
Hyaluronic acid nanocapsules for the intracellular delivery of ...
Upload
independentCategory
view
2download
0
Nanomedicine: Nanotechnology, Biology, and Medicine11 (2014) 263–273
Original Article
Albumin nanocapsules containing fenretinide: pre-clinical evaluation ofcytotoxic activity in experimental models of human non-small
cell lung cancerSara Pignatta, BSca, Isabella Orienti, PhDb,⁎, Mirella Falconi, MD, PhDc, Gabriella Teti, PhDc,
Chiara Arienti, BSca, Laura Medri, BScd, Michele Zanoni, BSca, Silvia Carloni, BSca,Wainer Zoli, BSca, Dino Amadori, MDa, Anna Tesei, MBiochem, PhDa
aIstituto Scientifico Romagnolo per lo Studio e la Cura dei Tumori, (IRST) IRCCS, Meldola, FC, ItalybFaBiT-Department of Pharmacy and Biotechnology, University of Bologna, Bologna, BO, Italy
cDIBINEM-Department of Biomedical and Neuromotor Sciences, University of Bologna, BO, ItalydPathology Unit, Morgagni-Pierantoni Hospital, Forlì, FC, Italy
Received 8 July 2014; accepted 16 October 2014
nanomedjournal.com
Abstract
The present study deals with the preparation of albumin nanocapsules containing fenretinide and their evaluation in experimental models ofhuman non-small cell lung cancer. These nanocapsules showed enhanced antitumor activity with respect to free fenretinide due to the solubilizationeffect of albumin on the hydrophobic drug, known to improve bioavailability. The high expression of caveolin-1 on the A549 cell surface furtherenhanced the antitumor activity of the nanoencapsulated fenretinide. Caveolin-1 favored albumin uptake and improved the efficacy of the fenretinide-loaded albumin nanocapsules, especially in 3-D cultureswhere the densely packed 3-D structures impaired drug diffusibility and severely reduced theactivity of the free drug. The efficacy of the fenretinide albumin nanocapsules was further confirmed in tumor xenograft models of A549 by thesignificant delay in tumor progression observed with respect to control after intravenous administration of the novel formulation.© 2014 Elsevier Inc. All rights reserved.
Key words: Nanocapsules; Fenretinide; Albumin; 3-D cell cultures; In vivo experiments
Background
Over recent years, one of the main challenges in the field ofoncology has been the development of new strategies to improvethe bioavailability of anticancer drugs, including those of thelatest generation. This is with a view to increasing the therapeuticindex of the drugs, prolonging their permanence at the tumor siteand at the same time reducing their toxic side effects, thusimproving the quality of life of patients.
Nanomedicine has been described as one of the mostimportant research and development frontiers of modern science.In particular, the use of nanoparticles in drug delivery has offeredconsiderable promise for the enhanced bioavailability of
Funds: This work was supported by the Italian Ministry of Research andTechnology (MURST) with an FIRB grant (RBAP10MLK7_005) and aPRIN 2009 grant.
Conflicts of interest: The authors have no conflicts of interest to declare.⁎Corresponding author at: University of Bologna, Dept. Pharmacy and
Biotechnology, Via S. Donato 19/2 40127 Bologna, Italy.E-mail address: [email protected] (I. Orienti).
http://dx.doi.org/10.1016/j.nano.2014.10.0041549-9634/© 2014 Elsevier Inc. All rights reserved.
chemotherapeutic agents. Encapsulation within or binding tosmall colloidal particles may enable drugs to circulate for longerperiods of time, to accumulate preferentially within tumor tissue,to have reduced systemic toxicity, to undergo controlled releaseand even to bypass certain cellular mechanism of drug resistance,such as MDR.1 However, potential toxicity associated with thenanoparticle itself can be a limitation. Toxicity of nanoparticlescan occur due to size, shape, charge, compositions, constituentleaching and triggering of immune reactions, and it should beconsidered when selecting the type of carrier for drug transport tothe tumor site.2
In order to overcome these concerns, a feasible approach isto use, as drug carriers, existing endogenous proteins insidethe human body. Albumin, the most abundant plasma proteinsynthesized by the liver, is emerging as a versatile tool for drugdelivery and for improving the pharmacokinetic profile ofantitumor drugs, especially peptide- or protein-based drugs. Therationale for its use in different drug delivery strategies is basedupon its long half-life in the body (about 19 days) and, overall, itspeculiar property of accumulating in malignant and inflamedtissues due to a leaky capillary combined with an absent or

264 S. Pignatta et al / Nanomedicine: Nanotechnology, Biology, and Medicine 11 (2014) 263–273
defective lymphatic drainage system. This is accompanied by thefact that tumors are able to trap plasma proteins and utilize theirdegradation products for proliferation.3 In this regard, it has beenhypothesized that albumin is amajor source of energy andnutrition fortumor growth on the basis of excessive plasma protein catabolism bythe tumor itself and an activemetabolic role of the liver,which seem tobe important factors for the genesis of cachexia.4 Finally, albumin isan extremely robust protein with respect to pH, temperature andorganic solvents and can be stored as a 5% or 20% solution for manyyears. The properties described abovemade albumin a very promisingdrug carrier as shown by its utilization in several anticancer drugformulations that have been clinically evaluated, including themethotrexate-albumin conjugate (MTX-HSA),5-7 albumin-bindingprodrug of doxorubicin (DOXO-EMCH)8,9 and albumin paclitaxelnanoparticle (Abraxane), the latter also approved by the FDA fortreating metastatic breast cancer.10-12
Retinoids are a class of chemical compounds including the activemetabolites of vitamin A as well as a diversified library of syntheticderivatives, some of which have been shown to possess anti-tumoractivity. These include fenretinide, or N-(4-hydroxyphenyl-retinamide) (4-HPR), which has emerged as one of the mostpromising retinoids endowed with higher anticancer activity and alower toxicity profile than those of other synthetic derivatives.In particular, 4-HPR has proved to hold cytotoxic activity on awide variety of experimental models belonging to different typesof cancer, including lung cancer.13-16
In spite of its excellent pharmacological profile, a majorlimitation to the clinical use of fenretinide is represented by itslow bioavailability due to insolubility in water and thus inaqueous body fluids. Numerous attempts have been made todevelop a fenretinide formulation capable of increasing itsbioavailability to a level that can elicit a therapeutic response. Anoral formulation of fenretinide consisting of soft gelatin capsulescontaining fenretinide (100 mg) in corn oil and polysorbate iscurrently available at the National Cancer Institute (NCI).
Clinical I–III evaluations of this formulation have shownminimal systemic toxicity limited to reduced night vision that isreversible by discontinuation of the drug,17 and good tolerabilityeven at high doses (2450 mg/m2/d).18,19 No limiting toxic effectshave been observed up to 4000 mg/m2/d.20 However, therapeuticefficacy has also proven inadequate after multiple and protractedadministrations as the plasma concentration of fenretinide remainsbelow the minimum threshold for the onset of antitumoractivity.18,20 Recently, an oral formulation of fenretinide designedto obtain increased bioavailability was developed in the USA21
and is currently undergoing evaluation in phase I clinical trials.Administration of very high doses (1700 mg/m2/d) of the novelformulation once again provides relatively low plasma concentra-tions. Other different injectable formulations based on fenretinideincorporation in micellar systems,22 in poly(lactic acid) (PLA)microspheres23or in cremophor-ethanol emulsions,24 have beenalso developed. These formulations provided good drug bio-availability but their transition to the clinical use may be hinderedby the tolerability of the excipients. From these premises it clearlyemerges the need for novel formulations able to increase thebioavailability and consequently the therapeutic efficacy offenretinide and the importance to use safe macromolecules suchas albumin in their production.
