
Optimization of anti-pseudomonal antibiotics for cystic fibrosis pulmonary exacerbations: III....
12
Pediatric Pulmonology State of the Art Optimization of Anti-pseudomonal Antibiotics for Cystic Fibrosis Pulmonary Exacerbations: I. Aztreonam and Carbapenems Jeffery T. Zobell, PharmD, 1,2 * David C. Young, PharmD, 3,4 C. Dustin Waters, PharmD, BCPS, 4,5 Chris Stockmann, MSc, 6,7 Krow Ampofo, MD, 6 Catherine M.T. Sherwin, PhD, 7 and Michael G. Spigarelli, MD, PhD 7 Summary. Acute pulmonary exacerbations (APE) in cystic fibrosis (CF) are associated with loss of lung function that may require aggressive management with intravenous antibiotics. The aim of this review is to provide an evidence-based summary of pharmacokinetic/pharmacodynamic (PK/PD), tolerability, and efficacy studies utilizing aztreonam and anti-pseudomonal carbape- nems (i.e., doripenem, imipenem–cilastatin, and meropenem) in the treatment of an APE, and to identify areas where further study is warranted. The current dosing recommendations in the United States and Europe for aztreonam are lower than the literature supported dosing range of 200–300 mg/kg/day divided every 6 hr, maximum 8–12 g/day. Invitro, PK/PD, and tolerability studies show the potential of doripenem 90 mg/kg/day divided every 8 hr, infused over 4 hr, maximum 6 g/day in the treatment of APE. Imipenem-cilastatin 100 mg/kg/day divided every 6 hr, maximum 4 g/day and meropenem 120 mg/kg/day divided every 8 hr, maximum 6 g/day have been shown to be tolerable and effective in the treatment of APE. With availability issues of new anti-pseudomonal agents and a large percentage of CF patients will not regain their lung function following an APE, we suggest the need to determine optimization of aztreonam and meropenem dosing in CF, as well as to determine the clinical efficacy of doripenem in the treatment of APE. The usefulness of imipenem-cilastatin may be limited due to the rapid devel- opment of resistance. Pediatr Pulmonol. ß 2012 Wiley Periodicals, Inc. Key words: beta-lactams; Pseudomonas aeruginosa; pharmacokinetics; pharmaco- dynamics. Funding source: none reported. 1 Pharmacy, Intermountain Primary Children’s Medical Center, Salt Lake City, Utah. 2 Intermountain Cystic Fibrosis Pediatric Center, Salt Lake City, Utah. 3 University of Utah College of Pharmacy, Salt Lake City, Utah. 4 Intermountain Cystic Fibrosis Adult Center, Salt Lake City, Utah. 5 Pharmacy, Intermountain McKay-Dee Hospital Center, Ogden, Utah. 6 Division of Pediatric Infectious Disease, University of Utah, Salt Lake City, Utah. 7 Division of Clinical Pharmacology and Clinical Trials Office, Depart- ment of Pediatrics, University of Utah School of Medicine, Salt Lake City, Utah. Conflict of interest: None A systematic review was conducted using Medline. MeSH and free text terms included: ‘‘Cystic fibrosis,’’ ‘‘antibiotics,’’ ‘‘pharmacokinetics,’’ ‘‘pharmacodynamics,’’ ‘‘aztreonam,’’ ‘‘doripenem,’’ ‘‘imipenem-cilasta- tin,’’ ‘‘meropenem’’. Search results were restricted to the English language without an age limit. Also, reference lists and conference proceedings were reviewed. *Correspondence to: Jeffery T. Zobell, PharmD, Department of Pharma- cy, Intermountain Primary Children’s Medical Center, 100 North Mario Capecchi Drive, Salt Lake City, UT 84113. E-mail: [email protected] Received 15 April 2012; Accepted 17 May 2012. DOI 10.1002/ppul.22655 Published online in Wiley Online Library (wileyonlinelibrary.com). ß 2012 Wiley Periodicals, Inc.
Transcript of Optimization of anti-pseudomonal antibiotics for cystic fibrosis pulmonary exacerbations: III....

Pediatric Pulmonology
State of the Art
Optimization of Anti-pseudomonal Antibiotics forCystic Fibrosis Pulmonary Exacerbations:
I. Aztreonam and Carbapenems
Jeffery T. Zobell, PharmD,1,2* David C. Young, PharmD,3,4 C. Dustin Waters, PharmD, BCPS,4,5
Chris Stockmann, MSc,6,7 Krow Ampofo, MD,6 Catherine M.T. Sherwin, PhD,7 andMichael G. Spigarelli, MD, PhD
7
Summary. Acute pulmonary exacerbations (APE) in cystic fibrosis (CF) are associated with loss
of lung function that may require aggressive management with intravenous antibiotics. The aim
of this review is to provide an evidence-based summary of pharmacokinetic/pharmacodynamic
(PK/PD), tolerability, and efficacy studies utilizing aztreonam and anti-pseudomonal carbape-
nems (i.e., doripenem, imipenem–cilastatin, and meropenem) in the treatment of an APE, and
to identify areas where further study is warranted. The current dosing recommendations in the
United States and Europe for aztreonam are lower than the literature supported dosing range
of 200–300 mg/kg/day divided every 6 hr, maximum 8–12 g/day. In vitro, PK/PD, and tolerability
studies show the potential of doripenem 90 mg/kg/day divided every 8 hr, infused over 4 hr,
maximum 6 g/day in the treatment of APE. Imipenem-cilastatin 100 mg/kg/day divided every
6 hr, maximum 4 g/day and meropenem 120 mg/kg/day divided every 8 hr, maximum 6 g/day
have been shown to be tolerable and effective in the treatment of APE. With availability issues
of new anti-pseudomonal agents and a large percentage of CF patients will not regain their
lung function following an APE, we suggest the need to determine optimization of aztreonam
and meropenem dosing in CF, as well as to determine the clinical efficacy of doripenem in the
treatment of APE. The usefulness of imipenem-cilastatin may be limited due to the rapid devel-
opment of resistance. Pediatr Pulmonol. � 2012 Wiley Periodicals, Inc.
Key words: beta-lactams; Pseudomonas aeruginosa; pharmacokinetics; pharmaco-
dynamics.
Funding source: none reported.
1Pharmacy, Intermountain Primary Children’s Medical Center, Salt Lake
City, Utah.
2Intermountain Cystic Fibrosis Pediatric Center, Salt Lake City, Utah.
3University of Utah College of Pharmacy, Salt Lake City, Utah.
4Intermountain Cystic Fibrosis Adult Center, Salt Lake City, Utah.
5Pharmacy, Intermountain McKay-Dee Hospital Center, Ogden, Utah.
6Division of Pediatric Infectious Disease, University of Utah, Salt Lake
City, Utah.
7Division of Clinical Pharmacology and Clinical Trials Office, Depart-
ment of Pediatrics, University of Utah School of Medicine, Salt Lake
City, Utah.
Conflict of interest: None
A systematic review was conducted using Medline. MeSH and free text
terms included: ‘‘Cystic fibrosis,’’ ‘‘antibiotics,’’ ‘‘pharmacokinetics,’’
‘‘pharmacodynamics,’’ ‘‘aztreonam,’’ ‘‘doripenem,’’ ‘‘imipenem-cilasta-
tin,’’ ‘‘meropenem’’. Search results were restricted to the English
language without an age limit. Also, reference lists and conference
proceedings were reviewed.
*Correspondence to: Jeffery T. Zobell, PharmD, Department of Pharma-
cy, Intermountain Primary Children’s Medical Center, 100 North Mario
Capecchi Drive, Salt Lake City, UT 84113.
E-mail: [email protected]
Received 15 April 2012; Accepted 17 May 2012.
DOI 10.1002/ppul.22655
Published online in Wiley Online Library
(wileyonlinelibrary.com).
� 2012 Wiley Periodicals, Inc.

INTRODUCTION
Cystic fibrosis (CF) is a common autosomal recessivedisorder affecting over 30,000 individuals in the UnitedStates.1,2 It is caused by mutations in a single gene onthe long arm of chromosome 7, which encodes thecystic fibrosis transmembrane conductance regulator(CFTR).1,2 CFTR is an active chloride transport channelthat helps maintain fluid balance across epithelialcells.1,2 Defective CFTR channels affect multiple organsystems in individuals with CF, including the gastroin-testinal, reproductive, endocrine, and pulmonarysystems.1,2
The pulmonary effects of CF typically have the larg-est impact on morbidity and mortality, and account for>90% of fatalities due to the disease.1–3 Detrimentaleffects of thick, dehydrated secretions, bacterial infec-tions, and inflammation result in bronchiectasis, andprogressive obstructive airway disease.1–3 Chronic ther-apies such as dornase alpha, hypertonic saline, andchest physiotherapy work to thin and mobilize mucussecretions.3–7 Aerosolized antibiotics (i.e., inhaledtobramycin or aztreonam) and oral azithromycin areused as chronic suppressive therapies and anti-inflam-matory agents, respectively.3,8–11 Acute pulmonaryexacerbations (APE) are managed with either oral oraerosolized antibiotics (mild exacerbations) or with in-travenous antibiotics (moderate to severe exacerbations)which can be administered in the hospital and/or athome.1–3
In 2009, the Cystic Fibrosis Foundation (CFF) re-leased guidelines for the treatment of APE.12 Theseguidelines recommend that APE be treated with twointravenous anti-pseudomonal antibiotics, each with adifferent mechanism of action in an effort to enhanceantibacterial activity and reduce resistance.12 The mostcommon antibiotic classes used in combination forAPE are anti-pseudomonal beta-lactams (98%) andaminoglycosides (61%) according to surveys of CFF-accredited care centers.12–14
Beta-lactam antibiotics share a common chemicalstructure (beta-lactam ring) and mechanism of action(inhibition of bacterial cell wall synthesis via bindingto penicillin binding proteins; Fig. 1).15 Various sidechains and derivatives of the beta-lactam ring charac-terize the different types of beta-lactam antibioticsincluding the penicillin (piperacillin–tazobactam andticarcillin–clavulanate), cephalosporin (ceftazidime andcefepime), carbapenem (doripenem, imipenem–cilastatin,and meropemen), and monobactam (aztreonam)agents.15 Beta-lactam antibiotics exhibit concentration-independent and time-dependent, (time above the mini-mum inhibitory concentration, T > MIC) bactericidalactivity against susceptible bacteria (Fig. 2).15,16 Theseagents achieve maximal microbiological efficacy when
a considerable portion of the penicillin binding proteinsare occupied which can occur at low multiples ofthe minimum inhibitory concentration (MIC) for therelevant pathogen (i.e., 3–4 times MIC) and when thebeta-lactam concentrations remain above the MIC for�20–70% of the dosing interval, depending on the
Fig. 1. Cellular targets for anti-pseudomonal drugs. Cell wall
synthesis is inhibited by beta-lactam agents. The fluoroquino-
lone agents interrupt DNA replication by trapping DNA bound
to the enzyme DNA gyrase. Protein synthesis at the ribosomal
level is targeted by the aminoglycoside agents. The polymixin
agents (i.e., colistimethate sodium) increase the permeability
of the cell membrane through electrostatic interactions.
