
Dose response to inhaled nitric oxide in pediatric patients with pulmonary hypertension and acute...
7
to inhaled nitric oxide in pediatric dmonary hypertension and acute ,ess syndrome Thomas A. Nakagawa, MD, Amelia Morris, RN, BSN, Robert J. Gomez, MD, Santa J. Johnston, MD, P. Timothy Sbarkey, t~, and Arno L. Zaritsky, MD Objective: To determine the pulmonary vascular functional dose response to inhaled nitric oxide (NO) for infants and children with acute respiratory distress syndrome and pulmonary artery hypertension. Design: Prospective, clinical observational study. Setting: Thirteen-bed pediatric intensive care unit at a 168-bed children's hospital. Patients: Infants and children requiring mechanical ventilation with an oxygenation index greater than 10. Methods: Children with severe acute respiratory distress syndrome received inhala- tion therapy with NO after conventional mechanical ventilation failed to result in im- provement. Inhaled NO was sequentially titrated from 10 parts per million to 20, 40, 60, and 80 ppm at 10-minute intervals. A reduction of at least 30% in the pulmonary vascular resistance index (PVRI), or a reduction in mean pulmonary artery pressure of at least 10%, or an increase in the hypoxemia score of at least 20%, or a decrease in the oxygenation index of at least 20% from pretreatment values was considered a thera- peutic response. After sequential titration, children who responded received continuous inhaled NO at the lowest dose associated with a therapeutic response. Continued on page 64 Acute respiratory distress syndrome re- mains a leading cause of morbidity and death in children) Contributing to this dis- ease process is a profound increase in pul- monary vascular resistance resulting in pul- monary hypertension. 2' 3 An elevated From the Divisionof PediatricCritical CareMedicineand the Departmentof Respiratory Care, ChiOren's Hospital of The King's Daughters, and the Departmentof Pediatrics, Eastern Virginia Medical Sehoo~No(olk, Virginia Submitted for publication June 26, 1996;accepted Jan. 29, 1997. Reprint requests: ThomasA. Nakagawa, MD, Children's Hospitalof The King'sDaughters, Divisionof Pediatric Critical Care, 601 Children's Lane, Norfolk,VA23507. J Pediatr 1997:131:63-9 Copyright© 1997 by Mosby-Year Book,Inc. 0022-3476/97/$5.00 + 0 9/21/80810 pulmonary vascular resistance results in right ventricular strain and diminishes car- diac output, 4 which results in impaired tis- sue oxygen delivery and subsequent multi- system organ dysfunction. This elevation in pulmonary vascular resistance results, in part, from damage to the vascular endotheli- urn, which diminishes production of endoge- nous nitric oxide. The vascular endothelium produces NO from a naturally occurring amino acid, L-arginine. N O activates soluble guanylate wclase, stimulating production of cyclic 3, 55monophosphate, which results in vascular and smooth muscle relaxation. 5 Studies show that exposure of constricted blood vessels to NO results in prompt relax- ation, with a short-lived effect of 3 to 5 sec- onds after removal of NO. 6 Endothelial dysfunction is considered to be a major contributing factor in the cause of pulmonary hypertension in adults with ARDS. 7-9 It is likely that the same mechanisms occur in infants and See related articles, pp. 55 and 70. children with severe lung disease. Inhalation of NO to replace deficient en- dogenous production resulting from in- jury to pulmonary endothelial cells pro- vides a rational therapeutic modality for the treatment of pulmonary hyperten- sion. Because inhaled NO selectively re- laxes the pulmonary microcirculation in ventilated areas of the lung, expected re- sults are improved pulmonary blood flow and correction of hypoxemia without systemic hypotension. These effects are well described in adults 7' 10, 11 and neo- nates, 12-14 but studies documenting the pulmonary vascular and oxygenation ef- fectslS, 16 and the optimal dose response to NO in pediatric patients with ARDS remain bruited. 63
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Dose response to inhaled nitric oxide in pediatric patients with pulmonary hypertension and acute...
to inhaled nitric oxide in pediatric dmonary hypertension and acute ,ess syndrome
Thomas A. Nakagawa, MD, Amelia Morris, RN, BSN, Robert J. Gomez, MD, Santa J. Johnston, MD, P. Timothy Sbarkey, t ~ , and Arno L. Zaritsky, MD
Objective: To determine the pulmonary vascular functional dose response to inhaled
nitric oxide (NO) for infants and children with acute respiratory distress syndrome
and pulmonary artery hypertension.
Design: Prospective, clinical observational study.
Setting: Thirteen-bed pediatric intensive care unit at a 168-bed children's hospital.
Patients: Infants and children requiring mechanical ventilation with an oxygenation
index greater than 10.
Methods: Children with severe acute respiratory distress syndrome received inhala-
tion therapy with NO after conventional mechanical ventilation failed to result in im-
provement. Inhaled NO was sequentially titrated from 10 parts per million to 20, 40,
60, and 80 ppm at 10-minute intervals. A reduction of at least 30% in the pulmonary
vascular resistance index (PVRI), or a reduction in mean pulmonary artery pressure of
at least 10%, or an increase in the hypoxemia score of at least 20%, or a decrease in the
oxygenation index of at least 20% from pretreatment values was considered a thera-
peutic response. After sequential titration, children who responded received continuous
inhaled N O at the lowest dose associated with a therapeutic response.