In this study, we prepared a novel formulation consisting ofalbumin nanocapsules containing fenretinide and evaluated itsanti-tumor activity in experimental models of non-small cell lungcancer (NSCLC).
Materials and methods
Drugs and chemicals
Human serum albumin (≥99% pure, HSA) was purchasedfrom Sigma-Aldrich; fenretinide (N-(4-hydroxyphenyl)retinamide)(4-HPR) was purchased from Fidia Solmag-Olon S.p.A. (Italy).
Preparation of albumin–fenretinide nanocapsules
The albumin–fenretinide nanocapsules (4-HPR-HSA)(Figure 1, A and B) were prepared by mixing a fenretinidesuspension in ethanol with an HSA solution in water. Thefenretinide suspension was obtained by dissolving 200 mg of thedrug in 1 ml of ethanol. This suspension was added to an HSAsolution obtained by dissolving 1g of HSA in 10 ml of water, thefinal mixture having an incorporated fenretinide content of 16.6%(w:w). After stirring for 10 min at room temperature in the dark,the mixture was sonicated in a Vibra-Cell VCX 400 Sonicator at40 kHz for 2 h. The temperature was kept constant at 40 °C by athermostatic circulating water bath. After sonication the mixturewas diluted with 40 ml phosphate buffer pH 7.4 and filteredthrough a 0.22 μm filter to obtain a clear solution of the albumin–fenretinide nanocapsules with a mean diameter below 0.22 μm.The fenretinide concentration in the final nanoencapsulatedformulation was determined by a spectrophotometric analysis ofthe filtered solution at 360 nm using as a blank a void albuminnanocapsule solution prepared by the samemethod but without thedrug. The solution containing the albumin–fenretinide nanocap-sules was lyophilized and the dry residue weighted to obtain ameasure of drug loading in the nanocapsules. The ratio between theamount of fenretinide in the solution before lyophilization and thefinal weight of the dry residuewas considered as a measure of drugloading in the nanocapsules. The stability of the nanoencapsulatedformulation was estimated by UV spectra (UV-1700 spectropho-tometer, Shimadzu, Milan Italy) in the 190-400 nm rangeperformed every 12 h for 3 days at 37 °C.
Cell lines
The lung adenocarcinoma cell line A549 was purchased bythe American Type Culture Collection (ATCC). The cells weregrown in F12K medium supplemented with 10% fetal bovineserum and checked periodically for mycoplasma contaminationby MycoAlert™ Mycoplasma Detection Kit (Lonza, Basel,Switzerland). The established cell line CAEP was isolated in ourlaboratory from a patient affected by epidermoid lung cancer25
and was grown in culture medium composed of DMEM/Ham’sF12 (1:1) supplemented with fetal calf serum (10%), glutamine(2 mM), non-essential amino acids (1%) (M-medical, Milan,Italy) and insulin (10 µg/ml) (Sigma-Aldrich, St. Louis, MO,USA). All experiments were performed on cells in theexponential growth phase.

Figure 1. (A) Chemical structure and molecular weight (MW) of N-(4-hydroxyphenyl-retinamide) (4-HPR, fenretinide). (B) Schematic representation of thealbumin nanoparticles containing fenretinide used in this study. (C) Images captured by transmission electron microscopy of emulsion droplet of albumin (HSA)nanocapsules containing fenretinide (4-HPR- HSA).
265S. Pignatta et al / Nanomedicine: Nanotechnology, Biology, and Medicine 11 (2014) 263–273
Three-dimensional cell culture bioreactor
A rotatory cell culture system (RCCS) (Synthecon, Houston,TX, USA) was used as previously described.26 All procedureswere performed in sterile conditions under a laminar flow hood.As no specific medium formulation was required for cell growthin the RCCS, we used the same medium as that used for themonolayer cell cultures. The culture medium was changed every4 days. Tumor spheroids of both cell lines were obtained inabout 15-20 days.
Drug testing
MTS Assay.For 2D monolayer proliferation assays, A549 and CAEP cells
were seeded onto wells of a 96-well plate at a density of 5 × 104
cells per well. The effects of the drugs on cell proliferation wereassessed by CellTiter 96® AQueous One Solution Cell ProliferatinAssay (Promega, Milan, Italy) and the assay was conducted after72 h of drug exposure. Three independent experiments wereperformed in octuplicate. The optical density (OD) of treated anduntreated cells was determined at a wavelength of 490 nm usinga fluorescence plate reader.
Trypan blue exclusion test
3D aggregates were removed from the RCCS vessels andplaced in single wells of a 96-well low attachment culture plate.Each spheroid was harvested, disrupted using trypsin/EDTA 1×
(GE Healthcare, Milan, Italy) and the trypan blue exclusion testwas used to verify the viability of the cells when counting cellswith the hemocytometer.
Microscopy analysis
Phase contrast imaging and morphological analyses ofspheroids in 96-well microplates were carried out manually onan Olympus IX51 microscope equipped with Nikon Digital SightDS-Vi1 camera.
Transmission electron microscopy (TEM)
10 μl of albumin–fenretinide nanocapsules was absorbedonto formvar-carbon coated grids (200 mesh size) for 40 minand stained with 2% aqueous phosphotungstic acid solutionbefore viewing with a Philips CM10 transmission electronmicroscope at 80kV (FEI Company, Eindhoven, the Netherlands).The images were digitally captured by SIS Megaview III CCDcamera (FEI Company).
Lysates and western blot analysis
Cells were treated according to the previously describedWestern blot procedure.27 The following antibodies were used:goat anti-rabbit IgG-HRP: sc-2004 1:5000 (Santa Cruz Biotech-nology, Santa Cruz, CA, USA), anti-actin 1:5000 (Sigma-Aldrich,Milan, Italy), Precision Protein™ StrepTactin-HRP Conjugate1:10,000 (Bio-Rad Laboratories), anti-caveolin 1 1:500 (Cell

266 S. Pignatta et al / Nanomedicine: Nanotechnology, Biology, and Medicine 11 (2014) 263–273
Signaling Technology, Inc., Beverly, MA, USA) and anti-Sparc1:500 (Cell Signaling Technology, Inc.). Densitometric analysiswas performed using Quantity One Software Version 4.6.7. (Bio-Rad Laboratories).
Immunohistochemistry
For histological analysis, the cell lines grown as monolayer or3-D spheroids were placed in 4% buffered formalin up to 24 h,dehydrated and embedded in paraffin. Serial sections were stainedwith hematoxylin–eosin or used for immunohistochemistry.The following antibodies were used: rabbit polyclonal antibodyanti-Caveolin-1(1:50, Cell Signaling Technology, Inc.) and rabbitpolyclonal antibody anti-sparc (1:1000, Cell Signaling Technol-ogy, Inc.). Immunoreactivity for active caveolin-1 or SPARC wasevaluated quantitatively by counting at least 1000 tumor cells at40 × magnification. Bound antibody was revealed using thesubstrate 3,3’-diaminobenzidine as chromogen and hematoxylincounterstaining. Positive and negative controls were included ineach batch. All samples were evaluated blindly using lightmicroscopy by two independent observers.