Fig. 2. Pharmacodynamic parameters of efficacy for anti-
pseudomonal antibiotics. Drug concentration versus time
curve. T > MIC—the duration of time in which serum concen-
trations exceed the MIC (this parameter best predicts microbi-
ologic efficacy for the beta-lactams). Cmax : MIC—the ratio of
the maximum serum drug concentration to the minimum inhib-
itory concentration (MIC) of P. aeruginosa (this parameter best
predicts microbiologic efficacy for the aminoglycosides). AUC:
MIC—the ratio of the area under the serum concentration
versus time curve to the MIC (this parameter best predicts
microbiologic efficacy for fluoroquinolones and colistimethate
sodium).
2 Zobell et al.
Pediatric Pulmonology

agent.16–19 Beta-lactams may be combined with otheranti-pseudomonal antibiotics (i.e., aminoglycosides,fluoroquinolones, and colistimethate sodium) whichexhibit different mechanisms of action and concentra-tion-dependent bactericidal activity, such as peak con-centration above the MIC (Cmax:MIC) or the ratio ofthe area under the serum concentration curve to theMIC (AUC:MIC).20–22
In the anti-pseudomonal beta-lactam utilization sur-vey, 93% of the respondents reported utilizing intermit-tent beta-lactam dosing (i.e., infused over 30 min),however, a majority of those (58%) chose dosing regi-mens lower than those recommended by the CFF andEuropean guidelines.13,23,24 The findings of this surveysuggest that recommended doses and dosing regimensare not used by a substantial number of CF centersdespite CFF, European, UK CF Trust Working Grouprecommendations, review articles, and literature con-firming the efficacy and safety of higher than Food andDrug Administration (FDA)-approved doses for anti-pseudomonal beta-lactam agents.1,23–32 Possible expla-nations may include concern for dose-related adverseeffects incurred from higher doses, lack of familiaritywith dosing guidelines among CF practitioners, lackof understanding of fundamental pharmacokinetic/pharmacodynamics (PK/PD) principles, and the use ofpublished dosing references which do not containCF-specific dosing recommendations.
This review serves as the first article in a comprehen-sive State of the Art series focusing on summarizing thePK/PD, efficacy, and tolerability studies utilizing anti-pseudomonal antibiotics in the treatment of APE. Thepurpose of this review is to provide a summary ofefficacious and tolerable dosing strategies based on theavailable literature for aztreonam and anti-pseudomonalcarbapenems which have been utilized in the treatmentof APE, and to identify areas where further study iswarranted.
Description of Beta-Lactam Agents
Monobactam
Aztreonam (Azactam1, Princeton, NJ), derived froma fungus, Chromobacterium violceum, contains a mono-cyclic beta-lactam nucleus with a wide-array of activityagainst aerobic gram negative bacteria, includingP. aeruginosa that is available as both an intravenousand aerosolized formulation. 15,33–36 Aztreonam achievesmaximal microbiological efficacy when the penicillinbinding proteins are occupied which can occur at lowmultiples of the MIC for the relevant pathogen (i.e.,3–4 times MIC) and when the beta-lactam concentra-tions remain above the MIC for �50–60% of the dosinginterval.16,17,19 The antimicrobial activity of aztreonamis different from other beta-lactam antibiotics but
similar to aminoglycosides, in that gram positive andanaerobic bacteria are intrinsically resistant to aztreo-nam.15 The most common toxicities related to aztreo-nam are phlebitis, diarrhea, nausea, vomiting, andrash.35 Due to the limited cross-reactivity of aztreonamwith other beta-lactam antibiotics, aztreonam may bewell tolerated by patients with hypersensitivity reac-tions to other beta-lactams.15
Carbapenems
Carbapenems have a wide range of antimicrobial ac-tivity against anaerobic, aerobic gram positive andgram negative bacteria, including activity againstP. aeruginosa. These agents achieve maximal microbio-logical efficacy when the penicillin binding proteins areoccupied which can occur at low multiples of the MICfor the relevant pathogen (i.e., 3–4 times MIC) andwhen the beta-lactam concentrations remain above theMIC for �20–40% of the dosing interval.16,17,19
Carbapenems were derived from thienamycin, a com-pound produced by Streptomyces cattleya.15 The mostcommon toxicities related to carbapenems are nausea,vomiting, seizures, and hypersensitivity in beta-lactamallergic patients.15 Anti-pseudomonal carbapenems in-clude doripenem (Doribax1, Raritan, NJ), imipenem–cilastatin (Primaxin1, Whitehouse Station, NJ), andmeropenem (Merrem1, Wilmington, DE). Ertapenem(Invanz1, Whitehouse Station, NJ) is another carbape-nem agent, but does not display any activity againstP. aeruginosa.37
Pharmacokinetics/Pharmacodynamics
Aztreonam
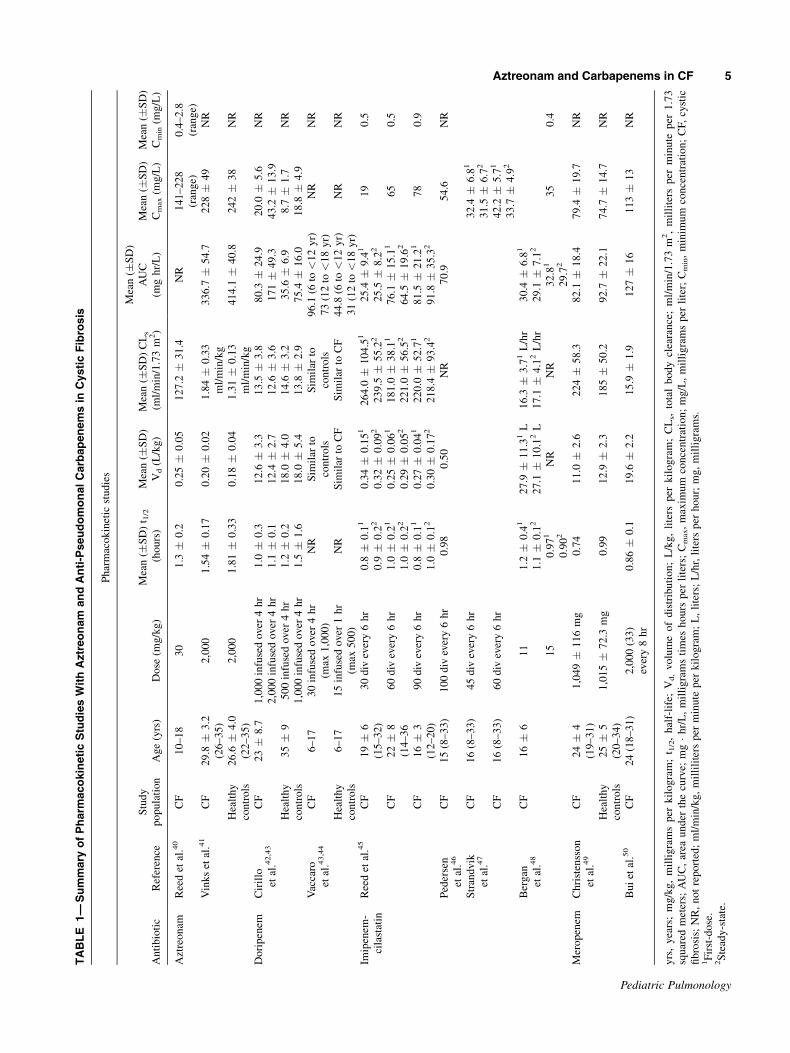
A PK analysis was performed in pediatric CFpatients who received a single 30 mg/kg intravenousdose of aztreonam. Based on the PK data, it was deter-mined that an aztreonam dose of 50 mg/kg/dose every6 hr would be required to maintain serum aztreonamconcentrations over pseudomonal isolates with higherMICs based on current MIC breakpoints from theEuropean Committee on Antimicrobial SusceptibilityTesting (EUCAST) and Clinical and Laboratory Stand-ards Institute (CLSI): S: �1 mg/L; R: >16 mg/L(EUCAST)38; S: �8 mg/L; R: >32 mg/L (CLSI)(Table 1).39,40
A population PK/PD analysis by Vinks et al.,41
showed that the maximum serum concentration (Cmax),half-life (t1/2), and steady-state volume of distribution(Vss) were not significantly different between patientswith CF and healthy controls. However, CF patientshad significantly increased mean total body clearance(CLs) values (41%; P < 0.01) as well as significantlylower mean area under the curve (AUC) values (23%)
Aztreonam and Carbapenems in CF 3
Pediatric Pulmonology

as compared to healthy controls (P < 0.01). Fornear-maximal bactericidal activity, the PK-PD MICbreakpoint for P. aeruginosa for aztreonam 1 g admin-istered every 8 hr was 2 mg/L. For aztreonam 2 gadministered every 8 hr, the PK-PD MIC breakpoint forP. aeruginosa was 4 mg/L. The authors concluded thatdue to significantly higher CLs in CF versus healthycontrols, aztreonam doses of 2 g every 8 hr may beneeded to achieve bactericidal effects among pseudo-monal isolates with MICs �4 mg/L, and are unlikely tobe effective against higher MIC isolates (Tables 1and 2).41