Cont inued on page 64
Acute respiratory distress syndrome re- mains a leading cause of morbidity and death in children) Contributing to this dis- ease process is a profound increase in pul- monary vascular resistance resulting in pul- monary hypertension. 2' 3 An elevated
From the Division of Pediatric Critical Care Medicine and the Department of Respiratory Care, ChiOren's Hospital of The King's Daughters, and the Department of Pediatrics, Eastern Virginia Medical Sehoo~ No(olk, Virginia
Submitted for publication June 26, 1996; accepted Jan. 29, 1997. Reprint requests: Thomas A. Nakagawa, MD, Children's Hospital of The King's Daughters, Division of Pediatric Critical Care, 601 Children's Lane, Norfolk, VA 23507. J Pediatr 1997:131:63-9 Copyright © 1997 by Mosby-Year Book, Inc. 0022-3476/97/$5.00 + 0 9/21/80810
pulmonary vascular resistance results in right ventricular strain and diminishes car- diac output, 4 which results in impaired tis- sue oxygen delivery and subsequent multi- system organ dysfunction. This elevation in pulmonary vascular resistance results, in part, from damage to the vascular endotheli- urn, which diminishes production of endoge- nous nitric oxide. The vascular endothelium produces NO from a naturally occurring amino acid, L-arginine. NO activates soluble guanylate wclase, stimulating production of cyclic 3, 55monophosphate, which results in vascular and smooth muscle relaxation. 5 Studies show that exposure of constricted blood vessels to NO results in prompt relax- ation, with a short-lived effect of 3 to 5 sec- onds after removal of NO. 6
Endothelial dysfunction is considered to be a major contributing factor in the cause of pulmonary hypertension in adults with ARDS. 7-9 It is likely that the same mechanisms occur in infants and
See related articles, pp. 55 and 70.
children with severe lung disease. Inhalation of N O to replace deficient en- dogenous production resulting from in- jury to pulmonary endothelial cells pro- vides a rational therapeutic modality for the treatment of pulmonary hyperten- sion. Because inhaled N O selectively re- laxes the pulmonary microcirculation in ventilated areas of the lung, expected re- sults are improved pulmonary blood flow and correction of hypoxemia without systemic hypotension. These effects are
well described in adults 7' 10, 11 and neo- nates, 12-14 but studies documenting the pulmonary vascular and oxygenation ef- fectslS, 16 and the optimal dose response to N O in pediatric patients with ARDS remain bruited.
63

NAKAGAWA ET AL.
Results: Fourteen children received 15 trials with inhaled N O (median age, 63.4
months; range, 0.4 to 201 months). One patient's condition deteriorated during the
titration phase, unrelated to NO treatment, and the patient was withdrawn from the
study protocol. The mean (+_SD) pretreatment oxygenation index was 35 +_ 15, which
decreased to 32 + 20 at 80 ppm of inhaled NO (p = 0.01). Ten children had pulmonary
artery catheter measurements. The PVRI decreased by 30% or greater in seven children
(70%). One child had a minimal decrease in PVRI during the titration phase but
demonstrated an increase of more than 30% after N O therapy was discontinued. Mean
pretreatment PVRI (270 _+ 105) decreased to 207 ± 92 dynes/see per cubic centimeter
per square meter at 80 ppm of inhaled N O (p = 0.06). Pretreatment mean pulmonary
artery pressure (31 _+ 7) decreased to 28 + 5 mm Hg at 80 ppm of inhaled NO (p = 0.04).
Six trials (43%) showed an increase of 20% or greater in their hypoxemia score.
Maximum improvement in the hypoxemia score and reduction in OI, PVRI, and mean
pulmonary artery pressure occurred at 20 to 40 ppm of NO. Ten trials led to continuous
inhaled NO therapy ranging from 7 to 661.5 hours, with a median of 47 hours.
Systemic hypotension was not observed in any patient, and the maximum
methemoglobin level was 5%.
Conclusion: Inhaled N O appears to be a safe, although variably effective, therapy for
the treatment of infants and children with acute respiratory distress syndrome. The max-
imu_m dose response occurs between 20 and 40 ppm of inhaled NO. Systemic side ef-
fects did not occur in any child who received NO therapy. (J Pediatr 1997;131:63-9)
Our study was designed to determine whether infants and children with ARDS and pulmonary hypertension respond to inhaled NO therapy titrated over a range of pharmacologic concentrations with a reduction in pulmonary artery pressures and improved oxygenation. Additionally, our study investigated whether hypoten- sion or methemoglobinemia occurred with inhaled N O therapy.
METHODS
This study protocol was approved by the institutional review board of Eastern Virginia Medical School and was in ac- cordance with the U.S. Food and Drug Administration's guidelines for an investi- gational new drug. Informed consent was obtained from the patient's parents or legal guardians before study enrollment.
Patients Infants and children with ARDS, de-
fined as acute hypoxemic respiratory fail- ure requiring mechanical ventilation as a result of diffuse parenchymal lung dis-
ease, 17 regardless of the cause, were in- cluded in this study. All children enrolled in this study had an oxygenation index of l0 or greater.
