
Endothelins and myocardial fibrosis
6
Basic Science and Experimental Studies Endothelins and Myocardial Fibrosis FELIX J. A. RAMIRES, MD, PhD, VERA L. NUNES, MD, FABIO FERNANDES, MD, PhD, CHARLES MADY, MD, PhD, JOSÉ A. F. RAMIRES, MD, PhD, FACC São Paulo, Brazil ABSTRACT Background: Endothelins are associated with cardiac remodeling. These peptides are the most powerful vasoconstrictor described—whether this remodeling is a direct effect of this hormone or indirect response to a relative ischemia promoted by vasoconstrictor effect. We evaluated the role of endothelin upon myocardial fibrosis despite of its hemodynamic effects and the benefits of its antagonism. Methods and Results: We used 40 Wistar rats: control, sham operated, rats had undergone myocardial infarction (MI) and MI rats treated with SB209670 which is an ET A /ET B endothelin antagonist. We evaluated tail systolic blood pressure (BP) and left ventricular end diastolic pressure (LVED) before surgery, just after, and at the end of the study. Remodeling was studied based on interstitial collagen and MI size by an image system analysis. BP decreased in MI groups after surgery, but did not differ between treated and untreated animals. LVED had increased levels in MI groups after surgery and did not differ between them. However, ICVF had an increase in MI group but significantly less in MISB209670. MI size was similar in both groups. Conclusions: Endothelin may have a pivotal role in the myocardial fibrosis by direct stimulation of collagen accumulation despite of its hemodynamic effects. Key Words: Endothelins, fibrosis, myocardial infarction, neurohormonal. For several years, heart failure was described as an exclusively hemodynamic disorder. According to this point of view, a myocardial injury would promote a mechanical change, which leads to progression of heart failure. 1,2 During the last decade, several studies have proved the significant importance of neurohormonal disorders related to abnormal matrix structure leading to myocardial remodeling and ventricular dysfunction. 3,4 Regarding this different pathophysiologic approach, heart failure has been recognized as a life-treating disorder despite relief of the congestive symptom. Different myocardial injuries may be responsible for the etiology of tissue remodeling. After myocardial infarction (MI), a wound healing response with repara- tive fibrosis occurs in the infarcted area and at the remote site. 5,6 Mediators of this myocardial fibrosis after MI were shown to be involved and attracted considerable interest. The tissue remodeling, including the interstitial and perivascular space, has been intensively investigated using a different model of fibrosis. A role for locally produced peptides in regulating collagen accumulation has been considered. Several studies have demonstrated the importance of renin-angiotensin II-aldosterone sys- tem in this process. 7–9 However, different substances From the Heart Institute (InCor)-University of São Paulo Medical School, São Paulo, Brazil. Manuscript received October 11, 2002; revised manuscript received December 27, 2002; revised manuscript accepted January 14, 2003. Reprint requests: Felix J. A. Ramires, MD, PhD, Instituto do Coração (InCor)-HCFMUSP, Av. Dr. Eneas de Carvalho Aguiar 44, Cerqueira Cesar, 05403-900 - São Paulo-SP, Brazil. © 2003 Elsevier Inc. All rights reserved. 1071-9164/03/0903-0012$30.00/0 doi:10.1054/jcaf.2003.26 Journal of Cardiac Failure Vol. 9 No. 3 2003 232
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Endothelins and myocardial fibrosis
Basic Science and Experimental Studies
Endothelins and Myocardial Fibrosis
FELIX J. A. RAMIRES, MD, PhD, VERA L. NUNES, MD,FABIO FERNANDES, MD, PhD, CHARLES MADY, MD, PhD,
JOSÉ A. F. RAMIRES, MD, PhD, FACC
São Paulo, Brazil
ABSTRACT
Background: Endothelins are associated with cardiac remodeling. These peptides are themost powerful vasoconstrictor described—whether this remodeling is a direct effect of thishormone or indirect response to a relative ischemia promoted by vasoconstrictor effect. Weevaluated the role of endothelin upon myocardial fibrosis despite of its hemodynamic effectsand the benefits of its antagonism.Methods and Results: We used 40 Wistar rats: control, sham operated, rats had undergonemyocardial infarction (MI) and MI rats treated with SB209670 which is an ETA/ETB
endothelin antagonist. We evaluated tail systolic blood pressure (BP) and left ventricular enddiastolic pressure (LVED) before surgery, just after, and at the end of the study. Remodelingwas studied based on interstitial collagen and MI size by an image system analysis. BPdecreased in MI groups after surgery, but did not differ between treated and untreated animals.LVED had increased levels in MI groups after surgery and did not differ between them.However, ICVF had an increase in MI group but significantly less in MI�SB209670. MI sizewas similar in both groups.Conclusions: Endothelin may have a pivotal role in the myocardial fibrosis by directstimulation of collagen accumulation despite of its hemodynamic effects.Key Words: Endothelins, fibrosis, myocardial infarction, neurohormonal.
