Role of angiotensin II in liver fibrosis-induced portal hypertension and therapeutic implications
10
Review Article Role of angiotensin II in liver fibrosis-induced portal hypertension and therapeutic implications Alejandro Lugo-Baruqui, 1 José Francisco Muñoz-Valle, 2 Sigifredo Arévalo-Gallegos 3 and Juan Armendáriz-Borunda 1,4 1 Institute of Molecular Biology in Medicine, Department of Molecular Biology and Genomics, CUCS, 2 Institute of Investigation in Rheumatology and Skeletal Muscle (IIRSME), 4 OPD Civil Hospital of Guadalajara, Guadalajara, and 3 Chemistry Faculty, University of Chihuahua, Mexico Angiotensin II (AT-II) is a peptide that plays an important role in the renin-angiotensin-aldosterone (RAA) system. Tradition- ally, the RAA system has been related with states of systemic hypertension and hypoperfusion as a counterbalance mecha- nism. Recently, AT-II has been studied for its properties in the process of fibrosis in several organs, especially in the liver. AT-II is capable to stimulate the activated hepatic stellate cells, which increase expression of profibrogenic molecules like tumor growth factor-b, tissue inhibitor of metalloproteinase-1 and collagen I, among others. At the same time, AT-II is implied in the hemodynamic balance of cirrhosis and portal hypertension. Due to its profibrogenic and vasoactive properties, blockade of AT-II actions constitutes an important therapeutic target to inhibit fibrotic processes and reduction of risk of complications of portal hypertension as well. Some drugs like angiotensin-converting enzyme inhibitors or the angiotensin II receptor blockers have been studied as alternatives for the treatment of patients with cirrhosis with promising results. Nonetheless, additional research is required in order to consider these drugs as a part of the integral treatment of the patient with cirrhosis and portal hypertension. Key words: angiotensin II, rennin-angiotensin-aldosterone system, therapeutic target, portal hypertension INTRODUCTION H EPATIC CIRRHOSIS CONSTITUTES a serious problem worldwide. Hepatic failure and portal hypertension are chief complications of liver cirrhosis, which represents the end stage of a cellular damage process which involves liver fibrosis and alteration of the regular hepatic architecture and function. 1 Recently, angiotensin II (AT-II) has been implied as an important molecule in the progression of liver fibrosis. The study of the molecular mechanisms by which AT-II enhances fibrosis represents the rationale for new therapeutic strategies. 2 AT-II is an octapeptide produced by the proteolytic degradation of its precursor, angiotensin I, by the action of the angiotensin converting enzyme (ACE). Tradition- ally, AT-II has been associated with systemic hyperten- sion for its role in the renin-angiotensin-aldosterone system (RAA). Due to this hemodynamic implication, the blockade of AT-II functions might constitute a prom- ising therapeutic target for the management of patients with systemic Hypertension. 3 In the clinical setting, there are two drug classes that inhibit the effects of AT-II in the RAA system. The first group is composed by the ACE inhibitors, which impedes degradation of angiotensin I into its active form AT-II. A newer class of drugs named angiotensin II receptor blockers (ARB) has been introduced for the management of systemic hypertension as an alternative for ACE inhibitors. The action of the ARB consists in the blockade of angiotensin receptor type 1 (ATR-1). The ATR-1 is a Gq type receptor protein that activates the phospolipase C pathway. It has been shown that most of the biological actions of AT-II are mediated by acti- vation of these receptors. The over stimulation of the ATR-1 caused by pathological conditions with high levels of circulating AT-II causes a down regulation in Correspondence: Dr Juan Armendáriz-Borunda, Apdo. Postal 2-123, Guadalajara, Jal. 44281, México. Email: [email protected] Received 21 April 2009; revision 9 June 2009; accepted 13 June 2009. Hepatology Research 2010; 40: 95–104 doi: 10.1111/j.1872-034X.2009.00581.x © 2009 The Japan Society of Hepatology 95
Transcript of Role of angiotensin II in liver fibrosis-induced portal hypertension and therapeutic implications
Review Article
Role of angiotensin II in liver fibrosis-induced portalhypertension and therapeutic implications
Alejandro Lugo-Baruqui,1 José Francisco Muñoz-Valle,2 Sigifredo Arévalo-Gallegos3 andJuan Armendáriz-Borunda1,4
1Institute of Molecular Biology in Medicine, Department of Molecular Biology and Genomics, CUCS, 2Institute ofInvestigation in Rheumatology and Skeletal Muscle (IIRSME), 4OPD Civil Hospital of Guadalajara, Guadalajara,and 3Chemistry Faculty, University of Chihuahua, Mexico
Angiotensin II (AT-II) is a peptide that plays an important rolein the renin-angiotensin-aldosterone (RAA) system. Tradition-ally, the RAA system has been related with states of systemichypertension and hypoperfusion as a counterbalance mecha-nism. Recently, AT-II has been studied for its properties inthe process of fibrosis in several organs, especially in theliver. AT-II is capable to stimulate the activated hepaticstellate cells, which increase expression of profibrogenicmolecules like tumor growth factor-b, tissue inhibitor ofmetalloproteinase-1 and collagen I, among others. At thesame time, AT-II is implied in the hemodynamic balance ofcirrhosis and portal hypertension. Due to its profibrogenicand vasoactive properties, blockade of AT-II actions
constitutes an important therapeutic target to inhibit fibroticprocesses and reduction of risk of complications of portalhypertension as well. Some drugs like angiotensin-convertingenzyme inhibitors or the angiotensin II receptor blockers havebeen studied as alternatives for the treatment of patientswith cirrhosis with promising results. Nonetheless, additionalresearch is required in order to consider these drugs as apart of the integral treatment of the patient with cirrhosis andportal hypertension.
