Triggers for emergency team activation: A multicenter assessment
8
Triggers for emergency team activation: A multicenter assessment ☆,☆☆ Jack Chen MBBS, PhD, MBA a, ⁎ , Rinaldo Bellomo FRACP, FJFICM, MD b , Ken Hillman MBBS, FRCA, FACA, FJFICM, MD a , Arthas Flabouris MBBS, FJFICM, FANZCA, PostGrad Dip Aviation Med c , Simon Finfer MBBS, FRCA, FRCP, FJFICM d the MERIT Study Investigators for the Simpson Centre and the ANZICS Clinical Trials Group a Simpson Centre for Health Services Research, University of New South Wales, Sydney, New South Wales, Australia b Intensive Care Unit, Austin Medical Centre, Melbourne, Victoria, Australia c Intensive Care Unit, Royal Adelaide Hospital, Adelaide, South Australia, Australia d Intensive Care Unit, Royal North Shore Hospital, Sydney, New South Wales, Australia Keywords: Medical emergency team; Rapid response system; Rapid response team; Critical care Abstract Purpose: The purpose of the study was to examine triggers for emergency team activation in hospitals with or without a medical emergency team (MET) system. Materials and Methods: Within a cluster randomized controlled trial examining the effect of introducing a MET system, we recorded the triggers for emergency team activation. We compared the proportion and rate of such triggers in hospitals with or without a MET system and in relation to type of hospital, type of patient ward, and time of day. Results: In control hospitals, the most common trigger for emergency team activation was a decrease in Glasgow Coma Score by 2 or more points (45.6%), whereas in MET hospitals, it was the fact that staff members were “worried” or the call occurred despite the lack of a “specified reason” (39.3%). In particular, MET hospitals were 35 times more likely to make a call because of staff being “worried” about the patient (14.1% vs 0.4%, P < .001). Control hospitals were also significantly more likely to call an emergency team because of a deteriorating respiratory (P = .003) or pulse (P < .001) rate, more calls had at least 3 triggers for activation (20.8% vs 10.2%, P = .036), and the average number of triggers per call was significantly higher (P = .013). Nonmetropolitan hospitals were more likely to call an ☆ The MERIT study is a collaboration of the Simpson Centre for Health Services Research and the Australian and New Zealand Intensive Care Society Clinical Trials Group. ☆☆ Sources of support for the study: The study was funded by grants from the National Health and Medical Research Council of Australia, the Australian Council for Safety and Quality in Health Care, and the Australian and New Zealand Intensive Care Foundation as part of the MERIT study. ⁎ Corresponding author. The Simpson Centre for Health Services Research, Liverpool Health Service, Liverpool BC, Sydney NSW 1871, Australia. Tel.: +61 2 9612 0635; fax: +61 2 9612 0742. E-mail address: [email protected] (J. Chen). 0883-9441/$ – see front matter © 2010 Elsevier Inc. All rights reserved. doi:10.1016/j.jcrc.2009.12.011 Journal of Critical Care (2010) 25, 359.e1–359.e7
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Triggers for emergency team activation: A multicenter assessment

Journal of Critical Care (2010) 25, 359.e1–359.e7
Triggers for emergency team activation:A multicenter assessment☆,☆☆
Jack Chen MBBS, PhD, MBAa,⁎, Rinaldo Bellomo FRACP, FJFICM, MDb,Ken Hillman MBBS, FRCA, FACA, FJFICM, MDa,Arthas Flabouris MBBS, FJFICM, FANZCA, PostGrad Dip Aviation Med c,Simon Finfer MBBS, FRCA, FRCP, FJFICMd
the MERIT Study Investigators for the Simpson Centre andthe ANZICS Clinical Trials GroupaSimpson Centre for Health Services Research, University of New South Wales, Sydney, New South Wales, AustraliabIntensive Care Unit, Austin Medical Centre, Melbourne, Victoria, AustraliacIntensive Care Unit, Royal Adelaide Hospital, Adelaide, South Australia, AustraliadIntensive Care Unit, Royal North Shore Hospital, Sydney, New South Wales, Australia
C
C
9
0d
Keywords:Medical emergency team;Rapid response system;Rapid response team;Critical care
AbstractPurpose: The purpose of the study was to examine triggers for emergency team activation in hospitalswith or without a medical emergency team (MET) system.Materials and Methods: Within a cluster randomized controlled trial examining the effect ofintroducing a MET system, we recorded the triggers for emergency team activation. We compared theproportion and rate of such triggers in hospitals with or without a MET system and in relation to type ofhospital, type of patient ward, and time of day.Results: In control hospitals, the most common trigger for emergency team activation was a decrease inGlasgow Coma Score by 2 or more points (45.6%), whereas in MET hospitals, it was the fact that staffmembers were “worried” or the call occurred despite the lack of a “specified reason” (39.3%). Inparticular, MET hospitals were 35 times more likely to make a call because of staff being “worried”about the patient (14.1% vs 0.4%, P < .001). Control hospitals were also significantly more likely to callan emergency team because of a deteriorating respiratory (P = .003) or pulse (P < .001) rate, more callshad at least 3 triggers for activation (20.8% vs 10.2%, P = .036), and the average number of triggers percall was significantly higher (P = .013). Nonmetropolitan hospitals were more likely to call an
☆ The MERIT study is a collaboration of the Simpson Centre for Health Services Research and the Australian and New Zealand Intensive Care Societylinical Trials Group.
