
Acute Respiratory Distress Syndrome
90
ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF – Fresno November 4, 2017
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Acute Respiratory Distress Syndrome

ACUTE RESPIRATORY DISTRESS SYNDROME
Angel Coz MD, FCCP, DCEAssistant Professor of Medicine
UCSF – FresnoNovember 4, 2017

• No disclosures

OBJECTIVES
• IdentifycurrenttrendsandriskfactorsofARDS
• Describethepathophysiology
• Definephasesduringdevelopment
• Listclinicalmanifestations
• Listcriteriathatmustbepresentfordiagnosis
• DescribetreatmentforpatientswithARDS
• 1821 – Laennec Idiopathic lung anasarca
• 1925 – Sir William OslerUncontrolled septicemia leads to frothy pulmonary edema
HISTORY

INTRODUCTION
• Acuterespiratorydistresssyndrome(ARDS)
wasdescribed50yearsago
• Alveolarspacesfilledwithhyalinemembranes
• Substantialoutcomeimprovementovertime
• Commonandlethal/disabling

DEFINITION
CRITERIA – 1994
• Acuteonset
• Bilateral InfiltratesonChest-X-ray
• PCWP≤18mmHgornoclinicalevidenceofvolumeoverload
• Oxygenation:• PaO2 /FiO2 ≤300à Acute LungInjury(ALI)
• PaO2 /FiO2 ≤200à ARDS

JAMA.2012;307(23):2526-2533
BerlinDefinition- 2012
• Timing within oneweek
• Imaging bilateralopacitiesonCXRorChestCT
• Edema not fullyexplainedbycardiacfailureorvolumeoverload
• Oxygenation- Mild- Moderate- Severe
OnPEEP≥5cmH20200<PaO2/FiO2 ≤300mmHg100<PaO2/FiO2 ≤200mmHg
PaO2/FiO2 ≤100mmHg

1994Definition Berlin– 2012
ALI ARDS Mild Moderate Severe
Mortality 26 % 37% 27% 32% 45%
Progressionfrommild 29% 4%
Progression frommoderate 13%
Ventilatorfreedays(d) 20 12 20 16 1
Duration ofMVsurvivors(d) 5 7 5 7 9
JAMA.2012;307(23):2526-2533

EPIDEMIOLOGY

EPIDEMIOLOGY
• Population-basedestimatesrangefrom10to86casesper100,000person– years
• About200,000casesperyear
• Likelyunderreportedindevelopingcountries
• Causescanbedirectorindirect
NEngl JMed2005;353:1685-93
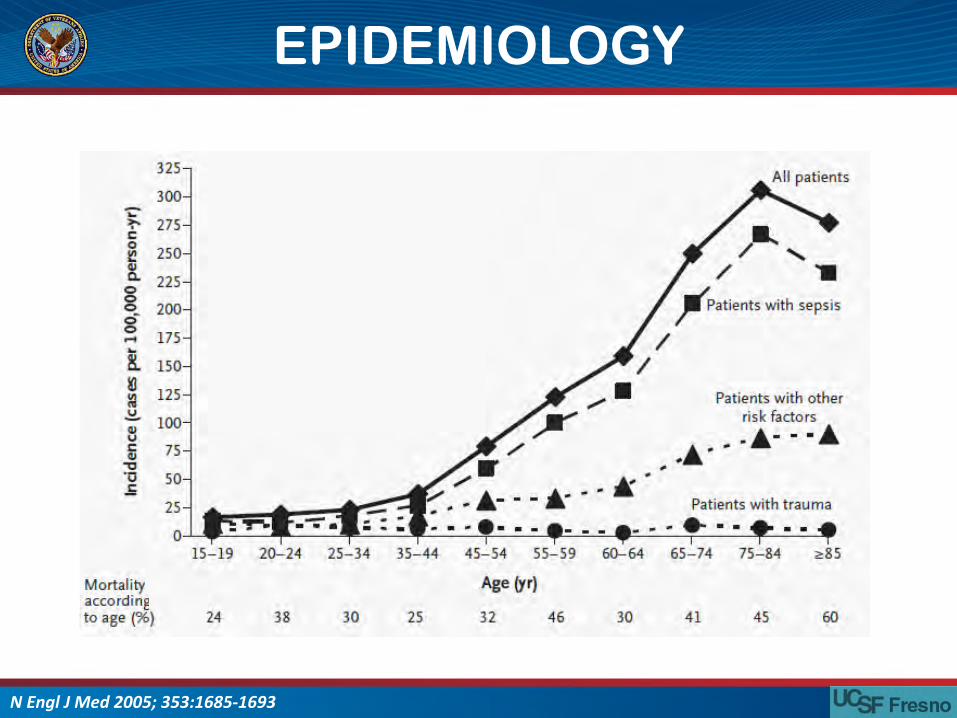
EPIDEMIOLOGY
NEngl JMed2005;353:1685-1693