Key words: angiotensin II, rennin-angiotensin-aldosteronesystem, therapeutic target, portal hypertension
INTRODUCTION
HEPATIC CIRRHOSIS CONSTITUTES a seriousproblem worldwide. Hepatic failure and portal
hypertension are chief complications of liver cirrhosis,which represents the end stage of a cellular damageprocess which involves liver fibrosis and alteration ofthe regular hepatic architecture and function.1 Recently,angiotensin II (AT-II) has been implied as an importantmolecule in the progression of liver fibrosis. The studyof the molecular mechanisms by which AT-II enhancesfibrosis represents the rationale for new therapeuticstrategies.2
AT-II is an octapeptide produced by the proteolyticdegradation of its precursor, angiotensin I, by the actionof the angiotensin converting enzyme (ACE). Tradition-
ally, AT-II has been associated with systemic hyperten-sion for its role in the renin-angiotensin-aldosteronesystem (RAA). Due to this hemodynamic implication,the blockade of AT-II functions might constitute a prom-ising therapeutic target for the management of patientswith systemic Hypertension.3
In the clinical setting, there are two drug classes thatinhibit the effects of AT-II in the RAA system. The firstgroup is composed by the ACE inhibitors, whichimpedes degradation of angiotensin I into its activeform AT-II. A newer class of drugs named angiotensin IIreceptor blockers (ARB) has been introduced for themanagement of systemic hypertension as an alternativefor ACE inhibitors. The action of the ARB consists inthe blockade of angiotensin receptor type 1 (ATR-1).The ATR-1 is a Gq type receptor protein that activates thephospolipase C pathway. It has been shown that mostof the biological actions of AT-II are mediated by acti-vation of these receptors. The over stimulation of theATR-1 caused by pathological conditions with highlevels of circulating AT-II causes a down regulation in
Correspondence: Dr Juan Armendáriz-Borunda, Apdo. Postal 2-123,Guadalajara, Jal. 44281, México. Email: [email protected] 21 April 2009; revision 9 June 2009; accepted 13 June2009.
Hepatology Research 2010; 40: 95–104 doi: 10.1111/j.1872-034X.2009.00581.x
© 2009 The Japan Society of Hepatology 95

the number of these receptors. This effect on ATR-1causes tachyphylaxis, along with over expression ofAT-II, causing an increase in the production of thishormone. This phenomenon is not seen with the actionof ARB.4 The role of AT-II receptor type 2 in the organ-ism is not yet understood and is believed to be impor-tant during the fetal development with actions thatopposes those of ATR-1. Because of their widespread useand long time experience with these drugs, many differ-ent publications highlight their application in differentconditions other than systemic Hypertension Both,ACE-inhibitors and ARB have been useful as cardiacremodeling drugs in patients with chronic cardiac fail-ure5,6 and as renal protectors in patients with diabeticnephropathy, reducing the mortality rate in thesepatients.7,8
MECHANISMS OF LIVER FIBROSISPROGRESSION
THE PROCESS OF hepatic fibrosis is the net result ofthe balance between synthesis and degradation of
extracellular matrix (ECM) proteins, especially collagenof several types. Degradation of these extracellular com-ponents is catalyzed by the action of matrix metallopro-teases (MMP). Proteolytic activity of these enzymes iscounterbalanced by tissue inhibitors of metallopro-teases (TIMP) which are responsible for sustainingthe equilibrium of MMP function. The importance ofTIMP-1 in the process of hepatic fibrosis has been high-lighted by several researchers.10
A key step in the process of liver fibrosis is the activa-tion of the hepatic stellate cells (HSC). Activation ofHSC is caused by metabolic damage, inflammatoryresponse to viral infection or other toxic injuries. Thisactivation promotes phenotypic differentiation of HSCinto myofibroblasts expressing surface marker a-smooth muscle antigen (SMA), increasing its prolifera-tion and production rate.9,11
Recently, it has been shown that activated HSCexpress AT-II receptors in vitro.12 Activation of ATR-1 inHSC renders release of intracellular Ca+2, promoting cel-lular contraction and proliferation. Different studieshave studied the molecular implications of intracellularpathways that promote hepatic fibrosis. Two potentcytokines that stimulate HSC in autocrine and paracrinefashion are transforming growth factor-b (TGF) andplatelet derived growth factor (PDGF). These cytokinesactivate different intracellular steps promoting liverfibrosis.13 The effects of AT-II over activated HSC includeexpression of collagen I by induction of the intracellular
MAPK/ERK pathway, in the same way that PDGF.14 Theactivation of ATR-1 by AT-II also promotes an increaseof TIMP-1 in the liver, producing disequilibrium withincreased collagen and protein deposition in the extra-cellular matrix (ECM).15
In bile-duct ligated rats undergoing liver cirrhosis, theadministration of an infusion of AT-II increases inflam-mation and stage of liver fibrosis.16 Among other puta-tive mechanisms for this effect, it is thought that AT-IIincreases oxidative stress, inducing a state of procoagu-lation, stimulating biliary duct proliferation and activa-tion of MAPK (mitogen -activated protein kinase)pathway in the liver.
Different cells in the organism are capable of produc-ing AT-II locally during a process of acute or chronicinjury such as mesangial glomerular cells or cardiacmyofibroblasts.17 This local production of AT-II pro-motes recruitment of inflammatory cells, inducesexpression and secretion of ECM proteins and inhibitscollagen degradation. These effects confirm the inflam-matory and profibrogenic actions of AT-II, which arenot exclusive of hepatic injury.18 A study performed byBataller and colleagues demonstrated that activated HSCexpressed an increased amount of RAA system compo-nents. Activated HSC were capable of expressing mRNAfor angiotensinogen, renin and ACE. At the same time,activated HSC showed an increase expression of surfaceATR-1 and ATR-2 as well as autocrine production ofAT-II. These changes were not observed in quiescentHSC. This fact implies that the phenotypic transforma-tion of activated HSC towards myofibroblastic cellsrenders augmentation of the production of proinflam-matory and profibrogenic factors in an independentmanner, everything due to the response to cellularinjury.19
IMPLICATIONS OF DIFFERENT RAA SYSTEMIN HEPATIC FIBROSIS
AS MENTIONED ABOVE, AT-II has multiple effectsas a hormone, besides the cardiovascular system
(Fig. 1). The RAA system is frequently activated inpatients with hepatic cirrhosis. This represents a com-pensatory response mechanism due to the state ofvasodilatation, systemic hypotension and renal hypop-erfusion.20 This hemodynamic response is accentuatedin patients with cirrhosis and ascites. This hormonalcounterbalance response implies an increase in plasmaAT-II. With the precedent of hepatic injury and fibrosisremodeling, the high levels of AT-II accelerate theprocess of tissue collagen deposition through the afore-
96 A. Lugo-Baruqui et al. Hepatology Research 2010; 40: 95–104
© 2009 The Japan Society of Hepatology

mentioned TGF-b1 pathway. This continuous stimula-tory effect of AT-II over activates HSC, promotes theirproliferation and perpetuates the priming of profibro-genic insult.
A common consequence of the remodeling andchanges in hepatic architecture secondary to hepatic cir-rhosis is the elevation of the hepatic vein wedge pressure(HVWP). Excess of collagen deposition in hepatic paren-chyma increases the resistance of hepatic microcircula-tion. The product of the diminished blood flow causesa retrograde increase in portal venous pressure (PVP)reflected in the sites of porto-systemic venous anasto-mosis. This increase in PVP represents an importantfactor for the development of cirrhosis complicationssuch as esophageal variceal bleeding. It has been proved
that infusion of AT-II produces a similar effect, mediat-ing an increase of the PVP.21 These observations suggestthat portal hypertension is a hemodynamic derange-ment caused by mechanical and humoral factors.