For several years, heart failure was described as anexclusively hemodynamic disorder. According to thispoint of view, a myocardial injury would promote amechanical change, which leads to progression of heartfailure.1,2 During the last decade, several studies haveproved the significant importance of neurohormonaldisorders related to abnormal matrix structure leading tomyocardial remodeling and ventricular dysfunction.3,4
Regarding this different pathophysiologic approach,heart failure has been recognized as a life-treatingdisorder despite relief of the congestive symptom.
Different myocardial injuries may be responsible forthe etiology of tissue remodeling. After myocardialinfarction (MI), a wound healing response with repara-tive fibrosis occurs in the infarcted area and at the remotesite.5,6 Mediators of this myocardial fibrosis after MIwere shown to be involved and attracted considerableinterest.
The tissue remodeling, including the interstitial andperivascular space, has been intensively investigatedusing a different model of fibrosis. A role for locallyproduced peptides in regulating collagen accumulationhas been considered. Several studies have demonstratedthe importance of renin-angiotensin II-aldosterone sys-tem in this process.7–9 However, different substances
From the Heart Institute (InCor)-University of São Paulo MedicalSchool, São Paulo, Brazil.
Manuscript received October 11, 2002; revised manuscript receivedDecember 27, 2002; revised manuscript accepted January 14, 2003.
Reprint requests: Felix J. A. Ramires, MD, PhD, Instituto do Coração(InCor)-HCFMUSP, Av. Dr. Eneas de Carvalho Aguiar 44, CerqueiraCesar, 05403-900 - São Paulo-SP, Brazil.
© 2003 Elsevier Inc. All rights reserved.1071-9164/03/0903-0012$30.00/0doi:10.1054/jcaf.2003.26
Journal of Cardiac Failure Vol. 9 No. 3 2003
232

such as endothelins are held responsible for the collagenaccumulation in different tissues, including heart.10,11
Many studies using in vivo and in vitro experiments haveshown a collagen turnover stimulation by endothelinI.12,13 Furthermore, an inhibition of collagenase activityby endothelins has been demonstrated that may have animportant contribution for inappropriate collagen accu-mulation.14 Some experimental studies suggested a pre-vention of collagen accumulation using bosentan, anendothelin (ETA and ETB) antagonist.15 During thepathologic states, the myofibroblast, a phenotypicallymodified fibroblast, has an important role related tocollagen production at the myocardium.16,17 This cellpopulation is extremely responsive to endothelin stimu-lation, promoting an increased collagen turnover.14,18 Onthe other hand, endothelins are the most powerful vaso-constrictor described. Therefore, their potential hemody-namic effect could be responsible for inducing myocar-dial fibrosis secondary to myocyte loss. Whether it is themain role of endothelins, regarding myocardial fibrosis,is related to its direct mediation as a peptide or becauseits vasoconstrictor effects causing myocyte damage.Many studies evaluated the role of endothelin antago-nism upon myocardial remodeling. However, most ofthem had an interference of the treatment on bloodpressure or on left ventricular filling pressure that couldbe the main trigger for the myocardial fibrosis.19 Someothers did not analyze the myocardial collagen related tohemodynamic changes.20 Therefore, this in vivo studywas performed in order to identify the role of endothelinsrelated to myocardial fibrosis after a MI despite hemo-dynamic changes, and evaluate the potential benefits ofendothelin antagonism regarding myocardial collagenaccumulation.
Materials and Methods
We studied male Wistar rats’ myocardium after a MI.These rats were divided into 4 groups (10 rats each): (1)normal control rats, (2) rats sham operated, (3) ratsundergoing to MI, and (4) rats undergoing to MI plusSB209670.
The MI was created with the left coronary arteryligation. The surgery was performed under ketamine (50mg/kg intraperitoneally) and pentobarbital (25 mg/kgintraperitoneally) anesthesia and followed recommenda-tions of COBEA (Brazilian College of ExperimentalAnimal Studies) and UFAW (The Universities Federa-tion for Animals Welfare).
