
Does subcutaneous adipose tissue behave as an (anti-)thixotropic material?

Bioceramic-collagen scaffolds loaded with human adipose-tissuederived stem cells for bone tissue engineering
Neda Daei-farshbaf • Abdolreza Ardeshirylajimi • Ehsan Seyedjafari •
Abbas Piryaei • Fatemeh Fadaei Fathabady • Mehdi Hedayati • Mohammad Salehi •
Masoud Soleimani • Hamid Nazarian • Sadegh-Lotfalah Moradi •
Mohsen Norouzian
Received: 22 June 2013 / Accepted: 16 December 2013
� Springer Science+Business Media Dordrecht 2013
Abstract The combination of bioceramics and stem cells
has attracted the interest of research community for bone
tissue engineering applications. In the present study, a
combination of Bio-Oss� and type 1 collagen gel as scaffold
were loaded with human adipose-tissue derived mesenchy-
mal stem cells (AT-MSCs) after isolation and characteriza-
tion, and the capacity of them for bone regeneration was
investigated in rat critical size defects using digital mam-
mography, multi-slice spiral computed tomography imaging
and histological analysis. 8 weeks after implantation, no
mortality or sign of inflammation was observed in the site of
defect. According to the results of imaging analysis, a higher
level of bone regeneration was observed in the rats receiving
Bio-Oss�-Gel compared to untreated group. In addition,
MSC-seeded Bio-Oss-Gel induced the highest bone recon-
struction among all groups. Histological staining confirmed
these findings and impressive osseointegration was observed
in MSC-seeded Bio-Oss-Gel compared with Bio-Oss-Gel.
On the whole, it was demonstrated that combination of AT-
MSCs, Bio-Oss and Gel synergistically enhanced bone
regeneration and reconstruction and also could serve as an
appropriate structure to bone regenerative medicine and
tissue engineering application.
Keywords Mesenchymal stem cells � Tissue
engineering � Bone � Bioceramic � Critical-size defect
Introduction
Thyroid hormones have critical functions for bone growth
and turnover process [1] which are induced by acting
directly or indirectly on bone cells including osteoblasts
and osteoclast precursors [2, 3]. In hypothyroidism, bone
resorption is increased because of the unknown mechanism
that causes osteoclast activation and growth, and finally
could lead to the development of osteoporosis. Clinical and
laboratory studies have revealed that in hypothyroid rats,
osteogenesis is decreased in the site of bone defects [4]. In
addition, patients prescribed a high dose of levothyroxine
for the treatment of thyroid hormones lackness, may
experience effects that mimic hyperthyroidism [5]. So
generally, thyroid hormones deficiency is considered to
cause abnormal skeletal regeneration [6].
There are several clinical methods such as bone grafting
and tissue engineering for the treatment of bone defects [7].
Bone graft methods are categorized into three subdivisions
N. Daei-farshbaf � A. Piryaei � F. Fadaei Fathabady �H. Nazarian � M. Norouzian (&)
Departments of Anatomy and Cell Biology, Shahid Beheshti
University of Medical Sciences, Tehran, Iran
e-mail: [email protected]
A. Ardeshirylajimi � S.-L. Moradi
Departments of Stem Cell Biology, Stem Cell Technology
Research Center, Tehran, Iran
e-mail: [email protected]
E. Seyedjafari
Department of Biotechnology, College of Science, University of
Tehran, Tehran, Iran
M. Hedayati
Endocrine Research Center, Shahid Beheshti University of
Medical Sciences, Tehran, Iran
M. Salehi
Department of Biotechnology, Faculty of Medicine, Shahid
Beheshti University of Medical Sciences, Tehran, Iran
M. Soleimani
Department of Hematology, Faculty of Medical Science, Tarbiat
Modares University, Tehran, Iran
123
Mol Biol Rep
DOI 10.1007/s11033-013-2913-8

including autologous, allogenic and xenogenic transplan-
tations. Autografts are in some way a gold standard
because they avoid most problems related to transfection
and rejection. However, they do involve significant donor
site morbidity and chronic donor shortages. Allografts are
made of tissue that derived from other individuals of the
same species. This tissue must be thoroughly sterilized in
order to avoid immunological reactions in the receiver and
infections. Their limitations include donor shortages and
risks of infections as mentioned above. Xenograft advan-
tage of being available in different shapes and sizes, but
they also have a non-negligible risk of immunological
reactions and infection. Therefore, scientists should take
the advantage of new methods referred to as tissue engi-
neering and regenerative medicine for the treatment of
patient’s tissue defects or damages [7, 8].