Doripenem
A single-dose of doripenem 1 and 2 g infused over4 hr was given to 34 adult patients (10 with CF, 24healthy volunteers) to define the PK/PD of doripenemin CF patients.42,43 All PK parameters in patients withCF were comparable to healthy controls. The predictedpercentage of time during which doripenem serum con-centrations remained over an minimum inhibitory con-centration (%T > MIC) of 4 mg/L for P. aeruginosawas shown to be 67% and 83% of the dosing intervalfor doripenem 1 and 2 g, respectively: S: �1 mg/L;R: >4 mg/L (EUCAST); S: �2 mg/L; R: NR (CLSI;Tables 1 and 4).38,39 Additionally, the PD of doripenem1 and 2 g doses infused over 4 hr given every 8 hr wereanalyzed. The PK/PD MIC breakpoint for doripenem1 g infused over 4 hr administered every 8 hr was8 mg/L versus 16 mg/L for doripenem 2 g infused over4 hr administered every 8 hr (Table 2). The authorsconcluded that doripenem 1 g infused over 4 hr admin-istered every 8 hr may be effective in the treatment ofAPEs caused by pseudomonal isolates with MICs�8 mg/L, whereas doripenem 2 g infused over 4 hradministered every 8 hr may be effective in the treat-ment of APEs caused by P. aeruginosa with MICs�16 mg/L.42,43
A PK study was performed with doripenem in 20pediatric CF patients receiving 30 mg/kg/dose, maxi-mum 1 g infused over 4 hr (Table 1). CLs was shownto increase with age, and the Vss was similar betweenthe CF and non-CF pediatric participants. The %T >MIC of 4 mg/L for P. aeruginosa was shown to be 63%of the dosing interval (Tables 1 and 4).43,44
Imipenem–Cilastatin
Four PK studies analyzing imipenem–cilastatin in 77CF patients (age range 8–33 years) have been per-formed utilizing doses ranging from 45–100 mg/kg/daydivided every 6 hr.45–48 The study by Reed et al.45 con-cluded that imipenem–cilastatin administered at a doseof 90–100 mg/kg/day divided every 6 hr would beadequate to maintain serum imipenem concentrations
above the MIC of the majority of P. aeruginosaisolates: S: �4 mg/L; R: >8 mg/L (EUCAST); S:�4 mg/L; R: >16 mg/L (CLSI; Tables 1 and 4).38,39,45
However, based on the short t½ of imipenem–cilastatinin patients with CF, the Pedersen et al.46 study conclud-ed that imipenem–cilastatin 100 mg/kg/day dividedevery 6 hr could not be recommended for the treatmentof P. aeruginosa in APE.46
Meropenem
A single-dose of meropenem 15 mg/kg was given in-travenously to CF patients and healthy controls with theintent to define the PK of meropenem in CF patients instable clinical condition. The AUC, Vss, and CLs, werenot different between CF patients and healthy controls.However, the authors found that CF patients haveshorter mean t½ (0.72 hr vs. 0.99 hr), mean residencetimes (1.09 hr vs. 1.39 hr, P < 0.007), and drug con-centrations above the MIC90 of P. aeruginosa <3.3 hrafter infusion: S: �2 mg/L; R: >8 mg/L (EUCAST);S: �4 mg/L; R: > 16 mg/L (CLSI) (Table 1).38,39
These variables show that meropenem concentrationsrapidly decline in some CF patients; therefore, shorterdosing intervals may be needed in order to maintainadequate meropenem serum concentration levels abovethe MIC90 of P. aeruginosa.49
A small PK study of meropenem 2 g (approximately33 mg/kg/dose) given intravenously every 8 hr was per-formed in six clinically stable CF patients to determineif the recommended maximum doses could sustainadequate serum concentrations above the MIC ofP. aeruginosa (Table 1). The meropenem plasma con-centrations remained above 4 mg/L for at least 50% ofthe dosing interval. The authors concluded that theutilization of high-dose meropenem (33 mg/kg/dose,maximum 2 g IV every 8 hr) optimizes the pharmaco-dynamics of meropenem and maximizes the chance ofachieving a positive clinical response.50
Efficacy/Tolerability
Aztreonam
Aztreonam is not a widely utilized anti-pseudomonalbeta-lactam (2/167 reported dosing regimens, 1%) forthe treatment of APE in CF patients.13 Half of the inter-mittent aztreonam regimens (1/2, 50%) were lower thanthe CFF (150 mg/kg/day div every 6–8 hr)24 and Euro-pean Consensus committee (150 mg/kg/day div every6 hr, maximum 8 g/day) doses for the treatment ofAPE in CF patients.13,23
Several efficacy and tolerability studies have beenperformed utilizing aztreonam (Tables 3 and 4).27,28,51–53
In a study by Scully et al.51 a dose of 2 g of aztreonamevery 8 hr was used. Improvement in clinical status
4 Zobell et al.
Pediatric Pulmonology
TABLE
1—
Summary
ofPharm
acokineticStudiesWithAztreonam
andAnti-PseudomonalCarbapenemsin
CysticFibrosis
Ph
arm
aco
kin
etic
stu
die
s
An
tib
ioti
cR
efer
ence
Stu
dy
po
pu
lati
on
Ag
e(y
rs)
Do
se(m
g/k
g)
Mea
n(�
SD
)t 1
/2
(ho
urs
)
Mea
n(�
SD
)
Vd
(L/k
g)
Mea
n(�
SD
)C
Ls
(ml/
min
/1.7
3m
2)
Mea
n(�
SD
)
AU
C
(mg
hr/
L)
Mea
n(�
SD
)
Cm
ax
(mg
/L)
Mea
n(�
SD
)
Cm
in(m
g/L
)
Azt
reo
nam
Ree
det
al.4
0C
F1
0–
18
30
1.3
�0
.20
.25�
0.0
51
27
.2�
31
.4N
R1
41
–2
28
(ran
ge)
0.4
–2
.8
(ran
ge)
Vin
ks
etal
.41
CF
29
.8�
3.2
(26
–3
5)
2,0
00
1.5
4�
0.1
70
.20�
0.0
21
.84�
0.3
3
ml/
min
/kg
33
6.7
�5
4.7
22
8�
49
NR
Hea
lth
y
con
tro
ls
26
.6�
4.0
(22
–3
5)
2,0
00
1.8
1�
0.3
30
.18�
0.0
41
.31�
0.1
3
ml/
min
/kg
41
4.1
�4
0.8
24
2�
38
NR
Do
rip
enem
Cir
illo
etal
.42
,43
CF
23�
8.7
1,0
00
infu
sed
over
4h
r1
.0�
0.3
12
.6�
3.3
13
.5�
3.8
80
.3�
24
.92
0.0
�5
.6N
R
2,0
00
infu
sed
over
4h
r1
.1�
0.1
12
.4�
2.7
12
.6�
3.6
17
1�
49
.34
3.2
�1
3.9
Hea
lth
y
con
tro
ls
35�
95
00
infu
sed
over
4h
r1
.2�
0.2
18
.0�
4.0
14
.6�
3.2
35
.6�
6.9
8.7
�1
.7N
R
1,0
00
infu
sed
over
4h
r1
.5�
1.6
18
.0�
5.4
13
.8�
2.9
75
.4�
16
.01
8.8
�4
.9
Vac
caro
etal
.43
,44
CF
6–
17
30
infu
sed
over
4h
r
(max
1,0
00
)
NR
Sim
ilar
to
con
tro
ls
Sim
ilar
to
con
tro
ls
96
.1(6
to<
12
yr)
NR
NR
73
(12
to<
18
yr)
Hea
lth
y
con
tro
ls
6–
17
15
infu
sed
over
1h
r
(max
50
0)
NR
Sim
ilar
toC
FS
imil
arto
CF
44
.8(6
to<
12
yr)
NR
NR
31
(12
to<
18
yr)
Imip
enem
-
cila
stat
in
Ree
det
al.4
5C
F1
9�
6
(15
–3
2)
30
div
ever
y6
hr
0.8
�0
.11
0.3
4�
0.1
51
26
4.0
�1
04
.51
25
.4�
9.4
11
90
.5
0.9
�0
.22
0.3
2�
0.0
92
23
9.5
�5
5.2
22
5.5
�8
.22
CF
22�
8
(14
–3
6
60
div
