
Thermoresponsive platforms for tissue engineering and regenerative medicine
Upload
independentCategory
view
2download
0
www.elsevier.com/locate/mser
Available online at www.sciencedirect.com
Materials Science and Engineering R 59 (2008) 1–37
Biomaterials in cardiac tissue engineering:
Ten years of research survey
Qi-Zhi Chen a,b,*, Sian E. Harding b, Nadire N. Ali b,Alexander R. Lyon b, Aldo R. Boccaccini a,*
a Department of Materials, Imperial College London, Prince Consort Road, London SW7 2AZ, UKb National Heart and Lung Institute, Imperial College London, Dovehouse Street, London SW3 6LY, UK
Received 24 June 2007; received in revised form 14 August 2007; accepted 14 August 2007
Available online 10 January 2008
Abstract
Driven by enormous clinical need, myocardial tissue engineering has become a prime focus of research within the field of tissue engineering.
Myocardial tissue engineering combines isolated functional cardiomyocytes and a biodegradable or nondegradable biomaterial to repair diseased
heart muscle. The challenges in heart muscle engineering include cell related issues (such as scale up in a short timeframe, efficiency of cell seeding
or cell survival rate, and immune rejection), the design and fabrication of myocardial tissue engineering substrates, and the engineering of tissue
constructs in vitro and in vivo. Several approaches have been put forward, and a number of models combining various polymeric biomaterials, cell
sources and bioreactors have been developed in the last 10 years for myocardial tissue engineering. This review provides a comprehensive update
on the biomaterials, as well as cells and biomimetic systems, used in the engineering of the cardiac muscle. The article is organized as follows. A
historic perspective of the evolution of cardiac medicine and emergence of cardiac tissue engineering is presented in the first section. Following a
review on the cells used in myocardial tissue engineering (second section), the third section presents a review on biomaterials used in myocardial
tissue engineering. This section starts with an overview of the development of tissue engineering substrates and goes on to discuss the selection of
biomaterials and design of solid and porous substrates. Then the applications of a variety of biomaterials used in different approaches of myocardial
tissue engineering are reviewed in great detail, and related issues and topics that remain challenges for the future progress of the field are identified
at the end of each subsection. This is followed by a brief review on the development of bioreactors (fourth section), which is an important
achievement in the field of myocardial tissue engineering, and which is also related to the biomaterials developed. At the end of this article, the
major achievements and remaining challenges are summarized, and the most promising paradigm for the future of heart muscle tissue engineering
is proposed (fifth section).
# 2007 Elsevier B.V. All rights reserved.
Keywords: Tissue engineering; Cardiac muscle; Biomaterials; Polymers; Cell therapy; Bioreactors
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
2. Cells applied in myocardial tissue engineering . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
2.1. Somatic muscle cells . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
2.1.1. Foetal or neonatal cardiomyocyte . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
2.1.2. Skeletal myoblast . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
2.2. Angiogenic cells. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
2.2.1. Fibroblasts. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
2.2.2. Endothelial progenitor cells . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
2.3. Stem cell-derived myocytes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
2.3.1. Basics of stem cells . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
* Corresponding authors. Tel.: +44 20 75946723; fax: +44 20 75946757.
E-mail addresses: [email protected] (Q.-Z. Chen), [email protected] (A.R. Boccaccini).
0927-796X/$ – see front matter # 2007 Elsevier B.V. All rights reserved.
doi:10.1016/j.mser.2007.08.001

Q.-Z. Chen et al. / Materials Science and Engineering R 59 (2008) 1–372
2.3.2. Bone marrow-derived stem cells. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
2.3.3. Adipose-derived stem cells . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
2.3.4. Native cardiac progenitor cells . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
2.3.5. Embryonic stem cells . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
2.3.6. Human embryonic stem cells . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
2.4. Strategies to address immune rejection in cells . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
2.5. Strategies of cell delivery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
2.6. Summary of cell-based therapy and their limitations. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
3. Biomaterials for myocardial tissue engineering . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
3.1. Overview of substrate development for tissue engineering . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
3.1.1. Criteria on tissue engineering substrates . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
3.1.2. Polymers used in soft tissue engineering . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
3.1.3. Fabrication of tissue engineering substrates . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
3.2. Biomaterials for myocardial tissue engineering . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
3.2.1. Selection of biomaterials and design of substrates . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
3.2.2. Biomaterials used in myocardial tissue engineering . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
4. Biomimetic tissue engineering—bioreactors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
4.1. Brief history of bioreactors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
4.2. Comparison of bioreactors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
4.3. Application of bioreactors in myocardial tissue engineering. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
4.4. Key issues . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30
5. Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30
Acknowledgements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31
1. Introduction
A historic perspective is presented in this section on the
evolution of cardiac medicine and the emergence of cardiac
tissue engineering as a major branch in the field of tissue
engineering. It is aimed to understand the rationale of cardiac
tissue engineering and related strategies. A general retrospect
on the history of tissue engineering has been given recently by
Vacanti [1].
Heart disease is the leading cause of death and disability in
both industrialised nations and the developing world, account-
ing for approximately 40% of all human mortality [2]. It is
estimated that 5 million Americans, 1.8 million Britons, and 25
million people worldwide suffer from heart failure, with
approximately 550,000 and 120,000 new cases diagnosed each
year in the United States (US) and the United Kingdom (UK),
respectively [3]. Prognosis is poor with 40% mortality within
12 months of diagnosis, and a 10% annual mortality rate
thereafter [4]. The economic burden imposed by this disease
has reached more than $33 billion in the US and more than £700
million in the UK annually [3].
Heart failure is a condition reflecting impairment of the
pumping efficiency of the heart, and it is caused by a variety of
underlying diseases, including ischemic heart disease with or
without an episode of acute myocardial infarction, hypertensive
heart disease, valvular heart disease, and primary myocardial
disease. The single most common cause of left-sided cardiac
failure is ischemic heart disease (also called coronary artery
disease) with an episode of acute myocardial infarction.
Myocardial infarction typically results in myocyte slippage.
The weakening of the collagen extracellular matrix results in
heart wall thinning and ventricular dilation. The impairment of
the heart wall muscle is permanent because, after a massive cell
loss due to infarction, the myocardial tissue lacks significant
intrinsic regenerative capability to replace the lost cells [5]. The
enlargement in ventricular volume leads to progressive
structural and functional changes in ventricles (called
ventricular remodelling) [5]. Ventricular remodelling is
initially compensatory, but adds further inefficiency to the
mechanical pumping of the ventricular muscle, predisposing
towards the end stage of congestive heart failure (CHF) (or just
heart failure) [5], a condition in which the heart cannot pump a
sufficient amount of blood to the meet the metabolic
requirements of the body [6].
Pharmacological therapy focuses on reduction of work load
(utilising diuretics, nitrates) and protection from the toxic
humoral factors which are overactivated in heart failure [7].
These include catecholamines (b-blockers), angiotensin-con-
verting enzyme (ACE inhibitors), and aldosterone (spirono-
lactone). Blockade of these humoral factors represents the
current standard conservative treatment for patients with mild
symptoms of heart failure and slight limitation during ordinary
activity [7]. Interventional therapy, such as surgery or
implantation of pacing devices to control electrical/mechanical
asynchrony, are now receiving more widespread application, in
particular for patients with marked symptoms and marked
limitation in activity [7–12]. However, both drug and
interventional therapies cannot adequately control disease
progression to the end stage [13]. Eventually, heart transplanta-
tion is the ultimate treatment option to end-stage heart failure.
Owing to the lack of organ donors and complications associated
with immune suppressive treatments, however, scientists and
surgeons constantly look for new strategies to repair the injured
heart [14].

Fig. 1. Heart–lung machine (http://heartonline.org/postpump.htm).
Q.-Z. Chen et al. / Materials Science and Engineering R 59 (2008) 1–37 3
Historically, all these surgical strategies started with the
development of the heart–lung machine (Fig. 1), which takes
over the functions of the heart and lungs during an open-heart
surgery [15], such as coronary bypass surgery and valve
replacement [16,17]. Cardiomyoplasty was an alternative
surgical approach for treating heart failure. Pre-prepared
skeletal muscle, which is able to function at power levels
analogous to those of the heart, was wrapped around the heart,
and paced to contract with the heart, thereby improving cardiac
pumping power [18,19]. Clinical studies reported that this
dynamic cardiomyoplasty could improve left ventricular
performance, reduce cardiac dilation, and interrupt disease
progression [20,21]. However, quantitative heamodynamic
analyses were not consistent, regarding the benefits of active
systolic assist, and mortality from the operation was
unacceptably high [22,23]. This prompted the suggestion that
passive mechanical constraint by the muscle wrap might halt or
even reverse the negative remodelling of the dilated ailing
heart. Inspired by this hypothesis, many studies have examined
Fig. 2. (a) Cardiac support device by Acorn CorCapTM, a typical approach of left ven
structure of the mesh [18]. Published with kind permission from Springer Science
the use of biomaterial supports to restrain the left ventricle [24].
Marlex mesh (polypropylene) [25], Merselene mesh (knitted
polyester) (26), Acorn CorCapTM heart mesh (knitted
polyester) (18) and MyocorTM Myosplint1 [18] are four
representative cardiac support devices that have been under
investigation. A typical approach of this strategy is illustrated in
Fig. 2. Although animal cardiomyoplasty showed distinct
benefits of the devices [27], these have not been translated to the
clinical setting, and currently evidence for their clinical benefit
is absent. None of these devices has received approval of the
Food and Drug Administration (FDA) [28].
Studies around the mid-1990s veered to an intriguing
strategy: the application of cell transplantation. Initially, it was
confirmed that diseased myocardium could be restored by the
transplantation of functional cardiac myocytes [29–31]. Since
then a number of research groups reproduced and refined
these pioneering experiments [32–45]. Most studies support the
conclusion that cell implantation in models of myocardial
infarction can improve contractile function. Clinical studies are
currently under way to investigate the safety and feasibility of
cell implantation in patients [39]. In the cell-based therapy,
isolated cells are injected to the infarct region via the
pericardium, coronary arteries, or endocardium.
In order to improve the site accuracy of cell delivery, an
alternative approach to deliver cells to the infarct region is to
rebuild 3D cell networks in vitro and to implant the cell bandage
onto the infarct heart, as shown in Fig. 3 [46].
The third approach involves the usage a man-made heart
patch (Fig. 4) [47–49], which is populated in vitro with cells and
implanted later in vivo. In this approach, the ring- or sheet-
shaped heart patch serves two functions: cell delivery and
mechanical support. According to theoretical simulations on
the effects of injected materials (Fig. 4b), the addition of a sheet
material to a damaged left ventricular wall could have
important effects on cardiac mechanics, with potentially
beneficial reduction of elevated myofibril stresses, as well as
tricle restraint. http://www.sciencedaily.com/releases/2004/11/. (b) The knitted
and Business Media.

Fig. 3. Schematic graph showing the transplantation of a myocardial cell-sheet graft, also called heart bandage [46]. Reproduced by permission of the MRS Bulletin.
Q.-Z. Chen et al. / Materials Science and Engineering R 59 (2008) 1–374
histological and functional changes to clinical left ventricular
metrics [50]. No simulation work has been reported yet, as far
as the authors are aware of, regarding the effects of epicardial
patches (Fig. 4a). The results may be similar in both cases.
A more ambitious strategy is the implantation of myocardial
tissue generated ex vivo, i.e. a 3D tissue regeneration strategy.
This classic strategy of tissue engineering is established on the
fact that living bodies have the potential of regeneration, and on
the supposition that the employment of natural biology (e.g.,
cells and biomolecules) will maximise the capacity for
regeneration and allow for greater success in developing
therapeutic strategies aimed at the replacement and repair of
tissue and the maintenance and enhancement of its function
[51–53]. The successful development of tissue engineering
constructs will have a profound impact in both the scientific
community and the public sphere. They could be used to
produce in vitro healthy cells for cell-based therapy. They may
also be used for many biomedical studies, such as cell biology,
organ development, functional cell differentiation from stem
cells, environment–cell interaction, cancer biology, new drug
treatment, and could ultimately be used for the repair of injured
or diseased tissues.
Fig. 4. Schematic illustrations of (a) epicardial and (b) endoventricular heart
patch approaches to deliver isolated cells to the infarct regions.
In essence, tissue engineering is a technique of imitating
nature. Natural tissues consist of three components: cells,
extracellular matrix (ECM), and signalling systems. The ECM
is made up of a complex of cell secretions immobilised in
spaces and thus forming a scaffold for its cells. Hence, it is
natural that the engineered tissue construct is a triad [54], the
three constitutes of which correspond to the above-mentioned
three basic components of natural tissues. Fig. 5 illustrates the
triad, i.e. a scaffold, living cells and signal molecules (such as
growth factors and cytokines).
The European Commission on Health and Consumer
Protection defined tissue engineering as ‘‘the persuasion of
the body to heal itself through the delivery, to the appropriate
site, independently or in synergy, of cells, biomolecules and
supporting structures’’ [53]. According to this definition, the
surgical approaches described above could be all classified into
the tissue engineering category, as listed in Table 1. It must be
mentioned that that these approaches are not independent of
one another. The heart patch approach, for example, is a
combinatory paradigm of passive diastolic constraint and cell
therapy. The classic 3D tissue engineering construction could
be optimised by the incorporation of drug and gene therapies.
The application of biomaterials has been mainly related with
the last four approaches listed in Table 1, i.e. left ventricular
constraint, scaffold-free cell sheet implantation, heart patch
implantation and 3D tissue engineering construction.
Cardiac tissue engineering covers heart valve, cardiovas-
cular and myocardial tissue engineering. This review focuses
on the myocardial tissue engineering. Recent reviews are
available on heart valve [55–58] and cardiovascular tissue
engineering [56,59–62].
In the past 10 years, many studies have been published using
different cells and different biomaterials for heart muscle
engineering [14,63–65], and excellent reviews focusing on
different aspects of cardiac muscle engineering are also
available [14,24,52,63–79]. In this article, we present a

Fig. 5. Triad of a classic tissue engineering construct.
Table 1
Currently applied or potential strategies for the treatment of heart failure
patients
1. Pharmaceutical therapy
2. Interventional therapy
(1) Reduction of the heart volume
(2) Implantation of a pace-maker
3. Heart transplantation
4. Tissue engineering strategy
(1) Cardiomyoplasty (active systolic assist)
(2) Cell-based therapy (isolated cell-delivery)
(3) Left ventricular restraint (passive diastolic constraint)
(4) Scaffold-free cell-sheet implantation
(5) Heart patch implantation (passive diastolic
constraint and cell delivery)
(6) 3D tissue engineering construction
(a scaffold + cells + macromolecules)
Q.-Z. Chen et al. / Materials Science and Engineering R 59 (2008) 1–37 5
comprehensive review on the achievements of myocardial
tissue engineering, including cells, biomaterials, and biomi-
metic approach (i.e. bioreactors). Our intention is to identify
what we consider significant challenges and the most promising
approaches in the future of heart muscle tissue engineering. At
the same time, we are aware of the possibility that our own
biases might be embedded in the opinions expressed in the
review. We also apologise in advance to any individuals whose
significant effort in the field of heart tissue engineering was
neglected due to our misunderstanding or oversight.
2. Cells applied in myocardial tissue engineering
This section is devoted to provide a concise review on cells
for heart tissue engineering, including key studies. Although it
is not biomaterial specific, this knowledge is essential to
biomaterials scientists in this field, as cell implantation plays a
pivotal role in the engineering of the heart muscle that lacks
significant intrinsic regenerative capability. After reading this
section, material scientists hopefully will have a guide to
browse the huge amounts of reports available on a variety of
cell types applied in cardiac muscle regeneration and
engineering.
As early as in 1978, Bader and Oberpriller demonstrated the
regenerative capacity of amphibian hearts after autologous
implantation of minced ventricular tissue samples (i.e.
nonisolated cells) into injured newt hearts [80]. In this study,
a partial regeneration of injured newt ventricles was observed.
However, grafted tissue fragments remained morphologically

Q.-Z. Chen et al. / Materials Science and Engineering R 59 (2008) 1–376
and functionally separated from the native myocardium. True
tissue engineering approaches emerged in early 1990s when
efforts to regenerate functional myocardial tissue were invested
in grafting of isolated cell [30,31]. Since then, numerous basic
studies on cells and several early-stage clinical trials have been
carried out using a variety of cell types with the hope of
improving myocardial function. So far, a variety of cell models
have been under intensive investigation. They can be
categorised into three groups (Table 2): (1) somatic muscle
cells, such as foetal or neonatal cardiomyocytes [42,44,45,81–
87] and skeletal myoblasts [88–92], (2) myocardium-generat-
ing cells, such as embryonic stem cells [93–97] (possibly) bone
marrow-derived mesenchymal stem cells [98–106] and adipose
stem cells [107]; and (3) angiogenesis-stimulating cells,
including fibroblasts [108] and endothelial progenitor cells.
Each of these cell types and cell delivery approaches are
reviewed in more detail in the following sections.
2.1. Somatic muscle cells
2.1.1. Foetal or neonatal cardiomyocyte
Early cell transplantation studies focused on using foetal or
neonatal rodent (rat or mouse) cardiomyocytes, as these cells
have the inherent electrophysiological, structural and contrac-
tile properties of cardiomyocytes and still retain some
proliferate capacity [31,81,87]. In their pioneering study,
Soonpaa et al. established the principles of cardiac cell
implantation in the heart. They demonstrated that foetal
cardiomyocyte could be transplanted and integrated within the
healthy myocardium of mice, and that the surviving donor cells
were aligned with recipient cells and formed cell-to-cell
contacts [31]. This group also reported the foetal cardiomyo-
cyte graft in the myocardium of dystrophic mice and dogs [87].
More studies have demonstrated that cardiac myocytes from
neonatal, embryonic or adult models can also be engrafted into
diseased (infarcted, cryoinjured or cardiomyopathic) hearts
Table 2
Potential cell sources for myocardial regeneration in human and their advantages
Cell source Autologous Easily
obtainable
Highly
expan
Somatic cells
Foetal cardiomyocytes No No No
Skeletal myoblasts Yes Yes Depen
Smooth muscle cells Yes Yes Yes
Fibroblasts Yes Yes Yes
Stem cells
Somatic stem cells
Mesenchymal stem cells Yes No Depen
Endothelial progenitor cells Yes Yes Depen
Crude bone marrow Yes Yes Depen
Umbilical cord cells No Yes Yes
(Hemaetopoietic stem cells)
Adipose stem cells
Yes Yes Yes
Embryonic stem cells
Human embryonic stem cells No No Yes
[30,42,44,45,81–83,85,86,109]. These results also indicate that
early-stage cardiomyocytes (foetal and neonatal) were better
candidates than more mature cardiac cells due to their superior
in vivo survival [42].
Time course studies for the survival of grafted cardiomyo-
cytes in the healthy heart were carried out by Muller-Ehmsen
et al. [34]. They isolated and injected male donor neonatal rat
cardiomyocytes into the left ventricular (LV) wall of adult
female inbred rats. They demonstrated that these cells could
survive and improve cardiac function for up to 6 months in a rat
model of chronic myocardial infarction [33]. Murry’s group
[110] showed, using syngeneic rat with cryoinjury, that cell
graft survival after 7 days could be up to 33%.
Cardiomyocyte transplantation, which was applied to
smaller infarcts [83], has been proved effective in the
prevention of cardiac dilation and remodelling following
infarction [36] and the improvement of the ventricular function
[44,85]. Several mechanisms have been proposed for improved
heart function following cardiac myocyte transplantation
[36,70,111,112]:
(1) d
and
dable
d on
d on
d on
d on
irect contribution of the transplanted myocytes to
contractility;
(2) a
ttenuation of infarct expansion by virtue of the elasticproperties of cardiomyocytes;
(3) a
ngiogenesis induced by growth factors secreted from thefoetal cells resulting in improved collateral flow;
(4) p
aracrine effects via the release of beneficial growth factorsfrom the transplanted cells, which support the cardiomyo-
cytes under strain in the failing heart, and may possibly
recruit residential cardiac progenitor cells.
However, the transplanted tissue decreased in size several
months after transplantation [42,83]. An electron microscopy
study revealed that dead cells had features of both necrosis and
apoptosis. Based on the most recent experiments, it is apparent
disadvantages for myocardial repair [63]
Cardiac
myogenesis
Clinical
trial
Safety
Yes No No
age Debated Yes Yes, arrhythmias
No No No
No No No
age Yes No Yes, fibrosis calcification
age Debated No Yes, calcification
age Debated Yes Yes, calcification
Debated No No
Yes No Yes
Yes No Yes, potential teratoma
if cells escape differentiation

Q.-Z. Chen et al. / Materials Science and Engineering R 59 (2008) 1–37 7
that cell death is rapid and extensive after cardiomyocyte
grafting, with most cell deaths occurring during the first 2 days.
However, after 1 week the graft is relatively stable [34,110].
Although this is important proof-of-concept work, there is no
realistic possibility of human or rat neonatal cardiomyocytes
coming to clinical application [110,113,114]. As a result,
several alternative approaches have been developed to over-
come the limitations of foetal cardiomyocyte transplantation
and to obviate the need for immunosuppressants.
2.1.2. Skeletal myoblast
Theoretically, skeletal muscle cells may be superior to
cardiomyocytes for infarct repair, because skeletal myoblasts
have almost all the properties of the ideal donor cell type except
their non-cardiac origin. Skeletal myoblast satellite cells can be
harvested from autologous sources, which obviate the need for
immune suppression. Satellite cells are mononuclear progenitor
cells found in mature muscle. In undamaged muscle, the
majority of satellite cells are quiescent. Upon muscle damage,
satellite cells become activated and are able to differentiate and
fuse to augment existing muscle fibres and to form new fibres.
They can be rapidly expanded in an undifferentiated state in
vitro to clinically applicable numbers of myoblasts without a
risk for tumourgenecity, and they have the capabilities to
withstand ischemia better than many other cell types.
Continued proliferation in vivo may be an advantage when
engrafting into an injured heart, since the input of a smaller
number of cells might give rise to a large graft [70,115].
Although it was originally hoped that skeletal myoblasts
would adapt a cardiac phenotype, it is now clear that within
heart tissue the skeletal myoblasts remain committed to form
only mature skeletal muscle cells that possess completely
different electromechanical properties than those of heart cells.
Moreover, given the inability of myoblasts to form electro-
mechanical connections with host cardiomyocytes (due to lack
of expression of adhesion and gap junction proteins), it is not
surprising that physiological studies failed to demonstrate
synchronous beating of the grafted cells within the host tissue
[116].
However, studies in small and large animal models of
infarction demonstrated beneficial effects of grafting of these
cells on ventricular performance [117,118]. The mechanisms
underlying the beneficial effects of skeletal myoblasts remain to
be elucidated. The improvement in heart wall motion could be
achieved by contraction of the transplanted cells, a local effect
on scar remodelling by mechanical support and/or paracrine
influences on the remodelling process.
Nevertheless, given their autologous origin, the capacity to
amplify primary myoblasts from human muscle biopsies, and
the encouraging preclinical results, skeletal myoblasts were the
first cell type to reach clinical application [92,119–126]. The
pioneering Phase I clinical trials were performed either using a
direct surgery approach (during coronary artery bypass graft
surgery) or using a percutaneous endocardial catheter-delivery
approach and have demonstrated both the feasibility of the
procedure and the ability of the cells to engraft in the infarcted
myocardium [92,119–121,123–128].
The clinical application of autologous skeletal myoblasts is
currently limited by several concerns [115,129,130].
(1) L
ack of myocardial phenotype. This has been blamed for thedisturbingly high incidence of life-threatening ventricular
arrhythmias noted in the initial post transplantation phase in
these trials [119,120].
(2) L
ow recovery of satellite cells. The recovery of satellitecells from muscle biopsies of elderly patients is low.
(3) E
fficiency. Grafting methods need be developed to improvethe efficiency of cell engraftment and survival.
(4) Q
uestionable beneficial effects. The efficacy of skeletalmyoblast therapy is still uncertain because of the following
facts. Firstly, the Phase I clinical trials were not randomised,
and might be placebo controlled. Secondly, widely different
cell transplantation protocols were used in a relatively small
number of patients. Finally, the trials were associated with
other confounding factors such as concomitant left ventricle
assistant device (LVAD) implantation or revascularisation.
Ongoing Phase II clinical trials will hopefully address these
concerns and thoroughly evaluate the safety and efficacy of
myoblast transplantation.
2.2. Angiogenic cells
2.2.1. Fibroblasts
Vascularisation is a key step in tissue repair. At sites of
injury, pheno-transformed fibroblast-like cells are responsible
for fibrous tissue formation. These cells are termed myofibro-
blasts because they contain alpha-smooth muscle actin
microfilaments and are contractile. In vivo studies of injured
rat cardiac tissues and in vitro cell culture studies [131] have
shown that such fibroblast-like cells contain requisite compo-
nents for angiotensin peptide generation and angiotensin II
receptors. Such locally generated angiotensin II acts in an
autocrine/paracrine manner to regulate collagen turnover and
thereby tissue homeostasis in injured tissue.
Human dermal fibroblasts have been applied for myocardial
regeneration to stimulate revascularisation and preserve left
ventricular (LV) function of the infarcted LV in mice [132]. It
has been shown that dermal fibroblasts functioned to attenuate
further loss of LV function accompanying acute myocardial
infarct and that this might be related in part to myocardial
revascularisation.
2.2.2. Endothelial progenitor cells
Endothelial progenitor cells (EPCs) are present in the bone
marrow and the peripheral blood and exhibit phenotypical
markers of mature endothelial cells [133]. It has been found that
rats with inflammatory-mediated cardiomyopathy exhibited a
significant mobilization of EPCs from the bone marrow to the
periphery and their ability to adhere to fibronectin, mature
endothelial cells and cultured cardiomyocytes was significantly
reduced when compared to healthy rats [134]. This result
prompted studies in the application of EPCs in attenuating
remodelling followed by acute myocardial infarction. Transfer
of EPCs resulted in a functional improvement in cardiac

Q.-Z. Chen et al. / Materials Science and Engineering R 59 (2008) 1–378
performance. EPC transfer is effective in attenuating myo-
cardial damage in a model of non-ischemic dilated cardiomyo-
pathy [134], and probably exert their beneficial effects via new
vessel growth and improved blood supply to the failing heart.
2.3. Stem cell-derived myocytes
2.3.1. Basics of stem cells
Stem cells are primal undifferentiated, and thus unspecia-
lized, cells that retain the ability to differentiate into multiple
cell lineages [135]. In principle stem cells are the optimal cell
source for tissue regeneration, including myocardium. Firstly,
they are capable of self-replication throughout life such that an
unlimited number of stem cells of similar properties can be
produced via expansion in vitro. Secondly, the stem cells are
clonogenic, and thus each cell can form a colony in which all
the cells are derived from this single cell and have identical
genetic constitution. Thirdly, they are able to differentiate into
one or more specialised cell types. Hence, after expansion stem
cells can be directed to differentiate into cardiomyogenic
lineage [94,136–138]. For these reasons, stem cell-based
therapy for cardiac muscle regeneration has been under
intensive research during the last decade.
Stem cells can be categorised according to their potency
(totipotent, pluripotent, multipotent, and unipotent) (Fig. 6),
anatomic source (adult, embryonic, foetus, cord blood, or
cancer), or by cell surface markers, transcription factors, and
proteins they express. Four basic stem cell types classified
according to their potency are briefly introduced as follows [135].
(1) T
otipotent stem cells are produced from the fusion of an eggand sperm cell. These cells can differentiate into embryonic
and extra-embryonic cell types.
(2) P
luripotent stem cells are the descendants of totipotent cellsand can differentiate into cells derived from the three germ
layers.
(3) M
ultipotent stem cells can produce only cells of a closelyrelated family of cells (e.g. haematopoietic stem cells
differentiate into red blood cells, white blood cells,
platelets, etc.).
(4) U
nipotent cells can produce only one cell type, but have theproperty of self-renewal which distinguishes them from
non-stem cells.
There are five sources for stem cells, as described below
[139].
� A
dult stem cells are undifferentiated cells found amongdifferentiated cells of a specific tissue and are mostly multi-
potent cells. They are more accurately called somatic stem
cells because foetal and umbilical cord stem cells also fall into
this category. They are present in all tissues and seem to survive
long time periods and harsh conditions. Important sources of
somatic stem cells include bone marrow-derived stem cells,
such as mesenchymal stem cells, and adipose stem cells.
� E
Fig. 6. Categories of stem cells in terms of potency [140].
mbryonic stem cells include early embryonic stem cells
(totipotent) and blastocyst embryonic stem cells (pluripotent)
(Fig. 6). Blastocyst embryonic stem cells are cultured cells
obtained from the undifferentiated inner cell mass of an early
stage pre-implantation embryo. Unlike somatic stem cells,
embryonic stem cells can differentiate into any one of the
body’s more than 200 cell types.
� F
oetal stem cells. After eighth week of development, thehuman embryo is referred to as a foetus. By this time it has
developed a human-like form. Stem cells in the foetus are
responsible for the initial development of all tissues before
birth. Like embryonic stem cells, foetal stem cells are
pluripotent.
� C
ord blood stem cells are derived from the blood of theplacenta and umbilical cord after birth. Umbilical cord stem
cells are multipotent.
� C
ancer stem cells arising through malignant transformationof adult stem cells are proposed to be the source of some or all
tumours and cause metastasis and relapse of the disease.
The common features of all stem cells include:
(1) A
bility to self renew, which means they can divide andproduce stem cell progeny with similar properties.

