Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
18
Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis Gregor Dueckers a , 1 , Nihal Guellac b , 1 , Martin Arbogast c , Guenther Dannecker d , Ivan Foeldvari e , Michael Frosch f , Gerd Ganser g , Arnd Heiligenhaus h , Gerd Horneff i , Arnold Illhardt g , Ina Kopp j , Ruediger Krauspe k , Barbara Markus l , Hartmut Michels m , Matthias Schneider n , Wolfram Singendonk o , Helmut Sitter p , Marianne Spamer m , Norbert Wagner q , Tim Niehues a , ⁎ a HELIOS Children's Hospital, Krefeld, Germany b German Federal Armed Forces central hospital, Koblenz, Germany c Rheumazentrum Oberammergau, Oberammergau, Germany d Olgahospital, Stuttgart, Germany e Hamburger Zentrum für Kinder- und Jugendrheumatologie am Schön Klinik Eilbeck, Hamburg, Germany f University Children's Hospital, Muenster, Germany g St. Josef Stift, Sendenhorst, Germany h St. Franziskus Hospital, Muenster, Germany i Asklepios Children's Hospital, St. Augustin, Germany j Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften (AWMF), Marburg, Germany k University Department of Orthopedics, Duesseldorf, Germany l Deutsche Rheuma Liga e.V., Bonn, Germany m German Centre for Pediatric and Adolescent Rheumatology, Garmisch Partenkirchen, Germany n University Department of Endocrinology, Diabetology and Rheumatology, Duesseldorf, Germany o Berlin-Schoeneberg, Germany p University Department of Surgical Research, Marburg, Germany q University Children's Hospital, Aachen, Germany Abbreviations: ACR, American College of Rheumatology; AE, adverse events; AGREE, appraisal of guidelines for research and evaluation; AWMF, Association of the Scientific Medical Associations; Bw, bodyweight; CAPS, cryopyrin-associated periodic syndromes; CD, cluster of dif- ferentiation; CIOMS, Council for International Organizations of Medical Sciences; CTLA-4, cytotoxic T-lymphocyte antigen 4; DELBI, German instrument for methodological guideline appraisal; DMARDs, disease modifying anti-rheumatic drugs; EBM, evidence based medicine; EMA, European Medical Agency; EULAR, European League against Rheumatism; FDA, Food and Drug Administration; GC, glucocorticoids; GKJR, Ger- man Society for Pediatric Rheumatology; GPs, general practitioners; IgG, immunoglobulin G; IL, interleukin; ILAR, International League of As- sociations for Rheumatology; JDM, juvenile dermatomyositis; JIA, juvenile idiopathic arthritis; MAS, macrophage activation syndrome; Max, maximum; MTX, methotrexate; NGT, nominal group technique; NSAID, nonsteroidal anti-inflammatory drug(s); SCT, stem cell transplanta- tion; SLE, systemic lupus erythematodes; SoJIA, systemic onset of juvenile idiopathic arthritis; TNF, tumor necrosis factor; TPMT, thiopurinmethyltransferase. ⁎ Corresponding author at: HELIOS Children's Hospital Krefeld, Lutherplatz 40-47805 Krefeld, Germany. Fax: + 49 2151 2334. E-mail address: [email protected] (T. Niehues). 1 Contributed equally. 1521-6616/$ - see front matter © 2011 Elsevier Inc. All rights reserved. doi:10.1016/j.clim.2011.10.003 available at www.sciencedirect.com Clinical Immunology www.elsevier.com/locate/yclim Clinical Immunology (2012) 142, 176–193
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis

ava i l ab l e a t wwwsc i enced i r ec t com
C l i n i ca l Immuno logy
wwwe l sev i e r com l oca te yc l im
Clinical Immunology (2012) 142 176ndash193
Evidence and consensus based GKJR guidelines for thetreatment of juvenile idiopathic arthritisGregor Dueckers a 1 Nihal Guellac b 1 Martin Arbogast cGuenther Dannecker d Ivan Foeldvari e Michael Frosch f Gerd Ganser gArnd Heiligenhaus h Gerd Horneff i Arnold Illhardt g Ina Kopp jRuediger Krauspe k Barbara Markus l Hartmut Michels mMatthias Schneider n Wolfram Singendonk o Helmut Sitter pMarianne Spamer m Norbert Wagner q Tim Niehues a
a HELIOS Childrens Hospital Krefeld Germanyb German Federal Armed Forces central hospital Koblenz Germanyc Rheumazentrum Oberammergau Oberammergau Germanyd Olgahospital Stuttgart Germanye Hamburger Zentrum fuumlr Kinder- und Jugendrheumatologie am Schoumln Klinik Eilbeck Hamburg Germanyf University Childrens Hospital Muenster Germanyg St Josef Stift Sendenhorst Germanyh St Franziskus Hospital Muenster Germanyi Asklepios Childrens Hospital St Augustin Germanyj Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften (AWMF) Marburg Germanyk University Department of Orthopedics Duesseldorf Germanyl Deutsche Rheuma Liga eV Bonn Germanym German Centre for Pediatric and Adolescent Rheumatology Garmisch Partenkirchen Germanyn University Department of Endocrinology Diabetology and Rheumatology Duesseldorf Germanyo Berlin-Schoeneberg Germanyp University Department of Surgical Research Marburg Germanyq University Childrens Hospital Aachen Germany
Abbreviations ACR American College of Rheumatology AE adverse events AGREE appraisal of guidelines for research and evaluationAWMF Association of the Scientific Medical Associations Bw bodyweight CAPS cryopyrin-associated periodic syndromes CD cluster of dif-ferentiation CIOMS Council for International Organizations of Medical Sciences CTLA-4 cytotoxic T-lymphocyte antigen 4 DELBI Germaninstrument for methodological guideline appraisal DMARDs disease modifying anti-rheumatic drugs EBM evidence based medicine EMAEuropean Medical Agency EULAR European League against Rheumatism FDA Food and Drug Administration GC glucocorticoids GKJR Ger-man Society for Pediatric Rheumatology GPs general practitioners IgG immunoglobulin G IL interleukin ILAR International League of As-sociations for Rheumatology JDM juvenile dermatomyositis JIA juvenile idiopathic arthritis MAS macrophage activation syndrome Maxmaximum MTX methotrexate NGT nominal group technique NSAID nonsteroidal anti-inflammatory drug(s) SCT stem cell transplanta-tion SLE systemic lupus erythematodes SoJIA systemic onset of juvenile idiopathic arthritis TNF tumor necrosis factor TPMTthiopurinmethyltransferase Corresponding author at HELIOS Childrens Hospital Krefeld Lutherplatz 40-47805 Krefeld Germany Fax +49 2151 2334E-mail address timniehueshelios-klinikende (T Niehues)
1 Contributed equally
1521-6616$ - see front matter copy 2011 Elsevier Inc All rights reserveddoi101016jclim201110003
177Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
Received 18 August 2011 accepted with revision 19 October 2011Available online 26 October 2011
KEYWORDSJuvenile idiopathic arthritisTreatmentGuidelineConsensusChildren and adolescents
Abstract Juvenile idiopathic arthritis (JIA) is the most common rheumatic disease in children andadolescents Immunomodulatory drugs are used frequently in its treatment Using the nominal grouptechnique (NGT) andDelphimethod we created amultidisciplinary evidence- and consensus-basedtreatment guideline for JIA based on a systematic literature analysis and three consensus confer-ences Conferenceswere headed by a professionalmoderator and were attended by representativeswho had been nominated by their scientific societies or organizations 15 statements regarding drugtherapy symptomatic and surgical management were generated It is recommended that initially
JIA is treated with NSAID followed by local glucocorticoids andor methotrexate if unresponsiveComplementing literature evidence with long-standing experience of caregivers allows creatingguidelines that may potentially improve the quality of care for children and adolescents with JIAcopy 2011 Elsevier Inc All rights reserved
1 Introduction
11 Background aims and addressees
Juvenile idiopathic arthritis (JIA) is defined by the InternationalLeague of Associations for Rheumatology (ILAR) [1] JIA is ahighly heterogeneous disorder Some of the subtypes of JIAare clearly distinct from others also in regard of immunopatho-physiology eg systemic onset of JIA is now thought to be anautoinflammatory disease Treatment of JIA subtypes maythus vary significantly [2] JIA shows substantial impact on pa-tients physical abilities psychological function and quality oflife [34] Therefore treatment goals are pain relief the elimi-nation of active disease the normalization of physical functionthe achievement of normal growth and development and im-provement of quality of life Appropriate initial managementcontinuous comprehensive and consistent care offer thechance of the prevention of long term sequels [56] The Ger-man consensus group for treatment of JIA systematically devel-oped guidelines for treatment of JIA in 1999 2005 and 2008[78] Our guideline is addressed to physicians in medical prac-tices and hospitals allied health professionals physiothera-pists occupational therapists and all people who are involvedin the treatment care and follow-up of children or adolescentswith JIA Our aim is to provide clear evidence- and consensusbased recommendations for the treatment of children and ado-lescents with JIA within a multidisciplinary setting The guide-line focuses on JIA and does not cover the issue of treatmentresistant cases complex or unusual forms of arthritis and doesnot consider all ILAR subtypes of JIA individually Subtype spe-cific recommendations are highlighted separately eg treat-ment schemes for oligo- polyarticular or systemic onset JIA
2 Methodology
21 Members of the consensus group and consensusconferences
Scientific societies and organizations (Table 1) representingpediatricians in medical practices and hospitals adult and
pediatric rheumatologists orthopedic surgeons ophthalmol-ogists surgeons physiotherapists psychologists nationaland local support-groups for parents and children nominatedrepresentatives for the participation in consensus confer-ences The scope of the conferences was the implementationof evidence and consensus based guideline for the treatmentof JIA in children and adolescents Consensus conferenceswere held at Duesseldorf respectively Krefeld (Germany) onthe 9th of May 2007 1st of August 2007 and 15th of January2010 and were all attended by N95 of the representatives
22 Literature search and literature review
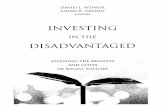
Based on existing guidelines [78] we conducted a systematicliterature search in Medline (httpwwwncbinlmnihgovpubmed) (deadline of search 15th January 2010 terms ldquoju-venile idiopathic (rheumatoid) arthritisrdquo and ldquotherapyrdquolimits ldquohumansrdquo ldquopublished in the last 3 yearsrdquo ldquoall child0ndash18 yearsrdquo ldquoclinical trialrdquo) Studies relating to diagnosis ofJIA uveitis vaccination transition rofecoxibe Ca-supplementation and costs were excluded manually The ex-clusion was necessary due to varying target groups and lossof market approval by European Medical agency (EMA) respec-tively [9] Final results of the literature review are as shown inFig 1 These studies were evaluated for quality of methodolo-gy following the definitions of evidence level and recommen-dation grade as published by Feldmann et al [10] (Table 2 andTable 3) Thirteen studies were judged as relevant for the2010 update of treatment guidelines for JIA (Table 4) Todraft guideline statements the core conclusions of studieswere discussed and formal consensus building followed thenominal group technique (NGT) [11] and Delphi method [12]
23 Consensus process
The consensus process was externally and independentlysupervised by the Association of the Scientific MedicalAssociations (AWMF) who has membership of Council for In-ternational Organizations of Medical Sciences (CIOMS) TheAWMF coordinates the systematic development of diagnostic
Table 1 Representatives nominated for the consensus group by scientific societies and professional organizations
Name Representing scientific societies or professional organisations
Arbogast M Association of Paediatric Orthopaedic SurgeonsDannecker G German Society of Paediatrics and Adolescent Medicine (DGKJ)Dueckers G (coordinator)Foeldvari I German Society for Paediatric Rheumatology (GKJR)Frosch M GKJRGanser G GKJRGuellac N (coordinator)Heiligenhaus A German Society for Ophthalmology (DOG)Horneff G GKJRIllhardt A German Society for Psychology (DGPs)Krauspe R Association of Paediatric Orthopaedic SurgeonsKopp I (moderator)Markus B National support group of parents and children with JIAmdashRheuma LigaMichels S GKJRNiehues T (coordinator) GKJRSchneider M German Society of Rheumatology (DGRh)Singendonk W Association of Paediatricians in private practice (BVKJ)Sitter H (moderator) Association of the Scientific Medical Associations (AWMF)Spamer M National Association of PhysiotherapistsWagner N German Society of Paediatrics and Adolescent Medicine (DGKJ)
178 G Dueckers et al
and treatment guidelines for medical scientific societiesand organizations in Germany
24 Consensus building nominal group technique(NGT)
Consensus building was headed by a professional moderators(HS IK) The moderator of the consensus conferences
Literature search 2007
(deadline June 30th 2007) [7]
Mesh terms ldquojuvenile idiopathic (rheumatoid)
arthritisrdquo and ldquotherapyrdquo
dArr n = 3138
Limits ldquohumansrdquo ldquopublished in the last 3
yearsrdquo ldquoall child 0-18rdquo
dArr n = 193
Limit ldquoclinical trialrdquo
dArr n = 52
Exclusion of studies relating to
diagnosis of JIA uveitis vaccination
transition rofecoxibe
rArr n = 22
Figure 1 Literature se
explained the purpose method and procedure of consensusfinding Representatives gave brief presentations of literatureand core conclusions for the guideline draft A formal consensusprocess led to adoption of guidelines for treatment of JIA Asformal consensus procedure we used NGT involving six stages
1 Silent review of the guideline draft and noting of comments andideas by the participants During this period participants did notconsult or discuss with others
Literature search 2010
(published June 30th 2007 ndash January 15th
2010)
Mesh terms ldquojuvenile idiopathic (rheumatoid)
arthritisrdquo and ldquotherapyrdquo
Limits ldquohumansrdquo ldquopublished in the last 3
yearsrdquo ldquoall child 0-18rdquo ldquoclinical trialrdquo
dArr n = 17
Exclusion of studies relating to
diagnosis of JIA uveitis vaccination
transition studies without control groups
Calcium supplementation costs
rArrrArr n = 13
arch 2007 and 2010
Table 3 Recommendation grade [10]
Recommendationgrade
Definition
A There is good evidence to support the recommendation that the intervention be performedB There is fair evidence to support the recommendation that the intervention be performedC There is poor evidence regarding the value or harm of the intervention recommendations may be made on
other groundsD There is fair evidence to support the recommendation that the intervention not be performedE There is good evidence to support the recommendation that the intervention not be performed
Table 2 Evidence level [10]
Evidencelevel
Definition
I Evidence obtained from at least one properly designed randomized controlled trialII Evidence obtained from well-designed controlled trials without randomization or from well-designed cohort or
casendashcontrol analytic studies preferably from more than one center or research group or from multiple time serieswith or without the intervention Dramatic results in uncontrolled trials might also be regarded as this type ofevidence
III Opinions of respected authorities based on clinical experience descriptive studies or reports of expertcommittees
179Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
2 Collocation of comments and ideas by the moderator using thewords of the participants
3 Clarification and substantiation of comments and ideas on alter-native guideline statements by the participants
4 Reconcilement of the manuscript and all alternative guidelinestatements
Table 4 Studies for 2010 update identified by the MEDLINE sear
Drugtreatment Mean age(age range) ofparticipants atstudy (years)
Totaof pa
Foeldvari et al [20] Celecoxibe 103 (2ndash16) 264Ceacutespedes-Cruzet al [33]
MTX 82 (np) 521
Lovell et al [45] Etanercept 104 (4ndash17) 58Horneff et al [83] Etanercept 129 (4ndash17) 20Giannini et al [46] Etanercept 99 (2ndash18) 594Lovell et al [40] Adalimumab 113 (4ndash17) 171Ruperto et al [31] Infliximab 112 (4ndash18) 121Lequerreacute et al [51] Anakinra 124 f (3ndash23) 20 f
Illowite et al [50] Anakinra 12 (2ndash17) 86Yokota et al [53] Tozilizumab 83 (2ndash19) 65Ruperto et al [54] Abatacept 124 (6ndash17) 190Singh-Grewal et al [58] Vigorous exercise
training116 (8ndash16) 80
Brinkmann et al [56] Stem celltransplantation
85 (4ndash18) 22
Abbreviations np = not provideda Not further specifiedb Only extended oligoarticular JIAc Pauciarticular onset with polyarticular coursed Extended oligoarticular JIA were included into polyarticular JIAe All JIA with polyarticular course with any type of onset not furthef Pediatric patients total number of patients in extended report wa
5 Discussion of statements and further explanation of any of thecomments that were not clear to all participants Each memberof the consensus group contributed to the discussion The moder-ator kept the process as neutral as possible avoiding judgmentand criticism
6 Final reconcilement for statements for guideline
ch algorithm (see Methodology)
l numbertients (n)
JIA
Oligoarticular Polyarticular Systemiconset
Othersubtypes
128 (53) a 114 (47) 22 (9)162 (31) b 284 (55) 75 (14)
5 (9) c 34 (58) 19 (33)2 (10) b 16 (80) 2
d 535 (90) 58 (97) 1171 (100) e
28 (23) c 74 (61) 19 (16)20 (100)
9 (10) c 62 (72) 15 (17)56 (100)
30 (16) 122 (64) 37 (20) 118 (23) 34 (43) 7 (9) 21 (26)
4 (18) 18 (82)
r specifieds 35 (15 were patients with adult onset of Still disease)
Consensus statement
NSAIDs are recommended for the treatmentof JIA Diclofenac Naproxen Ibuprofen andIndometacin (evidence level I respectively IIrecommendation grade A)If those drugs are contraindicated Celecoxibemight be used (evidence level I recommendationlevel BndashC)
Consensus statement
Intra-articular injections of crystalloid cortico-steroids (triamcinolone hexacetonide) are recom-mended and can be part of the first linetreatment Improvement of local inflammationpain swelling and range of joint movement hasbeen demonstrated (evidence level II recommen-dation grade A)Triamcinolone hexacetonide is more efficientthan triamcinolone acetonide inducing local remis-sion (evidence level I recommendation grade B)
180 G Dueckers et al
The conference guideline topics were reviewed andedited by working groups After the first consensus confer-ence statements were adopted by NGT and additional pro-posals for schemes of treatment strategies of JIA werecollated
25 Consensus finding method of Delphi
Three out of 15 statements remained without consensusafter NGT These statements comprise the utility of etaner-cept (treatment resistant polyarticular JIA) sulfasalazine(treatment resistant JIA) and anakinra (treatment for refrac-tory SoJIA) Therefore they were sent to all participants ofconsensus conferences via email To each of them partici-pants should state one of three votes (ldquoagreerdquo ldquodo notagreerdquo or ldquoalternative proposalrdquo) (1st round of Delphi)The results were summarized and the statements whichremained with no consensus after 1st round of Delphi weresent to participants again (2nd round of Delphi) After 2ndround of Delphi results were sent to external review
26 External review and adoption
The guideline manuscript has been reviewed in 2007 by na-tional experts in German Rheumatology Huppertz (BremenGermany) Michels (Garmisch Partenkirchen Germany) andSpecker (Essen Germany) The comments of external re-viewers (HI Huppertz) to the 2011 manuscript were in-volved within the 3rd round of Delphi External reviewenabled adoption of the guidelines core conclusions andstatements with strong consensus ie 95 agreement byrepresentatives of participating scientific societies andorganizations
3 Results treatment guidelines
31 Drug-based therapy
Drugs used in treatment of JIA are summarized in Table 5 Pro-posed schemes of treatment of JIA are shown in Fig 2 The fol-lowing paragraphs will highlight specific adverse reactions andintroduce the 13 studies relevant for the 2010 update of treat-ment guideline for JIA briefly For detailed information aboutprescribing information including indication contraindica-tion drug dosage route of administration monitoring andproduct characteristics the consensus group recommendsconsulting national drug data bases e g wwwrotelistede(German database of drugs with national market approval) orwwwfdaorg or wwwemaeuropaeu
311 Non-steroidal anti-inflammatory drugs (NSAIDs)Commonly NSAIDs are well tolerated Main side effects
of NSAIDs are stomach irritation dyspepsia andmdashin rarecasesmdashnephritis Cephalgia and behavioral changes can beassociated with the administration of ibuprofen Pseudo-porphyria is not uncommon in patients treated withnaproxen Pain relief has been demonstrated for Naproxen[13ndash15] Diclofenac [1516] and Ibuprofen [17] (evidencelevel I) and for Indometacin [18] and Meloxicam [19](evidence level II) Efficacy of Celecoxibe has been
demonstrated in a randomized double blind multicenterstudy [20] 95 of 212 patients entered the 12 week openlabel phase after a 12 week double blind phase in threetreatment groups (Celecoxibe 6 mgkgd versus Celecoxibe12 mgkgd versus Naproxen 15 mgkgd) Both dosages ofCelecoxibe showed comparable efficacy compared toNaproxen Safety ie number of adverse events (AE)did not differ significantly between Celecoxibe versusNaproxen
312 Glucocorticoids
3121 Glucocorticoids (GC)mdashlocal administration Theuse of intra-articular crystalline corticoids is highly potentand has a rather low rate of complications (evidence levelII) [2122] They might be administered as first line therapyResponse rate was significantly higher with triamcinolonehexacetonide than with triamcinolone acetonide at6 months and this difference was sustained to 24 months[2122] These findings were independent of duration andextent of disease [2122] Simultaneous intra-articular ste-roid injections are preferable to consecutive injections atdifferent time points (limited suppression of hypothalamicndashpituitaryndashadrenal axis) [23] Side effects eg local necrosisof fat tissue are seen in approximately 2 of injections [22]Working under sterile conditions the risk of infection is low
3122 GCmdashsystemic administration GC can be adminis-tered as a fast acting drug in highly active disease Indica-tions for their use are bridging time until DMARDs (diseasemodifying anti rheumatic drugs) become effective treat-ment of severe systemic features of systemic-onset JIA(SoJIA) induction of remission in polyarticular JIA and in se-vere forms of uveitis There are no controlled trials and nostandardized therapeutic regimes for the use of systemic
Table 5 Drugs for the treatment of JIA
Generic Dosage Age approval by Europeanmedical agency inpediatric rheumatology(EMA) a
Medical indication in pediatricrheumatology a b
Evidence levelrecommendationgrade [10]
Literature
NSAIDsDiclofenac 2ndash3 mgkg Bwd po (in 3 doses)
Retard formulation 1 dose14 years Arthritis IndashA Haapasiri [16] Laxer [14]
Ibuprofen 20ndash40 mgkg Bwd po in 3ndash4doses
6 months Pain fever IndashA Giannini [17]
Indometacin 1ndash3 mgkg Bwd po in 3 doses 2 years Arthritis IIndashA Stoeber [18]Meloxicam 0125ndash025 mgkg Bwd po 15 years Arthritis II Ruperto [19]Naproxen 10ndash15 mgkg Bwd po in 2 doses 1 year Arthritis IndashA Kvien [13] Laxer [14] Leak
[15]Celecoxibe 6 mgkg Bwd po in 2 doses or
12 mgkg Bwd in 1 doseNo approval for children Arthritis I B-C Foeldvari [20]
Glucocorticoids (GC)a) Systemic GCPrednisonePrednisolone
01ndash02 mgkg Bwd (max 5 mgd) JIA ie severe SoJIA severe peri-myokarditis severe uveitis (hypotoniaor cystoid macular edema) intoleranceto other drugs (ldquolow-doserdquo) or asldquobridgingrdquo therapy in higher doses eg2 mgkg Bwd until therapeutic effectof ldquoDMARDsrdquo
III Prieur [28]
Prednisone as an oralhigh-dose therapy
ge1ndash2 mgkg Bwd prednisolone-equivalent
III Prieur [28]
Prednisone as an oralmedium-dosetherapy
02 tob10 mgkg Bwdprednisolone-equivalent
III Kirwan [24] Prieur [28]
Prednisone as an orallow-dose therapy
b02 mgkg Bwd Prednisolone-equivalent or b4 mgmsup2 bodysurface
III Michels [25]
Prednisone as a ivpulse-therapy
N(5)ndash10 mgkg Bw (po)Prednisolone-equivalent10ndash30 mgkg Bwd Methyl-Prednisolone iv for 1ndash3 d(maximum 1 gdose)
III Miller [26] Picco [27]
b) Intra-articular GCTriamcinolonehexacetonide
05ndash1 mgkg Bw into large jointsdose adaption referring to size ofjoint (eg max 2 mg intointerphalangeal joints c)
5 months Arthritis tendo-vaginitis I Zulian [2122]
(continued on next page)(continued on next page)
181Evidence
andconsensus
basedGKJR
guidelinesfor
thetreatm
entof
juvenileidiopathic
arthritis
Table 5 (continued)
Generic Dosage Age approval by Europeanmedical agency inpediatric rheumatology(EMA) a
Medical indication in pediatricrheumatology a b
Evidence levelrecommendationgrade [10]
Literature
DMARDsSulfasalazine 30ndash50 mgkg Bwd in 2ndash3 doses 6 years Arthritis II Van Rossum [3637]Cytotoxic or immuno-suppressive drugsMethotrexate 10ndash15 (20) mgmsup2 body surface
once a week (po sc iv) e2 years Polyarticular JIA Psoriasis arthritis
uveitis CollagenosisI Giannini [84] Ravelli [85]
Woo [86]Cespedes-Cruz [33]Azathioprine 15ndash3 mgkg Bwd po in 1ndash2
dosesNo approval for children II Kvien [34]
Leflunomide No clear recommendation forchildren availableBwb20 kg d 1100 mgkg from d 2 10 mgkgdBw 20ndash40 kg d 1 to d 2 100 mgkgfrom d 3 10ndash20 mgkgdBwN40 kg d 1 to d 3 100 mgkgfrom d 3 20 mgkgd
No approval for children II Silverman [3587]
Biologic agentsa) TNFα inhibitorsEtanercept d 08 mgkg Bw sc 1timesweek
(max 50 mgweek) or 04 mgkgBw sc 2timesweek (max 50 mgweek)
4 years JIA Polyarthritis and insufficientefficacy of MTX
I Giannini [46] Horneff [49]Lovell [3888] Prince [41]
Adalimumab d 24 mgm2 body surface sc in 1dose every 2 weeks Bwb30 kg20 mgm2 body surface BwN30 kg40 mgm2 body surface(max 40 mg per dose)
4 years to 17 years Adalimumab in combination withmethotrexate is indicated for thetreatment of active polyarticularjuvenile idiopathic arthritis in childrenand adolescents who have had aninadequate response to one or moredisease-modifying anti-rheumatic drugs(DMARDs)
I Lovell [40]
182GDueckers
etal
Infliximab d 3ndash10 mgkg Bwdose iv Infusionat d 0 d 14 d 42 then every8 weeks intervals of applicationremain unclear
No approval for childrenwith JIA6 years (approval forMorbus Crohn)
III Ruperto [31]
b) IL-1 inhibitorsAnakinra d 1ndash4 mgkg Bwd sc in 1 dose No approval for children II Illowite [50] Lequerre [51]Canakinumab d 4 mgkg Bwsingle dose sc every
4 weeks (max 150 mg)No approval for childrenwith JIA 4 years (approvalfor CAPS)
III Ruperto [89]
Rilonacept d 1ndash2times44 mgkgweek sc (max320 mg) then 22 mgkgweek sc(max160 mg)
No approval for childrenwith JIA 12 years(approval for CAPS)
Lovell [889091]
c) IL-6 inhibitorsTocilizumab d 1 h Infusion every two 2 weeks
Bwb30 kg 8 mgkg BwN30 kg12 mgkg
2 years of age or older Since May 2011 EMA approval forpediatric patients with SoJIA who haveresponded inadequately to previoustherapy with NSAIDs and systemiccorticosteroids (Approval at Japan forSoJIA and polyarticular JIA since 2008) c
I Yokota [53] Ruperto [92]de Benedetti [62]
d) Co stimulatory-antagonistsAbatacept d 10 mgkg iv Infusion at d 0 d 14
d 28 then every 4 weeks6 years of age and older Abatacept in combination with
methotrexate is indicated for thetreatment of moderate to severe activepolyarticular (JIA) in pediatric patientswho have had an insufficient responseto other DMARDs including at least oneTNF inhibitor
I Ruperto [549394]
Abbreviations CAPS=Cryopyrine associated periodic fever syndrome JDM=juvenile dermatomyositis Bw=body weight SoJIA=systemic-onset of JIA SLE=systemic Lupus erythematodesa Compare wwwemaeuropaeub wwwrotelistede (German database of drugs with national market approval)c Intra-articular injection into same joint no more often than once every 3 monthsd A statement from insurance companies should be acquired before treatment initiation for off label treatment (if possible)e Oral application is most feasible in childhood
183Evidence
andconsensus
basedGKJR
guidelinesfor
thetreatm
entof
juvenileidiopathic
arthritis
Oligoarticular JIA
Polyarticular JIA
SoJIA
Figure 2 JIA treatment escalation schemes +=addition of the drug (abbreviations NSAIDs=non steroidal anti-inflammatory drugthotrexate)
Consensus statement
Long-term use of systemic GC is not recom-mended Continuous administration of ge02 mgPrednisolone equivalent per kg bodyweight (Bw)carries a high risk of adverse events and thereforeis not recommended (evidence level III recom-mendation grade A)
Consensus statement (continued)
184 G Dueckers et al
GC in JIA published thus leading to ldquojustrdquo evidence level IIIDifferent recommendations of dosage and therapy regimesare listed in Table 5 (evidence level III for all recommenda-tions) [1824ndash28] Frequency and seriousness of deleteriouseffects correlate mainly to duration of therapy and dosageof GC administered Main side effects are iatrogenicCushings syndrome growth disturbance weight gainmood changes Higher dosage carry the risk of increasedvulnerability to infection hypertension osteoporosisthrombosis diabetes gastro-intestinal ulceration cataractglaucoma atrophy of subcutaneous fatty tissue steroid in-duced acne To inform colleagues about GC treatment in acase of emergency and to reduce severe complications in longterm treated patients ie GC administrationN4 weeks thesupply of ldquoGlucocorticoid ID cardsrdquo for patients might be useful
GC=Glucocorticoids DMARDs=disease modifying drugs MTX=Me
Consensus statement
The systemic use of GC is recommended asfast acting drugs in highly active JIA GC areused for the treatment of children and adoles-cents with SoJIA organ manifestations of JIA(eg uveitis pericardial effusion) sero-positivepolyarticular JIA and for bridging time untilthe complete therapeutic effect of DMARDs(evidence level III recommendation grade A)
313 Methotrexate (MTX) biologic agents andimmunosuppressive agents
MTX biologic agents and immunosuppres-sive agents are used for the treatment of childrenand adolescents with polyarticular JIA ifNSAIDs or local GC treatment do not succeedThe combination of those drugs with NSAIDsand GC is feasible A common characteristic ofMTX biologic agents and immunosuppressiveagents is the delayed onset of therapeutic ef-fect ie up to 3 months or even longer aftercommencing treatment
185Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
Safe contraception is indicated during therapy with MTXAzathioprine or Leflunomide and in the following 3 to6 months after its discontinuation
Consensus statement
Administration of Sulfasalazine or Lefluno-mide is recommended if MTX or Etanercept donot show sufficient efficacy or cannot be used
3131 Methotrexate Among DMARDs MTX provides themainstay of long-term therapy in JIA [29ndash32] In case ofside effects eg dyspepsia or nausea prophylaxis withfolic acid can be recommended (1times1 mg per day or 5 mgonce a week 24ndash48 h after application of MTX) Safe contra-ception is mandatory while receiving MTX Safety and effica-cy of MTX and its impact on quality of life of children with JIAhave been investigated Significant positive impact of MTXon all health-related quality of life health conceptshas been shown although the study has its limit due to dif-ferent MTX dosages used within participating JIA patients[33]
Consensus statement
MTX administration can be recommendeddue to its proven safety and efficacy to reducedisease activity MTX is used in case of insuffi-cient therapeutic effect of NSAIDs andor localGC administration continuous need for system-ic GC andor highly active disease Efficacy ofMTX (orally or subcutaneously administered) isfrequently achievable with a dosage of 10ndash15 mgmsup2 body surface (evidence level I recom-mendation grade A)
for other reasons (evidence level II recommen-dation grade B)
3132 Purine analogs31321 Azathioprine Efficacy has been investigat-
ed in a double blind placebo controlled study (32 patients)After 8 weeks of therapy the changes in disease activitymeasurement indicated a minor improvement in the Azathi-oprine group compared to the placebo group At the end ofthe study statistically significant differences between thegroups were found for only 2 disease activity measurements[34] Two patients were taken out of study due to severeadverse events eg leucopenia Measurement of activityof Thiopurinmethyltransferase (TPMT) can be beneficial foravoidance of severe adverse events
3133 Pyrimidine analogs31331 Leflunomide Within a double blind study
(32 weeks 94 patients) efficacy of Leflunomide was inferiorin comparison to MTX but better than placebo Howeverdosing of Leflunomide may not have been adequate insome children [35] Contraindications for Leflunomide arerenal insufficiency severe immunodeficiency depressedmyelopoesis and pancytopenia An extensive half-life peri-od (approximately 14 days) has to be taken in accountwhen administering Leflunomide In combination with hepa-totoxic DMARDs the risk of severe adverse events might in-crease eg increased blood pressure is seen frequentlySafe contraception is mandatory
3134 Antibiotic analogs and Hydroxychloroquine andChloroquine
31341 Sulfasalazine Weak efficacy of Sulfasalazinewas demonstrated within a placebo-controlled randomizedstudy after 24 weeks (96 patients) [3637] One third of pa-tients enrolled in the study discontinued treatment with Sulfa-salazine due to side effects eg gastrointestinal symptomsleucopenia [36] Some experts use sulfasalazine in HLA-B27positive JIA Contraindications are Glucose-6-phosphatase de-ficiency and hypersensitivity against sulfonamides
31342 Hydroxychloroquine and chloroquine Hydrox-ychloroquine and Chloroquine have been subject to clinical tri-als for the treatment of JIA even though efficacy was limitedWithin three consensus conferences held in 2007 and 2010 theconsensus group decided not to give a consensus statementon the use of chloroquine or hydroxychloroquine treatmentdespite the fact that those drugs still might be used by somecaregivers
3135 Biologic agents Biologic agents are drugs whichselectively inhibit cytokines cytokine receptors or directlybind to receptors of lymphocytes eg CTLA-4 CD20 Theyinclude antibodies and fusion proteins So far allbiological therapies are administered subcutaneously orintravenously
31351 TNFα-inhibitors TNFα-inhibition with Adali-mumab and Etanercept is efficient and safe (evidencelevel I) [38ndash41] Both drugs have been approved for JIAwith polyarticular course TNFα-inhibitors have become anintegral part of the treatment of JIA Potential risks of therapyare vulnerability for infection andmdashin a rare occasionmdashthe in-duction of autoimmune disease Prior to the start of treatmentwith TNFα-inhibitors chronic infections needs to be excludedor treated sufficiently eg tuberculosis hepatitis B or C
In children with JIA treated with TNFα-inhibitors malig-nancies eg Lymphoma have been reported It remainsunclear if the rate of malignancies is increased in patientscompared to the risk by having JIA itself In response to aprevious letter of the FDA (as reviewed in [42]) the GermanSociety for Pediatric Rheumatology (GKJR) has published of-ficial statements [4344] The GKJR states that treatmentwith TNFα-inhibition should be used very carefully physi-cians need to be aware of co-medication e g immunosup-pressive drugs and should monitor those patientsclosely [43] There is insufficient data on all biologicagentsmdashincluding TNFα-inhibitionmdashto judge about the long-term risk for children and adolescents313511 Etanercept Etanercept is a fusion proteinconsisting of the extracellular binding domain of solubleTNFα-receptor and Fc chain of human IgG1 Etanercept in-hibits TNFα by direct binding of the cytokine Efficacy has
Consensus statement
The use of Anakinra or Tozilizumab can berecommended for treatment of children and ado-lescents with refractory SoJIA (evidence level IIrecommendation grade A)
186 G Dueckers et al
been demonstrated in a randomized controlled withdrawaldesign trial for patients with polyarticular JIA [38] Withinan open extension study long term efficacy and safety havebeen documented over 8 years in 1669 patients [3945]There is data on more than 2000 patients registered in Euro-pean registries [46ndash48] Currently retrospective data showsa somewhat better efficacy of combining MTX or otherDMARDs with TNFα-inhibition versus anti-TNFα therapy assingle therapy [49]313512 Adalimumab Adalimumab is a humanizedmonoclonal IgG1 antibody directed against TNFα whichbinds soluble and membrane bound TNFα A randomizedcontrolled withdrawal design trial demonstrated safety andefficacy of Adalimumab (24 mgmsup2 body surface every2 weeks max 40 mg) for children and adolescents withpolyarticular JIA (4ndash17 years of age n=171) [40] After16 weeks ldquowash inrdquo phase responders (n=144171) enteredthe 32 weeks randomized double blind phase After 48 weekstwice the number of patients in the verum group met ACR 70as compared to the control group (56 vs 28 pb001)Within the open extension phase Adalimumab dosage wasfixed ie 20 mgb30 kg Bw and 40 mgN30 kg Bw There islack of evidence showing superior efficacy of combiningMTX (DMARDs) with Adalimumab versus Adalimumab as sin-gle therapy [40]
Consensus statement
Efficacy of Etanercept and Adalimumab forthe treatment of polyarticular JIA has been dem-onstrated Therapy with TNFa-inhibition is indi-cated in case of insufficient therapeutic effectof NSAIDs and local GC administration and lackof response to MTX (evidence level I recom-mendation grade A)
Consensus statement
Patients with polyarticular JIA without sys-temic manifestation refractory to treatmentwith MTX and TNF inhibition might benefit fromthe use of Abatacept (evidence level III recom-mendation grade C)
313513 Infliximab Infliximab is a chimerical (humanmouse) monoclonal antibody which binds soluble and mem-brane bound TNFα A randomized controlled study in childrenand adolescents with JIA failed to demonstrate a significantdifference of efficacy after treatment with Infliximab com-pared to placebo [31]
31352 Interleukin-1-inhibitors None of interleukin-1-inhibitors are approved for the treatment of JIA or SoJIAThey are commonly used in an off label setting313521 Anakinra Anakinra is an IL-1 receptor antag-onist Within a randomized controlled trial no significant ef-ficacy of Anakinra for patients with polyarticular JIA couldbe demonstrated [50] 50 of 86 patients were enrolled intoblinded phase (11 Anakinra versus Placebo) No significantreduction of flare could be demonstrated in comparison toplacebo 29 of 50 patients completed the open label exten-sion study Two noncontrolled nonrandomized studieshave shown efficacy of anakinra in a proportion of patientswith systemic-onset of JIA (SoJIA) [5152]313522 Canakinumab Canakinumab an IL-1β anti-body binds IL-1β selectively without interfering with IL-1αor its physiological IL-1 receptor antagonist Canakinumabhas been approved for treatment of hereditary periodic IL-1 associated periodic fever syndromes ie Cryopyrin-
associated periodic syndromes There are ongoing studies in-vestigating safety and efficacy of Canakinumab for SoJIA
31353 Interleukin-6 inhibitors313531 Tozilizumab Tozilizumab is a humanizedanti-IL-6 receptor monoclonal antibody Efficacy has beendemonstrated within a 12 week double blind randomizedcontrolled withdrawal trial in children with SoJIA (n=562ndash19 years) in Japan [53] After a 48 week open extensionstudy ACR Pedi 30 was met by 47 patients (98) At thetime of our literature search Tocilizumab was approved fortreatment of SoJIA and polyarticular JIA since 2008 inJapan A multicenter European study investigating efficacyand safety of Tozilizumab in polyarticular JIA was ongoingat the deadline of literature search (wwwclinicaltrialsgov NCT00988221) No data on long term effects are cur-rently available
31354 Co-stimulation inhibitors313541 Abatacept Abatacept is a recombinant fu-sion protein of extracellular domain of human cytotoxic T-Lymphocyte Antigen 4 (CTLA-4) and IgG1-Fc-Fragment Itmodulates T-cell co-stimulation A randomized controlleddouble blind withdrawal design study of Ruperto et al [54]demonstrated efficacy of Abatacept in patients with polyar-ticular JIA 123 of 170 participants of study were enrolled inthe 6 month double blind phase Flares occurred in 33 of 62(53) patients who were given placebo versus 12 of 60(20) Abatacept patients during double blind phase Adverseevents (AE) did not differ in both groups ie 37 AE in Abata-cept versus 34 AE in placebo recipients Some children maytake 3 to 6 months or longer before their maximal responseis achieved 3 of patients developed reaction to the infu-sion [55] Abatacept is approved by FDA and EMA for pa-tients who did not respond to prior MTX treatment Nodata of long term effects of the use of Abatacept in JIA areavailable due to the low numbers of patients treated so far
314 Autologous stem cell transplantation (SCT)There are studies on autologous SCT for treatment of re-
fractory and severe forms of JIA (evidence level III) [56] 22
Consensus statement
187Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
patients were enrolled in one study 8 reached clinical re-mission 7 were assessed as partial responders 3 experi-enced relapse of the disease and 4 (18) died as aconsequence of MAS or immunosuppressive treatment [56]Due to serious adverse events including death this thera-peutic option is seen as the last treatment option
Exercise training is recommended dependingon the extent of inflammation number of affect-ed joints and global disease activity Sports withminor stress on joints is favorable (evidence levelI recommendation grade A)
32 Non-drug based therapy
321 Physiotherapy occupational therapy and thera-peutic appliances
Physio- and occupational therapy are integral parts of thetherapeutic concept in children and adolescents with JIA[5758] Therapeutic goals of physiotherapy are relaxationand pain relief preservation or rehabilitation of physiologi-cal range of joint movement prevention of contracturesstretching and activation of muscles build-up of muscleforce and training of physiological movements
Consensus statement
Structured treatment by a properly trainedphysiotherapistoccupational therapist in combi-nation with drug based therapy and instructionsfor disease adopted self-sufficient daily exercisesessions are recommended to keep and to im-prove joint mobility (evidence level II recom-mendation grade A)Custom-made therapeutic appliances for correc-tion of axial misalignment prevention of falseweight bearing stabilization of joints (eghand- finger- and foot-ortheses) are recom-mended individually The use of therapeutic ap-pliances follows individual physician-directedadvice Efficacy has been demonstrated (evi-dence level I recommendation grade B)
Consensus statement
In individual cases the indication for open orarthroscopic synovectomy can be considered ifconservative therapy does not succeed (evi-dence level III recommendation grade B)
Consensus statement
Other forms of non-drug based therapeutic approachesrely on experts opinion and are solely based on individualclinical experience No controlled studies are available
Consensus statement
The implementation of thermotherapy electro-or ultrasound therapy massage and lymph drain-age is recommended Application of cold appli-ances for acute joint inflammation is indicated(evidence level II recommendation grade A)Electro- and ultrasound therapy are recom-mended for patients with tendosynovitis (evi-dence level III recommendation grade B)
An early psychological support within stan-dard pediatric rheumatological care should beimplemented to apprehend and treat mental is-sues and behavioral syndromes associated withphysiological disturbances and physical factors(evidence level III recommendation grade A)
Consensus statement
A socio-pedagogical care with regard tointegration at school professional andeveryday life and formal education of parentsand patients is recommended (evidence levelIII recommendation grade A)
322 Sportive activity and exercise trainingPositive impact of sportive activity on the general physi-
cal condition and on oxygen consumption has been demon-strated (evidence level II) [57ndash60] Adequate exercise
training supports the physiological development and helpscoping with JIA [58] Prospective controlled long term stud-ies are currently not available
323 Surgical treatmentToledo et al investigated the role of arthroscopic syno-
vectomy in JIA They concluded that arthroscopy is a safebut only partially effective procedure in patients witholigoarticular JIA (evidence levelrecommendation gradeIIIB) [61]
324 Psychological social intervention orsocio-pedagogical care
There are no controlled or open studies focusing on psy-chological social andor socio-pedagogical intervention inchildren or adolescents with JIA Recommendations arebased on experts opinion and personal experience solely
188 G Dueckers et al
4 Addendum
Since the deadline January 15th 2010 new papers haveappeared that are of interest in the context of our guideline[5562ndash64] in particular we refer to the ACR recommenda-tions [65] and the most recent literature on the risk of malig-nancies in JIA in context with TNF blocking agent andindependent of medication [42] [66] Moreover there is arecent study on the use of Tocilizumab in polyarticular pa-tients [67] These papers will be discussed within the nextconsensus conference by NGT and considered for inclusioninto the next edition of this guideline On 6th of September2011 our advanced search on wwwclinicaltrialgov (searchterms juvenile idiopathic arthritis recruitment open stud-ies study type interventional study age group child(birthndash17) intervention drugs) led to 16 trials which are cur-rently recruiting or will soon start recruiting
5 Discussion
To develop clinical practice guidelines of high quality andvalidity a formal consensus process and explicit methodo-logical criteria for the production of guidelines are recom-mended [68ndash70] Our guideline for the treatment of JIA inchildren and adolescents implements all these issues Thesystematic literature search was terminated on 15th January2010 leading to the most up to date guideline for JIA whichis currently available The deadline of the ACR recommenda-tions as published recently by Beukelmann et al was 5th ofOctober 2009 [65] By exclusion of case reports trials with-out control groups preliminary results published as ab-stracts on conferences and the strict graduation of theliterature by the criteria of evidence based medicine weaimed to give our guideline statements additional strengthand a maximal validity Newer original studies providing ad-ditional evidence for the treatment of JIA became availableafter our consensus process was finished see AddendumThe results of these trials have to await the next NGT beforeinclusion into our recommendations
Our updated systematic literature search in 2010 led to13 relevant studies published after 30th June 2007 (Fig 1Table 4) Their results have to be interpreted with cautionFirst trials in JIA are mainly based on limited numbers of pe-diatric patients as the recruitment of a sufficient number ofpediatric patients remains challenging Second trials aremainly designed for patients with polyarticular JIA or witholigoarticular onset and a polyarticular course (Table 4)Most children with JIA do not have a polyarticular subtypeof JIA but an oligoarticular onset and course [71] Thus pa-tients with oligoarticular JIA are heavily underrepresentedin most of the current trials Third in 5 of the 13studies the withdrawal study design has been used[4045505354] Lehmann reviewed the bias of withdrawaldesign trials in 2008 [72] After a wash-in phase only re-sponders to treatment are eligible for randomization Thusthe design preselects responders to the placebo effect whomight retain their response throughout the entire study peri-od Further there is a carryover effect of AE into the place-bo group so that significant differences in AE betweengroups may not become apparent In the one placebo con-trolled trial without withdrawal design on TNFα-inhibition
(Infliximab) no significant efficacy could be demonstratedbetween verum and placebo [31]
To our knowledge there are two other guidelines that dealwith the management of JIA as a whole (Table 6) [65] [73]Other guidelines are limited to the use of single drugs in JIAeg biologic agents [74] etanercept [75] The Australian guide-line (wwwracgporgauguidelinejuvenileidiopathicarthritis)has not been published in a peer-reviewed journal It is to pro-vide recommendations for the early diagnosis and multidisci-plinary management of JIA in the primary care setting forgeneral practitioners (GPs) [73] No recommendations aremade regarding the use of GCs DMARDs immunosuppressivedrugs or biologic agents [73] The ACR recommendations usesthe Appraisal of Guidelines for Research and Evaluation(AGREE) instrument [65] [76] which does not fulfill criteria ofa proper consensus process and carries the risk that expertsvote for peer opinion which might not reflect the true valueWe used an advanced and linguistically validated version ofthe AGREE instrument the ldquoGerman Instrument for Methodo-logical Guideline Appraisal (DELBI)rdquo which has been developedin cooperation of the AWMF among others [7778] We followedthe highly structured Nominal Group Technique as described inMethodology Our consensus group only considered formallyboard nominated representatives of multidisciplinary scientificsocieties and organizations (Table 1) and included patients rep-resentatives as this has been strongly recommended by the Eu-ropean League against Rheumatism (EULAR) recently [79] TheACR mentions a parent representative within their task forcepanel but leaves this representative anonymous It remainsunclear how ACR experts were selected and involved [65]They defined treatment groups which have not been evaluatedsystematically so far We used the ILAR classification systemwhich has been repeatedly evaluated [80ndash82]
By content there are major differences between the ACRrecommendations and our guideline a) Our guideline pro-vides a detailed and systematic list of 20 drugs commonlyused in the treatment of JIA (Table 5) which has been an in-tegrative part of our consensus conferences The ACR recom-mendations do not provide information on approval status(Food and Drug Administration) indications for use and nospecific differences on dosage regimes or frequency ofdaily application [65] eg it refers to the 2008 ACR recom-mendations for the use of DMARDs in adult rheumatoid ar-thritis b) The ACR recommendations provide a more earlyaggressive approach in the treatment of JIA The ACR recom-mends MTX as first line treatment in patients (b4 joints) withhighly active disease [65] To our knowledge there are onlydata to recommend MTX administration in cases of insuffi-cient therapeutic effect of prior treatment with NSAIDandor GC [33] c) The ACR recommends the use of TNFα in-hibitors as escalation therapy for some patients with historyof arthritis of 4 or fewer joints and refer to publications[3840] conducted in patients with polyarticular JIA or pau-ciarticular JIA with polyarticular course [65] There is no ev-idence that TNF is safe and efficient in patients witholigoarticular JIA a systematic controlled clinical trial onthis issue has not been done yet d) We regard a brief trialof local or systemic administration of GC plus NSAID as a fea-sible first line treatment for patients with polyarticular JIAThe ACR recommends MTX without regard to disease activityat the initial stage [65] We reached consensus to recom-mend the use of GC as bridging therapy until full onset of
Table 6 Overview of recommendationsguidelines for treatment of JIA
USA Australia Germany
ACR recommendations[65]
RACGP recommendations[73]
GKJR guidelines
Deadline of literature search October 2009 January 2007 September 2010Source of publications Pub Med Pub Med
EMBASE CINHAL CochraneLibrary provisionalAustralian Guideline [95]
Pub MedPrevious German Guidelines [78]
Definition used for JIA subgroups Treatment groups definedby Core expert panel
Not specifically definedChildren withJIAb16 years
ILAR criteria [1]
Consensus processprocessvalidation
AGREE [76] AGREE [76] DELBI [77]RANDUCLA appropriatenessmethod [96]
NGT Delphi method
Conferences None None 3 Formal consensus conferencesAddressees Pediatric rheumatologists General practitioner Pediatric Rheumatologists
PediatriciansGeneral practitioners
Participating scientific societies or professional organizationsPediatric rheumatologist orrheumatologists for adolescents
Yes Yes Yes
General pediatrician- In hospital Yes Yes Yes- In private practice Yes Yes YesResearcher Yes No YesRheumatologists for adults No No YesOphthalmologists No No YesParentspatients support groups Yes No YesOrthopedic surgeons No No YesPediatric orthopedic surgeons No No YesPsychologists No No YesPhysiotherapists No No YesPediatric rheumatology nurses Yes No NoOther scientific societies ororganizations
ACR BSPAR PRINTO PReS RACGP NAMSCAG NHMRC DGKJ DGPs DGRh DGO AWMFBVKJ
(ACR=American College of Rheumatologists AGREE=Appraisal of Guidelines for Research amp Development AWMF=Association of the ScientificMedical Associations BSPAR=British Society for Pediatric Rheumatology BVJK=Association of Pediatricians in private practice CEP=Core expertpanel ILAR=International League against Rheumatism CINHAL=Cumulative Index to Nursing and Allied Health Literature DELBI=German In-strument for Methodological Guideline Appraisal DGKJ=German Society of Pediatrics and Adolescent Medicine DGO=German Society for Oph-thalmology DGPs=German society for Psychology DGRh=German Society for Rheumatology GKJR=German Society for Pediatric RheumatologyNAMSCAG=National Arthritis and Musculoskeletal Conditions Advisory Group NGT=Nominal Group Technique NHMRC=National Health andMedical Research Council PReS=Pediatric Rheumatology Society) PRINTO=Pediatric Rheumatology International Trial Organization RACG-P=Royal Australian College of General Practitioner RANDUCLA=Research and DevelopmentUniversity of California at Los Angeles)
189Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
therapeutic effect of DMARDs The ACR recommendations donot provide any recommendation for the use of systemic GCfor patients with oligo- or polyarticular course of JIA exceptsystemic onset of JIA e) The ACR recommendations do notcover the topic of non-drug based therapy at all althoughthere is strong evidence that eg exercise training is a usefuladdition to drug treatment [575860]
6 Conclusion
In summary we present a treatment guideline for JIA on a con-sensus conference basis We strongly advocate an interdisciplin-ary approach including surgery physiotherapy psychosocial
intervention physical therapy medications etc and a strictformal consensus process in order to create statements thatare most appropriate for the complex clinical situation of achild and family presenting with JIA and cover all aspects ofJIA care All German pediatric rheumatology sites are partici-pating at the national pediatric rheumatologic database in theDeutsche Rheuma-Forschungszentrum at Berlin (DRFZ wwwdrfzde) It aims at quality assurance in Germany and monitorstreatment behavior of pediatric rheumatologists by using inter-nationally agreed criteria (eg joint count global physician rat-ing of disease activity global parent rating of overall well-being CHAQ ESR ACR-ped response or JADAS) The databasewill be used as a tool to monitor the application of our treat-ment guidelines
190 G Dueckers et al
Conflict of interest statement
Gregor Dueckers Novartis Pharmaceuticals CorporationBaxter (for all travel grants for scientific meetings)Nihal Guellac no conflict of interestMartin Arbogast no conflict of interestGuumlnther Dannecker no conflict of interestIvan Foeldvari Wyeth Pfizer Abbott Immunology Pharma-ceuticals Chugai (for all advisory board member)Michael Frosch no conflict of interestGerd Ganser Abbott Immunology Pharmaceuticals (advisoryboard member grants for scientific meetings) Wyeth Pfizer(advisory board member grants for scientific meetings)ChugaiRoche (advisory board member grants for scientificmeetings) Merck (grants for scientific meetings) Actelios(grants for scientific meetings) Esaote (grants for scientificmeetings)Arnd Heiligenhaus Novartis Pharmaceuticals CorporationAbbott Immunology Pharmaceuticals Alcon (for all re-search grants)Gerd Horneff Abbott Immunology Pharmaceuticals (re-search grants consulting fees non-remunerative positionsof influence) Wyeth Pfizer (research grants consultingfees speakers bureau non-remunerative positions of influ-ence) Bristol-Myers Squibb (Consulting fees) Nycomed(Consulting fees non-remunerative positions of influence)RocheChugai (Consulting fees non-remunerative positionsof influence) Sandoz (Consulting fees) Genzyme (researchgrants consulting fees non-remunerative positions of influ-ence) Swedish Orphan (research grants consulting feesnon-remunerative positions of influence)Arnold Illhardt no conflict of interestRuumldiger Krauspe no conflict of interestBarbara Markus no conflict of interestHartmut Michels Abbott Immunology Pharmaceuticals (advi-sory board member and grants for scientific meeting)Matthias Schneider no conflict of interestWolfram Singendonk no conflict of interestHelmut Sitter no conflict of interestMarianne Spamer no conflict of interestNorbert Wagner no conflict of interestTim Niehues Abbott Immunology Pharmaceuticals EssexPharma Novartis Pharmaceutical Corporation WyethPfizer (for all research grants consulting fees non-remu-nerative positions of influence)
Acknowledgment
We like to express our grateful thanks to Prof Dr Hans IkoHuppertz for proof reading the article and for an excellentdiscussion on our work We like to express our thanks to HE-LIOS Clinic for funding the open access of the article
References
[1] RE Petty TR Southwood P Manners J Baum DN Glass JGoldenberg X He J Maldonado-Cocco J Orozco-Alcala AMPrieur ME Suarez-Almazor PWoo International League of Asso-ciations for Rheumatology classification of juvenile idiopathic ar-thritis second revision Edmonton 2001 J Rheumatol 31(2004) 390ndash392
[2] B Prakken S Albani A Martini Juvenile idiopathic arthritisLancet 377 (2011) 2138ndash2149
[3] KT April DE Feldman RW Platt CM Duffy Comparisonbetween children with juvenile idiopathic arthritis (JIA) andtheir parents concerning perceived quality of life Qual LifeRes 15 (2006) 655ndash661
[4] BM Feldman B Grundland L McCullough V Wright Distinc-tion of quality of life health related quality of life and healthstatus in children referred for rheumatologic care J Rheuma-tol 27 (2000) 226ndash233
[5] JC Packham MA Hall Long-term follow-up of 246 adultswith juvenile idiopathic arthritis functional outcomeRheumatology (Oxford) 41 (2002) 1428ndash1435
[6] C Sandborg Pediatric rheumatic disease standards of care forJIAmdashthe basic foundation for quality Nat Rev Rheumatol 6(2010) 389ndash390
[7] N Guellac T Niehues Interdisciplinary and evidence-basedtreatment guideline for juvenile idiopathic arthritis KlinPadiatr 220 (2008) 392ndash402
[8] K Schnakenburg Leitlinien in der Kinder- und JugendmedizinElsevier 2005 pp H1 1ndash15
[9] P Juni L Nartey S Reichenbach R Sterchi PA Dieppe MEgger Risk of cardiovascular events and rofecoxib cumulativemeta-analysis Lancet 364 (2004) 2021ndash2029
[10] W Feldman Evidence-based Pediatrics 1st ed BC DeckersHamilton 2000
[11] AH Van de Ven AL Delbecq The nominal group as a re-search instrument for exploratory health studies Am J PublicHealth 62 (1972) 337ndash342
[12] HA Linstone M Turoff The Delphi Method Techniques andApplications Addison-Wesley Pub 1975
[13] TK Kvien HM Hoyeraal B Sandstad Naproxen and acetyl-salicylic acid in the treatment of pauciarticular and polyarticu-lar juvenile rheumatoid arthritis Assessment of tolerance andefficacy in a single-centre 24-week double-blind parallelstudy Scand J Rheumatol 13 (1984) 342ndash350
[14] RM Laxer ED Silverman C St-Cyr MT Tran G Lingam Asix-month open safety assessment of a naproxen suspensionformulation in the therapy of juvenile rheumatoid arthritisClin Ther 10 (1988) 381ndash387
[15] AM Leak MR Richter LE Clemens MA Hall BM AnsellA crossover study of naproxen diclofenac and tolmetin in sero-negative juvenile chronic arthritis Clin Exp Rheumatol 6(1988) 157ndash160
[16] J Haapasaari E Wuolijoki H Ylijoki Treatment of juve-nile rheumatoid arthritis with diclofenac sodium Scand JRheumatol 12 (1983) 325ndash330
[17] EH Giannini EJ Brewer ML Miller D Gibbas MH PassoHM Hoyeraal B Bernstein DA Person CW Fink LA Sawyeret al Ibuprofen suspension in the treatment of juvenilerheumatoid arthritis Pediatric Rheumatology CollaborativeStudy Group J Pediatr 117 (1990) 645ndash652
[18] E Stoeber L Sanger Experiences with indomethacin in long-term therapy of juvenile rheumatoid arthritis Arzneimittel-forschung 21 (1971) 1865ndash1866
[19] N Ruperto I Nikishina ED Pachanov Y Shachbazian AMPrieur R Mouy R Joos F Zulian R Schwarz V ArtamonovaW Emminger M Bandeira A Buoncompagni I Foeldvari FFalcini E Baildam I Kone-Paut M Alessio V Gerloni ALenhardt A Martini G Hanft R Sigmund S Simianer Arandomized double-blind clinical trial of two doses ofmeloxicam compared with naproxen in children with juvenileidiopathic arthritis short- and long-term efficacy and safetyresults Arthritis Rheum 52 (2005) 563ndash572
[20] I Foeldvari IS Szer LS Zemel DJ Lovell EH Giannini JLRobbins CRWest G Steidle S Krishnaswami BJ Bloom A pro-spective study comparing celecoxib with naproxen in children withjuvenile rheumatoid arthritis J Rheumatol 36 (2009) 174ndash182
191Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
[21] F Zulian G Martini D Gobber C Agosto C Gigante FZacchello Comparison of intra-articular triamcinolone hexa-cetonide and triamcinolone acetonide in oligoarticular juve-nile idiopathic arthritis Rheumatology (Oxford) 42 (2003)1254ndash1259
[22] F Zulian G Martini D Gobber M Plebani F Zacchello PManners Triamcinolone acetonide and hexacetonide intra-articular treatment of symmetrical joints in juvenile idiopathicarthritis a double-blind trial Rheumatology (Oxford) 43 (2004)1288ndash1291
[23] GS Habib Systemic effects of intra-articular corticosteroidsClin Rheumatol 28 (2009) 749ndash756
[24] JR Kirwan The effect of glucocorticoids on joint destructionin rheumatoid arthritis The Arthritis and Rheumatism CouncilLow-Dose Glucocorticoid Study Group N Engl J Med 333(1995) 142ndash146
[25] H Michels What is low-dose corticosteroid therapy in juvenileidiopathic arthritis A worldwide questionnaire-based surveyZ Rheumatol 59 (Suppl 2) (2000) II127ndash130
[26] JJ Miller III Prolonged use of large intravenous steroid pulsesin the rheumatic diseases of children Pediatrics 65 (1980)989ndash994
[27] P Picco M Gattorno A Buoncompagni V Pistoia C Borrone6-methylprednisolone lsquomini-pulsesrsquo a newmodality of glucocor-ticoid treatment in systemic onset juvenile chronic arthritisScand J Rheumatol 25 (1996) 24ndash27
[28] AM Prieur The place of corticosteroid therapy in juvenilechronic arthritis in 1992 J Rheumatol Suppl 37 (1993)32ndash34
[29] JS Gao H Wu J Tian Treatment of patients with juvenilerheumatoid arthritis with combination of leflunomide andmethotrexate Zhonghua Er Ke Za Zhi 41 (2003) 435ndash438
[30] T Niehues G Horneff H Michels MS Hock L SchuchmannEvidence-based use of methotrexate in children with rheumat-ic diseases a consensus statement of the Working Groups Pedi-atric Rheumatology Germany (AGKJR) and PediatricRheumatology Austria Rheumatol Int 25 (2005) 169ndash178
[31] N Ruperto DJ Lovell R Cuttica N Wilkinson P Woo GEspada C Wouters ED Silverman Z Balogh M HenricksonMT Apaz E Baildam A Fasth V Gerloni P Lahdenne AMPrieur A Ravelli RK Saurenmann ML Gamir N WulffraatL Marodi RE Petty R Joos F Zulian D McCurdy BLMyones K Nagy P Reuman I Szer S Travers A BeutlerG Keenan J Clark S Visvanathan A Fasanmade A Ray-chaudhuri A Mendelsohn A Martini EH Giannini A random-ized placebo-controlled trial of infliximab plus methotrexatefor the treatment of polyarticular-course juvenile rheumatoidarthritis Arthritis Rheum 56 (2007) 3096ndash3106
[32] K Visser DM van der Heijde Risk and management of livertoxicity during methotrexate treatment in rheumatoid andpsoriatic arthritis a systematic review of the literature ClinExp Rheumatol 27 (2009) 1017ndash1025
[33] A Cespedes-Cruz R Gutierrez-Suarez A Pistorio A Ravelli ALoy KJ Murray V Gerloni N Wulffraat S Oliveira J WalshIC Penades MG Alpigiani P Lahdenne C Saad-Magalhaes ECortis L Lepore Y Kimura C Wouters A Martini N RupertoMethotrexate improves the health-related quality of life of chil-dren with juvenile idiopathic arthritis Ann Rheum Dis 67(2008) 309ndash314
[34] TK Kvien HM Hoyeraal B Sandstad Azathioprine versus place-bo in patients with juvenile rheumatoid arthritis a single centerdouble blind comparative study J Rheumatol 13 (1986) 118ndash123
[35] E Silverman R Mouy L Spiegel LK Jung RK SaurenmannP Lahdenne G Horneff I Calvo IS Szer K Simpson JAStewart V Strand Leflunomide or methotrexate for juvenilerheumatoid arthritis N Engl J Med 352 (2005) 1655ndash1666
[36] MA van Rossum TJ Fiselier MJ Franssen AH ZwindermanR ten Cate LW van Suijlekom-Smit WH van Luijk RM
van Soesbergen NM Wulffraat JC Oostveen W Kuis PFDijkstra CF van Ede BA Dijkmans Sulfasalazine in the treat-ment of juvenile chronic arthritis a randomized double-blindplacebo-controlled multicenter study Dutch Juvenile ChronicArthritis Study Group Arthritis Rheum 41 (1998) 808ndash816
[37] MA van Rossum RM van Soesbergen M Boers AHZwinderman TJ Fiselier MJ Franssen R ten Cate LW vanSuijlekom-Smit NM Wulffraat WH van Luijk JC OostveenW Kuis BA Dijkmans Long-term outcome of juvenile idiopathicarthritis following a placebo-controlled trial sustained benefits ofearly sulfasalazine treatment Ann Rheum Dis 66 (2007)1518ndash1524
[38] DJ Lovell EH Giannini A Reiff GD Cawkwell ED SilvermanJJ Nocton LD Stein A Gedalia NT Ilowite CA Wallace JWhitmore BK Finck Etanercept in children with polyarticularjuvenile rheumatoid arthritis Pediatric Rheumatology Collabora-tive Study Group N Engl J Med 342 (2000) 763ndash769
[39] DJ Lovell A Reiff OY Jones R Schneider J Nocton LDStein A Gedalia NT Ilowite CA Wallace JB WhitmoreB White EH Giannini Long-term safety and efficacy ofetanercept in children with polyarticular-course juvenile rheu-matoid arthritis Arthritis Rheum 54 (2006) 1987ndash1994
[40] DJ Lovell N Ruperto S Goodman A Reiff L Jung K JarosovaD Nemcova R Mouy C Sandborg J Bohnsack D Elewaut IFoeldvari V Gerloni J Rovensky K Minden RK Vehe LWWeiner G Horneff HI Huppertz NY Olson JR Medich RCarcereri-De-Prati MJ McIlraith EH Giannini A MartiniAdalimumab with or without methotrexate in juvenile rheuma-toid arthritis N Engl J Med 359 (2008) 810ndash820
[41] FH Prince M Twilt R ten Cate MA van RossumW ArmbrustEP Hoppenreijs M van Santen-Hoeufft Y Koopman-KeeminkNM Wulffraat LW van Suijlekom-Smit Long-term follow-upon effectiveness and safety of etanercept in juvenile idiopathicarthritis the Dutch National Register Ann Rheum Dis 68(2009) 635ndash641
[42] P Diak J Siegel L LaGrenade L Choi S Lemery AMcMahonTumor necrosis factor alpha blockers andmalignancy in childrenforty-eight cases reported to the Food and Drug AdministrationArthritis Rheum 62 (2010) 2517ndash2524
[43] G Horneff T Hospach G Dannecker D Foll JP Haas HJGirschick HI Huppertz R Keitzer HJ Laws H Michels KMinden R Trauzeddel Updated statement by the German So-ciety for Pediatric and Adolescent Rheumatology (GKJR) on theFDAs report regarding malignancies in anti-TNF-treated pa-tients from Aug 4 2009 Z Rheumatol 69 (2010) 561ndash567
[44] T Hospach JP Haas HI Huppertz R Keitzer H Michels RTrauzeddl D Foll G Dannecker G Horneff Comment of theSociety of Pediatric and Adolescent Rheumatology on the USFood and Drug Administration (FDA) announcement regardingcases of malignancy in anti-TNF-treated patients Z Rheumatol68 (2009) 162ndash164
[45] DJ Lovell A Reiff NT Ilowite CA Wallace Y Chon SL LinSW Baumgartner EH Giannini Safety and efficacy of up to eightyears of continuous etanercept therapy in patients with juvenilerheumatoid arthritis Arthritis Rheum 58 (2008) 1496ndash1504
[46] EH Giannini NT Ilowite DJ Lovell CA Wallace CERabinovich A Reiff G Higgins B Gottlieb NG Singer YChon SL Lin SW Baumgartner Long-term safety and effec-tiveness of etanercept in children with selected categories ofjuvenile idiopathic arthritis Arthritis Rheum 60 (2009)2794ndash2804
[47] G Horneff H Schmeling T Biedermann I Foeldvari G GanserHJ Girschick T Hospach HI Huppertz R Keitzer RM KusterH Michels D Moebius B Rogalski A Thon The German etaner-cept registry for treatment of juvenile idiopathic arthritis AnnRheum Dis 63 (2004) 1638ndash1644
[48] FH Prince M Twilt SC Simon MA van RossumW ArmbrustEP Hoppenreijs S Kamphuis M van Santen-Hoeufft Y
192 G Dueckers et al
Koopman-Keemink NM Wulffraat R ten Cate LW vanSuijlekom-Smit When and how to stop etanercept aftersuccessful treatment of patients with juvenile idiopathic ar-thritis Ann Rheum Dis 68 (2009) 1228ndash1229
[49] G Horneff F De Bock I Foeldvari HJ Girschick H MichelsD Moebius H Schmeling Safety and efficacy of combinationof etanercept and methotrexate compared to treatment withetanercept only in patients with juvenile idiopathic arthritis(JIA) preliminary data from the German JIA Registry AnnRheum Dis 68 (2009) 519ndash525
[50] N Ilowite O Porras A Reiff S Rudge M Punaro A Martin RAllen T Harville YN Sun T Bevirt G Aras B Appleton Ana-kinra in the treatment of polyarticular-course juvenile rheumatoidarthritis safety and preliminary efficacy results of a randomizedmulticenter study Clin Rheumatol 28 (2009) 129ndash137
[51] T Lequerre P Quartier D Rosellini F Alaoui M De BandtO Mejjad I Kone-Paut M Michel E Dernis M Khellaf NLimal C Job-Deslandre B Fautrel X Le Loet J Sibilia In-terleukin-1 receptor antagonist (anakinra) treatment in pa-tients with systemic-onset juvenile idiopathic arthritis oradult onset Still disease preliminary experience in FranceAnn Rheum Dis 67 (2008) 302ndash308
[52] M Gattorno A Piccini D Lasiglie S Tassi G Brisca S CartaL Delfino F Ferlito MA Pelagatti F Caroli A BuoncompagniS Viola A Loy M Sironi A Vecchi A Ravelli A Martini ARubartelli The pattern of response to anti-interleukin-1 treatmentdistinguishes two subsets of patients with systemic-onset juvenileidiopathic arthritis Arthritis Rheum 58 (2008) 1505ndash1515
[53] S Yokota T Imagawa M Mori T Miyamae Y Aihara STakei N Iwata H Umebayashi T Murata M Miyoshi MTomiita N Nishimoto T Kishimoto Efficacy and safety oftocilizumab in patients with systemic-onset juvenile idiopathicarthritis a randomised double-blind placebo-controlledwithdrawal phase III trial Lancet 371 (2008) 998ndash1006
[54] N Ruperto DJ Lovell P Quartier E Paz N Rubio-Perez CASilva C Abud-Mendoza R Burgos-Vargas V Gerloni JAMelo-Gomes C Saad-Magalhaes F Sztajnbok C Goldenstein-Schainberg M Scheinberg IC Penades M Fischbach J OrozcoPJ Hashkes C Hom L Jung L Lepore S Oliveira CAWallace LH Sigal AJ Block A Covucci A Martini EHGiannini Abatacept in children with juvenile idiopathic arthri-tis a randomised double-blind placebo-controlled withdrawaltrial Lancet 372 (2008) 383ndash391
[55] N Ruperto DJ Lovell P Quartier E Paz N Rubio-PerezCA Silva C Abud-Mendoza R Burgos-Vargas V GerloniJA Melo-Gomes C Saad-Magalhaes J Chavez-Corrales CHuemer A Kivitz FJ Blanco I Foeldvari M Hofer G HorneffHI Huppertz C Job-Deslandre A Loy K Minden M PunaroAF Nunez LH Sigal AJ Block M Nys A Martini EHGiannini Long-term safety and efficacy of abatacept inchildren with juvenile idiopathic arthritis Arthritis Rheum 62(2010) 1792ndash1802
[56] DM Brinkman IM de Kleer R ten Cate MA van RossumWP Bekkering A Fasth MJ van Tol W Kuis NM WulffraatJM Vossen Autologous stem cell transplantation in childrenwith severe progressive systemic or polyarticular juvenile idio-pathic arthritis long-term follow-up of a prospective clinicaltrial Arthritis Rheum 56 (2007) 2410ndash2421
[57] SE Klepper Effects of an eight-week physical conditioningprogram on disease signs and symptoms in children with chronicarthritis Arthritis Care Res 12 (1999) 52ndash60
[58] D Singh-Grewal J Schneiderman-Walker V Wright O Bar-OrJ Beyene H Selvadurai B Cameron RM Laxer R SchneiderED Silverman L Spiegel S Tse C Leblanc J Wong SStephens BM Feldman The effects of vigorous exercisetraining on physical function in children with arthritis arandomized controlled single-blinded trial ArthritisRheum 57 (2007) 1202ndash1210
[59] S Stephens D Singh-Grewal O Bar-Or J Beyene B CameronCM Leblanc R Schneider J Schneiderman-Walker HSelvadurai E Silverman L Spiegel SM Tse V WrightBM Feldman Reliability of exercise testing and functionalactivity questionnaires in children with juvenile arthritisArthritis Rheum 57 (2007) 1446ndash1452
[60] T Takken J van der Net W Kuis PJ Helders Physical ac-tivity and health related physical fitness in children with ju-venile idiopathic arthritis Ann Rheum Dis 62 (2003)885ndash889
[61] MM Toledo G Martini C Gigante L Da Dalt A TregnaghiF Zulian Is there a role for arthroscopic synovectomy in oli-goarticular juvenile idiopathic arthritis J Rheumatol 33(2006) 1868ndash1872
[62] F de Benedetti H Brunner N Ruperto SWright A KenwrightR Cuttica P Woo R Schneider DJ Lovell A Martini Efficacyand safety of Tocilizumab in patients with systemic juvenile idio-pathic arthritis (sJIA) 12-week data from the phase III TENDERtrial Ann Rheum Dis 69 (2010) 146
[63] P Quartier F Allantaz R Cimaz P Pillet C Messiaen CBardin X Bossuyt A Boutten J Bienvenu A Duquesne ORicher D Chaussabel A Mogenet J Banchereau JM Tre-luyer P Landais V Pascual A multicentre randomiseddouble-blind placebo-controlled trial with the interleukin-1receptor antagonist anakinra in patients with systemic-onsetjuvenile idiopathic arthritis (ANAJIS trial) Ann Rheum Dis70 (2011) 747ndash754
[64] DE Furst EC Keystone J Braun FC Breedveld GRBurmester F De Benedetti T Dorner P Emery R FleischmannA Gibofsky JR Kalden A Kavanaugh B Kirkham P Mease JSieper NG Singer JS Smolen PL Van Riel MH Weisman KWinthrop Updated consensus statement on biological agents forthe treatment of rheumatic diseases 2010 Ann Rheum Dis 70(Suppl 1) (2010) i2ndashi36
[65] T Beukelman NM Patkar KG Saag S Tolleson-RinehartRQ Cron EM Dewitt NT Ilowite Y Kimura RM LaxerDJ Lovell A Martini CE Rabinovich N Ruperto 2011 Ameri-can College of Rheumatology recommendations for the treatmentof juvenile idiopathic arthritis initiation and safety monitoring oftherapeutic agents for the treatment of arthritis and systemic fea-tures Arthritis Care Res 63 (2011) 465ndash482 (Hoboken)
[66] JF Simard M Neovius S Hagelberg J Askling Juvenile idi-opathic arthritis and risk of cancer a nationwide cohort studyArthritis Rheum 62 (2010) 3776ndash3782
[67] T Imagawa S Yokota M Mori T Miyamae S Takei H ImanakaY Nerome N Iwata T Murata M Miyoshi N Nishimoto TKishimoto Safety and efficacy of tocilizumab an anti-IL-6-receptor monoclonal antibody in patients with polyarticular-course juvenile idiopathic arthritis Mod Rheumatol (2011)doi102007s10165-011-0481-0
[68] TM Shaneyfelt MF Mayo-Smith J Rothwangl Are guide-lines following guidelines The methodological quality of clini-cal practice guidelines in the peer-reviewed medicalliterature Jama 281 (1999) 1900ndash1905
[69] R Grilli N Magrini A Penna G Mura A Liberati Practiceguidelines developed by specialty societies the need for a crit-ical appraisal Lancet 355 (2000) 103ndash106
[70] JS Burgers R Grol NS Klazinga M Makela J Zaat To-wards evidence-based clinical practice an international surveyof 18 clinical guideline programs Int J Qual Health Care 15(2003) 31ndash45
[71] JT Cassidy RE Petty Juvenile Idiopathic Rheumatic Arthri-tis 5th Edition WB Saunders Philadelphia 2005
[72] TJ Lehman Are withdrawal trials in paediatric rheumatic dis-ease helpful Lancet 372 (2008) 348ndash350
[73] J Munro Recommendations for the Diagnosis and Managementof Juvenile Idiopathic Arthritis The Royal Australian Collegeof General Practitioners South Melbourne 2009 pp 1ndash38
193Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
httpwwwnhmrcgovau_files_nhmrcpublicationsattachmentscp119-juvenile-arthritispdf
[74] MJ Santos JE Fonseca H Canhao M Conde M JoseVieira L Costa M Costa M Salgado JA Melo Gomes Guide-lines for prescribing and monitoring biologic therapies in juve-nile idiopathic arthritis Acta Reumatol Port 32 (2007) 43ndash47
[75] S Yokota M Mori T Imagawa T Murata M Tomiita Y ItohS Fujikawa S Takei Guidelines on the use of etanercept forjuvenile idiopathic arthritis in Japan Mod Rheumatol 20(2010) 107ndash113
[76] The AGREE Collaboration Appraisal of Guidelines for Researchamp Evaluation (AGREE) instrument wwwagreecollaborationorg
[77] I Kopp H Thole T Langer HK Selbmann G OllenschlaumlgerGerman Instrument for Methodological Guideline Appraisal(DELBI) wwwversorgungsleitliniende2008
[78] Auml Aumlrztliches Zentrum fuumlr Qualitaumlt in der Medizin A Arbeitsge-meinschaften der Wissenschaftlichen Fachgesellschaften in derMedizin Deutsches Instrument zur methodischen Leitlinien-Bewertung (DELBI) Fassung 20052006 Z Aumlrztl FortbildQualitaumltssich 99 (2005) 468ndash519
[79] MP de Wit SE Berlo GJ Aanerud D Aletaha JW BijlsmaL Croucher JA Da Silva B Glusing L Gossec S Hewlett MJongkees D Magnusson M Scholte-Voshaar P Richards CZiegler TA Abma European League Against Rheumatism rec-ommendations for the inclusion of patient representatives in sci-entific projects Ann Rheum Dis 70 (2011) 722ndash726
[80] I Foeldvari M Bidde Validation of the proposed ILAR classifi-cation criteria for juvenile idiopathic arthritis InternationalLeague of Associations for Rheumatology J Rheumatol 27(2000) 1069ndash1072
[81] R Merino J de Inocencio J Garcia-Consuegra Evaluation ofrevised International League of Associations for Rheumatologyclassification criteria for juvenile idiopathic arthritis in Spanishchildren (Edmonton 2001) J Rheumatol 32 (2005) 559ndash561
[82] SE Ramsey RK Bolaria DA Cabral PN Malleson REPetty Comparison of criteria for the classification of childhoodarthritis J Rheumatol 27 (2000) 1283ndash1286
[83] G Horneff A Ebert S Fitter K Minden I Foeldvari J Kum-merle-Deschner A Thon HJ Girschick F Weller HI Hup-pertz Safety and efficacy of once weekly etanercept 08mgkg in a multicentre 12 week trial in active polyarticularcourse juvenile idiopathic arthritis Rheumatology (Oxford) 48(2009) 916ndash919
[84] EH Giannini EJ Brewer N Kuzmina A Shaikov A Maxi-mov I Vorontsov CW Fink AJ Newman JT Cassidy LSZemel Methotrexate in resistant juvenile rheumatoid arthri-tis Results of the USAndashUSSR double-blind placebo-controlled trial The Pediatric Rheumatology CollaborativeStudy Group and The Cooperative Childrens Study GroupN Engl J Med 326 (1992) 1043ndash1049
[85] A Ravelli S Viola D Migliavacca N Ruperto A Pistorio AMartini The extended oligoarticular subtype is the best predic-tor of methotrexate efficacy in juvenile idiopathic arthritisJ Pediatr 135 (1999) 316ndash320
[86] P Woo TR Southwood AM Prieur CJ Dore J Grainger JDavid C Ryder N Hasson A Hall I Lemelle Randomizedplacebo-controlled crossover trial of low-dose oral
methotrexate in children with extended oligoarticular or sys-temic arthritis Arthritis Rheum 43 (2000) 1849ndash1857
[87] E Silverman L Spiegel D Hawkins R Petty D Goldsmith LSchanberg C Duffy P Howard V Strand Long-term open-label preliminary study of the safety and efficacy of lefluno-mide in patients with polyarticular-course juvenile rheumatoidarthritis Arthritis Rheum 52 (2005) 554ndash562
[88] DJ Lovell EH Giannini Y Kimura C Suzanne PJHashkes A Reiff Long-term safety and efficacy of rilonaceptin patients with systemic juvenile idiopathic arthritis (SJIA)Arthritis Rheum 60 (2009)
[89] N Ruperto P Quartier NWulffraat PWoo A Loy R Mouy BBader-Meunier BJ Prakken E Noseda R Belleli J Lecot CRordorf A Martini A Phase II Trial with canakinumab(ACZ885) a new IL-1-beta blocking monoclonal antibody toevaluate safety and preliminary efficacy in children with system-ic juvenile idiopathic arthritis Ann Rheum Dis 68 (2009) 170
[90] DJ Lovell EH Giannini Y Kimura et al Preliminary evi-dence for bioactivity of IL-1 trap (Rilonacept) a long actingIL-1 inhibitor in systemic juvenile idiopathic arthritis (sJIA)Arthritis Rheum 54 (2006) S325
[91] DJ Lovell EH Giannini Y Kimura et al Preliminary evi-dence for sustained bioactivity of IL-1 Trap (rilonacept) a longacting IL-1 inhibitor in systemic juvenile idiopathic arthritisArthritis Rheum 56 (2007) S514
[92] N Ruperto F De Benedetti H Brunner R Allen D Brown JChaitow E Cortis G Espada B Flato V Gerloni G HorneffS Wright A Kenwright R Schneider P Woo A Martini DJLovell Tocilizumab is efficacious in patients with systemic ju-venile idiopathic arthritis (sJIA) across baseline disease charac-teristics and priorbaseline treatments 12-week data from thephase II TENDER trial 17th PReS Congress Valencia Spain2010 2010
[93] N Ruperto DJ Lovell T Li F Sztajnbok C Goldenstein-Schainberg M Scheinberg IC Penades M Fischbach JOrozco PJ Hashkes C Hom L Jung L Lepore S OliveiraC Wallace M Alessio P Quartier E Cortis A Eberhard GSimonini I Lemelle E Chalom LH Sigal A Block A CovucciM Nys A Martini EH Giannini Abatacept improves health-related quality of life pain sleep quality and daily participationin subjects with juvenile idiopathic arthritis Arthritis Care Res(Hoboken) 62 (11) (2010) 1542ndash1551
[94] N Ruperto DJ Lovell P Quartier E Paz N Rubio-PerezCA Silva C Abud-Mendoza R Burgos-Vargas V GerloniJA Melo-Gomes C Saad-Magalhaes J Chavez C HuemerA Kivitz FJ Blanco I Foeldvari M Hofer G Horneff HIHuppertz CJ Deslandre A Loy K Minden M Punaro AFNunez LH Sigal AJ Block M Nys A Martini EH GianniniLong-term safety and efficacy of abatacept in children with ju-venile idiopathic arthritis Arthritis Rheum 62 (2010)1792ndash1802
[95] J Munro Juvenile Idiopathic Arthritis Management Guidelines(Provisional) Australian Paediatric Rheumatology Group 2006httpwwwnhmrcgovau
[96] K Fitch SJ Bernstein MD Aguilar B Burnand JR LaCalleP Lazaro M van het Loo J McDonnell JP Vader JPKahan The RANDUCLA Appropriateness Method Users ManualRAND Pittsburgh 2000

177Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
Received 18 August 2011 accepted with revision 19 October 2011Available online 26 October 2011
KEYWORDSJuvenile idiopathic arthritisTreatmentGuidelineConsensusChildren and adolescents
Abstract Juvenile idiopathic arthritis (JIA) is the most common rheumatic disease in children andadolescents Immunomodulatory drugs are used frequently in its treatment Using the nominal grouptechnique (NGT) andDelphimethod we created amultidisciplinary evidence- and consensus-basedtreatment guideline for JIA based on a systematic literature analysis and three consensus confer-ences Conferenceswere headed by a professionalmoderator and were attended by representativeswho had been nominated by their scientific societies or organizations 15 statements regarding drugtherapy symptomatic and surgical management were generated It is recommended that initially
JIA is treated with NSAID followed by local glucocorticoids andor methotrexate if unresponsiveComplementing literature evidence with long-standing experience of caregivers allows creatingguidelines that may potentially improve the quality of care for children and adolescents with JIAcopy 2011 Elsevier Inc All rights reserved
1 Introduction
11 Background aims and addressees
Juvenile idiopathic arthritis (JIA) is defined by the InternationalLeague of Associations for Rheumatology (ILAR) [1] JIA is ahighly heterogeneous disorder Some of the subtypes of JIAare clearly distinct from others also in regard of immunopatho-physiology eg systemic onset of JIA is now thought to be anautoinflammatory disease Treatment of JIA subtypes maythus vary significantly [2] JIA shows substantial impact on pa-tients physical abilities psychological function and quality oflife [34] Therefore treatment goals are pain relief the elimi-nation of active disease the normalization of physical functionthe achievement of normal growth and development and im-provement of quality of life Appropriate initial managementcontinuous comprehensive and consistent care offer thechance of the prevention of long term sequels [56] The Ger-man consensus group for treatment of JIA systematically devel-oped guidelines for treatment of JIA in 1999 2005 and 2008[78] Our guideline is addressed to physicians in medical prac-tices and hospitals allied health professionals physiothera-pists occupational therapists and all people who are involvedin the treatment care and follow-up of children or adolescentswith JIA Our aim is to provide clear evidence- and consensusbased recommendations for the treatment of children and ado-lescents with JIA within a multidisciplinary setting The guide-line focuses on JIA and does not cover the issue of treatmentresistant cases complex or unusual forms of arthritis and doesnot consider all ILAR subtypes of JIA individually Subtype spe-cific recommendations are highlighted separately eg treat-ment schemes for oligo- polyarticular or systemic onset JIA
2 Methodology
21 Members of the consensus group and consensusconferences
Scientific societies and organizations (Table 1) representingpediatricians in medical practices and hospitals adult and
pediatric rheumatologists orthopedic surgeons ophthalmol-ogists surgeons physiotherapists psychologists nationaland local support-groups for parents and children nominatedrepresentatives for the participation in consensus confer-ences The scope of the conferences was the implementationof evidence and consensus based guideline for the treatmentof JIA in children and adolescents Consensus conferenceswere held at Duesseldorf respectively Krefeld (Germany) onthe 9th of May 2007 1st of August 2007 and 15th of January2010 and were all attended by N95 of the representatives
22 Literature search and literature review
Based on existing guidelines [78] we conducted a systematicliterature search in Medline (httpwwwncbinlmnihgovpubmed) (deadline of search 15th January 2010 terms ldquoju-venile idiopathic (rheumatoid) arthritisrdquo and ldquotherapyrdquolimits ldquohumansrdquo ldquopublished in the last 3 yearsrdquo ldquoall child0ndash18 yearsrdquo ldquoclinical trialrdquo) Studies relating to diagnosis ofJIA uveitis vaccination transition rofecoxibe Ca-supplementation and costs were excluded manually The ex-clusion was necessary due to varying target groups and lossof market approval by European Medical agency (EMA) respec-tively [9] Final results of the literature review are as shown inFig 1 These studies were evaluated for quality of methodolo-gy following the definitions of evidence level and recommen-dation grade as published by Feldmann et al [10] (Table 2 andTable 3) Thirteen studies were judged as relevant for the2010 update of treatment guidelines for JIA (Table 4) Todraft guideline statements the core conclusions of studieswere discussed and formal consensus building followed thenominal group technique (NGT) [11] and Delphi method [12]
23 Consensus process
The consensus process was externally and independentlysupervised by the Association of the Scientific MedicalAssociations (AWMF) who has membership of Council for In-ternational Organizations of Medical Sciences (CIOMS) TheAWMF coordinates the systematic development of diagnostic
Table 1 Representatives nominated for the consensus group by scientific societies and professional organizations
Name Representing scientific societies or professional organisations
Arbogast M Association of Paediatric Orthopaedic SurgeonsDannecker G German Society of Paediatrics and Adolescent Medicine (DGKJ)Dueckers G (coordinator)Foeldvari I German Society for Paediatric Rheumatology (GKJR)Frosch M GKJRGanser G GKJRGuellac N (coordinator)Heiligenhaus A German Society for Ophthalmology (DOG)Horneff G GKJRIllhardt A German Society for Psychology (DGPs)Krauspe R Association of Paediatric Orthopaedic SurgeonsKopp I (moderator)Markus B National support group of parents and children with JIAmdashRheuma LigaMichels S GKJRNiehues T (coordinator) GKJRSchneider M German Society of Rheumatology (DGRh)Singendonk W Association of Paediatricians in private practice (BVKJ)Sitter H (moderator) Association of the Scientific Medical Associations (AWMF)Spamer M National Association of PhysiotherapistsWagner N German Society of Paediatrics and Adolescent Medicine (DGKJ)
178 G Dueckers et al
and treatment guidelines for medical scientific societiesand organizations in Germany
24 Consensus building nominal group technique(NGT)
Consensus building was headed by a professional moderators(HS IK) The moderator of the consensus conferences
Literature search 2007
(deadline June 30th 2007) [7]
Mesh terms ldquojuvenile idiopathic (rheumatoid)
arthritisrdquo and ldquotherapyrdquo
dArr n = 3138
Limits ldquohumansrdquo ldquopublished in the last 3
yearsrdquo ldquoall child 0-18rdquo
dArr n = 193
Limit ldquoclinical trialrdquo
dArr n = 52
Exclusion of studies relating to
diagnosis of JIA uveitis vaccination
transition rofecoxibe
rArr n = 22
Figure 1 Literature se
explained the purpose method and procedure of consensusfinding Representatives gave brief presentations of literatureand core conclusions for the guideline draft A formal consensusprocess led to adoption of guidelines for treatment of JIA Asformal consensus procedure we used NGT involving six stages
1 Silent review of the guideline draft and noting of comments andideas by the participants During this period participants did notconsult or discuss with others
Literature search 2010
(published June 30th 2007 ndash January 15th
2010)
Mesh terms ldquojuvenile idiopathic (rheumatoid)
arthritisrdquo and ldquotherapyrdquo
Limits ldquohumansrdquo ldquopublished in the last 3
yearsrdquo ldquoall child 0-18rdquo ldquoclinical trialrdquo
dArr n = 17
Exclusion of studies relating to
diagnosis of JIA uveitis vaccination
transition studies without control groups
Calcium supplementation costs
rArrrArr n = 13
arch 2007 and 2010
Table 3 Recommendation grade [10]
Recommendationgrade
Definition
A There is good evidence to support the recommendation that the intervention be performedB There is fair evidence to support the recommendation that the intervention be performedC There is poor evidence regarding the value or harm of the intervention recommendations may be made on
other groundsD There is fair evidence to support the recommendation that the intervention not be performedE There is good evidence to support the recommendation that the intervention not be performed
Table 2 Evidence level [10]
Evidencelevel
Definition
I Evidence obtained from at least one properly designed randomized controlled trialII Evidence obtained from well-designed controlled trials without randomization or from well-designed cohort or
casendashcontrol analytic studies preferably from more than one center or research group or from multiple time serieswith or without the intervention Dramatic results in uncontrolled trials might also be regarded as this type ofevidence
III Opinions of respected authorities based on clinical experience descriptive studies or reports of expertcommittees
179Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
2 Collocation of comments and ideas by the moderator using thewords of the participants
3 Clarification and substantiation of comments and ideas on alter-native guideline statements by the participants
4 Reconcilement of the manuscript and all alternative guidelinestatements
Table 4 Studies for 2010 update identified by the MEDLINE sear
Drugtreatment Mean age(age range) ofparticipants atstudy (years)
Totaof pa
Foeldvari et al [20] Celecoxibe 103 (2ndash16) 264Ceacutespedes-Cruzet al [33]
MTX 82 (np) 521
Lovell et al [45] Etanercept 104 (4ndash17) 58Horneff et al [83] Etanercept 129 (4ndash17) 20Giannini et al [46] Etanercept 99 (2ndash18) 594Lovell et al [40] Adalimumab 113 (4ndash17) 171Ruperto et al [31] Infliximab 112 (4ndash18) 121Lequerreacute et al [51] Anakinra 124 f (3ndash23) 20 f
Illowite et al [50] Anakinra 12 (2ndash17) 86Yokota et al [53] Tozilizumab 83 (2ndash19) 65Ruperto et al [54] Abatacept 124 (6ndash17) 190Singh-Grewal et al [58] Vigorous exercise
training116 (8ndash16) 80
Brinkmann et al [56] Stem celltransplantation
85 (4ndash18) 22
Abbreviations np = not provideda Not further specifiedb Only extended oligoarticular JIAc Pauciarticular onset with polyarticular coursed Extended oligoarticular JIA were included into polyarticular JIAe All JIA with polyarticular course with any type of onset not furthef Pediatric patients total number of patients in extended report wa
5 Discussion of statements and further explanation of any of thecomments that were not clear to all participants Each memberof the consensus group contributed to the discussion The moder-ator kept the process as neutral as possible avoiding judgmentand criticism
6 Final reconcilement for statements for guideline
ch algorithm (see Methodology)
l numbertients (n)
JIA
Oligoarticular Polyarticular Systemiconset
Othersubtypes
128 (53) a 114 (47) 22 (9)162 (31) b 284 (55) 75 (14)
5 (9) c 34 (58) 19 (33)2 (10) b 16 (80) 2
d 535 (90) 58 (97) 1171 (100) e
28 (23) c 74 (61) 19 (16)20 (100)
9 (10) c 62 (72) 15 (17)56 (100)
30 (16) 122 (64) 37 (20) 118 (23) 34 (43) 7 (9) 21 (26)
4 (18) 18 (82)
r specifieds 35 (15 were patients with adult onset of Still disease)
Consensus statement
NSAIDs are recommended for the treatmentof JIA Diclofenac Naproxen Ibuprofen andIndometacin (evidence level I respectively IIrecommendation grade A)If those drugs are contraindicated Celecoxibemight be used (evidence level I recommendationlevel BndashC)
Consensus statement
Intra-articular injections of crystalloid cortico-steroids (triamcinolone hexacetonide) are recom-mended and can be part of the first linetreatment Improvement of local inflammationpain swelling and range of joint movement hasbeen demonstrated (evidence level II recommen-dation grade A)Triamcinolone hexacetonide is more efficientthan triamcinolone acetonide inducing local remis-sion (evidence level I recommendation grade B)
180 G Dueckers et al
The conference guideline topics were reviewed andedited by working groups After the first consensus confer-ence statements were adopted by NGT and additional pro-posals for schemes of treatment strategies of JIA werecollated
25 Consensus finding method of Delphi
Three out of 15 statements remained without consensusafter NGT These statements comprise the utility of etaner-cept (treatment resistant polyarticular JIA) sulfasalazine(treatment resistant JIA) and anakinra (treatment for refrac-tory SoJIA) Therefore they were sent to all participants ofconsensus conferences via email To each of them partici-pants should state one of three votes (ldquoagreerdquo ldquodo notagreerdquo or ldquoalternative proposalrdquo) (1st round of Delphi)The results were summarized and the statements whichremained with no consensus after 1st round of Delphi weresent to participants again (2nd round of Delphi) After 2ndround of Delphi results were sent to external review
26 External review and adoption
The guideline manuscript has been reviewed in 2007 by na-tional experts in German Rheumatology Huppertz (BremenGermany) Michels (Garmisch Partenkirchen Germany) andSpecker (Essen Germany) The comments of external re-viewers (HI Huppertz) to the 2011 manuscript were in-volved within the 3rd round of Delphi External reviewenabled adoption of the guidelines core conclusions andstatements with strong consensus ie 95 agreement byrepresentatives of participating scientific societies andorganizations
3 Results treatment guidelines
31 Drug-based therapy
Drugs used in treatment of JIA are summarized in Table 5 Pro-posed schemes of treatment of JIA are shown in Fig 2 The fol-lowing paragraphs will highlight specific adverse reactions andintroduce the 13 studies relevant for the 2010 update of treat-ment guideline for JIA briefly For detailed information aboutprescribing information including indication contraindica-tion drug dosage route of administration monitoring andproduct characteristics the consensus group recommendsconsulting national drug data bases e g wwwrotelistede(German database of drugs with national market approval) orwwwfdaorg or wwwemaeuropaeu
311 Non-steroidal anti-inflammatory drugs (NSAIDs)Commonly NSAIDs are well tolerated Main side effects
of NSAIDs are stomach irritation dyspepsia andmdashin rarecasesmdashnephritis Cephalgia and behavioral changes can beassociated with the administration of ibuprofen Pseudo-porphyria is not uncommon in patients treated withnaproxen Pain relief has been demonstrated for Naproxen[13ndash15] Diclofenac [1516] and Ibuprofen [17] (evidencelevel I) and for Indometacin [18] and Meloxicam [19](evidence level II) Efficacy of Celecoxibe has been
demonstrated in a randomized double blind multicenterstudy [20] 95 of 212 patients entered the 12 week openlabel phase after a 12 week double blind phase in threetreatment groups (Celecoxibe 6 mgkgd versus Celecoxibe12 mgkgd versus Naproxen 15 mgkgd) Both dosages ofCelecoxibe showed comparable efficacy compared toNaproxen Safety ie number of adverse events (AE)did not differ significantly between Celecoxibe versusNaproxen
312 Glucocorticoids
3121 Glucocorticoids (GC)mdashlocal administration Theuse of intra-articular crystalline corticoids is highly potentand has a rather low rate of complications (evidence levelII) [2122] They might be administered as first line therapyResponse rate was significantly higher with triamcinolonehexacetonide than with triamcinolone acetonide at6 months and this difference was sustained to 24 months[2122] These findings were independent of duration andextent of disease [2122] Simultaneous intra-articular ste-roid injections are preferable to consecutive injections atdifferent time points (limited suppression of hypothalamicndashpituitaryndashadrenal axis) [23] Side effects eg local necrosisof fat tissue are seen in approximately 2 of injections [22]Working under sterile conditions the risk of infection is low
3122 GCmdashsystemic administration GC can be adminis-tered as a fast acting drug in highly active disease Indica-tions for their use are bridging time until DMARDs (diseasemodifying anti rheumatic drugs) become effective treat-ment of severe systemic features of systemic-onset JIA(SoJIA) induction of remission in polyarticular JIA and in se-vere forms of uveitis There are no controlled trials and nostandardized therapeutic regimes for the use of systemic
Table 5 Drugs for the treatment of JIA
Generic Dosage Age approval by Europeanmedical agency inpediatric rheumatology(EMA) a
Medical indication in pediatricrheumatology a b
Evidence levelrecommendationgrade [10]
Literature
NSAIDsDiclofenac 2ndash3 mgkg Bwd po (in 3 doses)
Retard formulation 1 dose14 years Arthritis IndashA Haapasiri [16] Laxer [14]
Ibuprofen 20ndash40 mgkg Bwd po in 3ndash4doses
6 months Pain fever IndashA Giannini [17]
Indometacin 1ndash3 mgkg Bwd po in 3 doses 2 years Arthritis IIndashA Stoeber [18]Meloxicam 0125ndash025 mgkg Bwd po 15 years Arthritis II Ruperto [19]Naproxen 10ndash15 mgkg Bwd po in 2 doses 1 year Arthritis IndashA Kvien [13] Laxer [14] Leak
[15]Celecoxibe 6 mgkg Bwd po in 2 doses or
12 mgkg Bwd in 1 doseNo approval for children Arthritis I B-C Foeldvari [20]
Glucocorticoids (GC)a) Systemic GCPrednisonePrednisolone
01ndash02 mgkg Bwd (max 5 mgd) JIA ie severe SoJIA severe peri-myokarditis severe uveitis (hypotoniaor cystoid macular edema) intoleranceto other drugs (ldquolow-doserdquo) or asldquobridgingrdquo therapy in higher doses eg2 mgkg Bwd until therapeutic effectof ldquoDMARDsrdquo
III Prieur [28]
Prednisone as an oralhigh-dose therapy
ge1ndash2 mgkg Bwd prednisolone-equivalent
III Prieur [28]
Prednisone as an oralmedium-dosetherapy
02 tob10 mgkg Bwdprednisolone-equivalent
III Kirwan [24] Prieur [28]
Prednisone as an orallow-dose therapy
b02 mgkg Bwd Prednisolone-equivalent or b4 mgmsup2 bodysurface
III Michels [25]
Prednisone as a ivpulse-therapy
N(5)ndash10 mgkg Bw (po)Prednisolone-equivalent10ndash30 mgkg Bwd Methyl-Prednisolone iv for 1ndash3 d(maximum 1 gdose)
III Miller [26] Picco [27]
b) Intra-articular GCTriamcinolonehexacetonide
05ndash1 mgkg Bw into large jointsdose adaption referring to size ofjoint (eg max 2 mg intointerphalangeal joints c)
5 months Arthritis tendo-vaginitis I Zulian [2122]
(continued on next page)(continued on next page)
181Evidence
andconsensus
basedGKJR
guidelinesfor
thetreatm
entof
juvenileidiopathic
arthritis
Table 5 (continued)
Generic Dosage Age approval by Europeanmedical agency inpediatric rheumatology(EMA) a
Medical indication in pediatricrheumatology a b
Evidence levelrecommendationgrade [10]
Literature
DMARDsSulfasalazine 30ndash50 mgkg Bwd in 2ndash3 doses 6 years Arthritis II Van Rossum [3637]Cytotoxic or immuno-suppressive drugsMethotrexate 10ndash15 (20) mgmsup2 body surface
once a week (po sc iv) e2 years Polyarticular JIA Psoriasis arthritis
uveitis CollagenosisI Giannini [84] Ravelli [85]
Woo [86]Cespedes-Cruz [33]Azathioprine 15ndash3 mgkg Bwd po in 1ndash2
dosesNo approval for children II Kvien [34]
Leflunomide No clear recommendation forchildren availableBwb20 kg d 1100 mgkg from d 2 10 mgkgdBw 20ndash40 kg d 1 to d 2 100 mgkgfrom d 3 10ndash20 mgkgdBwN40 kg d 1 to d 3 100 mgkgfrom d 3 20 mgkgd
No approval for children II Silverman [3587]
Biologic agentsa) TNFα inhibitorsEtanercept d 08 mgkg Bw sc 1timesweek
(max 50 mgweek) or 04 mgkgBw sc 2timesweek (max 50 mgweek)
4 years JIA Polyarthritis and insufficientefficacy of MTX
I Giannini [46] Horneff [49]Lovell [3888] Prince [41]
Adalimumab d 24 mgm2 body surface sc in 1dose every 2 weeks Bwb30 kg20 mgm2 body surface BwN30 kg40 mgm2 body surface(max 40 mg per dose)
4 years to 17 years Adalimumab in combination withmethotrexate is indicated for thetreatment of active polyarticularjuvenile idiopathic arthritis in childrenand adolescents who have had aninadequate response to one or moredisease-modifying anti-rheumatic drugs(DMARDs)
I Lovell [40]
182GDueckers
etal
Infliximab d 3ndash10 mgkg Bwdose iv Infusionat d 0 d 14 d 42 then every8 weeks intervals of applicationremain unclear
No approval for childrenwith JIA6 years (approval forMorbus Crohn)
III Ruperto [31]
b) IL-1 inhibitorsAnakinra d 1ndash4 mgkg Bwd sc in 1 dose No approval for children II Illowite [50] Lequerre [51]Canakinumab d 4 mgkg Bwsingle dose sc every
4 weeks (max 150 mg)No approval for childrenwith JIA 4 years (approvalfor CAPS)
III Ruperto [89]
Rilonacept d 1ndash2times44 mgkgweek sc (max320 mg) then 22 mgkgweek sc(max160 mg)
No approval for childrenwith JIA 12 years(approval for CAPS)
Lovell [889091]
c) IL-6 inhibitorsTocilizumab d 1 h Infusion every two 2 weeks
Bwb30 kg 8 mgkg BwN30 kg12 mgkg
2 years of age or older Since May 2011 EMA approval forpediatric patients with SoJIA who haveresponded inadequately to previoustherapy with NSAIDs and systemiccorticosteroids (Approval at Japan forSoJIA and polyarticular JIA since 2008) c
I Yokota [53] Ruperto [92]de Benedetti [62]
d) Co stimulatory-antagonistsAbatacept d 10 mgkg iv Infusion at d 0 d 14
d 28 then every 4 weeks6 years of age and older Abatacept in combination with
methotrexate is indicated for thetreatment of moderate to severe activepolyarticular (JIA) in pediatric patientswho have had an insufficient responseto other DMARDs including at least oneTNF inhibitor
I Ruperto [549394]
Abbreviations CAPS=Cryopyrine associated periodic fever syndrome JDM=juvenile dermatomyositis Bw=body weight SoJIA=systemic-onset of JIA SLE=systemic Lupus erythematodesa Compare wwwemaeuropaeub wwwrotelistede (German database of drugs with national market approval)c Intra-articular injection into same joint no more often than once every 3 monthsd A statement from insurance companies should be acquired before treatment initiation for off label treatment (if possible)e Oral application is most feasible in childhood
183Evidence
andconsensus
basedGKJR
guidelinesfor
thetreatm
entof
juvenileidiopathic
arthritis
Oligoarticular JIA
Polyarticular JIA
SoJIA
Figure 2 JIA treatment escalation schemes +=addition of the drug (abbreviations NSAIDs=non steroidal anti-inflammatory drugthotrexate)
Consensus statement
Long-term use of systemic GC is not recom-mended Continuous administration of ge02 mgPrednisolone equivalent per kg bodyweight (Bw)carries a high risk of adverse events and thereforeis not recommended (evidence level III recom-mendation grade A)
Consensus statement (continued)
184 G Dueckers et al
GC in JIA published thus leading to ldquojustrdquo evidence level IIIDifferent recommendations of dosage and therapy regimesare listed in Table 5 (evidence level III for all recommenda-tions) [1824ndash28] Frequency and seriousness of deleteriouseffects correlate mainly to duration of therapy and dosageof GC administered Main side effects are iatrogenicCushings syndrome growth disturbance weight gainmood changes Higher dosage carry the risk of increasedvulnerability to infection hypertension osteoporosisthrombosis diabetes gastro-intestinal ulceration cataractglaucoma atrophy of subcutaneous fatty tissue steroid in-duced acne To inform colleagues about GC treatment in acase of emergency and to reduce severe complications in longterm treated patients ie GC administrationN4 weeks thesupply of ldquoGlucocorticoid ID cardsrdquo for patients might be useful
GC=Glucocorticoids DMARDs=disease modifying drugs MTX=Me
Consensus statement
The systemic use of GC is recommended asfast acting drugs in highly active JIA GC areused for the treatment of children and adoles-cents with SoJIA organ manifestations of JIA(eg uveitis pericardial effusion) sero-positivepolyarticular JIA and for bridging time untilthe complete therapeutic effect of DMARDs(evidence level III recommendation grade A)
313 Methotrexate (MTX) biologic agents andimmunosuppressive agents
MTX biologic agents and immunosuppres-sive agents are used for the treatment of childrenand adolescents with polyarticular JIA ifNSAIDs or local GC treatment do not succeedThe combination of those drugs with NSAIDsand GC is feasible A common characteristic ofMTX biologic agents and immunosuppressiveagents is the delayed onset of therapeutic ef-fect ie up to 3 months or even longer aftercommencing treatment
185Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
Safe contraception is indicated during therapy with MTXAzathioprine or Leflunomide and in the following 3 to6 months after its discontinuation
Consensus statement
Administration of Sulfasalazine or Lefluno-mide is recommended if MTX or Etanercept donot show sufficient efficacy or cannot be used
3131 Methotrexate Among DMARDs MTX provides themainstay of long-term therapy in JIA [29ndash32] In case ofside effects eg dyspepsia or nausea prophylaxis withfolic acid can be recommended (1times1 mg per day or 5 mgonce a week 24ndash48 h after application of MTX) Safe contra-ception is mandatory while receiving MTX Safety and effica-cy of MTX and its impact on quality of life of children with JIAhave been investigated Significant positive impact of MTXon all health-related quality of life health conceptshas been shown although the study has its limit due to dif-ferent MTX dosages used within participating JIA patients[33]
Consensus statement
MTX administration can be recommendeddue to its proven safety and efficacy to reducedisease activity MTX is used in case of insuffi-cient therapeutic effect of NSAIDs andor localGC administration continuous need for system-ic GC andor highly active disease Efficacy ofMTX (orally or subcutaneously administered) isfrequently achievable with a dosage of 10ndash15 mgmsup2 body surface (evidence level I recom-mendation grade A)
for other reasons (evidence level II recommen-dation grade B)
3132 Purine analogs31321 Azathioprine Efficacy has been investigat-
ed in a double blind placebo controlled study (32 patients)After 8 weeks of therapy the changes in disease activitymeasurement indicated a minor improvement in the Azathi-oprine group compared to the placebo group At the end ofthe study statistically significant differences between thegroups were found for only 2 disease activity measurements[34] Two patients were taken out of study due to severeadverse events eg leucopenia Measurement of activityof Thiopurinmethyltransferase (TPMT) can be beneficial foravoidance of severe adverse events
3133 Pyrimidine analogs31331 Leflunomide Within a double blind study
(32 weeks 94 patients) efficacy of Leflunomide was inferiorin comparison to MTX but better than placebo Howeverdosing of Leflunomide may not have been adequate insome children [35] Contraindications for Leflunomide arerenal insufficiency severe immunodeficiency depressedmyelopoesis and pancytopenia An extensive half-life peri-od (approximately 14 days) has to be taken in accountwhen administering Leflunomide In combination with hepa-totoxic DMARDs the risk of severe adverse events might in-crease eg increased blood pressure is seen frequentlySafe contraception is mandatory
3134 Antibiotic analogs and Hydroxychloroquine andChloroquine
31341 Sulfasalazine Weak efficacy of Sulfasalazinewas demonstrated within a placebo-controlled randomizedstudy after 24 weeks (96 patients) [3637] One third of pa-tients enrolled in the study discontinued treatment with Sulfa-salazine due to side effects eg gastrointestinal symptomsleucopenia [36] Some experts use sulfasalazine in HLA-B27positive JIA Contraindications are Glucose-6-phosphatase de-ficiency and hypersensitivity against sulfonamides
31342 Hydroxychloroquine and chloroquine Hydrox-ychloroquine and Chloroquine have been subject to clinical tri-als for the treatment of JIA even though efficacy was limitedWithin three consensus conferences held in 2007 and 2010 theconsensus group decided not to give a consensus statementon the use of chloroquine or hydroxychloroquine treatmentdespite the fact that those drugs still might be used by somecaregivers
3135 Biologic agents Biologic agents are drugs whichselectively inhibit cytokines cytokine receptors or directlybind to receptors of lymphocytes eg CTLA-4 CD20 Theyinclude antibodies and fusion proteins So far allbiological therapies are administered subcutaneously orintravenously
31351 TNFα-inhibitors TNFα-inhibition with Adali-mumab and Etanercept is efficient and safe (evidencelevel I) [38ndash41] Both drugs have been approved for JIAwith polyarticular course TNFα-inhibitors have become anintegral part of the treatment of JIA Potential risks of therapyare vulnerability for infection andmdashin a rare occasionmdashthe in-duction of autoimmune disease Prior to the start of treatmentwith TNFα-inhibitors chronic infections needs to be excludedor treated sufficiently eg tuberculosis hepatitis B or C
In children with JIA treated with TNFα-inhibitors malig-nancies eg Lymphoma have been reported It remainsunclear if the rate of malignancies is increased in patientscompared to the risk by having JIA itself In response to aprevious letter of the FDA (as reviewed in [42]) the GermanSociety for Pediatric Rheumatology (GKJR) has published of-ficial statements [4344] The GKJR states that treatmentwith TNFα-inhibition should be used very carefully physi-cians need to be aware of co-medication e g immunosup-pressive drugs and should monitor those patientsclosely [43] There is insufficient data on all biologicagentsmdashincluding TNFα-inhibitionmdashto judge about the long-term risk for children and adolescents313511 Etanercept Etanercept is a fusion proteinconsisting of the extracellular binding domain of solubleTNFα-receptor and Fc chain of human IgG1 Etanercept in-hibits TNFα by direct binding of the cytokine Efficacy has
Consensus statement
The use of Anakinra or Tozilizumab can berecommended for treatment of children and ado-lescents with refractory SoJIA (evidence level IIrecommendation grade A)
186 G Dueckers et al
been demonstrated in a randomized controlled withdrawaldesign trial for patients with polyarticular JIA [38] Withinan open extension study long term efficacy and safety havebeen documented over 8 years in 1669 patients [3945]There is data on more than 2000 patients registered in Euro-pean registries [46ndash48] Currently retrospective data showsa somewhat better efficacy of combining MTX or otherDMARDs with TNFα-inhibition versus anti-TNFα therapy assingle therapy [49]313512 Adalimumab Adalimumab is a humanizedmonoclonal IgG1 antibody directed against TNFα whichbinds soluble and membrane bound TNFα A randomizedcontrolled withdrawal design trial demonstrated safety andefficacy of Adalimumab (24 mgmsup2 body surface every2 weeks max 40 mg) for children and adolescents withpolyarticular JIA (4ndash17 years of age n=171) [40] After16 weeks ldquowash inrdquo phase responders (n=144171) enteredthe 32 weeks randomized double blind phase After 48 weekstwice the number of patients in the verum group met ACR 70as compared to the control group (56 vs 28 pb001)Within the open extension phase Adalimumab dosage wasfixed ie 20 mgb30 kg Bw and 40 mgN30 kg Bw There islack of evidence showing superior efficacy of combiningMTX (DMARDs) with Adalimumab versus Adalimumab as sin-gle therapy [40]
Consensus statement
Efficacy of Etanercept and Adalimumab forthe treatment of polyarticular JIA has been dem-onstrated Therapy with TNFa-inhibition is indi-cated in case of insufficient therapeutic effectof NSAIDs and local GC administration and lackof response to MTX (evidence level I recom-mendation grade A)
Consensus statement
Patients with polyarticular JIA without sys-temic manifestation refractory to treatmentwith MTX and TNF inhibition might benefit fromthe use of Abatacept (evidence level III recom-mendation grade C)
313513 Infliximab Infliximab is a chimerical (humanmouse) monoclonal antibody which binds soluble and mem-brane bound TNFα A randomized controlled study in childrenand adolescents with JIA failed to demonstrate a significantdifference of efficacy after treatment with Infliximab com-pared to placebo [31]
31352 Interleukin-1-inhibitors None of interleukin-1-inhibitors are approved for the treatment of JIA or SoJIAThey are commonly used in an off label setting313521 Anakinra Anakinra is an IL-1 receptor antag-onist Within a randomized controlled trial no significant ef-ficacy of Anakinra for patients with polyarticular JIA couldbe demonstrated [50] 50 of 86 patients were enrolled intoblinded phase (11 Anakinra versus Placebo) No significantreduction of flare could be demonstrated in comparison toplacebo 29 of 50 patients completed the open label exten-sion study Two noncontrolled nonrandomized studieshave shown efficacy of anakinra in a proportion of patientswith systemic-onset of JIA (SoJIA) [5152]313522 Canakinumab Canakinumab an IL-1β anti-body binds IL-1β selectively without interfering with IL-1αor its physiological IL-1 receptor antagonist Canakinumabhas been approved for treatment of hereditary periodic IL-1 associated periodic fever syndromes ie Cryopyrin-
associated periodic syndromes There are ongoing studies in-vestigating safety and efficacy of Canakinumab for SoJIA
31353 Interleukin-6 inhibitors313531 Tozilizumab Tozilizumab is a humanizedanti-IL-6 receptor monoclonal antibody Efficacy has beendemonstrated within a 12 week double blind randomizedcontrolled withdrawal trial in children with SoJIA (n=562ndash19 years) in Japan [53] After a 48 week open extensionstudy ACR Pedi 30 was met by 47 patients (98) At thetime of our literature search Tocilizumab was approved fortreatment of SoJIA and polyarticular JIA since 2008 inJapan A multicenter European study investigating efficacyand safety of Tozilizumab in polyarticular JIA was ongoingat the deadline of literature search (wwwclinicaltrialsgov NCT00988221) No data on long term effects are cur-rently available
31354 Co-stimulation inhibitors313541 Abatacept Abatacept is a recombinant fu-sion protein of extracellular domain of human cytotoxic T-Lymphocyte Antigen 4 (CTLA-4) and IgG1-Fc-Fragment Itmodulates T-cell co-stimulation A randomized controlleddouble blind withdrawal design study of Ruperto et al [54]demonstrated efficacy of Abatacept in patients with polyar-ticular JIA 123 of 170 participants of study were enrolled inthe 6 month double blind phase Flares occurred in 33 of 62(53) patients who were given placebo versus 12 of 60(20) Abatacept patients during double blind phase Adverseevents (AE) did not differ in both groups ie 37 AE in Abata-cept versus 34 AE in placebo recipients Some children maytake 3 to 6 months or longer before their maximal responseis achieved 3 of patients developed reaction to the infu-sion [55] Abatacept is approved by FDA and EMA for pa-tients who did not respond to prior MTX treatment Nodata of long term effects of the use of Abatacept in JIA areavailable due to the low numbers of patients treated so far
314 Autologous stem cell transplantation (SCT)There are studies on autologous SCT for treatment of re-
fractory and severe forms of JIA (evidence level III) [56] 22
Consensus statement
187Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
patients were enrolled in one study 8 reached clinical re-mission 7 were assessed as partial responders 3 experi-enced relapse of the disease and 4 (18) died as aconsequence of MAS or immunosuppressive treatment [56]Due to serious adverse events including death this thera-peutic option is seen as the last treatment option
Exercise training is recommended dependingon the extent of inflammation number of affect-ed joints and global disease activity Sports withminor stress on joints is favorable (evidence levelI recommendation grade A)
32 Non-drug based therapy
321 Physiotherapy occupational therapy and thera-peutic appliances
Physio- and occupational therapy are integral parts of thetherapeutic concept in children and adolescents with JIA[5758] Therapeutic goals of physiotherapy are relaxationand pain relief preservation or rehabilitation of physiologi-cal range of joint movement prevention of contracturesstretching and activation of muscles build-up of muscleforce and training of physiological movements
Consensus statement
Structured treatment by a properly trainedphysiotherapistoccupational therapist in combi-nation with drug based therapy and instructionsfor disease adopted self-sufficient daily exercisesessions are recommended to keep and to im-prove joint mobility (evidence level II recom-mendation grade A)Custom-made therapeutic appliances for correc-tion of axial misalignment prevention of falseweight bearing stabilization of joints (eghand- finger- and foot-ortheses) are recom-mended individually The use of therapeutic ap-pliances follows individual physician-directedadvice Efficacy has been demonstrated (evi-dence level I recommendation grade B)
Consensus statement
In individual cases the indication for open orarthroscopic synovectomy can be considered ifconservative therapy does not succeed (evi-dence level III recommendation grade B)
Consensus statement
Other forms of non-drug based therapeutic approachesrely on experts opinion and are solely based on individualclinical experience No controlled studies are available
Consensus statement
The implementation of thermotherapy electro-or ultrasound therapy massage and lymph drain-age is recommended Application of cold appli-ances for acute joint inflammation is indicated(evidence level II recommendation grade A)Electro- and ultrasound therapy are recom-mended for patients with tendosynovitis (evi-dence level III recommendation grade B)
An early psychological support within stan-dard pediatric rheumatological care should beimplemented to apprehend and treat mental is-sues and behavioral syndromes associated withphysiological disturbances and physical factors(evidence level III recommendation grade A)
Consensus statement
A socio-pedagogical care with regard tointegration at school professional andeveryday life and formal education of parentsand patients is recommended (evidence levelIII recommendation grade A)
322 Sportive activity and exercise trainingPositive impact of sportive activity on the general physi-
cal condition and on oxygen consumption has been demon-strated (evidence level II) [57ndash60] Adequate exercise
training supports the physiological development and helpscoping with JIA [58] Prospective controlled long term stud-ies are currently not available
323 Surgical treatmentToledo et al investigated the role of arthroscopic syno-
vectomy in JIA They concluded that arthroscopy is a safebut only partially effective procedure in patients witholigoarticular JIA (evidence levelrecommendation gradeIIIB) [61]
324 Psychological social intervention orsocio-pedagogical care
There are no controlled or open studies focusing on psy-chological social andor socio-pedagogical intervention inchildren or adolescents with JIA Recommendations arebased on experts opinion and personal experience solely
188 G Dueckers et al
4 Addendum
Since the deadline January 15th 2010 new papers haveappeared that are of interest in the context of our guideline[5562ndash64] in particular we refer to the ACR recommenda-tions [65] and the most recent literature on the risk of malig-nancies in JIA in context with TNF blocking agent andindependent of medication [42] [66] Moreover there is arecent study on the use of Tocilizumab in polyarticular pa-tients [67] These papers will be discussed within the nextconsensus conference by NGT and considered for inclusioninto the next edition of this guideline On 6th of September2011 our advanced search on wwwclinicaltrialgov (searchterms juvenile idiopathic arthritis recruitment open stud-ies study type interventional study age group child(birthndash17) intervention drugs) led to 16 trials which are cur-rently recruiting or will soon start recruiting
5 Discussion
To develop clinical practice guidelines of high quality andvalidity a formal consensus process and explicit methodo-logical criteria for the production of guidelines are recom-mended [68ndash70] Our guideline for the treatment of JIA inchildren and adolescents implements all these issues Thesystematic literature search was terminated on 15th January2010 leading to the most up to date guideline for JIA whichis currently available The deadline of the ACR recommenda-tions as published recently by Beukelmann et al was 5th ofOctober 2009 [65] By exclusion of case reports trials with-out control groups preliminary results published as ab-stracts on conferences and the strict graduation of theliterature by the criteria of evidence based medicine weaimed to give our guideline statements additional strengthand a maximal validity Newer original studies providing ad-ditional evidence for the treatment of JIA became availableafter our consensus process was finished see AddendumThe results of these trials have to await the next NGT beforeinclusion into our recommendations
Our updated systematic literature search in 2010 led to13 relevant studies published after 30th June 2007 (Fig 1Table 4) Their results have to be interpreted with cautionFirst trials in JIA are mainly based on limited numbers of pe-diatric patients as the recruitment of a sufficient number ofpediatric patients remains challenging Second trials aremainly designed for patients with polyarticular JIA or witholigoarticular onset and a polyarticular course (Table 4)Most children with JIA do not have a polyarticular subtypeof JIA but an oligoarticular onset and course [71] Thus pa-tients with oligoarticular JIA are heavily underrepresentedin most of the current trials Third in 5 of the 13studies the withdrawal study design has been used[4045505354] Lehmann reviewed the bias of withdrawaldesign trials in 2008 [72] After a wash-in phase only re-sponders to treatment are eligible for randomization Thusthe design preselects responders to the placebo effect whomight retain their response throughout the entire study peri-od Further there is a carryover effect of AE into the place-bo group so that significant differences in AE betweengroups may not become apparent In the one placebo con-trolled trial without withdrawal design on TNFα-inhibition
(Infliximab) no significant efficacy could be demonstratedbetween verum and placebo [31]
To our knowledge there are two other guidelines that dealwith the management of JIA as a whole (Table 6) [65] [73]Other guidelines are limited to the use of single drugs in JIAeg biologic agents [74] etanercept [75] The Australian guide-line (wwwracgporgauguidelinejuvenileidiopathicarthritis)has not been published in a peer-reviewed journal It is to pro-vide recommendations for the early diagnosis and multidisci-plinary management of JIA in the primary care setting forgeneral practitioners (GPs) [73] No recommendations aremade regarding the use of GCs DMARDs immunosuppressivedrugs or biologic agents [73] The ACR recommendations usesthe Appraisal of Guidelines for Research and Evaluation(AGREE) instrument [65] [76] which does not fulfill criteria ofa proper consensus process and carries the risk that expertsvote for peer opinion which might not reflect the true valueWe used an advanced and linguistically validated version ofthe AGREE instrument the ldquoGerman Instrument for Methodo-logical Guideline Appraisal (DELBI)rdquo which has been developedin cooperation of the AWMF among others [7778] We followedthe highly structured Nominal Group Technique as described inMethodology Our consensus group only considered formallyboard nominated representatives of multidisciplinary scientificsocieties and organizations (Table 1) and included patients rep-resentatives as this has been strongly recommended by the Eu-ropean League against Rheumatism (EULAR) recently [79] TheACR mentions a parent representative within their task forcepanel but leaves this representative anonymous It remainsunclear how ACR experts were selected and involved [65]They defined treatment groups which have not been evaluatedsystematically so far We used the ILAR classification systemwhich has been repeatedly evaluated [80ndash82]
By content there are major differences between the ACRrecommendations and our guideline a) Our guideline pro-vides a detailed and systematic list of 20 drugs commonlyused in the treatment of JIA (Table 5) which has been an in-tegrative part of our consensus conferences The ACR recom-mendations do not provide information on approval status(Food and Drug Administration) indications for use and nospecific differences on dosage regimes or frequency ofdaily application [65] eg it refers to the 2008 ACR recom-mendations for the use of DMARDs in adult rheumatoid ar-thritis b) The ACR recommendations provide a more earlyaggressive approach in the treatment of JIA The ACR recom-mends MTX as first line treatment in patients (b4 joints) withhighly active disease [65] To our knowledge there are onlydata to recommend MTX administration in cases of insuffi-cient therapeutic effect of prior treatment with NSAIDandor GC [33] c) The ACR recommends the use of TNFα in-hibitors as escalation therapy for some patients with historyof arthritis of 4 or fewer joints and refer to publications[3840] conducted in patients with polyarticular JIA or pau-ciarticular JIA with polyarticular course [65] There is no ev-idence that TNF is safe and efficient in patients witholigoarticular JIA a systematic controlled clinical trial onthis issue has not been done yet d) We regard a brief trialof local or systemic administration of GC plus NSAID as a fea-sible first line treatment for patients with polyarticular JIAThe ACR recommends MTX without regard to disease activityat the initial stage [65] We reached consensus to recom-mend the use of GC as bridging therapy until full onset of
Table 6 Overview of recommendationsguidelines for treatment of JIA
USA Australia Germany
ACR recommendations[65]
RACGP recommendations[73]
GKJR guidelines
Deadline of literature search October 2009 January 2007 September 2010Source of publications Pub Med Pub Med
EMBASE CINHAL CochraneLibrary provisionalAustralian Guideline [95]
Pub MedPrevious German Guidelines [78]
Definition used for JIA subgroups Treatment groups definedby Core expert panel
Not specifically definedChildren withJIAb16 years
ILAR criteria [1]
Consensus processprocessvalidation
AGREE [76] AGREE [76] DELBI [77]RANDUCLA appropriatenessmethod [96]
NGT Delphi method
Conferences None None 3 Formal consensus conferencesAddressees Pediatric rheumatologists General practitioner Pediatric Rheumatologists
PediatriciansGeneral practitioners
Participating scientific societies or professional organizationsPediatric rheumatologist orrheumatologists for adolescents
Yes Yes Yes
General pediatrician- In hospital Yes Yes Yes- In private practice Yes Yes YesResearcher Yes No YesRheumatologists for adults No No YesOphthalmologists No No YesParentspatients support groups Yes No YesOrthopedic surgeons No No YesPediatric orthopedic surgeons No No YesPsychologists No No YesPhysiotherapists No No YesPediatric rheumatology nurses Yes No NoOther scientific societies ororganizations
ACR BSPAR PRINTO PReS RACGP NAMSCAG NHMRC DGKJ DGPs DGRh DGO AWMFBVKJ
(ACR=American College of Rheumatologists AGREE=Appraisal of Guidelines for Research amp Development AWMF=Association of the ScientificMedical Associations BSPAR=British Society for Pediatric Rheumatology BVJK=Association of Pediatricians in private practice CEP=Core expertpanel ILAR=International League against Rheumatism CINHAL=Cumulative Index to Nursing and Allied Health Literature DELBI=German In-strument for Methodological Guideline Appraisal DGKJ=German Society of Pediatrics and Adolescent Medicine DGO=German Society for Oph-thalmology DGPs=German society for Psychology DGRh=German Society for Rheumatology GKJR=German Society for Pediatric RheumatologyNAMSCAG=National Arthritis and Musculoskeletal Conditions Advisory Group NGT=Nominal Group Technique NHMRC=National Health andMedical Research Council PReS=Pediatric Rheumatology Society) PRINTO=Pediatric Rheumatology International Trial Organization RACG-P=Royal Australian College of General Practitioner RANDUCLA=Research and DevelopmentUniversity of California at Los Angeles)
189Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
therapeutic effect of DMARDs The ACR recommendations donot provide any recommendation for the use of systemic GCfor patients with oligo- or polyarticular course of JIA exceptsystemic onset of JIA e) The ACR recommendations do notcover the topic of non-drug based therapy at all althoughthere is strong evidence that eg exercise training is a usefuladdition to drug treatment [575860]
6 Conclusion
In summary we present a treatment guideline for JIA on a con-sensus conference basis We strongly advocate an interdisciplin-ary approach including surgery physiotherapy psychosocial
intervention physical therapy medications etc and a strictformal consensus process in order to create statements thatare most appropriate for the complex clinical situation of achild and family presenting with JIA and cover all aspects ofJIA care All German pediatric rheumatology sites are partici-pating at the national pediatric rheumatologic database in theDeutsche Rheuma-Forschungszentrum at Berlin (DRFZ wwwdrfzde) It aims at quality assurance in Germany and monitorstreatment behavior of pediatric rheumatologists by using inter-nationally agreed criteria (eg joint count global physician rat-ing of disease activity global parent rating of overall well-being CHAQ ESR ACR-ped response or JADAS) The databasewill be used as a tool to monitor the application of our treat-ment guidelines
190 G Dueckers et al
Conflict of interest statement
Gregor Dueckers Novartis Pharmaceuticals CorporationBaxter (for all travel grants for scientific meetings)Nihal Guellac no conflict of interestMartin Arbogast no conflict of interestGuumlnther Dannecker no conflict of interestIvan Foeldvari Wyeth Pfizer Abbott Immunology Pharma-ceuticals Chugai (for all advisory board member)Michael Frosch no conflict of interestGerd Ganser Abbott Immunology Pharmaceuticals (advisoryboard member grants for scientific meetings) Wyeth Pfizer(advisory board member grants for scientific meetings)ChugaiRoche (advisory board member grants for scientificmeetings) Merck (grants for scientific meetings) Actelios(grants for scientific meetings) Esaote (grants for scientificmeetings)Arnd Heiligenhaus Novartis Pharmaceuticals CorporationAbbott Immunology Pharmaceuticals Alcon (for all re-search grants)Gerd Horneff Abbott Immunology Pharmaceuticals (re-search grants consulting fees non-remunerative positionsof influence) Wyeth Pfizer (research grants consultingfees speakers bureau non-remunerative positions of influ-ence) Bristol-Myers Squibb (Consulting fees) Nycomed(Consulting fees non-remunerative positions of influence)RocheChugai (Consulting fees non-remunerative positionsof influence) Sandoz (Consulting fees) Genzyme (researchgrants consulting fees non-remunerative positions of influ-ence) Swedish Orphan (research grants consulting feesnon-remunerative positions of influence)Arnold Illhardt no conflict of interestRuumldiger Krauspe no conflict of interestBarbara Markus no conflict of interestHartmut Michels Abbott Immunology Pharmaceuticals (advi-sory board member and grants for scientific meeting)Matthias Schneider no conflict of interestWolfram Singendonk no conflict of interestHelmut Sitter no conflict of interestMarianne Spamer no conflict of interestNorbert Wagner no conflict of interestTim Niehues Abbott Immunology Pharmaceuticals EssexPharma Novartis Pharmaceutical Corporation WyethPfizer (for all research grants consulting fees non-remu-nerative positions of influence)
Acknowledgment
We like to express our grateful thanks to Prof Dr Hans IkoHuppertz for proof reading the article and for an excellentdiscussion on our work We like to express our thanks to HE-LIOS Clinic for funding the open access of the article
References
[1] RE Petty TR Southwood P Manners J Baum DN Glass JGoldenberg X He J Maldonado-Cocco J Orozco-Alcala AMPrieur ME Suarez-Almazor PWoo International League of Asso-ciations for Rheumatology classification of juvenile idiopathic ar-thritis second revision Edmonton 2001 J Rheumatol 31(2004) 390ndash392
[2] B Prakken S Albani A Martini Juvenile idiopathic arthritisLancet 377 (2011) 2138ndash2149
[3] KT April DE Feldman RW Platt CM Duffy Comparisonbetween children with juvenile idiopathic arthritis (JIA) andtheir parents concerning perceived quality of life Qual LifeRes 15 (2006) 655ndash661
[4] BM Feldman B Grundland L McCullough V Wright Distinc-tion of quality of life health related quality of life and healthstatus in children referred for rheumatologic care J Rheuma-tol 27 (2000) 226ndash233
[5] JC Packham MA Hall Long-term follow-up of 246 adultswith juvenile idiopathic arthritis functional outcomeRheumatology (Oxford) 41 (2002) 1428ndash1435
[6] C Sandborg Pediatric rheumatic disease standards of care forJIAmdashthe basic foundation for quality Nat Rev Rheumatol 6(2010) 389ndash390
[7] N Guellac T Niehues Interdisciplinary and evidence-basedtreatment guideline for juvenile idiopathic arthritis KlinPadiatr 220 (2008) 392ndash402
[8] K Schnakenburg Leitlinien in der Kinder- und JugendmedizinElsevier 2005 pp H1 1ndash15
[9] P Juni L Nartey S Reichenbach R Sterchi PA Dieppe MEgger Risk of cardiovascular events and rofecoxib cumulativemeta-analysis Lancet 364 (2004) 2021ndash2029
[10] W Feldman Evidence-based Pediatrics 1st ed BC DeckersHamilton 2000
[11] AH Van de Ven AL Delbecq The nominal group as a re-search instrument for exploratory health studies Am J PublicHealth 62 (1972) 337ndash342
[12] HA Linstone M Turoff The Delphi Method Techniques andApplications Addison-Wesley Pub 1975
[13] TK Kvien HM Hoyeraal B Sandstad Naproxen and acetyl-salicylic acid in the treatment of pauciarticular and polyarticu-lar juvenile rheumatoid arthritis Assessment of tolerance andefficacy in a single-centre 24-week double-blind parallelstudy Scand J Rheumatol 13 (1984) 342ndash350
[14] RM Laxer ED Silverman C St-Cyr MT Tran G Lingam Asix-month open safety assessment of a naproxen suspensionformulation in the therapy of juvenile rheumatoid arthritisClin Ther 10 (1988) 381ndash387
[15] AM Leak MR Richter LE Clemens MA Hall BM AnsellA crossover study of naproxen diclofenac and tolmetin in sero-negative juvenile chronic arthritis Clin Exp Rheumatol 6(1988) 157ndash160
[16] J Haapasaari E Wuolijoki H Ylijoki Treatment of juve-nile rheumatoid arthritis with diclofenac sodium Scand JRheumatol 12 (1983) 325ndash330
[17] EH Giannini EJ Brewer ML Miller D Gibbas MH PassoHM Hoyeraal B Bernstein DA Person CW Fink LA Sawyeret al Ibuprofen suspension in the treatment of juvenilerheumatoid arthritis Pediatric Rheumatology CollaborativeStudy Group J Pediatr 117 (1990) 645ndash652
[18] E Stoeber L Sanger Experiences with indomethacin in long-term therapy of juvenile rheumatoid arthritis Arzneimittel-forschung 21 (1971) 1865ndash1866
[19] N Ruperto I Nikishina ED Pachanov Y Shachbazian AMPrieur R Mouy R Joos F Zulian R Schwarz V ArtamonovaW Emminger M Bandeira A Buoncompagni I Foeldvari FFalcini E Baildam I Kone-Paut M Alessio V Gerloni ALenhardt A Martini G Hanft R Sigmund S Simianer Arandomized double-blind clinical trial of two doses ofmeloxicam compared with naproxen in children with juvenileidiopathic arthritis short- and long-term efficacy and safetyresults Arthritis Rheum 52 (2005) 563ndash572
[20] I Foeldvari IS Szer LS Zemel DJ Lovell EH Giannini JLRobbins CRWest G Steidle S Krishnaswami BJ Bloom A pro-spective study comparing celecoxib with naproxen in children withjuvenile rheumatoid arthritis J Rheumatol 36 (2009) 174ndash182
191Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
[21] F Zulian G Martini D Gobber C Agosto C Gigante FZacchello Comparison of intra-articular triamcinolone hexa-cetonide and triamcinolone acetonide in oligoarticular juve-nile idiopathic arthritis Rheumatology (Oxford) 42 (2003)1254ndash1259
[22] F Zulian G Martini D Gobber M Plebani F Zacchello PManners Triamcinolone acetonide and hexacetonide intra-articular treatment of symmetrical joints in juvenile idiopathicarthritis a double-blind trial Rheumatology (Oxford) 43 (2004)1288ndash1291
[23] GS Habib Systemic effects of intra-articular corticosteroidsClin Rheumatol 28 (2009) 749ndash756
[24] JR Kirwan The effect of glucocorticoids on joint destructionin rheumatoid arthritis The Arthritis and Rheumatism CouncilLow-Dose Glucocorticoid Study Group N Engl J Med 333(1995) 142ndash146
[25] H Michels What is low-dose corticosteroid therapy in juvenileidiopathic arthritis A worldwide questionnaire-based surveyZ Rheumatol 59 (Suppl 2) (2000) II127ndash130
[26] JJ Miller III Prolonged use of large intravenous steroid pulsesin the rheumatic diseases of children Pediatrics 65 (1980)989ndash994
[27] P Picco M Gattorno A Buoncompagni V Pistoia C Borrone6-methylprednisolone lsquomini-pulsesrsquo a newmodality of glucocor-ticoid treatment in systemic onset juvenile chronic arthritisScand J Rheumatol 25 (1996) 24ndash27
[28] AM Prieur The place of corticosteroid therapy in juvenilechronic arthritis in 1992 J Rheumatol Suppl 37 (1993)32ndash34
[29] JS Gao H Wu J Tian Treatment of patients with juvenilerheumatoid arthritis with combination of leflunomide andmethotrexate Zhonghua Er Ke Za Zhi 41 (2003) 435ndash438
[30] T Niehues G Horneff H Michels MS Hock L SchuchmannEvidence-based use of methotrexate in children with rheumat-ic diseases a consensus statement of the Working Groups Pedi-atric Rheumatology Germany (AGKJR) and PediatricRheumatology Austria Rheumatol Int 25 (2005) 169ndash178
[31] N Ruperto DJ Lovell R Cuttica N Wilkinson P Woo GEspada C Wouters ED Silverman Z Balogh M HenricksonMT Apaz E Baildam A Fasth V Gerloni P Lahdenne AMPrieur A Ravelli RK Saurenmann ML Gamir N WulffraatL Marodi RE Petty R Joos F Zulian D McCurdy BLMyones K Nagy P Reuman I Szer S Travers A BeutlerG Keenan J Clark S Visvanathan A Fasanmade A Ray-chaudhuri A Mendelsohn A Martini EH Giannini A random-ized placebo-controlled trial of infliximab plus methotrexatefor the treatment of polyarticular-course juvenile rheumatoidarthritis Arthritis Rheum 56 (2007) 3096ndash3106
[32] K Visser DM van der Heijde Risk and management of livertoxicity during methotrexate treatment in rheumatoid andpsoriatic arthritis a systematic review of the literature ClinExp Rheumatol 27 (2009) 1017ndash1025
[33] A Cespedes-Cruz R Gutierrez-Suarez A Pistorio A Ravelli ALoy KJ Murray V Gerloni N Wulffraat S Oliveira J WalshIC Penades MG Alpigiani P Lahdenne C Saad-Magalhaes ECortis L Lepore Y Kimura C Wouters A Martini N RupertoMethotrexate improves the health-related quality of life of chil-dren with juvenile idiopathic arthritis Ann Rheum Dis 67(2008) 309ndash314
[34] TK Kvien HM Hoyeraal B Sandstad Azathioprine versus place-bo in patients with juvenile rheumatoid arthritis a single centerdouble blind comparative study J Rheumatol 13 (1986) 118ndash123
[35] E Silverman R Mouy L Spiegel LK Jung RK SaurenmannP Lahdenne G Horneff I Calvo IS Szer K Simpson JAStewart V Strand Leflunomide or methotrexate for juvenilerheumatoid arthritis N Engl J Med 352 (2005) 1655ndash1666
[36] MA van Rossum TJ Fiselier MJ Franssen AH ZwindermanR ten Cate LW van Suijlekom-Smit WH van Luijk RM
van Soesbergen NM Wulffraat JC Oostveen W Kuis PFDijkstra CF van Ede BA Dijkmans Sulfasalazine in the treat-ment of juvenile chronic arthritis a randomized double-blindplacebo-controlled multicenter study Dutch Juvenile ChronicArthritis Study Group Arthritis Rheum 41 (1998) 808ndash816
[37] MA van Rossum RM van Soesbergen M Boers AHZwinderman TJ Fiselier MJ Franssen R ten Cate LW vanSuijlekom-Smit NM Wulffraat WH van Luijk JC OostveenW Kuis BA Dijkmans Long-term outcome of juvenile idiopathicarthritis following a placebo-controlled trial sustained benefits ofearly sulfasalazine treatment Ann Rheum Dis 66 (2007)1518ndash1524
[38] DJ Lovell EH Giannini A Reiff GD Cawkwell ED SilvermanJJ Nocton LD Stein A Gedalia NT Ilowite CA Wallace JWhitmore BK Finck Etanercept in children with polyarticularjuvenile rheumatoid arthritis Pediatric Rheumatology Collabora-tive Study Group N Engl J Med 342 (2000) 763ndash769
[39] DJ Lovell A Reiff OY Jones R Schneider J Nocton LDStein A Gedalia NT Ilowite CA Wallace JB WhitmoreB White EH Giannini Long-term safety and efficacy ofetanercept in children with polyarticular-course juvenile rheu-matoid arthritis Arthritis Rheum 54 (2006) 1987ndash1994
[40] DJ Lovell N Ruperto S Goodman A Reiff L Jung K JarosovaD Nemcova R Mouy C Sandborg J Bohnsack D Elewaut IFoeldvari V Gerloni J Rovensky K Minden RK Vehe LWWeiner G Horneff HI Huppertz NY Olson JR Medich RCarcereri-De-Prati MJ McIlraith EH Giannini A MartiniAdalimumab with or without methotrexate in juvenile rheuma-toid arthritis N Engl J Med 359 (2008) 810ndash820
[41] FH Prince M Twilt R ten Cate MA van RossumW ArmbrustEP Hoppenreijs M van Santen-Hoeufft Y Koopman-KeeminkNM Wulffraat LW van Suijlekom-Smit Long-term follow-upon effectiveness and safety of etanercept in juvenile idiopathicarthritis the Dutch National Register Ann Rheum Dis 68(2009) 635ndash641
[42] P Diak J Siegel L LaGrenade L Choi S Lemery AMcMahonTumor necrosis factor alpha blockers andmalignancy in childrenforty-eight cases reported to the Food and Drug AdministrationArthritis Rheum 62 (2010) 2517ndash2524
[43] G Horneff T Hospach G Dannecker D Foll JP Haas HJGirschick HI Huppertz R Keitzer HJ Laws H Michels KMinden R Trauzeddel Updated statement by the German So-ciety for Pediatric and Adolescent Rheumatology (GKJR) on theFDAs report regarding malignancies in anti-TNF-treated pa-tients from Aug 4 2009 Z Rheumatol 69 (2010) 561ndash567
[44] T Hospach JP Haas HI Huppertz R Keitzer H Michels RTrauzeddl D Foll G Dannecker G Horneff Comment of theSociety of Pediatric and Adolescent Rheumatology on the USFood and Drug Administration (FDA) announcement regardingcases of malignancy in anti-TNF-treated patients Z Rheumatol68 (2009) 162ndash164
[45] DJ Lovell A Reiff NT Ilowite CA Wallace Y Chon SL LinSW Baumgartner EH Giannini Safety and efficacy of up to eightyears of continuous etanercept therapy in patients with juvenilerheumatoid arthritis Arthritis Rheum 58 (2008) 1496ndash1504
[46] EH Giannini NT Ilowite DJ Lovell CA Wallace CERabinovich A Reiff G Higgins B Gottlieb NG Singer YChon SL Lin SW Baumgartner Long-term safety and effec-tiveness of etanercept in children with selected categories ofjuvenile idiopathic arthritis Arthritis Rheum 60 (2009)2794ndash2804
[47] G Horneff H Schmeling T Biedermann I Foeldvari G GanserHJ Girschick T Hospach HI Huppertz R Keitzer RM KusterH Michels D Moebius B Rogalski A Thon The German etaner-cept registry for treatment of juvenile idiopathic arthritis AnnRheum Dis 63 (2004) 1638ndash1644
[48] FH Prince M Twilt SC Simon MA van RossumW ArmbrustEP Hoppenreijs S Kamphuis M van Santen-Hoeufft Y
192 G Dueckers et al
Koopman-Keemink NM Wulffraat R ten Cate LW vanSuijlekom-Smit When and how to stop etanercept aftersuccessful treatment of patients with juvenile idiopathic ar-thritis Ann Rheum Dis 68 (2009) 1228ndash1229
[49] G Horneff F De Bock I Foeldvari HJ Girschick H MichelsD Moebius H Schmeling Safety and efficacy of combinationof etanercept and methotrexate compared to treatment withetanercept only in patients with juvenile idiopathic arthritis(JIA) preliminary data from the German JIA Registry AnnRheum Dis 68 (2009) 519ndash525
[50] N Ilowite O Porras A Reiff S Rudge M Punaro A Martin RAllen T Harville YN Sun T Bevirt G Aras B Appleton Ana-kinra in the treatment of polyarticular-course juvenile rheumatoidarthritis safety and preliminary efficacy results of a randomizedmulticenter study Clin Rheumatol 28 (2009) 129ndash137
[51] T Lequerre P Quartier D Rosellini F Alaoui M De BandtO Mejjad I Kone-Paut M Michel E Dernis M Khellaf NLimal C Job-Deslandre B Fautrel X Le Loet J Sibilia In-terleukin-1 receptor antagonist (anakinra) treatment in pa-tients with systemic-onset juvenile idiopathic arthritis oradult onset Still disease preliminary experience in FranceAnn Rheum Dis 67 (2008) 302ndash308
[52] M Gattorno A Piccini D Lasiglie S Tassi G Brisca S CartaL Delfino F Ferlito MA Pelagatti F Caroli A BuoncompagniS Viola A Loy M Sironi A Vecchi A Ravelli A Martini ARubartelli The pattern of response to anti-interleukin-1 treatmentdistinguishes two subsets of patients with systemic-onset juvenileidiopathic arthritis Arthritis Rheum 58 (2008) 1505ndash1515
[53] S Yokota T Imagawa M Mori T Miyamae Y Aihara STakei N Iwata H Umebayashi T Murata M Miyoshi MTomiita N Nishimoto T Kishimoto Efficacy and safety oftocilizumab in patients with systemic-onset juvenile idiopathicarthritis a randomised double-blind placebo-controlledwithdrawal phase III trial Lancet 371 (2008) 998ndash1006
[54] N Ruperto DJ Lovell P Quartier E Paz N Rubio-Perez CASilva C Abud-Mendoza R Burgos-Vargas V Gerloni JAMelo-Gomes C Saad-Magalhaes F Sztajnbok C Goldenstein-Schainberg M Scheinberg IC Penades M Fischbach J OrozcoPJ Hashkes C Hom L Jung L Lepore S Oliveira CAWallace LH Sigal AJ Block A Covucci A Martini EHGiannini Abatacept in children with juvenile idiopathic arthri-tis a randomised double-blind placebo-controlled withdrawaltrial Lancet 372 (2008) 383ndash391
[55] N Ruperto DJ Lovell P Quartier E Paz N Rubio-PerezCA Silva C Abud-Mendoza R Burgos-Vargas V GerloniJA Melo-Gomes C Saad-Magalhaes J Chavez-Corrales CHuemer A Kivitz FJ Blanco I Foeldvari M Hofer G HorneffHI Huppertz C Job-Deslandre A Loy K Minden M PunaroAF Nunez LH Sigal AJ Block M Nys A Martini EHGiannini Long-term safety and efficacy of abatacept inchildren with juvenile idiopathic arthritis Arthritis Rheum 62(2010) 1792ndash1802
[56] DM Brinkman IM de Kleer R ten Cate MA van RossumWP Bekkering A Fasth MJ van Tol W Kuis NM WulffraatJM Vossen Autologous stem cell transplantation in childrenwith severe progressive systemic or polyarticular juvenile idio-pathic arthritis long-term follow-up of a prospective clinicaltrial Arthritis Rheum 56 (2007) 2410ndash2421
[57] SE Klepper Effects of an eight-week physical conditioningprogram on disease signs and symptoms in children with chronicarthritis Arthritis Care Res 12 (1999) 52ndash60
[58] D Singh-Grewal J Schneiderman-Walker V Wright O Bar-OrJ Beyene H Selvadurai B Cameron RM Laxer R SchneiderED Silverman L Spiegel S Tse C Leblanc J Wong SStephens BM Feldman The effects of vigorous exercisetraining on physical function in children with arthritis arandomized controlled single-blinded trial ArthritisRheum 57 (2007) 1202ndash1210
[59] S Stephens D Singh-Grewal O Bar-Or J Beyene B CameronCM Leblanc R Schneider J Schneiderman-Walker HSelvadurai E Silverman L Spiegel SM Tse V WrightBM Feldman Reliability of exercise testing and functionalactivity questionnaires in children with juvenile arthritisArthritis Rheum 57 (2007) 1446ndash1452
[60] T Takken J van der Net W Kuis PJ Helders Physical ac-tivity and health related physical fitness in children with ju-venile idiopathic arthritis Ann Rheum Dis 62 (2003)885ndash889
[61] MM Toledo G Martini C Gigante L Da Dalt A TregnaghiF Zulian Is there a role for arthroscopic synovectomy in oli-goarticular juvenile idiopathic arthritis J Rheumatol 33(2006) 1868ndash1872
[62] F de Benedetti H Brunner N Ruperto SWright A KenwrightR Cuttica P Woo R Schneider DJ Lovell A Martini Efficacyand safety of Tocilizumab in patients with systemic juvenile idio-pathic arthritis (sJIA) 12-week data from the phase III TENDERtrial Ann Rheum Dis 69 (2010) 146
[63] P Quartier F Allantaz R Cimaz P Pillet C Messiaen CBardin X Bossuyt A Boutten J Bienvenu A Duquesne ORicher D Chaussabel A Mogenet J Banchereau JM Tre-luyer P Landais V Pascual A multicentre randomiseddouble-blind placebo-controlled trial with the interleukin-1receptor antagonist anakinra in patients with systemic-onsetjuvenile idiopathic arthritis (ANAJIS trial) Ann Rheum Dis70 (2011) 747ndash754
[64] DE Furst EC Keystone J Braun FC Breedveld GRBurmester F De Benedetti T Dorner P Emery R FleischmannA Gibofsky JR Kalden A Kavanaugh B Kirkham P Mease JSieper NG Singer JS Smolen PL Van Riel MH Weisman KWinthrop Updated consensus statement on biological agents forthe treatment of rheumatic diseases 2010 Ann Rheum Dis 70(Suppl 1) (2010) i2ndashi36
[65] T Beukelman NM Patkar KG Saag S Tolleson-RinehartRQ Cron EM Dewitt NT Ilowite Y Kimura RM LaxerDJ Lovell A Martini CE Rabinovich N Ruperto 2011 Ameri-can College of Rheumatology recommendations for the treatmentof juvenile idiopathic arthritis initiation and safety monitoring oftherapeutic agents for the treatment of arthritis and systemic fea-tures Arthritis Care Res 63 (2011) 465ndash482 (Hoboken)
[66] JF Simard M Neovius S Hagelberg J Askling Juvenile idi-opathic arthritis and risk of cancer a nationwide cohort studyArthritis Rheum 62 (2010) 3776ndash3782
[67] T Imagawa S Yokota M Mori T Miyamae S Takei H ImanakaY Nerome N Iwata T Murata M Miyoshi N Nishimoto TKishimoto Safety and efficacy of tocilizumab an anti-IL-6-receptor monoclonal antibody in patients with polyarticular-course juvenile idiopathic arthritis Mod Rheumatol (2011)doi102007s10165-011-0481-0
[68] TM Shaneyfelt MF Mayo-Smith J Rothwangl Are guide-lines following guidelines The methodological quality of clini-cal practice guidelines in the peer-reviewed medicalliterature Jama 281 (1999) 1900ndash1905
[69] R Grilli N Magrini A Penna G Mura A Liberati Practiceguidelines developed by specialty societies the need for a crit-ical appraisal Lancet 355 (2000) 103ndash106
[70] JS Burgers R Grol NS Klazinga M Makela J Zaat To-wards evidence-based clinical practice an international surveyof 18 clinical guideline programs Int J Qual Health Care 15(2003) 31ndash45
[71] JT Cassidy RE Petty Juvenile Idiopathic Rheumatic Arthri-tis 5th Edition WB Saunders Philadelphia 2005
[72] TJ Lehman Are withdrawal trials in paediatric rheumatic dis-ease helpful Lancet 372 (2008) 348ndash350
[73] J Munro Recommendations for the Diagnosis and Managementof Juvenile Idiopathic Arthritis The Royal Australian Collegeof General Practitioners South Melbourne 2009 pp 1ndash38
193Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
httpwwwnhmrcgovau_files_nhmrcpublicationsattachmentscp119-juvenile-arthritispdf
[74] MJ Santos JE Fonseca H Canhao M Conde M JoseVieira L Costa M Costa M Salgado JA Melo Gomes Guide-lines for prescribing and monitoring biologic therapies in juve-nile idiopathic arthritis Acta Reumatol Port 32 (2007) 43ndash47
[75] S Yokota M Mori T Imagawa T Murata M Tomiita Y ItohS Fujikawa S Takei Guidelines on the use of etanercept forjuvenile idiopathic arthritis in Japan Mod Rheumatol 20(2010) 107ndash113
[76] The AGREE Collaboration Appraisal of Guidelines for Researchamp Evaluation (AGREE) instrument wwwagreecollaborationorg
[77] I Kopp H Thole T Langer HK Selbmann G OllenschlaumlgerGerman Instrument for Methodological Guideline Appraisal(DELBI) wwwversorgungsleitliniende2008
[78] Auml Aumlrztliches Zentrum fuumlr Qualitaumlt in der Medizin A Arbeitsge-meinschaften der Wissenschaftlichen Fachgesellschaften in derMedizin Deutsches Instrument zur methodischen Leitlinien-Bewertung (DELBI) Fassung 20052006 Z Aumlrztl FortbildQualitaumltssich 99 (2005) 468ndash519
[79] MP de Wit SE Berlo GJ Aanerud D Aletaha JW BijlsmaL Croucher JA Da Silva B Glusing L Gossec S Hewlett MJongkees D Magnusson M Scholte-Voshaar P Richards CZiegler TA Abma European League Against Rheumatism rec-ommendations for the inclusion of patient representatives in sci-entific projects Ann Rheum Dis 70 (2011) 722ndash726
[80] I Foeldvari M Bidde Validation of the proposed ILAR classifi-cation criteria for juvenile idiopathic arthritis InternationalLeague of Associations for Rheumatology J Rheumatol 27(2000) 1069ndash1072
[81] R Merino J de Inocencio J Garcia-Consuegra Evaluation ofrevised International League of Associations for Rheumatologyclassification criteria for juvenile idiopathic arthritis in Spanishchildren (Edmonton 2001) J Rheumatol 32 (2005) 559ndash561
[82] SE Ramsey RK Bolaria DA Cabral PN Malleson REPetty Comparison of criteria for the classification of childhoodarthritis J Rheumatol 27 (2000) 1283ndash1286
[83] G Horneff A Ebert S Fitter K Minden I Foeldvari J Kum-merle-Deschner A Thon HJ Girschick F Weller HI Hup-pertz Safety and efficacy of once weekly etanercept 08mgkg in a multicentre 12 week trial in active polyarticularcourse juvenile idiopathic arthritis Rheumatology (Oxford) 48(2009) 916ndash919
[84] EH Giannini EJ Brewer N Kuzmina A Shaikov A Maxi-mov I Vorontsov CW Fink AJ Newman JT Cassidy LSZemel Methotrexate in resistant juvenile rheumatoid arthri-tis Results of the USAndashUSSR double-blind placebo-controlled trial The Pediatric Rheumatology CollaborativeStudy Group and The Cooperative Childrens Study GroupN Engl J Med 326 (1992) 1043ndash1049
[85] A Ravelli S Viola D Migliavacca N Ruperto A Pistorio AMartini The extended oligoarticular subtype is the best predic-tor of methotrexate efficacy in juvenile idiopathic arthritisJ Pediatr 135 (1999) 316ndash320
[86] P Woo TR Southwood AM Prieur CJ Dore J Grainger JDavid C Ryder N Hasson A Hall I Lemelle Randomizedplacebo-controlled crossover trial of low-dose oral
methotrexate in children with extended oligoarticular or sys-temic arthritis Arthritis Rheum 43 (2000) 1849ndash1857
[87] E Silverman L Spiegel D Hawkins R Petty D Goldsmith LSchanberg C Duffy P Howard V Strand Long-term open-label preliminary study of the safety and efficacy of lefluno-mide in patients with polyarticular-course juvenile rheumatoidarthritis Arthritis Rheum 52 (2005) 554ndash562
[88] DJ Lovell EH Giannini Y Kimura C Suzanne PJHashkes A Reiff Long-term safety and efficacy of rilonaceptin patients with systemic juvenile idiopathic arthritis (SJIA)Arthritis Rheum 60 (2009)
[89] N Ruperto P Quartier NWulffraat PWoo A Loy R Mouy BBader-Meunier BJ Prakken E Noseda R Belleli J Lecot CRordorf A Martini A Phase II Trial with canakinumab(ACZ885) a new IL-1-beta blocking monoclonal antibody toevaluate safety and preliminary efficacy in children with system-ic juvenile idiopathic arthritis Ann Rheum Dis 68 (2009) 170
[90] DJ Lovell EH Giannini Y Kimura et al Preliminary evi-dence for bioactivity of IL-1 trap (Rilonacept) a long actingIL-1 inhibitor in systemic juvenile idiopathic arthritis (sJIA)Arthritis Rheum 54 (2006) S325
[91] DJ Lovell EH Giannini Y Kimura et al Preliminary evi-dence for sustained bioactivity of IL-1 Trap (rilonacept) a longacting IL-1 inhibitor in systemic juvenile idiopathic arthritisArthritis Rheum 56 (2007) S514
[92] N Ruperto F De Benedetti H Brunner R Allen D Brown JChaitow E Cortis G Espada B Flato V Gerloni G HorneffS Wright A Kenwright R Schneider P Woo A Martini DJLovell Tocilizumab is efficacious in patients with systemic ju-venile idiopathic arthritis (sJIA) across baseline disease charac-teristics and priorbaseline treatments 12-week data from thephase II TENDER trial 17th PReS Congress Valencia Spain2010 2010
[93] N Ruperto DJ Lovell T Li F Sztajnbok C Goldenstein-Schainberg M Scheinberg IC Penades M Fischbach JOrozco PJ Hashkes C Hom L Jung L Lepore S OliveiraC Wallace M Alessio P Quartier E Cortis A Eberhard GSimonini I Lemelle E Chalom LH Sigal A Block A CovucciM Nys A Martini EH Giannini Abatacept improves health-related quality of life pain sleep quality and daily participationin subjects with juvenile idiopathic arthritis Arthritis Care Res(Hoboken) 62 (11) (2010) 1542ndash1551
[94] N Ruperto DJ Lovell P Quartier E Paz N Rubio-PerezCA Silva C Abud-Mendoza R Burgos-Vargas V GerloniJA Melo-Gomes C Saad-Magalhaes J Chavez C HuemerA Kivitz FJ Blanco I Foeldvari M Hofer G Horneff HIHuppertz CJ Deslandre A Loy K Minden M Punaro AFNunez LH Sigal AJ Block M Nys A Martini EH GianniniLong-term safety and efficacy of abatacept in children with ju-venile idiopathic arthritis Arthritis Rheum 62 (2010)1792ndash1802
[95] J Munro Juvenile Idiopathic Arthritis Management Guidelines(Provisional) Australian Paediatric Rheumatology Group 2006httpwwwnhmrcgovau
[96] K Fitch SJ Bernstein MD Aguilar B Burnand JR LaCalleP Lazaro M van het Loo J McDonnell JP Vader JPKahan The RANDUCLA Appropriateness Method Users ManualRAND Pittsburgh 2000

Table 1 Representatives nominated for the consensus group by scientific societies and professional organizations
Name Representing scientific societies or professional organisations
Arbogast M Association of Paediatric Orthopaedic SurgeonsDannecker G German Society of Paediatrics and Adolescent Medicine (DGKJ)Dueckers G (coordinator)Foeldvari I German Society for Paediatric Rheumatology (GKJR)Frosch M GKJRGanser G GKJRGuellac N (coordinator)Heiligenhaus A German Society for Ophthalmology (DOG)Horneff G GKJRIllhardt A German Society for Psychology (DGPs)Krauspe R Association of Paediatric Orthopaedic SurgeonsKopp I (moderator)Markus B National support group of parents and children with JIAmdashRheuma LigaMichels S GKJRNiehues T (coordinator) GKJRSchneider M German Society of Rheumatology (DGRh)Singendonk W Association of Paediatricians in private practice (BVKJ)Sitter H (moderator) Association of the Scientific Medical Associations (AWMF)Spamer M National Association of PhysiotherapistsWagner N German Society of Paediatrics and Adolescent Medicine (DGKJ)
178 G Dueckers et al
and treatment guidelines for medical scientific societiesand organizations in Germany
24 Consensus building nominal group technique(NGT)
Consensus building was headed by a professional moderators(HS IK) The moderator of the consensus conferences
Literature search 2007
(deadline June 30th 2007) [7]
Mesh terms ldquojuvenile idiopathic (rheumatoid)
arthritisrdquo and ldquotherapyrdquo
dArr n = 3138
Limits ldquohumansrdquo ldquopublished in the last 3
yearsrdquo ldquoall child 0-18rdquo
dArr n = 193
Limit ldquoclinical trialrdquo
dArr n = 52
Exclusion of studies relating to
diagnosis of JIA uveitis vaccination
transition rofecoxibe
rArr n = 22
Figure 1 Literature se
explained the purpose method and procedure of consensusfinding Representatives gave brief presentations of literatureand core conclusions for the guideline draft A formal consensusprocess led to adoption of guidelines for treatment of JIA Asformal consensus procedure we used NGT involving six stages
1 Silent review of the guideline draft and noting of comments andideas by the participants During this period participants did notconsult or discuss with others
Literature search 2010
(published June 30th 2007 ndash January 15th
2010)
Mesh terms ldquojuvenile idiopathic (rheumatoid)
arthritisrdquo and ldquotherapyrdquo
Limits ldquohumansrdquo ldquopublished in the last 3
yearsrdquo ldquoall child 0-18rdquo ldquoclinical trialrdquo
dArr n = 17
Exclusion of studies relating to
diagnosis of JIA uveitis vaccination
transition studies without control groups
Calcium supplementation costs
rArrrArr n = 13
arch 2007 and 2010
Table 3 Recommendation grade [10]
Recommendationgrade
Definition
A There is good evidence to support the recommendation that the intervention be performedB There is fair evidence to support the recommendation that the intervention be performedC There is poor evidence regarding the value or harm of the intervention recommendations may be made on
other groundsD There is fair evidence to support the recommendation that the intervention not be performedE There is good evidence to support the recommendation that the intervention not be performed
Table 2 Evidence level [10]
Evidencelevel
Definition
I Evidence obtained from at least one properly designed randomized controlled trialII Evidence obtained from well-designed controlled trials without randomization or from well-designed cohort or
casendashcontrol analytic studies preferably from more than one center or research group or from multiple time serieswith or without the intervention Dramatic results in uncontrolled trials might also be regarded as this type ofevidence
III Opinions of respected authorities based on clinical experience descriptive studies or reports of expertcommittees
179Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
2 Collocation of comments and ideas by the moderator using thewords of the participants
3 Clarification and substantiation of comments and ideas on alter-native guideline statements by the participants
4 Reconcilement of the manuscript and all alternative guidelinestatements
Table 4 Studies for 2010 update identified by the MEDLINE sear
Drugtreatment Mean age(age range) ofparticipants atstudy (years)
Totaof pa
Foeldvari et al [20] Celecoxibe 103 (2ndash16) 264Ceacutespedes-Cruzet al [33]
MTX 82 (np) 521
Lovell et al [45] Etanercept 104 (4ndash17) 58Horneff et al [83] Etanercept 129 (4ndash17) 20Giannini et al [46] Etanercept 99 (2ndash18) 594Lovell et al [40] Adalimumab 113 (4ndash17) 171Ruperto et al [31] Infliximab 112 (4ndash18) 121Lequerreacute et al [51] Anakinra 124 f (3ndash23) 20 f
Illowite et al [50] Anakinra 12 (2ndash17) 86Yokota et al [53] Tozilizumab 83 (2ndash19) 65Ruperto et al [54] Abatacept 124 (6ndash17) 190Singh-Grewal et al [58] Vigorous exercise
training116 (8ndash16) 80
Brinkmann et al [56] Stem celltransplantation
85 (4ndash18) 22
Abbreviations np = not provideda Not further specifiedb Only extended oligoarticular JIAc Pauciarticular onset with polyarticular coursed Extended oligoarticular JIA were included into polyarticular JIAe All JIA with polyarticular course with any type of onset not furthef Pediatric patients total number of patients in extended report wa
5 Discussion of statements and further explanation of any of thecomments that were not clear to all participants Each memberof the consensus group contributed to the discussion The moder-ator kept the process as neutral as possible avoiding judgmentand criticism
6 Final reconcilement for statements for guideline
ch algorithm (see Methodology)
l numbertients (n)
JIA
Oligoarticular Polyarticular Systemiconset
Othersubtypes
128 (53) a 114 (47) 22 (9)162 (31) b 284 (55) 75 (14)
5 (9) c 34 (58) 19 (33)2 (10) b 16 (80) 2
d 535 (90) 58 (97) 1171 (100) e
28 (23) c 74 (61) 19 (16)20 (100)
9 (10) c 62 (72) 15 (17)56 (100)
30 (16) 122 (64) 37 (20) 118 (23) 34 (43) 7 (9) 21 (26)
4 (18) 18 (82)
r specifieds 35 (15 were patients with adult onset of Still disease)
Consensus statement
NSAIDs are recommended for the treatmentof JIA Diclofenac Naproxen Ibuprofen andIndometacin (evidence level I respectively IIrecommendation grade A)If those drugs are contraindicated Celecoxibemight be used (evidence level I recommendationlevel BndashC)
Consensus statement
Intra-articular injections of crystalloid cortico-steroids (triamcinolone hexacetonide) are recom-mended and can be part of the first linetreatment Improvement of local inflammationpain swelling and range of joint movement hasbeen demonstrated (evidence level II recommen-dation grade A)Triamcinolone hexacetonide is more efficientthan triamcinolone acetonide inducing local remis-sion (evidence level I recommendation grade B)
180 G Dueckers et al
The conference guideline topics were reviewed andedited by working groups After the first consensus confer-ence statements were adopted by NGT and additional pro-posals for schemes of treatment strategies of JIA werecollated
25 Consensus finding method of Delphi
Three out of 15 statements remained without consensusafter NGT These statements comprise the utility of etaner-cept (treatment resistant polyarticular JIA) sulfasalazine(treatment resistant JIA) and anakinra (treatment for refrac-tory SoJIA) Therefore they were sent to all participants ofconsensus conferences via email To each of them partici-pants should state one of three votes (ldquoagreerdquo ldquodo notagreerdquo or ldquoalternative proposalrdquo) (1st round of Delphi)The results were summarized and the statements whichremained with no consensus after 1st round of Delphi weresent to participants again (2nd round of Delphi) After 2ndround of Delphi results were sent to external review
26 External review and adoption
The guideline manuscript has been reviewed in 2007 by na-tional experts in German Rheumatology Huppertz (BremenGermany) Michels (Garmisch Partenkirchen Germany) andSpecker (Essen Germany) The comments of external re-viewers (HI Huppertz) to the 2011 manuscript were in-volved within the 3rd round of Delphi External reviewenabled adoption of the guidelines core conclusions andstatements with strong consensus ie 95 agreement byrepresentatives of participating scientific societies andorganizations
3 Results treatment guidelines
31 Drug-based therapy
Drugs used in treatment of JIA are summarized in Table 5 Pro-posed schemes of treatment of JIA are shown in Fig 2 The fol-lowing paragraphs will highlight specific adverse reactions andintroduce the 13 studies relevant for the 2010 update of treat-ment guideline for JIA briefly For detailed information aboutprescribing information including indication contraindica-tion drug dosage route of administration monitoring andproduct characteristics the consensus group recommendsconsulting national drug data bases e g wwwrotelistede(German database of drugs with national market approval) orwwwfdaorg or wwwemaeuropaeu
311 Non-steroidal anti-inflammatory drugs (NSAIDs)Commonly NSAIDs are well tolerated Main side effects
of NSAIDs are stomach irritation dyspepsia andmdashin rarecasesmdashnephritis Cephalgia and behavioral changes can beassociated with the administration of ibuprofen Pseudo-porphyria is not uncommon in patients treated withnaproxen Pain relief has been demonstrated for Naproxen[13ndash15] Diclofenac [1516] and Ibuprofen [17] (evidencelevel I) and for Indometacin [18] and Meloxicam [19](evidence level II) Efficacy of Celecoxibe has been
demonstrated in a randomized double blind multicenterstudy [20] 95 of 212 patients entered the 12 week openlabel phase after a 12 week double blind phase in threetreatment groups (Celecoxibe 6 mgkgd versus Celecoxibe12 mgkgd versus Naproxen 15 mgkgd) Both dosages ofCelecoxibe showed comparable efficacy compared toNaproxen Safety ie number of adverse events (AE)did not differ significantly between Celecoxibe versusNaproxen
312 Glucocorticoids
3121 Glucocorticoids (GC)mdashlocal administration Theuse of intra-articular crystalline corticoids is highly potentand has a rather low rate of complications (evidence levelII) [2122] They might be administered as first line therapyResponse rate was significantly higher with triamcinolonehexacetonide than with triamcinolone acetonide at6 months and this difference was sustained to 24 months[2122] These findings were independent of duration andextent of disease [2122] Simultaneous intra-articular ste-roid injections are preferable to consecutive injections atdifferent time points (limited suppression of hypothalamicndashpituitaryndashadrenal axis) [23] Side effects eg local necrosisof fat tissue are seen in approximately 2 of injections [22]Working under sterile conditions the risk of infection is low
3122 GCmdashsystemic administration GC can be adminis-tered as a fast acting drug in highly active disease Indica-tions for their use are bridging time until DMARDs (diseasemodifying anti rheumatic drugs) become effective treat-ment of severe systemic features of systemic-onset JIA(SoJIA) induction of remission in polyarticular JIA and in se-vere forms of uveitis There are no controlled trials and nostandardized therapeutic regimes for the use of systemic
Table 5 Drugs for the treatment of JIA
Generic Dosage Age approval by Europeanmedical agency inpediatric rheumatology(EMA) a
Medical indication in pediatricrheumatology a b
Evidence levelrecommendationgrade [10]
Literature
NSAIDsDiclofenac 2ndash3 mgkg Bwd po (in 3 doses)
Retard formulation 1 dose14 years Arthritis IndashA Haapasiri [16] Laxer [14]
Ibuprofen 20ndash40 mgkg Bwd po in 3ndash4doses
6 months Pain fever IndashA Giannini [17]
Indometacin 1ndash3 mgkg Bwd po in 3 doses 2 years Arthritis IIndashA Stoeber [18]Meloxicam 0125ndash025 mgkg Bwd po 15 years Arthritis II Ruperto [19]Naproxen 10ndash15 mgkg Bwd po in 2 doses 1 year Arthritis IndashA Kvien [13] Laxer [14] Leak
[15]Celecoxibe 6 mgkg Bwd po in 2 doses or
12 mgkg Bwd in 1 doseNo approval for children Arthritis I B-C Foeldvari [20]
Glucocorticoids (GC)a) Systemic GCPrednisonePrednisolone
01ndash02 mgkg Bwd (max 5 mgd) JIA ie severe SoJIA severe peri-myokarditis severe uveitis (hypotoniaor cystoid macular edema) intoleranceto other drugs (ldquolow-doserdquo) or asldquobridgingrdquo therapy in higher doses eg2 mgkg Bwd until therapeutic effectof ldquoDMARDsrdquo
III Prieur [28]
Prednisone as an oralhigh-dose therapy
ge1ndash2 mgkg Bwd prednisolone-equivalent
III Prieur [28]
Prednisone as an oralmedium-dosetherapy
02 tob10 mgkg Bwdprednisolone-equivalent
III Kirwan [24] Prieur [28]
Prednisone as an orallow-dose therapy
b02 mgkg Bwd Prednisolone-equivalent or b4 mgmsup2 bodysurface
III Michels [25]
Prednisone as a ivpulse-therapy
N(5)ndash10 mgkg Bw (po)Prednisolone-equivalent10ndash30 mgkg Bwd Methyl-Prednisolone iv for 1ndash3 d(maximum 1 gdose)
III Miller [26] Picco [27]
b) Intra-articular GCTriamcinolonehexacetonide
05ndash1 mgkg Bw into large jointsdose adaption referring to size ofjoint (eg max 2 mg intointerphalangeal joints c)
5 months Arthritis tendo-vaginitis I Zulian [2122]
(continued on next page)(continued on next page)
181Evidence
andconsensus
basedGKJR
guidelinesfor
thetreatm
entof
juvenileidiopathic
arthritis
Table 5 (continued)
Generic Dosage Age approval by Europeanmedical agency inpediatric rheumatology(EMA) a
Medical indication in pediatricrheumatology a b
Evidence levelrecommendationgrade [10]
Literature
DMARDsSulfasalazine 30ndash50 mgkg Bwd in 2ndash3 doses 6 years Arthritis II Van Rossum [3637]Cytotoxic or immuno-suppressive drugsMethotrexate 10ndash15 (20) mgmsup2 body surface
once a week (po sc iv) e2 years Polyarticular JIA Psoriasis arthritis
uveitis CollagenosisI Giannini [84] Ravelli [85]
Woo [86]Cespedes-Cruz [33]Azathioprine 15ndash3 mgkg Bwd po in 1ndash2
dosesNo approval for children II Kvien [34]
Leflunomide No clear recommendation forchildren availableBwb20 kg d 1100 mgkg from d 2 10 mgkgdBw 20ndash40 kg d 1 to d 2 100 mgkgfrom d 3 10ndash20 mgkgdBwN40 kg d 1 to d 3 100 mgkgfrom d 3 20 mgkgd
No approval for children II Silverman [3587]
Biologic agentsa) TNFα inhibitorsEtanercept d 08 mgkg Bw sc 1timesweek
(max 50 mgweek) or 04 mgkgBw sc 2timesweek (max 50 mgweek)
4 years JIA Polyarthritis and insufficientefficacy of MTX
I Giannini [46] Horneff [49]Lovell [3888] Prince [41]
Adalimumab d 24 mgm2 body surface sc in 1dose every 2 weeks Bwb30 kg20 mgm2 body surface BwN30 kg40 mgm2 body surface(max 40 mg per dose)
4 years to 17 years Adalimumab in combination withmethotrexate is indicated for thetreatment of active polyarticularjuvenile idiopathic arthritis in childrenand adolescents who have had aninadequate response to one or moredisease-modifying anti-rheumatic drugs(DMARDs)
I Lovell [40]
182GDueckers
etal
Infliximab d 3ndash10 mgkg Bwdose iv Infusionat d 0 d 14 d 42 then every8 weeks intervals of applicationremain unclear
No approval for childrenwith JIA6 years (approval forMorbus Crohn)
III Ruperto [31]
b) IL-1 inhibitorsAnakinra d 1ndash4 mgkg Bwd sc in 1 dose No approval for children II Illowite [50] Lequerre [51]Canakinumab d 4 mgkg Bwsingle dose sc every
4 weeks (max 150 mg)No approval for childrenwith JIA 4 years (approvalfor CAPS)
III Ruperto [89]
Rilonacept d 1ndash2times44 mgkgweek sc (max320 mg) then 22 mgkgweek sc(max160 mg)
No approval for childrenwith JIA 12 years(approval for CAPS)
Lovell [889091]
c) IL-6 inhibitorsTocilizumab d 1 h Infusion every two 2 weeks
Bwb30 kg 8 mgkg BwN30 kg12 mgkg
2 years of age or older Since May 2011 EMA approval forpediatric patients with SoJIA who haveresponded inadequately to previoustherapy with NSAIDs and systemiccorticosteroids (Approval at Japan forSoJIA and polyarticular JIA since 2008) c
I Yokota [53] Ruperto [92]de Benedetti [62]
d) Co stimulatory-antagonistsAbatacept d 10 mgkg iv Infusion at d 0 d 14
d 28 then every 4 weeks6 years of age and older Abatacept in combination with
methotrexate is indicated for thetreatment of moderate to severe activepolyarticular (JIA) in pediatric patientswho have had an insufficient responseto other DMARDs including at least oneTNF inhibitor
I Ruperto [549394]
Abbreviations CAPS=Cryopyrine associated periodic fever syndrome JDM=juvenile dermatomyositis Bw=body weight SoJIA=systemic-onset of JIA SLE=systemic Lupus erythematodesa Compare wwwemaeuropaeub wwwrotelistede (German database of drugs with national market approval)c Intra-articular injection into same joint no more often than once every 3 monthsd A statement from insurance companies should be acquired before treatment initiation for off label treatment (if possible)e Oral application is most feasible in childhood
183Evidence
andconsensus
basedGKJR
guidelinesfor
thetreatm
entof
juvenileidiopathic
arthritis
Oligoarticular JIA
Polyarticular JIA
SoJIA
Figure 2 JIA treatment escalation schemes +=addition of the drug (abbreviations NSAIDs=non steroidal anti-inflammatory drugthotrexate)
Consensus statement
Long-term use of systemic GC is not recom-mended Continuous administration of ge02 mgPrednisolone equivalent per kg bodyweight (Bw)carries a high risk of adverse events and thereforeis not recommended (evidence level III recom-mendation grade A)
Consensus statement (continued)
184 G Dueckers et al
GC in JIA published thus leading to ldquojustrdquo evidence level IIIDifferent recommendations of dosage and therapy regimesare listed in Table 5 (evidence level III for all recommenda-tions) [1824ndash28] Frequency and seriousness of deleteriouseffects correlate mainly to duration of therapy and dosageof GC administered Main side effects are iatrogenicCushings syndrome growth disturbance weight gainmood changes Higher dosage carry the risk of increasedvulnerability to infection hypertension osteoporosisthrombosis diabetes gastro-intestinal ulceration cataractglaucoma atrophy of subcutaneous fatty tissue steroid in-duced acne To inform colleagues about GC treatment in acase of emergency and to reduce severe complications in longterm treated patients ie GC administrationN4 weeks thesupply of ldquoGlucocorticoid ID cardsrdquo for patients might be useful
GC=Glucocorticoids DMARDs=disease modifying drugs MTX=Me
Consensus statement
The systemic use of GC is recommended asfast acting drugs in highly active JIA GC areused for the treatment of children and adoles-cents with SoJIA organ manifestations of JIA(eg uveitis pericardial effusion) sero-positivepolyarticular JIA and for bridging time untilthe complete therapeutic effect of DMARDs(evidence level III recommendation grade A)
313 Methotrexate (MTX) biologic agents andimmunosuppressive agents
MTX biologic agents and immunosuppres-sive agents are used for the treatment of childrenand adolescents with polyarticular JIA ifNSAIDs or local GC treatment do not succeedThe combination of those drugs with NSAIDsand GC is feasible A common characteristic ofMTX biologic agents and immunosuppressiveagents is the delayed onset of therapeutic ef-fect ie up to 3 months or even longer aftercommencing treatment
185Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
Safe contraception is indicated during therapy with MTXAzathioprine or Leflunomide and in the following 3 to6 months after its discontinuation
Consensus statement
Administration of Sulfasalazine or Lefluno-mide is recommended if MTX or Etanercept donot show sufficient efficacy or cannot be used
3131 Methotrexate Among DMARDs MTX provides themainstay of long-term therapy in JIA [29ndash32] In case ofside effects eg dyspepsia or nausea prophylaxis withfolic acid can be recommended (1times1 mg per day or 5 mgonce a week 24ndash48 h after application of MTX) Safe contra-ception is mandatory while receiving MTX Safety and effica-cy of MTX and its impact on quality of life of children with JIAhave been investigated Significant positive impact of MTXon all health-related quality of life health conceptshas been shown although the study has its limit due to dif-ferent MTX dosages used within participating JIA patients[33]
Consensus statement
MTX administration can be recommendeddue to its proven safety and efficacy to reducedisease activity MTX is used in case of insuffi-cient therapeutic effect of NSAIDs andor localGC administration continuous need for system-ic GC andor highly active disease Efficacy ofMTX (orally or subcutaneously administered) isfrequently achievable with a dosage of 10ndash15 mgmsup2 body surface (evidence level I recom-mendation grade A)
for other reasons (evidence level II recommen-dation grade B)
3132 Purine analogs31321 Azathioprine Efficacy has been investigat-
ed in a double blind placebo controlled study (32 patients)After 8 weeks of therapy the changes in disease activitymeasurement indicated a minor improvement in the Azathi-oprine group compared to the placebo group At the end ofthe study statistically significant differences between thegroups were found for only 2 disease activity measurements[34] Two patients were taken out of study due to severeadverse events eg leucopenia Measurement of activityof Thiopurinmethyltransferase (TPMT) can be beneficial foravoidance of severe adverse events
3133 Pyrimidine analogs31331 Leflunomide Within a double blind study
(32 weeks 94 patients) efficacy of Leflunomide was inferiorin comparison to MTX but better than placebo Howeverdosing of Leflunomide may not have been adequate insome children [35] Contraindications for Leflunomide arerenal insufficiency severe immunodeficiency depressedmyelopoesis and pancytopenia An extensive half-life peri-od (approximately 14 days) has to be taken in accountwhen administering Leflunomide In combination with hepa-totoxic DMARDs the risk of severe adverse events might in-crease eg increased blood pressure is seen frequentlySafe contraception is mandatory
3134 Antibiotic analogs and Hydroxychloroquine andChloroquine
31341 Sulfasalazine Weak efficacy of Sulfasalazinewas demonstrated within a placebo-controlled randomizedstudy after 24 weeks (96 patients) [3637] One third of pa-tients enrolled in the study discontinued treatment with Sulfa-salazine due to side effects eg gastrointestinal symptomsleucopenia [36] Some experts use sulfasalazine in HLA-B27positive JIA Contraindications are Glucose-6-phosphatase de-ficiency and hypersensitivity against sulfonamides
31342 Hydroxychloroquine and chloroquine Hydrox-ychloroquine and Chloroquine have been subject to clinical tri-als for the treatment of JIA even though efficacy was limitedWithin three consensus conferences held in 2007 and 2010 theconsensus group decided not to give a consensus statementon the use of chloroquine or hydroxychloroquine treatmentdespite the fact that those drugs still might be used by somecaregivers
3135 Biologic agents Biologic agents are drugs whichselectively inhibit cytokines cytokine receptors or directlybind to receptors of lymphocytes eg CTLA-4 CD20 Theyinclude antibodies and fusion proteins So far allbiological therapies are administered subcutaneously orintravenously
31351 TNFα-inhibitors TNFα-inhibition with Adali-mumab and Etanercept is efficient and safe (evidencelevel I) [38ndash41] Both drugs have been approved for JIAwith polyarticular course TNFα-inhibitors have become anintegral part of the treatment of JIA Potential risks of therapyare vulnerability for infection andmdashin a rare occasionmdashthe in-duction of autoimmune disease Prior to the start of treatmentwith TNFα-inhibitors chronic infections needs to be excludedor treated sufficiently eg tuberculosis hepatitis B or C
In children with JIA treated with TNFα-inhibitors malig-nancies eg Lymphoma have been reported It remainsunclear if the rate of malignancies is increased in patientscompared to the risk by having JIA itself In response to aprevious letter of the FDA (as reviewed in [42]) the GermanSociety for Pediatric Rheumatology (GKJR) has published of-ficial statements [4344] The GKJR states that treatmentwith TNFα-inhibition should be used very carefully physi-cians need to be aware of co-medication e g immunosup-pressive drugs and should monitor those patientsclosely [43] There is insufficient data on all biologicagentsmdashincluding TNFα-inhibitionmdashto judge about the long-term risk for children and adolescents313511 Etanercept Etanercept is a fusion proteinconsisting of the extracellular binding domain of solubleTNFα-receptor and Fc chain of human IgG1 Etanercept in-hibits TNFα by direct binding of the cytokine Efficacy has
Consensus statement
The use of Anakinra or Tozilizumab can berecommended for treatment of children and ado-lescents with refractory SoJIA (evidence level IIrecommendation grade A)
186 G Dueckers et al
been demonstrated in a randomized controlled withdrawaldesign trial for patients with polyarticular JIA [38] Withinan open extension study long term efficacy and safety havebeen documented over 8 years in 1669 patients [3945]There is data on more than 2000 patients registered in Euro-pean registries [46ndash48] Currently retrospective data showsa somewhat better efficacy of combining MTX or otherDMARDs with TNFα-inhibition versus anti-TNFα therapy assingle therapy [49]313512 Adalimumab Adalimumab is a humanizedmonoclonal IgG1 antibody directed against TNFα whichbinds soluble and membrane bound TNFα A randomizedcontrolled withdrawal design trial demonstrated safety andefficacy of Adalimumab (24 mgmsup2 body surface every2 weeks max 40 mg) for children and adolescents withpolyarticular JIA (4ndash17 years of age n=171) [40] After16 weeks ldquowash inrdquo phase responders (n=144171) enteredthe 32 weeks randomized double blind phase After 48 weekstwice the number of patients in the verum group met ACR 70as compared to the control group (56 vs 28 pb001)Within the open extension phase Adalimumab dosage wasfixed ie 20 mgb30 kg Bw and 40 mgN30 kg Bw There islack of evidence showing superior efficacy of combiningMTX (DMARDs) with Adalimumab versus Adalimumab as sin-gle therapy [40]
Consensus statement
Efficacy of Etanercept and Adalimumab forthe treatment of polyarticular JIA has been dem-onstrated Therapy with TNFa-inhibition is indi-cated in case of insufficient therapeutic effectof NSAIDs and local GC administration and lackof response to MTX (evidence level I recom-mendation grade A)
Consensus statement
Patients with polyarticular JIA without sys-temic manifestation refractory to treatmentwith MTX and TNF inhibition might benefit fromthe use of Abatacept (evidence level III recom-mendation grade C)
313513 Infliximab Infliximab is a chimerical (humanmouse) monoclonal antibody which binds soluble and mem-brane bound TNFα A randomized controlled study in childrenand adolescents with JIA failed to demonstrate a significantdifference of efficacy after treatment with Infliximab com-pared to placebo [31]
31352 Interleukin-1-inhibitors None of interleukin-1-inhibitors are approved for the treatment of JIA or SoJIAThey are commonly used in an off label setting313521 Anakinra Anakinra is an IL-1 receptor antag-onist Within a randomized controlled trial no significant ef-ficacy of Anakinra for patients with polyarticular JIA couldbe demonstrated [50] 50 of 86 patients were enrolled intoblinded phase (11 Anakinra versus Placebo) No significantreduction of flare could be demonstrated in comparison toplacebo 29 of 50 patients completed the open label exten-sion study Two noncontrolled nonrandomized studieshave shown efficacy of anakinra in a proportion of patientswith systemic-onset of JIA (SoJIA) [5152]313522 Canakinumab Canakinumab an IL-1β anti-body binds IL-1β selectively without interfering with IL-1αor its physiological IL-1 receptor antagonist Canakinumabhas been approved for treatment of hereditary periodic IL-1 associated periodic fever syndromes ie Cryopyrin-
associated periodic syndromes There are ongoing studies in-vestigating safety and efficacy of Canakinumab for SoJIA
31353 Interleukin-6 inhibitors313531 Tozilizumab Tozilizumab is a humanizedanti-IL-6 receptor monoclonal antibody Efficacy has beendemonstrated within a 12 week double blind randomizedcontrolled withdrawal trial in children with SoJIA (n=562ndash19 years) in Japan [53] After a 48 week open extensionstudy ACR Pedi 30 was met by 47 patients (98) At thetime of our literature search Tocilizumab was approved fortreatment of SoJIA and polyarticular JIA since 2008 inJapan A multicenter European study investigating efficacyand safety of Tozilizumab in polyarticular JIA was ongoingat the deadline of literature search (wwwclinicaltrialsgov NCT00988221) No data on long term effects are cur-rently available
31354 Co-stimulation inhibitors313541 Abatacept Abatacept is a recombinant fu-sion protein of extracellular domain of human cytotoxic T-Lymphocyte Antigen 4 (CTLA-4) and IgG1-Fc-Fragment Itmodulates T-cell co-stimulation A randomized controlleddouble blind withdrawal design study of Ruperto et al [54]demonstrated efficacy of Abatacept in patients with polyar-ticular JIA 123 of 170 participants of study were enrolled inthe 6 month double blind phase Flares occurred in 33 of 62(53) patients who were given placebo versus 12 of 60(20) Abatacept patients during double blind phase Adverseevents (AE) did not differ in both groups ie 37 AE in Abata-cept versus 34 AE in placebo recipients Some children maytake 3 to 6 months or longer before their maximal responseis achieved 3 of patients developed reaction to the infu-sion [55] Abatacept is approved by FDA and EMA for pa-tients who did not respond to prior MTX treatment Nodata of long term effects of the use of Abatacept in JIA areavailable due to the low numbers of patients treated so far
314 Autologous stem cell transplantation (SCT)There are studies on autologous SCT for treatment of re-
fractory and severe forms of JIA (evidence level III) [56] 22
Consensus statement
187Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
patients were enrolled in one study 8 reached clinical re-mission 7 were assessed as partial responders 3 experi-enced relapse of the disease and 4 (18) died as aconsequence of MAS or immunosuppressive treatment [56]Due to serious adverse events including death this thera-peutic option is seen as the last treatment option
Exercise training is recommended dependingon the extent of inflammation number of affect-ed joints and global disease activity Sports withminor stress on joints is favorable (evidence levelI recommendation grade A)
32 Non-drug based therapy
321 Physiotherapy occupational therapy and thera-peutic appliances
Physio- and occupational therapy are integral parts of thetherapeutic concept in children and adolescents with JIA[5758] Therapeutic goals of physiotherapy are relaxationand pain relief preservation or rehabilitation of physiologi-cal range of joint movement prevention of contracturesstretching and activation of muscles build-up of muscleforce and training of physiological movements
Consensus statement
Structured treatment by a properly trainedphysiotherapistoccupational therapist in combi-nation with drug based therapy and instructionsfor disease adopted self-sufficient daily exercisesessions are recommended to keep and to im-prove joint mobility (evidence level II recom-mendation grade A)Custom-made therapeutic appliances for correc-tion of axial misalignment prevention of falseweight bearing stabilization of joints (eghand- finger- and foot-ortheses) are recom-mended individually The use of therapeutic ap-pliances follows individual physician-directedadvice Efficacy has been demonstrated (evi-dence level I recommendation grade B)
Consensus statement
In individual cases the indication for open orarthroscopic synovectomy can be considered ifconservative therapy does not succeed (evi-dence level III recommendation grade B)
Consensus statement
Other forms of non-drug based therapeutic approachesrely on experts opinion and are solely based on individualclinical experience No controlled studies are available
Consensus statement
The implementation of thermotherapy electro-or ultrasound therapy massage and lymph drain-age is recommended Application of cold appli-ances for acute joint inflammation is indicated(evidence level II recommendation grade A)Electro- and ultrasound therapy are recom-mended for patients with tendosynovitis (evi-dence level III recommendation grade B)
An early psychological support within stan-dard pediatric rheumatological care should beimplemented to apprehend and treat mental is-sues and behavioral syndromes associated withphysiological disturbances and physical factors(evidence level III recommendation grade A)
Consensus statement
A socio-pedagogical care with regard tointegration at school professional andeveryday life and formal education of parentsand patients is recommended (evidence levelIII recommendation grade A)
322 Sportive activity and exercise trainingPositive impact of sportive activity on the general physi-
cal condition and on oxygen consumption has been demon-strated (evidence level II) [57ndash60] Adequate exercise
training supports the physiological development and helpscoping with JIA [58] Prospective controlled long term stud-ies are currently not available
323 Surgical treatmentToledo et al investigated the role of arthroscopic syno-
vectomy in JIA They concluded that arthroscopy is a safebut only partially effective procedure in patients witholigoarticular JIA (evidence levelrecommendation gradeIIIB) [61]
324 Psychological social intervention orsocio-pedagogical care
There are no controlled or open studies focusing on psy-chological social andor socio-pedagogical intervention inchildren or adolescents with JIA Recommendations arebased on experts opinion and personal experience solely
188 G Dueckers et al
4 Addendum
Since the deadline January 15th 2010 new papers haveappeared that are of interest in the context of our guideline[5562ndash64] in particular we refer to the ACR recommenda-tions [65] and the most recent literature on the risk of malig-nancies in JIA in context with TNF blocking agent andindependent of medication [42] [66] Moreover there is arecent study on the use of Tocilizumab in polyarticular pa-tients [67] These papers will be discussed within the nextconsensus conference by NGT and considered for inclusioninto the next edition of this guideline On 6th of September2011 our advanced search on wwwclinicaltrialgov (searchterms juvenile idiopathic arthritis recruitment open stud-ies study type interventional study age group child(birthndash17) intervention drugs) led to 16 trials which are cur-rently recruiting or will soon start recruiting
5 Discussion
To develop clinical practice guidelines of high quality andvalidity a formal consensus process and explicit methodo-logical criteria for the production of guidelines are recom-mended [68ndash70] Our guideline for the treatment of JIA inchildren and adolescents implements all these issues Thesystematic literature search was terminated on 15th January2010 leading to the most up to date guideline for JIA whichis currently available The deadline of the ACR recommenda-tions as published recently by Beukelmann et al was 5th ofOctober 2009 [65] By exclusion of case reports trials with-out control groups preliminary results published as ab-stracts on conferences and the strict graduation of theliterature by the criteria of evidence based medicine weaimed to give our guideline statements additional strengthand a maximal validity Newer original studies providing ad-ditional evidence for the treatment of JIA became availableafter our consensus process was finished see AddendumThe results of these trials have to await the next NGT beforeinclusion into our recommendations
Our updated systematic literature search in 2010 led to13 relevant studies published after 30th June 2007 (Fig 1Table 4) Their results have to be interpreted with cautionFirst trials in JIA are mainly based on limited numbers of pe-diatric patients as the recruitment of a sufficient number ofpediatric patients remains challenging Second trials aremainly designed for patients with polyarticular JIA or witholigoarticular onset and a polyarticular course (Table 4)Most children with JIA do not have a polyarticular subtypeof JIA but an oligoarticular onset and course [71] Thus pa-tients with oligoarticular JIA are heavily underrepresentedin most of the current trials Third in 5 of the 13studies the withdrawal study design has been used[4045505354] Lehmann reviewed the bias of withdrawaldesign trials in 2008 [72] After a wash-in phase only re-sponders to treatment are eligible for randomization Thusthe design preselects responders to the placebo effect whomight retain their response throughout the entire study peri-od Further there is a carryover effect of AE into the place-bo group so that significant differences in AE betweengroups may not become apparent In the one placebo con-trolled trial without withdrawal design on TNFα-inhibition
(Infliximab) no significant efficacy could be demonstratedbetween verum and placebo [31]
To our knowledge there are two other guidelines that dealwith the management of JIA as a whole (Table 6) [65] [73]Other guidelines are limited to the use of single drugs in JIAeg biologic agents [74] etanercept [75] The Australian guide-line (wwwracgporgauguidelinejuvenileidiopathicarthritis)has not been published in a peer-reviewed journal It is to pro-vide recommendations for the early diagnosis and multidisci-plinary management of JIA in the primary care setting forgeneral practitioners (GPs) [73] No recommendations aremade regarding the use of GCs DMARDs immunosuppressivedrugs or biologic agents [73] The ACR recommendations usesthe Appraisal of Guidelines for Research and Evaluation(AGREE) instrument [65] [76] which does not fulfill criteria ofa proper consensus process and carries the risk that expertsvote for peer opinion which might not reflect the true valueWe used an advanced and linguistically validated version ofthe AGREE instrument the ldquoGerman Instrument for Methodo-logical Guideline Appraisal (DELBI)rdquo which has been developedin cooperation of the AWMF among others [7778] We followedthe highly structured Nominal Group Technique as described inMethodology Our consensus group only considered formallyboard nominated representatives of multidisciplinary scientificsocieties and organizations (Table 1) and included patients rep-resentatives as this has been strongly recommended by the Eu-ropean League against Rheumatism (EULAR) recently [79] TheACR mentions a parent representative within their task forcepanel but leaves this representative anonymous It remainsunclear how ACR experts were selected and involved [65]They defined treatment groups which have not been evaluatedsystematically so far We used the ILAR classification systemwhich has been repeatedly evaluated [80ndash82]
By content there are major differences between the ACRrecommendations and our guideline a) Our guideline pro-vides a detailed and systematic list of 20 drugs commonlyused in the treatment of JIA (Table 5) which has been an in-tegrative part of our consensus conferences The ACR recom-mendations do not provide information on approval status(Food and Drug Administration) indications for use and nospecific differences on dosage regimes or frequency ofdaily application [65] eg it refers to the 2008 ACR recom-mendations for the use of DMARDs in adult rheumatoid ar-thritis b) The ACR recommendations provide a more earlyaggressive approach in the treatment of JIA The ACR recom-mends MTX as first line treatment in patients (b4 joints) withhighly active disease [65] To our knowledge there are onlydata to recommend MTX administration in cases of insuffi-cient therapeutic effect of prior treatment with NSAIDandor GC [33] c) The ACR recommends the use of TNFα in-hibitors as escalation therapy for some patients with historyof arthritis of 4 or fewer joints and refer to publications[3840] conducted in patients with polyarticular JIA or pau-ciarticular JIA with polyarticular course [65] There is no ev-idence that TNF is safe and efficient in patients witholigoarticular JIA a systematic controlled clinical trial onthis issue has not been done yet d) We regard a brief trialof local or systemic administration of GC plus NSAID as a fea-sible first line treatment for patients with polyarticular JIAThe ACR recommends MTX without regard to disease activityat the initial stage [65] We reached consensus to recom-mend the use of GC as bridging therapy until full onset of
Table 6 Overview of recommendationsguidelines for treatment of JIA
USA Australia Germany
ACR recommendations[65]
RACGP recommendations[73]
GKJR guidelines
Deadline of literature search October 2009 January 2007 September 2010Source of publications Pub Med Pub Med
EMBASE CINHAL CochraneLibrary provisionalAustralian Guideline [95]
Pub MedPrevious German Guidelines [78]
Definition used for JIA subgroups Treatment groups definedby Core expert panel
Not specifically definedChildren withJIAb16 years
ILAR criteria [1]
Consensus processprocessvalidation
AGREE [76] AGREE [76] DELBI [77]RANDUCLA appropriatenessmethod [96]
NGT Delphi method
Conferences None None 3 Formal consensus conferencesAddressees Pediatric rheumatologists General practitioner Pediatric Rheumatologists
PediatriciansGeneral practitioners
Participating scientific societies or professional organizationsPediatric rheumatologist orrheumatologists for adolescents
Yes Yes Yes
General pediatrician- In hospital Yes Yes Yes- In private practice Yes Yes YesResearcher Yes No YesRheumatologists for adults No No YesOphthalmologists No No YesParentspatients support groups Yes No YesOrthopedic surgeons No No YesPediatric orthopedic surgeons No No YesPsychologists No No YesPhysiotherapists No No YesPediatric rheumatology nurses Yes No NoOther scientific societies ororganizations
ACR BSPAR PRINTO PReS RACGP NAMSCAG NHMRC DGKJ DGPs DGRh DGO AWMFBVKJ
(ACR=American College of Rheumatologists AGREE=Appraisal of Guidelines for Research amp Development AWMF=Association of the ScientificMedical Associations BSPAR=British Society for Pediatric Rheumatology BVJK=Association of Pediatricians in private practice CEP=Core expertpanel ILAR=International League against Rheumatism CINHAL=Cumulative Index to Nursing and Allied Health Literature DELBI=German In-strument for Methodological Guideline Appraisal DGKJ=German Society of Pediatrics and Adolescent Medicine DGO=German Society for Oph-thalmology DGPs=German society for Psychology DGRh=German Society for Rheumatology GKJR=German Society for Pediatric RheumatologyNAMSCAG=National Arthritis and Musculoskeletal Conditions Advisory Group NGT=Nominal Group Technique NHMRC=National Health andMedical Research Council PReS=Pediatric Rheumatology Society) PRINTO=Pediatric Rheumatology International Trial Organization RACG-P=Royal Australian College of General Practitioner RANDUCLA=Research and DevelopmentUniversity of California at Los Angeles)
189Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
therapeutic effect of DMARDs The ACR recommendations donot provide any recommendation for the use of systemic GCfor patients with oligo- or polyarticular course of JIA exceptsystemic onset of JIA e) The ACR recommendations do notcover the topic of non-drug based therapy at all althoughthere is strong evidence that eg exercise training is a usefuladdition to drug treatment [575860]
6 Conclusion
In summary we present a treatment guideline for JIA on a con-sensus conference basis We strongly advocate an interdisciplin-ary approach including surgery physiotherapy psychosocial
intervention physical therapy medications etc and a strictformal consensus process in order to create statements thatare most appropriate for the complex clinical situation of achild and family presenting with JIA and cover all aspects ofJIA care All German pediatric rheumatology sites are partici-pating at the national pediatric rheumatologic database in theDeutsche Rheuma-Forschungszentrum at Berlin (DRFZ wwwdrfzde) It aims at quality assurance in Germany and monitorstreatment behavior of pediatric rheumatologists by using inter-nationally agreed criteria (eg joint count global physician rat-ing of disease activity global parent rating of overall well-being CHAQ ESR ACR-ped response or JADAS) The databasewill be used as a tool to monitor the application of our treat-ment guidelines
190 G Dueckers et al
Conflict of interest statement
Gregor Dueckers Novartis Pharmaceuticals CorporationBaxter (for all travel grants for scientific meetings)Nihal Guellac no conflict of interestMartin Arbogast no conflict of interestGuumlnther Dannecker no conflict of interestIvan Foeldvari Wyeth Pfizer Abbott Immunology Pharma-ceuticals Chugai (for all advisory board member)Michael Frosch no conflict of interestGerd Ganser Abbott Immunology Pharmaceuticals (advisoryboard member grants for scientific meetings) Wyeth Pfizer(advisory board member grants for scientific meetings)ChugaiRoche (advisory board member grants for scientificmeetings) Merck (grants for scientific meetings) Actelios(grants for scientific meetings) Esaote (grants for scientificmeetings)Arnd Heiligenhaus Novartis Pharmaceuticals CorporationAbbott Immunology Pharmaceuticals Alcon (for all re-search grants)Gerd Horneff Abbott Immunology Pharmaceuticals (re-search grants consulting fees non-remunerative positionsof influence) Wyeth Pfizer (research grants consultingfees speakers bureau non-remunerative positions of influ-ence) Bristol-Myers Squibb (Consulting fees) Nycomed(Consulting fees non-remunerative positions of influence)RocheChugai (Consulting fees non-remunerative positionsof influence) Sandoz (Consulting fees) Genzyme (researchgrants consulting fees non-remunerative positions of influ-ence) Swedish Orphan (research grants consulting feesnon-remunerative positions of influence)Arnold Illhardt no conflict of interestRuumldiger Krauspe no conflict of interestBarbara Markus no conflict of interestHartmut Michels Abbott Immunology Pharmaceuticals (advi-sory board member and grants for scientific meeting)Matthias Schneider no conflict of interestWolfram Singendonk no conflict of interestHelmut Sitter no conflict of interestMarianne Spamer no conflict of interestNorbert Wagner no conflict of interestTim Niehues Abbott Immunology Pharmaceuticals EssexPharma Novartis Pharmaceutical Corporation WyethPfizer (for all research grants consulting fees non-remu-nerative positions of influence)
Acknowledgment
We like to express our grateful thanks to Prof Dr Hans IkoHuppertz for proof reading the article and for an excellentdiscussion on our work We like to express our thanks to HE-LIOS Clinic for funding the open access of the article
References
[1] RE Petty TR Southwood P Manners J Baum DN Glass JGoldenberg X He J Maldonado-Cocco J Orozco-Alcala AMPrieur ME Suarez-Almazor PWoo International League of Asso-ciations for Rheumatology classification of juvenile idiopathic ar-thritis second revision Edmonton 2001 J Rheumatol 31(2004) 390ndash392
[2] B Prakken S Albani A Martini Juvenile idiopathic arthritisLancet 377 (2011) 2138ndash2149
[3] KT April DE Feldman RW Platt CM Duffy Comparisonbetween children with juvenile idiopathic arthritis (JIA) andtheir parents concerning perceived quality of life Qual LifeRes 15 (2006) 655ndash661
[4] BM Feldman B Grundland L McCullough V Wright Distinc-tion of quality of life health related quality of life and healthstatus in children referred for rheumatologic care J Rheuma-tol 27 (2000) 226ndash233
[5] JC Packham MA Hall Long-term follow-up of 246 adultswith juvenile idiopathic arthritis functional outcomeRheumatology (Oxford) 41 (2002) 1428ndash1435
[6] C Sandborg Pediatric rheumatic disease standards of care forJIAmdashthe basic foundation for quality Nat Rev Rheumatol 6(2010) 389ndash390
[7] N Guellac T Niehues Interdisciplinary and evidence-basedtreatment guideline for juvenile idiopathic arthritis KlinPadiatr 220 (2008) 392ndash402
[8] K Schnakenburg Leitlinien in der Kinder- und JugendmedizinElsevier 2005 pp H1 1ndash15
[9] P Juni L Nartey S Reichenbach R Sterchi PA Dieppe MEgger Risk of cardiovascular events and rofecoxib cumulativemeta-analysis Lancet 364 (2004) 2021ndash2029
[10] W Feldman Evidence-based Pediatrics 1st ed BC DeckersHamilton 2000
[11] AH Van de Ven AL Delbecq The nominal group as a re-search instrument for exploratory health studies Am J PublicHealth 62 (1972) 337ndash342
[12] HA Linstone M Turoff The Delphi Method Techniques andApplications Addison-Wesley Pub 1975
[13] TK Kvien HM Hoyeraal B Sandstad Naproxen and acetyl-salicylic acid in the treatment of pauciarticular and polyarticu-lar juvenile rheumatoid arthritis Assessment of tolerance andefficacy in a single-centre 24-week double-blind parallelstudy Scand J Rheumatol 13 (1984) 342ndash350
[14] RM Laxer ED Silverman C St-Cyr MT Tran G Lingam Asix-month open safety assessment of a naproxen suspensionformulation in the therapy of juvenile rheumatoid arthritisClin Ther 10 (1988) 381ndash387
[15] AM Leak MR Richter LE Clemens MA Hall BM AnsellA crossover study of naproxen diclofenac and tolmetin in sero-negative juvenile chronic arthritis Clin Exp Rheumatol 6(1988) 157ndash160
[16] J Haapasaari E Wuolijoki H Ylijoki Treatment of juve-nile rheumatoid arthritis with diclofenac sodium Scand JRheumatol 12 (1983) 325ndash330
[17] EH Giannini EJ Brewer ML Miller D Gibbas MH PassoHM Hoyeraal B Bernstein DA Person CW Fink LA Sawyeret al Ibuprofen suspension in the treatment of juvenilerheumatoid arthritis Pediatric Rheumatology CollaborativeStudy Group J Pediatr 117 (1990) 645ndash652
[18] E Stoeber L Sanger Experiences with indomethacin in long-term therapy of juvenile rheumatoid arthritis Arzneimittel-forschung 21 (1971) 1865ndash1866
[19] N Ruperto I Nikishina ED Pachanov Y Shachbazian AMPrieur R Mouy R Joos F Zulian R Schwarz V ArtamonovaW Emminger M Bandeira A Buoncompagni I Foeldvari FFalcini E Baildam I Kone-Paut M Alessio V Gerloni ALenhardt A Martini G Hanft R Sigmund S Simianer Arandomized double-blind clinical trial of two doses ofmeloxicam compared with naproxen in children with juvenileidiopathic arthritis short- and long-term efficacy and safetyresults Arthritis Rheum 52 (2005) 563ndash572
[20] I Foeldvari IS Szer LS Zemel DJ Lovell EH Giannini JLRobbins CRWest G Steidle S Krishnaswami BJ Bloom A pro-spective study comparing celecoxib with naproxen in children withjuvenile rheumatoid arthritis J Rheumatol 36 (2009) 174ndash182
191Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
[21] F Zulian G Martini D Gobber C Agosto C Gigante FZacchello Comparison of intra-articular triamcinolone hexa-cetonide and triamcinolone acetonide in oligoarticular juve-nile idiopathic arthritis Rheumatology (Oxford) 42 (2003)1254ndash1259
[22] F Zulian G Martini D Gobber M Plebani F Zacchello PManners Triamcinolone acetonide and hexacetonide intra-articular treatment of symmetrical joints in juvenile idiopathicarthritis a double-blind trial Rheumatology (Oxford) 43 (2004)1288ndash1291
[23] GS Habib Systemic effects of intra-articular corticosteroidsClin Rheumatol 28 (2009) 749ndash756
[24] JR Kirwan The effect of glucocorticoids on joint destructionin rheumatoid arthritis The Arthritis and Rheumatism CouncilLow-Dose Glucocorticoid Study Group N Engl J Med 333(1995) 142ndash146
[25] H Michels What is low-dose corticosteroid therapy in juvenileidiopathic arthritis A worldwide questionnaire-based surveyZ Rheumatol 59 (Suppl 2) (2000) II127ndash130
[26] JJ Miller III Prolonged use of large intravenous steroid pulsesin the rheumatic diseases of children Pediatrics 65 (1980)989ndash994
[27] P Picco M Gattorno A Buoncompagni V Pistoia C Borrone6-methylprednisolone lsquomini-pulsesrsquo a newmodality of glucocor-ticoid treatment in systemic onset juvenile chronic arthritisScand J Rheumatol 25 (1996) 24ndash27
[28] AM Prieur The place of corticosteroid therapy in juvenilechronic arthritis in 1992 J Rheumatol Suppl 37 (1993)32ndash34
[29] JS Gao H Wu J Tian Treatment of patients with juvenilerheumatoid arthritis with combination of leflunomide andmethotrexate Zhonghua Er Ke Za Zhi 41 (2003) 435ndash438
[30] T Niehues G Horneff H Michels MS Hock L SchuchmannEvidence-based use of methotrexate in children with rheumat-ic diseases a consensus statement of the Working Groups Pedi-atric Rheumatology Germany (AGKJR) and PediatricRheumatology Austria Rheumatol Int 25 (2005) 169ndash178
[31] N Ruperto DJ Lovell R Cuttica N Wilkinson P Woo GEspada C Wouters ED Silverman Z Balogh M HenricksonMT Apaz E Baildam A Fasth V Gerloni P Lahdenne AMPrieur A Ravelli RK Saurenmann ML Gamir N WulffraatL Marodi RE Petty R Joos F Zulian D McCurdy BLMyones K Nagy P Reuman I Szer S Travers A BeutlerG Keenan J Clark S Visvanathan A Fasanmade A Ray-chaudhuri A Mendelsohn A Martini EH Giannini A random-ized placebo-controlled trial of infliximab plus methotrexatefor the treatment of polyarticular-course juvenile rheumatoidarthritis Arthritis Rheum 56 (2007) 3096ndash3106
[32] K Visser DM van der Heijde Risk and management of livertoxicity during methotrexate treatment in rheumatoid andpsoriatic arthritis a systematic review of the literature ClinExp Rheumatol 27 (2009) 1017ndash1025
[33] A Cespedes-Cruz R Gutierrez-Suarez A Pistorio A Ravelli ALoy KJ Murray V Gerloni N Wulffraat S Oliveira J WalshIC Penades MG Alpigiani P Lahdenne C Saad-Magalhaes ECortis L Lepore Y Kimura C Wouters A Martini N RupertoMethotrexate improves the health-related quality of life of chil-dren with juvenile idiopathic arthritis Ann Rheum Dis 67(2008) 309ndash314
[34] TK Kvien HM Hoyeraal B Sandstad Azathioprine versus place-bo in patients with juvenile rheumatoid arthritis a single centerdouble blind comparative study J Rheumatol 13 (1986) 118ndash123
[35] E Silverman R Mouy L Spiegel LK Jung RK SaurenmannP Lahdenne G Horneff I Calvo IS Szer K Simpson JAStewart V Strand Leflunomide or methotrexate for juvenilerheumatoid arthritis N Engl J Med 352 (2005) 1655ndash1666
[36] MA van Rossum TJ Fiselier MJ Franssen AH ZwindermanR ten Cate LW van Suijlekom-Smit WH van Luijk RM
van Soesbergen NM Wulffraat JC Oostveen W Kuis PFDijkstra CF van Ede BA Dijkmans Sulfasalazine in the treat-ment of juvenile chronic arthritis a randomized double-blindplacebo-controlled multicenter study Dutch Juvenile ChronicArthritis Study Group Arthritis Rheum 41 (1998) 808ndash816
[37] MA van Rossum RM van Soesbergen M Boers AHZwinderman TJ Fiselier MJ Franssen R ten Cate LW vanSuijlekom-Smit NM Wulffraat WH van Luijk JC OostveenW Kuis BA Dijkmans Long-term outcome of juvenile idiopathicarthritis following a placebo-controlled trial sustained benefits ofearly sulfasalazine treatment Ann Rheum Dis 66 (2007)1518ndash1524
[38] DJ Lovell EH Giannini A Reiff GD Cawkwell ED SilvermanJJ Nocton LD Stein A Gedalia NT Ilowite CA Wallace JWhitmore BK Finck Etanercept in children with polyarticularjuvenile rheumatoid arthritis Pediatric Rheumatology Collabora-tive Study Group N Engl J Med 342 (2000) 763ndash769
[39] DJ Lovell A Reiff OY Jones R Schneider J Nocton LDStein A Gedalia NT Ilowite CA Wallace JB WhitmoreB White EH Giannini Long-term safety and efficacy ofetanercept in children with polyarticular-course juvenile rheu-matoid arthritis Arthritis Rheum 54 (2006) 1987ndash1994
[40] DJ Lovell N Ruperto S Goodman A Reiff L Jung K JarosovaD Nemcova R Mouy C Sandborg J Bohnsack D Elewaut IFoeldvari V Gerloni J Rovensky K Minden RK Vehe LWWeiner G Horneff HI Huppertz NY Olson JR Medich RCarcereri-De-Prati MJ McIlraith EH Giannini A MartiniAdalimumab with or without methotrexate in juvenile rheuma-toid arthritis N Engl J Med 359 (2008) 810ndash820
[41] FH Prince M Twilt R ten Cate MA van RossumW ArmbrustEP Hoppenreijs M van Santen-Hoeufft Y Koopman-KeeminkNM Wulffraat LW van Suijlekom-Smit Long-term follow-upon effectiveness and safety of etanercept in juvenile idiopathicarthritis the Dutch National Register Ann Rheum Dis 68(2009) 635ndash641
[42] P Diak J Siegel L LaGrenade L Choi S Lemery AMcMahonTumor necrosis factor alpha blockers andmalignancy in childrenforty-eight cases reported to the Food and Drug AdministrationArthritis Rheum 62 (2010) 2517ndash2524
[43] G Horneff T Hospach G Dannecker D Foll JP Haas HJGirschick HI Huppertz R Keitzer HJ Laws H Michels KMinden R Trauzeddel Updated statement by the German So-ciety for Pediatric and Adolescent Rheumatology (GKJR) on theFDAs report regarding malignancies in anti-TNF-treated pa-tients from Aug 4 2009 Z Rheumatol 69 (2010) 561ndash567
[44] T Hospach JP Haas HI Huppertz R Keitzer H Michels RTrauzeddl D Foll G Dannecker G Horneff Comment of theSociety of Pediatric and Adolescent Rheumatology on the USFood and Drug Administration (FDA) announcement regardingcases of malignancy in anti-TNF-treated patients Z Rheumatol68 (2009) 162ndash164
[45] DJ Lovell A Reiff NT Ilowite CA Wallace Y Chon SL LinSW Baumgartner EH Giannini Safety and efficacy of up to eightyears of continuous etanercept therapy in patients with juvenilerheumatoid arthritis Arthritis Rheum 58 (2008) 1496ndash1504
[46] EH Giannini NT Ilowite DJ Lovell CA Wallace CERabinovich A Reiff G Higgins B Gottlieb NG Singer YChon SL Lin SW Baumgartner Long-term safety and effec-tiveness of etanercept in children with selected categories ofjuvenile idiopathic arthritis Arthritis Rheum 60 (2009)2794ndash2804
[47] G Horneff H Schmeling T Biedermann I Foeldvari G GanserHJ Girschick T Hospach HI Huppertz R Keitzer RM KusterH Michels D Moebius B Rogalski A Thon The German etaner-cept registry for treatment of juvenile idiopathic arthritis AnnRheum Dis 63 (2004) 1638ndash1644
[48] FH Prince M Twilt SC Simon MA van RossumW ArmbrustEP Hoppenreijs S Kamphuis M van Santen-Hoeufft Y
192 G Dueckers et al
Koopman-Keemink NM Wulffraat R ten Cate LW vanSuijlekom-Smit When and how to stop etanercept aftersuccessful treatment of patients with juvenile idiopathic ar-thritis Ann Rheum Dis 68 (2009) 1228ndash1229
[49] G Horneff F De Bock I Foeldvari HJ Girschick H MichelsD Moebius H Schmeling Safety and efficacy of combinationof etanercept and methotrexate compared to treatment withetanercept only in patients with juvenile idiopathic arthritis(JIA) preliminary data from the German JIA Registry AnnRheum Dis 68 (2009) 519ndash525
[50] N Ilowite O Porras A Reiff S Rudge M Punaro A Martin RAllen T Harville YN Sun T Bevirt G Aras B Appleton Ana-kinra in the treatment of polyarticular-course juvenile rheumatoidarthritis safety and preliminary efficacy results of a randomizedmulticenter study Clin Rheumatol 28 (2009) 129ndash137
[51] T Lequerre P Quartier D Rosellini F Alaoui M De BandtO Mejjad I Kone-Paut M Michel E Dernis M Khellaf NLimal C Job-Deslandre B Fautrel X Le Loet J Sibilia In-terleukin-1 receptor antagonist (anakinra) treatment in pa-tients with systemic-onset juvenile idiopathic arthritis oradult onset Still disease preliminary experience in FranceAnn Rheum Dis 67 (2008) 302ndash308
[52] M Gattorno A Piccini D Lasiglie S Tassi G Brisca S CartaL Delfino F Ferlito MA Pelagatti F Caroli A BuoncompagniS Viola A Loy M Sironi A Vecchi A Ravelli A Martini ARubartelli The pattern of response to anti-interleukin-1 treatmentdistinguishes two subsets of patients with systemic-onset juvenileidiopathic arthritis Arthritis Rheum 58 (2008) 1505ndash1515
[53] S Yokota T Imagawa M Mori T Miyamae Y Aihara STakei N Iwata H Umebayashi T Murata M Miyoshi MTomiita N Nishimoto T Kishimoto Efficacy and safety oftocilizumab in patients with systemic-onset juvenile idiopathicarthritis a randomised double-blind placebo-controlledwithdrawal phase III trial Lancet 371 (2008) 998ndash1006
[54] N Ruperto DJ Lovell P Quartier E Paz N Rubio-Perez CASilva C Abud-Mendoza R Burgos-Vargas V Gerloni JAMelo-Gomes C Saad-Magalhaes F Sztajnbok C Goldenstein-Schainberg M Scheinberg IC Penades M Fischbach J OrozcoPJ Hashkes C Hom L Jung L Lepore S Oliveira CAWallace LH Sigal AJ Block A Covucci A Martini EHGiannini Abatacept in children with juvenile idiopathic arthri-tis a randomised double-blind placebo-controlled withdrawaltrial Lancet 372 (2008) 383ndash391
[55] N Ruperto DJ Lovell P Quartier E Paz N Rubio-PerezCA Silva C Abud-Mendoza R Burgos-Vargas V GerloniJA Melo-Gomes C Saad-Magalhaes J Chavez-Corrales CHuemer A Kivitz FJ Blanco I Foeldvari M Hofer G HorneffHI Huppertz C Job-Deslandre A Loy K Minden M PunaroAF Nunez LH Sigal AJ Block M Nys A Martini EHGiannini Long-term safety and efficacy of abatacept inchildren with juvenile idiopathic arthritis Arthritis Rheum 62(2010) 1792ndash1802
[56] DM Brinkman IM de Kleer R ten Cate MA van RossumWP Bekkering A Fasth MJ van Tol W Kuis NM WulffraatJM Vossen Autologous stem cell transplantation in childrenwith severe progressive systemic or polyarticular juvenile idio-pathic arthritis long-term follow-up of a prospective clinicaltrial Arthritis Rheum 56 (2007) 2410ndash2421
[57] SE Klepper Effects of an eight-week physical conditioningprogram on disease signs and symptoms in children with chronicarthritis Arthritis Care Res 12 (1999) 52ndash60
[58] D Singh-Grewal J Schneiderman-Walker V Wright O Bar-OrJ Beyene H Selvadurai B Cameron RM Laxer R SchneiderED Silverman L Spiegel S Tse C Leblanc J Wong SStephens BM Feldman The effects of vigorous exercisetraining on physical function in children with arthritis arandomized controlled single-blinded trial ArthritisRheum 57 (2007) 1202ndash1210
[59] S Stephens D Singh-Grewal O Bar-Or J Beyene B CameronCM Leblanc R Schneider J Schneiderman-Walker HSelvadurai E Silverman L Spiegel SM Tse V WrightBM Feldman Reliability of exercise testing and functionalactivity questionnaires in children with juvenile arthritisArthritis Rheum 57 (2007) 1446ndash1452
[60] T Takken J van der Net W Kuis PJ Helders Physical ac-tivity and health related physical fitness in children with ju-venile idiopathic arthritis Ann Rheum Dis 62 (2003)885ndash889
[61] MM Toledo G Martini C Gigante L Da Dalt A TregnaghiF Zulian Is there a role for arthroscopic synovectomy in oli-goarticular juvenile idiopathic arthritis J Rheumatol 33(2006) 1868ndash1872
[62] F de Benedetti H Brunner N Ruperto SWright A KenwrightR Cuttica P Woo R Schneider DJ Lovell A Martini Efficacyand safety of Tocilizumab in patients with systemic juvenile idio-pathic arthritis (sJIA) 12-week data from the phase III TENDERtrial Ann Rheum Dis 69 (2010) 146
[63] P Quartier F Allantaz R Cimaz P Pillet C Messiaen CBardin X Bossuyt A Boutten J Bienvenu A Duquesne ORicher D Chaussabel A Mogenet J Banchereau JM Tre-luyer P Landais V Pascual A multicentre randomiseddouble-blind placebo-controlled trial with the interleukin-1receptor antagonist anakinra in patients with systemic-onsetjuvenile idiopathic arthritis (ANAJIS trial) Ann Rheum Dis70 (2011) 747ndash754
[64] DE Furst EC Keystone J Braun FC Breedveld GRBurmester F De Benedetti T Dorner P Emery R FleischmannA Gibofsky JR Kalden A Kavanaugh B Kirkham P Mease JSieper NG Singer JS Smolen PL Van Riel MH Weisman KWinthrop Updated consensus statement on biological agents forthe treatment of rheumatic diseases 2010 Ann Rheum Dis 70(Suppl 1) (2010) i2ndashi36
[65] T Beukelman NM Patkar KG Saag S Tolleson-RinehartRQ Cron EM Dewitt NT Ilowite Y Kimura RM LaxerDJ Lovell A Martini CE Rabinovich N Ruperto 2011 Ameri-can College of Rheumatology recommendations for the treatmentof juvenile idiopathic arthritis initiation and safety monitoring oftherapeutic agents for the treatment of arthritis and systemic fea-tures Arthritis Care Res 63 (2011) 465ndash482 (Hoboken)
[66] JF Simard M Neovius S Hagelberg J Askling Juvenile idi-opathic arthritis and risk of cancer a nationwide cohort studyArthritis Rheum 62 (2010) 3776ndash3782
[67] T Imagawa S Yokota M Mori T Miyamae S Takei H ImanakaY Nerome N Iwata T Murata M Miyoshi N Nishimoto TKishimoto Safety and efficacy of tocilizumab an anti-IL-6-receptor monoclonal antibody in patients with polyarticular-course juvenile idiopathic arthritis Mod Rheumatol (2011)doi102007s10165-011-0481-0
[68] TM Shaneyfelt MF Mayo-Smith J Rothwangl Are guide-lines following guidelines The methodological quality of clini-cal practice guidelines in the peer-reviewed medicalliterature Jama 281 (1999) 1900ndash1905
[69] R Grilli N Magrini A Penna G Mura A Liberati Practiceguidelines developed by specialty societies the need for a crit-ical appraisal Lancet 355 (2000) 103ndash106
[70] JS Burgers R Grol NS Klazinga M Makela J Zaat To-wards evidence-based clinical practice an international surveyof 18 clinical guideline programs Int J Qual Health Care 15(2003) 31ndash45
[71] JT Cassidy RE Petty Juvenile Idiopathic Rheumatic Arthri-tis 5th Edition WB Saunders Philadelphia 2005
[72] TJ Lehman Are withdrawal trials in paediatric rheumatic dis-ease helpful Lancet 372 (2008) 348ndash350
[73] J Munro Recommendations for the Diagnosis and Managementof Juvenile Idiopathic Arthritis The Royal Australian Collegeof General Practitioners South Melbourne 2009 pp 1ndash38
193Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
httpwwwnhmrcgovau_files_nhmrcpublicationsattachmentscp119-juvenile-arthritispdf
[74] MJ Santos JE Fonseca H Canhao M Conde M JoseVieira L Costa M Costa M Salgado JA Melo Gomes Guide-lines for prescribing and monitoring biologic therapies in juve-nile idiopathic arthritis Acta Reumatol Port 32 (2007) 43ndash47
[75] S Yokota M Mori T Imagawa T Murata M Tomiita Y ItohS Fujikawa S Takei Guidelines on the use of etanercept forjuvenile idiopathic arthritis in Japan Mod Rheumatol 20(2010) 107ndash113
[76] The AGREE Collaboration Appraisal of Guidelines for Researchamp Evaluation (AGREE) instrument wwwagreecollaborationorg
[77] I Kopp H Thole T Langer HK Selbmann G OllenschlaumlgerGerman Instrument for Methodological Guideline Appraisal(DELBI) wwwversorgungsleitliniende2008
[78] Auml Aumlrztliches Zentrum fuumlr Qualitaumlt in der Medizin A Arbeitsge-meinschaften der Wissenschaftlichen Fachgesellschaften in derMedizin Deutsches Instrument zur methodischen Leitlinien-Bewertung (DELBI) Fassung 20052006 Z Aumlrztl FortbildQualitaumltssich 99 (2005) 468ndash519
[79] MP de Wit SE Berlo GJ Aanerud D Aletaha JW BijlsmaL Croucher JA Da Silva B Glusing L Gossec S Hewlett MJongkees D Magnusson M Scholte-Voshaar P Richards CZiegler TA Abma European League Against Rheumatism rec-ommendations for the inclusion of patient representatives in sci-entific projects Ann Rheum Dis 70 (2011) 722ndash726
[80] I Foeldvari M Bidde Validation of the proposed ILAR classifi-cation criteria for juvenile idiopathic arthritis InternationalLeague of Associations for Rheumatology J Rheumatol 27(2000) 1069ndash1072
[81] R Merino J de Inocencio J Garcia-Consuegra Evaluation ofrevised International League of Associations for Rheumatologyclassification criteria for juvenile idiopathic arthritis in Spanishchildren (Edmonton 2001) J Rheumatol 32 (2005) 559ndash561
[82] SE Ramsey RK Bolaria DA Cabral PN Malleson REPetty Comparison of criteria for the classification of childhoodarthritis J Rheumatol 27 (2000) 1283ndash1286
[83] G Horneff A Ebert S Fitter K Minden I Foeldvari J Kum-merle-Deschner A Thon HJ Girschick F Weller HI Hup-pertz Safety and efficacy of once weekly etanercept 08mgkg in a multicentre 12 week trial in active polyarticularcourse juvenile idiopathic arthritis Rheumatology (Oxford) 48(2009) 916ndash919
[84] EH Giannini EJ Brewer N Kuzmina A Shaikov A Maxi-mov I Vorontsov CW Fink AJ Newman JT Cassidy LSZemel Methotrexate in resistant juvenile rheumatoid arthri-tis Results of the USAndashUSSR double-blind placebo-controlled trial The Pediatric Rheumatology CollaborativeStudy Group and The Cooperative Childrens Study GroupN Engl J Med 326 (1992) 1043ndash1049
[85] A Ravelli S Viola D Migliavacca N Ruperto A Pistorio AMartini The extended oligoarticular subtype is the best predic-tor of methotrexate efficacy in juvenile idiopathic arthritisJ Pediatr 135 (1999) 316ndash320
[86] P Woo TR Southwood AM Prieur CJ Dore J Grainger JDavid C Ryder N Hasson A Hall I Lemelle Randomizedplacebo-controlled crossover trial of low-dose oral
methotrexate in children with extended oligoarticular or sys-temic arthritis Arthritis Rheum 43 (2000) 1849ndash1857
[87] E Silverman L Spiegel D Hawkins R Petty D Goldsmith LSchanberg C Duffy P Howard V Strand Long-term open-label preliminary study of the safety and efficacy of lefluno-mide in patients with polyarticular-course juvenile rheumatoidarthritis Arthritis Rheum 52 (2005) 554ndash562
[88] DJ Lovell EH Giannini Y Kimura C Suzanne PJHashkes A Reiff Long-term safety and efficacy of rilonaceptin patients with systemic juvenile idiopathic arthritis (SJIA)Arthritis Rheum 60 (2009)
[89] N Ruperto P Quartier NWulffraat PWoo A Loy R Mouy BBader-Meunier BJ Prakken E Noseda R Belleli J Lecot CRordorf A Martini A Phase II Trial with canakinumab(ACZ885) a new IL-1-beta blocking monoclonal antibody toevaluate safety and preliminary efficacy in children with system-ic juvenile idiopathic arthritis Ann Rheum Dis 68 (2009) 170
[90] DJ Lovell EH Giannini Y Kimura et al Preliminary evi-dence for bioactivity of IL-1 trap (Rilonacept) a long actingIL-1 inhibitor in systemic juvenile idiopathic arthritis (sJIA)Arthritis Rheum 54 (2006) S325
[91] DJ Lovell EH Giannini Y Kimura et al Preliminary evi-dence for sustained bioactivity of IL-1 Trap (rilonacept) a longacting IL-1 inhibitor in systemic juvenile idiopathic arthritisArthritis Rheum 56 (2007) S514
[92] N Ruperto F De Benedetti H Brunner R Allen D Brown JChaitow E Cortis G Espada B Flato V Gerloni G HorneffS Wright A Kenwright R Schneider P Woo A Martini DJLovell Tocilizumab is efficacious in patients with systemic ju-venile idiopathic arthritis (sJIA) across baseline disease charac-teristics and priorbaseline treatments 12-week data from thephase II TENDER trial 17th PReS Congress Valencia Spain2010 2010
[93] N Ruperto DJ Lovell T Li F Sztajnbok C Goldenstein-Schainberg M Scheinberg IC Penades M Fischbach JOrozco PJ Hashkes C Hom L Jung L Lepore S OliveiraC Wallace M Alessio P Quartier E Cortis A Eberhard GSimonini I Lemelle E Chalom LH Sigal A Block A CovucciM Nys A Martini EH Giannini Abatacept improves health-related quality of life pain sleep quality and daily participationin subjects with juvenile idiopathic arthritis Arthritis Care Res(Hoboken) 62 (11) (2010) 1542ndash1551
[94] N Ruperto DJ Lovell P Quartier E Paz N Rubio-PerezCA Silva C Abud-Mendoza R Burgos-Vargas V GerloniJA Melo-Gomes C Saad-Magalhaes J Chavez C HuemerA Kivitz FJ Blanco I Foeldvari M Hofer G Horneff HIHuppertz CJ Deslandre A Loy K Minden M Punaro AFNunez LH Sigal AJ Block M Nys A Martini EH GianniniLong-term safety and efficacy of abatacept in children with ju-venile idiopathic arthritis Arthritis Rheum 62 (2010)1792ndash1802
[95] J Munro Juvenile Idiopathic Arthritis Management Guidelines(Provisional) Australian Paediatric Rheumatology Group 2006httpwwwnhmrcgovau
[96] K Fitch SJ Bernstein MD Aguilar B Burnand JR LaCalleP Lazaro M van het Loo J McDonnell JP Vader JPKahan The RANDUCLA Appropriateness Method Users ManualRAND Pittsburgh 2000