For tissue engineering, stem cells and scaffolds are the
two essential components [9]. There are many important
requirements for scaffolds such as biocompatibility, bio-
degradability and providing conditions resembling host
tissue in order to prevent the rejection of implanted cells or
tissues [10, 11]. In this study, we used a combination of
Bio-Oss� and type 1 collagen gel as scaffold for bone
regeneration applications. Bio-Oss is a deproteinized
bovine bone material and has unique features such as a
condensed strength of 35 Mpa and its highly porous nature
(75–80 % of the total volume) which increase the surface
area of the scaffolds. Bio-Oss is one of the several bioce-
ramics that are commonly used for treatment of osseous
defects, dental implant therapy, and periodontal defects
[10]. Furthermore, alternative to this sponge-type scaffold,
we used a type 1 collagen gel (from rat tail) which can
enhance the proliferating potential of stem cells and culture
mineralization [12]. Collagen is a fibrous protein that is
mostly found in skin, bone, tendons and other connective
tissues, and is consisted of three alpha-chains which can
combine to form a rope-like triple helix, providing tensile
strength to the extracellular matrix (ECM).
Stem cells have unique features such as intensive
regenerating potential, immunosuppressive features and
strong plasticity required for clinical trial and cell therapy
[13–15]. Mesenchymal stem cells (MSCs), especially with
the origin of bone marrow, are an efficient source for
regenerative medicine and tissue engineering applications
[16, 17]. However, preparation of MSCs from patient’s
bone marrow is an invasive procedure and suffers from
ethical issues. Nowadays, scientists have introduced other
MSCs sources such as human adipose tissue [18–20].
Isolation of MSCs from adipose (AT-MSCs) tissue is a
simple process and fat harvesting is much simpler versus
bone marrow aspiration. In addition, the yield of stem cells
from adipose tissue is higher than those from bone marrow
[21, 22]. Scarce morbidity of AT-MSCs during isolation
and low amount of needed factors for their growth and
expansion are other reasons for the priority of AT-MSCs
over BM.MSCs [19].
The purpose of the present study was to conduct tissue
engineering in hypothyroid models which suffers from
decreased bone regenerating ability using a combination of
Bio-Oss and collagen type I loaded with AT-MSCs.
Materials and methods
Isolation of human Ad-MSCs
The AT-MSCs were isolated from adipose tissue samples
collected at operations or liposuctions from five donors
(mean age 40 ± 5, Erfan Hospital, Tehran, Iran) after
informed consent according to guidelines of the Medical
Ethics Committee, Shahid Beheshti University of Medical
Sciences and Health services (Tehran, Iran). After washing
tissue, it was digested with collagenase type I (Sigma) and
incubated for about 1 h. After centrifugation, the supernatant
was removed and the cell pellet was treated with RBC lysis
buffer (Dako, Glostrup, Denmark) at room temperature (RT)
for 5 min. AT-MSCs were expanded in T-75 polystyrene
flasks in maintenance medium consisting of Dulbecco’s
modified Eagle’s medium (DMEM, Gibco, Grand Island,
NY, USA), 10 % fetal bovine serum (FBS, sigma), and
100 mg/mL streptomycin and 100 U/mL penicillin (1 %
antibiotics, Gibco). They were grown at 95 % air, 37 �C and
5 % CO2 atmosphere. Maintenance medium was replaced by
growth medium with 15 % FBS. Growth medium was
changed every 2 or 3 days. Unattached cells were discarded
by refreshing the medium. After reaching confluence (about
80–85 %) during 10 days, the cells were dissociated with
trypsin (2 min in 37 �C, 5 % CO2) and replated. Cells from
passages two were used for all procedure.
Characterization of isolated human Ad-MSCs
Flow cytometer surface markers
The human AT-MSCs were detached from the tissue cul-
ture flasks after 2 weeks in vitro with trypsin/EDTA and
counted. About 2 9 105 cells were divided into aliquots
and centrifuged at 1,200 rpm for 5 min at RT. The pellet
was resuspended in human serum and incubated for 30 min
on ice. After centrifugation at 1,000 rpm for 5 min, the
pellet was resuspended in 3 % (v/v) human serum albumin
(HSA)/PBS and incubated with appropriate antibodies
including fluorescent isothiocyanate (FITC)-conjugated
mouse anti-human CD45 (leukocyte common antigen),
Phycoerythrin (PE)-conjugated CD105 (Endoglin or SH2)
CD34, CD90and CD10 for 1 h on ice, washed twice in PBS
Mol Biol Rep
123

and centrifuged for 5 min. The cells were resuspended in
100 ll of PBS and studied by a Coulter Epics-XL flow
cytometer (Beckman Coulter, CA, USA). An isotype con-
trol with FITC- or PE-labeled antibodies was included in
each experiment, and specific staining was measured from
the cross point of the isotype using a specific antibody
graph. The corresponding histograms were created by Win
MDI 2.8 software (Scripps Institute, CA, USA).
Osteogenic and adipogenic differentiation
The potential of the isolated cells to differentiate into
osteogenic and adipogenic lineages was examined. For
osteogenic differentiation, human AT-MSCs were induced
for 3 weeks by DMEM supplemented with 10 % FBS,
0.1 mM dexamethasone, 10 mM b-glycerophosphate, and
50 mM ascorbate 2-phosphate. The medium was replaced
every 2 days up to 3 weeks. The cells were fixed with cold
4 % paraformaldehyde for 20 min at 4 �C and evaluated by
specific histochemical staining for mineralization with
alizarin red staining kit. The staining was examined with a
phasecontrast microscope (Nikon, Tokyo, Japan).