☆☆ Sources of support for the study: The study was funded by grants from the National Health and Medical Research Council of Australia, the Australianouncil for Safety and Quality in Health Care, and the Australian and New Zealand Intensive Care Foundation as part of the MERIT study.⁎ Corresponding author. The Simpson Centre for Health Services Research, Liverpool Health Service, Liverpool BC, Sydney NSW 1871, Australia. Tel.: +61 2
612 0635; fax: +61 2 9612 0742.E-mail address: [email protected] (J. Chen).
883-9441/$ – see front matter © 2010 Elsevier Inc. All rights reserved.oi:10.1016/j.jcrc.2009.12.011

359.e2 J. Chen et al.
emergency team because of respiratory rate abnormalities (33.6% vs 23.2%, P = .015). Coronary careunit calls were more likely to be triggered by abnormalities in pulse rate and systolic blood pressure, andmore calls occurred during the period from 6:00 AM to noon.Conclusions: In MET hospitals, more emergency team calls are triggered because staff members areworried about the patient; and fewer calls have multiple triggers. Type of hospital, type of ward, andtime of day also affect the nature and frequency of triggers for emergency team activation.© 2010 Elsevier Inc. All rights reserved.
1. Introduction
Medical emergency team (MET) or rapid response team(RRT) systems have been developed with the aim ofrecognizing seriously ill hospital patients early and,thereby, reducing adverse events through early intervention[1-4]. These systems have now been widely adoptedinternationally [5-8]. They have been extended to coverpediatric [7,9-12], obstetric [13-15], and emergency depart-ment patients [16-19]. Within these systems, nursing and/ormedical staff can call an emergency team based onprespecified vital sign abnormalities (“triggers”) or becausethey believe the patient is at risk of a serious adverse event(“worried” criterion). However, there is limited informa-tion concerning the nature and frequency of the callingcriteria used to activate an emergency response. Inparticular, there is no information as to whether theintroduction of a MET system affects the nature, frequency,and timing of such triggers and whether type of hospital,type of ward, and time of day also affect them. Suchinformation is important in helping understand how thesesystems affect care and where there may be deficiencies. Inthis study, we used the data from a 23-hospital clusterrandomized controlled trial of the introduction of a METsystem (the Medical Early Response Intervention Therapy[MERIT] study) [20] to test the hypotheses that thepresence of a MET system, the type of hospital, the type ofward, and the time of day would affect the triggersresponsible for emergency team activation.
2. Methods
The sample recruitment, size calculation, ethical approv-al, and randomization scheme for the MERIT study havebeen described previously [20]. The 23 hospitals wererandomized to introduction of a MET system or to a controlgroup. Data collection was conducted during a 2-monthbaseline period, followed by a 4-month standardizedimplementation period and a further 6-month study periodduring which the MET system was operational. Data werecollected from both MET and control hospitals throughoutthe study period. The conduct of the study was notpublicized in the control hospitals, and the managementand resuscitation committees of the control hospitals agreed
that the composition and operation of their cardiac arrestteams would not change during the implementation andstudy periods. For the purpose of comparing the reasons forcalling an emergency team, we used data collected duringthe study period.