ever
y6
hr
1.0
�0
.21
0.2
5�
0.0
61
18
1.0
�3
8.1
17
6.1
�1
5.1
16
50
.5
1.0
�0
.22
0.2
9�
0.0
52
22
1.0
�5
6.5
26
4.5
�1
9.6
2
CF
16�
3
(12
–2
0)
90
div
ever
y6
hr
0.8
�0
.11
0.2
7�
0.0
41
22
0.0
�5
2.7
18
1.5
�2
1.2
17
80
.9
1.0
�0
.12
0.3
0�
0.1
72
21
8.4
�9
3.4
29
1.8
�3
5.3
2
Ped
erse
n
etal
.46
CF
15
(8–
33
)1
00
div
ever
y6
hr
0.9
80
.50
NR
70
.95
4.6
NR
Str
and
vik
etal
.47
CF
16
(8–
33
)4
5d
ivev
ery
6h
r3
2.4
�6
.81
31
.5�
6.7
2
CF
16
(8–
33
)6
0d
ivev
ery
6h
r4
2.2
�5
.71
33
.7�
4.9
2
Ber
gan
etal
.48
CF
16�
61
11
.2�
0.4
12
7.9
�1
1.3
1L
16
.3�
3.7
1L
/hr
30
.4�
6.8
1
1.1
�0
.12
27
.1�
10
.12
L1
7.1
�4
.12
L/h
r2
9.1
�7
.12
15
0.9
71
NR
NR
32
.81
35
0.4
0.9
02
29
.72
Mer
op
enem
Ch
rist
enss
on
etal
.49
CF
24�
4
(19
–3
1)
1,0
49�
11
6m
g0
.74
11
.0�
2.6
22
4�
58
.38
2.1
�1
8.4
79
.4�
19
.7N
R
Hea
lth
y
con
tro
ls
25�
5
(20
–3
4)
1,0
15�
72
.3m
g0
.99
12
.9�
2.3
18
5�
50
.29
2.7
�2
2.1
74
.7�
14
.7N
R
Bu
iet
al.5
0C
F2
4(1
8–
31
)2
,00
0(3
3)
ever
y8
hr
0.8
6�
0.1
19
.6�
2.2
15
.9�
1.9
12
7�
16
11
3�
13
NR
yrs
,y
ears
;m
g/k
g,
mil
lig
ram
sp
erk
ilo
gra
m;
t 1/2
,h
alf-
life
;V
d,
vo
lum
eo
fd
istr
ibu
tio
n;
L/k
g,
lite
rsp
erk
ilo
gra
m;
CL
s,to
tal
bo
dy
clea
ran
ce;
ml/
min
/1.7
3m
2,
mil
lite
rsp
erm
inu
tep
er1
.73
squ
ared
met
ers;
AU
C,
area
un
der
the
curv
e;m
g�h
r/L
,m
illi
gra
ms
tim
esh
ou
rsp
erli
ters
;C
max,
max
imu
mco
nce
ntr
atio
n;
mg
/L,
mil
lig
ram
sp
erli
ter;
Cm
in,
min
imu
mco
nce
ntr
atio
n;
CF,
cyst
ic
fib
rosi
s;N
R,
no
tre
po
rted
;m
l/m
in/k
g,
mil
lili
ters
per
min
ute
per
kil
og
ram
;L
,li
ters
;L
/hr,
lite
rsp
erh
ou
r;m
g,
mil
lig
ram
s.1F
irst
-do
se.
2S
tead
y-s
tate
.
Aztreonam and Carbapenems in CF 5
Pediatric Pulmonology

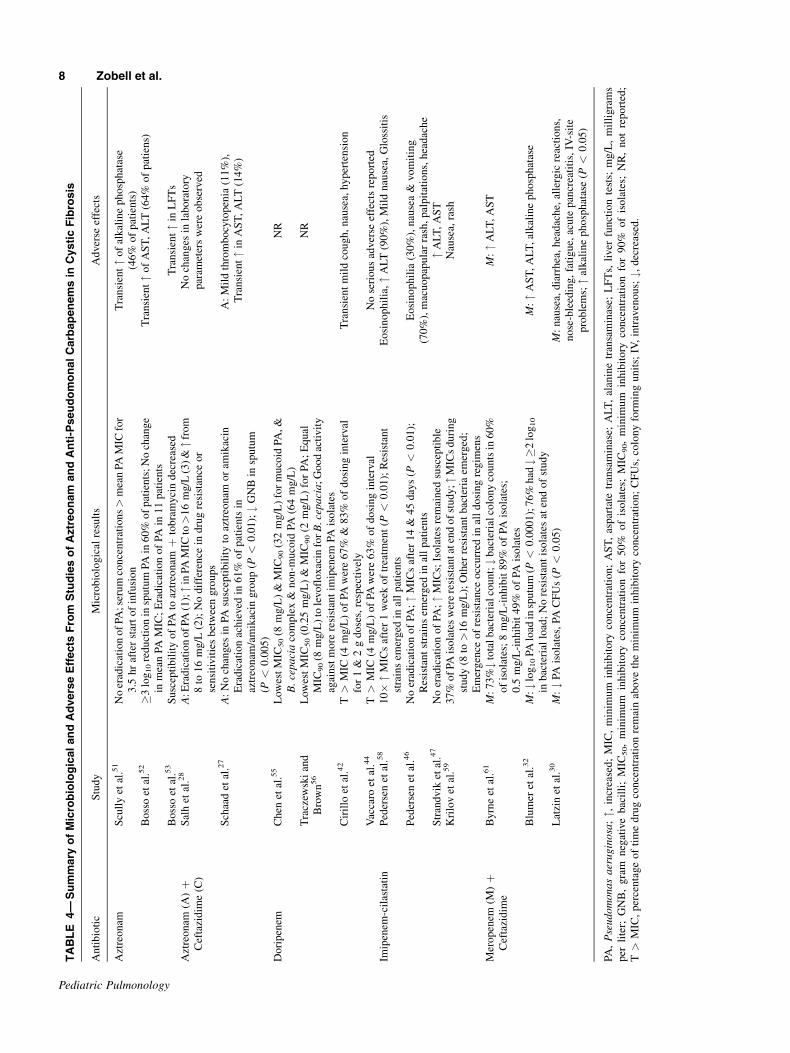
from baseline was observed; however, eradication ofP. aeruginosa was not achieved, and serum concentra-tions only exceeded the mean MIC for P. aeruginosaisolates for 3.5 hr after the start of infusion (Table 4).51
Based on the PK/PD study mentioned previously, thisdosing strategy may not be effective against pseudomo-nal isolates with higher MICs (Table 2).41 Larger andmore frequent aztreonam dosing strategies of 200–300 mg/kg/day divided every 6 hr, maximum 8–12 g/day utilized in four other studies showed clinical andmicrobiological efficacy in the treatment of APE due toP. aeruginosa, and were well-tolerated with no reportsof major adverse events (Tables 3 and 4).27,28,52,53 Theefficacy and tolerability of aerosolized aztreonam in thetreatment of APE is currently unknown, therefore fur-ther studies are warranted.
Doripenem
According to the utilization survey of anti-pseudomo-nal beta-lactams, no CFF-accredited centers reportedthe use of doripenem in the treatment of APE.13 It wasrecently approved by the FDA in 2007.54 The FDA-approved dose is 500 mg every 8 hr.54 No efficacy dataexists in CF and pediatric patients. There are also nodosing recommendations from the CFF, the EuropeanConsensus Committee, and the UK CF Trust. However,in vitro microbiological studies by Chen et al.,55 andTraczewski and Brown56 in CF patients show the poten-tial clinical efficacy of doripenem against P. aeruginosa(Table 4).55,56 The tolerability of doripenem in bothpediatric and adult CF patients was evaluated by Cirilloet al.42 and Vaccaro et al.44 both of which reported nomajor adverse events (Table 4).
Imipenem–Cilastatin
No CFF-accredited care center reported the use ofimipenem–cilastatin as their first-line anti-pseudomonalbeta-lactam in the treatment of APE in the beta-lactam
utilization survey.13 The FDA-approved dose for imipe-nem–cilastatin is very similar to the CFF dosing recom-mendations, the European Consensus Committeerecommendations, the UK CF Trust recommendations,and dosing recommendations from review articles forimipenem–cilastatin in CF patients.1,2,23–25,57 Multipleclinical efficacy and tolerability studies with imipenem–cilastatin in CF support these dosing recommendations(Tables 3 and 4).46,47,58,59
The imipenem–cilastatin dosing regimens utilized inthe four efficacy and tolerability studies ranged from30 to 100 mg/kg/day divided every 6 hr (Tables 3and 4).46,47,58,59 Although imipenem–cilastatin wasshown to be tolerable and efficacious in the treatmentof APE, resistance to P. aeruginosa developed rapidly,and the authors could not recommend imipenem–cilastatin for routine use for the treatment of APE.46,58,59
Meropenem
Meropenem is the only anti-pseudomonal carbape-nem that was reported to be utilized in a recent survey(21/167 reported dosing regimens, 13%) for the treat-ment of APE in CF patients.13 Approximately, half ofintermittent meropenem regimens (9/20, 45%) werelower than the FDA-approved meningitis (120 mg/kg/day div every 8 hr, maximum 6 g/day)60 and EuropeanConsensus guideline (60–120 mg/kg/day div every 8 hr,maximum 6 g/day)23 doses for the treatment of APE inCF patients.13 Three studies analyzing the tolerabilityand efficacy of meropenem in APE have been per-formed in 136 CF patients (age range 4–64 years)utilizing doses ranging from 75–120 mg/kg/day, up to3.75–6 g/day.30,32,61 These multicenter randomizedcomparative studies analyzed the clinical efficacy andtolerability of meropenem versus ceftazidime. Merope-nem was shown to be a well-tolerated and effectivealternative to ceftazidime alone and in combinationwith tobramycin in the treatment of APE secondary toP. aeruginosa, with recommendations that monitoring
TABLE 2—Summary of Pharmacodynamic Studies With Aztreonam and Anti-Pseudomonal Carbapenems in CysticFibrosis
Pharmacodynamic Studies
Antibiotic Study Dose (mg) Significant findings
Aztreonam Vinks et al.41 2,000 Higher CLs in CF vs. controls
Lower AUC in CF vs. controls
PK-PD MIC breakpoint (1 g every 8 hr) � 2 mg/L
PK-PD MIC breakpoint (2 g every 8 hr) � 4 mg/L
Doripenem Cirillo et al.42 1,000 every 8 hr, infused over 4 hr 1,000 mg ¼ PK/PD MIC breakpoint �8 mg/L
2,000 every 8 hr, infused over 4 hr 2,000 mg ¼ PK/PD MIC breakpoint �16 mg/L
CLs, total body clearance; CF, cystic fibrosis; AUC, area under the curve; mg, milligrams; PK-PD MIC breakpoint, pharmacokinetic/
pharmacodynamic minimum inhibitory concentration breakpoint (i.e., highest MIC with a PTA � 90%); mg/L, millgrams per liter.