TUNEL assay
At the end of treatment, the cells were fixed in 1%paraformaldehyde in PBS on ice for 15 min, suspended in icecold ethanol (70%) and stored overnight at −20 °C. The cellswere then washed twice in PBS and re-suspended in PBScontaining 0.1% Triton X-100 for 5 min at 4 °C. Thereafter, thepercentage of apoptotic cells was evaluated by flow cytometricanalysis (FACSanto flowcytometer, BectonDickinson, SanDiego,CA, USA) according to the previously described TUNEL assay.28
The samples were run in triplicate and 10,000 events werecollected for each replica. The data were the average of threeexperiments, with errors under 5%.
In vivo experiments
CD nu/nu female mice, weighing 20 to 25 g, were supplied byCharles River Laboratories (Harlan, Udine, Italy) and wereallowed unrestricted access to sterile food and water. Housingand all procedures involving animals were performed according tothe protocol approved by the ethics committee. Each experimentused the minimum number of mice needed to obtain statisticallymeaningful results. The mice were subcutaneously implanted inthe right flank with A549 cells (6 × 106 cells/mouse in a 200 μlvolume of serum-free medium). The dimensions of subcutaneoustumor mass were measured every 2 days in two perpendiculardirections using calipers. Tumor volume (mm3) was defined asfollows: (W1
2 × W2) × (π/6), whereW1 andW2 are the largest andsmallest tumor diameters (mm), respectively. The mice were thenrandomized into two groups of 10 animals. When the tumorsreached amean volume of 150 mm3, the animals were treated with4-HPR-HSA, HSA or vehicle alone (PBS), given slowly throughthe tail vein in a volume of 200 μL. The drug was administered atthe dose of 1 mg/kg every 3 days for a total of 12 administrations.The experiment was terminated 38 days after the start of treatment.We did not treat the animals with pure 4-HPR as its waterinsolubility would have required previous dissolution in ethanol orother water-mixable organic solvents followed by dilution with an
aqueous phase before injection. As is well known, dilution triggersdrug precipitation due to the mixing of the organic solvent withwater. Although this procedure iswidely used for in vitro studies ofpoorly soluble drugs, it is not a suitable experimental model inin vivo settings involving intravenous administrations. This isbecause drug particle precipitation, in addition to providing unevenbioavailability, can also randomly embolize blood vessels, especiallyafter repeated administrations, as in the case of our study.
Ethics statements
The animal experiments were carried out in the Department ofPharmacology of the University of Bologna with the approval ofthe local ethics committee (Veterinary Service of the Universityof Bologna, Italy) and in agreement with the National AnimalWelfare Act. All efforts were made to minimize animal sufferingand the number of animals used was kept to a minimum by theexperimental design. All the procedures followed in this workwere in compliance with the European Community CouncilDirective of 24 November 1986 (86/609/EEC) and wereapproved by the Ethics Committee of the University of Bologna(Prot. ARIC n. 4783-X/10).
Statistical analysis
The results were presented as the mean of at least two separateexperiments. The differences between values obtained by thevarious treatments were analyzed using the Student’s t test forunpaired observations. The statistical significance of the in vivoexperiments was analyzed via an unpaired two-tailed Student t testassuming equal variance. In addition, Hochberg’s method wasused to adjust P-values for multiple comparisons. P-values b0.05were considered significant.
Results
Ultrastructure of 4-HPR-HSA
TEM analysis showed several 4-HPR-HSA round particles withdiameters ranging from 80 to 100 nm. The round shape was regularand the distribution was highly homogeneous (Figure 1, C).
Drug loading and stability of the 4-HPR-HSA nanocapsulesDrug loading in the nanocapsules (14.5 ± 1.3% w:w) was
very close to the content incorporated in the preparative mixture(16.6% w:w), indicating that the preparative method used in thepresent work was highly efficient in favoring fenretinideentrapment in albumin nanocapsules. The stability of theformulation was maintained over time as no changes in UV spectrawere observed due to drug dissociation from the nanocapsules in anaqueous environment.
In vitro experiments
We first comparatively assessed the cytotoxic activity offenretinide (4-HPR) and fenretinide–albumin nanocapsules (4-HPR-HSA) in two human lung cancer cell lines CAEP andA549, grown as a single thickness cell layer by MTS assay(Figure 2). Cells were exposed to scalar drug concentrationsranging from 10 μM to 50 μM for 72 h. Both the pure drug and
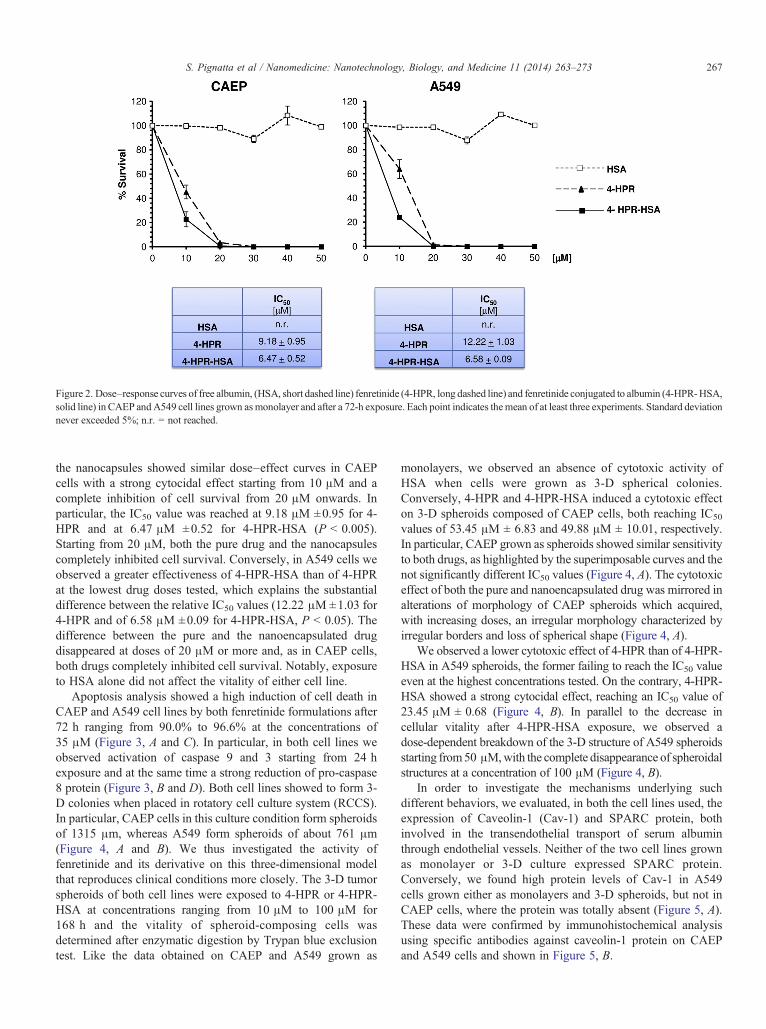
Figure 2. Dose–response curves of free albumin, (HSA, short dashed line) fenretinide (4-HPR, long dashed line) and fenretinide conjugated to albumin (4-HPR-HSA,solid line) in CAEP andA549 cell lines grown asmonolayer and after a 72-h exposure. Each point indicates themean of at least three experiments. Standard deviationnever exceeded 5%; n.r. = not reached.
