
Cystic fibrosis: a review of pulmonary and nutritional therapies
Upload
khangminh22Category
view
0download
0
1
National Clinical Guideline Centre
-
Diagnosis and management of idiopathic pulmonary fibrosis Appendices
Clinical Guideline
Appendices A-S
June 2013
-
Commissioned by the National Institute for Health and Care Excellence


3
Idiopathic Pulmonary Fibrosis Contents
1
Idiopathic Pulmonary Fibrosis
Disclaimer Healthcare professionals are expected to take NICE clinical guidelines fully into account when exercising their clinical judgement. However, the guidance does not override the responsibility of healthcare professionals to make decisions appropriate to the circumstances of each patient, in consultation with the patient and/or their guardian or carer.
Copyright National Clinical Guideline Centre, 2013. Confidential.
Funding National Institute for Health and Care Excellence

4
Idiopathic Pulmonary Fibrosis Scope
Contents
Appendices .................................................................................................................................. 5
Appendix A: Scope ........................................................................................................................... 5
Appendix B: Declarations of interest ............................................................................................ 12
Appendix C: Review protocols ...................................................................................................... 33
1.1 Diagnosis ............................................................................................................................. 33
1.2 Prognosis ............................................................................................................................. 36
1.3 Pulmonary rehabilitation .................................................................................................... 39
1.4 Best supportive care ........................................................................................................... 41
1.5 Psychosocial support ........................................................................................................... 42
1.6 Lung transplantation ........................................................................................................... 45
1.7 Ventilation ........................................................................................................................... 46
1.8 Review and follow-up ......................................................................................................... 47
1.9 Appended economic review protocol ................................................................................. 48
Appendix D: Literature search strategy ......................................................................................... 50
Appendix E: Forest plots ............................................................................................................... 87
Appendix F: Clinical evidence tables ........................................................................................... 117
Appendix G: Economic evidence tables ...................................................................................... 302
Appendix H: Interpreting post-test probabilities by considering prevalence/pre-test probability ............................................................................................................... 306
Appendix I: Calculations of standard errors from HR, RR and ORs ............................................ 307
Appendix J: Costing of a Multidisciplinary Team (MDT) in the Context of an Interstitial Lung Disease (ILD) Network: Finding the incremental cost of involving an MDT in the IPF diagnostic pathway. .......................................................................................... 319
Appendix K: Placing the diagnostic clinical evidence into an economic framework for decision making. ..................................................................................................... 327
Appendix L: Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis ................................................................................ 350
Appendix M: Model produced Median and Mean Life Expectancies for people diagnosed with IPF .................................................................................................. 401
Appendix N: Adverse events table .............................................................................................. 409
Appendix O: The cost of pharmacological interventions for IPF ................................................. 411
Appendix P: Research recommendations ................................................................................... 417
Appendix Q: Adapted Prisma Diagrams ...................................................................................... 430
Appendix R: Excluded Studies ..................................................................................................... 438
Appendix S: Reference list .......................................................................................................... 454
1

5
Idiopathic Pulmonary Fibrosis Scope
Appendices
Appendix A: Scope

6
Idiopathic Pulmonary Fibrosis Scope

7
Idiopathic Pulmonary Fibrosis Scope

8
Idiopathic Pulmonary Fibrosis Scope

9
Idiopathic Pulmonary Fibrosis Scope

10
Idiopathic Pulmonary Fibrosis Scope

11
Idiopathic Pulmonary Fibrosis Scope

12
Idiopathic Pulmonary Fibrosis Declarations of interest
Appendix B: Declarations of interest
B.1 Dr Nik Hirani
GDG meeting Declaration of Interests
Actions taken
On Application
NH declared he knew of no personal pecuniary interests or personal family interests in the past 12 months and had nothing to declare for the upcoming month.
NH declared non-personal pecuniary interests, which led to payments made directly to the University of Edinburgh:
NH received a non-commercial clinician scientist fellowship to study mechanisms of acute lung injury and repair. Funded by GlaxoSmithKlein from 2001to 2005.
NH was the principal investigator for local site in a multiple-centre phase 3 clinical trial of endothelin antagonist in IPF (ARTEMIS) study. Funded by Gilead, from 2010 to Dec 2011.
NH was the principal investigator in MRC/Industry-funded phase 1/2 clinical trial of CDK inhibitor. Funded by Astex, from 2010/2011 to January 2012.
NH was the principal investigator in collaborative research on pre-clinical models of lung injury and fibrosis. Funded by AstraZeneca, from 2010 to December 2011.
NH is the principal investigator for an MRC funded molecular imaging study in pulmonary fibrosis in partnership with AstraZeneca, which is due to commence in 2013.
NH declared personal non-pecuniary interests. NH is a member of the British Thoracic Society and Chair of ILD specialist advisory group. NH also belongs to the Advisory board EurlPFnet (European Registry of IPF).
None
First GDG meeting
(16/09/2011)
NH had no new interests to declare other than those declared at upon application to the GDG.
None
Second GDG Meeting
(21/10/11)
NH had no new interests to declare.
None
Third GDG Meeting
(02/12/11)
NH declared a non-personal pecuniary interest. NH attended a BTS meeting and gave a presentation on IPF. Travel and accommodation was provided for by the University of Edinburgh.
None
Fourth GDG Meeting
(12/01/12)
NH had no new interests to declare.
None
Fifth GDG Meeting
(24/02/12)
NH had no new interests to declare.
None
13
Idiopathic Pulmonary Fibrosis Declarations of interest
GDG meeting Declaration of Interests
Actions taken
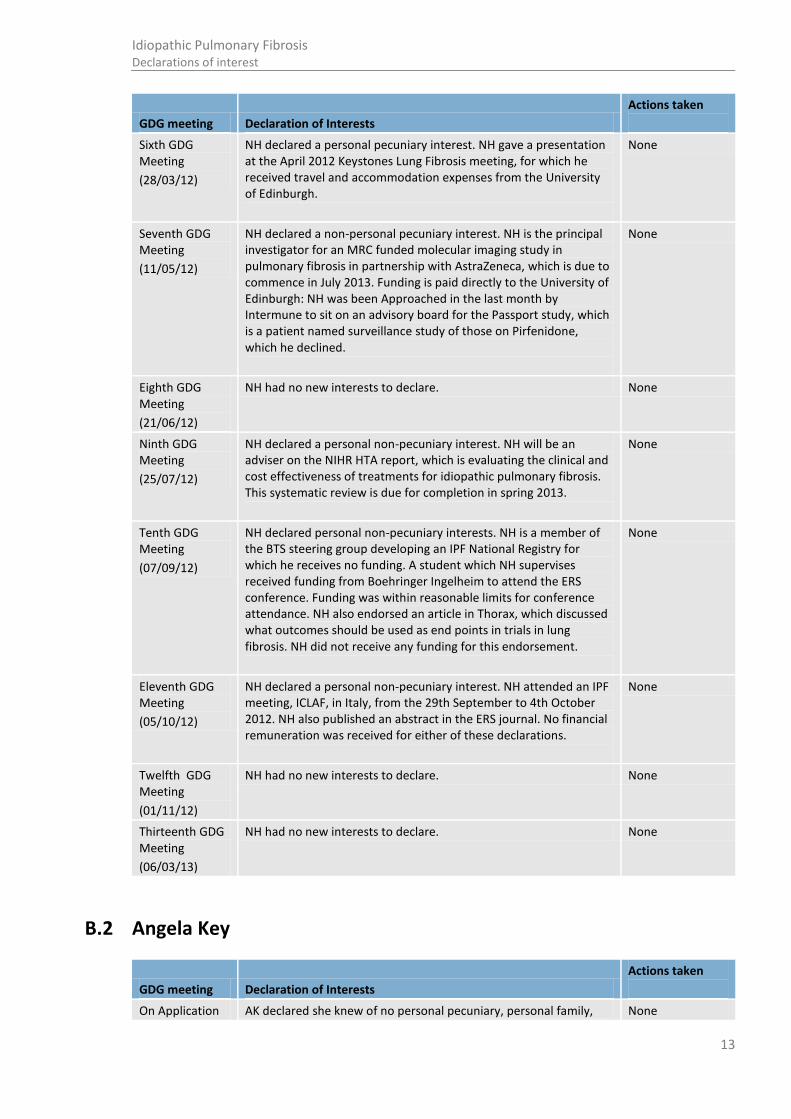
Sixth GDG Meeting
(28/03/12)
NH declared a personal pecuniary interest. NH gave a presentation at the April 2012 Keystones Lung Fibrosis meeting, for which he received travel and accommodation expenses from the University of Edinburgh.
None
Seventh GDG Meeting
(11/05/12)
NH declared a non-personal pecuniary interest. NH is the principal investigator for an MRC funded molecular imaging study in pulmonary fibrosis in partnership with AstraZeneca, which is due to commence in July 2013. Funding is paid directly to the University of Edinburgh: NH was been Approached in the last month by Intermune to sit on an advisory board for the Passport study, which is a patient named surveillance study of those on Pirfenidone, which he declined.
None
Eighth GDG Meeting
(21/06/12)
NH had no new interests to declare. None
Ninth GDG Meeting
(25/07/12)
NH declared a personal non-pecuniary interest. NH will be an adviser on the NIHR HTA report, which is evaluating the clinical and cost effectiveness of treatments for idiopathic pulmonary fibrosis. This systematic review is due for completion in spring 2013.
None
Tenth GDG Meeting
(07/09/12)
NH declared personal non-pecuniary interests. NH is a member of the BTS steering group developing an IPF National Registry for which he receives no funding. A student which NH supervises received funding from Boehringer Ingelheim to attend the ERS conference. Funding was within reasonable limits for conference attendance. NH also endorsed an article in Thorax, which discussed what outcomes should be used as end points in trials in lung fibrosis. NH did not receive any funding for this endorsement.
None
Eleventh GDG Meeting
(05/10/12)
NH declared a personal non-pecuniary interest. NH attended an IPF meeting, ICLAF, in Italy, from the 29th September to 4th October 2012. NH also published an abstract in the ERS journal. No financial remuneration was received for either of these declarations.
None
Twelfth GDG Meeting
(01/11/12)
NH had no new interests to declare. None
Thirteenth GDG Meeting
(06/03/13)
NH had no new interests to declare. None
B.2 Angela Key
GDG meeting Declaration of Interests
Actions taken
On Application AK declared she knew of no personal pecuniary, personal family, None

14
Idiopathic Pulmonary Fibrosis Declarations of interest
GDG meeting Declaration of Interests
Actions taken
non-personal pecuniary or personal non-pecuniary interests in the previous 12 months or upcoming month.
First GDG meeting
(16/09/2011)
AK had no new interests to declare other than those declared at upon application to the GDG.
None
Second GDG Meeting
(21/10/11)
AK had no new interests to declare.
None
Third GDG Meeting
(02/12/11)
AK had no new interests to declare.
None
Fourth GDG Meeting
(12/01/12)
AK had no new interests to declare.
None
Fifth GDG Meeting
(24/02/12)
Did not attend. None
Sixth GDG Meeting
(28/03/12)
AK had no new interests to declare.
None
Seventh GDG Meeting
(11/05/12)
AK had no new interests to declare.
None
Eighth GDG Meeting
(21/06/12)
AK had no new interests to declare.
None
Ninth GDG Meeting
(25/07/12)
AK had no new interests to declare.
None
Tenth GDG Meeting
(07/09/12)
AK had no new interests to declare. None
Eleventh GDG Meeting
(05/10/12)
AK had no new interests to declare None
Twelfth GDG Meeting
(01/11/12)
Did not attend. None
Thirteenth GDG Meeting
(06/03/13)
AK had no new interests to declare. None
B.3 Ann Millar

15
Idiopathic Pulmonary Fibrosis Declarations of interest
GDG meeting Declaration of Interests
Actions taken
On Application AM declared she knew of no personal pecuniary or personal family interests in the previous 12 months or upcoming month.
AM declared a non-personal pecuniary interest. AM is involved with trials of drug therapies for patients with IPF as recommended by the British Thoracic Society guidelines. These trials are funded by Boehringer Ingelheim and funding goes into a respiratory departmental research fund (on-going).
AM declared personal non-pecuniary interests. AM is the Chairman of the British Association for Lung Research and member of the Respiratory Expert Advisory Group for the MHRA (2009-2013.
None
First GDG meeting
(16/09/2011)
AM had no new interests to declare other than those declared at upon application to the GDG.
None
Second GDG Meeting
(21/10/11)
Did not attend.
None
Third GDG Meeting
(02/12/11)
Ann Millar declared she had written an editorial for the Thoracic Society on the PANTHER study.
None
Fourth GDG Meeting
(12/01/12)
AM had no new interests to declare. None
Fifth GDG Meeting
(24/02/12)
AM had no new interests to declare. None
Sixth GDG Meeting
(28/03/12)
AM had no new interests to declare. None
Seventh GDG Meeting
(11/05/12)
AM had no new interests to declare. None
Eighth GDG Meeting
(21/06/12)
Did not attend.
None
Ninth GDG Meeting
(25/07/12)
AM had no new interests to declare. None
Tenth GDG Meeting
(07/09/12)
AM declared a personal non-pecuniary interest. AM is a member of the BTS steering group developing an IPF National Registry, for which she receives no funding.
None
Eleventh GDG Meeting
(05/10/12)
AM had no new interests to declare. None
16
Idiopathic Pulmonary Fibrosis Declarations of interest
GDG meeting Declaration of Interests
Actions taken
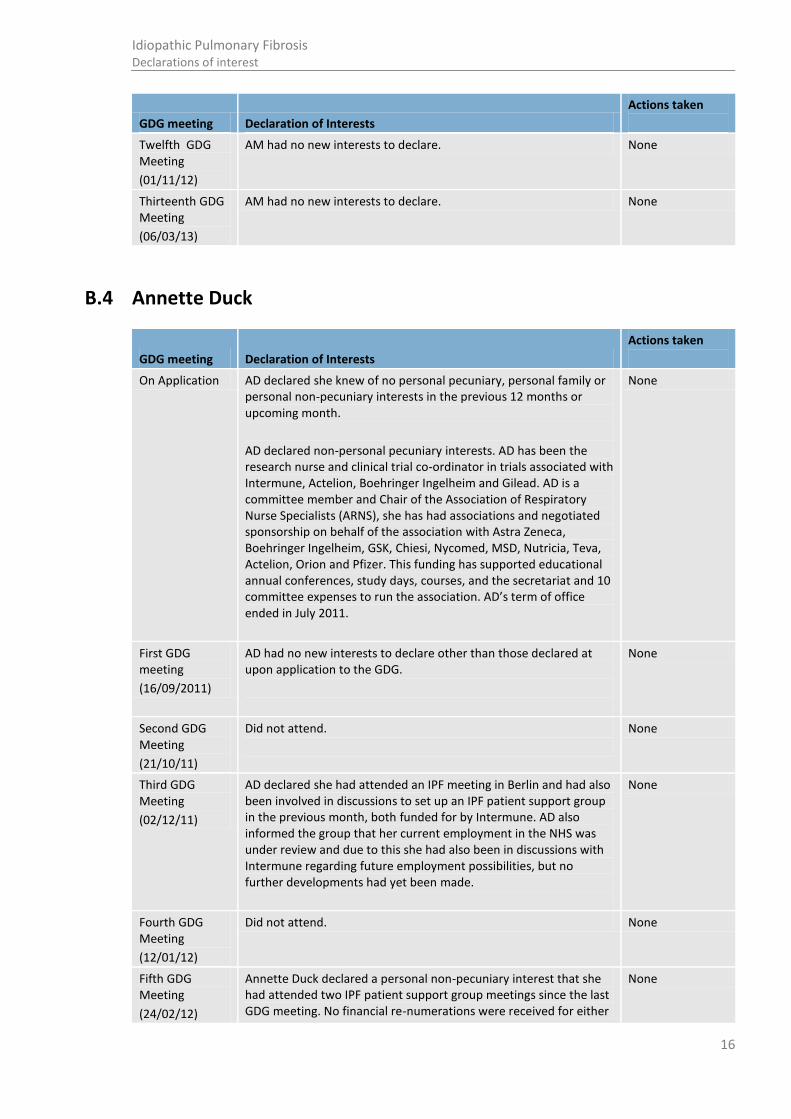
Twelfth GDG Meeting
(01/11/12)
AM had no new interests to declare. None
Thirteenth GDG Meeting
(06/03/13)
AM had no new interests to declare. None
B.4 Annette Duck
GDG meeting Declaration of Interests
Actions taken
On Application AD declared she knew of no personal pecuniary, personal family or personal non-pecuniary interests in the previous 12 months or upcoming month.
AD declared non-personal pecuniary interests. AD has been the research nurse and clinical trial co-ordinator in trials associated with Intermune, Actelion, Boehringer Ingelheim and Gilead. AD is a committee member and Chair of the Association of Respiratory Nurse Specialists (ARNS), she has had associations and negotiated sponsorship on behalf of the association with Astra Zeneca, Boehringer Ingelheim, GSK, Chiesi, Nycomed, MSD, Nutricia, Teva, Actelion, Orion and Pfizer. This funding has supported educational annual conferences, study days, courses, and the secretariat and 10 committee expenses to run the association. AD’s term of office ended in July 2011.
None
First GDG meeting
(16/09/2011)
AD had no new interests to declare other than those declared at upon application to the GDG.
None
Second GDG Meeting
(21/10/11)
Did not attend.
None
Third GDG Meeting
(02/12/11)
AD declared she had attended an IPF meeting in Berlin and had also been involved in discussions to set up an IPF patient support group in the previous month, both funded for by Intermune. AD also informed the group that her current employment in the NHS was under review and due to this she had also been in discussions with Intermune regarding future employment possibilities, but no further developments had yet been made.
None
Fourth GDG Meeting
(12/01/12)
Did not attend. None
Fifth GDG Meeting
(24/02/12)
Annette Duck declared a personal non-pecuniary interest that she had attended two IPF patient support group meetings since the last GDG meeting. No financial re-numerations were received for either
None

17
Idiopathic Pulmonary Fibrosis Declarations of interest
GDG meeting Declaration of Interests
Actions taken
of these days.
Sixth GDG Meeting
(28/03/12)
AD declared non-personal pecuniary interests. AD was involved in developing and speaking at a patient support group meeting on the 10th March 2012 and the 25th April at the BLF NW ILD networking day. No financial re-numerations were received for either of these days.
None
Seventh GDG Meeting
(11/05/12)
AD declared a personal pecuniary interest. AD acted as a freelance trainer on the ARNS End of Life course in Swansea 19th and 20th April 2012, for which she received £300.00 per day. AD also declared personal non-pecuniary interests. AD was a speaker at the North-West BLF ILD/IPF networking patient support group meeting on the 25th April. Ad also presented at the International Primary Care Respiratory Society Conference in Edinburgh on the 28th April. No financial re-numerations were received for either of these days.
None
Eighth GDG Meeting
(21/06/12)
AD declared a personal pecuniary interest. AD acted as a freelance trainer on the ARNS End of Life care in Cambridge in May, for which she received £300 per day.
None
Ninth GDG Meeting
(25/07/12)
AD declared a personal pecuniary interest for consulting at an IPF patient support day organised by Intermune on the 19th July 2012, for which she received a fee of £225. Intermune manufactures Pirfenidone, which is not a drug highlighted in the scope of this guideline. AD also declared non-personal pecuniary interests. AD attended a meeting to develop a national IPF support group in Nottingham on 20th July 2012 outside of her NHS commitments. No expenses or reimbursement was received for attending this meeting. AD is also a co-author on two articles, one on the benefits of a MDT in ILD diagnosis and another on the benefits of ambulatory oxygen in IPF, which have both been submitted to the European Respiratory Journal.
None
Tenth GDG Meeting
(07/09/12)
AD declared personal non-pecuniary interests. AD attended a study day organised by Intermune on 28th June. She received no financial remuneration for attendance. AD also presented a research poster at the ERS on 4th September on ‘Perceptions, experiences and information needs of patients with IPF’. The department in which AD works is taking part in the Pirfenidone Named Patient Programme, which commenced in September 2011 and for which there is no funding. AD declared a personal pecuniary interest that her hotel accommodation at the ERS was sponsored by Intermune. Her flight expenses were covered by her institution.
None
Eleventh GDG Meeting
(05/10/12)
AD declared personal pecuniary interests. AD acted as a freelance trainer on the ARNS ILD study day in Belfast for which she received trainer fee of £300.00. AD was also involved in a radio interview on South Manchester radio for which there was no financial renumeration. AD declared a personal non-pecuniary interest, as she was involved with IPF awareness week sponsored by Intermune. Intermune sponsored activities at UHSM that were
None

18
Idiopathic Pulmonary Fibrosis Declarations of interest
GDG meeting Declaration of Interests
Actions taken
associated with IPF Awareness week with £500.
Twelfth GDG Meeting
(01/11/12)
Did not attend None
Thirteenth GDG Meeting
(06/03/13)
AD declared personal pecuniary interests. AD acted as a freelance trainer for the ARNS 2-day end of life course in Cheltenham in November 2012, in Belfast in January 2013 and in Colchester in March 2013. AD also ran an ARNS ILD study day in Manchester and a BOC ILD oxygen talk in November 2012. AD received a fee for all of the training and study days she was involved with and all were deemed within reasonable limits.
AD declared personal non-pecuniary interests. AD was a co-author on two abstracts, one titled ‘real life experience of using pirfenidone’ and another on the quality of life in patients using pirfenidone. Both abstracts were submitted to the BTS.
None
B.5 Geraldine Burge
GDG meeting Declaration of Interests
Actions taken
On Application GB declared she knew of no personal pecuniary or personal family interests in the previous 12 months or upcoming month.
GB declared the following non-personal pecuniary interests. GB is involved with drug studies conducted at Birmingham NHS hospital; Inspire Study Gamma Interferon/ placebo in patients with UIP, funded by Intermune was completed in 2010; Capacity Study Pirfenidone /placebo in patients with UIP, funded by Intermune started in 2007; Recap study open labelled Pirfenidone , funded by Intermune; and Tomorrow Study Vargate/ Placebo in pts with UIP, funded by Boeringher and Ingleheim, started in 2009. All of these studies have now come to an end in 2012. All funding goes to the Medical Innovations research unit at the Birmingham Heartlands hospital (MIDRU).
GB declared a personal family interest, as her husband is the principle investigator of all the above studies mentioned since 2003 to 2012.
First GDG meeting
(16/09/2011)
GB had no new interests to declare other than those declared at upon application to the GDG.
None
Second GDG Meeting
(21/10/11)
GB declared a personal family interest that her husband is the principle investigator of all the IPF studies she has been involved with since 2003, which includes involvement with Pirfenedone, Vargate and Gamma interferone.
GB also declared personal non-pecuniary interests. GB
None

19
Idiopathic Pulmonary Fibrosis Declarations of interest
GDG meeting Declaration of Interests
Actions taken
attended two IPF meetings sponsored by Boeringher Ingleheim and one by Intermune at the ERS in September. GB also attended a Patient Group Advisory Panel in Manchester, organised by WG Consulting. GB is also due to give a lecture to regional physiotherapist on IPF in the upcoming month.
Third GDG Meeting
(02/12/11)
GB declared a personal pecuniary interest that she had attended an IPF meeting in Berlin during the previous month, for which travel and accommodation was funded by Intermune.
None
Fourth GDG Meeting
(12/01/12)
Did not attend. None
Fifth GDG Meeting
(24/02/12)
GB declared a personal non-pecuniary interest that she had attended an IPF patient support group since the last GDG meeting.
None
Sixth GDG Meeting
(28/03/12)
Did not attend. None
Seventh GDG Meeting
(11/05/12)
GB declared non-personal pecuniary interests. GB attended an ERS school meeting on the 4th May, for which she received travel and accommodation expenses. GB also attended a non-IPF related ARS conference funded by GlaxoSmithKlein, for which she received £300 to attend. GB also declared a personal non-pecuniary interest.
GB declared a personal non-pecuniary interest, as she attended an IPF support group meeting in Nottingham on the 10th March 2012, for which no funding was received.
None
Eighth GDG Meeting
(21/06/12)
GB had no new interests to declare. None
Ninth GDG Meeting
(25/07/12)
Did not attend. None
Tenth GDG Meeting
(07/09/12)
GB declared personal non-pecuniary interests. GB attended an IPF update in June, for which she received no funding and has also been involved with an IPF patient self-help group (query funding). She also attended an ERS conference, for which travel and accommodation was funded for by Intermune. All expenses were within reasonable limits.
None
Eleventh GDG Meeting
(05/10/12)
Did not attend. None
Twelfth GDG Meeting
(01/11/12)
Did not attend. None
Thirteenth GDG GB declared personal pecuniary interests. GB was involved in a None
20
Idiopathic Pulmonary Fibrosis Declarations of interest
GDG meeting Declaration of Interests
Actions taken
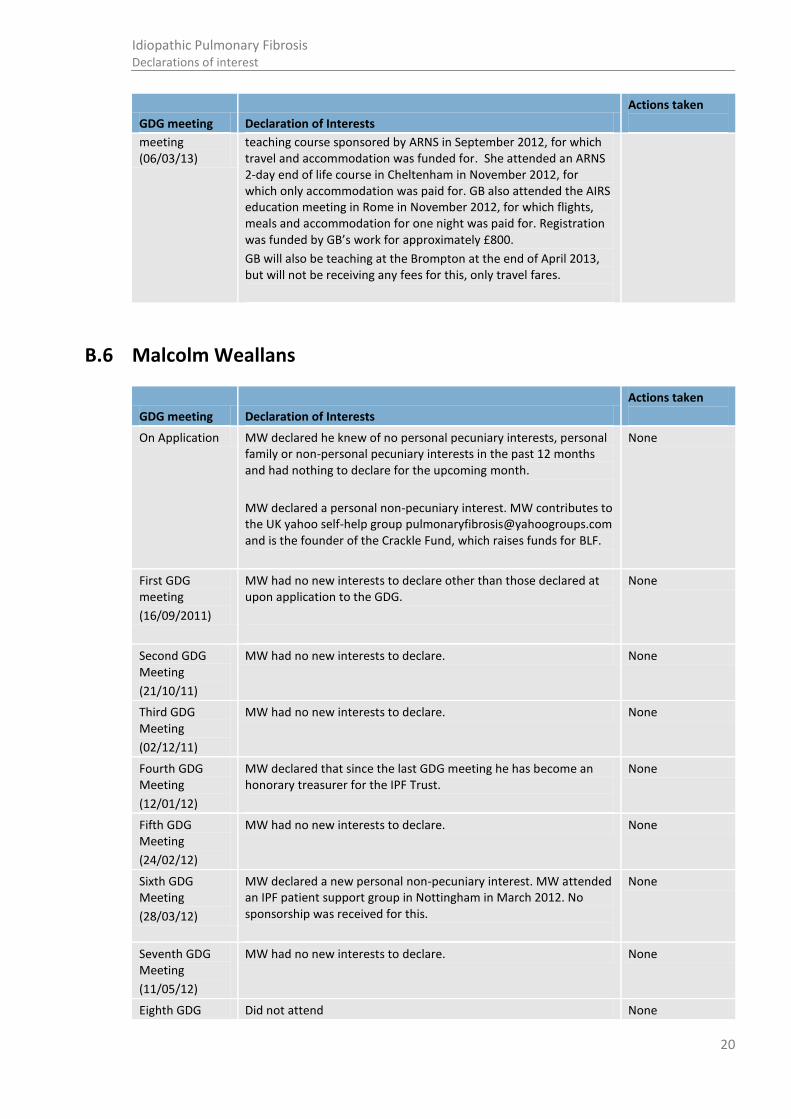
meeting (06/03/13)
teaching course sponsored by ARNS in September 2012, for which travel and accommodation was funded for. She attended an ARNS 2-day end of life course in Cheltenham in November 2012, for which only accommodation was paid for. GB also attended the AIRS education meeting in Rome in November 2012, for which flights, meals and accommodation for one night was paid for. Registration was funded by GB’s work for approximately £800.
GB will also be teaching at the Brompton at the end of April 2013, but will not be receiving any fees for this, only travel fares.
B.6 Malcolm Weallans
GDG meeting Declaration of Interests
Actions taken
On Application MW declared he knew of no personal pecuniary interests, personal family or non-personal pecuniary interests in the past 12 months and had nothing to declare for the upcoming month.
MW declared a personal non-pecuniary interest. MW contributes to the UK yahoo self-help group [email protected] and is the founder of the Crackle Fund, which raises funds for BLF.
None
First GDG meeting
(16/09/2011)
MW had no new interests to declare other than those declared at upon application to the GDG.
None
Second GDG Meeting
(21/10/11)
MW had no new interests to declare. None
Third GDG Meeting
(02/12/11)
MW had no new interests to declare. None
Fourth GDG Meeting
(12/01/12)
MW declared that since the last GDG meeting he has become an honorary treasurer for the IPF Trust.
None
Fifth GDG Meeting
(24/02/12)
MW had no new interests to declare. None
Sixth GDG Meeting
(28/03/12)
MW declared a new personal non-pecuniary interest. MW attended an IPF patient support group in Nottingham in March 2012. No sponsorship was received for this.
None
Seventh GDG Meeting
(11/05/12)
MW had no new interests to declare. None
Eighth GDG Did not attend None

21
Idiopathic Pulmonary Fibrosis Declarations of interest
GDG meeting Declaration of Interests
Actions taken
Meeting
(21/06/12)
Ninth GDG Meeting
(25/07/12)
MW had no new interests to declare. None
Tenth GDG Meeting
(07/09/12)
MW had no new interests to declare. None
Eleventh GDG Meeting
(05/10/12)
MW declared a personal non-pecuniary interest. MW is attending a research day at the Brompton, which is funded by Intermune, but for which MW does receive any financial remuneration. MW is also attending the Pirfenidone technology appraisal meeting in Manchester on the 24th October, for which travel expenses are funded by NICE.
None
Twelfth GDG Meeting
(01/11/12)
MW had no new interests to declare. None
Thirteenth GDG Meeting (06/03/13)
MW declared a personal pecuniary interest. He will be giving a presentation on IPF at the East Anglian University in April, for which travel expenses will be received.
None
B.7 Melissa Hippard
GDG meeting Declaration of Interests
Actions taken
On Application MH declared she knew of no personal pecuniary interests, personal family or non-personal pecuniary interests in the past 12 months and had nothing to declare for the upcoming month.
MH declared personal non-pecuniary interests.
MH is a member of an online support group: (http://health.groups.yahoo.com/group/pulmonaryfibrosis/) and has also posted in the past on other support groups: Huf’n’Puf (US group), PF Facebook group and the BLF support group. MH has attended the launch of and given donations to ‘Breathing Matters’ a charity set up to raise funds for research at the Centre for Respiratory Research, UCLH.
None
First GDG meeting
(16/09/2011)
Did not attend.
None
Second GDG Meeting
(21/10/11)
MH had no new interests to declare. None
Third GDG Meeting
MH had no new interests to declare. None

22
Idiopathic Pulmonary Fibrosis Declarations of interest
GDG meeting Declaration of Interests
Actions taken
(02/12/11)
Fourth GDG Meeting
(12/01/12)
MH had no new interests to declare. None
Fifth GDG Meeting
(24/02/12)
MH had no new interests to declare. None
Sixth GDG Meeting
(28/03/12)
MH had no new interests to declare. None
Seventh GDG Meeting
(11/05/12)
MH had no new interests to declare. None
Eighth GDG Meeting
(21/06/12)
Did not attend.
None
Ninth GDG Meeting
(25/07/12)
MH had no new interests to declare. None
Tenth GDG Meeting
(07/09/12)
MH declared a personal non-pecuniary interest that she has volunteered to be a patient expert on the Pirfenidone technology appraisal committee, due to take place in October 2012.
None
Eleventh GDG Meeting
(05/10/12)
Did not attend None
Twelfth GDG Meeting
(01/11/12)
MH had no new interests to declare. None
Thirteenth GDG Meeting (06/03/13)
MH declared a personal non-pecuniary interest. She was interviewed by Intermune to discuss the impact of IPF on her lifestyle and family. No fee was received.
None
B.8 Nicholas Kim Harrison
GDG meeting Declaration of Interests
Actions taken
On Application NKH declared he knew of no personal pecuniary interests or non-personal pecuniary interests in the past 12 months and had nothing to declare for the upcoming month.
NKH declared a personal family interest. NKH’s wife is an Assistant Medical Director (Primary Care) for Abertawe Bro Morgannwg University Health Board and is lead for the development of ‘Care Pathways’ (from 2010 to present).
None

23
Idiopathic Pulmonary Fibrosis Declarations of interest
GDG meeting Declaration of Interests
Actions taken
NKH declared personal pecuniary interests. NKH is the Lead for ‘Lung Research Wales’. NKH was the Chairman of the British Association for Lung Research from 2005 to 2009 and stepped down as a member of the BALR Committee in 2011. NKH represents Wales on the UK Respiratory Research Collaborative as well as the Respiratory Specialty Group of the National Institute for Health Research (NIHR) Clinical Research Network (from 2005 to present).
NKH enrolled patients into the following clinical trial: TIPAC (Treating Interstitial Pneumonia with the Addition of Co-Trimoxazole) – a phase III interventional study (funded by the NIHR Research for Patient Benefit and the East Anglia Thoracic Society and sponsored by the University of East Anglia). This study closed 31st December 2009
NKH enrolled patients into the following observational cohort study: Trent Lung Fibrosis Study – Does the presence of thrombophilia increase the risk of developing idiopathic pulmonary fibrosis? (Funded by the MRC and sponsored by the University of Nottingham, from 2009-2011).
First GDG meeting
(16/09/2011)
NKH had no new interests to declare other than those declared at upon application to the GDG.
None
Second GDG Meeting
(21/10/11)
NKH had no new interests to declare. None
Third GDG Meeting
(02/12/11)
NKH had no new interests to declare. None
Fourth GDG Meeting
(12/01/12)
NKH had no new interests to declare. None
Fifth GDG Meeting
(24/02/12)
NKH had no new interests to declare. None
Sixth GDG Meeting
(28/03/12)
NKH had no new interests to declare. None
Seventh GDG Meeting
(11/05/12)
NKH had no new interests to declare. None
Eighth GDG Meeting
(21/06/12)
NKH declared a non-personal pecuniary interest. NKH will be a co-investigator on a trial investigating the end of life needs of patients with IPF and their carers due to commence later in 2012 (date to be confirmed). The trial is funded by the Marie Curie Research Programme, and payment goes to a Palliative Care hospital.
None
Ninth GDG Meeting
NKH had no new interests to declare.
None
24
Idiopathic Pulmonary Fibrosis Declarations of interest
GDG meeting Declaration of Interests
Actions taken
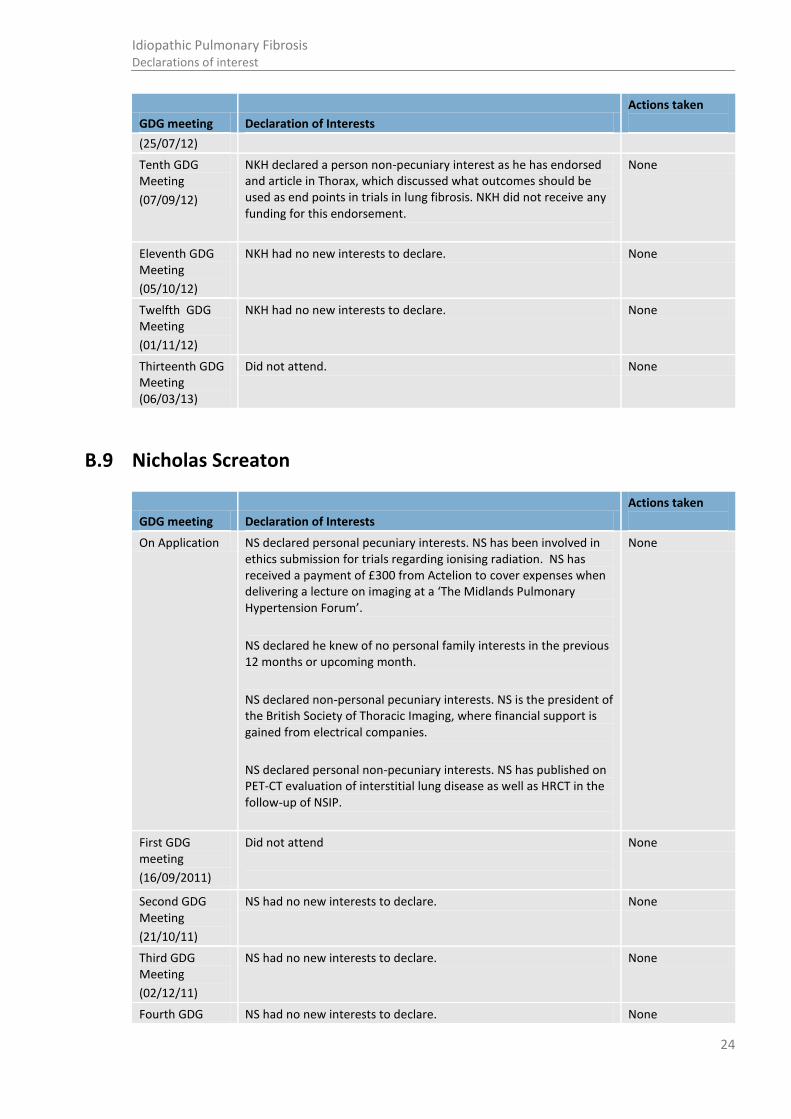
(25/07/12)
Tenth GDG Meeting
(07/09/12)
NKH declared a person non-pecuniary interest as he has endorsed and article in Thorax, which discussed what outcomes should be used as end points in trials in lung fibrosis. NKH did not receive any funding for this endorsement.
None
Eleventh GDG Meeting
(05/10/12)
NKH had no new interests to declare. None
Twelfth GDG Meeting
(01/11/12)
NKH had no new interests to declare. None
Thirteenth GDG Meeting (06/03/13)
Did not attend. None
B.9 Nicholas Screaton
GDG meeting Declaration of Interests
Actions taken
On Application NS declared personal pecuniary interests. NS has been involved in ethics submission for trials regarding ionising radiation. NS has received a payment of £300 from Actelion to cover expenses when delivering a lecture on imaging at a ‘The Midlands Pulmonary Hypertension Forum’.
NS declared he knew of no personal family interests in the previous 12 months or upcoming month.
NS declared non-personal pecuniary interests. NS is the president of the British Society of Thoracic Imaging, where financial support is gained from electrical companies.
NS declared personal non-pecuniary interests. NS has published on PET-CT evaluation of interstitial lung disease as well as HRCT in the follow-up of NSIP.
None
First GDG meeting
(16/09/2011)
Did not attend
None
Second GDG Meeting
(21/10/11)
NS had no new interests to declare. None
Third GDG Meeting
(02/12/11)
NS had no new interests to declare. None
Fourth GDG NS had no new interests to declare. None

25
Idiopathic Pulmonary Fibrosis Declarations of interest
GDG meeting Declaration of Interests
Actions taken
Meeting
(12/01/12)
Fifth GDG Meeting
(24/02/12)
NS had no new interests to declare. None
Sixth GDG Meeting
(28/03/12)
Did not attend None
Seventh GDG Meeting
(11/05/12)
NS had no new interests to declare. None
Eighth GDG Meeting
(21/06/12)
Did not attend
None
Ninth GDG Meeting
(25/07/12)
NS had no new interests to declare. None
Tenth GDG Meeting
(07/09/12)
NS declared a non-personal non-pecuniary interest. His department has received funding from GlaxoSmithKlein for one radiologist and one physicist positions.
None
Eleventh GDG Meeting
(05/10/12)
Did not attend None
Twelfth GDG Meeting
(01/11/12)
Did not attend None
Thirteenth GDG Meeting (06/03/13)
NS had no new interests to declare. None
B.10 Patrick Wilson
GDG meeting Declaration of Interests
Actions taken
On Application PW declared he knew of no personal pecuniary, personal family or non-personal pecuniary interests in the previous 12 months or upcoming month.
PW declared person non-pecuniary interests. PW has contributed to NICE scoping workshops involving inhaled mannitol and dry powder colistimethate sodium in cystic fibrosis. PW is involved though the United Kingdom Clinical Pharmacy Association in using web-based technology to deliver continuing education to pharmacists in the area of respiratory medicine.
None
First GDG PW had no new interests to declare other than those declared at None

26
Idiopathic Pulmonary Fibrosis Declarations of interest
GDG meeting Declaration of Interests
Actions taken
meeting
(16/09/2011)
upon application to the GDG.
Second GDG Meeting
(21/10/11)
PW had no new interests to declare. None
Third GDG Meeting
(02/12/11)
PW had no new interests to declare. None
Fourth GDG Meeting
(12/01/12)
PW had no new interests to declare. None
Fifth GDG Meeting
(24/02/12)
PW had no new interests to declare. None
Sixth GDG Meeting
(28/03/12)
Did not attend. None
Seventh GDG Meeting
(11/05/12)
PW had no new interests to declare. None
Eighth GDG Meeting
(21/06/12)
PW had no new interests to declare None
Ninth GDG Meeting
(25/07/12)
PW had no new interests to declare None
Tenth GDG Meeting
(07/09/12)
PW declared a non-personal pecuniary interest. PW has successfully applied for a Gilead Fellowship Grant to carry out a research project into improving adherence with nebulised antibiotic therapy in cystic fibrosis. This grant totals £10 000 and is to be paid directly into a departmental account on which PW is not named.
None
Eleventh GDG Meeting
(05/10/12)
PW declared a personal pecuniary interest. PW attended training on “Negotiating and Influencing”, which was paid for by Bayer Pharmaceuticals.
None
Twelfth GDG Meeting
(01/11/12)
Did not attend. None
Thirteenth GDG Meeting (06/03/13)
PW declared a personal pecuniary interest. He attended a training day discussing inhalers, funded by his department.
None
B.11 Richard Hubbard
GDG meeting Declaration of Interests
Actions taken
27
Idiopathic Pulmonary Fibrosis Declarations of interest
GDG meeting Declaration of Interests
Actions taken
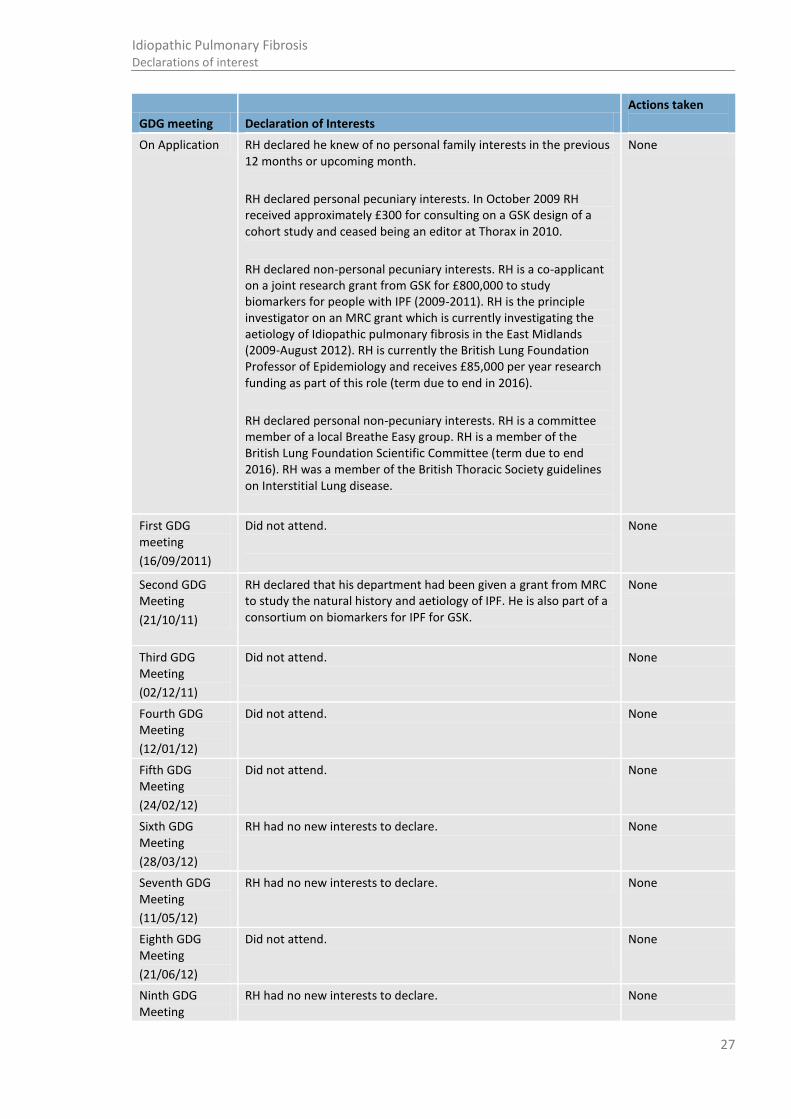
On Application RH declared he knew of no personal family interests in the previous 12 months or upcoming month.
RH declared personal pecuniary interests. In October 2009 RH received approximately £300 for consulting on a GSK design of a cohort study and ceased being an editor at Thorax in 2010.
RH declared non-personal pecuniary interests. RH is a co-applicant on a joint research grant from GSK for £800,000 to study biomarkers for people with IPF (2009-2011). RH is the principle investigator on an MRC grant which is currently investigating the aetiology of Idiopathic pulmonary fibrosis in the East Midlands (2009-August 2012). RH is currently the British Lung Foundation Professor of Epidemiology and receives £85,000 per year research funding as part of this role (term due to end in 2016).
RH declared personal non-pecuniary interests. RH is a committee member of a local Breathe Easy group. RH is a member of the British Lung Foundation Scientific Committee (term due to end 2016). RH was a member of the British Thoracic Society guidelines on Interstitial Lung disease.
None
First GDG meeting
(16/09/2011)
Did not attend.
None
Second GDG Meeting
(21/10/11)
RH declared that his department had been given a grant from MRC to study the natural history and aetiology of IPF. He is also part of a consortium on biomarkers for IPF for GSK.
None
Third GDG Meeting
(02/12/11)
Did not attend.
None
Fourth GDG Meeting
(12/01/12)
Did not attend. None
Fifth GDG Meeting
(24/02/12)
Did not attend. None
Sixth GDG Meeting
(28/03/12)
RH had no new interests to declare. None
Seventh GDG Meeting
(11/05/12)
RH had no new interests to declare. None
Eighth GDG Meeting
(21/06/12)
Did not attend.
None
Ninth GDG Meeting
RH had no new interests to declare. None
28
Idiopathic Pulmonary Fibrosis Declarations of interest
GDG meeting Declaration of Interests
Actions taken
(25/07/12)
Tenth GDG Meeting
(07/09/12)
Did not attend.
None
Eleventh GDG Meeting
(05/10/12)
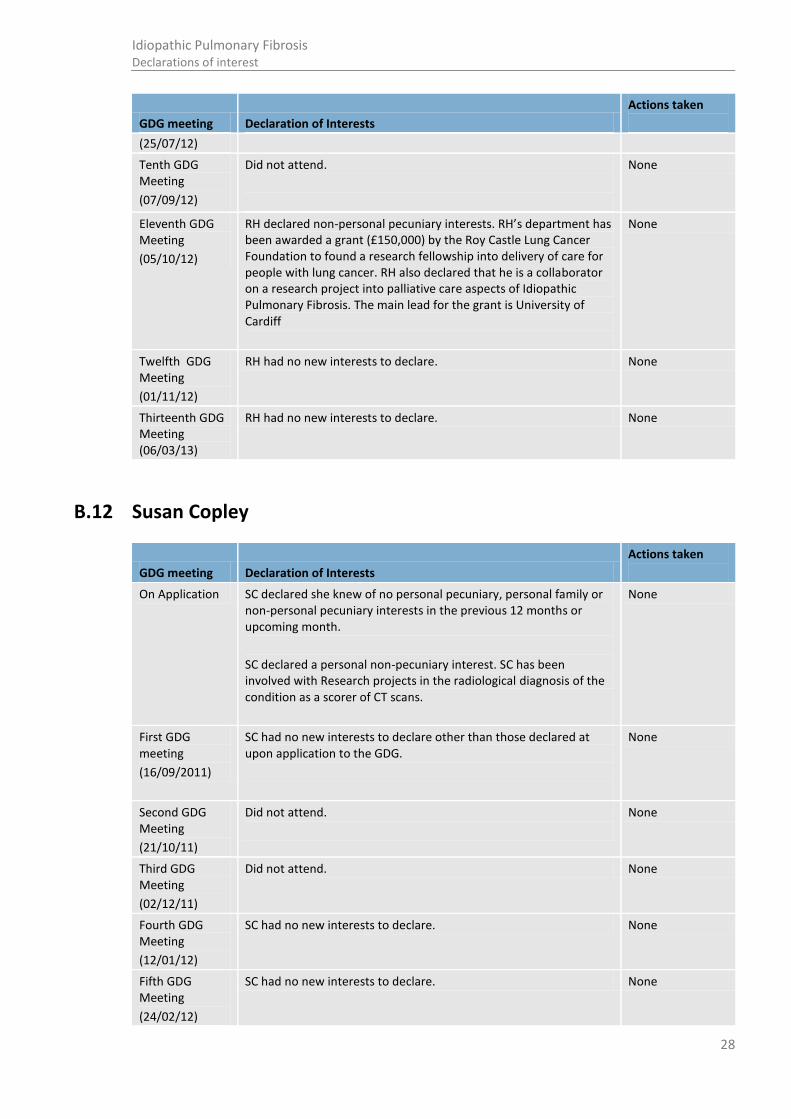
RH declared non-personal pecuniary interests. RH’s department has been awarded a grant (£150,000) by the Roy Castle Lung Cancer Foundation to found a research fellowship into delivery of care for people with lung cancer. RH also declared that he is a collaborator on a research project into palliative care aspects of Idiopathic Pulmonary Fibrosis. The main lead for the grant is University of Cardiff
None
Twelfth GDG Meeting
(01/11/12)
RH had no new interests to declare. None
Thirteenth GDG Meeting (06/03/13)
RH had no new interests to declare. None
B.12 Susan Copley
GDG meeting Declaration of Interests
Actions taken
On Application SC declared she knew of no personal pecuniary, personal family or non-personal pecuniary interests in the previous 12 months or upcoming month.
SC declared a personal non-pecuniary interest. SC has been involved with Research projects in the radiological diagnosis of the condition as a scorer of CT scans.
None
First GDG meeting
(16/09/2011)
SC had no new interests to declare other than those declared at upon application to the GDG.
None
Second GDG Meeting
(21/10/11)
Did not attend.
None
Third GDG Meeting
(02/12/11)
Did not attend. None
Fourth GDG Meeting
(12/01/12)
SC had no new interests to declare. None
Fifth GDG Meeting
(24/02/12)
SC had no new interests to declare. None

29
Idiopathic Pulmonary Fibrosis Declarations of interest
GDG meeting Declaration of Interests
Actions taken
Sixth GDG Meeting
(28/03/12)
Did not attend. None
Seventh GDG Meeting
(11/05/12)
SC had no new interests to declare. None
Eighth GDG Meeting
(21/06/12)
SC had no new interests to declare. None
Ninth GDG Meeting
(25/07/12)
SC had no new interests to declare. None
Tenth GDG Meeting
(07/09/12)
SC declared personal non-pecuniary interests. SC is a member of the BTS steering group developing an IPF National Registry, for which no funding is received, and is also a co-organizer of an ILD Educational Course, NHLI, which commenced in March 2013 and the funding goes to her department.
None
Eleventh GDG Meeting
(05/10/12)
Did not attend. None
Twelfth GDG Meeting
(01/11/12)
SC had no new interests to declare. None
Thirteenth GDG Meeting (06/03/13)
SC had no new interests to declare. None
B.13 Tessa Lewis
GDG meeting Declaration of Interests
Actions taken
On Application TL declared she knew of no personal pecuniary, personal family, non-personal pecuniary or personal non-pecuniary interests in the previous 12 months or upcoming month.
None
First GDG meeting
(16/09/2011)
TL had no new interests to declare other than those declared at upon application to the GDG.
None
Second GDG Meeting
(21/10/11)
TL had no new interests to declare. None
Third GDG Meeting
(02/12/11)
TL had no new interests to declare. None
Fourth GDG TL had no new interests to declare. None
30
Idiopathic Pulmonary Fibrosis Declarations of interest
GDG meeting Declaration of Interests
Actions taken
Meeting
(12/01/12)
Fifth GDG Meeting
(24/02/12)
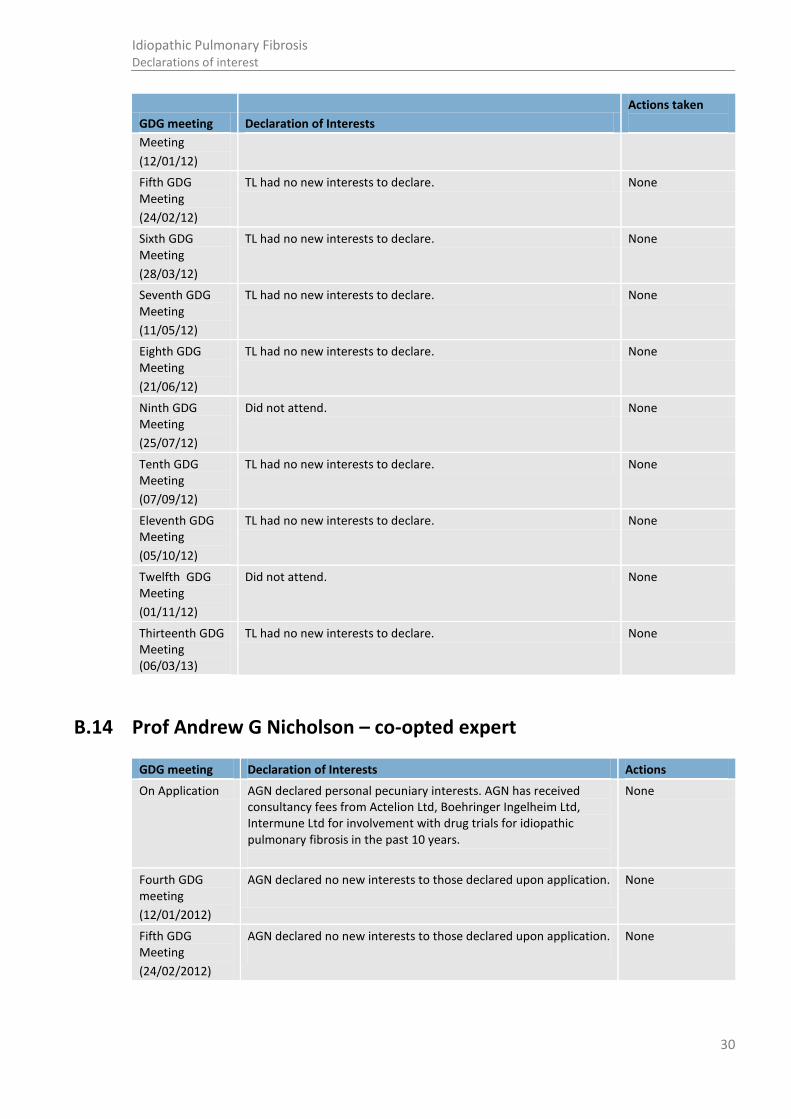
TL had no new interests to declare. None
Sixth GDG Meeting
(28/03/12)
TL had no new interests to declare. None
Seventh GDG Meeting
(11/05/12)
TL had no new interests to declare. None
Eighth GDG Meeting
(21/06/12)
TL had no new interests to declare. None
Ninth GDG Meeting
(25/07/12)
Did not attend. None
Tenth GDG Meeting
(07/09/12)
TL had no new interests to declare. None
Eleventh GDG Meeting
(05/10/12)
TL had no new interests to declare. None
Twelfth GDG Meeting
(01/11/12)
Did not attend. None
Thirteenth GDG Meeting (06/03/13)
TL had no new interests to declare. None
B.14 Prof Andrew G Nicholson – co-opted expert
GDG meeting Declaration of Interests Actions
On Application AGN declared personal pecuniary interests. AGN has received consultancy fees from Actelion Ltd, Boehringer Ingelheim Ltd, Intermune Ltd for involvement with drug trials for idiopathic pulmonary fibrosis in the past 10 years.
None
Fourth GDG meeting
(12/01/2012)
AGN declared no new interests to those declared upon application.
None
Fifth GDG Meeting
(24/02/2012)
AGN declared no new interests to those declared upon application.
None

31
Idiopathic Pulmonary Fibrosis Declarations of interest
B.15 Mr Stephen Clark – co-opted expert
GDG meeting Declaration of Interests Actions
On Application SC declared he had no conflicts of interests in the previous 12 months or upcoming month.
None
Tenth GDG Meeting
(07/09/12)
SC declared no new interests to those declared upon application.
None
B.16 Professor Sally Singh – co-opted expert
GDG meeting Declaration of Interests Actions
On Application SS declared she had no conflicts of interests in the previous 12 months or upcoming month.
None
Third GDG Meeting
(02/12/2011)
SS declared no new interests to those declared upon application.
None
Ninth GDG Meeting
(25/07/12)
SS declared a personal non-pecuniary interest. She will be an adviser on the NIHR HTA report, which is evaluating the clinical and cost effectiveness of treatments for idiopathic pulmonary fibrosis. This systematic review is due for completion in spring 2013.
None
B.17 NCGC technical team
GDG meeting
Declaration of Interests of the NCGC members
Actions
First GDG meeting
(16/09/2011)
No member of the NCGC knew of a personal pecuniary interests, personal family interests, non-personal pecuniary interests or personal non-pecuniary interests in the past 12 months or upcoming months.
None
Second GDG Meeting
(21/10/2011)
No interests to declare. None
Third GDG Meeting
(02/12/2011)
No interests to declare. None
Fourth GDG Meeting
(12/01/2012)
No interests to declare. None
Fifth GDG No interests to declare. None

32
Idiopathic Pulmonary Fibrosis Declarations of interest
GDG meeting
Declaration of Interests of the NCGC members
Actions
Meeting
(24/02/2012)
Sixth GDG Meeting
(28/03/2012)
No interests to declare. None
Seventh GDG Meeting
(11/05/2012)
No interests to declare. None
Eight GDG Meeting
(21/06/12)
VDN declared a non-personal pecuniary interest. VDN will be attending a meeting in St Petersburg, for which travel and accommodation is being funded by Pfizer. Consultancy fee will be paid into the NCGC account. Pfizer does not manufacture any IPF related drugs.
No other NCGC member had any interests to declare.
None
Ninth GDG Meeting
(25/07/12)
VDN declared a non-personal pecuniary interest. VDN attended a meeting in St Petersburg, for which travel and accommodation was funded by Pfizer. The consultancy fee was paid into the NCGC account. Pfizer does not manufacture any IPF related drugs.
No other NCGC member had any interests to declare
None
Tenth GDG Meeting
(07/09/12)
No interests to declare. None
Eleventh GDG Meeting
(05/10/12)
VN declared a non-personal non-pecuniary interest. VN is attending the Pirfenidone technology appraisal meeting in Manchester on the 24th October. No financial remuneration is being received for this.
No other NCGC member had any interests to declare
None
Twelfth GDG Meeting
(01/11/12)
No interests to declare. None
Thirteenth GDG Meeting (06/03/13)
No new interests to declare. None

33
Idiopathic Pulmonary Fibrosis Review protocols
Appendix C: Review protocols
1.1 Diagnosis
Table 1: Review protocols: biopsy
Review question
In suspected IPF what is the value of adding biopsy (bronchoscopic biopsy/transbronchial biopsy or surgical lung biopsy) and /or bronchoalveolar lavage, to clinical evaluation, PFTs and CT for confirming the diagnosis of IPF?
Objectives To determine the added benefit of a biopsy in the diagnosis of a patient with suspected IPF, when clinical history, PFTs, HRCT +/- bronchoalveolar lavage have all be conducted.
Criteria Population: Adults with suspected ILD
Interventions:
Baseline clinical assessment (history, PFTs, HRCT, +/- BAL), and:
o +/-Bronchoalveolar lavage
o Bronchoscopic biopsy/ transbronchial biopsy
o Surgical biopsy ( open lung or video assisted biopsy)
Comparisons: Baseline clinical assessment (history, PFTs, HRCT, +/- BAL)
Outcomes at following time intervals: original study definitions will be used and recorded Critical outcomes
All cause and IPF related mortality
1 and 3 year survival rates
Sensitivity
Specificity Other outcomes
Adverse events
Improvement in health-related quality of life
Population size and directness:
No limitations on sample size
Populations of people with IPF receiving pharmacological treatment will be included
Studies with indirect populations will not be considered
Setting: Secondary and tertiary care settings
Minimally important differences:
Please refer to section 3.3.9 Imprecision in the methodology chapter
Search Databases: Medline, Embase, the Cochrane Library
Date: Post 1994 data
Language: Restrict to English only
Population: ILDs
Study designs: Cohort studies
Review Appraisal of methodological quality: The methodological quality of each study will be assessed

34
Idiopathic Pulmonary Fibrosis Review protocols
strategy using NICE checklists.
Subgroups: People with co-existent emphysema
Type of analysis: Multivariable survival analysis
Table 2: Review protocols: MDT diagnostic consensus
Review question
In suspected IPF what is the additional value of adding multidisciplinary team (MDT) consensus to clinical assessment, PFTs and HRCT in the diagnosis of IPF?
Objectives To determine whether MDT consensus provides an additional benefit to diagnosis of IPF patients
Criteria Population: Adults with suspected ILD Interventions:
MDT 1: Clinical assessment + radiological assessment + MDT consensus
MDT 2: Clinical assessment + radiological assessment +/- bronchoaveolar lavage + MDT
consensus
MDT 3: Clinical assessment + radiological assessment +/- bronchoaveolar lavage +
bronchoscopic/ transbronchical biopsy surgical biopsy (open-lung or VATs) + MDT
Comparisons: The following procedures alone or in combination:
Clinical assessment
Radiological assessment
Bronchioalveolar lavage
Bronchscopic/ transbronchial biopsy
Surgical lung biopsy (open lung and video assisted biopsy)
Outcomes at following time intervals: original study definitions will be used and recorded Critical outcomes
All cause and IPF related mortality
1 and 3 year survival rates
Sensitivity
Specificity Other outcomes
Adverse events
Improvement in health-related quality of life
Population size and directness:
No limitations on sample size
Populations of people with IPF receiving pharmacological treatment will be included
Studies with indirect populations will not be considered
Setting: Secondary and tertiary care settings
Minimally important differences:
Please refer to section 3.3.9 Imprecision in the methodology chapter
Search Databases: Medline, Embase, the Cochrane Library
Date: Post 1994 data
Language: Restrict to English only
Population: ILDs
Study designs: Cohort studies
35
Idiopathic Pulmonary Fibrosis Review protocols
Review strategy
Appraisal of methodological quality: The methodological quality of each study will be assessed using NICE checklists.
Subgroups: People with co-existent emphysema
Type of analysis: Multivariable survival analysis
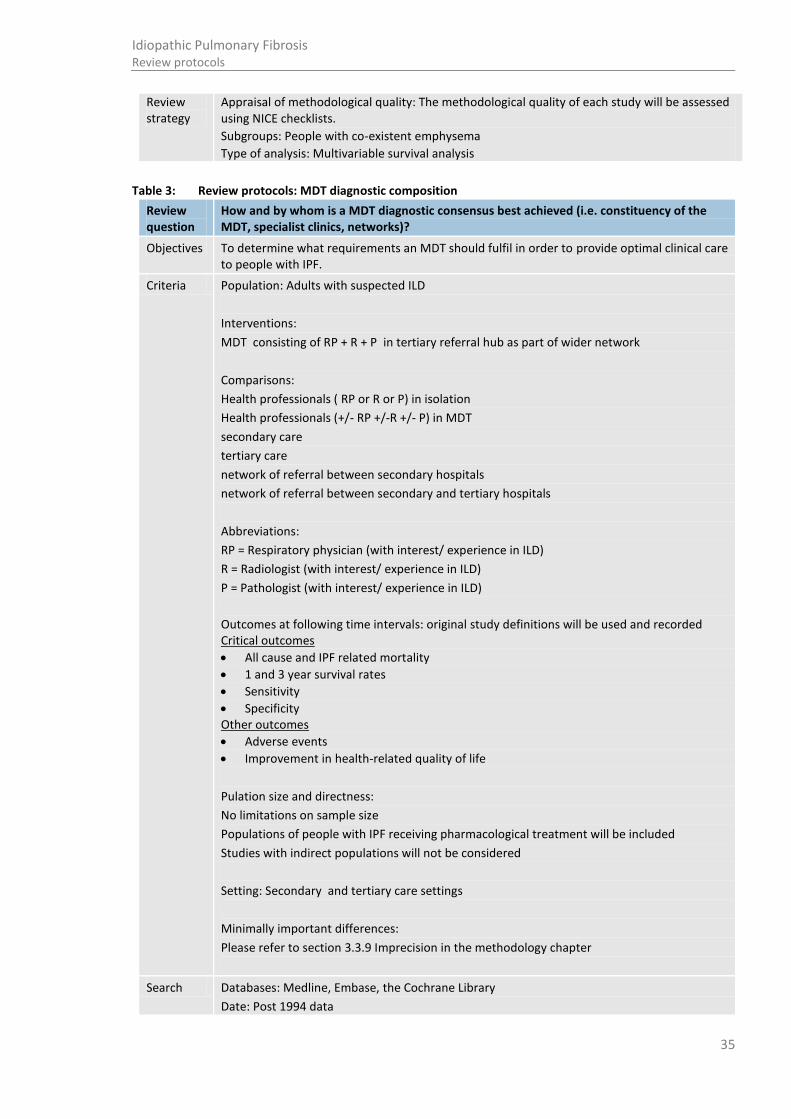
Table 3: Review protocols: MDT diagnostic composition
Review question
How and by whom is a MDT diagnostic consensus best achieved (i.e. constituency of the MDT, specialist clinics, networks)?
Objectives To determine what requirements an MDT should fulfil in order to provide optimal clinical care to people with IPF.
Criteria Population: Adults with suspected ILD
Interventions:
MDT consisting of RP + R + P in tertiary referral hub as part of wider network
Comparisons:
Health professionals ( RP or R or P) in isolation
Health professionals (+/- RP +/-R +/- P) in MDT
secondary care
tertiary care
network of referral between secondary hospitals
network of referral between secondary and tertiary hospitals
Abbreviations:
RP = Respiratory physician (with interest/ experience in ILD)
R = Radiologist (with interest/ experience in ILD)
P = Pathologist (with interest/ experience in ILD)
Outcomes at following time intervals: original study definitions will be used and recorded Critical outcomes
All cause and IPF related mortality
1 and 3 year survival rates
Sensitivity
Specificity Other outcomes
Adverse events
Improvement in health-related quality of life
Pulation size and directness:
No limitations on sample size
Populations of people with IPF receiving pharmacological treatment will be included
Studies with indirect populations will not be considered
Setting: Secondary and tertiary care settings
Minimally important differences:
Please refer to section 3.3.9 Imprecision in the methodology chapter
Search Databases: Medline, Embase, the Cochrane Library
Date: Post 1994 data
36
Idiopathic Pulmonary Fibrosis Review protocols
Language: Restrict to English only
Population: ILDs
Study designs: Cohort studies
Review strategy
Appraisal of methodological quality: The methodological quality of each study will be assessed using NICE checklists.
Subgroups: People with co-existent emphysema
Type of analysis: Multivariable survival analysis
1.2 Prognosis
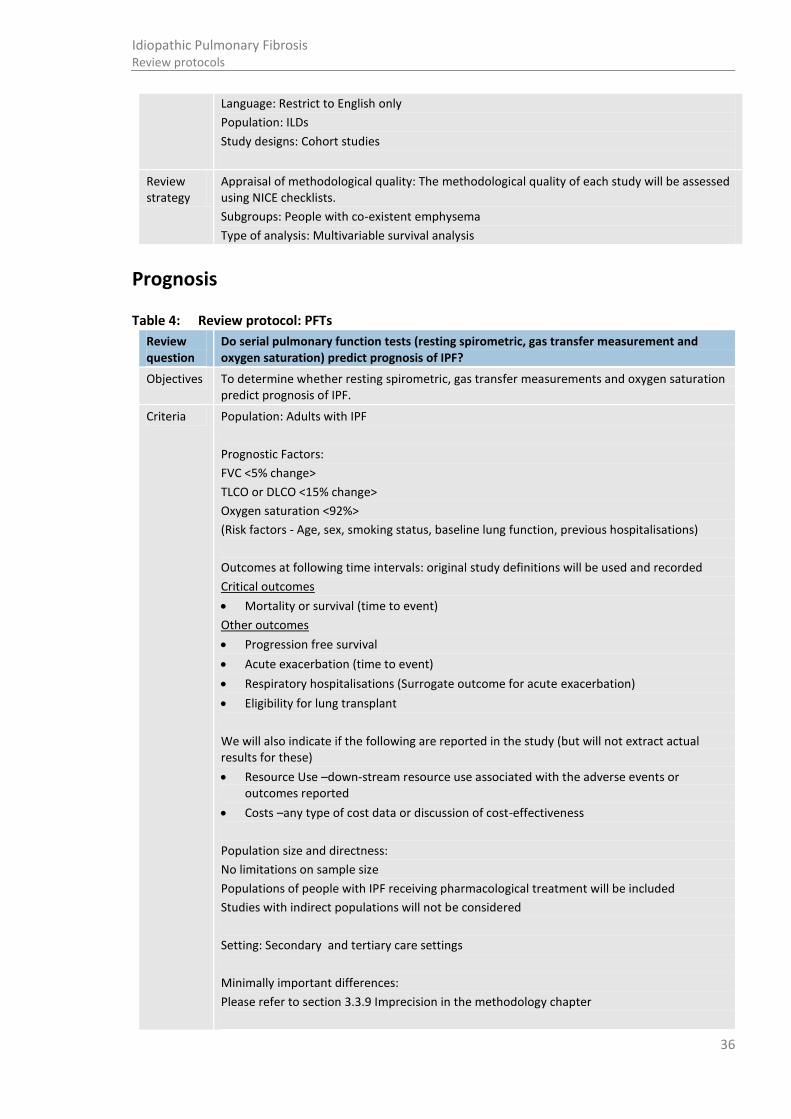
Table 4: Review protocol: PFTs
Review question
Do serial pulmonary function tests (resting spirometric, gas transfer measurement and oxygen saturation) predict prognosis of IPF?
Objectives To determine whether resting spirometric, gas transfer measurements and oxygen saturation predict prognosis of IPF.
Criteria Population: Adults with IPF
Prognostic Factors:
FVC <5% change>
TLCO or DLCO <15% change>
Oxygen saturation <92%>
(Risk factors - Age, sex, smoking status, baseline lung function, previous hospitalisations)
Outcomes at following time intervals: original study definitions will be used and recorded
Critical outcomes
Mortality or survival (time to event)
Other outcomes
Progression free survival
Acute exacerbation (time to event)
Respiratory hospitalisations (Surrogate outcome for acute exacerbation)
Eligibility for lung transplant
We will also indicate if the following are reported in the study (but will not extract actual results for these)
Resource Use –down-stream resource use associated with the adverse events or outcomes reported
Costs –any type of cost data or discussion of cost-effectiveness
Population size and directness:
No limitations on sample size
Populations of people with IPF receiving pharmacological treatment will be included
Studies with indirect populations will not be considered
Setting: Secondary and tertiary care settings
Minimally important differences:
Please refer to section 3.3.9 Imprecision in the methodology chapter

37
Idiopathic Pulmonary Fibrosis Review protocols
Search Databases: Medline, Embase, the Cochrane Library, CINAHL
Date: Post 1994 data
Language: Restrict to English only
Population: IPF only
Study designs: Cohorts
Review strategy
Appraisal of methodological quality: The methodological quality of each study will be assessed using NICE checklists.
Subgroups: People with co-existent emphysema
Type of analysis: Multivariable survival analysis
Table 5: Review protocol: Sub-maximal exercise testing
Review question Does baseline sub-maximal exercise testing predict prognosis of IPF?
Objectives To determine whether baseline sub-maximal exercise testing predicts prognosis of IPF.
Criteria Population: Adults with IPF
Prognostic factor: Sub-maximal exercise testing (threshold unknown – query <250m>)
(Risk factors - Age, sex, smoking status, baseline lung function)
Outcomes at following time intervals: original study definitions will be used and recorded
Critical outcomes
Mortality or survival (time to event)
Other outcomes
Progression free survival
Acute exacerbation (time to event)
Respiratory hospitalisations (Surrogate outcome for acute exacerbation)
Eligibility for lung transplant
We will also indicate if the following are reported in the study (but will not extract actual results for these)
Resource Use –down-stream resource use associated with the adverse events or outcomes reported
Costs –any type of cost data or discussion of cost-effectiveness
Population size and directness:
No limitations on sample size
Populations of people with IPF receiving pharmacological treatment will be included
Studies with indirect populations will not be considered
Setting: Secondary and tertiary care settings
Minimally important differences:
Please refer to section 3.3.9 Imprecision in the methodology chapter
Search Strategy
Databases: Medline, Embase, the Cochrane Library, CINAHL
Date: Post 1994 data

38
Idiopathic Pulmonary Fibrosis Review protocols
Language: Restrict to English only
Population: IPF only
Study designs: Cohort studies
Review Strategy
Appraisal of methodological quality: The methodological quality of each study will be assessed using NICE checklists.
Subgroups: People with co-existent emphysema
Type of analysis: Multivariable survival analysis
Table 6: Review protocol: echocardiography Review question
Does baseline echocardiography predict prognosis of IPF?
Objectives Does baseline echocardiography predict prognosis of IPF?
Criteria Population: Adults with IPF
Prognostic factor: Pulmonary arterial systolic pressure (threshold unknown)
(Risk factors - Age, sex, smoking status, baseline lung function)
Outcomes at following time intervals: original study definitions will be used and recorded
Critical outcomes
Mortality or survival (time to event)
Other outcomes
Progression free survival
Acute exacerbation (time to event)
Respiratory hospitalisations (Surrogate outcome for acute exacerbation)
Eligibility for lung transplant
We will also indicate if the following are reported in the study (but will not extract actual results for these)
Resource Use –down-stream resource use associated with the adverse events or
outcomes reported
Costs –any type of cost data or discussion of cost-effectiveness
Population size and directness:
No limitations on sample size
Populations of people with IPF receiving pharmacological treatment will be included
Studies with indirect populations will not be considered
Minimally important differences:
Please refer to section 3.3.9 Imprecision in the methodology chapter
Search Strategy
Databases: Medline, Embase, the Cochrane Library
Date: Post 1994 data
Language: Restrict to English only
Population: IPF only
Study designs: Cohort studies
Review Strategy
Appraisal of methodological quality: The methodological quality of each study will be assessed using NICE checklists.
Subgroups: People with co-existent emphysema
Type of analysis: Multivariable survival analysis
39
Idiopathic Pulmonary Fibrosis Review protocols
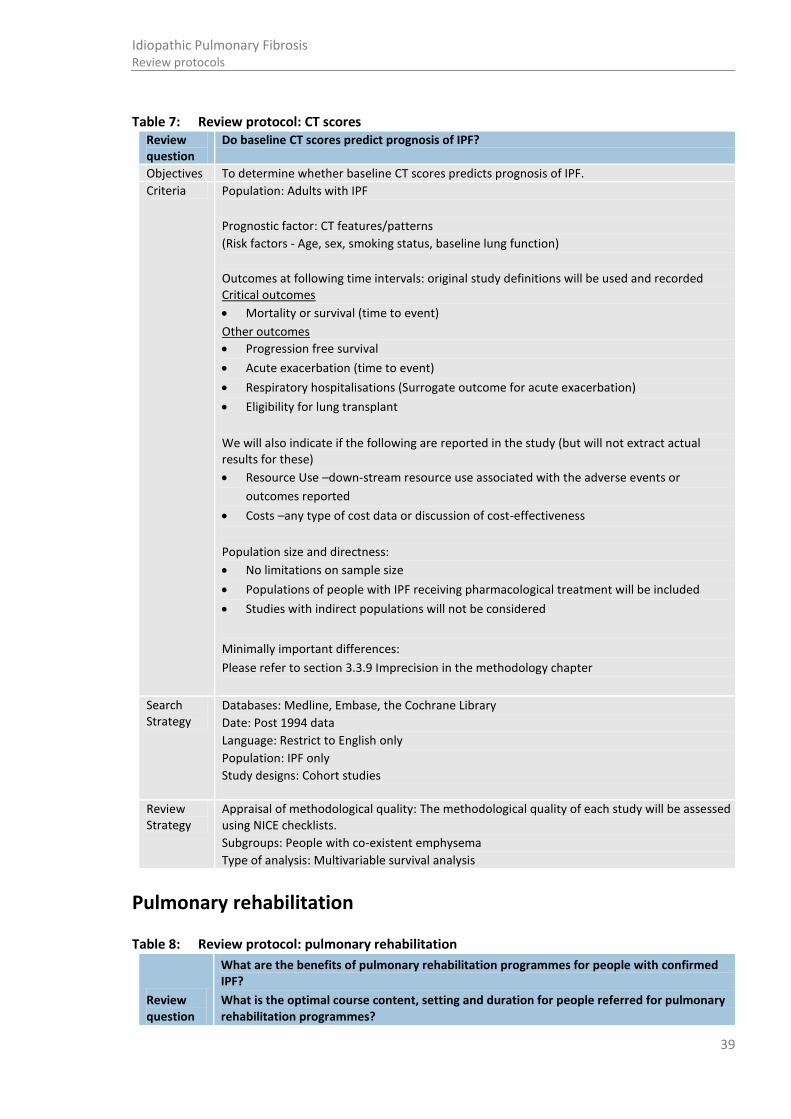
Table 7: Review protocol: CT scores Review question
Do baseline CT scores predict prognosis of IPF?
Objectives To determine whether baseline CT scores predicts prognosis of IPF.
Criteria Population: Adults with IPF
Prognostic factor: CT features/patterns
(Risk factors - Age, sex, smoking status, baseline lung function)
Outcomes at following time intervals: original study definitions will be used and recorded Critical outcomes
Mortality or survival (time to event)
Other outcomes
Progression free survival
Acute exacerbation (time to event)
Respiratory hospitalisations (Surrogate outcome for acute exacerbation)
Eligibility for lung transplant
We will also indicate if the following are reported in the study (but will not extract actual results for these)
Resource Use –down-stream resource use associated with the adverse events or
outcomes reported
Costs –any type of cost data or discussion of cost-effectiveness
Population size and directness:
No limitations on sample size
Populations of people with IPF receiving pharmacological treatment will be included
Studies with indirect populations will not be considered
Minimally important differences:
Please refer to section 3.3.9 Imprecision in the methodology chapter
Search Strategy
Databases: Medline, Embase, the Cochrane Library
Date: Post 1994 data
Language: Restrict to English only
Population: IPF only
Study designs: Cohort studies
Review Strategy
Appraisal of methodological quality: The methodological quality of each study will be assessed using NICE checklists.
Subgroups: People with co-existent emphysema
Type of analysis: Multivariable survival analysis
1.3 Pulmonary rehabilitation
Table 8: Review protocol: pulmonary rehabilitation
Review question
What are the benefits of pulmonary rehabilitation programmes for people with confirmed IPF?
What is the optimal course content, setting and duration for people referred for pulmonary rehabilitation programmes?

40
Idiopathic Pulmonary Fibrosis Review protocols
Objectives To determine the benefits or harms of pulmonary rehabilitation and the requirements of a pulmonary rehabilitation programme to provide optimal symptomatic relief people with IPF.
Criteria Population: Adult people with IPF
Interventions: Pulmonary rehabilitation
Comparisons:
• Best usual care/ usual medical management
• Self-management
Outcomes at following time intervals: original study definitions will be used and recorded
Critical outcomes
All cause and IPF related mortality
1 and 3 year survival rates
Other outcomes
Dyspnoea
Hospitalisations due to IPF complications (including IPF exacerbations)
Improvement in cough and breathlessness
Improvement in health-related quality of life
Performance on sub-maximal walk test (distance walked and lowest SaO2)
Improvement in psychosocial health (including depression)
We will also indicate if the following are reported in the study (but will not extract actual results for these)
Resource Use –down-stream resource use associated with the adverse events or outcomes reported
Costs –any type of cost data or discussion of cost-effectiveness
Population size and directness:
No limitations on sample size
Studies with indirect populations such as people with ILD and restrictive lung disease will be considered
Minimally important differences:
Please refer to section 3.3.9 Imprecision in the methodology chapter
Search Databases: Medline, Embase, the Cochrane Library, CINAHL, PsychInfo
Date: All years
Language: Restrict to English only
Population: Extended to ILDs
Study designs: RCTs, systematic reviews, cohort studies
Review strategy
Quality of life data: Collect all data for the stated QoL measure, for meta-analysis and GRADE report only overall scores
Appraisal of methodological quality: The methodological quality of each study will be assessed using NICE checklists and GRADE.
Data synthesis of RCT data: Meta-analysis where appropriate will be conducted. Meta-analysis where appropriate will be conducted.
Subgroups: People with co-existent emphysema

41
Idiopathic Pulmonary Fibrosis Review protocols
Type of analysis: Available case analysis
1.4 Best supportive care
Table 9: Review protocol: best supportive care
Review question
What is the clinical and cost effectiveness of best supportive care (palliation of cough, breathlessness and fatigue, and oxygen management) in the symptomatic relief of patients with IPF?
Objectives To determine the most clinically and cost effective best supportive care for patients with IPF
Criteria Population: Adults with confirmed IPF/ or ILD
Interventions:
• Oxygen management
• Palliation of cough
• Palliation of breathlessness
• Palliation of fatigue
Comparisons:
• No treatment
• Other treatments
Outcomes at following time intervals: original study definitions will be used and recorded
Critical outcome
Improvement in health-related quality of life
Other outcomes
Hospitalisations due to IPF complications (including IPF exacerbations)
Improvement in cough and breathlessness
Improvement in psychosocial health (including depression)
Mortality
Performance on sub-maximal walk test (distance walked and lowest SaO2)
Symptom relief
We will also indicate if the following are reported in the study (but will not extract actual results for these)
Resource Use –down-stream resource use associated with the adverse events or outcomes reported
Costs –any type of cost data or discussion of cost-effectiveness
Population size and directness:
• No limitations on sample size
• Studies with indirect populations will not be considered
Minimally important differences:
Please refer to section 3.3.9 Imprecision in the methodology chapter
Search Databases: Medline, Embase, the Cochrane Library, CINAHL, PsychInfo
Date: All years
Language: Restrict to English only
Study designs: RCTs, systematic reviews, cohort studies

42
Idiopathic Pulmonary Fibrosis Review protocols
Review strategy
Quality of life data: Collect all data for the stated QoL measure, for meta-analysis and GRADE report only overall scores
Appraisal of methodological quality: The methodological quality of each study will be assessed using NICE checklists and GRADE.
Data synthesis of RCT data: Meta-analysis where appropriate will be conducted. Meta-analysis where appropriate will be conducted.
Subgroups: People with co-existent emphysema
Type of analysis: Available case analysis
1.5 Psychosocial support
Table 10: Review protocol: psychosocial support
Review question
What is the specific type of psychosocial support and information that should be provided for patients diagnosed with IPF?
Objectives To determine what psychosocial support and information should be provided for patients diagnosed with IPF.
Criteria Population: Adults with confirmed IPF and/ or ILD
Intervention: Psychosocial support, Patient information
Comparison: None
Outcomes at following time intervals: original study definitions will be used and recorded
Critical outcomes
Improvement in health-related quality of life Other outcomes
Dyspnoea
Improvement in psychosocial health (including depression)
We will also indicate if the following are reported in the study (but will not extract actual results for these)
Resource Use –down-stream resource use associated with the adverse events or outcomes reported
Costs –any type of cost data or discussion of cost-effectiveness
Population size and directness:
No limitations on sample size
Studies with indirect populations will not be considered
Minimally important differences:
Please refer to section 3.3.9 Imprecision in the methodology chapter
Search Databases: Medline, Embase, the Cochrane Library, CINAHL, PsychInfo
Date: All years
Language: Restrict to English only
Study designs: RCTs, systematic reviews of RCTS, cohort studies
Review strategy
Quality of life data: Collect all data for the stated QoL measure, for meta-analysis and GRADE report only overall scores Appraisal of methodological quality: The methodological quality of each study will be assessed using NICE checklists and GRADE.

43
Idiopathic Pulmonary Fibrosis Review protocols
Data synthesis of RCT data: Meta-analysis where appropriate will be conducted. Meta-analysis where appropriate will be conducted. Subgroups: People with co-existent emphysema Type of analysis: Available case analysis
Table 11: Review protocol: pharmacological interventions
Review question
Which drug should be initiated first, for how long, and what combination in the treatment of IPF?
What is the clinical and cost effectiveness of pharmacological interventions to manage patients with suspected or confirmed IPF:
Objectives To determine which treatment should be initiated first, for how long and what are the benefits or harms of the different pharmacological therapies in treating patients with IPF.
Criteria Population: Adult patients with IPF
Interventions:
prednisolone
mycophenolate mofetil
warfarin
azathioprine
N-acetyl cysteine
proton-pump inhibitors
co-trimoxazole
ambrisentan
bosentan
sildenafil
drug combinations
Comparisons:
Other pharmacological treatments/ placebo
Outcomes at following time intervals: original study definitions will be used and recorded
Critical outcomes
All cause and IPF related mortality
1 and 3 year survival rates
Other outcomes
Adverse events (please see adverse events table listed in Appendix N)
Dyspnoea
Change in percent predicted DLCO
Hospitalisations due to IPF complications, including IPF exacerbations
Improvement in health-related quality of life
Change in percent predicted forced vital capacity
Performance on sub-maximal walk test (distance walked and lowest SaO2)
We will also indicate if the following are reported in the study (but will not extract actual results for these)
Resource Use –down-stream resource use associated with the adverse events or outcomes reported
Costs –any type of cost data or discussion of cost-effectiveness

44
Idiopathic Pulmonary Fibrosis Review protocols
Population size and directness:
• No limitations on sample size
• Studies with indirect populations will not be considered
Minimally important differences:
Please refer to section 3.3.9 Imprecision in the methodology chapter
Search Databases: Medline, Embase, the Cochrane Library
Date: All years
Language: Restrict to English only
Population: IPF only
Study designs: RCTs and systematic reviews of RCTs
Review strategy
Quality of life data: Collect all data for the stated QoL measure, for meta-analysis and GRADE report only overall scores
Appraisal of methodological quality: The methodological quality of each study will be assessed using NICE checklists and GRADE.
Data synthesis of RCT data: Meta-analysis where appropriate will be conducted. Meta-analysis where appropriate will be conducted.
Subgroups: People with co-existent emphysema
Type of analysis: Available case analysis
Table 12: Review protocol: minimising adverse events
Review question
Which measures can be taken to minimize the occurrence/severity of adverse events when undergoing pharmacological treatment for IPF?
Objectives To determine the severity of adverse events when undergoing pharmacological treatment for patients with confirmed IPF
Criteria Population: Adult patients with confirmed IPF consistent with ATS/ERS consensus
Interventions:
Assessing TPMT
Comparisons:
Not assessing TPMT
Outcomes at following time intervals: original study definitions will be used and recorded
Critical outcomes
All cause and IPF related mortality
1 and 3 year survival rates
Other outcomes
Adverse events (please see adverse events table listed in Appendix N)
Dyspnoea
Hospitalisations due to IPF complications, including IPF exacerbations
Improvement in health-related quality of life
Performance on sub-maximal walk test (distance walked and lowest SaO2)
We will also indicate if the following are reported in the study (but will not extract actual results for these)

45
Idiopathic Pulmonary Fibrosis Review protocols
Resource Use –down-stream resource use associated with the adverse events or outcomes reported
Costs –any type of cost data or discussion of cost-effectiveness
Population size and directness:
No limitations on sample size
Studies with indirect populations will not be considered
Minimally important differences:
Please refer to section 3.3.9 Imprecision in the methodology chapter
Search Databases: Medline, Embase, the Cochrane Library,
Date: All years
Language: Restrict to English only
Population: IPF only
Study designs: No restrictions on study designs
Review strategy
Quality of life data: Collect all data for the stated QoL measure, for meta-analysis and GRADE report only overall scores
Appraisal of methodological quality: The methodological quality of each study will be assessed using NICE checklists and GRADE.
Data synthesis of RCT data
Meta-analysis where appropriate will be conducted. Meta-analysis where appropriate will be conducted.
Subgroups: People with co-existent emphysema
Type of analysis: Available case analysis
1.6 Lung transplantation
Table 13: Review protocol: Lung transplantation
Review question
What is the optimal timing to consider a patient with IPF for lung transplantation referral?
Objectives To determine when in the IPF care pathway a patient should be considered for lung transplantation referral.
Criteria Population: Adults with confirmed IPF
Interventions: Time of assessment for lung/pulmonary transplantation
Comparisons:
Different timings in the IPF care pathway according to the different levels of disease severity
No assessment
Outcomes at following time intervals: original study definitions will be used and recorded
Critical outcomes
• All cause and IPF related Mortality
• 1 and 3 year survival rates
Other outcomes

46
Idiopathic Pulmonary Fibrosis Review protocols
• Cross-over time
• Hospitalisations due to IPF complications (including IPF exacerbations)
• Improvement of health-related quality of life
• Occurrence lung transplantation
We will also indicate if the following are reported in the study (but will not extract actual results for these)
Resource Use –down-stream resource use associated with the adverse events or outcomes reported
Costs –any type of cost data or discussion of cost-effectiveness
Population size and directness:
• No limitations on sample size
• Studies with indirect populations will not be considered
Minimally important differences:
Please refer to section 3.3.9 Imprecision in the methodology chapter
Search Databases: Medline, Embase, the Cochrane Library,
Date: All years
Language: Restrict to English only
Population: IPF only
Study designs: RCTs, systematic reviews of RCTs, cohorts
Review strategy
Quality of life data: Collect all data for the stated QoL measure, for meta-analysis and GRADE report only overall scores
Appraisal of methodological quality: The methodological quality of each study will be assessed using NICE checklists and GRADE.
Data synthesis of RCT data: Meta-analysis where appropriate will be conducted. Meta-analysis where appropriate will be conducted.
Type of analysis: Available case analysis
1.7 Ventilation
Table 14: Review protocol: ventilation
Review question
In acute or acute-on chronic respiratory failure in patients with IPF, what is the value of non-invasive and invasive ventilation?
Objectives To determine the benefit of non-invasive and invasive ventilation.
Criteria Population: Adults with confirmed IPF
Interventions: Invasive ventilation
Comparisons:
Non-invasive ventilation
No ventilation
Outcomes at following time intervals: original study definitions will be used and recorded
Critical outcome
Mortality (in hospital and post discharge)

47
Idiopathic Pulmonary Fibrosis Review protocols
Other outcomes
Improvement of health-related quality of life
Hospital length of stay
We will also indicate if the following are reported in the study (but will not extract actual results for these)
Resource Use –down-stream resource use associated with the adverse events or outcomes reported
Costs –any type of cost data or discussion of cost-effectiveness
Population size and directness:
• No limitations on sample size
• Studies with indirect populations will not be considered
Minimally important differences:
Please refer to section 3.3.9 Imprecision in the methodology chapter
Search Databases: Medline, Embase, the Cochrane Library,
Date: All years
Language: Restrict to English only
Population: IPF only
Study designs: RCTs, systematic reviews of RCTs, cohorts
Review strategy
Quality of life data: Collect all data for the stated QoL measure, for meta-analysis and GRADE report only overall scores
Appraisal of methodological quality: The methodological quality of each study will be assessed using NICE checklists and GRADE.
Data synthesis of RCT data: Meta-analysis where appropriate will be conducted. Meta-analysis where appropriate will be conducted.
Type of analysis: Available case analysis
1.8 Review and follow-up
Table 15: Review protocol: review and follow-up
Review question
a. How often should a patient with confirmed diagnosis of IPF be reviewed?
b. In which healthcare setting and by whom should a review appointment for patients with confirmed IPF be conducted?
Objectives To determine the frequency, healthcare setting and healthcare professionals that should conduct the following at a review appointment:
• Clinical history and examination
• Oxygen assessment
• Sub-maximal exercise testing
Criteria Population: Adults with confirmed IPF
Interventions:
• Review at 3 and 6 months
• Review earlier than 3 months if clinically indicated
• Review at yearly intervals
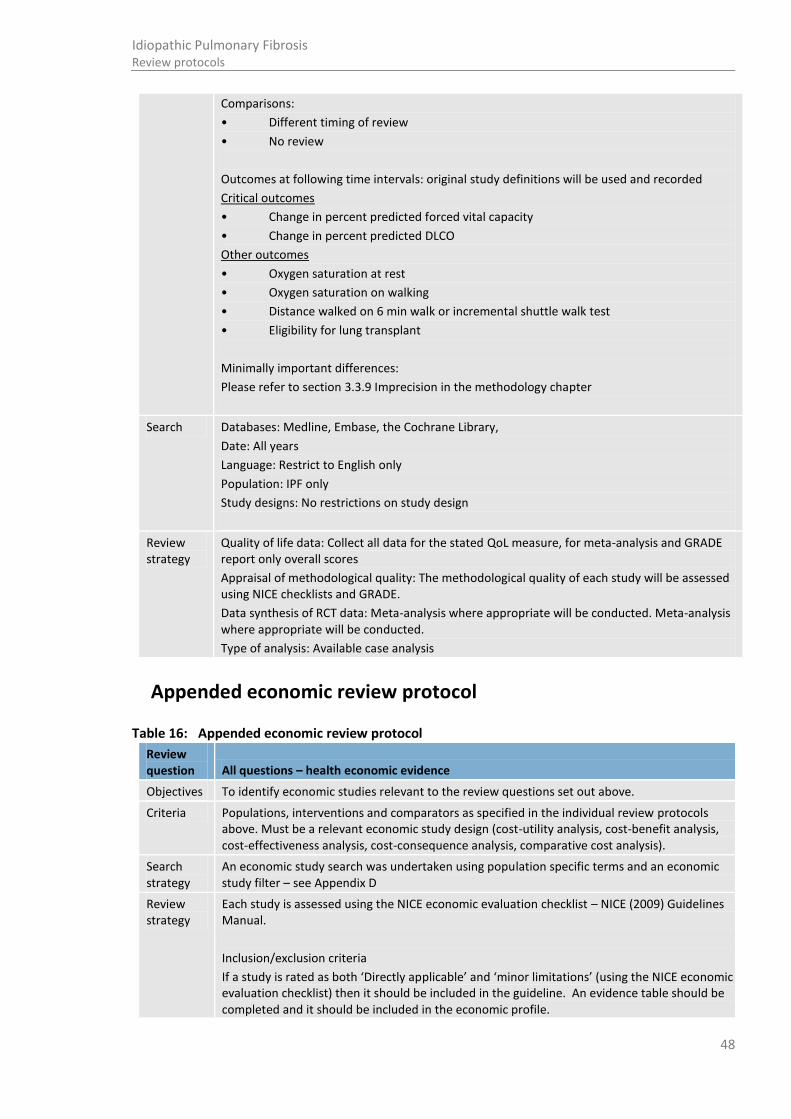
48
Idiopathic Pulmonary Fibrosis Review protocols
Comparisons:
• Different timing of review
• No review
Outcomes at following time intervals: original study definitions will be used and recorded
Critical outcomes
• Change in percent predicted forced vital capacity
• Change in percent predicted DLCO
Other outcomes
• Oxygen saturation at rest
• Oxygen saturation on walking
• Distance walked on 6 min walk or incremental shuttle walk test
• Eligibility for lung transplant
Minimally important differences:
Please refer to section 3.3.9 Imprecision in the methodology chapter
Search Databases: Medline, Embase, the Cochrane Library,
Date: All years
Language: Restrict to English only
Population: IPF only
Study designs: No restrictions on study design
Review strategy
Quality of life data: Collect all data for the stated QoL measure, for meta-analysis and GRADE report only overall scores
Appraisal of methodological quality: The methodological quality of each study will be assessed using NICE checklists and GRADE.
Data synthesis of RCT data: Meta-analysis where appropriate will be conducted. Meta-analysis where appropriate will be conducted.
Type of analysis: Available case analysis
1.9 Appended economic review protocol
Table 16: Appended economic review protocol
Review question All questions – health economic evidence
Objectives To identify economic studies relevant to the review questions set out above.
Criteria Populations, interventions and comparators as specified in the individual review protocols above. Must be a relevant economic study design (cost-utility analysis, cost-benefit analysis, cost-effectiveness analysis, cost-consequence analysis, comparative cost analysis).
Search strategy
An economic study search was undertaken using population specific terms and an economic study filter – see Appendix D
Review strategy
Each study is assessed using the NICE economic evaluation checklist – NICE (2009) Guidelines Manual.
Inclusion/exclusion criteria
If a study is rated as both ‘Directly applicable’ and ‘minor limitations’ (using the NICE economic evaluation checklist) then it should be included in the guideline. An evidence table should be completed and it should be included in the economic profile.
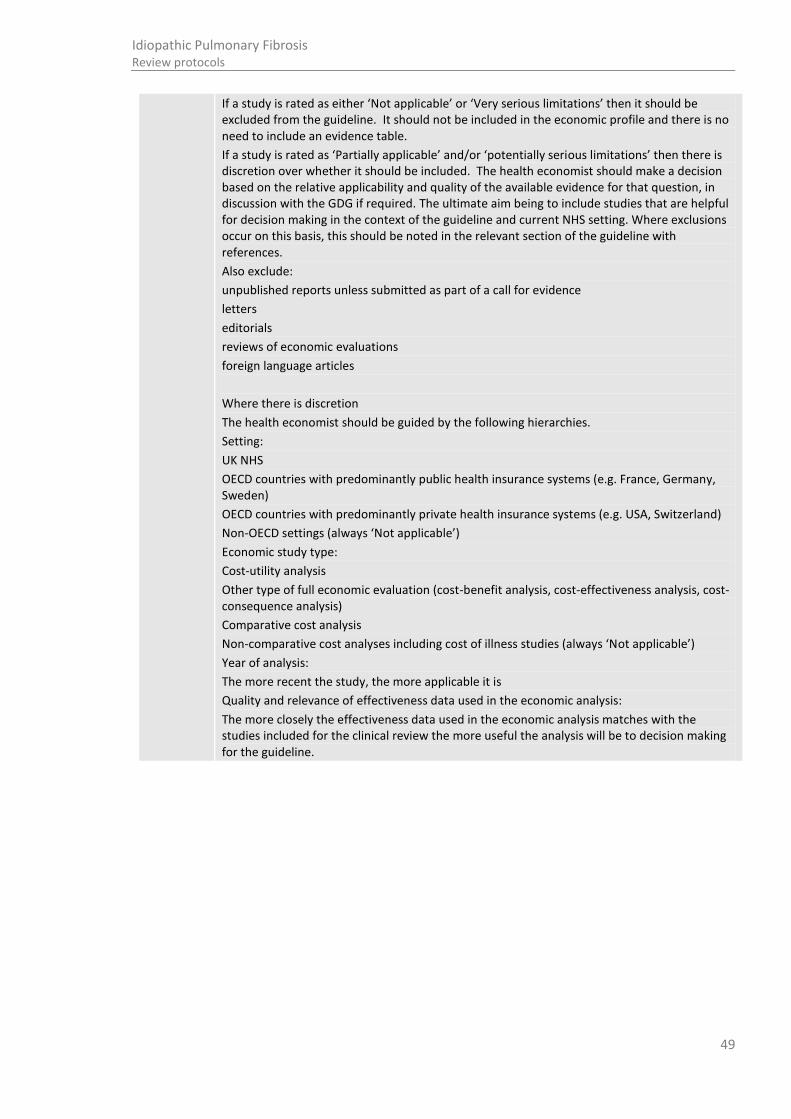
49
Idiopathic Pulmonary Fibrosis Review protocols
If a study is rated as either ‘Not applicable’ or ‘Very serious limitations’ then it should be excluded from the guideline. It should not be included in the economic profile and there is no need to include an evidence table.
If a study is rated as ‘Partially applicable’ and/or ‘potentially serious limitations’ then there is discretion over whether it should be included. The health economist should make a decision based on the relative applicability and quality of the available evidence for that question, in discussion with the GDG if required. The ultimate aim being to include studies that are helpful for decision making in the context of the guideline and current NHS setting. Where exclusions occur on this basis, this should be noted in the relevant section of the guideline with references.
Also exclude:
unpublished reports unless submitted as part of a call for evidence
letters
editorials
reviews of economic evaluations
foreign language articles
Where there is discretion
The health economist should be guided by the following hierarchies.
Setting:
UK NHS
OECD countries with predominantly public health insurance systems (e.g. France, Germany, Sweden)
OECD countries with predominantly private health insurance systems (e.g. USA, Switzerland)
Non-OECD settings (always ‘Not applicable’)
Economic study type:
Cost-utility analysis
Other type of full economic evaluation (cost-benefit analysis, cost-effectiveness analysis, cost-consequence analysis)
Comparative cost analysis
Non-comparative cost analyses including cost of illness studies (always ‘Not applicable’)
Year of analysis:
The more recent the study, the more applicable it is
Quality and relevance of effectiveness data used in the economic analysis:
The more closely the effectiveness data used in the economic analysis matches with the studies included for the clinical review the more useful the analysis will be to decision making for the guideline.

50
Idiopathic Pulmonary Fibrosis Literature search strategy
Appendix D: Literature search strategy Search strategies used for the idiopathic pulmonary fibrosis guideline are outlined below and were run as per the NICE Guidelines Manual 2009 http://www.nice.org.uk/media/5F2/44/The_guidelines_manual_2009_-_All_chapters.pdf .
Searches for the clinical reviews were run in Medline (Ovid), Embase (Ovid) and the Cochrane Library. Additional searches were run in Cinahl (EBSCO) and PsychInfo (Ovid) for some questions. Usually, searches were constructed in the following way:
• A PICO format was used for intervention searches where population (P) terms were combined with intervention (I) and sometimes comparison (C) terms. An intervention can be a drug, a procedure or a diagnostic test. Outcomes (O) are rarely used in search strategies for interventions. Search filters were also added to the search where appropriate.
• A PEO format was used for prognosis searches where population (P) terms were combined with exposure (E) terms and sometimes outcomes (O). Search filters were added to the search where appropriate.
Searches for the health economic reviews were run in Medline (Ovid), Embase (Ovid), the NHS Economic Evaluations Database (NHS EED), the Health Technology Assessment (HTA) database and the Health Economic Evaluation Database (HEED). Searches in NHS EED, HTA and HEED were constructed only using population terms. For Medline and Embase an economic filter (instead of a study type filter) was added to the same clinical search strategy.
All searches were run up to 1st November 2012 unless otherwise stated. Any studies added to the databases after this date were not included unless specifically stated in the text.
The search strategies are presented below in the following order:
Section D.1 Population terms by database. The same searches were used for all questions and for both clinical and health economic searches.
Section D.2 Study filter terms by database. These include filters for epidemiological study designs, health economic studies, quality of life studies and disease progression studies.
Section D.3 Searches run for specific questions with the intervention or exposure terms by database. Order as presented in guideline
Section D.3.1 Diagnosis: biopsy/lavage
Section D.3.2 Diagnosis: MDT
Section D.3.3 Prognosis: PFTs
Section D.3.4 Prognosis: sub maximal exercise testing
Section D.3.5 Prognosis: HRCT/echocardiography
Section D.3.6 Psychosocial support
Section D.3.7 Best supportive care/ patient review and follow up
Section D.3.8 Pulmonary rehabilitation
Section D.3.9 Pharmacological interventions
Section D.3.10
Pharmacological interventions: adverse events
Section D.3.11
Lung transplantation
Section D.3.12
Ventilation
Section D.4 Economics search
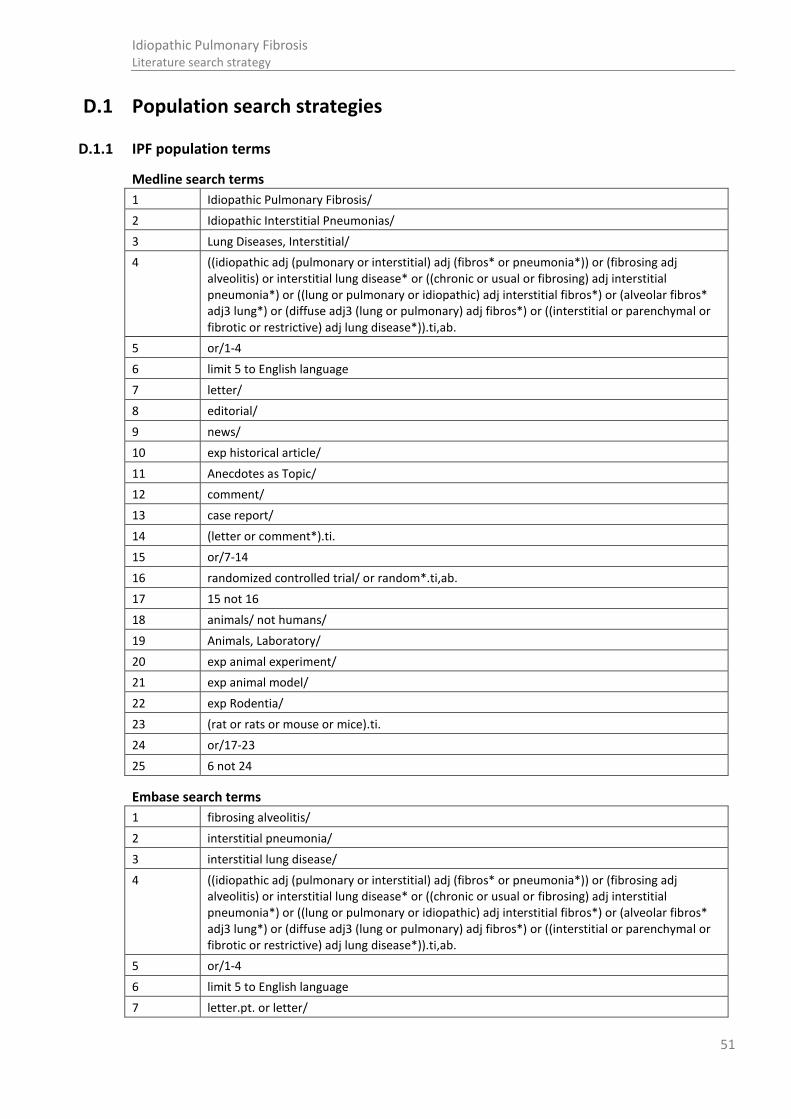
51
Idiopathic Pulmonary Fibrosis Literature search strategy
D.1 Population search strategies
D.1.1 IPF population terms
Medline search terms
1 Idiopathic Pulmonary Fibrosis/
2 Idiopathic Interstitial Pneumonias/
3 Lung Diseases, Interstitial/
4 ((idiopathic adj (pulmonary or interstitial) adj (fibros* or pneumonia*)) or (fibrosing adj alveolitis) or interstitial lung disease* or ((chronic or usual or fibrosing) adj interstitial pneumonia*) or ((lung or pulmonary or idiopathic) adj interstitial fibros*) or (alveolar fibros* adj3 lung*) or (diffuse adj3 (lung or pulmonary) adj fibros*) or ((interstitial or parenchymal or fibrotic or restrictive) adj lung disease*)).ti,ab.
5 or/1-4
6 limit 5 to English language
7 letter/
8 editorial/
9 news/
10 exp historical article/
11 Anecdotes as Topic/
12 comment/
13 case report/
14 (letter or comment*).ti.
15 or/7-14
16 randomized controlled trial/ or random*.ti,ab.
17 15 not 16
18 animals/ not humans/
19 Animals, Laboratory/
20 exp animal experiment/
21 exp animal model/
22 exp Rodentia/
23 (rat or rats or mouse or mice).ti.
24 or/17-23
25 6 not 24
Embase search terms
1 fibrosing alveolitis/
2 interstitial pneumonia/
3 interstitial lung disease/
4 ((idiopathic adj (pulmonary or interstitial) adj (fibros* or pneumonia*)) or (fibrosing adj alveolitis) or interstitial lung disease* or ((chronic or usual or fibrosing) adj interstitial pneumonia*) or ((lung or pulmonary or idiopathic) adj interstitial fibros*) or (alveolar fibros* adj3 lung*) or (diffuse adj3 (lung or pulmonary) adj fibros*) or ((interstitial or parenchymal or fibrotic or restrictive) adj lung disease*)).ti,ab.
5 or/1-4
6 limit 5 to English language
7 letter.pt. or letter/

52
Idiopathic Pulmonary Fibrosis Literature search strategy
8 note.pt.
9 editorial.pt.
10 case report/ or case study/
11 (letter or comment*).ti.
12 or/7-11
13 randomized controlled trial/ or random*.ti,ab.
14 12 not 13
15 animal/ not human/
16 nonhuman/
17 exp Animal Experiment/
18 exp Experimental Animal/
19 animal model/
20 exp Rodent/
21 (rat or rats or mouse or mice).ti.
22 or/14-21
23 5 not 22
Cinahl search terms
S1 (lung or pulmonary) n1 fibros*
S2 alveolitis n3 extrinsic
S3 lung disease* n3 (restrictive or interstitial)
S4 (MH "Pulmonary Fibrosis")
S5 S1 or S2 or S3 or S4
S6 PT anecdote or PT audiovisual or PT bibliography or PT biography or PT book or PT book review or PT brief item or PT cartoon or PT commentary or PT computer program or PT editorial or PT games or PT glossary or PT historical material or PT interview or PT letter or PT listservs or PT masters thesis or PT obituary or PT pamphlet or PT pamphlet chapter or PT pictorial or PT poetry or PT proceedings or PT “questions and answers” or PT response or PT software or PT teaching materials or PT website
S7 S5 NOT S6
Cochrane search terms
#1 MeSH descriptor Idiopathic Pulmonary Fibrosis, this term only
#2 MeSH descriptor Idiopathic Interstitial Pneumonias, this term only
#3 MeSH descriptor Lung Diseases, Interstitial, this term only
#4 ((idiopathic NEAR (pulmonary or interstitial) NEAR (fibros* or pneumonia*)) or (fibrosing NEAR alveolitis) or interstitial lung disease* or ((chronic or usual or fibrosing) NEAR interstitial pneumonia*) or ((lung or pulmonary or idiopathic) NEAR interstitial fibros*) or (alveolar fibros* NEAR/3 lung*) or (diffuse NEAR/3 (lung or pulmonary) adj fibros*) or ((interstitial or parenchymal or fibrotic or restrictive) NEAR lung disease*)):ti,ab
#5 (#1 OR #2 OR #3 OR #4)
PsychInfo search terms
1 ((idiopathic adj (pulmonary or interstitial) adj (fibros* or pneumonia*)) or (fibrosing adj alveolitis) or interstitial lung disease* or ((chronic or usual or fibrosing) adj interstitial pneumonia*) or ((lung or pulmonary or idiopathic) adj interstitial fibros*) or (alveolar fibros* adj3 lung*) or (diffuse adj3 (lung or pulmonary) adj fibros*) or ((interstitial or parenchymal or fibrotic or restrictive) adj lung disease*)).ti,ab.
2 ((lung or pulmonary) adj fibros*).ti,ab.

53
Idiopathic Pulmonary Fibrosis Literature search strategy
3 or/1-2
4 limit 3 to English language
D.1.2 ILD population terms
Medline search terms
1 Restrictive lung disease*.ti,ab.
2 Pulmonary fibrosis.ti,ab.
3 ((idiopathic adj (pulmonary or interstitial) adj (fibros* or pneumonia*)) or (fibrosing adj alveolitis) or interstitial lung disease* or ((chronic or usual or fibrosing) adj interstitial pneumonia*) or ((lung or pulmonary or idiopathic) adj interstitial fibros*) or (alveolar fibros* adj3 lung*) or (diffuse adj3 (lung or pulmonary) adj fibros*) or ((interstitial or parenchymal or fibrotic) adj lung disease*)).ti,ab.
4 Idiopathic Pulmonary Fibrosis/
5 Idiopathic Interstitial Pneumonias/
6 alveolitis, extrinsic allergic/
7 anti-glomerular basement membrane disease/
8 histiocytosis, langerhans-cell/
9 Idiopathic Interstitial Pneumonias/
10 Pneumoconiosis/
11 Radiation Pneumonitis/
12 Sarcoidosis, Pulmonary/
13 Wegener Granulomatosis/
14 pneumonitis, interstitial/
15 ((Lung disease* adj3 interstitial) or (Alveolitis adj3 Extrinsic) or anti Glomerular Basement Membrane Disease* or (Histiocytosis adj3 Langerhans*) or Idiopathic Interstitial Pneumonia* or pneumoconiosis or Radiation Pneumonitis or (Sarcoidosis adj3 Pulmonary) or Wegener Granulomatosis or (pneumoni* adj3 interstitial) or diffuse parenchymal lung disease*).ti,ab.
16 or/1-15
17 limit 16 to English language
18 letter/
19 editorial/
20 news/
21 exp historical article/
22 Anecdotes as Topic/
23 comment/
24 case report/
25 (letter or comment*).ti.
26 or/89-25
27 randomized controlled trial/ or random*.ti,ab.
28 26 not 287
29 animals/ not humans/
30 Animals, Laboratory/
31 exp animal experiment/
32 exp animal model/
33 exp Rodentia/
34 (rat or rats or mouse or mice).ti.

54
Idiopathic Pulmonary Fibrosis Literature search strategy
35 or/28-34
36 17 not 35
Embase search terms
1 ((idiopathic adj (pulmonary or interstitial) adj (fibros* or pneumonia*)) or (fibrosing adj alveolitis) or interstitial lung disease* or ((chronic or usual or fibrosing) adj interstitial pneumonia*) or ((lung or pulmonary or idiopathic) adj interstitial fibros*) or (alveolar fibros* adj3 lung*) or (diffuse adj3 (lung or pulmonary) adj fibros*) or ((interstitial or parenchymal or fibrotic) adj lung disease*)).ti,ab.
2 fibrosing alveolitis/
3 interstitial pneumonia/
4 ((Lung disease* adj3 interstitial) or (Alveolitis adj3 Extrinsic) or anti Glomerular Basement Membrane Disease* or (Histiocytosis adj3 Langerhans*) or Idiopathic Interstitial Pneumonia* or pneumoconiosis or Radiation Pneumonitis or (Sarcoidosis adj3 Pulmonary) or Wegener Granulomatosis or (pneumoni* adj3 interstitial) or diffuse parenchymal lung disease*).ti,ab.
5 lung alveolitis/
6 histiocytosis/
7 pneumoconiosis/
8 radiation pneumonia/
9 lung sarcoidosis/
10 Wegener granulomatosis/
11 Restrictive lung disease*.ti,ab.
12 Pulmonary fibrosis.ti,ab.
13 or/1-12
14 limit 13 to English language
15 letter.pt. or letter/
16 note.pt.
17 editorial.pt.
18 case report/ or case study/
19 (letter or comment*).ti.
20 or/15-19
21 randomized controlled trial/ or random*.ti,ab.
22 20 not 21
23 animal/ not human/
24 nonhuman/
25 exp Animal Experiment/
26 exp Experimental Animal/
27 animal model/
28 exp Rodent/
29 (rat or rats or mouse or mice).ti.
30 or/22-29
31 15 not 31
Cinahl search terms
S1 (lung or pulmonary) n1 fibros*
S2 Alveoliti* n2 fibrosing OR Alveoliti* n2 Extrinsic OR Wegener Granulomatosis OR Histiocytosis n3 Langerhans* OR anti Glomerular Basement Membrane Disease* OR pneumoconiosis OR Radiation Pneumonitis OR Sarcoidosis n3 Pulmonary OR alveolar fibros* n3 lung* OR

55
Idiopathic Pulmonary Fibrosis Literature search strategy
interstitial pneumonia*
S3 lung disease* n3 (restrictive or interstitial)
S4 (MH "Pulmonary Fibrosis") OR (MH "Lung Diseases, Interstitial+")
S5 S1 or S2 or S3 or S4
S6 PT anecdote or PT audiovisual or PT bibliography or PT biography or PT book or PT book review or PT brief item or PT cartoon or PT commentary or PT computer program or PT editorial or PT games or PT glossary or PT historical material or PT interview or PT letter or PT listservs or PT masters thesis or PT obituary or PT pamphlet or PT pamphlet chapter or PT pictorial or PT poetry or PT proceedings or PT “questions and answers” or PT response or PT software or PT teaching materials or PT website
S7 S5 NOT S6
Cochrane search terms
#1 (idiopathic NEXT (pulmonary or interstitial) NEXT (fibros* or pneumonia*)) or (fibrosing NEXT alveolitis) or (interstitial NEXT lung NEXT disease*) or ((chronic or usual or fibrosing) NEXT interstitial NEXT pneumonia*) or ((lung or pulmonary or idiopathic) NEXT (interstitial NEXT fibros*)) or (alveolar NEXT fibrosis NEAR/3 lung*) or (diffuse NEAR/3 (lung or pulmonary) NEXT fibros*) or ((interstitial or parenchymal or fibrotic) NEXT (lung NEXT disease*)):ti,ab
#2 Restrictive lung disease*:ti,ab
#3 Pulmonary fibrosis:ti,ab
#4 (Lung disease* NEAR/3 interstitial):ti,ab
#5 (Alveolitis NEAR/3 Extrinsic):ti,ab
#6 (Histiocytosis NEAR/3 Langerhans):ti,ab
#7 (Idiopathic Interstitial Pneumonia*):ti,ab
#8 Pneumoconiosis:ti,ab
#9 (Sarcoidosis NEAR/3 Pulmonary):ti,ab
#10 (Wegener NEXT Granulomatosis):ti,ab
#11 (pneumoni* NEAR/3 interstitial):ti,ab
#12 MeSH descriptor Lung Diseases, Interstitial explode all trees
#13 (#1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #12)
PsychInfo search terms
1 Restrictive lung disease*.ti,ab.
2 Pulmonary fibrosis.ti,ab.
3 ((idiopathic adj (pulmonary or interstitial) adj (fibros* or pneumonia*)) or (fibrosing adj alveolitis) or interstitial lung disease* or ((chronic or usual or fibrosing) adj interstitial pneumonia*) or ((lung or pulmonary or idiopathic) adj interstitial fibros*) or (alveolar fibros* adj3 lung*) or (diffuse adj3 (lung or pulmonary) adj fibros*) or ((interstitial or parenchymal or fibrotic) adj lung disease*)).ti,ab.
4 ((Lung disease* adj3 interstitial) or (Alveolitis adj3 Extrinsic) or anti Glomerular Basement Membrane Disease* or (Histiocytosis adj3 Langerhans*) or Idiopathic Interstitial Pneumonia* or pneumoconiosis or Radiation Pneumonitis or (Sarcoidosis adj3 Pulmonary) or Wegener Granulomatosis or (pneumoni* adj3 interstitial) or diffuse parenchymal lung disease*).ti,ab.
5 or/1-4
6 limit 5 to English language

56
Idiopathic Pulmonary Fibrosis Literature search strategy
D.2 Study filter search terms
D.2.1 Systematic review search terms
Medline search terms
1 Meta-Analysis/
2 Meta-Analysis as Topic/
3 (meta analy* or metanaly* or metaanaly*).ti,ab.
4 ((systematic* or evidence*) adj2 (review* or overview*)).ti,ab.
5 (reference list* or bibliograph* or hand search* or manual search* or relevant journals).ab.
6 (search strategy or search criteria or systematic search or study selection or data extraction).ab.
7 (search* adj4 literature).ab.
8 (medline or pubmed or cochrane or embase or psychlit or psyclit or psychinfo or psycinfo or cinahl or science citation index or bids or cancerlit).ab.
9 cochrane.jw.
10 ((indirect or mixed) adj2 comparison*).ti,ab.
11 or/1-10
Embase search terms
1 systematic review/
2 meta-analysis/
3 (meta analy* or metanaly* or metaanaly*).ti,ab.
4 ((systematic or evidence) adj2 (review* or overview*)).ti,ab.
5 (reference list* or bibliograph* or hand search* or manual search* or relevant journals).ab.
6 (search strategy or search criteria or systematic search or study selection or data extraction).ab.
7 (search* adj4 literature).ab.
8 (medline or pubmed or cochrane or embase or psychlit or psyclit or psychinfo or psycinfo or cinahl or science citation index or bids or cancerlit).ab.
9 ((pool* or combined) adj2 (data or trials or studies or results)).ab.
10 cochrane.jw.
11 ((indirect or mixed) adj2 comparison*).ti,ab.
12 or/1-11
D.2.2 Randomised controlled studies (RCTs) search terms
Medline search terms
1 randomized controlled trial.pt.
2 controlled clinical trial.pt.
3 randomi#ed.ab.
4 placebo.ab.
5 randomly.ab.
6 Clinical Trials as topic.sh.
7 trial.ti.
8 or/1-7
Embase search terms
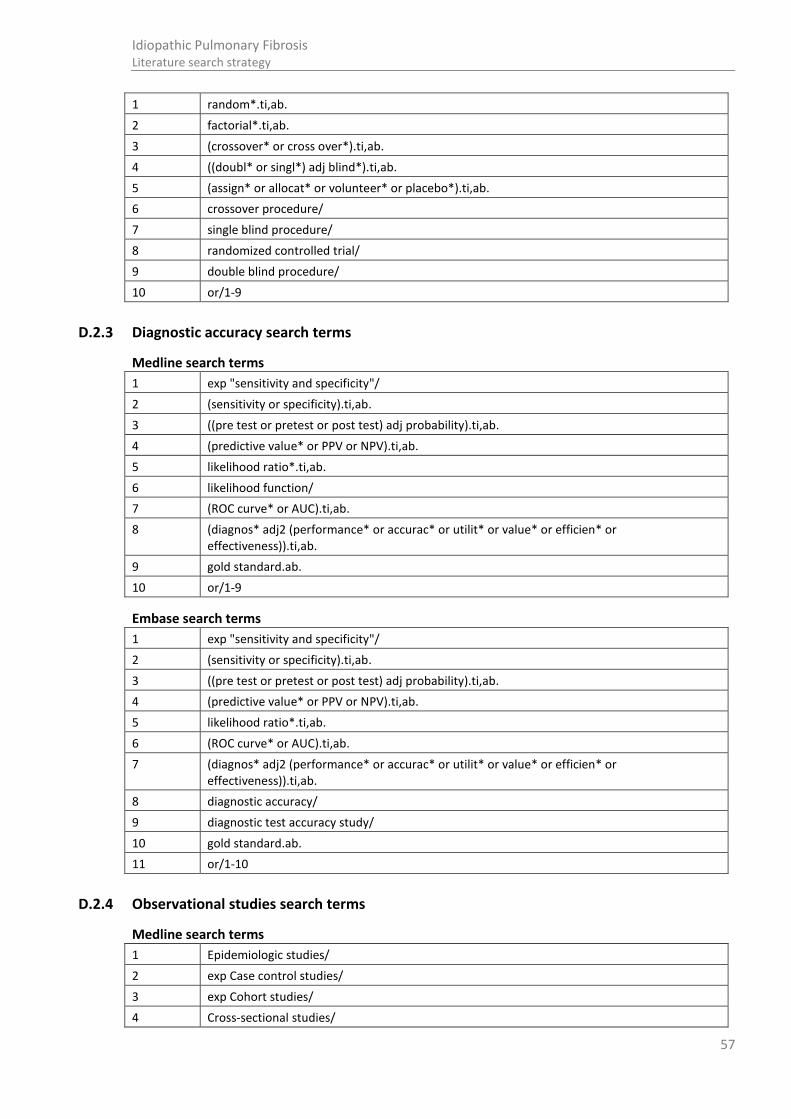
57
Idiopathic Pulmonary Fibrosis Literature search strategy
1 random*.ti,ab.
2 factorial*.ti,ab.
3 (crossover* or cross over*).ti,ab.
4 ((doubl* or singl*) adj blind*).ti,ab.
5 (assign* or allocat* or volunteer* or placebo*).ti,ab.
6 crossover procedure/
7 single blind procedure/
8 randomized controlled trial/
9 double blind procedure/
10 or/1-9
D.2.3 Diagnostic accuracy search terms
Medline search terms
1 exp "sensitivity and specificity"/
2 (sensitivity or specificity).ti,ab.
3 ((pre test or pretest or post test) adj probability).ti,ab.
4 (predictive value* or PPV or NPV).ti,ab.
5 likelihood ratio*.ti,ab.
6 likelihood function/
7 (ROC curve* or AUC).ti,ab.
8 (diagnos* adj2 (performance* or accurac* or utilit* or value* or efficien* or effectiveness)).ti,ab.
9 gold standard.ab.
10 or/1-9
Embase search terms
1 exp "sensitivity and specificity"/
2 (sensitivity or specificity).ti,ab.
3 ((pre test or pretest or post test) adj probability).ti,ab.
4 (predictive value* or PPV or NPV).ti,ab.
5 likelihood ratio*.ti,ab.
6 (ROC curve* or AUC).ti,ab.
7 (diagnos* adj2 (performance* or accurac* or utilit* or value* or efficien* or effectiveness)).ti,ab.
8 diagnostic accuracy/
9 diagnostic test accuracy study/
10 gold standard.ab.
11 or/1-10
D.2.4 Observational studies search terms
Medline search terms
1 Epidemiologic studies/
2 exp Case control studies/
3 exp Cohort studies/
4 Cross-sectional studies/
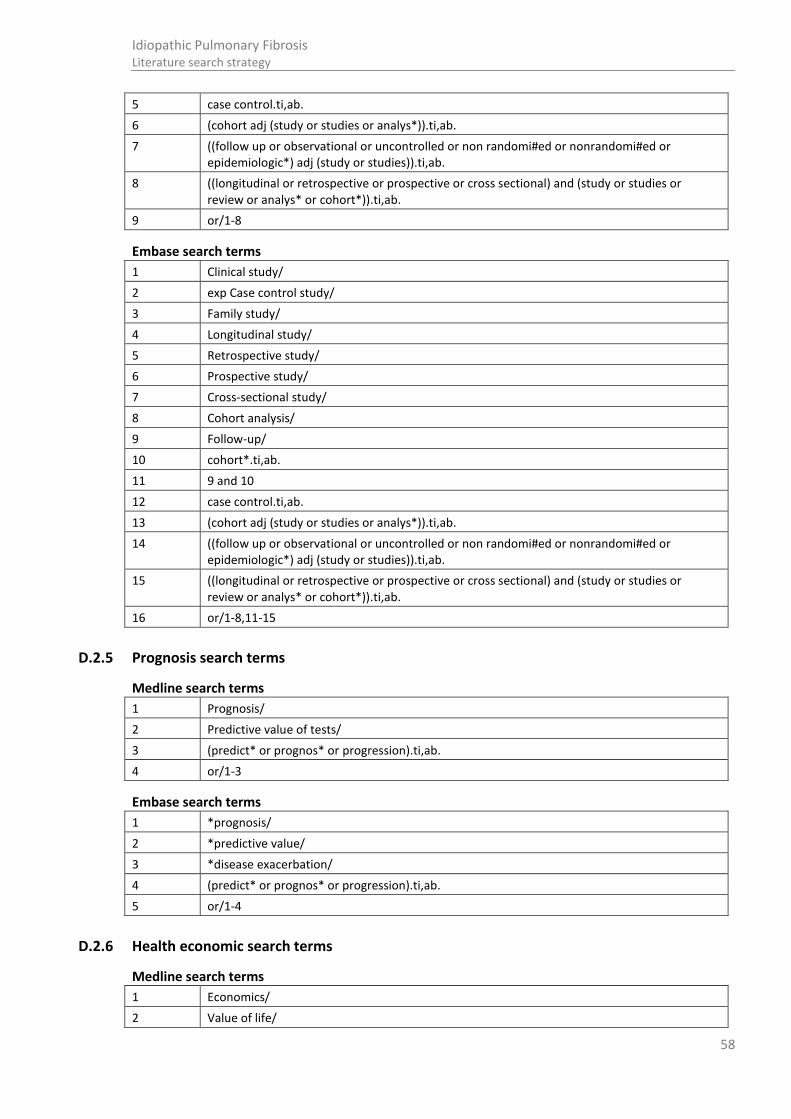
58
Idiopathic Pulmonary Fibrosis Literature search strategy
5 case control.ti,ab.
6 (cohort adj (study or studies or analys*)).ti,ab.
7 ((follow up or observational or uncontrolled or non randomi#ed or nonrandomi#ed or epidemiologic*) adj (study or studies)).ti,ab.
8 ((longitudinal or retrospective or prospective or cross sectional) and (study or studies or review or analys* or cohort*)).ti,ab.
9 or/1-8
Embase search terms
1 Clinical study/
2 exp Case control study/
3 Family study/
4 Longitudinal study/
5 Retrospective study/
6 Prospective study/
7 Cross-sectional study/
8 Cohort analysis/
9 Follow-up/
10 cohort*.ti,ab.
11 9 and 10
12 case control.ti,ab.
13 (cohort adj (study or studies or analys*)).ti,ab.
14 ((follow up or observational or uncontrolled or non randomi#ed or nonrandomi#ed or epidemiologic*) adj (study or studies)).ti,ab.
15 ((longitudinal or retrospective or prospective or cross sectional) and (study or studies or review or analys* or cohort*)).ti,ab.
16 or/1-8,11-15
D.2.5 Prognosis search terms
Medline search terms
1 Prognosis/
2 Predictive value of tests/
3 (predict* or prognos* or progression).ti,ab.
4 or/1-3
Embase search terms
1 *prognosis/
2 *predictive value/
3 *disease exacerbation/
4 (predict* or prognos* or progression).ti,ab.
5 or/1-4
D.2.6 Health economic search terms
Medline search terms
1 Economics/
2 Value of life/
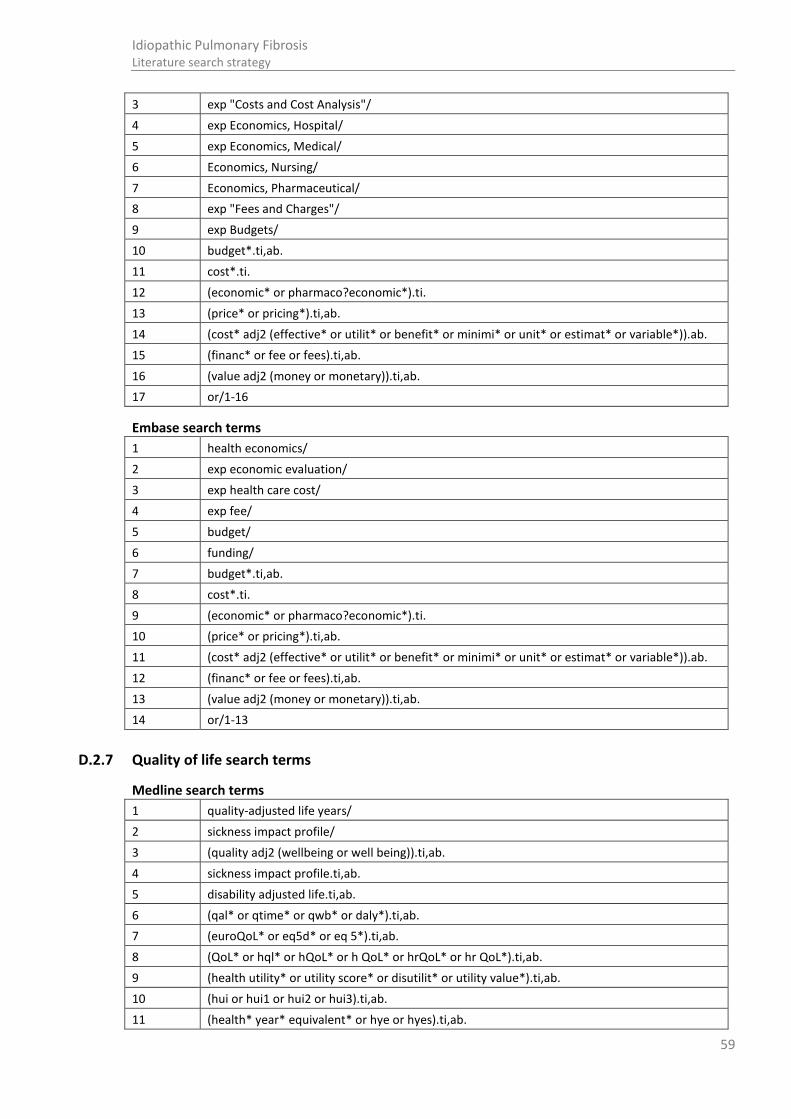
59
Idiopathic Pulmonary Fibrosis Literature search strategy
3 exp "Costs and Cost Analysis"/
4 exp Economics, Hospital/
5 exp Economics, Medical/
6 Economics, Nursing/
7 Economics, Pharmaceutical/
8 exp "Fees and Charges"/
9 exp Budgets/
10 budget*.ti,ab.
11 cost*.ti.
12 (economic* or pharmaco?economic*).ti.
13 (price* or pricing*).ti,ab.
14 (cost* adj2 (effective* or utilit* or benefit* or minimi* or unit* or estimat* or variable*)).ab.
15 (financ* or fee or fees).ti,ab.
16 (value adj2 (money or monetary)).ti,ab.
17 or/1-16
Embase search terms
1 health economics/
2 exp economic evaluation/
3 exp health care cost/
4 exp fee/
5 budget/
6 funding/
7 budget*.ti,ab.
8 cost*.ti.
9 (economic* or pharmaco?economic*).ti.
10 (price* or pricing*).ti,ab.
11 (cost* adj2 (effective* or utilit* or benefit* or minimi* or unit* or estimat* or variable*)).ab.
12 (financ* or fee or fees).ti,ab.
13 (value adj2 (money or monetary)).ti,ab.
14 or/1-13
D.2.7 Quality of life search terms
Medline search terms
1 quality-adjusted life years/
2 sickness impact profile/
3 (quality adj2 (wellbeing or well being)).ti,ab.
4 sickness impact profile.ti,ab.
5 disability adjusted life.ti,ab.
6 (qal* or qtime* or qwb* or daly*).ti,ab.
7 (euroQoL* or eq5d* or eq 5*).ti,ab.
8 (QoL* or hql* or hQoL* or h QoL* or hrQoL* or hr QoL*).ti,ab.
9 (health utility* or utility score* or disutilit* or utility value*).ti,ab.
10 (hui or hui1 or hui2 or hui3).ti,ab.
11 (health* year* equivalent* or hye or hyes).ti,ab.

60
Idiopathic Pulmonary Fibrosis Literature search strategy
12 discrete choice*.ti,ab.
13 rosser.ti,ab.
14 (willingness to pay or time tradeoff or time trade off or tto or standard gamble*).ti,ab.
15 (sf36* or sf 36* or short form 36* or shortform 36* or shortform36*).ti,ab.
16 (sf20 or sf 20 or short form 20 or shortform 20 or shortform20).ti,ab.
17 (sf12* or sf 12* or short form 12* or shortform 12* or shortform12*).ti,ab.
18 (sf8* or sf 8* or short form 8* or shortform 8* or shortform8*).ti,ab.
19 (sf6* or sf 6* or short form 6* or shortform 6* or shortform6*).ti,ab.
20 or/1-19
Embase search terms
1 quality adjusted life year/
2 "quality of life index"/
3 short form 12/ or short form 20/ or short form 36/ or short form 8/
4 sickness impact profile/
5 (quality adj2 (wellbeing or well being)).ti,ab.
6 sickness impact profile.ti,ab.
7 disability adjusted life.ti,ab.
8 (qal* or qtime* or qwb* or daly*).ti,ab.
9 (euroQoL* or eq5d* or eq 5*).ti,ab.
10 (QoL* or hql* or hQoL* or h QoL* or hrQoL* or hr QoL*).ti,ab.
11 (health utility* or utility score* or disutilit* or utility value*).ti,ab.
12 (hui or hui1 or hui2 or hui3).ti,ab.
13 (health* year* equivalent* or hye or hyes).ti,ab.
14 discrete choice*.ti,ab.
15 rosser.ti,ab.
16 (willingness to pay or time tradeoff or time trade off or tto or standard gamble*).ti,ab.
17 (sf36* or sf 36* or short form 36* or shortform 36* or shortform36*).ti,ab.
18 (sf20 or sf 20 or short form 20 or shortform 20 or shortform20).ti,ab.
19 (sf12* or sf 12* or short form 12* or shortform 12* or shortform12*).ti,ab.
20 (sf8* or sf 8* or short form 8* or shortform 8* or shortform8*).ti,ab.
21 (sf6* or sf 6* or short form 6* or shortform 6* or shortform6*).ti,ab.
22 or/1-21
D.2.8 Economic modelling search terms
Medline search terms
1 exp models, economic/
2 *Models, Theoretical/
3 *Models, Organizational/
4 markov chains/
5 monte carlo method/
6 exp Decision Theory/
7 (markov* or monte carlo).ti,ab.
8 econom* model*.ti,ab.
9 (decision* adj2 (tree* or analy* or model*)).ti,ab.

61
Idiopathic Pulmonary Fibrosis Literature search strategy
10 or/1-9
Embase search terms
1 statistical model/
2 exp economic aspect/
3 1 and 2
4 *theoretical model/
5 *nonbiological model/
6 stochastic model/
7 decision theory/
8 decision tree/
9 monte carlo method/
10 (markov* or monte carlo).ti,ab.
11 econom* model*.ti,ab.
12 (decision* adj2 (tree* or analy* or model*)).ti,ab.
13 or/3-12
D.2.9 Disease progression search terms
Medline search terms
1 exp disease progression/
2 exp "Severity of Illness Index"/
3 "International Classification of Diseases"/
4 (Disease* adj (classif* or progress* or course*)).ti,ab.
5 clinical course.ti,ab.
6 (disease adj (attribute* or development* or evolution*)).ti,ab.
7 Natural History/
8 (progress* adj2 (slow* or stable or rapid or fast or quick*)).ti,ab.
9 natural history.ti,ab.
10 (predict* adj3 (mortality or death)).ti,ab.
11 (acute adj (worse* or exacerbat*)).ti,ab.
12 or/1-11
Embase search terms
1 *disease classification/
2 *disease course/
3 *disease severity/
4 *disease association/
5 *disease exacerbation/
6 "international classification of diseases"/
7 (Disease* adj (classif* or progress* or course*)).ti,ab.
8 clinical course.ti,ab.
9 (disease adj (attribute* or development* or evolution*)).ti,ab.
10 (progress* adj2 (slow* or stable or rapid or fast or quick*)).ti,ab.
11 natural history.ti,ab.
12 (predict* adj3 (mortality or death)).ti,ab.
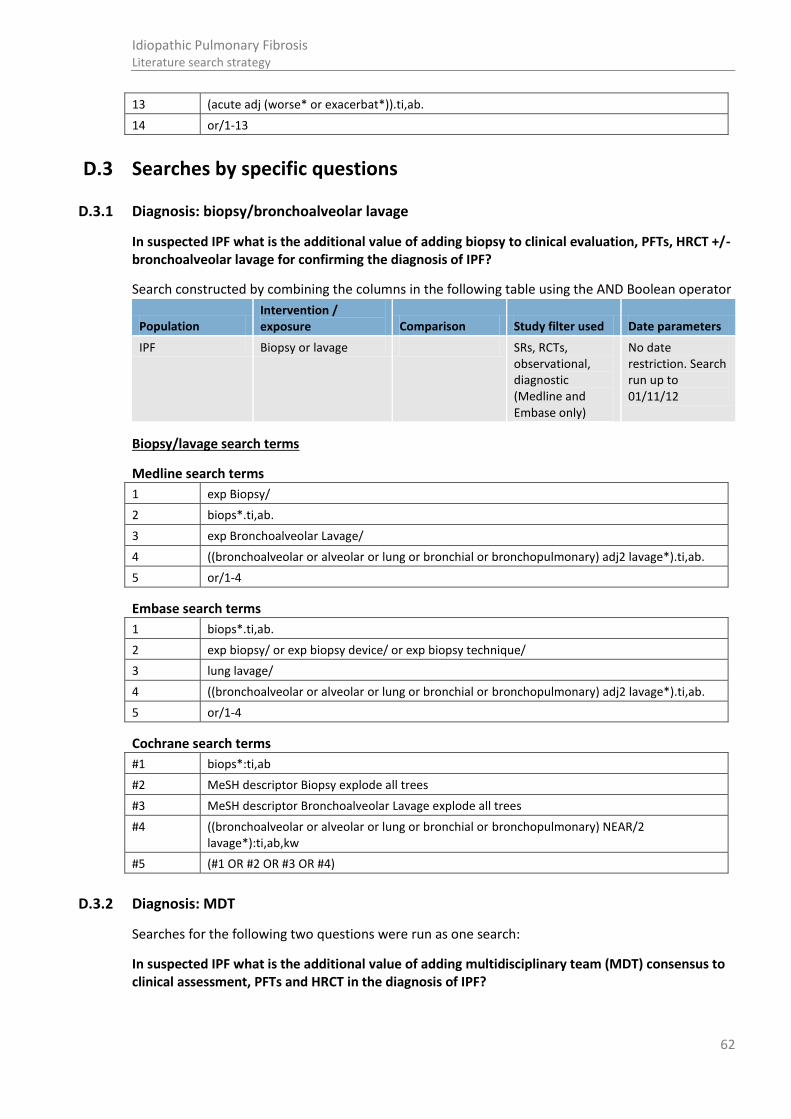
62
Idiopathic Pulmonary Fibrosis Literature search strategy
13 (acute adj (worse* or exacerbat*)).ti,ab.
14 or/1-13
D.3 Searches by specific questions
D.3.1 Diagnosis: biopsy/bronchoalveolar lavage
In suspected IPF what is the additional value of adding biopsy to clinical evaluation, PFTs, HRCT +/- bronchoalveolar lavage for confirming the diagnosis of IPF?
Search constructed by combining the columns in the following table using the AND Boolean operator
Population Intervention / exposure Comparison Study filter used Date parameters
IPF Biopsy or lavage SRs, RCTs, observational, diagnostic (Medline and Embase only)
No date restriction. Search run up to 01/11/12
Biopsy/lavage search terms
Medline search terms
1 exp Biopsy/
2 biops*.ti,ab.
3 exp Bronchoalveolar Lavage/
4 ((bronchoalveolar or alveolar or lung or bronchial or bronchopulmonary) adj2 lavage*).ti,ab.
5 or/1-4
Embase search terms
1 biops*.ti,ab.
2 exp biopsy/ or exp biopsy device/ or exp biopsy technique/
3 lung lavage/
4 ((bronchoalveolar or alveolar or lung or bronchial or bronchopulmonary) adj2 lavage*).ti,ab.
5 or/1-4
Cochrane search terms
#1 biops*:ti,ab
#2 MeSH descriptor Biopsy explode all trees
#3 MeSH descriptor Bronchoalveolar Lavage explode all trees
#4 ((bronchoalveolar or alveolar or lung or bronchial or bronchopulmonary) NEAR/2 lavage*):ti,ab,kw
#5 (#1 OR #2 OR #3 OR #4)
D.3.2 Diagnosis: MDT
Searches for the following two questions were run as one search:
In suspected IPF what is the additional value of adding multidisciplinary team (MDT) consensus to clinical assessment, PFTs and HRCT in the diagnosis of IPF?
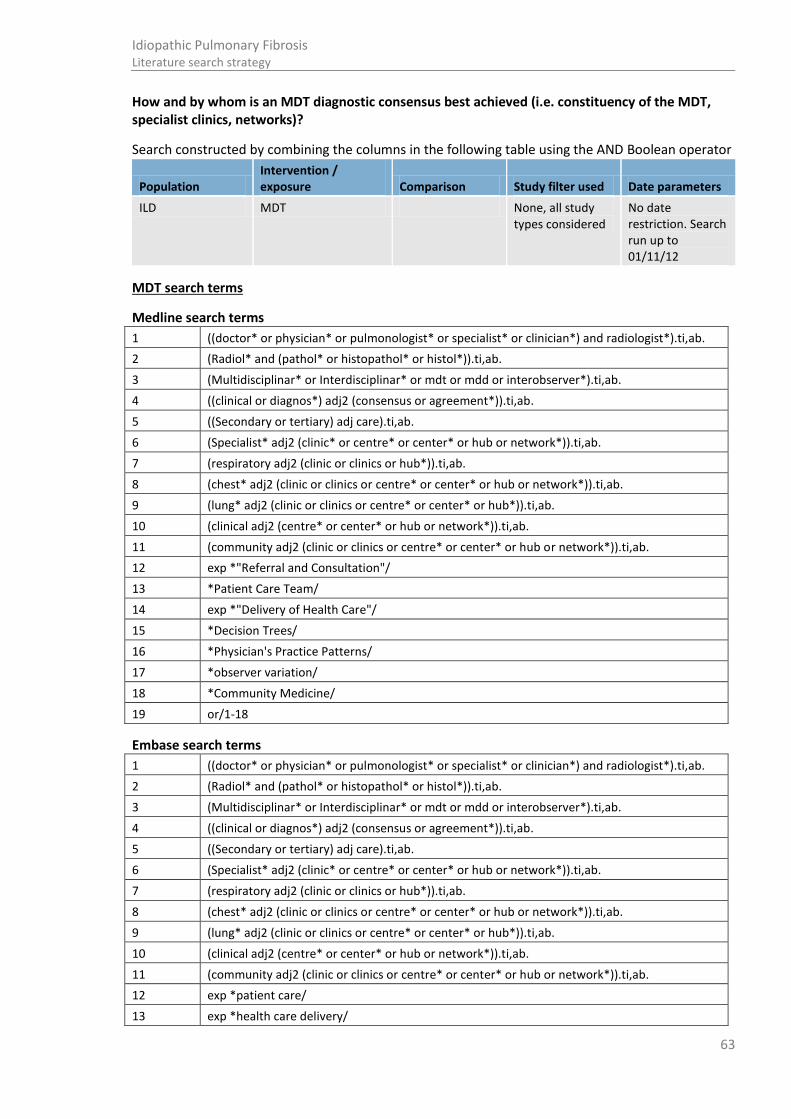
63
Idiopathic Pulmonary Fibrosis Literature search strategy
How and by whom is an MDT diagnostic consensus best achieved (i.e. constituency of the MDT, specialist clinics, networks)?
Search constructed by combining the columns in the following table using the AND Boolean operator
Population Intervention / exposure Comparison Study filter used Date parameters
ILD MDT None, all study types considered
No date restriction. Search run up to 01/11/12
MDT search terms
Medline search terms
1 ((doctor* or physician* or pulmonologist* or specialist* or clinician*) and radiologist*).ti,ab.
2 (Radiol* and (pathol* or histopathol* or histol*)).ti,ab.
3 (Multidisciplinar* or Interdisciplinar* or mdt or mdd or interobserver*).ti,ab.
4 ((clinical or diagnos*) adj2 (consensus or agreement*)).ti,ab.
5 ((Secondary or tertiary) adj care).ti,ab.
6 (Specialist* adj2 (clinic* or centre* or center* or hub or network*)).ti,ab.
7 (respiratory adj2 (clinic or clinics or hub*)).ti,ab.
8 (chest* adj2 (clinic or clinics or centre* or center* or hub or network*)).ti,ab.
9 (lung* adj2 (clinic or clinics or centre* or center* or hub*)).ti,ab.
10 (clinical adj2 (centre* or center* or hub or network*)).ti,ab.
11 (community adj2 (clinic or clinics or centre* or center* or hub or network*)).ti,ab.
12 exp *"Referral and Consultation"/
13 *Patient Care Team/
14 exp *"Delivery of Health Care"/
15 *Decision Trees/
16 *Physician's Practice Patterns/
17 *observer variation/
18 *Community Medicine/
19 or/1-18
Embase search terms
1 ((doctor* or physician* or pulmonologist* or specialist* or clinician*) and radiologist*).ti,ab.
2 (Radiol* and (pathol* or histopathol* or histol*)).ti,ab.
3 (Multidisciplinar* or Interdisciplinar* or mdt or mdd or interobserver*).ti,ab.
4 ((clinical or diagnos*) adj2 (consensus or agreement*)).ti,ab.
5 ((Secondary or tertiary) adj care).ti,ab.
6 (Specialist* adj2 (clinic* or centre* or center* or hub or network*)).ti,ab.
7 (respiratory adj2 (clinic or clinics or hub*)).ti,ab.
8 (chest* adj2 (clinic or clinics or centre* or center* or hub or network*)).ti,ab.
9 (lung* adj2 (clinic or clinics or centre* or center* or hub*)).ti,ab.
10 (clinical adj2 (centre* or center* or hub or network*)).ti,ab.
11 (community adj2 (clinic or clinics or centre* or center* or hub or network*)).ti,ab.
12 exp *patient care/
13 exp *health care delivery/

64
Idiopathic Pulmonary Fibrosis Literature search strategy
14 *"decision tree"/
15 *consensus/
16 *observer variation/
17 *community medicine/
18 *intermethod comparison/
19 *medical practice/
20 *differential diagnosis/
21 *quantitative diagnosis/
22 *diagnostic accuracy/
23 *"medical record review"/
24 *patient referral/
25 or/1-24
Cinahl search terms
S1 Multidisciplinar* OR Interdisciplinar* OR mdt OR mdd OR interobserv*
S2 clinical n2 consensus OR clinical n2 agreement* OR diagnos* n2 consensus OR diagnos* n2 agreement*
S3 doctor* OR physician* OR pulmonologist* OR specialist* OR clinician*
S4 radiologist*
S5 S3 and S4
S6 pathol* OR histopathol* OR histol*
S7 Radiol*
S8 S6 and S7
S9 Secondary care OR tertiary care OR Specialist* n2 clinic* OR Specialist* n2 centre* OR Specialist* n2 center* OR Specialist* n2 hub OR Specialist* n2 network* OR respiratory n2 clinic OR respiratory n2 clinics OR respiratory n2 hub*
S10 chest* n2 clinic OR chest* n2 clinics OR chest* n2 centre* OR chest* n2 center* OR chest* n2 hub* OR chest* n2 network* OR lung* n2 clinic OR lung* n2 clinics OR lung* n2 centre* OR lung* n2 center* OR lung* n2 hub* OR lung* n2 network*
S11 community n2 clinic OR community n2 clinics OR community n2 centre* OR community n2 center* OR community n2 hub* OR community n2 network* OR clinical n2 centre* OR clinical n2 center* OR clinical n2 hub* OR clinical n2 network*
S12 (MH "Referral and Consultation+")
S13 (MH "Multidisciplinary Care Team")
S14 (MM "Health Care Delivery+")
S15 (MM "Decision Support Techniques+")
S16 (MM "Practice Patterns")
S17 S1 or S2 or S5 or S8 or S9 or S10 or S11 or S12 or S13 or S14 or S15 or S16
Cochrane search terms
#1 ((doctor* or physician* or pulmonologist* or specialist* or clinician*) and radiologist*):ti,ab
#2 (Radiol* and (pathol* or histopathol* or histol*)):ti,ab
#3 (Multidisciplinar* or Interdisciplinar* or mdt or mdd or interobserver*):ti,ab
#4 ((clinical or diagnos*) NEAR/2 (consensus or agreement*)):ti,ab
#5 ((Secondary or tertiary) NEXT care):ti,ab
#6 (Specialist* NEAR/2 (clinic* or centre* or center* or hub or network*)):ti,ab
#7 (respiratory NEAR/2 (clinic or clinics or hub*)):ti,ab
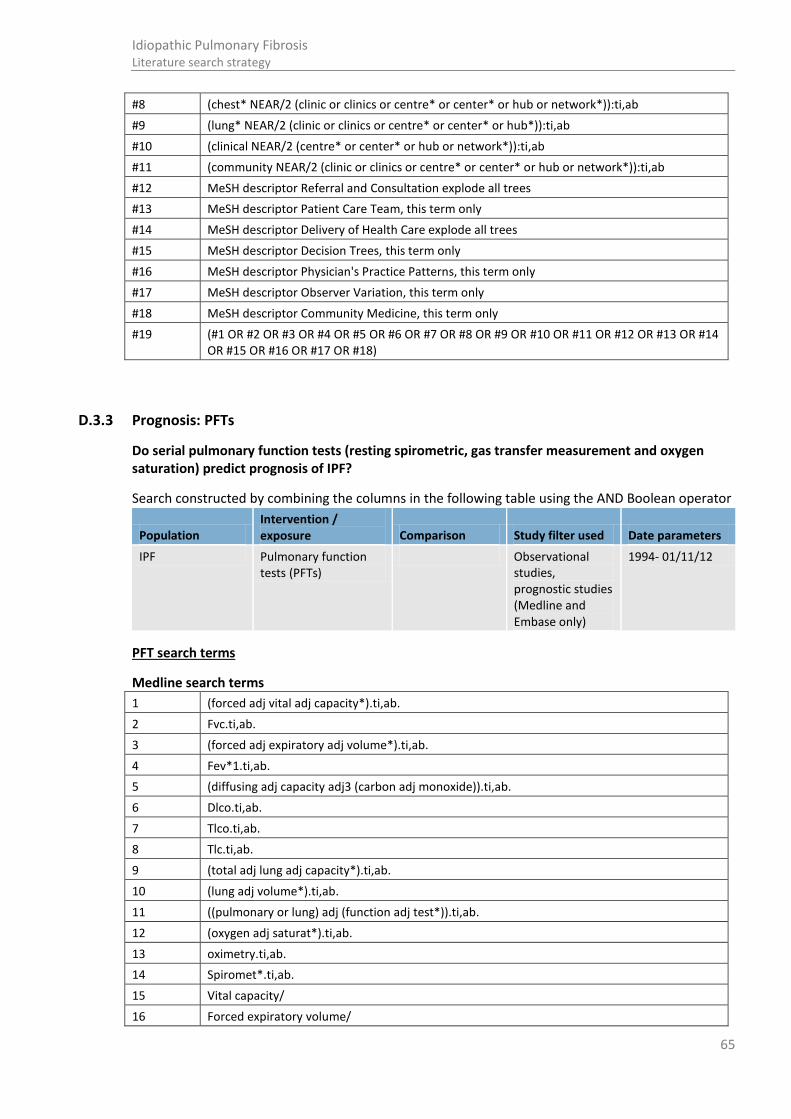
65
Idiopathic Pulmonary Fibrosis Literature search strategy
#8 (chest* NEAR/2 (clinic or clinics or centre* or center* or hub or network*)):ti,ab
#9 (lung* NEAR/2 (clinic or clinics or centre* or center* or hub*)):ti,ab
#10 (clinical NEAR/2 (centre* or center* or hub or network*)):ti,ab
#11 (community NEAR/2 (clinic or clinics or centre* or center* or hub or network*)):ti,ab
#12 MeSH descriptor Referral and Consultation explode all trees
#13 MeSH descriptor Patient Care Team, this term only
#14 MeSH descriptor Delivery of Health Care explode all trees
#15 MeSH descriptor Decision Trees, this term only
#16 MeSH descriptor Physician's Practice Patterns, this term only
#17 MeSH descriptor Observer Variation, this term only
#18 MeSH descriptor Community Medicine, this term only
#19 (#1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #12 OR #13 OR #14 OR #15 OR #16 OR #17 OR #18)
D.3.3 Prognosis: PFTs
Do serial pulmonary function tests (resting spirometric, gas transfer measurement and oxygen saturation) predict prognosis of IPF?
Search constructed by combining the columns in the following table using the AND Boolean operator
Population Intervention / exposure Comparison Study filter used Date parameters
IPF Pulmonary function tests (PFTs)
Observational studies, prognostic studies (Medline and Embase only)
1994- 01/11/12
PFT search terms
Medline search terms
1 (forced adj vital adj capacity*).ti,ab.
2 Fvc.ti,ab.
3 (forced adj expiratory adj volume*).ti,ab.
4 Fev*1.ti,ab.
5 (diffusing adj capacity adj3 (carbon adj monoxide)).ti,ab.
6 Dlco.ti,ab.
7 Tlco.ti,ab.
8 Tlc.ti,ab.
9 (total adj lung adj capacity*).ti,ab.
10 (lung adj volume*).ti,ab.
11 ((pulmonary or lung) adj (function adj test*)).ti,ab.
12 (oxygen adj saturat*).ti,ab.
13 oximetry.ti,ab.
14 Spiromet*.ti,ab.
15 Vital capacity/
16 Forced expiratory volume/
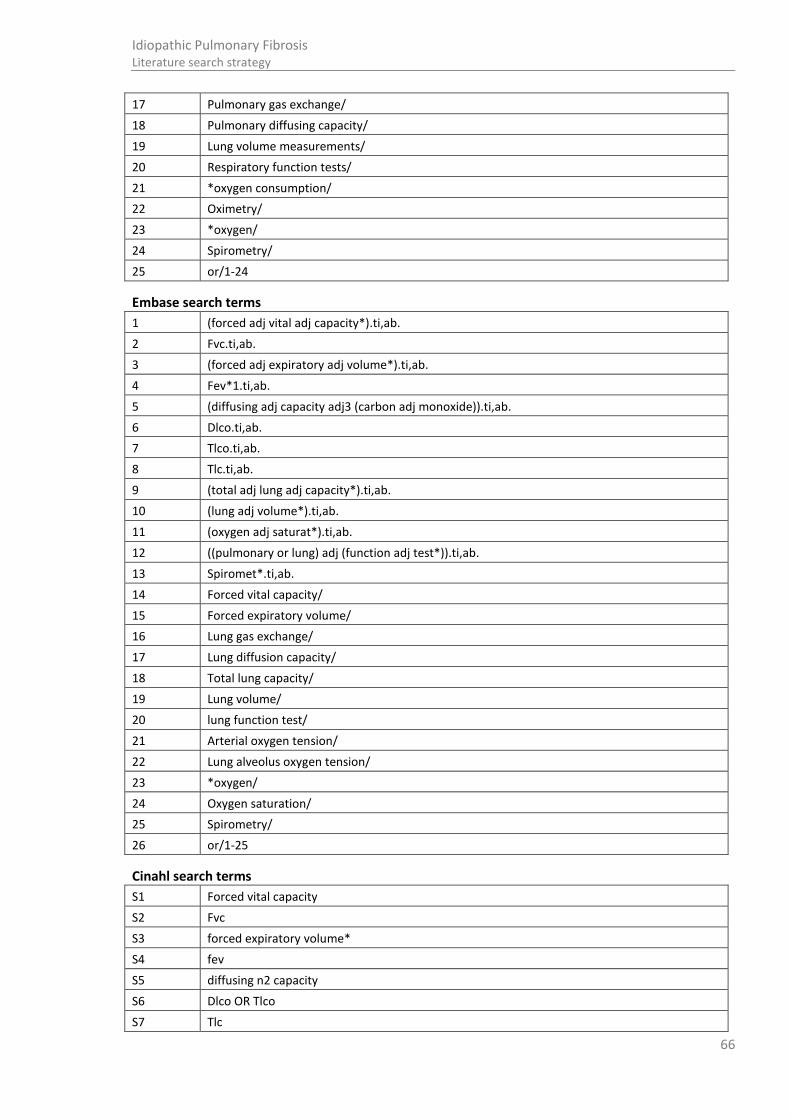
66
Idiopathic Pulmonary Fibrosis Literature search strategy
17 Pulmonary gas exchange/
18 Pulmonary diffusing capacity/
19 Lung volume measurements/
20 Respiratory function tests/
21 *oxygen consumption/
22 Oximetry/
23 *oxygen/
24 Spirometry/
25 or/1-24
Embase search terms
1 (forced adj vital adj capacity*).ti,ab.
2 Fvc.ti,ab.
3 (forced adj expiratory adj volume*).ti,ab.
4 Fev*1.ti,ab.
5 (diffusing adj capacity adj3 (carbon adj monoxide)).ti,ab.
6 Dlco.ti,ab.
7 Tlco.ti,ab.
8 Tlc.ti,ab.
9 (total adj lung adj capacity*).ti,ab.
10 (lung adj volume*).ti,ab.
11 (oxygen adj saturat*).ti,ab.
12 ((pulmonary or lung) adj (function adj test*)).ti,ab.
13 Spiromet*.ti,ab.
14 Forced vital capacity/
15 Forced expiratory volume/
16 Lung gas exchange/
17 Lung diffusion capacity/
18 Total lung capacity/
19 Lung volume/
20 lung function test/
21 Arterial oxygen tension/
22 Lung alveolus oxygen tension/
23 *oxygen/
24 Oxygen saturation/
25 Spirometry/
26 or/1-25
Cinahl search terms
S1 Forced vital capacity
S2 Fvc
S3 forced expiratory volume*
S4 fev
S5 diffusing n2 capacity
S6 Dlco OR Tlco
S7 Tlc
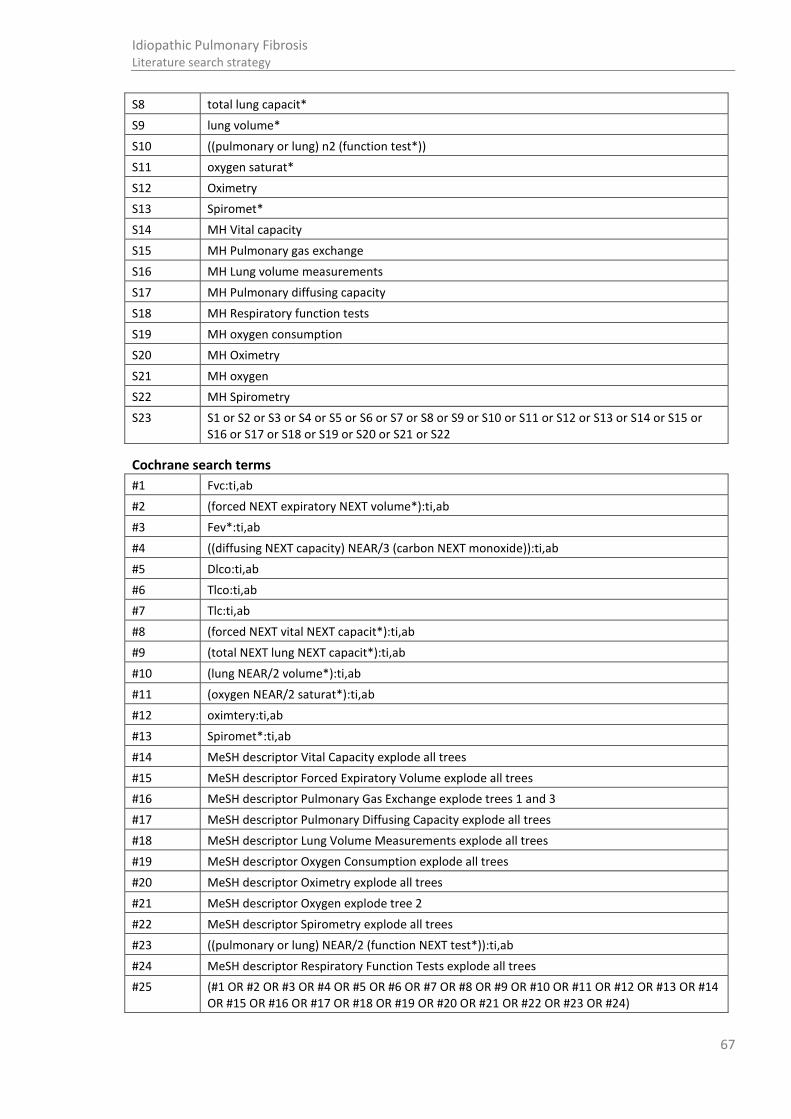
67
Idiopathic Pulmonary Fibrosis Literature search strategy
S8 total lung capacit*
S9 lung volume*
S10 ((pulmonary or lung) n2 (function test*))
S11 oxygen saturat*
S12 Oximetry
S13 Spiromet*
S14 MH Vital capacity
S15 MH Pulmonary gas exchange
S16 MH Lung volume measurements
S17 MH Pulmonary diffusing capacity
S18 MH Respiratory function tests
S19 MH oxygen consumption
S20 MH Oximetry
S21 MH oxygen
S22 MH Spirometry
S23 S1 or S2 or S3 or S4 or S5 or S6 or S7 or S8 or S9 or S10 or S11 or S12 or S13 or S14 or S15 or S16 or S17 or S18 or S19 or S20 or S21 or S22
Cochrane search terms
#1 Fvc:ti,ab
#2 (forced NEXT expiratory NEXT volume*):ti,ab
#3 Fev*:ti,ab
#4 ((diffusing NEXT capacity) NEAR/3 (carbon NEXT monoxide)):ti,ab
#5 Dlco:ti,ab
#6 Tlco:ti,ab
#7 Tlc:ti,ab
#8 (forced NEXT vital NEXT capacit*):ti,ab
#9 (total NEXT lung NEXT capacit*):ti,ab
#10 (lung NEAR/2 volume*):ti,ab
#11 (oxygen NEAR/2 saturat*):ti,ab
#12 oximtery:ti,ab
#13 Spiromet*:ti,ab
#14 MeSH descriptor Vital Capacity explode all trees
#15 MeSH descriptor Forced Expiratory Volume explode all trees
#16 MeSH descriptor Pulmonary Gas Exchange explode trees 1 and 3
#17 MeSH descriptor Pulmonary Diffusing Capacity explode all trees
#18 MeSH descriptor Lung Volume Measurements explode all trees
#19 MeSH descriptor Oxygen Consumption explode all trees
#20 MeSH descriptor Oximetry explode all trees
#21 MeSH descriptor Oxygen explode tree 2
#22 MeSH descriptor Spirometry explode all trees
#23 ((pulmonary or lung) NEAR/2 (function NEXT test*)):ti,ab
#24 MeSH descriptor Respiratory Function Tests explode all trees
#25 (#1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #12 OR #13 OR #14 OR #15 OR #16 OR #17 OR #18 OR #19 OR #20 OR #21 OR #22 OR #23 OR #24)

68
Idiopathic Pulmonary Fibrosis Literature search strategy
D.3.4 Prognosis: sub maximal exercise testing
Does baseline sub-maximal exercise testing predict prognosis of IPF?
Search constructed by combining the columns in the following table using the AND Boolean operator
Population Intervention / exposure Comparison Study filter used Date parameters
IPF Sub maximal exercise testing
Observational studies, prognostic studies (Medline and Embase only)
1994-01/11/12
Sub maximal exercise testing search terms
Medline search terms
1 ("Sub maximal" adj exercis*).ti,ab.
2 (Submaximal adj exercis*).ti,ab.
3 (walk* adj test*).ti,ab.
4 (walk adj distance).ti,ab.
5 (exercise adj test*).ti,ab.
6 (walk adj2 exercis*).ti,ab.
7 (fitness adj test*).ti,ab.
8 (shuttle adj test*).ti,ab.
9 (minute adj walk).ti,ab.
10 6mwt.ti,ab.
11 6mwd.ti,ab.
12 12MWT.ti,ab.
13 exp Exercise Therapy/
14 Exercise Tolerance/
15 Exercise Test/
16 or/1-15
Embase search terms
1 ("Sub maximal" adj exercis*).ti,ab.
2 (Submaximal adj exercis*).ti,ab.
3 (walk* adj test*).ti,ab.
4 (walk adj distance).ti,ab.
5 (exercise adj test*).ti,ab.
6 (walk adj2 exercis*).ti,ab.
7 (fitness adj test*).ti,ab.
8 (shuttle adj test*).ti,ab.
9 (minute adj walk).ti,ab.
10 6mwt.ti,ab.
11 6mwd.ti,ab.
12 12MWT.ti,ab.
13 exercise/
14 exercise test/
15 exercise tolerance/

69
Idiopathic Pulmonary Fibrosis Literature search strategy
16 cardiopulmonary exercise test/
17 or/1-16
Cinahl search terms
S1 Sub maximal exercis* OR Submaximal exercis*
S2 walk* n1 (test* or distance or exercise* or minute*)
S3 (exercise or fitness or shuttle) n1 test*
S4 6mwt OR 6mwd OR 12MWT
S5 (MH "Therapeutic Exercise") OR (MH "Exercise Therapy: Ambulation (Iowa NIC)") OR (MH "Exercise Tolerance+") OR (MH "Walking") OR (MH "Exercise Test+")
S6 S1 or S2 or S3 or S4 or S5
Cochrane search terms
#1 ((Sub NEXT maximal) NEXT exercis*):ti,ab
#2 (walk* NEXT test*):ti,ab
#3 (walk NEXT distance):ti,ab
#4 (walk NEXT exercis*):ti,ab
#5 (exercise NEXT test*):ti,ab
#6 (fitness NEXT test*):ti,ab
#7 (shuttle NEXT test*):ti,ab
#8 (minute NEXT walk):ti,ab
#9 6mwt:ti,ab
#10 6mwd:ti,ab
#11 12MWT:ti,ab
#12 MeSH descriptor Exercise Test explode trees 2 and 3
#13 MeSH descriptor Exercise Therapy explode all trees
#14 MeSH descriptor Exercise Tolerance explode all trees
#15 (#1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #12 OR #13 OR #14)
D.3.5 Prognosis: HRCT/echocardiography
Searches for the following two questions were run as one search:
Does baseline echocardiography predict prognosis of IPF?
Do baseline HRCT scores predict prognosis of IPF?
Search constructed by combining the columns in the following table using the AND Boolean operator
Population Intervention / exposure Comparison Study filter used Date parameters
IPF HRCT/ echocardiography
Observational studies, prognostic studies (Medline and Embase only)
1994-01/11/12
HRCT/ echocardiography search terms
Medline search terms
1 Hypertension, Pulmonary/di, ri, us [Diagnosis, Radionuclide Imaging, Ultrasonography]

70
Idiopathic Pulmonary Fibrosis Literature search strategy
2 *Hypertension, Pulmonary/
3 exp Echocardiography/
4 (echocardio* or tissue Doppler imag* or ((pulmonary or lung*) adj arter* adj2 pressure)).ti,ab.
5 exp Tomography, X-Ray Computed/
6 Lung/ra [Radiography]
7 Lung Diseases/ra [Radiography]
8 lung diseases, interstitial/ra [Radiography]
9 (hrct or (comput* adj3 tomograph*) or ((cat or ct) adj scan*)).ti,ab.
10 or/1-9
Embase search terms
1 *pulmonary hypertension/
2 pulmonary hypertension/di [Diagnosis]
3 exp echocardiography/
4 (echocardio* or tissue Doppler imag* or ((pulmonary or lung*) adj arter* adj2 pressure)).ti,ab.
5 exp computer assisted tomography/
6 (hrct or (comput* adj3 tomograph*) or ((cat or ct) adj scan*)).ti,ab.
7 or/1-6
Cinahl search terms
S1 (MM "Hypertension, Pulmonary") OR (MM "Pulmonary Arterial Hypertension")
S2 (MH "Echocardiography+")
S3 echocardio* OR tissue Doppler imag* OR pulmonary arter* n2 pressure OR lung* arter* n2 pressure
S4 (MH "Tomography, X-Ray Computed")
S5 (MH "Lung/RA") OR (MH "Lung Diseases/RA") OR (MH "Lung Diseases, Interstitial/RA")
S6 hrct OR comput* n3 tomograph* OR cat scan* OR ct scan*
S7 S1 or S2 or S3 or S4 or S5 or S6
Cochrane search terms
#1 MeSH descriptor Hypertension, Pulmonary, this term only
#2 MeSH descriptor Echocardiography explode all trees
#3 (echocardio* or tissue Doppler imag* or ((pulmonary or lung*) NEAR arter* NEAR/2 pressure)):ti,ab
#4 MeSH descriptor Tomography, X-Ray Computed explode all trees
#5 MeSH descriptor Lung, this term only with qualifier: RA
#6 MeSH descriptor Lung Diseases, this term only with qualifier: RA
#7 MeSH descriptor Lung Diseases, Interstitial, this term only with qualifier: RA
#8 (hrct or (comput* NEAR/3 tomograph*) or ((cat or ct) NEXT scan*)):ti,ab
#9 (#1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8)
D.3.6 Psychosocial support
What is the specific type of psychosocial support and information for patients diagnosed with IPF?
Search constructed by combining the columns in the following table using the AND Boolean operator. For PsychInfo only the population terms were used.