The rats were intubated and mechanically ventilated(Harvard Ventilator). A left thoracotomy was done, thepericardium opened, and the heart rapidly exteriorized toreach the coronary artery. The vessel was ligated using asilk 5-0 suture. After, the chest was closed and lungs re-
inflated using positive end-expiratory pressure.21 The ani-mals were sacrificed 4 weeks after surgery, and the heartswere fixed in 10% formalin. These hearts were mountedin paraffin and cross-sectioned at 5µm thickness.
The rats received SB209670, a potent endothelin ETA
and ETB antagonist,22 3 mg/kg intraperitoneally twiceper day23,24 starting after surgery, immediately aftercoronary ligation, according the protocols. The treatmentwas given for 4 weeks when the animals were sacrificed.
The structural remodeling of the myocardium wasevaluated by interstitial collagen volume fraction(ICVF), which was measured by videomorphometry(Quantimet Leica Imaging Analysis, Bannockburn, Illi-nois) using picosirius red-stained cross-sectionedhearts.25 We analyzed 1 section for each heart. Thesemeasurements were done at the interstitial space in thenoninfarcted site at the left ventricle (mean 17fields/section) and in the right ventricle (mean 5fields/section), separately. We calculated the percentageof collagen area over total area of the myocardium. Thegeometric changes were studied analyzing the infarctionsize, which was measured as described previously.21
Using an image analysis system (Quantimet Leica Imag-ing Analysis) we evaluated a cross-sectioned heart at thelargest surface length of infarcted ventricular wall andstained it with picosirius red. The epicardial circumfer-ential lengths of both infarcted and noninfarcted regionswere measured and the infarction size calculated as thepercentage of MI length relative to entire left ventricularcircumference.