Q.-Z. Chen et al. / Materials Science and Engineering R 59 (2008) 1–37 9
(2) C
lonogenic, which means that each cell can form a colonyin which all the cells are derived from this single cell and
have identical genetic constitution.
(3) B
road differentiation profile, which means they can growinto one or more mature cell types.
In this section, we focus on the applications of four types of
stem cells in myocardial tissue engineering: bone marrow-
derived stem cells, adipose stem cells, native cardiac progenitor
cells, and embryonic stem cells.
2.3.2. Bone marrow-derived stem cells
Bone marrow stem cells are the most primitive cells in the
marrow. These cells can be classified into: (1) bone marrow-
derived mesenchymal stem cell (MSC), and (2) haematopoietic
stem cell (HSC).
2.3.2.1. Bone marrow-derived mesenchymal stem cells. Bone
marrow-derived mesenchymal stem cells are a subset of bone
marrow stromal cells (the term ‘‘mesenchymal stem cell’’ is
now used to include multipotent cells that are derived from
either bone marrow or other tissues, such as adult muscle or the
Wharton’s jelly present in the umbilical cord). This potential
multipotent stem cell is derived from the non-haematopoietic,
stromal compartment of the bone marrow, which can grow into
non-marrow cells, such as bone, cartilage, tendon, adipose, and
endothelial cells [141].
A number of studies suggested that bone marrow-derived
MSCs could differentiate into cardiomyocytes both in vitro and
in vivo [38,40,136,137,142–145]. Makino et al. [137] treated
murine mesenchymal stem cells with 5-azacytidine and isolated
a cardiomyogenic cell line after repeated screening of
spontaneous beating cells. This result was confirmed by
Tomita et al. [146]. Later Orlic et al. [38] reported that a
subpopulation of bone marrow stem cells were capable of
generating myocardium in vivo in mice. More recently, it was
reported that transplantation of mesenchymal stem cells into
the infarcted myocardium of rats and pigs resulted in improved
myocardial performance [144,147].
One possible advantage of mesenchymal stem cells is their
ability to be either autotransplanted or allotransplanted, as some
reports suggested that they may be relatively privileged in terms
of immune compatibility [148].
2.3.2.2. Haematopoietic stem cells. In addition to the initial
hypothesis that bone marrow stem cells might be able to
differentiate into myocardium in vivo, another major rationale
behind the research of bone marrow stem cells for cardiac
muscle regeneration was the essential roles of vascularisation
and angiogenesis in tissue regeneration. Studies in the animal
models of ischemia and Phases I and II clinical trials suggested
that delivery of haematopoietic stem cells and circulating
endothelial progenitor cells, both originating from bone
marrow stem cells, may result in improvement in the ventricular
function in ischemic heart disease patients [115]. Furthermore,
since bone marrow stem cells reside in the bone marrow of all
patients, they can be obtained by a relatively simple procedure
of bone marrow aspiration, expanded in vitro with or without
differentiation, and re-transplanted into the patient, thus
eliminating the need for immunosuppressants [70].
The initial assumption, regarding the capability of bone
marrow-derived stem cells to regenerate the heart by
transdifferentiation into cardiomyocytes, has been challenged
by a number of recent studied. Balsam et al. [149,150] and
Murry et al. [151] demonstrated that the haematopoietic stem
cells continued to differentiate along the haematopoietic
lineage, suggesting the functional improvement observed
may not be related to transdifferentiation into the cardiac
lineage, but rather from indirect mechanisms. A considerable
body of data indicates that a specific subset of bone marrow-
derived angioblasts, expressing endothelial precursor markers,
is responsible for neovascularisation and angiogenesis [99,152–
157]. Kocher et al. [99] for example, demonstrated that an
intravenous injection of human bone marrow donor cells to the
infarcted myocardium of rats resulted in a significant increase
in neovascularisation of post-infarction myocardial tissue,
attenuation of cardiomyocyte apoptosis and left ventricular
remodelling. The potential of bone marrow stem cells to heal a
damaged heart by inducing vasculogenesis in the injured
myocardium, thereby increasing heart viability and restoring
cardiac function has promoted the studies on bone marrow stem
cells quickly from small animals to clinical trials [115,158].
At present, the results of three medium size clinical trials
(100–200 patients) show a variable and modest healing function
of autologous bone marrow stem cells in cardiac function [159–
161]. The application of bone marrow cells for cardiac disease
is still in its preliminary phase, as optimal cell type, delivery
route, dose and timing require further optimisation. The
application of bone marrow-derived stem cells is also limited
by a safety issue: obtaining adequate autologous cells from a
patient with myocardium infarction in time to prevent post-
infraction remodelling may be difficult. In addition, the
presence of stem cells for cardiomyocytes in other parts of
the body, including bone marrow, has not been widely accepted
yet. Caspi and Gepstein [115] have given an excellently
tabulated overview on the clinical trial results of using bone
marrow stem cells in the treatment of acute and chronic heart
diseases.
2.3.3. Adipose-derived stem cells
Human adipose tissue provides a uniquely abundant and
accessible source of adult stem cells for applications in tissue
engineering and regenerative medicine [162–165]. Adipose-
derived stem cells have the ability to differentiate along
multiple lineage pathways. The cardiomyocyte phenotype from
adipose-derived cells has been reported [107,166]. Animal trial
with rats showed that adipose tissue-derived regenerative cells
improved heart function following myocardial infarction [167].
2.3.4. Native cardiac progenitor cells
It had long been believed that the adult mammalian heart, a
terminally differentiated organ, had no self-renewal potential.
This notion about the adult heart, however, has been challenged
by accumulated evidence that myocardium itself contains a

Q.-Z. Chen et al. / Materials Science and Engineering R 59 (2008) 1–3710
resident progenitor cell population capable of giving rise to new
cardiomyocytes [168–172]. There are scientists who have
hypothesised that cardiac progenitor stem cells reside in the
hearts of neonatal animals, and that these progenitor stem cells
(if any) could eventually serve as the basis for cardiac cell
lineage formation and thus its application in the treatment of
cardiac disease in humans. Recently, cardiac progenitor cells
were found in the hearts of neonate humans, rats, and mice by a
multi-institution group of the United States and German
researchers [172].
Nonetheless, given the limited regeneration ability of the
adult heart, it is apparent that the existence of the above
mentioned cells within the adult heart do not translate to a
functionally significant cardiac differentiation following
myocardial infarction [115]. The role of these cells in the
normal adult heart is still to be elucidated. They may represent
an intrinsic repair system capable of replacing cells lost in the
normal process of ageing, or may simply reflect remnant cells
from organ development in early life. The existence of these
progenitor cells will no doubt open new opportunities for
myocardial repair, though many issues still need to be
addressed.
2.3.5. Embryonic stem cells
Embryonic stem cells are thought to have much greater
translational potential than other stem cells because of their
several advantages over other stem cells, in addition to the
common features shared by all stem cells as mentioned above.
First, they are pluripotent, which means they have a broader
multilineage expressing profile. Unlike adult stem cells, which
can differentiate to a relatively limited number of cell types,
embryonic stem cells have the potential to contribute to all adult
tissues. Second, they are robust. They have the long-term
proliferation ability with a normal karyotype, and can be
cryopreserved. Third, they can be genetically manipulated
[173]. Hence, research using embryonic stem cells remains at
the zenith of stem cell science.
The embryos, from which embryonic stem cells are derived,
are a hollow microscopic ball of cells called blastocyst. At this
blastocyst stage, a group of cells begins to separate from the
outer cell mass (or trophoblast) and forms the inner cell mass
(ICM) (also called embryoblast) (Fig. 6). While the outside
layer of cells of the blastocyst goes on to form the placenta, the
inner cell mass forms the embryo and will ultimately develop
into all the tissues in the body. Embryoblasts are, therefore,
truly pluripotent. In 1981, the inner embryoblasts were isolated
from mouse blastocysts and were successfully used to generate
pluripotent stem cell lines, which were termed embryonic stem
cells (ESC) [174,175]. However, the documentary world had
not seen a human embryonic stem cell line until 1998 when two
independent teams, Thomson et al. [94] and Shamblott et al.
[176], described the generation of human ESC lines.
The embryonic stem cell is capable of continuous
proliferation and self-renewal in vitro but also retains the
ability to differentiate into derivatives of all three germ layers
both in vitro and in vivo. Thus, following cultivation in
suspension, the ESCs tend to spontaneously create 3D
aggregates of differentiating tissue known as embryoid bodies
(EBs) [177]. Upon aggregation, differentiation is initiated and
the cells begin to a limited extent to recapitulate embryonic
development. Though they cannot form trophectodermal tissue
(which includes the placenta), cells of virtually every other type
present in the organism can develop. The aggregate at first
appears as a simple ball of cells, and then grow into an
increasingly more complex appearance. After a few days a
hollow ball (cystic embryoid body) forms, followed by the
appearance of internal structures, such as a yolk sac and heart
muscle cells (i.e. cardiomyocytes) which beat in a rhythmic
pattern to circulate nutrients within the increasingly larger
embryoid body.
The availability of the embryonic stem cell system has
boosted the hope of heart regeneration. The first study using
embryonic stem cell as a source for cell transplantation into the
myocardium was reported by Klug et al. [93]. By using
genetically selected mouse embryonic stem cell-derived
cardiomyocytes, Klug et al. showed that the differentiated
cells developed myofibrils and gap junctions between adjacent
cells and performed synchronous contractile activity in vitro for
up to 7 weeks. This study proved the feasibility to guide an
unlimited number of embryonic stem cells into cardiomyogenic
cell linage and to utilise them for myocardial regeneration.
Later studies [178–181], utilising the infarcted rat heart model,
demonstrated that transplantation of differentiated mouse
embryonic stem cell-derived cardiomyocytes can result in
short- and long-term improvement of myocardial performance.
Theoretically, the undifferentiated ESCs, which might be
able to differentiate in vivo into cardiomyocytes in the host
microenvironment containing cardiac-specific differentiation
signalling, could improve the heart function. However,
controversial results have been reported, regarding the in vivo
differentiation and outcome of the transplantation of undiffer-
entiated ESCs. Puceat’s group [182,183] showed that in
infarcted myocardium, grafted stem cells differentiated into
functional cardiomyocytes integrated with surrounding tissue,
improving contractile performance. However, Nussbaum et al.
[184] discovered that undifferentiated mouse ESCs consistently
formed cardiac teratomas in nude or immunocompetent
syngeneic mice, and that cardiac teratomas contained no more
cardiomyocytes than hind-limb teratomas, suggesting lack of
guided differentiation. Hence the authors concluded that
undifferentiated ESCs did not differentiate toward a cardio-
myocyte fate in either normal or infarcted hearts [184].
As regards immunogenicity of the transplantation of
undifferentiated ESCs, Menard et al. [185,186] reported that
cardiac committed mouse ESCs, which were transplanted to the
infarcted sheep heart following incubation with BMP-2,
differentiated to mature cardiomyocytes, and that cell
transplantation resulted in a significant improvement in cardiac
function independent of whether the sheep were immunosup-
pressed or not. However, another group [187] reported the
increased immunogenicity (i.e. rejection) of mouse ESCs upon
in vivo differentiation after transplantation into ischemic
myocardium of allogeneic animals, implying that clinical
transplantation of allogeneic ESCs or ESC derivatives for

Q.-Z. Chen et al. / Materials Science and Engineering R 59 (2008) 1–37 11
treatment of cardiac failure might require immunosuppressive
therapy. This result was confirmed by Nussbaum’s group [184],
who found no evidence for allogeneic immune tolerance of cell
derivatives. Hence, successful cardiac repair strategies invol-
ving ESCs will need to control cardiac differentiation, avoid
introducing undifferentiated cells, and will likely require
immune modulation to avoid rejection.
2.3.6. Human embryonic stem cells
The vast biomedical potential of human ESCs has stirred
enthusiasm in the field of tissue engineering. From human ESCs,
scientists hope to grow replacement tissues for people with
various diseases, including bone marrow for cancer patients,
neurons for people with Alzheimer’s disease, pancreatic cells for
people with diabetes, and cardiomyocytes for patients with heart
damage. Furthermore, establishment of a tissue-specific differ-
entiation system may have significant impact on the study of
early human tissue differentiation, functional genomics,
pharmacological testing, and cell therapy. Given these reasons,
we think that the utilisation of human ESCs in cardiac tissue
engineering is worthy of a separate section. An overview of the
relevant reports is given in Table 3. After the establishment of
human ESC lines in 1998 [94,176], other research groups have
been able to develop a reproducible cardiomyocyte differentia-
tion system from the human ESCs [138,188–191]. The detailed
protocols can be found in these reports.
It has been demonstrated that the human ESC-derived
cardiomyocytes displayed structural properties of early-stage
cardiomyocytes [138,188,189,192]. The presence cardiac-
specific proteins and the absence of skeletal muscle markers
have also been confirmed [192,193]. These studies also
demonstrated the progressive maturation from an irregular
myofilament distribution to a more mature (i.e. organized)
sarcomeric pattern [138,192,193]. The human ESC-derived
cardiomyocytes were also shown to display functional
properties, consistent with an early-stage cardiac phenotype
[138,189,190,194,195]. Functional improvement of heart
following cell transplantation would require structural,
electrophysiological, and mechanical coupling of donor cells
to the existing network of host cardiomyocytes [115]. Hence, it
is important to investigate whether cells derived from human
ESCs can restore myocardial electromechanical properties. A
study of Gepstein group [196,197] demonstrated tight
electrophysiological coupling between the engrafted human
ESCs and host rat (or swine) cardiomyocytes both in vitro and
in vivo.
In spite of the exciting potential of human ESCs, the cells are
also giving rise to daunting legal and ethical concerns. ESCs are
controversial because they are obtained from the destruction of
a potential human embryo. Technologies for therapeutic and,
especially, reproductive cloning add further ethical problems.
In addition, a number of technical issues need to be addressed
prior to clinical application [115], as discussed below.
(1) S
cale up. One of drawbacks of cell therapy is the difficultyin scaling up to meet larger production needs in clinical
applications.
(2) P
urification of the differentiating cardiomyocyte popula-tion is necessary.
(3) I
n vivo delivery and efficiency of grafting. Cell-deliveringtechniques should be developed to enable proper alignment
of the grafted tissue, high seeding rate of the transplanted
cells, and minimal damage to the host tissue.
(4) I
mmune rejection. Human ESCs (hESCs) are derived fromcell lines genetically distinct to the potential human
recipient. Therefore the potential for immune rejection
following hESC transplantation into an immunocompetent
adult recipient exists, as is observed with conventional solid
organ transplantation. As hESCs are therefore allogenic,
there is the potential requirement for co-administration of
immunosuppression [198–203]. Encouragingly there is
some evidence that hESCs have an immunopriviledged
status. Under certain conditions both in vitro and in vivo it
they display limited immunogenicity and are tolerated in
cross species (xeno-) transplantation without immunosup-
pression [204,205]. Reduced cell surface expression of both
major histocompatibility complex and accessory proteins is
believed to underlie this immunopriviledged status. How-
ever this is mainly observed in undifferentiated hESCs, and
with differentiation into specialised tissues such as
cardiomyocytes hESCs may acquire a greater immunogenic
phenotype. Strategies aimed at preventing immunological
rejection of the cells, such as genetic modification or graft-
recipient tissue type matching, should be explored.
2.4. Strategies to address immune rejection in cells
As mention above, the major limitation of cell therapy is
immune rejection associated with most used cell types.
Successful application of tissue engineering in man will
depend on the utilisation of an autologous or nonimmunogeneic
cell source, as well as synthetic scaffold materials, to avoid life
long immunosuppression. Several strategies aimed at achieving
immunological tolerance are being developed. These strategies
include [115]:
(1) E
stablishing banks of major histocompatibility complex(MHC) antigen-typed human ESC lines.
(2) G
enetically altering the human ESC to suppress theimmune response (e.g., by knocking out the major
histocompatibility complexes).
(3) T
he concept of haematopoietic chimerism.(4) G
enerating immune compatible ESC-derived cardiomyo-cytes with the patient’s own genetic information, known as
somatic cell nuclear transplantation or therapeutic cloning.
The successful application of nuclear transfer techniques to
a range of mammalian species has brought the possibility of
human therapeutic cloning significantly closer. The objective of
therapeutic cloning is to produce pluripotent stem cells that
carry the nuclear genome of the patient and then induce them to
differentiate into replacement cells, such as cardiomyocytes to
replace damaged heart tissue. In the process, a somatic cell
nucleus from a patient is transferred into an enucleated oocyte

Table 3
Differentiation of human ESCs towards cardiomyocytes
Method of hES differentiation Major results Reference
In vitro: via EBs in suspension ESCs differentiated into cardiomyocytes, even after long-term culture. Upon
differentiation, beating cells were observed after one week, increased in
numbers with time, and retained contractility for >70 days. The beating
cells expressed markers of cardiomyocytes
Carpenter and co-
workers [188]
In vitro: via EBs in suspension ESCs showed consistence in phenotype with early-stage cardiomyocytes,
and expression of several cardiac-specific genes and transcription factors
Gepstein and co-
workers [138]
In vitro: via EBs in suspension ESCs showed a progressive ultrastructural development from an irregular
myofibrillar distribution to an organized sarcomeric pattern at late stages
Snir et al. [193]
In vitro: via EBs in suspension ESC-derive myocytes at mid-stage development demonstrated the stable
presences of functional receptors and signalling pathways, and the presence
of cardiac-specific action potentials and ionic currents
Satin et al. [195]
In vitro: co-culture of differentiated
rat cardiomyocyte and hESC-
derived cardiomyocytes; In vivo:
transplantation of hESC-derived
cardiomyocytes into swine
Tight electrophysiological coupling between the engrafted hESC-derived
cardiomyocytes and rat cardiomyocytes was observed. The transplanted hES
cell-derived cardiomyocytes paced the hearts of swine
Kehat et al. [196]
In vitro: co-culture of
undifferentiated hESC
with mouse endoderm-like cells
ESCs differentiated to beating muscle. Sarcomeric marker proteins, chronotropic
responses, and ion channel expression and function were typical of cardiomyocytes.
Electrophysiology demonstrated that most cells resembled human foetal ventricular cells
Mummery et al. [189]
In vitro: via EBs in suspension ES cells differentiated into cardiomyocytes. Upon differentiation, beating cells were
observed after 9 days, and retained contractility for longer than 6 months
Harding et al. [206]
In vitro: co-culture of hESC-derived
cardiomyocytes with rat myocytes;
In vivo: differentiated hESC-
derived cardiomyocytes
transplanted into guinea pig
Electrically active, hESC-derived cardiomyocytes are capable of actively pacing quiescent,
recipient, ventricular cardiomyocytes in vitro and ventricular myocardium in vivo
Xue et al. [197]
In vivo: differentiated cardiac-
enriched hESC progeny
hESCs can form human myocardium in the rat heart, permitting studies of human
myocardial development and physiology and supporting the feasibility of their
use in myocardial repair
Laflamme et al. [192]
Q.-Z. Chen et al. / Materials Science and Engineering R 59 (2008) 1–3712
(i.e. its nucleus has been removed), as described in the cloning
of Dolly the sheep [207]. The oocyte containing the new
nucleus carries the genetic information of the patient. Using a
tiny pulse of electricity to cause the new nucleus to fuse with the
enucleated oocyte’s cytoplasm, this manipulated oocyte can
develop in vitro into a blastocyst. From this blastocyst,
embryonic stem cells with the genetics of the patient can be
isolated and expanded in vitro, and then differentiate in vitro
into genetically matched cardiomyocytes for transplantation.
Obviously, cloning would eliminate the critical problem of
immune incompatibility.
2.5. Strategies of cell delivery
In cell-based therapy, isolated cell suspensions are directly
injected into injured heart via the pericardium, coronary
arteries, or endocardium. Direct injection of isolated cells
avoids an open-heart surgery. However, it is difficult to control
the location of the grafted cells in the transplantation. To
address these problems, 2D and 3D cell delivery vehicles have
been under development using biomaterials. These strategies
are the core of the present review and will be discussed in great
detail in Section 3.
2.6. Summary of cell-based therapy and their limitations
Cell-based cardiac therapy represents an exciting strategy
in, for example, heart tissue regeneration and heart tissue
engineering. Huge efforts have been invested in the
development of cell sources for myocardial regeneration,
including foetal cardiomyocytes, skeletal myoblasts, bone
marrow stem cells, adipose stem cells, endothelial progeni-
tors, native cardiac progenitor cells, and embryonic stem cells
(ESC) (Table 2). A large amount of studies has also been
carried out to assess the roles of these potential cell types in
the regeneration of myocardial tissue, both in vitro and in
vivo. The translation of these basic scientific studies from
bench to bedside has been progressing. Among these cell
sources, embryonic stem cells possess the greatest potential
because of their intrinsic pluripotency. These pluripotent cells
can self-replicate tirelessly in the undifferentiated state in
vitro and be induced to differentiate into cell derivatives of all
three germ layers, including cardiomyocytes. The ability to
generate human cardiac tissue in vitro using embryonic stem
cells provides therefore the most exciting approach in the
field of cardiac tissue regenerative medicine and tissue
engineering.
Despite the enormous potential of cell-based therapy, a
number of technical issues need to be addressed prior to clinical
application. Key technical issues include (1) scaling up of cells,
(2) cell delivery, (3) efficiency of grafting, (4) suppression of
alternative unwanted cell phenotypes when ES cells are
applied, and (5) immune rejection. These issues, in particular
those associated with the efficiency of cell delivery and
grafting, could be potentially addressed by the strategies of
tissue engineering involving biomaterials.

Table 5
Selected polymeric biomaterials for tissue engineering [79,211–214]
Biomaterial Abbreviation
1. Synthetic polymers
Bulk biodegradable polymers
Aliphatic polyesters
Poly(lactic acid) PLA
Poly(D-lactic acid) PDLA
Poly(L-lactic acid) PLLA
Poly(D,L-lactic acid) PDLLA
Poly(glycolic acid) PGA
Poly(lactic-co-glycolic acid) PLGA
Poly(e-caprolactone) PCL
Poly(hydroxyalkanoate) PHA
Poly(3 or 4-hydroxybutyrate) PHB
Poly(3-hydroxyoctanoate) PHO
Poly(3-hydroxyvalerate) PHV
Poly ( p-dioxanone) PPD or PDS
Poly(propylene fumarate) PPF
Poly (1,3-trimethylene carbonate) PTMC
Poly(glycerol-sebacate) PGS
Poly (ester urethane) PEU
Surface bioerodible polymers
Poly(ortho ester) POE
Poly(anhydride) PA
Poly(phosphazene) PPHOS
Polyurethane PU
Nondegradable polymers
Poly(tetrafluoroethylene) PTFE
Poly(ethylene terephthalate) PET
Poly(propylene) PP
Poly(methyl methacrylate) PMMA
poly(N-isoproplylacrylamide PNIPAAm
2. Natural degradable polymers
Polysaccharides
Hyaluronan HyA
Alginate
Chitosan
Starch
Q.-Z. Chen et al. / Materials Science and Engineering R 59 (2008) 1–37 13
3. Biomaterials for myocardial tissue engineering
3.1. Overview of substrate development for tissue
engineering
The aim of this section is to provide an overview on the
development of substrates (scaffolds, matrices) for tissue
engineering, the principles of which also prevail in the
development of myocardial tissue engineering matrices.
3.1.1. Criteria on tissue engineering substrates
Being a very much fledgling discipline, tissue engineering
encounters a variety of challenges, which can be grouped into
three categories associated with the science and technology of
cells, materials, and interaction between them. The challenges
that the material scientists encounter are caused by the strict
requirements on the tissue engineering substrates, as listed in
Table 4. The first three requirements are directly associated
with the chemical and physical properties of biomaterials, and
the last three criteria are set for the fabrication technologies of
substrates. The criterion list is not exhaustive. Specific
requirements on a specific tissue engineering construct, such
as osteoconductivity of bone tissue engineering scaffolds and
electric conductivity for nerve tissue engineering, are not
included. Some listed criteria might not be essential in certain
approaches. Porosity, for example, is not essentially required in
the heart patch approach (Fig. 4), although a porous heart patch
can be used initially to grow vascular cells before seeding
cardiac muscle cells. Biodegradability is not demanded in the
treatment of congenital heart diseases either.
3.1.2. Polymers used in soft tissue engineering
Polymers are the major type of materials used in soft tissue
engineering. Selected biopolymers are listed in Table 5. They
can be naturally occurring or synthetic. Detailed reviews are
available in literature [79,211–214].
Table 4
Criteria for tissue engineering substrates [208–210]
1. Ability to deliver and foster cells
The material should not only be biocompatible (i.e. nontoxic), but also
foster cell attachment, differentiation, and proliferation
2. Biodegradability
The composition of the material should lead biodegradation in vivo at
rates appropriate to tissue regeneration
3. Mechanical properties
The substrate should provide mechanical support to cells until sufficient
new extracellular matrix is synthesised by cells
4. Porous structure
The scaffold should have an interconnected porous structure for cell
penetration, tissue ingrowth and vascularisation, and nutrient delivery
5. Fabrication
The material should possess desired fabrication capability, e.g., being readily
produced into irregular shapes of scaffolds that match the defects in bone of
individual patients
6. Commercialisation
The synthesis of the material and fabrication of the scaffold should be
suitable for commercialisation
Proteins
Collagen
Gelatin
Fibrin
3.1.2.1. Naturally occurring polymers. Natural extracellular
matrices of soft tissues are composed of various collagens. It is
not surprising that much research effort has been focused on
naturally occurring polymers such as collagen [215,216] and
chitosan [217] for tissue engineering applications. Theoretically,
naturally occurring polymers should not cause foreign materials
response when implanted in humans. They provide a natural
substrate for cellular attachment, proliferation, and differentia-
tion in its native state. For the above-mentioned reasons, natural
occurring polymers could be a favourite substrate for tissue
engineering [211,218]. Table 6 presents major naturally
occurring polymers, their sources and applications. Among
them, collagen, fibrin, gelatin and alginate have been extensively
investigated for myocardial tissue engineering [24,64]. Each of
these polymers will be reviewed in detail in Section 3.2, in terms
of their applications in myocardial tissue engineering.