DIRECT INDIRECT
• Pneumonia • Sepsis(nonpulmonary)
• Aspirationofgastriccontents • Nonthoracictrauma
• Pulmonarycontusion • Hemorrhagic shock
• Inhalationinjury • Pancreatitis
• Neardrowning • Major burninjury
• Transfusion
• Cardiopulmonarybypass
• Reperfusionedema aftertransplantorembolectomy
RISK FACTORS

ONSET TIME
AmJRespir Crit CareMed1995;151:293-301

PATHOPHYSIOLOGY

• DirectInjuryRegionalconsolidationfromdestructionofalveolararchitecture
• IndirectInjuryPulmonar vascularcongestion,interstitialedemaandlessseverealveolarinvolvement
PATHOPHYSIOLOGY

PHASES



• Systemicinflammation– Activationofcomplementandcoagulationsystems
– Stimulationofinflammatorycells– Releaseofproinflammatorymediators
• Sequestrationofneutrophilsinmicrovasculature
• Endothelialandepithelialdisruption
PATHOPHYSIOLOGY

• Exudationofproteinrichfluidfrommicrovasculatureintoalveolarandinterstitialspace
• Disruptionofsurfactant• Fibroticrepair• Failureofhypoxicvasoconstrictionresultinginseverehypoxemia
PATHOPHYSIOLOGY

PHASES

PHASES

CLINICAL PRESENTATION

• Pulmonary Edema
• Diffuse Alveolar
hemorrhage
• Pulmonary embolism
• Interstitial lung disease
• Pneumonia
• Pneumonitis
• Neoplasm
• Pulmonary contusion
• Atelectasis
• Emphysema
• Asthma
• Chronic Bronchitis
• Bronchiolitis
HYPOXEMIA

RADIOGRAPHIC FEATURES
• Diffuse bilateral infiltrates– Patchy, confluent– Alveolar, ground glass
• In contrast to heart failure, no prominence of – Cardiomegaly– Pleural effusion

CHEST CT

CHEST CT

• Hypoxia
• Tachypnea
• Decreasedcompliance
Δ VolumeC=
Δ Pressure
HALLMARKS OF DISEASE

SUMMARY
• Commonanddeadlydisease
• NewclassificationexcludesALI
• Causescanbeextrinsicorintrinsic
• Phases:exudative,proliferativeandfibrotic
• Hypoxemia,dyspneaandpoorlung
compliance

TREATMENT

• Treatunderlyingcondition
• Supportoxygenationandventilation
• Supportivenonventilatory therapy
• Rescueforrefractoryhypoxemia
TREATMENT

VENTILATOR SUPPORT

VENTILATOR ASSOCIATED LUNG INJURY
• Volutrauma
• Atelectotrauma
• Biotrauma

LUNG PROTECTIVE VENTILATION
NEngl JMed 2007;357:1113-20.

LUNG PROTECTIVE VENTILATION
• Lunginjuryisheterogeneous
BrJAnaesth2004;92:261±70

LUNG PROTECTIVE VENTILATION
NEngl JMed 2007;357:1113-20.

