Progression and regression in renal vascular and glomerular fibrosis
12
CURRENT STATUS REVIEW Progression and regression in renal vascular and glomerular fibrosis Christos Chatziantoniou, Jean-Jacques Boffa, Pierre-Louis Tharaux, Martin Flamant, Pierre Ronco and Jean-Claude Dussaule Inserm U489, Tenon Hospital, Paris, France I N T E R N AT I O N A L JOURNAL OF E X P E R I M E N TA L PAT H O L O G Y Summary End-stage renal disease (ESRD) is characterized by the development of fibrotic lesions in the glomerular, interstitial and vascular compartments. Renal fibrogenesis, a common complication of diabetes and hypertension, is a complex dynamic process involving several players such as inflammatory agents, cytokines, vasoactive agents and enzymes participating in extracellular matrix assembly, anchoring or degradation. The only available treatment today against chronic renal failure is dialysis or kidney transplant- ation, making thus ESRD one of the most expensive diseases to treat on a per-patient basis. An emerging challenge for clinicians, maybe the nephrologist’s Holy Grail in the 21st century, is to stop definitively the decline of renal function and, if possible, to achieve regression of renal fibrosis and restoration of renal structure. Over the last 5 years, different approaches have been tested in experimental models of nephropathy with variable degree of success. In this review, we will focus on the mechanisms of the hypertension-associated fibrosis and the few recent studies that gave promising results for a therapeutic intervention. Keywords angiotensin II, collagen I, progression, regression, renal vascular remodelling Diabetes and hypertension are amongst the leading causes of end- stage renal failure (ESRF), accounting for more than 60% of new cases (United States Renal Data System 1998; Valderrabano et al. 1996). Kidney disease can also develop from infection, inflamma- tion of renal blood vessels and glomeruli, kidney stones and cysts. ESRF is characterized by the development of fibrotic lesions in the glomerular, interstitial and vascular compartments. These lesions are defined by the abnormal accumulation of extracellular matrix (mainly fibrillar collagens) that substitutes normal kidney struc- ture. Under normal conditions, the formation of extracellular matrix is a dynamic equilibrium between systems that promote its synthesis and those that favour its degradation. In pathophysio- logical conditions that lead to the development of fibrosis, this equilibrium is broken due to exaggerated rates of extracellular matrix synthesis, to diminished capacity of degradation or to a combination of both. This process appears irrespective of the underlying disease and originating compartment, pointing out a final common pathway, independently of the primary cause. Under this view, identifying and targeting the systems participating in this pathway may provide an efficient treatment against renal fibrosis and failure regardless of the initiating pathology. Over the last years, an important progress has been made towards this Received for publication 7 January 2004 Accepted for publication 19 February 2004 Correspondence: Christos Chatziantoniou Inserm U489 Tenon Hospital 4 rue de la Chine 75020 Paris, France Tel.: +33 1 5601 6658 Fax: +33 1 4364 5448 E-mail: christos.chatziantoniou@tnn. ap-hop-paris.fr Int. J. Exp. Path. (2004), 85, 1–11 Ó 2004 Blackwell Publishing Ltd 1
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Progression and regression in renal vascular and glomerular fibrosis

CURRENT STATUSREVIEW
Progression and regression in renal vascular and glomerular fibrosis
Christos Chatziantoniou, Jean-Jacques Boffa, Pierre-Louis Tharaux, Martin Flamant, Pierre Ronco and
Jean-Claude Dussaule
Inserm U489, Tenon Hospital, Paris, France
I N T E R N AT I O N A LJOURNAL OFE X P E R I M E N TA LPAT H O L O G Y
Summary
End-stage renal disease (ESRD) is characterized by the development of fibrotic lesions in
the glomerular, interstitial and vascular compartments. Renal fibrogenesis, a common
complication of diabetes and hypertension, is a complex dynamic process involving
several players such as inflammatory agents, cytokines, vasoactive agents and enzymes
participating in extracellular matrix assembly, anchoring or degradation. The only
available treatment today against chronic renal failure is dialysis or kidney transplant-
ation, making thus ESRD one of the most expensive diseases to treat on a per-patient
basis. An emerging challenge for clinicians, maybe the nephrologist’s Holy Grail in the
21st century, is to stop definitively the decline of renal function and, if possible, to
achieve regression of renal fibrosis and restoration of renal structure. Over the last 5
years, different approaches have been tested in experimental models of nephropathy
with variable degree of success. In this review, we will focus on the mechanisms of the
hypertension-associated fibrosis and the few recent studies that gave promising results
for a therapeutic intervention.
Keywords
angiotensin II, collagen I, progression, regression, renal vascular remodelling
Diabetes and hypertension are amongst the leading causes of end-
stage renal failure (ESRF), accounting for more than 60% of new
cases (United States Renal Data System 1998; Valderrabano et al.
1996). Kidney disease can also develop from infection, inflamma-
tion of renal blood vessels and glomeruli, kidney stones and cysts.
ESRF is characterized by the development of fibrotic lesions in the
glomerular, interstitial and vascular compartments. These lesions
are defined by the abnormal accumulation of extracellular matrix
(mainly fibrillar collagens) that substitutes normal kidney struc-
ture. Under normal conditions, the formation of extracellular
matrix is a dynamic equilibrium between systems that promote
its synthesis and those that favour its degradation. In pathophysio-
logical conditions that lead to the development of fibrosis, this
equilibrium is broken due to exaggerated rates of extracellular
matrix synthesis, to diminished capacity of degradation or to a
combination of both. This process appears irrespective of the
underlying disease and originating compartment, pointing out a
final common pathway, independently of the primary cause.
Under this view, identifying and targeting the systems participating
in this pathway may provide an efficient treatment against renal
fibrosis and failure regardless of the initiating pathology. Over the
last years, an important progress has been made towards this
Received for publication 7 January
2004
Accepted for publication 19 February
2004
Correspondence:
Christos Chatziantoniou
Inserm U489
Tenon Hospital
4 rue de la Chine
75020 Paris, France
Tel.: +33 1 56016658
Fax: +33 143645448
E-mail: christos.chatziantoniou@tnn.
ap-hop-paris.fr
Int. J. Exp. Path. (2004), 85, 1–11
� 2004 Blackwell Publishing Ltd 1

direction, and it is now well established that various therapeutic
interventions can prevent the development of renal damage in
several experimental models. The challenge, however, remains to
go beyond slowing down the decline of renal function, and to
attempt to achieve regression of renal fibrosis and restoration of
the renal structure. Our group has contributed to the understand-
ing of the fibrotic mechanisms by focusing on experimental models
in which renal fibrosis originates from vascular dysfunction. The
present work aimed to review some of the most significant recent
developments concerning the mechanisms of progression and
regression of renal fibrosis.