Table 3 Recommendation grade [10]
Recommendationgrade
Definition
A There is good evidence to support the recommendation that the intervention be performedB There is fair evidence to support the recommendation that the intervention be performedC There is poor evidence regarding the value or harm of the intervention recommendations may be made on
other groundsD There is fair evidence to support the recommendation that the intervention not be performedE There is good evidence to support the recommendation that the intervention not be performed
Table 2 Evidence level [10]
Evidencelevel
Definition
I Evidence obtained from at least one properly designed randomized controlled trialII Evidence obtained from well-designed controlled trials without randomization or from well-designed cohort or
casendashcontrol analytic studies preferably from more than one center or research group or from multiple time serieswith or without the intervention Dramatic results in uncontrolled trials might also be regarded as this type ofevidence
III Opinions of respected authorities based on clinical experience descriptive studies or reports of expertcommittees
179Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
2 Collocation of comments and ideas by the moderator using thewords of the participants
3 Clarification and substantiation of comments and ideas on alter-native guideline statements by the participants
4 Reconcilement of the manuscript and all alternative guidelinestatements
Table 4 Studies for 2010 update identified by the MEDLINE sear
Drugtreatment Mean age(age range) ofparticipants atstudy (years)
Totaof pa
Foeldvari et al [20] Celecoxibe 103 (2ndash16) 264Ceacutespedes-Cruzet al [33]
MTX 82 (np) 521
Lovell et al [45] Etanercept 104 (4ndash17) 58Horneff et al [83] Etanercept 129 (4ndash17) 20Giannini et al [46] Etanercept 99 (2ndash18) 594Lovell et al [40] Adalimumab 113 (4ndash17) 171Ruperto et al [31] Infliximab 112 (4ndash18) 121Lequerreacute et al [51] Anakinra 124 f (3ndash23) 20 f
Illowite et al [50] Anakinra 12 (2ndash17) 86Yokota et al [53] Tozilizumab 83 (2ndash19) 65Ruperto et al [54] Abatacept 124 (6ndash17) 190Singh-Grewal et al [58] Vigorous exercise
training116 (8ndash16) 80
Brinkmann et al [56] Stem celltransplantation
85 (4ndash18) 22
Abbreviations np = not provideda Not further specifiedb Only extended oligoarticular JIAc Pauciarticular onset with polyarticular coursed Extended oligoarticular JIA were included into polyarticular JIAe All JIA with polyarticular course with any type of onset not furthef Pediatric patients total number of patients in extended report wa
5 Discussion of statements and further explanation of any of thecomments that were not clear to all participants Each memberof the consensus group contributed to the discussion The moder-ator kept the process as neutral as possible avoiding judgmentand criticism
6 Final reconcilement for statements for guideline
ch algorithm (see Methodology)
l numbertients (n)
JIA
Oligoarticular Polyarticular Systemiconset
Othersubtypes
128 (53) a 114 (47) 22 (9)162 (31) b 284 (55) 75 (14)
5 (9) c 34 (58) 19 (33)2 (10) b 16 (80) 2
d 535 (90) 58 (97) 1171 (100) e
28 (23) c 74 (61) 19 (16)20 (100)
9 (10) c 62 (72) 15 (17)56 (100)
30 (16) 122 (64) 37 (20) 118 (23) 34 (43) 7 (9) 21 (26)
4 (18) 18 (82)
r specifieds 35 (15 were patients with adult onset of Still disease)
Consensus statement
NSAIDs are recommended for the treatmentof JIA Diclofenac Naproxen Ibuprofen andIndometacin (evidence level I respectively IIrecommendation grade A)If those drugs are contraindicated Celecoxibemight be used (evidence level I recommendationlevel BndashC)
Consensus statement
Intra-articular injections of crystalloid cortico-steroids (triamcinolone hexacetonide) are recom-mended and can be part of the first linetreatment Improvement of local inflammationpain swelling and range of joint movement hasbeen demonstrated (evidence level II recommen-dation grade A)Triamcinolone hexacetonide is more efficientthan triamcinolone acetonide inducing local remis-sion (evidence level I recommendation grade B)
180 G Dueckers et al
The conference guideline topics were reviewed andedited by working groups After the first consensus confer-ence statements were adopted by NGT and additional pro-posals for schemes of treatment strategies of JIA werecollated
25 Consensus finding method of Delphi
Three out of 15 statements remained without consensusafter NGT These statements comprise the utility of etaner-cept (treatment resistant polyarticular JIA) sulfasalazine(treatment resistant JIA) and anakinra (treatment for refrac-tory SoJIA) Therefore they were sent to all participants ofconsensus conferences via email To each of them partici-pants should state one of three votes (ldquoagreerdquo ldquodo notagreerdquo or ldquoalternative proposalrdquo) (1st round of Delphi)The results were summarized and the statements whichremained with no consensus after 1st round of Delphi weresent to participants again (2nd round of Delphi) After 2ndround of Delphi results were sent to external review
26 External review and adoption
The guideline manuscript has been reviewed in 2007 by na-tional experts in German Rheumatology Huppertz (BremenGermany) Michels (Garmisch Partenkirchen Germany) andSpecker (Essen Germany) The comments of external re-viewers (HI Huppertz) to the 2011 manuscript were in-volved within the 3rd round of Delphi External reviewenabled adoption of the guidelines core conclusions andstatements with strong consensus ie 95 agreement byrepresentatives of participating scientific societies andorganizations
3 Results treatment guidelines
31 Drug-based therapy
Drugs used in treatment of JIA are summarized in Table 5 Pro-posed schemes of treatment of JIA are shown in Fig 2 The fol-lowing paragraphs will highlight specific adverse reactions andintroduce the 13 studies relevant for the 2010 update of treat-ment guideline for JIA briefly For detailed information aboutprescribing information including indication contraindica-tion drug dosage route of administration monitoring andproduct characteristics the consensus group recommendsconsulting national drug data bases e g wwwrotelistede(German database of drugs with national market approval) orwwwfdaorg or wwwemaeuropaeu
311 Non-steroidal anti-inflammatory drugs (NSAIDs)Commonly NSAIDs are well tolerated Main side effects
of NSAIDs are stomach irritation dyspepsia andmdashin rarecasesmdashnephritis Cephalgia and behavioral changes can beassociated with the administration of ibuprofen Pseudo-porphyria is not uncommon in patients treated withnaproxen Pain relief has been demonstrated for Naproxen[13ndash15] Diclofenac [1516] and Ibuprofen [17] (evidencelevel I) and for Indometacin [18] and Meloxicam [19](evidence level II) Efficacy of Celecoxibe has been
demonstrated in a randomized double blind multicenterstudy [20] 95 of 212 patients entered the 12 week openlabel phase after a 12 week double blind phase in threetreatment groups (Celecoxibe 6 mgkgd versus Celecoxibe12 mgkgd versus Naproxen 15 mgkgd) Both dosages ofCelecoxibe showed comparable efficacy compared toNaproxen Safety ie number of adverse events (AE)did not differ significantly between Celecoxibe versusNaproxen
312 Glucocorticoids
3121 Glucocorticoids (GC)mdashlocal administration Theuse of intra-articular crystalline corticoids is highly potentand has a rather low rate of complications (evidence levelII) [2122] They might be administered as first line therapyResponse rate was significantly higher with triamcinolonehexacetonide than with triamcinolone acetonide at6 months and this difference was sustained to 24 months[2122] These findings were independent of duration andextent of disease [2122] Simultaneous intra-articular ste-roid injections are preferable to consecutive injections atdifferent time points (limited suppression of hypothalamicndashpituitaryndashadrenal axis) [23] Side effects eg local necrosisof fat tissue are seen in approximately 2 of injections [22]Working under sterile conditions the risk of infection is low
3122 GCmdashsystemic administration GC can be adminis-tered as a fast acting drug in highly active disease Indica-tions for their use are bridging time until DMARDs (diseasemodifying anti rheumatic drugs) become effective treat-ment of severe systemic features of systemic-onset JIA(SoJIA) induction of remission in polyarticular JIA and in se-vere forms of uveitis There are no controlled trials and nostandardized therapeutic regimes for the use of systemic
Table 5 Drugs for the treatment of JIA
Generic Dosage Age approval by Europeanmedical agency inpediatric rheumatology(EMA) a
Medical indication in pediatricrheumatology a b
Evidence levelrecommendationgrade [10]
Literature
NSAIDsDiclofenac 2ndash3 mgkg Bwd po (in 3 doses)
Retard formulation 1 dose14 years Arthritis IndashA Haapasiri [16] Laxer [14]
Ibuprofen 20ndash40 mgkg Bwd po in 3ndash4doses
6 months Pain fever IndashA Giannini [17]
Indometacin 1ndash3 mgkg Bwd po in 3 doses 2 years Arthritis IIndashA Stoeber [18]Meloxicam 0125ndash025 mgkg Bwd po 15 years Arthritis II Ruperto [19]Naproxen 10ndash15 mgkg Bwd po in 2 doses 1 year Arthritis IndashA Kvien [13] Laxer [14] Leak
[15]Celecoxibe 6 mgkg Bwd po in 2 doses or
12 mgkg Bwd in 1 doseNo approval for children Arthritis I B-C Foeldvari [20]
Glucocorticoids (GC)a) Systemic GCPrednisonePrednisolone
01ndash02 mgkg Bwd (max 5 mgd) JIA ie severe SoJIA severe peri-myokarditis severe uveitis (hypotoniaor cystoid macular edema) intoleranceto other drugs (ldquolow-doserdquo) or asldquobridgingrdquo therapy in higher doses eg2 mgkg Bwd until therapeutic effectof ldquoDMARDsrdquo
III Prieur [28]
Prednisone as an oralhigh-dose therapy
ge1ndash2 mgkg Bwd prednisolone-equivalent
III Prieur [28]
Prednisone as an oralmedium-dosetherapy
02 tob10 mgkg Bwdprednisolone-equivalent
III Kirwan [24] Prieur [28]
Prednisone as an orallow-dose therapy
b02 mgkg Bwd Prednisolone-equivalent or b4 mgmsup2 bodysurface
III Michels [25]
Prednisone as a ivpulse-therapy
N(5)ndash10 mgkg Bw (po)Prednisolone-equivalent10ndash30 mgkg Bwd Methyl-Prednisolone iv for 1ndash3 d(maximum 1 gdose)
III Miller [26] Picco [27]
b) Intra-articular GCTriamcinolonehexacetonide
05ndash1 mgkg Bw into large jointsdose adaption referring to size ofjoint (eg max 2 mg intointerphalangeal joints c)
5 months Arthritis tendo-vaginitis I Zulian [2122]
(continued on next page)(continued on next page)
181Evidence
andconsensus
basedGKJR
guidelinesfor
thetreatm
entof
juvenileidiopathic
arthritis
Table 5 (continued)
Generic Dosage Age approval by Europeanmedical agency inpediatric rheumatology(EMA) a
Medical indication in pediatricrheumatology a b
Evidence levelrecommendationgrade [10]
Literature
DMARDsSulfasalazine 30ndash50 mgkg Bwd in 2ndash3 doses 6 years Arthritis II Van Rossum [3637]Cytotoxic or immuno-suppressive drugsMethotrexate 10ndash15 (20) mgmsup2 body surface
once a week (po sc iv) e2 years Polyarticular JIA Psoriasis arthritis
uveitis CollagenosisI Giannini [84] Ravelli [85]
Woo [86]Cespedes-Cruz [33]Azathioprine 15ndash3 mgkg Bwd po in 1ndash2
dosesNo approval for children II Kvien [34]
Leflunomide No clear recommendation forchildren availableBwb20 kg d 1100 mgkg from d 2 10 mgkgdBw 20ndash40 kg d 1 to d 2 100 mgkgfrom d 3 10ndash20 mgkgdBwN40 kg d 1 to d 3 100 mgkgfrom d 3 20 mgkgd
No approval for children II Silverman [3587]
Biologic agentsa) TNFα inhibitorsEtanercept d 08 mgkg Bw sc 1timesweek
(max 50 mgweek) or 04 mgkgBw sc 2timesweek (max 50 mgweek)
4 years JIA Polyarthritis and insufficientefficacy of MTX
I Giannini [46] Horneff [49]Lovell [3888] Prince [41]
Adalimumab d 24 mgm2 body surface sc in 1dose every 2 weeks Bwb30 kg20 mgm2 body surface BwN30 kg40 mgm2 body surface(max 40 mg per dose)
4 years to 17 years Adalimumab in combination withmethotrexate is indicated for thetreatment of active polyarticularjuvenile idiopathic arthritis in childrenand adolescents who have had aninadequate response to one or moredisease-modifying anti-rheumatic drugs(DMARDs)
I Lovell [40]
182GDueckers
etal
Infliximab d 3ndash10 mgkg Bwdose iv Infusionat d 0 d 14 d 42 then every8 weeks intervals of applicationremain unclear
No approval for childrenwith JIA6 years (approval forMorbus Crohn)
III Ruperto [31]
b) IL-1 inhibitorsAnakinra d 1ndash4 mgkg Bwd sc in 1 dose No approval for children II Illowite [50] Lequerre [51]Canakinumab d 4 mgkg Bwsingle dose sc every
4 weeks (max 150 mg)No approval for childrenwith JIA 4 years (approvalfor CAPS)
III Ruperto [89]
Rilonacept d 1ndash2times44 mgkgweek sc (max320 mg) then 22 mgkgweek sc(max160 mg)
No approval for childrenwith JIA 12 years(approval for CAPS)
Lovell [889091]
c) IL-6 inhibitorsTocilizumab d 1 h Infusion every two 2 weeks
Bwb30 kg 8 mgkg BwN30 kg12 mgkg
2 years of age or older Since May 2011 EMA approval forpediatric patients with SoJIA who haveresponded inadequately to previoustherapy with NSAIDs and systemiccorticosteroids (Approval at Japan forSoJIA and polyarticular JIA since 2008) c
I Yokota [53] Ruperto [92]de Benedetti [62]
d) Co stimulatory-antagonistsAbatacept d 10 mgkg iv Infusion at d 0 d 14
d 28 then every 4 weeks6 years of age and older Abatacept in combination with
methotrexate is indicated for thetreatment of moderate to severe activepolyarticular (JIA) in pediatric patientswho have had an insufficient responseto other DMARDs including at least oneTNF inhibitor
I Ruperto [549394]
Abbreviations CAPS=Cryopyrine associated periodic fever syndrome JDM=juvenile dermatomyositis Bw=body weight SoJIA=systemic-onset of JIA SLE=systemic Lupus erythematodesa Compare wwwemaeuropaeub wwwrotelistede (German database of drugs with national market approval)c Intra-articular injection into same joint no more often than once every 3 monthsd A statement from insurance companies should be acquired before treatment initiation for off label treatment (if possible)e Oral application is most feasible in childhood
183Evidence
andconsensus
basedGKJR
guidelinesfor
thetreatm
entof
juvenileidiopathic
arthritis
Oligoarticular JIA
Polyarticular JIA
SoJIA
Figure 2 JIA treatment escalation schemes +=addition of the drug (abbreviations NSAIDs=non steroidal anti-inflammatory drugthotrexate)
Consensus statement
Long-term use of systemic GC is not recom-mended Continuous administration of ge02 mgPrednisolone equivalent per kg bodyweight (Bw)carries a high risk of adverse events and thereforeis not recommended (evidence level III recom-mendation grade A)
Consensus statement (continued)
184 G Dueckers et al
GC in JIA published thus leading to ldquojustrdquo evidence level IIIDifferent recommendations of dosage and therapy regimesare listed in Table 5 (evidence level III for all recommenda-tions) [1824ndash28] Frequency and seriousness of deleteriouseffects correlate mainly to duration of therapy and dosageof GC administered Main side effects are iatrogenicCushings syndrome growth disturbance weight gainmood changes Higher dosage carry the risk of increasedvulnerability to infection hypertension osteoporosisthrombosis diabetes gastro-intestinal ulceration cataractglaucoma atrophy of subcutaneous fatty tissue steroid in-duced acne To inform colleagues about GC treatment in acase of emergency and to reduce severe complications in longterm treated patients ie GC administrationN4 weeks thesupply of ldquoGlucocorticoid ID cardsrdquo for patients might be useful
GC=Glucocorticoids DMARDs=disease modifying drugs MTX=Me
Consensus statement
The systemic use of GC is recommended asfast acting drugs in highly active JIA GC areused for the treatment of children and adoles-cents with SoJIA organ manifestations of JIA(eg uveitis pericardial effusion) sero-positivepolyarticular JIA and for bridging time untilthe complete therapeutic effect of DMARDs(evidence level III recommendation grade A)
313 Methotrexate (MTX) biologic agents andimmunosuppressive agents
MTX biologic agents and immunosuppres-sive agents are used for the treatment of childrenand adolescents with polyarticular JIA ifNSAIDs or local GC treatment do not succeedThe combination of those drugs with NSAIDsand GC is feasible A common characteristic ofMTX biologic agents and immunosuppressiveagents is the delayed onset of therapeutic ef-fect ie up to 3 months or even longer aftercommencing treatment
185Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
Safe contraception is indicated during therapy with MTXAzathioprine or Leflunomide and in the following 3 to6 months after its discontinuation
Consensus statement
Administration of Sulfasalazine or Lefluno-mide is recommended if MTX or Etanercept donot show sufficient efficacy or cannot be used
3131 Methotrexate Among DMARDs MTX provides themainstay of long-term therapy in JIA [29ndash32] In case ofside effects eg dyspepsia or nausea prophylaxis withfolic acid can be recommended (1times1 mg per day or 5 mgonce a week 24ndash48 h after application of MTX) Safe contra-ception is mandatory while receiving MTX Safety and effica-cy of MTX and its impact on quality of life of children with JIAhave been investigated Significant positive impact of MTXon all health-related quality of life health conceptshas been shown although the study has its limit due to dif-ferent MTX dosages used within participating JIA patients[33]
Consensus statement
MTX administration can be recommendeddue to its proven safety and efficacy to reducedisease activity MTX is used in case of insuffi-cient therapeutic effect of NSAIDs andor localGC administration continuous need for system-ic GC andor highly active disease Efficacy ofMTX (orally or subcutaneously administered) isfrequently achievable with a dosage of 10ndash15 mgmsup2 body surface (evidence level I recom-mendation grade A)
for other reasons (evidence level II recommen-dation grade B)
3132 Purine analogs31321 Azathioprine Efficacy has been investigat-
ed in a double blind placebo controlled study (32 patients)After 8 weeks of therapy the changes in disease activitymeasurement indicated a minor improvement in the Azathi-oprine group compared to the placebo group At the end ofthe study statistically significant differences between thegroups were found for only 2 disease activity measurements[34] Two patients were taken out of study due to severeadverse events eg leucopenia Measurement of activityof Thiopurinmethyltransferase (TPMT) can be beneficial foravoidance of severe adverse events
3133 Pyrimidine analogs31331 Leflunomide Within a double blind study
(32 weeks 94 patients) efficacy of Leflunomide was inferiorin comparison to MTX but better than placebo Howeverdosing of Leflunomide may not have been adequate insome children [35] Contraindications for Leflunomide arerenal insufficiency severe immunodeficiency depressedmyelopoesis and pancytopenia An extensive half-life peri-od (approximately 14 days) has to be taken in accountwhen administering Leflunomide In combination with hepa-totoxic DMARDs the risk of severe adverse events might in-crease eg increased blood pressure is seen frequentlySafe contraception is mandatory
3134 Antibiotic analogs and Hydroxychloroquine andChloroquine
31341 Sulfasalazine Weak efficacy of Sulfasalazinewas demonstrated within a placebo-controlled randomizedstudy after 24 weeks (96 patients) [3637] One third of pa-tients enrolled in the study discontinued treatment with Sulfa-salazine due to side effects eg gastrointestinal symptomsleucopenia [36] Some experts use sulfasalazine in HLA-B27positive JIA Contraindications are Glucose-6-phosphatase de-ficiency and hypersensitivity against sulfonamides
31342 Hydroxychloroquine and chloroquine Hydrox-ychloroquine and Chloroquine have been subject to clinical tri-als for the treatment of JIA even though efficacy was limitedWithin three consensus conferences held in 2007 and 2010 theconsensus group decided not to give a consensus statementon the use of chloroquine or hydroxychloroquine treatmentdespite the fact that those drugs still might be used by somecaregivers
3135 Biologic agents Biologic agents are drugs whichselectively inhibit cytokines cytokine receptors or directlybind to receptors of lymphocytes eg CTLA-4 CD20 Theyinclude antibodies and fusion proteins So far allbiological therapies are administered subcutaneously orintravenously
31351 TNFα-inhibitors TNFα-inhibition with Adali-mumab and Etanercept is efficient and safe (evidencelevel I) [38ndash41] Both drugs have been approved for JIAwith polyarticular course TNFα-inhibitors have become anintegral part of the treatment of JIA Potential risks of therapyare vulnerability for infection andmdashin a rare occasionmdashthe in-duction of autoimmune disease Prior to the start of treatmentwith TNFα-inhibitors chronic infections needs to be excludedor treated sufficiently eg tuberculosis hepatitis B or C
In children with JIA treated with TNFα-inhibitors malig-nancies eg Lymphoma have been reported It remainsunclear if the rate of malignancies is increased in patientscompared to the risk by having JIA itself In response to aprevious letter of the FDA (as reviewed in [42]) the GermanSociety for Pediatric Rheumatology (GKJR) has published of-ficial statements [4344] The GKJR states that treatmentwith TNFα-inhibition should be used very carefully physi-cians need to be aware of co-medication e g immunosup-pressive drugs and should monitor those patientsclosely [43] There is insufficient data on all biologicagentsmdashincluding TNFα-inhibitionmdashto judge about the long-term risk for children and adolescents313511 Etanercept Etanercept is a fusion proteinconsisting of the extracellular binding domain of solubleTNFα-receptor and Fc chain of human IgG1 Etanercept in-hibits TNFα by direct binding of the cytokine Efficacy has
Consensus statement
The use of Anakinra or Tozilizumab can berecommended for treatment of children and ado-lescents with refractory SoJIA (evidence level IIrecommendation grade A)
186 G Dueckers et al
been demonstrated in a randomized controlled withdrawaldesign trial for patients with polyarticular JIA [38] Withinan open extension study long term efficacy and safety havebeen documented over 8 years in 1669 patients [3945]There is data on more than 2000 patients registered in Euro-pean registries [46ndash48] Currently retrospective data showsa somewhat better efficacy of combining MTX or otherDMARDs with TNFα-inhibition versus anti-TNFα therapy assingle therapy [49]313512 Adalimumab Adalimumab is a humanizedmonoclonal IgG1 antibody directed against TNFα whichbinds soluble and membrane bound TNFα A randomizedcontrolled withdrawal design trial demonstrated safety andefficacy of Adalimumab (24 mgmsup2 body surface every2 weeks max 40 mg) for children and adolescents withpolyarticular JIA (4ndash17 years of age n=171) [40] After16 weeks ldquowash inrdquo phase responders (n=144171) enteredthe 32 weeks randomized double blind phase After 48 weekstwice the number of patients in the verum group met ACR 70as compared to the control group (56 vs 28 pb001)Within the open extension phase Adalimumab dosage wasfixed ie 20 mgb30 kg Bw and 40 mgN30 kg Bw There islack of evidence showing superior efficacy of combiningMTX (DMARDs) with Adalimumab versus Adalimumab as sin-gle therapy [40]
Consensus statement
Efficacy of Etanercept and Adalimumab forthe treatment of polyarticular JIA has been dem-onstrated Therapy with TNFa-inhibition is indi-cated in case of insufficient therapeutic effectof NSAIDs and local GC administration and lackof response to MTX (evidence level I recom-mendation grade A)
Consensus statement
Patients with polyarticular JIA without sys-temic manifestation refractory to treatmentwith MTX and TNF inhibition might benefit fromthe use of Abatacept (evidence level III recom-mendation grade C)
313513 Infliximab Infliximab is a chimerical (humanmouse) monoclonal antibody which binds soluble and mem-brane bound TNFα A randomized controlled study in childrenand adolescents with JIA failed to demonstrate a significantdifference of efficacy after treatment with Infliximab com-pared to placebo [31]
31352 Interleukin-1-inhibitors None of interleukin-1-inhibitors are approved for the treatment of JIA or SoJIAThey are commonly used in an off label setting313521 Anakinra Anakinra is an IL-1 receptor antag-onist Within a randomized controlled trial no significant ef-ficacy of Anakinra for patients with polyarticular JIA couldbe demonstrated [50] 50 of 86 patients were enrolled intoblinded phase (11 Anakinra versus Placebo) No significantreduction of flare could be demonstrated in comparison toplacebo 29 of 50 patients completed the open label exten-sion study Two noncontrolled nonrandomized studieshave shown efficacy of anakinra in a proportion of patientswith systemic-onset of JIA (SoJIA) [5152]313522 Canakinumab Canakinumab an IL-1β anti-body binds IL-1β selectively without interfering with IL-1αor its physiological IL-1 receptor antagonist Canakinumabhas been approved for treatment of hereditary periodic IL-1 associated periodic fever syndromes ie Cryopyrin-
associated periodic syndromes There are ongoing studies in-vestigating safety and efficacy of Canakinumab for SoJIA
31353 Interleukin-6 inhibitors313531 Tozilizumab Tozilizumab is a humanizedanti-IL-6 receptor monoclonal antibody Efficacy has beendemonstrated within a 12 week double blind randomizedcontrolled withdrawal trial in children with SoJIA (n=562ndash19 years) in Japan [53] After a 48 week open extensionstudy ACR Pedi 30 was met by 47 patients (98) At thetime of our literature search Tocilizumab was approved fortreatment of SoJIA and polyarticular JIA since 2008 inJapan A multicenter European study investigating efficacyand safety of Tozilizumab in polyarticular JIA was ongoingat the deadline of literature search (wwwclinicaltrialsgov NCT00988221) No data on long term effects are cur-rently available
31354 Co-stimulation inhibitors313541 Abatacept Abatacept is a recombinant fu-sion protein of extracellular domain of human cytotoxic T-Lymphocyte Antigen 4 (CTLA-4) and IgG1-Fc-Fragment Itmodulates T-cell co-stimulation A randomized controlleddouble blind withdrawal design study of Ruperto et al [54]demonstrated efficacy of Abatacept in patients with polyar-ticular JIA 123 of 170 participants of study were enrolled inthe 6 month double blind phase Flares occurred in 33 of 62(53) patients who were given placebo versus 12 of 60(20) Abatacept patients during double blind phase Adverseevents (AE) did not differ in both groups ie 37 AE in Abata-cept versus 34 AE in placebo recipients Some children maytake 3 to 6 months or longer before their maximal responseis achieved 3 of patients developed reaction to the infu-sion [55] Abatacept is approved by FDA and EMA for pa-tients who did not respond to prior MTX treatment Nodata of long term effects of the use of Abatacept in JIA areavailable due to the low numbers of patients treated so far
314 Autologous stem cell transplantation (SCT)There are studies on autologous SCT for treatment of re-
fractory and severe forms of JIA (evidence level III) [56] 22
Consensus statement
187Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
patients were enrolled in one study 8 reached clinical re-mission 7 were assessed as partial responders 3 experi-enced relapse of the disease and 4 (18) died as aconsequence of MAS or immunosuppressive treatment [56]Due to serious adverse events including death this thera-peutic option is seen as the last treatment option
Exercise training is recommended dependingon the extent of inflammation number of affect-ed joints and global disease activity Sports withminor stress on joints is favorable (evidence levelI recommendation grade A)
32 Non-drug based therapy
321 Physiotherapy occupational therapy and thera-peutic appliances
Physio- and occupational therapy are integral parts of thetherapeutic concept in children and adolescents with JIA[5758] Therapeutic goals of physiotherapy are relaxationand pain relief preservation or rehabilitation of physiologi-cal range of joint movement prevention of contracturesstretching and activation of muscles build-up of muscleforce and training of physiological movements
Consensus statement
Structured treatment by a properly trainedphysiotherapistoccupational therapist in combi-nation with drug based therapy and instructionsfor disease adopted self-sufficient daily exercisesessions are recommended to keep and to im-prove joint mobility (evidence level II recom-mendation grade A)Custom-made therapeutic appliances for correc-tion of axial misalignment prevention of falseweight bearing stabilization of joints (eghand- finger- and foot-ortheses) are recom-mended individually The use of therapeutic ap-pliances follows individual physician-directedadvice Efficacy has been demonstrated (evi-dence level I recommendation grade B)
Consensus statement
In individual cases the indication for open orarthroscopic synovectomy can be considered ifconservative therapy does not succeed (evi-dence level III recommendation grade B)
Consensus statement
Other forms of non-drug based therapeutic approachesrely on experts opinion and are solely based on individualclinical experience No controlled studies are available
Consensus statement
The implementation of thermotherapy electro-or ultrasound therapy massage and lymph drain-age is recommended Application of cold appli-ances for acute joint inflammation is indicated(evidence level II recommendation grade A)Electro- and ultrasound therapy are recom-mended for patients with tendosynovitis (evi-dence level III recommendation grade B)
An early psychological support within stan-dard pediatric rheumatological care should beimplemented to apprehend and treat mental is-sues and behavioral syndromes associated withphysiological disturbances and physical factors(evidence level III recommendation grade A)
Consensus statement
A socio-pedagogical care with regard tointegration at school professional andeveryday life and formal education of parentsand patients is recommended (evidence levelIII recommendation grade A)
322 Sportive activity and exercise trainingPositive impact of sportive activity on the general physi-
cal condition and on oxygen consumption has been demon-strated (evidence level II) [57ndash60] Adequate exercise
training supports the physiological development and helpscoping with JIA [58] Prospective controlled long term stud-ies are currently not available
323 Surgical treatmentToledo et al investigated the role of arthroscopic syno-
vectomy in JIA They concluded that arthroscopy is a safebut only partially effective procedure in patients witholigoarticular JIA (evidence levelrecommendation gradeIIIB) [61]
324 Psychological social intervention orsocio-pedagogical care
There are no controlled or open studies focusing on psy-chological social andor socio-pedagogical intervention inchildren or adolescents with JIA Recommendations arebased on experts opinion and personal experience solely
188 G Dueckers et al
4 Addendum
Since the deadline January 15th 2010 new papers haveappeared that are of interest in the context of our guideline[5562ndash64] in particular we refer to the ACR recommenda-tions [65] and the most recent literature on the risk of malig-nancies in JIA in context with TNF blocking agent andindependent of medication [42] [66] Moreover there is arecent study on the use of Tocilizumab in polyarticular pa-tients [67] These papers will be discussed within the nextconsensus conference by NGT and considered for inclusioninto the next edition of this guideline On 6th of September2011 our advanced search on wwwclinicaltrialgov (searchterms juvenile idiopathic arthritis recruitment open stud-ies study type interventional study age group child(birthndash17) intervention drugs) led to 16 trials which are cur-rently recruiting or will soon start recruiting
5 Discussion
To develop clinical practice guidelines of high quality andvalidity a formal consensus process and explicit methodo-logical criteria for the production of guidelines are recom-mended [68ndash70] Our guideline for the treatment of JIA inchildren and adolescents implements all these issues Thesystematic literature search was terminated on 15th January2010 leading to the most up to date guideline for JIA whichis currently available The deadline of the ACR recommenda-tions as published recently by Beukelmann et al was 5th ofOctober 2009 [65] By exclusion of case reports trials with-out control groups preliminary results published as ab-stracts on conferences and the strict graduation of theliterature by the criteria of evidence based medicine weaimed to give our guideline statements additional strengthand a maximal validity Newer original studies providing ad-ditional evidence for the treatment of JIA became availableafter our consensus process was finished see AddendumThe results of these trials have to await the next NGT beforeinclusion into our recommendations
Our updated systematic literature search in 2010 led to13 relevant studies published after 30th June 2007 (Fig 1Table 4) Their results have to be interpreted with cautionFirst trials in JIA are mainly based on limited numbers of pe-diatric patients as the recruitment of a sufficient number ofpediatric patients remains challenging Second trials aremainly designed for patients with polyarticular JIA or witholigoarticular onset and a polyarticular course (Table 4)Most children with JIA do not have a polyarticular subtypeof JIA but an oligoarticular onset and course [71] Thus pa-tients with oligoarticular JIA are heavily underrepresentedin most of the current trials Third in 5 of the 13studies the withdrawal study design has been used[4045505354] Lehmann reviewed the bias of withdrawaldesign trials in 2008 [72] After a wash-in phase only re-sponders to treatment are eligible for randomization Thusthe design preselects responders to the placebo effect whomight retain their response throughout the entire study peri-od Further there is a carryover effect of AE into the place-bo group so that significant differences in AE betweengroups may not become apparent In the one placebo con-trolled trial without withdrawal design on TNFα-inhibition
(Infliximab) no significant efficacy could be demonstratedbetween verum and placebo [31]
To our knowledge there are two other guidelines that dealwith the management of JIA as a whole (Table 6) [65] [73]Other guidelines are limited to the use of single drugs in JIAeg biologic agents [74] etanercept [75] The Australian guide-line (wwwracgporgauguidelinejuvenileidiopathicarthritis)has not been published in a peer-reviewed journal It is to pro-vide recommendations for the early diagnosis and multidisci-plinary management of JIA in the primary care setting forgeneral practitioners (GPs) [73] No recommendations aremade regarding the use of GCs DMARDs immunosuppressivedrugs or biologic agents [73] The ACR recommendations usesthe Appraisal of Guidelines for Research and Evaluation(AGREE) instrument [65] [76] which does not fulfill criteria ofa proper consensus process and carries the risk that expertsvote for peer opinion which might not reflect the true valueWe used an advanced and linguistically validated version ofthe AGREE instrument the ldquoGerman Instrument for Methodo-logical Guideline Appraisal (DELBI)rdquo which has been developedin cooperation of the AWMF among others [7778] We followedthe highly structured Nominal Group Technique as described inMethodology Our consensus group only considered formallyboard nominated representatives of multidisciplinary scientificsocieties and organizations (Table 1) and included patients rep-resentatives as this has been strongly recommended by the Eu-ropean League against Rheumatism (EULAR) recently [79] TheACR mentions a parent representative within their task forcepanel but leaves this representative anonymous It remainsunclear how ACR experts were selected and involved [65]They defined treatment groups which have not been evaluatedsystematically so far We used the ILAR classification systemwhich has been repeatedly evaluated [80ndash82]
By content there are major differences between the ACRrecommendations and our guideline a) Our guideline pro-vides a detailed and systematic list of 20 drugs commonlyused in the treatment of JIA (Table 5) which has been an in-tegrative part of our consensus conferences The ACR recom-mendations do not provide information on approval status(Food and Drug Administration) indications for use and nospecific differences on dosage regimes or frequency ofdaily application [65] eg it refers to the 2008 ACR recom-mendations for the use of DMARDs in adult rheumatoid ar-thritis b) The ACR recommendations provide a more earlyaggressive approach in the treatment of JIA The ACR recom-mends MTX as first line treatment in patients (b4 joints) withhighly active disease [65] To our knowledge there are onlydata to recommend MTX administration in cases of insuffi-cient therapeutic effect of prior treatment with NSAIDandor GC [33] c) The ACR recommends the use of TNFα in-hibitors as escalation therapy for some patients with historyof arthritis of 4 or fewer joints and refer to publications[3840] conducted in patients with polyarticular JIA or pau-ciarticular JIA with polyarticular course [65] There is no ev-idence that TNF is safe and efficient in patients witholigoarticular JIA a systematic controlled clinical trial onthis issue has not been done yet d) We regard a brief trialof local or systemic administration of GC plus NSAID as a fea-sible first line treatment for patients with polyarticular JIAThe ACR recommends MTX without regard to disease activityat the initial stage [65] We reached consensus to recom-mend the use of GC as bridging therapy until full onset of
Table 6 Overview of recommendationsguidelines for treatment of JIA
USA Australia Germany
ACR recommendations[65]
RACGP recommendations[73]
GKJR guidelines
Deadline of literature search October 2009 January 2007 September 2010Source of publications Pub Med Pub Med
EMBASE CINHAL CochraneLibrary provisionalAustralian Guideline [95]
Pub MedPrevious German Guidelines [78]
Definition used for JIA subgroups Treatment groups definedby Core expert panel
Not specifically definedChildren withJIAb16 years
ILAR criteria [1]
Consensus processprocessvalidation
AGREE [76] AGREE [76] DELBI [77]RANDUCLA appropriatenessmethod [96]
NGT Delphi method
Conferences None None 3 Formal consensus conferencesAddressees Pediatric rheumatologists General practitioner Pediatric Rheumatologists
PediatriciansGeneral practitioners
Participating scientific societies or professional organizationsPediatric rheumatologist orrheumatologists for adolescents
Yes Yes Yes
General pediatrician- In hospital Yes Yes Yes- In private practice Yes Yes YesResearcher Yes No YesRheumatologists for adults No No YesOphthalmologists No No YesParentspatients support groups Yes No YesOrthopedic surgeons No No YesPediatric orthopedic surgeons No No YesPsychologists No No YesPhysiotherapists No No YesPediatric rheumatology nurses Yes No NoOther scientific societies ororganizations
ACR BSPAR PRINTO PReS RACGP NAMSCAG NHMRC DGKJ DGPs DGRh DGO AWMFBVKJ
(ACR=American College of Rheumatologists AGREE=Appraisal of Guidelines for Research amp Development AWMF=Association of the ScientificMedical Associations BSPAR=British Society for Pediatric Rheumatology BVJK=Association of Pediatricians in private practice CEP=Core expertpanel ILAR=International League against Rheumatism CINHAL=Cumulative Index to Nursing and Allied Health Literature DELBI=German In-strument for Methodological Guideline Appraisal DGKJ=German Society of Pediatrics and Adolescent Medicine DGO=German Society for Oph-thalmology DGPs=German society for Psychology DGRh=German Society for Rheumatology GKJR=German Society for Pediatric RheumatologyNAMSCAG=National Arthritis and Musculoskeletal Conditions Advisory Group NGT=Nominal Group Technique NHMRC=National Health andMedical Research Council PReS=Pediatric Rheumatology Society) PRINTO=Pediatric Rheumatology International Trial Organization RACG-P=Royal Australian College of General Practitioner RANDUCLA=Research and DevelopmentUniversity of California at Los Angeles)
189Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
therapeutic effect of DMARDs The ACR recommendations donot provide any recommendation for the use of systemic GCfor patients with oligo- or polyarticular course of JIA exceptsystemic onset of JIA e) The ACR recommendations do notcover the topic of non-drug based therapy at all althoughthere is strong evidence that eg exercise training is a usefuladdition to drug treatment [575860]
6 Conclusion
In summary we present a treatment guideline for JIA on a con-sensus conference basis We strongly advocate an interdisciplin-ary approach including surgery physiotherapy psychosocial
intervention physical therapy medications etc and a strictformal consensus process in order to create statements thatare most appropriate for the complex clinical situation of achild and family presenting with JIA and cover all aspects ofJIA care All German pediatric rheumatology sites are partici-pating at the national pediatric rheumatologic database in theDeutsche Rheuma-Forschungszentrum at Berlin (DRFZ wwwdrfzde) It aims at quality assurance in Germany and monitorstreatment behavior of pediatric rheumatologists by using inter-nationally agreed criteria (eg joint count global physician rat-ing of disease activity global parent rating of overall well-being CHAQ ESR ACR-ped response or JADAS) The databasewill be used as a tool to monitor the application of our treat-ment guidelines
190 G Dueckers et al
Conflict of interest statement
Gregor Dueckers Novartis Pharmaceuticals CorporationBaxter (for all travel grants for scientific meetings)Nihal Guellac no conflict of interestMartin Arbogast no conflict of interestGuumlnther Dannecker no conflict of interestIvan Foeldvari Wyeth Pfizer Abbott Immunology Pharma-ceuticals Chugai (for all advisory board member)Michael Frosch no conflict of interestGerd Ganser Abbott Immunology Pharmaceuticals (advisoryboard member grants for scientific meetings) Wyeth Pfizer(advisory board member grants for scientific meetings)ChugaiRoche (advisory board member grants for scientificmeetings) Merck (grants for scientific meetings) Actelios(grants for scientific meetings) Esaote (grants for scientificmeetings)Arnd Heiligenhaus Novartis Pharmaceuticals CorporationAbbott Immunology Pharmaceuticals Alcon (for all re-search grants)Gerd Horneff Abbott Immunology Pharmaceuticals (re-search grants consulting fees non-remunerative positionsof influence) Wyeth Pfizer (research grants consultingfees speakers bureau non-remunerative positions of influ-ence) Bristol-Myers Squibb (Consulting fees) Nycomed(Consulting fees non-remunerative positions of influence)RocheChugai (Consulting fees non-remunerative positionsof influence) Sandoz (Consulting fees) Genzyme (researchgrants consulting fees non-remunerative positions of influ-ence) Swedish Orphan (research grants consulting feesnon-remunerative positions of influence)Arnold Illhardt no conflict of interestRuumldiger Krauspe no conflict of interestBarbara Markus no conflict of interestHartmut Michels Abbott Immunology Pharmaceuticals (advi-sory board member and grants for scientific meeting)Matthias Schneider no conflict of interestWolfram Singendonk no conflict of interestHelmut Sitter no conflict of interestMarianne Spamer no conflict of interestNorbert Wagner no conflict of interestTim Niehues Abbott Immunology Pharmaceuticals EssexPharma Novartis Pharmaceutical Corporation WyethPfizer (for all research grants consulting fees non-remu-nerative positions of influence)
Acknowledgment
We like to express our grateful thanks to Prof Dr Hans IkoHuppertz for proof reading the article and for an excellentdiscussion on our work We like to express our thanks to HE-LIOS Clinic for funding the open access of the article
References
[1] RE Petty TR Southwood P Manners J Baum DN Glass JGoldenberg X He J Maldonado-Cocco J Orozco-Alcala AMPrieur ME Suarez-Almazor PWoo International League of Asso-ciations for Rheumatology classification of juvenile idiopathic ar-thritis second revision Edmonton 2001 J Rheumatol 31(2004) 390ndash392
[2] B Prakken S Albani A Martini Juvenile idiopathic arthritisLancet 377 (2011) 2138ndash2149
[3] KT April DE Feldman RW Platt CM Duffy Comparisonbetween children with juvenile idiopathic arthritis (JIA) andtheir parents concerning perceived quality of life Qual LifeRes 15 (2006) 655ndash661
[4] BM Feldman B Grundland L McCullough V Wright Distinc-tion of quality of life health related quality of life and healthstatus in children referred for rheumatologic care J Rheuma-tol 27 (2000) 226ndash233
[5] JC Packham MA Hall Long-term follow-up of 246 adultswith juvenile idiopathic arthritis functional outcomeRheumatology (Oxford) 41 (2002) 1428ndash1435
[6] C Sandborg Pediatric rheumatic disease standards of care forJIAmdashthe basic foundation for quality Nat Rev Rheumatol 6(2010) 389ndash390
[7] N Guellac T Niehues Interdisciplinary and evidence-basedtreatment guideline for juvenile idiopathic arthritis KlinPadiatr 220 (2008) 392ndash402
[8] K Schnakenburg Leitlinien in der Kinder- und JugendmedizinElsevier 2005 pp H1 1ndash15
[9] P Juni L Nartey S Reichenbach R Sterchi PA Dieppe MEgger Risk of cardiovascular events and rofecoxib cumulativemeta-analysis Lancet 364 (2004) 2021ndash2029
[10] W Feldman Evidence-based Pediatrics 1st ed BC DeckersHamilton 2000
[11] AH Van de Ven AL Delbecq The nominal group as a re-search instrument for exploratory health studies Am J PublicHealth 62 (1972) 337ndash342
[12] HA Linstone M Turoff The Delphi Method Techniques andApplications Addison-Wesley Pub 1975
[13] TK Kvien HM Hoyeraal B Sandstad Naproxen and acetyl-salicylic acid in the treatment of pauciarticular and polyarticu-lar juvenile rheumatoid arthritis Assessment of tolerance andefficacy in a single-centre 24-week double-blind parallelstudy Scand J Rheumatol 13 (1984) 342ndash350
[14] RM Laxer ED Silverman C St-Cyr MT Tran G Lingam Asix-month open safety assessment of a naproxen suspensionformulation in the therapy of juvenile rheumatoid arthritisClin Ther 10 (1988) 381ndash387
[15] AM Leak MR Richter LE Clemens MA Hall BM AnsellA crossover study of naproxen diclofenac and tolmetin in sero-negative juvenile chronic arthritis Clin Exp Rheumatol 6(1988) 157ndash160
[16] J Haapasaari E Wuolijoki H Ylijoki Treatment of juve-nile rheumatoid arthritis with diclofenac sodium Scand JRheumatol 12 (1983) 325ndash330
[17] EH Giannini EJ Brewer ML Miller D Gibbas MH PassoHM Hoyeraal B Bernstein DA Person CW Fink LA Sawyeret al Ibuprofen suspension in the treatment of juvenilerheumatoid arthritis Pediatric Rheumatology CollaborativeStudy Group J Pediatr 117 (1990) 645ndash652
[18] E Stoeber L Sanger Experiences with indomethacin in long-term therapy of juvenile rheumatoid arthritis Arzneimittel-forschung 21 (1971) 1865ndash1866
[19] N Ruperto I Nikishina ED Pachanov Y Shachbazian AMPrieur R Mouy R Joos F Zulian R Schwarz V ArtamonovaW Emminger M Bandeira A Buoncompagni I Foeldvari FFalcini E Baildam I Kone-Paut M Alessio V Gerloni ALenhardt A Martini G Hanft R Sigmund S Simianer Arandomized double-blind clinical trial of two doses ofmeloxicam compared with naproxen in children with juvenileidiopathic arthritis short- and long-term efficacy and safetyresults Arthritis Rheum 52 (2005) 563ndash572
[20] I Foeldvari IS Szer LS Zemel DJ Lovell EH Giannini JLRobbins CRWest G Steidle S Krishnaswami BJ Bloom A pro-spective study comparing celecoxib with naproxen in children withjuvenile rheumatoid arthritis J Rheumatol 36 (2009) 174ndash182
191Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
[21] F Zulian G Martini D Gobber C Agosto C Gigante FZacchello Comparison of intra-articular triamcinolone hexa-cetonide and triamcinolone acetonide in oligoarticular juve-nile idiopathic arthritis Rheumatology (Oxford) 42 (2003)1254ndash1259
[22] F Zulian G Martini D Gobber M Plebani F Zacchello PManners Triamcinolone acetonide and hexacetonide intra-articular treatment of symmetrical joints in juvenile idiopathicarthritis a double-blind trial Rheumatology (Oxford) 43 (2004)1288ndash1291
[23] GS Habib Systemic effects of intra-articular corticosteroidsClin Rheumatol 28 (2009) 749ndash756
[24] JR Kirwan The effect of glucocorticoids on joint destructionin rheumatoid arthritis The Arthritis and Rheumatism CouncilLow-Dose Glucocorticoid Study Group N Engl J Med 333(1995) 142ndash146
[25] H Michels What is low-dose corticosteroid therapy in juvenileidiopathic arthritis A worldwide questionnaire-based surveyZ Rheumatol 59 (Suppl 2) (2000) II127ndash130
[26] JJ Miller III Prolonged use of large intravenous steroid pulsesin the rheumatic diseases of children Pediatrics 65 (1980)989ndash994
[27] P Picco M Gattorno A Buoncompagni V Pistoia C Borrone6-methylprednisolone lsquomini-pulsesrsquo a newmodality of glucocor-ticoid treatment in systemic onset juvenile chronic arthritisScand J Rheumatol 25 (1996) 24ndash27
[28] AM Prieur The place of corticosteroid therapy in juvenilechronic arthritis in 1992 J Rheumatol Suppl 37 (1993)32ndash34
[29] JS Gao H Wu J Tian Treatment of patients with juvenilerheumatoid arthritis with combination of leflunomide andmethotrexate Zhonghua Er Ke Za Zhi 41 (2003) 435ndash438
[30] T Niehues G Horneff H Michels MS Hock L SchuchmannEvidence-based use of methotrexate in children with rheumat-ic diseases a consensus statement of the Working Groups Pedi-atric Rheumatology Germany (AGKJR) and PediatricRheumatology Austria Rheumatol Int 25 (2005) 169ndash178
[31] N Ruperto DJ Lovell R Cuttica N Wilkinson P Woo GEspada C Wouters ED Silverman Z Balogh M HenricksonMT Apaz E Baildam A Fasth V Gerloni P Lahdenne AMPrieur A Ravelli RK Saurenmann ML Gamir N WulffraatL Marodi RE Petty R Joos F Zulian D McCurdy BLMyones K Nagy P Reuman I Szer S Travers A BeutlerG Keenan J Clark S Visvanathan A Fasanmade A Ray-chaudhuri A Mendelsohn A Martini EH Giannini A random-ized placebo-controlled trial of infliximab plus methotrexatefor the treatment of polyarticular-course juvenile rheumatoidarthritis Arthritis Rheum 56 (2007) 3096ndash3106
[32] K Visser DM van der Heijde Risk and management of livertoxicity during methotrexate treatment in rheumatoid andpsoriatic arthritis a systematic review of the literature ClinExp Rheumatol 27 (2009) 1017ndash1025
[33] A Cespedes-Cruz R Gutierrez-Suarez A Pistorio A Ravelli ALoy KJ Murray V Gerloni N Wulffraat S Oliveira J WalshIC Penades MG Alpigiani P Lahdenne C Saad-Magalhaes ECortis L Lepore Y Kimura C Wouters A Martini N RupertoMethotrexate improves the health-related quality of life of chil-dren with juvenile idiopathic arthritis Ann Rheum Dis 67(2008) 309ndash314
[34] TK Kvien HM Hoyeraal B Sandstad Azathioprine versus place-bo in patients with juvenile rheumatoid arthritis a single centerdouble blind comparative study J Rheumatol 13 (1986) 118ndash123
[35] E Silverman R Mouy L Spiegel LK Jung RK SaurenmannP Lahdenne G Horneff I Calvo IS Szer K Simpson JAStewart V Strand Leflunomide or methotrexate for juvenilerheumatoid arthritis N Engl J Med 352 (2005) 1655ndash1666
[36] MA van Rossum TJ Fiselier MJ Franssen AH ZwindermanR ten Cate LW van Suijlekom-Smit WH van Luijk RM
van Soesbergen NM Wulffraat JC Oostveen W Kuis PFDijkstra CF van Ede BA Dijkmans Sulfasalazine in the treat-ment of juvenile chronic arthritis a randomized double-blindplacebo-controlled multicenter study Dutch Juvenile ChronicArthritis Study Group Arthritis Rheum 41 (1998) 808ndash816
[37] MA van Rossum RM van Soesbergen M Boers AHZwinderman TJ Fiselier MJ Franssen R ten Cate LW vanSuijlekom-Smit NM Wulffraat WH van Luijk JC OostveenW Kuis BA Dijkmans Long-term outcome of juvenile idiopathicarthritis following a placebo-controlled trial sustained benefits ofearly sulfasalazine treatment Ann Rheum Dis 66 (2007)1518ndash1524
[38] DJ Lovell EH Giannini A Reiff GD Cawkwell ED SilvermanJJ Nocton LD Stein A Gedalia NT Ilowite CA Wallace JWhitmore BK Finck Etanercept in children with polyarticularjuvenile rheumatoid arthritis Pediatric Rheumatology Collabora-tive Study Group N Engl J Med 342 (2000) 763ndash769
[39] DJ Lovell A Reiff OY Jones R Schneider J Nocton LDStein A Gedalia NT Ilowite CA Wallace JB WhitmoreB White EH Giannini Long-term safety and efficacy ofetanercept in children with polyarticular-course juvenile rheu-matoid arthritis Arthritis Rheum 54 (2006) 1987ndash1994
[40] DJ Lovell N Ruperto S Goodman A Reiff L Jung K JarosovaD Nemcova R Mouy C Sandborg J Bohnsack D Elewaut IFoeldvari V Gerloni J Rovensky K Minden RK Vehe LWWeiner G Horneff HI Huppertz NY Olson JR Medich RCarcereri-De-Prati MJ McIlraith EH Giannini A MartiniAdalimumab with or without methotrexate in juvenile rheuma-toid arthritis N Engl J Med 359 (2008) 810ndash820
[41] FH Prince M Twilt R ten Cate MA van RossumW ArmbrustEP Hoppenreijs M van Santen-Hoeufft Y Koopman-KeeminkNM Wulffraat LW van Suijlekom-Smit Long-term follow-upon effectiveness and safety of etanercept in juvenile idiopathicarthritis the Dutch National Register Ann Rheum Dis 68(2009) 635ndash641
[42] P Diak J Siegel L LaGrenade L Choi S Lemery AMcMahonTumor necrosis factor alpha blockers andmalignancy in childrenforty-eight cases reported to the Food and Drug AdministrationArthritis Rheum 62 (2010) 2517ndash2524
[43] G Horneff T Hospach G Dannecker D Foll JP Haas HJGirschick HI Huppertz R Keitzer HJ Laws H Michels KMinden R Trauzeddel Updated statement by the German So-ciety for Pediatric and Adolescent Rheumatology (GKJR) on theFDAs report regarding malignancies in anti-TNF-treated pa-tients from Aug 4 2009 Z Rheumatol 69 (2010) 561ndash567
[44] T Hospach JP Haas HI Huppertz R Keitzer H Michels RTrauzeddl D Foll G Dannecker G Horneff Comment of theSociety of Pediatric and Adolescent Rheumatology on the USFood and Drug Administration (FDA) announcement regardingcases of malignancy in anti-TNF-treated patients Z Rheumatol68 (2009) 162ndash164
[45] DJ Lovell A Reiff NT Ilowite CA Wallace Y Chon SL LinSW Baumgartner EH Giannini Safety and efficacy of up to eightyears of continuous etanercept therapy in patients with juvenilerheumatoid arthritis Arthritis Rheum 58 (2008) 1496ndash1504
[46] EH Giannini NT Ilowite DJ Lovell CA Wallace CERabinovich A Reiff G Higgins B Gottlieb NG Singer YChon SL Lin SW Baumgartner Long-term safety and effec-tiveness of etanercept in children with selected categories ofjuvenile idiopathic arthritis Arthritis Rheum 60 (2009)2794ndash2804
[47] G Horneff H Schmeling T Biedermann I Foeldvari G GanserHJ Girschick T Hospach HI Huppertz R Keitzer RM KusterH Michels D Moebius B Rogalski A Thon The German etaner-cept registry for treatment of juvenile idiopathic arthritis AnnRheum Dis 63 (2004) 1638ndash1644
[48] FH Prince M Twilt SC Simon MA van RossumW ArmbrustEP Hoppenreijs S Kamphuis M van Santen-Hoeufft Y
192 G Dueckers et al
Koopman-Keemink NM Wulffraat R ten Cate LW vanSuijlekom-Smit When and how to stop etanercept aftersuccessful treatment of patients with juvenile idiopathic ar-thritis Ann Rheum Dis 68 (2009) 1228ndash1229
[49] G Horneff F De Bock I Foeldvari HJ Girschick H MichelsD Moebius H Schmeling Safety and efficacy of combinationof etanercept and methotrexate compared to treatment withetanercept only in patients with juvenile idiopathic arthritis(JIA) preliminary data from the German JIA Registry AnnRheum Dis 68 (2009) 519ndash525
[50] N Ilowite O Porras A Reiff S Rudge M Punaro A Martin RAllen T Harville YN Sun T Bevirt G Aras B Appleton Ana-kinra in the treatment of polyarticular-course juvenile rheumatoidarthritis safety and preliminary efficacy results of a randomizedmulticenter study Clin Rheumatol 28 (2009) 129ndash137
[51] T Lequerre P Quartier D Rosellini F Alaoui M De BandtO Mejjad I Kone-Paut M Michel E Dernis M Khellaf NLimal C Job-Deslandre B Fautrel X Le Loet J Sibilia In-terleukin-1 receptor antagonist (anakinra) treatment in pa-tients with systemic-onset juvenile idiopathic arthritis oradult onset Still disease preliminary experience in FranceAnn Rheum Dis 67 (2008) 302ndash308
[52] M Gattorno A Piccini D Lasiglie S Tassi G Brisca S CartaL Delfino F Ferlito MA Pelagatti F Caroli A BuoncompagniS Viola A Loy M Sironi A Vecchi A Ravelli A Martini ARubartelli The pattern of response to anti-interleukin-1 treatmentdistinguishes two subsets of patients with systemic-onset juvenileidiopathic arthritis Arthritis Rheum 58 (2008) 1505ndash1515
[53] S Yokota T Imagawa M Mori T Miyamae Y Aihara STakei N Iwata H Umebayashi T Murata M Miyoshi MTomiita N Nishimoto T Kishimoto Efficacy and safety oftocilizumab in patients with systemic-onset juvenile idiopathicarthritis a randomised double-blind placebo-controlledwithdrawal phase III trial Lancet 371 (2008) 998ndash1006
[54] N Ruperto DJ Lovell P Quartier E Paz N Rubio-Perez CASilva C Abud-Mendoza R Burgos-Vargas V Gerloni JAMelo-Gomes C Saad-Magalhaes F Sztajnbok C Goldenstein-Schainberg M Scheinberg IC Penades M Fischbach J OrozcoPJ Hashkes C Hom L Jung L Lepore S Oliveira CAWallace LH Sigal AJ Block A Covucci A Martini EHGiannini Abatacept in children with juvenile idiopathic arthri-tis a randomised double-blind placebo-controlled withdrawaltrial Lancet 372 (2008) 383ndash391
[55] N Ruperto DJ Lovell P Quartier E Paz N Rubio-PerezCA Silva C Abud-Mendoza R Burgos-Vargas V GerloniJA Melo-Gomes C Saad-Magalhaes J Chavez-Corrales CHuemer A Kivitz FJ Blanco I Foeldvari M Hofer G HorneffHI Huppertz C Job-Deslandre A Loy K Minden M PunaroAF Nunez LH Sigal AJ Block M Nys A Martini EHGiannini Long-term safety and efficacy of abatacept inchildren with juvenile idiopathic arthritis Arthritis Rheum 62(2010) 1792ndash1802
[56] DM Brinkman IM de Kleer R ten Cate MA van RossumWP Bekkering A Fasth MJ van Tol W Kuis NM WulffraatJM Vossen Autologous stem cell transplantation in childrenwith severe progressive systemic or polyarticular juvenile idio-pathic arthritis long-term follow-up of a prospective clinicaltrial Arthritis Rheum 56 (2007) 2410ndash2421
[57] SE Klepper Effects of an eight-week physical conditioningprogram on disease signs and symptoms in children with chronicarthritis Arthritis Care Res 12 (1999) 52ndash60
[58] D Singh-Grewal J Schneiderman-Walker V Wright O Bar-OrJ Beyene H Selvadurai B Cameron RM Laxer R SchneiderED Silverman L Spiegel S Tse C Leblanc J Wong SStephens BM Feldman The effects of vigorous exercisetraining on physical function in children with arthritis arandomized controlled single-blinded trial ArthritisRheum 57 (2007) 1202ndash1210
[59] S Stephens D Singh-Grewal O Bar-Or J Beyene B CameronCM Leblanc R Schneider J Schneiderman-Walker HSelvadurai E Silverman L Spiegel SM Tse V WrightBM Feldman Reliability of exercise testing and functionalactivity questionnaires in children with juvenile arthritisArthritis Rheum 57 (2007) 1446ndash1452
[60] T Takken J van der Net W Kuis PJ Helders Physical ac-tivity and health related physical fitness in children with ju-venile idiopathic arthritis Ann Rheum Dis 62 (2003)885ndash889
[61] MM Toledo G Martini C Gigante L Da Dalt A TregnaghiF Zulian Is there a role for arthroscopic synovectomy in oli-goarticular juvenile idiopathic arthritis J Rheumatol 33(2006) 1868ndash1872
[62] F de Benedetti H Brunner N Ruperto SWright A KenwrightR Cuttica P Woo R Schneider DJ Lovell A Martini Efficacyand safety of Tocilizumab in patients with systemic juvenile idio-pathic arthritis (sJIA) 12-week data from the phase III TENDERtrial Ann Rheum Dis 69 (2010) 146
[63] P Quartier F Allantaz R Cimaz P Pillet C Messiaen CBardin X Bossuyt A Boutten J Bienvenu A Duquesne ORicher D Chaussabel A Mogenet J Banchereau JM Tre-luyer P Landais V Pascual A multicentre randomiseddouble-blind placebo-controlled trial with the interleukin-1receptor antagonist anakinra in patients with systemic-onsetjuvenile idiopathic arthritis (ANAJIS trial) Ann Rheum Dis70 (2011) 747ndash754
[64] DE Furst EC Keystone J Braun FC Breedveld GRBurmester F De Benedetti T Dorner P Emery R FleischmannA Gibofsky JR Kalden A Kavanaugh B Kirkham P Mease JSieper NG Singer JS Smolen PL Van Riel MH Weisman KWinthrop Updated consensus statement on biological agents forthe treatment of rheumatic diseases 2010 Ann Rheum Dis 70(Suppl 1) (2010) i2ndashi36
[65] T Beukelman NM Patkar KG Saag S Tolleson-RinehartRQ Cron EM Dewitt NT Ilowite Y Kimura RM LaxerDJ Lovell A Martini CE Rabinovich N Ruperto 2011 Ameri-can College of Rheumatology recommendations for the treatmentof juvenile idiopathic arthritis initiation and safety monitoring oftherapeutic agents for the treatment of arthritis and systemic fea-tures Arthritis Care Res 63 (2011) 465ndash482 (Hoboken)
[66] JF Simard M Neovius S Hagelberg J Askling Juvenile idi-opathic arthritis and risk of cancer a nationwide cohort studyArthritis Rheum 62 (2010) 3776ndash3782
[67] T Imagawa S Yokota M Mori T Miyamae S Takei H ImanakaY Nerome N Iwata T Murata M Miyoshi N Nishimoto TKishimoto Safety and efficacy of tocilizumab an anti-IL-6-receptor monoclonal antibody in patients with polyarticular-course juvenile idiopathic arthritis Mod Rheumatol (2011)doi102007s10165-011-0481-0
[68] TM Shaneyfelt MF Mayo-Smith J Rothwangl Are guide-lines following guidelines The methodological quality of clini-cal practice guidelines in the peer-reviewed medicalliterature Jama 281 (1999) 1900ndash1905
[69] R Grilli N Magrini A Penna G Mura A Liberati Practiceguidelines developed by specialty societies the need for a crit-ical appraisal Lancet 355 (2000) 103ndash106
[70] JS Burgers R Grol NS Klazinga M Makela J Zaat To-wards evidence-based clinical practice an international surveyof 18 clinical guideline programs Int J Qual Health Care 15(2003) 31ndash45
[71] JT Cassidy RE Petty Juvenile Idiopathic Rheumatic Arthri-tis 5th Edition WB Saunders Philadelphia 2005
[72] TJ Lehman Are withdrawal trials in paediatric rheumatic dis-ease helpful Lancet 372 (2008) 348ndash350
[73] J Munro Recommendations for the Diagnosis and Managementof Juvenile Idiopathic Arthritis The Royal Australian Collegeof General Practitioners South Melbourne 2009 pp 1ndash38
193Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
httpwwwnhmrcgovau_files_nhmrcpublicationsattachmentscp119-juvenile-arthritispdf
[74] MJ Santos JE Fonseca H Canhao M Conde M JoseVieira L Costa M Costa M Salgado JA Melo Gomes Guide-lines for prescribing and monitoring biologic therapies in juve-nile idiopathic arthritis Acta Reumatol Port 32 (2007) 43ndash47
[75] S Yokota M Mori T Imagawa T Murata M Tomiita Y ItohS Fujikawa S Takei Guidelines on the use of etanercept forjuvenile idiopathic arthritis in Japan Mod Rheumatol 20(2010) 107ndash113
[76] The AGREE Collaboration Appraisal of Guidelines for Researchamp Evaluation (AGREE) instrument wwwagreecollaborationorg
[77] I Kopp H Thole T Langer HK Selbmann G OllenschlaumlgerGerman Instrument for Methodological Guideline Appraisal(DELBI) wwwversorgungsleitliniende2008
[78] Auml Aumlrztliches Zentrum fuumlr Qualitaumlt in der Medizin A Arbeitsge-meinschaften der Wissenschaftlichen Fachgesellschaften in derMedizin Deutsches Instrument zur methodischen Leitlinien-Bewertung (DELBI) Fassung 20052006 Z Aumlrztl FortbildQualitaumltssich 99 (2005) 468ndash519
[79] MP de Wit SE Berlo GJ Aanerud D Aletaha JW BijlsmaL Croucher JA Da Silva B Glusing L Gossec S Hewlett MJongkees D Magnusson M Scholte-Voshaar P Richards CZiegler TA Abma European League Against Rheumatism rec-ommendations for the inclusion of patient representatives in sci-entific projects Ann Rheum Dis 70 (2011) 722ndash726
[80] I Foeldvari M Bidde Validation of the proposed ILAR classifi-cation criteria for juvenile idiopathic arthritis InternationalLeague of Associations for Rheumatology J Rheumatol 27(2000) 1069ndash1072
[81] R Merino J de Inocencio J Garcia-Consuegra Evaluation ofrevised International League of Associations for Rheumatologyclassification criteria for juvenile idiopathic arthritis in Spanishchildren (Edmonton 2001) J Rheumatol 32 (2005) 559ndash561
[82] SE Ramsey RK Bolaria DA Cabral PN Malleson REPetty Comparison of criteria for the classification of childhoodarthritis J Rheumatol 27 (2000) 1283ndash1286
[83] G Horneff A Ebert S Fitter K Minden I Foeldvari J Kum-merle-Deschner A Thon HJ Girschick F Weller HI Hup-pertz Safety and efficacy of once weekly etanercept 08mgkg in a multicentre 12 week trial in active polyarticularcourse juvenile idiopathic arthritis Rheumatology (Oxford) 48(2009) 916ndash919
[84] EH Giannini EJ Brewer N Kuzmina A Shaikov A Maxi-mov I Vorontsov CW Fink AJ Newman JT Cassidy LSZemel Methotrexate in resistant juvenile rheumatoid arthri-tis Results of the USAndashUSSR double-blind placebo-controlled trial The Pediatric Rheumatology CollaborativeStudy Group and The Cooperative Childrens Study GroupN Engl J Med 326 (1992) 1043ndash1049
[85] A Ravelli S Viola D Migliavacca N Ruperto A Pistorio AMartini The extended oligoarticular subtype is the best predic-tor of methotrexate efficacy in juvenile idiopathic arthritisJ Pediatr 135 (1999) 316ndash320
[86] P Woo TR Southwood AM Prieur CJ Dore J Grainger JDavid C Ryder N Hasson A Hall I Lemelle Randomizedplacebo-controlled crossover trial of low-dose oral
methotrexate in children with extended oligoarticular or sys-temic arthritis Arthritis Rheum 43 (2000) 1849ndash1857
[87] E Silverman L Spiegel D Hawkins R Petty D Goldsmith LSchanberg C Duffy P Howard V Strand Long-term open-label preliminary study of the safety and efficacy of lefluno-mide in patients with polyarticular-course juvenile rheumatoidarthritis Arthritis Rheum 52 (2005) 554ndash562
[88] DJ Lovell EH Giannini Y Kimura C Suzanne PJHashkes A Reiff Long-term safety and efficacy of rilonaceptin patients with systemic juvenile idiopathic arthritis (SJIA)Arthritis Rheum 60 (2009)
[89] N Ruperto P Quartier NWulffraat PWoo A Loy R Mouy BBader-Meunier BJ Prakken E Noseda R Belleli J Lecot CRordorf A Martini A Phase II Trial with canakinumab(ACZ885) a new IL-1-beta blocking monoclonal antibody toevaluate safety and preliminary efficacy in children with system-ic juvenile idiopathic arthritis Ann Rheum Dis 68 (2009) 170
[90] DJ Lovell EH Giannini Y Kimura et al Preliminary evi-dence for bioactivity of IL-1 trap (Rilonacept) a long actingIL-1 inhibitor in systemic juvenile idiopathic arthritis (sJIA)Arthritis Rheum 54 (2006) S325
[91] DJ Lovell EH Giannini Y Kimura et al Preliminary evi-dence for sustained bioactivity of IL-1 Trap (rilonacept) a longacting IL-1 inhibitor in systemic juvenile idiopathic arthritisArthritis Rheum 56 (2007) S514
[92] N Ruperto F De Benedetti H Brunner R Allen D Brown JChaitow E Cortis G Espada B Flato V Gerloni G HorneffS Wright A Kenwright R Schneider P Woo A Martini DJLovell Tocilizumab is efficacious in patients with systemic ju-venile idiopathic arthritis (sJIA) across baseline disease charac-teristics and priorbaseline treatments 12-week data from thephase II TENDER trial 17th PReS Congress Valencia Spain2010 2010
[93] N Ruperto DJ Lovell T Li F Sztajnbok C Goldenstein-Schainberg M Scheinberg IC Penades M Fischbach JOrozco PJ Hashkes C Hom L Jung L Lepore S OliveiraC Wallace M Alessio P Quartier E Cortis A Eberhard GSimonini I Lemelle E Chalom LH Sigal A Block A CovucciM Nys A Martini EH Giannini Abatacept improves health-related quality of life pain sleep quality and daily participationin subjects with juvenile idiopathic arthritis Arthritis Care Res(Hoboken) 62 (11) (2010) 1542ndash1551
[94] N Ruperto DJ Lovell P Quartier E Paz N Rubio-PerezCA Silva C Abud-Mendoza R Burgos-Vargas V GerloniJA Melo-Gomes C Saad-Magalhaes J Chavez C HuemerA Kivitz FJ Blanco I Foeldvari M Hofer G Horneff HIHuppertz CJ Deslandre A Loy K Minden M Punaro AFNunez LH Sigal AJ Block M Nys A Martini EH GianniniLong-term safety and efficacy of abatacept in children with ju-venile idiopathic arthritis Arthritis Rheum 62 (2010)1792ndash1802
[95] J Munro Juvenile Idiopathic Arthritis Management Guidelines(Provisional) Australian Paediatric Rheumatology Group 2006httpwwwnhmrcgovau
[96] K Fitch SJ Bernstein MD Aguilar B Burnand JR LaCalleP Lazaro M van het Loo J McDonnell JP Vader JPKahan The RANDUCLA Appropriateness Method Users ManualRAND Pittsburgh 2000

Consensus statement
NSAIDs are recommended for the treatmentof JIA Diclofenac Naproxen Ibuprofen andIndometacin (evidence level I respectively IIrecommendation grade A)If those drugs are contraindicated Celecoxibemight be used (evidence level I recommendationlevel BndashC)
Consensus statement
Intra-articular injections of crystalloid cortico-steroids (triamcinolone hexacetonide) are recom-mended and can be part of the first linetreatment Improvement of local inflammationpain swelling and range of joint movement hasbeen demonstrated (evidence level II recommen-dation grade A)Triamcinolone hexacetonide is more efficientthan triamcinolone acetonide inducing local remis-sion (evidence level I recommendation grade B)
180 G Dueckers et al
The conference guideline topics were reviewed andedited by working groups After the first consensus confer-ence statements were adopted by NGT and additional pro-posals for schemes of treatment strategies of JIA werecollated
25 Consensus finding method of Delphi
Three out of 15 statements remained without consensusafter NGT These statements comprise the utility of etaner-cept (treatment resistant polyarticular JIA) sulfasalazine(treatment resistant JIA) and anakinra (treatment for refrac-tory SoJIA) Therefore they were sent to all participants ofconsensus conferences via email To each of them partici-pants should state one of three votes (ldquoagreerdquo ldquodo notagreerdquo or ldquoalternative proposalrdquo) (1st round of Delphi)The results were summarized and the statements whichremained with no consensus after 1st round of Delphi weresent to participants again (2nd round of Delphi) After 2ndround of Delphi results were sent to external review
26 External review and adoption
The guideline manuscript has been reviewed in 2007 by na-tional experts in German Rheumatology Huppertz (BremenGermany) Michels (Garmisch Partenkirchen Germany) andSpecker (Essen Germany) The comments of external re-viewers (HI Huppertz) to the 2011 manuscript were in-volved within the 3rd round of Delphi External reviewenabled adoption of the guidelines core conclusions andstatements with strong consensus ie 95 agreement byrepresentatives of participating scientific societies andorganizations
3 Results treatment guidelines
31 Drug-based therapy
Drugs used in treatment of JIA are summarized in Table 5 Pro-posed schemes of treatment of JIA are shown in Fig 2 The fol-lowing paragraphs will highlight specific adverse reactions andintroduce the 13 studies relevant for the 2010 update of treat-ment guideline for JIA briefly For detailed information aboutprescribing information including indication contraindica-tion drug dosage route of administration monitoring andproduct characteristics the consensus group recommendsconsulting national drug data bases e g wwwrotelistede(German database of drugs with national market approval) orwwwfdaorg or wwwemaeuropaeu
311 Non-steroidal anti-inflammatory drugs (NSAIDs)Commonly NSAIDs are well tolerated Main side effects
of NSAIDs are stomach irritation dyspepsia andmdashin rarecasesmdashnephritis Cephalgia and behavioral changes can beassociated with the administration of ibuprofen Pseudo-porphyria is not uncommon in patients treated withnaproxen Pain relief has been demonstrated for Naproxen[13ndash15] Diclofenac [1516] and Ibuprofen [17] (evidencelevel I) and for Indometacin [18] and Meloxicam [19](evidence level II) Efficacy of Celecoxibe has been
demonstrated in a randomized double blind multicenterstudy [20] 95 of 212 patients entered the 12 week openlabel phase after a 12 week double blind phase in threetreatment groups (Celecoxibe 6 mgkgd versus Celecoxibe12 mgkgd versus Naproxen 15 mgkgd) Both dosages ofCelecoxibe showed comparable efficacy compared toNaproxen Safety ie number of adverse events (AE)did not differ significantly between Celecoxibe versusNaproxen
312 Glucocorticoids
3121 Glucocorticoids (GC)mdashlocal administration Theuse of intra-articular crystalline corticoids is highly potentand has a rather low rate of complications (evidence levelII) [2122] They might be administered as first line therapyResponse rate was significantly higher with triamcinolonehexacetonide than with triamcinolone acetonide at6 months and this difference was sustained to 24 months[2122] These findings were independent of duration andextent of disease [2122] Simultaneous intra-articular ste-roid injections are preferable to consecutive injections atdifferent time points (limited suppression of hypothalamicndashpituitaryndashadrenal axis) [23] Side effects eg local necrosisof fat tissue are seen in approximately 2 of injections [22]Working under sterile conditions the risk of infection is low
3122 GCmdashsystemic administration GC can be adminis-tered as a fast acting drug in highly active disease Indica-tions for their use are bridging time until DMARDs (diseasemodifying anti rheumatic drugs) become effective treat-ment of severe systemic features of systemic-onset JIA(SoJIA) induction of remission in polyarticular JIA and in se-vere forms of uveitis There are no controlled trials and nostandardized therapeutic regimes for the use of systemic
Table 5 Drugs for the treatment of JIA
Generic Dosage Age approval by Europeanmedical agency inpediatric rheumatology(EMA) a
Medical indication in pediatricrheumatology a b
Evidence levelrecommendationgrade [10]
Literature
NSAIDsDiclofenac 2ndash3 mgkg Bwd po (in 3 doses)
Retard formulation 1 dose14 years Arthritis IndashA Haapasiri [16] Laxer [14]
Ibuprofen 20ndash40 mgkg Bwd po in 3ndash4doses
6 months Pain fever IndashA Giannini [17]
Indometacin 1ndash3 mgkg Bwd po in 3 doses 2 years Arthritis IIndashA Stoeber [18]Meloxicam 0125ndash025 mgkg Bwd po 15 years Arthritis II Ruperto [19]Naproxen 10ndash15 mgkg Bwd po in 2 doses 1 year Arthritis IndashA Kvien [13] Laxer [14] Leak
[15]Celecoxibe 6 mgkg Bwd po in 2 doses or
12 mgkg Bwd in 1 doseNo approval for children Arthritis I B-C Foeldvari [20]
Glucocorticoids (GC)a) Systemic GCPrednisonePrednisolone
01ndash02 mgkg Bwd (max 5 mgd) JIA ie severe SoJIA severe peri-myokarditis severe uveitis (hypotoniaor cystoid macular edema) intoleranceto other drugs (ldquolow-doserdquo) or asldquobridgingrdquo therapy in higher doses eg2 mgkg Bwd until therapeutic effectof ldquoDMARDsrdquo
III Prieur [28]
Prednisone as an oralhigh-dose therapy
ge1ndash2 mgkg Bwd prednisolone-equivalent
III Prieur [28]
Prednisone as an oralmedium-dosetherapy
02 tob10 mgkg Bwdprednisolone-equivalent
III Kirwan [24] Prieur [28]
Prednisone as an orallow-dose therapy
b02 mgkg Bwd Prednisolone-equivalent or b4 mgmsup2 bodysurface
III Michels [25]
Prednisone as a ivpulse-therapy
N(5)ndash10 mgkg Bw (po)Prednisolone-equivalent10ndash30 mgkg Bwd Methyl-Prednisolone iv for 1ndash3 d(maximum 1 gdose)
III Miller [26] Picco [27]
b) Intra-articular GCTriamcinolonehexacetonide
05ndash1 mgkg Bw into large jointsdose adaption referring to size ofjoint (eg max 2 mg intointerphalangeal joints c)
5 months Arthritis tendo-vaginitis I Zulian [2122]
(continued on next page)(continued on next page)
181Evidence
andconsensus
basedGKJR
guidelinesfor
thetreatm
entof
juvenileidiopathic
arthritis
Table 5 (continued)
Generic Dosage Age approval by Europeanmedical agency inpediatric rheumatology(EMA) a
Medical indication in pediatricrheumatology a b
Evidence levelrecommendationgrade [10]
Literature
DMARDsSulfasalazine 30ndash50 mgkg Bwd in 2ndash3 doses 6 years Arthritis II Van Rossum [3637]Cytotoxic or immuno-suppressive drugsMethotrexate 10ndash15 (20) mgmsup2 body surface
once a week (po sc iv) e2 years Polyarticular JIA Psoriasis arthritis
uveitis CollagenosisI Giannini [84] Ravelli [85]
Woo [86]Cespedes-Cruz [33]Azathioprine 15ndash3 mgkg Bwd po in 1ndash2
dosesNo approval for children II Kvien [34]
Leflunomide No clear recommendation forchildren availableBwb20 kg d 1100 mgkg from d 2 10 mgkgdBw 20ndash40 kg d 1 to d 2 100 mgkgfrom d 3 10ndash20 mgkgdBwN40 kg d 1 to d 3 100 mgkgfrom d 3 20 mgkgd
No approval for children II Silverman [3587]
Biologic agentsa) TNFα inhibitorsEtanercept d 08 mgkg Bw sc 1timesweek
(max 50 mgweek) or 04 mgkgBw sc 2timesweek (max 50 mgweek)
4 years JIA Polyarthritis and insufficientefficacy of MTX
I Giannini [46] Horneff [49]Lovell [3888] Prince [41]
Adalimumab d 24 mgm2 body surface sc in 1dose every 2 weeks Bwb30 kg20 mgm2 body surface BwN30 kg40 mgm2 body surface(max 40 mg per dose)
4 years to 17 years Adalimumab in combination withmethotrexate is indicated for thetreatment of active polyarticularjuvenile idiopathic arthritis in childrenand adolescents who have had aninadequate response to one or moredisease-modifying anti-rheumatic drugs(DMARDs)
I Lovell [40]
182GDueckers
etal
Infliximab d 3ndash10 mgkg Bwdose iv Infusionat d 0 d 14 d 42 then every8 weeks intervals of applicationremain unclear
No approval for childrenwith JIA6 years (approval forMorbus Crohn)
III Ruperto [31]
b) IL-1 inhibitorsAnakinra d 1ndash4 mgkg Bwd sc in 1 dose No approval for children II Illowite [50] Lequerre [51]Canakinumab d 4 mgkg Bwsingle dose sc every
4 weeks (max 150 mg)No approval for childrenwith JIA 4 years (approvalfor CAPS)
III Ruperto [89]
Rilonacept d 1ndash2times44 mgkgweek sc (max320 mg) then 22 mgkgweek sc(max160 mg)
No approval for childrenwith JIA 12 years(approval for CAPS)
Lovell [889091]
c) IL-6 inhibitorsTocilizumab d 1 h Infusion every two 2 weeks
Bwb30 kg 8 mgkg BwN30 kg12 mgkg
2 years of age or older Since May 2011 EMA approval forpediatric patients with SoJIA who haveresponded inadequately to previoustherapy with NSAIDs and systemiccorticosteroids (Approval at Japan forSoJIA and polyarticular JIA since 2008) c
I Yokota [53] Ruperto [92]de Benedetti [62]
d) Co stimulatory-antagonistsAbatacept d 10 mgkg iv Infusion at d 0 d 14
d 28 then every 4 weeks6 years of age and older Abatacept in combination with
methotrexate is indicated for thetreatment of moderate to severe activepolyarticular (JIA) in pediatric patientswho have had an insufficient responseto other DMARDs including at least oneTNF inhibitor
I Ruperto [549394]
Abbreviations CAPS=Cryopyrine associated periodic fever syndrome JDM=juvenile dermatomyositis Bw=body weight SoJIA=systemic-onset of JIA SLE=systemic Lupus erythematodesa Compare wwwemaeuropaeub wwwrotelistede (German database of drugs with national market approval)c Intra-articular injection into same joint no more often than once every 3 monthsd A statement from insurance companies should be acquired before treatment initiation for off label treatment (if possible)e Oral application is most feasible in childhood
183Evidence
andconsensus
basedGKJR
guidelinesfor
thetreatm
entof
juvenileidiopathic
arthritis
Oligoarticular JIA
Polyarticular JIA
SoJIA
Figure 2 JIA treatment escalation schemes +=addition of the drug (abbreviations NSAIDs=non steroidal anti-inflammatory drugthotrexate)
Consensus statement
Long-term use of systemic GC is not recom-mended Continuous administration of ge02 mgPrednisolone equivalent per kg bodyweight (Bw)carries a high risk of adverse events and thereforeis not recommended (evidence level III recom-mendation grade A)
Consensus statement (continued)
184 G Dueckers et al
GC in JIA published thus leading to ldquojustrdquo evidence level IIIDifferent recommendations of dosage and therapy regimesare listed in Table 5 (evidence level III for all recommenda-tions) [1824ndash28] Frequency and seriousness of deleteriouseffects correlate mainly to duration of therapy and dosageof GC administered Main side effects are iatrogenicCushings syndrome growth disturbance weight gainmood changes Higher dosage carry the risk of increasedvulnerability to infection hypertension osteoporosisthrombosis diabetes gastro-intestinal ulceration cataractglaucoma atrophy of subcutaneous fatty tissue steroid in-duced acne To inform colleagues about GC treatment in acase of emergency and to reduce severe complications in longterm treated patients ie GC administrationN4 weeks thesupply of ldquoGlucocorticoid ID cardsrdquo for patients might be useful
GC=Glucocorticoids DMARDs=disease modifying drugs MTX=Me
Consensus statement
The systemic use of GC is recommended asfast acting drugs in highly active JIA GC areused for the treatment of children and adoles-cents with SoJIA organ manifestations of JIA(eg uveitis pericardial effusion) sero-positivepolyarticular JIA and for bridging time untilthe complete therapeutic effect of DMARDs(evidence level III recommendation grade A)
313 Methotrexate (MTX) biologic agents andimmunosuppressive agents
MTX biologic agents and immunosuppres-sive agents are used for the treatment of childrenand adolescents with polyarticular JIA ifNSAIDs or local GC treatment do not succeedThe combination of those drugs with NSAIDsand GC is feasible A common characteristic ofMTX biologic agents and immunosuppressiveagents is the delayed onset of therapeutic ef-fect ie up to 3 months or even longer aftercommencing treatment
185Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
Safe contraception is indicated during therapy with MTXAzathioprine or Leflunomide and in the following 3 to6 months after its discontinuation
Consensus statement
Administration of Sulfasalazine or Lefluno-mide is recommended if MTX or Etanercept donot show sufficient efficacy or cannot be used
3131 Methotrexate Among DMARDs MTX provides themainstay of long-term therapy in JIA [29ndash32] In case ofside effects eg dyspepsia or nausea prophylaxis withfolic acid can be recommended (1times1 mg per day or 5 mgonce a week 24ndash48 h after application of MTX) Safe contra-ception is mandatory while receiving MTX Safety and effica-cy of MTX and its impact on quality of life of children with JIAhave been investigated Significant positive impact of MTXon all health-related quality of life health conceptshas been shown although the study has its limit due to dif-ferent MTX dosages used within participating JIA patients[33]
Consensus statement
MTX administration can be recommendeddue to its proven safety and efficacy to reducedisease activity MTX is used in case of insuffi-cient therapeutic effect of NSAIDs andor localGC administration continuous need for system-ic GC andor highly active disease Efficacy ofMTX (orally or subcutaneously administered) isfrequently achievable with a dosage of 10ndash15 mgmsup2 body surface (evidence level I recom-mendation grade A)
for other reasons (evidence level II recommen-dation grade B)
3132 Purine analogs31321 Azathioprine Efficacy has been investigat-
ed in a double blind placebo controlled study (32 patients)After 8 weeks of therapy the changes in disease activitymeasurement indicated a minor improvement in the Azathi-oprine group compared to the placebo group At the end ofthe study statistically significant differences between thegroups were found for only 2 disease activity measurements[34] Two patients were taken out of study due to severeadverse events eg leucopenia Measurement of activityof Thiopurinmethyltransferase (TPMT) can be beneficial foravoidance of severe adverse events
3133 Pyrimidine analogs31331 Leflunomide Within a double blind study
(32 weeks 94 patients) efficacy of Leflunomide was inferiorin comparison to MTX but better than placebo Howeverdosing of Leflunomide may not have been adequate insome children [35] Contraindications for Leflunomide arerenal insufficiency severe immunodeficiency depressedmyelopoesis and pancytopenia An extensive half-life peri-od (approximately 14 days) has to be taken in accountwhen administering Leflunomide In combination with hepa-totoxic DMARDs the risk of severe adverse events might in-crease eg increased blood pressure is seen frequentlySafe contraception is mandatory
3134 Antibiotic analogs and Hydroxychloroquine andChloroquine
31341 Sulfasalazine Weak efficacy of Sulfasalazinewas demonstrated within a placebo-controlled randomizedstudy after 24 weeks (96 patients) [3637] One third of pa-tients enrolled in the study discontinued treatment with Sulfa-salazine due to side effects eg gastrointestinal symptomsleucopenia [36] Some experts use sulfasalazine in HLA-B27positive JIA Contraindications are Glucose-6-phosphatase de-ficiency and hypersensitivity against sulfonamides
31342 Hydroxychloroquine and chloroquine Hydrox-ychloroquine and Chloroquine have been subject to clinical tri-als for the treatment of JIA even though efficacy was limitedWithin three consensus conferences held in 2007 and 2010 theconsensus group decided not to give a consensus statementon the use of chloroquine or hydroxychloroquine treatmentdespite the fact that those drugs still might be used by somecaregivers
3135 Biologic agents Biologic agents are drugs whichselectively inhibit cytokines cytokine receptors or directlybind to receptors of lymphocytes eg CTLA-4 CD20 Theyinclude antibodies and fusion proteins So far allbiological therapies are administered subcutaneously orintravenously
31351 TNFα-inhibitors TNFα-inhibition with Adali-mumab and Etanercept is efficient and safe (evidencelevel I) [38ndash41] Both drugs have been approved for JIAwith polyarticular course TNFα-inhibitors have become anintegral part of the treatment of JIA Potential risks of therapyare vulnerability for infection andmdashin a rare occasionmdashthe in-duction of autoimmune disease Prior to the start of treatmentwith TNFα-inhibitors chronic infections needs to be excludedor treated sufficiently eg tuberculosis hepatitis B or C
In children with JIA treated with TNFα-inhibitors malig-nancies eg Lymphoma have been reported It remainsunclear if the rate of malignancies is increased in patientscompared to the risk by having JIA itself In response to aprevious letter of the FDA (as reviewed in [42]) the GermanSociety for Pediatric Rheumatology (GKJR) has published of-ficial statements [4344] The GKJR states that treatmentwith TNFα-inhibition should be used very carefully physi-cians need to be aware of co-medication e g immunosup-pressive drugs and should monitor those patientsclosely [43] There is insufficient data on all biologicagentsmdashincluding TNFα-inhibitionmdashto judge about the long-term risk for children and adolescents313511 Etanercept Etanercept is a fusion proteinconsisting of the extracellular binding domain of solubleTNFα-receptor and Fc chain of human IgG1 Etanercept in-hibits TNFα by direct binding of the cytokine Efficacy has
Consensus statement
The use of Anakinra or Tozilizumab can berecommended for treatment of children and ado-lescents with refractory SoJIA (evidence level IIrecommendation grade A)
186 G Dueckers et al
been demonstrated in a randomized controlled withdrawaldesign trial for patients with polyarticular JIA [38] Withinan open extension study long term efficacy and safety havebeen documented over 8 years in 1669 patients [3945]There is data on more than 2000 patients registered in Euro-pean registries [46ndash48] Currently retrospective data showsa somewhat better efficacy of combining MTX or otherDMARDs with TNFα-inhibition versus anti-TNFα therapy assingle therapy [49]313512 Adalimumab Adalimumab is a humanizedmonoclonal IgG1 antibody directed against TNFα whichbinds soluble and membrane bound TNFα A randomizedcontrolled withdrawal design trial demonstrated safety andefficacy of Adalimumab (24 mgmsup2 body surface every2 weeks max 40 mg) for children and adolescents withpolyarticular JIA (4ndash17 years of age n=171) [40] After16 weeks ldquowash inrdquo phase responders (n=144171) enteredthe 32 weeks randomized double blind phase After 48 weekstwice the number of patients in the verum group met ACR 70as compared to the control group (56 vs 28 pb001)Within the open extension phase Adalimumab dosage wasfixed ie 20 mgb30 kg Bw and 40 mgN30 kg Bw There islack of evidence showing superior efficacy of combiningMTX (DMARDs) with Adalimumab versus Adalimumab as sin-gle therapy [40]
Consensus statement
Efficacy of Etanercept and Adalimumab forthe treatment of polyarticular JIA has been dem-onstrated Therapy with TNFa-inhibition is indi-cated in case of insufficient therapeutic effectof NSAIDs and local GC administration and lackof response to MTX (evidence level I recom-mendation grade A)
Consensus statement
Patients with polyarticular JIA without sys-temic manifestation refractory to treatmentwith MTX and TNF inhibition might benefit fromthe use of Abatacept (evidence level III recom-mendation grade C)
313513 Infliximab Infliximab is a chimerical (humanmouse) monoclonal antibody which binds soluble and mem-brane bound TNFα A randomized controlled study in childrenand adolescents with JIA failed to demonstrate a significantdifference of efficacy after treatment with Infliximab com-pared to placebo [31]
31352 Interleukin-1-inhibitors None of interleukin-1-inhibitors are approved for the treatment of JIA or SoJIAThey are commonly used in an off label setting313521 Anakinra Anakinra is an IL-1 receptor antag-onist Within a randomized controlled trial no significant ef-ficacy of Anakinra for patients with polyarticular JIA couldbe demonstrated [50] 50 of 86 patients were enrolled intoblinded phase (11 Anakinra versus Placebo) No significantreduction of flare could be demonstrated in comparison toplacebo 29 of 50 patients completed the open label exten-sion study Two noncontrolled nonrandomized studieshave shown efficacy of anakinra in a proportion of patientswith systemic-onset of JIA (SoJIA) [5152]313522 Canakinumab Canakinumab an IL-1β anti-body binds IL-1β selectively without interfering with IL-1αor its physiological IL-1 receptor antagonist Canakinumabhas been approved for treatment of hereditary periodic IL-1 associated periodic fever syndromes ie Cryopyrin-
associated periodic syndromes There are ongoing studies in-vestigating safety and efficacy of Canakinumab for SoJIA
31353 Interleukin-6 inhibitors313531 Tozilizumab Tozilizumab is a humanizedanti-IL-6 receptor monoclonal antibody Efficacy has beendemonstrated within a 12 week double blind randomizedcontrolled withdrawal trial in children with SoJIA (n=562ndash19 years) in Japan [53] After a 48 week open extensionstudy ACR Pedi 30 was met by 47 patients (98) At thetime of our literature search Tocilizumab was approved fortreatment of SoJIA and polyarticular JIA since 2008 inJapan A multicenter European study investigating efficacyand safety of Tozilizumab in polyarticular JIA was ongoingat the deadline of literature search (wwwclinicaltrialsgov NCT00988221) No data on long term effects are cur-rently available
31354 Co-stimulation inhibitors313541 Abatacept Abatacept is a recombinant fu-sion protein of extracellular domain of human cytotoxic T-Lymphocyte Antigen 4 (CTLA-4) and IgG1-Fc-Fragment Itmodulates T-cell co-stimulation A randomized controlleddouble blind withdrawal design study of Ruperto et al [54]demonstrated efficacy of Abatacept in patients with polyar-ticular JIA 123 of 170 participants of study were enrolled inthe 6 month double blind phase Flares occurred in 33 of 62(53) patients who were given placebo versus 12 of 60(20) Abatacept patients during double blind phase Adverseevents (AE) did not differ in both groups ie 37 AE in Abata-cept versus 34 AE in placebo recipients Some children maytake 3 to 6 months or longer before their maximal responseis achieved 3 of patients developed reaction to the infu-sion [55] Abatacept is approved by FDA and EMA for pa-tients who did not respond to prior MTX treatment Nodata of long term effects of the use of Abatacept in JIA areavailable due to the low numbers of patients treated so far
314 Autologous stem cell transplantation (SCT)There are studies on autologous SCT for treatment of re-
fractory and severe forms of JIA (evidence level III) [56] 22
Consensus statement
187Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
patients were enrolled in one study 8 reached clinical re-mission 7 were assessed as partial responders 3 experi-enced relapse of the disease and 4 (18) died as aconsequence of MAS or immunosuppressive treatment [56]Due to serious adverse events including death this thera-peutic option is seen as the last treatment option
Exercise training is recommended dependingon the extent of inflammation number of affect-ed joints and global disease activity Sports withminor stress on joints is favorable (evidence levelI recommendation grade A)
32 Non-drug based therapy
321 Physiotherapy occupational therapy and thera-peutic appliances
Physio- and occupational therapy are integral parts of thetherapeutic concept in children and adolescents with JIA[5758] Therapeutic goals of physiotherapy are relaxationand pain relief preservation or rehabilitation of physiologi-cal range of joint movement prevention of contracturesstretching and activation of muscles build-up of muscleforce and training of physiological movements
Consensus statement
Structured treatment by a properly trainedphysiotherapistoccupational therapist in combi-nation with drug based therapy and instructionsfor disease adopted self-sufficient daily exercisesessions are recommended to keep and to im-prove joint mobility (evidence level II recom-mendation grade A)Custom-made therapeutic appliances for correc-tion of axial misalignment prevention of falseweight bearing stabilization of joints (eghand- finger- and foot-ortheses) are recom-mended individually The use of therapeutic ap-pliances follows individual physician-directedadvice Efficacy has been demonstrated (evi-dence level I recommendation grade B)
Consensus statement
In individual cases the indication for open orarthroscopic synovectomy can be considered ifconservative therapy does not succeed (evi-dence level III recommendation grade B)
Consensus statement
Other forms of non-drug based therapeutic approachesrely on experts opinion and are solely based on individualclinical experience No controlled studies are available
Consensus statement
The implementation of thermotherapy electro-or ultrasound therapy massage and lymph drain-age is recommended Application of cold appli-ances for acute joint inflammation is indicated(evidence level II recommendation grade A)Electro- and ultrasound therapy are recom-mended for patients with tendosynovitis (evi-dence level III recommendation grade B)
An early psychological support within stan-dard pediatric rheumatological care should beimplemented to apprehend and treat mental is-sues and behavioral syndromes associated withphysiological disturbances and physical factors(evidence level III recommendation grade A)
Consensus statement
A socio-pedagogical care with regard tointegration at school professional andeveryday life and formal education of parentsand patients is recommended (evidence levelIII recommendation grade A)
322 Sportive activity and exercise trainingPositive impact of sportive activity on the general physi-
cal condition and on oxygen consumption has been demon-strated (evidence level II) [57ndash60] Adequate exercise
training supports the physiological development and helpscoping with JIA [58] Prospective controlled long term stud-ies are currently not available
323 Surgical treatmentToledo et al investigated the role of arthroscopic syno-
vectomy in JIA They concluded that arthroscopy is a safebut only partially effective procedure in patients witholigoarticular JIA (evidence levelrecommendation gradeIIIB) [61]
324 Psychological social intervention orsocio-pedagogical care
There are no controlled or open studies focusing on psy-chological social andor socio-pedagogical intervention inchildren or adolescents with JIA Recommendations arebased on experts opinion and personal experience solely
188 G Dueckers et al
4 Addendum
Since the deadline January 15th 2010 new papers haveappeared that are of interest in the context of our guideline[5562ndash64] in particular we refer to the ACR recommenda-tions [65] and the most recent literature on the risk of malig-nancies in JIA in context with TNF blocking agent andindependent of medication [42] [66] Moreover there is arecent study on the use of Tocilizumab in polyarticular pa-tients [67] These papers will be discussed within the nextconsensus conference by NGT and considered for inclusioninto the next edition of this guideline On 6th of September2011 our advanced search on wwwclinicaltrialgov (searchterms juvenile idiopathic arthritis recruitment open stud-ies study type interventional study age group child(birthndash17) intervention drugs) led to 16 trials which are cur-rently recruiting or will soon start recruiting
5 Discussion
To develop clinical practice guidelines of high quality andvalidity a formal consensus process and explicit methodo-logical criteria for the production of guidelines are recom-mended [68ndash70] Our guideline for the treatment of JIA inchildren and adolescents implements all these issues Thesystematic literature search was terminated on 15th January2010 leading to the most up to date guideline for JIA whichis currently available The deadline of the ACR recommenda-tions as published recently by Beukelmann et al was 5th ofOctober 2009 [65] By exclusion of case reports trials with-out control groups preliminary results published as ab-stracts on conferences and the strict graduation of theliterature by the criteria of evidence based medicine weaimed to give our guideline statements additional strengthand a maximal validity Newer original studies providing ad-ditional evidence for the treatment of JIA became availableafter our consensus process was finished see AddendumThe results of these trials have to await the next NGT beforeinclusion into our recommendations
Our updated systematic literature search in 2010 led to13 relevant studies published after 30th June 2007 (Fig 1Table 4) Their results have to be interpreted with cautionFirst trials in JIA are mainly based on limited numbers of pe-diatric patients as the recruitment of a sufficient number ofpediatric patients remains challenging Second trials aremainly designed for patients with polyarticular JIA or witholigoarticular onset and a polyarticular course (Table 4)Most children with JIA do not have a polyarticular subtypeof JIA but an oligoarticular onset and course [71] Thus pa-tients with oligoarticular JIA are heavily underrepresentedin most of the current trials Third in 5 of the 13studies the withdrawal study design has been used[4045505354] Lehmann reviewed the bias of withdrawaldesign trials in 2008 [72] After a wash-in phase only re-sponders to treatment are eligible for randomization Thusthe design preselects responders to the placebo effect whomight retain their response throughout the entire study peri-od Further there is a carryover effect of AE into the place-bo group so that significant differences in AE betweengroups may not become apparent In the one placebo con-trolled trial without withdrawal design on TNFα-inhibition
(Infliximab) no significant efficacy could be demonstratedbetween verum and placebo [31]
To our knowledge there are two other guidelines that dealwith the management of JIA as a whole (Table 6) [65] [73]Other guidelines are limited to the use of single drugs in JIAeg biologic agents [74] etanercept [75] The Australian guide-line (wwwracgporgauguidelinejuvenileidiopathicarthritis)has not been published in a peer-reviewed journal It is to pro-vide recommendations for the early diagnosis and multidisci-plinary management of JIA in the primary care setting forgeneral practitioners (GPs) [73] No recommendations aremade regarding the use of GCs DMARDs immunosuppressivedrugs or biologic agents [73] The ACR recommendations usesthe Appraisal of Guidelines for Research and Evaluation(AGREE) instrument [65] [76] which does not fulfill criteria ofa proper consensus process and carries the risk that expertsvote for peer opinion which might not reflect the true valueWe used an advanced and linguistically validated version ofthe AGREE instrument the ldquoGerman Instrument for Methodo-logical Guideline Appraisal (DELBI)rdquo which has been developedin cooperation of the AWMF among others [7778] We followedthe highly structured Nominal Group Technique as described inMethodology Our consensus group only considered formallyboard nominated representatives of multidisciplinary scientificsocieties and organizations (Table 1) and included patients rep-resentatives as this has been strongly recommended by the Eu-ropean League against Rheumatism (EULAR) recently [79] TheACR mentions a parent representative within their task forcepanel but leaves this representative anonymous It remainsunclear how ACR experts were selected and involved [65]They defined treatment groups which have not been evaluatedsystematically so far We used the ILAR classification systemwhich has been repeatedly evaluated [80ndash82]
By content there are major differences between the ACRrecommendations and our guideline a) Our guideline pro-vides a detailed and systematic list of 20 drugs commonlyused in the treatment of JIA (Table 5) which has been an in-tegrative part of our consensus conferences The ACR recom-mendations do not provide information on approval status(Food and Drug Administration) indications for use and nospecific differences on dosage regimes or frequency ofdaily application [65] eg it refers to the 2008 ACR recom-mendations for the use of DMARDs in adult rheumatoid ar-thritis b) The ACR recommendations provide a more earlyaggressive approach in the treatment of JIA The ACR recom-mends MTX as first line treatment in patients (b4 joints) withhighly active disease [65] To our knowledge there are onlydata to recommend MTX administration in cases of insuffi-cient therapeutic effect of prior treatment with NSAIDandor GC [33] c) The ACR recommends the use of TNFα in-hibitors as escalation therapy for some patients with historyof arthritis of 4 or fewer joints and refer to publications[3840] conducted in patients with polyarticular JIA or pau-ciarticular JIA with polyarticular course [65] There is no ev-idence that TNF is safe and efficient in patients witholigoarticular JIA a systematic controlled clinical trial onthis issue has not been done yet d) We regard a brief trialof local or systemic administration of GC plus NSAID as a fea-sible first line treatment for patients with polyarticular JIAThe ACR recommends MTX without regard to disease activityat the initial stage [65] We reached consensus to recom-mend the use of GC as bridging therapy until full onset of
Table 6 Overview of recommendationsguidelines for treatment of JIA
USA Australia Germany
ACR recommendations[65]
RACGP recommendations[73]
GKJR guidelines
Deadline of literature search October 2009 January 2007 September 2010Source of publications Pub Med Pub Med
EMBASE CINHAL CochraneLibrary provisionalAustralian Guideline [95]
Pub MedPrevious German Guidelines [78]
Definition used for JIA subgroups Treatment groups definedby Core expert panel
Not specifically definedChildren withJIAb16 years
ILAR criteria [1]
Consensus processprocessvalidation
AGREE [76] AGREE [76] DELBI [77]RANDUCLA appropriatenessmethod [96]
NGT Delphi method
Conferences None None 3 Formal consensus conferencesAddressees Pediatric rheumatologists General practitioner Pediatric Rheumatologists
PediatriciansGeneral practitioners
Participating scientific societies or professional organizationsPediatric rheumatologist orrheumatologists for adolescents
Yes Yes Yes
General pediatrician- In hospital Yes Yes Yes- In private practice Yes Yes YesResearcher Yes No YesRheumatologists for adults No No YesOphthalmologists No No YesParentspatients support groups Yes No YesOrthopedic surgeons No No YesPediatric orthopedic surgeons No No YesPsychologists No No YesPhysiotherapists No No YesPediatric rheumatology nurses Yes No NoOther scientific societies ororganizations
ACR BSPAR PRINTO PReS RACGP NAMSCAG NHMRC DGKJ DGPs DGRh DGO AWMFBVKJ
(ACR=American College of Rheumatologists AGREE=Appraisal of Guidelines for Research amp Development AWMF=Association of the ScientificMedical Associations BSPAR=British Society for Pediatric Rheumatology BVJK=Association of Pediatricians in private practice CEP=Core expertpanel ILAR=International League against Rheumatism CINHAL=Cumulative Index to Nursing and Allied Health Literature DELBI=German In-strument for Methodological Guideline Appraisal DGKJ=German Society of Pediatrics and Adolescent Medicine DGO=German Society for Oph-thalmology DGPs=German society for Psychology DGRh=German Society for Rheumatology GKJR=German Society for Pediatric RheumatologyNAMSCAG=National Arthritis and Musculoskeletal Conditions Advisory Group NGT=Nominal Group Technique NHMRC=National Health andMedical Research Council PReS=Pediatric Rheumatology Society) PRINTO=Pediatric Rheumatology International Trial Organization RACG-P=Royal Australian College of General Practitioner RANDUCLA=Research and DevelopmentUniversity of California at Los Angeles)
189Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
therapeutic effect of DMARDs The ACR recommendations donot provide any recommendation for the use of systemic GCfor patients with oligo- or polyarticular course of JIA exceptsystemic onset of JIA e) The ACR recommendations do notcover the topic of non-drug based therapy at all althoughthere is strong evidence that eg exercise training is a usefuladdition to drug treatment [575860]
6 Conclusion
In summary we present a treatment guideline for JIA on a con-sensus conference basis We strongly advocate an interdisciplin-ary approach including surgery physiotherapy psychosocial
intervention physical therapy medications etc and a strictformal consensus process in order to create statements thatare most appropriate for the complex clinical situation of achild and family presenting with JIA and cover all aspects ofJIA care All German pediatric rheumatology sites are partici-pating at the national pediatric rheumatologic database in theDeutsche Rheuma-Forschungszentrum at Berlin (DRFZ wwwdrfzde) It aims at quality assurance in Germany and monitorstreatment behavior of pediatric rheumatologists by using inter-nationally agreed criteria (eg joint count global physician rat-ing of disease activity global parent rating of overall well-being CHAQ ESR ACR-ped response or JADAS) The databasewill be used as a tool to monitor the application of our treat-ment guidelines
190 G Dueckers et al
Conflict of interest statement
Gregor Dueckers Novartis Pharmaceuticals CorporationBaxter (for all travel grants for scientific meetings)Nihal Guellac no conflict of interestMartin Arbogast no conflict of interestGuumlnther Dannecker no conflict of interestIvan Foeldvari Wyeth Pfizer Abbott Immunology Pharma-ceuticals Chugai (for all advisory board member)Michael Frosch no conflict of interestGerd Ganser Abbott Immunology Pharmaceuticals (advisoryboard member grants for scientific meetings) Wyeth Pfizer(advisory board member grants for scientific meetings)ChugaiRoche (advisory board member grants for scientificmeetings) Merck (grants for scientific meetings) Actelios(grants for scientific meetings) Esaote (grants for scientificmeetings)Arnd Heiligenhaus Novartis Pharmaceuticals CorporationAbbott Immunology Pharmaceuticals Alcon (for all re-search grants)Gerd Horneff Abbott Immunology Pharmaceuticals (re-search grants consulting fees non-remunerative positionsof influence) Wyeth Pfizer (research grants consultingfees speakers bureau non-remunerative positions of influ-ence) Bristol-Myers Squibb (Consulting fees) Nycomed(Consulting fees non-remunerative positions of influence)RocheChugai (Consulting fees non-remunerative positionsof influence) Sandoz (Consulting fees) Genzyme (researchgrants consulting fees non-remunerative positions of influ-ence) Swedish Orphan (research grants consulting feesnon-remunerative positions of influence)Arnold Illhardt no conflict of interestRuumldiger Krauspe no conflict of interestBarbara Markus no conflict of interestHartmut Michels Abbott Immunology Pharmaceuticals (advi-sory board member and grants for scientific meeting)Matthias Schneider no conflict of interestWolfram Singendonk no conflict of interestHelmut Sitter no conflict of interestMarianne Spamer no conflict of interestNorbert Wagner no conflict of interestTim Niehues Abbott Immunology Pharmaceuticals EssexPharma Novartis Pharmaceutical Corporation WyethPfizer (for all research grants consulting fees non-remu-nerative positions of influence)
Acknowledgment
We like to express our grateful thanks to Prof Dr Hans IkoHuppertz for proof reading the article and for an excellentdiscussion on our work We like to express our thanks to HE-LIOS Clinic for funding the open access of the article
References
[1] RE Petty TR Southwood P Manners J Baum DN Glass JGoldenberg X He J Maldonado-Cocco J Orozco-Alcala AMPrieur ME Suarez-Almazor PWoo International League of Asso-ciations for Rheumatology classification of juvenile idiopathic ar-thritis second revision Edmonton 2001 J Rheumatol 31(2004) 390ndash392
[2] B Prakken S Albani A Martini Juvenile idiopathic arthritisLancet 377 (2011) 2138ndash2149
[3] KT April DE Feldman RW Platt CM Duffy Comparisonbetween children with juvenile idiopathic arthritis (JIA) andtheir parents concerning perceived quality of life Qual LifeRes 15 (2006) 655ndash661
[4] BM Feldman B Grundland L McCullough V Wright Distinc-tion of quality of life health related quality of life and healthstatus in children referred for rheumatologic care J Rheuma-tol 27 (2000) 226ndash233
[5] JC Packham MA Hall Long-term follow-up of 246 adultswith juvenile idiopathic arthritis functional outcomeRheumatology (Oxford) 41 (2002) 1428ndash1435
[6] C Sandborg Pediatric rheumatic disease standards of care forJIAmdashthe basic foundation for quality Nat Rev Rheumatol 6(2010) 389ndash390
[7] N Guellac T Niehues Interdisciplinary and evidence-basedtreatment guideline for juvenile idiopathic arthritis KlinPadiatr 220 (2008) 392ndash402
[8] K Schnakenburg Leitlinien in der Kinder- und JugendmedizinElsevier 2005 pp H1 1ndash15
[9] P Juni L Nartey S Reichenbach R Sterchi PA Dieppe MEgger Risk of cardiovascular events and rofecoxib cumulativemeta-analysis Lancet 364 (2004) 2021ndash2029
[10] W Feldman Evidence-based Pediatrics 1st ed BC DeckersHamilton 2000
[11] AH Van de Ven AL Delbecq The nominal group as a re-search instrument for exploratory health studies Am J PublicHealth 62 (1972) 337ndash342
[12] HA Linstone M Turoff The Delphi Method Techniques andApplications Addison-Wesley Pub 1975
[13] TK Kvien HM Hoyeraal B Sandstad Naproxen and acetyl-salicylic acid in the treatment of pauciarticular and polyarticu-lar juvenile rheumatoid arthritis Assessment of tolerance andefficacy in a single-centre 24-week double-blind parallelstudy Scand J Rheumatol 13 (1984) 342ndash350
[14] RM Laxer ED Silverman C St-Cyr MT Tran G Lingam Asix-month open safety assessment of a naproxen suspensionformulation in the therapy of juvenile rheumatoid arthritisClin Ther 10 (1988) 381ndash387
[15] AM Leak MR Richter LE Clemens MA Hall BM AnsellA crossover study of naproxen diclofenac and tolmetin in sero-negative juvenile chronic arthritis Clin Exp Rheumatol 6(1988) 157ndash160
[16] J Haapasaari E Wuolijoki H Ylijoki Treatment of juve-nile rheumatoid arthritis with diclofenac sodium Scand JRheumatol 12 (1983) 325ndash330
[17] EH Giannini EJ Brewer ML Miller D Gibbas MH PassoHM Hoyeraal B Bernstein DA Person CW Fink LA Sawyeret al Ibuprofen suspension in the treatment of juvenilerheumatoid arthritis Pediatric Rheumatology CollaborativeStudy Group J Pediatr 117 (1990) 645ndash652
[18] E Stoeber L Sanger Experiences with indomethacin in long-term therapy of juvenile rheumatoid arthritis Arzneimittel-forschung 21 (1971) 1865ndash1866
[19] N Ruperto I Nikishina ED Pachanov Y Shachbazian AMPrieur R Mouy R Joos F Zulian R Schwarz V ArtamonovaW Emminger M Bandeira A Buoncompagni I Foeldvari FFalcini E Baildam I Kone-Paut M Alessio V Gerloni ALenhardt A Martini G Hanft R Sigmund S Simianer Arandomized double-blind clinical trial of two doses ofmeloxicam compared with naproxen in children with juvenileidiopathic arthritis short- and long-term efficacy and safetyresults Arthritis Rheum 52 (2005) 563ndash572
[20] I Foeldvari IS Szer LS Zemel DJ Lovell EH Giannini JLRobbins CRWest G Steidle S Krishnaswami BJ Bloom A pro-spective study comparing celecoxib with naproxen in children withjuvenile rheumatoid arthritis J Rheumatol 36 (2009) 174ndash182
191Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
[21] F Zulian G Martini D Gobber C Agosto C Gigante FZacchello Comparison of intra-articular triamcinolone hexa-cetonide and triamcinolone acetonide in oligoarticular juve-nile idiopathic arthritis Rheumatology (Oxford) 42 (2003)1254ndash1259
[22] F Zulian G Martini D Gobber M Plebani F Zacchello PManners Triamcinolone acetonide and hexacetonide intra-articular treatment of symmetrical joints in juvenile idiopathicarthritis a double-blind trial Rheumatology (Oxford) 43 (2004)1288ndash1291
[23] GS Habib Systemic effects of intra-articular corticosteroidsClin Rheumatol 28 (2009) 749ndash756
[24] JR Kirwan The effect of glucocorticoids on joint destructionin rheumatoid arthritis The Arthritis and Rheumatism CouncilLow-Dose Glucocorticoid Study Group N Engl J Med 333(1995) 142ndash146
[25] H Michels What is low-dose corticosteroid therapy in juvenileidiopathic arthritis A worldwide questionnaire-based surveyZ Rheumatol 59 (Suppl 2) (2000) II127ndash130
[26] JJ Miller III Prolonged use of large intravenous steroid pulsesin the rheumatic diseases of children Pediatrics 65 (1980)989ndash994
[27] P Picco M Gattorno A Buoncompagni V Pistoia C Borrone6-methylprednisolone lsquomini-pulsesrsquo a newmodality of glucocor-ticoid treatment in systemic onset juvenile chronic arthritisScand J Rheumatol 25 (1996) 24ndash27
[28] AM Prieur The place of corticosteroid therapy in juvenilechronic arthritis in 1992 J Rheumatol Suppl 37 (1993)32ndash34
[29] JS Gao H Wu J Tian Treatment of patients with juvenilerheumatoid arthritis with combination of leflunomide andmethotrexate Zhonghua Er Ke Za Zhi 41 (2003) 435ndash438
[30] T Niehues G Horneff H Michels MS Hock L SchuchmannEvidence-based use of methotrexate in children with rheumat-ic diseases a consensus statement of the Working Groups Pedi-atric Rheumatology Germany (AGKJR) and PediatricRheumatology Austria Rheumatol Int 25 (2005) 169ndash178
[31] N Ruperto DJ Lovell R Cuttica N Wilkinson P Woo GEspada C Wouters ED Silverman Z Balogh M HenricksonMT Apaz E Baildam A Fasth V Gerloni P Lahdenne AMPrieur A Ravelli RK Saurenmann ML Gamir N WulffraatL Marodi RE Petty R Joos F Zulian D McCurdy BLMyones K Nagy P Reuman I Szer S Travers A BeutlerG Keenan J Clark S Visvanathan A Fasanmade A Ray-chaudhuri A Mendelsohn A Martini EH Giannini A random-ized placebo-controlled trial of infliximab plus methotrexatefor the treatment of polyarticular-course juvenile rheumatoidarthritis Arthritis Rheum 56 (2007) 3096ndash3106
[32] K Visser DM van der Heijde Risk and management of livertoxicity during methotrexate treatment in rheumatoid andpsoriatic arthritis a systematic review of the literature ClinExp Rheumatol 27 (2009) 1017ndash1025
[33] A Cespedes-Cruz R Gutierrez-Suarez A Pistorio A Ravelli ALoy KJ Murray V Gerloni N Wulffraat S Oliveira J WalshIC Penades MG Alpigiani P Lahdenne C Saad-Magalhaes ECortis L Lepore Y Kimura C Wouters A Martini N RupertoMethotrexate improves the health-related quality of life of chil-dren with juvenile idiopathic arthritis Ann Rheum Dis 67(2008) 309ndash314
[34] TK Kvien HM Hoyeraal B Sandstad Azathioprine versus place-bo in patients with juvenile rheumatoid arthritis a single centerdouble blind comparative study J Rheumatol 13 (1986) 118ndash123
[35] E Silverman R Mouy L Spiegel LK Jung RK SaurenmannP Lahdenne G Horneff I Calvo IS Szer K Simpson JAStewart V Strand Leflunomide or methotrexate for juvenilerheumatoid arthritis N Engl J Med 352 (2005) 1655ndash1666
[36] MA van Rossum TJ Fiselier MJ Franssen AH ZwindermanR ten Cate LW van Suijlekom-Smit WH van Luijk RM
van Soesbergen NM Wulffraat JC Oostveen W Kuis PFDijkstra CF van Ede BA Dijkmans Sulfasalazine in the treat-ment of juvenile chronic arthritis a randomized double-blindplacebo-controlled multicenter study Dutch Juvenile ChronicArthritis Study Group Arthritis Rheum 41 (1998) 808ndash816
[37] MA van Rossum RM van Soesbergen M Boers AHZwinderman TJ Fiselier MJ Franssen R ten Cate LW vanSuijlekom-Smit NM Wulffraat WH van Luijk JC OostveenW Kuis BA Dijkmans Long-term outcome of juvenile idiopathicarthritis following a placebo-controlled trial sustained benefits ofearly sulfasalazine treatment Ann Rheum Dis 66 (2007)1518ndash1524
[38] DJ Lovell EH Giannini A Reiff GD Cawkwell ED SilvermanJJ Nocton LD Stein A Gedalia NT Ilowite CA Wallace JWhitmore BK Finck Etanercept in children with polyarticularjuvenile rheumatoid arthritis Pediatric Rheumatology Collabora-tive Study Group N Engl J Med 342 (2000) 763ndash769
[39] DJ Lovell A Reiff OY Jones R Schneider J Nocton LDStein A Gedalia NT Ilowite CA Wallace JB WhitmoreB White EH Giannini Long-term safety and efficacy ofetanercept in children with polyarticular-course juvenile rheu-matoid arthritis Arthritis Rheum 54 (2006) 1987ndash1994
[40] DJ Lovell N Ruperto S Goodman A Reiff L Jung K JarosovaD Nemcova R Mouy C Sandborg J Bohnsack D Elewaut IFoeldvari V Gerloni J Rovensky K Minden RK Vehe LWWeiner G Horneff HI Huppertz NY Olson JR Medich RCarcereri-De-Prati MJ McIlraith EH Giannini A MartiniAdalimumab with or without methotrexate in juvenile rheuma-toid arthritis N Engl J Med 359 (2008) 810ndash820
[41] FH Prince M Twilt R ten Cate MA van RossumW ArmbrustEP Hoppenreijs M van Santen-Hoeufft Y Koopman-KeeminkNM Wulffraat LW van Suijlekom-Smit Long-term follow-upon effectiveness and safety of etanercept in juvenile idiopathicarthritis the Dutch National Register Ann Rheum Dis 68(2009) 635ndash641
[42] P Diak J Siegel L LaGrenade L Choi S Lemery AMcMahonTumor necrosis factor alpha blockers andmalignancy in childrenforty-eight cases reported to the Food and Drug AdministrationArthritis Rheum 62 (2010) 2517ndash2524
[43] G Horneff T Hospach G Dannecker D Foll JP Haas HJGirschick HI Huppertz R Keitzer HJ Laws H Michels KMinden R Trauzeddel Updated statement by the German So-ciety for Pediatric and Adolescent Rheumatology (GKJR) on theFDAs report regarding malignancies in anti-TNF-treated pa-tients from Aug 4 2009 Z Rheumatol 69 (2010) 561ndash567
[44] T Hospach JP Haas HI Huppertz R Keitzer H Michels RTrauzeddl D Foll G Dannecker G Horneff Comment of theSociety of Pediatric and Adolescent Rheumatology on the USFood and Drug Administration (FDA) announcement regardingcases of malignancy in anti-TNF-treated patients Z Rheumatol68 (2009) 162ndash164
[45] DJ Lovell A Reiff NT Ilowite CA Wallace Y Chon SL LinSW Baumgartner EH Giannini Safety and efficacy of up to eightyears of continuous etanercept therapy in patients with juvenilerheumatoid arthritis Arthritis Rheum 58 (2008) 1496ndash1504
[46] EH Giannini NT Ilowite DJ Lovell CA Wallace CERabinovich A Reiff G Higgins B Gottlieb NG Singer YChon SL Lin SW Baumgartner Long-term safety and effec-tiveness of etanercept in children with selected categories ofjuvenile idiopathic arthritis Arthritis Rheum 60 (2009)2794ndash2804
[47] G Horneff H Schmeling T Biedermann I Foeldvari G GanserHJ Girschick T Hospach HI Huppertz R Keitzer RM KusterH Michels D Moebius B Rogalski A Thon The German etaner-cept registry for treatment of juvenile idiopathic arthritis AnnRheum Dis 63 (2004) 1638ndash1644
[48] FH Prince M Twilt SC Simon MA van RossumW ArmbrustEP Hoppenreijs S Kamphuis M van Santen-Hoeufft Y
192 G Dueckers et al
Koopman-Keemink NM Wulffraat R ten Cate LW vanSuijlekom-Smit When and how to stop etanercept aftersuccessful treatment of patients with juvenile idiopathic ar-thritis Ann Rheum Dis 68 (2009) 1228ndash1229
[49] G Horneff F De Bock I Foeldvari HJ Girschick H MichelsD Moebius H Schmeling Safety and efficacy of combinationof etanercept and methotrexate compared to treatment withetanercept only in patients with juvenile idiopathic arthritis(JIA) preliminary data from the German JIA Registry AnnRheum Dis 68 (2009) 519ndash525
[50] N Ilowite O Porras A Reiff S Rudge M Punaro A Martin RAllen T Harville YN Sun T Bevirt G Aras B Appleton Ana-kinra in the treatment of polyarticular-course juvenile rheumatoidarthritis safety and preliminary efficacy results of a randomizedmulticenter study Clin Rheumatol 28 (2009) 129ndash137
[51] T Lequerre P Quartier D Rosellini F Alaoui M De BandtO Mejjad I Kone-Paut M Michel E Dernis M Khellaf NLimal C Job-Deslandre B Fautrel X Le Loet J Sibilia In-terleukin-1 receptor antagonist (anakinra) treatment in pa-tients with systemic-onset juvenile idiopathic arthritis oradult onset Still disease preliminary experience in FranceAnn Rheum Dis 67 (2008) 302ndash308
[52] M Gattorno A Piccini D Lasiglie S Tassi G Brisca S CartaL Delfino F Ferlito MA Pelagatti F Caroli A BuoncompagniS Viola A Loy M Sironi A Vecchi A Ravelli A Martini ARubartelli The pattern of response to anti-interleukin-1 treatmentdistinguishes two subsets of patients with systemic-onset juvenileidiopathic arthritis Arthritis Rheum 58 (2008) 1505ndash1515
[53] S Yokota T Imagawa M Mori T Miyamae Y Aihara STakei N Iwata H Umebayashi T Murata M Miyoshi MTomiita N Nishimoto T Kishimoto Efficacy and safety oftocilizumab in patients with systemic-onset juvenile idiopathicarthritis a randomised double-blind placebo-controlledwithdrawal phase III trial Lancet 371 (2008) 998ndash1006
[54] N Ruperto DJ Lovell P Quartier E Paz N Rubio-Perez CASilva C Abud-Mendoza R Burgos-Vargas V Gerloni JAMelo-Gomes C Saad-Magalhaes F Sztajnbok C Goldenstein-Schainberg M Scheinberg IC Penades M Fischbach J OrozcoPJ Hashkes C Hom L Jung L Lepore S Oliveira CAWallace LH Sigal AJ Block A Covucci A Martini EHGiannini Abatacept in children with juvenile idiopathic arthri-tis a randomised double-blind placebo-controlled withdrawaltrial Lancet 372 (2008) 383ndash391
[55] N Ruperto DJ Lovell P Quartier E Paz N Rubio-PerezCA Silva C Abud-Mendoza R Burgos-Vargas V GerloniJA Melo-Gomes C Saad-Magalhaes J Chavez-Corrales CHuemer A Kivitz FJ Blanco I Foeldvari M Hofer G HorneffHI Huppertz C Job-Deslandre A Loy K Minden M PunaroAF Nunez LH Sigal AJ Block M Nys A Martini EHGiannini Long-term safety and efficacy of abatacept inchildren with juvenile idiopathic arthritis Arthritis Rheum 62(2010) 1792ndash1802
[56] DM Brinkman IM de Kleer R ten Cate MA van RossumWP Bekkering A Fasth MJ van Tol W Kuis NM WulffraatJM Vossen Autologous stem cell transplantation in childrenwith severe progressive systemic or polyarticular juvenile idio-pathic arthritis long-term follow-up of a prospective clinicaltrial Arthritis Rheum 56 (2007) 2410ndash2421
[57] SE Klepper Effects of an eight-week physical conditioningprogram on disease signs and symptoms in children with chronicarthritis Arthritis Care Res 12 (1999) 52ndash60
[58] D Singh-Grewal J Schneiderman-Walker V Wright O Bar-OrJ Beyene H Selvadurai B Cameron RM Laxer R SchneiderED Silverman L Spiegel S Tse C Leblanc J Wong SStephens BM Feldman The effects of vigorous exercisetraining on physical function in children with arthritis arandomized controlled single-blinded trial ArthritisRheum 57 (2007) 1202ndash1210
[59] S Stephens D Singh-Grewal O Bar-Or J Beyene B CameronCM Leblanc R Schneider J Schneiderman-Walker HSelvadurai E Silverman L Spiegel SM Tse V WrightBM Feldman Reliability of exercise testing and functionalactivity questionnaires in children with juvenile arthritisArthritis Rheum 57 (2007) 1446ndash1452
[60] T Takken J van der Net W Kuis PJ Helders Physical ac-tivity and health related physical fitness in children with ju-venile idiopathic arthritis Ann Rheum Dis 62 (2003)885ndash889
[61] MM Toledo G Martini C Gigante L Da Dalt A TregnaghiF Zulian Is there a role for arthroscopic synovectomy in oli-goarticular juvenile idiopathic arthritis J Rheumatol 33(2006) 1868ndash1872
[62] F de Benedetti H Brunner N Ruperto SWright A KenwrightR Cuttica P Woo R Schneider DJ Lovell A Martini Efficacyand safety of Tocilizumab in patients with systemic juvenile idio-pathic arthritis (sJIA) 12-week data from the phase III TENDERtrial Ann Rheum Dis 69 (2010) 146
[63] P Quartier F Allantaz R Cimaz P Pillet C Messiaen CBardin X Bossuyt A Boutten J Bienvenu A Duquesne ORicher D Chaussabel A Mogenet J Banchereau JM Tre-luyer P Landais V Pascual A multicentre randomiseddouble-blind placebo-controlled trial with the interleukin-1receptor antagonist anakinra in patients with systemic-onsetjuvenile idiopathic arthritis (ANAJIS trial) Ann Rheum Dis70 (2011) 747ndash754
[64] DE Furst EC Keystone J Braun FC Breedveld GRBurmester F De Benedetti T Dorner P Emery R FleischmannA Gibofsky JR Kalden A Kavanaugh B Kirkham P Mease JSieper NG Singer JS Smolen PL Van Riel MH Weisman KWinthrop Updated consensus statement on biological agents forthe treatment of rheumatic diseases 2010 Ann Rheum Dis 70(Suppl 1) (2010) i2ndashi36
[65] T Beukelman NM Patkar KG Saag S Tolleson-RinehartRQ Cron EM Dewitt NT Ilowite Y Kimura RM LaxerDJ Lovell A Martini CE Rabinovich N Ruperto 2011 Ameri-can College of Rheumatology recommendations for the treatmentof juvenile idiopathic arthritis initiation and safety monitoring oftherapeutic agents for the treatment of arthritis and systemic fea-tures Arthritis Care Res 63 (2011) 465ndash482 (Hoboken)
[66] JF Simard M Neovius S Hagelberg J Askling Juvenile idi-opathic arthritis and risk of cancer a nationwide cohort studyArthritis Rheum 62 (2010) 3776ndash3782
[67] T Imagawa S Yokota M Mori T Miyamae S Takei H ImanakaY Nerome N Iwata T Murata M Miyoshi N Nishimoto TKishimoto Safety and efficacy of tocilizumab an anti-IL-6-receptor monoclonal antibody in patients with polyarticular-course juvenile idiopathic arthritis Mod Rheumatol (2011)doi102007s10165-011-0481-0
[68] TM Shaneyfelt MF Mayo-Smith J Rothwangl Are guide-lines following guidelines The methodological quality of clini-cal practice guidelines in the peer-reviewed medicalliterature Jama 281 (1999) 1900ndash1905
[69] R Grilli N Magrini A Penna G Mura A Liberati Practiceguidelines developed by specialty societies the need for a crit-ical appraisal Lancet 355 (2000) 103ndash106
[70] JS Burgers R Grol NS Klazinga M Makela J Zaat To-wards evidence-based clinical practice an international surveyof 18 clinical guideline programs Int J Qual Health Care 15(2003) 31ndash45
[71] JT Cassidy RE Petty Juvenile Idiopathic Rheumatic Arthri-tis 5th Edition WB Saunders Philadelphia 2005
[72] TJ Lehman Are withdrawal trials in paediatric rheumatic dis-ease helpful Lancet 372 (2008) 348ndash350
[73] J Munro Recommendations for the Diagnosis and Managementof Juvenile Idiopathic Arthritis The Royal Australian Collegeof General Practitioners South Melbourne 2009 pp 1ndash38
193Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
httpwwwnhmrcgovau_files_nhmrcpublicationsattachmentscp119-juvenile-arthritispdf
[74] MJ Santos JE Fonseca H Canhao M Conde M JoseVieira L Costa M Costa M Salgado JA Melo Gomes Guide-lines for prescribing and monitoring biologic therapies in juve-nile idiopathic arthritis Acta Reumatol Port 32 (2007) 43ndash47
[75] S Yokota M Mori T Imagawa T Murata M Tomiita Y ItohS Fujikawa S Takei Guidelines on the use of etanercept forjuvenile idiopathic arthritis in Japan Mod Rheumatol 20(2010) 107ndash113
[76] The AGREE Collaboration Appraisal of Guidelines for Researchamp Evaluation (AGREE) instrument wwwagreecollaborationorg
[77] I Kopp H Thole T Langer HK Selbmann G OllenschlaumlgerGerman Instrument for Methodological Guideline Appraisal(DELBI) wwwversorgungsleitliniende2008
[78] Auml Aumlrztliches Zentrum fuumlr Qualitaumlt in der Medizin A Arbeitsge-meinschaften der Wissenschaftlichen Fachgesellschaften in derMedizin Deutsches Instrument zur methodischen Leitlinien-Bewertung (DELBI) Fassung 20052006 Z Aumlrztl FortbildQualitaumltssich 99 (2005) 468ndash519
[79] MP de Wit SE Berlo GJ Aanerud D Aletaha JW BijlsmaL Croucher JA Da Silva B Glusing L Gossec S Hewlett MJongkees D Magnusson M Scholte-Voshaar P Richards CZiegler TA Abma European League Against Rheumatism rec-ommendations for the inclusion of patient representatives in sci-entific projects Ann Rheum Dis 70 (2011) 722ndash726
[80] I Foeldvari M Bidde Validation of the proposed ILAR classifi-cation criteria for juvenile idiopathic arthritis InternationalLeague of Associations for Rheumatology J Rheumatol 27(2000) 1069ndash1072
[81] R Merino J de Inocencio J Garcia-Consuegra Evaluation ofrevised International League of Associations for Rheumatologyclassification criteria for juvenile idiopathic arthritis in Spanishchildren (Edmonton 2001) J Rheumatol 32 (2005) 559ndash561
[82] SE Ramsey RK Bolaria DA Cabral PN Malleson REPetty Comparison of criteria for the classification of childhoodarthritis J Rheumatol 27 (2000) 1283ndash1286
[83] G Horneff A Ebert S Fitter K Minden I Foeldvari J Kum-merle-Deschner A Thon HJ Girschick F Weller HI Hup-pertz Safety and efficacy of once weekly etanercept 08mgkg in a multicentre 12 week trial in active polyarticularcourse juvenile idiopathic arthritis Rheumatology (Oxford) 48(2009) 916ndash919
[84] EH Giannini EJ Brewer N Kuzmina A Shaikov A Maxi-mov I Vorontsov CW Fink AJ Newman JT Cassidy LSZemel Methotrexate in resistant juvenile rheumatoid arthri-tis Results of the USAndashUSSR double-blind placebo-controlled trial The Pediatric Rheumatology CollaborativeStudy Group and The Cooperative Childrens Study GroupN Engl J Med 326 (1992) 1043ndash1049
[85] A Ravelli S Viola D Migliavacca N Ruperto A Pistorio AMartini The extended oligoarticular subtype is the best predic-tor of methotrexate efficacy in juvenile idiopathic arthritisJ Pediatr 135 (1999) 316ndash320
[86] P Woo TR Southwood AM Prieur CJ Dore J Grainger JDavid C Ryder N Hasson A Hall I Lemelle Randomizedplacebo-controlled crossover trial of low-dose oral
methotrexate in children with extended oligoarticular or sys-temic arthritis Arthritis Rheum 43 (2000) 1849ndash1857
[87] E Silverman L Spiegel D Hawkins R Petty D Goldsmith LSchanberg C Duffy P Howard V Strand Long-term open-label preliminary study of the safety and efficacy of lefluno-mide in patients with polyarticular-course juvenile rheumatoidarthritis Arthritis Rheum 52 (2005) 554ndash562
[88] DJ Lovell EH Giannini Y Kimura C Suzanne PJHashkes A Reiff Long-term safety and efficacy of rilonaceptin patients with systemic juvenile idiopathic arthritis (SJIA)Arthritis Rheum 60 (2009)
[89] N Ruperto P Quartier NWulffraat PWoo A Loy R Mouy BBader-Meunier BJ Prakken E Noseda R Belleli J Lecot CRordorf A Martini A Phase II Trial with canakinumab(ACZ885) a new IL-1-beta blocking monoclonal antibody toevaluate safety and preliminary efficacy in children with system-ic juvenile idiopathic arthritis Ann Rheum Dis 68 (2009) 170
[90] DJ Lovell EH Giannini Y Kimura et al Preliminary evi-dence for bioactivity of IL-1 trap (Rilonacept) a long actingIL-1 inhibitor in systemic juvenile idiopathic arthritis (sJIA)Arthritis Rheum 54 (2006) S325
[91] DJ Lovell EH Giannini Y Kimura et al Preliminary evi-dence for sustained bioactivity of IL-1 Trap (rilonacept) a longacting IL-1 inhibitor in systemic juvenile idiopathic arthritisArthritis Rheum 56 (2007) S514
[92] N Ruperto F De Benedetti H Brunner R Allen D Brown JChaitow E Cortis G Espada B Flato V Gerloni G HorneffS Wright A Kenwright R Schneider P Woo A Martini DJLovell Tocilizumab is efficacious in patients with systemic ju-venile idiopathic arthritis (sJIA) across baseline disease charac-teristics and priorbaseline treatments 12-week data from thephase II TENDER trial 17th PReS Congress Valencia Spain2010 2010
[93] N Ruperto DJ Lovell T Li F Sztajnbok C Goldenstein-Schainberg M Scheinberg IC Penades M Fischbach JOrozco PJ Hashkes C Hom L Jung L Lepore S OliveiraC Wallace M Alessio P Quartier E Cortis A Eberhard GSimonini I Lemelle E Chalom LH Sigal A Block A CovucciM Nys A Martini EH Giannini Abatacept improves health-related quality of life pain sleep quality and daily participationin subjects with juvenile idiopathic arthritis Arthritis Care Res(Hoboken) 62 (11) (2010) 1542ndash1551
[94] N Ruperto DJ Lovell P Quartier E Paz N Rubio-PerezCA Silva C Abud-Mendoza R Burgos-Vargas V GerloniJA Melo-Gomes C Saad-Magalhaes J Chavez C HuemerA Kivitz FJ Blanco I Foeldvari M Hofer G Horneff HIHuppertz CJ Deslandre A Loy K Minden M Punaro AFNunez LH Sigal AJ Block M Nys A Martini EH GianniniLong-term safety and efficacy of abatacept in children with ju-venile idiopathic arthritis Arthritis Rheum 62 (2010)1792ndash1802
[95] J Munro Juvenile Idiopathic Arthritis Management Guidelines(Provisional) Australian Paediatric Rheumatology Group 2006httpwwwnhmrcgovau
[96] K Fitch SJ Bernstein MD Aguilar B Burnand JR LaCalleP Lazaro M van het Loo J McDonnell JP Vader JPKahan The RANDUCLA Appropriateness Method Users ManualRAND Pittsburgh 2000