For adipogenesis, the cells were incubated in adipogenic
inductive medium. This medium consisted of DMEM
supplemented with 10 % FBS, 1 mM dexamethasone,
200 mM indomethacin, 500 mM isobutyl-methyl xanthine
and ascorbate 2-phosphate for 18 days. After 18 days, the
cells were evaluated for adipocyte identification, using oil
red O-staining. Briefly, cells were fixed in cold 4 % para-
formaldehyde for 20 min at 4 �C, washed washed with
PBS two times, and stained with oil red O-solution for
5–10 min at 37 �C, the cells were washed again with PBS
three times and depicted by the light microscope. All
control groups without the differentiation inductive med-
ium were maintained in parallel to the differentiation
experiments and stained in the same manner.
Cell labeling
Before the cells seeded on scaffold, in passage two were
labeled. PKH26 red fluorescent cell linker kit (Sigma-
Aldrich) was used according to the manufacturer’s
instructions. In brief, human AT-MSCs were suspended in
a mixture of 1 mL of diluent C (Sigma-Aldrich) and 1 mL
of 4 9 10 - 6 molar PKH26 dye (Sigma-Aldrich) in
polypropylene tubes at room temperature. The samples
were then immediately mixed by pipetting and incubated at
25 �C for 3 min. At the end of this period, the staining
reaction was stopped by adding equal volumes of 1 % fetal
bovine serum for 1 min. Excessive staining solution was
removed by centrifugation of the cells at 400 g for 10 min.
The cells were resuspended in the complete medium and
examined by fluorescence microscopy for labeling.
Cell seeding on Bio-Oss� and type I collagen gel
After labeling stem cells, these cells were seeded on Bio-
Oss� particles (Geistlich Pharma AG, Switzerland) and
were incubated on 37 �C and 5 % CO2 about 8 h for
attaching. Then optimized protein concentration of Colla-
gen type I (GIBCO�) was provided according to the
manufacturer’s instructions. After collagen was provided,
appropriate numbers of AT-MSCs-seeded Bio-Oss� parti-
cles rinsed into it and then implanted in the site of rat
critical size calvarial defect immediately.
Animal model
All animal experiments were performed in accordance with
the Shahid Beheshti University of Medical Sciences and
Health services (Tehran, Iran) guidelines. Nine 6–7 weeks-
old male Wistar rats with a body weight of 190–200 g (five
animals per group, Razi Institute, Karaj, Iran) were used as
transplant recipients. Before surgery, the animals were kept
in clean and standard air conditions at a constant temperature
of 21 �C with a 12-h light/day cycle. They had ad libitum
access to drinking water and a standard laboratory rat food
pellet diet. Rats were anesthetized by intramuscular injec-
tion of 50 mg/kg ketamine hydrochloride with 5 mg/kg
diazepam under sterile conditions. After obtaining blood
samples from corner of their eyes, thyroid hormones (T3,
T4) were measured by radioimmunoassay kit. Digestion of
4 mg powdered methimazole (Tehran, Iran hormone) dis-
solved in 100 cc distilled water for 4 weeks induced hypo-
thyroidism. Thyroid hormones were determined again after
methimazole treatment. After 1 week interval, these rats
were watered with methimazole solution again for 4 weeks
and this schedule was performed all the period of study.
Surgery and transplantation procedure
According to the protocol is mentioned above hypothyroid
rats were anesthetized. Then, skin and periosteum were
raised to expose the calvaria. In all of the rats, an 8 mm
critical-size defect was made in the parietal bone by a
dental bur. Constant saline irrigation was provided and the
dura mater was kept intact. The procedure was performed
under sterile conditions. After transplantation, the skin
incision was closed with nylon sutures. The animals were
kept in sterile condition with enough water and foods. Nine
hypothyroid rats randomly divided into three groups:
control group with empty defect, first experimental group
defect filled with scaffold (Bio-Oss� and type I collagen
gel) only, second experimental group defect filled with
mentioned scaffold loaded with AT-MSCs. The rats were
sacrificed 6 weeks after transplantation and their calvarias
with grafts were harvested.
Mol Biol Rep
123
Digital mammography and multislice spiral computed
tomography (MSCT) imaging analysis
After 8 weeks, the animals were euthanized, and their
craniums were excised and placed in 10 % formalin. The
cranium samples were then radiographed under direct
digital mammography equipment (KonicaMinolta, Regius
model 110HQ) and were also scanned using a spiral high-
resolution computed tomography (CT) system (Siemens,
SOMATOM Sensation) in multislice mode. The radio-
graph images from digital mammography were scored by
two independent radiologists. To quantify the level of bone
regeneration via MSCT, a 9-mm circular region of interest
was placed in each CT image. The area of newly formed
bone was quantified relative to the original calvarial defect
[23].
Histological analysis
The fixed cranium samples were decalcified in ethylene
di-amine tetra acetic acid/HCl and embedded in paraffin.