During the MERIT study period, we collected data onthe reasons that triggered (triggers) an emergency team callfor both MET and control hospitals: (1) airway at risk, (2)seizure, (3) greater than 2 points decrease in GlasgowComa Score (GCS), (4) acute respiratory rate abnormalities,(5) acute pulse rate abnormalities, (6) acute blood pressureabnormalities, (7) staff member was “worried” about thepatient, and (8) not specified. We also collected data on thenumber of calls with more than one trigger. All the data ofvital signs and triggers were extracted from medical recordsby research nurses. Standardized data collection trainingwas provided and followed up with data auditing during theearlier stage of the study. We confirmed the “worried”category as the reason of calling an emergency team bythe formal documentation of concerns in the medicalrecords. For the purpose of this analysis, we also created acategory of “not specified” for those calls that did not fallinto any prespecified categories. This category capturedthose calls due to concern about patients but where nodocumentation was made of such concern in the charts. Italso included other reasons outside of prespecifiedphysiologic triggers such as chest pain, low urine output,and decreased oxygen saturation.
3. Statistical methods
To take hospital-specific effects into account, weconducted cluster-specific analyses. For descriptive analy-ses, the means and proportions were presented; and standarderrors were adjusted for cluster effect where appropriate. Totest the association between categorical variables, the Rao-Scott χ2 test or survey-adjusted logistic regression was usedwhere appropriate. For continuous variables, the survey-adjusted t test was used to test the difference between 2groups. The survey-adjusted multiple linear regressionapproach was used for multivariate analysis where appro-priate. A P value < .05 was considered indicative ofstatistical significance. All analyses were performed usingStata 9.2 (SE; StataCorp, College Station, TX).

Fig. 1 Number of reasons for each emergency team call in METand control hospitals.
359.e3Triggers for emergency team activation
4. Results
4.1. Reasons for triggering calls in the MET andcontrol hospitals
In control hospitals, a decrease in GCS by 2 or morepoints (45.6%) was the single most common trigger foremergency team activation, followed by abnormalities inpulse rate (34.8%) or respiratory rate (33.1%) (Table 1).Either being “worried” or “not specified” accounted for30.5% of all triggers. On the other hand, in MET hospitals,being “worried” or “not specified” were the commonesttrigger (39.3%), followed by a decrease in GCS (32.1%) andabnormalities in respiratory rate or pulse rate (bothapproximately 21%). Control hospitals were 1.6 timesmore likely to call an emergency team because of adeteriorating respiratory rate (P = .003) and 1.7 times morelikely to call an emergency team because of pulse rateabnormalities (P < .001). Conversely, MET hospitals were35 times more likely to make a call because of staff being“worried” (14.1% vs 0.4%, P < .001). In control hospitals,25% of calls did not have any specific reason stated for thecall in comparison to 15% of calls in the MET hospitals (P =.104), more calls occurred because of at least 3 triggers beingpresent (20.8% vs 10.2%, P = .036), and the average numberof triggers per call was =1.52 compared with 1.29 in METhospitals (P = .013, Table 1). Conversely, 55.8% of calls inMET hospitals had only one reason for activation comparedwith only 31.3% in control hospitals (P ≤ .001, Fig. 1).
Table 1 Reasons for emergency team calls for MET andcontrol hospitals
Reason Controlhospitals(n = 528)%
METhospitals(n = 1886)%
Total(N = 2414)P
Airway 11.0% 6.2% .309GCS 45.6% 32.1% .201Respiratory rate 33.1% 20.8% .003Pulse rate 34.8% 20.7% <.001Systolic blood pressure 22.2% 24.8% .608Staff “worried” aboutpatient
5.5% 24.2% .009
No reason but call wasmade
25.0% 15.2% .104
Either “worried” or nospecified reason butcall was made
30.5% 39.3% .201
“Worried” only 0.4% 14.1% <.001“Worried” and at least 1of other criteria
5.1% 10.1% .320
Average number oftriggers per call
1.52 1.29 .013
P values from Rao-Scott χ2 test or survey mean test. The sum of thepercentages exceeds 100% because multiple triggers were allowed.
