I
4 8 12 16
Time (weeks)
Figure 2. Mean provocative dose causing a 200/6 fall in forced expiratory volume in 1 second (PDzO) of inhaled methacholine recorded at baseline and 4, 8, 12, and 16 weeks after treatment with fluticasone propionate and/or nedocromil sodium. Significant differences (vs baseline PD,, values) detected for each of the 4 therapeutic regimens: *P -C 0.01; +P < 0.0001; *P < 0.05.
festations of asthma, the present study was designed to compare the anti- inflammatory action of 2 currently available inhaled antiasthma drugs-a ste- roidal (FP) and a nonsteroidal (NS) compound. For this reason, a simple, reproducible model of airway hyperresponsiveness-the bronchoconstrictive response to methacholine-was chosen for use in this study.
Although the effectiveness of inhaled corticosteroids in asthma therapy is well known, the occurrence of systemic side effects-albeit uncommon- cannot be ruled out, especially when used as long-term treatments at high doses. Therefore, we attempted to determine whether an alternative anti- inflammatory agent such as NS could be used by patients with mild, persistent asthma to replace or at least reduce the overall consumption of steroids.
Our findings suggested that FP exerted a more powerful effect than NS, thus confirming the results of recent studies.23*24 Svendsen and Jorgensen26 treated 2 groups of 20 patients with asthma using beclomethasone dipropionate (400 pg daily) or NS (8 mg daily) for 6 weeks followed by crossover of treat- ments for another 6 weeks. However, although beclomethasone dipropionate was more effective than NS, the duration of the trial may have been too short, since NS sometimes requires up to 8 weeks to be fully effective.*’ A similar
323

CURRENT THERAPEUTIC RESEARCH@
study of 2 groups of 14 patients with atopic asthma was conducted by Groot et a1.17 They used higher doses of both drugs (beclomethasone dipropionate, 800 pg daily; NS, 16 mg daily); according to an experimental design, a first treatment with beclomethasone or NS for 8 weeks was then followed by a 3-week washout period, and finally a further &week crossover treatment with NS or beclomethasone. With regard to lung function and bronchial hyper- responsiveness to histamine and distilled water, beclomethasone was signifi- cantly more effective than NS, but the washout period (3 weeks) may have been so long that the findings could not be used to assess the activity resulting from consecutive administration of the 2 drugs.
Our present data indicate that FP provided better control of bronchial hy- perresponsiveness to methacholine than NS. The association between airway hyperresponsiveness to methacholine and ongoing bronchial inflammation un- derlying asthma is strongly supported by the studf7 that demonstrated that PC,, (provocative concentration) for methacholine was inversely related to the average number of total leukocytes, mast cells, activated eosinophils, and T lymphocytes infiltrating the airways of patients with asthma. This implies that FP interferes more effectively than NS with the biological mechanisms responsible for airway inflammation. Indeed, inhaled steroids-but not NS-are able to decrease the level of exhaled nitric oxide, 28Y2g which is considered to be a reliable marker of airway inflammation in patients with asthma. Moreover, topical corticosteroids are stronger than NS in inhibiting eosinophil survival and the release of granulocyte/macrophage colony-stimulating factor and in- terleukins 6 and 8 from nasal polyp epithelial cells.30-33
However, our study has also shown that NS was effective in protecting the airways of patients with atopic asthma against methacholine-induced broncho- constriction after 8, 12, and 16 weeks of treatment. Furthermore, the protective effect of NS significantly improved throughout the trial, even between week 12 and week 16. A similar pharmacodynamic pattern was displayed by FP, sug- gesting that shorter-term studies may underestimate the efficacy of the anti- inflammatory action of these drugs.
