
IDIOPATHIC JUVENILE OSTEOPOROSIS - CiteSeerX
10
British Journal of Rheumatology 1995;34:6&-77 IDIOPATHIC JUVENILE OSTEOPOROSIS: EXPERIENCE OF TWENTY-ONE PATIENTS R. SMITH Nuffield Orthopaedic Centre, Windmill Road, Headmgton, Oxford OX3 7LD SUMMARY The features and outcome of 21 children (12 boys, nine girls) with idopathic juvenile osteoporosis (LJO) followed for up to 23 yr are described. The mean age of onset was 7 yr (range 1-13 yr)with no sex difference; the main presenting symptoms were long bone fractures, pain in the back and difficulty in walking. Typically, radiographs demonstrated compression of the vertebrae and metaphyses of the long bones; bone histology sometimes showed an excess of osteocytes associated with woven bone; routine biochemistry was normal for age; and with three exceptions no abnormalities of extracted dermal collagen or collagen synthesized by fibroblasts were detected. Where circulating vitamin D metabolites were measured they were within the normal range; and hip and spine bone mineral density (measured by DXA) was strikingly low. Five patients are still growing and two are currently untraceable. Of the remaining 14 who are now adults, 11 have substantially or completely recovered and three are disabled. Since spontaneous recovery occurs it remains impossible to assess the many forms of treatment given. KEY WORDS: Osteoporosis, Juvenile, Bone density, Bone histology, Collagen, Vitamin D. INTRODUCTION OSTEOPOROSIS is unusual in children and adolescents. Examples of known causes are prolonged immobiliz- ation, osteogenesis imperfecta, coeliac disease, Turner's syndrome and homocystinuria. Apart from osteogen- esis imperfecta, which requires special consideration (see Discussion) their exclusion is not difficult. Serious disorders such as leukaemia may also temporarily masquerade as osteoporosis. After all these possibilities are considered there is a form of osteoporosis with particular features, which include potential reversibility often at the time of adolescence, referred to as idio- pathic juvenile osteoporosis (UO) [1-4]. The cause of LJO is unknown although some have postulated a deficiency of 1,25(OH)JD [5-7]. Due to its rarity, descriptions of IJO have often been limited to single case reports or to a few patients followed for a short time. For this reason we know little of its natural history, and it remains difficult to predict the outcome in an individual child. This paper describes 21 patients followed for up to 23 yr from the time of onset. It provides information on presentation, treatment, prognosis and outcome. It includes five patients initially described in 1980 [2], when the literature up to that time was fully reviewed. PATIENTS AND METHODS Patients The patients are summarized in Table I. Thefirstfive correspond to those described 14 yr ago [2]; subsequent patients are arranged according to the date when they were first seen in Oxford. Several patients were investi- gated in detail elsewhere before referral. The diagnosis has been established as far as possible by the exclusion of known causes of osteoporosis. The results of appro- priate investigations are given in Tables II (bone Accepted 3 October 1994. histology, HI (collagen studies), FV (vitamin D metab- olites) and V (bone mineral density). For brevity, not all patients are described, but cases 17 and 18 are used as examples of LJO in childhood, case 14 ofreversibilitywithout treatment, and case 2 of one outcome in adult life. Apart from affected siblings (cases 12 and 13) and an apparently affected half- brother (case 9) there was no family history of bone disease. Case reports Patient 17. After a fall this previously well 5-yr-old girl had back pain and radiographs showed osteopenia with anterior wedging of D12. The pain improved but then recurred. Investigations (elsewhere) excluded known causes of osteoporosis. There was no significant family history. Transiliac bone biopsy showed active remodelling and some subperiosteal new bone for- mation. According to the pathologist there were some features of type IV osteogenesis imperfecta. The vert- ebral collapse initially worsened but then slowly im- proved on a cocktail of treatment which included oestrogen, anabolic steroids and a bisphosphonatc (clodronate). The density of the spine and hip was very low and the circulating concentrations of vitamin D metabolites normal. Radiographs at the age of lOyr showed that new bone had been laid down in the vertebrae with an outline of the previous shape (Fig. 1). Similar changes were present in the metaphyses. Patient 18. This previously well 9-yr-old girl had pain in her feet after landing off a see-saw. Subsequently she was unable to run and walked 'like an old lady'. Her parents noticed that her lower thoracic spine was prominent. She later sustained a fracture of the left femur and is now (aged 10 yr) confined to a wheel- chair. Her paediatrician excluded all known causes of osteoporosis and there were no features of osteogenesis imperfecta. Radiographs show the development of © 1995 British Society for Rheumatology 68 at Pennsylvania State University on May 9, 2016 http://rheumatology.oxfordjournals.org/ Downloaded from
-
Upload
khangminh22 -
Category
Documents
-
view
4 -
download
0
Transcript of IDIOPATHIC JUVENILE OSTEOPOROSIS - CiteSeerX

British Journal of Rheumatology 1995;34:6&-77
IDIOPATHIC JUVENILE OSTEOPOROSIS: EXPERIENCE OFTWENTY-ONE PATIENTS
R. SMITHNuffield Orthopaedic Centre, Windmill Road, Headmgton, Oxford OX3 7LD
SUMMARYThe features and outcome of 21 children (12 boys, nine girls) with idopathic juvenile osteoporosis (LJO) followed for up to 23 yrare described. The mean age of onset was 7 yr (range 1-13 yr)with no sex difference; the main presenting symptoms were longbone fractures, pain in the back and difficulty in walking. Typically, radiographs demonstrated compression of the vertebraeand metaphyses of the long bones; bone histology sometimes showed an excess of osteocytes associated with woven bone; routinebiochemistry was normal for age; and with three exceptions no abnormalities of extracted dermal collagen or collagen synthesizedby fibroblasts were detected. Where circulating vitamin D metabolites were measured they were within the normal range; andhip and spine bone mineral density (measured by DXA) was strikingly low. Five patients are still growing and two are currentlyuntraceable. Of the remaining 14 who are now adults, 11 have substantially or completely recovered and three are disabled. Sincespontaneous recovery occurs it remains impossible to assess the many forms of treatment given.