Progression of renal fibrosis of vascular origin
One of the most common complications associated with hyper-
tension is the development of renal sclerotic injury (Weistuch &
Dworkin 1992). For several years, the general belief was that
renal vascular and glomerular sclerosis were consequences of
the high blood pressure and that the exaggerated extracellular
matrix formation inmesangial and vascular smoothmuscle cells
was an adaptive response to the increased tension within the
renal vasculature (Figure1). This hypothesis postulates that the
systemic blood pressure increase is transmitted within renal
resistance vessels and glomeruli initiating an adaptive mechan-
ism that is subsequently extended to renal interstitium and that
ultimately leads to the development of renal fibrosis. Under this
schema, circulating or locally generated vasoconstrictors have a
primary (if not exclusive) action on the blood pressure increase.
However, over the last years, this belief was evolved to the
concept that vasoconstrictors have fibrogenic effects indepen-
dently of their constrictor action (Figure 1) and that an efficient
treatment against hypertension and its complications should
also address the issue of pathological structural remodelling (in
addition to simply lowering blood pressure). This concept is
based on data obtained mainly in the cardiac tissue with block-
ers of the renin–angiotensin system (Weber 2000). The follow-
ing lines will examine whether this concept can also apply to the
renal vasculature; the focus will be on the data concerning the
fibrogenic action of the most extensively studied peptides in this
field, angiotensin II, and endothelin and of the beneficial effects
of their inhibitors or antagonists; in addition, it will be exam-
ined whether inhibitors of the different growth factors (consid-
ered to mediate the fibrogenic action of vasoconstrictors) such
as transforming growth factor-b (TGFb) and tyrosine kinase
growth factors can be used against renal fibrosis.
Angiotensin II
A central role for the renin–angiotensin system in the vascular
remodelling and fibrosis is well established. Its involvement in
renal fibrosis was suggested from studies using pharmacological
blockade of the angiotensin II action. Thus, inhibition of the
angiotensin-converting enzyme (ACE) or antagonism of the
angiotensin AT1 receptors slowed or stopped the progression
of renal fibrosis in several models of experimental or genetic
hypertension. In the nitric oxide (NO) deficiency model of
hypertension (L-NAME model) for instance, inhibition or
antagonism of angiotensin II preserved kidney function and
morphology in addition to normalizing systolic pressure (Case-
llas et al. 1999; Michel et al. 1996). Treatment with a calcium
blocker and/or an ACE inhibitor improved renal haemody-
namics and protected against nephrosclerosis in spontaneously
hypertensive rat (SHR) treated with L-NAME (Francischetti
et al. 1998). To understand the underlying cellular mechan-
ism(s), we examined the hypothesis of whether angiotensin II
specifically activates genes of extracellular matrix proteins (such
as collagen I) within the renal cortical vasculature (Boffa et al.
1999). To this end, we used a transgenic strain of mice har-
bouring two reporter genes, the firefly luciferase and the
Escherichia coli B-galactosidase, under the control of the
promoter of the a2-chain of mouse collagen type I gene.
The choice of these mice was based on data showing that
the expression pattern of the two reporter genes closely
correlated with cell and tissue distribution of collagen I
(Bou-Gharios et al. 1996; Chatziantoniou et al. 1998). Due
to the sensibility of reporter gene assays, this model allows
changes in the expression of the collagen I gene to be
detected in a highly sensitive manner. Thus, the sensitivity
and reproducibility of luciferase activity measurements pro-
vided us with accurate estimates of tissular (afferent arter-
ioles or glomeruli vs. heart and aorta) and temporal
(before, during and after the establishment of pathology)
activation of collagen I gene. Hypertension and renal failure
were induced in these mice by inhibiting endogenous NO
synthesis in presence or absence of angiotensin blockade for
Intrinsic factors
Renal fibrogenesis
High blood pressureExtrinsic factors
NO ET-1 ANG II
–? +? +?
Figure 1 Classically, the development of renal fibrosis of vascular
origin was considered as an adaptive response to blood pressure
increase. This notion has been challenged lately by the concept
that vasoactive agents can control extracellular martrix synthesis
through a genetic action independent of their constrictor effects.
2 C. Chatziantoniou et al.
� 2004 Blackwell Publishing Ltd, International Journal of Experimental Pathology, 85, 1–11

a period of up to 14 weeks (Boffa et al. 1999). Systolic
blood pressure was increased after 6 weeks of treatment
and reached a plateau after 10 weeks (around 160mmHg).
Collagen I gene activity was increased in freshly isolated
afferent arterioles and glomeruli earlier than systolic pressure
(4 weeks of L-NAME treatment), indicating that the two phe-
nomena could be controlled by distinct mechanisms. The acti-
vation of collagen I gene became more pronounced with time,
and at 14 weeks, increased 10-fold compared with controls in
afferent arterioles and glomeruli. This activation of collagen I
gene was accompanied by the progressive accumulation of extra-
cellular matrix within glomeruli as evidenced by classical morpho-
logical methods. The kinetics of collagen I gene activation was
different in aorta and heart; it remained unchanged up to 8 weeks
and was increased slowly thereafter (in parallel with the systolic
pressure increase), suggesting that the early activation of col-
lagen I gene in renal resistance vessels and glomeruli was specific
to the renal tissue (Chatziantoniou et al. 1998). Pharmacologi-
cal blockade of angiotensin II action inhibited collagen I gene
activation in the renal cortical tissue and prevented the develop-
ment of renal vascular and glomerular fibrosis. This study,
summarized in Figure 2, provided an in vivo evidence that
angiotensin II is involved in the fibrogenic process by inducing
collagen gene activation within the renal tissue by a cellular
mechanism(s) partly independent of its systemic haemodynamic
actions (Boffa et al. 1999).
Endothelin
Several recent studies point to a major role for endothelin in
mediating renal fibrosis. Transgenic mice overexpressing human
endothelin 1 gene developed glomerulosclerosis and interstitial
fibrosis without change in arterial pressure (Hocher et al. 1997);
conversely, selective blockade of ETA receptors prevented pro-
teinuria and glomerular ischaemia and blunted the degree of
vascular and tubulointerstitial injuries during inhibition of NO
synthesis without normalizing blood pressure (Verhagen et al.