6 Zobell et al.
Pediatric Pulmonology

TABLE
3—
Summary
ofEfficacyStudiesofAztreonam
andAnti-PseudomonalCarbapenemsin
CysticFibrosis
An
tib
ioti
cS
tud
yM
ean
(�S
D)
age
(yrs
)D
ose
(mg
/kg
/day
)O
utc
om
es
Azt
reo
nam
Scu
lly
etal
.51
19
(12
–3
2)
2,0
00
mg
ever
y8
hr
wit
h
amin
og
lyco
sid
es
"cl
inic
alst
atu
s(8
5%
of
epis
od
es);
Mea
nin
terv
alo
f
imp
rovem
ent¼
7d
ays
Bo
sso
etal
.52
14
(6–
32
)2
00
div
ever
y6
hr
"cl
inic
alan
dp
ulm
on
ary
sco
res
&W
BC
(P<
0.0
5);
Mea
nin
terv
alo
f
imp
rovem
ent¼
12
.5d
ays
Bo
sso
etal
.53
14
20
0d
ivev
ery
6h
rþ
tob
ram
yci
no
r
azlo
cill
inþ
tob
ram
yci
n
"cl
inic
al&
pu
lmo
nar
ysc
ore
s,W
BC
,P
FT
s,X
-ray
s
Azt
reo
nam
(A)þ
Cef
tazi
dim
e(C
)
Sal
het
al.2
81
6–
32
(bo
thg
rou
ps)
2,0
00
mg
ever
y6
hr
(8g
/day
;b
oth
gro
up
s)
A:"
FE
V1%
pre
dic
ted
(P<
0.0
1);#s
pu
tum
wei
gh
t(P
<0
.05
);"
pat
ien
tw
ell-
bei
ng
(P<
0.0
01
)
Slo
wer
#in
FE
V1%
pre
dic
ted
inaz
treo
nam
vs.
ceft
azid
ime
atd
ay4
2
(P<
0.0
5)
Sch
aad
etal
.27
15
.4�
6.0
(2.3
–2
5.4
)
(bo
thg
rou
ps)
30
0d
ivev
ery
6h
r(m
ax1
2g
/day
)þ
amik
acin
(bo
thg
rou
ps)
A:#s
pu
tum
wei
gh
t(P
<0
.00
5),
WB
C,b
and
neu
tro
ph
ils
(P<
0.0
01
),
ES
R(P
<0
.05
)
"cli
nic
al/r
adio
gra
ph
ic&
rad
iolo
gic
sco
res,
FE
V1%
pre
dic
ted
,th
ora
cic
gas
vo
lum
e(P
<0
.05
),F
VC
%p
red
icte
d(P
<0
.01
),&
ox
yg
en
satu
rati
on
s(P
<0
.00
5)
Do
rip
enem
Cir
illo
etal
.42
23�
8.7
—D
ori
pen
em1
,00
0–
2,0
00
ever
y8
hr
infu
sed
over
4h
r
NR
35�
9—
Hea
lth
yco
ntr
ols
Vac
caro
etal
.44
6–
17
yea
rs9
0ev
ery
8h
r,in
fuse
dover
4h
r
(max
1,0
00
mg
/do
se)
NR
Imip
enem
-cil
asta
tin
Ped
erse
net
al.5
81
8(1
1–
30
)4
5d
ivev
ery
6h
r"
Sh
wac
hm
ansc
ore
s,ch
est
ausc
ula
tory
sco
res,
FV
C%
&F
EV
1%
pre
dic
ted
(P<
0.0
1)
#sp
utu
mp
rod
uct
ion
(P<
0.0
1),
WB
C(P
<0
.02
)&
rest
ing
pu
lse
rate
(P<
0.0
5)
Ped
erse
net
al.4
61
5(8
–3
3)
10
0d
ivev
ery
6h
rþ
tob
ram
yci
n"
FV
C%
&F
EV
1%
pre
dic
ted
;#
WB
C
Str
and
vik
etal
.47
16
(8–
33
)4
5–
60
div
ever
y6
hr
"S
hw
ach
man
sco
res,
FV
C%
&F
EV
1%
pre
dic
ted
,(P
<0
.00
1),
bo
dy
wei
gh
t(P
<0
.01
),b
loo
do
xy
gen
(P<
0.0
5);#
resp
irat
ory
&p
uls
e
rate
,W
BC
(P<
0.0
1),
spu
tum
pro
du
ctio
n
Kri
lov
etal
.59
12
–3
63
0–
90
div
ever
y6
hr
"S
hw
ach
man
,cl
inic
alsc
ore
s(P
<0
.00
1),
FV
C%
pre
dic
ted
(P<
0.0
1)
Mer
op
enem
þC
efta
zid
ime
By
rne
etal
.61
16
(6–
33
)—C
efta
zid
ime
(C)
(C)
15
0d
ivev
ery
8h
r(m
ax7
.5g
/day
)M
:9
8%
clin
ical
resp
on
sera
te;"F
EV
1%
&F
VC
%p
red
icte
d;#s
pu
tum
pro
du
ctio
n(P
<0
.05
)1
5(4
–2
8)—
Mer
op
enem
(M)
(M)
75
div
ever
y8
hr
(max
3.7
5g
/day
)
Blu
mer
etal
.32
5–
64
bo
thg
rou
ps
(C)
15
0d
ivev
ery
8h
r(m
ax6
g/d
ay)þ
tob
ram
yci
n
M:"
FE
V1%
pre
dic
ted
(P¼
0.0
00
2);#
AC
Ssc
ore
s(P
<0
.00
1);
96
%
clin
ical
resp
on
der
s;L
arg
erre
lati
ve
chan
ge
inF
EV
1%
pre
dic
ted
at
day
7v
s.ce
ftaz
idim
eg
rou
p(P
¼0
.07
)w
ith
maj
ori
tyo
f"
occ
urr
ing
in1
st7
day
s;L
arg
er"
FE
V1%
pre
dic
ted
vs.
ceft
azid
ime
(P<
0.0
01
);"
trea
tmen
tre
spo
nd
ers
atd
ay7
vs.
ceft
azid
ime
(P¼
0.0
4);
Sh
ort
erti
me
for
50
%cl
inic
alre
spo
nse
rate
(4d
ays
vs.
6
day
s)v
s.ce
ftaz
idim
e;ti
me
ton
ext
exac
erb
atio
n¼
17
6d
ays
(M)
12
0d
ivev
ery
8h
r(m
ax6
g/d
ay)þ
tob
ram
yci
n
Lat
zin
etal
.30
16
.9�
7.7
—ce
ftaz
idim
e(C
)2
00
–4
00
div
ever
y
8–
12
hrþ
tob
ram
yci
n
M:"
FE
V1%
,F
VC
%&
ME
F2
5%
pre
dic
ted
(P<
0.0
5);#
WB
C,C
RP
(P<
0.0
5)
17�
9—
mer
op
enem
(M)
12
0d
ivev
ery
8h
r
(max
6g
/day
)þ
tob
ram
yci
n
yrs
,y
ears
;m
g/k
g/d
ay,
mil
lig
ram
sp
erk
ilo
gra
mp
erd
ay;
mg
,m
illi
gra
ms;",
incr
ease
d;
WB
C,
wh
ite
blo
od
cou
nt;
PF
Ts,
pu
lmo
nar
yfu
nct
ion
test
s;F
EV
1%
pre
dic
ted
,fo
rced
exp
irat
ory
vo
lum
e
in1
sec
per
cen
tp
red
icte
d;#,
dec
reas
ed;
ES
R,
ery
thro
cyte
sed
imen
tati
on
rate
;F
VC
%p
red
icte
d,
forc
edv
ital
cap
acit
yp
erce
nt
pre
dic
ted
;N
R,
no
tre
po
rted
;A
CS
,ac
ute
clin
ical
sco
re;
ME
F2
5%
pre
dic
ted
,m
ean
exp
irat
ory
flow
of
25
%p
red
icte
d;
CR
P,C
-rea
ctiv
ep
rote
in.