Table 5 Drugs for the treatment of JIA
Generic Dosage Age approval by Europeanmedical agency inpediatric rheumatology(EMA) a
Medical indication in pediatricrheumatology a b
Evidence levelrecommendationgrade [10]
Literature
NSAIDsDiclofenac 2ndash3 mgkg Bwd po (in 3 doses)
Retard formulation 1 dose14 years Arthritis IndashA Haapasiri [16] Laxer [14]
Ibuprofen 20ndash40 mgkg Bwd po in 3ndash4doses
6 months Pain fever IndashA Giannini [17]
Indometacin 1ndash3 mgkg Bwd po in 3 doses 2 years Arthritis IIndashA Stoeber [18]Meloxicam 0125ndash025 mgkg Bwd po 15 years Arthritis II Ruperto [19]Naproxen 10ndash15 mgkg Bwd po in 2 doses 1 year Arthritis IndashA Kvien [13] Laxer [14] Leak
[15]Celecoxibe 6 mgkg Bwd po in 2 doses or
12 mgkg Bwd in 1 doseNo approval for children Arthritis I B-C Foeldvari [20]
Glucocorticoids (GC)a) Systemic GCPrednisonePrednisolone
01ndash02 mgkg Bwd (max 5 mgd) JIA ie severe SoJIA severe peri-myokarditis severe uveitis (hypotoniaor cystoid macular edema) intoleranceto other drugs (ldquolow-doserdquo) or asldquobridgingrdquo therapy in higher doses eg2 mgkg Bwd until therapeutic effectof ldquoDMARDsrdquo
III Prieur [28]
Prednisone as an oralhigh-dose therapy
ge1ndash2 mgkg Bwd prednisolone-equivalent
III Prieur [28]
Prednisone as an oralmedium-dosetherapy
02 tob10 mgkg Bwdprednisolone-equivalent
III Kirwan [24] Prieur [28]
Prednisone as an orallow-dose therapy
b02 mgkg Bwd Prednisolone-equivalent or b4 mgmsup2 bodysurface
III Michels [25]
Prednisone as a ivpulse-therapy
N(5)ndash10 mgkg Bw (po)Prednisolone-equivalent10ndash30 mgkg Bwd Methyl-Prednisolone iv for 1ndash3 d(maximum 1 gdose)
III Miller [26] Picco [27]
b) Intra-articular GCTriamcinolonehexacetonide
05ndash1 mgkg Bw into large jointsdose adaption referring to size ofjoint (eg max 2 mg intointerphalangeal joints c)
5 months Arthritis tendo-vaginitis I Zulian [2122]
(continued on next page)(continued on next page)
181Evidence
andconsensus
basedGKJR
guidelinesfor
thetreatm
entof
juvenileidiopathic
arthritis
Table 5 (continued)
Generic Dosage Age approval by Europeanmedical agency inpediatric rheumatology(EMA) a
Medical indication in pediatricrheumatology a b
Evidence levelrecommendationgrade [10]
Literature
DMARDsSulfasalazine 30ndash50 mgkg Bwd in 2ndash3 doses 6 years Arthritis II Van Rossum [3637]Cytotoxic or immuno-suppressive drugsMethotrexate 10ndash15 (20) mgmsup2 body surface
once a week (po sc iv) e2 years Polyarticular JIA Psoriasis arthritis
uveitis CollagenosisI Giannini [84] Ravelli [85]
Woo [86]Cespedes-Cruz [33]Azathioprine 15ndash3 mgkg Bwd po in 1ndash2
dosesNo approval for children II Kvien [34]
Leflunomide No clear recommendation forchildren availableBwb20 kg d 1100 mgkg from d 2 10 mgkgdBw 20ndash40 kg d 1 to d 2 100 mgkgfrom d 3 10ndash20 mgkgdBwN40 kg d 1 to d 3 100 mgkgfrom d 3 20 mgkgd
No approval for children II Silverman [3587]
Biologic agentsa) TNFα inhibitorsEtanercept d 08 mgkg Bw sc 1timesweek
(max 50 mgweek) or 04 mgkgBw sc 2timesweek (max 50 mgweek)
4 years JIA Polyarthritis and insufficientefficacy of MTX
I Giannini [46] Horneff [49]Lovell [3888] Prince [41]
Adalimumab d 24 mgm2 body surface sc in 1dose every 2 weeks Bwb30 kg20 mgm2 body surface BwN30 kg40 mgm2 body surface(max 40 mg per dose)
4 years to 17 years Adalimumab in combination withmethotrexate is indicated for thetreatment of active polyarticularjuvenile idiopathic arthritis in childrenand adolescents who have had aninadequate response to one or moredisease-modifying anti-rheumatic drugs(DMARDs)
I Lovell [40]
182GDueckers
etal
Infliximab d 3ndash10 mgkg Bwdose iv Infusionat d 0 d 14 d 42 then every8 weeks intervals of applicationremain unclear
No approval for childrenwith JIA6 years (approval forMorbus Crohn)
III Ruperto [31]
b) IL-1 inhibitorsAnakinra d 1ndash4 mgkg Bwd sc in 1 dose No approval for children II Illowite [50] Lequerre [51]Canakinumab d 4 mgkg Bwsingle dose sc every
4 weeks (max 150 mg)No approval for childrenwith JIA 4 years (approvalfor CAPS)
III Ruperto [89]
Rilonacept d 1ndash2times44 mgkgweek sc (max320 mg) then 22 mgkgweek sc(max160 mg)
No approval for childrenwith JIA 12 years(approval for CAPS)
Lovell [889091]
c) IL-6 inhibitorsTocilizumab d 1 h Infusion every two 2 weeks
Bwb30 kg 8 mgkg BwN30 kg12 mgkg
2 years of age or older Since May 2011 EMA approval forpediatric patients with SoJIA who haveresponded inadequately to previoustherapy with NSAIDs and systemiccorticosteroids (Approval at Japan forSoJIA and polyarticular JIA since 2008) c
I Yokota [53] Ruperto [92]de Benedetti [62]
d) Co stimulatory-antagonistsAbatacept d 10 mgkg iv Infusion at d 0 d 14
d 28 then every 4 weeks6 years of age and older Abatacept in combination with
methotrexate is indicated for thetreatment of moderate to severe activepolyarticular (JIA) in pediatric patientswho have had an insufficient responseto other DMARDs including at least oneTNF inhibitor
I Ruperto [549394]
Abbreviations CAPS=Cryopyrine associated periodic fever syndrome JDM=juvenile dermatomyositis Bw=body weight SoJIA=systemic-onset of JIA SLE=systemic Lupus erythematodesa Compare wwwemaeuropaeub wwwrotelistede (German database of drugs with national market approval)c Intra-articular injection into same joint no more often than once every 3 monthsd A statement from insurance companies should be acquired before treatment initiation for off label treatment (if possible)e Oral application is most feasible in childhood
183Evidence
andconsensus
basedGKJR
guidelinesfor
thetreatm
entof
juvenileidiopathic
arthritis
Oligoarticular JIA
Polyarticular JIA
SoJIA
Figure 2 JIA treatment escalation schemes +=addition of the drug (abbreviations NSAIDs=non steroidal anti-inflammatory drugthotrexate)
Consensus statement
Long-term use of systemic GC is not recom-mended Continuous administration of ge02 mgPrednisolone equivalent per kg bodyweight (Bw)carries a high risk of adverse events and thereforeis not recommended (evidence level III recom-mendation grade A)
Consensus statement (continued)
184 G Dueckers et al
GC in JIA published thus leading to ldquojustrdquo evidence level IIIDifferent recommendations of dosage and therapy regimesare listed in Table 5 (evidence level III for all recommenda-tions) [1824ndash28] Frequency and seriousness of deleteriouseffects correlate mainly to duration of therapy and dosageof GC administered Main side effects are iatrogenicCushings syndrome growth disturbance weight gainmood changes Higher dosage carry the risk of increasedvulnerability to infection hypertension osteoporosisthrombosis diabetes gastro-intestinal ulceration cataractglaucoma atrophy of subcutaneous fatty tissue steroid in-duced acne To inform colleagues about GC treatment in acase of emergency and to reduce severe complications in longterm treated patients ie GC administrationN4 weeks thesupply of ldquoGlucocorticoid ID cardsrdquo for patients might be useful
GC=Glucocorticoids DMARDs=disease modifying drugs MTX=Me
Consensus statement
The systemic use of GC is recommended asfast acting drugs in highly active JIA GC areused for the treatment of children and adoles-cents with SoJIA organ manifestations of JIA(eg uveitis pericardial effusion) sero-positivepolyarticular JIA and for bridging time untilthe complete therapeutic effect of DMARDs(evidence level III recommendation grade A)
313 Methotrexate (MTX) biologic agents andimmunosuppressive agents
MTX biologic agents and immunosuppres-sive agents are used for the treatment of childrenand adolescents with polyarticular JIA ifNSAIDs or local GC treatment do not succeedThe combination of those drugs with NSAIDsand GC is feasible A common characteristic ofMTX biologic agents and immunosuppressiveagents is the delayed onset of therapeutic ef-fect ie up to 3 months or even longer aftercommencing treatment
185Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
Safe contraception is indicated during therapy with MTXAzathioprine or Leflunomide and in the following 3 to6 months after its discontinuation
Consensus statement
Administration of Sulfasalazine or Lefluno-mide is recommended if MTX or Etanercept donot show sufficient efficacy or cannot be used
3131 Methotrexate Among DMARDs MTX provides themainstay of long-term therapy in JIA [29ndash32] In case ofside effects eg dyspepsia or nausea prophylaxis withfolic acid can be recommended (1times1 mg per day or 5 mgonce a week 24ndash48 h after application of MTX) Safe contra-ception is mandatory while receiving MTX Safety and effica-cy of MTX and its impact on quality of life of children with JIAhave been investigated Significant positive impact of MTXon all health-related quality of life health conceptshas been shown although the study has its limit due to dif-ferent MTX dosages used within participating JIA patients[33]
Consensus statement
MTX administration can be recommendeddue to its proven safety and efficacy to reducedisease activity MTX is used in case of insuffi-cient therapeutic effect of NSAIDs andor localGC administration continuous need for system-ic GC andor highly active disease Efficacy ofMTX (orally or subcutaneously administered) isfrequently achievable with a dosage of 10ndash15 mgmsup2 body surface (evidence level I recom-mendation grade A)
for other reasons (evidence level II recommen-dation grade B)
3132 Purine analogs31321 Azathioprine Efficacy has been investigat-
ed in a double blind placebo controlled study (32 patients)After 8 weeks of therapy the changes in disease activitymeasurement indicated a minor improvement in the Azathi-oprine group compared to the placebo group At the end ofthe study statistically significant differences between thegroups were found for only 2 disease activity measurements[34] Two patients were taken out of study due to severeadverse events eg leucopenia Measurement of activityof Thiopurinmethyltransferase (TPMT) can be beneficial foravoidance of severe adverse events
3133 Pyrimidine analogs31331 Leflunomide Within a double blind study
(32 weeks 94 patients) efficacy of Leflunomide was inferiorin comparison to MTX but better than placebo Howeverdosing of Leflunomide may not have been adequate insome children [35] Contraindications for Leflunomide arerenal insufficiency severe immunodeficiency depressedmyelopoesis and pancytopenia An extensive half-life peri-od (approximately 14 days) has to be taken in accountwhen administering Leflunomide In combination with hepa-totoxic DMARDs the risk of severe adverse events might in-crease eg increased blood pressure is seen frequentlySafe contraception is mandatory
3134 Antibiotic analogs and Hydroxychloroquine andChloroquine
31341 Sulfasalazine Weak efficacy of Sulfasalazinewas demonstrated within a placebo-controlled randomizedstudy after 24 weeks (96 patients) [3637] One third of pa-tients enrolled in the study discontinued treatment with Sulfa-salazine due to side effects eg gastrointestinal symptomsleucopenia [36] Some experts use sulfasalazine in HLA-B27positive JIA Contraindications are Glucose-6-phosphatase de-ficiency and hypersensitivity against sulfonamides
31342 Hydroxychloroquine and chloroquine Hydrox-ychloroquine and Chloroquine have been subject to clinical tri-als for the treatment of JIA even though efficacy was limitedWithin three consensus conferences held in 2007 and 2010 theconsensus group decided not to give a consensus statementon the use of chloroquine or hydroxychloroquine treatmentdespite the fact that those drugs still might be used by somecaregivers
3135 Biologic agents Biologic agents are drugs whichselectively inhibit cytokines cytokine receptors or directlybind to receptors of lymphocytes eg CTLA-4 CD20 Theyinclude antibodies and fusion proteins So far allbiological therapies are administered subcutaneously orintravenously
31351 TNFα-inhibitors TNFα-inhibition with Adali-mumab and Etanercept is efficient and safe (evidencelevel I) [38ndash41] Both drugs have been approved for JIAwith polyarticular course TNFα-inhibitors have become anintegral part of the treatment of JIA Potential risks of therapyare vulnerability for infection andmdashin a rare occasionmdashthe in-duction of autoimmune disease Prior to the start of treatmentwith TNFα-inhibitors chronic infections needs to be excludedor treated sufficiently eg tuberculosis hepatitis B or C
In children with JIA treated with TNFα-inhibitors malig-nancies eg Lymphoma have been reported It remainsunclear if the rate of malignancies is increased in patientscompared to the risk by having JIA itself In response to aprevious letter of the FDA (as reviewed in [42]) the GermanSociety for Pediatric Rheumatology (GKJR) has published of-ficial statements [4344] The GKJR states that treatmentwith TNFα-inhibition should be used very carefully physi-cians need to be aware of co-medication e g immunosup-pressive drugs and should monitor those patientsclosely [43] There is insufficient data on all biologicagentsmdashincluding TNFα-inhibitionmdashto judge about the long-term risk for children and adolescents313511 Etanercept Etanercept is a fusion proteinconsisting of the extracellular binding domain of solubleTNFα-receptor and Fc chain of human IgG1 Etanercept in-hibits TNFα by direct binding of the cytokine Efficacy has
Consensus statement
The use of Anakinra or Tozilizumab can berecommended for treatment of children and ado-lescents with refractory SoJIA (evidence level IIrecommendation grade A)
186 G Dueckers et al
been demonstrated in a randomized controlled withdrawaldesign trial for patients with polyarticular JIA [38] Withinan open extension study long term efficacy and safety havebeen documented over 8 years in 1669 patients [3945]There is data on more than 2000 patients registered in Euro-pean registries [46ndash48] Currently retrospective data showsa somewhat better efficacy of combining MTX or otherDMARDs with TNFα-inhibition versus anti-TNFα therapy assingle therapy [49]313512 Adalimumab Adalimumab is a humanizedmonoclonal IgG1 antibody directed against TNFα whichbinds soluble and membrane bound TNFα A randomizedcontrolled withdrawal design trial demonstrated safety andefficacy of Adalimumab (24 mgmsup2 body surface every2 weeks max 40 mg) for children and adolescents withpolyarticular JIA (4ndash17 years of age n=171) [40] After16 weeks ldquowash inrdquo phase responders (n=144171) enteredthe 32 weeks randomized double blind phase After 48 weekstwice the number of patients in the verum group met ACR 70as compared to the control group (56 vs 28 pb001)Within the open extension phase Adalimumab dosage wasfixed ie 20 mgb30 kg Bw and 40 mgN30 kg Bw There islack of evidence showing superior efficacy of combiningMTX (DMARDs) with Adalimumab versus Adalimumab as sin-gle therapy [40]
Consensus statement
Efficacy of Etanercept and Adalimumab forthe treatment of polyarticular JIA has been dem-onstrated Therapy with TNFa-inhibition is indi-cated in case of insufficient therapeutic effectof NSAIDs and local GC administration and lackof response to MTX (evidence level I recom-mendation grade A)
Consensus statement
Patients with polyarticular JIA without sys-temic manifestation refractory to treatmentwith MTX and TNF inhibition might benefit fromthe use of Abatacept (evidence level III recom-mendation grade C)
313513 Infliximab Infliximab is a chimerical (humanmouse) monoclonal antibody which binds soluble and mem-brane bound TNFα A randomized controlled study in childrenand adolescents with JIA failed to demonstrate a significantdifference of efficacy after treatment with Infliximab com-pared to placebo [31]
31352 Interleukin-1-inhibitors None of interleukin-1-inhibitors are approved for the treatment of JIA or SoJIAThey are commonly used in an off label setting313521 Anakinra Anakinra is an IL-1 receptor antag-onist Within a randomized controlled trial no significant ef-ficacy of Anakinra for patients with polyarticular JIA couldbe demonstrated [50] 50 of 86 patients were enrolled intoblinded phase (11 Anakinra versus Placebo) No significantreduction of flare could be demonstrated in comparison toplacebo 29 of 50 patients completed the open label exten-sion study Two noncontrolled nonrandomized studieshave shown efficacy of anakinra in a proportion of patientswith systemic-onset of JIA (SoJIA) [5152]313522 Canakinumab Canakinumab an IL-1β anti-body binds IL-1β selectively without interfering with IL-1αor its physiological IL-1 receptor antagonist Canakinumabhas been approved for treatment of hereditary periodic IL-1 associated periodic fever syndromes ie Cryopyrin-
associated periodic syndromes There are ongoing studies in-vestigating safety and efficacy of Canakinumab for SoJIA
31353 Interleukin-6 inhibitors313531 Tozilizumab Tozilizumab is a humanizedanti-IL-6 receptor monoclonal antibody Efficacy has beendemonstrated within a 12 week double blind randomizedcontrolled withdrawal trial in children with SoJIA (n=562ndash19 years) in Japan [53] After a 48 week open extensionstudy ACR Pedi 30 was met by 47 patients (98) At thetime of our literature search Tocilizumab was approved fortreatment of SoJIA and polyarticular JIA since 2008 inJapan A multicenter European study investigating efficacyand safety of Tozilizumab in polyarticular JIA was ongoingat the deadline of literature search (wwwclinicaltrialsgov NCT00988221) No data on long term effects are cur-rently available
31354 Co-stimulation inhibitors313541 Abatacept Abatacept is a recombinant fu-sion protein of extracellular domain of human cytotoxic T-Lymphocyte Antigen 4 (CTLA-4) and IgG1-Fc-Fragment Itmodulates T-cell co-stimulation A randomized controlleddouble blind withdrawal design study of Ruperto et al [54]demonstrated efficacy of Abatacept in patients with polyar-ticular JIA 123 of 170 participants of study were enrolled inthe 6 month double blind phase Flares occurred in 33 of 62(53) patients who were given placebo versus 12 of 60(20) Abatacept patients during double blind phase Adverseevents (AE) did not differ in both groups ie 37 AE in Abata-cept versus 34 AE in placebo recipients Some children maytake 3 to 6 months or longer before their maximal responseis achieved 3 of patients developed reaction to the infu-sion [55] Abatacept is approved by FDA and EMA for pa-tients who did not respond to prior MTX treatment Nodata of long term effects of the use of Abatacept in JIA areavailable due to the low numbers of patients treated so far
314 Autologous stem cell transplantation (SCT)There are studies on autologous SCT for treatment of re-
fractory and severe forms of JIA (evidence level III) [56] 22
Consensus statement
187Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
patients were enrolled in one study 8 reached clinical re-mission 7 were assessed as partial responders 3 experi-enced relapse of the disease and 4 (18) died as aconsequence of MAS or immunosuppressive treatment [56]Due to serious adverse events including death this thera-peutic option is seen as the last treatment option
Exercise training is recommended dependingon the extent of inflammation number of affect-ed joints and global disease activity Sports withminor stress on joints is favorable (evidence levelI recommendation grade A)
32 Non-drug based therapy
321 Physiotherapy occupational therapy and thera-peutic appliances
Physio- and occupational therapy are integral parts of thetherapeutic concept in children and adolescents with JIA[5758] Therapeutic goals of physiotherapy are relaxationand pain relief preservation or rehabilitation of physiologi-cal range of joint movement prevention of contracturesstretching and activation of muscles build-up of muscleforce and training of physiological movements
Consensus statement
Structured treatment by a properly trainedphysiotherapistoccupational therapist in combi-nation with drug based therapy and instructionsfor disease adopted self-sufficient daily exercisesessions are recommended to keep and to im-prove joint mobility (evidence level II recom-mendation grade A)Custom-made therapeutic appliances for correc-tion of axial misalignment prevention of falseweight bearing stabilization of joints (eghand- finger- and foot-ortheses) are recom-mended individually The use of therapeutic ap-pliances follows individual physician-directedadvice Efficacy has been demonstrated (evi-dence level I recommendation grade B)
Consensus statement
In individual cases the indication for open orarthroscopic synovectomy can be considered ifconservative therapy does not succeed (evi-dence level III recommendation grade B)
Consensus statement
Other forms of non-drug based therapeutic approachesrely on experts opinion and are solely based on individualclinical experience No controlled studies are available
Consensus statement
The implementation of thermotherapy electro-or ultrasound therapy massage and lymph drain-age is recommended Application of cold appli-ances for acute joint inflammation is indicated(evidence level II recommendation grade A)Electro- and ultrasound therapy are recom-mended for patients with tendosynovitis (evi-dence level III recommendation grade B)
An early psychological support within stan-dard pediatric rheumatological care should beimplemented to apprehend and treat mental is-sues and behavioral syndromes associated withphysiological disturbances and physical factors(evidence level III recommendation grade A)
Consensus statement
A socio-pedagogical care with regard tointegration at school professional andeveryday life and formal education of parentsand patients is recommended (evidence levelIII recommendation grade A)
322 Sportive activity and exercise trainingPositive impact of sportive activity on the general physi-
cal condition and on oxygen consumption has been demon-strated (evidence level II) [57ndash60] Adequate exercise
training supports the physiological development and helpscoping with JIA [58] Prospective controlled long term stud-ies are currently not available
323 Surgical treatmentToledo et al investigated the role of arthroscopic syno-
vectomy in JIA They concluded that arthroscopy is a safebut only partially effective procedure in patients witholigoarticular JIA (evidence levelrecommendation gradeIIIB) [61]
324 Psychological social intervention orsocio-pedagogical care
There are no controlled or open studies focusing on psy-chological social andor socio-pedagogical intervention inchildren or adolescents with JIA Recommendations arebased on experts opinion and personal experience solely
188 G Dueckers et al
4 Addendum
Since the deadline January 15th 2010 new papers haveappeared that are of interest in the context of our guideline[5562ndash64] in particular we refer to the ACR recommenda-tions [65] and the most recent literature on the risk of malig-nancies in JIA in context with TNF blocking agent andindependent of medication [42] [66] Moreover there is arecent study on the use of Tocilizumab in polyarticular pa-tients [67] These papers will be discussed within the nextconsensus conference by NGT and considered for inclusioninto the next edition of this guideline On 6th of September2011 our advanced search on wwwclinicaltrialgov (searchterms juvenile idiopathic arthritis recruitment open stud-ies study type interventional study age group child(birthndash17) intervention drugs) led to 16 trials which are cur-rently recruiting or will soon start recruiting
5 Discussion
To develop clinical practice guidelines of high quality andvalidity a formal consensus process and explicit methodo-logical criteria for the production of guidelines are recom-mended [68ndash70] Our guideline for the treatment of JIA inchildren and adolescents implements all these issues Thesystematic literature search was terminated on 15th January2010 leading to the most up to date guideline for JIA whichis currently available The deadline of the ACR recommenda-tions as published recently by Beukelmann et al was 5th ofOctober 2009 [65] By exclusion of case reports trials with-out control groups preliminary results published as ab-stracts on conferences and the strict graduation of theliterature by the criteria of evidence based medicine weaimed to give our guideline statements additional strengthand a maximal validity Newer original studies providing ad-ditional evidence for the treatment of JIA became availableafter our consensus process was finished see AddendumThe results of these trials have to await the next NGT beforeinclusion into our recommendations
Our updated systematic literature search in 2010 led to13 relevant studies published after 30th June 2007 (Fig 1Table 4) Their results have to be interpreted with cautionFirst trials in JIA are mainly based on limited numbers of pe-diatric patients as the recruitment of a sufficient number ofpediatric patients remains challenging Second trials aremainly designed for patients with polyarticular JIA or witholigoarticular onset and a polyarticular course (Table 4)Most children with JIA do not have a polyarticular subtypeof JIA but an oligoarticular onset and course [71] Thus pa-tients with oligoarticular JIA are heavily underrepresentedin most of the current trials Third in 5 of the 13studies the withdrawal study design has been used[4045505354] Lehmann reviewed the bias of withdrawaldesign trials in 2008 [72] After a wash-in phase only re-sponders to treatment are eligible for randomization Thusthe design preselects responders to the placebo effect whomight retain their response throughout the entire study peri-od Further there is a carryover effect of AE into the place-bo group so that significant differences in AE betweengroups may not become apparent In the one placebo con-trolled trial without withdrawal design on TNFα-inhibition
(Infliximab) no significant efficacy could be demonstratedbetween verum and placebo [31]
To our knowledge there are two other guidelines that dealwith the management of JIA as a whole (Table 6) [65] [73]Other guidelines are limited to the use of single drugs in JIAeg biologic agents [74] etanercept [75] The Australian guide-line (wwwracgporgauguidelinejuvenileidiopathicarthritis)has not been published in a peer-reviewed journal It is to pro-vide recommendations for the early diagnosis and multidisci-plinary management of JIA in the primary care setting forgeneral practitioners (GPs) [73] No recommendations aremade regarding the use of GCs DMARDs immunosuppressivedrugs or biologic agents [73] The ACR recommendations usesthe Appraisal of Guidelines for Research and Evaluation(AGREE) instrument [65] [76] which does not fulfill criteria ofa proper consensus process and carries the risk that expertsvote for peer opinion which might not reflect the true valueWe used an advanced and linguistically validated version ofthe AGREE instrument the ldquoGerman Instrument for Methodo-logical Guideline Appraisal (DELBI)rdquo which has been developedin cooperation of the AWMF among others [7778] We followedthe highly structured Nominal Group Technique as described inMethodology Our consensus group only considered formallyboard nominated representatives of multidisciplinary scientificsocieties and organizations (Table 1) and included patients rep-resentatives as this has been strongly recommended by the Eu-ropean League against Rheumatism (EULAR) recently [79] TheACR mentions a parent representative within their task forcepanel but leaves this representative anonymous It remainsunclear how ACR experts were selected and involved [65]They defined treatment groups which have not been evaluatedsystematically so far We used the ILAR classification systemwhich has been repeatedly evaluated [80ndash82]
By content there are major differences between the ACRrecommendations and our guideline a) Our guideline pro-vides a detailed and systematic list of 20 drugs commonlyused in the treatment of JIA (Table 5) which has been an in-tegrative part of our consensus conferences The ACR recom-mendations do not provide information on approval status(Food and Drug Administration) indications for use and nospecific differences on dosage regimes or frequency ofdaily application [65] eg it refers to the 2008 ACR recom-mendations for the use of DMARDs in adult rheumatoid ar-thritis b) The ACR recommendations provide a more earlyaggressive approach in the treatment of JIA The ACR recom-mends MTX as first line treatment in patients (b4 joints) withhighly active disease [65] To our knowledge there are onlydata to recommend MTX administration in cases of insuffi-cient therapeutic effect of prior treatment with NSAIDandor GC [33] c) The ACR recommends the use of TNFα in-hibitors as escalation therapy for some patients with historyof arthritis of 4 or fewer joints and refer to publications[3840] conducted in patients with polyarticular JIA or pau-ciarticular JIA with polyarticular course [65] There is no ev-idence that TNF is safe and efficient in patients witholigoarticular JIA a systematic controlled clinical trial onthis issue has not been done yet d) We regard a brief trialof local or systemic administration of GC plus NSAID as a fea-sible first line treatment for patients with polyarticular JIAThe ACR recommends MTX without regard to disease activityat the initial stage [65] We reached consensus to recom-mend the use of GC as bridging therapy until full onset of
Table 6 Overview of recommendationsguidelines for treatment of JIA
USA Australia Germany
ACR recommendations[65]
RACGP recommendations[73]
GKJR guidelines
Deadline of literature search October 2009 January 2007 September 2010Source of publications Pub Med Pub Med
EMBASE CINHAL CochraneLibrary provisionalAustralian Guideline [95]
Pub MedPrevious German Guidelines [78]
Definition used for JIA subgroups Treatment groups definedby Core expert panel
Not specifically definedChildren withJIAb16 years
ILAR criteria [1]
Consensus processprocessvalidation
AGREE [76] AGREE [76] DELBI [77]RANDUCLA appropriatenessmethod [96]
NGT Delphi method
Conferences None None 3 Formal consensus conferencesAddressees Pediatric rheumatologists General practitioner Pediatric Rheumatologists
PediatriciansGeneral practitioners
Participating scientific societies or professional organizationsPediatric rheumatologist orrheumatologists for adolescents
Yes Yes Yes
General pediatrician- In hospital Yes Yes Yes- In private practice Yes Yes YesResearcher Yes No YesRheumatologists for adults No No YesOphthalmologists No No YesParentspatients support groups Yes No YesOrthopedic surgeons No No YesPediatric orthopedic surgeons No No YesPsychologists No No YesPhysiotherapists No No YesPediatric rheumatology nurses Yes No NoOther scientific societies ororganizations
ACR BSPAR PRINTO PReS RACGP NAMSCAG NHMRC DGKJ DGPs DGRh DGO AWMFBVKJ
(ACR=American College of Rheumatologists AGREE=Appraisal of Guidelines for Research amp Development AWMF=Association of the ScientificMedical Associations BSPAR=British Society for Pediatric Rheumatology BVJK=Association of Pediatricians in private practice CEP=Core expertpanel ILAR=International League against Rheumatism CINHAL=Cumulative Index to Nursing and Allied Health Literature DELBI=German In-strument for Methodological Guideline Appraisal DGKJ=German Society of Pediatrics and Adolescent Medicine DGO=German Society for Oph-thalmology DGPs=German society for Psychology DGRh=German Society for Rheumatology GKJR=German Society for Pediatric RheumatologyNAMSCAG=National Arthritis and Musculoskeletal Conditions Advisory Group NGT=Nominal Group Technique NHMRC=National Health andMedical Research Council PReS=Pediatric Rheumatology Society) PRINTO=Pediatric Rheumatology International Trial Organization RACG-P=Royal Australian College of General Practitioner RANDUCLA=Research and DevelopmentUniversity of California at Los Angeles)
189Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
therapeutic effect of DMARDs The ACR recommendations donot provide any recommendation for the use of systemic GCfor patients with oligo- or polyarticular course of JIA exceptsystemic onset of JIA e) The ACR recommendations do notcover the topic of non-drug based therapy at all althoughthere is strong evidence that eg exercise training is a usefuladdition to drug treatment [575860]
6 Conclusion
In summary we present a treatment guideline for JIA on a con-sensus conference basis We strongly advocate an interdisciplin-ary approach including surgery physiotherapy psychosocial
intervention physical therapy medications etc and a strictformal consensus process in order to create statements thatare most appropriate for the complex clinical situation of achild and family presenting with JIA and cover all aspects ofJIA care All German pediatric rheumatology sites are partici-pating at the national pediatric rheumatologic database in theDeutsche Rheuma-Forschungszentrum at Berlin (DRFZ wwwdrfzde) It aims at quality assurance in Germany and monitorstreatment behavior of pediatric rheumatologists by using inter-nationally agreed criteria (eg joint count global physician rat-ing of disease activity global parent rating of overall well-being CHAQ ESR ACR-ped response or JADAS) The databasewill be used as a tool to monitor the application of our treat-ment guidelines
190 G Dueckers et al
Conflict of interest statement
Gregor Dueckers Novartis Pharmaceuticals CorporationBaxter (for all travel grants for scientific meetings)Nihal Guellac no conflict of interestMartin Arbogast no conflict of interestGuumlnther Dannecker no conflict of interestIvan Foeldvari Wyeth Pfizer Abbott Immunology Pharma-ceuticals Chugai (for all advisory board member)Michael Frosch no conflict of interestGerd Ganser Abbott Immunology Pharmaceuticals (advisoryboard member grants for scientific meetings) Wyeth Pfizer(advisory board member grants for scientific meetings)ChugaiRoche (advisory board member grants for scientificmeetings) Merck (grants for scientific meetings) Actelios(grants for scientific meetings) Esaote (grants for scientificmeetings)Arnd Heiligenhaus Novartis Pharmaceuticals CorporationAbbott Immunology Pharmaceuticals Alcon (for all re-search grants)Gerd Horneff Abbott Immunology Pharmaceuticals (re-search grants consulting fees non-remunerative positionsof influence) Wyeth Pfizer (research grants consultingfees speakers bureau non-remunerative positions of influ-ence) Bristol-Myers Squibb (Consulting fees) Nycomed(Consulting fees non-remunerative positions of influence)RocheChugai (Consulting fees non-remunerative positionsof influence) Sandoz (Consulting fees) Genzyme (researchgrants consulting fees non-remunerative positions of influ-ence) Swedish Orphan (research grants consulting feesnon-remunerative positions of influence)Arnold Illhardt no conflict of interestRuumldiger Krauspe no conflict of interestBarbara Markus no conflict of interestHartmut Michels Abbott Immunology Pharmaceuticals (advi-sory board member and grants for scientific meeting)Matthias Schneider no conflict of interestWolfram Singendonk no conflict of interestHelmut Sitter no conflict of interestMarianne Spamer no conflict of interestNorbert Wagner no conflict of interestTim Niehues Abbott Immunology Pharmaceuticals EssexPharma Novartis Pharmaceutical Corporation WyethPfizer (for all research grants consulting fees non-remu-nerative positions of influence)
Acknowledgment
We like to express our grateful thanks to Prof Dr Hans IkoHuppertz for proof reading the article and for an excellentdiscussion on our work We like to express our thanks to HE-LIOS Clinic for funding the open access of the article
References
[1] RE Petty TR Southwood P Manners J Baum DN Glass JGoldenberg X He J Maldonado-Cocco J Orozco-Alcala AMPrieur ME Suarez-Almazor PWoo International League of Asso-ciations for Rheumatology classification of juvenile idiopathic ar-thritis second revision Edmonton 2001 J Rheumatol 31(2004) 390ndash392
[2] B Prakken S Albani A Martini Juvenile idiopathic arthritisLancet 377 (2011) 2138ndash2149
[3] KT April DE Feldman RW Platt CM Duffy Comparisonbetween children with juvenile idiopathic arthritis (JIA) andtheir parents concerning perceived quality of life Qual LifeRes 15 (2006) 655ndash661
[4] BM Feldman B Grundland L McCullough V Wright Distinc-tion of quality of life health related quality of life and healthstatus in children referred for rheumatologic care J Rheuma-tol 27 (2000) 226ndash233
[5] JC Packham MA Hall Long-term follow-up of 246 adultswith juvenile idiopathic arthritis functional outcomeRheumatology (Oxford) 41 (2002) 1428ndash1435
[6] C Sandborg Pediatric rheumatic disease standards of care forJIAmdashthe basic foundation for quality Nat Rev Rheumatol 6(2010) 389ndash390
[7] N Guellac T Niehues Interdisciplinary and evidence-basedtreatment guideline for juvenile idiopathic arthritis KlinPadiatr 220 (2008) 392ndash402
[8] K Schnakenburg Leitlinien in der Kinder- und JugendmedizinElsevier 2005 pp H1 1ndash15
[9] P Juni L Nartey S Reichenbach R Sterchi PA Dieppe MEgger Risk of cardiovascular events and rofecoxib cumulativemeta-analysis Lancet 364 (2004) 2021ndash2029
[10] W Feldman Evidence-based Pediatrics 1st ed BC DeckersHamilton 2000
[11] AH Van de Ven AL Delbecq The nominal group as a re-search instrument for exploratory health studies Am J PublicHealth 62 (1972) 337ndash342
[12] HA Linstone M Turoff The Delphi Method Techniques andApplications Addison-Wesley Pub 1975
[13] TK Kvien HM Hoyeraal B Sandstad Naproxen and acetyl-salicylic acid in the treatment of pauciarticular and polyarticu-lar juvenile rheumatoid arthritis Assessment of tolerance andefficacy in a single-centre 24-week double-blind parallelstudy Scand J Rheumatol 13 (1984) 342ndash350
[14] RM Laxer ED Silverman C St-Cyr MT Tran G Lingam Asix-month open safety assessment of a naproxen suspensionformulation in the therapy of juvenile rheumatoid arthritisClin Ther 10 (1988) 381ndash387
[15] AM Leak MR Richter LE Clemens MA Hall BM AnsellA crossover study of naproxen diclofenac and tolmetin in sero-negative juvenile chronic arthritis Clin Exp Rheumatol 6(1988) 157ndash160
[16] J Haapasaari E Wuolijoki H Ylijoki Treatment of juve-nile rheumatoid arthritis with diclofenac sodium Scand JRheumatol 12 (1983) 325ndash330
[17] EH Giannini EJ Brewer ML Miller D Gibbas MH PassoHM Hoyeraal B Bernstein DA Person CW Fink LA Sawyeret al Ibuprofen suspension in the treatment of juvenilerheumatoid arthritis Pediatric Rheumatology CollaborativeStudy Group J Pediatr 117 (1990) 645ndash652
[18] E Stoeber L Sanger Experiences with indomethacin in long-term therapy of juvenile rheumatoid arthritis Arzneimittel-forschung 21 (1971) 1865ndash1866
[19] N Ruperto I Nikishina ED Pachanov Y Shachbazian AMPrieur R Mouy R Joos F Zulian R Schwarz V ArtamonovaW Emminger M Bandeira A Buoncompagni I Foeldvari FFalcini E Baildam I Kone-Paut M Alessio V Gerloni ALenhardt A Martini G Hanft R Sigmund S Simianer Arandomized double-blind clinical trial of two doses ofmeloxicam compared with naproxen in children with juvenileidiopathic arthritis short- and long-term efficacy and safetyresults Arthritis Rheum 52 (2005) 563ndash572
[20] I Foeldvari IS Szer LS Zemel DJ Lovell EH Giannini JLRobbins CRWest G Steidle S Krishnaswami BJ Bloom A pro-spective study comparing celecoxib with naproxen in children withjuvenile rheumatoid arthritis J Rheumatol 36 (2009) 174ndash182
191Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
[21] F Zulian G Martini D Gobber C Agosto C Gigante FZacchello Comparison of intra-articular triamcinolone hexa-cetonide and triamcinolone acetonide in oligoarticular juve-nile idiopathic arthritis Rheumatology (Oxford) 42 (2003)1254ndash1259
[22] F Zulian G Martini D Gobber M Plebani F Zacchello PManners Triamcinolone acetonide and hexacetonide intra-articular treatment of symmetrical joints in juvenile idiopathicarthritis a double-blind trial Rheumatology (Oxford) 43 (2004)1288ndash1291
[23] GS Habib Systemic effects of intra-articular corticosteroidsClin Rheumatol 28 (2009) 749ndash756
[24] JR Kirwan The effect of glucocorticoids on joint destructionin rheumatoid arthritis The Arthritis and Rheumatism CouncilLow-Dose Glucocorticoid Study Group N Engl J Med 333(1995) 142ndash146
[25] H Michels What is low-dose corticosteroid therapy in juvenileidiopathic arthritis A worldwide questionnaire-based surveyZ Rheumatol 59 (Suppl 2) (2000) II127ndash130
[26] JJ Miller III Prolonged use of large intravenous steroid pulsesin the rheumatic diseases of children Pediatrics 65 (1980)989ndash994
[27] P Picco M Gattorno A Buoncompagni V Pistoia C Borrone6-methylprednisolone lsquomini-pulsesrsquo a newmodality of glucocor-ticoid treatment in systemic onset juvenile chronic arthritisScand J Rheumatol 25 (1996) 24ndash27
[28] AM Prieur The place of corticosteroid therapy in juvenilechronic arthritis in 1992 J Rheumatol Suppl 37 (1993)32ndash34
[29] JS Gao H Wu J Tian Treatment of patients with juvenilerheumatoid arthritis with combination of leflunomide andmethotrexate Zhonghua Er Ke Za Zhi 41 (2003) 435ndash438
[30] T Niehues G Horneff H Michels MS Hock L SchuchmannEvidence-based use of methotrexate in children with rheumat-ic diseases a consensus statement of the Working Groups Pedi-atric Rheumatology Germany (AGKJR) and PediatricRheumatology Austria Rheumatol Int 25 (2005) 169ndash178
[31] N Ruperto DJ Lovell R Cuttica N Wilkinson P Woo GEspada C Wouters ED Silverman Z Balogh M HenricksonMT Apaz E Baildam A Fasth V Gerloni P Lahdenne AMPrieur A Ravelli RK Saurenmann ML Gamir N WulffraatL Marodi RE Petty R Joos F Zulian D McCurdy BLMyones K Nagy P Reuman I Szer S Travers A BeutlerG Keenan J Clark S Visvanathan A Fasanmade A Ray-chaudhuri A Mendelsohn A Martini EH Giannini A random-ized placebo-controlled trial of infliximab plus methotrexatefor the treatment of polyarticular-course juvenile rheumatoidarthritis Arthritis Rheum 56 (2007) 3096ndash3106
[32] K Visser DM van der Heijde Risk and management of livertoxicity during methotrexate treatment in rheumatoid andpsoriatic arthritis a systematic review of the literature ClinExp Rheumatol 27 (2009) 1017ndash1025
[33] A Cespedes-Cruz R Gutierrez-Suarez A Pistorio A Ravelli ALoy KJ Murray V Gerloni N Wulffraat S Oliveira J WalshIC Penades MG Alpigiani P Lahdenne C Saad-Magalhaes ECortis L Lepore Y Kimura C Wouters A Martini N RupertoMethotrexate improves the health-related quality of life of chil-dren with juvenile idiopathic arthritis Ann Rheum Dis 67(2008) 309ndash314
[34] TK Kvien HM Hoyeraal B Sandstad Azathioprine versus place-bo in patients with juvenile rheumatoid arthritis a single centerdouble blind comparative study J Rheumatol 13 (1986) 118ndash123
[35] E Silverman R Mouy L Spiegel LK Jung RK SaurenmannP Lahdenne G Horneff I Calvo IS Szer K Simpson JAStewart V Strand Leflunomide or methotrexate for juvenilerheumatoid arthritis N Engl J Med 352 (2005) 1655ndash1666
[36] MA van Rossum TJ Fiselier MJ Franssen AH ZwindermanR ten Cate LW van Suijlekom-Smit WH van Luijk RM
van Soesbergen NM Wulffraat JC Oostveen W Kuis PFDijkstra CF van Ede BA Dijkmans Sulfasalazine in the treat-ment of juvenile chronic arthritis a randomized double-blindplacebo-controlled multicenter study Dutch Juvenile ChronicArthritis Study Group Arthritis Rheum 41 (1998) 808ndash816
[37] MA van Rossum RM van Soesbergen M Boers AHZwinderman TJ Fiselier MJ Franssen R ten Cate LW vanSuijlekom-Smit NM Wulffraat WH van Luijk JC OostveenW Kuis BA Dijkmans Long-term outcome of juvenile idiopathicarthritis following a placebo-controlled trial sustained benefits ofearly sulfasalazine treatment Ann Rheum Dis 66 (2007)1518ndash1524
[38] DJ Lovell EH Giannini A Reiff GD Cawkwell ED SilvermanJJ Nocton LD Stein A Gedalia NT Ilowite CA Wallace JWhitmore BK Finck Etanercept in children with polyarticularjuvenile rheumatoid arthritis Pediatric Rheumatology Collabora-tive Study Group N Engl J Med 342 (2000) 763ndash769
[39] DJ Lovell A Reiff OY Jones R Schneider J Nocton LDStein A Gedalia NT Ilowite CA Wallace JB WhitmoreB White EH Giannini Long-term safety and efficacy ofetanercept in children with polyarticular-course juvenile rheu-matoid arthritis Arthritis Rheum 54 (2006) 1987ndash1994
[40] DJ Lovell N Ruperto S Goodman A Reiff L Jung K JarosovaD Nemcova R Mouy C Sandborg J Bohnsack D Elewaut IFoeldvari V Gerloni J Rovensky K Minden RK Vehe LWWeiner G Horneff HI Huppertz NY Olson JR Medich RCarcereri-De-Prati MJ McIlraith EH Giannini A MartiniAdalimumab with or without methotrexate in juvenile rheuma-toid arthritis N Engl J Med 359 (2008) 810ndash820
[41] FH Prince M Twilt R ten Cate MA van RossumW ArmbrustEP Hoppenreijs M van Santen-Hoeufft Y Koopman-KeeminkNM Wulffraat LW van Suijlekom-Smit Long-term follow-upon effectiveness and safety of etanercept in juvenile idiopathicarthritis the Dutch National Register Ann Rheum Dis 68(2009) 635ndash641
[42] P Diak J Siegel L LaGrenade L Choi S Lemery AMcMahonTumor necrosis factor alpha blockers andmalignancy in childrenforty-eight cases reported to the Food and Drug AdministrationArthritis Rheum 62 (2010) 2517ndash2524
[43] G Horneff T Hospach G Dannecker D Foll JP Haas HJGirschick HI Huppertz R Keitzer HJ Laws H Michels KMinden R Trauzeddel Updated statement by the German So-ciety for Pediatric and Adolescent Rheumatology (GKJR) on theFDAs report regarding malignancies in anti-TNF-treated pa-tients from Aug 4 2009 Z Rheumatol 69 (2010) 561ndash567
[44] T Hospach JP Haas HI Huppertz R Keitzer H Michels RTrauzeddl D Foll G Dannecker G Horneff Comment of theSociety of Pediatric and Adolescent Rheumatology on the USFood and Drug Administration (FDA) announcement regardingcases of malignancy in anti-TNF-treated patients Z Rheumatol68 (2009) 162ndash164
[45] DJ Lovell A Reiff NT Ilowite CA Wallace Y Chon SL LinSW Baumgartner EH Giannini Safety and efficacy of up to eightyears of continuous etanercept therapy in patients with juvenilerheumatoid arthritis Arthritis Rheum 58 (2008) 1496ndash1504
[46] EH Giannini NT Ilowite DJ Lovell CA Wallace CERabinovich A Reiff G Higgins B Gottlieb NG Singer YChon SL Lin SW Baumgartner Long-term safety and effec-tiveness of etanercept in children with selected categories ofjuvenile idiopathic arthritis Arthritis Rheum 60 (2009)2794ndash2804
[47] G Horneff H Schmeling T Biedermann I Foeldvari G GanserHJ Girschick T Hospach HI Huppertz R Keitzer RM KusterH Michels D Moebius B Rogalski A Thon The German etaner-cept registry for treatment of juvenile idiopathic arthritis AnnRheum Dis 63 (2004) 1638ndash1644
[48] FH Prince M Twilt SC Simon MA van RossumW ArmbrustEP Hoppenreijs S Kamphuis M van Santen-Hoeufft Y
192 G Dueckers et al
Koopman-Keemink NM Wulffraat R ten Cate LW vanSuijlekom-Smit When and how to stop etanercept aftersuccessful treatment of patients with juvenile idiopathic ar-thritis Ann Rheum Dis 68 (2009) 1228ndash1229
[49] G Horneff F De Bock I Foeldvari HJ Girschick H MichelsD Moebius H Schmeling Safety and efficacy of combinationof etanercept and methotrexate compared to treatment withetanercept only in patients with juvenile idiopathic arthritis(JIA) preliminary data from the German JIA Registry AnnRheum Dis 68 (2009) 519ndash525
[50] N Ilowite O Porras A Reiff S Rudge M Punaro A Martin RAllen T Harville YN Sun T Bevirt G Aras B Appleton Ana-kinra in the treatment of polyarticular-course juvenile rheumatoidarthritis safety and preliminary efficacy results of a randomizedmulticenter study Clin Rheumatol 28 (2009) 129ndash137
[51] T Lequerre P Quartier D Rosellini F Alaoui M De BandtO Mejjad I Kone-Paut M Michel E Dernis M Khellaf NLimal C Job-Deslandre B Fautrel X Le Loet J Sibilia In-terleukin-1 receptor antagonist (anakinra) treatment in pa-tients with systemic-onset juvenile idiopathic arthritis oradult onset Still disease preliminary experience in FranceAnn Rheum Dis 67 (2008) 302ndash308
[52] M Gattorno A Piccini D Lasiglie S Tassi G Brisca S CartaL Delfino F Ferlito MA Pelagatti F Caroli A BuoncompagniS Viola A Loy M Sironi A Vecchi A Ravelli A Martini ARubartelli The pattern of response to anti-interleukin-1 treatmentdistinguishes two subsets of patients with systemic-onset juvenileidiopathic arthritis Arthritis Rheum 58 (2008) 1505ndash1515
[53] S Yokota T Imagawa M Mori T Miyamae Y Aihara STakei N Iwata H Umebayashi T Murata M Miyoshi MTomiita N Nishimoto T Kishimoto Efficacy and safety oftocilizumab in patients with systemic-onset juvenile idiopathicarthritis a randomised double-blind placebo-controlledwithdrawal phase III trial Lancet 371 (2008) 998ndash1006
[54] N Ruperto DJ Lovell P Quartier E Paz N Rubio-Perez CASilva C Abud-Mendoza R Burgos-Vargas V Gerloni JAMelo-Gomes C Saad-Magalhaes F Sztajnbok C Goldenstein-Schainberg M Scheinberg IC Penades M Fischbach J OrozcoPJ Hashkes C Hom L Jung L Lepore S Oliveira CAWallace LH Sigal AJ Block A Covucci A Martini EHGiannini Abatacept in children with juvenile idiopathic arthri-tis a randomised double-blind placebo-controlled withdrawaltrial Lancet 372 (2008) 383ndash391
[55] N Ruperto DJ Lovell P Quartier E Paz N Rubio-PerezCA Silva C Abud-Mendoza R Burgos-Vargas V GerloniJA Melo-Gomes C Saad-Magalhaes J Chavez-Corrales CHuemer A Kivitz FJ Blanco I Foeldvari M Hofer G HorneffHI Huppertz C Job-Deslandre A Loy K Minden M PunaroAF Nunez LH Sigal AJ Block M Nys A Martini EHGiannini Long-term safety and efficacy of abatacept inchildren with juvenile idiopathic arthritis Arthritis Rheum 62(2010) 1792ndash1802
[56] DM Brinkman IM de Kleer R ten Cate MA van RossumWP Bekkering A Fasth MJ van Tol W Kuis NM WulffraatJM Vossen Autologous stem cell transplantation in childrenwith severe progressive systemic or polyarticular juvenile idio-pathic arthritis long-term follow-up of a prospective clinicaltrial Arthritis Rheum 56 (2007) 2410ndash2421
[57] SE Klepper Effects of an eight-week physical conditioningprogram on disease signs and symptoms in children with chronicarthritis Arthritis Care Res 12 (1999) 52ndash60
[58] D Singh-Grewal J Schneiderman-Walker V Wright O Bar-OrJ Beyene H Selvadurai B Cameron RM Laxer R SchneiderED Silverman L Spiegel S Tse C Leblanc J Wong SStephens BM Feldman The effects of vigorous exercisetraining on physical function in children with arthritis arandomized controlled single-blinded trial ArthritisRheum 57 (2007) 1202ndash1210
[59] S Stephens D Singh-Grewal O Bar-Or J Beyene B CameronCM Leblanc R Schneider J Schneiderman-Walker HSelvadurai E Silverman L Spiegel SM Tse V WrightBM Feldman Reliability of exercise testing and functionalactivity questionnaires in children with juvenile arthritisArthritis Rheum 57 (2007) 1446ndash1452
[60] T Takken J van der Net W Kuis PJ Helders Physical ac-tivity and health related physical fitness in children with ju-venile idiopathic arthritis Ann Rheum Dis 62 (2003)885ndash889
[61] MM Toledo G Martini C Gigante L Da Dalt A TregnaghiF Zulian Is there a role for arthroscopic synovectomy in oli-goarticular juvenile idiopathic arthritis J Rheumatol 33(2006) 1868ndash1872
[62] F de Benedetti H Brunner N Ruperto SWright A KenwrightR Cuttica P Woo R Schneider DJ Lovell A Martini Efficacyand safety of Tocilizumab in patients with systemic juvenile idio-pathic arthritis (sJIA) 12-week data from the phase III TENDERtrial Ann Rheum Dis 69 (2010) 146
[63] P Quartier F Allantaz R Cimaz P Pillet C Messiaen CBardin X Bossuyt A Boutten J Bienvenu A Duquesne ORicher D Chaussabel A Mogenet J Banchereau JM Tre-luyer P Landais V Pascual A multicentre randomiseddouble-blind placebo-controlled trial with the interleukin-1receptor antagonist anakinra in patients with systemic-onsetjuvenile idiopathic arthritis (ANAJIS trial) Ann Rheum Dis70 (2011) 747ndash754
[64] DE Furst EC Keystone J Braun FC Breedveld GRBurmester F De Benedetti T Dorner P Emery R FleischmannA Gibofsky JR Kalden A Kavanaugh B Kirkham P Mease JSieper NG Singer JS Smolen PL Van Riel MH Weisman KWinthrop Updated consensus statement on biological agents forthe treatment of rheumatic diseases 2010 Ann Rheum Dis 70(Suppl 1) (2010) i2ndashi36
[65] T Beukelman NM Patkar KG Saag S Tolleson-RinehartRQ Cron EM Dewitt NT Ilowite Y Kimura RM LaxerDJ Lovell A Martini CE Rabinovich N Ruperto 2011 Ameri-can College of Rheumatology recommendations for the treatmentof juvenile idiopathic arthritis initiation and safety monitoring oftherapeutic agents for the treatment of arthritis and systemic fea-tures Arthritis Care Res 63 (2011) 465ndash482 (Hoboken)
[66] JF Simard M Neovius S Hagelberg J Askling Juvenile idi-opathic arthritis and risk of cancer a nationwide cohort studyArthritis Rheum 62 (2010) 3776ndash3782
[67] T Imagawa S Yokota M Mori T Miyamae S Takei H ImanakaY Nerome N Iwata T Murata M Miyoshi N Nishimoto TKishimoto Safety and efficacy of tocilizumab an anti-IL-6-receptor monoclonal antibody in patients with polyarticular-course juvenile idiopathic arthritis Mod Rheumatol (2011)doi102007s10165-011-0481-0
[68] TM Shaneyfelt MF Mayo-Smith J Rothwangl Are guide-lines following guidelines The methodological quality of clini-cal practice guidelines in the peer-reviewed medicalliterature Jama 281 (1999) 1900ndash1905
[69] R Grilli N Magrini A Penna G Mura A Liberati Practiceguidelines developed by specialty societies the need for a crit-ical appraisal Lancet 355 (2000) 103ndash106
[70] JS Burgers R Grol NS Klazinga M Makela J Zaat To-wards evidence-based clinical practice an international surveyof 18 clinical guideline programs Int J Qual Health Care 15(2003) 31ndash45
[71] JT Cassidy RE Petty Juvenile Idiopathic Rheumatic Arthri-tis 5th Edition WB Saunders Philadelphia 2005
[72] TJ Lehman Are withdrawal trials in paediatric rheumatic dis-ease helpful Lancet 372 (2008) 348ndash350
[73] J Munro Recommendations for the Diagnosis and Managementof Juvenile Idiopathic Arthritis The Royal Australian Collegeof General Practitioners South Melbourne 2009 pp 1ndash38
193Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
httpwwwnhmrcgovau_files_nhmrcpublicationsattachmentscp119-juvenile-arthritispdf
[74] MJ Santos JE Fonseca H Canhao M Conde M JoseVieira L Costa M Costa M Salgado JA Melo Gomes Guide-lines for prescribing and monitoring biologic therapies in juve-nile idiopathic arthritis Acta Reumatol Port 32 (2007) 43ndash47
[75] S Yokota M Mori T Imagawa T Murata M Tomiita Y ItohS Fujikawa S Takei Guidelines on the use of etanercept forjuvenile idiopathic arthritis in Japan Mod Rheumatol 20(2010) 107ndash113
[76] The AGREE Collaboration Appraisal of Guidelines for Researchamp Evaluation (AGREE) instrument wwwagreecollaborationorg
[77] I Kopp H Thole T Langer HK Selbmann G OllenschlaumlgerGerman Instrument for Methodological Guideline Appraisal(DELBI) wwwversorgungsleitliniende2008
[78] Auml Aumlrztliches Zentrum fuumlr Qualitaumlt in der Medizin A Arbeitsge-meinschaften der Wissenschaftlichen Fachgesellschaften in derMedizin Deutsches Instrument zur methodischen Leitlinien-Bewertung (DELBI) Fassung 20052006 Z Aumlrztl FortbildQualitaumltssich 99 (2005) 468ndash519
[79] MP de Wit SE Berlo GJ Aanerud D Aletaha JW BijlsmaL Croucher JA Da Silva B Glusing L Gossec S Hewlett MJongkees D Magnusson M Scholte-Voshaar P Richards CZiegler TA Abma European League Against Rheumatism rec-ommendations for the inclusion of patient representatives in sci-entific projects Ann Rheum Dis 70 (2011) 722ndash726
[80] I Foeldvari M Bidde Validation of the proposed ILAR classifi-cation criteria for juvenile idiopathic arthritis InternationalLeague of Associations for Rheumatology J Rheumatol 27(2000) 1069ndash1072
[81] R Merino J de Inocencio J Garcia-Consuegra Evaluation ofrevised International League of Associations for Rheumatologyclassification criteria for juvenile idiopathic arthritis in Spanishchildren (Edmonton 2001) J Rheumatol 32 (2005) 559ndash561
[82] SE Ramsey RK Bolaria DA Cabral PN Malleson REPetty Comparison of criteria for the classification of childhoodarthritis J Rheumatol 27 (2000) 1283ndash1286
[83] G Horneff A Ebert S Fitter K Minden I Foeldvari J Kum-merle-Deschner A Thon HJ Girschick F Weller HI Hup-pertz Safety and efficacy of once weekly etanercept 08mgkg in a multicentre 12 week trial in active polyarticularcourse juvenile idiopathic arthritis Rheumatology (Oxford) 48(2009) 916ndash919
[84] EH Giannini EJ Brewer N Kuzmina A Shaikov A Maxi-mov I Vorontsov CW Fink AJ Newman JT Cassidy LSZemel Methotrexate in resistant juvenile rheumatoid arthri-tis Results of the USAndashUSSR double-blind placebo-controlled trial The Pediatric Rheumatology CollaborativeStudy Group and The Cooperative Childrens Study GroupN Engl J Med 326 (1992) 1043ndash1049
[85] A Ravelli S Viola D Migliavacca N Ruperto A Pistorio AMartini The extended oligoarticular subtype is the best predic-tor of methotrexate efficacy in juvenile idiopathic arthritisJ Pediatr 135 (1999) 316ndash320
[86] P Woo TR Southwood AM Prieur CJ Dore J Grainger JDavid C Ryder N Hasson A Hall I Lemelle Randomizedplacebo-controlled crossover trial of low-dose oral
methotrexate in children with extended oligoarticular or sys-temic arthritis Arthritis Rheum 43 (2000) 1849ndash1857
[87] E Silverman L Spiegel D Hawkins R Petty D Goldsmith LSchanberg C Duffy P Howard V Strand Long-term open-label preliminary study of the safety and efficacy of lefluno-mide in patients with polyarticular-course juvenile rheumatoidarthritis Arthritis Rheum 52 (2005) 554ndash562
[88] DJ Lovell EH Giannini Y Kimura C Suzanne PJHashkes A Reiff Long-term safety and efficacy of rilonaceptin patients with systemic juvenile idiopathic arthritis (SJIA)Arthritis Rheum 60 (2009)
[89] N Ruperto P Quartier NWulffraat PWoo A Loy R Mouy BBader-Meunier BJ Prakken E Noseda R Belleli J Lecot CRordorf A Martini A Phase II Trial with canakinumab(ACZ885) a new IL-1-beta blocking monoclonal antibody toevaluate safety and preliminary efficacy in children with system-ic juvenile idiopathic arthritis Ann Rheum Dis 68 (2009) 170
[90] DJ Lovell EH Giannini Y Kimura et al Preliminary evi-dence for bioactivity of IL-1 trap (Rilonacept) a long actingIL-1 inhibitor in systemic juvenile idiopathic arthritis (sJIA)Arthritis Rheum 54 (2006) S325
[91] DJ Lovell EH Giannini Y Kimura et al Preliminary evi-dence for sustained bioactivity of IL-1 Trap (rilonacept) a longacting IL-1 inhibitor in systemic juvenile idiopathic arthritisArthritis Rheum 56 (2007) S514
[92] N Ruperto F De Benedetti H Brunner R Allen D Brown JChaitow E Cortis G Espada B Flato V Gerloni G HorneffS Wright A Kenwright R Schneider P Woo A Martini DJLovell Tocilizumab is efficacious in patients with systemic ju-venile idiopathic arthritis (sJIA) across baseline disease charac-teristics and priorbaseline treatments 12-week data from thephase II TENDER trial 17th PReS Congress Valencia Spain2010 2010
[93] N Ruperto DJ Lovell T Li F Sztajnbok C Goldenstein-Schainberg M Scheinberg IC Penades M Fischbach JOrozco PJ Hashkes C Hom L Jung L Lepore S OliveiraC Wallace M Alessio P Quartier E Cortis A Eberhard GSimonini I Lemelle E Chalom LH Sigal A Block A CovucciM Nys A Martini EH Giannini Abatacept improves health-related quality of life pain sleep quality and daily participationin subjects with juvenile idiopathic arthritis Arthritis Care Res(Hoboken) 62 (11) (2010) 1542ndash1551
[94] N Ruperto DJ Lovell P Quartier E Paz N Rubio-PerezCA Silva C Abud-Mendoza R Burgos-Vargas V GerloniJA Melo-Gomes C Saad-Magalhaes J Chavez C HuemerA Kivitz FJ Blanco I Foeldvari M Hofer G Horneff HIHuppertz CJ Deslandre A Loy K Minden M Punaro AFNunez LH Sigal AJ Block M Nys A Martini EH GianniniLong-term safety and efficacy of abatacept in children with ju-venile idiopathic arthritis Arthritis Rheum 62 (2010)1792ndash1802
[95] J Munro Juvenile Idiopathic Arthritis Management Guidelines(Provisional) Australian Paediatric Rheumatology Group 2006httpwwwnhmrcgovau
[96] K Fitch SJ Bernstein MD Aguilar B Burnand JR LaCalleP Lazaro M van het Loo J McDonnell JP Vader JPKahan The RANDUCLA Appropriateness Method Users ManualRAND Pittsburgh 2000