4.2. The impact of teaching hospital status, patientlocation, and time
Compared with metropolitan hospitals, nonmetropolitanhospitals were more likely to call an emergency teambecause of respiratory rate abnormalities (33.6% vs 23.2%,P = .015, Table 2). An alteration in the GCS score was themost common trigger for all hospital areas (Table 3). How-ever, calls originating from the coronary care unit (CCU)were more likely to be triggered by abnormalities in pulserate (55.7%) and systolic blood pressure (39.3%). Comparedwith CCUs, other units were more likely to have a calltriggered by either being “worried” or for “not specified”reasons (P = .008, Table 3). More calls occurred during theperiod from 6:00 AM to noon (747/2417 = 30.9%) thanduring the period from midnight to 6:00 AM (443/2417 = 18.3%). The time slot of noon to 6:00 PM, however, had thehighest proportion of calls (42.8%) due to staff either being“worried” or for “not specified” reasons compared with otherperiods (P = .012).
5. Discussion
Using the data from the MERIT study, we examined thenature and frequency of triggers for emergency teamactivation in hospitals with or without a MET system. Wefound that MET hospitals had a significantly higher numberand percentage of calls due to nurses or physicians being”worried” about the patient or for “not specified” reasons.On the other hand, in control hospitals, more of the callswere due to a specific physiologic trigger (with GCSbeing most common), more calls were triggered by 2 ormore physiologic criteria being present, and the averagenumber of triggers for each call was higher. We also foundthat nonmetropolitan hospitals were more likely to have
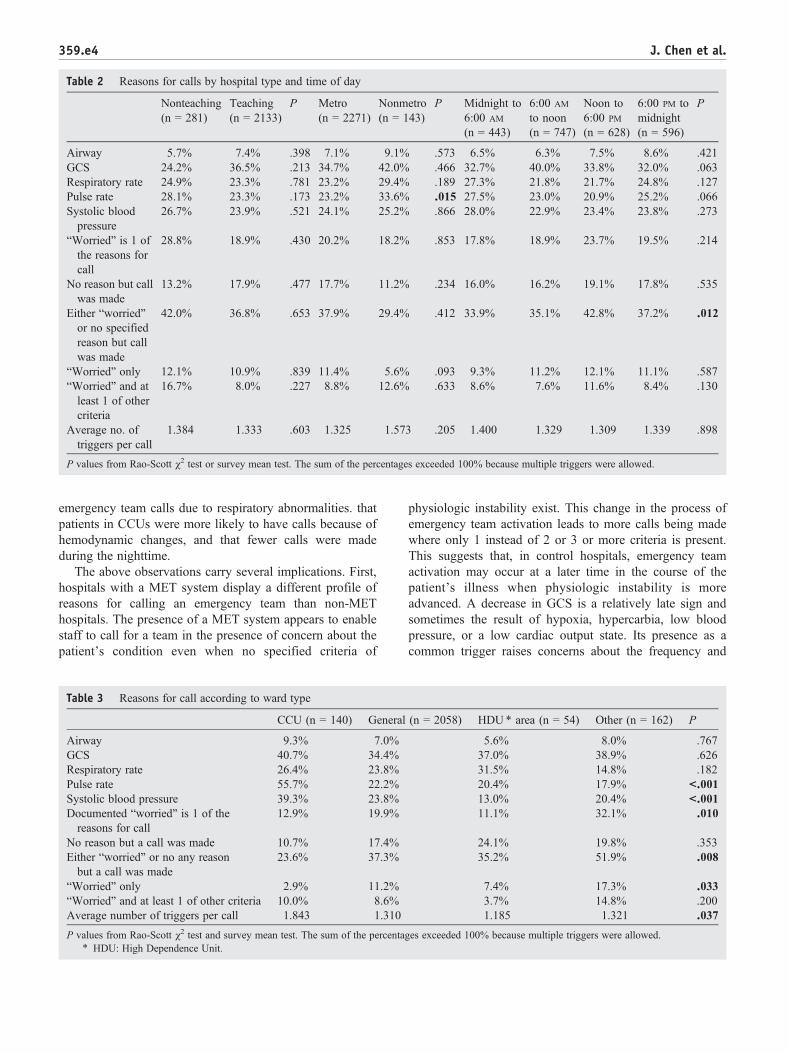
Table 2 Reasons for calls by hospital type and time of day
Nonteaching(n = 281)
Teaching(n = 2133)
P Metro(n = 2271)
Nonmetro(n = 143)
P Midnight to6:00 AM
(n = 443)
6:00 AM
to noon(n = 747)
Noon to6:00 PM
(n = 628)
6:00 PM tomidnight(n = 596)
P
Airway 5.7% 7.4% .398 7.1% 9.1% .573 6.5% 6.3% 7.5% 8.6% .421GCS 24.2% 36.5% .213 34.7% 42.0% .466 32.7% 40.0% 33.8% 32.0% .063Respiratory rate 24.9% 23.3% .781 23.2% 29.4% .189 27.3% 21.8% 21.7% 24.8% .127Pulse rate 28.1% 23.3% .173 23.2% 33.6% .015 27.5% 23.0% 20.9% 25.2% .066Systolic bloodpressure
26.7% 23.9% .521 24.1% 25.2% .866 28.0% 22.9% 23.4% 23.8% .273
“Worried” is 1 ofthe reasons forcall
28.8% 18.9% .430 20.2% 18.2% .853 17.8% 18.9% 23.7% 19.5% .214
No reason but callwas made
13.2% 17.9% .477 17.7% 11.2% .234 16.0% 16.2% 19.1% 17.8% .535