Hemodynamic changes were evaluated with noninva-sive blood pressure determination in the rats’ tail (IndirectBlood Pressure Measuring System, Letica) before and af-ter the surgery and at the end of the experiment. The ani-mals were training and warmed 1 week before the experi-ment to avoid interference during blood pressure readings.Before and just after surgery and at the end of the study,using a carotid introduced catheter, we measured the leftventricular end diastolic pressure using a signal acquisi-tion system (Biopac Systems, Goleta, California).
Results
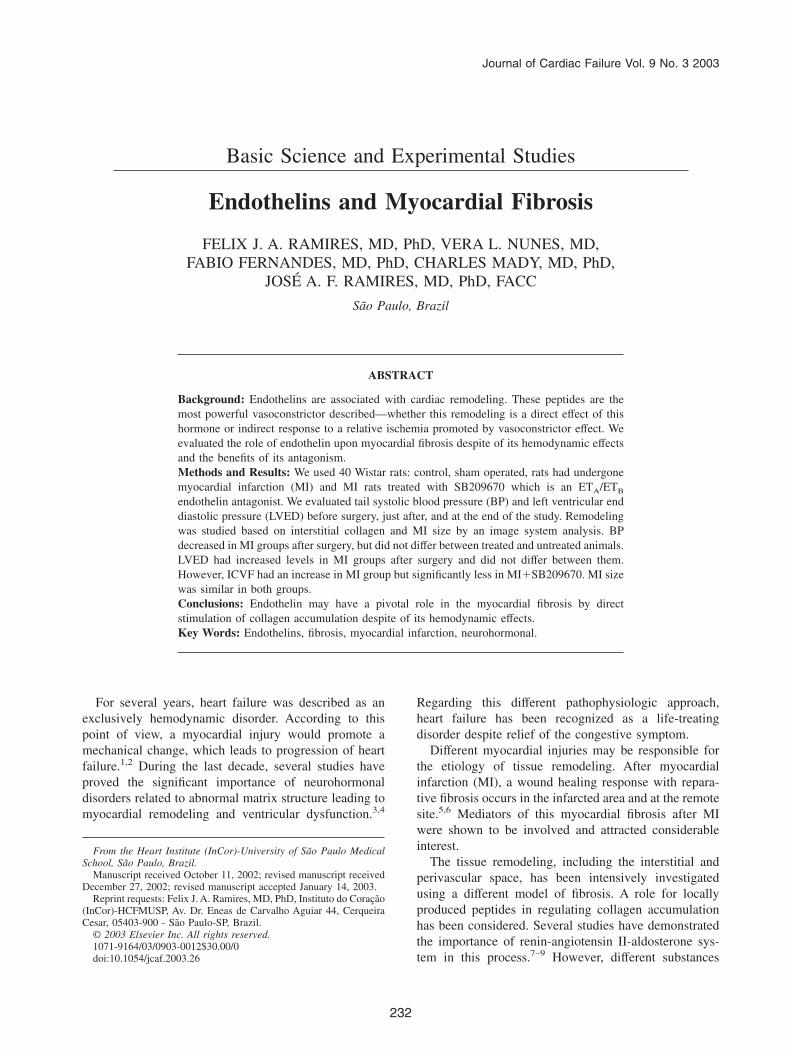
Regarding the behavior of left ventricular end-diastolic pressure in each group, we observed a rise in itslevels in MI groups right after surgery and at the fourthweek compared with baseline. This variable remainedunchanged in the sham and control group (Fig. 1). Wedid not observe any difference between groups at thebaseline, but did observe a significant increase of the leftventricular end-diastolic pressure right after surgery andat the end of the study in MI groups compared with shamand control. We found differences but they were notstatistically significant (P < .06) between treated and not
Endothelins and Myocardial Fibrosis O Ramires et al 233
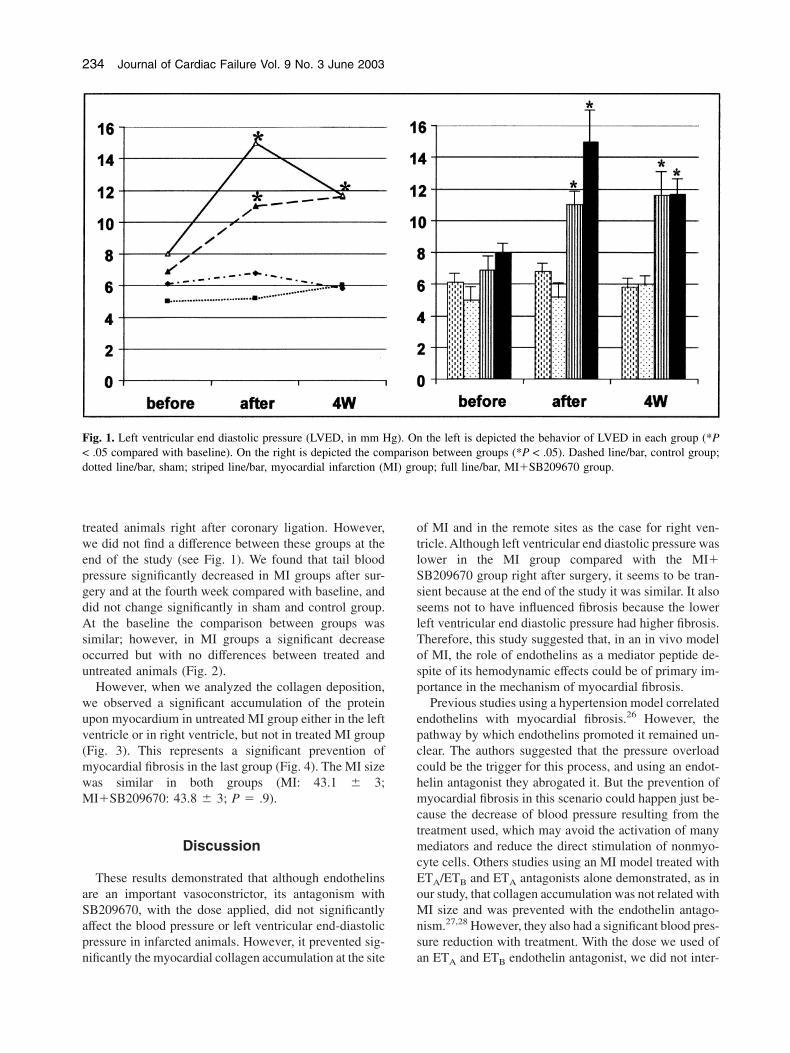
treated animals right after coronary ligation. However,we did not find a difference between these groups at theend of the study (see Fig. 1). We found that tail bloodpressure significantly decreased in MI groups after sur-gery and at the fourth week compared with baseline, anddid not change significantly in sham and control group.At the baseline the comparison between groups wassimilar; however, in MI groups a significant decreaseoccurred but with no differences between treated anduntreated animals (Fig. 2).
