
Induction immunotherapy in pediatric heart transplant recipients: a multicenter study
Upload
independentCategory
view
6download
0
CLINICAL THERAPEUTICSWOL. 20, NO. 5, 1998
Multicenter Comparative Trial of Ciprofloxacin Versus Cefuroxime Axetil in the Treatment of Acute Rhinosinusitis in a Primary Care Setting
Mark Weis, MD,’ Kim Hendrick, MD,2 Glenn Tillotson, MS,3 Kathleen Gravelle,3 and the Rhinosinusitis Investigation Group* ‘Private practice, Scottsville, Kentucky, 2Private practice, Flushing, Michigan, and 3Bayer Corporation, Phamaceutical Division, West Haven, Connecticut
ABSTRACT
In a primary care setting, the efficacy and safety of ciprofloxacin (CIP) 500 mg BID were compared with those of cefuroxime axetil (CA) 250 mg BID, each given for 10 days, in a nationwide, open, prospective,
randomized trial of 1414 adults with acute sinusitis. Patients were enrolled if they had clinically documented acute sinusitis (ie, rhinosinusitis) (~4 weeks’ duration), based on the 1997 American Academy of Otorhi- nolaryngology-Head and Neck Surgery cri- teria of either two major or one major and two minor symptoms. The primary efficacy variable was clinical response (resolution
or failure) at the posttherapy assessment on study days 14 through 26. The most com- mon presenting major signs and symptoms of acute rhinosinusitis were facial conges- tion, nasal drainage/purulence, facial pain/ pressure, and nasal obstruction/blockage. The minor symptom, headache, was more common and severe than was nasal ob- struction/blockage. A total of 12 19 patients were clinically evaluable. Clinical resolu- tion was observed in 559 of 613 (91.2%)
*The members of the Rhinosinusitis Investigation
Group are listed in the Acknowledgments.
0149.2918/98/$19.00
CIP-treated patients and 546 of 606 (90.1%) CA-treated patients. The two regimens were statistically equivalent (95% confidence in- terval, -2.16% to 4.71%). There were 80
drug-related adverse events reported in the (X-treated patients and 8 1 drug-related ad- verse events reported in the CA-treated pa- tients. The main adverse events were nau- sea (n = 18) and diarrhea (n = 7) in patients treated with CIP and diarrhea (n = 14) nau-
sea (n = 12), headache (n = 7) and vagini- tis (n = 7) in those treated with CA. CIP 500 mg BID was found to be statistically equivalent to CA 250 mg BID in the treat- ment of acute rhinosinusitis. Key words: ciprofloxacin, cefuroxime axetil, acute si- nusitis, primary care.
INTRODUCTION
Sinusitis is an inflammatory condition in- volving the accumulation of excessive mu-
cus, with nasal ostia blockage and the po- tential for the development of secondary bacterial infection.’ Acute sinusitis is of- ten a complication of a common cold or viral upper respiratory tract infection and is frequently preceded by rhinitis. This as- sociation has recently led experts to intro- duce the term “rhinosinusitis,” which more
921
CLINICAL THERAPEUTICS”
accurately describes the condition.2 Re- gardless of the underlying cause, rhinosi-
nusitis is associated with considerable morbidity and thus deserves appropriate diagnosis and treatment.
Acute rhinosinusitis is the most com- mon health complaint in the United States.2
It has been estimated that more than 1 bil- lion people are affected worldwide annu- ally.’ In the United States, approximately 0.5% to 2% of viral upper respiratory tract infections are believed to precipitate at least 20 million cases a year of acute commu- nity-acquired bacterial sinusitis.’ However,
it is difficult to establish the true incidence of rhinosinusitis, partially because it is a complex and challenging clinical diagno- sis.2 Many practitioners are familiar with
the characteristic symptoms and signs of acute rhinosinusitis, which may include nasal congestion, nasal obstruction, puru- lent drainage, tenderness over the affected sinuses, headache, and dental pain. Ac- cording to the Rhinosinusitis Task Force Committee convened by the American Academy of Otorhinolaryngology-Head
and Neck Surgery (AAOHNS), these and other major and minor factors associated with acute rhinosinusitis must be recog- nized to make the correct diagnosis.2 Ac- cording to the task force committee crite- ria, acute rhinosinusitis is considered a probable diagnosis if two major factors (symptoms) or one major and two or more minor factors are present.2 The symptoms and signs of acute rhinosinusitis are sud- den in onset and of limited duration (~4 weeks).2 After the symptoms resolve, the nasal mucosa returns to normal.