Table 6
List of naturally occurring polymers, their sources and main application fields [219]
Polymer Source Main application fields
Collagen Tendons and ligament Multi-applications, including cardiac tissue engineering
Collagen-GAG
(alginate) copolymers
Artificial skin grafts for skin replacement
Albumin In blood Transporting protein, used as coating to form a thromboresistant surface
Hyaluronic acid In the ECM of all higher animals An important starting material for preparation of new biocompatible and
biodegradable polymers that have applications in drug delivery and tissue
engineering, including cardiac tissue engineering
Fibrinogen-fibrin Purified from plasma in blood Multi-applications, including cardiac tissue engineering
Gelatin Extracted from the collagen inside
animals’ connective tissue
Multi-applications, including cardiac tissue engineering
Chitosan Shells of shrimp and crabs Multi-applications, including cardiac tissue engineering
MatrigelTM (gelatinous
protein mixture)
Mouse tumor cells Myocardial tissue regeneration
Alginate Abundant in the cell walls of
brown algae
Multi-applications, including cardiac tissue engineering
Polyhydroxyalkanoates By fermentation Cardiovascular and bone tissue engineering
Q.-Z. Chen et al. / Materials Science and Engineering R 59 (2008) 1–3714
3.1.2.2. Synthetic polymers. Although naturally occurring
polymers possess the above-mentioned advantages, their poor
mechanical properties and variable physical properties with
different sources of the protein matrices have hampered the
progress with these approaches. Concerns have also arisen
regarding immunogenic problems associated with the intro-
duction of foreign collagen [220].
Following the developmental efforts using naturally
occurring polymers as scaffold materials, much attention has
been paid to synthetic polymers. Synthetic polymers are
essential materials for tissue engineering not only due to their
excellent processing characteristics, which can ensure the off-
the-shelf availability; but also because of their advantage of
being biocompatible and biodegradable [220,221]. Synthetic
polymers have predictable and reproducible mechanical and
physical properties (e.g., tensile strength, elastic modulus, and
degradation rate), and they can be manufactured with great
precision. Although they are unfamiliar to cells and many suffer
some shortcomings, such as eliciting persistent inflammatory
reactions, being eroded, not be compliant or able to integrate
with host tissues, they may be replaced in vivo in a timely
Table 7
Selected properties of synthetic, biodegradable polymers investigated as scaffold m
Polymers Melting point,
Tm (8C)
Glass transition
point, Tg (8C)
Degra
1. Bulk degradable polymers
PDLLA Amorphous 55-60 Sutur
PLLA 173–178 60–65 Sutur
PGA 225–230 35–40 Sutur
PLGA Amorphous 45–55 Sutur
PPF <140 �20 Not a
PCL 58 70–72 Not a
PHB 177 4 Much
2. Surface erodible polymers
Poly(anhydrides) 150–200 Surfa
Poly(ortho-esters) 30–100 Surfa
Polyphosphazene �66 to 50 242 Surfa
fashion by native extracellular matrices built by the cells seeded
into them. It has become widely realised that an ideal tissue
engineered substitute should be made from a synthetic scaffold.
Table 5 has listed most synthetic polymers used in tissue
engineering. Table 7 provides selected properties of synthetic,
biocompatible and biodegradable polymers that have been
intensively investigated as substrate materials for tissue
engineering, type I collagen fibres being included for
comparison. Among them, aliphatic polyesters (PLA, PGA,
and PCL) have widely been applied as scaffolding materials for
3D tissue engineering constructs, an approach listed in Table 1.
Degradability is generally a desired characteristic in tissue
engineering substrates because the second surgery to remove
them (such as a heart patch) would be averted if the substrate
could be removed by the physiological system of the host body.
The biodegradable suture is a successful example of the
applications of biodegradable polymers. Moreover, in many
applications 3D tissue engineering constructs cannot be
removed, and the non-degradable biomaterials would act as
barriers to new tissue ingrowth and blood flow. Nonetheless, a
few nondegradable polymers, including PTFE and PET, have
aterials
dation kinetics Reference
es are absorbed completely in vivo in 12–16 months [221,224,225]
es can be absorbed completely in vivo after 24 months [221,224]
es are absorbed completely in vivo in 6-12 months [221,226,227]
es are absorbed completely in vivo in 2-12 months [211]
vailable [211,228]
vailable [229–231]
slower than PLA,PGA and PLGA [232,233]
ce erosion [211,228,234]
ce erosion [211,235]
ce erosion [236,237]

Table 8
Advantages and disadvantages of polymeric biomaterials for tissue engineering
Biomaterial Positive Negative
Naturally occurring polymers Excellent biocompatibility
(nor foreign body reactions)
(1) Poor processability
Biodegradable (with a wide range
of degradation rates)
(2) Poor mechanical properties
Bioresorbable (3) Immunogenic problem (i.e. poor immune compatibility)
(4) Disease transfection
Bulk biodegradable synthetic polymers (1) Good biocompatibility (1) Inflammatory caused by acid degradation products
Poly(lactic acid) (2) Biodegradable (with a wide
range of degradation rates).
(2) Accelerated degradation rates cause collapse of scaffolds
Poly(glycolic acid) (3) Bioresorbable.
Poly(lactic-co-glycolic acid) (4) Off-the-shelf availability
Poly(propylene fumarate) (5) Good processability
(6) Good ductility
Surface bioerodible synthetic polymers (1) Good biocompatibility (1) They cannot be completely replaced by new tissue
Poly(ortho esters) (2) Retention of mechanical integrity
over the degradative lifetime of the device
(2) Concern associated with the long-term effect
Poly(anhydrides) (3) Significantly enhanced tissue
ingrowth into the porous scaffolds,
owing to the increment in pore size
Poly(phosphazene) (4) Good processability
(5) Off-the-shelf availability
Nondegradable synthetic polymers (1) No foreign body reactions (1) Second surgery is required, or
(2) Tailorable mechanical properties (2) Concern associated with the long-term effect if they
have to stay in the host organ for a lifetime
(3) Good processability
(4) Off-the-shelf availability
Q.-Z. Chen et al. / Materials Science and Engineering R 59 (2008) 1–37 15
been investigated for certain tissue engineering approaches,
such as passive diastolic restraint (Fig. 2) [24], congenital heart
disease [222], and especially vascular tissue engineering
[24,52,79].
Table 9
3D fabrication technologies of polymer scaffolds [238]
Fabrication technology Required properties
of materials
Available po
size (mm)
Melting-based
Melt moulding Thermoplastic 50-500
Extrusion/particle leaching Thermoplastic <100
Solvent-based
Solvent casting/particle leaching Soluble 30–300
Paraffin template Soluble 100–700
Emulsion freeze drying Soluble <200
Thermally induced phase
separation/freeze drying
Soluble <200
Electrospinning Soluble 20–100
Membrane lamination Soluble 30–300
Gas foaming
Chemical reactant gas foaming Amorphous 100–700
Physical induced gas foaming/
particle leaching
Amorphous Micropores
Macropores
Rapid prototyping
3D Printing Soluble 45–150
Fused deposition modelling
Direct rapid prototyping
To design a tissue engineering substrate, it is necessary to
weight up the ‘‘pros and cons’’ of the potential precursor
materials, which are summarised in Table 8. None of polymers
is universally suitable for all tissues. Actually no single material
re Porosity
(%)
Porous structure
<80 Spherical pores/low interconnectivity
<84 Spherical pores/low interconnectivity
20–50 Irregular pores
>90% Spherical pores
<97 High volume of interconnected micropores
<97 High volume of interconnected micropores
<95 Fibrous
<85 Irregular pores
>90% High volume of non-interconnected micropores
<50 <97 Low volume of non-interconnected micropores
combined with high volume of interconnected
macropores
<400
<70 100% interconnected macrospores

Q.-Z. Chen et al. / Materials Science and Engineering R 59 (2008) 1–3716
can provide all necessary properties required by a particular
application. In these instances, a hybrid of natural and synthetic
polymers designed to combine the advantages of both natural
and synthetic materials, such as a porous synthetic polymeric
scaffold filled with naturally occurring biomolecules [223],
may be most appropriate.
3.1.3. Fabrication of tissue engineering substrates
In general, the polymers used for tissue engineering are
either in gel or in solid states. Solid polymers are usually
applied as sheets (or films), knitted meshes, or 3D porous
scaffolds. The processing of polymer sheets/films and knitted
meshes is relative simple, and standard procedures are available
in many polymeric processing handbooks [239]. In the field of
tissue engineering, huge effort has been invested on the
development of fabrication technologies of 3D porous networks
for engineering of tissue constructs, and numerous techniques
have been developed to process porous polymeric, ceramic, and
composite scaffolds. A number of reviews are available in the
literature [238,240–246].
Polymeric scaffold processing methods could be classified
into four groups, as listed in Table 9 which is adapted from Ref.
Fig. 7. Typical porous structures produced by different scaffolding techniques. (a)
Elsevier; (b) extrusion with gas blowing (starch-based), reproduced from ref. [249],
(PLA) http://www.cbmm.lodz.pl/res/sppb_big2.jpg (accessed in May 2007); (d) par
permission from Springer Science and Business Media; (e) chemical reactant gas
drying (PLA), reprinted from ref. [251], with permission from Elsevier; (g) electrosp
May 2007); (h) 3D Printing (PLGA) http://www-bioc.rice.edu/bios576/scaffolds/Sca
reproduced with permission of J. Wiley and Sons Ltd.
[238]: (i) melted-polymer based, (ii) solvent based, (iii) gas-
foaming, and (iv) rapid prototyping (RP). The first three
processing methods are manual techniques, and the last one is
computer-aided technique. Fig. 7 illustrates typical porous
structures of 3D scaffolds fabricated by the techniques listed in
Table 9.
Melted-derived polymer-based methods seldom produce
satisfying porous structure, as shown in Fig. 7a and b. In the
particle leaching processing, it is a tricky task to control the
quality of scaffolds when using salt or sugar, due to the irregular
shape of the particles (Fig. 7c). However, this problem could be
addressed by using nearly perfect microspheres, such as
paraffin microspheres, as illustrated in Fig. 7d. Chemical
reactant gas foaming always produces controlled porous
structure (Fig. 7e), but it is limited to few polymers that could
produce gases during synthesis. It seems that among the
currently available techniques the microsphere-template
technique is the best one to fabricate spherical porous
networks, because it is controllable, low-cost, easy to operate,
and applicable to all soluble polymers, as listed in Table 10.
The freeze-drying and electrospinning methods produce
interesting aligned textures and porous structures (Fig. 7f and
Inject melt moulding (starch-based), reprint from ref. [248] with permission of
copyright by Mary Ann Liebert, Inc., publichers; (c) salt/sugar particle leaching
affin template (paraffin microsphere leaching (PLA) [250], published with kind
foaming (polyurethane); (f) thermally induced phase separation (TIPS)/freeze
inning (PCL), http://www.chem.pku.edu.cn/liangdh/eresearch.html (accessed in
ffolds.htm (accessed in May 2007); (i) fused deposition modelling (PCL) [252],

Table 10
Advantages and disadvantages of polymer scaffolding techniques
Techniques Advantages Disadvantages
Melted-polymer based Mass product ability Very poor quality
Solvent-based
Particle-leaching Simple, low cost, and suitable for many soluble polymers Poor in quality control
Microsphere-template Simple, low cost, suitable for many soluble polymers,
controlled quality, and controlled pore size and porosity
Using organic chemicals
Freeze-drying and
electrospinning
Simple, low cost, suitable for many soluble polymers,
and aligned structure
The aligned texture might not
be always desirable
Gas-foaming Simple, low cost, controlled quality, and controlled pore size and porosity Limited to few polymers
Rapid prototyping Controlled quality, controlled pore size and porosity,
and suitable for many soluble polymers
Expensive
Q.-Z. Chen et al. / Materials Science and Engineering R 59 (2008) 1–37 17
g). In order to guide cells in soft tissue engineering, such as
myocardial tissue which has an aligned texture, scaffolds with
an aligned texture are desirable. Specialised cells in these
tissues may maintain their appropriate phenotypes and lay
down extracellular matrix better on the textured scaffolds [247].
Rapid prototyping (RP), also known as solid free-form (SFF)
techniques, are a computer-aided fabrication processes. They
can rapidly produce highly complex 3D objects using date
generated by computer aided design (CAD) systems. An image
of a defect in a patient can be taken, which is used to develop a
3D CAD computer model. The computer can then reduce the
model to slices or layers. The 3D objects are constructed layer-
by-layer using rapid prototyping techniques of fused deposition
Table 11
Overview of biomaterials used in cardiac tissue engineering
Biomaterials Physical state
Naturally occurring (also degradable)
Collagen based Gel
Fibrin glue Injectable gel
Peptide nanofibre Injectable gel
Collagen mesh 3D porous me
Collagen-glycosaminoglycan 3D porous me
Gelatin mesh 3D porous me
Alginate mesh 3D porous me
Synthetic
Biodegradable
PGA and copolymer with PLA 3D porous me
PLLA 3D porous me
PCL and copolymer with PLA 3D porous me
PGS 3D porous foa
Polyurethane (PU) 3D porous foa
Poly(ester urethane) (PEU)
[or poly(ester urethane)urea (PEUU)]
Solid sheet
Nondegradable
Poly(ethylene terepthalate) (PET).
The fibers are manufactured under
trade names Dacron, Terylene & Trevira
Knitted mesh
Solid sheet
Polypropylene (PP) Solid
Poly(tetrafluoroethylene) (PTFE) with or without PGA/PLA Solid sheet
Poly(N-isopropyl acrylamide) (PNIPAAm or PIPAAm) Solid sheet
modelling (FDM) (Fig. 7i), selective laser sintering (SLS), 3D
printing (3D-P) (Fig. 7h), stereo lithography, or extrusion free-
forming [253].
Rapid prototyping was developed as an inexpensive
technology for the manufacture industry. The idea behind this
is that a new machine could be entirely manufactured and
assembled quite inexpensively from the same polymer filament
feed stock that the rapid prototyping machine uses to make
prototypes by the owner of an existing one. Such a self-
replication technique will considerably reduce the cost of
prototyping machines [254]. However, this idea does not fit into
tissue engineering, as no patients have organs or tissues of
exactly the same geometric size and shape. Hence, rapid
s Tissue engineering approaches Reference
Epicardial heart patch [64,256]
Endoventricular heart patch [257]
Endoventricular heart patch [258]
sh 3D tissue engineering construction [259–261]
sh 3D tissue engineering construction [262]
sh 3D tissue engineering construction [263]
sh 3D tissue engineering construction [264]
[74,265]
sh 3D tissue engineering construction
sh 3D tissue engineering construction [266]
sh 3D tissue engineering construction [267]
m (sponge) 3D tissue engineering construction
and Epicardial heart patch
[268,269]
m (sponge) 2D tissue engineering films that could
be used as heart patches
[270,271]
Cardiovascular grafting [272,273]
Left ventricular constrain [18,274–293]
Cardiovascular grafting [294,295]
Left ventricular constrain [25,26,296,297]
Treatment of congenital heart disease [222]
Cardiovascular grafting [294,298–303]
Scaffold-free cell sheet [304–315]

Fig. 8. Parameters in Laplace’s law. R is the radius of a cylinder-shaped
ventricle, t the thickness of the wall, T the stress in the wall, and DP =
Pinside � Poutside.
Q.-Z. Chen et al. / Materials Science and Engineering R 59 (2008) 1–3718
prototyping processing can be an expensive fabrication
technique for the application of tissue engineering.
In summary, a variety of fabrication techniques have been
developed to produce polymeric scaffolds for tissue engineer-
ing. The microsphere-template method could be the most
promising one for producing spherical porous networks. The
freeze-drying and electrospinning methods could produce
aligned 3D pore textures, which might be desirable in most soft
tissue engineering applications, such as muscles. Although the
computer-aided technology is expensive, it is probably the most
advanced in terms of precise structural design and quality
control.
3.2. Biomaterials for myocardial tissue engineering
3.2.1. Selection of biomaterials and design of substrates
In general, the selection of biomaterials and the design of
substrates for heart muscle engineering could be guided by the
first three criteria listed in Table 4, i.e. (i) ability to deliver and
foster cells, (ii) biodegradability, and (iii) appropriate
mechanical properties. Porosity is another important factor
to be considered, in particular, for 3D tissue engineering
constructs.
3.2.1.1. Biocompatibility. The first and foremost function of a
substrate for tissue engineering is its role as substratum for cell
attachment. Indeed, the ability to support and foster cells is one
of essential properties of a biomaterial used in tissue
engineering [208,210,255]. Hence, the first step in achieving
a successful substrate is to design and produce an extracellular
matrix-like biomaterial that cells would like to attach to. Hence,
it is not surprising that almost all polymers applied for cardiac
muscle engineering are included in Table 5, which are polymers
initially developed for engineering tissues other than heart
tissue and have been well documented for their good
biocompatibilities.
3.2.1.2. Biodegradability. Biodegradability is not always
essential, depending on the applied approaches for cardiac
tissue engineering (Table 11). In general, nondegradable
polymers are selected in the approach of passive diastolic
constraint and the treatment of congenital heart disease, as well
as cardiovascular grafting. Degradable polymers, including
natural and synthetic, are applied in the heart patch approach
and, in particular, in 3D tissue engineering construction. One of
the important challenges encountered by materials scientists is
to design a material for 3D tissue engineering that could
biodegrade in a rate matching the growth kinetics of a specific
tissue at a specific anatomic position.
3.2.1.3. Mechanical properties. In general, different
approaches of myocardial tissue engineering have different
requirements on the mechanical properties of the biomaterials
applied.
Passive diastolic constraint. The idea behind this approach
is Laplace’s law [18], which gives the relation between the
stress T in a wall and the pressure difference across the wall
(DP = Pinside � Poutside), as illustrated in Eq. (1) and Fig. 8.
T ¼ R � DP
t: (1)
In the case of passive diastolic constraint (diastole is the
process of blood filling into a heart), T is the stress in the heart
wall, being named diastolic wall stress. Assuming that the
blood pressure in the left ventricle at the end of diastole (LVED)
is PLVED, and the supporting pressure provided by a cardiac
support device (CSD) is PCSD, then DP, which is also called
transmural pressure, equals PLVED when no CSD is applied, or
PLVED � PCSD when a CSD is implanted. Therefore, the law of
Laplace’s can be expressed by
diastolic wall stress ¼ R � PLVED
tðwithout a CSDÞ (2)
or
diastolic wall stress ¼ RðPLVED � PCSDÞt
ðwith a CSDÞ: (3)
Myocardial infarction typically results in heart wall thinning
(a reduction in t) and ventricular dilation (an increase in R),
which cause a significant increase in the heart wall stress
according to Eq. (2). Overstressed heart wall leads to
progressive structural and functional changes in ventricles
(ventricular remodelling), predisposing towards the end stage
of heart failure [5]. Hence, to prevent negative ventricular
remodelling, it is important to reduce the heart wall stress. This
could be achieved through a heart-supporting device according
to Eq. (3).
Eq. (3) indicates that theoretically there are no strict
requirements on the mechanical properties of the biomaterials
of a CSD, as long as it could provide a mechanical support at the
end of diastole. Practically, however, a CSD should have
optimal compliance so as to smoothly fit on the surface of heart.

Fig. 9. (a) Representative stress–strain curve of a collagen matrix from skin tested at a strain rate of 38.5% min�1. The stress-strain curve can be separated into three
distinct regions designated ‘‘toe’’, ‘‘linear’’, and ‘‘failure’’, reproduced from ref. [321] with permission of ASME International. (b) A typical stress-strain curve of
collagen fibres from tendon, the strain rate being 0.42% min�1, published from ref. [322] with permission of American Society for Clinical Investigation. Note: stress
level is kPa and MPa, in (a) and (b), respectively.
Table 12
Types I/III collagen ratio in heart muscle
Types I/III collagen ratio Measuring technique Reference
Healthy
heart
Heart with
DCM
0.60 1.27 Cyanogen bromide
analysis
[316]
0.58 1.12 Spectrophotometry [316]
No data 6.4–8.4 mRNA [318]
3.76 6.14 Sirius red positive
staining
[319]
0.3 1.25 mRNA [320]
DCM stands for dilated cardiomyopathy.
Q.-Z. Chen et al. / Materials Science and Engineering R 59 (2008) 1–37 19
The compliance can be achieved, for example, through the
knitting of polymer fibres (Fig. 2). It would also be ideal that the
supporting device exhibits a nonlinear elasticity of heart muscle
such that it could reshape with the heart and thus provide
mechanical support to the heart throughout the beating
processes, rather than only at the end of diastole [18].
Heart patch. One specific benefit of the heart patch approach
could be simple changes in ventricular geometry and mechanics
leading to a reduction of elevated local wall stresses. According
to theoretical simulations, the addition of a heart patch to the
bonder-zone could decrease the heart wall stress [50]. In these
simulations, added materials are noncontractile and have 1–
200% of the average stiffness of passive myocardium. The
reduction in wall stress was calculated to be proportional to the
fractional volume added, with stiffer materials improving this
attenuation better [50].
The simulation work apparently indicates that a heart patch
could be designed to be stiffer than the heart muscle. On the
other hand, it is reasonable to assume that a polymer that is too
stiff may induce diastolic dysfunction. The maximum value of
the stiffness of a heart patch material (i.e. what percentage of
the average stiffness of passive myocardium) is an open
question. Therefore, it would be worthy to carry out in vivo
(e.g. on a suitable animal model) investigations on the effects
of heart patch stiffness on the cardiac functions of an infarct
heart.
Classic 3D tissue engineering approach (scaffold + cells). In
this classic approach of tissue engineering, the regenerative
ability of the host body is enhanced through a designed
construct that is populated with isolated cells and signalling
molecules, aiming at regenerating functional tissue as an
alternative to conventional organ transplantation and tissue
reconstruction. 3D tissue engineering constructs could also be
used to produce in vitro healthy cells for cell-based therapy.
They may also be applied for many biomedical studies, such as
cell biology, organ development, functional cell differentiation
from stem cells, environment–cell interaction, cancer biology
and new drug treatment.
In essence, 3D tissue engineering is a technique of imitating
extracellular matrix. Hence, a construct should display some of
the mechanical properties of native myocardium. This is
another major challenge encountered by materials scientists, in
addition to the controlled degradation kinetics. Since the
extracellular matrix of myocytes is collagen, we hypothesize
that cardiomyocytes would be able to beat adequately in a
scaffolding material with mechanical properties similar
(although impossible to be exactly equal) to those of
myocardial collagen.
The myocardium collagen matrix mainly consists of types I
and III collagens, which form a structural continuum.
Synthesised by cardiac fibroblasts, types I and III collagens
have different physical properties. type I collagen mainly
provides rigidity, whereas type III collagen contributes to
elasticity [316]. The two types of collagens jointly support and
tether myocytes to maintain their alignment, whereas their tensile
strength and resilience resist the deformation, maintain the shape
and thickness, prevent the rupture and contribute to the passive
and active stiffness of the myocardium [317]. The ratio of
collagen types within the heart is of significance. Table 12 shows
values for the types I/III collage ratios reported in the literature.
Fig. 9 shows two typical stress–strain curves of type I
collagen, from which the most important property, elastic

Table 13
Selected mechanical properties of type I collagens
Source of collagen Stiffness Failure stress Failure strain Reference
Calf skin 2–22 kPa 1–9 kPa 0.5–0.7 [321]
Tendon, cartilage,
ligament or bone
25–250 MPa 1–7 MPa 0.24–68 [322,323]
Q.-Z. Chen et al. / Materials Science and Engineering R 59 (2008) 1–3720
modulus (stiffness or Young’s modulus), as well as two other
mechanical properties, failure stress (also called mechanical
strength) and failure strain, can be determined, as listed in
Table 13.
As regards the mechanical properties of type III collagen,
there has been no reported data, as far as the present authors are
aware of. It is well known that tissues with predominance of
type I collagen (such as tendon) are characterised by relatively
higher strength and stiffness, whereas tissues containing large
amount of type III collagen (such as skin) are characterised by
greater flexibility (compliance) [318]. Hence, it can be
predicted that the increase of collagen type I would result in
an increase in tissue stiffness. This has been demonstrated by
diseased heart muscle with different levels of dilation, as shown
in Fig. 10 [320]. In general, the stiffness of collagen increases
with stress linearly, i.e. ds/de = ks, where the coefficient k is
termed stiffness constant. A larger stiffness constant k gives rise
to a more rapidly rising curve with increasing stresses. Hence
the increase of stiffness constant with increasing ratio types I/III
collagen (Fig. 10) indicates stiffening of heart muscle.
According to Fig. 10, the stiffness constant of healthy heart
muscle with a types I–III collagen ratio of 0.5 is about 2.
A more direct reference for the mechanical design is the
mechanical properties of heart muscle. Typically, the passive
strains of the heart muscle could reach up to 15–22% at the end
of diastole [324–328]. Hence, the heart muscle mainly works
within the nonlinear elastic region, as indicated by Figs. 9 and
11. The stiffness of the heart muscle is around 10–20 kPa at the
early stage of diastole, and rises up to 50 kPa (healthy hearts) or
200–300 kPa (CHF hearts) at the end of diastole [324–328].
Fig. 10. Relation between Collagen I/III ratio and stiffness in myocardium
given by the stiffness constant k [320]. Reproduced with permission from
Elsevier.
These data could be used as the lower and upper bounds of
stiffness in the selection of materials for 3D tissue engineering
scaffolds.
3.2.1.4. Design of porous structures for 3D tissue engineer-
ing. The classic approach of tissue engineering is based on the
supposition that the employment of extracellular matrix-like
scaffold, natural biology (e.g., cells and biomolecules) of the
living body will induce the regeneration tissue or organ ex vivo
[51–53]. However, in the absence of true vascularisation, in
vitro engineering approaches face the problem of critical
thickness: mass transportation into tissue is difficult beyond a
thin peripheral layer of a tissue construct even with artificial
means to supply engineered tissue constructs with nutrients and
oxygen (<100 mm without the use of bioreactor, and<200 mm
with the support of bioreactor) [74]. Diffusion barriers that are
present in vitro are most likely to become more deleterious in
vivo due to lack of vascularisation. Once the engineered tissue
construct is placed in the body, vascularisation becomes a key
issue for further remodelling in the in vivo environment.
It was initially thought that a pore size in the range of 50–
100 mm was sufficient to allow the vascularisation of a scaffold
following transplantation [71]. Later Radisic and Vunjak-
Novakovic [74] suggested a larger (�100 mm) pore size for
Fig. 11. Typical passive stress–strain curves of heart muscles of different
murine and human. The stiffness of the heart muscle is around 10–20 kPa at
the early stage of diastole (strain<10%), and rises up to 50 kPa (healthy hearts)
or 200–300 kPa (CHF hearts) at the end of diastole (strain being 15–22%).