Aztreonam and Carbapenems in CF 7
Pediatric Pulmonology
TABLE
4—
Summary
ofMicrobiologicalandAdverseEffects
From
StudiesofAztreonam
andAnti-PseudomonalCarbapenemsin
CysticFibrosis
An
tib
ioti
cS
tud
yM
icro
bio
log
ical
resu
lts
Ad
ver
seef
fect
s
Azt
reo
nam
Scu
lly
etal
.51
No
erad
icat
ion
of
PA
;se
rum
con
cen
trat
ion
s>
mea
nPA
MIC
for
3.5
hr
afte
rst
art
of
infu
sio
n
Tra
nsi
ent"
of
alk
alin
ep
ho
sph
atas
e
(46
%o
fp
atie
nts
)
Bo
sso
etal
.52
�3
log
10
red
uct
ion
insp
utu
mPA
in6
0%
of
pat
ien
ts;
No
chan
ge
inm
ean
PA
MIC
;E
rad
icat
ion
of
PA
in1
1p
atie
nts
Tra
nsi
ent"
of
AS
T,
AL
T(6
4%
of
pat
ien
s)
Bo
sso
etal
.53
Su
scep
tib
ilit
yo
fPA
toaz
treo
nam
þto
bra
my
cin
dec
reas
edT
ran
sien
t"
inL
FT
s
Azt
reo
nam
(A)þ
Cef
tazi
dim
e(C
)
Sal
het
al.2
8A
:E
rad
icat
ion
of
PA
(1);"i
nPA
MIC
to>
16
mg
/L(3
)&"f
rom
8to
16
mg
/L(2
);N
od
iffe
ren
cein
dru
gre
sist
ance
or
sen
siti
vit
ies
bet
wee
ng
rou
ps
No
chan
ges
inla
bo
rato
ry
par
amet
ers
wer
eo
bse
rved
Sch
aad
etal
.27
A:
No
chan
ges
inPA
susc
epti
bil
ity
toaz
treo
nam
or
amik
acin
Era
dic
atio
nac
hie
ved
in6
1%
of
pat
ien
tsin
aztr
eon
am/a
mik
acin
gro
up
(P<
0.0
1);#
GN
Bin
spu
tum
(P<
0.0
05
)
A:
Mil
dth
rom
bo
cyto
pen
ia(1
1%
),
Tra
nsi
ent"
inA
ST
,A
LT
(14
%)
Do
rip
enem
Ch
enet
al.5
5L
ow
est
MIC
50
(8m
g/L
)&
MIC
90
(32
mg
/L)
for
mu
coid
PA
,&
B.cepacia
com
ple
x&
no
n-m
uco
idPA
(64
mg
/L)
NR
Tra
czew
ski
and
Bro
wn
56
Low
est
MIC
50
(0.2
5m
g/L
)&
MIC
90
(2m
g/L
)fo
rPA
;E
qu
al
MIC
90
(8m
g/L
)to
levo
flo
xac
info
rB.cepacia
;G
oo
dac
tiv
ity
agai
nst
mo
rere
sist
ant
imip
enem
PA
iso
late
s
NR
Cir
illo
etal
.42
T>
MIC
(4m
g/L
)o
fPA
wer
e6
7%
&8
3%
of
do
sin
gin
terv
al
for
1&
2g
do
ses,
resp
ecti
vel
y
Tra
nsi
ent
mil
dco
ug
h,
nau
sea,
hy
per
ten
sio
n
Vac
caro
etal
.44
T>
MIC
(4m
g/L
)o
fPA
wer
e6
3%
of
do
sin
gin
terv
alN
ose
rio
us
adver
seef
fect
sre
po
rted
Imip
enem
-cil
asta
tin
Ped
erse
net
al.5
81
0�
"M
ICs
afte
r1
wee
ko
ftr
eatm
ent
(P<
0.0
1);
Res
ista
nt
stra
ins
emer
ged
inal
lp
atie
nts
Eo
sin
op
hil
ia,"
AL
T(9
0%
),M
ild
nau
sea,
Glo
ssit
is
Ped
erse
net
al.4
6N
oer
adic
atio
no
fPA
;"
MIC
saf
ter
14
&4
5d
ays
(P<
0.0
1);
Res
ista
nt
stra
ins
emer
ged
inal
lp
atie
nts
Eo
sin
op
hil
ia(3
0%
),n
ause
a&
vo
mit
ing
(70
%),
mac
uo
pap
ula
rra
sh,
pal
pit
atio
ns,
hea
dac
he
Str
and
vik
etal
.47
No
erad
icat
ion
of
PA
;"
MIC
s;Is
ola
tes
rem
ain
edsu
scep
tib
le"
AL
T,
AS
T
Kri
lov
etal
.59
37
%o
fPA
iso
late
sw
ere
resi
stan
tat
end
of
stu
dy
;"M
ICs
du
rin
g
stu
dy
(8to
>1
6m
g/L
);O
ther
resi
stan
tb
acte
ria
emer
ged
;
Em
erg
ence
of
resi
stan
ceo
ccu
rred
inal
ld
osi
ng
reg
imen
s
Nau
sea,
rash
Mer
op
enem
(M)þ
Cef
tazi
dim
e
By
rne
etal
.61
M:
73
%#
tota
lb
acte
rial
cou
nt;#
bac
teri
alco
lony
cou
nts
in6
0%
of
iso
late
s;8
mg
/L-i
nh
ibit
89
%o
fPA
iso
late
s;
0.5
mg
/L-i
nh
ibit
49
%o
fPA
iso
late
s
M:"
AL
T,
AS
T
Blu
mer
etal
.32
M:#l
og
10
PA
load
insp
utu
m(P
<0
.00
01
);7
6%
had
#�2
log
10
inb
acte
rial
load
;N
ore
sist
ant
iso
late
sat
end
of
stu
dy
M:"
AS
T,
AL
T,
alk
alin
ep
ho
sph
atas
e
Lat
zin
etal
.30
M:#
PA
iso
late
s,PA
CF
Us
(P<
0.0
5)
M:
nau
sea,
dia
rrh
ea,
hea
dac
he,
alle
rgic
reac
tio
ns,
no
se-b
leed
ing
,fa
tig
ue,
acu
tep
ancr
eati
tis,
IV-s
ite
pro
ble
ms;"
alk
alin
ep
ho
sph
atas
e(P
<0
.05
)
PA
,Pseudomonasaeruginosa
;",
incr
ease
d;
MIC
,m
inim
um
inh
ibit
ory
con
cen
trat
ion
;A
ST
,as
par
tate
tran
sam
inas
e;A
LT
,al
anin
etr
ansa
min
ase;
LF
Ts,
liver
fun
ctio
nte
sts;
mg
/L,
mil
lig
ram
s
per
lite
r;G
NB
,g
ram
neg
ativ
eb
acil
li;
MIC
50,
min
imu
min
hib
ito
ryco
nce
ntr
atio
nfo
r5
0%
of
iso
late
s;M
IC9
0,
min
imu
min
hib
ito
ryco
nce
ntr
atio
nfo
r9
0%
of
iso
late
s;N
R,
no
tre
po
rted
;
T>
MIC
,p
erce
nta
ge
of
tim
ed
rug
con
cen
trat
ion
rem
ain
above
the
min
imu
min
hib
ito
ryco
nce
ntr
atio
n;
CF
Us,
colo
ny
form
ing
un
its;
IV,
intr
aven
ou
s;#,
dec
reas
ed.
8 Zobell et al.
Pediatric Pulmonology

of hepatic function may be warranted (Tables 3and 4).30,32,61
Evidenced-Based Summary of Anti-PseudomonalBeta-Lactams
Aztreonam
The literature does not support the CFF and Europe-an Consensus Committee dosing recommendations ofaztreonam 150 mg/kg/day divided every 6–8 hr, maxi-mum 8 g/day.23,24 The UK CF Trust Working Grouprecommendation is 90–200 mg/kg/day divided 6–8 hr,maximum 8 g/day.25 An intravenous aztreonam dosingregimen of 200–300 mg/kg/day divided every 6 hr,maximum 8–12 g/day, was shown to be a well-toleratedand effective dosing regimen for the treatment ofP. aeruginosa in APE in 133 patients (Tables 3 and 4),although this exceeds the current FDA labeling recom-mendation (Tables 3–5).35 Further study is needed todefine the maximum dose, and optimal PK/PD param-eters of aztreonam in CF for the treatment of APE.
Doripenem
As doripenem was recently approved (2007) for usein the US, limited literature evidence exists describingthe use of doripenem in CF. However, the literature inCF does not support the FDA-approved54 dosing recom-mendation of intravenous doripenem 500 mg every8 hr. The literature supports a dosing recommendationof intravenous doripenem 90 mg/kg/day divided every8 hr, infused over 4 hr, maximum 6 g/day, as a tolera-ble and potentially optimal dosing regimen for the treat-ment of P. aeruginosa in APE (Tables 1, 2, 4,and 5).42,44 Future study is needed to determine theclinical efficacy of this dosing regimen in APE.
Imipenem–Cilastatin
The literature supports the FDA-approved, CFF,European Consensus Committee, and UK CF TrustWorking Group dosing recommendations of intravenous
imipenem–cilastatin 100 mg/kg/day divided every 6 hr,maximum 4 g/day, as a tolerable and effective dosingregimen for the treatment of P. aeruginosa in APE,though the development of resistance may be an issue(Tables 3–5).23,24,46,57–59 In addition to the developmentof resistance, imipenem–cilastatin use is limited by itsrisk of lowering the seizure threshold and the presenceof strict hospital/institutional formularies limitingaccess to this antibiotic.57,62–64 Although there are gapsin the literature, the development of resistance has lim-ited the usefulness of this medication for the treatmentAPE secondary to P. aeruginosa in CF patients.46,58,59
Meropenem
The literature supports the FDA-approved meningitis,European Consensus Committee, and UK CF TrustWorking Group dosing recommendations of intravenousmeropenem 120 mg/kg/day divided every 8 hr, maxi-mum 6 g/day, as a tolerable and effective dosing regi-men for the treatment of P. aeruginosa in APE(Tables 1, 3–5).23,25,30,32,50,60 CFF guideline recommen-dations do not exist for meropenem, as this agent wasnot marketed when the CFF guidelines were ap-proved.24 No PD modeling studies exist for pediatricand adult CF populations making determination of opti-mal dosing recommendations difficult.