When NS was administered after treatment with FP, a significant reduction in the bronchoprotective effect obtained with the first drug was observed be- tween weeks 8 and 12. However, NS was able to maintain approximately the same level of protection between weeks 12 and 16, with no further significant decrease in methacholine PD,,, which remained well above the baseline values. This indicates that NS afforded a degree of control of airway inflammation at least up to 8 weeks after FP withdrawal, thus reducing the potentially negative impact due to the progressive loss of the carryover effect of inhaled steroids. Of course, abrupt interruption of FP was not totally compensated by subse- quent treatment with NS, but the latter drug provided a valid alternative to FP in patients with mild asthma. However, 8 weeks of treatment with FP adminis- tered as the second drug (after 8 weeks of treatment with NS, when the PD,, was higher than at baseline) did not improve PD,, as much as 8 weeks of
324

A. Vatrelia et al.
treatment with FP administered as the first drug (before 8 weeks of treatment with NS). This suggests that the anti-inflammatory mechanisms responsible for the effects of NS might partially overlap with those of glucocorticoids.
CONCLUSIONS In this selected population of patients with asthma, FP was effective in decreas- ing airway hyperresponsiveness to methacholine, and NS exerted progressive protection against methacholineinduced bronchoconstriction, thereby par- tially limiting the negative consequences of FP withdrawal.
1.
2.
3.
4.
8.
9.
10.
11.
12.
13.
14.
Laitinen LA, Laitinen A, Haahtela T. Airway mucosal inflammation even in patients with newly diagnosed asthma. Am Rev Respir Dis. 1993;147:697-704.
Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention. National Heart, Lung, and Blood Institute/World Health Organization Workshop Re- port. Bethesda, Md: National Institutes of Health; 1995. Publication no. 95-3659.
Barnes PJ, Pedersen S, Busse WW. Efficacy and safety of inhaled corticosteroids: New developments. Am J Respir Crit Care Med. 1998;157:Sl-S53. Edsblcker S, Szefler SJ. Glucocorticoid pharmacokinetics: Principles and clinical implications. In: Schleimer RP, Busse WW, O’Byrne PM, eds. Inhaled Glucocotiicoids in Asthma. New York: Marcel Dekker; 1997:381-426.
Rabe KF, Schmidt DT. Pharmacological treatment of asthma today. Eur Respir J 2001;18(supp1 34):34HOS.
Corin RE. Nedocromil sodium: A review of the evidence for a dual mechanism of action. Clin Exp Allergy. 2000;30:461-468.
Stelmach 1, Jerzynska J, Brzozowska A, Kuna P. Double-blind, randomized, placebo- controlled trial of effect of nedocromil sodium on clinical and inflammatory param- eters of asthma in children allergic to dust mite. Allergy. 2001;56:518-524.
Aalbers R, Kauffman HF, Groen H, et al. The effect of nedocromil sodium on the early and late reaction and allergen-induced bronchial hyperresponsiveness. JAllergy Clin Immunol. 1991;87:993-1001.
Konig P, Hordvik NL, Kreutz C. The preventive effect and duration of action of nedocromil sodium and cromolyn sodium on exercise-induced asthma (EIA) in adults. J Allergy Clin Immunol. 1987;79:64-68.
Spooner C, Rowe BH, Saunders LD. Nedocromil sodium in the treatment of exercise- induced asthma: A meta-analysis. Eur Respir J. 2000;16:30-37.
Jackson DM, Eady RP. Acute transient SO,-induced airway hyperreactivity: Effects of nedocromil sodium. J Appl Physiol. 1988;65:1119-1124.
Juniper EF, Kline PA, Morris MM, Hargreave FE. Airway constriction by isocapnic hyperventilation of cold, dry air: Comparison of magnitude and duration of protec- tion by nedocromil sodium and sodium cromoglycate. Clin Allergy. 1987;17:523-528.
Robuschi M, Simone P, Vaghi P, Bianco S. Prevention of fog-induced bronchocon- striction by nedocromil sodium. Eur J Respir Dis. 1986;69(Suppl 147):286-288.
Lavorini M, Fontana GA, Pantaleo T, et al. Fog-induced respiratory responses are attenuated by nedocromil sodium in humans. Am J Respir Crit Care Med. 2001;163: 1117-1120.
325

15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
CURRENT THERAPEUTIC RESEARCH@
Crimi N, Palermo F, Olivieri R, et al. Effect of nedocromil on bronchospasm induced by inhalation of substance P in asthmatic subjects. Clin Allergy. 1988;18:375-382.
Phillips CD, Scott VL, Richards R, Holgate ST. Effect of nedocromil sodium and sodium cromoglycate against bronchoconstriction induced by inhaled adenosine 5’ monophosphate. Eur Respir J. 1989;2:210-217.