Table 14
Investigated or potential biomaterials used in cardiac muscle engineering
Polymer Elastomer (E)
or thermoplastic (T)
Young’s modulus
(or stiffness)
Tensile
strength
Degradation
(month)
Reference
Synthetic, nondegradable
PET T or E 4 GPa Nondegradable [323]
PET/DLA E 2–3 MPa Nondegradable
Synthetic, degradable
PGA T 7–10 GPa 70 MPa 2–12 [214,228,244,334]
PLLA or PDLLA T 1–4 GPa 30–80 MPa 2–12 [214,228,244,334]
PHB E 2–3 GPa 36 MPa Degradable [232,334]
PPD (= PDS) E 0.6 GPa = 600 MPa 12 MPa 6 [334,335]
PU E 5–60 MPa 20–45 MPa Surface errodible [336]
PEUU E Not available Not available Degradable
TMC E 6 MPa 12 MPa Degradable [337]
TMC-PDLLA(50:50) E 16 MPa 10 MPa Degradable [337]
POC T 1–16 MPa 6.7 MPa Degradable [334,338]
PGS E 0.04–0.282 MPa 0.5 MPa Degradable [48,334,339]
Naturally occurring
Collagen fibre
(tendon/cartilage/
ligament/bone)
E 2–46 MPa 1–7 MPa Degradable [322,323,334]
Collagen gel (calf skin) E 0.002–0.022 MPa 1–9 kPa Degradable [321]
Heart muscle
Myocardium of rat E 0.14 MPa (at the end of diastole) 30-70 kPa Not Applicable [340–342]
Myocardium of human E 0.2–0.5 MPa (at the end of diastole) 3–15 kPa Not Applicable [324,343,344]
Q.-Z. Chen et al. / Materials Science and Engineering R 59 (2008) 1–37 21
cardiac tissue constructs. It has been also suggested that pore
size larger than 300 mm is necessary for long-term survival, i.e.
vascularisation [238,329–331]. But excessively large pores
could impair vascularisation, because endothelial cells are
unable to bridge pores greater than a cell diameter [258]. A
potential approach to address this problem is to fill a highly
porous scaffold with a cell-seeded and/or gene-containing
collagen gel, as it has been reported that collagen gels do not
obstruct vascularisation while providing substrata for cells to
attach [77].
3.2.2. Biomaterials used in myocardial tissue engineering
The majority of polymeric biomaterials used in the fields of
cardiac muscle tissue engineering have been listed in Table 11.
Among the natural polymers, collagen, alginate and gelatin
have been under intensive investigation for myocardial tissue
engineering by research groups in Germany [64,66,77], Israel
[63,70,71], and Canada [263,332], respectively. Among the
synthetic biodegradable polymers, PGA and copolymers with
PLLA, and PCL have been studied systematically using
bioreactors for myocardial tissue engineering at MIT
[74,76,269] and Harvard [267,333]. The thermo-responsive
polymer PNIPAAM was applied to cardiac tissue engineering
by researchers in Japan [304–314]. The cardiac devices made
from nondegradable polymers have been under intensive
animal and human clinical trials by surgeons mainly in USA
[18,274–285], Germany [286–291] and Sweden [292,293].
Selected properties of most materials mentioned above are
given in Table 14. Sections 3.2.2.1–3.2.2.5 provide an accurate
and thorough assessment of the state-of-the-art of each of these
materials applied in the field of myocardial tissue engineering.
At the end of each section, critical discussions are given on the
important research issues and topics that remain challenges to
the advancement of the field, aiming to stimulate new insights
and perspectives that may be most useful for material scientists
involved in this field.
3.2.2.1. Materials used in the heart patch approach. In this
application, the major function of a heart patch is to deliver
healthy, functional cardiomyocytes to the infarct area of the
heart (Fig. 4), and the patch is then expected to degrade at the
end of the cell-delivery. These requirements could be achieved
with biological gels [47]. It would be ideal that a heart patch
could also provide mechanical support to the left ventricle. For
this purpose, stiffer synthetic heart patches have also been
applied [48].
Collagen gel. In 1997, Eschenhagen et al. [47] reported, for
the first time, an artificial heart tissue, which was termed
engineered heart tissue (EHT). Several years later, a similar
artificial tissue, ‘Engineered Cardiac Tissue’ (ECT) was
reported by a Chinese research group [345,346]. In Eschenha-
gen et al.’s work, embryonic chick cardiomyocytes were mixed
with collagen solution and allowed to gel. By culturing the
cardiomyocytes in the collagen matrix, they produced a
spontaneously and coherently contracting 3D heart tissue in
vitro. Immunohistochemistry and electron microscopy revealed
a highly organized myocardium-like structure exhibiting
typical cross-striation, sarcomeric myofilaments, intercalated
discs, desmosomes, and tight junctions.
Later the same group reported the long-term survival of
neonatal rat cardiomyocytes in the matrix and its functional and
physiological characteristics in vitro [347]. They detected an
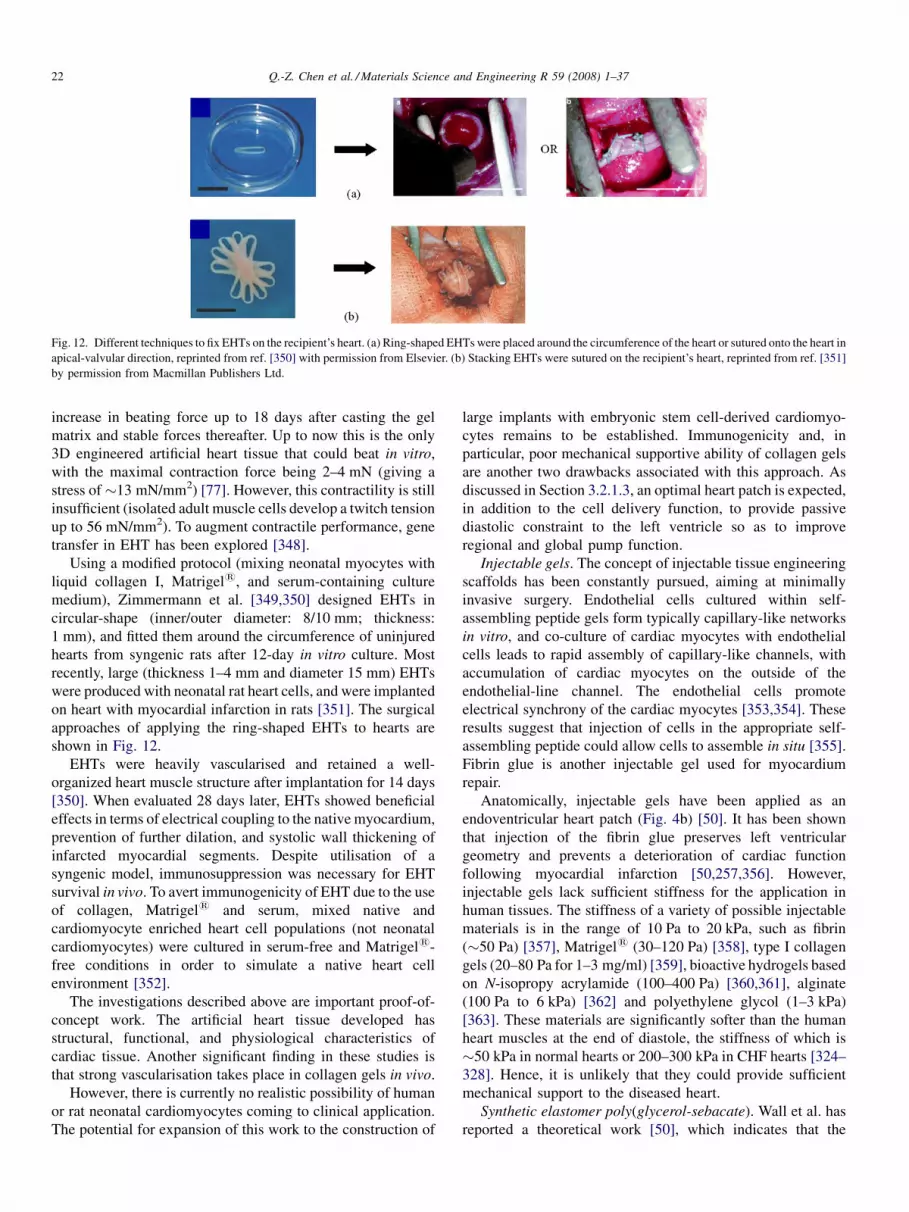
Fig. 12. Different techniques to fix EHTs on the recipient’s heart. (a) Ring-shaped EHTs were placed around the circumference of the heart or sutured onto the heart in
apical-valvular direction, reprinted from ref. [350] with permission from Elsevier. (b) Stacking EHTs were sutured on the recipient’s heart, reprinted from ref. [351]
by permission from Macmillan Publishers Ltd.
Q.-Z. Chen et al. / Materials Science and Engineering R 59 (2008) 1–3722
increase in beating force up to 18 days after casting the gel
matrix and stable forces thereafter. Up to now this is the only
3D engineered artificial heart tissue that could beat in vitro,
with the maximal contraction force being 2–4 mN (giving a
stress of�13 mN/mm2) [77]. However, this contractility is still
insufficient (isolated adult muscle cells develop a twitch tension
up to 56 mN/mm2). To augment contractile performance, gene
transfer in EHT has been explored [348].
Using a modified protocol (mixing neonatal myocytes with
liquid collagen I, Matrigel1, and serum-containing culture
medium), Zimmermann et al. [349,350] designed EHTs in
circular-shape (inner/outer diameter: 8/10 mm; thickness:
1 mm), and fitted them around the circumference of uninjured
hearts from syngenic rats after 12-day in vitro culture. Most
recently, large (thickness 1–4 mm and diameter 15 mm) EHTs
were produced with neonatal rat heart cells, and were implanted
on heart with myocardial infarction in rats [351]. The surgical
approaches of applying the ring-shaped EHTs to hearts are
shown in Fig. 12.
EHTs were heavily vascularised and retained a well-
organized heart muscle structure after implantation for 14 days
[350]. When evaluated 28 days later, EHTs showed beneficial
effects in terms of electrical coupling to the native myocardium,
prevention of further dilation, and systolic wall thickening of
infarcted myocardial segments. Despite utilisation of a
syngenic model, immunosuppression was necessary for EHT
survival in vivo. To avert immunogenicity of EHT due to the use
of collagen, Matrigel1 and serum, mixed native and
cardiomyocyte enriched heart cell populations (not neonatal
cardiomyocytes) were cultured in serum-free and Matrigel1-
free conditions in order to simulate a native heart cell
environment [352].
The investigations described above are important proof-of-
concept work. The artificial heart tissue developed has
structural, functional, and physiological characteristics of
cardiac tissue. Another significant finding in these studies is
that strong vascularisation takes place in collagen gels in vivo.
However, there is currently no realistic possibility of human
or rat neonatal cardiomyocytes coming to clinical application.
The potential for expansion of this work to the construction of
large implants with embryonic stem cell-derived cardiomyo-
cytes remains to be established. Immunogenicity and, in
particular, poor mechanical supportive ability of collagen gels
are another two drawbacks associated with this approach. As
discussed in Section 3.2.1.3, an optimal heart patch is expected,
in addition to the cell delivery function, to provide passive
diastolic constraint to the left ventricle so as to improve
regional and global pump function.
Injectable gels. The concept of injectable tissue engineering
scaffolds has been constantly pursued, aiming at minimally
invasive surgery. Endothelial cells cultured within self-
assembling peptide gels form typically capillary-like networks
in vitro, and co-culture of cardiac myocytes with endothelial
cells leads to rapid assembly of capillary-like channels, with
accumulation of cardiac myocytes on the outside of the
endothelial-line channel. The endothelial cells promote
electrical synchrony of the cardiac myocytes [353,354]. These
results suggest that injection of cells in the appropriate self-
assembling peptide could allow cells to assemble in situ [355].
Fibrin glue is another injectable gel used for myocardium
repair.
Anatomically, injectable gels have been applied as an
endoventricular heart patch (Fig. 4b) [50]. It has been shown
that injection of the fibrin glue preserves left ventricular
geometry and prevents a deterioration of cardiac function
following myocardial infarction [50,257,356]. However,
injectable gels lack sufficient stiffness for the application in
human tissues. The stiffness of a variety of possible injectable
materials is in the range of 10 Pa to 20 kPa, such as fibrin
(�50 Pa) [357], Matrigel1 (30–120 Pa) [358], type I collagen
gels (20–80 Pa for 1–3 mg/ml) [359], bioactive hydrogels based
on N-isopropy acrylamide (100–400 Pa) [360,361], alginate
(100 Pa to 6 kPa) [362] and polyethylene glycol (1–3 kPa)
[363]. These materials are significantly softer than the human
heart muscles at the end of diastole, the stiffness of which is
�50 kPa in normal hearts or 200–300 kPa in CHF hearts [324–
328]. Hence, it is unlikely that they could provide sufficient
mechanical support to the diseased heart.
Synthetic elastomer poly(glycerol-sebacate). Wall et al. has
reported a theoretical work [50], which indicates that the

Q.-Z. Chen et al. / Materials Science and Engineering R 59 (2008) 1–37 23
addition of a sheet material to a damaged left ventricular wall
could have important effects on cardiac mechanics, with
potentially beneficial reduction of elevated myofibril stresses,
as well as confounding changes to clinical left ventricular
metrics. The reduction in wall stress was calculated to be
proportional to the fractional volume added, with stiffer
materials improving this attenuation better [50]. Stimulated by
the theoretical simulation of Wall et al. [50], the present authors
have designed a heart patch (Fig. 4a) from a biocompatible and
biodegradable poly(glycerol-sebacate) (PGS) [364].
PGS was recently developed for the field of soft tissue
engineering [339,365]. This polymer is a biodegradable,
biocompatible, and inexpensive elastomer [366], and has
already shown potential in nerve [367] and vascular tissue
engineering [368–371]. PGS also has superior mechanical
properties, being capable of sustaining and recovering from
deformation due to its intrinsic elasticity, and thus it is well
suited to work in a mechanically dynamic environment, such as
the heart [268,269].
The PGS developed by the present authors shows a wide
range of stiffness values (several 10 kPa to 1.2 MPa) that could
be tailored to be either softer or stiffer than the heart muscles of
various animals [364]. Hence, this material could offer the most
convenient tool to carry out in vivo studies on the mechanical
effects of heart patches on the cardiac function of an infarct
heart and to address the following fundamental questions: (1)
Should a heart patch be softer or stiffer than the heart muscle?
(2) What is the maximum stiffness of a heart patch that would
not cause heart dysfunction?
Polyurethane (PU) and poly(ester-urethane) (PEU) rubbers.
Polyurethane rubbers are segmented copolymers having the
characters of thermoplastic elastomers. These copolymers
contain two types of segments: one type of blocks, i.e. A blocks,
is above its glass transition temperature Tg and forms soft
segments, and the other type, i.e. B blocks, is below its Tg and
forms hard segments. In poly(ester-urethane) elastomers, the
hard polyurethane segments tend to aggregate to give ordered
crystalline domains aided by the possibility of forming
hydrogen bonds between adjacent hard segment units. In
contrast, the soft polyester segments remain amorphous at
ambient temperature.
PU can be tailored to have a broad range of mechanical
properties and good biocompatibility, which makes them ideal
for many implantable devices [372,373]. A major problem of
PU composed with di-isocyanate may be the toxicity of
degradation products. However, in vitro and in vivo studies have
reported good cell adhesion and proliferation and no adverse
tissue reaction [374]. Because these materials are subject to in
vivo degradation, they are no longer applicable in long-term
implanted devices. On the other hand, it is because of their
biodegradability and elasticity that polyurethane elastomers
have gained new attention for the field of tissue engineering.
Since the early 1990s polyurethane elastomers have been
studied for soft, in particular, vascular tissue engineering [375–
377]. Recently, the elasticity of polyurethane elastomers has
made them also attractive for cardiac muscle engineering
[49,270,271].
The Young’s modulus of PU is typically in the range of 5–
60 MPa [378], which is much higher than that of the heart
muscle at the end of diastole. However, PU can be processed
into very thin films (10–15 mm in thickness) [270,271] and
highly porous network [49] which makes PU flexible and
compliant. Researchers at Toronto University [270,271] carried
out in vitro studies on the integrity of the cardiomyocyte
patterns on a thin polyurethane film. In these studies, adult or
ESC-derived cardiomyocytes were seeded onto the patterned
films and cultured for up to 4 weeks or 30 days. At the end of
culture, multilayered (approximately 2–3 cell layers) and
patterned cardiomyocytes were formed on the films. The dense
and highly aligned cardiomyocytes were able to contract the
thin polyurethane films [271]. These results indicate that the PU
and PEU films could be promising heart-patch materials,
although this was not explicitly pointed out by the researchers
[270,271].
Most recently, Fujimoto et al. [49] reported a successful
animal trial using a biodegradable, porous PU heart patch. The
heart patch was sutured to the infarct region of the rat heart. The
implanted PU patch promoted contractile phenotype smooth
muscle tissue formation and improved cardiac remodelling and
contractile function at the chronic stage. This work suggests
that the heart patch approach could be a new therapeutic option
against post-infarct cardiac failure.
Major challenges. The most important challenge that
material scientists currently encounter in the heart patch
approach, as well as in 3D tissue engineering scaffold design, is
to achieve, with synthetic polymers, a nonlinear elasticity that
is similar to that of heart muscle. Such a nonlinear elasticity
would ensure that the heart patch can ‘beat’ together with the
recipient heart, thus providing appropriate restraints to the left
ventricle throughout the beating process. To successfully
design such a nonlinear elasticity, material scientists need to
gain fundamental understanding of the nonlinear elasticity of
collagen-based muscles [379–388] and, in particular, the
mechanical behaviours of collagen or collagen gels at a single
molecule level [389,390].
3.2.2.2. Polymers used for 3D tissue engineering scaffold-
s. As discussed in Section 4.1.3, the mechanical requirement
on the materials used for 3D tissue engineering construction is
that they should have mechanical properties similar to those of
native myocardium. The anisotropic, nonlinear elasticity of
heart muscles makes this task the most challenging. In the field
of myocardial tissue engineering, the development of 3D tissue
engineering constructs did not follow what we think today
should be required. Instead, most 3D tissue engineering
constructs investigated for heart muscle engineering were
adopted from other areas of tissue engineering, even from bone
tissue engineering (e.g. bioceramic TiO2 [391]). This is one of
the reasons why the utilisation of artificial matrices to engineer
myocardium has been rather disappointing, with no examples
of human application to date. Nevertheless, it is the following
pioneering work that deepened our understanding of the fate of
implanted materials and cells in the myocardium of both
healthy and diseased hearts.

Q.-Z. Chen et al. / Materials Science and Engineering R 59 (2008) 1–3724
Collagen fibrous mesh (or collagen sponge). The application
of collagen gel matrix is limited by its insufficient mechanical
strength. Hence, alternatives are being sought. 3D solid
collagen mesh, for example, is commercially available for
scaffold applications, such as Tissue Fleece by Baxter
Deutschland, Heidelberg, Germany [392] and Collagen type
I matrix from Biomaterials Research B.V. Vaals, The Nether-
lands [393,394].
Kofodis et al. [259,260] seeded neonatal rat cardiomyocytes
in vitro into this commercially available collagen sponge, and
called the product artificial myocardial tissue (AMT). The
myocardial tissue generated in the 3D scaffolds in vitro
possesses structural, mechanical, physiological and biologic
characteristics similar to native cardiac tissue [259,260].
Undifferentiated embryonic stem cells were seeded into
collagen mesh scaffolds [395], the construct being called
‘Bioartificial Myocardial Tissue’ (BMT). The bioartificial
mixtures were implanted in the infarct area of rat hearts
(Fig. 13). It was revealed that embryonic stem cells formed
stable intramyocardial grafts that were incorporated into the
surrounding area without distorting myocardial geometry,
thereby preventing ventricular wall thinning. Fractional short-
ening was better in embryonic stem cell-treated animals than in
those which had received matrix implants without cells.
The studies of van Luyn et al. [393] confirmed that
contracting cells (not contracting constructs) were present after
seeding neonatal rat heart ventricular cell fractions and were
able to survive in collagen type I sponges for up to 135 days. In
the subsequent investigation of the same group [394], Collagen-
I scaffolds were directly sutured to healthy or injured left
ventricles of mice without in vitro cell culture. Encouraging
results were reported, in terms of vascularisation, degradation
of scaffolds and foreign body reactions.
To summarize this section, although positive results were
obtained from the histological analysis on the retrieved hearts,
no significant improvement was reported regarding ventricular
function in hearts receiving collagen sponge grafts. Moreover,
no beating constructs have been achieved in vitro with collagen
sponges.
Gelatin mesh. Gelatin mesh is the second type of solid
scaffold applied in cardiac muscle engineering [263]. Gelatin
Fig. 13. Intramural transplantation of a bioartificial, embryonic stem cells-
containing matrix [395]. Reprinted with permission from Elsevier.
mesh is also commercially available as foam (e.g. Gelfoam
prepared from purified pork skin and supplied by Upjohn,
Ontario, Canada). Li et al. [263] seeded foetal rat ventricular
muscle (not isolated cells) into Gelfoam to form grafts. The grafts
were cultured in vitro for 7 days, forming a beating cardiac tissue
in vitro in the grafts. Then the grafts were implanted either into
the subcutaneous tissue of adult rat legs or onto myocardial scar
tissue in a cryoinjured rat heart. In both the subcutaneous tissue
and the myocardial scar, blood vessels grew into the grafts from
the surrounding tissue. The grafts implanted into the sub-
cutaneous tissue contracted regularly and spontaneously. When
implanted onto myocardial scar tissue, the cells within the grafts
survived and formed junctions with the recipient heart cells. Like
in the case of collagen scaffolds, the researchers did not note any
improvement of ventricular function in hearts receiving either
cell-seeded or unseeded gelatin grafts.
In a subsequent investigation, the same research group [396]
seeded various isolated cells into gelatin meshes separately,
including foetal rat ventricular cardiomyocytes, stomach
smooth muscle cells, skin fibroblasts, and adult human atrial
cells, and cultured them in vitro. The important facts revealed
by this investigation include: (1) grafts seeded with foetal rat
ventricular cells exhibited spontaneous rhythmic contractility
in vitro; (2) the gelatin mesh was slowly degraded; (3) all cell
types preferentially migrated to the uppermost surface of each
graft and formed a 300–500 mm thick layer. The last point
indicates a critical issue in 3D tissue engineering, i.e. critical
size. Readers will see from the rest of this section that all 3D
tissue engineering constructs face the problem of critical
thickness: mass transportation into tissue is difficult beyond a
thin peripheral layer of a tissue construct even with artificial
means to supply engineered tissue constructs with nutrients and
oxygen [74]. The usage of a bioreactor can ameliorate the
situation [261,397] but the problem is not totally solved. In fact,
vascularisation is one of the greatest challenges in 3D tissue
engineering construction [398]. This topic will be further
discussed at the end of Section 3.2.2.2 (Challenges in 3D
engineered myocardial constructs).
In another series of interesting studies [399–403], gelatin
and other synthetic (PCL, PGA and PCL-co-PLLA) patches
were combined with foetal, adult rat heart or rat aortic smooth
muscle cells and cultured in vitro to expand the number of cells.
Then the patches were used to replace the right ventricular
outflow tract (RVOT) in syngeneic rats and stayed in vivo for up
to 22 weeks. The gelatin patches, which started to dissolve at 4
weeks, had completely dissolved at 12 weeks [399], while the
patches made from PCL, PGL or PCL-co-PLLA did not thin or
dilate in vivo due to their relatively slow degradation kinetics
[401–403]. The seeded cells survived in the right ventricular
outflow tract. The patches encouraged the ingrowth of fibrous
tissue and remained endothelialized [399–403]. However, a
significant inflammatory reaction was noted in the gelatin patch
after 4 weeks as the scaffold started to dissolve [399]. But the
inflammatory response did not happen with PCL, PGA and
PCL-co-PLLA patches, among which PCL-co-PLLA patches
permitted better cellular penetration in vitro than PCL and PGA
patches [401–403].