CONCLUSIONS
This review has provided an overview of the PK/PD,tolerability, and efficacy studies utilizing intravenousaztreonam and anti-pseudomonal carbapenems ap-proved in the US in the treatment of APE. Studies haveshown that approximately 25% of CF patients will notregain their lung function following a pulmonaryexacerbation despite aggressive treatment with two ormore anti-pseudomonal antibiotics.65,66 It is possiblethat currently available anti-pseudomonal antibiotics,including beta-lactams are being used sub-optimally byCF clinicians, which has been suggested by recent sur-veys.13,14 Multiple explanations may exist ranging from
TABLE 5—Evidence-Based Dosing Summary of Intravenous Anti-Pseudomonal Beta-Lactams for Pediatric and Adult CFPatients
Antibiotic Dose (mg/kg/day) Maximum dose (grams/day)
Monobactam
Aztreonam25,27,28,40,52,53 200–300 div every 6 hr 8–12
Carbapenems
Doripenem42,44 90 div every 8 hr, infused over 4 hr 6
Imipenem–cilastatin23,24,45,46 100 div every 6 hr1 4
Meropenem23,25,30,32,50 120 div every 8 hr 6
mg/kg/day, milligrams per kilogram per day; div, divided.1Limited usefulness due to development of resistance.
Aztreonam and Carbapenems in CF 9
Pediatric Pulmonology

concern for adverse effects due to higher doses to useof published dosing references which do not containCF-specific dosing recommendations. As new anti-pseudomonal agents are scarce, standardization of boththe dosing and dosing regimens of currently availableanti-pseudomonal antibiotics used to treat APE, as wellas additional education, implementation strategies, andrandomized, controlled trials with these standardizeddosing regimens to analyze clinical endpoints may behelpful for CF practitioners in optimizing the treatmentof APE secondary to P aeruginosa (Table 5).
ACKNOWLEDGMENTS
The authors would like to thank Dr. Kevin Epps,Pharm.D., BCPS, from the Pharmacy Department atSt. Vincent’s Medical Center Riverside, Jacksonville,FL, Dr. Jared Cash, Pharm.D., BCPS from the Pharma-cy Department at Intermountain Primary Children’sMedical Center, Salt Lake City, UT, and Dr. BarbaraChatfield, M.D., Director of the Intermountain CysticFibrosis Pediatric Center, Salt Lake City, UT, for theircontributions to the editing and reviewing of this manu-script. The authors would like extend a special thanksto Dr. Lisa Saiman, MD, MPH, Professor of ClinicalPediatrics, Pediatric Infectious Diseases, ColumbiaUniversity Medical Center, New York, NY for the con-ception and design of this manuscript, for the extensivereview and editing, and the overall success of thisseries.
REFERENCES
1. Ramsey BW. Management of pulmonary disease in patients
with cystic fibrosis. N Engl J Med 1996;335:179–188.
2. Gibson RL, Burns JL, Ramsey BW. Pathophysiology and man-
agement of pulmonary infections in cystic fibrosis. Am J Respir
Crit Care Med 2003;168:918–951.
3. Flume PA, O’Sullivan BP, Robinson KA, Goss CH, Mogayzel
PJ, Willey-Courand DB, Bujan J, Finder J, Lester M, Quittell L,
et al. Cystic fibrosis pulmonary guidelines: chronic medications
for maintenance of lung health. Am J Respir Crit Care Med
2007;176:957–969.
4. McCool FD, Rosen MJ. Nonpharmacologic airway clearance
therapies: ACCP evidence-based clinical practice guidelines.
Chest 2006;129:250S–259S.
5. Flume PA, Robinson KA, O’Sullivan BP, Finder JD, Vender
RL, Willey-Courand DB, White TB, Marshall BC. Cystic fibro-
sis pulmonary guidelines: Airway clearance therapies. Respir
Care 2009;54:522–537.
6. Fuchs HJ, Borowitz DS, Christiansen DH, Morris EM, Nash
ML, Ramsey BW, Rosenstein BJ, Smith AL, Wohl ME. Effect
of aerosolized recombinant human DNase on exacerbations of
respiratory symptoms and on pulmonary function in patients
with cystic fibrosis. The Pulmozyme Study Group. N Engl J
Med 1994;331:637–642.
7. Elkins MR, Robinson M, Rose BR, Harbour C, Moriarty CP,
Marks GB, Belousova EG, Xuan W, Bye PTP. A controlled trial
of long-term inhaled hypertonic saline in patients with cystic
fibrosis. N Engl J Med 2006;354:229–240.
8. Ramsey BW, Pepe MS, Quan JM, Otto KL, Montgomery
AB, Williams-Warren J, Vasiljev-K M, Borowitz D, Bowman
CM, Marshall BC, et al. Intermittent administration of inhaled
tobramycin in patients with cystic fibrosis. Cystic Fibrosis
Inhaled Tobramycin Study Group. N Engl J Med 1999;340:
23–30.
9. Retsch-Bogart GZ, Quittner AL, Gibson RL, Oemann CM,
McCoy KS, Montgomery AB, Cooper PJ. Efficacy and safety of
inhaled aztreonam lysine for airway pseudomonas in cystic
fibrosis. Chest 2009;135:1223–1232.
10. Saiman L, Marshall BC, Mayer-Hamblett N, Burns JL, Quittner
AL, Cibene DA, Coquillette S, Fieberg AY, Accurso FJ,
Campbell PW. Azithromycin in patients with cystic fibrosis
chronically infected with Pseudomonas aeruginosa: A random-
ized controlled trial. JAMA 2003;290:1749–1756.
11. Saiman L, Anstead M, Mayer-Hamblett N, Lands LC, Kloster
M, Hocevar-Trnka J, Goss CH, Rose LM, Burns JL, Marshall
BC, et al. Effect of azithromycin on pulmonary function in
patients with cystic fibrosis uninfected with Pseudomonas
aeruginosa: A randomized controlled trial. JAMA 2010;303:
1707–1715.
12. Flume PA, Mogayzel PJ, Robinson KA, Goss CH, Rosenblatt
RL, Kuhn RJ, Marshall BC. Cystic fibrosis pulmonary guide-
lines: Treatment of pulmonary exacerbations. Am J Respir Crit
Care Med 2009;180:802–808.
13. Zobell JT, Young DC, Waters CD, Ampofo K, Cash J, Marshall
BC, Olson J, Chatfield BA. A survey of the utilization of anti-
pseudomonal beta-lactam therapy in cystic fibrosis patients.
Pediatr Pulmonol 2011;46:987–990.
14. Van Meter DJ, Corriveau M, Ahern JW, Lahiri T. A survey of
once-daily dosage tobramycin therapy in patients with cystic
fibrosis. Pediatr Pulmonol 2009;44:325–329.
15. Petri WA. In: Hardman JG, Limbird LE, editors. Chapter 45:
Antimicrobial agents: Penicillins, Cephalosporins, and Other
Beta-Lactam Antibiotics, in Goodman and Gilman’s The
Pharmacological Basis of Therapeutics. New York: McGraw-
Hill; 2001. pp 1189–1218.
16. Burgess DS. Use of pharmacokinetics and pharmacodynamics
to optimize antimicrobial treatment of Pseudomonas aeruginosa
infections. Clin Infect Dis 2005;40:S99–S104.
17. Craig WA. Pharmacokinetic/pharmacodynamic parameters:
rationale for antibacterial dosing of mice and men. Clin Infect
Dis 1998;26:1–10; quiz 11–12.
18. Burgess DS, Hastings RW, Hardin TC. Pharmacokinetics and
pharmacodynamics of cefepime administered by intermittent
and continuous infusion. Clin Ther 2000;22:66–75.
19. Drusano GL. Antimicrobial pharmacodynamics: critical inter-
actions of ‘bug and drug’. Nat Rev Microbiol 2004;2:289–
300.
20. Chambers HF. In: Hardman JG, Limbird LE, editors. Chapter
46: Antimicrobial agents: the Aminoglycosides, in Goodman
and Gilman’s the pharmacological basis of therapeutics. New
York: McGraw-Hill; 2001. pp 1219–1238.
21. Ambrose PG, Bhavnani SM, Rubino CM, Louie A, Gumbo T,
Forrest A, Drusano GL. Pharmacokinetics-pharmacodynamics
of antimicrobial therapy: it’s not just for mice anymore. Clin
Infect Dis 2007;44:79–86.
22. Colistimethate sodium approved package labeling. 2010. X-Gen
Pharmaceuticals, Big Flats, NY.
23. Doring G, Conway SP, Heijerman HGM, Hodson ME, Hoiby N,
Smyth A, Touw DJ. Antibiotic therapy against Pseudomonas
aeruginosa in cystic fibrosis: a European consensus. Eur
Respir J 2000;16:749–767.
10 Zobell et al.
Pediatric Pulmonology

24. Foundation CF. Microbiology and infectious disease in cystic
fibrosis in Cystic Fibrosis Foundation Consensus Conference.
1994.
25. Trust UCF. Antibiotic treatment for cystic fibrosis in UK Cystic
Fibrosis Trust Antibiotic Working Group. 2009.
26. Zobell JT, Ampofo K, Cash J, Korgenski K, Chatfield BA. High
dose intermittent ticarcillin-clavulanate administration in pediat-
ric cystic fibrosis patients. J Cystic Fibrosis 2010;9:280–283.