267S. Pignatta et al / Nanomedicine: Nanotechnology, Biology, and Medicine 11 (2014) 263–273
the nanocapsules showed similar dose–effect curves in CAEPcells with a strong cytocidal effect starting from 10 μM and acomplete inhibition of cell survival from 20 μM onwards. Inparticular, the IC50 value was reached at 9.18 μM ±0.95 for 4-HPR and at 6.47 μM ±0.52 for 4-HPR-HSA (P b 0.005).Starting from 20 μM, both the pure drug and the nanocapsulescompletely inhibited cell survival. Conversely, in A549 cells weobserved a greater effectiveness of 4-HPR-HSA than of 4-HPRat the lowest drug doses tested, which explains the substantialdifference between the relative IC50 values (12.22 μM ±1.03 for4-HPR and of 6.58 μM ±0.09 for 4-HPR-HSA, P b 0.05). Thedifference between the pure and the nanoencapsulated drugdisappeared at doses of 20 μM or more and, as in CAEP cells,both drugs completely inhibited cell survival. Notably, exposureto HSA alone did not affect the vitality of either cell line.
Apoptosis analysis showed a high induction of cell death inCAEP and A549 cell lines by both fenretinide formulations after72 h ranging from 90.0% to 96.6% at the concentrations of35 μM (Figure 3, A and C). In particular, in both cell lines weobserved activation of caspase 9 and 3 starting from 24 hexposure and at the same time a strong reduction of pro-caspase8 protein (Figure 3, B and D). Both cell lines showed to form 3-D colonies when placed in rotatory cell culture system (RCCS).In particular, CAEP cells in this culture condition form spheroidsof 1315 μm, whereas A549 form spheroids of about 761 μm(Figure 4, A and B). We thus investigated the activity offenretinide and its derivative on this three-dimensional modelthat reproduces clinical conditions more closely. The 3-D tumorspheroids of both cell lines were exposed to 4-HPR or 4-HPR-HSA at concentrations ranging from 10 μM to 100 μM for168 h and the vitality of spheroid-composing cells wasdetermined after enzymatic digestion by Trypan blue exclusiontest. Like the data obtained on CAEP and A549 grown as
monolayers, we observed an absence of cytotoxic activity ofHSA when cells were grown as 3-D spherical colonies.Conversely, 4-HPR and 4-HPR-HSA induced a cytotoxic effecton 3-D spheroids composed of CAEP cells, both reaching IC50
values of 53.45 μM ± 6.83 and 49.88 μM ± 10.01, respectively.In particular, CAEP grown as spheroids showed similar sensitivityto both drugs, as highlighted by the superimposable curves and thenot significantly different IC50 values (Figure 4, A). The cytotoxiceffect of both the pure and nanoencapsulated drug was mirrored inalterations of morphology of CAEP spheroids which acquired,with increasing doses, an irregular morphology characterized byirregular borders and loss of spherical shape (Figure 4, A).
We observed a lower cytotoxic effect of 4-HPR than of 4-HPR-HSA in A549 spheroids, the former failing to reach the IC50 valueeven at the highest concentrations tested. On the contrary, 4-HPR-HSA showed a strong cytocidal effect, reaching an IC50 value of23.45 μM ± 0.68 (Figure 4, B). In parallel to the decrease incellular vitality after 4-HPR-HSA exposure, we observed adose-dependent breakdown of the 3-D structure of A549 spheroidsstarting from50 μM,with the complete disappearance of spheroidalstructures at a concentration of 100 μM (Figure 4, B).
In order to investigate the mechanisms underlying suchdifferent behaviors, we evaluated, in both the cell lines used, theexpression of Caveolin-1 (Cav-1) and SPARC protein, bothinvolved in the transendothelial transport of serum albuminthrough endothelial vessels. Neither of the two cell lines grownas monolayer or 3-D culture expressed SPARC protein.Conversely, we found high protein levels of Cav-1 in A549cells grown either as monolayers and 3-D spheroids, but not inCAEP cells, where the protein was totally absent (Figure 5, A).These data were confirmed by immunohistochemical analysisusing specific antibodies against caveolin-1 protein on CAEPand A549 cells and shown in Figure 5, B.
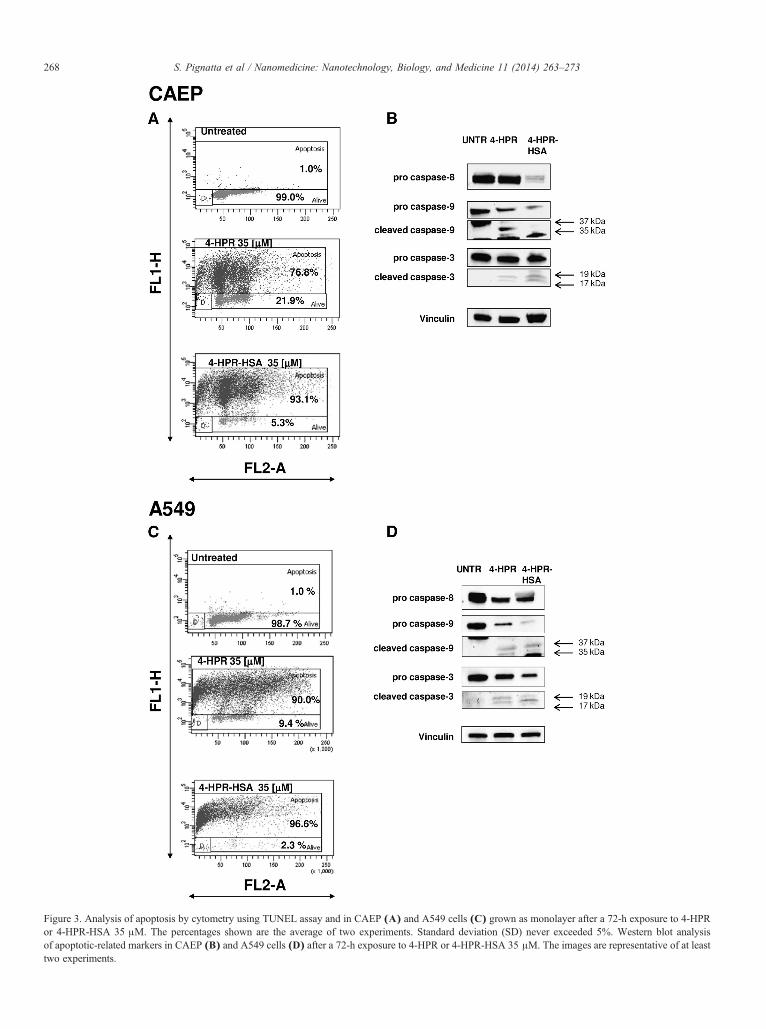
Figure 3. Analysis of apoptosis by cytometry using TUNEL assay and in CAEP (A) and A549 cells (C) grown as monolayer after a 72-h exposure to 4-HPRor 4-HPR-HSA 35 μM. The percentages shown are the average of two experiments. Standard deviation (SD) never exceeded 5%. Western blot analysisof apoptotic-related markers in CAEP (B) and A549 cells (D) after a 72-h exposure to 4-HPR or 4-HPR-HSA 35 μM. The images are representative of at leasttwo experiments.