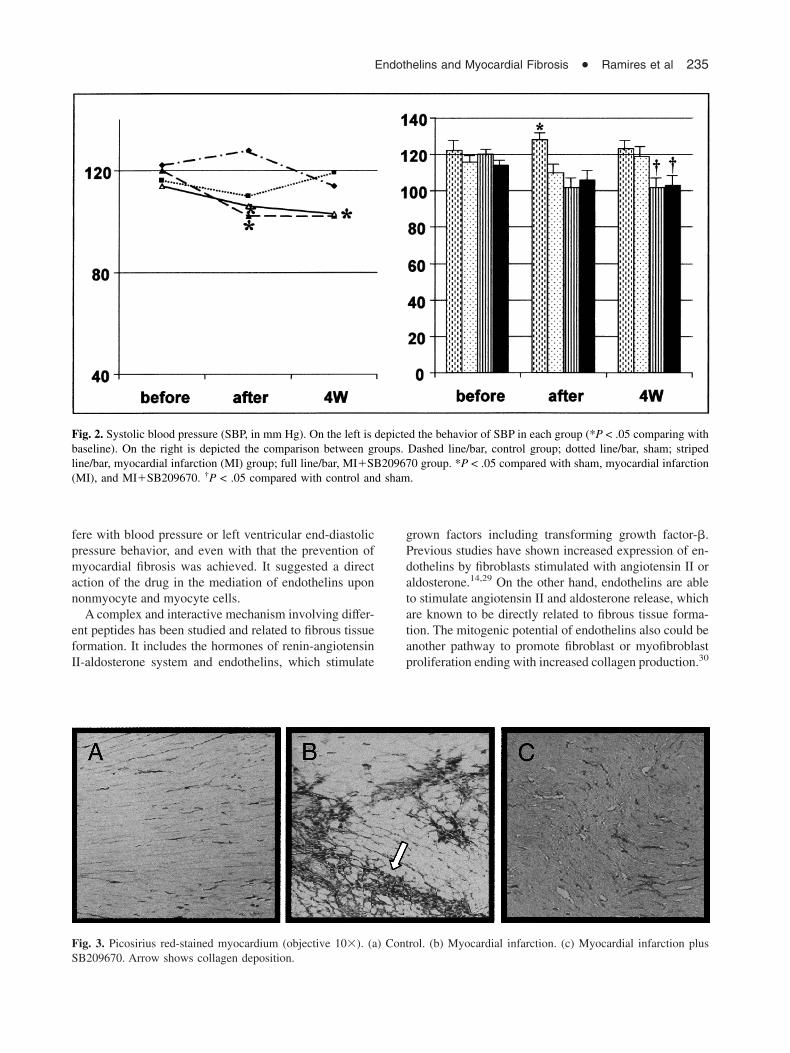
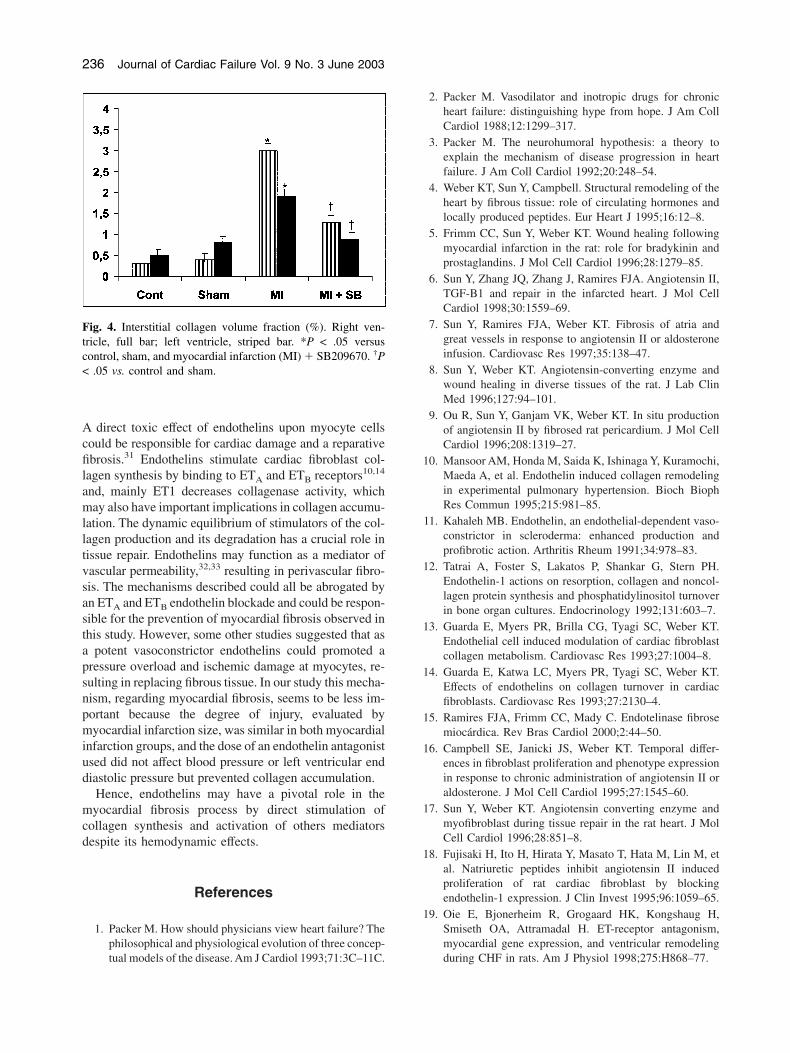
However, when we analyzed the collagen deposition,we observed a significant accumulation of the proteinupon myocardium in untreated MI group either in the leftventricle or in right ventricle, but not in treated MI group(Fig. 3). This represents a significant prevention ofmyocardial fibrosis in the last group (Fig. 4). The MI sizewas similar in both groups (MI: 43.1 � 3;MI�SB209670: 43.8 � 3; P � .9).