Table 5 (continued)
Generic Dosage Age approval by Europeanmedical agency inpediatric rheumatology(EMA) a
Medical indication in pediatricrheumatology a b
Evidence levelrecommendationgrade [10]
Literature
DMARDsSulfasalazine 30ndash50 mgkg Bwd in 2ndash3 doses 6 years Arthritis II Van Rossum [3637]Cytotoxic or immuno-suppressive drugsMethotrexate 10ndash15 (20) mgmsup2 body surface
once a week (po sc iv) e2 years Polyarticular JIA Psoriasis arthritis
uveitis CollagenosisI Giannini [84] Ravelli [85]
Woo [86]Cespedes-Cruz [33]Azathioprine 15ndash3 mgkg Bwd po in 1ndash2
dosesNo approval for children II Kvien [34]
Leflunomide No clear recommendation forchildren availableBwb20 kg d 1100 mgkg from d 2 10 mgkgdBw 20ndash40 kg d 1 to d 2 100 mgkgfrom d 3 10ndash20 mgkgdBwN40 kg d 1 to d 3 100 mgkgfrom d 3 20 mgkgd
No approval for children II Silverman [3587]
Biologic agentsa) TNFα inhibitorsEtanercept d 08 mgkg Bw sc 1timesweek
(max 50 mgweek) or 04 mgkgBw sc 2timesweek (max 50 mgweek)
4 years JIA Polyarthritis and insufficientefficacy of MTX
I Giannini [46] Horneff [49]Lovell [3888] Prince [41]
Adalimumab d 24 mgm2 body surface sc in 1dose every 2 weeks Bwb30 kg20 mgm2 body surface BwN30 kg40 mgm2 body surface(max 40 mg per dose)
4 years to 17 years Adalimumab in combination withmethotrexate is indicated for thetreatment of active polyarticularjuvenile idiopathic arthritis in childrenand adolescents who have had aninadequate response to one or moredisease-modifying anti-rheumatic drugs(DMARDs)
I Lovell [40]
182GDueckers
etal
Infliximab d 3ndash10 mgkg Bwdose iv Infusionat d 0 d 14 d 42 then every8 weeks intervals of applicationremain unclear
No approval for childrenwith JIA6 years (approval forMorbus Crohn)
III Ruperto [31]
b) IL-1 inhibitorsAnakinra d 1ndash4 mgkg Bwd sc in 1 dose No approval for children II Illowite [50] Lequerre [51]Canakinumab d 4 mgkg Bwsingle dose sc every
4 weeks (max 150 mg)No approval for childrenwith JIA 4 years (approvalfor CAPS)
III Ruperto [89]
Rilonacept d 1ndash2times44 mgkgweek sc (max320 mg) then 22 mgkgweek sc(max160 mg)
No approval for childrenwith JIA 12 years(approval for CAPS)
Lovell [889091]
c) IL-6 inhibitorsTocilizumab d 1 h Infusion every two 2 weeks
Bwb30 kg 8 mgkg BwN30 kg12 mgkg
2 years of age or older Since May 2011 EMA approval forpediatric patients with SoJIA who haveresponded inadequately to previoustherapy with NSAIDs and systemiccorticosteroids (Approval at Japan forSoJIA and polyarticular JIA since 2008) c
I Yokota [53] Ruperto [92]de Benedetti [62]
d) Co stimulatory-antagonistsAbatacept d 10 mgkg iv Infusion at d 0 d 14
d 28 then every 4 weeks6 years of age and older Abatacept in combination with
methotrexate is indicated for thetreatment of moderate to severe activepolyarticular (JIA) in pediatric patientswho have had an insufficient responseto other DMARDs including at least oneTNF inhibitor
I Ruperto [549394]
Abbreviations CAPS=Cryopyrine associated periodic fever syndrome JDM=juvenile dermatomyositis Bw=body weight SoJIA=systemic-onset of JIA SLE=systemic Lupus erythematodesa Compare wwwemaeuropaeub wwwrotelistede (German database of drugs with national market approval)c Intra-articular injection into same joint no more often than once every 3 monthsd A statement from insurance companies should be acquired before treatment initiation for off label treatment (if possible)e Oral application is most feasible in childhood
183Evidence
andconsensus
basedGKJR
guidelinesfor
thetreatm
entof
juvenileidiopathic
arthritis
Oligoarticular JIA
Polyarticular JIA
SoJIA
Figure 2 JIA treatment escalation schemes +=addition of the drug (abbreviations NSAIDs=non steroidal anti-inflammatory drugthotrexate)
Consensus statement
Long-term use of systemic GC is not recom-mended Continuous administration of ge02 mgPrednisolone equivalent per kg bodyweight (Bw)carries a high risk of adverse events and thereforeis not recommended (evidence level III recom-mendation grade A)
Consensus statement (continued)
184 G Dueckers et al
GC in JIA published thus leading to ldquojustrdquo evidence level IIIDifferent recommendations of dosage and therapy regimesare listed in Table 5 (evidence level III for all recommenda-tions) [1824ndash28] Frequency and seriousness of deleteriouseffects correlate mainly to duration of therapy and dosageof GC administered Main side effects are iatrogenicCushings syndrome growth disturbance weight gainmood changes Higher dosage carry the risk of increasedvulnerability to infection hypertension osteoporosisthrombosis diabetes gastro-intestinal ulceration cataractglaucoma atrophy of subcutaneous fatty tissue steroid in-duced acne To inform colleagues about GC treatment in acase of emergency and to reduce severe complications in longterm treated patients ie GC administrationN4 weeks thesupply of ldquoGlucocorticoid ID cardsrdquo for patients might be useful
GC=Glucocorticoids DMARDs=disease modifying drugs MTX=Me
Consensus statement
The systemic use of GC is recommended asfast acting drugs in highly active JIA GC areused for the treatment of children and adoles-cents with SoJIA organ manifestations of JIA(eg uveitis pericardial effusion) sero-positivepolyarticular JIA and for bridging time untilthe complete therapeutic effect of DMARDs(evidence level III recommendation grade A)
313 Methotrexate (MTX) biologic agents andimmunosuppressive agents
MTX biologic agents and immunosuppres-sive agents are used for the treatment of childrenand adolescents with polyarticular JIA ifNSAIDs or local GC treatment do not succeedThe combination of those drugs with NSAIDsand GC is feasible A common characteristic ofMTX biologic agents and immunosuppressiveagents is the delayed onset of therapeutic ef-fect ie up to 3 months or even longer aftercommencing treatment
185Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
Safe contraception is indicated during therapy with MTXAzathioprine or Leflunomide and in the following 3 to6 months after its discontinuation
Consensus statement
Administration of Sulfasalazine or Lefluno-mide is recommended if MTX or Etanercept donot show sufficient efficacy or cannot be used
3131 Methotrexate Among DMARDs MTX provides themainstay of long-term therapy in JIA [29ndash32] In case ofside effects eg dyspepsia or nausea prophylaxis withfolic acid can be recommended (1times1 mg per day or 5 mgonce a week 24ndash48 h after application of MTX) Safe contra-ception is mandatory while receiving MTX Safety and effica-cy of MTX and its impact on quality of life of children with JIAhave been investigated Significant positive impact of MTXon all health-related quality of life health conceptshas been shown although the study has its limit due to dif-ferent MTX dosages used within participating JIA patients[33]
Consensus statement
MTX administration can be recommendeddue to its proven safety and efficacy to reducedisease activity MTX is used in case of insuffi-cient therapeutic effect of NSAIDs andor localGC administration continuous need for system-ic GC andor highly active disease Efficacy ofMTX (orally or subcutaneously administered) isfrequently achievable with a dosage of 10ndash15 mgmsup2 body surface (evidence level I recom-mendation grade A)
for other reasons (evidence level II recommen-dation grade B)
3132 Purine analogs31321 Azathioprine Efficacy has been investigat-
ed in a double blind placebo controlled study (32 patients)After 8 weeks of therapy the changes in disease activitymeasurement indicated a minor improvement in the Azathi-oprine group compared to the placebo group At the end ofthe study statistically significant differences between thegroups were found for only 2 disease activity measurements[34] Two patients were taken out of study due to severeadverse events eg leucopenia Measurement of activityof Thiopurinmethyltransferase (TPMT) can be beneficial foravoidance of severe adverse events
3133 Pyrimidine analogs31331 Leflunomide Within a double blind study
(32 weeks 94 patients) efficacy of Leflunomide was inferiorin comparison to MTX but better than placebo Howeverdosing of Leflunomide may not have been adequate insome children [35] Contraindications for Leflunomide arerenal insufficiency severe immunodeficiency depressedmyelopoesis and pancytopenia An extensive half-life peri-od (approximately 14 days) has to be taken in accountwhen administering Leflunomide In combination with hepa-totoxic DMARDs the risk of severe adverse events might in-crease eg increased blood pressure is seen frequentlySafe contraception is mandatory
3134 Antibiotic analogs and Hydroxychloroquine andChloroquine
31341 Sulfasalazine Weak efficacy of Sulfasalazinewas demonstrated within a placebo-controlled randomizedstudy after 24 weeks (96 patients) [3637] One third of pa-tients enrolled in the study discontinued treatment with Sulfa-salazine due to side effects eg gastrointestinal symptomsleucopenia [36] Some experts use sulfasalazine in HLA-B27positive JIA Contraindications are Glucose-6-phosphatase de-ficiency and hypersensitivity against sulfonamides
31342 Hydroxychloroquine and chloroquine Hydrox-ychloroquine and Chloroquine have been subject to clinical tri-als for the treatment of JIA even though efficacy was limitedWithin three consensus conferences held in 2007 and 2010 theconsensus group decided not to give a consensus statementon the use of chloroquine or hydroxychloroquine treatmentdespite the fact that those drugs still might be used by somecaregivers
3135 Biologic agents Biologic agents are drugs whichselectively inhibit cytokines cytokine receptors or directlybind to receptors of lymphocytes eg CTLA-4 CD20 Theyinclude antibodies and fusion proteins So far allbiological therapies are administered subcutaneously orintravenously
31351 TNFα-inhibitors TNFα-inhibition with Adali-mumab and Etanercept is efficient and safe (evidencelevel I) [38ndash41] Both drugs have been approved for JIAwith polyarticular course TNFα-inhibitors have become anintegral part of the treatment of JIA Potential risks of therapyare vulnerability for infection andmdashin a rare occasionmdashthe in-duction of autoimmune disease Prior to the start of treatmentwith TNFα-inhibitors chronic infections needs to be excludedor treated sufficiently eg tuberculosis hepatitis B or C
In children with JIA treated with TNFα-inhibitors malig-nancies eg Lymphoma have been reported It remainsunclear if the rate of malignancies is increased in patientscompared to the risk by having JIA itself In response to aprevious letter of the FDA (as reviewed in [42]) the GermanSociety for Pediatric Rheumatology (GKJR) has published of-ficial statements [4344] The GKJR states that treatmentwith TNFα-inhibition should be used very carefully physi-cians need to be aware of co-medication e g immunosup-pressive drugs and should monitor those patientsclosely [43] There is insufficient data on all biologicagentsmdashincluding TNFα-inhibitionmdashto judge about the long-term risk for children and adolescents313511 Etanercept Etanercept is a fusion proteinconsisting of the extracellular binding domain of solubleTNFα-receptor and Fc chain of human IgG1 Etanercept in-hibits TNFα by direct binding of the cytokine Efficacy has
Consensus statement
The use of Anakinra or Tozilizumab can berecommended for treatment of children and ado-lescents with refractory SoJIA (evidence level IIrecommendation grade A)
186 G Dueckers et al
been demonstrated in a randomized controlled withdrawaldesign trial for patients with polyarticular JIA [38] Withinan open extension study long term efficacy and safety havebeen documented over 8 years in 1669 patients [3945]There is data on more than 2000 patients registered in Euro-pean registries [46ndash48] Currently retrospective data showsa somewhat better efficacy of combining MTX or otherDMARDs with TNFα-inhibition versus anti-TNFα therapy assingle therapy [49]313512 Adalimumab Adalimumab is a humanizedmonoclonal IgG1 antibody directed against TNFα whichbinds soluble and membrane bound TNFα A randomizedcontrolled withdrawal design trial demonstrated safety andefficacy of Adalimumab (24 mgmsup2 body surface every2 weeks max 40 mg) for children and adolescents withpolyarticular JIA (4ndash17 years of age n=171) [40] After16 weeks ldquowash inrdquo phase responders (n=144171) enteredthe 32 weeks randomized double blind phase After 48 weekstwice the number of patients in the verum group met ACR 70as compared to the control group (56 vs 28 pb001)Within the open extension phase Adalimumab dosage wasfixed ie 20 mgb30 kg Bw and 40 mgN30 kg Bw There islack of evidence showing superior efficacy of combiningMTX (DMARDs) with Adalimumab versus Adalimumab as sin-gle therapy [40]
Consensus statement
Efficacy of Etanercept and Adalimumab forthe treatment of polyarticular JIA has been dem-onstrated Therapy with TNFa-inhibition is indi-cated in case of insufficient therapeutic effectof NSAIDs and local GC administration and lackof response to MTX (evidence level I recom-mendation grade A)
Consensus statement
Patients with polyarticular JIA without sys-temic manifestation refractory to treatmentwith MTX and TNF inhibition might benefit fromthe use of Abatacept (evidence level III recom-mendation grade C)
313513 Infliximab Infliximab is a chimerical (humanmouse) monoclonal antibody which binds soluble and mem-brane bound TNFα A randomized controlled study in childrenand adolescents with JIA failed to demonstrate a significantdifference of efficacy after treatment with Infliximab com-pared to placebo [31]
31352 Interleukin-1-inhibitors None of interleukin-1-inhibitors are approved for the treatment of JIA or SoJIAThey are commonly used in an off label setting313521 Anakinra Anakinra is an IL-1 receptor antag-onist Within a randomized controlled trial no significant ef-ficacy of Anakinra for patients with polyarticular JIA couldbe demonstrated [50] 50 of 86 patients were enrolled intoblinded phase (11 Anakinra versus Placebo) No significantreduction of flare could be demonstrated in comparison toplacebo 29 of 50 patients completed the open label exten-sion study Two noncontrolled nonrandomized studieshave shown efficacy of anakinra in a proportion of patientswith systemic-onset of JIA (SoJIA) [5152]313522 Canakinumab Canakinumab an IL-1β anti-body binds IL-1β selectively without interfering with IL-1αor its physiological IL-1 receptor antagonist Canakinumabhas been approved for treatment of hereditary periodic IL-1 associated periodic fever syndromes ie Cryopyrin-
associated periodic syndromes There are ongoing studies in-vestigating safety and efficacy of Canakinumab for SoJIA
31353 Interleukin-6 inhibitors313531 Tozilizumab Tozilizumab is a humanizedanti-IL-6 receptor monoclonal antibody Efficacy has beendemonstrated within a 12 week double blind randomizedcontrolled withdrawal trial in children with SoJIA (n=562ndash19 years) in Japan [53] After a 48 week open extensionstudy ACR Pedi 30 was met by 47 patients (98) At thetime of our literature search Tocilizumab was approved fortreatment of SoJIA and polyarticular JIA since 2008 inJapan A multicenter European study investigating efficacyand safety of Tozilizumab in polyarticular JIA was ongoingat the deadline of literature search (wwwclinicaltrialsgov NCT00988221) No data on long term effects are cur-rently available
31354 Co-stimulation inhibitors313541 Abatacept Abatacept is a recombinant fu-sion protein of extracellular domain of human cytotoxic T-Lymphocyte Antigen 4 (CTLA-4) and IgG1-Fc-Fragment Itmodulates T-cell co-stimulation A randomized controlleddouble blind withdrawal design study of Ruperto et al [54]demonstrated efficacy of Abatacept in patients with polyar-ticular JIA 123 of 170 participants of study were enrolled inthe 6 month double blind phase Flares occurred in 33 of 62(53) patients who were given placebo versus 12 of 60(20) Abatacept patients during double blind phase Adverseevents (AE) did not differ in both groups ie 37 AE in Abata-cept versus 34 AE in placebo recipients Some children maytake 3 to 6 months or longer before their maximal responseis achieved 3 of patients developed reaction to the infu-sion [55] Abatacept is approved by FDA and EMA for pa-tients who did not respond to prior MTX treatment Nodata of long term effects of the use of Abatacept in JIA areavailable due to the low numbers of patients treated so far
314 Autologous stem cell transplantation (SCT)There are studies on autologous SCT for treatment of re-
fractory and severe forms of JIA (evidence level III) [56] 22
Consensus statement
187Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
patients were enrolled in one study 8 reached clinical re-mission 7 were assessed as partial responders 3 experi-enced relapse of the disease and 4 (18) died as aconsequence of MAS or immunosuppressive treatment [56]Due to serious adverse events including death this thera-peutic option is seen as the last treatment option
Exercise training is recommended dependingon the extent of inflammation number of affect-ed joints and global disease activity Sports withminor stress on joints is favorable (evidence levelI recommendation grade A)
32 Non-drug based therapy
321 Physiotherapy occupational therapy and thera-peutic appliances
Physio- and occupational therapy are integral parts of thetherapeutic concept in children and adolescents with JIA[5758] Therapeutic goals of physiotherapy are relaxationand pain relief preservation or rehabilitation of physiologi-cal range of joint movement prevention of contracturesstretching and activation of muscles build-up of muscleforce and training of physiological movements
Consensus statement
Structured treatment by a properly trainedphysiotherapistoccupational therapist in combi-nation with drug based therapy and instructionsfor disease adopted self-sufficient daily exercisesessions are recommended to keep and to im-prove joint mobility (evidence level II recom-mendation grade A)Custom-made therapeutic appliances for correc-tion of axial misalignment prevention of falseweight bearing stabilization of joints (eghand- finger- and foot-ortheses) are recom-mended individually The use of therapeutic ap-pliances follows individual physician-directedadvice Efficacy has been demonstrated (evi-dence level I recommendation grade B)
Consensus statement
In individual cases the indication for open orarthroscopic synovectomy can be considered ifconservative therapy does not succeed (evi-dence level III recommendation grade B)
Consensus statement
Other forms of non-drug based therapeutic approachesrely on experts opinion and are solely based on individualclinical experience No controlled studies are available
Consensus statement
The implementation of thermotherapy electro-or ultrasound therapy massage and lymph drain-age is recommended Application of cold appli-ances for acute joint inflammation is indicated(evidence level II recommendation grade A)Electro- and ultrasound therapy are recom-mended for patients with tendosynovitis (evi-dence level III recommendation grade B)
An early psychological support within stan-dard pediatric rheumatological care should beimplemented to apprehend and treat mental is-sues and behavioral syndromes associated withphysiological disturbances and physical factors(evidence level III recommendation grade A)
Consensus statement
A socio-pedagogical care with regard tointegration at school professional andeveryday life and formal education of parentsand patients is recommended (evidence levelIII recommendation grade A)
322 Sportive activity and exercise trainingPositive impact of sportive activity on the general physi-
cal condition and on oxygen consumption has been demon-strated (evidence level II) [57ndash60] Adequate exercise
training supports the physiological development and helpscoping with JIA [58] Prospective controlled long term stud-ies are currently not available
323 Surgical treatmentToledo et al investigated the role of arthroscopic syno-
vectomy in JIA They concluded that arthroscopy is a safebut only partially effective procedure in patients witholigoarticular JIA (evidence levelrecommendation gradeIIIB) [61]
324 Psychological social intervention orsocio-pedagogical care
There are no controlled or open studies focusing on psy-chological social andor socio-pedagogical intervention inchildren or adolescents with JIA Recommendations arebased on experts opinion and personal experience solely
188 G Dueckers et al
4 Addendum
Since the deadline January 15th 2010 new papers haveappeared that are of interest in the context of our guideline[5562ndash64] in particular we refer to the ACR recommenda-tions [65] and the most recent literature on the risk of malig-nancies in JIA in context with TNF blocking agent andindependent of medication [42] [66] Moreover there is arecent study on the use of Tocilizumab in polyarticular pa-tients [67] These papers will be discussed within the nextconsensus conference by NGT and considered for inclusioninto the next edition of this guideline On 6th of September2011 our advanced search on wwwclinicaltrialgov (searchterms juvenile idiopathic arthritis recruitment open stud-ies study type interventional study age group child(birthndash17) intervention drugs) led to 16 trials which are cur-rently recruiting or will soon start recruiting
5 Discussion
To develop clinical practice guidelines of high quality andvalidity a formal consensus process and explicit methodo-logical criteria for the production of guidelines are recom-mended [68ndash70] Our guideline for the treatment of JIA inchildren and adolescents implements all these issues Thesystematic literature search was terminated on 15th January2010 leading to the most up to date guideline for JIA whichis currently available The deadline of the ACR recommenda-tions as published recently by Beukelmann et al was 5th ofOctober 2009 [65] By exclusion of case reports trials with-out control groups preliminary results published as ab-stracts on conferences and the strict graduation of theliterature by the criteria of evidence based medicine weaimed to give our guideline statements additional strengthand a maximal validity Newer original studies providing ad-ditional evidence for the treatment of JIA became availableafter our consensus process was finished see AddendumThe results of these trials have to await the next NGT beforeinclusion into our recommendations
Our updated systematic literature search in 2010 led to13 relevant studies published after 30th June 2007 (Fig 1Table 4) Their results have to be interpreted with cautionFirst trials in JIA are mainly based on limited numbers of pe-diatric patients as the recruitment of a sufficient number ofpediatric patients remains challenging Second trials aremainly designed for patients with polyarticular JIA or witholigoarticular onset and a polyarticular course (Table 4)Most children with JIA do not have a polyarticular subtypeof JIA but an oligoarticular onset and course [71] Thus pa-tients with oligoarticular JIA are heavily underrepresentedin most of the current trials Third in 5 of the 13studies the withdrawal study design has been used[4045505354] Lehmann reviewed the bias of withdrawaldesign trials in 2008 [72] After a wash-in phase only re-sponders to treatment are eligible for randomization Thusthe design preselects responders to the placebo effect whomight retain their response throughout the entire study peri-od Further there is a carryover effect of AE into the place-bo group so that significant differences in AE betweengroups may not become apparent In the one placebo con-trolled trial without withdrawal design on TNFα-inhibition
(Infliximab) no significant efficacy could be demonstratedbetween verum and placebo [31]
To our knowledge there are two other guidelines that dealwith the management of JIA as a whole (Table 6) [65] [73]Other guidelines are limited to the use of single drugs in JIAeg biologic agents [74] etanercept [75] The Australian guide-line (wwwracgporgauguidelinejuvenileidiopathicarthritis)has not been published in a peer-reviewed journal It is to pro-vide recommendations for the early diagnosis and multidisci-plinary management of JIA in the primary care setting forgeneral practitioners (GPs) [73] No recommendations aremade regarding the use of GCs DMARDs immunosuppressivedrugs or biologic agents [73] The ACR recommendations usesthe Appraisal of Guidelines for Research and Evaluation(AGREE) instrument [65] [76] which does not fulfill criteria ofa proper consensus process and carries the risk that expertsvote for peer opinion which might not reflect the true valueWe used an advanced and linguistically validated version ofthe AGREE instrument the ldquoGerman Instrument for Methodo-logical Guideline Appraisal (DELBI)rdquo which has been developedin cooperation of the AWMF among others [7778] We followedthe highly structured Nominal Group Technique as described inMethodology Our consensus group only considered formallyboard nominated representatives of multidisciplinary scientificsocieties and organizations (Table 1) and included patients rep-resentatives as this has been strongly recommended by the Eu-ropean League against Rheumatism (EULAR) recently [79] TheACR mentions a parent representative within their task forcepanel but leaves this representative anonymous It remainsunclear how ACR experts were selected and involved [65]They defined treatment groups which have not been evaluatedsystematically so far We used the ILAR classification systemwhich has been repeatedly evaluated [80ndash82]
By content there are major differences between the ACRrecommendations and our guideline a) Our guideline pro-vides a detailed and systematic list of 20 drugs commonlyused in the treatment of JIA (Table 5) which has been an in-tegrative part of our consensus conferences The ACR recom-mendations do not provide information on approval status(Food and Drug Administration) indications for use and nospecific differences on dosage regimes or frequency ofdaily application [65] eg it refers to the 2008 ACR recom-mendations for the use of DMARDs in adult rheumatoid ar-thritis b) The ACR recommendations provide a more earlyaggressive approach in the treatment of JIA The ACR recom-mends MTX as first line treatment in patients (b4 joints) withhighly active disease [65] To our knowledge there are onlydata to recommend MTX administration in cases of insuffi-cient therapeutic effect of prior treatment with NSAIDandor GC [33] c) The ACR recommends the use of TNFα in-hibitors as escalation therapy for some patients with historyof arthritis of 4 or fewer joints and refer to publications[3840] conducted in patients with polyarticular JIA or pau-ciarticular JIA with polyarticular course [65] There is no ev-idence that TNF is safe and efficient in patients witholigoarticular JIA a systematic controlled clinical trial onthis issue has not been done yet d) We regard a brief trialof local or systemic administration of GC plus NSAID as a fea-sible first line treatment for patients with polyarticular JIAThe ACR recommends MTX without regard to disease activityat the initial stage [65] We reached consensus to recom-mend the use of GC as bridging therapy until full onset of
Table 6 Overview of recommendationsguidelines for treatment of JIA
USA Australia Germany
ACR recommendations[65]
RACGP recommendations[73]
GKJR guidelines
Deadline of literature search October 2009 January 2007 September 2010Source of publications Pub Med Pub Med
EMBASE CINHAL CochraneLibrary provisionalAustralian Guideline [95]
Pub MedPrevious German Guidelines [78]
Definition used for JIA subgroups Treatment groups definedby Core expert panel
Not specifically definedChildren withJIAb16 years
ILAR criteria [1]
Consensus processprocessvalidation
AGREE [76] AGREE [76] DELBI [77]RANDUCLA appropriatenessmethod [96]
NGT Delphi method
Conferences None None 3 Formal consensus conferencesAddressees Pediatric rheumatologists General practitioner Pediatric Rheumatologists
PediatriciansGeneral practitioners
Participating scientific societies or professional organizationsPediatric rheumatologist orrheumatologists for adolescents
Yes Yes Yes
General pediatrician- In hospital Yes Yes Yes- In private practice Yes Yes YesResearcher Yes No YesRheumatologists for adults No No YesOphthalmologists No No YesParentspatients support groups Yes No YesOrthopedic surgeons No No YesPediatric orthopedic surgeons No No YesPsychologists No No YesPhysiotherapists No No YesPediatric rheumatology nurses Yes No NoOther scientific societies ororganizations
ACR BSPAR PRINTO PReS RACGP NAMSCAG NHMRC DGKJ DGPs DGRh DGO AWMFBVKJ
(ACR=American College of Rheumatologists AGREE=Appraisal of Guidelines for Research amp Development AWMF=Association of the ScientificMedical Associations BSPAR=British Society for Pediatric Rheumatology BVJK=Association of Pediatricians in private practice CEP=Core expertpanel ILAR=International League against Rheumatism CINHAL=Cumulative Index to Nursing and Allied Health Literature DELBI=German In-strument for Methodological Guideline Appraisal DGKJ=German Society of Pediatrics and Adolescent Medicine DGO=German Society for Oph-thalmology DGPs=German society for Psychology DGRh=German Society for Rheumatology GKJR=German Society for Pediatric RheumatologyNAMSCAG=National Arthritis and Musculoskeletal Conditions Advisory Group NGT=Nominal Group Technique NHMRC=National Health andMedical Research Council PReS=Pediatric Rheumatology Society) PRINTO=Pediatric Rheumatology International Trial Organization RACG-P=Royal Australian College of General Practitioner RANDUCLA=Research and DevelopmentUniversity of California at Los Angeles)
189Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
therapeutic effect of DMARDs The ACR recommendations donot provide any recommendation for the use of systemic GCfor patients with oligo- or polyarticular course of JIA exceptsystemic onset of JIA e) The ACR recommendations do notcover the topic of non-drug based therapy at all althoughthere is strong evidence that eg exercise training is a usefuladdition to drug treatment [575860]
6 Conclusion
In summary we present a treatment guideline for JIA on a con-sensus conference basis We strongly advocate an interdisciplin-ary approach including surgery physiotherapy psychosocial
intervention physical therapy medications etc and a strictformal consensus process in order to create statements thatare most appropriate for the complex clinical situation of achild and family presenting with JIA and cover all aspects ofJIA care All German pediatric rheumatology sites are partici-pating at the national pediatric rheumatologic database in theDeutsche Rheuma-Forschungszentrum at Berlin (DRFZ wwwdrfzde) It aims at quality assurance in Germany and monitorstreatment behavior of pediatric rheumatologists by using inter-nationally agreed criteria (eg joint count global physician rat-ing of disease activity global parent rating of overall well-being CHAQ ESR ACR-ped response or JADAS) The databasewill be used as a tool to monitor the application of our treat-ment guidelines
190 G Dueckers et al
Conflict of interest statement
Gregor Dueckers Novartis Pharmaceuticals CorporationBaxter (for all travel grants for scientific meetings)Nihal Guellac no conflict of interestMartin Arbogast no conflict of interestGuumlnther Dannecker no conflict of interestIvan Foeldvari Wyeth Pfizer Abbott Immunology Pharma-ceuticals Chugai (for all advisory board member)Michael Frosch no conflict of interestGerd Ganser Abbott Immunology Pharmaceuticals (advisoryboard member grants for scientific meetings) Wyeth Pfizer(advisory board member grants for scientific meetings)ChugaiRoche (advisory board member grants for scientificmeetings) Merck (grants for scientific meetings) Actelios(grants for scientific meetings) Esaote (grants for scientificmeetings)Arnd Heiligenhaus Novartis Pharmaceuticals CorporationAbbott Immunology Pharmaceuticals Alcon (for all re-search grants)Gerd Horneff Abbott Immunology Pharmaceuticals (re-search grants consulting fees non-remunerative positionsof influence) Wyeth Pfizer (research grants consultingfees speakers bureau non-remunerative positions of influ-ence) Bristol-Myers Squibb (Consulting fees) Nycomed(Consulting fees non-remunerative positions of influence)RocheChugai (Consulting fees non-remunerative positionsof influence) Sandoz (Consulting fees) Genzyme (researchgrants consulting fees non-remunerative positions of influ-ence) Swedish Orphan (research grants consulting feesnon-remunerative positions of influence)Arnold Illhardt no conflict of interestRuumldiger Krauspe no conflict of interestBarbara Markus no conflict of interestHartmut Michels Abbott Immunology Pharmaceuticals (advi-sory board member and grants for scientific meeting)Matthias Schneider no conflict of interestWolfram Singendonk no conflict of interestHelmut Sitter no conflict of interestMarianne Spamer no conflict of interestNorbert Wagner no conflict of interestTim Niehues Abbott Immunology Pharmaceuticals EssexPharma Novartis Pharmaceutical Corporation WyethPfizer (for all research grants consulting fees non-remu-nerative positions of influence)
Acknowledgment
We like to express our grateful thanks to Prof Dr Hans IkoHuppertz for proof reading the article and for an excellentdiscussion on our work We like to express our thanks to HE-LIOS Clinic for funding the open access of the article
References
[1] RE Petty TR Southwood P Manners J Baum DN Glass JGoldenberg X He J Maldonado-Cocco J Orozco-Alcala AMPrieur ME Suarez-Almazor PWoo International League of Asso-ciations for Rheumatology classification of juvenile idiopathic ar-thritis second revision Edmonton 2001 J Rheumatol 31(2004) 390ndash392
[2] B Prakken S Albani A Martini Juvenile idiopathic arthritisLancet 377 (2011) 2138ndash2149
[3] KT April DE Feldman RW Platt CM Duffy Comparisonbetween children with juvenile idiopathic arthritis (JIA) andtheir parents concerning perceived quality of life Qual LifeRes 15 (2006) 655ndash661
[4] BM Feldman B Grundland L McCullough V Wright Distinc-tion of quality of life health related quality of life and healthstatus in children referred for rheumatologic care J Rheuma-tol 27 (2000) 226ndash233
[5] JC Packham MA Hall Long-term follow-up of 246 adultswith juvenile idiopathic arthritis functional outcomeRheumatology (Oxford) 41 (2002) 1428ndash1435
[6] C Sandborg Pediatric rheumatic disease standards of care forJIAmdashthe basic foundation for quality Nat Rev Rheumatol 6(2010) 389ndash390
[7] N Guellac T Niehues Interdisciplinary and evidence-basedtreatment guideline for juvenile idiopathic arthritis KlinPadiatr 220 (2008) 392ndash402
[8] K Schnakenburg Leitlinien in der Kinder- und JugendmedizinElsevier 2005 pp H1 1ndash15
[9] P Juni L Nartey S Reichenbach R Sterchi PA Dieppe MEgger Risk of cardiovascular events and rofecoxib cumulativemeta-analysis Lancet 364 (2004) 2021ndash2029
[10] W Feldman Evidence-based Pediatrics 1st ed BC DeckersHamilton 2000
[11] AH Van de Ven AL Delbecq The nominal group as a re-search instrument for exploratory health studies Am J PublicHealth 62 (1972) 337ndash342
[12] HA Linstone M Turoff The Delphi Method Techniques andApplications Addison-Wesley Pub 1975
[13] TK Kvien HM Hoyeraal B Sandstad Naproxen and acetyl-salicylic acid in the treatment of pauciarticular and polyarticu-lar juvenile rheumatoid arthritis Assessment of tolerance andefficacy in a single-centre 24-week double-blind parallelstudy Scand J Rheumatol 13 (1984) 342ndash350
[14] RM Laxer ED Silverman C St-Cyr MT Tran G Lingam Asix-month open safety assessment of a naproxen suspensionformulation in the therapy of juvenile rheumatoid arthritisClin Ther 10 (1988) 381ndash387
[15] AM Leak MR Richter LE Clemens MA Hall BM AnsellA crossover study of naproxen diclofenac and tolmetin in sero-negative juvenile chronic arthritis Clin Exp Rheumatol 6(1988) 157ndash160
[16] J Haapasaari E Wuolijoki H Ylijoki Treatment of juve-nile rheumatoid arthritis with diclofenac sodium Scand JRheumatol 12 (1983) 325ndash330
[17] EH Giannini EJ Brewer ML Miller D Gibbas MH PassoHM Hoyeraal B Bernstein DA Person CW Fink LA Sawyeret al Ibuprofen suspension in the treatment of juvenilerheumatoid arthritis Pediatric Rheumatology CollaborativeStudy Group J Pediatr 117 (1990) 645ndash652
[18] E Stoeber L Sanger Experiences with indomethacin in long-term therapy of juvenile rheumatoid arthritis Arzneimittel-forschung 21 (1971) 1865ndash1866
[19] N Ruperto I Nikishina ED Pachanov Y Shachbazian AMPrieur R Mouy R Joos F Zulian R Schwarz V ArtamonovaW Emminger M Bandeira A Buoncompagni I Foeldvari FFalcini E Baildam I Kone-Paut M Alessio V Gerloni ALenhardt A Martini G Hanft R Sigmund S Simianer Arandomized double-blind clinical trial of two doses ofmeloxicam compared with naproxen in children with juvenileidiopathic arthritis short- and long-term efficacy and safetyresults Arthritis Rheum 52 (2005) 563ndash572
[20] I Foeldvari IS Szer LS Zemel DJ Lovell EH Giannini JLRobbins CRWest G Steidle S Krishnaswami BJ Bloom A pro-spective study comparing celecoxib with naproxen in children withjuvenile rheumatoid arthritis J Rheumatol 36 (2009) 174ndash182
191Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
[21] F Zulian G Martini D Gobber C Agosto C Gigante FZacchello Comparison of intra-articular triamcinolone hexa-cetonide and triamcinolone acetonide in oligoarticular juve-nile idiopathic arthritis Rheumatology (Oxford) 42 (2003)1254ndash1259
[22] F Zulian G Martini D Gobber M Plebani F Zacchello PManners Triamcinolone acetonide and hexacetonide intra-articular treatment of symmetrical joints in juvenile idiopathicarthritis a double-blind trial Rheumatology (Oxford) 43 (2004)1288ndash1291
[23] GS Habib Systemic effects of intra-articular corticosteroidsClin Rheumatol 28 (2009) 749ndash756
[24] JR Kirwan The effect of glucocorticoids on joint destructionin rheumatoid arthritis The Arthritis and Rheumatism CouncilLow-Dose Glucocorticoid Study Group N Engl J Med 333(1995) 142ndash146
[25] H Michels What is low-dose corticosteroid therapy in juvenileidiopathic arthritis A worldwide questionnaire-based surveyZ Rheumatol 59 (Suppl 2) (2000) II127ndash130
[26] JJ Miller III Prolonged use of large intravenous steroid pulsesin the rheumatic diseases of children Pediatrics 65 (1980)989ndash994
[27] P Picco M Gattorno A Buoncompagni V Pistoia C Borrone6-methylprednisolone lsquomini-pulsesrsquo a newmodality of glucocor-ticoid treatment in systemic onset juvenile chronic arthritisScand J Rheumatol 25 (1996) 24ndash27
[28] AM Prieur The place of corticosteroid therapy in juvenilechronic arthritis in 1992 J Rheumatol Suppl 37 (1993)32ndash34
[29] JS Gao H Wu J Tian Treatment of patients with juvenilerheumatoid arthritis with combination of leflunomide andmethotrexate Zhonghua Er Ke Za Zhi 41 (2003) 435ndash438
[30] T Niehues G Horneff H Michels MS Hock L SchuchmannEvidence-based use of methotrexate in children with rheumat-ic diseases a consensus statement of the Working Groups Pedi-atric Rheumatology Germany (AGKJR) and PediatricRheumatology Austria Rheumatol Int 25 (2005) 169ndash178
[31] N Ruperto DJ Lovell R Cuttica N Wilkinson P Woo GEspada C Wouters ED Silverman Z Balogh M HenricksonMT Apaz E Baildam A Fasth V Gerloni P Lahdenne AMPrieur A Ravelli RK Saurenmann ML Gamir N WulffraatL Marodi RE Petty R Joos F Zulian D McCurdy BLMyones K Nagy P Reuman I Szer S Travers A BeutlerG Keenan J Clark S Visvanathan A Fasanmade A Ray-chaudhuri A Mendelsohn A Martini EH Giannini A random-ized placebo-controlled trial of infliximab plus methotrexatefor the treatment of polyarticular-course juvenile rheumatoidarthritis Arthritis Rheum 56 (2007) 3096ndash3106
[32] K Visser DM van der Heijde Risk and management of livertoxicity during methotrexate treatment in rheumatoid andpsoriatic arthritis a systematic review of the literature ClinExp Rheumatol 27 (2009) 1017ndash1025
[33] A Cespedes-Cruz R Gutierrez-Suarez A Pistorio A Ravelli ALoy KJ Murray V Gerloni N Wulffraat S Oliveira J WalshIC Penades MG Alpigiani P Lahdenne C Saad-Magalhaes ECortis L Lepore Y Kimura C Wouters A Martini N RupertoMethotrexate improves the health-related quality of life of chil-dren with juvenile idiopathic arthritis Ann Rheum Dis 67(2008) 309ndash314
[34] TK Kvien HM Hoyeraal B Sandstad Azathioprine versus place-bo in patients with juvenile rheumatoid arthritis a single centerdouble blind comparative study J Rheumatol 13 (1986) 118ndash123
[35] E Silverman R Mouy L Spiegel LK Jung RK SaurenmannP Lahdenne G Horneff I Calvo IS Szer K Simpson JAStewart V Strand Leflunomide or methotrexate for juvenilerheumatoid arthritis N Engl J Med 352 (2005) 1655ndash1666
[36] MA van Rossum TJ Fiselier MJ Franssen AH ZwindermanR ten Cate LW van Suijlekom-Smit WH van Luijk RM
van Soesbergen NM Wulffraat JC Oostveen W Kuis PFDijkstra CF van Ede BA Dijkmans Sulfasalazine in the treat-ment of juvenile chronic arthritis a randomized double-blindplacebo-controlled multicenter study Dutch Juvenile ChronicArthritis Study Group Arthritis Rheum 41 (1998) 808ndash816
[37] MA van Rossum RM van Soesbergen M Boers AHZwinderman TJ Fiselier MJ Franssen R ten Cate LW vanSuijlekom-Smit NM Wulffraat WH van Luijk JC OostveenW Kuis BA Dijkmans Long-term outcome of juvenile idiopathicarthritis following a placebo-controlled trial sustained benefits ofearly sulfasalazine treatment Ann Rheum Dis 66 (2007)1518ndash1524
[38] DJ Lovell EH Giannini A Reiff GD Cawkwell ED SilvermanJJ Nocton LD Stein A Gedalia NT Ilowite CA Wallace JWhitmore BK Finck Etanercept in children with polyarticularjuvenile rheumatoid arthritis Pediatric Rheumatology Collabora-tive Study Group N Engl J Med 342 (2000) 763ndash769
[39] DJ Lovell A Reiff OY Jones R Schneider J Nocton LDStein A Gedalia NT Ilowite CA Wallace JB WhitmoreB White EH Giannini Long-term safety and efficacy ofetanercept in children with polyarticular-course juvenile rheu-matoid arthritis Arthritis Rheum 54 (2006) 1987ndash1994
[40] DJ Lovell N Ruperto S Goodman A Reiff L Jung K JarosovaD Nemcova R Mouy C Sandborg J Bohnsack D Elewaut IFoeldvari V Gerloni J Rovensky K Minden RK Vehe LWWeiner G Horneff HI Huppertz NY Olson JR Medich RCarcereri-De-Prati MJ McIlraith EH Giannini A MartiniAdalimumab with or without methotrexate in juvenile rheuma-toid arthritis N Engl J Med 359 (2008) 810ndash820
[41] FH Prince M Twilt R ten Cate MA van RossumW ArmbrustEP Hoppenreijs M van Santen-Hoeufft Y Koopman-KeeminkNM Wulffraat LW van Suijlekom-Smit Long-term follow-upon effectiveness and safety of etanercept in juvenile idiopathicarthritis the Dutch National Register Ann Rheum Dis 68(2009) 635ndash641
[42] P Diak J Siegel L LaGrenade L Choi S Lemery AMcMahonTumor necrosis factor alpha blockers andmalignancy in childrenforty-eight cases reported to the Food and Drug AdministrationArthritis Rheum 62 (2010) 2517ndash2524
[43] G Horneff T Hospach G Dannecker D Foll JP Haas HJGirschick HI Huppertz R Keitzer HJ Laws H Michels KMinden R Trauzeddel Updated statement by the German So-ciety for Pediatric and Adolescent Rheumatology (GKJR) on theFDAs report regarding malignancies in anti-TNF-treated pa-tients from Aug 4 2009 Z Rheumatol 69 (2010) 561ndash567
[44] T Hospach JP Haas HI Huppertz R Keitzer H Michels RTrauzeddl D Foll G Dannecker G Horneff Comment of theSociety of Pediatric and Adolescent Rheumatology on the USFood and Drug Administration (FDA) announcement regardingcases of malignancy in anti-TNF-treated patients Z Rheumatol68 (2009) 162ndash164
[45] DJ Lovell A Reiff NT Ilowite CA Wallace Y Chon SL LinSW Baumgartner EH Giannini Safety and efficacy of up to eightyears of continuous etanercept therapy in patients with juvenilerheumatoid arthritis Arthritis Rheum 58 (2008) 1496ndash1504
[46] EH Giannini NT Ilowite DJ Lovell CA Wallace CERabinovich A Reiff G Higgins B Gottlieb NG Singer YChon SL Lin SW Baumgartner Long-term safety and effec-tiveness of etanercept in children with selected categories ofjuvenile idiopathic arthritis Arthritis Rheum 60 (2009)2794ndash2804
[47] G Horneff H Schmeling T Biedermann I Foeldvari G GanserHJ Girschick T Hospach HI Huppertz R Keitzer RM KusterH Michels D Moebius B Rogalski A Thon The German etaner-cept registry for treatment of juvenile idiopathic arthritis AnnRheum Dis 63 (2004) 1638ndash1644
[48] FH Prince M Twilt SC Simon MA van RossumW ArmbrustEP Hoppenreijs S Kamphuis M van Santen-Hoeufft Y
192 G Dueckers et al
Koopman-Keemink NM Wulffraat R ten Cate LW vanSuijlekom-Smit When and how to stop etanercept aftersuccessful treatment of patients with juvenile idiopathic ar-thritis Ann Rheum Dis 68 (2009) 1228ndash1229
[49] G Horneff F De Bock I Foeldvari HJ Girschick H MichelsD Moebius H Schmeling Safety and efficacy of combinationof etanercept and methotrexate compared to treatment withetanercept only in patients with juvenile idiopathic arthritis(JIA) preliminary data from the German JIA Registry AnnRheum Dis 68 (2009) 519ndash525
[50] N Ilowite O Porras A Reiff S Rudge M Punaro A Martin RAllen T Harville YN Sun T Bevirt G Aras B Appleton Ana-kinra in the treatment of polyarticular-course juvenile rheumatoidarthritis safety and preliminary efficacy results of a randomizedmulticenter study Clin Rheumatol 28 (2009) 129ndash137
[51] T Lequerre P Quartier D Rosellini F Alaoui M De BandtO Mejjad I Kone-Paut M Michel E Dernis M Khellaf NLimal C Job-Deslandre B Fautrel X Le Loet J Sibilia In-terleukin-1 receptor antagonist (anakinra) treatment in pa-tients with systemic-onset juvenile idiopathic arthritis oradult onset Still disease preliminary experience in FranceAnn Rheum Dis 67 (2008) 302ndash308
[52] M Gattorno A Piccini D Lasiglie S Tassi G Brisca S CartaL Delfino F Ferlito MA Pelagatti F Caroli A BuoncompagniS Viola A Loy M Sironi A Vecchi A Ravelli A Martini ARubartelli The pattern of response to anti-interleukin-1 treatmentdistinguishes two subsets of patients with systemic-onset juvenileidiopathic arthritis Arthritis Rheum 58 (2008) 1505ndash1515
[53] S Yokota T Imagawa M Mori T Miyamae Y Aihara STakei N Iwata H Umebayashi T Murata M Miyoshi MTomiita N Nishimoto T Kishimoto Efficacy and safety oftocilizumab in patients with systemic-onset juvenile idiopathicarthritis a randomised double-blind placebo-controlledwithdrawal phase III trial Lancet 371 (2008) 998ndash1006
[54] N Ruperto DJ Lovell P Quartier E Paz N Rubio-Perez CASilva C Abud-Mendoza R Burgos-Vargas V Gerloni JAMelo-Gomes C Saad-Magalhaes F Sztajnbok C Goldenstein-Schainberg M Scheinberg IC Penades M Fischbach J OrozcoPJ Hashkes C Hom L Jung L Lepore S Oliveira CAWallace LH Sigal AJ Block A Covucci A Martini EHGiannini Abatacept in children with juvenile idiopathic arthri-tis a randomised double-blind placebo-controlled withdrawaltrial Lancet 372 (2008) 383ndash391
[55] N Ruperto DJ Lovell P Quartier E Paz N Rubio-PerezCA Silva C Abud-Mendoza R Burgos-Vargas V GerloniJA Melo-Gomes C Saad-Magalhaes J Chavez-Corrales CHuemer A Kivitz FJ Blanco I Foeldvari M Hofer G HorneffHI Huppertz C Job-Deslandre A Loy K Minden M PunaroAF Nunez LH Sigal AJ Block M Nys A Martini EHGiannini Long-term safety and efficacy of abatacept inchildren with juvenile idiopathic arthritis Arthritis Rheum 62(2010) 1792ndash1802
[56] DM Brinkman IM de Kleer R ten Cate MA van RossumWP Bekkering A Fasth MJ van Tol W Kuis NM WulffraatJM Vossen Autologous stem cell transplantation in childrenwith severe progressive systemic or polyarticular juvenile idio-pathic arthritis long-term follow-up of a prospective clinicaltrial Arthritis Rheum 56 (2007) 2410ndash2421
[57] SE Klepper Effects of an eight-week physical conditioningprogram on disease signs and symptoms in children with chronicarthritis Arthritis Care Res 12 (1999) 52ndash60
[58] D Singh-Grewal J Schneiderman-Walker V Wright O Bar-OrJ Beyene H Selvadurai B Cameron RM Laxer R SchneiderED Silverman L Spiegel S Tse C Leblanc J Wong SStephens BM Feldman The effects of vigorous exercisetraining on physical function in children with arthritis arandomized controlled single-blinded trial ArthritisRheum 57 (2007) 1202ndash1210
[59] S Stephens D Singh-Grewal O Bar-Or J Beyene B CameronCM Leblanc R Schneider J Schneiderman-Walker HSelvadurai E Silverman L Spiegel SM Tse V WrightBM Feldman Reliability of exercise testing and functionalactivity questionnaires in children with juvenile arthritisArthritis Rheum 57 (2007) 1446ndash1452
[60] T Takken J van der Net W Kuis PJ Helders Physical ac-tivity and health related physical fitness in children with ju-venile idiopathic arthritis Ann Rheum Dis 62 (2003)885ndash889
[61] MM Toledo G Martini C Gigante L Da Dalt A TregnaghiF Zulian Is there a role for arthroscopic synovectomy in oli-goarticular juvenile idiopathic arthritis J Rheumatol 33(2006) 1868ndash1872
[62] F de Benedetti H Brunner N Ruperto SWright A KenwrightR Cuttica P Woo R Schneider DJ Lovell A Martini Efficacyand safety of Tocilizumab in patients with systemic juvenile idio-pathic arthritis (sJIA) 12-week data from the phase III TENDERtrial Ann Rheum Dis 69 (2010) 146
[63] P Quartier F Allantaz R Cimaz P Pillet C Messiaen CBardin X Bossuyt A Boutten J Bienvenu A Duquesne ORicher D Chaussabel A Mogenet J Banchereau JM Tre-luyer P Landais V Pascual A multicentre randomiseddouble-blind placebo-controlled trial with the interleukin-1receptor antagonist anakinra in patients with systemic-onsetjuvenile idiopathic arthritis (ANAJIS trial) Ann Rheum Dis70 (2011) 747ndash754
[64] DE Furst EC Keystone J Braun FC Breedveld GRBurmester F De Benedetti T Dorner P Emery R FleischmannA Gibofsky JR Kalden A Kavanaugh B Kirkham P Mease JSieper NG Singer JS Smolen PL Van Riel MH Weisman KWinthrop Updated consensus statement on biological agents forthe treatment of rheumatic diseases 2010 Ann Rheum Dis 70(Suppl 1) (2010) i2ndashi36
[65] T Beukelman NM Patkar KG Saag S Tolleson-RinehartRQ Cron EM Dewitt NT Ilowite Y Kimura RM LaxerDJ Lovell A Martini CE Rabinovich N Ruperto 2011 Ameri-can College of Rheumatology recommendations for the treatmentof juvenile idiopathic arthritis initiation and safety monitoring oftherapeutic agents for the treatment of arthritis and systemic fea-tures Arthritis Care Res 63 (2011) 465ndash482 (Hoboken)
[66] JF Simard M Neovius S Hagelberg J Askling Juvenile idi-opathic arthritis and risk of cancer a nationwide cohort studyArthritis Rheum 62 (2010) 3776ndash3782
[67] T Imagawa S Yokota M Mori T Miyamae S Takei H ImanakaY Nerome N Iwata T Murata M Miyoshi N Nishimoto TKishimoto Safety and efficacy of tocilizumab an anti-IL-6-receptor monoclonal antibody in patients with polyarticular-course juvenile idiopathic arthritis Mod Rheumatol (2011)doi102007s10165-011-0481-0
[68] TM Shaneyfelt MF Mayo-Smith J Rothwangl Are guide-lines following guidelines The methodological quality of clini-cal practice guidelines in the peer-reviewed medicalliterature Jama 281 (1999) 1900ndash1905
[69] R Grilli N Magrini A Penna G Mura A Liberati Practiceguidelines developed by specialty societies the need for a crit-ical appraisal Lancet 355 (2000) 103ndash106
[70] JS Burgers R Grol NS Klazinga M Makela J Zaat To-wards evidence-based clinical practice an international surveyof 18 clinical guideline programs Int J Qual Health Care 15(2003) 31ndash45
[71] JT Cassidy RE Petty Juvenile Idiopathic Rheumatic Arthri-tis 5th Edition WB Saunders Philadelphia 2005
[72] TJ Lehman Are withdrawal trials in paediatric rheumatic dis-ease helpful Lancet 372 (2008) 348ndash350
[73] J Munro Recommendations for the Diagnosis and Managementof Juvenile Idiopathic Arthritis The Royal Australian Collegeof General Practitioners South Melbourne 2009 pp 1ndash38
193Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
httpwwwnhmrcgovau_files_nhmrcpublicationsattachmentscp119-juvenile-arthritispdf
[74] MJ Santos JE Fonseca H Canhao M Conde M JoseVieira L Costa M Costa M Salgado JA Melo Gomes Guide-lines for prescribing and monitoring biologic therapies in juve-nile idiopathic arthritis Acta Reumatol Port 32 (2007) 43ndash47
[75] S Yokota M Mori T Imagawa T Murata M Tomiita Y ItohS Fujikawa S Takei Guidelines on the use of etanercept forjuvenile idiopathic arthritis in Japan Mod Rheumatol 20(2010) 107ndash113
[76] The AGREE Collaboration Appraisal of Guidelines for Researchamp Evaluation (AGREE) instrument wwwagreecollaborationorg
[77] I Kopp H Thole T Langer HK Selbmann G OllenschlaumlgerGerman Instrument for Methodological Guideline Appraisal(DELBI) wwwversorgungsleitliniende2008
[78] Auml Aumlrztliches Zentrum fuumlr Qualitaumlt in der Medizin A Arbeitsge-meinschaften der Wissenschaftlichen Fachgesellschaften in derMedizin Deutsches Instrument zur methodischen Leitlinien-Bewertung (DELBI) Fassung 20052006 Z Aumlrztl FortbildQualitaumltssich 99 (2005) 468ndash519
[79] MP de Wit SE Berlo GJ Aanerud D Aletaha JW BijlsmaL Croucher JA Da Silva B Glusing L Gossec S Hewlett MJongkees D Magnusson M Scholte-Voshaar P Richards CZiegler TA Abma European League Against Rheumatism rec-ommendations for the inclusion of patient representatives in sci-entific projects Ann Rheum Dis 70 (2011) 722ndash726
[80] I Foeldvari M Bidde Validation of the proposed ILAR classifi-cation criteria for juvenile idiopathic arthritis InternationalLeague of Associations for Rheumatology J Rheumatol 27(2000) 1069ndash1072
[81] R Merino J de Inocencio J Garcia-Consuegra Evaluation ofrevised International League of Associations for Rheumatologyclassification criteria for juvenile idiopathic arthritis in Spanishchildren (Edmonton 2001) J Rheumatol 32 (2005) 559ndash561
[82] SE Ramsey RK Bolaria DA Cabral PN Malleson REPetty Comparison of criteria for the classification of childhoodarthritis J Rheumatol 27 (2000) 1283ndash1286
[83] G Horneff A Ebert S Fitter K Minden I Foeldvari J Kum-merle-Deschner A Thon HJ Girschick F Weller HI Hup-pertz Safety and efficacy of once weekly etanercept 08mgkg in a multicentre 12 week trial in active polyarticularcourse juvenile idiopathic arthritis Rheumatology (Oxford) 48(2009) 916ndash919
[84] EH Giannini EJ Brewer N Kuzmina A Shaikov A Maxi-mov I Vorontsov CW Fink AJ Newman JT Cassidy LSZemel Methotrexate in resistant juvenile rheumatoid arthri-tis Results of the USAndashUSSR double-blind placebo-controlled trial The Pediatric Rheumatology CollaborativeStudy Group and The Cooperative Childrens Study GroupN Engl J Med 326 (1992) 1043ndash1049
[85] A Ravelli S Viola D Migliavacca N Ruperto A Pistorio AMartini The extended oligoarticular subtype is the best predic-tor of methotrexate efficacy in juvenile idiopathic arthritisJ Pediatr 135 (1999) 316ndash320
[86] P Woo TR Southwood AM Prieur CJ Dore J Grainger JDavid C Ryder N Hasson A Hall I Lemelle Randomizedplacebo-controlled crossover trial of low-dose oral
methotrexate in children with extended oligoarticular or sys-temic arthritis Arthritis Rheum 43 (2000) 1849ndash1857
[87] E Silverman L Spiegel D Hawkins R Petty D Goldsmith LSchanberg C Duffy P Howard V Strand Long-term open-label preliminary study of the safety and efficacy of lefluno-mide in patients with polyarticular-course juvenile rheumatoidarthritis Arthritis Rheum 52 (2005) 554ndash562
[88] DJ Lovell EH Giannini Y Kimura C Suzanne PJHashkes A Reiff Long-term safety and efficacy of rilonaceptin patients with systemic juvenile idiopathic arthritis (SJIA)Arthritis Rheum 60 (2009)
[89] N Ruperto P Quartier NWulffraat PWoo A Loy R Mouy BBader-Meunier BJ Prakken E Noseda R Belleli J Lecot CRordorf A Martini A Phase II Trial with canakinumab(ACZ885) a new IL-1-beta blocking monoclonal antibody toevaluate safety and preliminary efficacy in children with system-ic juvenile idiopathic arthritis Ann Rheum Dis 68 (2009) 170
[90] DJ Lovell EH Giannini Y Kimura et al Preliminary evi-dence for bioactivity of IL-1 trap (Rilonacept) a long actingIL-1 inhibitor in systemic juvenile idiopathic arthritis (sJIA)Arthritis Rheum 54 (2006) S325
[91] DJ Lovell EH Giannini Y Kimura et al Preliminary evi-dence for sustained bioactivity of IL-1 Trap (rilonacept) a longacting IL-1 inhibitor in systemic juvenile idiopathic arthritisArthritis Rheum 56 (2007) S514
[92] N Ruperto F De Benedetti H Brunner R Allen D Brown JChaitow E Cortis G Espada B Flato V Gerloni G HorneffS Wright A Kenwright R Schneider P Woo A Martini DJLovell Tocilizumab is efficacious in patients with systemic ju-venile idiopathic arthritis (sJIA) across baseline disease charac-teristics and priorbaseline treatments 12-week data from thephase II TENDER trial 17th PReS Congress Valencia Spain2010 2010
[93] N Ruperto DJ Lovell T Li F Sztajnbok C Goldenstein-Schainberg M Scheinberg IC Penades M Fischbach JOrozco PJ Hashkes C Hom L Jung L Lepore S OliveiraC Wallace M Alessio P Quartier E Cortis A Eberhard GSimonini I Lemelle E Chalom LH Sigal A Block A CovucciM Nys A Martini EH Giannini Abatacept improves health-related quality of life pain sleep quality and daily participationin subjects with juvenile idiopathic arthritis Arthritis Care Res(Hoboken) 62 (11) (2010) 1542ndash1551
[94] N Ruperto DJ Lovell P Quartier E Paz N Rubio-PerezCA Silva C Abud-Mendoza R Burgos-Vargas V GerloniJA Melo-Gomes C Saad-Magalhaes J Chavez C HuemerA Kivitz FJ Blanco I Foeldvari M Hofer G Horneff HIHuppertz CJ Deslandre A Loy K Minden M Punaro AFNunez LH Sigal AJ Block M Nys A Martini EH GianniniLong-term safety and efficacy of abatacept in children with ju-venile idiopathic arthritis Arthritis Rheum 62 (2010)1792ndash1802
[95] J Munro Juvenile Idiopathic Arthritis Management Guidelines(Provisional) Australian Paediatric Rheumatology Group 2006httpwwwnhmrcgovau
[96] K Fitch SJ Bernstein MD Aguilar B Burnand JR LaCalleP Lazaro M van het Loo J McDonnell JP Vader JPKahan The RANDUCLA Appropriateness Method Users ManualRAND Pittsburgh 2000

Infliximab d 3ndash10 mgkg Bwdose iv Infusionat d 0 d 14 d 42 then every8 weeks intervals of applicationremain unclear
No approval for childrenwith JIA6 years (approval forMorbus Crohn)
III Ruperto [31]
b) IL-1 inhibitorsAnakinra d 1ndash4 mgkg Bwd sc in 1 dose No approval for children II Illowite [50] Lequerre [51]Canakinumab d 4 mgkg Bwsingle dose sc every
4 weeks (max 150 mg)No approval for childrenwith JIA 4 years (approvalfor CAPS)
III Ruperto [89]
Rilonacept d 1ndash2times44 mgkgweek sc (max320 mg) then 22 mgkgweek sc(max160 mg)
No approval for childrenwith JIA 12 years(approval for CAPS)
Lovell [889091]
c) IL-6 inhibitorsTocilizumab d 1 h Infusion every two 2 weeks
Bwb30 kg 8 mgkg BwN30 kg12 mgkg
2 years of age or older Since May 2011 EMA approval forpediatric patients with SoJIA who haveresponded inadequately to previoustherapy with NSAIDs and systemiccorticosteroids (Approval at Japan forSoJIA and polyarticular JIA since 2008) c
I Yokota [53] Ruperto [92]de Benedetti [62]
d) Co stimulatory-antagonistsAbatacept d 10 mgkg iv Infusion at d 0 d 14
d 28 then every 4 weeks6 years of age and older Abatacept in combination with
methotrexate is indicated for thetreatment of moderate to severe activepolyarticular (JIA) in pediatric patientswho have had an insufficient responseto other DMARDs including at least oneTNF inhibitor
I Ruperto [549394]
Abbreviations CAPS=Cryopyrine associated periodic fever syndrome JDM=juvenile dermatomyositis Bw=body weight SoJIA=systemic-onset of JIA SLE=systemic Lupus erythematodesa Compare wwwemaeuropaeub wwwrotelistede (German database of drugs with national market approval)c Intra-articular injection into same joint no more often than once every 3 monthsd A statement from insurance companies should be acquired before treatment initiation for off label treatment (if possible)e Oral application is most feasible in childhood
183Evidence
andconsensus
basedGKJR
guidelinesfor
thetreatm
entof
juvenileidiopathic
arthritis
Oligoarticular JIA
Polyarticular JIA
SoJIA
Figure 2 JIA treatment escalation schemes +=addition of the drug (abbreviations NSAIDs=non steroidal anti-inflammatory drugthotrexate)
Consensus statement
Long-term use of systemic GC is not recom-mended Continuous administration of ge02 mgPrednisolone equivalent per kg bodyweight (Bw)carries a high risk of adverse events and thereforeis not recommended (evidence level III recom-mendation grade A)
Consensus statement (continued)
184 G Dueckers et al
GC in JIA published thus leading to ldquojustrdquo evidence level IIIDifferent recommendations of dosage and therapy regimesare listed in Table 5 (evidence level III for all recommenda-tions) [1824ndash28] Frequency and seriousness of deleteriouseffects correlate mainly to duration of therapy and dosageof GC administered Main side effects are iatrogenicCushings syndrome growth disturbance weight gainmood changes Higher dosage carry the risk of increasedvulnerability to infection hypertension osteoporosisthrombosis diabetes gastro-intestinal ulceration cataractglaucoma atrophy of subcutaneous fatty tissue steroid in-duced acne To inform colleagues about GC treatment in acase of emergency and to reduce severe complications in longterm treated patients ie GC administrationN4 weeks thesupply of ldquoGlucocorticoid ID cardsrdquo for patients might be useful
GC=Glucocorticoids DMARDs=disease modifying drugs MTX=Me
Consensus statement
The systemic use of GC is recommended asfast acting drugs in highly active JIA GC areused for the treatment of children and adoles-cents with SoJIA organ manifestations of JIA(eg uveitis pericardial effusion) sero-positivepolyarticular JIA and for bridging time untilthe complete therapeutic effect of DMARDs(evidence level III recommendation grade A)
313 Methotrexate (MTX) biologic agents andimmunosuppressive agents
MTX biologic agents and immunosuppres-sive agents are used for the treatment of childrenand adolescents with polyarticular JIA ifNSAIDs or local GC treatment do not succeedThe combination of those drugs with NSAIDsand GC is feasible A common characteristic ofMTX biologic agents and immunosuppressiveagents is the delayed onset of therapeutic ef-fect ie up to 3 months or even longer aftercommencing treatment
185Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
Safe contraception is indicated during therapy with MTXAzathioprine or Leflunomide and in the following 3 to6 months after its discontinuation
Consensus statement
Administration of Sulfasalazine or Lefluno-mide is recommended if MTX or Etanercept donot show sufficient efficacy or cannot be used
3131 Methotrexate Among DMARDs MTX provides themainstay of long-term therapy in JIA [29ndash32] In case ofside effects eg dyspepsia or nausea prophylaxis withfolic acid can be recommended (1times1 mg per day or 5 mgonce a week 24ndash48 h after application of MTX) Safe contra-ception is mandatory while receiving MTX Safety and effica-cy of MTX and its impact on quality of life of children with JIAhave been investigated Significant positive impact of MTXon all health-related quality of life health conceptshas been shown although the study has its limit due to dif-ferent MTX dosages used within participating JIA patients[33]
Consensus statement
MTX administration can be recommendeddue to its proven safety and efficacy to reducedisease activity MTX is used in case of insuffi-cient therapeutic effect of NSAIDs andor localGC administration continuous need for system-ic GC andor highly active disease Efficacy ofMTX (orally or subcutaneously administered) isfrequently achievable with a dosage of 10ndash15 mgmsup2 body surface (evidence level I recom-mendation grade A)
for other reasons (evidence level II recommen-dation grade B)
3132 Purine analogs31321 Azathioprine Efficacy has been investigat-
ed in a double blind placebo controlled study (32 patients)After 8 weeks of therapy the changes in disease activitymeasurement indicated a minor improvement in the Azathi-oprine group compared to the placebo group At the end ofthe study statistically significant differences between thegroups were found for only 2 disease activity measurements[34] Two patients were taken out of study due to severeadverse events eg leucopenia Measurement of activityof Thiopurinmethyltransferase (TPMT) can be beneficial foravoidance of severe adverse events
3133 Pyrimidine analogs31331 Leflunomide Within a double blind study
(32 weeks 94 patients) efficacy of Leflunomide was inferiorin comparison to MTX but better than placebo Howeverdosing of Leflunomide may not have been adequate insome children [35] Contraindications for Leflunomide arerenal insufficiency severe immunodeficiency depressedmyelopoesis and pancytopenia An extensive half-life peri-od (approximately 14 days) has to be taken in accountwhen administering Leflunomide In combination with hepa-totoxic DMARDs the risk of severe adverse events might in-crease eg increased blood pressure is seen frequentlySafe contraception is mandatory
3134 Antibiotic analogs and Hydroxychloroquine andChloroquine
31341 Sulfasalazine Weak efficacy of Sulfasalazinewas demonstrated within a placebo-controlled randomizedstudy after 24 weeks (96 patients) [3637] One third of pa-tients enrolled in the study discontinued treatment with Sulfa-salazine due to side effects eg gastrointestinal symptomsleucopenia [36] Some experts use sulfasalazine in HLA-B27positive JIA Contraindications are Glucose-6-phosphatase de-ficiency and hypersensitivity against sulfonamides
31342 Hydroxychloroquine and chloroquine Hydrox-ychloroquine and Chloroquine have been subject to clinical tri-als for the treatment of JIA even though efficacy was limitedWithin three consensus conferences held in 2007 and 2010 theconsensus group decided not to give a consensus statementon the use of chloroquine or hydroxychloroquine treatmentdespite the fact that those drugs still might be used by somecaregivers
3135 Biologic agents Biologic agents are drugs whichselectively inhibit cytokines cytokine receptors or directlybind to receptors of lymphocytes eg CTLA-4 CD20 Theyinclude antibodies and fusion proteins So far allbiological therapies are administered subcutaneously orintravenously
31351 TNFα-inhibitors TNFα-inhibition with Adali-mumab and Etanercept is efficient and safe (evidencelevel I) [38ndash41] Both drugs have been approved for JIAwith polyarticular course TNFα-inhibitors have become anintegral part of the treatment of JIA Potential risks of therapyare vulnerability for infection andmdashin a rare occasionmdashthe in-duction of autoimmune disease Prior to the start of treatmentwith TNFα-inhibitors chronic infections needs to be excludedor treated sufficiently eg tuberculosis hepatitis B or C
In children with JIA treated with TNFα-inhibitors malig-nancies eg Lymphoma have been reported It remainsunclear if the rate of malignancies is increased in patientscompared to the risk by having JIA itself In response to aprevious letter of the FDA (as reviewed in [42]) the GermanSociety for Pediatric Rheumatology (GKJR) has published of-ficial statements [4344] The GKJR states that treatmentwith TNFα-inhibition should be used very carefully physi-cians need to be aware of co-medication e g immunosup-pressive drugs and should monitor those patientsclosely [43] There is insufficient data on all biologicagentsmdashincluding TNFα-inhibitionmdashto judge about the long-term risk for children and adolescents313511 Etanercept Etanercept is a fusion proteinconsisting of the extracellular binding domain of solubleTNFα-receptor and Fc chain of human IgG1 Etanercept in-hibits TNFα by direct binding of the cytokine Efficacy has
Consensus statement
The use of Anakinra or Tozilizumab can berecommended for treatment of children and ado-lescents with refractory SoJIA (evidence level IIrecommendation grade A)
186 G Dueckers et al
been demonstrated in a randomized controlled withdrawaldesign trial for patients with polyarticular JIA [38] Withinan open extension study long term efficacy and safety havebeen documented over 8 years in 1669 patients [3945]There is data on more than 2000 patients registered in Euro-pean registries [46ndash48] Currently retrospective data showsa somewhat better efficacy of combining MTX or otherDMARDs with TNFα-inhibition versus anti-TNFα therapy assingle therapy [49]313512 Adalimumab Adalimumab is a humanizedmonoclonal IgG1 antibody directed against TNFα whichbinds soluble and membrane bound TNFα A randomizedcontrolled withdrawal design trial demonstrated safety andefficacy of Adalimumab (24 mgmsup2 body surface every2 weeks max 40 mg) for children and adolescents withpolyarticular JIA (4ndash17 years of age n=171) [40] After16 weeks ldquowash inrdquo phase responders (n=144171) enteredthe 32 weeks randomized double blind phase After 48 weekstwice the number of patients in the verum group met ACR 70as compared to the control group (56 vs 28 pb001)Within the open extension phase Adalimumab dosage wasfixed ie 20 mgb30 kg Bw and 40 mgN30 kg Bw There islack of evidence showing superior efficacy of combiningMTX (DMARDs) with Adalimumab versus Adalimumab as sin-gle therapy [40]
Consensus statement
Efficacy of Etanercept and Adalimumab forthe treatment of polyarticular JIA has been dem-onstrated Therapy with TNFa-inhibition is indi-cated in case of insufficient therapeutic effectof NSAIDs and local GC administration and lackof response to MTX (evidence level I recom-mendation grade A)
Consensus statement
Patients with polyarticular JIA without sys-temic manifestation refractory to treatmentwith MTX and TNF inhibition might benefit fromthe use of Abatacept (evidence level III recom-mendation grade C)
313513 Infliximab Infliximab is a chimerical (humanmouse) monoclonal antibody which binds soluble and mem-brane bound TNFα A randomized controlled study in childrenand adolescents with JIA failed to demonstrate a significantdifference of efficacy after treatment with Infliximab com-pared to placebo [31]
31352 Interleukin-1-inhibitors None of interleukin-1-inhibitors are approved for the treatment of JIA or SoJIAThey are commonly used in an off label setting313521 Anakinra Anakinra is an IL-1 receptor antag-onist Within a randomized controlled trial no significant ef-ficacy of Anakinra for patients with polyarticular JIA couldbe demonstrated [50] 50 of 86 patients were enrolled intoblinded phase (11 Anakinra versus Placebo) No significantreduction of flare could be demonstrated in comparison toplacebo 29 of 50 patients completed the open label exten-sion study Two noncontrolled nonrandomized studieshave shown efficacy of anakinra in a proportion of patientswith systemic-onset of JIA (SoJIA) [5152]313522 Canakinumab Canakinumab an IL-1β anti-body binds IL-1β selectively without interfering with IL-1αor its physiological IL-1 receptor antagonist Canakinumabhas been approved for treatment of hereditary periodic IL-1 associated periodic fever syndromes ie Cryopyrin-
associated periodic syndromes There are ongoing studies in-vestigating safety and efficacy of Canakinumab for SoJIA
31353 Interleukin-6 inhibitors313531 Tozilizumab Tozilizumab is a humanizedanti-IL-6 receptor monoclonal antibody Efficacy has beendemonstrated within a 12 week double blind randomizedcontrolled withdrawal trial in children with SoJIA (n=562ndash19 years) in Japan [53] After a 48 week open extensionstudy ACR Pedi 30 was met by 47 patients (98) At thetime of our literature search Tocilizumab was approved fortreatment of SoJIA and polyarticular JIA since 2008 inJapan A multicenter European study investigating efficacyand safety of Tozilizumab in polyarticular JIA was ongoingat the deadline of literature search (wwwclinicaltrialsgov NCT00988221) No data on long term effects are cur-rently available
31354 Co-stimulation inhibitors313541 Abatacept Abatacept is a recombinant fu-sion protein of extracellular domain of human cytotoxic T-Lymphocyte Antigen 4 (CTLA-4) and IgG1-Fc-Fragment Itmodulates T-cell co-stimulation A randomized controlleddouble blind withdrawal design study of Ruperto et al [54]demonstrated efficacy of Abatacept in patients with polyar-ticular JIA 123 of 170 participants of study were enrolled inthe 6 month double blind phase Flares occurred in 33 of 62(53) patients who were given placebo versus 12 of 60(20) Abatacept patients during double blind phase Adverseevents (AE) did not differ in both groups ie 37 AE in Abata-cept versus 34 AE in placebo recipients Some children maytake 3 to 6 months or longer before their maximal responseis achieved 3 of patients developed reaction to the infu-sion [55] Abatacept is approved by FDA and EMA for pa-tients who did not respond to prior MTX treatment Nodata of long term effects of the use of Abatacept in JIA areavailable due to the low numbers of patients treated so far
314 Autologous stem cell transplantation (SCT)There are studies on autologous SCT for treatment of re-
fractory and severe forms of JIA (evidence level III) [56] 22
Consensus statement
187Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
patients were enrolled in one study 8 reached clinical re-mission 7 were assessed as partial responders 3 experi-enced relapse of the disease and 4 (18) died as aconsequence of MAS or immunosuppressive treatment [56]Due to serious adverse events including death this thera-peutic option is seen as the last treatment option
Exercise training is recommended dependingon the extent of inflammation number of affect-ed joints and global disease activity Sports withminor stress on joints is favorable (evidence levelI recommendation grade A)
32 Non-drug based therapy
321 Physiotherapy occupational therapy and thera-peutic appliances
Physio- and occupational therapy are integral parts of thetherapeutic concept in children and adolescents with JIA[5758] Therapeutic goals of physiotherapy are relaxationand pain relief preservation or rehabilitation of physiologi-cal range of joint movement prevention of contracturesstretching and activation of muscles build-up of muscleforce and training of physiological movements
Consensus statement
Structured treatment by a properly trainedphysiotherapistoccupational therapist in combi-nation with drug based therapy and instructionsfor disease adopted self-sufficient daily exercisesessions are recommended to keep and to im-prove joint mobility (evidence level II recom-mendation grade A)Custom-made therapeutic appliances for correc-tion of axial misalignment prevention of falseweight bearing stabilization of joints (eghand- finger- and foot-ortheses) are recom-mended individually The use of therapeutic ap-pliances follows individual physician-directedadvice Efficacy has been demonstrated (evi-dence level I recommendation grade B)
Consensus statement
In individual cases the indication for open orarthroscopic synovectomy can be considered ifconservative therapy does not succeed (evi-dence level III recommendation grade B)
Consensus statement
Other forms of non-drug based therapeutic approachesrely on experts opinion and are solely based on individualclinical experience No controlled studies are available
Consensus statement
The implementation of thermotherapy electro-or ultrasound therapy massage and lymph drain-age is recommended Application of cold appli-ances for acute joint inflammation is indicated(evidence level II recommendation grade A)Electro- and ultrasound therapy are recom-mended for patients with tendosynovitis (evi-dence level III recommendation grade B)
An early psychological support within stan-dard pediatric rheumatological care should beimplemented to apprehend and treat mental is-sues and behavioral syndromes associated withphysiological disturbances and physical factors(evidence level III recommendation grade A)
Consensus statement
A socio-pedagogical care with regard tointegration at school professional andeveryday life and formal education of parentsand patients is recommended (evidence levelIII recommendation grade A)
322 Sportive activity and exercise trainingPositive impact of sportive activity on the general physi-
cal condition and on oxygen consumption has been demon-strated (evidence level II) [57ndash60] Adequate exercise
training supports the physiological development and helpscoping with JIA [58] Prospective controlled long term stud-ies are currently not available
323 Surgical treatmentToledo et al investigated the role of arthroscopic syno-
vectomy in JIA They concluded that arthroscopy is a safebut only partially effective procedure in patients witholigoarticular JIA (evidence levelrecommendation gradeIIIB) [61]
324 Psychological social intervention orsocio-pedagogical care
There are no controlled or open studies focusing on psy-chological social andor socio-pedagogical intervention inchildren or adolescents with JIA Recommendations arebased on experts opinion and personal experience solely
188 G Dueckers et al
4 Addendum
Since the deadline January 15th 2010 new papers haveappeared that are of interest in the context of our guideline[5562ndash64] in particular we refer to the ACR recommenda-tions [65] and the most recent literature on the risk of malig-nancies in JIA in context with TNF blocking agent andindependent of medication [42] [66] Moreover there is arecent study on the use of Tocilizumab in polyarticular pa-tients [67] These papers will be discussed within the nextconsensus conference by NGT and considered for inclusioninto the next edition of this guideline On 6th of September2011 our advanced search on wwwclinicaltrialgov (searchterms juvenile idiopathic arthritis recruitment open stud-ies study type interventional study age group child(birthndash17) intervention drugs) led to 16 trials which are cur-rently recruiting or will soon start recruiting
5 Discussion
To develop clinical practice guidelines of high quality andvalidity a formal consensus process and explicit methodo-logical criteria for the production of guidelines are recom-mended [68ndash70] Our guideline for the treatment of JIA inchildren and adolescents implements all these issues Thesystematic literature search was terminated on 15th January2010 leading to the most up to date guideline for JIA whichis currently available The deadline of the ACR recommenda-tions as published recently by Beukelmann et al was 5th ofOctober 2009 [65] By exclusion of case reports trials with-out control groups preliminary results published as ab-stracts on conferences and the strict graduation of theliterature by the criteria of evidence based medicine weaimed to give our guideline statements additional strengthand a maximal validity Newer original studies providing ad-ditional evidence for the treatment of JIA became availableafter our consensus process was finished see AddendumThe results of these trials have to await the next NGT beforeinclusion into our recommendations
Our updated systematic literature search in 2010 led to13 relevant studies published after 30th June 2007 (Fig 1Table 4) Their results have to be interpreted with cautionFirst trials in JIA are mainly based on limited numbers of pe-diatric patients as the recruitment of a sufficient number ofpediatric patients remains challenging Second trials aremainly designed for patients with polyarticular JIA or witholigoarticular onset and a polyarticular course (Table 4)Most children with JIA do not have a polyarticular subtypeof JIA but an oligoarticular onset and course [71] Thus pa-tients with oligoarticular JIA are heavily underrepresentedin most of the current trials Third in 5 of the 13studies the withdrawal study design has been used[4045505354] Lehmann reviewed the bias of withdrawaldesign trials in 2008 [72] After a wash-in phase only re-sponders to treatment are eligible for randomization Thusthe design preselects responders to the placebo effect whomight retain their response throughout the entire study peri-od Further there is a carryover effect of AE into the place-bo group so that significant differences in AE betweengroups may not become apparent In the one placebo con-trolled trial without withdrawal design on TNFα-inhibition
(Infliximab) no significant efficacy could be demonstratedbetween verum and placebo [31]
To our knowledge there are two other guidelines that dealwith the management of JIA as a whole (Table 6) [65] [73]Other guidelines are limited to the use of single drugs in JIAeg biologic agents [74] etanercept [75] The Australian guide-line (wwwracgporgauguidelinejuvenileidiopathicarthritis)has not been published in a peer-reviewed journal It is to pro-vide recommendations for the early diagnosis and multidisci-plinary management of JIA in the primary care setting forgeneral practitioners (GPs) [73] No recommendations aremade regarding the use of GCs DMARDs immunosuppressivedrugs or biologic agents [73] The ACR recommendations usesthe Appraisal of Guidelines for Research and Evaluation(AGREE) instrument [65] [76] which does not fulfill criteria ofa proper consensus process and carries the risk that expertsvote for peer opinion which might not reflect the true valueWe used an advanced and linguistically validated version ofthe AGREE instrument the ldquoGerman Instrument for Methodo-logical Guideline Appraisal (DELBI)rdquo which has been developedin cooperation of the AWMF among others [7778] We followedthe highly structured Nominal Group Technique as described inMethodology Our consensus group only considered formallyboard nominated representatives of multidisciplinary scientificsocieties and organizations (Table 1) and included patients rep-resentatives as this has been strongly recommended by the Eu-ropean League against Rheumatism (EULAR) recently [79] TheACR mentions a parent representative within their task forcepanel but leaves this representative anonymous It remainsunclear how ACR experts were selected and involved [65]They defined treatment groups which have not been evaluatedsystematically so far We used the ILAR classification systemwhich has been repeatedly evaluated [80ndash82]
By content there are major differences between the ACRrecommendations and our guideline a) Our guideline pro-vides a detailed and systematic list of 20 drugs commonlyused in the treatment of JIA (Table 5) which has been an in-tegrative part of our consensus conferences The ACR recom-mendations do not provide information on approval status(Food and Drug Administration) indications for use and nospecific differences on dosage regimes or frequency ofdaily application [65] eg it refers to the 2008 ACR recom-mendations for the use of DMARDs in adult rheumatoid ar-thritis b) The ACR recommendations provide a more earlyaggressive approach in the treatment of JIA The ACR recom-mends MTX as first line treatment in patients (b4 joints) withhighly active disease [65] To our knowledge there are onlydata to recommend MTX administration in cases of insuffi-cient therapeutic effect of prior treatment with NSAIDandor GC [33] c) The ACR recommends the use of TNFα in-hibitors as escalation therapy for some patients with historyof arthritis of 4 or fewer joints and refer to publications[3840] conducted in patients with polyarticular JIA or pau-ciarticular JIA with polyarticular course [65] There is no ev-idence that TNF is safe and efficient in patients witholigoarticular JIA a systematic controlled clinical trial onthis issue has not been done yet d) We regard a brief trialof local or systemic administration of GC plus NSAID as a fea-sible first line treatment for patients with polyarticular JIAThe ACR recommends MTX without regard to disease activityat the initial stage [65] We reached consensus to recom-mend the use of GC as bridging therapy until full onset of
Table 6 Overview of recommendationsguidelines for treatment of JIA
USA Australia Germany
ACR recommendations[65]
RACGP recommendations[73]
GKJR guidelines
Deadline of literature search October 2009 January 2007 September 2010Source of publications Pub Med Pub Med
EMBASE CINHAL CochraneLibrary provisionalAustralian Guideline [95]
Pub MedPrevious German Guidelines [78]
Definition used for JIA subgroups Treatment groups definedby Core expert panel
Not specifically definedChildren withJIAb16 years
ILAR criteria [1]
Consensus processprocessvalidation
AGREE [76] AGREE [76] DELBI [77]RANDUCLA appropriatenessmethod [96]
NGT Delphi method
Conferences None None 3 Formal consensus conferencesAddressees Pediatric rheumatologists General practitioner Pediatric Rheumatologists
PediatriciansGeneral practitioners
Participating scientific societies or professional organizationsPediatric rheumatologist orrheumatologists for adolescents
Yes Yes Yes
General pediatrician- In hospital Yes Yes Yes- In private practice Yes Yes YesResearcher Yes No YesRheumatologists for adults No No YesOphthalmologists No No YesParentspatients support groups Yes No YesOrthopedic surgeons No No YesPediatric orthopedic surgeons No No YesPsychologists No No YesPhysiotherapists No No YesPediatric rheumatology nurses Yes No NoOther scientific societies ororganizations
ACR BSPAR PRINTO PReS RACGP NAMSCAG NHMRC DGKJ DGPs DGRh DGO AWMFBVKJ
(ACR=American College of Rheumatologists AGREE=Appraisal of Guidelines for Research amp Development AWMF=Association of the ScientificMedical Associations BSPAR=British Society for Pediatric Rheumatology BVJK=Association of Pediatricians in private practice CEP=Core expertpanel ILAR=International League against Rheumatism CINHAL=Cumulative Index to Nursing and Allied Health Literature DELBI=German In-strument for Methodological Guideline Appraisal DGKJ=German Society of Pediatrics and Adolescent Medicine DGO=German Society for Oph-thalmology DGPs=German society for Psychology DGRh=German Society for Rheumatology GKJR=German Society for Pediatric RheumatologyNAMSCAG=National Arthritis and Musculoskeletal Conditions Advisory Group NGT=Nominal Group Technique NHMRC=National Health andMedical Research Council PReS=Pediatric Rheumatology Society) PRINTO=Pediatric Rheumatology International Trial Organization RACG-P=Royal Australian College of General Practitioner RANDUCLA=Research and DevelopmentUniversity of California at Los Angeles)
189Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
therapeutic effect of DMARDs The ACR recommendations donot provide any recommendation for the use of systemic GCfor patients with oligo- or polyarticular course of JIA exceptsystemic onset of JIA e) The ACR recommendations do notcover the topic of non-drug based therapy at all althoughthere is strong evidence that eg exercise training is a usefuladdition to drug treatment [575860]
6 Conclusion
In summary we present a treatment guideline for JIA on a con-sensus conference basis We strongly advocate an interdisciplin-ary approach including surgery physiotherapy psychosocial
intervention physical therapy medications etc and a strictformal consensus process in order to create statements thatare most appropriate for the complex clinical situation of achild and family presenting with JIA and cover all aspects ofJIA care All German pediatric rheumatology sites are partici-pating at the national pediatric rheumatologic database in theDeutsche Rheuma-Forschungszentrum at Berlin (DRFZ wwwdrfzde) It aims at quality assurance in Germany and monitorstreatment behavior of pediatric rheumatologists by using inter-nationally agreed criteria (eg joint count global physician rat-ing of disease activity global parent rating of overall well-being CHAQ ESR ACR-ped response or JADAS) The databasewill be used as a tool to monitor the application of our treat-ment guidelines
190 G Dueckers et al
Conflict of interest statement
Gregor Dueckers Novartis Pharmaceuticals CorporationBaxter (for all travel grants for scientific meetings)Nihal Guellac no conflict of interestMartin Arbogast no conflict of interestGuumlnther Dannecker no conflict of interestIvan Foeldvari Wyeth Pfizer Abbott Immunology Pharma-ceuticals Chugai (for all advisory board member)Michael Frosch no conflict of interestGerd Ganser Abbott Immunology Pharmaceuticals (advisoryboard member grants for scientific meetings) Wyeth Pfizer(advisory board member grants for scientific meetings)ChugaiRoche (advisory board member grants for scientificmeetings) Merck (grants for scientific meetings) Actelios(grants for scientific meetings) Esaote (grants for scientificmeetings)Arnd Heiligenhaus Novartis Pharmaceuticals CorporationAbbott Immunology Pharmaceuticals Alcon (for all re-search grants)Gerd Horneff Abbott Immunology Pharmaceuticals (re-search grants consulting fees non-remunerative positionsof influence) Wyeth Pfizer (research grants consultingfees speakers bureau non-remunerative positions of influ-ence) Bristol-Myers Squibb (Consulting fees) Nycomed(Consulting fees non-remunerative positions of influence)RocheChugai (Consulting fees non-remunerative positionsof influence) Sandoz (Consulting fees) Genzyme (researchgrants consulting fees non-remunerative positions of influ-ence) Swedish Orphan (research grants consulting feesnon-remunerative positions of influence)Arnold Illhardt no conflict of interestRuumldiger Krauspe no conflict of interestBarbara Markus no conflict of interestHartmut Michels Abbott Immunology Pharmaceuticals (advi-sory board member and grants for scientific meeting)Matthias Schneider no conflict of interestWolfram Singendonk no conflict of interestHelmut Sitter no conflict of interestMarianne Spamer no conflict of interestNorbert Wagner no conflict of interestTim Niehues Abbott Immunology Pharmaceuticals EssexPharma Novartis Pharmaceutical Corporation WyethPfizer (for all research grants consulting fees non-remu-nerative positions of influence)
Acknowledgment
We like to express our grateful thanks to Prof Dr Hans IkoHuppertz for proof reading the article and for an excellentdiscussion on our work We like to express our thanks to HE-LIOS Clinic for funding the open access of the article
References
[1] RE Petty TR Southwood P Manners J Baum DN Glass JGoldenberg X He J Maldonado-Cocco J Orozco-Alcala AMPrieur ME Suarez-Almazor PWoo International League of Asso-ciations for Rheumatology classification of juvenile idiopathic ar-thritis second revision Edmonton 2001 J Rheumatol 31(2004) 390ndash392
[2] B Prakken S Albani A Martini Juvenile idiopathic arthritisLancet 377 (2011) 2138ndash2149
[3] KT April DE Feldman RW Platt CM Duffy Comparisonbetween children with juvenile idiopathic arthritis (JIA) andtheir parents concerning perceived quality of life Qual LifeRes 15 (2006) 655ndash661
[4] BM Feldman B Grundland L McCullough V Wright Distinc-tion of quality of life health related quality of life and healthstatus in children referred for rheumatologic care J Rheuma-tol 27 (2000) 226ndash233
[5] JC Packham MA Hall Long-term follow-up of 246 adultswith juvenile idiopathic arthritis functional outcomeRheumatology (Oxford) 41 (2002) 1428ndash1435
[6] C Sandborg Pediatric rheumatic disease standards of care forJIAmdashthe basic foundation for quality Nat Rev Rheumatol 6(2010) 389ndash390
[7] N Guellac T Niehues Interdisciplinary and evidence-basedtreatment guideline for juvenile idiopathic arthritis KlinPadiatr 220 (2008) 392ndash402
[8] K Schnakenburg Leitlinien in der Kinder- und JugendmedizinElsevier 2005 pp H1 1ndash15
[9] P Juni L Nartey S Reichenbach R Sterchi PA Dieppe MEgger Risk of cardiovascular events and rofecoxib cumulativemeta-analysis Lancet 364 (2004) 2021ndash2029
[10] W Feldman Evidence-based Pediatrics 1st ed BC DeckersHamilton 2000
[11] AH Van de Ven AL Delbecq The nominal group as a re-search instrument for exploratory health studies Am J PublicHealth 62 (1972) 337ndash342
[12] HA Linstone M Turoff The Delphi Method Techniques andApplications Addison-Wesley Pub 1975
[13] TK Kvien HM Hoyeraal B Sandstad Naproxen and acetyl-salicylic acid in the treatment of pauciarticular and polyarticu-lar juvenile rheumatoid arthritis Assessment of tolerance andefficacy in a single-centre 24-week double-blind parallelstudy Scand J Rheumatol 13 (1984) 342ndash350
[14] RM Laxer ED Silverman C St-Cyr MT Tran G Lingam Asix-month open safety assessment of a naproxen suspensionformulation in the therapy of juvenile rheumatoid arthritisClin Ther 10 (1988) 381ndash387
[15] AM Leak MR Richter LE Clemens MA Hall BM AnsellA crossover study of naproxen diclofenac and tolmetin in sero-negative juvenile chronic arthritis Clin Exp Rheumatol 6(1988) 157ndash160
[16] J Haapasaari E Wuolijoki H Ylijoki Treatment of juve-nile rheumatoid arthritis with diclofenac sodium Scand JRheumatol 12 (1983) 325ndash330
[17] EH Giannini EJ Brewer ML Miller D Gibbas MH PassoHM Hoyeraal B Bernstein DA Person CW Fink LA Sawyeret al Ibuprofen suspension in the treatment of juvenilerheumatoid arthritis Pediatric Rheumatology CollaborativeStudy Group J Pediatr 117 (1990) 645ndash652
[18] E Stoeber L Sanger Experiences with indomethacin in long-term therapy of juvenile rheumatoid arthritis Arzneimittel-forschung 21 (1971) 1865ndash1866
[19] N Ruperto I Nikishina ED Pachanov Y Shachbazian AMPrieur R Mouy R Joos F Zulian R Schwarz V ArtamonovaW Emminger M Bandeira A Buoncompagni I Foeldvari FFalcini E Baildam I Kone-Paut M Alessio V Gerloni ALenhardt A Martini G Hanft R Sigmund S Simianer Arandomized double-blind clinical trial of two doses ofmeloxicam compared with naproxen in children with juvenileidiopathic arthritis short- and long-term efficacy and safetyresults Arthritis Rheum 52 (2005) 563ndash572
[20] I Foeldvari IS Szer LS Zemel DJ Lovell EH Giannini JLRobbins CRWest G Steidle S Krishnaswami BJ Bloom A pro-spective study comparing celecoxib with naproxen in children withjuvenile rheumatoid arthritis J Rheumatol 36 (2009) 174ndash182
191Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
[21] F Zulian G Martini D Gobber C Agosto C Gigante FZacchello Comparison of intra-articular triamcinolone hexa-cetonide and triamcinolone acetonide in oligoarticular juve-nile idiopathic arthritis Rheumatology (Oxford) 42 (2003)1254ndash1259
[22] F Zulian G Martini D Gobber M Plebani F Zacchello PManners Triamcinolone acetonide and hexacetonide intra-articular treatment of symmetrical joints in juvenile idiopathicarthritis a double-blind trial Rheumatology (Oxford) 43 (2004)1288ndash1291
[23] GS Habib Systemic effects of intra-articular corticosteroidsClin Rheumatol 28 (2009) 749ndash756
[24] JR Kirwan The effect of glucocorticoids on joint destructionin rheumatoid arthritis The Arthritis and Rheumatism CouncilLow-Dose Glucocorticoid Study Group N Engl J Med 333(1995) 142ndash146
[25] H Michels What is low-dose corticosteroid therapy in juvenileidiopathic arthritis A worldwide questionnaire-based surveyZ Rheumatol 59 (Suppl 2) (2000) II127ndash130
[26] JJ Miller III Prolonged use of large intravenous steroid pulsesin the rheumatic diseases of children Pediatrics 65 (1980)989ndash994
[27] P Picco M Gattorno A Buoncompagni V Pistoia C Borrone6-methylprednisolone lsquomini-pulsesrsquo a newmodality of glucocor-ticoid treatment in systemic onset juvenile chronic arthritisScand J Rheumatol 25 (1996) 24ndash27
[28] AM Prieur The place of corticosteroid therapy in juvenilechronic arthritis in 1992 J Rheumatol Suppl 37 (1993)32ndash34
[29] JS Gao H Wu J Tian Treatment of patients with juvenilerheumatoid arthritis with combination of leflunomide andmethotrexate Zhonghua Er Ke Za Zhi 41 (2003) 435ndash438
[30] T Niehues G Horneff H Michels MS Hock L SchuchmannEvidence-based use of methotrexate in children with rheumat-ic diseases a consensus statement of the Working Groups Pedi-atric Rheumatology Germany (AGKJR) and PediatricRheumatology Austria Rheumatol Int 25 (2005) 169ndash178
[31] N Ruperto DJ Lovell R Cuttica N Wilkinson P Woo GEspada C Wouters ED Silverman Z Balogh M HenricksonMT Apaz E Baildam A Fasth V Gerloni P Lahdenne AMPrieur A Ravelli RK Saurenmann ML Gamir N WulffraatL Marodi RE Petty R Joos F Zulian D McCurdy BLMyones K Nagy P Reuman I Szer S Travers A BeutlerG Keenan J Clark S Visvanathan A Fasanmade A Ray-chaudhuri A Mendelsohn A Martini EH Giannini A random-ized placebo-controlled trial of infliximab plus methotrexatefor the treatment of polyarticular-course juvenile rheumatoidarthritis Arthritis Rheum 56 (2007) 3096ndash3106
[32] K Visser DM van der Heijde Risk and management of livertoxicity during methotrexate treatment in rheumatoid andpsoriatic arthritis a systematic review of the literature ClinExp Rheumatol 27 (2009) 1017ndash1025
[33] A Cespedes-Cruz R Gutierrez-Suarez A Pistorio A Ravelli ALoy KJ Murray V Gerloni N Wulffraat S Oliveira J WalshIC Penades MG Alpigiani P Lahdenne C Saad-Magalhaes ECortis L Lepore Y Kimura C Wouters A Martini N RupertoMethotrexate improves the health-related quality of life of chil-dren with juvenile idiopathic arthritis Ann Rheum Dis 67(2008) 309ndash314
[34] TK Kvien HM Hoyeraal B Sandstad Azathioprine versus place-bo in patients with juvenile rheumatoid arthritis a single centerdouble blind comparative study J Rheumatol 13 (1986) 118ndash123
[35] E Silverman R Mouy L Spiegel LK Jung RK SaurenmannP Lahdenne G Horneff I Calvo IS Szer K Simpson JAStewart V Strand Leflunomide or methotrexate for juvenilerheumatoid arthritis N Engl J Med 352 (2005) 1655ndash1666
[36] MA van Rossum TJ Fiselier MJ Franssen AH ZwindermanR ten Cate LW van Suijlekom-Smit WH van Luijk RM
van Soesbergen NM Wulffraat JC Oostveen W Kuis PFDijkstra CF van Ede BA Dijkmans Sulfasalazine in the treat-ment of juvenile chronic arthritis a randomized double-blindplacebo-controlled multicenter study Dutch Juvenile ChronicArthritis Study Group Arthritis Rheum 41 (1998) 808ndash816
[37] MA van Rossum RM van Soesbergen M Boers AHZwinderman TJ Fiselier MJ Franssen R ten Cate LW vanSuijlekom-Smit NM Wulffraat WH van Luijk JC OostveenW Kuis BA Dijkmans Long-term outcome of juvenile idiopathicarthritis following a placebo-controlled trial sustained benefits ofearly sulfasalazine treatment Ann Rheum Dis 66 (2007)1518ndash1524
[38] DJ Lovell EH Giannini A Reiff GD Cawkwell ED SilvermanJJ Nocton LD Stein A Gedalia NT Ilowite CA Wallace JWhitmore BK Finck Etanercept in children with polyarticularjuvenile rheumatoid arthritis Pediatric Rheumatology Collabora-tive Study Group N Engl J Med 342 (2000) 763ndash769
[39] DJ Lovell A Reiff OY Jones R Schneider J Nocton LDStein A Gedalia NT Ilowite CA Wallace JB WhitmoreB White EH Giannini Long-term safety and efficacy ofetanercept in children with polyarticular-course juvenile rheu-matoid arthritis Arthritis Rheum 54 (2006) 1987ndash1994
[40] DJ Lovell N Ruperto S Goodman A Reiff L Jung K JarosovaD Nemcova R Mouy C Sandborg J Bohnsack D Elewaut IFoeldvari V Gerloni J Rovensky K Minden RK Vehe LWWeiner G Horneff HI Huppertz NY Olson JR Medich RCarcereri-De-Prati MJ McIlraith EH Giannini A MartiniAdalimumab with or without methotrexate in juvenile rheuma-toid arthritis N Engl J Med 359 (2008) 810ndash820
[41] FH Prince M Twilt R ten Cate MA van RossumW ArmbrustEP Hoppenreijs M van Santen-Hoeufft Y Koopman-KeeminkNM Wulffraat LW van Suijlekom-Smit Long-term follow-upon effectiveness and safety of etanercept in juvenile idiopathicarthritis the Dutch National Register Ann Rheum Dis 68(2009) 635ndash641
[42] P Diak J Siegel L LaGrenade L Choi S Lemery AMcMahonTumor necrosis factor alpha blockers andmalignancy in childrenforty-eight cases reported to the Food and Drug AdministrationArthritis Rheum 62 (2010) 2517ndash2524
[43] G Horneff T Hospach G Dannecker D Foll JP Haas HJGirschick HI Huppertz R Keitzer HJ Laws H Michels KMinden R Trauzeddel Updated statement by the German So-ciety for Pediatric and Adolescent Rheumatology (GKJR) on theFDAs report regarding malignancies in anti-TNF-treated pa-tients from Aug 4 2009 Z Rheumatol 69 (2010) 561ndash567
[44] T Hospach JP Haas HI Huppertz R Keitzer H Michels RTrauzeddl D Foll G Dannecker G Horneff Comment of theSociety of Pediatric and Adolescent Rheumatology on the USFood and Drug Administration (FDA) announcement regardingcases of malignancy in anti-TNF-treated patients Z Rheumatol68 (2009) 162ndash164
[45] DJ Lovell A Reiff NT Ilowite CA Wallace Y Chon SL LinSW Baumgartner EH Giannini Safety and efficacy of up to eightyears of continuous etanercept therapy in patients with juvenilerheumatoid arthritis Arthritis Rheum 58 (2008) 1496ndash1504
[46] EH Giannini NT Ilowite DJ Lovell CA Wallace CERabinovich A Reiff G Higgins B Gottlieb NG Singer YChon SL Lin SW Baumgartner Long-term safety and effec-tiveness of etanercept in children with selected categories ofjuvenile idiopathic arthritis Arthritis Rheum 60 (2009)2794ndash2804
[47] G Horneff H Schmeling T Biedermann I Foeldvari G GanserHJ Girschick T Hospach HI Huppertz R Keitzer RM KusterH Michels D Moebius B Rogalski A Thon The German etaner-cept registry for treatment of juvenile idiopathic arthritis AnnRheum Dis 63 (2004) 1638ndash1644
[48] FH Prince M Twilt SC Simon MA van RossumW ArmbrustEP Hoppenreijs S Kamphuis M van Santen-Hoeufft Y
192 G Dueckers et al
Koopman-Keemink NM Wulffraat R ten Cate LW vanSuijlekom-Smit When and how to stop etanercept aftersuccessful treatment of patients with juvenile idiopathic ar-thritis Ann Rheum Dis 68 (2009) 1228ndash1229
[49] G Horneff F De Bock I Foeldvari HJ Girschick H MichelsD Moebius H Schmeling Safety and efficacy of combinationof etanercept and methotrexate compared to treatment withetanercept only in patients with juvenile idiopathic arthritis(JIA) preliminary data from the German JIA Registry AnnRheum Dis 68 (2009) 519ndash525
[50] N Ilowite O Porras A Reiff S Rudge M Punaro A Martin RAllen T Harville YN Sun T Bevirt G Aras B Appleton Ana-kinra in the treatment of polyarticular-course juvenile rheumatoidarthritis safety and preliminary efficacy results of a randomizedmulticenter study Clin Rheumatol 28 (2009) 129ndash137
[51] T Lequerre P Quartier D Rosellini F Alaoui M De BandtO Mejjad I Kone-Paut M Michel E Dernis M Khellaf NLimal C Job-Deslandre B Fautrel X Le Loet J Sibilia In-terleukin-1 receptor antagonist (anakinra) treatment in pa-tients with systemic-onset juvenile idiopathic arthritis oradult onset Still disease preliminary experience in FranceAnn Rheum Dis 67 (2008) 302ndash308
[52] M Gattorno A Piccini D Lasiglie S Tassi G Brisca S CartaL Delfino F Ferlito MA Pelagatti F Caroli A BuoncompagniS Viola A Loy M Sironi A Vecchi A Ravelli A Martini ARubartelli The pattern of response to anti-interleukin-1 treatmentdistinguishes two subsets of patients with systemic-onset juvenileidiopathic arthritis Arthritis Rheum 58 (2008) 1505ndash1515
[53] S Yokota T Imagawa M Mori T Miyamae Y Aihara STakei N Iwata H Umebayashi T Murata M Miyoshi MTomiita N Nishimoto T Kishimoto Efficacy and safety oftocilizumab in patients with systemic-onset juvenile idiopathicarthritis a randomised double-blind placebo-controlledwithdrawal phase III trial Lancet 371 (2008) 998ndash1006
[54] N Ruperto DJ Lovell P Quartier E Paz N Rubio-Perez CASilva C Abud-Mendoza R Burgos-Vargas V Gerloni JAMelo-Gomes C Saad-Magalhaes F Sztajnbok C Goldenstein-Schainberg M Scheinberg IC Penades M Fischbach J OrozcoPJ Hashkes C Hom L Jung L Lepore S Oliveira CAWallace LH Sigal AJ Block A Covucci A Martini EHGiannini Abatacept in children with juvenile idiopathic arthri-tis a randomised double-blind placebo-controlled withdrawaltrial Lancet 372 (2008) 383ndash391
[55] N Ruperto DJ Lovell P Quartier E Paz N Rubio-PerezCA Silva C Abud-Mendoza R Burgos-Vargas V GerloniJA Melo-Gomes C Saad-Magalhaes J Chavez-Corrales CHuemer A Kivitz FJ Blanco I Foeldvari M Hofer G HorneffHI Huppertz C Job-Deslandre A Loy K Minden M PunaroAF Nunez LH Sigal AJ Block M Nys A Martini EHGiannini Long-term safety and efficacy of abatacept inchildren with juvenile idiopathic arthritis Arthritis Rheum 62(2010) 1792ndash1802
[56] DM Brinkman IM de Kleer R ten Cate MA van RossumWP Bekkering A Fasth MJ van Tol W Kuis NM WulffraatJM Vossen Autologous stem cell transplantation in childrenwith severe progressive systemic or polyarticular juvenile idio-pathic arthritis long-term follow-up of a prospective clinicaltrial Arthritis Rheum 56 (2007) 2410ndash2421
[57] SE Klepper Effects of an eight-week physical conditioningprogram on disease signs and symptoms in children with chronicarthritis Arthritis Care Res 12 (1999) 52ndash60
[58] D Singh-Grewal J Schneiderman-Walker V Wright O Bar-OrJ Beyene H Selvadurai B Cameron RM Laxer R SchneiderED Silverman L Spiegel S Tse C Leblanc J Wong SStephens BM Feldman The effects of vigorous exercisetraining on physical function in children with arthritis arandomized controlled single-blinded trial ArthritisRheum 57 (2007) 1202ndash1210
[59] S Stephens D Singh-Grewal O Bar-Or J Beyene B CameronCM Leblanc R Schneider J Schneiderman-Walker HSelvadurai E Silverman L Spiegel SM Tse V WrightBM Feldman Reliability of exercise testing and functionalactivity questionnaires in children with juvenile arthritisArthritis Rheum 57 (2007) 1446ndash1452
[60] T Takken J van der Net W Kuis PJ Helders Physical ac-tivity and health related physical fitness in children with ju-venile idiopathic arthritis Ann Rheum Dis 62 (2003)885ndash889
[61] MM Toledo G Martini C Gigante L Da Dalt A TregnaghiF Zulian Is there a role for arthroscopic synovectomy in oli-goarticular juvenile idiopathic arthritis J Rheumatol 33(2006) 1868ndash1872
[62] F de Benedetti H Brunner N Ruperto SWright A KenwrightR Cuttica P Woo R Schneider DJ Lovell A Martini Efficacyand safety of Tocilizumab in patients with systemic juvenile idio-pathic arthritis (sJIA) 12-week data from the phase III TENDERtrial Ann Rheum Dis 69 (2010) 146
[63] P Quartier F Allantaz R Cimaz P Pillet C Messiaen CBardin X Bossuyt A Boutten J Bienvenu A Duquesne ORicher D Chaussabel A Mogenet J Banchereau JM Tre-luyer P Landais V Pascual A multicentre randomiseddouble-blind placebo-controlled trial with the interleukin-1receptor antagonist anakinra in patients with systemic-onsetjuvenile idiopathic arthritis (ANAJIS trial) Ann Rheum Dis70 (2011) 747ndash754
[64] DE Furst EC Keystone J Braun FC Breedveld GRBurmester F De Benedetti T Dorner P Emery R FleischmannA Gibofsky JR Kalden A Kavanaugh B Kirkham P Mease JSieper NG Singer JS Smolen PL Van Riel MH Weisman KWinthrop Updated consensus statement on biological agents forthe treatment of rheumatic diseases 2010 Ann Rheum Dis 70(Suppl 1) (2010) i2ndashi36
[65] T Beukelman NM Patkar KG Saag S Tolleson-RinehartRQ Cron EM Dewitt NT Ilowite Y Kimura RM LaxerDJ Lovell A Martini CE Rabinovich N Ruperto 2011 Ameri-can College of Rheumatology recommendations for the treatmentof juvenile idiopathic arthritis initiation and safety monitoring oftherapeutic agents for the treatment of arthritis and systemic fea-tures Arthritis Care Res 63 (2011) 465ndash482 (Hoboken)
[66] JF Simard M Neovius S Hagelberg J Askling Juvenile idi-opathic arthritis and risk of cancer a nationwide cohort studyArthritis Rheum 62 (2010) 3776ndash3782
[67] T Imagawa S Yokota M Mori T Miyamae S Takei H ImanakaY Nerome N Iwata T Murata M Miyoshi N Nishimoto TKishimoto Safety and efficacy of tocilizumab an anti-IL-6-receptor monoclonal antibody in patients with polyarticular-course juvenile idiopathic arthritis Mod Rheumatol (2011)doi102007s10165-011-0481-0
[68] TM Shaneyfelt MF Mayo-Smith J Rothwangl Are guide-lines following guidelines The methodological quality of clini-cal practice guidelines in the peer-reviewed medicalliterature Jama 281 (1999) 1900ndash1905
[69] R Grilli N Magrini A Penna G Mura A Liberati Practiceguidelines developed by specialty societies the need for a crit-ical appraisal Lancet 355 (2000) 103ndash106
[70] JS Burgers R Grol NS Klazinga M Makela J Zaat To-wards evidence-based clinical practice an international surveyof 18 clinical guideline programs Int J Qual Health Care 15(2003) 31ndash45
[71] JT Cassidy RE Petty Juvenile Idiopathic Rheumatic Arthri-tis 5th Edition WB Saunders Philadelphia 2005
[72] TJ Lehman Are withdrawal trials in paediatric rheumatic dis-ease helpful Lancet 372 (2008) 348ndash350
[73] J Munro Recommendations for the Diagnosis and Managementof Juvenile Idiopathic Arthritis The Royal Australian Collegeof General Practitioners South Melbourne 2009 pp 1ndash38
193Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
httpwwwnhmrcgovau_files_nhmrcpublicationsattachmentscp119-juvenile-arthritispdf
[74] MJ Santos JE Fonseca H Canhao M Conde M JoseVieira L Costa M Costa M Salgado JA Melo Gomes Guide-lines for prescribing and monitoring biologic therapies in juve-nile idiopathic arthritis Acta Reumatol Port 32 (2007) 43ndash47
[75] S Yokota M Mori T Imagawa T Murata M Tomiita Y ItohS Fujikawa S Takei Guidelines on the use of etanercept forjuvenile idiopathic arthritis in Japan Mod Rheumatol 20(2010) 107ndash113
[76] The AGREE Collaboration Appraisal of Guidelines for Researchamp Evaluation (AGREE) instrument wwwagreecollaborationorg
[77] I Kopp H Thole T Langer HK Selbmann G OllenschlaumlgerGerman Instrument for Methodological Guideline Appraisal(DELBI) wwwversorgungsleitliniende2008
[78] Auml Aumlrztliches Zentrum fuumlr Qualitaumlt in der Medizin A Arbeitsge-meinschaften der Wissenschaftlichen Fachgesellschaften in derMedizin Deutsches Instrument zur methodischen Leitlinien-Bewertung (DELBI) Fassung 20052006 Z Aumlrztl FortbildQualitaumltssich 99 (2005) 468ndash519
[79] MP de Wit SE Berlo GJ Aanerud D Aletaha JW BijlsmaL Croucher JA Da Silva B Glusing L Gossec S Hewlett MJongkees D Magnusson M Scholte-Voshaar P Richards CZiegler TA Abma European League Against Rheumatism rec-ommendations for the inclusion of patient representatives in sci-entific projects Ann Rheum Dis 70 (2011) 722ndash726
[80] I Foeldvari M Bidde Validation of the proposed ILAR classifi-cation criteria for juvenile idiopathic arthritis InternationalLeague of Associations for Rheumatology J Rheumatol 27(2000) 1069ndash1072
[81] R Merino J de Inocencio J Garcia-Consuegra Evaluation ofrevised International League of Associations for Rheumatologyclassification criteria for juvenile idiopathic arthritis in Spanishchildren (Edmonton 2001) J Rheumatol 32 (2005) 559ndash561
[82] SE Ramsey RK Bolaria DA Cabral PN Malleson REPetty Comparison of criteria for the classification of childhoodarthritis J Rheumatol 27 (2000) 1283ndash1286
[83] G Horneff A Ebert S Fitter K Minden I Foeldvari J Kum-merle-Deschner A Thon HJ Girschick F Weller HI Hup-pertz Safety and efficacy of once weekly etanercept 08mgkg in a multicentre 12 week trial in active polyarticularcourse juvenile idiopathic arthritis Rheumatology (Oxford) 48(2009) 916ndash919
[84] EH Giannini EJ Brewer N Kuzmina A Shaikov A Maxi-mov I Vorontsov CW Fink AJ Newman JT Cassidy LSZemel Methotrexate in resistant juvenile rheumatoid arthri-tis Results of the USAndashUSSR double-blind placebo-controlled trial The Pediatric Rheumatology CollaborativeStudy Group and The Cooperative Childrens Study GroupN Engl J Med 326 (1992) 1043ndash1049
[85] A Ravelli S Viola D Migliavacca N Ruperto A Pistorio AMartini The extended oligoarticular subtype is the best predic-tor of methotrexate efficacy in juvenile idiopathic arthritisJ Pediatr 135 (1999) 316ndash320
[86] P Woo TR Southwood AM Prieur CJ Dore J Grainger JDavid C Ryder N Hasson A Hall I Lemelle Randomizedplacebo-controlled crossover trial of low-dose oral
methotrexate in children with extended oligoarticular or sys-temic arthritis Arthritis Rheum 43 (2000) 1849ndash1857
[87] E Silverman L Spiegel D Hawkins R Petty D Goldsmith LSchanberg C Duffy P Howard V Strand Long-term open-label preliminary study of the safety and efficacy of lefluno-mide in patients with polyarticular-course juvenile rheumatoidarthritis Arthritis Rheum 52 (2005) 554ndash562
[88] DJ Lovell EH Giannini Y Kimura C Suzanne PJHashkes A Reiff Long-term safety and efficacy of rilonaceptin patients with systemic juvenile idiopathic arthritis (SJIA)Arthritis Rheum 60 (2009)
[89] N Ruperto P Quartier NWulffraat PWoo A Loy R Mouy BBader-Meunier BJ Prakken E Noseda R Belleli J Lecot CRordorf A Martini A Phase II Trial with canakinumab(ACZ885) a new IL-1-beta blocking monoclonal antibody toevaluate safety and preliminary efficacy in children with system-ic juvenile idiopathic arthritis Ann Rheum Dis 68 (2009) 170
[90] DJ Lovell EH Giannini Y Kimura et al Preliminary evi-dence for bioactivity of IL-1 trap (Rilonacept) a long actingIL-1 inhibitor in systemic juvenile idiopathic arthritis (sJIA)Arthritis Rheum 54 (2006) S325
[91] DJ Lovell EH Giannini Y Kimura et al Preliminary evi-dence for sustained bioactivity of IL-1 Trap (rilonacept) a longacting IL-1 inhibitor in systemic juvenile idiopathic arthritisArthritis Rheum 56 (2007) S514
[92] N Ruperto F De Benedetti H Brunner R Allen D Brown JChaitow E Cortis G Espada B Flato V Gerloni G HorneffS Wright A Kenwright R Schneider P Woo A Martini DJLovell Tocilizumab is efficacious in patients with systemic ju-venile idiopathic arthritis (sJIA) across baseline disease charac-teristics and priorbaseline treatments 12-week data from thephase II TENDER trial 17th PReS Congress Valencia Spain2010 2010
[93] N Ruperto DJ Lovell T Li F Sztajnbok C Goldenstein-Schainberg M Scheinberg IC Penades M Fischbach JOrozco PJ Hashkes C Hom L Jung L Lepore S OliveiraC Wallace M Alessio P Quartier E Cortis A Eberhard GSimonini I Lemelle E Chalom LH Sigal A Block A CovucciM Nys A Martini EH Giannini Abatacept improves health-related quality of life pain sleep quality and daily participationin subjects with juvenile idiopathic arthritis Arthritis Care Res(Hoboken) 62 (11) (2010) 1542ndash1551
[94] N Ruperto DJ Lovell P Quartier E Paz N Rubio-PerezCA Silva C Abud-Mendoza R Burgos-Vargas V GerloniJA Melo-Gomes C Saad-Magalhaes J Chavez C HuemerA Kivitz FJ Blanco I Foeldvari M Hofer G Horneff HIHuppertz CJ Deslandre A Loy K Minden M Punaro AFNunez LH Sigal AJ Block M Nys A Martini EH GianniniLong-term safety and efficacy of abatacept in children with ju-venile idiopathic arthritis Arthritis Rheum 62 (2010)1792ndash1802
[95] J Munro Juvenile Idiopathic Arthritis Management Guidelines(Provisional) Australian Paediatric Rheumatology Group 2006httpwwwnhmrcgovau
[96] K Fitch SJ Bernstein MD Aguilar B Burnand JR LaCalleP Lazaro M van het Loo J McDonnell JP Vader JPKahan The RANDUCLA Appropriateness Method Users ManualRAND Pittsburgh 2000