Groot CAR, Lammers JW, Molema J, et al. Effect of inhaled beclomethasone and nedocromil sodium on bronchial hyperresponsiveness to histamine and distilled water. Eur Respir J. 1992;5:1075-1082.
Be1 EH, Timmers MC, Hermans J, et al. The long-term effects of nedocromil sodium and beclomethasone dipropionate on bronchial responsiveness to methacholine in nonatopic asthmatic subjects. Am Rev Respir Dis. 1990;141:21-28.
Orefice U, Struzzo P, Dorigo R, Peratoner A. Long-term treatment with sodium cro- moglycate, nedocromil sodium and beclomethasone dipropionate reduces bronchi- al hyperresponsiveness in asthmatic subjects. Respiration. 1992;59:97-101.
Becker JW, Bierman W. Prophylactic anti-asthma drugs. In: Page CP, Metzger WJ, eds. Drugs and the Lung. New York: Raven Press; 1994:221-256.
Juniper EF, Kline PA, Vanzieleghem MA, et al. Long-term effects of budesonide on air- way hyperresponsiveness and clinical asthma severity in inhaled steroid-dependent asthmatics. Eur Respir J. 1990;3:1122-1127.
North American Tilade Study Group. A double-blind multicenter group comparative study of the efficacy and safety of nedocromil sodium in the management of asthma. Chest. 1990;97:1299-1306.
Di Franc0 A, Giannini D, Bacci E, et al. Comparison of different long-term asthma treatments in subjects with mild-to-moderate asthma. Monaldi Arch Chest Dis. 1999; 54:390-393.
Long-term effects of budesonide or nedocromil in children with asthma. The Child- hood Asthma Management Program Research Group. N Engl J Med. 2000;343:1054- 1063.
Jarvis B, Faulds D. Inhaled fluticasone propionate: A review of its therapeutic effi- cacy at dosages < or = 500 microg/day in adults and adolescents with mild to moderate asthma. Drugs. 1999;57:769-803.
Svendsen UG, Jorgensen H. Inhaled nedocromil sodium as additional treatment to high dose inhaled corticosteroids in the management of bronchial asthma. Eur Respir J. 199 1;4:992-999.
Sont JK, Han J, van Krieken JM, et al. Relationship between the inflammatory infil- trate in bronchial biopsy specimens and clinical severity of asthma in patients treated with inhaled steroids. Thorax. 1996;51:496-502.
Gratziou C, Rovina N, Lignos M, et al. Exhaled nitric oxide in seasonal allergic rhi- nitis: Influence of pollen season and therapy. Clin Exp Allergy. 2001;31:409-416.
Carra S, Gagliardi L, Zanconato S, et al. Budesonide but not nedocromil sodium reduces exhaled nitric oxide levels in asthmatic children. Respir Med. 2001;95:734- 739.
Rota-Ferrer J, Mull01 J, Lopez E, et al. Effect of topical anti-inflammatory drugs on epithelial cell-induced eosinophil survival and GM-CSF secretion. Eur Respir J. 1997; 10:1489-1495.
Mull01 J, Lopez E, Rota-Ferrer J, et al. Effects of topical anti-inflammatory drugs on eosinophil survival primed by epithelial cells. Additive effect of glucocorticoids and nedocromil sodium. Clin Exp Allergy. 1997;27:1432-1441.
326

A. VatreNa et a/.
32. Mull01 J, Rota-Ferrer J, Xaubet A, et al. Inhibition of CM-CSF secretion by topical corticosteroids and nedocromil sodium. A comparison study using nasal polyp epi- thelial cells. Respir Med. 2000;94:428-431.
33. Xaubet A, Mull01 J, Rota-Ferrer J, et al. Effect of budesonide and nedocromil sodium on IL-6 and IL-8 release from human nasal mucosa and polyp epithelial cells. Respir Med. 2001:95:40!3-414.
Address correspondence to: Girolamo Pelaia, MD Policlinico Universitario “Mater Domini” Via T. Campanella 88100 Catanzaro Italy E-mail: [email protected]
327