1998). These results corroborate the hypothesis that the
endothelin-mediated fibrogenic mechanisms are independent
of systemic haemodynamics. We have observed that mRNA
175
150
125
100
75
200
150
100
50
0
Without AT1 antagonistWith AT1 antagonist
Glomeruli
Control LN 8 w LN 14 w
Control LN 8 w LN 14 w
Col
lage
n I g
ene
activ
atio
nS
ysto
lic p
ress
ure
(mm
Hg)
L-NAME 14 w
L-NAME + AT1 antagonist 14 w
Figure 2 Antagonism of angiotensin II action inhibited collagen I gene activation within the renal vasculature (glomeruli and afferent
arterioles) and prevented the development of glomerulosclerosis without normalizing systolic pressure increase (Boffa et al. 1999).
Renal vascular and glomerular fibrosis 3
� 2004 Blackwell Publishing Ltd, International Journal of Experimental Pathology, 85, 1–11

expression and peptide content of endothelin in renal resistance
vessels and endothelin urinary excretion rate were increased in
rats developing renal vascular fibrosis (Tharaux et al. 1999). We
pursued the hypothesis of an endothelin–collagen I gene inter-
action using the same transgenic strain and a similar to the
above-described protocol with the exception that an endothelin
receptor blocker was used instead of the AT1 receptor antago-
nist. Endothelin blockade prevented the collagen I gene activa-
tion and protected kidneys from the development of fibrosis
without altering the blood pressure increase induced by NO
inhibition (Chatziantoniou et al. 1998). These studies provided
an additional support to the hypothesis that the fibrogenic
action of vasoactive peptides is local and independent of sys-
temic haemodynamics; on the other hand, these findings raised a
number of important questions such as to identify the way (if
any) of the interaction between angiotensin II and endothelin
that leads to collagen I gene activation and the development of
renal fibrosis. We have addressed this issue in subsequent
experiments by investigating the role of some pro-fibrogenic
and/or mitogenic transduction pathways that are known to
interact with angiotensin II, such as TGF-b/SMAD, MAP/ERK
and tyrosine kinase receptors of growth factors.
TGF-�
TGF-b is a well-known agent promoting extracellular matrix
synthesis and is considered to play a major role as mediator of
the fibrogenic action of several vasoconstrictor peptides, parti-
cularly of the angiotensin II (Border & Noble 1998). The angio-
tensin II–TGF-b interaction does not appear to depend on
systemic haemodymamics. In the L-NAME model, TGF-bmRNA expression was increased locally in the renal cortex;
treatment with an ACE inhibitor, but not with hydralazine,
reduced the exaggerated expression of TGF-b and improved
renal histology, despite a similar reduction of systolic blood
pressure with both treatments (Kashiwagi et al. 2000). More
controversial is the issue of whether TGF-b mediates the fibro-
genic actions of endothelin. In two models of experimental
fibrotic nephropathy (the streptozotocin-induced diabetes or
the 5/6 nephrectomy), ETA/B antagonism had no effect on the
exaggerated expression of TGF-b or collagen IV and the pro-
gression of fibrosis in glomeruli and tubules (Kelly et al. 2000).
In other studies that used similar models of chronic renal failure
(5/6 nephrectomy), ETA/B antagonismmarkedly reduced extra-
cellular matrix synthesis, protected renal structure and
improved the survival of 5/6 nephrectomized rats (Benigni et al.
1993). We studied the interactions between angiotensin II,
endothelin and TGF-b on collagen I gene activation in acute in
vivo experiments. To this end, we tested whether exogenous
administration of angiotensin II, endothelin or TGF-b activated
collagen I gene in the aortic and renal cortical tissue andwhether
a cross-reaction of blockers of these systems affected collagen I
gene activation (Fakhouri et al. 2001). The main conclusion of
these studies was that cooperation and/or synergy between
endothelin and TGF-b are required and mediate the fibrogenic
action of angiotensin II. The molecular events that lead from the
angiotensin II receptor to collagen I gene activation were
subsequently examined by focusing on the role ofMAPKpathway.
MAP kinases and intracellular signalling mediators of
fibrogenesis
The MAP/ER kinase cascade is considered as a major intracel-
lular signalling pathway mediating the mitogenic actions of
most vasoconstrictors. We tested if this pathway could also
mediate fibrogenesis in the renal and vascular tissues in col-
lagen I gene transgenic mice. Angiotensin II produced an early
stimulation of collagen I gene activity in freshly isolated aortas
and renal cortical slices followed by similar increase in col-
lagen I gene mRNA levels (Tharaux et al. 2000). This effect of
angiotensin II was inhibited by AT1 receptor antagonism and
blockade of the MAPK/ERK cascade, but not by inhibition of
the P38 kinase pathway or blockade of the transcription factor
NFkB. The angiotensin II-induced increase of the MAPK/ERK
activity was accompanied by increased expression of the c-fos
proto-oncogene; inversely, inactivation of the transcriptional
factor AP-1 cancelled the effect of angiotensin II on the col-
lagen I gene (Figure 3). Similar data have been obtained in a
transgenic model of rat harbouring both human renin and
angiotensinogen genes (Muller et al. 2000). In this model,
characterized by angiotensin II–induced end-organ damage in
heart and kidney, AP-1 expression and several genes regulated
by this complex (such as intercellular adhesion molecule-1 and
vascular cell adhesion molecule-1) were locally overexpressed
in the renal and cardiac tissues; treatment with angiotensin II
or endothelin antagonists, but not with hydralazine, improved
albuminuria and renal injury and reduced mortality rates;
these functional improvements were independent of blood
pressure effects and were associated to significant reduction
of AP-1 (and AP-1-regulated genes) expression in the kidney.
Tyrosine kinase receptors of growth factors
A relatively novel concept regarding the signalling pathways of
potent vasoconstrictors such as angiotensin II or endothelin is
that they can transactivate the receptors of growth factors
(Berk 1999). Increased expression or levels, or activation of
these receptors have been observed during the development of
several forms of nephropathies (Klahr & Morrisey 2000),
making thus attractive the hypothesis that this activation
4 C. Chatziantoniou et al.
� 2004 Blackwell Publishing Ltd, International Journal of Experimental Pathology, 85, 1–11
could participate in the progression of renal fibrotic disease.