Oligoarticular JIA
Polyarticular JIA
SoJIA
Figure 2 JIA treatment escalation schemes +=addition of the drug (abbreviations NSAIDs=non steroidal anti-inflammatory drugthotrexate)
Consensus statement
Long-term use of systemic GC is not recom-mended Continuous administration of ge02 mgPrednisolone equivalent per kg bodyweight (Bw)carries a high risk of adverse events and thereforeis not recommended (evidence level III recom-mendation grade A)
Consensus statement (continued)
184 G Dueckers et al
GC in JIA published thus leading to ldquojustrdquo evidence level IIIDifferent recommendations of dosage and therapy regimesare listed in Table 5 (evidence level III for all recommenda-tions) [1824ndash28] Frequency and seriousness of deleteriouseffects correlate mainly to duration of therapy and dosageof GC administered Main side effects are iatrogenicCushings syndrome growth disturbance weight gainmood changes Higher dosage carry the risk of increasedvulnerability to infection hypertension osteoporosisthrombosis diabetes gastro-intestinal ulceration cataractglaucoma atrophy of subcutaneous fatty tissue steroid in-duced acne To inform colleagues about GC treatment in acase of emergency and to reduce severe complications in longterm treated patients ie GC administrationN4 weeks thesupply of ldquoGlucocorticoid ID cardsrdquo for patients might be useful
GC=Glucocorticoids DMARDs=disease modifying drugs MTX=Me
Consensus statement
The systemic use of GC is recommended asfast acting drugs in highly active JIA GC areused for the treatment of children and adoles-cents with SoJIA organ manifestations of JIA(eg uveitis pericardial effusion) sero-positivepolyarticular JIA and for bridging time untilthe complete therapeutic effect of DMARDs(evidence level III recommendation grade A)
313 Methotrexate (MTX) biologic agents andimmunosuppressive agents
MTX biologic agents and immunosuppres-sive agents are used for the treatment of childrenand adolescents with polyarticular JIA ifNSAIDs or local GC treatment do not succeedThe combination of those drugs with NSAIDsand GC is feasible A common characteristic ofMTX biologic agents and immunosuppressiveagents is the delayed onset of therapeutic ef-fect ie up to 3 months or even longer aftercommencing treatment
185Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
Safe contraception is indicated during therapy with MTXAzathioprine or Leflunomide and in the following 3 to6 months after its discontinuation
Consensus statement
Administration of Sulfasalazine or Lefluno-mide is recommended if MTX or Etanercept donot show sufficient efficacy or cannot be used
3131 Methotrexate Among DMARDs MTX provides themainstay of long-term therapy in JIA [29ndash32] In case ofside effects eg dyspepsia or nausea prophylaxis withfolic acid can be recommended (1times1 mg per day or 5 mgonce a week 24ndash48 h after application of MTX) Safe contra-ception is mandatory while receiving MTX Safety and effica-cy of MTX and its impact on quality of life of children with JIAhave been investigated Significant positive impact of MTXon all health-related quality of life health conceptshas been shown although the study has its limit due to dif-ferent MTX dosages used within participating JIA patients[33]
Consensus statement
MTX administration can be recommendeddue to its proven safety and efficacy to reducedisease activity MTX is used in case of insuffi-cient therapeutic effect of NSAIDs andor localGC administration continuous need for system-ic GC andor highly active disease Efficacy ofMTX (orally or subcutaneously administered) isfrequently achievable with a dosage of 10ndash15 mgmsup2 body surface (evidence level I recom-mendation grade A)
for other reasons (evidence level II recommen-dation grade B)
3132 Purine analogs31321 Azathioprine Efficacy has been investigat-
ed in a double blind placebo controlled study (32 patients)After 8 weeks of therapy the changes in disease activitymeasurement indicated a minor improvement in the Azathi-oprine group compared to the placebo group At the end ofthe study statistically significant differences between thegroups were found for only 2 disease activity measurements[34] Two patients were taken out of study due to severeadverse events eg leucopenia Measurement of activityof Thiopurinmethyltransferase (TPMT) can be beneficial foravoidance of severe adverse events
3133 Pyrimidine analogs31331 Leflunomide Within a double blind study
(32 weeks 94 patients) efficacy of Leflunomide was inferiorin comparison to MTX but better than placebo Howeverdosing of Leflunomide may not have been adequate insome children [35] Contraindications for Leflunomide arerenal insufficiency severe immunodeficiency depressedmyelopoesis and pancytopenia An extensive half-life peri-od (approximately 14 days) has to be taken in accountwhen administering Leflunomide In combination with hepa-totoxic DMARDs the risk of severe adverse events might in-crease eg increased blood pressure is seen frequentlySafe contraception is mandatory
3134 Antibiotic analogs and Hydroxychloroquine andChloroquine
31341 Sulfasalazine Weak efficacy of Sulfasalazinewas demonstrated within a placebo-controlled randomizedstudy after 24 weeks (96 patients) [3637] One third of pa-tients enrolled in the study discontinued treatment with Sulfa-salazine due to side effects eg gastrointestinal symptomsleucopenia [36] Some experts use sulfasalazine in HLA-B27positive JIA Contraindications are Glucose-6-phosphatase de-ficiency and hypersensitivity against sulfonamides
31342 Hydroxychloroquine and chloroquine Hydrox-ychloroquine and Chloroquine have been subject to clinical tri-als for the treatment of JIA even though efficacy was limitedWithin three consensus conferences held in 2007 and 2010 theconsensus group decided not to give a consensus statementon the use of chloroquine or hydroxychloroquine treatmentdespite the fact that those drugs still might be used by somecaregivers
3135 Biologic agents Biologic agents are drugs whichselectively inhibit cytokines cytokine receptors or directlybind to receptors of lymphocytes eg CTLA-4 CD20 Theyinclude antibodies and fusion proteins So far allbiological therapies are administered subcutaneously orintravenously
31351 TNFα-inhibitors TNFα-inhibition with Adali-mumab and Etanercept is efficient and safe (evidencelevel I) [38ndash41] Both drugs have been approved for JIAwith polyarticular course TNFα-inhibitors have become anintegral part of the treatment of JIA Potential risks of therapyare vulnerability for infection andmdashin a rare occasionmdashthe in-duction of autoimmune disease Prior to the start of treatmentwith TNFα-inhibitors chronic infections needs to be excludedor treated sufficiently eg tuberculosis hepatitis B or C
In children with JIA treated with TNFα-inhibitors malig-nancies eg Lymphoma have been reported It remainsunclear if the rate of malignancies is increased in patientscompared to the risk by having JIA itself In response to aprevious letter of the FDA (as reviewed in [42]) the GermanSociety for Pediatric Rheumatology (GKJR) has published of-ficial statements [4344] The GKJR states that treatmentwith TNFα-inhibition should be used very carefully physi-cians need to be aware of co-medication e g immunosup-pressive drugs and should monitor those patientsclosely [43] There is insufficient data on all biologicagentsmdashincluding TNFα-inhibitionmdashto judge about the long-term risk for children and adolescents313511 Etanercept Etanercept is a fusion proteinconsisting of the extracellular binding domain of solubleTNFα-receptor and Fc chain of human IgG1 Etanercept in-hibits TNFα by direct binding of the cytokine Efficacy has
Consensus statement
The use of Anakinra or Tozilizumab can berecommended for treatment of children and ado-lescents with refractory SoJIA (evidence level IIrecommendation grade A)
186 G Dueckers et al
been demonstrated in a randomized controlled withdrawaldesign trial for patients with polyarticular JIA [38] Withinan open extension study long term efficacy and safety havebeen documented over 8 years in 1669 patients [3945]There is data on more than 2000 patients registered in Euro-pean registries [46ndash48] Currently retrospective data showsa somewhat better efficacy of combining MTX or otherDMARDs with TNFα-inhibition versus anti-TNFα therapy assingle therapy [49]313512 Adalimumab Adalimumab is a humanizedmonoclonal IgG1 antibody directed against TNFα whichbinds soluble and membrane bound TNFα A randomizedcontrolled withdrawal design trial demonstrated safety andefficacy of Adalimumab (24 mgmsup2 body surface every2 weeks max 40 mg) for children and adolescents withpolyarticular JIA (4ndash17 years of age n=171) [40] After16 weeks ldquowash inrdquo phase responders (n=144171) enteredthe 32 weeks randomized double blind phase After 48 weekstwice the number of patients in the verum group met ACR 70as compared to the control group (56 vs 28 pb001)Within the open extension phase Adalimumab dosage wasfixed ie 20 mgb30 kg Bw and 40 mgN30 kg Bw There islack of evidence showing superior efficacy of combiningMTX (DMARDs) with Adalimumab versus Adalimumab as sin-gle therapy [40]
Consensus statement
Efficacy of Etanercept and Adalimumab forthe treatment of polyarticular JIA has been dem-onstrated Therapy with TNFa-inhibition is indi-cated in case of insufficient therapeutic effectof NSAIDs and local GC administration and lackof response to MTX (evidence level I recom-mendation grade A)
Consensus statement
Patients with polyarticular JIA without sys-temic manifestation refractory to treatmentwith MTX and TNF inhibition might benefit fromthe use of Abatacept (evidence level III recom-mendation grade C)
313513 Infliximab Infliximab is a chimerical (humanmouse) monoclonal antibody which binds soluble and mem-brane bound TNFα A randomized controlled study in childrenand adolescents with JIA failed to demonstrate a significantdifference of efficacy after treatment with Infliximab com-pared to placebo [31]
31352 Interleukin-1-inhibitors None of interleukin-1-inhibitors are approved for the treatment of JIA or SoJIAThey are commonly used in an off label setting313521 Anakinra Anakinra is an IL-1 receptor antag-onist Within a randomized controlled trial no significant ef-ficacy of Anakinra for patients with polyarticular JIA couldbe demonstrated [50] 50 of 86 patients were enrolled intoblinded phase (11 Anakinra versus Placebo) No significantreduction of flare could be demonstrated in comparison toplacebo 29 of 50 patients completed the open label exten-sion study Two noncontrolled nonrandomized studieshave shown efficacy of anakinra in a proportion of patientswith systemic-onset of JIA (SoJIA) [5152]313522 Canakinumab Canakinumab an IL-1β anti-body binds IL-1β selectively without interfering with IL-1αor its physiological IL-1 receptor antagonist Canakinumabhas been approved for treatment of hereditary periodic IL-1 associated periodic fever syndromes ie Cryopyrin-
associated periodic syndromes There are ongoing studies in-vestigating safety and efficacy of Canakinumab for SoJIA
31353 Interleukin-6 inhibitors313531 Tozilizumab Tozilizumab is a humanizedanti-IL-6 receptor monoclonal antibody Efficacy has beendemonstrated within a 12 week double blind randomizedcontrolled withdrawal trial in children with SoJIA (n=562ndash19 years) in Japan [53] After a 48 week open extensionstudy ACR Pedi 30 was met by 47 patients (98) At thetime of our literature search Tocilizumab was approved fortreatment of SoJIA and polyarticular JIA since 2008 inJapan A multicenter European study investigating efficacyand safety of Tozilizumab in polyarticular JIA was ongoingat the deadline of literature search (wwwclinicaltrialsgov NCT00988221) No data on long term effects are cur-rently available
31354 Co-stimulation inhibitors313541 Abatacept Abatacept is a recombinant fu-sion protein of extracellular domain of human cytotoxic T-Lymphocyte Antigen 4 (CTLA-4) and IgG1-Fc-Fragment Itmodulates T-cell co-stimulation A randomized controlleddouble blind withdrawal design study of Ruperto et al [54]demonstrated efficacy of Abatacept in patients with polyar-ticular JIA 123 of 170 participants of study were enrolled inthe 6 month double blind phase Flares occurred in 33 of 62(53) patients who were given placebo versus 12 of 60(20) Abatacept patients during double blind phase Adverseevents (AE) did not differ in both groups ie 37 AE in Abata-cept versus 34 AE in placebo recipients Some children maytake 3 to 6 months or longer before their maximal responseis achieved 3 of patients developed reaction to the infu-sion [55] Abatacept is approved by FDA and EMA for pa-tients who did not respond to prior MTX treatment Nodata of long term effects of the use of Abatacept in JIA areavailable due to the low numbers of patients treated so far
314 Autologous stem cell transplantation (SCT)There are studies on autologous SCT for treatment of re-
fractory and severe forms of JIA (evidence level III) [56] 22
Consensus statement
187Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
patients were enrolled in one study 8 reached clinical re-mission 7 were assessed as partial responders 3 experi-enced relapse of the disease and 4 (18) died as aconsequence of MAS or immunosuppressive treatment [56]Due to serious adverse events including death this thera-peutic option is seen as the last treatment option
Exercise training is recommended dependingon the extent of inflammation number of affect-ed joints and global disease activity Sports withminor stress on joints is favorable (evidence levelI recommendation grade A)
32 Non-drug based therapy
321 Physiotherapy occupational therapy and thera-peutic appliances
Physio- and occupational therapy are integral parts of thetherapeutic concept in children and adolescents with JIA[5758] Therapeutic goals of physiotherapy are relaxationand pain relief preservation or rehabilitation of physiologi-cal range of joint movement prevention of contracturesstretching and activation of muscles build-up of muscleforce and training of physiological movements
Consensus statement
Structured treatment by a properly trainedphysiotherapistoccupational therapist in combi-nation with drug based therapy and instructionsfor disease adopted self-sufficient daily exercisesessions are recommended to keep and to im-prove joint mobility (evidence level II recom-mendation grade A)Custom-made therapeutic appliances for correc-tion of axial misalignment prevention of falseweight bearing stabilization of joints (eghand- finger- and foot-ortheses) are recom-mended individually The use of therapeutic ap-pliances follows individual physician-directedadvice Efficacy has been demonstrated (evi-dence level I recommendation grade B)
Consensus statement
In individual cases the indication for open orarthroscopic synovectomy can be considered ifconservative therapy does not succeed (evi-dence level III recommendation grade B)
Consensus statement
Other forms of non-drug based therapeutic approachesrely on experts opinion and are solely based on individualclinical experience No controlled studies are available
Consensus statement
The implementation of thermotherapy electro-or ultrasound therapy massage and lymph drain-age is recommended Application of cold appli-ances for acute joint inflammation is indicated(evidence level II recommendation grade A)Electro- and ultrasound therapy are recom-mended for patients with tendosynovitis (evi-dence level III recommendation grade B)
An early psychological support within stan-dard pediatric rheumatological care should beimplemented to apprehend and treat mental is-sues and behavioral syndromes associated withphysiological disturbances and physical factors(evidence level III recommendation grade A)
Consensus statement
A socio-pedagogical care with regard tointegration at school professional andeveryday life and formal education of parentsand patients is recommended (evidence levelIII recommendation grade A)
322 Sportive activity and exercise trainingPositive impact of sportive activity on the general physi-
cal condition and on oxygen consumption has been demon-strated (evidence level II) [57ndash60] Adequate exercise
training supports the physiological development and helpscoping with JIA [58] Prospective controlled long term stud-ies are currently not available
323 Surgical treatmentToledo et al investigated the role of arthroscopic syno-
vectomy in JIA They concluded that arthroscopy is a safebut only partially effective procedure in patients witholigoarticular JIA (evidence levelrecommendation gradeIIIB) [61]
324 Psychological social intervention orsocio-pedagogical care
There are no controlled or open studies focusing on psy-chological social andor socio-pedagogical intervention inchildren or adolescents with JIA Recommendations arebased on experts opinion and personal experience solely
188 G Dueckers et al
4 Addendum
Since the deadline January 15th 2010 new papers haveappeared that are of interest in the context of our guideline[5562ndash64] in particular we refer to the ACR recommenda-tions [65] and the most recent literature on the risk of malig-nancies in JIA in context with TNF blocking agent andindependent of medication [42] [66] Moreover there is arecent study on the use of Tocilizumab in polyarticular pa-tients [67] These papers will be discussed within the nextconsensus conference by NGT and considered for inclusioninto the next edition of this guideline On 6th of September2011 our advanced search on wwwclinicaltrialgov (searchterms juvenile idiopathic arthritis recruitment open stud-ies study type interventional study age group child(birthndash17) intervention drugs) led to 16 trials which are cur-rently recruiting or will soon start recruiting
5 Discussion
To develop clinical practice guidelines of high quality andvalidity a formal consensus process and explicit methodo-logical criteria for the production of guidelines are recom-mended [68ndash70] Our guideline for the treatment of JIA inchildren and adolescents implements all these issues Thesystematic literature search was terminated on 15th January2010 leading to the most up to date guideline for JIA whichis currently available The deadline of the ACR recommenda-tions as published recently by Beukelmann et al was 5th ofOctober 2009 [65] By exclusion of case reports trials with-out control groups preliminary results published as ab-stracts on conferences and the strict graduation of theliterature by the criteria of evidence based medicine weaimed to give our guideline statements additional strengthand a maximal validity Newer original studies providing ad-ditional evidence for the treatment of JIA became availableafter our consensus process was finished see AddendumThe results of these trials have to await the next NGT beforeinclusion into our recommendations
Our updated systematic literature search in 2010 led to13 relevant studies published after 30th June 2007 (Fig 1Table 4) Their results have to be interpreted with cautionFirst trials in JIA are mainly based on limited numbers of pe-diatric patients as the recruitment of a sufficient number ofpediatric patients remains challenging Second trials aremainly designed for patients with polyarticular JIA or witholigoarticular onset and a polyarticular course (Table 4)Most children with JIA do not have a polyarticular subtypeof JIA but an oligoarticular onset and course [71] Thus pa-tients with oligoarticular JIA are heavily underrepresentedin most of the current trials Third in 5 of the 13studies the withdrawal study design has been used[4045505354] Lehmann reviewed the bias of withdrawaldesign trials in 2008 [72] After a wash-in phase only re-sponders to treatment are eligible for randomization Thusthe design preselects responders to the placebo effect whomight retain their response throughout the entire study peri-od Further there is a carryover effect of AE into the place-bo group so that significant differences in AE betweengroups may not become apparent In the one placebo con-trolled trial without withdrawal design on TNFα-inhibition
(Infliximab) no significant efficacy could be demonstratedbetween verum and placebo [31]
To our knowledge there are two other guidelines that dealwith the management of JIA as a whole (Table 6) [65] [73]Other guidelines are limited to the use of single drugs in JIAeg biologic agents [74] etanercept [75] The Australian guide-line (wwwracgporgauguidelinejuvenileidiopathicarthritis)has not been published in a peer-reviewed journal It is to pro-vide recommendations for the early diagnosis and multidisci-plinary management of JIA in the primary care setting forgeneral practitioners (GPs) [73] No recommendations aremade regarding the use of GCs DMARDs immunosuppressivedrugs or biologic agents [73] The ACR recommendations usesthe Appraisal of Guidelines for Research and Evaluation(AGREE) instrument [65] [76] which does not fulfill criteria ofa proper consensus process and carries the risk that expertsvote for peer opinion which might not reflect the true valueWe used an advanced and linguistically validated version ofthe AGREE instrument the ldquoGerman Instrument for Methodo-logical Guideline Appraisal (DELBI)rdquo which has been developedin cooperation of the AWMF among others [7778] We followedthe highly structured Nominal Group Technique as described inMethodology Our consensus group only considered formallyboard nominated representatives of multidisciplinary scientificsocieties and organizations (Table 1) and included patients rep-resentatives as this has been strongly recommended by the Eu-ropean League against Rheumatism (EULAR) recently [79] TheACR mentions a parent representative within their task forcepanel but leaves this representative anonymous It remainsunclear how ACR experts were selected and involved [65]They defined treatment groups which have not been evaluatedsystematically so far We used the ILAR classification systemwhich has been repeatedly evaluated [80ndash82]
By content there are major differences between the ACRrecommendations and our guideline a) Our guideline pro-vides a detailed and systematic list of 20 drugs commonlyused in the treatment of JIA (Table 5) which has been an in-tegrative part of our consensus conferences The ACR recom-mendations do not provide information on approval status(Food and Drug Administration) indications for use and nospecific differences on dosage regimes or frequency ofdaily application [65] eg it refers to the 2008 ACR recom-mendations for the use of DMARDs in adult rheumatoid ar-thritis b) The ACR recommendations provide a more earlyaggressive approach in the treatment of JIA The ACR recom-mends MTX as first line treatment in patients (b4 joints) withhighly active disease [65] To our knowledge there are onlydata to recommend MTX administration in cases of insuffi-cient therapeutic effect of prior treatment with NSAIDandor GC [33] c) The ACR recommends the use of TNFα in-hibitors as escalation therapy for some patients with historyof arthritis of 4 or fewer joints and refer to publications[3840] conducted in patients with polyarticular JIA or pau-ciarticular JIA with polyarticular course [65] There is no ev-idence that TNF is safe and efficient in patients witholigoarticular JIA a systematic controlled clinical trial onthis issue has not been done yet d) We regard a brief trialof local or systemic administration of GC plus NSAID as a fea-sible first line treatment for patients with polyarticular JIAThe ACR recommends MTX without regard to disease activityat the initial stage [65] We reached consensus to recom-mend the use of GC as bridging therapy until full onset of
Table 6 Overview of recommendationsguidelines for treatment of JIA
USA Australia Germany
ACR recommendations[65]
RACGP recommendations[73]
GKJR guidelines
Deadline of literature search October 2009 January 2007 September 2010Source of publications Pub Med Pub Med
EMBASE CINHAL CochraneLibrary provisionalAustralian Guideline [95]
Pub MedPrevious German Guidelines [78]
Definition used for JIA subgroups Treatment groups definedby Core expert panel
Not specifically definedChildren withJIAb16 years
ILAR criteria [1]
Consensus processprocessvalidation
AGREE [76] AGREE [76] DELBI [77]RANDUCLA appropriatenessmethod [96]
NGT Delphi method
Conferences None None 3 Formal consensus conferencesAddressees Pediatric rheumatologists General practitioner Pediatric Rheumatologists
PediatriciansGeneral practitioners
Participating scientific societies or professional organizationsPediatric rheumatologist orrheumatologists for adolescents
Yes Yes Yes
General pediatrician- In hospital Yes Yes Yes- In private practice Yes Yes YesResearcher Yes No YesRheumatologists for adults No No YesOphthalmologists No No YesParentspatients support groups Yes No YesOrthopedic surgeons No No YesPediatric orthopedic surgeons No No YesPsychologists No No YesPhysiotherapists No No YesPediatric rheumatology nurses Yes No NoOther scientific societies ororganizations
ACR BSPAR PRINTO PReS RACGP NAMSCAG NHMRC DGKJ DGPs DGRh DGO AWMFBVKJ
(ACR=American College of Rheumatologists AGREE=Appraisal of Guidelines for Research amp Development AWMF=Association of the ScientificMedical Associations BSPAR=British Society for Pediatric Rheumatology BVJK=Association of Pediatricians in private practice CEP=Core expertpanel ILAR=International League against Rheumatism CINHAL=Cumulative Index to Nursing and Allied Health Literature DELBI=German In-strument for Methodological Guideline Appraisal DGKJ=German Society of Pediatrics and Adolescent Medicine DGO=German Society for Oph-thalmology DGPs=German society for Psychology DGRh=German Society for Rheumatology GKJR=German Society for Pediatric RheumatologyNAMSCAG=National Arthritis and Musculoskeletal Conditions Advisory Group NGT=Nominal Group Technique NHMRC=National Health andMedical Research Council PReS=Pediatric Rheumatology Society) PRINTO=Pediatric Rheumatology International Trial Organization RACG-P=Royal Australian College of General Practitioner RANDUCLA=Research and DevelopmentUniversity of California at Los Angeles)
189Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
therapeutic effect of DMARDs The ACR recommendations donot provide any recommendation for the use of systemic GCfor patients with oligo- or polyarticular course of JIA exceptsystemic onset of JIA e) The ACR recommendations do notcover the topic of non-drug based therapy at all althoughthere is strong evidence that eg exercise training is a usefuladdition to drug treatment [575860]
6 Conclusion
In summary we present a treatment guideline for JIA on a con-sensus conference basis We strongly advocate an interdisciplin-ary approach including surgery physiotherapy psychosocial
intervention physical therapy medications etc and a strictformal consensus process in order to create statements thatare most appropriate for the complex clinical situation of achild and family presenting with JIA and cover all aspects ofJIA care All German pediatric rheumatology sites are partici-pating at the national pediatric rheumatologic database in theDeutsche Rheuma-Forschungszentrum at Berlin (DRFZ wwwdrfzde) It aims at quality assurance in Germany and monitorstreatment behavior of pediatric rheumatologists by using inter-nationally agreed criteria (eg joint count global physician rat-ing of disease activity global parent rating of overall well-being CHAQ ESR ACR-ped response or JADAS) The databasewill be used as a tool to monitor the application of our treat-ment guidelines
190 G Dueckers et al
Conflict of interest statement
Gregor Dueckers Novartis Pharmaceuticals CorporationBaxter (for all travel grants for scientific meetings)Nihal Guellac no conflict of interestMartin Arbogast no conflict of interestGuumlnther Dannecker no conflict of interestIvan Foeldvari Wyeth Pfizer Abbott Immunology Pharma-ceuticals Chugai (for all advisory board member)Michael Frosch no conflict of interestGerd Ganser Abbott Immunology Pharmaceuticals (advisoryboard member grants for scientific meetings) Wyeth Pfizer(advisory board member grants for scientific meetings)ChugaiRoche (advisory board member grants for scientificmeetings) Merck (grants for scientific meetings) Actelios(grants for scientific meetings) Esaote (grants for scientificmeetings)Arnd Heiligenhaus Novartis Pharmaceuticals CorporationAbbott Immunology Pharmaceuticals Alcon (for all re-search grants)Gerd Horneff Abbott Immunology Pharmaceuticals (re-search grants consulting fees non-remunerative positionsof influence) Wyeth Pfizer (research grants consultingfees speakers bureau non-remunerative positions of influ-ence) Bristol-Myers Squibb (Consulting fees) Nycomed(Consulting fees non-remunerative positions of influence)RocheChugai (Consulting fees non-remunerative positionsof influence) Sandoz (Consulting fees) Genzyme (researchgrants consulting fees non-remunerative positions of influ-ence) Swedish Orphan (research grants consulting feesnon-remunerative positions of influence)Arnold Illhardt no conflict of interestRuumldiger Krauspe no conflict of interestBarbara Markus no conflict of interestHartmut Michels Abbott Immunology Pharmaceuticals (advi-sory board member and grants for scientific meeting)Matthias Schneider no conflict of interestWolfram Singendonk no conflict of interestHelmut Sitter no conflict of interestMarianne Spamer no conflict of interestNorbert Wagner no conflict of interestTim Niehues Abbott Immunology Pharmaceuticals EssexPharma Novartis Pharmaceutical Corporation WyethPfizer (for all research grants consulting fees non-remu-nerative positions of influence)
Acknowledgment
We like to express our grateful thanks to Prof Dr Hans IkoHuppertz for proof reading the article and for an excellentdiscussion on our work We like to express our thanks to HE-LIOS Clinic for funding the open access of the article
References
[1] RE Petty TR Southwood P Manners J Baum DN Glass JGoldenberg X He J Maldonado-Cocco J Orozco-Alcala AMPrieur ME Suarez-Almazor PWoo International League of Asso-ciations for Rheumatology classification of juvenile idiopathic ar-thritis second revision Edmonton 2001 J Rheumatol 31(2004) 390ndash392
[2] B Prakken S Albani A Martini Juvenile idiopathic arthritisLancet 377 (2011) 2138ndash2149
[3] KT April DE Feldman RW Platt CM Duffy Comparisonbetween children with juvenile idiopathic arthritis (JIA) andtheir parents concerning perceived quality of life Qual LifeRes 15 (2006) 655ndash661
[4] BM Feldman B Grundland L McCullough V Wright Distinc-tion of quality of life health related quality of life and healthstatus in children referred for rheumatologic care J Rheuma-tol 27 (2000) 226ndash233
[5] JC Packham MA Hall Long-term follow-up of 246 adultswith juvenile idiopathic arthritis functional outcomeRheumatology (Oxford) 41 (2002) 1428ndash1435
[6] C Sandborg Pediatric rheumatic disease standards of care forJIAmdashthe basic foundation for quality Nat Rev Rheumatol 6(2010) 389ndash390
[7] N Guellac T Niehues Interdisciplinary and evidence-basedtreatment guideline for juvenile idiopathic arthritis KlinPadiatr 220 (2008) 392ndash402
[8] K Schnakenburg Leitlinien in der Kinder- und JugendmedizinElsevier 2005 pp H1 1ndash15
[9] P Juni L Nartey S Reichenbach R Sterchi PA Dieppe MEgger Risk of cardiovascular events and rofecoxib cumulativemeta-analysis Lancet 364 (2004) 2021ndash2029
[10] W Feldman Evidence-based Pediatrics 1st ed BC DeckersHamilton 2000
[11] AH Van de Ven AL Delbecq The nominal group as a re-search instrument for exploratory health studies Am J PublicHealth 62 (1972) 337ndash342
[12] HA Linstone M Turoff The Delphi Method Techniques andApplications Addison-Wesley Pub 1975
[13] TK Kvien HM Hoyeraal B Sandstad Naproxen and acetyl-salicylic acid in the treatment of pauciarticular and polyarticu-lar juvenile rheumatoid arthritis Assessment of tolerance andefficacy in a single-centre 24-week double-blind parallelstudy Scand J Rheumatol 13 (1984) 342ndash350
[14] RM Laxer ED Silverman C St-Cyr MT Tran G Lingam Asix-month open safety assessment of a naproxen suspensionformulation in the therapy of juvenile rheumatoid arthritisClin Ther 10 (1988) 381ndash387
[15] AM Leak MR Richter LE Clemens MA Hall BM AnsellA crossover study of naproxen diclofenac and tolmetin in sero-negative juvenile chronic arthritis Clin Exp Rheumatol 6(1988) 157ndash160
[16] J Haapasaari E Wuolijoki H Ylijoki Treatment of juve-nile rheumatoid arthritis with diclofenac sodium Scand JRheumatol 12 (1983) 325ndash330
[17] EH Giannini EJ Brewer ML Miller D Gibbas MH PassoHM Hoyeraal B Bernstein DA Person CW Fink LA Sawyeret al Ibuprofen suspension in the treatment of juvenilerheumatoid arthritis Pediatric Rheumatology CollaborativeStudy Group J Pediatr 117 (1990) 645ndash652
[18] E Stoeber L Sanger Experiences with indomethacin in long-term therapy of juvenile rheumatoid arthritis Arzneimittel-forschung 21 (1971) 1865ndash1866
[19] N Ruperto I Nikishina ED Pachanov Y Shachbazian AMPrieur R Mouy R Joos F Zulian R Schwarz V ArtamonovaW Emminger M Bandeira A Buoncompagni I Foeldvari FFalcini E Baildam I Kone-Paut M Alessio V Gerloni ALenhardt A Martini G Hanft R Sigmund S Simianer Arandomized double-blind clinical trial of two doses ofmeloxicam compared with naproxen in children with juvenileidiopathic arthritis short- and long-term efficacy and safetyresults Arthritis Rheum 52 (2005) 563ndash572
[20] I Foeldvari IS Szer LS Zemel DJ Lovell EH Giannini JLRobbins CRWest G Steidle S Krishnaswami BJ Bloom A pro-spective study comparing celecoxib with naproxen in children withjuvenile rheumatoid arthritis J Rheumatol 36 (2009) 174ndash182
191Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
[21] F Zulian G Martini D Gobber C Agosto C Gigante FZacchello Comparison of intra-articular triamcinolone hexa-cetonide and triamcinolone acetonide in oligoarticular juve-nile idiopathic arthritis Rheumatology (Oxford) 42 (2003)1254ndash1259
[22] F Zulian G Martini D Gobber M Plebani F Zacchello PManners Triamcinolone acetonide and hexacetonide intra-articular treatment of symmetrical joints in juvenile idiopathicarthritis a double-blind trial Rheumatology (Oxford) 43 (2004)1288ndash1291
[23] GS Habib Systemic effects of intra-articular corticosteroidsClin Rheumatol 28 (2009) 749ndash756
[24] JR Kirwan The effect of glucocorticoids on joint destructionin rheumatoid arthritis The Arthritis and Rheumatism CouncilLow-Dose Glucocorticoid Study Group N Engl J Med 333(1995) 142ndash146
[25] H Michels What is low-dose corticosteroid therapy in juvenileidiopathic arthritis A worldwide questionnaire-based surveyZ Rheumatol 59 (Suppl 2) (2000) II127ndash130
[26] JJ Miller III Prolonged use of large intravenous steroid pulsesin the rheumatic diseases of children Pediatrics 65 (1980)989ndash994
[27] P Picco M Gattorno A Buoncompagni V Pistoia C Borrone6-methylprednisolone lsquomini-pulsesrsquo a newmodality of glucocor-ticoid treatment in systemic onset juvenile chronic arthritisScand J Rheumatol 25 (1996) 24ndash27
[28] AM Prieur The place of corticosteroid therapy in juvenilechronic arthritis in 1992 J Rheumatol Suppl 37 (1993)32ndash34
[29] JS Gao H Wu J Tian Treatment of patients with juvenilerheumatoid arthritis with combination of leflunomide andmethotrexate Zhonghua Er Ke Za Zhi 41 (2003) 435ndash438
[30] T Niehues G Horneff H Michels MS Hock L SchuchmannEvidence-based use of methotrexate in children with rheumat-ic diseases a consensus statement of the Working Groups Pedi-atric Rheumatology Germany (AGKJR) and PediatricRheumatology Austria Rheumatol Int 25 (2005) 169ndash178
[31] N Ruperto DJ Lovell R Cuttica N Wilkinson P Woo GEspada C Wouters ED Silverman Z Balogh M HenricksonMT Apaz E Baildam A Fasth V Gerloni P Lahdenne AMPrieur A Ravelli RK Saurenmann ML Gamir N WulffraatL Marodi RE Petty R Joos F Zulian D McCurdy BLMyones K Nagy P Reuman I Szer S Travers A BeutlerG Keenan J Clark S Visvanathan A Fasanmade A Ray-chaudhuri A Mendelsohn A Martini EH Giannini A random-ized placebo-controlled trial of infliximab plus methotrexatefor the treatment of polyarticular-course juvenile rheumatoidarthritis Arthritis Rheum 56 (2007) 3096ndash3106
[32] K Visser DM van der Heijde Risk and management of livertoxicity during methotrexate treatment in rheumatoid andpsoriatic arthritis a systematic review of the literature ClinExp Rheumatol 27 (2009) 1017ndash1025
[33] A Cespedes-Cruz R Gutierrez-Suarez A Pistorio A Ravelli ALoy KJ Murray V Gerloni N Wulffraat S Oliveira J WalshIC Penades MG Alpigiani P Lahdenne C Saad-Magalhaes ECortis L Lepore Y Kimura C Wouters A Martini N RupertoMethotrexate improves the health-related quality of life of chil-dren with juvenile idiopathic arthritis Ann Rheum Dis 67(2008) 309ndash314
[34] TK Kvien HM Hoyeraal B Sandstad Azathioprine versus place-bo in patients with juvenile rheumatoid arthritis a single centerdouble blind comparative study J Rheumatol 13 (1986) 118ndash123
[35] E Silverman R Mouy L Spiegel LK Jung RK SaurenmannP Lahdenne G Horneff I Calvo IS Szer K Simpson JAStewart V Strand Leflunomide or methotrexate for juvenilerheumatoid arthritis N Engl J Med 352 (2005) 1655ndash1666
[36] MA van Rossum TJ Fiselier MJ Franssen AH ZwindermanR ten Cate LW van Suijlekom-Smit WH van Luijk RM
van Soesbergen NM Wulffraat JC Oostveen W Kuis PFDijkstra CF van Ede BA Dijkmans Sulfasalazine in the treat-ment of juvenile chronic arthritis a randomized double-blindplacebo-controlled multicenter study Dutch Juvenile ChronicArthritis Study Group Arthritis Rheum 41 (1998) 808ndash816
[37] MA van Rossum RM van Soesbergen M Boers AHZwinderman TJ Fiselier MJ Franssen R ten Cate LW vanSuijlekom-Smit NM Wulffraat WH van Luijk JC OostveenW Kuis BA Dijkmans Long-term outcome of juvenile idiopathicarthritis following a placebo-controlled trial sustained benefits ofearly sulfasalazine treatment Ann Rheum Dis 66 (2007)1518ndash1524
[38] DJ Lovell EH Giannini A Reiff GD Cawkwell ED SilvermanJJ Nocton LD Stein A Gedalia NT Ilowite CA Wallace JWhitmore BK Finck Etanercept in children with polyarticularjuvenile rheumatoid arthritis Pediatric Rheumatology Collabora-tive Study Group N Engl J Med 342 (2000) 763ndash769
[39] DJ Lovell A Reiff OY Jones R Schneider J Nocton LDStein A Gedalia NT Ilowite CA Wallace JB WhitmoreB White EH Giannini Long-term safety and efficacy ofetanercept in children with polyarticular-course juvenile rheu-matoid arthritis Arthritis Rheum 54 (2006) 1987ndash1994
[40] DJ Lovell N Ruperto S Goodman A Reiff L Jung K JarosovaD Nemcova R Mouy C Sandborg J Bohnsack D Elewaut IFoeldvari V Gerloni J Rovensky K Minden RK Vehe LWWeiner G Horneff HI Huppertz NY Olson JR Medich RCarcereri-De-Prati MJ McIlraith EH Giannini A MartiniAdalimumab with or without methotrexate in juvenile rheuma-toid arthritis N Engl J Med 359 (2008) 810ndash820
[41] FH Prince M Twilt R ten Cate MA van RossumW ArmbrustEP Hoppenreijs M van Santen-Hoeufft Y Koopman-KeeminkNM Wulffraat LW van Suijlekom-Smit Long-term follow-upon effectiveness and safety of etanercept in juvenile idiopathicarthritis the Dutch National Register Ann Rheum Dis 68(2009) 635ndash641
[42] P Diak J Siegel L LaGrenade L Choi S Lemery AMcMahonTumor necrosis factor alpha blockers andmalignancy in childrenforty-eight cases reported to the Food and Drug AdministrationArthritis Rheum 62 (2010) 2517ndash2524
[43] G Horneff T Hospach G Dannecker D Foll JP Haas HJGirschick HI Huppertz R Keitzer HJ Laws H Michels KMinden R Trauzeddel Updated statement by the German So-ciety for Pediatric and Adolescent Rheumatology (GKJR) on theFDAs report regarding malignancies in anti-TNF-treated pa-tients from Aug 4 2009 Z Rheumatol 69 (2010) 561ndash567
[44] T Hospach JP Haas HI Huppertz R Keitzer H Michels RTrauzeddl D Foll G Dannecker G Horneff Comment of theSociety of Pediatric and Adolescent Rheumatology on the USFood and Drug Administration (FDA) announcement regardingcases of malignancy in anti-TNF-treated patients Z Rheumatol68 (2009) 162ndash164
[45] DJ Lovell A Reiff NT Ilowite CA Wallace Y Chon SL LinSW Baumgartner EH Giannini Safety and efficacy of up to eightyears of continuous etanercept therapy in patients with juvenilerheumatoid arthritis Arthritis Rheum 58 (2008) 1496ndash1504
[46] EH Giannini NT Ilowite DJ Lovell CA Wallace CERabinovich A Reiff G Higgins B Gottlieb NG Singer YChon SL Lin SW Baumgartner Long-term safety and effec-tiveness of etanercept in children with selected categories ofjuvenile idiopathic arthritis Arthritis Rheum 60 (2009)2794ndash2804
[47] G Horneff H Schmeling T Biedermann I Foeldvari G GanserHJ Girschick T Hospach HI Huppertz R Keitzer RM KusterH Michels D Moebius B Rogalski A Thon The German etaner-cept registry for treatment of juvenile idiopathic arthritis AnnRheum Dis 63 (2004) 1638ndash1644
[48] FH Prince M Twilt SC Simon MA van RossumW ArmbrustEP Hoppenreijs S Kamphuis M van Santen-Hoeufft Y
192 G Dueckers et al
Koopman-Keemink NM Wulffraat R ten Cate LW vanSuijlekom-Smit When and how to stop etanercept aftersuccessful treatment of patients with juvenile idiopathic ar-thritis Ann Rheum Dis 68 (2009) 1228ndash1229
[49] G Horneff F De Bock I Foeldvari HJ Girschick H MichelsD Moebius H Schmeling Safety and efficacy of combinationof etanercept and methotrexate compared to treatment withetanercept only in patients with juvenile idiopathic arthritis(JIA) preliminary data from the German JIA Registry AnnRheum Dis 68 (2009) 519ndash525
[50] N Ilowite O Porras A Reiff S Rudge M Punaro A Martin RAllen T Harville YN Sun T Bevirt G Aras B Appleton Ana-kinra in the treatment of polyarticular-course juvenile rheumatoidarthritis safety and preliminary efficacy results of a randomizedmulticenter study Clin Rheumatol 28 (2009) 129ndash137
[51] T Lequerre P Quartier D Rosellini F Alaoui M De BandtO Mejjad I Kone-Paut M Michel E Dernis M Khellaf NLimal C Job-Deslandre B Fautrel X Le Loet J Sibilia In-terleukin-1 receptor antagonist (anakinra) treatment in pa-tients with systemic-onset juvenile idiopathic arthritis oradult onset Still disease preliminary experience in FranceAnn Rheum Dis 67 (2008) 302ndash308
[52] M Gattorno A Piccini D Lasiglie S Tassi G Brisca S CartaL Delfino F Ferlito MA Pelagatti F Caroli A BuoncompagniS Viola A Loy M Sironi A Vecchi A Ravelli A Martini ARubartelli The pattern of response to anti-interleukin-1 treatmentdistinguishes two subsets of patients with systemic-onset juvenileidiopathic arthritis Arthritis Rheum 58 (2008) 1505ndash1515
[53] S Yokota T Imagawa M Mori T Miyamae Y Aihara STakei N Iwata H Umebayashi T Murata M Miyoshi MTomiita N Nishimoto T Kishimoto Efficacy and safety oftocilizumab in patients with systemic-onset juvenile idiopathicarthritis a randomised double-blind placebo-controlledwithdrawal phase III trial Lancet 371 (2008) 998ndash1006
[54] N Ruperto DJ Lovell P Quartier E Paz N Rubio-Perez CASilva C Abud-Mendoza R Burgos-Vargas V Gerloni JAMelo-Gomes C Saad-Magalhaes F Sztajnbok C Goldenstein-Schainberg M Scheinberg IC Penades M Fischbach J OrozcoPJ Hashkes C Hom L Jung L Lepore S Oliveira CAWallace LH Sigal AJ Block A Covucci A Martini EHGiannini Abatacept in children with juvenile idiopathic arthri-tis a randomised double-blind placebo-controlled withdrawaltrial Lancet 372 (2008) 383ndash391
[55] N Ruperto DJ Lovell P Quartier E Paz N Rubio-PerezCA Silva C Abud-Mendoza R Burgos-Vargas V GerloniJA Melo-Gomes C Saad-Magalhaes J Chavez-Corrales CHuemer A Kivitz FJ Blanco I Foeldvari M Hofer G HorneffHI Huppertz C Job-Deslandre A Loy K Minden M PunaroAF Nunez LH Sigal AJ Block M Nys A Martini EHGiannini Long-term safety and efficacy of abatacept inchildren with juvenile idiopathic arthritis Arthritis Rheum 62(2010) 1792ndash1802
[56] DM Brinkman IM de Kleer R ten Cate MA van RossumWP Bekkering A Fasth MJ van Tol W Kuis NM WulffraatJM Vossen Autologous stem cell transplantation in childrenwith severe progressive systemic or polyarticular juvenile idio-pathic arthritis long-term follow-up of a prospective clinicaltrial Arthritis Rheum 56 (2007) 2410ndash2421
[57] SE Klepper Effects of an eight-week physical conditioningprogram on disease signs and symptoms in children with chronicarthritis Arthritis Care Res 12 (1999) 52ndash60
[58] D Singh-Grewal J Schneiderman-Walker V Wright O Bar-OrJ Beyene H Selvadurai B Cameron RM Laxer R SchneiderED Silverman L Spiegel S Tse C Leblanc J Wong SStephens BM Feldman The effects of vigorous exercisetraining on physical function in children with arthritis arandomized controlled single-blinded trial ArthritisRheum 57 (2007) 1202ndash1210
[59] S Stephens D Singh-Grewal O Bar-Or J Beyene B CameronCM Leblanc R Schneider J Schneiderman-Walker HSelvadurai E Silverman L Spiegel SM Tse V WrightBM Feldman Reliability of exercise testing and functionalactivity questionnaires in children with juvenile arthritisArthritis Rheum 57 (2007) 1446ndash1452
[60] T Takken J van der Net W Kuis PJ Helders Physical ac-tivity and health related physical fitness in children with ju-venile idiopathic arthritis Ann Rheum Dis 62 (2003)885ndash889
[61] MM Toledo G Martini C Gigante L Da Dalt A TregnaghiF Zulian Is there a role for arthroscopic synovectomy in oli-goarticular juvenile idiopathic arthritis J Rheumatol 33(2006) 1868ndash1872
[62] F de Benedetti H Brunner N Ruperto SWright A KenwrightR Cuttica P Woo R Schneider DJ Lovell A Martini Efficacyand safety of Tocilizumab in patients with systemic juvenile idio-pathic arthritis (sJIA) 12-week data from the phase III TENDERtrial Ann Rheum Dis 69 (2010) 146
[63] P Quartier F Allantaz R Cimaz P Pillet C Messiaen CBardin X Bossuyt A Boutten J Bienvenu A Duquesne ORicher D Chaussabel A Mogenet J Banchereau JM Tre-luyer P Landais V Pascual A multicentre randomiseddouble-blind placebo-controlled trial with the interleukin-1receptor antagonist anakinra in patients with systemic-onsetjuvenile idiopathic arthritis (ANAJIS trial) Ann Rheum Dis70 (2011) 747ndash754
[64] DE Furst EC Keystone J Braun FC Breedveld GRBurmester F De Benedetti T Dorner P Emery R FleischmannA Gibofsky JR Kalden A Kavanaugh B Kirkham P Mease JSieper NG Singer JS Smolen PL Van Riel MH Weisman KWinthrop Updated consensus statement on biological agents forthe treatment of rheumatic diseases 2010 Ann Rheum Dis 70(Suppl 1) (2010) i2ndashi36
[65] T Beukelman NM Patkar KG Saag S Tolleson-RinehartRQ Cron EM Dewitt NT Ilowite Y Kimura RM LaxerDJ Lovell A Martini CE Rabinovich N Ruperto 2011 Ameri-can College of Rheumatology recommendations for the treatmentof juvenile idiopathic arthritis initiation and safety monitoring oftherapeutic agents for the treatment of arthritis and systemic fea-tures Arthritis Care Res 63 (2011) 465ndash482 (Hoboken)
[66] JF Simard M Neovius S Hagelberg J Askling Juvenile idi-opathic arthritis and risk of cancer a nationwide cohort studyArthritis Rheum 62 (2010) 3776ndash3782
[67] T Imagawa S Yokota M Mori T Miyamae S Takei H ImanakaY Nerome N Iwata T Murata M Miyoshi N Nishimoto TKishimoto Safety and efficacy of tocilizumab an anti-IL-6-receptor monoclonal antibody in patients with polyarticular-course juvenile idiopathic arthritis Mod Rheumatol (2011)doi102007s10165-011-0481-0
[68] TM Shaneyfelt MF Mayo-Smith J Rothwangl Are guide-lines following guidelines The methodological quality of clini-cal practice guidelines in the peer-reviewed medicalliterature Jama 281 (1999) 1900ndash1905
[69] R Grilli N Magrini A Penna G Mura A Liberati Practiceguidelines developed by specialty societies the need for a crit-ical appraisal Lancet 355 (2000) 103ndash106
[70] JS Burgers R Grol NS Klazinga M Makela J Zaat To-wards evidence-based clinical practice an international surveyof 18 clinical guideline programs Int J Qual Health Care 15(2003) 31ndash45
[71] JT Cassidy RE Petty Juvenile Idiopathic Rheumatic Arthri-tis 5th Edition WB Saunders Philadelphia 2005
[72] TJ Lehman Are withdrawal trials in paediatric rheumatic dis-ease helpful Lancet 372 (2008) 348ndash350
[73] J Munro Recommendations for the Diagnosis and Managementof Juvenile Idiopathic Arthritis The Royal Australian Collegeof General Practitioners South Melbourne 2009 pp 1ndash38
193Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
httpwwwnhmrcgovau_files_nhmrcpublicationsattachmentscp119-juvenile-arthritispdf
[74] MJ Santos JE Fonseca H Canhao M Conde M JoseVieira L Costa M Costa M Salgado JA Melo Gomes Guide-lines for prescribing and monitoring biologic therapies in juve-nile idiopathic arthritis Acta Reumatol Port 32 (2007) 43ndash47
[75] S Yokota M Mori T Imagawa T Murata M Tomiita Y ItohS Fujikawa S Takei Guidelines on the use of etanercept forjuvenile idiopathic arthritis in Japan Mod Rheumatol 20(2010) 107ndash113
[76] The AGREE Collaboration Appraisal of Guidelines for Researchamp Evaluation (AGREE) instrument wwwagreecollaborationorg
[77] I Kopp H Thole T Langer HK Selbmann G OllenschlaumlgerGerman Instrument for Methodological Guideline Appraisal(DELBI) wwwversorgungsleitliniende2008
[78] Auml Aumlrztliches Zentrum fuumlr Qualitaumlt in der Medizin A Arbeitsge-meinschaften der Wissenschaftlichen Fachgesellschaften in derMedizin Deutsches Instrument zur methodischen Leitlinien-Bewertung (DELBI) Fassung 20052006 Z Aumlrztl FortbildQualitaumltssich 99 (2005) 468ndash519
[79] MP de Wit SE Berlo GJ Aanerud D Aletaha JW BijlsmaL Croucher JA Da Silva B Glusing L Gossec S Hewlett MJongkees D Magnusson M Scholte-Voshaar P Richards CZiegler TA Abma European League Against Rheumatism rec-ommendations for the inclusion of patient representatives in sci-entific projects Ann Rheum Dis 70 (2011) 722ndash726
[80] I Foeldvari M Bidde Validation of the proposed ILAR classifi-cation criteria for juvenile idiopathic arthritis InternationalLeague of Associations for Rheumatology J Rheumatol 27(2000) 1069ndash1072
[81] R Merino J de Inocencio J Garcia-Consuegra Evaluation ofrevised International League of Associations for Rheumatologyclassification criteria for juvenile idiopathic arthritis in Spanishchildren (Edmonton 2001) J Rheumatol 32 (2005) 559ndash561
[82] SE Ramsey RK Bolaria DA Cabral PN Malleson REPetty Comparison of criteria for the classification of childhoodarthritis J Rheumatol 27 (2000) 1283ndash1286
[83] G Horneff A Ebert S Fitter K Minden I Foeldvari J Kum-merle-Deschner A Thon HJ Girschick F Weller HI Hup-pertz Safety and efficacy of once weekly etanercept 08mgkg in a multicentre 12 week trial in active polyarticularcourse juvenile idiopathic arthritis Rheumatology (Oxford) 48(2009) 916ndash919
[84] EH Giannini EJ Brewer N Kuzmina A Shaikov A Maxi-mov I Vorontsov CW Fink AJ Newman JT Cassidy LSZemel Methotrexate in resistant juvenile rheumatoid arthri-tis Results of the USAndashUSSR double-blind placebo-controlled trial The Pediatric Rheumatology CollaborativeStudy Group and The Cooperative Childrens Study GroupN Engl J Med 326 (1992) 1043ndash1049
[85] A Ravelli S Viola D Migliavacca N Ruperto A Pistorio AMartini The extended oligoarticular subtype is the best predic-tor of methotrexate efficacy in juvenile idiopathic arthritisJ Pediatr 135 (1999) 316ndash320
[86] P Woo TR Southwood AM Prieur CJ Dore J Grainger JDavid C Ryder N Hasson A Hall I Lemelle Randomizedplacebo-controlled crossover trial of low-dose oral
methotrexate in children with extended oligoarticular or sys-temic arthritis Arthritis Rheum 43 (2000) 1849ndash1857
[87] E Silverman L Spiegel D Hawkins R Petty D Goldsmith LSchanberg C Duffy P Howard V Strand Long-term open-label preliminary study of the safety and efficacy of lefluno-mide in patients with polyarticular-course juvenile rheumatoidarthritis Arthritis Rheum 52 (2005) 554ndash562
[88] DJ Lovell EH Giannini Y Kimura C Suzanne PJHashkes A Reiff Long-term safety and efficacy of rilonaceptin patients with systemic juvenile idiopathic arthritis (SJIA)Arthritis Rheum 60 (2009)
[89] N Ruperto P Quartier NWulffraat PWoo A Loy R Mouy BBader-Meunier BJ Prakken E Noseda R Belleli J Lecot CRordorf A Martini A Phase II Trial with canakinumab(ACZ885) a new IL-1-beta blocking monoclonal antibody toevaluate safety and preliminary efficacy in children with system-ic juvenile idiopathic arthritis Ann Rheum Dis 68 (2009) 170
[90] DJ Lovell EH Giannini Y Kimura et al Preliminary evi-dence for bioactivity of IL-1 trap (Rilonacept) a long actingIL-1 inhibitor in systemic juvenile idiopathic arthritis (sJIA)Arthritis Rheum 54 (2006) S325
[91] DJ Lovell EH Giannini Y Kimura et al Preliminary evi-dence for sustained bioactivity of IL-1 Trap (rilonacept) a longacting IL-1 inhibitor in systemic juvenile idiopathic arthritisArthritis Rheum 56 (2007) S514
[92] N Ruperto F De Benedetti H Brunner R Allen D Brown JChaitow E Cortis G Espada B Flato V Gerloni G HorneffS Wright A Kenwright R Schneider P Woo A Martini DJLovell Tocilizumab is efficacious in patients with systemic ju-venile idiopathic arthritis (sJIA) across baseline disease charac-teristics and priorbaseline treatments 12-week data from thephase II TENDER trial 17th PReS Congress Valencia Spain2010 2010
[93] N Ruperto DJ Lovell T Li F Sztajnbok C Goldenstein-Schainberg M Scheinberg IC Penades M Fischbach JOrozco PJ Hashkes C Hom L Jung L Lepore S OliveiraC Wallace M Alessio P Quartier E Cortis A Eberhard GSimonini I Lemelle E Chalom LH Sigal A Block A CovucciM Nys A Martini EH Giannini Abatacept improves health-related quality of life pain sleep quality and daily participationin subjects with juvenile idiopathic arthritis Arthritis Care Res(Hoboken) 62 (11) (2010) 1542ndash1551
[94] N Ruperto DJ Lovell P Quartier E Paz N Rubio-PerezCA Silva C Abud-Mendoza R Burgos-Vargas V GerloniJA Melo-Gomes C Saad-Magalhaes J Chavez C HuemerA Kivitz FJ Blanco I Foeldvari M Hofer G Horneff HIHuppertz CJ Deslandre A Loy K Minden M Punaro AFNunez LH Sigal AJ Block M Nys A Martini EH GianniniLong-term safety and efficacy of abatacept in children with ju-venile idiopathic arthritis Arthritis Rheum 62 (2010)1792ndash1802
[95] J Munro Juvenile Idiopathic Arthritis Management Guidelines(Provisional) Australian Paediatric Rheumatology Group 2006httpwwwnhmrcgovau
[96] K Fitch SJ Bernstein MD Aguilar B Burnand JR LaCalleP Lazaro M van het Loo J McDonnell JP Vader JPKahan The RANDUCLA Appropriateness Method Users ManualRAND Pittsburgh 2000

185Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
Safe contraception is indicated during therapy with MTXAzathioprine or Leflunomide and in the following 3 to6 months after its discontinuation
Consensus statement
Administration of Sulfasalazine or Lefluno-mide is recommended if MTX or Etanercept donot show sufficient efficacy or cannot be used
3131 Methotrexate Among DMARDs MTX provides themainstay of long-term therapy in JIA [29ndash32] In case ofside effects eg dyspepsia or nausea prophylaxis withfolic acid can be recommended (1times1 mg per day or 5 mgonce a week 24ndash48 h after application of MTX) Safe contra-ception is mandatory while receiving MTX Safety and effica-cy of MTX and its impact on quality of life of children with JIAhave been investigated Significant positive impact of MTXon all health-related quality of life health conceptshas been shown although the study has its limit due to dif-ferent MTX dosages used within participating JIA patients[33]
Consensus statement
MTX administration can be recommendeddue to its proven safety and efficacy to reducedisease activity MTX is used in case of insuffi-cient therapeutic effect of NSAIDs andor localGC administration continuous need for system-ic GC andor highly active disease Efficacy ofMTX (orally or subcutaneously administered) isfrequently achievable with a dosage of 10ndash15 mgmsup2 body surface (evidence level I recom-mendation grade A)
for other reasons (evidence level II recommen-dation grade B)
3132 Purine analogs31321 Azathioprine Efficacy has been investigat-
ed in a double blind placebo controlled study (32 patients)After 8 weeks of therapy the changes in disease activitymeasurement indicated a minor improvement in the Azathi-oprine group compared to the placebo group At the end ofthe study statistically significant differences between thegroups were found for only 2 disease activity measurements[34] Two patients were taken out of study due to severeadverse events eg leucopenia Measurement of activityof Thiopurinmethyltransferase (TPMT) can be beneficial foravoidance of severe adverse events
3133 Pyrimidine analogs31331 Leflunomide Within a double blind study
(32 weeks 94 patients) efficacy of Leflunomide was inferiorin comparison to MTX but better than placebo Howeverdosing of Leflunomide may not have been adequate insome children [35] Contraindications for Leflunomide arerenal insufficiency severe immunodeficiency depressedmyelopoesis and pancytopenia An extensive half-life peri-od (approximately 14 days) has to be taken in accountwhen administering Leflunomide In combination with hepa-totoxic DMARDs the risk of severe adverse events might in-crease eg increased blood pressure is seen frequentlySafe contraception is mandatory
3134 Antibiotic analogs and Hydroxychloroquine andChloroquine
31341 Sulfasalazine Weak efficacy of Sulfasalazinewas demonstrated within a placebo-controlled randomizedstudy after 24 weeks (96 patients) [3637] One third of pa-tients enrolled in the study discontinued treatment with Sulfa-salazine due to side effects eg gastrointestinal symptomsleucopenia [36] Some experts use sulfasalazine in HLA-B27positive JIA Contraindications are Glucose-6-phosphatase de-ficiency and hypersensitivity against sulfonamides
31342 Hydroxychloroquine and chloroquine Hydrox-ychloroquine and Chloroquine have been subject to clinical tri-als for the treatment of JIA even though efficacy was limitedWithin three consensus conferences held in 2007 and 2010 theconsensus group decided not to give a consensus statementon the use of chloroquine or hydroxychloroquine treatmentdespite the fact that those drugs still might be used by somecaregivers
3135 Biologic agents Biologic agents are drugs whichselectively inhibit cytokines cytokine receptors or directlybind to receptors of lymphocytes eg CTLA-4 CD20 Theyinclude antibodies and fusion proteins So far allbiological therapies are administered subcutaneously orintravenously
31351 TNFα-inhibitors TNFα-inhibition with Adali-mumab and Etanercept is efficient and safe (evidencelevel I) [38ndash41] Both drugs have been approved for JIAwith polyarticular course TNFα-inhibitors have become anintegral part of the treatment of JIA Potential risks of therapyare vulnerability for infection andmdashin a rare occasionmdashthe in-duction of autoimmune disease Prior to the start of treatmentwith TNFα-inhibitors chronic infections needs to be excludedor treated sufficiently eg tuberculosis hepatitis B or C
In children with JIA treated with TNFα-inhibitors malig-nancies eg Lymphoma have been reported It remainsunclear if the rate of malignancies is increased in patientscompared to the risk by having JIA itself In response to aprevious letter of the FDA (as reviewed in [42]) the GermanSociety for Pediatric Rheumatology (GKJR) has published of-ficial statements [4344] The GKJR states that treatmentwith TNFα-inhibition should be used very carefully physi-cians need to be aware of co-medication e g immunosup-pressive drugs and should monitor those patientsclosely [43] There is insufficient data on all biologicagentsmdashincluding TNFα-inhibitionmdashto judge about the long-term risk for children and adolescents313511 Etanercept Etanercept is a fusion proteinconsisting of the extracellular binding domain of solubleTNFα-receptor and Fc chain of human IgG1 Etanercept in-hibits TNFα by direct binding of the cytokine Efficacy has
Consensus statement
The use of Anakinra or Tozilizumab can berecommended for treatment of children and ado-lescents with refractory SoJIA (evidence level IIrecommendation grade A)
186 G Dueckers et al
been demonstrated in a randomized controlled withdrawaldesign trial for patients with polyarticular JIA [38] Withinan open extension study long term efficacy and safety havebeen documented over 8 years in 1669 patients [3945]There is data on more than 2000 patients registered in Euro-pean registries [46ndash48] Currently retrospective data showsa somewhat better efficacy of combining MTX or otherDMARDs with TNFα-inhibition versus anti-TNFα therapy assingle therapy [49]313512 Adalimumab Adalimumab is a humanizedmonoclonal IgG1 antibody directed against TNFα whichbinds soluble and membrane bound TNFα A randomizedcontrolled withdrawal design trial demonstrated safety andefficacy of Adalimumab (24 mgmsup2 body surface every2 weeks max 40 mg) for children and adolescents withpolyarticular JIA (4ndash17 years of age n=171) [40] After16 weeks ldquowash inrdquo phase responders (n=144171) enteredthe 32 weeks randomized double blind phase After 48 weekstwice the number of patients in the verum group met ACR 70as compared to the control group (56 vs 28 pb001)Within the open extension phase Adalimumab dosage wasfixed ie 20 mgb30 kg Bw and 40 mgN30 kg Bw There islack of evidence showing superior efficacy of combiningMTX (DMARDs) with Adalimumab versus Adalimumab as sin-gle therapy [40]
Consensus statement
Efficacy of Etanercept and Adalimumab forthe treatment of polyarticular JIA has been dem-onstrated Therapy with TNFa-inhibition is indi-cated in case of insufficient therapeutic effectof NSAIDs and local GC administration and lackof response to MTX (evidence level I recom-mendation grade A)
Consensus statement
Patients with polyarticular JIA without sys-temic manifestation refractory to treatmentwith MTX and TNF inhibition might benefit fromthe use of Abatacept (evidence level III recom-mendation grade C)
313513 Infliximab Infliximab is a chimerical (humanmouse) monoclonal antibody which binds soluble and mem-brane bound TNFα A randomized controlled study in childrenand adolescents with JIA failed to demonstrate a significantdifference of efficacy after treatment with Infliximab com-pared to placebo [31]
31352 Interleukin-1-inhibitors None of interleukin-1-inhibitors are approved for the treatment of JIA or SoJIAThey are commonly used in an off label setting313521 Anakinra Anakinra is an IL-1 receptor antag-onist Within a randomized controlled trial no significant ef-ficacy of Anakinra for patients with polyarticular JIA couldbe demonstrated [50] 50 of 86 patients were enrolled intoblinded phase (11 Anakinra versus Placebo) No significantreduction of flare could be demonstrated in comparison toplacebo 29 of 50 patients completed the open label exten-sion study Two noncontrolled nonrandomized studieshave shown efficacy of anakinra in a proportion of patientswith systemic-onset of JIA (SoJIA) [5152]313522 Canakinumab Canakinumab an IL-1β anti-body binds IL-1β selectively without interfering with IL-1αor its physiological IL-1 receptor antagonist Canakinumabhas been approved for treatment of hereditary periodic IL-1 associated periodic fever syndromes ie Cryopyrin-
associated periodic syndromes There are ongoing studies in-vestigating safety and efficacy of Canakinumab for SoJIA
31353 Interleukin-6 inhibitors313531 Tozilizumab Tozilizumab is a humanizedanti-IL-6 receptor monoclonal antibody Efficacy has beendemonstrated within a 12 week double blind randomizedcontrolled withdrawal trial in children with SoJIA (n=562ndash19 years) in Japan [53] After a 48 week open extensionstudy ACR Pedi 30 was met by 47 patients (98) At thetime of our literature search Tocilizumab was approved fortreatment of SoJIA and polyarticular JIA since 2008 inJapan A multicenter European study investigating efficacyand safety of Tozilizumab in polyarticular JIA was ongoingat the deadline of literature search (wwwclinicaltrialsgov NCT00988221) No data on long term effects are cur-rently available
31354 Co-stimulation inhibitors313541 Abatacept Abatacept is a recombinant fu-sion protein of extracellular domain of human cytotoxic T-Lymphocyte Antigen 4 (CTLA-4) and IgG1-Fc-Fragment Itmodulates T-cell co-stimulation A randomized controlleddouble blind withdrawal design study of Ruperto et al [54]demonstrated efficacy of Abatacept in patients with polyar-ticular JIA 123 of 170 participants of study were enrolled inthe 6 month double blind phase Flares occurred in 33 of 62(53) patients who were given placebo versus 12 of 60(20) Abatacept patients during double blind phase Adverseevents (AE) did not differ in both groups ie 37 AE in Abata-cept versus 34 AE in placebo recipients Some children maytake 3 to 6 months or longer before their maximal responseis achieved 3 of patients developed reaction to the infu-sion [55] Abatacept is approved by FDA and EMA for pa-tients who did not respond to prior MTX treatment Nodata of long term effects of the use of Abatacept in JIA areavailable due to the low numbers of patients treated so far
314 Autologous stem cell transplantation (SCT)There are studies on autologous SCT for treatment of re-
fractory and severe forms of JIA (evidence level III) [56] 22
Consensus statement
187Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
patients were enrolled in one study 8 reached clinical re-mission 7 were assessed as partial responders 3 experi-enced relapse of the disease and 4 (18) died as aconsequence of MAS or immunosuppressive treatment [56]Due to serious adverse events including death this thera-peutic option is seen as the last treatment option
Exercise training is recommended dependingon the extent of inflammation number of affect-ed joints and global disease activity Sports withminor stress on joints is favorable (evidence levelI recommendation grade A)
32 Non-drug based therapy
321 Physiotherapy occupational therapy and thera-peutic appliances
Physio- and occupational therapy are integral parts of thetherapeutic concept in children and adolescents with JIA[5758] Therapeutic goals of physiotherapy are relaxationand pain relief preservation or rehabilitation of physiologi-cal range of joint movement prevention of contracturesstretching and activation of muscles build-up of muscleforce and training of physiological movements
Consensus statement
Structured treatment by a properly trainedphysiotherapistoccupational therapist in combi-nation with drug based therapy and instructionsfor disease adopted self-sufficient daily exercisesessions are recommended to keep and to im-prove joint mobility (evidence level II recom-mendation grade A)Custom-made therapeutic appliances for correc-tion of axial misalignment prevention of falseweight bearing stabilization of joints (eghand- finger- and foot-ortheses) are recom-mended individually The use of therapeutic ap-pliances follows individual physician-directedadvice Efficacy has been demonstrated (evi-dence level I recommendation grade B)
Consensus statement
In individual cases the indication for open orarthroscopic synovectomy can be considered ifconservative therapy does not succeed (evi-dence level III recommendation grade B)
Consensus statement
Other forms of non-drug based therapeutic approachesrely on experts opinion and are solely based on individualclinical experience No controlled studies are available
Consensus statement
The implementation of thermotherapy electro-or ultrasound therapy massage and lymph drain-age is recommended Application of cold appli-ances for acute joint inflammation is indicated(evidence level II recommendation grade A)Electro- and ultrasound therapy are recom-mended for patients with tendosynovitis (evi-dence level III recommendation grade B)
An early psychological support within stan-dard pediatric rheumatological care should beimplemented to apprehend and treat mental is-sues and behavioral syndromes associated withphysiological disturbances and physical factors(evidence level III recommendation grade A)
Consensus statement
A socio-pedagogical care with regard tointegration at school professional andeveryday life and formal education of parentsand patients is recommended (evidence levelIII recommendation grade A)
322 Sportive activity and exercise trainingPositive impact of sportive activity on the general physi-
cal condition and on oxygen consumption has been demon-strated (evidence level II) [57ndash60] Adequate exercise
training supports the physiological development and helpscoping with JIA [58] Prospective controlled long term stud-ies are currently not available
323 Surgical treatmentToledo et al investigated the role of arthroscopic syno-
vectomy in JIA They concluded that arthroscopy is a safebut only partially effective procedure in patients witholigoarticular JIA (evidence levelrecommendation gradeIIIB) [61]
324 Psychological social intervention orsocio-pedagogical care
There are no controlled or open studies focusing on psy-chological social andor socio-pedagogical intervention inchildren or adolescents with JIA Recommendations arebased on experts opinion and personal experience solely
188 G Dueckers et al
4 Addendum
Since the deadline January 15th 2010 new papers haveappeared that are of interest in the context of our guideline[5562ndash64] in particular we refer to the ACR recommenda-tions [65] and the most recent literature on the risk of malig-nancies in JIA in context with TNF blocking agent andindependent of medication [42] [66] Moreover there is arecent study on the use of Tocilizumab in polyarticular pa-tients [67] These papers will be discussed within the nextconsensus conference by NGT and considered for inclusioninto the next edition of this guideline On 6th of September2011 our advanced search on wwwclinicaltrialgov (searchterms juvenile idiopathic arthritis recruitment open stud-ies study type interventional study age group child(birthndash17) intervention drugs) led to 16 trials which are cur-rently recruiting or will soon start recruiting
5 Discussion
To develop clinical practice guidelines of high quality andvalidity a formal consensus process and explicit methodo-logical criteria for the production of guidelines are recom-mended [68ndash70] Our guideline for the treatment of JIA inchildren and adolescents implements all these issues Thesystematic literature search was terminated on 15th January2010 leading to the most up to date guideline for JIA whichis currently available The deadline of the ACR recommenda-tions as published recently by Beukelmann et al was 5th ofOctober 2009 [65] By exclusion of case reports trials with-out control groups preliminary results published as ab-stracts on conferences and the strict graduation of theliterature by the criteria of evidence based medicine weaimed to give our guideline statements additional strengthand a maximal validity Newer original studies providing ad-ditional evidence for the treatment of JIA became availableafter our consensus process was finished see AddendumThe results of these trials have to await the next NGT beforeinclusion into our recommendations
Our updated systematic literature search in 2010 led to13 relevant studies published after 30th June 2007 (Fig 1Table 4) Their results have to be interpreted with cautionFirst trials in JIA are mainly based on limited numbers of pe-diatric patients as the recruitment of a sufficient number ofpediatric patients remains challenging Second trials aremainly designed for patients with polyarticular JIA or witholigoarticular onset and a polyarticular course (Table 4)Most children with JIA do not have a polyarticular subtypeof JIA but an oligoarticular onset and course [71] Thus pa-tients with oligoarticular JIA are heavily underrepresentedin most of the current trials Third in 5 of the 13studies the withdrawal study design has been used[4045505354] Lehmann reviewed the bias of withdrawaldesign trials in 2008 [72] After a wash-in phase only re-sponders to treatment are eligible for randomization Thusthe design preselects responders to the placebo effect whomight retain their response throughout the entire study peri-od Further there is a carryover effect of AE into the place-bo group so that significant differences in AE betweengroups may not become apparent In the one placebo con-trolled trial without withdrawal design on TNFα-inhibition
(Infliximab) no significant efficacy could be demonstratedbetween verum and placebo [31]
To our knowledge there are two other guidelines that dealwith the management of JIA as a whole (Table 6) [65] [73]Other guidelines are limited to the use of single drugs in JIAeg biologic agents [74] etanercept [75] The Australian guide-line (wwwracgporgauguidelinejuvenileidiopathicarthritis)has not been published in a peer-reviewed journal It is to pro-vide recommendations for the early diagnosis and multidisci-plinary management of JIA in the primary care setting forgeneral practitioners (GPs) [73] No recommendations aremade regarding the use of GCs DMARDs immunosuppressivedrugs or biologic agents [73] The ACR recommendations usesthe Appraisal of Guidelines for Research and Evaluation(AGREE) instrument [65] [76] which does not fulfill criteria ofa proper consensus process and carries the risk that expertsvote for peer opinion which might not reflect the true valueWe used an advanced and linguistically validated version ofthe AGREE instrument the ldquoGerman Instrument for Methodo-logical Guideline Appraisal (DELBI)rdquo which has been developedin cooperation of the AWMF among others [7778] We followedthe highly structured Nominal Group Technique as described inMethodology Our consensus group only considered formallyboard nominated representatives of multidisciplinary scientificsocieties and organizations (Table 1) and included patients rep-resentatives as this has been strongly recommended by the Eu-ropean League against Rheumatism (EULAR) recently [79] TheACR mentions a parent representative within their task forcepanel but leaves this representative anonymous It remainsunclear how ACR experts were selected and involved [65]They defined treatment groups which have not been evaluatedsystematically so far We used the ILAR classification systemwhich has been repeatedly evaluated [80ndash82]
By content there are major differences between the ACRrecommendations and our guideline a) Our guideline pro-vides a detailed and systematic list of 20 drugs commonlyused in the treatment of JIA (Table 5) which has been an in-tegrative part of our consensus conferences The ACR recom-mendations do not provide information on approval status(Food and Drug Administration) indications for use and nospecific differences on dosage regimes or frequency ofdaily application [65] eg it refers to the 2008 ACR recom-mendations for the use of DMARDs in adult rheumatoid ar-thritis b) The ACR recommendations provide a more earlyaggressive approach in the treatment of JIA The ACR recom-mends MTX as first line treatment in patients (b4 joints) withhighly active disease [65] To our knowledge there are onlydata to recommend MTX administration in cases of insuffi-cient therapeutic effect of prior treatment with NSAIDandor GC [33] c) The ACR recommends the use of TNFα in-hibitors as escalation therapy for some patients with historyof arthritis of 4 or fewer joints and refer to publications[3840] conducted in patients with polyarticular JIA or pau-ciarticular JIA with polyarticular course [65] There is no ev-idence that TNF is safe and efficient in patients witholigoarticular JIA a systematic controlled clinical trial onthis issue has not been done yet d) We regard a brief trialof local or systemic administration of GC plus NSAID as a fea-sible first line treatment for patients with polyarticular JIAThe ACR recommends MTX without regard to disease activityat the initial stage [65] We reached consensus to recom-mend the use of GC as bridging therapy until full onset of
Table 6 Overview of recommendationsguidelines for treatment of JIA
USA Australia Germany
ACR recommendations[65]
RACGP recommendations[73]
GKJR guidelines
Deadline of literature search October 2009 January 2007 September 2010Source of publications Pub Med Pub Med
EMBASE CINHAL CochraneLibrary provisionalAustralian Guideline [95]
Pub MedPrevious German Guidelines [78]
Definition used for JIA subgroups Treatment groups definedby Core expert panel
Not specifically definedChildren withJIAb16 years
ILAR criteria [1]
Consensus processprocessvalidation
AGREE [76] AGREE [76] DELBI [77]RANDUCLA appropriatenessmethod [96]
NGT Delphi method
Conferences None None 3 Formal consensus conferencesAddressees Pediatric rheumatologists General practitioner Pediatric Rheumatologists
PediatriciansGeneral practitioners
Participating scientific societies or professional organizationsPediatric rheumatologist orrheumatologists for adolescents
Yes Yes Yes
General pediatrician- In hospital Yes Yes Yes- In private practice Yes Yes YesResearcher Yes No YesRheumatologists for adults No No YesOphthalmologists No No YesParentspatients support groups Yes No YesOrthopedic surgeons No No YesPediatric orthopedic surgeons No No YesPsychologists No No YesPhysiotherapists No No YesPediatric rheumatology nurses Yes No NoOther scientific societies ororganizations
ACR BSPAR PRINTO PReS RACGP NAMSCAG NHMRC DGKJ DGPs DGRh DGO AWMFBVKJ
(ACR=American College of Rheumatologists AGREE=Appraisal of Guidelines for Research amp Development AWMF=Association of the ScientificMedical Associations BSPAR=British Society for Pediatric Rheumatology BVJK=Association of Pediatricians in private practice CEP=Core expertpanel ILAR=International League against Rheumatism CINHAL=Cumulative Index to Nursing and Allied Health Literature DELBI=German In-strument for Methodological Guideline Appraisal DGKJ=German Society of Pediatrics and Adolescent Medicine DGO=German Society for Oph-thalmology DGPs=German society for Psychology DGRh=German Society for Rheumatology GKJR=German Society for Pediatric RheumatologyNAMSCAG=National Arthritis and Musculoskeletal Conditions Advisory Group NGT=Nominal Group Technique NHMRC=National Health andMedical Research Council PReS=Pediatric Rheumatology Society) PRINTO=Pediatric Rheumatology International Trial Organization RACG-P=Royal Australian College of General Practitioner RANDUCLA=Research and DevelopmentUniversity of California at Los Angeles)
189Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
therapeutic effect of DMARDs The ACR recommendations donot provide any recommendation for the use of systemic GCfor patients with oligo- or polyarticular course of JIA exceptsystemic onset of JIA e) The ACR recommendations do notcover the topic of non-drug based therapy at all althoughthere is strong evidence that eg exercise training is a usefuladdition to drug treatment [575860]
6 Conclusion
In summary we present a treatment guideline for JIA on a con-sensus conference basis We strongly advocate an interdisciplin-ary approach including surgery physiotherapy psychosocial
intervention physical therapy medications etc and a strictformal consensus process in order to create statements thatare most appropriate for the complex clinical situation of achild and family presenting with JIA and cover all aspects ofJIA care All German pediatric rheumatology sites are partici-pating at the national pediatric rheumatologic database in theDeutsche Rheuma-Forschungszentrum at Berlin (DRFZ wwwdrfzde) It aims at quality assurance in Germany and monitorstreatment behavior of pediatric rheumatologists by using inter-nationally agreed criteria (eg joint count global physician rat-ing of disease activity global parent rating of overall well-being CHAQ ESR ACR-ped response or JADAS) The databasewill be used as a tool to monitor the application of our treat-ment guidelines
190 G Dueckers et al
Conflict of interest statement
Gregor Dueckers Novartis Pharmaceuticals CorporationBaxter (for all travel grants for scientific meetings)Nihal Guellac no conflict of interestMartin Arbogast no conflict of interestGuumlnther Dannecker no conflict of interestIvan Foeldvari Wyeth Pfizer Abbott Immunology Pharma-ceuticals Chugai (for all advisory board member)Michael Frosch no conflict of interestGerd Ganser Abbott Immunology Pharmaceuticals (advisoryboard member grants for scientific meetings) Wyeth Pfizer(advisory board member grants for scientific meetings)ChugaiRoche (advisory board member grants for scientificmeetings) Merck (grants for scientific meetings) Actelios(grants for scientific meetings) Esaote (grants for scientificmeetings)Arnd Heiligenhaus Novartis Pharmaceuticals CorporationAbbott Immunology Pharmaceuticals Alcon (for all re-search grants)Gerd Horneff Abbott Immunology Pharmaceuticals (re-search grants consulting fees non-remunerative positionsof influence) Wyeth Pfizer (research grants consultingfees speakers bureau non-remunerative positions of influ-ence) Bristol-Myers Squibb (Consulting fees) Nycomed(Consulting fees non-remunerative positions of influence)RocheChugai (Consulting fees non-remunerative positionsof influence) Sandoz (Consulting fees) Genzyme (researchgrants consulting fees non-remunerative positions of influ-ence) Swedish Orphan (research grants consulting feesnon-remunerative positions of influence)Arnold Illhardt no conflict of interestRuumldiger Krauspe no conflict of interestBarbara Markus no conflict of interestHartmut Michels Abbott Immunology Pharmaceuticals (advi-sory board member and grants for scientific meeting)Matthias Schneider no conflict of interestWolfram Singendonk no conflict of interestHelmut Sitter no conflict of interestMarianne Spamer no conflict of interestNorbert Wagner no conflict of interestTim Niehues Abbott Immunology Pharmaceuticals EssexPharma Novartis Pharmaceutical Corporation WyethPfizer (for all research grants consulting fees non-remu-nerative positions of influence)
Acknowledgment
We like to express our grateful thanks to Prof Dr Hans IkoHuppertz for proof reading the article and for an excellentdiscussion on our work We like to express our thanks to HE-LIOS Clinic for funding the open access of the article
References
[1] RE Petty TR Southwood P Manners J Baum DN Glass JGoldenberg X He J Maldonado-Cocco J Orozco-Alcala AMPrieur ME Suarez-Almazor PWoo International League of Asso-ciations for Rheumatology classification of juvenile idiopathic ar-thritis second revision Edmonton 2001 J Rheumatol 31(2004) 390ndash392
[2] B Prakken S Albani A Martini Juvenile idiopathic arthritisLancet 377 (2011) 2138ndash2149
[3] KT April DE Feldman RW Platt CM Duffy Comparisonbetween children with juvenile idiopathic arthritis (JIA) andtheir parents concerning perceived quality of life Qual LifeRes 15 (2006) 655ndash661
[4] BM Feldman B Grundland L McCullough V Wright Distinc-tion of quality of life health related quality of life and healthstatus in children referred for rheumatologic care J Rheuma-tol 27 (2000) 226ndash233
[5] JC Packham MA Hall Long-term follow-up of 246 adultswith juvenile idiopathic arthritis functional outcomeRheumatology (Oxford) 41 (2002) 1428ndash1435
[6] C Sandborg Pediatric rheumatic disease standards of care forJIAmdashthe basic foundation for quality Nat Rev Rheumatol 6(2010) 389ndash390
[7] N Guellac T Niehues Interdisciplinary and evidence-basedtreatment guideline for juvenile idiopathic arthritis KlinPadiatr 220 (2008) 392ndash402
[8] K Schnakenburg Leitlinien in der Kinder- und JugendmedizinElsevier 2005 pp H1 1ndash15
[9] P Juni L Nartey S Reichenbach R Sterchi PA Dieppe MEgger Risk of cardiovascular events and rofecoxib cumulativemeta-analysis Lancet 364 (2004) 2021ndash2029
[10] W Feldman Evidence-based Pediatrics 1st ed BC DeckersHamilton 2000
[11] AH Van de Ven AL Delbecq The nominal group as a re-search instrument for exploratory health studies Am J PublicHealth 62 (1972) 337ndash342
[12] HA Linstone M Turoff The Delphi Method Techniques andApplications Addison-Wesley Pub 1975
[13] TK Kvien HM Hoyeraal B Sandstad Naproxen and acetyl-salicylic acid in the treatment of pauciarticular and polyarticu-lar juvenile rheumatoid arthritis Assessment of tolerance andefficacy in a single-centre 24-week double-blind parallelstudy Scand J Rheumatol 13 (1984) 342ndash350
[14] RM Laxer ED Silverman C St-Cyr MT Tran G Lingam Asix-month open safety assessment of a naproxen suspensionformulation in the therapy of juvenile rheumatoid arthritisClin Ther 10 (1988) 381ndash387
[15] AM Leak MR Richter LE Clemens MA Hall BM AnsellA crossover study of naproxen diclofenac and tolmetin in sero-negative juvenile chronic arthritis Clin Exp Rheumatol 6(1988) 157ndash160
[16] J Haapasaari E Wuolijoki H Ylijoki Treatment of juve-nile rheumatoid arthritis with diclofenac sodium Scand JRheumatol 12 (1983) 325ndash330
[17] EH Giannini EJ Brewer ML Miller D Gibbas MH PassoHM Hoyeraal B Bernstein DA Person CW Fink LA Sawyeret al Ibuprofen suspension in the treatment of juvenilerheumatoid arthritis Pediatric Rheumatology CollaborativeStudy Group J Pediatr 117 (1990) 645ndash652
[18] E Stoeber L Sanger Experiences with indomethacin in long-term therapy of juvenile rheumatoid arthritis Arzneimittel-forschung 21 (1971) 1865ndash1866
[19] N Ruperto I Nikishina ED Pachanov Y Shachbazian AMPrieur R Mouy R Joos F Zulian R Schwarz V ArtamonovaW Emminger M Bandeira A Buoncompagni I Foeldvari FFalcini E Baildam I Kone-Paut M Alessio V Gerloni ALenhardt A Martini G Hanft R Sigmund S Simianer Arandomized double-blind clinical trial of two doses ofmeloxicam compared with naproxen in children with juvenileidiopathic arthritis short- and long-term efficacy and safetyresults Arthritis Rheum 52 (2005) 563ndash572
[20] I Foeldvari IS Szer LS Zemel DJ Lovell EH Giannini JLRobbins CRWest G Steidle S Krishnaswami BJ Bloom A pro-spective study comparing celecoxib with naproxen in children withjuvenile rheumatoid arthritis J Rheumatol 36 (2009) 174ndash182
191Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
[21] F Zulian G Martini D Gobber C Agosto C Gigante FZacchello Comparison of intra-articular triamcinolone hexa-cetonide and triamcinolone acetonide in oligoarticular juve-nile idiopathic arthritis Rheumatology (Oxford) 42 (2003)1254ndash1259
[22] F Zulian G Martini D Gobber M Plebani F Zacchello PManners Triamcinolone acetonide and hexacetonide intra-articular treatment of symmetrical joints in juvenile idiopathicarthritis a double-blind trial Rheumatology (Oxford) 43 (2004)1288ndash1291
[23] GS Habib Systemic effects of intra-articular corticosteroidsClin Rheumatol 28 (2009) 749ndash756
[24] JR Kirwan The effect of glucocorticoids on joint destructionin rheumatoid arthritis The Arthritis and Rheumatism CouncilLow-Dose Glucocorticoid Study Group N Engl J Med 333(1995) 142ndash146
[25] H Michels What is low-dose corticosteroid therapy in juvenileidiopathic arthritis A worldwide questionnaire-based surveyZ Rheumatol 59 (Suppl 2) (2000) II127ndash130
[26] JJ Miller III Prolonged use of large intravenous steroid pulsesin the rheumatic diseases of children Pediatrics 65 (1980)989ndash994
[27] P Picco M Gattorno A Buoncompagni V Pistoia C Borrone6-methylprednisolone lsquomini-pulsesrsquo a newmodality of glucocor-ticoid treatment in systemic onset juvenile chronic arthritisScand J Rheumatol 25 (1996) 24ndash27
[28] AM Prieur The place of corticosteroid therapy in juvenilechronic arthritis in 1992 J Rheumatol Suppl 37 (1993)32ndash34
[29] JS Gao H Wu J Tian Treatment of patients with juvenilerheumatoid arthritis with combination of leflunomide andmethotrexate Zhonghua Er Ke Za Zhi 41 (2003) 435ndash438
[30] T Niehues G Horneff H Michels MS Hock L SchuchmannEvidence-based use of methotrexate in children with rheumat-ic diseases a consensus statement of the Working Groups Pedi-atric Rheumatology Germany (AGKJR) and PediatricRheumatology Austria Rheumatol Int 25 (2005) 169ndash178
[31] N Ruperto DJ Lovell R Cuttica N Wilkinson P Woo GEspada C Wouters ED Silverman Z Balogh M HenricksonMT Apaz E Baildam A Fasth V Gerloni P Lahdenne AMPrieur A Ravelli RK Saurenmann ML Gamir N WulffraatL Marodi RE Petty R Joos F Zulian D McCurdy BLMyones K Nagy P Reuman I Szer S Travers A BeutlerG Keenan J Clark S Visvanathan A Fasanmade A Ray-chaudhuri A Mendelsohn A Martini EH Giannini A random-ized placebo-controlled trial of infliximab plus methotrexatefor the treatment of polyarticular-course juvenile rheumatoidarthritis Arthritis Rheum 56 (2007) 3096ndash3106
[32] K Visser DM van der Heijde Risk and management of livertoxicity during methotrexate treatment in rheumatoid andpsoriatic arthritis a systematic review of the literature ClinExp Rheumatol 27 (2009) 1017ndash1025
[33] A Cespedes-Cruz R Gutierrez-Suarez A Pistorio A Ravelli ALoy KJ Murray V Gerloni N Wulffraat S Oliveira J WalshIC Penades MG Alpigiani P Lahdenne C Saad-Magalhaes ECortis L Lepore Y Kimura C Wouters A Martini N RupertoMethotrexate improves the health-related quality of life of chil-dren with juvenile idiopathic arthritis Ann Rheum Dis 67(2008) 309ndash314
[34] TK Kvien HM Hoyeraal B Sandstad Azathioprine versus place-bo in patients with juvenile rheumatoid arthritis a single centerdouble blind comparative study J Rheumatol 13 (1986) 118ndash123
[35] E Silverman R Mouy L Spiegel LK Jung RK SaurenmannP Lahdenne G Horneff I Calvo IS Szer K Simpson JAStewart V Strand Leflunomide or methotrexate for juvenilerheumatoid arthritis N Engl J Med 352 (2005) 1655ndash1666
[36] MA van Rossum TJ Fiselier MJ Franssen AH ZwindermanR ten Cate LW van Suijlekom-Smit WH van Luijk RM
van Soesbergen NM Wulffraat JC Oostveen W Kuis PFDijkstra CF van Ede BA Dijkmans Sulfasalazine in the treat-ment of juvenile chronic arthritis a randomized double-blindplacebo-controlled multicenter study Dutch Juvenile ChronicArthritis Study Group Arthritis Rheum 41 (1998) 808ndash816
[37] MA van Rossum RM van Soesbergen M Boers AHZwinderman TJ Fiselier MJ Franssen R ten Cate LW vanSuijlekom-Smit NM Wulffraat WH van Luijk JC OostveenW Kuis BA Dijkmans Long-term outcome of juvenile idiopathicarthritis following a placebo-controlled trial sustained benefits ofearly sulfasalazine treatment Ann Rheum Dis 66 (2007)1518ndash1524
[38] DJ Lovell EH Giannini A Reiff GD Cawkwell ED SilvermanJJ Nocton LD Stein A Gedalia NT Ilowite CA Wallace JWhitmore BK Finck Etanercept in children with polyarticularjuvenile rheumatoid arthritis Pediatric Rheumatology Collabora-tive Study Group N Engl J Med 342 (2000) 763ndash769
[39] DJ Lovell A Reiff OY Jones R Schneider J Nocton LDStein A Gedalia NT Ilowite CA Wallace JB WhitmoreB White EH Giannini Long-term safety and efficacy ofetanercept in children with polyarticular-course juvenile rheu-matoid arthritis Arthritis Rheum 54 (2006) 1987ndash1994
[40] DJ Lovell N Ruperto S Goodman A Reiff L Jung K JarosovaD Nemcova R Mouy C Sandborg J Bohnsack D Elewaut IFoeldvari V Gerloni J Rovensky K Minden RK Vehe LWWeiner G Horneff HI Huppertz NY Olson JR Medich RCarcereri-De-Prati MJ McIlraith EH Giannini A MartiniAdalimumab with or without methotrexate in juvenile rheuma-toid arthritis N Engl J Med 359 (2008) 810ndash820
[41] FH Prince M Twilt R ten Cate MA van RossumW ArmbrustEP Hoppenreijs M van Santen-Hoeufft Y Koopman-KeeminkNM Wulffraat LW van Suijlekom-Smit Long-term follow-upon effectiveness and safety of etanercept in juvenile idiopathicarthritis the Dutch National Register Ann Rheum Dis 68(2009) 635ndash641
[42] P Diak J Siegel L LaGrenade L Choi S Lemery AMcMahonTumor necrosis factor alpha blockers andmalignancy in childrenforty-eight cases reported to the Food and Drug AdministrationArthritis Rheum 62 (2010) 2517ndash2524
[43] G Horneff T Hospach G Dannecker D Foll JP Haas HJGirschick HI Huppertz R Keitzer HJ Laws H Michels KMinden R Trauzeddel Updated statement by the German So-ciety for Pediatric and Adolescent Rheumatology (GKJR) on theFDAs report regarding malignancies in anti-TNF-treated pa-tients from Aug 4 2009 Z Rheumatol 69 (2010) 561ndash567
[44] T Hospach JP Haas HI Huppertz R Keitzer H Michels RTrauzeddl D Foll G Dannecker G Horneff Comment of theSociety of Pediatric and Adolescent Rheumatology on the USFood and Drug Administration (FDA) announcement regardingcases of malignancy in anti-TNF-treated patients Z Rheumatol68 (2009) 162ndash164
[45] DJ Lovell A Reiff NT Ilowite CA Wallace Y Chon SL LinSW Baumgartner EH Giannini Safety and efficacy of up to eightyears of continuous etanercept therapy in patients with juvenilerheumatoid arthritis Arthritis Rheum 58 (2008) 1496ndash1504
[46] EH Giannini NT Ilowite DJ Lovell CA Wallace CERabinovich A Reiff G Higgins B Gottlieb NG Singer YChon SL Lin SW Baumgartner Long-term safety and effec-tiveness of etanercept in children with selected categories ofjuvenile idiopathic arthritis Arthritis Rheum 60 (2009)2794ndash2804
[47] G Horneff H Schmeling T Biedermann I Foeldvari G GanserHJ Girschick T Hospach HI Huppertz R Keitzer RM KusterH Michels D Moebius B Rogalski A Thon The German etaner-cept registry for treatment of juvenile idiopathic arthritis AnnRheum Dis 63 (2004) 1638ndash1644
[48] FH Prince M Twilt SC Simon MA van RossumW ArmbrustEP Hoppenreijs S Kamphuis M van Santen-Hoeufft Y
192 G Dueckers et al
Koopman-Keemink NM Wulffraat R ten Cate LW vanSuijlekom-Smit When and how to stop etanercept aftersuccessful treatment of patients with juvenile idiopathic ar-thritis Ann Rheum Dis 68 (2009) 1228ndash1229
[49] G Horneff F De Bock I Foeldvari HJ Girschick H MichelsD Moebius H Schmeling Safety and efficacy of combinationof etanercept and methotrexate compared to treatment withetanercept only in patients with juvenile idiopathic arthritis(JIA) preliminary data from the German JIA Registry AnnRheum Dis 68 (2009) 519ndash525
[50] N Ilowite O Porras A Reiff S Rudge M Punaro A Martin RAllen T Harville YN Sun T Bevirt G Aras B Appleton Ana-kinra in the treatment of polyarticular-course juvenile rheumatoidarthritis safety and preliminary efficacy results of a randomizedmulticenter study Clin Rheumatol 28 (2009) 129ndash137
[51] T Lequerre P Quartier D Rosellini F Alaoui M De BandtO Mejjad I Kone-Paut M Michel E Dernis M Khellaf NLimal C Job-Deslandre B Fautrel X Le Loet J Sibilia In-terleukin-1 receptor antagonist (anakinra) treatment in pa-tients with systemic-onset juvenile idiopathic arthritis oradult onset Still disease preliminary experience in FranceAnn Rheum Dis 67 (2008) 302ndash308
[52] M Gattorno A Piccini D Lasiglie S Tassi G Brisca S CartaL Delfino F Ferlito MA Pelagatti F Caroli A BuoncompagniS Viola A Loy M Sironi A Vecchi A Ravelli A Martini ARubartelli The pattern of response to anti-interleukin-1 treatmentdistinguishes two subsets of patients with systemic-onset juvenileidiopathic arthritis Arthritis Rheum 58 (2008) 1505ndash1515
[53] S Yokota T Imagawa M Mori T Miyamae Y Aihara STakei N Iwata H Umebayashi T Murata M Miyoshi MTomiita N Nishimoto T Kishimoto Efficacy and safety oftocilizumab in patients with systemic-onset juvenile idiopathicarthritis a randomised double-blind placebo-controlledwithdrawal phase III trial Lancet 371 (2008) 998ndash1006
[54] N Ruperto DJ Lovell P Quartier E Paz N Rubio-Perez CASilva C Abud-Mendoza R Burgos-Vargas V Gerloni JAMelo-Gomes C Saad-Magalhaes F Sztajnbok C Goldenstein-Schainberg M Scheinberg IC Penades M Fischbach J OrozcoPJ Hashkes C Hom L Jung L Lepore S Oliveira CAWallace LH Sigal AJ Block A Covucci A Martini EHGiannini Abatacept in children with juvenile idiopathic arthri-tis a randomised double-blind placebo-controlled withdrawaltrial Lancet 372 (2008) 383ndash391
[55] N Ruperto DJ Lovell P Quartier E Paz N Rubio-PerezCA Silva C Abud-Mendoza R Burgos-Vargas V GerloniJA Melo-Gomes C Saad-Magalhaes J Chavez-Corrales CHuemer A Kivitz FJ Blanco I Foeldvari M Hofer G HorneffHI Huppertz C Job-Deslandre A Loy K Minden M PunaroAF Nunez LH Sigal AJ Block M Nys A Martini EHGiannini Long-term safety and efficacy of abatacept inchildren with juvenile idiopathic arthritis Arthritis Rheum 62(2010) 1792ndash1802
[56] DM Brinkman IM de Kleer R ten Cate MA van RossumWP Bekkering A Fasth MJ van Tol W Kuis NM WulffraatJM Vossen Autologous stem cell transplantation in childrenwith severe progressive systemic or polyarticular juvenile idio-pathic arthritis long-term follow-up of a prospective clinicaltrial Arthritis Rheum 56 (2007) 2410ndash2421
[57] SE Klepper Effects of an eight-week physical conditioningprogram on disease signs and symptoms in children with chronicarthritis Arthritis Care Res 12 (1999) 52ndash60
[58] D Singh-Grewal J Schneiderman-Walker V Wright O Bar-OrJ Beyene H Selvadurai B Cameron RM Laxer R SchneiderED Silverman L Spiegel S Tse C Leblanc J Wong SStephens BM Feldman The effects of vigorous exercisetraining on physical function in children with arthritis arandomized controlled single-blinded trial ArthritisRheum 57 (2007) 1202ndash1210
[59] S Stephens D Singh-Grewal O Bar-Or J Beyene B CameronCM Leblanc R Schneider J Schneiderman-Walker HSelvadurai E Silverman L Spiegel SM Tse V WrightBM Feldman Reliability of exercise testing and functionalactivity questionnaires in children with juvenile arthritisArthritis Rheum 57 (2007) 1446ndash1452
[60] T Takken J van der Net W Kuis PJ Helders Physical ac-tivity and health related physical fitness in children with ju-venile idiopathic arthritis Ann Rheum Dis 62 (2003)885ndash889
[61] MM Toledo G Martini C Gigante L Da Dalt A TregnaghiF Zulian Is there a role for arthroscopic synovectomy in oli-goarticular juvenile idiopathic arthritis J Rheumatol 33(2006) 1868ndash1872
[62] F de Benedetti H Brunner N Ruperto SWright A KenwrightR Cuttica P Woo R Schneider DJ Lovell A Martini Efficacyand safety of Tocilizumab in patients with systemic juvenile idio-pathic arthritis (sJIA) 12-week data from the phase III TENDERtrial Ann Rheum Dis 69 (2010) 146
[63] P Quartier F Allantaz R Cimaz P Pillet C Messiaen CBardin X Bossuyt A Boutten J Bienvenu A Duquesne ORicher D Chaussabel A Mogenet J Banchereau JM Tre-luyer P Landais V Pascual A multicentre randomiseddouble-blind placebo-controlled trial with the interleukin-1receptor antagonist anakinra in patients with systemic-onsetjuvenile idiopathic arthritis (ANAJIS trial) Ann Rheum Dis70 (2011) 747ndash754
[64] DE Furst EC Keystone J Braun FC Breedveld GRBurmester F De Benedetti T Dorner P Emery R FleischmannA Gibofsky JR Kalden A Kavanaugh B Kirkham P Mease JSieper NG Singer JS Smolen PL Van Riel MH Weisman KWinthrop Updated consensus statement on biological agents forthe treatment of rheumatic diseases 2010 Ann Rheum Dis 70(Suppl 1) (2010) i2ndashi36
[65] T Beukelman NM Patkar KG Saag S Tolleson-RinehartRQ Cron EM Dewitt NT Ilowite Y Kimura RM LaxerDJ Lovell A Martini CE Rabinovich N Ruperto 2011 Ameri-can College of Rheumatology recommendations for the treatmentof juvenile idiopathic arthritis initiation and safety monitoring oftherapeutic agents for the treatment of arthritis and systemic fea-tures Arthritis Care Res 63 (2011) 465ndash482 (Hoboken)
[66] JF Simard M Neovius S Hagelberg J Askling Juvenile idi-opathic arthritis and risk of cancer a nationwide cohort studyArthritis Rheum 62 (2010) 3776ndash3782
[67] T Imagawa S Yokota M Mori T Miyamae S Takei H ImanakaY Nerome N Iwata T Murata M Miyoshi N Nishimoto TKishimoto Safety and efficacy of tocilizumab an anti-IL-6-receptor monoclonal antibody in patients with polyarticular-course juvenile idiopathic arthritis Mod Rheumatol (2011)doi102007s10165-011-0481-0
[68] TM Shaneyfelt MF Mayo-Smith J Rothwangl Are guide-lines following guidelines The methodological quality of clini-cal practice guidelines in the peer-reviewed medicalliterature Jama 281 (1999) 1900ndash1905
[69] R Grilli N Magrini A Penna G Mura A Liberati Practiceguidelines developed by specialty societies the need for a crit-ical appraisal Lancet 355 (2000) 103ndash106
[70] JS Burgers R Grol NS Klazinga M Makela J Zaat To-wards evidence-based clinical practice an international surveyof 18 clinical guideline programs Int J Qual Health Care 15(2003) 31ndash45
[71] JT Cassidy RE Petty Juvenile Idiopathic Rheumatic Arthri-tis 5th Edition WB Saunders Philadelphia 2005
[72] TJ Lehman Are withdrawal trials in paediatric rheumatic dis-ease helpful Lancet 372 (2008) 348ndash350
[73] J Munro Recommendations for the Diagnosis and Managementof Juvenile Idiopathic Arthritis The Royal Australian Collegeof General Practitioners South Melbourne 2009 pp 1ndash38
193Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
httpwwwnhmrcgovau_files_nhmrcpublicationsattachmentscp119-juvenile-arthritispdf
[74] MJ Santos JE Fonseca H Canhao M Conde M JoseVieira L Costa M Costa M Salgado JA Melo Gomes Guide-lines for prescribing and monitoring biologic therapies in juve-nile idiopathic arthritis Acta Reumatol Port 32 (2007) 43ndash47
[75] S Yokota M Mori T Imagawa T Murata M Tomiita Y ItohS Fujikawa S Takei Guidelines on the use of etanercept forjuvenile idiopathic arthritis in Japan Mod Rheumatol 20(2010) 107ndash113
[76] The AGREE Collaboration Appraisal of Guidelines for Researchamp Evaluation (AGREE) instrument wwwagreecollaborationorg
[77] I Kopp H Thole T Langer HK Selbmann G OllenschlaumlgerGerman Instrument for Methodological Guideline Appraisal(DELBI) wwwversorgungsleitliniende2008
[78] Auml Aumlrztliches Zentrum fuumlr Qualitaumlt in der Medizin A Arbeitsge-meinschaften der Wissenschaftlichen Fachgesellschaften in derMedizin Deutsches Instrument zur methodischen Leitlinien-Bewertung (DELBI) Fassung 20052006 Z Aumlrztl FortbildQualitaumltssich 99 (2005) 468ndash519
[79] MP de Wit SE Berlo GJ Aanerud D Aletaha JW BijlsmaL Croucher JA Da Silva B Glusing L Gossec S Hewlett MJongkees D Magnusson M Scholte-Voshaar P Richards CZiegler TA Abma European League Against Rheumatism rec-ommendations for the inclusion of patient representatives in sci-entific projects Ann Rheum Dis 70 (2011) 722ndash726
[80] I Foeldvari M Bidde Validation of the proposed ILAR classifi-cation criteria for juvenile idiopathic arthritis InternationalLeague of Associations for Rheumatology J Rheumatol 27(2000) 1069ndash1072
[81] R Merino J de Inocencio J Garcia-Consuegra Evaluation ofrevised International League of Associations for Rheumatologyclassification criteria for juvenile idiopathic arthritis in Spanishchildren (Edmonton 2001) J Rheumatol 32 (2005) 559ndash561
[82] SE Ramsey RK Bolaria DA Cabral PN Malleson REPetty Comparison of criteria for the classification of childhoodarthritis J Rheumatol 27 (2000) 1283ndash1286
[83] G Horneff A Ebert S Fitter K Minden I Foeldvari J Kum-merle-Deschner A Thon HJ Girschick F Weller HI Hup-pertz Safety and efficacy of once weekly etanercept 08mgkg in a multicentre 12 week trial in active polyarticularcourse juvenile idiopathic arthritis Rheumatology (Oxford) 48(2009) 916ndash919
[84] EH Giannini EJ Brewer N Kuzmina A Shaikov A Maxi-mov I Vorontsov CW Fink AJ Newman JT Cassidy LSZemel Methotrexate in resistant juvenile rheumatoid arthri-tis Results of the USAndashUSSR double-blind placebo-controlled trial The Pediatric Rheumatology CollaborativeStudy Group and The Cooperative Childrens Study GroupN Engl J Med 326 (1992) 1043ndash1049
[85] A Ravelli S Viola D Migliavacca N Ruperto A Pistorio AMartini The extended oligoarticular subtype is the best predic-tor of methotrexate efficacy in juvenile idiopathic arthritisJ Pediatr 135 (1999) 316ndash320
[86] P Woo TR Southwood AM Prieur CJ Dore J Grainger JDavid C Ryder N Hasson A Hall I Lemelle Randomizedplacebo-controlled crossover trial of low-dose oral
methotrexate in children with extended oligoarticular or sys-temic arthritis Arthritis Rheum 43 (2000) 1849ndash1857
[87] E Silverman L Spiegel D Hawkins R Petty D Goldsmith LSchanberg C Duffy P Howard V Strand Long-term open-label preliminary study of the safety and efficacy of lefluno-mide in patients with polyarticular-course juvenile rheumatoidarthritis Arthritis Rheum 52 (2005) 554ndash562
[88] DJ Lovell EH Giannini Y Kimura C Suzanne PJHashkes A Reiff Long-term safety and efficacy of rilonaceptin patients with systemic juvenile idiopathic arthritis (SJIA)Arthritis Rheum 60 (2009)
[89] N Ruperto P Quartier NWulffraat PWoo A Loy R Mouy BBader-Meunier BJ Prakken E Noseda R Belleli J Lecot CRordorf A Martini A Phase II Trial with canakinumab(ACZ885) a new IL-1-beta blocking monoclonal antibody toevaluate safety and preliminary efficacy in children with system-ic juvenile idiopathic arthritis Ann Rheum Dis 68 (2009) 170
[90] DJ Lovell EH Giannini Y Kimura et al Preliminary evi-dence for bioactivity of IL-1 trap (Rilonacept) a long actingIL-1 inhibitor in systemic juvenile idiopathic arthritis (sJIA)Arthritis Rheum 54 (2006) S325
[91] DJ Lovell EH Giannini Y Kimura et al Preliminary evi-dence for sustained bioactivity of IL-1 Trap (rilonacept) a longacting IL-1 inhibitor in systemic juvenile idiopathic arthritisArthritis Rheum 56 (2007) S514
[92] N Ruperto F De Benedetti H Brunner R Allen D Brown JChaitow E Cortis G Espada B Flato V Gerloni G HorneffS Wright A Kenwright R Schneider P Woo A Martini DJLovell Tocilizumab is efficacious in patients with systemic ju-venile idiopathic arthritis (sJIA) across baseline disease charac-teristics and priorbaseline treatments 12-week data from thephase II TENDER trial 17th PReS Congress Valencia Spain2010 2010
[93] N Ruperto DJ Lovell T Li F Sztajnbok C Goldenstein-Schainberg M Scheinberg IC Penades M Fischbach JOrozco PJ Hashkes C Hom L Jung L Lepore S OliveiraC Wallace M Alessio P Quartier E Cortis A Eberhard GSimonini I Lemelle E Chalom LH Sigal A Block A CovucciM Nys A Martini EH Giannini Abatacept improves health-related quality of life pain sleep quality and daily participationin subjects with juvenile idiopathic arthritis Arthritis Care Res(Hoboken) 62 (11) (2010) 1542ndash1551
[94] N Ruperto DJ Lovell P Quartier E Paz N Rubio-PerezCA Silva C Abud-Mendoza R Burgos-Vargas V GerloniJA Melo-Gomes C Saad-Magalhaes J Chavez C HuemerA Kivitz FJ Blanco I Foeldvari M Hofer G Horneff HIHuppertz CJ Deslandre A Loy K Minden M Punaro AFNunez LH Sigal AJ Block M Nys A Martini EH GianniniLong-term safety and efficacy of abatacept in children with ju-venile idiopathic arthritis Arthritis Rheum 62 (2010)1792ndash1802
[95] J Munro Juvenile Idiopathic Arthritis Management Guidelines(Provisional) Australian Paediatric Rheumatology Group 2006httpwwwnhmrcgovau
[96] K Fitch SJ Bernstein MD Aguilar B Burnand JR LaCalleP Lazaro M van het Loo J McDonnell JP Vader JPKahan The RANDUCLA Appropriateness Method Users ManualRAND Pittsburgh 2000

