Physical parameters affecting ultrasound/microbubble-mediated gene delivery efficiency in vitro
11
doi:10.1016/j.ultrasmedbio.2006.04.014 ● Original Contribution PHYSICAL PARAMETERS AFFECTING ULTRASOUND/MICROBUBBLE- MEDIATED GENE DELIVERY EFFICIENCY IN VITRO AHAD RAHIM,* SARAH L. TAYLOR,* NIGEL L. BUSH, † GAIL R. TER HAAR, † JEFFREY C. BAMBER, † and COLIN D. PORTER* *The Institute of Cancer Research, Gene Therapy Group, Section of Cell and Molecular Biology, London; and † The Institute of Cancer Research and The Royal Marsden NHS Trust, Joint Department of Physics, Sutton, UK (Received 25 January 2006; revised 4 April 2006; in final form 13 April 2006) Abstract—Ultrasound (US)/microbubble-mediated gene delivery is a technology with many potential advantages suited to clinical application. Previous studies have demonstrated transfection but many are unsatisfactory in respect to the exposure apparatus, lack of definition of the US field or the limitations on parameters that can be explored using clinical diagnostic US machines. We investigated individual exposure parameters using a system minimising experimental artefacts and allowing control of many parameters of the US field. Using a 1-MHz transducer we systematically varied US parameters, the duration of exposure and the microbubble and DNA concentrations to optimise gene delivery. Delivery was achieved, using lipid microbubbles (SonoVue ® ) and clinically acceptable US exposures, to adherent cells at efficiencies of 4%. The acoustic pressure amplitude (0.25 MPa peak-negative), pulse repetition frequency (1-kHz) and duration of exposure (10 s) were important in optimising gene delivery with minimal impact on cell viability. These findings support the hypothesis that varying the physical parameters of US-mediated gene delivery has an affect on both efficiency and cell viability. These data are the first in terms of their thorough exploration of the US parameter space and will be the basis for more-informed approaches to developing clinical applications of this technology. (E-mail: [email protected]) © 2006 World Federation for Ultrasound in Medicine & Biology. Key Words: Ultrasound, Microbubble contrast agent, Nonviral vector. INTRODUCTION To date, a number of physical methods for delivery of nonviral vectors to cells, such as electroporation, hydro- dynamic delivery, ballistic delivery and microinjection, have been investigated (Wells 2004). A more recent method that is being developed is the combined use of ultrasound (US) and medical imaging microbubble con- trast agents (Newman et al. 2001; Unger et al. 2001). The major advantage that US/microbubble-mediated gene de- livery has over other physical force protocols is that it allows targeted and site-specific gene delivery with min- imal procedural invasiveness: the plasmid and micro- bubbles can be administered intravenously or directly to the tissue of interest and gene delivery limited to the area subsequently exposed to US, avoiding delivery to non- target cells. In addition, both US and microbubble con- trast agents are used routinely in the clinic (Blomley et al. 2001; Lindner 2004). The precision with which a US beam can be targeted has already been demonstrated in clinical approaches such as focused US ablation (ter Haar 2001), albeit at much higher intensities than those used for nondestructive gene delivery. The ultimate goal would be a systemic approach. Given the vascular reten- tion of microbubbles, the method will be particularly suited to delivery to endothelial cells, such as for the treatment of cardiovascular disease or cancer. The use of US alone to deliver DNA into cells has been studied (Kim et al. 1996; Lawrie et al. 1999). For example, Lawrie et al. demonstrated a 7.5-fold enhance- ment in naked plasmid luciferase gene expression when porcine vascular smooth muscle cells were exposed to continuous wave 1-MHz US for 60-s compared with that seen with plasmid alone (Lawrie et al. 1999); the same study demonstrated enhancement of lipofection by 2.4- fold. The mechanism by which US enhances gene deliv- ery is not fully understood but is thought to be linked to a bioeffect, called sonoporation, in which transient pores in the cell membrane are created as a consequence of Address correspondence to: Dr. Ahad Rahim, The Institute of Cancer Research, 237 Fulham Road, London, SW3 6JB, UK. E-mail: [email protected] Ultrasound in Med. & Biol., Vol. 32, No. 8, pp. 1269 –1279, 2006 Copyright © 2006 World Federation for Ultrasound in Medicine & Biology Printed in the USA. All rights reserved 0301-5629/06/$–see front matter 1269