As mentioned earlier, most of the biological responsesto AT-II are mediated by the ATR-1. In the liver, theprofibrogenic effect of AT-II is regulated by the activa-tion of the same receptors. In a study carried out in ananimal model of cirrhosis, the expression of truncatedATR-1 demonstrated a decrease in the hepatic concen-tration of TGF-b1, a reduction in the number of inflam-matory cells and cytokines, and a decrease in lipidperoxidation as well as a reduced phosphorilation inthe c-Jun and MAPK pathways.22 These results confirmthe importance of the role of ATR-1 in the process of
Normal liver
End stage liver
fibrosis
Portal hypertension
Stimulates proliferation
and activation of HSC.
Main action site of
ace inhibitors;
cellular proliferation
and activation of HSC
* Systemic vasoconstriction
* Increase in TPR
* Increase in PVP
* Mesangial cell proliferation
* Increase in GFR
* Decrease in RPF
Cardiac
remodeling
Afferent artericle
Glomerular
ultrafiltrate
Protein
Other
solutes
Glomerular
(bowman’s capsule)Efferent
arteriole
AT II
Figure 1 The figure displays the effects of angiotensin (AT) II on the kidney by constricting the efferent arteriole in the glomerulus,with a resulting increase in glomerular filtration rate (GFR) and decrease in renal plasma flow (RPF). ATII also acts in cardiac fibersprovoking cardiac remodeling, making the rationale for the use of angiotensin-converting enzyme (ACE) inhibitors for thetreatment of post-miocardial infarction adverse remodeling effects. He lungs are the mail site for ATI conversion into ATII by theeffect of ACE, although this enzyme is also found in endothelial cells. In the periphery AT II is a potent vasoconstrictor, elevatingtotal peripheral resistance and is usually released as part of the RAS system in response to hypotension. Finally, recent works explainits role in the activation and proliferation of hepatic stellate cells (HSC) of chronically injured liver which leads to cirrhosis and itscomplications such as portal hypertension and liver failure.
Hepatology Research 2010; 40: 95–104 Angiotensin II therapy in portal hypertension 97
© 2009 The Japan Society of Hepatology

inflammation and fibrosis and the initiation of thisactivation via AT-II stimulation.
In an animal model of cirrhosis by bile duct ligation,it was observed that treatment with the ACE inhibitor,captopril, was effective in reducing fibrosis stage andinflammatory grading by reducing the number ofa-SMA positive cells. Additionally, there was an impor-tant reduction in the profibrogenic proteins expressionsuch as TGF-b1 and a1-procollagen. Likewise, the quan-tity of MMP-2 and MMP-9 were reduced, revealing adecrease in the need for their expression, which is com-monly up-regulated in chronic hepatic diseases as acompensatory mechanism for degradation of ECM pro-teins.23 With these results, the effect of AT-II blockadeshowed potential benefit in preventing and reversing thefibrosis process.
The comparative effects of ACE inhibitors against ARBwere studied in rats with liver fibrosis induced byadministration of pig serum. This revealed that the inter-vention with perindopril vs. candesartan resulted insimilar findings. Both groups of animals showed amarked decrease in fibrosis, when measured by directdensitometry when compared against a control groupwithout induced fibrosis. The levels of hydroxyprolinein the liver, and the serum fibrotic markers, i.e.7s-collagen, hialuronic acid, and procollagen-III-peptide were also reduced. In the immunological analy-sis reduced amounts of a-SMA positive cells, as well as aconcomitant reduction in the levels of expression forTGF-b1 mRNA were reported. These results did not havea statistically relevant difference between the groupstreated with perindopril or candesartan. The similaritiesof results demonstrate that the effects of AT-II blockadeare obtained either by enzymatic inhibition or by recep-tor blockade.
Since therapeutic interventions were started after4 weeks from the beginning of toxic injury, this studyclearly mimicked the common clinical setting in whicha patient with chronic liver injury has a profibrogenicprocess already established. As a side observation, theauthors discussed that the sole effect of AT-II over itsreceptors, is by itself incapable of inducing liver cirrho-sis. In this setting, there must be a previous injurycausing the activation of HSC, in order for AT-II toexacerbate the fibrotic process.24
The knowledge of the activation pathway of HSCrenders an important step in understanding overproduc-tion of profibrogenic proteins. In this process, the acti-vation signal induced by the TGF-b/Smad pathway hasclearly been related to stimulation or inhibition of thefibrosis process. It has been described that after activa-
tion of the membrane receptor for TGF-b, different pro-teins of the Smad family activates. After activation ofTGFb type 1 receptor, the first response consists in theinduction of Smad 2 and Smad 3 to bind together toform the activator complex Smad 4. There are previousreports in which activation of ATR-1 by AT-II, stimulateexpression of TGF-b, promoting an autocrine stimula-tion of HSC.25 Once activated by AT-II, there is a nucleartranslocation of Smad 2. This process results in the samemolecular mechanism perpetuating the fibrotic pro-cess.26 It has been observed that treatment with ACEinhibitors and ARB in cirrhotic rats reduces expressionof Smad3 by HSC, increasing at the same time expres-sion of Smad7, which represents the main counterregu-latory protein within the Smad family.27 The inhibitoryeffect of Smad 7 is observed normally after activation ofTGF-b receptor as a compensatory mechanism for theprofibrogenic stimulus of Smad 4.28 In this manner,antifibrotic intervention of the AT-II signalization block-ade could follow the same intracellular mechanisms asthe TGF-b blockade.
Different experimental studies have demonstrated therole of VEGF (vascular endothelial growth factor-1) inthe process of hepatic fibrosis and carcinogenesis bymediation of angiogenesis. Recent observations statethat molecular mechanisms associated with angiogen-esis and fibrosis occur in a simultaneous manner, actingsynergistically between them.29 It has been previouslysuggested that AT-II induces an increase of VEGF expres-sion in the HSC.30 The selective blockade of VEGF recep-tors by specific antibodies reduces expression of VEGFmRNA in the liver of cirrhotic rats. This inhibition andreduced expression reduces the hepatic fibrosis processby means of neovascularization arrest, diminished HSCproliferation and reduced pro-collagen mRNA. Inter-vention with ACE inhibitors blocks the AT-II signaling,reducing VEGF expression. As a consequence of treat-ment, intracellular fibrotic processes of VEGF activationcan be effectively inhibited, resulting in an additionalstep for the treatment of hepatic fibrosis as well as forthe prevention of neoplasias, including hepatocellularcarcinoma.31
HEMODYNAMIC CONSIDERATIONS
RAA SYSTEM IS found to be frequently up-regulatedin patients with chronic hepatic disease. AT-II is
considered to be an important mediator in the increaseof portal venous pressure. The administration of AT-IIalone induces an elevation in portal venous pressure.21
Since hepatic cirrhosis induces a state of hyperdynamic
98 A. Lugo-Baruqui et al. Hepatology Research 2010; 40: 95–104
© 2009 The Japan Society of Hepatology

systemic circulation with increased levels of AT-II, therole of this hormone could be implicated in some of thecomplications of portal venous Hypertension.