All patients had mechanical ventilation, with an FIo 2 of 0.7 or greater in the pres- sure control mode with either a Servo 900 C ventilator (Siemens Critical Care, Laurel, N.J.), a Newport Wave ventilator (Newport Medical Instruments, New- port, Calif.), or an Infant Star ventilator (Infrasonics Inc., San Diego, Calif.), ex- cept one child whose lungs were ventilat- ed with a SensorMedics model 3100a high-frequency oscillatory ventilator (SensorMedics Corp., Yorba Linda, Calif.). Peak inspiratory pressures were adjusted to maintain the partial pressure of carbon dioxide at 40 to 50 mm Hg. There was no predetermined upper limit of PIP or positive end-expiratory pres- sure. Arterial oxygen saturation measured by pulse o~,netry was maintained at 90% or greater with the use of PEEP or by in- creasing the FIo 2 .
A hypoxemia score (partial pressure of arterial oxygen/FIo 2 ratio) was calculated for each child before, during, and after
THE JOUP, NAL OF PEDmA'rRICS JUt.'( 1997
therapy with inhaled NO. Pulmonary artery catheters were used for continuous pulmonary artery pressure monitoring in children weighing more than 10 kg. Hemodynamic parameters derived from a pulmonary artery thermodilution catheter (Baxter Healthcare, Irvine, Calif.) were calculated with standard formulas and in- eluded pulmonary vascular resistance index, systemic vascular resistance index, pulmonary artery occlusion and mean pulmonary artery pressures, and cardiac index. An indwelling arterial catheter was used for continuous systemic arterial blood pressure monitoring as well as in- termittent sampling of arterial blood for blood gas analysis performed with stan- dard electrodes (model 288 blood gas an- alyzer, Ciba Coming, Medfield, Mass.). Methemoglobin levels were measured be- fore and during treatment with N O at 40 and 80 ppm by co-oximetry (model 270 co-oximeter analyzer, Ciba Corning).
Administration of Nitric Oxide Inhaled N O (Airco Gases, Murray
Hill, New Jersey), certified as medical grade with a concentration of 800 _+ 5 ppm blended with nitrogen, was administered through a closed ventilator circuit before use of the humidifier. Intermittent-flow ventilators were adapted so that continu- ous flow could be added in-line. Electrochemical analyzers (Dr~tger, Dragerwerk AG, Ltibeck, Germany) were used for continuous in-line monitor- ing of N O and nitrogen dioxide levels. Analyzers were placed before the humidi- tier, 24 inches distal to the NO adminis- tration port to allow adequate mixing of gases. The NO and NO 2 analyzers were calibrated with a reference standard gas of N O and N O 2 supplied by the manu- facturer. A low-flow meter (Bird Products, Palm Springs, Calif.) was used to control the concentration of N O ad- ministered. Exhaled gases were scav- enged through a suction unit connected to the wall vacuum line.
Study Protocol Baseline data included ventilator set-
tings, FIo 2, arterial blood gas analysis, methemoglobin level, and mean and pha-
64
THE JOURNAL OF PEDIATRICS Volume 1 3 I, N u m b e r I, Part I
NAKAGAWA ET AL.
sic arterial blood pressure. When a pul- monary artery catheter was used, addi- tional baseline data included mean and phasic pulmonary artery pressures, pul- monary artery occlusion pressure, cardiac index, PVRI, and SVRI. All patients had continuous monitoring of their heart rate, blood pressure, central venous pressure, respiratory rate, and pulse oxlrneter and end-tldal CO 2 measurements (Nellcor Inc., Hayward, Calif.).