Transcript of Physical parameters affecting ultrasound/microbubble-mediated gene delivery efficiency in vitro

Ultrasound in Med. & Biol., Vol. 32, No. 8, pp. 1269–1279, 2006Copyright © 2006 World Federation for Ultrasound in Medicine & Biology
Printed in the USA. All rights reserved0301-5629/06/$–see front matter
doi:10.1016/j.ultrasmedbio.2006.04.014
● Original Contribution
PHYSICAL PARAMETERS AFFECTING ULTRASOUND/MICROBUBBLE-MEDIATED GENE DELIVERY EFFICIENCY IN VITRO
AHAD RAHIM,* SARAH L. TAYLOR,* NIGEL L. BUSH,† GAIL R. TER HAAR,†
JEFFREY C. BAMBER,† and COLIN D. PORTER**The Institute of Cancer Research, Gene Therapy Group, Section of Cell and Molecular Biology, London; and †The
Institute of Cancer Research and The Royal Marsden NHS Trust, Joint Department of Physics, Sutton, UK
(Received 25 January 2006; revised 4 April 2006; in final form 13 April 2006)
Abstract—Ultrasound (US)/microbubble-mediated gene delivery is a technology with many potential advantagessuited to clinical application. Previous studies have demonstrated transfection but many are unsatisfactory inrespect to the exposure apparatus, lack of definition of the US field or the limitations on parameters that can beexplored using clinical diagnostic US machines. We investigated individual exposure parameters using a systemminimising experimental artefacts and allowing control of many parameters of the US field. Using a 1-MHztransducer we systematically varied US parameters, the duration of exposure and the microbubble and DNAconcentrations to optimise gene delivery. Delivery was achieved, using lipid microbubbles (SonoVue®) andclinically acceptable US exposures, to adherent cells at efficiencies of �4%. The acoustic pressure amplitude (0.25MPa peak-negative), pulse repetition frequency (1-kHz) and duration of exposure (10 s) were important inoptimising gene delivery with minimal impact on cell viability. These findings support the hypothesis that varyingthe physical parameters of US-mediated gene delivery has an affect on both efficiency and cell viability. Thesedata are the first in terms of their thorough exploration of the US parameter space and will be the basis formore-informed approaches to developing clinical applications of this technology. (E-mail: [email protected])© 2006 World Federation for Ultrasound in Medicine & Biology.
Key Words: Ultrasound, Microbubble contrast agent, Nonviral vector.
INTRODUCTION
To date, a number of physical methods for delivery ofnonviral vectors to cells, such as electroporation, hydro-dynamic delivery, ballistic delivery and microinjection,have been investigated (Wells 2004). A more recentmethod that is being developed is the combined use ofultrasound (US) and medical imaging microbubble con-trast agents (Newman et al. 2001; Unger et al. 2001). Themajor advantage that US/microbubble-mediated gene de-livery has over other physical force protocols is that itallows targeted and site-specific gene delivery with min-imal procedural invasiveness: the plasmid and micro-bubbles can be administered intravenously or directly tothe tissue of interest and gene delivery limited to the areasubsequently exposed to US, avoiding delivery to non-target cells. In addition, both US and microbubble con-trast agents are used routinely in the clinic (Blomley et
Address correspondence to: Dr. Ahad Rahim, The Institute of
Cancer Research, 237 Fulham Road, London, SW3 6JB, UK. E-mail:[email protected]1269
al. 2001; Lindner 2004). The precision with which a USbeam can be targeted has already been demonstrated inclinical approaches such as focused US ablation (terHaar 2001), albeit at much higher intensities than thoseused for nondestructive gene delivery. The ultimate goalwould be a systemic approach. Given the vascular reten-tion of microbubbles, the method will be particularlysuited to delivery to endothelial cells, such as for thetreatment of cardiovascular disease or cancer.