KEY WORDS: Osteoporosis, Juvenile, Bone density, Bone histology, Collagen, Vitamin D.
INTRODUCTIONOSTEOPOROSIS is unusual in children and adolescents.Examples of known causes are prolonged immobiliz-ation, osteogenesis imperfecta, coeliac disease, Turner'ssyndrome and homocystinuria. Apart from osteogen-esis imperfecta, which requires special consideration(see Discussion) their exclusion is not difficult. Seriousdisorders such as leukaemia may also temporarilymasquerade as osteoporosis. After all these possibilitiesare considered there is a form of osteoporosis withparticular features, which include potential reversibilityoften at the time of adolescence, referred to as idio-pathic juvenile osteoporosis (UO) [1-4].
The cause of LJO is unknown although some havepostulated a deficiency of 1,25(OH)JD [5-7]. Due to itsrarity, descriptions of IJO have often been limited tosingle case reports or to a few patients followed for ashort time. For this reason we know little of its naturalhistory, and it remains difficult to predict the outcomein an individual child.
This paper describes 21 patients followed for up to23 yr from the time of onset. It provides information onpresentation, treatment, prognosis and outcome. Itincludes five patients initially described in 1980 [2],when the literature up to that time was fully reviewed.
PATIENTS AND METHODSPatients
The patients are summarized in Table I. The first fivecorrespond to those described 14 yr ago [2]; subsequentpatients are arranged according to the date when theywere first seen in Oxford. Several patients were investi-gated in detail elsewhere before referral. The diagnosishas been established as far as possible by the exclusionof known causes of osteoporosis. The results of appro-priate investigations are given in Tables II (bone
Accepted 3 October 1994.
histology, HI (collagen studies), FV (vitamin D metab-olites) and V (bone mineral density).
For brevity, not all patients are described, but cases17 and 18 are used as examples of LJO in childhood,case 14 of reversibility without treatment, and case 2 ofone outcome in adult life. Apart from affected siblings(cases 12 and 13) and an apparently affected half-brother (case 9) there was no family history of bonedisease.
Case reportsPatient 17. After a fall this previously well 5-yr-old
girl had back pain and radiographs showed osteopeniawith anterior wedging of D12. The pain improved butthen recurred. Investigations (elsewhere) excludedknown causes of osteoporosis. There was no significantfamily history. Transiliac bone biopsy showed activeremodelling and some subperiosteal new bone for-mation. According to the pathologist there were somefeatures of type IV osteogenesis imperfecta. The vert-ebral collapse initially worsened but then slowly im-proved on a cocktail of treatment which includedoestrogen, anabolic steroids and a bisphosphonatc(clodronate). The density of the spine and hip was verylow and the circulating concentrations of vitamin Dmetabolites normal. Radiographs at the age of lOyrshowed that new bone had been laid down in thevertebrae with an outline of the previous shape (Fig. 1).Similar changes were present in the metaphyses.
Patient 18. This previously well 9-yr-old girl had painin her feet after landing off a see-saw. Subsequently shewas unable to run and walked 'like an old lady'. Herparents noticed that her lower thoracic spine wasprominent. She later sustained a fracture of the leftfemur and is now (aged 10 yr) confined to a wheel-chair. Her paediatrician excluded all known causes ofosteoporosis and there were no features of osteogenesisimperfecta. Radiographs show the development of
© 1995 British Society for Rheumatology68
at Pennsylvania State University on M
ay 9, 2016http://rheum
atology.oxfordjournals.org/D
ownloaded from

SMITH: IDIOPATHIC JUVENILE OSTEOPOROSIS 69
CaseNo.