Inhaled NO was continuously adminis- tered and sequentially titrated at 10-mlnute intervals from concentrations of 10 ppm to 20, 40, 60, and 80 ppm. Hemodynarrfic pa- rameters were measured and arterial blood gases were analyzed after each change in NO concentration. Methernoglobin levels were measured before and during N O titration at 40 and 80 ppm. Cardiac output was measured by thermodilution tech- nique and recorded as the average of five values obtained after injections of iced saline solution. Ventilator settings and in- otropic support remained unchanged dur- ing the titration phase of NO.
A therapeutic response to inhaled NO was defined by the following criteria: a re- duction in PVRI of at least 30%, or a re- duction in mean PAP of at least 10%, 18 or an improvement in the hypoxemia score or OI by 20% or greater. Those patients who demonstrated a therapeutic response to N O during the titration phase subse- quently received continuous N O therapy at the lowest close associated with a thera- peutic response. Patients receiving con- tinuous NO therapy had serial methemo- globin levels measured every 8 hours to monitor for toxic effects. Additionally, NO and NO 2 levels were continuously monitored by in-line electrochemical ana- lyzers. Nitrogen dioxide levels greater than 5 ppm were defined as toxic on the basis of the Centers for Disease Control and Prevention criteria. 19 Patients were weaned from NO therapy, at the discre- tion of the attending physician in the pe- diatric intensive care unit, when they were medically stable and able to tolerate a decrease in N O concentrations without an adverse affect on hemodynamic or oxygenation parameters. Patients were weaned from N O therapy by 10 ppm at
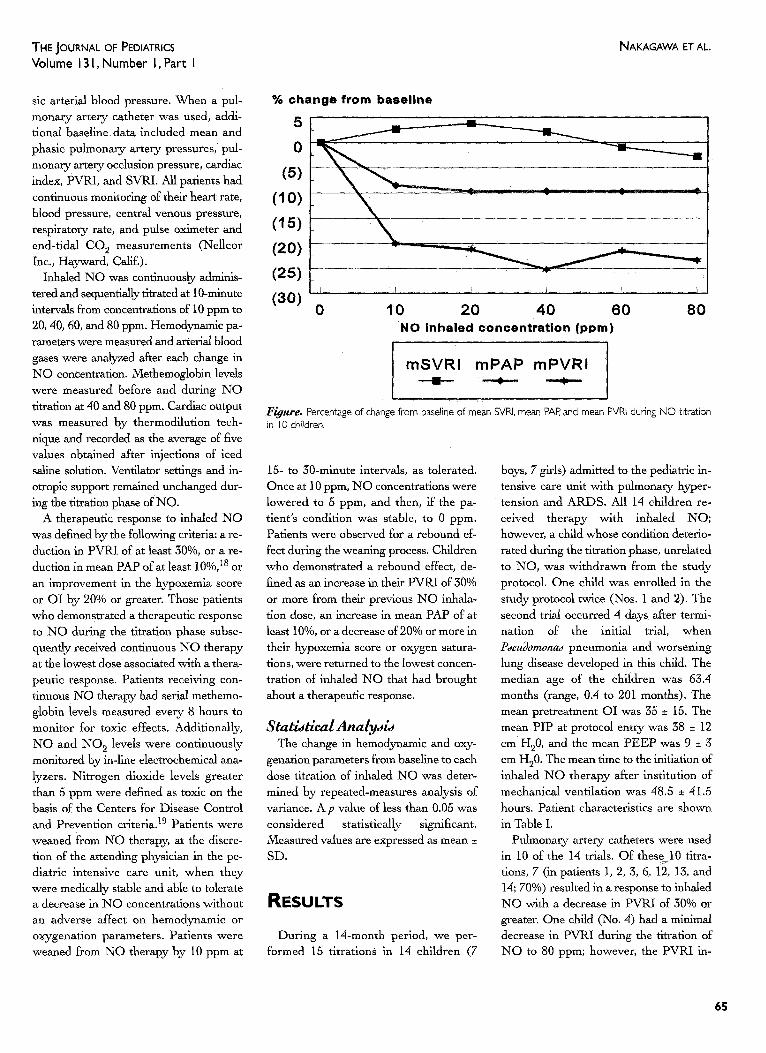
% change from basel ine
51 _ _ _
0
(5) (10)
(15) (20)
(25)
(30) 0 10 20 40 60
NO inhaled concentrat ion (ppm) 80
rnSVRI m P A P m P V R I
F~ure. Percentage of change from baseline of mean SVRI. mean PAR and mean PVRI during NO titration in I 0 children.
15- to 30-rninute intervals, as tolerated. Once at 10 ppm, N O concentrations were lowered to 5 ppm, and then, if the pa- tient's condition was stable, to 0 ppm. Patients were observed for a rebound ef- fect during the weaning process. Children who demonstrated a rebound effect, de- fined as an increase in their PVRI of 30% or more from their previous NO inhala- tion dose, an increase in mean PAP of at least 10%, or a decrease of 20% or more in their hypoxemia score or oxygen satura- tions, were returned to the lowest concen- tration of inhaled N O that had brought about a therapeutic response.
Statistical Analysis The change in hemodynamic arid oxy-
genation parameters from baseline to each dose titration of inhaled NO was deter- mined by repeated-measures analysis of variance. A p value of less than 0.05 was considered statistically significant. Measured values are expressed as mean ± SD.
R E S U L T S
During a 14-month period, we per- formed 15 titrations in 14 children (7
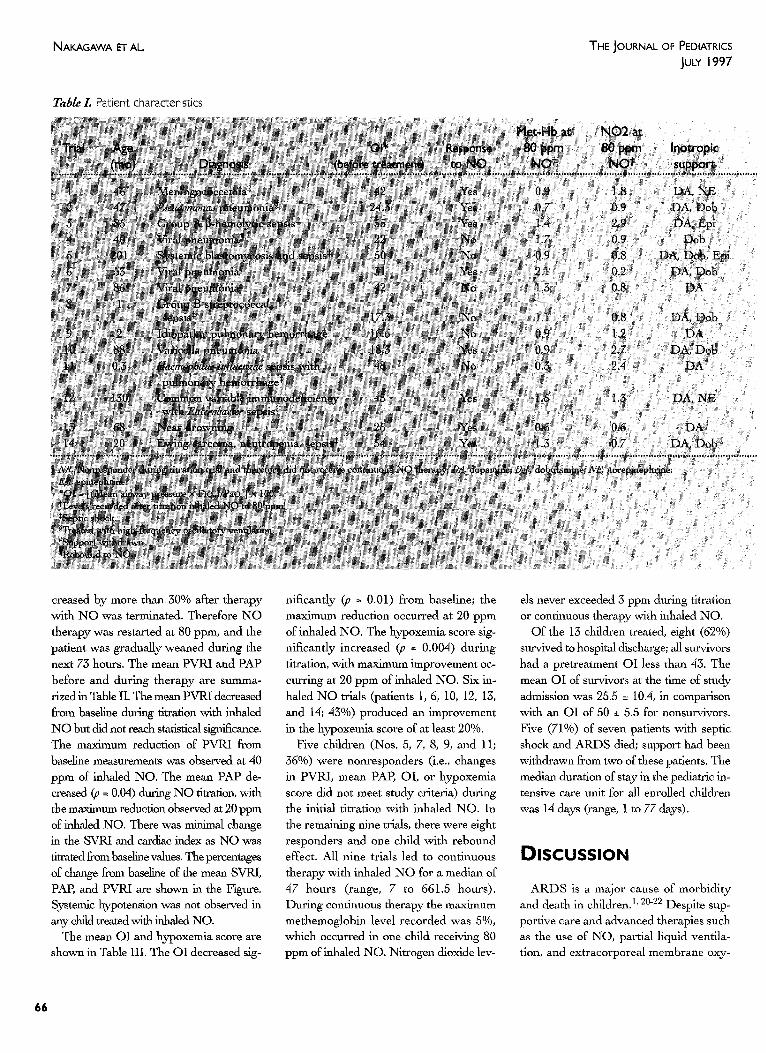
boys, 7 girls) admitted to the pediatric in- tensive care unit with pulmonary hyper- tension and ARDS. All 14 children re- ceived therapy with inhaled NO; however, a child whose condition deterio- rated during the titrafon phase, unrelated to NO, was withdrawn from the study protocol. One child was enrolled in the study protocol twice (Nos. 1 and 2). The second trial occurred 4 days after termi- nation of the initial trial, when Pseudomonas pneumonia and worsening lung disease developed in this child. The median age of the children was 63.4 months (range, 0.4 to 201 months), The mean pretreatment OI was 35 ± 15. The mean PIP at protocol entry was 38 ± 12 cm H20, and the mean PEEP was 9 ± 3 cm H20. The mean time to the initiation of inhaled N O therapy after institution of mechanical ventilation was 48.5 ± 41.5 hours. Patient characteristics are shown in Table I.