For light microscopy studies, histological sections with
3–5 lm thickness were obtained and stained with
hematoxylin and eosin (H&E). The area of newly formed
bone was quantified using a computer-assisted Image-Pro
Plus System (Media Cybernetics, Silver Springs, MD,
USA).
Statistical analysis
Each experiment was performed at least 3 times in vivo.
MSCT and H&E data were reported as mean ± standard
deviation (SD). One-way analysis of variance (ANOVA)
was used to compare the results. All analyses were per-
formed using SPSS 17.0 software. P values of\0.05 were
considered as statistically significant.
Results
Characterization of isolated AT-MSCs
Isolated AT-MSCs were passaged two times and then were
evaluated through its morphology and surface markers.
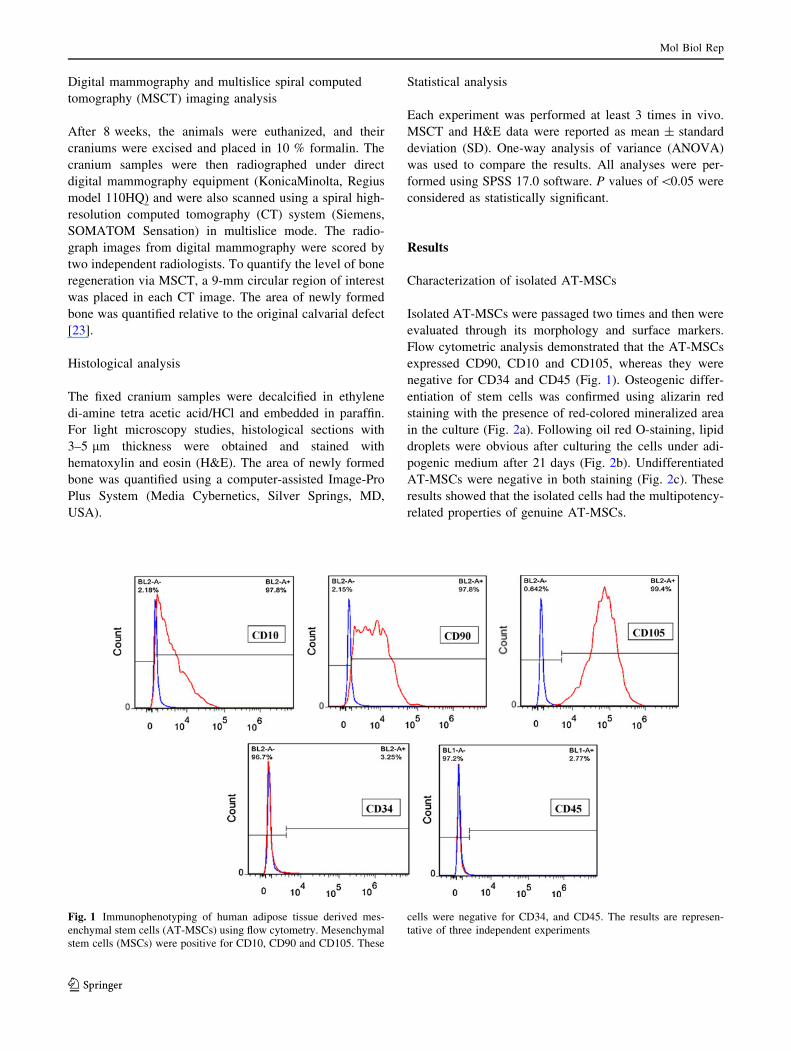
Flow cytometric analysis demonstrated that the AT-MSCs
expressed CD90, CD10 and CD105, whereas they were
negative for CD34 and CD45 (Fig. 1). Osteogenic differ-
entiation of stem cells was confirmed using alizarin red
staining with the presence of red-colored mineralized area
in the culture (Fig. 2a). Following oil red O-staining, lipid
droplets were obvious after culturing the cells under adi-
pogenic medium after 21 days (Fig. 2b). Undifferentiated
AT-MSCs were negative in both staining (Fig. 2c). These
results showed that the isolated cells had the multipotency-
related properties of genuine AT-MSCs.
Fig. 1 Immunophenotyping of human adipose tissue derived mes-
enchymal stem cells (AT-MSCs) using flow cytometry. Mesenchymal
stem cells (MSCs) were positive for CD10, CD90 and CD105. These
cells were negative for CD34, and CD45. The results are represen-
tative of three independent experiments
Mol Biol Rep
123

In vivo bone regeneration
Gross examinations
No mortality or sign of complication was observed during
study in any of the animals. As we showed in Fig. 3a, no
sign of wound fester, bleeding, infection, effusion, or scalp
edema was observed at the site of osseous defects after
surgery. After 8 weeks of implantation, all samples were
retrieved for evaluation of new bone reconstruction. No
sign of inflammation or Bio-Oss particle disintegration was
observed at the site of calvarial defects (Fig. 3b). Evalua-
tion of the untreated control group showed negative
spontaneous mineralization and bone healing in the osse-
ous defect after the period of study (Fig. 3b). As we
showed in Fig. 4c, all implanted particles were well inte-
grated into the calvarial osseous defect with no sign of
encapsulation or prominent foreign body reaction. More-
over, the Bio-Oss particles also adhered strongly to the host
bone tissue without any fixation.