Advances in the diagnosis of rhinosi- nusitis using a rhinolaryngoscope have led to better assessment, care, and surgi- cal management.3 However, although rhi- nosinusitis is diagnosed by physician ex-
tenders, otorhinolaryngologists, allergists, and pulmonologists, it is in the primary care setting that acute rhinosinusitis is
most often recognized.2 Diagnosis is fol- lowed by appropriate treatment, often in- cluding antimicrobial agents.2
The objectives of treating acute rhinosi- nusitis include eradication of the infection, decreasing the duration of illness, and pre- venting complications (eg, chronic sinusitis
and central nervous system [CNS] infec- tions). Effective therapy should restore sterility and normal mucociliary function to the sinus cavity. Antimicrobial therapy should be instituted only for suspected bacterial infection. Antimicrobial therapy
has included beta-lactams, cephalosporins, trimethoprim-sulfamethoxazole, and, more recently, clarithromycin and fluoro- quinolones. However, only nine agents are
approved by the US Food and Drug Ad- ministration for the treatment of acute rhi- nosinusitis: cefuroxime axetil (CA),* amoxicillin/clavulanic acid,+ cefprozil,* lo-
racarbef,* clarithromycin,” levofloxacin,q ciprofloxacin (CIP),# trovafloxacin,** and sparfloxacin.t+ To varying degrees, these agents provide coverage of the most com-
*Trademark: Ceftin” (Glaxo Wellcome Inc., Re-
search Triangle Park, North Carolina).
tTrademark: Augmentin@ (SmithKline Beecham,
Philadelphia, Pennsylvania).
*Trademark: Cefzil’s (Bristol-Myers Squibb, Prince-
ton, New Jersey).
~Trademark Lorabid” (Eli Lilly & Company, Indi-
anapolis, Indiana).
“Trademark: Biaxin@ (Abbott Laboratories, Abbott
Park, Illinois).
ITrademark: Levaquin@ (Ortho-McNeil Pharmaceu-
tical, Raritan, New Jersey).
#Trademark: Cipro@ (Bayer Corporation, Pharma- ceutical Division, West Haven, Connecticut).
“Trademark: Trovan@ @‘fixer Inc., New York New York). +tTrademark: Zagam” @bone-Poulenc Rorer Phar-
maceuticals Inc., Collegeville, Pennsylvania).
922
M. WEIS ET AL.
monly implicated organisms in acute sinus
infections, including Haemophilus injluen- zae, Moraxella catarrhalis, Streptococcus pneumoniae, and Staphylococcus aureus.‘*4 The two drugs used in the present trial (CIP and CA) are indicated for the first three organisms. The increasing national preva-
lence of beta-lactamase-producing H in- fluenzae and M catarrhalis and pneu- monococci resistant to penicillin and other
drugs has spurred the search for alternative antimicrobial treatments for acute episodes of bacterial rhinosinusitis.s
Three recent studies have documented the effectiveness of CIP for the treatment of patients with clinically documented and radiologically confirmed acute sinusi- tis.9-1’ Collectively, these studies estab- lished that a lo-day course of oral CIP 500 mg BID was of comparable efficacy to a lo-day course of CA 250 mg BID or a 14-day course of clarithromycin 500 mg BID. In one of these trials,10 laboratory
studies confirmed bacterial infection in approximately 40% of patients; the in- fecting species included H influenzae (1 l%), M catarrhalis (18%), S pneumo- niae (7%), and S aureus (17%). Eradica- tion of the causative organisms was re- ported in 97% of CIP-treated and 95% of CA-treated patients. lo These three studies were designed and conducted before the recent recommendations of the Rhinosi- nusitis Task Force Committee.2
The present study was undertaken in a primary care setting to compare the effi- cacy and safety of lo-day oral regimens of CIP and CA in the treatment of clini- cally confirmed acute rhinosinusitis in adults. To the best of our knowledge, this is the first large community-based study to use the Rhinosinusitis Task Force Com- mittee’s recent recommendations for the diagnosis of acute rhinosinusitis.
PATIENTS AND METHODS
Study Participants
Adults of both sexes with a primary di- agnosis of clinically documented acute rhi- nosinusitis of ~4 weeks’ duration were en- rolled. Eligible adults were 218 years of age and presented with clinical signs and symptoms of acute rhinosinusitis, includ- ing at least two of the major diagnostic
factors or one of the major factors and two of the minor factors listed in Table I. The presenting symptoms were evaluated on a 5-point scale ranging from 0 = normal to 4 = severe. The study investigators also identified patients with a history of aller- gic rhinitis and the frequency of allergic rhinitis in these patients so that their clin- ical response could be analyzed separately.
Patients with any of the following were excluded from the study: hypersensitivity to carboxyquinolones or beta-lactam
agents or development of type I anaphy- laxis in response to penicillin or its deriv- atives; a history of chronic sinusitis (~4 weeks of continuous symptoms or two or more recurrences of acute rhinosinusitis, despite adequate treatment, in the previ- ous 6 months); a recent history (c4 weeks) of dental complications (eg, maxillary ab- scess); known or suspected bacteremia or meningitis; previous enrollment in this study; pregnancy or lactation; a baseline serum creatinine level of >3.0 mg/dL; or receipt of an investigational drug within 30 days of enrollment. Patients were also excluded if they had received an antimi- crobial agent within 1 week of study en- rollment, unless treatment had failed or they had received less than two doses of the antibiotic. Use of adjunctive medica- tions, such as antihistamines, deconges- tants, antipyretics, or expectorants, was
923

CLINICAL THERAPEUTICS”
Table I. Presenting symptoms of acute rhinosinusitis.