Q.-Z. Chen et al. / Materials Science and Engineering R 59 (2008) 1–37 25
In summary, unlike collagen meshes, gelatin meshes seeded
with foetal rat ventricular cells were reported to exhibit
spontaneous rhythmic contractility in vitro. Like collagen
meshes, no improvement of ventricular function was noted in
hearts receiving either cell-seeded or unseeded gelatin grafts.
Critical size is a major issue in the 3D tissue engineering
approach.
Alginate mesh. In addition to protein-based materials, there
is intensive research activity in the area of natural poly-
saccharides. Alginate, a negatively charged polysaccharide
from seaweed that forms hydrogels in the presence of calcium
ions, was initially developed for drug delivery [404,405] and it
is now under development for tissue engineering [406,407].
Alginate sponges with porosity being 90% and pore size in
the range of 50–150 mm were produced by the group of Cohen
and co-workers [408,409], using freeze-drying technique. The
collaborators Leor et al. [264] seeded foetal rat myocardial cells
into this sponge to form an engineered heart construct. After 4-
day culture in vitro, the engineered constructs were implanted
into the rat hearts with myocardial infarct, which were
harvested 9 weeks after implantation. A large number of
blood vessels were found in the grafting area, indicating
intensive neovascularisation. The specimens showed almost
complete disappearance of the scaffold and good integration
into the host.
In contrast to the control animals which developed
significant left ventricular dilatation accompanied by progres-
sive deterioration in left ventricular contractility, the graft-
treated rats showed attenuation of left ventricular dilatation and
unchanged contractility in the left ventricle [264]. To optimise
the alginate scaffolds, efforts have been invested to achieve 3D
high-density cardiac constructs with a uniform cell distribution
[410] and to enhance the vascularisation of the alginate
scaffolds by incorporating controlled release basic fibroblast
growth factor (bFGF) microspheres [411]. This was the first 3D
scaffold that was reported to improve the cardiac function of the
left ventricle.
Poly(glycolic acid) (PGA) and its copolymer with poly(-
lactic acid) (PLA). Scaffolds made by the electrospinning
technique from PGA, PLA or their copolymers (PLGA) have
long been investigated for the engineering of a variety of tissue
types by the MIT and Harvard Medical School collaboration
since 1991 [65,73,412,413]. The first formally published work on
a synthetic polymer-based scaffold designed for cardiac muscle
engineering was produced by Freed and Vunjak-Novakovic in
1997 [265]. In this pioneering work, it was demonstrated that
cultivation of primary neonatal rat cardiomyocytes on highly
porous (porosity being 97%) PGA scaffolds in bioreactors could
result in contractile 3D cardiac-like tissues (not constructs),
which consisted of cardiomyocytes with cardiac-specific
structural and electrophysiological properties, contracting
spontaneously and synchronously [265,414]. To the knowledge
of the present authors, this is the first achievement of engineered
beating tissue on synthetic polymers, though the visible
spontaneous contractions in constructs were not comparable
to those of native ventricles and eventually ceased after 4 days of
cultivation [414].
The drawback associated with the critical thickness of the
engineered tissue constructs was investigated systematically by
this group. After one week, a peripheral tissue-like region (50–
70 mm thick) was observed [414]. The small thickness of the
cardiac muscle-like zone in constructs, including both synthetic
and natural polymer scaffolds, was attributed to the poor mass
transportation in the construct centre [74,415]. In the
subsequent studies, efforts were invested to overcome the
limitation on the thickness of engineered tissue through
improving cell seeding and tissue culturing conditions as
follows:
(1) c
ell seeding density [416–418];(2) c
ell seeding vessel, using rotating vessels (laminar flow)rather than mixed flasks (turbulent flow) [416,419];
(3) t
issue culture vessel, using dynamic (i.e. rotating) ratherthan static conditions [416,419,420];
(4) i
mprovement of gas exchange [421,422];(5) p
erfusion of medium through the construct (perfusionbioreactor) [417,422,423];
(6) l
aminin-coated PGA sponge [414,416,419];(7) u
se of collagen scaffolds instead of PGA scaffolds[417,418].
In summary, with three investigated scaffolds (including
collagen sponges, gels or PGA), cultivations performed in
dishes, static or mixed (turbulent flow) flasks or rotating
(laminar flow) bioreactors yielded constructs with a thin (0.1–
0.2 mm) peripheral layer [419] of tissue expressing markers of
cardiac differentiation and able to propagate electrical signals.
The non-uniform cell distribution is a result of oxygen
diffusional limitations within the constructs. It was also found
that cultivation with perfusion of culture medium through the
construct could enhance the convective-diffusive oxygen
supply and yield a 1–2 mm thick construct [423] (this equals
to a 0.5–1 mm thick peripheral layer) with physiologically high
and spatially uniform distribution of viable cells expressing
cardiac markers [74,269].
Poly(e-caprolactone) (PCL) and its copolymer with poly(-
lactic acid) (PLA). PCL is another important member of the
aliphatic polyester family. It has been used to effectively entrap
antibiotic drugs, and constructs made with PCL have been
considered as drug delivery systems. The degradation of PCL
and its copolymers involves similar mechanisms to PLA,
proceeding in two stages: random hydrolytic ester cleavage and
weight loss through the diffusion of oligometric species from
the bulk.
Vacanti’s group [267] demonstrated the formation of
contractile cardiac grafts in vitro using a nanofibrous PCL
mesh. The nanofibrous mesh, which was produced by the
electrospinning technique, had an extracellular matrix-like
topography. The average fibre diameter of the scaffold was
about 250 nm, well below the size of an individual
cardiomyocyte. After neonatal rat cardiomyocytes were seeded
in the nanofibrous mesh, the construct was cultured, while
being suspended across a wire ring that acted as a passive load
to contracting cardiomyocytes. The cardiomyocytes started

Q.-Z. Chen et al. / Materials Science and Engineering R 59 (2008) 1–3726
beating after 3 days and were cultured in vitro for 14 days. The
cardiomyocytes attached well on the PCL meshes and
expressed cardiac-specific proteins such as alpha-myosin
heavy chain, connexin-43 and cardiac troponin I. This work
indicated that using this technique, cardiac grafts can be
matured in vitro to obtain sufficient function prior to
implantation [267].
The subsequent work of the same group [333] demonstrated
the formation of thick cardiac grafts in vitro and the versatility
of biodegradable electrospun meshes for cardiac tissue
engineering. To construct 3D cardiac grafts, the cell-seeded
cardiac nanofibrous PCL meshes were overlaid between days 5
and 7 of the in vitro culture period. In addition to well-attached
and strongly beating cells throughout the experimental period,
constructs with up to five layers could be cultured without any
incidence of core necrosis. The layers adhered intimately, with
morphologic and electrical communication being established
between the layers, as verified by means of histology and
immunohistochemistry as well as synchronized beating. It is
envisioned that cardiac grafts with clinically relevant dimen-
sions can be created by using this approach and combining it
with new technologies to induce vascularisation.
Along with the gelatin meshes, PCL, PGL or PCL-co-PLLA
have also been investigated in vivo to replace the right
ventricular outflow tract due to their relatively slow degradation
kinetics [401–403].
Poly(glycerol-sebacate) (PGS). As discussed in Section
3.2.1.3, the mechanical and structural properties of a 3D tissue
engineered construct should closely resemble those of living
tissues that they intend to replace. To engineer the myocardial
tissue, which beats cyclically and constantly throughout life,
the biomaterial should be as soft and elastic as heart muscle.
These mechanical characteristics are impossible to reproduce
with polyester-based thermoplastic polymers, such as PGA,
PLA, PCL and their copolymers, because they undergo
plastic deformation and failure when exposed to long-term
cyclic strain. The limitation of their use in engineering soft
tissues has made scientists turn to elastomers for cardiac tissue
engineering.
It has been mentioned that PGS with a wide range of
stiffness has been developed for the heart patch approach by the
present authors [364]. Actually this material could also be
applied to build 3D tissue engineering scaffolds, and perhaps is
the most promising material to date. The PGS synthesised at
110 8C has stiffness of several tens kPa, which is in the range of
passive stiffness of the healthy human heart muscle. PGS also
has a tailorable biodegradability, from being degradable in a
couple of weeks to being nearly non-degradable. Initial in vitro
cell culture showed that PGS was biocompatible with
cardiomyocytes, with the human embryonic stem cell-derived
cardiomyocytes beating for at least 2 months when cultured on
the synthesised PGS. Hence, PGS is a very promising soft
elastomer for heart tissue engineering.
Poly(ester urethane) urea (PEUU) and poly(1,3-trymethy-
lene carbonate) (PTMC). 3D PEUU scaffolds have been
fabricated by the electrospinning technique [378,424,425].
Electrospun PEUU is elastomeric and allows for the control of
fibre diameter, porosity, and degradation rate through a variety
of fabrication parameters. The PEUU constructs integrated with
smooth muscle cells were flexible and have anisotropic
mechanical properties, with stiffness ranging form 1.7 to
2.5 MPa on the material axis, which is close to that of the
human heart muscle at the end of diastole [378]. To the
knowledge of the present authors, the use of 3D electrospun
PEUU scaffolds in the myocardial tissue engineering has not
been explored, and would be an interesting topic.
Poly(TMC) is surface erodible elastomers designed for soft
tissue engineering. It has been copolymerised with epsilon-
caprolactone (CL) [337] and DLLA [426,427] to modify its
biodegradability and mechanical properties. The application of
poly(TMC) for heart muscle engineering has been investigated
to a very limited extent [427].
Challenges in 3D engineered myocardial constructs. No
matter what types of biomaterials they are built from, the
utilisation of artificial matrices (scaffolds) to engineer
myocardium has been rather disappointing, with no examples
of human application to date. The limitations are not only set by
cell related issues (such as scale up in a rather short period,
efficiency of cell seeding or cell survival rate, and immune
rejection), but also caused by the quality of the engineered
tissue construct.
First of all, engineered heart muscle must develop systolic
(contractive) force with appropriate compliance, at the same
time it must withstand diastolic (expansive) loads. This
mechanical requirement on the engineered construct is proved
to be a tough task for biomaterial scientists, as discussed
below. The material used to build the construct has no ability
to beat without cells. The contractile movement of the
engineered construct is completely driven by the seeded
myocardial cells that inherently have a beating ability. One
can envisage that the transfer of mechanical signals from cells
to the scaffold would be jeopardized if the scaffold material is
too stiff. Then the question is how soft the material should be?
The obvious answer is that the compliance should be that of
the collagen matrix of the heart muscle. One can see from
Table 14 that most of these biomaterials, including collagen
fibres, are much stronger than myocardium. This explains
why most solid engineered constructs lack contractile
function. An exception is the beating collagen rings produced
by Zimmermann et al. [64]. On the other hand, collagen gels
are too weak. The data in the table indicates that PGS could be
the most promising candidate from the mechanical compat-
ibility point of view. However, there is another hurdle,
nonlinear elasticity of heart muscle. Given the complex
anisotropic mechanical behaviour of heart muscle, it is by no
means an easy task to synthesize a polymer that responses to
stresses the way heart muscle does. Without an adequate
mechanical environment, the engineered tissue would develop
into poor tissue organisation. This is because the potential of
cardiac myocytes to organise into a 3D force-generating unit
is limited when they are forced to seed a structurally defined
environment when solid matrices are employed. The poor
organisation of cardiomyocytes in turn leads to a weak
electrical and functional syncytium.

Fig. 14. Schematic illustration showing surgical procedure of heterotypic heart
transplantation using PTFE. After cold cardioplegia and explantation, (A) a 6-
mm long ventriculotomy was created lateral to the left anterior descending
artery, and (B) the 4 mm � 4 mm � 2 mm patches were implanted into the left
ventricle (C) to enlarge the ventricular cavity [222]. Reprinted with permission
from Elsevier.
Q.-Z. Chen et al. / Materials Science and Engineering R 59 (2008) 1–37 27
Another equally critical issue is size limitation, which is
still a barrier common to most tissue engineering approaches.
Perfusion in vitro may improve the nutrient supply to augment
the size of the engineered constructs. However, once they are
implanted in vivo, the thick tissue will need to be vascularised
so that the cells within will receive the necessary nutrients and
waste products will be removed. Hence, vascularisation will
be a crucial step in the development of any engineered tissue
construct. Previous work [238,329–331] has shown that
angiogenesis, which can occur in many biological tissues
without large pores, does not always succeed with synthetic
scaffolds. It has been reported that necrosis occurs in the core
regions of synthetic scaffolds of low porosity due to the
obstruction of the material [74]. To ensure the smooth
regeneration of the vascular tissue without blocking by the
biomaterial, a 3D scaffold should have reasonably large pore
size (perhaps >300 mm) [238,329–331], as discussed in
Section 3.2.1.4. However, the highly open porosity in the
scaffolds ironically would provide insufficient surface areas
for cells to attach and proliferate. This issue could probably be
addressed by filling the scaffolds with cell-seeded collagen
gels, as previous work has shown that collagen gels do not
obstruct mass transportation and vascularisation [77]. To
promote vascularisation, vascular growth factors (VGF)
incorporated by the gene delivery techniques and an optimal
stem cell type (i.e. mesenchymal stem cells) could be applied
to engineer the constructs. This combinatorial paradigm
might ultimately bring tissue engineering into clinical
application.
3.2.2.3. Nondegradable polymers used for the treatment of
congenital heart diseases. It is well documented that
polytetrafluoroethylene persist at the site of reconstruction
for the life of the repair [222]. For the treatment of certain
congenital heart diseases, Krupnick et al. [222] have developed
an in vivo model of ventricular tissue engineering using
heterotypic heart transplantation and polytetrafluoroethylene
(PTFE)–polylactide meshes combined with types I and IV
collagen gels. In this work, solid scaffolds were made of PGA–
PTFE or PLLA–PTFE. Liquid types I and IV collagen hydrogel
mixture was poured into 4 mm � 4 mm � 2 mm PGA- or
PLLA-based meshes to produce initial scaffolds. Then isolated
mesenchymal progenitor cells were seeded into the above
constructs to form patches. This was followed by overnight
incubation before implantation into syngeneic rats.
The surgical procedure is shown in Fig. 14. In brief, after
cold cardioplegia and explantation, a 6-mm long ventriculot-
omy was created in lateral position to the left anterior
descending artery, and the 4 mm � 4 mm � 2mm cell-seeded
patches were sutured into the left ventricle to enlarge the
ventricular cavity. The assessment duration was up to 1 month.
Successful transplantation and differentiation of mesenchymal
progenitor cells were accomplished using this approach [222].
The outcomes were also encouraging:
(1) T
he constructs resulted in minimal inflammation withoutaneurysmal dilatation.
(2) N
o ventricular arrhythmias resulted from this surgicalmanipulation and echocardiography revealed both end
systolic and diastolic volume augmentation with ventricular
expansion (note: ventricular expansion is desirable in the
case of systolic dysfunction).
3.2.2.4. Nondegradable polymers used for passive diastolic
constraint. To prevent the negative left ventricular remodel-
ling and left ventricular dilation associated with myocardial
infarction, many studies have examined the use of biomaterial
supports to restrain the left ventricle.
Poly( propylene) (PP) used as heart patches. Kelley et al.
[25] first demonstrated that restraining expansion of acute
myocardial infarctions preserves left ventricle geometry and
function. In this work, a poly(propylene) (Marlex) mesh was
sutured onto the myocardium of sheep at the location of a
subsequently induced myocardial infarction (Fig. 4a without
cells). Bowen et al. [296] demonstrated that restraining acute
infarct expansion with poly(propylene) decreases collagenase
activity in borderzone myocardium. However, the matrix
components of the heart muscle were unchanged within the
infarct region. The work by Enomoto et al. [26] indicated that
stiffening only the infarct region may not be sufficient.
Poly(ethylene terephthalate) (PET) used as heart wrapping
jackets. Other type of left ventricle restraint consisting of a
knitted PET mesh has been developed by Acorn Cardiovascular
Inc. The cardiac support device (CSD) is fitted around both
ventricles (Fig. 2). Investigations with canine and ovine models
showed that CSD decreased left ventricular end-diastolic
volume, myocyte hypertrophy and interstitial fibrosis
[275,276], and increased ejection fraction after myocardial
infarction [27,277,280,282,283,428]. Saavedra et al. [274]
further demonstrated that reverse remodelling with reduced
systolic wall stress and improved adrenergic signalling could be

Q.-Z. Chen et al. / Materials Science and Engineering R 59 (2008) 1–3728
achieved by passive external support that does not generate
diastolic constriction.
Key issues. Acorn’s clinical trial encompassing 300 patients
initially reported that the CSD reduced left ventricle diastolic
volume, improved the life quality of patients [18,286].
However, the significance of the study has been questioned
because of the partial recruitment of patients in an unblended
way, the influence of missing data, and the conflicting results on
beneficial effects [24]. Therefore, this strategy should be taken
with caution, and there exists a need for more long-term follow-
up data and a more thorough investigation on the exact
mechanisms behind left ventral restraint [24].
3.2.2.5. Scaffold-free myocardial tissue engineering. This
strategy is based on the self-assembling properties of
cardiomyocytes, aiming to generate scaffold-free 3D tissue
constructs. The materials involved in this approach are used as
cell culture supports in vitro.
Polystyrene (culture plates and microcarrier beads). Akins
et al. [429,430] made a first attempt to generate scaffold-free
myocardial tissue constructs, using polystyrene tissue culture
plates and polystyrene microcarrier beads. Kelm et al. [431]
further refined this approach and obtained highly organized 3D
micro-tissue with cardiac phenotypic characteristics. In a
similar approach, Baar et al. [432] obtained spontaneously
beating cylindrical construct.
Thermo-responsive poly(N-isoproplylacrylamide) (PNI-
PAAm). PNIPAAm is a special biocompatible polymer shown
to be temperature-responsive. This material was developed by a
research group in Japan [312,433–439] as a cell culture
substrate ex vivo, rather than used as an implant in the body.
This culture surface is slightly hydrophobic and cell-adhesive
under culture condition at 37 8C and change reversely to
become hydrophilic and non-cell-adhesive below 32 8C due to
rapid hydration and swelling of grafted PNIPAAm. Unlike the
cells undergoing enzymatic digestion (e.g. trypsinisation), cell-
to-cell junction and adhesive proteins within confluent cultured
cells are completely preserved during detachment from
PNIPAAm surface. Eventually an intact cell sheet is produced.
The monolayer sheets can be overlaid to form multi-layered
sheets, which are eventually grafted to the heart without any
artificial scaffolds. So far, this group has produced cell sheets
using various types of cells [310,311,315,440–443], including
cardiomyocytes [310,311,315].
The myocardial cell sheets were first built by Shimizu et al,
and assessed both in vitro and in vivo [310,311,444]. Neonatal
rat cardiomyocyte sheets detached from PNIPAAm-grafted
surfaces were overlaid to construct multilayer cardiac grafts.
Layered cell sheets began to pulse simultaneously and
morphological communication was established between the
sheets. In vivo, layered cardiomyocyte sheets were transplanted
into subcutaneous tissues of nude rats. The microvasculature of
the grafts was rapidly organized within a few days with graft
beatings observed by naked eyes 3 days after transplantation.
The macroscopic beating of the grafts was preserved up to 1
year [444], confirming their ability for long-term survival.
Histological studies showed characteristic structures of heart
tissue, including elongated cardiomyocytes, well-differentiated
sarcomeres, and gap junctions within the grafts. These results
demonstrate that electrically communicative pulsatile 3D
cardiac constructs were achieved both in vitro and in vivo by
layering cardiomyocyte sheets. [310,311,444].
Recently, autologous myocardial cell sheets were grafted to
rats [445] and hamsters [446] with myocardial infarction
(Fig. 3) [46]. The cardiomyocyte sheets became attached to and
integrated with the infarcted myocardium, showed angiogen-
esis, expressed connexin-43, and appeared as homogeneous
tissue in the myocardium. Overall, cardiomyocyte sheets
improved cardiac performance in ischemic myocardium when
compared with fibroblast sheets in infarcted myocardium [445],
myoblast injection, and sham operation [446]. The prolonged
life expectancy was considered due to a reduction in
myocardial fibrosis and re-organization of the cytoskeletal
proteins in hamsters.
Without the use of any additional materials such as carrier
substrates or scaffolds, cell-sheet engineering avoids the
complications associated with traditional tissue engineering
approaches such as host inflammatory responses to implanted
polymer materials. Cell sheet engineering thus presents
significant advantages and can overcome some of the problems
that have restricted tissue engineering with biodegradable
scaffolds [46,447]. The above-described approach holds an
enormous potential in cardiac tissue engineering if combined
with the computer-aided design (CAD) technology [52].
4. Biomimetic tissue engineering—bioreactors
4.1. Brief history of bioreactors
A bioreactor is an apparatus that attempts to mimic
biological conditions in order to maintain and encourage
tissue regeneration [448]. In a bioreactor, a dynamic culture
environment, which mimics in vivo physiochemical (e.g.
temperature, pO2, pH, and pCO2), electrical and mechanical
conditions, is constantly maintained.
The development of bioreactors used for research in tissue
engineering was fuelled by the rather disappointing results of in
vitro tissue regeneration in dishes. Under static culture
conditions, cell growth rates are diffusionally limited due to
increasing cell mass and decreasing effective implant porosity
resulting from extracellular matrix regeneration. It has been
widely recognised that bioreactors are essential for the research
in tissue engineering. In the body, cells are always stimulated
by mechanical, electrical and chemical signals that influence
their biological behaviour. If these signals are inadequate or
non-existent, cells dedifferentiate, become disorganised, and
eventually die. In fact, biological tissues adapt their structure
and composition to surrounding specifically functional
demands [448]. Placing cells alone or only in contact with
materials in culture medium is not enough to obtain a functional
tissue. Therefore, bioreactors are particularly crucial for the
regeneration of complex 3D tissues, such as heart.
The world saw the first tissue engineering bioreactor in
1993, which was invented by Langer’s group for cartilage tissue

Fig. 15. Schematics of four types of tissue engineering bioreactors: (a) static; (b) mixed; (c) rotating; (d) perfusion bioreactors [412].
Q.-Z. Chen et al. / Materials Science and Engineering R 59 (2008) 1–37 29
engineering [412]. Since then, studies on the development and
application of tissue engineering bioreactors have been rapidly
spreading throughout the world, involving actually all types of
tissues in the body. With the use of bioreactors, the products of
in vitro engineered skin and cartilage are commercially
available. Bioreactors have also improved the quality of
engineered corneas, bones, urethras, and pancreatic islets such
that they are currently under in vivo trial in humans [448]. A
number of comprehensive reviews on bioreactors are available
[74,269,448–450].
4.2. Comparison of bioreactors
Bioreactors can be grouped into four types: i.e. static, mixed
(turbulent flow), rotating (laminar flow), and perfusion
bioreactors [269]. Fig. 15, which is adapted from Ref. [451],
shows the four types of bioreactors. The major characters of
these four types of bioreactors are summarised as follows (see
Table 15 as well) [269,449]:
(1) I
Tabl
Cha
Bior
Stati
Mix
Rota
Perf
n a static flask, the cultured tissue is fixed in place and
exposed to motionless medium. Hence, mass transportation
occurs through molecular diffusion, and there is no shear
stress on the cells.
(2) I
n a mixed flask, tissues are fixed in place and exposed to awell-mixed medium. The mixing is achieved via flask
spinning. Hence, the mass transportation in the medium
occurs via turbulence. Turbulent flow can produce severe
shear stresses on cells at the construct surface such that it
might cause cell damage or death. Within the tissue
construct, the mass transportation is governed by molecular
diffusion.
(3) I
n a rotation chamber, the tissue constructs are suspended inculture medium. The lateral chamber rotates slowly such
that the tissue constructs can fall by gravity. The slow
e 15
racters of four types of bioreactors
eactor Mass transportation
c No fluid flow in the culture media, so mass transportation occ
ed Mass transportation occurs via turbulent fluid flow in medium
diffusion within the construct
ting Fluid flow is laminar, so mass transportation is by convection
governed by diffusion within the constructs
usion Mass transfer is by pressing a medium to flow through a tissu
transportation is by convection both in the medium and withi
rotation encourages the uniform growth of the tissues. In the
meantime, it decreases mechanical flow stresses in the
medium, and thus alleviates the situation of surface cell
damage and death. The slow rotation also protects fragile
tissues from cracking. However, the mass transportation
with the constructs is still controlled by molecular diffusion.
(4) I
n a perfusion bioreactor, constructs are cultivated withdirect perfusion of culture medium through the cultured
tissue construct, in order to achieve convective-diffusive
oxygen transportation throughout the construct volume
[269].
Most recently, Bilodeau and Mantovani [448] made a specific
review, focusing on the mechanical environment of various types
of bioreactors and its effects on cultured tissue. They concluded
that rotating bioreactors are more suitable for the culture of
fragile tissues, such as cartilage, while static perfusion
bioreactors are better for the culture of tissues with complex
geometry that normally subjects to higher mechanical constrains
in the body. Advantages and disadvantages of these two types of
bioreactors for different tissue cultures are given in Table 16.
4.3. Application of bioreactors in myocardial tissue
engineering
In myocardial tissue engineering bioreactors are very
important to grow the constructs in which the regeneration
of lost cardiac functions is achieved via providing the right
mechanical and physiological properties. However, studies on
the in vitro culture of cardiac muscle constructs are more
complex, less advanced and rarer than those on cartilage. The
effects of culture parameters and their mechanisms are still
largely unknown. The advantage with using bioreactors is the
possibility of obtaining a better understanding of various
phenomena.
Mechanical condition
urs via molecular diffusion No shear stress on the cells
, and is governed by Severe shear stress on the cells
at the surface of the construct
in the medium, and is Mild shear stress
e construct. So mass
n the constructs
Mild shear stress

Table 16
Comparison of bioreactors used for different tissues [448]
Tissues Static/perfusion bioreactor Rotating bioreactor
Cartilage, bone, and ligament Possible application of mechanical stress Adequate exchange of nutrients and glass
Complex shape feasible Insufficient mechanical stresses
Blood vessels Possible application of mechanical stresses and strains Uniform culture
Complex shape feasible Insufficient mechanical stresses and strains
Myocardial tissues Mechanical stress too substantial A free-falling environment protests fragile issues
Heart valves Complex shapes feasible Insufficient mechanical stresses
Possible application of a flow
Q.-Z. Chen et al. / Materials Science and Engineering R 59 (2008) 1–3730
The bioreactor-based investigations on 3D cardiac muscle
constructs have experienced the processes of applying rotating
and then perfusion bioreactors. The first report on culturing
cardiac muscle constructs in bioreactors was by Freed and
Vunjak-Novakovic in 1997 [265]. In this work, mixed
bioreactors were used. Using this type of bioreactors, the
largest engineered tissue that could be achieved was a 50–
70 mm thick peripheral tissue-like layer [414]. The small
thickness of the cardiac muscle-like zone in constructs,
including both synthetic and natural polymer scaffolds, was
attributed to the poor mass transportation in the construct centre
[74,415]. Later Carrier et al. [416] discovered that a rotating
bioreactor improved cell quality, distribution, and metabolism
compared to static and mixed culture vessel. However, the
thickness of culture muscle tissue was still very limited. With
three types of scaffolds (including collagen sponges, gels or
PGA) cultivated in rotating (laminar flow) bioreactors, the best
result yielded constructs with a thin (100–200 mm = 0.1–
0.2 mm) peripheral layer [419]. The non-uniform cell
distribution was a result of oxygen diffusional limitations
within the constructs, although the mass transportation in the
medium was improved by the rotating condition.
In the subsequent studies, the group invested great efforts to
overcome the limitation on the thickness of engineered tissue
through improving cell seeding and bioreactor design [416–
423], as mentioned in Section 3.2.2.2 (PLA–PGA part).
Eventually, cultivations with perfusion of culture medium
through the construct enhance the convective-diffusive oxygen
supply and yield a 1–2 mm thick construct [423] (note: this
equals to a 0.5–1 mm thick peripheral layer) with physiolo-
gically high and spatially uniform distribution of viable cells
expressing cardiac markers [74,269].
It has been discovered that shear stresses as low as 0.1 Pa are
sufficient to harm cardiac myocytes. Adequate stresses to
encourage growth and differentiation of these cells are around
0.001 Pa, which can be obtained with a laminar flow in a
rotating bioreactor [448].
Fink et al. [452] studied the effects of strain (elongation)
instead of shear stresses. Instead being deteriorated, the cardiac
tissues responded to a 20% strain by hypertrophy. These tissues
had an increase of DNA and protein/cell ratios and an improved
organisation of the cells into parallel arrays. Also, the stretched
cells were longer and wider and the thickness distribution of
cells was more uniform than in the control tissues. Hence, it
would be of importance to investigate 3D heart muscle
regeneration by applying an elastomeric material and dynamic
mechanical conditions, which are similar to the mechanical
properties of the cardiac muscle and the heart beating process,
respectively.
4.4. Key issues
Although bioreactors have improved the in vitro tissue
culture, there are several limitations on their applications. They
do not regenerate completely native-like tissues. During
culture, there is always a period when the properties stop
improving, remain constant for a short periods, and then begin
to decline. Dynamic culture lessens this phenomenon, but it
does not eradicate it. The maximum volume of tissue that can
be regenerated without developing an appropriate vessel tree
into the tissue is approximately 3 mm [448]. From the clinical
point of view, engineered tissue constructs could be used in situ
to enhance its function. The body would be its own bioreactor
and allow for infiltration of cells within the scaffold matrix to
regenerate myocardial muscle and blood vessels. However,
necrosis has been reported at the core regions of implanted 3D
scaffolds. Hence, vascularisation is also one of key issues in the
development of 3D tissue culture system.
In addition, specific tissue culture requires specific design
parameters on bioreactors. The physiological, biochemical,
electrical and mechanical controls, which are essential in cell
and tissue cultures, have not been achieved for most tissue
cultures. For myocardial tissue engineering, the bioreactor that
mimics contractile and electrical activities of the heart is a
particularly important issue.
5. Summary
Heart muscle engineering aims to regenerate functional
myocardium to repair diseased and injured heart. Several
strategies and their approaches have been established over the
last decade (Table 1). Among all types of cells applied so far,
embryonic stem cells and cloned cells seem to be most
promising. Different approaches have different requirements on
biomaterials. Hence, material scientists should select and
design biomaterials according to the specific approach they
have adopted. Myocardial tissue engineering encounters a
variety of challenges, which are grouped into three categories
associated with cells, materials and vascularisation, as
summarised in Table 17. A combinatory paradigm, which