Parameter Conventional Protective
BAL%PMN ↑ ↓
BALTNF– α ↑ ↓
BALIL– 1β ↑ ↓
BALIL– 6 ↑ ↓
BALIL– 8 NoΔ ↓
PlasmaTNF– α ↑ NoΔ
PlasmaIL– 6 ↑ ↓
PlasmaIL– 8 NoΔ NoΔ
JAMA1999;282:54-61

LOW TIDAL VOLUME

NEngl JMed 1998;338:347-54

NEngl JMed 2000;342:1301-8
• Tidalvolume6ml/Kg(Idealbodyweight)
• Pplat<30cmH20
• AimforpH>7.2byincreasingRR
• AddbicarbonateifpH<7.15

P
t
V
t
PeakP
30
Vti =402Vte =400
HighPressure
PlatP
26
Ppeak =Pplat +Pres

NEngl JMed 2000;342:1301-8

NEngl JMed 2000;342:1301-8

Crit Care Med 2004;32:1260–1265

JournalofCriticalCare44(2018)72–76

RECRUITMENT MANEUVER

RECRUITMENT MANEUVER
WorldJCrit CareMed2015November4;4(4):278-286

NEngl JMed 2006;354:1775-86

CochraneDatabaseofSystematicReviews2016,Issue11.Art.No.:CD006667

JAMA.2017;318(14):1335-1345

PEEP

NEngl JMed2004;351:327-36
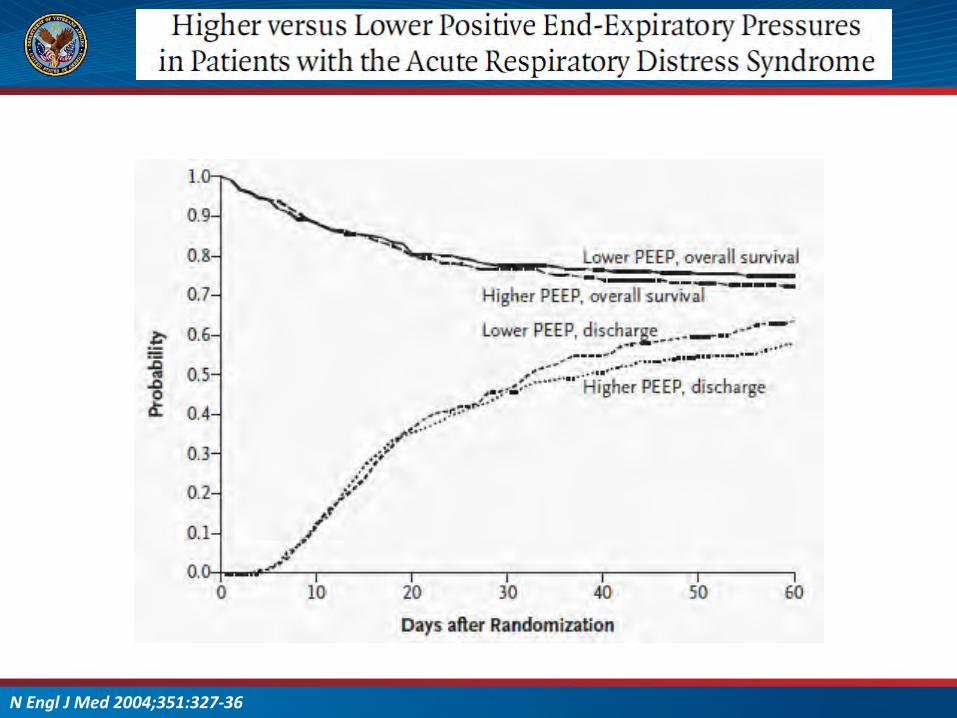
NEngl JMed2004;351:327-36

VENTILATORYSUPPORT
• Protectivelungstrategy:improvesmortality,organfailureandventilatordays– LowTV(<6ml/KgIBW)– Plateaupressure<30cmH20
• PEEPimprovesoxygenationbutnotmortality
• Recruitmentmaneuverscanworsenoutcomes

NON VENTILATORY SUPPORT

VOLUME STATUS

NEngl JMed2006;354:2564-75.

NEngl JMed2006;354:2564-75.

NEngl JMed2006;354:2564-75.

STEROIDS

NEngl JMed2006;354:1671-84.