71
Idiopathic Pulmonary Fibrosis Literature search strategy
Population Intervention / exposure Comparison Study filter used Date parameters
ILD Psychosocial support None, all study types considered
No date restriction. Search run up to 01/11/12
Psychosocial support search terms
Medline search terms
1 exp Information Services/ or exp Publications/ or Counseling/ or Directive Counseling/
2 Patient Education as Topic/ or Patient Education Handout/
3 "patient acceptance of health care"/ or exp patient satisfaction/
4 Communication/
5 exp Consumer Health Information/
6 exp Psychotherapy/
7 Social support/
8 ((patient or patients) adj3 (education or educate or educating or information or literature or leaflet* or booklet* or pamphlet* or website* or knowledge)).ti,ab.
9 (information* adj3 (patient* or need* or requirement* or support* or seek* or access* or disseminat*)).ti,ab.
10 ((client* or patient* or user* or carer* or consumer* or customer*) adj2 (attitud* or priorit* or perception* or preferen* or expectation* or choice* or perspective* or view* or satisfact* or inform* or experience or experiences or opinion*)).ti,ab.
11 (psycholog* or council* or counsel* or psychotherap* or psychosocial).ti,ab.
12 ((support* or advice or advise) adj3 (telephone* or internet or program* or group*)).ti,ab.
13 or/1-12
Embase search terms
1 patient attitude/ or patient preference/ or patient satisfaction/ or consumer attitude/
2 consumer health information/
3 Information Service/ or Information center/ or Publication/ or Book/
4 Patient information/ or Patient education/
5 medical information/
6 health literacy/
7 exp *interpersonal communication/
8 exp Counseling/
9 exp psychotherapy/
10 psychosocial care/
11 *social support/
12 ((patient or patients) adj3 (education or educate or educating or information or literature or leaflet* or booklet* or pamphlet* or website* or knowledge)).ti,ab.
13 (information* adj3 (patient* or need* or requirement* or support* or seek* or access* or disseminat*)).ti,ab.
14 ((client* or patient* or user* or carer* or consumer* or customer*) adj2 (attitud* or priorit* or perception* or preferen* or expectation* or choice* or perspective* or view* or satisfact* or inform* or experience or experiences or opinion*)).ti,ab.
15 (psycholog* or council* or counsel* or psychotherap* or psychosocial).ti,ab.
16 ((support* or advice or advise) adj3 (telephone* or internet or program*or group*)).ti,ab.

72
Idiopathic Pulmonary Fibrosis Literature search strategy
17 or/1-16
Cinahl search terms
S1 (MH "Information Services+") OR (MH "Counseling+") OR (MH "Patient Education") OR (MH "Patient Discharge Education") OR (MH "Health Education") OR (MH "Death Education") OR (MH "Patient Attitudes") OR (MH "Communication+")
S2 (MH "Consumer Health Information") OR (MH "Psychotherapy+")
S3 ((patient or patients) n3 (education or educate or educating or information or literature or leaflet* or booklet* or pamphlet* or website* or knowledge))
S4 (information* n3 (patient* or need* or requirement* or support* or seek* or access* or disseminat*))
S5 ((client* or patient* or user* or carer* or consumer* or customer*) n2 (attitud* or priorit* or perception* or preferen* or expectation* or choice* or perspective* or view* or satisfact* or inform* or experience or experiences or opinion*))
S6 psycholog* or council* or counsel* or psychotherap* or psychosocial
S7 ((support* or advice or advise) n3 (telephone* or internet or program* or group*))
S8 S1 or S2 or S3 or S4 or S5 or S6 or S7
Cochrane search terms
#1 MeSH descriptor Information Services explode all trees
#2 MeSH descriptor Publications explode all trees
#3 MeSH descriptor Counseling, this term only
#4 MeSH descriptor Directive Counseling, this term only
#5 MeSH descriptor Patient Education as Topic, this term only
#6 MeSH descriptor Patient Acceptance of Health Care, this term only
#7 MeSH descriptor Patient Satisfaction explode all trees
#8 MeSH descriptor Communication, this term only
#9 MeSH descriptor Consumer Health Information explode all trees
#10 MeSH descriptor Psychotherapy explode all trees
#11 MeSH descriptor Social Support, this term only
#12 ((patient or patients) NEAR/3 (education or educate or educating or information or literature or leaflet* or booklet* or pamphlet* or website* or knowledge)):ti,ab
#13 (information* NEAR/3 (patient* or need* or requirement* or support* or seek* or access* or disseminat*)):ti,ab
#14 ((client* or patient* or user* or carer* or consumer* or customer*) NEAR/2 (attitud* or priorit* or perception* or preferen* or expectation* or choice* or perspective* or view* or satisfact* or inform* or experience or experiences or opinion*)):ti,ab
#15 (psycholog* or council* or counsel* or psychotherap* or psychosocial):ti,ab
#16 ((support* or advice or advise) NEAR/3 (telephone* or internet or program* or group*)):ti,ab
#17 (#1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #12 OR #13 OR #14 OR #15 OR #16)
D.3.7 Best supportive care/ patient review and follow up
Searches for the following three questions were run as one search:
What is the clinical and cost effectiveness of best supportive care (palliation of cough, breathlessness and fatigue, and oxygen management) in the symptomatic relief of patients with IPF?

73
Idiopathic Pulmonary Fibrosis Literature search strategy
How often should a patient with confirmed diagnosis of IPF be reviewed?
In which healthcare setting and by whom should a review appointment for patients with confirmed IPF be conducted?
Search constructed by combining the columns in the following table using the AND Boolean operator. For PsychInfo only the population terms were used.
Population Intervention / exposure Comparison Study filter used Date parameters
ILD Best supportive care (BSC) or patient review
SRs, RCTs, observational (Medline and Embase only)
No date restriction. Search run up to 01/11/12
BSC/ patient review search terms
Medline search terms
1 exp oximetry/
2 Oxygen Inhalation Therapy/
3 Oxygen/
4 ((oxygen or o2) adj3 (manag* or assess* or saturation* or sats or therap* or review* or ambulat* or nocturnal* or measur* or transcutaneous)).ti,ab.
5 (oximetr* or ptc02 or tcp02 or ltot).ti,ab.
6 or/1-5
7 Dyspnea/
8 (breathless* or dyspnea* or (short* adj2 breath*)).ti,ab.
9 or/7-8
10 Cough/
11 cough*.ti,ab.
12 or/10-11
13 Fatigue/
14 (fatigue* or lassitude).ti,ab.
15 or/13-14
16 Palliative Care/
17 (((best supportive or palliat*) adj2 (care or treat* or therap*)) or (symptom* adj2 (relie* or palliat*))).ti,ab.
18 or/16-17
19 ((review or reviews or "follow up*" or follow-up* or "check up*" or check-up* or monit*) adj3 (patient* or appoint* or clinic* or gp or routine or regular or assess* or hospital* or primary care or consult*)).ti,ab.
20 ((hospital or frequent or frequency or periodic* or standardiz* or standardis* or out-patient or patient-initiated or GP-initiated or rheumatologist-initiated) adj2 (review or reviews or "follow up*" or follow-up* or "check up*" or check-up*)).ti,ab.
21 or/19-20
22 6 or 9 or 12 or 15 or 18 or 21
Embase search terms
1 exp oximetry/
2 oxygen therapy/ or exp home oxygen therapy/
3 oxygen saturation/

74
Idiopathic Pulmonary Fibrosis Literature search strategy
4 *oxygen/
5 ((oxygen or o2) adj3 (manag* or assess* or saturation* or sats or therap* or review* or ambulat* or nocturnal* or measur* or transcutaneous)).ti,ab.
6 (oximetr* or ptc02 or tcp02 or ltot).ti,ab.
7 or/1-6
8 (breathless* or dyspnea* or (short* adj2 breath*)).ti,ab.
9 *dyspnea/
10 or/8-9
11 cough*.ti,ab.
12 *coughing/
13 or/11-12
14 fatigue/ or exp lassitude/
15 (fatigue* or lassitude).ti,ab.
16 or/14-15
17 palliative therapy/
18 (((best supportive or palliat*) adj2 (care or treat* or therap*)) or (symptom* adj2 (relie* or palliat*))).ti,ab.
19 or/17-18
20 ((review or reviews or "follow up*" or follow-up* or "check up*" or check-up* or monit*) adj3 (patient* or appoint* or clinic* or gp or routine or regular or assess* or hospital* or primary care or consult*)).ti,ab.
21 ((hospital or frequent or frequency or periodic* or standardiz* or standardis* or out-patient or patient-initiated or GP-initiated or rheumatologist-initiated) adj2 (review or reviews or "follow up*" or follow-up* or "check up*" or check-up*)).ti,ab.
22 or/20-21
23 7 or 10 or 13 or 16 or 19 or 22
Cinahl search terms
S1 (MH "Oximetry+") OR (MH "Oxygen Therapy") OR (MH "Home Oxygen Therapy") OR (MH "Oxygen Saturation") OR (MH "Oxygen")
S2 ((oxygen or o2) n3 (manag* or assess* or saturation* or sats or therap* or review* or ambulat* or nocturnal* or measur* or transcutaneous))
S3 oximetr* or ptc02 or tcp02 or ltot
S4 (MH "Dyspnea") OR (MH "Cough") OR (MH "Fatigue") OR (MH "Palliative Care") OR (MH "After Care")
S5 (breathless* or dyspnea* or (short* n2 breath*))
S6 cough* OR fatigue* OR lassitude
S7 (((best supportive or palliat*) n2 (care or treat* or therap*)) or (symptom* n2 (relie* or palliat*)))
S8 ((review or reviews or "follow up*" or follow-up* or "check up*" or check-up* or monit*) n3 (patient* or appoint* or clinic* or gp or routine or regular or assess* or hospital* or primary care or consult*))
S9 ((hospital or frequent or frequency or periodic* or standardiz* or standardis* or out-patient or patient-initiated or GP-initiated or rheumatologist-initiated) n2 (review or reviews or "follow up*" or follow-up* or "check up*" or check-up*))
S10 S1 or S2 or S3 or S4 or S5 or S6 or S7 or S8 or S9
Cochrane search terms
#1 MeSH descriptor Oximetry explode all trees

75
Idiopathic Pulmonary Fibrosis Literature search strategy
#2 MeSH descriptor Oxygen Inhalation Therapy, this term only
#3 MeSH descriptor Oxygen, this term only
#4 ((oxygen or o2) NEAR/3 (manag* or assess* or saturation* or sats or therap* or review* or ambulat* or nocturnal* or measur* or transcutaneous)):ti,ab
#5 (oximetr* or ptc02 or tcp02 or ltot):ti,ab
#6 MeSH descriptor Dyspnea, this term only
#7 (breathless* or dyspnea* or (short* NEAR/2 breath*)):ti,ab
#8 MeSH descriptor Cough, this term only
#9 cough*:ti,ab
#10 MeSH descriptor Fatigue, this term only
#11 (fatigue* or lassitude):ti,ab
#12 MeSH descriptor Palliative Care, this term only
#13 (((best supportive or palliat*) NEAR/2 (care or treat* or therap*)) or (symptom* NEAR/2 (relie* or palliat*))):ti,ab
#14 ((review or reviews or "follow up*" or follow-up* or "check up*" or check-up* or monit*) NEAR/3 (patient* or appoint* or clinic* or gp or routine or regular or assess* or hospital* or primary care or consult*)):ti,ab
#15 ((hospital or frequent or frequency or periodic* or standardiz* or standardis* or out-patient or patient-initiated or GP-initiated or rheumatologist-initiated) NEAR/2 (review or reviews or "follow up*" or follow-up* or "check up*" or check-up*)):ti,ab
#16 (#1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #12 OR #13 OR #14 OR #15)
D.3.8 Pulmonary rehabilitation
Searches for the following two questions were run as one search:
What are the benefits of pulmonary rehabilitation programmes for patients with confirmed IPF?
What is the optimal course content, setting and duration for patients referred for pulmonary rehab programmes?
Search constructed by combining the columns in the following table using the AND Boolean operator. For PsychInfo only the population terms were used.
Population Intervention / exposure Comparison Study filter used Date parameters
ILD Pulmonary rehabilitation
None, all study types considered
No date restriction. Search run up to 01/11/12
Pulmonary rehabilitation search terms
Medline search terms
1 (fatigue severity scale* or visual analog* scale*).ti,ab.
2 (Borg adj2 scale*).ti,ab.
3 ((Dyspn?ea or illness) adj index).ti,ab.
4 (Daily adj2 activit* adj2 (life or living)).ti,ab.
5 (Exercise or Treadmill or bicycle or stepper or weights or ergometer or walk*).ti,ab.
6 ((Physical or aerobic or endurance or strength or fitness or resistance) adj2 (activit* or train* or condition* or program* or regime*)).ti,ab.

76
Idiopathic Pulmonary Fibrosis Literature search strategy
7 ((minute walk adj (test or distance)) or 6MWT or 6MWD).ti,ab.
8 (cycle ergometry or ICET).ti,ab.
9 Shuttle walk*.ti,ab.
10 ((Pulmonary adj2 rehabilitat*) or (rehabilitat* adj2 program*)).ti,ab.
11 Written disclosure therap*.ti,ab.
12 (psycholog* or council* or counsel* or psychotherap*).ti,ab.
13 ((Emotional or psychosocial) adj2 support).ti,ab.
14 ((patient* or carer*) adj2 (information or education* or knowledge)).ti,ab.
15 ((patient* or carer*) adj5 (leaflet* or pamphlet* or booklet* or website* or web site*)).ti,ab.
16 ((multifactor* or multifacet* or managed care) adj program*).ti,ab.
17 (Diet* or nutrition*).ti,ab.
18 (((Respiratory disease or George* respiratory) adj questionnaire*) or sgrq).ti,ab.
19 (WHOQOL-100 or whoQoL100).ti,ab.
20 (Support adj group*).ti,ab.
21 (disease adj management adj program*).ti,ab.
22 *Exercise Test/
23 exp Exercise Tolerance/
24 exp Exercise Movement Techniques/
25 *Exercise/
26 *Walking/
27 Physical endurance/
28 Exercise therapy/
29 Rehabilitation/
30 Rehabilitation centers/
31 Severity of illness index/
32 Activities of daily living/
33 Managed care programs/
34 Patient Education as Topic/
35 exp Consumer Health Information/
36 Access to Information/
37 Information services/
38 Pamphlets/
39 Counseling/
40 exp Psychotherapy/
41 exp diet/
42 exp nutrition therapy/
43 or/1-42
Embase search terms
1 (fatigue severity scale* or visual analog* scale*).ti,ab.
2 (Borg adj2 scale*).ti,ab.
3 ((Dyspn?ea or illness) adj index).ti,ab.
4 (Daily adj2 activit* adj2 (life or living)).ti,ab.
5 (Exercise or Treadmill or bicycle or stepper or weights or ergometer or walk*).ti,ab.
6 ((Physical or aerobic or endurance or strength or fitness or resistance) adj2 (activit* or train*
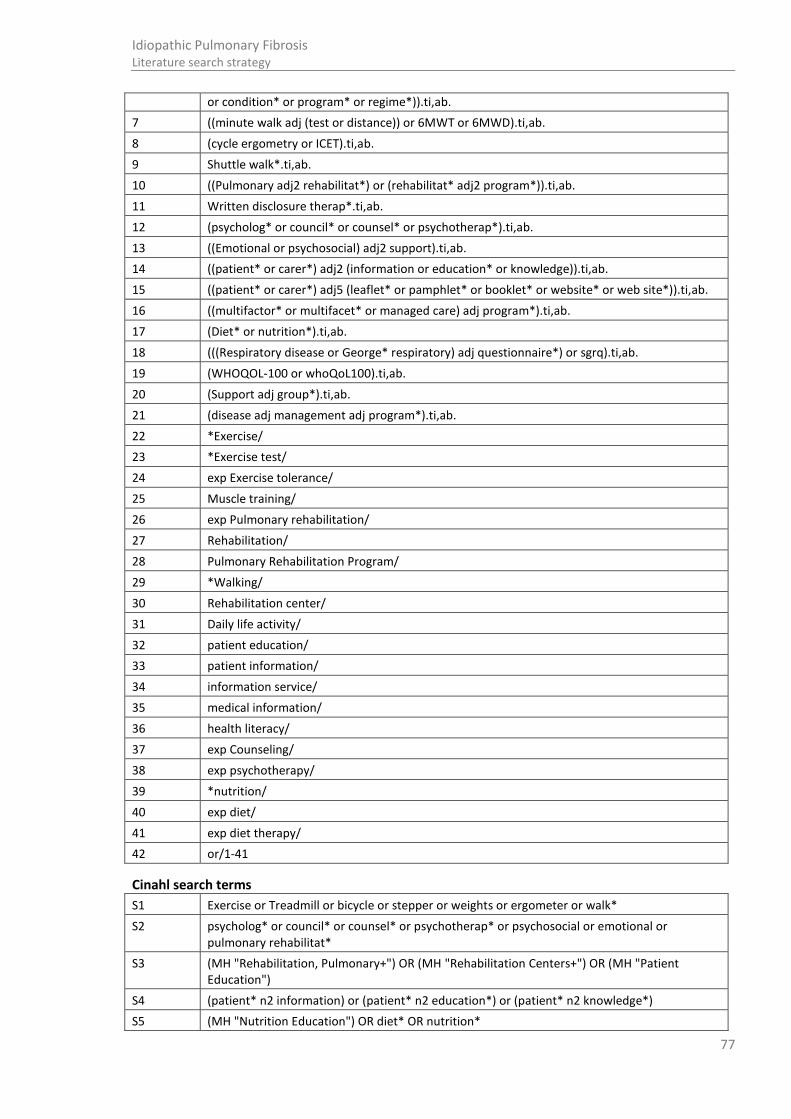
77
Idiopathic Pulmonary Fibrosis Literature search strategy
or condition* or program* or regime*)).ti,ab.
7 ((minute walk adj (test or distance)) or 6MWT or 6MWD).ti,ab.
8 (cycle ergometry or ICET).ti,ab.
9 Shuttle walk*.ti,ab.
10 ((Pulmonary adj2 rehabilitat*) or (rehabilitat* adj2 program*)).ti,ab.
11 Written disclosure therap*.ti,ab.
12 (psycholog* or council* or counsel* or psychotherap*).ti,ab.
13 ((Emotional or psychosocial) adj2 support).ti,ab.
14 ((patient* or carer*) adj2 (information or education* or knowledge)).ti,ab.
15 ((patient* or carer*) adj5 (leaflet* or pamphlet* or booklet* or website* or web site*)).ti,ab.
16 ((multifactor* or multifacet* or managed care) adj program*).ti,ab.
17 (Diet* or nutrition*).ti,ab.
18 (((Respiratory disease or George* respiratory) adj questionnaire*) or sgrq).ti,ab.
19 (WHOQOL-100 or whoQoL100).ti,ab.
20 (Support adj group*).ti,ab.
21 (disease adj management adj program*).ti,ab.
22 *Exercise/
23 *Exercise test/
24 exp Exercise tolerance/
25 Muscle training/
26 exp Pulmonary rehabilitation/
27 Rehabilitation/
28 Pulmonary Rehabilitation Program/
29 *Walking/
30 Rehabilitation center/
31 Daily life activity/
32 patient education/
33 patient information/
34 information service/
35 medical information/
36 health literacy/
37 exp Counseling/
38 exp psychotherapy/
39 *nutrition/
40 exp diet/
41 exp diet therapy/
42 or/1-41
Cinahl search terms
S1 Exercise or Treadmill or bicycle or stepper or weights or ergometer or walk*
S2 psycholog* or council* or counsel* or psychotherap* or psychosocial or emotional or pulmonary rehabilitat*
S3 (MH "Rehabilitation, Pulmonary+") OR (MH "Rehabilitation Centers+") OR (MH "Patient Education")
S4 (patient* n2 information) or (patient* n2 education*) or (patient* n2 knowledge*)
S5 (MH "Nutrition Education") OR diet* OR nutrition*
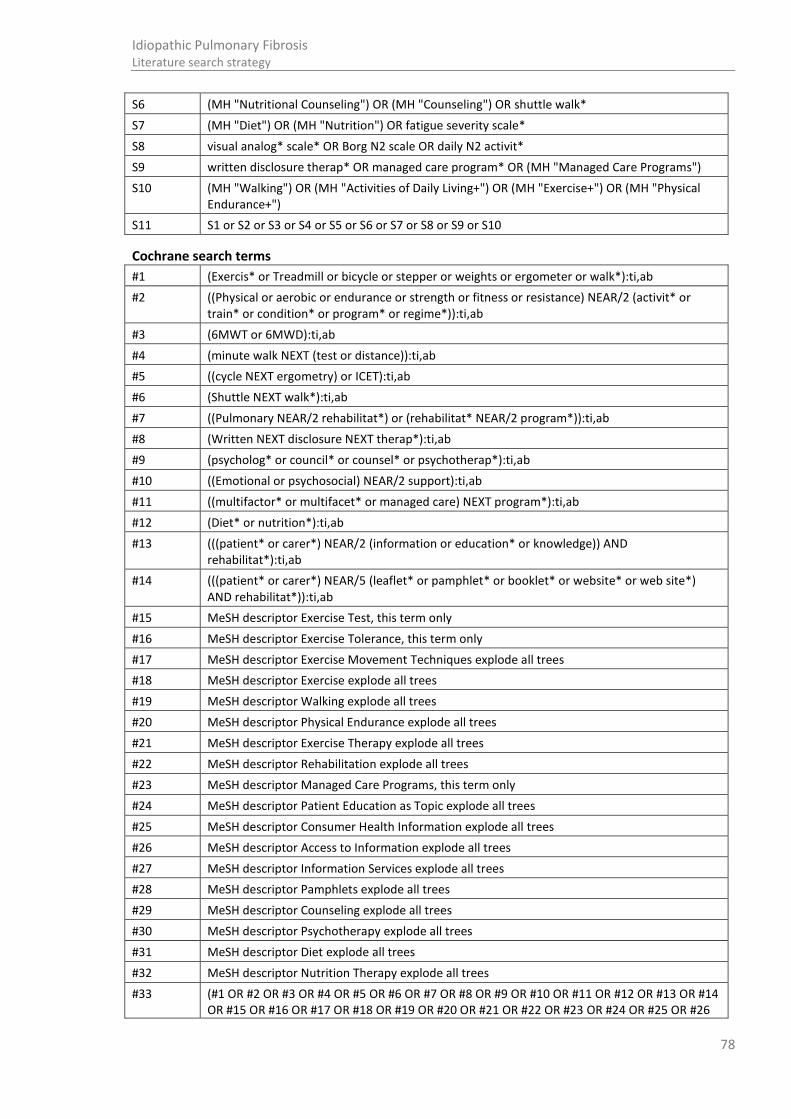
78
Idiopathic Pulmonary Fibrosis Literature search strategy
S6 (MH "Nutritional Counseling") OR (MH "Counseling") OR shuttle walk*
S7 (MH "Diet") OR (MH "Nutrition") OR fatigue severity scale*
S8 visual analog* scale* OR Borg N2 scale OR daily N2 activit*
S9 written disclosure therap* OR managed care program* OR (MH "Managed Care Programs")
S10 (MH "Walking") OR (MH "Activities of Daily Living+") OR (MH "Exercise+") OR (MH "Physical Endurance+")
S11 S1 or S2 or S3 or S4 or S5 or S6 or S7 or S8 or S9 or S10
Cochrane search terms
#1 (Exercis* or Treadmill or bicycle or stepper or weights or ergometer or walk*):ti,ab
#2 ((Physical or aerobic or endurance or strength or fitness or resistance) NEAR/2 (activit* or train* or condition* or program* or regime*)):ti,ab
#3 (6MWT or 6MWD):ti,ab
#4 (minute walk NEXT (test or distance)):ti,ab
#5 ((cycle NEXT ergometry) or ICET):ti,ab
#6 (Shuttle NEXT walk*):ti,ab
#7 ((Pulmonary NEAR/2 rehabilitat*) or (rehabilitat* NEAR/2 program*)):ti,ab
#8 (Written NEXT disclosure NEXT therap*):ti,ab
#9 (psycholog* or council* or counsel* or psychotherap*):ti,ab
#10 ((Emotional or psychosocial) NEAR/2 support):ti,ab
#11 ((multifactor* or multifacet* or managed care) NEXT program*):ti,ab
#12 (Diet* or nutrition*):ti,ab
#13 (((patient* or carer*) NEAR/2 (information or education* or knowledge)) AND rehabilitat*):ti,ab
#14 (((patient* or carer*) NEAR/5 (leaflet* or pamphlet* or booklet* or website* or web site*) AND rehabilitat*)):ti,ab
#15 MeSH descriptor Exercise Test, this term only
#16 MeSH descriptor Exercise Tolerance, this term only
#17 MeSH descriptor Exercise Movement Techniques explode all trees
#18 MeSH descriptor Exercise explode all trees
#19 MeSH descriptor Walking explode all trees
#20 MeSH descriptor Physical Endurance explode all trees
#21 MeSH descriptor Exercise Therapy explode all trees
#22 MeSH descriptor Rehabilitation explode all trees
#23 MeSH descriptor Managed Care Programs, this term only
#24 MeSH descriptor Patient Education as Topic explode all trees
#25 MeSH descriptor Consumer Health Information explode all trees
#26 MeSH descriptor Access to Information explode all trees
#27 MeSH descriptor Information Services explode all trees
#28 MeSH descriptor Pamphlets explode all trees
#29 MeSH descriptor Counseling explode all trees
#30 MeSH descriptor Psychotherapy explode all trees
#31 MeSH descriptor Diet explode all trees
#32 MeSH descriptor Nutrition Therapy explode all trees
#33 (#1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #12 OR #13 OR #14 OR #15 OR #16 OR #17 OR #18 OR #19 OR #20 OR #21 OR #22 OR #23 OR #24 OR #25 OR #26

79
Idiopathic Pulmonary Fibrosis Literature search strategy
OR #27 OR #28 OR #29 OR #30 OR #31 OR #32)
D.3.9 Pharmacological interventions
Searches for the following two questions were run as one search:
Which drug should be initiated first, for how long, and what combination in the treatment of IPF?
(Sub-question) What is the clinical and cost effectiveness of pharmacological interventions to manage patients with suspected or confirmed IPF?
Search constructed by combining the columns in the following table using the AND Boolean operator
Population Intervention / exposure Comparison Study filter used Date parameters
IPF Pharmacological interventions
SRs, RCTs (Medline and Embase only)
No date restriction. Search run up to 01/11/12
Pharmacological intervention search terms
Medline search terms
1 Acetylcysteine/
2 (acetylcystein* or acetyl cystein* or acetadote or parvolex).ti,ab.
3 Azathioprine/
4 exp Immunosuppressive Agents/
5 (azathioprine or imuran or azasan or immunosuppress*).ti,ab.
6 (ambrisentan or volibris or letairis or bosentan or tracleer).ti,ab.
7 Glucocorticoids/ or Adrenal cortex hormones/ or Pregnadienetriols/ or Pregnenediones/
8 Prednisolone/ or betamethasone/ or cortisone/ or dexamethasone/ or hydrocortisone/ or methylprednisolone/ or prednisone/ or triamcinolone/ or beclomethasone/ or budesonide/
9 (Prednisolone or prednisone or deltacotril or (pred adj forte) or methylprednisolone or depo medrol or lodotra or Deltastab or betamethasone or betnelan or betnesol).ti,ab.
10 (cortisone or deflazacort or calcort or dexamethasone or hydrocortisone).ti,ab.
11 (triamcinolone or Nasacort or adcortyl or kenalog or triderm or triacet or trivaris or triesence).ti,ab.
12 (Efcortesol or (Solu adj Cortef) or Medrone or (Solu adj Medrone) or Hydrocortistab or (Depo adj Medrone) or Adcortyl).ti,ab.
13 (beclometasone or beclomethasone or qvar or fostair or clenil or asmabec or beconase or pulvinal or becodisks or budesonide or budelin or budenofalk or pulmicort or symbicort or rhinocort or entocort).ti,ab.
14 (ciclesonide or alvesco or omnaris or fluticasone or flixotide or seretide or evohaler or veramyst or flovent or flonase or cutivate or advair or avamys or flixonase or pirinase or asmanex or elocon or nasonex).ti,ab.
15 (Glucocorticoid* or Corticosteroid* or Adrenal cortex hormone*).ti,ab.
16 Trimethoprim-Sulfamethoxazole Combination/
17 ((trimethoprim adj2 sulfamethoxazole) or co trimoxazole or septrin).ti,ab.
18 (arzip or cellcept or mycophenolic or myfortic or mycophenolate).ti,ab.
19 mycophenolic acid/
20 Warfarin/
21 warfarin.ti,ab.

80
Idiopathic Pulmonary Fibrosis Literature search strategy
22 anticoagulants/ or antithrombins/
23 exp Acenocoumarol/
24 exp Phenindione/
25 exp Coumarins/
26 phenprocoumon/
27 (acenocoumarol or nicoumalone or phenprocoumon or phenindione or nicoumalone or acenocoumarin or sinthrome or sintrom or coumadin or coumarin* or hydroxycoumarin* or (anti adj coagulant*)).ti,ab.
28 Proton pump inhibitors/
29 (proton adj3 pump* adj3 (inhibitor* or antagonist*)).ti,ab.
30 Omeprazole/
31 (omeprazole or prilosec or nexium or esomeprazole or vimovo or losec or pantoprazole or protium or protonix or lansoprazole or prevacid or zoton or rabeprazole or pariet).ti,ab.
32 (sildenafil or viagra or revatio).ti,ab.
33 vasodilator*.ti,ab.
34 *Vasodilator Agents/
35 ((phosphodiesterase adj2 inhibitor*) or avanafil or beminafil or dasantafil or gisadenafil or lodenafil or mirodenafil or tadalafil or udenafil or vardenafil).ti,ab.
36 or/1-35
Embase search terms
1 acetylcysteine/
2 (acetylcystein* or acetyl cystein* or acetadote or parvolex).ti,ab.
3 (azathioprine or imuran or azasan or immunosuppress*).ti,ab.
4 azathioprine/ or immunosuppressive agent/
5 (ambrisentan or volibris or letairis or bosentan or tracleer).ti,ab.
6 Glucocorticoid/
7 Corticosteroid/
8 Corticosteroid derivative/
9 Pregnane derivative/
10 Prednisolone/ or betamethasone/ or cortisone/deflazacort or dexamethasone/ or hydrocortisone/ or methylprednisolone/ or prednisone/ or triamcinolone/ or beclometasone/ or beclometasone diproprionate/ or beclometasone dipropionate plus salbutamol/ or budesonide/ or ciclesonide/
11 (Prednisolone or prednisone or deltacotril or (pred adj forte) or methylprednisolone or depo medrol or lodotra or Deltastab or betamethasone or betnelan or betnesol).ti,ab.
12 (cortisone or deflazacort or calcort or dexamethasone or hydrocortisone).ti,ab.
13 (triamcinolone or Nasacort or adcortyl or kenalog or triderm or triacet or trivaris or triesence).ti,ab.
14 (Efcortesol or (Solu adj Cortef) or Medrone or (Solu adj Medrone) or Hydrocortistab or (Depo adj Medrone) or Adcortyl).ti,ab.
15 (beclometasone or beclomethasone or qvar or fostair or clenil or asmabec or beconase or pulvinal or becodisks or budesonide or budelin or budenofalk or pulmicort or symbicort or rhinocort or entocort).ti,ab.
16 (ciclesonide or alvesco or omnaris or fluticasone or flixotide or seretide or evohaler or veramyst or flovent or flonase or cutivate or advair or avamys or flixonase or pirinase or asmanex or elocon or nasonex).ti,ab.
17 (Glucocorticoid* or Corticosteroid* or Adrenal cortex hormone*).ti,ab.

81
Idiopathic Pulmonary Fibrosis Literature search strategy
18 ((trimethoprim adj2 sulfamethoxazole) or co trimoxazole or septrin).ti,ab.
19 cotrimoxazole/
20 (arzip or cellcept or mycophenolic or myfortic or mycophenolate).ti,ab.
21 mycophenolic acid 2 morpholinoethyl ester/
22 warfarin/
23 warfarin.ti,ab.
24 (acenocoumarol or nicoumalone or phenindione or nicoumalone or acenocoumarin or sinthrome or sintrom or coumadin or coumarin* or hydroxycoumarin* or (anti adj coagulant*)).ti,ab.
25 exp coumarin/
26 anticoagulant agent/
27 exp phenindione/
28 exp acenocoumarol/
29 phenprocoumon/
30 exp coumarin anticoagulant/
31 phenprocoumon.ti,ab.
32 exp Proton pump inhibitor/
33 (proton adj3 pump* adj3 (inhibitor* or antagonist*)).ti,ab.
34 Esomeprazole/
35 Omeprazole/
36 Lansoprazole/
37 Rabeprazole/
38 pantoprazole/
39 (omeprazole or prilosec or nexium or esomeprazole or vimovo or losec or pantoprazole or protium or protonix or lansoprazole or prevacid or zoton or rabeprazole or pariet).ti,ab.
40 (sildenafil or viagra or revatio).ti,ab.
41 *sildenafil/
42 *phosphodiesterase V inhibitor/
43 phosphodiesterase v inhibitor/ or *avanafil/ or *beminafil/ or *dasantafil/ or *gisadenafil/ or *lodenafil/ or *mirodenafil/ or *sildenafil/ or *sildenafil nitrate/ or *tadalafil/ or *udenafil/ or *vardenafil/
44 ((phosphodiesterase adj2 inhibitor*) or avanafil or beminafil or dasantafil or gisadenafil or lodenafil or mirodenafil or tadalafil or udenafil or vardenafil).ti,ab.
45 or/1-44
Cochrane search terms
#1 (acetylcystein* or (acetyl NEXT cystein*) or acetadote or parvolex):ti,ab
#2 MeSH descriptor Acetylcysteine explode all trees
#3 (azathioprine or imuran or azasan or immunosuppress*):ti,ab
#4 MeSH descriptor Azathioprine explode all trees
#5 MeSH descriptor Immunosuppressive Agents explode all trees
#6 (ambrisentan or volibris or letairis or bosentan or tracleer):ti,ab,kw
#7 MeSH descriptor Glucocorticoids explode all trees
#8 MeSH descriptor Adrenal Cortex Hormones explode all trees
#9 MeSH descriptor Pregnadienetriols explode all trees
#10 MeSH descriptor Pregnenediones explode all trees

82
Idiopathic Pulmonary Fibrosis Literature search strategy
#11 MeSH descriptor Prednisolone explode all trees
#12 MeSH descriptor Betamethasone explode all trees
#13 MeSH descriptor Cortisone explode all trees
#14 MeSH descriptor Dexamethasone explode all trees
#15 MeSH descriptor Hydrocortisone explode all trees
#16 MeSH descriptor Methylprednisolone explode all trees
#17 MeSH descriptor Prednisone explode all trees
#18 MeSH descriptor Triamcinolone explode all trees
#19 MeSH descriptor Beclomethasone explode all trees
#20 MeSH descriptor Budesonide explode all trees
#21 (Prednisolone or prednisone or deltacotril or (pred adj forte) or methylprednisolone or (depo medrol) or lodotra or Deltastab or betamethasone or betnelan or betnesol):ti,ab
#22 (cortisone or deflazacort or calcort or dexamethasone or hydrocortisone):ti,ab
#23 (triamcinolone or Nasacort or adcortyl or kenalog or triderm or triacet or trivaris or triesence):ti,ab
#24 (Efcortesol or (Solu NEXT Cortef) or Medrone or (Solu NEXT Medrone) or Hydrocortistab or (Depo NEXT Medrone) or Adcortyl):ti,ab
#25 (beclometasone or beclomethasone or qvar or fostair or clenil or asmabec or beconase or pulvinal or becodisks or budesonide or budelin or budenofalk or pulmicort or symbicort or rhinocort or entocort):ti,ab
#26 (ciclesonide or alvesco or omnaris or fluticasone or flixotide or seretide or evohaler or veramyst or flovent or flonase or cutivate or advair or avamys or flixonase or pirinase or asmanex or elocon or nasonex):ti,ab
#27 (Glucocorticoid* or Corticosteroid* or (Adrenal cortex hormone*)):ti,ab
#28 ((trimethoprim adj2 sulfamethoxazole) or (co trimoxazole)):ti,ab
#29 MeSH descriptor Trimethoprim-Sulfamethoxazole Combination explode all trees
#30 (arzip or cellcept or mycophenolic or myfortic or mycophenolate):ti,ab
#31 MeSH descriptor Mycophenolic Acid explode all trees
#32 (warfarin):ti,ab,kw
#33 MeSH descriptor Warfarin, this term only
#34 (acenocoumarol or nicoumalone or phenprocoumon or phenindione or nicoumalone or acenocoumarin or sinthrome or sintrom or coumadin or coumarin* or hydroxycoumarin* or (anti adj coagulant*)):ti,ab
#35 MeSH descriptor Anticoagulants explode all trees
#36 MeSH descriptor Antithrombins explode all trees
#37 MeSH descriptor Acenocoumarol explode all trees
#38 MeSH descriptor Phenindione, this term only
#39 MeSH descriptor Coumarins explode all trees
#40 MeSH descriptor Phenprocoumon, this term only
#41 MeSH descriptor Proton Pump Inhibitors explode all trees
#42 MeSH descriptor Omeprazole explode all trees
#43 (omeprazole or prilosec or nexium or esomeprazole or vimovo or losec or pantoprazole or protium or protonix or lansoprazole or prevacid or zoton or rabeprazole or pariet):ti,ab
#44 ((phosphodiesterase adj2 inhibitor*) or avanafil or beminafil or dasantafil or gisadenafil or lodenafil or mirodenafil or tadalafil or udenafil or vardenafil or sildenafil or viagra or revatio or vasodilator*):ti,ab,kw
#45 MeSH descriptor Vasodilator Agents explode all trees

83
Idiopathic Pulmonary Fibrosis Literature search strategy
#46 (proton NEAR/3 pump* NEAR/3 (inhibitor* or antagonist*)):ti,ab
#47 (#1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #12 OR #13 OR #14 OR #15 OR #16 OR #17 OR #18 OR #19 OR #20 OR #21 OR #22 OR #23 OR #24 OR #25 OR #26 OR #27 OR #28 OR #29 OR #30 OR #31 OR #32 OR #33 OR #34 OR #35 OR #36 OR #37 OR #38 OR #39 OR #40 OR #41 OR #42 OR #43 OR #44 OR #45 OR #46)
D.3.10 Pharmacological interventions: adverse events
Which measures can be taken to minimize the occurrence/severity of adverse events when undergoing pharmacological treatment for IPF?"
Search constructed by combining the columns in the following table using the AND Boolean operator
Population Intervention / exposure Comparison Study filter used Date parameters
IPF OR Azazthioprine
TPMT None, all study types considered
No date restriction. Search run up to 01/11/12
Azathioprine search terms
Medline search terms
1 (az#thiopri* or azasan or azamune or im?uran or imure#).ti,ab.
2 exp Azathioprine/
3 1 or 2
Embase search terms
1 exp azathioprine/
2 (az#thiopri* or azasan or azamune or im?uran or imure#).ti,ab.
3 1 or 2
Cochrane search terms
#1 (az?thiopri* or azasan or azamune or imuran or immuran or imurel or imurek or imuren):ti,ab
#2 MeSH descriptor Azathioprine explode all trees
#3 #1 OR #2
TMPT search terms
Medline search terms
1 *Methyltransferases/
2 ((thiopurine adj2 methyltransferase) or (methyl adj2 methyl transferase) or tpmt).ti,ab.
3 1 or 2
Embase search terms
1 exp thiopurine methyltransferase/ or *methyltransferase/
2 ((thiopurine adj2 methyltransferase) or (thiopurine adj2 methyl transferase) or tpmt).ti,ab.
3 1 or 2
Cochrane search terms
#1 ((thiopurine NEAR/2 methyl) NEXT transferase):ti,ab
#2 tpmt:ti,ab
#3 (thiopurine NEAR/2 methyltransferase):ti,ab
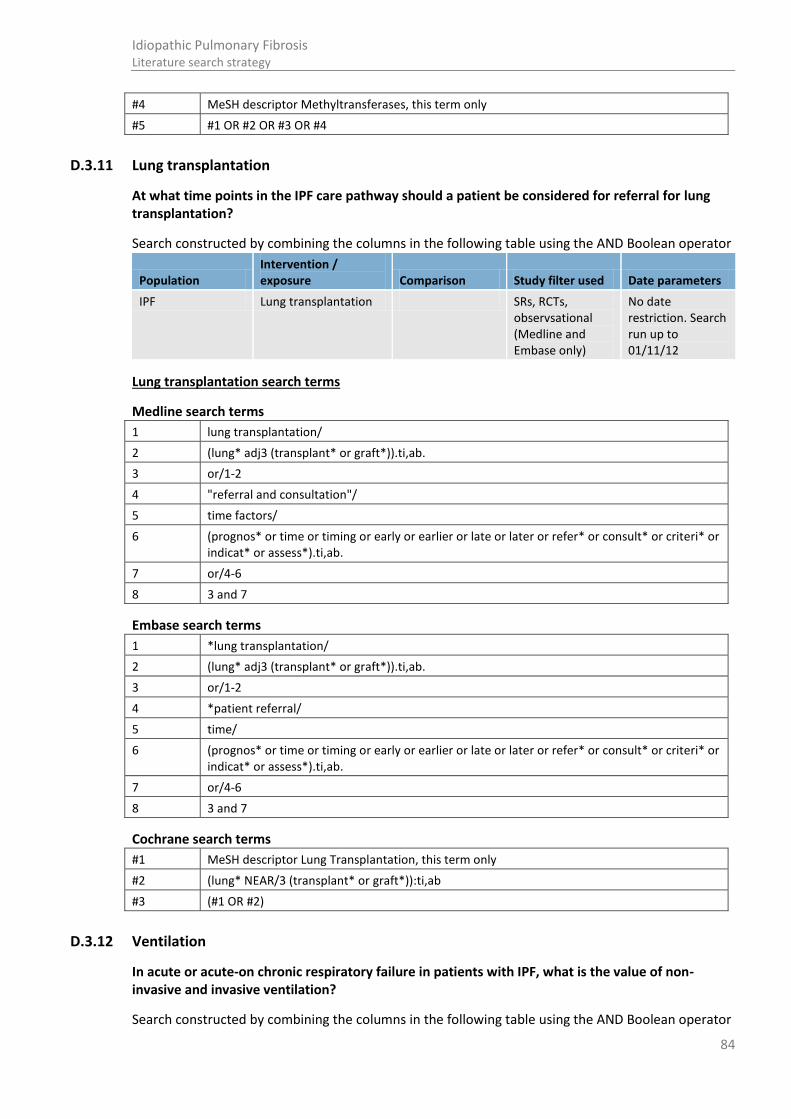
84
Idiopathic Pulmonary Fibrosis Literature search strategy
#4 MeSH descriptor Methyltransferases, this term only
#5 #1 OR #2 OR #3 OR #4
D.3.11 Lung transplantation
At what time points in the IPF care pathway should a patient be considered for referral for lung transplantation?
Search constructed by combining the columns in the following table using the AND Boolean operator
Population Intervention / exposure Comparison Study filter used Date parameters
IPF Lung transplantation SRs, RCTs, observsational (Medline and Embase only)
No date restriction. Search run up to 01/11/12
Lung transplantation search terms
Medline search terms
1 lung transplantation/
2 (lung* adj3 (transplant* or graft*)).ti,ab.
3 or/1-2
4 "referral and consultation"/
5 time factors/
6 (prognos* or time or timing or early or earlier or late or later or refer* or consult* or criteri* or indicat* or assess*).ti,ab.
7 or/4-6
8 3 and 7
Embase search terms
1 *lung transplantation/
2 (lung* adj3 (transplant* or graft*)).ti,ab.
3 or/1-2
4 *patient referral/
5 time/
6 (prognos* or time or timing or early or earlier or late or later or refer* or consult* or criteri* or indicat* or assess*).ti,ab.
7 or/4-6
8 3 and 7
Cochrane search terms
#1 MeSH descriptor Lung Transplantation, this term only
#2 (lung* NEAR/3 (transplant* or graft*)):ti,ab
#3 (#1 OR #2)
D.3.12 Ventilation
In acute or acute-on chronic respiratory failure in patients with IPF, what is the value of non-invasive and invasive ventilation?
Search constructed by combining the columns in the following table using the AND Boolean operator
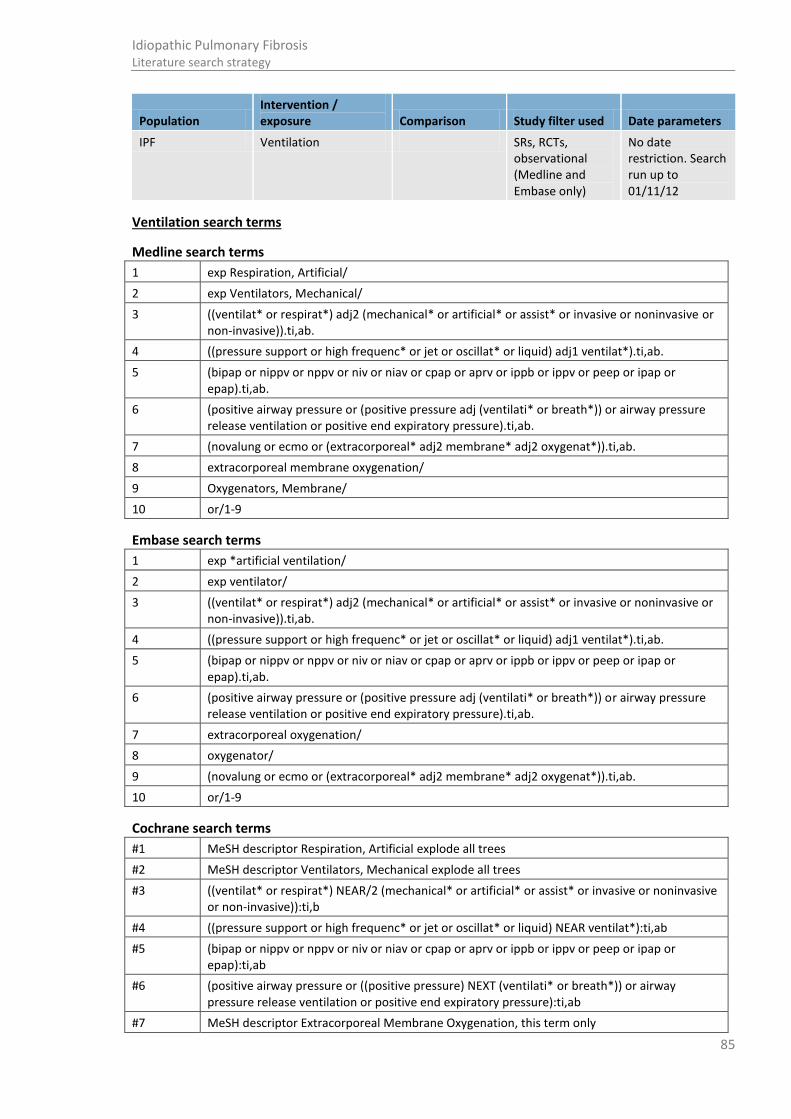
85
Idiopathic Pulmonary Fibrosis Literature search strategy
Population Intervention / exposure Comparison Study filter used Date parameters
IPF Ventilation SRs, RCTs, observational (Medline and Embase only)
No date restriction. Search run up to 01/11/12
Ventilation search terms
Medline search terms
1 exp Respiration, Artificial/
2 exp Ventilators, Mechanical/
3 ((ventilat* or respirat*) adj2 (mechanical* or artificial* or assist* or invasive or noninvasive or non-invasive)).ti,ab.
4 ((pressure support or high frequenc* or jet or oscillat* or liquid) adj1 ventilat*).ti,ab.
5 (bipap or nippv or nppv or niv or niav or cpap or aprv or ippb or ippv or peep or ipap or epap).ti,ab.
6 (positive airway pressure or (positive pressure adj (ventilati* or breath*)) or airway pressure release ventilation or positive end expiratory pressure).ti,ab.
7 (novalung or ecmo or (extracorporeal* adj2 membrane* adj2 oxygenat*)).ti,ab.
8 extracorporeal membrane oxygenation/
9 Oxygenators, Membrane/
10 or/1-9
Embase search terms
1 exp *artificial ventilation/
2 exp ventilator/
3 ((ventilat* or respirat*) adj2 (mechanical* or artificial* or assist* or invasive or noninvasive or non-invasive)).ti,ab.
4 ((pressure support or high frequenc* or jet or oscillat* or liquid) adj1 ventilat*).ti,ab.
5 (bipap or nippv or nppv or niv or niav or cpap or aprv or ippb or ippv or peep or ipap or epap).ti,ab.
6 (positive airway pressure or (positive pressure adj (ventilati* or breath*)) or airway pressure release ventilation or positive end expiratory pressure).ti,ab.
7 extracorporeal oxygenation/
8 oxygenator/
9 (novalung or ecmo or (extracorporeal* adj2 membrane* adj2 oxygenat*)).ti,ab.
10 or/1-9
Cochrane search terms
#1 MeSH descriptor Respiration, Artificial explode all trees
#2 MeSH descriptor Ventilators, Mechanical explode all trees
#3 ((ventilat* or respirat*) NEAR/2 (mechanical* or artificial* or assist* or invasive or noninvasive or non-invasive)):ti,b
#4 ((pressure support or high frequenc* or jet or oscillat* or liquid) NEAR ventilat*):ti,ab
#5 (bipap or nippv or nppv or niv or niav or cpap or aprv or ippb or ippv or peep or ipap or epap):ti,ab
#6 (positive airway pressure or ((positive pressure) NEXT (ventilati* or breath*)) or airway pressure release ventilation or positive end expiratory pressure):ti,ab
#7 MeSH descriptor Extracorporeal Membrane Oxygenation, this term only

86
Idiopathic Pulmonary Fibrosis Literature search strategy
#8 MeSH descriptor Oxygenators, Membrane, this term only
#9 (novalung or ecmo or (extracorporeal* NEAR/2 membrane* NEAR/2 oxygenat*)):ti,ab
#10 (#1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8 OR #9)
D.4 Economics search
Economic searches were conducted in Medline, Embase, HEED and CRD for NHS EED and HTA.
Population Intervention / exposure Comparison Study filter used Date parameters
ILD Economic, economic modelling, quality of life, disease progression (Medline and Embase only)
No date restriction. Search run up to 01/11/12.
Economic filter in Medline and Embase limited to 2010 - 01/11/12
CRD search terms
#1 MeSH DESCRIPTOR Lung Diseases, Interstitial EXPLODE ALL TREES WITH QUALIFIER undefined
#2 MeSH DESCRIPTOR Pulmonary Fibrosis EXPLODE ALL TREES WITH QUALIFIER undefined
#3 (interstitial near pneumonia*) IN NHSEED, HTA
#4 (interstitial near lung disease*) IN NHSEED, HTA
#5 (pulmonary near fibros*) IN NHSEED, HTA
#6 (alveoliti* ) IN NHSEED, HTA
#7 #1 OR #2 OR #3 OR #4 OR #5 OR #6
HEED search terms
1 ax=interstitial
2 ax=pulmonary AND fibros*
3 ax=alveoliti*
4 ax=Pneumoconiosis
5 ax=Pneumonitis
6 ax=Sarcoidosis
7 ax=Wegener Granulomatosis
8 ax=lung AND fibros*
9 ax=organizing AND pneumonia
10 cs=1 or 2 or 3 or 4 or 5 or 6 or 7 or 8

87
Idiopathic Pulmonary Fibrosis Forest plots
Appendix E: Forest plots
E.1 Diagnosis
The data from these studies were not meta- analysable therefore forest plots for these outcomes could not be provided; see the clinical evidence profile and the evidence tables for further information
E.2 Prognosis
Note: For graphical purposes only, results have been presented in forest plots.
• Only the results of the multivariable analysis have been reported in evidence tables and included in the final analysis.
• Inversed hazard ratios were calculated to present declines of PFT measures/ predicted values
• Hazard ratios were also calculated per 5% decline for FVC and per 10% decline for DLCO
(See Appendix I for calculations of standard errors from hazard ratios, risk ratios and odds ratios)
Please note evidence from the same dataset was used for DuBois201118, Dubois2011A117 and DuBois2011B121,
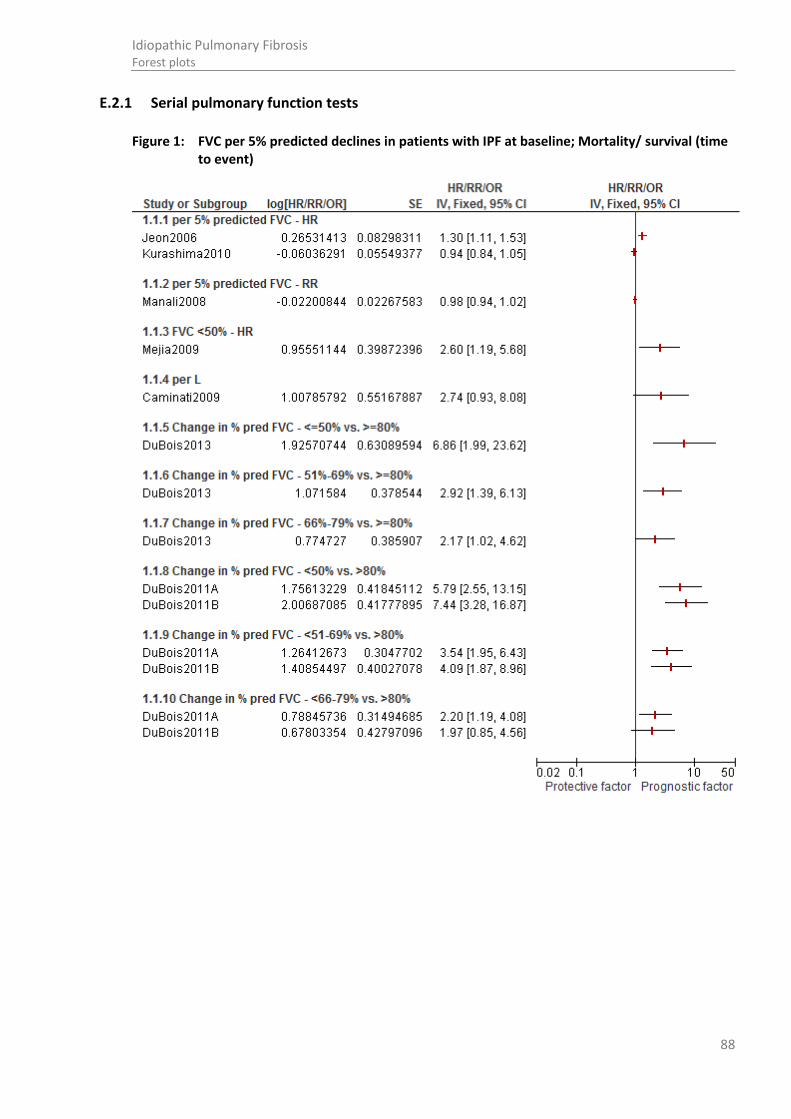
88
Idiopathic Pulmonary Fibrosis Forest plots
E.2.1 Serial pulmonary function tests
Figure 1: FVC per 5% predicted declines in patients with IPF at baseline; Mortality/ survival (time to event)

89
Idiopathic Pulmonary Fibrosis Forest plots
Figure 2: Relative declines in mortality/survival (time to event)
Figure 3: DLCO per 10% predicted declines in patients with IPF at baseline; Mortality/ survival (time to event)
Study or Subgroup
1.5.11 FVC at 12 months - >/=5% predicted decline
Richeldi 2012
1.5.12 FVC at 12 months - >/=10% predicted decline
Richeldi 2012
1.5.13 FVC at 12 months - >/=15% predicted decline
Richeldi 2012
log[HR/RR/OR]
0.47623418
1.01160091
1.1568812
SE
0.30309118
0.32256027
0.43004086
IV, Fixed, 95% CI
1.61 [0.89, 2.92]
2.75 [1.46, 5.17]
3.18 [1.37, 7.39]
HR/RR/OR HR/RR/OR
IV, Fixed, 95% CI
0.01 0.1 1 10 100Protective factor Prognostic factor
Study or Subgroup
1.3.2 per mL/min/Hgmm
Caminati2009
1.3.3 Low DLCO <40% - RR
Hamada2007
1.3.9 per 10% predicted DLCO - HR
Jeon2006
Kurashima2010
Lynch 2005
Mogulkoc 2001A
log[HR/RR/OR]
0.32434606
0.99325177
0.40546511
-0.1308524
0.61875404
0.43951888
SE
0.14142561
0.31352027
0.02219678
0.08017044
0.21723931
0.15724058
IV, Fixed, 95% CI
1.38 [1.05, 1.82]
2.70 [1.46, 4.99]
1.50 [1.44, 1.57]
0.88 [0.75, 1.03]
1.86 [1.21, 2.84]
1.55 [1.14, 2.11]
HR/RR/OR HR/RR/OR
IV, Fixed, 95% CI
0.2 0.5 1 2 5Protective factor Prognostic factor

90
Idiopathic Pulmonary Fibrosis Forest plots
Figure 4: Absolute declines in FVC in patients with IPF; Mortality/ survival (time to event)

91
Idiopathic Pulmonary Fibrosis Forest plots
Figure 5: Absolute declines in DLCO in patients with IPF; mortality/ survival (time to event)
Figure 6: Baseline oxygen saturation in patients with IPF; mortality/ survival (time to event)
Figure 7: Absolute change in oxygen saturation at 12 months; mortality/ survival (time to event)
Study or Subgroup
1.4.1 DLCO at 6 months - -15% vs. -10%
Schmidt2011
1.4.6 DLCO at 6 months - -20% vs. -10%
Schmidt2011
1.4.7 DLCO at 6 months - -25% vs. -10%
Schmidt2011
1.4.8 DLCO at 12 months - -15% vs. -10%
Schmidt2011
1.4.12 DLCO at 12 months - -20% vs. -10%
Schmidt2011
1.4.13 DLCO at 12 months - -25% vs. -10%
Schmidt2011
1.4.14 per 10% predicted DLCO over 12 months
Caminati2009
1.4.16 per 10% predicted DLCO over 2yrs
Mogulkoc 2001A
log[HR/RR/OR]
0.47000363
0.58778666
0.83290912
0.83290912
1.09861229
1.25276297
0.71334989
0.80126044
SE
0.20943381
0.25594442
0.31958239
0.2303234
0.25547157
0.2844749
0.38173088
0.34507145
IV, Fixed, 95% CI
1.60 [1.06, 2.41]
1.80 [1.09, 2.97]
2.30 [1.23, 4.30]
2.30 [1.46, 3.61]
3.00 [1.82, 4.95]
3.50 [2.00, 6.11]
2.04 [0.97, 4.31]
2.23 [1.13, 4.38]
HR/RR/OR HR/RR/OR
IV, Fixed, 95% CI
0.1 0.2 0.5 1 2 5 10Protective factor Prognostic factor
Study or Subgroup
2.1.1 Multivariable analysis O2 Sat - continuous HR
Caminati2009
Hallstrand2005
log[HR/ OR/ RR]
-0.20334092
0.05826891
SE
0.21369252
0.12784192
IV, Fixed, 95% CI
0.82 [0.54, 1.24]
1.06 [0.83, 1.36]
HR/ OR/ RR HR/ OR/ RR
IV, Fixed, 95% CI
0.5 0.7 1 1.5 2Protective factor Prognostic factor
Study or Subgroup
2.2.1 Multivariable analysis O2 Sat at 12 months vs. baseline
Caminati2009
log[HR/ OR/ RR]
-1.38629436
SE
0.61539183
IV, Fixed, 95% CI
0.25 [0.07, 0.84]
HR/ OR/ RR HR/ OR/ RR
IV, Fixed, 95% CI
0.05 0.2 1 5 20Protective factor Prognostic factor

92
Idiopathic Pulmonary Fibrosis Forest plots
Figure 8: Percentage predicted decline in FVC (5-10%) adjusted for DLCO compared to stable disease in patients with IPF; progression free survival
E.2.2 Sub maximal exercise testing
Figure 9: Baseline 6MWD: mortality
Figure 10: Serial change in 6MWD: mortality
E.2.3 Echocardiography
Figure 11: Baseline pulmonary arterial pressure: mortality
Study or Subgroup
Zappala2010
log[HR/ OR/ RR]
0.94000726
SE
0.33499288
IV, Fixed, 95% CI
2.56 [1.33, 4.94]
HR/ OR/ RR HR/ OR/ RR
IV, Fixed, 95% CI
0.2 0.5 1 2 5Protective factor Prognostic factor
Study or Subgroup
1.1.2 Multivariable analysis ESPAP >75mmHg - HR
Mejia 2009
log[HR/RR/OR]
0.81093
SE
0.35704
IV, Fixed, 95% CI
2.25 [1.12, 4.53]
HR/RR/OR HR/RR/OR
IV, Fixed, 95% CI
0.1 0.2 0.5 1 2 5 10
Protective factor Prognostic factor

93
Idiopathic Pulmonary Fibrosis Forest plots
E.2.4 HRCT scores
Figure 12: Baseline HRCT features: mortality
Study or Subgroup
1.1.1 Multivariable analysis kurtosis-OR
Best2008
1.1.2 Multivariable analysis fibrosis - OR
Best2008
1.1.3 fibrosis score- multivariable analysis
Lynch 2005
1.1.4 fibrosis score- multivariable analysis
Mogulkoc 2001A
1.1.11 Multivariable analysis: traction bronchiectasis
Sumikawa 2008
1.1.12 Multivariable analysis: fibrosis score
Sumikawa 2008
log[HR/RR/OR]
-0.54645
0.09894
0.996949
0.726098
0.262364
0.09531
SE
0.302875
0.041534
0.265024
0.208866
0.04902
0.036835
IV, Fixed, 95% CI
0.58 [0.32, 1.05]
1.10 [1.02, 1.20]
2.71 [1.61, 4.56]
2.07 [1.37, 3.11]
1.30 [1.18, 1.43]
1.10 [1.02, 1.18]
HR/RR/OR HR/RR/OR
IV, Fixed, 95% CI
0.1 0.2 0.5 1 2 5 10
Protective factor Prognostic factor
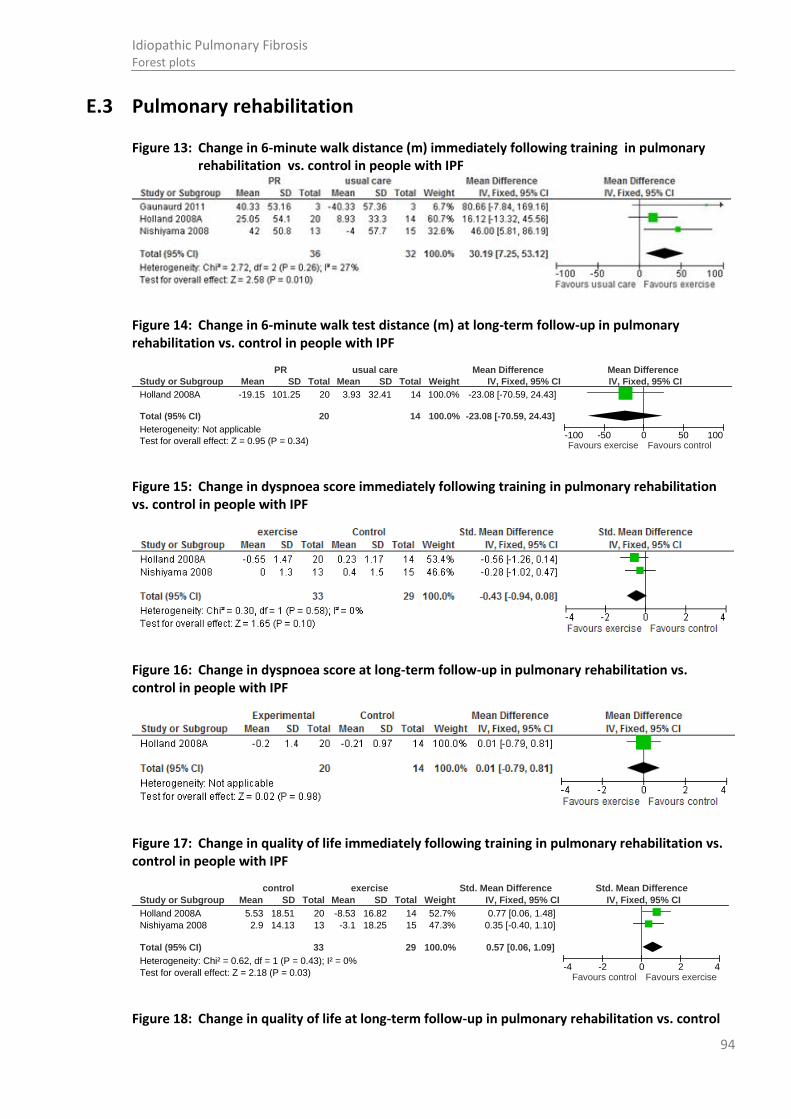
94
Idiopathic Pulmonary Fibrosis Forest plots
E.3 Pulmonary rehabilitation
Figure 13: Change in 6-minute walk distance (m) immediately following training in pulmonary rehabilitation vs. control in people with IPF
Figure 14: Change in 6-minute walk test distance (m) at long-term follow-up in pulmonary rehabilitation vs. control in people with IPF
Figure 15: Change in dyspnoea score immediately following training in pulmonary rehabilitation vs. control in people with IPF
Figure 16: Change in dyspnoea score at long-term follow-up in pulmonary rehabilitation vs. control in people with IPF
Figure 17: Change in quality of life immediately following training in pulmonary rehabilitation vs. control in people with IPF
Figure 18: Change in quality of life at long-term follow-up in pulmonary rehabilitation vs. control
Study or Subgroup
Holland 2008A
Total (95% CI)
Heterogeneity: Not applicable
Test for overall effect: Z = 0.95 (P = 0.34)
Mean
-19.15
SD
101.25
Total
20
20
Mean
3.93
SD
32.41
Total
14
14
Weight
100.0%
100.0%
IV, Fixed, 95% CI
-23.08 [-70.59, 24.43]
-23.08 [-70.59, 24.43]
PR usual care Mean Difference Mean Difference
IV, Fixed, 95% CI
-100 -50 0 50 100Favours exercise Favours control
Study or Subgroup
Holland 2008A
Nishiyama 2008
Total (95% CI)
Heterogeneity: Chi² = 0.62, df = 1 (P = 0.43); I² = 0%
Test for overall effect: Z = 2.18 (P = 0.03)
Mean
5.53
2.9
SD
18.51
14.13
Total
20
13
33
Mean
-8.53
-3.1
SD
16.82
18.25
Total
14
15
29
Weight
52.7%
47.3%
100.0%
IV, Fixed, 95% CI
0.77 [0.06, 1.48]
0.35 [-0.40, 1.10]
0.57 [0.06, 1.09]
control exercise Std. Mean Difference Std. Mean Difference
IV, Fixed, 95% CI
-4 -2 0 2 4Favours control Favours exercise

95
Idiopathic Pulmonary Fibrosis Forest plots
in people with IPF
Figure 19: Six month survival in pulmonary rehabilitation vs. control in people with IPF
Figure 20: QoL: SF36 domain: physical functioning score immediately following training in pulmonary rehabilitation vs. usual care in people with IPF
Figure 21: QoL: SF36 domain: physical role functioning score immediately following training in pulmonary rehabilitation vs. usual care in people with IPF
Figure 22: QoL: SF36 domain: vitality score immediately following training in pulmonary rehabilitation vs. usual care in people with IPF
Figure 23: QoL: SF36 domain: bodily pain score immediately following training in pulmonary rehabilitation vs. usual care in people with IPF
Study or Subgroup
Holland 2008A
Total (95% CI)
Heterogeneity: Not applicable
Test for overall effect: Z = 0.90 (P = 0.37)
Mean
-3.06
SD
29.49
Total
20
20
Mean
-10.11
SD
15.79
Total
14
14
Weight
100.0%
100.0%
IV, Fixed, 95% CI
7.05 [-8.29, 22.39]
7.05 [-8.29, 22.39]
Experimental Control Mean Difference Mean Difference
IV, Fixed, 95% CI
-50 -25 0 25 50Favours control Favours exercise
Study or Subgroup
Holland 2008A
Total (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.38 (P = 0.70)
Events
2
2
Total
20
20
Events
2
2
Total
14
14
Weight
100.0%
100.0%
M-H, Fixed, 95% CI
0.70 [0.11, 4.39]
0.70 [0.11, 4.39]
PR usual care Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.005 0.1 1 10 200Favours PR Favours usual care
Study or Subgroup
Holland 2008A
Total (95% CI)
Heterogeneity: Not applicable
Test for overall effect: Z = 1.50 (P = 0.13)
Mean
45.56
SD
23.63
Total
30
30
Mean
36.67
SD
21.17
Total
27
27
Weight
100.0%
100.0%
IV, Fixed, 95% CI
8.89 [-2.74, 20.52]
8.89 [-2.74, 20.52]
PR Usual care Mean Difference Mean Difference
IV, Fixed, 95% CI
-100 -50 0 50 100Favours PR Favours usual care
Study or Subgroup
Holland 2008A
Total (95% CI)
Heterogeneity: Not applicable
Test for overall effect: Z = 0.09 (P = 0.93)
Mean
24.07
SD
39.52
Total
30
30
Mean
25
SD
36.69
Total
27
27
Weight
100.0%
100.0%
IV, Fixed, 95% CI
-0.93 [-20.72, 18.86]
-0.93 [-20.72, 18.86]
PR Usual care Mean Difference Mean Difference
IV, Fixed, 95% CI
-100 -50 0 50 100Favours PR Favours usual care
Study or Subgroup
Holland 2008A
Total (95% CI)
Heterogeneity: Not applicable
Test for overall effect: Z = 1.94 (P = 0.05)
Mean
52.31
SD
17.79
Total
30
30
Mean
42.04
SD
21.76
Total
27
27
Weight
100.0%
100.0%
IV, Fixed, 95% CI
10.27 [-0.12, 20.66]
10.27 [-0.12, 20.66]
PR Usual care Mean Difference Mean Difference
IV, Fixed, 95% CI
-100 -50 0 50 100Favours PR Favours usual care
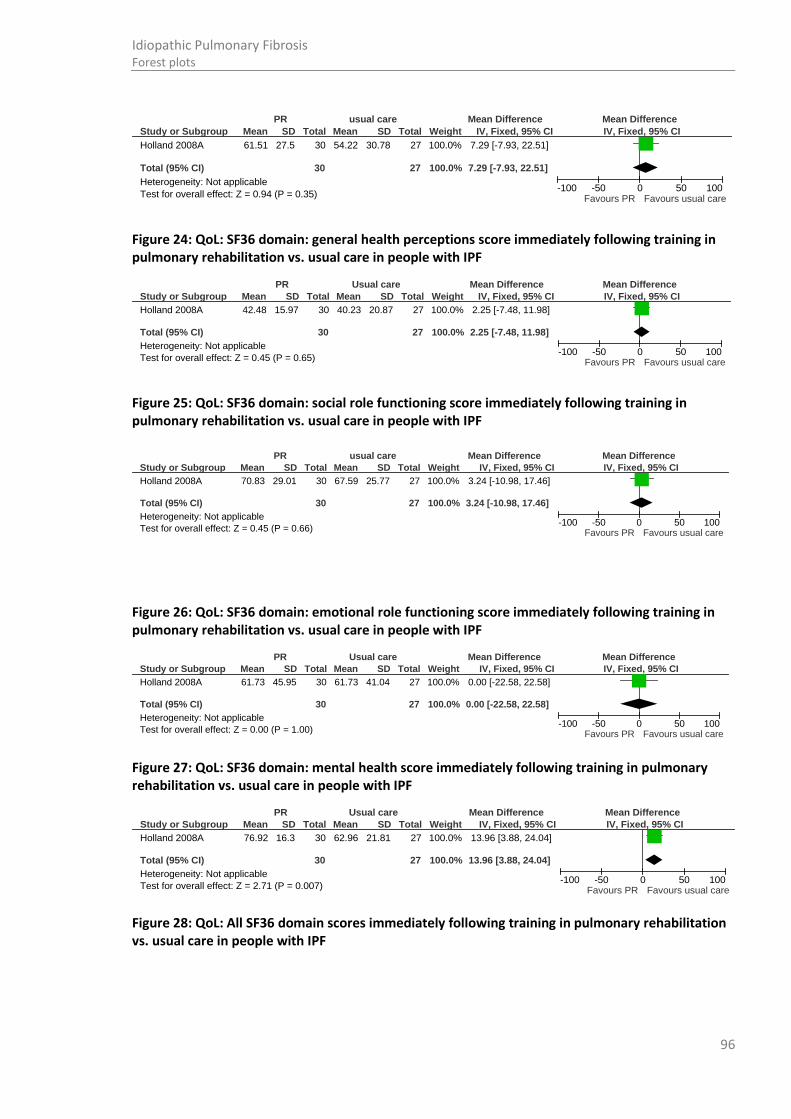
96
Idiopathic Pulmonary Fibrosis Forest plots
Figure 24: QoL: SF36 domain: general health perceptions score immediately following training in pulmonary rehabilitation vs. usual care in people with IPF
Figure 25: QoL: SF36 domain: social role functioning score immediately following training in pulmonary rehabilitation vs. usual care in people with IPF
Figure 26: QoL: SF36 domain: emotional role functioning score immediately following training in pulmonary rehabilitation vs. usual care in people with IPF
Figure 27: QoL: SF36 domain: mental health score immediately following training in pulmonary rehabilitation vs. usual care in people with IPF
Figure 28: QoL: All SF36 domain scores immediately following training in pulmonary rehabilitation vs. usual care in people with IPF
Study or Subgroup
Holland 2008A
Total (95% CI)
Heterogeneity: Not applicable
Test for overall effect: Z = 0.94 (P = 0.35)
Mean
61.51
SD
27.5
Total
30
30
Mean
54.22
SD
30.78
Total
27
27
Weight
100.0%
100.0%
IV, Fixed, 95% CI
7.29 [-7.93, 22.51]
7.29 [-7.93, 22.51]
PR usual care Mean Difference Mean Difference
IV, Fixed, 95% CI
-100 -50 0 50 100Favours PR Favours usual care
Study or Subgroup
Holland 2008A
Total (95% CI)
Heterogeneity: Not applicable
Test for overall effect: Z = 0.45 (P = 0.65)
Mean
42.48
SD
15.97
Total
30
30
Mean
40.23
SD
20.87
Total
27
27
Weight
100.0%
100.0%
IV, Fixed, 95% CI
2.25 [-7.48, 11.98]
2.25 [-7.48, 11.98]
PR Usual care Mean Difference Mean Difference
IV, Fixed, 95% CI
-100 -50 0 50 100Favours PR Favours usual care
Study or Subgroup
Holland 2008A
Total (95% CI)
Heterogeneity: Not applicable
Test for overall effect: Z = 0.45 (P = 0.66)
Mean
70.83
SD
29.01
Total
30
30
Mean
67.59
SD
25.77
Total
27
27
Weight
100.0%
100.0%
IV, Fixed, 95% CI
3.24 [-10.98, 17.46]
3.24 [-10.98, 17.46]
PR usual care Mean Difference Mean Difference
IV, Fixed, 95% CI
-100 -50 0 50 100Favours PR Favours usual care
Study or Subgroup
Holland 2008A
Total (95% CI)
Heterogeneity: Not applicable
Test for overall effect: Z = 0.00 (P = 1.00)
Mean
61.73
SD
45.95
Total
30
30
Mean
61.73
SD
41.04
Total
27
27
Weight
100.0%
100.0%
IV, Fixed, 95% CI
0.00 [-22.58, 22.58]
0.00 [-22.58, 22.58]
PR Usual care Mean Difference Mean Difference
IV, Fixed, 95% CI
-100 -50 0 50 100Favours PR Favours usual care
Study or Subgroup
Holland 2008A
Total (95% CI)
Heterogeneity: Not applicable
Test for overall effect: Z = 2.71 (P = 0.007)
Mean
76.92
SD
16.3
Total
30
30
Mean
62.96
SD
21.81
Total
27
27
Weight
100.0%
100.0%
IV, Fixed, 95% CI
13.96 [3.88, 24.04]
13.96 [3.88, 24.04]
PR Usual care Mean Difference Mean Difference
IV, Fixed, 95% CI
-100 -50 0 50 100Favours PR Favours usual care

97
Idiopathic Pulmonary Fibrosis Forest plots
E.4 Best supportive care
E.4.1 Oxygen management
Figure 29: Mortality (12 months) in patients receiving oxygen vs. air in people with IPF
Figure 30: Mortality (24 months) in patients receiving oxygen vs. air in people with IPF
Figure 31: Mortality (3 years) in patients receiving oxygen vs. air in people with IPF
Study or Subgroup
Holland2008A- PhysFx
Holland2008A-GenHealth
Holland2008A-MentalHealth
Holland2008A-Pain
Holland2008A-RoleEmot
Holland2008A-RolePhys
Holland2008A-SocialFx
Holland2008A-Vitality
Mean
45.56
42.48
76.92
61.51
61.73
24.07
70.83
52.31
SD
23.63
15.97
16.3
27.5
45.95
39.52
29.01
17.79
Total
30
30
30
30
30
30
30
30
Mean
36.67
40.23
62.96
54.22
61.73
25
67.59
42.04
SD
21.17
20.87
21.81
30.78
41.04
36.69
25.77
21.76
Total
27
27
27
27
27
27
27
27
IV, Fixed, 95% CI
8.89 [-2.74, 20.52]
2.25 [-7.48, 11.98]
13.96 [3.88, 24.04]
7.29 [-7.93, 22.51]
0.00 [-22.58, 22.58]
-0.93 [-20.72, 18.86]
3.24 [-10.98, 17.46]
10.27 [-0.12, 20.66]
PR Usual care Mean Difference Mean Difference
IV, Fixed, 95% CI
-50 -25 0 25 50Favours usual care Favours PR
Study or Subgroup
Crockett 2001
Total (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 1.17 (P = 0.24)
Events
7
7
Total
37
37
Events
8
8
Total
25
25
Weight
100.0%
100.0%
M-H, Fixed, 95% CI
0.59 [0.25, 1.42]
0.59 [0.25, 1.42]
Oxygen Air Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.2 0.5 1 2 5Favours oxygen Favours air
Study or Subgroup
Crockett 2001
Total (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 1.06 (P = 0.29)
Events
23
23
Total
37
37
Events
12
12
Total
25
25
Weight
100.0%
100.0%
M-H, Fixed, 95% CI
1.30 [0.80, 2.09]
1.30 [0.80, 2.09]
Oxygen Air Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.2 0.5 1 2 5Favours oxygen Favours air
Study or Subgroup
Crockett 2001
Total (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.02 (P = 0.99)
Events
34
34
Total
37
37
Events
23
23
Total
25
25
Weight
100.0%
100.0%
M-H, Fixed, 95% CI
1.00 [0.86, 1.16]
1.00 [0.86, 1.16]
Oxygen Air Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.2 0.5 1 2 5Favours oxygen Favours air

98
Idiopathic Pulmonary Fibrosis Forest plots
Figure 32: Arterial oxygen saturation in patients receiving oxygen vs. air in people with IPF immediately after treatment period
Figure 33: Dyspnoea (VAS) in patients receiving oxygen vs. air in people with IPF immediately after treatment period
E.4.2 Prednisolone for the palliation of cough
The data from these studies were not meta- analysable therefore forest plots for these outcomes could not be provided; see the clinical evidence profile and the evidence tables for further information.
E.4.3 Thalidomide for the palliation of cough
The data from these studies were not meta- analysable therefore forest plots for these outcomes could not be provide; see the clinical evidence profile and the evidence tables for further information.
E.4.4 Morphine for the palliation of breathlessness
The data from these studies were not meta- analysable therefore forest plots for these outcomes could not be provided; see the clinical evidence profile and the evidence tables for further information.
E.5 Pharmacological interventions
(See Appendix I for calculations of standard errors from hazard ratios, risk ratios and odds ratios)
Study or Subgroup
Swinburn 1991
Total (95% CI)
Heterogeneity: Not applicable
Test for overall effect: Z = 4.78 (P < 0.00001)
Mean
94.7
SD
2.85
Total
10
10
Mean
85.5
SD
5.38
Total
10
10
Weight
100.0%
100.0%
IV, Fixed, 95% CI
9.20 [5.43, 12.97]
9.20 [5.43, 12.97]
Oxygen Air Mean Difference Mean Difference
IV, Fixed, 95% CI
-20 -10 0 10 20Favours oxygen Favours air
Study or Subgroup
Swinburn 1991
Total (95% CI)
Heterogeneity: Not applicable
Test for overall effect: Z = 2.64 (P = 0.008)
Mean
30.2
SD
16.3
Total
10
10
Mean
48.1
SD
13.91
Total
10
10
Weight
100.0%
100.0%
IV, Fixed, 95% CI
-17.90 [-31.18, -4.62]
-17.90 [-31.18, -4.62]
Oxygen Air Mean Difference Mean Difference
IV, Fixed, 95% CI
-50 -25 0 25 50Favours oxygen Favours air
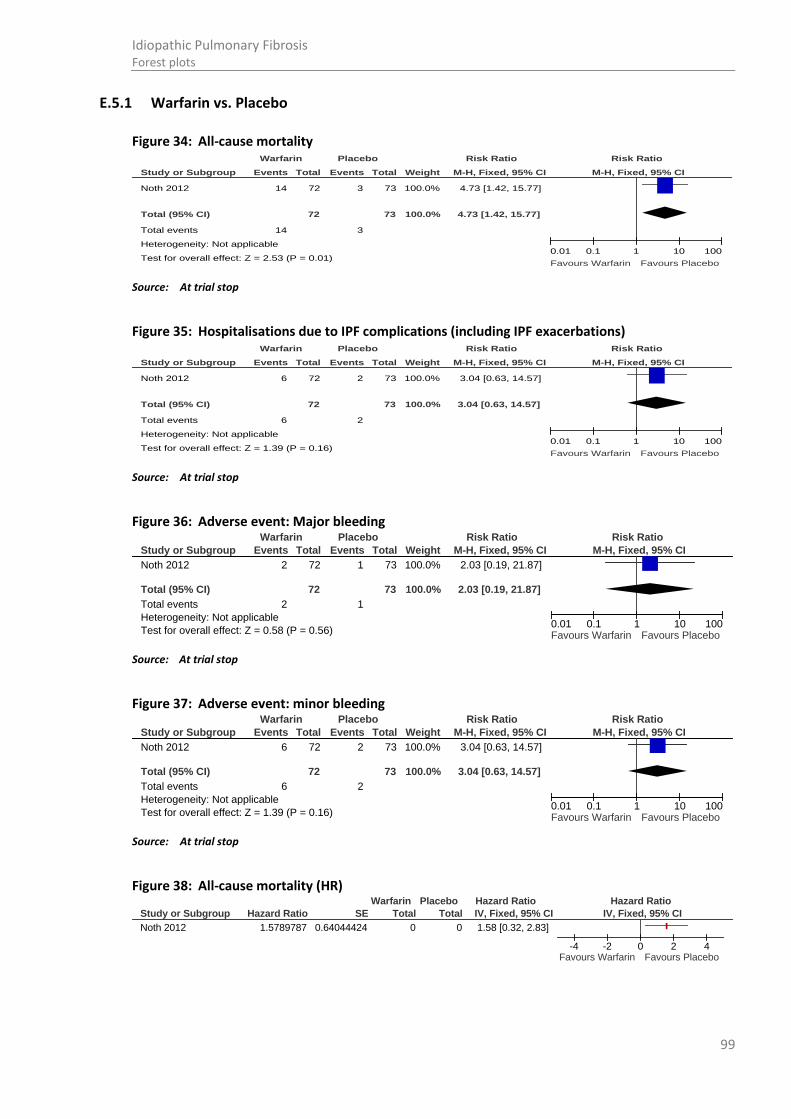
99
Idiopathic Pulmonary Fibrosis Forest plots
E.5.1 Warfarin vs. Placebo
Figure 34: All-cause mortality
Source: At trial stop
Figure 35: Hospitalisations due to IPF complications (including IPF exacerbations)
Source: At trial stop
Figure 36: Adverse event: Major bleeding
Source: At trial stop
Figure 37: Adverse event: minor bleeding
Source: At trial stop
Figure 38: All-cause mortality (HR)
Study or Subgroup
Noth 2012
Total (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 2.53 (P = 0.01)
Events
14
14
Total
72
72
Events
3
3
Total
73
73
Weight
100.0%
100.0%
M-H, Fixed, 95% CI
4.73 [1.42, 15.77]
4.73 [1.42, 15.77]
Warfarin Placebo Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.01 0.1 1 10 100
Favours Warfarin Favours Placebo
Study or Subgroup
Noth 2012
Total (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 1.39 (P = 0.16)
Events
6
6
Total
72
72
Events
2
2
Total
73
73
Weight
100.0%
100.0%
M-H, Fixed, 95% CI
3.04 [0.63, 14.57]
3.04 [0.63, 14.57]
Warfarin Placebo Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.01 0.1 1 10 100
Favours Warfarin Favours Placebo
Study or Subgroup
Noth 2012
Total (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.58 (P = 0.56)
Events
2
2
Total
72
72
Events
1
1
Total
73
73
Weight
100.0%
100.0%
M-H, Fixed, 95% CI
2.03 [0.19, 21.87]
2.03 [0.19, 21.87]
Warfarin Placebo Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.01 0.1 1 10 100Favours Warfarin Favours Placebo
Study or Subgroup
Noth 2012
Total (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 1.39 (P = 0.16)
Events
6
6
Total
72
72
Events
2
2
Total
73
73
Weight
100.0%
100.0%
M-H, Fixed, 95% CI
3.04 [0.63, 14.57]
3.04 [0.63, 14.57]
Warfarin Placebo Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.01 0.1 1 10 100Favours Warfarin Favours Placebo
Study or Subgroup
Noth 2012
Hazard Ratio
1.5789787
SE
0.64044424
Total
0
Total
0
IV, Fixed, 95% CI
1.58 [0.32, 2.83]
Warfarin Placebo Hazard Ratio Hazard Ratio
IV, Fixed, 95% CI
-4 -2 0 2 4Favours Warfarin Favours Placebo
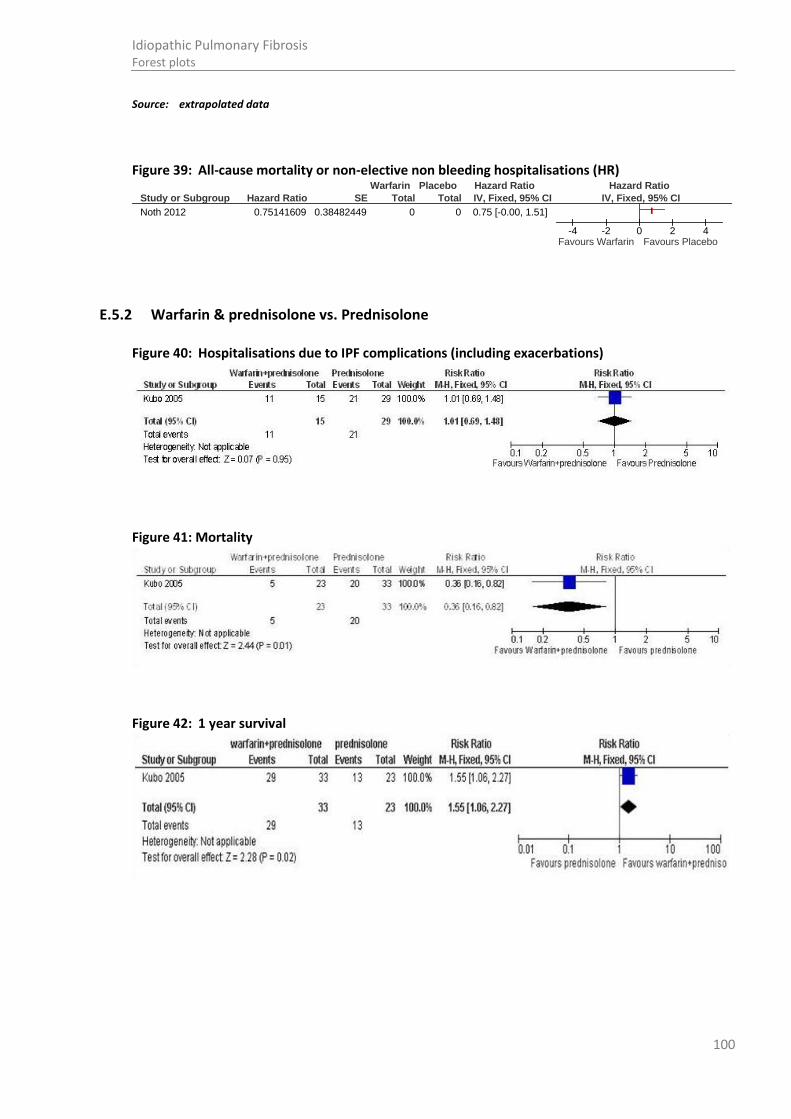
100
Idiopathic Pulmonary Fibrosis Forest plots
Source: extrapolated data
Figure 39: All-cause mortality or non-elective non bleeding hospitalisations (HR)
E.5.2 Warfarin & prednisolone vs. Prednisolone
Figure 40: Hospitalisations due to IPF complications (including exacerbations)
Figure 41: Mortality
Figure 42: 1 year survival
Study or Subgroup
Noth 2012
Hazard Ratio
0.75141609
SE
0.38482449
Total
0
Total
0
IV, Fixed, 95% CI
0.75 [-0.00, 1.51]
Warfarin Placebo Hazard Ratio Hazard Ratio
IV, Fixed, 95% CI
-4 -2 0 2 4Favours Warfarin Favours Placebo
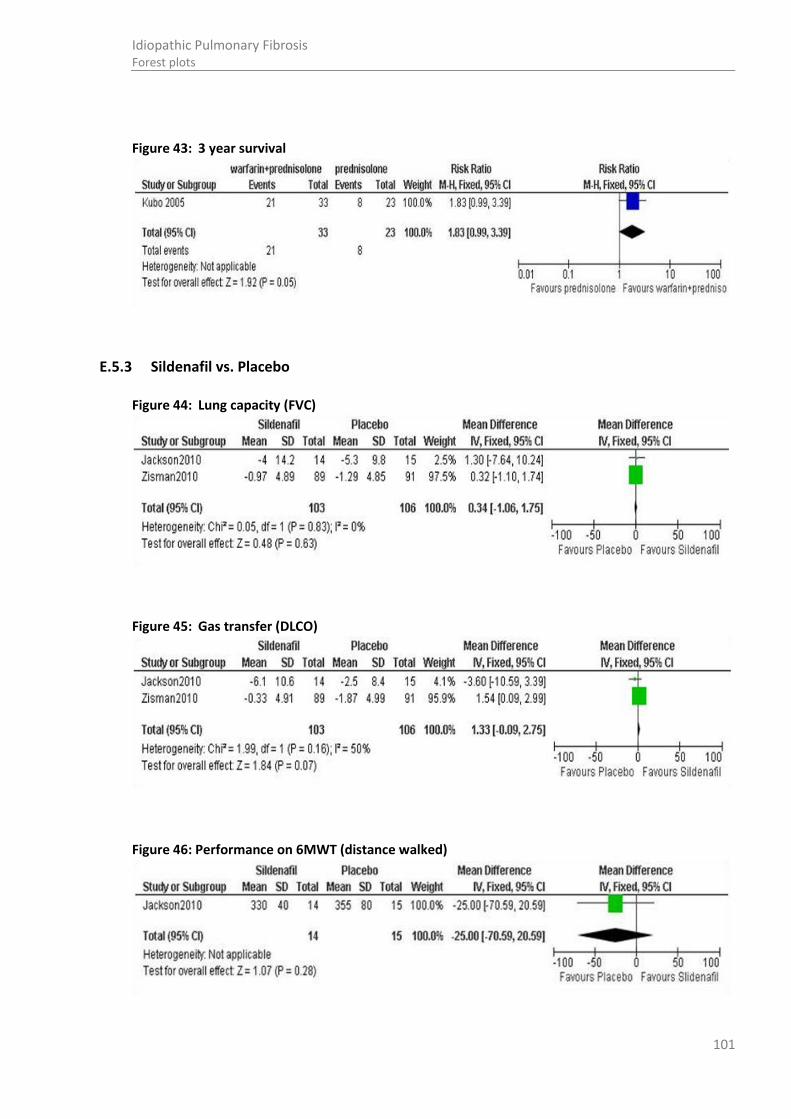
101
Idiopathic Pulmonary Fibrosis Forest plots
Figure 43: 3 year survival
E.5.3 Sildenafil vs. Placebo
Figure 44: Lung capacity (FVC)
Figure 45: Gas transfer (DLCO)
Figure 46: Performance on 6MWT (distance walked)

102
Idiopathic Pulmonary Fibrosis Forest plots
Figure 47: Mortality
Figure 48: Adverse events: chest pain/coronary artery disease
Figure 49: Adverse events: facial flushing
Figure 50: Adverse events: visual disturbance
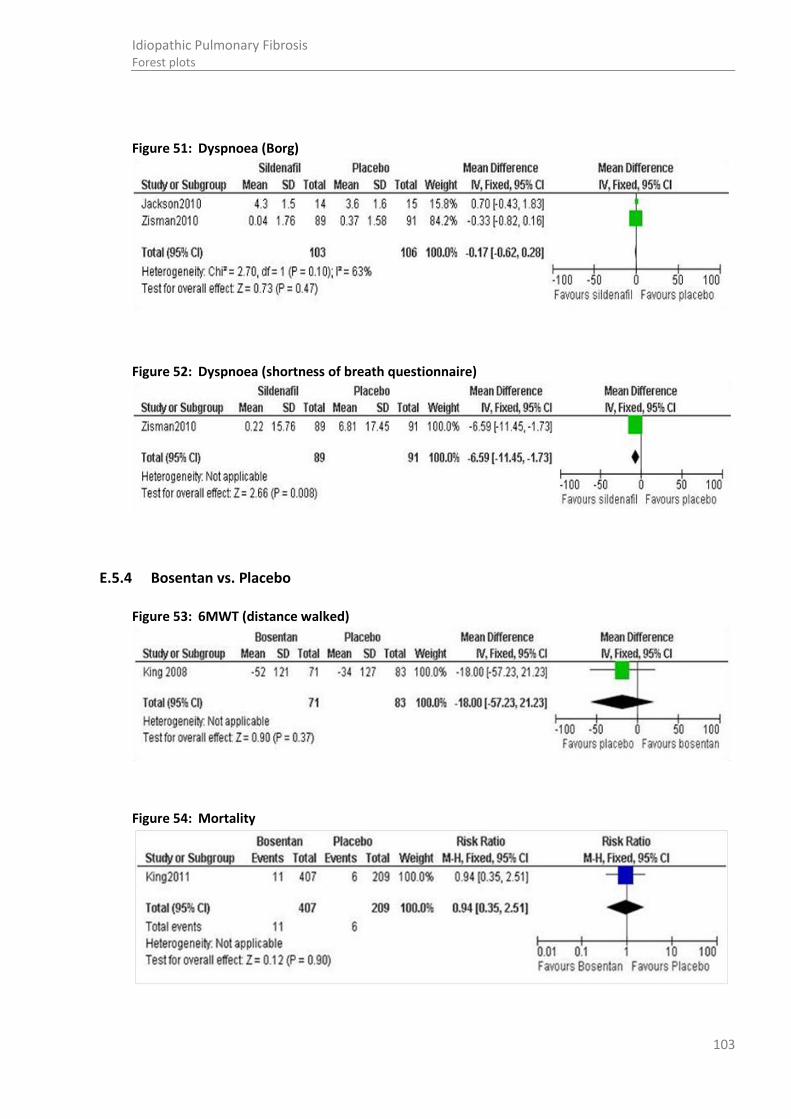
103
Idiopathic Pulmonary Fibrosis Forest plots
Figure 51: Dyspnoea (Borg)
Figure 52: Dyspnoea (shortness of breath questionnaire)
E.5.4 Bosentan vs. Placebo
Figure 53: 6MWT (distance walked)
Figure 54: Mortality

104
Idiopathic Pulmonary Fibrosis Forest plots
Figure 55: Adverse events (abnormal LFTs)
Figure 56: Adverse events (drug hypersensitivity)
Figure 57: Dyspnoea
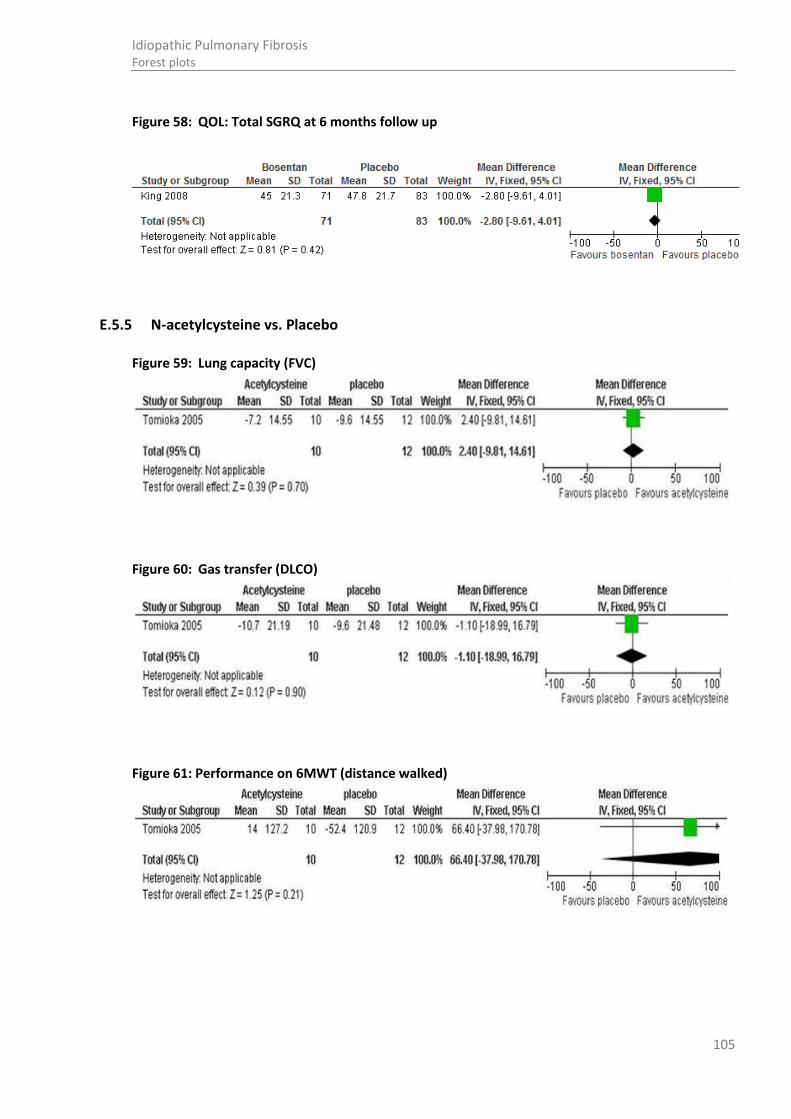
105
Idiopathic Pulmonary Fibrosis Forest plots
Figure 58: QOL: Total SGRQ at 6 months follow up
E.5.5 N-acetylcysteine vs. Placebo
Figure 59: Lung capacity (FVC)
Figure 60: Gas transfer (DLCO)
Figure 61: Performance on 6MWT (distance walked)

106
Idiopathic Pulmonary Fibrosis Forest plots
Figure 62: Performance on 6MWT (lowest SaO2)
Figure 63: QOL: SF36: Physical function
Figure 64: QOL: SF36: Physical role functioning
Figure 65: QOL: SF36: Vitality
Figure 66: QOL: SF36: Bodily pain

107
Idiopathic Pulmonary Fibrosis Forest plots
Figure 67: QOL: SF36: general health perceptions
Figure 68: QOL: SF36: Social role functioning
Figure 69: QOL: SF36: emotional role functioning
Figure 70: QOL: SF36: Mental health
E.5.6 N-acetylcysteine vs. no treatment
Figure 71: Lung capacity (FVC)

108
Idiopathic Pulmonary Fibrosis Forest plots
Figure 72: Hospitalisations due to IPF complications (including IPF exacerbations)
Figure 73: Dyspnoea
E.5.7 Co-trimoxazole vs. Placebo
Figure 74: Mortality (ITT)
Figure 75: Mortality (per-protocol)
Figure 76: Lung capacity: FVC (ml)
Study or Subgroup
Homma 2012
Total (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 1.22 (P = 0.22)
Events
1
1
Total
44
44
Events
4
4
Total
46
46
Weight
100.0%
100.0%
M-H, Fixed, 95% CI
0.26 [0.03, 2.25]
0.26 [0.03, 2.25]
NAC Placebo Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.01 0.1 1 10 100Favours NAC Favours Placebo
Study or Subgroup
Homma 2012
Total (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.33 (P = 0.74)
Events
33
33
Total
38
38
Events
32
32
Total
38
38
Weight
100.0%
100.0%
M-H, Fixed, 95% CI
1.03 [0.86, 1.24]
1.03 [0.86, 1.24]
NAC Placebo Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.01 0.1 1 10 100Favours NAC Favours Placebo

109
Idiopathic Pulmonary Fibrosis Forest plots
Figure 77: Lung capacity: FVC (% predicted)
Figure 78: Gas transfer: DLCO (mmol/min/KPa)
Figure 79: Gas transfer: DLCO % predicted
Figure 80: Health related quality of life: SGRQ total (units)
Figure 81: Performance on sub-maximal walk test: 6MWT (distance walked)

110
Idiopathic Pulmonary Fibrosis Forest plots
Figure 82: Performance on sub-maximal walk test: 6MWT (desaturation of 4% or more)
Figure 83: Dyspnoea: MRC score (units)
E.5.8 Ambrisentan vs. Placebo
Figure 84: Mortality
Figure 85: Decrease in lung function
E.5.9 Combination: Prednisolone & azathioprine vs. Prednisolone & placebo
Figure 86: Lung capacity (FVC)

111
Idiopathic Pulmonary Fibrosis Forest plots
Figure 87: Gas transfer (DLCO)
Figure 88: Mortality
Figure 89: Adverse events: elevated liver enzymes
Figure 90: Adverse events: infections
E.5.10 Combination: Prednisolone & azathioprine & n-acetylcysteine vs. Azathioprine & prednisolone

112
Idiopathic Pulmonary Fibrosis Forest plots
Figure 91: lung capacity (FVC)- Available case analysis
Figure 92: lung capacity (FVC)- Intention to treat analysis
Figure 93: gas transfer (DLCO)- Available case analysis
Figure 94: DLCO- Intention to treat analysis
Figure 95: Mortality (all cause)

113
Idiopathic Pulmonary Fibrosis Forest plots
Figure 96: Adverse events: abnormal liver function tests
E.5.11 Combination: Prednisolone & azathioprine & n-acetylcysteine vs. Placebo
Figure 97: All-cause mortality at trial stop
Source: At trial stop
Figure 98: Hospitalisations due to IPF exacerbations
Source: At trial stop
Figure 99: Adverse events (infections)
Source: At trial stop
Figure 100: Adverse events (GI)
Study or Subgroup
Panther 2012
Total (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 2.00 (P = 0.05)
Events
8
8
Total
77
77
Events
1
1
Total
78
78
Weight
100.0%
100.0%
M-H, Fixed, 95% CI
8.10 [1.04, 63.26]
8.10 [1.04, 63.26]
Pred, AZA and NAC Placebo Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.01 0.1 1 10 100Favours Pred, AZA and NAC Favours Placebo
Study or Subgroup
Panther 2012
Total (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 1.64 (P = 0.10)
Events
5
5
Total
77
77
Events
0
0
Total
78
78
Weight
100.0%
100.0%
M-H, Fixed, 95% CI
11.14 [0.63, 198.09]
11.14 [0.63, 198.09]
Pred, AZA and NAC Placebo Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.001 0.1 1 10 1000Favours Pred, AZA and NAC Favours Placebo
Study or Subgroup
Panther 2012
Total (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 1.50 (P = 0.13)
Events
5
5
Total
77
77
Events
1
1
Total
78
78
Weight
100.0%
100.0%
M-H, Fixed, 95% CI
5.06 [0.61, 42.36]
5.06 [0.61, 42.36]
Pred, AZA and NAC Placebo Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.01 0.1 1 10 100Favours Pred, AZA and NAC Favours Placebo
Study or Subgroup
Panther 2012
Total (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.95 (P = 0.34)
Events
1
1
Total
77
77
Events
3
3
Total
78
78
Weight
100.0%
100.0%
M-H, Fixed, 95% CI
0.34 [0.04, 3.18]
0.34 [0.04, 3.18]
Pred, AZA and NAC Placebo Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.01 0.1 1 10 100Favours Pred, AZA and NAC Favours Placebo
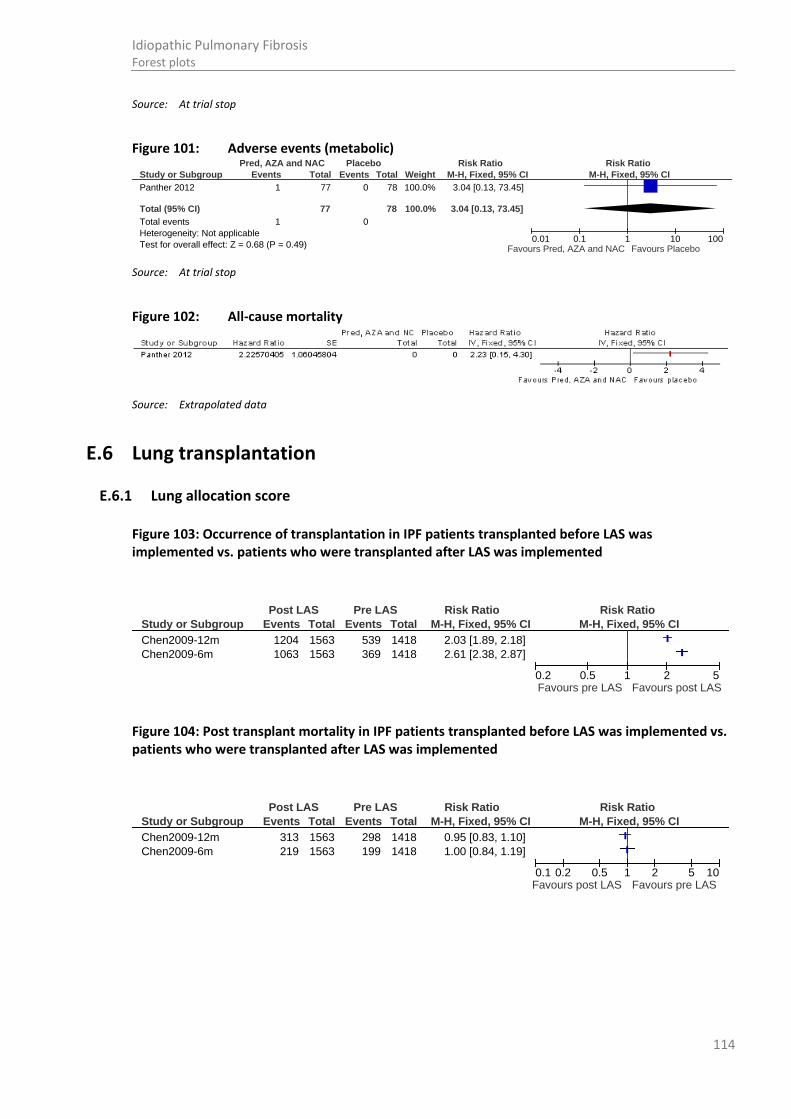
114
Idiopathic Pulmonary Fibrosis Forest plots
Source: At trial stop
Figure 101: Adverse events (metabolic)
Source: At trial stop
Figure 102: All-cause mortality
Source: Extrapolated data
E.6 Lung transplantation
E.6.1 Lung allocation score
Figure 103: Occurrence of transplantation in IPF patients transplanted before LAS was implemented vs. patients who were transplanted after LAS was implemented
Figure 104: Post transplant mortality in IPF patients transplanted before LAS was implemented vs. patients who were transplanted after LAS was implemented
Study or Subgroup
Panther 2012
Total (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.68 (P = 0.49)
Events
1
1
Total
77
77
Events
0
0
Total
78
78
Weight
100.0%
100.0%
M-H, Fixed, 95% CI
3.04 [0.13, 73.45]
3.04 [0.13, 73.45]
Pred, AZA and NAC Placebo Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.01 0.1 1 10 100Favours Pred, AZA and NAC Favours Placebo
Study or Subgroup
Chen2009-12m
Chen2009-6m
Events
1204
1063
Total
1563
1563
Events
539
369
Total
1418
1418
M-H, Fixed, 95% CI
2.03 [1.89, 2.18]
2.61 [2.38, 2.87]
Post LAS Pre LAS Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.2 0.5 1 2 5Favours pre LAS Favours post LAS
Study or Subgroup
Chen2009-12m
Chen2009-6m
Events
313
219
Total
1563
1563
Events
298
199
Total
1418
1418
M-H, Fixed, 95% CI
0.95 [0.83, 1.10]
1.00 [0.84, 1.19]
Post LAS Pre LAS Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.1 0.2 0.5 1 2 5 10Favours post LAS Favours pre LAS

115
Idiopathic Pulmonary Fibrosis Forest plots
Figure 105: Waiting list mortality in IPF patients transplanted before LAS was implemented vs. patients who were transplanted after LAS was implemented
Figure 106: 1 year survival in IPF patients transplanted before LAS was implemented vs. patients who were transplanted after LAS was implemented
Figure 107: 3 year survival in IPF patients transplanted before LAS was implemented vs. patients who were transplanted after LAS was implemented
Figure 108: Readmission <30 days in IPF patients transplanted before LAS was implemented vs. patients who were transplanted after LAS was implemented
Figure 109: Hospital mortality in IPF patients transplanted before LAS was implemented vs. patients who were transplanted after LAS was implemented
Study or Subgroup
Chen2009-12m
Chen2009-6m
Events
172
141
Total
1563
1563
Events
298
213
Total
1418
1418
M-H, Fixed, 95% CI
0.52 [0.44, 0.62]
0.60 [0.49, 0.73]
Post LAS Pre LAS Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.1 0.2 0.5 1 2 5 10Favours post LAS Favours pre LAS
Study or Subgroup
De Oliveira 2012
Total (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.69 (P = 0.49)
Events
27
27
Total
32
32
Events
28
28
Total
36
36
Weight
100.0%
100.0%
M-H, Fixed, 95% CI
1.08 [0.86, 1.36]
1.08 [0.86, 1.36]
Post LAS Pre LAS Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.1 0.2 0.5 1 2 5 10Favours post LAS Favours pre LAS
Study or Subgroup
De Oliveira 2012
Total (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.43 (P = 0.67)
Events
3
3
Total
4
4
Events
17
17
Total
26
26
Weight
100.0%
100.0%
M-H, Fixed, 95% CI
1.15 [0.61, 2.16]
1.15 [0.61, 2.16]
Post LAS Pre LAS Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.1 0.2 0.5 1 2 5 10Favours post LAS Favours pre LAS
Study or Subgroup
De Oliveira 2012
Total (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.28 (P = 0.78)
Events
11
11
Total
46
46
Events
7
7
Total
33
33
Weight
100.0%
100.0%
M-H, Fixed, 95% CI
1.13 [0.49, 2.60]
1.13 [0.49, 2.60]
Post LAS Pre LAS Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.1 0.2 0.5 1 2 5 10Favours post LAS Favours pre LAS
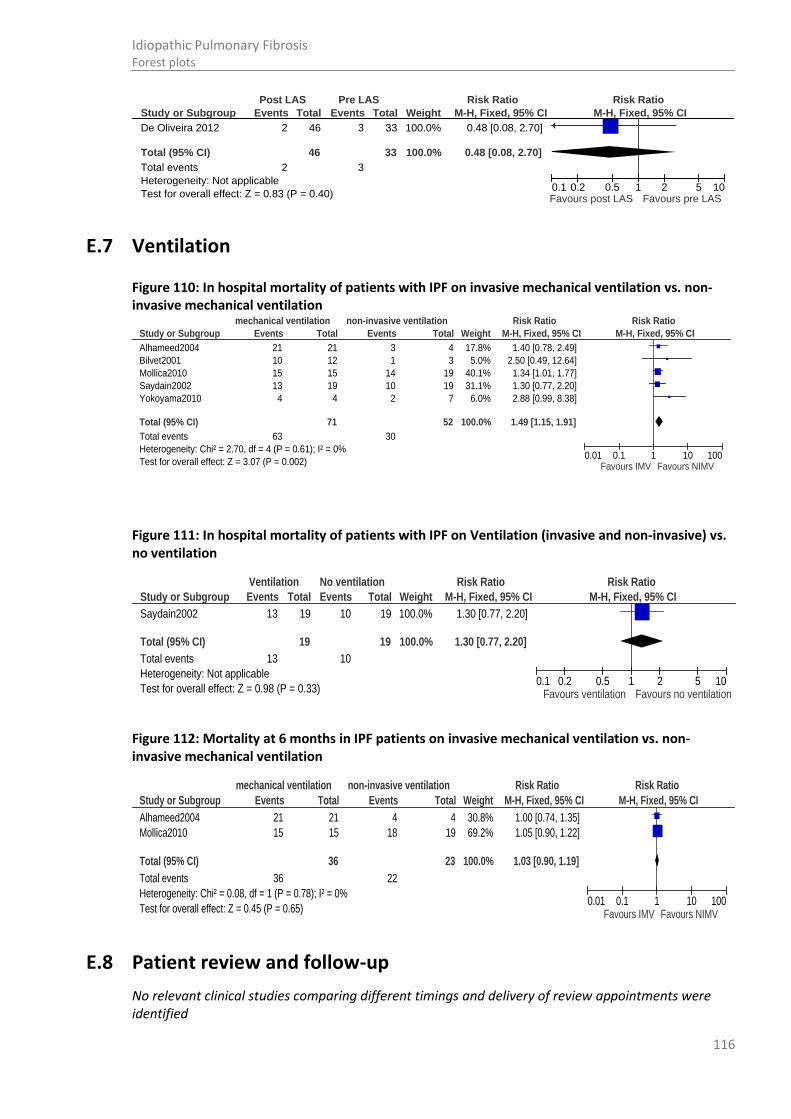
116
Idiopathic Pulmonary Fibrosis Forest plots
E.7 Ventilation
Figure 110: In hospital mortality of patients with IPF on invasive mechanical ventilation vs. non-invasive mechanical ventilation
Figure 111: In hospital mortality of patients with IPF on Ventilation (invasive and non-invasive) vs. no ventilation
Figure 112: Mortality at 6 months in IPF patients on invasive mechanical ventilation vs. non-invasive mechanical ventilation
E.8 Patient review and follow-up
No relevant clinical studies comparing different timings and delivery of review appointments were identified
Study or Subgroup
Alhameed2004
Bilvet2001
Mollica2010
Saydain2002
Yokoyama2010
Total (95% CI)
Total events
Heterogeneity: Chi² = 2.70, df = 4 (P = 0.61); I² = 0%
Test for overall effect: Z = 3.07 (P = 0.002)
Events
21
10
15
13
4
63
Total
21
12
15
19
4
71
Events
3
1
14
10
2
30
Total
4
3
19
19
7
52
Weight
17.8%
5.0%
40.1%
31.1%
6.0%
100.0%
M-H, Fixed, 95% CI
1.40 [0.78, 2.49]
2.50 [0.49, 12.64]
1.34 [1.01, 1.77]
1.30 [0.77, 2.20]
2.88 [0.99, 8.38]
1.49 [1.15, 1.91]
mechanical ventilation non-invasive ventilation Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.01 0.1 1 10 100Favours IMV Favours NIMV
Study or Subgroup
Saydain2002
Total (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.98 (P = 0.33)
Events
13
13
Total
19
19
Events
10
10
Total
19
19
Weight
100.0%
100.0%
M-H, Fixed, 95% CI
1.30 [0.77, 2.20]
1.30 [0.77, 2.20]
Ventilation No ventilation Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.1 0.2 0.5 1 2 5 10Favours ventilation Favours no ventilation
Study or Subgroup
Alhameed2004
Mollica2010
Total (95% CI)
Total events
Heterogeneity: Chi² = 0.08, df = 1 (P = 0.78); I² = 0%
Test for overall effect: Z = 0.45 (P = 0.65)
Events
21
15
36
Total
21
15
36
Events
4
18
22
Total
4
19
23
Weight
30.8%
69.2%
100.0%
M-H, Fixed, 95% CI
1.00 [0.74, 1.35]
1.05 [0.90, 1.22]
1.03 [0.90, 1.19]
mechanical ventilation non-invasive ventilation Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.01 0.1 1 10 100Favours IMV Favours NIMV
Study or Subgroup
De Oliveira 2012
Total (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.83 (P = 0.40)
Events
2
2
Total
46
46
Events
3
3
Total
33
33
Weight
100.0%
100.0%
M-H, Fixed, 95% CI
0.48 [0.08, 2.70]
0.48 [0.08, 2.70]
Post LAS Pre LAS Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.1 0.2 0.5 1 2 5 10Favours post LAS Favours pre LAS

117
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Appendix F: Clinical evidence tables
F.1 Diagnosis
F.1.1 Bronchoalveolar lavage
Table 17: Ohshimo 2009 365
Study
details
Population Methods Outcome measures Effect size Comments
Ohshimo 2009
365
Country of study: Germany
Study design:
retrospective
Setting: Ruhrlandklinik, Essen, Germany
Duration of follow-up:
NR
Patient group: suspected IPF on HRCT
Patient characteristics: mean (SD)
N: 101 (suspicious IPF based on HRCT findings)
Excluded:
17- no evidence of restriction
3- no impairment of gas exchange
5- evidence of collagen vascular disease- associated interstitial pneumonia or drug-induced pneumonia
2- lacked clinical history for IPF
N after exclusions: 74 (all had a clinical diagnosis of IPF according to ATS/ERS criteria)
M:F: 60:14
All patients
HRCT findings were evaluated by observers blinded to BAL results and other clinical data.
Intervention: BAL
Final diagnosis IPF 68
NSIP 3
EAA 3
Funding: Arbeitsgemeinscaft zur Foderung der Pneumologie an der Ruhrlandklinik (AFPR)
Limitations:
Concurrent medication use
Additional outcomes: BAL findings
Notes:
Year: 2003-2007
Change in diagnosis after BAL
6/74

118
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Study
details
Population Methods Outcome measures Effect size Comments
Age: 69 (8)
Smoking status, current/ex/ non: 4/40/29
Duration of symptoms before diagnosis, years: 3.2 (4.5)
Relevant concomitant medications, n (%):
Corticosteroids and/ or immunosuppressants: 17 (23)
Oxygen use: 7 (9)
Inclusion criteria: criteria recommended in 2002 ATS/ERS consensus statement
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon monoxide diffusing capacity , IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 6MWT= 6 minute walking test RBILD/ DIP= respiratory bronchiolitis interstitial lung disease/ desquamative interstitial pneumonia, UIP= usual interstitial pneumonia, NSIP= non-specific interstitial pneumonia
F.1.2 Transbronchial biopsy/ surgical lung biopsy
Table 18: Aalokken 20126
Study
details
Population Methods Outcome measures Effect size Comments
Aalokken 2012
6
Setting: regional and
Patient group: clinical suspicion of ILD who had undergone both HRCT and SLB
Inclusion criteria:
All patients underwent SLB (open thoracotomy or thoracoscopy) and thin-section CT.
Histological diagnosis Funding: NR
Limitations:
details of clinical information known to
Sensitivity 73%
Specificity 74%
PPV 83%
NPV 61%

119
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Study
details
Population Methods Outcome measures Effect size Comments
national centre for chronic lung diseases, Norway 1992-2007
Duration of follow-up: 3-17 years (range), 7.2 (median)
Design: retrospective cohort
CT examinations were judged to be consistent
The lung disease was not associated with connective tissue disease, environmental exposure and/ or drug toxicity
Exclusion criteria:
Histopathologic specimens not available or of suboptimal quality
All patients n=91 initially, n=64 had a composite reference diagnosis established and were included in the analysis.
M/F: 49/42
Mean age: 53.2 years, range 23-79
Follow up: 3-17 years (range), 7.2 (median)
Criteria for CT
Images were reviewed separately and in random order by two chest radiologists. Observers were blinded to clinical information and histological diagnosis. CT features were classified according to the Nomenclature Committee of the Fleischner Society.
Criteria for histopathology
Specimens were retrospectively studied by light microscopy in consensus by two experienced lung pathologists who were blinded to clinical and radiological features. Classification was according to ATS criteria.
A composite reference standard was used to
reviewers unclear
Additional outcomes:
Inter-observer variation for the evaluation of first choice HRCT diagnosis
Inter-observer variation for the extent of HRCT abnormalities
Thin section CT readings, comparison between UIP and non-UIP patients
Sensitivity, specificity, PPV and NPV of CT diagnosis
Notes:
During the follow-up period 45 patients died and 5 patients underwent lung transplantation due to respiratory failure
MDT consisted of a pulmonologist and a radiologist.
Consensus CT reading
Overall correct diagnosis
37/64 (58%), including 26 (63%) in people with UIP
Histological consensus (correct diagnosis)
34/64 (53%), including 30 (73%) cases of UIP
Diagnostic yield (histology)
64 people with IIP
TP 30/64 (73%)
TN 4/64
FP 6/64
FN unclear

120
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Study
details
Population Methods Outcome measures Effect size Comments
provide an overall clinical diagnosis at the end of the study. A multidisciplinary team (pulmonologist and a radiologist). The team was blinded to the results of the retrospective review of the initial thin-section CT scans and retrospective histological evaluation made for the purpose of this study.
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon monoxide diffusing capacity , IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 6MWT= 6 minute walking test RBILD/ DIP= respiratory bronchiolitis interstitial lung disease/ desquamative interstitial pneumonia, UIP= usual interstitial pneumonia, NSIP= non-specific interstitial pneumonia
Table 19: Coutinho 2008 89
Study
details
Population Methods Outcome measures Effect size Comments
Coutinho 2008
89
Country of study: Portugal
Patient group: diffuse parenchymal lung disease (DPLD)
Exclusion criteria:
NR
Patient characteristics: mean (SD)
N: 120
All patients
Previous investigations included:
Clinical assessment
CXR/ CT/ HRCT
Bronchoscopic exam and
Mortality 0 Funding: NR
Limitations:
Retrospective study- difficult to know the real accuracy of the
Diagnosis IIP 42
Hypersensitivity pneumonitis 21
Pneumoconiosis 18
Sarcoidosis 16
Organizing pneumonia 5

121
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Study
details
Population Methods Outcome measures Effect size Comments
Study design:
Retrospective review
Who was blinded: no- one
Setting:
Centre of Cardiothoracic Surgery, University Hospital, Coimbra, Portugal
Duration of follow-up:
NR
Age: 55.8 (14.0) range 17-77
M:F: 50:50
Smoking status (%): 37.5
Immunosuppressed (%): 30.8
Symptomatic (%): 67.5
related procedures (BAL/ TBB)
Microbiology culture
Intervention:
SLB (VATS/ OLB)
Respiratory bronchiolitis 5
Connective tissue associated 4
Amiodarone associated 3
Histiocytosis 2
Eosinophilic pneumonia 1
Others 3
clinical/ imagiological examination due to patients being treated conservatively and others with a correct pathological diagnosis obtained by less invasive procedures not included in the study.
Not all patients originated in the same institution, many being referred from other centres, meaning the clinical and imagiological observations were not uniform for all patients, with a probable impact on accuracy.
Correlation between clinical/ imagiological and histopathological diagnosis
Correct diagnosis 76% (n=80)
New diagnosis 21% (n=22)
Biopsy inconclusive 3% (n=3)
Sensitivity % (95% CI) of clinical diagnosis
67 (57-75)
Specificity % (95% CI) of clinical diagnosis
90 (85-93)
PPV % (95% CI) of clinical diagnosis
76 (67-84)
NPV % (95% CI) of clinical diagnosis
85 (80-89)
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon monoxide diffusing capacity , IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 6MWT= 6 minute walking test RBILD/ DIP= respiratory bronchiolitis interstitial lung disease/ desquamative interstitial pneumonia, UIP= usual interstitial pneumonia, NSIP= non-specific interstitial pneumonia
Table 20: Flaherty 2002 150
Study
details
Population Methods Outcome measures Effect size Comments
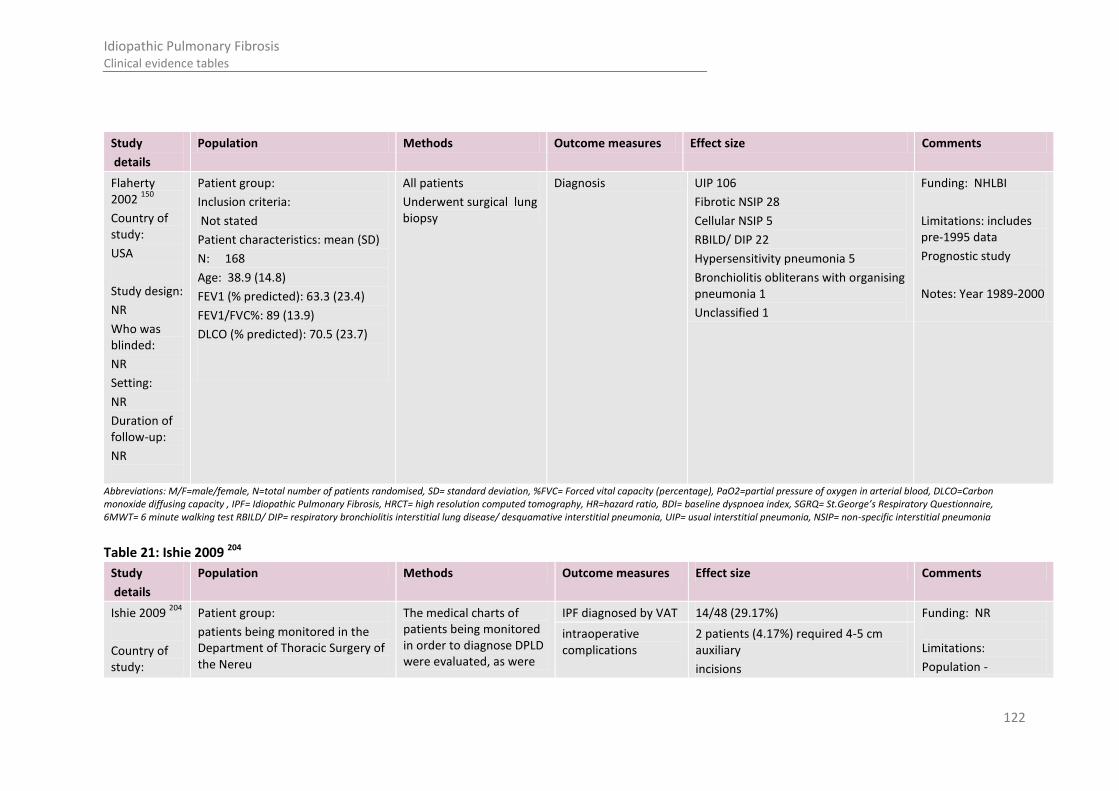
122
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Study
details
Population Methods Outcome measures Effect size Comments
Flaherty 2002
150
Country of study:
USA
Study design:
NR
Who was blinded:
NR
Setting:
NR
Duration of follow-up:
NR
Patient group:
Inclusion criteria:
Not stated
Patient characteristics: mean (SD)
N: 168
Age: 38.9 (14.8)
FEV1 (% predicted): 63.3 (23.4)
FEV1/FVC%: 89 (13.9)
DLCO (% predicted): 70.5 (23.7)
All patients
Underwent surgical lung biopsy
Diagnosis UIP 106
Fibrotic NSIP 28
Cellular NSIP 5
RBILD/ DIP 22
Hypersensitivity pneumonia 5
Bronchiolitis obliterans with organising pneumonia 1
Unclassified 1
Funding: NHLBI
Limitations: includes pre-1995 data
Prognostic study
Notes: Year 1989-2000
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon monoxide diffusing capacity , IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 6MWT= 6 minute walking test RBILD/ DIP= respiratory bronchiolitis interstitial lung disease/ desquamative interstitial pneumonia, UIP= usual interstitial pneumonia, NSIP= non-specific interstitial pneumonia
Table 21: Ishie 2009 204
Study
details
Population Methods Outcome measures Effect size Comments
Ishie 2009 204
Country of study:
Patient group:
patients being monitored in the Department of Thoracic Surgery of the Nereu
The medical charts of patients being monitored in order to diagnose DPLD were evaluated, as were
IPF diagnosed by VAT 14/48 (29.17%) Funding: NR
Limitations:
Population -
intraoperative complications
2 patients (4.17%) required 4-5 cm auxiliary
incisions
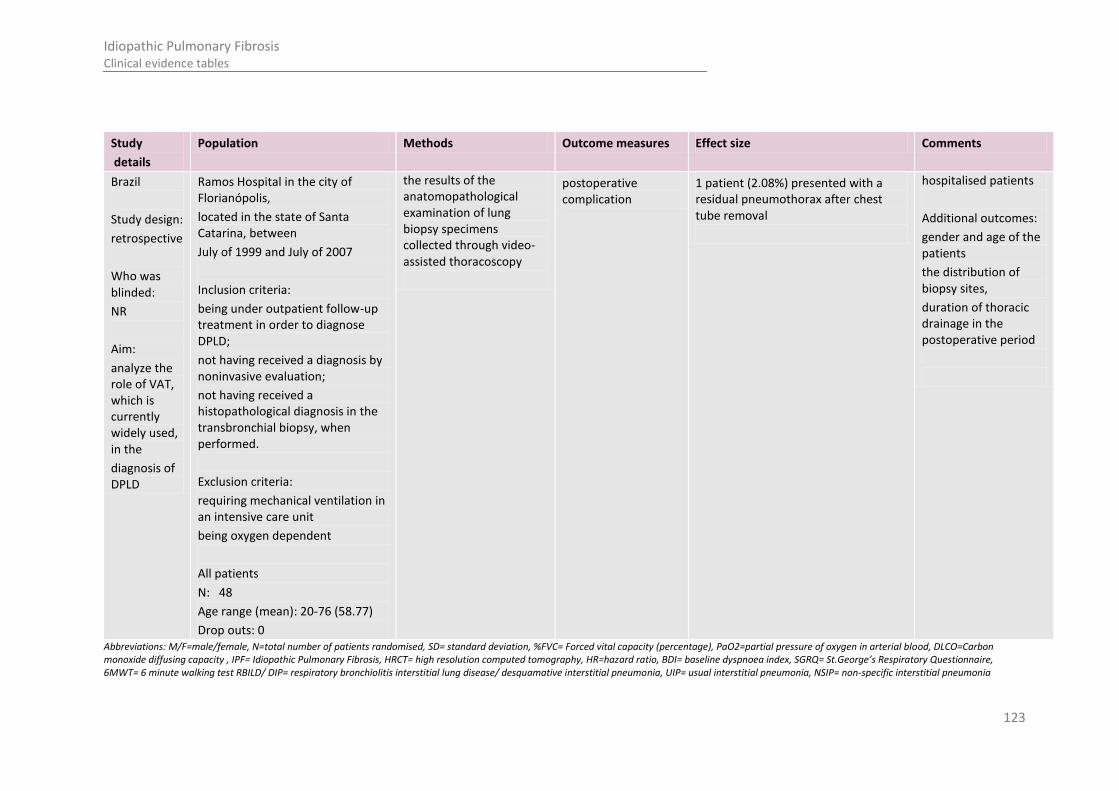
123
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Study
details
Population Methods Outcome measures Effect size Comments
Brazil
Study design:
retrospective
Who was blinded:
NR
Aim:
analyze the role of VAT, which is currently widely used, in the
diagnosis of DPLD
Ramos Hospital in the city of Florianópolis,
located in the state of Santa Catarina, between
July of 1999 and July of 2007
Inclusion criteria:
being under outpatient follow-up treatment in order to diagnose DPLD;
not having received a diagnosis by noninvasive evaluation;
not having received a histopathological diagnosis in the transbronchial biopsy, when performed.
Exclusion criteria:
requiring mechanical ventilation in an intensive care unit
being oxygen dependent
All patients
N: 48
Age range (mean): 20-76 (58.77)
Drop outs: 0
the results of the anatomopathological examination of lung biopsy specimens collected through video-assisted thoracoscopy
postoperative complication
1 patient (2.08%) presented with a residual pneumothorax after chest tube removal
hospitalised patients
Additional outcomes:
gender and age of the patients
the distribution of biopsy sites,
duration of thoracic drainage in the postoperative period
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon monoxide diffusing capacity , IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 6MWT= 6 minute walking test RBILD/ DIP= respiratory bronchiolitis interstitial lung disease/ desquamative interstitial pneumonia, UIP= usual interstitial pneumonia, NSIP= non-specific interstitial pneumonia

124
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Table 22: Jamaati 2006 210
Study
details
Population Methods Outcome measures Effect size Comments
Jamaati 2006 210
Country of study:
Iran
Study design:
retrospective
Who was blinded: no- one
Setting: Masih Daneshvari Hospital
Patient group: IPF
Inclusion criteria:
Not stated
Patient characteristics: mean (SD)
N: 50 (27M, 23 F)
Age: 56.25 (15.86)
Clinical features: frequency, %
Dyspnoea: 50 (100%)
Cough: 45 (90%)
Weight loss: 28 (56%)
Orthopnoea, PND: 22 (44%)
Chest pain: 16 (32%)
Oedema: 10 (20%)
Haemoptysis: 2 (8%)
Clinical signs: frequency, %
Crackles: 45 (90%)
Tachpnoea: 29 (58%)
Cyanosis: 16 (32%)
Clubbing : 15 (30%)
HRCT pattern
Reticular pattern: 21 (42%)
Honeycomb: 15 (30%)
Ground glass: 3 (6%)
Reticulo-nodular: 8 (16%)
Increased pleural thickening: 8
All patients
Transbronchial biopsy (70%)
OLB (26%)
Video assisted thoracoscopic lung biopsy (4%)
Diagnosis All patients showed UIP on microscopy Funding: NR
Limitations:
Pathological findings not well described.
Additional outcomes: HRCT pattern
Notes:
Occupational/ environmental exposure described in patient characteristics- some cases may not be IPF.

125
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Study
details
Population Methods Outcome measures Effect size Comments
(16%)
Lymphadenopathy: 7 (14%)
Normal: 0
Occupational/ environmental exposure
Farming: 9 (18%)
Cigarette smoking: 9 (18%)
History of baking: 7 (14%)
Contact with metal dust: 4 (8%)
Contact with chemicals: 1 (2%)
Contact with dust: 3 (6%)
Contact with asbestos: 1 (2%)
Indefinite contact: 16 (32%)
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon monoxide diffusing capacity , IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 6MWT= 6 minute walking test RBILD/ DIP= respiratory bronchiolitis interstitial lung disease/ desquamative interstitial pneumonia, UIP= usual interstitial pneumonia, NSIP= non-specific interstitial pneumonia
Table 23: Lettieri 2005A 279
Study
details
Population Methods Outcome measures Effect size Comments
Lettieri 2005A
279
Country of study: USA
Study design: retrospective
Patient group: suspected ILD
Exclusion criteria:
<18 years of age
History of biopsy proven ILD
All patients
Data were abstracted regarding demographics, factors known to increase perioperative mortality, pulmonary function, spirometry.
Mortality- all patients
4/83 (4.8%) at 30 days
5/83 (6.0%) at 90 days
Funding: NR
Limitations:
Retrospective study- likely to be confounded by recall and coding bias
Mortality- IPF patients
3/42 (7.1%) at 30 days
4/42 (9.5%) at 90 days (of these, only one was suspected to have IPF based on clinical and radiographic findings)
Mortality- non-IPF 1/41 (2.4%) at 30 days

126
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Study
details
Population Methods Outcome measures Effect size Comments
cohort
Who was blinded: no- one
Setting: tertiary care university affiliated medical centre
Duration of follow-up: 90 days
Patient characteristics: mean (SD)
N: 88 underwent SLB; 5 patients excluded due to incomplete data.
Final number: 83
Age: 57.3 (14.2)
FVC (% predicted): 69.8 (15.1)
FEV1 (% predicted): 67.9 (15.9)
DLCO (% predicted): 42.7 (14.8)
Male (%): 57.8
Tobacco use(%): 53.0
Supplemental oxygen: 45.8 %
Immunosuppressed: 16.9%
Mechanically ventilated: 9.6%
It was noted whether the patient required supplemental oxygen at the time of SLB, and whether they were in ICU receiving mechanical ventilation.
SLB (OLB 27.7%)
patients 1/41 (2.4%) at 90 days Small sample size
Institution in study not an IPF referral centre
Referral for SLB was not protocolled
Selection bias may mean that some very ill patients were never considered to be candidates for SLB- may have led to an overestimate of SLB safety
Diagnosis IPF: 42/83
Non-IPF: 41/83
40% of subjects in whom IPF was eventually diagnosed per ATS guidelines were thought to have had other conditions pre-operatively.
Adverse events 7/83 (8.4%), of which 2 were in IPF patients
Acute MI 2
Nosocomial pneumonia 2
Stroke 1
Pancreatitis 1
Prolonged mechanical ventilation 1
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon monoxide diffusing capacity , IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 6MWT= 6 minute walking test RBILD/ DIP= respiratory bronchiolitis interstitial lung disease/ desquamative interstitial pneumonia, UIP= usual interstitial pneumonia, NSIP= non-specific interstitial pneumonia
Table 24: Lettieri 2005 280
Study
details
Population Methods Outcome measures Effect size Comments
Lettieri 2005 280
Country of study: USA
Study design:
retrospective
Patient group: subjects presenting to the pulmonary clinic with both clinical and radiographic evidence of ILD
Inclusion criteria:
Not stated
Patient characteristics: mean (SD)
All patients
Underwent SLB. A general pathologist initially reviewed all SLB specimens. In some instances, specimens were further reviewed by pathologists with expertise
Diagnosis Achieved in 93.2% of pts by the general pathologist, and in all cases by the specialist
UIP 17 (specialists), 22 (general pathologists)
NSIP 10 (specialists), 7 (general pathologists)
Sarcoidosis 4 (specialists), 0 (general
Funding: NR
Limitations: None reported
Notes: Gold standard was the findings of the

127
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Study
details
Population Methods Outcome measures Effect size Comments
Setting:
Walter Reed Army Medical Centre, Washington DC (large, multidisciplinary, tertiary care referral centre)
Duration of follow-up:
N: 83 underwent SLB. Of these, samples from 44 patients were further reviewed by pathologists specialising in pulmonary diseases.
N=44
Age: 58.5 (14.2)
% male: 47.7%
FVC, % predicted: 70.2 (14.3)
FEV1, % predicted: 68.6 (15.4)
DLCO: 43.7 (13.5)
% requiring supplemental O2 at time of biopsy: 54.5%
in ILD. Only those patients whose samples were examined by a pathologist specialising in pulmonary diseases were included in the final cohort.
Each patient had multiple sites sampled by either OLB or VATS.
The final diagnosis represented the consensus of several pulmonary pathologists.
pathologists)
Cryptogenic organising pneumonia 3 (specialists), 3 (general pathologists)
Diffuse alveolar damage 2 (specialists), 1 (general pathologists)
Infection 2 (specialists), 1 (general pathologists)
Malignancy 2 (specialists), 0 (general pathologists)
Other 5(specialists) 10 (general pathologists)
specialist pathologist
Difference in histopathological interpretation between general and specialist pathologists
Occurred in 52.3% of cases (kappa 0.21), leading to a change in clinical management in 60% of cases.
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon monoxide diffusing capacity , IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 6MWT= 6 minute walking test RBILD/ DIP= respiratory bronchiolitis interstitial lung disease/ desquamative interstitial pneumonia, UIP= usual interstitial pneumonia, NSIP= non-specific interstitial pneumonia
Table 25: Oliveira 2011 366
Study
details
Population Methods Outcome measures Effect size Comments
Oliveira 2011 366
Country of study: Brazil
Study design:
Patient group: suspected ILD
Inclusion criteria:
Not stated
Exclusion criteria:
Incomplete clinical history/ examination
All patients
Clinical suspicion of ILD was defined as the presence of dyspnoea or dry cough accompanied by radiological findings of nodules or reticular
Diagnosis 11/56 (19.6%) had a definitive diagnosis of IPF
45/56 non-IPF diagnosis
Funding: None
Limitations:
Additional outcomes:
Sensitivity, specificity, PPV, NPV, likelihood
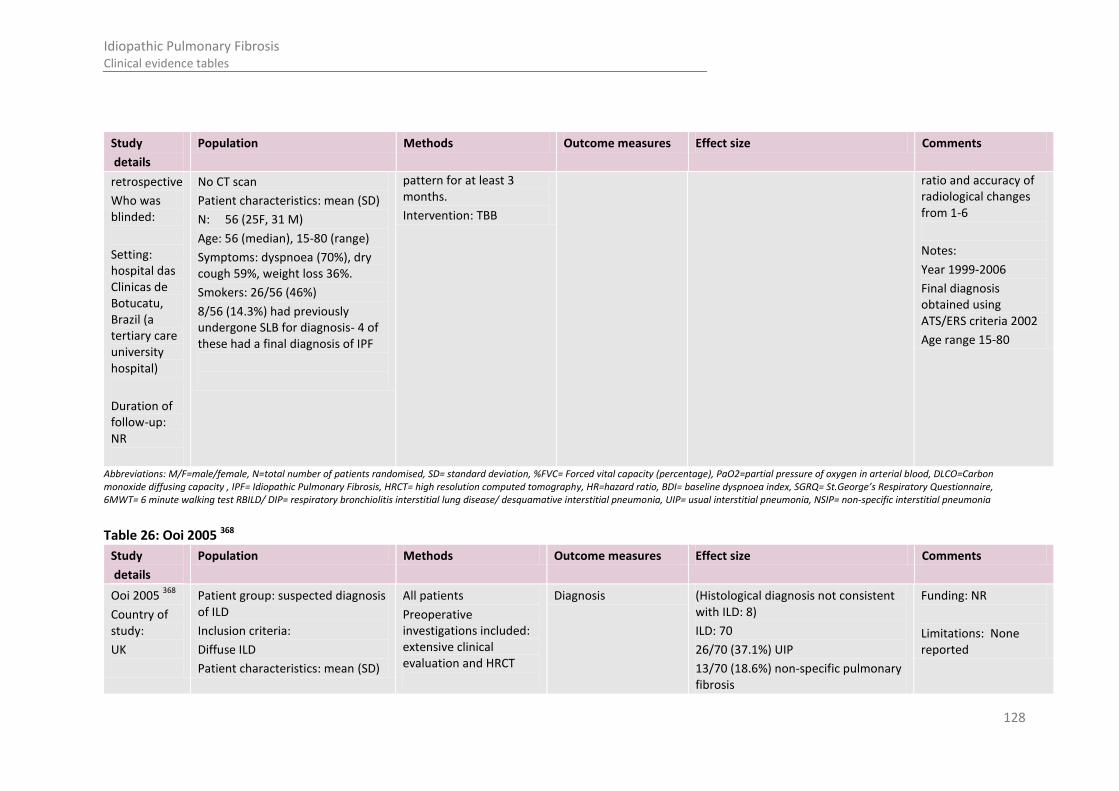
128
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Study
details
Population Methods Outcome measures Effect size Comments
retrospective
Who was blinded:
Setting: hospital das Clinicas de Botucatu, Brazil (a tertiary care university hospital)
Duration of follow-up: NR
No CT scan
Patient characteristics: mean (SD)
N: 56 (25F, 31 M)
Age: 56 (median), 15-80 (range)
Symptoms: dyspnoea (70%), dry cough 59%, weight loss 36%.
Smokers: 26/56 (46%)
8/56 (14.3%) had previously undergone SLB for diagnosis- 4 of these had a final diagnosis of IPF
pattern for at least 3 months.
Intervention: TBB
ratio and accuracy of radiological changes from 1-6
Notes:
Year 1999-2006
Final diagnosis obtained using ATS/ERS criteria 2002
Age range 15-80
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon monoxide diffusing capacity , IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 6MWT= 6 minute walking test RBILD/ DIP= respiratory bronchiolitis interstitial lung disease/ desquamative interstitial pneumonia, UIP= usual interstitial pneumonia, NSIP= non-specific interstitial pneumonia
Table 26: Ooi 2005 368
Study
details
Population Methods Outcome measures Effect size Comments
Ooi 2005 368
Country of study:
UK
Patient group: suspected diagnosis of ILD
Inclusion criteria:
Diffuse ILD
Patient characteristics: mean (SD)
All patients
Preoperative investigations included: extensive clinical evaluation and HRCT
Diagnosis (Histological diagnosis not consistent with ILD: 8)
ILD: 70
26/70 (37.1%) UIP
13/70 (18.6%) non-specific pulmonary fibrosis
Funding: NR
Limitations: None reported
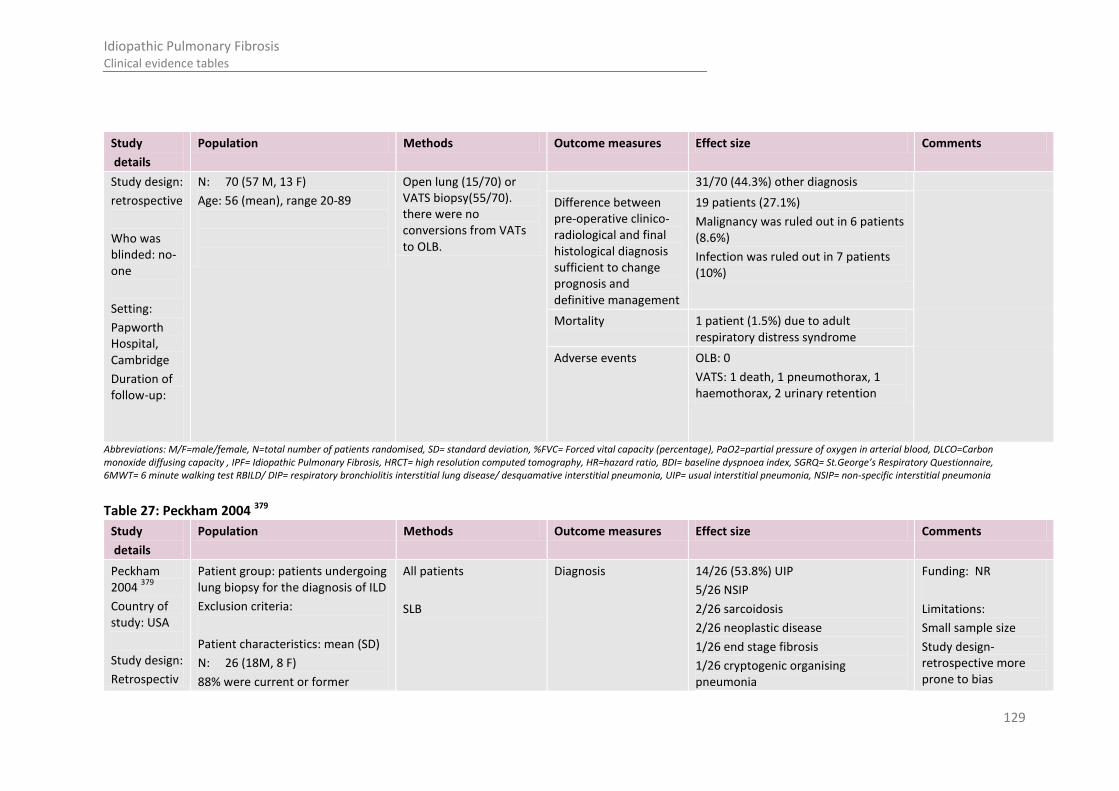
129
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Study
details
Population Methods Outcome measures Effect size Comments
Study design:
retrospective
Who was blinded: no- one
Setting:
Papworth Hospital, Cambridge
Duration of follow-up:
N: 70 (57 M, 13 F)
Age: 56 (mean), range 20-89
Open lung (15/70) or VATS biopsy(55/70). there were no conversions from VATs to OLB.
31/70 (44.3%) other diagnosis
Difference between pre-operative clinico-radiological and final histological diagnosis sufficient to change prognosis and definitive management
19 patients (27.1%)
Malignancy was ruled out in 6 patients (8.6%)
Infection was ruled out in 7 patients (10%)
Mortality 1 patient (1.5%) due to adult respiratory distress syndrome
Adverse events OLB: 0
VATS: 1 death, 1 pneumothorax, 1 haemothorax, 2 urinary retention
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon monoxide diffusing capacity , IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 6MWT= 6 minute walking test RBILD/ DIP= respiratory bronchiolitis interstitial lung disease/ desquamative interstitial pneumonia, UIP= usual interstitial pneumonia, NSIP= non-specific interstitial pneumonia
Table 27: Peckham 2004 379
Study
details
Population Methods Outcome measures Effect size Comments
Peckham 2004
379
Country of study: USA
Study design:
Retrospectiv
Patient group: patients undergoing lung biopsy for the diagnosis of ILD
Exclusion criteria:
Patient characteristics: mean (SD)
N: 26 (18M, 8 F)
88% were current or former
All patients
SLB
Diagnosis 14/26 (53.8%) UIP
5/26 NSIP
2/26 sarcoidosis
2/26 neoplastic disease
1/26 end stage fibrosis
1/26 cryptogenic organising pneumonia
Funding: NR
Limitations:
Small sample size
Study design- retrospective more prone to bias
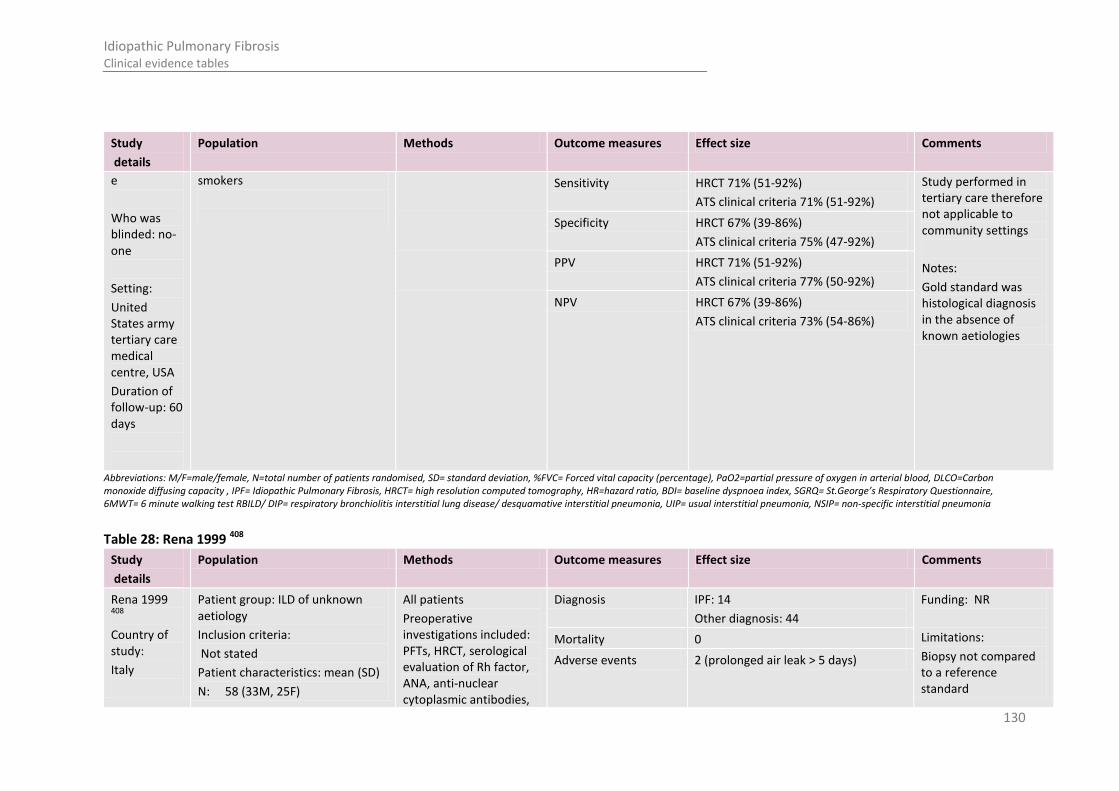
130
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Study
details
Population Methods Outcome measures Effect size Comments
e
Who was blinded: no- one
Setting:
United States army tertiary care medical centre, USA
Duration of follow-up: 60 days
smokers
Sensitivity HRCT 71% (51-92%)
ATS clinical criteria 71% (51-92%)
Study performed in tertiary care therefore not applicable to community settings
Notes:
Gold standard was histological diagnosis in the absence of known aetiologies
Specificity HRCT 67% (39-86%)
ATS clinical criteria 75% (47-92%)
PPV HRCT 71% (51-92%)
ATS clinical criteria 77% (50-92%)
NPV HRCT 67% (39-86%)
ATS clinical criteria 73% (54-86%)
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon monoxide diffusing capacity , IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 6MWT= 6 minute walking test RBILD/ DIP= respiratory bronchiolitis interstitial lung disease/ desquamative interstitial pneumonia, UIP= usual interstitial pneumonia, NSIP= non-specific interstitial pneumonia
Table 28: Rena 1999 408
Study
details
Population Methods Outcome measures Effect size Comments
Rena 1999 408
Country of study:
Italy
Patient group: ILD of unknown aetiology
Inclusion criteria:
Not stated
Patient characteristics: mean (SD)
N: 58 (33M, 25F)
All patients
Preoperative investigations included: PFTs, HRCT, serological evaluation of Rh factor, ANA, anti-nuclear cytoplasmic antibodies,
Diagnosis IPF: 14
Other diagnosis: 44
Funding: NR
Limitations:
Biopsy not compared to a reference standard
Mortality 0
Adverse events 2 (prolonged air leak > 5 days)

131
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Study
details
Population Methods Outcome measures Effect size Comments
Study design: prospective cohort
Who was blinded: no- one
Setting:
Duration of follow-up: NR
Age: 49.6 (12.0)
angiotensin converting enzyme.
Bronchoscopy and BAL were carried out and specimens sent for cell count, cytological examination, lymphocyte subtyping and microbiological studies.
Video-assisted thoracoscopic lung biopsy
Study is pre-2002 therefore ATS/ERS criteria not used
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon monoxide diffusing capacity , IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 6MWT= 6 minute walking test RBILD/ DIP= respiratory bronchiolitis interstitial lung disease/ desquamative interstitial pneumonia, UIP= usual interstitial pneumonia, NSIP= non-specific interstitial pneumonia
Table 29: Sigurdsson 2009 442
Study
details
Population Methods Outcome measures Effect size Comments
Sigurdsson 2009
442
Country of study: Iceland
Study design:
retrospective
Patient group: suspected ILD
Exclusion criteria: people with a solitary pulmonary nodule or patients in whom the surgery was used to remove foreign bodies or for treatment of recurrent pulmonary infections.
All patients
Information collected:
Clinical symptoms, smoking history, clinical examination, spiromentry, DLCO, lab results, chest radiographs CT results,
Mortality 2/73 (3%) at 30 days
3/73 (4%) at 90 days
Funding: NR
Limitations: not all patients had a CT scan (81%) prior to biopsy
Additional outcomes:
Notes:
Diagnosis UIP23/72 (32%), of which 12 were nonspecific fibrosis (16% of total)
Noninterstitial diagnosis: 8/73 (11%)
Adverse events Total 12/73 (16%)
Prolonged air leakage 9/73 (12%)
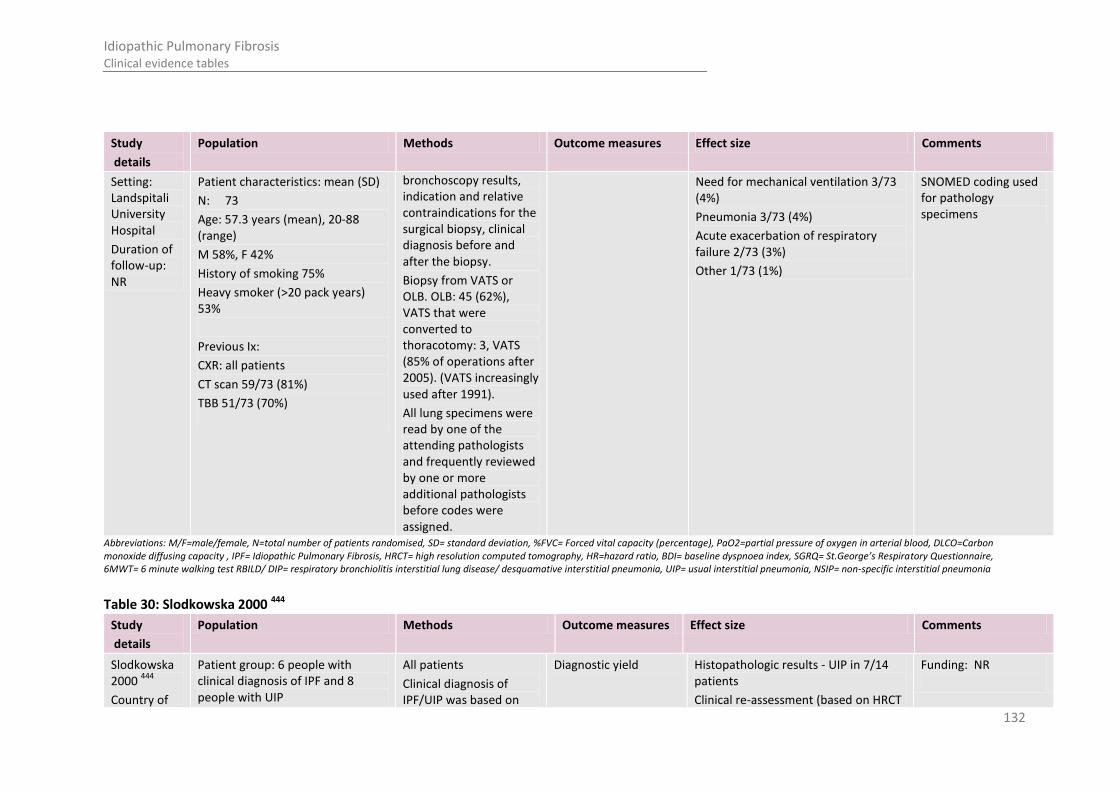
132
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Study
details
Population Methods Outcome measures Effect size Comments
Setting: Landspitali University Hospital
Duration of follow-up: NR
Patient characteristics: mean (SD)
N: 73
Age: 57.3 years (mean), 20-88 (range)
M 58%, F 42%
History of smoking 75%
Heavy smoker (>20 pack years) 53%
Previous Ix:
CXR: all patients
CT scan 59/73 (81%)
TBB 51/73 (70%)
bronchoscopy results, indication and relative contraindications for the surgical biopsy, clinical diagnosis before and after the biopsy.
Biopsy from VATS or OLB. OLB: 45 (62%), VATS that were converted to thoracotomy: 3, VATS (85% of operations after 2005). (VATS increasingly used after 1991).
All lung specimens were read by one of the attending pathologists and frequently reviewed by one or more additional pathologists before codes were assigned.
Need for mechanical ventilation 3/73 (4%)
Pneumonia 3/73 (4%)
Acute exacerbation of respiratory failure 2/73 (3%)
Other 1/73 (1%)
SNOMED coding used for pathology specimens
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon monoxide diffusing capacity , IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 6MWT= 6 minute walking test RBILD/ DIP= respiratory bronchiolitis interstitial lung disease/ desquamative interstitial pneumonia, UIP= usual interstitial pneumonia, NSIP= non-specific interstitial pneumonia
Table 30: Slodkowska 2000 444
Study
details
Population Methods Outcome measures Effect size Comments
Slodkowska 2000
444
Country of
Patient group: 6 people with clinical diagnosis of IPF and 8 people with UIP
All patients
Clinical diagnosis of IPF/UIP was based on
Diagnostic yield Histopathologic results - UIP in 7/14 patients
Clinical re-assessment (based on HRCT
Funding: NR

133
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Study
details
Population Methods Outcome measures Effect size Comments
study:
Poland
Study design:
Retrospective
Who was blinded: not reported
Setting: analysis of patient records from Chinese literature and data from Drum Tower Hospital, Nanjing, China
Duration of follow-up: Follow-up ranged from 1-4 years.
Exclusion criteria: people without any underlying medical conditions or potential causes of pulmonary abnormalities e.g. connective tissue disease, exposure to organic or inorganic dust, toxic fumes and history of specific drug intake (no further details reported)
Patient characteristics: mean (SD)
N: 14 (6F and 8M)
Age range: 28-73yrs
clinical symptoms, chest radiographs, HRCT and lung function tests.
Histologic re-examination of open lung biopsy specimens performed for all patients
Separate analysis of HRCT findings. No further details.
and pathology reports - UIP 12/14 patients
Histopathology and HRCT analysis - UIP 7/14 patients
Limitations:
Specific time period between clinical diagnosis, histologic and HRCT analysis not reported.
Small sample size
Study is pre-2002 therefore ATS/ERS criteria not used
Notes:
Authors note that discrepancy between histology and HRCT was due to a sampling problem observed in 2/12 (14%) patients. Authors conclude this is due to disease progression.
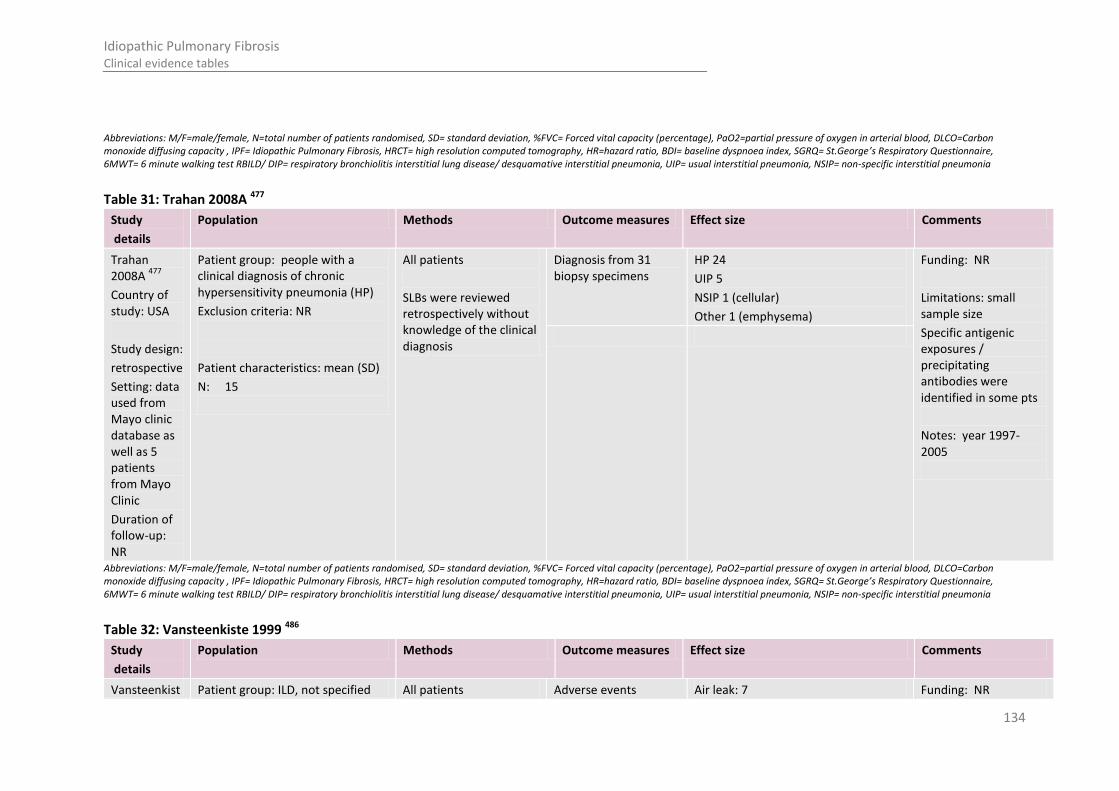
134
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon monoxide diffusing capacity , IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 6MWT= 6 minute walking test RBILD/ DIP= respiratory bronchiolitis interstitial lung disease/ desquamative interstitial pneumonia, UIP= usual interstitial pneumonia, NSIP= non-specific interstitial pneumonia
Table 31: Trahan 2008A 477
Study
details
Population Methods Outcome measures Effect size Comments
Trahan 2008A
477
Country of study: USA
Study design:
retrospective
Setting: data used from Mayo clinic database as well as 5 patients from Mayo Clinic
Duration of follow-up: NR
Patient group: people with a clinical diagnosis of chronic hypersensitivity pneumonia (HP)
Exclusion criteria: NR
Patient characteristics: mean (SD)
N: 15
All patients
SLBs were reviewed retrospectively without knowledge of the clinical diagnosis
Diagnosis from 31 biopsy specimens
HP 24
UIP 5
NSIP 1 (cellular)
Other 1 (emphysema)
Funding: NR
Limitations: small sample size
Specific antigenic exposures / precipitating antibodies were identified in some pts
Notes: year 1997-2005
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon monoxide diffusing capacity , IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 6MWT= 6 minute walking test RBILD/ DIP= respiratory bronchiolitis interstitial lung disease/ desquamative interstitial pneumonia, UIP= usual interstitial pneumonia, NSIP= non-specific interstitial pneumonia
Table 32: Vansteenkiste 1999 486
Study
details
Population Methods Outcome measures Effect size Comments
Vansteenkist Patient group: ILD, not specified All patients Adverse events Air leak: 7 Funding: NR
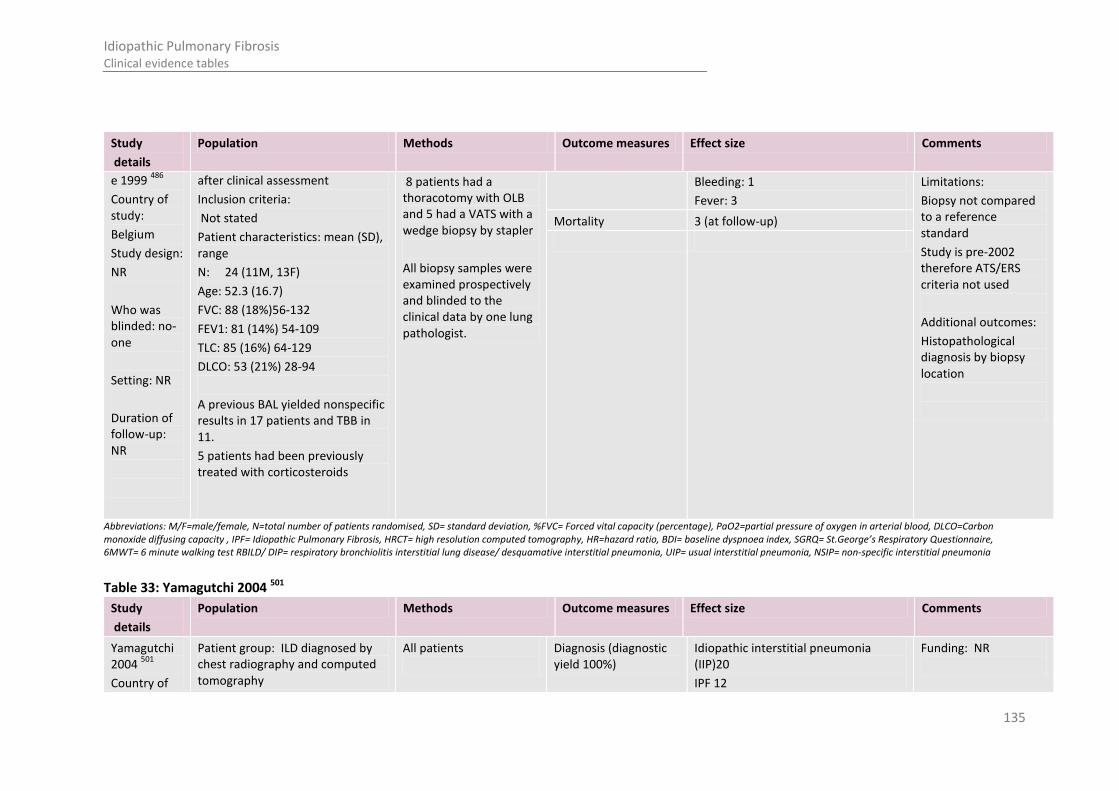
135
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Study
details
Population Methods Outcome measures Effect size Comments
e 1999 486
Country of study:
Belgium
Study design:
NR
Who was blinded: no- one
Setting: NR
Duration of follow-up: NR
after clinical assessment
Inclusion criteria:
Not stated
Patient characteristics: mean (SD), range
N: 24 (11M, 13F)
Age: 52.3 (16.7)
FVC: 88 (18%)56-132
FEV1: 81 (14%) 54-109
TLC: 85 (16%) 64-129
DLCO: 53 (21%) 28-94
A previous BAL yielded nonspecific results in 17 patients and TBB in 11.
5 patients had been previously treated with corticosteroids
8 patients had a thoracotomy with OLB and 5 had a VATS with a wedge biopsy by stapler
All biopsy samples were examined prospectively and blinded to the clinical data by one lung pathologist.
Bleeding: 1
Fever: 3
Limitations:
Biopsy not compared to a reference standard
Study is pre-2002 therefore ATS/ERS criteria not used
Additional outcomes:
Histopathological diagnosis by biopsy location
Mortality 3 (at follow-up)
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon monoxide diffusing capacity , IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 6MWT= 6 minute walking test RBILD/ DIP= respiratory bronchiolitis interstitial lung disease/ desquamative interstitial pneumonia, UIP= usual interstitial pneumonia, NSIP= non-specific interstitial pneumonia
Table 33: Yamagutchi 2004 501
Study
details
Population Methods Outcome measures Effect size Comments
Yamagutchi 2004
501
Country of
Patient group: ILD diagnosed by chest radiography and computed tomography
All patients
Diagnosis (diagnostic yield 100%)
Idiopathic interstitial pneumonia (IIP)20
IPF 12
Funding: NR
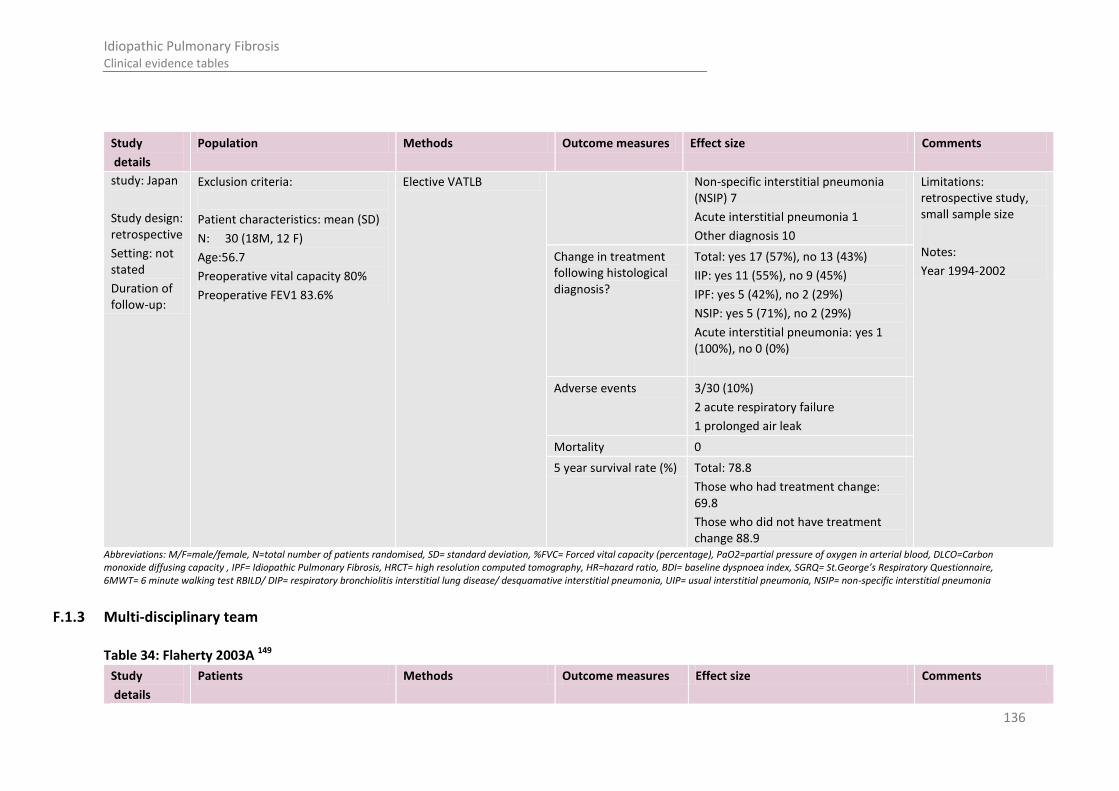
136
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Study
details
Population Methods Outcome measures Effect size Comments
study: Japan
Study design: retrospective
Setting: not stated
Duration of follow-up:
Exclusion criteria:
Patient characteristics: mean (SD)
N: 30 (18M, 12 F)
Age:56.7
Preoperative vital capacity 80%
Preoperative FEV1 83.6%
Elective VATLB Non-specific interstitial pneumonia (NSIP) 7
Acute interstitial pneumonia 1
Other diagnosis 10
Limitations: retrospective study, small sample size
Notes:
Year 1994-2002 Change in treatment following histological diagnosis?
Total: yes 17 (57%), no 13 (43%)
IIP: yes 11 (55%), no 9 (45%)
IPF: yes 5 (42%), no 2 (29%)
NSIP: yes 5 (71%), no 2 (29%)
Acute interstitial pneumonia: yes 1 (100%), no 0 (0%)
Adverse events 3/30 (10%)
2 acute respiratory failure
1 prolonged air leak
Mortality 0
5 year survival rate (%) Total: 78.8
Those who had treatment change: 69.8
Those who did not have treatment change 88.9
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon monoxide diffusing capacity , IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 6MWT= 6 minute walking test RBILD/ DIP= respiratory bronchiolitis interstitial lung disease/ desquamative interstitial pneumonia, UIP= usual interstitial pneumonia, NSIP= non-specific interstitial pneumonia
F.1.3 Multi-disciplinary team
Table 34: Flaherty 2003A 149
Study
details
Patients Methods Outcome measures Effect size Comments