268 S. Pignatta et al / Nanomedicine: Nanotechnology, Biology, and Medicine 11 (2014) 263–273
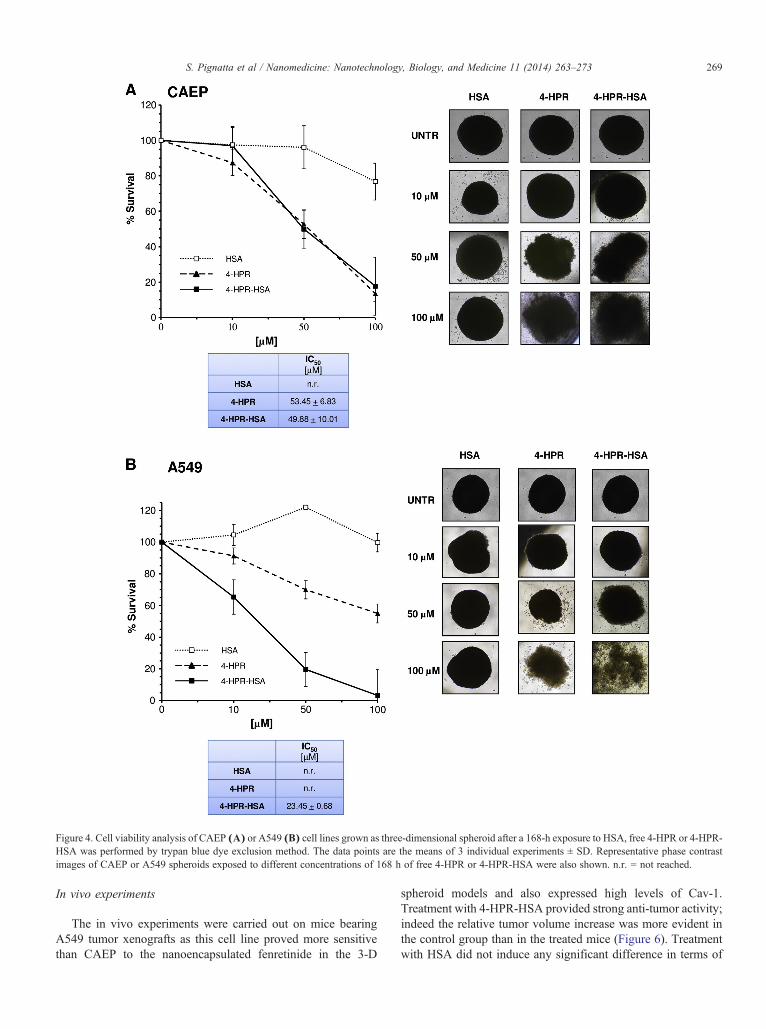
Figure 4. Cell viability analysis of CAEP (A) or A549 (B) cell lines grown as three-dimensional spheroid after a 168-h exposure to HSA, free 4-HPR or 4-HPR-HSA was performed by trypan blue dye exclusion method. The data points are the means of 3 individual experiments ± SD. Representative phase contrastimages of CAEP or A549 spheroids exposed to different concentrations of 168 h of free 4-HPR or 4-HPR-HSA were also shown. n.r. = not reached.
269S. Pignatta et al / Nanomedicine: Nanotechnology, Biology, and Medicine 11 (2014) 263–273
In vivo experiments
The in vivo experiments were carried out on mice bearingA549 tumor xenografts as this cell line proved more sensitivethan CAEP to the nanoencapsulated fenretinide in the 3-D
spheroid models and also expressed high levels of Cav-1.Treatment with 4-HPR-HSA provided strong anti-tumor activity;indeed the relative tumor volume increase was more evident inthe control group than in the treated mice (Figure 6). Treatmentwith HSA did not induce any significant difference in terms of

Figure 5. (A)Western blot analysis of Cav-1 and SPARC expression in A549 and CAEP cell lines grown as three-dimensional spheroid. The human cancer celllines, NCI-N87 and HUVEC, were used as positive controls (Ctr +) for Cav-1 and SPARC protein expression, respectively. Actin was used as loading control.The images are representative of at least two experiments. (B) Immunohistochemical (IHC) detection of Caveolin-1 positive cells in CAEP or A549 cell linesgrown as monolayer or 3-D spheroids using a primary anti cav-1 protein antibody.
270 S. Pignatta et al / Nanomedicine: Nanotechnology, Biology, and Medicine 11 (2014) 263–273
tumor growth with respect to the controls (Figure 6). In particular,we observed that after 20 days, tumor growth was significantlyslower in the treated mice than in the control group (P b 0.05) andthis trend persisted throughout the whole observation period.Average sizes of the tumors at sacrifice were as follows:control = 1578.58 mm3 ± 635.96 (mean ± S.E.M), HSA =1613.40 mm3 ± 387.19 (mean ± S.E.M), 4-HPR-HSA =588.90 mm3 ± 257.52 (mean ± S.E.M., P b 0.05 compared withcontrol). This indicated a reduction in tumor volume of 62.6% by 4-HPR-HSA vs control. No weight loss or signs of toxicity were observedduring the treatment period indicating good tolerability of 4-HPR-HSA.
Discussion
Lung cancer is the leading cause of cancer-related mortalityworldwide29 and non-small cell lung cancer (NSCLC) accounts
for over 80% of lung cancer deaths.30 In addition to the traditionallung cancer treatments of surgery, radiation and chemotherapy,molecularly targeted drugs such as EGFR tyrosine kinase inhibitors(gefitinib and erlotinib),31 and anaplastic lymphoma kinase (ALK)tyrosine kinase inhibitors (crizotinib)32 have recently emergedas viable therapeutic options. However, therapeutic outcomesappear to have reached a plateau, with response rates of 20%-35% and a median survival of 8-12 months.33-35 Thus, newapproaches are urgently needed to improve the therapeuticoutcome of this tumor.