Either “worried”or no specifiedreason but callwas made
42.0% 36.8% .653 37.9% 29.4% .412 33.9% 35.1% 42.8% 37.2% .012
“Worried” only 12.1% 10.9% .839 11.4% 5.6% .093 9.3% 11.2% 12.1% 11.1% .587“Worried” and atleast 1 of othercriteria
16.7% 8.0% .227 8.8% 12.6% .633 8.6% 7.6% 11.6% 8.4% .130
Average no. oftriggers per call
1.384 1.333 .603 1.325 1.573 .205 1.400 1.329 1.309 1.339 .898
P values from Rao-Scott χ2 test or survey mean test. The sum of the percentages exceeded 100% because multiple triggers were allowed.
359.e4 J. Chen et al.
emergency team calls due to respiratory abnormalities. thatpatients in CCUs were more likely to have calls because ofhemodynamic changes, and that fewer calls were madeduring the nighttime.
The above observations carry several implications. First,hospitals with a MET system display a different profile ofreasons for calling an emergency team than non-METhospitals. The presence of a MET system appears to enablestaff to call for a team in the presence of concern about thepatient's condition even when no specified criteria of
Table 3 Reasons for call according to ward type
CCU (n = 140) General
Airway 9.3% 7.0%GCS 40.7% 34.4%Respiratory rate 26.4% 23.8%Pulse rate 55.7% 22.2%Systolic blood pressure 39.3% 23.8%Documented “worried” is 1 of thereasons for call
12.9% 19.9%
No reason but a call was made 10.7% 17.4%Either “worried” or no any reasonbut a call was made
23.6% 37.3%
“Worried” only 2.9% 11.2%“Worried” and at least 1 of other criteria 10.0% 8.6%Average number of triggers per call 1.843 1.310
P values from Rao-Scott χ2 test and survey mean test. The sum of the percenta⁎ HDU: High Dependence Unit.
physiologic instability exist. This change in the process ofemergency team activation leads to more calls being madewhere only 1 instead of 2 or 3 or more criteria is present.This suggests that, in control hospitals, emergency teamactivation may occur at a later time in the course of thepatient's illness when physiologic instability is moreadvanced. A decrease in GCS is a relatively late sign andsometimes the result of hypoxia, hypercarbia, low bloodpressure, or a low cardiac output state. Its presence as acommon trigger raises concerns about the frequency and
(n = 2058) HDU ⁎ area (n = 54) Other (n = 162) P
5.6% 8.0% .76737.0% 38.9% .62631.5% 14.8% .18220.4% 17.9% <.00113.0% 20.4% <.00111.1% 32.1% .010
24.1% 19.8% .35335.2% 51.9% .008
7.4% 17.3% .0333.7% 14.8% .2001.185 1.321 .037
ges exceeded 100% because multiple triggers were allowed.