Pulmonary artery catheters were used in 10 of the 14 trials. Of these 10 titra- tions, 7 (in patients 1, 2, 3, 6, 12, 13, and 14; 70%) resulted in a response to inhaled NO with a decrease in PVRI of 30% or greater. One child (No. 4) had a minimal decrease in PVRI during the titration of N O to 80 ppm; however, the PVRI in-
65
NAKAGAWA ET AL. THE JOURNAL OF PEDIATRICS JuLY 1997
TaMe/. Patient characteristics
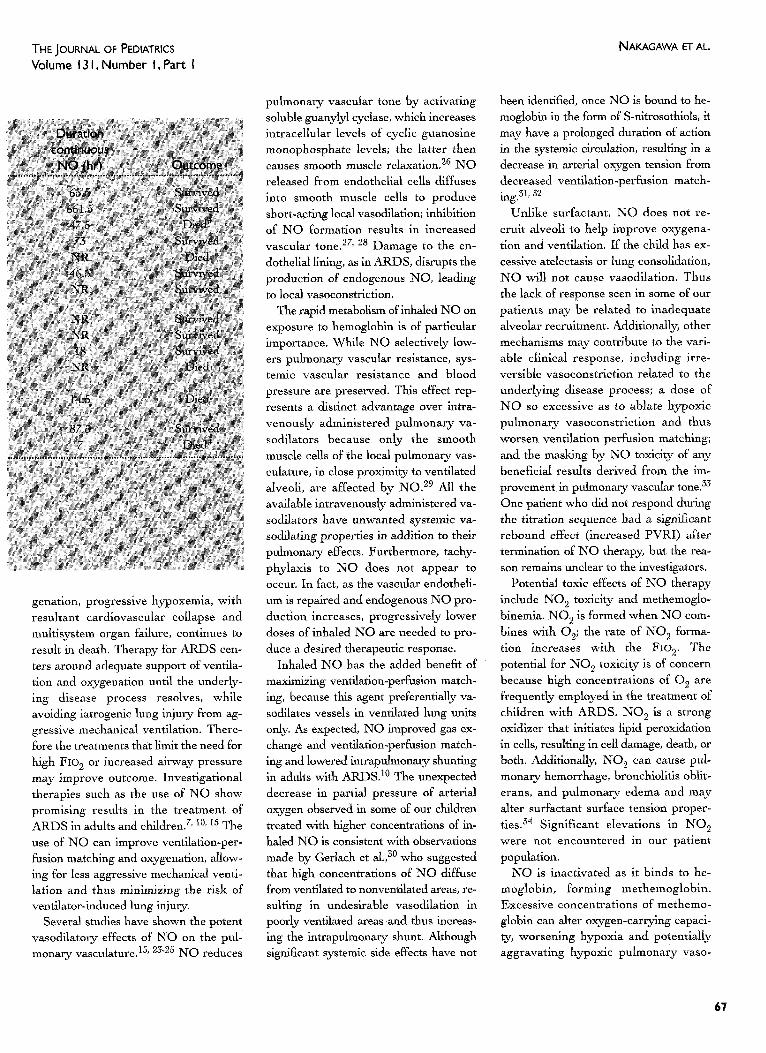
creased by more than 30% after therapy with N O was terminated. Therefore NO therapy was restarted at 80 ppm, and the patient was gradually weaned during the next 73 hours. The mean PVRI and PAP before and during therapy are summa- rized in Table II. The mean PVRI decreased from baseline during titration with inhaled NO but did not reach statistical significance. The maximum reduction of PVRI from baseline measurements was observed at 40 ppm of' inhaled NO. The mean PAP de- creased (p = 0.04) during NO titration, with the maximum reduction observed at 20 ppm of inhaled NO. There was minimal change in the SVRI and cardiac index as NO was titrated from baseline values. The percentages of change from baseline of the mean SVRI, PAP, and PVRI are shown in the Figure. Systemic hypotension was not observed in any child treated with inhaled NO.