Evaluation of bone regeneration
Quantification of newly formed bone on the fixed calvar-
ium specimens after 8 weeks of implantation was per-
formed by digital mammography and MSCT. Results of the
radiological analysis of different groups have been shown
in Fig. 4. Qualitatively, the data revealed reconstruction of
calvarial osseous defects after implantation of particles.
Results of the quantitative analysis of the regenerated bone
areas demonstrated that a higher amount of new mineral-
ized osseous tissue was observed in the groups that
received stem cell-seeded Bio-Oss-Gel compared to Bio-
Oss-Gel and untreated control groups (P \ 0.05). Results
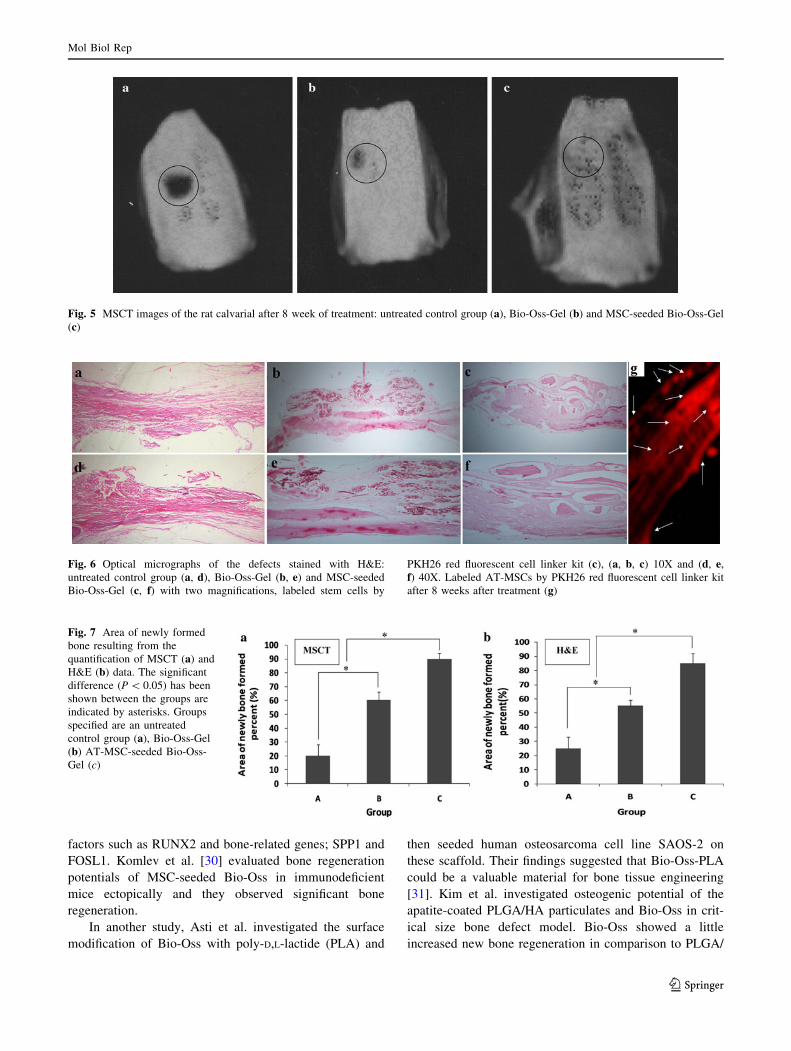
of MSCT have shown that the area of newly formed bone
in stem cell-seeded Bio-Oss-Gel exhibited a complete
regeneration of the calvarial osseous defect compared to
other groups (Fig. 5). In addition, different levels of void
defects were detected in all control groups with no treat-
ment. In both CT and digital mammography, bone regen-
eration was observed to begin from the edges of the
osseous defect toward the center. Since the area of newly
bone formed in untreated groups was not significant, so the
8-mm-diameter osseous defects were demonstrated to be a
critical-size rat calvarial osseous defect in this study.
Finally, histological evaluation was performed to trace
AT-MSCs in the area of newly bone formed in calvarial
osseous defect (Fig. 6). The area of newly formed bone
was revealed as mean ± SD and is shown in Fig. 7. The
highest amount of newly formed bone tissue was perceived
in the rats treated with AT-MSC-seeded Bio-Oss-Gel
(P \ 0.05). Although the healing pattern of calvarial
osseous defects was similar in animals that treated with
Bio-Oss-Gel and AT-MSC-seeded Bio-Oss�-Gel, but in
the latter group, the healing was much more significant
than animals received cell-free Bio-Oss-Gel and control
groups (P \ 0.05).
Discussion
Bone defects are one of the most important and frequent
problems in human health care. Since, bone turnover is a
complicated and long process, biomimetic approach in
tissue engineering and regenerative medicine have been
shown to be an efficient way to design biocompatible and
osteoinductive scaffolds for bone implants applications.