1
2
3
•4
5
6
7
8
9
10
Sex andbirthdate
F, 1963
M, 1963
M, 1956
M, 1960
F, 1964
M, 1960
F, 1969
F, 1967
F, 1969
F, 1952
Age firstsymptoms
(yr)4
7
7
12
9
13
7
7
11
8
TABLE IClinical details, roatine i
Period offollow-up
(yr)
9
23
21
19
6
18
16
8
9
23
Main symptoms
Backache
Painful feetSlow walkingRecurrent long bone
fracture
Kyphosii
Pain in back
Pain in back
Pain in back
Pain in feet"Stress' fractures in
long bones
Long bone fractures
Pain in backLong bone fractures
Difficulty inwalking
Fracture R femur
nvestigations and outcome
Radiographs
Vertebral collapse
Biconcave vertebraeLong bone fractures
Vertebra] fracture
Vertebral fractures
Vertebral wedgefractures
Concave lumbarvertebrae
Fractures femur, tibia.metaphyses, vertebrae
FracturesBiconcave vertebrae
Vertebral collapseFractures
Metatarsal fracturesWedge fractures
several vertebrae
Outcome
Complete radiographkal andclinical recovery
Severe scoliosisLong bone fracturesDisabled. Confined to
wheelchair at age 30
Clinically wellRadiological osteoporosis
WellAnterior wedging of vertebrae
persists
Improved within 2 VT
Well
Still disabledMany orthopaedic procedures.Confined to wheelchair at age 24
Wen
Concurrent diabetesLost to follow up
Recurrent ankle pain. Lost tofollow up
11 M, 1963 17 Long bone fracture Fractures Continued multiple long bonefractures
Disabled, with scoliosis.Confined to wheelchair
12
13
14
15
16
17
18
19
20
21
M, 1971
M, 1974
M, 1975
M, 1974
M, 1980
F, 1982
F, 1983
M, 1981
M, 1978
F, 1987
8
5
11
9 months
9
5
9
11
1.5
2
13
15
7
18
4
6
1
1
15
4
Fractures forearm,wrist, tibia andfibular
Kyphosis
Fractures toes andfingers
Pain L hip.Difficulty in
walking. Growthfailure
Fractures longbones
Fracture L femurafter minor injury
Back pain followingfall
Pain in feetPeculiar gaitThen fracture L
femur
Pain in back
Multiple long bonefractures
Long bone fracturesFailure to thriveShort
Spine; bone within abone—evidence ofgrowth arrest;vertebral collapse
Vertebral wedging
"Stress' fracture femur.Metaphyseal fractures.Biconcave vertebrae
Wedged thoracicvertebrae
Metaphyses abnormalVertebrae irregular
Multiple vertebralcompression
Metaphyseal fractures.Progressive vertebral
bkoncavity
Biconcave. vertebraeLoss of vertebral height
Long bone fracturesVertebral compression
Biconcave collapsedvertebrae. Numerouslines of growth arrest
No further fractures. (Brotherof case 13)
Spontaneous rupture ringertendons. (Brother of case 12;has cryoglobulinaemia)
Complete recovery
Recovery
Still has symptoms. Previousneonatal hypoglycaemia
Bilateral cataractsUndetectable plasma CT.Normal pentagastrin response
Improvement Multipletreatments given
Still disabled
Improving clinically andradiologically
Complete recovery
No changeMild partial villus atrophy
at Pennsylvania State University on M
ay 9, 2016http://rheum
atology.oxfordjournals.org/D
ownloaded from

70 BRITISH JOURNAL OF RHEUMATOLOGY VOL. 34 NO. 1
TABLE DBone histology
Case No. Description
1-5
7
8
14
16
17
18
See Smith [2]
Trabeculae variable thickness, some very thin. Osteocyte density in trabculae increased
Bone taken from femoral fracture site. Some woven bone. Increased osteocyte number
Increased osteocytes in cortical bone. Some woven bone
Irregular cement lines, variable Haversian size, patchy excess of osteocytes
Cortex thin, wide Haversian canals, numerous small osteons, active remodelling, subperiosteal new bone, increase in osteocytenumbers. Some features of OI type IV
Trabeculae thin and normally calcified. No excess of osteocytes
symmetrically biconcave vertebral bodies and meta-physeal compression fractures of the long bones(Fig. 2). Bone biopsy (Table II) showed osteoporosiswith no excess of osteocytes. Measured hip and spinebone mineral densities were very low (Table V). Treat-ment (elsewhere) included intermittent nasal calcitonin,additional oral calcium and physiological amounts ofvitamin D. The circulating vitamin D metabolite con-centrations were normal (Table IV).