Portal hypertension is a common complication of cir-rhosis. This represents an important step in the patho-genesis of esophageal variceal bleeding. A commonpathway that results in elevated portal venous pressureis represented by an increase in intrahepatic portal resis-tance rendering retrograde venous blood flow in theporto-systemic anastomoses. The morphologic alter-ations in the hepatic parenchyma are responsible for theincrease in the intrahepatic vascular resistance. The com-bination of alterations seen in chronic liver injuries suchas tissue remodeling due to fibrosis, endothelial dys-function by endothelial nitric oxide synthase deficiency,along with increased levels of vasoactive hormones suchas catecholamines and AT-II, induce dysregulation ofthe circulatory homeostasis. Increased basal serumlevels of AT-II causes a down-regulation of the ATR-1due to overactivation of this receptor. The clinical impli-cations of this loss of regulatory mechanisms in circula-tion, produces a diminished response to vasodilatorydrugs like ARB.32
In the clinical setting, portal venous pressure (PVP) isbest characterized by the use of hepatic vein pressuregradient (HVPG). HVPG is the product of the portalblood flow and intrahepatic resistance. It is consideredthat a HVPG < 12 mmHg, or a decrease of 20% or moreof its basal values, confers primary protection againstbleeding from esophageal variceal bleeding.33 Tradition-ally, intervention with a non-specific beta-blocker suchas propranolol has been employed to reduce the risk ofvariceal bleeding.34 Previous works report that patientstreated with beta-blockers show a decrease in the HVPGof only 15%. Due to this moderate reduction, a com-bined treatment strategy has been employed with beta-blockers and the addition of vasodilatory nitrates.35
Nonetheless, when this strategy is applied in patientswith ascites and fluid retention, serious renal failure hasbeen reported. The look for new and safe strategies thateffectively reduce the HVPG is important to reduce therisk of developing serious complications.
RENAL ACTION OF AT-II
IN THE RENAL vasculature, AT-II produces changesthat alter the function of glomerular arterioles. Physi-
ologically, AT-II selectively increases the vascular tone ofefferent arterioles in the glomeruli. The use of ACEinhibitors, or the blockade of ATR-1 produce a dilation ofthe efferent arteriole with a secondary decrease of glom-
erular hydrostatic pressure and a reduced plasma bloodflow. The inhibitory effects of these drugs in the renalvasculature are accompanied by a reduced filtration frac-tion. This leads to a mild renal failure with azotemia aftera patient begins treatment for conditions like systemicHypertension The reduced filtration fraction can also bebeneficial in patients with Diabetes Mellitus (DM) inwhich the blockade of AT-II action can reduce theexisting proteinuria in diabetic nephropathy.36
Another hormone of the RAA implied in the renalfunction is aldosterone. In response to a hypotensivestate, aldosterone secretion promotes sodium resorp-tion in the collecting tubule with consequent fluidretention and expansion of intravascular volume. Theblockade of this effect caused by ACE inhibitors andARB is an important mediator of the antihypertensivecharacteristics of these drugs. It has been described thatpatients with cirrhosis without ascites have alterationsin their sodium-handling mechanisms. These patientspresent a net positive sodium balance with a dietaryingestion greater than 200 mmol/day, due to ineffectivenatriuresis because of elevated serum aldosterone lev-els.37 The altered sodium handling mechanism couldplay a role in the progress of portal hypertension incirrhotic patients and could also explain the beneficialeffects of AT-II blockade as a strategy for control of thesepatients.
AT-II BLOCKADE IN CLINICAL TRIALS
ADDITIONAL EVIDENCE SUGGESTS that renalsodium handling can be also improved in patients
treated with ARB. In a small study conducted in 9 cir-rhotic patients without ascites, with a daily diet of200 mmol of sodium, it was found that administrationof losartan in small doses (7.5 mg/day) normalized therenal sodium excretion to 202 mmol/day, achieving aslightly negative net sodium balance. These patients pre-sented improvements in fluid management withoutimportant alterations in mean arterial blood pressure,glomerular filtration rate or renal plasma flow.38 Thisevidence suggests that AT-II is not the main regulatorymechanisms in cirrhotic patients who have not yetdeveloped ascites. The treatment with ACE inhibitors ofARB could result beneficial in patients in early stages ofhepatic fibrosis, without endangering the patients toserious adverse effects. Usually the dose of losartanadministered for the treatment of systemic hypertensionis between 25 and 100 mg/day. The smaller doses used inthis trial evidence the enhanced sensibility in thesepatients of the renal function towards the effects of AT-II.
Hepatology Research 2010; 40: 95–104 Angiotensin II therapy in portal hypertension 99
© 2009 The Japan Society of Hepatology

Patients with hepatic cirrhosis present importanthemodynamic alterations. The presence of ascites is ofbad prognosis because it reflects the failure of compen-satory mechanisms in the underlying increased vascularresistance, decreased plasma oncotic pressure andimportant intravascular volume expansion with a con-sequent high output heart failure. The role of At-II hasbeen described as an important factor that could beeffective at a multifunctional level, including regula-tion of the hyperdynamic state present in cirrhoticpatients.
The intervention of AT-II blockade has been studiedin clinical trials. In a previous study including 45 cir-rhotic patients with portal hypertension (defined assevere in patients with HVPG 3 20 mmHg or moderatein patients with HVPG > 12 but < 20 mmHg) the thera-peutical intervention with losartan (ARB) in small doses(25 mg/day) resulted effective in lowering the PVP.The results reported a decrease in the HVPG from24.8 1 3.6 mmHg to 13.1 1 4.1 mm Hg in the groupwith severe portal hypertension and from 17.9 11.4 mmHg to 10.0 1 2.7 mmHg of HVPG in patientswith moderate portal Hypertension Both groupsshowed an important decrease in the hepatic wedgepressure. An effective reduction greater than 20 mmHgin the HVPG was observed in 44 patients (98%).Authors reported only one case of severe hypotensionpresented after the first dose administered and resolvedafter adequate management. There were no reports ofelectrolyte disturbances or renal failure.39 This studyreflects that intervention with ARB could be used as analternative for b-blockers as a primary prevention strat-egy against variceal bleeding due to their effective reduc-tion in HVPG and portal Hypertension.