137
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Study
details
Patients Methods Outcome measures Effect size Comments
Flaherty 2003A
149
Country of study:
USA
Study design:
Retrospective
Who was blinded:
Setting:
Aim:
examines whether HRCT features add prognostic
information to the histological classification in the differential
diagnosis of UIP and
Patient group:
consecutively referred Patients from the University of Michigan Specialized Center of
Research in the Pathobiology of Fibrotic Lung Disease database. Who underwent surgical lung biopsy between October 1989 and February 2000.
Inclusion criteria:
people with a histological diagnosis of UIP or NSIP (by surgical lung biopsy)
HRCT scan within 6 months of the biopsy
Exclusion criteria:
Associated collagen vascular illness
All patients
N: 73 (histological UIP) 23 (histological NSIP)
Age (mean±SD): NR
Drop outs: 0
Radiological classification
Two thoracic radiologists independently reviewed each HRCT scan and recorded each case as either
definite UIP,
probable UIP,
indeterminate (equal probability of UIP or NSIP),
probable NSIP,
definite NSIP.
The finding felt by the radiologists to indicate probable or definite UIP was honeycombing, as this finding correlates strongly with pathological fibrosis and impaired survival.
The absence of honeycombing, the presence of ground glass opacity, and an apical or non-subpleural distribution favoured NSIP
Pathological classification
Three pathologists blinded to the clinical and radiological features reviewed the biopsy
Differential HRCT consensus diagnosis of people with a histological diagnosis of UIP
Definite UIP : 16/73
Probable UIP : 11/73
Indeterminate: 20/73
Probable NSIP : 17/73
Definite NSIP : 9/73
Funding: NR Limitations:
Study design- retrospective more prone to bias
Notes:
Interobserver agreement of the radiological diagnoses was described using kappa and
weighted kappa statistics, where weighted kappa statistics confer partial agreement for assignment of adjacent diagnoses—for example, definite and probable UIP, or probable UIP and indeterminate assignments.23 Interobserver agreement between radiologists was first evaluated across all five diagnostic categories (definite UIP, probable UIP,
Radiologist complete agreement
35/96 (36%)
Kappa = 0.20 p<0.0001
Weighted kappa = 0.43 p<0.0001
Radiological diagnosis of definite /probable UIP
27/73 total cases of histologically diagnosed UIP
Radiologists specificity
100%
Radiologists sensitivity
37% (SD 6)

138
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Study
details
Patients Methods Outcome measures Effect size Comments
NSIP, and determines whether the
current radiological criteria for NSIP are useful in histologically
proven cases of NSIP
specimens.
Each specimen was assigned a histological diagnosis of UIP or NSIP using defined criteria.
A patient received a diagnosis of UIP when one or more biopsy specimens showed UIP.
Cases of cellular NSIP (n=3) and fibrotic NSIP (n=20) were collectively classified as NSIP
indeterminate, probable NSIP, and definite NSIP).
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon monoxide diffusing capacity , IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 6MWT= 6 minute walking test RBILD/ DIP= respiratory bronchiolitis interstitial lung disease/ desquamative interstitial pneumonia, UIP= usual interstitial pneumonia, NSIP= non-specific interstitial pneumonia
Table 35: Flaherty 2007152
Study
details
Population Methods Outcome measures Effect size Comments
Flaherty 2007 152
Country of study:
USA
Study design:
Patient group:
Data from patients referred to the University of Michigan Specialized Centre of Research in the Pathobiology of Fibrotic Lung Disease between August 2002 and December 2003. People with suspected IIP were referred to the study centre by participants in the University of Michigan Fibrotic
Patients underwent a history, physical examination, complete pulmonary function testing, HRCT, and SLB.
Case information was provided to three groups (community 1, community 2, and the University of Michigan) on separate
Inter observer Agreement κ Score
Step 5: Consensus diagnosis
Academic centre
Clinical: 0.71 (± 0.03 SE)
Radiological: 0.55 (± 0.08 SE)
Pathology: 0.57 (± 0.05 SE)
Funding: National institute of health, National Heart, Lung and Blood Institute grants
Limitations:
Study design- retrospective more prone to bias
Inter observer Agreement κ Score
Step 5: Consensus diagnosis
Community centre
Clinical: 0.44 (±0.07 SE)
Radiological: 0.32 (±0.11 SE)
Pathology: 0.41 (±0.13 SE)

139
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Study
details
Population Methods Outcome measures Effect size Comments
Retrospective review
Who was blinded:
NR
Setting:
2 community locations and 1
academic location
Aim: Evaluated
the agreement in classification of people with suspected IIP in community and academic settings. And
examined the influence
Lung Disease Network
Inclusion criteria:
NR
Exclusion criteria:
People without an HRCT
scan or an SLB were excluded
All patients
N: 39
Age (mean±SD): NR
Drop outs: 0
days.
Participants at the University of Michigan were expert clinicians, radiologists, and pathologists from five centres (within and outside the United States).
On average, participants at the University of Michigan had been in practice longer and spend a greater amount of time in the evaluation and treatment of people with interstitial lung disease
The cases were presented with the same information and in the same order at each institution.
Provided participants incremental information through five stages
clinicians and radiologists independently reviewed HRCT,
clinicians and radiologists independently reviewed clinical information & HRCT
clinicians and radiologists
Clinicians: Sensitivity without MDT#
Community : 65%-74%
Academic: 50%-55%
Overall:55%- 62%
Notes:
McNemar tests were used to test whether two probabilities of agreement conducted during different steps or by different raters were equal.
A κ statistic allowing for multiple raters was used to assess agreement in diagnosis.
κ Scores are rated as almost perfect agreement (above 0.8), substantial agreement (scores between 0.6 and 0.8), moderate agreement (scores between 0.4 and 0.6), fair agreement (scores between 0.2 and 0.4), slight agreement (scores between 0.0 and 0.2), and poor agreement (scores below 0.0)
Radiologists: Sensitivity without MDT#
Community : 80%- 85%
Academic: 48%-73%
Overall: 64%-79%
Pathologists: Sensitivity without MDT#
Community : 90%- 92%
Academic: 86%-98%
Overall: 96%-88%
Clinicans and radiologists Sensitivity without MDT#
Community : 71%- 78%
Academic: 49%-60%
Overall: 58%-67%
Clinicans, radiologists and pathologist: Sensitivity without MDT#
Community : 82%- 87%
Academic: 72%-78%
Overall: 76%-81%
Clinicians: Specificity without MDT#
Community : 72%- 81%
Academic: 88%-94%
Overall: 83%-90%
Radiologists: Specificity without MDT#
Community : 65%- 78%
Academic: 97%-98%
Overall: 82%-88%
Pathologists: Specificity without MDT#
Community :43%- 53%
Academic: 67%-81%
Overall: 59%-72%
Clinicans and Community :70%- 80%

140
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Study
details
Population Methods Outcome measures Effect size Comments
of an iterative diagnostic approach on
diagnostic agreement in a community compared with an academic
setting, and addressed features that influenced diagnostic
approaches
discussed, as a group, the clinical and HRCT features
As this was occurring, the pathologists were independently reviewing SLB
specimens and assigning an independent histopathologic diagnosis.
Clinicians, radiologists, and pathologists discussion of the findings of HRCT, clinical data and SLB.
an attempt was made to reach a consensus diagnosis.
radiologists Specificity without MDT#
Academic: 90%-95%
Overall: 82%-89%
An estimating equation approach to the analysis of correlated κ statistics was used in comparisons of κ statistics estimated throughout the study and in producing confidence intervals for the κ statistics
# NCGC calculated using data reported in paper
Clinicans, radiologists and pathologist: Specificity without MDT#
Community :64%- 72%
Academic: 83%-90%
Overall: 78%-84%
Clinicians: Sensitivity with MDT#
Community :85%- 87%
Academic: 74%-100%
Overall: 78%-96%
Radiologists: Sensitivity with MDT#
Community :90%- 92%
Academic: 53%-77%
Overall: 71%-85%
Pathologists: Sensitivity with MDT#
Community :95%- 100%
Academic: 80%-98%
Overall: 85%-99%
Clinicians and radiologists Sensitivity with MDT#
Community :87%- 89%
Academic: 69%-94%
Overall: 76%-92%
Clinicians, radiologists and pathologist: Sensitivity with MDT#
Community :89%- 92%
Academic: 73%-96%
Overall: 79%-94%
Clinicians: Specificity with MDT#
Community :67%- 81%
Academic: 91%-97%
Overall: 83%-92%
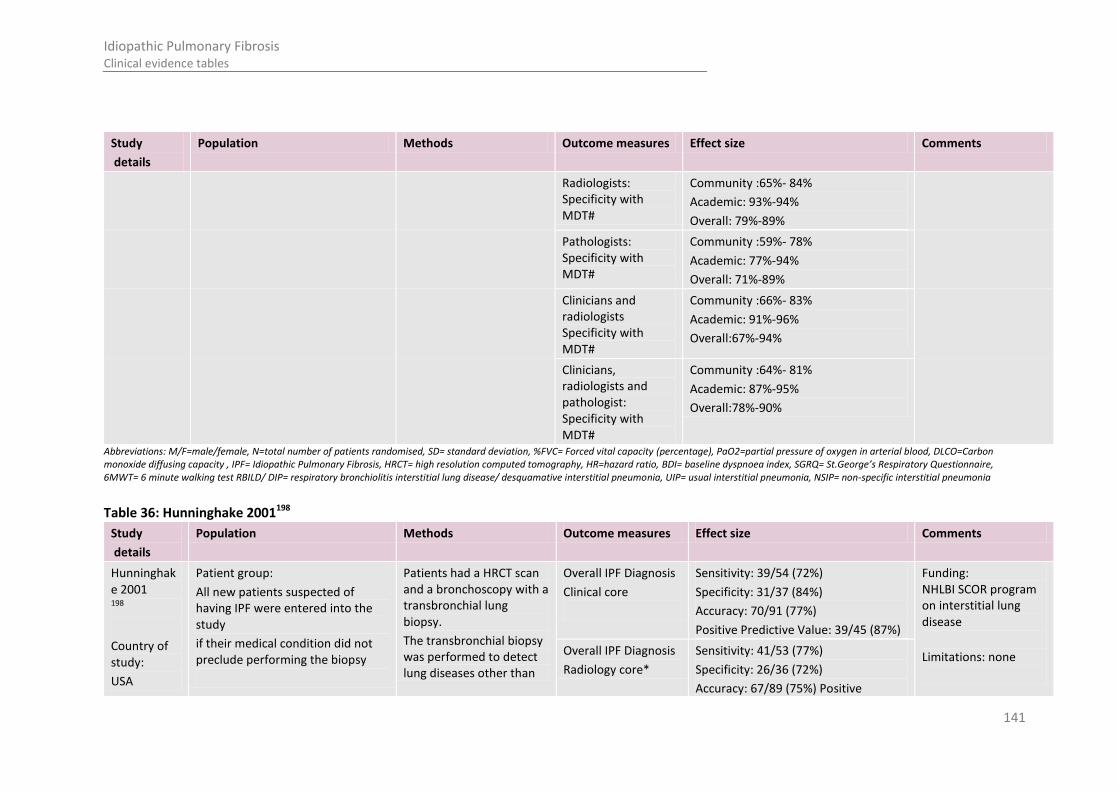
141
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Study
details
Population Methods Outcome measures Effect size Comments
Radiologists: Specificity with MDT#
Community :65%- 84%
Academic: 93%-94%
Overall: 79%-89%
Pathologists: Specificity with MDT#
Community :59%- 78%
Academic: 77%-94%
Overall: 71%-89%
Clinicians and radiologists Specificity with MDT#
Community :66%- 83%
Academic: 91%-96%
Overall:67%-94%
Clinicians, radiologists and pathologist: Specificity with MDT#
Community :64%- 81%
Academic: 87%-95%
Overall:78%-90%
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon monoxide diffusing capacity , IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 6MWT= 6 minute walking test RBILD/ DIP= respiratory bronchiolitis interstitial lung disease/ desquamative interstitial pneumonia, UIP= usual interstitial pneumonia, NSIP= non-specific interstitial pneumonia
Table 36: Hunninghake 2001198
Study
details
Population Methods Outcome measures Effect size Comments
Hunninghake 2001 198
Country of study:
USA
Patient group:
All new patients suspected of having IPF were entered into the study
if their medical condition did not preclude performing the biopsy
Patients had a HRCT scan and a bronchoscopy with a transbronchial lung biopsy.
The transbronchial biopsy was performed to detect lung diseases other than
Overall IPF Diagnosis
Clinical core
Sensitivity: 39/54 (72%)
Specificity: 31/37 (84%)
Accuracy: 70/91 (77%)
Positive Predictive Value: 39/45 (87%)
Funding: NHLBI SCOR program on interstitial lung disease
Limitations: none
Overall IPF Diagnosis
Radiology core*
Sensitivity: 41/53 (77%)
Specificity: 26/36 (72%)
Accuracy: 67/89 (75%) Positive

142
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Study
details
Population Methods Outcome measures Effect size Comments
Study design:
prospective, blinded study
Who was blinded:
NR
Setting:
eight referring centres
Aim: determined the value of clinical and radiologic findings for the diagnosis of IPF.
Inclusion criteria:
Patients able to undergo biopsy
Exclusion criteria:
People with an underlying connective tissue disorder
Exposure to environmental agents or drugs known to cause pulmonary fibrosis
Other underlying disorders known to cause pulmonary fibrosis
All patients
N: 91 patients
Age (mean±SD): NR
Drop outs: 0
IPF.
If the transbronchial biopsy did not provide a specific diagnosis, patients underwent a surgical (open or thoracoscopic) lung biopsy.
The lung HRCT scan was not used to determine if a patient should undergo a surgical biopsy.
Before the surgical biopsy but after the results of the lung HRCT scan and transbronchial biopsy, one pulmonologist at each of the referring centres rated the certainty of the diagnosis of IPF (as certain, uncertain, or unlikely) and provided an overall clinical diagnosis, even if the diagnosis was uncertain.
The centre investigators could use any clinical information that was available for the patient to provide this assessment.
No predetermined clinical or radiologic criteria were used to make a clinical
Predictive Value: 41/48 (85%) Additional outcomes:
Sensitivity, specificity, accuracy and positive predictive value of a confident diagnosis of IPF (excluding cases where the investigator was uncertain of the diagnosis of IPF)
Bayesian posterior conditional predicative probability of IPF (A prior probability of 0.60 of having IPF among new suspected patients that presented for diagnosis was used in the calculation of the posterior probability.)
Notes:
* Excludes two patients for whom the radiology core provided no diagnosis
The kappa coefficient used to measure agreement within the cores was based on
Overall IPF Diagnosis
Referring centre
Sensitivity: 46/54 (85%)
Specificity: 16/37 (43%)
Accuracy: 62/91 (68%)
Positive Predictive Value: 46/67 (69%)
Probability Of Agreement Within The Cores
IPF versus Non-IPF
Agreement
Clinical: 0.79
Radiological: 0.77
Pathology: 0.85
Probability Of Agreement Within The Cores
IPF versus Non-IPF
Kappa score
Clinical: 0.59 (±0.06 SE)
Radiological: 0.54 (±0.06 SE)
Pathology: 0.68 (±0.06 SE)
Probability Of Agreement Within The Cores
Specific Diagnosis of ILD
Agreement
Clinical: 0.49
Radiological: 0.54
Pathology: 0.72
Probability Of Agreement Within The Cores
Specific Diagnosis of ILD
Kappa score
Clinical: 0.32 (±0.05 SE)
Radiological: 0.31 (±0.05 SE)
Pathology: 0.55 (±0.05 SE)

143
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Study
details
Population Methods Outcome measures Effect size Comments
diagnosis or to determine the level of certainty of the diagnosis of IPF.
The following information was provided by the referring centres for review by a clinical core of three pulmonologists: presence and duration of cough; presence and duration of dyspnea; history of smoking; history of fever, weight loss, myalgias, arthralgias, rash, and arthritis; presence of finger clubbing; and pulmonary function tests.
The clinical core directly evaluated chest radiographs and HRCT scans.
Each independently rated their certainty of the diagnosis of IPF (as certain, uncertain, or unlikely) and provided an overall clinical diagnosis, even if the diagnosis was uncertain.
A core of four chest radiologists independently evaluated the HRCT scans.
the form proposed by Kraemer which allowed for unequal numbers of observations per subject.
The probability of agreement between any two members of a core, estimated as the average proportion of concordant pairs for all possible pairings of raters per subject, was also estimated.
Using the pathology diagnosis of IPF as the gold standard, sensitivity, specificity, accuracy, and positive predictive value of the diagnosis of IPF of the cores and centres were calculated.
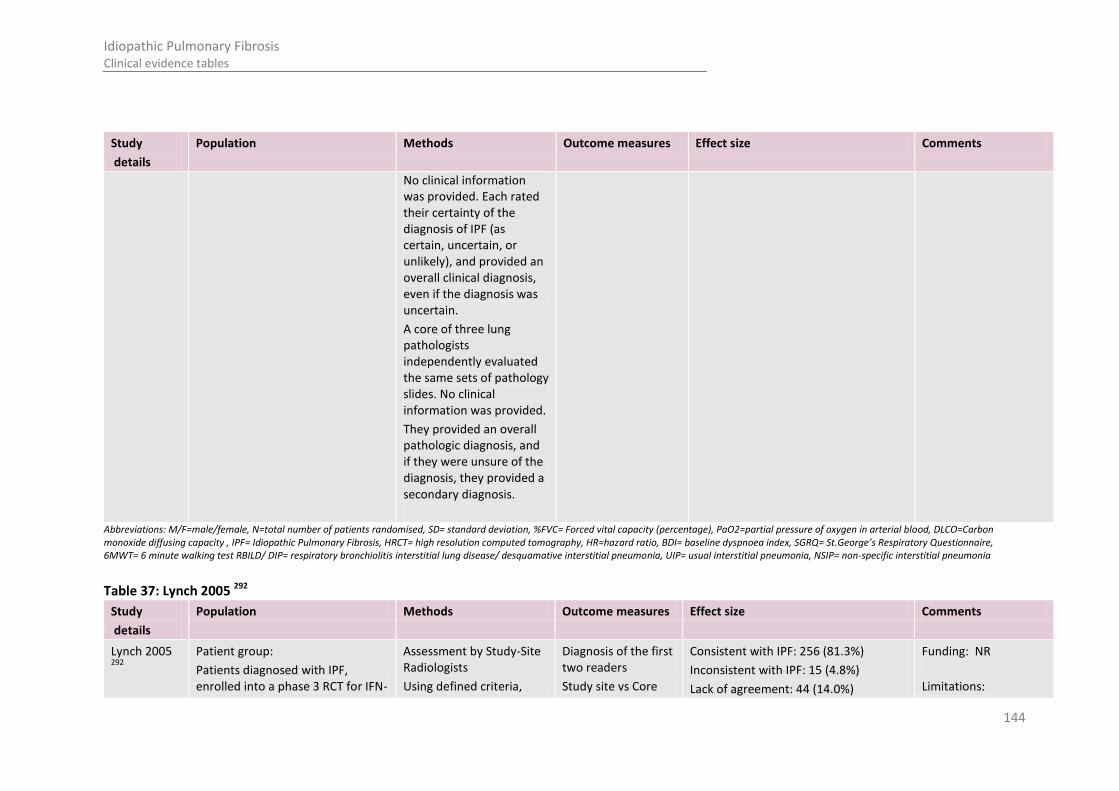
144
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Study
details
Population Methods Outcome measures Effect size Comments
No clinical information was provided. Each rated their certainty of the diagnosis of IPF (as certain, uncertain, or unlikely), and provided an overall clinical diagnosis, even if the diagnosis was uncertain.
A core of three lung pathologists independently evaluated the same sets of pathology slides. No clinical information was provided.
They provided an overall pathologic diagnosis, and if they were unsure of the diagnosis, they provided a secondary diagnosis.
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon monoxide diffusing capacity , IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 6MWT= 6 minute walking test RBILD/ DIP= respiratory bronchiolitis interstitial lung disease/ desquamative interstitial pneumonia, UIP= usual interstitial pneumonia, NSIP= non-specific interstitial pneumonia
Table 37: Lynch 2005 292
Study
details
Population Methods Outcome measures Effect size Comments
Lynch 2005 292
Patient group:
Patients diagnosed with IPF, enrolled into a phase 3 RCT for IFN-
Assessment by Study-Site Radiologists
Using defined criteria,
Diagnosis of the first two readers
Study site vs Core
Consistent with IPF: 256 (81.3%)
Inconsistent with IPF: 15 (4.8%)
Lack of agreement: 44 (14.0%)
Funding: NR
Limitations:

145
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Study
details
Population Methods Outcome measures Effect size Comments
Country of study:
USA, Europe, Canada, and South
Africa (RCT)
Study design:
Retrospective review of RCT data
Who was blinded:
Core radiologists
Setting:
Aim: To describe HRCT features in patients
with mild to moderate IPF, compare diagnostic evaluations
y1b, who had a baseline HRCT scan available for evaluation
Inclusion criteria:
Baseline HRCT was performed within 60 days before the first dose of study drug in the phase 3 trial.
Exclusion criteria:
NR
All patients
N: 315
Age (mean±SD): NR
Drop outs: 0
radiologists were asked to determine if either “definite” or “probable” IPF was present.
A radiographic diagnosis of “definite IPF” required all three of the following criteria:
presence of reticular abnormality and/or traction bronchiectasis with basal and peripheral predominance;
presence of honeycombing with basal and peripheral predominance;
absence of atypical features, such as micronodules, peribronchovascular nodules, consolidation, isolated (nonhoneycomb) cysts, extensive ground glass attenuation, or extensive mediastinal adenopathy.
The presence of the first and third criterion only qualified as “probable” IPF (i.e., honeycombing was
radiologists Clinical information may have been provided and the study-site radiologists knew that IPF was a consideration.
The core radiologists were blinded to clinical data and treatment group assignment; however, they knew that the patients had met non-radiologic inclusion criteria for the study, and that a study-site radiologist had interpreted the HRCT scan as at least probable IPF on the basis of predefined criteria.
Notes:
The simple κ coefficient, ranging from –1 to +1, was used to assess the degree of interrater agreement in specific comparisons.
The Wilcoxon rank
Consensus diagnosis of the three readers
Study site vs Core radiologists
Consistent with IPF: 283 (89.8%)
Inconsistent with IPF: 30 (9.5%)
Lack of agreement: 2 (0.6%)
Concordant interpretations by the first two readers
271/315 (86.0%)
Κ = 0.33 (95% CI, 0.18–0.48)
Classification of definite IPF cases by core radiologist
Consistent with IPF 245/263 (93.2%)
p = 0.001
Classification of probable IPF cases by core radiologist
probable IPF: 37/49
(75.5%)
p = 0.001
Agreement with IPF diagnosis by core radiologists according to study site location (academic/community)
Academic: 206 /228 (90.4%)
Community: 76/84 (90.5%)
p = 1.0
Histologic confirmation of UIP on SLB
205/315 (65%)
HRCT classification of IPF diagnosis by core radiologist consensus of cases with histologically confirmed UIP on
Consistent with IPF: 181/205 (88.3%)
Inconsistent with IPF: 24/205 (11.7%)
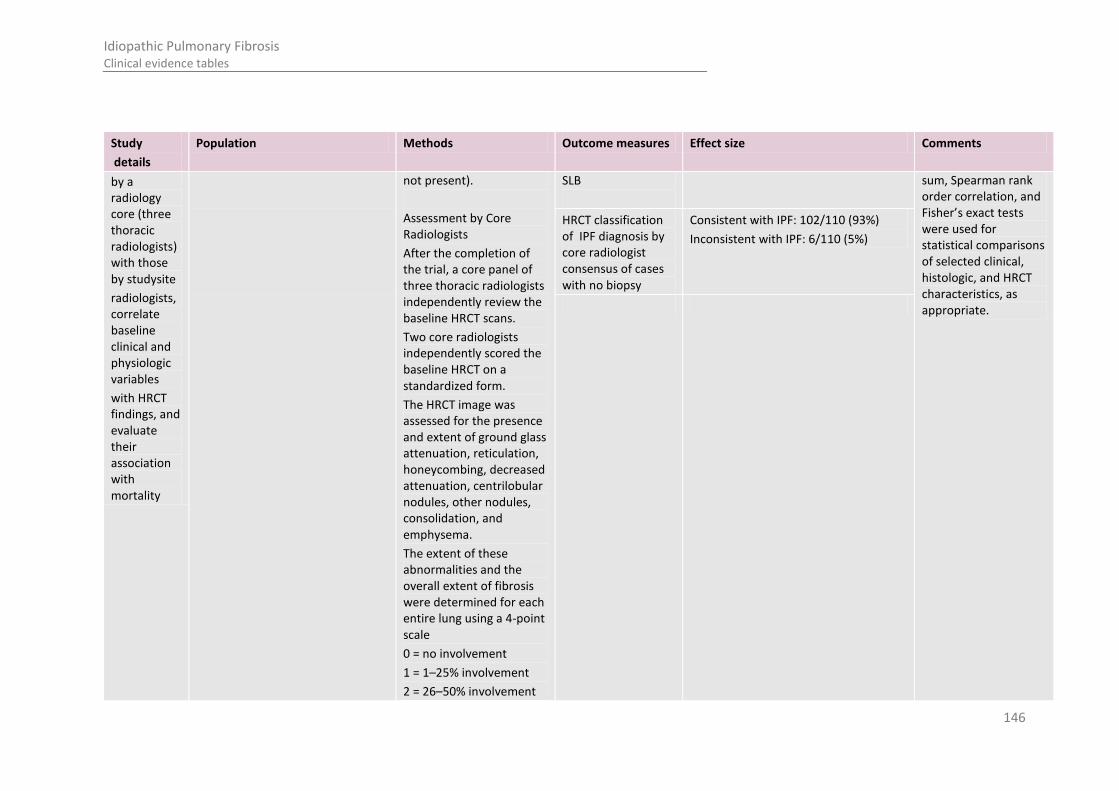
146
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Study
details
Population Methods Outcome measures Effect size Comments
by a radiology core (three thoracic radiologists) with those by studysite
radiologists, correlate baseline clinical and physiologic variables
with HRCT findings, and evaluate their association with mortality
not present).
Assessment by Core Radiologists
After the completion of the trial, a core panel of three thoracic radiologists independently review the baseline HRCT scans.
Two core radiologists independently scored the baseline HRCT on a standardized form.
The HRCT image was assessed for the presence and extent of ground glass attenuation, reticulation, honeycombing, decreased attenuation, centrilobular nodules, other nodules, consolidation, and emphysema.
The extent of these abnormalities and the overall extent of fibrosis were determined for each entire lung using a 4-point scale
0 = no involvement
1 = 1–25% involvement
2 = 26–50% involvement
SLB
sum, Spearman rank order correlation, and Fisher’s exact tests were used for statistical comparisons of selected clinical, histologic, and HRCT characteristics, as appropriate.
HRCT classification of IPF diagnosis by core radiologist consensus of cases with no biopsy
Consistent with IPF: 102/110 (93%)
Inconsistent with IPF: 6/110 (5%)
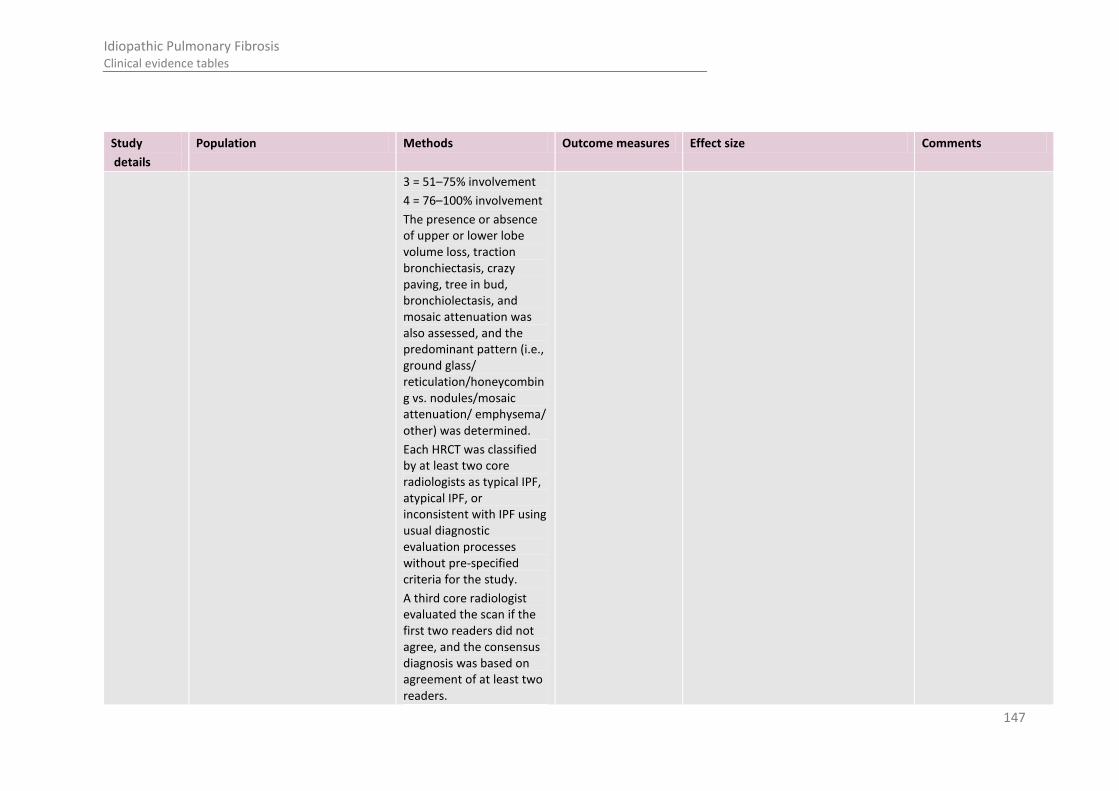
147
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Study
details
Population Methods Outcome measures Effect size Comments
3 = 51–75% involvement
4 = 76–100% involvement
The presence or absence of upper or lower lobe volume loss, traction bronchiectasis, crazy paving, tree in bud, bronchiolectasis, and mosaic attenuation was also assessed, and the predominant pattern (i.e., ground glass/ reticulation/honeycombing vs. nodules/mosaic attenuation/ emphysema/ other) was determined.
Each HRCT was classified by at least two core radiologists as typical IPF, atypical IPF, or inconsistent with IPF using usual diagnostic evaluation processes without pre-specified criteria for the study.
A third core radiologist evaluated the scan if the first two readers did not agree, and the consensus diagnosis was based on agreement of at least two readers.

148
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Study
details
Population Methods Outcome measures Effect size Comments
Only two readers were used for pattern extent scores, including honeycombing.
Neither discussion nor adjudication was used for any result.
In the event of disagreement between the readers, the result was recorded as missing.
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon monoxide diffusing capacity , IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 6MWT= 6 minute walking test RBILD/ DIP= respiratory bronchiolitis interstitial lung disease/ desquamative interstitial pneumonia, UIP= usual interstitial pneumonia, NSIP= non-specific interstitial pneumonia
Table 38: Raghu 1999 402
Study
details
Population Methods Outcome measures Effect size Comments
Raghu 1999 402
Country of study:
USA
Study design:
Prospective
Who was blinded:
Patient group:
all symptomatic, adult,
untreated people with ILD consecutively referred to a senior ILD specialist for diagnostic evaluation of new-onset ILD without a specific diagnosis at the University of Washington
Medical Centre in Seattle
Inclusion criteria:
Exclusion criteria:
All patients referred during the period from 1992 to 1997 for further diagnostic evaluation of nonspecific ILD were considered potential candidates.
Patients meeting the criteria were prospectively evaluated by the senior ILD specialist
A detailed and thorough clinical assessment was
Histological diagnosis of IPF
IPF= 29/59 Funding: NR Limitations:
Referral of patients from 1992-1997 (pre 1995 outdated?)
Notes:
The histologic features of SLB were used as the reference standard for an accurate diagnosis to compare
Clinical diagnosis of ILD other than IPF
Accuracy = 61% of cases
Sensitivity = 88.8%
Specificity = 40%
Positive predictive value = 94%
Negative predictive value = 25%
Clinical diagnosis
of IPF
Accuracy = 62% of cases
Sensitivity = 62%%
Specificity = 97%
Positive predictive value = 95%
Negative predictive value = 73%
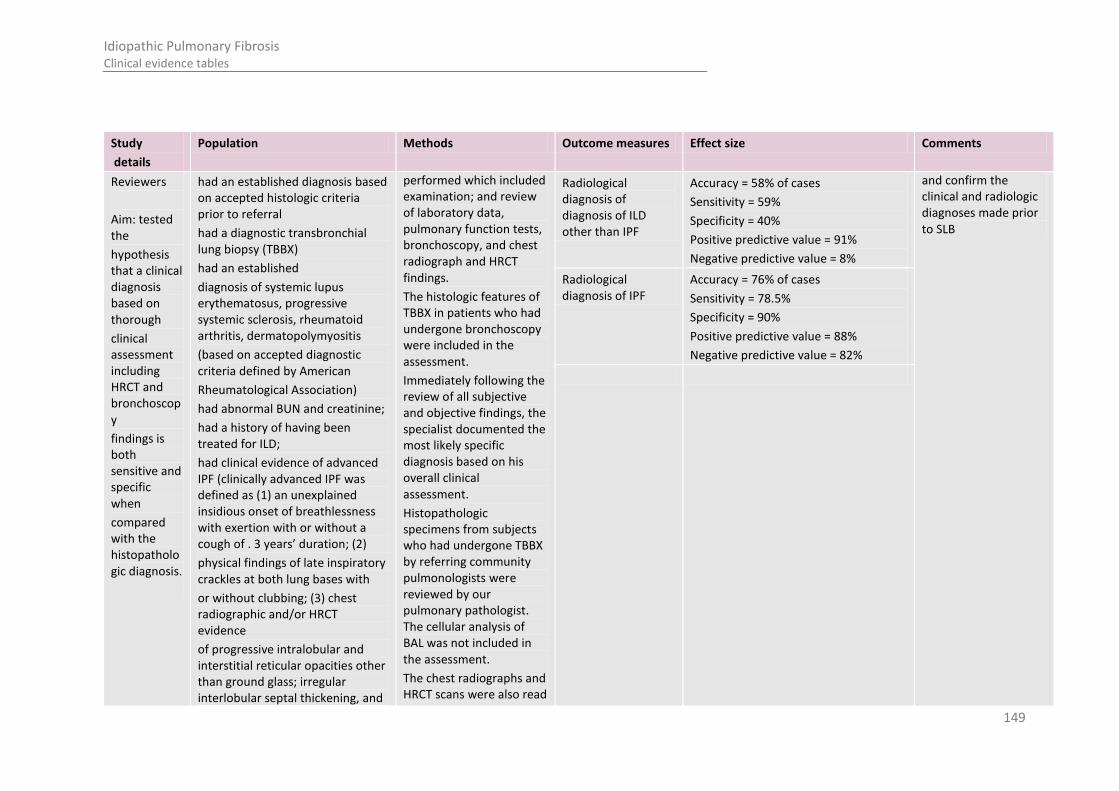
149
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Study
details
Population Methods Outcome measures Effect size Comments
Reviewers
Aim: tested the
hypothesis that a clinical diagnosis based on thorough
clinical assessment including HRCT and bronchoscopy
findings is both sensitive and specific when
compared with the histopathologic diagnosis.
had an established diagnosis based on accepted histologic criteria prior to referral
had a diagnostic transbronchial lung biopsy (TBBX)
had an established
diagnosis of systemic lupus erythematosus, progressive systemic sclerosis, rheumatoid arthritis, dermatopolymyositis
(based on accepted diagnostic criteria defined by American
Rheumatological Association)
had abnormal BUN and creatinine;
had a history of having been treated for ILD;
had clinical evidence of advanced IPF (clinically advanced IPF was defined as (1) an unexplained insidious onset of breathlessness with exertion with or without a cough of . 3 years’ duration; (2)
physical findings of late inspiratory crackles at both lung bases with
or without clubbing; (3) chest radiographic and/or HRCT evidence
of progressive intralobular and interstitial reticular opacities other than ground glass; irregular interlobular septal thickening, and
performed which included examination; and review of laboratory data, pulmonary function tests, bronchoscopy, and chest radiograph and HRCT findings.
The histologic features of TBBX in patients who had undergone bronchoscopy were included in the assessment.
Immediately following the review of all subjective and objective findings, the specialist documented the most likely specific diagnosis based on his overall clinical assessment.
Histopathologic specimens from subjects who had undergone TBBX by referring community pulmonologists were reviewed by our pulmonary pathologist. The cellular analysis of BAL was not included in the assessment.
The chest radiographs and HRCT scans were also read
Radiological diagnosis of diagnosis of ILD other than IPF
Accuracy = 58% of cases
Sensitivity = 59%
Specificity = 40%
Positive predictive value = 91%
Negative predictive value = 8%
and confirm the clinical and radiologic diagnoses made prior to SLB
Radiological diagnosis of IPF
Accuracy = 76% of cases
Sensitivity = 78.5%
Specificity = 90%
Positive predictive value = 88%
Negative predictive value = 82%

150
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Study
details
Population Methods Outcome measures Effect size Comments
diffuse honeycombing in both lungs (not restricted to
the subpleural and lower lung zones) associated with traction bronchiectasis on HRCT;
had evidence of overt right or left heart failure on physical examination;
refused SLB
All patients
N: 59
Age range (median): 24-78 (53)
Drop outs: 0
independently by a senior chest radiologist who made a most likely specific diagnosis based solely on radiographic and HRCT features. The radiologist was only aware that the chest radiographs and HRCT scans were being obtained to rule out ILD.
Prior to SLB, neither the radiologist’s report nor the clinical diagnosis independently made by the ILD specialist was made available to one another or to the pathologist.
All consenting patients in whom a diagnosis was not clearly established by characteristic histologic features on TBBX underwent SLB within 1 month of their initial clinical assessment.
The biopsy slides were interpreted by a senior pulmonary pathologist. The pathologist was aware that the SLB was obtained for diagnosis of ILD, but
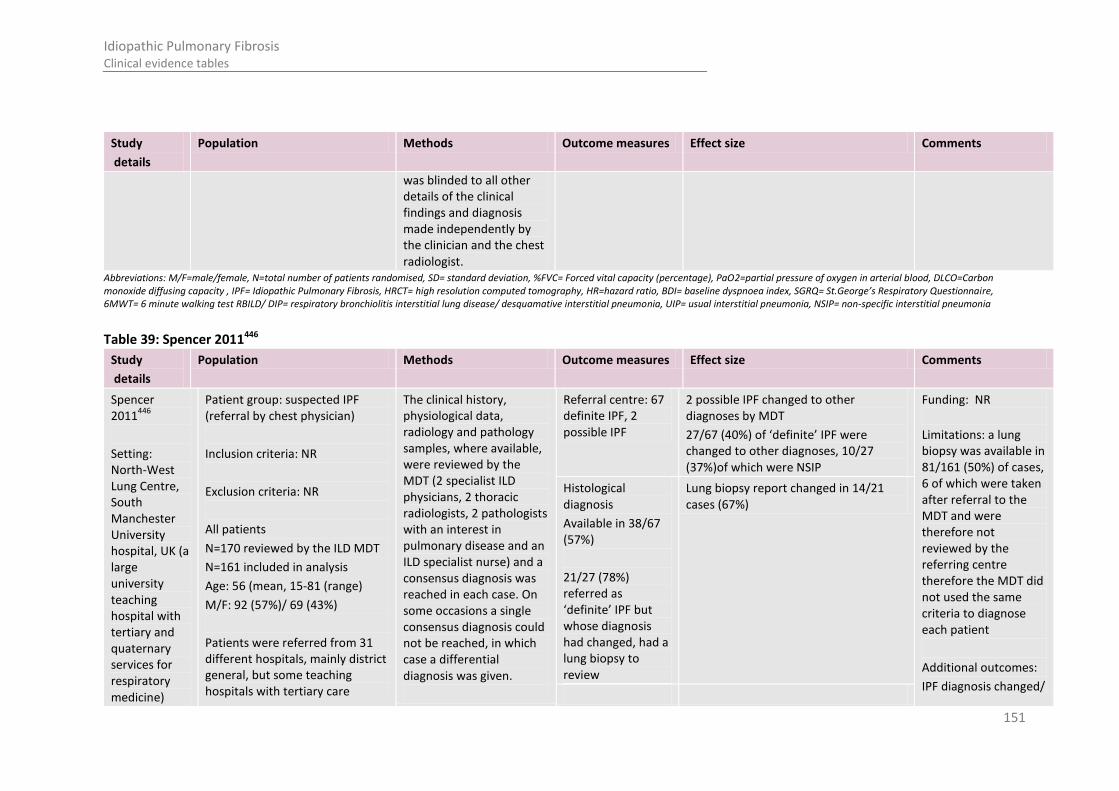
151
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Study
details
Population Methods Outcome measures Effect size Comments
was blinded to all other details of the clinical findings and diagnosis made independently by the clinician and the chest radiologist.
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon monoxide diffusing capacity , IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 6MWT= 6 minute walking test RBILD/ DIP= respiratory bronchiolitis interstitial lung disease/ desquamative interstitial pneumonia, UIP= usual interstitial pneumonia, NSIP= non-specific interstitial pneumonia
Table 39: Spencer 2011446
Study
details
Population Methods Outcome measures Effect size Comments
Spencer 2011
446
Setting: North-West Lung Centre, South Manchester University hospital, UK (a large university teaching hospital with tertiary and quaternary services for respiratory medicine)
Patient group: suspected IPF (referral by chest physician)
Inclusion criteria: NR
Exclusion criteria: NR
All patients
N=170 reviewed by the ILD MDT
N=161 included in analysis
Age: 56 (mean, 15-81 (range)
M/F: 92 (57%)/ 69 (43%)
Patients were referred from 31 different hospitals, mainly district general, but some teaching hospitals with tertiary care
The clinical history, physiological data, radiology and pathology samples, where available, were reviewed by the MDT (2 specialist ILD physicians, 2 thoracic radiologists, 2 pathologists with an interest in pulmonary disease and an ILD specialist nurse) and a consensus diagnosis was reached in each case. On some occasions a single consensus diagnosis could not be reached, in which case a differential diagnosis was given.
Referral centre: 67 definite IPF, 2 possible IPF
2 possible IPF changed to other diagnoses by MDT
27/67 (40%) of ‘definite’ IPF were changed to other diagnoses, 10/27 (37%)of which were NSIP
Funding: NR
Limitations: a lung biopsy was available in 81/161 (50%) of cases, 6 of which were taken after referral to the MDT and were therefore not reviewed by the referring centre therefore the MDT did not used the same criteria to diagnose each patient
Additional outcomes:
IPF diagnosis changed/
Histological diagnosis
Available in 38/67 (57%)
21/27 (78%) referred as ‘definite’ IPF but whose diagnosis had changed, had a lung biopsy to review
Lung biopsy report changed in 14/21 cases (67%)

152
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Study
details
Population Methods Outcome measures Effect size Comments
Duration of follow-up:
Design: retrospective cohort
services
Had HRCT of the thorax and their cases had been reviewed by an ILD physician.
unchanged by:
patients age
Number of months from MDT to follow-up
Lung function at time of MDT meeting
Change in HRCT report following MDT
Change in pathology report following MDT
Number of cases agreed/ disagreed between centres
Survival benefit from change of diagnosis from IPF to other ILD
Notes: some patients were <18 years old
The MDT consisted of 2 specialist ILD physicians, 2 thoracic radiologists, 2 pathologists with an interest in pulmonary disease and an ILD specialist nurse, all of

153
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Study
details
Population Methods Outcome measures Effect size Comments
whom, bar 1 chest physician, had more than 10 years experience in a tertiary referral ILD clinic.
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon monoxide diffusing capacity , IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 6MWT= 6 minute walking test RBILD/ DIP= respiratory bronchiolitis interstitial lung disease/ desquamative interstitial pneumonia, UIP= usual interstitial pneumonia, NSIP= non-specific interstitial pneumonia
Table 40: Sumikawa 2008454
Study
details
Population Methods Outcome measures Effect size Comments
Sumikawa 2008 454
Country of study:
Japan
Study design:
retrospective review
Who was blinded:
No blinding
Patient group:
154 patients who underwent surgical biopsies at three institutions and who met the clinical and histologic criteria for diagnosis recommended by the ATS/ERS consensus classification of the IIPs were identified. Of which only 112 cases confirmed as confident UIP by a second pathologist where studied
Inclusion criteria:
NR
Exclusion criteria:
NR
Patient selection: All 154 cases were originally diagnosed histologically as diagnostic of UIP by a lung pathologist at each of the contributing institutions. All biopsy specimens were also reviewed by a second lung pathologist and classified into the following four categories by the certainty of the diagnosis of UIP:
confident UIP,
probable UIP,
probably not UIP
Classification by second lung pathologist(patient selection)
Confident UIP: 112 cases (73%)
Probable UIP: 19 cases (12%)
Probably not UIP: 16 cases (10%)
Confident not UIP: 7 cases (5%)
Funding: NR
Limitations:
All radiologists and the pathologist were informed about pathological and clinical UIP diagnosis of the patient
Additional outcomes:
The relationship between survival duration and the three CT categories as subtypes was
Radiologists classification of UIP
Definite UIP: 33/112(34%)
Consistent with UIP: 36/112
Suggestive of alternative diagnosis: 21/112 (21%)
Unclassified findings: 8/112 (8%)
The inter-observer agreement of CT diagnosis into consistent with UIP (definite or probable) or suggestive of
moderate (k 5 0.60)

154
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Study
details
Population Methods Outcome measures Effect size Comments
Aim:
to revisit the thin-section CT findings of IPF and to
clarify the correlation between CT findings and mortality
All patients
N: 154 (pathological review) 112 (radiological review)
Age (mean±SD): NR
Drop outs: 0
confident not UIP.
A confident diagnosis of UIP was made if all the ATS/ERS criteria were fulfilled: patchy involvement with clear evidence of chronic scarring/honeycombing and the presence of fibroblast foci in the absence of features against the diagnosis of UIP, such as granulomas and etc.
A confident diagnosis of ‘‘not UIP’’ was made if there were clear features of an alternative diagnosis, or if none of the ATS/ERS criteria for UIP were present.
Diagnoses of ‘‘probable UIP’’ and ‘‘probably not UIP’’ were more subjective; most commonly the former represented cases of extensive honeycombing without good evidence of patchy involvement in the sample reviewed, and the
alternate diagnosis (suggestive of NSIP or indeterminate)
evaluated
Notes:
The inter-observer variation of the existence of predominant distribution and the overall impression of the findings was analyzed using the k statistic. Inter-observer agreement was classified as follows:
poor (k 5 0–0.20),
fair (k 5 0.21–0.40),
moderate (k 5 0.41–0.60),
good (k 5 0.61–0.80),
excellent (k 5 0.81–1.00).
Comparison between definite UIP and the other two CT categories of abnormality was made using univariable analysis

155
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Study
details
Population Methods Outcome measures Effect size Comments
latter were cases in which the histology was more suggestive of an alternative diagnosis.
Only the 112 cases interpreted by the second lung pathologist as definitely being UIP were considered acceptable for the study
Thin-section CT scans of all patients were reviewed in a random order by four radiologists
All radiologists were informed about pathological and clinical UIP diagnosis.
The radiologist evaluated the presence, extent, and distribution of CT findings and radiologic abnormalities, excluding emphysema, that were present in both lungs to determine the percentage of lung parenchyma occupied by the disease.
After review of the
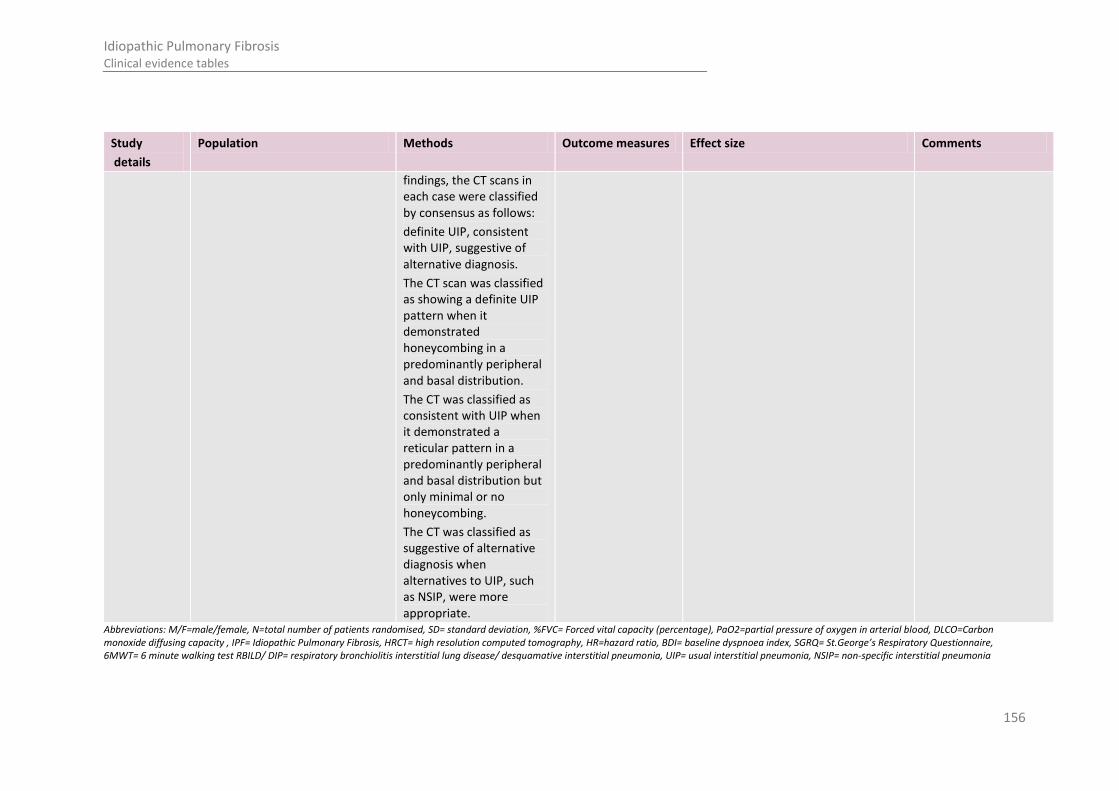
156
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Study
details
Population Methods Outcome measures Effect size Comments
findings, the CT scans in each case were classified by consensus as follows:
definite UIP, consistent with UIP, suggestive of alternative diagnosis.
The CT scan was classified as showing a definite UIP pattern when it demonstrated honeycombing in a predominantly peripheral and basal distribution.
The CT was classified as consistent with UIP when it demonstrated a reticular pattern in a predominantly peripheral and basal distribution but only minimal or no honeycombing.
The CT was classified as suggestive of alternative diagnosis when alternatives to UIP, such as NSIP, were more appropriate.
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon monoxide diffusing capacity , IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 6MWT= 6 minute walking test RBILD/ DIP= respiratory bronchiolitis interstitial lung disease/ desquamative interstitial pneumonia, UIP= usual interstitial pneumonia, NSIP= non-specific interstitial pneumonia
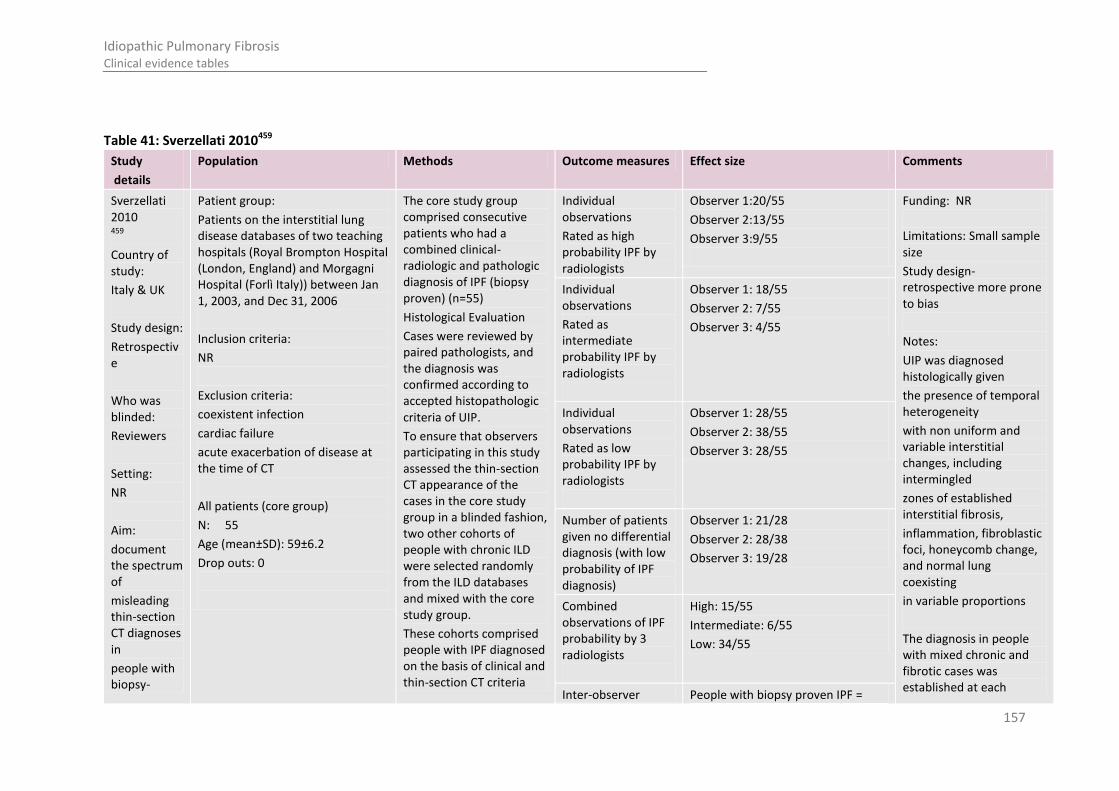
157
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Table 41: Sverzellati 2010459
Study
details
Population Methods Outcome measures Effect size Comments
Sverzellati 2010 459
Country of study:
Italy & UK
Study design:
Retrospective
Who was blinded:
Reviewers
Setting:
NR
Aim:
document the spectrum of
misleading thin-section CT diagnoses in
people with biopsy-
Patient group:
Patients on the interstitial lung disease databases of two teaching hospitals (Royal Brompton Hospital (London, England) and Morgagni Hospital (Forlì Italy)) between Jan 1, 2003, and Dec 31, 2006
Inclusion criteria:
NR
Exclusion criteria:
coexistent infection
cardiac failure
acute exacerbation of disease at the time of CT
All patients (core group)
N: 55
Age (mean±SD): 59±6.2
Drop outs: 0
The core study group comprised consecutive patients who had a combined clinical-radiologic and pathologic diagnosis of IPF (biopsy proven) (n=55)
Histological Evaluation
Cases were reviewed by paired pathologists, and the diagnosis was confirmed according to accepted histopathologic criteria of UIP.
To ensure that observers participating in this study assessed the thin-section CT appearance of the cases in the core study group in a blinded fashion, two other cohorts of people with chronic ILD were selected randomly from the ILD databases and mixed with the core study group.
These cohorts comprised people with IPF diagnosed on the basis of clinical and thin-section CT criteria
Individual observations
Rated as high probability IPF by radiologists
Observer 1:20/55
Observer 2:13/55
Observer 3:9/55
Funding: NR
Limitations: Small sample size
Study design- retrospective more prone to bias
Notes:
UIP was diagnosed histologically given
the presence of temporal heterogeneity
with non uniform and variable interstitial changes, including intermingled
zones of established interstitial fibrosis,
inflammation, fibroblastic foci, honeycomb change, and normal lung coexisting
in variable proportions
The diagnosis in people with mixed chronic and fibrotic cases was established at each
Individual observations
Rated as intermediate probability IPF by radiologists
Observer 1: 18/55
Observer 2: 7/55
Observer 3: 4/55
Individual observations
Rated as low probability IPF by radiologists
Observer 1: 28/55
Observer 2: 38/55
Observer 3: 28/55
Number of patients given no differential diagnosis (with low probability of IPF diagnosis)
Observer 1: 21/28
Observer 2: 28/38
Observer 3: 19/28
Combined observations of IPF probability by 3 radiologists
High: 15/55
Intermediate: 6/55
Low: 34/55
Inter-observer People with biopsy proven IPF =

158
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Study
details
Population Methods Outcome measures Effect size Comments
proved IPF (n=20) & a mixed group of subjects with various chronic and fibrotic interstitial lung diseases (n=48)
In the mixed group, subjects had diseases such as NSIP (n = 17), sarcoidosis (n = 6), chronic hypersensitivity pneumonitis (HP (n = 8)), desquamative interstitial pneumonia (n = 5), fibrotic Langerhans cell histiocytosis (n = 4), organizing pneumonia (n = 3), mixed NSIP and organizing pneumonia (n = 3), and lymphoid interstitial pneumonia (n = 2).
Clinical data (eg, absence of previous environmental exposures and connective tissue disease) were reviewed by two chest physicians
Lung biopsy specimens with a histologic diagnosis of UIP were reviewed by paired pathologists
Decisions were made with
agreement of first choice diagnosis
Moderate: ( k = 0.45 (95%
CI: 0.32, 0.58))
Whole study population= Fair: ( k = 0.39 (95% CI: 0.34, 0.44))
participating institution on the basis of compatible clinical and histologic findings obtained by means of surgical lung biopsy (for HP, NSIP, organizing pneumonia, desquamative interstitial pneumonia, and lymphoid interstitial pneumonia) or transbronchial biopsy (for sarcoidosis).
Unadjusted k coefficients of agreement were computed for the first-choice diagnosis in the entire study population and in the cohort of people with biopsy proved IPF. The weighted k (k w) coefficient of agreement was used to calculate the observer variation for the estimation of the probability of IPF diagnosis in the entire cohort and in the cohort of people with biopsy-proved IPF between paired observers ( n = 3). To do this, the percentage
159
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Study
details
Population Methods Outcome measures Effect size Comments
consensus.
UIP was diagnosed by using the ATS and ERS criteria.
Image Evaluation
Images were reviewed independently by three thoracic radiologists
They did not provide any cases included in the study population, and had no knowledge of clinical findings or details of the patient population and were not aware of the purpose of the study.
The observers were asked to list their differential diagnoses (with no limit to the number of possible diagnoses) and to assign likelihood to each diagnosis (to the nearest 5%, totalling 100%).
Specific diagnostic criteria for ILDs were not provided, so the diagnoses were based on each observer’s own experience and understanding of the current CT literature.
likelihood given to each diagnosis was assigned a grade of 0 to 4, representing clinically useful probabilities: grade 0, condition not included in the differential diagnosis;
grade 1, unlikely (5%–25 %);
grade 2, intermediate probability (30%–65%); grade 3, high probability (70%–95%); grade 4, definite (100%).
Observer agreement was categorized according to k values as:
Poor ( less than 0.20)
fair (0.21–0.40)
moderate,( 0.41–0.60)
good ( 0.61–0.80)
excellent (0.81–1.00)

160
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Study
details
Population Methods Outcome measures Effect size Comments
However, the
observers used the terminology of the
ATS and ERS classification for the diagnosis of idiopathic interstitial pneumonias.
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon monoxide diffusing capacity , IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 6MWT= 6 minute walking test RBILD/ DIP= respiratory bronchiolitis interstitial lung disease/ desquamative interstitial pneumonia, UIP= usual interstitial pneumonia, NSIP= non-specific interstitial pneumonia
Table 42: Thomeer 2008 470
Study
details
Population Methods Outcome measures Effect size Comments
Thomeer 2008
470
Country of study:
6 European countries (IFIGENIA RCT)
Study design:
Retrospective review
Who was blinded:
Patient group:
All of the patients included in the Idiopathic Pulmonary Fibrosis International Group Exploring N-Acetylcysteine I Annual (IFIGENIA) trial. All patients diagnosed with IPF by a specialist respiratory physician
Inclusion criteria:
Diagnosis of IPF was based on the international consensus criteria
Aged 18–75 yrs.
Newly diagnosed (<6 months) as well as previously diagnosed (>6 months) patients
Review by the radiological committee:
The copies of the HRCT scans were reviewed independently by 3 members of the radiology committee, without knowledge of clinical, physiological or pathological parameters.
Each member of the committee confirmed the diagnosis of UIP on thoracic HRCT based on the criteria of the international consensus statement.
Diagnosis of IPF by HRCT
Present: 165 (92.7%)
Absent: 14 (7.3%)
Funding: NR
Limitations: none
Additional outcomes:
Diagnosis of IPF by HRCT and/or biopsy for subgroups of patients (grouped by recruiting country)
Inter-observer agreement between histology reviewers sub grouped by presence UIP in HRCT and % predicted FVC
Inter-observer agreement between radiology
Diagnosis of IPF by OLB/TLB
Present: 68 (84.0%)
Absent: 14 (16.0%)
Definite diagnosis of IPF*
Present: 156 (87.2%)
Absent: 23 (12.8%)
Inter-observer agreement between reviewers (mean weighted kappa coefficients)
HRCT reviewers:
0.33-0.46 ((0.23-0.36)-(0.44-0.56)) (95% CIs)
Histology reviewers:
0.30 (0.12–0.48)

161
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Reviewers
Setting:
NR
Aim: evaluate the diagnostic accuracy of respiratory physicians in IPF, and to calculate the interobserver agreement between HRCT
reviewers and histology reviewers in the diagnosis of UIP
Exclusion criteria:
NR
All patients
N:
Age (mean±SD):
Drop outs: NR
The degree of confidence in the diagnosis was recorded in terms of the scan being very suggestive, probable or unlikely for the diagnosis.
The UIP diagnosis on thoracic HRCT was confirmed if the scan was scored as very suggestive or probable for UIP, and rejected if it was scored as unlikely.
If disagreement occurred between the three members of the radiology committee, the UIP diagnosis agreed by the majority of the three members was accepted as definite.
Review by the histology committee:
The diagnosis of UIP according to the criteria of the ATS/ERS consensus classification was assessed by an independent panel of three pathology experts.
The slides were reviewed independently without knowledge of clinical or
reviewers sub grouped by presence UIP in biopsy and no biopsy and % predicted FVC
Notes: *defined as agreement of the histology and radiology committees with the diagnosis of IPF based on OLB/TLB and thoracic HRCT, or of the radiology committee when only HRCT scans were available.
Weighted kappa coefficients (kw) were used to measure the level of inter-observer agreement. The kw were calculated using a method recommended for comparing level of agreement with categorical data along with their respective 95% CI
162
Idiopathic Pulmonary Fibrosis Clinical evidence tables
physiological parameters.
All slides were graded as being very suggestive, probable or unlikely for the diagnosis of UIP.
For each observer, the UIP diagnosis on lung biopsy was confirmed if the slide was scored as very suggestive or probable for UIP and rejected if it was scored as unlikely.
If the two reviewers disagreed as to diagnosis of UIP, the slides were sent to the third member of the pathology committee and assessed in an identical fashion.
The diagnosis agreed by the majority of the three members was accepted as final.
The diagnosis of UIP was rejected when one or both committees did not confirm a diagnosis of UIP.
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon monoxide diffusing capacity , IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 6MWT= 6 minute walking test RBILD/ DIP= respiratory bronchiolitis interstitial lung disease/ desquamative interstitial pneumonia, UIP= usual interstitial pneumonia, NSIP= non-specific interstitial pneumonia
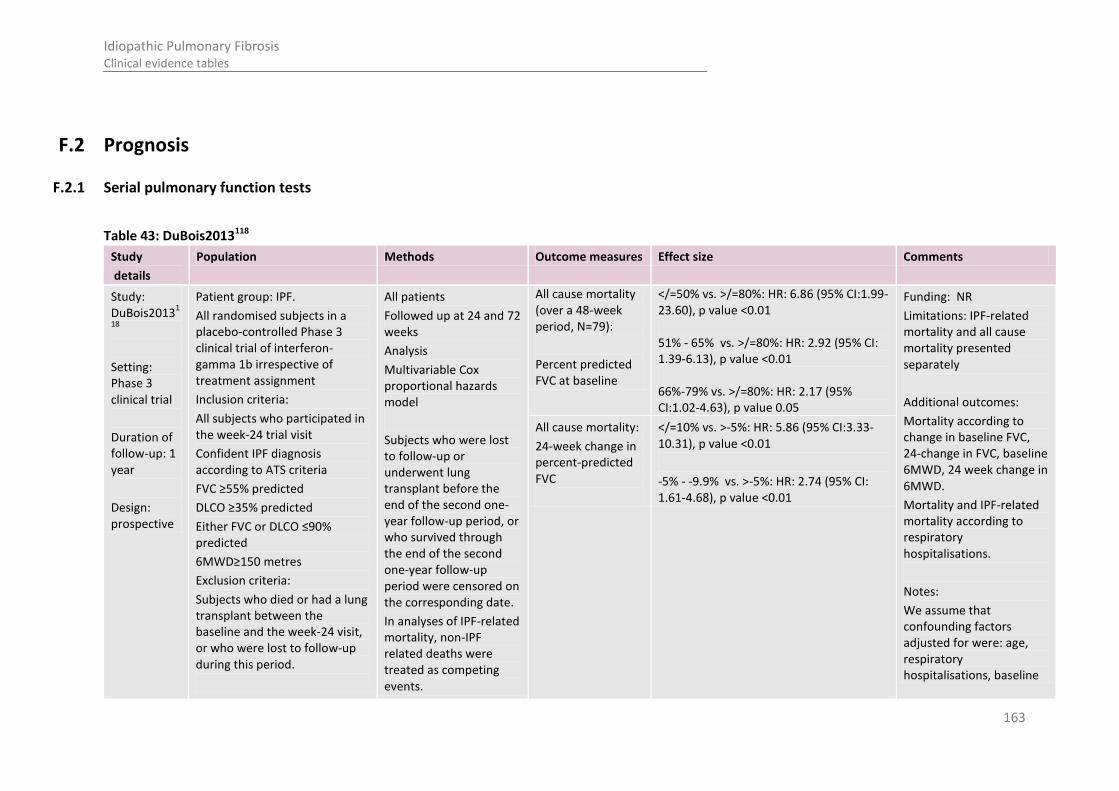
163
Idiopathic Pulmonary Fibrosis Clinical evidence tables
F.2 Prognosis
F.2.1 Serial pulmonary function tests
Table 43: DuBois2013118
Study
details
Population Methods Outcome measures Effect size Comments
Study: DuBois2013
1
18
Setting: Phase 3 clinical trial
Duration of follow-up: 1 year
Design: prospective
Patient group: IPF.
All randomised subjects in a placebo-controlled Phase 3 clinical trial of interferon-gamma 1b irrespective of treatment assignment
Inclusion criteria:
All subjects who participated in the week-24 trial visit
Confident IPF diagnosis according to ATS criteria
FVC ≥55% predicted
DLCO ≥35% predicted
Either FVC or DLCO ≤90% predicted
6MWD≥150 metres
Exclusion criteria:
Subjects who died or had a lung transplant between the baseline and the week-24 visit, or who were lost to follow-up during this period.
All patients
Followed up at 24 and 72 weeks
Analysis
Multivariable Cox proportional hazards model
Subjects who were lost to follow-up or underwent lung transplant before the end of the second one-year follow-up period, or who survived through the end of the second one-year follow-up period were censored on the corresponding date.
In analyses of IPF-related mortality, non-IPF related deaths were treated as competing events.
All cause mortality (over a 48-week period, N=79):
Percent predicted FVC at baseline
</=50% vs. >/=80%: HR: 6.86 (95% CI:1.99-23.60), p value <0.01 51% - 65% vs. >/=80%: HR: 2.92 (95% CI: 1.39-6.13), p value <0.01 66%-79% vs. >/=80%: HR: 2.17 (95% CI:1.02-4.63), p value 0.05
Funding: NR
Limitations: IPF-related mortality and all cause mortality presented separately
Additional outcomes:
Mortality according to change in baseline FVC, 24-change in FVC, baseline 6MWD, 24 week change in 6MWD.
Mortality and IPF-related mortality according to respiratory hospitalisations.
Notes:
We assume that confounding factors adjusted for were: age, respiratory hospitalisations, baseline
All cause mortality:
24-week change in percent-predicted FVC
</=10% vs. >-5%: HR: 5.86 (95% CI:3.33-10.31), p value <0.01
-5% - -9.9% vs. >-5%: HR: 2.74 (95% CI: 1.61-4.68), p value <0.01
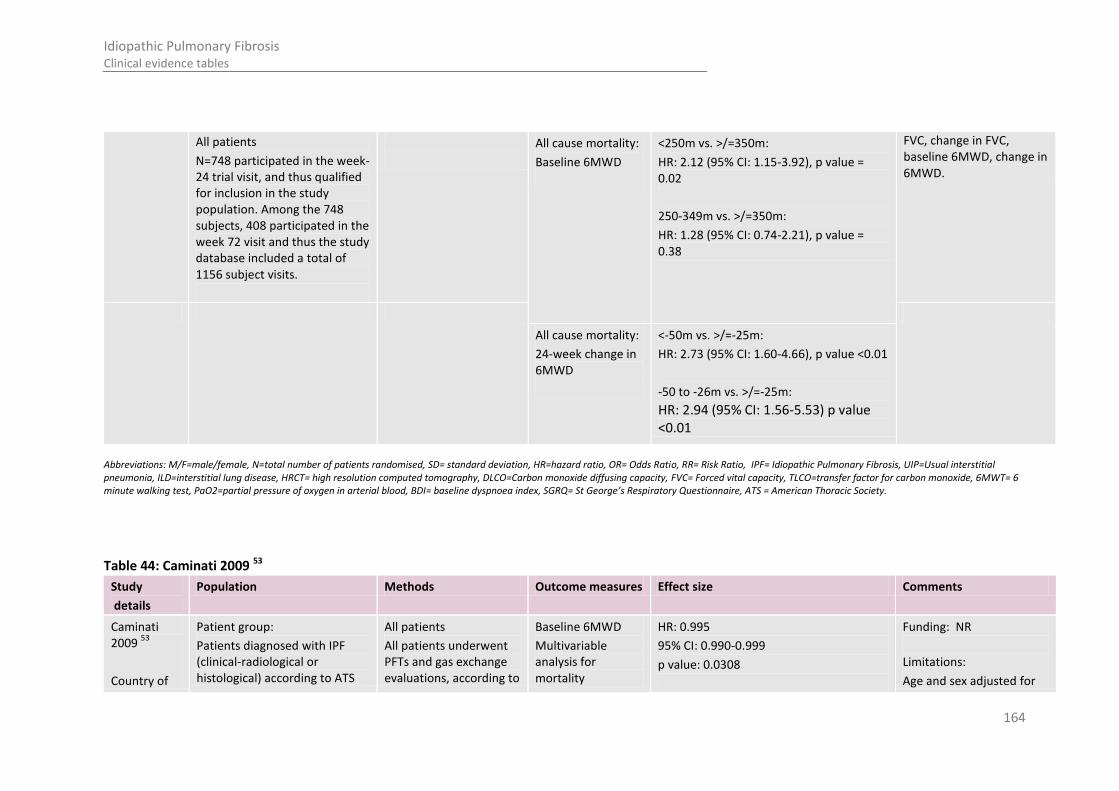
164
Idiopathic Pulmonary Fibrosis Clinical evidence tables
All patients
N=748 participated in the week-24 trial visit, and thus qualified for inclusion in the study population. Among the 748 subjects, 408 participated in the week 72 visit and thus the study database included a total of 1156 subject visits.
All cause mortality:
Baseline 6MWD
<250m vs. >/=350m:
HR: 2.12 (95% CI: 1.15-3.92), p value = 0.02
250-349m vs. >/=350m:
HR: 1.28 (95% CI: 0.74-2.21), p value = 0.38
FVC, change in FVC, baseline 6MWD, change in 6MWD.
All cause mortality:
24-week change in 6MWD
<-50m vs. >/=-25m:
HR: 2.73 (95% CI: 1.60-4.66), p value <0.01
-50 to -26m vs. >/=-25m:
HR: 2.94 (95% CI: 1.56-5.53) p value <0.01
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, HR=hazard ratio, OR= Odds Ratio, RR= Risk Ratio, IPF= Idiopathic Pulmonary Fibrosis, UIP=Usual interstitial pneumonia, ILD=interstitial lung disease, HRCT= high resolution computed tomography, DLCO=Carbon monoxide diffusing capacity, FVC= Forced vital capacity, TLCO=transfer factor for carbon monoxide, 6MWT= 6 minute walking test, PaO2=partial pressure of oxygen in arterial blood, BDI= baseline dyspnoea index, SGRQ= St George’s Respiratory Questionnaire, ATS = American Thoracic Society.
Table 44: Caminati 2009 53
Study
details
Population Methods Outcome measures Effect size Comments
Caminati 2009
53
Country of
Patient group:
Patients diagnosed with IPF (clinical-radiological or histological) according to ATS
All patients
All patients underwent PFTs and gas exchange evaluations, according to
Baseline 6MWD
Multivariable analysis for mortality
HR: 0.995
95% CI: 0.990-0.999
p value: 0.0308
Funding: NR
Limitations:
Age and sex adjusted for

165
Idiopathic Pulmonary Fibrosis Clinical evidence tables
study:
Italy
Study design:
Retrospective cohort
Who was blinded:
NA
Setting:
NR
Duration of follow-up:
Mean 19.8 months (range 3.2-46.4)
criteria that underwent a 6 minute walk test on room air.
Inclusion criteria:
NR
Exclusion criteria:
Underlying connective tissue disease
Exposure to environmental agents or drugs known to cause pulmonary fibrosis
Underlying disorder known to cause pulmonary fibrosis
If resting saturation was less then 90% on room air, patients were not considered eligible for 6MWT
All patients
N: 44
Age (mean): 61.9±1.5
M/F: 23/21
Drop outs: Unclear
ATS criteria, at baseline and 6 months.
6MWT: Patients walked on level ground using standardized instructions. The test was symptom limited and was stopped for safety purposes if the arterial oxygen saturation dropped to <86%
Clinical data and survival data were obtained from medical records
Analysis:
Univariable Cox proportional hazard model was used to analyse the relationship between 6MWT and mortality (results not reported). Multivariate Cox proportional hazards model was used for each parameter adjusting for covariables, age and sex.
Oxygen saturation at rest
Multivariable analysis for mortality
HR: 0.816
95% CI: 0.537-1.241
P value: 0.3416
in analysis, no other confounding factors considered
Additional outcomes:
The paper reports the correlation between physiologic and 6MWT parameters multivariable analysis of physiologic and 6MWT parameters associated with mortality
Notes: 35 patients received drug therapy during the study period.
During the follow-up period, 11/44 patients died for causes related to disease. 3 patients fulfil criteria for acute exacerbation of disease.
Baseline FVC
Multivariable analysis for mortality
HR: 0.365
95% CI: 0.124-1.078
p value: 0.0681
Baseline DLCO
Multivariable analysis for mortality
HR: 0.723
95% CI: 0.548-0.954
p value: 0.0219
Change in 6MWD at 12 months
Multivariable analysis for mortality
HR: 0.994
95% CI: 0.988-1
P value: 0.05
Change in oxygen saturation at rest, at 12 months
Multivariable analysis for mortality
HR: 0.25
95% CI: 0.075-0.837
P value: 0.02
Change in FVC at 12 months
Multivariable analysis for mortality
HR: 0.142
95% CI: 0.018-1.1
P value: 0.06
Change in DLCO at 12 months
Multivariable
HR: 0.49
95% CI: 0.232-1.036
P value: 0.06
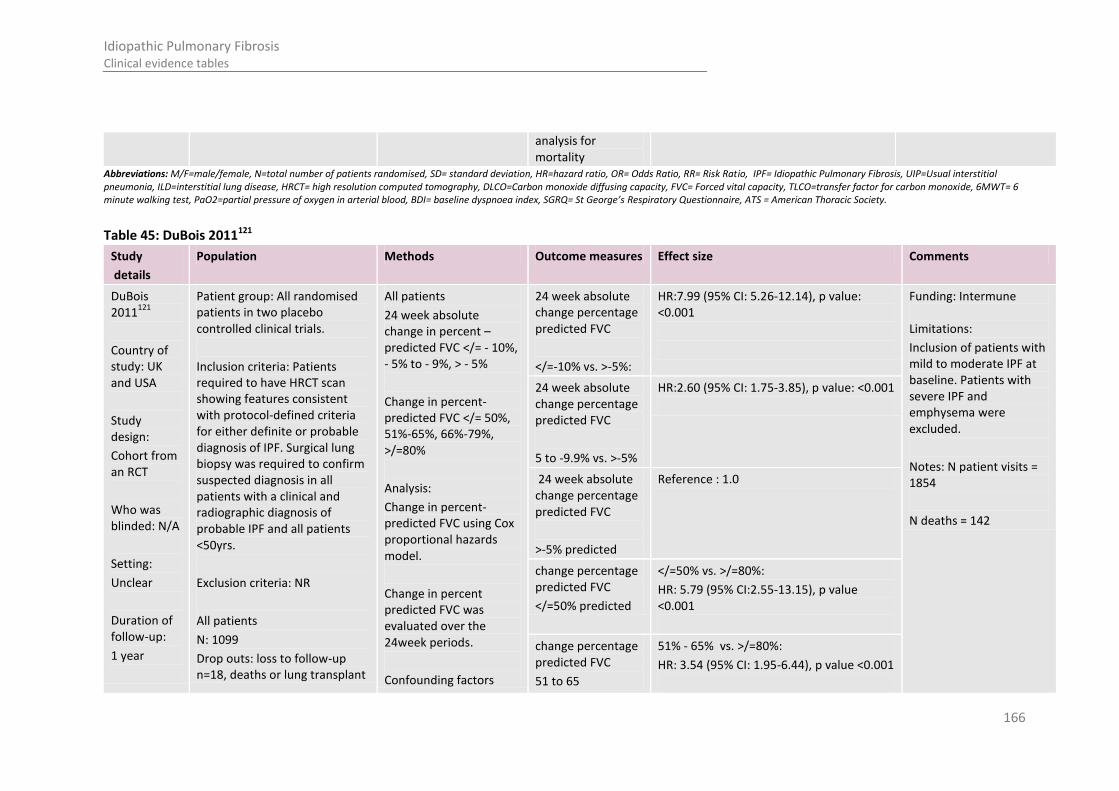
166
Idiopathic Pulmonary Fibrosis Clinical evidence tables
analysis for mortality
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, HR=hazard ratio, OR= Odds Ratio, RR= Risk Ratio, IPF= Idiopathic Pulmonary Fibrosis, UIP=Usual interstitial pneumonia, ILD=interstitial lung disease, HRCT= high resolution computed tomography, DLCO=Carbon monoxide diffusing capacity, FVC= Forced vital capacity, TLCO=transfer factor for carbon monoxide, 6MWT= 6 minute walking test, PaO2=partial pressure of oxygen in arterial blood, BDI= baseline dyspnoea index, SGRQ= St George’s Respiratory Questionnaire, ATS = American Thoracic Society.
Table 45: DuBois 2011121
Study
details
Population Methods Outcome measures Effect size Comments
DuBois 2011
121
Country of study: UK and USA
Study design:
Cohort from an RCT
Who was blinded: N/A
Setting:
Unclear
Duration of follow-up:
1 year
Patient group: All randomised patients in two placebo controlled clinical trials.
Inclusion criteria: Patients required to have HRCT scan showing features consistent with protocol-defined criteria for either definite or probable diagnosis of IPF. Surgical lung biopsy was required to confirm suspected diagnosis in all patients with a clinical and radiographic diagnosis of probable IPF and all patients <50yrs.
Exclusion criteria: NR
All patients
N: 1099
Drop outs: loss to follow-up n=18, deaths or lung transplant
All patients
24 week absolute change in percent –predicted FVC </= - 10%, - 5% to - 9%, > - 5%
Change in percent-predicted FVC </= 50%, 51%-65%, 66%-79%, >/=80%
Analysis:
Change in percent-predicted FVC using Cox proportional hazards model.
Change in percent predicted FVC was evaluated over the 24week periods.
Confounding factors
24 week absolute change percentage predicted FVC
</=-10% vs. >-5%:
HR:7.99 (95% CI: 5.26-12.14), p value: <0.001
Funding: Intermune Limitations:
Inclusion of patients with mild to moderate IPF at baseline. Patients with severe IPF and emphysema were excluded.
Notes: N patient visits = 1854
N deaths = 142
24 week absolute change percentage predicted FVC
5 to -9.9% vs. >-5%
HR:2.60 (95% CI: 1.75-3.85), p value: <0.001
24 week absolute change percentage predicted FVC
>-5% predicted
Reference : 1.0
change percentage predicted FVC
</=50% predicted
</=50% vs. >/=80%:
HR: 5.79 (95% CI:2.55-13.15), p value <0.001
change percentage predicted FVC
51 to 65
51% - 65% vs. >/=80%:
HR: 3.54 (95% CI: 1.95-6.44), p value <0.001
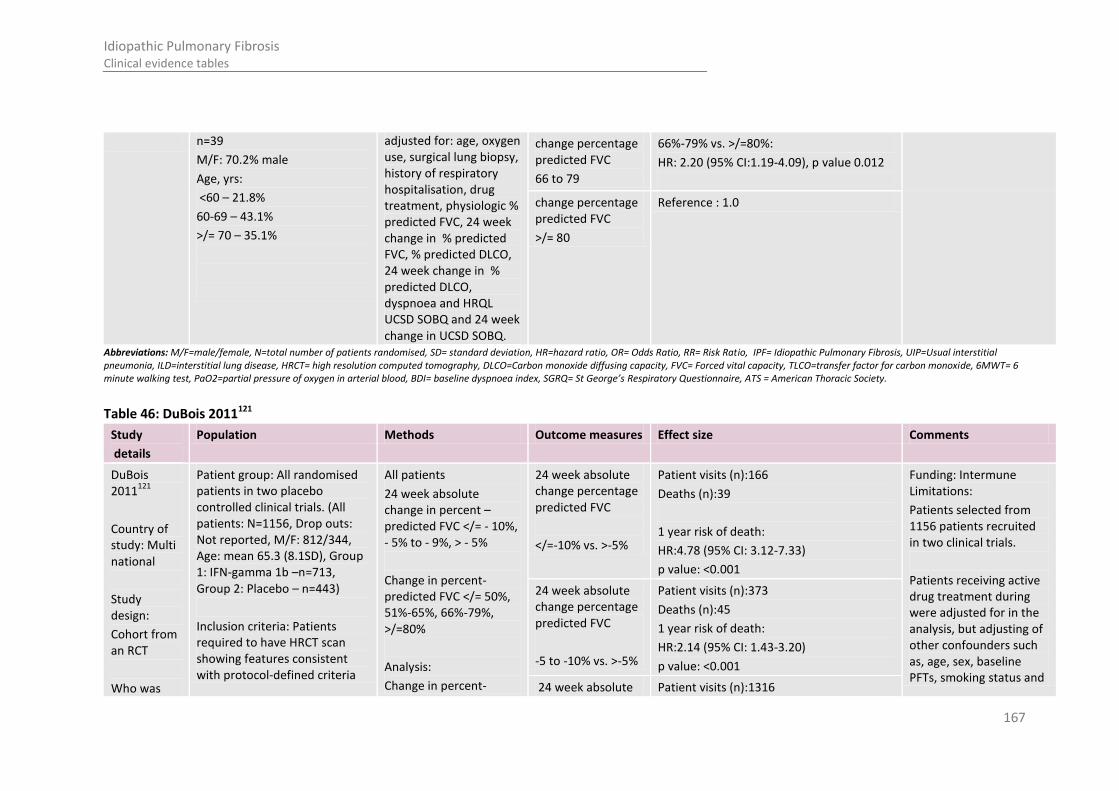
167
Idiopathic Pulmonary Fibrosis Clinical evidence tables
n=39
M/F: 70.2% male
Age, yrs:
<60 – 21.8%
60-69 – 43.1%
>/= 70 – 35.1%
adjusted for: age, oxygen use, surgical lung biopsy, history of respiratory hospitalisation, drug treatment, physiologic % predicted FVC, 24 week change in % predicted FVC, % predicted DLCO, 24 week change in % predicted DLCO, dyspnoea and HRQL UCSD SOBQ and 24 week change in UCSD SOBQ.
change percentage predicted FVC
66 to 79
66%-79% vs. >/=80%:
HR: 2.20 (95% CI:1.19-4.09), p value 0.012
change percentage predicted FVC
>/= 80
Reference : 1.0
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, HR=hazard ratio, OR= Odds Ratio, RR= Risk Ratio, IPF= Idiopathic Pulmonary Fibrosis, UIP=Usual interstitial pneumonia, ILD=interstitial lung disease, HRCT= high resolution computed tomography, DLCO=Carbon monoxide diffusing capacity, FVC= Forced vital capacity, TLCO=transfer factor for carbon monoxide, 6MWT= 6 minute walking test, PaO2=partial pressure of oxygen in arterial blood, BDI= baseline dyspnoea index, SGRQ= St George’s Respiratory Questionnaire, ATS = American Thoracic Society.
Table 46: DuBois 2011121
Study
details
Population Methods Outcome measures Effect size Comments
DuBois 2011
121
Country of study: Multi national
Study design:
Cohort from an RCT
Who was
Patient group: All randomised patients in two placebo controlled clinical trials. (All patients: N=1156, Drop outs: Not reported, M/F: 812/344, Age: mean 65.3 (8.1SD), Group 1: IFN-gamma 1b –n=713, Group 2: Placebo – n=443)
Inclusion criteria: Patients required to have HRCT scan showing features consistent with protocol-defined criteria
All patients
24 week absolute change in percent –predicted FVC </= - 10%, - 5% to - 9%, > - 5%
Change in percent-predicted FVC </= 50%, 51%-65%, 66%-79%, >/=80%
Analysis:
Change in percent-
24 week absolute change percentage predicted FVC
</=-10% vs. >-5%
Patient visits (n):166
Deaths (n):39
1 year risk of death:
HR:4.78 (95% CI: 3.12-7.33)
p value: <0.001
Funding: Intermune Limitations:
Patients selected from 1156 patients recruited in two clinical trials.
Patients receiving active drug treatment during were adjusted for in the analysis, but adjusting of other confounders such as, age, sex, baseline PFTs, smoking status and
24 week absolute change percentage predicted FVC
-5 to -10% vs. >-5%
Patient visits (n):373
Deaths (n):45
1 year risk of death:
HR:2.14 (95% CI: 1.43-3.20)
p value: <0.001
24 week absolute Patient visits (n):1316

168
Idiopathic Pulmonary Fibrosis Clinical evidence tables
blinded: N/A
Setting:
Unclear
Duration of follow-up:
1 year
for either definite or probable diagnosis of IPF. Surgical lung biopsy was required to confirm suspected diagnosis in all patients with a clinical and radiographic diagnosis of probable IPF and all patients <50yrs.
Exclusion criteria: NR
All patients
N: 1156
Drop outs: Not reported
M/F: 812/ 344 (70.2%/ 29.8%)
Age (mean, SD): 65.3 years (8.1)
predicted FVC taken at week 24 and 1 year risk using Cox proportional hazards model.
Change in percent predicted FVC was evaluated over the 24week periods immediately preceding the week 24 and week 72 trial visits, respectively and defined categorically based on prior research.
change percentage predicted FVC
>-5% predicted
Deaths (n):56
Reference : 1.0
previous hospitalisations, not reported.
Notes: Authors report that all deaths occurring over 48weeks of the trail were included in the analysis; subjects who were lost to follow-up and those who underwent lung transplant during follow-up were censored on the corresponding date.
change percentage predicted FVC
</=50% predicted
Patient visits (n):203
Deaths (n):42
1 year risk of death:
HR:7.44 (95% CI: 3.28-16.87)
p value: <0.001
change percentage predicted FVC
51 to 65
Patient visits (n):691
Deaths (n):65
1 year risk of death:
HR:4.09 (95% CI: 1.87-8.98)
p value: <0.001
change percentage predicted FVC
66 to 79
Patient visits (n):594
Deaths (n):26
1 year risk of death:
HR: 1.97 (95% CI: 1.87-8.98)
p value: 0.111
change percentage predicted FVC
>/= 80
Patient visits (n):374
Deaths (n):7
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, HR=hazard ratio, OR= Odds Ratio, RR= Risk Ratio, IPF= Idiopathic Pulmonary Fibrosis, UIP=Usual interstitial pneumonia, ILD=interstitial lung disease, HRCT= high resolution computed tomography, DLCO=Carbon monoxide diffusing capacity, FVC= Forced vital capacity, TLCO=transfer factor for carbon monoxide, 6MWT= 6 minute walking test, PaO2=partial pressure of oxygen in arterial blood, BDI= baseline dyspnoea index, SGRQ= St George’s Respiratory Questionnaire, ATS = American Thoracic Society.
Table 47: Hallstrand 2005172
Study Population Methods Outcome measures Effect size Comments

169
Idiopathic Pulmonary Fibrosis Clinical evidence tables
details
Hallstrand 2005
172
Country of study:
USA
Study design:
Prospective cohort
Who was blinded:
NR
Setting:
the Interstitial Lung Disease
Clinic, University of Washington Medical Center, Seattle,
WA, USA, and for further evaluation
Patient group:
Consecutive new referrals for further management of IPF. Patients with IPF who were entered into this study had progressive symptomatic and/or physiological deterioration, despite treatment with prednisone with or without immunosuppressives.
Inclusion criteria:
Consented to the study
met the diagnostic criteria for IPF*
Exclusion criteria:
Collagen vascular disease, occupational lung disease, sarcoid, hypersensitivity pneumonitis and other idiopathic interstitial pneumonias
Patients with concurrent emphysema were excluded based on elevated residual volume of ≥120% and (FEV1)/ (FVC) ratio of f 0.60.
All patients
All patients:
Timed walk test (TWT):
TWT on a 30-m-long level course.
Patients walked at a pace comfortable to them until they became too fatigued, up to a maximum of 6 min**
The test was stopped when saturation reached 80%, the lowest saturation was recorded if the saturation continued to decline.
FVC and DLCO were performed were performed within 24 hours of the TWT according to ATS criteria.
Analysis:
Survival time was measured in days from enrolment until death or censoring (patients censored at the end of the follow-up period or if patients underwent lung transplantation). Multivariable Cox
Multivariable analysis
Walk distance 30-m units to mortality
Relative hazard (95% CI): 0.91 (0.81–1.02)
P value: 0.098
Funding: NR
Limitations:
Baseline characteristics for each group not reported
Effect could be due to confounding
Selection bias
Unclear cut-off for distance walked
Additional outcomes:
Effect of supplementary oxygen on walk distance, velocity and saturation
Association of the timed walk test with pulmonary function
Notes: *The diagnosis of IPF was ascertained by typical clinical, radiographical, non-diagnostic transbronchial biopsy, and physiological features consistent with IPF; surgical lung biopsy demonstrating histological features of usual interstitial
Multivariable analysis
Resting room air arterial oxygen saturation to mortality
Relative hazard (95% CI): 1.06(0.83–1.37)
P value: 0.637
Multivariable analysis
DLCO % pred to mortality
Relative hazard (95% CI): 0.92(0.87–0.98)
P value: 0.005
Multivariable analysis
FVC % pred to mortality
Relative hazard (95% CI): 0.94(0.97–1.02)
P value: 0.646

170
Idiopathic Pulmonary Fibrosis Clinical evidence tables
and management in the Interstitial Lung Disease/Sarcoid/Pulmonary Fibrosis
Program at the University of Washington
Duration of follow-up:
Median (range) 5.4 years (4.3-6.2)
N: 28
Drop outs: 5 (underwent lung transplantation)
Age (mean): 62.7(57-69)
M/F: 19/9
Smokers: 19 (67.9%)
proportional hazards models were adjusted for age, sex, FVC % pred, time from the onset of symptoms and supplemental oxygen administration during the test.
pneumonia was accepted for the diagnosis of IPF in patients not meeting the major and minor clinical criteria.
** Patients with resting room air saturation of 88% had TWT in room air and with 2 L of oxygen. Patients with resting saturation ≤88% were tested only on 2 L of oxygen. The test was stopped for safety if the patient had signs of overt fatigue and/or asked to stop, or the saturation dropped to <80%.
Survival time was measured in days from enrolment until death or censoring. Patients were censored at the end of the follow-up period or if they underwent lung transplantation
19 out of 28 (67.9%) patients died within 2 yrs from the time of the

171
Idiopathic Pulmonary Fibrosis Clinical evidence tables
baseline TWT, 22 out of 28 (78.6%) died over the entire follow-up period at an average (range) of 1.2 yrs (0.2–3.0) from enrolment. During the study period, five patients underwent single-lung transplant at an average of 1.5 yrs (1.0–2.4) from enrolment and were censored in the analysis at the time of transplantation.
Disease severity ranged from FVC ≥70% predicted in eight patients and ≤40% predicted in five.
All patients had progressive disease based on symptoms or pulmonary function tests, despite treatment with prednisone with or without Azathioprine.

172
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, HR=hazard ratio, OR= Odds Ratio, RR= Risk Ratio, IPF= Idiopathic Pulmonary Fibrosis, UIP=Usual interstitial pneumonia, ILD=interstitial lung disease, HRCT= high resolution computed tomography, DLCO=Carbon monoxide diffusing capacity, FVC= Forced vital capacity, TLCO=transfer factor for carbon monoxide, 6MWT= 6 minute walking test, PaO2=partial pressure of oxygen in arterial blood, BDI= baseline dyspnoea index, SGRQ= St George’s Respiratory Questionnaire, ATS = American Thoracic Society.
Table 48: Hamada2007 173
Study
details
Population Methods Outcome measures Effect size Comments
Hamada2007
173
Country of study: Japan
Study design:
Prospective cohort
Who was blinded:
NR
Setting:
University hospital
Duration of follow-up: 5 years
Patient group: Patients with IPF diagnosed by pathology, “none of whom were receiving corticosteroids or immunosuppressive agents at the time of workup”.
Inclusion criteria: As above
Exclusion criteria:
Patients who died within a month of open lung biopsy, had collagen vascular diseases, asbestosis, venoocculusive disease with Langerhans cell histocytosis. Other disorders that could cause secondary PAH were excluded, including pulmonary arterial thromboembolism, connective tissue disease, chronic liver dieases and obstructive sleep apnea syndrome.
All patients
N: 78
All patients
Right hearted catherisation and PFTs were performed in the same week in most patients. No further details on measurements reported.
Analysis
Survival rates estimated using Kaplan-Meier nonparametric survival model. Regression analysis performed to evaluate factors contributing to survival: age, gender, mean pulmonary arterial pressure, Pa02, P02 in mixed venous blood, FVC % predicted, DLCO% predicted and cardiac index.
Preserved DLCO (%DLCO>/=40%, n=27)
19/27 (70.4%) survived for 5 years compared to low DLCO group (p value<0.001)
Funding: NR
Limitations: Small sample analysed.
Notes: Study objectives were to evaluate long term clinical course of patients with IPF complicated with pulmonary arterial hypertension
Low DLCO
(<40, n=25)
5/25 (20%) survived for 5 years
RR2.70 (95% CI: 1.46 to 4.99) p value < 0.001
Causes of death Respiratory failure due to IPF: 33/52
Pulmonary infection: 1
Lung cancer: 9
Other malignancies: 3
Cardiac disorders: 4
Cerebrovascular disorders: 1
Unknown: 1

173
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Age (mean): 62+/-8 years
Drop outs: unclear
M/F: 53/8 Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, HR=hazard ratio, OR= Odds Ratio, RR= Risk Ratio, IPF= Idiopathic Pulmonary Fibrosis, UIP=Usual interstitial pneumonia, ILD=interstitial lung disease, HRCT= high resolution computed tomography, DLCO=Carbon monoxide diffusing capacity, FVC= Forced vital capacity, TLCO=transfer factor for carbon monoxide, 6MWT= 6 minute walking test, PaO2=partial pressure of oxygen in arterial blood, BDI= baseline dyspnoea index, SGRQ= St George’s Respiratory Questionnaire, ATS = American Thoracic Society.
Table 49: Jeon 2006219
Study
details
Population Methods Outcome measures Effect size Comments
Jeon 2006219
Country of study: South Korea
Study design:
Retrospective cohort
Who was blinded: Not reported
Setting:
Hospital
Duration of follow-up: >1 year (unclear)
Patient group: Patients pathologically confirmed to have UIP on surgical lung biopsy and patients diagnosed as IPF positive by diagnostic American Thoracic Society criteria
Inclusion criteria: As above
Exclusion criteria: Clinical evidence of connective tissue disease, occupational or environmental exposure, or a history of ingestion of a drug known to cause ILD
All patients
N: 88
Drop outs: Not reported
Age: 60.3 mean (+/-7.5 SD))
M:F – 69:19
All patients
FVC and DLCO as continuous variables
PFTs were obtained within 2 weeks at the time of diagnosis and measured as recommended by ATS criteria.
Analysis:
Patients grouped according to whether they were managed by pharmacological treatment or symptomatic supportive care only.
Cox proportional hazards regression was used to identify
Baseline PFTs (mean+/-SD %predicted):
FVC: 74.0 +/- 19.2
DLCO: 65.2 +/- 21.4
FVC
Specific treatment group: 74.6 +/- 18.1
Symptomatic supportive care: 73.2 +/- 20.8
p value: 0.758
DLCO
Specific treatment group: 64.7 +/- 20.5
Symptomatic supportive care: 65.8 +/- 22.9
p value: 0.834
Funding: NR Limitations: Patients with UIP and IPF grouped together in analysis
Predictors of mortality for patients with IPF by multivariable analysis not presented by treatment group compared to supportive care group.
Adjusted for age, sex, severity of dyspnoea, FVC and DLCO and treatment, multivariable survival analysis.
Predictors of mortality of IPF patients by multivariable analysis (% predicted)
FVC
HR: 1.7 (95% CI: 1.2-2.3)
p value: 0.004
DLCO
HR: 1.5 (95% CI: 1.1-2.1)
p value: 0.033
Causes of death in Respiratory failure 34 (68%)

174
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Group 1: Specific treatment group
N: 49
Age (mean): 58.9 (+/-7.1 SD)
Drop outs: Not reported
Group 2: Symptomatic supportive care
N: 39
Age (mean): 62.1 (+/-7.8 SD)
Drop outs: Not reported
variables associated with survival rate. Hazard ratios were reported for these analyses.
patients with IPF (n=50)
Acute exacerbation 23
Slow progression 11
Infection 7 (14%)
HAP 4
CAP 2
Wound infection 1
Lung cancer 4 (8%)
Pulmonary embolism 1 (2%)
Cardiovascular disease 1 (2%)
Variceal bleeding 1 (2%)
Unknown 2 (4%) Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, HR=hazard ratio, OR= Odds Ratio, RR= Risk Ratio, IPF= Idiopathic Pulmonary Fibrosis, UIP=Usual interstitial pneumonia, ILD=interstitial lung disease, HRCT= high resolution computed tomography, DLCO=Carbon monoxide diffusing capacity, FVC= Forced vital capacity, TLCO=transfer factor for carbon monoxide, 6MWT= 6 minute walking test, PaO2=partial pressure of oxygen in arterial blood, BDI= baseline dyspnoea index, SGRQ= St George’s Respiratory Questionnaire, ATS = American Thoracic Society.
Table 50: Kurashima 2010 260
Study
details
Population Methods Outcome measures Effect size Comments
Kurashima 2010 260
Country of study: Japan
Study design:
Retrospective cohort
Who was
Patient group: Patients previously diagnosed with UIP based on HRCT findings, with or without emphysema.
Inclusion criteria: Medical records, PFT results and laboratory tests reviewed and patients selected according to following criteria: patients who underwent HRCT for clinical symptoms or other medical reasons and who were
All patients
FVC and DLCO as continuous variables
PFTs performed according to the ATS criteria.
Analysis:
Survival analysis was performed by the Kaplan Meier method, with end points being death or censoring of data. A univariable Cox’s
Baseline characteristics in patients with UIP
%FVC (n=348): 71.8 +/- 19.4
%DLCO (n=202): 74.3 +/- 20.1
Funding: NR Limitations:
Confounding factors adjusted for in multivariable survival analysis were emphysema, FVC % predicted, FEV/FVC per 1% and DLCO% predicted.
Patients receiving treatment were not adjusted for in analysis
Multivariable Cox’s proportional hazards regression model for risk of death in patients with UIP
%FVC predicted per 1% (n=362)
HR:0.988 (95% CI: 0.967-1.010)
p value: 0.27
%DLCO predicted per 1% (n=251):
HR: 0.987 (95%CI: 0.971-1.002)
p value: 0.21
Causes of death in patients with UIP
Lung cancer 8 (12.1%)
Acute exacerbation 21 (31.8%)

175
Idiopathic Pulmonary Fibrosis Clinical evidence tables
blinded: Thoracic radiologists blinded to clinical details
Setting:
Hospital
Duration of follow-up: 0
diagnosed with UIP by radiologists.
Exclusion criteria: Connective tissue disease, diagnosis of other ILD, such as drug-induced ILD.
Patients without PFT results and patient with lung cancer were excluded from analysis of PFT and HRCT findings and from survival analysis
All patients
N: 660 (UIP, n=439: UIP with emphysema, n=221)
Drop outs: Unclear
M/F: 336/103
Age: 72.9 years +/-8.1
Patients receiving treatment: n=8
proportional hazards regression model followed by multivariable analysis was used to identify risk factors for mortality.
Chronic Respiratory failure 26 (39.4%)
Other causes 11 (16.6%)
Notes:
Total of 1050 patients with possible diagnosis of UIP on HRCT were screened. For 660 patients (UIP with and without emphysema) the diagnostic findings were compatible with IPF. Of these 238 patients had lung cancer at diagnosis and PFT results were not available for 131 patients.
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, HR=hazard ratio, OR= Odds Ratio, RR= Risk Ratio, IPF= Idiopathic Pulmonary Fibrosis, UIP=Usual interstitial pneumonia, ILD=interstitial lung disease, HRCT= high resolution computed tomography, DLCO=Carbon monoxide diffusing capacity, FVC= Forced vital capacity, TLCO=transfer factor for carbon monoxide, 6MWT= 6 minute walking test, PaO2=partial pressure of oxygen in arterial blood, BDI= baseline dyspnoea index, SGRQ= St George’s Respiratory Questionnaire, ATS = American Thoracic Society.
Table 51: Lynch 2005 292
Study
details
Population Methods Outcome measures Effect size Comments
Lynch 2005 292
Patient group: mild to moderate IPF
HRCT features
Overall extent of fibrosis score- multivariable analysis
Hazard ratio (calculated by the Cox proportional hazards model, stratifying by smoking status): 2.71
Funding: InterMune

176
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Country of study: multi-national (United states, Europe, Canada and South Africa)
Study design:
(e.g. RCT) patients from an RCT
Who was blinded: (if RCT) N/A
Setting: 58 medical centres (39 academic, 19 community based) in the USA, Europe, Canada and South Africa
Inclusion criteria: as above
Exclusion criteria: NR
All patients:
N: 315
Age (mean): NR
Drop outs: unclear
Baseline FVC and DLCO results presented, but no details provided on these measurements.
Analysis:
Stepwise logistic regression (stratified by smoking status) model built using variables with a univariable p values <0.2. These were overall disease extent score on HRCT, reticulation pattern score, honeycomb pattern score, predominant pattern reticulation, A_a gradient and current O2 use.
95% confidence interval of hazard ratio: 1.61, 4.55
p value: <0.0001
Limitations:
Possible bias from radiologists who knew patients were being entered into a trial of treatment for IPF
Additional outcomes:
Agreement on diagnosis between radiologists
HRCT characteristics according to HRCT classified as consistent with, or not consistent with IPF
Clinical features according to HRCT classified as consistent with, or not consistent with IPF
Correlation between baseline HRCT and baseline clinical characteristics
Notes:
Patients were enrolled in a trial of Interferon
Baseline % predicted DLCO – multivariable analysis
Hazard ratio: 0.94
95% confidence interval of hazard ratio: 0.90, 0.98
p value: 0.004

177
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Duration of follow-up: NR
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, HR=hazard ratio, OR= Odds Ratio, RR= Risk Ratio, IPF= Idiopathic Pulmonary Fibrosis, UIP=Usual interstitial pneumonia, ILD=interstitial lung disease, HRCT= high resolution computed tomography, DLCO=Carbon monoxide diffusing capacity, FVC= Forced vital capacity, TLCO=transfer factor for carbon monoxide, 6MWT= 6 minute walking test, PaO2=partial pressure of oxygen in arterial blood, BDI= baseline dyspnoea index, SGRQ= St George’s Respiratory Questionnaire, ATS = American Thoracic Society.
Table 52: Manali 2008300
Study
details Population Methods Outcome measures Effect size Comments
Manali 2008
300
Country of study: Greece
Study design:
Retrospective cohort
Who was blinded: Not reported
Setting:
Respiratory outpatient clinic
Duration of
Patient group: 25 consecutive patients with IPF recruited from respiratory outpatients clinic
Inclusion criteria: All patients had IPF based on American Thoracic Society criteria and lung biopsies obtained by video assisted thoracoscopic surgery which showed UIP
Exclusion criteria: Secondary causes of lung fibrosis: none of the patients had a history of environmental or occupational exposure, drug toxicity or connective tissue disease as documented by history, clinical and immunological tests.
All patients
N:25
Drop outs: 12/25 deaths
All patients:
FVC as a continuous
variables
Lung function tests were measured during the diagnostic approach.
Analysis:
The patients still alive during the reporting of this study were censored for survival analysis (13/22..
Univariable and multivariable Cox regression analysis was conducted for survival.
Impact on survival using multivariable Cox regression analysis
FVC
RR 1.045 (95% CI: 0.956-1.142)
p value: 0.033
Funding: Thorax Foundation, Athens
Limitations:
Multivariable survival analysis adjusting for confounders not clearly reported
Additional outcomes: Deaths 12/25
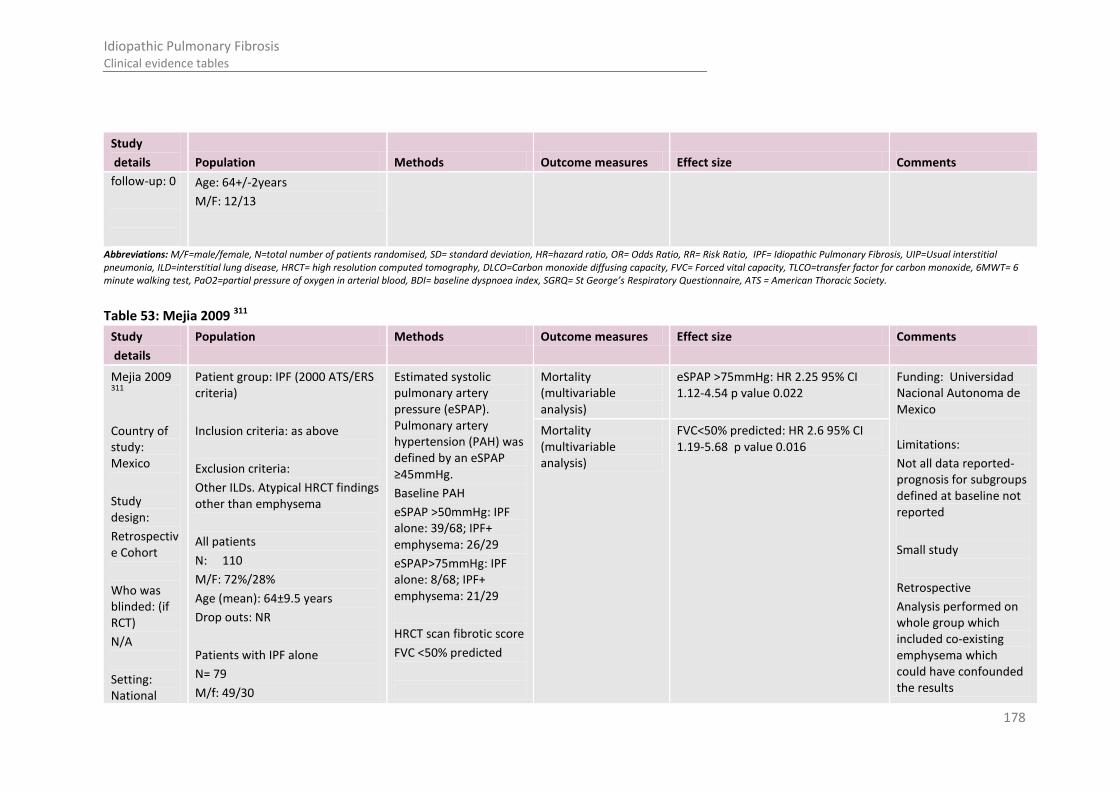
178
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Study
details Population Methods Outcome measures Effect size Comments
follow-up: 0
Age: 64+/-2years
M/F: 12/13
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, HR=hazard ratio, OR= Odds Ratio, RR= Risk Ratio, IPF= Idiopathic Pulmonary Fibrosis, UIP=Usual interstitial pneumonia, ILD=interstitial lung disease, HRCT= high resolution computed tomography, DLCO=Carbon monoxide diffusing capacity, FVC= Forced vital capacity, TLCO=transfer factor for carbon monoxide, 6MWT= 6 minute walking test, PaO2=partial pressure of oxygen in arterial blood, BDI= baseline dyspnoea index, SGRQ= St George’s Respiratory Questionnaire, ATS = American Thoracic Society.
Table 53: Mejia 2009 311
Study
details
Population Methods Outcome measures Effect size Comments
Mejia 2009 311
Country of study: Mexico
Study design:
Retrospective Cohort
Who was blinded: (if RCT)
N/A
Setting: National
Patient group: IPF (2000 ATS/ERS criteria)
Inclusion criteria: as above
Exclusion criteria:
Other ILDs. Atypical HRCT findings other than emphysema
All patients
N: 110
M/F: 72%/28%
Age (mean): 64±9.5 years
Drop outs: NR
Patients with IPF alone
N= 79
M/f: 49/30
Estimated systolic pulmonary artery pressure (eSPAP). Pulmonary artery hypertension (PAH) was defined by an eSPAP ≥45mmHg.
Baseline PAH
eSPAP >50mmHg: IPF alone: 39/68; IPF+ emphysema: 26/29
eSPAP>75mmHg: IPF alone: 8/68; IPF+ emphysema: 21/29
HRCT scan fibrotic score
FVC <50% predicted
Mortality (multivariable analysis)
eSPAP >75mmHg: HR 2.25 95% CI 1.12-4.54 p value 0.022
Funding: Universidad Nacional Autonoma de Mexico
Limitations:
Not all data reported- prognosis for subgroups defined at baseline not reported
Small study
Retrospective
Analysis performed on whole group which included co-existing emphysema which could have confounded the results
Mortality (multivariable analysis)
FVC<50% predicted: HR 2.6 95% CI 1.19-5.68 p value 0.016

179
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Institute of Respiratory Diseases, Mexico
Duration of follow-up: NR
Age, year: 63±10
Smoking status:
Yes: 36
No: 40
Pack years: 0 (0-78).
Subgroup: Patients with IPF and Emphysema
N= 31
M/f: 30/1
Age, year: 67±7
Smoking status:
Yes: 24
No: 7
Pack years: 5 (0-60)
Additional outcomes:
Univariable analysis for male gender
Notes: Multivariable analysis performed with the variables showing influence on mortality as identified with univariable analysis
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, HR=hazard ratio, OR= Odds Ratio, RR= Risk Ratio, IPF= Idiopathic Pulmonary Fibrosis, UIP=Usual interstitial pneumonia, ILD=interstitial lung disease, HRCT= high resolution computed tomography, DLCO=Carbon monoxide diffusing capacity, FVC= Forced vital capacity, TLCO=transfer factor for carbon monoxide, 6MWT= 6 minute walking test, PaO2=partial pressure of oxygen in arterial blood, BDI= baseline dyspnoea index, SGRQ= St George’s Respiratory Questionnaire, ATS = American Thoracic Society.
Table 54: Mogulkoc 2001A 327
Study
details
Population Methods Outcome measures Effect size Comments
Mogulkoc 2001A
327
Country of study: UK
Study design:
cohort
Patient group: mild to moderate IPF; age <65 years; potentially eligible for lung transplantation
Inclusion criteria: as above
Exclusion criteria: (1) the presence of known histories of collagen vascular disease, allergic
DLCO
HRCT score, n (%)
HRCT fibrosis score: 2.1±0.7
HRCT ground glass score: 3.0±1.3
HRCT fibrosis score at baseline- multivariable analysis (n=85)
HRCT fibrosis score- baseline
HR/ OR: 2.067
95% CI: 1.726- 3.914
p value: 0.026
Funding: NR Limitations: patients were all <65 years
Additional outcomes:
Survival probability according to method of diagnosis
DLCO % predicted at baseline (n=85)
HR/ OR: 0.957
95% CI: 0.928- 0.987
p value: 0.005
DLCO % predicted at 2 year follow-up (n=70)
HR/ OR: 0.923
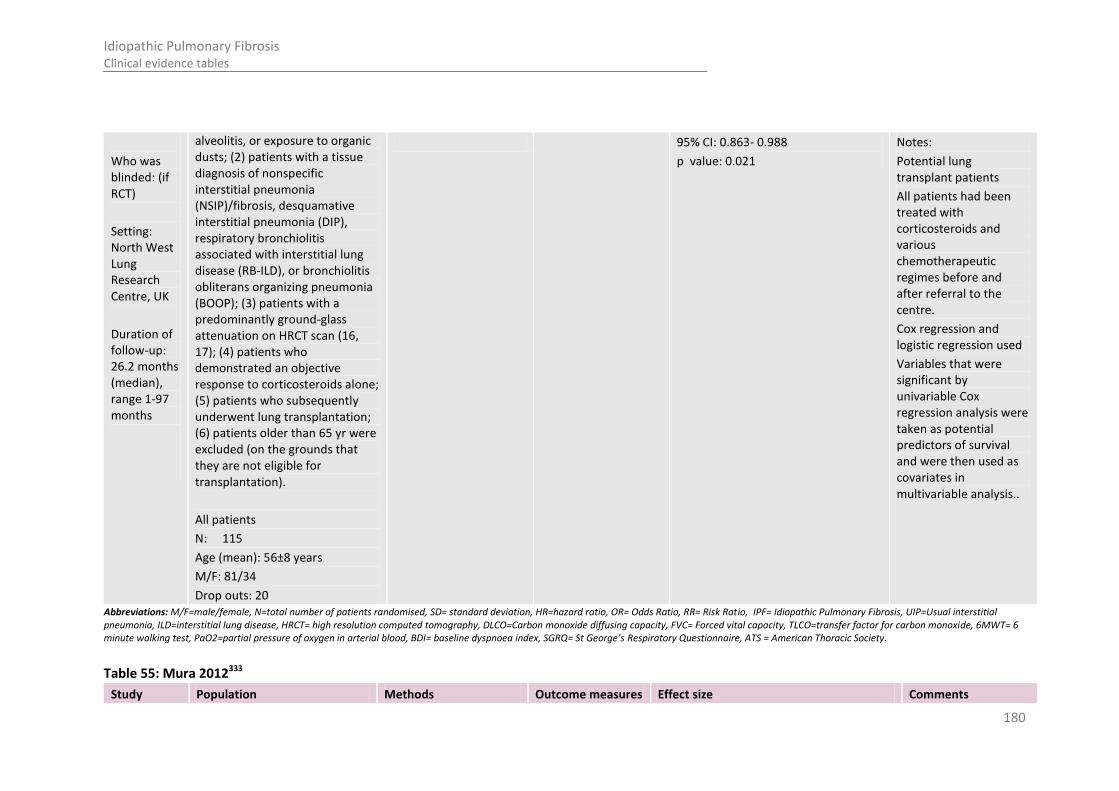
180
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Who was blinded: (if RCT)
Setting: North West Lung Research Centre, UK
Duration of follow-up: 26.2 months (median), range 1-97 months
alveolitis, or exposure to organic dusts; (2) patients with a tissue diagnosis of nonspecific interstitial pneumonia (NSIP)/fibrosis, desquamative interstitial pneumonia (DIP), respiratory bronchiolitis associated with interstitial lung disease (RB-ILD), or bronchiolitis obliterans organizing pneumonia (BOOP); (3) patients with a predominantly ground-glass attenuation on HRCT scan (16, 17); (4) patients who demonstrated an objective response to corticosteroids alone; (5) patients who subsequently underwent lung transplantation; (6) patients older than 65 yr were excluded (on the grounds that they are not eligible for transplantation).
All patients
N: 115
Age (mean): 56±8 years
M/F: 81/34
Drop outs: 20
95% CI: 0.863- 0.988
p value: 0.021
Notes:
Potential lung transplant patients
All patients had been treated with corticosteroids and various chemotherapeutic regimes before and after referral to the centre.
Cox regression and logistic regression used
Variables that were significant by univariable Cox regression analysis were taken as potential predictors of survival and were then used as covariates in multivariable analysis..
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, HR=hazard ratio, OR= Odds Ratio, RR= Risk Ratio, IPF= Idiopathic Pulmonary Fibrosis, UIP=Usual interstitial pneumonia, ILD=interstitial lung disease, HRCT= high resolution computed tomography, DLCO=Carbon monoxide diffusing capacity, FVC= Forced vital capacity, TLCO=transfer factor for carbon monoxide, 6MWT= 6 minute walking test, PaO2=partial pressure of oxygen in arterial blood, BDI= baseline dyspnoea index, SGRQ= St George’s Respiratory Questionnaire, ATS = American Thoracic Society.
Table 55: Mura 2012333
Study Population Methods Outcome measures Effect size Comments
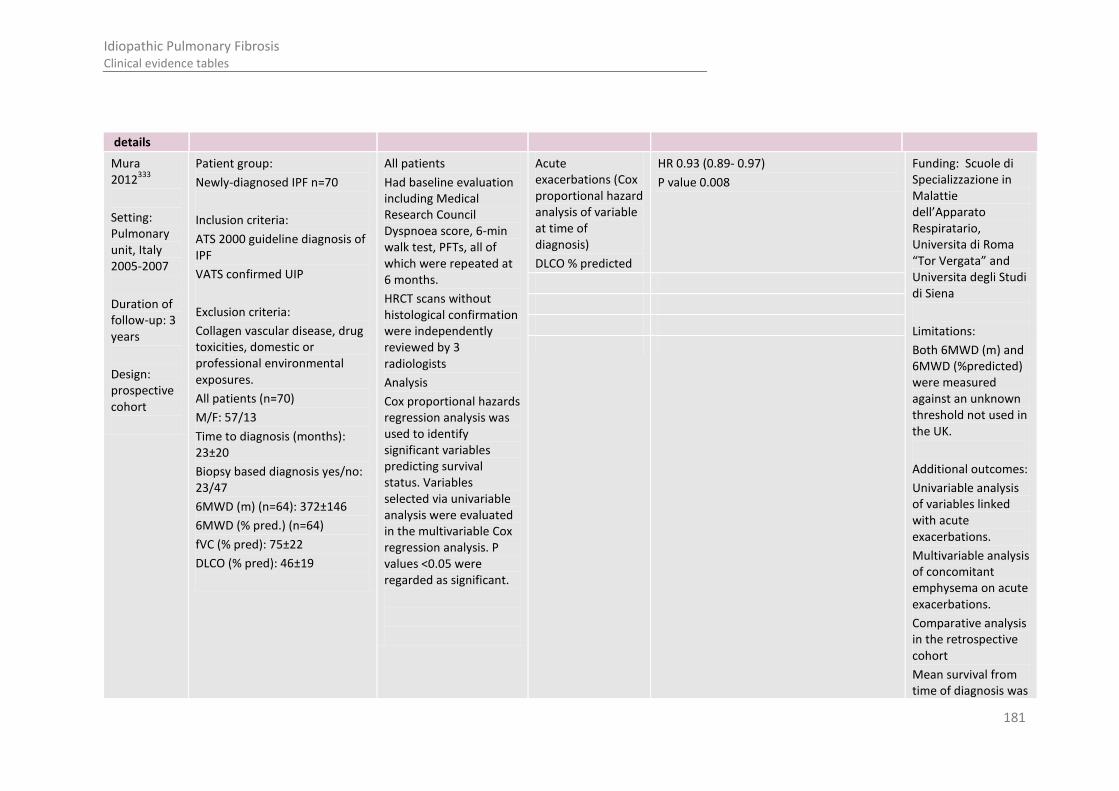
181
Idiopathic Pulmonary Fibrosis Clinical evidence tables
details
Mura 2012
333
Setting: Pulmonary unit, Italy 2005-2007
Duration of follow-up: 3 years
Design: prospective cohort
Patient group:
Newly-diagnosed IPF n=70
Inclusion criteria:
ATS 2000 guideline diagnosis of IPF
VATS confirmed UIP
Exclusion criteria:
Collagen vascular disease, drug toxicities, domestic or professional environmental exposures.
All patients (n=70)
M/F: 57/13
Time to diagnosis (months): 23±20
Biopsy based diagnosis yes/no: 23/47
6MWD (m) (n=64): 372±146
6MWD (% pred.) (n=64)
fVC (% pred): 75±22
DLCO (% pred): 46±19
All patients
Had baseline evaluation including Medical Research Council Dyspnoea score, 6-min walk test, PFTs, all of which were repeated at 6 months.
HRCT scans without histological confirmation were independently reviewed by 3 radiologists
Analysis
Cox proportional hazards regression analysis was used to identify significant variables predicting survival status. Variables selected via univariable analysis were evaluated in the multivariable Cox regression analysis. P values <0.05 were regarded as significant.
Acute exacerbations (Cox proportional hazard analysis of variable at time of diagnosis)
DLCO % predicted
HR 0.93 (0.89- 0.97)
P value 0.008
Funding: Scuole di Specializzazione in Malattie dell’Apparato Respiratario, Universita di Roma “Tor Vergata” and Universita degli Studi di Siena
Limitations:
Both 6MWD (m) and 6MWD (%predicted) were measured against an unknown threshold not used in the UK.
Additional outcomes:
Univariable analysis of variables linked with acute exacerbations.
Multivariable analysis of concomitant emphysema on acute exacerbations.
Comparative analysis in the retrospective cohort
Mean survival from time of diagnosis was

182
Idiopathic Pulmonary Fibrosis Clinical evidence tables
30 months
3 year mortality was 46%
Mortality (Cox proportional hazard analysis of variable at time of diagnosis)
6MWD <72% predicted - HR 3.27 (1.25-8.82)
P value 0.0162
Notes: 24 (34%) subjects had concomitant emphysema.
Survival was defined as the time to death or lung transplant.
Multivariable survival analysis adjusted for: BMI, MRC dyspnoea score, 6MWD, desaturation at 6MWD, PaO2, FV % predicted, DLCO % predicted, composite physiologic index, HRCT fibrosis score, BAL total cell counts and concomitant emphysema.
A retrospective

183
Idiopathic Pulmonary Fibrosis Clinical evidence tables
cohort of 68 patients was used for confirmation.
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, HR=hazard ratio, OR= Odds Ratio, RR= Risk Ratio, IPF= Idiopathic Pulmonary Fibrosis, UIP=Usual interstitial pneumonia, ILD=interstitial lung disease, HRCT= high resolution computed tomography, DLCO=Carbon monoxide diffusing capacity, FVC= Forced vital capacity, TLCO=transfer factor for carbon monoxide, 6MWT= 6 minute walking test, PaO2=partial pressure of oxygen in arterial blood, BDI= baseline dyspnoea index, SGRQ= St George’s Respiratory Questionnaire, ATS = American Thoracic Society.
Table 56: Richeldi 2012A410
Study
details
Population Methods Outcome measures Effect size Comments
Richeldi 2012A
410
Setting:
Two independent longitudinal cohorts, USA
Duration of follow-up: 12 months
Design: cohort
Patient group: newly-diagnosed IPF (ATS 2000 guideline)
Inclusion criteria:
Two serial FVC measurements 12 months apart
Exclusion criteria: NR
All patients n=142
Age: 67 years (mean)
Male: 74%
History of smoking: 69%
Biopsy proven disease: 56%
FVC (L): 2.70 mean, SD 0.78
FVC, % predicted: 67.6 mean, SD 16.1
All patients
Analysis
Logistic regression was used to determine the association of dichotomised decline in FVC with 2 year transplant-free survival. Unadjusted analyses were performed, followed by adjustment for age, gender, O2 use and baseline % predicted FVC and DLCO (only adjusted results presented in this table)
Death or transplant (time to event)
≥10% decline in FVC (L) at 12 months (adjusted OR/HR)
OR/HR3.54 (2.04 to 6.15) no p value Funding: NIH grant HL086516
Limitations: none
Additional outcomes:
Frequency of ≥5%, ≥10% and ≥15% decline in FVC at 12 months for whole cohort, and excluding patients with severe disease.
Unadjusted OR/HRs for all death/ death or transplant outcomes
Transplant-free survival at 2 years for 12 month FVC
Death (time to event)
≥10% decline in FVC (L) at 12 months (adjusted OR/HR)
OR/HR2.78 (1.48 to 2.54) no p value
Death or transplant at 2 years (time to event)
≥5% decline in % predicted FVC at 12 months (adjusted OR/HR)
1.91 (1.12-3.26) relative change
3.24 (1.84-5.69) absolute change
Death at 2 years 1.61 (0.89-2.92) relative change
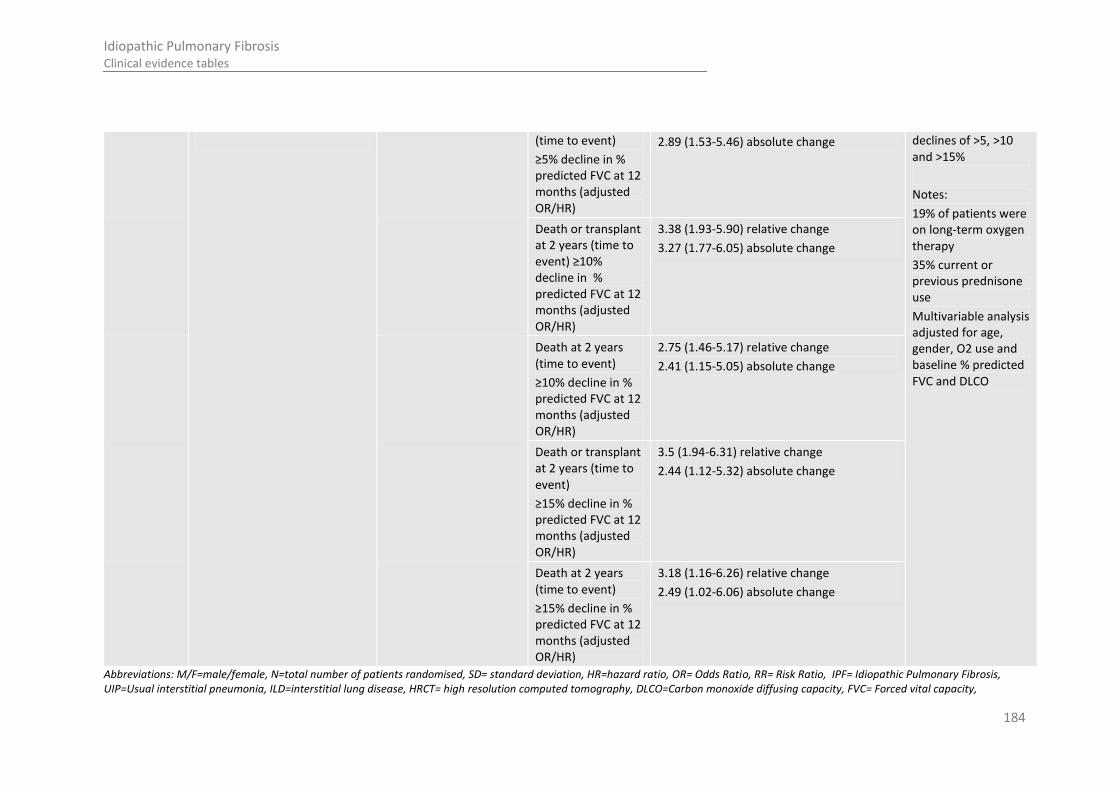
184
Idiopathic Pulmonary Fibrosis Clinical evidence tables
(time to event)
≥5% decline in % predicted FVC at 12 months (adjusted OR/HR)
2.89 (1.53-5.46) absolute change declines of >5, >10 and >15%
Notes:
19% of patients were on long-term oxygen therapy
35% current or previous prednisone use
Multivariable analysis adjusted for age, gender, O2 use and baseline % predicted FVC and DLCO
Death or transplant at 2 years (time to event) ≥10% decline in % predicted FVC at 12 months (adjusted OR/HR)
3.38 (1.93-5.90) relative change
3.27 (1.77-6.05) absolute change
Death at 2 years (time to event)
≥10% decline in % predicted FVC at 12 months (adjusted OR/HR)
2.75 (1.46-5.17) relative change
2.41 (1.15-5.05) absolute change
Death or transplant at 2 years (time to event)
≥15% decline in % predicted FVC at 12 months (adjusted OR/HR)
3.5 (1.94-6.31) relative change
2.44 (1.12-5.32) absolute change
Death at 2 years (time to event)
≥15% decline in % predicted FVC at 12 months (adjusted OR/HR)
3.18 (1.16-6.26) relative change
2.49 (1.02-6.06) absolute change
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, HR=hazard ratio, OR= Odds Ratio, RR= Risk Ratio, IPF= Idiopathic Pulmonary Fibrosis, UIP=Usual interstitial pneumonia, ILD=interstitial lung disease, HRCT= high resolution computed tomography, DLCO=Carbon monoxide diffusing capacity, FVC= Forced vital capacity,

185
Idiopathic Pulmonary Fibrosis Clinical evidence tables
TLCO=transfer factor for carbon monoxide, 6MWT= 6 minute walking test, PaO2=partial pressure of oxygen in arterial blood, BDI= baseline dyspnoea index, SGRQ= St George’s Respiratory Questionnaire, ATS = American Thoracic Society.
Table 57: Schmidt 2011 424
Study
details
Population Methods Outcome measures Effect size Comments
Schmidt 2011
424
Country of study:
USA
Study design:
Retrospective cohort
Who was blinded:
NR
Setting:
Secondary care
Duration of follow-up:
5.2-6.6 years
Patient group:
Patients with IPF were selected from the university of Michigan interstitial lung disease database. Diagnosis made with either surgical lung biopsy or HRCT scan diagnostic of UIP using standard criteria.
Inclusion criteria:
PFT performed within 3 months of diagnosis.
Exclusion criteria:
NR
All patients: Baseline
N: 321
Age: 63.9±9.7
Drop outs: 0
M/F:217/104
Ever tobacco use: 236 (73.5%)
All patients: 6 months
All patients
FVC and DLCO as continuous variables
PFT measured at diagnosis and at least one PFT after baseline
Analysis
Longitudinal analysis:
For 6 months; PFTs included from 3-9 months included in analysis. An estimated PFT value was obtained from regression
For 12 months; PFTs included from 9-15 months after diagnosis
Cox proportional hazard models used to evaluate changes in Composite
Longitudinal HR for mortality by absolute decrease in PFTs:
% FVC predicted
Over 6 months (n=211)
5%: HR 1.8(95% CI: 1.2-2.7), p value 0.002
10%: HR 1.4(95% CI: 0.9-2.1), p value 0.122
15%: HR 1.1(95% CI: 0.6-1.8), p value 0.857
20%: HR 2.0(95% CI: 1.0-4.0), p value 0.051
Funding: National institutes for health
National heart, lung and blood institute
Limitations: none
Additional outcomes:
Longitudinal hazard ratios for mortality associated with absolute increases in composite physiologic index (CPI) and relative decreases in individual PFTs over 6 and 12 months in patients with combined IPF and emphysema.
Notes:
Mortality data were confirmed through social security death registry index
Longitudinal HR for mortality by absolute decrease in PFTs:
% DLCO predicted
Over 6 months (n=211)
10%:- HR 1.7(95% CI: 1.1-2.5), p value 0.011
15%: HR 1.6(95% CI: 1.1-2.5), p value 0.029
20%: HR 1.8(95% CI: 1.1-3.0), p value 0.030
25%: HR 2.3(95% CI: 1.2-4.2), p value 0.010
Longitudinal HR for mortality by absolute decrease in PFTs:
% FVC predicted
Over 12 months (n=144)
5%: HR 1.8(95% CI: 1.1-2.9), p value 0.012
10%: HR 2.4(95% CI: 1.5-3.8), p value <0.001
15%: HR 2.6(95% CI: 1.6-4.5), p value <0.001
20%: HR 3.6(95% CI: 1.9-6.9), p value <0.001
Longitudinal HR for mortality by absolute decrease in PFTs:
% DLCO predicted
10%:- HR 2.2(95% CI: 1.4-3.5), p value 0.001
15%: HR 2.3(95% CI: 1.5-3.7), p value <0.001
20%: HR 3.0(95% CI: 1.8-4.9), p value <0.001

186
Idiopathic Pulmonary Fibrosis Clinical evidence tables
N: 211
Age (mean): 63.2±10
Drop outs: 0
M/F:151/60
Ever tobacco use: 162(76%)
All patients: 12 months
N: 144
Age (mean): 62.3±10
Drop outs: 0
M/F:102/42
Ever tobacco use: 109 (75.7%)
physiologic index and PFTs in patients stratified by amount of emphysema.
Over 12 months (n=144)
25%: HR 3.5(95% CI: 2.0-6.1), p value <0.001
censured by 3 months to account for reporting lag.
Follow up time was determined from date of baseline PFT to date of death or censure
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, HR=hazard ratio, OR= Odds Ratio, RR= Risk Ratio, IPF= Idiopathic Pulmonary Fibrosis, UIP=Usual interstitial pneumonia, ILD=interstitial lung disease, HRCT= high resolution computed tomography, DLCO=Carbon monoxide diffusing capacity, FVC= Forced vital capacity, TLCO=transfer factor for carbon monoxide, 6MWT= 6 minute walking test, PaO2=partial pressure of oxygen in arterial blood, BDI= baseline dyspnoea index, SGRQ= St George’s Respiratory Questionnaire, ATS = American Thoracic Society.
Table 58: Zappala 2010507
Study
details
Population Methods Outcome measures Effect size Comments
Zappala 2010
507
Country of study:
UK and Australia
Study design:
Retrospective Cohort
Patient group:
January 1978-June 2005 patients who met the histological criteria at surgical biopsy for IPF.
Inclusion criteria:
ATS/ERS diagnostic criteria
Exclusion criteria:
Patients without serial PFT data
All patients
Serial PFT trends at 6(±2)months expressed as percentages of baseline values, were evaluated for FVC (measured using spirometer) and DLCO (measured by single breath/re-breathing technique using respirometer) relative trends were defined a priori as significant (FVC
Progression free survival patients with 5-10% decline in FVC compared with stable disease
HR; 1.82 (0.97-3.40)
P value; 0.06
Funding: NR
Limitations:
Additional outcomes:
Study looked at patients with NSIP too but did some separate analysis for IPF patients (for which data has been extracted)
Progression free survival patients with 5-10% decline in FVC compared with stable disease- adjusted for baseline DLCO
HR; 2.56 (1.17-4.38)
P value; 0.02

187
Idiopathic Pulmonary Fibrosis Clinical evidence tables
Setting:
Secondary care
Duration of follow-up:
6 months ±2
N: 84 (only IPF excluding NSIP)
Age (mean): 57.4±8.50
Drop outs: 0
m/f: 69/15
smokers (n): ever/never: 62/22
> 10% predicted, DLCO > 15% predicted)or marginal (FVC 5-10% predicted; DLCO 7.5-15% predicted) compared with baseline. Criteria for marginal decline were chosen to allow rapid computation in clinical practice reflecting the rational of current ATS criteria for significant PFT change.
PFT trends analysed using proportional hazards analysis and multivariable analysis adjusting for age, sex, smoking status and baseline disease severity
Notes: Transplanted patients n=4 were censored as alive at date of transplant
Treatment regimes included combination immunosuppressant treatment including low dose prednisolone (10mg) or high dose prednisolone (40-60mg) initially reducing to maintenance average of 10mg
* includes NSIP patients n=72
** excluding patients with a significant decline in FVC
HR; 2.34 (1.19-4.60)
P value; 0.01
HR; 2.31 (1.19-4.50)
P value; 0.014
HR;3.33 (1.61-6.88)
P value; <0.001 Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, HR=hazard ratio, OR= Odds Ratio, RR= Risk Ratio, IPF= Idiopathic Pulmonary Fibrosis, UIP=Usual interstitial pneumonia, ILD=interstitial lung disease, HRCT= high resolution computed tomography, DLCO=Carbon monoxide diffusing capacity, FVC= Forced vital capacity, TLCO=transfer factor for carbon monoxide, 6MWT= 6 minute walking test, PaO2=partial pressure of oxygen in arterial blood, BDI= baseline dyspnoea index, SGRQ= St George’s Respiratory Questionnaire, ATS = American Thoracic Society

188
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
18
8
F.2.2 Sub-maximal exercise tests 1
Some studies reported on more than one prognostic factor the information for sub-maximal exercise tests is in the following evidence tables located in the 2 serial pulmonary function test subsection: 3
Table 43: 4
Table 44: Caminati 2009 5
Table 47: Hallstrand 2005 6
F.2.3 Echocardiography 7
Some studies reported on more than one prognostic factor the information for echocardiography is in the following evidence tables located in the serial 8 pulmonary function test subsection: 9
Table 37: Mejia 2009 311 10
F.2.4 CT scores 11
Some studies reported on more than one prognostic factor the information for CT scores is in the following evidence tables located in the serial pulmonary 12 function test subsection: 13
Table 35: Lynch 2005 292 14
Table 54: Mogulkoc 2001A 15
Table 59: Best 200838 16
Study
details Population Methods Outcome measures Effect size Comments

189
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
18
9
Study
details Population Methods Outcome measures Effect size Comments 38
Country of study: USA
Study design:
Retrospective cohort
Who was blinded: N/A
Setting: Hospital
Duration of follow-up: 0.9-2.7 years (median follow-up, 1.5years)
Patient group: Patients enrolled in a clinical trial of interferon β-1a for treatment of IPF. (IPF diagnosed using American Thoracic Society criteria).
Inclusion criteria:
Progression of IPF, defined as meeting at least one of the following:
>10% relative decrease in TLC or FVC or >15% relative decrease in DLCO
>3% decrease in resting oxygen saturation level, a 3mm Hg increase in the resting gradient between the partial pressure of oxygen in the artery and that in the alveoli, or a 5% decrease in oxygen saturation with exercise
Radiologic progression of disease as assessed on chest radiographs or thin-CT images
Exclusion criteria:
Environmental or drug exposures likely to cause ILD
Connective tissue disease
Emphysema occupying more than 50% of the lung
End stage IPF defined as meeting at least two of the following:
TLC less than 45% of predicted volume
Haemoglobin-corrected DLCO <25% of predicted capacity
All patients:
CT visual score: fibrosis (%), ground glass opacity (GGO) %, emphysema (%)
Analysis:
Survival analysis performed to assess value of each variable accounting for differences in duration of follow-up. Potential predictors were used in the Cox proportional hazards model for univariable analysis. No further details provided
Mortality prediction (multivariable logistic regression analysis)
Fibrosis
OR estimate: 1.104
95% cI: 1.018, 1.198
P value: 0.017
Funding: NR
Limitations:
Outcome measures not clearly reported in paper.
Paper reports that univariable analysis for treatment assignment conducted, but results unclear.
Paper reports that univariable and multivariable logistic regression analysis was performed to predict mortality, however multivariable analysis data for FVC was not presented.
Additional outcomes:
Mortality: 35/167 (21.0%)
Abstract reports that at multivariable analysis, FVC (P=0.006). This is not presented in the paper. No further details provided.
Notes: N/A

190
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
19
0
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, HR=hazard ratio, OR= Odds Ratio, RR= Risk Ratio, IPF= Idiopathic Pulmonary Fibrosis, UIP=Usual interstitial 1 pneumonia, ILD=interstitial lung disease, HRCT= high resolution computed tomography, DLCO=Carbon monoxide diffusing capacity, FVC= Forced vital capacity, TLCO=transfer factor for carbon monoxide, 6MWT= 6 2 minute walking test, PaO2=partial pressure of oxygen in arterial blood, BDI= baseline dyspnoea index, SGRQ= St George’s Respiratory Questionnaire, ATS = American Thoracic Society. 3
Table 60: Sumikawa 2008454 4
Study
details
Population Methods Outcome measures Effect size Comments
Sumikawa 2008
454
Country of study: USA
Study design:
Retrospectivecohort
Who was blinded: N/A
Setting: unclear
Duration of follow-up:
79 months (mean)
63 months (median)
Patient group: IPF
Inclusion criteria: as above
Exclusion criteria: NR
All patients
N: 98
Age (mean): 63 years (range 36-75)
M/F: 71/27
Drop outs: 46 died, 10 lost to follow-up
HRCT findings
Analysis:
Cox proportional hazards regression models used
Confounding factors adjusted for: each one of the following CT findings: presence of ground-glass attenuation; airspace consolidation; nodules; interlobular septal thickening; thickening of bronchovascular bundles; intralobular reticular opacities; irregular interlobular septal thickening; nonseptal linear or platelike opacities; presence of honeycombing, cysts, emphysema, architectural distortion, or traction
Traction bronchiectasis- multivariable analysis
HR 1.30 95% CI 1.18-1.43 Funding: NR
Limitations:
Additional outcomes:
Interobserver agreement for CT findings
Fibrosis score - multivariable analysis
HR 1.10 95% CI 1.03-1.19

191
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
19
1
bronchiectasis; fibrosis score; the extent of disease close to the hilum; and upper, lower, peripheral, dependent, peribronchovascular, and asymmetric predominant distribution.
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, HR=hazard ratio, OR= Odds Ratio, RR= Risk Ratio, IPF= Idiopathic Pulmonary Fibrosis, UIP=Usual interstitial 1 pneumonia, ILD=interstitial lung disease, HRCT= high resolution computed tomography, DLCO=Carbon monoxide diffusing capacity, FVC= Forced vital capacity, TLCO=transfer factor for carbon monoxide, 6MWT= 6 2 minute walking test, PaO2=partial pressure of oxygen in arterial blood, BDI= baseline dyspnoea index, SGRQ= St George’s Respiratory Questionnaire, ATS = American Thoracic Society. 3
F.3 Pulmonary rehabilitation 4
Table 61: Almoamary 201211 5
Study
details
Population Methods Outcome measures Effect size Comments
Almoamary 2012
11
Country of study:
Saudi Arabia
Study design:
retrospective study
Who was blinded:
Patient group:
The medical records of people referred for pulmonary rehabilitation between 1 July 2004 and 15 January 2008 were reviewed. Only ILD patient data recorded in this table.
Inclusion criteria:
≥18 years,
Diagnoses of bronchiectasis, severe uncontrolled asthma, interstitial lung diseases (ILD)* or scoliosis.
All people
People were initially interviewed by a pulmonary rehabilitation physiotherapist as part of the initial assessment on entry in the programme.
Adherence to the pulmonary rehabilitation programme required the patient to complete the
6-min. walking distance (m)
Mean (SD)
Pre-rehab: 179 (74)
Post-rehab: 293 (97)
Difference: 114 (58)
p value: 0.006
Funding: NR
Limitations:
Retrospective design
Bias
Doesn’t account for confounding
No blinding
Additional outcomes:
Adherence to rehabilitation programme: 11/21
Distance on treadmill (m)
Mean (SD)
Pre-rehab: 114 (66)
Post-rehab: 371 (199)
Difference: 257 (163)
p value: 0.001
Distance on bicycle (m)
Mean (SD)
Pre-rehab: 1031 (358)
Post-rehab: 2532 (1120)
Difference: 1503 (962)
p value: 0.004
Distance on ergometer Pre-rehab: 555 (136)
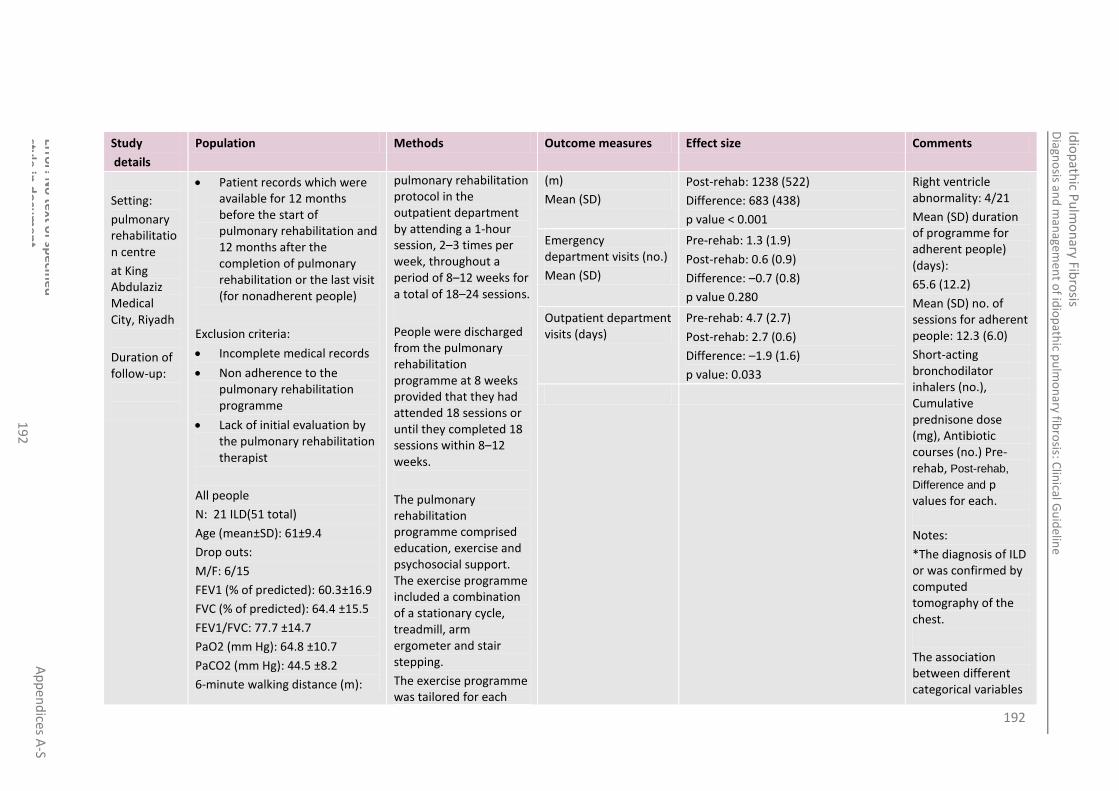
192
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
19
2
Study
details
Population Methods Outcome measures Effect size Comments
Setting:
pulmonary rehabilitation centre
at King Abdulaziz Medical City, Riyadh
Duration of follow-up:
Patient records which were available for 12 months before the start of pulmonary rehabilitation and 12 months after the completion of pulmonary rehabilitation or the last visit (for nonadherent people)
Exclusion criteria:
Incomplete medical records
Non adherence to the pulmonary rehabilitation programme
Lack of initial evaluation by the pulmonary rehabilitation therapist
All people
N: 21 ILD(51 total)
Age (mean±SD): 61±9.4
Drop outs:
M/F: 6/15
FEV1 (% of predicted): 60.3±16.9
FVC (% of predicted): 64.4 ±15.5
FEV1/FVC: 77.7 ±14.7
PaO2 (mm Hg): 64.8 ±10.7
PaCO2 (mm Hg): 44.5 ±8.2
6-minute walking distance (m):
pulmonary rehabilitation protocol in the outpatient department by attending a 1-hour session, 2–3 times per week, throughout a period of 8–12 weeks for a total of 18–24 sessions.
People were discharged from the pulmonary rehabilitation programme at 8 weeks provided that they had attended 18 sessions or until they completed 18 sessions within 8–12 weeks.
The pulmonary rehabilitation programme comprised education, exercise and psychosocial support. The exercise programme included a combination of a stationary cycle, treadmill, arm ergometer and stair stepping.
The exercise programme was tailored for each
(m)
Mean (SD)
Post-rehab: 1238 (522)
Difference: 683 (438)
p value < 0.001
Right ventricle abnormality: 4/21
Mean (SD) duration of programme for adherent people) (days):
65.6 (12.2)
Mean (SD) no. of sessions for adherent people: 12.3 (6.0)
Short-acting bronchodilator inhalers (no.), Cumulative prednisone dose (mg), Antibiotic courses (no.) Pre-rehab, Post-rehab,
Difference and p values for each.
Notes:
*The diagnosis of ILD or was confirmed by computed tomography of the chest.
The association between different categorical variables
Emergency department visits (no.)
Mean (SD)
Pre-rehab: 1.3 (1.9)
Post-rehab: 0.6 (0.9)
Difference: –0.7 (0.8)
p value 0.280
Outpatient department visits (days)
Pre-rehab: 4.7 (2.7)
Post-rehab: 2.7 (0.6)
Difference: –1.9 (1.6)
p value: 0.033

193
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
19
3
Study
details
Population Methods Outcome measures Effect size Comments
189 ±95 patient based on their physiological parameters and the physiotherapist’s judgement.
Specific exercises for the upper and lower extremities were included, as well as strength and flexibility exercises.
Small group education sessions were conducted by the appropriate specialist
was assessed using the chi-squared test, whereas the paired and unpaired t-test was used to test differences between continuous variables. A P-value of < 0.05 was regarded as statistically significant
Abbreviations: M/F=male/female, N=total number of people randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon 1 monoxide diffusing capacity, IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 2 6MWT= 6 minute walking test 3
Table 62: Ferreira 2009141 4
Study
details
Population Methods Outcome measures Effect size Comments
Ferreira 2009
141
Country of study:
USA
Patient group:
Records of people with a diagnosis of ILD who had been
referred for PR between January 2003 and March 2008 were retrospectively collected and analyzed from 3 study
All people
PR programs were multidisciplinary, outpatient programs that consisted of two or three sessions per week
Borg score (n = 99)
mean (SD)
Baseline: 3.6 (2.0)
After PR: 2.7 (1.7)
Change: -1.0 (1.7)
P: > 0.0001
Funding: NR
Limitations:
No control group
Blinding is not reported
Data available did not
UCSD questionnaire (n =29) mean (SD)
Baseline: 57.4 (25)
After PR: 49.1 (25)
Change: - 8.3 (14)

194
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
19
4
Study
details
Population Methods Outcome measures Effect size Comments
Study design:
Retrospective observational study
Who was blinded: NR
Setting: hospital
Duration of follow-up:
NR
centres
Inclusion criteria:
a referring diagnosis of ILD and documentation of pre- and post-PR variables
Exclusion criteria:
NR
All people
N: 99
Age (mean ±SD): 66± 13
M/F: 54/45
FVC (L, ±SD): 2.2 ±0.9
FVC (% predicted, ±SD): 62 ±20
DLCO (%, ±SD):40 ±14
6MWD (m): NR
BDI score:NR
SGRQ score (total):NR
Lowest oxygen saturation on baseline 6MWT (%,±SD): 89 ±6
Never-smoker: n=41 (41%)
LTOT (±SD): 65 ±66
Drop outs: 0
(2 to 3 h each) of exercise and educational activities for 6 to 8 weeks. The exercise sessions included endurance, strength, and respiratory muscles training, along with pacing and breathing techniques. The educational topics included medication and oxygen use, nutrition, panic control and relaxation techniques, as well as psychosocial support and end-of-life issues.
P: 0.005 include information on comorbidities, the onset of a respiratory exacerbation
or an acute illness during the PR program, current medications, and specific ILD diagnosis, all of which could potentially influence the results.
Data on the level of oxygen used during walk testing were not available for all people. While standard practice was to use a stable level of oxygen throughout the period of PR, it is possible that some people could have received varying levels.
Important differences between participating centres could be present that were missed due to inadequate numbers.
6MWT distance, m (n = 99) mean (SD)
Baseline: 335 (131)
After PR: 391 (118)
Change: 56 (69)
P: > 0.0001
CES-D score (n =27) mean (SD)
Baseline: 15.7 (8)
After PR: 13.6 (8)
Change: 2.2 (5)
P: 0.046
6MWT distance, % change (n =99) Median (25th percentile, 75th percentile).
Change: 14 (2, 33)
P: 0.002

195
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
19
5
Study
details
Population Methods Outcome measures Effect size Comments
Notes:
Variables recorded included age, gender, baseline pulmonary function test values, specifically FVC and diffusion capacity of the lung for carbon monoxide (Dlco), smoking history, use of long-term oxygen therapy (LTOT), pre- and post-PR Borg dyspnoea score, pre- and post-PR 6-min walk test (6MWT) distance, and the PR centre attended. Pre- and post-PR University of California San Diego (UCSD) shortness of breath questionnaire scores and Centre for Epidemiologic Studies-Depression (CES-D) scores were available for some people.