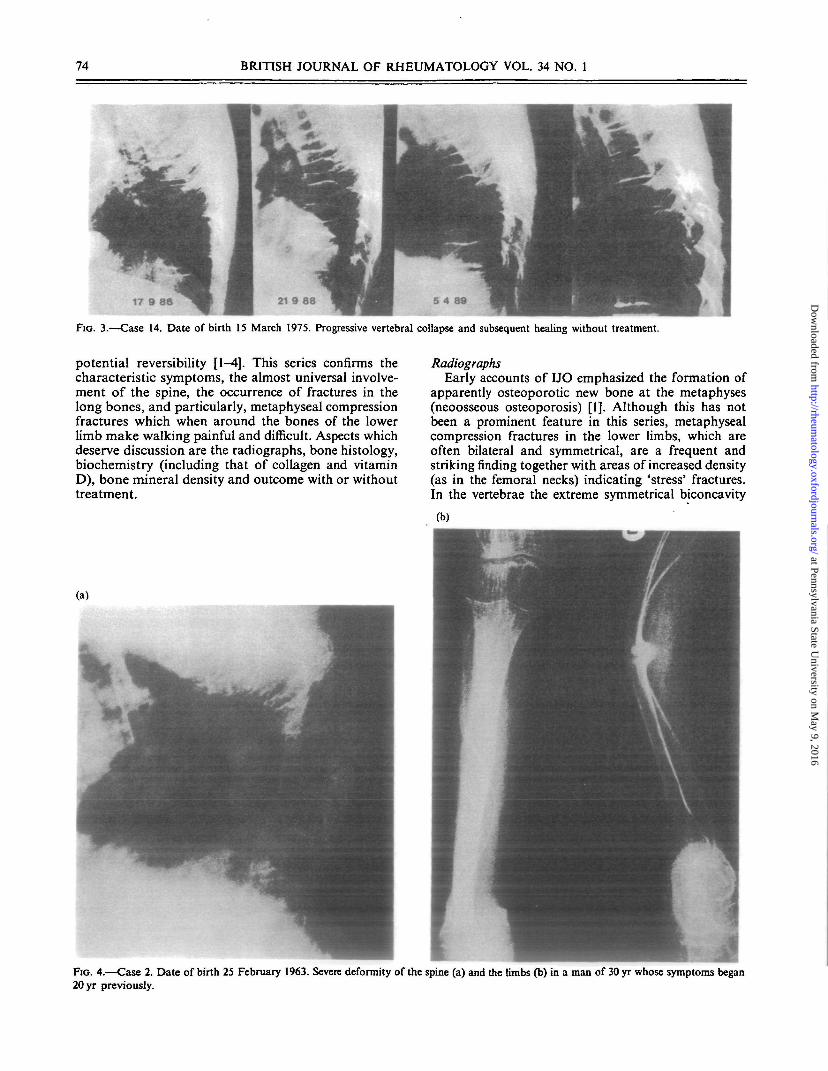
Patient 14. This previously well 11-yr-old boy hadpain in his left hip and knee, difficulty in walking andgrowth failure. There was a stress fracture of the leftfemoral neck, metaphyseal fractures of the long bonesand progressive biconcavity of the vertebrae (Fig. 3). Atransiliac bone biopsy (decalcified in error) showedsome areas of increased osteocyte numbers and focalwoven bone. Symptoms improved without treatmentand by the age of 13 yr growth in height resumed. Twoyears later he was quite well and the vertebral appear-ances were near normal. Spine, hip and forearm BMD(aged 18 yr) were all within the normal range for age(Table V). Interestingly, the collagen synthesized bydermal fibroblasts showed mild abnormalities (below).
Patient 2. In this patient (subject No. 2, [2D painfulfeet with difficulty in walking began at the age of 7 yr,to be followed 2 yr later by fractures of the right radiusand femur. He has subsequently continued to fracture,without any improvement when growth ceased. In 1990forearm BMD was significantly low. Currently (aged30 yr) he is confined to a wheelchair with severescoliosis and lower limb deformity (Fig. 4).
MethodsRoutine biochemical methods were used for in-
vestigation. Bone biopsies were examined before andafter decalcification. In early studies, the ratio of alpha1(1) to alpha l(lil) in extracted polymeric dermalcollagen was measured [2]; subsequently the amountand type of collagen synthesized by dermal fibroblastswas examined according to methods described else-where [8].
RESULTSClinical
Of 22 patients initially referred one was excludedbecause he was blind from infancy and probably hadthe osteoporosis psuedoglioma syndrome [9]. Twopatients are brothers (12 and 13) so the diagnosis ofLTO must remain in doubt; however they had nofeatures of osteogenesis imperfecta. In three patients(15, 20 and 21) fractures began in infancy which isunusual for LJO; and patient 9 had a half brother withnumerous fractures whose daughter has osteogenesisimperfecta.
The age of onset of the first symptoms varied from9 months to 13 yr in the whole group. There was nosignificant difference between the 12 boys (mean age7.7, range 0.75-13 yr) and the nine girls (mean age 7.0,range 2-11 yr).