TREATMENT OF LIVER FIBROSIS CAUSED BYDIFFERENT ETIOLOGIES
THE UNDERSTANDING OF molecular basis govern-ing the role of AT-II in the process of hepatic cirrho-
sis has been facilitated by a great deal of research usinganimal models and could be applied in patients withchronic liver damage of various etiologies. Some ofthe presumed benefits of the intervention include thereduction of portal hypertension comorbilities such asvariceal bleeding or spontaneous bacterial peritonitis.The observed effects of the intervention on the histo-logic and hemodynamic parameters set the basis for theapplication of these drugs in liver fibrosis secondary tometabolic or viral injury.
Chronic infection with hepatitis C virus (HCV) repre-sents a global health problem, affecting more than 170million people worldwide, with a total estimated preva-lence of 3% of the total globe population.40 Interventionwith ARB has been studied in patients with HCV infec-tion in early stages of cirrhosis. It has been observed that50 mg of losartan effectively reduced fibrosis degree aswell as serum levels of collagen type IV and TGF-b1. Thestudy did not show important serious adverse effects inthe intervention group; neither had it revealed a higherincidence of hypotension as expected.41 Decreased levelsof profibrotic markers could represent an additionalalternative for the chronic treatment of these patients. Ina retrospective study conducted on patients infectedwith hepatitis C virus, a group of patients with systemicarterial hypertension was analyzed. Hypertensivepatients showed significantly higher levels of liver fibro-sis, possibly due to the effect of At-II in circulation. Thesubgroup of patients who were receiving treatment withACE inhibitors had less fibrosis compared with the restof the patients. This shows an association with hyper-tension and a beneficial role of ACE for the inhibition ofliver fibrosis in HCV infected patients.42
Another study performed in 62 patients with portalhypertension due to of liver cirrhosis of different etiolo-gies, compared directly the efficacy of captopril (ACEinhibitor) vs. propranolol to evaluate the effect onHVPG. The results report that caprotpril did not reducesignificantly the HVPG.43 In an analysis realized apartfrom the primary end point, it was observed that capto-pril was useful in reducing 20% the basal values ofHVPG in about a third of patients treated with this drug.Captopril also reduced the hepatic wedge pressure, sug-gesting that it influences intrahepatic vascular resistance,improving by this mechanism the portal venous flow.This effect was not observed in the propranolol group.Similar results were reported in patients with chronicliver disease that received candesartan for a year, obtain-ing a reduction in the HVPG greater than 20% in 25% ofthe patients with adequate toleration to the drug.44
These findings confirmed the action of AT-II not onlyin systemic circulation, leaving background for moreresearch in this matter.
Due to the beneficial results of ACE inhibitors inpatients with liver cirrhosis, different treatment combi-nations have been employed. The immune systemmodulator interferon alpha (IFN-a) has been tradition-ally employed for the treatment of chronic infectionwith HCV. Recently, it has been reported that IFN-aimproves the fibrosis index, reducing the expression ofcollagen type I in patients with HCV infection.45 In a
100 A. Lugo-Baruqui et al. Hepatology Research 2010; 40: 95–104
© 2009 The Japan Society of Hepatology

report by Yoshiji and cols. the intervention with perin-dopril was combined with IFN-a to treat patients whowere non-responders to the treatment with high dosesof IFN alone. The group of patients with combinedtreatment showed reductions in the plasma levels ofhyaluronic acid, collagen type IV 7S, as well as pro-collagen type III peptide (P-III-P). This implied that thecombined treatment with perindopril and IFN-a at lowdoses could result in an alternative for the patients thatcould not tolerate or that did not respond to regular orhigh doses of IFN.46
Another studied combined the strategy of blockingthe signaling pathway of TGF-b and consists in thedual use of ACE inhibitor together with PDGF receptorinhibitor. TGF-b is an important cytokine for the devel-opment of fibrosis, and PDGF is an important stimu-lus for the proliferation of activated HSC. In an animalmodel of liver cirrhosis induced with CCl4, combinedblockade of the TGF-b signaling with perindopril aswell as the kinase inhibitor of PDGF receptor, imatinib,demonstrated a synergistic effect in the improvementof liver fibrosis in molecular and morphological analy-sis. The intervention resulted in a decrease of TGF-bmRNA levels, reduced hydroxiproline liver contentand diminished serum values of fibrosis markers. At amolecular level, it was reported a diminished phos-phorylation and signal activation by PDGF, reducingthe fibrosis process and inhibiting activation of HSC.47
This trial used drugs that are currently available in theclinical setting and that resulted in an interestingcombination for patients with liver cirrhosis of variousetiologies.
Recently, studies have underlined the important rela-tion between the progression of non-alcoholic steato-hepatitis (NASH) and insulin resistance with the RAAsystem.48 Obesity and type 2 DM are considered themain risk factors for the development of NASH, boththese conditions are associated with elevated insulinblood levels.49 In diabetic rat models, the interventionwith ARB olmesartan and losartan attenuated the pro-gression of hepatic steatosis and diminished the expres-sion of lipogenic genes, together with a decrease inoxidative stress in the liver.50–52 Different single nucle-otide polymorphisms in the ART-1 gene have beendescribed in patients with NASH, highlighting theimportance of AT-II as a mediator of the progression ofliver disease.53 Since there are no effective therapeuticalinterventions for the treatment of NASH and liver fibro-sis progression, the use of ARB in clinical trials couldprovide a new alternative for the management of liversteatosis and metabolic syndrome.
FUTURE DIRECTIONS AND CONCLUSIONS
LIVER FIBROSIS IS an intensively studied subject inwhich numerous factors are involved, including
stimulus from the RAA system like AT-II. Blockade ofAT-II effects results in a diminished response tochronic injury and slower progression of hepatic fibro-sis. This intervention also affects positively the hemo-dynamic conditions of patients with cirrhosis such asportal Hypertension Recent studies with patients withchronic liver disease have revealed improved clinicalconditions, reduction in histologic damage and dimin-ished profibrotic markers with the blockade of AT-IIaction by means of ACE inhibitors or ARB. Evidencesuggest that patients with early stages of liver diseasewithout ascites get maximum benefits of these inter-ventions rendering diminished portal pressure values,showing an adequate security profile without seriousside-effects. Nonetheless, in patients in which the liverdamage shows marked progression clinically evidentwith the presence of ascites, blockade of RAA systemcould result in severe hypotension and acute renalfailure.