Consensus statement
The use of Anakinra or Tozilizumab can berecommended for treatment of children and ado-lescents with refractory SoJIA (evidence level IIrecommendation grade A)
186 G Dueckers et al
been demonstrated in a randomized controlled withdrawaldesign trial for patients with polyarticular JIA [38] Withinan open extension study long term efficacy and safety havebeen documented over 8 years in 1669 patients [3945]There is data on more than 2000 patients registered in Euro-pean registries [46ndash48] Currently retrospective data showsa somewhat better efficacy of combining MTX or otherDMARDs with TNFα-inhibition versus anti-TNFα therapy assingle therapy [49]313512 Adalimumab Adalimumab is a humanizedmonoclonal IgG1 antibody directed against TNFα whichbinds soluble and membrane bound TNFα A randomizedcontrolled withdrawal design trial demonstrated safety andefficacy of Adalimumab (24 mgmsup2 body surface every2 weeks max 40 mg) for children and adolescents withpolyarticular JIA (4ndash17 years of age n=171) [40] After16 weeks ldquowash inrdquo phase responders (n=144171) enteredthe 32 weeks randomized double blind phase After 48 weekstwice the number of patients in the verum group met ACR 70as compared to the control group (56 vs 28 pb001)Within the open extension phase Adalimumab dosage wasfixed ie 20 mgb30 kg Bw and 40 mgN30 kg Bw There islack of evidence showing superior efficacy of combiningMTX (DMARDs) with Adalimumab versus Adalimumab as sin-gle therapy [40]
Consensus statement
Efficacy of Etanercept and Adalimumab forthe treatment of polyarticular JIA has been dem-onstrated Therapy with TNFa-inhibition is indi-cated in case of insufficient therapeutic effectof NSAIDs and local GC administration and lackof response to MTX (evidence level I recom-mendation grade A)
Consensus statement
Patients with polyarticular JIA without sys-temic manifestation refractory to treatmentwith MTX and TNF inhibition might benefit fromthe use of Abatacept (evidence level III recom-mendation grade C)
313513 Infliximab Infliximab is a chimerical (humanmouse) monoclonal antibody which binds soluble and mem-brane bound TNFα A randomized controlled study in childrenand adolescents with JIA failed to demonstrate a significantdifference of efficacy after treatment with Infliximab com-pared to placebo [31]
31352 Interleukin-1-inhibitors None of interleukin-1-inhibitors are approved for the treatment of JIA or SoJIAThey are commonly used in an off label setting313521 Anakinra Anakinra is an IL-1 receptor antag-onist Within a randomized controlled trial no significant ef-ficacy of Anakinra for patients with polyarticular JIA couldbe demonstrated [50] 50 of 86 patients were enrolled intoblinded phase (11 Anakinra versus Placebo) No significantreduction of flare could be demonstrated in comparison toplacebo 29 of 50 patients completed the open label exten-sion study Two noncontrolled nonrandomized studieshave shown efficacy of anakinra in a proportion of patientswith systemic-onset of JIA (SoJIA) [5152]313522 Canakinumab Canakinumab an IL-1β anti-body binds IL-1β selectively without interfering with IL-1αor its physiological IL-1 receptor antagonist Canakinumabhas been approved for treatment of hereditary periodic IL-1 associated periodic fever syndromes ie Cryopyrin-
associated periodic syndromes There are ongoing studies in-vestigating safety and efficacy of Canakinumab for SoJIA
31353 Interleukin-6 inhibitors313531 Tozilizumab Tozilizumab is a humanizedanti-IL-6 receptor monoclonal antibody Efficacy has beendemonstrated within a 12 week double blind randomizedcontrolled withdrawal trial in children with SoJIA (n=562ndash19 years) in Japan [53] After a 48 week open extensionstudy ACR Pedi 30 was met by 47 patients (98) At thetime of our literature search Tocilizumab was approved fortreatment of SoJIA and polyarticular JIA since 2008 inJapan A multicenter European study investigating efficacyand safety of Tozilizumab in polyarticular JIA was ongoingat the deadline of literature search (wwwclinicaltrialsgov NCT00988221) No data on long term effects are cur-rently available
31354 Co-stimulation inhibitors313541 Abatacept Abatacept is a recombinant fu-sion protein of extracellular domain of human cytotoxic T-Lymphocyte Antigen 4 (CTLA-4) and IgG1-Fc-Fragment Itmodulates T-cell co-stimulation A randomized controlleddouble blind withdrawal design study of Ruperto et al [54]demonstrated efficacy of Abatacept in patients with polyar-ticular JIA 123 of 170 participants of study were enrolled inthe 6 month double blind phase Flares occurred in 33 of 62(53) patients who were given placebo versus 12 of 60(20) Abatacept patients during double blind phase Adverseevents (AE) did not differ in both groups ie 37 AE in Abata-cept versus 34 AE in placebo recipients Some children maytake 3 to 6 months or longer before their maximal responseis achieved 3 of patients developed reaction to the infu-sion [55] Abatacept is approved by FDA and EMA for pa-tients who did not respond to prior MTX treatment Nodata of long term effects of the use of Abatacept in JIA areavailable due to the low numbers of patients treated so far
314 Autologous stem cell transplantation (SCT)There are studies on autologous SCT for treatment of re-
fractory and severe forms of JIA (evidence level III) [56] 22
Consensus statement
187Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
patients were enrolled in one study 8 reached clinical re-mission 7 were assessed as partial responders 3 experi-enced relapse of the disease and 4 (18) died as aconsequence of MAS or immunosuppressive treatment [56]Due to serious adverse events including death this thera-peutic option is seen as the last treatment option
Exercise training is recommended dependingon the extent of inflammation number of affect-ed joints and global disease activity Sports withminor stress on joints is favorable (evidence levelI recommendation grade A)
32 Non-drug based therapy
321 Physiotherapy occupational therapy and thera-peutic appliances
Physio- and occupational therapy are integral parts of thetherapeutic concept in children and adolescents with JIA[5758] Therapeutic goals of physiotherapy are relaxationand pain relief preservation or rehabilitation of physiologi-cal range of joint movement prevention of contracturesstretching and activation of muscles build-up of muscleforce and training of physiological movements
Consensus statement
Structured treatment by a properly trainedphysiotherapistoccupational therapist in combi-nation with drug based therapy and instructionsfor disease adopted self-sufficient daily exercisesessions are recommended to keep and to im-prove joint mobility (evidence level II recom-mendation grade A)Custom-made therapeutic appliances for correc-tion of axial misalignment prevention of falseweight bearing stabilization of joints (eghand- finger- and foot-ortheses) are recom-mended individually The use of therapeutic ap-pliances follows individual physician-directedadvice Efficacy has been demonstrated (evi-dence level I recommendation grade B)
Consensus statement
In individual cases the indication for open orarthroscopic synovectomy can be considered ifconservative therapy does not succeed (evi-dence level III recommendation grade B)
Consensus statement
Other forms of non-drug based therapeutic approachesrely on experts opinion and are solely based on individualclinical experience No controlled studies are available
Consensus statement
The implementation of thermotherapy electro-or ultrasound therapy massage and lymph drain-age is recommended Application of cold appli-ances for acute joint inflammation is indicated(evidence level II recommendation grade A)Electro- and ultrasound therapy are recom-mended for patients with tendosynovitis (evi-dence level III recommendation grade B)
An early psychological support within stan-dard pediatric rheumatological care should beimplemented to apprehend and treat mental is-sues and behavioral syndromes associated withphysiological disturbances and physical factors(evidence level III recommendation grade A)
Consensus statement
A socio-pedagogical care with regard tointegration at school professional andeveryday life and formal education of parentsand patients is recommended (evidence levelIII recommendation grade A)
322 Sportive activity and exercise trainingPositive impact of sportive activity on the general physi-
cal condition and on oxygen consumption has been demon-strated (evidence level II) [57ndash60] Adequate exercise
training supports the physiological development and helpscoping with JIA [58] Prospective controlled long term stud-ies are currently not available
323 Surgical treatmentToledo et al investigated the role of arthroscopic syno-
vectomy in JIA They concluded that arthroscopy is a safebut only partially effective procedure in patients witholigoarticular JIA (evidence levelrecommendation gradeIIIB) [61]
324 Psychological social intervention orsocio-pedagogical care
There are no controlled or open studies focusing on psy-chological social andor socio-pedagogical intervention inchildren or adolescents with JIA Recommendations arebased on experts opinion and personal experience solely
188 G Dueckers et al
4 Addendum
Since the deadline January 15th 2010 new papers haveappeared that are of interest in the context of our guideline[5562ndash64] in particular we refer to the ACR recommenda-tions [65] and the most recent literature on the risk of malig-nancies in JIA in context with TNF blocking agent andindependent of medication [42] [66] Moreover there is arecent study on the use of Tocilizumab in polyarticular pa-tients [67] These papers will be discussed within the nextconsensus conference by NGT and considered for inclusioninto the next edition of this guideline On 6th of September2011 our advanced search on wwwclinicaltrialgov (searchterms juvenile idiopathic arthritis recruitment open stud-ies study type interventional study age group child(birthndash17) intervention drugs) led to 16 trials which are cur-rently recruiting or will soon start recruiting
5 Discussion
To develop clinical practice guidelines of high quality andvalidity a formal consensus process and explicit methodo-logical criteria for the production of guidelines are recom-mended [68ndash70] Our guideline for the treatment of JIA inchildren and adolescents implements all these issues Thesystematic literature search was terminated on 15th January2010 leading to the most up to date guideline for JIA whichis currently available The deadline of the ACR recommenda-tions as published recently by Beukelmann et al was 5th ofOctober 2009 [65] By exclusion of case reports trials with-out control groups preliminary results published as ab-stracts on conferences and the strict graduation of theliterature by the criteria of evidence based medicine weaimed to give our guideline statements additional strengthand a maximal validity Newer original studies providing ad-ditional evidence for the treatment of JIA became availableafter our consensus process was finished see AddendumThe results of these trials have to await the next NGT beforeinclusion into our recommendations
Our updated systematic literature search in 2010 led to13 relevant studies published after 30th June 2007 (Fig 1Table 4) Their results have to be interpreted with cautionFirst trials in JIA are mainly based on limited numbers of pe-diatric patients as the recruitment of a sufficient number ofpediatric patients remains challenging Second trials aremainly designed for patients with polyarticular JIA or witholigoarticular onset and a polyarticular course (Table 4)Most children with JIA do not have a polyarticular subtypeof JIA but an oligoarticular onset and course [71] Thus pa-tients with oligoarticular JIA are heavily underrepresentedin most of the current trials Third in 5 of the 13studies the withdrawal study design has been used[4045505354] Lehmann reviewed the bias of withdrawaldesign trials in 2008 [72] After a wash-in phase only re-sponders to treatment are eligible for randomization Thusthe design preselects responders to the placebo effect whomight retain their response throughout the entire study peri-od Further there is a carryover effect of AE into the place-bo group so that significant differences in AE betweengroups may not become apparent In the one placebo con-trolled trial without withdrawal design on TNFα-inhibition
(Infliximab) no significant efficacy could be demonstratedbetween verum and placebo [31]
To our knowledge there are two other guidelines that dealwith the management of JIA as a whole (Table 6) [65] [73]Other guidelines are limited to the use of single drugs in JIAeg biologic agents [74] etanercept [75] The Australian guide-line (wwwracgporgauguidelinejuvenileidiopathicarthritis)has not been published in a peer-reviewed journal It is to pro-vide recommendations for the early diagnosis and multidisci-plinary management of JIA in the primary care setting forgeneral practitioners (GPs) [73] No recommendations aremade regarding the use of GCs DMARDs immunosuppressivedrugs or biologic agents [73] The ACR recommendations usesthe Appraisal of Guidelines for Research and Evaluation(AGREE) instrument [65] [76] which does not fulfill criteria ofa proper consensus process and carries the risk that expertsvote for peer opinion which might not reflect the true valueWe used an advanced and linguistically validated version ofthe AGREE instrument the ldquoGerman Instrument for Methodo-logical Guideline Appraisal (DELBI)rdquo which has been developedin cooperation of the AWMF among others [7778] We followedthe highly structured Nominal Group Technique as described inMethodology Our consensus group only considered formallyboard nominated representatives of multidisciplinary scientificsocieties and organizations (Table 1) and included patients rep-resentatives as this has been strongly recommended by the Eu-ropean League against Rheumatism (EULAR) recently [79] TheACR mentions a parent representative within their task forcepanel but leaves this representative anonymous It remainsunclear how ACR experts were selected and involved [65]They defined treatment groups which have not been evaluatedsystematically so far We used the ILAR classification systemwhich has been repeatedly evaluated [80ndash82]
By content there are major differences between the ACRrecommendations and our guideline a) Our guideline pro-vides a detailed and systematic list of 20 drugs commonlyused in the treatment of JIA (Table 5) which has been an in-tegrative part of our consensus conferences The ACR recom-mendations do not provide information on approval status(Food and Drug Administration) indications for use and nospecific differences on dosage regimes or frequency ofdaily application [65] eg it refers to the 2008 ACR recom-mendations for the use of DMARDs in adult rheumatoid ar-thritis b) The ACR recommendations provide a more earlyaggressive approach in the treatment of JIA The ACR recom-mends MTX as first line treatment in patients (b4 joints) withhighly active disease [65] To our knowledge there are onlydata to recommend MTX administration in cases of insuffi-cient therapeutic effect of prior treatment with NSAIDandor GC [33] c) The ACR recommends the use of TNFα in-hibitors as escalation therapy for some patients with historyof arthritis of 4 or fewer joints and refer to publications[3840] conducted in patients with polyarticular JIA or pau-ciarticular JIA with polyarticular course [65] There is no ev-idence that TNF is safe and efficient in patients witholigoarticular JIA a systematic controlled clinical trial onthis issue has not been done yet d) We regard a brief trialof local or systemic administration of GC plus NSAID as a fea-sible first line treatment for patients with polyarticular JIAThe ACR recommends MTX without regard to disease activityat the initial stage [65] We reached consensus to recom-mend the use of GC as bridging therapy until full onset of
Table 6 Overview of recommendationsguidelines for treatment of JIA
USA Australia Germany
ACR recommendations[65]
RACGP recommendations[73]
GKJR guidelines
Deadline of literature search October 2009 January 2007 September 2010Source of publications Pub Med Pub Med
EMBASE CINHAL CochraneLibrary provisionalAustralian Guideline [95]
Pub MedPrevious German Guidelines [78]
Definition used for JIA subgroups Treatment groups definedby Core expert panel
Not specifically definedChildren withJIAb16 years
ILAR criteria [1]
Consensus processprocessvalidation
AGREE [76] AGREE [76] DELBI [77]RANDUCLA appropriatenessmethod [96]
NGT Delphi method
Conferences None None 3 Formal consensus conferencesAddressees Pediatric rheumatologists General practitioner Pediatric Rheumatologists
PediatriciansGeneral practitioners
Participating scientific societies or professional organizationsPediatric rheumatologist orrheumatologists for adolescents
Yes Yes Yes
General pediatrician- In hospital Yes Yes Yes- In private practice Yes Yes YesResearcher Yes No YesRheumatologists for adults No No YesOphthalmologists No No YesParentspatients support groups Yes No YesOrthopedic surgeons No No YesPediatric orthopedic surgeons No No YesPsychologists No No YesPhysiotherapists No No YesPediatric rheumatology nurses Yes No NoOther scientific societies ororganizations
ACR BSPAR PRINTO PReS RACGP NAMSCAG NHMRC DGKJ DGPs DGRh DGO AWMFBVKJ
(ACR=American College of Rheumatologists AGREE=Appraisal of Guidelines for Research amp Development AWMF=Association of the ScientificMedical Associations BSPAR=British Society for Pediatric Rheumatology BVJK=Association of Pediatricians in private practice CEP=Core expertpanel ILAR=International League against Rheumatism CINHAL=Cumulative Index to Nursing and Allied Health Literature DELBI=German In-strument for Methodological Guideline Appraisal DGKJ=German Society of Pediatrics and Adolescent Medicine DGO=German Society for Oph-thalmology DGPs=German society for Psychology DGRh=German Society for Rheumatology GKJR=German Society for Pediatric RheumatologyNAMSCAG=National Arthritis and Musculoskeletal Conditions Advisory Group NGT=Nominal Group Technique NHMRC=National Health andMedical Research Council PReS=Pediatric Rheumatology Society) PRINTO=Pediatric Rheumatology International Trial Organization RACG-P=Royal Australian College of General Practitioner RANDUCLA=Research and DevelopmentUniversity of California at Los Angeles)
189Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
therapeutic effect of DMARDs The ACR recommendations donot provide any recommendation for the use of systemic GCfor patients with oligo- or polyarticular course of JIA exceptsystemic onset of JIA e) The ACR recommendations do notcover the topic of non-drug based therapy at all althoughthere is strong evidence that eg exercise training is a usefuladdition to drug treatment [575860]
6 Conclusion
In summary we present a treatment guideline for JIA on a con-sensus conference basis We strongly advocate an interdisciplin-ary approach including surgery physiotherapy psychosocial
intervention physical therapy medications etc and a strictformal consensus process in order to create statements thatare most appropriate for the complex clinical situation of achild and family presenting with JIA and cover all aspects ofJIA care All German pediatric rheumatology sites are partici-pating at the national pediatric rheumatologic database in theDeutsche Rheuma-Forschungszentrum at Berlin (DRFZ wwwdrfzde) It aims at quality assurance in Germany and monitorstreatment behavior of pediatric rheumatologists by using inter-nationally agreed criteria (eg joint count global physician rat-ing of disease activity global parent rating of overall well-being CHAQ ESR ACR-ped response or JADAS) The databasewill be used as a tool to monitor the application of our treat-ment guidelines
190 G Dueckers et al
Conflict of interest statement
Gregor Dueckers Novartis Pharmaceuticals CorporationBaxter (for all travel grants for scientific meetings)Nihal Guellac no conflict of interestMartin Arbogast no conflict of interestGuumlnther Dannecker no conflict of interestIvan Foeldvari Wyeth Pfizer Abbott Immunology Pharma-ceuticals Chugai (for all advisory board member)Michael Frosch no conflict of interestGerd Ganser Abbott Immunology Pharmaceuticals (advisoryboard member grants for scientific meetings) Wyeth Pfizer(advisory board member grants for scientific meetings)ChugaiRoche (advisory board member grants for scientificmeetings) Merck (grants for scientific meetings) Actelios(grants for scientific meetings) Esaote (grants for scientificmeetings)Arnd Heiligenhaus Novartis Pharmaceuticals CorporationAbbott Immunology Pharmaceuticals Alcon (for all re-search grants)Gerd Horneff Abbott Immunology Pharmaceuticals (re-search grants consulting fees non-remunerative positionsof influence) Wyeth Pfizer (research grants consultingfees speakers bureau non-remunerative positions of influ-ence) Bristol-Myers Squibb (Consulting fees) Nycomed(Consulting fees non-remunerative positions of influence)RocheChugai (Consulting fees non-remunerative positionsof influence) Sandoz (Consulting fees) Genzyme (researchgrants consulting fees non-remunerative positions of influ-ence) Swedish Orphan (research grants consulting feesnon-remunerative positions of influence)Arnold Illhardt no conflict of interestRuumldiger Krauspe no conflict of interestBarbara Markus no conflict of interestHartmut Michels Abbott Immunology Pharmaceuticals (advi-sory board member and grants for scientific meeting)Matthias Schneider no conflict of interestWolfram Singendonk no conflict of interestHelmut Sitter no conflict of interestMarianne Spamer no conflict of interestNorbert Wagner no conflict of interestTim Niehues Abbott Immunology Pharmaceuticals EssexPharma Novartis Pharmaceutical Corporation WyethPfizer (for all research grants consulting fees non-remu-nerative positions of influence)
Acknowledgment
We like to express our grateful thanks to Prof Dr Hans IkoHuppertz for proof reading the article and for an excellentdiscussion on our work We like to express our thanks to HE-LIOS Clinic for funding the open access of the article
References
[1] RE Petty TR Southwood P Manners J Baum DN Glass JGoldenberg X He J Maldonado-Cocco J Orozco-Alcala AMPrieur ME Suarez-Almazor PWoo International League of Asso-ciations for Rheumatology classification of juvenile idiopathic ar-thritis second revision Edmonton 2001 J Rheumatol 31(2004) 390ndash392
[2] B Prakken S Albani A Martini Juvenile idiopathic arthritisLancet 377 (2011) 2138ndash2149
[3] KT April DE Feldman RW Platt CM Duffy Comparisonbetween children with juvenile idiopathic arthritis (JIA) andtheir parents concerning perceived quality of life Qual LifeRes 15 (2006) 655ndash661
[4] BM Feldman B Grundland L McCullough V Wright Distinc-tion of quality of life health related quality of life and healthstatus in children referred for rheumatologic care J Rheuma-tol 27 (2000) 226ndash233
[5] JC Packham MA Hall Long-term follow-up of 246 adultswith juvenile idiopathic arthritis functional outcomeRheumatology (Oxford) 41 (2002) 1428ndash1435
[6] C Sandborg Pediatric rheumatic disease standards of care forJIAmdashthe basic foundation for quality Nat Rev Rheumatol 6(2010) 389ndash390
[7] N Guellac T Niehues Interdisciplinary and evidence-basedtreatment guideline for juvenile idiopathic arthritis KlinPadiatr 220 (2008) 392ndash402
[8] K Schnakenburg Leitlinien in der Kinder- und JugendmedizinElsevier 2005 pp H1 1ndash15
[9] P Juni L Nartey S Reichenbach R Sterchi PA Dieppe MEgger Risk of cardiovascular events and rofecoxib cumulativemeta-analysis Lancet 364 (2004) 2021ndash2029
[10] W Feldman Evidence-based Pediatrics 1st ed BC DeckersHamilton 2000
[11] AH Van de Ven AL Delbecq The nominal group as a re-search instrument for exploratory health studies Am J PublicHealth 62 (1972) 337ndash342
[12] HA Linstone M Turoff The Delphi Method Techniques andApplications Addison-Wesley Pub 1975
[13] TK Kvien HM Hoyeraal B Sandstad Naproxen and acetyl-salicylic acid in the treatment of pauciarticular and polyarticu-lar juvenile rheumatoid arthritis Assessment of tolerance andefficacy in a single-centre 24-week double-blind parallelstudy Scand J Rheumatol 13 (1984) 342ndash350
[14] RM Laxer ED Silverman C St-Cyr MT Tran G Lingam Asix-month open safety assessment of a naproxen suspensionformulation in the therapy of juvenile rheumatoid arthritisClin Ther 10 (1988) 381ndash387
[15] AM Leak MR Richter LE Clemens MA Hall BM AnsellA crossover study of naproxen diclofenac and tolmetin in sero-negative juvenile chronic arthritis Clin Exp Rheumatol 6(1988) 157ndash160
[16] J Haapasaari E Wuolijoki H Ylijoki Treatment of juve-nile rheumatoid arthritis with diclofenac sodium Scand JRheumatol 12 (1983) 325ndash330
[17] EH Giannini EJ Brewer ML Miller D Gibbas MH PassoHM Hoyeraal B Bernstein DA Person CW Fink LA Sawyeret al Ibuprofen suspension in the treatment of juvenilerheumatoid arthritis Pediatric Rheumatology CollaborativeStudy Group J Pediatr 117 (1990) 645ndash652
[18] E Stoeber L Sanger Experiences with indomethacin in long-term therapy of juvenile rheumatoid arthritis Arzneimittel-forschung 21 (1971) 1865ndash1866
[19] N Ruperto I Nikishina ED Pachanov Y Shachbazian AMPrieur R Mouy R Joos F Zulian R Schwarz V ArtamonovaW Emminger M Bandeira A Buoncompagni I Foeldvari FFalcini E Baildam I Kone-Paut M Alessio V Gerloni ALenhardt A Martini G Hanft R Sigmund S Simianer Arandomized double-blind clinical trial of two doses ofmeloxicam compared with naproxen in children with juvenileidiopathic arthritis short- and long-term efficacy and safetyresults Arthritis Rheum 52 (2005) 563ndash572
[20] I Foeldvari IS Szer LS Zemel DJ Lovell EH Giannini JLRobbins CRWest G Steidle S Krishnaswami BJ Bloom A pro-spective study comparing celecoxib with naproxen in children withjuvenile rheumatoid arthritis J Rheumatol 36 (2009) 174ndash182
191Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
[21] F Zulian G Martini D Gobber C Agosto C Gigante FZacchello Comparison of intra-articular triamcinolone hexa-cetonide and triamcinolone acetonide in oligoarticular juve-nile idiopathic arthritis Rheumatology (Oxford) 42 (2003)1254ndash1259
[22] F Zulian G Martini D Gobber M Plebani F Zacchello PManners Triamcinolone acetonide and hexacetonide intra-articular treatment of symmetrical joints in juvenile idiopathicarthritis a double-blind trial Rheumatology (Oxford) 43 (2004)1288ndash1291
[23] GS Habib Systemic effects of intra-articular corticosteroidsClin Rheumatol 28 (2009) 749ndash756
[24] JR Kirwan The effect of glucocorticoids on joint destructionin rheumatoid arthritis The Arthritis and Rheumatism CouncilLow-Dose Glucocorticoid Study Group N Engl J Med 333(1995) 142ndash146
[25] H Michels What is low-dose corticosteroid therapy in juvenileidiopathic arthritis A worldwide questionnaire-based surveyZ Rheumatol 59 (Suppl 2) (2000) II127ndash130
[26] JJ Miller III Prolonged use of large intravenous steroid pulsesin the rheumatic diseases of children Pediatrics 65 (1980)989ndash994
[27] P Picco M Gattorno A Buoncompagni V Pistoia C Borrone6-methylprednisolone lsquomini-pulsesrsquo a newmodality of glucocor-ticoid treatment in systemic onset juvenile chronic arthritisScand J Rheumatol 25 (1996) 24ndash27
[28] AM Prieur The place of corticosteroid therapy in juvenilechronic arthritis in 1992 J Rheumatol Suppl 37 (1993)32ndash34
[29] JS Gao H Wu J Tian Treatment of patients with juvenilerheumatoid arthritis with combination of leflunomide andmethotrexate Zhonghua Er Ke Za Zhi 41 (2003) 435ndash438
[30] T Niehues G Horneff H Michels MS Hock L SchuchmannEvidence-based use of methotrexate in children with rheumat-ic diseases a consensus statement of the Working Groups Pedi-atric Rheumatology Germany (AGKJR) and PediatricRheumatology Austria Rheumatol Int 25 (2005) 169ndash178
[31] N Ruperto DJ Lovell R Cuttica N Wilkinson P Woo GEspada C Wouters ED Silverman Z Balogh M HenricksonMT Apaz E Baildam A Fasth V Gerloni P Lahdenne AMPrieur A Ravelli RK Saurenmann ML Gamir N WulffraatL Marodi RE Petty R Joos F Zulian D McCurdy BLMyones K Nagy P Reuman I Szer S Travers A BeutlerG Keenan J Clark S Visvanathan A Fasanmade A Ray-chaudhuri A Mendelsohn A Martini EH Giannini A random-ized placebo-controlled trial of infliximab plus methotrexatefor the treatment of polyarticular-course juvenile rheumatoidarthritis Arthritis Rheum 56 (2007) 3096ndash3106
[32] K Visser DM van der Heijde Risk and management of livertoxicity during methotrexate treatment in rheumatoid andpsoriatic arthritis a systematic review of the literature ClinExp Rheumatol 27 (2009) 1017ndash1025
[33] A Cespedes-Cruz R Gutierrez-Suarez A Pistorio A Ravelli ALoy KJ Murray V Gerloni N Wulffraat S Oliveira J WalshIC Penades MG Alpigiani P Lahdenne C Saad-Magalhaes ECortis L Lepore Y Kimura C Wouters A Martini N RupertoMethotrexate improves the health-related quality of life of chil-dren with juvenile idiopathic arthritis Ann Rheum Dis 67(2008) 309ndash314
[34] TK Kvien HM Hoyeraal B Sandstad Azathioprine versus place-bo in patients with juvenile rheumatoid arthritis a single centerdouble blind comparative study J Rheumatol 13 (1986) 118ndash123
[35] E Silverman R Mouy L Spiegel LK Jung RK SaurenmannP Lahdenne G Horneff I Calvo IS Szer K Simpson JAStewart V Strand Leflunomide or methotrexate for juvenilerheumatoid arthritis N Engl J Med 352 (2005) 1655ndash1666
[36] MA van Rossum TJ Fiselier MJ Franssen AH ZwindermanR ten Cate LW van Suijlekom-Smit WH van Luijk RM
van Soesbergen NM Wulffraat JC Oostveen W Kuis PFDijkstra CF van Ede BA Dijkmans Sulfasalazine in the treat-ment of juvenile chronic arthritis a randomized double-blindplacebo-controlled multicenter study Dutch Juvenile ChronicArthritis Study Group Arthritis Rheum 41 (1998) 808ndash816
[37] MA van Rossum RM van Soesbergen M Boers AHZwinderman TJ Fiselier MJ Franssen R ten Cate LW vanSuijlekom-Smit NM Wulffraat WH van Luijk JC OostveenW Kuis BA Dijkmans Long-term outcome of juvenile idiopathicarthritis following a placebo-controlled trial sustained benefits ofearly sulfasalazine treatment Ann Rheum Dis 66 (2007)1518ndash1524
[38] DJ Lovell EH Giannini A Reiff GD Cawkwell ED SilvermanJJ Nocton LD Stein A Gedalia NT Ilowite CA Wallace JWhitmore BK Finck Etanercept in children with polyarticularjuvenile rheumatoid arthritis Pediatric Rheumatology Collabora-tive Study Group N Engl J Med 342 (2000) 763ndash769
[39] DJ Lovell A Reiff OY Jones R Schneider J Nocton LDStein A Gedalia NT Ilowite CA Wallace JB WhitmoreB White EH Giannini Long-term safety and efficacy ofetanercept in children with polyarticular-course juvenile rheu-matoid arthritis Arthritis Rheum 54 (2006) 1987ndash1994
[40] DJ Lovell N Ruperto S Goodman A Reiff L Jung K JarosovaD Nemcova R Mouy C Sandborg J Bohnsack D Elewaut IFoeldvari V Gerloni J Rovensky K Minden RK Vehe LWWeiner G Horneff HI Huppertz NY Olson JR Medich RCarcereri-De-Prati MJ McIlraith EH Giannini A MartiniAdalimumab with or without methotrexate in juvenile rheuma-toid arthritis N Engl J Med 359 (2008) 810ndash820
[41] FH Prince M Twilt R ten Cate MA van RossumW ArmbrustEP Hoppenreijs M van Santen-Hoeufft Y Koopman-KeeminkNM Wulffraat LW van Suijlekom-Smit Long-term follow-upon effectiveness and safety of etanercept in juvenile idiopathicarthritis the Dutch National Register Ann Rheum Dis 68(2009) 635ndash641
[42] P Diak J Siegel L LaGrenade L Choi S Lemery AMcMahonTumor necrosis factor alpha blockers andmalignancy in childrenforty-eight cases reported to the Food and Drug AdministrationArthritis Rheum 62 (2010) 2517ndash2524
[43] G Horneff T Hospach G Dannecker D Foll JP Haas HJGirschick HI Huppertz R Keitzer HJ Laws H Michels KMinden R Trauzeddel Updated statement by the German So-ciety for Pediatric and Adolescent Rheumatology (GKJR) on theFDAs report regarding malignancies in anti-TNF-treated pa-tients from Aug 4 2009 Z Rheumatol 69 (2010) 561ndash567
[44] T Hospach JP Haas HI Huppertz R Keitzer H Michels RTrauzeddl D Foll G Dannecker G Horneff Comment of theSociety of Pediatric and Adolescent Rheumatology on the USFood and Drug Administration (FDA) announcement regardingcases of malignancy in anti-TNF-treated patients Z Rheumatol68 (2009) 162ndash164
[45] DJ Lovell A Reiff NT Ilowite CA Wallace Y Chon SL LinSW Baumgartner EH Giannini Safety and efficacy of up to eightyears of continuous etanercept therapy in patients with juvenilerheumatoid arthritis Arthritis Rheum 58 (2008) 1496ndash1504
[46] EH Giannini NT Ilowite DJ Lovell CA Wallace CERabinovich A Reiff G Higgins B Gottlieb NG Singer YChon SL Lin SW Baumgartner Long-term safety and effec-tiveness of etanercept in children with selected categories ofjuvenile idiopathic arthritis Arthritis Rheum 60 (2009)2794ndash2804
[47] G Horneff H Schmeling T Biedermann I Foeldvari G GanserHJ Girschick T Hospach HI Huppertz R Keitzer RM KusterH Michels D Moebius B Rogalski A Thon The German etaner-cept registry for treatment of juvenile idiopathic arthritis AnnRheum Dis 63 (2004) 1638ndash1644
[48] FH Prince M Twilt SC Simon MA van RossumW ArmbrustEP Hoppenreijs S Kamphuis M van Santen-Hoeufft Y
192 G Dueckers et al
Koopman-Keemink NM Wulffraat R ten Cate LW vanSuijlekom-Smit When and how to stop etanercept aftersuccessful treatment of patients with juvenile idiopathic ar-thritis Ann Rheum Dis 68 (2009) 1228ndash1229
[49] G Horneff F De Bock I Foeldvari HJ Girschick H MichelsD Moebius H Schmeling Safety and efficacy of combinationof etanercept and methotrexate compared to treatment withetanercept only in patients with juvenile idiopathic arthritis(JIA) preliminary data from the German JIA Registry AnnRheum Dis 68 (2009) 519ndash525
[50] N Ilowite O Porras A Reiff S Rudge M Punaro A Martin RAllen T Harville YN Sun T Bevirt G Aras B Appleton Ana-kinra in the treatment of polyarticular-course juvenile rheumatoidarthritis safety and preliminary efficacy results of a randomizedmulticenter study Clin Rheumatol 28 (2009) 129ndash137
[51] T Lequerre P Quartier D Rosellini F Alaoui M De BandtO Mejjad I Kone-Paut M Michel E Dernis M Khellaf NLimal C Job-Deslandre B Fautrel X Le Loet J Sibilia In-terleukin-1 receptor antagonist (anakinra) treatment in pa-tients with systemic-onset juvenile idiopathic arthritis oradult onset Still disease preliminary experience in FranceAnn Rheum Dis 67 (2008) 302ndash308
[52] M Gattorno A Piccini D Lasiglie S Tassi G Brisca S CartaL Delfino F Ferlito MA Pelagatti F Caroli A BuoncompagniS Viola A Loy M Sironi A Vecchi A Ravelli A Martini ARubartelli The pattern of response to anti-interleukin-1 treatmentdistinguishes two subsets of patients with systemic-onset juvenileidiopathic arthritis Arthritis Rheum 58 (2008) 1505ndash1515
[53] S Yokota T Imagawa M Mori T Miyamae Y Aihara STakei N Iwata H Umebayashi T Murata M Miyoshi MTomiita N Nishimoto T Kishimoto Efficacy and safety oftocilizumab in patients with systemic-onset juvenile idiopathicarthritis a randomised double-blind placebo-controlledwithdrawal phase III trial Lancet 371 (2008) 998ndash1006
[54] N Ruperto DJ Lovell P Quartier E Paz N Rubio-Perez CASilva C Abud-Mendoza R Burgos-Vargas V Gerloni JAMelo-Gomes C Saad-Magalhaes F Sztajnbok C Goldenstein-Schainberg M Scheinberg IC Penades M Fischbach J OrozcoPJ Hashkes C Hom L Jung L Lepore S Oliveira CAWallace LH Sigal AJ Block A Covucci A Martini EHGiannini Abatacept in children with juvenile idiopathic arthri-tis a randomised double-blind placebo-controlled withdrawaltrial Lancet 372 (2008) 383ndash391
[55] N Ruperto DJ Lovell P Quartier E Paz N Rubio-PerezCA Silva C Abud-Mendoza R Burgos-Vargas V GerloniJA Melo-Gomes C Saad-Magalhaes J Chavez-Corrales CHuemer A Kivitz FJ Blanco I Foeldvari M Hofer G HorneffHI Huppertz C Job-Deslandre A Loy K Minden M PunaroAF Nunez LH Sigal AJ Block M Nys A Martini EHGiannini Long-term safety and efficacy of abatacept inchildren with juvenile idiopathic arthritis Arthritis Rheum 62(2010) 1792ndash1802
[56] DM Brinkman IM de Kleer R ten Cate MA van RossumWP Bekkering A Fasth MJ van Tol W Kuis NM WulffraatJM Vossen Autologous stem cell transplantation in childrenwith severe progressive systemic or polyarticular juvenile idio-pathic arthritis long-term follow-up of a prospective clinicaltrial Arthritis Rheum 56 (2007) 2410ndash2421
[57] SE Klepper Effects of an eight-week physical conditioningprogram on disease signs and symptoms in children with chronicarthritis Arthritis Care Res 12 (1999) 52ndash60
[58] D Singh-Grewal J Schneiderman-Walker V Wright O Bar-OrJ Beyene H Selvadurai B Cameron RM Laxer R SchneiderED Silverman L Spiegel S Tse C Leblanc J Wong SStephens BM Feldman The effects of vigorous exercisetraining on physical function in children with arthritis arandomized controlled single-blinded trial ArthritisRheum 57 (2007) 1202ndash1210
[59] S Stephens D Singh-Grewal O Bar-Or J Beyene B CameronCM Leblanc R Schneider J Schneiderman-Walker HSelvadurai E Silverman L Spiegel SM Tse V WrightBM Feldman Reliability of exercise testing and functionalactivity questionnaires in children with juvenile arthritisArthritis Rheum 57 (2007) 1446ndash1452
[60] T Takken J van der Net W Kuis PJ Helders Physical ac-tivity and health related physical fitness in children with ju-venile idiopathic arthritis Ann Rheum Dis 62 (2003)885ndash889
[61] MM Toledo G Martini C Gigante L Da Dalt A TregnaghiF Zulian Is there a role for arthroscopic synovectomy in oli-goarticular juvenile idiopathic arthritis J Rheumatol 33(2006) 1868ndash1872
[62] F de Benedetti H Brunner N Ruperto SWright A KenwrightR Cuttica P Woo R Schneider DJ Lovell A Martini Efficacyand safety of Tocilizumab in patients with systemic juvenile idio-pathic arthritis (sJIA) 12-week data from the phase III TENDERtrial Ann Rheum Dis 69 (2010) 146
[63] P Quartier F Allantaz R Cimaz P Pillet C Messiaen CBardin X Bossuyt A Boutten J Bienvenu A Duquesne ORicher D Chaussabel A Mogenet J Banchereau JM Tre-luyer P Landais V Pascual A multicentre randomiseddouble-blind placebo-controlled trial with the interleukin-1receptor antagonist anakinra in patients with systemic-onsetjuvenile idiopathic arthritis (ANAJIS trial) Ann Rheum Dis70 (2011) 747ndash754
[64] DE Furst EC Keystone J Braun FC Breedveld GRBurmester F De Benedetti T Dorner P Emery R FleischmannA Gibofsky JR Kalden A Kavanaugh B Kirkham P Mease JSieper NG Singer JS Smolen PL Van Riel MH Weisman KWinthrop Updated consensus statement on biological agents forthe treatment of rheumatic diseases 2010 Ann Rheum Dis 70(Suppl 1) (2010) i2ndashi36
[65] T Beukelman NM Patkar KG Saag S Tolleson-RinehartRQ Cron EM Dewitt NT Ilowite Y Kimura RM LaxerDJ Lovell A Martini CE Rabinovich N Ruperto 2011 Ameri-can College of Rheumatology recommendations for the treatmentof juvenile idiopathic arthritis initiation and safety monitoring oftherapeutic agents for the treatment of arthritis and systemic fea-tures Arthritis Care Res 63 (2011) 465ndash482 (Hoboken)
[66] JF Simard M Neovius S Hagelberg J Askling Juvenile idi-opathic arthritis and risk of cancer a nationwide cohort studyArthritis Rheum 62 (2010) 3776ndash3782
[67] T Imagawa S Yokota M Mori T Miyamae S Takei H ImanakaY Nerome N Iwata T Murata M Miyoshi N Nishimoto TKishimoto Safety and efficacy of tocilizumab an anti-IL-6-receptor monoclonal antibody in patients with polyarticular-course juvenile idiopathic arthritis Mod Rheumatol (2011)doi102007s10165-011-0481-0
[68] TM Shaneyfelt MF Mayo-Smith J Rothwangl Are guide-lines following guidelines The methodological quality of clini-cal practice guidelines in the peer-reviewed medicalliterature Jama 281 (1999) 1900ndash1905
[69] R Grilli N Magrini A Penna G Mura A Liberati Practiceguidelines developed by specialty societies the need for a crit-ical appraisal Lancet 355 (2000) 103ndash106
[70] JS Burgers R Grol NS Klazinga M Makela J Zaat To-wards evidence-based clinical practice an international surveyof 18 clinical guideline programs Int J Qual Health Care 15(2003) 31ndash45
[71] JT Cassidy RE Petty Juvenile Idiopathic Rheumatic Arthri-tis 5th Edition WB Saunders Philadelphia 2005
[72] TJ Lehman Are withdrawal trials in paediatric rheumatic dis-ease helpful Lancet 372 (2008) 348ndash350
[73] J Munro Recommendations for the Diagnosis and Managementof Juvenile Idiopathic Arthritis The Royal Australian Collegeof General Practitioners South Melbourne 2009 pp 1ndash38
193Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
httpwwwnhmrcgovau_files_nhmrcpublicationsattachmentscp119-juvenile-arthritispdf
[74] MJ Santos JE Fonseca H Canhao M Conde M JoseVieira L Costa M Costa M Salgado JA Melo Gomes Guide-lines for prescribing and monitoring biologic therapies in juve-nile idiopathic arthritis Acta Reumatol Port 32 (2007) 43ndash47
[75] S Yokota M Mori T Imagawa T Murata M Tomiita Y ItohS Fujikawa S Takei Guidelines on the use of etanercept forjuvenile idiopathic arthritis in Japan Mod Rheumatol 20(2010) 107ndash113
[76] The AGREE Collaboration Appraisal of Guidelines for Researchamp Evaluation (AGREE) instrument wwwagreecollaborationorg
[77] I Kopp H Thole T Langer HK Selbmann G OllenschlaumlgerGerman Instrument for Methodological Guideline Appraisal(DELBI) wwwversorgungsleitliniende2008
[78] Auml Aumlrztliches Zentrum fuumlr Qualitaumlt in der Medizin A Arbeitsge-meinschaften der Wissenschaftlichen Fachgesellschaften in derMedizin Deutsches Instrument zur methodischen Leitlinien-Bewertung (DELBI) Fassung 20052006 Z Aumlrztl FortbildQualitaumltssich 99 (2005) 468ndash519
[79] MP de Wit SE Berlo GJ Aanerud D Aletaha JW BijlsmaL Croucher JA Da Silva B Glusing L Gossec S Hewlett MJongkees D Magnusson M Scholte-Voshaar P Richards CZiegler TA Abma European League Against Rheumatism rec-ommendations for the inclusion of patient representatives in sci-entific projects Ann Rheum Dis 70 (2011) 722ndash726
[80] I Foeldvari M Bidde Validation of the proposed ILAR classifi-cation criteria for juvenile idiopathic arthritis InternationalLeague of Associations for Rheumatology J Rheumatol 27(2000) 1069ndash1072
[81] R Merino J de Inocencio J Garcia-Consuegra Evaluation ofrevised International League of Associations for Rheumatologyclassification criteria for juvenile idiopathic arthritis in Spanishchildren (Edmonton 2001) J Rheumatol 32 (2005) 559ndash561
[82] SE Ramsey RK Bolaria DA Cabral PN Malleson REPetty Comparison of criteria for the classification of childhoodarthritis J Rheumatol 27 (2000) 1283ndash1286
[83] G Horneff A Ebert S Fitter K Minden I Foeldvari J Kum-merle-Deschner A Thon HJ Girschick F Weller HI Hup-pertz Safety and efficacy of once weekly etanercept 08mgkg in a multicentre 12 week trial in active polyarticularcourse juvenile idiopathic arthritis Rheumatology (Oxford) 48(2009) 916ndash919
[84] EH Giannini EJ Brewer N Kuzmina A Shaikov A Maxi-mov I Vorontsov CW Fink AJ Newman JT Cassidy LSZemel Methotrexate in resistant juvenile rheumatoid arthri-tis Results of the USAndashUSSR double-blind placebo-controlled trial The Pediatric Rheumatology CollaborativeStudy Group and The Cooperative Childrens Study GroupN Engl J Med 326 (1992) 1043ndash1049
[85] A Ravelli S Viola D Migliavacca N Ruperto A Pistorio AMartini The extended oligoarticular subtype is the best predic-tor of methotrexate efficacy in juvenile idiopathic arthritisJ Pediatr 135 (1999) 316ndash320
[86] P Woo TR Southwood AM Prieur CJ Dore J Grainger JDavid C Ryder N Hasson A Hall I Lemelle Randomizedplacebo-controlled crossover trial of low-dose oral
methotrexate in children with extended oligoarticular or sys-temic arthritis Arthritis Rheum 43 (2000) 1849ndash1857
[87] E Silverman L Spiegel D Hawkins R Petty D Goldsmith LSchanberg C Duffy P Howard V Strand Long-term open-label preliminary study of the safety and efficacy of lefluno-mide in patients with polyarticular-course juvenile rheumatoidarthritis Arthritis Rheum 52 (2005) 554ndash562
[88] DJ Lovell EH Giannini Y Kimura C Suzanne PJHashkes A Reiff Long-term safety and efficacy of rilonaceptin patients with systemic juvenile idiopathic arthritis (SJIA)Arthritis Rheum 60 (2009)
[89] N Ruperto P Quartier NWulffraat PWoo A Loy R Mouy BBader-Meunier BJ Prakken E Noseda R Belleli J Lecot CRordorf A Martini A Phase II Trial with canakinumab(ACZ885) a new IL-1-beta blocking monoclonal antibody toevaluate safety and preliminary efficacy in children with system-ic juvenile idiopathic arthritis Ann Rheum Dis 68 (2009) 170
[90] DJ Lovell EH Giannini Y Kimura et al Preliminary evi-dence for bioactivity of IL-1 trap (Rilonacept) a long actingIL-1 inhibitor in systemic juvenile idiopathic arthritis (sJIA)Arthritis Rheum 54 (2006) S325
[91] DJ Lovell EH Giannini Y Kimura et al Preliminary evi-dence for sustained bioactivity of IL-1 Trap (rilonacept) a longacting IL-1 inhibitor in systemic juvenile idiopathic arthritisArthritis Rheum 56 (2007) S514
[92] N Ruperto F De Benedetti H Brunner R Allen D Brown JChaitow E Cortis G Espada B Flato V Gerloni G HorneffS Wright A Kenwright R Schneider P Woo A Martini DJLovell Tocilizumab is efficacious in patients with systemic ju-venile idiopathic arthritis (sJIA) across baseline disease charac-teristics and priorbaseline treatments 12-week data from thephase II TENDER trial 17th PReS Congress Valencia Spain2010 2010
[93] N Ruperto DJ Lovell T Li F Sztajnbok C Goldenstein-Schainberg M Scheinberg IC Penades M Fischbach JOrozco PJ Hashkes C Hom L Jung L Lepore S OliveiraC Wallace M Alessio P Quartier E Cortis A Eberhard GSimonini I Lemelle E Chalom LH Sigal A Block A CovucciM Nys A Martini EH Giannini Abatacept improves health-related quality of life pain sleep quality and daily participationin subjects with juvenile idiopathic arthritis Arthritis Care Res(Hoboken) 62 (11) (2010) 1542ndash1551
[94] N Ruperto DJ Lovell P Quartier E Paz N Rubio-PerezCA Silva C Abud-Mendoza R Burgos-Vargas V GerloniJA Melo-Gomes C Saad-Magalhaes J Chavez C HuemerA Kivitz FJ Blanco I Foeldvari M Hofer G Horneff HIHuppertz CJ Deslandre A Loy K Minden M Punaro AFNunez LH Sigal AJ Block M Nys A Martini EH GianniniLong-term safety and efficacy of abatacept in children with ju-venile idiopathic arthritis Arthritis Rheum 62 (2010)1792ndash1802
[95] J Munro Juvenile Idiopathic Arthritis Management Guidelines(Provisional) Australian Paediatric Rheumatology Group 2006httpwwwnhmrcgovau
[96] K Fitch SJ Bernstein MD Aguilar B Burnand JR LaCalleP Lazaro M van het Loo J McDonnell JP Vader JPKahan The RANDUCLA Appropriateness Method Users ManualRAND Pittsburgh 2000

Consensus statement
187Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
patients were enrolled in one study 8 reached clinical re-mission 7 were assessed as partial responders 3 experi-enced relapse of the disease and 4 (18) died as aconsequence of MAS or immunosuppressive treatment [56]Due to serious adverse events including death this thera-peutic option is seen as the last treatment option
Exercise training is recommended dependingon the extent of inflammation number of affect-ed joints and global disease activity Sports withminor stress on joints is favorable (evidence levelI recommendation grade A)
32 Non-drug based therapy
321 Physiotherapy occupational therapy and thera-peutic appliances
Physio- and occupational therapy are integral parts of thetherapeutic concept in children and adolescents with JIA[5758] Therapeutic goals of physiotherapy are relaxationand pain relief preservation or rehabilitation of physiologi-cal range of joint movement prevention of contracturesstretching and activation of muscles build-up of muscleforce and training of physiological movements
Consensus statement
Structured treatment by a properly trainedphysiotherapistoccupational therapist in combi-nation with drug based therapy and instructionsfor disease adopted self-sufficient daily exercisesessions are recommended to keep and to im-prove joint mobility (evidence level II recom-mendation grade A)Custom-made therapeutic appliances for correc-tion of axial misalignment prevention of falseweight bearing stabilization of joints (eghand- finger- and foot-ortheses) are recom-mended individually The use of therapeutic ap-pliances follows individual physician-directedadvice Efficacy has been demonstrated (evi-dence level I recommendation grade B)
Consensus statement
In individual cases the indication for open orarthroscopic synovectomy can be considered ifconservative therapy does not succeed (evi-dence level III recommendation grade B)
Consensus statement
Other forms of non-drug based therapeutic approachesrely on experts opinion and are solely based on individualclinical experience No controlled studies are available
Consensus statement
The implementation of thermotherapy electro-or ultrasound therapy massage and lymph drain-age is recommended Application of cold appli-ances for acute joint inflammation is indicated(evidence level II recommendation grade A)Electro- and ultrasound therapy are recom-mended for patients with tendosynovitis (evi-dence level III recommendation grade B)
An early psychological support within stan-dard pediatric rheumatological care should beimplemented to apprehend and treat mental is-sues and behavioral syndromes associated withphysiological disturbances and physical factors(evidence level III recommendation grade A)
Consensus statement
A socio-pedagogical care with regard tointegration at school professional andeveryday life and formal education of parentsand patients is recommended (evidence levelIII recommendation grade A)
322 Sportive activity and exercise trainingPositive impact of sportive activity on the general physi-
cal condition and on oxygen consumption has been demon-strated (evidence level II) [57ndash60] Adequate exercise
training supports the physiological development and helpscoping with JIA [58] Prospective controlled long term stud-ies are currently not available
323 Surgical treatmentToledo et al investigated the role of arthroscopic syno-
vectomy in JIA They concluded that arthroscopy is a safebut only partially effective procedure in patients witholigoarticular JIA (evidence levelrecommendation gradeIIIB) [61]
324 Psychological social intervention orsocio-pedagogical care
There are no controlled or open studies focusing on psy-chological social andor socio-pedagogical intervention inchildren or adolescents with JIA Recommendations arebased on experts opinion and personal experience solely
188 G Dueckers et al
4 Addendum
Since the deadline January 15th 2010 new papers haveappeared that are of interest in the context of our guideline[5562ndash64] in particular we refer to the ACR recommenda-tions [65] and the most recent literature on the risk of malig-nancies in JIA in context with TNF blocking agent andindependent of medication [42] [66] Moreover there is arecent study on the use of Tocilizumab in polyarticular pa-tients [67] These papers will be discussed within the nextconsensus conference by NGT and considered for inclusioninto the next edition of this guideline On 6th of September2011 our advanced search on wwwclinicaltrialgov (searchterms juvenile idiopathic arthritis recruitment open stud-ies study type interventional study age group child(birthndash17) intervention drugs) led to 16 trials which are cur-rently recruiting or will soon start recruiting
5 Discussion
To develop clinical practice guidelines of high quality andvalidity a formal consensus process and explicit methodo-logical criteria for the production of guidelines are recom-mended [68ndash70] Our guideline for the treatment of JIA inchildren and adolescents implements all these issues Thesystematic literature search was terminated on 15th January2010 leading to the most up to date guideline for JIA whichis currently available The deadline of the ACR recommenda-tions as published recently by Beukelmann et al was 5th ofOctober 2009 [65] By exclusion of case reports trials with-out control groups preliminary results published as ab-stracts on conferences and the strict graduation of theliterature by the criteria of evidence based medicine weaimed to give our guideline statements additional strengthand a maximal validity Newer original studies providing ad-ditional evidence for the treatment of JIA became availableafter our consensus process was finished see AddendumThe results of these trials have to await the next NGT beforeinclusion into our recommendations
Our updated systematic literature search in 2010 led to13 relevant studies published after 30th June 2007 (Fig 1Table 4) Their results have to be interpreted with cautionFirst trials in JIA are mainly based on limited numbers of pe-diatric patients as the recruitment of a sufficient number ofpediatric patients remains challenging Second trials aremainly designed for patients with polyarticular JIA or witholigoarticular onset and a polyarticular course (Table 4)Most children with JIA do not have a polyarticular subtypeof JIA but an oligoarticular onset and course [71] Thus pa-tients with oligoarticular JIA are heavily underrepresentedin most of the current trials Third in 5 of the 13studies the withdrawal study design has been used[4045505354] Lehmann reviewed the bias of withdrawaldesign trials in 2008 [72] After a wash-in phase only re-sponders to treatment are eligible for randomization Thusthe design preselects responders to the placebo effect whomight retain their response throughout the entire study peri-od Further there is a carryover effect of AE into the place-bo group so that significant differences in AE betweengroups may not become apparent In the one placebo con-trolled trial without withdrawal design on TNFα-inhibition
(Infliximab) no significant efficacy could be demonstratedbetween verum and placebo [31]
To our knowledge there are two other guidelines that dealwith the management of JIA as a whole (Table 6) [65] [73]Other guidelines are limited to the use of single drugs in JIAeg biologic agents [74] etanercept [75] The Australian guide-line (wwwracgporgauguidelinejuvenileidiopathicarthritis)has not been published in a peer-reviewed journal It is to pro-vide recommendations for the early diagnosis and multidisci-plinary management of JIA in the primary care setting forgeneral practitioners (GPs) [73] No recommendations aremade regarding the use of GCs DMARDs immunosuppressivedrugs or biologic agents [73] The ACR recommendations usesthe Appraisal of Guidelines for Research and Evaluation(AGREE) instrument [65] [76] which does not fulfill criteria ofa proper consensus process and carries the risk that expertsvote for peer opinion which might not reflect the true valueWe used an advanced and linguistically validated version ofthe AGREE instrument the ldquoGerman Instrument for Methodo-logical Guideline Appraisal (DELBI)rdquo which has been developedin cooperation of the AWMF among others [7778] We followedthe highly structured Nominal Group Technique as described inMethodology Our consensus group only considered formallyboard nominated representatives of multidisciplinary scientificsocieties and organizations (Table 1) and included patients rep-resentatives as this has been strongly recommended by the Eu-ropean League against Rheumatism (EULAR) recently [79] TheACR mentions a parent representative within their task forcepanel but leaves this representative anonymous It remainsunclear how ACR experts were selected and involved [65]They defined treatment groups which have not been evaluatedsystematically so far We used the ILAR classification systemwhich has been repeatedly evaluated [80ndash82]
By content there are major differences between the ACRrecommendations and our guideline a) Our guideline pro-vides a detailed and systematic list of 20 drugs commonlyused in the treatment of JIA (Table 5) which has been an in-tegrative part of our consensus conferences The ACR recom-mendations do not provide information on approval status(Food and Drug Administration) indications for use and nospecific differences on dosage regimes or frequency ofdaily application [65] eg it refers to the 2008 ACR recom-mendations for the use of DMARDs in adult rheumatoid ar-thritis b) The ACR recommendations provide a more earlyaggressive approach in the treatment of JIA The ACR recom-mends MTX as first line treatment in patients (b4 joints) withhighly active disease [65] To our knowledge there are onlydata to recommend MTX administration in cases of insuffi-cient therapeutic effect of prior treatment with NSAIDandor GC [33] c) The ACR recommends the use of TNFα in-hibitors as escalation therapy for some patients with historyof arthritis of 4 or fewer joints and refer to publications[3840] conducted in patients with polyarticular JIA or pau-ciarticular JIA with polyarticular course [65] There is no ev-idence that TNF is safe and efficient in patients witholigoarticular JIA a systematic controlled clinical trial onthis issue has not been done yet d) We regard a brief trialof local or systemic administration of GC plus NSAID as a fea-sible first line treatment for patients with polyarticular JIAThe ACR recommends MTX without regard to disease activityat the initial stage [65] We reached consensus to recom-mend the use of GC as bridging therapy until full onset of
Table 6 Overview of recommendationsguidelines for treatment of JIA
USA Australia Germany
ACR recommendations[65]
RACGP recommendations[73]
GKJR guidelines
Deadline of literature search October 2009 January 2007 September 2010Source of publications Pub Med Pub Med
EMBASE CINHAL CochraneLibrary provisionalAustralian Guideline [95]
Pub MedPrevious German Guidelines [78]
Definition used for JIA subgroups Treatment groups definedby Core expert panel
Not specifically definedChildren withJIAb16 years
ILAR criteria [1]
Consensus processprocessvalidation
AGREE [76] AGREE [76] DELBI [77]RANDUCLA appropriatenessmethod [96]
NGT Delphi method
Conferences None None 3 Formal consensus conferencesAddressees Pediatric rheumatologists General practitioner Pediatric Rheumatologists
PediatriciansGeneral practitioners
Participating scientific societies or professional organizationsPediatric rheumatologist orrheumatologists for adolescents
Yes Yes Yes
General pediatrician- In hospital Yes Yes Yes- In private practice Yes Yes YesResearcher Yes No YesRheumatologists for adults No No YesOphthalmologists No No YesParentspatients support groups Yes No YesOrthopedic surgeons No No YesPediatric orthopedic surgeons No No YesPsychologists No No YesPhysiotherapists No No YesPediatric rheumatology nurses Yes No NoOther scientific societies ororganizations
ACR BSPAR PRINTO PReS RACGP NAMSCAG NHMRC DGKJ DGPs DGRh DGO AWMFBVKJ
(ACR=American College of Rheumatologists AGREE=Appraisal of Guidelines for Research amp Development AWMF=Association of the ScientificMedical Associations BSPAR=British Society for Pediatric Rheumatology BVJK=Association of Pediatricians in private practice CEP=Core expertpanel ILAR=International League against Rheumatism CINHAL=Cumulative Index to Nursing and Allied Health Literature DELBI=German In-strument for Methodological Guideline Appraisal DGKJ=German Society of Pediatrics and Adolescent Medicine DGO=German Society for Oph-thalmology DGPs=German society for Psychology DGRh=German Society for Rheumatology GKJR=German Society for Pediatric RheumatologyNAMSCAG=National Arthritis and Musculoskeletal Conditions Advisory Group NGT=Nominal Group Technique NHMRC=National Health andMedical Research Council PReS=Pediatric Rheumatology Society) PRINTO=Pediatric Rheumatology International Trial Organization RACG-P=Royal Australian College of General Practitioner RANDUCLA=Research and DevelopmentUniversity of California at Los Angeles)
189Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
therapeutic effect of DMARDs The ACR recommendations donot provide any recommendation for the use of systemic GCfor patients with oligo- or polyarticular course of JIA exceptsystemic onset of JIA e) The ACR recommendations do notcover the topic of non-drug based therapy at all althoughthere is strong evidence that eg exercise training is a usefuladdition to drug treatment [575860]
6 Conclusion
In summary we present a treatment guideline for JIA on a con-sensus conference basis We strongly advocate an interdisciplin-ary approach including surgery physiotherapy psychosocial
intervention physical therapy medications etc and a strictformal consensus process in order to create statements thatare most appropriate for the complex clinical situation of achild and family presenting with JIA and cover all aspects ofJIA care All German pediatric rheumatology sites are partici-pating at the national pediatric rheumatologic database in theDeutsche Rheuma-Forschungszentrum at Berlin (DRFZ wwwdrfzde) It aims at quality assurance in Germany and monitorstreatment behavior of pediatric rheumatologists by using inter-nationally agreed criteria (eg joint count global physician rat-ing of disease activity global parent rating of overall well-being CHAQ ESR ACR-ped response or JADAS) The databasewill be used as a tool to monitor the application of our treat-ment guidelines
190 G Dueckers et al
Conflict of interest statement
Gregor Dueckers Novartis Pharmaceuticals CorporationBaxter (for all travel grants for scientific meetings)Nihal Guellac no conflict of interestMartin Arbogast no conflict of interestGuumlnther Dannecker no conflict of interestIvan Foeldvari Wyeth Pfizer Abbott Immunology Pharma-ceuticals Chugai (for all advisory board member)Michael Frosch no conflict of interestGerd Ganser Abbott Immunology Pharmaceuticals (advisoryboard member grants for scientific meetings) Wyeth Pfizer(advisory board member grants for scientific meetings)ChugaiRoche (advisory board member grants for scientificmeetings) Merck (grants for scientific meetings) Actelios(grants for scientific meetings) Esaote (grants for scientificmeetings)Arnd Heiligenhaus Novartis Pharmaceuticals CorporationAbbott Immunology Pharmaceuticals Alcon (for all re-search grants)Gerd Horneff Abbott Immunology Pharmaceuticals (re-search grants consulting fees non-remunerative positionsof influence) Wyeth Pfizer (research grants consultingfees speakers bureau non-remunerative positions of influ-ence) Bristol-Myers Squibb (Consulting fees) Nycomed(Consulting fees non-remunerative positions of influence)RocheChugai (Consulting fees non-remunerative positionsof influence) Sandoz (Consulting fees) Genzyme (researchgrants consulting fees non-remunerative positions of influ-ence) Swedish Orphan (research grants consulting feesnon-remunerative positions of influence)Arnold Illhardt no conflict of interestRuumldiger Krauspe no conflict of interestBarbara Markus no conflict of interestHartmut Michels Abbott Immunology Pharmaceuticals (advi-sory board member and grants for scientific meeting)Matthias Schneider no conflict of interestWolfram Singendonk no conflict of interestHelmut Sitter no conflict of interestMarianne Spamer no conflict of interestNorbert Wagner no conflict of interestTim Niehues Abbott Immunology Pharmaceuticals EssexPharma Novartis Pharmaceutical Corporation WyethPfizer (for all research grants consulting fees non-remu-nerative positions of influence)
Acknowledgment
We like to express our grateful thanks to Prof Dr Hans IkoHuppertz for proof reading the article and for an excellentdiscussion on our work We like to express our thanks to HE-LIOS Clinic for funding the open access of the article
References
[1] RE Petty TR Southwood P Manners J Baum DN Glass JGoldenberg X He J Maldonado-Cocco J Orozco-Alcala AMPrieur ME Suarez-Almazor PWoo International League of Asso-ciations for Rheumatology classification of juvenile idiopathic ar-thritis second revision Edmonton 2001 J Rheumatol 31(2004) 390ndash392
[2] B Prakken S Albani A Martini Juvenile idiopathic arthritisLancet 377 (2011) 2138ndash2149
[3] KT April DE Feldman RW Platt CM Duffy Comparisonbetween children with juvenile idiopathic arthritis (JIA) andtheir parents concerning perceived quality of life Qual LifeRes 15 (2006) 655ndash661
[4] BM Feldman B Grundland L McCullough V Wright Distinc-tion of quality of life health related quality of life and healthstatus in children referred for rheumatologic care J Rheuma-tol 27 (2000) 226ndash233
[5] JC Packham MA Hall Long-term follow-up of 246 adultswith juvenile idiopathic arthritis functional outcomeRheumatology (Oxford) 41 (2002) 1428ndash1435
[6] C Sandborg Pediatric rheumatic disease standards of care forJIAmdashthe basic foundation for quality Nat Rev Rheumatol 6(2010) 389ndash390
[7] N Guellac T Niehues Interdisciplinary and evidence-basedtreatment guideline for juvenile idiopathic arthritis KlinPadiatr 220 (2008) 392ndash402
[8] K Schnakenburg Leitlinien in der Kinder- und JugendmedizinElsevier 2005 pp H1 1ndash15
[9] P Juni L Nartey S Reichenbach R Sterchi PA Dieppe MEgger Risk of cardiovascular events and rofecoxib cumulativemeta-analysis Lancet 364 (2004) 2021ndash2029
[10] W Feldman Evidence-based Pediatrics 1st ed BC DeckersHamilton 2000
[11] AH Van de Ven AL Delbecq The nominal group as a re-search instrument for exploratory health studies Am J PublicHealth 62 (1972) 337ndash342
[12] HA Linstone M Turoff The Delphi Method Techniques andApplications Addison-Wesley Pub 1975
[13] TK Kvien HM Hoyeraal B Sandstad Naproxen and acetyl-salicylic acid in the treatment of pauciarticular and polyarticu-lar juvenile rheumatoid arthritis Assessment of tolerance andefficacy in a single-centre 24-week double-blind parallelstudy Scand J Rheumatol 13 (1984) 342ndash350
[14] RM Laxer ED Silverman C St-Cyr MT Tran G Lingam Asix-month open safety assessment of a naproxen suspensionformulation in the therapy of juvenile rheumatoid arthritisClin Ther 10 (1988) 381ndash387
[15] AM Leak MR Richter LE Clemens MA Hall BM AnsellA crossover study of naproxen diclofenac and tolmetin in sero-negative juvenile chronic arthritis Clin Exp Rheumatol 6(1988) 157ndash160
[16] J Haapasaari E Wuolijoki H Ylijoki Treatment of juve-nile rheumatoid arthritis with diclofenac sodium Scand JRheumatol 12 (1983) 325ndash330
[17] EH Giannini EJ Brewer ML Miller D Gibbas MH PassoHM Hoyeraal B Bernstein DA Person CW Fink LA Sawyeret al Ibuprofen suspension in the treatment of juvenilerheumatoid arthritis Pediatric Rheumatology CollaborativeStudy Group J Pediatr 117 (1990) 645ndash652
[18] E Stoeber L Sanger Experiences with indomethacin in long-term therapy of juvenile rheumatoid arthritis Arzneimittel-forschung 21 (1971) 1865ndash1866
[19] N Ruperto I Nikishina ED Pachanov Y Shachbazian AMPrieur R Mouy R Joos F Zulian R Schwarz V ArtamonovaW Emminger M Bandeira A Buoncompagni I Foeldvari FFalcini E Baildam I Kone-Paut M Alessio V Gerloni ALenhardt A Martini G Hanft R Sigmund S Simianer Arandomized double-blind clinical trial of two doses ofmeloxicam compared with naproxen in children with juvenileidiopathic arthritis short- and long-term efficacy and safetyresults Arthritis Rheum 52 (2005) 563ndash572
[20] I Foeldvari IS Szer LS Zemel DJ Lovell EH Giannini JLRobbins CRWest G Steidle S Krishnaswami BJ Bloom A pro-spective study comparing celecoxib with naproxen in children withjuvenile rheumatoid arthritis J Rheumatol 36 (2009) 174ndash182
191Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
[21] F Zulian G Martini D Gobber C Agosto C Gigante FZacchello Comparison of intra-articular triamcinolone hexa-cetonide and triamcinolone acetonide in oligoarticular juve-nile idiopathic arthritis Rheumatology (Oxford) 42 (2003)1254ndash1259
[22] F Zulian G Martini D Gobber M Plebani F Zacchello PManners Triamcinolone acetonide and hexacetonide intra-articular treatment of symmetrical joints in juvenile idiopathicarthritis a double-blind trial Rheumatology (Oxford) 43 (2004)1288ndash1291
[23] GS Habib Systemic effects of intra-articular corticosteroidsClin Rheumatol 28 (2009) 749ndash756
[24] JR Kirwan The effect of glucocorticoids on joint destructionin rheumatoid arthritis The Arthritis and Rheumatism CouncilLow-Dose Glucocorticoid Study Group N Engl J Med 333(1995) 142ndash146
[25] H Michels What is low-dose corticosteroid therapy in juvenileidiopathic arthritis A worldwide questionnaire-based surveyZ Rheumatol 59 (Suppl 2) (2000) II127ndash130
[26] JJ Miller III Prolonged use of large intravenous steroid pulsesin the rheumatic diseases of children Pediatrics 65 (1980)989ndash994
[27] P Picco M Gattorno A Buoncompagni V Pistoia C Borrone6-methylprednisolone lsquomini-pulsesrsquo a newmodality of glucocor-ticoid treatment in systemic onset juvenile chronic arthritisScand J Rheumatol 25 (1996) 24ndash27
[28] AM Prieur The place of corticosteroid therapy in juvenilechronic arthritis in 1992 J Rheumatol Suppl 37 (1993)32ndash34
[29] JS Gao H Wu J Tian Treatment of patients with juvenilerheumatoid arthritis with combination of leflunomide andmethotrexate Zhonghua Er Ke Za Zhi 41 (2003) 435ndash438
[30] T Niehues G Horneff H Michels MS Hock L SchuchmannEvidence-based use of methotrexate in children with rheumat-ic diseases a consensus statement of the Working Groups Pedi-atric Rheumatology Germany (AGKJR) and PediatricRheumatology Austria Rheumatol Int 25 (2005) 169ndash178
[31] N Ruperto DJ Lovell R Cuttica N Wilkinson P Woo GEspada C Wouters ED Silverman Z Balogh M HenricksonMT Apaz E Baildam A Fasth V Gerloni P Lahdenne AMPrieur A Ravelli RK Saurenmann ML Gamir N WulffraatL Marodi RE Petty R Joos F Zulian D McCurdy BLMyones K Nagy P Reuman I Szer S Travers A BeutlerG Keenan J Clark S Visvanathan A Fasanmade A Ray-chaudhuri A Mendelsohn A Martini EH Giannini A random-ized placebo-controlled trial of infliximab plus methotrexatefor the treatment of polyarticular-course juvenile rheumatoidarthritis Arthritis Rheum 56 (2007) 3096ndash3106
[32] K Visser DM van der Heijde Risk and management of livertoxicity during methotrexate treatment in rheumatoid andpsoriatic arthritis a systematic review of the literature ClinExp Rheumatol 27 (2009) 1017ndash1025
[33] A Cespedes-Cruz R Gutierrez-Suarez A Pistorio A Ravelli ALoy KJ Murray V Gerloni N Wulffraat S Oliveira J WalshIC Penades MG Alpigiani P Lahdenne C Saad-Magalhaes ECortis L Lepore Y Kimura C Wouters A Martini N RupertoMethotrexate improves the health-related quality of life of chil-dren with juvenile idiopathic arthritis Ann Rheum Dis 67(2008) 309ndash314
[34] TK Kvien HM Hoyeraal B Sandstad Azathioprine versus place-bo in patients with juvenile rheumatoid arthritis a single centerdouble blind comparative study J Rheumatol 13 (1986) 118ndash123
[35] E Silverman R Mouy L Spiegel LK Jung RK SaurenmannP Lahdenne G Horneff I Calvo IS Szer K Simpson JAStewart V Strand Leflunomide or methotrexate for juvenilerheumatoid arthritis N Engl J Med 352 (2005) 1655ndash1666
[36] MA van Rossum TJ Fiselier MJ Franssen AH ZwindermanR ten Cate LW van Suijlekom-Smit WH van Luijk RM
van Soesbergen NM Wulffraat JC Oostveen W Kuis PFDijkstra CF van Ede BA Dijkmans Sulfasalazine in the treat-ment of juvenile chronic arthritis a randomized double-blindplacebo-controlled multicenter study Dutch Juvenile ChronicArthritis Study Group Arthritis Rheum 41 (1998) 808ndash816
[37] MA van Rossum RM van Soesbergen M Boers AHZwinderman TJ Fiselier MJ Franssen R ten Cate LW vanSuijlekom-Smit NM Wulffraat WH van Luijk JC OostveenW Kuis BA Dijkmans Long-term outcome of juvenile idiopathicarthritis following a placebo-controlled trial sustained benefits ofearly sulfasalazine treatment Ann Rheum Dis 66 (2007)1518ndash1524
[38] DJ Lovell EH Giannini A Reiff GD Cawkwell ED SilvermanJJ Nocton LD Stein A Gedalia NT Ilowite CA Wallace JWhitmore BK Finck Etanercept in children with polyarticularjuvenile rheumatoid arthritis Pediatric Rheumatology Collabora-tive Study Group N Engl J Med 342 (2000) 763ndash769
[39] DJ Lovell A Reiff OY Jones R Schneider J Nocton LDStein A Gedalia NT Ilowite CA Wallace JB WhitmoreB White EH Giannini Long-term safety and efficacy ofetanercept in children with polyarticular-course juvenile rheu-matoid arthritis Arthritis Rheum 54 (2006) 1987ndash1994
[40] DJ Lovell N Ruperto S Goodman A Reiff L Jung K JarosovaD Nemcova R Mouy C Sandborg J Bohnsack D Elewaut IFoeldvari V Gerloni J Rovensky K Minden RK Vehe LWWeiner G Horneff HI Huppertz NY Olson JR Medich RCarcereri-De-Prati MJ McIlraith EH Giannini A MartiniAdalimumab with or without methotrexate in juvenile rheuma-toid arthritis N Engl J Med 359 (2008) 810ndash820
[41] FH Prince M Twilt R ten Cate MA van RossumW ArmbrustEP Hoppenreijs M van Santen-Hoeufft Y Koopman-KeeminkNM Wulffraat LW van Suijlekom-Smit Long-term follow-upon effectiveness and safety of etanercept in juvenile idiopathicarthritis the Dutch National Register Ann Rheum Dis 68(2009) 635ndash641
[42] P Diak J Siegel L LaGrenade L Choi S Lemery AMcMahonTumor necrosis factor alpha blockers andmalignancy in childrenforty-eight cases reported to the Food and Drug AdministrationArthritis Rheum 62 (2010) 2517ndash2524
[43] G Horneff T Hospach G Dannecker D Foll JP Haas HJGirschick HI Huppertz R Keitzer HJ Laws H Michels KMinden R Trauzeddel Updated statement by the German So-ciety for Pediatric and Adolescent Rheumatology (GKJR) on theFDAs report regarding malignancies in anti-TNF-treated pa-tients from Aug 4 2009 Z Rheumatol 69 (2010) 561ndash567
[44] T Hospach JP Haas HI Huppertz R Keitzer H Michels RTrauzeddl D Foll G Dannecker G Horneff Comment of theSociety of Pediatric and Adolescent Rheumatology on the USFood and Drug Administration (FDA) announcement regardingcases of malignancy in anti-TNF-treated patients Z Rheumatol68 (2009) 162ndash164
[45] DJ Lovell A Reiff NT Ilowite CA Wallace Y Chon SL LinSW Baumgartner EH Giannini Safety and efficacy of up to eightyears of continuous etanercept therapy in patients with juvenilerheumatoid arthritis Arthritis Rheum 58 (2008) 1496ndash1504
[46] EH Giannini NT Ilowite DJ Lovell CA Wallace CERabinovich A Reiff G Higgins B Gottlieb NG Singer YChon SL Lin SW Baumgartner Long-term safety and effec-tiveness of etanercept in children with selected categories ofjuvenile idiopathic arthritis Arthritis Rheum 60 (2009)2794ndash2804
[47] G Horneff H Schmeling T Biedermann I Foeldvari G GanserHJ Girschick T Hospach HI Huppertz R Keitzer RM KusterH Michels D Moebius B Rogalski A Thon The German etaner-cept registry for treatment of juvenile idiopathic arthritis AnnRheum Dis 63 (2004) 1638ndash1644
[48] FH Prince M Twilt SC Simon MA van RossumW ArmbrustEP Hoppenreijs S Kamphuis M van Santen-Hoeufft Y
192 G Dueckers et al
Koopman-Keemink NM Wulffraat R ten Cate LW vanSuijlekom-Smit When and how to stop etanercept aftersuccessful treatment of patients with juvenile idiopathic ar-thritis Ann Rheum Dis 68 (2009) 1228ndash1229
[49] G Horneff F De Bock I Foeldvari HJ Girschick H MichelsD Moebius H Schmeling Safety and efficacy of combinationof etanercept and methotrexate compared to treatment withetanercept only in patients with juvenile idiopathic arthritis(JIA) preliminary data from the German JIA Registry AnnRheum Dis 68 (2009) 519ndash525
[50] N Ilowite O Porras A Reiff S Rudge M Punaro A Martin RAllen T Harville YN Sun T Bevirt G Aras B Appleton Ana-kinra in the treatment of polyarticular-course juvenile rheumatoidarthritis safety and preliminary efficacy results of a randomizedmulticenter study Clin Rheumatol 28 (2009) 129ndash137
[51] T Lequerre P Quartier D Rosellini F Alaoui M De BandtO Mejjad I Kone-Paut M Michel E Dernis M Khellaf NLimal C Job-Deslandre B Fautrel X Le Loet J Sibilia In-terleukin-1 receptor antagonist (anakinra) treatment in pa-tients with systemic-onset juvenile idiopathic arthritis oradult onset Still disease preliminary experience in FranceAnn Rheum Dis 67 (2008) 302ndash308
[52] M Gattorno A Piccini D Lasiglie S Tassi G Brisca S CartaL Delfino F Ferlito MA Pelagatti F Caroli A BuoncompagniS Viola A Loy M Sironi A Vecchi A Ravelli A Martini ARubartelli The pattern of response to anti-interleukin-1 treatmentdistinguishes two subsets of patients with systemic-onset juvenileidiopathic arthritis Arthritis Rheum 58 (2008) 1505ndash1515
[53] S Yokota T Imagawa M Mori T Miyamae Y Aihara STakei N Iwata H Umebayashi T Murata M Miyoshi MTomiita N Nishimoto T Kishimoto Efficacy and safety oftocilizumab in patients with systemic-onset juvenile idiopathicarthritis a randomised double-blind placebo-controlledwithdrawal phase III trial Lancet 371 (2008) 998ndash1006
[54] N Ruperto DJ Lovell P Quartier E Paz N Rubio-Perez CASilva C Abud-Mendoza R Burgos-Vargas V Gerloni JAMelo-Gomes C Saad-Magalhaes F Sztajnbok C Goldenstein-Schainberg M Scheinberg IC Penades M Fischbach J OrozcoPJ Hashkes C Hom L Jung L Lepore S Oliveira CAWallace LH Sigal AJ Block A Covucci A Martini EHGiannini Abatacept in children with juvenile idiopathic arthri-tis a randomised double-blind placebo-controlled withdrawaltrial Lancet 372 (2008) 383ndash391
[55] N Ruperto DJ Lovell P Quartier E Paz N Rubio-PerezCA Silva C Abud-Mendoza R Burgos-Vargas V GerloniJA Melo-Gomes C Saad-Magalhaes J Chavez-Corrales CHuemer A Kivitz FJ Blanco I Foeldvari M Hofer G HorneffHI Huppertz C Job-Deslandre A Loy K Minden M PunaroAF Nunez LH Sigal AJ Block M Nys A Martini EHGiannini Long-term safety and efficacy of abatacept inchildren with juvenile idiopathic arthritis Arthritis Rheum 62(2010) 1792ndash1802
[56] DM Brinkman IM de Kleer R ten Cate MA van RossumWP Bekkering A Fasth MJ van Tol W Kuis NM WulffraatJM Vossen Autologous stem cell transplantation in childrenwith severe progressive systemic or polyarticular juvenile idio-pathic arthritis long-term follow-up of a prospective clinicaltrial Arthritis Rheum 56 (2007) 2410ndash2421
[57] SE Klepper Effects of an eight-week physical conditioningprogram on disease signs and symptoms in children with chronicarthritis Arthritis Care Res 12 (1999) 52ndash60
[58] D Singh-Grewal J Schneiderman-Walker V Wright O Bar-OrJ Beyene H Selvadurai B Cameron RM Laxer R SchneiderED Silverman L Spiegel S Tse C Leblanc J Wong SStephens BM Feldman The effects of vigorous exercisetraining on physical function in children with arthritis arandomized controlled single-blinded trial ArthritisRheum 57 (2007) 1202ndash1210
[59] S Stephens D Singh-Grewal O Bar-Or J Beyene B CameronCM Leblanc R Schneider J Schneiderman-Walker HSelvadurai E Silverman L Spiegel SM Tse V WrightBM Feldman Reliability of exercise testing and functionalactivity questionnaires in children with juvenile arthritisArthritis Rheum 57 (2007) 1446ndash1452
[60] T Takken J van der Net W Kuis PJ Helders Physical ac-tivity and health related physical fitness in children with ju-venile idiopathic arthritis Ann Rheum Dis 62 (2003)885ndash889
[61] MM Toledo G Martini C Gigante L Da Dalt A TregnaghiF Zulian Is there a role for arthroscopic synovectomy in oli-goarticular juvenile idiopathic arthritis J Rheumatol 33(2006) 1868ndash1872
[62] F de Benedetti H Brunner N Ruperto SWright A KenwrightR Cuttica P Woo R Schneider DJ Lovell A Martini Efficacyand safety of Tocilizumab in patients with systemic juvenile idio-pathic arthritis (sJIA) 12-week data from the phase III TENDERtrial Ann Rheum Dis 69 (2010) 146
[63] P Quartier F Allantaz R Cimaz P Pillet C Messiaen CBardin X Bossuyt A Boutten J Bienvenu A Duquesne ORicher D Chaussabel A Mogenet J Banchereau JM Tre-luyer P Landais V Pascual A multicentre randomiseddouble-blind placebo-controlled trial with the interleukin-1receptor antagonist anakinra in patients with systemic-onsetjuvenile idiopathic arthritis (ANAJIS trial) Ann Rheum Dis70 (2011) 747ndash754
[64] DE Furst EC Keystone J Braun FC Breedveld GRBurmester F De Benedetti T Dorner P Emery R FleischmannA Gibofsky JR Kalden A Kavanaugh B Kirkham P Mease JSieper NG Singer JS Smolen PL Van Riel MH Weisman KWinthrop Updated consensus statement on biological agents forthe treatment of rheumatic diseases 2010 Ann Rheum Dis 70(Suppl 1) (2010) i2ndashi36
[65] T Beukelman NM Patkar KG Saag S Tolleson-RinehartRQ Cron EM Dewitt NT Ilowite Y Kimura RM LaxerDJ Lovell A Martini CE Rabinovich N Ruperto 2011 Ameri-can College of Rheumatology recommendations for the treatmentof juvenile idiopathic arthritis initiation and safety monitoring oftherapeutic agents for the treatment of arthritis and systemic fea-tures Arthritis Care Res 63 (2011) 465ndash482 (Hoboken)
[66] JF Simard M Neovius S Hagelberg J Askling Juvenile idi-opathic arthritis and risk of cancer a nationwide cohort studyArthritis Rheum 62 (2010) 3776ndash3782
[67] T Imagawa S Yokota M Mori T Miyamae S Takei H ImanakaY Nerome N Iwata T Murata M Miyoshi N Nishimoto TKishimoto Safety and efficacy of tocilizumab an anti-IL-6-receptor monoclonal antibody in patients with polyarticular-course juvenile idiopathic arthritis Mod Rheumatol (2011)doi102007s10165-011-0481-0
[68] TM Shaneyfelt MF Mayo-Smith J Rothwangl Are guide-lines following guidelines The methodological quality of clini-cal practice guidelines in the peer-reviewed medicalliterature Jama 281 (1999) 1900ndash1905
[69] R Grilli N Magrini A Penna G Mura A Liberati Practiceguidelines developed by specialty societies the need for a crit-ical appraisal Lancet 355 (2000) 103ndash106
[70] JS Burgers R Grol NS Klazinga M Makela J Zaat To-wards evidence-based clinical practice an international surveyof 18 clinical guideline programs Int J Qual Health Care 15(2003) 31ndash45
[71] JT Cassidy RE Petty Juvenile Idiopathic Rheumatic Arthri-tis 5th Edition WB Saunders Philadelphia 2005
[72] TJ Lehman Are withdrawal trials in paediatric rheumatic dis-ease helpful Lancet 372 (2008) 348ndash350
[73] J Munro Recommendations for the Diagnosis and Managementof Juvenile Idiopathic Arthritis The Royal Australian Collegeof General Practitioners South Melbourne 2009 pp 1ndash38
193Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
httpwwwnhmrcgovau_files_nhmrcpublicationsattachmentscp119-juvenile-arthritispdf
[74] MJ Santos JE Fonseca H Canhao M Conde M JoseVieira L Costa M Costa M Salgado JA Melo Gomes Guide-lines for prescribing and monitoring biologic therapies in juve-nile idiopathic arthritis Acta Reumatol Port 32 (2007) 43ndash47
[75] S Yokota M Mori T Imagawa T Murata M Tomiita Y ItohS Fujikawa S Takei Guidelines on the use of etanercept forjuvenile idiopathic arthritis in Japan Mod Rheumatol 20(2010) 107ndash113
[76] The AGREE Collaboration Appraisal of Guidelines for Researchamp Evaluation (AGREE) instrument wwwagreecollaborationorg
[77] I Kopp H Thole T Langer HK Selbmann G OllenschlaumlgerGerman Instrument for Methodological Guideline Appraisal(DELBI) wwwversorgungsleitliniende2008
[78] Auml Aumlrztliches Zentrum fuumlr Qualitaumlt in der Medizin A Arbeitsge-meinschaften der Wissenschaftlichen Fachgesellschaften in derMedizin Deutsches Instrument zur methodischen Leitlinien-Bewertung (DELBI) Fassung 20052006 Z Aumlrztl FortbildQualitaumltssich 99 (2005) 468ndash519
[79] MP de Wit SE Berlo GJ Aanerud D Aletaha JW BijlsmaL Croucher JA Da Silva B Glusing L Gossec S Hewlett MJongkees D Magnusson M Scholte-Voshaar P Richards CZiegler TA Abma European League Against Rheumatism rec-ommendations for the inclusion of patient representatives in sci-entific projects Ann Rheum Dis 70 (2011) 722ndash726
[80] I Foeldvari M Bidde Validation of the proposed ILAR classifi-cation criteria for juvenile idiopathic arthritis InternationalLeague of Associations for Rheumatology J Rheumatol 27(2000) 1069ndash1072
[81] R Merino J de Inocencio J Garcia-Consuegra Evaluation ofrevised International League of Associations for Rheumatologyclassification criteria for juvenile idiopathic arthritis in Spanishchildren (Edmonton 2001) J Rheumatol 32 (2005) 559ndash561
[82] SE Ramsey RK Bolaria DA Cabral PN Malleson REPetty Comparison of criteria for the classification of childhoodarthritis J Rheumatol 27 (2000) 1283ndash1286
[83] G Horneff A Ebert S Fitter K Minden I Foeldvari J Kum-merle-Deschner A Thon HJ Girschick F Weller HI Hup-pertz Safety and efficacy of once weekly etanercept 08mgkg in a multicentre 12 week trial in active polyarticularcourse juvenile idiopathic arthritis Rheumatology (Oxford) 48(2009) 916ndash919
[84] EH Giannini EJ Brewer N Kuzmina A Shaikov A Maxi-mov I Vorontsov CW Fink AJ Newman JT Cassidy LSZemel Methotrexate in resistant juvenile rheumatoid arthri-tis Results of the USAndashUSSR double-blind placebo-controlled trial The Pediatric Rheumatology CollaborativeStudy Group and The Cooperative Childrens Study GroupN Engl J Med 326 (1992) 1043ndash1049
[85] A Ravelli S Viola D Migliavacca N Ruperto A Pistorio AMartini The extended oligoarticular subtype is the best predic-tor of methotrexate efficacy in juvenile idiopathic arthritisJ Pediatr 135 (1999) 316ndash320
[86] P Woo TR Southwood AM Prieur CJ Dore J Grainger JDavid C Ryder N Hasson A Hall I Lemelle Randomizedplacebo-controlled crossover trial of low-dose oral
methotrexate in children with extended oligoarticular or sys-temic arthritis Arthritis Rheum 43 (2000) 1849ndash1857
[87] E Silverman L Spiegel D Hawkins R Petty D Goldsmith LSchanberg C Duffy P Howard V Strand Long-term open-label preliminary study of the safety and efficacy of lefluno-mide in patients with polyarticular-course juvenile rheumatoidarthritis Arthritis Rheum 52 (2005) 554ndash562
[88] DJ Lovell EH Giannini Y Kimura C Suzanne PJHashkes A Reiff Long-term safety and efficacy of rilonaceptin patients with systemic juvenile idiopathic arthritis (SJIA)Arthritis Rheum 60 (2009)
[89] N Ruperto P Quartier NWulffraat PWoo A Loy R Mouy BBader-Meunier BJ Prakken E Noseda R Belleli J Lecot CRordorf A Martini A Phase II Trial with canakinumab(ACZ885) a new IL-1-beta blocking monoclonal antibody toevaluate safety and preliminary efficacy in children with system-ic juvenile idiopathic arthritis Ann Rheum Dis 68 (2009) 170
[90] DJ Lovell EH Giannini Y Kimura et al Preliminary evi-dence for bioactivity of IL-1 trap (Rilonacept) a long actingIL-1 inhibitor in systemic juvenile idiopathic arthritis (sJIA)Arthritis Rheum 54 (2006) S325
[91] DJ Lovell EH Giannini Y Kimura et al Preliminary evi-dence for sustained bioactivity of IL-1 Trap (rilonacept) a longacting IL-1 inhibitor in systemic juvenile idiopathic arthritisArthritis Rheum 56 (2007) S514
[92] N Ruperto F De Benedetti H Brunner R Allen D Brown JChaitow E Cortis G Espada B Flato V Gerloni G HorneffS Wright A Kenwright R Schneider P Woo A Martini DJLovell Tocilizumab is efficacious in patients with systemic ju-venile idiopathic arthritis (sJIA) across baseline disease charac-teristics and priorbaseline treatments 12-week data from thephase II TENDER trial 17th PReS Congress Valencia Spain2010 2010
[93] N Ruperto DJ Lovell T Li F Sztajnbok C Goldenstein-Schainberg M Scheinberg IC Penades M Fischbach JOrozco PJ Hashkes C Hom L Jung L Lepore S OliveiraC Wallace M Alessio P Quartier E Cortis A Eberhard GSimonini I Lemelle E Chalom LH Sigal A Block A CovucciM Nys A Martini EH Giannini Abatacept improves health-related quality of life pain sleep quality and daily participationin subjects with juvenile idiopathic arthritis Arthritis Care Res(Hoboken) 62 (11) (2010) 1542ndash1551
[94] N Ruperto DJ Lovell P Quartier E Paz N Rubio-PerezCA Silva C Abud-Mendoza R Burgos-Vargas V GerloniJA Melo-Gomes C Saad-Magalhaes J Chavez C HuemerA Kivitz FJ Blanco I Foeldvari M Hofer G Horneff HIHuppertz CJ Deslandre A Loy K Minden M Punaro AFNunez LH Sigal AJ Block M Nys A Martini EH GianniniLong-term safety and efficacy of abatacept in children with ju-venile idiopathic arthritis Arthritis Rheum 62 (2010)1792ndash1802
[95] J Munro Juvenile Idiopathic Arthritis Management Guidelines(Provisional) Australian Paediatric Rheumatology Group 2006httpwwwnhmrcgovau
[96] K Fitch SJ Bernstein MD Aguilar B Burnand JR LaCalleP Lazaro M van het Loo J McDonnell JP Vader JPKahan The RANDUCLA Appropriateness Method Users ManualRAND Pittsburgh 2000

188 G Dueckers et al
4 Addendum
Since the deadline January 15th 2010 new papers haveappeared that are of interest in the context of our guideline[5562ndash64] in particular we refer to the ACR recommenda-tions [65] and the most recent literature on the risk of malig-nancies in JIA in context with TNF blocking agent andindependent of medication [42] [66] Moreover there is arecent study on the use of Tocilizumab in polyarticular pa-tients [67] These papers will be discussed within the nextconsensus conference by NGT and considered for inclusioninto the next edition of this guideline On 6th of September2011 our advanced search on wwwclinicaltrialgov (searchterms juvenile idiopathic arthritis recruitment open stud-ies study type interventional study age group child(birthndash17) intervention drugs) led to 16 trials which are cur-rently recruiting or will soon start recruiting
5 Discussion
To develop clinical practice guidelines of high quality andvalidity a formal consensus process and explicit methodo-logical criteria for the production of guidelines are recom-mended [68ndash70] Our guideline for the treatment of JIA inchildren and adolescents implements all these issues Thesystematic literature search was terminated on 15th January2010 leading to the most up to date guideline for JIA whichis currently available The deadline of the ACR recommenda-tions as published recently by Beukelmann et al was 5th ofOctober 2009 [65] By exclusion of case reports trials with-out control groups preliminary results published as ab-stracts on conferences and the strict graduation of theliterature by the criteria of evidence based medicine weaimed to give our guideline statements additional strengthand a maximal validity Newer original studies providing ad-ditional evidence for the treatment of JIA became availableafter our consensus process was finished see AddendumThe results of these trials have to await the next NGT beforeinclusion into our recommendations
Our updated systematic literature search in 2010 led to13 relevant studies published after 30th June 2007 (Fig 1Table 4) Their results have to be interpreted with cautionFirst trials in JIA are mainly based on limited numbers of pe-diatric patients as the recruitment of a sufficient number ofpediatric patients remains challenging Second trials aremainly designed for patients with polyarticular JIA or witholigoarticular onset and a polyarticular course (Table 4)Most children with JIA do not have a polyarticular subtypeof JIA but an oligoarticular onset and course [71] Thus pa-tients with oligoarticular JIA are heavily underrepresentedin most of the current trials Third in 5 of the 13studies the withdrawal study design has been used[4045505354] Lehmann reviewed the bias of withdrawaldesign trials in 2008 [72] After a wash-in phase only re-sponders to treatment are eligible for randomization Thusthe design preselects responders to the placebo effect whomight retain their response throughout the entire study peri-od Further there is a carryover effect of AE into the place-bo group so that significant differences in AE betweengroups may not become apparent In the one placebo con-trolled trial without withdrawal design on TNFα-inhibition
(Infliximab) no significant efficacy could be demonstratedbetween verum and placebo [31]
To our knowledge there are two other guidelines that dealwith the management of JIA as a whole (Table 6) [65] [73]Other guidelines are limited to the use of single drugs in JIAeg biologic agents [74] etanercept [75] The Australian guide-line (wwwracgporgauguidelinejuvenileidiopathicarthritis)has not been published in a peer-reviewed journal It is to pro-vide recommendations for the early diagnosis and multidisci-plinary management of JIA in the primary care setting forgeneral practitioners (GPs) [73] No recommendations aremade regarding the use of GCs DMARDs immunosuppressivedrugs or biologic agents [73] The ACR recommendations usesthe Appraisal of Guidelines for Research and Evaluation(AGREE) instrument [65] [76] which does not fulfill criteria ofa proper consensus process and carries the risk that expertsvote for peer opinion which might not reflect the true valueWe used an advanced and linguistically validated version ofthe AGREE instrument the ldquoGerman Instrument for Methodo-logical Guideline Appraisal (DELBI)rdquo which has been developedin cooperation of the AWMF among others [7778] We followedthe highly structured Nominal Group Technique as described inMethodology Our consensus group only considered formallyboard nominated representatives of multidisciplinary scientificsocieties and organizations (Table 1) and included patients rep-resentatives as this has been strongly recommended by the Eu-ropean League against Rheumatism (EULAR) recently [79] TheACR mentions a parent representative within their task forcepanel but leaves this representative anonymous It remainsunclear how ACR experts were selected and involved [65]They defined treatment groups which have not been evaluatedsystematically so far We used the ILAR classification systemwhich has been repeatedly evaluated [80ndash82]
By content there are major differences between the ACRrecommendations and our guideline a) Our guideline pro-vides a detailed and systematic list of 20 drugs commonlyused in the treatment of JIA (Table 5) which has been an in-tegrative part of our consensus conferences The ACR recom-mendations do not provide information on approval status(Food and Drug Administration) indications for use and nospecific differences on dosage regimes or frequency ofdaily application [65] eg it refers to the 2008 ACR recom-mendations for the use of DMARDs in adult rheumatoid ar-thritis b) The ACR recommendations provide a more earlyaggressive approach in the treatment of JIA The ACR recom-mends MTX as first line treatment in patients (b4 joints) withhighly active disease [65] To our knowledge there are onlydata to recommend MTX administration in cases of insuffi-cient therapeutic effect of prior treatment with NSAIDandor GC [33] c) The ACR recommends the use of TNFα in-hibitors as escalation therapy for some patients with historyof arthritis of 4 or fewer joints and refer to publications[3840] conducted in patients with polyarticular JIA or pau-ciarticular JIA with polyarticular course [65] There is no ev-idence that TNF is safe and efficient in patients witholigoarticular JIA a systematic controlled clinical trial onthis issue has not been done yet d) We regard a brief trialof local or systemic administration of GC plus NSAID as a fea-sible first line treatment for patients with polyarticular JIAThe ACR recommends MTX without regard to disease activityat the initial stage [65] We reached consensus to recom-mend the use of GC as bridging therapy until full onset of
Table 6 Overview of recommendationsguidelines for treatment of JIA
USA Australia Germany
ACR recommendations[65]
RACGP recommendations[73]
GKJR guidelines
Deadline of literature search October 2009 January 2007 September 2010Source of publications Pub Med Pub Med
EMBASE CINHAL CochraneLibrary provisionalAustralian Guideline [95]
Pub MedPrevious German Guidelines [78]
Definition used for JIA subgroups Treatment groups definedby Core expert panel
Not specifically definedChildren withJIAb16 years
ILAR criteria [1]
Consensus processprocessvalidation
AGREE [76] AGREE [76] DELBI [77]RANDUCLA appropriatenessmethod [96]
NGT Delphi method
Conferences None None 3 Formal consensus conferencesAddressees Pediatric rheumatologists General practitioner Pediatric Rheumatologists
PediatriciansGeneral practitioners
Participating scientific societies or professional organizationsPediatric rheumatologist orrheumatologists for adolescents
Yes Yes Yes
General pediatrician- In hospital Yes Yes Yes- In private practice Yes Yes YesResearcher Yes No YesRheumatologists for adults No No YesOphthalmologists No No YesParentspatients support groups Yes No YesOrthopedic surgeons No No YesPediatric orthopedic surgeons No No YesPsychologists No No YesPhysiotherapists No No YesPediatric rheumatology nurses Yes No NoOther scientific societies ororganizations
ACR BSPAR PRINTO PReS RACGP NAMSCAG NHMRC DGKJ DGPs DGRh DGO AWMFBVKJ
(ACR=American College of Rheumatologists AGREE=Appraisal of Guidelines for Research amp Development AWMF=Association of the ScientificMedical Associations BSPAR=British Society for Pediatric Rheumatology BVJK=Association of Pediatricians in private practice CEP=Core expertpanel ILAR=International League against Rheumatism CINHAL=Cumulative Index to Nursing and Allied Health Literature DELBI=German In-strument for Methodological Guideline Appraisal DGKJ=German Society of Pediatrics and Adolescent Medicine DGO=German Society for Oph-thalmology DGPs=German society for Psychology DGRh=German Society for Rheumatology GKJR=German Society for Pediatric RheumatologyNAMSCAG=National Arthritis and Musculoskeletal Conditions Advisory Group NGT=Nominal Group Technique NHMRC=National Health andMedical Research Council PReS=Pediatric Rheumatology Society) PRINTO=Pediatric Rheumatology International Trial Organization RACG-P=Royal Australian College of General Practitioner RANDUCLA=Research and DevelopmentUniversity of California at Los Angeles)
189Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
therapeutic effect of DMARDs The ACR recommendations donot provide any recommendation for the use of systemic GCfor patients with oligo- or polyarticular course of JIA exceptsystemic onset of JIA e) The ACR recommendations do notcover the topic of non-drug based therapy at all althoughthere is strong evidence that eg exercise training is a usefuladdition to drug treatment [575860]
6 Conclusion
In summary we present a treatment guideline for JIA on a con-sensus conference basis We strongly advocate an interdisciplin-ary approach including surgery physiotherapy psychosocial
intervention physical therapy medications etc and a strictformal consensus process in order to create statements thatare most appropriate for the complex clinical situation of achild and family presenting with JIA and cover all aspects ofJIA care All German pediatric rheumatology sites are partici-pating at the national pediatric rheumatologic database in theDeutsche Rheuma-Forschungszentrum at Berlin (DRFZ wwwdrfzde) It aims at quality assurance in Germany and monitorstreatment behavior of pediatric rheumatologists by using inter-nationally agreed criteria (eg joint count global physician rat-ing of disease activity global parent rating of overall well-being CHAQ ESR ACR-ped response or JADAS) The databasewill be used as a tool to monitor the application of our treat-ment guidelines
190 G Dueckers et al
Conflict of interest statement
Gregor Dueckers Novartis Pharmaceuticals CorporationBaxter (for all travel grants for scientific meetings)Nihal Guellac no conflict of interestMartin Arbogast no conflict of interestGuumlnther Dannecker no conflict of interestIvan Foeldvari Wyeth Pfizer Abbott Immunology Pharma-ceuticals Chugai (for all advisory board member)Michael Frosch no conflict of interestGerd Ganser Abbott Immunology Pharmaceuticals (advisoryboard member grants for scientific meetings) Wyeth Pfizer(advisory board member grants for scientific meetings)ChugaiRoche (advisory board member grants for scientificmeetings) Merck (grants for scientific meetings) Actelios(grants for scientific meetings) Esaote (grants for scientificmeetings)Arnd Heiligenhaus Novartis Pharmaceuticals CorporationAbbott Immunology Pharmaceuticals Alcon (for all re-search grants)Gerd Horneff Abbott Immunology Pharmaceuticals (re-search grants consulting fees non-remunerative positionsof influence) Wyeth Pfizer (research grants consultingfees speakers bureau non-remunerative positions of influ-ence) Bristol-Myers Squibb (Consulting fees) Nycomed(Consulting fees non-remunerative positions of influence)RocheChugai (Consulting fees non-remunerative positionsof influence) Sandoz (Consulting fees) Genzyme (researchgrants consulting fees non-remunerative positions of influ-ence) Swedish Orphan (research grants consulting feesnon-remunerative positions of influence)Arnold Illhardt no conflict of interestRuumldiger Krauspe no conflict of interestBarbara Markus no conflict of interestHartmut Michels Abbott Immunology Pharmaceuticals (advi-sory board member and grants for scientific meeting)Matthias Schneider no conflict of interestWolfram Singendonk no conflict of interestHelmut Sitter no conflict of interestMarianne Spamer no conflict of interestNorbert Wagner no conflict of interestTim Niehues Abbott Immunology Pharmaceuticals EssexPharma Novartis Pharmaceutical Corporation WyethPfizer (for all research grants consulting fees non-remu-nerative positions of influence)
Acknowledgment
We like to express our grateful thanks to Prof Dr Hans IkoHuppertz for proof reading the article and for an excellentdiscussion on our work We like to express our thanks to HE-LIOS Clinic for funding the open access of the article
References
[1] RE Petty TR Southwood P Manners J Baum DN Glass JGoldenberg X He J Maldonado-Cocco J Orozco-Alcala AMPrieur ME Suarez-Almazor PWoo International League of Asso-ciations for Rheumatology classification of juvenile idiopathic ar-thritis second revision Edmonton 2001 J Rheumatol 31(2004) 390ndash392
[2] B Prakken S Albani A Martini Juvenile idiopathic arthritisLancet 377 (2011) 2138ndash2149
[3] KT April DE Feldman RW Platt CM Duffy Comparisonbetween children with juvenile idiopathic arthritis (JIA) andtheir parents concerning perceived quality of life Qual LifeRes 15 (2006) 655ndash661
[4] BM Feldman B Grundland L McCullough V Wright Distinc-tion of quality of life health related quality of life and healthstatus in children referred for rheumatologic care J Rheuma-tol 27 (2000) 226ndash233
[5] JC Packham MA Hall Long-term follow-up of 246 adultswith juvenile idiopathic arthritis functional outcomeRheumatology (Oxford) 41 (2002) 1428ndash1435
[6] C Sandborg Pediatric rheumatic disease standards of care forJIAmdashthe basic foundation for quality Nat Rev Rheumatol 6(2010) 389ndash390
[7] N Guellac T Niehues Interdisciplinary and evidence-basedtreatment guideline for juvenile idiopathic arthritis KlinPadiatr 220 (2008) 392ndash402
[8] K Schnakenburg Leitlinien in der Kinder- und JugendmedizinElsevier 2005 pp H1 1ndash15
[9] P Juni L Nartey S Reichenbach R Sterchi PA Dieppe MEgger Risk of cardiovascular events and rofecoxib cumulativemeta-analysis Lancet 364 (2004) 2021ndash2029
[10] W Feldman Evidence-based Pediatrics 1st ed BC DeckersHamilton 2000
[11] AH Van de Ven AL Delbecq The nominal group as a re-search instrument for exploratory health studies Am J PublicHealth 62 (1972) 337ndash342
[12] HA Linstone M Turoff The Delphi Method Techniques andApplications Addison-Wesley Pub 1975
[13] TK Kvien HM Hoyeraal B Sandstad Naproxen and acetyl-salicylic acid in the treatment of pauciarticular and polyarticu-lar juvenile rheumatoid arthritis Assessment of tolerance andefficacy in a single-centre 24-week double-blind parallelstudy Scand J Rheumatol 13 (1984) 342ndash350
[14] RM Laxer ED Silverman C St-Cyr MT Tran G Lingam Asix-month open safety assessment of a naproxen suspensionformulation in the therapy of juvenile rheumatoid arthritisClin Ther 10 (1988) 381ndash387
[15] AM Leak MR Richter LE Clemens MA Hall BM AnsellA crossover study of naproxen diclofenac and tolmetin in sero-negative juvenile chronic arthritis Clin Exp Rheumatol 6(1988) 157ndash160
[16] J Haapasaari E Wuolijoki H Ylijoki Treatment of juve-nile rheumatoid arthritis with diclofenac sodium Scand JRheumatol 12 (1983) 325ndash330
[17] EH Giannini EJ Brewer ML Miller D Gibbas MH PassoHM Hoyeraal B Bernstein DA Person CW Fink LA Sawyeret al Ibuprofen suspension in the treatment of juvenilerheumatoid arthritis Pediatric Rheumatology CollaborativeStudy Group J Pediatr 117 (1990) 645ndash652
[18] E Stoeber L Sanger Experiences with indomethacin in long-term therapy of juvenile rheumatoid arthritis Arzneimittel-forschung 21 (1971) 1865ndash1866
[19] N Ruperto I Nikishina ED Pachanov Y Shachbazian AMPrieur R Mouy R Joos F Zulian R Schwarz V ArtamonovaW Emminger M Bandeira A Buoncompagni I Foeldvari FFalcini E Baildam I Kone-Paut M Alessio V Gerloni ALenhardt A Martini G Hanft R Sigmund S Simianer Arandomized double-blind clinical trial of two doses ofmeloxicam compared with naproxen in children with juvenileidiopathic arthritis short- and long-term efficacy and safetyresults Arthritis Rheum 52 (2005) 563ndash572
[20] I Foeldvari IS Szer LS Zemel DJ Lovell EH Giannini JLRobbins CRWest G Steidle S Krishnaswami BJ Bloom A pro-spective study comparing celecoxib with naproxen in children withjuvenile rheumatoid arthritis J Rheumatol 36 (2009) 174ndash182
191Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
[21] F Zulian G Martini D Gobber C Agosto C Gigante FZacchello Comparison of intra-articular triamcinolone hexa-cetonide and triamcinolone acetonide in oligoarticular juve-nile idiopathic arthritis Rheumatology (Oxford) 42 (2003)1254ndash1259
[22] F Zulian G Martini D Gobber M Plebani F Zacchello PManners Triamcinolone acetonide and hexacetonide intra-articular treatment of symmetrical joints in juvenile idiopathicarthritis a double-blind trial Rheumatology (Oxford) 43 (2004)1288ndash1291
[23] GS Habib Systemic effects of intra-articular corticosteroidsClin Rheumatol 28 (2009) 749ndash756
[24] JR Kirwan The effect of glucocorticoids on joint destructionin rheumatoid arthritis The Arthritis and Rheumatism CouncilLow-Dose Glucocorticoid Study Group N Engl J Med 333(1995) 142ndash146
[25] H Michels What is low-dose corticosteroid therapy in juvenileidiopathic arthritis A worldwide questionnaire-based surveyZ Rheumatol 59 (Suppl 2) (2000) II127ndash130
[26] JJ Miller III Prolonged use of large intravenous steroid pulsesin the rheumatic diseases of children Pediatrics 65 (1980)989ndash994
[27] P Picco M Gattorno A Buoncompagni V Pistoia C Borrone6-methylprednisolone lsquomini-pulsesrsquo a newmodality of glucocor-ticoid treatment in systemic onset juvenile chronic arthritisScand J Rheumatol 25 (1996) 24ndash27
[28] AM Prieur The place of corticosteroid therapy in juvenilechronic arthritis in 1992 J Rheumatol Suppl 37 (1993)32ndash34
[29] JS Gao H Wu J Tian Treatment of patients with juvenilerheumatoid arthritis with combination of leflunomide andmethotrexate Zhonghua Er Ke Za Zhi 41 (2003) 435ndash438
[30] T Niehues G Horneff H Michels MS Hock L SchuchmannEvidence-based use of methotrexate in children with rheumat-ic diseases a consensus statement of the Working Groups Pedi-atric Rheumatology Germany (AGKJR) and PediatricRheumatology Austria Rheumatol Int 25 (2005) 169ndash178
[31] N Ruperto DJ Lovell R Cuttica N Wilkinson P Woo GEspada C Wouters ED Silverman Z Balogh M HenricksonMT Apaz E Baildam A Fasth V Gerloni P Lahdenne AMPrieur A Ravelli RK Saurenmann ML Gamir N WulffraatL Marodi RE Petty R Joos F Zulian D McCurdy BLMyones K Nagy P Reuman I Szer S Travers A BeutlerG Keenan J Clark S Visvanathan A Fasanmade A Ray-chaudhuri A Mendelsohn A Martini EH Giannini A random-ized placebo-controlled trial of infliximab plus methotrexatefor the treatment of polyarticular-course juvenile rheumatoidarthritis Arthritis Rheum 56 (2007) 3096ndash3106
[32] K Visser DM van der Heijde Risk and management of livertoxicity during methotrexate treatment in rheumatoid andpsoriatic arthritis a systematic review of the literature ClinExp Rheumatol 27 (2009) 1017ndash1025
[33] A Cespedes-Cruz R Gutierrez-Suarez A Pistorio A Ravelli ALoy KJ Murray V Gerloni N Wulffraat S Oliveira J WalshIC Penades MG Alpigiani P Lahdenne C Saad-Magalhaes ECortis L Lepore Y Kimura C Wouters A Martini N RupertoMethotrexate improves the health-related quality of life of chil-dren with juvenile idiopathic arthritis Ann Rheum Dis 67(2008) 309ndash314
[34] TK Kvien HM Hoyeraal B Sandstad Azathioprine versus place-bo in patients with juvenile rheumatoid arthritis a single centerdouble blind comparative study J Rheumatol 13 (1986) 118ndash123
[35] E Silverman R Mouy L Spiegel LK Jung RK SaurenmannP Lahdenne G Horneff I Calvo IS Szer K Simpson JAStewart V Strand Leflunomide or methotrexate for juvenilerheumatoid arthritis N Engl J Med 352 (2005) 1655ndash1666
[36] MA van Rossum TJ Fiselier MJ Franssen AH ZwindermanR ten Cate LW van Suijlekom-Smit WH van Luijk RM
van Soesbergen NM Wulffraat JC Oostveen W Kuis PFDijkstra CF van Ede BA Dijkmans Sulfasalazine in the treat-ment of juvenile chronic arthritis a randomized double-blindplacebo-controlled multicenter study Dutch Juvenile ChronicArthritis Study Group Arthritis Rheum 41 (1998) 808ndash816
[37] MA van Rossum RM van Soesbergen M Boers AHZwinderman TJ Fiselier MJ Franssen R ten Cate LW vanSuijlekom-Smit NM Wulffraat WH van Luijk JC OostveenW Kuis BA Dijkmans Long-term outcome of juvenile idiopathicarthritis following a placebo-controlled trial sustained benefits ofearly sulfasalazine treatment Ann Rheum Dis 66 (2007)1518ndash1524
[38] DJ Lovell EH Giannini A Reiff GD Cawkwell ED SilvermanJJ Nocton LD Stein A Gedalia NT Ilowite CA Wallace JWhitmore BK Finck Etanercept in children with polyarticularjuvenile rheumatoid arthritis Pediatric Rheumatology Collabora-tive Study Group N Engl J Med 342 (2000) 763ndash769
[39] DJ Lovell A Reiff OY Jones R Schneider J Nocton LDStein A Gedalia NT Ilowite CA Wallace JB WhitmoreB White EH Giannini Long-term safety and efficacy ofetanercept in children with polyarticular-course juvenile rheu-matoid arthritis Arthritis Rheum 54 (2006) 1987ndash1994
[40] DJ Lovell N Ruperto S Goodman A Reiff L Jung K JarosovaD Nemcova R Mouy C Sandborg J Bohnsack D Elewaut IFoeldvari V Gerloni J Rovensky K Minden RK Vehe LWWeiner G Horneff HI Huppertz NY Olson JR Medich RCarcereri-De-Prati MJ McIlraith EH Giannini A MartiniAdalimumab with or without methotrexate in juvenile rheuma-toid arthritis N Engl J Med 359 (2008) 810ndash820
[41] FH Prince M Twilt R ten Cate MA van RossumW ArmbrustEP Hoppenreijs M van Santen-Hoeufft Y Koopman-KeeminkNM Wulffraat LW van Suijlekom-Smit Long-term follow-upon effectiveness and safety of etanercept in juvenile idiopathicarthritis the Dutch National Register Ann Rheum Dis 68(2009) 635ndash641
[42] P Diak J Siegel L LaGrenade L Choi S Lemery AMcMahonTumor necrosis factor alpha blockers andmalignancy in childrenforty-eight cases reported to the Food and Drug AdministrationArthritis Rheum 62 (2010) 2517ndash2524
[43] G Horneff T Hospach G Dannecker D Foll JP Haas HJGirschick HI Huppertz R Keitzer HJ Laws H Michels KMinden R Trauzeddel Updated statement by the German So-ciety for Pediatric and Adolescent Rheumatology (GKJR) on theFDAs report regarding malignancies in anti-TNF-treated pa-tients from Aug 4 2009 Z Rheumatol 69 (2010) 561ndash567
[44] T Hospach JP Haas HI Huppertz R Keitzer H Michels RTrauzeddl D Foll G Dannecker G Horneff Comment of theSociety of Pediatric and Adolescent Rheumatology on the USFood and Drug Administration (FDA) announcement regardingcases of malignancy in anti-TNF-treated patients Z Rheumatol68 (2009) 162ndash164
[45] DJ Lovell A Reiff NT Ilowite CA Wallace Y Chon SL LinSW Baumgartner EH Giannini Safety and efficacy of up to eightyears of continuous etanercept therapy in patients with juvenilerheumatoid arthritis Arthritis Rheum 58 (2008) 1496ndash1504
[46] EH Giannini NT Ilowite DJ Lovell CA Wallace CERabinovich A Reiff G Higgins B Gottlieb NG Singer YChon SL Lin SW Baumgartner Long-term safety and effec-tiveness of etanercept in children with selected categories ofjuvenile idiopathic arthritis Arthritis Rheum 60 (2009)2794ndash2804
[47] G Horneff H Schmeling T Biedermann I Foeldvari G GanserHJ Girschick T Hospach HI Huppertz R Keitzer RM KusterH Michels D Moebius B Rogalski A Thon The German etaner-cept registry for treatment of juvenile idiopathic arthritis AnnRheum Dis 63 (2004) 1638ndash1644
[48] FH Prince M Twilt SC Simon MA van RossumW ArmbrustEP Hoppenreijs S Kamphuis M van Santen-Hoeufft Y
192 G Dueckers et al
Koopman-Keemink NM Wulffraat R ten Cate LW vanSuijlekom-Smit When and how to stop etanercept aftersuccessful treatment of patients with juvenile idiopathic ar-thritis Ann Rheum Dis 68 (2009) 1228ndash1229
[49] G Horneff F De Bock I Foeldvari HJ Girschick H MichelsD Moebius H Schmeling Safety and efficacy of combinationof etanercept and methotrexate compared to treatment withetanercept only in patients with juvenile idiopathic arthritis(JIA) preliminary data from the German JIA Registry AnnRheum Dis 68 (2009) 519ndash525
[50] N Ilowite O Porras A Reiff S Rudge M Punaro A Martin RAllen T Harville YN Sun T Bevirt G Aras B Appleton Ana-kinra in the treatment of polyarticular-course juvenile rheumatoidarthritis safety and preliminary efficacy results of a randomizedmulticenter study Clin Rheumatol 28 (2009) 129ndash137
[51] T Lequerre P Quartier D Rosellini F Alaoui M De BandtO Mejjad I Kone-Paut M Michel E Dernis M Khellaf NLimal C Job-Deslandre B Fautrel X Le Loet J Sibilia In-terleukin-1 receptor antagonist (anakinra) treatment in pa-tients with systemic-onset juvenile idiopathic arthritis oradult onset Still disease preliminary experience in FranceAnn Rheum Dis 67 (2008) 302ndash308
[52] M Gattorno A Piccini D Lasiglie S Tassi G Brisca S CartaL Delfino F Ferlito MA Pelagatti F Caroli A BuoncompagniS Viola A Loy M Sironi A Vecchi A Ravelli A Martini ARubartelli The pattern of response to anti-interleukin-1 treatmentdistinguishes two subsets of patients with systemic-onset juvenileidiopathic arthritis Arthritis Rheum 58 (2008) 1505ndash1515
[53] S Yokota T Imagawa M Mori T Miyamae Y Aihara STakei N Iwata H Umebayashi T Murata M Miyoshi MTomiita N Nishimoto T Kishimoto Efficacy and safety oftocilizumab in patients with systemic-onset juvenile idiopathicarthritis a randomised double-blind placebo-controlledwithdrawal phase III trial Lancet 371 (2008) 998ndash1006
[54] N Ruperto DJ Lovell P Quartier E Paz N Rubio-Perez CASilva C Abud-Mendoza R Burgos-Vargas V Gerloni JAMelo-Gomes C Saad-Magalhaes F Sztajnbok C Goldenstein-Schainberg M Scheinberg IC Penades M Fischbach J OrozcoPJ Hashkes C Hom L Jung L Lepore S Oliveira CAWallace LH Sigal AJ Block A Covucci A Martini EHGiannini Abatacept in children with juvenile idiopathic arthri-tis a randomised double-blind placebo-controlled withdrawaltrial Lancet 372 (2008) 383ndash391
[55] N Ruperto DJ Lovell P Quartier E Paz N Rubio-PerezCA Silva C Abud-Mendoza R Burgos-Vargas V GerloniJA Melo-Gomes C Saad-Magalhaes J Chavez-Corrales CHuemer A Kivitz FJ Blanco I Foeldvari M Hofer G HorneffHI Huppertz C Job-Deslandre A Loy K Minden M PunaroAF Nunez LH Sigal AJ Block M Nys A Martini EHGiannini Long-term safety and efficacy of abatacept inchildren with juvenile idiopathic arthritis Arthritis Rheum 62(2010) 1792ndash1802
[56] DM Brinkman IM de Kleer R ten Cate MA van RossumWP Bekkering A Fasth MJ van Tol W Kuis NM WulffraatJM Vossen Autologous stem cell transplantation in childrenwith severe progressive systemic or polyarticular juvenile idio-pathic arthritis long-term follow-up of a prospective clinicaltrial Arthritis Rheum 56 (2007) 2410ndash2421
[57] SE Klepper Effects of an eight-week physical conditioningprogram on disease signs and symptoms in children with chronicarthritis Arthritis Care Res 12 (1999) 52ndash60
[58] D Singh-Grewal J Schneiderman-Walker V Wright O Bar-OrJ Beyene H Selvadurai B Cameron RM Laxer R SchneiderED Silverman L Spiegel S Tse C Leblanc J Wong SStephens BM Feldman The effects of vigorous exercisetraining on physical function in children with arthritis arandomized controlled single-blinded trial ArthritisRheum 57 (2007) 1202ndash1210
[59] S Stephens D Singh-Grewal O Bar-Or J Beyene B CameronCM Leblanc R Schneider J Schneiderman-Walker HSelvadurai E Silverman L Spiegel SM Tse V WrightBM Feldman Reliability of exercise testing and functionalactivity questionnaires in children with juvenile arthritisArthritis Rheum 57 (2007) 1446ndash1452
[60] T Takken J van der Net W Kuis PJ Helders Physical ac-tivity and health related physical fitness in children with ju-venile idiopathic arthritis Ann Rheum Dis 62 (2003)885ndash889
[61] MM Toledo G Martini C Gigante L Da Dalt A TregnaghiF Zulian Is there a role for arthroscopic synovectomy in oli-goarticular juvenile idiopathic arthritis J Rheumatol 33(2006) 1868ndash1872
[62] F de Benedetti H Brunner N Ruperto SWright A KenwrightR Cuttica P Woo R Schneider DJ Lovell A Martini Efficacyand safety of Tocilizumab in patients with systemic juvenile idio-pathic arthritis (sJIA) 12-week data from the phase III TENDERtrial Ann Rheum Dis 69 (2010) 146
[63] P Quartier F Allantaz R Cimaz P Pillet C Messiaen CBardin X Bossuyt A Boutten J Bienvenu A Duquesne ORicher D Chaussabel A Mogenet J Banchereau JM Tre-luyer P Landais V Pascual A multicentre randomiseddouble-blind placebo-controlled trial with the interleukin-1receptor antagonist anakinra in patients with systemic-onsetjuvenile idiopathic arthritis (ANAJIS trial) Ann Rheum Dis70 (2011) 747ndash754
[64] DE Furst EC Keystone J Braun FC Breedveld GRBurmester F De Benedetti T Dorner P Emery R FleischmannA Gibofsky JR Kalden A Kavanaugh B Kirkham P Mease JSieper NG Singer JS Smolen PL Van Riel MH Weisman KWinthrop Updated consensus statement on biological agents forthe treatment of rheumatic diseases 2010 Ann Rheum Dis 70(Suppl 1) (2010) i2ndashi36
[65] T Beukelman NM Patkar KG Saag S Tolleson-RinehartRQ Cron EM Dewitt NT Ilowite Y Kimura RM LaxerDJ Lovell A Martini CE Rabinovich N Ruperto 2011 Ameri-can College of Rheumatology recommendations for the treatmentof juvenile idiopathic arthritis initiation and safety monitoring oftherapeutic agents for the treatment of arthritis and systemic fea-tures Arthritis Care Res 63 (2011) 465ndash482 (Hoboken)
[66] JF Simard M Neovius S Hagelberg J Askling Juvenile idi-opathic arthritis and risk of cancer a nationwide cohort studyArthritis Rheum 62 (2010) 3776ndash3782
[67] T Imagawa S Yokota M Mori T Miyamae S Takei H ImanakaY Nerome N Iwata T Murata M Miyoshi N Nishimoto TKishimoto Safety and efficacy of tocilizumab an anti-IL-6-receptor monoclonal antibody in patients with polyarticular-course juvenile idiopathic arthritis Mod Rheumatol (2011)doi102007s10165-011-0481-0
[68] TM Shaneyfelt MF Mayo-Smith J Rothwangl Are guide-lines following guidelines The methodological quality of clini-cal practice guidelines in the peer-reviewed medicalliterature Jama 281 (1999) 1900ndash1905
[69] R Grilli N Magrini A Penna G Mura A Liberati Practiceguidelines developed by specialty societies the need for a crit-ical appraisal Lancet 355 (2000) 103ndash106
[70] JS Burgers R Grol NS Klazinga M Makela J Zaat To-wards evidence-based clinical practice an international surveyof 18 clinical guideline programs Int J Qual Health Care 15(2003) 31ndash45
[71] JT Cassidy RE Petty Juvenile Idiopathic Rheumatic Arthri-tis 5th Edition WB Saunders Philadelphia 2005
[72] TJ Lehman Are withdrawal trials in paediatric rheumatic dis-ease helpful Lancet 372 (2008) 348ndash350
[73] J Munro Recommendations for the Diagnosis and Managementof Juvenile Idiopathic Arthritis The Royal Australian Collegeof General Practitioners South Melbourne 2009 pp 1ndash38
193Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
httpwwwnhmrcgovau_files_nhmrcpublicationsattachmentscp119-juvenile-arthritispdf
[74] MJ Santos JE Fonseca H Canhao M Conde M JoseVieira L Costa M Costa M Salgado JA Melo Gomes Guide-lines for prescribing and monitoring biologic therapies in juve-nile idiopathic arthritis Acta Reumatol Port 32 (2007) 43ndash47
[75] S Yokota M Mori T Imagawa T Murata M Tomiita Y ItohS Fujikawa S Takei Guidelines on the use of etanercept forjuvenile idiopathic arthritis in Japan Mod Rheumatol 20(2010) 107ndash113
[76] The AGREE Collaboration Appraisal of Guidelines for Researchamp Evaluation (AGREE) instrument wwwagreecollaborationorg
[77] I Kopp H Thole T Langer HK Selbmann G OllenschlaumlgerGerman Instrument for Methodological Guideline Appraisal(DELBI) wwwversorgungsleitliniende2008
[78] Auml Aumlrztliches Zentrum fuumlr Qualitaumlt in der Medizin A Arbeitsge-meinschaften der Wissenschaftlichen Fachgesellschaften in derMedizin Deutsches Instrument zur methodischen Leitlinien-Bewertung (DELBI) Fassung 20052006 Z Aumlrztl FortbildQualitaumltssich 99 (2005) 468ndash519
[79] MP de Wit SE Berlo GJ Aanerud D Aletaha JW BijlsmaL Croucher JA Da Silva B Glusing L Gossec S Hewlett MJongkees D Magnusson M Scholte-Voshaar P Richards CZiegler TA Abma European League Against Rheumatism rec-ommendations for the inclusion of patient representatives in sci-entific projects Ann Rheum Dis 70 (2011) 722ndash726
[80] I Foeldvari M Bidde Validation of the proposed ILAR classifi-cation criteria for juvenile idiopathic arthritis InternationalLeague of Associations for Rheumatology J Rheumatol 27(2000) 1069ndash1072
[81] R Merino J de Inocencio J Garcia-Consuegra Evaluation ofrevised International League of Associations for Rheumatologyclassification criteria for juvenile idiopathic arthritis in Spanishchildren (Edmonton 2001) J Rheumatol 32 (2005) 559ndash561
[82] SE Ramsey RK Bolaria DA Cabral PN Malleson REPetty Comparison of criteria for the classification of childhoodarthritis J Rheumatol 27 (2000) 1283ndash1286
[83] G Horneff A Ebert S Fitter K Minden I Foeldvari J Kum-merle-Deschner A Thon HJ Girschick F Weller HI Hup-pertz Safety and efficacy of once weekly etanercept 08mgkg in a multicentre 12 week trial in active polyarticularcourse juvenile idiopathic arthritis Rheumatology (Oxford) 48(2009) 916ndash919
[84] EH Giannini EJ Brewer N Kuzmina A Shaikov A Maxi-mov I Vorontsov CW Fink AJ Newman JT Cassidy LSZemel Methotrexate in resistant juvenile rheumatoid arthri-tis Results of the USAndashUSSR double-blind placebo-controlled trial The Pediatric Rheumatology CollaborativeStudy Group and The Cooperative Childrens Study GroupN Engl J Med 326 (1992) 1043ndash1049
[85] A Ravelli S Viola D Migliavacca N Ruperto A Pistorio AMartini The extended oligoarticular subtype is the best predic-tor of methotrexate efficacy in juvenile idiopathic arthritisJ Pediatr 135 (1999) 316ndash320
[86] P Woo TR Southwood AM Prieur CJ Dore J Grainger JDavid C Ryder N Hasson A Hall I Lemelle Randomizedplacebo-controlled crossover trial of low-dose oral
methotrexate in children with extended oligoarticular or sys-temic arthritis Arthritis Rheum 43 (2000) 1849ndash1857
[87] E Silverman L Spiegel D Hawkins R Petty D Goldsmith LSchanberg C Duffy P Howard V Strand Long-term open-label preliminary study of the safety and efficacy of lefluno-mide in patients with polyarticular-course juvenile rheumatoidarthritis Arthritis Rheum 52 (2005) 554ndash562
[88] DJ Lovell EH Giannini Y Kimura C Suzanne PJHashkes A Reiff Long-term safety and efficacy of rilonaceptin patients with systemic juvenile idiopathic arthritis (SJIA)Arthritis Rheum 60 (2009)
[89] N Ruperto P Quartier NWulffraat PWoo A Loy R Mouy BBader-Meunier BJ Prakken E Noseda R Belleli J Lecot CRordorf A Martini A Phase II Trial with canakinumab(ACZ885) a new IL-1-beta blocking monoclonal antibody toevaluate safety and preliminary efficacy in children with system-ic juvenile idiopathic arthritis Ann Rheum Dis 68 (2009) 170
[90] DJ Lovell EH Giannini Y Kimura et al Preliminary evi-dence for bioactivity of IL-1 trap (Rilonacept) a long actingIL-1 inhibitor in systemic juvenile idiopathic arthritis (sJIA)Arthritis Rheum 54 (2006) S325
[91] DJ Lovell EH Giannini Y Kimura et al Preliminary evi-dence for sustained bioactivity of IL-1 Trap (rilonacept) a longacting IL-1 inhibitor in systemic juvenile idiopathic arthritisArthritis Rheum 56 (2007) S514
[92] N Ruperto F De Benedetti H Brunner R Allen D Brown JChaitow E Cortis G Espada B Flato V Gerloni G HorneffS Wright A Kenwright R Schneider P Woo A Martini DJLovell Tocilizumab is efficacious in patients with systemic ju-venile idiopathic arthritis (sJIA) across baseline disease charac-teristics and priorbaseline treatments 12-week data from thephase II TENDER trial 17th PReS Congress Valencia Spain2010 2010
[93] N Ruperto DJ Lovell T Li F Sztajnbok C Goldenstein-Schainberg M Scheinberg IC Penades M Fischbach JOrozco PJ Hashkes C Hom L Jung L Lepore S OliveiraC Wallace M Alessio P Quartier E Cortis A Eberhard GSimonini I Lemelle E Chalom LH Sigal A Block A CovucciM Nys A Martini EH Giannini Abatacept improves health-related quality of life pain sleep quality and daily participationin subjects with juvenile idiopathic arthritis Arthritis Care Res(Hoboken) 62 (11) (2010) 1542ndash1551
[94] N Ruperto DJ Lovell P Quartier E Paz N Rubio-PerezCA Silva C Abud-Mendoza R Burgos-Vargas V GerloniJA Melo-Gomes C Saad-Magalhaes J Chavez C HuemerA Kivitz FJ Blanco I Foeldvari M Hofer G Horneff HIHuppertz CJ Deslandre A Loy K Minden M Punaro AFNunez LH Sigal AJ Block M Nys A Martini EH GianniniLong-term safety and efficacy of abatacept in children with ju-venile idiopathic arthritis Arthritis Rheum 62 (2010)1792ndash1802
[95] J Munro Juvenile Idiopathic Arthritis Management Guidelines(Provisional) Australian Paediatric Rheumatology Group 2006httpwwwnhmrcgovau
[96] K Fitch SJ Bernstein MD Aguilar B Burnand JR LaCalleP Lazaro M van het Loo J McDonnell JP Vader JPKahan The RANDUCLA Appropriateness Method Users ManualRAND Pittsburgh 2000