Major Facial ~ongestio~~llness Nasal drainage/purulence/discoloration Hyposmia/anosmia Facial pain/pressure Fever Nasal obstruction/blockage
Minor Headache Halitosis Fatigue Dental pain Cough Ear p~~p~ssurel~llness
permitted. The study was approved by an independent institutional review board. Written informed consent was obtained from each patient before enrollment.
Sbdy Design
This was an open-label, prospective, randomized, nationwide, multicenter, out- patient comparative trial. Clinical assess- ments were performed at study enrollment to establish the clinical diagnosis of acute rhinosinusitis and on days 2 through 6 of
therapy (by telephone) to assess each pa- tient’s progress and inquire about adverse
events. Assessments were also performed at the end of therapy (4 to 16 days post- therapy) to assess ~timic~bial effective- ness and safety.
Ra~damiza~~ and Therapy
Patients were randomly assigned to one of two treatment groups through the use of a block-design random code computer-
924
generated at Bayer Corporation. CIP was supplied as 500-mg tablets, and CA was supplied as 250-mg tablets. All patients were to receive one tablet BID for 10 days. Patients were instructed to take study medication with or without food, but with at least 120 mL of water.
Eficacy Assessment
For a course of therapy to be judged valid for efficacy assessment, the follow- ing criteria must have been satisfied: (1) the diagnosis of acute infection was con-
firmed by clinical signs and symptoms of acute rhinosinusitis (ie, two major factors or one major and two minor factors); (2) the study antibiotic was given for 10 full days with >80% compliance (assessed by tablet count at follow-up), unless treat- ment was a failure; and (3) no other an- timi~robi~ agent was administered con- comitantly with the study antibiotic or during the 4- to 16-day posttreatment pe- riod. Patients who received fewer than 16
M. WEIS ET AL.
doses of study antibiotic were not valid for efficacy assessment.
The effectiveness of therapy was deter- mined based on the patient’s clinical re- sponse at the end-of-therapy assessment (posttherapy days 4 through 16). Clinical response was determined based on the observation of the following in serial ex- aminations of the patient: decrease in post- nasal drainage, decrease in nasal obstruc- tion, decrease in facial tenderness/pain, decrease in frequency of cough or throat clearing, disappearance of or lessening
severity of headache, or reduction in any other presenting symptom. At the end of therapy, clinical response was defined as resolution (absence of or significant im- provement in all signs and symptoms of infection, as assessed by investigator, such that additional antimicrobial therapy was
not required), failure (no change, worsen- ing, or reappearance of the presenting signs and symptoms of infection, such that additional antimicrobial therapy was required), or indeterminate (no assessment possible because of missing data or pa- tient unavailability).
Safety Assessment
All patients who received at least one
dose of study medication constituted the safety (intent-to-treat) population. Safety of drug treatment was assessed by clinical observations, including evaluation of pos- sible CNS effects, and by conventional laboratory tests of renal, hepatic, and hematopoietic function, as indicated. Ad- verse events were rated by the unmasked investigator according to their severity (mild, moderate, severe, or serious/life threatening) and their potential relation- ship to the study drug (probable, possible, remote, or none). Countermeasures and
length of time to resolution of each ad-
verse event were also recorded.
Statistical Analysis
The goal of this study was to demon- strate that the CIP regimen was statisti- cally equivalent to that of the CA regi- men. The primary measure of efficacy was the proportion of patients in each treat- ment group with clinical resolution at the end of therapy. The estimated clinical res- olution rate in each treatment group was 80%. With the sample size enrolled, the
study had a power of more than 90% to detect equivalence between CIP and CA (a = 0.05, two-sided). Further, the study had a power of 90% to exclude the possi- bility that CA was 210% better.
Demographic and baseline medical characteristics were summarized by treat- ment group, using the mean and standard deviation, median, range (quantitative data), or frequency counts (qualitative data). To test the comparability of the study-drug groups, categorical variables (eg, race) were analyzed using a chi- square test. For continuous variables such as age, an analysis of variance model was fitted, with treatment-group, center, and
treatment-by-center interaction as factors. For end-of-therapy clinical responses,
95% two-sided confidence intervals (95% CI) were calculated for the differences between resolution rates; the Cochran- Mantel-Haenszel weighting procedure was used to adjust for the multicenter na- ture of the trial, The two treatments were considered equivalent at the 2.5% signif- icance level if the lower confidence limit was c-0.10. The 95% CI was calculated using a normal approximation to the bi- nomial distribution with a correction for continuity. These analyses were per-
925
CLINICAL THERAPEUTICS”
formed for both the efficacy-valid and intent-to-treat populations.