Recently, another enzyme has been related in theRAA system, called the angiotensina convertingenzyme type 2 (ACE-2). The supposed function of theACE-2 is the degradation of AT-II into AT1–7 which isbelieved to have vasodilatory properties accompaniedwith tisular protection with antifibrogenic characteris-tics.54 AT1–7 represents an alternative enzymaticpathway in the RAA system that could mediate andcounterbalance the effects of AT-II. It has beendescribed the up-regulation of the ACE-2 in humanpatients with liver cirrhosis.55 In animal models withliver cirrhosis where the receptor for AT1–7 has beenblocked a greater degree of fibrogenic activity wasobserved.56 These findings make ACE-2 and AT1–7 veryattractive as therapeutic targets for future strategies. Thebalance between profibrogenic and antifibrogenic sig-naling pathways in the HSC, are mediated by AT-IIreceptors type 1 and type 2, among others (Fig. 2).57
Evidence shows that AT-II receptor type 2 is expressedin chronically inflamed tissue like the live and heart,with antifibrogenic effect on its activation.58,59 Overall,the complete implications of the RAA system in theprocess of fibrosis are not yet fully understood, but it isclear that important implications are involved in theprogression of the disease.
In order to give clear recommendations about the useof ACE inhibitors or ARB for the treatment of patientswith chronic liver disease, larger, randomized, double
Hepatology Research 2010; 40: 95–104 Angiotensin II therapy in portal hypertension 101
© 2009 The Japan Society of Hepatology
blinded studies are needed. Complete guidelines thatissue the type of drug as well as the dose and duration oftreatment are necessary in order to consider this inter-vention as part of the integral treatment of the cirrhoticpatient. Previous results with ACE inhibitors and ARBhave resulted promising. The combination of thesedrugs with other agents previously used like IFN andPDGF blocker, show synergistic effects in the end pointsstudied. Another plausible combination not yet tested isthe use of ARB with an antifibrotic agent like pirfeni-done (PFD). There are previous reports that describe themechanism of action of PFD by means of blockadeof TGF-b biological function. PFD has been used inpatients with liver cirrhosis achieving important regres-sion of hepatic fibrosis and improvement of the necro-
inflammatory index in patients with advanced disease,without serious adverse effects.60 Also, an improvementof quality of life, as measured by SF-36 questionnaires,was noted.
According to all the previous works and findings, it isclear that the use of ACE inhibitors of ARB represents apromising intervention for patients with liver cirrhosisand other pathologic conditions in which fibrotic pro-cesses are implied. More research is needed in order toinclude these drugs as a part of the conventional treat-ment for every patient with chronic hepatic disease,especially those with increased portal pressure. Thisshows the idiosyncratic effects of old drugs and theunderstanding we have to accomplish before we inte-grally manage these patients.
Procollagen α1(1)
PA1-1
TIMP-1
MCP-1/rantes
PDFGR
PKC
VEGF
++
MAP/ERKCA+
IP3
Smad 2Smad 3
Smad 7
AT-II R2
AT-II R1 receptor
ACE inhibitors
TGF-β1
Angiotensin 1-7
ARB
AT-II
AT-II
AT-I
ACE-2
(+)(+)
(–)
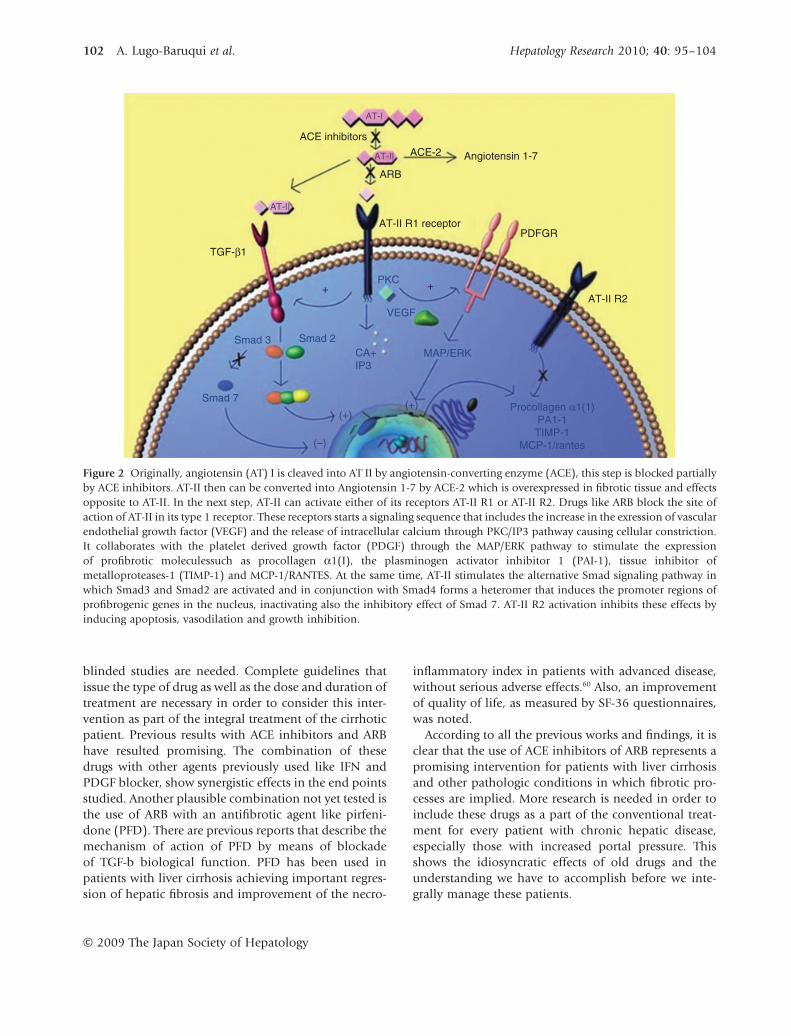
Figure 2 Originally, angiotensin (AT) I is cleaved into AT II by angiotensin-converting enzyme (ACE), this step is blocked partiallyby ACE inhibitors. AT-II then can be converted into Angiotensin 1-7 by ACE-2 which is overexpressed in fibrotic tissue and effectsopposite to AT-II. In the next step, AT-II can activate either of its receptors AT-II R1 or AT-II R2. Drugs like ARB block the site ofaction of AT-II in its type 1 receptor. These receptors starts a signaling sequence that includes the increase in the exression of vascularendothelial growth factor (VEGF) and the release of intracellular calcium through PKC/IP3 pathway causing cellular constriction.It collaborates with the platelet derived growth factor (PDGF) through the MAP/ERK pathway to stimulate the expressionof profibrotic moleculessuch as procollagen a1(I), the plasminogen activator inhibitor 1 (PAI-1), tissue inhibitor ofmetalloproteases-1 (TIMP-1) and MCP-1/RANTES. At the same time, AT-II stimulates the alternative Smad signaling pathway inwhich Smad3 and Smad2 are activated and in conjunction with Smad4 forms a heteromer that induces the promoter regions ofprofibrogenic genes in the nucleus, inactivating also the inhibitory effect of Smad 7. AT-II R2 activation inhibits these effects byinducing apoptosis, vasodilation and growth inhibition.