Table 6 Overview of recommendationsguidelines for treatment of JIA
USA Australia Germany
ACR recommendations[65]
RACGP recommendations[73]
GKJR guidelines
Deadline of literature search October 2009 January 2007 September 2010Source of publications Pub Med Pub Med
EMBASE CINHAL CochraneLibrary provisionalAustralian Guideline [95]
Pub MedPrevious German Guidelines [78]
Definition used for JIA subgroups Treatment groups definedby Core expert panel
Not specifically definedChildren withJIAb16 years
ILAR criteria [1]
Consensus processprocessvalidation
AGREE [76] AGREE [76] DELBI [77]RANDUCLA appropriatenessmethod [96]
NGT Delphi method
Conferences None None 3 Formal consensus conferencesAddressees Pediatric rheumatologists General practitioner Pediatric Rheumatologists
PediatriciansGeneral practitioners
Participating scientific societies or professional organizationsPediatric rheumatologist orrheumatologists for adolescents
Yes Yes Yes
General pediatrician- In hospital Yes Yes Yes- In private practice Yes Yes YesResearcher Yes No YesRheumatologists for adults No No YesOphthalmologists No No YesParentspatients support groups Yes No YesOrthopedic surgeons No No YesPediatric orthopedic surgeons No No YesPsychologists No No YesPhysiotherapists No No YesPediatric rheumatology nurses Yes No NoOther scientific societies ororganizations
ACR BSPAR PRINTO PReS RACGP NAMSCAG NHMRC DGKJ DGPs DGRh DGO AWMFBVKJ
(ACR=American College of Rheumatologists AGREE=Appraisal of Guidelines for Research amp Development AWMF=Association of the ScientificMedical Associations BSPAR=British Society for Pediatric Rheumatology BVJK=Association of Pediatricians in private practice CEP=Core expertpanel ILAR=International League against Rheumatism CINHAL=Cumulative Index to Nursing and Allied Health Literature DELBI=German In-strument for Methodological Guideline Appraisal DGKJ=German Society of Pediatrics and Adolescent Medicine DGO=German Society for Oph-thalmology DGPs=German society for Psychology DGRh=German Society for Rheumatology GKJR=German Society for Pediatric RheumatologyNAMSCAG=National Arthritis and Musculoskeletal Conditions Advisory Group NGT=Nominal Group Technique NHMRC=National Health andMedical Research Council PReS=Pediatric Rheumatology Society) PRINTO=Pediatric Rheumatology International Trial Organization RACG-P=Royal Australian College of General Practitioner RANDUCLA=Research and DevelopmentUniversity of California at Los Angeles)
189Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
therapeutic effect of DMARDs The ACR recommendations donot provide any recommendation for the use of systemic GCfor patients with oligo- or polyarticular course of JIA exceptsystemic onset of JIA e) The ACR recommendations do notcover the topic of non-drug based therapy at all althoughthere is strong evidence that eg exercise training is a usefuladdition to drug treatment [575860]
6 Conclusion
In summary we present a treatment guideline for JIA on a con-sensus conference basis We strongly advocate an interdisciplin-ary approach including surgery physiotherapy psychosocial
intervention physical therapy medications etc and a strictformal consensus process in order to create statements thatare most appropriate for the complex clinical situation of achild and family presenting with JIA and cover all aspects ofJIA care All German pediatric rheumatology sites are partici-pating at the national pediatric rheumatologic database in theDeutsche Rheuma-Forschungszentrum at Berlin (DRFZ wwwdrfzde) It aims at quality assurance in Germany and monitorstreatment behavior of pediatric rheumatologists by using inter-nationally agreed criteria (eg joint count global physician rat-ing of disease activity global parent rating of overall well-being CHAQ ESR ACR-ped response or JADAS) The databasewill be used as a tool to monitor the application of our treat-ment guidelines
190 G Dueckers et al
Conflict of interest statement
Gregor Dueckers Novartis Pharmaceuticals CorporationBaxter (for all travel grants for scientific meetings)Nihal Guellac no conflict of interestMartin Arbogast no conflict of interestGuumlnther Dannecker no conflict of interestIvan Foeldvari Wyeth Pfizer Abbott Immunology Pharma-ceuticals Chugai (for all advisory board member)Michael Frosch no conflict of interestGerd Ganser Abbott Immunology Pharmaceuticals (advisoryboard member grants for scientific meetings) Wyeth Pfizer(advisory board member grants for scientific meetings)ChugaiRoche (advisory board member grants for scientificmeetings) Merck (grants for scientific meetings) Actelios(grants for scientific meetings) Esaote (grants for scientificmeetings)Arnd Heiligenhaus Novartis Pharmaceuticals CorporationAbbott Immunology Pharmaceuticals Alcon (for all re-search grants)Gerd Horneff Abbott Immunology Pharmaceuticals (re-search grants consulting fees non-remunerative positionsof influence) Wyeth Pfizer (research grants consultingfees speakers bureau non-remunerative positions of influ-ence) Bristol-Myers Squibb (Consulting fees) Nycomed(Consulting fees non-remunerative positions of influence)RocheChugai (Consulting fees non-remunerative positionsof influence) Sandoz (Consulting fees) Genzyme (researchgrants consulting fees non-remunerative positions of influ-ence) Swedish Orphan (research grants consulting feesnon-remunerative positions of influence)Arnold Illhardt no conflict of interestRuumldiger Krauspe no conflict of interestBarbara Markus no conflict of interestHartmut Michels Abbott Immunology Pharmaceuticals (advi-sory board member and grants for scientific meeting)Matthias Schneider no conflict of interestWolfram Singendonk no conflict of interestHelmut Sitter no conflict of interestMarianne Spamer no conflict of interestNorbert Wagner no conflict of interestTim Niehues Abbott Immunology Pharmaceuticals EssexPharma Novartis Pharmaceutical Corporation WyethPfizer (for all research grants consulting fees non-remu-nerative positions of influence)
Acknowledgment
We like to express our grateful thanks to Prof Dr Hans IkoHuppertz for proof reading the article and for an excellentdiscussion on our work We like to express our thanks to HE-LIOS Clinic for funding the open access of the article
References
[1] RE Petty TR Southwood P Manners J Baum DN Glass JGoldenberg X He J Maldonado-Cocco J Orozco-Alcala AMPrieur ME Suarez-Almazor PWoo International League of Asso-ciations for Rheumatology classification of juvenile idiopathic ar-thritis second revision Edmonton 2001 J Rheumatol 31(2004) 390ndash392
[2] B Prakken S Albani A Martini Juvenile idiopathic arthritisLancet 377 (2011) 2138ndash2149
[3] KT April DE Feldman RW Platt CM Duffy Comparisonbetween children with juvenile idiopathic arthritis (JIA) andtheir parents concerning perceived quality of life Qual LifeRes 15 (2006) 655ndash661
[4] BM Feldman B Grundland L McCullough V Wright Distinc-tion of quality of life health related quality of life and healthstatus in children referred for rheumatologic care J Rheuma-tol 27 (2000) 226ndash233
[5] JC Packham MA Hall Long-term follow-up of 246 adultswith juvenile idiopathic arthritis functional outcomeRheumatology (Oxford) 41 (2002) 1428ndash1435
[6] C Sandborg Pediatric rheumatic disease standards of care forJIAmdashthe basic foundation for quality Nat Rev Rheumatol 6(2010) 389ndash390
[7] N Guellac T Niehues Interdisciplinary and evidence-basedtreatment guideline for juvenile idiopathic arthritis KlinPadiatr 220 (2008) 392ndash402
[8] K Schnakenburg Leitlinien in der Kinder- und JugendmedizinElsevier 2005 pp H1 1ndash15
[9] P Juni L Nartey S Reichenbach R Sterchi PA Dieppe MEgger Risk of cardiovascular events and rofecoxib cumulativemeta-analysis Lancet 364 (2004) 2021ndash2029
[10] W Feldman Evidence-based Pediatrics 1st ed BC DeckersHamilton 2000
[11] AH Van de Ven AL Delbecq The nominal group as a re-search instrument for exploratory health studies Am J PublicHealth 62 (1972) 337ndash342
[12] HA Linstone M Turoff The Delphi Method Techniques andApplications Addison-Wesley Pub 1975
[13] TK Kvien HM Hoyeraal B Sandstad Naproxen and acetyl-salicylic acid in the treatment of pauciarticular and polyarticu-lar juvenile rheumatoid arthritis Assessment of tolerance andefficacy in a single-centre 24-week double-blind parallelstudy Scand J Rheumatol 13 (1984) 342ndash350
[14] RM Laxer ED Silverman C St-Cyr MT Tran G Lingam Asix-month open safety assessment of a naproxen suspensionformulation in the therapy of juvenile rheumatoid arthritisClin Ther 10 (1988) 381ndash387
[15] AM Leak MR Richter LE Clemens MA Hall BM AnsellA crossover study of naproxen diclofenac and tolmetin in sero-negative juvenile chronic arthritis Clin Exp Rheumatol 6(1988) 157ndash160
[16] J Haapasaari E Wuolijoki H Ylijoki Treatment of juve-nile rheumatoid arthritis with diclofenac sodium Scand JRheumatol 12 (1983) 325ndash330
[17] EH Giannini EJ Brewer ML Miller D Gibbas MH PassoHM Hoyeraal B Bernstein DA Person CW Fink LA Sawyeret al Ibuprofen suspension in the treatment of juvenilerheumatoid arthritis Pediatric Rheumatology CollaborativeStudy Group J Pediatr 117 (1990) 645ndash652
[18] E Stoeber L Sanger Experiences with indomethacin in long-term therapy of juvenile rheumatoid arthritis Arzneimittel-forschung 21 (1971) 1865ndash1866
[19] N Ruperto I Nikishina ED Pachanov Y Shachbazian AMPrieur R Mouy R Joos F Zulian R Schwarz V ArtamonovaW Emminger M Bandeira A Buoncompagni I Foeldvari FFalcini E Baildam I Kone-Paut M Alessio V Gerloni ALenhardt A Martini G Hanft R Sigmund S Simianer Arandomized double-blind clinical trial of two doses ofmeloxicam compared with naproxen in children with juvenileidiopathic arthritis short- and long-term efficacy and safetyresults Arthritis Rheum 52 (2005) 563ndash572
[20] I Foeldvari IS Szer LS Zemel DJ Lovell EH Giannini JLRobbins CRWest G Steidle S Krishnaswami BJ Bloom A pro-spective study comparing celecoxib with naproxen in children withjuvenile rheumatoid arthritis J Rheumatol 36 (2009) 174ndash182
191Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
[21] F Zulian G Martini D Gobber C Agosto C Gigante FZacchello Comparison of intra-articular triamcinolone hexa-cetonide and triamcinolone acetonide in oligoarticular juve-nile idiopathic arthritis Rheumatology (Oxford) 42 (2003)1254ndash1259
[22] F Zulian G Martini D Gobber M Plebani F Zacchello PManners Triamcinolone acetonide and hexacetonide intra-articular treatment of symmetrical joints in juvenile idiopathicarthritis a double-blind trial Rheumatology (Oxford) 43 (2004)1288ndash1291
[23] GS Habib Systemic effects of intra-articular corticosteroidsClin Rheumatol 28 (2009) 749ndash756
[24] JR Kirwan The effect of glucocorticoids on joint destructionin rheumatoid arthritis The Arthritis and Rheumatism CouncilLow-Dose Glucocorticoid Study Group N Engl J Med 333(1995) 142ndash146
[25] H Michels What is low-dose corticosteroid therapy in juvenileidiopathic arthritis A worldwide questionnaire-based surveyZ Rheumatol 59 (Suppl 2) (2000) II127ndash130
[26] JJ Miller III Prolonged use of large intravenous steroid pulsesin the rheumatic diseases of children Pediatrics 65 (1980)989ndash994
[27] P Picco M Gattorno A Buoncompagni V Pistoia C Borrone6-methylprednisolone lsquomini-pulsesrsquo a newmodality of glucocor-ticoid treatment in systemic onset juvenile chronic arthritisScand J Rheumatol 25 (1996) 24ndash27
[28] AM Prieur The place of corticosteroid therapy in juvenilechronic arthritis in 1992 J Rheumatol Suppl 37 (1993)32ndash34
[29] JS Gao H Wu J Tian Treatment of patients with juvenilerheumatoid arthritis with combination of leflunomide andmethotrexate Zhonghua Er Ke Za Zhi 41 (2003) 435ndash438
[30] T Niehues G Horneff H Michels MS Hock L SchuchmannEvidence-based use of methotrexate in children with rheumat-ic diseases a consensus statement of the Working Groups Pedi-atric Rheumatology Germany (AGKJR) and PediatricRheumatology Austria Rheumatol Int 25 (2005) 169ndash178
[31] N Ruperto DJ Lovell R Cuttica N Wilkinson P Woo GEspada C Wouters ED Silverman Z Balogh M HenricksonMT Apaz E Baildam A Fasth V Gerloni P Lahdenne AMPrieur A Ravelli RK Saurenmann ML Gamir N WulffraatL Marodi RE Petty R Joos F Zulian D McCurdy BLMyones K Nagy P Reuman I Szer S Travers A BeutlerG Keenan J Clark S Visvanathan A Fasanmade A Ray-chaudhuri A Mendelsohn A Martini EH Giannini A random-ized placebo-controlled trial of infliximab plus methotrexatefor the treatment of polyarticular-course juvenile rheumatoidarthritis Arthritis Rheum 56 (2007) 3096ndash3106
[32] K Visser DM van der Heijde Risk and management of livertoxicity during methotrexate treatment in rheumatoid andpsoriatic arthritis a systematic review of the literature ClinExp Rheumatol 27 (2009) 1017ndash1025
[33] A Cespedes-Cruz R Gutierrez-Suarez A Pistorio A Ravelli ALoy KJ Murray V Gerloni N Wulffraat S Oliveira J WalshIC Penades MG Alpigiani P Lahdenne C Saad-Magalhaes ECortis L Lepore Y Kimura C Wouters A Martini N RupertoMethotrexate improves the health-related quality of life of chil-dren with juvenile idiopathic arthritis Ann Rheum Dis 67(2008) 309ndash314
[34] TK Kvien HM Hoyeraal B Sandstad Azathioprine versus place-bo in patients with juvenile rheumatoid arthritis a single centerdouble blind comparative study J Rheumatol 13 (1986) 118ndash123
[35] E Silverman R Mouy L Spiegel LK Jung RK SaurenmannP Lahdenne G Horneff I Calvo IS Szer K Simpson JAStewart V Strand Leflunomide or methotrexate for juvenilerheumatoid arthritis N Engl J Med 352 (2005) 1655ndash1666
[36] MA van Rossum TJ Fiselier MJ Franssen AH ZwindermanR ten Cate LW van Suijlekom-Smit WH van Luijk RM
van Soesbergen NM Wulffraat JC Oostveen W Kuis PFDijkstra CF van Ede BA Dijkmans Sulfasalazine in the treat-ment of juvenile chronic arthritis a randomized double-blindplacebo-controlled multicenter study Dutch Juvenile ChronicArthritis Study Group Arthritis Rheum 41 (1998) 808ndash816
[37] MA van Rossum RM van Soesbergen M Boers AHZwinderman TJ Fiselier MJ Franssen R ten Cate LW vanSuijlekom-Smit NM Wulffraat WH van Luijk JC OostveenW Kuis BA Dijkmans Long-term outcome of juvenile idiopathicarthritis following a placebo-controlled trial sustained benefits ofearly sulfasalazine treatment Ann Rheum Dis 66 (2007)1518ndash1524
[38] DJ Lovell EH Giannini A Reiff GD Cawkwell ED SilvermanJJ Nocton LD Stein A Gedalia NT Ilowite CA Wallace JWhitmore BK Finck Etanercept in children with polyarticularjuvenile rheumatoid arthritis Pediatric Rheumatology Collabora-tive Study Group N Engl J Med 342 (2000) 763ndash769
[39] DJ Lovell A Reiff OY Jones R Schneider J Nocton LDStein A Gedalia NT Ilowite CA Wallace JB WhitmoreB White EH Giannini Long-term safety and efficacy ofetanercept in children with polyarticular-course juvenile rheu-matoid arthritis Arthritis Rheum 54 (2006) 1987ndash1994
[40] DJ Lovell N Ruperto S Goodman A Reiff L Jung K JarosovaD Nemcova R Mouy C Sandborg J Bohnsack D Elewaut IFoeldvari V Gerloni J Rovensky K Minden RK Vehe LWWeiner G Horneff HI Huppertz NY Olson JR Medich RCarcereri-De-Prati MJ McIlraith EH Giannini A MartiniAdalimumab with or without methotrexate in juvenile rheuma-toid arthritis N Engl J Med 359 (2008) 810ndash820
[41] FH Prince M Twilt R ten Cate MA van RossumW ArmbrustEP Hoppenreijs M van Santen-Hoeufft Y Koopman-KeeminkNM Wulffraat LW van Suijlekom-Smit Long-term follow-upon effectiveness and safety of etanercept in juvenile idiopathicarthritis the Dutch National Register Ann Rheum Dis 68(2009) 635ndash641
[42] P Diak J Siegel L LaGrenade L Choi S Lemery AMcMahonTumor necrosis factor alpha blockers andmalignancy in childrenforty-eight cases reported to the Food and Drug AdministrationArthritis Rheum 62 (2010) 2517ndash2524
[43] G Horneff T Hospach G Dannecker D Foll JP Haas HJGirschick HI Huppertz R Keitzer HJ Laws H Michels KMinden R Trauzeddel Updated statement by the German So-ciety for Pediatric and Adolescent Rheumatology (GKJR) on theFDAs report regarding malignancies in anti-TNF-treated pa-tients from Aug 4 2009 Z Rheumatol 69 (2010) 561ndash567
[44] T Hospach JP Haas HI Huppertz R Keitzer H Michels RTrauzeddl D Foll G Dannecker G Horneff Comment of theSociety of Pediatric and Adolescent Rheumatology on the USFood and Drug Administration (FDA) announcement regardingcases of malignancy in anti-TNF-treated patients Z Rheumatol68 (2009) 162ndash164
[45] DJ Lovell A Reiff NT Ilowite CA Wallace Y Chon SL LinSW Baumgartner EH Giannini Safety and efficacy of up to eightyears of continuous etanercept therapy in patients with juvenilerheumatoid arthritis Arthritis Rheum 58 (2008) 1496ndash1504
[46] EH Giannini NT Ilowite DJ Lovell CA Wallace CERabinovich A Reiff G Higgins B Gottlieb NG Singer YChon SL Lin SW Baumgartner Long-term safety and effec-tiveness of etanercept in children with selected categories ofjuvenile idiopathic arthritis Arthritis Rheum 60 (2009)2794ndash2804
[47] G Horneff H Schmeling T Biedermann I Foeldvari G GanserHJ Girschick T Hospach HI Huppertz R Keitzer RM KusterH Michels D Moebius B Rogalski A Thon The German etaner-cept registry for treatment of juvenile idiopathic arthritis AnnRheum Dis 63 (2004) 1638ndash1644
[48] FH Prince M Twilt SC Simon MA van RossumW ArmbrustEP Hoppenreijs S Kamphuis M van Santen-Hoeufft Y
192 G Dueckers et al
Koopman-Keemink NM Wulffraat R ten Cate LW vanSuijlekom-Smit When and how to stop etanercept aftersuccessful treatment of patients with juvenile idiopathic ar-thritis Ann Rheum Dis 68 (2009) 1228ndash1229
[49] G Horneff F De Bock I Foeldvari HJ Girschick H MichelsD Moebius H Schmeling Safety and efficacy of combinationof etanercept and methotrexate compared to treatment withetanercept only in patients with juvenile idiopathic arthritis(JIA) preliminary data from the German JIA Registry AnnRheum Dis 68 (2009) 519ndash525
[50] N Ilowite O Porras A Reiff S Rudge M Punaro A Martin RAllen T Harville YN Sun T Bevirt G Aras B Appleton Ana-kinra in the treatment of polyarticular-course juvenile rheumatoidarthritis safety and preliminary efficacy results of a randomizedmulticenter study Clin Rheumatol 28 (2009) 129ndash137
[51] T Lequerre P Quartier D Rosellini F Alaoui M De BandtO Mejjad I Kone-Paut M Michel E Dernis M Khellaf NLimal C Job-Deslandre B Fautrel X Le Loet J Sibilia In-terleukin-1 receptor antagonist (anakinra) treatment in pa-tients with systemic-onset juvenile idiopathic arthritis oradult onset Still disease preliminary experience in FranceAnn Rheum Dis 67 (2008) 302ndash308
[52] M Gattorno A Piccini D Lasiglie S Tassi G Brisca S CartaL Delfino F Ferlito MA Pelagatti F Caroli A BuoncompagniS Viola A Loy M Sironi A Vecchi A Ravelli A Martini ARubartelli The pattern of response to anti-interleukin-1 treatmentdistinguishes two subsets of patients with systemic-onset juvenileidiopathic arthritis Arthritis Rheum 58 (2008) 1505ndash1515
[53] S Yokota T Imagawa M Mori T Miyamae Y Aihara STakei N Iwata H Umebayashi T Murata M Miyoshi MTomiita N Nishimoto T Kishimoto Efficacy and safety oftocilizumab in patients with systemic-onset juvenile idiopathicarthritis a randomised double-blind placebo-controlledwithdrawal phase III trial Lancet 371 (2008) 998ndash1006
[54] N Ruperto DJ Lovell P Quartier E Paz N Rubio-Perez CASilva C Abud-Mendoza R Burgos-Vargas V Gerloni JAMelo-Gomes C Saad-Magalhaes F Sztajnbok C Goldenstein-Schainberg M Scheinberg IC Penades M Fischbach J OrozcoPJ Hashkes C Hom L Jung L Lepore S Oliveira CAWallace LH Sigal AJ Block A Covucci A Martini EHGiannini Abatacept in children with juvenile idiopathic arthri-tis a randomised double-blind placebo-controlled withdrawaltrial Lancet 372 (2008) 383ndash391
[55] N Ruperto DJ Lovell P Quartier E Paz N Rubio-PerezCA Silva C Abud-Mendoza R Burgos-Vargas V GerloniJA Melo-Gomes C Saad-Magalhaes J Chavez-Corrales CHuemer A Kivitz FJ Blanco I Foeldvari M Hofer G HorneffHI Huppertz C Job-Deslandre A Loy K Minden M PunaroAF Nunez LH Sigal AJ Block M Nys A Martini EHGiannini Long-term safety and efficacy of abatacept inchildren with juvenile idiopathic arthritis Arthritis Rheum 62(2010) 1792ndash1802
[56] DM Brinkman IM de Kleer R ten Cate MA van RossumWP Bekkering A Fasth MJ van Tol W Kuis NM WulffraatJM Vossen Autologous stem cell transplantation in childrenwith severe progressive systemic or polyarticular juvenile idio-pathic arthritis long-term follow-up of a prospective clinicaltrial Arthritis Rheum 56 (2007) 2410ndash2421
[57] SE Klepper Effects of an eight-week physical conditioningprogram on disease signs and symptoms in children with chronicarthritis Arthritis Care Res 12 (1999) 52ndash60
[58] D Singh-Grewal J Schneiderman-Walker V Wright O Bar-OrJ Beyene H Selvadurai B Cameron RM Laxer R SchneiderED Silverman L Spiegel S Tse C Leblanc J Wong SStephens BM Feldman The effects of vigorous exercisetraining on physical function in children with arthritis arandomized controlled single-blinded trial ArthritisRheum 57 (2007) 1202ndash1210
[59] S Stephens D Singh-Grewal O Bar-Or J Beyene B CameronCM Leblanc R Schneider J Schneiderman-Walker HSelvadurai E Silverman L Spiegel SM Tse V WrightBM Feldman Reliability of exercise testing and functionalactivity questionnaires in children with juvenile arthritisArthritis Rheum 57 (2007) 1446ndash1452
[60] T Takken J van der Net W Kuis PJ Helders Physical ac-tivity and health related physical fitness in children with ju-venile idiopathic arthritis Ann Rheum Dis 62 (2003)885ndash889
[61] MM Toledo G Martini C Gigante L Da Dalt A TregnaghiF Zulian Is there a role for arthroscopic synovectomy in oli-goarticular juvenile idiopathic arthritis J Rheumatol 33(2006) 1868ndash1872
[62] F de Benedetti H Brunner N Ruperto SWright A KenwrightR Cuttica P Woo R Schneider DJ Lovell A Martini Efficacyand safety of Tocilizumab in patients with systemic juvenile idio-pathic arthritis (sJIA) 12-week data from the phase III TENDERtrial Ann Rheum Dis 69 (2010) 146
[63] P Quartier F Allantaz R Cimaz P Pillet C Messiaen CBardin X Bossuyt A Boutten J Bienvenu A Duquesne ORicher D Chaussabel A Mogenet J Banchereau JM Tre-luyer P Landais V Pascual A multicentre randomiseddouble-blind placebo-controlled trial with the interleukin-1receptor antagonist anakinra in patients with systemic-onsetjuvenile idiopathic arthritis (ANAJIS trial) Ann Rheum Dis70 (2011) 747ndash754
[64] DE Furst EC Keystone J Braun FC Breedveld GRBurmester F De Benedetti T Dorner P Emery R FleischmannA Gibofsky JR Kalden A Kavanaugh B Kirkham P Mease JSieper NG Singer JS Smolen PL Van Riel MH Weisman KWinthrop Updated consensus statement on biological agents forthe treatment of rheumatic diseases 2010 Ann Rheum Dis 70(Suppl 1) (2010) i2ndashi36
[65] T Beukelman NM Patkar KG Saag S Tolleson-RinehartRQ Cron EM Dewitt NT Ilowite Y Kimura RM LaxerDJ Lovell A Martini CE Rabinovich N Ruperto 2011 Ameri-can College of Rheumatology recommendations for the treatmentof juvenile idiopathic arthritis initiation and safety monitoring oftherapeutic agents for the treatment of arthritis and systemic fea-tures Arthritis Care Res 63 (2011) 465ndash482 (Hoboken)
[66] JF Simard M Neovius S Hagelberg J Askling Juvenile idi-opathic arthritis and risk of cancer a nationwide cohort studyArthritis Rheum 62 (2010) 3776ndash3782
[67] T Imagawa S Yokota M Mori T Miyamae S Takei H ImanakaY Nerome N Iwata T Murata M Miyoshi N Nishimoto TKishimoto Safety and efficacy of tocilizumab an anti-IL-6-receptor monoclonal antibody in patients with polyarticular-course juvenile idiopathic arthritis Mod Rheumatol (2011)doi102007s10165-011-0481-0
[68] TM Shaneyfelt MF Mayo-Smith J Rothwangl Are guide-lines following guidelines The methodological quality of clini-cal practice guidelines in the peer-reviewed medicalliterature Jama 281 (1999) 1900ndash1905
[69] R Grilli N Magrini A Penna G Mura A Liberati Practiceguidelines developed by specialty societies the need for a crit-ical appraisal Lancet 355 (2000) 103ndash106
[70] JS Burgers R Grol NS Klazinga M Makela J Zaat To-wards evidence-based clinical practice an international surveyof 18 clinical guideline programs Int J Qual Health Care 15(2003) 31ndash45
[71] JT Cassidy RE Petty Juvenile Idiopathic Rheumatic Arthri-tis 5th Edition WB Saunders Philadelphia 2005
[72] TJ Lehman Are withdrawal trials in paediatric rheumatic dis-ease helpful Lancet 372 (2008) 348ndash350
[73] J Munro Recommendations for the Diagnosis and Managementof Juvenile Idiopathic Arthritis The Royal Australian Collegeof General Practitioners South Melbourne 2009 pp 1ndash38
193Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
httpwwwnhmrcgovau_files_nhmrcpublicationsattachmentscp119-juvenile-arthritispdf
[74] MJ Santos JE Fonseca H Canhao M Conde M JoseVieira L Costa M Costa M Salgado JA Melo Gomes Guide-lines for prescribing and monitoring biologic therapies in juve-nile idiopathic arthritis Acta Reumatol Port 32 (2007) 43ndash47
[75] S Yokota M Mori T Imagawa T Murata M Tomiita Y ItohS Fujikawa S Takei Guidelines on the use of etanercept forjuvenile idiopathic arthritis in Japan Mod Rheumatol 20(2010) 107ndash113
[76] The AGREE Collaboration Appraisal of Guidelines for Researchamp Evaluation (AGREE) instrument wwwagreecollaborationorg
[77] I Kopp H Thole T Langer HK Selbmann G OllenschlaumlgerGerman Instrument for Methodological Guideline Appraisal(DELBI) wwwversorgungsleitliniende2008
[78] Auml Aumlrztliches Zentrum fuumlr Qualitaumlt in der Medizin A Arbeitsge-meinschaften der Wissenschaftlichen Fachgesellschaften in derMedizin Deutsches Instrument zur methodischen Leitlinien-Bewertung (DELBI) Fassung 20052006 Z Aumlrztl FortbildQualitaumltssich 99 (2005) 468ndash519
[79] MP de Wit SE Berlo GJ Aanerud D Aletaha JW BijlsmaL Croucher JA Da Silva B Glusing L Gossec S Hewlett MJongkees D Magnusson M Scholte-Voshaar P Richards CZiegler TA Abma European League Against Rheumatism rec-ommendations for the inclusion of patient representatives in sci-entific projects Ann Rheum Dis 70 (2011) 722ndash726
[80] I Foeldvari M Bidde Validation of the proposed ILAR classifi-cation criteria for juvenile idiopathic arthritis InternationalLeague of Associations for Rheumatology J Rheumatol 27(2000) 1069ndash1072
[81] R Merino J de Inocencio J Garcia-Consuegra Evaluation ofrevised International League of Associations for Rheumatologyclassification criteria for juvenile idiopathic arthritis in Spanishchildren (Edmonton 2001) J Rheumatol 32 (2005) 559ndash561
[82] SE Ramsey RK Bolaria DA Cabral PN Malleson REPetty Comparison of criteria for the classification of childhoodarthritis J Rheumatol 27 (2000) 1283ndash1286
[83] G Horneff A Ebert S Fitter K Minden I Foeldvari J Kum-merle-Deschner A Thon HJ Girschick F Weller HI Hup-pertz Safety and efficacy of once weekly etanercept 08mgkg in a multicentre 12 week trial in active polyarticularcourse juvenile idiopathic arthritis Rheumatology (Oxford) 48(2009) 916ndash919
[84] EH Giannini EJ Brewer N Kuzmina A Shaikov A Maxi-mov I Vorontsov CW Fink AJ Newman JT Cassidy LSZemel Methotrexate in resistant juvenile rheumatoid arthri-tis Results of the USAndashUSSR double-blind placebo-controlled trial The Pediatric Rheumatology CollaborativeStudy Group and The Cooperative Childrens Study GroupN Engl J Med 326 (1992) 1043ndash1049
[85] A Ravelli S Viola D Migliavacca N Ruperto A Pistorio AMartini The extended oligoarticular subtype is the best predic-tor of methotrexate efficacy in juvenile idiopathic arthritisJ Pediatr 135 (1999) 316ndash320
[86] P Woo TR Southwood AM Prieur CJ Dore J Grainger JDavid C Ryder N Hasson A Hall I Lemelle Randomizedplacebo-controlled crossover trial of low-dose oral
methotrexate in children with extended oligoarticular or sys-temic arthritis Arthritis Rheum 43 (2000) 1849ndash1857
[87] E Silverman L Spiegel D Hawkins R Petty D Goldsmith LSchanberg C Duffy P Howard V Strand Long-term open-label preliminary study of the safety and efficacy of lefluno-mide in patients with polyarticular-course juvenile rheumatoidarthritis Arthritis Rheum 52 (2005) 554ndash562
[88] DJ Lovell EH Giannini Y Kimura C Suzanne PJHashkes A Reiff Long-term safety and efficacy of rilonaceptin patients with systemic juvenile idiopathic arthritis (SJIA)Arthritis Rheum 60 (2009)
[89] N Ruperto P Quartier NWulffraat PWoo A Loy R Mouy BBader-Meunier BJ Prakken E Noseda R Belleli J Lecot CRordorf A Martini A Phase II Trial with canakinumab(ACZ885) a new IL-1-beta blocking monoclonal antibody toevaluate safety and preliminary efficacy in children with system-ic juvenile idiopathic arthritis Ann Rheum Dis 68 (2009) 170
[90] DJ Lovell EH Giannini Y Kimura et al Preliminary evi-dence for bioactivity of IL-1 trap (Rilonacept) a long actingIL-1 inhibitor in systemic juvenile idiopathic arthritis (sJIA)Arthritis Rheum 54 (2006) S325
[91] DJ Lovell EH Giannini Y Kimura et al Preliminary evi-dence for sustained bioactivity of IL-1 Trap (rilonacept) a longacting IL-1 inhibitor in systemic juvenile idiopathic arthritisArthritis Rheum 56 (2007) S514
[92] N Ruperto F De Benedetti H Brunner R Allen D Brown JChaitow E Cortis G Espada B Flato V Gerloni G HorneffS Wright A Kenwright R Schneider P Woo A Martini DJLovell Tocilizumab is efficacious in patients with systemic ju-venile idiopathic arthritis (sJIA) across baseline disease charac-teristics and priorbaseline treatments 12-week data from thephase II TENDER trial 17th PReS Congress Valencia Spain2010 2010
[93] N Ruperto DJ Lovell T Li F Sztajnbok C Goldenstein-Schainberg M Scheinberg IC Penades M Fischbach JOrozco PJ Hashkes C Hom L Jung L Lepore S OliveiraC Wallace M Alessio P Quartier E Cortis A Eberhard GSimonini I Lemelle E Chalom LH Sigal A Block A CovucciM Nys A Martini EH Giannini Abatacept improves health-related quality of life pain sleep quality and daily participationin subjects with juvenile idiopathic arthritis Arthritis Care Res(Hoboken) 62 (11) (2010) 1542ndash1551
[94] N Ruperto DJ Lovell P Quartier E Paz N Rubio-PerezCA Silva C Abud-Mendoza R Burgos-Vargas V GerloniJA Melo-Gomes C Saad-Magalhaes J Chavez C HuemerA Kivitz FJ Blanco I Foeldvari M Hofer G Horneff HIHuppertz CJ Deslandre A Loy K Minden M Punaro AFNunez LH Sigal AJ Block M Nys A Martini EH GianniniLong-term safety and efficacy of abatacept in children with ju-venile idiopathic arthritis Arthritis Rheum 62 (2010)1792ndash1802
[95] J Munro Juvenile Idiopathic Arthritis Management Guidelines(Provisional) Australian Paediatric Rheumatology Group 2006httpwwwnhmrcgovau
[96] K Fitch SJ Bernstein MD Aguilar B Burnand JR LaCalleP Lazaro M van het Loo J McDonnell JP Vader JPKahan The RANDUCLA Appropriateness Method Users ManualRAND Pittsburgh 2000

190 G Dueckers et al
Conflict of interest statement
Gregor Dueckers Novartis Pharmaceuticals CorporationBaxter (for all travel grants for scientific meetings)Nihal Guellac no conflict of interestMartin Arbogast no conflict of interestGuumlnther Dannecker no conflict of interestIvan Foeldvari Wyeth Pfizer Abbott Immunology Pharma-ceuticals Chugai (for all advisory board member)Michael Frosch no conflict of interestGerd Ganser Abbott Immunology Pharmaceuticals (advisoryboard member grants for scientific meetings) Wyeth Pfizer(advisory board member grants for scientific meetings)ChugaiRoche (advisory board member grants for scientificmeetings) Merck (grants for scientific meetings) Actelios(grants for scientific meetings) Esaote (grants for scientificmeetings)Arnd Heiligenhaus Novartis Pharmaceuticals CorporationAbbott Immunology Pharmaceuticals Alcon (for all re-search grants)Gerd Horneff Abbott Immunology Pharmaceuticals (re-search grants consulting fees non-remunerative positionsof influence) Wyeth Pfizer (research grants consultingfees speakers bureau non-remunerative positions of influ-ence) Bristol-Myers Squibb (Consulting fees) Nycomed(Consulting fees non-remunerative positions of influence)RocheChugai (Consulting fees non-remunerative positionsof influence) Sandoz (Consulting fees) Genzyme (researchgrants consulting fees non-remunerative positions of influ-ence) Swedish Orphan (research grants consulting feesnon-remunerative positions of influence)Arnold Illhardt no conflict of interestRuumldiger Krauspe no conflict of interestBarbara Markus no conflict of interestHartmut Michels Abbott Immunology Pharmaceuticals (advi-sory board member and grants for scientific meeting)Matthias Schneider no conflict of interestWolfram Singendonk no conflict of interestHelmut Sitter no conflict of interestMarianne Spamer no conflict of interestNorbert Wagner no conflict of interestTim Niehues Abbott Immunology Pharmaceuticals EssexPharma Novartis Pharmaceutical Corporation WyethPfizer (for all research grants consulting fees non-remu-nerative positions of influence)
Acknowledgment
We like to express our grateful thanks to Prof Dr Hans IkoHuppertz for proof reading the article and for an excellentdiscussion on our work We like to express our thanks to HE-LIOS Clinic for funding the open access of the article
References
[1] RE Petty TR Southwood P Manners J Baum DN Glass JGoldenberg X He J Maldonado-Cocco J Orozco-Alcala AMPrieur ME Suarez-Almazor PWoo International League of Asso-ciations for Rheumatology classification of juvenile idiopathic ar-thritis second revision Edmonton 2001 J Rheumatol 31(2004) 390ndash392
[2] B Prakken S Albani A Martini Juvenile idiopathic arthritisLancet 377 (2011) 2138ndash2149
[3] KT April DE Feldman RW Platt CM Duffy Comparisonbetween children with juvenile idiopathic arthritis (JIA) andtheir parents concerning perceived quality of life Qual LifeRes 15 (2006) 655ndash661
[4] BM Feldman B Grundland L McCullough V Wright Distinc-tion of quality of life health related quality of life and healthstatus in children referred for rheumatologic care J Rheuma-tol 27 (2000) 226ndash233
[5] JC Packham MA Hall Long-term follow-up of 246 adultswith juvenile idiopathic arthritis functional outcomeRheumatology (Oxford) 41 (2002) 1428ndash1435
[6] C Sandborg Pediatric rheumatic disease standards of care forJIAmdashthe basic foundation for quality Nat Rev Rheumatol 6(2010) 389ndash390
[7] N Guellac T Niehues Interdisciplinary and evidence-basedtreatment guideline for juvenile idiopathic arthritis KlinPadiatr 220 (2008) 392ndash402
[8] K Schnakenburg Leitlinien in der Kinder- und JugendmedizinElsevier 2005 pp H1 1ndash15
[9] P Juni L Nartey S Reichenbach R Sterchi PA Dieppe MEgger Risk of cardiovascular events and rofecoxib cumulativemeta-analysis Lancet 364 (2004) 2021ndash2029
[10] W Feldman Evidence-based Pediatrics 1st ed BC DeckersHamilton 2000
[11] AH Van de Ven AL Delbecq The nominal group as a re-search instrument for exploratory health studies Am J PublicHealth 62 (1972) 337ndash342
[12] HA Linstone M Turoff The Delphi Method Techniques andApplications Addison-Wesley Pub 1975
[13] TK Kvien HM Hoyeraal B Sandstad Naproxen and acetyl-salicylic acid in the treatment of pauciarticular and polyarticu-lar juvenile rheumatoid arthritis Assessment of tolerance andefficacy in a single-centre 24-week double-blind parallelstudy Scand J Rheumatol 13 (1984) 342ndash350
[14] RM Laxer ED Silverman C St-Cyr MT Tran G Lingam Asix-month open safety assessment of a naproxen suspensionformulation in the therapy of juvenile rheumatoid arthritisClin Ther 10 (1988) 381ndash387
[15] AM Leak MR Richter LE Clemens MA Hall BM AnsellA crossover study of naproxen diclofenac and tolmetin in sero-negative juvenile chronic arthritis Clin Exp Rheumatol 6(1988) 157ndash160
[16] J Haapasaari E Wuolijoki H Ylijoki Treatment of juve-nile rheumatoid arthritis with diclofenac sodium Scand JRheumatol 12 (1983) 325ndash330
[17] EH Giannini EJ Brewer ML Miller D Gibbas MH PassoHM Hoyeraal B Bernstein DA Person CW Fink LA Sawyeret al Ibuprofen suspension in the treatment of juvenilerheumatoid arthritis Pediatric Rheumatology CollaborativeStudy Group J Pediatr 117 (1990) 645ndash652
[18] E Stoeber L Sanger Experiences with indomethacin in long-term therapy of juvenile rheumatoid arthritis Arzneimittel-forschung 21 (1971) 1865ndash1866
[19] N Ruperto I Nikishina ED Pachanov Y Shachbazian AMPrieur R Mouy R Joos F Zulian R Schwarz V ArtamonovaW Emminger M Bandeira A Buoncompagni I Foeldvari FFalcini E Baildam I Kone-Paut M Alessio V Gerloni ALenhardt A Martini G Hanft R Sigmund S Simianer Arandomized double-blind clinical trial of two doses ofmeloxicam compared with naproxen in children with juvenileidiopathic arthritis short- and long-term efficacy and safetyresults Arthritis Rheum 52 (2005) 563ndash572
[20] I Foeldvari IS Szer LS Zemel DJ Lovell EH Giannini JLRobbins CRWest G Steidle S Krishnaswami BJ Bloom A pro-spective study comparing celecoxib with naproxen in children withjuvenile rheumatoid arthritis J Rheumatol 36 (2009) 174ndash182
191Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
[21] F Zulian G Martini D Gobber C Agosto C Gigante FZacchello Comparison of intra-articular triamcinolone hexa-cetonide and triamcinolone acetonide in oligoarticular juve-nile idiopathic arthritis Rheumatology (Oxford) 42 (2003)1254ndash1259
[22] F Zulian G Martini D Gobber M Plebani F Zacchello PManners Triamcinolone acetonide and hexacetonide intra-articular treatment of symmetrical joints in juvenile idiopathicarthritis a double-blind trial Rheumatology (Oxford) 43 (2004)1288ndash1291
[23] GS Habib Systemic effects of intra-articular corticosteroidsClin Rheumatol 28 (2009) 749ndash756
[24] JR Kirwan The effect of glucocorticoids on joint destructionin rheumatoid arthritis The Arthritis and Rheumatism CouncilLow-Dose Glucocorticoid Study Group N Engl J Med 333(1995) 142ndash146
[25] H Michels What is low-dose corticosteroid therapy in juvenileidiopathic arthritis A worldwide questionnaire-based surveyZ Rheumatol 59 (Suppl 2) (2000) II127ndash130
[26] JJ Miller III Prolonged use of large intravenous steroid pulsesin the rheumatic diseases of children Pediatrics 65 (1980)989ndash994
[27] P Picco M Gattorno A Buoncompagni V Pistoia C Borrone6-methylprednisolone lsquomini-pulsesrsquo a newmodality of glucocor-ticoid treatment in systemic onset juvenile chronic arthritisScand J Rheumatol 25 (1996) 24ndash27
[28] AM Prieur The place of corticosteroid therapy in juvenilechronic arthritis in 1992 J Rheumatol Suppl 37 (1993)32ndash34
[29] JS Gao H Wu J Tian Treatment of patients with juvenilerheumatoid arthritis with combination of leflunomide andmethotrexate Zhonghua Er Ke Za Zhi 41 (2003) 435ndash438
[30] T Niehues G Horneff H Michels MS Hock L SchuchmannEvidence-based use of methotrexate in children with rheumat-ic diseases a consensus statement of the Working Groups Pedi-atric Rheumatology Germany (AGKJR) and PediatricRheumatology Austria Rheumatol Int 25 (2005) 169ndash178
[31] N Ruperto DJ Lovell R Cuttica N Wilkinson P Woo GEspada C Wouters ED Silverman Z Balogh M HenricksonMT Apaz E Baildam A Fasth V Gerloni P Lahdenne AMPrieur A Ravelli RK Saurenmann ML Gamir N WulffraatL Marodi RE Petty R Joos F Zulian D McCurdy BLMyones K Nagy P Reuman I Szer S Travers A BeutlerG Keenan J Clark S Visvanathan A Fasanmade A Ray-chaudhuri A Mendelsohn A Martini EH Giannini A random-ized placebo-controlled trial of infliximab plus methotrexatefor the treatment of polyarticular-course juvenile rheumatoidarthritis Arthritis Rheum 56 (2007) 3096ndash3106
[32] K Visser DM van der Heijde Risk and management of livertoxicity during methotrexate treatment in rheumatoid andpsoriatic arthritis a systematic review of the literature ClinExp Rheumatol 27 (2009) 1017ndash1025
[33] A Cespedes-Cruz R Gutierrez-Suarez A Pistorio A Ravelli ALoy KJ Murray V Gerloni N Wulffraat S Oliveira J WalshIC Penades MG Alpigiani P Lahdenne C Saad-Magalhaes ECortis L Lepore Y Kimura C Wouters A Martini N RupertoMethotrexate improves the health-related quality of life of chil-dren with juvenile idiopathic arthritis Ann Rheum Dis 67(2008) 309ndash314
[34] TK Kvien HM Hoyeraal B Sandstad Azathioprine versus place-bo in patients with juvenile rheumatoid arthritis a single centerdouble blind comparative study J Rheumatol 13 (1986) 118ndash123
[35] E Silverman R Mouy L Spiegel LK Jung RK SaurenmannP Lahdenne G Horneff I Calvo IS Szer K Simpson JAStewart V Strand Leflunomide or methotrexate for juvenilerheumatoid arthritis N Engl J Med 352 (2005) 1655ndash1666
[36] MA van Rossum TJ Fiselier MJ Franssen AH ZwindermanR ten Cate LW van Suijlekom-Smit WH van Luijk RM
van Soesbergen NM Wulffraat JC Oostveen W Kuis PFDijkstra CF van Ede BA Dijkmans Sulfasalazine in the treat-ment of juvenile chronic arthritis a randomized double-blindplacebo-controlled multicenter study Dutch Juvenile ChronicArthritis Study Group Arthritis Rheum 41 (1998) 808ndash816
[37] MA van Rossum RM van Soesbergen M Boers AHZwinderman TJ Fiselier MJ Franssen R ten Cate LW vanSuijlekom-Smit NM Wulffraat WH van Luijk JC OostveenW Kuis BA Dijkmans Long-term outcome of juvenile idiopathicarthritis following a placebo-controlled trial sustained benefits ofearly sulfasalazine treatment Ann Rheum Dis 66 (2007)1518ndash1524
[38] DJ Lovell EH Giannini A Reiff GD Cawkwell ED SilvermanJJ Nocton LD Stein A Gedalia NT Ilowite CA Wallace JWhitmore BK Finck Etanercept in children with polyarticularjuvenile rheumatoid arthritis Pediatric Rheumatology Collabora-tive Study Group N Engl J Med 342 (2000) 763ndash769
[39] DJ Lovell A Reiff OY Jones R Schneider J Nocton LDStein A Gedalia NT Ilowite CA Wallace JB WhitmoreB White EH Giannini Long-term safety and efficacy ofetanercept in children with polyarticular-course juvenile rheu-matoid arthritis Arthritis Rheum 54 (2006) 1987ndash1994
[40] DJ Lovell N Ruperto S Goodman A Reiff L Jung K JarosovaD Nemcova R Mouy C Sandborg J Bohnsack D Elewaut IFoeldvari V Gerloni J Rovensky K Minden RK Vehe LWWeiner G Horneff HI Huppertz NY Olson JR Medich RCarcereri-De-Prati MJ McIlraith EH Giannini A MartiniAdalimumab with or without methotrexate in juvenile rheuma-toid arthritis N Engl J Med 359 (2008) 810ndash820
[41] FH Prince M Twilt R ten Cate MA van RossumW ArmbrustEP Hoppenreijs M van Santen-Hoeufft Y Koopman-KeeminkNM Wulffraat LW van Suijlekom-Smit Long-term follow-upon effectiveness and safety of etanercept in juvenile idiopathicarthritis the Dutch National Register Ann Rheum Dis 68(2009) 635ndash641
[42] P Diak J Siegel L LaGrenade L Choi S Lemery AMcMahonTumor necrosis factor alpha blockers andmalignancy in childrenforty-eight cases reported to the Food and Drug AdministrationArthritis Rheum 62 (2010) 2517ndash2524
[43] G Horneff T Hospach G Dannecker D Foll JP Haas HJGirschick HI Huppertz R Keitzer HJ Laws H Michels KMinden R Trauzeddel Updated statement by the German So-ciety for Pediatric and Adolescent Rheumatology (GKJR) on theFDAs report regarding malignancies in anti-TNF-treated pa-tients from Aug 4 2009 Z Rheumatol 69 (2010) 561ndash567
[44] T Hospach JP Haas HI Huppertz R Keitzer H Michels RTrauzeddl D Foll G Dannecker G Horneff Comment of theSociety of Pediatric and Adolescent Rheumatology on the USFood and Drug Administration (FDA) announcement regardingcases of malignancy in anti-TNF-treated patients Z Rheumatol68 (2009) 162ndash164
[45] DJ Lovell A Reiff NT Ilowite CA Wallace Y Chon SL LinSW Baumgartner EH Giannini Safety and efficacy of up to eightyears of continuous etanercept therapy in patients with juvenilerheumatoid arthritis Arthritis Rheum 58 (2008) 1496ndash1504
[46] EH Giannini NT Ilowite DJ Lovell CA Wallace CERabinovich A Reiff G Higgins B Gottlieb NG Singer YChon SL Lin SW Baumgartner Long-term safety and effec-tiveness of etanercept in children with selected categories ofjuvenile idiopathic arthritis Arthritis Rheum 60 (2009)2794ndash2804
[47] G Horneff H Schmeling T Biedermann I Foeldvari G GanserHJ Girschick T Hospach HI Huppertz R Keitzer RM KusterH Michels D Moebius B Rogalski A Thon The German etaner-cept registry for treatment of juvenile idiopathic arthritis AnnRheum Dis 63 (2004) 1638ndash1644
[48] FH Prince M Twilt SC Simon MA van RossumW ArmbrustEP Hoppenreijs S Kamphuis M van Santen-Hoeufft Y
192 G Dueckers et al
Koopman-Keemink NM Wulffraat R ten Cate LW vanSuijlekom-Smit When and how to stop etanercept aftersuccessful treatment of patients with juvenile idiopathic ar-thritis Ann Rheum Dis 68 (2009) 1228ndash1229
[49] G Horneff F De Bock I Foeldvari HJ Girschick H MichelsD Moebius H Schmeling Safety and efficacy of combinationof etanercept and methotrexate compared to treatment withetanercept only in patients with juvenile idiopathic arthritis(JIA) preliminary data from the German JIA Registry AnnRheum Dis 68 (2009) 519ndash525
[50] N Ilowite O Porras A Reiff S Rudge M Punaro A Martin RAllen T Harville YN Sun T Bevirt G Aras B Appleton Ana-kinra in the treatment of polyarticular-course juvenile rheumatoidarthritis safety and preliminary efficacy results of a randomizedmulticenter study Clin Rheumatol 28 (2009) 129ndash137
[51] T Lequerre P Quartier D Rosellini F Alaoui M De BandtO Mejjad I Kone-Paut M Michel E Dernis M Khellaf NLimal C Job-Deslandre B Fautrel X Le Loet J Sibilia In-terleukin-1 receptor antagonist (anakinra) treatment in pa-tients with systemic-onset juvenile idiopathic arthritis oradult onset Still disease preliminary experience in FranceAnn Rheum Dis 67 (2008) 302ndash308
[52] M Gattorno A Piccini D Lasiglie S Tassi G Brisca S CartaL Delfino F Ferlito MA Pelagatti F Caroli A BuoncompagniS Viola A Loy M Sironi A Vecchi A Ravelli A Martini ARubartelli The pattern of response to anti-interleukin-1 treatmentdistinguishes two subsets of patients with systemic-onset juvenileidiopathic arthritis Arthritis Rheum 58 (2008) 1505ndash1515
[53] S Yokota T Imagawa M Mori T Miyamae Y Aihara STakei N Iwata H Umebayashi T Murata M Miyoshi MTomiita N Nishimoto T Kishimoto Efficacy and safety oftocilizumab in patients with systemic-onset juvenile idiopathicarthritis a randomised double-blind placebo-controlledwithdrawal phase III trial Lancet 371 (2008) 998ndash1006
[54] N Ruperto DJ Lovell P Quartier E Paz N Rubio-Perez CASilva C Abud-Mendoza R Burgos-Vargas V Gerloni JAMelo-Gomes C Saad-Magalhaes F Sztajnbok C Goldenstein-Schainberg M Scheinberg IC Penades M Fischbach J OrozcoPJ Hashkes C Hom L Jung L Lepore S Oliveira CAWallace LH Sigal AJ Block A Covucci A Martini EHGiannini Abatacept in children with juvenile idiopathic arthri-tis a randomised double-blind placebo-controlled withdrawaltrial Lancet 372 (2008) 383ndash391
[55] N Ruperto DJ Lovell P Quartier E Paz N Rubio-PerezCA Silva C Abud-Mendoza R Burgos-Vargas V GerloniJA Melo-Gomes C Saad-Magalhaes J Chavez-Corrales CHuemer A Kivitz FJ Blanco I Foeldvari M Hofer G HorneffHI Huppertz C Job-Deslandre A Loy K Minden M PunaroAF Nunez LH Sigal AJ Block M Nys A Martini EHGiannini Long-term safety and efficacy of abatacept inchildren with juvenile idiopathic arthritis Arthritis Rheum 62(2010) 1792ndash1802
[56] DM Brinkman IM de Kleer R ten Cate MA van RossumWP Bekkering A Fasth MJ van Tol W Kuis NM WulffraatJM Vossen Autologous stem cell transplantation in childrenwith severe progressive systemic or polyarticular juvenile idio-pathic arthritis long-term follow-up of a prospective clinicaltrial Arthritis Rheum 56 (2007) 2410ndash2421
[57] SE Klepper Effects of an eight-week physical conditioningprogram on disease signs and symptoms in children with chronicarthritis Arthritis Care Res 12 (1999) 52ndash60
[58] D Singh-Grewal J Schneiderman-Walker V Wright O Bar-OrJ Beyene H Selvadurai B Cameron RM Laxer R SchneiderED Silverman L Spiegel S Tse C Leblanc J Wong SStephens BM Feldman The effects of vigorous exercisetraining on physical function in children with arthritis arandomized controlled single-blinded trial ArthritisRheum 57 (2007) 1202ndash1210
[59] S Stephens D Singh-Grewal O Bar-Or J Beyene B CameronCM Leblanc R Schneider J Schneiderman-Walker HSelvadurai E Silverman L Spiegel SM Tse V WrightBM Feldman Reliability of exercise testing and functionalactivity questionnaires in children with juvenile arthritisArthritis Rheum 57 (2007) 1446ndash1452
[60] T Takken J van der Net W Kuis PJ Helders Physical ac-tivity and health related physical fitness in children with ju-venile idiopathic arthritis Ann Rheum Dis 62 (2003)885ndash889
[61] MM Toledo G Martini C Gigante L Da Dalt A TregnaghiF Zulian Is there a role for arthroscopic synovectomy in oli-goarticular juvenile idiopathic arthritis J Rheumatol 33(2006) 1868ndash1872
[62] F de Benedetti H Brunner N Ruperto SWright A KenwrightR Cuttica P Woo R Schneider DJ Lovell A Martini Efficacyand safety of Tocilizumab in patients with systemic juvenile idio-pathic arthritis (sJIA) 12-week data from the phase III TENDERtrial Ann Rheum Dis 69 (2010) 146
[63] P Quartier F Allantaz R Cimaz P Pillet C Messiaen CBardin X Bossuyt A Boutten J Bienvenu A Duquesne ORicher D Chaussabel A Mogenet J Banchereau JM Tre-luyer P Landais V Pascual A multicentre randomiseddouble-blind placebo-controlled trial with the interleukin-1receptor antagonist anakinra in patients with systemic-onsetjuvenile idiopathic arthritis (ANAJIS trial) Ann Rheum Dis70 (2011) 747ndash754
[64] DE Furst EC Keystone J Braun FC Breedveld GRBurmester F De Benedetti T Dorner P Emery R FleischmannA Gibofsky JR Kalden A Kavanaugh B Kirkham P Mease JSieper NG Singer JS Smolen PL Van Riel MH Weisman KWinthrop Updated consensus statement on biological agents forthe treatment of rheumatic diseases 2010 Ann Rheum Dis 70(Suppl 1) (2010) i2ndashi36
[65] T Beukelman NM Patkar KG Saag S Tolleson-RinehartRQ Cron EM Dewitt NT Ilowite Y Kimura RM LaxerDJ Lovell A Martini CE Rabinovich N Ruperto 2011 Ameri-can College of Rheumatology recommendations for the treatmentof juvenile idiopathic arthritis initiation and safety monitoring oftherapeutic agents for the treatment of arthritis and systemic fea-tures Arthritis Care Res 63 (2011) 465ndash482 (Hoboken)
[66] JF Simard M Neovius S Hagelberg J Askling Juvenile idi-opathic arthritis and risk of cancer a nationwide cohort studyArthritis Rheum 62 (2010) 3776ndash3782
[67] T Imagawa S Yokota M Mori T Miyamae S Takei H ImanakaY Nerome N Iwata T Murata M Miyoshi N Nishimoto TKishimoto Safety and efficacy of tocilizumab an anti-IL-6-receptor monoclonal antibody in patients with polyarticular-course juvenile idiopathic arthritis Mod Rheumatol (2011)doi102007s10165-011-0481-0
[68] TM Shaneyfelt MF Mayo-Smith J Rothwangl Are guide-lines following guidelines The methodological quality of clini-cal practice guidelines in the peer-reviewed medicalliterature Jama 281 (1999) 1900ndash1905
[69] R Grilli N Magrini A Penna G Mura A Liberati Practiceguidelines developed by specialty societies the need for a crit-ical appraisal Lancet 355 (2000) 103ndash106
[70] JS Burgers R Grol NS Klazinga M Makela J Zaat To-wards evidence-based clinical practice an international surveyof 18 clinical guideline programs Int J Qual Health Care 15(2003) 31ndash45
[71] JT Cassidy RE Petty Juvenile Idiopathic Rheumatic Arthri-tis 5th Edition WB Saunders Philadelphia 2005
[72] TJ Lehman Are withdrawal trials in paediatric rheumatic dis-ease helpful Lancet 372 (2008) 348ndash350
[73] J Munro Recommendations for the Diagnosis and Managementof Juvenile Idiopathic Arthritis The Royal Australian Collegeof General Practitioners South Melbourne 2009 pp 1ndash38
193Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
httpwwwnhmrcgovau_files_nhmrcpublicationsattachmentscp119-juvenile-arthritispdf
[74] MJ Santos JE Fonseca H Canhao M Conde M JoseVieira L Costa M Costa M Salgado JA Melo Gomes Guide-lines for prescribing and monitoring biologic therapies in juve-nile idiopathic arthritis Acta Reumatol Port 32 (2007) 43ndash47
[75] S Yokota M Mori T Imagawa T Murata M Tomiita Y ItohS Fujikawa S Takei Guidelines on the use of etanercept forjuvenile idiopathic arthritis in Japan Mod Rheumatol 20(2010) 107ndash113
[76] The AGREE Collaboration Appraisal of Guidelines for Researchamp Evaluation (AGREE) instrument wwwagreecollaborationorg
[77] I Kopp H Thole T Langer HK Selbmann G OllenschlaumlgerGerman Instrument for Methodological Guideline Appraisal(DELBI) wwwversorgungsleitliniende2008
[78] Auml Aumlrztliches Zentrum fuumlr Qualitaumlt in der Medizin A Arbeitsge-meinschaften der Wissenschaftlichen Fachgesellschaften in derMedizin Deutsches Instrument zur methodischen Leitlinien-Bewertung (DELBI) Fassung 20052006 Z Aumlrztl FortbildQualitaumltssich 99 (2005) 468ndash519
[79] MP de Wit SE Berlo GJ Aanerud D Aletaha JW BijlsmaL Croucher JA Da Silva B Glusing L Gossec S Hewlett MJongkees D Magnusson M Scholte-Voshaar P Richards CZiegler TA Abma European League Against Rheumatism rec-ommendations for the inclusion of patient representatives in sci-entific projects Ann Rheum Dis 70 (2011) 722ndash726
[80] I Foeldvari M Bidde Validation of the proposed ILAR classifi-cation criteria for juvenile idiopathic arthritis InternationalLeague of Associations for Rheumatology J Rheumatol 27(2000) 1069ndash1072
[81] R Merino J de Inocencio J Garcia-Consuegra Evaluation ofrevised International League of Associations for Rheumatologyclassification criteria for juvenile idiopathic arthritis in Spanishchildren (Edmonton 2001) J Rheumatol 32 (2005) 559ndash561
[82] SE Ramsey RK Bolaria DA Cabral PN Malleson REPetty Comparison of criteria for the classification of childhoodarthritis J Rheumatol 27 (2000) 1283ndash1286
[83] G Horneff A Ebert S Fitter K Minden I Foeldvari J Kum-merle-Deschner A Thon HJ Girschick F Weller HI Hup-pertz Safety and efficacy of once weekly etanercept 08mgkg in a multicentre 12 week trial in active polyarticularcourse juvenile idiopathic arthritis Rheumatology (Oxford) 48(2009) 916ndash919
[84] EH Giannini EJ Brewer N Kuzmina A Shaikov A Maxi-mov I Vorontsov CW Fink AJ Newman JT Cassidy LSZemel Methotrexate in resistant juvenile rheumatoid arthri-tis Results of the USAndashUSSR double-blind placebo-controlled trial The Pediatric Rheumatology CollaborativeStudy Group and The Cooperative Childrens Study GroupN Engl J Med 326 (1992) 1043ndash1049
[85] A Ravelli S Viola D Migliavacca N Ruperto A Pistorio AMartini The extended oligoarticular subtype is the best predic-tor of methotrexate efficacy in juvenile idiopathic arthritisJ Pediatr 135 (1999) 316ndash320
[86] P Woo TR Southwood AM Prieur CJ Dore J Grainger JDavid C Ryder N Hasson A Hall I Lemelle Randomizedplacebo-controlled crossover trial of low-dose oral
methotrexate in children with extended oligoarticular or sys-temic arthritis Arthritis Rheum 43 (2000) 1849ndash1857
[87] E Silverman L Spiegel D Hawkins R Petty D Goldsmith LSchanberg C Duffy P Howard V Strand Long-term open-label preliminary study of the safety and efficacy of lefluno-mide in patients with polyarticular-course juvenile rheumatoidarthritis Arthritis Rheum 52 (2005) 554ndash562
[88] DJ Lovell EH Giannini Y Kimura C Suzanne PJHashkes A Reiff Long-term safety and efficacy of rilonaceptin patients with systemic juvenile idiopathic arthritis (SJIA)Arthritis Rheum 60 (2009)
[89] N Ruperto P Quartier NWulffraat PWoo A Loy R Mouy BBader-Meunier BJ Prakken E Noseda R Belleli J Lecot CRordorf A Martini A Phase II Trial with canakinumab(ACZ885) a new IL-1-beta blocking monoclonal antibody toevaluate safety and preliminary efficacy in children with system-ic juvenile idiopathic arthritis Ann Rheum Dis 68 (2009) 170
[90] DJ Lovell EH Giannini Y Kimura et al Preliminary evi-dence for bioactivity of IL-1 trap (Rilonacept) a long actingIL-1 inhibitor in systemic juvenile idiopathic arthritis (sJIA)Arthritis Rheum 54 (2006) S325
[91] DJ Lovell EH Giannini Y Kimura et al Preliminary evi-dence for sustained bioactivity of IL-1 Trap (rilonacept) a longacting IL-1 inhibitor in systemic juvenile idiopathic arthritisArthritis Rheum 56 (2007) S514
[92] N Ruperto F De Benedetti H Brunner R Allen D Brown JChaitow E Cortis G Espada B Flato V Gerloni G HorneffS Wright A Kenwright R Schneider P Woo A Martini DJLovell Tocilizumab is efficacious in patients with systemic ju-venile idiopathic arthritis (sJIA) across baseline disease charac-teristics and priorbaseline treatments 12-week data from thephase II TENDER trial 17th PReS Congress Valencia Spain2010 2010
[93] N Ruperto DJ Lovell T Li F Sztajnbok C Goldenstein-Schainberg M Scheinberg IC Penades M Fischbach JOrozco PJ Hashkes C Hom L Jung L Lepore S OliveiraC Wallace M Alessio P Quartier E Cortis A Eberhard GSimonini I Lemelle E Chalom LH Sigal A Block A CovucciM Nys A Martini EH Giannini Abatacept improves health-related quality of life pain sleep quality and daily participationin subjects with juvenile idiopathic arthritis Arthritis Care Res(Hoboken) 62 (11) (2010) 1542ndash1551
[94] N Ruperto DJ Lovell P Quartier E Paz N Rubio-PerezCA Silva C Abud-Mendoza R Burgos-Vargas V GerloniJA Melo-Gomes C Saad-Magalhaes J Chavez C HuemerA Kivitz FJ Blanco I Foeldvari M Hofer G Horneff HIHuppertz CJ Deslandre A Loy K Minden M Punaro AFNunez LH Sigal AJ Block M Nys A Martini EH GianniniLong-term safety and efficacy of abatacept in children with ju-venile idiopathic arthritis Arthritis Rheum 62 (2010)1792ndash1802
[95] J Munro Juvenile Idiopathic Arthritis Management Guidelines(Provisional) Australian Paediatric Rheumatology Group 2006httpwwwnhmrcgovau
[96] K Fitch SJ Bernstein MD Aguilar B Burnand JR LaCalleP Lazaro M van het Loo J McDonnell JP Vader JPKahan The RANDUCLA Appropriateness Method Users ManualRAND Pittsburgh 2000

191Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
[21] F Zulian G Martini D Gobber C Agosto C Gigante FZacchello Comparison of intra-articular triamcinolone hexa-cetonide and triamcinolone acetonide in oligoarticular juve-nile idiopathic arthritis Rheumatology (Oxford) 42 (2003)1254ndash1259
[22] F Zulian G Martini D Gobber M Plebani F Zacchello PManners Triamcinolone acetonide and hexacetonide intra-articular treatment of symmetrical joints in juvenile idiopathicarthritis a double-blind trial Rheumatology (Oxford) 43 (2004)1288ndash1291
[23] GS Habib Systemic effects of intra-articular corticosteroidsClin Rheumatol 28 (2009) 749ndash756
[24] JR Kirwan The effect of glucocorticoids on joint destructionin rheumatoid arthritis The Arthritis and Rheumatism CouncilLow-Dose Glucocorticoid Study Group N Engl J Med 333(1995) 142ndash146
[25] H Michels What is low-dose corticosteroid therapy in juvenileidiopathic arthritis A worldwide questionnaire-based surveyZ Rheumatol 59 (Suppl 2) (2000) II127ndash130
[26] JJ Miller III Prolonged use of large intravenous steroid pulsesin the rheumatic diseases of children Pediatrics 65 (1980)989ndash994
[27] P Picco M Gattorno A Buoncompagni V Pistoia C Borrone6-methylprednisolone lsquomini-pulsesrsquo a newmodality of glucocor-ticoid treatment in systemic onset juvenile chronic arthritisScand J Rheumatol 25 (1996) 24ndash27
[28] AM Prieur The place of corticosteroid therapy in juvenilechronic arthritis in 1992 J Rheumatol Suppl 37 (1993)32ndash34
[29] JS Gao H Wu J Tian Treatment of patients with juvenilerheumatoid arthritis with combination of leflunomide andmethotrexate Zhonghua Er Ke Za Zhi 41 (2003) 435ndash438
[30] T Niehues G Horneff H Michels MS Hock L SchuchmannEvidence-based use of methotrexate in children with rheumat-ic diseases a consensus statement of the Working Groups Pedi-atric Rheumatology Germany (AGKJR) and PediatricRheumatology Austria Rheumatol Int 25 (2005) 169ndash178
[31] N Ruperto DJ Lovell R Cuttica N Wilkinson P Woo GEspada C Wouters ED Silverman Z Balogh M HenricksonMT Apaz E Baildam A Fasth V Gerloni P Lahdenne AMPrieur A Ravelli RK Saurenmann ML Gamir N WulffraatL Marodi RE Petty R Joos F Zulian D McCurdy BLMyones K Nagy P Reuman I Szer S Travers A BeutlerG Keenan J Clark S Visvanathan A Fasanmade A Ray-chaudhuri A Mendelsohn A Martini EH Giannini A random-ized placebo-controlled trial of infliximab plus methotrexatefor the treatment of polyarticular-course juvenile rheumatoidarthritis Arthritis Rheum 56 (2007) 3096ndash3106
[32] K Visser DM van der Heijde Risk and management of livertoxicity during methotrexate treatment in rheumatoid andpsoriatic arthritis a systematic review of the literature ClinExp Rheumatol 27 (2009) 1017ndash1025
[33] A Cespedes-Cruz R Gutierrez-Suarez A Pistorio A Ravelli ALoy KJ Murray V Gerloni N Wulffraat S Oliveira J WalshIC Penades MG Alpigiani P Lahdenne C Saad-Magalhaes ECortis L Lepore Y Kimura C Wouters A Martini N RupertoMethotrexate improves the health-related quality of life of chil-dren with juvenile idiopathic arthritis Ann Rheum Dis 67(2008) 309ndash314
[34] TK Kvien HM Hoyeraal B Sandstad Azathioprine versus place-bo in patients with juvenile rheumatoid arthritis a single centerdouble blind comparative study J Rheumatol 13 (1986) 118ndash123
[35] E Silverman R Mouy L Spiegel LK Jung RK SaurenmannP Lahdenne G Horneff I Calvo IS Szer K Simpson JAStewart V Strand Leflunomide or methotrexate for juvenilerheumatoid arthritis N Engl J Med 352 (2005) 1655ndash1666
[36] MA van Rossum TJ Fiselier MJ Franssen AH ZwindermanR ten Cate LW van Suijlekom-Smit WH van Luijk RM
van Soesbergen NM Wulffraat JC Oostveen W Kuis PFDijkstra CF van Ede BA Dijkmans Sulfasalazine in the treat-ment of juvenile chronic arthritis a randomized double-blindplacebo-controlled multicenter study Dutch Juvenile ChronicArthritis Study Group Arthritis Rheum 41 (1998) 808ndash816
[37] MA van Rossum RM van Soesbergen M Boers AHZwinderman TJ Fiselier MJ Franssen R ten Cate LW vanSuijlekom-Smit NM Wulffraat WH van Luijk JC OostveenW Kuis BA Dijkmans Long-term outcome of juvenile idiopathicarthritis following a placebo-controlled trial sustained benefits ofearly sulfasalazine treatment Ann Rheum Dis 66 (2007)1518ndash1524
[38] DJ Lovell EH Giannini A Reiff GD Cawkwell ED SilvermanJJ Nocton LD Stein A Gedalia NT Ilowite CA Wallace JWhitmore BK Finck Etanercept in children with polyarticularjuvenile rheumatoid arthritis Pediatric Rheumatology Collabora-tive Study Group N Engl J Med 342 (2000) 763ndash769
[39] DJ Lovell A Reiff OY Jones R Schneider J Nocton LDStein A Gedalia NT Ilowite CA Wallace JB WhitmoreB White EH Giannini Long-term safety and efficacy ofetanercept in children with polyarticular-course juvenile rheu-matoid arthritis Arthritis Rheum 54 (2006) 1987ndash1994
[40] DJ Lovell N Ruperto S Goodman A Reiff L Jung K JarosovaD Nemcova R Mouy C Sandborg J Bohnsack D Elewaut IFoeldvari V Gerloni J Rovensky K Minden RK Vehe LWWeiner G Horneff HI Huppertz NY Olson JR Medich RCarcereri-De-Prati MJ McIlraith EH Giannini A MartiniAdalimumab with or without methotrexate in juvenile rheuma-toid arthritis N Engl J Med 359 (2008) 810ndash820
[41] FH Prince M Twilt R ten Cate MA van RossumW ArmbrustEP Hoppenreijs M van Santen-Hoeufft Y Koopman-KeeminkNM Wulffraat LW van Suijlekom-Smit Long-term follow-upon effectiveness and safety of etanercept in juvenile idiopathicarthritis the Dutch National Register Ann Rheum Dis 68(2009) 635ndash641
[42] P Diak J Siegel L LaGrenade L Choi S Lemery AMcMahonTumor necrosis factor alpha blockers andmalignancy in childrenforty-eight cases reported to the Food and Drug AdministrationArthritis Rheum 62 (2010) 2517ndash2524
[43] G Horneff T Hospach G Dannecker D Foll JP Haas HJGirschick HI Huppertz R Keitzer HJ Laws H Michels KMinden R Trauzeddel Updated statement by the German So-ciety for Pediatric and Adolescent Rheumatology (GKJR) on theFDAs report regarding malignancies in anti-TNF-treated pa-tients from Aug 4 2009 Z Rheumatol 69 (2010) 561ndash567
[44] T Hospach JP Haas HI Huppertz R Keitzer H Michels RTrauzeddl D Foll G Dannecker G Horneff Comment of theSociety of Pediatric and Adolescent Rheumatology on the USFood and Drug Administration (FDA) announcement regardingcases of malignancy in anti-TNF-treated patients Z Rheumatol68 (2009) 162ndash164
[45] DJ Lovell A Reiff NT Ilowite CA Wallace Y Chon SL LinSW Baumgartner EH Giannini Safety and efficacy of up to eightyears of continuous etanercept therapy in patients with juvenilerheumatoid arthritis Arthritis Rheum 58 (2008) 1496ndash1504
[46] EH Giannini NT Ilowite DJ Lovell CA Wallace CERabinovich A Reiff G Higgins B Gottlieb NG Singer YChon SL Lin SW Baumgartner Long-term safety and effec-tiveness of etanercept in children with selected categories ofjuvenile idiopathic arthritis Arthritis Rheum 60 (2009)2794ndash2804
[47] G Horneff H Schmeling T Biedermann I Foeldvari G GanserHJ Girschick T Hospach HI Huppertz R Keitzer RM KusterH Michels D Moebius B Rogalski A Thon The German etaner-cept registry for treatment of juvenile idiopathic arthritis AnnRheum Dis 63 (2004) 1638ndash1644
[48] FH Prince M Twilt SC Simon MA van RossumW ArmbrustEP Hoppenreijs S Kamphuis M van Santen-Hoeufft Y
192 G Dueckers et al
Koopman-Keemink NM Wulffraat R ten Cate LW vanSuijlekom-Smit When and how to stop etanercept aftersuccessful treatment of patients with juvenile idiopathic ar-thritis Ann Rheum Dis 68 (2009) 1228ndash1229
[49] G Horneff F De Bock I Foeldvari HJ Girschick H MichelsD Moebius H Schmeling Safety and efficacy of combinationof etanercept and methotrexate compared to treatment withetanercept only in patients with juvenile idiopathic arthritis(JIA) preliminary data from the German JIA Registry AnnRheum Dis 68 (2009) 519ndash525
[50] N Ilowite O Porras A Reiff S Rudge M Punaro A Martin RAllen T Harville YN Sun T Bevirt G Aras B Appleton Ana-kinra in the treatment of polyarticular-course juvenile rheumatoidarthritis safety and preliminary efficacy results of a randomizedmulticenter study Clin Rheumatol 28 (2009) 129ndash137
[51] T Lequerre P Quartier D Rosellini F Alaoui M De BandtO Mejjad I Kone-Paut M Michel E Dernis M Khellaf NLimal C Job-Deslandre B Fautrel X Le Loet J Sibilia In-terleukin-1 receptor antagonist (anakinra) treatment in pa-tients with systemic-onset juvenile idiopathic arthritis oradult onset Still disease preliminary experience in FranceAnn Rheum Dis 67 (2008) 302ndash308
[52] M Gattorno A Piccini D Lasiglie S Tassi G Brisca S CartaL Delfino F Ferlito MA Pelagatti F Caroli A BuoncompagniS Viola A Loy M Sironi A Vecchi A Ravelli A Martini ARubartelli The pattern of response to anti-interleukin-1 treatmentdistinguishes two subsets of patients with systemic-onset juvenileidiopathic arthritis Arthritis Rheum 58 (2008) 1505ndash1515
[53] S Yokota T Imagawa M Mori T Miyamae Y Aihara STakei N Iwata H Umebayashi T Murata M Miyoshi MTomiita N Nishimoto T Kishimoto Efficacy and safety oftocilizumab in patients with systemic-onset juvenile idiopathicarthritis a randomised double-blind placebo-controlledwithdrawal phase III trial Lancet 371 (2008) 998ndash1006
[54] N Ruperto DJ Lovell P Quartier E Paz N Rubio-Perez CASilva C Abud-Mendoza R Burgos-Vargas V Gerloni JAMelo-Gomes C Saad-Magalhaes F Sztajnbok C Goldenstein-Schainberg M Scheinberg IC Penades M Fischbach J OrozcoPJ Hashkes C Hom L Jung L Lepore S Oliveira CAWallace LH Sigal AJ Block A Covucci A Martini EHGiannini Abatacept in children with juvenile idiopathic arthri-tis a randomised double-blind placebo-controlled withdrawaltrial Lancet 372 (2008) 383ndash391
[55] N Ruperto DJ Lovell P Quartier E Paz N Rubio-PerezCA Silva C Abud-Mendoza R Burgos-Vargas V GerloniJA Melo-Gomes C Saad-Magalhaes J Chavez-Corrales CHuemer A Kivitz FJ Blanco I Foeldvari M Hofer G HorneffHI Huppertz C Job-Deslandre A Loy K Minden M PunaroAF Nunez LH Sigal AJ Block M Nys A Martini EHGiannini Long-term safety and efficacy of abatacept inchildren with juvenile idiopathic arthritis Arthritis Rheum 62(2010) 1792ndash1802
[56] DM Brinkman IM de Kleer R ten Cate MA van RossumWP Bekkering A Fasth MJ van Tol W Kuis NM WulffraatJM Vossen Autologous stem cell transplantation in childrenwith severe progressive systemic or polyarticular juvenile idio-pathic arthritis long-term follow-up of a prospective clinicaltrial Arthritis Rheum 56 (2007) 2410ndash2421
[57] SE Klepper Effects of an eight-week physical conditioningprogram on disease signs and symptoms in children with chronicarthritis Arthritis Care Res 12 (1999) 52ndash60
[58] D Singh-Grewal J Schneiderman-Walker V Wright O Bar-OrJ Beyene H Selvadurai B Cameron RM Laxer R SchneiderED Silverman L Spiegel S Tse C Leblanc J Wong SStephens BM Feldman The effects of vigorous exercisetraining on physical function in children with arthritis arandomized controlled single-blinded trial ArthritisRheum 57 (2007) 1202ndash1210
[59] S Stephens D Singh-Grewal O Bar-Or J Beyene B CameronCM Leblanc R Schneider J Schneiderman-Walker HSelvadurai E Silverman L Spiegel SM Tse V WrightBM Feldman Reliability of exercise testing and functionalactivity questionnaires in children with juvenile arthritisArthritis Rheum 57 (2007) 1446ndash1452
[60] T Takken J van der Net W Kuis PJ Helders Physical ac-tivity and health related physical fitness in children with ju-venile idiopathic arthritis Ann Rheum Dis 62 (2003)885ndash889
[61] MM Toledo G Martini C Gigante L Da Dalt A TregnaghiF Zulian Is there a role for arthroscopic synovectomy in oli-goarticular juvenile idiopathic arthritis J Rheumatol 33(2006) 1868ndash1872
[62] F de Benedetti H Brunner N Ruperto SWright A KenwrightR Cuttica P Woo R Schneider DJ Lovell A Martini Efficacyand safety of Tocilizumab in patients with systemic juvenile idio-pathic arthritis (sJIA) 12-week data from the phase III TENDERtrial Ann Rheum Dis 69 (2010) 146
[63] P Quartier F Allantaz R Cimaz P Pillet C Messiaen CBardin X Bossuyt A Boutten J Bienvenu A Duquesne ORicher D Chaussabel A Mogenet J Banchereau JM Tre-luyer P Landais V Pascual A multicentre randomiseddouble-blind placebo-controlled trial with the interleukin-1receptor antagonist anakinra in patients with systemic-onsetjuvenile idiopathic arthritis (ANAJIS trial) Ann Rheum Dis70 (2011) 747ndash754
[64] DE Furst EC Keystone J Braun FC Breedveld GRBurmester F De Benedetti T Dorner P Emery R FleischmannA Gibofsky JR Kalden A Kavanaugh B Kirkham P Mease JSieper NG Singer JS Smolen PL Van Riel MH Weisman KWinthrop Updated consensus statement on biological agents forthe treatment of rheumatic diseases 2010 Ann Rheum Dis 70(Suppl 1) (2010) i2ndashi36
[65] T Beukelman NM Patkar KG Saag S Tolleson-RinehartRQ Cron EM Dewitt NT Ilowite Y Kimura RM LaxerDJ Lovell A Martini CE Rabinovich N Ruperto 2011 Ameri-can College of Rheumatology recommendations for the treatmentof juvenile idiopathic arthritis initiation and safety monitoring oftherapeutic agents for the treatment of arthritis and systemic fea-tures Arthritis Care Res 63 (2011) 465ndash482 (Hoboken)
[66] JF Simard M Neovius S Hagelberg J Askling Juvenile idi-opathic arthritis and risk of cancer a nationwide cohort studyArthritis Rheum 62 (2010) 3776ndash3782
[67] T Imagawa S Yokota M Mori T Miyamae S Takei H ImanakaY Nerome N Iwata T Murata M Miyoshi N Nishimoto TKishimoto Safety and efficacy of tocilizumab an anti-IL-6-receptor monoclonal antibody in patients with polyarticular-course juvenile idiopathic arthritis Mod Rheumatol (2011)doi102007s10165-011-0481-0
[68] TM Shaneyfelt MF Mayo-Smith J Rothwangl Are guide-lines following guidelines The methodological quality of clini-cal practice guidelines in the peer-reviewed medicalliterature Jama 281 (1999) 1900ndash1905
[69] R Grilli N Magrini A Penna G Mura A Liberati Practiceguidelines developed by specialty societies the need for a crit-ical appraisal Lancet 355 (2000) 103ndash106
[70] JS Burgers R Grol NS Klazinga M Makela J Zaat To-wards evidence-based clinical practice an international surveyof 18 clinical guideline programs Int J Qual Health Care 15(2003) 31ndash45
[71] JT Cassidy RE Petty Juvenile Idiopathic Rheumatic Arthri-tis 5th Edition WB Saunders Philadelphia 2005
[72] TJ Lehman Are withdrawal trials in paediatric rheumatic dis-ease helpful Lancet 372 (2008) 348ndash350
[73] J Munro Recommendations for the Diagnosis and Managementof Juvenile Idiopathic Arthritis The Royal Australian Collegeof General Practitioners South Melbourne 2009 pp 1ndash38
193Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
httpwwwnhmrcgovau_files_nhmrcpublicationsattachmentscp119-juvenile-arthritispdf
[74] MJ Santos JE Fonseca H Canhao M Conde M JoseVieira L Costa M Costa M Salgado JA Melo Gomes Guide-lines for prescribing and monitoring biologic therapies in juve-nile idiopathic arthritis Acta Reumatol Port 32 (2007) 43ndash47
[75] S Yokota M Mori T Imagawa T Murata M Tomiita Y ItohS Fujikawa S Takei Guidelines on the use of etanercept forjuvenile idiopathic arthritis in Japan Mod Rheumatol 20(2010) 107ndash113
[76] The AGREE Collaboration Appraisal of Guidelines for Researchamp Evaluation (AGREE) instrument wwwagreecollaborationorg
[77] I Kopp H Thole T Langer HK Selbmann G OllenschlaumlgerGerman Instrument for Methodological Guideline Appraisal(DELBI) wwwversorgungsleitliniende2008
[78] Auml Aumlrztliches Zentrum fuumlr Qualitaumlt in der Medizin A Arbeitsge-meinschaften der Wissenschaftlichen Fachgesellschaften in derMedizin Deutsches Instrument zur methodischen Leitlinien-Bewertung (DELBI) Fassung 20052006 Z Aumlrztl FortbildQualitaumltssich 99 (2005) 468ndash519
[79] MP de Wit SE Berlo GJ Aanerud D Aletaha JW BijlsmaL Croucher JA Da Silva B Glusing L Gossec S Hewlett MJongkees D Magnusson M Scholte-Voshaar P Richards CZiegler TA Abma European League Against Rheumatism rec-ommendations for the inclusion of patient representatives in sci-entific projects Ann Rheum Dis 70 (2011) 722ndash726
[80] I Foeldvari M Bidde Validation of the proposed ILAR classifi-cation criteria for juvenile idiopathic arthritis InternationalLeague of Associations for Rheumatology J Rheumatol 27(2000) 1069ndash1072
[81] R Merino J de Inocencio J Garcia-Consuegra Evaluation ofrevised International League of Associations for Rheumatologyclassification criteria for juvenile idiopathic arthritis in Spanishchildren (Edmonton 2001) J Rheumatol 32 (2005) 559ndash561
[82] SE Ramsey RK Bolaria DA Cabral PN Malleson REPetty Comparison of criteria for the classification of childhoodarthritis J Rheumatol 27 (2000) 1283ndash1286
[83] G Horneff A Ebert S Fitter K Minden I Foeldvari J Kum-merle-Deschner A Thon HJ Girschick F Weller HI Hup-pertz Safety and efficacy of once weekly etanercept 08mgkg in a multicentre 12 week trial in active polyarticularcourse juvenile idiopathic arthritis Rheumatology (Oxford) 48(2009) 916ndash919
[84] EH Giannini EJ Brewer N Kuzmina A Shaikov A Maxi-mov I Vorontsov CW Fink AJ Newman JT Cassidy LSZemel Methotrexate in resistant juvenile rheumatoid arthri-tis Results of the USAndashUSSR double-blind placebo-controlled trial The Pediatric Rheumatology CollaborativeStudy Group and The Cooperative Childrens Study GroupN Engl J Med 326 (1992) 1043ndash1049
[85] A Ravelli S Viola D Migliavacca N Ruperto A Pistorio AMartini The extended oligoarticular subtype is the best predic-tor of methotrexate efficacy in juvenile idiopathic arthritisJ Pediatr 135 (1999) 316ndash320
[86] P Woo TR Southwood AM Prieur CJ Dore J Grainger JDavid C Ryder N Hasson A Hall I Lemelle Randomizedplacebo-controlled crossover trial of low-dose oral
methotrexate in children with extended oligoarticular or sys-temic arthritis Arthritis Rheum 43 (2000) 1849ndash1857
[87] E Silverman L Spiegel D Hawkins R Petty D Goldsmith LSchanberg C Duffy P Howard V Strand Long-term open-label preliminary study of the safety and efficacy of lefluno-mide in patients with polyarticular-course juvenile rheumatoidarthritis Arthritis Rheum 52 (2005) 554ndash562
[88] DJ Lovell EH Giannini Y Kimura C Suzanne PJHashkes A Reiff Long-term safety and efficacy of rilonaceptin patients with systemic juvenile idiopathic arthritis (SJIA)Arthritis Rheum 60 (2009)
[89] N Ruperto P Quartier NWulffraat PWoo A Loy R Mouy BBader-Meunier BJ Prakken E Noseda R Belleli J Lecot CRordorf A Martini A Phase II Trial with canakinumab(ACZ885) a new IL-1-beta blocking monoclonal antibody toevaluate safety and preliminary efficacy in children with system-ic juvenile idiopathic arthritis Ann Rheum Dis 68 (2009) 170
[90] DJ Lovell EH Giannini Y Kimura et al Preliminary evi-dence for bioactivity of IL-1 trap (Rilonacept) a long actingIL-1 inhibitor in systemic juvenile idiopathic arthritis (sJIA)Arthritis Rheum 54 (2006) S325
[91] DJ Lovell EH Giannini Y Kimura et al Preliminary evi-dence for sustained bioactivity of IL-1 Trap (rilonacept) a longacting IL-1 inhibitor in systemic juvenile idiopathic arthritisArthritis Rheum 56 (2007) S514
[92] N Ruperto F De Benedetti H Brunner R Allen D Brown JChaitow E Cortis G Espada B Flato V Gerloni G HorneffS Wright A Kenwright R Schneider P Woo A Martini DJLovell Tocilizumab is efficacious in patients with systemic ju-venile idiopathic arthritis (sJIA) across baseline disease charac-teristics and priorbaseline treatments 12-week data from thephase II TENDER trial 17th PReS Congress Valencia Spain2010 2010
[93] N Ruperto DJ Lovell T Li F Sztajnbok C Goldenstein-Schainberg M Scheinberg IC Penades M Fischbach JOrozco PJ Hashkes C Hom L Jung L Lepore S OliveiraC Wallace M Alessio P Quartier E Cortis A Eberhard GSimonini I Lemelle E Chalom LH Sigal A Block A CovucciM Nys A Martini EH Giannini Abatacept improves health-related quality of life pain sleep quality and daily participationin subjects with juvenile idiopathic arthritis Arthritis Care Res(Hoboken) 62 (11) (2010) 1542ndash1551
[94] N Ruperto DJ Lovell P Quartier E Paz N Rubio-PerezCA Silva C Abud-Mendoza R Burgos-Vargas V GerloniJA Melo-Gomes C Saad-Magalhaes J Chavez C HuemerA Kivitz FJ Blanco I Foeldvari M Hofer G Horneff HIHuppertz CJ Deslandre A Loy K Minden M Punaro AFNunez LH Sigal AJ Block M Nys A Martini EH GianniniLong-term safety and efficacy of abatacept in children with ju-venile idiopathic arthritis Arthritis Rheum 62 (2010)1792ndash1802
[95] J Munro Juvenile Idiopathic Arthritis Management Guidelines(Provisional) Australian Paediatric Rheumatology Group 2006httpwwwnhmrcgovau
[96] K Fitch SJ Bernstein MD Aguilar B Burnand JR LaCalleP Lazaro M van het Loo J McDonnell JP Vader JPKahan The RANDUCLA Appropriateness Method Users ManualRAND Pittsburgh 2000

192 G Dueckers et al
Koopman-Keemink NM Wulffraat R ten Cate LW vanSuijlekom-Smit When and how to stop etanercept aftersuccessful treatment of patients with juvenile idiopathic ar-thritis Ann Rheum Dis 68 (2009) 1228ndash1229
[49] G Horneff F De Bock I Foeldvari HJ Girschick H MichelsD Moebius H Schmeling Safety and efficacy of combinationof etanercept and methotrexate compared to treatment withetanercept only in patients with juvenile idiopathic arthritis(JIA) preliminary data from the German JIA Registry AnnRheum Dis 68 (2009) 519ndash525
[50] N Ilowite O Porras A Reiff S Rudge M Punaro A Martin RAllen T Harville YN Sun T Bevirt G Aras B Appleton Ana-kinra in the treatment of polyarticular-course juvenile rheumatoidarthritis safety and preliminary efficacy results of a randomizedmulticenter study Clin Rheumatol 28 (2009) 129ndash137
[51] T Lequerre P Quartier D Rosellini F Alaoui M De BandtO Mejjad I Kone-Paut M Michel E Dernis M Khellaf NLimal C Job-Deslandre B Fautrel X Le Loet J Sibilia In-terleukin-1 receptor antagonist (anakinra) treatment in pa-tients with systemic-onset juvenile idiopathic arthritis oradult onset Still disease preliminary experience in FranceAnn Rheum Dis 67 (2008) 302ndash308
[52] M Gattorno A Piccini D Lasiglie S Tassi G Brisca S CartaL Delfino F Ferlito MA Pelagatti F Caroli A BuoncompagniS Viola A Loy M Sironi A Vecchi A Ravelli A Martini ARubartelli The pattern of response to anti-interleukin-1 treatmentdistinguishes two subsets of patients with systemic-onset juvenileidiopathic arthritis Arthritis Rheum 58 (2008) 1505ndash1515
[53] S Yokota T Imagawa M Mori T Miyamae Y Aihara STakei N Iwata H Umebayashi T Murata M Miyoshi MTomiita N Nishimoto T Kishimoto Efficacy and safety oftocilizumab in patients with systemic-onset juvenile idiopathicarthritis a randomised double-blind placebo-controlledwithdrawal phase III trial Lancet 371 (2008) 998ndash1006
[54] N Ruperto DJ Lovell P Quartier E Paz N Rubio-Perez CASilva C Abud-Mendoza R Burgos-Vargas V Gerloni JAMelo-Gomes C Saad-Magalhaes F Sztajnbok C Goldenstein-Schainberg M Scheinberg IC Penades M Fischbach J OrozcoPJ Hashkes C Hom L Jung L Lepore S Oliveira CAWallace LH Sigal AJ Block A Covucci A Martini EHGiannini Abatacept in children with juvenile idiopathic arthri-tis a randomised double-blind placebo-controlled withdrawaltrial Lancet 372 (2008) 383ndash391
[55] N Ruperto DJ Lovell P Quartier E Paz N Rubio-PerezCA Silva C Abud-Mendoza R Burgos-Vargas V GerloniJA Melo-Gomes C Saad-Magalhaes J Chavez-Corrales CHuemer A Kivitz FJ Blanco I Foeldvari M Hofer G HorneffHI Huppertz C Job-Deslandre A Loy K Minden M PunaroAF Nunez LH Sigal AJ Block M Nys A Martini EHGiannini Long-term safety and efficacy of abatacept inchildren with juvenile idiopathic arthritis Arthritis Rheum 62(2010) 1792ndash1802
[56] DM Brinkman IM de Kleer R ten Cate MA van RossumWP Bekkering A Fasth MJ van Tol W Kuis NM WulffraatJM Vossen Autologous stem cell transplantation in childrenwith severe progressive systemic or polyarticular juvenile idio-pathic arthritis long-term follow-up of a prospective clinicaltrial Arthritis Rheum 56 (2007) 2410ndash2421
[57] SE Klepper Effects of an eight-week physical conditioningprogram on disease signs and symptoms in children with chronicarthritis Arthritis Care Res 12 (1999) 52ndash60
[58] D Singh-Grewal J Schneiderman-Walker V Wright O Bar-OrJ Beyene H Selvadurai B Cameron RM Laxer R SchneiderED Silverman L Spiegel S Tse C Leblanc J Wong SStephens BM Feldman The effects of vigorous exercisetraining on physical function in children with arthritis arandomized controlled single-blinded trial ArthritisRheum 57 (2007) 1202ndash1210
[59] S Stephens D Singh-Grewal O Bar-Or J Beyene B CameronCM Leblanc R Schneider J Schneiderman-Walker HSelvadurai E Silverman L Spiegel SM Tse V WrightBM Feldman Reliability of exercise testing and functionalactivity questionnaires in children with juvenile arthritisArthritis Rheum 57 (2007) 1446ndash1452
[60] T Takken J van der Net W Kuis PJ Helders Physical ac-tivity and health related physical fitness in children with ju-venile idiopathic arthritis Ann Rheum Dis 62 (2003)885ndash889
[61] MM Toledo G Martini C Gigante L Da Dalt A TregnaghiF Zulian Is there a role for arthroscopic synovectomy in oli-goarticular juvenile idiopathic arthritis J Rheumatol 33(2006) 1868ndash1872
[62] F de Benedetti H Brunner N Ruperto SWright A KenwrightR Cuttica P Woo R Schneider DJ Lovell A Martini Efficacyand safety of Tocilizumab in patients with systemic juvenile idio-pathic arthritis (sJIA) 12-week data from the phase III TENDERtrial Ann Rheum Dis 69 (2010) 146
[63] P Quartier F Allantaz R Cimaz P Pillet C Messiaen CBardin X Bossuyt A Boutten J Bienvenu A Duquesne ORicher D Chaussabel A Mogenet J Banchereau JM Tre-luyer P Landais V Pascual A multicentre randomiseddouble-blind placebo-controlled trial with the interleukin-1receptor antagonist anakinra in patients with systemic-onsetjuvenile idiopathic arthritis (ANAJIS trial) Ann Rheum Dis70 (2011) 747ndash754
[64] DE Furst EC Keystone J Braun FC Breedveld GRBurmester F De Benedetti T Dorner P Emery R FleischmannA Gibofsky JR Kalden A Kavanaugh B Kirkham P Mease JSieper NG Singer JS Smolen PL Van Riel MH Weisman KWinthrop Updated consensus statement on biological agents forthe treatment of rheumatic diseases 2010 Ann Rheum Dis 70(Suppl 1) (2010) i2ndashi36
[65] T Beukelman NM Patkar KG Saag S Tolleson-RinehartRQ Cron EM Dewitt NT Ilowite Y Kimura RM LaxerDJ Lovell A Martini CE Rabinovich N Ruperto 2011 Ameri-can College of Rheumatology recommendations for the treatmentof juvenile idiopathic arthritis initiation and safety monitoring oftherapeutic agents for the treatment of arthritis and systemic fea-tures Arthritis Care Res 63 (2011) 465ndash482 (Hoboken)
[66] JF Simard M Neovius S Hagelberg J Askling Juvenile idi-opathic arthritis and risk of cancer a nationwide cohort studyArthritis Rheum 62 (2010) 3776ndash3782
[67] T Imagawa S Yokota M Mori T Miyamae S Takei H ImanakaY Nerome N Iwata T Murata M Miyoshi N Nishimoto TKishimoto Safety and efficacy of tocilizumab an anti-IL-6-receptor monoclonal antibody in patients with polyarticular-course juvenile idiopathic arthritis Mod Rheumatol (2011)doi102007s10165-011-0481-0
[68] TM Shaneyfelt MF Mayo-Smith J Rothwangl Are guide-lines following guidelines The methodological quality of clini-cal practice guidelines in the peer-reviewed medicalliterature Jama 281 (1999) 1900ndash1905
[69] R Grilli N Magrini A Penna G Mura A Liberati Practiceguidelines developed by specialty societies the need for a crit-ical appraisal Lancet 355 (2000) 103ndash106
[70] JS Burgers R Grol NS Klazinga M Makela J Zaat To-wards evidence-based clinical practice an international surveyof 18 clinical guideline programs Int J Qual Health Care 15(2003) 31ndash45
[71] JT Cassidy RE Petty Juvenile Idiopathic Rheumatic Arthri-tis 5th Edition WB Saunders Philadelphia 2005
[72] TJ Lehman Are withdrawal trials in paediatric rheumatic dis-ease helpful Lancet 372 (2008) 348ndash350
[73] J Munro Recommendations for the Diagnosis and Managementof Juvenile Idiopathic Arthritis The Royal Australian Collegeof General Practitioners South Melbourne 2009 pp 1ndash38
193Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
httpwwwnhmrcgovau_files_nhmrcpublicationsattachmentscp119-juvenile-arthritispdf
[74] MJ Santos JE Fonseca H Canhao M Conde M JoseVieira L Costa M Costa M Salgado JA Melo Gomes Guide-lines for prescribing and monitoring biologic therapies in juve-nile idiopathic arthritis Acta Reumatol Port 32 (2007) 43ndash47
[75] S Yokota M Mori T Imagawa T Murata M Tomiita Y ItohS Fujikawa S Takei Guidelines on the use of etanercept forjuvenile idiopathic arthritis in Japan Mod Rheumatol 20(2010) 107ndash113
[76] The AGREE Collaboration Appraisal of Guidelines for Researchamp Evaluation (AGREE) instrument wwwagreecollaborationorg
[77] I Kopp H Thole T Langer HK Selbmann G OllenschlaumlgerGerman Instrument for Methodological Guideline Appraisal(DELBI) wwwversorgungsleitliniende2008
[78] Auml Aumlrztliches Zentrum fuumlr Qualitaumlt in der Medizin A Arbeitsge-meinschaften der Wissenschaftlichen Fachgesellschaften in derMedizin Deutsches Instrument zur methodischen Leitlinien-Bewertung (DELBI) Fassung 20052006 Z Aumlrztl FortbildQualitaumltssich 99 (2005) 468ndash519
[79] MP de Wit SE Berlo GJ Aanerud D Aletaha JW BijlsmaL Croucher JA Da Silva B Glusing L Gossec S Hewlett MJongkees D Magnusson M Scholte-Voshaar P Richards CZiegler TA Abma European League Against Rheumatism rec-ommendations for the inclusion of patient representatives in sci-entific projects Ann Rheum Dis 70 (2011) 722ndash726
[80] I Foeldvari M Bidde Validation of the proposed ILAR classifi-cation criteria for juvenile idiopathic arthritis InternationalLeague of Associations for Rheumatology J Rheumatol 27(2000) 1069ndash1072
[81] R Merino J de Inocencio J Garcia-Consuegra Evaluation ofrevised International League of Associations for Rheumatologyclassification criteria for juvenile idiopathic arthritis in Spanishchildren (Edmonton 2001) J Rheumatol 32 (2005) 559ndash561
[82] SE Ramsey RK Bolaria DA Cabral PN Malleson REPetty Comparison of criteria for the classification of childhoodarthritis J Rheumatol 27 (2000) 1283ndash1286
[83] G Horneff A Ebert S Fitter K Minden I Foeldvari J Kum-merle-Deschner A Thon HJ Girschick F Weller HI Hup-pertz Safety and efficacy of once weekly etanercept 08mgkg in a multicentre 12 week trial in active polyarticularcourse juvenile idiopathic arthritis Rheumatology (Oxford) 48(2009) 916ndash919
[84] EH Giannini EJ Brewer N Kuzmina A Shaikov A Maxi-mov I Vorontsov CW Fink AJ Newman JT Cassidy LSZemel Methotrexate in resistant juvenile rheumatoid arthri-tis Results of the USAndashUSSR double-blind placebo-controlled trial The Pediatric Rheumatology CollaborativeStudy Group and The Cooperative Childrens Study GroupN Engl J Med 326 (1992) 1043ndash1049
[85] A Ravelli S Viola D Migliavacca N Ruperto A Pistorio AMartini The extended oligoarticular subtype is the best predic-tor of methotrexate efficacy in juvenile idiopathic arthritisJ Pediatr 135 (1999) 316ndash320
[86] P Woo TR Southwood AM Prieur CJ Dore J Grainger JDavid C Ryder N Hasson A Hall I Lemelle Randomizedplacebo-controlled crossover trial of low-dose oral
methotrexate in children with extended oligoarticular or sys-temic arthritis Arthritis Rheum 43 (2000) 1849ndash1857
[87] E Silverman L Spiegel D Hawkins R Petty D Goldsmith LSchanberg C Duffy P Howard V Strand Long-term open-label preliminary study of the safety and efficacy of lefluno-mide in patients with polyarticular-course juvenile rheumatoidarthritis Arthritis Rheum 52 (2005) 554ndash562
[88] DJ Lovell EH Giannini Y Kimura C Suzanne PJHashkes A Reiff Long-term safety and efficacy of rilonaceptin patients with systemic juvenile idiopathic arthritis (SJIA)Arthritis Rheum 60 (2009)
[89] N Ruperto P Quartier NWulffraat PWoo A Loy R Mouy BBader-Meunier BJ Prakken E Noseda R Belleli J Lecot CRordorf A Martini A Phase II Trial with canakinumab(ACZ885) a new IL-1-beta blocking monoclonal antibody toevaluate safety and preliminary efficacy in children with system-ic juvenile idiopathic arthritis Ann Rheum Dis 68 (2009) 170
[90] DJ Lovell EH Giannini Y Kimura et al Preliminary evi-dence for bioactivity of IL-1 trap (Rilonacept) a long actingIL-1 inhibitor in systemic juvenile idiopathic arthritis (sJIA)Arthritis Rheum 54 (2006) S325
[91] DJ Lovell EH Giannini Y Kimura et al Preliminary evi-dence for sustained bioactivity of IL-1 Trap (rilonacept) a longacting IL-1 inhibitor in systemic juvenile idiopathic arthritisArthritis Rheum 56 (2007) S514
[92] N Ruperto F De Benedetti H Brunner R Allen D Brown JChaitow E Cortis G Espada B Flato V Gerloni G HorneffS Wright A Kenwright R Schneider P Woo A Martini DJLovell Tocilizumab is efficacious in patients with systemic ju-venile idiopathic arthritis (sJIA) across baseline disease charac-teristics and priorbaseline treatments 12-week data from thephase II TENDER trial 17th PReS Congress Valencia Spain2010 2010
[93] N Ruperto DJ Lovell T Li F Sztajnbok C Goldenstein-Schainberg M Scheinberg IC Penades M Fischbach JOrozco PJ Hashkes C Hom L Jung L Lepore S OliveiraC Wallace M Alessio P Quartier E Cortis A Eberhard GSimonini I Lemelle E Chalom LH Sigal A Block A CovucciM Nys A Martini EH Giannini Abatacept improves health-related quality of life pain sleep quality and daily participationin subjects with juvenile idiopathic arthritis Arthritis Care Res(Hoboken) 62 (11) (2010) 1542ndash1551
[94] N Ruperto DJ Lovell P Quartier E Paz N Rubio-PerezCA Silva C Abud-Mendoza R Burgos-Vargas V GerloniJA Melo-Gomes C Saad-Magalhaes J Chavez C HuemerA Kivitz FJ Blanco I Foeldvari M Hofer G Horneff HIHuppertz CJ Deslandre A Loy K Minden M Punaro AFNunez LH Sigal AJ Block M Nys A Martini EH GianniniLong-term safety and efficacy of abatacept in children with ju-venile idiopathic arthritis Arthritis Rheum 62 (2010)1792ndash1802
[95] J Munro Juvenile Idiopathic Arthritis Management Guidelines(Provisional) Australian Paediatric Rheumatology Group 2006httpwwwnhmrcgovau
[96] K Fitch SJ Bernstein MD Aguilar B Burnand JR LaCalleP Lazaro M van het Loo J McDonnell JP Vader JPKahan The RANDUCLA Appropriateness Method Users ManualRAND Pittsburgh 2000

193Evidence and consensus based GKJR guidelines for the treatment of juvenile idiopathic arthritis
httpwwwnhmrcgovau_files_nhmrcpublicationsattachmentscp119-juvenile-arthritispdf
[74] MJ Santos JE Fonseca H Canhao M Conde M JoseVieira L Costa M Costa M Salgado JA Melo Gomes Guide-lines for prescribing and monitoring biologic therapies in juve-nile idiopathic arthritis Acta Reumatol Port 32 (2007) 43ndash47
[75] S Yokota M Mori T Imagawa T Murata M Tomiita Y ItohS Fujikawa S Takei Guidelines on the use of etanercept forjuvenile idiopathic arthritis in Japan Mod Rheumatol 20(2010) 107ndash113
[76] The AGREE Collaboration Appraisal of Guidelines for Researchamp Evaluation (AGREE) instrument wwwagreecollaborationorg
[77] I Kopp H Thole T Langer HK Selbmann G OllenschlaumlgerGerman Instrument for Methodological Guideline Appraisal(DELBI) wwwversorgungsleitliniende2008
[78] Auml Aumlrztliches Zentrum fuumlr Qualitaumlt in der Medizin A Arbeitsge-meinschaften der Wissenschaftlichen Fachgesellschaften in derMedizin Deutsches Instrument zur methodischen Leitlinien-Bewertung (DELBI) Fassung 20052006 Z Aumlrztl FortbildQualitaumltssich 99 (2005) 468ndash519
[79] MP de Wit SE Berlo GJ Aanerud D Aletaha JW BijlsmaL Croucher JA Da Silva B Glusing L Gossec S Hewlett MJongkees D Magnusson M Scholte-Voshaar P Richards CZiegler TA Abma European League Against Rheumatism rec-ommendations for the inclusion of patient representatives in sci-entific projects Ann Rheum Dis 70 (2011) 722ndash726
[80] I Foeldvari M Bidde Validation of the proposed ILAR classifi-cation criteria for juvenile idiopathic arthritis InternationalLeague of Associations for Rheumatology J Rheumatol 27(2000) 1069ndash1072
[81] R Merino J de Inocencio J Garcia-Consuegra Evaluation ofrevised International League of Associations for Rheumatologyclassification criteria for juvenile idiopathic arthritis in Spanishchildren (Edmonton 2001) J Rheumatol 32 (2005) 559ndash561
[82] SE Ramsey RK Bolaria DA Cabral PN Malleson REPetty Comparison of criteria for the classification of childhoodarthritis J Rheumatol 27 (2000) 1283ndash1286
[83] G Horneff A Ebert S Fitter K Minden I Foeldvari J Kum-merle-Deschner A Thon HJ Girschick F Weller HI Hup-pertz Safety and efficacy of once weekly etanercept 08mgkg in a multicentre 12 week trial in active polyarticularcourse juvenile idiopathic arthritis Rheumatology (Oxford) 48(2009) 916ndash919
[84] EH Giannini EJ Brewer N Kuzmina A Shaikov A Maxi-mov I Vorontsov CW Fink AJ Newman JT Cassidy LSZemel Methotrexate in resistant juvenile rheumatoid arthri-tis Results of the USAndashUSSR double-blind placebo-controlled trial The Pediatric Rheumatology CollaborativeStudy Group and The Cooperative Childrens Study GroupN Engl J Med 326 (1992) 1043ndash1049
[85] A Ravelli S Viola D Migliavacca N Ruperto A Pistorio AMartini The extended oligoarticular subtype is the best predic-tor of methotrexate efficacy in juvenile idiopathic arthritisJ Pediatr 135 (1999) 316ndash320
[86] P Woo TR Southwood AM Prieur CJ Dore J Grainger JDavid C Ryder N Hasson A Hall I Lemelle Randomizedplacebo-controlled crossover trial of low-dose oral
methotrexate in children with extended oligoarticular or sys-temic arthritis Arthritis Rheum 43 (2000) 1849ndash1857
[87] E Silverman L Spiegel D Hawkins R Petty D Goldsmith LSchanberg C Duffy P Howard V Strand Long-term open-label preliminary study of the safety and efficacy of lefluno-mide in patients with polyarticular-course juvenile rheumatoidarthritis Arthritis Rheum 52 (2005) 554ndash562
[88] DJ Lovell EH Giannini Y Kimura C Suzanne PJHashkes A Reiff Long-term safety and efficacy of rilonaceptin patients with systemic juvenile idiopathic arthritis (SJIA)Arthritis Rheum 60 (2009)
[89] N Ruperto P Quartier NWulffraat PWoo A Loy R Mouy BBader-Meunier BJ Prakken E Noseda R Belleli J Lecot CRordorf A Martini A Phase II Trial with canakinumab(ACZ885) a new IL-1-beta blocking monoclonal antibody toevaluate safety and preliminary efficacy in children with system-ic juvenile idiopathic arthritis Ann Rheum Dis 68 (2009) 170
[90] DJ Lovell EH Giannini Y Kimura et al Preliminary evi-dence for bioactivity of IL-1 trap (Rilonacept) a long actingIL-1 inhibitor in systemic juvenile idiopathic arthritis (sJIA)Arthritis Rheum 54 (2006) S325
[91] DJ Lovell EH Giannini Y Kimura et al Preliminary evi-dence for sustained bioactivity of IL-1 Trap (rilonacept) a longacting IL-1 inhibitor in systemic juvenile idiopathic arthritisArthritis Rheum 56 (2007) S514
[92] N Ruperto F De Benedetti H Brunner R Allen D Brown JChaitow E Cortis G Espada B Flato V Gerloni G HorneffS Wright A Kenwright R Schneider P Woo A Martini DJLovell Tocilizumab is efficacious in patients with systemic ju-venile idiopathic arthritis (sJIA) across baseline disease charac-teristics and priorbaseline treatments 12-week data from thephase II TENDER trial 17th PReS Congress Valencia Spain2010 2010
[93] N Ruperto DJ Lovell T Li F Sztajnbok C Goldenstein-Schainberg M Scheinberg IC Penades M Fischbach JOrozco PJ Hashkes C Hom L Jung L Lepore S OliveiraC Wallace M Alessio P Quartier E Cortis A Eberhard GSimonini I Lemelle E Chalom LH Sigal A Block A CovucciM Nys A Martini EH Giannini Abatacept improves health-related quality of life pain sleep quality and daily participationin subjects with juvenile idiopathic arthritis Arthritis Care Res(Hoboken) 62 (11) (2010) 1542ndash1551
[94] N Ruperto DJ Lovell P Quartier E Paz N Rubio-PerezCA Silva C Abud-Mendoza R Burgos-Vargas V GerloniJA Melo-Gomes C Saad-Magalhaes J Chavez C HuemerA Kivitz FJ Blanco I Foeldvari M Hofer G Horneff HIHuppertz CJ Deslandre A Loy K Minden M Punaro AFNunez LH Sigal AJ Block M Nys A Martini EH GianniniLong-term safety and efficacy of abatacept in children with ju-venile idiopathic arthritis Arthritis Rheum 62 (2010)1792ndash1802
[95] J Munro Juvenile Idiopathic Arthritis Management Guidelines(Provisional) Australian Paediatric Rheumatology Group 2006httpwwwnhmrcgovau
[96] K Fitch SJ Bernstein MD Aguilar B Burnand JR LaCalleP Lazaro M van het Loo J McDonnell JP Vader JPKahan The RANDUCLA Appropriateness Method Users ManualRAND Pittsburgh 2000