Nanoparticle delivery systems have attracted increasingattention in recent years, especially for cancer therapies. Inparticular, nanoencapsulation of active peptides and proteins canprotect these sensitive drugs from degradation and simulta-neously prolong or modify their release, maintaining effectiveplasma concentration for prolonged time periods. Furthermore,nanoencapsulation represents a valuable tool to improve the
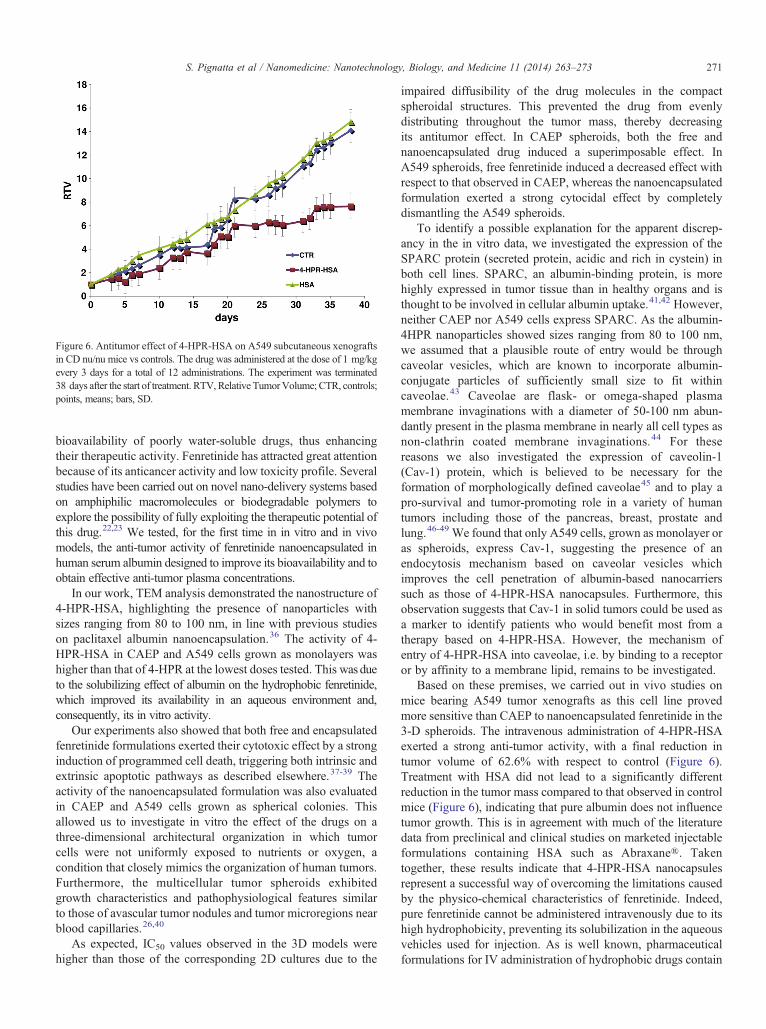
Figure 6. Antitumor effect of 4-HPR-HSA on A549 subcutaneous xenograftsin CD nu/nu mice vs controls. The drug was administered at the dose of 1 mg/kgevery 3 days for a total of 12 administrations. The experiment was terminated38 days after the start of treatment. RTV, Relative TumorVolume; CTR, controls;points, means; bars, SD.
271S. Pignatta et al / Nanomedicine: Nanotechnology, Biology, and Medicine 11 (2014) 263–273
bioavailability of poorly water-soluble drugs, thus enhancingtheir therapeutic activity. Fenretinide has attracted great attentionbecause of its anticancer activity and low toxicity profile. Severalstudies have been carried out on novel nano-delivery systems basedon amphiphilic macromolecules or biodegradable polymers toexplore the possibility of fully exploiting the therapeutic potential ofthis drug.22,23 We tested, for the first time in in vitro and in vivomodels, the anti-tumor activity of fenretinide nanoencapsulated inhuman serum albumin designed to improve its bioavailability and toobtain effective anti-tumor plasma concentrations.
In our work, TEM analysis demonstrated the nanostructure of4-HPR-HSA, highlighting the presence of nanoparticles withsizes ranging from 80 to 100 nm, in line with previous studieson paclitaxel albumin nanoencapsulation.36 The activity of 4-HPR-HSA in CAEP and A549 cells grown as monolayers washigher than that of 4-HPR at the lowest doses tested. This was dueto the solubilizing effect of albumin on the hydrophobic fenretinide,which improved its availability in an aqueous environment and,consequently, its in vitro activity.
Our experiments also showed that both free and encapsulatedfenretinide formulations exerted their cytotoxic effect by a stronginduction of programmed cell death, triggering both intrinsic andextrinsic apoptotic pathways as described elsewhere.37-39 Theactivity of the nanoencapsulated formulation was also evaluatedin CAEP and A549 cells grown as spherical colonies. Thisallowed us to investigate in vitro the effect of the drugs on athree-dimensional architectural organization in which tumorcells were not uniformly exposed to nutrients or oxygen, acondition that closely mimics the organization of human tumors.Furthermore, the multicellular tumor spheroids exhibitedgrowth characteristics and pathophysiological features similarto those of avascular tumor nodules and tumor microregions nearblood capillaries.26,40
As expected, IC50 values observed in the 3D models werehigher than those of the corresponding 2D cultures due to the
impaired diffusibility of the drug molecules in the compactspheroidal structures. This prevented the drug from evenlydistributing throughout the tumor mass, thereby decreasingits antitumor effect. In CAEP spheroids, both the free andnanoencapsulated drug induced a superimposable effect. InA549 spheroids, free fenretinide induced a decreased effect withrespect to that observed in CAEP, whereas the nanoencapsulatedformulation exerted a strong cytocidal effect by completelydismantling the A549 spheroids.
To identify a possible explanation for the apparent discrep-ancy in the in vitro data, we investigated the expression of theSPARC protein (secreted protein, acidic and rich in cystein) inboth cell lines. SPARC, an albumin-binding protein, is morehighly expressed in tumor tissue than in healthy organs and isthought to be involved in cellular albumin uptake.41,42 However,neither CAEP nor A549 cells express SPARC. As the albumin-4HPR nanoparticles showed sizes ranging from 80 to 100 nm,we assumed that a plausible route of entry would be throughcaveolar vesicles, which are known to incorporate albumin-conjugate particles of sufficiently small size to fit withincaveolae.43 Caveolae are flask- or omega-shaped plasmamembrane invaginations with a diameter of 50-100 nm abun-dantly present in the plasma membrane in nearly all cell types asnon-clathrin coated membrane invaginations.44 For thesereasons we also investigated the expression of caveolin-1(Cav-1) protein, which is believed to be necessary for theformation of morphologically defined caveolae45 and to play apro-survival and tumor-promoting role in a variety of humantumors including those of the pancreas, breast, prostate andlung.46-49 We found that only A549 cells, grown as monolayer oras spheroids, express Cav-1, suggesting the presence of anendocytosis mechanism based on caveolar vesicles whichimproves the cell penetration of albumin-based nanocarrierssuch as those of 4-HPR-HSA nanocapsules. Furthermore, thisobservation suggests that Cav-1 in solid tumors could be used asa marker to identify patients who would benefit most from atherapy based on 4-HPR-HSA. However, the mechanism ofentry of 4-HPR-HSA into caveolae, i.e. by binding to a receptoror by affinity to a membrane lipid, remains to be investigated.