These problems are much increased in patients with
hypothyroidism. Over the four decades, bioceramics have
been known as classic bone graft substitutes. In addition,
there are many polymers that have been used in tissue
engineering and their number are increasing However,
Fig. 2 Morphology of stem cells under two induction medium, after
a 21-day culture under basal medium (a), oil red O-staining of stem
cells after a 21-day culture under adipogenic induction medium
(b) and alizarin red staining of stem cells after a 21-day under
osteogenic induction medium (c), all with low magnification
Mol Biol Rep
123

findings showed that combination of stem cells and bi-
oceramics has been shown more efficient to reconstruct the
bone in osseous defects than when used individually [24–
26].
In the present study, we aimed to evaluate the osteoin-
ductivity of human MSCs seeded on natural bioceramic
implanted in hypothyroid rat calvarial defects. One of the
most important bioceramics that has been studied in bone
tissue engineering and regenerative medicine is calcium-
phosphate based ceramics. Among them, many studies
have reported the highly efficient in vitro and in vivo
performance of hydroxyapatite (HA) as bone implants. HA
could be used in two ways: as scaffolds or as nanoparticles
for coating the surface of other scaffolds. Finding of Bigi
et al. [27] showed the improved adherent of bone to the
surface of HA-coated alloy implant. Dinarvand et al. have
used a combination of bioceramics (HA, bioactive glass
(BG) tricalcium phosphate (TCP) particles) and polymeric
nanofibers (electrospun poly(L-lactic acid) (PLLA) nanof-
ibers) to evaluate their osteogenic potential in vivo. Their
findings showed the highest bone reconstruction in animals
treated with nanofibers coated simultaneously with HA and
BG [28]. In another study, Sollazzo et al. [29] demon-
strated the increased osteogenic differentiation of periph-
eral blood human MSCs seed on Bio-Oss. They evaluated
the in vitro expression of osteoblastic transcriptional
Fig. 3 Critical-size defect created in rat calvaria without (a) or with (b) implanted scaffold and after 8 week treatment (c)
Fig. 4 Digital mammography images of the rat calvarial 8 weeks after treatment: untreated control group (a), Bio-Oss-Gel (b) and MSC-seeded
Bio-Oss-Gel (c)
Mol Biol Rep
123
factors such as RUNX2 and bone-related genes; SPP1 and
FOSL1. Komlev et al. [30] evaluated bone regeneration
potentials of MSC-seeded Bio-Oss in immunodeficient
mice ectopically and they observed significant bone
regeneration.
In another study, Asti et al. investigated the surface
modification of Bio-Oss with poly-D,L-lactide (PLA) and
then seeded human osteosarcoma cell line SAOS-2 on
these scaffold. Their findings suggested that Bio-Oss-PLA
could be a valuable material for bone tissue engineering
[31]. Kim et al. investigated osteogenic potential of the
apatite-coated PLGA/HA particulates and Bio-Oss in crit-
ical size bone defect model. Bio-Oss showed a little
increased new bone regeneration in comparison to PLGA/
Fig. 5 MSCT images of the rat calvarial after 8 week of treatment: untreated control group (a), Bio-Oss-Gel (b) and MSC-seeded Bio-Oss-Gel
(c)
Fig. 6 Optical micrographs of the defects stained with H&E:
untreated control group (a, d), Bio-Oss-Gel (b, e) and MSC-seeded
Bio-Oss-Gel (c, f) with two magnifications, labeled stem cells by
PKH26 red fluorescent cell linker kit (c), (a, b, c) 10X and (d, e,
f) 40X. Labeled AT-MSCs by PKH26 red fluorescent cell linker kit
after 8 weeks after treatment (g)
Fig. 7 Area of newly formed
bone resulting from the
quantification of MSCT (a) and
H&E (b) data. The significant
difference (P \ 0.05) has been
shown between the groups are
indicated by asterisks. Groups
specified are an untreated
control group (a), Bio-Oss-Gel
(b) AT-MSC-seeded Bio-Oss-
Gel (c)
Mol Biol Rep
123

HA particulates in the site of defect [32]. From a gross
view, after 8 weeks, no sign of inflammation or bleeding
was observed in the site of implantation for any of the
animals. This observation was confirmed by histological
study and showed the in vivo biocompatibility of our
scaffolds in the animal model. Two independent quantita-
tive methods were used to evaluate the amount of miner-
alization and bone reconstruction during the treatment
period. Interestingly, similar results were found from both
X-ray imaging and MSCT which demonstrated that MSC-
Bio-Oss-Gel scaffold induced the highest level of bone
reconstruction compared to that result from scaffolds
without stem cells. These results demonstrated that not
only human MSCs were not rejected, also bone regenera-
tion was enhanced via these cells in the site of osseous
defect. Presence of human MSCs in the newly formed bone
in the site of defect was confirmed by PKH26 red staining
results.
As the Bio-Oss collagen product has not received suf-
ficient attention in the tissue engineering literatures, in the
present study we used rat critical-size calvarial model for
evaluation of stem cell-seeded Bio-Oss effects on bone
regeneration. By the way, our data demonstrated that
combination of AT-MSCs, Bio-Oss and Gel synergistically
enhanced osseous regeneration and reconstruction higher
than that observed for Bio-Oss and Gel.