Table 17
Major challenges in myocardial tissue engineering
1. Challenges associated with cells
Cell sourcing, cell scale-up, cell delivery and immune rejection
2. Challenges associated with biomaterials and scaffolds
One of the challenges in myocardial tissue engineering is to design and fabricate mechanically compatible materials and scaffolds that have nonlinear
elasticity similar to the heart muscle and thus can develop synchronically beating with the recipient heart
3. Challenges associated with vascularisation
After transplantation, rapid vascularisation is the critical step for the subsequent events: adequate mass transportation, cell survival, integration and function of
the engineered cardiac constructs. The maximum volume of tissue that can be regenerated without developing an appropriate vessel tree into the tissue is
approximately 3 mm, which is far too smaller than clinical required size. Vascularisation remains the key factor in the transition of in vitro achievements into
effective therapeutic tool
Q.-Z. Chen et al. / Materials Science and Engineering R 59 (2008) 1–37 31
uses stem cells, signalling molecules (such as genes) and novel
biomaterials to enhance cell growth and proliferate, to
encourage vascularisation and to support the damaged heart,
will be needed to bring heart tissue engineering into clinical
application.
Acknowledgements
The authors would like to acknowledge financial support
from the UK Biotechnology and Biological Sciences Research
Council (BBSRC) (grant number BB/D011027/1).
References
[1] C.A. Vacanti, Tissue Eng. 12 (5) (2006) 1137–1142.
[2] http://en.wikipedia.org/wiki/List_of_causes_of_death_by_rate
(accessed in July 2007).
[3] http://www.acorncv.com/patients_families/heart_failure.cfm (accessed
in July 2007).
[4] M.R. Cowie, D.A. Wood, A.J.S. Coats, S.G. Thompson, V. Suresh, P.A.
Poole-Wilson, et al. Heart 83 (5) (2000) 505–510.
[5] M.K. Baig, N. Mahon, W.J. McKenna, A.L.P. Caforio, R.O. Bonow, G.S.
Francis, et al. Heart Lung 28 (2) (1999) 87–101.
[6] D.K. Burns, V. Kumar, in: V. Kumar, R.S. Cotran, S.L. Robbins (Eds.),
Robbins Basic Pathology, 7th ed., Saunders, Philadelphia, PA, 2003, pp.
361–394.
[7] J.B. Young, R.M. Mills, Clinical Management of Heart Failure, Profes-
sional Communications, Caddo, Okla, 2004.
[8] F.Y. Chen, L.H. Cohn, Cardiol. Rev. 10 (6) (2002) 326–333.
[9] M. Loebe, E. Soltero, V. Thohan, J.A. Lafuente, G.P. Noon, Curr. Opin.
Cardiol. 18 (3) (2003) 194–198.
[10] N.M. Hawkins, M.C. Petrie, M.R. MacDonald, K.J. Hogg, J.J.V. McMur-
ray, Eur. Heart J. 27 (11) (2006) 1270–1281.
[11] C. Martinez, A. Tzur, H. Hrachian, J. Zebede, G.A. Lamas, Am. J. Geriat.
Cardiol. 15 (2) (2006) 82–87.
[12] S.K. Kohli, P. Elliott, Br. J. Hosp. Med. 66 (8) (2005) 469–473.
[13] M. Packer, J. Card. Fail. 8 (4) (2002) 193–196.
[14] P. Zammaretti, M. Jaconi, Curr. Opin. Biotechnol. 15 (5) (2004) 430–
434.
[15] B.J. Miller, J.H. Gibbon, C. Fineberg, Med. Clin. North Am. 1 (1953)
1603–1624.
[16] D.N. Ross, Lancet 2 (1962) 487.
[17] A. Senning, J. Thorac. Cardiovasc. Surg. 54 (1967) 465–470.
[18] R.G. Walsh, Heart Fail. Rev. 10 (2) (2005) 101–107.
[19] S.L. Moainie, J.H. Gorman, T.S. Guy, F.W. Bowen, B.M. Jackson, T.
Plappert, et al. Ann. Thorac. Surg. 74 (3) (2002) 753–760.
[20] J.C. Chachques, A. Berrebi, A. Hernigou, A. CohenSolal, T. Lavergne,
J.P. Marino, et al. J. Heart Lung Transpl. 16 (8) (1997) 854–868.
[21] R. Lorusso, E. Milan, M. Volterrani, R. Giubbini, F.H. vanderVeen, J.J.
Schreuder, et al. Eur. J. Cardio-Thorac. Surg. 11 (2) (1997) 363–371.
[22] J.H. Oh, V. Badhwar, R.C.J. Chiu, J. Cardiac Surg. 11 (3) (1996) 194–
199.
[23] R.M. Eloakley, J.C. Jarvis, Circulation 90 (4) (1994) 2085–2090.
[24] K.L. Christman, R.J. Lee, J. Am. Coll. Cardiol. 48 (5) (2006) 907–
913.
[25] S.T. Kelley, R. Malekan, J.H. Gorman, B.M. Jackson, R.C. Gorman, Y.
Suzuki, et al. Circulation 99 (1) (1999) 135–142.
[26] Y. Enomoto, J.H. Gorman, S.L. Moainie, B.M. Jackson, L.M. Parish, T.
Plappert, et al. Ann. Thorac. Surg. 79 (3) (2005) 881–887.
[27] H.N. Sabbah, Ann. Thorac. Surg. 75 (6) (2003) S13–S19.
[28] www.acorncv.com/newsrelease12-08-06disputeresolutionpanelNO-
FINAL.pdf.
[29] G.Y. Koh, M.G. Klug, M.H. Soonpaa, L.J. Field, J. Clin. Invest. 92 (3)
(1993) 1548–1554.
[30] G.Y. Koh, M.H. Soonpaa, M.G. Klug, L.J. Field, Am. J. Physiol. 264 (5)
(1993) H1727–H1733.
[31] M.H. Soonpaa, G.Y. Koh, M.G. Klug, L.J. Field, Science 264 (5155)
(1994) 98–101.
[32] W. Roell, Z.J. Lu, W. Bloch, S. Siedner, K. Tiemann, Y. Xia, et al.
Circulation 105 (20) (2002) 2435–2441.
[33] J. Muller-Ehmsen, K.L. Peterson, L. Kedes, P. Whittaker, J.S. Dow, T.I.
Long, et al. Circulation 105 (14) (2002) 1720–1726.
[34] J. Muller-Ehmsen, P. Whittaker, R.A. Kloner, J.S. Dow, T. Sakoda, T.I.
Long, et al. J. Mol. Cell. Cardiol. 34 (2) (2002) 107–116.
[35] J. Muller-Ehmsen, K.L. Peterson, L. Kedes, P. Whittaker, J.S. Dow, T.I.
Long, P.W. Laird, R.A. Kloner, Circulation 105 (14) (2002) 1720–1726.
[36] S. Etzion, A. Battler, I.M. Barbash, E. Cagnano, P. Zarin, Y. Granot, et al.
J. Mol. Cell. Cardiol. 33 (7) (2001) 1321–1330.
[37] G. Condorelli, U. Borello, L. De Angelis, M. Latronico, D Sirabella, M.
Coletta, et al. Proc. Natl. Acad. Sci. U.S.A. 98 (19) (2001) 10733–10738.
[38] D. Orlic, J. Kajstura, S. Chimenti, I. Jakoniuk, S.M. Anderson, B.S. Li,
et al. Nature 410 (6829) (2001) 701–705.
[39] P. Menasche, A.A. Hagege, M. Scorsin, B. Pouzet, M. Desnos, D. Duboc,
et al. Lancet 357 (9252) (2001) 279–280.
[40] S. Tomita, R.K. Li, R.D. Weisel, D.A.G. Mickle, E.J. Kim, T. Sakai, et al.
Circulation 100 (19) (1999) 247–256.
[41] T. Sakai, R.K. Li, R.D. Weisel, D.A.G. Mickle, Z.Q. Jia, S. Tomita, et al.
J. Thorac. Cardiovasc. Surg. 118 (4) (1999) 715–724.
[42] H. Reinecke, M. Zhang, T. Bartosek, C.E. Murry, Circulation 100 (2)
(1999) 193–202.
[43] D.A. Taylor, B.Z. Atkins, P. Hungspreugs, T.R. Jones, M.C. Reedy, K.A.
Hutchinson, et al. Nat. Med. 4 (10) (1998) 1200–11200.
[44] M. Scorsin, A.A. Hagege, F. Marotte, N. Mirochnik, H. Copin, M.
Barnoux, et al. Circulation 96 (9) (1997) 188–193.
[45] R.K. Li, D.A.G. Mickle, R.D. Weisel, J. Zhang, M.K. Mohabeer, Circ.
Res. 78 (2) (1996) 283–288.
[46] J. Yang, M. Yamato, T. Okano, MRS Bull. 30 (3) (2005) 189–193.
[47] T. Eschenhagen, C. Fink, U. Remmers, H. Scholz, J. Wattchow, J. Weil,
et al. FASEB J. 11 (8) (1997) 683–694.

Q.-Z. Chen et al. / Materials Science and Engineering R 59 (2008) 1–3732
[48] Q.Z. Chen, S.E. Harding, N.N. Ali, A.R. Boccaccini, Chap 16: Myo-
cardial tissue engineering, in: A.R. Boccaccini, J. Gough (Eds.), Tissue
Engineering Using Ceramics and Polymers, Woodhead Publishing Lim-
ited, 2008.
[49] K.L. Fujimoto, K. Tobita, W.D. Merryman, J.J. Guan, N. Momoi, D.B.
Stolz, et al. J. Am. Coll. Cardiol. 49 (23) (2007) 2292–2300.
[50] S.T. Wall, J.C. Walker, K.E. Healy, M.B. Ratcliffe, J.M. Guccione,
Circulation 114 (24) (2006) 2627–2635.
[51] R.M. Nerem, in: R.P. Lanza, R. Langer, J.P. Vacanti (Eds.), Principles of
Tissue Engineering, 2nd ed., Academic Press, California, 2000, pp. 9–15.
[52] M.N. Giraud, C. Armbuster, T. Carrel, H.T. Tevaearai, Tissue Eng. 13 (8)
(2007) 1825–1836.
[53] Opinion on the State of the Art Concerning Tissue Engineering, Eur-
opean Commission health and Consumer Protection, http://ec.europa.eu,
2001.
[54] E. Bell, in: R.P. Lanza, R. Langer, J.P. Vacanti (Eds.), Principles of Tissue
Engineering, 2nd ed., Academic Press, California, 2000, pp. xxxv–xli.
[55] K. Mendelson, F.J. Schoen, Ann. Biomed. Eng. 34 (12) (2006) 1799–
1819.
[56] D. Schmidt, S.P. Hoerstrup, Swiss Med. Weekly 136 (39/40) (2006) 618–
623.
[57] I. Vesely, Circ. Res. 97 (8) (2005) 743–755.
[58] P.S. Malchesky, Artif. Organs 30 (3) (2006) 192–207.
[59] D.S. Vara, H.J. Salacinski, R.Y. Kannan, L. Bordenave, G. Hamilton,
A.M. Seifalian, Pathol. Biol. 53 (10) (2005) 599–612.
[60] S. Sarkar, T. Schmitz-Rixen, G. Hamilton, A.M. Seifalian, Med. Biol.
Eng. Comput. 45 (4) (2007) 327–336.
[61] L. Hecker, R.K. Birla, Regenerat. Med. 2 (2) (2007) 125–144.
[62] X.W. Wang, P. Lin, Q.H. Yao, C.Y. Chen, World J. Surg. 31 (4) (2007)
682–689.
[63] J. Leor, Y. Amsalem, S. Cohen, Pharmacol. Therapeut. 105 (2) (2005)
151–163.
[64] W.H. Zimmermann, I. Melnychenko, T. Eschenhagen, Biomaterials 25
(9) (2004) 1639–1647.
[65] L.G. Cima, J.P. Vacanti, C. Vacanti, D. Ingber, D. Mooney, J. Biomech.
Eng.-Trans. ASME 113 (2) (1991) 143–151.
[66] W.H. Zimmermann, T. Eschenhagen, Heart Fail. Rev. 8 (3) (2003) 259–
269.
[67] T. Eschenhagen, M. Didie, J. Heubach, U. Ravens, W.H. Zimmermann,
Transpl. Immunol. 9 (2–4) (2002) 315–321.
[68] T. Eschenhagen, J. Biotechnol. 118 (2005) S65–S165.
[69] M.J. Yost, R.L. Price, D.G. Simpson, W. Yan, L. Terracio, in: G.E. Wnek,
G.L. Bowlin (Eds.), Encyclopedia of Biomaterials and Biomedical
Engineering, Marcel Dekker, New York, 2004, pp. 273–282.
[70] S. Etzion, L.H. Kedes, R.A. Kloner, J. Leor, Am. J. Cardiovasc. Drugs 1
(4) (2001) 233–244.
[71] M. Shachar, S. Cohen, Heart Fail. Rev. 8 (3) (2003) 271–276.
[72] J. Leor, S. Cohen, Cardiac Engineering: From Genes and Cells to
Structure Function, New York Academic Sciences, New York, 2004 ,
pp. 312–319.
[73] J.J. Marler, J. Upton, R. Langer, J.P. Vacanti, Adv. Drug Deliv. Rev. 33 (1/
2) (1998) 165–182.
[74] M. Radisic, G. Vunjak-Novakovic, J. Serbian Chem. Soc. 70 (3) (2005)
541–556.
[75] S. Gerecht-Nir, M. Radisic, H. Park, C. Cannizzaro, J. Boublik, R.
Langer, et al. Int. J. Dev. Biol. 50 (2/3) (2006) 233–243.
[76] M. Papadaki, R. Langer, Basic Appl. Myol. 9 (4) (1999) 151–159.
[77] W.H. Zimmermann, M. Didie, S. Doker, I. Melnychenko, H. Naito, C.
Rogge, et al. Cardiovasc. Res. 71 (3) (2006) 419–429.
[78] M.E. Davis, P.C.H. Hsieh, A.J. Grodzinsky, R.T. Lee, Circ. Res. 97 (1)
(2005) 8–15.
[79] H.M. Nugent, E.R. Edelman, Circ. Res. 92 (10) (2003) 1068–1078.
[80] D. Bader, J.O. Oberpriller, J. Morphol. 155 (3) (1978) 349–357.
[81] J. Leor, M. Patterson, M.J. Quinones, L.H. Kedes, R.A. Kloner, Circula-
tion 94 (9) (1996) 332–336.
[82] R.K. Li, Z.Q. Jia, R.D. Weisel, D.A.G. Mickle, J. Zhang, M.K. Mohab-
eer, et al. Ann. Thorac. Surg. 62 (3) (1996) 654–660.
[83] R.K. Li, D.A.G. Mickle, R.D. Weisel, M.K. Mohabeer, J. Zhang, V. Rao,
et al. Circulation 96 (9) (1997) 179–186.
[84] M. Scorsin, F. Marotte, A. Sabri, O. LeDref, M. Demirag, J.L. Samuel,
et al. Circulation 94 (9 Suppl) (1996) II337–II340.
[85] M. Scorsin, A.A. Hagege, I. Dolizy, F. Marotte, N. Mirochnik, H. Copin,
et al. Circulation 98 (19) (1998) II151–II155.
[86] C.E. Murry, M.L. Whitney, M.A. Laflamme, H. Reinecke, L.J. Field,
Cold Spring Harbor Symp. Quan. Biol. 67 (2002) 519–526.
[87] G.Y. Koh, M.H. Soonpaa, M.G. Klug, H.P. Pride, B.J. Cooper, D.P. Zipes,
et al. J. Clin. Invest. 96 (4) (1995) 2034–2042.
[88] R.C. Chiu, Adv. Cardiovasc. Surg. 11 (1999) 69–98.
[89] J. Dorfman, M. Duong, A. Zibaitis, M.P. Pelletier, D. Shum-Tim, C. Li,
et al. J. Thorac. Cardiovasc. Surg. 116 (5) (1998) 744–751.
[90] B. Pouzet, J.T. Vilquin, A.A. Hagege, M. Scorsin, E. Messas, M. Fisz-
man, et al. Circulation 102 (19) (2000) 210–215.
[91] C.E. Murry, R.W. Wiseman, S.M. Schwartz, S.D. Hauschka, J. Clin.
Invest. 98 (11) (1996) 2512–2523.
[92] P. Menasche, Coronary Artery Dis. 16 (2) (2005) 105–110.
[93] M.G. Klug, M.H. Soonpaa, G.Y. Koh, L.J. Field, J. Clin. Invest. 98 (1)
(1996) 216–224.
[94] J.A. Thomson, J. Itskovitz-Eldor, S.S. Shapiro, M.A. Waknitz, J.J.
Swiergiel, V.S. Marshall, et al. Science 282 (5391) (1998) 1145–1147.
[95] C.S. McLachlan, B. Hambly, Z. Almsherqi, R. El Oakley, M.A. McGuire,
Lancet 367 (9507) (2006) 301–302.
[96] D.K. Singla, T.A. Hacker, L.N. Ma, P.S. Douglas, R. Sullivan, G.E.
Lyons, et al. J. Mol. Cell. Cardiol. 40 (1) (2006) 195–200.
[97] B.C. Heng, H. Liu, T. Cao, Med. Hypotheses 64 (6) (2005) 1085–1088.
[98] R.E. Bittner, C. Schofer, K. Weipoltshammer, S. Ivanova, B. Streubel, E.
Hauser, et al. Anat. Embryol. 199 (5) (1999) 391–396.
[99] A.A. Kocher, M.D. Schuster, M.J. Szabolcs, S. Takuma, D. Burkhoff, J.
Wang, et al. Nat. Med. 7 (4) (2001) 430–436.
[100] S. Itescu, M.D. Schuster, A.A. Kocher, Int. J. Artif. Organs 25 (7) (2002)
647–653.
[101] J. Bartunek, J.D. Croissant, B. De Bruyne, W. Wijns, M. Penicka, M.
Vanderheyden, et al. Circulation 110 (17) (2004) 69–169.
[102] N. Noiseux, M. Lopez-Iiasaca, M. Gnecchi, L.N. Zhang, S.D. Solomon,
V.J. Dzau, et al. Circulation 110 (17) (2004) 68–168.
[103] J. Yoon, B.G. Min, Y.H. Kim, W.J. Shim, Y.M. Ro, D.S. Lim, Acta
Cardiologica 60 (3) (2005) 277–284.
[104] S.L. Beeres, D.E. Atsma, A. van der Laarse, D.A. Pijnappels, J. van Tuyn,
W.E. Fibbe, A.A.F. de Vries, D.L. Ypey, E.E. van der Wall, M.J. Schalij,
J. Am. Coll. Cardiol. 46 (10) (2005) 1943–1952.
[105] Y.S. Yoon, N. Lee, H. Scadova, Biol. Cell 97 (4) (2005) 253–263.
[106] H.K. Haider, M. Ashraf, Am. J. Physiol.-Heart Circ. Physiol. 288 (6)
(2005) H2557–H2567.
[107] V. Planat-Benard, C. Menard, M. Andre, M. Puceat, A. Perez, J.M.
Garcia-Verdugo, et al. Circ. Res. 94 (2) (2004) 223–229.
[108] S. Etzion, I.M. Barbash, M.S. Feinberg, P. Zarin, L. Miller, E. Guetta, R.
Holbova, R.A. Kloner, L.H. Kedes, J. Leor, Circulation 106 (12 Suppl 1)
(2002) I125–I130.
[109] M. Scorsin, A. Hagege, J.T. Vilquin, I. Garcin, M. Fiszman, F. Marotte,
et al. Circulation 98 (17) (1998) 200–1200.
[110] M. Zhang, D. Methot, V. Poppa, Y. Fujio, K. Walsh, C.E. Murry, J. Mol.
Cell. Cardiol. 33 (5) (2001) 907–921.
[111] L. Reinlib, L. Field, Circulation 101 (18) (2000) E182–E187.
[112] P.D. Kessler, B.J. Byrne, Annu. Rev. Physiol. 61 (1999) 219–242.
[113] N. Varda-Bloom, J. Leor, D.G. Ohad, Y. Hasin, M. Amar, R. Fixler, et al.
J. Mol. Cell. Cardiol. 32 (12) (2000) 2141–2149.
[114] J.D. Hosenpud, L.E. Bennett, B.M. Keck, B. Fiol, M.M. Boucek, R.J.
Novick, J. Heart Lung Transpl. 18 (7) (1999) 611–626.
[115] O. Caspi, L. Gepstein, Eur. Heart J. Suppl. 8 (Suppl. E) (2006) E43–E54.
[116] M. Rubart, M.H. Soonpaa, H. Nakajima, L.J. Field, J. Clin. Invest. 114
(6) (2004) 775–783.
[117] D.A. Taylor, B.Z. Atkins, P. Hungspreugs, T.R. Jones, M.C. Reedy, K.A.
Hutcheson, et al. Nat. Med. 4 (8) (1998) 929–933.
[118] M. Scorsin, A. Hagege, J.T. Vilquin, M. Fiszman, F. Marotte, J.L.
Samuel, et al. J. Thorac. Cardiovasc. Surg. 119 (6) (2000) 1169–1175.