RESULTS
a preexisting condition, equally distrib- uted between the two treatment groups. Clinical outcome did not appear to be in-
fluenced by this underlying condition.
Study Demographics
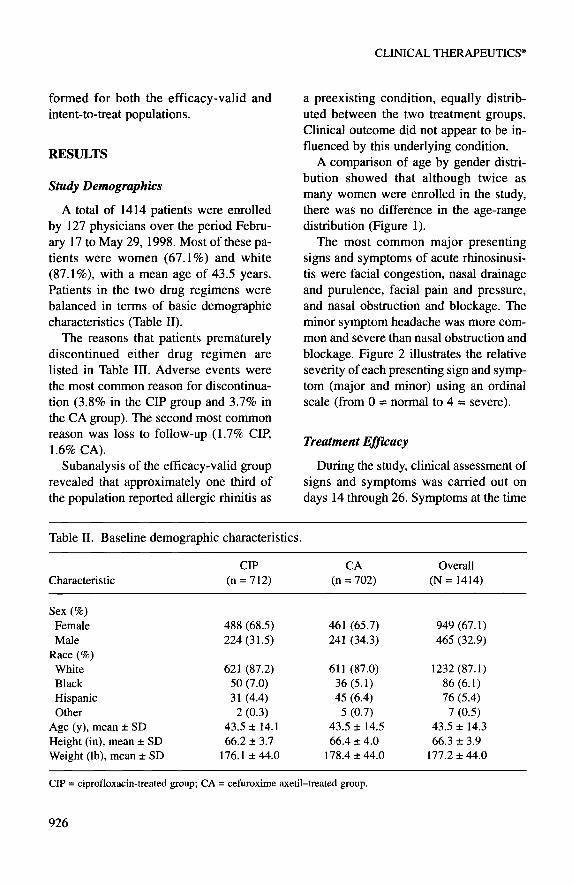
A total of 1414 patients were enrolled by 127 physicians over the period Febru- ary 17 to May 29,1998. Most of these pa- tients were women (67.1%) and white (87.1%), with a mean age of 43.5 years. Patients in the two drug regimens were balanced in terms of basic demographic
characteristics (Table II).
A comparison of age by gender distri- bution showed that although twice as many women were enrolled in the study, there was no difference in the age-range distribution (Figure 1).
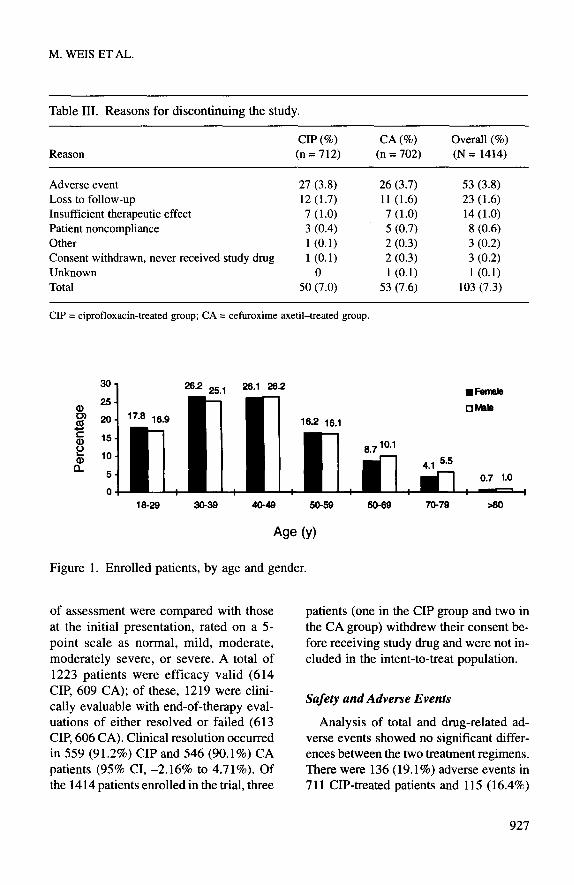
The reasons that patients prematurely discontinued either drug regimen are listed in Table III. Adverse events were the most common reason for discontinua- tion (3.8% in the CIP group and 3.7% in the CA group). The second most common reason was loss to follow-up (1.7% CIP, 1.6% CA).
The most common major presenting
signs and symptoms of acute rhinosinusi- tis were facial congestion, nasal drainage and purulence, facial pain and pressure, and nasal obstruction and blockage. The minor symptom headache was more com- mon and severe than nasal obstruction and blockage. Figure 2 illustrates the relative
severity of each presenting sign and symp- tom (major and minor) using an ordinal scale (from 0 = normal to 4 = severe).
Treatment E@acy
Subanalysis of the efficacy-valid group During the study, clinical assessment of revealed that approximately one third of signs and symptoms was carried out on the population reported allergic rhinitis as days 14 through 26. Symptoms at the time
Table II. Baseline demographic characteristics.