196
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
19
6
Study
details
Population Methods Outcome measures Effect size Comments
The Borg dyspnoea score, UCSD
shortness of breath questionnaire, and the CES-D score were all
performed according to published standards.18–20 The 6MWTs were performed according to modified guidelines of the American Thoracic Society.21 Supplemental oxygen was used during the test in people who were already on LTOT or in those who desaturated below 88%
All people had ILD diagnosed, which was recorded as idiopathic pulmonary fibrosis (n = 50),
unspecified ILD (n =42), scleroderma (n =3), nonspecific interstitial
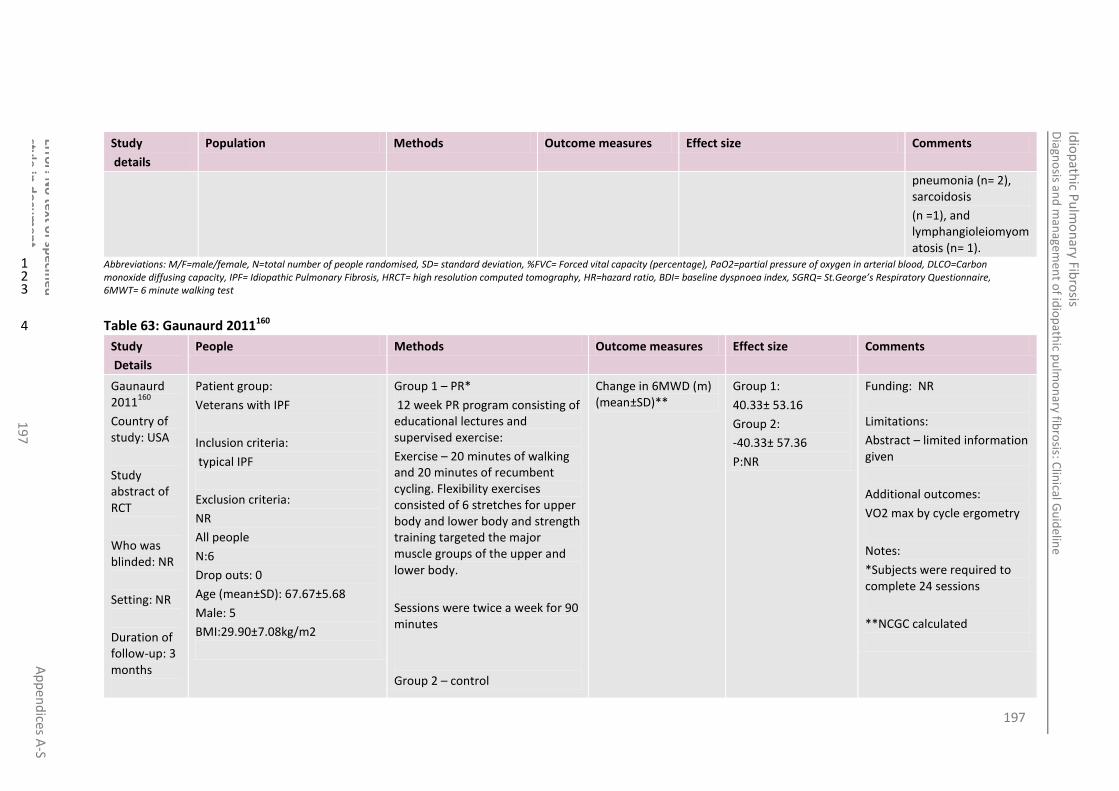
197
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
19
7
Study
details
Population Methods Outcome measures Effect size Comments
pneumonia (n= 2), sarcoidosis
(n =1), and lymphangioleiomyomatosis (n= 1).
Abbreviations: M/F=male/female, N=total number of people randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon 1 monoxide diffusing capacity, IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 2 6MWT= 6 minute walking test 3
Table 63: Gaunaurd 2011160 4
Study
Details
People Methods Outcome measures Effect size Comments
Gaunaurd 2011
160
Country of study: USA
Study abstract of RCT
Who was blinded: NR
Setting: NR
Duration of follow-up: 3 months
Patient group:
Veterans with IPF
Inclusion criteria:
typical IPF
Exclusion criteria:
NR
All people
N:6
Drop outs: 0
Age (mean±SD): 67.67±5.68
Male: 5
BMI:29.90±7.08kg/m2
Group 1 – PR*
12 week PR program consisting of educational lectures and supervised exercise:
Exercise – 20 minutes of walking and 20 minutes of recumbent cycling. Flexibility exercises consisted of 6 stretches for upper body and lower body and strength training targeted the major muscle groups of the upper and lower body.
Sessions were twice a week for 90 minutes
Group 2 – control
Change in 6MWD (m) (mean±SD)**
Group 1:
40.33± 53.16
Group 2:
-40.33± 57.36
P:NR
Funding: NR
Limitations:
Abstract – limited information given
Additional outcomes:
VO2 max by cycle ergometry
Notes:
*Subjects were required to complete 24 sessions
**NCGC calculated

198
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
19
8
Study
Details
People Methods Outcome measures Effect size Comments
Abbreviations: M/F=male/female, N=total number of people randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon 1 monoxide diffusing capacity, IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 2 6MWT= 6 minute walking test 3
Table 64: Holland 2008185(including unpublished data provided by authors) & Holland 2008 186 4
Study details
People Methods Outcome measures
Effect size Comments
Holland 2008 185
(including unpublished data provided by authors) , Holland 2008
186
(Cochrane review) &
Country of study:
Australia
Study design:
Randomised controlled trial
Patient group:
Total n=57, including IPF n=34, IIP n=4 diffuse parenchymal lung disease of unknown cause n=14, granulotamous lung disease n=4. Only IPF people will be reported on in this table.
Inclusion criteria:
>18 years and sypmtomatic
People ambulent and reported dyspnoea on exertion, on stable medical therapy.
Exclusion criteria:
History of syncope on exertion or any comorbities which precluded exercise
Group 1 - Exercise group
8 week outpatient exercise program, twice weekly supervised sessions by a physiotherapist. Consisting of 30 minutes endurance exercise (cycling and walking) with initial intensity at 80% of walking speed on initial 6-minute walk test and progressed according to protocol. Upper limb endurance and functional strength training for lower limbs also performed. Supplemental oxygen provided for SpO2≥85%. Once established on supervised programme a unsupervised home exercise program prescribed 3 times per week. Aim to achieve 5 exercise sessions per week.
Group 2 - Control group
Change in 6-minute walk test immediately following PR
(taken from Cochrane)
Group 1: 25.05
Group 2: 8.93
Mean difference: 16.12
95% CI: -13.32, 45.56
P-value: NR
Funding: Victorian Tuberculosis and Lung Association (Holland 2008
185)
Limitations:
Large numbers of drop outs
The effect of disease aetiology and severity on response to exercise training could not be fully characterised – the study was not powered to adequately assess this outcome.
Small sample size
Notes:
IPF diagnosis criteria in line with international consensus statement
Stratified for IPF – raw data
Chang e in 6-minute walk test long term follow up
(taken from Cochrane)
Group 1: -19.15
Group 2: 3.93
Mean difference: -23.08
95% CI: -70.59, 24.43
P-value: 0.34
Change in dyspnoea score immediately following training
(taken from Cochrane)
Group 1: -0.55
Group 2: 0.23
Standard Mean difference: -0.56
95% CI: -1.26, 0.14
P-value: NR

199
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
19
9
Study details
People Methods Outcome measures
Effect size Comments
Who was blinded:
Single blinded
Setting:
outpatient
Duration of follow-up
9 &26 weeks
training (such as severe orthopaedic or neurological deficits or unstable cardiac disease). Had participated in a pulmonary rehabilitation programme in the last 12 months
All people
N: =34 (IPF)
Age (mean±SD): NR for IPF alone – all people: 67±13
Drop outs for all participants NR for IPF alone: 8
Group 1 Exercise group
N: =30
Age (mean±SD): 70(8)
Drop outs for all participants NR for IPF alone:
Exercise training programme dropouts: 6 (1=IPF exacerbation, 2=unwell non respiratory, anxiety disorder and back pain 3= didn’t want to complete)
Loss to follow up :9 week follow up: 2 (declined)
26 week follow up:5
Weekly telephone calls for general health advice and support.
Change in dyspnoea score long term follow up
(taken from Cochrane)
Group 1: -0.2
Group 2: -0.21
Mean difference: 0.01
95% CI: -0.79, 0.81
P-value: 0.98
not reported in paper for all outcomes in IPF only group
Measured pre and post intervention period. 6 minute walk test and questionnaires repeated at 6 month follow up.
Computer generated random number sequence generation.
Allocation concealment in a central location, sealed opaque envelope, by an individual unrelated to the study. (randomisation was done separately for IPF to other ILD people to ensure even distribution across groups)
Data collector blinded to treatment allocation.
Intention to treat analysis, last observation carried forward.
All data available at all time points
Change in quality of life immediately following training (taken from Cochrane)
Group 1: 5.53
Group 2: -8.53
Standard Mean difference: 0.77
95% CI: 0.06, 1.48
P-value: NR
Change in quality of life long term follow up (taken from Cochrane)
Group 1: -3.06
Group 2: -10.11
Mean difference: 7.05
95% CI: -8.29, 22.39
P-value: 0.37
Six month survival
(taken from Cochrane)
Group 1: 2/20
Group 2: 2/14
RR: 0.7
95% CI: 0.11, 4.39
P-value: 0.70
SF36 domain: physical functioning (unpublished
Group 1 post treatment : 36.67±21.17
Group1 long term follow up:

200
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
20
0
Study details
People Methods Outcome measures
Effect size Comments
(declined 3 deceased 2)
TLCO: 50(19)
SF36 domains (mean±SD):
Vitality: 40.38±17.43
physical functioning: 40.02±22.45
bodily pain: 59.78±23.21
general health perceptions: 42.19±18.05
physical role functioning: 19.44±28.87
emotional role functioning: 55.56±42.37
social role functioning: 64.35±29.36
mental health: 69.08±16.49
Group 2 Control group
N: =27
Age (mean±SD): 67(13)
Drop outs for all participants NR for IPF alone:
Loss to follow up : 9 week follow up: 2 (1=deceased, 1=Unwell lymphoma)
26 week follow up: 9 (1= declined, 2 =deceased, 2=unwell IPF related 1=unwell lymphoma)
data) mean±SD 31.11±18.93
Group 2 post treatment : 45.56±23.63
Group 2 long term follow up: 38.70±25.89
All data reported in the original paper (Holland 2008
185)did not give IPF data
separately from the total
SF36 domain:
physical role functioning (unpublished data) mean±SD
Group 1 post treatment : 25.00±36.69
Group1 long term follow up: 20.37±30.25
Group 2 post treatment : 24.07±39.52
Group 2 long term follow up: 14.81±33.44
SF36 domain: vitality (unpublished data) mean±SD
Group 1 post treatment : 42.04±21.76
Group1 long term follow up: 41.48±19.41
Group 2 post treatment : 52.31±17.79
Group 2 long term follow up: 45.38±23.11
SF36 domain: bodily pain (unpublished data) mean±SD
Group 1 post treatment : 54.22±30.78
Group1 long term follow up: 55.22±33.93
Group 2 post treatment : 61.51±27.50
Group 2 long term follow up: 63.22±29.23
SF36 domain: Group 1 post treatment :
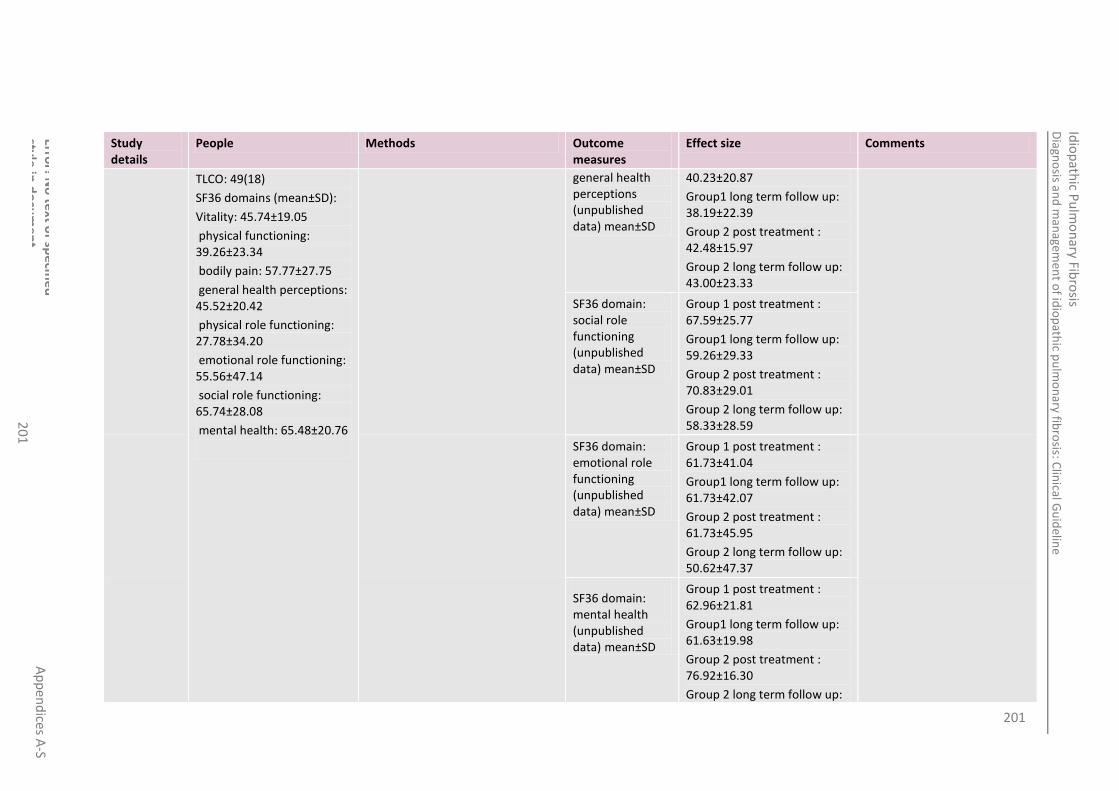
201
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
20
1
Study details
People Methods Outcome measures
Effect size Comments
TLCO: 49(18)
SF36 domains (mean±SD):
Vitality: 45.74±19.05
physical functioning: 39.26±23.34
bodily pain: 57.77±27.75
general health perceptions: 45.52±20.42
physical role functioning: 27.78±34.20
emotional role functioning: 55.56±47.14
social role functioning: 65.74±28.08
mental health: 65.48±20.76
general health perceptions (unpublished data) mean±SD
40.23±20.87
Group1 long term follow up: 38.19±22.39
Group 2 post treatment : 42.48±15.97
Group 2 long term follow up: 43.00±23.33
SF36 domain: social role functioning (unpublished data) mean±SD
Group 1 post treatment : 67.59±25.77
Group1 long term follow up: 59.26±29.33
Group 2 post treatment : 70.83±29.01
Group 2 long term follow up: 58.33±28.59
SF36 domain: emotional role functioning (unpublished data) mean±SD
Group 1 post treatment : 61.73±41.04
Group1 long term follow up: 61.73±42.07
Group 2 post treatment : 61.73±45.95
Group 2 long term follow up: 50.62±47.37
SF36 domain: mental health (unpublished data) mean±SD
Group 1 post treatment : 62.96±21.81
Group1 long term follow up: 61.63±19.98
Group 2 post treatment : 76.92±16.30
Group 2 long term follow up:

202
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
20
2
Study details
People Methods Outcome measures
Effect size Comments
72.92±17.65 Abbreviations: M/F=male/female, N=total number of people randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon 1 monoxide diffusing capacity, IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 2 6MWT= 6 minute walking test 3
Table 65: Holland 2012187 4
Study
details
Population Methods Outcome measures Effect size Comments
Holland 2012
187
Design:
Observational Study
Setting:
People recruited from two tertiary centres in Australia
Who was blinded?:
No one
Duration of follow-up:
People
Patient group:
44 participants (25 of whom had IPF)
Only IPF data presented here
Inclusion criteria:
Ambulant people reporting dyspnoea on stable medical therapy.
Exclusion criteria:
History of syncope on exertion; any comorbidities precluding exercise training; participation in a pulmonary rehabilitation program in the last two years
IPF people
N: 25
Age (mean): 72.9
FVC (% predicted) mean +/- SD: 76.4 +/- 20.3
All people
The pulmonary rehabilitation consisted of a twice weekly, eight week exercise program of endurance and strength training which was prescribed and progressed according to a previously defined standard protocol. Supplemental O2 was provided to maintain SaO2 ≥ 85%
An unsupervised home exercise program was also prescribed with the aim of achieving five sessions per week in total. People who had been prescribed supplemental O2 were encouraged to use this during home exercise.
Participants also attended an education and self-management
Dyspnoea: Change in CRQ dyspnoea domain (at 8 weeks)
Mean (SD): 2.7 (5.6)
Significantly improved from baseline
p˂0.5
Funding: No conflicts of interest declared
Limitations:
Confounding factors weren’t accounted for
Small sample size
No control
Non randomised
Additional outcomes:
Change in FVC at 6 months
Change in DLCO at 6 months
No hazard ratios, odds rations or risk ratios reported to inform prognosis.
Notes:
Only IPF data presented
MID: 6MWD 34m (within
Dyspnoea: Change in CRQ dyspnoea domain (at 6 months)
NS change from baseline
Mean improvement in 6MWD (at 8 weeks)
Mean (SD): 21 (58)
Significantly improved from baseline
p˂0.5
Change in 6MWD (at 6 months)
NS change from baseline
Number of people achieving gains exceeding the MID for 6MWD at 8 weeks
“improvements that exceeded the MID occurred in 40% of participants”
Number of people achieving gains exceeding the MID for 6MWD at 6 months
“improvements that exceeded the MID occurred in 35% of participants”
Number of people “improvements that

203
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
20
3
undertook 8 weeks of pulmonary rehab and were assessed after 8 weeks and six months
TLCO (% predicted): mean +/- SD: 48.5 (19.1)
Drop outs: “6 participants (in whole group) did not complete the rehab program due to respiratory illness (n=1), other illness (n=1), musculoskeletal pain (n=1) and lack of motivation (n=3). Two of these participants (both with IPF) declined further participation in the study”
One participant with IPF died prior to 6 month follow up
program.
achieving gains exceeding the MID for CRQ dyspnoea at 8 weeks
exceeded the MID occurred in 59% of participants”
our MID range 24-45m)
MID: CRQ dyspnoea 2.5 points (we use standard MIDs)
Number of people achieving gains exceeding the MID for CRQ dyspnoea at 6 months
“improvements that exceeded the MID occurred in 24% of participants”
Abbreviations: M/F=male/female, N=total number of people randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon 1 monoxide diffusing capacity, IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 2 6MWT= 6 minute walking test 3
Table 66: Jastrzebski 2006213 4
Study
details
Population Methods Outcome measures Effect size Comments
Jastrzebski 2006
213
Country of study: Poland
Study design: cohort
Patient group: ILD
Inclusion criteria:
· interstitial lung disease was diagnosed on the basis of radioclinical criteria
· people reported at least 2 years of disease symptoms
· people did not require home oxygen therapy
All people
The rehabilitation programme was composed of 4 weeks of rehabilitation held in the hospital and later continued by people themselves at home. The exercise programme was formed on the basis of the American Society, the British Thorax Society, and the American
Dyspnoea (MRC scale)- 5 grade scale
Baseline: 2.3±0.8
After rehab: 2.0±0.9
P: 0.06
Funding: NR
Limitations:
No baseline data provided
Confounding factors weren’t accounted for
Small sample size
No control
Non randomised
Dyspnoea (oxygen cost diagram)
Baseline: 72.2±14.6
After rehab: 77.2±15.9
Dyspnoea (baseline dyspnoea index): sum of functional impairment, magnitude and effort and
Baseline: 6.3±2.8
After rehab: 6.8±3.3

204
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
20
4
Study
details
Population Methods Outcome measures Effect size Comments
Who was blinded: no one
Setting: Department of Lung diseases and Tuberculosis of an academic hospital in Zabrze, Poland
Duration of follow-up: 6 weeks
· people were able to perform exercises on a bicycle ergometer
· treatment with no more than 20 mg of prednisone per day
· people were at a stable stage of disease, free of infection
Exclusion criteria:
All people
N: 38 (began programme; 31 completed)*
M/F: 19/12
Mean age: 48.7 years
Drop outs: 7
Society of Cardiologic
and Respiratory Rehabilitation recommendations, which were for COPD people.
The people were informed about the rules and aims of the planned programme. A diary was provided in which they were obliged to note any deviations from, or problems with, the execution of the exercise programme. In the hospital environment, the programme was introduced to the patient under the supervision of an experienced instructor of rehabilitation, and exercise was preceded by instruction and demonstration of the planned tasks.
The timing and intensity of the exercise program was prepared individually for each patient.
The programme consisted of general exercise, performed twice a week for 30 min, (movements of the thorax, correctional exercise, isometric exercise), respiratory muscle exercise, consisting of 6 series of 5-breath cycles interspersed with
magnitude of task
Additional outcomes:
BDI domains – functional impairment, magnitude of task, magnitude of effort
Notes:
3 people terminated the rehabilitation due to disease exacerbation caused by infection that led to hospitalization, 2 people resigned from the training programme after 2 and 4 weeks because of discouragement to exercise, although they did not manifest any side effects, and 2 others were excluded from the analysis, since they did not report to the control examination due to personal reasons.
*THE SAMPLE INCLUDED: · 21 people with idiopathic interstitial pneumonia
· 13 people with idiopathic pulmonary fibrosis
· 8 people with nonspecific
Dyspnoea (Borg scale of 1 to 10)
Baseline: 3.0±1.4
After rehab: 2.5±1.4
SF36 domain: physical functioning (mean-taken from graph)
Baseline: 55
After rehab:65
P: <0.05
SF36 domain: physical role functioning (mean-taken from graph)
Baseline: 40
After rehab:55
P: NR
SF36 domain: vitality (mean-taken from graph)
Baseline: 53
After rehab:58
P: <0.05
SF36 domain: bodily pain (mean-taken from graph)
Baseline: 69
After rehab:67
P: NR
SF36 domain: general health perceptions (mean-taken from graph)
Baseline: 38
After rehab: 41
P: NR
SF36 domain: social role functioning (mean-taken from graph)
Baseline: 58
After rehab:70
P: <0.05
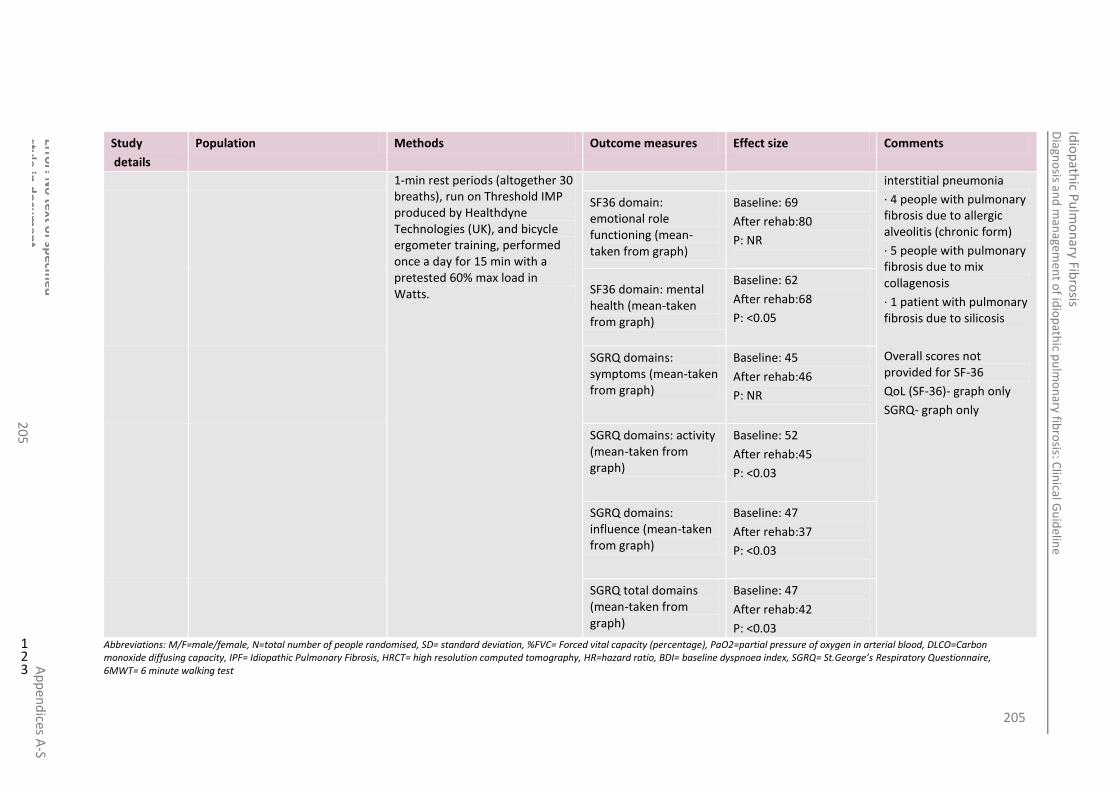
205
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
20
5
Study
details
Population Methods Outcome measures Effect size Comments
1-min rest periods (altogether 30 breaths), run on Threshold IMP produced by Healthdyne Technologies (UK), and bicycle ergometer training, performed once a day for 15 min with a pretested 60% max load in Watts.
interstitial pneumonia
· 4 people with pulmonary fibrosis due to allergic alveolitis (chronic form)
· 5 people with pulmonary fibrosis due to mix collagenosis
· 1 patient with pulmonary fibrosis due to silicosis
Overall scores not provided for SF-36
QoL (SF-36)- graph only
SGRQ- graph only
SF36 domain: emotional role functioning (mean-taken from graph)
Baseline: 69
After rehab:80
P: NR
SF36 domain: mental health (mean-taken from graph)
Baseline: 62
After rehab:68
P: <0.05
SGRQ domains: symptoms (mean-taken from graph)
Baseline: 45
After rehab:46
P: NR
SGRQ domains: activity (mean-taken from graph)
Baseline: 52
After rehab:45
P: <0.03
SGRQ domains: influence (mean-taken from graph)
Baseline: 47
After rehab:37
P: <0.03
SGRQ total domains (mean-taken from graph)
Baseline: 47
After rehab:42
P: <0.03 Abbreviations: M/F=male/female, N=total number of people randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon 1 monoxide diffusing capacity, IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 2 6MWT= 6 minute walking test 3
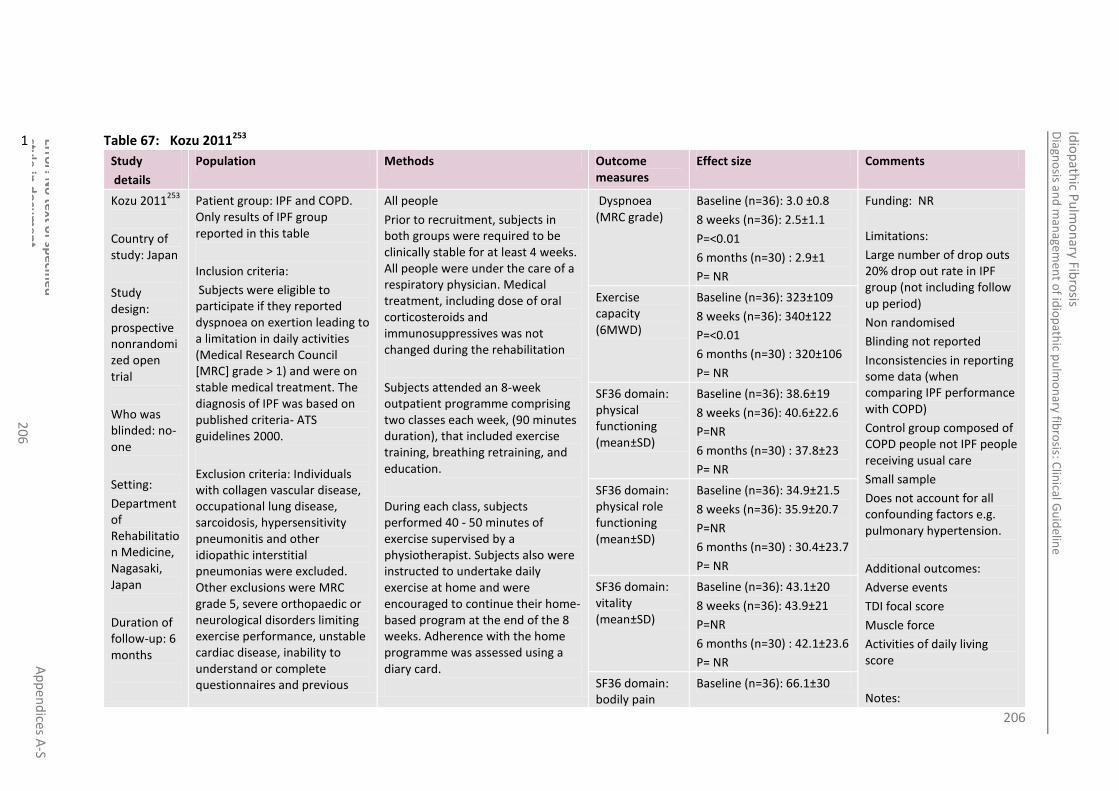
206
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
20
6
Table 67: Kozu 2011253 1
Study
details
Population Methods Outcome measures
Effect size Comments
Kozu 2011253
Country of study: Japan
Study design:
prospective nonrandomized open trial
Who was blinded: no-one
Setting:
Department of Rehabilitation Medicine, Nagasaki, Japan
Duration of follow-up: 6 months
Patient group: IPF and COPD. Only results of IPF group reported in this table
Inclusion criteria:
Subjects were eligible to participate if they reported dyspnoea on exertion leading to a limitation in daily activities (Medical Research Council [MRC] grade > 1) and were on stable medical treatment. The diagnosis of IPF was based on published criteria- ATS guidelines 2000.
Exclusion criteria: Individuals with collagen vascular disease, occupational lung disease, sarcoidosis, hypersensitivity pneumonitis and other idiopathic interstitial pneumonias were excluded. Other exclusions were MRC grade 5, severe orthopaedic or neurological disorders limiting exercise performance, unstable cardiac disease, inability to understand or complete questionnaires and previous
All people
Prior to recruitment, subjects in both groups were required to be clinically stable for at least 4 weeks. All people were under the care of a respiratory physician. Medical treatment, including dose of oral corticosteroids and immunosuppressives was not changed during the rehabilitation
Subjects attended an 8-week outpatient programme comprising two classes each week, (90 minutes duration), that included exercise training, breathing retraining, and education.
During each class, subjects performed 40 - 50 minutes of exercise supervised by a physiotherapist. Subjects also were instructed to undertake daily exercise at home and were encouraged to continue their home-based program at the end of the 8 weeks. Adherence with the home programme was assessed using a diary card.
Dyspnoea (MRC grade)
Baseline (n=36): 3.0 ±0.8
8 weeks (n=36): 2.5±1.1
P=<0.01
6 months (n=30) : 2.9±1
P= NR
Funding: NR
Limitations:
Large number of drop outs 20% drop out rate in IPF group (not including follow up period)
Non randomised
Blinding not reported
Inconsistencies in reporting some data (when comparing IPF performance with COPD)
Control group composed of COPD people not IPF people receiving usual care
Small sample
Does not account for all confounding factors e.g. pulmonary hypertension.
Additional outcomes:
Adverse events
TDI focal score
Muscle force
Activities of daily living score
Notes:
Exercise capacity (6MWD)
Baseline (n=36): 323±109
8 weeks (n=36): 340±122
P=<0.01
6 months (n=30) : 320±106
P= NR
SF36 domain: physical functioning (mean±SD)
Baseline (n=36): 38.6±19
8 weeks (n=36): 40.6±22.6
P=NR
6 months (n=30) : 37.8±23
P= NR
SF36 domain: physical role functioning (mean±SD)
Baseline (n=36): 34.9±21.5
8 weeks (n=36): 35.9±20.7
P=NR
6 months (n=30) : 30.4±23.7
P= NR
SF36 domain: vitality (mean±SD)
Baseline (n=36): 43.1±20
8 weeks (n=36): 43.9±21
P=NR
6 months (n=30) : 42.1±23.6
P= NR
SF36 domain: bodily pain
Baseline (n=36): 66.1±30

207
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
20
7
Study
details
Population Methods Outcome measures
Effect size Comments
participation in a pulmonary rehabilitation programme.
All people
N: 90
Drop outs:
Group 1 (IPF)- only results of this group reported in this table
N: 45 (36 completed programme(discontinued due to exacerbation =3, didn’t wish to complete = 3 other reasons =3), 30 completed 6 month follow-up (deceased = 4 declined = 2))
Age (mean): 67.5 ±7.8
Gender, M/F: 37/8
Time since diagnosis, years: 1.8±1.8
Oral corticosteroids 20 (44%)
Cough: 30 (67%)
FVC, litres: 2.0 ±0.6
FVc, % predicted: 68.6 ±16
DLCO:, ml/min/mmHg: 6.0±2.5
DLCO, % predicted: 38.8±20
Drop outs: 9 (exacerbation: 3, did not wish to complete: 3, other reasons:3)
Exercise training included stretches and endurance and strength training. Lower limb endurance training was performed using a cycle ergometer with the initial workload prescribed at 50% of the PWR achieved on the baseline cycle ergometer test. In the early stages of the program, cycling was limited to 5 to 10 minutes and progressively increased, within symptom tolerance, to 20 minutes of continuous cycling. Once subjects had achieved 20 minutes cycling, the workload was increased. Upper limb endurance training comprised repetitive bilateral shoulder flexion and abduction using a light weight and synchronized with expiration for 2 minutes. Strength training was accomplished using free weights or the subject’s own body weight. One set of 10 repetitions was initially prescribed increasing to 3 sets when the subject could perform the exercises without any difficulty. Arterial oxygen saturation was monitored during each session, and supplemental oxygen was given as necessary, to maintain arterial oxygen saturation above 85%. We recorded the duration of cycle-
(mean±SD) 8 weeks (n=36): 63.4±28.1
P=NR
6 months (n=30) : 62.5±30.3
P= <0.05
No adverse events were recorded during this programme.
Supervised sessions attended by IPF people: 13.3±3.8 p=0.24
Average number of home based exercise sessions completed each week 3.9±1.9 p=0.59
20% drop out rate in IPF group
SF36 domain: general health perceptions (mean±SD)
Baseline (n=36): 37.1±20
8 weeks (n=36): 36.9±21.1
P=NR
6 months (n=30) : 34.4±21.5
P= <0.05
SF36 domain: social role functioning (mean±SD)
Baseline (n=36): 51±23.8
8 weeks (n=36): 50.3±25.3
P=NR
6 months (n=30) : 45.8±26.9
P= <0.05
SF36 domain: emotional role functioning (mean±SD)
Baseline (n=36): 39.6±30.7
8 weeks (n=36): 38.7±31.3
P=NR
6 months (n=30) : 35.8±29.8
P= NR
SF36 domain: mental health (mean±SD)
Baseline (n=36): 50.7±18.7
8 weeks (n=36): 52.6±20.5
P=NR
6 months (n=30) : 47.5±21.8
P= NR

208
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
20
8
Study
details
Population Methods Outcome measures
Effect size Comments
Group 2 (COPD- control)- results not reported in this table
N: 45 (40 completed programme, 37 completed 6 month follow-up)
Age (mean):
Drop outs: 5 (exacerbation: 1, did not wish to complete: 2, other reasons: 2)
based exercise (in minutes) and workload (in Watts) of all subjects for each of the exercise sessions.
Breathing retraining consisted of relaxation with breathing control, pursed-lip breathing and pacing during exercise training and ADL. The rationale for pursed-lip breathing in the IPF cohort was to assist subjects to control their breathing by reducing respiratory frequency. All subjects received the same instructions.
The education component was provided by a physiotherapist at each class and consisted of the benefits and importance of daily exercise, pacing and energy conservation techniques to manage ADL and self-management strategies for coping with an exacerbation.
Subjects were considered to have completed the programme if they attended at least 12 (75%) of
the 16 supervised sessions. At the end of the 8 week programme, all subjects were encouraged to

209
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
20
9
Study
details
Population Methods Outcome measures
Effect size Comments
continue with their home exercise program however no formal maintenance programme was provided.
Abbreviations: M/F=male/female, N=total number of people randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon 1 monoxide diffusing capacity, IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 2 6MWT= 6 minute walking test 3
Table 68: Naji 2006338 4
Study
details
Population Methods Outcome measures
Effect size Comments
Naji 2006338
Country of study:
Ireland
Study design:
Retrospective chart review
Who was blinded:
NR
Setting:
Hospital
Patient group:
People with restrictive lung disease referred to a pulmonary rehabilitation centre over the past 8 years. Only the data for ILD people is presented here.
Inclusion criteria:
NR
Exclusion criteria:
Significant airflow obstruction
Noncompliant
Unable to perform pulmonary function tests or exercise endurance tests
All people
People initially admitted to hospital for 3 days for baseline assessments and to commence on the programme.
The programme consisted of exercise and education * was continued post discharge 2/week over a period of 8 weeks.
Shuttle test (m)
mean±SD
Baseline**:171±102
8 weeks:232±118
1 year: NR
Funding: NR
Limitations: Some figures related to dropouts and survival data doesn’t add up correctly. Very unclearly reported.
Small sample size
Single centre
High dropout rate – 46%
Blinding is not reported
Retrospective observational study-
No control group
Additional outcomes: Survival (accurate and reliable data was not extractable from the paper)
treadmill test
Anxiety and depression were also measured using the hospital anxiety questionnaire.
Results for all outcomes for all people with
CRDQ (dyspnoea)
Median (ranges)
Baseline**: 15.6 (9.7, 22.6)
8 weeks:17.2(14.6, 27.1)
1 year: NR
SGRQ
Median (ranges)
Baseline**: 48.1 (23, 82)
8 weeks: 26.4(17.4, 69.4)
1 year: NR
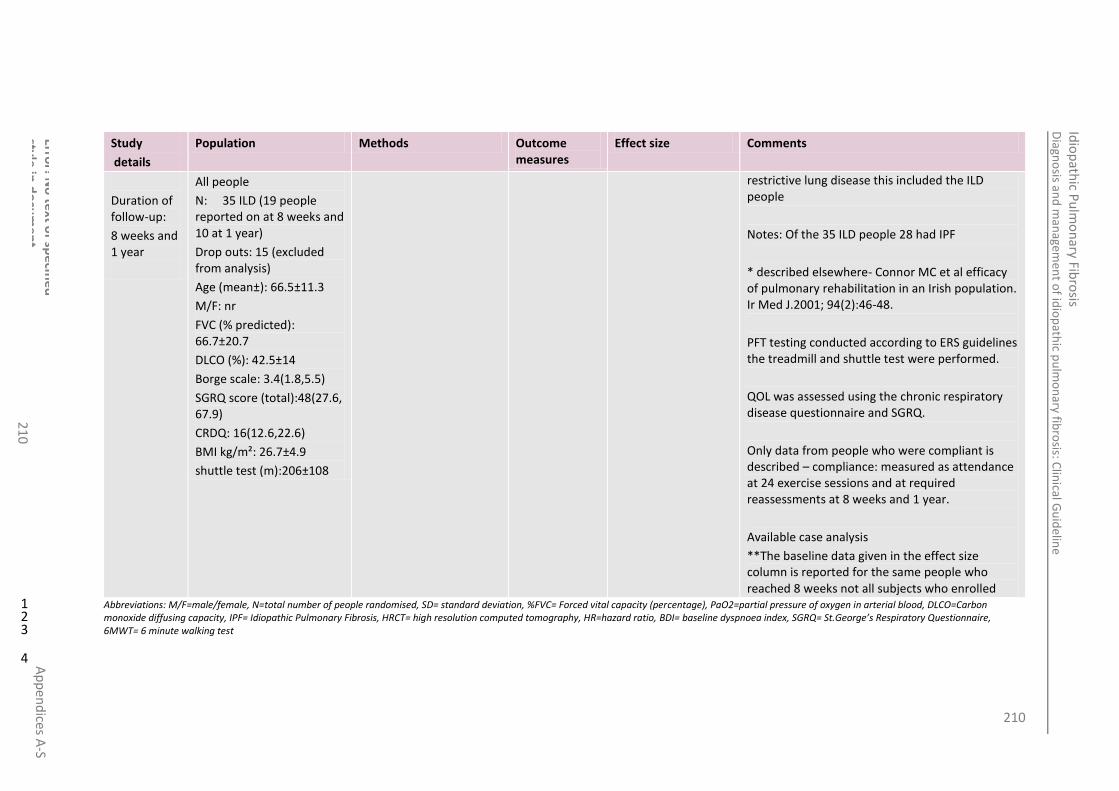
210
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
21
0
Study
details
Population Methods Outcome measures
Effect size Comments
Duration of follow-up:
8 weeks and 1 year
All people
N: 35 ILD (19 people reported on at 8 weeks and 10 at 1 year)
Drop outs: 15 (excluded from analysis)
Age (mean±): 66.5±11.3
M/F: nr
FVC (% predicted): 66.7±20.7
DLCO (%): 42.5±14
Borge scale: 3.4(1.8,5.5)
SGRQ score (total):48(27.6, 67.9)
CRDQ: 16(12.6,22.6)
BMI kg/m²: 26.7±4.9
shuttle test (m):206±108
restrictive lung disease this included the ILD people
Notes: Of the 35 ILD people 28 had IPF
* described elsewhere- Connor MC et al efficacy of pulmonary rehabilitation in an Irish population. Ir Med J.2001; 94(2):46-48.
PFT testing conducted according to ERS guidelines the treadmill and shuttle test were performed.
QOL was assessed using the chronic respiratory disease questionnaire and SGRQ.
Only data from people who were compliant is described – compliance: measured as attendance at 24 exercise sessions and at required reassessments at 8 weeks and 1 year.
Available case analysis
**The baseline data given in the effect size column is reported for the same people who reached 8 weeks not all subjects who enrolled
Abbreviations: M/F=male/female, N=total number of people randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon 1 monoxide diffusing capacity, IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 2 6MWT= 6 minute walking test 3
4
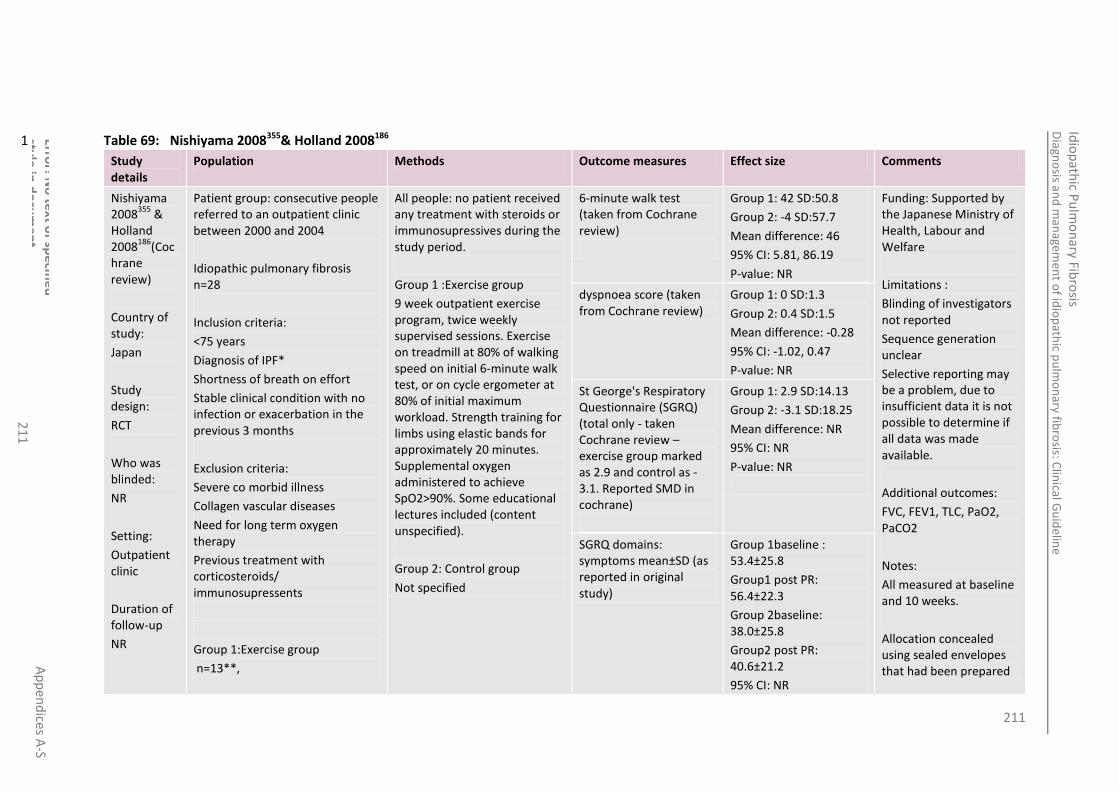
211
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
21
1
Table 69: Nishiyama 2008355& Holland 2008186 1
Study details
Population Methods Outcome measures Effect size Comments
Nishiyama 2008
355 &
Holland 2008
186(Coc
hrane review)
Country of study:
Japan
Study design:
RCT
Who was blinded:
NR
Setting:
Outpatient clinic
Duration of follow-up
NR
Patient group: consecutive people referred to an outpatient clinic between 2000 and 2004
Idiopathic pulmonary fibrosis n=28
Inclusion criteria:
<75 years
Diagnosis of IPF*
Shortness of breath on effort
Stable clinical condition with no infection or exacerbation in the previous 3 months
Exclusion criteria:
Severe co morbid illness
Collagen vascular diseases
Need for long term oxygen therapy
Previous treatment with corticosteroids/ immunosupressents
Group 1:Exercise group
n=13**,
All people: no patient received any treatment with steroids or immunosupressives during the study period.
Group 1 :Exercise group
9 week outpatient exercise program, twice weekly supervised sessions. Exercise on treadmill at 80% of walking speed on initial 6-minute walk test, or on cycle ergometer at 80% of initial maximum workload. Strength training for limbs using elastic bands for approximately 20 minutes. Supplemental oxygen administered to achieve SpO2>90%. Some educational lectures included (content unspecified).
Group 2: Control group
Not specified
6-minute walk test (taken from Cochrane review)
Group 1: 42 SD:50.8
Group 2: -4 SD:57.7
Mean difference: 46
95% CI: 5.81, 86.19
P-value: NR
Funding: Supported by the Japanese Ministry of Health, Labour and Welfare
Limitations :
Blinding of investigators not reported
Sequence generation unclear
Selective reporting may be a problem, due to insufficient data it is not possible to determine if all data was made available.
Additional outcomes:
FVC, FEV1, TLC, PaO2, PaCO2
Notes:
All measured at baseline and 10 weeks.
Allocation concealed using sealed envelopes that had been prepared
dyspnoea score (taken from Cochrane review)
Group 1: 0 SD:1.3
Group 2: 0.4 SD:1.5
Mean difference: -0.28
95% CI: -1.02, 0.47
P-value: NR
St George's Respiratory Questionnaire (SGRQ) (total only - taken Cochrane review – exercise group marked as 2.9 and control as -3.1. Reported SMD in cochrane)
Group 1: 2.9 SD:14.13
Group 2: -3.1 SD:18.25
Mean difference: NR
95% CI: NR
P-value: NR
SGRQ domains: symptoms mean±SD (as reported in original study)
Group 1baseline : 53.4±25.8
Group1 post PR: 56.4±22.3
Group 2baseline: 38.0±25.8
Group2 post PR: 40.6±21.2
95% CI: NR
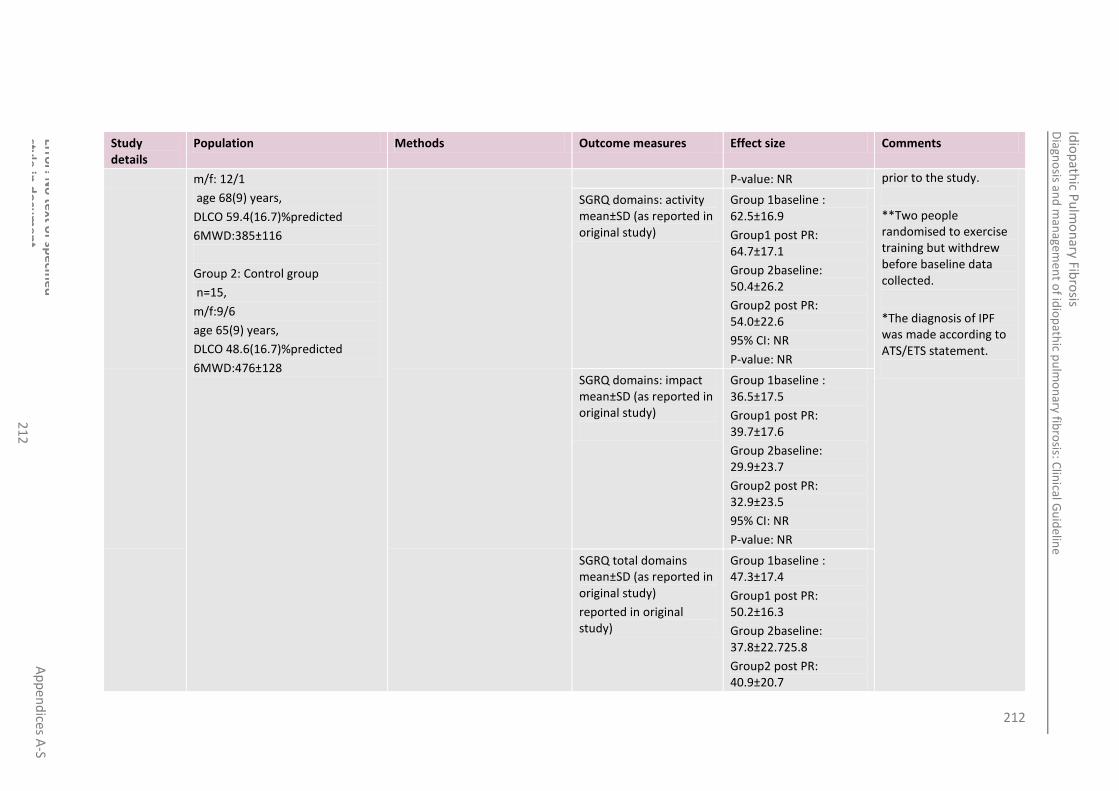
212
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
21
2
Study details
Population Methods Outcome measures Effect size Comments
m/f: 12/1
age 68(9) years,
DLCO 59.4(16.7)%predicted
6MWD:385±116
Group 2: Control group
n=15,
m/f:9/6
age 65(9) years,
DLCO 48.6(16.7)%predicted
6MWD:476±128
P-value: NR prior to the study.
**Two people randomised to exercise training but withdrew before baseline data collected.
*The diagnosis of IPF was made according to ATS/ETS statement.
SGRQ domains: activity mean±SD (as reported in original study)
Group 1baseline : 62.5±16.9
Group1 post PR: 64.7±17.1
Group 2baseline: 50.4±26.2
Group2 post PR: 54.0±22.6
95% CI: NR
P-value: NR
SGRQ domains: impact mean±SD (as reported in original study)
Group 1baseline : 36.5±17.5
Group1 post PR: 39.7±17.6
Group 2baseline: 29.9±23.7
Group2 post PR: 32.9±23.5
95% CI: NR
P-value: NR
SGRQ total domains mean±SD (as reported in original study)
reported in original study)
Group 1baseline : 47.3±17.4
Group1 post PR: 50.2±16.3
Group 2baseline: 37.8±22.725.8
Group2 post PR: 40.9±20.7

213
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
21
3
Study details
Population Methods Outcome measures Effect size Comments
95% CI: NR
P-value: NR
Abbreviations: M/F=male/female, N=total number of people randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon 1 monoxide diffusing capacity, IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 2 6MWT= 6 minute walking test 3
Table 70: Ozalevli 2010373 4
Study
Details
Population Methods Outcome measures Effect size Comments
Ozalevli 2010
373
Country of study: Turkey
Study design: prospective cohort
Who was blinded: no-one
Setting:
Patient group: IPF, diagnosed using ATS/ERS criteria
Inclusion criteria:
Clinically stable
Treatment with no more than 20mg of prednisone per day
No pulmonary infections in the last 6 weeks
No serious cardiological or psychological problems
Not receiving supplementary O2 therapy
No neurological, inner ear or orthopaedic disease
Able to ambulate without assistance or assistive devices
All people
Home-based PR programme lasting 12 weeks.
All people received a booklet giving instructions on the programme. The programme consisted of pursed-lips breathing, thoracic expansion exercises, upper and lower extremity exercises combined with breathing control and a walking programme (15-30 min/day).
Breathing control training, coping strategies to deal with shortness of breath and relaxation training were given. People were instructed to
6MWD Before: 390.3
After: 430.5
P=0.04
Funding: NR
Limitations:
Small study size
No blinding or randomisation
Did not account for confounding factors
No control group
Generalisability
Additional outcomes:
FEV1
FEV1/FVC
6MWD-SpO2 and heart rate, dyspnoea, leg fatigue
Dyspnoea (MRC scale) Before:2.3±1.2
After: 1.4±1.3
P=0.003
SF36 domain: physical functioning (mean±SD)
Before: 57.00±5.7
After: 58.7±7.3
P:0.24
SF36 domain: physical role functioning (mean±SD)
Before: 56.00±1.7
After: 68.3±1.6
P:0.01
SF36 domain: vitality (mean±SD)
Before: 52.00±4.9
After: 55±4.2
P:0.40
SF36 domain: bodily pain Before: 25.00±2.6

214
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
21
4
Home-based, Izmir, Turkey
Duration of follow-up: 12 weeks
Willing to participate in the study
Exclusion criteria:
Obstructive lung disease (FEV1/FVC <80%)
Acute coronary artery disease
Collagen vascular disease
Pneumoconiosis
Sarcoidosis
Cancer
Non-parenchymal restrictive lung disease
Other severe co morbid conditions
All people
N: 17 (15 completed)
Drop outs: 2 (infectious disease)
Age (mean): 62.8±8.5
M/F: 10/5
Disease duration, years: 5.0 ±3.8
Smoking history: 6/13 (40%)
perform all exercises 5 days a week, in 3 sessions per day with 10 repeats.
Supervision was done by phone calls once a week and a daily exercise query.
(mean±SD) After: 72±2.2
P:0.40
FVC
DLCO
Notes:
Those who did not complete the home based pulmonary rehabilitation programme or voluntarily left were excluded
6MWT administered to ATS criteria
SF-36 (no total provided)
Mean number of weekly completed session: 13.2±2.1
SF36 domain: general health perceptions (mean±SD)
Before: 67.30±4.6
After: 74±4.7
P:0.04
SF36 domain: social role functioning (mean±SD)
Before: 75.80±2.7
After: 89.1±1.8
P:0.17
SF36 domain: emotional role functioning (mean±SD)
Before: 29.00±1.3
After: 65±1.4
P:0.02
SF36 domain: mental health (mean±SD)
Before: 49.90±6.7
After: 56.8±5.4
P:0.14
Abbreviations: M/F=male/female, N=total number of people randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon 1 monoxide diffusing capacity, IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 2 6MWT= 6 minute walking test 3
4
Table 71: Rammaert 2011 404 5
Study Population Methods Outcome measures Effect size Comments

215
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
21
5
Details
Rammaert 2011
404
Country of study: France
Study design:
Prospective observational
Who was blinded: no-one
Setting: Calmette Hospital (part of Lille University Hospital)
Duration of follow-up: 8 weeks
Patient group: stable people with IPF
Inclusion criteria:
ATS/ERS diagnosis of IPF
The ability to perform a walk test and use a cycle ergometer
The motivation and agreement of the patient for the setting up of a home based rehabilitation programme
Exclusion criteria:
Contraindications to functional exercise testing
Acute exacerbation of IPF
Changes in therapy planned in the coming 8 weeks
People not requiring oxygen therapy during exercise
All people
N: 17 began programme, 14 completed, 13 evaluable
Age (mean): 67±13
Male: 9/13 (62%):
Drop outs: 3 (3 presented exacerbation of fibrosis- 2 of whom died; one patient developed a gluteal abscess)
All people
All examinations were carried out as part of the usual management of people with IPF.
Pulmonary rehabilitation was based on the French Society of Pneumonology recommendations for people with COPD. All people underwent prior cardiopulmonary exercise testing to establish a personalised prescription for training.
Home-based PR was carried out for 8 consecutive weeks, lasting 30-45 minutes per day and included:
Endurance training
Muscle strengthening
Activities of daily living, walking and learning to climb stairs
Compliance with the programme was evaluated every week by a team member.
A patient education programme was also implemented with a picture folder and fact sheets.
6MWT breathing room air (n=13)
Before: 383±115
After: 375±01
Funding: NR
Limitations:
Small sample size
QoL scores not adequately reported
Doesn’t account for confounding
Large number of drop outs – 41%
Generalisability – single centre
No comparison group
Additional outcomes:
Cycle endurance
6 minute step test
Timed up and go
Nadir SpO2
Chair stands
FVC, DLCO and FEV1 before and after
VAS domains: impact on everyday life, treatment constraints anxiety, breathlessness, quality of sleep, physical capabilities and sense of wellbeing.
Notes:
Oxygen therapy was
Dyspnoea (MRC score)- median
Before: 1.5 (1-3)
After: 2 (1-3)
Dyspnoea (Borg scale) evaluated during step test
Before:4 (2-8)
After: 3 (2-9)
Visual Analogue Scale (total)-assessing anxiety and sense of wellbeing.
Before: 38±8
After: 42±12
p=0.004
QoL (SF-36, SGRQ & HAD)
“Perceived physical limitation during exercise as described in the SF-36 decreased after PR (P=0.047). no significant differences were observed for the other SF-36 parameters, the SGRQ or the HAD scale
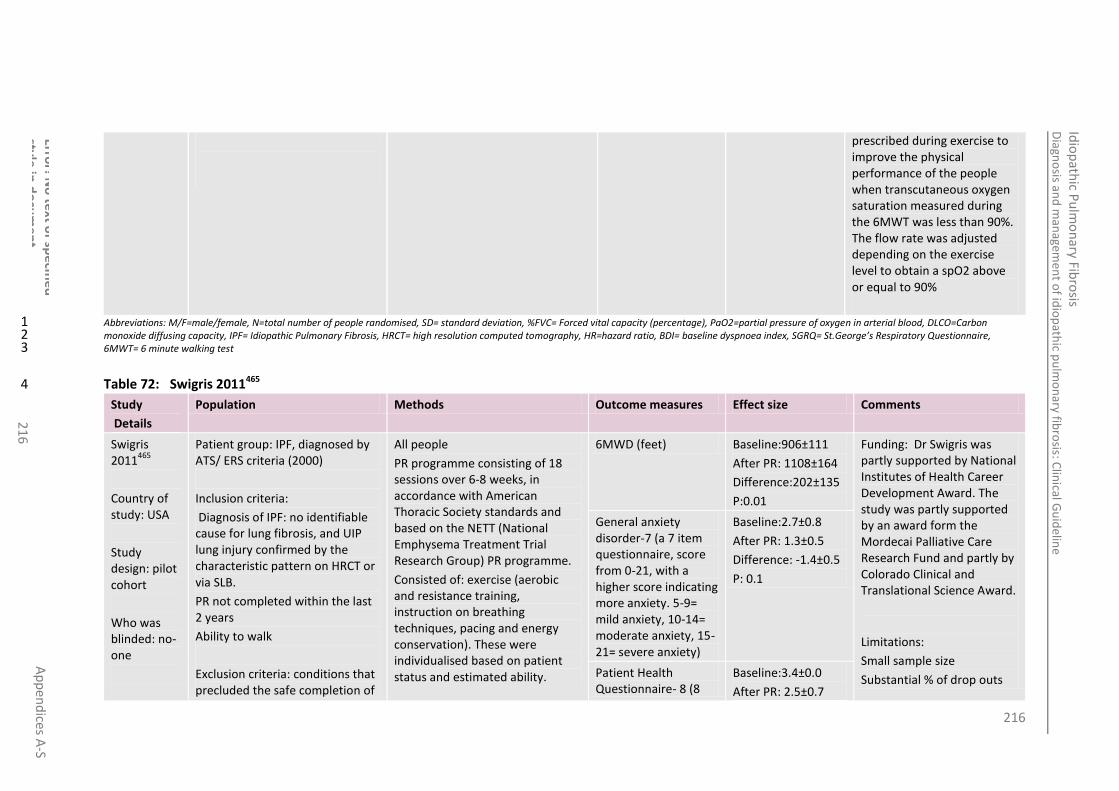
216
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
21
6
prescribed during exercise to improve the physical performance of the people when transcutaneous oxygen saturation measured during the 6MWT was less than 90%. The flow rate was adjusted depending on the exercise level to obtain a spO2 above or equal to 90%
Abbreviations: M/F=male/female, N=total number of people randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon 1 monoxide diffusing capacity, IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 2 6MWT= 6 minute walking test 3
Table 72: Swigris 2011465 4
Study
Details
Population Methods Outcome measures Effect size Comments
Swigris 2011
465
Country of study: USA
Study design: pilot cohort
Who was blinded: no-one
Patient group: IPF, diagnosed by ATS/ ERS criteria (2000)
Inclusion criteria:
Diagnosis of IPF: no identifiable cause for lung fibrosis, and UIP lung injury confirmed by the characteristic pattern on HRCT or via SLB.
PR not completed within the last 2 years
Ability to walk
Exclusion criteria: conditions that precluded the safe completion of
All people
PR programme consisting of 18 sessions over 6-8 weeks, in accordance with American Thoracic Society standards and based on the NETT (National Emphysema Treatment Trial Research Group) PR programme.
Consisted of: exercise (aerobic and resistance training, instruction on breathing techniques, pacing and energy conservation). These were individualised based on patient status and estimated ability.
6MWD (feet) Baseline:906±111
After PR: 1108±164
Difference:202±135
P:0.01
Funding: Dr Swigris was partly supported by National Institutes of Health Career Development Award. The study was partly supported by an award form the Mordecai Palliative Care Research Fund and partly by Colorado Clinical and Translational Science Award.
Limitations:
Small sample size
Substantial % of drop outs
General anxiety disorder-7 (a 7 item questionnaire, score from 0-21, with a higher score indicating more anxiety. 5-9= mild anxiety, 10-14= moderate anxiety, 15-21= severe anxiety)
Baseline:2.7±0.8
After PR: 1.3±0.5
Difference: -1.4±0.5
P: 0.1
Patient Health Questionnaire- 8 (8
Baseline:3.4±0.0
After PR: 2.5±0.7

217
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
21
7
Study
Details
Population Methods Outcome measures Effect size Comments
Setting:
6 centres certified by the American Association of Cardiovascular and Pulmonary Rehabilitation
Duration of follow-up: 6-8 weeks
PR (e.g. unstable coronary artery disease)
All people
N: 21 had baseline data collected, 14 had data collected after PR
Drop outs: 7 (2 died with IPF exacerbation, 4 did not enrol in PR, 1 withdrew from PR due to back pain)
Age (mean): 71.5±7.4
Male: 18
FVC (% predicted): 73±22 (41-113)
DLCO (%): 38±13 (12-63)
6MWD (m): 906±488 (110-1755)
SLB: 14
Supplemental O2, 24 h/d: 7
Supplemental O2 only on exertion: 7
Ever smoked: 13
Taking prednisone: 7
Stable coronary artery disease: 3
Systemic hypertension: 7
Osteoarthritis: 13
COPD: 7
Diabetes mellitus: 5
The aerobic component was begun at a level to achieve a heart rate 60% of the predicted maximum for the age; intensity and duration was gradually increased to build tolerance and confidence, with the goal of reaching maximum tolerated workload during each exercise period (goal at least 30min of continuous exercise). Prior to PR as part of routine care, each subject performed walk oximetry with oxygen titration to maintain Spo2 of ≥90%. During PR Spo2 and titrated oxygen flow were monitored to ensure saturation was >89%
The education component included sessions on oxygen use, medications, relaxation, psychosocial support, energy, nutrition and end of life issues.
item questionnaire from 0-24, where a higher score indicates more severe depression. 5-9=mild, 10-14= moderate, 15-19= moderately severe, 20-24= severe depression)
Difference: -0.9±0.7
P:0.2
PR was paid for through people’ insurance therefore were a highly motivated group
Additional outcomes:
Fatigue severity scale
Pittsburgh Sleep total
Notes:
7/21 people had co-existing COPD
The comparison group was COPD people results taken from another trial (results not reported in this table)
SF36 domain: physical functioning (mean±SE)
Baseline: 31.9±2.4
After PR: 33.1±2.8
Difference: 1.2±2.2
P:0.6
SF36 domain: physical role functioning (mean±SE)
Baseline: 36.4±2.3
After PR: 38±2.8
Difference: 1.5±2.0
P:0.5
SF36 domain: vitality (mean±SE)
Baseline: 47.2±2.2
After PR: 50.8±2.6
Difference: 3.6±2.2
P:0.1
SF36 domain: bodily pain (mean±SE)
Baseline: 45±2.2
After PR: 47.6±2.7
Difference: 2.7±2.7
P:0.3
SF36 domain: general health perceptions (mean±SE)
Baseline: 38.3±1.7
After PR: 39.8±2.9
Difference: 1.4±2.8
P:0.6

218
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
21
8
Study
Details
Population Methods Outcome measures Effect size Comments
SF36 domain: social role functioning (mean±SE)
Baseline: 45.1±2
After PR: 47.1±3
Difference: 1.9±2.2
P:0.4
SF36 domain: emotional role functioning (mean±SE)
Baseline: 45.7±2.6
After PR: 43.8±4
Difference: -1.9±4.3
P:0.7
SF36 domain: mental health (mean±SE)
Baseline: 51.8±2
After PR: 53.3±1.4
Difference: 1.6±1.7
P:0.4
Abbreviations: M/F=male/female, N=total number of people randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon 1 monoxide diffusing capacity, IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 2 6MWT= 6 minute walking test 3
F.4 Best supportive care 4
F.4.1 Oxygen management 5
Table 73: Crockett 200192 & Zielinski 2000509 6
Study
details
Population Methods Outcome measures Effect size Comments
Crockett 2001
92 &
Zielinski 2000
509
Patient group: Patients diagnosed with interstitial pulmonary Fibrosis. The patients were followed over a four year period.
Compared long-term oxygen therapy to a control, no oxygen therapy group
Mortality at 12 months
Group1: 7/37
Group 2: 8/25
p value: 0.24
Funding: NR
Limitations:
Mortality at 24 Group1: 23/37

219
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
21
9
Study
details
Population Methods Outcome measures Effect size Comments
review of Braghiroli 2000 unpublished data
Country of study:
International
Study design:
Controlled multi-centre study
Who was blinded: NR
Setting: NR
Duration of follow-up: 3 years
(study commenced in 1988)
Inclusion criteria:
either gender
under 79 years of age
diagnosis on X-ray examination of interstitial pulmonary Fibrosis,
clinically stable,
not previously treated with oxygen,
Arterial oxygen tension (PaO2) between 45-60 mm Hg (6.0-8.0 kPa) on 4 consecutive weekly determinations.
Total lung capacity (TLC) was < 80% predicted
Exclusion criteria:
without other major causes of morbidity and mortality such as malignancy, unstable angina, or recent myocardial infarction, congestive cardiac failure, alcoholism, recent pulmonary embolism, diabetes or pregnancy.
All patients
N: 62
Drop outs:
Group 1
Treatment with long-term domiciliary oxygen therapy
Group 2 no oxygen therapy
All patients
Pharmacological treatment was kept steady for as long as possible during the study
Pulmonary artery catheterisation was performed using a swan-ganz thermodilution catheter. After initial measurements were taken, patients received oxygen at a flow of ≥2L/min to increase PaO2 to > 65mmHg. Second measurements were taken after one
months Group 2: 12/25
p value: 0.27
The method of randomisation for the study was not stated. The method of blinding was not described. However, random sampling was set up by blocks, each with six cases allocated to the treatment group and five cases to the control group
Missing baseline data per group
Additional outcomes:
Pulmonary artery pressure, cardiac output, pulmonary vascular resistance, arterial oxygen tension for patients on oxygen and room air.
Mortality at 12 months: Peto Odds Ratio (Peto, Fixed, 95% CI): 0.50 [0.15, 1.61], Mortality at 24 months: Peto Odds Ratio (Peto, Fixed, 95% CI): 1.76 [0.64, 4.86], Mortality at 3 years:Peto Odds Ratio (Peto, Fixed, 95% CI): 0.99 [0.16, 6.26]
Notes:
Crockett 2001 92
& Zielinski 2000 509
present the findings of the unpublished work of Braghiroli et al. information has been taken from both reviews. Results and
Mortality at 3 years Group1: 34/37
Group 2: 23/25
p value: 0.99

220
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
22
0
Study
details
Population Methods Outcome measures Effect size Comments
Age: 62±7
Mean vital capacity: 51±13% of predicted
Ratio of FEV in the first second to the VC: 103±12%
Total lung capacity: 65±18%of predicted
DLCO: 43±10% of predicted
Mean PaO2: 54±10 mmHg
Mean PaCO2: 36±5 mmHg
Group 1
N: 37*
Age (mean): NR
M/F: 17/20
Drop outs: 0
Group 2
N: 25*
Age (mean): NR
Drop outs: 0
M/F: 14/11
hour of oxygen information on methodology have been taken from Crockett 2001
92
and only information on metholodoly was taken from Zielinski 2000
509
Forty nine of the patients (28 treated and
21 controls) had a diagnosis of idiopathic pulmonary fibrosis, and
13 (9 treated and 4 controls) had pulmonary fibrosis secondary to
other diseases
Only mortality data with both disease groups combined
was provided for the included patients
The effect of oxygen therapy on physiological parameters was not indicated & data on quality of life was not reported in crockett 2001 review of Braghiroli 2000 study.
Abbreviations: M/F=male/female, N=total number of people randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon 1 monoxide diffusing capacity, IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 2 6MWT= 6 minute walking test 3

221
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
22
1
Table 74: Obi 2010363 1
Study
details
Population Methods Outcome measures Effect size Comments
Obi 2010363
Design:
Retrospective review
Country of study:
Setting:
Inova Fairfax Hospital, VA, USA
Duration of follow-up:
Comparison of 6MWT done with and without O2 on the same day
Patient group:
Advanced chronic lung diseases
Only IPF data presented
Inclusion criteria:
NR
Exclusion criteria:
NR
IPF Patients
N: 24
Baseline characteristics: NR
Drop outs: NR
Group 1:
With Supplementary O2
Group 2:
Without O2
Mean difference change in 6MWD (m) between groups
19.17
NS difference
Funding:
NR
Limitations:
Abstract only
No baseline characteristics
No blinding
No randomisation
Small sample size
No description of sample given
Additional outcomes:
Mean O2 requirement
Notes:
Abstract only
Mean difference change in lowest SaO2 (%) between groups
4.83
p˂0.05
Dyspnoea: Mean change in Borg max (score) between groups
-1.04
p˂0.05
Abbreviations: M/F=male/female, N=total number of people randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon 2 monoxide diffusing capacity, IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 3 6MWT= 6 minute walking test 4
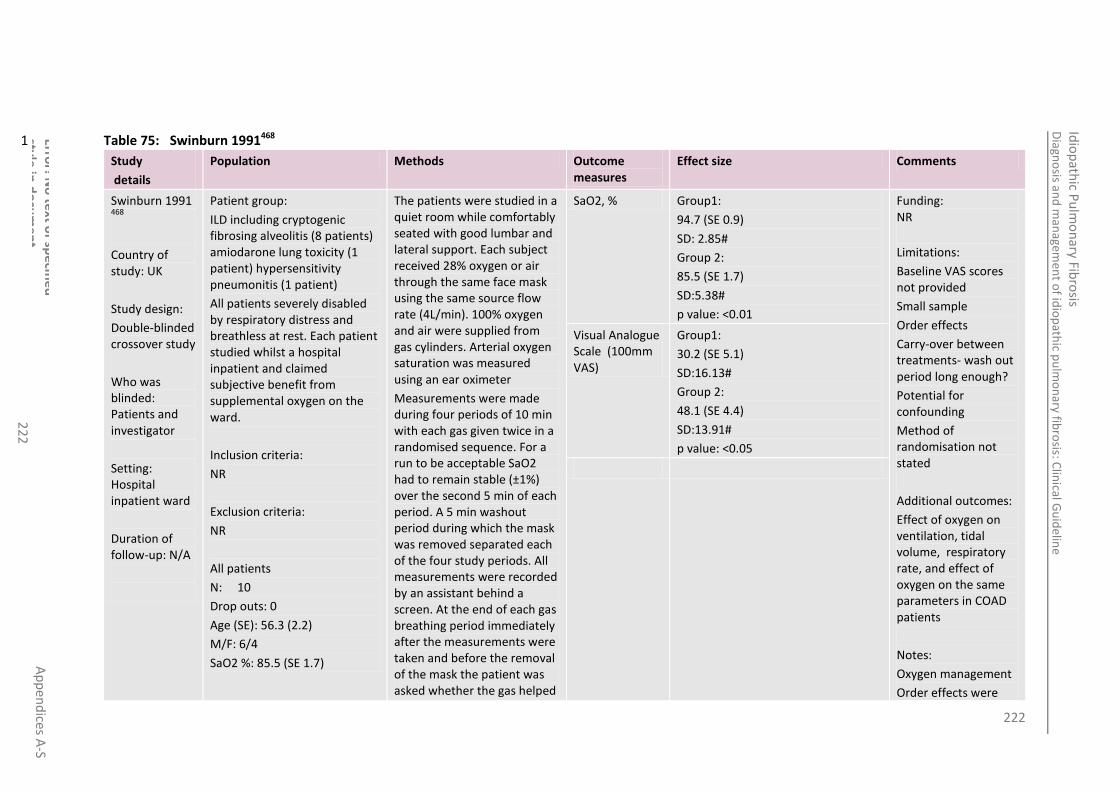
222
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
22
2
Table 75: Swinburn 1991468 1
Study
details
Population Methods Outcome measures
Effect size Comments
Swinburn 1991 468
Country of study: UK
Study design:
Double-blinded crossover study
Who was blinded: Patients and investigator
Setting: Hospital inpatient ward
Duration of follow-up: N/A
Patient group:
ILD including cryptogenic fibrosing alveolitis (8 patients) amiodarone lung toxicity (1 patient) hypersensitivity pneumonitis (1 patient)
All patients severely disabled by respiratory distress and breathless at rest. Each patient studied whilst a hospital inpatient and claimed subjective benefit from supplemental oxygen on the ward.
Inclusion criteria:
NR
Exclusion criteria:
NR
All patients
N: 10
Drop outs: 0
Age (SE): 56.3 (2.2)
M/F: 6/4
SaO2 %: 85.5 (SE 1.7)
The patients were studied in a quiet room while comfortably seated with good lumbar and lateral support. Each subject received 28% oxygen or air through the same face mask using the same source flow rate (4L/min). 100% oxygen and air were supplied from gas cylinders. Arterial oxygen saturation was measured using an ear oximeter
Measurements were made during four periods of 10 min with each gas given twice in a randomised sequence. For a run to be acceptable SaO2 had to remain stable (±1%) over the second 5 min of each period. A 5 min washout period during which the mask was removed separated each of the four study periods. All measurements were recorded by an assistant behind a screen. At the end of each gas breathing period immediately after the measurements were taken and before the removal of the mask the patient was asked whether the gas helped
SaO2, % Group1:
94.7 (SE 0.9)
SD: 2.85#
Group 2:
85.5 (SE 1.7)
SD:5.38#
p value: <0.01
Funding: NR
Limitations:
Baseline VAS scores not provided
Small sample
Order effects
Carry-over between treatments- wash out period long enough?
Potential for confounding
Method of randomisation not stated
Additional outcomes:
Effect of oxygen on ventilation, tidal volume, respiratory rate, and effect of oxygen on the same parameters in COAD patients
Notes:
Oxygen management
Order effects were
Visual Analogue Scale (100mm VAS)
Group1:
30.2 (SE 5.1)
SD:16.13#
Group 2:
48.1 (SE 4.4)
SD:13.91#
p value: <0.05

223
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
22
3
Study
details
Population Methods Outcome measures
Effect size Comments
his/her breathing (y/n) and to record the severity of breathlessness on a 100-mm visual analogue scale with limits marked “not at all breathless” and “extremely breathless”
Group 1 (oxygen)
28% oxygen by venture face mask
Group 2 (air) air by venturi face mask
All patients
Received both gases twice
analysed by ANOVA
#NCGC calculated
Abbreviations: M/F=male/female, N=total number of people randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon 1 monoxide diffusing capacity, IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 2 6MWT= 6 minute walking test 3
F.4.2 Prednisolone for the palliation of cough 4
Table 76: Hope-Gill 2003 191 5
Study
details
Population Methods Outcome measures
Effect size Comments
Hope-Gill 2003
191
Country of study: UK
Patient group:
IPF patients with disabling cough (all had a visual analogue score
All patients
Prednisolone 40-60 mg/day for least 4 weeks.
visual analogue scale score of cough intensity using a 10 cm scale
Baseline: 7.2±0.8
Post treatment: 2.2±2.5
p value: <0.05
Funding: supported by a grant from lechyd morgannwg health R&D consortium. Asta Zeneca pharmaceuticals donated the omeprazole used in this study.
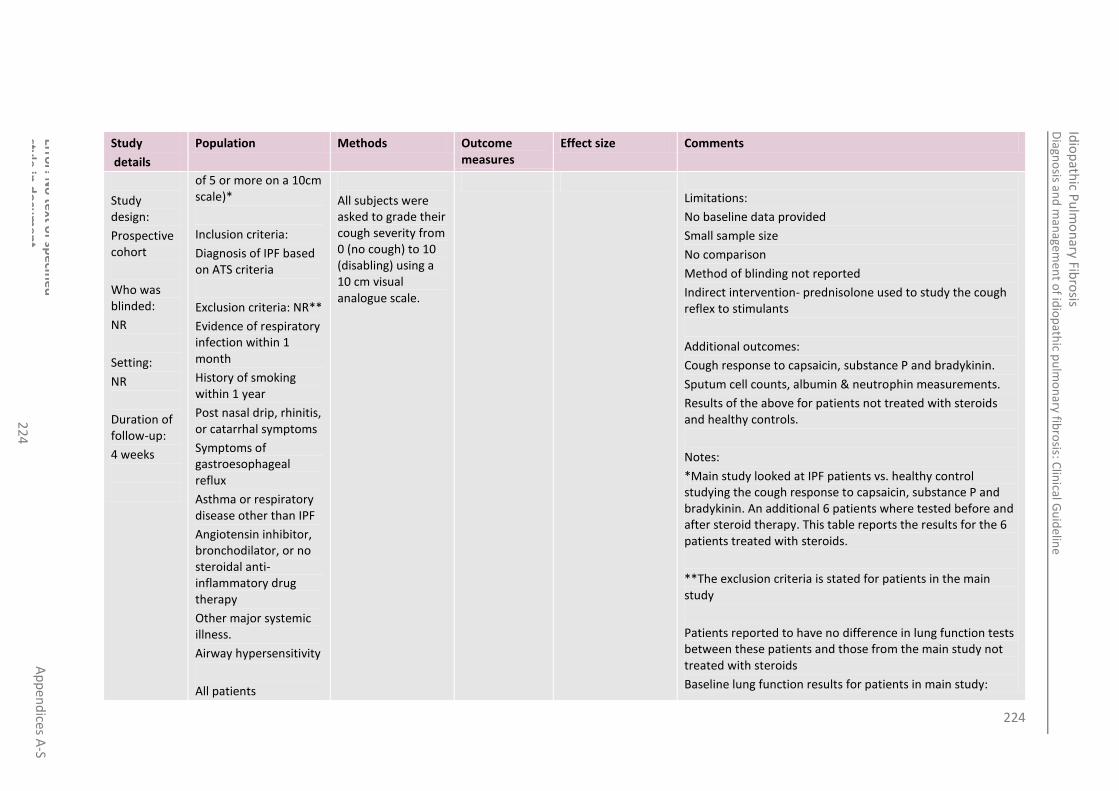
224
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
22
4
Study
details
Population Methods Outcome measures
Effect size Comments
Study design:
Prospective cohort
Who was blinded:
NR
Setting:
NR
Duration of follow-up:
4 weeks
of 5 or more on a 10cm scale)*
Inclusion criteria:
Diagnosis of IPF based on ATS criteria
Exclusion criteria: NR**
Evidence of respiratory infection within 1 month
History of smoking within 1 year
Post nasal drip, rhinitis, or catarrhal symptoms
Symptoms of gastroesophageal reflux
Asthma or respiratory disease other than IPF
Angiotensin inhibitor, bronchodilator, or no steroidal anti-inflammatory drug therapy
Other major systemic illness.
Airway hypersensitivity
All patients
All subjects were asked to grade their cough severity from 0 (no cough) to 10 (disabling) using a 10 cm visual analogue scale.
Limitations:
No baseline data provided
Small sample size
No comparison
Method of blinding not reported
Indirect intervention- prednisolone used to study the cough reflex to stimulants
Additional outcomes:
Cough response to capsaicin, substance P and bradykinin.
Sputum cell counts, albumin & neutrophin measurements.
Results of the above for patients not treated with steroids and healthy controls.
Notes:
*Main study looked at IPF patients vs. healthy control studying the cough response to capsaicin, substance P and bradykinin. An additional 6 patients where tested before and after steroid therapy. This table reports the results for the 6 patients treated with steroids.
**The exclusion criteria is stated for patients in the main study
Patients reported to have no difference in lung function tests between these patients and those from the main study not treated with steroids
Baseline lung function results for patients in main study:

225
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
22
5
Study
details
Population Methods Outcome measures
Effect size Comments
N: 6
Drop outs: 0
N=10
FVC % predicted: 77.43
TLC % predicted: 67.02
DLCO % predicted: 42.44 Abbreviations: M/F=male/female, N=total number of people randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon 1 monoxide diffusing capacity, IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 2 6MWT= 6 minute walking test 3
F.4.3 Thalidomide for the palliation of cough 4
Table 77: Horton 2008192 5
Study
details
Population Methods Outcome measures Effect size Comments
Horton 2008192
Country of study:
USA
Study design:
Prospective cohort
Open label phase II trial
Abstract
Who was
Patient group:
11 patients with chronic cough
Inclusion criteria:
As above
Exclusion criteria:
NR
All patients
N:11
Drop outs: 5
All patients
Thalidomide administered daily in 100-400mg doses.
Patients were followed with interval histories, physical examinations and quality of life questionnaires.
Cough score Baseline:4.9±0.3
Follow up at 3 months: 2.2±1.6
P = 0.03
(data from 6 patients for who there was complete data)
Funding: NR
Limitations:
Abstract
Limited information given on methodology, no baseline data, and post treatment
Large dropout rate
Additional outcomes:
quantification of cough was recorded by subjects on question 2 of SGRQ

226
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
22
6
Study
details
Population Methods Outcome measures Effect size Comments
blinded:
NR
Setting: Hospital
Duration of follow-up:
3 months
Side effects; most commonly reported adverse event was dizziness and constipation.
Abbreviations: M/F=male/female, N=total number of people randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon 1 monoxide diffusing capacity, IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 2 6MWT= 6 minute walking test 3
Table 78: Horton 2012193 4
Study
details
Population Methods Outcome measures Effect size Comments
Horton 2012
193
Country of study: USA
Study design:
Double blind 2 treatment 2 period crossover trial
Patient group:
Consecutive eligible patients between February 2008 and March 2011
Inclusion criteria:
>50 years
Clinical history consistent with IPF (symptom duration >3 months <5 years)
chronic cough (defined by cough of more than 8 weeks duration that adversely affected QOL and was not due to identifiable causes)
All patients
Patients received each treatment for 12 weeks in the crossover design with a 2 week washout period
All patients began on 50mg of thalidomide orally at bedtime, the does was increased to 100mg if not improvement in cough was seen after 2 weeks*
QOL: cough quality of life questionnaire
(mean±SD)
Baseline:60.5±12
Post treatment placebo:58.7±14.0
Post treatment thalidomide:47.2±13.4
Mean difference (95% CI):-11.4(-15.7to-7)
P value:<0.001
Funding: Celgene corporation provided the study drug and funding but had no role in study design, conduct, analysis or manuscript
Limitations:
Treatment crossover was the washout period adequate
Unclear allocation concealment
QOL: Visual analogue scale
(mean±SD)
Baseline:64.8±21.4
Post treatment placebo:61.9±26.5
Post treatment thalidomide: 32.2±26.1
Mean difference (95% CI):-31.2(-45.2to-17.2)
P value:<0.001

227
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
22
7
Study
details
Population Methods Outcome measures Effect size Comments
Who was blinded: double blind study investigators and participants
Setting: hospital
Duration of follow-up: 12 weeks
HRCT consistent with IPF or SLB results confirming interstitial pneumonia
FVC between 40-90%predicted
TLC between 40-80% predicted
DLCO between 80-90% predicted at screening
Exclusion criteria:
Pregnancy
Female with childbearing potential
Toxic or environmental exposure to respiratory irritants
Collagen vascular disease
Airflow obstruction
Active narcotic antitussive use
Peripheral vascular disease
Neuropathy
Inability to give informed consent
Allergy or intolerance to thalidomide
Life expectancy less than 6 months in the opinion of investigators
All patients
N: 24
Drop outs: 4(1 patient withdrew before receiving treatment, 3
All patients received sodium docusate 100mg orally during the trial for constipation and vitamin b complex supplement for any undiagnosied deficiency.
Any prescription for cough was discountinued 2 weeks before the trial and no patients began benzonatate therapy or reported changes in ACEi/ARB GERD or sinus therapies during the trial.
SGRQ total
(mean±SD)
Baseline:57.4±18.8
Post treatment placebo:56.9±17.1
Post treatment thalidomide: 43.9±16.0
Mean difference (95% CI):-11.7(-18.6to-4.8)
P value:0.001
Small sample size
Single centre study
Short duration of study
Additional outcomes:
Adverse events
Notes:
Randomisation schedula prepared by using manual algorithm. A random seed number was generated by using RAND function in excel. The pharmacist dispensing the drug was the only person who had access to the treatment.
This happened in 21/22 patient’s receiving thalidomide and all placebo patients
SGRQ symptom domain
(mean±SD)
Baseline:67.7±19.7
Post treatment placebo:62±18.3
Post treatment thalidomide: 50.3±20.9
Mean difference (95% CI):-12.1(-22.2to-2.0)
P value:0.018
SGRQ impact domain
(mean±SD)
Baseline:48.1±20.7
Post treatment placebo:49.0±19.4
Post treatment thalidomide:34.3±16.1
Mean difference (95% CI):-13.1 (-19.7to-6.6)
P value:<0.001
SGRQ activity domain
(mean±SD)
Baseline:64.3±22.7
Post treatment placebo:65.8±18.7
Post treatment thalidomide: 60.9±14.2
Mean difference (95% CI):-3.3(-9.8 to-3.2)
P value:0.31
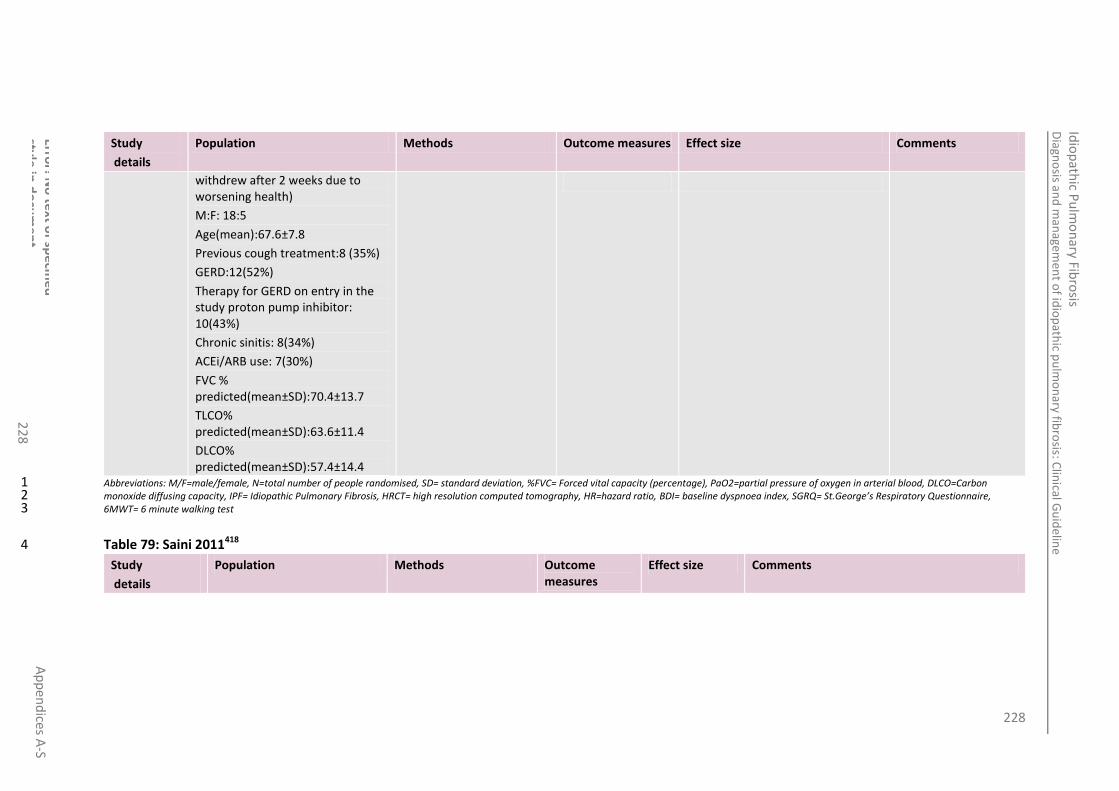
228
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
22
8
Study
details
Population Methods Outcome measures Effect size Comments
withdrew after 2 weeks due to worsening health)
M:F: 18:5
Age(mean):67.6±7.8
Previous cough treatment:8 (35%)
GERD:12(52%)
Therapy for GERD on entry in the study proton pump inhibitor: 10(43%)
Chronic sinitis: 8(34%)
ACEi/ARB use: 7(30%)
FVC % predicted(mean±SD):70.4±13.7
TLCO% predicted(mean±SD):63.6±11.4
DLCO% predicted(mean±SD):57.4±14.4
Abbreviations: M/F=male/female, N=total number of people randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon 1 monoxide diffusing capacity, IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 2 6MWT= 6 minute walking test 3
Table 79: Saini 2011418 4
Study
details
Population Methods Outcome measures
Effect size Comments

229
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
22
9
Study
details
Population Methods Outcome measures
Effect size Comments
Saini 2011418
Country of study: UK
Study design: prospective cohort
Who was blinded: NR
Setting: hospital
Duration of follow-up: NR
Patient group:
9 Patients referred to ILD clinic between 2009 -2011for assessment for their cough
Inclusion criteria:
Patients with IPF who had “significant cough”*
Exclusion criteria:
All patients
N: 6 (4 IPF, 1 hypersensitivity pneumonitis, 1 fibrotic cryptogenic organising pneumonia)
Drop outs: NR
Male: 72%
Age (mean (range)): 69 (51-88)
All patients
Treated with thalidomide – no details of starting dosages given (“two patients are currently stable on 50mg once daily and 1 with 50mg alternate daily”)*
Cough score:
(Leicester cough questionnaire)
Median (IQR)
Baseline (pre-thalidomide):
74.5(13.25)
Post-treatment: 51.5(49.25)
P=0.046
Funding: NR
Limitations:
Abstract limited information on methodology and results, baseline data, treatment and post treatment.
All patients had been treated with other drugs for cough before starting thalidomide therapy, no washout period stated
Additional outcomes:
None
Notes:
*the 9 patients who were initially referred for assessment were assessed using a modified version of Leicester cough questionnaire in conjunction with subjective symptoms. A trail of PPI (omeprazole 40mg) and prednisolone 10mg for 6 weeks – two subjects were excluded as they did not have a significant cough and one patient declined thalidomide after initial screening.
*3 patients stopped thalidomide subsequent to rash.
Abbreviations: M/F=male/female, N=total number of people randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon 1 monoxide diffusing capacity, IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 2 6MWT= 6 minute walking test 3

230
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
23
0
F.4.4 Morphine for the palliation of breathlessness 1
Table 80: Currow 2011 93 2
Study
details
Population Methods Outcome measures Effect size Comments
Currow 2011 93
Country of study: Australia
Study design:
Cohort. Phase II was an open-label prospective study
Who was blinded: N/A
Setting: outpatients from 4 tertiary university teaching hospitals in two states
Patient group:
Patients with a palliative diagnosis (only ILD reported in this table). Recruited from 4 tertiary university hospitals between July 2007- October 2009.
Inclusion criteria:
Opioid-naïve
Palliative diagnosis
Age ≥ 18 years
Ongoing dyspnoea (3 or 4 on the modified Medical Research Council [MMRC] Dyspnoea Scale)
Any underlying reversible causes of dyspnoea must have been maximally treated
On stable medications and oxygen (if required) for the seven days before commencing the study, with an estimated prognosis of > 1 month.
Exclusion criteria:
Regular use of any opioid medication in the 2 weeks before
All patients
N= 10
3 week titration period.
Received 10mg daily of sustained-release morphine sulphate, which was increased in non-responders by 10mg daily each week to a maximum of 30mg daily. Administered with laxatives (sodium docusate with sennnosides). The participant was withdrawn if there were unacceptable side effects or no response to maximum dose.
Morning and evening dyspnoea VAS scores were recorded on days 5-7 of each seven-day week (i.e. during steady-state) were averaged and contributed to assessments of the number of people who responded to morphine and the dose at which they responded; an individual
VAS intensity of dyspnoea at baseline
100mm VAS scale “right now” (hence, at rest) anchored at 0mm as “no breathlessness” and at 100mm as “worst imaginable breathlessness”. Participants recorded dyspnoea twice daily in a purpose-printed diary.
Baseline
Average: 44.8
SD: 15.4
Range: 18-61
Difference- first and last measured VAS in Phase II
Average: 3.2
SD: 32.7
Range: -33 to 46
Funding: National Health and Medical Research Council
Limitations:
Small sample size
Additional outcomes:
Improvement in dyspnoea (VAS scale) for COPD and cancer.
Side effects
Participant ranked ‘physical symptoms or problems that have been the biggest problem for you over the past two days’(McGill Quality of life questionnaire) data not reported for ILD separately
Indirect intervention results taken from phase II of a pharmacovigilance study

231
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
23
1
Study
details
Population Methods Outcome measures Effect size Comments
of Australia
Duration of follow-up: N/A
screening
A true hypersensitivity reaction to opioids
History of substance misuse
Use of monoamine oxidase inhibitors in the last 2 weeks
Functional status <50 on the Australian –modified Karnofsky Performance Scale (AKPS)
A calculated creatinine clearance of <15mL/ min
Pregnancy
Confusion (< 24/30 on a Mini Mental State Examination)
Unwilling/ unable to complete the study measures.
All patients
N: 83 (total), 10 ILD
Drop outs: 4 (toxicity), 2 (other reason)
4 patients proceeded to Phase IV
improvement of 10% over baseline was considered, a priori, as a clinically significant improvement.
Notes:
Phase II part of study only
Study withdrawal initiated at any time by the participant. Other reason included AKPS falling below 30, sudden increase dyspnoea, or participant death.
Abbreviations: M/F=male/female, N=total number of people randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon 1 monoxide diffusing capacity, IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 2 6MWT= 6 minute walking test 3
4

232
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
23
2
F.5 Psychosocial support 1
2
Study
details Patients Interventions Outcome measures Qualitative statement Comments
Collard 2007
78
Country of study:
Study design:
Qualitative
Questionnaire survey
Who was blinded:
None
Setting:
NR
Duration of follow-up:
NR
Patient group:
Patients and careers of current and deceased for which address were available between July 2003 and December 2004
Inclusion criteria:
NR
Exclusion criteria:
NR
All patients
N: 1448
Patients :1251
Caregivers: 197
Age (median): 65
Drop outs: 0
All patients
A questionnaire survey* was distributed to over 2000 members, in both paper and via email with a link to a web based survey site. The survey was also made available to CPF** members online and in paper form through the CPF website, sponsored seminars and institutional partners.
The completed surveys were compiled by Michaels Opinions Research Inc.
Results from this publication are based on responses from living patients or caregivers of living patients.
Two authors reviewed the raw data and directed the analysis
Education and resources
63% somewhat/ strongly agreed with the statements there was a clear lack of information and resources about PF
51.2% reported being generally/very well informed regarding the treatment options available at the present time.
38.7% reported being generally/very well informed regarding the benefits of pulmonary rehabilitation.
42.5% reported being generally/very well informed regarding the benefits of managing supplemental oxygen.
32.5% reported being generally/very well informed regarding the risks and benefits of lung transplantation.
Funding: DuBrul family Fund and the family of Helen and Michael Gavin
Limitations:
Sampling: self identified no confirmation of diagnosis, non probability sampling- sampling bias
Generalisability – external validity
Large proportion of non-responses- response rate 50% .
Responder bias- responders may be substantially different to non-responders.
Recall bias.
Misinformation bias.
Additional outcomes:
Incorrect diagnosis’s
Experiences with diagnosis: procedures undertaken
Experience with treatment:
Types of treatments being received currently and in the past; prednisolone, cyclophosphamide,
Experience with diagnosis
54.6% reported at least a 1 year delay between earliest indications of a potential breathing problem and the diagnosis of PF.
38.2% reported seeing 2 or more physicians before a diagnosis of PF was established
53.2% sought a second opinion
84.4% consulted a pulmonologist at some stage during their diagnostic evaluation
Experience with treatment
74.7% of respondents reported current pharmacologic therapy for PF
Common reasons for not receiving
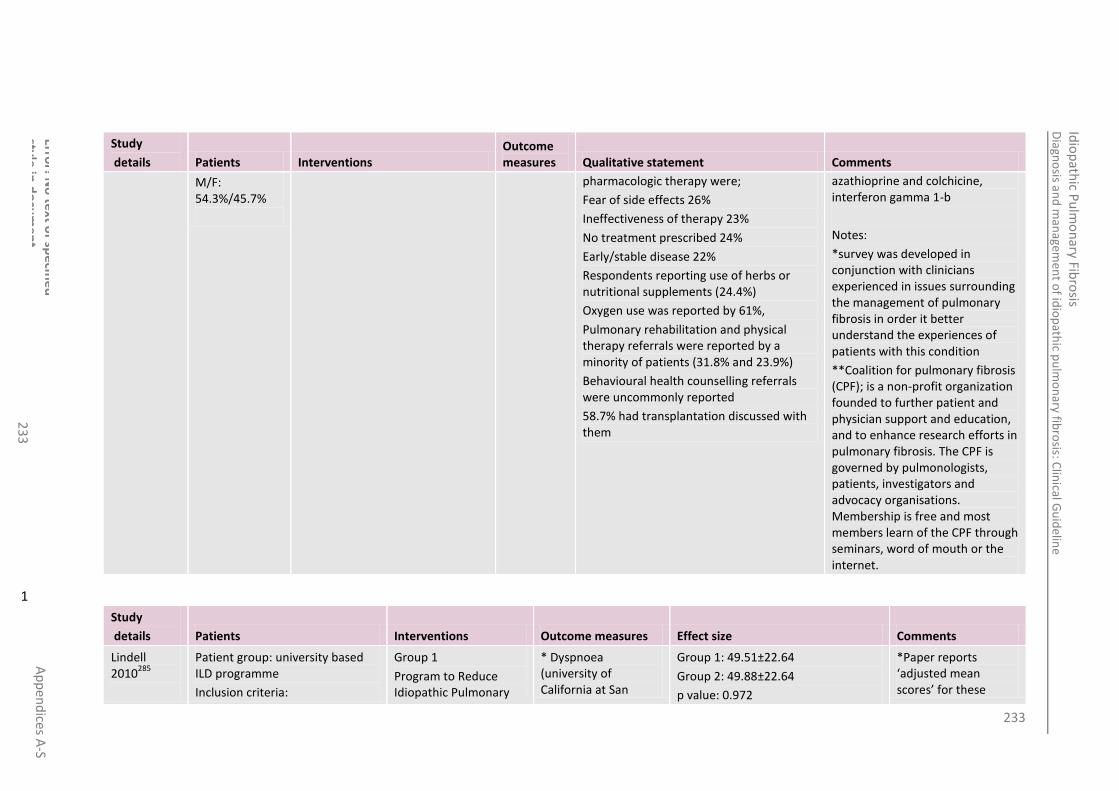
233
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
23
3
Study
details Patients Interventions Outcome measures Qualitative statement Comments
M/F: 54.3%/45.7%
pharmacologic therapy were;
Fear of side effects 26%
Ineffectiveness of therapy 23%
No treatment prescribed 24%
Early/stable disease 22%
Respondents reporting use of herbs or nutritional supplements (24.4%)
Oxygen use was reported by 61%,
Pulmonary rehabilitation and physical therapy referrals were reported by a minority of patients (31.8% and 23.9%)
Behavioural health counselling referrals were uncommonly reported
58.7% had transplantation discussed with them
azathioprine and colchicine, interferon gamma 1-b
Notes:
*survey was developed in conjunction with clinicians experienced in issues surrounding the management of pulmonary fibrosis in order it better understand the experiences of patients with this condition
**Coalition for pulmonary fibrosis (CPF); is a non-profit organization founded to further patient and physician support and education, and to enhance research efforts in pulmonary fibrosis. The CPF is governed by pulmonologists, patients, investigators and advocacy organisations. Membership is free and most members learn of the CPF through seminars, word of mouth or the internet.
1
Study
details Patients Interventions Outcome measures Effect size Comments
Lindell 2010
285
Patient group: university based ILD programme
Inclusion criteria:
Group 1
Program to Reduce Idiopathic Pulmonary
* Dyspnoea (university of California at San
Group 1: 49.51±22.64
Group 2: 49.88±22.64
p value: 0.972
*Paper reports ‘adjusted mean scores’ for these

234
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
23
4
Study
details Patients Interventions Outcome measures Effect size Comments
Country of study: USA
Study design:
RCT (quantitatively driven concurrent nested mixed-method design)
Who was blinded: no-one
Setting:
Centre for Interstitial Lung Disease, University of Pittsburgh medical centre
Duration of follow-up:
Patients:
age >21 years
able to read and understand English
diagnosis of IPF
have an FVC reflecting moderate (FVC 55%-70% predicted) or severe (FVC <55% predicted) disease
Care partners:
Age >21 years
Able to read and understand English
Lives with or cares for the patient with IPF
Exclusion criteria: NR
All patients
N: 42
Drop outs: 2 patients and 3 care partners
Group 1
N: 10
Age (mean): 65.2±10.28
% male: 33.33%
Diagnosis:
Biopsy: 14.29%
HRCT: 33.33%
Fibrosis Symptoms and Improve Management (PRISIM) intervention
6 weekly group sessions attended by patients and care partners. The content for these sessions was developed by a pulmonary clinical nurse specialist, a psychiatric clinical specialist with training as a cognitive behavioural therapist and an advanced care planning instructor.
Group 2 usual care only
Patients were seen by members of the clinical care team consisting of a pulmonary clinical nurse specialist and physicians with expertise in the management of IPF, typically at intervals of every3 to 6 months. The pulmonary clinical nurse specialist was available by phone to answer questions and
Diego Shortness of breath Questionnaire): 6 point scale where 0=not at all to 5=maximal or unable to do) during 21 activities of daily living associated with varying exertion. Total score out of 120
outcomes- raw data not reported therefore unable to meta-analyse
Funding: Fairbanks-Horix Foundation
Limitations:
Reporting of outcomes: pre scores reported more fully than post treatment scores (graphical data only)
Small sample size
Discrepancy in method of diagnosis between the two groups- ATS/ERS criteria not used
Additional outcomes:
Care partner outcomes for anxiety, depression, perceived stress and SF-36 physical and mental.
SF-36 physical and
*Anxiety (Beck Anxiety Inventory): a standardised 21 item tool that uses a 4 point scale (0=absent/not at all disturbing to 3= I could barely stand it). Total score ranged from 0-63. 0-7= no anxiety, 8-15= mild anxiety, 16-25= moderate anxiety, >26= severe anxiety
Group1:15.13±6.92
Group 2:8.56±6.95
p value: 0.077
*Depression (Beck Depression Inventory-II), a 21 item validated self-report instrument designed to measure the severity of depression in adults
Group1: 9.71±4.43
Group 2: 9.44±4.35
p value: 0.894

235
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
23
5
Study
details Patients Interventions Outcome measures Effect size Comments
FVC>55%: 40%
FVC 50-55%: 5%
FVC <50%: 5%
Current or prior depression: 9.52%
Drop outs: 0
Group 2
N: 11
Age (mean):
% male: 42.9%
Diagnosis:
Biopsy: 42.86%
HRCT: 9.52%
FVC>55%: 30%
FVC 50-55%: 10%
FVC <50%: 10%
Current or prior depression: 9.52%
Drop outs: 4.76%
conducted a monthly support group for those wanting to attend. Psychologic counselling was provided if indicated but was not offered on a routine basis
and adolescents aged 13 and over. a score of 0-13= minimal depression, 14-19= mild depression, 20-28= moderate depression, 29-63= severe depression.
mental domains (totals not given)
Qualitative outcomes (interviews)
Notes:
Randomisation: permuted block design
Pilot study therefore sample size not based on a power calculation
*Perceived stress- designed to measure the degree to which subjects find their lives unpredictable, uncontrollable and overloading. Total scores range from 0 to 40 with higher scores indicating more stress.
Group1:19.32±3.64
Group 2: 18.20±3.65
p value: 0.531
Qualitative analysis
1
Study
details Patients Interventions Outcome measures Qualitative statement Comments
Shoenheit 2011
426
Patient group:
Patients with a physician-
All patients
Patients participated in an in-depth interview conducted by a
Diagnostic pathway
58% (26 of 45) of patients reported ‘protracted route’ to confirmed diagnosis was characterized by an initial dismissal of the presenting symptoms, with repeated
Doxa Pharma S.r.l. was commissioned to execute the research protocol, which was conducted in accordance with the

236
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
23
6
Study
details Patients Interventions Outcome measures Qualitative statement Comments
Country of study:
Germany, France,
Italy, Spain, and the United Kingdom.
Study design:
qualitative
in-depth interviews
Who was blinded:
None
Setting:
Patients home
Duration of follow-up:
N/A
confirmed diagnosis of IPF
Inclusion criteria: As above
Exclusion criteria: NR
All patients
N: 45
Age (median): 67
Drop outs: 0
M/F: 22/23
trained facilitator. Whenever possible, the caregivers were encouraged to participate as well.
Whenever possible, the caregivers were encouraged to participate as well (care givers participated in 18 [40%] of the 45 interviews).
All interviews were performed in the respondents’ homes and typically lasted for 1 hour in length or longer.
The interviews were conducted using a qualitative discussion guide*; participants were asked to recount their IPF-related health care experience in an open and free-ranging manner.
The interviews were structured to include two projective techniques: an associative technique, whereby respondents are asked to select images that express their feelings; and a constructive technique in which respondents are asked to recall what was said in a particular situation such as the moment that the diagnosis was communicated**
Informed consent was obtained from each subject and family member prior to the interview.
physician for further evaluation and testing. This was commonly interrupted by an ‘acute event,’ which was often initially attributed to other causes this frequently resulted in an emergency room visit and subsequent hospitalization, where a detailed evaluation by a pulmonologist would eventually result in a diagnosis of IPF. This process reportedly took as long as 2–12 years, despite repeated visits to health care practitioners during this period. Patients who were subjected to this protracted route to diagnosis were often critical of the care they received, citing both a lack of empathy and emotional support and an apparent lack of competence among health care practitioners. There was a tendency among these patients to perceive the initial diagnosis not as a working hypothesis but rather as an erroneous or missed diagnosis. In a minority of cases (16%), the diagnosis was made within a month of the patient’s initial presentation. Early detection was attributed to a well-informed patient researching their symptoms online, a well-informed physician detecting the distinctive ‘Velcro1 rales’ on chest auscultation, which prompted further evaluation for possible interstitial lung disease, or routine surveillance of known drug toxicities (e.g.
International Chamber of Commerce (ICC)/The European Society for Opinion and Market Research (ESCOMAR) International Code on Market and Social Research and other ESOMAR/ European Pharmaceutical Market Research Association (EphMRA) professional standards. Data was processed in accordance with Legislative Decree No.196 (30 June 2003), as well as the ESOMAR Standards and the ‘Code of Ethics and Conduct’ issued by the Guarantor of Privacy (16 June 2004).
Funding: InterMune
Limitations:
IPF diagnosis wasn’t confirmed using current criteria
Recall bias
Small sample size
Generalisability
Additional outcomes:
demographics

237
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
23
7
Study
details Patients Interventions Outcome measures Qualitative statement Comments
Audio recordings were made during each of these interviews and used to assist with accurate and thorough data capture and analysis. Audio recordings of the interviews were transcribed and all individual data were then collated in content analysis grids with data from other respondents and presented in aggregate with complete confidentiality maintained for each participant.
Researchers from all five counties analyzed the raw data in a collaborative process aimed at identifying the primary themes emerging from the results of the survey.
At the onset of each interview, the moderator read a scripted introduction that described the purpose and nature of the discussion as follows: ‘The overall purpose of this discussion is to understand how your IPF is managed, and what your current needs are. The discussion will take the form of an interactive session, with exercises/ tasks which are designed to be enjoyable as well as informative for us; they allow us to
amiodarone). most commonly reported presenting symptoms
median time from initial presentation and diagnosis
number of physicians consulted before receiving a confirmed diagnosis
patients expectations of available treatments
commonly reported misdiagnoses
Notes:
*The discussion guide was developed after a comprehensive review of the limited relevant medical literature and with input from health care practitioners with expertise in IPF.
** The choices of images and the output of the constructive task were not considered to have any interpretive value except in the context of what the respondents verbalized on completion of the task.
Diagnosis “Patients expressed a dissatisfaction with the manner in which the diagnosis was divulged, citing insensitivity on the part of the health care practitioner and insufficient time during the consultation to address the full range of patients’ questions and concerns”
Quality of care in tertiary centre
“Patients treated in a tertiary care center consistently reported greater satisfaction with the quality of care, the availability of treatment options (including enrolment in a clinical trial), the knowledge and expertise of health care practitioners, and the frequency of follow-up visits and routine monitoring. Additionally, patients treated in a tertiary care center commonly reported that the opportunity to interact with other IPF patients provided important benefits, including psychological support and practical disease management tips”
Quality of care in community practice
“Patients treated in the community practice setting consistently reported infrequent follow-up visits (typically once per year), short duration of visits (generally less than 10 minutes), and a lack of available treatment options. In general, these patients were less well informed about their disease and the available treatment options, including pulmonary rehabilitation, lung transplantation, and

238
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
23
8
Study
details Patients Interventions Outcome measures Qualitative statement Comments
access information that we would not be able to access by asking a straight question. In particular, we are interested in understanding not just what you think but why you think it.’
Because of the exploratory nature of the research objectives, wherever possible, attempts were made to elicit spontaneous responses, with prompts being used only as necessary to advance the discussion and to glean the study elements of interest.
enrolment in a clinical trial”
Patients aims for disease management
“Focused on disease stability and efforts to slow progression if feasible. For only a small minority of those surveyed, the emphasis was either on lung transplantation
as the ‘hope’ for future survival beyond IPF, or some belief that their particular condition was atypical and associated with a less dire prognosis”
Commonly reported unmet medical needs
Improved access to Centres of Excellence
Clear and understandable disease education resources
Comprehensive family support/counselling programs
Fewer bureaucratic barriers to scheduling specialist appointments and obtaining supplemental oxygen
Patient advocacy and public education
improved diagnostic techniques
more effective treatment options
IPF on Patients’ Quality of Life and
Emotional Well-Being
personal independence
Loss of independence that coincided with the deterioration in health and inability to perform routine daily tasks. The requirement for supplemental oxygen was commonly identified as a milestone in the patients’ loss of independence, as it is at this point that the disease becomes highly visible to others and excursions outside the

239
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
23
9
Study
details Patients Interventions Outcome measures Qualitative statement Comments
home begin to require significant logistical planning. In many cases, this loss of independence has a notable impact on the patient’s emotional well-being, as they begin to perceive themselves as a burden to both their family and society
relationships with others
considerable difficulty in continuing relationships with friends and acquaintances
due to their worsening pulmonary status and
immobility, as well as a general lack of awareness and understanding of the disease
financial status
20% of respondents reported financial difficulties as a result of their inability to work and the consequent reduction in income. This further served as a stressor, as well as the concern that they were now an increasing burden to their families and loved ones
1
2

240
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
24
0
F.6 Pharmacological interventions 1
F.6.1 Warfarin vs. Placebo 2
Table 81: Noth 2012359 3
Study
details
Patients Methods Outcome measures Effect size Comments
Noth 2012359
Comparison:
Warfarin
versus placebo
Setting:
Multicentre trial;
22 centres in the USA
Duration of follow-up:
48 weeks planned:
Study was stopped by Independent safety and monitoring board with a mean follow up of 28 weeks
Design:
Parallel group
Patient group:
Patients aged 35 to 80 meeting ATS/ERS diagnostic criteria for IPF
Inclusion criteria:
Progressive IPF patients i.e. those with a history of 1) worsening dyspnoea or 2) physiologic deterioration defined as an absolute of either FVC ≥ 10% or DLCO ≥ 15%, progression of radiographic findings a reduction is SaO2 of ≥ 5%. Patients must be willing to do home INR testing.
Exclusion criteria:
Current indication for or treatment with warfarin, prasugrel, or clopidogrel combined with aspirin; presence of an increased
Group 1: (n=72)
Oral warfarin dose adjusted to maintain an INR of 2-3
Group 2: (n=73)
Sham dose adjusted placebo
All-cause mortality at trial stop (RR)
Group 1: 14
Group 2: 3
RR [95%CI]: 4.73 [1.42, 15.77]
p=0.01
Funding:
Unclear
Limitations:
All disclosures on online appendix and not presented in paper
High risk of attrition bias as trial stopped prior to completion for safety thus all available results analysed together and high overall dropout rate
Additional outcomes:
Plasma D-Dimer levels
Combined all-cause mortality and non-elective non bleeding hospitalisations at trial stop (RR)
Group 1: 21
Group 2: 10
RR [95%CI]: 2.13 [1.08, 4.20]
p=0.03
Respiratory cause mortality at trial end (RR)
Group 1: 11
Group 2: 3
RR [95%CI]: 3.72 [1.08, 12.77]
p=0.04
Cardiac cause mortality at trial end (RR)
Group 1: 3
Group 2: 0
NS difference
All-cause mortality at trial stop (HR)
HR: 4.85
SE:
Combined all-cause mortality and non-
HR:2.12

241
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
24
1
risk of bleeding; a recent CVA or GI bleed; any signs and symptoms of a severe, progressive or uncontrolled comorbid illness; presence on active list for lung transplantation.
All patients
N:145
Age (mean): 67
Male/female (%): 63/27
Mean predicted FVC (%): 59
Mean predicted DLCO (%): 34
Drop outs:
Group 1:
N: 72
Age (mean): 67.3 +/- 7.1
Male/female (%): 67/33
FVC, % predicted (mean +/- SD): 58.9 +/- 16.2
DLCO % predicted (mean +/- SD): 33.8 +/- 12.4
Drop outs:
Group 2:
N: 73
Age (mean): 66.7 +/- 7.4
elective non bleeding hospitalisations at trial stop (HR)
SE:
Notes:
Change in 6MWD (m),FVC (%) and DLCO (%)at 48 weeks (extrapolated)
Non-significant difference between groups reported in text narrative. No data given
QoL Non-significant between groups reported in text narrative. No data given
Number of participants with IPF exacerbations at trial end
Group 1: 6
Group 2: 2
Non-significant difference
Number of participants with major bleeds at trial end
Group 1: 2
Group 2: 1
Non-significant difference
Number of participants with minor bleeds at trial end
Group 1: 6
Group 2: 2
Non-significant difference
1 and 3 year survival rate NR
Hospitalisations due to IPF
NR
Dyspnoea NR
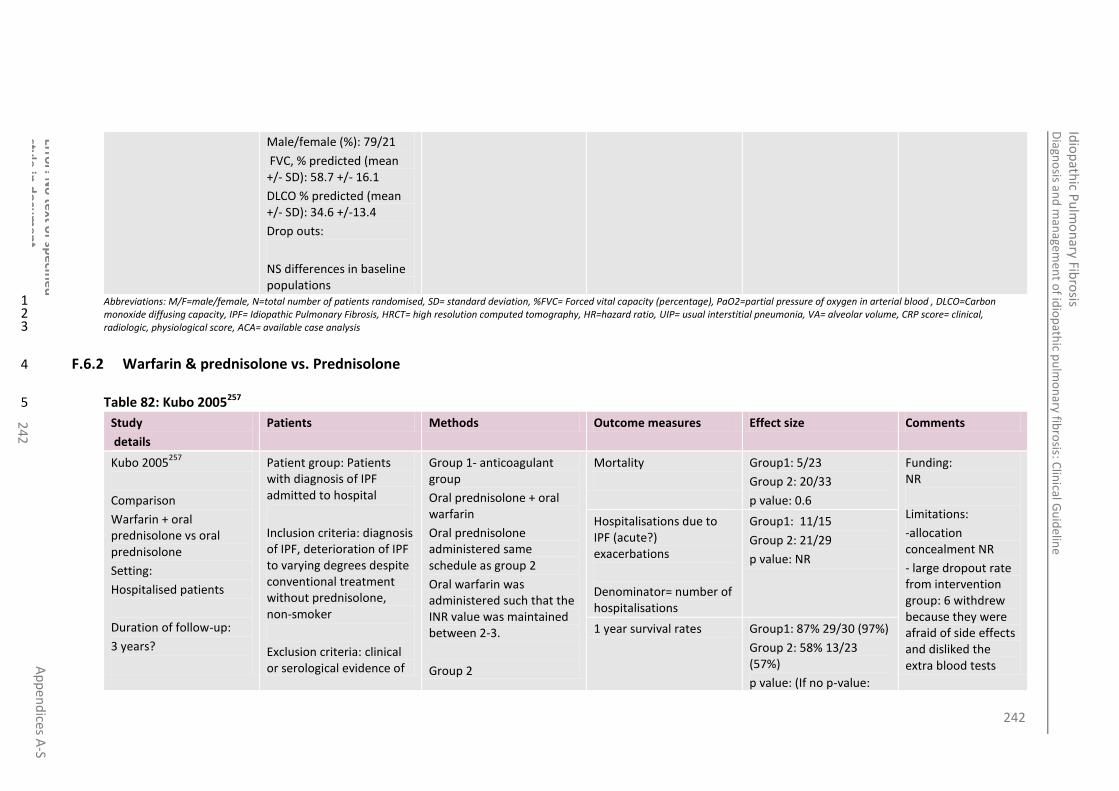
242
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
24
2
Male/female (%): 79/21
FVC, % predicted (mean +/- SD): 58.7 +/- 16.1
DLCO % predicted (mean +/- SD): 34.6 +/-13.4
Drop outs:
NS differences in baseline populations
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood , DLCO=Carbon 1 monoxide diffusing capacity, IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, UIP= usual interstitial pneumonia, VA= alveolar volume, CRP score= clinical, 2 radiologic, physiological score, ACA= available case analysis 3
F.6.2 Warfarin & prednisolone vs. Prednisolone 4
Table 82: Kubo 2005257 5
Study
details
Patients Methods Outcome measures Effect size Comments
Kubo 2005257
Comparison
Warfarin + oral prednisolone vs oral prednisolone
Setting:
Hospitalised patients
Duration of follow-up:
3 years?
Patient group: Patients with diagnosis of IPF admitted to hospital
Inclusion criteria: diagnosis of IPF, deterioration of IPF to varying degrees despite conventional treatment without prednisolone, non-smoker
Exclusion criteria: clinical or serological evidence of
Group 1- anticoagulant group
Oral prednisolone + oral warfarin
Oral prednisolone administered same schedule as group 2
Oral warfarin was administered such that the INR value was maintained between 2-3.
Group 2
Mortality
Group1: 5/23
Group 2: 20/33
p value: 0.6
Funding: NR
Limitations:
-allocation concealment NR
- large dropout rate from intervention group: 6 withdrew because they were afraid of side effects and disliked the extra blood tests
Hospitalisations due to IPF (acute?) exacerbations
Denominator= number of hospitalisations
Group1: 11/15
Group 2: 21/29
p value: NR
1 year survival rates Group1: 87% 29/30 (97%)
Group 2: 58% 13/23 (57%)
p value: (If no p-value:
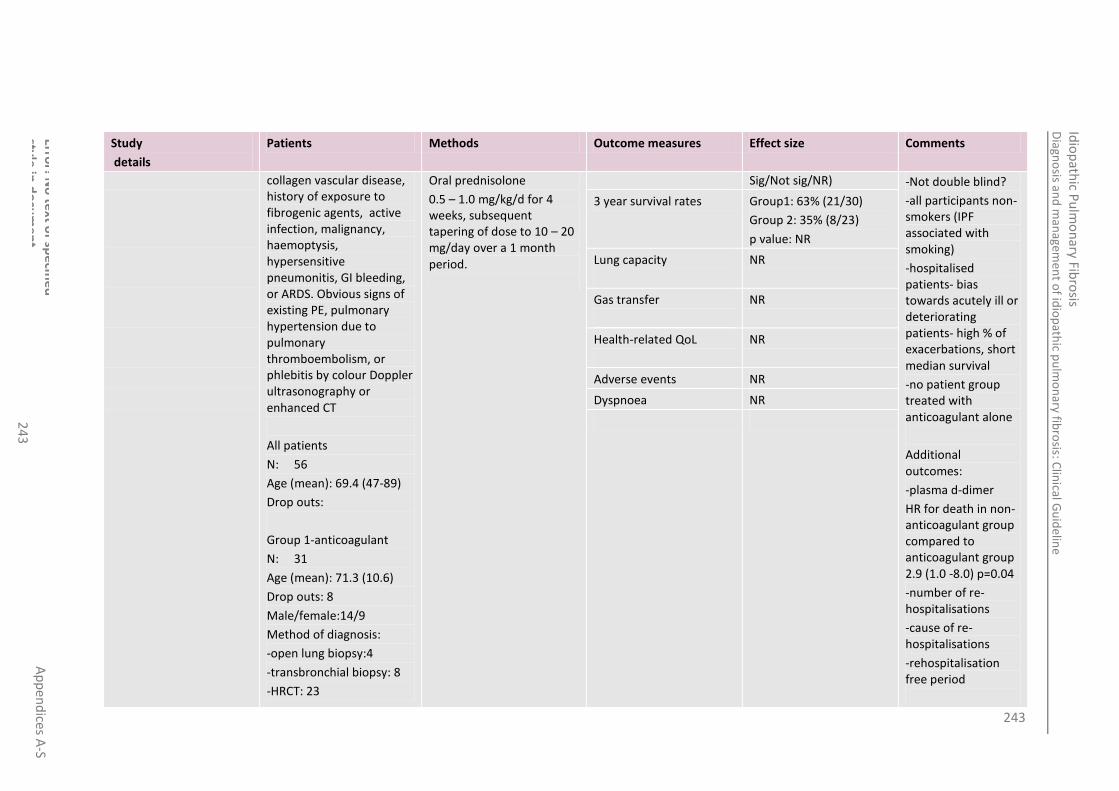
243
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
24
3
Study
details
Patients Methods Outcome measures Effect size Comments
collagen vascular disease, history of exposure to fibrogenic agents, active infection, malignancy, haemoptysis, hypersensitive pneumonitis, GI bleeding, or ARDS. Obvious signs of existing PE, pulmonary hypertension due to pulmonary thromboembolism, or phlebitis by colour Doppler ultrasonography or enhanced CT
All patients
N: 56
Age (mean): 69.4 (47-89)
Drop outs:
Group 1-anticoagulant
N: 31
Age (mean): 71.3 (10.6)
Drop outs: 8
Male/female:14/9
Method of diagnosis:
-open lung biopsy:4
-transbronchial biopsy: 8
-HRCT: 23
Oral prednisolone
0.5 – 1.0 mg/kg/d for 4 weeks, subsequent tapering of dose to 10 – 20 mg/day over a 1 month period.
Sig/Not sig/NR) -Not double blind?
-all participants non-smokers (IPF associated with smoking)
-hospitalised patients- bias towards acutely ill or deteriorating patients- high % of exacerbations, short median survival
-no patient group treated with anticoagulant alone
Additional outcomes:
-plasma d-dimer
HR for death in non-anticoagulant group compared to anticoagulant group 2.9 (1.0 -8.0) p=0.04
-number of re-hospitalisations
-cause of re-hospitalisations
-rehospitalisation free period
3 year survival rates Group1: 63% (21/30)
Group 2: 35% (8/23)
p value: NR
Lung capacity
NR
Gas transfer
NR
Health-related QoL
NR
Adverse events NR
Dyspnoea NR
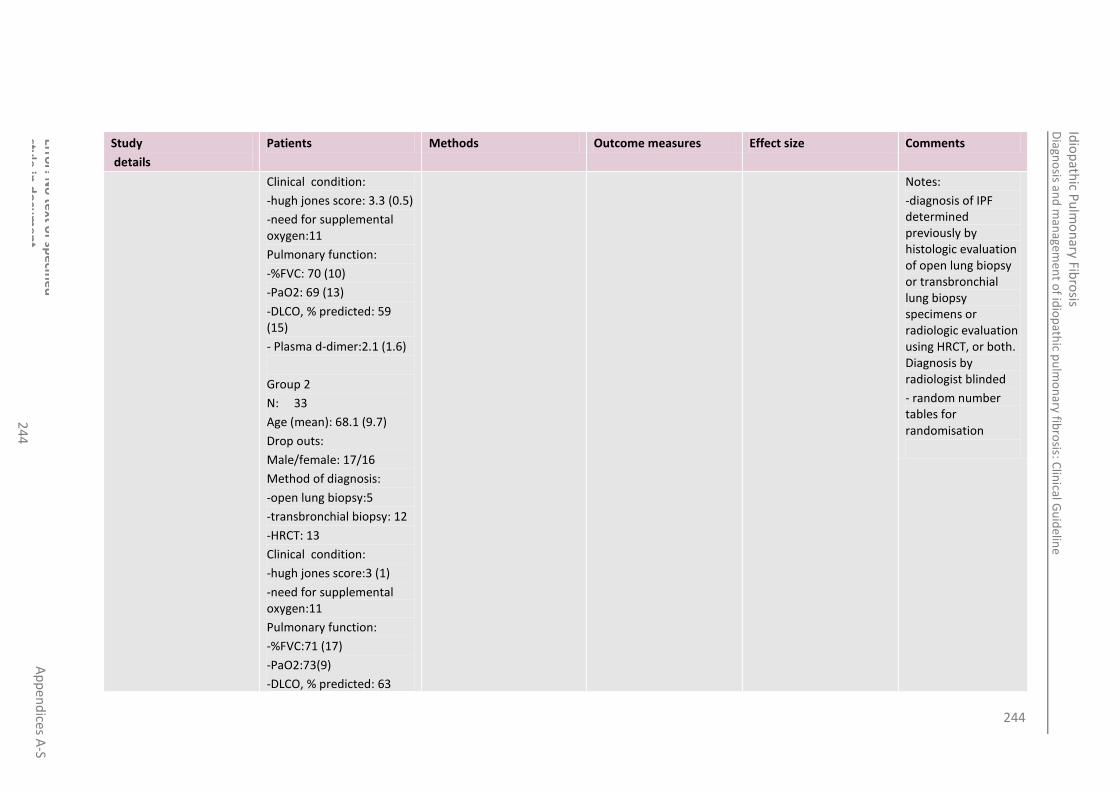
244
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
24
4
Study
details
Patients Methods Outcome measures Effect size Comments
Clinical condition:
-hugh jones score: 3.3 (0.5)
-need for supplemental oxygen:11
Pulmonary function:
-%FVC: 70 (10)
-PaO2: 69 (13)
-DLCO, % predicted: 59 (15)
- Plasma d-dimer:2.1 (1.6)
Group 2
N: 33
Age (mean): 68.1 (9.7)
Drop outs:
Male/female: 17/16
Method of diagnosis:
-open lung biopsy:5
-transbronchial biopsy: 12
-HRCT: 13
Clinical condition:
-hugh jones score:3 (1)
-need for supplemental oxygen:11
Pulmonary function:
-%FVC:71 (17)
-PaO2:73(9)
-DLCO, % predicted: 63
Notes:
-diagnosis of IPF determined previously by histologic evaluation of open lung biopsy or transbronchial lung biopsy specimens or radiologic evaluation using HRCT, or both. Diagnosis by radiologist blinded
- random number tables for randomisation

245
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
24
5
Study
details
Patients Methods Outcome measures Effect size Comments
(14)
-Plasma d-dimer:1.9 (1.3) Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood , DLCO=Carbon 1 monoxide diffusing capacity, IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, UIP= usual interstitial pneumonia, VA= alveolar volume, CRP score= clinical, 2 radiologic, physiological score, ACA= available case analysis 3
F.6.3 Sildenafil vs. Placebo 4
Table 83: Jackson 2010207 5
Study
details
Patients Methods Outcome measures Effect size Comments
Jackson 2010
207
Country of study:
USA
Study design:
single-centre, double blind,
placebo-controlled trial (RCT)
Who was blinded:
Treatment assignments
Patient group:
Typical patients with IPF, who fulfilled the clinical diagnostic criteria of the American Thoracic and European Respiratory Societies. Subjects recruited from August 2006 to November 2008.
Inclusion criteria:
IPF onset between 3 -36 months before screening
Diagnosis must be made by HRCT scan showing definite / probable IPF and VATS lung biopsy showing definite/ probable UIP
RVSP or PAsys 25–50 mmHg, based on echocardiography and absence of decompensated right heart failure (NYHA class I or II acceptable)
Age 21 -85 years, inclusive. Patients aged 21–40 years must have diagnosis by open or video-assisted thorascopic surgery lung biopsy
Group 1
Subjects were treated with sildenafil citrate tablets orally in an escalating dose schedule: 20 mg daily for 3 days, 20 mg twice daily for 3 days, and then 20 mg three times daily for the remainder of the trial.
Patients took the study drug at home after receiving verbal and written
6MWD: metres
(Approximation read off graph) (Mean ±SD)
Group1: 330 ±40
Group 2: 355±80
Relative risk [95% CI]: NR
p value: NR
Funding: Supported by a grant from the Veterans Administration Research Service. Pfizer UK provided sildenafil and placebo donation.
Limitations:
Unclear allocation concealment
Small sample size
Study of short duration
21.4% drop out rate in placebo arm
Lung capacity
FVC (% of predicted value) (mean change ± SD)
Group1: -4 ± 14.2
Group 2: -5.3 ± 9.8
Relative risk [95% CI]: NR
p value: 0.79
Gas transfer
DLCO (% of predicted value) (mean change ± SD)
Group1: -6.1 ± 10.6
Group 2: -2.5 ± 8.4
Relative risk [95% CI]: NR
p value: 0.341
Dyspnoea: 10 point Borg scale (after exercise stress test)
Group1: 4.3±1.5
Group 2: 3.6±1.6
Relative risk [95%

246
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
24
6
Study
details
Patients Methods Outcome measures Effect size Comments
and personnel
Setting:
Clinical
Duration of follow-up:
6 months
FVC 40–90% predicted or DLCO 30–90% predicted or impaired gas exchange with rest or exercise
6MWT (distance) ≥150 m and ≤500 m
Worsening of one of the following in the last year :>10% decrease in percent predicted FVC or worsening dyspnoea at rest/ on exertion
Ability to understand and sign a written informed consent form and comply with the requirements of the study
Absence of clinical features suggesting infection, neoplasm, sarcoidosis, collagen-vascular disease or exposure to known fibrogenic environmental factors
Exclusion criteria:
PAsys>50 mmHg, based on echocardiography or TR velocity≥ 3.2 m/s
Severe heart failure (NYHA class III or IV or LVEF<25%)
6MWD <150 m />500 m
FEV1/FVC ratio <0.5 at screening (post-bronchodilator)
Residual volume>120% predicted
Any condition other than IPF likely to result in the death of the patient within 2 years
History of unstable or deteriorating cardiac or neurologic disease
Pregnancy or lactation.
instruction
Group 2
Identical placebo
(Mean ±SD) CI]:NR
p value: 0.202
Additional outcomes:
Exercise stress test times before and after intervention.
PFTs; TLC, RVSP, SaO2
Notes:
Randomly assigned, in a ratio as close as 1:1 as possible, used blocked randomization, with varying size of the blocks
Double blind. Active and placebo compounds were identically packaged and labelled. Study personnel involved in obtaining 6MWT were blinded to adverse events, symptoms, and possible side effects. Treatment assignments were unblinded only at the completion of the
Adverse events: chest pain
Group1: 1/14
Group 2: 0/15
Relative risk [95% CI]:NR
p value: NR
Adverse events: facial flushing
Group1: 1/14
Group 2: 1/15
Relative risk [95% CI]:NR
p value: NR
Adverse events: visual disturbance
Group1: 1/14
Group 2: 0/15
Relative risk [95% CI]:NR
p value: NR

247
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
24
7
Study
details
Patients Methods Outcome measures Effect size Comments
Current treatment with corticosteroids (oral or inhaled), Cytoxan, azathioprine, 247nblended247s, pirfenidone, interferon gamma or beta, anti-tumour necrosis factor therapy, or with endothelin receptor blockers. There must be at least 4 weeks of treatment washout before inclusion in this study
Investigational therapy for any indication within 28 days before treatment
Creatinine>1.5 9 upper limit of normal at screening
WBC<2,500/mm3 or neutrophil count<1500, hematocrit<30% or>59%, platelets<100,000/mm3 at screening
Total bilirubin >2.0 X upper limit of normal; aspartate or alanine aminotransferases (AST, SGOT or ALT, SGPT) >3 X upper limit of normal; alkaline phosphatise>3 X upper limit of normal; albumin <3.0 mg/dl at screening
Degenerative arthritis, cerebrovascular accident, or other limitation to mobility preventing completion of the 6MWT
Oxygen saturation on room air<80% at rest
All patients
N: 29
Age (mean): NR
Drop outs: 4
Group 1
study.
Statistical analyses were performed on intent-to treat basis. All statistical tests were two-sided tests at a nominal 5% level of significance.
Drug compliance ranged from 89%-100%.for the sildenafil and placebo groups respectively
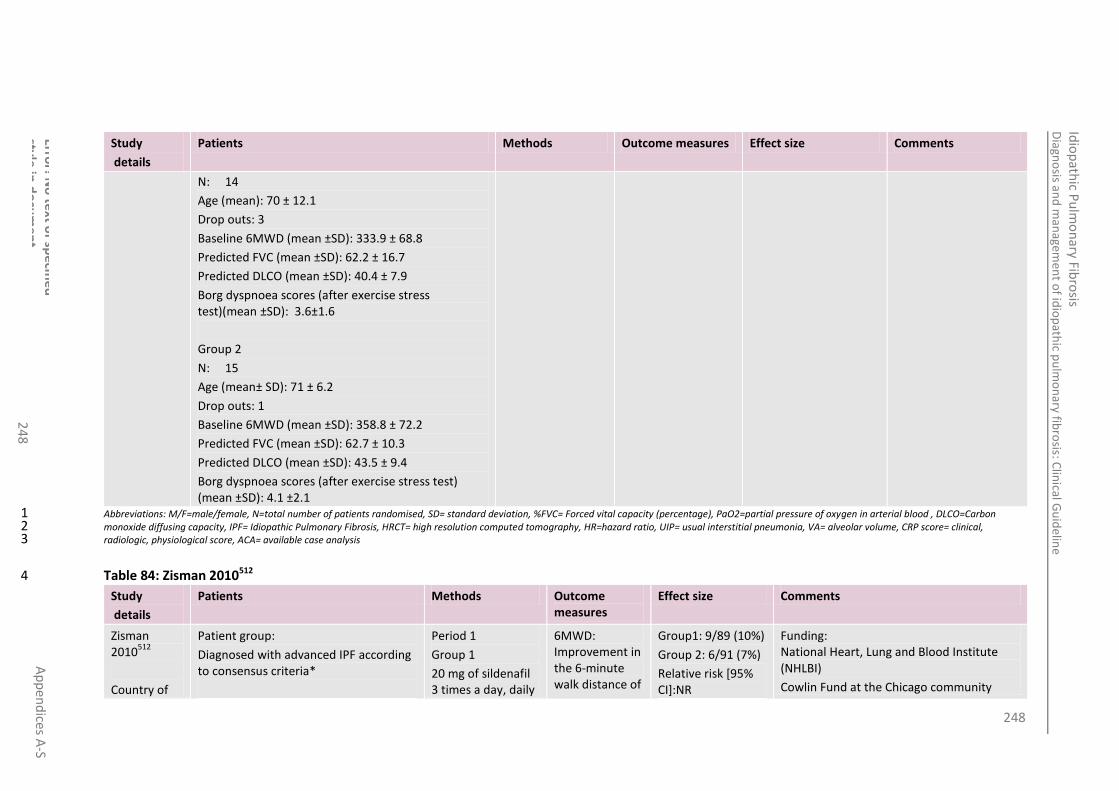
248
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
24
8
Study
details
Patients Methods Outcome measures Effect size Comments
N: 14
Age (mean): 70 ± 12.1
Drop outs: 3
Baseline 6MWD (mean ±SD): 333.9 ± 68.8
Predicted FVC (mean ±SD): 62.2 ± 16.7
Predicted DLCO (mean ±SD): 40.4 ± 7.9
Borg dyspnoea scores (after exercise stress test)(mean ±SD): 3.6±1.6
Group 2
N: 15
Age (mean± SD): 71 ± 6.2
Drop outs: 1
Baseline 6MWD (mean ±SD): 358.8 ± 72.2
Predicted FVC (mean ±SD): 62.7 ± 10.3
Predicted DLCO (mean ±SD): 43.5 ± 9.4
Borg dyspnoea scores (after exercise stress test) (mean ±SD): 4.1 ±2.1
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood , DLCO=Carbon 1 monoxide diffusing capacity, IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, UIP= usual interstitial pneumonia, VA= alveolar volume, CRP score= clinical, 2 radiologic, physiological score, ACA= available case analysis 3
Table 84: Zisman 2010512 4
Study
details
Patients Methods Outcome measures
Effect size Comments
Zisman 2010
512
Country of
Patient group:
Diagnosed with advanced IPF according to consensus criteria*
Period 1
Group 1
20 mg of sildenafil 3 times a day, daily
6MWD: Improvement in the 6-minute walk distance of
Group1: 9/89 (10%)
Group 2: 6/91 (7%)
Relative risk [95% CI]:NR
Funding: National Heart, Lung and Blood Institute (NHLBI)
Cowlin Fund at the Chicago community

249
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
24
9
Study
details
Patients Methods Outcome measures
Effect size Comments
study:
USA
Study design:
Multi-center, randomized, double-blind, placebo-controlled period (period 1), followed by open-label period (period 2).
Who was blinded:
Double -blind
Setting:
Clinical
14 IPFnet centres
Duration of follow-up:
12 weeks
Inclusion criteria:
Diagnosis of IPF, as defined by consensus criteria*, in an advanced stage, which was defined as a diffusing capacity for carbon monoxide of <35% of the predicted value.
Exclusion criteria:
6MWD <50m (164 ft)
A difference of more than 15% in the 6MWD between two pre-randomization walks;
Extent of emphysema greater than the extent of fibrotic change, determined by HRCT;
Treatment with medications containing nitrates
The presence of aortic stenosis/ idiopathic hypertrophic subaortic stenosis;
The initiation of pulmonary rehabilitation within 30 days after screening;
The initiation or change in the dose of any investigational treatment for idiopathic pulmonary fibrosis within 30 days after screening;
Treatment for pulmonary hypertension with prostaglandins, endothelin-1 antagonists, or other
for 12 weeks, then 20 mg of sildenafil 3 times a day, daily for 12 weeks
Group 2 matched placebo
Period 2
All subjects took part in a second 12-week open-label phase of the protocol once they had completed the first period. This second study period assigned all subjects to
sildenafil 20 mg 3 times daily and evaluated the short-term effects of treatment and longer-term
(24-week) safety profile
20% or more over baseline
p value: 0.39 Trust
Pfizer (donated sildenafil and matching placebo)
Masimo (donated pulse oximeters)
Limitations:
Blinding not reported
Findings are applicable only to patients with advanced idiopathic pulmonary fibrosis
Unknown whether the treatment effect was driven by a particular subgroup of patients (e.g., those with more severe pulmonary vascular disease)
Small sample size
Study of short duration
improvements in subjective outcomes, such as quality of life, may be due to incomplete masking
SD have not been reported for all outcomes
Additional outcomes:
PFT; partial pressure of oxygen, partial pressure of carbon dioxide, alveolar-arterial gradient, arterial oxygen saturation.
Acute exacerbations
Quality of life: SF-36
Dyspnoea: Shortness of breath questionnaire –mean change (95% CI) (higher score indicates worse function)
Group1: 0.22 (-3.10 to 3.54) SD: 15.76*
Group 2: 6.81 (3.53 to 10.08) SD: 17.45*
#Absolute difference: -6.58 (-11.25 to -1.92)
p value: 0.006
Dyspnoea: Score on Borg Dyspnoea Index after walk test- mean change (95% CI) (higher score indicates worse function)
Group1: 0.04(-0.30 to 0.37) SD: 1.76*
Group 2: 0.37(0.04 to 0.70) SD: 1.58*
#Absolute difference:-0.34 (-0.81 to 0.14)
p value: 0.16
Quality of life: St Georges Respiratory Questionnaire, total score –mean change (95% CI) (higher score indicates worse function)
Group1: -1.64 (-3.91 to 0.64) SD: 10.8*
Group 2: 2.45 (0.17 to 4.72) SD: 10.92*
#Absolute difference: -4.08 (-7.30 to -0.86)
p value: 0.01
Quality of life: EQ-5D self-
Group1: −0.01 (−0.06 to 0.03)

250
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
25
0
Study
details
Patients Methods Outcome measures
Effect size Comments
phosphodiesterase inhibitors within 30 days after screening;
A resting SpO2 < 92% while breathing 6 litres of supplemental oxygen;
Listed for lung transplantation
All patients
N: 180
Age (mean): 69
Drop outs: 14
M/F: 83%/17%
Baseline 6MWD (mean): 265m
Predicted FVC (mean): 56.8%
Predicted DLCO (mean):26.3%
Group 1
N: 89
Age (mean): 69.76 ± 8.71
Drop outs: 8 (4 adverse event 2 died 2 lost to follow up)
M/F: 73 (82%)/16(18%)
Baseline 6MWD (mean): 246.39m ±103.40m
Predicted FVC (mean): 54.89% ±14.00%
Predicted DLCO (mean): 25.81% ±6.03%
Group 2
report questionnaire
mean change (95% CI)
Group 2: −0.03 (−0.08 to 0.01)
#Absolute difference: 0.02 (−0.04 to 0.08)
p value: 0.54
Quality of life: EQ-5D visual-analogue scale
Notes:
Supplementary Appendix:
http://www.nejm.org/doi/suppl/10.1056/NEJMoa1002110/suppl_file/nejmoa1002110_appendix.pdf
Randomisation: 1:1 with the use of a permuted block design, with stratification according to clinical centre.
Calculations based on chi squared test of equal proportions
Intention to treat analysis - patients were deemed to have had no response if the rate of improvement was less than 20% at 12 weeks or if they died, withdrew from the study, or had missing data
All P values are two-sided, and no adjustment has been made for multiple comparisons
*Consensus criteria:
The presence of all major criteria and 3 of the 4 minor criteria are required to meet study criteria for the diagnosis of IPF.
Major Criteria
1. Clinical: exclusion of other known causes
Lung capacity:
FVC (% of predicted value) –mean change (95% CI)
Group1: -0.97 (-2.00 to 0.06) SD: 4.89*
Group 2: -1.29 (-2.30 to -0.28) SD:4.85*
#Absolute difference:0.32 (-1.12 to 1.76)
p value: 0.66
Gas transfer
DLCO (% of predicted value)–mean change (95% CI)
Group1: -0.33 (-1.36 to 0.71) SD: 4.91*
Group 2: -1.86 (-2.91 to -0.83) SD: 4.99*
#Absolute difference: 1.55 (0.08 to 3.01)
p value: 0.04
Mortality (Death from any cause)
Group1: 2/89 (2%)
Group 2: 4/91 (4%)
Relative risk [95% CI]: NR

251
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
25
1
Study
details
Patients Methods Outcome measures
Effect size Comments
N: 91
Age (mean): 68.20 ± 9.25
Drop outs: 6 (4 adverse events 1, died, 1 underwent lung transplantation)
M/F: 77(84%)/14(16%)
Baseline 6MWD (mean): 269.55m ±129.83m
Predicted FVC (mean): 58.73% ±14.12%
Predicted DLCO (mean): 26.73% ±6.16%
p value: 0.43 (connective tissue diseases,
environmental and drug exposures) of ILD
2. Physiologic: restriction on pulmonary function testing (PFT) and/or evidence of
impaired gas exchange (decreased DLCO or increased alveolar-arterial partial
pressure of oxygen difference [A-aPO2] at rest or with exercise)
3. Radiographic: HRCT with bibasilar reticular abnormality and honeycomb
change with minimal ground glass opacities
Minor Criteria
1. Age > 50 years
2. Insidious onset of unexplained dyspnoea
3. Duration of illness for ≥ 3 months
4. Bibasilar, inspiratory crackles
# Absolute difference: this value is the absolute difference between sildenafil group and the placebo group in the change from baseline
*Calculated by NCGC
Adverse events (all adverse events classed as ‘serious’): coronary artery disease
Group1: 0/89(0%)
Group 2: 1/91 (1.1%)
Relative risk [95% CI]:NR
p value: NR
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood , DLCO=Carbon 1 monoxide diffusing capacity, IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, UIP= usual interstitial pneumonia, VA= alveolar volume, CRP score= clinical, 2 radiologic, physiological score, ACA= available case analysis 3
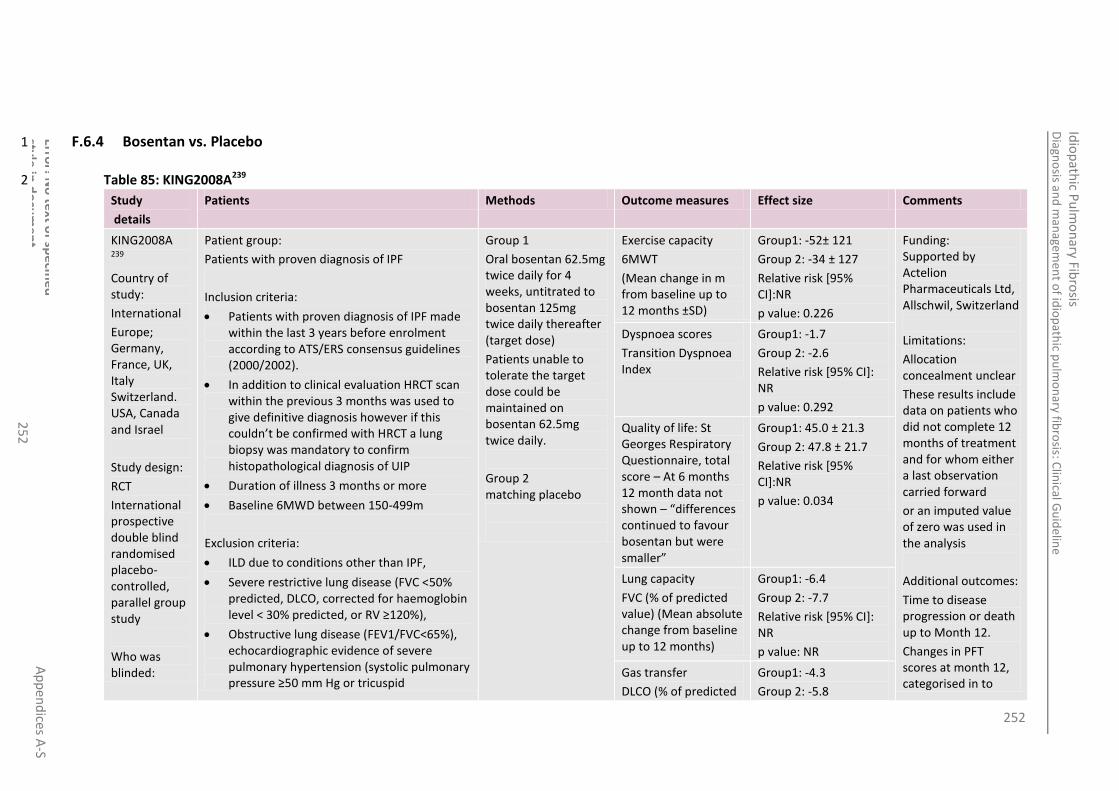
252
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
25
2
F.6.4 Bosentan vs. Placebo 1
Table 85: KING2008A239 2
Study
details
Patients Methods Outcome measures Effect size Comments
KING2008A 239
Country of study:
International
Europe; Germany, France, UK, Italy Switzerland. USA, Canada and Israel
Study design:
RCT
International prospective double blind randomised placebo-controlled, parallel group study
Who was blinded:
Patient group:
Patients with proven diagnosis of IPF
Inclusion criteria:
Patients with proven diagnosis of IPF made within the last 3 years before enrolment according to ATS/ERS consensus guidelines (2000/2002).
In addition to clinical evaluation HRCT scan within the previous 3 months was used to give definitive diagnosis however if this couldn’t be confirmed with HRCT a lung biopsy was mandatory to confirm histopathological diagnosis of UIP
Duration of illness 3 months or more
Baseline 6MWD between 150-499m
Exclusion criteria:
ILD due to conditions other than IPF,
Severe restrictive lung disease (FVC <50% predicted, DLCO, corrected for haemoglobin level < 30% predicted, or RV ≥120%),
Obstructive lung disease (FEV1/FVC<65%), echocardiographic evidence of severe pulmonary hypertension (systolic pulmonary pressure ≥50 mm Hg or tricuspid
Group 1
Oral bosentan 62.5mg twice daily for 4 weeks, untitrated to bosentan 125mg twice daily thereafter (target dose)
Patients unable to tolerate the target dose could be maintained on bosentan 62.5mg twice daily.
Group 2 matching placebo
Exercise capacity
6MWT
(Mean change in m from baseline up to 12 months ±SD)
Group1: -52± 121
Group 2: -34 ± 127
Relative risk [95% CI]:NR
p value: 0.226
Funding: Supported by Actelion Pharmaceuticals Ltd, Allschwil, Switzerland
Limitations:
Allocation concealment unclear
These results include data on patients who did not complete 12 months of treatment and for whom either a last observation carried forward
or an imputed value of zero was used in the analysis
Additional outcomes:
Time to disease progression or death up to Month 12.
Changes in PFT scores at month 12, categorised in to
Dyspnoea scores
Transition Dyspnoea Index
Group1: -1.7
Group 2: -2.6
Relative risk [95% CI]: NR
p value: 0.292
Quality of life: St Georges Respiratory Questionnaire, total score – At 6 months 12 month data not shown – “differences continued to favour bosentan but were smaller”
Group1: 45.0 ± 21.3
Group 2: 47.8 ± 21.7
Relative risk [95% CI]:NR
p value: 0.034
Lung capacity
FVC (% of predicted value) (Mean absolute change from baseline up to 12 months)
Group1: -6.4
Group 2: -7.7
Relative risk [95% CI]: NR
p value: NR
Gas transfer
DLCO (% of predicted
Group1: -4.3
Group 2: -5.8
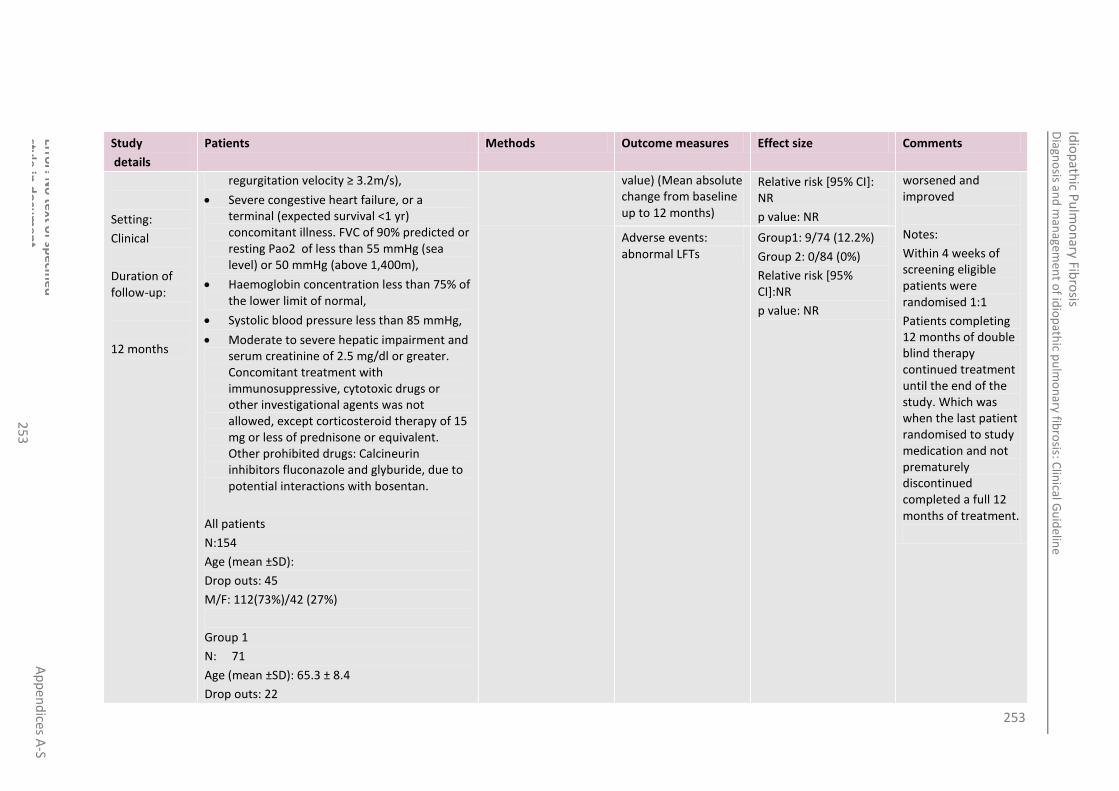
253
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
25
3
Study
details
Patients Methods Outcome measures Effect size Comments
Setting:
Clinical
Duration of follow-up:
12 months
regurgitation velocity ≥ 3.2m/s),
Severe congestive heart failure, or a terminal (expected survival <1 yr) concomitant illness. FVC of 90% predicted or resting Pao2 of less than 55 mmHg (sea level) or 50 mmHg (above 1,400m),
Haemoglobin concentration less than 75% of the lower limit of normal,
Systolic blood pressure less than 85 mmHg,
Moderate to severe hepatic impairment and serum creatinine of 2.5 mg/dl or greater. Concomitant treatment with immunosuppressive, cytotoxic drugs or other investigational agents was not allowed, except corticosteroid therapy of 15 mg or less of prednisone or equivalent. Other prohibited drugs: Calcineurin inhibitors fluconazole and glyburide, due to potential interactions with bosentan.
All patients
N:154
Age (mean ±SD):
Drop outs: 45
M/F: 112(73%)/42 (27%)
Group 1
N: 71
Age (mean ±SD): 65.3 ± 8.4
Drop outs: 22
value) (Mean absolute change from baseline up to 12 months)
Relative risk [95% CI]: NR
p value: NR
worsened and improved
Notes:
Within 4 weeks of screening eligible patients were randomised 1:1
Patients completing 12 months of double blind therapy continued treatment until the end of the study. Which was when the last patient randomised to study medication and not prematurely discontinued completed a full 12 months of treatment.
Adverse events: abnormal LFTs
Group1: 9/74 (12.2%)
Group 2: 0/84 (0%)
Relative risk [95% CI]:NR
p value: NR
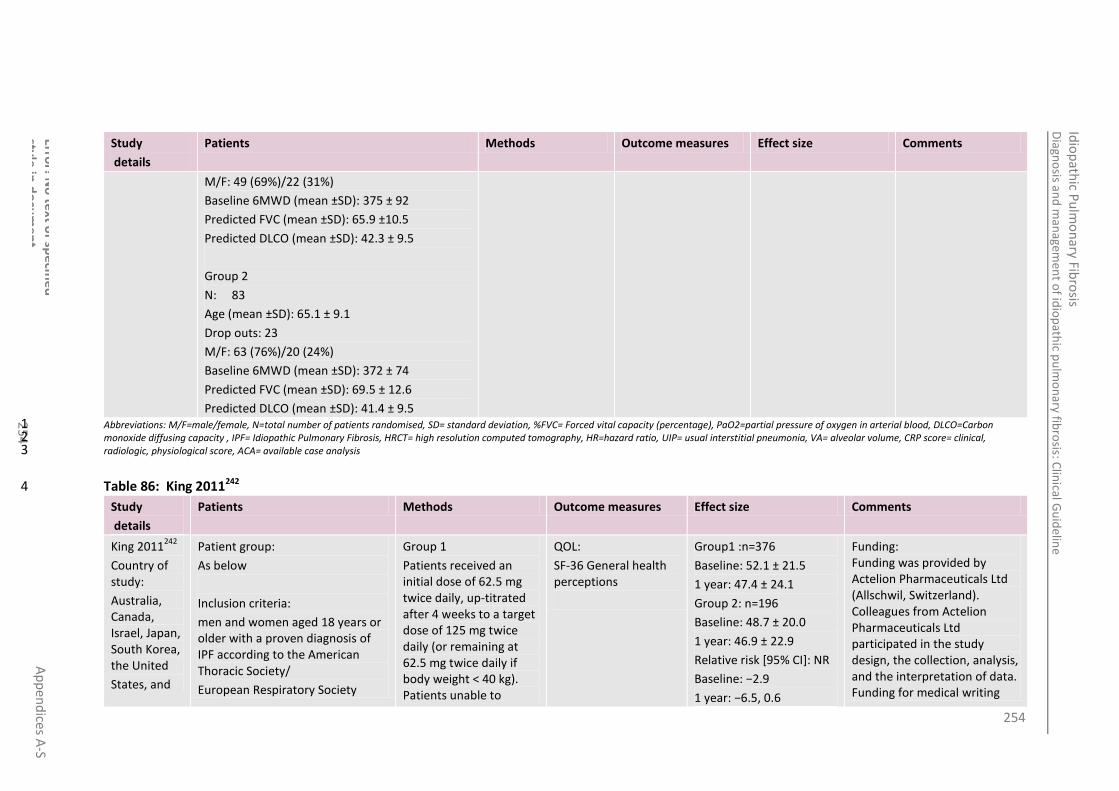
254
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
25
4
Study
details
Patients Methods Outcome measures Effect size Comments
M/F: 49 (69%)/22 (31%)
Baseline 6MWD (mean ±SD): 375 ± 92
Predicted FVC (mean ±SD): 65.9 ±10.5
Predicted DLCO (mean ±SD): 42.3 ± 9.5
Group 2
N: 83
Age (mean ±SD): 65.1 ± 9.1
Drop outs: 23
M/F: 63 (76%)/20 (24%)
Baseline 6MWD (mean ±SD): 372 ± 74
Predicted FVC (mean ±SD): 69.5 ± 12.6
Predicted DLCO (mean ±SD): 41.4 ± 9.5 Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon 1 monoxide diffusing capacity , IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, UIP= usual interstitial pneumonia, VA= alveolar volume, CRP score= clinical, 2 radiologic, physiological score, ACA= available case analysis 3
Table 86: King 2011242 4
Study
details
Patients Methods Outcome measures Effect size Comments
King 2011242
Country of study:
Australia, Canada, Israel, Japan, South Korea, the United
States, and
Patient group:
As below
Inclusion criteria:
men and women aged 18 years or older with a proven diagnosis of IPF according to the American Thoracic Society/
European Respiratory Society
Group 1
Patients received an initial dose of 62.5 mg twice daily, up-titrated after 4 weeks to a target dose of 125 mg twice daily (or remaining at 62.5 mg twice daily if body weight < 40 kg). Patients unable to
QOL:
SF-36 General health perceptions
Group1 :n=376
Baseline: 52.1 ± 21.5
1 year: 47.4 ± 24.1
Group 2: n=196
Baseline: 48.7 ± 20.0
1 year: 46.9 ± 22.9
Relative risk [95% CI]: NR
Baseline: −2.9
1 year: −6.5, 0.6
Funding: Funding was provided by Actelion Pharmaceuticals Ltd (Allschwil, Switzerland). Colleagues from Actelion Pharmaceuticals Ltd participated in the study design, the collection, analysis, and the interpretation of data. Funding for medical writing

255
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
25
5
Study
details
Patients Methods Outcome measures Effect size Comments
13 countries in Europe
Study design:
prospective, multicentre, randomised, double-blind,
placebo-controlled, parallel-group, event-driven, morbidity–mortality
trial
Who was blinded: (if RCT)
Setting:
teaching and community hospitals
Duration of follow-up:
1 year
statement, of less than 3 years’ duration, and with diagnosis confirmed by surgical lung biopsy
Exclusion criteria:
Severe concomitant illness limiting life expectancy (<1 year); severe restrictive lung disease (forced vital capacity [FVC] <50% of predicted or <1.2 L [formula reported in E1], diffusing capacity for carbon monoxide [DLCO] <30% of predicted or residual volume [RV] ≥120% of obstructive lung disease (forced expiratory volume in 1 second [FEV1] ÷ FVC <0.65); a documented, sustained improvement in IPF up to 12 months prior to randomisation; recent pulmonary or upper respiratory tract infection (≤4 weeks prior to randomisation); acute or chronic impairment (other than dyspnoea) limiting ability to comply with study requirements; chronic heart failure; serum levels of alanine
aminotransferase or aspartate aminotransferase >1.5 × upper limit of normal; moderate-to-severe hepatic impairment; and, serum creatinine ≥2.5 mg·dL−1.
tolerate target dose could be maintained on initial dose
Group 2
matching placebo
p value: NR assistance during the preparation of this manuscript was provided by Actelion Pharmaceuticals Ltd
Limitations:
None
Additional outcomes:
None
Notes:
Eligible patients were randomized 2:1 to receive oral bosentan or matching placebo, respectively.
Intention to treat analysis performed,
Patients were assessed at baseline, at randomization, and every 4 months thereafter until BUILD-3 End of Study, which was scheduled to be declared when 202 primary endpoint events were confirmed. In cases of premature discontinuation of study treatment, patients underwent an End of Study Treatment assessment and
Dyspnoea
Transition dyspnoea index at 1 year
Group1: −1.7 ± 3.5
N= 383
Group 2: −1.7 ± 3.6
N= 199
Relative risk [95% CI]: 0.1 (−0.5, 0.7)
p value: NR
Mortality Group1: 11/407
Group 2: 6/209
Relative risk [95% CI]: NR
p value: NR
Adverse events (observed in ≥5% of bosentan treated patients): abnormal LFTs
Group1: 30/406 (7.4%)
Group 2: 0/209 (0%)
Relative risk [95% CI]: NR
p value: NR
Adverse events (observed in ≥5% of bosentan treated patients): drug hypersensitivity
Group1: 1/406 (7.4%)
Group 2: 0/209 (0%)
Relative risk [95% CI]: NR
p value: NR
Time to IPF worsening (excluding death).
HR (95% CI): 0.85 (0.654-1.107)
Time to death up to BUILD-3 End of Study.
HR (95% CI): 1.039 (0.6-1.798)

256
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
25
6
Study
details
Patients Methods Outcome measures Effect size Comments
Also patients were not enrolled if, within 4 weeks preceding randomization, they received chronic treatment for IPF with: oral corticosteroids (>20 mg per day prednisone or equivalent), immunosuppressive or cytotoxic drugs, antifibrotic drugs, or N-acetylcysteine. Patients treated using glibenclamide (glyburide) and calcineurin inhibitors within 1 week preceding randomization were also not enrolled
All patients
N: 616
Age (mean):
Drop outs: 95
M/F: 429(69.6%)/187 (30.4%)
Group 1
N: 407
Age (mean): 63.8 ± 8.4
Drop outs: 75
M/F: 296 (72.7%) /111(27.3%)
Predicted FVC (mean ±SD): 74.9 ±14.8
Predicted DLCO (mean ±SD): 47.7 ±11.9
remained in the trial until the BUILD-3 End of Study was declared.
Patients were assigned a unique randomization number via a centralized Interactive Randomization System which designated which study treatment was to be dispensed at randomization, at each patient visit to the site, and each time a patient’s dose was adjusted. The randomization code was generated using Visual Basic 6.0. The investigators, study staff, patients, monitors, and study sponsor remained blinded to treatment assignment until study database closure
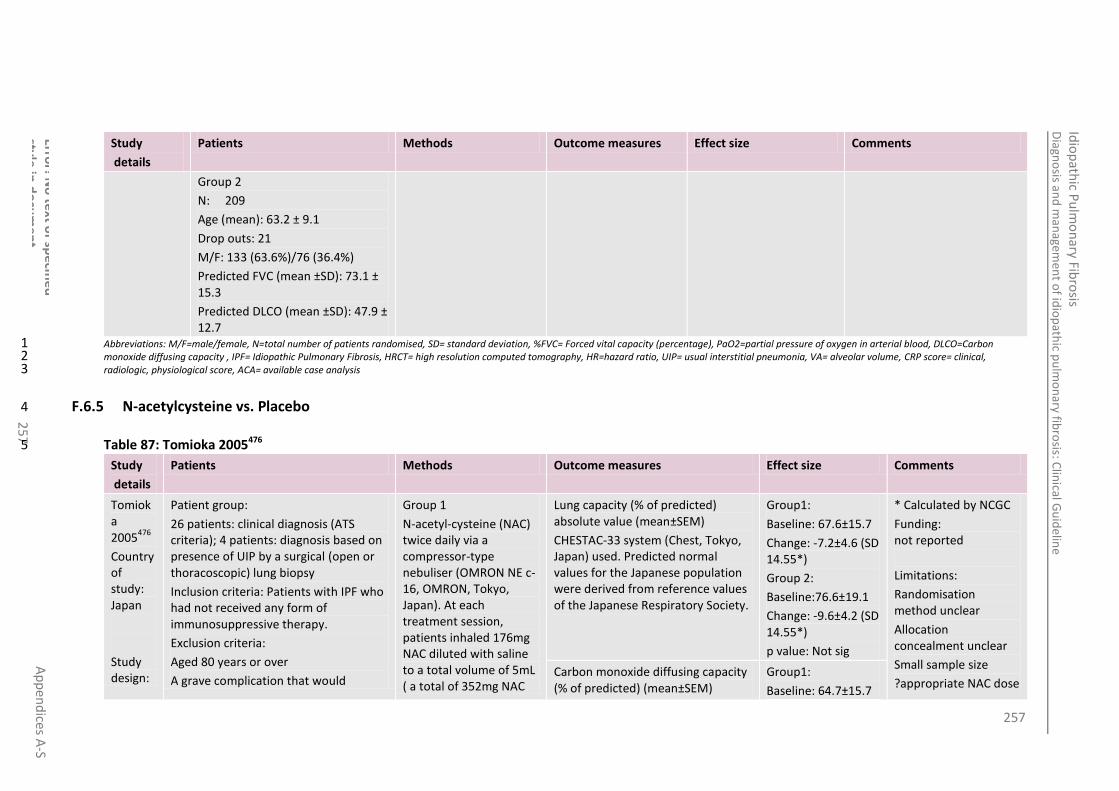
257
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
25
7
Study
details
Patients Methods Outcome measures Effect size Comments
Group 2
N: 209
Age (mean): 63.2 ± 9.1
Drop outs: 21
M/F: 133 (63.6%)/76 (36.4%)
Predicted FVC (mean ±SD): 73.1 ± 15.3
Predicted DLCO (mean ±SD): 47.9 ± 12.7
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon 1 monoxide diffusing capacity , IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, UIP= usual interstitial pneumonia, VA= alveolar volume, CRP score= clinical, 2 radiologic, physiological score, ACA= available case analysis 3
F.6.5 N-acetylcysteine vs. Placebo 4
Table 87: Tomioka 2005476 5
Study
details
Patients Methods Outcome measures Effect size Comments
Tomioka 2005
476
Country of study: Japan
Study design:
Patient group:
26 patients: clinical diagnosis (ATS criteria); 4 patients: diagnosis based on presence of UIP by a surgical (open or thoracoscopic) lung biopsy
Inclusion criteria: Patients with IPF who had not received any form of immunosuppressive therapy.
Exclusion criteria:
Aged 80 years or over
A grave complication that would
Group 1
N-acetyl-cysteine (NAC) twice daily via a compressor-type nebuliser (OMRON NE c-16, OMRON, Tokyo, Japan). At each treatment session, patients inhaled 176mg NAC diluted with saline to a total volume of 5mL ( a total of 352mg NAC
Lung capacity (% of predicted) absolute value (mean±SEM)
CHESTAC-33 system (Chest, Tokyo, Japan) used. Predicted normal values for the Japanese population were derived from reference values of the Japanese Respiratory Society.
Group1:
Baseline: 67.6±15.7
Change: -7.2±4.6 (SD 14.55*)
Group 2:
Baseline:76.6±19.1
Change: -9.6±4.2 (SD 14.55*)
p value: Not sig
* Calculated by NCGC
Funding: not reported
Limitations:
Randomisation method unclear
Allocation concealment unclear
Small sample size
?appropriate NAC dose Carbon monoxide diffusing capacity (% of predicted) (mean±SEM)
Group1:
Baseline: 64.7±15.7
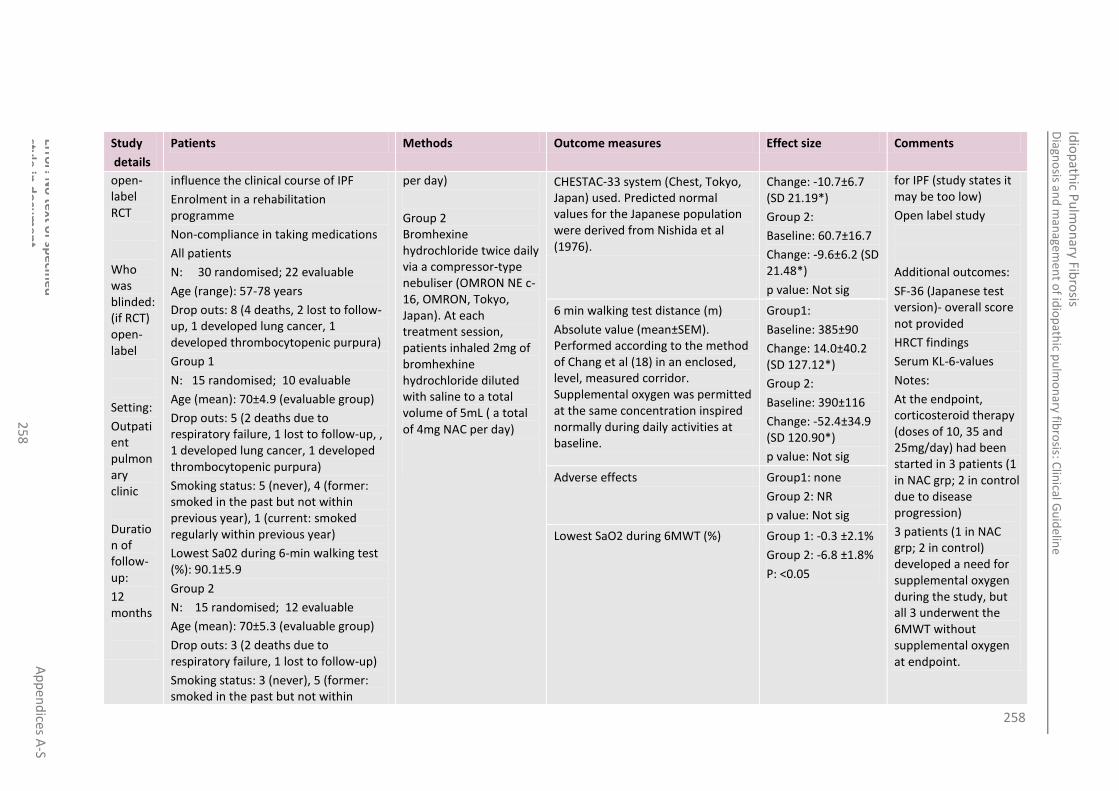
258
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
25
8
Study
details
Patients Methods Outcome measures Effect size Comments
open-label RCT
Who was blinded: (if RCT) open-label
Setting:
Outpatient pulmonary clinic
Duration of follow-up:
12 months
influence the clinical course of IPF
Enrolment in a rehabilitation programme
Non-compliance in taking medications
All patients
N: 30 randomised; 22 evaluable
Age (range): 57-78 years
Drop outs: 8 (4 deaths, 2 lost to follow-up, 1 developed lung cancer, 1 developed thrombocytopenic purpura)
Group 1
N: 15 randomised; 10 evaluable
Age (mean): 70±4.9 (evaluable group)
Drop outs: 5 (2 deaths due to respiratory failure, 1 lost to follow-up, , 1 developed lung cancer, 1 developed thrombocytopenic purpura)
Smoking status: 5 (never), 4 (former: smoked in the past but not within previous year), 1 (current: smoked regularly within previous year)
Lowest Sa02 during 6-min walking test (%): 90.1±5.9
Group 2
N: 15 randomised; 12 evaluable
Age (mean): 70±5.3 (evaluable group)
Drop outs: 3 (2 deaths due to respiratory failure, 1 lost to follow-up)
Smoking status: 3 (never), 5 (former: smoked in the past but not within
per day)
Group 2 Bromhexine hydrochloride twice daily via a compressor-type nebuliser (OMRON NE c-16, OMRON, Tokyo, Japan). At each treatment session, patients inhaled 2mg of bromhexhine hydrochloride diluted with saline to a total volume of 5mL ( a total of 4mg NAC per day)
CHESTAC-33 system (Chest, Tokyo, Japan) used. Predicted normal values for the Japanese population were derived from Nishida et al (1976).
Change: -10.7±6.7 (SD 21.19*)
Group 2:
Baseline: 60.7±16.7
Change: -9.6±6.2 (SD 21.48*)
p value: Not sig
for IPF (study states it may be too low)
Open label study
Additional outcomes:
SF-36 (Japanese test version)- overall score not provided
HRCT findings
Serum KL-6-values
Notes:
At the endpoint, corticosteroid therapy (doses of 10, 35 and 25mg/day) had been started in 3 patients (1 in NAC grp; 2 in control due to disease progression)
3 patients (1 in NAC grp; 2 in control) developed a need for supplemental oxygen during the study, but all 3 underwent the 6MWT without supplemental oxygen at endpoint.
6 min walking test distance (m)
Absolute value (mean±SEM). Performed according to the method of Chang et al (18) in an enclosed, level, measured corridor. Supplemental oxygen was permitted at the same concentration inspired normally during daily activities at baseline.
Group1:
Baseline: 385±90
Change: 14.0±40.2 (SD 127.12*)
Group 2:
Baseline: 390±116
Change: -52.4±34.9 (SD 120.90*)
p value: Not sig
Adverse effects Group1: none
Group 2: NR
p value: Not sig
Lowest SaO2 during 6MWT (%) Group 1: -0.3 ±2.1%
Group 2: -6.8 ±1.8%
P: <0.05

259
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
25
9
Study
details
Patients Methods Outcome measures Effect size Comments
previous year), 4 (current: smoked regularly within previous year)
Lowest Sa02 during 6-min walking test (%): 91.1±5.9
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood , DLCO=Carbon 1 monoxide diffusing capacity, IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, UIP= usual interstitial pneumonia, VA= alveolar volume, CRP score= clinical, 2 radiologic, physiological score, ACA= available case analysis 3
F.6.6 N-acetylcysteine vs. no treatment 4
Table 88: Homma 2012189 5
Study
details
Patients Methods Outcome measures Effect size Comments
Homma 2012189
Comparison:
NAC therapy
versus nil NAC therapy
Setting:
Multicentre trial;
27 centres in Japan
Duration of follow-up:
48 weeks
Design:
Parallel group
Patient group:
Early stage (I or II) IPF patients aged between 50-79 years as diagnosed by ATS/ERS consensus. HRCT evidence of UIP mandatory.
Inclusion criteria:
Firm clinical and radiological diagnosis of IPF at stage I or II and a lowest arterial O2 saturation of > 90% during 6MWD test.
Group 1: (n=44)
352.4mg N-Acetylcysteine (NAC) diluted with saline to a volume of 4ml nebulised twice daily with microair nebulisers (NE-U222, Omron, Tokyo, Japan)
Group 2: (n=46)
‘No treatment (or placebo)’
Number of patients who subjectively felt their dyspnoea had improved compared to deteriorated at 48 weeks
Group 1: 33/38
Group2:32/38
NS Difference
Funding:
Grant from Ministry of Health, Labour and Welfare of Japan. Authors thank Pharma KK and Niphix KK for their help with study management and data analysis
Limitations:
Very High Risk of Bias overall
High risk selection bias:
Mean change in FVC (l) from baseline (mean +/- SD) at 48 weeks
Group 1: -0.09 +/- 0.3
Group2: -0.15 +/- 0.2
NS Difference
Change in lowest SaO2 (%) during 6MWT, 6MWD (m), VC (%) and (% of predicted, DLCO (%) and (% of predicted), TLC (%) and (%) of predicted at 48 weeks
No data presented but narrative text says NS difference between group 1 and 2.
Number of patients with IPF exacerbation
Group 1: 1
Group 2: 4
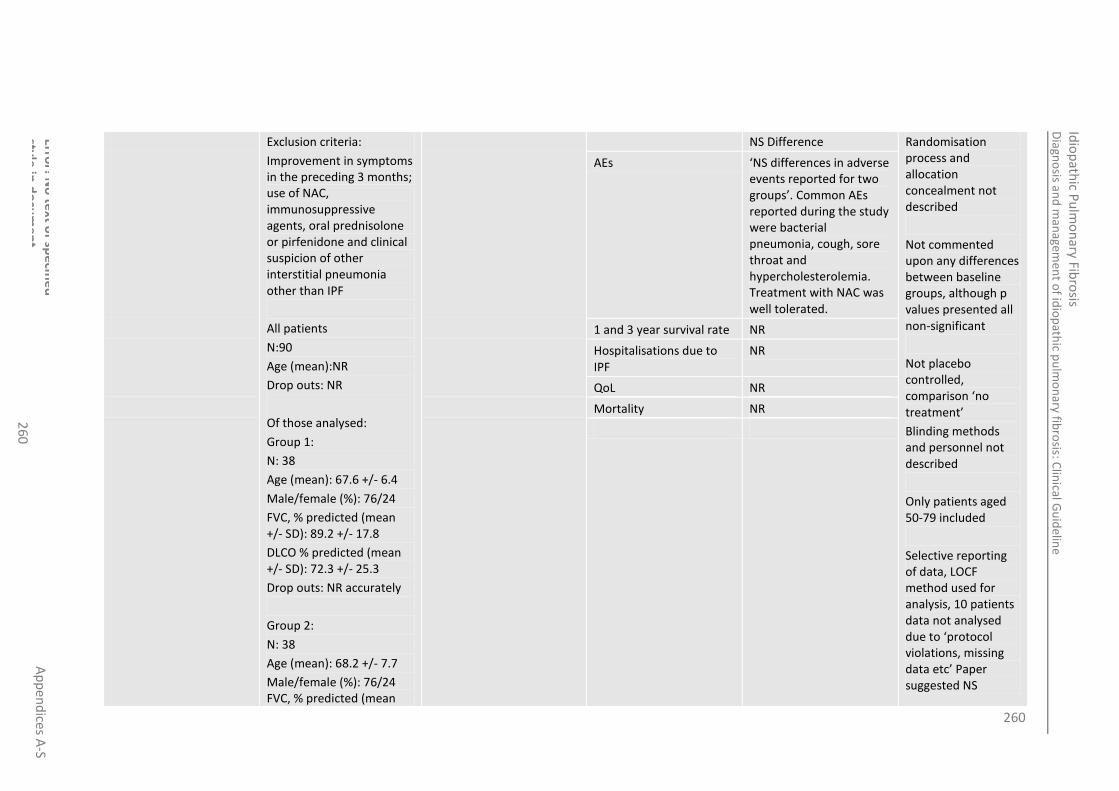
260
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
26
0
Exclusion criteria:
Improvement in symptoms in the preceding 3 months; use of NAC, immunosuppressive agents, oral prednisolone or pirfenidone and clinical suspicion of other interstitial pneumonia other than IPF
All patients
N:90
Age (mean):NR
Drop outs: NR
Of those analysed:
Group 1:
N: 38
Age (mean): 67.6 +/- 6.4
Male/female (%): 76/24
FVC, % predicted (mean +/- SD): 89.2 +/- 17.8
DLCO % predicted (mean +/- SD): 72.3 +/- 25.3
Drop outs: NR accurately
Group 2:
N: 38
Age (mean): 68.2 +/- 7.7
Male/female (%): 76/24 FVC, % predicted (mean
NS Difference Randomisation process and allocation concealment not described
Not commented upon any differences between baseline groups, although p values presented all non-significant
Not placebo controlled, comparison ‘no treatment’
Blinding methods and personnel not described
Only patients aged 50-79 included
Selective reporting of data, LOCF method used for analysis, 10 patients data not analysed due to ‘protocol violations, missing data etc’ Paper suggested NS
AEs ‘NS differences in adverse events reported for two groups’. Common AEs reported during the study were bacterial pneumonia, cough, sore throat and hypercholesterolemia. Treatment with NAC was well tolerated.
1 and 3 year survival rate NR
Hospitalisations due to IPF
NR
QoL NR
Mortality NR

261
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
26
1
+/- SD): 88.7 +/-15.5
DLCO % predicted (mean +/- SD):64.4 +/-20.1
Drop outs: NR accurately
See limitations section for discussion of dropouts and selective reporting
difference in excluded from analysis population between arms. Reason for Dropouts not given and selective analysed subset.
Serum markers of pneumocyte injury (KL-6, surfactant proteins A and D)
Disease progression as determined by HRCT
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood , DLCO=Carbon 1 monoxide diffusing capacity, IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, UIP= usual interstitial pneumonia, VA= alveolar volume, CRP score= clinical, 2 radiologic, physiological score, ACA= available case analysis 3
F.6.7 Co-trimoxazole vs. Placebo 4
Table 89: Shulgina 2013441 5
Study
details
Patients Methods Outcome measures Effect size Comments
Shulgina 2013 441
Country of study:
Patient group: Fibrotic idiopathic interstitial pneumonia (89% with definite/probable IPF)
Inclusion criteria:
Age : >40 years
MRC dyspnoea score ≥2
Group 1: co-trimoxazole 960mg twice daily orally in addition to usual care
Group 2: Placebo tablets, twice daily
Mortality (ITT analysis) Group1: 18/95 (19%)
Group 2: 19/86 (22%)
p value: 0.379
Funding:
East Anglia Thoracic Society
NIHR Research for Patient benefit programme
Boehringer Ingelheim Mortality (per-protocol analysis) Group1: 3/53
Group 2: 14/65

262
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
26
2
Study
details
Patients Methods Outcome measures Effect size Comments
UK
Study design:RCT
Who was blinded: (if RCT) double-blind
Setting: 28 university and district hospital in England and Wales
Duration of follow-up:
Treatment regimens had remained unchanged for at least 6 weeks
A protocol amendment was made to include patients not receiving immunosuppressive therapy as long as they had progressive disease with deteriorating lung function and those receiving anti-oxidants to reflect changes in UK prescribing practice.
Exclusion criteria:
Child-bearing potential
Secondary cause for pulmonary fibrosis identified
Receiving immunosuppressant medication other than prednisolone, azathioprine or mycophenolate mofetil
Co-trimoxazole allergy or intolerance
Untreated folate or B12 deficiency
Respiratory tract infection within 2 months prior to randomisation
Significant concomitant disease that could affect subject safety or influence study outcome.
All patients
N: 181 (ITT analysis)
Age: 71.6 ±8.5 years (mean)
FVc (% predicted): 70.7 ±21.2
p value: 0.02 non-commercial educational grant Limitations:
Not all patients had IPF
Patients in the co-trimoxazole group may have had shorter disease duration
Additional outcomes:
Hospital days
Medicine increase/ decrease
Oxygen increase/ decrease
Notes:
Outcomes presented as ‘adjusted for baseline’
ITT and per-protocol analysis both used
Randomisation: performed centrally using a computer generated randomisation code and the site research pharmacist was
FVC (ml) ITT analysis Group1: -195.67 (SD 288.82)
Group 2:-182.22 (SD 330.15)
p value: 0.988 (95% CI -0.11, 0.11)
FVC % predicted ITT analysis Group1: -4.65 (SD 9.96)
Group 2: -4.79 (SD 8.7)
p value: 0.978 (95% CI -3.22, 3.32)
DLCO (mmol/min/KPa) ITT analysis Group 1: -0.3 (SD0.68)
Group 2: -0.22 (SD 0.81)
P value: 0.48 (95% CI -0.4, 0.19)
DLCO % predicted ITT analysis Group 1: -3.67
Group 2: -3.88
P value: 0.459 (85% CI -4.88, 2.21)
SGRQ total (units) Group 1: 0.71
Group 2: 1.78
P value: 0.599 (95% CI -6.13, 3.54)
6MWD (metres) Group 1: -18.7
Group 2: -19.48

263
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
26
3
Study
details
Patients Methods Outcome measures Effect size Comments
DLCO (% predicted): 37.5±11.5
Drop outs:
Group 1 (co-trimoxazole)
N: 95
Age (mean): 72.38 (SD 8.45)
Definite IPF (UIP histopathology, honeycombing on HRCT or in report on destroyed HRCT): 37
Probable IPF (Fell probability score ≥0.6): 46
Probable IPF (all features consistent with UIP except honeycombing on HRCT or in report on destroyed HRCT): 46
Co-existing emphysema: 6 (6.3%)
Drop outs: 4% did not receive more than 80% of the scheduled study drug doses
Group 2 (placebo)
N: 86
Age (mean): 70.65 (SD 8.56)
Definite IPF (UIP histopathology, honeycombing on HRCT or in report on
P value: 0.835 (95% CI -53.55, 43.24)
informed of the code by email via Norwich Clinical Trials Unit.
Patients were randomised with stratification for the site and the use of azathioprine/ mycophenolate mofetil.
A blinded retrospective radiological review was undertaken by 2 specialist respiratory radiologists using the criteria of Silva et al., 2008 for those patients where a histopathological diagnosis of UIP or NSIP was not available. In addition, HRCT scans of patients without definite IPF were scored according to the algorithm
6MW desaturation of 4% or more Group 1: 16/20 (80%)
Group 2: 31/35 (88.6%)
P value: 0.634 (95% CI -2.37, 4.1)
MRC score Group 1: 0.07 (SD 0.72)
Group 2: 0.21 (SD 0.82)
P value: 0.533 (95% CI -0.37, 0.19)
Adverse events (GI), number of individuals with 1 or more
Group 1: 41 (44.6%)
Group 2: 21 (24.4%)
P value: 0.005
Adverse events (nausea), number of individuals with 1 or more
Group 1: 17 (18.5%)
Group 2: 6 (7%)
P value: 0.022
Adverse events (immune system disorder), number of individuals with 1 or more
Group 1: 0
Group 2: 1 (1.2%)
p value: 0.483
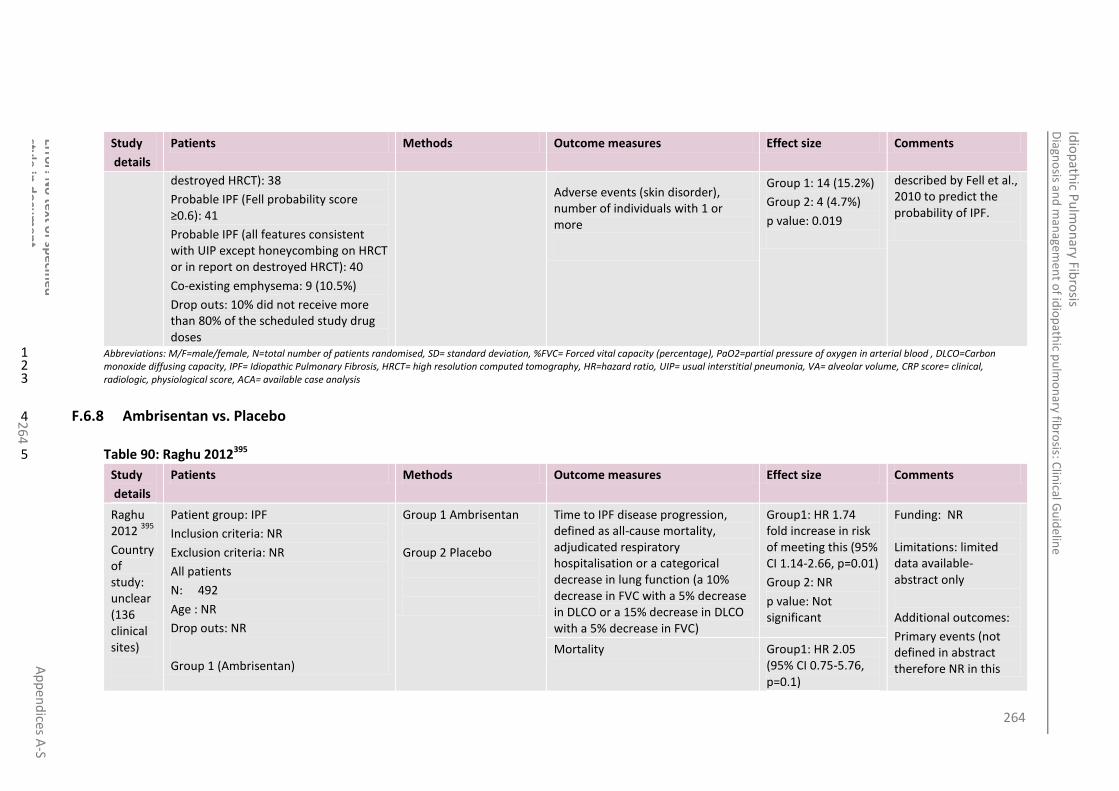
264
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
26
4
Study
details
Patients Methods Outcome measures Effect size Comments
destroyed HRCT): 38
Probable IPF (Fell probability score ≥0.6): 41
Probable IPF (all features consistent with UIP except honeycombing on HRCT or in report on destroyed HRCT): 40
Co-existing emphysema: 9 (10.5%)
Drop outs: 10% did not receive more than 80% of the scheduled study drug doses
Adverse events (skin disorder), number of individuals with 1 or more
Group 1: 14 (15.2%)
Group 2: 4 (4.7%)
p value: 0.019
described by Fell et al., 2010 to predict the probability of IPF.
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood , DLCO=Carbon 1 monoxide diffusing capacity, IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, UIP= usual interstitial pneumonia, VA= alveolar volume, CRP score= clinical, 2 radiologic, physiological score, ACA= available case analysis 3
F.6.8 Ambrisentan vs. Placebo 4
Table 90: Raghu 2012395 5
Study
details
Patients Methods Outcome measures Effect size Comments
Raghu 2012
395
Country of study: unclear (136 clinical sites)
Patient group: IPF
Inclusion criteria: NR
Exclusion criteria: NR
All patients
N: 492
Age : NR
Drop outs: NR
Group 1 (Ambrisentan)
Group 1 Ambrisentan
Group 2 Placebo
Time to IPF disease progression, defined as all-cause mortality, adjudicated respiratory hospitalisation or a categorical decrease in lung function (a 10% decrease in FVC with a 5% decrease in DLCO or a 15% decrease in DLCO with a 5% decrease in FVC)
Group1: HR 1.74 fold increase in risk of meeting this (95% CI 1.14-2.66, p=0.01)
Group 2: NR
p value: Not significant
Funding: NR Limitations: limited data available- abstract only
Additional outcomes:
Primary events (not defined in abstract therefore NR in this
Mortality Group1: HR 2.05 (95% CI 0.75-5.76, p=0.1)

265
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
26
5
Study
details
Patients Methods Outcome measures Effect size Comments
Study design:RCT
Who was blinded: (if RCT) double-blind
Setting:
136 clinical sites
Duration of follow-up: 34 weeks
N: NR
Age (mean): NR
Drop outs: NR
Group 2 (Placebo)
N: NR
Age (mean): NR
Drop outs: NR
Group 2: NR
p value: Not significant
table)
Respiratory hospitalisations
Notes:
Abstract only
11% of patients in each group had pulmonary hypertension
Categorical decrease in lung function (a 10% decrease in FVC with a 5% decrease in DLCO or a 15% decrease in DLCO with a 5% decrease in FVC)
Group1: HR 1.53 (95% CI 0.84- 2.78, p=0.109)
Group 2: NR
p value: Not significant
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon 1 monoxide diffusing capacity, IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, UIP= usual interstitial pneumonia, VA= alveolar volume, CRP score= clinical, 2 radiologic, physiological score, ACA= available case analysis 3
4

266
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
26
6
F.6.9 Combination: Prednisolone & azathioprine vs. Prednisolone & placebo 1
Table 91: Raghu 1991400 2
Study
details
Patients Methods Outcome measures Effect size Comments
Raghu 1991
400
Country of study:
USA
Study design:
RCT
Who was blinded: (if RCT) Patients and clinicians
Setting:
Outpatient
Duration of follow-up:
12 months
Patient group:
Newly diagnosed patients with IPF
Symptomatic adult patients with diffuse pulmonary infiltrates
Diagnosis:
Supported by lung biopsy in all patients (23 OLB, 4 transbronchial). All fulfilled:
Progressive dyspnoea from day of onset
Progressive roentgenographic parenchymal abnormality
10% or greater decrease in FVC or total lung capacity compared with previous values; or
20% or greater reduction in DLCO compared with previous values
Inclusion criteria:
Exclusion criteria:
NR
All patients
N: 27
M:F: 12:15
Drop outs: 8
Group 1
Azathioprine plus prednisolone.
Azathioprine was administered at a daily dose of 3mg/kg/day (not to exceed 200mg/day) to the nearest 25mg dose increment for the duration of the trial.
Group 2 Prednisone plus placebo.
Oral prednisone dose: in an initial dose of 1.5mg/kg/day to a maximum of 100mg/day for the first 2 weeks followed by a fortnightly decrease of according to participants’ tolerance until a maintenance dose of 20mg/day or less was reached. A similar number of placebo tablets were dispensed.
All patients
Change in lung capacity (FVC) (% predicted) after 1 year of therapy (mean± SE) measured using an Ohio spirometer and interpreted according to Schoenberg 1978
Group1: +6.5 ±5.3 (*SD 19.83)
Group 2: +1.7 ±7.4 (*SD 26.68)
Mean difference: 6.4 *
p value: 0.87
*Calculated by NCGC
Funding: Virginia Mason Research Centre, Seattle, WA
Limitations:
Unclear allocation concealment
Patients were allowed to cross over between groups
ATS diagnostic criteria not used (HRCT not mandatory)
Additional outcomes:
Change in rest P[A-a]O2 (mmHg)
Numbers who had improved/unchanged or deteriorated
Change in gas transfer (DLCOSB) (% predicted) (mean± SE) after 1 year of therapy measured with a Medscience Model 572 Diffusion corrected for haemoglobin concentration and interpreted according to Ogilvie 1957 and Dinkara 1970
Group1: +7.3 ±5.3 (*SD 19.83)
Group 2: +0.9 ±5.7 (*SD 20.55)
Relative risk [95% CI]:NR
p value: 0.70
Overall survival at 1 year, probability (mean± SE) (estimated from graph therefore only reported here)
Group 1: 0.72
Group 2: 0.70
Overall survival at 3 years, probability
Group1: 0.6
Group 2: 0.55
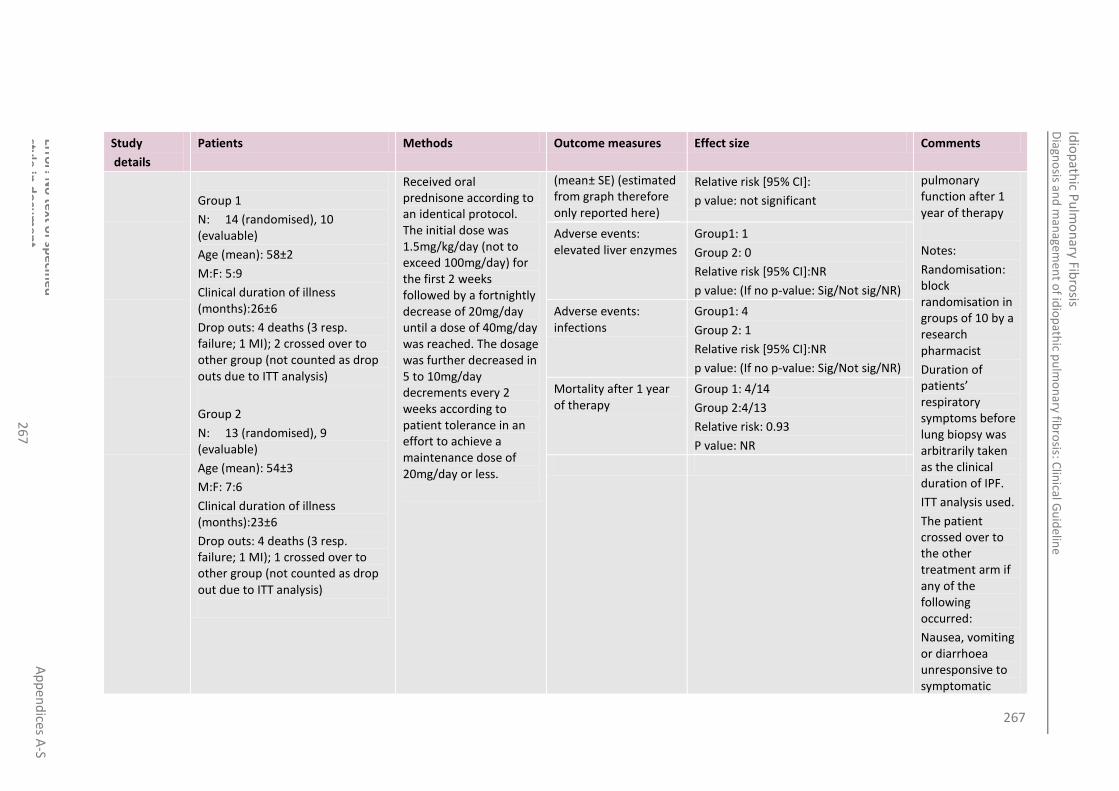
267
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
26
7
Study
details
Patients Methods Outcome measures Effect size Comments
Group 1
N: 14 (randomised), 10 (evaluable)
Age (mean): 58±2
M:F: 5:9
Clinical duration of illness (months):26±6
Drop outs: 4 deaths (3 resp. failure; 1 MI); 2 crossed over to other group (not counted as drop outs due to ITT analysis)
Group 2
N: 13 (randomised), 9 (evaluable)
Age (mean): 54±3
M:F: 7:6
Clinical duration of illness (months):23±6
Drop outs: 4 deaths (3 resp. failure; 1 MI); 1 crossed over to other group (not counted as drop out due to ITT analysis)
Received oral prednisone according to an identical protocol. The initial dose was 1.5mg/kg/day (not to exceed 100mg/day) for the first 2 weeks followed by a fortnightly decrease of 20mg/day until a dose of 40mg/day was reached. The dosage was further decreased in 5 to 10mg/day decrements every 2 weeks according to patient tolerance in an effort to achieve a maintenance dose of 20mg/day or less.
(mean± SE) (estimated from graph therefore only reported here)
Relative risk [95% CI]:
p value: not significant
pulmonary function after 1 year of therapy
Notes:
Randomisation: block randomisation in groups of 10 by a research pharmacist
Duration of patients’ respiratory symptoms before lung biopsy was arbitrarily taken as the clinical duration of IPF.
ITT analysis used.
The patient crossed over to the other treatment arm if any of the following occurred:
Nausea, vomiting or diarrhoea unresponsive to symptomatic
Adverse events: elevated liver enzymes
Group1: 1
Group 2: 0
Relative risk [95% CI]:NR
p value: (If no p-value: Sig/Not sig/NR)
Adverse events: infections
Group1: 4
Group 2: 1
Relative risk [95% CI]:NR
p value: (If no p-value: Sig/Not sig/NR)
Mortality after 1 year of therapy
Group 1: 4/14
Group 2:4/13
Relative risk: 0.93
P value: NR

268
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
26
8
Study
details
Patients Methods Outcome measures Effect size Comments
therapy
WBC<3500/ml
Platelet count<80,000/ml
Respiratory failure requiring mechanical ventilation
Coma
Abnormal LFTs
Rapid disease progression
Patient’s request Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood , DLCO=Carbon 1 monoxide diffusing capacity, IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, UIP= usual interstitial pneumonia, VA= alveolar volume, CRP score= clinical, 2 radiologic, physiological score, ACA= available case analysis 3
F.6.10 Combination: Prednisolone & azathioprine & n-acetylcysteine vs. Azathioprine & prednisolone 4
Table 92: Demedts 2005105 5
Study
details
Patients Methods Outcome measures Effect size Comments
Demedts 2005
105
Country of study:
Multinational: 36 centres in 6
Patient group:
IPF
Inclusion criteria:
Age 18-75 years with a histological or radiologic pattern of UIP, with other causes ruled out
Group 1
Corticosteroids, azathioprine and acetylcysteine
N-acetylcysteine (Fluimucil, Zambon Group) in 600mg
Mortality (12 month follow-up) ITT analysis
Group1: 7/80 (8.8%)
Group 2: 8/75 (10.7%)
Relative risk [95% CI]:0.82 (0.31-2.15)
p value: 0.69
Funding: Zambon Group
Limitations:
High drop-out rate: only 30% of initially
FVC (litres) (12 month follow-up) ACA
Baseline
Group1: 2.29±0.68
Group 2:2.36±0.74

269
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
26
9
Study
details
Patients Methods Outcome measures Effect size Comments
countries (Germany, France, Spain, Belgium, the Netherlands and Italy)
Study design:
RCT
Who was blinded: patients, clinicians and investigators
Setting:
Duration of follow-up:
1 year
HRCT very suggestive of, or consistent with, a diagnosis of UIP
Patients <50 years: open or thorascopic lung biopsy was mandatory and showed a pattern of UIP
Bronchoalveolar lavage must have been performed at any time before inclusion and must have failed to show features supporting alternative diagnoses.
Duration of disease >3 months
Bibasilar inspiratory crackles
Dyspnoea scores of at least 2 on a scale of 0 (min) and 20 (max)
Vital capacity no more than 80% predicted
Single breath DLCO <80% predicted
At least 2 of the 3 members of each committee or at least 2 members of the radiology committee (if no biopsy was available) had to confirm the diagnosis of UIP.
Exclusion criteria:
effervescent tablets 3 times daily.
Group 2 Corticosteroids and azathioprine
Matched placebo
All patients
Usual care, as recommended by ATS/ERS plus:
Prednisone:
starting dose 0.5 per kg of body weight per day
month 2: 0.4mg/kg/day
month 3: 0.3 mg/kg/day
dose progressively reduced to 10mg per day in months 4,5 and 6 and this dose was maintained until month 12.
Azathioprine:
2mg/kg/day
12 months
Group1: 2.31±0.79 n=55
Group 2: 2.26±0.72 n=51
randomised patients available for follow-up after 1 year
Patients excluded after randomisation
Total dose of N-acetylcysteine was 1800mg/day which is 3-9x the usual approved dose when administered in COPD
Results for some outcomes not reported fully
Additional outcomes:
FVC (% predicted value)
DLCO (% predicted value)
DLCO:VA
Maximum exercise load
Maximum oxygen uptake
Maximum
FVC (litres) (12 month follow-up) ITT
Baseline
Group1: 2.29±0.68
Group 2:2.36±0.74
12 months
Group1: 2.22±0.77 n=71
Group 2: 2.17±0.71 n=68
DLCO (mmol/min/kPa) (12 month follow-up) ACA
Baseline
Group1: 3.85±1.41
Group 2: 3.90±1.39
12 months
Group1: 4.20± 2.07 n=55
Group 2: 3.46± 1.22 n=51
DLCO (mmol/min/kPa) (12 month follow-up) ITT
Baseline
Group1: 3.85±1.41
Group 2: 3.90±1.39
12 months
Group1: 3.74± 1.99 n=68
Group 2: 3.20± 1.26 n=63
Adverse events: abnormal LFTs
ITT analysis
Group1: 14/80 (18%)
Group 2: 11/75 (15%)

270
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
27
0
Study
details
Patients Methods Outcome measures Effect size Comments
Contraindication to, or no justification for standard regimen of prednisone and azathioprine
Treatment with prednisone at a dose of at least 0.5mg/kg/day or with azathioprine at a dose of at least 2 mg/kg/day during the month before inclusion in the study, or treatment with acetylcysteine at a dose of >600mg/day for >3 months in the previous 3 years.
Concomitant/ pre-existing diseases, abnormalities or treatment at study entry or in the past with drugs (such as antioxidants or anti-fibrotic drugs) that interfere with the diagnosis, severity, therapy or prognosis of IPF.
All patients
N: 182 (randomised)
Group 1
N: 92 (randomised), 80 (confirmed and included)57/80 (71%) completed study
Age (mean): 62±9
M:F (%):69:31
Drop outs: 23 (prohibited therapy:3, withdrawn by
exercise ventilation
CRP score
HRCT score
Dyspnoea
Notes:
1:1 randomisation performed centrally with computer-generated randomisation list stratified in blocks of 4 according to country and whether vital capacity was less than or more than 60% of the predicted value.