The main presenting symptoms were long bonefracture (7), back pain (7), difficulty in walking (5),progressive kyphosis (I), and failure to thrive (1). Somepatients had more than one of these symptoms
TABLE HICollagen studies
Case No. Result
1-5
7
8
10
11
12
13
14
16
18
Normal ratio type I:III in extracted dermal collagen (see [2] for method and normal range)
Normal Ill/I ratio. Collagen synthesized by fibroblasts showed no abnormality
m/I ratio 0.247
in/I ratio 0.150
m/I ratio normal
Apparently abnormal synthesis of type I collagen by skin fibroblasts [10]
Apparently abnormal synthesis of type I collagen by skin fibroblasts [10]
Apparently abnormal synthesis of type I collagen by skin fibroblasts [10]
Normal synthesized collagen
Normal synthesized collagen
at Pennsylvania State University on M
ay 9, 2016http://rheum
atology.oxfordjournals.org/D
ownloaded from

SMITH: IDIOPATHIC JUVENILE OSTEOPOROSIS 71
Case No.
7
81014
1617
181921
Circulating
Date ofmeasurement
19781980
1981
1982
19921994
1989
199319931994
1993
1993
1989
TABLE IVvitamin D metabolites
25 OHD(ng/ml)
2.716.3
9.2'Normal'
16.9 (3-30)20.6 (5-30)
88 (10-120)
7.3 (7-50)9.9 (5-30)
15.7 (5-30)
25.2
31.3
'Normal'
l ^ O H W D(pg/ml)
20.3
57—
76 (20-50)
—
35 (20-50)24 (24-50)
3344
'Normal'
Numbers in parentheses are the reference values where given. Intwo patients (10 and 21) the only information available is that theresults were 'normal'.
simultaneously. Although pain in the back was not aconstant first symptom, the vertebrae were alwaysradiologically abnormal. In the absence of overt frac-ture the most striking sign was pain and difficulty inwalking. Apart from bony fragility no patient hadfeatures of osteogenesis imperfecta.
RadiographsThese showed metaphyseal compression fractures in
the long bones and progressive loss of height in thevertebrae. When improvement occurred this was first inthe vertebral bodies. In some cases there were multiplelines of growth arrest indicating the previous size of the
vertebrae (Fig. 5). None of the patients had Wormianbones.
Bone biopsy (Table II)The bone biopsy appearances either showed the
features of osteoporosis alone, or of an excess ofosteocytes sometimes associated with woven bone, or(as in cases 16 and 17) those seen previously in patientswith known type IV osteogenesis imperfecta. Wherequantitative histomorphometry was performed thissuggested a failure of osteoblastic activity.
BiochemistryRoutine biochemical measurements were within
the normal range when due account was taken ofthe normal increase in alkaline phosphatase andurine hydroxyproline in the pre-adolescent growthphase.
Collagen studiesIn most patients, the amount of extracted polymeric
collagen and the ratio of alpha 1(1) to alpha 1(111)collagen was normal; likewise the alpha chains of typeI collagen synthesized by the skin fibroblasts showedno clear quantitative or qualitative abnormality. How-ever, minor abnormalities were found in cases 12, 13and 14, A. E. Pocock, unpublished.
Vitamin D metabolitesWhen measured circulating vitamin D metabolites
were within the normal range (Table IV).
Bone mineral density (Table V)Bone density was measured by different methods at
different times in the course of the disease. The lowestvalues were found in the spine and hip soon after theonset of symptoms (cases 17,18 and 21). Forearm bone
CaseNo.
26
14
15
1617
18
2021
Date ofmeasurement
1990
1991
1990
1994
19901991
1989
1993/4
1993
1993
1993
Forearm
0.32 g/cm1
0.66 g/cm2
0.39 g/cm2
0.32 g/cm2
0.33 g/cm2
—
0.27 g/cm2
—
0.41 g/cm2
—
TABLEMeasurements of bone
Part of skeleton
Spine
——
-0.81
—
Normal
-2 .32
-5.37
—
-11
Hip
——
-0 .84 (T)-1 .37 (W)
—
—
-4 .29 ( D-3.37 (W)
- 6 . 9 (T)-5 .42 (W)
——
Vmineral density
Method
Single isotope
Single isotope
Single isotope
DXA
Single isotope
CT
Single isotope and DXA
DXA
Single isotope
DXA
Comments
Significantly low
Normal value. Clinicallyrecovered
Probably low. Subsequentforearm BMD measurements:1992—0.46; 1994—0.52
Spine and hip T scores normal
Probably low
Spine Z and hip T scores very low
Spine Z and hip T scores very low
Possibly low. Clinically recovered
Very low (0.23 g/cm2)
Values are expressed in relation to age-matched controls Z scores where these are available and in relation to peak bone mass, T scores, wherethese are not; or as g/cm2.
For hip (T) «total and (W) = Ward's triangle.
at Pennsylvania State University on M
ay 9, 2016http://rheum
atology.oxfordjournals.org/D
ownloaded from

72 BRITISH JOURNAL OF RHEUMATOLOGY VOL. 34 NO. 1
FIG. 1.—Case 17. Date of birth: 12 July 1982. Sequential changes in the vertebral bodies with lines of growth arrest which mark the previousoutline of the vertebrae before improvement, (a) 2 March 1993. (b) 24 June 1993. Similar changes are present in the metaphyses (c) 4 March1993.
density was less reduced but difficult to interpret in theabsence of a normal reference range for age. Theapparently 'normal' vertebral density by CT in case 16is unexpected.