102 A. Lugo-Baruqui et al. Hepatology Research 2010; 40: 95–104
© 2009 The Japan Society of Hepatology

REFERENCES
1 Bosch J, García-Pagán JC. Complications of cirrhosis. I.Portal Hypertension J Hepatol 2000; 32 (Suppl. 1): 141–56.
2 Yoshiji H, Noguchi R, Ikenaka Y et al. Renin-Angiotensinsystem inhibitors as therapeutic alternatives in the treat-ment of chronic liver diseases. Curr Med Chem 2007; 14:2749–54.
3 Johnston CI. Renin-angiotensin system: a dual tissue andhormonal system for cardiovascular control. J HypertensSuppl 1992; 10: S13–26.
4 Goodfriend TL, Elliott ME, Catt KJ. Angiotensin receptorsand their antagonists. N Engl J Med 1996; 334: 1649–54.
5 Konstam MA, Rousseau MF, Kronenberg MW et al. Effectsof the angiotensin converting enzyme inhibitor enalaprilon the long-term progression of ventricular dysfunction inpatients with heart failure. Circulation 1992; 86: 431–8.
6 Cohn JN, Tognoni G. A randomized trial of theangiotensin-receptor blocker valsartan in chronic heartfailure. N Engl J Med 2001; 345: 1667.
7 Lewis EJ, Hunsicker LG, Bain RP, Rohde RD. The effect ofangiotensin- converting–enzyme inhibition on diabeticnephropathy. N Engl J Med 1993; 329: 1456–62.
8 Barnett AH, Bain SC, Bouter P et al. Angiotensin-ReceptorBlockade versus Converting–Enzyme Inhibition in Type 2Diabetes and Nephropathy. N Engl J Med 2004; 351: 1952.
9 Parsons CJ, Takashima M, Rippe RA. Molecular mecha-nisms of hepatic fibrogenesis. J Gastroenterol Hepatol 2007;22: 79–84.
10 Bataller R, Brenner DA. Liver fibrosis. J Clin Invest 2005;115: 209–18. Erratum in J Clin Invest 2005; 115: 1100.
11 Weiner FR, Giambrone MA, Czaja MJ et al. Ito-cell geneexpression and collagen regulation. Hepatology 1990; 11:111–17.
12 Bataller R, Gines P, Nicolas JM et al. Angiotensin II inducescontraction and proliferation of human hepatic stellatecells. Gastroenterology 2000; 118: 1149–56.
13 Verrecchia F, Mauviel A. Transforming growth factor-b andfibrosis. World J Gastroenterol 2007; 13: 3056–62.
14 Tharaux PL, Chatziantoniou C, Fakhouri F, Dussaule JC.Angiotensin II activates collagen I gene through a mecha-nism involving the MAP/ER kinase pathway. Hypertension2000; 36: 330–6.
15 Yoshiji H, Kuriyama S, Yoshii J et al. Angiotensin-II inducesthe tissue inhibitor of metalloproteinases-1 through theprotein kinase-C signaling pathway in rat liver fibrosisdevelopment. Hepatol Res 2003; 27: 51–6.
16 Bataller R, Gabele E, Parsons CJ et al. Systemic infusion ofangiotensin II exacerbates liver fibrosis in bile duct-ligatedrats. Hepatology 2005; 41: 1046–55.
17 Mezzano SA, Ruiz-Ortega M, Egido J. Angiotensin II andrenal fibrosis. Hypertension 2001; 38: 635–8.
18 Weber KT, Sun Y, Katwa LC, Cleutjens JP. Tissue repair andangiotensin II generated at sites of healing. Basic Res Cardiol1997; 92: 75–8.
19 Bataller R, Sancho-Bru P, Gines P et al. Activated humanhepatic stellate cells express the renin-angiotensin systemand synthesize angiotensin II. Gastroenterology 2003; 125:117–25.
20 Ballet F, Chretien Y, Rey C et al. Differential response ofnormal and cirrhotic liver to vasoactive agents. A study inthe isolated perfused rat liver. J Pharmacol Exp Ther 1988;244: 233–5.
21 Helmy A, Jalan R, Newby DE, Hayes PC, Webb DJ. Role ofangiotensin II in regulation of basal and sympatheticallystimulated vascular tone in early and advanced cirrhosis.Gastroenterology 2000; 118: 565–72.
22 Yang L, Bataller R, Dulyx J et al. Attenuated hepatic inflam-mation and fibrosis in angiotensin type 1a receptor-deficient mice. J Hepatol 2005; 43: 317–23.
23 Jonsson JR, Clouston AD, Ando Y et al. Angiotensin-converting enzyme inhibition attenuates the progressionof rat hepatic fibrosis. Gastroenterology 2001; 121: 148–55.
24 Yoshiji H, Kuriyama S, Yoshii J et al. Angiotensin-II type 1receptor interaction is a major regulator for liver fibrosisdevelopment in rats. Hepatology 2001; 34: 745–50.
25 Dooley S, Delvoux B, Streckert M et al. Transforminggrowth factor beta signal transduction in hepatic stellatecells via Smad2/3 phosphorylation, a pathway that isabrogated during in vitro progression to myofibroblasts.TGFbeta signal transduction during transdifferentiation ofhepatic stellate cells. FEBS Lett 2001; 502: 4–10.
26 Kamada Y, Tamura S, Kiso S et al. Angiotensin II stimulatesthe nuclear translocation of Smad2 and induces PAI-1mRNA in rat hepatic stellate cells. Hepatol Res 2003; 25:296–305.
27 Xu W, Song S, Huang Y, Gong Z. Effects of perindopril andvalsartan on expression of transforming growth factorb-Smads in experimental hepatic fibrosis in rats. J Gastroen-terol Hepatol 2006; 21: 1250–6.
28 Nakao A, Afrakhte M, Moren A et al. Identification ofSmad7, a TGFbeta- inducible antagonist of TGF-beta sig-naling. Nature 1997; 389: 631–5.
29 Corpechot C, Barbu V, Wendum D et al. Hypoxia-inducedVEGF and collagen I expressions are associated with angio-genesis and fibrogenesis in experimental cirrhosis. Hepatol-ogy 2002; 35: 1010–21.
30 Yoshiji H, Kuriyama S, Yoshii J et al. Vascular endothelialgrowth factor and receptor interaction is a prerequisite formurine hepatic fibrogenesis. Gut 2003; 52: 1347–54.
31 Yoshiji H, Kuriyama S, Kawata M et al. The angiotensin-I-converting enzyme inhibitor perindopril suppresses tumorgrowth and angiogenesis: possible role of the vascularendothelial growth factor. Clin Cancer Res 2001; 7:1073–8.