The mean OI and hypoxemia score are shown in Table III. The OI decreased sig-
nificantly (p = 0.01) from baseline; the maximum reduction occurred at 20 ppm of inhaled NO. The hypoxemia score sig- nificantly increased (p = 0.004) during titration, with maximum improvement oc- curring at 20 ppm of inhaled NO. Six in- haled N O trials (patients 1, 6, 10, 12, 13, and 14; 43%) produced an improvement in the hypoxemia score of at least 20%.
Five children (Nos. 5, 7, 8, 9, and 11; 36%) were nonresponders (i.e., changes in PVRI, mean PAP, OI, or hypoxemia score did not meet study criteria) during the initial titration with inhaled NO. In the remaining nine trials, there were eight responders and one child with rebound effect. All nine trials led to continuous therapy with inhaled N O for a median of 47 hours (range, 7 to 661.5 hours). During continuous therapy the maximum methemoglobin level recorded was 5%, which occurred in one child receiving 80 ppm of inhaled NO. Nitrogen dioxide lev-
els never exceeded 3 ppm during titration or continuous therapy with inhaled NO.
Of the 13 children treated, eight (62%) survived to hospital discharge; all survivors had a pretreatment OI less than 43. The mean OI of survivors at the time of study admission was 25.5 ± 10.4, in comparison with an OI of 50 _+ 5.5 for nonsurvivors. Five (71%) of seven patients with septic shock and ARDS died; support had been withdrawn from two of these patients. The median duration of stay in the pediatric in- tensive care unit for all enrolled children was 14 days (range, 1 to 77 days).
DISCUSSION
ARDS is a major cause of morbidity and death in children)' 20-22 Despite sup- portive care and advanced therapies such as the use of NO, partial liquid ventila- tion, and extracorporeal membrane oxy-
66
THE JOURNAL OF PEDIATRICS Volume 13 I, Number I, Part I
NAKAGAWA ET AL.
genation, progressive bypoxemia, with resultant cardiovascular collapse and multisystem organ failure, continues to result in death. Therapy for ARDS cen- ters around adequate support of ventila- tion and oxygenation until the underly- ing disease process resolves, while avoiding iatrogenic lung injury from ag- gressive mechanical ventilation. There- fore the treatments that limit the need for high FIO 2 or increased airway pressure may improve outcome. Investigational therapies such as the use of NO show promising results in the treatment of ARDS in adults and children. 7' 10, 15 The use of NO can improve ventilation-per- fusion matching and oxygenation, allow- ing for less aggressive mechanical venti- lation and thus minimizing the risk of ventilator-induced lung injury.
Several studies have shown the potent vasodilatory effects of NO on the pul- monary vasculature. 15' 23.25 NO reduces
pulmonary vascular tone by activating soluble guanylyl cyclase, which increases intracellular levels of cyclic guanosine monophosphate levels; the latter then causes smooth muscle relaxation. 26 NO released from endothelial cells diffuses into smooth muscle cells to produce short-acting local vasodilation; inhibition of NO formation results in increased vascular t o n e . 27' 28 Damage to the en- dothelial lining, as in ARDS, disrupts the production of endogenous NO, leading to local vasoconstriction.
The rapid metabolism of inhaled NO on exposure to hemoglobin is of particular importance. While NO selectively low- ers pulmonary vascular resistance, sys- temic vascular resistance and blood pressure are preserved. This effect rep- resents a distinct advantage over intra- venously administered pulmonary va- sodilators because only the smooth muscle cells of the local pulmonary vas- eulature, in close proximity to ventilated alveoli, are affected by NO. 29 All the available intravenously administered va- sodilators have unwanted systemic va- soclilating properties in a d d i t i o n to their pulmonary effects. Furthermore, tachy- phylaxis to N O does not appear to occur. In fact, as the vascular endotheli- um is repaired and endogenous NO pro- duction increases, progressively lower doses of inhaled NO are needed to pro- duce a desired therapeutic response.
Inhaled NO has the added benefit of maximizing ventilatlon-perfusion match- ing, because this agent preferentially van sodilates vessels in ventilated lung units only. As expected, NO improved gas ex- change and ventilafion-perfusion match- ing and lowered intrapulmonary shunting in adults with ARDS. 10 The unexpected decrease in partial pressure of arterial oxygen observed in some of our children treated with higher concentrations of in- haled NO is consistent with observations made by Gerlach et al., ~0 who suggested that high concentrations of NO diffuse from ventilated to nonventilated areas, re- sulting in undesirable vasodilation in poorly ventilated areas and thus increas- ing the intrapulmonary shunt. Although significant systemic side effects have not
been identified, once NO is bound to he- moglobin in the form of S-nitrosothiols, it may have a prolonged duration of action in the systemic circulation, resulting in a decrease in arterial oxygen tension from decreased ventilation-perfusion match- ing.31, 52
Unlike surfactant, NO does not re- cruit alveoli to help improve oxygena- tion and ventilation. If the child has ex- cessive atelectasis or lung consolidation, NO will not cause vasodilation. Thus the lack of response seen in some of our patients may be related to inadequate alveolar recruitment. Additionally, other mechanisms may contribute to the vari- able clinical response, including irre- versible vasoconstriction related to the underlying disease process; a dose of NO so excessive as to ablate hypoxic pulmonary vasoconstriction and thus worsen ventilation perfusion matching; and the masking by NO toxicity of any beneficial results derived from the im- provement in pulmonary vascular tone. 33 One patient who did not respond during the titration sequence had a significant rebound effect (increased PVRI) after termination of NO therapy, but the rea- son remains unclear to the investigators.