Discussion
These results demonstrated that although endothelinsare an important vasoconstrictor, its antagonism withSB209670, with the dose applied, did not significantlyaffect the blood pressure or left ventricular end-diastolicpressure in infarcted animals. However, it prevented sig-nificantly the myocardial collagen accumulation at the site
of MI and in the remote sites as the case for right ven-tricle. Although left ventricular end diastolic pressure waslower in the MI group compared with the MI�SB209670 group right after surgery, it seems to be tran-sient because at the end of the study it was similar. It alsoseems not to have influenced fibrosis because the lowerleft ventricular end diastolic pressure had higher fibrosis.Therefore, this study suggested that, in an in vivo modelof MI, the role of endothelins as a mediator peptide de-spite of its hemodynamic effects could be of primary im-portance in the mechanism of myocardial fibrosis.
Previous studies using a hypertension model correlatedendothelins with myocardial fibrosis.26 However, thepathway by which endothelins promoted it remained un-clear. The authors suggested that the pressure overloadcould be the trigger for this process, and using an endot-helin antagonist they abrogated it. But the prevention ofmyocardial fibrosis in this scenario could happen just be-cause the decrease of blood pressure resulting from thetreatment used, which may avoid the activation of manymediators and reduce the direct stimulation of nonmyo-cyte cells. Others studies using an MI model treated withETA/ETB and ETA antagonists alone demonstrated, as inour study, that collagen accumulation was not related withMI size and was prevented with the endothelin antago-nism.27,28 However, they also had a significant blood pres-sure reduction with treatment. With the dose we used ofan ETA and ETB endothelin antagonist, we did not inter-
Fig. 1. Left ventricular end diastolic pressure (LVED, in mm Hg). On the left is depicted the behavior of LVED in each group (*P< .05 compared with baseline). On the right is depicted the comparison between groups (*P < .05). Dashed line/bar, control group;dotted line/bar, sham; striped line/bar, myocardial infarction (MI) group; full line/bar, MI�SB209670 group.
234 Journal of Cardiac Failure Vol. 9 No. 3 June 2003
fere with blood pressure or left ventricular end-diastolicpressure behavior, and even with that the prevention ofmyocardial fibrosis was achieved. It suggested a directaction of the drug in the mediation of endothelins uponnonmyocyte and myocyte cells.
A complex and interactive mechanism involving differ-ent peptides has been studied and related to fibrous tissueformation. It includes the hormones of renin-angiotensinII-aldosterone system and endothelins, which stimulate
grown factors including transforming growth factor-�.Previous studies have shown increased expression of en-dothelins by fibroblasts stimulated with angiotensin II oraldosterone.14,29 On the other hand, endothelins are ableto stimulate angiotensin II and aldosterone release, whichare known to be directly related to fibrous tissue forma-tion. The mitogenic potential of endothelins also could beanother pathway to promote fibroblast or myofibroblastproliferation ending with increased collagen production.30
Fig. 2. Systolic blood pressure (SBP, in mm Hg). On the left is depicted the behavior of SBP in each group (*P < .05 comparing withbaseline). On the right is depicted the comparison between groups. Dashed line/bar, control group; dotted line/bar, sham; stripedline/bar, myocardial infarction (MI) group; full line/bar, MI�SB209670 group. *P < .05 compared with sham, myocardial infarction(MI), and MI�SB209670. †P < .05 compared with control and sham.
Fig. 3. Picosirius red-stained myocardium (objective 10�). (a) Control. (b) Myocardial infarction. (c) Myocardial infarction plusSB209670. Arrow shows collagen deposition.