359.e5Triggers for emergency team activation
quality of patient monitoring. Second, the type of hospitalaffects the call triggers, with respiratory abnormalities beingmore common in nonmetropolitan hospitals. Given thatnonmetropolitan hospitals are typically smaller and lessresourced in comparison to metropolitan hospitals in termsof staff and intensive care beds, this observation suggeststhat, in particular, the management of respiratory instabilityis affected by these factors. The type of ward affects theprocess of calling for the emergency team, with wards likeCCUs calling the team because of hemodynamic instability.This is logical and reflects the emphasis placed on thecardiovascular monitoring in such units. It also indirectlyindicates that monitoring and clinical vigilance, its fre-quency, and its nature are likely to be major driving forcesfor emergency team activation. This notion is confirmed bythe fact that as monitoring decreases at night, so doesemergency team activation.
The pattern of call triggers for a MET has been reported inother smaller studies. An audit from a single-center METhospital reported that the most common triggers were a fall inGCS greater than 2, a systolic blood pressure less than 90mm Hg; and a respiratory rate greater than 35 [21]. A 2-hospital Australian study reported that a low systolic bloodpressure and staff being “worried” were the most frequenttriggers [22], whereas a study across 6 hospitals showed thatthe “worried” criterion was the most common trigger [23]. Astudy from the United States reported that the most commonreasons for activating an RRT were cardiac, respiratory, andneurologic conditions [24]. In a review of 400 MET calls,Jones et al [25] reported that an altered conscious stateaccounted for 23% of calls. However, in another studyreviewing the relationship between MET activities andmortality, Jones et al [26] reported that hypotension,hypoxia, and tachypnea were the most common triggersfor activation. A respiratory rate trigger applied to 33.1% ofpatients in control hospitals and 20.8% of patients in METhospitals in our study. Mailey et al [27] found that 30% of1335 patients triggering an RRT activation had respiratorydistress and that 20% had respiratory rate triggers. Thesereports are broadly consistent; and the above local variationsare likely influenced by case-mix, type of the wards, hospitalpolicies, RRT/MET maturation, and ease of activation. Theyhighlight the kind of problems that an emergency team islikely to encounter and can inform the type of training thatsuch teams are likely to benefit from.
The importance of the subjective “worried” category asa trigger for MET activations in our study was consistentwith other studies that explored calling triggers in METhospitals [21-23,28]. For example, Jones et al [28] reportedthat more than half of the nurses would make a MET callif they were worried about a patient even if the patient'svital signs were normal. Our study showed that close toa quarter of calls in MET hospitals had “worried” as theonly trigger for MET activation. Our estimate is likely tobe conservative, as the “worried” criterion required thedocumentation in patient's medical record. Our study,
however, is the first of its kind to report that a quarter ofthe calls made in control hospitals were without anyspecific reason. These findings may be explained by thefact that the introduction of the MET systems affects docu-mentation or that it legitimized clinical concern and itsexpression or both. Beyond such speculations, thesefindings imply that, in control hospitals during theMERIT study, cardiac arrest teams were also used as abroad emergency response system.
The variable documentation of physiologic parameters isone of the important confounding factors in understandingthe triggers for an emergency team call. Monitoring anddocumentation of vital signs are important to emergencyteam activation. Even with proper documentation, abnormalvital signs may still be ignored [20]. Our observations thatthe worried criterion was so widely used suggest thatcreating systems where triggering of emergency teamintervention relies only on physiologic calling criteriamay lead to underutilization of the MET. In this regard,data showing that essentially all MET interventions in theMERIT study entailed some kind of critical care interven-tion (in press, Resuscitation) reinforce the notion that thisdelayed use or underuse might have occurred during theMERIT trial.
Our study has several strengths. It is the first of its kindin providing a comprehensive description of the calltriggers for emergency teams within both hospitals withand without a MET system. The study was across 23hospitals with a standardized data collection process.Furthermore, we provided description of physiologic andobservational triggers as well as the subjective “worried”criterion. The limitations of the study include the fact that itwas a post hoc analysis and that no information wasavailable to more specifically describe the reason for callingin those patients where neither the worried criterion nor theobjective criteria applied. Furthermore, for simplicity, wedid not include the baseline distribution of triggers in ouranalysis. We have previously shown that the baselinedistributions of both control and MET hospitals wererelatively balanced and that adjustment according tobaseline distribution made no material difference to theresults at the study period [20]. However, caution needs tobe exercised before making causal inferences.