To this end, a tyrosine kinase inhibitor attenuated the devel-
opment of fibrosis in the model of unilateral ureteral obstruc-
tion (Ludewig et al. 2000). More recently, use of nuclease
resistant high-affinity aptamers that neutralized the effects of
PDGF-B inhibited glomerular and interstitial fibrosis in a rat
model of mesangioproliferative glomerulosclerosis (Ostendorf
et al. 2001). We tested the interaction between vasoconstrict-
ors, epidermal growth factor (EGF) receptor transactivation
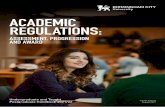
and collagen I gene (Flamant et al. 2003), and we found that
endothelin induced a rapid phosphorylation of the EGF recep-
tor associated to activation of the MAP/ERK pathway and to
increased collagen I gene activity in freshly isolated aortic and
renal cortical tissue (Figure 3). In subsequent in vivo studies,
we observed that EGF receptor was activated within glomeruli
concomitantly to the development of glomerulosclerosis in the
NO deficiency model. In this model, an EGF receptor-tyrosine
kinase inhibitor, normalized the MAPK activation, inhibited
the abnormal increase of collagen I gene expression, decreased
proteinuria and creatininaemia and prevented the develop-
ment of renal vascular and glomerular fibrosis (Francois et al.
2003). It appears, thus, that EGF receptor activation is a major
step in the fibrogenic process, at least in the model of NO
deficiency. These observations provide a novel perspective for
the eventual use of growth factor receptor inhibitors as anti-
fibrotic agents.
Regression of renal fibrosis
Blockade of the renin–angiotensin system
Figure 3 summarizes the signalling pathways that have been
characterized by our studies as mediators of the angiotensin II-
induced activation of collagen I gene. These studies were
mainly focused on the mechanisms leading to the progression
of renal vascular fibrosis. From a therapeutic point of view,
however, the challenge remains to go beyond prevention and
to attempt to achieve regression of renal fibrosis and restor-
ation of the renal structure. Over the last years, several studies
in humans gave promising results indicating that anti-
hypertensive treatments can have beneficial effects regarding
renoprotection. Thus, blockade of the angiotensin II action
protected against the progression of renal insufficiency in
patients with various renal diseases (such as glomerulopathies,
interstitial nephritis, nephrosclerosis, polycystic kidney disease
or diabetic nephropathy) (Maschio et al. 1996). This initial
Figure 3 Angiotensin II-induced signalling pathways that lead to activation of collagen I gene. Interruption of one of these cascades is
sufficient to inhibit collagen I synthesis and to prevent the development of fibrosis (dash arrows indicate the targets used in experimental
studies to block collagen I formation).
Renal vascular and glomerular fibrosis 5
� 2004 Blackwell Publishing Ltd, International Journal of Experimental Pathology, 85, 1–11

report was validated with the publication of three large-scale
studies concerning hypertensive patients with type 2 diabetes
(Brenner et al. 2001; Lewis et al. 2001; Parving et al. 2001).
Angiotensin II receptor antagonism was effective in protecting
against the progression of nephropathy by reducing micro-
albuminuria and slowing down the rate of decline of filtration
rate; interestingly, these renoprotective effects were independ-
ent of the blood-pressure-lowering effect, providing an add-
itional argument supporting the dissociation between the
contractile and the fibrotic actions of angiotensin II in the
renal tissue. These observations are corroborated by a mor-
phometric analysis performed in a limited number of type 2
diabetic patients with glomerulosclerosis. After 2 years of
follow-up, mean cortical interstitial fractional volume (a marker
of progression of renal fibrosis) was increased significantly
in the placebo group, whereas it remained unchanged in the
ACE inhibitor-treated patients (Cordonnier et al. 1999).
We have addressed the issue of renoprotection by investigat-
ing the mechanisms by which AT1 receptor antagonists make
possible the regression of renal vascular and glomerular fibro-
sis (Boffa et al. 2003). To this end, hypertension and renal
failure were induced by inhibiting NO synthesis. After 1
month of hypertension, animals displayed a decline of renal
function (evidenced by increased levels of proteinuria and
plasma creatinine), an exaggerated gene and protein expres-
sion of TGF-b, collagen I and collagen IV within the renal
vasculature and an abnormal accumulation of extracellular
matrix in glomeruli (Figure 4). These structural and functional
alterations were accompanied by increased activities of matrix
metalloproteinases (MMPs) 2 and 9. Administration of an
angiotensin II receptor antagonist immediately decreased col-
lagen I, collagen IV and TGF-b gene and protein expressions,
without affecting activities of metalloproteinases 2 and 9.
These cellular alterations were accompanied by a gradual
regression of glomerulosclerosis and restoration of renal func-
tion; after 1 month of anti-hypertensive treatment, all func-
tional and structural parameters of kidney were normalized
(Figure 4). Hydralazine failed to improve renal function and/or
structure despite a similar degree of systolic pressure decrease,
providing another element to support the hypothesis that sys-
temic pressure regulation and renal vascular fibrosis follow
distinct mechanisms. These data are among the first studies
2.5
2.0
1.5
1.0
0.5
0
150
125
100
75
50
25
4
3
2
1
0Protein/creatinine (mg/µmol) Plasma creatinine (µmol/l) Sclerotic index
Control L-NAME 4w L-NAME 4w +L-NAME 4w + Los 4w
Figure 4 Chronic inhibition of nitric oxide is accompanied by the development of renal failure as evidenced by the increase of urinary
protein excretion, plasma creatinine and the exaggerated extracellular matrix accumulation in renal cortex. Treatment of the diseased
animals with an angiotensin receptor antagonist normalized renal functional and structural parameters indicating that renal fibrosis is a
reversible phenomenon, at least in this experimental model (white, black and grey bars represent control animals and animals treated for
4 weeks with L-NAME or 4 weeks with L-NAME followed by 4 weeks L-NAME+ losartan, respectively; L-NAME: a NO synthase
inhibitor; Los: losartan, an AT1 receptor antagonist; w: weeks (Boffa et al. 2003).