Q.-Z. Chen et al. / Materials Science and Engineering R 59 (2008) 1–37 33
[119] P. Menasche, A.A. Hagege, J.T. Vilquin, M. Desnos, E. Abergel, B.
Pouzet, et al. J. Am. Coll. Cardiol. 41 (7) (2003) 1078–1083.
[120] P.C. Smits, R.J.M. van Geuns, D. Poldermans, M. Bountioukos, E.E.M.
Onderwater, C.H. Lee, et al. J. Am. Coll. Cardiol. 42 (12) (2003) 2063–
2069.
[121] J. Herreros, F. Prosper, A. Perez, J.J. Gavira, M.J. Garcia-Velloso, J.
Barba, et al. Eur. Heart J. 24 (22) (2003) 2012–2020.
[122] F.D. Pagani, H. DerSimonian, A. Zawadzka, K. Wetzel, A.S.B.
Edge, D.B. Jacoby, et al. J. Am. Coll. Cardiol. 41 (5) (2003) 879–
888.
[123] T. Siminiak, R. Kalawski, D. Fiszer, O. Jerzykowska, J. Rzezniczak, N.
Rozwadowska, et al. Am. Heart J. 148 (3) (2004) 531–537.
[124] T. Siminiak, D. Fiszer, O. Jerzykowska, B. Grygielska, N. Rozwadowska,
P. Kalmucki, et al. Eur. Heart J. 26 (12) (2005) 1188–1195.
[125] T. Siminiak, D. Fiszer, O. Jerzykowska, M. Majewski, M. Kurpisz, J.
Am. Coll. Cardiol. 45 (3) (2005) 57A.
[126] N. Dib, R.E. Michler, F.D. Pagani, S. Wright, D.J. Kereiakes, R.
Lengerich, et al. Circulation 112 (12) (2005) 1748–1755.
[127] F.D. Pagani, H. DerSimonian, A. Zawadzka, D.B. Jacoby, J. Dinsmore, S.
Wright, et al. Circulation 106 (19) (2002) 463–1463.
[128] A.A. Hagege, J.P. Marolleau, J.T. Vilquin, A. Alheritiere, S. Peyrard, D.
Duboc, et al. Circulation 114 (2006) I108–I113.
[129] M.A. Laflamme, C.E. Murry, Nat. Biotechnol. 23 (7) (2005) 845–
856.
[130] C.E. Murry, L.J. Field, P. Menasche, Circulation 112 (20) (2005) 3174–
3183.
[131] K.T. Weber, Y. Sun, L.C. Katwa, Int. J. Biochem. Cell Biol. 29 (1) (1997)
31–42.
[132] R.S. Kellar, B.R. Shepherd, D.F. Larson, G.K. Naughton, S.K. Williams,
Tissue Eng. 11 (11/12) (2005) 1678–1687.
[133] C. Urbich, S. Dimmeler, Circ. Res. 95 (4) (2004) 343–353.
[134] L. Werner, V. Deutsch, I. Barshack, H. Miller, G. Keren, J. George, J.
Mol. Cell. Cardiol. 39 (4) (2005) 691–697.
[135] M.R. Alison, R. Poulsom, S. Forbes, N.A. Wright, J. Pathol. 197 (4)
(2002) 419–423.
[136] S. Wakitani, T. Saito, A.I. Caplan, Muscle Nerve 18 (12) (1995) 1417–
1426.
[137] S. Makino, K. Fukuda, S. Miyoshi, F. Konishi, H. Kodama, J. Pan, et al.
J. Clin. Invest. 103 (5) (1999) 697–705.
[138] I. Kehat, D. Kenyagin-Karsenti, M. Snir, H. Segev, M. Amit, A. Gepstein,
et al. J. Clin. Invest. 108 (3) (2001) 407–414.
[139] A. Vats, N.S. Tolley, J.M. Polak, L.D.K. Buttery, Clin. Otolaryngol. 27
(4) (2002) 227–232.
[140] A.M. Wobus, K.R. Boheler, Physiol. Rev. 85 (2) (2005) 635–678.
[141] M.F. Pittenger, A.M. Mackay, S.C. Beck, R.K. Jaiswal, R. Douglas, J.D.
Mosca, et al. Science 284 (5411) (1999) 143–147.
[142] D. Orlic, J. Kajstura, S. Chimenti, D.M. Bodine, A. Leri, P. Anversa,
Hematopoietic Stem Cells 2000 Basic and Clinical Sciences, New York
Academic Sciences, New York, 2001, pp. 221–230.
[143] C. Toma, M.F. Pittenger, K.S. Cahill, B.J. Byrne, P.D. Kessler, Circula-
tion 105 (1) (2002) 93–98.
[144] A.A. Mangi, N. Noiseux, D.L. Kong, H.M. He, M. Rezvani, J.S. Ingwall,
et al. Nat. Med. 9 (9) (2003) 1195–1201.
[145] M.F. Pittenger, B.J. Martin, Circ. Res. 95 (1) (2004) 9–20.
[146] S. Tomita, L. Ren-Ke, Z.Q. Jia, D.A.G. Mickle, R.D. Weisel, T. Sakai,
et al. Circulation 100 (18) (1999) 91–92.
[147] L.C. Amado, A.P. Saliaris, K.H. Schuleri, M. St John, J.S. Xie, S.
Cattaneo, et al. Proc. Natl. Acad. Sci. U.S.A. 102 (32) (2005)
11474–11479.
[148] K. Le Blanc, Cytotherapy 5 (6) (2003) 485–489.
[149] L.B. Balsam, A.J. Wagers, T. Kofidis, I.L. Weissman, R.C. Robbins, Am.
J. Transpl. 4 (2004) 469–1469.
[150] L.B. Balsam, A.J. Wagers, J.L. Christensen, T. Kofidis, I.L. Weissman,
R.C. Robbins, Nature 428 (6983) (2004) 668–673.
[151] C.E. Murry, M.H. Soonpaa, H. Reinecke, H. Nakajima, H.O. Nakajima,
M. Rubart, et al. Nature 428 (6983) (2004) 664–668.
[152] T. Asahara, T. Murohara, A. Sullivan, M. Silver, R. vanderZee, T. Li,
et al. Science 275 (5302) (1997) 964–967.
[153] T. Takahashi, C. Kalka, H. Masuda, D. Chen, M. Silver, M. Kearney, et al.
Nat. Med. 5 (4) (1999) 434–438.
[154] S. Shintani, T. Murohara, H. Ikeda, T. Ueno, K. Sasaki, J.L. Duan, et al.
Circulation 103 (6) (2001) 897–903.
[155] H. Kamihata, H. Matsubara, T. Nishiue, S. Fujiyama, Y. Tsutsumi, R.
Ozono, et al. Circulation 104 (9) (2001) 1046–1052.
[156] A. Kawamoto, T. Tkebuchava, J.I. Yamaguchi, H. Nishimura, C. Milli-
ken, O. Masuo, et al. Circulation 104 (17) (2001) 443–1443.
[157] A. Kawamoto, H.C. Gwon, H. Iwaguro, H. Masuda, S.I. Hayashi, C.
Kalka, et al. Circulation 102 (18) (2000) 5–15.
[158] S. Dimmeler, A.M. Zeiher, M.D. Schneider, J. Clin. Invest. 115 (3)
(2005) 572–583.
[159] B. Assmus, J. Honold, V. Schachinger, M.B. Britten, U. Fischer-Rasokat,
R. Lehmann, et al. N. Engl. J. Med. 355 (12) (2006) 1222–1232.
[160] V. Schachinger, S. Erbs, A. Elsasser, W. Haberbosch, R. Hambrecht, H.
Holschermann, et al. N. Engl. J. Med. 355 (12) (2006) 1210–1221.
[161] K. Lunde, S. Solheim, S. Aakhus, H. Arnesen, M. Abdelnoor, T. Egeland,
et al. N. Engl. J. Med. 355 (12) (2006) 1199–1209.
[162] J.M. Gimble, Exp. Opin. Biol. Ther. 3 (5) (2003) 705–713.
[163] J.M. Gimble, F. Guilak, Current Topics in Developmental Biology, vol.
58, Academic Press Inc., San Diego, 2003, pp. 137–160.
[164] A.M. Rodriguez, C. Elabd, E.Z. Amri, G. Ailhaud, C. Dani, Biochimie 87
(1) (2005) 125–128.
[165] J.M. Gimble, A.J. Katz, B.A. Bunnell, Circ. Res. 100 (9) (2007) 1249–
1260.
[166] J.B. Liu, Q.S. Hu, Z.L. Wang, C.S. Xu, X.H. Wang, G.R. Gong, et al.
Am. J. Physiol.-Heart Circ. Physiol. 287 (2) (2004) H501–H511.
[167] L. Wang, J. Deng, G. Li, J. Wang, B. Xiang, T. Kashour, et al. J. Mol.
Cell. Cardiol. 42 (2007) S97–S197.
[168] A.P. Beltrami, L. Barlucchi, D. Torella, M. Baker, F. Limana, S.
Chimenti, et al. Cell 114 (6) (2003) 763–776.
[169] H. Oh, S.B. Bradfute, T.D. Gallardo, T. Nakamura, V. Gaussin, Y.
Mishina, et al. Proc. Natl. Acad. Sci. U.S.A. 100 (21) (2003) 12313–
12318.
[170] O. Pfister, F. Mouquet, M. Jain, R. Summer, M. Helmes, A. Fine, et al.
Circ. Res. 97 (1) (2005) 52–61.
[171] E. Messina, L. De Angelis, G. Frati, S. Morrone, S. Chimenti, F.
Fiordaliso, et al. Circ. Res. 95 (9) (2004) 911–921.
[172] K.L. Laugwitz, A. Moretti, J. Lam, P. Gruber, Y.H. Chen, S. Woodard,
et al. Nature 433 (7026) (2005) 647–653.
[173] M.J. Shamblott, J. Axelman, J.W. Littlefield, P.D. Blumenthal, G.R.
Huggins, Y. Cui, et al. Proc. Natl. Acad. Sci. U.S.A. 98 (1) (2001) 113–
118.
[174] M.J. Evans, M.H. Kaufman, Nature 292 (5819) (1981) 154–156.
[175] G.R. Martin, Proc. Natl. Acad. Sci. U.S.A.-Biol. Sci. 78 (12) (1981)
7634–7638.
[176] M.J. Shamblott, J. Axelman, S.P. Wang, E.M. Bugg, J.W. Littlefield, P.J.
Donovan, et al. Proc. Natl. Acad. Sci. U.S.A. 95 (23) (1998) 13726–
13731.
[177] T.C. Doetschman, H. Eistetter, M. Katz, W. Schmidt, R. Kemler, J.
Embryol. Exp. Morphol. 87 (June) (1985) 27–45.
[178] J.Y. Min, Y.K. Yang, K.L. Converso, L.X. Liu, Q. Huang, J.P. Morgan,
et al. J. Appl. Physiol. 92 (1) (2002) 288–296.
[179] J.Y. Min, Y.K. Yang, M.F. Sullivan, Q.E. Ke, K.L. Converso, Y. Chen,
et al. J. Thorac. Cardiovasc. Surg. 125 (2) (2003) 361–369.
[180] J.Y. Min, Y. Chen, S. Malek, A. Meissner, M.X. Xiang, Q. Ke, et al. J.
Thorac. Cardiovasc. Surg. 130 (2) (2005) 547–553.
[181] J.Y. Min, X.L. Huang, M.X. Xiang, A. Meissner, Y. Chen, Q.G. Ke, et al.
J. Thorac. Cardiovasc. Surg. 131 (4) (2006) 889–897.
[182] A. Behfar, L.V. Zingman, D.M. Hodgson, J.M. Rauzier, G.C. Kane, A.
Terzic, et al. FASEB J. 16 (12) (2002) 1558–1566.
[183] A. Behfar, D.M. Hodgson, L.V. Zingman, C. Perez-Terzic, S. Yamada,
G.C. Kane, et al., Stem Cell Biology: Development and Plasticity, New
York Academic Sciences, New York, 2005, pp. 189–198.
[184] J. Nussbaum, E. Minami, M.A. Laflamme, J.A. Virag, C.B. Ware, A.
Masino, et al. FASEB J. 21 (7) (2007) 1345–1357.
[185] C. Menard, A.A. Hagege, O. Agbulut, M. Barro, M.C. Morichetti, C.
Brasselet, et al. Lancet 366 (9490) (2005) 1005–1012.

Q.-Z. Chen et al. / Materials Science and Engineering R 59 (2008) 1–3734
[186] C. Menard, C. Grey, A. Mery, D. Zeineddine, F. Aimond, M. Puceat, J.
Cell. Biochem. 93 (4) (2004) 681–687.
[187] R.J. Swijnenburg, M. Tanaka, H. Vogel, J. Baker, T. Kofidis, F. Gunawan,
et al. Circulation 112 (9) (2005) I166–I172.
[188] C.H. Xu, S. Police, N. Rao, M.K. Carpenter, Circ. Res. 91 (6) (2002)
501–508.
[189] C. Mummery, D. Ward-van Oostwaard, P. Doevendans, R. Spijker, S. van
den Brink, R. Hassink, et al. Circulation 107 (21) (2003) 2733–2740.
[190] I. Kehat, L. Gepstein, Heart Fail. Rev. 8 (3) (2003) 229–236.
[191] C.H. Xu, E. Rosler, J.J. Jiang, J.S. Lebkowski, J.D. Gold, C. O’Sullivan,
et al. Stem Cells 23 (3) (2005) 315–323.
[192] M.A. Laflamme, J. Gold, C.H. Xu, M. Hassanipour, E. Rosler, S. Police,
et al. Am. J. Pathol. 167 (3) (2005) 663–671.
[193] M. Snir, I. Kehat, A. Gepstein, R. Coleman, J. Itskovitz-Eldor, E. Livne,
et al. Am. J. Physiol.-Heart Circ. Physiol. 285 (6) (2003) H2355–H2363.
[194] L. Kehat, A. Gepstein, A. Spira, J. Itskovitz-Eldor, L. Gepstein, Circ.
Res. 91 (8) (2002) 659–661.
[195] J. Satin, L. Kehat, O. Caspi, I. Huber, G. Arbel, I. Itzhaki, et al. J.
Physiol.-Lond. 559 (2) (2004) 479–496.
[196] I. Kehat, L. Khimovich, O. Caspi, A. Gepstein, R. Shofti, G. Arbel, et al.
Nat. Biotechnol. 22 (10) (2004) 1282–1289.
[197] T. Xue, H.C. Cho, F.G. Akar, S.Y. Tsang, S.P. Jones, E. Marban, et al.
Circulation 111 (1) (2005) 11–20.
[198] R.J. Hassink, J.D. Dowell, A.B. de la Riviere, P.A. Doevendans, L.J.
Field, Trends Mol. Med. 9 (10) (2003) 436–441.
[199] J.D. Dowell, M. Rubart, K.B.S. Pasumarthi, M.H. Soonpaa, L.J. Field,
Cardiovasc. Res. 58 (2) (2003) 336–350.
[200] T. Reffelmann, R.A. Kloner, Cardiovasc. Res. 58 (2) (2003) 358–368.
[201] T. Reffelmann, J. Leor, J. Muller-Ehmsen, L. Kedes, R.A. Kloner, Heart
Fail. Rev. 8 (3) (2003) 201–211.
[202] J. Leor, I.M. Barbash, Exp. Opin. Biol. Ther. 3 (7) (2003) 1023–1039.
[203] J.A. Bradley, E.M. Bolton, R.A. Pedersen, Nat. Rev. Immunol. 2 (11)
(2002) 859–871.
[204] M. Drukker, G. Katz, A. Urbach, M. Schuldiner, G. Markel, J. Itskovitz-
Eldor, et al. Proc. Natl. Acad. Sci. U.S.A. 99 (15) (2002) 9864–9869.
[205] M. Drukkera, H. Katchmanb, G.F.S. Katzc, E.-T. Shezenb, E.E. Horn-
steina, et al. Stem Cells 24 (2006) 221–229.
[206] S.E. Harding, N.N. Ali, M. Brito-Martins, J. Gorelik, Pharmacol. Ther-
apeut. 113 (2) (2007) 341–353.
[207] I. Wilmut, A.E. Schnieke, J. McWhir, A.J. Kind, K.H.S. Campbell,
Nature 386 (6621) (1997) 200–1200.
[208] S.P. Bruder, A.I. Caplan, in: R.P. Lanza, R. Langer, J.P. Vacanti (Eds.),
Principles of Tissue Engineering, 2nd ed., Academic Press, California,
2000, pp. 683–696.
[209] J.R. Jones, L.L. Hench, Curr. Opin. Solid State Mater. Sci. 7 (4/5) (2003)
301–307.
[210] J.R. Jones, A.R. Boccaccini, in: M. Scheffler, P. Colombo (Eds.), Cellular
Ceramics: Structure, Manufacturing, Processing and Applications,
Wiley–VCH Verlag GmbH & Co. KGaA, Weinheim, 2005, pp. 550–573.
[211] B.L. Seal, T.C. Otero, A. Panitch, Mater. Sci. Eng. R-Rep. 34 (4/5) (2001)
147–230.
[212] A. Atala, R.P. Lanza, Methods of Tissue Engineering, Academic Press,
California, 2002.
[213] P.A. Gunatillak, R. Adhikari, Eur. Cells Mater. 5 (2003) 1–16.
[214] D. Garlotta, J. Polym. Environ. 9 (2001) 63–84.
[215] M.B. Yaylaoglu, C. Yildiz, F. Korkusuz, V. Hasirci, Biomaterials 20 (16)
(1999) 1513–1520.
[216] C. Du, F.Z. Cui, X.D. Zhu, K. de Groot, J. Biomed. Mater. Res. 44 (4)
(1999) 407–415.
[217] C.D. Brown, A.S. Hoffman, in: A. Atala, R.P. Lanza (Eds.), Methods of
Tissue Engineering, Academic Press, California, 2002, pp. 565–574.
[218] S.F. Badylak, Biomaterials 28 (25) (2007) 3587–3593.
[219] A. Atala, R.P. Lanza (Eds.), Methods of Tissue Engineering, Academic
Press, California, 2002.
[220] C.A. Vacanti, L.J. Bonassar, J.P. Vacanti, in: R.P. Lanza, R. Langer, J.P.
Vacanti (Eds.), Principles of Tissue Engineering, 2nd ed., Academic
Press, California, 2000, pp. 671–682.
[221] J.C. Middleton, A.J. Tipton, Biomaterials 21 (23) (2000) 2335–2346.
[222] A.S. Krupnick, D. Kreisel, F.H. Engels, W.Y. Szeto, T. Plappert, S.H.
Popma, et al. J. Heart Lung Transpl. 21 (2) (2002) 233–243.
[223] M. Taira, Y. Araki, J. Takahashi, J. Mater. Sci. Lett. 20 (2004) 1773–
1774.
[224] L.C. Lu, A.G. Mikos, in: J.E. Mark (Ed.), Polymer Data Handbook,
Oxford Press, Oxford, 1999, pp. 527–533.
[225] S.F. Yang, K.F. Leong, Z.H. Du, C.K. Chua, Tissue Engg. 7 (6) (2001)
679–689.
[226] L.C. Lu, A.G. Mikos, in: J.E. Mark (Ed.), Polymer Data Handbook,
Oxford Press, Oxford, 1999, pp. 566–569.
[227] S. Ramakrishna, Z.M. Huang, G.V. Kumar, A.W. Batchelor, J. Mayer, An
Introduction to Biocomposites, Imperial College Press, London, 2004.
[228] P.A. Gunatillake, R. Adhikari, Eur. Cells Mater. 5 (2003) 1–16.
[229] J.O. Iroh, in: J.E. Mark (Ed.), Polymer Data Handbook, Oxford Press,
Oxford, 1999, pp. 361–362.
[230] A. Baji, S.C. Wong, T.S. Srivatsan, G.O. Njus, G. Mathur, Mater. Manuf.
Process. 21 (2) (2006) 211–218.
[231] L. Calandrelli, B. Immirzi, M. Malinconico, S. Luessenheide, I. Pas-
saro, R. Di Pasquale, et al. J. Bioact. Compat. Polym. 19 (4) (2004) 301–
313.
[232] B.A. Ramsay, V. Langlade, P.J. Carreau, J.A. Ramsay, Appl. Environ.
Microbiol. 59 (4) (1993) 1242–1246.
[233] G.Q. Chen, Q. Wu, Biomaterials 26 (33) (2005) 6565–6578.
[234] N. Yoda, Die Markromol. Chem. 32 (2003) 1–12.
[235] M. Kellomaki, J. Heller, P. Tormala, J. Mater. Sci.-Mater. Med. 11 (6)
(2000) 345–355.
[236] J.H. Magill, in: J.E. Mark (Ed.), Polymer Data Handbook, Oxford Press,
Oxford, 1999, pp. 746–749.
[237] C.T. Laurencin, S. Lakshmi, in: Proceedings of the NATOASI Confer-
ence, Antalya, Turkey, September 1–12, (2003), pp. 281–300.
[238] D.W. Hutmacher, Biomaterials 21 (24) (2000) 2529–2543.
[239] Handbook of applied polymer processing technology, M. Dekker, New
York, 1996.
[240] L.C. Lu, A.G. Mikos, MRS Bull. 21 (11) (1996) 28–32.
[241] R.C. Thomas, A.K. Shung, M.J. Yaszemski, in: R.P. Lanza, R. Langer,
J.P. Vacanti (Eds.), Principles of Tissue Engineering, 2nd ed., Academic
Press, California, USA, 2000, pp. 251–262.
[242] M.S. Widmer, A.G. Mikos, in: C.W. Patrick, Jr., A.G. Mikos, L.V.
Mcintire (Eds.), Frontier in Tissue Engineering, Elsevier Science,
New York, 1998, pp. 107–120.
[243] A. Atala, R.P. Lanza (Eds.), Methods of Tissue Engineering, Academic
Press, California, 2002, pp. 681–740.
[244] S.F. Yang, K.F. Leong, Z.H. Du, C.K. Chua, Tissue Eng. 7 (6) (2001)
679–689.
[245] S.F. Yang, K.F. Leong, Z.H. Du, C.K. Chua, Tissue Eng. 8 (1) (2002) 1–
11.
[246] Q.Z. Chen, O. Bretcanu, A.R. Boccaccini, in: X. Liu, P. Chu (Eds.),
Handbook of Fabrication and Processing of Biomaterials, CRC Press
LLC, Boca Raton, FL, 2008, in press.
[247] A. Khademhosseini, G. Eng, J. Yeh, P.A. Kucharczyk, R. Langer, G.
Vunjak-Novakovic, et al. Biomed. Microdev. 9 (2) (2007) 149–157.
[248] M.E. Gomes, A.S. Ribeiro, P.B. Malafaya, R.L. Reis, A.M. Cunha,
Biomaterials 22 (9) (2001) 883–889.
[249] A.J. Salgado, O.P. Coutinho, R.L. Reis, Tissue Eng. 10 (3/4) (2004) 465–
474.
[250] X.H. Liu, P.X. Ma, Ann. Biomed. Eng. 32 (3) (2004) 477–486.
[251] J.J. Blaker, V. Maquet, R. Jerome, A.R. Boccaccini, S.N. Nazhat, Acta
Biomater. 1 (6) (2005) 643–652.
[252] D.W. Hutmacher, T. Schantz, I. Zein, K.W. Ng, S.H. Teoh, K.C. Tan, J.
Biomed. Mater. Res. 55 (2) (2001) 203–216.
[253] K.F. Leong, C.M. Cheah, C.K. Chua, Biomaterials 24 (13) (2003) 2363–
2378.
[254] C.M. Cheah, C.K. Chua, C.W. Lee, C. Feng, K. Totong, Int. J. Adv.
Manuf. Technol. 25 (3/4) (2005) 308–320.
[255] J.S. Temenoff, L. Lu, A.G. Mikos, in: J.E. Davies (Ed.), Bone Engineer-
ing, EM Squared, Toronto, 2000, pp. 455–462.
[256] T. Eschenhagen, W.H. Zimmermann, Circ. Res. 97 (12) (2005) 1220–
1231.

Q.-Z. Chen et al. / Materials Science and Engineering R 59 (2008) 1–37 35
[257] K.L. Christman, Q.Z. Fang, M.S. Yee, K.R. Johnson, R.E. Sievers, R.J.
Lee, Biomaterials 26 (10) (2005) 1139–1144.
[258] M.E. Davis, J.P.M. Motion, D.A. Narmoneva, T. Takahashi, D. Hakuno,
R.D. Kamm, et al. Circulation 111 (4) (2005) 442–450.
[259] T. Kofidis, P. Akhyari, B. Wachsmann, J. Boublik, K. Mueller-Stahl, R.
Leyh, et al. Eur. J. Cardio-Thorac. Surg. 22 (2) (2002) 238–243.
[260] T. Kofidis, P. Akhyari, J. Boublik, P. Theodorou, U. Martin, A. Ruhpar-
war, et al. J. Thorac. Cardiovasc. Surg. 124 (1) (2002) 63–69.
[261] T. Kofidis, A. Lenz, J. Boublik, P. Akhyari, B. Wachsmann, K.M. Stahl,
et al. Eur. J. Cardio-Thorac. Surg. 24 (6) (2003) 906–911.
[262] Z. Xiang, R.L. Liao, M.S. Kelly, M. Spector, Tissue Eng. 12 (9) (2006)
2467–2478.
[263] R.K. Li, Z.Q. Jia, R.D. Weisel, D.A.G. Mickle, A. Choi, T.M. Yau,
Circulation 100 (19) (1999) 63–69.
[264] J. Leor, S. Aboulafia-Etzion, A. Dar, L. Shapiro, I.M. Barbash, A. Battler,
et al. Circulation 102 (19) (2000) 56–61.
[265] L.E. Freed, G. VunjakNovakovic, In Vitro Cell. Dev. Biol.-Anim. 33 (5)
(1997) 381–385.
[266] O. Caspi, A. Lesman, Y. Basevitch, A. Gepstein, G. Arbel, I. Huber, et al.
Circ. Res. 100 (2) (2007) 263–272.
[267] M. Shin, O. Ishii, T. Sueda, J.P. Vacanti, Biomaterials 25 (17) (2004)
3717–3723.
[268] M. Radisic, W. Deen, R. Langer, G. Vunjak-Novakovic, Am. J. Physiol.
Heart Circ. Physiol. 288 (3) (2005) H1278–H1289.
[269] G. Vunjak-Novakovic, M. Radisic, B. Obradovic, J. Chem. Technol.
Biotechnol. 81 (4) (2006) 485–490.
[270] C. Alperin, P.W. Zandstra, K.A. Woodhouse, Biomaterials 26 (35) (2005)
7377–7386.
[271] T.C. McDevitt, K.A. Woodhouse, S.D. Hauschka, C.E. Murry, P.S.
Stayton, J. Biomed. Mater. Res. Part A 66 (3) (2003) 586–595.
[272] M.R. Brunstedt, N.P. Ziats, S.P. Robertson, A. Hiltner, J.M. Anderson,
G.A. Lodoen, et al. J. Biomed. Mater. Res. 27 (3) (1993) 367–377.
[273] M.R. Brunstedt, N.P. Ziats, M. Schubert, P.A. Hiltner, J.M. Anderson,
G.A. Lodoen, et al. J. Biomed. Mater. Res. 27 (2) (1993) 255–267.
[274] W.F. Saavedra, R.S. Tunin, N. Paolocci, T. Mishima, G. Suzuki, C.W.
Emala, et al. J. Am. Coll. Cardiol. 39 (12) (2002) 2069–2076.
[275] P.A. Chaudhry, P.V. Anagnostopouls, T. Mishima, G. Suzuki, H. Nair, H.
Morita, et al. J. Cardiac Surg. 16 (2) (2001) 118–126.
[276] P.A. Chaudhry, T. Mishima, V.G. Sharov, J. Hawkins, C. Alferness, G.
Paone, et al. Ann. Thorac. Surg. 70 (4) (2000) 1275–1280.
[277] J.J. Pilla, A.S. Blom, D.J. Brockman, V.A. Ferrari, D. Yuan, M.A. Acker,
J. Thorac. Cardiovasc. Surg. 126 (5) (2003) 1467–1476.
[278] H.N. Sabbah, Heart Fail. Rev. 10 (2) (2005) 109–115.
[279] S. Rastogi, R.C. Gupta, S. Mishra, H. Morita, E.J. Tanhehco, H.N.
Sabbah, J. Heart Lung Transpl. 24 (10) (2005) 1619–1625.
[280] H.N. Sabbah, J. Cardiac Fail. 10 (6) (2004) S207–S214.
[281] D.L. Mann, M.A. Acker, M. Jessup, H.N. Sabbah, R.C. Starling, S.H.
Kubo, J. Cardiac Fail. 10 (3) (2004) 185–192.
[282] J.J. Pilla, A.S. Blom, D.J. Brockman, F. Bowen, Q. Yuan, J. Giammarco,
et al. Circulation 106 (13) (2002) I207–I211.
[283] J.J. Pilla, A.S. Blom, J.H. Gorman, D.J. Brockman, J. Affuso, L.M.
Parish, et al. Ann. Thorac. Surg. 80 (6) (2005) 2257–2262.
[284] A.S. Blom, J.J. Pilla, R.C. Gorman, J.H. Gorman, R. Mukherjee, F.G.
Spinale, et al. Heart Fail. Rev. 10 (2) (2005) 125–139.
[285] A.S. Blom, R. Mukherjee, J.J. Pilla, A.S. Lowry, W.M. Yarbrough, J.T.
Mingoia, et al. Circulation 112 (9) (2005) 1274–1283.
[286] W.F. Konertz, J.E. Shapland, H. Hotz, S. Dushe, J.P. Braun, K. Stantke,
et al. Circulation 104 (12) (2001) I270–I275.
[287] A. Lembcke, S. Dushe, P.M. Dohmen, U. Hoffmann, B. Wegner, C.
Kloeters, et al. J. Heart Lung Transpl. 25 (1) (2006) 90–98.
[288] A. Lembcke, P.M. Dohmen, T.H. Wiese, D.E. Kivelitz, P. Rogalla, M.
Dewey, et al. Rofo-Fortschritte Auf Dem Gebiet Der Rontgenstrahlen
Der Bildgebenden Verfahren 177 (7) (2005) 946–954.
[289] A. Lembcke, S. Dushe, S. Sonntag, C. Kloeters, C.N.H. Enzweiler, T.H.
Wiese, et al. Ann. Thorac. Surg. 78 (3) (2004) 900–905.
[290] A. Lembcke, S. Dushe, C.N.H. Enzweiler, C. Kloeters, T.H. Wiese,
K.G.A. Hermann, et al. Eur. J. Cardio-Thorac. Surg. 25 (1) (2004)
84–90.
[291] A. Lembcke, T.H. Wiese, S. Dushe, H. Hotz, C.N.H. Enzweiler, B.
Hamm, et al. J. Heart Lung Transpl. 23 (1) (2004) 11–19.
[292] A. Franco-Cereceda, U. Lockwandt, A. Olsson, F. Bredin, G. Forssell, A.
Owall, et al. Scand. Cardiovasc. J. 38 (3) (2004) 159–163.
[293] A. Olsson, F. Bredin, A. Franco-Cereceda, Eur. J. Cardio-Thorac. Surg.
28 (3) (2005) 448–453.
[294] R.J. Pitsch, D.J. Minion, M.L. Goman, J.A. vanAalst, P.L. Fox, L.M.
Graham, J. Vasc. Surg. 26 (1) (1997) 70–78.
[295] R.E. Schmidt, D.R. Reavill, J. Exot. Pet Med. 16 (1) (2007) 49–51.
[296] F.W. Bowen, S.C. Jones, N. Narula, M. Sutton, T. Plappert, L.H.
Edmunds, et al. Ann. Thorac. Surg. 72 (6) (2001) 1950–1956.
[297] S.L. Moainie, S. Guy, J.H. Gorman, T. Plappert, B.M. Jackson, M.G.
St John-Sutton, et al. Ann. Thorac. Surg. 74 (2) (2002) 444–
449.
[298] S.P. Schmidt, T.J. Hunter, M. Hirko, T.A. Belden, M.M. Evancho, W.V.
Sharp, et al. J. Vasc. Surg. 2 (2) (1985) 292–297.
[299] K.J. Pawlowski, S.E. Rittgers, S.P. Schmidt, G.L. Bowlin, Frontiers
Biosci. 9 (2004) 1412–1421.
[300] J.C. Zhang, J. Wojta, B.R. Binder, J. Thorac. Cardiovasc. Surg. 109 (6)
(1995) 1059–1065.
[301] J.M. Anderson, L.G. Cima, S.G. Eskin, L.M. Graham, H. Greisler,
J. Hubbell, et al. J. Biomed. Mater. Res. 29 (12) (1995) 1473–
1475.
[302] C.L. Mesh, A. Majors, D. Mistele, L.M. Graham, L.A. Ehrhart, J. Vasc.
Surg. 22 (2) (1995) 142–149.
[303] D.A. Margolin, B.R. Kaufman, D.J. Deluca, P.L. Fox, L.M. Graham, J.
Vasc. Surg. 17 (5) (1993) 858–867.
[304] Y.M. Lim, J.P. Jeun, J.H. Lee, Y.M. Lee, Y.C. Nho, J. Ind. Eng. Chem. 13
(1) (2007) 21–26.
[305] J.Y. Lai, P.L. Lu, K.H. Chen, Y. Tabata, G.H. Hsiue, Biomacromolecules
7 (6) (2006) 1836–1844.
[306] G.H. Hsiue, J.Y. Lai, K.H. Chen, W.M. Hsu, Transplantation 81 (3)
(2006) 473–476.
[307] K. Takamizawa, K. Shoda, T. Matsuda, J. Biomater. Sci.-Polym. Ed. 13
(1) (2002) 81–94.
[308] M. Yamazaki, M. Tsuchida, K.Y. Kobayashi, T. Takezawa, Y. Mori,
Biotechnol. Bioeng. 48 (1) (1995) 17–24.
[309] M. Yamazaki, M. Tsuchida, K.Y. Kobayashi, T. Takezawa, Y. Mori,
Biotechnol. Bioeng. 44 (1) (1994) 38–44.
[310] T. Shimizu, M. Yamato, T. Akutsu, T. Shibata, Y. Isoi, A. Kikuchi, et al.
J. Biomed. Mater. Res. 60 (1) (2002) 110–117.
[311] T. Shimizu, M. Yamato, Y. Isoi, T. Akutsu, T. Setomaru, K. Abe, et al.
Circ. Res. 90 (3) (2002) E40–E48.
[312] O.H. Kwon, A. Kikuchi, M. Yamato, Y. Sakurai, T. Okano, J. Biomed.
Mater. Res. 50 (1) (2000) 82–89.
[313] O.H. Kwon, A. Kikuchi, M. Yamato, T. Okano, Biomaterials 24 (7)
(2003) 1223–1232.
[314] H. Hatakeyama, A. Kikuchi, M. Yamato, T. Okano, Biomaterials 27 (29)
(2006) 5069–5078.
[315] T. Shimizu, M. Yamoto, A. Kikuchi, T. Okano, Tissue Eng. 7 (2) (2001)
141–151.
[316] M.M.H. Marijianowski, P. Teeling, J. Mann, A.E. Becker, J. Am. Coll.
Cardiol. 25 (6) (1995) 1263–1272.
[317] K.T. Weber, J. Am. Coll. Cardiol. 13 (7) (1989) 1637–1652.
[318] M. Pauschinger, D. Knopf, S. Petschauer, A. Doerner, W. Poller, P.L.
Schwimmbeck, et al. Circulation 99 (21) (1999) 2750–2756.
[319] A. Brooks, V. Schinde, A.C. Bateman, P.J. Gallagher, Heart 89 (10)
(2003) 1255–1256.
[320] N. Nishikawa, T. Masuyama, K. Yamamoto, Y. Sakata, T. Mano, T.
Miwa, et al. J. Am. Coll. Cardiol. 38 (5) (2001) 1539–1545.
[321] B.A. Roeder, K. Kokini, J.E. Sturgis, J.P. Robinson, S.L. Voytik-Harbin,
J. Biomech. Eng.-Trans. ASME 124 (2) (2002) 214–222.
[322] K. Misof, W.J. Landis, K. Klaushofer, P. Fratzl, J. Clin. Invest. 100 (1)
(1997) 40–45.
[323] C. Kumudine, J.K. Premachandra, Polymer Data Handbook, Oxford
Press, Oxford, 1999.
[324] S.F. Nagueh, G. Shah, Y. Wu, G. Torre-Amione, N.M.P. King, S.
Lahmers, et al. Circulation 110 (2) (2004) 155–162.

Q.-Z. Chen et al. / Materials Science and Engineering R 59 (2008) 1–3736
[325] S.M. Weis, J.L. Emery, K.D. Becker, D.J. McBride, J.H. Omens, A.D.
McCulloch, Circ. Res. 87 (8) (2000) 663–669.
[326] C. Coirault, J.L. Samuel, D. Chemla, J.C. Pourny, F. Lambert, F. Marotte,
et al. J. Appl. Physiol. 85 (5) (1998) 1762–1769.
[327] J.H. Omens, Prog. Biophys. Mol. Biol. 69 (2/3) (1998) 559–572.
[328] R. Verheggen, W.J. SchulteBaumann, G. Hahm, J. Lang, S. Freudentha-
ler, T. Schaake, et al. Acta Neurochir. 139 (11) (1997) 1074–1079.
[329] K. Rezwan, Q.Z. Chen, J.J. Blaker, A.R. Boccaccini, Biomaterials 27
(18) (2006) 3413–3431.
[330] J.S. Temenoff, L. Lu, A.G. Mikos, in: J.E. Davies (Ed.), Bone Tissue
Engineering, EM Squared, Toronto, 2000, pp. 455–462.
[331] V. Karageorgiou, D. Kaplan, Biomaterials 26 (27) (2005) 5474–5491.
[332] S. Madai, S. De Girolamo, D.M. Munoz, R.K. Li, G. Sweeney, Cardi-
ovasc Res. 69 (3) (2006) 716–725.
[333] O. Ishii, M. Shin, T. Sueda, J.P. Vacanti, J. Thorac. Cardiovasc. Surg. 130
(5) (2005) 1358–1363.
[334] A.R. Webb, J. Yang, G.A. Ameer, Exp. Opin. Biol. Ther. 4 (6) (2004)
801–812.
[335] A.P.T. Pezzin, G. van Ekenstein, C.A.C. Zavaglia, G. ten Brinke, E.A.R.
Deuk, J. Appl. Polym. Sci. 88 (12) (2003) 2744–2755.
[336] S.S. Narine, X.H. Kong, L. Bouzidi, P. Sporns, J. Am. Oil Chem. Soc. 84
(1) (2007) 55–63.
[337] A.P. Pego, A.A. Poot, D.W. Grijpma, J. Feijen, J. Controlled Release 87
(1–3) (2003) 69–79.
[338] J. Yang, A.R. Webb, G.A. Ameer, Adv. Mater. 16 (6) (2004) 511–
516.
[339] Y.D. Wang, G.A. Ameer, B.J. Sheppard, R. Langer, Nat. Biotechnol. 20
(6) (2002) 602–606.
[340] O.H.L. Bing, S. Matsushita, B.L. Fanburg, H.J. Levine, Circ. Res. 28 (2)
(1971) 234–245.
[341] F.C. Yin, H.A. Dpurgeon, M.L. Weisfeldt, E.G. Lakatta, Circ. Res. 46
(1980) 292–300.
[342] H. Takaoka, G. Esposito, L. Mao, H. Suga, H.A. Rockman, Am. J.
Physiol.-Heart Circ. Physiol. 282 (6) (2002) H2190–H2197.
[343] K. Nakano, M. Sugawara, K. Ishihara, S. Kanazawa, W. Corin, S.
Denslow, et al. Circulation 82 (4) (1990) 1352–1361.
[344] S. Watanabe, J. Shite, H. Takaoka, T. Shinke, Y. Imuro, T. Ozawa, et al.
Eur. Heart J. 27 (7) (2006) 832–838.
[345] Y.S. Zhao, C.Y. Wang, D.X. Li, X.Z. Zhang, Y. Qiao, X.M. Guo, et al. J.
Heart Lung Transpl. 24 (8) (2005) 1091–1097.
[346] X.M. Guo, Y.S. Zhao, H.X. Chang, C.Y. Wang, E. Ling-Ling, X.A.
Zhang, et al. Circulation 113 (18) (2006) 2229–2237.
[347] W.H. Zimmermann, C. Fink, D. Kralisch, U. Remmers, J. Weil, T.
Eschenhagen, Biotechnol. Bioeng. 68 (1) (2000) 106–114.
[348] A. Remppis, S.T. Pleger, P. Most, J. Lindenkamp, P. Ehlermann, C.
Schweda, et al. J. Gene Med. 6 (4) (2004) 387–394.
[349] W.H. Zimmermann, K. Schneiderbanger, P. Schubert, M. Didie, F.
Munzel, J.F. Heubach, et al. Circ. Res. 90 (2) (2002) 223–230.
[350] W.H. Zimmermann, M. Didie, G.H. Wasmeier, U. Nixdorff, A. Hess, I.
Melnychenko, et al. Circulation 106 (13) (2002) I151–I157.
[351] W.H. Zimmermann, I. Melnychenko, G. Wasmeier, M. Didie, H. Naito,
U. Nixdorff, et al. Nat. Med. 12 (4) (2006) 452–458.
[352] H. Naito, I. Melnychenko, M. Didie, K. Schneiderbanger, P. Schubert, S.
Rosenkranz, et al. Circulation 114 (2006) I72–I78.
[353] D.A. Narmoneva, R. Vukmirovic, M.E. Davis, R.D. Kamm, R.T. Lee,
Circulation 110 (8) (2004) 962–968.
[354] D.A. Narmoneva, O. Oni, A.L. Sieminski, S.G. Zhang, J.P. Gertler, R.D.
Kamm, et al. Biomaterials 26 (23) (2005) 4837–4846.
[355] P.C.H. Hsieh, M.E. Davis, R.T. Lee, Circulation 112 (17) (2005) U28–
U29.
[356] K.L. Christman, A.J. Vardanian, Q.Z. Fang, R.E. Sievers, H.H. Fok, R.J.
Lee, J. Am. Coll. Cardiol. 44 (3) (2004) 654–660.
[357] L. Urech, A.G. Bittermann, J.A. Hubbell, H. Hall, Biomaterials 26 (12)
(2005) 1369–1379.
[358] E.J. Semler, C.S. Ranucci, P.V. Moghe, Biotechnol. Bioeng. 69 (4) (2000)
359–369.
[359] V.H. Barocas, A.G. Moon, R.T. Tranquillo, J. Biomech. Eng.-Trans.
ASME 117 (2) (1995) 161–170.
[360] R.A. Stile, E. Chung, W.R. Burghardt, K.E. Healy, J. Biomater. Sci.-
Polym. Ed. 15 (7) (2004) 865–878.
[361] S. Kim, K.E. Healy, Biomacromolecules 4 (5) (2003) 1214–1223.
[362] B.T. Stokke, K.I. Draget, O. Smidsrod, Y. Yuguchi, H. Urakawa, K.
Kajiwara, Macromolecules 33 (5) (2000) 1853–1863.
[363] S.C. Rizzi, M. Ehrbar, S. Halstenberg, G.P. Raeber, H.G. Schmoekel,
H. Hagenmuller, et al. Biomacromolecules 7 (11) (2006) 3019–3029.
[364] Q.Z. Chen, A. Bismarck, U. Hansen, S. Junaid, M.Q. Tran, S.E. Harding,
N.N. Ali, A.R. Boccaccini, Biomaterials 29 (1) (2008) 47–57.
[365] J. Gao, P.M. Crapo, Y.D. Wang, Tissue Eng. 12 (4) (2006) 917–925.
[366] Y.D. Wang, Y.M. Kim, R. Langer, J. Biomed. Mater. Res. Part A 66 (1)
(2003) 192–197.
[367] C.A. Sundback, J.Y. Shyu, Y.D. Wang, W.C. Faquin, R.S. Langer, J.P.
Vacanti, et al. Biomaterials 26 (27) (2005) 5454–5464.
[368] D. Motlagh, J. Yang, K.Y. Lui, A.R. Webb, G.A. Ameer, Biomaterials 27
(24) (2006) 4315–4324.
[369] C.J. Bettinger, B. Orrick, A. Misra, R. Langer, J.T. Borenstein, Bioma-
terials 27 (12) (2006) 2558–2565.
[370] C.J. Bettinger, E.J. Weinberg, K.M. Kulig, J.P. Vacanti, Y.D. Wang, J.T.
Borenstein, et al. Adv. Mater. 18 (2) (2006) 165–169.
[371] C. Fidkowski, M.R. Kaazempur-Mofrad, J. Borenstein, J.P. Vacanti, R.
Langer, Y.D. Wang, Tissue Eng. 11 (1/2) (2005) 302–309.
[372] K. Stokes, R. McVenes, J.M. Anderson, J. Biomater. Appl. 9 (4) (1995)
321–354.
[373] R. Yoda, J. Biomater. Sci.-Polym. Ed. 9 (6) (1998) 561–626.
[374] R.J. Zdrahala, I.J. Zdrahala, J. Biomater. Appl. 14 (1) (1999) 67–
90.
[375] W.L.J. Hinrichs, J. Kuit, H. Feil, C.R.H. Wildevuur, J. Feijen, Biomater-
ials 13 (9) (1992) 585–593.
[376] R.J. Zdrahala, J. Biomater. Appl. 11 (1) (1996) 37–61.
[377] J.D. Fromstein, K.A. Woodhouse, J. Biomater. Sci.-Polym. Ed. 13 (4)
(2002) 391–406.
[378] J.J. Stankus, J.J. Guan, K. Fujimoto, W.R. Wagner, Biomaterials 27 (5)
(2006) 735–744.
[379] N.R. Alpert, B.B. Hamrell, L.A. Mulieri, Annu. Rev. Physiol. 41 (1979)
521–537.
[380] Y.C. Fung, J. Biomech. 3 (4) (1970) 381–404.
[381] J.G. Pinto, Y.C. Fung, J. Biomech. 6 (6) (1973) 597–616.
[382] Y.C. Fung, J. Biomech. 4 (4) (1971) 289–295.
[383] E. Meyhofer, J. Exp. Biol. 185 (1993) 207–249.
[384] C. Tasche, E. Meyhofer, B. Brenner, Am. J. Physiol.-Heart Circ. Physiol.
277 (6) (1999) H2400–H2408.
[385] C. Tasche, E. Meyhofer, B. Brenner, Biophys. J. 74 (2) (1998) A350.
[386] H.W. Haslach, Biomech. Model. Mechanobiol. 3 (3) (2005) 172–
189.
[387] R. Sinkus, J. Bercoff, M. Tanter, J.L. Gennisson, C. El Khoury, V.
Servois, et al. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 53
(11) (2006) 2009–2018.
[388] Y.C. Fung, Am. Zool. 24 (1) (1984) 13–22.
[389] Z.P. Luo, Y.L. Sun, T. Fujii, K.N. An, Biorheology 41 (3/4) (2004) 247–
254.
[390] C. Storm, J.J. Pastore, F.C. MacKintosh, T.C. Lubensky, P.A. Janmey,
Nature 435 (7039) (2005) 191–194.
[391] L. Polonchuk, J. Elbel, L. Eckert, J. Blum, E. Wintermantel, H.M.
Eppenberger, Biomaterials 21 (6) (2000) 539–550.
[392] T. Kofidis, P. Akhyari, B. Wachsmann, K. Mueller-Stahl, J. Boublik, A.
Ruhparwar, et al. Tissue Eng. 9 (3) (2003) 517–523.
[393] M.J.A. van Luyn, R.A. Tio, X. van Seijen, J.A. Plantinga, L. de Leij,
M.J.L. DeJongste, et al. Biomaterials 23 (24) (2002) 4793–4801.
[394] M.J. van Amerongen, M.C. Harmsen, A.H. Petersen, G. Kors, M.J.A. van
Luyn, Biomaterials 27 (10) (2006) 2247–2257.
[395] T. Kofidis, J.L. de Bruin, G. Hoyt, Y. Ho, M. Tanaka, T. Yamane, et al. J.
Heart Lung Transpl. 24 (6) (2005) 737–744.
[396] R.K. Li, T.M. Yau, R.D. Weisel, D.A.G. Mickle, T. Sakai, A. Choi, et al.
J. Thorac. Cardiovasc. Surg. 119 (2) (2000) 368–375.
[397] T. Kofidis, A. Lenz, J. Boublik, P. Akhyari, B. Wachsmann, K. Mueller-
Stahl, et al. Biomaterials 24 (27) (2003) 5009–5014.
[398] R.M. Nerem, Tissue Eng. 12 (5) (2006) 1143–1150.

Q.-Z. Chen et al. / Materials Science and Engineering R 59 (2008) 1–37 37
[399] T. Sakai, R.K. Li, R.D. Weisel, D.A.G. Mickle, E.T.J. Kim, Z.Q. Jia, et al.
J. Thorac. Cardiovasc. Surg. 121 (5) (2001) 932–942.
[400] T. Ozawa, D.A.G. Mickle, R.D. Weisel, N. Koyama, H. Wong, S. Ozawa,
et al. J. Thorac. Cardiovasc. Surg. 124 (6) (2002) 1157–1164.
[401] T. Ozawa, D.A.G. Mickle, R.D. Weisel, N. Koyama, S. Ozawa, R.K. Li,
Circulation 106 (13) (2002) I176–I182.
[402] K. Matsubayashi, P.W.M. Fedak, D.A.G. Mickle, R.D. Weisel, T. Ozawa,
R.K. Li, Circulation 108 (10) (2003) 219–225.
[403] T. Ozawa, D.A.G. Mickle, R.D. Weisel, K. Matsubayashi, T. Fujii,
P.W.M. Fedak, et al. Cell Transpl. 13 (2) (2004) 169–177.
[404] E. Tziampazis, A. Sambanis, Biotechnol. Prog. 11 (2) (1995) 115–126.
[405] A.C. Jen, M.C. Wake, A.G. Mikos, Biotechnol. Bioeng. 50 (4) (1996)
357–364.
[406] S.K. Ashiku, M.A. Randolph, C.A. Vacanti, Porous Materials for Tissue
Engineering, Transtec Publications Ltd., Zurich-Uetikon, 1997, pp. 129–
150.
[407] K.H. Bouhadir, I. Yue, L. Chen, D. Hausman, D.J. Mooney, Abstr. Pap.
Am. Chem. Soc. 216 (1998) U266–U267.
[408] L. Shapiro, S. Cohen, Biomaterials 18 (8) (1997) 583–590.
[409] S. Zmora, R. Glicklis, S. Cohen, Biomaterials 23 (20) (2002) 4087–
4094.
[410] A. Dar, M. Shachar, J. Leor, S. Cohen, Biotechnol. Bioeng. 80 (3) (2002)
305–312.
[411] A. Perets, Y. Baruch, F. Weisbuch, G. Shoshany, G. Neufeld, S. Cohen, J.
Biomed. Mater. Res. Part A 65 (4) (2003) 489–497.
[412] L.E. Freed, G. Vunjaknovakovic, R. Langer, J. Cell. Biochem. 51 (3)
(1993) 257–264.
[413] A.G. Mikos, G. Sarakinos, M.D. Lyman, D.E. Ingber, J.P. Vacanti, R.
Langer, Biotechnol. Bioeng. 42 (6) (1993) 716–723.
[414] N. Bursac, M. Papadaki, R.J. Cohen, F.J. Schoen, S.R. Eisenberg, R.
Carrier, et al. Am. J. Physiol.-Heart Circ. Physiol. 277 (2) (1999) H433–
H444.
[415] J. Folkman, M. Hochberg, J. Exp. Med. 138 (4) (1973) 745–753.
[416] R.L. Carrier, M. Papadaki, M. Rupnick, F.J. Schoen, N. Bursac, R.
Langer, et al. Biotechnol. Bioeng. 64 (5) (1999) 580–589.
[417] M. Radisic, M. Euloth, L.M. Yang, R. Langer, L.E. Freed, G. Vunjak-
Novakovic, Biotechnol. Bioeng. 82 (4) (2003) 403–414.
[418] M. Radisic, H. Park, H. Shing, T. Consi, F.J. Schoen, R. Langer, et al.
Proc. Natl. Acad. Sci. U.S.A. 101 (52) (2004) 18129–18134.
[419] M. Papadaki, N. Bursac, R. Langer, J. Merok, G. Vunjak-Novakovic,
L.E. Freed, Am. J. Physiol.-Heart Circ. Physiol. 280 (1) (2001) H168–
H178.
[420] N. Bursac, M. Papadaki, J.A. White, S.R. Eisenberg, G. Vunjak-Nova-
kovic, L.E. Freed, Tissue Eng. 9 (6) (2003) 1243–1253.
[421] B. Obradovic, R.L. Carrier, G. Vunjak-Novakovic, L.E. Freed, Biotech-
nol. Bioeng. 63 (2) (1999) 197–205.
[422] R.L. Carrier, M. Rupnick, R. Langer, F.J. Schoen, L.E. Freed, G. Vunjak-
Novakovic, Biotechnol. Bioeng. 78 (6) (2002) 617–625.
[423] R.L. Carrier, M. Rupnick, R. Langer, F.J. Schoen, L.E. Freed, G. Vunjak-
Novakovic, Tissue Eng. 8 (2) (2002) 175–188.
[424] J.J. Stankus, J.J. Guan, W.R. Wagner, J. Biomed. Mater. Res. Part A 70
(4) (2004) 603–614.
[425] T. Courtney, M.S. Sacks, J. Stankus, J. Guan, W.R. Wagner, Biomaterials
27 (19) (2006) 3631–3638.
[426] A.P. Pego, A.A. Poot, D.W. Grijpma, J. Feijen, Macromol. Biosci. 2 (9)
(2002) 411–419.
[427] A.P. Pego, B. Siebum, M.J.A. Van Luyn, X. Van Seijen, A.A. Poot, D.W.
Grijpma, et al. Tissue Eng. 9 (5) (2003) 981–994.
[428] H.N. Sabbah, V.G. Sharov, R.C. Gupta, S. Mishra, S. Rastogi, A.I.
Undrovinas, et al. Circ. Res. 93 (11) (2003) 1095–1101.
[429] R.E. Akins, N.A. Schroedl, S.R. Gonda, C.R. Hartzell, In Vitro Cell. Dev.
Biol.-Anim. 33 (5) (1997) 337–343.
[430] R.E. Akins, R.A. Boyce, M.L. Madonna, N.A. Schroedl, S.R. Gonda,
T.A. McLaughlin, et al. Tissue Eng. 5 (2) (1999) 103–118.
[431] J.M. Kelm, E. Ehler, L.K. Nielsen, S. Schlatter, J.C. Perriard, M.
Fussenegger, Tissue Eng. 10 (1/2) (2004) 201–214.
[432] K. Baar, R. Birla, M.O. Boluyt, G.H. Borschel, E.M. Arruda, R.G.
Dennis, FASEB J. 19 (2) (2005) 275–277.
[433] T. Okano, N. Yamada, H. Sakai, Y. Sakurai, J. Biomed. Mater. Res. 27
(10) (1993) 1243–1251.
[434] T. Aoki, Y. Nagao, E. Terada, K. Sanui, N. Ogata, N. Yamada, et al. J.
Biomater. Sci.-Polym. Ed. 7 (7) (1995) 539–550.
[435] T. Okano, N. Yamada, M. Okuhara, H. Sakai, Y. Sakurai, Biomaterials 16
(4) (1995) 297–303.
[436] T. Shimizu, M. Yamato, A. Kikuchi, T. Okano, J. Artif. Organs 5 (2002)
216–222.
[437] H. Hatakeyama, A. Kikuchi, M. Yamato, T. Okano, Biomaterials 28 (25)
(2007) 3632–3643.
[438] M. Hirose, M. Yamato, O.H. Kwon, M. Harimoto, A. Kushida, T.
Shimizu, et al. Yonsei Med. J. 41 (6) (2000) 803–813.
[439] A. Kushida, M. Yamato, C. Konno, A. Kikuchi, Y. Sakurai, T. Okano, J.
Biomed. Mater. Res. 51 (2) (2000) 216–223.
[440] A. Kikuchi, M. Okuhara, F. Karikusa, Y. Sakurai, T. Okano, J. Biomater.
Sci.-Polym. Ed. 9 (12) (1998) 1331–1348.
[441] A. Kushida, M. Yamato, A. Kikuchi, T. Okano, J. Biomed. Mater. Res. 54
(1) (2001) 37–46.
[442] M. Yamato, M. Utsumi, A. Kushida, C. Konno, A. Kikuchi, T. Okano,
Tissue Eng. 7 (4) (2001) 473–480.
[443] M. Harimoto, M. Yamato, M. Hirose, C. Takahashi, Y. Isoi, A. Kikuchi,
et al. J. Biomed. Mater. Res. 62 (3) (2002) 464–470.
[444] T. Shimizu, H. Sekine, Y. Isoi, M. Yamato, A. Kikuchi, T. Okano, Tissue
Eng. 12 (3) (2006) 499–507.
[445] S. Miyagawa, Y. Sawa, S. Sakakida, S. Taketani, H. Kondoh, I.A.
Memon, et al. Transplantation 80 (11) (2005) 1586–1595.
[446] H. Kondoh, Y. Sawa, S. Miyagawa, S. Sakakida-Kitagawa, M.A.
Memon, N. Kawaguchi, et al. Cardiovasc. Res. 69 (2) (2006) 466–475.
[447] J. Yang, M. Yamato, C. Kohno, A. Nishimoto, H. Sekine, F. Fukai, et al.
Biomaterials 26 (33) (2005) 6415–6422.
[448] K. Bilodeau, D. Mantovani, Tissue Eng. 12 (8) (2006) 2367–2383.
[449] V. Barron, E. Lyons, C. Stenson-Cox, P.E. McHugh, A. Pandit, Ann.
Biomed. Eng. 31 (9) (2003) 1017–1030.
[450] E. Lyons, A. Pandit, in: N. Ashammakhi, R.L. Reis (Eds.), Topics of
Tissue Engineering: e-Book, 2005 (Chapter 7).
[451] L.E. Freed, G. Vunjak-Novakovic, in: R.Z. Lanza, R.S. Langer, J.P.
Vacanti (Eds.), Principles of Tissue Engineering, 2nd ed., Academic
Press, California, 2000, pp. 143–156.
[452] C. Fink, S. Ergun, D. Kralisch, U. Remmers, J. Weil, T. Eschenhagen,
FASEB J. 14 (5) (2000) 669–679.
Copyright © 2022 FDOKUMEN




