Based on these premises, we carried out in vivo studies onmice bearing A549 tumor xenografts as this cell line provedmore sensitive than CAEP to nanoencapsulated fenretinide in the3-D spheroids. The intravenous administration of 4-HPR-HSAexerted a strong anti-tumor activity, with a final reduction intumor volume of 62.6% with respect to control (Figure 6).Treatment with HSA did not lead to a significantly differentreduction in the tumor mass compared to that observed in controlmice (Figure 6), indicating that pure albumin does not influencetumor growth. This is in agreement with much of the literaturedata from preclinical and clinical studies on marketed injectableformulations containing HSA such as Abraxane®. Takentogether, these results indicate that 4-HPR-HSA nanocapsulesrepresent a successful way of overcoming the limitations causedby the physico-chemical characteristics of fenretinide. Indeed,pure fenretinide cannot be administered intravenously due to itshigh hydrophobicity, preventing its solubilization in the aqueousvehicles used for injection. As is well known, pharmaceuticalformulations for IV administration of hydrophobic drugs contain

272 S. Pignatta et al / Nanomedicine: Nanotechnology, Biology, and Medicine 11 (2014) 263–273
water-mixable organic solvents such as ethanol or benzyl alcoholplus tensides such as cremophor or polysorbate to solubilize thedrug. Apart from the serious concerns about the tolerability ofthese excipients, the major problem is the vehicle dilution thattakes place in the bloodstream immediately after IV administra-tion. This causes dilution of the co-solvents and the consequentprecipitation of the drug, with a significant decrease in itsbioavailability and the risk of embolism, especially for repeatedand frequent administrations.
Conversely, drug encapsulation in albumin nanoparticlesprevents drug precipitation upon dilution because of the presenceof characteristic hydrophobic pockets in the structure of the proteinthat stabilize the interaction between albumin and the hydrophobicdrugs. This, in fact, represents the physiological role of albumin,which is that of hosting hydrophobic molecules, e.g. fatty acids,hormones etc., and of transporting them throughout the body.50
Moreover, the improved penetration of the 4-HPR-HSA nanocap-sules into the tumor mass due to the presence of Cav-1 on the cellsurface makes this formulation a promising tool for the exploitationof fenretinide in antitumor therapy.
In conclusion, this new pharmaceutical system could provideunexpected opportunities for cancer treatment. In particular, theimproved availability of fenretinide, together with its limitedtoxicity, could permit prolonged administration of the drug andlead to better disease control, especially in minimal residualdisease which often becomes resistant to conventional therapy.
Acknowledgments
The authors wish to thank Dr. Catia Barboni (DIMEVET,University of Bologna) for her invaluable help in performing thein vivo experiments. The authors also thank Ursula Elbling forediting the manuscript.
References
1. Brigger I, Dubernet C, Couvreur P. Nanoparticles in cancer therapy anddiagnosis. Adv Drug Deliv Rev 2002;54:631-51.
2. Singh S, Sharma A, Robertson GP. Realizing the clinical potential ofcancer nanotechnology by minimizing toxicologic and targeted deliveryconcerns. Cancer Res 2012;72:5663-8.
3. Matsumura Y, Maeda H. A new concept for macromoleculartherapeutics in cancer chemotherapy: mechanism of tumoritropicaccumulation of proteins and the antitumor agent smancs. Cancer Res1986;46:6387-92.
4. Stehle G, Sinn H, Wunder A, Schrenk HH, Stewart JC, Hartung G, et al.Plasma protein (albumin) catabolism by the tumor itself-implications fortumor metabolism and the genesis of cachexia. Crit Rev Oncol Hematol1997;26:77-100.
5. Hartung G, Stehle G, Sinn H, Wunder A, Schrenk HH, Heeger S, et al.Phase I trial of methotrexate-albumin in a weekly intravenous bolusregimen in cancer patients. Phase I Study Group of the Association forMedical Oncology of the German Cancer Society. Clin Cancer Res1999;5:753-9.
6. Vis AN, van der Gaast A, van Rhijn BW, Catsburg TK, Schmidt C,Mickisch GH. A phase II trial of methotrexate-human serum albumin(MTX-HSA) in patients with metastatic renal cell carcinoma whoprogressed under immunotherapy. Cancer Chemother Pharmacol2002;49:342-5.
7. Bolling C, Graefe T, Lübbing C, Jankevicius F, Uktveris S, Cesas A, et al.Phase II study of MTX-HSA in combination with cisplatin as first linetreatment in patients with advanced or metastatic transitional cellcarcinoma. Invest New Drugs 2006;24:521-7.
8. Unger C, Häring B, Medinger M, Drevs J, Steinbild S, Kratz F, et al.Phase I and pharmacokinetic study of the (6-maleimidocaproyl)hydra-zone derivative of doxorubicin. Clin Cancer Res 2007;13:4858-66.
9. Kratz F. DOXO-EMCH (INNO-206): the first albumin-binding prodrug ofdoxorubicin to enter clinical trials.Expert Opin InvestigDrugs 2007;16:855-66.
10. Ibrahim NK, Desai N, Legha S, Soon-Shiong P, Theriault RL, Rivera E,et al. Phase I and pharmacokinetic study of ABI-007, a Cremophor-free,protein-stabilized, nanoparticle formulation of paclitaxel. Clin CancerRes 2002;8:1038-44.
11. Ibrahim NK, Samuels B, Page R, Doval D, Patel KM, Rao SC, et al.Multicenter phase II trial of ABI-007, an albumin-bound paclitaxel, inwomen with metastatic breast cancer. J Clin Oncol 2005;23:6019-26.
12. Gradishar WJ, Tjulandin S, Davidson N, Shaw H, Desai N, Bhar P, et al.Phase III trial of nanoparticle albumin-bound paclitaxel compared withpolyethylated castor oil-based paclitaxel in women with breast cancer. JClin Oncol 2005;23:7794-803.
13. Hong WK, Lippman SM, Itri LM, Karp DD, Lee JS, Byers RM, et al.Prevention of second primary tumors with isotretinoin in squamous-cellcarcinoma of the head and neck. N Engl J Med 1990;323:795-801.
14. Kalemkerian GP, Slusher R, Ramalingam S, Gadgeel S, Mabry M.Growth inhibition and induction of apoptosis by fenretinide in small celllung cancer cell lines. J Natl Cancer Inst 1995;87:1674-80.
15. Ulukaya E, Wood EJ. Fenretinide and its relation to cancer. CancerTreat Rev 1999;25:229-35.
16. Zou CP, Kurie JM, Lotan D, Zou CC, Hong WK, Lotan R. Higherpotency of n-(4-hydroxyphenyl)retinamide than alltrans-retinoic acid ininduction of apoptosis in non-small cell lung cancer cell lines. ClinCancer Res 1998;4:1345-55.
17. Torrisi R, Parodi S, Fontana V, Rondanina G, Formelli F, Costa A, et al.Factors affecting plasma retinol decline during long term administrationof the synthetic retinoid fenretined in breast cancer patients. CancerEpidemiol Biomarkers Prev 1994;3:507-10.
18. Jasti BR, Lo Russo PM, Parchment RE. Phase I clinical trial offenretinide (NSC374551) in advanced solid tumors. Proc Am Soc ClinOncol 2001;20:122a.
19. Villablanca JG, Krailo MD, Ames MM, Reid JM, Reaman GH,Reynolds CP. Phase I trial of oral fenretinide in children with high risksolid tumors: a report from the Children’s Oncology Group(CCG09709). J Clin Oncol 2006;24:3423-30.
20. Garaventa A, Luksch R, Lo Piccolo MS, Cavadini E, Montaldo PG,Pizzitola MR, et al. Phase I trial and pharmacokinetics of fenretinide inchildren with neuroblastoma. Clin Cancer Res 2003;9:2032-9.