271
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
27
1
Study
details
Patients Methods Outcome measures Effect size Comments
investigator: 3, consent withdrawn: 4, adverse events: 2, noncompliance 1, other: 3, deaths due to disease progression:3 , deaths due to respiratory tract infection: 3, deaths due to heart failure: 1)
Group 2
N: 90 (randomised), 75 (confirmed and included), 51/75 (68%) completed study
Age (mean): 64±9
M:F (%):75:25
Drop outs: 24 (prohibited therapy:2, withdrawn by investigator: 2, consent withdrawn: 4, adverse events: 2, noncompliance 2, ineffective treatment or worsening condition: 4, deaths due to disease progression:4 , deaths due to respiratory tract infection: 1, deaths due to cardiac arrest: 1, deaths due to MI: 1, deaths due to cancer: 1)
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial 1 blood, DLCO=Carbon monoxide diffusing capacity , IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, UIP= usual interstitial pneumonia, VA= 2 alveolar volume, CRP score= clinical, radiologic, physiological score, ACA= available case analysis 3
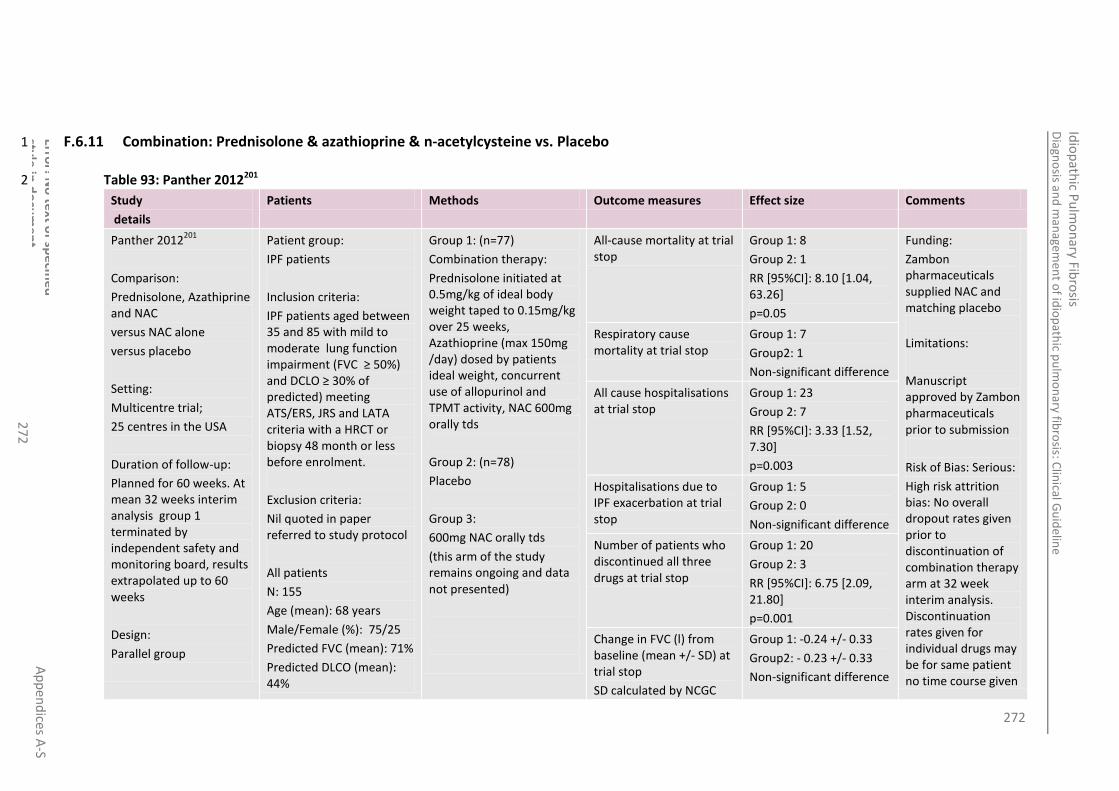
272
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
27
2
F.6.11 Combination: Prednisolone & azathioprine & n-acetylcysteine vs. Placebo 1
Table 93: Panther 2012201 2
Study
details
Patients Methods Outcome measures Effect size Comments
Panther 2012201
Comparison:
Prednisolone, Azathiprine and NAC
versus NAC alone
versus placebo
Setting:
Multicentre trial;
25 centres in the USA
Duration of follow-up:
Planned for 60 weeks. At mean 32 weeks interim analysis group 1 terminated by independent safety and monitoring board, results extrapolated up to 60 weeks
Design:
Parallel group
Patient group:
IPF patients
Inclusion criteria:
IPF patients aged between 35 and 85 with mild to moderate lung function impairment (FVC ≥ 50%) and DCLO ≥ 30% of predicted) meeting ATS/ERS, JRS and LATA criteria with a HRCT or biopsy 48 month or less before enrolment.
Exclusion criteria:
Nil quoted in paper referred to study protocol
All patients
N: 155
Age (mean): 68 years
Male/Female (%): 75/25
Predicted FVC (mean): 71%
Predicted DLCO (mean): 44%
Group 1: (n=77)
Combination therapy:
Prednisolone initiated at 0.5mg/kg of ideal body weight taped to 0.15mg/kg over 25 weeks, Azathioprine (max 150mg /day) dosed by patients ideal weight, concurrent use of allopurinol and TPMT activity, NAC 600mg orally tds
Group 2: (n=78)
Placebo
Group 3:
600mg NAC orally tds
(this arm of the study remains ongoing and data not presented)
All-cause mortality at trial stop
Group 1: 8
Group 2: 1
RR [95%CI]: 8.10 [1.04, 63.26]
p=0.05
Funding:
Zambon pharmaceuticals supplied NAC and matching placebo
Limitations:
Manuscript approved by Zambon pharmaceuticals prior to submission
Risk of Bias: Serious:
High risk attrition bias: No overall dropout rates given prior to discontinuation of combination therapy arm at 32 week interim analysis. Discontinuation rates given for individual drugs may be for same patient no time course given
Respiratory cause mortality at trial stop
Group 1: 7
Group2: 1
Non-significant difference
All cause hospitalisations at trial stop
Group 1: 23
Group 2: 7
RR [95%CI]: 3.33 [1.52, 7.30]
p=0.003
Hospitalisations due to IPF exacerbation at trial stop
Group 1: 5
Group 2: 0
Non-significant difference
Number of patients who discontinued all three drugs at trial stop
Group 1: 20
Group 2: 3
RR [95%CI]: 6.75 [2.09, 21.80]
p=0.001
Change in FVC (l) from baseline (mean +/- SD) at trial stop
SD calculated by NCGC
Group 1: -0.24 +/- 0.33
Group2: - 0.23 +/- 0.33
Non-significant difference
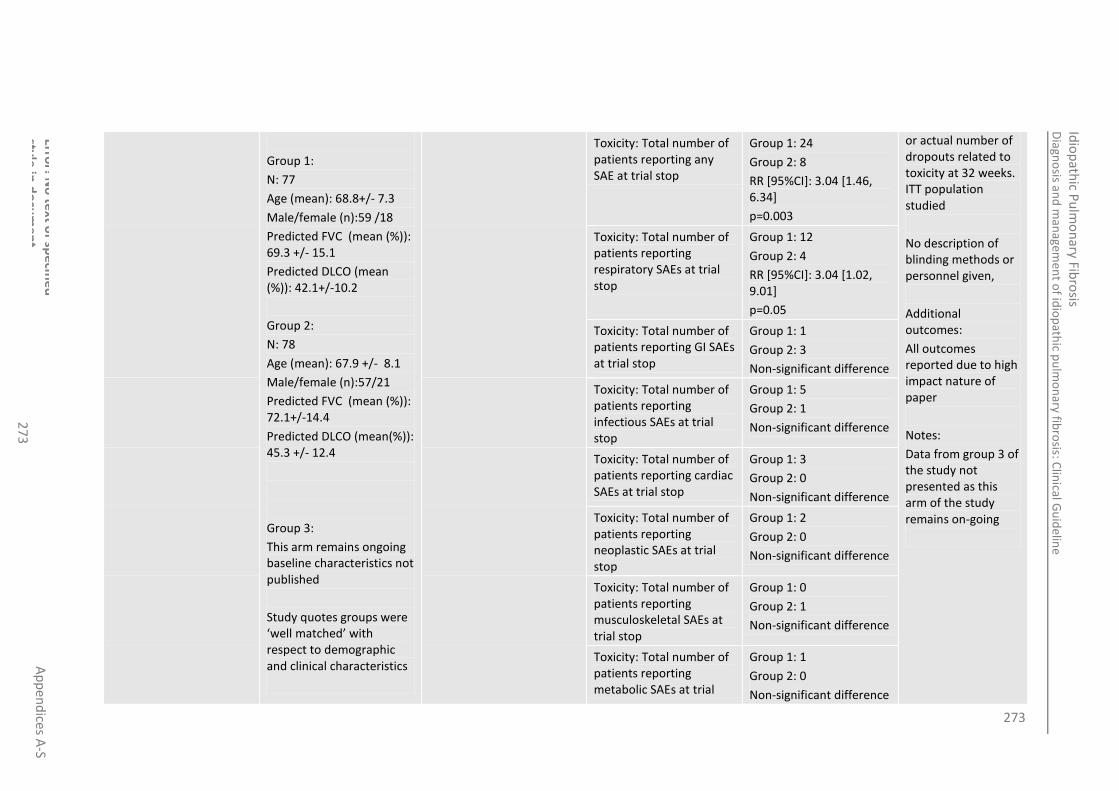
273
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
27
3
Group 1:
N: 77
Age (mean): 68.8+/- 7.3
Male/female (n):59 /18
Predicted FVC (mean (%)): 69.3 +/- 15.1
Predicted DLCO (mean (%)): 42.1+/-10.2
Group 2:
N: 78
Age (mean): 67.9 +/- 8.1
Male/female (n):57/21
Predicted FVC (mean (%)): 72.1+/-14.4
Predicted DLCO (mean(%)): 45.3 +/- 12.4
Group 3:
This arm remains ongoing baseline characteristics not published
Study quotes groups were ‘well matched’ with respect to demographic and clinical characteristics
Toxicity: Total number of patients reporting any SAE at trial stop
Group 1: 24
Group 2: 8
RR [95%CI]: 3.04 [1.46, 6.34]
p=0.003
or actual number of dropouts related to toxicity at 32 weeks. ITT population studied
No description of blinding methods or personnel given,
Additional outcomes:
All outcomes reported due to high impact nature of paper
Notes:
Data from group 3 of the study not presented as this arm of the study remains on-going
Toxicity: Total number of patients reporting respiratory SAEs at trial stop
Group 1: 12
Group 2: 4
RR [95%CI]: 3.04 [1.02, 9.01]
p=0.05
Toxicity: Total number of patients reporting GI SAEs at trial stop
Group 1: 1
Group 2: 3
Non-significant difference
Toxicity: Total number of patients reporting infectious SAEs at trial stop
Group 1: 5
Group 2: 1
Non-significant difference
Toxicity: Total number of patients reporting cardiac SAEs at trial stop
Group 1: 3
Group 2: 0
Non-significant difference
Toxicity: Total number of patients reporting neoplastic SAEs at trial stop
Group 1: 2
Group 2: 0
Non-significant difference
Toxicity: Total number of patients reporting musculoskeletal SAEs at trial stop
Group 1: 0
Group 2: 1
Non-significant difference
Toxicity: Total number of patients reporting metabolic SAEs at trial
Group 1: 1
Group 2: 0
Non-significant difference

274
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
27
4
See limitations for notes on dropout and attrition bias
stop
Toxicity: Total number of patients reporting nervous system SAEs at trial stop
Group 1: 1
Group 2: 0
Non-significant difference
Toxicity: Total number of patients reporting reproductive system SAEs at trial stop
Group 1: 1
Group 2: 0
Non-significant difference
Toxicity: Total number of patients reporting any AEs at trial stop
Group 1: 68
Group 2: 61
Non-significant difference
Toxicity: Total number of patients reporting skin AEs at trial stop
Group 1: 13
Group 2: 4
RR [95%CI]: 3.29 [1.12, 9.65]
p=0.03
Toxicity: Total number of patients reporting renal/urinary AEs at trial stop
Group 1: 10
Group 2: 1
RR [95%CI]: 10.13 [1.33, 77.24]
p=0.03
All-cause mortality at 60 weeks (extrapolated)
HR: 9.26
SE:
All-cause mortality or hospitalisation at 60 weeks (extrapolated)
HR:3.74
SE:
All-cause mortality or ≥10% decline in FVC at 60 weeks (extrapolated)
HR:1.46
SE:
1 and 3 year survival rates NR

275
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
27
5
Dyspnoea NR
Gas transfer NR
QoL NR
Performance on sub-maximal walk test
NR
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood , DLCO=Carbon 1 monoxide diffusing capacity, IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, UIP= usual interstitial pneumonia, VA= alveolar volume, CRP score= clinical, 2 radiologic, physiological score, ACA= available case analysis 3
F.7 Lung transplantation 4
Table 94: Charman 200262 5
Study
details
Patients Methods Outcome measures
Effect size Comments
Charman2002
62
Country of study:
UK
Study design:
Retrospective cohort
Who was blinded:
NR
Patient group:
Patients accepted for single, double and heart lung transplant between April 1984-september 1999
Inclusion criteria:
Patients were required to have a life expectancy of 12-24 months, or severely impaired quality of life despite maximal medical therapy.
Acceptance criteria for LTX in line with ATS, ERS and ISHLT
Exclusion criteria:
All patients
Patient data was routinely collected from the time they were accepted for LTX.
Cohort collected from April 1984 – September 1999*
Data is analysed separately for the following groups:
ALL Patients n=100
Single LTX patients n=63
Double/Heart Lung Transplant patients n=37
Died on Waiting List (n)
All Patients: 33
Single LTX patients: 18
Double/Heart Lung Transplant patients: 15
Funding: NR
Limitations:
Doesn’t specify IPF: Cohort is all Pulmonary Fibrosis
Doesn’t account for any confounders – no data given on disease severity at baseline.
Presented as crude data
Additional outcomes:
The same outcomes reported for other diseases
Equity point
Risk profiles
Removed or still waiting (n)
All Patients: 7
Single LTX patients: 3
Double/Heart Lung Transplant patients: 4
Transplanted (n)
All Patients: 60
Single LTX patients: 42
Double/Heart Lung Transplant patients: 18
Days Waiting (Median (IQR))
All Patients: 117 (43, 231)
Single LTX patients: 104 (5,194)
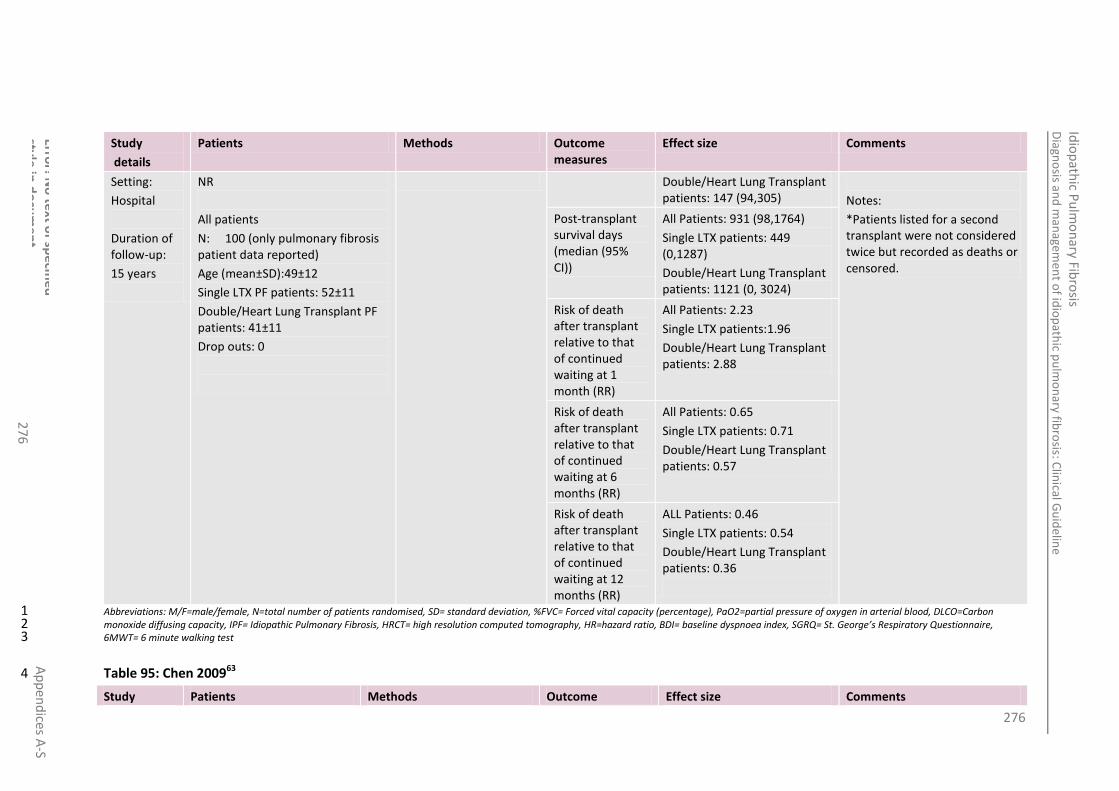
276
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
27
6
Study
details
Patients Methods Outcome measures
Effect size Comments
Setting:
Hospital
Duration of follow-up:
15 years
NR
All patients
N: 100 (only pulmonary fibrosis patient data reported)
Age (mean±SD):49±12
Single LTX PF patients: 52±11
Double/Heart Lung Transplant PF patients: 41±11
Drop outs: 0
Double/Heart Lung Transplant patients: 147 (94,305)
Notes:
*Patients listed for a second transplant were not considered twice but recorded as deaths or censored.
Post-transplant survival days (median (95% CI))
All Patients: 931 (98,1764)
Single LTX patients: 449 (0,1287)
Double/Heart Lung Transplant patients: 1121 (0, 3024)
Risk of death after transplant relative to that of continued waiting at 1 month (RR)
All Patients: 2.23
Single LTX patients:1.96
Double/Heart Lung Transplant patients: 2.88
Risk of death after transplant relative to that of continued waiting at 6 months (RR)
All Patients: 0.65
Single LTX patients: 0.71
Double/Heart Lung Transplant patients: 0.57
Risk of death after transplant relative to that of continued waiting at 12 months (RR)
ALL Patients: 0.46
Single LTX patients: 0.54
Double/Heart Lung Transplant patients: 0.36
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon 1 monoxide diffusing capacity, IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St. George’s Respiratory Questionnaire, 2 6MWT= 6 minute walking test 3
Table 95: Chen 200963 4
Study Patients Methods Outcome Effect size Comments

277
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
27
7
details measures
Chen200963
Country of study:
USA
Study design:
Retrospective cohort
Who was blinded:
NR
Setting:
Hospital
Duration of follow-up:
12 months
Patient group:
All lung transplantation registrants in the United States listed from May 4, 2002 to May 3, 2008 – IPF patient data is presented only
Inclusion criteria:
Age 18 or older with one of four primary diagnoses defined in the OPTN database:
Primary Pulmonary Hypertension
Idiopathic Pulmonary Fibrosis
COPD/Emphysema
Cystic Fibrosis.
Exclusion criteria:
patients classified as secondary pulmonary hypertension
Listings for combined heart-lung
All patients
N: 2981
Drop outs: 0
Group 1
National data from United Network for Organ Sharing used to describe waiting list and post-transplant outcomes for patients before and after implementation of the LAS.
The total cohort was divided by “pre-LAS’’ cohort and a ‘‘post-LAS’’ cohort based on their initial date of registration for lung transplant.
Group 1 - pre LAS
The pre-LAS time frame was defined as the 3-year period before implementation of the LAS (May 4, 2002 to May 3, 2005).
Group 2 – post LAS
The post-LAS time frame was defined as the 3-year period after implementation of the LAS (May 4, 2005 to May 3, 2008).
LTX % 6 months from initial listing for LTX
(Cumulative incidence (95 % CI))
Group 1: 26(23-28)
Group 2: 68 (65-70)
95% CI:NR
P: <0.001
Funding:
Supported in part by NHLBI grant K23 HL086585 (H.C.) and NCRR UCSF-CTSI grant UL1 RR024131 (S.C.S.), and Health Resources and Services Administration contract 231-00-0115. The content is the responsibility of the authors alone and does not necessarily reflect the views or policies of the U.S. Department of Health and Human Services. Conflict of Interest Statement: H.C. served as a consultant to United Therapeutics and received $1,000 in 2007 and 2008. S.C.S. does not have a financial relationship with a commercial entity that has an interest in the subject of this manuscript. J.A.G. has received $205,000 in research funding from Actelion
Pharmaceuticals Ltd. in 2007 and 2008. M.K.G. does not have a financial relationship with a commercial entity that has an interest in the subject of this manuscript. S.R.H. does not have a financial relationship with a commercial entity that has an interest in the subject of
LTX % 12 months from initial listing for LTX
(Cumulative incidence (95 % CI))
Group 1: 38(36-41)
Group 2: 77(74-79)
95% CI:NR
P: <0.001
Waiting list mortality % 6 months from initial listing for LTX
(Cumulative incidence (95 % CI))
Group 1: 15(13-17)
Group 2: 9(8-11)
95% CI:NR
P: <0.001
Waiting list mortality % 12 months from initial listing for LTX
(Cumulative incidence (95 % CI))
Group 1: 21(19-23)
Group 2: 11(10-13)
95% CI:NR
P: <0.001
Post LTX mortality 6 months from initial listing for LTX
Group 1: 14 (11-17)
Group 2: 14 (12-16)
95% CI:NR
P: 0.494

278
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
27
8
N: 1418
Age (mean): 55-9
M/F: 895 /523
Lung request
Right: 907
Left: 974
Bilateral:683
LAS score at listing: NA
Drop outs: 0
Group 2
N: 1563
Age (mean): 58-9
M/F: /506
Lung request
Right:758
Left:865
Bilateral:945
LAS score at listing: 40.9 (39.0-48.3)
Drop outs: 0
(Cumulative incidence (95 % CI))
this manuscript. C.W.H. does not have a financial relationship with a commercial entity that has an interest in the subject
Limitations:
Changing in referral patterns
Secular trends
Factors determined at organ matching may have a large impact on who receives the LTX
No indication of disease severity at baseline
Additional outcomes:
All listed outcomes also reported for: Primary Pulmonary Hypertension, COPD/Emphysema and Cystic Fibrosis
Cumulative incidence curves and comparisons of outcomes results between diseases.
Notes:
In the United States, donor lung allocation is overseen by the Organ Procurement and Transplantation Network (OPTN), which is operated by the United Network for Organ Sharing (UNOS)
Post LTX mortality 6 months from initial listing for LTX
(Cumulative incidence (95 % CI))
Group 1: 21(18-25)
Group 2: 20 (17-22)
95% CI:NR
P: 0.494

279
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
27
9
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon 1 monoxide diffusing capacity, IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St. George’s Respiratory Questionnaire, 2 6MWT= 6 minute walking test 3
Table 96: De Oliveira 201210 4
Study
details
Patients Methods Outcome measures Effect size Comments
De Oliveira 2012
103
Country of study:
USA
Study design:
Retrospective cohort
Who was blinded:
NR
Setting:
Hospital
Duration of follow-up: 5 years
Patient group:
LTX registrants consecutive patients with advanced ILD from Jan 93- Jan 09
Inclusion criteria:
As above
Exclusion criteria:
NR
All patients
N: 79 (107 total- only IPF data presented here)
Drop outs: 0
Group 1
N: 33
Age (mean): 52.5-9.9
M/F: 27/6
FVC (% predicted): 47±16
History of smoking: 17 (51%)
History of diabetes: 4 (12.1%)
Group 1 pre LAS
Data collected from January 1993-april 2005
Group 2 LAS
Data collected from May 2005- march 2009
Hospital mortality
Group 1: 3 (9.1%)
Group 2: 2 (4.3%)
95% CI:NR
P: 0.64
Funding: NR
Limitations:
Similar baseline characteristics however higher frequency of history of diabetes, and smoking in LAS group (p=0.02)
Sample size
Single centre – lack of generalisability
Changes in medical management
Additional outcomes:
Post-operative outcomes
Kaplan Meier graphs
Notes:
Medians displayed for data which was skewed
Survival at 1 year
Group 1: 78.8%
Group 2: 85.8%
95% CI: NR
P: 0.98
Survival at 3 years
Group 1: 63.6%
Group 2: 62.8%
95% CI: NR
P: 0.98
Survival at 5 years
Group 1: 63.6%
Group 2: NR
95% CI: NR
P: NR
Time on waiting list (days median (IQR))
Group 1: 209(113-379)
Group 2: 65(14-209)
95% CI:
P: <0.01
Length of ICU stay (days median (IQR))
Group 1: 6(4-16)
Group 2: 3(2-7)
95% CI:

280
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
28
0
Study
details
Patients Methods Outcome measures Effect size Comments
LAS score:40.3(IQR; 36.7-45.1)
Drop outs: 0
Group 2
N: 46
Age (mean): 57.9±6.5
M/F: 37/9
FVC (L): 48±16
History of smoking: 35 (76.1%)
History of diabetes: 16 (34.8%)
LAS score: 43.5 (IQR; 38.8-48.9)
Drop outs: 0
P: <0.01
Length of hospital stay median (IQR))
Group 1: 23(16-42)
Group 2: 11(9-17)
95% CI:
P: <0.01
Readmission <30 days (%)
Group 1: 7 (21.2%)
Group 2: 11 (23.9%)
95% CI:
P: 0.78
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon 1 monoxide diffusing capacity, IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St. George’s Respiratory Questionnaire, 2 6MWT= 6 minute walking test 3
Table 97: Kadikar 1997225 4
Study
details
Patients Methods Outcome measures Effect size Comments
Kadikar 1997
225
Country of study:
Canada
Study design:
Retrospective chart
Patient group:
From January 1991 to June 1995, patients who were assessed for lung transplantation by the Toronto lung transplantation program.*
Inclusion criteria:
NR
All patients
Patient data was collected from a retrospective chart review of patients who were evaluated for the program.
6MWD test;
Conducted in an
Transplanted (n)
6/26 Funding: NR
Limitations:
6MWD not documented for 7/26 IPF patients and no analysis conducted for IPF alone
Single centre
Did not account for confounding factors
Remained on waiting list (n)
9/26
Died on waiting list (n)
11/26
6MWD Patients on waiting list/transplanted:364.3±122.8

281
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
28
1
Study
details
Patients Methods Outcome measures Effect size Comments
review
Who was blinded:
NR
Setting:
Hospital
Duration of follow-up:
5 years
Exclusion criteria:
NR
All patients
N: 26 IPF patients (144 total cohort )
Age (mean):52.1±6.0
Drop outs: NR
enclosed hospital corridor of 52.7m. Patients were asked to walk quickly but comfortably with encouragement along the way and rests if necessary.
N=13
Patient who died: 214.9±143.6
N=6
P=0.057
Sensitivity, specificity PPV, NPV of the 6MWT in the prediction of death – using <300m and <400 m thresholds for total cohort – not IPF alone.
Additional outcomes:
Lung function
Cardiac function
The above and reported outcomes were also given for other disease populations in the cohort.
Notes:
*included patients diagnosed with emphysema, alpha-1-antitrypsin deficiency, IPF, primary pulmonary hypertension, eisenmengers syndrome and cystic fibrosis.
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon 1 monoxide diffusing capacity, IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St. George’s Respiratory Questionnaire, 2 6MWT= 6 minute walking test 3
Table 98: Paik 2012374 4
Study
details
Patients Methods Outcome measures Effect size Comments
Paik 2012374
Patient group:
From May 1996 to May 2011,
All patients
Patient data was
Transplanted (n (%))
23/61 (37.7%) Funding: NR
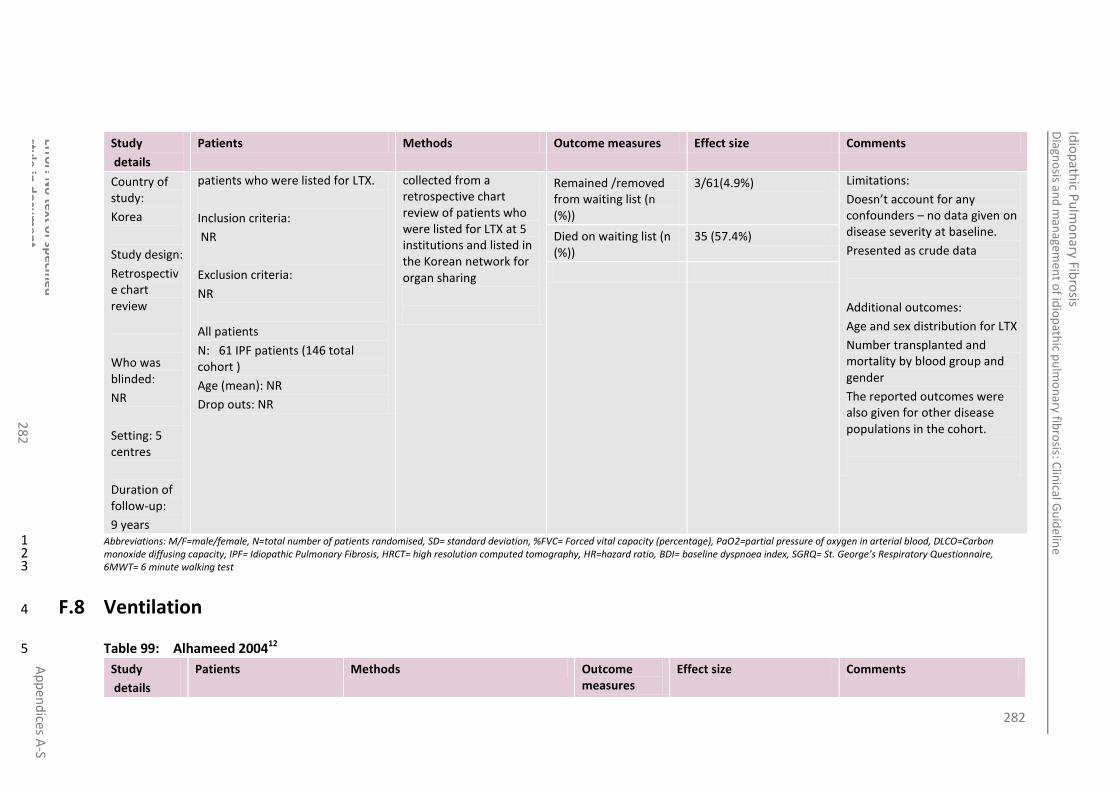
282
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
28
2
Study
details
Patients Methods Outcome measures Effect size Comments
Country of study:
Korea
Study design:
Retrospective chart review
Who was blinded:
NR
Setting: 5 centres
Duration of follow-up:
9 years
patients who were listed for LTX.
Inclusion criteria:
NR
Exclusion criteria:
NR
All patients
N: 61 IPF patients (146 total cohort )
Age (mean): NR
Drop outs: NR
collected from a retrospective chart review of patients who were listed for LTX at 5 institutions and listed in the Korean network for organ sharing
Remained /removed from waiting list (n (%))
3/61(4.9%) Limitations:
Doesn’t account for any confounders – no data given on disease severity at baseline.
Presented as crude data
Additional outcomes:
Age and sex distribution for LTX
Number transplanted and mortality by blood group and gender
The reported outcomes were also given for other disease populations in the cohort.
Died on waiting list (n (%))
35 (57.4%)
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon 1 monoxide diffusing capacity, IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St. George’s Respiratory Questionnaire, 2 6MWT= 6 minute walking test 3
F.8 Ventilation 4
Table 99: Alhameed 200412 5
Study
details
Patients Methods Outcome measures
Effect size Comments
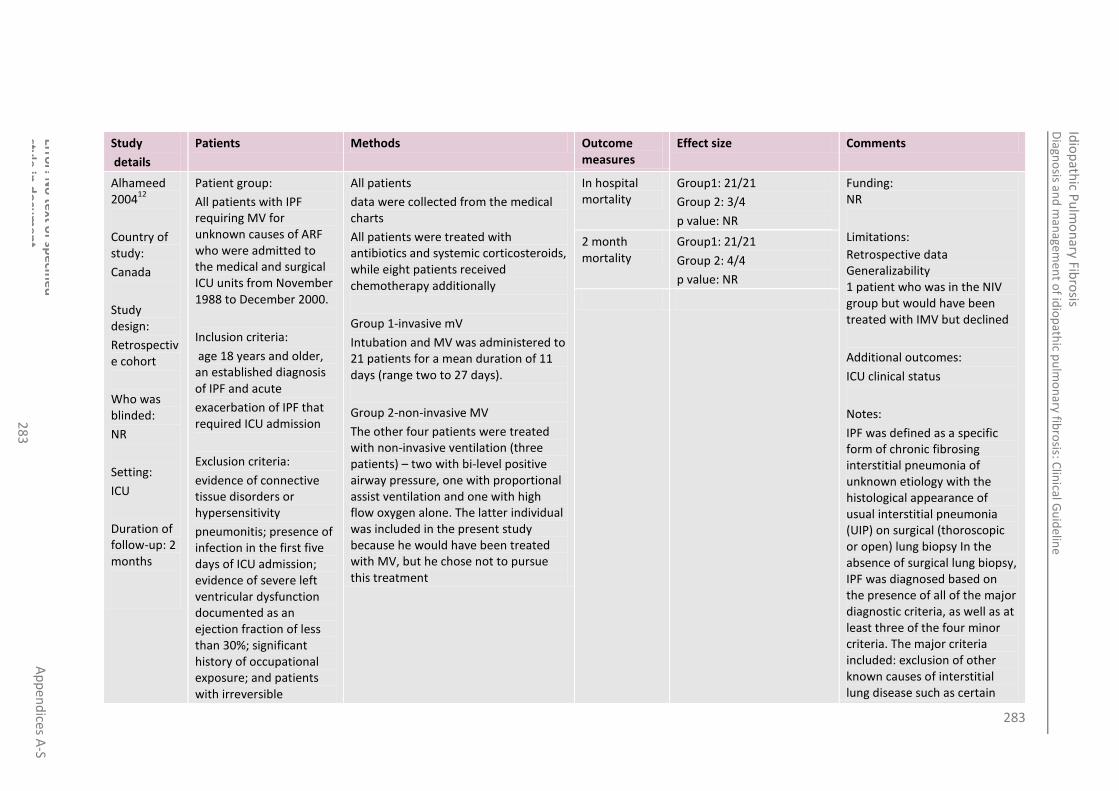
283
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
28
3
Study
details
Patients Methods Outcome measures
Effect size Comments
Alhameed 2004
12
Country of study:
Canada
Study design:
Retrospective cohort
Who was blinded:
NR
Setting:
ICU
Duration of follow-up: 2 months
Patient group:
All patients with IPF requiring MV for unknown causes of ARF who were admitted to the medical and surgical ICU units from November 1988 to December 2000.
Inclusion criteria:
age 18 years and older, an established diagnosis of IPF and acute
exacerbation of IPF that required ICU admission
Exclusion criteria:
evidence of connective tissue disorders or hypersensitivity
pneumonitis; presence of infection in the first five days of ICU admission; evidence of severe left ventricular dysfunction documented as an ejection fraction of less than 30%; significant history of occupational exposure; and patients with irreversible
All patients
data were collected from the medical charts
All patients were treated with antibiotics and systemic corticosteroids, while eight patients received chemotherapy additionally
Group 1-invasive mV
Intubation and MV was administered to 21 patients for a mean duration of 11 days (range two to 27 days).
Group 2-non-invasive MV
The other four patients were treated with non-invasive ventilation (three patients) – two with bi-level positive airway pressure, one with proportional assist ventilation and one with high flow oxygen alone. The latter individual was included in the present study because he would have been treated with MV, but he chose not to pursue this treatment
In hospital mortality
Group1: 21/21
Group 2: 3/4
p value: NR
Funding: NR
Limitations:
Retrospective data Generalizability 1 patient who was in the NIV group but would have been treated with IMV but declined
Additional outcomes:
ICU clinical status
Notes:
IPF was defined as a specific form of chronic fibrosing interstitial pneumonia of unknown etiology with the histological appearance of usual interstitial pneumonia (UIP) on surgical (thoroscopic or open) lung biopsy In the absence of surgical lung biopsy, IPF was diagnosed based on the presence of all of the major diagnostic criteria, as well as at least three of the four minor criteria. The major criteria included: exclusion of other known causes of interstitial lung disease such as certain
2 month mortality
Group1: 21/21
Group 2: 4/4
p value: NR

284
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
28
4
Study
details
Patients Methods Outcome measures
Effect size Comments
systemic disease, e.g. end-stage neoplasm
All patients
N: 25
M/F: 23/2
Age (mean): 69±11
Drop outs: 0
Group 1
N: 21
M/F:NR
Age (mean): NR
Drop outs: NR
Group 2
N: 4
M/F: NR
Age (mean): NR
Drop outs: NR
drug toxicities, environmental exposures and connective tissue diseases; abnormal pulmonary function studies that included evidence of restriction (reduced vital capacity, often with an increased forced expiratory volume in 1 s/forced vital capacity ratio) and impaired gas exchange (increased alveolar to arterial oxygen gradient of the partial pressure of oxygen [PaO2] at rest or exercise or decreased diffusion capacity of the lung for carbon monoxide); bibasilar reticular abnormalities with minimal ground glass opacities on high resolution computed tomography (HRCT) scan; and transbronchial lung biopsy or bronchoalveolar lavage showing no features supporting an alternative diagnosis. The minor criteria included: age older than 50 years; insidious onset of otherwise unexplained dyspnoea on exertion; duration of illness three months or longer; and bilateral inspiratory crackles.

285
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
28
5
Study
details
Patients Methods Outcome measures
Effect size Comments
Acute exacerbation of IPF was defined by the following criteria: exacerbation of dyspnoea within eight to 12 weeks; development of adult respiratory distress syndrome (ARDS) criteria (based on the American and European consensus conference
absence of apparent infectious agents; and ICU admission for further diagnostic workup and management
Infections were ruled out by extensive surveillance cultures (including sputum, blood and urine cultures) and/or bronchoscopy with BAL in the first five days of ICU admission. The diagnosis of pneumonia was considered if the patient met the following criteria: fever and deterioration of pulmonary status with appearance of a new pulmonary infiltrate on chest radiograph, and documented pulmonary pathogens.
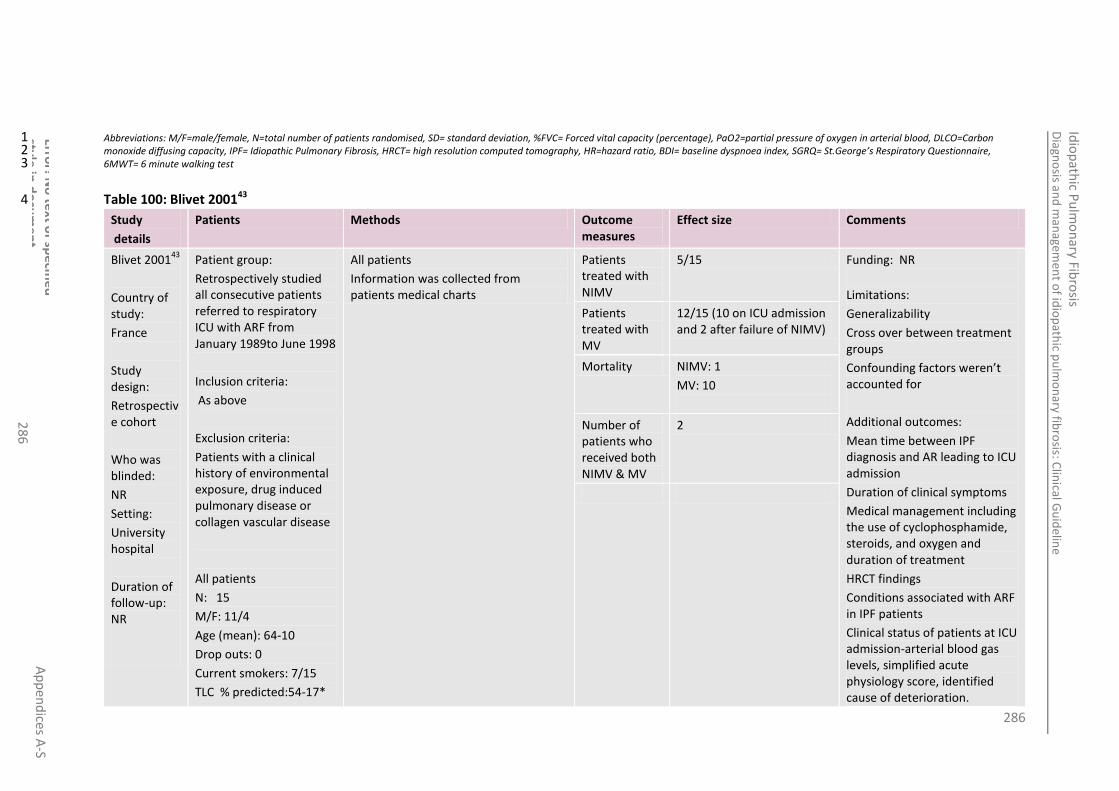
286
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
28
6
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon 1 monoxide diffusing capacity, IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 2 6MWT= 6 minute walking test 3
Table 100: Blivet 200143 4
Study
details
Patients Methods Outcome measures
Effect size Comments
Blivet 200143
Country of study:
France
Study design:
Retrospective cohort
Who was blinded:
NR
Setting:
University hospital
Duration of follow-up: NR
Patient group:
Retrospectively studied all consecutive patients referred to respiratory ICU with ARF from January 1989to June 1998
Inclusion criteria:
As above
Exclusion criteria:
Patients with a clinical history of environmental exposure, drug induced pulmonary disease or collagen vascular disease
All patients
N: 15
M/F: 11/4
Age (mean): 64-10
Drop outs: 0
Current smokers: 7/15
TLC % predicted:54-17*
All patients
Information was collected from patients medical charts
Patients treated with NIMV
5/15 Funding: NR
Limitations:
Generalizability
Cross over between treatment groups
Confounding factors weren’t accounted for
Additional outcomes:
Mean time between IPF diagnosis and AR leading to ICU admission
Duration of clinical symptoms
Medical management including the use of cyclophosphamide, steroids, and oxygen and duration of treatment
HRCT findings
Conditions associated with ARF in IPF patients
Clinical status of patients at ICU admission-arterial blood gas levels, simplified acute physiology score, identified cause of deterioration.
Patients treated with MV
12/15 (10 on ICU admission and 2 after failure of NIMV)
Mortality NIMV: 1
MV: 10
Number of patients who received both NIMV & MV
2

287
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
28
7
Study
details
Patients Methods Outcome measures
Effect size Comments
FVC % predicted:55-15*
FEV1 % predicted: 61-22*
Duration of ventilation
Cause of death
Length of ICU stay of all patients
Mortality of all patients
Notes:
The definition ARF is: exacerbation of dyspnoea within a few days, deterioration of hypoxemia(PaO2/fraction of inspired oxygen <250), MV requirement
IPF diagnosis: based on a combination of the following; persistent bilateral dry crackles on auscultation, widespread bilateral shadowing on chest radiographs or IPF related abnormalities on HRCT, PFT results showing a restrictive ventilatory defect and decreased single breath carbon monoxide diffusing capacity and /or pathologic criteria on open lung biopsy specimen.
* PFTs performed a year before ARF

288
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
28
8
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon 1 monoxide diffusing capacity, IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 2 6MWT= 6 minute walking test 3
Table 101: Fumeaux 2001157 4
Study
details
Patients Methods Outcome measures
Effect size Comments
Fumeaux 2001
157
Country of study:
Switzerland
Study design:
Retrospective observational case series
Who was blinded:
NR
Setting:
Hospital
Duration of follow-up:
Patient group:
Patients diagnosed with PF from December 96- to march 2001.
Inclusion criteria:
Patients requiring MV for ARF during their ICU stay.
Exclusion criteria:
NR
All patients
N: 14
M/F: 7/7
Age (mean): 72-8.2
Drop outs: 0
TLC 60-8
FVC 72-19
FEV 69-19
All patients
Patients data was retrieved from a computerized database
Patients treated with NIMV
11/14 Funding: NR
Limitations:
The population includes patients who have secondary PF – 3/14 patients had secondary PF associated with sarcoidosis and rheumatoid arthritis
Single centre-results may be influenced by variations in the management of patients
Additional outcomes:
results of biopsy, HRCT and BAL
Medical management including the use of azathioprine, steroids, no pharma and oxygen - duration of treatment and last dosage
Disease severity- dyspnoea ranked as mild to moderate in all
Symptom of ARF
Time between first symptom and admission
Patients treated with MV
14/14
Number of patients who received both NIMV & MV
11/14
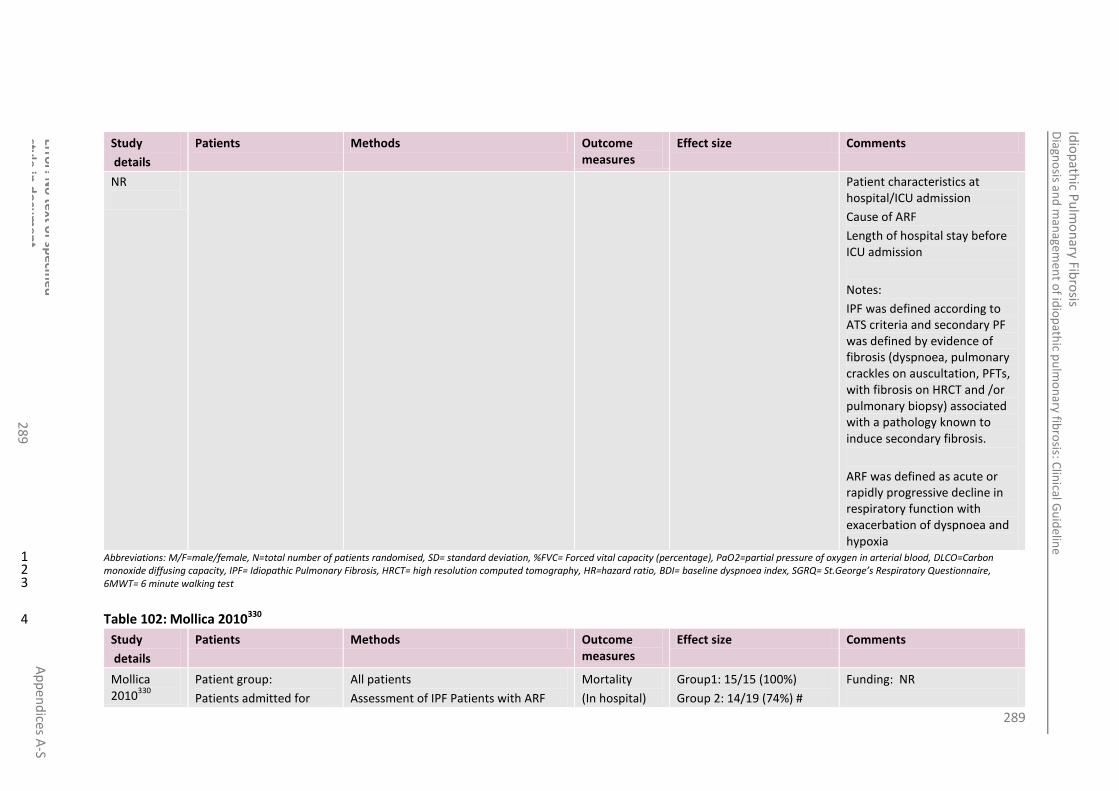
289
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
28
9
Study
details
Patients Methods Outcome measures
Effect size Comments
NR
Patient characteristics at hospital/ICU admission
Cause of ARF
Length of hospital stay before ICU admission
Notes:
IPF was defined according to ATS criteria and secondary PF was defined by evidence of fibrosis (dyspnoea, pulmonary crackles on auscultation, PFTs, with fibrosis on HRCT and /or pulmonary biopsy) associated with a pathology known to induce secondary fibrosis.
ARF was defined as acute or rapidly progressive decline in respiratory function with exacerbation of dyspnoea and hypoxia
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon 1 monoxide diffusing capacity, IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 2 6MWT= 6 minute walking test 3
Table 102: Mollica 2010330 4
Study
details
Patients Methods Outcome measures
Effect size Comments
Mollica 2010
330
Patient group:
Patients admitted for
All patients
Assessment of IPF Patients with ARF
Mortality
(In hospital)
Group1: 15/15 (100%)
Group 2: 14/19 (74%) #
Funding: NR
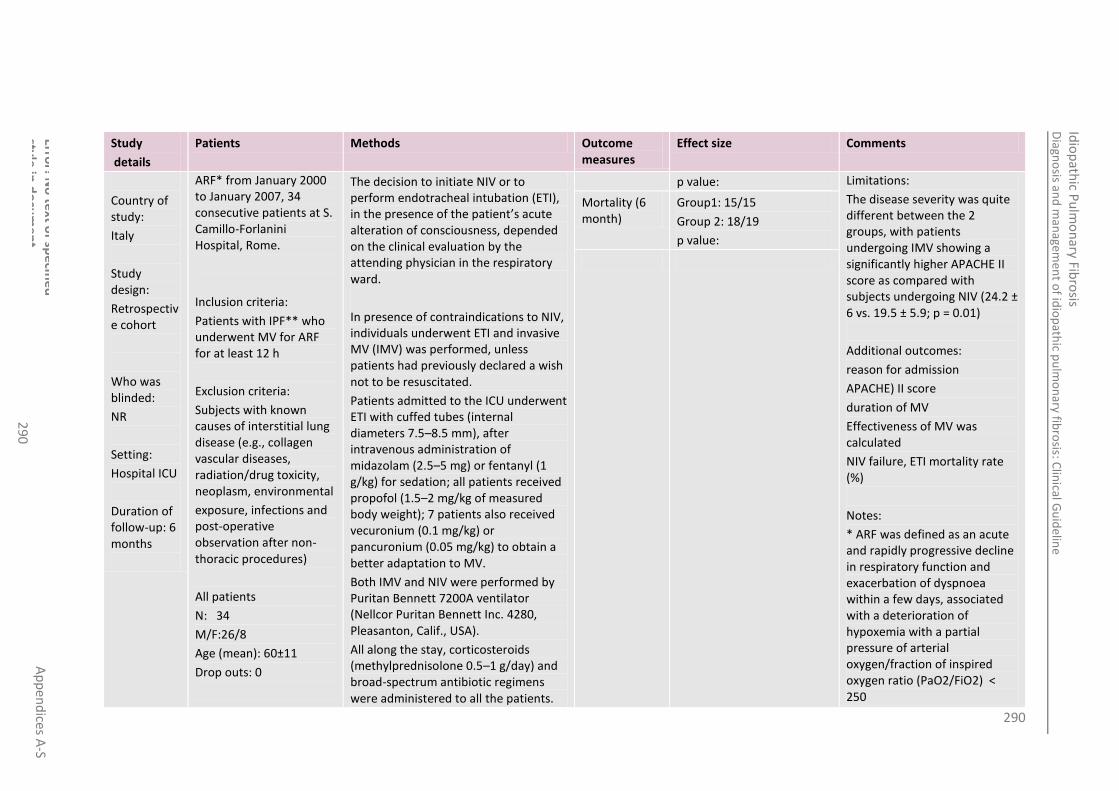
290
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
29
0
Study
details
Patients Methods Outcome measures
Effect size Comments
Country of study:
Italy
Study design:
Retrospective cohort
Who was blinded:
NR
Setting:
Hospital ICU
Duration of follow-up: 6 months
ARF* from January 2000 to January 2007, 34 consecutive patients at S. Camillo-Forlanini Hospital, Rome.
Inclusion criteria:
Patients with IPF** who underwent MV for ARF for at least 12 h
Exclusion criteria:
Subjects with known causes of interstitial lung disease (e.g., collagen vascular diseases, radiation/drug toxicity, neoplasm, environmental
exposure, infections and post-operative observation after non-thoracic procedures)
All patients
N: 34
M/F:26/8
Age (mean): 60±11
Drop outs: 0
The decision to initiate NIV or to perform endotracheal intubation (ETI), in the presence of the patient’s acute alteration of consciousness, depended on the clinical evaluation by the attending physician in the respiratory ward.
In presence of contraindications to NIV, individuals underwent ETI and invasive MV (IMV) was performed, unless patients had previously declared a wish not to be resuscitated.
Patients admitted to the ICU underwent ETI with cuffed tubes (internal diameters 7.5–8.5 mm), after intravenous administration of midazolam (2.5–5 mg) or fentanyl (1 g/kg) for sedation; all patients received propofol (1.5–2 mg/kg of measured body weight); 7 patients also received vecuronium (0.1 mg/kg) or pancuronium (0.05 mg/kg) to obtain a better adaptation to MV.
Both IMV and NIV were performed by Puritan Bennett 7200A ventilator (Nellcor Puritan Bennett Inc. 4280, Pleasanton, Calif., USA).
All along the stay, corticosteroids (methylprednisolone 0.5–1 g/day) and broad-spectrum antibiotic regimens were administered to all the patients.
p value: Limitations:
The disease severity was quite different between the 2 groups, with patients undergoing IMV showing a significantly higher APACHE II score as compared with subjects undergoing NIV (24.2 ± 6 vs. 19.5 ± 5.9; p = 0.01)
Additional outcomes:
reason for admission
APACHE) II score
duration of MV
Effectiveness of MV was calculated
NIV failure, ETI mortality rate (%)
Notes:
* ARF was defined as an acute and rapidly progressive decline in respiratory function and exacerbation of dyspnoea within a few days, associated with a deterioration of hypoxemia with a partial pressure of arterial oxygen/fraction of inspired oxygen ratio (PaO2/FiO2) < 250
Mortality (6 month)
Group1: 15/15
Group 2: 18/19
p value:

291
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
29
1
Study
details
Patients Methods Outcome measures
Effect size Comments
Group 1- invasive MV
N: 15
M/F: NR
Age (mean):64.6±10
Drop outs: 0
Group 2- non-invasive MV
N: 19
M/F: NR
Age (mean):56±11
Drop outs:
Group 1
IMV was applied in a volume-controlled mode with a mean delivered tidal volume (TV) value of 7.5ml/kg (range 6–9) of measured body weight. Positive end expiratory pressure (PEEP) was set in order to obtain the best oxygenation with the fewest side effects on haemodynamics
Group2
NIV was performed in pressure support mode (NIPSV); a helmet (CaSta; Starmed, Mirandola, Italy) was used as an interface for all patients. Pressure support, PEEP and flow-by trigger values were adjusted in order to obtain the best oxygenation and to reduce RR and were modified on the basis of blood gas data.
The criteria for NIPSV discontinuation and shift to IMV were: onset of coma, cardiovascular instability or poor compliance to NIV device.
Sepsis and shock diagnoses were based on American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference (1992) criteria
** In 16 subjects, the diagnosis was obtained by lung biopsy, and in the remaining 18 by the presence of all major and at least 3 minor European Respiratory Society/American Thoracic Society criteria for IPF diagnosis
All patients had severe functional and radiological impairment. On hospital admission, microbiological investigations for a suspected pulmonary infection (sputum culture and/or endotracheal aspiration and/or BAL) were performed upon all patients, before the introduction of an empirical antibiotic treatment.
# despite the observed improvement in oxygenation, NIV was withdrawn because of

292
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
29
2
Study
details
Patients Methods Outcome measures
Effect size Comments
poor compliance (3 patients), pneumothorax (1 patient) and blood emesis (1 patient). All of them requested not to be resuscitated and died after 16 ± 5.4 days. NIV failed to improve PaO2 /FiO2 in 9 individuals: 5 underwent IMV and died after 8.8 ± 5.8 days and 4 died before undergoing ETI.
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon 1 monoxide diffusing capacity, IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 2 6MWT= 6 minute walking test 3
Table 103: Stern 2001449 4
Study
details
Patients Methods Outcome measures
Effect size Comments
Stern 2001
449
Country of study:
France
Study design:
retrospective cohort
Who was
Patient group:
27 consecutive patients with pulmonary fibrosis requiring MV for ARF admitted between
September 1990 and October 1999 were retrospectively examined.
Inclusion criteria:
A diagnosis of IPF was based on the association of the three
following criteria: (1)
All patients
The decision of initiating IMV depended on the attending physician**
The patients were receiving mechanical ventilation using Cesar (Taema; Paris, France), Erica (Engstro¨m; Bromma, Sweden), or Evita 2 (Dra¨ger Medical; Lübeck, Germany) ventilators. The initial settings of the ventilator were adjusted in order to minimize peak airway pressure and to maintain adequate ventilation. To accomplish the goal of limiting peak airway pressure, Paco2 was permitted to rise.
In hospital Mortality
Group1: 22/23*
p value: NR
Funding: NR
Limitations:
Blinding
No comparison/ control group
Observational data
Retrospective
Single centre
Small sample size
Additional outcomes:
The presence of organ
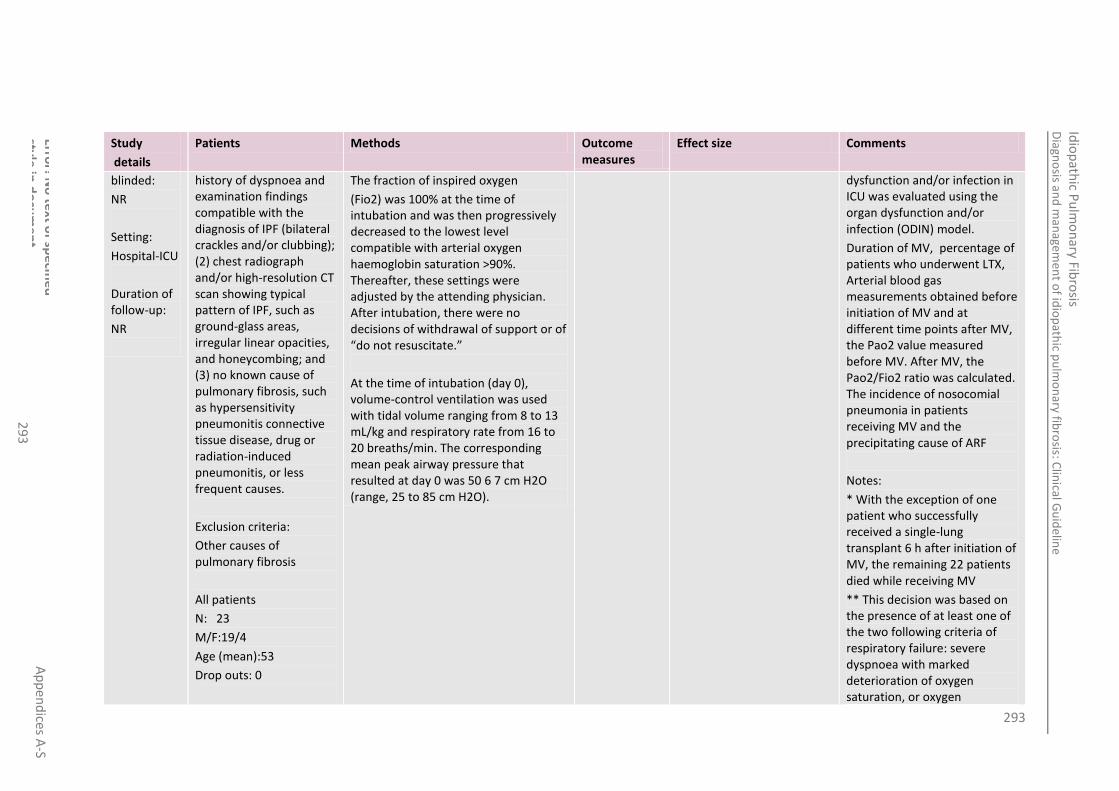
293
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
29
3
Study
details
Patients Methods Outcome measures
Effect size Comments
blinded:
NR
Setting:
Hospital-ICU
Duration of follow-up:
NR
history of dyspnoea and examination findings compatible with the diagnosis of IPF (bilateral crackles and/or clubbing); (2) chest radiograph and/or high-resolution CT scan showing typical pattern of IPF, such as ground-glass areas, irregular linear opacities, and honeycombing; and (3) no known cause of pulmonary fibrosis, such as hypersensitivity pneumonitis connective tissue disease, drug or radiation-induced pneumonitis, or less frequent causes.
Exclusion criteria:
Other causes of pulmonary fibrosis
All patients
N: 23
M/F:19/4
Age (mean):53
Drop outs: 0
The fraction of inspired oxygen
(Fio2) was 100% at the time of intubation and was then progressively decreased to the lowest level compatible with arterial oxygen haemoglobin saturation >90%. Thereafter, these settings were adjusted by the attending physician. After intubation, there were no decisions of withdrawal of support or of “do not resuscitate.”
At the time of intubation (day 0), volume-control ventilation was used with tidal volume ranging from 8 to 13 mL/kg and respiratory rate from 16 to 20 breaths/min. The corresponding mean peak airway pressure that resulted at day 0 was 50 6 7 cm H2O (range, 25 to 85 cm H2O).
dysfunction and/or infection in ICU was evaluated using the organ dysfunction and/or infection (ODIN) model.
Duration of MV, percentage of patients who underwent LTX, Arterial blood gas measurements obtained before initiation of MV and at different time points after MV, the Pao2 value measured before MV. After MV, the Pao2/Fio2 ratio was calculated. The incidence of nosocomial pneumonia in patients receiving MV and the precipitating cause of ARF
Notes:
* With the exception of one patient who successfully received a single-lung transplant 6 h after initiation of MV, the remaining 22 patients died while receiving MV
** This decision was based on the presence of at least one of the two following criteria of respiratory failure: severe dyspnoea with marked deterioration of oxygen saturation, or oxygen
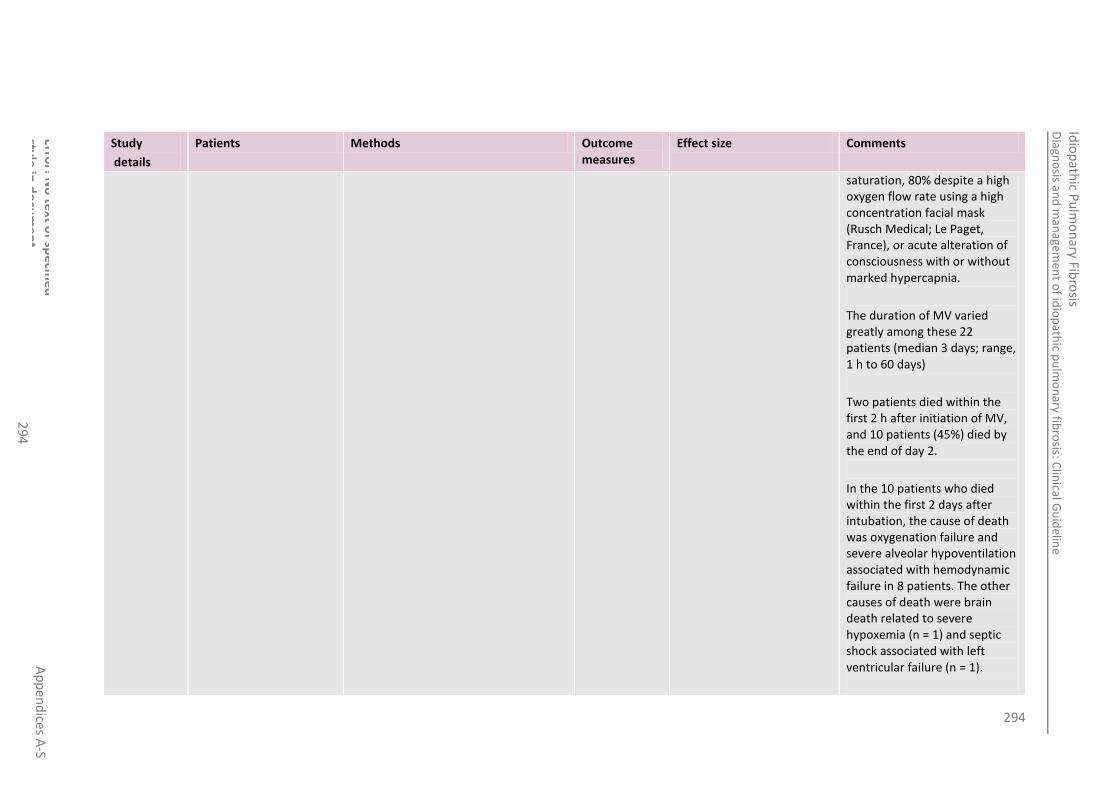
294
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
29
4
Study
details
Patients Methods Outcome measures
Effect size Comments
saturation, 80% despite a high oxygen flow rate using a high concentration facial mask (Rusch Medical; Le Paget, France), or acute alteration of consciousness with or without marked hypercapnia.
The duration of MV varied greatly among these 22 patients (median 3 days; range, 1 h to 60 days)
Two patients died within the first 2 h after initiation of MV, and 10 patients (45%) died by the end of day 2.
In the 10 patients who died within the first 2 days after intubation, the cause of death was oxygenation failure and severe alveolar hypoventilation associated with hemodynamic failure in 8 patients. The other causes of death were brain death related to severe hypoxemia (n = 1) and septic shock associated with left ventricular failure (n = 1).

295
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
29
5
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon 1 monoxide diffusing capacity, IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 2 6MWT= 6 minute walking test 3
Table 104: Saydain 2002423 4
Study
details
Patients Methods Outcome measures
Effect size Comments
Saydain 2002
423
Country of study: USA
Study design:
Retrospective cohort
Who was blinded: NR
Setting:
ICU
Duration of follow-up: NR
Patient group:
patients with IPF admitted to the ICU between January 1995 and July 2000
Inclusion criteria:
had IPF based on the following criteria: (1) surgical biopsy showing usual interstitial pneumonitis (UIP); (2) abnormal pulmonary function studies that included evidence of restriction, and/or increased alveolar-arterial oxygen tension gradient at rest or during exercise, or decreased diffusing capacity for carbon monoxide; and (3) chest radio graph or high-resolution computed tomography suggestive of UIP. In the absence of surgical biopsy, patients had to fulfil all of the major criteria and at least three of the four minor criteria of the ATS & ERS
Exclusion criteria:
This study was aimed to describe the clinical course and outcome of patients with IPF admitted to the ICU.
Group 1- ventilated patients (invasive and non-invasive)
Group 2- no ventilation
In hospital mortality*
Group1: 13/19
Group 2: 10/19
p value: NR
Funding: Robert N. brewer family foundation and the mayo foundation
Limitations: Observational data
Generalizability – single centre data
Additional outcomes:
Observational data recorded throughout ICU stay.
Notes:
Of the 32 patients admitted for respiratory failure, 10 (31%) had pneumonia, 2 (6%) pulmonary embolism, 2 (6%) congestive heart failure, and 2 (6%) pneumothorax. One patient developed acute on chronic respiratory failure following surgery for mitral valve replacement. The remaining 15 (47%) patients with respiratory

296
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
29
6
Study
details
Patients Methods Outcome measures
Effect size Comments
Patients who have known causes of interstitial lung disease, such as collagen vascular disease, drug toxicity, and environmental exposure, Patients who were admitted to ICU for electrocardiographic
monitoring or postoperative observation after non thoracic procedures
All patients
N: 38
M/F: 25/13
Age (mean): 69±11
Drop outs: 0
Group 1
N: 19
M/F: NR
Age (mean): NR
Drop outs: 0
Group 2
N: 19
M/F:NR
Age (mean): NR
Drop outs: 0
failure had no immediate precipitating factor, and the worsening respiratory failure was attributed to progression of IPF
*Nineteen patients (50%) received mechanical ventilation for an average of 10.5 ± 12.4 (median 5) days. Six patients received invasive as well as non-invasive positive pressure ventilation, whereas one patient received non-invasive positive pressure ventilation only. Fifteen patients (39%) requested not to be resuscitated. Life support was withdrawn from eight patients (21%) at the request of next of kin. Ten of the 19 patients (53%) who did not receive mechanical ventilation died compared with 13 of the 19 patients (68%) who received mechanical ventilation p=0.51
There was no significant difference in the duration of mechanical ventilation between survivors and no survivors
(p = 0.10). (median of 4.5 for

297
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
29
7
Study
details
Patients Methods Outcome measures
Effect size Comments
survivors and of 11.0 for no survivors, p =0.66)
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon 1 monoxide diffusing capacity, IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 2 6MWT= 6 minute walking test 3
Table 105: Yokoyama 2010504 4
Study
details
Patients Methods Outcome measures
Effect size Comments
Yokoyama 2010 504
Country of study:
Japan
Study design:
retrospective cohort
Who was blinded:
No one
Setting:
Hospital
Patient group:
Patients included in the study diagnosed with IPF and were who fulfilled the proposed Japanese Respiratory Society criteria for acute exacerbation-IPF* during the period between April 1998 and June 2004 at Tosei General Hospital.
Inclusion criteria:
NIV was initiated in cases of a respiratory failure of PaO2/FIO2 less than 300,
Exclusion criteria:
Patients had contraindications of NIV use such as severe coma and pneumothorax.
All patients
Standard microbiological investigations with blood and sputum cultures were performed to exclude pulmonary infection in all patients#
BAL was performed on admission to rule out infectious disease except in patients with severe pulmonary function impairment before AE, marked honeycombing on HRCT, or rejection of BAL##.
High-dose corticosteroid therapy was introduced as general therapy for AE-IPF. Another immunosuppressive therapy such as cyclophosphamide or cyclosporine A was concurrently or subsequently used###.
Ventilatory managements
BiPAP Vision (Respironics Inc, Murrysville, PA, USA) was used for NIV. The initial setting for NIV was CPAP
Mortality (all) Group1: 6/11
p value: NR
Funding: Grant from Japanese ministry of health, labour and welfare.
Limitations:
No comparison/ control group
Observational data
Retrospective
Single centre
Small sample size
Post hoc analysis of NIMV vs. IMV
Baseline data not given per group
Notes:
*IPF was defined according to American Thoracic Society (ATS)/European Respiratory Society (ERS) Consensus Statement Criteria. The criteria
Mortality (non-intubated cases)-NIMV
Group1: 2/7
p value: NR
Mortality (intubated cases)- MV
Group1: 4/4
p value: NR

298
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
29
8
Study
details
Patients Methods Outcome measures
Effect size Comments
Duration of follow-up:
3 months
All patients
N: 11**
M/F:7/4
Age (mean): 72.3± 7.7 years
Drop outs: 0
mode and the CPAP level was gradually increased to 12 cmH2O. Pressure support was given if high respiratory frequency or respiratory acidosis was found, and FIO2 was set at the lowest value to keep PaO2 at more than 60 mmHg.
Endotracheal intubation was performed in patients with any of the following criteria: decreased alertness or major agitation requiring sedation, clinical signs of exhaustion (active contraction of the accessory muscles of respiration with paradoxical abdominal or thoracic motion), hemodynamic instability, cardiac arrest, or refractory hypoxemia.
The criteria for the end of NIV use were defined as follows: PaO2/FIO2 >200, respiration rate <20, clinical improvement of the radiological findings
for AE-IPF were as follows: During the chronic course of IPF, there was 1) acute worsening of dyspnoea within the course of one month, 2) bibasilar honeycombing with newly developing ground glass attenuation and/or consolidation on HRCT scans, 3) deterioration of PaO2 of more than 10 mmHg under the same condition, and 4) exclusion of other known causes of exacerbation, such as pulmonary infection, pneumothorax, malignancy, pulmonary thromboembolism, and heart failure
** Ten patients were diagnosed with IPF before acute exacerbation and one patient was diagnosed with IPF in acute exacerbation
#All blood cultures were negative, and neither sputum Gram staining nor culture was contributory. After these diagnostic investigations, broad-spectrum antibiotics were administered as empiric

299
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
29
9
Study
details
Patients Methods Outcome measures
Effect size Comments
therapy until the offending pathogen was identified or ruled out.
##BAL was performed during acute exacerbation before antibiotics were introduced in 6 patients. In all 6 cases, BAL fluid studies for routine bacterial organisms, opportunistic pathogens, as well as common viral pathogens revealed no evidence of infection.
###After diagnosis of AE-IPF, all patients were treated with steroid pulse therapy and/or methyl-prednisolone 2 mg/kg/day, followed by tapering corticosteroid with or without an immunosuppressant.
The time from introduction of NIV to steroid therapy was 2.2±1.2 days
Duration of NIV was 5.4±3.8 days in all cases
Intubation was required in 4 of 11 patients, who failed NIV.
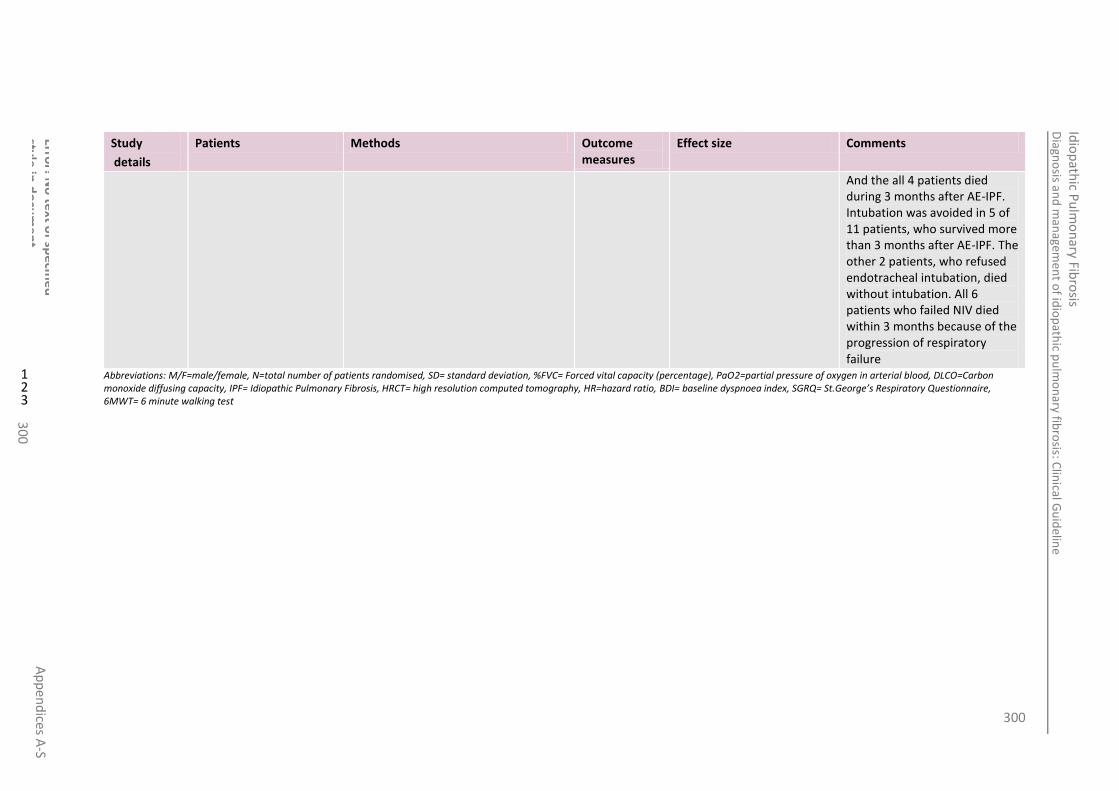
300
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Error! N
o te
xt of sp
ecifie
d
style in
do
cum
en
t. A
pp
end
ices A-S
30
0
Study
details
Patients Methods Outcome measures
Effect size Comments
And the all 4 patients died during 3 months after AE-IPF. Intubation was avoided in 5 of 11 patients, who survived more than 3 months after AE-IPF. The other 2 patients, who refused endotracheal intubation, died without intubation. All 6 patients who failed NIV died within 3 months because of the progression of respiratory failure
Abbreviations: M/F=male/female, N=total number of patients randomised, SD= standard deviation, %FVC= Forced vital capacity (percentage), PaO2=partial pressure of oxygen in arterial blood, DLCO=Carbon 1 monoxide diffusing capacity, IPF= Idiopathic Pulmonary Fibrosis, HRCT= high resolution computed tomography, HR=hazard ratio, BDI= baseline dyspnoea index, SGRQ= St.George’s Respiratory Questionnaire, 2 6MWT= 6 minute walking test3

301
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Gu
idelin
e nam
e A
pp
end
ices A-S
30
1
F.9 Patient review and follow-up 1
No relevant clinical studies comparing different timings and delivery of review appointments were identified 2
3
4 5

302
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Gu
idelin
e nam
e A
pp
end
ices A-S
30
2
Appendix G: Economic evidence tables 1
G.1 Diagnosis 2
No relevant economic evaluations were identified that assessed the value of a biopsy, multidisciplinary team consensus in the diagnosis of IPF or how this 3 should best be achieved. 4
G.2 Prognosis 5
No health economic literature assessing an intervention for a prognostic purpose in an IPF population was identified. 6
G.3 Pulmonary rehabilitation 7
No relevant economic evaluations that assessed pulmonary rehabilitation in an IPF population were identified. 8
G.4 Best supportive care 9
No relevant economic evaluations comparing strategies of oxygen management, or palliation of cough, breathlessness or fatigue were identified. 10
G.5 Pharmacological interventions 11
G.5.1 Combination: Prednisolone & azathioprine & n-acetylcysteine vs. Conservative treatment and thiopurine S-methyltransferase testing 12
Table 106: Hagaman 2010171 13
J. T. Hagaman, B. W. Kinder, and M. H. Eckman. Thiopurine S-methyltranferase testing in idiopathic pulmonary fibrosis: a pharmacogenetic cost-effectiveness analysis. Lung 188 (2):125-132, 2010.
Study details Population & interventions Costs Health outcomes
Cost effectiveness

303
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Gu
idelin
e nam
e A
pp
end
ices A-S
30
3
J. T. Hagaman, B. W. Kinder, and M. H. Eckman. Thiopurine S-methyltranferase testing in idiopathic pulmonary fibrosis: a pharmacogenetic cost-effectiveness analysis. Lung 188 (2):125-132, 2010.
Economic analysis: CUA
Study design:
Analytic decision model
Approach to analysis:
Decision tree structure depicted however assumed Markov based on description. Based on published estimates and expert opinion
Perspective: USA, Medicare
Time horizon: Lifetime, with key intervention related events captured only in first year. Events assumed to occur every 0.5 years
Treatment effect duration: Assumed to be continuous with use of drug
Discounting: NR
Population:
IPF patients
Cohort settings:
Start age = NR
M =NR
Intervention 1:
Conservative therapy, medical history and exam.
Intervention 2:
Azathioprine, NAC, and steroids at standard dose [dose NR], medical history and exam 3 times annually, monthly CBC for 1 year and bimonthly after, LFT and renal function biannually, PFT and CT scan annually, DEXA scanning, bisphosphate therapy, calcium, and Vitamin D, TMP/sulfa 3 times weekly
Intervention 3:
Azathioprine, NAC, and steroids at reduced dose [dose NR], medical history and exam 3 times annually, monthly CBC for 1 year and bimonthly after, LFT and renal function biannually, PFT and CT scan annually, DEXA scanning, bisphosphate therapy, calcium, and Vitamin D, TMP/sulfa 3 times weekly
Total costs (mean per patient):
Intvn 1: £6,249.78
Intvn 2: £10,190.81
Intvn 3: £10,201.12
Currency & cost year:
2007 US dollars (presented here as 2007 UK pounds‡)
Cost components incorporated:
TPMT assay:£193.47
Cost of delivering Intvn. 1 per month = £42.56
Cost of delivering Intvn. 2 per month = £191.54
Cost of delivering Intvn. 3 per month = £154.78
Complicated leukopenia = £6,536.77
Complicated leukopenia leading to death = £9,458.19
Uncomplicated leukopenia = £272.80
Cost of IPF progression (Interstitial lung disease DRG code 93, additional CT and PFT per year, additional comprehensive medical
Primary outcome measure:
QALYs (mean per patient)
Intvn 1: 2.50
Intvn 2: 2.61
Intvn 3: 2.62
Primary ICER (Intvn 2 vs. Intvn 1):
Intervention 2 was subject to extended dominance
ICER of Intvn3 vs. 1: £31,701.per QALY gained
CI: NR
Probability cost-effective: NR
Other:
If conservative treatment is excluded from the incremental analysis due to lack of applicability to the UK context, the ICER of Intvn 3 vs. 2 is £19,129.85
Subgroup analyses: NA
Analysis of uncertainty:
Deterministic sensitivity performed for majority of inputs except costs.
A threshold analysis was conducted for prevalence of abnormal activity. Inspection from graph suggests that in order for TPMT testing to be cost effective compared to no testing, the prevalence of abnormal TPMT activity needs to be 2.5%. At prevalence above 13.5% TPMT testing dominates.
The sensitivity analysis also showed that results were sensitive to the probability of leukopenia. If the probability of leukopenia on low dose of azathioprine increases above 12% over the base case value (21.4% with intermediate TPMT activity) then testing is no longer cost effective at $50,000 threshold [results not reported]
A two way sensitivity analysis assessing cumulative probability of disease progression on conservative therapy and that of the drug regimen. This showed with lower estimates of disease progression on conservative therapy the less favourable the drug regimen was in comparison.

304
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Gu
idelin
e nam
e A
pp
end
ices A-S
30
4
J. T. Hagaman, B. W. Kinder, and M. H. Eckman. Thiopurine S-methyltranferase testing in idiopathic pulmonary fibrosis: a pharmacogenetic cost-effectiveness analysis. Lung 188 (2):125-132, 2010.
exam every 6 months) = £9,527.20
Authors reported no other parameters tested influenced the results significantly.
Data sources
Health outcomes: Respective 1 year cumulative probability of developing leucopoenia with standard dose was 1%, 21.4%, 100% for normal, intermediate and absent TPMT activity. Respective 1 year cumulative probability of developing leucopoenia with reduced dose was 1%, 10%, and NA for normal, intermediate and absent TPMT activity. 1 year probability of miscellaneous complications on azathioprine was 2.5%. In patients with leucopoenia the probability of complicated leukopenia was 16% and 8% probability of death. The one year probability of disease progression for patients on the pharmacological regimens was 37% and 51% for those without. The respective quality of life estimates used was 0.63, 0.95 and 0.76 for patients with progression of IPF, leucopoenia and complicated leucopoenia. Excess mortality due to IPF was 9% per year. Life expectancy after IPF diagnosis was 3 years. All values were subject to sensitivity analysis.
Effectiveness data for the drug regimen was derived from one RCT and two observational trials - Demedts et al (2005), Raghu et al (1991), Winterbaurer et al (1978)
Quality-of-life weights: IPF weights derived from Japanese population using SF36. Other weights derived from Eldar-Lissai et al (2008), Vogel et al (2005), Talcott (2000)
Cost sources: Drug costs from www.drugstore.com; other costs from average Medicare reimbursement for the corresponding Current Procedural Terminology or Diagnosis Related Group codes.
Comments
Source of funding: Not reported; Limitations: Lifetime horizon used with no events associated with the intervention occurring beyond the first year, potentially not capturing some of the benefits of having appropriate dose beyond first year. Implicit assumption that if you have an adverse event due to inappropriate dosage this will occur in first year of treatment. Relevant health outcomes are included. Where possible RCT data is used, supplemented by observational data and expert opinion. Unclear if cost estimates come from the best source of data. Deterministic sensitivity performed and incremental analysis presented. No probabilistic sensitivity analysis. Other: Unclear whether marginal cost between conservative treatment and triple therapy applicable to UK context.
Overall applicability*: Partially applicable Overall quality**: Potentially serious limitations
Abbreviations: CBC = Complete Blood Count; CI = confidence interval; CT = Computer-aided Tomography CUA = cost-utility analysis; ICER = incremental cost-effectiveness ratio; LFT = Liver 1 Function Test; NA = Not applicable; NAC = N-acetylcysteine; NR = not reported; pa = probabilistic analysis; PFT = Pulmonary Function Test; QALY = Quality Adjusted Life Year; RCT = 2 Randomised Control Trial; TPMT = Thiopurine S-methyltranferase; ‡ Converted using 2007 Purchasing Power Parities 3 * Directly applicable / partially applicable / Not applicable; ** Minor limitations /potentially serious Limitations / Very serious limitations 4
5
G.6 Lung transplantation 6
No relevant economic evaluations comparing different timing of LTX in a population of IPF were identified. 7
305
Diagn
osis an
d m
anagem
ent o
f idio
path
ic pu
lmo
nary fib
rosis: C
linical G
uid
eline
Idio
path
ic Pu
lmo
nary Fib
rosis
Gu
idelin
e nam
e A
pp
end
ices A-S
30
5
G.7 Ventilation 1
No relevant economic evaluations comparing invasive and non-invasive ventilation strategies were identified. 2
G.8 Patient review and follow-up 3
No relevant economic evaluations comparing different review and monitoring strategies were identified. 4
5

306
Idiopathic Pulmonary Fibrosis Interpreting post-test probabilities by considering prevalence/pre-test probability
Appendix H: Interpreting post-test probabilities 1
by considering prevalence/pre-test probability 2
Predictive values or post-test probabilities address the chances of a person having a particular 3 diagnosis given the known test result. However, the values are only accurate for a population with 4 similar prevalence to the population tested because the prevalence of disease in the population can 5 have a large effect on the calculated predictive value. Therefore, the predictive values are not 6 independent of prevalence and are not intrinsic to the test itself. 7
Consequently, it is necessary to consider the prevalence when interpreting the positive and negative 8 predictive values. In this report, the modified positive and negative predictive values have been 9 calculated, which represent the value-added predictive figures: 10
Value-added PPV = PPV – prevalence 11
Value-added NPV = NPV – (1 – prevalence) 12
These figures convey the additional certainty of the diagnosis that is contributed by a positive or 13 negative test result over the starting probability of a diagnosis (the prevalence in the sample). 14 However, it is important to bear in mind that if there is only a small amount of uncertainty in the 15 diagnosis before the test a small absolute increase in certainty may be important for diagnostic 16 decisions. 17
Below is a summary matrix to aid interpretation of these values when the post-test probability is 18 high, which superficially suggests a high diagnostic accuracy. Note that if the PPV or NPV is low then 19 the test is unlikely to be useful as it will be unable to accurately discriminate a positive from a 20 negative diagnosis in the majority of cases. 21
Table 107: Interpreting high post-test probabilities 22
Prevalence (pre-test probability)
Post-test probability (predictive values)
PPV high NPV high
High Little value added: limited additional certainty in the diagnosis and so uncertain in the discriminative ability of the test (accurately detected those with disease but there was a large proportion of positives in the sample)
Large value added: considerable additional certainty in the negative diagnosis and so high value of the test (accurately detected those without disease from a small total number of negatives)
Low Large value added: considerable additional certainty in the positive diagnosis and so high value of the test (accurately detected those with disease from a small total number of positives)
Little value added: limited additional certainty in the diagnosis and so limited value of the test (accurately detected those with disease but there was a large proportion of negatives in the sample)
23
24

307
Idiopathic Pulmonary Fibrosis Calculations of standard errors from HR, RR and ORs
Appendix I: Calculations of standard errors 1
from HR, RR and ORs 2
These formulae were applied for any ratio measures including HR, RR and OR 3
Using the Confidence Interval for the RR/OR/HR to find the SE
OR/RR/HR =
0.48
Upper CI limit =
0.69 Lower CI limit =
0.33
% CI (enter 0.95 for 95%; or 0.90 for 90%CI or 0.99 for 99%CI) = 0.95
No. of participants in Group 1 = 107 No. of participants in Group 2 = 2911
(divisor = 3.92 )
ln (RR) SE(ln RR)
-0.7339692 0.188163
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19

308
Idiopathic Pulmonary Fibrosis Calculations of standard errors from HR, RR and ORs
I.1.1 Calculations of SE 1
Guideline section Study ID Outcome & Prognostic factor RR/OR/HR Lower CI Upper CI ln(RR/OR/HR)
SE (In RR RR/OR/HR)
Prognosis: PFTs
DuBois2012A4 All-cause mortality:
Baseline FVC
</=50% vs. >/=80%:
- - - - -
All-cause mortality:
Baseline FVC
51% - 65% vs. >/=80%:
- - - - -
All-cause mortality:
Baseline FVC
66%-79% vs. >/=80%:
- - - - -
Caminati 2009 53
Mortality:
Baseline resting room air arterial oxygen saturation
0.816 0.537 1.241 -0.203340924 0.21369252
Mortality:
Baseline FVC (L)
2.73972603 8.064516 0.927644 1.007857925 -0.55167887
Mortality:
Baseline DLCO (mL/min/mmHg)
1.38312586 1.824818 1.048218 0.324346057 -0.14142561
DuBois2011A 117
Mortality:
Change in percent-predicted FVC
5.79 2.55 13.15 1.756132292 0.41845112
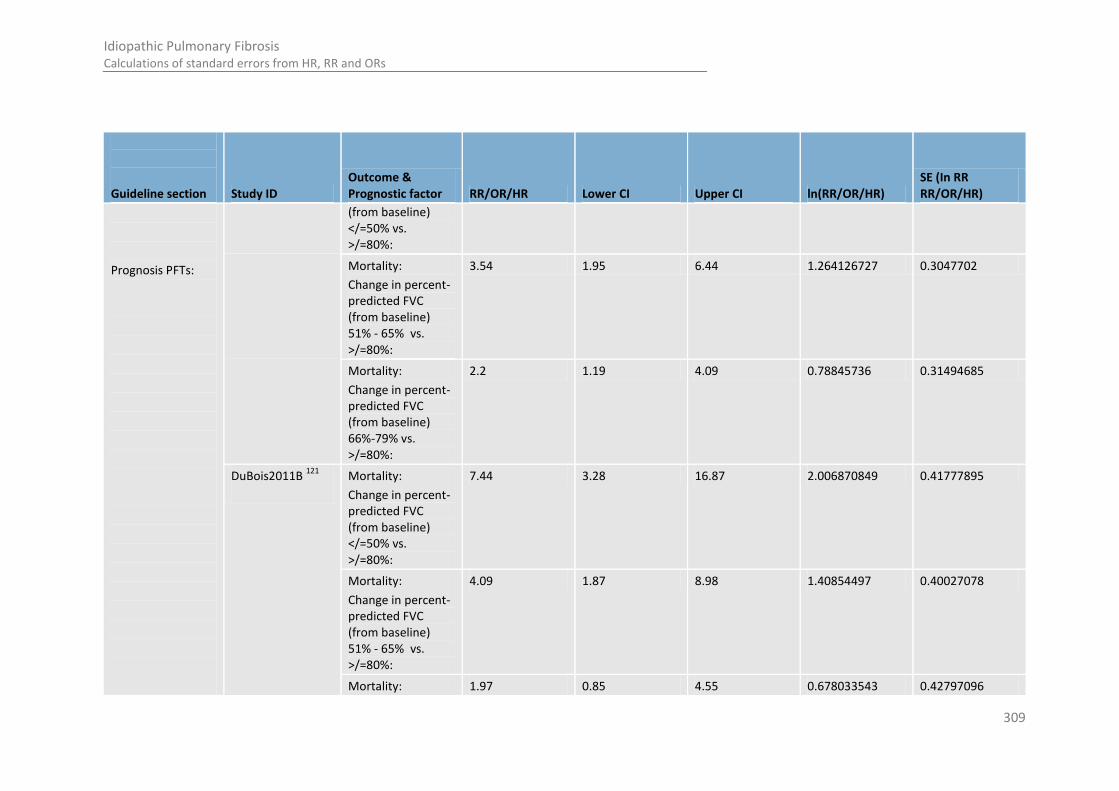
309
Idiopathic Pulmonary Fibrosis Calculations of standard errors from HR, RR and ORs
Guideline section Study ID Outcome & Prognostic factor RR/OR/HR Lower CI Upper CI ln(RR/OR/HR)
SE (In RR RR/OR/HR)
Prognosis PFTs:
(from baseline) </=50% vs. >/=80%:
Mortality:
Change in percent-predicted FVC (from baseline) 51% - 65% vs. >/=80%:
3.54 1.95 6.44 1.264126727 0.3047702
Mortality:
Change in percent-predicted FVC (from baseline) 66%-79% vs. >/=80%:
2.2 1.19 4.09 0.78845736 0.31494685
DuBois2011B 121
Mortality:
Change in percent-predicted FVC (from baseline) </=50% vs. >/=80%:
7.44 3.28 16.87 2.006870849 0.41777895
Mortality:
Change in percent-predicted FVC (from baseline) 51% - 65% vs. >/=80%:
4.09 1.87 8.98 1.40854497 0.40027078
Mortality: 1.97 0.85 4.55 0.678033543 0.42797096
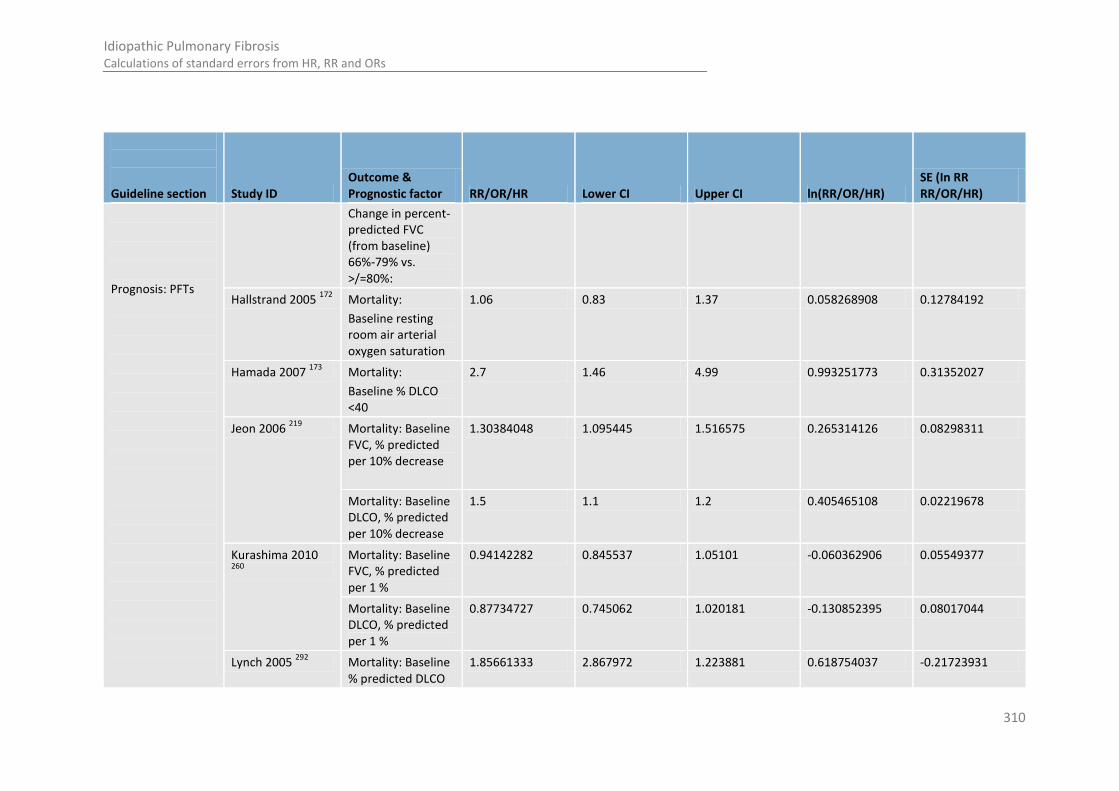
310
Idiopathic Pulmonary Fibrosis Calculations of standard errors from HR, RR and ORs
Guideline section Study ID Outcome & Prognostic factor RR/OR/HR Lower CI Upper CI ln(RR/OR/HR)
SE (In RR RR/OR/HR)
Prognosis: PFTs
Change in percent-predicted FVC (from baseline) 66%-79% vs. >/=80%:
Hallstrand 2005 172
Mortality:
Baseline resting room air arterial oxygen saturation
1.06 0.83 1.37 0.058268908 0.12784192
Hamada 2007 173
Mortality:
Baseline % DLCO <40
2.7 1.46 4.99 0.993251773 0.31352027
Jeon 2006 219
Mortality: Baseline FVC, % predicted per 10% decrease
1.30384048 1.095445 1.516575 0.265314126 0.08298311
Mortality: Baseline DLCO, % predicted per 10% decrease
1.5 1.1 1.2 0.405465108 0.02219678
Kurashima 2010 260
Mortality: Baseline FVC, % predicted per 1 %
0.94142282 0.845537 1.05101 -0.060362906 0.05549377
Mortality: Baseline DLCO, % predicted per 1 %
0.87734727 0.745062 1.020181 -0.130852395 0.08017044
Lynch 2005 292
Mortality: Baseline % predicted DLCO
1.85661333 2.867972 1.223881 0.618754037 -0.21723931
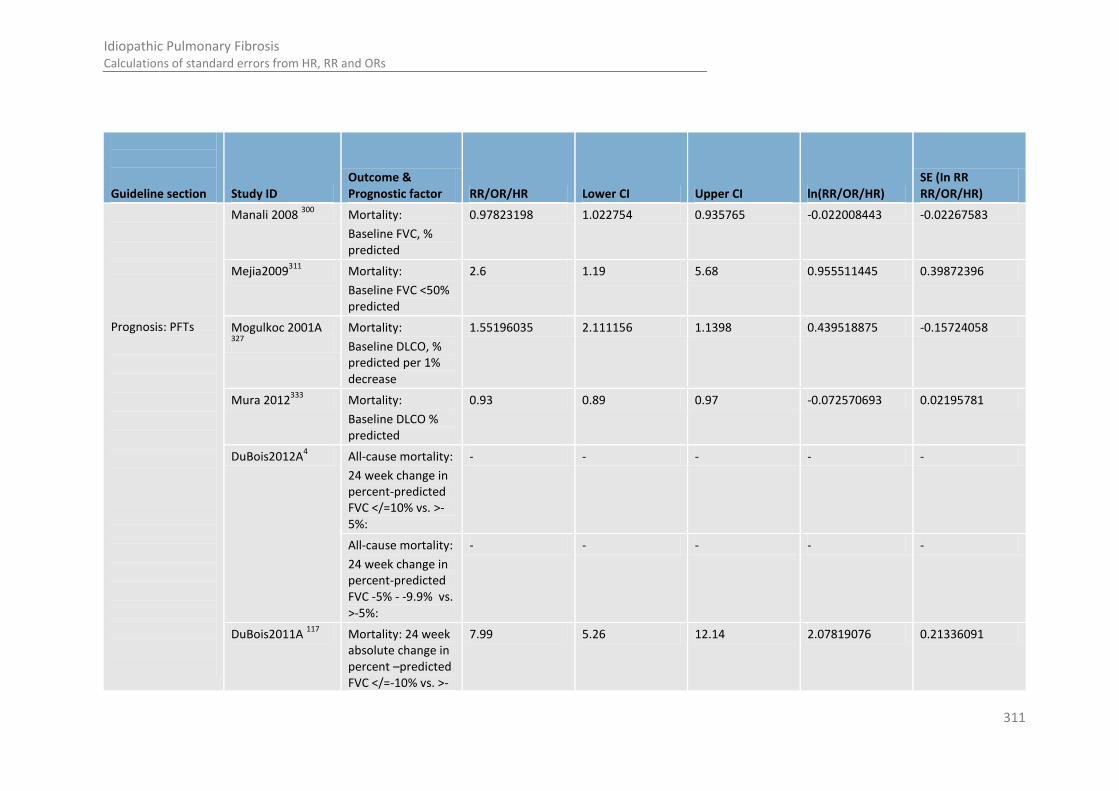
311
Idiopathic Pulmonary Fibrosis Calculations of standard errors from HR, RR and ORs
Guideline section Study ID Outcome & Prognostic factor RR/OR/HR Lower CI Upper CI ln(RR/OR/HR)
SE (In RR RR/OR/HR)
Prognosis: PFTs
Manali 2008 300
Mortality:
Baseline FVC, % predicted
0.97823198 1.022754 0.935765 -0.022008443 -0.02267583
Mejia2009311
Mortality:
Baseline FVC <50% predicted
2.6 1.19 5.68 0.955511445 0.39872396
Mogulkoc 2001A 327
Mortality:
Baseline DLCO, % predicted per 1% decrease
1.55196035 2.111156 1.1398 0.439518875 -0.15724058
Mura 2012333
Mortality:
Baseline DLCO % predicted
0.93 0.89 0.97 -0.072570693 0.02195781
DuBois2012A4 All-cause mortality:
24 week change in percent-predicted FVC </=10% vs. >-5%:
- - - - -
All-cause mortality:
24 week change in percent-predicted FVC -5% - -9.9% vs. >-5%:
- - - - -
DuBois2011A 117
Mortality: 24 week absolute change in percent –predicted FVC </=-10% vs. >-
7.99 5.26 12.14 2.07819076 0.21336091

312
Idiopathic Pulmonary Fibrosis Calculations of standard errors from HR, RR and ORs
Guideline section Study ID Outcome & Prognostic factor RR/OR/HR Lower CI Upper CI ln(RR/OR/HR)
SE (In RR RR/OR/HR)
Prognosis: PFTs
5%
Mortality: 24 week absolute change in percent –predicted FVC -5 to -9.9% vs. >-5%
2.6 1.75 3.85 0.955511445 0.20113708
DuBois2011B 121
Mortality: 24 week absolute change percentage predicted FVC </=-10% vs. >-5%:
4.78 3.12 7.33 1.564440547 0.2178935
Mortality: 24 week absolute change percentage predicted FVC -5 to -10% vs. >-5%
2.14 1.43 2.3 0.760805829 0.12123334
Caminati 2009 53
Change in oxygen saturation over 12 months follow up compared to baseline
4 13.33333 1.194743 1.386294361 -0.61539183
Mortality: Change in FVC at 12 months
7.04225352 55.55556 0.909091 1.951928221 -1.04915656
Mortality: Change in DLCO at 12 months
2.04081633 4.310345 0.965251 0.713349888 -0.38173088
Mogulkoc 2001A DLCO % predicted 2.22834787 4.364073 1.128315 0.801260445 -0.34507145
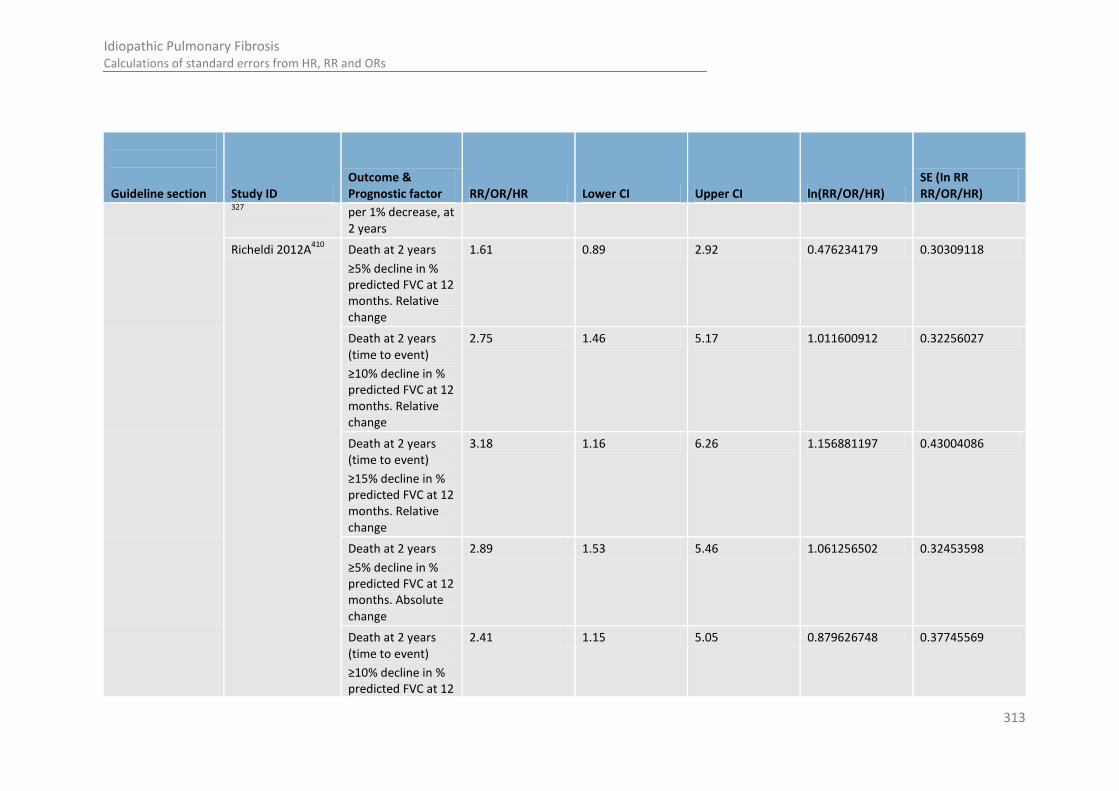
313
Idiopathic Pulmonary Fibrosis Calculations of standard errors from HR, RR and ORs
Guideline section Study ID Outcome & Prognostic factor RR/OR/HR Lower CI Upper CI ln(RR/OR/HR)
SE (In RR RR/OR/HR)
327 per 1% decrease, at
2 years
Richeldi 2012A410
Death at 2 years
≥5% decline in % predicted FVC at 12 months. Relative change
1.61 0.89 2.92 0.476234179 0.30309118
Death at 2 years (time to event)
≥10% decline in % predicted FVC at 12 months. Relative change
2.75 1.46 5.17 1.011600912 0.32256027
Death at 2 years (time to event)
≥15% decline in % predicted FVC at 12 months. Relative change
3.18 1.16 6.26 1.156881197 0.43004086
Death at 2 years
≥5% decline in % predicted FVC at 12 months. Absolute change
2.89 1.53 5.46 1.061256502 0.32453598
Death at 2 years (time to event)
≥10% decline in % predicted FVC at 12
2.41 1.15 5.05 0.879626748 0.37745569
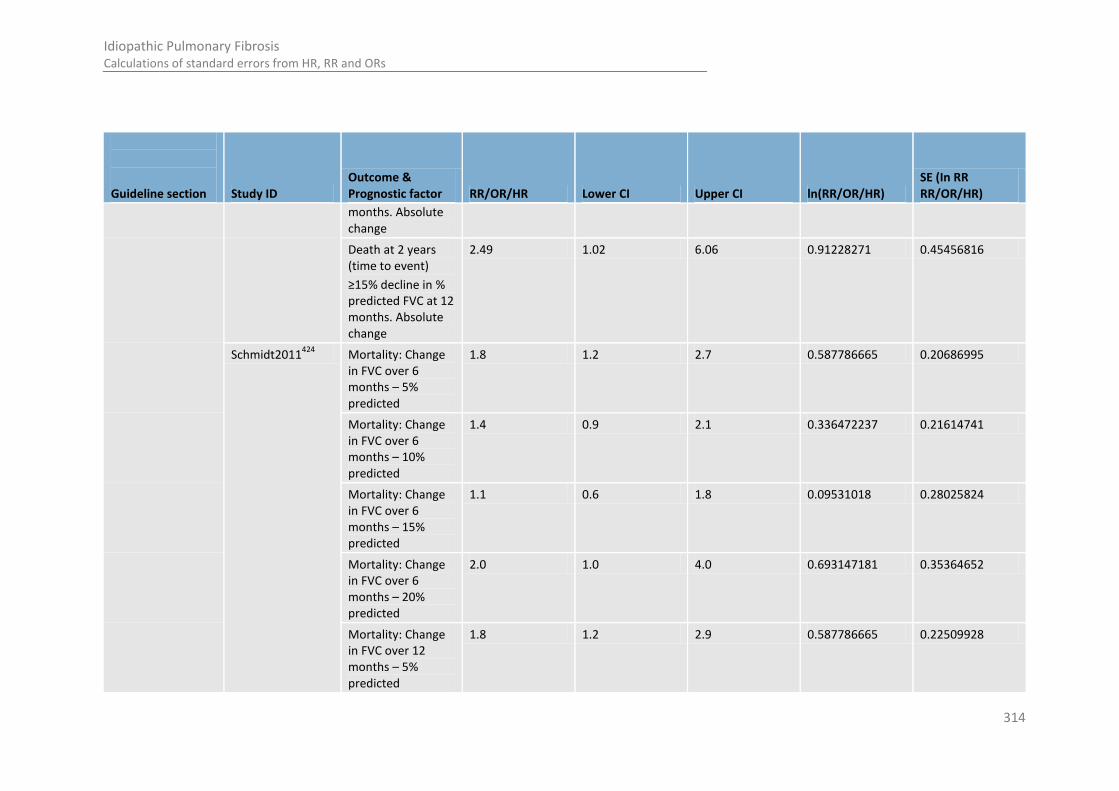
314
Idiopathic Pulmonary Fibrosis Calculations of standard errors from HR, RR and ORs
Guideline section Study ID Outcome & Prognostic factor RR/OR/HR Lower CI Upper CI ln(RR/OR/HR)
SE (In RR RR/OR/HR)
months. Absolute change
Death at 2 years (time to event)
≥15% decline in % predicted FVC at 12 months. Absolute change
2.49 1.02 6.06 0.91228271 0.45456816
Schmidt2011424
Mortality: Change in FVC over 6 months – 5% predicted
1.8 1.2 2.7 0.587786665 0.20686995
Mortality: Change in FVC over 6 months – 10% predicted
1.4 0.9 2.1 0.336472237 0.21614741
Mortality: Change in FVC over 6 months – 15% predicted
1.1 0.6 1.8 0.09531018 0.28025824
Mortality: Change in FVC over 6 months – 20% predicted
2.0 1.0 4.0 0.693147181 0.35364652
Mortality: Change in FVC over 12 months – 5% predicted
1.8 1.2 2.9 0.587786665 0.22509928

315
Idiopathic Pulmonary Fibrosis Calculations of standard errors from HR, RR and ORs
Guideline section Study ID Outcome & Prognostic factor RR/OR/HR Lower CI Upper CI ln(RR/OR/HR)
SE (In RR RR/OR/HR)
Mortality: Change in FVC over 12 months – 10% predicted
2.4 1.5 3.8 0.875468737 0.23712652
Mortality: Change in FVC over 12 months – 15% predicted
2.6 1.6 4.5 0.955511445 0.26379433
Mortality: Change in FVC over 12 months – 20% predicted
3.6 1.9 6.9 1.280933845 0.32899682
Mortality: Change in DLCO over 6 months – 10% predicted:
1.7 1.1 2.5 0.530628251 0.20943381
Mortality: Change in DLCO over 6 months – 15% predicted :
1.6 1.1 2.5 0.470003629 0.20943381
Mortality: Change in DLCO over 6 months – 20% predicted :
1.8 1.1 3.0 0.587786665 0.25594442
Mortality: Change in DLCO over 6 months – 25% predicted :
2.3 1.2 4.2 0.832909123 0.31958239

316
Idiopathic Pulmonary Fibrosis Calculations of standard errors from HR, RR and ORs
Guideline section Study ID Outcome & Prognostic factor RR/OR/HR Lower CI Upper CI ln(RR/OR/HR)
SE (In RR RR/OR/HR)
Mortality: Change in DLCO over 12 months – 10% predicted
2.2 1.4 3.5 0.78845736 0.23374764
Mortality: Change in DLCO over 12 months – 15% predicted
2.3 1.5 3.7 0.832909123 0.2303234
Mortality: Change in DLCO over 12 months – 20% predicted
3.0 1.8 4.9 1.098612289 0.25547157
Mortality: Change in DLCO over 12 months – 25% predicted
3.5 2.0 6.1 1.252762968 0.2844749
Zappala2010507
Decline in FVC at 6 months -adjusted for DLCO
3.33 1.61 6.88 1.202972304 0.37050624
Progression free survival patients with 5-10% decline in FVC compared with stable disease- adjusted for baseline DLCO
2.56 1.17 4.38 0.940007258 0.33674617
Prognosis: Sub maximal exercise DuBois2012A4
All-cause mortality:
Baseline 6MWD
- - - - -
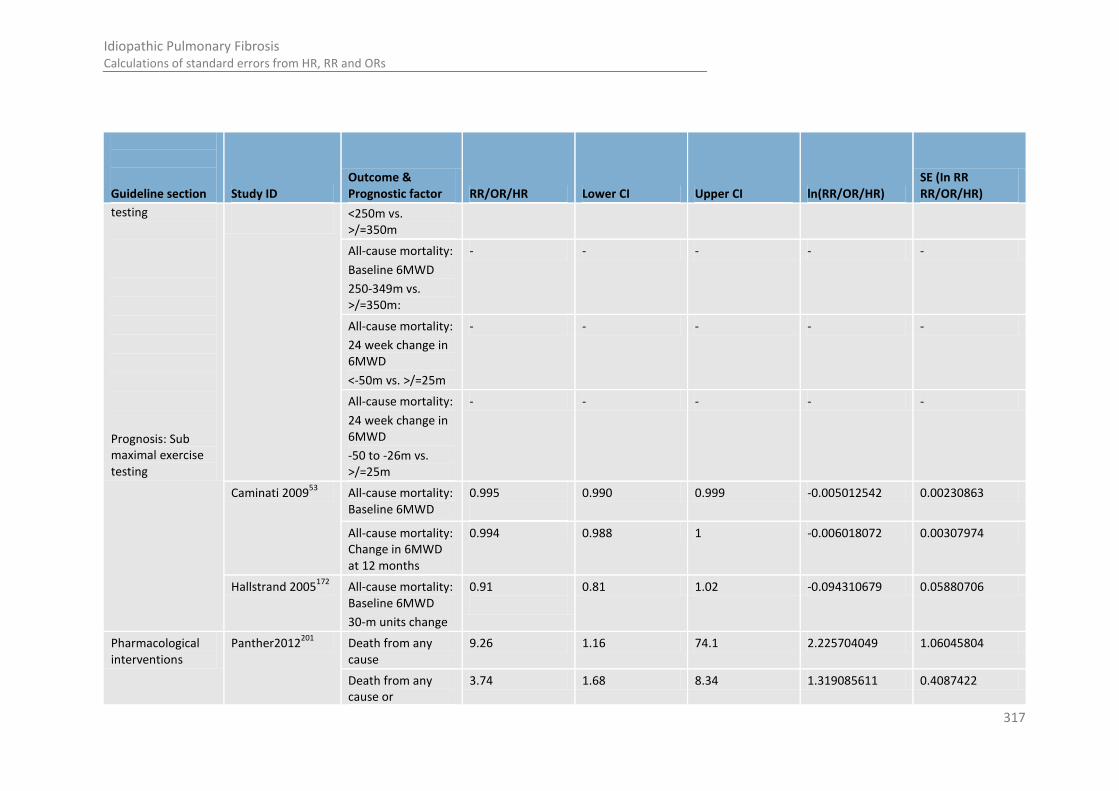
317
Idiopathic Pulmonary Fibrosis Calculations of standard errors from HR, RR and ORs
Guideline section Study ID Outcome & Prognostic factor RR/OR/HR Lower CI Upper CI ln(RR/OR/HR)
SE (In RR RR/OR/HR)
testing
Prognosis: Sub maximal exercise testing
<250m vs. >/=350m
All-cause mortality:
Baseline 6MWD
250-349m vs. >/=350m:
- - - - -
All-cause mortality:
24 week change in 6MWD
<-50m vs. >/=25m
- - - - -
All-cause mortality:
24 week change in 6MWD
-50 to -26m vs. >/=25m
- - - - -
Caminati 200953
All-cause mortality: Baseline 6MWD
0.995
0.990 0.999 -0.005012542 0.00230863
All-cause mortality: Change in 6MWD at 12 months
0.994 0.988 1 -0.006018072 0.00307974
Hallstrand 2005172
All-cause mortality: Baseline 6MWD
30-m units change
0.91
0.81 1.02 -0.094310679 0.05880706
Pharmacological interventions
Panther2012201
Death from any cause
9.26 1.16 74.1 2.225704049 1.06045804
Death from any cause or
3.74 1.68 8.34 1.319085611 0.4087422

318
Idiopathic Pulmonary Fibrosis Calculations of standard errors from HR, RR and ORs
Guideline section Study ID Outcome & Prognostic factor RR/OR/HR Lower CI Upper CI ln(RR/OR/HR)
SE (In RR RR/OR/HR)
hospitalisation
Death from any cause or >/=10% decline in FVC
1.46 0.7 3.05 0.378436436 0.3754634
Noth2012359
Primary endpoint 1.32 0.7 2.47 0.277631737 0.3216564
All-cause mortality 4.85 1.38 16.99 1.578978705 0.64044424
Combined all-cause mortality or non-elective, non-bleeding hospitalisations
2.12 1 4.52 0.751416089 0.38482449
Combined all-cause mortality or >/=10% FVC drop
1.44 0.69 2.99 0.364643114 0.37406558
1

319
Idiopathic Pulmonary Fibrosis Costing of a Multidisciplinary Team (MDT) in the Context of an Interstitial Lung Disease (ILD) Network: Finding the incremental cost of involving an MDT in the IPF diagnostic pathway.
Appendix J: Costing of a Multidisciplinary Team 1
(MDT) in the Context of an Interstitial Lung 2
Disease (ILD) Network: Finding the incremental 3
cost of involving an MDT in the IPF diagnostic 4
pathway. 5
6
J.1 Introduction 7
The addition of the MDT to the diagnostic pathway will mean extra resources will need to be made 8 available to enable staff to attend the MDT. In recognition that the specialist staff who form an MDT 9 may be geographically widely distributed, the economic consideration of adding an MDT to the 10 diagnostic pathway is undertaken with the assumption that MDTs will evolve within an ILD network 11 configuration. 12
In an ILD network, we could assume that two forms of MDTs occur: a local level MDT in secondary 13 care and a specialist level MDT in a tertiary care referral hub. The cost per IPF patient diagnosed 14 through a network of MDTs will depend on the implementation costs and on the number of ILD 15 patients (including IPF patients) diagnosed in the network. 16
The below sections propose a possible configuration for a network and estimate an incremental cost 17 of £682 per IPF patient diagnosed with MDT involvement, or £227 per ILD (including IPF) diagnosis 18 made. To note these estimated costs may cover up to one local and three tertiary MDT meetings as 19 part of the diagnostic pathway. The costing assumes that there would be one specialist MDT and six 20 local MDTs in each network, serving a population of 1.5 million. Other configurations may result in 21 different cost per diagnosis. 22
J.2 Implementation costs of local and specialist level MDTs 23
J.2.1 The type, number and location of staff involved in local MDT meetings 24
It is envisioned that at a local MDT would consist of a radiologist and respiratory medical consultant 25 as a minimum. Although there is potential involvement of a pathologist and ILD nurse (band 6), the 26 costing does not include the time of these members as part of the local team, as it is envisioned they 27 would be a shared resource across the network and included only as part of the specialist team. 28
J.2.2 The type, number and location of staff involved in specialist MDT meetings 29
It is envisioned that a specialist MDT would consist of a radiologist, chest physician and pathologist at 30 consultant grade and with a specialist interest in ILD. A nurse with a specialist interest in ILD could 31 also be present (band 6). Further, additional clerical staff could be employed to coordinate the MDTs 32 at tertiary level and provide support for local level centres. The role of the administrative staff could 33 include managing meetings, continuity of patient care, patient notes and potentially management of 34 information for audit and research purposes. 35

320
Idiopathic Pulmonary Fibrosis Costing of a Multidisciplinary Team (MDT) in the Context of an Interstitial Lung Disease (ILD) Network: Finding the incremental cost of involving an MDT in the IPF diagnostic pathway.
J.2.3 Unit cost of staff and time involvement 1
The unit cost of each cadre of staff, alongside the cost of their time for their membership in an MDT 2 meeting, is provided in Table 108. These meeting costs represent opportunity costs of the increased 3 time commitment of already employed staff to the MDT; however, the unit cost where qualification 4 has been incorporated is presented in parenthesis for information and in recognition that additional 5 staffing levels may be needed. 6
We assume that a local MDT meeting, including any additional preparation time, will involve 3 hours 7 for each clinical staff member. We assume local level MDT members are not present at specialist 8 level MDTs, and no additional referral time is costed. We assume that a specialist MDT meeting, 9 including any additional preparation time, will involve 2 hours for each clinical staff member. We 10 have not taken into account the potential for staff members to have less than 100% attendance at 11 MDT meetings. In a sensitivity analysis, the time per weekly specialist MDT was increased to 3 hours. 12
Depending on the configuration of the network it is possible some staff members will need to travel, 13 the costs (including time) of which would be in part dependent on the distances involved between 14 centres and the frequency and duration of the meetings. However, the potential to use of 15 information technology and teleconference facilities may mitigate this need. Therefore, the time and 16 cost of travel has not been considered further. 17
18
19

321
Idiopathic Pulmonary Fibrosis Costing of a Multidisciplinary Team (MDT) in the Context of an Interstitial Lung Disease (ILD) Network: Finding the incremental cost of involving an MDT in the IPF diagnostic pathway.
Table 108: Unit cost of MDT staff 1
Cadre of staff Per contract hour
Per local MDT meeting
Per specialist MDT meeting
Annual cost per member of staff for local MDT meetings
Annual cost per member of staff for specialist MDT meetings
Source
Number of meetings per year Number of meetings per year
52 26 12 52 26 12
Consultant (Medical, Radiologist, Pathologist)
£110 £330 £220 £17,160 £8,580 £3,960 £11,440 £5,720 £2,640 PSSRU (2010)
381
With Qualification £127 £381 £254 £19,812 £9,906 £4,572 £13,208 £6,604 £3,048
Specialist respiratory nurse (band 6)
£28 £84 £56 £4,368 £2,184 £1,008 £2,912 £1,456 £672 PSSRU (2010)
381
With Qualification £31 £93 £62 £4,836 £2,418 £1,116 £3,224 £1,612 £744
MDT coordinator - (Band 4 – agenda for Change point 16)
£13 (a) £489 £489 (b) £25,411 £25,411 £12,706 £25,411 £25,411 £12,706 Estimate (c)
With Qualification £13 £489 £489 £25,411 £25,411 £12,706 £25,411 £25,411 £12,706
MDT composition
3 consultants, specialist nurse and MDT coordinator
£371 £1,563 £1,205 £81,259 £53,335 £25,594 £62,643 £44,027 £21,298 Calculated
With Qualification £425 £1,725 £1,313 £89,683 £57,547 £27,538 £68,259 £46,835 £22,594
3 consultants and MDT coordinator
£343 £1,479 £1,149 £76,891 £51,151 £24,586 £59,731 £42,571 £20,626 Calculated
With Qualification £394 £1,632 £1,251 £84,847 £55,129 £26,422 £65,035 £45,223 £21,850
2 consultants £220 £660 £440 £34,320 £17,160 £7,920 £22,880 £11,440 £5,280 Calculated
With Qualification £254 £762 £508 £39,624 £19,812 £9,144 £26,416 £13,208 £6,096
(a) Per contract hour based on full annual salary plus on cost and 37.5 hour week. 2 (b) Per meeting cost based on full annual salary plus on cost divided by 52 meetings 3 (c) 52 meetings based on £21,176 annual salary with 20% employers on cost of £4235. 12 meetings based on 0.5 WTE of £21,176 per annum salary with 20% employers on cost. 4

322
Idiopathic Pulmonary Fibrosis Costing of a Multidisciplinary Team (MDT) in the Context of an Interstitial Lung Disease (ILD) Network: Finding the incremental cost of involving an MDT in the IPF diagnostic pathway.
Note: For information, cost estimates of staff time have been provided in full for information and completeness (as provided in development of the analysis). However, costs for staff not 1 used in the costing are indicated in a lighter colour. For example the cost of an ILD specialist nurse or MDT coordinator was not included in the cost of a local MDT as their input is 2 assumed only to be required for a specialist MDT. 3
4
323
Idiopathic Pulmonary Fibrosis Costing of a Multidisciplinary Team (MDT) in the Context of an Interstitial Lung Disease (ILD) Network: Finding the incremental cost of involving an MDT in the IPF diagnostic pathway.
Based on the unit costs presented in Table 108 and taking into account qualification, we could 1 estimate the annual staff cost for weekly specialist MDTs (consisting of 3 consultants, a respiratory 2 nurse and full time coordinator support) to be £62,643 (£1,351 per meeting with audio-visual 3 included). If these meetings were monthly with coordinator support (0.5 WTE), the annual staff cost 4 would be £22,594. 5
The annual staff cost for a fortnightly local MDTs consisting of only 2 consultants (i.e. a radiologist 6 and chest physician) would be £19,812 (£785 per meeting with audio-visual included). The annual 7 staff cost for monthly local MDTs consisting of only 2 consultants (i.e. a radiologist and chest 8 physician) would be £9,144 (£812 per meeting with audio-visual included). 9
J.2.4 The availability and cost of teleconferencing facilities. 10
The cost of videoconferencing will depend in part on the type of system specified and the number of 11 sites involved. Additional costs would include line rentals and potentially additional IT equipment. An 12 additional consideration is whether further administrative support or training would be required in 13 the operation of the teleconferencing facility and in preparing slides and papers for electronic 14 distribution in a timely manner. The cost of the video conferencing system would depend on the 15 number and type of inputs and outputs as well as the quality requirement. Dependent on these 16 factors commercial quotes for medical audio-visual teleconferencing range from £10,000 to £30,000 17 per centre. However, with many centres already utilising MDTs for other conditions, rooms may 18 already be set up for MDT purposes. In this case, where the ILD network could “piggy back” on 19 capital and arrangements already made, running and installation costs could be as low as £1324 20 installation fee for the hub and £45 per month fee for each participating unit (Confidential 21 communication with provider of audio-visual equipment to NHS, 2012). For the purposes of costing, 22 we have allowed a budget of £600 per local centre and £2000 for the specialist centre to invest in 23 audio-visual equipment per year. 24
J.2.5 The number of teams needed to serve the network and the configuration of MDTs within 25
the network. 26
There is diversity and variation in the existing arrangements for MDTs and referral for the diagnosis 27 of IPF patients. The incremental cost of adding an MDT into the diagnostic pathway is likely to vary 28 depending on the existing architecture, the local incidence of IPF and potential best configuration 29 (for instance, whether the MDTs at different levels are combined or done in isolation). However, in 30 the sections below we use prevalence and incidence estimates, alongside assumptions of the role of 31 the local and specialist MDTs, to provide a possible configuration of MDTs within the network for 32 costing purposes. 33
In accordance with the information presented in sections below, we could assume that a network 34 serves a population of 1.5 million. This network would have one specialist weekly MDT which would 35 review 9 patients, of which 2 or 3 would be diagnosed with IPF. In order to achieve this number of 36 referred patients per week, the network could consist of 6 local centres which would have fortnightly 37 MDTs, reviewing 25 ILD patients per MDT (either to diagnose new cases or to discuss management 38 plans). In any given month, it would be expected that a local MDT will need to refer an ILD patient to 39 a specialist MDT to confirm diagnosis of IPF. 40

324
Idiopathic Pulmonary Fibrosis Costing of a Multidisciplinary Team (MDT) in the Context of an Interstitial Lung Disease (ILD) Network: Finding the incremental cost of involving an MDT in the IPF diagnostic pathway.
J.3 The population served by each MDT and across a network 1
J.3.1 Prevalence and incidence of IPF in the UK population. 2
It has been estimated that there are around 15,000 people in the UK with a diagnosis of IPF and each 3 year 5000 new cases are identified. In 2010 the UK population was estimated to be 62.3 million (ONS 4 2011). This would give a prevalence estimate of 24 IPF patients per 100,000 population, with an 5 expected 8 newly diagnosed cases per 100,000 per year. 6
J.3.2 The number of patients reviewed and managed by local level MDTs. 7
According to the population size a network serves, the below table gives estimates on the number of 8 IPF and ILD patients (including IPF patients) that could present and be managed by the local centres 9 within a network serving the population size specified. It is assumed that IPF patients form one third 10 of the ILD patients presenting. 11
It is acknowledged that the role of the MDT may not purely be to diagnose ILD patients, but also to 12 manage their care. Although this additional role of the MDT is outside of the scope of the guideline, 13 it is considered due its potential to bring health benefit and to estimate the number of patients 14 reviewed by the MDT on a weekly or monthly basis. For costing purposes, we therefore assume that 15 local MDTs will be responsible for reviewing on the care management of all diagnosed ILD patients 16 within their catchment area. We assume that, on average, an ILD patient’s management plan is 17 reviewed by their local MDT three times per year. 18
Table 109: The number of IPF and ILD (including IPF) patients reviewed and managed by local 19 level MDTs 20
Size of population served by network
Number of new IPF cases presenting in a network
Number of diagnosed IPF patients served by a network
Number of IPF patient management plans discussed by local level MDTs in a network
Total number of IPF patients discussed by local level MDTs in a network
a=annually m=monthly wk=weekly
a m wk a m wk a m wk a m wk
62,000,000 (UK population)
5000 417 96 15, 000
1250 288 45,
000
3750 865 20,
000
1667 50,
000
100000 8 1 0 24 2 0 73 6 1 32 3 81
500000 40 3.4 1 121 10 2 363 30 7 161 13 403
750000 60 5 1 181 15 3 544 45 10 242 20 605
1000000 81 7 2 242 20 5 726 60 14 323 27 806
1500000 121 10 2 363 30 7 1089 91 21 484 40 1210
2000000 161 13 3 484 40 9 1452 121 28 645 54 1613
2500000 202 17 4 605 50 12 1815 151 35 806 67 2016
62,000,000 15,
000
1250 288 45,
000
3750 865 135,
000
11,
250
2596 150,
000
12,
500
2885
100000 24 2 0 73 6 1 218 18 4 242 20 5
500000 121 10 2 363 30 7 1089 91 21 1210 101 23
750000 181 15 3 544 45 10 1633 136 31 1815 151 35
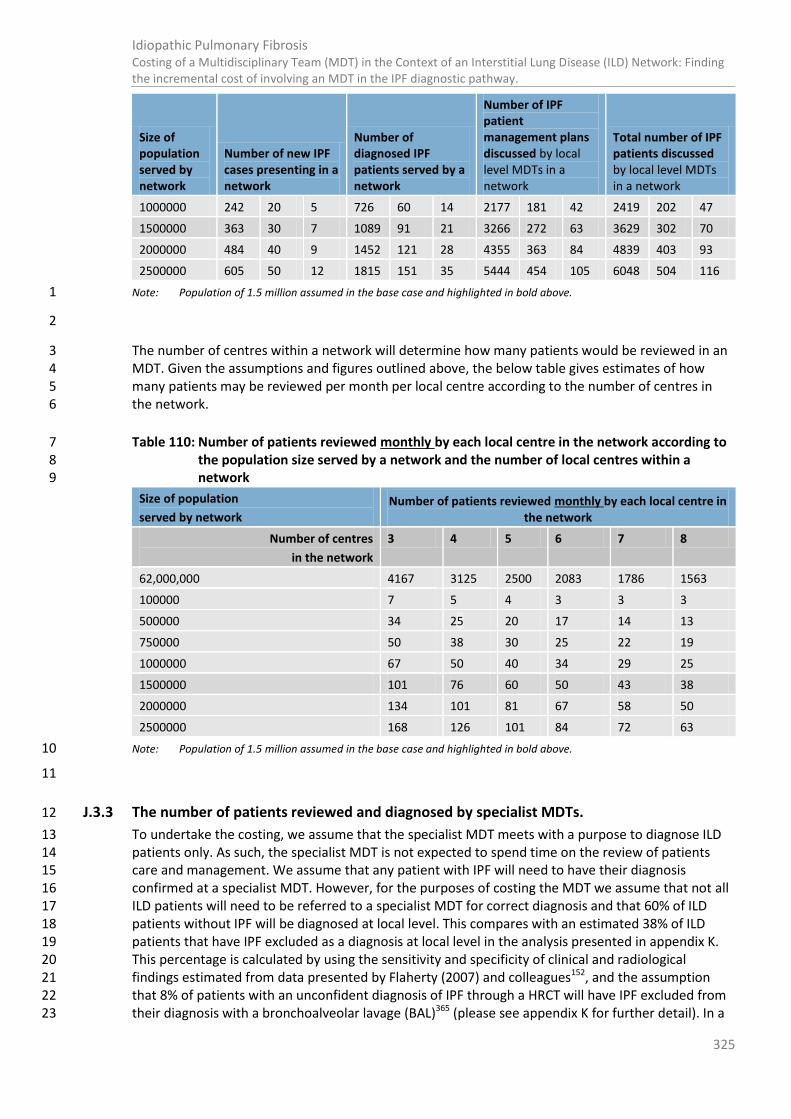
325
Idiopathic Pulmonary Fibrosis Costing of a Multidisciplinary Team (MDT) in the Context of an Interstitial Lung Disease (ILD) Network: Finding the incremental cost of involving an MDT in the IPF diagnostic pathway.
Size of population served by network
Number of new IPF cases presenting in a network
Number of diagnosed IPF patients served by a network
Number of IPF patient management plans discussed by local level MDTs in a network
Total number of IPF patients discussed by local level MDTs in a network
1000000 242 20 5 726 60 14 2177 181 42 2419 202 47
1500000 363 30 7 1089 91 21 3266 272 63 3629 302 70
2000000 484 40 9 1452 121 28 4355 363 84 4839 403 93
2500000 605 50 12 1815 151 35 5444 454 105 6048 504 116
Note: Population of 1.5 million assumed in the base case and highlighted in bold above. 1
2
The number of centres within a network will determine how many patients would be reviewed in an 3 MDT. Given the assumptions and figures outlined above, the below table gives estimates of how 4 many patients may be reviewed per month per local centre according to the number of centres in 5 the network. 6
Table 110: Number of patients reviewed monthly by each local centre in the network according to 7 the population size served by a network and the number of local centres within a 8 network 9
Size of population
served by network Number of patients reviewed monthly by each local centre in
the network
Number of centres
in the network
3 4 5 6 7 8
62,000,000 4167 3125 2500 2083 1786 1563
100000 7 5 4 3 3 3
500000 34 25 20 17 14 13
750000 50 38 30 25 22 19
1000000 67 50 40 34 29 25
1500000 101 76 60 50 43 38
2000000 134 101 81 67 58 50
2500000 168 126 101 84 72 63
Note: Population of 1.5 million assumed in the base case and highlighted in bold above. 10
11
J.3.3 The number of patients reviewed and diagnosed by specialist MDTs. 12
To undertake the costing, we assume that the specialist MDT meets with a purpose to diagnose ILD 13 patients only. As such, the specialist MDT is not expected to spend time on the review of patients 14 care and management. We assume that any patient with IPF will need to have their diagnosis 15 confirmed at a specialist MDT. However, for the purposes of costing the MDT we assume that not all 16 ILD patients will need to be referred to a specialist MDT for correct diagnosis and that 60% of ILD 17 patients without IPF will be diagnosed at local level. This compares with an estimated 38% of ILD 18 patients that have IPF excluded as a diagnosis at local level in the analysis presented in appendix K. 19 This percentage is calculated by using the sensitivity and specificity of clinical and radiological 20 findings estimated from data presented by Flaherty (2007) and colleagues152, and the assumption 21 that 8% of patients with an unconfident diagnosis of IPF through a HRCT will have IPF excluded from 22 their diagnosis with a bronchoalveolar lavage (BAL)365 (please see appendix K for further detail). In a 23
326
Idiopathic Pulmonary Fibrosis Costing of a Multidisciplinary Team (MDT) in the Context of an Interstitial Lung Disease (ILD) Network: Finding the incremental cost of involving an MDT in the IPF diagnostic pathway.
sensitivity analysis, the time requirement of the weekly specialist MDT was increased from 2 to 3 1 hours, to take into account that local expertise and level of referral. 2
It is possible that a specialist MDT could need to review the diagnosis of a patient up to three time to 3 confirm a diagnosis (i.e. to decide the need for bronchoaveolar lavage or transbronchial biopsy, to 4 interpret the results of the biopsy and consider the need for further surgical biopsy and then if 5 applicable to interpret the results of surgical biopsy). For the purposes of costing the MDT using the 6 clinical experience of the GDG we assume that: 7
70% of patients are reviewed by specialist MDT only one time (i.e. biopsy is not needed or 8 inappropriate) 9
25% of patients are reviewed by specialist MDT two times (i.e. the patient has required one 10 biopsy) 11
5% of patients are reviewed by specialist MDT three times (i.e. the patient has required two 12 biopsies) 13
If we use the sensitivity and specificity for the diagnostic interventions as extracted for the clinical 14 review from Flaherty (2007)152, Ohshimo (2009)365, Flaherty (2002) 150and Coutinho (2008)89 we could 15 estimate 53% of patients are diagnosed with clinical exam and HRCT, 43% of patients are diagnosed 16 after a first biopsy, and 4% of patients are diagnosed with a final surgical lung biopsy (please see 17 appendix K for further detail). 18
19
Table 111: Number of patients reviewed at specialist level MDT according to size of 20 population served by a network. 21
Size of population served by network
Number of patients referred weekly to specialist MDT
Number of patients on 2
nd
review
Number of patients on 3
rd
review
Total number of patients reviewed at weekly meeting
Number of ILD patients diagnosed per week
Number of IPF patients diagnosed per week
Approximate number of specialist MDTs needed to serve UK population.
62000000 231 115 23 369 231 96 1
100000 0 0 0 1 0 0 620
500000 2 1 0 3 2 1 124
750000 3 1 0 4 3 1 83
1000000 4 2 0 6 4 2 62
1500000 6 3 1 9 6 2 41
2000000 7 4 1 12 7 3 31
2500000 9 5 1 15 9 4 25
Note: Population of 1.5 million assumed in the base case and highlighted in bold above. 22
23
24
J.4 Summary 25
Based on the above information, we could argue a potential configuration for an ILD MDT network 26 configuration in the UK as follows: 27

327
Idiopathic Pulmonary Fibrosis Placing the diagnostic clinical evidence into an economic framework for decision making.
Those 41 networks across the UK could serve a population of 1.5 million each. Each network would 1 have one specialist weekly MDT which would review 4 to 5 patients, of which 2 to 3 patients would 2 be diagnosed with IPF. In order to achieve this number of patients per week, the network could 3 consist of 6 local centres which would have fortnightly MDTs, reviewing 25 ILD patients per MDT 4 (either to diagnose new cases or to discuss management plans). Each local MDT would serve a 5 population of approximately 250,000. In any given month, it would be expected that a local MDT will 6 need to refer four ILD patients to a specialist MDT to confirm diagnosis. 7
The annual opportunity cost of MDT staff across such a network would be approximately £187,131 8 (£68,259 for weekly specialist MDTs and £118,872 for fortnightly local MDTs in 6 local centres). 9 However, if we were to assume that local MDTs only spent 10 percent of time on diagnostic activity, 10 the opportunity of staff time per year would be £80,146. When an additional cost of audio-visual is 11 also accounted for, the total annual cost rises to £192,731 or £82,506 when considering diagnostic 12 time only. 13
With 121 new presentations of IPF expected annually within the network, the incremental cost of 14 running an ILD network of MDTs per IPF diagnosis would be approximately£682; or £227 per ILD 15 (including IPF) diagnosis made. This assumes that the MDT has a hundred percent diagnostic yield. 16
It is important to note that these are estimates for only one form of network configuration and 17 composition, with an assumption that 60% of ILD patients without IPF could be diagnosed at local 18 level. If less patients can be diagnosed at local level, the time requirement and cost of the specialist 19 MDT would increase If 3 hours was allowed for the specialist MDT instead of 2, the additional cost 20 per ILD (including IPF) patient diagnosed through MDT discussion would rise to £286.The incremental 21 cost would increase if the ILD network could not use facilities already in place for the cancer network 22 that utilises an MDT approach. It is likely that the most cost effective configuration will depend on 23 local need and commissioning arrangements. 24
25
Appendix K: Placing the diagnostic clinical 26
evidence into an economic framework for 27
decision making. 28
29
K.1 Introduction 30
An economic model to assess the cost effectiveness of diagnostic interventions for IPF was not 31 prioritised in this guideline; in part this was due to the fact that treatment pathways that follow a 32 correct diagnosis are still emerging and uncertain. As such the health benefit that could be obtained 33 from a correct diagnosis of IPF and the opportunity cost of an incorrect diagnosis would also be 34 uncertain. However, placing the clinical evidence in an economic framework for analysis can allow 35 estimation of the number of correct and incorrect diagnoses that result from a diagnostic strategy. 36 From these estimations it is possible to demonstrate which potential diagnostic strategies may create 37 fewer successful diagnostic outcomes than others. In addition, when the outcome of a diagnostic 38 strategy is considered alongside its cost, it is possible to demonstrate that some strategies are less 39 successful but more costly – that is to say they are dominated options and should not be 40 recommended on the grounds of cost effectiveness. 41
328
Idiopathic Pulmonary Fibrosis Placing the diagnostic clinical evidence into an economic framework for decision making.
K.1.1 Population 1
The population considered in the analysis are ILD patients presenting within a diagnostic ILD network 2 assumed to have a population of 1.5 million. We assume IPF patients form one third of all ILD 3 patients presenting within the network, and on this basis estimate that there will be approximately 4 121 new presentations per annum. We assume all of the starting population is fit enough to biopsy. 5
K.1.2 The comparators 6
Eight diagnostic strategies are compared in the analysis. These strategies are based on four 7 scenarios, as outlined below. Each scenario was considered with and without MDT involvement. 8
Scenario 1: Clinical examination (including PFTs) and HRCT only. 9
Scenario 2: Clinical examination (including PFTs) and HRCT, with the addition of BAL for any patients 10 which could not have a confident diagnosis using HRCT findings. 11
Scenario 3: Clinical examination (including PFTs) and HRCT, with the addition of BAL for any patients 12 which could not have a confident diagnosis using HRCT findings. Where BAL could not exclude IPF 13 with certainty, these patients would have a biopsy. That is to say only patients which had an 14 unconfident diagnosis would be referred for biopsy. 15
Scenario 4: Clinical examination (including PFTs) and HRCT, with the addition of BAL for any patients 16 which could not have a confident diagnosis using HRCT findings. With the exception of patients that 17 were diagnosed with an alternative ILD at BAL, all patients have a biopsy to confirm diagnosis of 18 HRCT. 19
K.2 Clinical Effectiveness inputs in the primary analysis 20
The analysis is based on clinical evidence identified in the diagnostic systematic review undertaken 21 for the guideline, supplemented by additional data sources as required. A summary of the inputs 22 used in the base-case (primary) analysis is provided in the table below. 23
Table 112: Inputs to estimate diagnostic accuracy of interventions in the diagnostic pathway in the 24 base-case analysis 25
Intervention
Value Source Notes
Clinical examination and HRCT
Confident diagnosis Sensitivity 67% Calculation using data presented by Flaherty (2007)
MDT final agreement used as reference standard. All questionable cases are excluded in the calculation. Calculation used data from community and academic clinicians and radiologists.
Specificity 89%
Unconfident diagnosis
Specificity 58% Calculation using data presented by Flaherty (2007)
MDT final agreement used as reference standard. All questionable cases are included in the calculation. Calculation used data from community and academic clinicians and radiologists.
Specificity 82%
Clinical examination and HRCT + MDT
Confident diagnosis Sensitivity 92% Calculation using MDT final agreement used as

329
Idiopathic Pulmonary Fibrosis Placing the diagnostic clinical evidence into an economic framework for decision making.
Intervention
Value Source Notes
Specificity 94% data presented by Flaherty (2007)
reference standard. All questionable cases are excluded in the calculation. Calculation used data from community and academic clinicians and radiologists.
Unconfident diagnosis
Sensitivity 76% Calculation using data presented by Flaherty (2007)
MDT final agreement used as reference standard. All questionable cases are included in the calculation. Calculation used data from community and academic clinicians and radiologists.
Specificity 67%
Bronchoalveolar lavage (BAL)
Percentage of IPF cases confirmed at HRCT that will be rediagnosed as not having IPF with BAL
8% Ohshimo (2009) This percentage applies to the total number diagnosed with IPF at HRCT, but is only composed of the false positives
Percentage of cases suspected without IPF, confirmed negative with BAL
25% Expert opinion This percentage applies to the total number diagnosed without IPF at HRCT, but is only composed of the true negatives
Accuracy of biopsy after clinical exam, HRCT.
After a confident HRCT diagnosis
Sensitivity 96% Calculation using data presented by Flaherty (2007)
MDT final agreement used as reference standard. All questionable cases are excluded in the calculation. Calculation used data from community and academic pathologists.
Specificity 72%
After an unconfident HRCT diagnosis
Sensitivity 88%
Calculation using data presented by Flaherty (2007)
MDT final agreement used as reference standard. All questionable cases are included in the calculation. Calculation used data from community and academic pathologists.
Specificity 59%
Accuracy of biopsy after clinical exam, HRCT + MDT
After a confident HRCT diagnosis Sensitivity 99%
Calculation using data presented by Flaherty (2007)
MDT final agreement used as reference standard. All questionable cases are excluded in the calculation. Calculation used data from community and academic pathologists.
Specificity 89%
After an unconfident HRCT diagnosis
Sensitivity 85% Calculation using data presented by Flaherty (2007)
MDT final agreement used as reference standard. All questionable cases are included in the calculation. Calculation used data from community and academic pathologists.
Specificity 71%
Probability that diagnosis will be confident at clinical exam and HRCT
when patient has IPF 74%
Calculated from