Finally, our data from radiology photography and
MSCT were confirmed by pathological analysis. In addi-
tion, penetration of the newly formed bone into the scaf-
folds obviously indicated the capability of AT-MSC-Bio-
Oss-Gel scaffolds to induce an efficient amount of osteo-
integration which is critical for an absolute healing of
osseous lesions and defects.
Conclusion
In this study, we demonstrated that AT-MSC-seeded Bio-
Oss-Gel could be used as an appropriate support to guide
bone reconstruction. In addition, Bio-Oss-Gel could be a
suitable tissue-engineered matrix to support stem cells for
bone regenerative applications.
References
1. Williams GR (2009) Actions of thyroid hormones in bone. En-
dokrynol Pol 60(5):380–388
2. Abe E, Marians RC, Yu W, Wu X-B, Ando T, Li Y, Iqbal J,
Eldeiry L, Rajendren G, Blair HC (2003) TSH is a negative
regulator of skeletal remodeling. Cell 115(2):151–162
3. Tsai J, Janson A, Bucht E, Kindmark H, Marcus C, Stark A,
Zemack HR, Torring O (2004) Weak evidence of thyrotropin
receptors in primary cultures of human osteoblast-like cells.
Calcif Tissue Int 74(5):486–491
4. Fadaei Fathabady F, Norouzian M, Azizi F (2005) Effect of
Hypothyroidism on Bone Repair inMature Female Rats. Int J
Endocrinol Metab 1:126–129
5. Vaidya B, Pearce SH (2008) Management of hypothyroidism in
adults. BMJ 337:a801
6. Bassett JD, Williams AJ, Murphy E, Boyde A, Howell PG,
Swinhoe R, Archanco M, Flamant F, Samarut J, Costagliola S
(2008) A lack of thyroid hormones rather than excess thyrotropin
causes abnormal skeletal development in hypothyroidism. Mol
Endocrinol 22(2):501–512
7. Ardeshirylajimi A, Dinarvand P, Seyedjafari E, Langroudi L,
Adegani FJ, Soleimani M (2013) Enhanced reconstruction of rat
calvarial defects achieved by plasma-treated electrospun scaf-
folds and induced pluripotent stem cells. Cell Tissue Res
354(3):849–860
8. Dinarvand P, Farhadian S, Seyedjafari E, Shafiee A, Jalali A,
Sanaei-rad P, Dinarvand B, Soleimani M (2013) Novel approach
to reduce postsurgical adhesions to a minimum: administration of
losartan plus atorvastatin intraperitoneally. J Surg Res
181(1):91–98
9. Arvidson K, Abdallah B, Applegate L, Baldini N, Cenni E, Go-
mez-Barrena E, Granchi D, Kassem M, Konttinen Y, Mustafa K
(2011) Bone regeneration and stem cells. J Cell Mol Med
15(4):718–746
10. Araujo MG, Liljenberg B, Lindhe J (2010) Dynamics of Bio-
Oss� collagen incorporation in fresh extraction wounds: an
experimental study in the dog. Clin Oral Implant Res 21(1):55–64
11. Dinarvand P, Hashemi SM, Seyedjafari E, Shabani I, Moham-
madi-Sangcheshmeh A, Farhadian S, Soleimani M (2012)
Function of poly (lactic-co-glycolic acid) nanofiber in reduction
of adhesion bands. J Surg Res 172(1):e1–e9
12. Eslaminejad MB, Mirzadeh H, Nickmahzar A, Mohamadi Y,
Mivehchi H (2009) Type I collagen gel in seeding medium
improves murine mesencymal stem cell loading onto the scaffold,
increases their subsequent proliferation, and enhances culture
mineralization. J Biomed Mater Res B Appl Biomater
90(2):659–667
13. Levi B, James AW, Wan DC, Glotzbach JP, Commons GW,
Longaker MT (2010) Regulation of human adipose-derived
stromal cell osteogenic differentiation by insulin-like growth
factor-1 and platelet-derived growth factor-alpha. Plast Reconstr
Surg 126(1):41
14. Yoon E, Dhar S, Chun DE, Gharibjanian NA, Evans GR (2007)
In vivo osteogenic potential of human adipose-derived stem cells/
poly lactide-co-glycolic acid constructs for bone regeneration in a
rat critical-sized calvarial defect model. Tissue Eng
13(3):619–627
15. Kode JA, Mukherjee S, Joglekar MV, Hardikar AA (2009)
Mesenchymal stem cells: immunobiology and role in immuno-
modulation and tissue regeneration. Cytotherapy 11(4):377–391
16. Kon E, Muraglia A, Corsi A, Bianco P, Marcacci M, Martin I,
Boyde A, Ruspantini I, Chistolini P, Rocca M (2000) Autologous
bone marrow stromal cells loaded onto porous hydroxyapatite
ceramic accelerate bone repair in critical-size defects of sheep
long bones. J Biomed Mater Res 49(3):328–337
17. Cui L, Liu B, Liu G, Zhang W, Cen L, Sun J, Yin S, Liu W, Cao
Y (2007) Repair of cranial bone defects with adipose derived
stem cells and coral scaffold in a canine model. Biomaterials
28(36):5477–5486
18. Løken S, Jakobsen RB, Arøen A, Heir S, Shahdadfar A,
Brinchmann J, Engebretsen L, Reinholt F (2008) Bone marrow
mesenchymal stem cells in a hyaluronan scaffold for treatment of
an osteochondral defect in a rabbit model. Knee Surg Sports
Traumatol Arthrosc 16(10):896–903
Mol Biol Rep
123
19. Zuk PA, Zhu M, Mizuno H, Huang J, Futrell JW, Katz AJ,
Benhaim P, Lorenz HP, Hedrick MH (2001) Multilineage cells
from human adipose tissue: implications for cell-based therapies.