Characteristic CIP
(n = 712) CA
(n = 702) Overall
(N = 1414)
Sex (%) Female Male
Race (%) White Black Hispanic Other
Age (y), mean f SD Height (in), mean f SD Weight (lb), mean f SD
488 (68.5) 461 (65.7) 949 (67.1) 224 (31.5) 241 (34.3) 465 (32.9)
621 (87.2) 611 (87.0) 1232 (87.1) 50 (7.0) 36 (5.1) 86 (6.1) 31 (4.4) 45 (6.4) 76 (5.4)
2 (0.3) 5 (0.7) 7 (0.5) 43.5 f 14.1 43.5 f 14.5 43.5 f 14.3 66.2 + 3.7 66.4 rtr 4.0 66.3 f 3.9
176.1 + 44.0 178.4 * 44.0 177.2 f 44.0
CIP = ciprofloxacin-treated group; CA = cefuroxime axetil-treated group.
926
M. WEIS ET AL.
Table III. Reasons for discontinuing the study.
Reason CIP (%) (n=712)
CA (%) Overall (%) (n = 702) (N = 1414)
Adverse event 27 (3.8) Loss to follow-up 12 (1.7) Insufficient therapeutic effect 7 (1.0) Patient noncompliance 3 (0.4) Other 1 (0.1) Consent withdrawn, never received study drug l(O.1) Unknown 0 Total 50 (7.0)
26 (3.7) 11 (1.6) 7 (1.0) 5 (0.7) 2 (0.3) 2 (0.3) l(O.1)
53 (7.6)
53 (3.8) 23 (1.6) 14 (1.0) 8 (0.6) 3 (0.2) 3 (0.2) l(O.1)
103 (7.3)
CIP = ciprofloxacin-treated group; CA = cefuroxime axetil-treated group.
Age (Y)
Figure 1. Enrolled patients, by age and gender.
of assessment were compared with those at the initial presentation, rated on a 5-
point scale as normal, mild, moderate, moderately severe, or severe. A total of
1223 patients were efficacy valid (614 CIP, 609 CA); of these, 1219 were clini- tally evaluable with end-of-therapy evaI- uations of either resolved or failed (613 CIP, 606 CA). Clinical resolution occurred in 559 (91.2%) CIP and 546 (90.1%) CA patients (95% CI, -2.16% to 4.71%). Of the 1414 patients enrolled in the trial, three
patients (one in the CIP group and two in the CA group) withdrew their consent be- fore receiving study drug and were not in- eluded in the intent-to-treat population.
Safety and Adverse Events
Analysis of total and drug-related ad- verse events showed no significant differ- ences between the two treatment regimens. There were 136 (19.1%) adverse events in 7 11 CIP-treated patients and 115 (16.4%)
927

CLINICAL THERAPEUTICS”
zi?
4
P Major Symptoms Minor Symptoms
Figure 2. Mean severity of presenting symptoms in acute rhinosinusitis. 0 = normal; 1 = mild; 2 = moderate; 3 = moderately severe; 4 = severe.
in 700 CA-treated patients, with 80
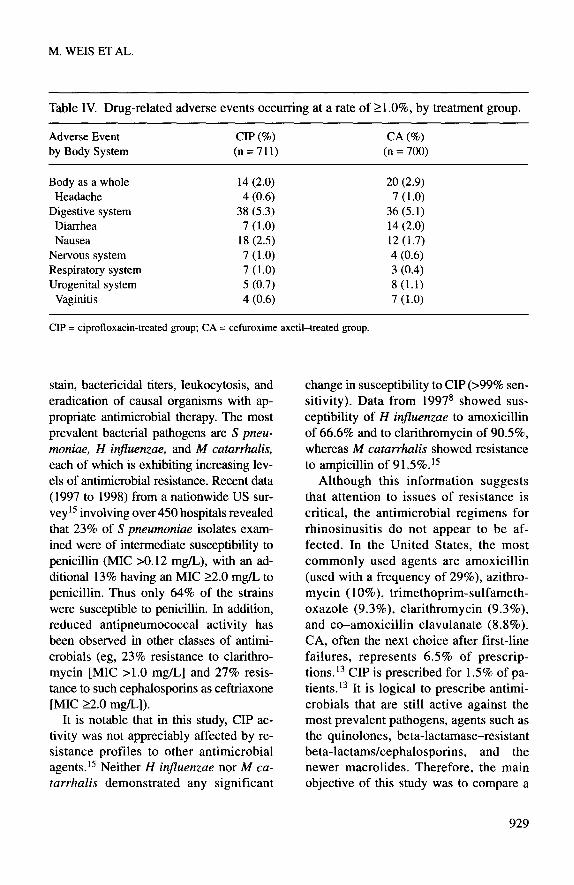
(11.3%) and 81 (11.6%), respectively, con- sidered possibly or probably drug related. The most common drug-related events were nausea (18 CIP, 12 CA), diarrhea (7 CIP, 14 CA), headache (4 CIP, 7 CA), and vaginitis (4 CIP, 7 CA). Table IV lists drug- related events that occurred at a rate of 21 .O% in either treatment group.