6 C. Chatziantoniou et al.
� 2004 Blackwell Publishing Ltd, International Journal of Experimental Pathology, 85, 1–11

implying that the progression of renal vascular fibrosis is a
reversible process. The mechanism of the regression (at least in
the NO deficiency model) appears to be dual: inhibition of
collagen synthesis due to AT1 receptor antagonism and acti-
vation of metalloproteinases that is probably associated with
the degree of fibrosis independently of AT1 blockade. In a
subsequent study, other investigators confirmed the reversibil-
ity of vascular lesions after angiotensin II blockade in the
model of 5/6 nephrectomy (Adamczak et al. 2003). In this
study, delayed treatment with an ACE inhibitor regressed
preexisting glomerular, tubular and vascular lesions, and
reversed glomerular hypertrophy. However, the initially
decreased number of podocytes (following renal ablation)
was not restored by the pharmacological treatment indicating
that the limiting step of glomerular regeneration depends on
the degree of damage of glomerular podocytes. In agreement
to this notion, mesangial proliferation was reduced and inter-
stitial changes were reversed after favourable treatment,
whereas the number of sclerotic glomeruli remained
unchanged in biopsies of immunoglobulin A (IgA) nephro-
pathy patients (Hotta et al. 2002). These observations are con-
sistent with the notion that the no-return point is associated to
podocyte alterations and underline the importance of finding
markers to detect these alterations as early as possible.
Blockade of the TGF-� pathway
Despite the reservations, exposed in the first part of the
review, of whether TGF-b is a common fibrogenic mediator
of all vasoconstrictor peptides, its involvement in the angio-
tensin II-induced fibrogenesis is well established. For this rea-
son, anti-fibrogenic strategies have been proposed that block
the action of TGF-b. Exogenous administration of decorin
mimicked the effect of chronic anti-TGF-b antibody infusion
by blunting the formation of extracellular matrix within the
renal cortex and protecting rat kidneys from the development
of glomerulonephritis (Border et al. 1992). In addition, endo-
genous overexpression of decorin in the skeletal muscle of rats
by gene transfer technology inhibited the fibrogenic action of
TGF-b and protected kidneys against glomerulosclerosis
(Isaka et al. 1996). However, an important limitation for the
generalized use of decorin is that increased concentrations of
decorin lack the anti-TGF-b specificity and can produce sec-
ondary effects. An alternative approach could be to block the
TGF-b action at the receptor level (exogenous administration of
anti-TGF-b receptor antibody or soluble receptors of TGF-b) orat the intracellular signalling pathway (SMADs, the intracellu-
lar mediators of TGF-b actions); both treatments gave promis-
ing results by preventing the development of renal and cardiac
fibrosis (Kasuga et al. 2001; Wang et al. 2002).
Another more recent option is to use bone morphogenic
protein-7 (BMP-7), a 35-kDa homodimeric protein and a
member of the TGF-b superfamily that antagonizes the action
of TGF-b. BMP-7 is highly expressed in the kidney, and its
genetic deletion in mice leads to severe impairment of eye,
skeletal and kidney development (Hogan 1996). Ischaemic
kidneys showed a marked decrease of BMP-7 mRNA, whereas
BMP-7 enhanced recovery when infused into rats with ischaemia-
induced acute renal failure (Simon et al. 1999). More
importantly, BMP-7 treatment in a preventive or curative
way preserved or restored renal histology and renal func-
tion in a rat model of unilateral ureteral obstruction; these
effects of BMP-7 were slightly better compared to the pro-
tection obtained with an ACE inhibitor (Hruska et al.
2000; Morrissey et al. 2002). In addition, systemic admin-
istration of recombinant human BMP-7 in mice with
nephrotoxic serum nephritis leads to repair of severely
damaged renal tubular epithelial cells, in association with
reversal of chronic renal injury (Zeisberg et al. 2003). These
results indicate the potential of BMP-7 to reverse the TGF-
b-induced injury and to repair renal tissue in a variety of
experimental models.
An additional endogenous ligand antagonizing the effects of
TGF-b is the ‘Hepatocyte Growth Factor’ (HGF). The therapeu-
tic potential of HGF has been tested in the unilateral ureteral
obstruction model, a model of renal interstitial fibrosis (Yang&
Liu 2003). Delayed administration of recombinant HGF
retarded the progression of renal lesions by blunting the myofi-
broblast accumulation and collagen deposition within the
kidney. This action of HGF is probably related to a mitogen-
activated protein kinase-dependent blockade of TGF-b-inducednuclear translocation of SMADs (Yang et al. 2003). Continuous
infusion of HGF in the rat remnant kidney model decreased
tubulointerstitial collagen deposition and ameliorated renal
fibrosis; in contrast, blocking of endogenous HGF by an anti-
HGF-neutralizing antibody increased interstitial collagen and
aggravated the degree of renal fibrosis. Interestingly, HGF infu-
sion increased, and conversely HGF antibody suppressed, the in
situ gelatinolytic activity in remnant kidneys thus, supporting
our hypothesis that MMPs play a beneficial role in renal fibrosis
by facilitating collagen degradation (Gong et al. 2003)
Stem cells
A very important issue when one addresses the problem of
regression of renal fibrosis is whether sclerotic glomeruli can
regenerate, and if so, what cells are or can be used as progeni-
tors. As mentioned above, a limiting step factor for the rever-
sibility of renal fibrosis appears to be podocyte differentiation.
Considerable progress has been made over the last years to this
Renal vascular and glomerular fibrosis 7
� 2004 Blackwell Publishing Ltd, International Journal of Experimental Pathology, 85, 1–11

direction, and emerging data demonstrated that bone marrow
cells can serve as progenitors for a variety of cells such as
vascular smooth, endothelial, hepatic or osteoblastic cells
(Prockop 1997). Furthermore, it has been demonstrated that
these marrow-derived cells can migrate into areas of induced
tissue degeneration, undergo differentiation and participate in
the regeneration of the damaged tissue (Asahara et al. 1997;
Ferrari et al. 1998). This innovative therapeutic approach has
been successfully applied in myocardial ischaemia (Kawamoto
et al. 2001) and in osteogenesis imperfecta, a genetic disorder
in which osteoblasts produce defective type I collagen (Horwitz
et al. 1999).
Bone marrow-derived cells may have the potential to differ-
entiate into glomerular mesangial cells (Imasawa et al. 2001).
However, this efficiency to differentiate can act as double-edge
feature, depending on whether the conditions favour hyper-
plasia and/or proliferation or recovery and/or regeneration.
Thus, the sclerotic phenotype was carried by mesangial cell
progenitors, and this phenotype could be derived from the
bone marrow in a genetic model of diffuse glomerulosclerosis
and glomerular hypertrophy (Cornacchia et al. 2001), or in
IgA nephropathy (Imasawa et al. 1999). Inversely, healthy
bone marrow cells gave rise to mesangial cells in vivo and
participated in the regeneration of glomeruli in the anti-Thy1
antibody-mediated glomerulonephritis (Ito et al. 2001); in
addition, use of genetically modified bone marrow-derived
cells to deliver an interleukin-1 receptor antagonist prevented
the phenotypic alterations of interstitial cells and protected kid-
neys in the model of unilateral ureteral obstruction (Yamagishi
et al. 2001).