OutcomeThe clinical outcome cannot be assessed in those
patients who have not finished growing (cases 16-19and 21). In two patients follow-up details are not
at Pennsylvania State University on M
ay 9, 2016http://rheum
atology.oxfordjournals.org/D
ownloaded from

SMITH: IDIOPATHIC JUVENILE OSTEOPOROSIS
(a)
FIG. 2.—Case 18. Date of birth 21 November 1993. Radiographs of the spine show the development of biconcave vertebral bodies, (a) 28 October1992. (b) 24 June 1993. Radiographs of the knees (c) show multiple compression fractures.
complete (cases 9 and 10). Of the remaining 14, 11 haveimproved substantially or completely (cases 1, 3-6, 8,12-15 and 20) but three (cases 2, 7 and 11) are disabledin their adult life (Table I).
DISCUSSION
Previous accounts of IJO have emphasized its re-lation to the pre-adolescent time of growth and its
at Pennsylvania State University on M
ay 9, 2016http://rheum
atology.oxfordjournals.org/D
ownloaded from
74 BRITISH JOURNAL OF RHEUMATOLOGY VOL. 34 NO. 1
17 9 86
FIG. 3.—Case 14. Date of birth 15 March 1975. Progressive vertebral collapse and subsequent healing without treatment.
potential reversibility [1-4]. This series confirms thecharacteristic symptoms, the almost universal involve-ment of the spine, the occurrence of fractures in thelong bones, and particularly, metaphyseal compressionfractures which when around the bones of the lowerlimb make walking painful and difficult. Aspects whichdeserve discussion are the radiographs, bone histology,biochemistry (including that of collagen and vitaminD), bone mineral density and outcome with or withouttreatment.
RadiographsEarly accounts of IJO emphasized the formation of
apparently osteoporotic new bone at the metaphyses(neoosseous osteoporosis) [1]. Although this has notbeen a prominent feature in this series, metaphysealcompression fractures in the lower limbs, which areoften bilateral and symmetrical, are a frequent andstriking finding together with areas of increased density(as in the femoral necks) indicating 'stress' fractures.In the vertebrae the extreme symmetrical biconcavity
FIG. 4.—Case 2. Date of birth 25 February 1963. Severe deformity of the spine (a) and the limbs (b) in a man of 30 yr whose symptoms began20 yr previously.
at Pennsylvania State University on M
ay 9, 2016http://rheum
atology.oxfordjournals.org/D
ownloaded from

SMITH: IDIOPATHIC JUVENILE OSTEOPOROSIS 75
FIG. 5.—Case 20. Date of birth 22 July 1978. This 1994 radiographdemonstrates the previous outline of the vertebral bodies in a patientwho has recovered from IJO.
corresponds with previous descriptions. Perhaps themost striking appearances are seen after healing (withor without treatment) where the previous size of thevertebrae are outlined, sometimes in a sequentialmanner (Fig. 5).
Bone histologyThe histology of bone is difficult to interpret in IJO.
Previous quantitative histomorphometry suggestedtemporary failure of osteoblast function [2], but in oursubsequent biopsies the qualitative appearances werevariable. In particular, bone from two patients showedan excess of osteocytes in the trabecular (case 7) andcortical (case 14) bone.
Excessive numbers of osteocytes occur in wovenbone, but this is also a feature of lamellar bone in themild forms of osteogenesis imperfecta (01) [10]. Thus,OI is a possibility in case 7 in which improvement hasnot occurred. In patient 14, who had apparently com-pletely recovered, the increase in osteocytes was associ-ated with focal areas of woven bone.
Collagen biochemistrySince many mutations in the type I collagen genes
have been described in osteogenesis imperfecta [11]which, in its mild form, may be regarded as an inherited
form of osteoporosis in childhood, it was appropriateto look for collagen abnormalities in IJO.
Early studies showed no quantitative abnormality ofpolymeric collagen extracted from skin or in the ratiosof type I to type III collagen, derived from the relativeabundance of their alpha chains. The results of fibro-blast culture have on the whole supported this normal-ity. However, cyanogen bromide pep tide analysis ofsynthesized collagens suggested minor abnormalities inparts of the collagen chains in two brothers (cases 12and 13) and in patient 14. The possible significance ofthese minor findings is discussed below.