330
Idiopathic Pulmonary Fibrosis Placing the diagnostic clinical evidence into an economic framework for decision making.
Intervention
Value Source Notes
when patient has not got IPF 38%
Hunninghake (2007)
K.3 Analytical Overview 1
K.3.1 Placing the clinical effectiveness data into an analytical framework 2
Using the inputs identified by systematic review and listed above, a series of 2 by 2 tables were 3 constructed for each intervention in the diagnostic pathway to calculate the number of true 4 positives, true negatives, false negatives and false positives that could be expected for each scenario. 5 Those constructed for the diagnostic pathway without MDT involvement are depicted in Figure 113 6 and Figure 114; however the exact same structure was used for the pathway with MDT involvement. 7 The figures in the table have been rounded to 2 decimal places as calculated by the pathway; 8 however, for explanatory purposes the text below explains the figures in whole numbers which may 9 differ slightly due to rounding error. 10
To note, the information shown in Figure 114 shows the level of agreement between the diagnosis 11 by clinical exam and HRCT, and the diagnosis made by biopsy. So for example, 60 patients were 12 correctly and confidently diagnosed with IPF by HRCT, and subsequent biopsy would correctly 13 diagnose a further 26 patients, and as such assumed to be in agreement in 60 true positive cases. 14 HRCT correctly and confidently diagnosed 81 patients to not have IPF, whereas a biopsy only 15 correctly diagnosed 66 patients to not have IPF, therefore HRCT and biopsy agreed 66 true negative 16 cases. Further HRCT and biopsy agreed in 3 false negative cases and 10 false positive cases (i.e. both 17 interventions diagnosed incorrectly). 18
Therefore in patients where a confident diagnosis was made by HRCT, the biopsy agrees with the 19 diagnostic conclusion in 138 out of 181 cases (77%). In the other 43 cases HRCT and biopsy will 20 disagree and the diagnosis will be uncertain. The level of agreement is affected by the prior 21 prevalence of disease, as the two tests could come to the same conclusion by chance. Therefore, for 22 information the kappa statistic was calculated to measure interobserver agreement. So for instance 23 when HRCT findings are confident, the level of agreement adjusting for chance is 0.56 (the kappa 24 statistic). 25
The pathway allowed four different scenarios to be explored. 26
The first scenario is that where the patient is only offered a HRCT scan. It considered only the 27 outcomes from the 2 by 2 tables constructed for the confident and unconfident HRCT. These tables 28 can be seen in Figure 113. 29
The second scenario is that where the patient is offered a HRCT scan, and if the diagnosis is 30 unconfident they are then offered BAL. Scenario 2 considered only the outcomes seen in the 2 by 2 31 table constructed for confident HRCT findings and those after BAL had been performed on patients 32 with unconfident HRCT findings. These tables can be seen in Figure 113 33
The third scenario is that where the patient is offered a HRCT scan, and if the diagnosis is 34 unconfident is offered BAL to rule out IPF. Those which are not ruled out with BAL are offered biopsy. 35 This scenario considered the outcomes seen in the 2 by 2 table constructed for confident HRCT 36 findings and the patients which had left the pathway after BAL (i.e. patients which BAL confirmed as 37 true negatives). In addition this scenario considered the outcomes in the 2 by 2 table constructed 38 using the cases where uncertain HRCT findings and biopsy agreed or disagreed, as shown in Figure 39 114. 40
331
Idiopathic Pulmonary Fibrosis Placing the diagnostic clinical evidence into an economic framework for decision making.
The fourth scenario is that where every patient is offered an additional diagnostic procedure after 1 HRCT. If the diagnosis is confident at HRCT, the patient is offered biopsy to confirm. If the diagnosis is 2 unconfident at HRCT, the patient is offered BAL to rule out IPF, and if IPF is still suspected is offered 3 biopsy. This scenario considered the patients which had left the pathway after BAL (as seen in Figure 4 113) as well as the outcomes in the 2 by 2 table constructed using the cases where uncertain and 5 certain HRCT findings and biopsy agreed or disagreed (as shown in Figure 114). 6
When only HRCT or BAL was considered in the pathway (scenarios 1 and 2), the outcomes were to be 7 diagnosed with or without IPF, either correctly or incorrectly. When biopsy was considered as an 8 additional step (scenarios 3 and 4), there was also the possibility of an uncertain diagnosis as an 9 outcome (whereby HRCT and biopsy disagreed). The outcomes for each of the scenarios with MDT 10 involvement were considered in the same manner as described above. 11
12
13
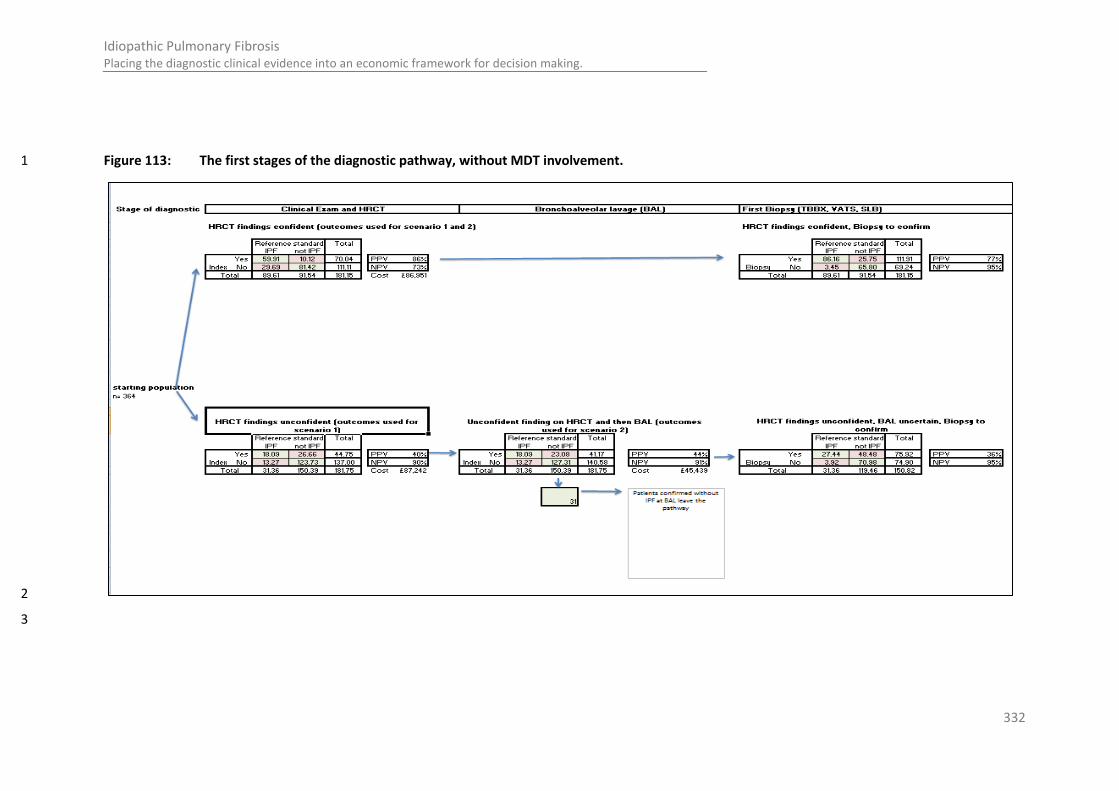
332
Idiopathic Pulmonary Fibrosis Placing the diagnostic clinical evidence into an economic framework for decision making.
Figure 113: The first stages of the diagnostic pathway, without MDT involvement. 1
2
3

333
Idiopathic Pulmonary Fibrosis Placing the diagnostic clinical evidence into an economic framework for decision making.
Figure 114: The level of agreement between the diagnostic conclusion of the HRCT and biopsy (post HRCT) which would be found with no MDT 1 involvement. 2
3

334
Idiopathic Pulmonary Fibrosis Placing the diagnostic clinical evidence into an economic framework for decision making.
1

335
Idiopathic Pulmonary Fibrosis Placing the diagnostic clinical evidence into an economic framework for decision making.
K.4 Calculating the cost of each diagnostic strategy 1
From the series of 2 by 2 tables, the number of patients undertaking each diagnostic intervention in 2 both the pathways with and without MDT involvement could be calculated. To find the total cost of 3 diagnostic pathway in each scenario, the unit cost of each diagnostic intervention was multiplied by 4 the number of patients having the intervention. The cost of staff time was used to estimate the cost 5 of the MDT, with the cost of audiovisual equipement is incorporated in the cost of a specialist MDT . 6
To incorporate the cost of MDT involvement in the diagnostic model, the assumption is made that 7 everyone entering the pathway is fit enough to benefit from biopsy. This differs from the approach 8 used in the MDT costing presented Appendix J where clinical members considered the likelihood of 9 being fit enough to biopsy in their estimate of the likelihood of being reviewed more than once by a 10 specialist MDT. 11
With the assumption that everyone entering the pathway is fit enough to benefit from biopsy, the 12 proportion of patients being reviewed by a local MDT or specialist MDT can be derived by the 13 diagnostic pathways. In scenario 1, every patient has a HRCT but no further intervention, therefore 14 the patient is reviewed once by a local level MDT. In scenario 2, every patient has a HRCT and a 15 proportion with a confident diagnosis will be diagnosed at local level MDT – the remainder will be 16 reviewed by a specialist level MDT (i.e. with a pathologist) before BAL and post BAL. In the third 17 scenario, again a proportion will have a confident diagnosis at local level MDT – the remainder will be 18 reviewed by a specialist MDT (i.e. with a pathologist) before BAL and post BAL, and in some cases 19 post biopsy where applicable. In the fourth scenario, every patient will be reviewed at least one 20 review by a specialist MDT as every patient undergoes BAL or biopsy (mirroring the assumption made 21 in the MDT costing outlined in Appendix J. The number of diagnostic patient reviews at each level is 22 therefore dependent on the assumptions made in the scenario and the accuracy/level of confidence 23 at each stage in the pathway. 24
The table below also details the number of patients that require a diagnostic review per monthly 25 MDT meeting at a local level, or at a weekly meeting at a specialist level. This was calculated based 26 on the number of patients requiring a diagnostic review given the incidence of IPF within a network 27 of 1.5 million. 28
Table 113: Data generated from and used in costing of MDT diagnostic pathways 29 Scenario
1 2 3 4
% of IPF patients which are diagnosed at local level 100% 74% 74% 0%
% of non IPF patients which are excluded at local level 100% 38% 38% 0%
% of all patients diagnosed at local level 100% 50% 50% 0%
Of those patients who have not been diagnosed at local level
% of patients which are reviewed three times by specialist MDT
0% 0% 86% 93%
% of patients which are reviewed twice by specialist MDT 0% 100% 14% 7%
% of patients which are reviewed once by specialist MDT (%) 0% 0% 0% 0%
Number of diagnostic reviews undertaken in an MDT
In one local MDT per month 50 50 50 50
In one specialist MDT per week (including first, second and third reviews) 0 9 13 27
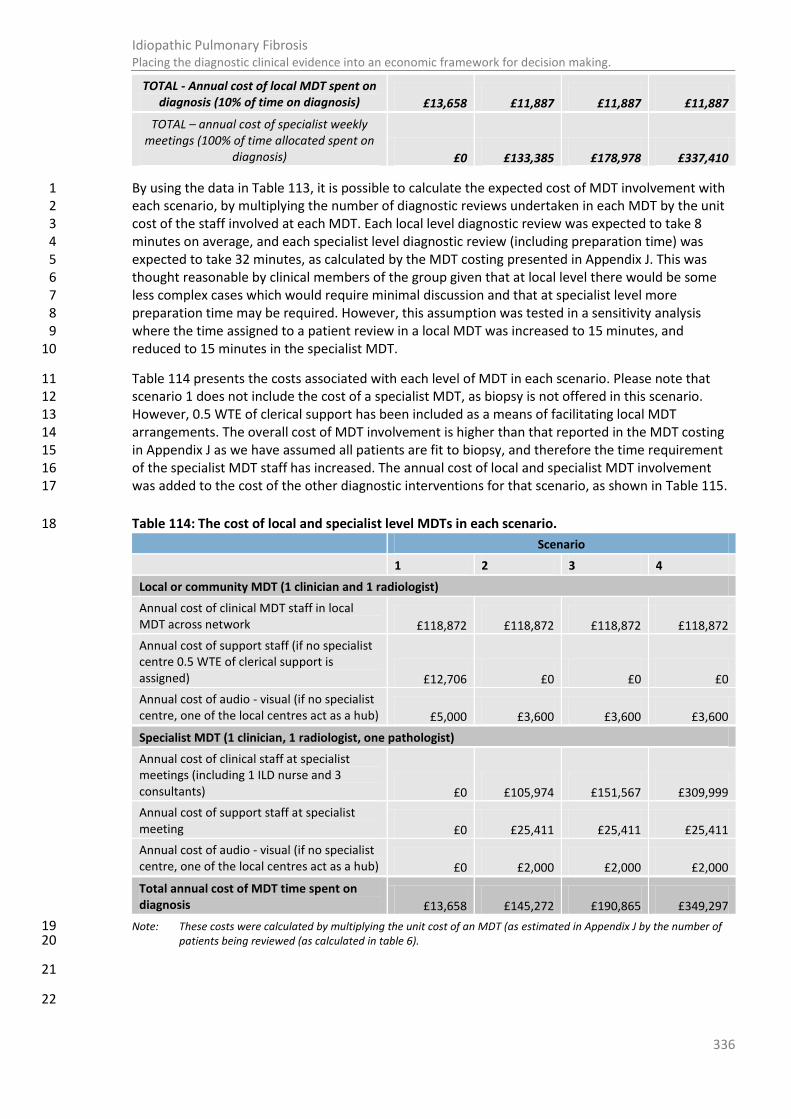
336
Idiopathic Pulmonary Fibrosis Placing the diagnostic clinical evidence into an economic framework for decision making.
By using the data in Table 113, it is possible to calculate the expected cost of MDT involvement with 1 each scenario, by multiplying the number of diagnostic reviews undertaken in each MDT by the unit 2 cost of the staff involved at each MDT. Each local level diagnostic review was expected to take 8 3 minutes on average, and each specialist level diagnostic review (including preparation time) was 4 expected to take 32 minutes, as calculated by the MDT costing presented in Appendix J. This was 5 thought reasonable by clinical members of the group given that at local level there would be some 6 less complex cases which would require minimal discussion and that at specialist level more 7 preparation time may be required. However, this assumption was tested in a sensitivity analysis 8 where the time assigned to a patient review in a local MDT was increased to 15 minutes, and 9 reduced to 15 minutes in the specialist MDT. 10
Table 114 presents the costs associated with each level of MDT in each scenario. Please note that 11 scenario 1 does not include the cost of a specialist MDT, as biopsy is not offered in this scenario. 12 However, 0.5 WTE of clerical support has been included as a means of facilitating local MDT 13 arrangements. The overall cost of MDT involvement is higher than that reported in the MDT costing 14 in Appendix J as we have assumed all patients are fit to biopsy, and therefore the time requirement 15 of the specialist MDT staff has increased. The annual cost of local and specialist MDT involvement 16 was added to the cost of the other diagnostic interventions for that scenario, as shown in Table 115. 17
Table 114: The cost of local and specialist level MDTs in each scenario. 18
Scenario
1 2 3 4
Local or community MDT (1 clinician and 1 radiologist)
Annual cost of clinical MDT staff in local MDT across network £118,872 £118,872 £118,872 £118,872
Annual cost of support staff (if no specialist centre 0.5 WTE of clerical support is assigned) £12,706 £0 £0 £0
Annual cost of audio - visual (if no specialist centre, one of the local centres act as a hub) £5,000 £3,600 £3,600 £3,600
Specialist MDT (1 clinician, 1 radiologist, one pathologist)
Annual cost of clinical staff at specialist meetings (including 1 ILD nurse and 3 consultants) £0 £105,974 £151,567 £309,999
Annual cost of support staff at specialist meeting £0 £25,411 £25,411 £25,411
Annual cost of audio - visual (if no specialist centre, one of the local centres act as a hub) £0 £2,000 £2,000 £2,000
Total annual cost of MDT time spent on diagnosis £13,658 £145,272 £190,865 £349,297
Note: These costs were calculated by multiplying the unit cost of an MDT (as estimated in Appendix J by the number of 19 patients being reviewed (as calculated in table 6). 20
21
22
TOTAL - Annual cost of local MDT spent on diagnosis (10% of time on diagnosis) £13,658 £11,887 £11,887 £11,887
TOTAL – annual cost of specialist weekly meetings (100% of time allocated spent on
diagnosis) £0 £133,385 £178,978 £337,410
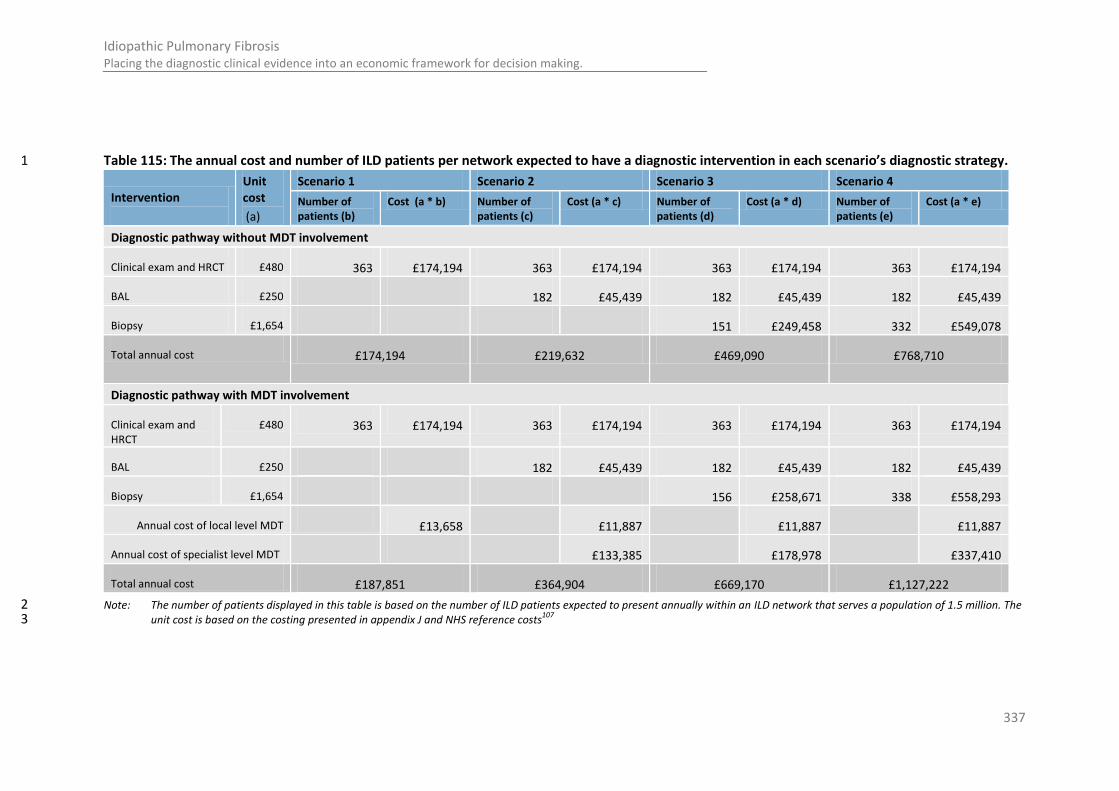
337
Idiopathic Pulmonary Fibrosis Placing the diagnostic clinical evidence into an economic framework for decision making.
Table 115: The annual cost and number of ILD patients per network expected to have a diagnostic intervention in each scenario’s diagnostic strategy. 1
Intervention
Unit cost
(a)
Scenario 1 Scenario 2 Scenario 3 Scenario 4
Number of patients (b)
Cost (a * b) Number of patients (c)
Cost (a * c) Number of patients (d)
Cost (a * d) Number of patients (e)
Cost (a * e)
Diagnostic pathway without MDT involvement
Clinical exam and HRCT £480 363 £174,194 363 £174,194 363 £174,194 363 £174,194
BAL £250 182 £45,439 182 £45,439 182 £45,439
Biopsy £1,654 151 £249,458 332 £549,078
Total annual cost £174,194 £219,632 £469,090 £768,710
Diagnostic pathway with MDT involvement
Clinical exam and HRCT
£480 363 £174,194 363 £174,194 363 £174,194 363 £174,194
BAL £250 182 £45,439 182 £45,439 182 £45,439
Biopsy £1,654 156 £258,671 338 £558,293
Annual cost of local level MDT £13,658
£11,887
£11,887
£11,887
Annual cost of specialist level MDT
£133,385
£178,978
£337,410
Total annual cost £187,851 £364,904 £669,170 £1,127,222
Note: The number of patients displayed in this table is based on the number of ILD patients expected to present annually within an ILD network that serves a population of 1.5 million. The 2 unit cost is based on the costing presented in appendix J and NHS reference costs
107 3

338
Idiopathic Pulmonary Fibrosis Placing the diagnostic clinical evidence into an economic framework for decision making.
K.4.1 Estimation of the health benefit of the diagnostic outcomes 1
The outcome of a diagnostic strategy can be placed in four categories: true positives (IPF patients 2 correctly diagnosed with IPF), true negatives (ILD patients without IPF correctly excluded of an IPF 3 diagnosis), false negatives (IPF patients incorrectly excluded of an IPF diagnosis) and false positives 4 (ILD patients without IPF incorrectly being diagnosed with IPF). The health benefit and cost 5 associated with each of these outcomes in the IPF population is not known, as effective management 6 of IPF are still emerging and are uncertain. However, the potential consequences of the various 7 diagnostic outcomes should be given due consideration. One means of doing so is by attaching a 8 hypothetical Quality Adjusted Life Year to each outcome and explore how the impact of changing the 9 QALY associated with each outcome influences the results of the analysis. 10
The below table gives a qualitative summary of the potential consequences of each diagnostic 11 outcome, and details the QALY given to each diagnostic outcome found in the analyses. To note, the 12 downstream cost which could be required to achieve the downstream health benefit has not been 13 considered further in the analysis, and therefore the results should be interpreted with caution. 14
Table 116: Estimation of the health benefit which could be found with each diagnostic outcome. 15
Diagnostic Outcome
Potential downstream cost and health benefit
Hypothetical QALY associated with each diagnostic outcome
Base case analysis (a)
Sensitivity Analysis 1(b)
Sensitivity Analysis 2 (c)
Sensitivity Analysis 3 (d)
True positives
Timely IPF management plan with health benefit (QoL)
Utility of correct prognosis
+0.08 QALY
+ 0.7 QALY +0.7 QALY 0
True negatives
Possible diagnosis of alternative condition with health benefit of appropriate management
Appropriate onward referral and associated benefit (outside scope)
+0.08 QALY
+0.7 QALY +0.7 QALY +0.7 QALY
False negatives
Delayed diagnosis of IPF with possible less effective management options (i.e. reduced QoL for longer time)
Inappropriate onward referral, further investigative tests
-0.08 QALY -0.7 QALY 0 0
False positives
Patients with conditions other than IPF may miss out on health benefit of alternative treatment
Patient “disutility” of incorrect prognosis for other patients
-0.08 QALY -0.7 QALY 0 0
(a) 0.08 is the minimally important difference used in this guideline for a quality of life improvement. In this analysis we 16 assume that a correct diagnosis will improve the quality of life of an ILD patient for one year. 17
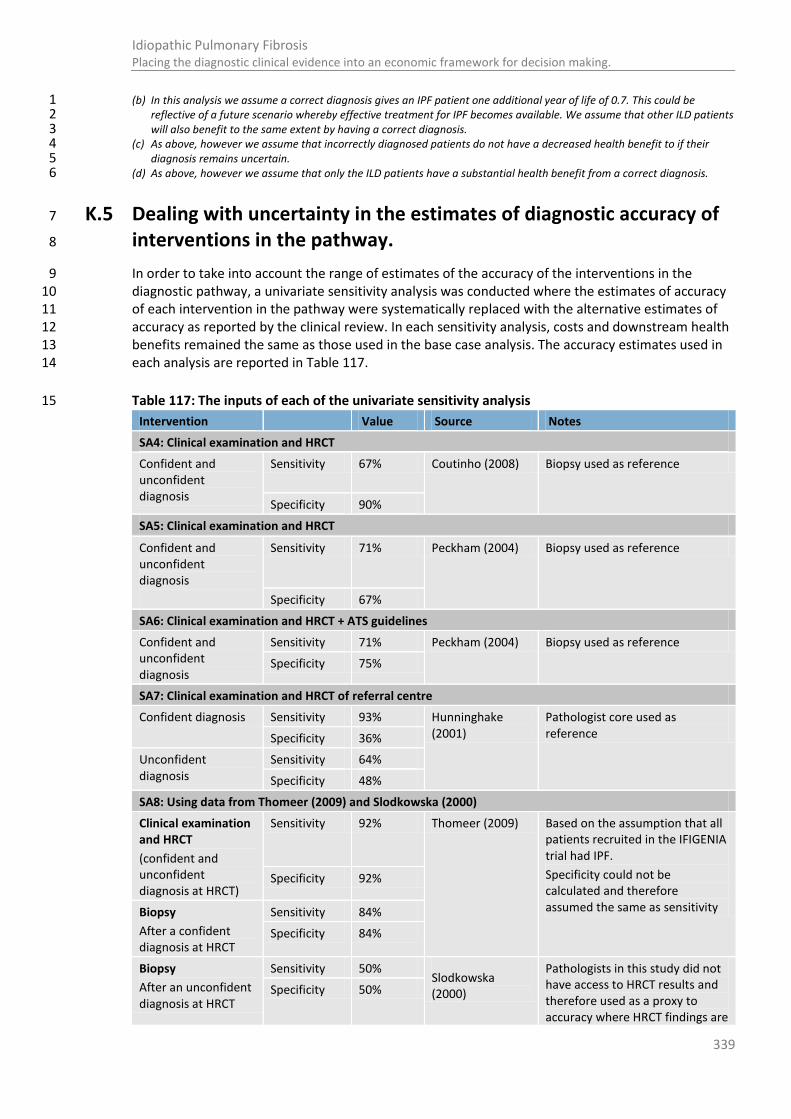
339
Idiopathic Pulmonary Fibrosis Placing the diagnostic clinical evidence into an economic framework for decision making.
(b) In this analysis we assume a correct diagnosis gives an IPF patient one additional year of life of 0.7. This could be 1 reflective of a future scenario whereby effective treatment for IPF becomes available. We assume that other ILD patients 2 will also benefit to the same extent by having a correct diagnosis. 3
(c) As above, however we assume that incorrectly diagnosed patients do not have a decreased health benefit to if their 4 diagnosis remains uncertain. 5
(d) As above, however we assume that only the ILD patients have a substantial health benefit from a correct diagnosis. 6
K.5 Dealing with uncertainty in the estimates of diagnostic accuracy of 7
interventions in the pathway. 8
In order to take into account the range of estimates of the accuracy of the interventions in the 9 diagnostic pathway, a univariate sensitivity analysis was conducted where the estimates of accuracy 10 of each intervention in the pathway were systematically replaced with the alternative estimates of 11 accuracy as reported by the clinical review. In each sensitivity analysis, costs and downstream health 12 benefits remained the same as those used in the base case analysis. The accuracy estimates used in 13 each analysis are reported in Table 117. 14
Table 117: The inputs of each of the univariate sensitivity analysis 15
Intervention
Value Source Notes
SA4: Clinical examination and HRCT
Confident and unconfident diagnosis
Sensitivity 67% Coutinho (2008) Biopsy used as reference
Specificity 90%
SA5: Clinical examination and HRCT
Confident and unconfident diagnosis
Sensitivity 71% Peckham (2004) Biopsy used as reference
Specificity 67%
SA6: Clinical examination and HRCT + ATS guidelines
Confident and unconfident diagnosis
Sensitivity 71% Peckham (2004) Biopsy used as reference
Specificity 75%
SA7: Clinical examination and HRCT of referral centre
Confident diagnosis Sensitivity 93% Hunninghake (2001)
Pathologist core used as reference Specificity 36%
Unconfident diagnosis
Sensitivity 64%
Specificity 48%
SA8: Using data from Thomeer (2009) and Slodkowska (2000)
Clinical examination and HRCT
(confident and unconfident diagnosis at HRCT)
Sensitivity 92% Thomeer (2009) Based on the assumption that all patients recruited in the IFIGENIA trial had IPF.
Specificity could not be calculated and therefore assumed the same as sensitivity
Specificity 92%
Biopsy
After a confident diagnosis at HRCT
Sensitivity 84%
Specificity 84%
Biopsy
After an unconfident diagnosis at HRCT
Sensitivity 50% Slodkowska (2000)
Pathologists in this study did not have access to HRCT results and therefore used as a proxy to accuracy where HRCT findings are
Specificity 50%

340
Idiopathic Pulmonary Fibrosis Placing the diagnostic clinical evidence into an economic framework for decision making.
Intervention
Value Source Notes
unconfident. Specificity could not be calculated and therefore assumed the same as sensitivity
SA9: Clinical exam, HRCT and Biopsy
Biopsy
After a confident diagnosis at HRCT
Sensitivity 63% Flaherty (2002) All patients assumed IIP, SLB + HRCT, but this is not clearly
reported in paper. Specificity could not be calculated and therefore assumed the same as sensitivity
Specificity 63%
Biopsy
After an unconfident diagnosis at HRCT
Sensitivity 50% Slodkowska (2000)
Pathologists in this study did not have access to HRCT results and therefore used as a proxy to accuracy where HRCT findings are unconfident. Specificity could not be calculated and therefore assumed the same as sensitivity
Specificity 50%
K.6 Examining the effect of community versus academic clinical staff in 1
the diagnostic pathway. 2
Flaherty et al (2007) provided patient level data which showed the frequency at which a clinician, 3 radiologist and pathologist would amend their diagnosis post an MDT consensus. Data was 4 disaggregated according to whether the consultant worked in a community or academic setting. 5 Using the MDT consensus as a reference standard, it was possible to calculate the sensitivity and 6 specificity of the radiologist and clinician, or pathologist, in obtaining the diagnosis eventually 7 arrived by MDT consensus in both a community setting and an academic setting. In a sensitivity 8 analysis this data is explored further to examine the impact the setting in which the consultant works 9 may have on their accuracy of diagnosis. To note all other inputs, including all unit costs, remained 10 the same as the base-case. 11
Table 118: Diagnostic accuracy estimates derived for community and academic clinical staff 12
Intervention
Value Notes
Community setting - Clinical examination and HRCT
Confident diagnosis Sensitivity 78% Calculation used data from community clinicians and radiologists only.
Specificity 80%
Unconfident diagnosis Sensitivity 71%
Specificity 70%
Academic setting - Clinical examination and HRCT
Confident diagnosis Sensitivity 60% Calculation used data from academic clinicians and radiologists only.
Specificity 95%
Unconfident diagnosis Sensitivity 49%
Specificity 90%
Community setting - Clinical examination and HRCT, + MDT
Confident diagnosis Sensitivity 89% Calculation used data from community clinicians and radiologists only.
Specificity 83%
Unconfident diagnosis Sensitivity 87%

341
Idiopathic Pulmonary Fibrosis Placing the diagnostic clinical evidence into an economic framework for decision making.
Intervention
Value Notes
Specificity 66%
Academic setting - Clinical examination and HRCT, +MDT
Confident diagnosis Sensitivity 94% Calculation used data from academic clinicians and radiologists only. Specificity 96%
Unconfident diagnosis Sensitivity 69%
Specificity 91%
Community setting - Accuracy of biopsy after clinical exam and HRCT.
After a confident HRCT diagnosis Sensitivity 92% Calculation used data from community pathologists only. Specificity 53%
After an unconfident HRCT diagnosis Sensitivity 90%
Specificity 43%
Academic setting - Accuracy of biopsy after clinical exam and HRCT.
After a confident HRCT diagnosis Sensitivity 98% Calculation used data from academic pathologists only.
Specificity 81%
After an unconfident HRCT diagnosis Sensitivity 86%
Specificity 67%
Community setting – Accuracy of biopsy after clinical exam and HRCT + MDT.
After a confident HRCT diagnosis Sensitivity 100% Calculation used data from community pathologists only. Specificity 78%
After an unconfident HRCT diagnosis Sensitivity 95%
Specificity 59%
Academic setting – Accuracy of biopsy after clinical exam and HRCT + MDT.
After a confident HRCT diagnosis Sensitivity 98% Calculation used data from academic pathologists only. Specificity 94%
After an unconfident HRCT diagnosis Sensitivity 80%
Specificity 71%
Source/Note: Calculation using data presented by Flaherty (2007). MDT final consensus was used as a 1 reference standard. For confident HRCT diagnosis, all questionable cases which final MDT could not make a 2 firm diagnosis were excluded from the calculation. For unconfident HRCT diagnosis, all questionable cases 3 which final MDT could not make a firm diagnosis were included in the calculation. 4
K.7 Estimation of cost effectiveness 5
The widely used cost-effectiveness metric is the incremental cost-effectiveness ratio (ICER). This is 6 calculated by dividing the difference in costs associated with two alternatives by the difference in 7 QALYs. The decision rule then applied is that if the ICER falls below a given cost per QALY threshold 8 the result is considered to be cost effective. If both costs are lower and QALYs are higher the option 9 is said to dominate and an ICER is not calculated. 10
)()(
)()(
AQALYsBQALYs
ACostsBCostsICER
Where: Costs/QALYs(X) = total costs/QALYs for option X
Cost-effective if: ICER < Threshold

342
Idiopathic Pulmonary Fibrosis Placing the diagnostic clinical evidence into an economic framework for decision making.
When there are more than two comparators, as in this analysis, options must be ranked in order of 1 increasing cost then options ruled out by dominance or extended dominance before calculating ICERs 2 excluding these options. An option is said to be dominated, and ruled out, if another intervention is 3 less costly and more effective. An option is said to be extendedly dominated if a combination of two 4 other options would prove to be less costly and more effective. 5
It is also possible, for a particular cost-effectiveness threshold, to re-express cost-effectiveness 6 results in term of net monetary benefit (NMB). This is calculated by multiplying the total QALYs for a 7 comparator by the threshold cost per QALY value (for example, £20,000) and then subtracting the 8 total costs (formula below). The decision rule then applied is that the comparator with the highest 9 NMB is the most cost-effective option at the specified threshold. That is the option that provides the 10 highest number of QALYs at an acceptable cost. 11
)()()( XCostsXQALYsXBenefitNet
Where: Costs/QALYs(X) = total costs/QALYs for option X; λ = threshold
Cost-effective if: highest net benefit
Both methods of determining cost effectiveness will identify exactly the same optimal strategy. For 12 ease of computation NMB is used in this analysis to identify the optimal strategy. 13
Results are also presented graphically where total costs and total QALYs for each diagnostic strategy 14 are shown. Comparisons not ruled out by dominance or extended dominance are joined by a line on 15 the graph where the slope represents the incremental cost-effectiveness ratio. 16
K.7.1 Interpreting Results 17
NICE’s report ‘Social value judgements: principles for the development of NICE guidance’ sets out the 18 principles that GDGs should consider when judging whether an intervention offers good value for 19 money. In general, an intervention was considered to be cost effective if either of the following 20 criteria applied (given that the estimate was considered plausible): 21
The intervention dominated other relevant strategies (that is, it was both less costly in terms of 22 resource use and more clinically effective compared with all the other relevant alternative 23 strategies), or 24
The intervention costs less than £20,000 per quality-adjusted life-year (QALY) gained compared 25 with the next best strategy. 26
As we have several interventions, we use the NMB to rank the strategies on the basis of their relative 27 cost-effectiveness. The highest NMB identifies the optimal strategy at a willingness to pay of £20,000 28 per QALY gained. 29
K.8 Results and interpretation of the analysis 30
The result of the base case analysis is given in Table 119 and represented graphically in Figure 115. 31 The base-case results show that the only non-dominated strategies are scenario 1 with MDT, 32 scenario 2 with MDT, scenario 3 with MDT, and scenario 4 with MDT. Using a cost effectiveness 33 threshold of £20,000, the base case analysis suggests the most likely cost effective option is to have a 34 clinical exam, PFTs, and HRCT with a multidisciplinary discussion at local level (scenario 1 with MDT). 35 Varying the time required to review a patient in a local MDT and specialist MDT to 15 minutes 36 respectively did not change the conclusions of the results (see Table 120). However, care should be 37 taken when interpreting the results as the true QALY associated with each outcome is unknown, and 38 further no downstream costs that would follow a diagnostic outcome have been incorporated into 39 the analysis. 40

343
Idiopathic Pulmonary Fibrosis Placing the diagnostic clinical evidence into an economic framework for decision making.
Table 121 gives the results of the sensitivity analyses where the value of the QALYs associated with 1 each diagnostic outcome varied. Table 122 gives the results of the sensitivity analyses where 2 estimates of diagnostic accuracy of various interventions in the pathway were replaced by alternative 3 estimates derived by the clinical review. The results show that scenario 3 without MDT and scenario 4 4 without MDT remained dominated options in all of these sensitivity analyses. It is therefore unlikely 5 these strategies are cost effective. 6
Table 123 show results of the sensitivity analysis where the setting in where the diagnostic clinical 7 staff worked was considered. It shows that staff working in academic settings achieve greater 8 diagnostic success than those working in the community both with and without an MDT. Scenarios 9 with an academic MDT in this analysis dominate scenarios without MDT or community MDT. A 10 limitation, however, is that any potential difference in staff costs between the academic or 11 community setting were considered. Therefore the results of this analysis are only informative if the 12 additional expertise of academic staff compared to community staff can be achieved with no 13 additional cost to the NHS. 14
No analysis suggested that a strategy with biopsy was optimal. However, if a greater QALY gain could 15 be associated with a correct diagnostic outcome; or alternatively a greater QALY or monetary loss 16 could be associated with an incorrect diagnostic outcome, strategies involving biopsy would become 17 more cost effective. It is worth noting that scenario 4, where everyone was offered biopsy post HRCT, 18 ranked less optimal than scenario 3 in all analyses when using a threshold of £20,000. This gives 19 greater strength to the argument that if biopsy is considered, it should only be offered to patients 20 who have an unconfident diagnosis at HRCT. Also to note that scenarios with biopsy appeared more 21 cost effective with MDT involvement than without, as MDT involvement reduced the number of 22 cases where findings did not agree with HRCT findings. 23
A key limitation of this analysis is that it does not explore the impact of downstream costs associated 24 with each diagnostic outcome. The addition of downstream cost is likely to further accentuate the 25 patterns already seen in the analysis, as there is likely to be a greater cost to the NHS is associated 26 with incorrect diagnoses. However, the findings of this analysis may not be reflective of a scenario 27 where there is substantial cost associated with effective treatment of IPF patients. The cost 28 effectiveness of diagnostic interventions is in part dependent on the cost effectiveness of the 29 management strategies that follow a particular diagnostic result. A further consideration is that the 30 analyses did not explore a QALY gain or loss associated to cases where no agreement. 31
32
K.9 Conclusion = Evidence Statement 33
It is likely that involvement of a multidisciplinary team at each stage of the diagnostic pathway for IPF 34 patients is cost effective when compared to no involvement. This is based on evidence with direct 35 applicability but with potentially serious limitations. 36
It is likely that with the involvement of a multidisciplinary team at each stage of the diagnostic 37 pathway a diagnosis using clinical and radiological findings alone is more cost effective than a 38 diagnosis using clinical and radiological findings with biopsy. This is based on evidence with direct 39 applicability but with potentially serious limitations. 40 41 42
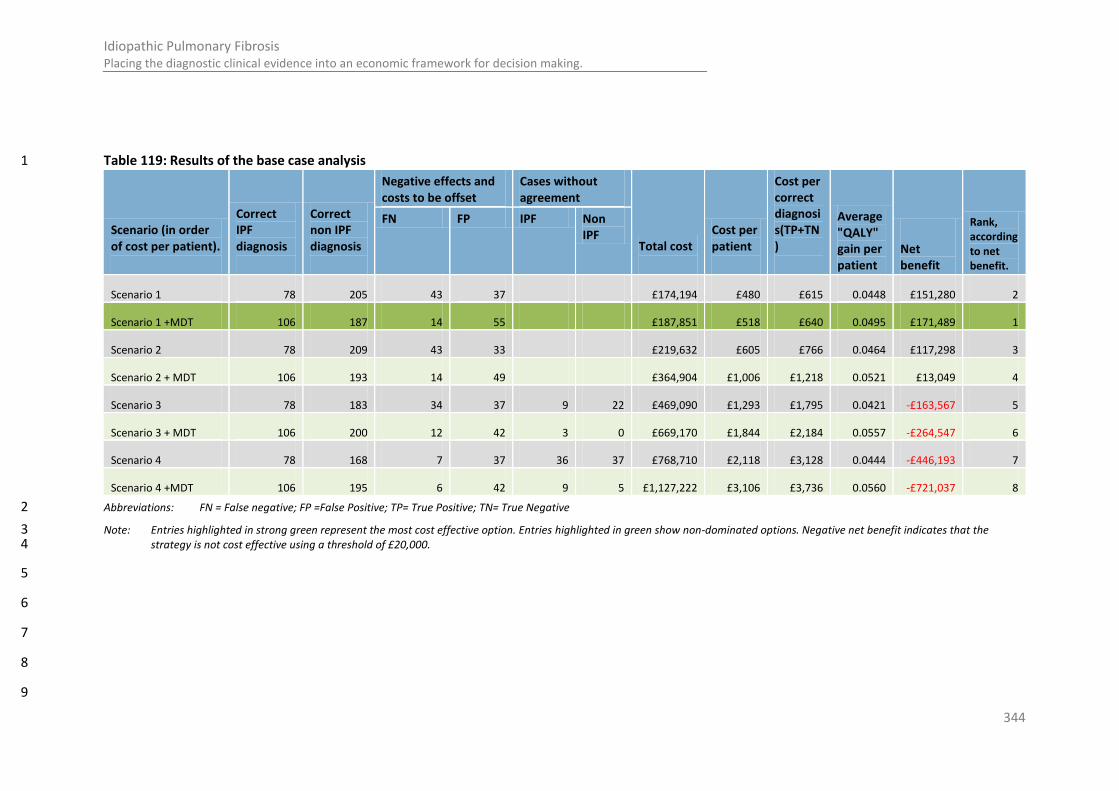
344
Idiopathic Pulmonary Fibrosis Placing the diagnostic clinical evidence into an economic framework for decision making.
Table 119: Results of the base case analysis 1
Scenario (in order of cost per patient).
Correct IPF diagnosis
Correct non IPF diagnosis
Negative effects and costs to be offset
Cases without agreement
Total cost
Cost per patient
Cost per correct diagnosis(TP+TN)
Average "QALY" gain per patient
Net benefit
Rank, according to net benefit.
FN FP IPF Non IPF
Scenario 1 78 205 43 37 £174,194 £480 £615 0.0448 £151,280 2
Scenario 1 +MDT 106 187 14 55 £187,851 £518 £640 0.0495 £171,489 1
Scenario 2 78 209 43 33 £219,632 £605 £766 0.0464 £117,298 3
Scenario 2 + MDT 106 193 14 49 £364,904 £1,006 £1,218 0.0521 £13,049 4
Scenario 3 78 183 34 37 9 22 £469,090 £1,293 £1,795 0.0421 -£163,567 5
Scenario 3 + MDT 106 200 12 42 3 0 £669,170 £1,844 £2,184 0.0557 -£264,547 6
Scenario 4 78 168 7 37 36 37 £768,710 £2,118 £3,128 0.0444 -£446,193 7
Scenario 4 +MDT 106 195 6 42 9 5 £1,127,222 £3,106 £3,736 0.0560 -£721,037 8
Abbreviations: FN = False negative; FP =False Positive; TP= True Positive; TN= True Negative 2
Note: Entries highlighted in strong green represent the most cost effective option. Entries highlighted in green show non-dominated options. Negative net benefit indicates that the 3 strategy is not cost effective using a threshold of £20,000. 4
5
6
7
8
9
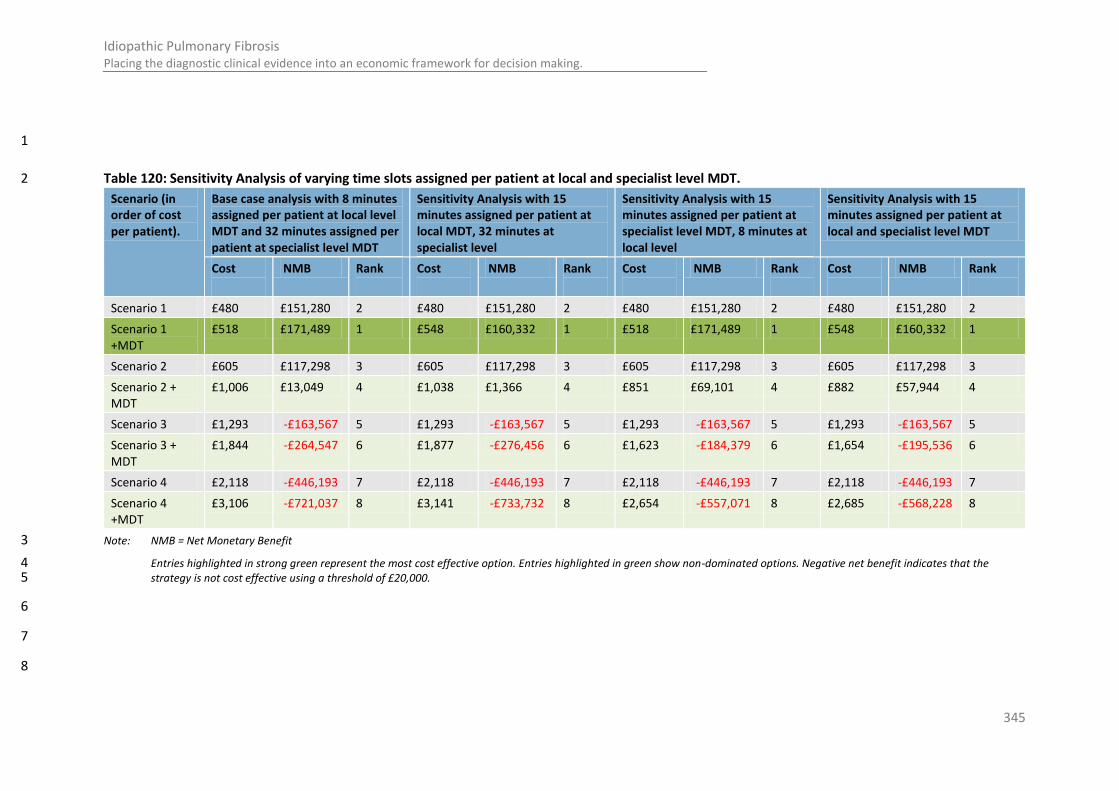
345
Idiopathic Pulmonary Fibrosis Placing the diagnostic clinical evidence into an economic framework for decision making.
1
Table 120: Sensitivity Analysis of varying time slots assigned per patient at local and specialist level MDT. 2
Scenario (in order of cost per patient).
Base case analysis with 8 minutes assigned per patient at local level MDT and 32 minutes assigned per patient at specialist level MDT
Sensitivity Analysis with 15 minutes assigned per patient at local MDT, 32 minutes at specialist level
Sensitivity Analysis with 15 minutes assigned per patient at specialist level MDT, 8 minutes at local level
Sensitivity Analysis with 15 minutes assigned per patient at local and specialist level MDT
Cost
NMB Rank
Cost
NMB Rank
Cost
NMB Rank
Cost
NMB Rank
Scenario 1 £480 £151,280 2 £480 £151,280 2 £480 £151,280 2 £480 £151,280 2
Scenario 1 +MDT
£518 £171,489 1 £548 £160,332 1 £518 £171,489 1 £548 £160,332 1
Scenario 2 £605 £117,298 3 £605 £117,298 3 £605 £117,298 3 £605 £117,298 3
Scenario 2 + MDT
£1,006 £13,049 4 £1,038 £1,366 4 £851 £69,101 4 £882 £57,944 4
Scenario 3 £1,293 -£163,567 5 £1,293 -£163,567 5 £1,293 -£163,567 5 £1,293 -£163,567 5
Scenario 3 + MDT
£1,844 -£264,547 6 £1,877 -£276,456 6 £1,623 -£184,379 6 £1,654 -£195,536 6
Scenario 4 £2,118 -£446,193 7 £2,118 -£446,193 7 £2,118 -£446,193 7 £2,118 -£446,193 7
Scenario 4 +MDT
£3,106 -£721,037 8 £3,141 -£733,732 8 £2,654 -£557,071 8 £2,685 -£568,228 8
Note: NMB = Net Monetary Benefit 3
Entries highlighted in strong green represent the most cost effective option. Entries highlighted in green show non-dominated options. Negative net benefit indicates that the 4 strategy is not cost effective using a threshold of £20,000. 5
6
7
8

346
Idiopathic Pulmonary Fibrosis Placing the diagnostic clinical evidence into an economic framework for decision making.
Table 121: Results of the sensitivity analyses where the QALY weighting associated with each outcome varied (cost per patient unchanged) 1
Scenario (in order of cost per patient).
Base case analysis Sensitivity Analysis 1 Sensitivity Analysis 2 Sensitivity Analysis 3
Average "QALY" gain per patient
Net benefit
Rank, according to net benefit.
Average "QALY" gain per patient
Net benefit
Rank, according to net benefit.
Average "QALY" gain per patient
Net benefit
Rank, according to net benefit.
Average "QALY" gain per patient
Net benefit
Rank, according to net benefit.
Scenario 1 0.0448 £151,280 2 0.3924 £2,673,700 5 0.5462 £3,790,076 4 0.3957 £2,697,973 2
Scenario 1 +MDT 0.0495 £171,489 1 0.4332 £2,956,378 2 0.5666 £3,924,586 1 0.3612 £2,433,926 3
Scenario 2 0.0464 £117,298 3 0.4062 £2,728,505 4 0.5531 £3,794,759 3 0.4026 £2,702,656 1
Scenario 2 + MDT 0.0521 £13,049 4 0.4556 £2,974,878 1 0.5778 £3,861,654 2 0.3724 £2,370,993 4
Scenario 3 0.0421 -£163,567 5 0.3683 £2,204,230 7 0.5041 £3,189,730 7 0.3536 £2,097,627 6
Scenario 3 + MDT 0.0557 -£264,547 6 0.4878 £2,920,484 3 0.5911 £3,670,312 5 0.3857 £2,179,652 5
Scenario 4 0.0444 -£446,193 7 0.3888 £2,053,311 8 0.4740 £2,671,374 8 0.3235 £1,579,271 8
Scenario 4 +MDT 0.0560 -£721,037 8 0.4897 £2,526,532 6 0.5819 £3,195,945 6 0.3765 £1,705,285 7
Note: Entries highlighted in strong green represent the most cost effective option. Entries highlighted in light green show non-dominated options. Negative net benefit indicates that the 2 strategy is not cost effective using a threshold of £20,000. 3
4
5
6
7
8
9

347
Idiopathic Pulmonary Fibrosis Placing the diagnostic clinical evidence into an economic framework for decision making.
Table 122: Results of the sensitivity analyses where the diagnostic accuracy estimates where changed in line with different sources used in the clinical 1 review (QALY associated with each diagnostic outcome as per the base case) 2
Scenario (in order of cost per patient).
Sensitivity Analysis 4 – Coutinho: HRCT
Sensitivity Analysis 5 - Peckham (HRCT)
Sensitivity Analysis 6 – Peckham (HRCT+ ATS)
Sensitivity Analysis 7 – Hunninghake (HRCT)
Sensitivity Analysis 8 – Thomeer & Slodkowska (HRCT+biopsy)
Sensitivity Analysis 9 – Flaherty &Slodkowska (biopsy)
Cost QALY Rank Cost
QALY Rank
Cost
QALY Rank
Cost QALY Rank Cost QALY Rank Cost QALY Rank
Scenario 1 £480 0.052 1 £480 0.029 2 £480 0.038 2 £480 0.012 3 £480 0.067 1 £480 0.045 2
Scenario 1 +MDT
£518 0.050 2 £518 0.050 1 £518 0.050 1 £518 0.050 1 £518 0.050 3 £518 0.050 1
Scenario 2 £605 0.053 3 £605 0.032 4 £605 0.040 3 £605 0.015 4 £605 0.069 2 £605 0.046 3
Scenario 2 + MDT
£1,006 0.052 4 £1,006 0.052 3 £1,006 0.052 4 £1,006 0.052 2 £1,006 0.052 4 £1,006 0.052 4
Scenario 3 £1,279 0.046 5 £1,319 0.030 5 £1,305 0.036 5 £1,352 0.023 6 £1,276 0.054 5 £1,293 0.037 5
Scenario 3 + MDT
£1,844 0.056 6 £1,844 0.056 6 £1,844 0.056 6 £1,844 0.056 5 £1,844 0.056 6 £1,844 0.056 6
Scenario 4 £2,105 0.048 7 £2,144 0.036 7 £2,131 0.041 7 £2,177 0.031 7 £2,102 0.051 7 £2,118 0.031 7
Scenario 4 +MDT
£3,106 0.056 8 £3,106 0.056 8 £3,106 0.056 8 £3,106 0.056 8 £3,106 0.056 8 £3,106 0.056 8
Note: Costs and QALYs presented are mean per patient. Rank is based on calculated net monetary benefit (using a threshold of £20,000) with 1 representing the most optimal strategy. 3 Options which are not dominated appear in light green. These options would improve in rank if the net monetary benefit was calculated with a higher threshold per QALY. 4
5
6
Table 123: Results of the sensitivity analyses where the diagnostic accuracy estimates are based on either community clinicians or academic clinicians. 7
Scenario (in order of cost per patient).
Correct IPF diagnosis
Correct non IPF diagno
Negative effects and costs to be offset
Cases without agreement
Total cost
Cost per patient
Cost per successful outcome
Average "QALY" gain per
Net
Rank, according to net

348
Idiopathic Pulmonary Fibrosis Placing the diagnostic clinical evidence into an economic framework for decision making.
sis
FN FP IPF Non
IPF
(TP+TN)
patient Monetary Benefit
benefit.
Community Scenario 1 93 178 28 64 0 0 £174,194 £480 £644 0.039 £110,532 6
Academic Scenario 1 69 222 52 20 0 0 £174,194 £480 £598 0.048 £176,748 2
Community Scenario 1 +MDT 107 175 14 67 0 0 £187,851 £518 £666 0.044 £134,395 4
Academic Scenario 1 +MDT 106 225 15 17 0 0 £187,851 £518 £567 0.066 £291,598 1
Community Scenario 2 93 183 28 59 0 0 £219,632 £605 £796 0.042 £82,511 7
Academic Scenario 2 69 225 52 17 0 0 £219,632 £605 £748 0.049 £139,040 3
Academic Scenario 2 + MDT 106 228 15 14 0 0 £364,904 £1,006 £1,092 0.067 £123,413 5
Community Scenario 2 + MDT 107 181 14 61 0 0 £364,904 £1,006 £1,265 0.047 -£22,616 8
Academic Scenario 3 69 199 40 20 12 23 £464,150 £1,279 £1,733 0.046 -£131,934 9
Community Scenario 3 93 153 22 64 6 24 £476,993 £1,314 £1,939 0.035 -£221,853 11
Academic Scenario 3 + MDT 106 205 10 17 5 21 £651,726 £1,796 £2,097 0.063 -£197,025 10
Community Scenario 3 + MDT 107 190 14 52 1 0 £670,172 £1,847 £2,263 0.051 -£302,168 12
Academic Scenario 4 69 187 6 20 46 35 £763,770 £2,105 £2,987 0.051 -£395,865 13
Community Scenario 4 93 129 10 64 18 49 £776,613 £2,140 £3,508 0.032 -£540,985 14
Academic Scenario 4 +MDT 106 198 6 17 9 27 £1,109,777 £3,058 £3,653 0.062 -£659,705 15
Community Scenario 4 +MDT 107 190 5 47 9 6 £1,128,223 £3,109 £3,810 0.054 -£737,769 16
Note: Costs and QALYs presented are mean per patient. Rank is based on calculated net monetary benefit (using a threshold of £20,000) with 1 representing the most optimal strategy. 1 Options which are not dominated appear in light green. These options would improve in rank if the net monetary benefit was calculated with a higher threshold per QALY. 2
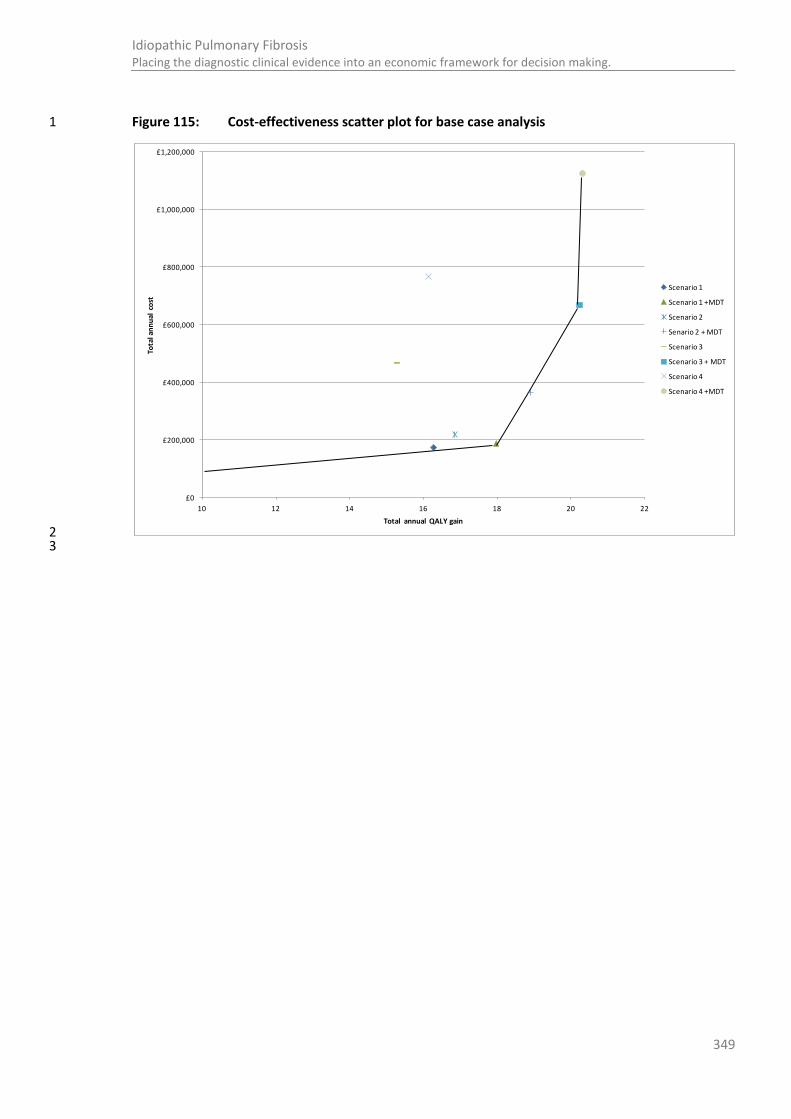
349
Idiopathic Pulmonary Fibrosis Placing the diagnostic clinical evidence into an economic framework for decision making.
Figure 115: Cost-effectiveness scatter plot for base case analysis 1
2 3
£0
£200,000
£400,000
£600,000
£800,000
£1,000,000
£1,200,000
10 12 14 16 18 20 22
Tota
l an
nu
al c
ost
Total annual QALY gain
Scenario 1
Scenario 1 +MDT
Scenario 2
Senario 2 + MDT
Scenario 3
Scenario 3 + MDT
Scenario 4
Scenario 4 +MDT

350
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
1
Appendix L: Cost-effectiveness analysis – 2
Pulmonary rehabilitation for patients with 3
Idiopathic Pulmonary Fibrosis 4
L.1 Introduction 5
Pulmonary rehabilitation aims to reduce disability in people with lung disease and to improve their 6 quality of life while diminishing the health care burden. Provided by a multiprofessional team, 7 pulmonary rehabilitation comprises of physical training, education, dietetics, occupational therapy, 8 psychology, and social support. The benefits include improvements in exercise performance, health 9 status, dyspnoea, and reduction in usage of health services. There can be involvement from the 10 patient’s family or carer. It assumes that optimal medical management has been achieved or 11 continues alongside the programme, and thus rehabilitation should be seen as an adjunct rather than 12 a comparator to other interventions 47. 13
Currently in the UK, pulmonary rehabilitation designed and provided specifically for the IPF 14 population is not known to exist. Either patients are not offered pulmonary rehabilitation, or are 15 offered places on pulmonary rehabilitation courses for patients with Chronic Obstructive Pulmonary 16 Disease (COPD). Content in programmes designed for COPD may be inappropriate for an IPF 17 population. Unlike COPD, a dry cough (which can become debilitating), shortness of breath, and 18 fatigue are common symptoms of restrictive lung disease such as IPF and may not be addressed 19 sufficiently in programmes designed for COPD patients. IPF patients do not need instruction on 20 inhalers. Whilst COPD patients can have problems with high-flow supplemental oxygen, patients with 21 restrictive lung diseases need as much oxygen as possible. Furthermore, pulmonary fibrosis 22 progresses more rapidly than COPD, and the only “cure” currently available is a lung transplant. With 23 a shorter median life expectancy on diagnosis, IPF patients need different consideration in 24 pulmonary rehabilitation in managing expectations in end of life care and psychosocial support. As 25 IPF is less common than COPD, patient members of the group expressed that a key benefit of a 26 pulmonary rehabilitation programme provided for IPF patients could only be a reduction in the 27 feeling of isolation in experiencing the condition, mitigating some of the associated anxiety and 28 depression associated with IPF. 29
The reasons why pulmonary rehabilitation for IPF is lacking in the UK are complex, but may include 30 medical indifference to non-pharmacological management, lack of scientific evidence, poor funding, 31 and ineffective consumer demand. Clinical guidelines also appear to be lagging behind the strength 32 of evidence in respect of rehabilitation 47. No studies on the cost effectiveness of pulmonary 33 rehabilitation in the IPF population were identified. 34
Pulmonary rehabilitation could be underutilised as a means of improving quality of life in people who 35 live with IPF, including both patients and carers. Further, pulmonary rehabilitation programmes 36 provided and designed specifically for IPF patients could prove to have additional benefit to 37 programmes designed principally for COPD patients, although provision of IPF programmes would 38 come at additional cost. It is suspected that rehabilitation could potentially prevent unnecessary 39 contacts with the NHS as patients learnt how to self-manage symptoms of IPF, and therefore could 40 reduce costs; however, there is currently an absence of evidence to demonstrate this. Overall the 41 Guideline Development Group (GDG) considered a cost utility analysis to explore the cost 42 effectiveness of offering IPF patients pulmonary rehabilitation in the current UK context to be a 43 priority. 44
351
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
Pulmonary rehabilitation can be defined as a multi professional team led programme involving 1 exercise, education and psychosocial support. The typical duration of one programme is 6-8 weeks, 2 although some do run for longer. IPF patients could be defined as having category C rehabilitation 3 needs, and therefore require a category 3a rehabilitation service. Having said this, the prevalence of 4 IPF is lower than that of many other respiratory conditions for which pulmonary rehabilitation is 5 offered. As such, we would expect only large district general hospitals or tertiary care centres to have 6 a sufficiently large catchment area of referral to recruit the required number of patients to make use 7 of economies of scale and make programmes offered exclusively to IPF patients viable in terms of 8 cost effectiveness. 9
Patients with Category C rehabilitation needs: 10
• Patient goals are typically focused in restoration of function / independence and co-ordinated 11 discharge planning with a view to continuing rehabilitation in the community. 12
• Patients require rehabilitation in the context of their specialist treatment as part of a specific 13 diagnostic group (e.g. stroke). 14
• Patients may be medically unstable or require specialist medical investigation / procedures for the 15 specific condition. 16
• Patients usually require less intensive rehabilitation intervention from 1-3 therapy disciplines in 17 relatively short rehabilitation programmes (i.e. up to 6 weeks). 18
• Patients are treated by a local specialist team (i.e. Level 3a service) which may be led by 19 consultants in specialties other than Rehabilitative Medicine (e.g. neurology / stroke medicine) and 20 staffed by therapy and nursing teams with specialist expertise in the target condition. 21
Source: Cambridgeshire Joint Prescribing Group, 2010 52
22
Therefore, it is felt appropriate to explore all strategies in the context of a network of referral, 23 allowing patients managed in smaller providers to be able to access the service provided. As IPF is 24 relatively rare ( we approximate 24 per 100,000 population [see Appendix J 349]), IPF patients are 25 usually under the outpatient care of a consultant in a large hospital and therefore we would expect 26 any implementation cost of referral to be low given that a referral system should already be in place. 27 To note, we would expect coordination of referral to sit comfortably within the context of the 28 Multidisciplinary Team (MDT) (inclusive a full time coordinator and ILD nurse in each specialist hub); 29 which is recommended and costed as part of the diagnostic pathway for IPF patients in this guideline. 30
The evidence base to inform the clinical course of IPF and the treatment effect in the health 31 economic model is limited. The implications of a lack of available evidence to populate the model 32 were considered, however, the developers felt a health economic model would still add value in 33 determining thresholds and scenarios whereby certain strategies become more or less likely to be 34 cost effective given that pulmonary rehabilitation is felt to be one of the few interventions that could 35 benefit people with IPF. 36
L.2 Methods 37
L.2.1 Model overview 38
A cost-utility analysis was undertaken to evaluate the cost-effectiveness of a pulmonary 39 rehabilitation course with IPF participants compared to a strategy of no offer of pulmonary 40 rehabilitation. Lifetime quality-adjusted life years (QALYs) and costs were estimated from a current 41 UK NHS and personal social services perspective. Both costs and QALYS were discounted at a rate of 42

352
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
3.5% per annum in line with NICE methodological guidance 348. The cost effectiveness outcome of the 1 model is cost per QALY gained. 2
The following general principles were adhered to in developing the cost-effectiveness analysis: 3
The GDG was consulted during the construction and interpretation of the model. 4
Model inputs were based on the systematic review of the clinical literature supplemented with 5 other published data sources where possible. 6
When published data was not available expert opinion was used to populate the model. 7
Model inputs and assumptions were reported fully and transparently. 8
The results were subject to sensitivity analysis and limitations were discussed. 9
The model was peer-reviewed by another health economist at the NCGC. 10
L.2.1.1 Comparators 11
The below comparators were identified 12
1. No pulmonary rehabilitation 13
2. Community rehabilitation with exercise component 14
3. Pulmonary rehabilitation with exercise component and an educational component specifically 15 designed for IPF patients. 16
Community rehabilitation is defined as a programme of exercise and physiotherapy only. It consists 17 of bi-weekly attendance at pulmonary rehabilitation exercise session conducted weekly by 18 community physiotherapist in local proximity to patients’ residence. It is expected these sessions 19 could be shared with other patient populations with respiratory conditions such as those with COPD, 20 so long as safety of the patient in the case of over exertion was taken into account. 21
Pulmonary rehabilitation specifically designed for IPF patients is considered to be the exercise 22 programme offered by community rehabilitation, with the addition of an educational component 23 which would be delivered and overseen by a clinician (registrar or consultant level) with a specialist 24 interest in IPF, alongside a ILD respiratory nurse, as well as one or more of the rehabilitation 25 disciplines (physiotherapy, occupational therapy, psychology, dietetics, social work, vocational / 26 educational support etc.). 27
L.2.1.2 Population 28
The base case considers a population of patients with a diagnosis of suspected or confirmed IPF. The 29 analysis considers three subgroups of patients with IPF that have differential rates of disease 30 progression. This is to allow for further analysis of the impact treatment effect duration on cost 31 effectiveness. The proportion of patients in each subgroup is explored in a sensitivity analysis 32
L.2.1.3 Time horizon and cycle length. 33
The Markov model takes a lifetime horizon (maximum of 20 years post diagnosis) with a cycle length 34 of 1 month to allow for changes in treatment effect duration. 35
L.2.1.4 Deviations from NICE reference case 36
The analysis will follow the standard assumptions of the reference case including discounting at 3.5% 37 for costs and health effects, and incremental analysis is conducted. A sensitivity analysis using a 38 discount rate of 1.5% for both costs and health benefit is conducted. 39
353
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
L.2.2 Approach to modelling 1
L.2.2.1 Model structure 2
The cost utility analysis uses a decision tree with Markov states which are based on a continuum of 3 absolute Forced Vital Capacity Percentage (FVC %) predicted values ranging from 100% to 35%. A 4 cohort of IPF patients with suspected or confirmed diagnosis of differing rates of disease progression 5 is offered one of the compared strategies (in correspondence of the decision node of the tree) and 6 then enters the Markov model which is depicted in Figure 116. It illustrates the health states in the 7 model and possible transitions between them in each cycle. There is implicit time dependency within 8 the model due to the increased risk of mortality as the cohort increases with age. 9
In a Markov model a set of mutually exclusive health states are defined that describe what can 10 happen to the population of interest over time. People in the model can only exist in one of these 11 health states at a time. Possible transitions are defined between each of the health states and the 12 probability of each transition occurring within a defined period of time (a cycle) is assigned to each 13 possible transition. 14
The health states are fixed according to categories of absolute FVC% predicted values. The cohort is 15 subject to a probability of respiratory hospitalisation (which may include acute exacerbation), which 16 acts as a transition event that moves the cohort to tunnel states that are also fixed on absolute FVC% 17 predicted values. The tunnel states, however, have a higher associated probability of mortality due 18 to the history of prior hospitalisation. The event of a respiratory hospitalisation occurs at the 19 beginning of a cycle. Therefore from the first cycle, a patient may move to a health state with a lower 20 FVC% predicted value without experiencing a hospitalisation, move to a lower FVC% predicted value 21 having experienced hospitalisation or die. If a patient has a respiratory hospitalisation in the first 22 month, for example, the probability of death in that cycle will take into account that the patient has 23 experienced a hospitalisation. Additionally a half cycle correction is applied to all life years and costs 24 accrued to reflect movement between states throughout the time of the cycle. 25
The rate at which the cohort progresses through the health states is determined by the probability of 26 being in a subgroup experiencing a predefined rate of disease progression, as measured by a unit 27 drop in FVC% predicted. The event of hospitalisation does not influence the rate of disease 28 progression, and therefore the rate of disease progression for each subgroup is the same in pre and 29 post hospitalisation states. This is due to a lack of data to parameterise this correlation. However, in 30 line with evidence retrieved for the prognostic review, hospitalisation does influence probability of 31 mortality and this has been captured in the model accordingly. To note, as a simplification to model 32 disease progression, FVC% predicted can only deteriorate with time. In reality, some patients with 33 IPF may experience an increase in FVC% predicted, however it is likely this is due to co morbidity such 34 as emphysema or inaccuracies of the test. As there is no data to inform probability of mortality for 35 this group of patients a sensitivity analysis was conducted where we assume this group experience 36 mortality rates similar to patients with a slow, moderate or rapid rate of disease progression (please 37 refer to ‘Rate of disease progression’ in section L.2.3.3 for further detail). 38
The rate of mortality is dependent on the age of the cohort, the absolute FVC% predicted value, the 39 rate of disease progression and the history of hospitalisation 117. Additionally it is assumed that the 40 patient would not be in a state below 35% FVC% predicted as this is assumed to be unsustainable to 41 life; therefore, movement beyond this is directed to the dead state. The intervention of pulmonary 42 rehabilitation is only expected to influence QoL and a cost accrued within the model and does not 43 influence any transition probability contained within the Markov model. 44

354
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
Figure 116: Simplified graphic of the Markov Model 1
2 Note: FVC%x denotes the starting lung function status of the cohort as measured by FVC% predicted. The diagram 3
depicts a continuum of health states defined by FVC% predicted values. In the basecase, for example, the cohort 4 starts in a health state of 75% FVC% predicted, and have a probability of moving to health states of 74% FVC% 5 predicted, 73% FVC% predicted, 72% FVC% predicted and so on. 6
A one month cycle duration was used in this model to capture the potential decline in lung function 7 and reflect disease progression. All the probabilities and on-going costs associated with community 8 rehabilitation were converted to reflect the one month cycle length in the model. The model was run 9 for repeated cycles, and the time spent in each health state was calculated. By attributing costs and 10 quality of life weights to the time spent in each health state, total resource costs and QALYs can be 11 calculated. There were no secondary outcomes recorded, however for clinical validation the median 12 and mean life expectancy, alongside Kaplan Meier curves were produced for cohorts with differing 13 starting characteristics. The model was run for 10,000 cycles in order to calculate costs and QALYs 14 over a lifetime horizon. 15
To take into account the impact of disease progression on the ability to participate, it was assumed 16 that pulmonary rehabilitation will not be of benefit when FVC% predicted is very low (approximately 17 45%) when patients would be unlikely to participate. To note, the patient’s FVC% predicted value is 18 used in this case as a proxy marker for the ability to participate for the purposes of modelling 19 participation, and does not infer that an offer of rehabilitation should not be made for these patients 20 as currently evidence does not exist to validate this assumption. A sensitivity analysis explores the 21 scenarios whereby patients cannot participate in pulmonary rehabilitation within the cycle 22 immediately post hospitalisation, and secondly whereby only a proportion of patients return to 23 rehabilitation post any respiratory hospitalisation. 24
An assessment cost is applied at the beginning of each course of rehabilitation for every patient who 25 is still alive in the model, regardless of the patient’s assumed ability to participate due to prior 26
355
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
hospitalisation, low FVC% predicted value or otherwise. For the proportion of patients passing 1 assessment and returning to rehabilitation, a cost for a place throughout the duration of the course 2 is applied. The cost of pulmonary rehabilitation is not assumed to change in regard to the patient’s 3 clinical status or timing of the offer. As the probability of respiratory hospitalisation is the same in all 4 compared strategies, the cost of the hospitalisation is not considered in the model. 5
A patient’s quality of life is dependent on the time since the start of the model, treatment effect of 6 the pulmonary rehabilitation course and the time period that has occurred since the beginning of the 7 course. Quality of life is not adjusted according to FVC% predicted value. In case of death, the patient 8 remains in the dead health state which is associated with no cost and a Health Related Quality of Life 9 (HRQoL) equal to 0. In strategies where the cohort has had pulmonary rehabilitation an improved 10 quality of life is added to the baseline quality of life. 11
The base case assumes that the maximum effect in quality of life recorded at follow up by the 12 literature is only realised at the end of the programme (i.e. after 2 months) with a linear increase in 13 quality of life until that point. This maximal benefit is sustained for a period of time after the 14 programme finishes, and then declines to the point where the last long term follow up of quality of 15 life was recorded by the literature (i.e. 6 months). From this point forth quality of life declines to 16 baseline. Therefore, after the longest treatment effect duration has expired, the patient experiences 17 the same quality of life as a patient at the same time period in the model that had not had the 18 rehabilitation course. 19
For each strategy the expected healthcare resource costs and expected QALYs were calculated by 20 estimating the costs and quality adjusted month for each state and then multiplying them by the 21 proportion of patients who would be in that state (as determined by the differing transition 22 probabilities associated with the strategy taken). Quality adjusted months were converted into 23 quality adjusted life years. 24
The number of patients entering the Markov model for each subgroup was in accordance to the 25 proportion the subgroup assumed in the population. In order to assess the cost-utility of 26 implementing the compared strategies for a population, the resource costs and QALYs were summed 27 for all subgroups in the cohort. The total costs and QALYs for a strategy were divided by the number 28 of patients in the cohort, allowing an average cost and QALY per patient to be calculated. Comparing 29 these results allows us to identify which strategy is the most cost-effective. 30
L.2.2.2 Uncertainty 31
The model was built probabilistically to take account of the uncertainty around input parameter 32 point estimates. A probability distribution was defined for each model input parameter. When the 33 model was run, a value for each input was randomly selected simultaneously from its respective 34 probability distribution; mean costs and mean QALYs were calculated using these values. The model 35 was run repeatedly – 10,000 times for the base case and 2500 times for each sensitivity analysis – 36 and results were summarised. The number of simulations used was chosen considering the Monte 37 Carlo error of the incremental costs, QALYs and net monetary benefit using methods as described by 38 Koehler et al247. It was set to ensure that the Monte Carlo error was not more than 5% of the 39 standard error for each of these outcomes in all analyses, with the base case having an improved 40 accuracy due to the greater number of simulations. 41
The way in which distributions are defined reflects the nature of the data, so for example utilities 42 were given a beta distribution, which is bounded by zero and one, reflecting that a QoL weighting will 43 not be outside this range. All of the variables that were probabilistic in the model and their 44 distributional parameters are detailed in Table 124 and in the relevant input summary tables in 45 section L.2.3. Probability distributions in the analysis were parameterised using error estimates from 46 data sources. 47

356
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
Table 124: Description of the type and properties of distributions used in the probabilistic 1 sensitivity analysis 2
Parameter Type of distribution Properties of distribution
Probability of being in a particular subgroup (i.e. having a certain rate of disease progression)
Dirichlet Fitted to multinomial data. Represents a series of conditional distributions, bounded on 0-1 interval. Derived by the number of patients in the sample and the number of patients in a particular subgroup.
Mortality Uniform The risk calculator for mortality gave a range for a one year risk of mortality given four risk factors. A uniform distribution was taken to select from the range of the one year risk quoted for a given set of risk factors, before conversion to the appropriate probability for the cycle length.
Hospitalisation probability
Beta Bounded between 0 and 1. As the sample size and the number of events were specified alpha and Beta values were calculated as follows:
Alpha=(number of patients hospitalised)
Beta=(Number of patients)-(number of patients hospitalised)
Utility Beta
Bounded between 0 and 1. Derived from mean of a domain or total quality of life score and its standard error, using the method of moments.
Alpha and Beta values were calculated as follows:
Alpha = mean2 *(1-(mean/SE
2)-mean
Beta = Alpha *((1-mean)/mean)
The following variables, were left deterministic (i.e. were not varied in the probabilistic analysis): 3 cost-effectiveness threshold (which was deemed to be fixed by NICE), the resource, including time 4 and cost of staff, required to implement each strategy (assumed to be fixed according to national pay 5 scales and programme content) and the rate of disease progression (which was assumed to be 6 linear). 7
In addition, various deterministic sensitivity analyses were undertaken to test the robustness of 8 model assumptions. In these, one or more inputs were changed and the analysis rerun to evaluate 9 the impact on results and whether conclusions on which intervention should be recommended 10 would change. 11
L.2.3 Model inputs 12
L.2.3.1 Summary table of model inputs 13
Model inputs were based on clinical evidence identified in the reviews undertaken for the guideline, 14 supplemented by additional data sources (including expert opinion) as required. In particular, 15 estimates of treatment effect were derived from the only two RCTs identified by the systematic 16 review conducted specifically for pulmonary rehabilitation, whereas other data sources were 17 selectively chosen from the evidence retrieved as discussed in the following sections of this report. 18 Model inputs were discussed and validated with clinical members of the GDG. A summary of the 19 model inputs used in the base-case (primary) analysis is provided in the table below. More details 20 about sources, calculations and rationale for selection can be found in the sections following this 21 summary table. 22

357
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
Table 125: Summary table of model inputs 1
Input Data Source Probability distribution
Comparators Pulmonary rehabilitation with educational component
Community rehabilitation
No rehabilitation
n/a n/a
Population and subgroups
People diagnosed with IPF with
a) rapid disease progression
b) moderate disease progression
c) slow disease progression
Expert opinion n/a
Perspective UK NHS & PSS NICE reference case348
n/a
Time horizon Lifetime NICE reference case348
n/a
Discount rate Costs: 3.5%
Outcomes: 3.5%
NICE reference case348
n/a
Cohort settings
Age on entry to model
70 years Expert opinion Fixed
FVC% predicted absolute value on entry to the model
75% Expert opinion Fixed
Mortality
Mortality rate Dependent on age, history of respiratory hospitalisation, baseline FVC% predicted value and 6 month change in FVC% predicted value.
Du Bois 2011 117
Uniform. Please see Table 124 for further explanation.
Quality of life (utility)
Without rehabilitation
Time dependent , linear rate of decline between time points
Year 0
Year 1
Year 2
Year 3
Year 4
Year 5
Year 6
Year 7
Year 8 onwards
0.892
0.852
0.821
0.769
0.720
0.677
0.607
0.569
0.488
Tzanakis, 2005 482
Beta
Community rehabilitation (exercise only) Holland, 2008 185
Absolute change at 3 months
0.068 Beta
Absolute change at 6 months
0.058 Beta
IPF rehabilitation (exercise with educational component) Nishiyama, 2008 355
Absolute change at 3 months
0.060 Beta
Absolute change at 6 months
0.060 Beta
Long term utility Treatment effect diminishes at linear Assumption n/a
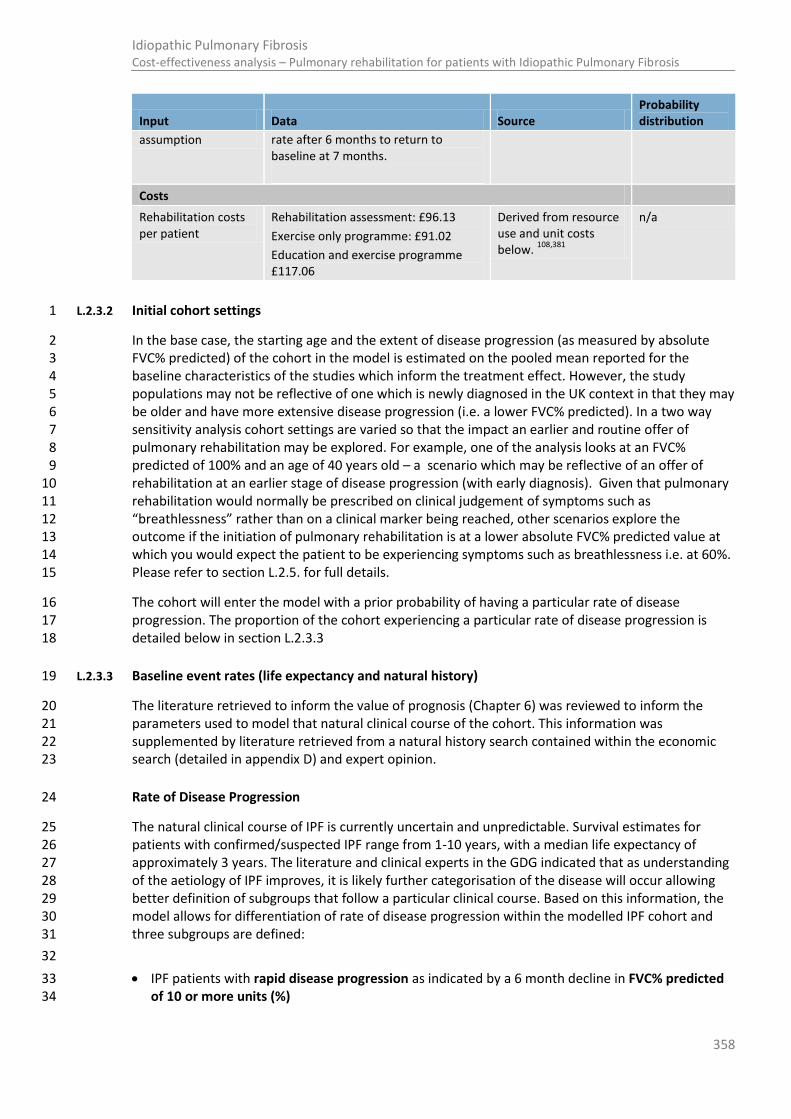
358
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
Input Data Source Probability distribution
assumption rate after 6 months to return to baseline at 7 months.
Costs
Rehabilitation costs per patient
Rehabilitation assessment: £96.13
Exercise only programme: £91.02
Education and exercise programme £117.06
Derived from resource use and unit costs below.
108,381
n/a
L.2.3.2 Initial cohort settings 1
In the base case, the starting age and the extent of disease progression (as measured by absolute 2 FVC% predicted) of the cohort in the model is estimated on the pooled mean reported for the 3 baseline characteristics of the studies which inform the treatment effect. However, the study 4 populations may not be reflective of one which is newly diagnosed in the UK context in that they may 5 be older and have more extensive disease progression (i.e. a lower FVC% predicted). In a two way 6 sensitivity analysis cohort settings are varied so that the impact an earlier and routine offer of 7 pulmonary rehabilitation may be explored. For example, one of the analysis looks at an FVC% 8 predicted of 100% and an age of 40 years old – a scenario which may be reflective of an offer of 9 rehabilitation at an earlier stage of disease progression (with early diagnosis). Given that pulmonary 10 rehabilitation would normally be prescribed on clinical judgement of symptoms such as 11 “breathlessness” rather than on a clinical marker being reached, other scenarios explore the 12 outcome if the initiation of pulmonary rehabilitation is at a lower absolute FVC% predicted value at 13 which you would expect the patient to be experiencing symptoms such as breathlessness i.e. at 60%. 14 Please refer to section L.2.5. for full details. 15
The cohort will enter the model with a prior probability of having a particular rate of disease 16 progression. The proportion of the cohort experiencing a particular rate of disease progression is 17 detailed below in section L.2.3.3 18
L.2.3.3 Baseline event rates (life expectancy and natural history) 19
The literature retrieved to inform the value of prognosis (Chapter 6) was reviewed to inform the 20 parameters used to model that natural clinical course of the cohort. This information was 21 supplemented by literature retrieved from a natural history search contained within the economic 22 search (detailed in appendix D) and expert opinion. 23
Rate of Disease Progression 24
The natural clinical course of IPF is currently uncertain and unpredictable. Survival estimates for 25 patients with confirmed/suspected IPF range from 1-10 years, with a median life expectancy of 26 approximately 3 years. The literature and clinical experts in the GDG indicated that as understanding 27 of the aetiology of IPF improves, it is likely further categorisation of the disease will occur allowing 28 better definition of subgroups that follow a particular clinical course. Based on this information, the 29 model allows for differentiation of rate of disease progression within the modelled IPF cohort and 30 three subgroups are defined: 31
32
IPF patients with rapid disease progression as indicated by a 6 month decline in FVC% predicted 33 of 10 or more units (%) 34

359
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
IPF patients with moderate disease progression as indicated by a 6 month decline in FVC% 1 predicted of 5 to 9 units (%) 2
IPF patients with slow disease progression as indicated by a 6 month decline in FVC% predicted 3 of less than 5 units (%) 4
The probability of moving between health states of an absolute FVC% predicted value was calculated 5 for each subgroup according to the rate of FVC% predicted decline specified above. To do this, it was 6 assumed that at 6 months the subgroup would have equal chance of experiencing an absolute unit 7 change within the range specified. The unit decline per month and subsequently per cycle was 8 calculated, assuming that decline was linear and rounding the unit decline per cycle to the nearest 9 one percent of FVC% predicted (as the health states are defined per percent). Due to the rounding to 10 the nearest percent, the model applies the below in the deterministic analysis: 11
All IPF patients with rapid disease progression experience a decline of 2% per month leading to a 12 6 month decline in FVC% predicted of 12 units (%) 13
IPF patients with moderate disease progression have an 80% chance of experiencing a decline of 14 1% per month leading to a 6 month decline in FVC% predicted of 6 units (%) and 20% chance of 15 experiencing a decline of 2 units change per month leading to a 6 month decline in FVC% 16 predicted of 12 units (%). Across the subgroup, a mean decline of 1.2 units is applied per month, 17 or a 7.2 unit decline per 6 months 18
IPF patients with stable disease progression have a 60% chance of experiencing a decline of 0% 19 per month leading to a 6 month decline in FVC% predicted of 0 units (%) and 40% chance of 20 experiencing a decline of 1 unit change per month leading to a 6 month decline in FVC% predicted 21 of 6 units (%).Across the subgroup, a mean decline of 0.6 units is applied per month, or a 3.6 unit 22 decline per 6 months. 23
In the probabilistic analysis, rounding error is accounted for so that the mean unit decline 24 experienced in each subgroup is exactly the midpoint of the range over a large number of 25 simulations. 26
It is recognised that the above subgroups are not inclusive of all IPF patients, as some patient’s FVC% 27 predicted may improve post diagnosis. This improvement may in part be explained by co-morbidities 28 such as emphysema, or by variation or discrepancy in pulmonary function testing. However, no 29 evidence was retrieved to inform the duration of improvement in FVC in IPF patients or the impact 30 this improvement would have on future rate of disease progression, hospitalisation or mortality. On 31 the premise that other factors (such as co morbidity) could mask IPF disease progression (when 32 measured by a change in FVC% predicted), it was agreed reasonable to assume patients with 33 improved IPF would incur the same or more risk of mortality as patients with slow disease 34 progression. 35
The proportion of the cohort entering the model with a particular rate of disease progression was 36 estimated by averaging the proportion of patients with each rate of disease progression observed in 37 the BUILD1 trial464 and UK unpublished hospital data provided by a clinical member of the GDG 38 (Table 126). The calculation of the proportion of patients in each subgroup in the base case excluded 39 data retrieved from patients whom FVC% predicted improved. In a sensitivity analysis, the proportion 40 of patients in each subgroup was explored, firstly by assuming patients who had an improved FVC% 41 predicted had the same mortality risk as those with slow disease progression and secondly by 42 assuming a patients mortality risk was influenced by the rate of change (improvement or decline) in 43 FVC% predicted, with those experiencing a small improvement experiencing the same mortality risk 44 as those with a small decline, and patients with moderate improvement experiencing the same 45 mortality risk as those with moderate decline(SA1 and SA2 respectively in the table below). 46

360
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
Table 126: The proportion of patients experiencing a given rate of disease progression according to 1 FVC% predicted (per unit of %) 2
Disease progression within 6 months
(defined by FVC% predicted unit change)
Swigris (2010) [a]
UK data source [b]
Base case estimate [c] SA1 [d] SA2 [e] SA3 SA4 SA5
Moderate improvement
6% (n=8) 13% (n=24)
Small improvement
8% (n=10)
24%
(n=45)
Slow disease progression
53% (n=68)
33% (n=60)
57% (n=128)
69% (n=215)
58% (n=183)
100%
Moderate disease progression
20% (n=26)
15%
(n=28)
24% (n=54)
17% (n=54)
27% (n=86)
100%
Rapid disease progression
13% (n=17)
15%
(n=27)
19% (n=44)
14% (n=44)
14% (n=44)
100%
(a) Swigris et al(2010) categorisation of disease progression in absolute change of FVC% predicted: Moderate improvement 3 = >+12%; Small improvement=+7% to +12%; Slow disease progression=-7% to+7%; Moderate disease progression = - 4 12% to -7% ; Rapid disease progression=>-12% 5
(b) The UK data source categorisation of disease progression in absolute change of FVC% predicted: Moderate improvement 6 =>+5%; Small improvement=0% to 5%; Slow disease progression=0% to -5%; Moderate disease progression =-5% to -7 10%; Rapid disease progression=>-10% 8
(c) Base case categorisation of disease progression: Slow disease progression=0 to 5 unit decrease; Moderate disease 9 progression =5 to 10 unit decrease; Rapid disease progression=>10 unit decrease. Proportions are an average of data 10 sources, excluding with patients with improved FVC% predicted. 11
(d) Assumption that all patients with improved FVC experience same mortality risk as those with slow disease progression. 12 (e) Assumption that only patients with small improvement in FVC experience the same mortality risk as those with slow 13
disease progression, and the remainder experience the same mortality risk as those with moderate disease progression. 14
Rate of Respiratory Hospitalisation (including acute exacerbation) 15
Findings from Du Bois et al (2011) 117 indicate that previous hospitalisation for a respiratory cause is a 16 prognostic risk factor for mortality. Further, hospitalisation was indicated as a potential event that 17 would prevent participation in a programme. A natural history search retrieved three papers which 18 potentially could inform the rate of hospitalisation from respiratory causes in the IPF population, 19 taking into account disease progression as measured by FVC% predicted. 20
Kondoh et al (2010)248 found a 10% decline in FVC% predicted at 6 months found to be independent 21 risk factor of AE, reporting a hazard ratio of 2.60 (95% CI 1.01-7.45). Additionally these authors found 22 that acute exacerbation, when adjusted for FVC% predicted and decline in FVC % predicted, was an 23 independent predictor of survival (with a hazard ration of 2.79 [95% CI 1.59-4.88]). In a multivariate 24 analysis, Song et al. (2011) 445 reported a hazard ratio of 0.979 (0.964-0.995) for “low” FVC% 25 predicted values. Whilst both papers were informative, neither papers specified the comparator 26 used in the calculation of the hazard ratio, making the use of their data unviable in the model. 27
Martinez et al. (2005) 304 reported that 38 of 168 patients had respiratory hospitalization. The 28 authors report that 82 patients had an FVC % predicted value of less than 63%, and 25 of these 29 patients had a respiratory hospitalisation within 18 months of follow up. 86 patients had an FVC % 30 predicted value of over 62%, 13 of whom had a respiratory hospitalisation in the same time. Using 31 this data, the following probability of hospitalisation in the model was derived. 32

361
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
Table 127: Probability of respiratory hospitalisation according to FVC% predicted value. Source: 1 Martinez et al. (2005). 2
N
Number of hospitalisations (over 18 month period)
Probability of 1st hospitalisation (over 18 month period) alpha Beta Rate
Probability of hospitalisation over a one month cycle
Complete cohort
168 38 0.23 38 130 0.0142 0.01
FVC% predicted
<=62% (n=82) 82 25 0.30 25 57 0.0202 0.02
FVC% predicted
>62% (n=86) 86 13 0.15 13 73 0.0091 0.009
Rate of Mortality 3
Du Bois et al (2011) 117 provide a mortality risk scoring system taking into account 4 risk factors (age, 4 history of hospitalisation, FVC% predicted and 24 week change in FVC% predicted) providing baseline 5 risk data of mortality. The hazard ratio derived by multiple regression and score assigned to each risk 6 factor is given in Table 128, and the risk of 1 year mortality by composite score is given in Table 129. 7
Table 128: Multivariate analysis of predictors of all-cause mortality among patients with idiopathic 8 pulmonary fibrosis 9
Heading HR LCI UCI Score
Age
>=70 2.21 1.35 3.62 8
60-69 1.49 0.90 2.46 4
<60 1 0
History of respiratory hospitalisation
yes 4.11 2.57 6.58 14
no 1 0
FVC% predicted
<=50 5.79 2.55 13.15 18
51-65 3.54 1.95 6.44 13
66-79 2.2 1.19 4.09 8
>=80 1 0
24 week change in FVC% predicted
<=-10 7.99 5.26 12.14 21
-5 to-9.9 2.60 1.75 3.85 10
>-5 1 0
Table 129: Expected 1-year probability of death corresponding to total risk score shown in Table 10 128 11
Total Risk score Expected 1 year Risk of death
0-4 <2%

362
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
Total Risk score Expected 1 year Risk of death
8-14 2-5%
16-21 5-10%
22-29 10-20%
30-33 20-30%
34-37 30-40%
38-40 40-50%
41-43 50-60%
44-45 60-70%
47-49 70-80%
>50 >80%
1
The model uses the one year risk of mortality calculator detailed in Table 129 to estimate the 2 probability of mortality in each cycle of each health state. This was done by determining the score 3 each subgroup would have at any particular time point in the model by taking into account increasing 4 age as the cohort progressed through the model, whether the event of hospitalisation had occurred 5 through use of tunnel states and a decreasing absolute FVC % predicted as the FVC% declined in 6 accordance to which subgroup they were in. For simplicity as the model cycle was 1 month in 7 duration, we assume that a 6 month decline in FVC% predicted is interchangeable and equivalent to 8 the 24 week decline in FVC% predicted specified by the Du Bois study. The probability of mortality in 9 one cycle was calculated from the one year risk using methods outlined in section L.2.4 10
The nature of the Markov model, the use of the Du Bois data and the model structure imposes 11 several assumptions regarding the natural history of the IPF patients: 12
The rate of disease progression is linear and we can divide into subgroups accordingly. If the rate 13 of disease progression increases with time, the model may underestimate the mortality risk in 14 later cycles of the model. 15
The risk of hospitalisation is only influenced by absolute FVC% predicted values, and not by rate of 16 disease progression (as there is an absence of evidence to suggest this). If hospitalisation 17 increases with an increased rate of disease progression, the model may underestimate mortality 18 risk. 19
Due to computational complexity, the model only has the capacity to have memory of one 20 previous hospitalisation, which may have occurred at any point since entry of the cohort. Using 21 the hazard ratios specified by Du Bois et al (2011) 117 could result in overestimation of mortality 22 risk in cycles post 24 weeks. However, this overestimation may be mitigated by the fact that 25% 23 of patients with history of hospitalisation will be expected to have multiple episodes 445. 24
The model assumes that previous hospitalisation only affects the risk of mortality, it does not 25 decrease FVC % predicted value or increase rate of disease progression. If hospitalisation does 26 result in a rapid drop in FVC% predicted value, the model may underestimate mortality risk post 27 hospitalisation and overestimate life expectancy, as a lower proportion of the cohort surviving a 28 hospitalisation will reach an FVC% predicted value of <35% (the dead through disease progression 29 state) in the time period expected. 30
The assumptions outlined above were discussed in light of findings from the prognostic clinical 31 review. In order to clinically validate the model output, the median life expectancy and disease 32 trajectory of cohorts with differing baseline characteristics was produced. The median life 33 expectancies mean life years gained per patient and Kaplan Meier curves are given for cohorts of 34 differing age and FVC% predicted at baseline in Appendix M: M. 35

363
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
L.2.3.4 Quality of Life (Utilities) 1
The Quality Adjusted Life Year (QALY) is a measure of a person’s length of life weighted by a 2 valuation of their Health Related Quality of Life (HRQoL) over that period. Utilities are a 3 measurement of the preference for a particular health state, with a score ranging from 0 (death) to 1 4 (perfect health). To inform the utility of the time spent in the model; a search of the economic and 5 quality of life literature identified utilities which have been used in previous economic evaluations 6 regarding idiopathic pulmonary fibrosis. 7
A number of instruments are used in assessing the HRQoL associated with interventions in IPF. Two 8 commonly instruments are the generic SF36 and the disease specific SRGQ questionnaires. 9
The SF36 has been validated in the IPF population 305,464 and can be mapped to EQ5D using the 10 methods cited by Ara and Brazier [20 equation 1]. The use of SRGQ (St Georges Respiratory 11 Questionnaire) has also been suggested as a valid tool to assess quality of life in the IPF population 12 464,482,510 and can also be mapped to the EQ5D by the algorithm developed by Starkie and 13 colleagues447. Where estimates of utility either directly from EQ5D estimates or from values mapped 14 from SF36 are not obtainable, consideration will be given to mapping SRGQ scores to the EQ5D. 15
Uncertainty associated with any reported scores can also be taken into account in the mapped EQ5D 16 estimate by using probabilistic methods and simulation. The mapped EQ5D estimate, with 17 confidence interval, is a composite score that will allow an assessment of the change in quality of life 18 provided by an intervention. For full details of the method and calculations used in mapping to the 19 EQ5D, please refer to section L.2.4. When assessing the evidence, the limitations of both the HRQoL 20 instruments and mapping methods were taken into consideration, and these are outlined in section 0 21
Estimating quality of life throughout the natural clinical course of IPF (baseline QoL) 22
The quality of life search and the history search retrieved two studies 464 482 that provided potential 23 means of estimating the quality of life throughout the natural clinical course of IPF. The two data 24 sources lend themselves to two different approaches to estimating the baseline QoL of patients in 25 the no rehabilitation strategy of the model. 26
Estimating baseline utility – approach 1: 27
Swigris et al. (2010) 464 used data from the BUILD-1 trial in a retrospective analysis to determine a 28 minimally important difference in QoL of IPF patients as measured by the SF36 and SRGQ. The 29 authors used distributional and anchor based methods, and report regression equations for each 30 SF36 domain for a unit change in FVC% predicted. These are shown alongside the expected decline in 31 the value of the SF36 domain for a unit decline in FVC% predicted in Table 130. The final row gives 32 the decline in utility you would expect with the associated decline in FVC% predicted if these values 33 were mapped to the EQ5D. 34
Table 130: Regression equation for a change in SF36 domain and FVC% predicted. Source: Swigris 35 et al (2010)/ 36
SF36 domain Regression equation
Decline in SF36 domain score that corresponds to a raw change in FVC% predicted of:
5% 10% 15%
Physical Functioning (PF) 1.6 2.5 (1.1-3.9) 3.4
Physical Role (RP) 2.5 3.3 (1.3 – 5.4) 4.1
Bodily Pain (BP) 0.5 1.2 (0.5 – 3.0) 1.9
General Health (GH) 0.33 0.7 (-0.5-1.8) 1.03

364
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
SF36 domain Regression equation
Decline in SF36 domain score that corresponds to a raw change in FVC% predicted of:
5% 10% 15%
Vitality (VT) 1.27 2.1 (0.8 – 3.4) 2.87
Social Functioning (SF) 3.15 5.0 (2.1- 7.0) 6.85
Emotional Role (RE) 2.35 3.7 (1.4-6.1) 5.05
Mental Health (MH) 1.16 1.3 (0.8 – 2.8) 1.56
Estimated decline in utility (as mapped by to the EQ5D)
0.0457116 0.0534191 0.0611266
(a) The study used data recorded at baseline and 6 months. Note that the range was only reported for a decline of 10% in 1 FVC% predicted value. 2
Table 131 shows the expected FVC% predicted value at given time points in the model for the 3 different subgroups, such that it gives the predicted utility of a patient at a given time point in the 4 model if the utility decrements specified for a given decline in FVC% predicted (of that subgroup) 5 were used. It was decided that it would become to0 computationally burdensome to find the utility 6 decrement associated with each FVC% predicted unit change within the model, given the number of 7 health states and tunnel health states required to represent a continuum and all 8 SF36 domains 8 would need to be taken into account before mapping to the EQ5D. Further, although application of a 9 different baseline utility may influence the accuracy of total QALY gain, as the treatment effect is 10 added to the baseline in the model, assumptions regarding baseline utility would not impact greatly 11 on the incremental effect calculated. 12
Table 131: Predicted QoL according to decline in FVC% predicted per year 13
Time (years)
Slow decline
(2.5% every 6 months)
Moderate decline
(7.5% every 6 months)
Fast decline
(12.5% every 6 months)
FVC% predicted QoL estimate
FVC% predicted QoL estimate
FVC% predicted
QoL estimate
0 100% 1.00 100% 1 100% 1
1 95% 0.92 85% 0.90 0.75 0.89
2 90% 0.83 69% 0.80 0.5 0.77
3 85% 0.75 52% 0.70 0.25 0.66
4 80% 0.67 34% 0.60
5 75% 0.58
6 70% 0.50
7 65% 0.41
8 60% 0.33
Estimating baseline utility – approach 2: 14
Tzanakis et al (2005) 482 reports on a cross sectional study examining the correlation between quality 15 of life measures and pulmonary function tests. The authors found that duration of disease was 16 significantly correlated with SGRQ scores (r=0.483, p=0.01). Using the methodology outlined in 17 section L.2.3.4, utilities for each year post diagnosis are given in Table 132. 18
Table 132: Quality of Life of IPF patients over an 8 year time horizon. Source: Tzanakis et al. (2005). 19
Time (years) SRGQ score EQ5D Utility Estimates (mapped from SRGQ)

365
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
Time (years) SRGQ score EQ5D Utility Estimates (mapped from SRGQ)
Estimate SEM LCI UCI
0 24 0.89 0.02 0.84 0.93
1 30 0.85 0.03 0.79 0.90
2 34 0.82 0.03 0.75 0.87
3 40 0.77 0.04 0.70 0.83
4 45 0.72 0.04 0.64 0.79
5 49 0.68 0.04 0.59 0.75
6 55 0.61 0.05 0.51 0.69
7 58 0.57 0.05 0.47 0.66
8 64 0.49 0.05 0.38 0.59
Note: Sample size (n) = 25; Male = 84%; Age = 66±11(sd); FVC% pred = 68.8±16 (sd). Rate of FVC% pred. decline = NR; 1 No participating subjects had any significant medical history or co morbidity. 32% had supplemental oxygen use. 2 SGRQ = 37.7 ± 18.9(sd). SRGQ standard error approximated at 3.78 = (18.9/ 25). Please note that SRGQ scores 3 were read from graph as exact values were not provided on request. 4
In the model, each life year in the no rehabilitation strategy is weighted with the respective utility 5 detailed in Table 132. It was not possible to estimate from the paper the quality of life beyond the 8th 6 year, it was assumed that the quality of life for patients living beyond 8 years was the same as that 7 derived for the 8th year of the model. The model assumes that baseline quality of life is not 8 influenced by the patient’s FVC% predicted, hospitalisation or rate of disease progression. If quality 9 of life does decline with these factors, the model is likely to overestimate the total QALY gain of the 10 subgroups with moderate and rapid decline across all strategies. To take this limitation into account, 11 and to avoid error in estimating the incremental QALY gain between those receiving pulmonary 12 rehabilitation and those without, the model adds a mean difference of effect found by the clinical 13 review, rather than applying a relative treatment effect (i.e. QoL improves by 25%). 14
L.2.3.5 Treatment effect 15
The clinical review identified two RCTs 185 355 and 6 cohort studies 213,253,373,404,465 to inform the 16 treatment effect of pulmonary rehabilitation for an IPF and ILD population. A further study that 17 looked at only psychosocial support specifically285. Three of the cohort studies that gave SF36 values 18 at baseline and post intervention213,253,373. Due to the quality of these observational studies, it was 19 decided that only the programmes specified by the RCTs should be used to inform the model. 20
One RCT185 suggested there may be a small improvement in 6 month survival following an exercise 21 programme, however there was too much uncertainty to determine whether there was a difference 22 in this parameter. As such, it is not expected that pulmonary rehabilitation will delay disease 23 progression; rather that it improves the quality of life throughout the first stages of disease 24 progression. Therefore the only treatment effect examined in the model is the quality of life 25 improvement found with pulmonary rehabilitation. Pulmonary rehabilitation does not influence the 26 probability of disease progression, respiratory hospitalisation (including acute exacerbation) or 27 death. This means that the life expectancy and the number of hospitalisations will be the same 28 across compared strategies. For this reason the number and cost of healthcare contacts is not 29 recorded by the model. 30
The two RCTs 355 185 suggested that pulmonary rehabilitation improved quality of life. 31
Nishiyama et al (2008) 355 showed that quality of life, as measured by the St Georges Respiratory 32 questionnaire, improved moderately by a nine week programme that had some educational 33 elements (not specified). Table 133 gives the St Georges Respiratory Questionnaire scores presented 34 by Nishiyama et al. 2008, and Table 134 shows the utility estimates used in the model when these 35

366
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
scores were mapped to the EQ5D using the methods stated in section L.2.4.1. An absolute effect 1 difference in utility of 0.060 was found at the end of the pulmonary rehabilitation programme 2 between the control and intervention arm. 3
Table 133: St Georges Respiratory Questionnaire Scores presented by Nishiyama et al (2008) 4
SGRQ Domain Control (n=15) Rehab (n=13)
Difference between groups in change from baseline
Baseline
SD Post intervention
SD Baseline SD Post intervention
SD
Symptoms 38.0 25.8 40.6 21.2 53.4 25.8 56.4 22.3 -5.7
Activity 50.4 26.2 54.0 22.6 62.5 16.9 64.7 17.1 -5.8
Impacts 29.9 23.7 32.9 23.5 36.5 17.5 39.7 17.6 -6.2
Total 37.8 22.7 40.9 20.7 47.3 17.4 50.2 16.3 -6.1
Note: SD = Standard deviation 5
6
Table 134: Utility estimates used in the model, as derived by mapping the SGRQ scores to the EQ5D 7
Total SGRQ
Mapped to the EQ5D from SGRQ
SE of SGRQ α β
Control - baseline 37.800 0.786 5.861 40.314 66.337
Rehab - baseline 50.200 0.661 4.826 49.297 48.904
Control - post 40.900 0.757 5.345 44.857 64.817
Rehab - post 47.300 0.693 13.923 46.313 51.601
Difference - control 3.100 -0.028
Difference - rehab -2.900 0.032
Absolute mean difference
0.060
Note: Percentage male = not reported, therefore assumed at 70%; SE = Standard error calculated by dividing standard 8 deviation by the square root of the sample size. Alpha and Beta calculated using standard error. A beta 9 distribution was used in the probabilistic sensitivity analysis. 10
Holland et al (2008) showed that quality of life as measured by the SF36 improved to a similar extent 11 to that found by Nishiyama et al. (2008). Table 135 gives the mean SF36 scores (provided as summary 12 data from the authors), with the mapped values as calculated in the methodology stated in section 13 L.2.4. The data shows that at three months follow up, an absolute effect difference in utility of 0.068 14 was found between the control and intervention arm, and at six months follow up the absolute 15 difference in effect had decreased to 0.058. Table 136 gives the uncertainty estimates used in the 16 probabilistic sensitivity analysis for this parameter. 17
Table 135: Treatment effect of exercise programme as detailed by Holland et al (2008) 185 18
Mean SF36 Dimension Score Utility (Mappe Sam Time PH RP BP GH SF RE MH V
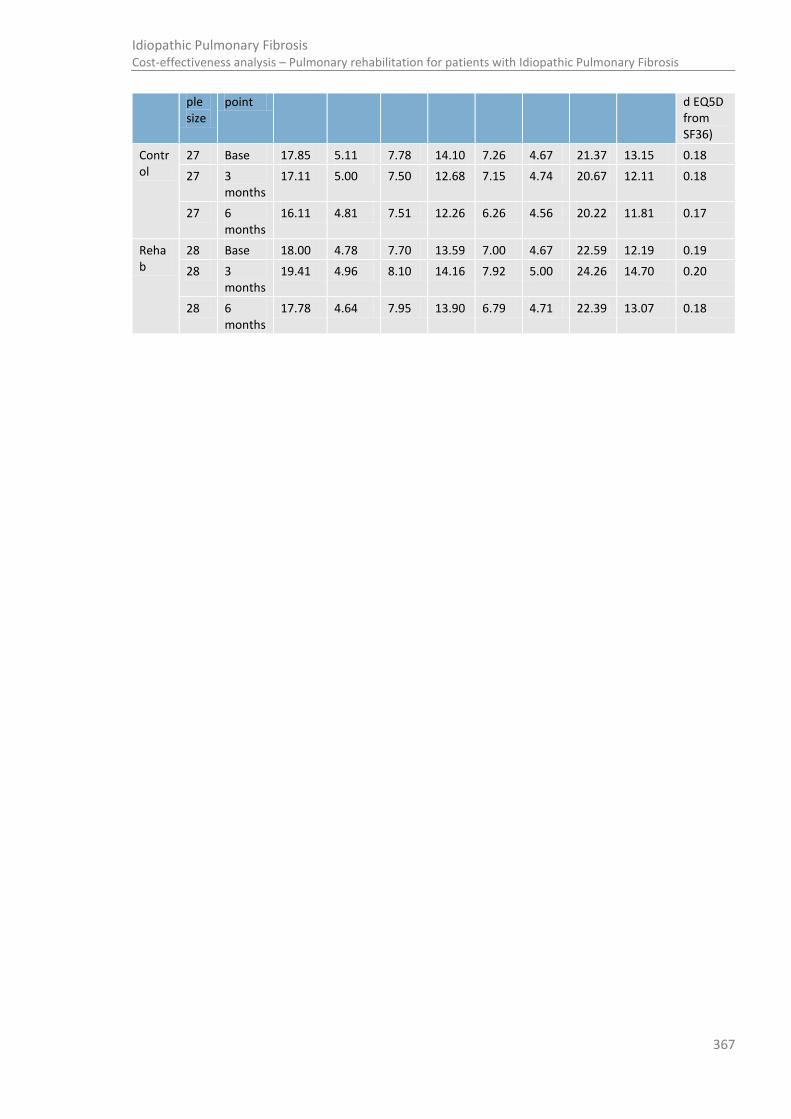
367
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
ple size
point d EQ5D from SF36)
Control
27 Base 17.85 5.11 7.78 14.10 7.26 4.67 21.37 13.15 0.18
27 3 months
17.11 5.00 7.50 12.68 7.15 4.74 20.67 12.11 0.18
27 6 months
16.11 4.81 7.51 12.26 6.26 4.56 20.22 11.81 0.17
Rehab
28 Base 18.00 4.78 7.70 13.59 7.00 4.67 22.59 12.19 0.19
28 3 months
19.41 4.96 8.10 14.16 7.92 5.00 24.26 14.70 0.20
28 6 months
17.78 4.64 7.95 13.90 6.79 4.71 22.39 13.07 0.18

368
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
Table 136: Uncertainty estimates for the SF36 values provided by Holland for use in the probabilistic sensitivity analysis 1
Arm of trail
t
[a]
Standard Error for each SF36 domain
Alpha and Beta values derived by method of moments (Briggs)
PH RP BP GH SF RE MH V
PH RP BP GH SF RE MH V α β α β α β α β α β α β α β α β
Control
0 4.49 6.58 5.34 3.93 5.40 9.07 4.00 3.67 46 71 13 33 49 36 73 87 50 26 16 13 92 49 84 100
3 4.07 7.06 5.92 4.02 4.96 7.90 4.20 4.19 51 88 9 27 38 32 60 88 60 29 23 14 83 49 58 80
6
4.07 5.82 6.53 4.31 5.64 8.10 3.85 3.74 40 88 10 37 31 26 48 78 44 30 22 13 98 61 72 101
Rehab
0
4.24 5.46 4.39 3.41 5.55 8.01 3.12 3.29 53 79 10 42 74 50 88 121 47 26 21 17 151 68 89 132
3
4.47 7.47 5.20 3.02 5.48 8.68 3.08 3.36 56 67 8 24 53 33 114 154 48 20 19 12 143 43 115 105
6
4.47 6.32 5.52 4.41 5.40 8.95 3.34 4.37 46 72 5 26 48 28 54 71 48 34 15 15 129 48 59 70
Note: Standard error calculated by dividing the standard deviation by square root of the sample size. T= time since programme start (months). Alpha and Beta values derived by method of 2 moments
46 . A beta distribution was used in the probabilistic sensitivity analysis. 3
4
5
369
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
Treatment effect duration 1
No evidence was retrieved to inform treatment effect duration or the impact of pulmonary 2 rehabilitation maintenance. The base case takes the conservative assumption that utility increases at 3 a linear rate from baseline to the maximum absolute difference seen by the RCT at the end of the 4 pulmonary rehabilitation course (2 months). At this point the maximum absolute difference in utility 5 is sustained until the midpoint follow-up period of 3 months specified by Holland et al. (2008) has 6 surpassed. From this midpoint the utility difference between those who do not have rehabilitation 7 and those who have had rehabilitation declines at a linear rate until the observed difference in utility 8 at the long term follow up time point at 6 months is achieved. In the base case, it is assumed no 9 further treatment effect will be observed past this time period, and the rehabilitation cohort then 10 experiences the same utility as the cohort that did not have rehabilitation. In a sensitivity analysis, a 11 long term treatment effect diminishing at a linear rate is tested, with treatment effect completely 12 disappearing after 6 months (base case), 9 months, 12 months, 15 months, 18 months and 24 13 months. 14
Treatment effect of repeated programmes 15
There was no evidence to inform whether patients undergoing a repeated programme would 16 experience the same increase in quality of life as they had experienced with the first programme. A 17 sensitivity analysis was conducted whereby the treatment effect was reduced by a given percentage 18 compared to that experienced by completing a previous programme by applying a treatment effect 19 multiplier powered to the number of programmes previously undertaken. So for example, a patient 20 on their second programme of rehabilitation will only experience 80% of the quality of life 21 improvement that they had experienced on the first programme. A patient on their third programme 22 would experience 80% of the quality of life improvement they had experienced on their second 23 programme and so on. 24
A three-way deterministic sensitivity analysis explores the impact of differing treatment effect 25 assumptions as outlined in section L.2.5 to aid decision making regarding the viability of offering 26 pulmonary rehabilitation more than once. The graphs below illustrate the utility applied for the 27 programmes given a 12 month long term treatment effect with an offer of rehabilitation every 12 28 months and every 9 months. Figure 117 and Figure 118 illustrate this with the treatment effect 29 multiplier set to 100% so no difference in effect was observed between repeated programmes, and 30 Figure 119 and Figure 120 show the same over a longer time horizon, with the treatment effect 31 multiplier set to 80% which shows the decline in effect with each repeated programme. 32
In some cases, where the long-term treatment effect was long and the magnitude of treatment 33 effect with each repeated offer decreased substantially, it was possible that at the time point of the 34 repeated programme the utility arising from sustained effect of the first programme was higher than 35 that produced by the second programme. The model was programmed to ensure that in such 36 instances the sustained treatment effect was applied appropriately by modelling the utility gain in 37 each repeated course (according to magnitude of effect and treatment effect duration) and selecting 38 the highest utility possible in each cycle. 39

370
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
Figure 117: Utility estimates applied in the first 24 months of the model, whereby the 1 pulmonary rehabilitation course was repeated at 12 months, and long term treatment 2 effect duration of 12 months was applied. 3
4
Figure 118: Utility estimates applied in the first 24 months of the model, whereby the 5 pulmonary rehabilitation course was repeated at 9 months, and long term treatment 6 effect duration of 12 months was applied. 7
8
0.800
0.820
0.840
0.860
0.880
0.900
0.920
0.940
0.960
0.980
0 3 6 9 12 15 18 21 24
Uti
lity
Time (months)
No rehab
Exercise only
Exercise and education
0.800
0.820
0.840
0.860
0.880
0.900
0.920
0.940
0.960
0.980
0 3 6 9 12 15 18 21 24
Uti
lity
Time (months)
No rehab
Exercise only
Exercise and education

371
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
Figure 119: Utility estimates applied in the first 60 months of the model, whereby the 1 pulmonary rehabilitation course was repeated at 12 months, and long term treatment 2 effect duration of 12 months was applied. Each subsequent programme is 80% as 3 effective as the previous programme experienced before. 4
5
6
Figure 120: Utility estimates applied in the first 60 months of the model, whereby the 7 pulmonary rehabilitation course was repeated at 9 months, and long term treatment 8 effect duration of 12 months was applied. Each subsequent programme is 80% as 9 effective as the previous programme experienced before. 10
11
12
13
0.400
0.500
0.600
0.700
0.800
0.900
1.000
0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45 48 51 54 57 60
Uti
lity
Time (months)
No rehab
Exercise only
Exercise and education
0.400
0.500
0.600
0.700
0.800
0.900
1.000
0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45 48 51 54 57 60
Uti
lity
Time (months)
No rehab
Exercise only
Exercise and education

372
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
Figure 121: Utility estimates applied in the first 60 months of the model, whereby the 1 pulmonary rehabilitation course was repeated at 9 months, and long term treatment 2 effect duration of 24 months was applied. Each subsequent programme is 80% as 3 effective as the previous programme experienced before. 4
5
6
L.2.3.6 Participation and drop out 7
The ability to participate in a programme will influence the cost effectiveness, however there was no 8 evidence to inform this element of the model. The clinical experience of the group was that if the 9 patient’s needs were fully identified at assessment for pulmonary rehabilitation, it was likely that a 10 patient would be able to fully participate throughout the course and experience any long term 11 benefit effect thereafter. However, hospitalisation could influence a patient’s ability to be “fit” to 12 participate and subsequently benefit of pulmonary rehabilitation. 13
For this reason various participation scenarios were tested. The base case assumes so long as the 14 patient is alive, they may participate in pulmonary rehabilitation, regardless of their hospitalised 15 status. Participation scenario one assumes that a patient will not be able to participate or feel the 16 benefit of pulmonary rehabilitation (i.e. their utility is the same as baseline) in the cycle post 17 hospitalisation. Participation scenario two assumes that a proportion of the cohort could not return 18 to participate in or benefit from pulmonary rehabilitation if they have had a previous hospitalisation. 19 Within this scenario the proportion of patients with prior hospitalisation not returning to pulmonary 20 rehabilitation was tested, from 100% of patients that had experienced hospitalisation not returning 21 to the programme to 0% of patients (i.e. all patients could continue to participate which mirrored the 22 base case participation setting). If a patient did not return to pulmonary rehabilitation, they would 23 still be assessed (and incur assessment costs), however they would not incur programme costs or 24 benefit from an improved quality of life from the programme. 25
L.2.3.7 Resource use and cost 26
There was no evidence identified that examined the impact pulmonary rehabilitaton may have on 27 downstream healthcare resource use such as hospital admission or other healthcare contacts. 28 Although in reality you would expect some costs to be associated with treatment, hospitalisation etc 29 with no rehabilitation, there was no evidence to confirm whether these would be different from 30
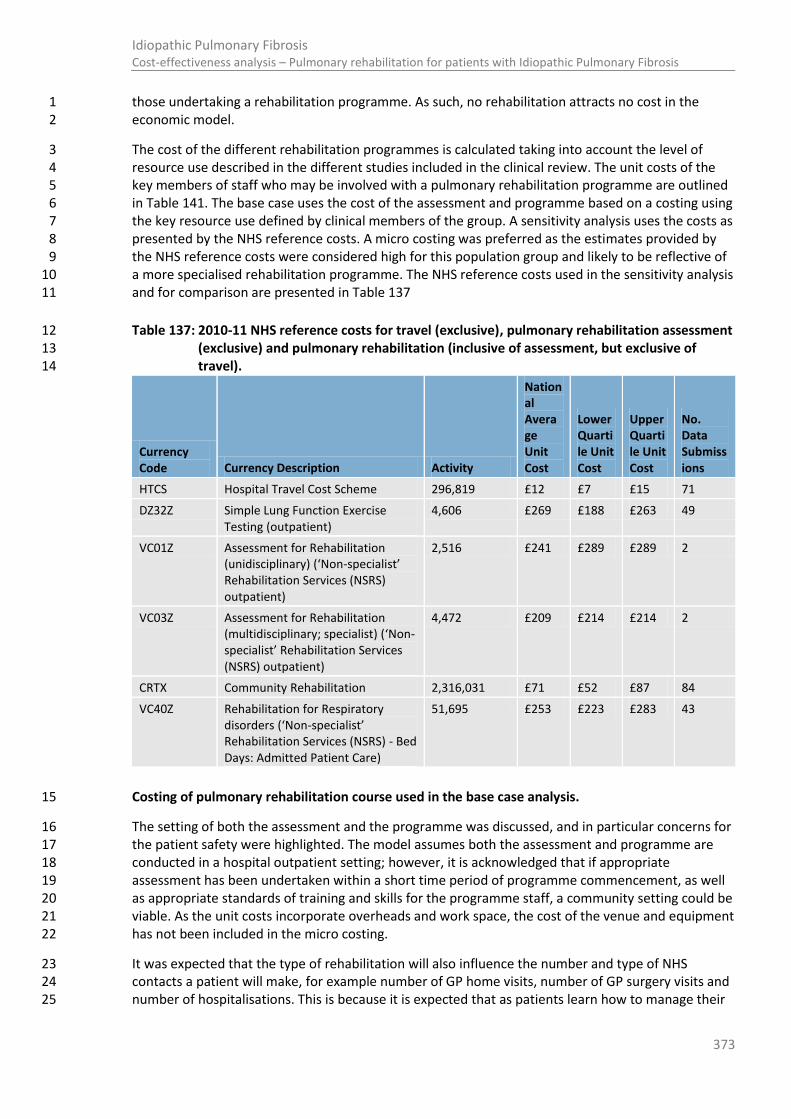
373
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
those undertaking a rehabilitation programme. As such, no rehabilitation attracts no cost in the 1 economic model. 2
The cost of the different rehabilitation programmes is calculated taking into account the level of 3 resource use described in the different studies included in the clinical review. The unit costs of the 4 key members of staff who may be involved with a pulmonary rehabilitation programme are outlined 5 in Table 141. The base case uses the cost of the assessment and programme based on a costing using 6 the key resource use defined by clinical members of the group. A sensitivity analysis uses the costs as 7 presented by the NHS reference costs. A micro costing was preferred as the estimates provided by 8 the NHS reference costs were considered high for this population group and likely to be reflective of 9 a more specialised rehabilitation programme. The NHS reference costs used in the sensitivity analysis 10 and for comparison are presented in Table 137 11
Table 137: 2010-11 NHS reference costs for travel (exclusive), pulmonary rehabilitation assessment 12 (exclusive) and pulmonary rehabilitation (inclusive of assessment, but exclusive of 13 travel). 14
Currency Code Currency Description Activity
National Average Unit Cost
Lower Quartile Unit Cost
Upper Quartile Unit Cost
No. Data Submissions
HTCS Hospital Travel Cost Scheme 296,819 £12 £7 £15 71
DZ32Z Simple Lung Function Exercise Testing (outpatient)
4,606 £269 £188 £263 49
VC01Z Assessment for Rehabilitation (unidisciplinary) (‘Non-specialist’ Rehabilitation Services (NSRS) outpatient)
2,516 £241 £289 £289 2
VC03Z Assessment for Rehabilitation (multidisciplinary; specialist) (‘Non-specialist’ Rehabilitation Services (NSRS) outpatient)
4,472 £209 £214 £214 2
CRTX Community Rehabilitation 2,316,031 £71 £52 £87 84
VC40Z Rehabilitation for Respiratory disorders (‘Non-specialist’ Rehabilitation Services (NSRS) - Bed Days: Admitted Patient Care)
51,695 £253 £223 £283 43
Costing of pulmonary rehabilitation course used in the base case analysis. 15
The setting of both the assessment and the programme was discussed, and in particular concerns for 16 the patient safety were highlighted. The model assumes both the assessment and programme are 17 conducted in a hospital outpatient setting; however, it is acknowledged that if appropriate 18 assessment has been undertaken within a short time period of programme commencement, as well 19 as appropriate standards of training and skills for the programme staff, a community setting could be 20 viable. As the unit costs incorporate overheads and work space, the cost of the venue and equipment 21 has not been included in the micro costing. 22
It was expected that the type of rehabilitation will also influence the number and type of NHS 23 contacts a patient will make, for example number of GP home visits, number of GP surgery visits and 24 number of hospitalisations. This is because it is expected that as patients learn how to manage their 25

374
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
symptoms, the number of NHS contacts will decrease. However, no data was found to inform this 1 aspect of the planned model, and therefore this decrease in resource use has not been considered. 2
Two different approaches to costing were explored. The base case assumes the patient incurs the 3 cost of the assessment and the course up front. This reflects the scenario of diminishing class size 4 with drop out due to inability to participate due to disease progression, hospitalisation or death. A 5 second approach assumes that the programme is rolling, with patients being able to participate at 6 any time (i.e. have maximal benefit from the intervention throughout the time horizon of the model 7 when participating) and that the class is at full capacity. This is presented as a scenario in the 8 sensitivity analysis. 9
Assessment for pulmonary rehabilitation 10
Assessment for pulmonary rehabilitation is assumed to be the same for all programmes. It is 11 assumed that patients would be referred for assessment following diagnosis at specialist MDT, and 12 thereby the role of the MDT coordinator and ILD nurse will extend into this care pathway. 13 Alternatively referral may come from Primary Care e.g. GPs, practice nurses, community 14 pharmacists; and Secondary care e.g. consultants, nurses, Early Supported Discharge (ESD) teams; 15 respiratory clinics, wards, physiotherapists. The Administration clerk will contact patients for 16 assessment & re-assessment (and may need to send a follow-up letter to those who don't respond). 17 This is assumed to take 10 minutes. 18
Clinical experts stressed the importance of the assessment for pulmonary rehabilitation. The IPF 19 patient's desaturation profile should be fully understood at assessment in order to prevent an 20 emergency scenario arising within the pulmonary rehabilitation class. Therefore both a submaximal 21 and endurance test may be appropriate to ascertain the patient's needs when undertaking the 22 course. It was agreed that the assessment should occur in a hospital setting so that in the 23 unlikelihood of over exertion or emergency appropriate care would be available. To ensure access, 24 the requirement for transport for a certain percentage of patients to be able to access the hospital 25 outpatient setting is included in the costing. Using the group’s experience, it was thought 10% of 26 patients would require transport. It is assumed that oxygen requirements are already established 27 and catered for, and as such oxygen assessment and oxygen use has not been included in the costing. 28 It was acknowledged oxygen reassessment may be required within a short timeframe prior to the 29 rehabilitation assessment. It was also assumed that lung function tests would have already been 30 recently performed and were also not included in the assessment costs. 31
Clinical members advised that assessment would require 1.5 hours of a physiotherapist's time (band 32 6) due to the requirement for a practice exercise test and a real test, the need for the patient to rest 33 between exercise tests and the need for the physiotherapist to be present throughout and conduct 34 any associated paperwork. The same resource use will occur for first and repeat assessments. The 35 costing assumes a frequency of 1.33 to allow for one third of patients to have more than one 36 appointment (due to attendance failure or to complete the session). 37
Table 138: Unit cost of pulmonary rehabilitation assessment 38
Activity Frequency Cadre of staff Band Unit cost per hour
Time required (hour)
Group size
Cost per patient
Contacting patient for assessment
1.33 Clerical coordinator
4 26 0.17 1 6
Assessment 1.33 Physiotherapist 6 44 1.50 1 88
0.13 Transport na 19 1 3
Total £96.13

375
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
1
Pulmonary Rehabilitation Programme Costs 2
Nishiyama2008355 gave a treatment effect for a nine week outpatient exercise program, with twice 3 weekly supervised sessions. Exercise on treadmill at 80% of walking speed on initial 6-minute walk 4 test, or on cycle ergometer at 80% of initial maximum workload. Strength training for limbs using 5 elastic bands for approximately 20 minutes. Supplemental oxygen administered to achieve 6 SpO2>90%. Some educational lectures were included but the content was not specified. Thus in the 7 costing, we have the conservative assumption that both a nurse and physiotherapist (at band 6) are 8 required throughout the course. In addition a clinician of registrar grade and two hospital based 9 allied health professionals (at band 5) are each required to undertake an hour educational session 10 per course programme. Transport is provided for 10% of patients. The costing of this programme is 11 outlined in Table 139. 12
Table 139: Resource use for the programme cited by Nishiyama et al (2008) 13
Activity Frequency Cadre of staff Band
Unit cost per hour
Time required (hour)
Group size
Cost per patient
Pulmonary Rehab Course
18 Physiotherapist - hospital
6 £44 0.50 10 £39
18 Nurse (team leader) - hospital
6 £45 0.50 10 £41
1 Band 5 allied hospital based allied work professional (i.e. hospital dietician)
5 £37 2.00 10 £7
1 Registrar na £73 1.00 10 £7
18 Transport na £12 1.00 10 £22
Total £117.06
Holland et al (2008) gave a treatment effect for an eight week outpatient exercise program, twice 14 weekly supervised sessions consisting of 30 minutes endurance exercise (cycling and walking) with 15 initial intensity at 80% of walking speed on initial 6-minute walk test and progressed according to 16 protocol. Upper limb endurance and functional strength training for lower limbs also performed. 17 Supplemental oxygen provided for SpO2>85%. Unsupervised home exercise program prescribed 3 18 times per week. In the costing, we have the conservative assumption that both a nurse and 19 physiotherapist (at band 6) are required throughout the course. Transport is provided for 10% of 20 patients. The costing of this programme is outlined in Table 140. 21
Table 140: Resource use for the programme cited by Holland et al (2008). 22
23
Activity Frequency Cadre of staff Band
Unit cost per hour
Time required (hour)
Group size
Cost per patient
Pulmonary Rehab Course
16 Physiotherapist - hospital
6 £44 0.50 10.00 £35
16 Nurse (team leader) - hospital
6 £45 0.50 10.00 £36

376
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
Activity Frequency Cadre of staff Band
Unit cost per hour
Time required (hour)
Group size
Cost per patient
16 Transport na £12 1.00 10.00 £20
Total £91.02

377
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
Table 141: Unit cost of NHS staff who may be involved with a pulmonary rehabilitation programme. 1
Staff NHS Band
Hours per annum [a]
Direct salary [b]
On cost [c]
Qualification and on-going training [d]
Staff overhead [e]
Non staff overhead [f]
Capital [g] Total
Per hour of working time
Hospital staff
Hospital physiotherapist 6 1549 £29,464 £6,947 £4,927 £6,954 £15,147 £4,541 £67,980 £44
Hospital dietician 5 1549 £24,554 £5,789 £5,059 £5,796 £12,623 £3,535 £57,355 £37
Nurse team leader 6 1549 £29,464 £6,947 £9,356 £6,954 £15,147 £2,307 £70,175 £45
Registrar * PSSRU estimate for 2011 on mean full time equivalent earnings
- 1987 £55,600 £14,169 £28,711 £13,325 £29,024 £3,297 £144,126 £73
Clerical coordinator 4 1549 £20,433 £4,818 £0 £4,823 £10,504 £0 £40,578 £26
(a) Source: PSSRU (2011)95
2 (b) Source: For staff on NHS band pay scales these figures have been taken from 'Pay Circular (AfC) 2/2012'. Pay and conditions for NHS
352. For consultants and the community pharmacist, 3
these figures are taken from PSSRU (2011)95
and have not been inflated. 4 (c) Employers’ national insurance is included plus 14 per cent of salary for employers’ contribution to superannuation. This equates to approximately 24 per cent of direct salary cost. 5 (d) Annual cost of qualification (estimated at 3.5 per cent of total qualification cost), and where appropriate on-going training cost, is as reported by PSSRU (2011)
95 6
(e) Direct overheads cover the resources required to deliver services to users or patients and are directly related to the level of service activity. Indirect overheads include functions of the 7 organisation which support the services and allow the organisation to operate; examples would be the Human Resources or Finance Departments. Unfortunately, the information 8 provided in the Summarised Accounts does not identify these categories separately, and we have adapted our estimation method to obtain a percentage figure that reflects the 9 relationship between all overheads and direct salary costs. The Summarised Accounts show the number of care (direct) and non‐care (indirect) staff and costs for the latter group were 10 estimated using the average salary for NHS management and administrative staff
344 The calculation resulted in an additional 19.1 per cent on care staff costs to cover management, 11
estates and administrative staff. 12 (f) The non-staff overheads are the remaining costs to the provider (office costs, travelling subsistence, leased and contract hire, advertising, transport and moveable plant, telephone rentals 13
etc.), supplies and services (clinical and general), utilities and premises costs (water, sewerage, electricity and gas, cleaning, air conditioning) and education and training costs for the 14 professional staff. These account for an additional 41.6 per cent of direct care staff salary costs, making a total of overheads ‘multiplier’ for direct salary costs of 60.7 per cent. More 15 information on NHS accounting procedures can be found in the NHS Costing Manual
106 95
16 (g) Based on the new‐build and land requirements, plus additional space for shared facilities. Capital costs have been annuitised over 60 years at a discount rate of 3.5 per cent (PSSRU 17
2011)95
18
19

378
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
L.2.4 Computations 1
The model was constructed in Microsoft Excel and was evaluated by cohort simulation. Time 2 dependency was built in by cross referencing the cohorts age as a respective risk factor for mortality. 3 Baseline utility was also time dependent and was conditional on the number of years post entry to 4 the model. 5
Patients start in cycle 0 in an alive health state. Patients moved to the dead health state at the end of 6 each cycle as defined by the mortality transition probabilities and if the rate of disease progression 7 indicated the patient should deteriorate to a state with a FVC% predicted value of less than 35%. 8
Transition probabilities for respiratory hospitalisation (including acute exacerbation) and death were 9 derived from the literature. Transition probabilities for the rate of disease progression were based on 10 an assumption of a fixed rate of decline in FVC% predicted for each subgroup. For mortality, hazard 11 ratios for four risk factors within the same multivariate analysis were reported. However, as the 12 regression equation, mean, variance and covariance matrix of beta coefficients from the regression 13 equation was not obtained, it was not possible to calculate a composite hazard ratio to calculate the 14 adjusted rate of mortality for the IPF patient given their respective risk factors. Instead, the risk 15 calculator provided for an individual patient was used. These mortality rates were converted into 16 transition probabilities for the respective cycle length (1 month in the base case) before inputting 17 into the Markov model. For respiratory hospitalisation, the probability of the event over the time 18 horizon specified by the literature was converted into a rate, before being converted into a 19 probability appropriate for the cycle length. The above conversions were done using the following 20 formulae: 21
Where
r = selected rate
t= cycle length (months)
Where
P=probability of event over time t
t=time over which probability occurs
Life years for the cohort were computed each cycle. To calculate QALYs for each cycle, Q(t), the time 22 spent (i.e. 1 month or 0.08 years) in the alive state of the model was weighted by a utility value that 23 is dependent on the time spent in the model and the treatment effect. A half-cycle correction was 24 applied. QALYs were then discounted to reflect time preference (discount rate = r). QALYs during the 25 first cycle were not discounted. The total discounted QALYs were the sum of the discounted QALYs 26 per cycle. The total discounted QALYs were the sum of the discounted QALYs per cycle. 27
Costs per cycle, C(t), were calculated in the same way as QALYs. In the base case, rehabilitation costs 28 were applied in cycle 1 only. If a difference in post-rehabilitation costs was being included, this was 29 applied in cycle two and beyond. Costs were discounted to reflect time preference (discount rate = r) 30 in the same way as QALYs using the following formula: 31
Discount formula: 32
nr
1
Total totalDiscounted
Where:
r = discount rate per annum
n = time (years)
In the deterministic and probabilistic analysis, the total number of QALYs and resource costs accrued 33 by each subgroup was recorded. These subtotals were summed across all subgroups to ascertain the 34
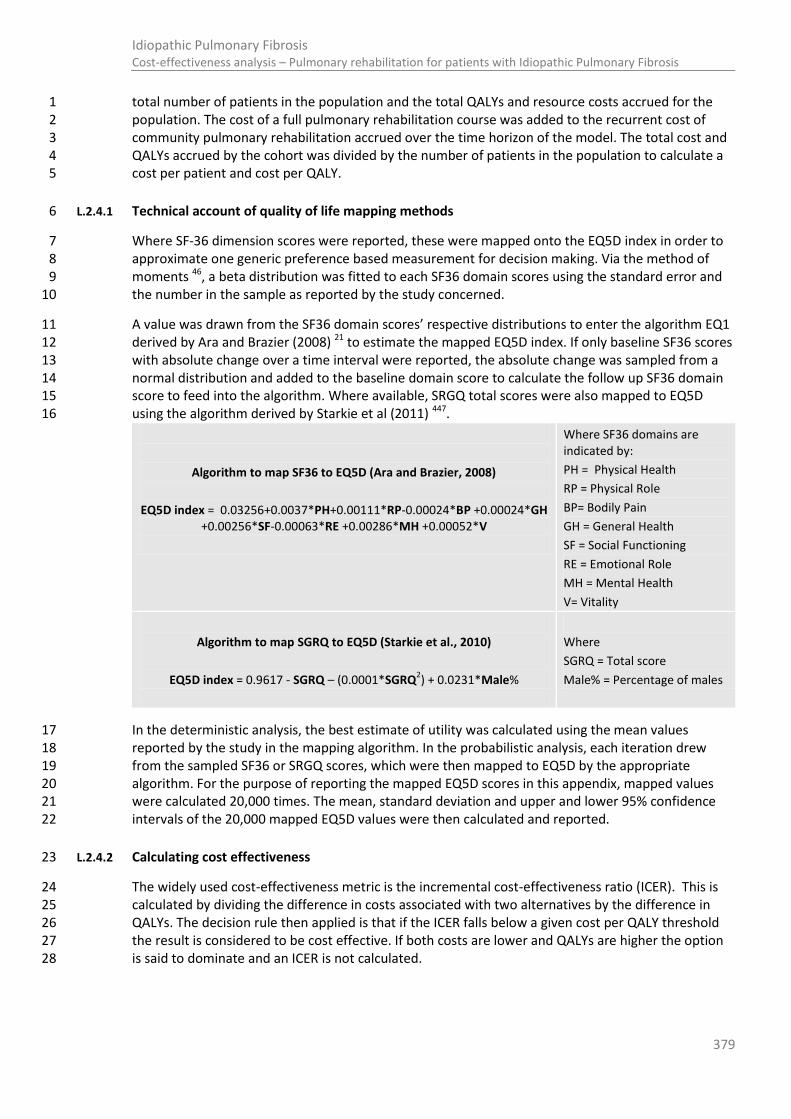
379
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
total number of patients in the population and the total QALYs and resource costs accrued for the 1 population. The cost of a full pulmonary rehabilitation course was added to the recurrent cost of 2 community pulmonary rehabilitation accrued over the time horizon of the model. The total cost and 3 QALYs accrued by the cohort was divided by the number of patients in the population to calculate a 4 cost per patient and cost per QALY. 5
L.2.4.1 Technical account of quality of life mapping methods 6
Where SF-36 dimension scores were reported, these were mapped onto the EQ5D index in order to 7 approximate one generic preference based measurement for decision making. Via the method of 8 moments 46, a beta distribution was fitted to each SF36 domain scores using the standard error and 9 the number in the sample as reported by the study concerned. 10
A value was drawn from the SF36 domain scores’ respective distributions to enter the algorithm EQ1 11 derived by Ara and Brazier (2008) 21 to estimate the mapped EQ5D index. If only baseline SF36 scores 12 with absolute change over a time interval were reported, the absolute change was sampled from a 13 normal distribution and added to the baseline domain score to calculate the follow up SF36 domain 14 score to feed into the algorithm. Where available, SRGQ total scores were also mapped to EQ5D 15 using the algorithm derived by Starkie et al (2011) 447. 16
Algorithm to map SF36 to EQ5D (Ara and Brazier, 2008)
EQ5D index = 0.03256+0.0037*PH+0.00111*RP-0.00024*BP +0.00024*GH +0.00256*SF-0.00063*RE +0.00286*MH +0.00052*V
Where SF36 domains are indicated by:
PH = Physical Health
RP = Physical Role
BP= Bodily Pain
GH = General Health
SF = Social Functioning
RE = Emotional Role
MH = Mental Health
V= Vitality
Algorithm to map SGRQ to EQ5D (Starkie et al., 2010)
EQ5D index = 0.9617 - SGRQ – (0.0001*SGRQ2) + 0.0231*Male%
Where
SGRQ = Total score
Male% = Percentage of males
In the deterministic analysis, the best estimate of utility was calculated using the mean values 17 reported by the study in the mapping algorithm. In the probabilistic analysis, each iteration drew 18 from the sampled SF36 or SRGQ scores, which were then mapped to EQ5D by the appropriate 19 algorithm. For the purpose of reporting the mapped EQ5D scores in this appendix, mapped values 20 were calculated 20,000 times. The mean, standard deviation and upper and lower 95% confidence 21 intervals of the 20,000 mapped EQ5D values were then calculated and reported. 22
L.2.4.2 Calculating cost effectiveness 23
The widely used cost-effectiveness metric is the incremental cost-effectiveness ratio (ICER). This is 24 calculated by dividing the difference in costs associated with two alternatives by the difference in 25 QALYs. The decision rule then applied is that if the ICER falls below a given cost per QALY threshold 26 the result is considered to be cost effective. If both costs are lower and QALYs are higher the option 27 is said to dominate and an ICER is not calculated. 28
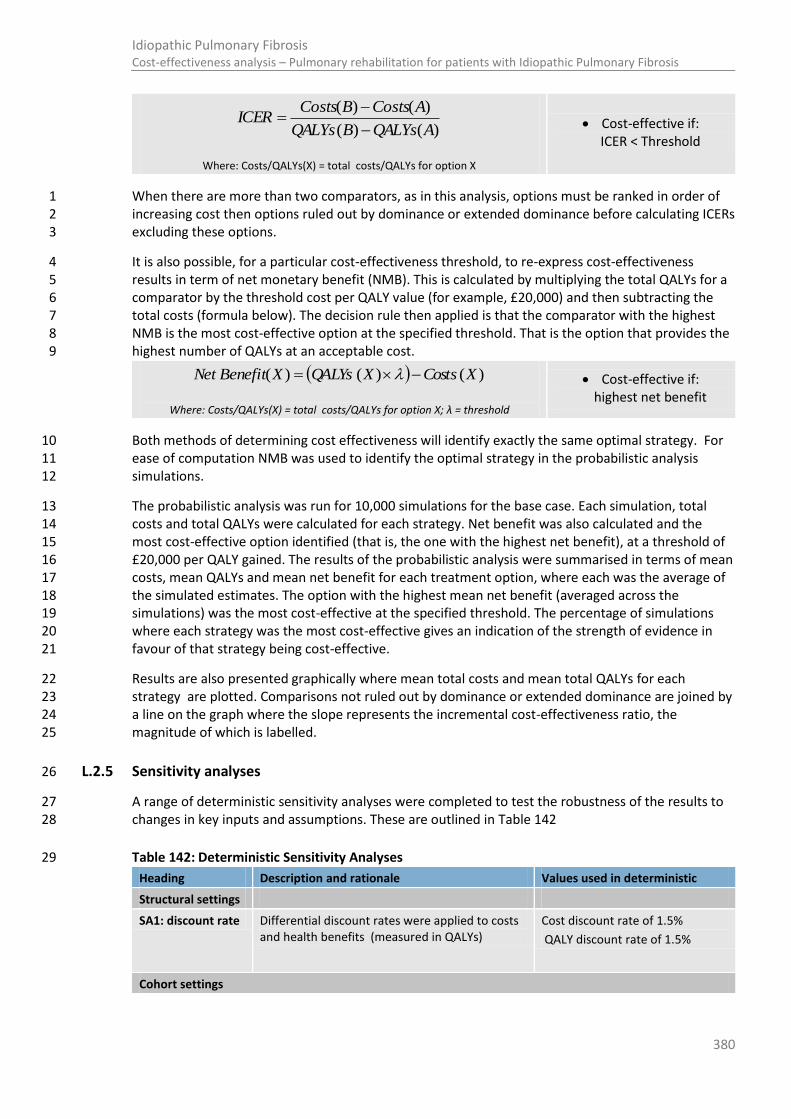
380
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
)()(
)()(
AQALYsBQALYs
ACostsBCostsICER
Where: Costs/QALYs(X) = total costs/QALYs for option X
Cost-effective if: ICER < Threshold
When there are more than two comparators, as in this analysis, options must be ranked in order of 1 increasing cost then options ruled out by dominance or extended dominance before calculating ICERs 2 excluding these options. 3
It is also possible, for a particular cost-effectiveness threshold, to re-express cost-effectiveness 4 results in term of net monetary benefit (NMB). This is calculated by multiplying the total QALYs for a 5 comparator by the threshold cost per QALY value (for example, £20,000) and then subtracting the 6 total costs (formula below). The decision rule then applied is that the comparator with the highest 7 NMB is the most cost-effective option at the specified threshold. That is the option that provides the 8 highest number of QALYs at an acceptable cost. 9
)()()( XCostsXQALYsXBenefitNet
Where: Costs/QALYs(X) = total costs/QALYs for option X; λ = threshold
Cost-effective if: highest net benefit
Both methods of determining cost effectiveness will identify exactly the same optimal strategy. For 10 ease of computation NMB was used to identify the optimal strategy in the probabilistic analysis 11 simulations. 12
The probabilistic analysis was run for 10,000 simulations for the base case. Each simulation, total 13 costs and total QALYs were calculated for each strategy. Net benefit was also calculated and the 14 most cost-effective option identified (that is, the one with the highest net benefit), at a threshold of 15 £20,000 per QALY gained. The results of the probabilistic analysis were summarised in terms of mean 16 costs, mean QALYs and mean net benefit for each treatment option, where each was the average of 17 the simulated estimates. The option with the highest mean net benefit (averaged across the 18 simulations) was the most cost-effective at the specified threshold. The percentage of simulations 19 where each strategy was the most cost-effective gives an indication of the strength of evidence in 20 favour of that strategy being cost-effective. 21
Results are also presented graphically where mean total costs and mean total QALYs for each 22 strategy are plotted. Comparisons not ruled out by dominance or extended dominance are joined by 23 a line on the graph where the slope represents the incremental cost-effectiveness ratio, the 24 magnitude of which is labelled. 25
L.2.5 Sensitivity analyses 26
A range of deterministic sensitivity analyses were completed to test the robustness of the results to 27 changes in key inputs and assumptions. These are outlined in Table 142 28
Table 142: Deterministic Sensitivity Analyses 29
Heading Description and rationale Values used in deterministic
Structural settings
SA1: discount rate Differential discount rates were applied to costs and health benefits (measured in QALYs)
Cost discount rate of 1.5%
QALY discount rate of 1.5%
Cohort settings

381
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
Heading Description and rationale Values used in deterministic
SA2: age We assume that the average age of patients commencing pulmonary rehabilitation is 70. However, this sensitivity analysis is conducted in the recognition that changes in identification and diagnosis of IPF may identify patients at earlier stages of disease progression and at a younger age.
Results from this analysis inform whether prompt referral to pulmonary rehabilitation at an early diagnosis is more cost effective than a later referral.
40 years old
50 years old
60 years old
70 years old (base case)
80 years old
SA3: Starting FVC% predicted
We assume an initial FVC% predicted value for the cohort which one would hope to have at diagnosis of 100%. However, in recognition that diagnosis of IPF is often delayed, this assumption will be tested through sensitivity analysis with varying proportions of the cohort starting in the model with different FVC% predicted values. Results from this analysis inform whether prompt referral to pulmonary rehabilitation at an early stage of disease progression is more cost effective than a later referral.
100%
90%
80%
70%
60%
50%
SA4: The proportion in each subgroup.
The proportion of people with IPF experiencing a given rate of disease progression is uncertain, especially regarding the expected decline in patients who may in the first year in prognosis experience an increase in percentage predicted FVC% predicted. Therefore a sensitivity analysis was conducted to explore the impact a given rate of disease progression would have on the cost effectiveness of the intervention.
Base case:
Stable = 57% (n=128)
Moderate decline = 24% (n=54)
Rapid decline = 19% (n=44)
SA4.1
Assumption that all patients with improved FVC% predicted experience same mortality risk as those with slow disease progression.
Stable = 69% (n=215)
Moderate decline = 17% (n=54)
Rapid decline = 14% (n=44)
SA4.2
Assumption that only patients with small improvement in FVC% predicted experience the same mortality risk as those with slow disease progression, and the remainder with a larger improvement in FVC experience the same mortality risk as those with moderate disease progression. This reflects the possibility that it is the degree of instability of FVC which could be prognostic.
Stable = 58% (n=183)
Moderate decline = 27% (n=86)
Rapid decline = 14% (n=44)
SA4.3 All patients offered pulmonary rehabilitation have stable disease
Stable: 100%
SA4.4 All patients offered pulmonary rehabilitation have moderate disease
Moderate: 100%
SA4.5 All patients offered pulmonary rehabilitation have rapid disease
Rapid: 100%
Participation assumptions
Base case The base case assumes that all patients who are alive can participate in pulmonary rehabilitation,

382
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
Heading Description and rationale Values used in deterministic
regardless of whether they have been hospitalised in the same cycle in which they may be undertaking rehabilitation.
Participation scenario 1
In this scenario, we assume that patients cannot benefit from pulmonary rehabilitation in the cycle of hospitalisation. Treatment effect of pulmonary rehabilitation returns in the cycles post hospitalisation.
Participation scenario 2
Base case
In this scenario, we assume that only a proportion of patients cannot participate or benefit from pulmonary rehabilitation post hospitalisation. For these patients the treatment effect of pulmonary rehabilitation does not return in the cycles post hospitalisation. They are costed for the assessment but not for any places on subsequent rehabilitation courses.
100%
80%
70%
60%
40%
20%
0% (base case participation effect)
Treatment effect scenarios
SA5: Treatment effect duration (months)
This sensitivity analysis specifies the time period from the start of the programme until the treatment effect diminishes to baseline.
6 (base case)
9
12
15
18
24
SA6: Treatment effect of repeated pulmonary rehabilitation programmes
This sensitivity analysis applies a treatment effect multiplier so that repeated programmes are proportionally less effective than the one undertaken previously.
100% as effective (base case)
90% as effective
80% as effective
70% as effective
60% as effective
50% as effective
40% as effective
30% as effective
20% as effective
10% as effective
SA7: Time period between repeating the rehabilitation programme (months)
This sensitivity analysis examines the impact of varying the time period between the beginning of one programme and starting the subsequent programme.
6 months
12 months (base case)
18 months
24 months
36 months
48 months
Intervention Cost and resource use
SA.8: Use of NHS reference costs rather than micro costing
NHS reference costs (assumed to be inclusive of assessment) used instead of micro costing.
Community rehabilitation = £71
Respiratory rehabilitation = £253
383
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
Parameters associated with the programme composition and resource use (i.e. programme 1 duration, staff levels, patients requiring transport) were not tested in a sensitivity analysis for two 2 main reasons. Firstly adjustments were unlikely to make programme costs higher than those 3 estimated through use of NHS reference costs and secondly the impact a change on resource use 4 would have on programme effect is unknown. 5
L.2.6 Model validation 6
The model was developed in consultation with the GDG; model structure, inputs and results were 7 presented to and discussed with the GDG for clinical validation and interpretation. In particular, the 8 median life expectancy calculated for the subgroups with differential rates of disease progression 9 were of interest to the GDG. For this reason, survival curves calculated from the model were 10 produced for clinical validation. 11
The model was systematically checked by the health economist undertaking the analysis; this 12 included inputting null and extreme values and checking that results were plausible given inputs. The 13 model was peer reviewed by a second experienced health economist; this included systematic 14 checking of the model calculations. 15
L.2.7 Interpreting results 16
NICE’s report ‘Social value judgements: principles for the development of NICE guidance’ sets out the 17 principles that GDGs should consider when judging whether an intervention offers good value for 18 money347. 19
In general, an intervention was considered to be cost effective if either of the following criteria 20 applied: 21
a) The intervention dominated other relevant strategies (that is, it was both less costly in terms of 22 resource use and more clinically effective compared with all the other relevant alternative 23 strategies), or 24
b) The intervention cost less than £20,000 per quality-adjusted life-year (QALY) gained compared 25 with the next best strategy. 26
As the analysis is based on two RCTs with a selected population and specified intervention it had 27 limited applicability to the overall IPF population and current UK practice. It was felt that the analysis 28 could help evaluate the likelihood that an offer of pulmonary rehabilitation at diagnosis, with 29 continued community rehabilitation, was cost-effective and provide useful information to feed into 30 decision making; however, it was also noted that it would not be able to provide definitive 31 conclusions given these limitations. 32
L.3 Results 33
Detailed results are presented over the next few pages for the base case and various sensitivity 34 analyses. 35
The results of the deterministic analyses showed the exercise and educational programme to be 36 dominated by the exercise only programme, with the exercise only programme proving to be most 37 cost effective at the £20,000 threshold throughout all analysis. 38
The results of the probabilistic analyses showed that the exercise and educational programme, and 39 the exercise only programme, were comparable in their probability of being the optimal programme 40 determined by the highest net monetary benefit, with no rehabilitation being the least optimal 41 throughout. 42

384
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
L.3.1 Base case 1
The base case shows that pulmonary rehabilitation is cost effective when compared to no pulmonary 2 rehabilitation, with both programmes having similar chance of being cost effective using the £20000 3 threshold when uncertainty of treatment effect is taken into account, with exercise programmes 4 ranking optimal in 48% of simulations and exercise with education ranking optimal in 47% 5 simulations. The highest incremental net benefit was achieved for the exercise programme of 6 pulmonary rehabilitation. The results of the base case are shown in Figure 122, Figure 123 and Table 7 143. 8
Figure 122: Cost effectiveness plane for the base case results (deterministic) 9
10
£-
£100
£200
£300
£400
£500
£600
£700
£800
2.340 2.360 2.380 2.400 2.420 2.440 2.460
Tota
l cos
t pe
r pa
tien
t (£
)
Total QALY per patient
Cost Effectiveness Plane
Exercise only
Education and Exercise
No rehab
ICER = £7004

385
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
Figure 123: Cost effectiveness plane for the base case results (probabilistic) 1
2
£-
£100
£200
£300
£400
£500
£600
£700
£800
£900
2.450 2.500 2.550 2.600
Tota
l co
st p
er
pat
ien
t (£
)
Total QALY per patient
Cost Effectiveness Plane
Exercise only
Education and Exercise
No rehab
ICER = £6841

386
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
Table 143: Probabilistic results for the base case analysis, with results of sensitivity analysis looking at structural assumptions regarding participation 1 and benefit post hospitalisation. 2
Participation scenarios
Intervention Cost Cost discounted
QALY QALY discounted
NMB (£20K)
NMB (£30k)
% of times ranked optimal at 20K
% of times ranked optimal at 30K
Base case (a)
No rehab £- £- 2.713 2.474 £49,480 £74,220 5% 4%
Exercise only £741 £678 2.817 2.573 £50,785 £76,453 48% 48%
Education and Exercise £841 £770 2.802 2.559 £50,413 £75,933 47% 48%
Scenario 1 (b)
No rehab £- £- 2.713 2.474 £49,480 £74,220 6% 0%
Exercise only £741 £678 2.816 2.572 £50,676 £83,739 46% 51%
Education and Exercise £841 £770 2.801 2.558 £50,398 £83,204 48% 49%
Scenario 2 (c)
No rehab £- £- 2.713 2.474 £49,480 £74,220 6% 4%
Exercise only £741 £678 2.798 2.557 £50,457 £76,025 47% 48%
Education and Exercise £841 £770 2.785 2.544 £50,118 £75,562 47% 48% (a) Base case participation scenario: Patients benefit from and participate in pulmonary rehabilitation regardless of hospitalisation. 3 (b) Participation scenario 1: Patients do not benefit from pulmonary rehabilitation in the cycle post hospitalisation 4 (c) Participation scenario 2: Patients do not benefit from or return to pulmonary rehabilitation post hospitalisation (all subsequent cycles) – however all patients undertake assessment 5
regardless of previous hospitalisation. 6
387
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
1
L.3.2 Sensitivity analyses 2
L.3.2.1 Sensitivity analysis on structural assumptions regarding treatment effect and participation. 3
The results of the sensitivity analysis on different scenarios of participation are reported in Table 143. 4 In no scenario was no rehabilitation optimal, and when only considering the mean net monetary 5 benefit achieved the exercise only programme appeared more cost effective than the exercise and 6 educational programme. It becomes more likely that the exercise only programme is cost effective in 7 comparison to exercise and when patients are less likely to benefit from pulmonary rehabilitation 8 post hospitalisation. 9
Participation scenarios were tested across all sensitivity analyses reported below to check that 10 conclusions of the analysis did not change regardless of these baseline assumptions. The results from 11 the sensitivity analyses using alternative participation scenarios did not indicate a different 12 conclusion to the basecase. Due to this fact, and the quanity of results across all analyses, only the 13 results from the basecase participation scenario are presented below. 14
L.3.2.2 Sensitivity analysis on differing rates of mortality post hospitalisation 15
Due the changes in treatment effect requiring a monthly cycle, the model took the conservative 16 assumption by applying a higher mortality rate to patients who had experienced a respiratory 17 hospitalisation, regardless of when that hospitalisation occurred. This assumption may reduce the 18 number of patients who accumulate benefit of the programme once the programme has come to an 19 end, favouring no rehabilitation. 20
To assess the impact this may have had on the potential life expectancy the model was rerun with a 6 21 month cycle, and a higher mortality rate was only applied in the cycle post hospitalisation. This 22 allowed the scoring system presented by Du Bois in predicting mortality to be applied with greater 23 accuracy; however the rate of movement through the health states slows with the longer cycle 24 length. For information and clinical validation, Kaplan Meier curves for each cohort evaluated in this 25 analysis were produced. These, alongside the mean and median life expectancy of each cohort are 26 presented in Appendix M. Due to the changes in treatment effect requiring a cycle length less than 6 27 months, it was not possible to evaluate the potential increase in cost effectiveness of the pulmonary 28 rehabilitation programmes that a change in this structural assumption may have. 29
If we assume only one hospitalisation per patient once diagnosed the results in Appendix M show 30 that mortality is likely to be overestimated, and life expectancy is likely to be underestimated in the 31 model. However, it is likely the model results are more reflective of the typical survival of people 32 with IPF post diagnosis if people with IPF, once having experienced a respiratory hospitalisation, are 33 likely to have a hospitalisation at least once every 6 months thereafter. When applying a higher 34 mortality rate for only one month post hospitalisation, this favoured the pulmonary rehabilitation 35 programmes in terms of cost effectiveness (see Table 145). 36
37
L.3.2.3 Sensitivity analysis of the discount factor 38
The change in discount factor did not change the conclusions of the analysis. Results are shown in 39 Table 145. 40

388
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
L.3.2.4 Sensitivity analysis of the FVC% predicted and age 1
This analysis explored the impact that differing starting characteristics of the cohort may have on the 2 cost effectiveness of the programme. The analysis shows that pulmonary rehabilitation in 3 comparison to no rehabilitation is cost effective regardless of age of stage of disease progression. 4 The exception is that the higher cost of the education and exercise programme meant it was not cost 5 effective in cohorts which were older than 60 years of age and who also had an FVC% predicted 6 baseline of 50%. In general, cost effectiveness is reduced in cohorts that have a higher starting risk of 7 mortality and hospitalisation as these cohorts are less likely to accrue the benefit of the programme 8 once it has ended. The deterministic results of this analysis are presented in Table 144. 9
For information and clinical validation, Kaplan Meier curves for each cohort evaluated in this analysis 10 were produced. These, alongside the mean and median life expectancy of each cohort are presented 11 in appendix M. 12
L.3.2.5 Sensitivity analysis on the proportion of people in each subgroup 13
The rate of disease progression of the cohort did not change the conclusions of the analysis, however 14 the programmes are more cost effective when the cohort is more likely to be able to benefit from 15 any long term treatment effect once the course has ended (i.e. with more stable rate of disease 16 progression). Results are shown in Table 145. 17
L.3.2.6 Sensitivity analysis on the number of people able to rejoin and benefit from pulmonary 18 rehabilitation post hospitalisation (extension of participation scenario 2) 19
The change in the number of people able to rejoin and benefit from pulmonary rehabilitation did not 20 change the conclusions of the analysis. However, the programmes are more cost effective when the 21 cohort is more likely to be able to benefit from any long term treatment effect once the course has 22 ended (i.e. if more patients are able to experience a higher quality of life after pulmonary 23 rehabilitation despite hospitalisation). Results are shown in Table 145. 24
L.3.2.7 Sensitivity analysis on the cost of the programme. 25
Use of NHS reference costs, which were higher for the educational programme than estimated 26 through the costing of staff time, did not change the conclusion of the analysis. Results are shown in 27 Table 145. 28
29
30
31
32
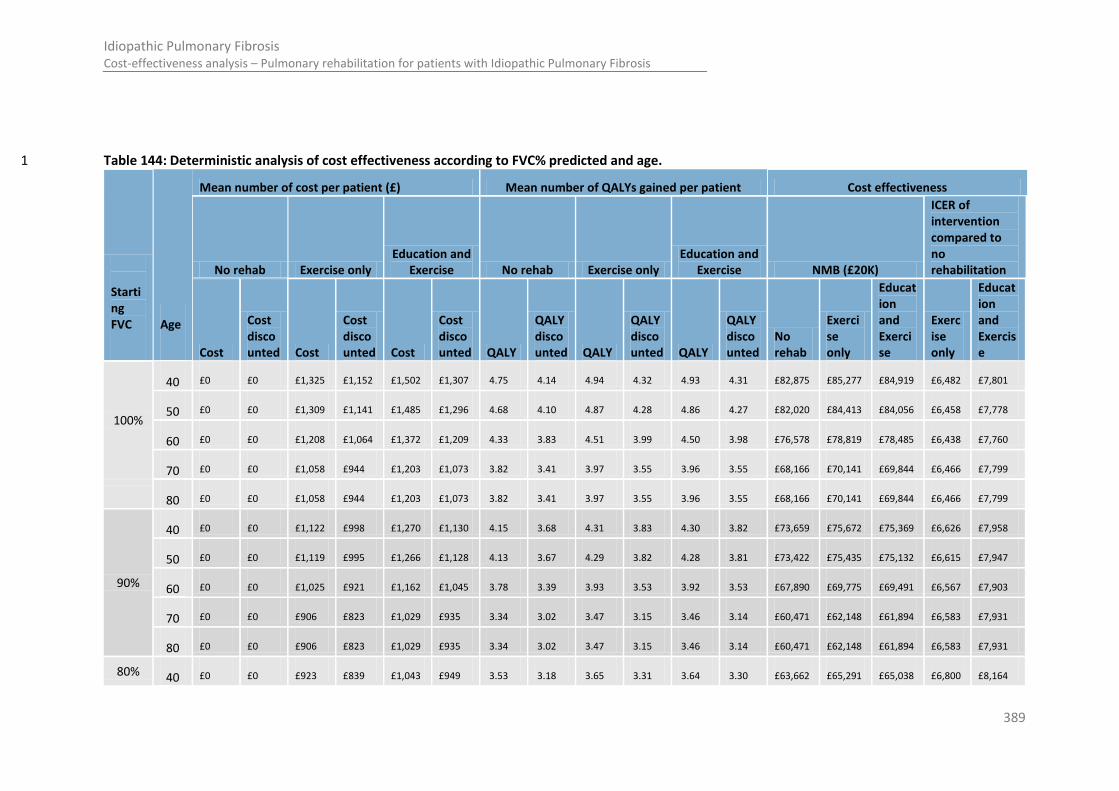
389
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
Table 144: Deterministic analysis of cost effectiveness according to FVC% predicted and age. 1
Starting FVC
Age
Mean number of cost per patient (£) Mean number of QALYs gained per patient Cost effectiveness
No rehab Exercise only Education and
Exercise No rehab Exercise only Education and
Exercise NMB (£20K)
ICER of intervention compared to no rehabilitation
Cost
Cost discounted Cost
Cost discounted Cost
Cost discounted QALY
QALY discounted QALY
QALY discounted QALY
QALY discounted
No rehab
Exercise only
Education and Exercise
Exercise only
Education and Exercise
100%
40 £0 £0 £1,325 £1,152 £1,502 £1,307 4.75 4.14 4.94 4.32 4.93 4.31 £82,875 £85,277 £84,919 £6,482 £7,801
50 £0 £0 £1,309 £1,141 £1,485 £1,296 4.68 4.10 4.87 4.28 4.86 4.27 £82,020 £84,413 £84,056 £6,458 £7,778
60 £0 £0 £1,208 £1,064 £1,372 £1,209 4.33 3.83 4.51 3.99 4.50 3.98 £76,578 £78,819 £78,485 £6,438 £7,760
70 £0 £0 £1,058 £944 £1,203 £1,073 3.82 3.41 3.97 3.55 3.96 3.55 £68,166 £70,141 £69,844 £6,466 £7,799
80 £0 £0 £1,058 £944 £1,203 £1,073 3.82 3.41 3.97 3.55 3.96 3.55 £68,166 £70,141 £69,844 £6,466 £7,799
90%
40 £0 £0 £1,122 £998 £1,270 £1,130 4.15 3.68 4.31 3.83 4.30 3.82 £73,659 £75,672 £75,369 £6,626 £7,958
50 £0 £0 £1,119 £995 £1,266 £1,128 4.13 3.67 4.29 3.82 4.28 3.81 £73,422 £75,435 £75,132 £6,615 £7,947
60 £0 £0 £1,025 £921 £1,162 £1,045 3.78 3.39 3.93 3.53 3.92 3.53 £67,890 £69,775 £69,491 £6,567 £7,903
70 £0 £0 £906 £823 £1,029 £935 3.34 3.02 3.47 3.15 3.46 3.14 £60,471 £62,148 £61,894 £6,583 £7,931
80 £0 £0 £906 £823 £1,029 £935 3.34 3.02 3.47 3.15 3.46 3.14 £60,471 £62,148 £61,894 £6,583 £7,931
80% 40 £0 £0 £923 £839 £1,043 £949 3.53 3.18 3.65 3.31 3.64 3.30 £63,662 £65,291 £65,038 £6,800 £8,164
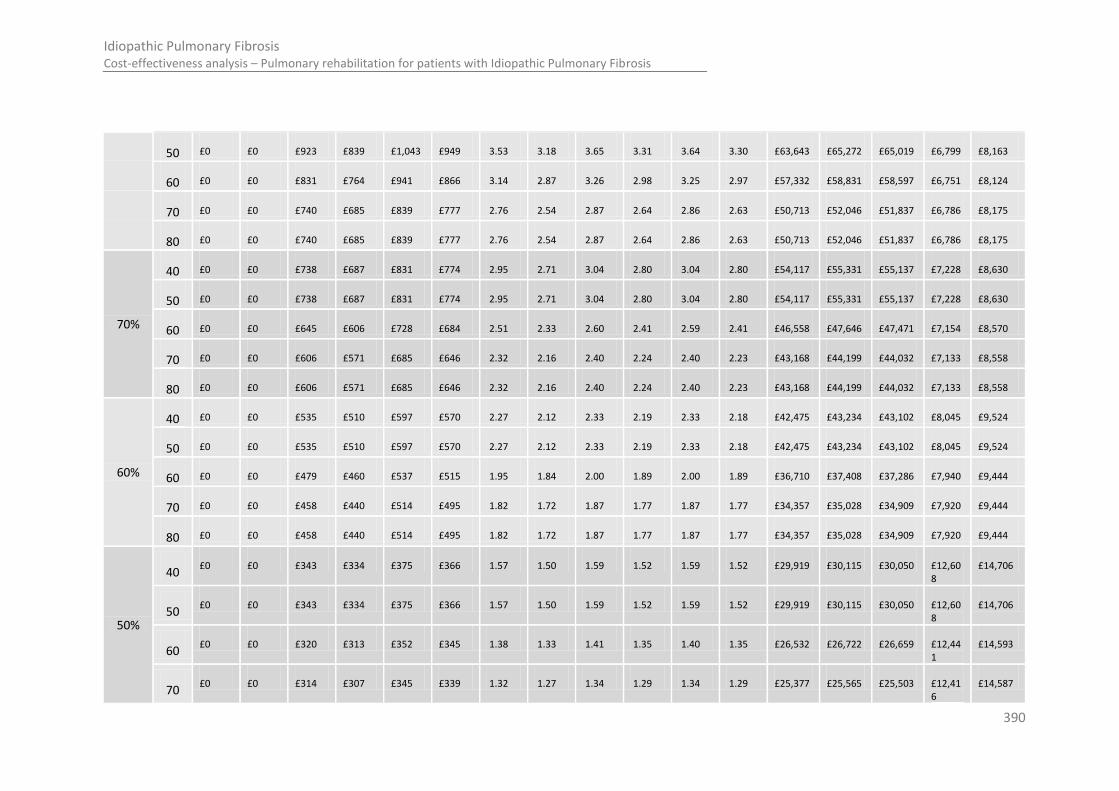
390
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
50 £0 £0 £923 £839 £1,043 £949 3.53 3.18 3.65 3.31 3.64 3.30 £63,643 £65,272 £65,019 £6,799 £8,163
60 £0 £0 £831 £764 £941 £866 3.14 2.87 3.26 2.98 3.25 2.97 £57,332 £58,831 £58,597 £6,751 £8,124
70 £0 £0 £740 £685 £839 £777 2.76 2.54 2.87 2.64 2.86 2.63 £50,713 £52,046 £51,837 £6,786 £8,175
80 £0 £0 £740 £685 £839 £777 2.76 2.54 2.87 2.64 2.86 2.63 £50,713 £52,046 £51,837 £6,786 £8,175
70%
40 £0 £0 £738 £687 £831 £774 2.95 2.71 3.04 2.80 3.04 2.80 £54,117 £55,331 £55,137 £7,228 £8,630
50 £0 £0 £738 £687 £831 £774 2.95 2.71 3.04 2.80 3.04 2.80 £54,117 £55,331 £55,137 £7,228 £8,630
60 £0 £0 £645 £606 £728 £684 2.51 2.33 2.60 2.41 2.59 2.41 £46,558 £47,646 £47,471 £7,154 £8,570
70 £0 £0 £606 £571 £685 £646 2.32 2.16 2.40 2.24 2.40 2.23 £43,168 £44,199 £44,032 £7,133 £8,558
80 £0 £0 £606 £571 £685 £646 2.32 2.16 2.40 2.24 2.40 2.23 £43,168 £44,199 £44,032 £7,133 £8,558
60%
40 £0 £0 £535 £510 £597 £570 2.27 2.12 2.33 2.19 2.33 2.18 £42,475 £43,234 £43,102 £8,045 £9,524
50 £0 £0 £535 £510 £597 £570 2.27 2.12 2.33 2.19 2.33 2.18 £42,475 £43,234 £43,102 £8,045 £9,524
60 £0 £0 £479 £460 £537 £515 1.95 1.84 2.00 1.89 2.00 1.89 £36,710 £37,408 £37,286 £7,940 £9,444
70 £0 £0 £458 £440 £514 £495 1.82 1.72 1.87 1.77 1.87 1.77 £34,357 £35,028 £34,909 £7,920 £9,444
80 £0 £0 £458 £440 £514 £495 1.82 1.72 1.87 1.77 1.87 1.77 £34,357 £35,028 £34,909 £7,920 £9,444
50%
40 £0 £0 £343 £334 £375 £366 1.57 1.50 1.59 1.52 1.59 1.52 £29,919 £30,115 £30,050 £12,60
8 £14,706
50 £0 £0 £343 £334 £375 £366 1.57 1.50 1.59 1.52 1.59 1.52 £29,919 £30,115 £30,050 £12,60
8 £14,706
60 £0 £0 £320 £313 £352 £345 1.38 1.33 1.41 1.35 1.40 1.35 £26,532 £26,722 £26,659 £12,44
1 £14,593
70 £0 £0 £314 £307 £345 £339 1.32 1.27 1.34 1.29 1.34 1.29 £25,377 £25,565 £25,503 £12,41
6 £14,587