Endothelins and Myocardial Fibrosis O Ramires et al 235
A direct toxic effect of endothelins upon myocyte cellscould be responsible for cardiac damage and a reparativefibrosis.31 Endothelins stimulate cardiac fibroblast col-lagen synthesis by binding to ETA and ETB receptors10,14
and, mainly ET1 decreases collagenase activity, whichmay also have important implications in collagen accumu-lation. The dynamic equilibrium of stimulators of the col-lagen production and its degradation has a crucial role intissue repair. Endothelins may function as a mediator ofvascular permeability,32,33 resulting in perivascular fibro-sis. The mechanisms described could all be abrogated byan ETA and ETB endothelin blockade and could be respon-sible for the prevention of myocardial fibrosis observed inthis study. However, some other studies suggested that asa potent vasoconstrictor endothelins could promoted apressure overload and ischemic damage at myocytes, re-sulting in replacing fibrous tissue. In our study this mecha-nism, regarding myocardial fibrosis, seems to be less im-portant because the degree of injury, evaluated bymyocardial infarction size, was similar in both myocardialinfarction groups, and the dose of an endothelin antagonistused did not affect blood pressure or left ventricular enddiastolic pressure but prevented collagen accumulation.
Hence, endothelins may have a pivotal role in themyocardial fibrosis process by direct stimulation ofcollagen synthesis and activation of others mediatorsdespite its hemodynamic effects.
References
1. Packer M. How should physicians view heart failure? Thephilosophical and physiological evolution of three concep-tual models of the disease. Am J Cardiol 1993;71:3C–11C.
2. Packer M. Vasodilator and inotropic drugs for chronicheart failure: distinguishing hype from hope. J Am CollCardiol 1988;12:1299–317.
3. Packer M. The neurohumoral hypothesis: a theory toexplain the mechanism of disease progression in heartfailure. J Am Coll Cardiol 1992;20:248–54.
4. Weber KT, Sun Y, Campbell. Structural remodeling of theheart by fibrous tissue: role of circulating hormones andlocally produced peptides. Eur Heart J 1995;16:12–8.
5. Frimm CC, Sun Y, Weber KT. Wound healing followingmyocardial infarction in the rat: role for bradykinin andprostaglandins. J Mol Cell Cardiol 1996;28:1279–85.
6. Sun Y, Zhang JQ, Zhang J, Ramires FJA. Angiotensin II,TGF-B1 and repair in the infarcted heart. J Mol CellCardiol 1998;30:1559–69.
7. Sun Y, Ramires FJA, Weber KT. Fibrosis of atria andgreat vessels in response to angiotensin II or aldosteroneinfusion. Cardiovasc Res 1997;35:138–47.
8. Sun Y, Weber KT. Angiotensin-converting enzyme andwound healing in diverse tissues of the rat. J Lab ClinMed 1996;127:94–101.
9. Ou R, Sun Y, Ganjam VK, Weber KT. In situ productionof angiotensin II by fibrosed rat pericardium. J Mol CellCardiol 1996;208:1319–27.
10. Mansoor AM, Honda M, Saida K, Ishinaga Y, Kuramochi,Maeda A, et al. Endothelin induced collagen remodelingin experimental pulmonary hypertension. Bioch BiophRes Commun 1995;215:981–85.
11. Kahaleh MB. Endothelin, an endothelial-dependent vaso-constrictor in scleroderma: enhanced production andprofibrotic action. Arthritis Rheum 1991;34:978–83.
12. Tatrai A, Foster S, Lakatos P, Shankar G, Stern PH.Endothelin-1 actions on resorption, collagen and noncol-lagen protein synthesis and phosphatidylinositol turnoverin bone organ cultures. Endocrinology 1992;131:603–7.
13. Guarda E, Myers PR, Brilla CG, Tyagi SC, Weber KT.Endothelial cell induced modulation of cardiac fibroblastcollagen metabolism. Cardiovasc Res 1993;27:1004–8.
14. Guarda E, Katwa LC, Myers PR, Tyagi SC, Weber KT.Effects of endothelins on collagen turnover in cardiacfibroblasts. Cardiovasc Res 1993;27:2130–4.
15. Ramires FJA, Frimm CC, Mady C. Endotelinase fibrosemiocárdica. Rev Bras Cardiol 2000;2:44–50.
16. Campbell SE, Janicki JS, Weber KT. Temporal differ-ences in fibroblast proliferation and phenotype expressionin response to chronic administration of angiotensin II oraldosterone. J Mol Cell Cardiol 1995;27:1545–60.