Potential toxic effects of NO therapy include NO 2 toxicity and methemoglo- binemia. NO 2 is formed when NO com- bines with 02; the rate of NO~ forma- tion increases with the F~o 2. The potential for NO 2 toxicity is of concern because high concentrations of 0 2 are frequently employed in the treatment of children with ARDS. NO 2 is a strong oxidizer that initiates lipid peroxidation in cells, resulting in cell damage, death, or both. Additionally, NO 2 can cause pul- monary hemorrhage, bronchlolitis ohlit- erans, and pulmonary edema and may alter surfactant surface tension proper- ties. 54 Significant elevations in NO 2 were not encountered in our patient population.
NO is inactivated as it binds to he- moglobin, forming methemoglobin. Excessive concentrations of methemo- globin can alter oxygen-carrying capaci- ty, worsening hypoxia and potentially aggravating hypoxic pulmonary vaso-
67
NAKAGAWA El" AL. THE JOURNAL OF PEDIATRICS JULY 1997
Table II. Hemodynamic dose-response to inhaled NO in I0 children with pulmonary artery catheters
Tab& III. Change in oxygenation index and hypoxemia score in i4 children treated with inhaled NO
constriction. The NADH-dependent en- zyme responsible for reducing methemo- globin to hemoglobin is methemoglobln reductase. Neonates, American Indians, and Eskimos have limited methemoglo- bin reductase activity and are potentially at greater risk of having methemoglo- binemia than the general population, a5 Methemoglobin levels in excess of 5% were not appreciated during the t i trat ion phase in any of the children who partici- pated in our study. The one child with a methemoglobin level of 5% during con- tinuous N O therapy at 80 ppm required no treatment other than a decrease in the concentration of inhaled NO.
The overall mortality rate of all children enrolled in this study was 38%. This study was not designed to determine whether NO had any effect on the mortality rate; however, the high rate in children with an OI of more than 42 is consistent with ob- servations by Arnold et al.a6 Additionally, we observed a poor survival rate in pa- tients with septic shock complicated by ARDS, consistent with observations by DeBruin et al. 3z
Inhaled N O shows promise as a selec- tive pulmonary vasodilator in some chil- dren with pulmonary hypertension and ARDS. Inhaled N O appears safe with no apparent side effects, making it a more at- tractive agent for use in the treatment of pulmonary hypertension when compared with intravenously administered vasodila- tors. The maximum response to inhaled N O occurs between 20 and 40 ppm; high- er concentrations fail to decrease further the PVRI or mean PAP or to improve oxygenation.
, , a ¢ , ~,~ , > :
REFERENCES 1. Timmons OD, Dean JM, Vernon D.
Mortality rates and prognostic variables in children with aduk respiratory distress syn- drome. J Pedlatr 1991;119:896-9.
2. Zapol ZNI, Snyder MT. Pulmonary artery hypertension in severe acute respiratory failure. N Engl J Med 1977;296:476-80.
3. Katz R, Pollack M, Spady D. Cardio- pulmonary abnormalities in severe acute res- piratory failure. J Pedlatr 1984;104:357-64.
4. Fierobe L, Brunet F, Dhainaut J, Belghith M, Jira J, Santucci D, et al. Effect of in-
haled nitric oxide on right ventricular func- tion in adult respirato W distress syndrome. Am J Respir Crit Care Med 1995;181: 1414-9.
5. Palmer R, Ashton D, Moncada S. Vascular endothelial cells synthesize nitric oxide from L-arginlne. Nature 1988;333:664-6.
6. Griffith TM, Edward DH, Lewis M J, Newby AC, Henderson AH. The nature of endothelium-derlvad vascular relaxant fac- tor. Nature 1984;308:645-7.
7. Rossaint R, Herwig G, Schmidt-Ruhnke H, Dirk P, Lewandowski K, et al. Efficacy of inhaled nitric oxide in patients with se- vere ARDS. Chest 1995;107'.1107-15.
8. Cioffe W,, Hiroshi O. Inhaled nitric oxide in acute lung disease. New Horizons 1995; 3:73-85.
9. Moncada S, Higgs A. The L-arginine-nitric oxide pathway. N Engl O IVied 1993;329: 2002-12.
10. Rossaint R, Falke K, Lopez E Slama K, Pison U, Zapol W. Inhaled nkric oxide for the adult respiratory distress syndrome. N Engl J Ivied 1993;328:379-405.
11. Frostell C, Blomqvist H, Hedenstierna G, Lundberg J, Zapol WM. Inhaled nitric oxide selectively reverses human hypoxic pulmonary vasoconstriction without caus- ing systemic vasodilatinn. Anesthesiology 1993;78:427-35.
12, Roberts JD Jr, Chen T'L, Wain J, Polaner D, Dupuay P, Zapol WM. Inhaled nitric oxide is a selective pulmonary vasodilator of the hypoxic newborn lamb. Am Rev Respir Dis 1992;145:A208.
13. Kinsella JE Neish SR, Ivy DD, Shaffer, E, Abman SH. Clinical responses to prolonged treatment of persistent pulmonary hyperten- sion of the newborn with low doses of in- haled nitric oxide. J Pediatr 1993;123:103-8.