21. Maurer BJ, Kalous O, Yesair DW, Wu X, Janeba J, Maldonado V, et al.Improved oral delivery of N-(4-hydroxyphenyl) retinamide with a novelLYM-X-SORB organized lipid complex.Clin Cancer Res 2007;13:3079-86.
22. Orienti I, Zuccari G, Falconi M, Teti G, Illingworth NA, Veal GJ. Novelmicelles based on amphiphilic branched PEG as carriers for fenretinide.Nanomedicine 2012;8:880-90.
23. Falconi M, Focaroli S, Teti G, Salvatore V, Durante S, Nicolini B, et al.Novel PLA microspheres with hydrophilic and bioadhesive surfaces forthe controlled delivery of fenretinide. J Microencapsul 2014;31:41-8.
24. Mohrbacher A, Gutierrez M, Murgo AJ, Kummar S, Reynolds CP,Maurer BJ, et al. Phase I trial of fenretinide (4-HPR) intravenousemulsion for hematologic malignancies. Proc Am Soc Clin Oncol2007;25:13007 [Abstr.].
25. Gasperi-Campani A, Roncuzzi L, Ricotti L, Lenzi L, Gruppioni R, Sensi A, et al.Molecular and biological features of two new human squamous andadenocarcinoma of the lung cell lines.Cancer Genet Cytogenet 1998;107:11-20.
26. Tesei A, Sarnelli A, Arienti C, Menghi E, Medri L, Gabucci E, et al. In vitroirradiation system for radiobiological experiments.Radiat Oncol 2013;8:257-69.
27. Pignatta S, Arienti C, Zoli W, Di Donato M, Castoria G, Gabucci E, et al.Prolonged exposure to (R)-bicalutamide generates a LNCaP subclone

273S. Pignatta et al / Nanomedicine: Nanotechnology, Biology, and Medicine 11 (2014) 263–273
with alteration of mitochondrial genome. Mol Cell Endocrinol2014;382:314-24.
28. Rosetti M, Tesei A, Ulivi P, Fabbri F, Vannini I, Brigliadori G, et al.Molecular characterization of cytotoxic and resistance mechanismsinduced by NCX 4040, a novel NO-NSAID, in pancreatic cancer celllines. Apoptosis 2006;11:1321-30.
29. Ramalingam SS, Owonikoko TK, Khuri FR. Lung cancer: newbiological insights and recent therapeutic advances. CA Cancer J Clin2011;61:91-112.
30. Favaretto AG, Pasello G, Magro C. Second and third line treatment inadvanced non small cell lung cancer. Discov Med 2009;8:204-9.
31. Maione P, Rossi A, Sacco PC, Bareschino MA, Schettino C, Gridelli C.Advances in chemotherapy in advanced non-small-cell lung cancer.Expert Opin Pharmacother 2010;11:2997-3007.
32. Kwak EL, Bang YJ, Camidge DR, Shaw AT, Solomon B, Maki RG, etal. Anaplastic lymphoma kinase inhibition in non-small-cell lung cancer.N Engl J Med 2010;363:1693-703.
33. Sandler A, Gray R, Perry MC, Brahmer J, Schiller JH, Dowlati A, et al.Paclitaxel-carboplatin alone or with bevacizumab for non-small-cell lungcancer. N Engl J Med 2006;355:2542-50.
34. Scagliotti GV, Parikh P, von Pawel J, BiesmaB, Vansteenkiste J,Manegold C,et al. Phase III study comparing cisplatin plus gemcitabine with cisplatinplus pemetrexed in chemotherapynaive patients with advanced-stage non-small-cell lung cancer. J Clin Oncol 2008;26:3543-51.
35. Schiller JH, Harrington D, Belani CP, Langer C, Sandler A, Krook J, et al.Comparison of four chemotherapy regimens for advanced non-small-celllung cancer. N Engl J Med 2002;346:92-8.
36. Ma P, Mumper RJ. Paclitaxel nano-delivery systems: a comprehensivereview. J Nanomed Nanotechnol 2013;4:1000164-79.
37. Wu JM, DiPietrantonio AM, Hsieh TC. Mechanism of fenretinide (4-HPR)-induced cell death. Apoptosis 2001;6:377-88.
38. Kalli KR, Devine KE, CabotMC,Arnt CR,HeldebrantMP, Svingen PA, et al.Heterogeneous role of caspase-8 in fenretinide-induced apoptosis in epithelialovarian carcinoma cell lines.Mol Pharmacol 2003;64:1434-43.
39. Raguénez G, Mühlethaler-Mottet A,Meier R, Duros C, Bénard J, Gross N.Fenretinide-induced caspase-8 activation and apoptosis in an establishedmodel of metastatic neuroblastoma. BMC Cancer 2009;9:97-109.
40. Friedrich J, Ebner R, Kunz-Schughart LA. Experimental anti-tumortherapy in 3-D: spheroids— old hat or new challenge? Int J Radiat Biol2007;83:849-71.
41. Desai NP, Trieu V, Hwang LY, Wu R, Soon-Shiong P, Gradishar WJ.Improved effectiveness of nanoparticle albumin-bound (nab) paclitaxelversus polysorbate-based docetaxel in multiple xenografts as a functionof HER2 and SPARC status. Anticancer Drugs 2008;19:899-909.
42. Frei E. Albumin binding ligands and albumin conjugate uptake by cancercells. Diabetol Metab Syndr 2001;3:11-4.
43. Oh P, Borgstrom P,Witkiewicz H, Li Y, Borgstrom BJ, Chrastina A, et al.Live dynamic imaging of caveolae pumping targeted antibody rapidlyand specifically across endothelium in the lung. Nat Biotechnol2007;25:327-37.
44. Jasmin JF, Frank PG, Lisanti MC. Caveolins and caveolae. Roles insignaling and disease mechanisms. Advances in Experimental Medicineand Biology, vol. 729; 20124-5 [Springer Editions].
45. Sternberg PW, Schmid SL. Caveolin-1, cholesterol and Ras signalling.Nat Cell Biol 1999;1:98-105.
46. Williams TM, Lisanti MP. Caveolin-1 in oncogenic transformation,cancer, and metastasis. Am J Physiol Cell Physiol 2005;288:494-506.
47. Yang G, Truong LD, Timme TL, Ren C, Wheeler TM, Park SH, et al.Elevated expression of caveolin is associated with prostate and breastcancer. Clin Cancer Res 1998;4:1873-80.
48. Shatz M, Liscovitch M. Caveolin-1: a tumor-promoting role in humancancer. Int J Radiat Biol 2008;84:177-89.
49. Pancotti F, Roncuzzi L, Maggiolini M, Gasperi-Campani A. Caveolin-1silencing arrests the proliferation of metastatic lung cancer cells throughthe inhibition of STAT3 signaling. Cell Signal 2012;24:1390-7.
50. Simard JR, Zunszain PA, Hamilton JA, Curry S. Location of high andlow affinity fatty acid binding sites on human serum albumin revealed byNMR drug-competition analysis. J Mol Biol 2006;361:336-51.
Copyright © 2022 FDOKUMEN




