DISCUSSION
Rhinosinusitis comprises a complex array of disorders, ranging from the simply in- convenient to the potentially life threaten- ing. It is defined as an inflammatory re- sponse involving the mucous membranes of the nasal cavity and paranasal sinuses, the fluids in these cavities, and the under- lying bone and is associated with a multi- tude of symptoms (Figure 2). Acute rhi- nosinusitis in adults is sudden in onset. Symptoms last at least 5 days but no more than 4 weeks, with complete resolution.
928
Further, the recognition of rhinosinusitis is increasing, although most available na- tional data do not differentiate between acute, recurrent, or chronic disease.
The growing incidence of this disease is evidenced by the rapidly increasing numbers of antimicrobial prescriptions. Over the period 1992 to 1997, prescrip- tions for rhinosinusitis doubled from 13 million in 1992 to 28 million in 1997.‘2q13 This represents a fivefold increase from 1985 (5.8 million prescriptions).14 In view
of this burgeoning problem, a better ap- preciation of the complex nature of rhi- nosinusitis was clearly needed. Thus a Rhinosinusitis Task Force Committee was convened by the AAOHNS to address sev- eral issues, including a detailed classifi- cation of the different disease entities, that would allow physicians to manage the condition more appropriately.
Previous investigators have demon- strated the role of infection, viral or bacte- rial, in rhinosinusitis by correlating Gram’s
M. WEIS ET AL.
Table IV. Drug-related adverse events occurring at a rate of 21 .O%, by treatment group.
Adverse Event CIP (%) CA (%) by Body System (n=711) (n = 700)
Body as a whole Headache
Digestive system Diarrhea Nausea
Nervous system Respiratory system Urogenital system
Vaginitis
14 (2.0) 4 (0.6)
38 (5.3) 7 (1.0)
18 (2.5) 7 (1.0) 7 (1.0) 5 (0.7) 4 (0.6)
20 (2.9) 7 (1.0)
36 (5.1) 14 (2.0) 12 (1.7) 4 (0.6) 3 (0.4) 8 (1.1) 7 (1.0)
CIP = ciprofloxacin-treated group; CA = cefuroxime axetil-treated group.
stain, bactericidal titers, leukocytosis, and eradication of causal organisms with ap- propriate antimicrobial therapy. The most prevalent bacterial pathogens are S pneu- moniae, H injluenzae, and A4 catarrhalis, each of which is exhibiting increasing lev- els of antimicrobial resistance. Recent data (1997 to 1998) from a nationwide US sur-
vey15 involving over 450 hospitals revealed that 23% of S pneumoniae isolates exam- ined were of intermediate susceptibility to penicillin (MIC ~0.12 mg/L), with an ad- ditional 13% having an MIC 22.0 mg/L to penicillin. Thus only 64% of the strains were susceptible to penicillin. In addition, reduced antipneumococcal activity has been observed in other classes of antimi-
crobials (eg, 23% resistance to clarithro- mycin [MIC ~1.0 mg/L] and 27% resis- tance to such cephalosporins as ceftriaxone [MIC 22.0 mg/L]).
It is notable that in this study, CIP ac- tivity was not appreciably affected by re- sistance profiles to other antimicrobial agents. l5 Neither H injluenzae nor M ca- tarrhalis demonstrated any significant
change in susceptibility to CIP (>99% sen-
sitivity). Data from 19978 showed sus- ceptibility of H inji’uenzae to amoxicillin of 66.6% and to clarithromycin of 90.5%, whereas M catarrhulis showed resistance to ampicillin of 91.5%.15
Although this information suggests that attention to issues of resistance is
critical, the antimicrobial regimens for rhinosinusitis do not appear to be af- fected. In the United States, the most commonly used agents are amoxicillin (used with a frequency of 29%), azithro- mycin (1 O%), trimethoprim-sulfameth- oxazole (9.3%), clarithromycin (9.3%), and co-amoxicillin clavulanate (8.8%). CA, often the next choice after first-line
failures, represents 6.5% of prescrip- tions.13 CIP is prescribed for 1.5% of pa- tients.13 It is logical to prescribe antimi- crobials that are still active against the most prevalent pathogens, agents such as the quinolones, beta-lactamase-resistant beta-lactams/cephalosporins, and the newer macrolides. Therefore, the main objective of this study was to compare a
929
CLINICAL THERAPEUTICS”
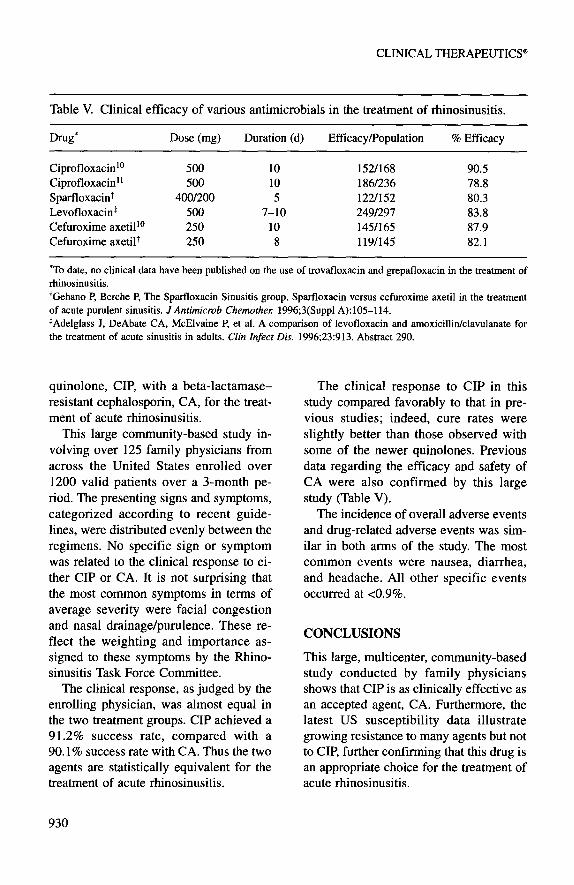
Table V. Clinical efficacy of various antimicrobials in the treatment of rhinosinusitis.