Vitamin D metabolitesWhen measured, the circulating concentrations of
25 OHD and 1,25(OH)2D were not significantly differ-ent from normal. Patient 18 was on physiological dosesof vitamin D. In previous accounts which have de-scribed low concentrations of 1,25(OH)2D in the pres-ence of normal circulating 25 OHD, the skeletalimprovement which occurred when calcitriol was givensometimes coincided with the onset of puberty, and itis therefore difficult to attribute the improvement to thecalcitriol itself [5-7]. In a single patient there was adissociation in concentrations of the vitamin D metab-olites (raised 1,25(OH)2D and reduced 25 OHD and24,25(OH)2D) which was corrected with skeletal recov-ery and treatment with calcium and 25 OHD3 [12].Further in a boy of 17 yr with apparent IJO and muscleweakness the administration of calcitriol produced arapid increase in strength [7].
Bone mineral densityOur results demonstrate that the bone mineral den-
sity, particularly of the spine, can be very low. Thereare not sufficient data to demonstrate whether thisreduction is corrected or at what speed, although wherethere is clear radiological improvement a similar im-provement in BMD might be expected. The relativelysmaller reduction in forearm bone density reflects themajor effect of IJO on the spine. In a CT assessmentof vertebral bone mineral in a large group of childrenit was found that in seven with IJO, those four withactive IJO had low values whereas in three who hadclinically resolved the values were normal [13]. A casereport [14] followed the development and recovery ofspinal osteoporosis in a girl from 3-9 yr of age withconsecutive CT scans which showed spontaneous im-provement in bone density. It has also been reportedthat total body calcium is significantly reduced (com-pared with age-matched controls) in IJO children [15].
OutcomeIn most patients followed up after adolescence sig-
nificant improvement has occurred, although mildkyphosis and probably a low normal bone density maypersist. The most convincing evidence of reversibility isshown by patient 14, in which complete reconstructionof the biconcave vertebrae occurred without treatment.Similar changes are described in single patients in the
at Pennsylvania State University on M
ay 9, 2016http://rheum
atology.oxfordjournals.org/D
ownloaded from

76 BRITISH JOURNAL OF RHEUMATOLOGY VOL. 34 NO. 1
European literature (reviewed in [2]). Since it is clearthat improvement may occur spontaneously it isdifficult to assess the effectiveness (or otherwise) of themany treatments given. These include appropriate sexhormones, additional calcium, physiological amountsof vitamin D, bisphosphonates [16, 17] and intermittentcalcitonin [18] given separately or together.
Occasionally, disability and fracture can persist intoadult life (cases 2, 7, 9 and 11) and the reason for thisis obscure. One may be that the diagnosis is wrong;certainly not all relevant evidence may be availablewhen the patient is first seen.
Hyperosteocytosis (as in case 7) may suggest osteo-genesis imperfecta, although the difficulty in interpret-ation has been referred to. In case 9 the subsequentoffspring of a half-brother has now developed typicalosteogenesis imperfecta.
CauseThe cause of LTO remains obscure. Several case
reports suggest that there is a lack of 1,25(OH)2D butthis is clearly not a universal feature and the apparentimprovement associated with giving this metabolite atthe time of adolescence may be coincidental. It isalmost impossible to be sure that any form of treatmentgiven at this time alters the course of the disease,although a striking improvement of myopathy by1,25(OH)2D has been described [7]. For this reason, thereports of spontaneous remission with remodelling andremodelling of bone are important (ref. [2] and case 14).The proposal that the major cause of LTO is transientosteoblast failure is not supported by recent experimen-tal work which shows that osteoblasts from suchpatients repond in a normal way to 1,25(OH)2D3stimulation [19].
Finally, it is possible that in LTO the major com-ponent of the bone matrix, collagen, could (by analogywith OI) harbour important mutations but our studiesdo not support this. Minor non-glycine mutations ordefects in collagen gene control could also contributeto LTO. In a recent study Spotila et al. [20] found thatin 26 patients with low bone density three had non-glycine collagen gene mutations. The biological effectof such mutations is difficult to assess and there is apaucity of clinical information.
This review provides some points of practicalclinical importance and suggests directions for futureresearch.
Since IJO is very uncommon the first step is toexclude the known causes of osteoporosis in childhood;and to make sure that disorders such as leukaemia arenot missed. If LTO then seems likely it is important todo certain investigations as soon as possible (or arrangefor them to be done at a specialized centre). Theseinclude a skin biopsy for fibroblast culture and collagenbiosynthetic studies; measurement of circulating vita-min D metabolites; and a transiliac bone biopsy, fromwhich decalcified and undecalcified sections should beprepared. Where there is clear evidence of a reductionin the amount of type I collagen, or of an abnormalmutant collagen chain this makes osteogenesis imper-
fecta likely. If there is a reduction in vitamin Dmetabolite concentrations this suggests that it is worth-while administering them. The results of a bone biopsymay be difficult to interpret, unless they are veryabnormal, but at least they will exclude obviousalternative diagnoses, such as osteomalacia or haema-tological disorders.
Provided that the diagnosis of LIO is establishedthere is probably no indication for specific treat-ment with, for instance, anti-resorptive agents or sexhormones, but symptomatic treatment should not beneglected.