In summary, we found that both physiologic triggersand the subjective (“worried”) criteria were importanttriggers for emergency team intervention; that, in METhospitals, more emergency team calls are triggered becausestaff members are worried about the patient; and that fewercalls have multiple triggers. Furthermore, type of hospital,type of ward, and time of day affected the nature andfrequency of triggers for emergency team activation. Ourfindings demonstrate that hospitals with a MET systemdisplayed a different profile in the nature and frequency ofemergency team activation and suggest that, when suchactivations occur, they occur earlier in the course of thepatient's illness.

359.e6 J. Chen et al.
Appendix A
Writing Committee: Jack Chen, Rinaldo Bellomo,Kenneth Hillman, Arthas Flabouris, Simon Finfer
Management Committee: Ken Hillman (Study Chair),Simon Finfer (Study Vice-chair), Rinaldo Bellomo, DanielBrown, Michelle Cretikos, Jack Chen, Gordon Doig, ArthasFlabouris, and David Sanchez
Steering Committee: Ken Hillman (Chair), JenniferBartlett, Rinaldo Bellomo, Daniel Brown, Michael Buist,Jack Chen, Michelle Cretikos, Michael Corkeron, GordonDoig, Simon Finfer, Arthas Flabouris, Michael Parr, SandraPeake, and John Santamaria
Site Investigators and Research Coordinators (in alpha-betical order):
Australian Capital Territory:Calvary Hospital–Marielle Ruigrok, Margaret WillshireCanberra Hospital–David Elliott, John Gowardman,
Imogen Mitchell, Carolyn Paini, Gillian TurnerNew South Wales:Broken Hill Hospital–Coral Bennett, Linda Lynott, Mathew
Oliver, Linda Peel Sittampalam Ragavan, Russell SchedlichGosford Hospital–John Albury, Sean KellyJohn Hunter Hospital–Ken Havill, Jane O'BrienPrince ofWales Hospital–Harriet Adamson, Yahya Shehabi,Royal North Shore Hospital–Simeon Dale, Simon FinferWollongong Hospital–Sundaram Rachakonda, Kathryn
Rhodes, E. Grant SimmonsWyong Hospital–John Albury, Sean KellyQueensland:Mackay Hospital–Kathryn Crane, Judy StruikRedcliffe Hospital–Matthys Campher, Raymond
Johnson, Sharon Ragau, Neil WiddicombeRedland Hospital–Susan Carney, David MillerTownsville Hospital–Michelle Barrett, Michael
Corkeron, Sue WaltersSouth Australia:Flinders Hospital–Tamara Hunt, Gerard O'CallaghanQueen Elizabeth Hospital–Jonathan Foote, Sandra PeakeRepatriation General Hospital–Gerard O'Callaghan,
Vicki RobbRoyal Adelaide Hospital–Marianne Chapman, Arthas
Flabouris, Deborah Herewane, Sandy JansenVictoria:Bendigo Hospital–John Edington, Kathleen PayneBox Hill Hospital–David Ernest, Angela HamiltonGeelong Hospital–David Green, Jill Mann, Gary PriscoMonash Hospital–Laura Lister, Ramesh Nagappan,St. Vincent's Hospital–Jenny Holmes, John SantamariaWangaratta Hospital–Chris Giles, Debbie Hobijn
References
[1] Hillman K, Chen J, Brown D. A clinical model for health servicesresearch—the medical emergency team. J Crit Care 2003;18:195-9.
[2] Hillman K, Parr M, Flabouris A, Bishop G, Stewart A. Redefining in-hospital resuscitation: the concept of the medical emergency team.Resuscitation 2001;48:105-10.
[3] Braithwaite RS, DeVita MA, Mahidhara R, Simmons RL, Stuart S,Foraida M. Use of medical emergency team (MET) responses to detectmedical errors. Qual Saf Health Care 2004;13:255-9.
[4] Lee A, Bishop G, Hillman K, Daffurn K. The medical emergencyteam. Anaesth Intensive Care 1995;23:183-6.
[5] Barbetti J, Lee G. Medical emergency team: a review of the literature.Nurs Crit Care 2008;13:80-5.
[6] Burns B, Beckett J, Jones D, Webb S. Using a medical emergencyteam to manage anaphylactic shock. Jt Comm J Qual Patient Saf 2008;34:360-3.
[7] Dean BS, Decker MJ, Hupp D, Urbach AH, Lewis E, es-Stickle J.Condition HELP: a paediatric rapid response team triggered bypatients and parents. J Healthc Qual 2008;30:28-31.