391
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
80 £0 £0 £314 £307 £345 £339 1.32 1.27 1.34 1.29 1.34 1.29 £25,377 £25,565 £25,503 £12,41
6 £14,587
Table 145: Deterministic results of sensitivity analyses testing assumptions and data sources of the model. 1
Name of sensitivity analysis
Mean cost per patient (£) Mean number of QALYs gained per patient Cost Effectiveness
No rehab Exercise only Education
and Exercise No rehab Exercise only Education
and Exercise NMB (£20K)
ICER of intervention when compared to no rehabilitation.
Cost
Cost discounte
d Cost
Cost discounte
d Cost
Cost discounte
d QALY
QALY discounte
d QALY
QALY discounte
d QALY
QALY discounte
d No
rehab Exercise only
Education and Exercis
e
Exercise only
Education and
Exercise
Base case £0 £0 £672 £628 £762 £712 2.54 2.35 2.63 2.44 2.63 2.43 £46,972 £48,137 £47,949 £7,005 £8,427
No half cycle correction applied
£0 £0 £672 £628 £762 £712 2.58 2.38 2.67 2.47 2.66 2.46 £47,541 £48,731 £48,542 £6,907 £8,311
Discount rate of 1.5% applied to costs and 1.5%
applied to benefits
£0 £0 £672 £652 £762 £739 2.55 2.46 2.63 2.55 2.63 2.54 £49,129 £50,262 £50,068 £7,309 £8,813
Sub grouping based on assumption all observed to
have increasing FVC% predicted have slow disease progression
£0 £0 £741 £688 £839 £780 2.82 2.59 2.92 2.69 2.91 2.69 £51,823 £53,132 £52,925 £6,891 £8,287
Sub grouping based on assumption all observed to
have increasing FVC% predicted have slow to
moderate disease progression
£0 £0 £689 £643 £781 £729 2.62 2.42 2.71 2.51 2.71 2.51 £48,404 £49,606 £49,414 £6,972 £8,385
Cohort consists only of people with slow disease
progression
£0 £0 £918 £844 £1,039
£957 3.53 3.22 3.66 3.35 3.65 3.34 £64,425 £66,108 £65,851 £6,680 £8,030
Cohort consists only of people with moderate
disease progression
£0 £0 £418 £407 £473 £461 1.61 1.55 1.66 1.60 1.66 1.60 £30,977 £31,615 £31,501 £7,785 £9,357

392
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
Cohort consists only of people with rapid disease
progression
£0 £0 £271 £268 £308 £305 0.81 0.79 0.84 0.82 0.83 0.82 £15,832 £16,132 £16,058 £9,442 £11,487
35% FVC% predicted cut off point for participation
(no cut off point for participation)
£0 £0 £699 £649 £796 £739 2.54 2.35 2.64 2.45 2.64 2.44 £46,972 £48,304 £48,099 £6,554 £7,922
40% FVC% predicted cut off point for participation
£0 £0 £689 £642 £784 £730 2.54 2.35 2.64 2.44 2.63 2.44 £46,972 £48,240 £48,041 £6,721 £8,116
50% FVC% predicted cut off point for participation
£0 £0 £646 £605 £728 £683 2.54 2.35 2.63 2.43 2.62 2.43 £46,972 £48,044 £47,870 £7,218 £8,637
60% FVC% predicted cut off point for participation
£0 £0 £570 £538 £630 £596 2.54 2.35 2.60 2.41 2.60 2.41 £46,972 £47,681 £47,553 £8,629 £10,130
100% of patients do not return to or benefit from pulmonary rehabilitation
post hospitalisation
£0 £0 £672 £628 £762 £712 2.54 2.35 2.62 2.42 2.61 2.42 £46,972 £47,868 £47,696 £8,242 £9,912
80% of patients do not return to or benefit from pulmonary rehabilitation
post hospitalisation
£0 £0 £610 £569 £681 £636 2.54 2.35 2.62 2.43 2.62 2.42 £46,972 £47,980 £47,823 £7,216 £8,559
60% of patients do not return to or benefit from pulmonary rehabilitation
post hospitalisation
£0 £0 £547 £510 £601 £561 2.54 2.35 2.62 2.43 2.62 2.43 £46,972 £48,093 £47,949 £6,259 £7,296
40% of patients do not return to or benefit from pulmonary rehabilitation
post hospitalisation
£0 £0 £485 £452 £521 £485 2.54 2.35 2.63 2.43 2.62 2.43 £46,972 £48,205 £48,075 £5,362 £6,112
20% of patients do not return to or benefit from pulmonary rehabilitation
post hospitalisation
£0 £0 £422 £393 £440 £410 2.54 2.35 2.63 2.44 2.63 2.43 £46,972 £48,318 £48,201 £4,521 £5,002
Higher mortality risk applied only one cycle post
hospitalisation
£0 £0 £768 £707 £867 £799 2.96 2.69 3.06 2.79 3.05 2.79 £53,831 £55,115 £54,909 £7,106 £8,517
Cost of programme using NHS reference costs
£0 £0 £244 £229 £868 £815 2.54 2.35 2.63 2.44 2.63 2.43 £46,972 £48,535 £47,846 £2,556 £9,656

393
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
L.3.2.8 Sensitivity analysis on treatment effect duration, a declining treatment effect on each subsequent 1 offer of pulmonary rehabilitation and time between repeated programmes of pulmonary 2 rehabilitation. 3
There was no evidence to inform the duration of effect that pulmonary rehabilitation has on 4 improving quality of life in people with pulmonary rehabilitation, with the longest reported follow up 5 being 6 months, 4 months after the programme finished. 185) As this study showed quality of life had 6 not returned to baseline at this point, there is reason to believe that treatment effect lasts for a 7 longer time period than 6 months, however the duration and rate of diminishing effect remains 8 unknown. The optimal time between repeated offers of pulmonary rehabilitation to sustain a 9 treatment effect given the additional cost of offering repeated programmes is dependent on the 10 duration and rate of diminishing effect, as well as knowledge whether a repeated programme will 11 achieve the same effect as the first programme the patient undertakes. 12
A three way sensitivity analysis was conducted to estimate the optimal time period between offers 13 of repeated programmes given varying assumptions regarding duration and rate of diminishing long 14 term treatment effect , and a potential decline in the magnitude of treatment effect with each 15 additional programme. The analysis looked at repeating the programmes every 6, 12, 18, 24, 36 and 16 48 months, and identified which strategy (including no rehabilitation) obtained the highest net 17 monetary benefit for a given combination treatment effect duration and magnitude of effect on 18 repeated programmes. Table 146 details which strategy is optimal for a given combination of 19 treatment effect assumptions, as well as the optimal time interval (in terms of highest net benefit) 20 which the programme should be repeated for a combination of assumptions. An aspect of this 21 analysis to keep in mind is that the more frequently the programme is repeated, the more 22 programmes at a reduced efficacy (due to each subsequent programme having less effect) the 23 patient will experience in the same timeframe. Further, when it is assumed that long term treatment 24 effect is sustained over a lengthy time (i.e. 24 months), the repeated programme could give a lower 25 treatment effect than what would have been observed at the same time point had the programme 26 not been repeated. 27
28
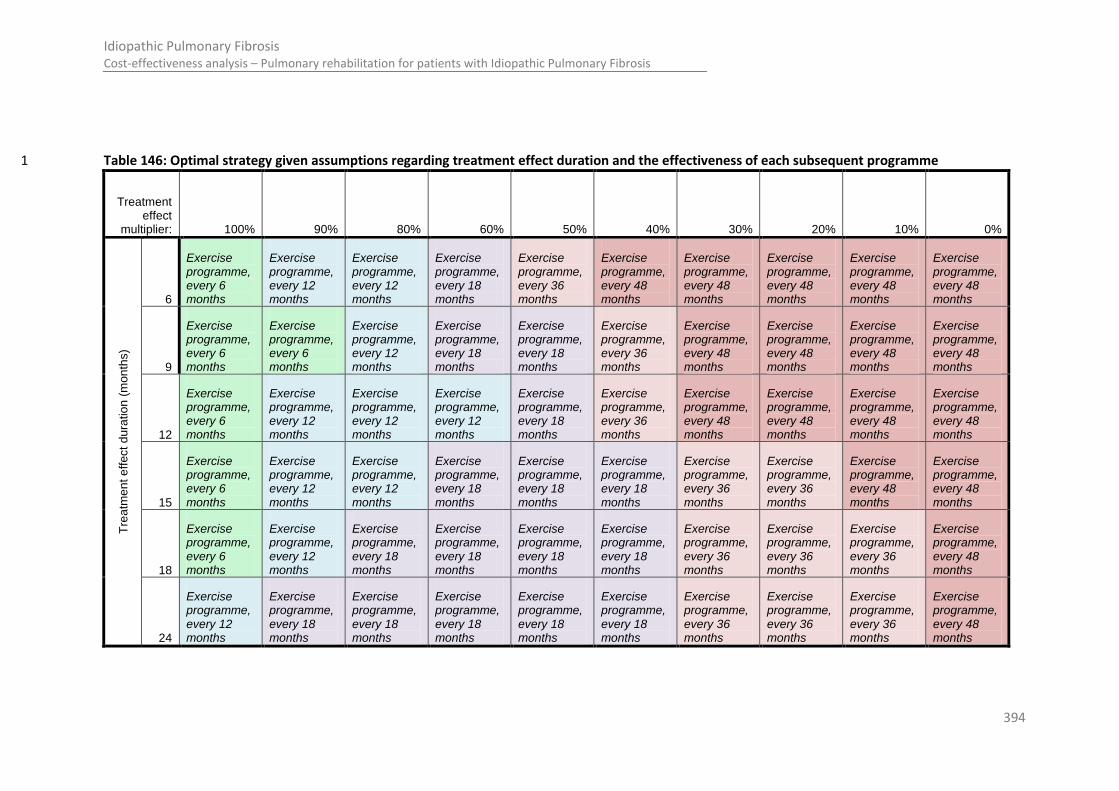
394
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
Table 146: Optimal strategy given assumptions regarding treatment effect duration and the effectiveness of each subsequent programme 1
Treatment effect
multiplier: 100% 90% 80% 60% 50% 40% 30% 20% 10% 0%
Tre
atm
en
t e
ffect
du
ratio
n (
mon
ths)
6
Exercise programme, every 6 months
Exercise programme, every 12 months
Exercise programme, every 12 months
Exercise programme, every 18 months
Exercise programme, every 36 months
Exercise programme, every 48 months
Exercise programme, every 48 months
Exercise programme, every 48 months
Exercise programme, every 48 months
Exercise programme, every 48 months
9
Exercise programme, every 6 months
Exercise programme, every 6 months
Exercise programme, every 12 months
Exercise programme, every 18 months
Exercise programme, every 18 months
Exercise programme, every 36 months
Exercise programme, every 48 months
Exercise programme, every 48 months
Exercise programme, every 48 months
Exercise programme, every 48 months
12
Exercise programme, every 6 months
Exercise programme, every 12 months
Exercise programme, every 12 months
Exercise programme, every 12 months
Exercise programme, every 18 months
Exercise programme, every 36 months
Exercise programme, every 48 months
Exercise programme, every 48 months
Exercise programme, every 48 months
Exercise programme, every 48 months
15
Exercise programme, every 6 months
Exercise programme, every 12 months
Exercise programme, every 12 months
Exercise programme, every 18 months
Exercise programme, every 18 months
Exercise programme, every 18 months
Exercise programme, every 36 months
Exercise programme, every 36 months
Exercise programme, every 48 months
Exercise programme, every 48 months
18
Exercise programme, every 6 months
Exercise programme, every 12 months
Exercise programme, every 18 months
Exercise programme, every 18 months
Exercise programme, every 18 months
Exercise programme, every 18 months
Exercise programme, every 36 months
Exercise programme, every 36 months
Exercise programme, every 36 months
Exercise programme, every 48 months
24
Exercise programme, every 12 months
Exercise programme, every 18 months
Exercise programme, every 18 months
Exercise programme, every 18 months
Exercise programme, every 18 months
Exercise programme, every 18 months
Exercise programme, every 36 months
Exercise programme, every 36 months
Exercise programme, every 36 months
Exercise programme, every 48 months

395
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
The deterministic analysis shows that across the range of treatment effect assumptions tested, the 1 exercise programme had the potential to produce the highest net benefit if offered at the optimal 2 time interval. If the same treatment effect is observed on repeated offers, unless duration of 3 treatment effect is very long (i.e. 24 months), it is most cost effective to repeat the programme every 4 6 months. If it is expected that each repeated programme is at least 80% as effective as the one 5 previously undertaken, it is likely that repeating the programme every 12 months will be cost 6 effective. This is with the exception when the treatment effect is likely to be less than 18 months. 7 Once the magnitude of effect started to decrease by 60% on each subsequent programme the 8 optimal time interval between programmes extends to 18 months or more. If the effectiveness of 9 programmes more than halve on each offer, it is increasingly likely that the programme should not 10 be repeated. 11
L.4 Discussion 12
L.4.1 Summary of results 13
It is highly likely that pulmonary rehabilitation compared to no rehabilitation is cost effective as a 14 means to improve quality of life for people with IPF. It is uncertain whether pulmonary rehabilitation 15 with exercise alone is cost effective when compared to a programme with an educational 16 component, with both types of programmes having a comparable probability of being optimal in 17 terms of cost effectiveness. 18
L.4.2 Limitations & interpretation 19
The conclusion that pulmonary rehabilitation compared to no rehabilitation proved to be robust over 20 a wide range of sensitivity analyses. This gives reassurance that the conclusion of the analysis would 21 not change had alternative assumptions in the model been made. However, the findings of the 22 sensitivity analyses have practical implications in terms of how to make the programmes most cost 23 effective and indicate the type of further research that could aid to resolve some of the limitations of 24 the current model. 25
L.4.2.1 When and to whom to offer pulmonary rehabilitation 26
The two way sensitivity analysis on the age and FVC% predicted of the cohort as they entered the 27 model showed that the programmes were most cost effective for patients who were likely to benefit 28 from the longer term treatment effect. The sensitivity analysis on the proportion of patients in each 29 subgroup of rate of disease progression supported this conclusion, with rehabilitation proving not 30 cost effective for a cohort only consisting of people with rapid disease progression. 31
This finding has two implications for policy. Firstly, that an early diagnosis and referral to pulmonary 32 rehabilitation is likely to improve the cost effectiveness of the programmes. Secondly, it is important 33 to consider whether the patient group being referred to pulmonary rehabilitation is likely to able to 34 experience the benefit of the course after it has ended, with a likely indicator of this being the 35 patient’s short term prognosis (i.e. whether the disease is progressing rapidly). However, the 36 population diagnosed with IPF are heterogeneous and the disease course unpredictable. Because of 37 this, recommendations that refer only specific subgroups to rehabilitation on the account of cost 38 effectiveness are unlikely to be appropriate, and further may reduce the cost effectiveness of the 39 programme as a whole due to delays in establishing a prognosis. 40
396
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
L.4.2.2 The optimal time interval between programmes 1
Generally, the longer the treatment effect duration the less cost effective it is to shorten the interval 2 between programmes; and the less effective each subsequent offer is, the less cost effective it is to 3 undertake the repeat programme. 4
If the programme is repeated frequently with a short time interval between programmes, the cohort 5 will experience more programmes which are less effective than if there were less programmes in the 6 same period of time (given each subsequent programme reduces in effect). For this reason repeating 7 the programme every 6 months only becomes optimal if the effectiveness of each repeated 8 programme is high and we assume the programme would not necessarily carry a long term 9 treatment effect once the course ended. This scenario could be reflective of a maintenance exercise 10 programme. 11
When a programme carries a longer term effect, it becomes more cost effective to have a longer 12 time interval between programmes, especially if you assume each subsequent programme becomes 13 less effective. This scenario could be reflective of an educational programme, where the knowledge 14 gained would improve quality of life for a longer period, and unlikely to improve quality of life 15 substantially if repeated. 16
In this population group, the natural history of the disease also plays a part in determining the 17 optimal time period between programmes – which may in part explain why in some cases a more 18 frequent programme is optimal despite an assumption that long term effect duration is longer. The 19 impact of a reduced effect in each subsequent programme on results is mitigated to some extent by 20 the fact the median life expectancy of people with IPF is relatively low and a low proportion of the 21 cohort will start and participate in the less effective repeated programmes. If the life expectancy of 22 people with IPF were to dramatically increase, the magnitude of effect of repeated programmes 23 would be more influential on results. 24
The stable subgroup are most likely to be able to start, participate and benefit from repeated 25 programmes, especially where there longer time intervals between programmes are explored. The 26 analysis of FVC% predicted and age, as well as that for the subgroups, show it is the stable patients 27 that potentially benefit most from pulmonary rehabilitation as they are most likely to be able to 28 participate and accrue benefit after the programme has ended (due to reduced mortality and/or 29 hospitalisation). The time period between programmes should therefore be sufficiently long to 30 capitalise on any residing long term treatment effect, however should not be so long that the stable 31 group which benefits most has become an age or entered a stage of disease progression (lower 32 absolute FVC% predicted) where they have a higher risk of mortality or hospitalisation which would 33 prevent them from benefiting from the long term treatment effect. 34
The probabilistic analysis suggested that the two types of programmes were equally as effective 35 using the same treatment effect assumptions and when offered at the same time interval; however it 36 is possible that one type of programme may carry a different long term effect than the other. If 37 education has a longer treatment effect than the exercise programme, it would not be as cost 38 effective as the exercise programme when offered in shorter time intervals. If this assertion is true, 39 the practical implication is that the educational programme should be offered over a longer time 40 period i.e. every 12 months, whereas an exercise programme should be repeated more regularly i.e. 41 every 6 months. 42
43
44

397
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
L.4.2.3 The role of assessment for pulmonary rehabilitation 1
The assessment for pulmonary rehabilitation is of importance in determining which patients are 2 most likely to benefit from pulmonary rehabilitation. An important factor to consider at assessment 3 is whether a patient is likely to be able to benefit from the rehabilitation programme after the 4 programme ends. 5
6
L.4.3 Summary of key limitations 7
It is likely that the model underestimates the cost effectiveness of the pulmonary rehabilitation 8 programmes in the base case for a variety of reasons. Firstly, the mortality is likely to be 9 overestimated in the base case, as demonstrated from the discrepancy in modelled life expectancy 10 between the results using the base case settings and a higher risk of mortality applied only for 6 11 months post hospitalisation (see Appendix M:). A higher mortality would mean fewer patients will 12 have benefited from long term treatment effect, and the programmes would appear less cost 13 effective. It is worth noting however, the results shown in appendix M do not allow for a second 14 hospitalisation. Secondly, the long term treatment effect in the base case was 6 months, and in 15 practice this may be longer which would raise the cost effectiveness of the programme if offered at 16 an appropriate time interval accordingly. 17
The quality of life assumed for people not undertaking rehabilitation was relatively high. In 18 simulation runs where the educational programme had a large positive effect, it was possible the 19 cohort experienced full health and any additional benefit beyond this was not captured, whereas it 20 would have been if the quality of life associated with no rehabilitation was lower. Further, the quality 21 of life improvement of the programmes may understate some important benefits described by 22 patients (please refer to detail in the below sections). 23
The costing of the programme took the conservative assumption that only 10 patients would 24 participate in each class, whereas in practice some class sizes may be greater than this, decreasing 25 the cost per patient and improving the cost effectiveness of the programme. Further, we did not 26 assume that rehabilitation influenced the number of healthcare contacts. If rehabilitation does 27 reduce the number of healthcare contacts a patient makes, it could potentially be cost saving. 28
Thus although the model is robust in determining that rehabilitation is more cost effective than no 29 rehabilitation through the incremental analysis, the exact accuracy of the total QALY gain and cost of 30 the respective comparators is likely to be low. 31
L.4.3.1 Limitations of assumptions and simplifications made in order to model disease progression. 32
Subgroups are identified based upon their rates of disease progression at six months. It is assumed 33 that the rate of disease progression at 6 months is indicative of future progression, and this rate is 34 applied as a constant monthly probability throughout the model lifetime, with adjustment within 35 subgroups to capture time-varying rates of progression. There is a strong assumption that the rate of 36 disease is linear, posing a potential limitation in the validity of results. 37
In order to be as transparent as possible, median life expectancies and survival curves calculated by 38 the models inputs are given in Appendix M. It is acknowledged that the median life expectancies 39 given in Appendix M appear generally on the low side –e.g. a median life expectancy of 2.33 years for 40 the population with 70% starting FVC% predicted (M.1 table 1) (cf. 2-5 years cited by Noble et al 41 2011 in the CAPACITY study358). However, as shown in the sensitivity analysis regarding age and 42 starting FVC% predicted, as well as in section L.3.2.4 which details the natural history assumptions, 43
398
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
cost effectiveness is in general reduced in cohorts that have a higher starting risk of mortality and so 1 these assumptions are unlikely to alter the conclusions of the analysis. In this regard the model is 2 likely to make a conservative estimation of cost effectiveness. 3
4
L.4.3.2 Limitations of using FVC% predicted as a marker for disease progression in the IPF population, and 5 as a proxy for ability to participate and benefit from the pulmonary rehabilitation programme. 6
Clinical members expressed concern in the use of FVC% predicted as a marker for disease 7 progression in the IPF population, and as a proxy for ability to participate and benefit from the 8 pulmonary rehabilitation programme. They felt that FVC% predicted was much less indicative of to 9 reflect these factors than it may be for other populations which have a respiratory condition. 10 However, given that the decline in FVC% predicted was found to be the best predictor of mortality 11 (see chapter 6), and evidence was retrieved to link FVC to hospitalisation, a consensus was made it 12 was suitable for modelling purposes. 13
Clinical members of the group noted that emphysema may mask disease progression if measured by 14 FVC% predicted, and this co morbidity may in part explain why the baseline data to estimate the 15 proportion of patients in each subgroup may have rises in FVC% predicted. There was insufficient 16 data on clinical course and treatment effect to allow consideration of a subgroup of patients with IPF 17 and emphysema, and it was not possible to explore whether these patients may benefit more from a 18 pulmonary rehabilitation alongside COPD patients than IPF patients without the co morbidity. 19
L.4.3.3 Limitations of applying the same absolute treatment effect across all subgroups. 20
The treatment effect and baseline QoL was a mean taken across what developers assumed to be 21 patients from all subgroups, An absolute, rather than a relative treatment effect was applied. The use 22 of PSA explored the uncertainty surrounding this point estimate and the range covered may be 23 indicative of the different rates of declines in the studies used to derive the inputs for the model. 24 However it may not be reasonable to assume the same absolute QoL treatment benefit across all 25 subgroups, with patients with varying rate of declines potentially benefiting more or less from 26 pulmonary rehabilitation. Unfortunately, no evidence currently exists to inform how rate of decline 27 may be correlated with outcomes of rehabilitation and as such developers felt a sensitivity analysis 28 would not be useful. It was noted the subgroup sensitivity analysis could be misleading if the rate of 29 disease progression did influence treatment outcome, however at this time developers felt there was 30 not sufficient information to estimate the impact on conclusions. Overall, developers any range of 31 inputs to modify the sensitivity analysis which would be estimated without further evidence unlikely 32 to change final conclusions at this time. 33
L.4.3.4 Limitations of the instruments that measure quality of life in an IPF population 34
To our knowledge, validated instruments that measure quality of life in the IPF population are not in 35 widespread use. However, the SF-36 generic HRQoL instrument and the SRGQ have been commonly 36 used in clinical trials that have an IPF population. Both instruments have an evidence base to support 37 their use in an IPF population 61 482 26 290,305,464,475,510 and scores from both instruments can be mapped 38 to the EQ5D using standard methodology. However, a number of criticisms of the instruments for 39 use in the IPF population exist. 40
The SF36 has been criticized for limited coverage of aspects that concern IPF patients 467. For 41 example the SF36 does not include any items focusing on therapy, sleep, forethought, employment 42 and finances, dependence, sexual relations, or mortality. There is no mention of cough or 43 breathlessness on the SF36, and pain which is included on the SF36 was not mentioned by IPF 44

399
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
patients. The SRGQ has also been criticized for limited coverage of aspects that concern IPF patients 1 (in particular its lack of focus on social relationships), in addition to dubious face validity 104. Overall 2 the clinical members of the group felt that the HRQoL tools to assess QoL in IPF in the studies may 3 not have captured all the important benefits that pulmonary rehabilitation may bring, for example 4 reduced feeling of social isolation and improved social relationships. Such concerns have also been 5 noted in the literature 104,467. 6
L.4.3.5 Limitations of mapping algorithms 7
The mapping function of SF-36 to EQ5D has been validated using a wide array of datasets from 8 conditions such as asthma, coronary heart disease, diabetes, depression, renal transplant, pain, 9 walking impairment, psoriasis etc. Authors of the algorithm note that caution should be taken when 10 applying the algorithm for scores that are likely to produce very low utility values. They also note that 11 a different algorithm may be preferable when looking at incremental differences between study 12 arms or over time. However, when we have compared results from the two algorithms, the 13 incremental difference calculated from the mean results from the first algorithm appears to be a 14 closer match than the second. 15
The mapping function of the SRGQ score to EQ5D was developed using datasets for COPD patients, 16 who were categorised by disease severity (moderate, severe, very severe). Authors found that the 17 mapped QALY was slightly greater than the observed (Table 1). 18
Table 147: Mean (SD) observed and predicted utility scores by disease severity 19
Heading Moderate Severe Very Severe
QALYs observed 2.16 (0.68) 1.99 (0.74) 1.75 (0.75)
QALYs predicted 2.18 (0.52) 2.01 (0.57) 1.80 (0.58)
The difference between the estimated QALY for the moderate and severe disease category was the 20 same as the observed, however the estimated difference between the severe and very severe 21 disease category was slightly smaller than observed. The difference in QALY gain between the most 22 and least effective treatment was the same in predicted and observed values, however the authors 23 note some of the ranking of strategies between these treatments changed. The mean values 24 between observed and predicted did not differ more than 0.05, and each of the standard deviations 25 associated with the mean value were greater than 0.05. It is likely that quality of life associated with 26 more severe states may be lower than the mapped estimates suggest. Although uncertainty intervals 27 will be provided with the mapped estimate, these will not be reflective of the potential error that 28 may have been introduced by the mapping method. 29
L.4.3.6 Limitations regarding programme setting and resource use 30
A lack of clinical data meant that it was not possible to explore the cost effectiveness of rehabilitation 31 in different settings. The potential settings of the pulmonary rehabilitation programmes include the 32 outpatient, community and home setting, as well as potentially a residential course. The setting of 33 the pulmonary rehabilitation programme could influence the cost of running the programme, 34 accessibility for the patient and potentially the uptake and/or participation in the programme, and 35 the efficacy of the programme. 36
It was expected that the type of rehabilitation would influence the number and type of NHS contacts 37 a patient will make, for example number of GP home visits, number of GP surgery visits and number 38 of hospitalisations. This is because it is expected that as patients learn how to manage their 39 symptoms, the number of NHS contacts will decrease. However, no data was found to inform this 40 aspect of the planned model, and therefore this decrease in resource use has not been considered. If 41

400
Idiopathic Pulmonary Fibrosis Cost-effectiveness analysis – Pulmonary rehabilitation for patients with Idiopathic Pulmonary Fibrosis
a healthcare resource use decrease is found with pulmonary rehabilitation, it is possible 1 rehabilitation could be cost saving. 2
L.4.4 Comparisons with published studies 3
No economic evaluations comparing pulmonary rehabilitation programmes for patients with IPF to 4 any other strategy was identified in the literature. One study in the UK, which was excluded at the 5 sifting stage on the account of inappropriate population (predominately with COPD), found the 6 programme to increase the mean number of QALYs generated by 0.03 per patient (p=0.03) and 7 found a non-significant mean “cost saving” of £152 per patient (p=0.68). This study took into account 8 potential reductions in healthcare resource use (such as GP visits) whereas the IPF model did not. 9 Thus the cost effectiveness of rehabilitation for IPF patients appears lower despite the quality of life 10 gain being similar and the cost per patient being higher than this models estimation (due to 11 increased staff involvement on the programme). Even without reduction in healthcare resource use, 12 however, the IPF model finds pulmonary rehabilitation to be cost effective using the £20,000 13 threshold. 14
L.4.5 Implications for future research 15
The economic model produced was based on many assumptions which future research may be able 16 to inform. Future studies should consider the following to provide information which would improve 17 future economic evaluations of pulmonary rehabilitation for people with IPF: 18
a) Collection of quality of life data using the EQ5D 19 b) The correlation between quality of life and any key outcomes of the study, such as change in 20
FVC% predicted and walking distance achieved, with subsequent analysis adjusting for 21 confounding factors appropriately. 22
c) Analysis of treatment effect and potential confounding factors such as stage and rate of 23 disease progression. 24
d) Analysis of healthcare resource use with and without pulmonary rehabilitation. 25 e) Analysis of the factors which impact uptake, participation and sustaining treatment effect. 26 f) Analysis of the effectiveness of different types of pulmonary rehabilitation programme 27
including that which could be shared with patients with COPD, with clear detail regarding the 28 composition and setting of the programme, and resource use involved. 29
g) The duration and magnitude of the long term effect of pulmonary rehabilitation and the 30 requirement of maintenance rehabilitation to sustain effect. 31
Only one economic model 171 evaluating a treatment strategy for people with IPF was identified to 32 inform this guideline. In order for future economic models assessing any treatment strategy in this 33 population group, information regarding the natural history of the disease, including information on 34 prognostic risk factors for differing rates of disease progression and likelihood of acute exacerbation 35 and/or respiratory hospitalisation is likely to improve future attempts at modelling the IPF disease 36 pathway - which still remains relatively unknown. 37
L.4.6 Conclusion = evidence statement 38
It is highly likely that pulmonary rehabilitation is cost effective as a means to improve quality of life 39 for people with IPF. 40
It is uncertain whether pulmonary rehabilitation with exercise alone is cost effective when compared 41 to a programme with an educational component. Both programmes are highly likely to be cost 42 effective when compared to no rehabilitation. 43

401
Idiopathic Pulmonary Fibrosis Model produced Median and Mean Life Expectancies for people diagnosed with IPF
Pulmonary rehabilitation could be cost effective if offered at 6 to 12 month intervals to people with 1 IPF, given appropriate assessment of the patient prior to the programme. If the duration of long term 2 effect is shorter in the exercise programme than the educational programme, it is likely it is more 3 cost effective to repeat this component of pulmonary rehabilitation in shorter time intervals (i.e. 6 4 months) than an educational component (i.e. 12 months or more). 5
6
Appendix M: Model produced Median and Mean 7
Life Expectancies for people diagnosed with IPF 8
9
M.1 Median and mean life expectancy of people diagnosed with IPF 10
Table 148: Natural history results from the deterministic analysis in the model using base case 11 assumptions and 1 month cycle length 12
Starting FVC% predicted Age Median life expectancy Mean Life years
Slow decline
Moderate decline
Rapid decline
Population
Slow decline
Moderate decline
Rapid decline
Population
100%
40 10.33 4.08 2.33 5.25 9.83 3.66 2.08 6.09
50 10.25 4.08 2.33 5.25 9.60 3.66 2.08 6.09
60 8.83 3.75 1.92 4.75 8.68 3.47 1.83 5.69
70 7.25 3.25 1.67 4.33 7.40 3.10 1.67 4.97
80 7.25 3.25 1.67 4.33 7.40 3.10 1.67 4.97
90%
40 8.83 3.50 2.00 4.08 8.33 3.09 1.75 5.51
50 8.83 3.50 2.00 4.08 8.28 3.09 1.75 5.51
60 7.42 3.25 1.58 4.00 7.36 2.90 1.54 5.02
70 6.08 2.75 1.33 3.58 6.31 2.63 1.38 4.37
80 6.08 2.75 1.33 3.58 6.31 2.63 1.38 4.37
80%
40 7.33 2.92 1.67 3.33 6.86 2.50 1.41 4.72
50 7.33 2.92 1.67 3.33 6.86 2.50 1.41 4.72
60 5.92 2.67 1.25 3.17 5.91 2.31 1.24 4.12
70 5.00 2.25 1.00 2.83 5.07 2.12 1.07 3.58
80 5.00 2.25 1.00 2.83 5.07 2.12 1.07 3.58
70%
40 5.92 2.25 1.33 2.75 5.53 1.96 1.07 3.81
50 5.92 2.25 1.33 2.75 5.53 1.96 1.07 3.81
60 4.42 2.17 1.00 2.42 4.50 1.88 0.95 3.18
70 4.08 1.83 0.75 2.33 4.18 1.67 0.80 2.92
80 4.08 1.83 0.75 2.33 4.18 1.67 0.80 2.92
60% 40 4.33 1.67 0.92 1.92 4.05 1.48 0.80 2.80
50 4.33 1.67 0.92 1.92 4.05 1.48 0.80 2.80

402
Idiopathic Pulmonary Fibrosis Model produced Median and Mean Life Expectancies for people diagnosed with IPF
60 3.42 1.58 0.83 1.75 3.36 1.41 0.72 2.38
70 3.00 1.50 0.58 1.67 3.16 1.28 0.61 2.22
80 3.00 1.50 0.58 1.67 3.16 1.28 0.61 2.22
50%
40 2.83 1.00 0.58 1.25 2.70 0.97 0.52 1.86
50 2.83 1.00 0.58 1.25 2.70 0.97 0.52 1.86
60 2.50 1.00 0.58 1.08 2.34 0.92 0.49 1.64
70 2.42 0.92 0.42 1.08 2.26 0.86 0.42 1.57
80 2.42 0.92 0.42 1.08 2.26 0.86 0.42 1.57
Table 149: Natural history results from the deterministic analysis in the model using base case 1 assumptions, but with a 6 month cycle length and application of the higher post 2 hospitalisation mortality risk only in the cycle of hospitalisation 3
Starting FVC% predicted
Age Median life expectancy Mean Life years
Slow decline
Moderate decline
Rapid decline
Population
Slow decline
Moderate decline
Rapid decline
Population
100%
40 14.50 4.00 2.00 8.00 13.78 3.97 2.18 9.18
50 13.50 4.00 2.00 8.00 13.09 3.97 2.18 8.79
60 12.50 4.00 2.00 7.00 12.37 3.80 1.94 8.29
70 11.00 3.50 1.50 4.50 10.78 3.39 1.80 7.26
80 11.00 3.50 1.50 4.50 10.78 3.39 1.80 7.26
90%
40 12.00 3.00 1.50 6.50 11.57 3.34 1.81 7.71
50 12.00 3.00 1.50 6.50 11.29 3.34 1.81 7.54
60 10.50 3.00 1.50 5.00 10.20 3.17 1.62 6.85
70 9.00 3.00 1.50 4.00 8.96 2.86 1.49 6.05
80 9.00 3.00 1.50 4.00 8.96 2.86 1.49 6.05
80%
40 10.00 2.50 1.50 4.50 9.32 2.72 1.48 6.21
50 10.00 2.50 1.50 4.50 9.26 2.72 1.48 6.18
60 8.00 2.50 1.00 3.50 7.95 2.58 1.35 5.38
70 7.00 2.50 1.00 3.00 7.05 2.35 1.25 4.80
80 7.00 2.50 1.00 3.00 7.05 2.35 1.25 4.80
70%
40 7.50 2.00 1.00 3.50 7.30 2.11 1.19 4.87
50 7.50 2.00 1.00 3.50 7.30 2.11 1.19 4.87
60 6.00 2.00 1.00 2.50 5.90 1.99 1.09 4.03
70 5.50 1.50 1.00 2.00 5.61 1.83 0.98 3.81
80 5.50 1.50 1.00 2.00 5.61 1.83 0.98 3.81
60%
40 5.50 1.50 0.50 2.50 5.27 1.54 0.87 3.52
50 5.50 1.50 0.50 2.50 5.27 1.54 0.87 3.52
60 4.50 1.00 0.50 1.50 4.32 1.48 0.81 2.96
70 4.00 1.00 0.50 1.50 4.25 1.35 0.73 2.87
80 4.00 1.00 0.50 1.50 4.25 1.35 0.73 2.87
50%
40 3.00 0.50 0.50 1.50 3.29 1.01 0.62 2.23
50 3.00 0.50 0.50 1.50 3.29 1.01 0.62 2.23
60 2.50 0.50 0.50 1.00 2.83 0.96 0.59 1.94
70 2.50 0.50 0.00 1.00 2.80 0.90 0.51 1.90
80 2.50 0.50 0.00 1.00 2.80 0.90 0.51 1.90

403
Idiopathic Pulmonary Fibrosis Model produced Median and Mean Life Expectancies for people diagnosed with IPF
Figure 124: Kaplan Meier curves produced by using the base case probabilities of the economic model (1 month cycle)
Figure 125:Kaplan Meier curves produced by using the higher risk of hospitalisation for only one cycle post hospitalisation (6month cycle)
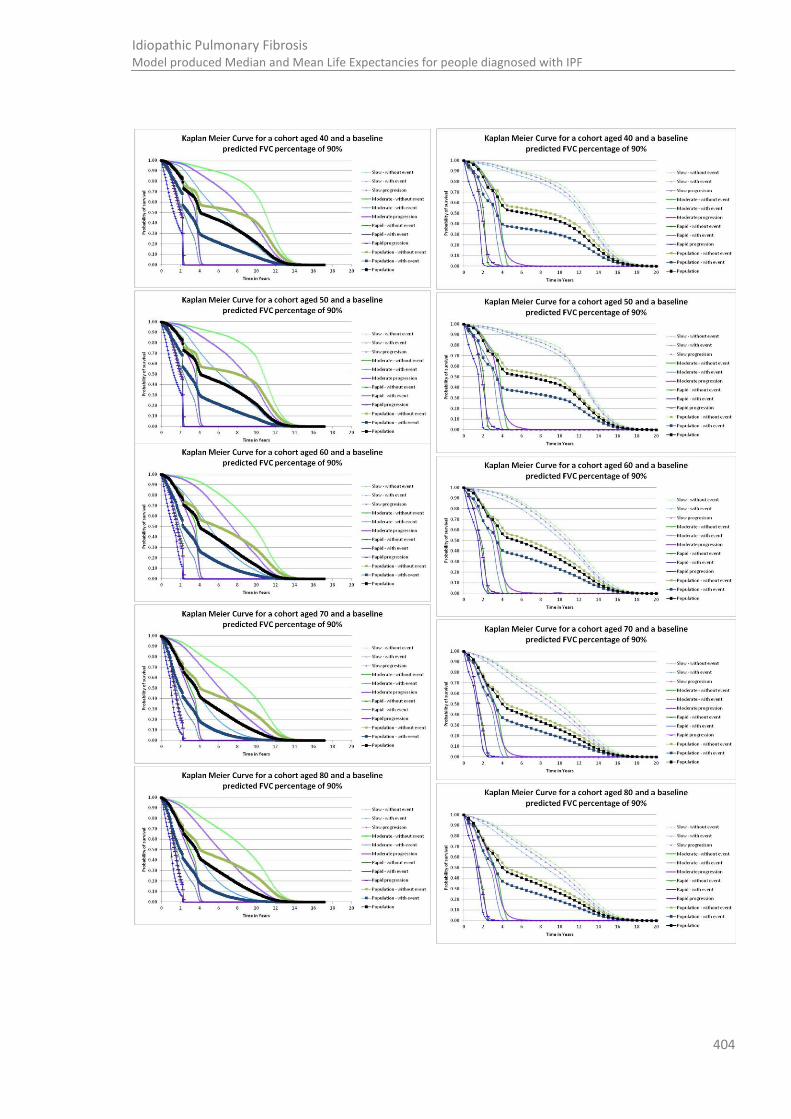
404
Idiopathic Pulmonary Fibrosis Model produced Median and Mean Life Expectancies for people diagnosed with IPF
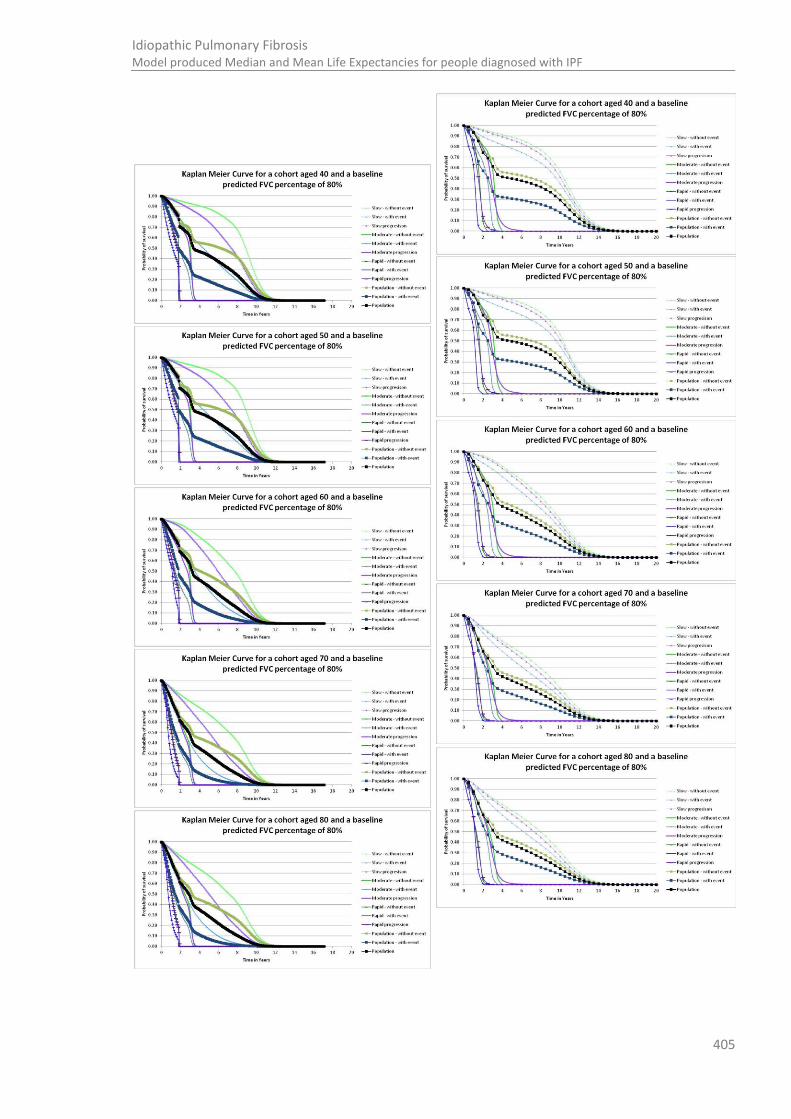
405
Idiopathic Pulmonary Fibrosis Model produced Median and Mean Life Expectancies for people diagnosed with IPF

406
Idiopathic Pulmonary Fibrosis Model produced Median and Mean Life Expectancies for people diagnosed with IPF

407
Idiopathic Pulmonary Fibrosis Model produced Median and Mean Life Expectancies for people diagnosed with IPF
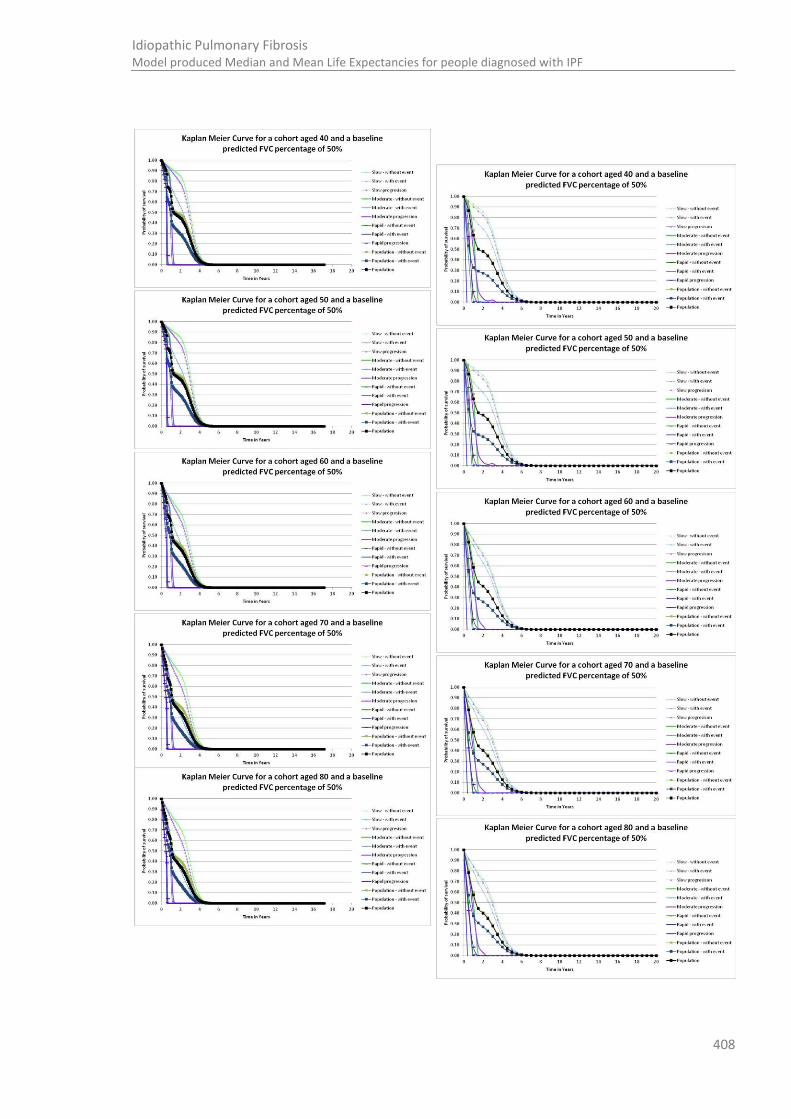
408
Idiopathic Pulmonary Fibrosis Model produced Median and Mean Life Expectancies for people diagnosed with IPF
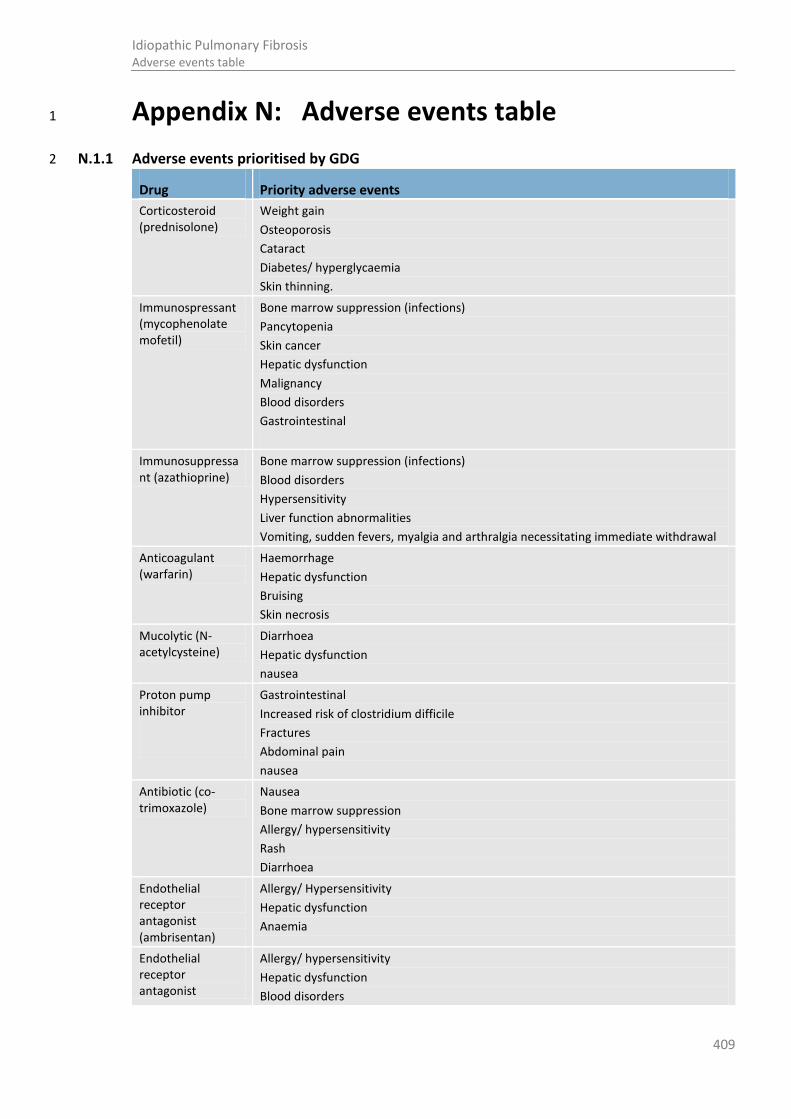
409
Idiopathic Pulmonary Fibrosis Adverse events table
Appendix N: Adverse events table 1
N.1.1 Adverse events prioritised by GDG 2
Drug Priority adverse events
Corticosteroid (prednisolone)
Weight gain
Osteoporosis
Cataract
Diabetes/ hyperglycaemia
Skin thinning.
Immunospressant (mycophenolate mofetil)
Bone marrow suppression (infections)
Pancytopenia
Skin cancer
Hepatic dysfunction
Malignancy
Blood disorders
Gastrointestinal
Immunosuppressant (azathioprine)
Bone marrow suppression (infections)
Blood disorders
Hypersensitivity
Liver function abnormalities
Vomiting, sudden fevers, myalgia and arthralgia necessitating immediate withdrawal
Anticoagulant (warfarin)
Haemorrhage
Hepatic dysfunction
Bruising
Skin necrosis
Mucolytic (N-acetylcysteine)
Diarrhoea
Hepatic dysfunction
nausea
Proton pump inhibitor
Gastrointestinal
Increased risk of clostridium difficile
Fractures
Abdominal pain
nausea
Antibiotic (co-trimoxazole)
Nausea
Bone marrow suppression
Allergy/ hypersensitivity
Rash
Diarrhoea
Endothelial receptor antagonist (ambrisentan)
Allergy/ Hypersensitivity
Hepatic dysfunction
Anaemia
Endothelial receptor antagonist
Allergy/ hypersensitivity
Hepatic dysfunction
Blood disorders

410
Idiopathic Pulmonary Fibrosis Adverse events table
Drug Priority adverse events (bosentan)
PDE inhibitor (sildenafil)
Visual impairment
Cardiovascular disease
Flushing
Dry mouth
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21

411
Idiopathic Pulmonary Fibrosis The cost of pharmacological interventions for IPF
Appendix O: The cost of pharmacological interventions for IPF 1
Intervention; with assumed dose/duration of treatment for typical IPF patient [a]
Unit cost of pharmacological intervention [based on drug tariff, March 2013, and unless otherwise stated]
351 5
Additional Costs; monitoring/prevention of complications [b]
Expected cost per patient per year (nearest pound) Notes
Prednisolone
40 mg daily for first 4 weeks
30 mg daily for weeks 4-8
20mg daily for weeks 8-12
10mg thereafter
NB: this dosage differs from that cited in the BNF and was agreed to be typical by clinical members of the GDG
Cost per 5mg 28 tab pack = £0.96
Cost per week
For wks 1-4: £1.92
For wks 4-8: £1.44
For wks 8-12: £0.96
For weeks 12+:£0.48
Cost per 1st year = £36.48
Cost per year thereafter = £24.96
Monitoring
Assessment for corticosteroid complications, once on initiation and twice per year thereafter as a minimum. Assessment would include screening for contraindications, as well as regular blood pressure and urine testing Vitamin D supplementation may be offered. A Dexa bone scan is sometimes offered to patients considered at risk of osteoporosis.
Dexa scan = £77 107
General practice nurse time per consultation = £10381
Urine testing: Costs vary depending on how many substances can be detected and on the supplier. Typical price per Clinistix® (and similar) is approximately 5-8 pence per stick. Strips detecting 7 or 10 different substances can cost up to 20 pence per strip.
Calcium and Ergocalciferol (10mg) (Calcium and Vitamin D) 28 tab pack costs £7.91. A year of one tablet daily = £143.11
For the costing it is assumed that monitoring occurs via 4 primary care nurse consultation per year and that staff time is the only significant cost.
Cost of monitoring + supplements per year + dexa = (4*£10) + £103.11+£77 = £220.11
Cost of drug = £36 (1st year)
Additional costs = £220
Total = £256
Alternative drugs in the same class.
Betamethasone; cortisone acetate; deflazacort; dexamethasone; hydrocortisone; methylprednisolone; prednisone; triamcinolone

412
Idiopathic Pulmonary Fibrosis The cost of pharmacological interventions for IPF
Intervention; with assumed dose/duration of treatment for typical IPF patient [a]
Unit cost of pharmacological intervention [based on drug tariff, March 2013, and unless otherwise stated]
351 5
Additional Costs; monitoring/prevention of complications [b]
Expected cost per patient per year (nearest pound) Notes
Mycophenolate mofetil
1g twice daily
Cost per 500mg 50-tab pack=£7.11
Cost per day = £0.57
Cost per week = £3.98
Cost per year = £207.04
Monitoring
Patients monitored for neutropenia, concomitant medications, viral infections, or some combination of these causes. Complete blood counts weekly during the first month, twice monthly for the second and third months of treatment, then monthly through the first year.
Cost of full blood count: £2.49112
Cost of nurse time per procedure in primary care: £9381
Assumed number of tests per year: 19
Cost of tests per year: £47.31+£171 =£218.31
Cost of drug = £207
Additional costs = £218
Total = £425
Brands include:
Arzip®
Cellcept®
Myfortic® [ NB higher dosage may be required]
Warfarin
Dose according to INR
Assumed dose of 3mg daily
Cost per 3mg 28-tab pack=£0.78
Cost per day = £0.03
Cost per week = £0.20
Cost per year = £10.14
Monitoring
INR be determined daily or on alternate days in early days of treatment, then at longer intervals, 4-6 weeks, then up to every 12 weeks. INR testing may be done by NHS in clinic or primary care. The NHS reference cost takes data from both settings.
Estimates from literature
Cost per year of INR monitoring = £155223,223
Cost per year, clinic setting = £98.47 80,146
Cost per year, primary care setting = £283.10 345,346
Estimate from NHS reference cost
Number of visits per year, assuming daily for first week and monthly thereafter: 7+12 = 19
Anticoagulation clinics [non consultant led – service code 324]: £22 first visit; £10 for each follow-up visit cost per year = £22+£180 = £202
107
Assuming no adverse event
Cost of drug = £10
Additional costs = £202
Total = £210

413
Idiopathic Pulmonary Fibrosis The cost of pharmacological interventions for IPF
Intervention; with assumed dose/duration of treatment for typical IPF patient [a]
Unit cost of pharmacological intervention [based on drug tariff, March 2013, and unless otherwise stated]
351 5
Additional Costs; monitoring/prevention of complications [b]
Expected cost per patient per year (nearest pound) Notes
Azathioprine
2mg/kg – max 150mg per day
Assume 125 mg per day
Cost per 25mg 28-tab pack=£4.41
Cost per 50mg 56 tab-pack = £4.36
Cost per day = £0.31
Cost per week = £2.20
Cost per year = £114
Monitoring
Monitor for toxicity throughout treatment (including routine liver tests); monitor full blood count weekly (more frequently with higher doses or if severe hepatic or renal impairment) for first 4 weeks, at least every 3 months. Consider measuring TPMT activity before starting azathioprine
Estimated cost of TPMT assay: £20 [price for service quoted by City Hospital, Birmingham]
68
Cost of nurse time per procedure in primary care: £9381
Cost of TPMT = £29
Full Blood Count
Cost of full blood count: £2.49112
Cost of nurse time per procedure in primary care: £9381
Assumed number of tests per year: 7
Cost of tests per year: £17.43+£63.00 =£80.43
Liver Function Tests
Cost of liver function test: £4.12112
Cost of nurse time per procedure in primary care: £9381
Assumed number of tests per year: 13
Cost of tests per year: £53.56+£117 =£170.56
Cost of drug = £114
Additional costs (inc TPMT) = £280
Total = £394
Brands include
Azamune®, Imuran®
N-acetyl cysteine
600mg 3 times daily
N-acetylcysteine, as an oral agent, is only available as an unlicensed generic. The following is an example
No additional monitoring required Cost of drug = £158.34
Total = £158
Oral form not licensed in the UK – therefore not quoted in BNF or tariff.
Used as adjunctive
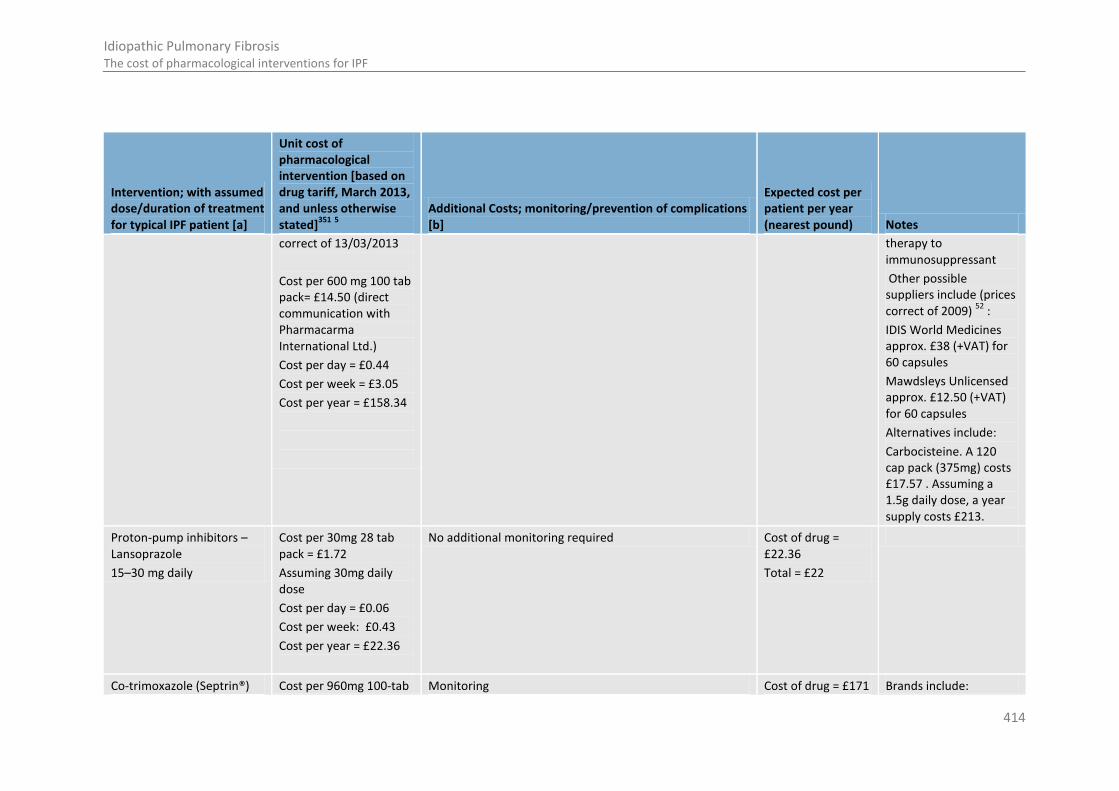
414
Idiopathic Pulmonary Fibrosis The cost of pharmacological interventions for IPF
Intervention; with assumed dose/duration of treatment for typical IPF patient [a]
Unit cost of pharmacological intervention [based on drug tariff, March 2013, and unless otherwise stated]
351 5
Additional Costs; monitoring/prevention of complications [b]
Expected cost per patient per year (nearest pound) Notes
correct of 13/03/2013
Cost per 600 mg 100 tab pack= £14.50 (direct communication with Pharmacarma International Ltd.)
Cost per day = £0.44
Cost per week = £3.05
Cost per year = £158.34
therapy to immunosuppressant
Other possible suppliers include (prices correct of 2009)
52 :
IDIS World Medicines approx. £38 (+VAT) for 60 capsules
Mawdsleys Unlicensed approx. £12.50 (+VAT) for 60 capsules
Alternatives include:
Carbocisteine. A 120 cap pack (375mg) costs £17.57 . Assuming a 1.5g daily dose, a year supply costs £213.
Proton-pump inhibitors – Lansoprazole
15–30 mg daily
Cost per 30mg 28 tab pack = £1.72
Assuming 30mg daily dose
Cost per day = £0.06
Cost per week: £0.43
Cost per year = £22.36
No additional monitoring required Cost of drug = £22.36
Total = £22
Co-trimoxazole (Septrin®) Cost per 960mg 100-tab Monitoring Cost of drug = £171 Brands include:

415
Idiopathic Pulmonary Fibrosis The cost of pharmacological interventions for IPF
Intervention; with assumed dose/duration of treatment for typical IPF patient [a]
Unit cost of pharmacological intervention [based on drug tariff, March 2013, and unless otherwise stated]
351 5
Additional Costs; monitoring/prevention of complications [b]
Expected cost per patient per year (nearest pound) Notes
960mg given twice daily
pack = £23.46
Cost per day = £0.47
Cost per week = £3.28
Cost per year = £170.79
Monitor blood counts on prolonged treatment
Cost of full blood count: £2.49112
Cost of nurse time per procedure in primary care: £9381
Assumed number of tests per year: 12
Cost of tests per year: £29.88+£108=£137.88
Additional costs = £138
Total = £309
Fectrim®, Fectrim® Forte
Ambrisentan - Volibris®
5mg given daily
Cost per 5 or 10 mg 30-tab pack = £1,651.07
Cost per day = £55.04
Cost per week = £385.25
Cost per year = £20,032 .98
For treatment using HRG code XD01Z: £215 per unit
107
Monitoring
Patients should be monitored for signs of hepatic injury and monthly monitoring of ALT and AST is recommended.
Cost of liver function test: £4.12112
Cost of nurse procedure in primary care: £9381
Assumed number of tests per year: 13
Cost of tests per year: £53.56+£117 =£170.56
It is recommended that haemoglobin and/or haematocrit levels are measured during treatment e.g. at 1 month, 3 months and periodically thereafter in line with clinical practice.
Cost of full blood count: £2.49112
Cost of nurse procedure in primary care: £9381
Assumed number of tests per year: 5
Cost of tests per year: £12.45+£45 =£57.45
Cost of drug = £20033
Additional costs = £228
Total = £20261
Excluded from tariff
Cost sourced by MIMS
Unbundled HCD (OPSC code X821)
No non-proprietary form available
Bosanten - Tracleer®
Initially 62.5 mg twice daily increased after 4 weeks to 125 mg twice daily; max. 250 mg twice daily
Cost per 62.5 mg 56-tab pack = £1,510.21
3
Cost per 125mg 56-tab pack = £1,510.21
3
Cost per day = £26.97
Self-administered
Monitoring
Liver aminotransferase levels measured prior to initiation of treatment and subsequently at monthly intervals for the duration of treatment with Tracleer. In addition, liver
Cost of drug = £19,633
Additional costs = £171
Total = £19,804
Excluded from tariff when used for IPF
Cost sourced by MIMS
Unbundled HCD (OPSC code X822)
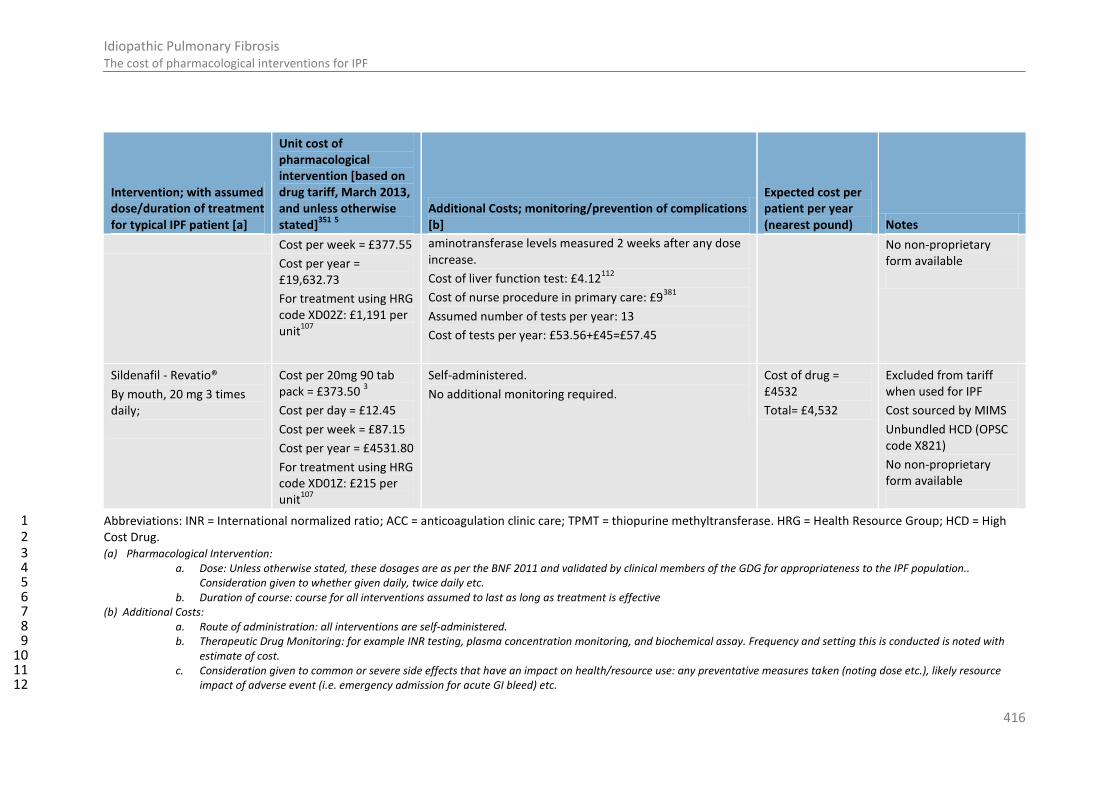
416
Idiopathic Pulmonary Fibrosis The cost of pharmacological interventions for IPF
Intervention; with assumed dose/duration of treatment for typical IPF patient [a]
Unit cost of pharmacological intervention [based on drug tariff, March 2013, and unless otherwise stated]
351 5
Additional Costs; monitoring/prevention of complications [b]
Expected cost per patient per year (nearest pound) Notes
Cost per week = £377.55
Cost per year = £19,632.73
For treatment using HRG code XD02Z: £1,191 per unit
107
aminotransferase levels measured 2 weeks after any dose increase.
Cost of liver function test: £4.12112
Cost of nurse procedure in primary care: £9381
Assumed number of tests per year: 13
Cost of tests per year: £53.56+£45=£57.45
No non-proprietary form available
Sildenafil - Revatio®
By mouth, 20 mg 3 times daily;
Cost per 20mg 90 tab pack = £373.50
3
Cost per day = £12.45
Cost per week = £87.15
Cost per year = £4531.80
For treatment using HRG code XD01Z: £215 per unit
107
Self-administered.
No additional monitoring required.
Cost of drug = £4532
Total= £4,532
Excluded from tariff when used for IPF
Cost sourced by MIMS
Unbundled HCD (OPSC code X821)
No non-proprietary form available
Abbreviations: INR = International normalized ratio; ACC = anticoagulation clinic care; TPMT = thiopurine methyltransferase. HRG = Health Resource Group; HCD = High 1 Cost Drug. 2 (a) Pharmacological Intervention: 3
a. Dose: Unless otherwise stated, these dosages are as per the BNF 2011 and validated by clinical members of the GDG for appropriateness to the IPF population.. 4 Consideration given to whether given daily, twice daily etc. 5
b. Duration of course: course for all interventions assumed to last as long as treatment is effective 6 (b) Additional Costs: 7
a. Route of administration: all interventions are self-administered. 8 b. Therapeutic Drug Monitoring: for example INR testing, plasma concentration monitoring, and biochemical assay. Frequency and setting this is conducted is noted with 9
estimate of cost. 10 c. Consideration given to common or severe side effects that have an impact on health/resource use: any preventative measures taken (noting dose etc.), likely resource 11
impact of adverse event (i.e. emergency admission for acute GI bleed) etc. 12

417
Idiopathic Pulmonary Fibrosis Research recommendations
Appendix P: Research recommendations 1
P.1 The value of bronchoalveolar lavage 2
Research question: 3
What is the value of bronchoalveolar lavage in people in whom idiopathic pulmonary fibrosis is 4 considered the most likely diagnosis when clinical and computed tomography findings are 5 insufficient to support a confident diagnosis? 6
Why this is important: A confident diagnosis of idiopathic pulmonary fibrosis needs integration of 7 clinical and computed tomography findings in a multidisciplinary setting. However, a consensus 8 diagnosis cannot always be made with confidence. In some people with ‘probable idiopathic 9 pulmonary fibrosis’, bronchoalveolar lavage alone may help attain a more confident diagnosis while 10 in others, a subsequent surgical lung biopsy may be needed. It is not known whether the benefits of 11 attaining a more confident diagnosis by bronchoalveolar lavage outweigh the risks of the procedure. 12 A randomised controlled trial should be conducted to determine the potential benefits and risks of 13 bronchoalveolar lavage with regard to increasing diagnostic certainty and avoiding the need for 14 surgical lung biopsy. The study should incorporate outcomes that include diagnostic certainty 15 (sensitivity, specificity), mortality (all-cause and idiopathic pulmonary fibrosis-related), health-related 16 quality of life and change in lung function. Adjustments should be made for differences in baseline 17 clinical and radiological features. Clinical studies should be of sufficient power and duration and 18 include a health economic evaluation 19
Criteria for selecting high-priority research recommendations: 20
PICO question What is the value of bronchoalveolar lavage in patients in patients in
whom IPF is suspected clinically, but the CT findings are insufficient to
support a confident diagnosis?
Importance to patients or the population
Results would inform recommendations for, or against routine BAL when diagnosing people with IPF
Relevance to NICE guidance
Future NICE guidance may recommend BAL as a first line option before SLB.
Relevance to the NHS If outcomes are positive (high sensitivity and specificity), then BAL may prove to increase diagnostic certainty for people with IPF. BAL analysis may not be routinely available in all secondary care centres and will require additional resource
National priorities None
Current evidence base There are no suitable studies addressing this.
Equality The research question has no particular equality issues.
Study design A controlled trial should be conducted to determine the potential benefits and risks of BAL in adults.
Feasibility There are specialist secondary care facilities which offer BAL and its analysis routinely, so there will be an adequate infrastructure for a study.
Other comments None
Importance High: the research is essential to inform future updates of key recommendations in the guideline.
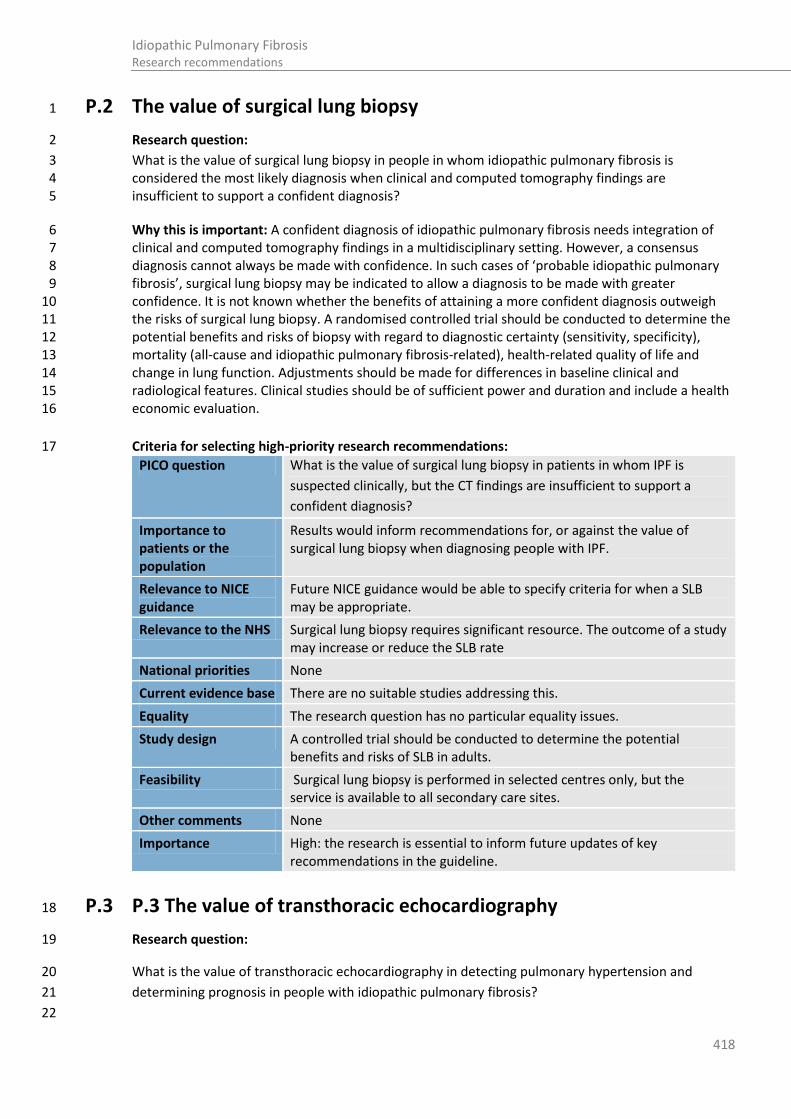
418
Idiopathic Pulmonary Fibrosis Research recommendations
P.2 The value of surgical lung biopsy 1
Research question: 2
What is the value of surgical lung biopsy in people in whom idiopathic pulmonary fibrosis is 3 considered the most likely diagnosis when clinical and computed tomography findings are 4 insufficient to support a confident diagnosis? 5
Why this is important: A confident diagnosis of idiopathic pulmonary fibrosis needs integration of 6 clinical and computed tomography findings in a multidisciplinary setting. However, a consensus 7 diagnosis cannot always be made with confidence. In such cases of ‘probable idiopathic pulmonary 8 fibrosis’, surgical lung biopsy may be indicated to allow a diagnosis to be made with greater 9 confidence. It is not known whether the benefits of attaining a more confident diagnosis outweigh 10 the risks of surgical lung biopsy. A randomised controlled trial should be conducted to determine the 11 potential benefits and risks of biopsy with regard to diagnostic certainty (sensitivity, specificity), 12 mortality (all-cause and idiopathic pulmonary fibrosis-related), health-related quality of life and 13 change in lung function. Adjustments should be made for differences in baseline clinical and 14 radiological features. Clinical studies should be of sufficient power and duration and include a health 15 economic evaluation. 16
Criteria for selecting high-priority research recommendations: 17
PICO question What is the value of surgical lung biopsy in patients in whom IPF is
suspected clinically, but the CT findings are insufficient to support a
confident diagnosis?
Importance to patients or the population
Results would inform recommendations for, or against the value of surgical lung biopsy when diagnosing people with IPF.
Relevance to NICE guidance
Future NICE guidance would be able to specify criteria for when a SLB may be appropriate.
Relevance to the NHS Surgical lung biopsy requires significant resource. The outcome of a study may increase or reduce the SLB rate
National priorities None
Current evidence base There are no suitable studies addressing this.
Equality The research question has no particular equality issues.
Study design A controlled trial should be conducted to determine the potential benefits and risks of SLB in adults.
Feasibility Surgical lung biopsy is performed in selected centres only, but the service is available to all secondary care sites.
Other comments None
Importance High: the research is essential to inform future updates of key recommendations in the guideline.
P.3 P.3 The value of transthoracic echocardiography 18
Research question: 19
What is the value of transthoracic echocardiography in detecting pulmonary hypertension and 20
determining prognosis in people with idiopathic pulmonary fibrosis? 21
22

419
Idiopathic Pulmonary Fibrosis Research recommendations
Why this is important: People with IPF sometimes develop pulmonary hypertension. This may be an 1
indicator of poor prognosis. Pulmonary artery pressure (PAP) can only be accurately measured by 2
right heart catheter which is an invasive procedure. Transthoracic doppler echocardiography (TCC) is 3
a non-invasive technique for estimating PAP although values correlate poorly with those obtained by 4
right heart catheterisation. The benefits of estimating PAP in people with IPF, at the time of diagnosis 5
or serially thereafter, is not known. A study should be undertaken to determine whether estimation 6
of PAP is a useful predictor of prognosis for disease progression in IPF. The study should address the 7
additive value of TCC over other routinely performed tests, by measuring rates of survival, mortality 8
(all-cause and IPF-related); hospitalisation (all-cause, non-elective and IPF-related); change in lung 9
function (vital capacity and diffusion capacity for carbon monoxide); 6 minute walk distance; 10
breathlessness score; health related quality of life measures (ideally employing a tool validated in IPF 11
patients); and development of pulmonary hypertension as measured by right heart catheterisation. 12
Clinical studies should be of sufficient power and duration and include health economic evaluation. 13
Criteria for selecting high-priority research recommendations: 14
PICO question What is the value of transthoracic echocardiography (TCC) in detecting
pulmonary hypertension and determining prognosis in people with IPF?
Importance to patients or the population
People with IPF may present with co-existing pulmonary hypertension, or may develop pulmonary hypertension over time. Several studies have suggested that pulmonary hypertension is a poor prognostic indicator in IPF.
Relevance to NICE guidance
Future NICE guidance may recommend routine TCC in order to predict prognosis in people with IPF.
Relevance to the NHS TCC is widely available but requires resource. Most centres do not perform TTC routinely in all patients with IPF.
National priorities None.
Current evidence base The NICE IPF guideline development systematic review found no adequate evidence to support or condemn the use of transthoracic echocardiography. No research has been done to modern standards.
Equality The research question has no particular equality issues.
Study design Cohort studies investigating the prognostic value of TCC in adults should be adequately powered and measure mortality/ survival (time to event data).
Feasibility TCC is available in most secondary care centres.
Other comments None.
Importance Medium: the research is relevant to the recommendations in the guideline, but the research recommendations are not key to future updates.
15
P.4 Agreement between radiologists in the interpretation of CT 16
17
Research question: 18
What is the agreement between radiologists in the interpretation of CT in patients with suspected 19
idiopathic pulmonary fibrosis? 20
21

420
Idiopathic Pulmonary Fibrosis Research recommendations
Why this is important: Interpretation of the computed tomography (CT) is of pivotal importance in 1
the diagnosis of IPF. Patients with a consistent clinical history can be confidently diagnosed with IPF if 2
the CT is considered indicative of the usual interstitial pneumonia (UIP) pattern of disease. Previous 3
studies from North America have attempted to determine the agreement between radiologists in 4
interpreting CT images in patients with suspected IPF, but these predated the most recently 5
published international consensus criteria for the diagnosis of IPF and these previous studies may not 6
reflect current practice in the UK. A multicentre study should be performed to determine the level of 7
agreement between radiologists of varying expertise for the diagnosis of UIP pattern of disease on 8
CT. Clinical studies should be of sufficient power and duration, and should routinely include health 9
economic evaluation. 10
Criteria for selecting high-priority research recommendations: 11
PICO question What is the agreement between radiologists in the interpretation of CT in
patients with suspected IPF?
Importance to patients or the population
CT appearances are pivotal in the diagnosis of IPF. Uniformity of CT interpretation would ensure that IPF is diagnosed appropriately and accurately.
Relevance to NICE guidance
None.
Relevance to the NHS It is not known if there is adequate expertise in CT interpretation in all secondary care centres. Expert chest CT interpretation requires resource.
National priorities None.
Current evidence base The NICE IPF guideline development systematic review found no adequate evidence to support or condemn the use of computed tomography. No research has been done to modern standards.
Equality The research question has no particular equality issues.
Study design A multicentre study should determine the level of agreement between radiologists when assessing the diagnosis of UIP pattern of disease.
Feasibility CT scans are digitally archived and can be independently reviewed
Other comments None.
Importance Medium: the research is relevant to the recommendations in the guideline, but the research recommendations are not key to future updates.
12
P.5 CT scoring systems 13
Research question: 14
What is the feasibility of a formal ‘CT scoring system’ to assess disease severity in patients with 15
suspected idiopathic pulmonary fibrosis? 16
17
Why this is important: There are a number of published ‘CT scoring systems’ that have been 18
validated to varying extents. Scoring of CT consumes resources. There is no data comparing different 19
CT scoring systems in terms of inter- and intra-observer agreement, functional correlation and ease 20
of use. There are no data comparing observers at MDTs in secondary and tertiary care for inter- and 21
intra-observer agreement of CT scoring. Studies should be performed that compare different CT 22

421
Idiopathic Pulmonary Fibrosis Research recommendations
scoring systems in terms of ease of use, observer agreement and correlation with functional indices. 1
Clinical studies should be of sufficiently long duration, sufficiently powered and should include health 2
economic evaluation. 3
Criteria for selecting high-priority research recommendations: 4
PICO question What is the feasibility of a formal ‘CT scoring system’ to assess disease
severity in patients with suspected IPF?
Importance to patients or the population
There are a number of CT scoring systems used for research purposes but the applicability in clinical practice is not known
Relevance to NICE guidance
Future NICE guidance may include formal CT scoring or quantification if it is found to be valuable in determining disease severity
Relevance to the NHS Formal CT scoring is routinely performed and requires resource
National priorities None
Current evidence base The NICE IPF guideline development systematic review found no adequate evidence to support or condemn the use of computed tomography scoring. No research has been done to modern standards.
Equality The research question has no particular equality issues.
Study design A blinded study of independently scored CT scans
Feasibility CT scans are digitally archived and can be independently reviewed
Other comments None
Importance Medium: the research is relevant to the recommendations in the guideline, but the research recommendations are not key to future updates.
5
P.6 Utility of a formal CT scoring system in determining outcomes 6
Research question: 7
What is the utility of a formal CT scoring system in determining outcome in patients with suspected 8
idiopathic pulmonary fibrosis? 9
10
Why this is important: Some evidence suggests that composite score systems (including CT scoring) 11
are of value in predicting prognosis in IPF. There is little information on whether a score suggesting 12
CT abnormalities at the time of diagnosis or whether scoring a change in CT appearance at follow-up 13
might independently predict prognosis. Studies should be undertaken to compare different CT 14
scoring systems in patients with IPF evaluating the extent, pattern and ancillary features of fibrosis 15
(including any co-existing conditions such as emphysema) at diagnosis. Furthermore, longitudinal 16
observational studies should measure inter-observer agreement comparing observers with different 17
levels of expertise at multi-disciplinary teams (MDTs) of secondary and tertiary care level. Primary 18
outcomes should include a correlation between CT scores and survival. Study length should be 5 19
years and also be sufficiently powered and include health economic evaluation. 20
Criteria for selecting high-priority research recommendations: 21
PICO question What is the utility of a formal CT scoring system in determining outcome

422
Idiopathic Pulmonary Fibrosis Research recommendations
in patients with suspected IPF?
Importance to patients or the population
Severity of disease in IPF is generally assessed by symptoms and lung function testing. The value of quantifying CT abnormalities by CT scoring in predicting outcome, or for monitoring disease progression is not known
Relevance to NICE guidance
Future NICE guidance may include formal CT scoring or quantification if it is found to be valuable in determining disease progression
Relevance to the NHS Formal CT scoring is routinely performed and requires resource
National priorities None
Current evidence base The NICE IPF guideline development systematic review found no adequate evidence to support or condemn the use of computed tomography scoring systems. No research has been done to modern standards.
Equality The research question has no particular equality issues.
Study design Longitudinal observational studies should measure CT scores against disease progression. Primary outcomes should include association between CT scores and survival. Adjustments should be made for variables known to predict outcome in IPF.
Feasibility CT scans are digitally archived and can be independently reviewed
Other comments None
Importance Medium: the research is relevant to the recommendations in the guideline, but the research recommendations are not key to future updates.
1
P.7 Pulmonary rehabilitation 2
Research question: 3
Does pulmonary rehabilitation improve outcomes for patients with idiopathic pulmonary fibrosis? 4
5
Why this is important: There is evidence that patients with idiopathic pulmonary fibrosis may benefit 6
from pulmonary rehabilitation. However this evidence is mostly derived from programmes designed 7
principally for patients with chronic obstructive pulmonary disease. It is likely that the needs of 8
people with idiopathic pulmonary fibrosis and chronic obstructive pulmonary disease differ. 9
Randomised controlled trials should be carried out to determine the effects of pulmonary 10
rehabilitation programmes tailored to idiopathic pulmonary fibrosis, compared with currently 11
offered pulmonary rehabilitation programmes, on quality of life, walking distance and lung function 12
with analysis adjusting for confounding factors appropriately. Trials should analyse benefits of the 13
different aspects of pulmonary rehabilitation including the components, setting and location of the 14
programme, and healthcare resources involved. End points may include: 6-minute walk distance; 15
breathlessness score; a measure of health-related quality of life (ideally employing a tool validated in 16
people with idiopathic pulmonary fibrosis): mortality (all-cause and idiopathic pulmonary fibrosis-17
related); hospitalisation (all-cause, non-elective and idiopathic pulmonary fibrosis -related); lung 18
function (vital capacity and diffusion capacity for carbon monoxide). Studies should be of sufficient 19
power and duration and include a health economic evaluation. 20
21

423
Idiopathic Pulmonary Fibrosis Research recommendations
Criteria for selecting high-priority research recommendations: 1
PICO question Does pulmonary rehabilitation improve outcomes for patients with IPF?
Importance to patients or the population
Pulmonary rehabilitation may consist of various exercise or educational components Currently, patients with IPF are most likely to be offered pulmonary rehabilitation tailored to people with COPD, if at all.
Relevance to NICE guidance
Future NICE guidance may be able to specify components of pulmonary rehabilitation programmes which are proven to improve quality or life outcomes specifically for people with IPF.
Relevance to the NHS Pulmonary rehabilitation specifically designed for IPF would have resource implications
National priorities None
Current evidence base There are no suitable studies addressing the components of pulmonary rehabilitation programmes in people with IPF.
Equality The availability, setting and locations of pulmonary rehabilitation programmes should be tailored to all people with IPF, including those with disabilities.
Study design Controlled trials should investigate the benefit of pulmonary rehabilitation components in adults, be adequately powered and measure patient centred outcomes.
Feasibility Pulmonary rehabilitation facilities are widely available.
Other comments None
Importance High: the research is essential to inform future updates of key recommendations in the guideline.
2
P.8 Nocturnal oxygen 3
Research question: 4
Does nocturnal oxygen improve outcomes in idiopathic pulmonary fibrosis? 5
6
Why this is important: Oxygen desaturation during sleep is known to occur in many patients with IPF 7
even if they do not desaturate on exercise. The detection of nocturnal hypoxaemia and its treatment 8
with supplemental oxygen is not currently part of routine clinical practice. A randomised control trial 9
should establish the benefits of supplementary nocturnal oxygen therapy in patients with IPF who 10
develop hypoxia during sleep and include a placebo arm. Endpoints in phase 3 clinical trials in IPF 11
should reflect patient survival, quality of life and functional status. Appropriate endpoints may 12
include 6 minute walk distance; transthoracic echocardiogram to estimate pulmonary artery 13
pressure; breathlessness score; a measure of health related quality of life (ideally employing a tool 14
validated in IPF patients), mortality (all-cause and IPF-related); hospitalisation (all-cause, non-elective 15
and IPF-related). Phase 3 trials should have a duration of greater than 12 months and include health 16
economic evaluation. 17
Criteria for selecting high-priority research recommendations: 18
PICO question Does nocturnal oxygen improve outcomes in IPF?
Importance to patients or the population
Oxygen desaturation during sleep is known to occur in many patients with IPF even if they do not desaturate on exercise. The significance of this is not known

424
Idiopathic Pulmonary Fibrosis Research recommendations
Relevance to NICE guidance
NICE would provide guidance on nocturnal oxygen
Relevance to the NHS Nocturnal oxygen therapy requires resource
National priorities None
Current evidence base There are no suitable studies addressing this.
Equality The research question has no particular equality issues.
Study design A randomised control trial should establish the benefits of supplementary nocturnal oxygen therapy versus placebo.
Feasibility Oxygen therapy is readily available
Other comments None
Importance Medium: the research is relevant to the recommendations in the guideline, but the research recommendations are not key to future updates.
1
P.9 Ambulatory oxygen 2
Research question: 3
Does ambulatory oxygen improve outcomes in idiopathic pulmonary fibrosis? 4
5
Why this is important: People with idiopathic pulmonary fibrosis frequently demonstrate a fall in 6
oxygen saturation during exercise even though they are not hypoxic at rest. In such people, 7
ambulatory oxygen is often provided to improve exercise capacity, enhance mobility and enable 8
activities of daily living in order to improve quality of life. However, there are no randomised 9
controlled trials to demonstrate that ambulatory oxygen therapy is effective in achieving these aims 10
in patients with idiopathic pulmonary fibrosis. A randomised controlled trial should be conducted to 11
determine the effects of ambulatory oxygen on quality of life in people with idiopathic pulmonary 12
fibrosis and consideration given to the use of a placebo arm. This should include a standardised 13
protocol for assessing exercise such as the 6-minute walk test. The end points may include 6-minute 14
walk distance; breathlessness score; a measure of health-related quality of life (ideally employing a 15
tool validated in idiopathic pulmonary fibrosis patients). Phase III trials should have a duration of 16
greater than 12 months and include a health economic evaluation. 17
Criteria for selecting high-priority research recommendations: 18
PICO question Does ambulatory oxygen improve outcomes in IPF?
Importance to patients or the population
Patients with IPF frequently demonstrate a fall in oxygen saturation during exercise even though they are not hypoxia at rest. Ambulatory oxygen is often prescribed to patients that desaturate on exercise, but its value is not known
Relevance to NICE guidance
NICE would recommend ambulatory oxygen if future guidelines
Relevance to the NHS Ambulatory oxygen requires resource
National priorities None
Current evidence base There are no suitable studies addressing this.
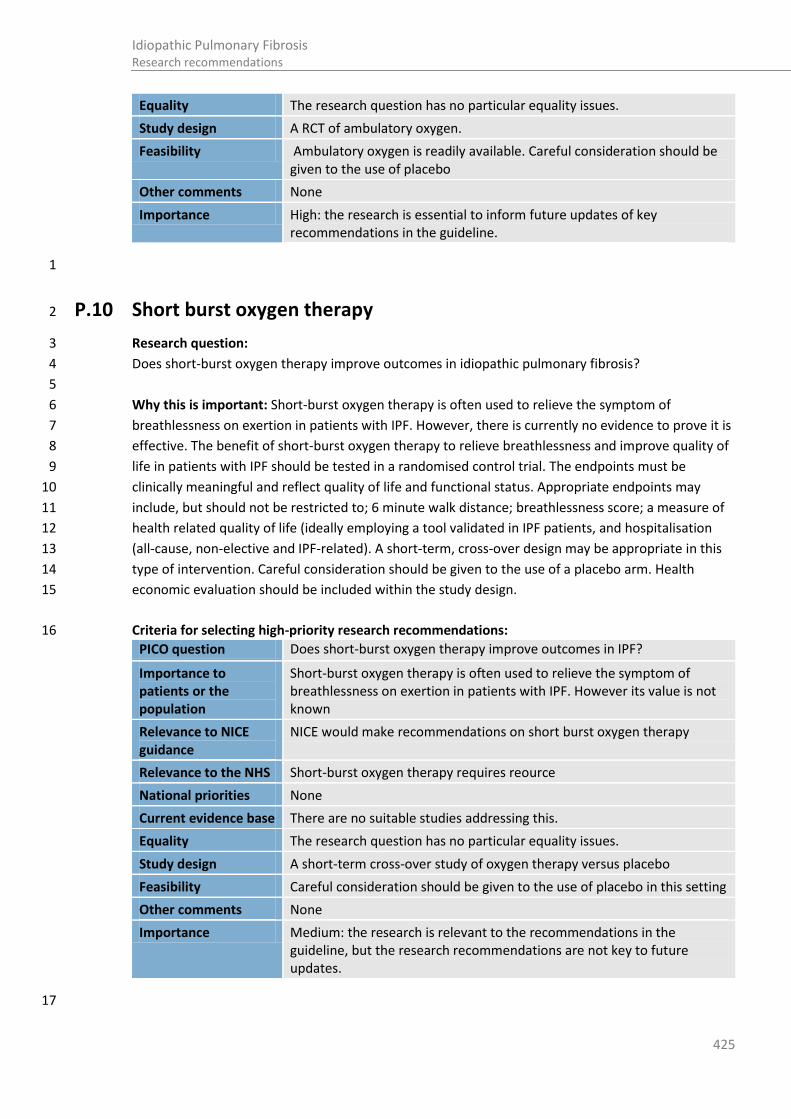
425
Idiopathic Pulmonary Fibrosis Research recommendations
Equality The research question has no particular equality issues.
Study design A RCT of ambulatory oxygen.
Feasibility Ambulatory oxygen is readily available. Careful consideration should be given to the use of placebo
Other comments None
Importance High: the research is essential to inform future updates of key recommendations in the guideline.
1
P.10 Short burst oxygen therapy 2
Research question: 3
Does short-burst oxygen therapy improve outcomes in idiopathic pulmonary fibrosis? 4
5
Why this is important: Short-burst oxygen therapy is often used to relieve the symptom of 6
breathlessness on exertion in patients with IPF. However, there is currently no evidence to prove it is 7
effective. The benefit of short-burst oxygen therapy to relieve breathlessness and improve quality of 8
life in patients with IPF should be tested in a randomised control trial. The endpoints must be 9
clinically meaningful and reflect quality of life and functional status. Appropriate endpoints may 10
include, but should not be restricted to; 6 minute walk distance; breathlessness score; a measure of 11
health related quality of life (ideally employing a tool validated in IPF patients, and hospitalisation 12
(all-cause, non-elective and IPF-related). A short-term, cross-over design may be appropriate in this 13
type of intervention. Careful consideration should be given to the use of a placebo arm. Health 14
economic evaluation should be included within the study design. 15
Criteria for selecting high-priority research recommendations: 16
PICO question Does short-burst oxygen therapy improve outcomes in IPF?
Importance to patients or the population
Short-burst oxygen therapy is often used to relieve the symptom of breathlessness on exertion in patients with IPF. However its value is not known
Relevance to NICE guidance
NICE would make recommendations on short burst oxygen therapy
Relevance to the NHS Short-burst oxygen therapy requires reource
National priorities None
Current evidence base There are no suitable studies addressing this.
Equality The research question has no particular equality issues.
Study design A short-term cross-over study of oxygen therapy versus placebo
Feasibility Careful consideration should be given to the use of placebo in this setting
Other comments None
Importance Medium: the research is relevant to the recommendations in the guideline, but the research recommendations are not key to future updates.
17
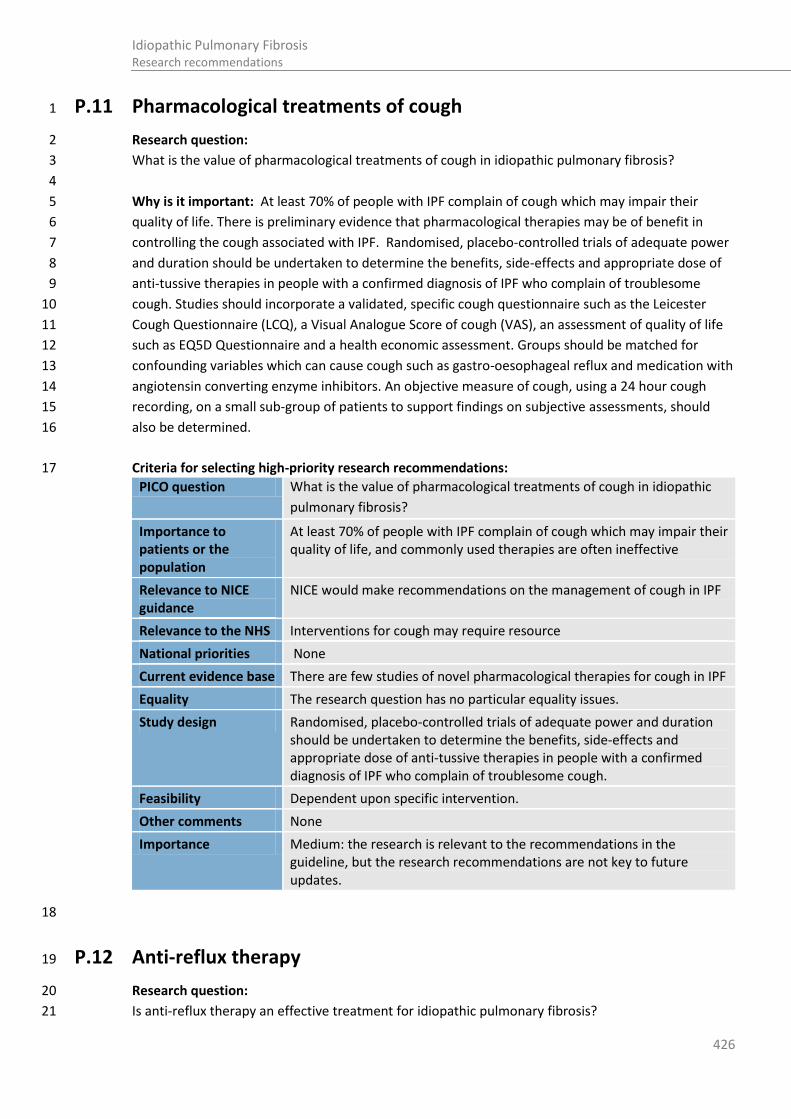
426
Idiopathic Pulmonary Fibrosis Research recommendations
P.11 Pharmacological treatments of cough 1
Research question: 2
What is the value of pharmacological treatments of cough in idiopathic pulmonary fibrosis? 3
4
Why is it important: At least 70% of people with IPF complain of cough which may impair their 5
quality of life. There is preliminary evidence that pharmacological therapies may be of benefit in 6
controlling the cough associated with IPF. Randomised, placebo-controlled trials of adequate power 7
and duration should be undertaken to determine the benefits, side-effects and appropriate dose of 8
anti-tussive therapies in people with a confirmed diagnosis of IPF who complain of troublesome 9
cough. Studies should incorporate a validated, specific cough questionnaire such as the Leicester 10
Cough Questionnaire (LCQ), a Visual Analogue Score of cough (VAS), an assessment of quality of life 11
such as EQ5D Questionnaire and a health economic assessment. Groups should be matched for 12
confounding variables which can cause cough such as gastro-oesophageal reflux and medication with 13
angiotensin converting enzyme inhibitors. An objective measure of cough, using a 24 hour cough 14
recording, on a small sub-group of patients to support findings on subjective assessments, should 15
also be determined. 16
Criteria for selecting high-priority research recommendations: 17
PICO question What is the value of pharmacological treatments of cough in idiopathic
pulmonary fibrosis?
Importance to patients or the population
At least 70% of people with IPF complain of cough which may impair their quality of life, and commonly used therapies are often ineffective
Relevance to NICE guidance
NICE would make recommendations on the management of cough in IPF
Relevance to the NHS Interventions for cough may require resource
National priorities None
Current evidence base There are few studies of novel pharmacological therapies for cough in IPF
Equality The research question has no particular equality issues.
Study design Randomised, placebo-controlled trials of adequate power and duration should be undertaken to determine the benefits, side-effects and appropriate dose of anti-tussive therapies in people with a confirmed diagnosis of IPF who complain of troublesome cough.
Feasibility Dependent upon specific intervention.
Other comments None
Importance Medium: the research is relevant to the recommendations in the guideline, but the research recommendations are not key to future updates.
18
P.12 Anti-reflux therapy 19
Research question: 20
Is anti-reflux therapy an effective treatment for idiopathic pulmonary fibrosis? 21

427
Idiopathic Pulmonary Fibrosis Research recommendations
1
Why this is important: There is evidence from observational studies, and uncontrolled interventional 2
trials, that microaspiration of gastric/oesophageal contents contribute to disease progression, and 3
perhaps even cause idiopathic pulmonary fibrosis. There have been no randomised controlled trials 4
of anti-reflux therapy in idiopathic pulmonary fibrosis but proton-pump inhibitors are often 5
prescribed for symptoms of acid-reflux. A randomised, placebo-controlled trial of adequate power 6
and duration of greater than 12 months should be undertaken to determine the benefits and side 7
effects of anti-reflux therapy, including proton pump inhibition in people with a confirmed diagnosis 8
of idiopathic pulmonary fibrosis. Appropriate end points may include mortality (all-cause and 9
idiopathic pulmonary fibrosis-related); hospitalisation (all-cause, non-elective and idiopathic 10
pulmonary fibrosis-related); lung function (vital capacity and diffusion capacity for carbon 11
monoxide); 6-minute walk distance; breathlessness score; a measure of health-related quality of life 12
(ideally employing a tool validated in idiopathic pulmonary fibrosis patients). Phase III trials should 13
include a health economic evaluation. 14
Criteria for selecting high-priority research recommendations: 15
PICO question Is anti-reflux therapy an effective treatment for IPF?
Importance to patients or the population
There is evidence from observational studies, and uncontrolled interventional trials, that microaspiration of gastric/oesophageal contents contribute to disease progression, and perhaps even cause IPF.
Relevance to NICE guidance
NICE would provide guidance on the value of reflux therapy in IPF
Relevance to the NHS Anti-reflux therapies may require resource
National priorities None
Current evidence base There are no suitable studies to address this
Equality The research question has no particular equality issues.
Study design A randomised, placebo-controlled trial of adequate power and duration should be undertaken to determine the benefits and side-effects of anti-reflux therapy, including proton pump inhibition in people with a confirmed diagnosis of IPF
Feasibility Dependent upon specific anti-reflux strategy
Other comments None
Importance High: the research is essential to inform future updates of key recommendations in the guideline.
16
P.13 Corticosteriod therapy 17
Research question: 18
Is corticosteroid therapy an effective treatment for IPF? 19
20
Why this is important: Historically, high dose oral corticosteroids (≥60mg daily) were used to treat 21
IPF. However, there is recent evidence to suggest that the combination of prednisolone and 22
azathioprine may be harmful and lead to increased mortality. There have been no placebo-controlled 23
trials of corticosteroids as monotherapy in IPF. A randomised, placebo-controlled trial of adequate 24

428
Idiopathic Pulmonary Fibrosis Research recommendations
power and duration should be undertaken to determine the benefits and side-effects of 1
prednisolone to treat people with IPF. Since high doses of corticosteroids may be harmful, careful 2
consideration should be given to the most appropriate dose to employ. Endpoints in phase 3 clinical 3
trials must reflect patient survival, quality of life and functional status. Appropriate endpoints may 4
include mortality (all-cause and IPF-related); hospitalisation (all-cause, non-elective and IPF-related); 5
lung function (vital capacity and diffusion capacity for carbon monoxide); 6 minute walk distance; 6
and a measure of health related quality of life (ideally employing a tool validated in IPF patients). 7
Phase 3 trials should have a duration of greater than 12 months and include a health economic 8
evaluation. 9
Criteria for selecting high-priority research recommendations: 10
PICO question Is corticosteroid therapy an effective treatment for IPF?
Importance to patients or the population
Historically, high dose oral corticosteroids (≥60mg daily) were used to treat IPF. However, there is recent evidence to suggest that the combination of prednisolone and azathioprine may be harmful and lead to increased mortality. There have been no placebo-controlled trials of corticosteroids as monotherapy in IPF
Relevance to NICE guidance
NICE may recommend corticosteroids for IPF if found to be valuable
Relevance to the NHS Corticosteroids usage is likely to require resource
National priorities None
Current evidence base There are no suitable studies to address this
Equality The research question has no particular equality issues.
Study design A randomised, placebo-controlled trial of adequate power and duration should be undertaken to determine the benefits and side-effects of prednisolone to treat people with IPF.
Feasibility The study is feasible
Other comments None
Importance Medium: the research is relevant to the recommendations in the guideline, but the research recommendations are not key to future updates.
11
P.14 Co-trimoxazole 12
13
Research question: 14
Is co-trimoxazole an effective treatment for IPF? 15
16
Why this is important: Co-trimoxazole is an antibiotic that may also have immunomodulatory 17
function. In a randomised placebo-controlled trial, treatment with co-trimoxazole did not affect the 18
primary end-point, and change in forced vital capacity over 12 months. The majority of participants 19
had IPF, but some had other idiopathic fibrotic lung diseases. Over one third of participants were 20
taking azathioprine and/or prednisolone. In the subgroup of participants who completed the study as 21
per protocol, co-trimoxazole therapy was associated with fewer deaths. A randomised, placebo-22
controlled trial should be undertaken to determine if co-trimoxazole therapy reduces mortality in 23
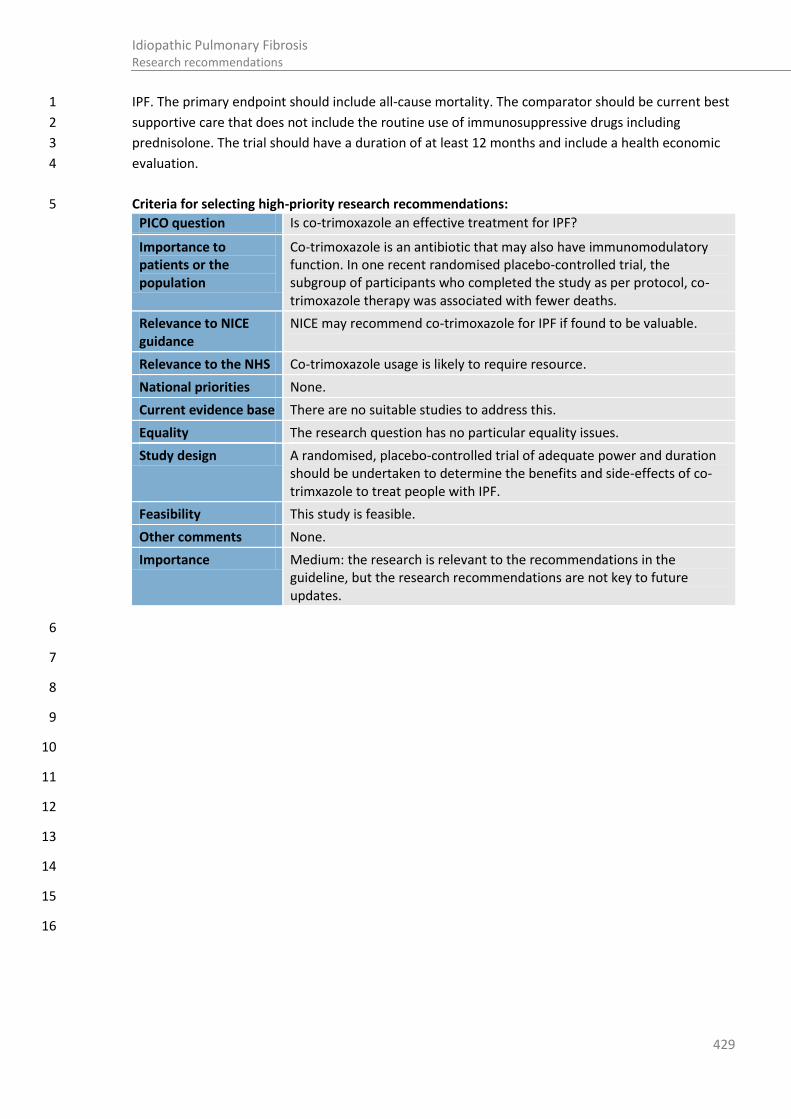
429
Idiopathic Pulmonary Fibrosis Research recommendations
IPF. The primary endpoint should include all-cause mortality. The comparator should be current best 1
supportive care that does not include the routine use of immunosuppressive drugs including 2
prednisolone. The trial should have a duration of at least 12 months and include a health economic 3
evaluation. 4
Criteria for selecting high-priority research recommendations: 5
PICO question Is co-trimoxazole an effective treatment for IPF?
Importance to patients or the population
Co-trimoxazole is an antibiotic that may also have immunomodulatory function. In one recent randomised placebo-controlled trial, the subgroup of participants who completed the study as per protocol, co-trimoxazole therapy was associated with fewer deaths.
Relevance to NICE guidance
NICE may recommend co-trimoxazole for IPF if found to be valuable.
Relevance to the NHS Co-trimoxazole usage is likely to require resource.
National priorities None.
Current evidence base There are no suitable studies to address this.
Equality The research question has no particular equality issues.
Study design A randomised, placebo-controlled trial of adequate power and duration should be undertaken to determine the benefits and side-effects of co-trimxazole to treat people with IPF.
Feasibility This study is feasible.
Other comments None.
Importance Medium: the research is relevant to the recommendations in the guideline, but the research recommendations are not key to future updates.
6
7
8
9
10
11
12
13
14
15
16
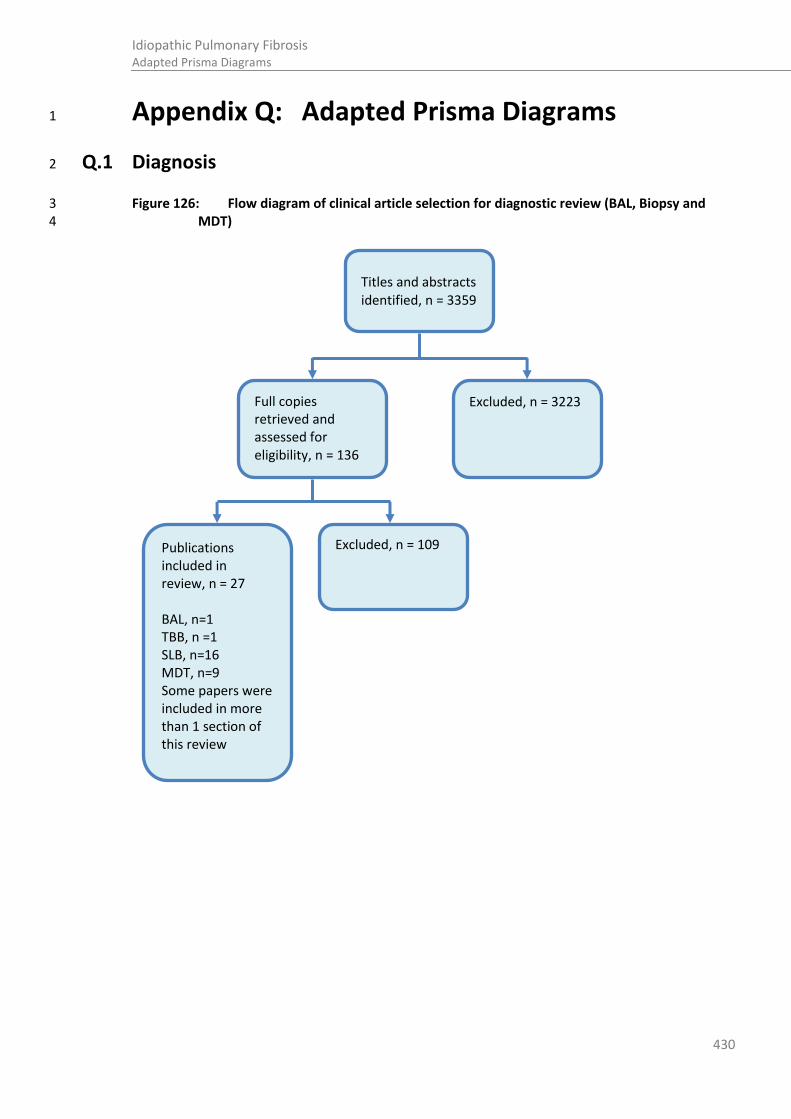
430
Idiopathic Pulmonary Fibrosis Adapted Prisma Diagrams
Titles and abstracts identified, n = 3359
Full copies retrieved and assessed for eligibility, n = 136
Excluded, n = 3223
Publications included in review, n = 27 BAL, n=1 TBB, n =1 SLB, n=16 MDT, n=9 Some papers were included in more than 1 section of this review
Excluded, n = 109
Appendix Q: Adapted Prisma Diagrams 1
Q.1 Diagnosis 2
Figure 126: Flow diagram of clinical article selection for diagnostic review (BAL, Biopsy and 3 MDT) 4

431
Idiopathic Pulmonary Fibrosis Adapted Prisma Diagrams
Q.2 Prognosis 1
Figure 127: Flow diagram of clinical article selection for prognosis review 2
3
4
5
6
7
8
9
10
Titles and abstracts identified, n = 3428
Full copies retrieved and assessed for eligibility, n = 108
Excluded, n =3320
Publications included in review, n=18 Some studies had information on more than 1 prognostic factor
PFTs, n=16
6MWD, n=3
Echocardiography, n=1
CT, n=4
Excluded, n = 90
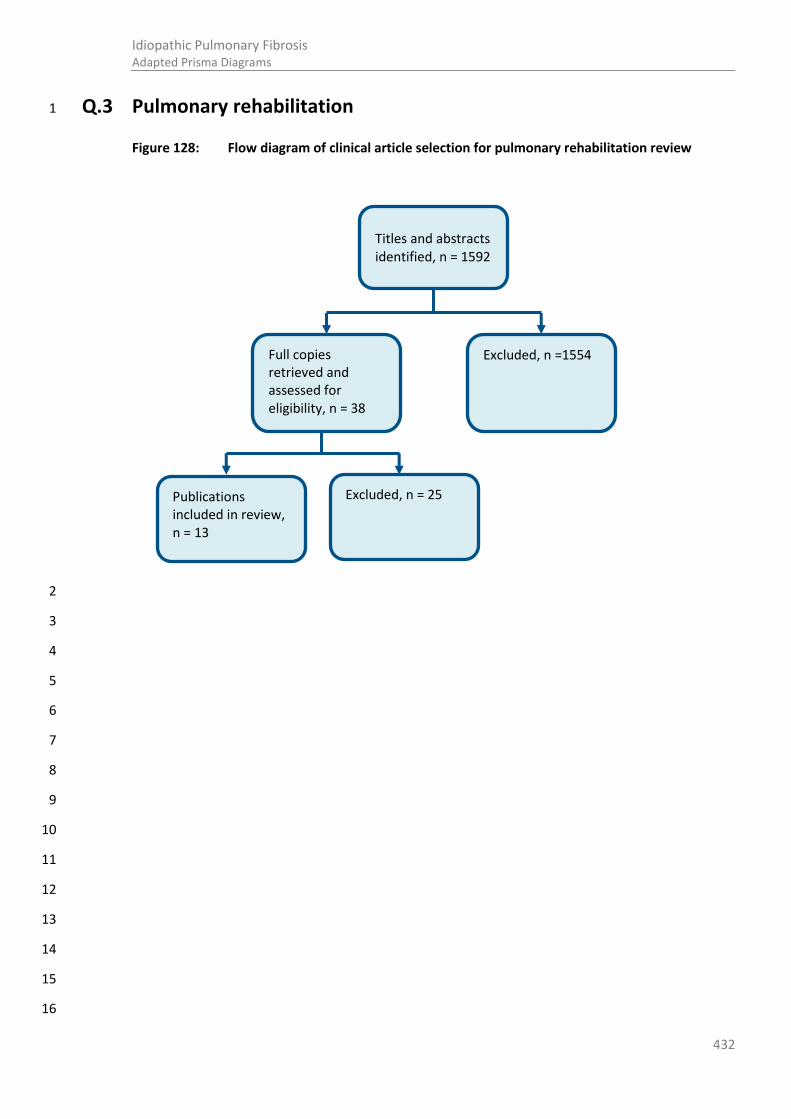
432
Idiopathic Pulmonary Fibrosis Adapted Prisma Diagrams
Q.3 Pulmonary rehabilitation 1
Figure 128: Flow diagram of clinical article selection for pulmonary rehabilitation review
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
Titles and abstracts identified, n = 1592
Full copies retrieved and assessed for eligibility, n = 38
Excluded, n =1554
Publications included in review, n = 13
Excluded, n = 25

433
Idiopathic Pulmonary Fibrosis Adapted Prisma Diagrams
Q.4 Best supportive care 1
Figure 129: Flow diagram of clinical article selection for best supportive care
2
Titles and abstracts identified, n = 2443
Full copies retrieved and assessed for eligibility, n = 87
Excluded, n = 2356
Publications included in review, n = 9
Excluded, n = 78
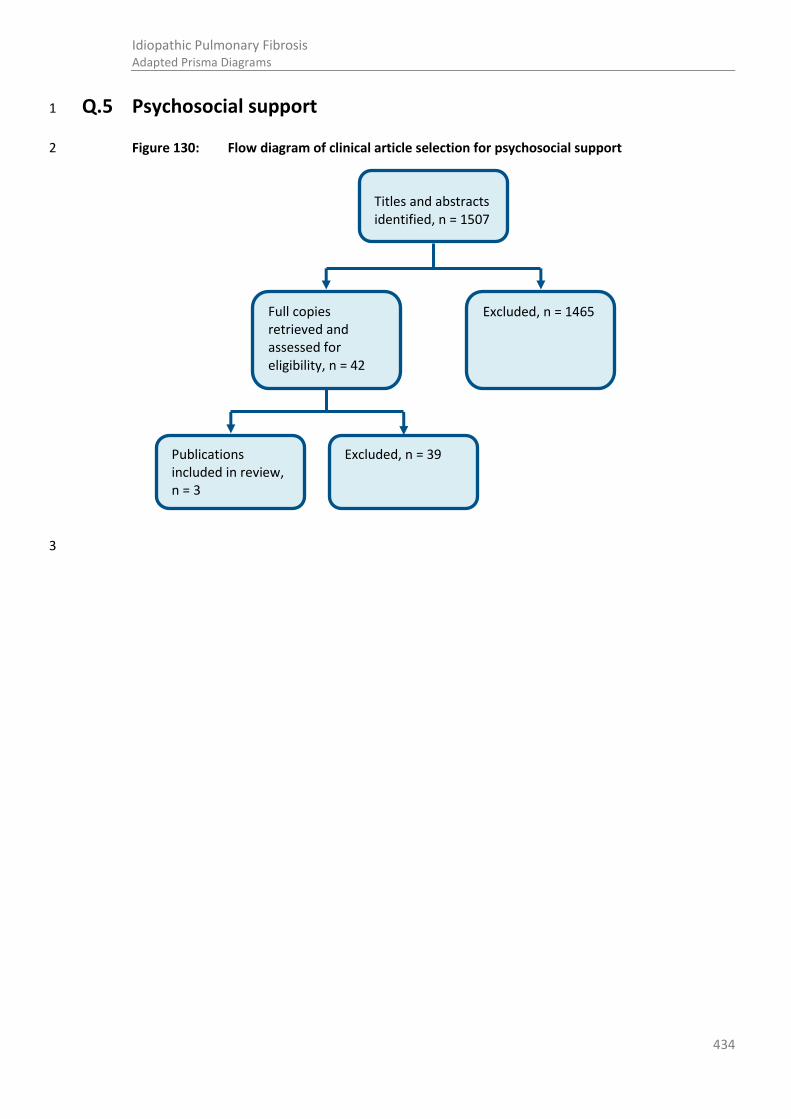
434
Idiopathic Pulmonary Fibrosis Adapted Prisma Diagrams
Q.5 Psychosocial support 1
Figure 130: Flow diagram of clinical article selection for psychosocial support 2
3
Titles and abstracts identified, n = 1507
Full copies retrieved and assessed for eligibility, n = 42
Excluded, n = 1465
Publications included in review, n = 3
Excluded, n = 39

435
Idiopathic Pulmonary Fibrosis Adapted Prisma Diagrams
Q.6 Pharmacological interventions 1
Figure 131: Flow diagram of clinical article selection for pharmacological interventions review 2
3
4
5
6
7
8
9
10
11
12
13
14
Titles and abstracts identified, n = 2058
Full copies retrieved and assessed for eligibility, n = 51
Excluded, n = 2007
Publications included in review, n = 13 TPMT, n=0
Excluded, n = 38

436
Idiopathic Pulmonary Fibrosis Adapted Prisma Diagrams
Q.7 Lung transplantation 1
Figure 132: Flow diagram of clinical article selection for timing of referral for lung 2 transplantation review 3
4
Q.8 Ventilation 5
Figure 133: Flow diagram of clinical article selection for ventilation review 6
7
Titles and abstracts identified, n = 300
Full copies retrieved and assessed for eligibility, n =56
Excluded, n = 244
Publications included in review, n = 6
Excluded, n = 50
Titles and abstracts identified, n = 175
Full copies retrieved and assessed for eligibility, n = 34
Excluded, n = 141
Publications included in review, n = 7
Excluded, n = 27

437
Idiopathic Pulmonary Fibrosis Adapted Prisma Diagrams
Q.9 Review and follow-up 1
Figure 134: Flow diagram of clinical article selection for review and follow-up 2
3
4
5
6
7
8
9
10
11
12
13
14
15
Titles and abstracts identified, n = 2442
Full copies retrieved and assessed for eligibility, n = 84
Excluded, n = 2358
Publications included in review, n = 0
Excluded, n = 84
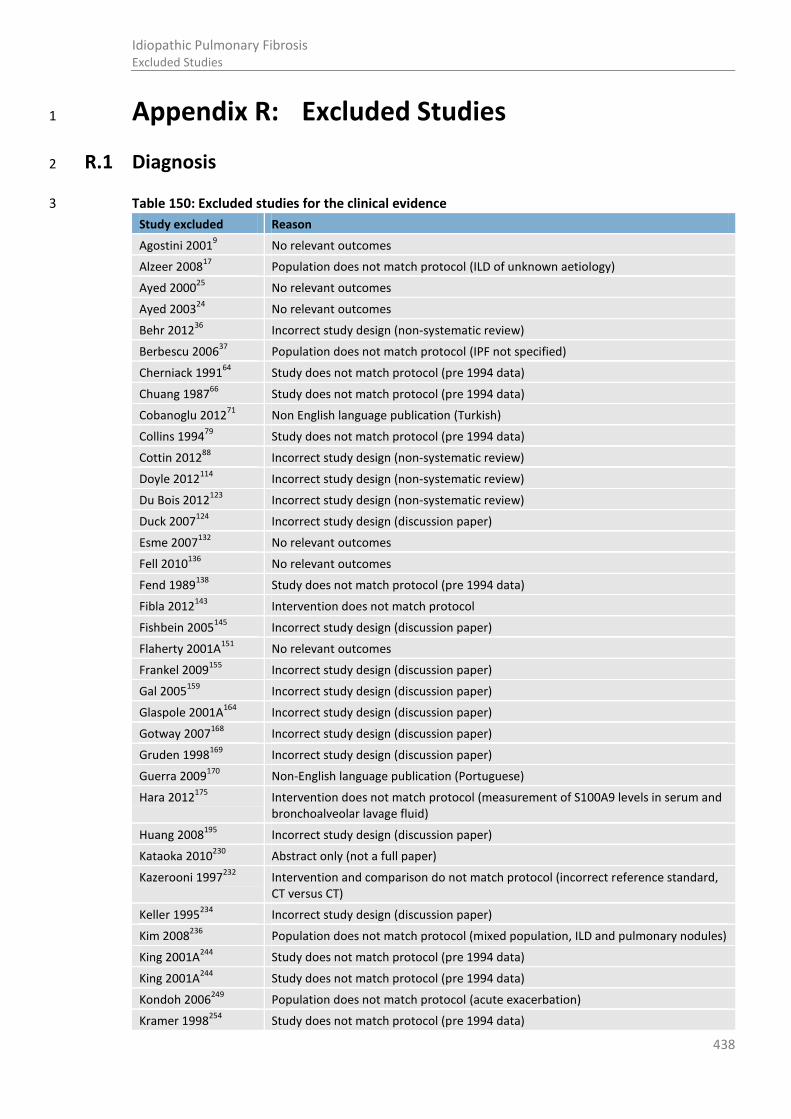
438
Idiopathic Pulmonary Fibrosis Excluded Studies
Appendix R: Excluded Studies 1
R.1 Diagnosis 2
Table 150: Excluded studies for the clinical evidence 3
Study excluded Reason
Agostini 20019 No relevant outcomes
Alzeer 200817
Population does not match protocol (ILD of unknown aetiology)
Ayed 200025
No relevant outcomes
Ayed 200324
No relevant outcomes
Behr 201236
Incorrect study design (non-systematic review)
Berbescu 200637
Population does not match protocol (IPF not specified)
Cherniack 199164
Study does not match protocol (pre 1994 data)
Chuang 198766
Study does not match protocol (pre 1994 data)
Cobanoglu 201271
Non English language publication (Turkish)
Collins 199479
Study does not match protocol (pre 1994 data)
Cottin 201288
Incorrect study design (non-systematic review)
Doyle 2012114
Incorrect study design (non-systematic review)
Du Bois 2012123
Incorrect study design (non-systematic review)
Duck 2007124
Incorrect study design (discussion paper)
Esme 2007132
No relevant outcomes
Fell 2010136
No relevant outcomes
Fend 1989138
Study does not match protocol (pre 1994 data)
Fibla 2012143
Intervention does not match protocol
Fishbein 2005145
Incorrect study design (discussion paper)
Flaherty 2001A151
No relevant outcomes
Frankel 2009155
Incorrect study design (discussion paper)
Gal 2005159
Incorrect study design (discussion paper)
Glaspole 2001A164
Incorrect study design (discussion paper)
Gotway 2007168
Incorrect study design (discussion paper)
Gruden 1998169
Incorrect study design (discussion paper)
Guerra 2009170
Non-English language publication (Portuguese)
Hara 2012175
Intervention does not match protocol (measurement of S100A9 levels in serum and bronchoalveolar lavage fluid)
Huang 2008195
Incorrect study design (discussion paper)
Kataoka 2010230
Abstract only (not a full paper)
Kazerooni 1997232
Intervention and comparison do not match protocol (incorrect reference standard, CT versus CT)
Keller 1995234
Incorrect study design (discussion paper)
Kim 2008236
Population does not match protocol (mixed population, ILD and pulmonary nodules)
King 2001A244
Study does not match protocol (pre 1994 data)
King 2001A244
Study does not match protocol (pre 1994 data)
Kondoh 2006249
Population does not match protocol (acute exacerbation)
Kramer 1998254
Study does not match protocol (pre 1994 data)

439
Idiopathic Pulmonary Fibrosis Excluded Studies
Study excluded Reason
Kreider 2007255
No relevant outcomes
Kulshres 2012258
No relevant outcomes
Lee 2009274
Abstract only (not a full paper)
Lee 2010273
Population does not match protocol (cryptogenic organizing pneumonia)
Lee 2012271
Intervention does not match protocol (assessing the levels of pepsin in BAL fluid in IPF patients with acute exacerbation compared to stable disease)
Leslie 2006275
Incorrect study design (discussion paper)
Leslie 2012276
Incorrect study design (non systematic review)
Lynch 2000291
Incorrect study design (discussion paper)
Magpantay 2010294
Population does not match protocol (pulmonary tuberculosis)
Mahajan 2002295
Incorrect study design (discussion paper)
Maher 2008A296
Incorrect study design (discussion paper)
Margaritopoulos 2012
303
Incorrect study design (non systematic review)
Matsuo 1996308
Study does not match protocol (pre 1994 data)
Mazuranic 1996309
No relevant outcomes
Melo 2009312
Non English language publication (Portuguese)
Meyer 2004315
Incorrect study design (discussion paper)
Meyer 2012316
Intervention does not match protocol (clinical practice guideline outlining technique for BAL)
Miller 2000319
Intervention and comparison do not match protocol (comparison of two biopsy techniques)
Milman 1994320
Study does not match protocol (pre 1994 data)
Milman 1995322
Population does not match protocol (diffuse pulmonary lesions)
Misumi 2006323
Incorrect study design (discussion paper)
Mouroux 1997332
Study does not match protocol (pre 1994 data)
Nicholson 2002353
Incorrect study design (discussion paper)
Noth 2007360
Incorrect study design (discussion paper)
Orens 1995369
Intervention does not match protocol (Incorrect reference standard, HRCT)
Park 2007A378
No relevant outcomes
Poletti 2004382
Incorrect study design (Discussion paper)
Polychronopoulos 2009
385
Abstract only (not a full paper)
Popp 1992386
Study does not match protocol (pre 1994 data)
Popper 2001387
Incorrect study design (discussion paper)
Quadrelli 2010390
No relevant outcomes
Quigley 2006391
Incorrect study design (discussion paper)
Qureshi 2002394
No relevant outcomes
Qureshira 2003393
No relevant outcomes
Raghu 2004A399
Incorrect study design (discussion paper)
Raghu 2004B396
Incorrect study design (discussion paper)
Ryu 2007A417
Incorrect study design (discussion paper)
Sawy 2004422
Population does not match protocol (all patients undergoing a bronchoscopy)
Schmidt 2009A425
Incorrect study design (discussion paper)
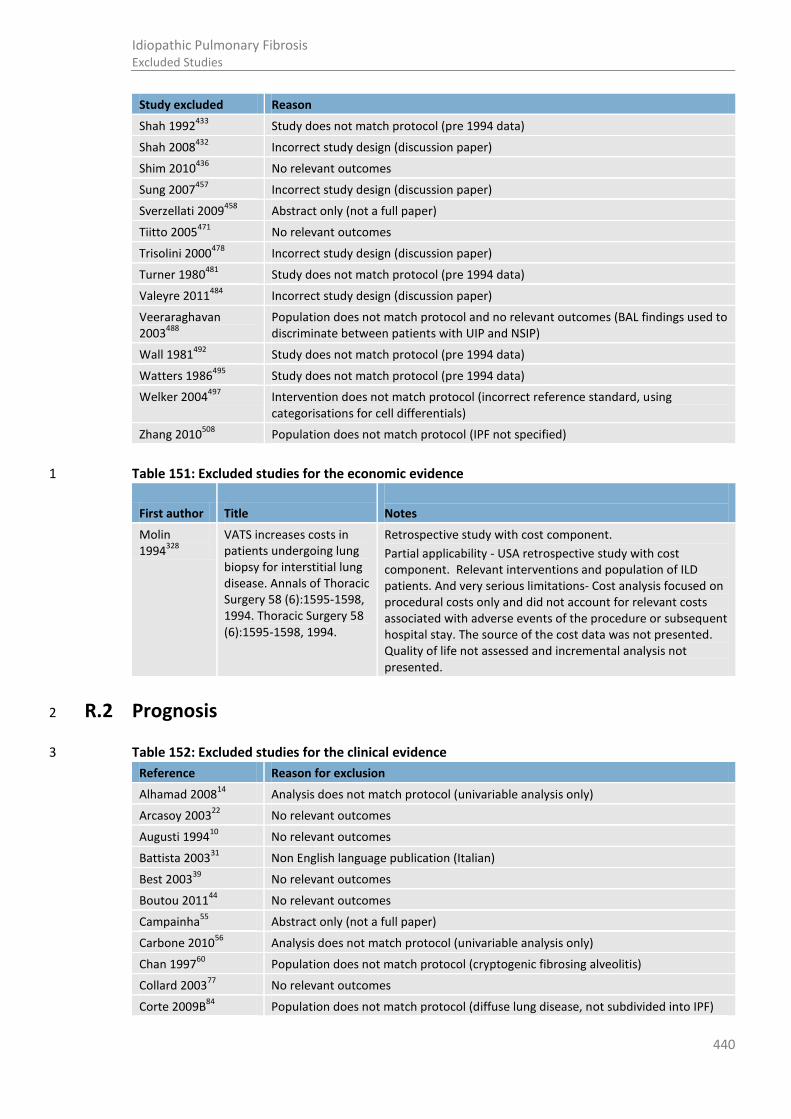
440
Idiopathic Pulmonary Fibrosis Excluded Studies
Study excluded Reason
Shah 1992433
Study does not match protocol (pre 1994 data)
Shah 2008432
Incorrect study design (discussion paper)
Shim 2010436
No relevant outcomes
Sung 2007457
Incorrect study design (discussion paper)
Sverzellati 2009458
Abstract only (not a full paper)
Tiitto 2005471
No relevant outcomes
Trisolini 2000478
Incorrect study design (discussion paper)
Turner 1980481
Study does not match protocol (pre 1994 data)
Valeyre 2011484
Incorrect study design (discussion paper)
Veeraraghavan 2003
488
Population does not match protocol and no relevant outcomes (BAL findings used to discriminate between patients with UIP and NSIP)
Wall 1981492
Study does not match protocol (pre 1994 data)
Watters 1986495
Study does not match protocol (pre 1994 data)
Welker 2004497
Intervention does not match protocol (incorrect reference standard, using categorisations for cell differentials)
Zhang 2010508
Population does not match protocol (IPF not specified)
Table 151: Excluded studies for the economic evidence 1
First author Title
Notes
Molin 1994
328
VATS increases costs in patients undergoing lung biopsy for interstitial lung disease. Annals of Thoracic Surgery 58 (6):1595-1598, 1994. Thoracic Surgery 58 (6):1595-1598, 1994.
Retrospective study with cost component.
Partial applicability - USA retrospective study with cost component. Relevant interventions and population of ILD patients. And very serious limitations- Cost analysis focused on procedural costs only and did not account for relevant costs associated with adverse events of the procedure or subsequent hospital stay. The source of the cost data was not presented. Quality of life not assessed and incremental analysis not presented.
R.2 Prognosis 2
Table 152: Excluded studies for the clinical evidence 3
Reference Reason for exclusion
Alhamad 200814
Analysis does not match protocol (univariable analysis only)
Arcasoy 200322
No relevant outcomes
Augusti 199410
No relevant outcomes
Battista 200331
Non English language publication (Italian)
Best 200339
No relevant outcomes
Boutou 201144
No relevant outcomes
Campainha55
Abstract only (not a full paper)
Carbone 201056
Analysis does not match protocol (univariable analysis only)
Chan 199760
Population does not match protocol (cryptogenic fibrosing alveolitis)
Collard 200377
No relevant outcomes
Corte 2009B84
Population does not match protocol (diffuse lung disease, not subdivided into IPF)

441
Idiopathic Pulmonary Fibrosis Excluded Studies
Reference Reason for exclusion
Corte 2010A83
Population does not match protocol (only 16/90 had IPF; analyses not presented for IPF separately)
Corte 201285
Population does not match protocol (includes IIP considered as IPF, NSIP and interdeterminate IIP; analyses not presented for IPF separately)
Dancer 201296
Incorrect study design (non systematic review)
Devaraj 2009 109
Abstract (not a full paper)
Doherty 1997111
Population does not match protocol (cryptogenic fibrosing alveolitis)
DuBois 2011 122
Analysis does not match protocol (univariable analysis only)
Du Bois 2012123
Incorrect study design (non systematic review)
Edey 2011128
Population does not match protocol (fibrotic IIP; analyses not presented for IPF separately)
Erbes 1997131
Study does not match protocol (pre 1994)
Fakharian 2010 133
Abstract only (not a full paper)
Fasano 1999 134
Non English language publication (Italian)
Fell 2010136
No relevant outcomes
Fernandezperez 2010 139
No relevant outcomes
Flaherty 2002150
Analysis does not match protocol (univariable analysis only)
Flaherty 2003147
Population does not match protocol (fibrotic IIP -UIP and NSIP not distinguished)
Flaherty 2003A149
No relevant outcomes
Flaherty 2006153
No relevant outcomes
Fujimoto 2012 156
Population does not match protocol (all IPF patients with acute exacerbation)
Gay 1998 161
Analysis does not match protocol (univariable analysis only)
Harari 1997 176
Study does not match protocol (pre 1994)
Holland 2008A185
Intervention does not match protocol (RCT looking at the effects of exercise training)
Holland 2010184
Abstract (not a full paper)
Hubbard 1998196
Population does not match protocol (cryptogenic fibrosing alveolitis)
Huie 2011 197
Abstract only (not a full paper)
Hwang 2011199
Population does not match protocol (IPF not specified)
Ichikado 2002 200
Population does not match protocol (acute interstitial pneumonia)
Iwasawa 2008 205
Non English language publication (Japanese)
Iwasawa 2009 206
Intervention does not match protocol (used the Gaussian histogram normalised correlation system to determine the extent of disease on CT images)
Jastrzebski 2005A215
Population and prognostic factor does not match protocol (all lung transplant referrals and left ventricular ejection fraction)
Jegal 2005218
Population does not match protocol (fibrotic IIP, UIP and NSIP not distinguished)
Jeong 2005 220
Analysis does not match protocol (univariable analysis only)
Kaminsky 2007228
No extractable data (No OR, RR or HR)
Kim 2010B237
Abstract only (not a full paper)
King 2001243
No relevant outcomes
Kishaba 2012245
No relevant outcomes
Kurashima 2010 260
Abstract only (not a full paper)
Kawut 2005231
Population does not match protocol (indirect population, 55% UIP only)
Lama 2003262
No relevant outcomes

442
Idiopathic Pulmonary Fibrosis Excluded Studies
Reference Reason for exclusion
Laz 2011 269
Abstract only (not a full paper)
Lederer 2006270
No relevant outcomes
Lettieri 2006 277
Intervention does not match protocol (right heart catherterisation to measure PAH)
Lettieri 2006A278
No relevant outcomes
Ley 2012282
Intervention does not match protocol (development and validation of a staging system, data not presented for FVC in patient's with IPF alone)
Manali 2010299
No relevant outcomes
Miller 2012318
Incorrect study design (non-systematic review)
Moloney 2003331
Intervention does not match protocol (reliability of the SWT measuring functional capacity in patients with IPF)
Nadrous 2005 335
No relevant outcomes
Nadrous2005A 334
No relevant outcomes
Nagao 2002 337
Study does not match protocol (pre 1994)
Nathan 2007341
No relevant outcomes
Nathan 2008A 343
No relevant outcomes
Nathan 2011A 342
No relevant outcomes
Latsi 2003267
No relevant outcomes and population does not match protocol (UIP versus NSIP)
Peelen 2010380
Population does not match protocol (fibrotic IIP, UIP and NSIP not distinguished)
Riha 2002411
No relevant outcomes and population does not match protocol (UIP versus NSIP)
Ryerson 2011414
No relevant outcomes
Screaton 2005 430
Population does not match protocol (not IPF)
Shabbier 2012 Intervention does not match protocol (sensitivity and specificty of HRCT scans, not the prognostic implications of HRCT features and patterns)
Shin 2008 437
Population does not match protocol (not IPF)
Sumikawa 2006 455
No relevant outcomes
Schwartz1994A428
Schwartz1994B429
No relevant outcomes
Swigris 2010A463
No relevant outcomes
Swigris 2009 462
No relevant outcomes
Valeyre 2010485
Intervention does not match protocol (responsiveness to pharmacological treatment)
Xaubet 1998 500
No relevant outcomes
Yang 2009 502
Non English language publication (Chinese)
Zisman 2007 513
No relevant outcomes
Zisman 2007A 514
Intervention does not match protocol (prediction of pulmonary hypertension)
Zompatori 2003515
No relevant outcomes
Excluded studies for the economic evidence: 1
No health economic literature assessing an intervention for a prognostic purpose in an IPF population 2 was identified. No studies were selectively excluded. 3
4

443
Idiopathic Pulmonary Fibrosis Excluded Studies
R.3 Pulmonary rehabilitation 1
Table 153: Excluded studies for the clinical evidence 2 Reference Reason for exclusion
Bausewein2008C34
Intervention and population do not match protocol (Cochrane review, no studies included had IPF/ILD people or used PR as an intervention)
Bevelaqua201140
Population do not match protocol (ILD not specified)
Budweiser2006 50
Population does not match protocol (restrictive lung disease doesn’t analysis results for ILD/IPF separately)
Butcher200151
Population does not match protocol (primarily COPD, 9/49 pulmonary fibrosis and were not analysed separately)
Cockcroft198173
Population does not match protocol (coal workers with pneumoconiosis and chronic obstructive airway disease)
Cockcroft198272
Population does not match protocol (people had coal workers pneumoconiosis and COPD)
Connor 200781
Population does not match protocol (restrictive lung disease which includes ILD and thoracic skeletal abnormalities, ILD not analysed separately)
Dierich2010110
Population and outcomes do not match protocol (mixed ILD population and analyses of VC and 6MWT is not presented for IPF separately)
Ferreira 2000142
Population does not match protocol (COPD vs. non COPD, does not analyse results for IPF/ILD separately)
Fowler2011154
Population and outcomes do not match protocol (ILD proportion of included population not specified and results for shuttle walk test not presented)
Ho2010182
Population does not match protocol (ILD not specified)
Holden 1990183
Population does not match protocol (not IPF)
Jastrzebski2007A216
Intervention does not match protocol (inspiratory muscle training versus no inspiratory muscle training in isolation)
Jastrzebski2008217
Non-English language publication (Polish)
Kagaya 2009227
Population does not match protocol (cannot determine proportion of people with IPF/ILD)
Kozu 2011B252
Intervention does not match protocol (effectiveness of PR programmes according to the severity of dyspnoea)
Lindell 2010285
Intervention does not match protocol (psychosocial support no PR is included; this paper has been included in the psychosocial support section of the guideline).
Marciniak2010302
Intervention and population does not match protocol (weight management programme for people with obesity people and no further information provided on population)
Mittal 2011324
Population does not match protocol (did not analyse results for people with IPF/ILD people separately)
Ochmann2012364
Incorrect study design (non systematic review)
Rozanski2012413
Population and outcomes do not match protocol (mixed ILD population post lung tranplantation and analyses of 6MWT is not presented for IPF separately)
Salhi 2010420
Population does not match protocol (restrictive lung disease, 6/31 people had pulmonary fibrosis and results have not been analysed separately for IPF/ILD)

444
Idiopathic Pulmonary Fibrosis Excluded Studies
Reference Reason for exclusion
Verrill2008490
Population does not match protocol (does not specify if people with IPF/ILD are included)
Verrill2008A491
Intervention does not match protocol (validating a prediction equation)
Warrington 2010494
Intervention does not match protocol (PR with and without oxygen)
Excluded studies for the economic evidence: 1
No relevant economic evaluations that assessed pulmonary rehabilitation in an IPF population were 2 identified. No studies were selectively excluded. 3
4
R.4 Best supportive care 5
Table 154: Excluded studies for the clinical evidence 6
Reference Reason for exclusion
Agarwal 20098 Not relevant to clinical question (review of ILD and sleep)
Alhamad 200913
Population does not match protocol (sarcoidosis)
Allen 200515
Incorrect study design (not an intervention study)
Annane 200718
Population and intervention do not match protocol and intervention (no IPF/ILD and intervention is mechanical ventilation)
Aversa 199323
Population does not match protocol (only 6/73 pulmonary fibrosis; majority COPD)
Bailey 201027
Incorrect study design (not an intervention study)
Bajwah 201229
Incorrect study design (not an intervention study)
Barlo 200930
Non English language publication (Dutch)
Baughman 200532
Population does not match protocol (sarcoidosis)
Baughman 2006A33
Population and intervention does not match protocol (infliximab therapy in sarcoidosis)
Bevelaqua 201140
Population does not match protocol (end stage lung disease, ILD/IPF not specified)
Braghiroli 199345
No relevant outcomes. (This study contains the protocol of a study which is included in Crockett 2001
22 & Zielinski 2000
83)
Brown 200649
Incorrect study design (not an intervention study)
Cerri 201258
Incorrect study design (not an intervention study)
Chailleux 199659
Does not match review question (not relevant to patient review or best supportive care)
Chang 199961
Does not match review question (description of HRQoL)
Choi 200865
Incorrect study design (dissertation)
Cima 201067
Population does not match protocol (not IPF)
Clark 200169
Does not match review question (descriptive study of prevalence of cough in IPF)
Coelho 201074
Does not match review question (QOL in IPF and no intervention)
Corte 200982
Does not match review question (mortality prediction by nocturnal desaturation)
Crockett 199191
Population does not match protocol (majority COPD)
Currow 200894
Population does not match protocol and does not match review question (majority COPD)
Dayton 199399
Does not match review question and study does not match protocol (pre-1994)

445
Idiopathic Pulmonary Fibrosis Excluded Studies
Reference Reason for exclusion
Dayton 199399
Does not match review question (not relevant to patient review or best supportive care)
Douglas 2000113
Incorrect study design and does not match review question (observational study looking at prognostic factors)
Dubois 1999120
Population does not match protocol (sarcoidosis)
Duck 2008125
Incorrect study design (non-systematics review)
Duck 2009126
Incorrect study design (non-systematics review)
Eaton 2001127
Population does not match protocol (majority COPD)
Fasciolo 1994135
Population does not match protocol (only 17/104 pulmonary fibrosis; majority COPD/ cancer)
Fakharian 2010133
Does not match review question (not best supportive care)
Harris-Eze 1994177
No relevant outcomes
Harris-Eze 1995178
No relevant outcomes
Hira 1997180
Incorrect study design (not an intervention study)
Hirst 2001181
Does not match review question (insomnia)
Ho 2010182
Population does not match protocol (restrictive lung disease, ILD/IPF not specified)
Hook 2012190
Does not match review question (not relevant to patient review or best supportive care)
Irwin 1998203
Does not match review question (management of cough; not specific to IPF)
Janssen 2010211
Incorrect study design and population does not match protocol (case series and majority COPD)
Janssens 1996212
Comparison does not match protocol (comparative evaluation with COPD patients)
Jastrzebski 2005214
Does not match review question (QOL in patientss awaiting lung transplantation)
Johnson 1989222
Does not match review question and study does not match protocol (pharmacological study, pre-1994)
Judson 2006224
Population does not match protocol (sarcoidosis)
Kagan 1976226
Population does not match protocol (not IPF/ILD)
Kastelik 2005229
Does not match review question (chronic cough; not specific to IPF)
Krishnan 2008256
Does not match review question (sleep quality and HRQoL description only)
Kumar 2010259
Incorrect study design and population does not match protocol (not an intervention study and not IPF)
Kyeong 1999261
Non English language publication (Korean)
Lamas 2011264
Does not match review question (delay in initial assessment)
Lancaster 2009265
Incorrect study design (descriptive study only, no intervention)
Lindell 2007283
Incorrect study design (no intervention)
Louly 2009287
Incorrect study design (case study)
Lower 2008288
Population does not match protocol (sarcoidosis)
Mahler 1989298
Population does not match protocol (ILD population only)
Martinez 2000305
Does not match review question (evaluation of SF36 in IPF)
Martinez 2005304
Does not match review question (clinical course of IPF)
Masjedi 2010306
Incorrect study design (no intervention)
Mermigkis 2009314
Incorrect study design (observational study, no intervention)
Milman 1994A321
Population does not match protocol (sarcoidosis)
Papiris 2005377
Incorrect study design (descriptive study only, no intervention)
Polosa 2002384
Does not match review question (X

446
Idiopathic Pulmonary Fibrosis Excluded Studies
Reference Reason for exclusion
Polonski 1994383
No relevant outcomes
Rank 2007406
Incorrect study design (no intervention)
Ryerson 2011414
Does not match review question (prognostic study of cough)
Ryerson 2012416
Incorrect study design (no intervention)
Ryerson 2012A415
Systematic review- all relevant papers have been included in the guideline
Saydain 2002423
Incorrect study design (descriptive study only, no intervention)
Sharifabad 2010435
Population does not match protocol (chronic lung disease, IPF not specified)
Shulgina 2011440
Does not match review question (not relevant to patient review or best supportive care)
Simon2012443
Population does not match protocol (not IPF)
Sundar 2010456
Does not match review question (prevalence of cough in conditions other than IPF)
Swigris 2005A466
Does not match review question (background to IPF QoL tools)
Swigris 2005B461
Does not match review question (not relevant to patient review or best supportive care)
Swigris 2011465
Does not match review question (not relevant to patient review or best supportive care)
Troy 2012479
Does not match review question (sleep disordered breathing in IPF)
Wee 2011496
Population does not match protocol (no ILD /IPF populations included in any of the studies included in this review)
Xaubet 2001499
Does not match review question (delay in initial assessment)
Table 155: Excluded studies for the economic evidence 1
Reference Reason for exclusion
M. Neri, L. Fedi, A. Spanevello, G. Mazzucchelli, M. Grandi, M. Ambrosetti, S. Conti, and G. B. Migliori. Savings obtained using an oxygen economizer device: a cost-minimization analysis. Monaldi Archives for Chest Disease 54 (4):311-314, 1999.
This cost minimisation analysis evaluates the use of oxygen minimiser device in the administration of liquid oxygen. This study was selectively excluded on not assessing a relevant population (Only 4 of 29 patients in the sample had restrictive lung disease).
2
R.5 Psychosocial support 3
Table 156: Studies excluded from the clinical review 4
Reference Reason for exclusion
Anon 20052 Does not match review question (patient information on a clinical trial)
Bajwah 201128
Poster presentation only (not a full paper)
Blake 199041
Population does not match protocol (chronic lung disease, IPF not specified)
Carroll 199957
Incorrect study design (no intervention)
Coffman 200275
Does not match review question (review of psychiatric issues and pulmonary disease, no intervention)
Cox 200490
Population does not match protocol (no ILD/ IPF patients)
Daniels 200697
Intervention does not match protocol (review of management of patients with IPF)
Drent 1998115
Population does not match protocol (sarcoidosis)
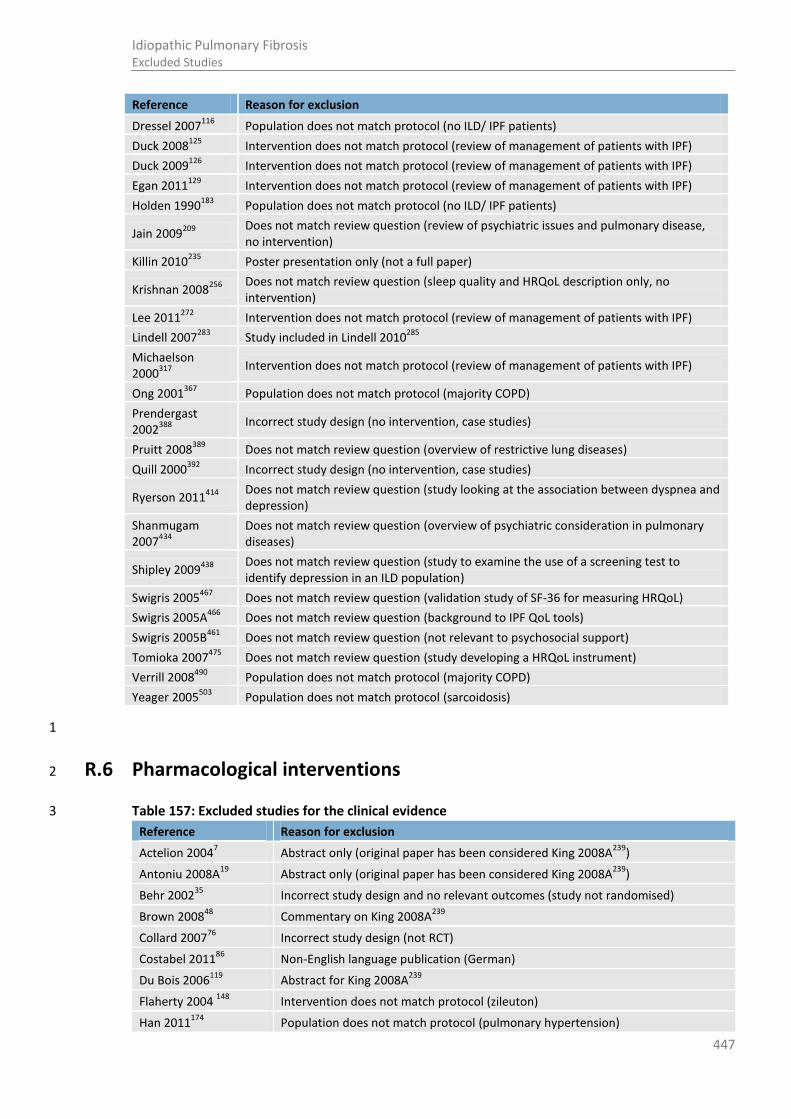
447
Idiopathic Pulmonary Fibrosis Excluded Studies
Reference Reason for exclusion
Dressel 2007116
Population does not match protocol (no ILD/ IPF patients)
Duck 2008125
Intervention does not match protocol (review of management of patients with IPF)
Duck 2009126
Intervention does not match protocol (review of management of patients with IPF)
Egan 2011129
Intervention does not match protocol (review of management of patients with IPF)
Holden 1990183
Population does not match protocol (no ILD/ IPF patients)
Jain 2009209
Does not match review question (review of psychiatric issues and pulmonary disease, no intervention)
Killin 2010235
Poster presentation only (not a full paper)
Krishnan 2008256
Does not match review question (sleep quality and HRQoL description only, no intervention)
Lee 2011272
Intervention does not match protocol (review of management of patients with IPF)
Lindell 2007283
Study included in Lindell 2010285
Michaelson 2000
317
Intervention does not match protocol (review of management of patients with IPF)
Ong 2001367
Population does not match protocol (majority COPD)
Prendergast 2002
388
Incorrect study design (no intervention, case studies)
Pruitt 2008389
Does not match review question (overview of restrictive lung diseases)
Quill 2000392
Incorrect study design (no intervention, case studies)
Ryerson 2011414
Does not match review question (study looking at the association between dyspnea and depression)
Shanmugam 2007
434
Does not match review question (overview of psychiatric consideration in pulmonary diseases)
Shipley 2009438
Does not match review question (study to examine the use of a screening test to identify depression in an ILD population)
Swigris 2005467
Does not match review question (validation study of SF-36 for measuring HRQoL)
Swigris 2005A466
Does not match review question (background to IPF QoL tools)
Swigris 2005B461
Does not match review question (not relevant to psychosocial support)
Tomioka 2007475
Does not match review question (study developing a HRQoL instrument)
Verrill 2008490
Population does not match protocol (majority COPD)
Yeager 2005503
Population does not match protocol (sarcoidosis)
1
R.6 Pharmacological interventions 2
Table 157: Excluded studies for the clinical evidence 3
Reference Reason for exclusion
Actelion 20047 Abstract only (original paper has been considered King 2008A
239)
Antoniu 2008A19
Abstract only (original paper has been considered King 2008A239
)
Behr 200235
Incorrect study design and no relevant outcomes (study not randomised)
Brown 200848
Commentary on King 2008A239
Collard 200776
Incorrect study design (not RCT)
Costabel 201186
Non-English language publication (German)
Du Bois 2006119
Abstract for King 2008A239
Flaherty 2004 148
Intervention does not match protocol (zileuton)
Han 2011174
Population does not match protocol (pulmonary hypertension)
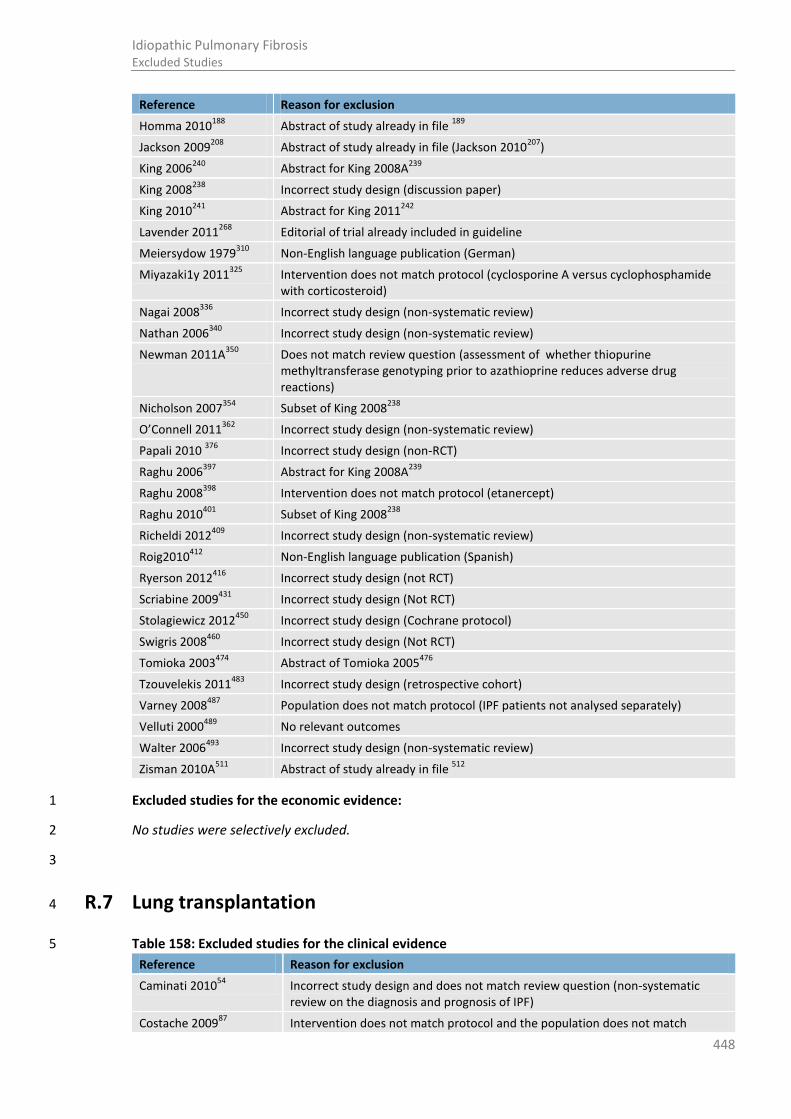
448
Idiopathic Pulmonary Fibrosis Excluded Studies
Reference Reason for exclusion
Homma 2010188
Abstract of study already in file 189
Jackson 2009208
Abstract of study already in file (Jackson 2010207
)
King 2006240
Abstract for King 2008A239
King 2008238
Incorrect study design (discussion paper)
King 2010241
Abstract for King 2011242
Lavender 2011268
Editorial of trial already included in guideline
Meiersydow 1979310
Non-English language publication (German)
Miyazaki1y 2011325
Intervention does not match protocol (cyclosporine A versus cyclophosphamide with corticosteroid)
Nagai 2008336
Incorrect study design (non-systematic review)
Nathan 2006340
Incorrect study design (non-systematic review)
Newman 2011A350
Does not match review question (assessment of whether thiopurine methyltransferase genotyping prior to azathioprine reduces adverse drug reactions)
Nicholson 2007354
Subset of King 2008238
O’Connell 2011362
Incorrect study design (non-systematic review)
Papali 2010 376
Incorrect study design (non-RCT)
Raghu 2006397
Abstract for King 2008A239
Raghu 2008398
Intervention does not match protocol (etanercept)
Raghu 2010401
Subset of King 2008238
Richeldi 2012409
Incorrect study design (non-systematic review)
Roig2010412
Non-English language publication (Spanish)
Ryerson 2012416
Incorrect study design (not RCT)
Scriabine 2009431
Incorrect study design (Not RCT)
Stolagiewicz 2012450
Incorrect study design (Cochrane protocol)
Swigris 2008460
Incorrect study design (Not RCT)
Tomioka 2003474
Abstract of Tomioka 2005476
Tzouvelekis 2011483
Incorrect study design (retrospective cohort)
Varney 2008487
Population does not match protocol (IPF patients not analysed separately)
Velluti 2000489
No relevant outcomes
Walter 2006493
Incorrect study design (non-systematic review)
Zisman 2010A511
Abstract of study already in file 512
Excluded studies for the economic evidence: 1
No studies were selectively excluded. 2
3
R.7 Lung transplantation 4
Table 158: Excluded studies for the clinical evidence 5
Reference Reason for exclusion
Caminati 201054
Incorrect study design and does not match review question (non-systematic review on the diagnosis and prognosis of IPF)
Costache 200987
Intervention does not match protocol and the population does not match

449
Idiopathic Pulmonary Fibrosis Excluded Studies
Reference Reason for exclusion
protocol (study does not look at referral times/severity level of disease and results for IPF not separated)
Daniels 200697
Incorrect study design (non-systematic review)
Davis 199498
Intervention does not match protocol (investigates the results after lung transplantation)
Demeester 2001100
Intervention does not match protocol and population does not match protocol (life expectancy and lung transplant effect and results for IPF not separated)
Deoliveira 2012a102
Intervention does not match protocol (effectiveness of type of lung transplant, single versus bilateral)
Deoliveira 2012b101
Intervention and population do not match the protocol (ILD population with no stratification for IPF, outcomes of patients who underwent single lung and bilateral LTX)
Egan 1991130
Intervention does not match protocol (analyses referrals to a single centre for lung transplantation)
Feltrim 2008137
Intervention does not match protocol (QoL of patients on lung transplantation waiting list)
Fioret 2011144
Incorrect study design (non-systematic review on the management of IPF)
Genao 2012162
Intervention does not match protocol (trajectory of function after lung transplantation in old and young recipients in the post lung allocation score era and abstract only)
George 2011163
Intervention does not match protocol (no information on stage or timing of referral)
Gottlieb 2012167
Intervention does not match protocol (outcomes of ventilated transplant patients and the results aren’t separated out for IPF patients)
Gomez 2003165
Population does not match protocol (does not specify IPF)
Hayden 1993179
Population does not match protocol (does not analyse IPF patients separately)
Jastrzebski 2005214
Intervention does not match protocol (QoL of patients on a lung transplantation waiting list)
Jastrzebski 2005a215
Population does not match protocol (does not analyse IPF patients separately)
Keating 2009233
Intervention does not match protocol (no mention of timing of referral)
King 2001243
Intervention does not match protocol (prognostic study looking at survival in IPF patients)
Klooster 2011246
Abstract only (not a full paper)
Kozower 2008251
Intervention does not match protocol (survival of IPF patients is not captured pre and post LAS implementation)
Lalaatsp 19981 Guideline: all relevant papers have already been included/considered
Lamas 2011264
Intervention does not match protocol (referral time to sub-speciality care not specifically LTX referral)
Lamas 2011a263
Abstract only (full paper assessed LAMAS 2011264
)
Langer 2012266
Intervention does not match protocol (investigates the level of activity in patients who are candidates for lung transplantation)
Lederer 2006270
Intervention does not match protocol (does not look at referral times/severity level of disease)
Levvey 2009281
Abstract only (not a full paper)
Ley 2011264
Intervention does not match protocol (development of a staging system)
Lingaraju 2006286
Intervention does not match protocol (survival of IPF patients is not captured pre and post LAS implementation)

450
Idiopathic Pulmonary Fibrosis Excluded Studies
Reference Reason for exclusion
Lutogniewska 2010290
Intervention does not match protocol (QoL and dyspnoea in patients referred for lung transplantation)
Mackay 2007293
Population does not match protocol (does not analyse IPF patients separately)
Mahida 2012297
Incorrect study design (non-systematic review)
Mansour 2011301
Abstract only and intervention does not match protocol (difference in outcomes for lung transplantation in patients with IPF who had an acute exacerbation)
Martinez 2005304
Intervention does not match protocol (clinical course of IPF patients, no mention of referral times)
Mason 2007307
Intervention does not match protocol does (compares survival of IPF patients versus non IPF receiving lung transplantation)
Merlo 2009313
Intervention does not match protocol (of IPF patients is not captured pre and post LAS implementation)
Nathan 2005b339
Incorrect study design (non-systematic review)
Obeirne 2010361
Incorrect study design (non-systematic review)
Orens 2006370
Guideline: all relevant papers have already been included/considered
Osaki 2009372
Abstract only and population does not match protocol (does not analyse IPF patients)
Osaki 2010371
Population does not match protocol ( does not analyse IPF patients separately)
Reed 2006407
Intervention does not match protocol (does not analyse IPF patients separately)
Santana 2009421
Intervention does not match protocol (improvements in QOL after transplantation)
Shitrit 2009439
Intervention does not match protocol (study on the 15-step oximetry test)
Stavem 2000448
Intervention does not match protocol (QoL of patients on lung transplantation waiting list and recipients)
Studer 2000451
Incorrect study design (non-systematic review)
Thabut 2003469
Intervention does not match protocol (survival benefits of lung transplantation)
Titman 2009472
P population does not match protocol (diffuse parenchymal lung disease, doesn’t specify IPF)
Tuppin 2008480
Population does not match protocol (does not analyse IPF patients separately)
Whelan 2005498
Does not match review question (prognostic value of pulmonary artery pressure)
Table 159: Excluded studies for the economic evidence 1
Reference Reason for exclusion
S. D. Ramsey, D. L. Patrick, R. K. Albert, E. B. Larson, D. E. Wood, and G. Raghu. The cost-effectiveness of lung transplantation: a pilot study. Anonymous. Anonymous. Chest 108(6):1594-1601, 1995.
Within trial CUA from USA Medicare perspective based on case findings. Excluded due to a low proportion of the sample having IPF (n=5/26)
2
R.8 Ventilation 3
Table 160: Excluded studies for the clinical evidence 4
Reference Reason for exclusion
Altinoz 201016
Non-English language publication (Turkish)