The use of US alone to deliver DNA into cells hasbeen studied (Kim et al. 1996; Lawrie et al. 1999). Forexample, Lawrie et al. demonstrated a 7.5-fold enhance-ment in naked plasmid luciferase gene expression whenporcine vascular smooth muscle cells were exposed tocontinuous wave 1-MHz US for 60-s compared with thatseen with plasmid alone (Lawrie et al. 1999); the samestudy demonstrated enhancement of lipofection by 2.4-fold. The mechanism by which US enhances gene deliv-ery is not fully understood but is thought to be linked toa bioeffect, called sonoporation, in which transient pores
in the cell membrane are created as a consequence of
1270 Ultrasound in Medicine and Biology Volume 32, Number 8, 2006
acoustic cavitation. Cavitation can be divided into twotypes: stable (noninertial) and inertial. Stable cavitationrefers to the US-induced steady oscillation of endoge-nous gas microbubbles that may be found in liquids ormay be formed as dissolved gas comes out of solutionduring the negative pressure cycles of the acoustic wave.Increasing the intensity of US may lead to inertial cav-itation, in which the oscillation of the microbubblesbecomes increasingly violent until they break up. Stableand inertial cavitation generate pressure gradients andlocal shear forces thought to cause the formation of smalltransient pores in the cell membrane, through whichplasmid DNA can enter. On the basis that acoustic cav-itation is required for gene delivery, the transfectionmedium has been supplemented with exogenous micro-bubbles in the form of agents used regularly in the clinicto increase echo image signal from blood, particularlywhen imaging the heart (Greenleaf et al. 1998; Lawrie etal. 2000). E.g., Lawrie et al. showed that Optison™microbubbles and US resulted in a 300-fold increase innaked plasmid gene expression over plasmid alone(Lawrie et al. 2000). However, the attraction of usingmicrobubbles lies not only in reducing the cavitationthreshold but also in their potential utility as vehicles fordrug or gene delivery in a clinical setting, most logicallyfor systemic administration.
A number of other in vitro (Frenkel et al. 2002; Guo etal. 2004; Lawrie et al. 2003; Miller et al. 2003), ex vivo(Akowuah et al. 2005) and in vivo (Bekeredjian et al. 2003;Christiansen et al. 2003; Lu et al. 2003; Miao et al. 2005)studies have been published using various transgenes anddisease models. However, the literature lacks a detailedstudy of how the physical characteristics of the US beamaffect gene delivery efficiency, in part because many studieshave used diagnostic scanners or physiotherapy machinesas the source of US, which allow very limited user controlover exposure parameters. More generally, the machinesettings or exposure conditions that have been reported areinstrument dependent, with no common point of referenceand, therefore, it is impossible to draw any general conclu-sions from this body of work, e.g., intensity (or energyexposure) in W/cm2 (J/cm2) or mechanical index are oftencited but fundamental parameters are often missing. Inparticular, acoustic pressures, for which marked local vari-ations occur depending on the position in the sound fieldrelative to the transducer, despite constant intensity, haveonly rarely been documented accurately. Consequently, un-derstanding of the process of US-mediated gene deliveryhas been compromised. Moreover, for the majority of invitro studies, the cells were adherent to plastic tissue culturevessels with attendant (but unaddressed) impact on dosim-etry and the potential for surface heating effects. Manystudies have also adopted a set-up allowing for US reflec-
tion from a medium/air interface, often very close to the celllayer, with profound implications for the field conditions towhich the cells are exposed; in particular, the occurrence ofstrong standing waves, which are conducive to cavitation inthese experiments, is an in vitro phenomenon. