Nanofiber-reinforced myocardial tissue-construct as ventricular assist device
10
http://aan.sagepub.com/ Asian Cardiovascular and Thoracic Annals http://aan.sagepub.com/content/early/2014/02/18/0218492314523627 The online version of this article can be found at: DOI: 10.1177/0218492314523627 published online 18 February 2014 Asian Cardiovascular and Thoracic Annals Soma Guhathakurta, Santosh Mathapati, Dillip Kumar Bishi, Suneel Rallapalli and Kotturathu Mammen Cherian Nanofiber-reinforced myocardial tissue-construct as ventricular assist device Published by: http://www.sagepublications.com On behalf of: The Asian Society for Cardiovascular Surgery can be found at: Asian Cardiovascular and Thoracic Annals Additional services and information for http://aan.sagepub.com/cgi/alerts Email Alerts: http://aan.sagepub.com/subscriptions Subscriptions: http://www.sagepub.com/journalsReprints.nav Reprints: http://www.sagepub.com/journalsPermissions.nav Permissions: What is This? - Feb 18, 2014 OnlineFirst Version of Record >> by guest on February 21, 2014 aan.sagepub.com Downloaded from by guest on February 21, 2014 aan.sagepub.com Downloaded from
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Nanofiber-reinforced myocardial tissue-construct as ventricular assist device

http://aan.sagepub.com/Asian Cardiovascular and Thoracic Annals
http://aan.sagepub.com/content/early/2014/02/18/0218492314523627The online version of this article can be found at:
DOI: 10.1177/0218492314523627
published online 18 February 2014Asian Cardiovascular and Thoracic AnnalsSoma Guhathakurta, Santosh Mathapati, Dillip Kumar Bishi, Suneel Rallapalli and Kotturathu Mammen Cherian
Nanofiber-reinforced myocardial tissue-construct as ventricular assist device
Published by:
http://www.sagepublications.com
On behalf of:
The Asian Society for Cardiovascular Surgery
can be found at:Asian Cardiovascular and Thoracic AnnalsAdditional services and information for
http://aan.sagepub.com/cgi/alertsEmail Alerts:
http://aan.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
What is This?
- Feb 18, 2014OnlineFirst Version of Record >>
by guest on February 21, 2014aan.sagepub.comDownloaded from by guest on February 21, 2014aan.sagepub.comDownloaded from

XML Template (2014) [12.2.2014–10:34am] [1–9]//blrnas3/cenpro/ApplicationFiles/Journals/SAGE/3B2/AANJ/Vol00000/140022/APPFile/SG-AANJ140022.3d (AAN) [PREPRINTER stage]
Original Article
Nanofiber-reinforced myocardialtissue-construct as ventricularassist device
Soma Guhathakurta1, Santosh Mathapati2, Dillip Kumar Bishi2,Suneel Rallapalli1 and Kotturathu Mammen Cherian2
Abstract
Objectives: This study aimed to create a myocardial tissue construct by tissue engineering to repair, replace, and
regenerate damaged cardiac tissue.
Methods and results: Human cardiac muscles harvested from a homograft heart retrieval system were decellularized
followed by coating with electrospun nanofibers to make them amenable to scaffolding. These processed cardiac tissues
were nourished in modified media having ischemic cardiac tissue conditioned media in 6 separate experimental variants,
and cord blood mononuclear cells were injected into 4 of them. On the 17th day of culture, the nanofiber-coated
scaffolds injected with mononuclear cells and/or reinforced by electrical and mechanical forces, started contracting
spontaneously at varying rates, while the control remain noncontractile. Histological staining confirmed the pre-culture
acellularity as well as post-culture stem cell viability, and revealed expression of troponin I and cardiac myosin. The
acellular processed scaffold when implanted into sheep ischemic myocardial apex revealed transformation into sheep
myocardium after 4 months of implantation.
Conclusion: These results provide direct evidence for the re-cellularization of decellularized cardiac tissue grafts
reinforced with a polymer nanofiber coating, by human mononuclear cells injection, leading to generation of a tissue-
engineered myocardial construct.
Keywords
Heart failure, heart ventricles, prostheses and implants, regenerative medicine, stem cells, tissue engineering
Introduction
Tissue engineering aims to repair, replace, and regener-ate damaged tissues, and ex-vivo creation of tissue con-structs is challenging.1,2 Cell transplantation with bonemarrow mesenchymal stem cells or mononuclear cellsat the transitional zone of full-thickness scar and viablemyocardium is the preferred modality of treatment, butthe efficacy of cell homing remains a question.Injectable biomaterials in the form of biocompatiblehydrogel loaded with target cells have been taken ser-iously because it may be a less-invasive modality formyocardial regeneration.3 A regenerative approach topatients at risk of cardiac failure seems to be moreeffective in preventing infarct expansion, ventriculardilatation, and post-ischemic adverse remodeling.4
Cell transplantation, growth factors, and gene
therapy represent emerging biological treatments toimprove myocardial viability in ischemic heart failure.5
However, effective functionality may be questionablebecause the muscle mass generated is inadequate.Treatment under the category of a cardiac assistdevice with Marceline mesh to support the heart frombulging appears to be more physiological but not afoolproof system. Myosplint and Acorn assist devices
Asian Cardiovascular & Thoracic Annals
0(0) 1–9
� The Author(s) 2014
Reprints and permissions:
sagepub.co.uk/journalsPermissions.nav
DOI: 10.1177/0218492314523627
aan.sagepub.com
1Department of Engineering Design, Indian Institute of Technology
Madras, Chennai, India2International Centre for Cardiothoracic and Vascular Diseases, Frontier
Lifeline Hospital, Chennai, India
Corresponding author:
Soma Guhathakurta, Department of Engineering Design, Indian Institute
of Technology Madras, Chennai 600036, India.
Email: [email protected]
by guest on February 21, 2014aan.sagepub.comDownloaded from

XML Template (2014) [12.2.2014–10:34am] [1–9]//blrnas3/cenpro/ApplicationFiles/Journals/SAGE/3B2/AANJ/Vol00000/140022/APPFile/SG-AANJ140022.3d (AAN) [PREPRINTER stage]
have their own problem of non-pliability during dia-stolic relaxation. Geometric reconstruction of theheart, which should be elliptical in shape and contracteffectively from apex to base, was conceptualized byJatene6 in 1985, and Dor’s left ventriculoplasty hasnow been modified with a Gore-Tex or Dacron graftas a patch material during endoventricular patch-plasty. This is routinely practiced because a foolproofbiological alternative is not available. The geometricreconstruction by Gore-Tex or Dacron gives the heartthe required shape, but the patch, being synthetic, doesnot contract. For effective myocardial tissue engineer-ing, a range of natural and synthetic polymers havebeen chosen either alone or in combination with vari-ous cell types from skeletal myoblasts to cardiac stemcells.7 In this study, the processed myocardial patch wassubjected to similar forces to those the myocardiumexperiences, such as pacemaker current for rhythmiccontraction, along with alternate contraction and relax-ation, by a pulsating balloon after mononuclear cell(MNC) injection. Although the biomimetic approachto produce functional cardiac grafts has faced seriouschallenges, it is nevertheless a pressing objective in car-diac regenerative medicine. The cardiac tissue con-structs could provide an effective treatment for severalcardiac disorders in which one ventricle is functional,and also in the one and a half ventricle situation. In thisstudy, the tissue chosen was dead myocardium whichwas processed into an acellular crosslinked scaffold.Our objective was to find out whether a natural acellu-lar scaffold might be an amenable substrate for in-vivoregeneration of myocardial cells. We also investigatedhow migrating progenitor cells from the circulation orcardiac stem cells might play a role in regeneration atthe site of injury when appropriate forces and cues weredelivered to the scaffold.
Materials and methods
For preparation of the acellular composite tissue con-struct (ACTC) from natural homologous myocardialtissue, approval of the regulatory board of the institu-tion was obtained for harvesting the tissue. Cardiacmuscle tissues were harvested from adult humanhearts within 24 h of death. The cardiac muscle tissueswere cut into rectangular sheets of 3mm thickness, andcylindrical scaffolds of 5-mm diameter and were subse-quently made acellular with indigenous methods ofdecellularization. The decellularization protocol wasmodified to preserve the extracellular matrix proteins(ECM). Briefly, decellularization was performed using1% deoxycholic acid (pH 7.4) for 20–30 h at 37�C (thedwelling time was dependent on the thickness). Thiswas followed by DNase and RNase treatment toremove the cellular materials, and washing with
phosphate-buffered saline (PBS). The acellular scaffoldwas coated with electrospun nanofibers of poly-(L)lactic acid (Sigma, St. Louis, MO, USA), polycaprono-lactone (Sigma, St. Louis, MO, USA), and collagenblend (Sigma, St. Louis, MO, USA).8 The nanofiberswere generated at random to coat the processed musclesheet. The nanofiber coating was evaluated by scanningelectron microscopy, and porosity was also determined.Finally, the coated acellular processed myo-patch wascrosslinked by dye-mediated photooxidation to gainfurther strength.9 Briefly, the processed myo-patchcoated with nanofibers was treated with 1% methyleneblue and medium-wave ultraviolet light in an oxygen-rich atmosphere. The tissues were fixed with 10% phos-phate-buffered formalin, embedded in paraffin, cut into5-mm-thick sections, and fixed on glass slides. The cutsections were stained with hematoxylin and eosin(H&E). Immunohistochemical analysis was carriedout to determine the presence of troponin I and cardiacactinin.
Human umbilical cord blood was obtained fromobstetrics and gynecology units of various hospitals inChennai, India, with due approval from institutionalethics committees and informed consent from donors.The MNC fraction was isolated using Ficoll-Paque(1.077 g cm�3; GE Healthcare) density-gradient centri-fugation. Briefly, anticoagulated cord blood wasdiluted 3 times with PBS, and approximately 35 mLof diluted blood was layered over 15 mL Ficoll in a50 mL conical tube. Centrifugation was carried out at400 g for 30min at 4�C in a swinging bucket rotor with-out brake. The upper plasma layer was carefully aspi-rated off, and the interphase containing mononuclearcells was transferred to a fresh tube, and washed twicewith PBS by centrifuging at 300 g for 10min. MNCwere plated at a density of 1� 107 cellsmL�1 inDulbecco minimal essential medium (DMEM) supple-mented with 2 mmol glutamine, 0.001% b-mercap-toethanol, 1% nonessential amino acids, 10% fetalcalf serum, and 1% penicillin/streptomycin, and main-tained for 48 h at 37�C in a humidified atmosphere of5% CO2 and 95% air. MNC positive for CD34 andCD45 were quantified by fluorescence-activated cellsorting.
Right atrial cardiac tissues were collected frompatients during decannulation, with prior informedconsent, and characterized as ischemic tissue samplesbecause they were collected from patients undergoingcoronary artery bypass graft surgery. Fresh cardiac tis-sues were processed within 6 h of the harvest. Each car-diac tissue sample was weighed under sterile conditions,chopped into small pieces not exceeding 1 mm in size,and incubated with 10 mL DMEM and 10% fetalbovine serum for 7 days under 5% CO2 at 37�C. Themedium from each tissue was centrifuged and filtered to
2 Asian Cardiovascular & Thoracic Annals 0(0)
by guest on February 21, 2014aan.sagepub.comDownloaded from

XML Template (2014) [12.2.2014–10:34am] [1–9]//blrnas3/cenpro/ApplicationFiles/Journals/SAGE/3B2/AANJ/Vol00000/140022/APPFile/SG-AANJ140022.3d (AAN) [PREPRINTER stage]
remove the cardiac tissues and myocytes. The mediafree of cells from the ischemic samples were pooledtogether and stored at �80�C.
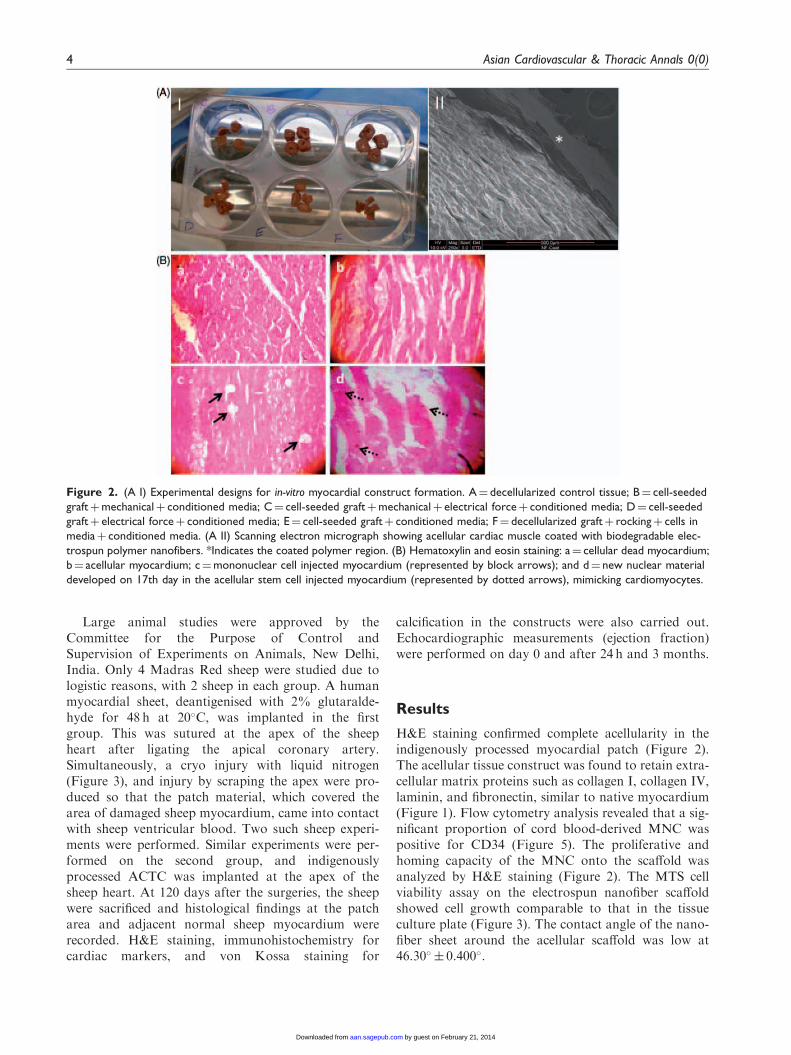
For cell seeding onto the scaffolds, approximately2� 106 MNC were seeded onto the processed sterilescaffold using 28G insulin needles, by multiple punc-tures. The MNC-loaded scaffolds were placed intissue culture dishes in low-glucose DMEM alongwith indigenous cardiac conditioned medium, a 9:1v/v ratio of DMEM: culture medium with 10% fetalbovine serum and antibiotics, designated modifiedmedia (MM). Tissue culture was conducted in custo-mized cell culture dishes to allow for cultivation of thecells seeded onto scaffolds. Our aim was to examine theeffect of electrical and mechanical stimulation on thecardiac-differentiation potential of cord blood-derivedMNC. Mechanical forces would promote the formationof cell aggregates that enhanced the kinetics of cellattachment without compromising the uniformity ofcell distribution. We hypothesized that cells stressedby external electrical fields would undergo remodelingcaused by electromechanical stresses. Six variants ofstimulation protocols were studied as follows(Figure 2). Group A: a static scaffold with no cellsinjected was incubated in MM and served as negativecontrol; in group B, the scaffold loaded with MNC wasmaintained in MM and subjected to mechanical forcescontinuously for 2 weeks. The forces were withdrawnafter 2 weeks, and the cell-seeded scaffold was main-tained in conditioned medium with regular mediumchanges. In group C, the cell-seeded scaffold was main-tained in MM and subjected to electrical forces with nomechanical force applied. In group D, the cell-seededscaffold was maintained in MM and subjected to sim-ultaneous mechanical and electrical forces. The elec-trical forces characteristic of native myocardium weregenerated from a single-chamber pulse generator at arate of 60 beatsmin�1 (this allowed us to electrically
stimulate the cell population while applying kineticforces to the cells); in group E, a static cell-seeded scaf-fold was maintained in MM with no electrical andmechanical forces applied. In group F, the scaffoldwith no cells injected was maintained in MM.However, cells were seeded onto the culture dish inwhich the scaffold was placed. A rocking movementwas imparted to the plate to investigate whether kin-etics influence possible mechanisms of cell adhesiononto the scaffold. In groups B, C, and D, the mechan-ical force was delivered by alternate inflation and defla-tion of balloon inside the myocardial scaffold. Theelectrical forces were generated by a pacemaker currentthrough an implantable pulse generator. The mediumwas replenished every 3rd day, and external forces wereremoved after 2 weeks. Cell seeding in the scaffold wasconfirmed by microscopic observation (Figure 2). Afterdiscontinuation of the external forces, all the scaffoldswere placed in the 6 well plates labeled A to F(Figure 2). From the 15th day onward, the 6 wellplates were observed daily under an inverted micro-scope for any changes. Four such experiments wereperformed consecutively, and the microscopic evidencewas noted. Biochemical parameters (troponin I, potas-sium, and calcium) were evaluated from the respectivemedia of the culture wells on the 3rd week of culture,depending on a critical observation. A cell viabilityassay based on 3-(4,5-dimethylthiazol-2-yl)-5-(3-car-boxymethoxyphenyl)-2-(4-sulfophenyl)-2H-tetrazolium(MTS) was conducted on the nanofiber scaffolds atvarious time points (Figure 3). Expression of cardiacmarkers such as troponin I was determined by immu-nohistochemistry. Contractile activity in response toisoprenaline or without isoprenaline was measured byvideomicroscopy. Isoprenaline was used because itenhances cardiac contractility and can cause myocar-dial fibrillation which is dose-dependent as well as elec-trolyte-dependent.
Figure 1. Immunohistochemical analysis of extracellular matrix proteins for (a–d) native and (e–h) acellular myocardium.
Scale bars¼ 50 mm.
Guhathakurta et al. 3
by guest on February 21, 2014aan.sagepub.comDownloaded from
XML Template (2014) [12.2.2014–10:34am] [1–9]//blrnas3/cenpro/ApplicationFiles/Journals/SAGE/3B2/AANJ/Vol00000/140022/APPFile/SG-AANJ140022.3d (AAN) [PREPRINTER stage]
Large animal studies were approved by theCommittee for the Purpose of Control andSupervision of Experiments on Animals, New Delhi,India. Only 4 Madras Red sheep were studied due tologistic reasons, with 2 sheep in each group. A humanmyocardial sheet, deantigenised with 2% glutaralde-hyde for 48 h at 20�C, was implanted in the firstgroup. This was sutured at the apex of the sheepheart after ligating the apical coronary artery.Simultaneously, a cryo injury with liquid nitrogen(Figure 3), and injury by scraping the apex were pro-duced so that the patch material, which covered thearea of damaged sheep myocardium, came into contactwith sheep ventricular blood. Two such sheep experi-ments were performed. Similar experiments were per-formed on the second group, and indigenouslyprocessed ACTC was implanted at the apex of thesheep heart. At 120 days after the surgeries, the sheepwere sacrificed and histological findings at the patcharea and adjacent normal sheep myocardium wererecorded. H&E staining, immunohistochemistry forcardiac markers, and von Kossa staining for
calcification in the constructs were also carried out.Echocardiographic measurements (ejection fraction)were performed on day 0 and after 24 h and 3 months.
Results
H&E staining confirmed complete acellularity in theindigenously processed myocardial patch (Figure 2).The acellular tissue construct was found to retain extra-cellular matrix proteins such as collagen I, collagen IV,laminin, and fibronectin, similar to native myocardium(Figure 1). Flow cytometry analysis revealed that a sig-nificant proportion of cord blood-derived MNC waspositive for CD34 (Figure 5). The proliferative andhoming capacity of the MNC onto the scaffold wasanalyzed by H&E staining (Figure 2). The MTS cellviability assay on the electrospun nanofiber scaffoldshowed cell growth comparable to that in the tissueculture plate (Figure 3). The contact angle of the nano-fiber sheet around the acellular scaffold was low at46.30� � 0.400�.
Figure 2. (A I) Experimental designs for in-vitro myocardial construct formation. A¼ decellularized control tissue; B¼ cell-seeded
graftþmechanicalþ conditioned media; C¼ cell-seeded graftþmechanicalþ electrical forceþ conditioned media; D¼ cell-seeded
graftþ electrical forceþ conditioned media; E¼ cell-seeded graftþ conditioned media; F¼ decellularized graftþ rockingþ cells in
mediaþ conditioned media. (A II) Scanning electron micrograph showing acellular cardiac muscle coated with biodegradable elec-
trospun polymer nanofibers. *Indicates the coated polymer region. (B) Hematoxylin and eosin staining: a¼ cellular dead myocardium;
b¼ acellular myocardium; c¼mononuclear cell injected myocardium (represented by block arrows); and d¼ new nuclear material
developed on 17th day in the acellular stem cell injected myocardium (represented by dotted arrows), mimicking cardiomyocytes.
4 Asian Cardiovascular & Thoracic Annals 0(0)
by guest on February 21, 2014aan.sagepub.comDownloaded from

XML Template (2014) [12.2.2014–10:34am] [1–9]//blrnas3/cenpro/ApplicationFiles/Journals/SAGE/3B2/AANJ/Vol00000/140022/APPFile/SG-AANJ140022.3d (AAN) [PREPRINTER stage]
After 3 weeks of culture, our biomimetic approachresulted in myocardial sheets which contained electro-mechanically stimulated cells expressing cardiac differ-entiation markers with spontaneous and rhythmiccontraction without isoprenaline. In the 3rd week ofculture, it was noted that the scaffolds which wereseeded or in contact with cells regained contractile abil-ity. The most effective contractions were noted in cul-ture groups B (mechanical force), C (electrical force),and D (electromechanical force). All these contractionswere spontaneous, and all of them started in the 3rdweek of culture and maintenance in MM. Rhythmiccontractions were noticed in all scaffolds. However,rhythmic contractions of lesser impact with a longgap between contractions were observed in group C(electrical forces alone). When the contracting musclesheets were subjected to isoprenaline treatment, theydisplayed fibrillatory motion followed by a standstill.H&E staining of the scaffolds after acquiring contract-ile ability (groups B to F) showed the same histologicalfeatures as native human myocardium (Figure 2). Thesame tissues from each group were analyzed by immu-nohistochemistry, which revealed strong expression ofcardiac myosin and faint expression of troponin T(Figure 4). The biochemical analysis of the mediumindicated the presence of troponin I, and the level of
troponin I was significantly higher in the medium afterisoprenaline injection (Table 1).
The indigenously processed acellular myo-patchACTC was excised from the sheep heart 120 days afterimplantation, and revealed no calcification. Re-cellular-ization of the processed acellular human myocardialpatch by sheep myocardial cells was noted (Figure 4).The indigenous patch was further subjected to immuno-histochemistry; it was strongly positive for cardiactroponin T and cardiac actinin (Figure 4). The explantsof ACTC were positive for von Willebrand factor andnegative for von Kossa staining after 120 days ofimplantation, whereas the glutaraldehyde-treatedhuman myocardial patch showed severe calcification,immune reactions, fibrosis, and encapsulation(Figure 3). Preoperative and 24-h post-surgery ejectionfraction was 65%� 1.18% and 53.2%� 1.14%, respect-ively, in the indigenously processed acellular myo-patchACTC group. A normalization of ejection fraction(68.1%� 1.21%) was observed after 90 days in the indi-genously processed acellular myo-patch ACTC group.
Discussion
Tissue engineering with stem cells is a known phenom-enon that requires an appropriate scaffold and milieu
Figure 3. In-vivo large animal experiments: (a) tying the apical coronary artery to produce infarction at the apex of normal sheep
heart; (b) inflicting added injury to the same sheep heart apex by liquid nitrogen and scraping; (c) application of the acellular myocardial
scaffold at the injured apex of the sheep heart, and (d) the implanted glutaraldehyde-treated patch showing calcification on explant
(von Kossa staining). Scale bars¼ 50 mm. *Indicates the infarcted cryo-injured apex. (e) Human mesenchymal stem cell proliferation
assays in 3 different conditions; the polymer-blend scaffold was included to prove its efficacy.
Guhathakurta et al. 5
by guest on February 21, 2014aan.sagepub.comDownloaded from

XML Template (2014) [12.2.2014–10:35am] [1–9]//blrnas3/cenpro/ApplicationFiles/Journals/SAGE/3B2/AANJ/Vol00000/140022/APPFile/SG-AANJ140022.3d (AAN) [PREPRINTER stage]
for the stem cells to differentiate into the required celltype. Worldwide effort is on to develop a scaffold thatwould mimic the extracellular matrix for regenerationof tissues or organs.10 The application of defined
mechanical stimuli to cultured cardiac fibroblasts hasbeen associated with ECM gene expression and bio-activity. Dynamic stretching of cardiac fibroblastsresulted in the activation of b1-integrin-dependent
Figure 4. (A) Explanted acellular processed human myocardial scaffold after 120 days. a¼ hematoxylin and eosin staining of the
section taken from the explant; b¼ elastic Van Gieson staining of the section; c and d¼ immunohistochemistry of the explants
revealing cardiac troponin T (c) expression and positive expression of cardiac actinin (d) in the explant. Scale bars¼ 50 mm. (B).
Immunohistochemistry images: a¼ positive expression for cardiac myosin in native cardiac tissue before processing; b¼ positive for
cardiac troponin T in native human myocardial tissue; c¼ strongly positive expression of cardiac myosin in processed acellular cardiac
tissue after 14th day of stem cell injection and force application; d¼ faintly positive expression of cardiac troponin T in processed
acellular cardiac tissue after 14th day of stem cell injection and force application. Scale bars¼ 50 mm.
6 Asian Cardiovascular & Thoracic Annals 0(0)
by guest on February 21, 2014aan.sagepub.comDownloaded from

XML Template (2014) [12.2.2014–10:35am] [1–9]//blrnas3/cenpro/ApplicationFiles/Journals/SAGE/3B2/AANJ/Vol00000/140022/APPFile/SG-AANJ140022.3d (AAN) [PREPRINTER stage]
extracellular signal-regulated kinases and c-Jun N-terminal kinase pathways, as well as the expression ofcollagen III and fibronectin.11,12
In-vitro formation of functional cardiac-like tissuestructures were observed when the cells cultured onscaffolds were stimulated by applying electrical signalssimilar to those in the native heart, or by applyingdirect mechanical stimulation.13,14 The present effortwas towards making a biological myocardial assistdevice that would become incorporated into theimplanted biological system without any immune reac-tion. The idea was to retain the basic architecture andECM of the construct and subject it to similar dynamicforces and a chemical environment that a live myocar-dium experiences. To test our hypothesis, we designedan in-vitro culture system that maintained efficient elec-trical and mechanical stimuli to the cells and thehoming scaffold continuously for 2 weeks. Cell-seededconstructs were assessed at timed intervals with respectto cell number, distribution, viability, presence of con-tractile proteins (troponin I), contractile function inresponse to electrical and/or mechanical stimulation,and response to drugs such as isoprenaline.
The origin of the biomaterial was human myocar-dium, and as our previously published data substanti-ates that the indigenous procedure of decellularizationretains the native tissue ECM, similar results wereobtained in these experiments.11 The presence ofECM proteins such as collagen I and IV, laminin,and fibronectin in the matrix of the scaffold in compar-able quantum were demonstrated by immunohisto-chemistry (Figure 1). In addition, coating of theelectrospun nanofibers of the hybrid polymer blendwas reinforced to impart extra strength to the processedmyocardial sheet and effective homing of mononuclearcells which were seeded. We coated the myo-patch withpoly-L-lactic acid, polycapronolactone, and collagenblended electrospun nanofibers with an average diam-eter of 347 nanometers (Figure 2). The cell populationseeded had a mixture of precursor cells, a very small
percentage of mesenchymal stem cells and probablyvery small embryonic-like cells, which could differenti-ate into myocardial-like cells under the designed experi-mental conditions. The ability of MNC-derivedprogenitor to proliferate in acellular scaffold wasproved by the MTS assay results. Moreover, the nano-fiber-coated scaffold would also enhance cell attach-ment. This observation is based on in-situ cellmigration and proliferation assays performed on nano-fiber-coated scaffolds (Figure 3). The Ca2þ cycling fromthe medium occurred by diffusion and this was quiteevident by the consumption of calcium from themedium, as demonstrated by biochemical analysis(Table 1).15 We attempted to enhance the cardio-myogenic differentiation of progenitor cells using car-diac conditioned medium under electromechanicalstimulation. Furthermore, these forces might have sti-mulated the Kinesin family of proteins in the adult pro-genitor cells, very small embryonic-like cells,16 andmesenchymal stem cells present in the injected mono-nuclear cells, to guide them for proliferation and sub-sequent differentiation in the congenial scaffold ofmyocardial origin. In the human heart, electricalwaves propagate through the cardiac tissue along thegap junctions, and produce contractility. This effect wasmimicked by a pacemaker current in the medium-nur-tured acellular myocardium. In addition to electricalimpulse, mechanical stress applied on the cell-seededscaffold might have triggered the complex feedbacksystem known as mechanoelectrical feedback, which isbelieved to be derived from mechanically sensitive ionchannels such as stretch-activated channels.17 That iswhy the greatest rhythmic contraction was noticed inthe ACTC that had received both forces.
Previously published data indicated that a biomim-etic system designed to deliver electrical signals mimick-ing those in native heart tissue resulted in progressivedevelopment of the conductive and contractile proper-ties characteristic of cardiac tissue.13 In another study,the effect of electrical stimulation on the cardiac
Figure 5. Flow cytometry data (scatter plot) for positive expression of (a) CD45 and (b) CD34 in cord blood mononuclear cells.
Guhathakurta et al. 7
by guest on February 21, 2014aan.sagepub.comDownloaded from

XML Template (2014) [12.2.2014–10:35am] [1–9]//blrnas3/cenpro/ApplicationFiles/Journals/SAGE/3B2/AANJ/Vol00000/140022/APPFile/SG-AANJ140022.3d (AAN) [PREPRINTER stage]
differentiation potential of cardiac adipose tissue-derived progenitor cells was evaluated. In response toelectrical stimulation, progenitor cells elongated, andboth cardiac and progenitor cells became aligned fol-lowing the linear surface pattern of the construct, andelectrical cell training within an engineered tissue seemsto be an advisable strategy.
Native ECM is complex combinations ofproteoglycans, interconnected fibrous proteins, glyco-saminoglycans, and other molecules.18 Cardiac immu-nohistochemistry analysis revealed that troponin T wasfaintly positive in cells present on the myocardial patch3 weeks after the initiation of force application in cellculture. It was reported that the differentiation andmaturational changes in the expression of troponin Tisoforms may be a key determinant of overall musclefunction.19 This possibly indicates that a small percent-age of cells on the myocardial patch were in the earlystages of differentiation and maturation. The largeanimal experiments were designed to prove the conceptin vivo. Two ACTC scaffolds and 2 glutaraldehyde-treated antigen-free cellular human myocardiumscaffolds in two different groups delivered completelydifferent results due to the biocompatibility results ofthe two different materials. No calcification or encap-sulation was seen after 120 days in the ACTC group,and integration of the scaffold into the normal myocar-dium was noticed with areas showing re-cellularizationof the acellular scaffold into cardiac muscle along withneoangiogenesis, as demonstrated by immunohisto-chemistry. As established by the large animal studies,the presence of ECM proteins collagen I and IV, fibro-nectin, and laminin would have helped to maintain theintegrity of the scaffold, and might have stimulated hostcell migration (Figure 4). Left ventricular ejection frac-tion showed a recovery to better than the preoperativeejection fraction, although negligible, but the dampen-ing on ejection fraction immediately after surgical inter-vention showed considerable recovery. However, theglutaraldehyde-treated patches revealed severe calcifi-cation in the other group. Along with calcification,encapsulation was also noticed, with von Kossa stainbeing strongly positive (Figure 3). Although glutaralde-hyde-fixation causes less antigenicity in a cellular scaf-fold, the cytotoxicity of glutaraldehyde and its leachingas a mono-aldehyde later produces calcification, andautologous cell deposition does not happen due to thecytotoxicity.20
Based on our observations, a nanofiber-coated myo-cardial tissue construct can be layered with autologouspericardium and may be inserted as an all-biologicalcomposite myocardial patch instead of using Dacronor ePTFE, as described in the Dor procedure, in casesof aneurysm repair and escharectomy. This probablywould invite effective cell migration from theT
ab
le1.
Bio
chem
ical
anal
ysis
of
diff
ere
nt
experi
menta
lgr
oups.
Tro
ponin
IKþ
(mm
olL�
1)
Caþþ
(mg
dL�
1)
Contr
action
Gro
up
Experi
ment
Without
isopre
nal
ine
With
isopre
nal
ine
Without
isopre
nal
ine
With
isopre
nal
ine
Without
isopre
nal
ine
AD
e-c
ellu
lari
zed
contr
oltiss
ueþ
MM
0.1
4�
0.0
40.1
3�
0.2
43.9
6�
1.0
46.3
2�
3.0
210.5
1�
1.2
4N
ilin
all4
experi
ments
BC
ell-
seeded
graf
tþ
mech
anic
alan
dele
ctri
cfo
rceþ
MM
4.2�
0.5
217.9
9�
0.2
25.8
6�
0.1
46.4
9�
1.0
97.9
3�
.08
þþþþ
CC
ell-
seeded
graf
tþ
mech
anic
alfo
rceþ
MM
3.5
3�
0.6
313.9
5�
0.5
05.2
6�
0.0
46.3
6�
3.0
47.5
1�
0.3
6þþþþ
DC
ell-
seeded
graf
tþ
ele
ctri
cfo
rceþ
MM
3.8
1�
1.2
819.8
3�
0.3
25.4
7�
0.0
16.2
7�
2.4
77.3
2�
1.0
2þþþ
EC
ell-
seeded
graf
tþ
MM
4.7
6�
0.0
217.9
2�
0.0
24.2
2�
2.0
36.3�
2.2
39.6
7�
0.0
1þþ
FD
e-c
ellu
lari
zed
graf
tþ
rock
ingþ
cells
inm
ediaþ
MM
3.5
2�
1.0
22.7
8�
0.5
25.0
8�
0.1
76.3
3�
1.2
37.6
2�
2.0
9þþ
in2
of
4
MM
:m
odifi
ed
card
iac
conditio
ned
media
.
8 Asian Cardiovascular & Thoracic Annals 0(0)
by guest on February 21, 2014aan.sagepub.comDownloaded from

XML Template (2014) [12.2.2014–10:35am] [1–9]//blrnas3/cenpro/ApplicationFiles/Journals/SAGE/3B2/AANJ/Vol00000/140022/APPFile/SG-AANJ140022.3d (AAN) [PREPRINTER stage]
transitional zone of damaged myocardial tissue totransform the ACTC into live myocardium. If in acompromised patient, this procedure of cardiomyo-plasty with the described myocardial patch is carriedout, then 3–4 weeks of cardiorespiratory support maydeliver a rhythmically contracting cardiac tissue con-struct with better functionality. This could potentiallyopen an arena for biventricular repair in one and halfventricle situations and also in many more indications.
Our concept evidently worked efficiently in the sheepexperiment as well as in in-vitro experiments. Furthermarker studies and immunohistochemistry at differentstages of maturation of the so-called ‘‘neomyocardium’’have to be assessed. The mechanical strength and fati-gue testing has to be conducted elaborately. The forceapplied during balloon inflation and deflation for twoweeks was not enough to derive a fatigability result.The concept of retraining and re-cellularization of anacellular myocardial scaffold in situ requires proof ofacquiring a similar conduction rhythm to that of thenative heart. We concluded that if retraining of skeletalmuscle to cardiac muscle is a possibility (skeletal cardi-omyoplasty by latissimus dorsi muscle), retrainingshould be successful in this sector as well, which is in-built in the system.
Funding
This research received no specific grant from any fundingagency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
None declared.
References
1. Robinson KA, Li J, Mathison M, et al. Extracellularmatrix scaffold for cardiac repair. Circulation 2005;
112(Suppl I): 135–143.2. Badylak SF. The extracellular matrix as a biologic scaffold
material. Biomaterials 2007; 28: 3587–3593.
3. Rosenblatt J, Devereux B and Wallace DG. Injectable col-lagen as a pH-sensitive hydrogel [Review]. Biomaterials1994; 15: 985–995.
4. Chiu RC, Zibaitis A and Kao RL. Cellular cardiomyo-
plasty: myocardial regeneration with satellite cell implant-ation. Ann Thorac Surg 1995; 60: 12–18.
5. Enomoto Y, Gorman JH, 3rd, Moainie SL, et al. Early
ventricular restraint after myocardial infarction: extent ofthe wrap determines the outcome of remodeling. AnnThorac Surg 2005; 79: 881–887.
6. Jatene AD. Left ventricular aneurysmectomy. Resection orreconstruction. J Thorac Cardiovasc Surg 1985; 89:321–331.
7. Kubo H, Jaleel N, Kumarapeli A, et al. Increased cardiacmyocyte progenitors in failing human hearts. Circulation2008; 118: 649–657.
8. Guhathakurta S, Galla S, Ramesh B, Venugopal JR,Ramakrishna S and Cherian KM. Nanofiber-reinforcedbiological conduit in cardiac surgery: preliminary report.Asian Cardiovasc Thorac Ann 2011; 19: 207–212.
9. Ramesh B, Mathapati S, Galla S, Cherian KM andGuhathakurta S. Crosslinked acellular saphenous veinfor small-diameter vascular graft. Asian Cardiovasc
Thorac Ann 2013; 21: 293–302.10. Song JJ and Ott HC. Organ engineering based on decel-
lularized matrix scaffolds [Review]. Trends Mol Med
2011; 17: 424–432.11. Guhathakurta S, Varghese S, Balasubramanian V, et al.
Technique to process xenogenic tissues for cardiovascular
implantation-a preliminary report. Current Science2006;91:1068–73. Available at: http://www.currentscience.ac.in/php/toc.php?vol¼091&issue¼08. Accessed January16, 2014.
12. Gerecht-Nir S, Radisic M, Park H, et al. Biophysicalregulation during cardiac development and applicationto tissue engineering. Int J Dev Biol 2006; 50: 233–243.
13. Radisic M, Park H, Shing H, et al. Functional assemblyof engineered myocardium by electrical stimulation ofcardiac myocytes cultured on scaffolds. Proc Natl Acad
Sci U S A 2004; 101: 18129–18134.14. Zimmermann WH, Tiburcy M and Eschenhagen T.
Cardiac tissue engineering: a clinical perspective[Review]. Future Cardiol 2007; 3: 435–445.
15. Ramesh B, Bishi DK, Rallapalli S, Arumugam S,Cherian KM and Guhathakurta S. Ischemic cardiactissue conditioned media induced differentiation of
human mesenchymal stem cells into early stage cardio-myocytes. Cytotechnology 2012; 64: 563–575.
16. Ratajczak MZ, Zuba-Surma EK, Wysoczynski M,
Ratajczak J and Kucia M. Very small embryonic-likestem cells: characterization, developmental origin, andbiological significance. Exper Hematol 2008; 36: 742–751.
17. Keldermann RH, Nash MP, Gelderblom H, Wang VYand Panfilov AV. Electromechanical wavebreak in amodel of the human left ventricle. Am J Physiol HeartCirc Physiol 2010; 299: H134–H143.
18. Fitzhugh G and Marden J. Maturational changes introponin T expression, Ca2þ-sensitivity and twitch con-traction kinetics in dragonfly flight muscle. J Exper Biol
1997; 200: 1473–1482.19. Etzion S, Barbash IM, Feinberg MS, et al. Cellular car-
diomyoplasty of cardiac fibroblasts by adenoviral deliv-
ery of MyoD ex vivo: an unlimited source of cells formyocardial repair. Circulation 2002; 106(Suppl I):125–130.
20. Zilla P, Brink J, Human P and Bezuidenhout D.
Prosthetic heart valves: catering for the few.Biomaterials 2008; 29: 385–406.
Guhathakurta et al. 9
by guest on February 21, 2014aan.sagepub.comDownloaded from