17. Sun Y, Weber KT. Angiotensin converting enzyme andmyofibroblast during tissue repair in the rat heart. J MolCell Cardiol 1996;28:851–8.
18. Fujisaki H, Ito H, Hirata Y, Masato T, Hata M, Lin M, etal. Natriuretic peptides inhibit angiotensin II inducedproliferation of rat cardiac fibroblast by blockingendothelin-1 expression. J Clin Invest 1995;96:1059–65.
19. Oie E, Bjonerheim R, Grogaard HK, Kongshaug H,Smiseth OA, Attramadal H. ET-receptor antagonism,myocardial gene expression, and ventricular remodelingduring CHF in rats. Am J Physiol 1998;275:H868–77.
Fig. 4. Interstitial collagen volume fraction (%). Right ven-tricle, full bar; left ventricle, striped bar. *P < .05 versuscontrol, sham, and myocardial infarction (MI) � SB209670. †P< .05 vs. control and sham.
236 Journal of Cardiac Failure Vol. 9 No. 3 June 2003

20. Sakai S, Miyauchi T, Kobayashi M, Yamaguchi I, Goto K,Sugishita Y. Inhibition of myocardial endothelin pathwayimproves long-term survival in heart failure. Nature1996;384:353–5.
21. Frimm CC, Sun Y, Weber KT. Angiotensin II receptorblockade and myocardial fibrosis of the infarcted ratheart. J Lab Clin Med 1997;129:439–45.
22. Ohlstein EH, Nambi P, Douglas SA, Edwards RM, GellaiM, Lago A, et al. SB 209670, a rationally designed potentnonpeptide endothelin receptor antagonist. Proc Nat AcadSci U S A 1994;91(17):8052–6.
23. Klemm P, Warner TD, Corder R, Vane JR. Endothelin-1mediates coronary vasoconstriction caused by exogenousand endogenous cytokines. J Cardiovasc Pharmacol 1995;26(Suppl 3):S419–21.
24. Douglas SA, Louden C, Vickery-Clark LM, Storer BL,Hart T, Feuerstein GZ, et al. A role for endogenousendothelin-1 in neointimal formation after rat carotid ar-tery balloon angioplasty. Protective effects of the novelnonpeptide endothelin receptor antagonist SB 209670. CircRes 1994;75(1):190–7.
25. Ramires FJA, Sun Y, Weber KT. Myocardial fibrosisassociated with aldosterone or angiotensin II administra-tion: attenuation by calcium channel blockade. J Mol CellCardiol 1998;30(3):475–83.
26. Hart CYT, Meyer DM, Tazelaar HD, Grande JP, BurnettJC Jr, Housmans PR, Redfield MM. Load versus humoralactivation in the genesis of early hypertensive heartdisease. Circulation 2001;104(2):215–20.
27. Mulder P, Richard V, Derumeaux G. Role of endogenousendothelin in chronic heart failure: effect of a long termtreatment with an endothelin antagonist on survival, he-modynamics and cardiac remodeling. Circulation 1997;96:1976–82.
28. Mulder P, Richard V, Bouchart F, Derumeaux G, MunterK, Thuillez C. Selective ETA receptor blockade preventsleft ventricular remodeling and deterioration of cardiacfunction in experimental heart failure. Cardiovasc Res1998;39:600–8.
29. Katwa LC, Guarda E, Weber KT. Endothelin receptors incultured adult rat cardiac fibroblasts: Cardiovasc Res 1993;27:2125–9.
30. Rizvi MAD, Katwa L, Spadone DP, Myers PR. Theeffects of endothelin-1 on collagen type I and type IIIsynthesis in cultured porcine coronary artery vascularsmooth muscle cells. J Mol Cell Cardiol 1996;28:243–52.
31. Prasad MR. Endothelin stimulates degeneration of phos-pholipids in isolated rat hearts. Biophys Res Commun1991;174:952–7.
32. Lopez-Belmonte J, Whittle BJ: The involvement of en-dothelial dysfunction, nitric oxide and prostanoids in therat gastric microcirculatory responses to endothelin-1. BrJ Pharmacol 1994;112:267–71.
33. Filep JG, Fournier A, Foldes-Filep E. Acute pro-inflammatory actions of endothelin-1 in the guinea-piglung: involvement of ETA and ETB receptors. Br JPharmacol 1995;115:227–36.
Endothelins and Myocardial Fibrosis O Ramires et al 237




