[8] Downey AW, Quach JL, Haase M, Haase-Fielitz A, Jones D, BellomoR. Characteristics and outcomes of patients receiving a medicalemergency team review for acute change in conscious state orarrhythmias. Crit Care Med 2008;36:477-81.
[9] Hunt EA, Zimmer KP, Rinke ML, et al. Transition from a traditionalcode team to a medical emergency team and categorization ofcardiopulmonary arrests in a children's center. Arch Pediatr AdolescMed 2008;162:117-22.
[10] Kinney S, Tibballs J, Johnston L, Duke T. Clinical profile ofhospitalized children provided with urgent assistance from a medicalemergency team. Pediatrics 2008;121.
[11] Avent Y, Dycus P, Henderson N, et al. Utilizing a performanceimprovement team to plan and implement a rapid response teamfor pediatric oncology patients. Pediatr Intensive Care Nurs 2007;8:11-6.
[12] Brilli RJ, Gibson R, Luria JW, et al. Implementation of a medicalemergency team in a large pediatric teaching hospital preventsrespiratory and cardiopulmonary arrests outside the intensive careunit. Pediatr Crit Care Med 2007;8:236-46.
[13] Gosman GG, Baldisseri MR, Stein KL, et al. Introduction ofan obstetric-specific medical emergency team for obstetriccrises: implementation and experience. Am J Obstet Gynecol2008;198.
[14] Skupski DW, Lowenwirt IP, Weinbaum FI, Brodsky D, Danek M,Eglinton GS. Improving hospital systems for the care of women withmajor obstetric hemorrhage. Obstet Gynecol 2006;107:977-83.
[15] Meyer J, Reinartz I, Pichon A, Zerr V. Regulation of extra hospitaldelivery and pre hospital care by the emergency medical carecoordinator. Urgences Medicales 1996;15:269-75.
[16] Deasy C, Ryan D, O'Donnell C, Cusack S. The impact of a pre-hospital medical response unit on patient care and emergencydepartment attendances. Ir Med J 2008;101:44-6.
[17] Etter R, Ludwig R, Lersch F, Takala J, Merz TM. Early prognosticvalue of the medical emergency team calling criteria in patientsadmitted to intensive care from the emergency department. Crit CareMed 2008;36:775-81.
[18] Carter C. Implementing the severe sepsis care bundles outside the ICUby outreach. Nurs Crit Care 2007;12:225-30.
[19] Subbe CP, Slater A, Menon D, Gemmell L. Validation ofphysiological scoring systems in the accident and emergencydepartment. Emerg Med J 2006;23:841-5.
[20] The MERIT Study Investigators. Introduction of the medicalemergency team (MET) system: a cluster-randomised controlledtrial. Lancet 2005;365:2091-7.
[21] Parr MJA, Hadfield JH, Flabouris A, Bishop G, Hillman K. Themedical emergency team: 12 month analysis of reasons for activation,immediate outcome and not-for-resuscitation orders. Resuscitation2001;50:39-44.
[22] Young L, Donald M, Parr M, Hillman K. The medical emergencyteam system: a two hospital comparison. Resuscitation 2008;77:180-8.

359.e7Triggers for emergency team activation
[23] Santiano N, Young L, Hillman K, et al. Analysis of medical emergencyteam calls comparing subjective to “objective” call criteria. Resusci-tation 2009;80:44-9.
[24] King E, Horvath R, Shulkin DJ. Establishing a rapid response team(RRT) in an academic hospital: one year's experience. J Hosp Med(Online) 2006;1:296-305.
[25] Jones D, Duke G, Green J, et al. Medical emergency teamsyndromes and an approach to their management. Crit Care2006;10.
[26] Jones DA, McIntyre T, Baldwin I, Mercer I, Kattula A, Bellomo R.The medical emergency team and end-of-life care: a pilot study. CritCare Resusc 2007;9:151-6.
[27] Mailey J, Digiovine B, Baillod D, Gnam G, Jordan J, Rubinfeld I.Reducing hospital standardized mortality rate with early interven-tions. J Trauma Nurs 2006;13:178-82.
[28] Jones D, Baldwin I, McIntyre T, et al. Nurses' attitudes to a medicalemergency team service in a teaching hospital. Qual Saf Health Care2006;15:427-32.

Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.