Perspectives
Figure 5 summarizes the factors that have been identified to
play a crucial role in the mechanisms controlling extracellular
matrix formation in the renal vascular and glomerular tissue.
Although encouraging data have been obtained lately, the
issue still remains open on how to cure renal fibrosis. In this
context, some critical steps of the fibrotic mechanisms need to
be first well defined. Can the same treatment, for instance, be
applied to all stages of renal fibrosis, or does it depend on the
degree, severity and nature (type and supramolecular organi-
zation of collagen) of lesions? Are all stages of fibrosis rever-
sible or is there a no-return point, and in this case, how this
point will be clinically defined and what markers can be used
for its definition? Because the abnormal formation of col-
lagens is a common phenomenon of chronic renal failure
independently of cause and initiating mechanisms, is it possi-
ble to achieve regression by targeting a common step (blocking
collagen synthesis)? In that sense, angiotensin II appears as an
appropriate target, and the recently obtained data point to this
direction. However, anti-angiotensin treatments have been
widely used for several years now, and it becomes clear that
blocking angiotensin II action alone is not as much efficient in
regressing renal fibrosis in humans as it is in animals. Does this
mean that the prescribed doses of angiotensin blockers (based
on anti-hypertensive efficency) are not sufficient enough to
block the locally generated angiotensin? Or, may it be better
to associate angiotensin blockade to specific anti-fibrotic treat-
ments (anti-TGF-b or anti-tyrosine kinase growth factors) and/
or to agents that can degrade specifically the abnormally
formed extracellular matrix? Is it reasonable to believe that
the technological advance based on stem cells will permit to
reconstruct and regenerate completely a fibrotic kidney, even
if it is beyond on what we call today a no-return point?
Certainly, it is still a long way to go before making a fibrotic
kidney operational again; however, the progress made over the
last years and the continuously novel options emerging in the
horizon are sufficient reasons for optimism that is not far from
the day in which the regression of renal fibrosis will no more
considered as a myth but as a reality.
Factors involved in progression Factors facilitating regression
Angiotensin II
Endothelin
TGFβTyrosine kinase growth factors
NO
Activation of MMPs
BMP-7
Hepatic growth factor
Stem cells?
Extracellular matrix formation
Figure 5 Factors controlling the formation of extracellular matrix and the development of renal vascular and glomerular fibrosis.
Inhibition of pro-fibrogenic agents and/or activation of anti-fibrogenic systems have been accompanied by regression of fibrosis and
restoration of renal function in experimental nephropathies.
8 C. Chatziantoniou et al.
� 2004 Blackwell Publishing Ltd, International Journal of Experimental Pathology, 85, 1–11

References
Adamczak M., Gross M.L., Krtil J., Koch A., Tyralla K., Amann K.,
Ritz E. (2003) Reversal of glomerulosclerosis after high-dose
enalapril treatment in subtotally nephrectomized rats. J. Am.
Soc. Nephrol. 14, 2833–2842.
Asahara T., Murohara T., Sullivan A., Silver M., van der Zee R.,
Li T., Witzenbichler B., Schatteman G., Isner J.M. (1997)
Isolation of putative progenitor endothelial cells for angiogen-
esis. Science 275, 964–967.
Benigni A., Zoja C., Corna D., Orisio S., Longaretti L., Bertani T.,
Remuzzi G. (1993) A specific endothelin subtype A receptor
antagonist protects against injury in renal disease progression.
Kidney Int. 44, 440–444.
Berk B.C. (1999) Angiotensin II signal transduction in vascular
smooth muscle: pathways activated by specific tyrosine kinases.
J. Am. Soc. Nephrol. 10 (Suppl. 11), S62–S68.
Boffa J.J., Tharaux P.L., Placier S., Ardaillou R., Dussaule J.C.,
Chatziantoniou C. (1999) Angiotensin II activates collagen type
I gene in the renal vasculature of transgenic mice during
inhibition of nitric oxide synthesis: evidence for an endothelin-
mediated mechanism. Circulation 100, 1901–1908.
Boffa J.J., Ying L., Placier S., Stefanski A., Dussaule J.C.,
Chatziantoniou C. (2003) Regression of renal vascular and
glomerular fibrosis: Role of angiotensin II receptor antagonism
and metalloproteinases. J. Am. Soc. Nephrol. 14, 1132–1144
(editorial comment 1411–1414).
Border W.A. & Noble N.A. (1998) Interactions of transforming
growth factor-b and angiotensin II in renal fibrosis. Hyperten-
sion 31, 181–188.
Border W.A., Noble N.A., Yamamoto T., Harper J.R.,
Yamaguchi Y., Pierschbacher M.D., Ruoslahti E. (1992) Natural
inhibitor of transforming growth factor-b protects against
scarring in experimental kidney disease. Nature 360, 361–364.
Bou-Gharios G., Garrett L.A., Rossert J., Niederreither K.,
Eberspaecher H., Smith C., Black C., de Crombrugghe B.
(1996) A potent far-upstream enhancer in the mouse proa2 (I)
collagen gene regulates expression of reporter genes in
transgenic mice. J. Cell Biol. 134, 1333–1344.
Brenner B.M., Cooper M.E., de Zeeuw D., KeaneW.F., Mitch W.E.,
Parving H.H., Remuzzi G., Snapinn S.M., Zhang Z., Shahinfar S.,
RENAAL Study Investigators. (2001) Effects of losartan on renal
and cardiovascular outcomes in patients with type 2 diabetes and
nephropathy. N. Engl. J. Med. 345, 861–869.
Casellas D., Benhamed S., Artuso A., Jover B. (1999) Candesartan
and progression of preglomerular lesions in L-NAME hyper-
tensive rats. J. Am. Soc. Nephrol. 10, S230–S233.
Chatziantoniou C., Boffa J.J., Ardaillou R., Dussaule J.C. (1998)
Nitric oxide inhibition induces early activation of type I
collagen gene in renal resistance vessels and glomeruli in
transgenic mice: role of endothelin. J. Clin. Invest. 101,
2780–2789.
Cordonnier D.J., Pinel N., Barro C., Maynard M., Zaoui P.,
Halimi S., Hurault de Ligny B., Reznic Y., Simon D., Bilous R.W.