451
Idiopathic Pulmonary Fibrosis Excluded Studies
Reference Reason for exclusion
Blancal 201042
Abstract only and intervention does not match the protocol (studies the clinical feature and prognostic factors of acute exacerbation of IPF)
Claudett 201070
Intervention does not match protocol (protocol used for NIMV)
Fernandez 2008140
Intervention does not match protocol (setting for MV)
Fumeaux 2003158
Non-English language publication (French)
Gottlieb 2010166
Abstract only (the original paper Gottlieb 201211
has been considered)
Gottlieb 2012167
Population and intervcention does not match protocol (analysis of prognostic markers of ventilated patients who are lung transplantation candidates and IPF not separated in the analysis)
Howard 2009194
Abstract only and intervention does not match protocol (overview of NIMV and its effectiveness in a range of conditions)
Iotti 2010202
Population and intervention does not match protocol, the study does not specify if IPF patients are present in the sample. And the Intervention does not match protocol the study compares two different types of MV
Jin 2008221
Non-English language publication (Korean).
Koschel 2010250
Population and intervention does not match protocol (IPF not separated and study looks at the acute effects of NIMV)
Lunt 2011289
Abstract only and population does not match protocol (ILD, n=1)
Moderno 2010326
Intervention does not match protocol (effects of NIMV on exercise performance)
Mollica 2008329
Incorrect study design (non-systematic review)
Niwa 2010356
Abstract only and population does not match protocol (acute respiratory distress syndrome)
Niwa 2011357
Intervention does not match protocol (safety of a new ventilation system in patients with interstitial pneumonia)
Pandey 2011375
Population and intervention does not match protocol (ILD, n=1 and benefits of NIMV)
Rai 2004403
Population does not match protocol (ILD, n=2)
Rangappa 2009405
Intervention does not match protocol (outcomes of IPF patients admitted to ICU)
Ryerson 2012416
Systematic review (all relevant papers have already been included/considered)
Sakamoto 2011419
Intervention does not match protocol (incidence of acute exacerbation after lung transplantation)
Schönhofer 1997427
Intervention does not match protocol (use of MV during the day versus the night)
Su 2010452
Non-English language publication (Chinese)
Suh 2006453
Population does not match protocol (interstitial pneumonia)
Tomii 2010473
Population does not match protocol (interstitial pneumonia)
Yokoyama 2011505
Abstract only and intervention and population do not match the protocol (effect of early NIMV in acute exacerbation of interstitial pneumonia)
Yokoyama 2012506
Population does not match protocol (interstitial pneumonia)
Excluded studies for the economic evidence: 1
No relevant economic evaluations comparing invasive and non-invasive ventilation strategies were 2 identified. No studies were selectively excluded. 3
4
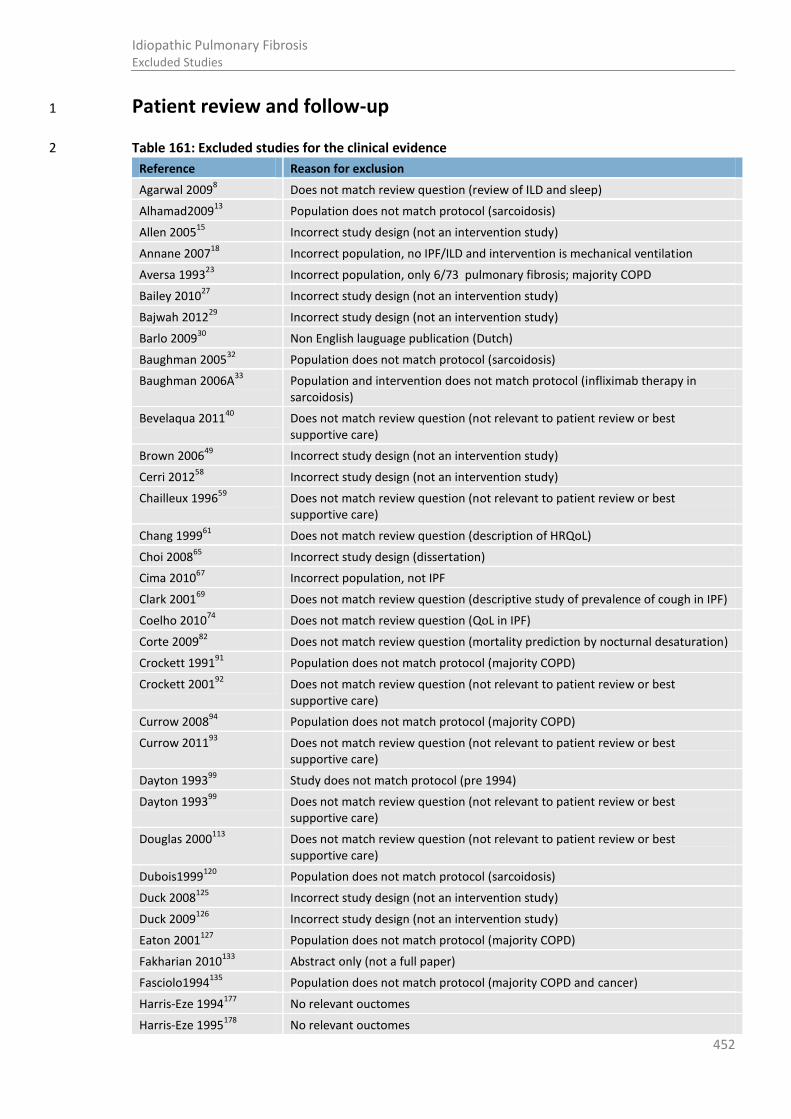
452
Idiopathic Pulmonary Fibrosis Excluded Studies
Patient review and follow-up 1
Table 161: Excluded studies for the clinical evidence 2
Reference Reason for exclusion
Agarwal 20098 Does not match review question (review of ILD and sleep)
Alhamad200913
Population does not match protocol (sarcoidosis)
Allen 200515
Incorrect study design (not an intervention study)
Annane 200718
Incorrect population, no IPF/ILD and intervention is mechanical ventilation
Aversa 199323
Incorrect population, only 6/73 pulmonary fibrosis; majority COPD
Bailey 201027
Incorrect study design (not an intervention study)
Bajwah 201229
Incorrect study design (not an intervention study)
Barlo 200930
Non English lauguage publication (Dutch)
Baughman 200532
Population does not match protocol (sarcoidosis)
Baughman 2006A33
Population and intervention does not match protocol (infliximab therapy in sarcoidosis)
Bevelaqua 201140
Does not match review question (not relevant to patient review or best supportive care)
Brown 200649
Incorrect study design (not an intervention study)
Cerri 201258
Incorrect study design (not an intervention study)
Chailleux 199659
Does not match review question (not relevant to patient review or best supportive care)
Chang 199961
Does not match review question (description of HRQoL)
Choi 200865
Incorrect study design (dissertation)
Cima 201067
Incorrect population, not IPF
Clark 200169
Does not match review question (descriptive study of prevalence of cough in IPF)
Coelho 201074
Does not match review question (QoL in IPF)
Corte 200982
Does not match review question (mortality prediction by nocturnal desaturation)
Crockett 199191
Population does not match protocol (majority COPD)
Crockett 200192
Does not match review question (not relevant to patient review or best supportive care)
Currow 200894
Population does not match protocol (majority COPD)
Currow 201193
Does not match review question (not relevant to patient review or best supportive care)
Dayton 199399
Study does not match protocol (pre 1994)
Dayton 199399
Does not match review question (not relevant to patient review or best supportive care)
Douglas 2000113
Does not match review question (not relevant to patient review or best supportive care)
Dubois1999120
Population does not match protocol (sarcoidosis)
Duck 2008125
Incorrect study design (not an intervention study)
Duck 2009126
Incorrect study design (not an intervention study)
Eaton 2001127
Population does not match protocol (majority COPD)
Fakharian 2010133
Abstract only (not a full paper)
Fasciolo1994135
Population does not match protocol (majority COPD and cancer)
Harris-Eze 1994177
No relevant ouctomes
Harris-Eze 1995178
No relevant ouctomes
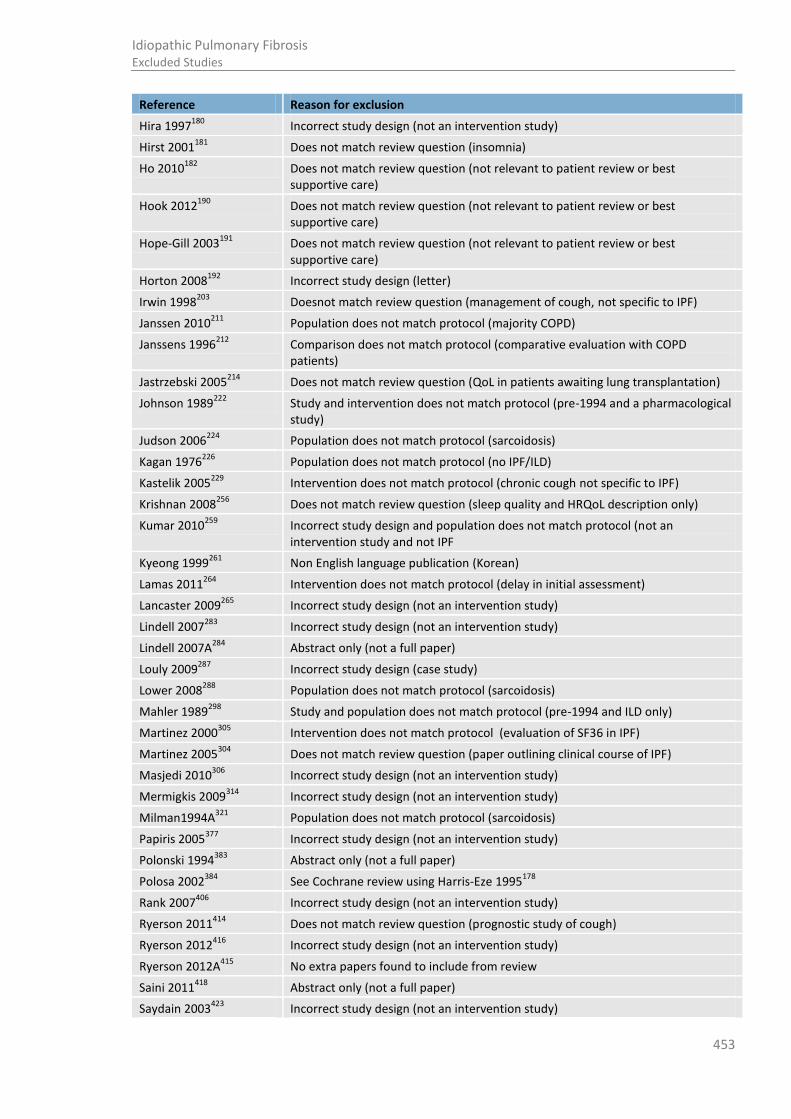
453
Idiopathic Pulmonary Fibrosis Excluded Studies
Reference Reason for exclusion
Hira 1997180
Incorrect study design (not an intervention study)
Hirst 2001181
Does not match review question (insomnia)
Ho 2010182
Does not match review question (not relevant to patient review or best supportive care)
Hook 2012190
Does not match review question (not relevant to patient review or best supportive care)
Hope-Gill 2003191
Does not match review question (not relevant to patient review or best supportive care)
Horton 2008192
Incorrect study design (letter)
Irwin 1998203
Doesnot match review question (management of cough, not specific to IPF)
Janssen 2010211
Population does not match protocol (majority COPD)
Janssens 1996212
Comparison does not match protocol (comparative evaluation with COPD patients)
Jastrzebski 2005214
Does not match review question (QoL in patients awaiting lung transplantation)
Johnson 1989222
Study and intervention does not match protocol (pre-1994 and a pharmacological study)
Judson 2006224
Population does not match protocol (sarcoidosis)
Kagan 1976226
Population does not match protocol (no IPF/ILD)
Kastelik 2005229
Intervention does not match protocol (chronic cough not specific to IPF)
Krishnan 2008256
Does not match review question (sleep quality and HRQoL description only)
Kumar 2010259
Incorrect study design and population does not match protocol (not an intervention study and not IPF
Kyeong 1999261
Non English language publication (Korean)
Lamas 2011264
Intervention does not match protocol (delay in initial assessment)
Lancaster 2009265
Incorrect study design (not an intervention study)
Lindell 2007283
Incorrect study design (not an intervention study)
Lindell 2007A284
Abstract only (not a full paper)
Louly 2009287
Incorrect study design (case study)
Lower 2008288
Population does not match protocol (sarcoidosis)
Mahler 1989298
Study and population does not match protocol (pre-1994 and ILD only)
Martinez 2000305
Intervention does not match protocol (evaluation of SF36 in IPF)
Martinez 2005304
Does not match review question (paper outlining clinical course of IPF)
Masjedi 2010306
Incorrect study design (not an intervention study)
Mermigkis 2009314
Incorrect study design (not an intervention study)
Milman1994A321
Population does not match protocol (sarcoidosis)
Papiris 2005377
Incorrect study design (not an intervention study)
Polonski 1994383
Abstract only (not a full paper)
Polosa 2002384
See Cochrane review using Harris-Eze 1995178
Rank 2007406
Incorrect study design (not an intervention study)
Ryerson 2011414
Does not match review question (prognostic study of cough)
Ryerson 2012416
Incorrect study design (not an intervention study)
Ryerson 2012A415
No extra papers found to include from review
Saini 2011418
Abstract only (not a full paper)
Saydain 2003423
Incorrect study design (not an intervention study)

454
Idiopathic Pulmonary Fibrosis Reference list
Reference Reason for exclusion
Sharifabad 2010435
Population does not match protocol (majority COPD)
Shulgina 2011440
Does not match review question (not relevant to patient review or best supportive care)
Simon 2010443
Population does not match protocol (not IPF)
Sundar 2010456
Does not match review question (prevalence of cough in conditions other than IPF)
Swigris 2005A466
Does not match review question (background to IPF QoL tools)
Swigris 2005B461
Does not match review question (not relevant to patient review or best supportive care)
Swigris 2011465
Does not match review question (not relevant to patient review or best supportive care)
Swinburn 1991468
Does not match review question (effect of O2 on ILD)
Troy 2012479
Does not match review question (sleep disordered breathing in IPF)
Xaubet 2001499
Does not match review question (delay in initial assessment)
Zielinski 2000509
See Crockett Cochrane review89
1
Excluded studies for the economic evidence: 2
No relevant economic evaluations comparing different review and monitoring strategies were 3 identified. No studies were selectively excluded. 4
5
Appendix S: Reference list 6
1 International guidelines for the selection of lung transplant candidates. The American Society for 7 Transplant Physicians (ASTP)/American Thoracic Society(ATS)/European Respiratory 8 Society(ERS)/International Society for Heart and Lung Transplantation(ISHLT). American Journal 9 of Respiratory and Critical Care Medicine. 1998; 158(1):335-339. (Guideline Ref ID 10 LALAATSP1998) 11
2 Summaries for patients. What is the natural course of idiopathic pulmonary fibrosis? Annals of 12 Internal Medicine. 2005; 142(12 Pt 1):I23. (Guideline Ref ID ANON2005) 13
3 British National Formulary. 59 edition. London: BMJ Group Pharmaceutical Press; 2010. Available 14 from: http://bnf.org/bnf/bnf/current/index.htm (Guideline Ref ID BNF2010) 15
4 6MWD and Risk of Mortality in IPF. 2012 (Guideline Ref ID DUBOIS2012A) 16
5 MIMS. 2013. Available from: http://www.mims.co.uk/home/ [Last accessed: 13 March 2013] 17 (Guideline Ref ID MIMS2013) 18
6 Aalokken TM, Naalsund A, Mynarek G, Berstad AE, Solberg S, Strom EH et al. Diagnostic accuracy 19 of computed tomography and histopathology in the diagnosis of usual interstitial pneumonia. 20 Acta Radiologica. 2012; 53(3):296-302. (Guideline Ref ID AALOKKEN2012) 21
7 Actelion. Efficacy and safety of oral bosentan in patients with idiopathic pulmonary fibrosis. 22 Clinicaltrials Gov. 2004. (Guideline Ref ID ACTELION2004A) 23
455
Idiopathic Pulmonary Fibrosis Reference list
8 Agarwal S, Richardson B, Krishnan V, Schneider H, Collop NA, Danoff SK. Interstitial lung disease 1 and sleep: What is known? Sleep Medicine. 2009; 10(9):947-951. (Guideline Ref ID 2 AGARWAL2009) 3
9 Agostini C, Albera C, Bariffi F, De Palma M, Harari S, Lusuardi M et al. First report of the Italian 4 register for diffuse infiltrative lung disorders (RIPID). Monaldi Archives for Chest Disease - 5 Pulmonary Series. 2001; 56(4):364-368. (Guideline Ref ID AGOSTINI2001) 6
10 Agusti C, Xaubet A, Agusti AG, Roca J, Ramirez J, Rodriguez-Roisin R. Clinical and functional 7 assessment of patients with idiopathic pulmonary fibrosis: results of a 3 year follow-up. 8 European Respiratory Journal. 1994; 7(4):643-650. (Guideline Ref ID AGUSTI1994) 9
11 Al Moamary MS. Impact of a pulmonary rehabilitation programme on respiratory parameters 10 and health care utilization in patients with chronic lung diseases other than COPD. Eastern 11 Mediterranean Health Journal. 2012; 18(2):120-126. (Guideline Ref ID ALMOAMARY2012) 12
12 Al-Hameed FM, Sharma S. Outcome of patients admitted to the intensive care unit for acute 13 exacerbation of idiopathic pulmonary fibrosis. Canadian Respiratory Journal. 2004; 11(2):117-14 122. (Guideline Ref ID ALHAMEED2004) 15
13 Alhamad EH. The six-minute walk test in patients with pulmonary sarcoidosis. Annals of Thoracic 16 Medicine. 2009; 4(2):60-64. (Guideline Ref ID ALHAMAD2009) 17
14 Alhamad EH, Masood M, Shaik SA, Arafah M. Clinical and functional outcomes in Middle Eastern 18 patients with idiopathic pulmonary fibrosis. Clinical Respiratory Journal. 2008; 2(4):220-226. 19 (Guideline Ref ID ALHAMAD2008) 20
15 Allen S, Raut S, Woollard J, Vassallo M. Low dose diamorphine reduces breathlessness without 21 causing a fall in oxygen saturation in elderly patients with end-stage idiopathic pulmonary 22 fibrosis. Palliative Medicine. 2005; 19(2):128-130. (Guideline Ref ID ALLEN2005) 23
16 Altinoz H, Adiguzel N, Karakurt Z, Yarkin T, Ozmen I, Gungor G. Results of patients invasively 24 mechanically ventilated for acute respiratory failure due to obstructive and restrictive lung 25 disease. Journal of Medical and Surgical Intensive Care Medicine. 2010; 1(2):31-34. (Guideline Ref 26 ID ALTINOZ2010) 27
17 Alzeer AH, Al-Otair HA, Al-Hajjaj MS. Yield and complications of flexible fiberoptic bronchoscopy 28 in a teaching hospital. Saudi Medical Journal. 2008; 29(1):55-59. (Guideline Ref ID ALZEER2008) 29
18 Annane D, Orlikowski D, Chevret S, Chevrolet JC, Raphaël JC. Nocturnal mechanical ventilation for 30 chronic hypoventilation in patients with neuromuscular and chest wall disorders. Cochrane 31 Database of Systematic Reviews. 2007; Issue 4:CD001941. 32 DOI:10.1002/14651858.CD001941.pub2. (Guideline Ref ID ANNANE2007) 33
19 Antoniu SA. Bosentan for the treatment of idiopathic pulmonary fibrosis. Expert Opinion on 34 Investigational Drugs. 2008; 17(4):611-614. (Guideline Ref ID ANTONIU2008A) 35
20 Ara R, Brazier J. Deriving an algorithm to convert the eight mean SF-36 dimension scores into a 36 mean EQ-5D preference-based score from published studies (where patient level data are not 37 available). Value in Health.: Blackwell Publishing Inc. 2008; 11(7):1131-1143. (Guideline Ref ID 38 ARA2008) 39
21 Ara R, Brazier J. Predicting the short form-6D preference-based index using the eight mean short 40 form-36 health dimension scores: estimating preference-based health-related utilities when 41
456
Idiopathic Pulmonary Fibrosis Reference list
patient level data are not available. Value in Health. 2009; 12(2):346-353. (Guideline Ref ID 1 ARA2009) 2
22 Arcasoy SM, Christie JD, Ferrari VA, Sutton MSJ, Zisman DA, Blumenthal NP et al. 3 Echocardiographic assessment of pulmonary hypertension in patients with advanced lung 4 disease. American Journal of Respiratory and Critical Care Medicine. 2003; 167(5):735-740. 5 (Guideline Ref ID ARCASOY2003) 6
23 Aversa C, Cazzola M, Clini V, Dal Negro R, Maiorano V, Tana F et al. Clinical trial of the efficacy 7 and safety of moguisteine in patients with cough associated with chronic respiratory diseases. 8 Drugs Under Experimental and Clinical Research. 1993; 19(6):273-279. (Guideline Ref ID 9 AVERSA1993) 10
24 Ayed AK. Video-assisted thoracoscopic lung biopsy in the diagnosis of diffuse interstitial lung 11 disease. A prospective study. Journal of Cardiovascular Surgery. 2003; 44(1):115-118. (Guideline 12 Ref ID AYED2003) 13
25 Ayed AK, Raghunathan R. Thoracoscopy versus open lung biopsy in the diagnosis of interstitial 14 lung disease: a randomised controlled trial. Journal of the Royal College of Surgeons of 15 Edinburgh. 2000; 45(3):159-163. (Guideline Ref ID AYED2000) 16
26 Baddini Martinez JA, Martinez TY, Lovetro Galhardo FP, de Castro Pereira CA. Dyspnea scales as a 17 measure of health-related quality of life in patients with idiopathic pulmonary fibrosis. Medical 18 Science Monitor. 2002; 8(6):CR405-CR410. (Guideline Ref ID BADDINIZ2002) 19
27 Bailey CD, Wagland R, Dabbour R, Caress A, Smith J, Molassiotis A. An integrative review of 20 systematic reviews related to the management of breathlessness in respiratory illnesses. BMC 21 Pulmonary Medicine. 2010; 10. (Guideline Ref ID BAILEY2010) 22
28 Bajwah S, Koffman J, Higginson IJ, Ross JR, Wells AU, Birring SS et al. The needs and experiences 23 of progressive idiopathic fibrotic interstitial lung disease patients, Informal caregivers and health 24 professionals: a qualitative study. Thorax. 2011; 66(Suppl 4):A103. (Guideline Ref ID 25 BAJWAH2011) 26
29 Bajwah S, Higginson IJ, Ross JR, Wells AU, Birring SS, Patel A et al. Specialist palliative care is more 27 than drugs: a retrospective study of ILD patients. Lung. 2012; 190(2):215-220. (Guideline Ref ID 28 BAJWAH2012) 29
30 Barlo NP, van Moorsel CH, van den Bosch JM, van de Graaf EA, Kwakkel-van Erp JM, Grutters JC. 30 Idiopathic pulmonary fibrosis; description of a Dutch cohort. Nederlands Tijdschrift Voor 31 Geneeskunde. 2009; 153:B425. (Guideline Ref ID BARLO2009) 32
31 Battista G, Zompatori M, Fasano L, Pacilli A, Basile B. Progressive worsening of idiopathic 33 pulmonary fibrosis. High resolution computed tomography (HRCT) study with functional 34 correlations. Radiologia Medica. 2003; 105(1-2):2-11. (Guideline Ref ID BATTISTA2003A) 35
32 Baughman RP, Barnathan E. Dyspnea in patients with chronic sarcoidosis with pulmonary 36 involvement enrolled in a multicenter randomized double-blind placebo-controlled trial. 37 American Thoracic Society 2005 International Conference. May 20-25 San Diego, California 38 2005;D33. (Guideline Ref ID BAUGHMAN2005) 39
33 Baughman RP, Drent M, Kavuru M, Judson MA, Costabel U, du Bois R et al. Infliximab therapy in 40 patients with chronic sarcoidosis and pulmonary involvement. American Journal of Respiratory 41 and Critical Care Medicine. 2006; 174(7):795-802. (Guideline Ref ID BAUGHMAN2006A) 42

457
Idiopathic Pulmonary Fibrosis Reference list
34 Bausewein C, Booth S, Gysels M, Higginson IJ. Non-pharmacological interventions for 1 breathlessness in advanced stages of malignant and non-malignant diseases. Cochrane Database 2 of Systematic Reviews. 2008; Issue 2:CD005623. (Guideline Ref ID BAUSEWEIN2008C) 3
35 Behr J, Degenkolb B, Krombach F, Vogelmeier C. Intracellular glutathione and bronchoalveolar 4 cells in fibrosing alveolitis: effects of N-acetylcysteine. European Respiratory Journal. 2002; 5 19(5):906-911. (Guideline Ref ID BEHR2002) 6
36 Behr J. Approach to the diagnosis of interstitial lung disease. Clinics in Chest Medicine. 2012; 7 33(1):1-10. (Guideline Ref ID BEHR2012) 8
37 Berbescu EA, Katzenstein AL, Snow JL, Zisman DA. Transbronchial biopsy in usual interstitial 9 pneumonia. Chest. 2006; 129(5):1126-1131. (Guideline Ref ID BERBESCU2006) 10
38 Best AC, Meng J, Lynch AM, Bozic CM, Miller D, Grunwald GK et al. Idiopathic pulmonary fibrosis: 11 physiologic tests, quantitative CT indexes, and CT visual scores as predictors of mortality. 12 Radiology. 2008; 246(3):935-940. (Guideline Ref ID BEST2008) 13
39 Best AC, Lynch AM, Bozic CM, Miller D, Grunwald GK, Lynch DA. Quantitative CT indexes in 14 idiopathic pulmonary fibrosis: relationship with physiologic impairment. Radiology. 2003; 15 228(2):407-414. (Guideline Ref ID BEST2003) 16
40 Bevelaqua A-C, Armstrong H, Bartels MN, Layton AM. Pulmonary rehabilitation for patients with 17 severe end-stage lung disease awaiting transplantation. PM and R. 2011; 3(10 Suppl 1):S186. 18 (Guideline Ref ID BEVELAQUA2011) 19
41 Blake RL, Vandiver TA, Braun S, Bertuso DD, Straub V. A randomized controlled evaluation of a 20 psychosocial intervention in adults with chronic lung disease. Family Medicine. 1990; 22(5):365-21 370. (Guideline Ref ID BLAKE1990) 22
42 Blancal V, Nunes H, Freynet O, Bouvry D, Cohen Y, Vincent F et al. Acute exacerbation of 23 idiopathic pulmonary fibrosis: Analysis of clinical features and prognosis factors. American 24 Journal of Respiratory and Critical Care Medicine. 2010; 181(1 MeetingAbstracts). (Guideline Ref 25 ID BLANCAL2010) 26
43 Blivet S, Philit F, Sab JM, Langevin B, Paret M, Guerin C et al. Outcome of patients with idiopathic 27 pulmonary fibrosis admitted to the ICU for respiratory failure. Chest. 2001; 120(1):209-212. 28 (Guideline Ref ID BLIVET2001) 29
44 Boutou AK, Pitsiou GG, Trigonis I, Papakosta D, Kontou PK, Chavouzis N et al. Exercise capacity in 30 idiopathic pulmonary fibrosis: the effect of pulmonary hypertension. Respirology. 2011; 31 16(3):451-458. (Guideline Ref ID BOUTOU2011) 32
45 Braghiroli A, Ioli F, Spada EL, Vecchio C, Donner CF. LTOT in pulmonary fibrosis. Monaldi Archives 33 for Chest Disease. 1993; 48(5):437-440. (Guideline Ref ID BRAGHIROLI1993) 34
46 Briggs A, Claxton K, Sculpher M. Decision modelling for health economic evaluation. Oxford: OUP; 35 2006 (Guideline Ref ID BRIGGS2006) 36
47 British Thoracic Society Standards of Care Subcommittee on Pulmonary Rehabilitation. 37 Pulmonary rehabilitation. Thorax. 2001; 56(11):827-834. (Guideline Ref ID BTS2001) 38
48 Brown KK, Wells AU. Recent clinical trials in idiopathic pulmonary fibrosis and the BUILD-1 study. 39 European Respiratory Review. 2008; 17(109):116-122. (Guideline Ref ID BROWN2008) 40

458
Idiopathic Pulmonary Fibrosis Reference list
49 Brown KK. Chronic cough due to chronic interstitial pulmonary diseases: ACCP evidence-based 1 clinical practice guidelines. Chest. 2006; 129(1 Suppl):180S-185S. (Guideline Ref ID BROWN2006) 2
50 Budweiser S, Moertl M, Jörres RA, Windisch W, Heinemann F, Pfeifer M. Respiratory muscle 3 training in restrictive thoracic disease: a randomized controlled trial. Archives of Physical 4 Medicine and Rehabilitation. 2006; 87(12):1559-1565. (Guideline Ref ID BUDWEISER2006) 5
51 Butcher K, McCron T, Madeley C, Ross D. Lakeridge health Respiratory Rehabilitation Program. 6 Outcomes at one year: an outpatient, interdisciplinary Respiratory Rehabilitation Program. 7 Canadian Journal of Respiratory Therapy. 2001; 37(4):26-35. (Guideline Ref ID BUTCHER2001) 8
52 Cambridgeshire Joint Prescibing Group. Recommendation made by CJPG to Commissioners and 9 Prescribers: N-Acetylcysteine (Fluimucil®, Elder Pharmaceuticals (Zambon Group) - not licensed 10 in the UK) as adjunctive therapy to immunosuppressants in idiopathic pulmonary fibrosis. 2010. 11 Available from: http://www.cambsphn.nhs.uk/Libraries/Decision_Documents/N-Acetylcysteine_-12 _Decision_May_2010.sflb.ashx (Guideline Ref ID CJPG2010) 13
53 Caminati A, Bianchi A, Cassandro R, Mirenda MR, Harari S. Walking distance on 6-MWT is a 14 prognostic factor in idiopathic pulmonary fibrosis. Respiratory Medicine. 2009; 103(1):117-123. 15 (Guideline Ref ID CAMINATI2009) 16
54 Caminati A, Harari S. IPF: new insight in diagnosis and prognosis. Respiratory Medicine. 2010; 104 17 Suppl 1:S2-10. (Guideline Ref ID CAMINATI2010) 18
55 Campainha S, Goncalves I, Sanches A, Costa F, Brito MC, Torres S et al. Idiopathic pulmonary 19 fibrosis - characterization of a population and assessment of prognostic markers. Sarcoidosis 20 Vasculitis and Diffuse Lung Diseases. 2011; 28(Suppl):23-24. (Guideline Ref ID CAMPAINHA2011) 21
56 Carbone R, Bottino G, Paredi P, Shah P, Meyer KC. Predictors of survival in idiopathic interstitial 22 pneumonia. European Review for Medical and Pharmacological Sciences. 2010; 14(8):695-704. 23 (Guideline Ref ID CARBONE2010) 24
57 Carroll M. Viewpoint self-help groups. Appalachian coal miners combine mutual help and 25 advocacy. Public Health Reports. 1999; 114(4):326-327. (Guideline Ref ID CARROLL1999) 26
58 Cerri S, Spagnolo P, Luppi F, Richeldi L. Management of idiopathic pulmonary fibrosis. Clinics in 27 Chest Medicine. 2012; 33(1):85-94. (Guideline Ref ID CERRI2012) 28
59 Chailleux E, Fauroux B, Binet F, Dautzenberg B, Polu J. Predictors of survival in patients receiving 29 domiciliary oxygen therapy of mechanical ventilation: a 10-year analysis of ANTADIR observatory. 30 Chest. 1996; 109(3):741-749. (Guideline Ref ID CHAILLEUX1996) 31
60 Chan TY, Hansell DM, Rubens MB, du Bois RM, Wells AU. Cryptogenic fibrosing alveolitis and the 32 fibrosing alveolitis of systemic sclerosis: morphological differences on computed tomographic 33 scans. Thorax. 1997; 52(3):265-270. (Guideline Ref ID CHAN1997) 34
61 Chang JA, Curtis JR, Patrick DL, Raghu G. Assessment of health-related quality of life in patients 35 with interstitial lung disease. Chest. 1999; 116(5):1175-1182. (Guideline Ref ID CHANG1999) 36
62 Charman SC, Sharples LD, McNeil KD, Wallwork J. Assessment of survival benefit after lung 37 transplantation by patient diagnosis. Journal of Heart and Lung Transplantation. 2002; 21(2):226-38 232. (Guideline Ref ID CHARMAN2002) 39
459
Idiopathic Pulmonary Fibrosis Reference list
63 Chen H, Shiboski SC, Golden JA, Gould MK, Hays SR, Hoopes CW et al. Impact of the lung 1 allocation score on lung transplantation for pulmonary arterial hypertension. American Journal of 2 Respiratory and Critical Care Medicine. 2009; 180(5):468-474. (Guideline Ref ID CHEN2009) 3
64 Cherniack RM, Colby TV, Flint A, Thurlbeck WM, Waldron J, Ackerson L et al. Quantitative 4 assessment of lung pathology in idiopathic pulmonary fibrosis. The BAL Cooperative Group 5 Steering Committee. American Review of Respiratory Disease. 1991; 144(4):892-900. (Guideline 6 Ref ID CHERNIACK1991) 7
65 Choi J. Exhaled nitric oxide in patients with interstitial lung disease: a pilot study University of 8 Pittsburgh; 2008. (Guideline Ref ID CHOI2008) 9
66 Chuang MT, Raskin J, Krellenstein DJ, Teirstein AS. Bronchoscopy in diffuse lung disease: 10 evaluation by open lung biopsy in nondiagnostic transbronchial lung biopsy. Annals of Otology, 11 Rhinology, and Laryngology. 1987; 96(6):654-657. (Guideline Ref ID CHUANG1987) 12
67 Cima MA. Pulmonary fibrosis: long-term survival with pulsed cyclophosphamide and 13 methylprednisolone without daily steroids. Twenty years follow up. Lupus. 2010; 19(1 Suppl):80. 14 (Guideline Ref ID CIMA2010) 15
68 Cityassays. Clinical biochemistry, City Hospital, Birmingham TPMT test. 2011. Available from: 16 http://www.cityassays.org.uk/tpmt.html [Last accessed: 27 October 2011] (Guideline Ref ID 17 CITYASSAYS2011) 18
69 Clark M, Cooper B, Singh S, Cooper M, Carr A, Hubbard R. A survey of nocturnal hypoxaemia and 19 health related quality of life in patients with cryptogenic fibrosing alveolitis. Thorax. 2001; 20 56(6):482-486. (Guideline Ref ID CLARK2001) 21
70 Claudett KB, Claudett MB, Sang MC, Maiguashca HA, Pico DC, Andrade MG et al. Noinvasive 22 ventilation in relapse of acute respiratory failure outside ICU. Internet Journal of Pulmonary 23 Medicine. 2010; 12(1). (Guideline Ref ID CLAUDETT2010) 24
71 Cobanoglu U, Sayir F, Mergan D. An ideal choice in the diagnosis of interstitial lung diseases: 25 Video-assisted thoracoscopic surgery. Journal of Clinical and Analytical Medicine. 2012; 3(1):46-26 50. (Guideline Ref ID COBANOGLU2012) 27
72 Cockcroft A, Berry G, Brown EB, Exall C. Psychological changes during a controlled trial of 28 rehabilitation in chronic respiratory disability. Thorax. 1982; 37(6):413-416. (Guideline Ref ID 29 COCKCROFT1982) 30
73 Cockcroft AE, Saunders MJ, Berry G. Randomised controlled trial of rehabilitation in chronic 31 respiratory disability. Thorax. 1981; 36(3):200-203. (Guideline Ref ID COCKCROFT1981) 32
74 Coelho AC, Knorst MM, Gazzana MB, Barreto SSM. Predictors of physical and mental health-33 related quality of life in patients with interstitial lung disease: a multifactorial analysis. Jornal 34 Brasileiro De Pneumologia. 2010; 36(5):562-570. (Guideline Ref ID COELHO2010) 35
75 Coffman K. Psychiatric issues in pulmonary disease. Psychiatric Clinics of North America. 2002; 36 25(1):89-127. (Guideline Ref ID COFFMAN2002) 37
76 Collard HR, Anstrom KJ, Schwarz MI, Zisman DA. Sildenafil improves walk distance in idiopathic 38 pulmonary fibrosis. Chest. 2007; 131(3):897-899. (Guideline Ref ID COLLARD2007) 39
460
Idiopathic Pulmonary Fibrosis Reference list
77 Collard HR, King TE, Jr., Bartelson BB, Vourlekis JS, Schwarz MI, Brown KK. Changes in clinical and 1 physiologic variables predict survival in idiopathic pulmonary fibrosis. American Journal of 2 Respiratory & Critical Care Medicine. 2003; 168(5):538-542. (Guideline Ref ID COLLARD2003) 3
78 Collard HR, Tino G, Noble PW, Shreve MA, Michaels M, Carlson B et al. Patient experiences with 4 pulmonary fibrosis. Respiratory Medicine. 2007; 101(6):1350-1354. (Guideline Ref ID 5 COLLARD2007A) 6
79 Collins CD, Wells AU, Hansell DM, Morgan RA, MacSweeney JE, du Bois RM et al. Observer 7 variation in pattern type and extent of disease in fibrosing alveolitis on thin section computed 8 tomography and chest radiography. Clinical Radiology. 1994; 49(4):236-240. (Guideline Ref ID 9 COLLINS1994) 10
80 Connock M, Stevens C, Fry-Smith A, Jowett S, Fitzmaurice D, Moore D et al. Clinical effectiveness 11 and cost-effectiveness of different models of managing long-term oral anticoagulation therapy: a 12 systematic review and economic modelling. Health Technology Assessment.: NICE. 2007; 11(38). 13 (Guideline Ref ID CONNOCK2007) 14
81 Connor M, Naji N, Donnelly S, McDonnell T. Effectiveness of pulmonary rehabilitation in 15 restrictive lung disease. Physiotherapy Ireland. 2007; 28(1):43. (Guideline Ref ID CONNOR2007) 16
82 Corte TJ, Talbot S, Wort SJ. Elevated nocturnal oxygen desaturation index predicts higher short-17 term mortality in interstitial lung disease. Thorax. 2009; 64(Suppl 4):A5. (Guideline Ref ID 18 CORTE2009) 19
83 Corte TJ, Wort SJ, Gatzoulis MA, Engel R, Giannakoulas G, Macdonald PM et al. Elevated brain 20 natriuretic peptide predicts mortality in interstitial lung disease. European Respiratory Journal. 21 2010; 36(4):819-825. (Guideline Ref ID CORTE2010A) 22
84 Corte TJ, Wort SJ, Gatzoulis MA, Macdonald P, Hansell DM, Wells AU. Pulmonary vascular 23 resistance predicts early mortality in patients with diffuse fibrotic lung disease and suspected 24 pulmonary hypertension. Thorax. 2009; 64(10):883-888. (Guideline Ref ID CORTE2009B) 25
85 Corte TJ, Wort SJ, Macdonald PS, Edey A, Hansell DM, Renzoni E et al. Pulmonary function 26 vascular index predicts prognosis in idiopathic interstitial pneumonia. Respirology. 2012; 27 17(4):674-680. (Guideline Ref ID CORTE2012) 28
86 Costabel U, Bonella F. Treatment of pulmonary fibrosis. New substances and new interventions. 29 Internist. 2011; 52(12):1422-1428. (Guideline Ref ID COSTABEL2011) 30
87 Costache V, Chavanon O, St Raymond C, Sessa C, Durand M, Duret J et al. Dramatic improvement 31 in survival after lung transplantation over time: a single center experience. Transplantation 32 Proceedings. 2009; 41(2):687-691. (Guideline Ref ID COSTACHE2009) 33
88 Cottin V, Cordier JF. Combined pulmonary fibrosis and emphysema in connective tissue disease. 34 Current Opinion in Pulmonary Medicine. 2012; 18(5):418-427. (Guideline Ref ID COTTIN2012) 35
89 Coutinho GF, Pancas R, Magalhaes E, Bernardo JE, Eugenio L, Antunes MJ. Diagnostic value of 36 surgical lung biopsy: comparison with clinical and radiological diagnosis. European Journal of 37 Cardio-Thoracic Surgery. 2008; 33(5):781-785. (Guideline Ref ID COUTINHO2008) 38
90 Cox CE, Donohue JF, Brown CD, Kataria YP, Judson MA. Health-related quality of life of persons 39 with sarcoidosis. Chest. 2004; 125(3):997-1004. (Guideline Ref ID COX2004) 40
461
Idiopathic Pulmonary Fibrosis Reference list
91 Crockett AJ, Alpers JH, Moss JR. Home oxygen therapy: an audit of survival. Australian and New 1 Zealand Journal of Medicine. 1991; 21(2):217-221. (Guideline Ref ID CROCKETT1991) 2
92 Crockett AJ, Cranston JM, Antic N. Domiciliary oxygen for interstitial lung disease. Cochrane 3 Database of Systematic Reviews. 2001; Issue 3:CD002883. (Guideline Ref ID CROCKETT2001) 4
93 Currow DC, McDonald C, Oaten S, Kenny B, Allcroft P, Frith P et al. Once-daily opioids for chronic 5 dyspnea: a dose increment and pharmacovigilance study. Journal of Pain and Symptom 6 Management. 2011; 42(3):388-399. (Guideline Ref ID CURROW2011) 7
94 Currow DC, Ward A, Clark K, Burns CM, Abernethy AP. Caregivers for people with end-stage lung 8 disease: characteristics and unmet needs in the whole population. International Journal of 9 Chronic Obstructive Pulmonary Disease. 2008; 3(4):753-762. (Guideline Ref ID CURROW2008) 10
95 Curtis L. Unit costs of health and social care. Canterbury: Personal Social Services Reseach Unit, 11 University of Kent; 2011. Available from: http://www.pssru.ac.uk/project-pages/unit-12 costs/2011/index.php (Guideline Ref ID PSSRU2011) 13
96 Dancer R, Thickett D. Pulmonary function tests. Medicine. 2012; 40(4):186-189. (Guideline Ref ID 14 DANCER2012) 15
97 Daniels CE, Ryu JH. Treatment of idiopathic pulmonary fibrosis. Seminars in Respiratory and 16 Critical Care Medicine. 2006; 27(6):668-676. (Guideline Ref ID DANIELS2006) 17
98 Davis RDJ, Trulock EP, Manley J, Pasque MK, Sundaresan S, Cooper JD et al. Differences in early 18 results after single-lung transplantation. Annals of Thoracic Surgery. 1994; 58(5):1327-5. 19 (Guideline Ref ID DAVIS1994) 20
99 Dayton CS, Schwartz DA, Helmers RA, Pueringer RJ, Gilbert SR, Merchant RK et al. Outcome of 21 subjects with idiopathic pulmonary fibrosis who fail corticosteroid therapy. Implications for 22 further studies. Chest. 1993; 103(1):69-73. (Guideline Ref ID DAYTON1993) 23
100 De Meester J, Smits JM, Persijn GG, Haverich A. Listing for lung transplantation: life expectancy 24 and transplant effect, stratified by type of end-stage lung disease, the Eurotransplant experience. 25 Journal of Heart and Lung Transplantation. 2001; 20(5):518-524. (Guideline Ref ID 26 DEMEESTER2001) 27
101 De Oliveira NC, Osaki S, Maloney J, Cornwell RD, Meyer KC. Lung transplant for interstitial lung 28 disease: outcomes for single versus bilateral lung transplantation. Interactive Cardiovascular and 29 Thoracic Surgery. 2012; 14(3):263-267. (Guideline Ref ID DEOLIVEIRA2012B) 30
102 De Oliveira NC, Osaki S, Maloney J, Cornwell RD, Meyer KC. Lung transplant for interstitial lung 31 disease: outcomes before and after implementation of the united network for organ sharing lung 32 allocation scoring system. European Journal of Cardio-Thoracic Surgery. 2012; 41(3):680-685. 33 (Guideline Ref ID DEOLIVEIRA2012A) 34
103 De Oliveira NC, Osaki S, Maloney J, Cornwell RD, Meyer KC. Lung transplant for interstitial lung 35 disease: outcomes for single versus bilateral lung transplantation. Interactive Cardiovascular and 36 Thoracic Surgery. 2012; 14(3):263-267. (Guideline Ref ID DEOLIVEIRA2012) 37
104 De Vries J, Seebregts A, Drent M. Assessing health status and quality of life in idiopathic 38 pulmonary fibrosis: which measure should be used? Respiratory Medicine. 2000; 94(3):273-278. 39 (Guideline Ref ID DEVRIES2000) 40

462
Idiopathic Pulmonary Fibrosis Reference list
105 Demedts M, Behr J, Buhl R, Costabel U, Dekhuijzen R, Jansen HM et al. High-dose acetylcysteine 1 in idiopathic pulmonary fibrosis. New England Journal of Medicine. 2005; 353(21):2229-2242. 2 (Guideline Ref ID DEMEDTS2005) 3
106 Department of Health. NHS costing manual 2010-11, 2011 Available from: 4 http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance5 /DH_126450 (Guideline Ref ID DOH2011A) 6
107 Department of Health. NHS reference costs 2009-2010: Appendix NSRC04: NHS trust and PCT 7 combined reference cost schedules, 2011 Available from: 8 http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance9 /DH_123459 (Guideline Ref ID NHSNSRC2011) 10
108 Department of Health. NHS reference costs 2010-11. 2012. Available from: 11 http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance12 /DH_131140 [Last accessed: 27 March 2012] (Guideline Ref ID DOH2012) 13
109 Devaraj A, Wells AU, Meister MG, Corte T, Wort J, Hansell DM. The prognostic significance of CT 14 signs of pulmonary hypertension in patients with idiopathic pulmonary fibrosis. Journal of 15 Thoracic Imaging. 2009; 24(3):w8. (Guideline Ref ID DEVARAJ2009) 16
110 Dierich MG, Geldmacher H, Fuehner T, Simon A, Welte T, Gottlieb J. Effect of a 3 week in-patient 17 rehabilitation program following lung transplantation on body composition and exercise 18 performance. American Journal of Respiratory and Critical Care Medicine. 2010; 181(1 19 MeetingAbstracts). (Guideline Ref ID DIERICH2010) 20
111 Doherty MJ, Pearson MG, O'Grady EA, Pellegrini V, Calverley PMA. Cryptogenic fibrosing 21 alveolitis with preserved lung volumes. Thorax. 1997; 52(11):998-1002. (Guideline Ref ID 22 DOHERTY1997) 23
112 Donnan PT, McLernon D, Dillon JF, Ryder S, Ryder S, Roderick P et al. Development of a decision 24 support tool for primary care management of patients with abnormal liver function tests without 25 clinically apparent liver disease: a record-linkage population cohort study and decision analysis 26 (ALFIE). Health Technology Assessment. 2009; 13(25). (Guideline Ref ID DONNAN2009) 27
113 Douglas WW, Ryu JH, Schroeder DR. Idiopathic pulmonary fibrosis: Impact of oxygen and 28 colchicine, prednisone, or no therapy on survival. American Journal of Respiratory and Critical 29 Care Medicine. 2000; 161(4 Pt 1):1172-1178. (Guideline Ref ID DOUGLAS2000) 30
114 Doyle TJ, Hunninghake GM, Rosas IO. Subclinical interstitial lung disease: why you should care. 31 American Journal of Respiratory and Critical Care Medicine. 2012; 185(11):1147-1153. (Guideline 32 Ref ID DOYLE2012) 33
115 Drent M, Wirnsberger RM, Breteler MH, Kock LM, De Vries J, Wouters EF. Quality of life and 34 depressive symptoms in patients suffering from sarcoidosis. Sarcoidosis, Vasculitis, and Diffuse 35 Lung Diseases. 1998; 15(1):59-66. (Guideline Ref ID DRENT1998) 36
116 Dressel H, Gross C, de la Motte D, Sültz J, Jörres RA, Nowak D. Educational intervention decreases 37 exhaled nitric oxide in farmers with occupational asthma. European Respiratory Journal : Official 38 Journal of the European Society for Clinical Respiratory Physiology. 2007; 30(3):545-548. 39 (Guideline Ref ID DRESSEL2007) 40

463
Idiopathic Pulmonary Fibrosis Reference list
117 Du Bois R, Weycker D, Albera C, Bradford WZ, Costabel U, Kartashov A et al. Ascertainment of 1 individual risk of mortality for patients with idiopathic pulmonary fibrosis. American Journal of 2 Respiratory and Critical Care Medicine. 2011; 184(4):459-466. (Guideline Ref ID DUBOIS2011A) 3
118 du Bois RM, Albera C, Bradford WZ, Costabel U, Noble PW, Sahn SA et al. A Novel Clinical 4 Prediction Model For Near-Term Mortality In Patients With Idiopathic Pulmonary Fibrosis (IPF). 5 American Journal of Respiratory & Critical Care Medicine. American Thoracic Society 6 International Conference Abstracts: American Thoracic Society. 2013; 187:A2357. (Guideline Ref 7 ID DUBOIS2013) 8
119 du Bois RM, Behr J, Brown KK, Raghu G, King TE. Bosentan in idiopathic pulmonary fibrosis (IPF) 9 patients the BUILD 1 study. European Respiratory Journal. 2006; 28(Suppl 50):383s. (Guideline 10 Ref ID DUBOIS2006) 11
120 du Bois RM, Greenhalgh PM, Southcott AM, Johnson NM, Harris TA. Randomized trial of inhaled 12 fluticasone propionate in chronic stable pulmonary sarcoidosis: a pilot study. European 13 Respiratory Journal. 1999; 13(6):1345-1350. (Guideline Ref ID DUBOIS1999) 14
121 du Bois RM, Weycker D, Albera C, Bradford WZ, Costabel U, Kartashov A et al. Forced vital 15 capacity in patients with idiopathic pulmonary fibrosis: test properties and minimal clinically 16 important difference. American Journal of Respiratory & Critical Care Medicine. 2011; 17 184(12):1382-1389. (Guideline Ref ID DUBOIS2011B) 18
122 du Bois RM, Weycker D, Albera C, Bradford WZ, Costabel U, Kartashov A et al. Six-minute-walk 19 test in idiopathic pulmonary fibrosis: test validation and minimal clinically important difference. 20 American Journal of Respiratory & Critical Care Medicine. 2011; 183(9):1231-1237. (Guideline Ref 21 ID DUBOIS2011) 22
123 du Bois RM. An earlier and more confident diagnosis of idiopathic pulmonary fibrosis. European 23 Respiratory Review. 2012; 21(124):141-146. (Guideline Ref ID DUBOIS2012) 24
124 Duck A. Interstitial lung diseases 1: diagnosis and investigation. Nursing Times. 2007; 103(43):28-25 29. (Guideline Ref ID DUCK2007) 26
125 Duck A. Respiratory nursing. Nursing patients with interstitial lung disease. Nursing Times. 2008; 27 104(9):46-49. (Guideline Ref ID DUCK2008) 28
126 Duck A. Principles to effectively manage people with interstitial lung disease in the community. 29 Nursing Times. 2009; 105(49-50):29-30. (Guideline Ref ID DUCK2009) 30
127 Eaton TE, Grey C, Garrett JE. An evaluation of short-term oxygen therapy: the prescription of 31 oxygen to patients with chronic lung disease hypoxic at discharge from hospital. Respiratory 32 Medicine. 2001; 95(7):582-587. (Guideline Ref ID EATON2001) 33
128 Edey AJ, Devaraj AA, Barker RP, Nicholson AG, Wells AU, Hansell DM. Fibrotic idiopathic 34 interstitial pneumonias: HRCT findings that predict mortality. European Radiology. 2011; 35 21(8):1586-1593. (Guideline Ref ID EDEY2011) 36
129 Egan JJ. Follow-up and nonpharmacological management of the idiopathic pulmonary fibrosis 37 patient. European Respiratory Review. 2011; 20(120):114-117. (Guideline Ref ID EGAN2011) 38
130 Egan TM, Trulock EP, Boychuk J, Ochoa L, Cooper JD. Analysis of referrals for lung 39 transplantation. Chest. 1991; 99(4):867-870. (Guideline Ref ID EGAN1991) 40

464
Idiopathic Pulmonary Fibrosis Reference list
131 Erbes R, Schaberg T, Loddenkemper R. Lung function tests in patients with idiopathic pulmonary 1 fibrosis. Are they helpful for predicting outcome? Chest. 1997; 111(1):51-57. (Guideline Ref ID 2 ERBES1997) 3
132 Esme H, Sezer M, Solak O, Sahin O. Importance of open lung biopsy in patients suspected 4 interstitial lung disease. European Journal of General Medicine. 2007; 4(1):16-18. (Guideline Ref 5 ID ESME2007) 6
133 Fakharian A, Masjedi MR, Hashemi N, Marashian SM. Clinical pattern of idiopathic pulmonary 7 fibrosis in Iran: A retrospective study. Respirology. 2010; 15(Suppl 2):29. (Guideline Ref ID 8 FAKHARIAN2010) 9
134 Fasano L, Zompatori M, Monetti N, Battista G, Pacilli AMG, Di Scioscio VD et al. Usual interstitial 10 pneumonitis (UIP) presenting with Wells grade III. Can imaging methods help predict further 11 progression of disease? Radiologia Medica. 1999; 98(4):268-274. (Guideline Ref ID FASANO1999) 12
135 Fasciolo G, Nicolini A, Vacca N, Viglierchio P. Efficacy and safety of moguisteine in comparison 13 with levodropropizine in patients with cough assoclated with chronic obstructive pulmonary 14 disease, lung cancer, or pulmonary fibrosis. Current Therapeutic Research - Clinical and 15 Experimental. 1994; 55(3):251-261. (Guideline Ref ID FASCIOLO1994) 16
136 Fell CD, Martinez FJ, Liu LX, Murray S, Han MK, Kazerooni EA et al. Clinical predictors of a 17 diagnosis of idiopathic pulmonary fibrosis. American Journal of Respiratory and Critical Care 18 Medicine. 2010; 181(8):832-837. (Guideline Ref ID FELL2010) 19
137 Feltrim MIZ, Rozanski A, Borges ACS, Cardoso CA, Caramori ML, Pego-Fernandes P. The quality of 20 life of patients on the lung transplantation waiting list. Transplantation Proceedings. 2008; 21 40(3):819-821. (Guideline Ref ID FELTRIM2008) 22
138 Fend F, Mikuz G, Ott G, Rothmund J. Diagnostic value of combined bronchoalveolar lavage and 23 transbronchial lung biopsy. Pathology, Research and Practice. 1989; 184(3):312-317. (Guideline 24 Ref ID FEND1989) 25
139 Fernandez Perez ER, Daniels CE, Schroeder DR, St Sauver J, Hartman TE, Bartholmai BJ et al. 26 Incidence, prevalence, and clinical course of idiopathic pulmonary fibrosis: a population-based 27 study. Chest. 2010; 137(1):129-137. (Guideline Ref ID FERNANDEZ2010) 28
140 Fernandez-Perez ER, Yilmaz M, Jenad H, Daniels CE, Ryu JH, Hubmayr RD et al. Ventilator settings 29 and outcome of respiratory failure in chronic interstitial lung disease. Chest. 2008; 133(5):1113-30 1119. (Guideline Ref ID FERNANDEZ2008) 31
141 Ferreira A, Garvey C, Connors GL, Hilling L, Rigler J, Farrell S et al. Pulmonary rehabilitation in 32 interstitial lung disease: benefits and predictors of response. Chest. 2009; 135(2):442-447. 33 (Guideline Ref ID FERREIRA2009) 34
142 Ferreira G, Feuerman M, Spiegler P. Results of an 8-week, outpatient pulmonary rehabilitation 35 program on patients with and without chronic obstructive pulmonary disease. J Cardiopulm 36 Rehabil. 2006; 26(1):54-60. (Guideline Ref ID FERREIRA2006) 37
143 Fibla JJ, Molins L, Blanco A, Royo I, Martinez Vallina P, Martinez N et al. Video-assisted 38 thoracoscopic lung biopsy in the diagnosis of interstitial lung disease: a prospective, multi-center 39 study in 224 patients. Archivos De Bronconeumologia. 2012; 48(3):81-85. (Guideline Ref ID 40 FIBLA2012) 41
465
Idiopathic Pulmonary Fibrosis Reference list
144 Fioret D, Perez RL, Roman J. Management of idiopathic pulmonary fibrosis. American Journal of 1 the Medical Sciences. 2011; 341(6):450-453. (Guideline Ref ID FIORET2011) 2
145 Fishbein MC. Diagnosis: to biopsy or not to biopsy: assessing the role of surgical lung biopsy in 3 the diagnosis of idiopathic pulmonary fibrosis. Chest. 2005; 128(5 Suppl 1):520S-525S. (Guideline 4 Ref ID FISHBEIN2005) 5
146 Fitzmaurice DA, Murray ET, McCahon D, Holder R, Raftery JP, Hussain S et al. Self management of 6 oral anticoagulation: randomised trial. BMJ. 2005; 331(7524):1057-1062. (Guideline Ref ID 7 FITZMAURICE2005) 8
147 Flaherty KR, Mumford JA, Murray S, Kazerooni EA, Gross BH, Colby TV et al. Prognostic 9 implications of physiologic and radiographic changes in idiopathic interstitial pneumonia. 10 American Journal of Respiratory and Critical Care Medicine. 2003; 168(5):543-548. (Guideline Ref 11 ID FLAHERTY2003) 12
148 Flaherty KR, Perters-Golden M, Travis W, Colby T, Gross B, Kazerooni E et al. Zileuton versus 13 azathioprine /prednisone in idiopathic pulmonary fibrosis. European Respiratory Journal. 2004; 14 24(Suppl 48):254s. (Guideline Ref ID FLAHERTY2004) 15
149 Flaherty KR, Thwaite EL, Kazerooni EA, Gross BH, Toews GB, Colby TV et al. Radiological versus 16 histological diagnosis in UIP and NSIP: survival implications. Thorax. 2003; 58(2):143-148. 17 (Guideline Ref ID FLAHERTY2003A) 18
150 Flaherty KR, Toews GB, Travis WD, Colby TV, Kazerooni EA, Gross BH et al. Clinical significance of 19 histological classification of idiopathic interstitial pneumonia. European Respiratory Journal. 20 2002; 19(2):275-283. (Guideline Ref ID FLAHERTY2002) 21
151 Flaherty KR, Travis WD, Colby TV, Toews GB, Kazerooni EA, Gross BH et al. Histopathologic 22 variability in usual and nonspecific interstitial pneumonias. American Journal of Respiratory and 23 Critical Care Medicine. 2001; 164(9):1722-1727. (Guideline Ref ID FLAHERTY2001A) 24
152 Flaherty KR, Andrei AC, King TEJ, Raghu G, Colby TV, Wells A et al. Idiopathic interstitial 25 pneumonia: do community and academic physicians agree on diagnosis? American Journal of 26 Respiratory and Critical Care Medicine. 2007; 175(10):1054-1060. (Guideline Ref ID 27 FLAHERTY2007) 28
153 Flaherty KR, Andrei AC, Murray S, Fraley C, Colby TV, Travis WD et al. Idiopathic pulmonary 29 fibrosis: prognostic value of changes in physiology and six-minute-walk test. American Journal of 30 Respiratory and Critical Care Medicine. 2006; 174(7):803-809. (Guideline Ref ID FLAHERTY2006) 31
154 Fowler RP, Ardelean D, Ingram KI, Clark AL, Marns PL, Kon C et al. Assessing the educational 32 impact of pulmonary rehabilitation in non-copd patients using the lung information needs 33 questionnaire. Thorax. 2011; 66:A16. (Guideline Ref ID FOWLER2011) 34
155 Frankel SK, Schwarz MI. Update in idiopathic pulmonary fibrosis. Current Opinion in Pulmonary 35 Medicine. 2009; 15(5):463-469. (Guideline Ref ID FRANKEL2009) 36
156 Fujimoto K, Taniguchi H, Johkoh T, Kondoh Y, Ichikado K, Sumikawa H et al. Acute exacerbation of 37 idiopathic pulmonary fibrosis: high-resolution CT scores predict mortality. European Radiology. 38 2012; 22(1):83-92. (Guideline Ref ID FUJIMOTO2012) 39

466
Idiopathic Pulmonary Fibrosis Reference list
157 Fumeaux T, Rothmeier C, Jolliet P. Outcome of mechanical ventilation for acute respiratory 1 failure in patients with pulmonary fibrosis. Intensive Care Medicine. 2001; 27(12):1868-1874. 2 (Guideline Ref ID FUMEAUX2001) 3
158 Fumeaux T, Rothmeier C, Jolliet P. Pulmonary fibrosis in the intensive care unit. Reanimation. 4 2003; 12(1):37-45. (Guideline Ref ID FUMEAUX2003) 5
159 Gal AA. Use and abuse of lung biopsy. Advances in Anatomic Pathology. 2005; 12(4):195-202. 6 (Guideline Ref ID GAL2005) 7
160 Gaunaurd I, Eustis N, Cohen M, Ramos C, Sol C, Cardenas D et al. Rehabilitation of patients with 8 idiopathic pulmonary fibrosis: changes in quality of life, functional mobility, and oxygen 9 metabolism. Cardiopulmonary Physical Therapy Journal. 2011; 22(4):30-31. (Guideline Ref ID 10 GAUNAURD2011) 11
161 Gay SE, Kazerooni EA, Toews GB, Lynch JP, Gross BH, Cascade PN et al. Idiopathic pulmonary 12 fibrosis: predicting response to therapy and survival. American Journal of Respiratory and Critical 13 Care Medicine. 1998; 157(4 Pt 1):1063-1072. (Guideline Ref ID GAY1998) 14
162 Genao L, Whitson H, Zaas D, Sanders L, Schmader K. Functional status after lung transplantation 15 in older adults in the post allocation score era. American Journal of Transplantation. 2012; 16 12(Suppl s3):49. (Guideline Ref ID GENAO2012) 17
163 George TJ, Arnaoutakis GJ, Shah AS. Lung transplant in idiopathic pulmonary fibrosis. Archives of 18 Surgery. 2011; 146(10):1204-1209. (Guideline Ref ID GEORGE2011) 19
164 Glaspole IN, Wells AU, du Bois RM. Lung biopsy in diffuse parenchymal lung disease. Monaldi 20 Archives for Chest Disease. 2001; 56(3):225-232. (Guideline Ref ID GLASPOLE2001A) 21
165 Gomez FJ, Planas A, Ussetti P, Tejada JJ, Varela A. Prognostic factors of early morbidity and 22 mortality after lung transplantation. Archivos De Bronconeumologia. 2003; 39(8):353-360. 23 (Guideline Ref ID GOMEZ2003) 24
166 Gottlieb J, Simon AR, Hadem J, Dierich M, Wiesner O, Strueber M et al. Outcome of lung 25 transplant candidates on mechanical ventilation or extracorporal support. Journal of Heart and 26 Lung Transplantation. 2010; 29(2 Suppl 1):S16-S17. (Guideline Ref ID GOTTLIEB2010) 27
167 Gottlieb J, Warnecke G, Hadem J, Dierich M, Wiesner O, Fuhner T et al. Outcome of critically ill 28 lung transplant candidates on invasive respiratory support. Intensive Care Medicine. 2012; 29 38(6):968-975. (Guideline Ref ID GOTTLIEB2012) 30
168 Gotway MB, Freemer MM, King TEJ. Challenges in pulmonary fibrosis. 1: Use of high resolution 31 CT scanning of the lung for the evaluation of patients with idiopathic interstitial pneumonias. 32 Thorax. 2007; 62(6):546-553. (Guideline Ref ID GOTWAY2007) 33
169 Gruden JF, Naidich DP. High-resolution CT: Can it obviate lung biopsy? Clinical Pulmonary 34 Medicine. 1998; 5(1):23-35. (Guideline Ref ID GRUDEN1998) 35
170 Guerra M, Miranda JA, Leal F, Vouga L. Interstitial lung disease: diagnostic accuracy and safety of 36 surgical lung biopsy. Revista Portuguesa De Pneumologia. 2009; 15(3):433-442. (Guideline Ref ID 37 GUERRA2009) 38

467
Idiopathic Pulmonary Fibrosis Reference list
171 Hagaman JT, Kinder BW, Eckman MH. Thiopurine S-methyltranferase testing in idiopathic 1 pulmonary fibrosis: a pharmacogenetic cost-effectiveness analysis. Lung. United States 2010; 2 188(2):125-132. (Guideline Ref ID HAGAMAN2010) 3
172 Hallstrand TS, Boitano LJ, Johnson WC, Spada CA, Hayes JG, Raghu G. The timed walk test as a 4 measure of severity and survival in idiopathic pulmonary fibrosis. European Respiratory Journal. 5 2005; 25(1):96-103. (Guideline Ref ID HALLSTRAND2005) 6
173 Hamada K, Nagai S, Tanaka S, Handa T, Shigematsu M, Nagao T et al. Significance of pulmonary 7 arterial pressure and diffusion capacity of the lung as prognosticator in patients with idiopathic 8 pulmonary fibrosis. Chest. 2007; 131(3):650-656. (Guideline Ref ID HAMADA2007) 9
174 Han MK, Bach D, Hagan P, Schmidt SL, Flaherty KR, Toews GB et al. Presence of right ventricular 10 dysfunction modifies treatment response to sildenafil in the step-IPF trial. American Journal of 11 Respiratory and Critical Care Medicine. 2011; 183(1 MeetingAbstracts). (Guideline Ref ID 12 HAN2011) 13
175 Hara A, Sakamoto N, Ishimatsu Y, Kakugawa T, Nakashima S, Hara S et al. S100A9 in BALF is a 14 candidate biomarker of idiopathic pulmonary fibrosis. Respiratory Medicine. 2012; 106(4):571-15 580. (Guideline Ref ID HARA2012) 16
176 Harari S, Simonneau G, De Juli E, Brenot F, Cerrina J, Colombo P et al. Prognostic value of 17 pulmonary hypertension in patients with chronic interstitial lung disease referred for lung or 18 heart-lung transplantation. Journal of Heart and Lung Transplantation. 1997; 16(4):460-463. 19 (Guideline Ref ID HARARI1997) 20
177 Harris-Eze AO, Sridhar G, Clemens RE, Gallagher CG, Marciniuk DD. Oxygen improves maximal 21 exercise performance in interstitial lung disease. American Journal of Respiratory and Critical 22 Care Medicine. 1994; 150(6 Pt 1):1616-1622. (Guideline Ref ID HARRISEZE1994) 23
178 Harris-Eze AO, Sridhar G, Clemens RE, Zintel TA, Gallagher CG, Marciniuk DD. Low-dose nebulized 24 morphine does not improve exercise in interstitial lung disease. American Journal of Respiratory 25 and Critical Care Medicine. 1995; 152(6 Pt 1):1940-1945. (Guideline Ref ID HARRISEZE1995) 26
179 Hayden AM, Robert RC, Kriett JM, Smith CM, Nicholson K, Jamieson SW. Primary diagnosis 27 predicts prognosis of lung transplant candidates. Transplantation. 1993; 55(5):1048-1050. 28 (Guideline Ref ID HAYDEN1993) 29
180 Hira HS, Sharma RK. Study of oxygen saturation, breathing pattern and arrhythmias in patients of 30 interstitial lung disease during sleep. Indian Journal of Chest Diseases and Allied Sciences. 1997; 31 39(3):157-162. (Guideline Ref ID HIRA1997) 32
181 Hirst A, Sloan R. Benzodiazepines and related drugs for insomnia in palliative care. Cochrane 33 Database of Systematic Reviews. 2001; Issue 4:CD003346. DOI:10.1002/14651858.CD003346. 34 (Guideline Ref ID HIRST2001) 35
182 Ho S-C, Chen L-F, Sheng T-F, Jao W-C, Kuo H-P, Lin H-C. Effects of negative ventilation and 36 exercise training on dyspnea sensation and exercise tolerance in patients with restrictive lung 37 diseases. American Journal of Respiratory and Critical Care Medicine. 2010; 181(Meeting 38 Abstracts):A3768. (Guideline Ref ID HO2010) 39
183 Holden DA, Stelmach KD, Curtis PS, Beck GJ, Stoller JK. The impact of a rehabilitation program on 40 functional status of patients with chronic lung disease. Respiratory Care. 1990; 35(4):332-341. 41 (Guideline Ref ID HOLDEN1990) 42

468
Idiopathic Pulmonary Fibrosis Reference list
184 Holland A, Knapman L, Brazzale DJ, Conron M, Glaspole I, Goh N. The 6-minute walk test elicits 1 high but submaximal cardiorespiratory responses in interstitial lung disease. American Journal of 2 Respiratory and Critical Care Medicine. 2010; 181(Meeting Abstracts):A2968. (Guideline Ref ID 3 HOLLAND2010) 4
185 Holland AE, Hill CJ, Conron M, Munro P, McDonald CF. Short term improvement in exercise 5 capacity and symptoms following exercise training in interstitial lung disease. Thorax. 2008; 6 63(6):549-554. (Guideline Ref ID HOLLAND2008A) 7
186 Holland A, Hill C. Physical training for interstitial lung disease. Cochrane Database of Systematic 8 Reviews. 2008; Issue 4:CD006322. (Guideline Ref ID HOLLAND2008) 9
187 Holland AE, Hill CJ, Glaspole I, Goh N, McDonald CF. Predictors of benefit following pulmonary 10 rehabilitation for interstitial lung disease. Respiratory Medicine. 2012; 106(3):429-435. (Guideline 11 Ref ID HOLLAND2012) 12
188 Homma SA, Azuma A, Taniguchi H, Ogura T, Mochizuki Y, Sugiyama Y. A randomized, bouble-13 blind, multicentre, controlled trial of inhaled N-acetylcysteine in patients with the early stage of 14 idiopathic pulmonary fibrosis in Japan. American Journal of Respiratory and Critical Care 15 Medicine. 2010; 181(Meeting Abstracts):A3986. (Guideline Ref ID HOMMA2010) 16
189 Homma S, Azuma A, Taniguchi H, Ogura T, Mochiduki Y, Sugiyama Y et al. Efficacy of inhaled N-17 acetylcysteine monotherapy in patients with early stage idiopathic pulmonary fibrosis. 18 Respirology. 2012; 17(3):467-477. (Guideline Ref ID HOMMA2012) 19
190 Hook JL, Arcasoy SM, Zemmel D, Bartels MN, Kawut SM, Lederer DJ. Titrated oxygen requirement 20 and prognostication in idiopathic pulmonary fibrosis. European Respiratory Journal. 2012; 21 39(2):359-365. (Guideline Ref ID HOOK2012) 22
191 Hope-Gill BDM, Hilldrup S, Davies C, Newton RP, Harrison NK. A study of the cough reflex in 23 idiopathic pulmonary fibrosis. American Journal of Respiratory and Critical Care Medicine. 2003; 24 168(8):995-1002. (Guideline Ref ID HOPEGILL2003) 25
192 Horton MR, Danoff SK, Lechtzin N. Thalidomide inhibits the intractable cough of idiopathic 26 pulmonary fibrosis. Thorax. 2008; 63(8):749. (Guideline Ref ID HORTON2008) 27
193 Horton MR, Santopietro V, Mathew L, Horton KM, Polito AJ, Liu MC et al. Thalidomide for the 28 treatment of cough in idiopathic pulmonary fibrosis: a randomized trial. Annals of Internal 29 Medicine. 2012; 157(6):398-406. (Guideline Ref ID HORTON2012) 30
194 Howard M. The evidence for domiciliary noninvasive ventilation. Sleep and Biological Rhythms. 31 2009; 7(Suppl s1):A9. (Guideline Ref ID HOWARD2009) 32
195 Huang SK, Myers JL, Flaherty KR. The role of lung biopsy in the diagnosis and management of 33 idiopathic interstitial pneumonia. Expert Opinion on Medical Diagnostics. 2008; 2(2):183-190. 34 (Guideline Ref ID HUANG2008) 35
196 Hubbard R, Johnston I, Britton J. Survival in patients with cryptogenic fibrosing alveolitis: a 36 population-based cohort study. Chest. 1998; 113(2):396-400. (Guideline Ref ID HUBBARD1998) 37
197 Huie T, Collard H, Solomon J, Sahin H, Woods A, Kinder B et al. Serologies and chest CT findings 38 predict prognosis in interstitial lung disease. Chest. 2011; 140(4 Meeting Abstracts). (Guideline 39 Ref ID HUIE2011) 40

469
Idiopathic Pulmonary Fibrosis Reference list
198 Hunninghake GW, Zimmerman MB, Schwartz DA, King TE, Jr., Lynch J, Hegele R et al. Utility of a 1 lung biopsy for the diagnosis of idiopathic pulmonary fibrosis. American Journal of Respiratory & 2 Critical Care Medicine. 2001; 164(2):193-196. (Guideline Ref ID HUNNINGHAKE2001) 3
199 Hwang JH, Misumi S, Curran-Everett D, Brown KK, Sahin H, Lynch DA. Longitudinal follow-up of 4 fibrosing interstitial pneumonia: relationship between physiologic testing, computed tomography 5 changes, and survival rate. Journal of Thoracic Imaging. 2011; 26(3):209-217. (Guideline Ref ID 6 HWANG2011) 7
200 Ichikado K, Suga M, Muller NL, Taniguchi H, Kondoh Y, Akira M et al. Acute interstitial 8 pneumonia: comparison of high-resolution computed tomography findings between survivors 9 and nonsurvivors. American Journal of Respiratory and Critical Care Medicine. 2002; 10 165(11):1551-1556. (Guideline Ref ID ICHIKADO2002) 11
201 Idiopathic Pulmonary Fibrosis Clinical Research Network, Raghu G, Anstrom KJ, King TEJ, Lasky JA, 12 Martinez FJ. Prednisone, azathioprine, and N-acetylcysteine for pulmonary fibrosis. New England 13 Journal of Medicine. 2012; 366(21):1968-1977. (Guideline Ref ID PANTHER2012) 14
202 Iotti GA, Polito A, Belliato M, Pasero D, Beduneau G, Wysocki M et al. Adaptive support 15 ventilation versus conventional ventilation for total ventilatory support in acute respiratory 16 failure. Intensive Care Medicine. 2010; 36(8):1371-1379. (Guideline Ref ID IOTTI2010) 17
203 Irwin RS, Boulet L-P, Cloutier MM, Gold PM, Ing AJ, O'Byrne P et al. Managing cough as a defense 18 mechanism and as a symptom: a consensus panel report of the American college of chest 19 physicians. Chest. 1998; 114(2 Suppl I):133S-181S. (Guideline Ref ID IRWIN1998) 20
204 Ishie RT, Cardoso JJdD, Silveira RJ, Stocco L. Video-assisted thoracoscopy for the diagnosis of 21 diffuse parenchymal lung disease. Jornal Brasileiro De Pneumologia. 2009; 35(3):234-241. 22 (Guideline Ref ID ISHIE2009) 23
205 Iwasawa T, Nishimura J, Ogura T, Asakura A, Goto T, Yazawa T et al. Quantitative analysis of thin-24 section CT; correlation with prognosis of patients with idiopathic pulmonary fibrosis. Japanese 25 Journal of Clinical Radiology. 2008; 53(1):194-202. (Guideline Ref ID IWASAWA2008) 26
206 Iwasawa T, Asakura A, Sakai F, Kanauchi T, Gotoh T, Ogura T et al. Assessment of prognosis of 27 patients with idiopathic pulmonary fibrosis by computer-aided analysis of CT images. Journal of 28 Thoracic Imaging. 2009; 24(3):216-222. (Guideline Ref ID IWASAWA2009) 29
207 Jackson RM, Glassberg MK, Ramos CF, Bejarano PA, Butrous G, Gomez-Marin O. Sildenafil 30 therapy and exercise tolerance in idiopathic pulmonary fibrosis. Lung. 2010; 188(2):115-123. 31 (Guideline Ref ID JACKSON2010) 32
208 Jackson RM, Ramos CF, Glassberg M, Bejarano P, Gomez-Marin O. Effects of sildenafil on exercise 33 and dyspnea in IPF patients. American Thoracic Society International Conference, May 15-20, 34 2009, San Diego. 2009; 179(Meeting Abstracts):A1134. (Guideline Ref ID JACKSON2009) 35
209 Jain A, Lolak S. Psychiatric aspects of chronic lung disease. Current Psychiatry Reports. 2009; 36 11(3):219-225. (Guideline Ref ID JAIN2009) 37
210 Jamaati HR, Tabarsi P, Emami M, Mohammadi F, Bakhshayesh KM, Masjedi MR. Clinical pattern 38 of idiopathic pulmonary fibrosis: a retrospective study. Tanaffos. 2006; 5(2):27-32. (Guideline Ref 39 ID JAMAATI2006) 40

470
Idiopathic Pulmonary Fibrosis Reference list
211 Janssen DJA, Spruit MA, Alsemgeest TPG, Does JD, Schols JMGA, Wouters EFM. A patient-centred 1 interdisciplinary palliative care programme for end-stage chronic respiratory diseases. 2 International Journal of Palliative Nursing. 2010; 16(4):189-194. (Guideline Ref ID JANSSEN2010) 3
212 Janssens JP, Penalosa B, Degive C, Rabeus M, Rochat T. Quality of life of patients under home 4 mechanical ventilation for restrictive lung diseases: a comparative evaluation with COPD 5 patients. Monaldi Archives for Chest Disease. 1996; 51(3):178-184. (Guideline Ref ID 6 JANSSENS1996) 7
213 Jastrzebski D, Gumola A, Gawlik R, Kozielski J. Dyspnea and quality of life in patients with 8 pulmonary fibrosis after six weeks of respiratory rehabilitation. Journal of Physiology and 9 Pharmacology. 2006; 57 Suppl 4:139-148. (Guideline Ref ID JASTRZEBSKI2006) 10
214 Jastrzebski D, Kozielski J, Banas A, Cebula T, Gumola A, Ziora D et al. Quality of life during one-11 year observation of patients with idiopathic pulmonary fibrosis awaiting lung transplantation. 12 Journal of Physiology and Pharmacology. 2005; 56 Suppl 4:99-105. (Guideline Ref ID 13 JASTRZEBSKI2005) 14
215 Jastrzebski D, Kozielski J, Nowak J, Zielinska-Les I, Ziora D, Szulik B et al. Prognostic risk factors in 15 patients with interstitial lung disease referred for lung transplantation. Journal of Physiology and 16 Pharmacology. 2005; 56(Suppl 4):107-113. (Guideline Ref ID JASTRZEBSKI2005A) 17
216 Jastrzebski D, Kozielski J, Zebrowska A. Pulmonary rehabilitation in patients with idiopathic 18 pulmonary fibrosis (IPF) with inspiratory muscle training. European Respiratory Journal. 2007; 19 30(Suppl 51):767s. (Guideline Ref ID JASTRZEBSKI2007A) 20
217 Jastrzebski D, Kozielski J, Zebrowska A. Pulmonary rehabilitation in patients with idiopathic 21 pulmonary fibrosis with inspiratory muscle training. Pneumonologia i Alergologia Polska : Organ 22 Polskiego Towarzystwa Ftyzjopneumonologicznego, Polskiego Towarzystwa Alergologicznego, i 23 Instytutu Gruand#378. licy i Chorób Pand#322 2008; 76(3):131-141. (Guideline Ref ID 24 JASTRZEBSKI2008) 25
218 Jegal Y, Kim DS, Shim TS, Lim CM, Do Lee S, Koh Y et al. Physiology is a stronger predictor of 26 survival than pathology in fibrotic interstitial pneumonia. American Journal of Respiratory and 27 Critical Care Medicine. 2005; 171(6):639-644. (Guideline Ref ID JEGAL2005) 28
219 Jeon K, Chung MP, Lee KS, Chung MJ, Han J, Koh W-J et al. Prognostic factors and causes of death 29 in Korean patients with idiopathic pulmonary fibrosis. Respiratory Medicine. 2006; 100(3):451-30 457. (Guideline Ref ID JEON2006) 31
220 Jeong YJ, Lee KS, Muller NL, Chung MP, Chung MJ, Han J et al. Usual interstitial pneumonia and 32 non-specific interstitial pneumonia: serial thin-section CT findings correlated with pulmonary 33 function. Korean Journal of Radiology. 2005; 6(3):143-152. (Guideline Ref ID JEONG2005) 34
221 Jin WS, Choi C-M, Hong S-B, Oh Y-M, Tae SS, Lim C-M et al. Analysis of characteristics and 35 prognostic factors in adult patients receiving mechanical ventilation in the medical intensive care 36 unit of a university hospital. Tuberculosis and Respiratory Diseases. 2008; 65(4):292-300. 37 (Guideline Ref ID JIN2008) 38
222 Johnson MA, Kwan S, Snell NJ, Nunn AJ, Darbyshire JH, Turner-Warwick M. Randomised 39 controlled trial comparing prednisolone alone with cyclophosphamide and low dose 40 prednisolone in combination in cryptogenic fibrosing alveolitis. Thorax. 1989; 44(4):280-288. 41 (Guideline Ref ID JOHNSON1989) 42

471
Idiopathic Pulmonary Fibrosis Reference list
223 Jowett S, Bryan S, Murray E, McCahon D, Raftery J, Hobbs FDR et al. Patient self-management of 1 anticoagulation therapy: a trial-based cost-effectiveness analysis. British Journal of 2 Haematology.: Blackwell Publishing Ltd. 2006; 134(6):632-639. (Guideline Ref ID JOWETT2006) 3
224 Judson MA, Silvestri J, Hartung C, Byars T, Cox CE. The effect of thalidomide on corticosteroid-4 dependent pulmonary sarcoidosis. Sarcoidosis, Vasculitis, and Diffuse Lung Diseases. 2006; 5 23(1):51-57. (Guideline Ref ID JUDSON2006) 6
225 Kadikar A, Maurer J, Kesten S. The six-minute walk test: a guide to assessment for lung 7 transplantation. Journal of Heart and Lung Transplantation. 1997; 16(3):313-319. (Guideline Ref 8 ID KADIKAR1997) 9
226 Kagan G, Rose R. Double-blind trial of a long-acting bronchodilator preparation ("Nethaprin 10 Dospan") in bronchospastic disease. Current Medical Research and Opinion. 1976; 4(6):436-441. 11 (Guideline Ref ID KAGAN1976) 12
227 Kagaya H, Takahashi H, Sugawara K, Kasai C, Kiyokawa N, Shioya T. Effective home-based 13 pulmonary rehabilitation in patients with restrictive lung diseases. Tohoku Journal of 14 Experimental Medicine. 2009; 218(3):215-219. (Guideline Ref ID KAGAYA2009) 15
228 Kaminsky DA, Whitman T, Callas PW. DLCO versus DLCO/VA as predictors of pulmonary gas 16 exchange. Respiratory Medicine. 2007; 101(5):989-994. (Guideline Ref ID KAMINSKY2007) 17
229 Kastelik JA, Aziz I, Ojoo JC, Thompson RH, Redington AE, Morice AH. Investigation and 18 management of chronic cough using a probability-based algorithm. European Respiratory 19 Journal. 2005; 25(2):235-243. (Guideline Ref ID KASTELIK2005) 20
230 Kataoka K, Taniguchi H, Kondoh Y, Fujimoto K, Kitaichi M, Kondo M et al. Accuracy of clinical-21 radiological diagnosis of interstitial pneumonia by physicians with different levels of experience. 22 Respirology. 2010; 15(Suppl 2):83. (Guideline Ref ID KATAOKA2010) 23
231 Kawut SM, O'Shea MK, Bartels MN, Wilt JS, Sonett JR, Arcasoy SM. Exercise testing determines 24 survival in patients with diffuse parenchymal lung disease evaluated for lung transplantation. 25 Respiratory Medicine. 2005; 99(11):1431-1439. (Guideline Ref ID KAWUT2005) 26
232 Kazerooni EA, Martinez FJ, Flint A, Jamadar DA, Gross BH, Spizarny DL et al. Thin-section CT 27 obtained at 10-mm increments versus limited three-level thin-section CT for idiopathic 28 pulmonary fibrosis: correlation with pathologic scoring. AJR American Journal of Roentgenology. 29 1997; 169(4):977-983. (Guideline Ref ID KAZEROONI1997) 30
233 Keating D, Levvey B, Kotsimbos T, Whitford H, Westall G, Williams T et al. Lung transplantation in 31 pulmonary fibrosis: challenging early outcomes counterbalanced by surprisingly good outcomes 32 beyond 15 years. Transplantation Proceedings. 2009; 41(1):289-291. (Guideline Ref ID 33 KEATING2009) 34
234 Keller R. Diagnostic strategies of lung biopsy. Monaldi Archives for Chest Disease. 1995; 35 50(6):464-468. (Guideline Ref ID KELLER1995) 36
235 Killin CR, Hayes J, Byrne A, Hope-Gill B. Quality of care for patients with idiopathic pulmonary 37 fibrosis-perspectives from patients and carers. Palliative Medicine. 2010; 24(4 Suppl 1):S178-38 S179. (Guideline Ref ID KILLIN2010) 39

472
Idiopathic Pulmonary Fibrosis Reference list
236 Kim HK, Jo WM, Jung JH, Chung WJ, Shim JH, Choi YH et al. Needlescopic lung biopsy for 1 interstitial lung disease and indeterminate pulmonary nodules: a report on 65 cases. Annals of 2 Thoracic Surgery. 2008; 86(4):1098-1103. (Guideline Ref ID KIM2008) 3
237 Kim J-H, Lee J-H, Ryu YJ, Chun EM, Chang JH. Clinical predictors of survival in idiopathic 4 pulmonary fibrosis. Chest. 2010; 138(4). (Guideline Ref ID KIM2010B) 5
238 King TE, Jr. Bosentan for idiopathic pulmonary fibrosis. Current Opinion in Investigational Drugs. 6 2008; 9(11):1171-1179. (Guideline Ref ID KING2008) 7
239 King TE, Jr., Behr J, Brown KK, du Bois RM, Lancaster L, de Andrade JA et al. BUILD-1: a 8 randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis. American 9 Journal of Respiratory & Critical Care Medicine. 2008; 177(1):75-81. (Guideline Ref ID 10 KING2008A) 11
240 King TE, Behr J, Brown KK, du Bois RM, Raghu G. Bosentan use in idiopathic pulmonary fibrosis 12 (IPF): results of the placebo-controlled BUILD-1 study. Proceedings of the American Thoracic 13 Society. 2006; 3:A524. (Guideline Ref ID KING2006) 14
241 King TE, Jr., Brown KK, Raghu G, du Bois RM, Lynch DA, Martinez FJ ea. The BUILD-3 trial: a 15 prospective, randomized, double-blind, placebo-controlled study of bosentan in idiopathic 16 pulmonary fibrosis. American Journal of Respiratory and Critical Care Medicine. 2010; 17 181(Meeting Abstracts):A6838. (Guideline Ref ID KING2010) 18
242 King TE, Jr., Brown KK, Raghu G, du Bois RM, Lynch DA, Martinez F et al. BUILD-3: a randomized, 19 controlled trial of bosentan in idiopathic pulmonary fibrosis. American Journal of Respiratory & 20 Critical Care Medicine. 2011; 184(1):92-99. (Guideline Ref ID KING2011) 21
243 King TE, Jr., Tooze JA, Schwarz MI, Brown KR, Cherniack RM. Predicting survival in idiopathic 22 pulmonary fibrosis: scoring system and survival model. American Journal of Respiratory & Critical 23 Care Medicine. 2001; 164(7):1171-1181. (Guideline Ref ID KING2001) 24
244 King TEJ, Schwarz MI, Brown K, Tooze JA, Colby TV, Waldron JAJ et al. Idiopathic pulmonary 25 fibrosis: relationship between histopathologic features and mortality. American Journal of 26 Respiratory and Critical Care Medicine. 2001; 164(6):1025-1032. (Guideline Ref ID KING2001A) 27
245 Kishaba T, Shimaoka Y, Fukuyama H, Yoshida K, Tanaka M, Yamashiro S et al. A cohort study of 28 mortality predictors and characteristics of patients with combined pulmonary fibrosis and 29 emphysema. BMJ Open. 2012; 2(3). (Guideline Ref ID KISHABA2012) 30
246 Klooster TL, van Moorsel CHM, van Kessel DA, van de Graaf EA, Kwakkel-van Erp JM, Luijk HD et 31 al. Mortality in idiopathic pulmonary fibrosis (IPF) on the waiting list for lung transplantation in 32 the Netherlands. Sarcoidosis Vasculitis and Diffuse Lung Diseases. 2011; 28:22. (Guideline Ref ID 33 KLOOSTER2011) 34
247 Koehler E, Brown E, Haneuse J-PA. On the assessment of Monte Carlo error in simulation-based 35 statistical analyses. The American Statistician. 2009; 63(2):155-162. (Guideline Ref ID 36 KOEHLER2009) 37
248 Kondoh Y, Taniguchi H, Katsuta T, Kataoka K, Kimura T, Nishiyama O et al. Risk factors of acute 38 exacerbation of idiopathic pulmonary fibrosis. Sarcoidosis, Vasculitis, and Diffuse Lung Diseases. 39 2010; 27(2):103-110. (Guideline Ref ID KONDOH2010) 40

473
Idiopathic Pulmonary Fibrosis Reference list
249 Kondoh Y, Taniguchi H, Kitaichi M, Yokoi T, Johkoh T, Oishi T et al. Acute exacerbation of 1 interstitial pneumonia following surgical lung biopsy. Respiratory Medicine. 2006; 100(10):1753-2 1759. (Guideline Ref ID KONDOH2006) 3
250 Koschel D, Handzhiev S, Wiedemann B, Hoffken G. Acute effects of NPPV in interstitial lung 4 disease with chronic hypercapnic respiratory failure. Respiratory Medicine. 2010; 104(2):291-5 295. (Guideline Ref ID KOSCHEL2010) 6
251 Kozower BD, Meyers BF, Smith MA, De Oliveira NC, Cassivi SD, Guthrie TJ et al. The impact of the 7 lung allocation score on short-term transplantation outcomes: a multicenter study. Journal of 8 Thoracic and Cardiovascular Surgery. 2008; 135(1):166-171. (Guideline Ref ID KOZOWER2008) 9
252 Kozu R, Jenkins S, Senjyu H. Effect of disability on response to pulmonary rehabilitation (PR) in 10 individuals with idiopathic pulmonary fibrosis (IPF). Respirology. 2011; 16(Suppl s1):20. 11 (Guideline Ref ID KOZU2011B) 12
253 Kozu R, Senjyu H, Jenkins SC, Mukae H, Sakamoto N, Kohno S. Differences in response to 13 pulmonary rehabilitation in idiopathic pulmonary fibrosis and chronic obstructive pulmonary 14 disease. Respiration; International Review of Thoracic Diseases. 2011; 81(3):196-205. (Guideline 15 Ref ID KOZU2011) 16
254 Kramer MR, Berkman N, Mintz B, Godfrey S, Saute M, Amir G. The role of open lung biopsy in the 17 management and outcome of patients with diffuse lung disease. Annals of Thoracic Surgery. 18 1998; 65(1):198-202. (Guideline Ref ID KRAMER1998) 19
255 Kreider ME, Hansen-Flaschen J, Ahmad NN, Rossman MD, Kaiser LR, Kucharczuk JC et al. 20 Complications of video-assisted thoracoscopic lung biopsy in patients with interstitial lung 21 disease. Annals of Thoracic Surgery. 2007; 83(3):1140-1144. (Guideline Ref ID KREIDER2007) 22
256 Krishnan V, McCormack MC, Mathai SC, Agarwal S, Richardson B, Horton MR et al. Sleep quality 23 and health-related quality of life in idiopathic pulmonary fibrosis. Chest. 2008; 134(4):693-698. 24 (Guideline Ref ID KRISHNAN2008) 25
257 Kubo H, Nakayama K, Yanai M, Suzuki T, Yamaya M, Watanabe M et al. Anticoagulant therapy for 26 idiopathic pulmonary fibrosis. Chest. 2005; 128(3):1475-1482. (Guideline Ref ID KUBO2005) 27
258 Kulshrestha R, Menon BK, Rajkumar, Vijayan VK. Role of a pattern-based approach in 28 interpretation of transbronchoscopic lung biopsy and its clinical implications. Indian Journal of 29 Chest Diseases and Allied Sciences. 2012; 54(1):9-17. (Guideline Ref ID KULSHRES2012) 30
259 Kumar SP, Jim A. Physical therapy in palliative care: from symptom control to quality of life: a 31 critical review. Indian Journal of Palliative Care. 2010; 16(3):138-146. (Guideline Ref ID 32 KUMAR2010) 33
260 Kurashima K, Takayanagi N, Tsuchiya N, Kanauchi T, Ueda M, Hoshi T et al. The effect of 34 emphysema on lung function and survival in patients with idiopathic pulmonary fibrosis. 35 Respirology. 2010; 15(5):843-848. (Guideline Ref ID KURASHIMA2010) 36
261 Kyeong WK, Sang JP, Young MK, Sang PL, Gee YS, Man PC et al. Short-term efficacy of steroid and 37 immunosuppressive drugs in patients with idiopathic pulmonary fibrosis and pre-treatment 38 factors associated with favorable response. Tuberculosis and Respiratory Diseases. 1999; 39 46(5):685-696. (Guideline Ref ID KYEONG1999) 40

474
Idiopathic Pulmonary Fibrosis Reference list
262 Lama VN, Flaherty KR, Toews GB, Colby TV, Travis WD, Long Q et al. Prognostic value of 1 desaturation during a 6-minute walk test in idiopathic interstitial pneumonia. American Journal 2 of Respiratory and Critical Care Medicine. 2003; 168(9):1084-1090. (Guideline Ref ID LAMA2003) 3
263 Lamas DJ, Kawut SM, Philip N, Arcasoy SM, Lederer DJ. Delayed referral to a tertiary care center 4 is associated with higher mortality in idiopathic pulmonary fibrosis. American Journal of 5 Respiratory and Critical Care Medicine. 2011; 183(1 MeetingAbstracts). (Guideline Ref ID 6 LAMAS2011A) 7
264 Lamas DJ, Kawut SM, Bagiella E, Philip N, Arcasoy SM, Lederer DJ. Delayed access and survival in 8 idiopathic pulmonary fibrosis: a cohort study. American Journal of Respiratory and Critical Care 9 Medicine. 2011; 184(7):842-847. (Guideline Ref ID LAMAS2011) 10
265 Lancaster LH, Mason WR, Parnell JA, Rice TW, Loyd JE, Milstone AP et al. Obstructive sleep apnea 11 is common in idiopathic pulmonary fibrosis. Chest. 2009; 136(3):772-778. (Guideline Ref ID 12 LANCASTER2009) 13
266 Langer D, Iranzo MA, Burtin C, Verleden SE, Vanaudenaerde BM, Troosters T et al. Determinants 14 of physical activity in daily life in candidates for lung transplantation. Respiratory Medicine. 2012; 15 106(5):747-754. (Guideline Ref ID LANGER2012) 16
267 Latsi PI, du Bois RM, Nicholson AG, Colby TV, Bisirtzoglou D, Nikolakopoulou A et al. Fibrotic 17 idiopathic interstitial pneumonia: The prognostic value of longitudinal functional trends. 18 American Journal of Respiratory and Critical Care Medicine. 2003; 168(5):531-537. (Guideline Ref 19 ID LATSI2003) 20
268 Lavender M. Sildenafil does not improve 6 min walk distance in advanced idiopathic pulmonary 21 fibrosis. Thorax. 2011; 66(3):239. (Guideline Ref ID LAVENDER2011) 22
269 Laz N, Ahmed Y. Clinical profiles of patients with idiopathic pulmonary fibrosis and pulmonary 23 arterial hypertension. Chest. 2011; 140(4 Meeting Abstracts). (Guideline Ref ID LAZ2011) 24
270 Lederer DJ, Arcasoy SM, Wilt JS, D'Ovidio F, Sonett JR, Kawut SM. Six-minute-walk distance 25 predicts waiting list survival in idiopathic pulmonary fibrosis. American Journal of Respiratory and 26 Critical Care Medicine. 2006; 174(6):659-664. (Guideline Ref ID LEDERER2006) 27
271 Lee JS, Song JW, Wolters PJ, Elicker BM, King TEJ, Kim DS et al. Bronchoalveolar lavage pepsin in 28 acute exacerbation of idiopathic pulmonary fibrosis. European Respiratory Journal. 2012; 29 39(2):352-358. (Guideline Ref ID LEE2012) 30
272 Lee J, McLaughlin S, Collard H. Comprehensive care of the patient with idiopathic pulmonary 31 fibrosis. Current Opinion in Pulmonary Medicine. 2011; 17(5):348-354. (Guideline Ref ID LEE2011) 32
273 Lee JW, Lee KS, Lee HY, Chung MP, Yi CA, Kim TS et al. Cryptogenic organizing pneumonia: serial 33 high-resolution CT findings in 22 patients. American Journal of Roentgenology. 2010; 195(4):916-34 922. (Guideline Ref ID LEE2010) 35
274 Lee SN, Lee N, Lee WY, Jung SH, Kown W, Noh JK et al. Feasibility of CT guided percutaneous 36 needle biopsy in diffuse parenchymal lung disease. Respirology. 2009; 14(Suppl s3):A210. 37 (Guideline Ref ID LEE2009) 38
275 Leslie KO. Pulmonary pathology for the clinician. Clinics in Chest Medicine. 2006; 27(Suppl):S1-39 S10. (Guideline Ref ID LESLIE2006) 40
475
Idiopathic Pulmonary Fibrosis Reference list
276 Leslie KO. Idiopathic pulmonary fibrosis may be a disease of recurrent, tractional injury to the 1 periphery of the aging lung: a unifying hypothesis regarding etiology and pathogenesis. Archives 2 of Pathology and Laboratory Medicine. 2012; 136(6):591-600. (Guideline Ref ID LESLIE2012) 3
277 Lettieri CJ, Nathan SD, Barnett SD, Ahmad S, Shorr AF. Prevalence and outcomes of pulmonary 4 arterial hypertension in advanced idiopathic pulmonary fibrosis. Chest. 2006; 129(3):746-752. 5 (Guideline Ref ID LETTIERI2006) 6
278 Lettieri CJ, Nathan SD, Browning RF, Barnett SD, Ahmad S, Shorr AF. The distance-saturation 7 product predicts mortality in idiopathic pulmonary fibrosis. Respiratory Medicine. 2006; 8 100(10):1734-1741. (Guideline Ref ID LETTIERI2006A) 9
279 Lettieri CJ, Veerappan GR, Helman DL, Mulligan CR, Shorr AF. Outcomes and safety of surgical 10 lung biopsy for interstitial lung disease. Chest. 2005; 127(5):1600-1605. (Guideline Ref ID 11 LETTIERI2005A) 12
280 Lettieri CJ, Veerappan GR, Parker JM, Franks TJ, Hayden D, Travis WD et al. Discordance between 13 general and pulmonary pathologists in the diagnosis of interstitial lung disease. Respiratory 14 Medicine. 2005; 99(11):1425-1430. (Guideline Ref ID LETTIERI2005) 15
281 Levvey BJ, Keating D, Griffiths A, Oto T, Snell GI. The lung allocation score predicts lung transplant 16 short-term waiting list and late (3yr) post-transplant mortality in a Non-US Center. Journal of 17 Heart and Lung Transplantation. 2009; 28(2 Suppl 1):S316. (Guideline Ref ID LEVVEY2009) 18
282 Ley B, Ryerson CJ, Vittinghoff E, Ryu JH, Tomassetti S, Lee JS et al. A multidimensional index and 19 staging system for idiopathic pulmonary fibrosis. Annals of Internal Medicine. 2012; 156(10):684-20 691. (Guideline Ref ID LEY2012) 21
283 Lindell KO. Improving end-of-life care for patients with idiopathic pulmonary fibrosis and their 22 care partners University of Pittsburgh; 2007. (Guideline Ref ID LINDELL2007) 23
284 Lindell KO, Hoffman LH, Zullo TJ, Olshansky E, Gibson KF, Kaminski N. Palliative care in patients 24 with idiopathic pulmonary fibrosis and their care partners. American Journal of Respiratory and 25 Critical Care Medicine. 2007; 175:A92. (Guideline Ref ID LINDELL2007A) 26
285 Lindell KO, Olshansky E, Song MK, Zullo TG, Gibson KF, Kaminski N et al. Impact of a disease-27 management program on symptom burden and health-related quality of life in patients with 28 idiopathic pulmonary fibrosis and their care partners. Heart and Lung. 2010; 39(4):304-313. 29 (Guideline Ref ID LINDELL2010) 30
286 Lingaraju R, Blumenthal NP, Kotloff RM, Christie J, Ahya VN, Sager JS et al. Effects of lung 31 allocation score on waiting list rankings and transplant procedures. Journal of Heart and Lung 32 Transplantation. 2006; 25(9):1167-1170. (Guideline Ref ID LINGARAJU2006) 33
287 Louly PG, Medeiros-Souza P, Santos-Neto L. N-of-1 double-blind, randomized controlled trial of 34 tramadol to treat chronic cough. Clinical Therapeutics. 2009; 31(5):1007-1013. (Guideline Ref ID 35 LOULY2009) 36
288 Lower EE, Harman S, Baughman RP. Double-blind, randomized trial of dexmethylphenidate 37 hydrochloride for the treatment of sarcoidosis-associated fatigue. Chest. 2008; 133(5):1189-38 1195. (Guideline Ref ID LOWER2008) 39

476
Idiopathic Pulmonary Fibrosis Reference list
289 Lunt D, Winship P, Bostock S, Musk M, Hill K. The effects of bi-level positive pressure ventilation 1 on exercise capacity in patients awaiting lung transplant. Respirology. 2011; 16(Suppl s1):80. 2 (Guideline Ref ID LUNT2011) 3
290 Lutogniewska W, Jastrzebski D, Wyrwol J, Ksiazek B, Ochman M, Kowalski K et al. Dyspnea and 4 quality of life in patients referred for lung transplantation. European Journal of Medical 5 Research. 2010; 15 Suppl 2:76-78. (Guideline Ref ID LUTOGNIEWSKA2010) 6
291 Lynch III JP, Martinez FJ, Travis WD. Idiopathic pulmonary fibrosis: Is lung biopsy essential? 7 Journal of Respiratory Diseases. 2000; 21(3):197-214. (Guideline Ref ID LYNCH2000) 8
292 Lynch DA, Godwin JD, Safrin S, Starko KM, Hormel P, Brown KK et al. High-resolution computed 9 tomography in idiopathic pulmonary fibrosis: diagnosis and prognosis. American Journal of 10 Respiratory and Critical Care Medicine. 2005; 172(4):488-493. (Guideline Ref ID LYNCH2005) 11
293 Mackay LS, Anderson RL, Parry G, Lordan J, Corris PA, Fisher AJ. Pulmonary fibrosis: rate of 12 disease progression as a trigger for referral for lung transplantation. Thorax. 2007; 62(12):1069-13 1073. (Guideline Ref ID MACKAY2007) 14
294 Magpantay FK, De Guia T. The unusual usual lung disease. Respirology. 2010; 15(Suppl 2):84. 15 (Guideline Ref ID MAGPANTAY2010) 16
295 Mahajan R, Daga MK, Tiwari N. Diffuse parenchymal lung disease: an approach to diagnosis. 17 Journal of the Association of Physicians of India. 2002; 50(October):1285-1294. (Guideline Ref ID 18 MAHAJAN2002) 19
296 Maher TM. Diffuse parenchymal lung disease. Medicine. 2008; 36(5):265-272. (Guideline Ref ID 20 MAHER2008A) 21
297 Mahida RY, Wiscombe S, Fisher AJ. Current status of lung transplantation. Chronic Respiratory 22 Disease. 2012; 9(2):131-145. (Guideline Ref ID MAHIDA2012) 23
298 Mahler DA, Harver A, Rosiello R, Daubenspeck JA. Measurement of respiratory sensation in 24 interstitial lung disease: evaluation of clinical dyspnea ratings and magnitude scaling. Chest. 25 1989; 96(4):767-771. (Guideline Ref ID MAHLER1989) 26
299 Manali ED, Lyberopoulos P, Triantafillidou C, Kolilekas LF, Sotiropoulou C, Milic-Emili J et al. MRC 27 chronic Dyspnea Scale: Relationships with cardiopulmonary exercise testing and 6-minute walk 28 test in idiopathic pulmonary fibrosis patients: a prospective study. BMC Pulmonary Medicine. 29 2010; 10:32. (Guideline Ref ID MANALI2010) 30
300 Manali ED, Stathopoulos GT, Kollintza A, Kalomenidis I, Emili JM, Sotiropoulou C et al. The 31 Medical Research Council chronic dyspnea score predicts the survival of patients with idiopathic 32 pulmonary fibrosis. Respiratory Medicine. 2008; 102(4):586-592. (Guideline Ref ID MANALI2008) 33
301 Mansour A, Nair K, Barrios R, Kesavan R, Parulekar A, Loebe M et al. Clinical outcomes in patients 34 with acute exacerbation of idiopathic pulmonary fibrosis undergoing lung transplantation. Chest. 35 2011; 140(4 Meeting Abstracts). (Guideline Ref ID MANSOUR2011) 36
302 Marciniak E, Blackstone A, Doehrel J, Ezzie M, Diaz PT, Lucarelli MR. Use of a structured weight 37 management program for obese patients participating in phase 2 pulmonary rehabilitation. 38 American Journal of Respiratory and Critical Care Medicine. 2010; 181(1 MeetingAbstracts). 39 (Guideline Ref ID MARCINIAK2010) 40
477
Idiopathic Pulmonary Fibrosis Reference list
303 Margaritopoulos GA, Romagnoli M, Poletti V, Siafakas NM, Wells AU, Antoniou KM. Recent 1 advances in the pathogenesis and clinical evaluation of pulmonary fibrosis. European Respiratory 2 Review. 2012; 21(123):48-56. (Guideline Ref ID MARGARITOPOULOS2012) 3
304 Martinez FJ, Safrin S, Weycker D, Starko KM, Bradford WZ, King TEJ et al. The clinical course of 4 patients with idiopathic pulmonary fibrosis. Annals of Internal Medicine. 2005; 142(12 Pt 1):963-5 967. (Guideline Ref ID MARTINEZ2005) 6
305 Martinez TY, Pereira CA, dos Santos ML, Ciconelli RM, Guimaraes SM, Martinez JA. Evaluation of 7 the short-form 36-item questionnaire to measure health-related quality of life in patients with 8 idiopathic pulmonary fibrosis. Chest. 2000; 117(6):1627-1632. (Guideline Ref ID MARTINEZ2000) 9
306 Masjedi MR, Hashemi N, Fakharian A, Marashian M. Idiopathic pulmonary fibrosis in Iran. Annals 10 of Thoracic Medicine. 2010; 5(3):184. (Guideline Ref ID MASJEDI2010) 11
307 Mason DP, Brizzio ME, Alster JM, McNeill AM, Murthy SC, Budev MM et al. Lung transplantation 12 for idiopathic pulmonary fibrosis. Annals of Thoracic Surgery. 2007; 84(4):1121-1128. (Guideline 13 Ref ID MASON2007) 14
308 Matsuo K, Tada S, Shibayama T, Ueno Y, Miyake T, Takehara H et al. Factors affecting prognosis 15 of idiopathic interstitial pneumonia. Acta Medica Okayama. 1996; 50(1):37-46. (Guideline Ref ID 16 MATSUO1996) 17
309 Mazuranic I, Ivanovi-Herceg Z. Complementariness of the radiological finding and transbronchial 18 lung biopsy for definitive diagnosis of diffuse interstitial lung diseases. Radiology and Oncology. 19 1996; 30(2):89-94. (Guideline Ref ID MAZURANIC1996) 20
310 Meier-Sydow J, Rust M, Kronenberger H, Thiel C, Amthor M, Riemann H. Long-term follow-up of 21 lung function parameters in patients with idiopathic pulmonary fibrosis treated with prednisone 22 and azathioprin or d-penicillamine. Praxis Und Klinik Der Pneumologie. 1979; 33 Suppl 1:680-688. 23 (Guideline Ref ID MEIERSYDOW1979) 24
311 Mejia M, Carrillo G, Rojas-Serrano J, Estrada A, Suarez T, Alonso D et al. Idiopathic pulmonary 25 fibrosis and emphysema: decreased survival associated with severe pulmonary arterial 26 hypertension. Chest. 2009; 136(1):10-15. (Guideline Ref ID MEJIA2009) 27
312 Melo N, Figueiredo S, Morais A, Moura CS, Pinho P, Bastos P et al. Open lung biopsy in patients 28 on mechanical ventilation with suspected diffuse lung disease. Revista Portuguesa De 29 Pneumologia. 2009; 15(4):597-611. (Guideline Ref ID MELO2009) 30
313 Merlo CA, Weiss ES, Orens JB, Borja MC, Diener-West M, Conte JV et al. Impact of U.S. Lung 31 Allocation Score on survival after lung transplantation. Journal of Heart and Lung 32 Transplantation. 2009; 28(8):769-775. (Guideline Ref ID MERLO2009) 33
314 Mermigkis C, Stagaki E, Amfilochiou A, Polychronopoulos V, Korkonikitas P, Mermigkis D et al. 34 Sleep quality and associated daytime consequences in patients with idiopathic pulmonary 35 fibrosis. Medical Principles and Practice. 2009; 18(1):10-15. (Guideline Ref ID MERMIGKIS2009) 36
315 Meyer KC. The role of bronchoalveolar lavage in interstitial lung disease. Clinics in Chest 37 Medicine. 2004; 25(4 Special Issue):637-649. (Guideline Ref ID MEYER2004) 38
316 Meyer KC, Raghu G, Baughman RP, Brown KK, Costabel U, du Bois RM et al. An official American 39 Thoracic Society clinical practice guideline: the clinical utility of bronchoalveolar lavage cellular 40

478
Idiopathic Pulmonary Fibrosis Reference list
analysis in interstitial lung disease. American Journal of Respiratory and Critical Care Medicine. 1 2012; 185(9):1004-1014. (Guideline Ref ID MEYER2012) 2
317 Michaelson JE, Aguayo SM, Roman J. Idiopathic pulmonary fibrosis: A practical approach for 3 diagnosis and management. Chest. 2000; 118(3):788-794. (Guideline Ref ID MICHAELSON2000) 4
318 Miller A, Enright P. PFT Interpretive Strategies: American Thoracic Society/ European Respiratory 5 Society 2005 Guideline Gaps... includes discussion. Respiratory Care. 2012; 57(1):127-135. 6 (Guideline Ref ID MILLER2012) 7
319 Miller JD, Urschel JD, Cox G, Olak J, Young JE, Kay JM et al. A randomized, controlled trial 8 comparing thoracoscopy and limited thoracotomy for lung biopsy in interstitial lung disease. 9 Annals of Thoracic Surgery. 2000; 70(5):1647-1650. (Guideline Ref ID MILLER2000) 10
320 Milman N, Faurschou P, Munch EP, Grode G. Transbronchial lung biopsy through the fibre optic 11 bronchoscope. Results and complications in 452 examinations. Respiratory Medicine. 1994; 12 88(10):749-753. (Guideline Ref ID MILMAN1994) 13
321 Milman N, Graudal N, Grode G, Munch E. No effect of high-dose inhaled steroids in pulmonary 14 sarcoidosis: a double-blind, placebo-controlled study. Journal of Internal Medicine. 1994; 15 236(3):285-290. (Guideline Ref ID MILMAN1994A) 16
322 Milman N, Graudal N, Jacobsen GK. Bronchoalveolar lavage in radiologically detected diffuse lung 17 disease. Diagnostic value of total and differential cell count in a series of 130 patients. APMIS. 18 1995; 103(10):764-768. (Guideline Ref ID MILMAN1995) 19
323 Misumi S, Lynch DA. Idiopathic pulmonary fibrosis/usual interstitial pneumonia: imaging 20 diagnosis, spectrum of abnormalities, and temporal progression. Proceedings of the American 21 Thoracic Society. 2006; 3(4):307-314. (Guideline Ref ID MISUMI2006) 22
324 Mittal N, Raj R, Nugent K, Islam E. Frailty in patients with chronic lung diseases undergoing 23 pulmonary rehabilitation. Journal of Investigative Medicine. 2011; 59(2):535. (Guideline Ref ID 24 MITTAL2011) 25
325 Miyazaki1 Y, Azuma A, Inase N, Ogura T, Taniguchi H, Yoshizawa Y. A randomized, double-blind, 26 multi-centered controlled trial of cyclosporine A vs. cyclophosphamide with corticosteroid in 27 patients with idiopathic pulmonary fibrosis in Japan. American Journal of Respiratory and Critical 28 Care Medicine. 2011; 183(Meeting Abstracts):A3812. (Guideline Ref ID MIYAZAKI1Y2011) 29
326 Moderno EV, Yamaguti WPS, Schettino GPP, Kairalla RA, Martins MA, Carvalho CRR et al. Effects 30 of proportional assisted ventilation on exercise performance in idiopathic pulmonary fibrosis 31 patients. Respiratory Medicine. 2010; 104(1):134-141. (Guideline Ref ID MODERNO2010) 32
327 Mogulkoc N, Brutsche MH, Bishop PW, Greaves SM, Horrocks AW, Egan JJ et al. Pulmonary 33 function in idiopathic pulmonary fibrosis and referral for lung transplantation. American Journal 34 of Respiratory and Critical Care Medicine. 2001; 164(1):103-108. (Guideline Ref ID 35 MOGULKOC2001A) 36
328 Molin LJ, Steinberg JB, Lanza LA. VATS increases costs in patients undergoing lung biopsy for 37 interstitial lung disease. Annals of Thoracic Surgery. United States 1994; 58(6):1595-1598. 38 (Guideline Ref ID MOLIN1994) 39

479
Idiopathic Pulmonary Fibrosis Reference list
329 Mollica C. Acute exacerbation of pulmonary fibrosis: Does mechanical ventilation have a role? 1 Rassegna Di Patologia Dell'Apparato Respiratorio. 2008; 23(6):347-349. (Guideline Ref ID 2 MOLLICA2008) 3
330 Mollica C, Paone G, Conti V, Ceccarelli D, Schmid G, Mattia P et al. Mechanical ventilation in 4 patients with end-stage idiopathic pulmonary fibrosis. Respiration; International Review of 5 Thoracic Diseases. 2010; 79(3):209-215. (Guideline Ref ID MOLLICA2010) 6
331 Moloney ED, Clayton N, Mukherjee DK, Gallagher CG, Egan JJ. The shuttle walk exercise test in 7 idiopathic pulmonary fibrosis. Respiratory Medicine. 2003; 97(6):682-687. (Guideline Ref ID 8 MOLONEY2003) 9
332 Mouroux J, Clary-Meinesz C, Padovani B, Perrin C, Rotomondo C, Chavaillon JM et al. Efficacy and 10 safety of videothoracoscopic lung biopsy in the diagnosis of interstitial lung disease. European 11 Journal of Cardio-Thoracic Surgery. 1997; 11(1):22-26. (Guideline Ref ID MOUROUX1997) 12
333 Mura M, Porretta MA, Bargagli E, Sergiacomi G, Zompatori M, Sverzellati N et al. Predicting 13 survival in newly diagnosed idiopathic pulmonary fibrosis: a 3-year prospective study. European 14 Respiratory Journal. 2012; 40(1):101-109. (Guideline Ref ID MURA2012) 15
334 Nadrous HF, Myers JL, Decker PA, Ryu JH. Idiopathic pulmonary fibrosis in patients younger than 16 50 years. Mayo Clinic Proceedings. 2005; 80(1):37-40. (Guideline Ref ID NADROUS2005A) 17
335 Nadrous HF, Pellikka PA, Krowka MJ, Swanson KL, Chaowalit N, Decker PA et al. Pulmonary 18 hypertension in patients with idiopathic pulmonary fibrosis. Chest. 2005; 128(4):2393-2399. 19 (Guideline Ref ID NADROUS2005) 20
336 Nagai S, Handa T, Kim D. Pharmacotherapy in patients with idiopathic pulmonary fibrosis. Expert 21 Opinion on Pharmacotherapy. 2008; 9(11):1909-1925. (Guideline Ref ID NAGAI2008) 22
337 Nagao T, Nagai S, Hiramoto Y, Hamada K, Shigematsu M, Hayashi M et al. Serial evaluation of 23 high-resolution computed tomography findings in patients with idiopathic pulmonary fibrosis in 24 usual interstitial pneumonia. Respiration; International Review of Thoracic Diseases. 2002; 25 69(5):413-419. (Guideline Ref ID NAGAO2002) 26
338 Naji NA, Connor MC, Donnelly SC, McDonnell TJ. Effectiveness of pulmonary rehabilitation in 27 restrictive lung disease. Journal of Cardiopulmonary Rehabilitation. 2006; 26(4):237-243. 28 (Guideline Ref ID NAJI2006) 29
339 Nathan S. Lung transplant candidate selection and clinical outcomes: Strategies for improvement 30 in prioritization. Current Opinion in Organ Transplantation. 2005; 10(3):216-220. (Guideline Ref 31 ID NATHAN2005B) 32
340 Nathan SD. Therapeutic management of idiopathic pulmonary fibrosis: An evidence-based 33 approach. Clinics in Chest Medicine. 2006; 27(Suppl):S27-S35. (Guideline Ref ID NATHAN2006) 34
341 Nathan SD, Shlobin OA, Ahmad S, Urbanek S, Barnett SD. Pulmonary hypertension and 35 pulmonary function testing in idiopathic pulmonary fibrosis. Chest. 2007; 131(3):657-663. 36 (Guideline Ref ID NATHAN2007) 37
342 Nathan SD, Shlobin OA, Weir N, Ahmad S, Kaldjob JM, Battle E et al. Long-term course and 38 prognosis of idiopathic pulmonary fibrosis in the new millennium. Chest. 2011; 140(1):221-229. 39 (Guideline Ref ID NATHAN2011A) 40

480
Idiopathic Pulmonary Fibrosis Reference list
343 Nathan SD, Shlobin OA, Barnett SD, Saggar R, Belperio JA, Ross DJ et al. Right ventricular systolic 1 pressure by echocardiography as a predictor of pulmonary hypertension in idiopathic pulmonary 2 fibrosis. Respiratory Medicine. 2008; 102(9):1305-1310. (Guideline Ref ID NATHAN2008A) 3
344 National Audit Office. NHS (England) Summarised Accounts 2009-2010. London. The Stationery 4 Office, 2010 Available from: http://www.official-5 documents.gov.uk/document/hc1011/hc04/0410/0410.pdf (Guideline Ref ID NAO2010) 6
345 National Collaborating Centre for Chronic Conditions. Stroke: national clinical guideline for 7 diagnosis and initial management of acute stroke and transient ischaemic attack (TIA). London. 8 Royal College of Physicians, 2008 Available from: 9 http://www.nice.org.uk/nicemedia/live/12018/41363/41363.pdf (Guideline Ref ID NCCCC2008) 10
346 National Institute for Health and Clinical Excellence. Clinical Guideline 36: National cost impact 11 report to accompany 'Atrial fibrillation: the management of atrial fibrillation', 2006 Available 12 from: http://www.nice.org.uk/nicemedia/live/10982/30061/30061.pdf (Guideline Ref ID 13 NICE2006) 14
347 National Institute for Health and Clinical Excellence. Guideline development methods: 15 information for national collaborating centres and guideline developers. 2008. [Last accessed: 24 16 December 2008] (Guideline Ref ID NICE2008A) 17
348 National Institute for Health and Clinical Excellence. The guidelines manual 2009. 2009. Available 18 from: 19 http://www.nice.org.uk/aboutnice/howwework/developingniceclinicalguidelines/clinicalguidelin20 edevelopmentmethods/GuidelinesManual2009.jsp [Last accessed: 13 January 2009] (Guideline 21 Ref ID NICE2009) 22
349 Navaratnam V, Fleming KM, West J, Smith CJ, Jenkins RG, Fogarty A et al. The rising incidence of 23 idiopathic pulmonary fibrosis in the U.K. Thorax. 2011; 66(6):462-467. (Guideline Ref ID 24 NAVARATNAM2011) 25
350 Newman WG, Payne K, Tricker K, Roberts SA, Fargher E, Pushpakom S et al. A pragmatic 26 randomized controlled trial of thiopurine methyltransferase genotyping prior to azathioprine 27 treatment: The TARGET study. Pharmacogenomics. 2011; 12(6):815-826. (Guideline Ref ID 28 NEWMAN2011A) 29
351 NHS Business Services Authority. NHS electronic drug tariff. 2013. Available from: 30 http://www.ppa.org.uk/edt/March_2013/mindex.htm (Guideline Ref ID NHS2013) 31
352 NHS Employers. Pay Circular (AforC) 2/2011. NHS terms and conditions of service handbook 32 (amendment number 23): pay and conditions for NHS staff covered by the Agenda for Change 33 agreement, 2011 Available from: 34 http://www.nhsemployers.org/Aboutus/Publications/PayCirculars/Pages/Pay-Circular-AforC-2-35 2011.aspx (Guideline Ref ID NHS2011A) 36
353 Nicholson AG. Classification of idiopathic interstitial pneumonias: making sense of the alphabet 37 soup. Histopathology. 2002; 41(5):381-391. (Guideline Ref ID NICHOLSON2002) 38
354 Nicholson AG, Behr J, Brown KK, du Bois RM, King jr TE, Raghu G et al. Effect of bosentan in 39 patients with confirmed usual interstitial pneumonia (UIP) on surgical lung biopsy (SLB): subset 40 analysis of the randomised controlled BUILD 1 trial in IPF. European Respiratory Journal. 2007; 41 30(Suppl 51):112s. (Guideline Ref ID NICHOLSON2007) 42

481
Idiopathic Pulmonary Fibrosis Reference list
355 Nishiyama O, Kondoh Y, Kimura T, Kato K, Kataoka K, Ogawa T et al. Effects of pulmonary 1 rehabilitation in patients with idiopathic pulmonary fibrosis. Respirology. 2008; 13(3):394-399. 2 (Guideline Ref ID NISHIYAMA2008) 3
356 Niwa T, Hasegawa R, Kawase M, Kondoh Y, Taniguchi H. Effectiveness and adverse events of high 4 frequency oscillatory ventilation for the patients with acute respiratory distress syndrome. 5 Intensive Care Medicine. 2010; 36(Suppl 2):S106. (Guideline Ref ID NIWA2010) 6
357 Niwa T, Hasegawa R, Ryuge M, Kawase M, Kondoh Y, Taniguchi H. Benefits and risks associated 7 with the R100 high frequency oscillatory ventilator for patients with severe hypoxaemic 8 respiratory failure. Anaesthesia and Intensive Care. 2011; 39(6):1111-1119. (Guideline Ref ID 9 NIWA2011) 10
358 Noble PW, Albera C, Bradford WZ, Costabel U, Glassberg MK, Kardatzke D et al. Pirfenidone in 11 patients with idiopathic pulmonary fibrosis (CAPACITY): two randomised trials. Lancet. 2011; 12 377(9779):1760-1769. (Guideline Ref ID NOBLE2011) 13
359 Noth I, Anstrom KJ, Calvert SB, de Andrade JA, Flaherty KR, Glazer C et al. A placebo-controlled 14 randomized trial of warfarin in idiopathic pulmonary fibrosis. American Journal of Respiratory 15 and Critical Care Medicine. 2012; 186(1):88-95. (Guideline Ref ID NOTH2012) 16
360 Noth I, Martinez FJ. Recent advances in idiopathic pulmonary fibrosis. Chest. 2007; 132(2):637-17 650. (Guideline Ref ID NOTH2007) 18
361 O'Beirne S, Counihan IP, Keane MP. Interstitial lung disease and lung transplantation. Seminars in 19 Respiratory and Critical Care Medicine. 2010; 31(2):139-146. (Guideline Ref ID OBEIRNE2010) 20
362 O'Connell OJ, Kennedy MP, Henry MT. Idiopathic pulmonary fibrosis: treatment update. 21 Advances in Therapy. 2011; 28(11):986-999. (Guideline Ref ID OCONNELL2011) 22
363 Obi I, Shlobin OA, Weir N, Ahmad S, Barnett S, Nathan SD. Effects of oxygen therapy in patients 23 with advanced lung diseases. American Journal of Respiratory and Critical Care Medicine. 2010; 24 181(1 MeetingAbstracts). (Guideline Ref ID OBI2010) 25
364 Ochmann U, Jorres RA, Nowak D. Long-term efficacy of pulmonary rehabilitation: A state-of-the-26 art review. Journal of Cardiopulmonary Rehabilitation and Prevention. 2012; 32(3):117-126. 27 (Guideline Ref ID OCHMANN2012) 28
365 Ohshimo S, Bonella F, Cui A, Beume M, Kohno N, Guzman J et al. Significance of bronchoalveolar 29 lavage for the diagnosis of idiopathic pulmonary fibrosis. American Journal of Respiratory and 30 Critical Care Medicine. 2009; 179(11):1043-1047. (Guideline Ref ID OHSHIMO2009) 31
366 Oliveira CC, Fabro AT, Ribeiro SM, Defaveri J, Capelozzi VL, Queluz THT et al. Evaluation of the use 32 of transbronchial biopsy in patients with clinical suspicion of interstitial lung disease. Jornal 33 Brasileiro De Pneumologia. 2011; 37(2):168-175. (Guideline Ref ID OLIVEIRA2011) 34
367 Ong KC, Wong WP, Jailani AR, Sew S, Ong YY. Effects of a pulmonary rehabilitation programme on 35 physiologic and psychosocial outcomes in patients with chronic respiratory disorders. Annals of 36 the Academy of Medicine, Singapore. 2001; 30(1):15-21. (Guideline Ref ID ONG2001) 37
368 Ooi A, Iyenger S, Ferguson J, Ritchie AJ. VATS lung biopsy in suspected, diffuse interstitial lung 38 disease provides diagnosis, and alters management strategies. Heart, Lung and Circulation. 2005; 39 14(2):90-92. (Guideline Ref ID OOI2005) 40

482
Idiopathic Pulmonary Fibrosis Reference list
369 Orens JB, Kazerooni EA, Martinez FJ, Curtis JL, Gross BH, Flint A et al. The sensitivity of high-1 resolution CT in detecting idiopathic pulmonary fibrosis proved by open lung biopsy: A 2 prospective study. Chest. 1995; 108(1):109-115. (Guideline Ref ID ORENS1995) 3
370 Orens JB, Estenne M, Arcasoy S, Conte JV, Corris P, Egan JJ et al. International guidelines for the 4 selection of lung transplant candidates: 2006 update--a consensus report from the Pulmonary 5 Scientific Council of the International Society for Heart and Lung Transplantation. Journal of 6 Heart and Lung Transplantation. 2006; 25(7):745-755. (Guideline Ref ID ORENS2006) 7
371 Osaki S, Maloney J, Cornwel RD, Meyer KC, Edwards NM. Impact of the UNOS lung allocation 8 scoring system on lung transplantation for interstitial lung disease. Journal of Heart and Lung 9 Transplantation. 2010; 29(2 Suppl 1):S112-S113. (Guideline Ref ID OSAKI2010) 10
372 Osaki S, Maloney JD, Meyer KC, Cornwell RD, Edwards NM, De Oliveira NC. The impact of the 11 lung allocation scoring system at the single national Veterans Affairs Hospital lung 12 transplantation program. European Journal of Cardio-Thoracic Surgery. 2009; 36(3):497-501. 13 (Guideline Ref ID OSAKI2009) 14
373 Ozalevli S, Karaali HK, Ilgin D, Ucan ES. Effect of home-based pulmonary rehabilitation in patients 15 with idiopathic pulmonary fibrosis. Multidisciplinary Respiratory Medicine. 2010; 5(1):31-37. 16 (Guideline Ref ID OZALEVLI2010) 17
374 Paik HC, Haam SJ, Lee DY, Yi GJ, Song SW, Kim YT et al. The fate of patients on the waiting list for 18 lung transplantation in Korea. Transplantation Proceedings. 2012; 44(4):865-869. (Guideline Ref 19 ID PAIK2012) 20
375 Pandey R, Chokhani R, Kc N. Use of non invasive vantilation in patients with respiratory failure in 21 Nepal. Kathmandu University Medical Journal. 2011; 9(36):256-259. (Guideline Ref ID 22 PANDEY2011) 23
376 Papali A, Lemme M, Shlobin OA, Weir N, Brown K, Huber C et al. Effect Of N-Acetylcysteine on 24 mortality and functional status in patients with IPF. American Journal of Respiratory and Critical 25 Care Medicine. 2010; 181(1 MeetingAbstracts). (Guideline Ref ID PAPALI2010) 26
377 Papiris SA, Daniil ZD, Malagari K, Kapotsis GE, Sotiropoulou C, Milic-Emili J et al. The Medical 27 Research Council dyspnea scale in the estimation of disease severity in idiopathic pulmonary 28 fibrosis. Respiratory Medicine. 2005; 99(6):755-761. (Guideline Ref ID PAPIRIS2005) 29
378 Park JH, Kim DK, Kim DS, Koh Y, Lee SD, Kim WS et al. Mortality and risk factors for surgical lung 30 biopsy in patients with idiopathic interstitial pneumonia. European Journal of Cardio-Thoracic 31 Surgery. 2007; 31(6):1115-1119. (Guideline Ref ID PARK2007A) 32
379 Peckham RM, Shorr AF, Helman DLJ. Potential limitations of clinical criteria for the diagnosis of 33 idiopathic pulmonary fibrosis/cryptogenic fibrosing alveolitis. Respiration; International Review 34 of Thoracic Diseases. 2004; 71(2):165-169. (Guideline Ref ID PECKHAM2004) 35
380 Peelen L, Wells AU, Prijs M, Blumenthal JP, Van Steenwijk RP, Jonkers RE et al. Fibrotic idiopathic 36 interstitial pneumonias: Mortality is linked to a decline in gas transfer. Respirology. 2010; 37 15(8):1233-1243. (Guideline Ref ID PEELEN2010) 38
381 Personal Social Services Research Unit. Unit Costs of Health and Social Care 2010. University of 39 Kent: 2010 Available from: http://www.pssru.ac.uk/uc/uc2010contents.htm (Guideline Ref ID 40 PSSRU2010) 41

483
Idiopathic Pulmonary Fibrosis Reference list
382 Poletti V, Chilosi M, Olivieri D. Diagnostic invasive procedures in diffuse infiltrative lung diseases. 1 Respiration; International Review of Thoracic Diseases. 2004; 71(2):107-119. (Guideline Ref ID 2 POLETTI2004) 3
383 Polonski L, Kusnierz B, Tendera N, Krzywiecki A, Polonska A, Oklek K. Long term oxygen therapy 4 attenuates progression of pathologic changes in pulmonary circulation and the heart in patients 5 with idiopathic interstitial lung fibrosis. European Respiratory Journal - Supplement. 1994; 6 7(Suppl 18):80s. (Guideline Ref ID POLONSKI1994) 7
384 Polosa R, Simidchiev A, Walters EH. Nebulised morphine for severe interstitial lung disease. 8 Cochrane Database of Systematic Reviews. 2002; Issue 3:CD002872. (Guideline Ref ID 9 POLOSA2002) 10
385 Polychronopoulos VS. Diffuse lung diseases (DLDS): Differential approach. Respirology. 2009; 11 14(Suppl 3):A118. (Guideline Ref ID POLYCHRONOPOULOS2009) 12
386 Popp W, Rauscher H, Ritschka L, Braun O, Scherak O, Kolarz G et al. Prediction of interstitial lung 13 involvement in rheumatoid arthritis; The value of clinical data, chest roentgenogram, lung 14 function, and serologic parameters. Chest. 1992; 102(2):391-394. (Guideline Ref ID POPP1992) 15
387 Popper HH. Which biopsies in diffuse infiltrative lung diseases and when are these necessary? 16 Monaldi Archives for Chest Disease - Pulmonary Series. 2001; 56(5):446-452. (Guideline Ref ID 17 POPPER2001) 18
388 Prendergast TJ, Puntillo KA. Perspectives on care at the close of life. Withdrawal of life support: 19 intensive caring at the end of life. Journal of the American Medical Association. 2002; 20 288(21):2732-2740. (Guideline Ref ID PRENDERGAST2002) 21
389 Pruitt B. Loosening the bonds of restrictive lung disease. Nursing. 2008; 38(8):34-40. (Guideline 22 Ref ID PRUITT2008) 23
390 Quadrelli S, Molinari L, Ciallella L, Spina JC, Sobrino E, Chertcoff J. Radiological versus 24 histopathological diagnosis of usual interstitial pneumonia in the clinical practice: does it have 25 any survival difference? Respiration; International Review of Thoracic Diseases. 2010; 79(1):32-26 37. (Guideline Ref ID QUADRELLI2010) 27
391 Quigley M, Hansell DM, Nicholson AG. Interstitial lung disease--the new synergy between 28 radiology and pathology. Histopathology. 2006; 49(4):334-342. (Guideline Ref ID QUIGLEY2006) 29
392 Quill TE. Initiating end-of-life discussions with seriously ill patients: Addressing the "elephant in 30 the room". JAMA: Journal of the American Medical Association. 2000; 284(19):2502-2507. 31 (Guideline Ref ID QUILL2000) 32
393 Qureshi RA SA. Efficacy of thoracoscopic lung biopsy in interstitial lung diseases: comparison with 33 open lung biopsy. Journal of the College of Physicians and Surgeons - Pakistan. 2003; 13(10):600-34 603. (Guideline Ref ID QURESHIRA2003) 35
394 Qureshi RA, Ahmed TA, Grayson AD, Soorae AS, Drakeley MJ, Page RD. Does lung biopsy help 36 patients with interstitial lung disease? European Journal of Cardio-Thoracic Surgery. 2002; 37 21(4):621-626. (Guideline Ref ID QURESHI2002) 38
395 Raghu G, Behr J, Brown KK, Egan JJ, Kawut SM, Flaherty KR et al. Artemis-Ipf: a placebo-39 controlled trial of ambrisentan in idiopathic pulmonary fibrosis. American Journal of Respiratory 40 & Critical Care Medicine. 2012; 185(Suppl):A3632. (Guideline Ref ID RAGHU2012) 41
484
Idiopathic Pulmonary Fibrosis Reference list
396 Raghu G, Brown KK. Interstitial lung disease: Clinical evaluation and keys to an accurate 1 diagnosis. Clinics in Chest Medicine. 2004; 25(3):409-419. (Guideline Ref ID RAGHU2004B) 2
397 Raghu G, Brown KK, Behr J, du Bois RM, King TE. Bosentan in idiopathic pulmonary fibrosis (IPF) 3 quality of life (QOL) results of the BUILD 1 study. European Respiratory Journal. 2006; 28(Suppl 4 50):571s. (Guideline Ref ID RAGHU2006) 5
398 Raghu G, Brown KK, Costabel U, Cottin V, du Bois RM, Lasky JA et al. Treatment of idiopathic 6 pulmonary fibrosis with etanercept: An exploratory, placebo-controlled trial. American Journal of 7 Respiratory and Critical Care Medicine. 2008; 178(9):948-955. (Guideline Ref ID RAGHU2008) 8
399 Raghu G, Chang J. Idiopathic pulmonary fibrosis: Current trends in management. Clinics in Chest 9 Medicine. 2004; 25(4 Special Issue):621-636. (Guideline Ref ID RAGHU2004A) 10
400 Raghu G, Depaso WJ, Cain K, Hammar SP, Wetzel CE, Dreis DF et al. Azathioprine combined with 11 prednisone in the treatment of idiopathic pulmonary fibrosis: a prospective double-blind, 12 randomized, placebo-controlled clinical trial. American Review of Respiratory Disease. 1991; 13 144(2):291-296. (Guideline Ref ID RAGHU1991) 14
401 Raghu G, King TE, Jr., Behr J, Brown KK, du Bois RM, Leconte I et al. Quality of life and dyspnoea 15 in patients treated with bosentan for idiopathic pulmonary fibrosis (BUILD-1). European 16 Respiratory Journal. 2010; 35(1):118-123. (Guideline Ref ID RAGHU2010) 17
402 Raghu G, Mageto YN, Lockhart D, Schmidt RA, Wood DE, Godwin JD. The accuracy of the clinical 18 diagnosis of new-onset idiopathic pulmonary fibrosis and other interstitial lung disease: A 19 prospective study. Chest. 1999; 116(5):1168-1174. (Guideline Ref ID RAGHU1999) 20
403 Rai SP, Panda BN, Upadhyay KK. Noninvasive positive pressure ventilation in patients with acute 21 respiratory failure. Medical Journal Armed Forces India. 2004; 60(3):224-226. (Guideline Ref ID 22 RAI2004) 23
404 Rammaert B, Leroy S, Cavestri B, Wallaert B, Grosbois JM. Home-based pulmonary rehabilitation 24 in idiopathic pulmonary fibrosis. Revue Des Maladies Respiratoires. 2011; 28(7):e52-e57. 25 (Guideline Ref ID RAMMAERT2011) 26
405 Rangappa P, Moran JL. Outcomes of patients admitted to the intensive care unit with idiopathic 27 pulmonary fibrosis. Critical Care and Resuscitation. 2009; 11(2):102-109. (Guideline Ref ID 28 RANGAPPA2009) 29
406 Rank MA, Kelkar P, Oppenheimer JJ. Taming chronic cough. Annals of Allergy, Asthma and 30 Immunology. 2007; 98(4):305-313. (Guideline Ref ID RANK2007) 31
407 Reed A, Snell GI, McLean C, Williams TJ. Outcomes of patients with interstitial lung disease 32 referred for lung transplant assessment. Internal Medicine Journal. 2006; 36(7):423-430. 33 (Guideline Ref ID REED2006) 34
408 Rena O, Casadio C, Leo F, Giobbe R, Cianci R, Baldi S et al. Videothoracoscopic lung biopsy in the 35 diagnosis of interstitial lung disease. European Journal of Cardio-Thoracic Surgery. 1999; 36 16(6):624-627. (Guideline Ref ID RENA1999) 37
409 Richeldi L. Assessing the treatment effect from multiple trials in idiopathic pulmonary fibrosis. 38 European Respiratory Review. 2012; 21(124):147-151. (Guideline Ref ID RICHELDI2012) 39

485
Idiopathic Pulmonary Fibrosis Reference list
410 Richeldi L, Ryerson CJ, Lee JS, Wolters PJ, Koth LL, Ley B et al. Relative versus absolute change in 1 forced vital capacity in idiopathic pulmonary fibrosis. Thorax. 2012; 67(5):407-411. (Guideline Ref 2 ID RICHELDI2012A) 3
411 Riha RL, Duhig EE, Clarke BE, Steele RH, Slaughter RE, Zimmerman PV. Survival of patients with 4 biopsy-proven usual interstitial pneumonia and nonspecific interstitial pneumonia. European 5 Respiratory Journal. 2002; 19(6):1114-1118. (Guideline Ref ID RIHA2002) 6
412 Roig V, Herrero A, Arroyo-Cozar M, Vielba D, Juarros S, Macias E. Comparative study between 7 oral azathioprine and intravenous cyclophosphamide pulses in the treatment of idiopathic 8 pulmonary fibrosis. Archivos De Bronconeumologia. 2010; 46(1):15-19. (Guideline Ref ID 9 ROIG2010) 10
413 Rozanski A, Ferrante FA, Alves PHB, Ribas RTB, Caramori ML, Pego-Fernandes PM et al. 11 Comparison between supervised and unsupervised exercise program after lung transplantation. 12 Journal of Heart and Lung Transplantation. 2012; 31(4 SUPPL. 1):S81-S82. (Guideline Ref ID 13 ROZANSKI2012) 14
414 Ryerson CJ, Abbritti M, Ley B, Elicker BM, Jones KD, Collard HR. Cough predicts prognosis in 15 idiopathic pulmonary fibrosis. Respirology. 2011; 16(6):969-975. (Guideline Ref ID RYERSON2011) 16
415 Ryerson CJ, Arean PA, Berkeley J, Carrieri-Kohlman VL, Pantilat SZ, Landefeld CS et al. Depression 17 is a common and chronic comorbidity in patients with interstitial lung disease. Respirology. 2012; 18 17(3):525-532. (Guideline Ref ID RYERSON2012A) 19
416 Ryerson CJ, Donesky D, Pantilat SZ, Collard HR. Dyspnea in idiopathic pulmonary fibrosis: a 20 systematic review. Journal of Pain and Symptom Management. 2012; 43(4):771-782. (Guideline 21 Ref ID RYERSON2012) 22
417 Ryu JH, Daniels CE, Hartman TE, Yi ES. Diagnosis of interstitial lung diseases. Mayo Clinic 23 Proceedings. 2007; 82(8):976-986. (Guideline Ref ID RYU2007A) 24
418 Saini G, McKeever T, Johnson S, Jenkins G. Thalidomide as treatment for IPF associated cough. 25 Thorax. 2011; 66(Suppl 4):A103. (Guideline Ref ID SAINI2011) 26
419 Sakamoto S, Homma S, Mun M, Fujii T, Kurosaki A, Yoshimura K. Acute exacerbation of idiopathic 27 interstitial pneumonia following lung surgery in 3 of 68 consecutive patients: a retrospective 28 study. Internal Medicine. 2011; 50(2):77-85. (Guideline Ref ID SAKAMOTO2011) 29
420 Salhi B, Troosters T, Behaegel M, Joos G, Derom E. Effects of pulmonary rehabilitation in patients 30 with restrictive lung diseases. Chest. 2010; 137(2):273-279. (Guideline Ref ID SALHI2010) 31
421 Santana M-J, Feeny D, Jackson K, Weinkauf J, Lien D. Improvement in health-related quality of 32 life after lung transplantation. Canadian Respiratory Journal. 2009; 16(5):153-158. (Guideline Ref 33 ID SANTANA2009) 34
422 Sawy MS, Jayakrishnan B, Behbehani N, Abal AT, El-Shamy A, Nair MGP. Flexible fiberoptic 35 bronchoscopy. Diagnostic yield. Saudi Medical Journal. 2004; 25(10):1459-1463. (Guideline Ref ID 36 SAWY2004) 37
423 Saydain G, Islam A, Afessa B, Ryu JH, Scott JP, Peters SG. Outcome of patients with idiopathic 38 pulmonary fibrosis admitted to the intensive care unit. American Journal of Respiratory and 39 Critical Care Medicine. 2002; 166(6):839-842. (Guideline Ref ID SAYDAIN2002) 40
486
Idiopathic Pulmonary Fibrosis Reference list
424 Schmidt SL, Nambiar AM, Tayob N, Sundaram B, Han MK, Gross BH et al. Pulmonary function 1 measures predict mortality differently in IPF versus combined pulmonary fibrosis and 2 emphysema. European Respiratory Journal. 2011; 38(1):176-183. (Guideline Ref ID 3 SCHMIDT2011) 4
425 Schmidt SL, Sundaram B, Flaherty KR. Diagnosing fibrotic lung disease: when is high-resolution 5 computed tomography sufficient to make a diagnosis of idiopathic pulmonary fibrosis? 6 Respirology. 2009; 14(7):934-939. (Guideline Ref ID SCHMIDT2009A) 7
426 Schoenheit G, Becattelli I, Cohen AH. Living with idiopathic pulmonary fibrosis: an in-depth 8 qualitative survey of European patients. Chronic Respiratory Disease. 2011; 8(4):225-231. 9 (Guideline Ref ID SCHOENHEIT2011) 10
427 Schönhofer B, Geibel M, Sonneborn M, Haidl P, Köhler D. Daytime mechanical ventilation in 11 chronic respiratory insufficiency. European Respiratory Journal : Official Journal of the European 12 Society for Clinical Respiratory Physiology. 1997; 10(12):2840-2846. (Guideline Ref ID 13 SCHÖNHOFER1997) 14
428 Schwartz DA, Helmers RA, Galvin JR, Van Fossen DS, Frees KL, Dayton CS et al. Determinants of 15 survival in idiopathic pulmonary fibrosis. American Journal of Respiratory and Critical Care 16 Medicine. 1994; 149(2 Pt 1):450-454. (Guideline Ref ID SCHWARTZ1994A) 17
429 Schwartz DA, Van Fossen DS, Davis CS, Helmers RA, Dayton CS, Burmeister LF et al. Determinants 18 of progression in idiopathic pulmonary fibrosis. American Journal of Respiratory and Critical Care 19 Medicine. 1994; 149(2 Pt 1):444-449. (Guideline Ref ID SCHWARTZ1994B) 20
430 Screaton NJ, Hiorns MP, Lee KS, Franquet T, Johkoh T, Fujimoto K et al. Serial high resolution CT 21 in non-specific interstitial pneumonia: prognostic value of the initial pattern. Clinical Radiology. 22 2005; 60(1):96-104. (Guideline Ref ID SCREATON2005) 23
431 Scriabine A, Rabin DU. New developments in the therapy of pulmonary fibrosis. Advances in 24 Pharmacology. 2009; 57:419-464. (Guideline Ref ID SCRIABINE2009) 25
432 Shah PL. Flexible bronchoscopy. Medicine. 2008; 36(3):151-154. (Guideline Ref ID SHAH2008) 26
433 Shah SS, Tsang V, Goldstraw P. Open lung biopsy: a safe, reliable and accurate method for 27 diagnosis in diffuse lung disease. Respiration; International Review of Thoracic Diseases. 1992; 28 59(4):243-246. (Guideline Ref ID SHAH1992) 29
434 Shanmugam G, Bhutani S, Khan DA, Brown ES. Psychiatric considerations in pulmonary disease. 30 Psychiatric Clinics of North America. 2007; 30(4):761-780. (Guideline Ref ID SHANMUGAM2007) 31
435 Sharifabad MA, Hurewitz A, Spiegler P, Bernstein M, Feuerman M, Smyth JM. Written disclosure 32 therapy for patients with chronic lung disease undergoing pulmonary rehabilitation. Journal of 33 Cardiopulmonary Rehabilitation and Prevention. 2010; 30(5):340-345. (Guideline Ref ID 34 SHARIFABAD2010) 35
436 Shim HS, Park MS, Park IK. Histopathologic findings of transbronchial biopsy in usual interstitial 36 pneumonia. Pathology International. 2010; 60(5):373-377. (Guideline Ref ID SHIM2010) 37
437 Shin KM, Lee KS, Chung MP, Han J, Bae YA, Kim TS et al. Prognostic determinants among clinical, 38 thin-section CT, and histopathologic findings for fibrotic idiopathic interstitial pneumonias: 39 tertiary hospital study. Radiology. 2008; 249(1):328-337. (Guideline Ref ID SHIN2008) 40

487
Idiopathic Pulmonary Fibrosis Reference list
438 Shipley MD, Hardy T, Heslop K, Forrest IA. Identifying anxiety and depression in interstitial lung 1 disease: Use of a simple outpatient screening tool. Thorax. 2009; 64(Suppl 4):A6-A7. (Guideline 2 Ref ID SHIPLEY2009) 3
439 Shitrit D, Rusanov V, Peled N, Amital A, Fuks L, Kramer MR. The 15-step oximetry test: a reliable 4 tool to identify candidates for lung transplantation among patients with idiopathic pulmonary 5 fibrosis. Journal of Heart and Lung Transplantation. 2009; 28(4):328-333. (Guideline Ref ID 6 SHITRIT2009) 7
440 Shulgina L, Cahn A, Chilvers E, Parfrey H, Clark A, Wilson E et al. Treating idiopathic pulmonary 8 fibrosis with the addition of Co-trimoxazole. Thorax. 2011; 66(Suppl 4):A63-A64. (Guideline Ref ID 9 SHULGINA2011) 10
441 Shulgina L, Cahn AP, Chilvers ER, Parfrey H, Clark AB, Wilson ECF et al. Treating idiopathic 11 pulmonary fibrosis with the addition of co-trimoxazole: a randomised controlled trial. Thorax. 12 2013; 68(2):155-162. (Guideline Ref ID SHULGINA2013) 13
442 Sigurdsson MI, Isaksson HJ, Gudmundsson G, Gudbjartsson T. Diagnostic surgical lung biopsies 14 for suspected interstitial lung diseases: a retrospective study. Annals of Thoracic Surgery. 2009; 15 88(1):227-232. (Guideline Ref ID SIGURDSSON2009A) 16
443 Simon ST, Higginson IJ, Booth S, Harding R, Bausewein C. Benzodiazepines for the relief of 17 breathlessness in advanced malignant and non-malignant diseases in adults. Cochrane Database 18 of Systematic Reviews. 2010; Issue 1:CD007354. (Guideline Ref ID SIMON2010) 19
444 Slodkowska J, Wesolowski S, Onish K, Kus J. Usual interstitial pneumonia: A comparative analysis 20 of histopathology and high resolution computed tomography (HRCT) in relation to the clinical 21 course of the disease. Electronic Journal of Pathology and Histology. 2000; 6(4):88-99. (Guideline 22 Ref ID SLODKOWSKA2000) 23
445 Song JW, Hong SB, Lim CM, Koh Y, Kim DS. Acute exacerbation of idiopathic pulmonary fibrosis: 24 incidence, risk factors and outcome. European Respiratory Journal. 2011; 37(2):356-363. 25 (Guideline Ref ID SONG2011) 26
446 Spencer L, Grundy S, Greaves M, Bishop P, Duck A, Leonard C. Demonstration of diagnostic and 27 prognostic benefits of an interstitial lung disease (ILD) multidisciplinary team meeting. European 28 Respiratory Society Congress 2011 2011. (Guideline Ref ID SPENCER2011) 29
447 Starkie HJ, Briggs AH, Chambers MG, Jones P. Predicting EQ-5D values using the SGRQ. Value in 30 Health. 2011; 14(2):354-360. (Guideline Ref ID STARKIE2011) 31
448 Stavem K, Bjortuft O, Lund MB, Kongshaug K, Geiran O, Boe J. Health-related quality of life in 32 lung transplant candidates and recipients. Respiration; International Review of Thoracic Diseases. 33 2000; 67(2):159-165. (Guideline Ref ID STAVEM2000) 34
449 Stern JB, Mal H, Groussard O, Brugiere O, Marceau A, Jebrak G et al. Prognosis of patients with 35 advanced idiopathic pulmonary fibrosis requiring mechanical ventilation for acute respiratory 36 failure. Chest. 2001; 120(1):213-219. (Guideline Ref ID STERN2001) 37
450 Stolagiewicz NE, Draper A, Schomberg Lucy EE, Chua F. Mycophenolate mofetil (MMF) for the 38 treatment of connective tissue disease-associated interstitial lung disease (ILD). Cochrane 39 Database of Systematic Reviews. 2012; Issue 6:CD009911. DOI:10.1002/14651858.CD009911. 40 (Guideline Ref ID STOLAGIEWICZ2012) 41

488
Idiopathic Pulmonary Fibrosis Reference list
451 Studer SM, Orens JB. Optimal timing of lung transplantation in end-stage lung disease. Clinical 1 Pulmonary Medicine. 2000; 7(2):97-103. (Guideline Ref ID STUDER2000) 2
452 Su J, Dai HP, Ban CJ, Ye Q, Zhan QY, Wang C. Causes of respiratory failure complicating interstitial 3 lung disease and application value of mechanical ventilation. Zhonghua Yi Xue Za Zhi. 2010; 4 90(12):799-803. (Guideline Ref ID SU2010) 5
453 Suh GY, Kang EH, Chung MP, Lee KS, Han J, Kitaichi M et al. Early intervention can improve clinical 6 outcome of acute interstitial pneumonia. Chest. 2006; 129(3):753-761. (Guideline Ref ID 7 SUH2006) 8
454 Sumikawa H, Johkoh T, Colby TV, Ichikado K, Suga M, Taniguchi H et al. Computed tomography 9 findings in pathological usual interstitial pneumonia: relationship to survival. American Journal of 10 Respiratory and Critical Care Medicine. 2008; 177(4):433-439. (Guideline Ref ID SUMIKAWA2008) 11
455 Sumikawa H, Johkoh T, Ichikado K, Taniguchi H, Kondoh Y, Fujimoto K et al. Usual interstitial 12 pneumonia and chronic idiopathic interstitial pneumonia: analysis of CT appearance in 92 13 patients. Radiology. 2006; 241(1):258-266. (Guideline Ref ID SUMIKAWA2006) 14
456 Sundar KM, Daly SE, Pearce MJ, Alward WT. Chronic cough and obstructive sleep apnea in a 15 community-based pulmonary practice. Cough. 2010; 6(1):2. (Guideline Ref ID SUNDAR2010) 16
457 Sung A, Swigris J, Saleh A, Raoof S. High-resolution chest tomography in idiopathic pulmonary 17 fibrosis and nonspecific interstitial pneumonia: utility and challenges. Current Opinion in 18 Pulmonary Medicine. 2007; 13(5):451-457. (Guideline Ref ID SUNG2007) 19
458 Sverzellati N, Wells AU, Tomassetti S, Desai SR, Copley SJ, Aziz ZA et al. Idiopathic pulmonary 20 fibrosis: Spectrum of HRCT appearances of diagnostically misleading cases. Journal of Thoracic 21 Imaging. 2009; 24(3):w27. (Guideline Ref ID SVERZELLATI2009) 22
459 Sverzellati N, Wells AU, Tomassetti S, Desai SR, Copley SJ, Aziz ZA et al. Biopsy-proved idiopathic 23 pulmonary fibrosis: spectrum of nondiagnostic thin-section CT diagnoses. Radiology. 2010; 24 254(3):957-964. (Guideline Ref ID SVERZELLATI2010) 25
460 Swigris JJ, Brown KK. Evaluation of bosentan for idiopathic pulmonary fibrosis. Expert Review of 26 Respiratory Medicine. 2008; 2(3):315-321. (Guideline Ref ID SWIGRIS2008) 27
461 Swigris JJ, Kuschner WG, Jacobs SS, Wilson SR, Gould MK. Health-related quality of life in patients 28 with idiopathic pulmonary fibrosis: a systematic review. Thorax. 2005; 60(7):588-594. (Guideline 29 Ref ID SWIGRIS2005B) 30
462 Swigris JJ, Swick J, Wamboldt FS, Sprunger D, Du Bois R, Fischer A et al. Heart rate recovery after 31 6-min walk test predicts survival in patients with idiopathic pulmonary fibrosis. Chest. 2009; 32 136(3):841-848. (Guideline Ref ID SWIGRIS2009) 33
463 Swigris JJ, Wamboldt FS, Behr J, du Bois RM, King TE, Raghu G et al. The 6 minute walk in 34 idiopathic pulmonary fibrosis: longitudinal changes and minimum important difference. Thorax. 35 2010; 65(2):173-177. (Guideline Ref ID SWIGRIS2010A) 36
464 Swigris JJ, Brown KK, Behr J, du Bois RM, King TE, Raghu G et al. The SF-36 and SGRQ: validity and 37 first look at minimum important differences in IPF. Respiratory Medicine. 2010; 104(2):296-304. 38 (Guideline Ref ID SWIGRIS2010) 39

489
Idiopathic Pulmonary Fibrosis Reference list
465 Swigris JJ, Fairclough DL, Morrison M, Make B, Kozora E, Brown KK et al. Benefits of pulmonary 1 rehabilitation in idiopathic pulmonary fibrosis. Respiratory Care. 2011; 56(6):783-789. (Guideline 2 Ref ID SWIGRIS2011) 3
466 Swigris JJ, Gould MK, Wilson SR. Health-related quality of life among patients with idiopathic 4 pulmonary fibrosis. Chest. 2005; 127(1):284-294. (Guideline Ref ID SWIGRIS2005A) 5
467 Swigris JJ, Stewart AL, Gould MK, Wilson SR. Patients' perspectives on how idiopathic pulmonary 6 fibrosis affects the quality of their lives. Health and Quality of Life Outcomes. 2005; 3:61. 7 (Guideline Ref ID SWIGRIS2005) 8
468 Swinburn CR, Mould H, Stone TN, Corris PA, Gibson GJ. Symptomatic benefit of supplemental 9 oxygen in hypoxemic patients with chronic lung disease. American Review of Respiratory 10 Disease. 1991; 143(5 Pt 1):913-915. (Guideline Ref ID SWINBURN1991) 11
469 Thabut G, Mal H, Castier Y, Groussard O, Brugiere O, Marrash-Chahla R et al. Survival benefit of 12 lung transplantation for patients with idiopathic pulmonary fibrosis. Journal of Thoracic and 13 Cardiovascular Surgery. 2003; 126(2):469-475. (Guideline Ref ID THABUT2003) 14
470 Thomeer M, Verschakelen J, Laurent F, Nicholson AG, Verbeken EK, Capron F et al. 15 Multidisciplinary interobserver agreement in the diagnosis of idiopathic pulmonary fibrosis. 16 European Respiratory Journal. 2008; 31(3):585-591. (Guideline Ref ID THOMEER2008) 17
471 Tiitto L, Heiskanen U, Bloigu R, Paakko P, Kinnula V, Kaarteenaho-Wiik R. Thoracoscopic lung 18 biopsy is a safe procedure in diagnosing usual interstitial pneumonia. Chest. 2005; 128(4):2375-19 2380. (Guideline Ref ID TIITTO2005) 20
472 Titman A, Rogers CA, Bonser RS, Banner NR, Sharples LD. Disease-specific survival benefit of lung 21 transplantation in adults: a national cohort study. American Journal of Transplantation. 2009; 22 9(7):1640-1649. (Guideline Ref ID TITMAN2009) 23
473 Tomii K, Tachikawa R, Chin K, Murase K, Handa T, Mishima M et al. Role of non-invasive 24 ventilation in managing life-threatening acute exacerbation of interstitial pneumonia. Internal 25 Medicine. 2010; 49(14):1341-1347. (Guideline Ref ID TOMII2010) 26
474 Tomioka H, Kuwata Y, Imanaka K, Hashimoto K, Ohnishi H, Tada K et al. Randomized, open-label 27 pilot study of aerosolized administration of N-acetylcysteine for idiopathic pulmonary fibrosis. 28 American Journal of Respiratory & Critical Care Medicine. 2003; 167(Meeting Abstracts):A091. 29 (Guideline Ref ID TOMIOKA2003) 30
475 Tomioka H, Imanaka K, Hashimoto K, Iwasaki H. Health-related quality of life in patients with 31 idiopathic pulmonary fibrosis--cross-sectional and longitudinal study. Internal Medicine. 2007; 32 46(18):1533-1542. (Guideline Ref ID TOMIOKA2007) 33
476 Tomioka H, Kuwata Y, Imanaka K, Hashimoto K, Ohnishi H, Tada K et al. A pilot study of 34 aerosolized N-acetylcysteine for idiopathic pulmonary fibrosis. Respirology. 2005; 10(4):449-455. 35 (Guideline Ref ID TOMIOKA2005) 36
477 Trahan S, Hanak V, Ryu JH, Myers JL. Role of surgical lung biopsy in separating chronic 37 hypersensitivity pneumonia from usual interstitial pneumonia/idiopathic pulmonary fibrosis. 38 Chest. 2008; 134(1):126-132. (Guideline Ref ID TRAHAN2008A) 39

490
Idiopathic Pulmonary Fibrosis Reference list
478 Trisolini R, Poletti V. The clinical role of bronchoalveolar lavage in the setting of idiopathic 1 interstitial pneumonias. Monaldi Archives for Chest Disease. 2000; 55(6):455-458. (Guideline Ref 2 ID TRISOLINI2000) 3
479 Troy L, Honeysett L, Lau E, Wong K, Yee B, Grunstein R et al. Sleep-disordered breathing in 4 patients with interstitial lung disease. Respirology. 2012; 17(Suppl s1):75. (Guideline Ref ID 5 TROY2012) 6
480 Tuppin MP, Paratz JD, Chang AT, Seale HE, Walsh JR, Kermeeen FD et al. Predictive utility of the 7 6-minute walk distance on survival in patients awaiting lung transplantation. Journal of Heart and 8 Lung Transplantation. 2008; 27(7):729-734. (Guideline Ref ID TUPPIN2008) 9
481 Turner-Warwick M, Burrows B, Johnson A. Cryptogenic fibrosing alveolitis: Clinical features and 10 their influence on survival. Thorax. 1980; 35(3):171-180. (Guideline Ref ID TURNER1980) 11
482 Tzanakis N, Samiou M, Lambiri I, Antoniou K, Siafakas N, Bouros D. Evaluation of health-related 12 quality-of-life and dyspnea scales in patients with idiopathic pulmonary fibrosis. Correlation with 13 pulmonary function tests. European Journal of Internal Medicine. 2005; 16(2):105-112. 14 (Guideline Ref ID TZANAKIS2005) 15
483 Tzouvelekis A, Bouros E, Oikonomou A, Ntolios P, Zacharis G, Kolios G et al. Effect and safety of 16 mycophenolate mofetil in idiopathic pulmonary fibrosis. Pulmonary Medicine. 2011; 17 2011:849035. (Guideline Ref ID TZOUVELEKIS2011) 18
484 Valeyre D. Towards a better diagnosis of idiopathic pulmonary fibrosis. European Respiratory 19 Review. 2011; 20(120):108-113. (Guideline Ref ID VALEYRE2011) 20
485 Valeyre D, Albera C, du Bois RM, Bradford WZ, Costabel U, King TE, Jr. 6 minute walk distance 21 (6MWD) and forced vital capacity (FVC) in patients with idiopathic pulmonary fibrosis (IPF): 22 similar pattern of pirfenidone response. American Journal of Respiratory and Critical Care 23 Medicine. 2010; 181(Meeting Abstracts):A6026. (Guideline Ref ID VALEYRE2010) 24
486 Vansteenkiste J, Verbeken E, Thomeer M, Van Haecke P, Eeckhout AV, Demedts M. Medical 25 thoracoscopic lung biopsy in interstitial lung disease: a prospective study of biopsy quality. 26 European Respiratory Journal. 1999; 14(3):585-590. (Guideline Ref ID VANSTEENKISTE1999) 27
487 Varney VA, Parnell HM, Salisbury DT, Ratnatheepan S, Tayar RB. A double blind randomised 28 placebo controlled pilot study of oral co-trimoxazole in advanced fibrotic lung disease. 29 Pulmonary Pharmacology and Therapeutics. 2008; 21(1):178-187. (Guideline Ref ID VARNEY2008) 30
488 Veeraraghavan S, Latsi PI, Wells AU, Pantelidis P, Nicholson AG, Colby TV et al. BAL findings in 31 idiopathic nonspecific interstitial pneumonia and usual interstitial pneumonia. European 32 Respiratory Journal. 2003; 22(2):239-244. (Guideline Ref ID VEERARAGHAVAN2003) 33
489 Velluti G, Luppi F, Covi M, Bonucchi ME. Co-trimoxazole: an old drug for a new treatment of the 34 usual interstitial pneumonia? European Respiratory Journal. 2000; 16(Suppl 31):430s. (Guideline 35 Ref ID VELLUTI2000) 36
490 Verrill DE, Moretz C. Depression characteristics following 12 weeks of pulmonary rehabilitation in 37 a greater metropolitan area. Journal of Cardiopulmonary Rehabilitation and Prevention. 2008; 38 28(4):274. (Guideline Ref ID VERRILL2008) 39
491 Verrill DE, Moretz C, Lippard WM. Predicting 12-week follow-up 6-minute walk test performance 40 in men and women of north carolina pulmonary rehabilitation programs. Journal of 41

491
Idiopathic Pulmonary Fibrosis Reference list
Cardiopulmonary Rehabilitation and Prevention. 2008; 28(4):269. (Guideline Ref ID 1 VERRILL2008A) 2
492 Wall CP, Gaensler EA, Carrington CB, Hayes JA. Comparison of transbronchial and open biopsies 3 in chronic infiltrative lung diseases. American Review of Respiratory Disease. 1981; 123(3):280-4 285. (Guideline Ref ID WALL1981) 5
493 Walter N, Collard HR, King TE, Jr. Current perspectives on the treatment of idiopathic pulmonary 6 fibrosis. Proceedings of the American Thoracic Society. 2006; 3(4):330-338. (Guideline Ref ID 7 WALTER2006) 8
494 Warrington VL, Scullion J, Sewell L, Williams J, Singh S. Outcomes following pulmonary 9 rehabilitation for patients with restrictive lung diseases with or without oxygen therapy. Thorax. 10 2010; 65(Suppl 4):A96. (Guideline Ref ID WARRINGTON2010) 11
495 Watters LC, King TE, Schwarz MI, Waldron JA, Stanford RE, Cherniack RM. A clinical, radiographic, 12 and physiologic scoring system for the longitudinal assessment of patients with idiopathic 13 pulmonary fibrosis. American Review of Respiratory Disease. 1986; 133(1):97-103. (Guideline Ref 14 ID WATTERS1986) 15
496 Wee B, Browning J, Adams A, Benson D, Howard P, Klepping G et al. Management of chronic 16 cough in patients receiving palliative care: review of evidence and recommendations by a task 17 group of the Association for Palliative Medicine of Great Britain and Ireland. Palliative Medicine. 18 2011. (Guideline Ref ID WEE2011) 19
497 Welker L, Jorres RA, Costabel U, Magnussen H. Predictive value of BAL cell differentials in the 20 diagnosis of interstitial lung diseases. European Respiratory Journal. 2004; 24(6):1000-1006. 21 (Guideline Ref ID WELKER2004) 22
498 Whelan TPM, Dunitz JM, Kelly RF, Edwards LB, Herrington CS, Hertz MI et al. Effect of 23 preoperative pulmonary artery pressure on early survival after lung transplantation for idiopathic 24 pulmonary fibrosis. Journal of Heart and Lung Transplantation. 2005; 24(9):1269-1274. (Guideline 25 Ref ID WHELAN2005) 26
499 Xaubet A, Agusti C, Luburich P, Roca J, Ayuso MC, Marrades RM et al. Is it necessary to treat all 27 patients with idiopathic pulmonary fibrosis? Sarcoidosis, Vasculitis, and Diffuse Lung Diseases. 28 2001; 18(3):289-295. (Guideline Ref ID XAUBET2001) 29
500 Xaubet A, Agusti C, Luburich P, Roca J, Monton C, Ayuso MC et al. Pulmonary function tests and 30 CT scan in the management of idiopathic pulmonary fibrosis. American Journal of Respiratory 31 and Critical Care Medicine. 1998; 158(2):431-436. (Guideline Ref ID XAUBET1998) 32
501 Yamaguchi M, Yoshino I, Suemitsu R, Osoegawa A, Kameyama T, Tagawa T et al. Elective video-33 assisted thoracoscopic lung biopsy for interstitial lung disease. Asian Cardiovascular and Thoracic 34 Annals. 2004; 12(1):65-68. (Guideline Ref ID YAMAGUCHI2004) 35
502 Yang W, He B, Shan Y. High-resolution CT semi-quantitative score may have a role in predicting 36 short-term response to corticosteroid therapy in idiopathic interstitial pneumonias. Zhonghua Jie 37 He He Hu Xi Za Zhi = Zhonghua Jiehe He Huxi Zazhi = Chinese Journal of Tuberculosis and 38 Respiratory Diseases. 2009; 32(2):124-127. (Guideline Ref ID YANG2009) 39
503 Yeager H, Rossman MD, Baughman RP, Teirstein AS, Judson MA, Rabin DL et al. Pulmonary and 40 psychosocial findings at enrollment in the ACCESS study. Sarcoidosis, Vasculitis, and Diffuse Lung 41 Diseases. 2005; 22(2):147-153. (Guideline Ref ID YEAGER2005) 42

492
Idiopathic Pulmonary Fibrosis Reference list
504 Yokoyama T, Kondoh Y, Taniguchi H, Kataoka K, Kato K, Nishiyama O et al. Noninvasive 1 ventilation in acute exacerbation of idiopathic pulmonary fibrosis. Internal Medicine. 2010; 2 49(15):1509-1514. (Guideline Ref ID YOKOYAMA2010) 3
505 Yokoyama T, Tsushima K, Yamamoto H, Koizumi T, Kubo K. Beneficial effects of early intervention 4 with non-invasive ventilation for acute exacerbation of interstitial pneumonia. American Journal 5 of Respiratory and Critical Care Medicine. 2011; 183(1 MeetingAbstracts). (Guideline Ref ID 6 YOKOYAMA2011) 7
506 Yokoyama T, Tsushima K, Yamamoto H, Koizumi T, Kubo K. Potential benefits of early continuous 8 positive pressure ventilation in patients with rapidly progressive interstitial pneumonia. 9 Respirology. 2012; 17(2):315-321. (Guideline Ref ID YOKOYAMA2012) 10
507 Zappala CJ, Latsi PI, Nicholson AG, Colby TV, Cramer D, Renzoni EA et al. Marginal decline in 11 forced vital capacity is associated with a poor outcome in idiopathic pulmonary fibrosis. 12 European Respiratory Journal : Official Journal of the European Society for Clinical Respiratory 13 Physiology. 2010; 35(4):830-836. (Guideline Ref ID ZAPPALA2010) 14
508 Zhang D, Liu Y. Surgical lung biopsies in 418 patients with suspected interstitial lung disease in 15 China. Internal Medicine. 2010; 49(12):1097-1102. (Guideline Ref ID ZHANG2010) 16
509 Zielinski J. Long-term oxygen therapy in conditions other than chronic obstructive pulmonary 17 disease. State-of-the-art conference on long-term oxygen therapy, part II. Respiratory Care. 18 2000; 45(2):172-177. (Guideline Ref ID ZIELINSKI2000) 19
510 Zimmermann CS, Carvalho CRF, Silveira KR, Yamaguti WPS, Moderno EV, Salge JM et al. 20 Comparison of two questionnaires which measure the health-related quality of life of idiopathic 21 pulmonary fibrosis patients. Brazilian Journal of Medical and Biological Research = Revista 22 Brasileira De Pesquisas Medicas e Biologicas / Sociedade Brasileira De Biofisica [Et Al ]. 2007; 23 40(2):179-187. (Guideline Ref ID ZIMMERMANN2007) 24
511 Zisman DA. The STEP-IPF Trial: Sildenafil Trial Of Exercise Performance In Idiopathic Pulmonary 25 Fibrosis. American Journal of Respiratory and Critical Care Medicine. 2010; 181(Meeting 26 Abstracts):A3992. (Guideline Ref ID ZISMAN2010A) 27
512 Zisman DA, Schwarz M, Anstrom KJ, Collard HR, Flaherty KR, Hunninghake GW. A controlled trial 28 of sildenafil in advanced idiopathic pulmonary fibrosis. New England Journal of Medicine. 2010; 29 363(7):620-628. (Guideline Ref ID ZISMAN2010) 30
513 Zisman DA, Karlamangla AS, Ross DJ, Keane MP, Belperio JA, Saggar R et al. High-resolution chest 31 CT findings do not predict the presence of pulmonary hypertension in advanced idiopathic 32 pulmonary fibrosis. Chest. 2007; 132(3):773-779. (Guideline Ref ID ZISMAN2007) 33
514 Zisman DA, Ross DJ, Belperio JA, Saggar R, Lynch JP, Ardehali A et al. Prediction of pulmonary 34 hypertension in idiopathic pulmonary fibrosis. Respiratory Medicine. 2007; 101(10):2153-2159. 35 (Guideline Ref ID ZISMAN2007A) 36
515 Zompatori M, Calabro E, Chetta A, Chiari G, Marangio E, Olivieri D. Chronic hypersensitivity 37 pneumonitis or idiopathic pulmonary fibrosis? Diagnostic role of high resolution Computed 38 Tomography (HRCT). La Radiologia Medica. 2003; 106(3):135-146. (Guideline Ref ID 39 ZOMPATORI2003) 40
41

493
Idiopathic Pulmonary Fibrosis Reference list
1
Copyright © 2022 FDOKUMEN




