14. Roberts JD Jr, Polaner DM, Todres D, Lang P, Zapol WM. Inhaled nitric oxide: a selective pulmonary vasodilatur for the treatment of persistent pulmonary hyper-
68
THE JOURNAL OF PEDIATRICS Volume 13 I, Number I, Part I
NAKAGAWA ET AL.
tension of the newborn [abstract]. Circulation 1991;84:321.
15. Ahman S, Griebel J, Parker D, Schmidt J, Swanton D, Kinsella J. Acute effects of in- haled nitric oxide in children with severe hypoxemic respiratory failure. J Pediatr 1994;124:881-8.
16. Day R, Guarin M, Lynch J, Vernon D, Dean J. Inhaled nitric oxide in children with severe lung disease: results of acute and prolonged therapy with two concentra- tions. Crit Care Med 1996;24:215-21.
17. Bernard G, Arfgas A, Brigham K, Carlet J, Falke K, Hudson L, et al. Report of the American-European Consensus Conference on acute respiratory distress syndrome: deft- nitions, mechanism, relevant outcomes, and clinical trial coordination. J Crit Care 1994;9:72-81.
18. Palevsky H, Schloo B, Pietra G, Weber KT, Janicld JS, Rubin E, et al. Primary pul- monary hypertension: vascular structure, morphometry, and responsiveness to va- sodilating agents. Circulation 1989;80: 1207-21.
19. Centers for Disease Control. NIOSH rec- ommendations for occupational safety and health standards. MMWR Moth Mortal Wldy Rep 1988;37:1-29.
20. Tamburro RE, Bugnitz ME), Stidham GL. Alveolar:arterial oxygen gradient as a pre- dictor of outcome in patients with non- neonatal pediatric respiratory failure. J Pediatr 1991;119:935-8.
21. Davis SL, Furman DE Costarino AT. Adult respiratory distress syndrome in children: associated disease, clinical course and pre- dictors of death, d Pediatr 1993;123:35-45.
22. Lyrene RK, Truog WE. Adult respiratory distress syndrome in a pediatric intensive care unit: predisposing conditions, clinical course and outcome. Pediatrics 1982;6:790-5.
23. Kinsella JP, Neish SR, Shaffer E, Abman SH. Low-dose inhalation nitric oxide thera- py in persistent pulmonary hypertension of the newborn. Lancet 1992;340:819-20.
24. Roberts JD Jr, Lang P, Bigatello L, Vlahakes G J, Zapol WM. Inhaled nitric oxide in congenital heart disease. Circulation 1993;87:447-53.
25. Wessel D, Adatia I, Giglia M, Thompson J, Kulik T. Use of inhaled nitric oxide and acetylcholine in the evaluation of pulmonary hypertension and endothelial function after cardiopulmonary bypass. Circulation 1993; 88:2128-38.
26. Fratacci MD, Frostell CG, Chen TY, Wain JC, Robinson DR, Zapol WM. Inhaled ni- tric oxide: a selective pulmonary vasodilator of heparin-protamine vasoconstriction in sheep. Anesthesiology 1991;75:990-9.
27. Martin W, Villani G, Jothianandaus D, Furehgott R. Selective blockade of en- dothelium-dependent and glyceryl trini- trate-induced relaxation by hemoglobin and by methylene blue in the rabbit aorta. J Pharmacol Exp Ther 1985;232:708-16.
28. Cobb JP, Darmer RL. Nitric oxide and sep- tic shock. JAMA 1996;275:1192-6.
29. Frostell C, Fratacci MD, Wain JC, Jones R, Zapol WM. Inhaled nitric oxide: a selec- tive pulmonary vasodilator reversing hypoxic pulmonary vasoconstriction. Circulation 1991;83:2038-47.
30. Gerlach H, Rossalnt R, Pappert D, Falke KJ. Time course and dose-response of hi-
tric oxide inhalation for systemic oxygena- tion and pulmonary hypertension in pa- tients with adult respiratory distress syn- drome. Eur J Clin Invest 1993;23:499- 502.
31. Body S, HHartigan P, Sheman S, Forman V, Hurford W. Nitric oxide: delivery, measure- ment, and clinical application. J Cardio- thorac Vasc Anesth 1995;9:748-63.
32. Upchureh G, Welch G, Loscalzo J. S nl- trosothiols: chemistry, biochemistry, and bi- ologic actions. Adv Pharmacol 1995;34: 343-9.
33. Abman S, KinseUa J. Inhaled nitric oxide for persistent pulmonary hypertension of the newborn: the physiology matters. Pediatrics 1995;96:1153-5.
34. Azoulay E, Dupuls E, Torres M, Soler P. Pulmonary NO 2 toxicity in neonate and adult guinea pigs and rats. Environ Res 1983;30:322-9.
35. Bunn t-IF. Human hemoglobins: normal and abnurmal-methemoglobinemia. In: Nathan DG, Oski FA, editors. Hematology of infancy and childhood. 4th ed. Philadelphia: WB Saunders; 1993.
36. Arnold JN, Hanson JH, Toro-Figuero If), Gutierrez J, Berens R J, Anglin DL. Prospective, randomized comparison of high- frequency oscillatory ventilation and conven- tional mechanical ventilation in pediatric res- piratory failure. Crit Care Med 1994; 22:1530-9.
37. DeBruin W, Notterman D, Magid M, Godwin T, Johnston S. Acute hypoxemic respiratory failure in infants and children: clinical and pathologic characteristics. Crit Care Med 1995;20:1223-34.
69




