(1999) Expansion of cortical interstitium is limited by
converting enzyme inhibition in type 2 diabetic patients with
glomerulosclerosis. The Diabiopsies Group. J. Am. Soc.
Nephrol. 10, 1253–1263.
Cornacchia F., Fornoni A., Plati A.R., Thomas A., Wang Y.,
Inverardi L., Striker L.J., Striker G.E. (2001) Glomerulo-
sclerosis is transmitted by bone marrow-derived mesangial cell
progenitors. J. Clin. Invest. 108, 1649–1656.
Fakhouri F., Placier S., Ardaillou R., Dussaule J.C.,
Chatziantoniou C. (2001) Angiotensin II activates collagen
type I gene in the renal cortex and aorta of transgenic mice
through interaction with endothelin and TGFb. J. Am. Soc.
Nephrol. 12, 2701–2710.
Ferrari G., Cusella-De Angelis G., Coletta M., Paolucci E.,
Stornaiuolo A., Cossu G., Mavilio F. (1998) Muscle regener-
ation by bone marrow-derived myogenic progenitors. Science
279, 1528–1530.
Flamant M., Tharaux P.L., Placier S., Henrion D., Coffman T.,
Chatziantoniou C., Dussaule J.C. (2003) Epidermal Growth
Factor Transactivation Mediates the Tonic and Fibrogenic
Effects of Endothelin in the Aortic Wall of Transgenic Mice.
FASEB J. 17, 327–329 (Epub 02–0115fje, December 2002).
Francischetti A., Ono H., Frohlich E.D. (1998) Renoprotective
effects of felodipine and/or enalapril in spontaneously hyper-
tensive rats with and without L-NAME. Hypertension 31,
795–801.
Francois H., Placier S., Parvez-Braun L., Dussaule J.C., Chat-
ziantoniou C. (2003) Prevention of renal vascular and
glomerular fibrosis by inhibiting tyrosine-kinase growth factor
receptors. J. Am. Soc. Nephrol. 14, 20A.
Gong R., Rifai A., Tolbert E.M., Centracchio J.N., Dworkin L.D.
(2003) Hepatocyte growth factor modulates matrix metallo-
proteinases and plasminogen activator/plasmin proteolytic
pathways in progressive renal interstitial fibrosis. J. Am. Soc.
Nephrol. 14, 3047–3060.
Hocher B., Thone-Reineke C., Rohmeiss P., Schmager F.,
Slowinski T., Burst V., Siegmund F., Quertermous T., Bauer C.,
Neumayer H.H., Schleuning W.D., Theuring F. (1997)
Endothelin-1 transgenic mice develops glomerulosclerosis,
interstitial fibrosis, and renal cysts but not hypertension.
J. Clin. Invest. 99, 1380–1389.
Hogan B.L. (1996) Bone morphogenic proteins in development
Curr. Opin. Genet. Dev. 6, 432–438.
Horwitz E.M., Prockop D.J., Fitzpatrick L.A., Koo W.W.,
Gordon P.L., Neel M., Sussman M., Orchard P., Marx J.C.,
PyeritZ. R.E., Brenner M.K. (1999) Transplantability and
therapeutic effects of bone marrow-derived mesenchymal cells
in children with osteogenesis imperfecta. Nat. Med. 5,
309–313.
Renal vascular and glomerular fibrosis 9
� 2004 Blackwell Publishing Ltd, International Journal of Experimental Pathology, 85, 1–11
Hotta O., Furuta T., Chiba S., Tomioka S., Taguma Y. (2002)
Regression of IgA nephropathy: a repeat biopsy study. Am. J.
Kidney Dis. 39, 493–502.
Hruska K.A., Guo G., Wozniak M., Martin D., Miller S., Liapis H.,
Loveday K., Klahr S., Sampath T.K., Morrissey J. (2000)
Osteogenic protein-1 prevents renal fibrogenesis associated
with ureteral obstruction. Am. J. Physiol. Renal Physiol. 279,
F130–F143.
Imasawa T., Nagasawa R., Utsunomiya Y., Kawamura T., Zhong Y.,
Makita N., Muso E., Miyawaki S., Maruyama N., Hosoya T.,
Sakai O., Ohno T. (1999) Bone marrow transplantation
attenuates murine IgA nephropathy: The role of a stem cell
disorder. Kidney Int. 56, 1809–1817.
Imasawa T., Utsunomiya Y., Kawamura T., Zhong Y., Nagasawa R.,
Okabe M., Maruyama N., Hosoya T., Ohno T. (2001) The
potential of bone marrow-derived cells to differentiate to
glomerular mesangial cells. J. Am. Soc. Nephrol. 12,
1401–1409.
Isaka Y., Brees D., Ikegaya K., Kaneda Y., Imai E., Noble N.A.,
Border W.A. (1996) Gene therapy by skeletal muscle expres-
sion of decorin prevents fibrotic disease in rat kidney. Nat.
Med. 2, 418–423.
Ito T., Suzuki A., Imai E., Okabe M., Hori M. (2001) Bone
marrow is a reservoir of repopulating mesangial cells during
glomerular remodeling. J. Am. Soc. Nephrol. 12, 2625–2635.
Kashiwagi M., Shinozaki M., Hirakata H., Tamaki K., Hirano T.,
Tokumoto M., Goto H., Okuda S., Fujishima M. (2000)
Locally activated renin-angiotensin system associated with
TGFb as a major factor for renal injury induced by chronic
inhibition of nitric oxide synthase in rats. J. Am. Soc. Nephrol.
11, 616–624.
Kasuga H., Ito Y., Sakamoto S., Kawachi H., Shimizu F., Yuzawa Y.,
Matsuo S. (2001) Effects of anti-TGF-beta type II receptor
antibody on experimental glomerulonephritis. Kidney Int. 60,
1745–1755.
Kawamoto A., Gwon H.C., Iwaguro H., Yamaguchi J.I., Uchida S.,
Masuda H., Silver M., Ma H., Kearney M., Isner J.M., Asahara T.
(2001) Therapeutic potential of ex vivo expanded endothelial
progenitor cells for myocardial ischemia. Circulation 103,
634–637.
Kelly D.J., Skinner S.L., Gilbert R.E., Cox A.J., Cooper M.E.,
Wilkinson-Berka J.L. (2000) Effects of endothelin or angio-
tensin II receptor blockade on diabetes in the transgenic (mRen-2),
27 rat. Kidney Int. 57, 1882–1894.