NEngl JMed2006;354:1671-84.
PARAMETER Methylprednisolone Placebo Pvalue
60day mortality 29.2 28.6 1
180daymortality 31.5 31.9 1
Ventilatorfreedays(throughday28) 11.2 6.8 <0.001

PARALYTICS

• 340patients• Within48hoursofonset
• PaO2/FiO2 <150• Cisatracurium vsplacebo
NEngl JMed2010;363:1107-16

NEngl JMed2010;363:1107-16

PRONE POSITIONING


NEngl JMed2001;345:568-73

• 466patients
• PaO2/FiO2 <150
• Pronepositionwithin
firsthourof
randomization
• Pronefor≥16h/day
NEngl JMed2013;368:2159-68

NEngl JMed2013;368:2159-68

NON- VENTILATORYSUPPORT
• Fluidmanagement:decreasesdaysonventilator
• Corticosteroids:decreasesdaysonventilatorCanworsenmortalityifinitiatedafter14days
• ParalyticsinPaO2/FiO2 <150improvemortality
• PronepositioninginPaO2/FiO2 <150improvemortality

RESCUE STRATEGIES

OSCILLATORY VENTILATION

NEngl JMed 2013;368:806-13

NEngl JMed2013;368:795-805.
• Plannedfor1200
patients
• PaO2/FiO2 <200
• Stoppedat548patients

NEngl JMed2013;368:795-805.

INHALED NITRIC OXIDE

NEngl JMed2005;353:2683-95.

BMJ.2007Apr14;334(7597):779

Crit CareMed2014;42:404–412

Crit CareMed2014;42:404–412
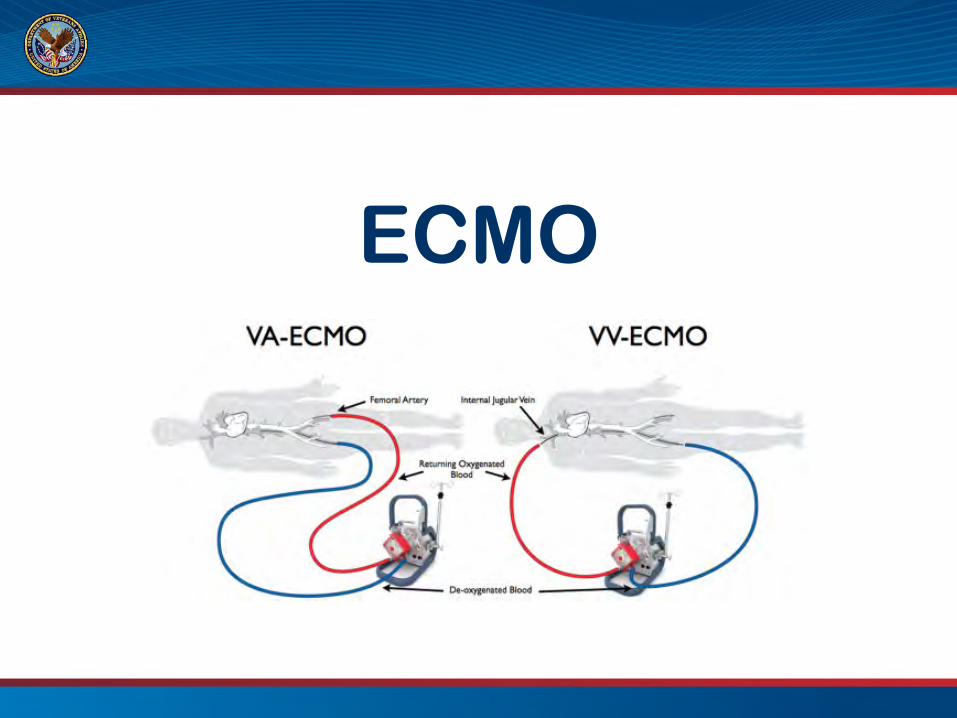
ECMO


• 180 patients PaO2/FiO2 <80• Conventional management vs referral for ECMO consideration
Lancet2009;374:1351–63

Lancet2009;374:1351–63
93% 70%PROTECTIVELUNGSTRATEGY

RESCUETHERAPIES
• HFOVcanworsenmortality.Increasesuseofsedativesandparalytics
• iNO:Improvesoxygenation.Noevidenceofmortalitybenefit
• ECMO:ConsiderinPaO2/FiO2 <80

FINALSUMMARY
• Hypoxemia,opacitiesandlowlungcompliance• Threephases:exudative,proliferativeandfibrotic• Lowtidalvolume:improvessurvival• PEEP:Improvesoxygenation• RecruitmentandHFOV:Couldbeharmful• Keepthemdryandsteroidsbutnotpast14days• ParalyticsandpronepositionforPaO2/FiO2 <150• iNO:improvesoxigenation butnotmortality• ECMO:Considerinsevere….moredataneeded

THANK [email protected]






