The main features of IJO, namely a form of transientosteoporosis associated with growth, should continueto provide many questions for research. For instance,how important are any biochemical changes in colla-gen; why does LJO improve so rapidly in adolescence;and is there any specific form of treatment?
ACKNOWLEDGEMENTS
I am indebted to the many colleagues who havereferred patients to me and to those who have helpedwith their investigation, care and management; inparticular to Colin Woods and Nick Athanasou (bonehistology); to Martin Francis and Andrew Pocock(collagen studies) and to Sarah Vipond for her clinicaland biochemical help and measurements of bone den-sity; and to the patients themselves for their willingcooperation in this study.
REFERENCES1. Dent CE, Friedman M. Idiopathic juvenile osteoporosis.
QJMed 1965^4:177-210.2. Smith R. Idiopathic osteoporosis in the young. J Bone
Joint Surg 1980;62B:417-27.3. Smith R. Idiopathic juvenile osteoporosis. Am J Dis
Children 1979;133:889-91.4. Evans AA, Dunstan CR, Hills E. Bone metabolism in
idiopathic juvenile osteoporosis. Calcified Tissue Int1983^5:5-8.
5. Marder HK, Tsang RG, Hug G, Crawford AC. Ca\-citriol deficiency in idiopathic juvenile osteoporosis. AmJ Dis Children 1982;136.-917.
6. Saggesse G, Bertelloni S, Baroncelli GI, Perri P, Calder-azzi A. Mineral metabolism and cakitriol therapy inidiopathic juvenile osteoporosis. Am J Dis Children1991;145:457-62.
7. Rosskamp R, Sell G, Emons D, Issa S, Burmeister W.Idiopathic juvenile osteoporosis: report of two cases. KlinPadiat 1987:199:457-61.
8. Pocock AE, Francis MJO, Smith R. Severe osteogenesisimperfecta. Type I collagen abnormalities in 17 skinfibroblast cell lines. Biochem Soc Trans 1991;19:382S.
9. Swoboda W, Grill F. The osteoporosis pseudogliomasyndrome: update and report on two affected siblings.Paediat Radiol 1988;1&399-4O4.
10. Bullough PG. Orthopaedic pathology, 2nd edn. NewYork: Gower, 1992.
11. Byers PH. Osteogenesis imperfecta. In: Royce PM andSteinmann B, eds. Connective tissue and its heritabledisorders. New York: Wiley-Liss, 1993:317-50.
12. Leroy D, Garabedian M, Guillozo H, Bourdeau A,Sauvegrain J, Balsan S. Evolution des concentrations
at Pennsylvania State University on M
ay 9, 2016http://rheum
atology.oxfordjournals.org/D
ownloaded from

SMITH: IDIOPATHIC JUVENILE OSTEOPOROSIS 77
scriques en metabolites de la vitamine D (25)OH)D, 24,25-{OH)jD, l ^ O H ^ D ) dans un cas d'osteoporose ju-venile idiopathique. Arch FT Pediatr 1981;38:165-70.
13. Fredericks BJ, De Campo JF, Sephton R, McCredie DA.Computed tomographic assessment of vertebral bonemineral in childhood. Skeletal Radiogr 1990;19#9-102.
14. Exner GU, Prader A, Elsasser U, Anliker M. Idiopathicosteoporosis in a three year old girl. Hetv Paediat Ada1984^:517-28.
15. Lorenc RS, Wieczorek E, Marowska J, Olszaniecka M,Tatajko A. Diagnostics and monitoring of idiopathicjuvenile osteoporosis by means of densitometry andbiochemical testa. Bone and tooth society meeting, March1992 (Abstract).
16. Hoekman K, Papapoulos SE, Peters ACB, Bijvoet OLM.Characteristics of bisphosphonate treatment of a patient
with juvenile osteoporosis. / Clin Endocrinol Metab1985;61:952-6.
17. Levis S, Gruber HE, Conn D, Howard GA, Roos BA.Juvenile osteoporosis treated with pamidronate. CalcifiedTissue Int 1993^2 (Supplement 2):S41 (Abstract).
18. Jackson EC, Strife CF, Tsang RC, Marder HK. Effect ofcalcitonin replacement therapy in idiopathic juvenileosteoporosis. Am J Dis Children 1988; 142:1237-9.
19. Bertelloni S, Baroncelli GI, Nero GD, Saggesse G.Idiopathic juvenile osteoporosis: evidence of normalosteoblast function by 1,25 dihydroxy vitamin D3 stimu-lation test. Calcified Tissue Int 1992^1^0-3.
20. Spotila LD, Colige A, Sereda L, Constantinou-Deltas CD, Whyte MP et al. Mutation analysis of codingsequences for Type I procollagen in individuals with lowbone density. J Bone Mineral'Res 1994^h923-32.
at Pennsylvania State University on M
ay 9, 2016http://rheum
atology.oxfordjournals.org/D
ownloaded from




