Klahr S. & Morrisey J.J. (2000) The role of vasoactive
compounds, growth factors and cytokines in the progression
of renal disease. Kidney Int. 57 (Suppl. 75), S7–S14.
Lewis E.J., Hunsicker L.G., Clarke W.R., Berl T., Pohl M.A.,
Lewis J.B., Ritz E., Atkins R.C., Rohde R., Raz I. (2001)
Renoprotective effect of the angiotensin-receptor antagonist
irbesartan in patients with nephropathy due to type 2 diabetes.
N. Engl. J. Med. 345, 851–860.
Ludewig D., Kosmehl H., Sommer M., Bohmer F.D., Stein G.
(2000) PDGF receptor kinase blocker AG1295 attenuates
interstitial fibrosis in rat kidney after unilateral obstruction.
Cell Tissue Res. 299, 97–103.
Maschio G., Alberti D., Janin G., Locatelli F., Mann J.F.,
Motolese M., Ponticelli C., Ritz E., Zucchelli P. (1996) Effect
of the angiotensin-converting-enzyme inhibitor benazepril on
the progression of chronic renal insufficiency. The Angiotensin-
Converting-Enzyme Inhibition in Progressive Renal Insuffi-
ciency Study Group. N. Engl. J. Med. 334, 939–945.
Michel J.B., Xu Y., Blot S., Philippe M., Chatelier G. (1996)
Improved survival in rats administered L-NAME due to
converting enzyme inhibition. J. Cardiovasc. Pharmacol. 28
(142–148), 1996.
Morrissey J., Hruska K., Guo G., Wang S., Chen Q., Klahr S.
(2002) Bone morphogenetic protein-7 improves renal fibrosis
and accelerates the return of renal function. J. Am. Soc.
Nephrol. 13 Suppl, S14–S21.
Muller D.N., Mervaala E.M., Schmidt F., Park J.K., Dechend R.,
Genersch E., Breu V., Loffler B.M., Ganten D., Schneider W.,
Haller H., Luft F.C. (2000) Effect of bosentan on NF-kB,inflammation, and tissue factor in angiotensin II-induced end-
organ damage. Hypertension 36, 282–290.
Ostendorf T., Kunter U., Grone H.J., Bahlmann F., Kawachi H.,
Shimizu F., Koch K.M., Janjic N., Floege J. (2001) Specific
antagonism of PDGF prevents renal scarring in experimental
glomerulonephritis. J. Am. Soc. Nephrol. 12, 909–918.
Parving H.H., Lehnert H., Brochner-Mortensen J., Gomis R.,
Andersen S., Arner P., Irbesartan in Patients with Type 2
Diabetes and Microalbuminuria Study Group. (2001) The
effect of irbesartan on the development of diabetic nephropathy
in patients with type 2 diabetes. N. Engl. J. Med. 345,
870–878.
Prockop D.J. (1997) Marrow stromal cells as stem cells for
nonhematopoietic tissues. Science 276, 71–74.
Simon M., Maresh J.G., Harris S.E., HernandeZ. J.D., Arar M.,
Olson M.S., Abboud H.E. (1999) Expression of bone
morphogenetic protein-7 mRNA in normal and ischemic adult
rat kidney. Am. J. Physiol. 276, F382–F389.
Tharaux P.L., Chatziantoniou C., Casellas D., Fouassier L.,
Ardaillou R., Dussaule J.C. (1999) Vascular endothelin-1 gene
expression, synthesis and effect on renal type I collagen
synthesis and nephroangiosclerosis during nitric oxide synthase
inhibition in rats. Circulation 99, 2185–2191.
Tharaux P.L., Chatziantoniou C., Fakhouri F., Dussaule J.C.
(2000) Angiotensin II activates collagen I gene through a
mechanism involving the MAP/ER kinase pathway. Hyperten-
sion 36, 330–336.
United States Renal Data System. (1998) Incidence and pre-
valence of ESRD. Am. J. Kidney Dis. 32 (Suppl. 1), S38–S49.
Valderrabano F., Berthoux F.C., Jones E.H., Mehls O. (1996)
Report on management of renal failure in Europe, XXV, 1994
10 C. Chatziantoniou et al.
� 2004 Blackwell Publishing Ltd, International Journal of Experimental Pathology, 85, 1–11

end stage renal disease and dialysis report. The EDTA-ERA
Registry. Nephrol. Dial. Transplant. 11 (Suppl. 1), 2–21.
Verhagen A.M., Rabelink T.J., Braam B., Opgenorth T.J.,
Grone H.J., Koomans H.A., Joles J.A. (1998) Endothelin A
receptor blockade alleviates hypertension and renal lesions
associated with chronic nitric oxide synthase inhibition. J. Am.
Soc. Nephrol. 9, 755–762.
Wang B., Hao J., Jones S.C., Yee M.S., Roth J.C., Dixon I.M.
(2002) Decreased Smad 7 expression contributes to cardiac
fibrosis in the infarcted rat heart. Am. J. Physiol. Heart Circ.
Physiol. 282, H1685–H1696.
Weber K.T. (2000) Targeting pathological remodelling: concepts
of cardioprotection and reparation. Circulation 102,
1342–1345.
Weistuch J.M. & Dworkin L.D. (1992) Does essential hyperten-
sion cause end- stage renal disease? Kidney Int. 41, S33–S37.
Yamagishi H., Yokoo T., Imasawa T., Mitarai T., Kawamura T.,
Utsunomiya Y. (2001) Genetically modified bone marrow-
derived vehicle cells site specifically deliver an anti-inflammatory
cytokine to inflamed interstitium of obstructive nephropathy.
J. Immunol. 166, 609–616.
Yang J., Dai C., Liu Y. (2003) Hepatocyte growth factor
suppresses renal interstitial myofibroblast activation and
intercepts Smad signal transduction. Am. J. Pathol. 163,
621–632.
Yang J. & Liu Y. (2003) Delayed administration of hepatocyte
growth factor reduces renal fibrosis in obstructive nephro-
pathy. Am. J. Physiol. Renal Physiol. 284, F349–F357.
Zeisberg M., Hanai J., Sugimoto H., Mammoto T., Charytan D.,
Strut Z.F., Kalluri R. (2003) BMP-7 counteracts TGF-beta
1-inducedepithelial-to-mesenchymal transitionandreverses
chronic renal injury. Nat. Med. 9, 964–968.
Renal vascular and glomerular fibrosis 11
� 2004 Blackwell Publishing Ltd, International Journal of Experimental Pathology, 85, 1–11