Drug* Dose (mg) Duration (d) Efficacy/Population % Efficacy
Ciprofloxacinl” 500 10 1521168 90.5 Ciprofloxacin” 500 10 1861236 78.8 Sparfloxacin+ 4OOl200 5 122/152 80.3 Levofloxacin+ 500 7-10 2491297 83.8 Cefuroxime axetill 250 10 1451165 87.9 Cefuroxime axetil+ 250 8 119/145 82.1
‘To date, no clinical data have been published on the use of trovafloxacin and grepafloxacin in the treatment of
rhinosinusitis.
+Gehano P, Berche P, The Sparfloxacin Sinusitis group. Sparfloxacin versus cefuroxime axetil in the treatment
of acute purulent sinusitis. JAntimicrob Chemorhe,: 1996;3(Suppl A):105114.
*Adelglass J, DeAbate CA, McElvaine P, et al. A comparison of levofloxacin and amoxicillinklavulanate for
the treatment of acute sinusitis in adults. Chin Infect Dis. 1996;23:913. Abstract 290.
quinolone, CIP, with a beta-lactamase- resistant cephalosporin, CA, for the treat- ment of acute rhinosinusitis.
This large community-based study in- volving over 125 family physicians from
across the United States enrolled over 1200 valid patients over a 3-month pe- riod. The presenting signs and symptoms, categorized according to recent guide- lines, were distributed evenly between the regimens. No specific sign or symptom was related to the clinical response to ei- ther CIP or CA. It is not surprising that the most common symptoms in terms of average severity were facial congestion and nasal drainage/purulence. These re- flect the weighting and importance as- signed to these symptoms by the Rhino- sinusitis Task Force Committee.
The clinical response, as judged by the enrolling physician, was almost equal in the two treatment groups. CIP achieved a 91.2% success rate, compared with a 90.1% success rate with CA. Thus the two agents are statistically equivalent for the treatment of acute rhinosinusitis.
930
The clinical response to CIP in this study compared favorably to that in pre- vious studies; indeed, cure rates were slightly better than those observed with some of the newer quinolones. Previous
data regarding the efficacy and safety of CA were also confirmed by this large study (Table V).
The incidence of overall adverse events and drug-related adverse events was sim- ilar in both arms of the study. The most common events were nausea, diarrhea, and headache. All other specific events occurred at ~0.9%.
CONCLUSIONS
This large, multicenter, community-based study conducted by family physicians shows that CIP is as clinically effective as an accepted agent, CA. Furthermore, the latest US susceptibility data illustrate growing resistance to many agents but not to CIP, further confirming that this drug is an appropriate choice for the treatment of acute rhinosinusitis.
M. WEIS ET AL.
ACKNOWLEDGMENTS
This study was supported by a research grant from Bayer Corporation, Pharmaceu-
tical Division, West Haven, Connecticut. The authors wish to thank Blair Robert-
son, PhD, and Teresa Tartaglione, PharmD, for editorial and scientific con- tributions. The following were members of the Rhinosinusitis Investigation Group:
Mark Bartz, MD; Charles Berg, MD; Stephen Bills, MD; Patricia Buchanan, MD; Brent Clark, MD; James Farrell, MD; Brian First, MD; Lawrence Gernon, MD; Steven Goldberg, MD; William Grace, DO; Catherine Grellet, MD; Har- vey Hart, MD; Roger Ingham, MD; Rod-
ney Ison, MD; James Kinahan, MD; Thomas Kinstrey, MD; George Klein, MD; Kris Kostrzewski, MD; Michael Ko- vacich, MD; Craig Krause, DO; Thomas Lehner, MD; Gary Levinson, MD; Jerry L. Miller, MD; R. Louis Murphy, MD; Edward Myers, DO; Seymour Myers, MD; Sunita Narang, MD; Alan Paul, MD; Luis Quintero, MD; Jonathan Reimer, MD; Louis Reznick, DO; Kenneth Roberts, MD; Rajeev Saini, MD; James Sarrett, MD; Carlos Say, MD; Carlos Scott, MD; Vincent Sghiatti, MD; Thomas Shetter, MD; Donald Shushan, MD; Sunil Sinha, MD; and Louis Tsarouhas, MD.