Tissue Eng 7(2):211–228
20. Haimi S, Suuriniemi N, Haaparanta A-M, Ella V, Lindroos B,
Huhtala H, Raty S, Kuokkanen H, Sandor GK, Kellomaki M
(2008) Growth and osteogenic differentiation of adipose stem
cells on PLA/bioactive glass and PLA/b-TCP scaffolds. Tissue
Eng Part A 15(7):1473–1480
21. Mitchell JB, McIntosh K, Zvonic S, Garrett S, Floyd ZE, Kloster
A, Di Halvorsen Y, Storms RW, Goh B, Kilroy G (2006)
Immunophenotype of human adipose-derived cells: temporal
changes in stromal-associated and stem cell-associated markers.
Stem cells 24(2):376–385
22. Fraser JK, Schreiber R, Strem B, Zhu M, Alfonso Z, Wulur I,
Hedrick MH (2006) Plasticity of human adipose stem cells
toward endothelial cells and cardiomyocytes. Nat Clin Pract
Cardiovasc Med 3:S33–S37
23. Ardeshirylajimi A, Hosseinkhani S, Parivar K, Yaghmaie P,
Soleimani M (2013) Nanofiber-based polyethersulfone scaffold
and efficient differentiation of human induced pluripotent stem
cells into osteoblastic lineage. Mol Biol Rep 40(7):4287–4294
24. Marcacci M, Kon E, Moukhachev V, Lavroukov A, Kutepov S,
Quarto R, Mastrogiacomo M, Cancedda R (2007) Stem cells
associated with macroporous bioceramics for long bone repair:
6-to 7-year outcome of a pilot clinical study. Tissue Eng
13(5):947–955
25. Ohgushi H, Miyake J, Tateishi T (1999) Mesenchymal stem cells
and bioceramics: strategies to regenerate the skeleton. In:
Novartis foundation symposium, 2003. Wiley, New York,
pp 118–126
26. Takahashi Y, Yamamoto M, Tabata Y (2005) Osteogenic dif-
ferentiation of mesenchymal stem cells in biodegradable sponges
composed of gelatin and \i[b\/i[-tricalcium phosphate. Bio-
materials 26(17):3587–3596
27. Bigi A, Fini M, Bracci B, Boanini E, Torricelli P, Giavaresi G,
Aldini NN, Facchini A, Sbaiz F, Giardino R (2008) The response
of bone to nanocrystalline hydroxyapatite-coated Ti13Nb11Zr
alloy in an animal model. Biomaterials 29(11):1730–1736
28. Dinarvand P, Seyedjafari E, Shafiee A, Babaei Jandaghi A,
Doostmohammadi A, Fathi MH, Farhadian S, Soleimani M
(2011) New approach to bone tissue engineering: simultaneous
application of hydroxyapatite and bioactive glass coated on a
poly (L-lactic acid) scaffold. ACS Appl Mater Interfaces
3(11):4518–4524
29. Sollazzo V, Palmieri A, Scapoli L, Martinelli M, Girardi A, Al-
viano F, Pellati A, Perrotti V, Carinci F (2010) Bio-Oss� acts on
Stem cells derived from peripheral blood. Oman Med J 25(1):26
30. Komlev V, Mastrogiacomo M, Pereira R, Peyrin F, Rustichelli F,
Cancedda R (2010) Biodegradation of porous calcium phosphate
scaffolds in an ectopic bone formation model studied by X-ray
computed microtomography. Eur Cell Mater 19:136–146
31. Asti A, Visai L, Dorati R, Conti B, Saino E, Sbarra S, Gastaldi G,
Benazzo F (2008) Improved cell growth by Bio-Oss/PLA scaffolds
for use as a bone substitute. Technol Health Care 16(6):401–413
32. Kim S–S, Kim B-S (2008) Comparison of osteogenic potential
between apatite-coated poly (lactide-co-glycolide)/hydroxyapa-
tite particulates and Bio-Oss. Dent Mater J 27(3):368–375
Mol Biol Rep
123
Copyright © 2022 FDOKUMEN




