32 Töx U, Steffen HM. Impact of inhibitors of the renin-angiotensin-aldosterone system on liver fibrosis and portalhypertension. Curr Med Chem 2006; 13: 3649–61.
33 Groszmann RJ, Bosch J, Grace ND, Conn HO, Garcia-TsaoG. Hemodynamic events in a prospective randomized trial
Hepatology Research 2010; 40: 95–104 Angiotensin II therapy in portal hypertension 103
© 2009 The Japan Society of Hepatology

of propranolol versus placebo in the prevention of a firstvariceal hemorrhage. Gastroenterology 1990; 99: 1401–7.
34 Poynard T, Calés P, Pasta L et al. Beta-adrenergic antagonistdrugs in the prevention of gastrointestinal bleeding inpatients with cirrhosis and esophageal varices. An analysisof data and prognostic factors from 589 patients fromfour randomized clinical trials. N Engl J Med 1991; 324:1532–8.
35 Morillas RM, Planas R, Cabré E et al. Propranolol plusisosorbide-5-mononitrate for portal hypertension in cir-rhosis: long-term hemodynamic and renal effects. Hepatol-ogy 1994; 20: 1502–8.
36 Arroyo V, Bosch J, Mauri M, Ribera F, Navarro-López F,Rodés J. Effect of angiotensin-II blockade on systemic andhepatic hemodynamics and on the renin-angiotensin-aldosterone system in cirrhosis with ascites. Eur J Clin Invest1981; 11: 221–9.
37 Wong F, Liu P, Allidina Y et al. Pattern of sodium handlingand its consequences in pre-ascitic cirrhosis. Gastroenterol-ogy 1995; 108: 1820–7.
38 Girgrah N, Liu P, Collier J, Blendis L, Wong F. Haemody-namic, renal sodium handling, and neurohumoral effectsof acute administration of losartan, an angiotensin IIreceptor antagonist, in preascitic cirrhosis. Gut 2000; 46:114–20.
39 Schneider AW, Kalk JF, Klein CP. Effect of losartan, anangiotensin II receptor antagonist, on portal pressure incirrhosis. Hepatology 1999; 29: 334–9.
40 World Health Organization. Hepatitis C-global prevalence(update). Wkly Epidemiol Rec 1999; 74: 425.
41 Terui Y, Saito T, Watanabe H et al. Effect of angiotensinreceptor antagonist on liver fibrosis in early stages ofchronic hepatitis C. Hepatology 2002; 36 (4 Pt 1): 1022.
42 Corey KE, Shah N, Misdraji J et al. The effect ofangiotensin-blocking agents on liver fibrosis in patientswith hepatitis C. Liver Int 2009; 29: 748–53.
43 Baik SK, Park DH, Kim MY et al. Captopril reduces portalpressure effectively in portal hypertensive patients withlow portal venous velocity. J Gastroenterol 2003; 38:1150–4.
44 Debernardi-Venon W, Martini S, Biasi F et al. AT1 receptorantagonist Candesartan in selected cirrhotic patients: effecton portal pressure and liver fibrosis markers. J Hepatol2007; 47: 426–7.
45 Inagaki Y, Nemoto T, Kushida M et al. Interferon alfadown-regulates collagen gene transcription and suppressesexperimental hepatic fibrosis in mice. Hepatology 2003; 38:890–9.
46 Yoshiji H, Noguchi R, Fukui H. Combined effect of anACE inhibitor, perindopril and interferon on liver fibrosis
markers in patients with chronic hepatitis C. J Gastroenterol2005; 40: 215–16.
47 Yoshiji H, Kuriyama S, Noguchi R et al. Amelioration ofliver fibrogenesis by dual inhibition of PDGF and TGF-betawith a combination of imatinib mesylate and ACE inhibi-tor in rats. Int J Mol Med 2006; 17: 899–904.
48 Lubel JS, Herath CB, Burrell LM, Angus PW. Liver diseaseand the renin-angiotensin system: recent discoveries andclinical implications. J Gastroenterol Hepatol 2008; 23:1327–38.
49 Angulo P. Nonalcoholic fatty liver disease. N Engl J Med2002; 346: 1221.
50 Kurita S, Takamura T, Ota T et al. Olmesartan ameliorates adietary rat model of non-alcoholic steatohepatitis throughits pleiotropic effects. Eur J Pharmacol 2008; 588: 316–24.
51 Yokozawa J, Sasaki T, Ohwada K et al. Down-regulation ofhepatic stearoyl-CoA desaturase 1 expression by angio-tensin II receptor blocker in the obese fa/fa Zucker rat:possible role in amelioration of insulin resistance andhepatic steatosis. J Gastroenterol 2009; 44: 583–91.
52 Yoshiji H, Noguchi R, Ikenaka Y et al. Losartan, anangiotensin-II type 1 receptor blocker, attenuates the liverfibrosis development of non-alcoholic steatohepatitis inthe rat. BMC Res Notes 2009; 2: 70.
53 Yoneda M, Hotta K, Nozaki Y et al. Association betweenangiotensin II type 1 receptor polymorphisms and theoccurrence of nonalcoholic fatty liver disease. Liver Int2009; 29: 1078–85.
54 Ferrario CM, Chappell MC, Tallant EA et al. Counterregu-latory actions of angiotensin-(1-7). Hypertension 1997; 30:535–41.
55 Paizis G, Tikellis C, Cooper ME et al. Chronic liver injury inrats and humans upregulates the novel enzyme angio-tensin converting enzyme 2. Gut 2005; 54: 1790–6.
56 Moreno M, Bataller R. Cytokines and renin-angiotensinsystem signaling in hepatic fibrosis. Clin Liver Dis 2008; 12:825–52, ix.
57 Pereira RM, Dos Santos RA, Teixeira MM et al. The renin-angiotensin system in a rat model of hepatic fibrosis: evi-dence for a protective role of Angiotensin-(1-7). J Hepatol2007; 46: 674–81.
58 Kaschina E, Unger T. Angiotensin AT1/AT2 receptors:regulation, signalling and function. Blood Press 2003; 12:70–88.
59 Kurisu S, Ozono R, Oshima T et al. Cardiac angiotensin IItype 2 receptor activates the kinin/NO system and inhibitsfibrosis. Hypertension 2003; 41: 99–107.
60 Armendáriz-Borunda J, Islas-Carbajal MC, Meza-García Eet al. A pilot study in patients with established advancedliver fibrosis using pirfenidone. Gut 2006; 55: 1663–5.
104 A. Lugo-Baruqui et al. Hepatology Research 2010; 40: 95–104
© 2009 The Japan Society of Hepatology