27. Schaad UB, Wedgwood-Krucko J, Guenin K, Buehlmann U,
Kraemer R. Antipseudomonal therapy in cystic fibrosis: aztreo-
nam and amikacin versus ceftazidime and amikacin adminis-
tered intravenously followed by oral ciprofloxacin. Eur J Clin
Microbiol Infect Dis 1989;8:858–865.
28. Salh B, Bilton D, Dodd M, Abbot J, Webb K. A comparison of
aztreonam and ceftazidime in the treatment of respiratory infec-
tions in adults with cystic fibrosis. Scand J Infect Dis 1992;
24:215–218.
29. Reed MD, Stern RC, Myers CM, Klinger JD, Yamashita TS,
Blumer JL. Therapeutic evaluation of piperacillin for acute
pulmonary exacerbations in cystic fibrosis. Pediatr Pulmonol
1987;3:101–109.
30. Latzin P, Fehling M, Bauernfeind A, Reinhardt D, Kappler M,
Griese M. Efficacy and safety of intravenous meropenem and
tobramycin versus ceftazidime and tobramycin in cystic fibrosis.
J Cystic Fibrosis 2008;7:142–146.
31. Hubert D, Le Roux E, Lavrut T, Wallaert B, Scheid P, Manach
D, Grenet D, Sermet-Gaudelus I, Ramel S, Cracowski C. et al.
Continuous versus intermittent infusions of ceftazidime for
treating exacerbation of cystic fibrosis. Antimicrob Agents
Chemother 2009;53:3650–3656.
32. Blumer JL, Saiman L, Konstan MW, Melnick D. The efficacy
and safety of meropenem and tobramycin vs ceftazidime and
tobramycin in the treatment of acute pulmonary exacerbations
in patients with cystic fibrosis. Chest 2005;128:2336–2346.
33. Lacy CF, Armstrong LL, Goldman MP, Lance LL. Drug infor-
mation handbook. 2011. Hudson, OH: Lexi-Comp, Inc.
34. Taketomo CK, Hodding JH, Kraus DM. Pediatric dosage hand-
book. Hudson, OH: Lexi-Comp, Inc; 2011.
35. Azactam1 approved package labeling. Princeton, NJ: Bristol
Meyers Squibb; 2010.
36. Cayston1 approved package labeling. Foster City, CA: Gilead
Sciences, Inc; 2010.
37. Invanz1 approved package labeling. Whitehouse Station, NJ:
Merck & Co., Inc; 2011.
38. Testing ECoAS. Breakpoint tables for interpretation of MICs
and zone diameters. Basel, Switzerland: EUCAST; 2011.
39. Institute CaLS. Performance standards for antimicrobial suscep-
tibility testing: Twenty-first international supplement m 100-
S21. 2011. Wayne, PA: CLSI.
40. Reed MD, Aronoff SC, Stern RC, Yamashita TS, Myers CM,
Friedhoff LT, Blumer JL. Single-dose pharmacokinetics of
aztreonam in children with cystic fibrosis. Pediatr Pulmonol
1986;2:282–286.
41. Vinks AA, van Rossem RN, Mathot RA, Heijerman HG,
Mouton JW. Pharmacokinetics of aztreonam in healthy subjects
and patients with cystic fibrosis and evaluation of dose-exposure
relationships using monte carlo simulation. Antimicrob Agents
Chemother 2007;51:3049–3055.
42. Cirillo I, Vaccaro N, Redman R, Black PL, Kearns GL. Pharma-
cokinetics of single-dose doripenem in adults with cystic fibro-
sis. J Clin Pharmacol 2011; DOI 10.1177/0091270011427564.
43. Cirillo I, Vaccaro N, Turner K, Solanki B, Natarajan J, Redman
R. Pharmacokinetics, safety, and tolerability of doripenem after
0.5-, 1-, and 4-hour infusions in healthy volunteers. J Clin
Pharmacol 2009;49:798–806.
44. Vaccaro NCI, Redman R, Black P, Kearns GL. Pharmacokinet-
ics of doripenem in pediatric patients with cystic fibrosis. Am J
Respir Crit Care Med 2011;183:A5728.
45. Reed MD, Stern RC, O’Brien CA, Yamashita TS, Myers CM,
Blumer JL. Pharmacokinetics of imipenem and cilastatin in
patients with cystic fibrosis. Antimicrob Agents Chemother
1985;27:583–588.
46. Pedersen SS, Pressler T, Jensen T, Rosdahl VT, Bentzon
MW, Hoiby N, Koch C. Combined imipenem/cilastatin and
tobramycin therapy of multiresistant Pseudomonas aeruginosa
in cystic fibrosis. J Antimicrob Chemother 1987;19:101–107.
47. Strandvik B, Malmborg AS, Bergan T, Michalsen H, Storrosten
OT, Wretlind B. Imipenem/cilastatin, an alternative treatment of
pseudomonas infection in cystic fibrosis. J Antimicrob Chemo-
ther 1988;21:471–480.
48. Bergan T, Michalsen H, Malmborg AS, Pedersen SS, Pressler T,
Storrosten OT, Strandvik B. Pharmacokinetic evaluation of
imipenem combined with cilastatin in cystic fibrosis. Chemo-
therapy 1993;39:369–373.
49. Christensson BA, Ljungberg B, Eriksson L, Nilsson-Ehle I.
Pharmacokinetics of meropenem in patients with cystic fibrosis.
Eur J Clin Microbiol Infect Dis 1998;17:873–876.
50. Bui KQ, Ambrose PG, Nicolau DP, Lapin CD, Nightingale
CH, Quintiliani R. Pharmacokinetics of high-dose meropenem
in adult cystic fibrosis patients. Chemotherapy 2001;47:153–
156.
51. Scully BE, Ores CN, Prince AS, Neu HC. Treatment of lower
respiratory tract infections due to Pseudomonas aeruginosa in
patients with cystic fibrosis. Rev Infect Dis 1985;7:S669–S674.
52. Bosso JA, Black PG, Matsen JM. Efficacy of aztreonam in
pulmonary exacerbations of cystic fibrosis. Pediatr Infect Dis J
1987;6:393–397.
53. Bosso JA, Black PG. Controlled trial of aztreonam vs. tobramy-
cin and azlocillin for acute pulmonary exacerbations of cystic
fibrosis. Pediatr Infect Dis J 1988;7:171–176.
54. Doribax1 approved package labeling. Raritan, NJ: Ortho
McNeil Janssen; 2009.
55. Chen Y, Garber E, Zhao Q, Ge Y, Wikler MA, Kaniga K,
Saiman L. In vitro activity of doripenem (S-4661) against multi-
drug-resistant gram-negative bacilli isolated from patients with
cystic fibrosis. Antimicrob Agents Chemother 2005;49:2510–
2511.
56. Traczewski MM, Brown SD. In vitro activity of doripenem
against Pseudomonas aeruginosa and Burkholderia cepacia
isolates from both cystic fibrosis and non-cystic fibrosis patients.
Antimicrob Agents Chemother 2006;50:819–821.
57. Primaxin1 approved package labeling. Whitehouse Station, NJ:
Merck; 2009.
58. Pedersen SS, Pressler T, Hoiby N, Bentzon MW, Koch C.
Imipenem/cilastatin treatment of multiresistant Pseudomonas
aeruginosa lung infection in cystic fibrosis. J Antimicrob
Chemother 1985;16:629–635.
59. Krilov LR, Blumer JL, Stern RC, Hartstein AI, Iglewski BN.
Imipenem/cilastatin in acute pulmonary exacerbations of cystic
fibrosis. Rev Infect Dis 1985;7:S482–S489.
60. Merrem1 approved package labeling. Wilmington, DE: Astra-
Zeneca; 2009.
61. Byrne S, Maddison J, Connor P, Doughty I, Dodd M, Jenney M,
Webb AK, David TJ. Clinical evaluation of meropenem versus
ceftazidime for the treatment of Pseudomonas spp. infections in
cystic fibrosis patients. J Antimicrob Chemother 1995;36:135–
143.
62. Lima AL, Oliveira PR, Paula AP, Dal-Paz K, Almeida JN, Felix
Cda S, Rossi F. Carbapenem stewardship: positive impact on
hospital ecology. Braz J Infect Dis 2011;15:1–5.
Aztreonam and Carbapenems in CF 11
Pediatric Pulmonology

63. Nicolau DP, Carmeli Y, Crank CW, Goff DA, Graber CJ, Lima
AL, Goldstein EJ. Carbapenem stewardship: does ertapenem
affect Pseudomonas susceptibility to other carbapenems? A
review of the evidence. Int J Antimicrob Agents 2012;39:
11–15.
64. Dellit TH, Owens RC, McGowan JE, Gerding DN, Weinstein
RA, Burke JP, Huskins WC, Paterson DL, Fishman NO,
Carpenter CF. et al. Infectious Diseases Society of America
and the Society for Healthcare Epidemiology of America
guidelines for developing an institutional program to en-
hance antimicrobial stewardship. Clin Infect Dis 2007;44:159–
177.
65. Sanders DB, Hoffman LR, Emerson J, Gibson RL, Rosenfeld
M, Redding GJ, Goss CH. Return of FEV1 after pulmonary ex-
acerbation in children with cystic fibrosis. Pediatr Pulmonol
2010;45:127–134.
66. Sanders DB, Bittner RC, Rosenfeld M, Hoffman LR, Redding
GJ, Goss CH. Failure to recover to baseline pulmonary function
after cystic fibrosis pulmonary exacerbation. Am J Respir Crit
Care Med 2010;182:627–632.
12 Zobell et al.
Pediatric Pulmonology




