Address correspondence to: Mark Weis, MD, Family Health Center, 456 Bumey Road, Scottsville, KY 42164.
REFERENCES
1. Gwaltney JM. Acute community-acquired sinusitis. Clin Infect Dis. 1996;23: 1209-1225.
2. Lanza DC, Kennedy DW. Adult rhinosi- nusitis defined. Otolaryngol Head Neck
Surg. 1997;117:51-57.
3. Orlandi RR, Kennedy DW. Surgical man- agement of rhinosinusitis. Am J Med Sci.
1998:316:29-38.
4. Gwaltney JM Jr, Scheld WM, Sande MA, Sydnor A Jr. The microbial etiology and antimicrobial therapy of adults with acute community-acquired sinusitis: A fifteen- year experience at the University of Vir- ginia and review of other selected studies. J Allergy Clin Immunol. 1992;90:457462.
5. Doem GV, Brueggemann AB, Pierce G, et al. Antibiotic resistance among clinical
isolates of Haemophilus injluenzae in the United States in 1994 and 1995 and de- tection of beta-lactamase positive strains resistant to amoxicillin-clavulanate: Re-
sults of a national multicenter study. An- timicrob Agents Chemothe,: 1997;41: 292-297.
6. Doem GV, Brueggemann AB, Pierce G, et al. Prevalence of antimicrobial resistance among 723 outpatient clinical isolates of Moraxella catarrhalis in the United States in 1994 and 1995: Results of a 30-center national surveillance study. Antimicrob
Agents Chemothe,: 1996;40:2884-2886.
7. Doem GV, Brueggemann AB, Holley HP Jr, Rauch AM. Antimicrobial resistance of Streptococcus pneumoniae recovered from outpatients in the United States dur- ing the winter months of 1994 to 1995: Results of a 30-center national surveil- lance study. Antimicrob Agents Chemo- the,: 1996:40:1208-1213.
8. Thomsberry C, Ogilvie P, Kahn J, et al. Surveillance of antimicrobial resistance in Streptococcus pneumoniae, Haemophilus injluenzae, and Moraxella catarrhalis in the United States in 19961997 respira-
931

CLINICAL THERAPEUTICS”
tory season. Diagn Microbial Infect Dis.
1997;29:249-257.
9. Klein GL, Whalen E, Echols RM, Heyd A. Ciprofloxacin versus cefuroxime axetil in the treatment of adult patients with acute bacterial sinusitis. J Otolaryngol.
1998;27:10-16.
10. Heyd A, Echols R, Shan M, et al. Oral ciprofloxacin vs cefuroxime axetil in the treatment of acute sinusitis. Presented at 35th Interscience Conference on Antimi-
crobial Agents and Chemotherapy; Sep- tember 17-20, 1995; San Francisco, Cali-
fornia. Abstract LM-3 1.
11. Huck W, Shan M, Tosiello R, et al. Dou- ble-blind comparative trial of ciprofloxa- tin (CIP) vs clarithromycin (CLR) in the treatment of acute bacterial sinusitis. Pre-
sented at American College of Allergy Asthma and Immunology Meeting; No- vember 8-9, 1997; San Diego, California. Abstract P57.
12. Kalliner MA, Osguthorpe DJ, Fireman P, et al. Sinusitis: Bench to bedside. J Allergy Clin Immunol. 1997;99(Suppl):
S829-S848.
13. National Data Trends Inc. Antibiotic Pre-
scriptions-USA. Plymouth, Pennsylva- nia: IMS; 1998.
14. McCraig LF, Hughes JM. Trends in an- timicrobial drug prescribing among of- fice-based physicians in the United States. JAMA. 1995:273:21&219.
15. Hickey ML, Thornsberry C, Diakun DR, et al. Activity of ciprofloxacin against S pneumoniae (Sp), H inj7uenzae (Hi), and M catarrhalis (MC): Has it changed in the last decade? 1998. Presented at 38th In- terscience Conference on Antimicrobial Agents and Chemotherapy; September 24-27, 1998; San Diego, California. Ab- stract 16545, poster E020.
932
Copyright © 2022 FDOKUMEN















![[Distribution of blaOXA genes in Acinetobacter baumannii strains: a multicenter study]](https://static.fdokumen.com/doc/165x107/6337b5c66f78ac31240eb601/distribution-of-blaoxa-genes-in-acinetobacter-baumannii-strains-a-multicenter.jpg)




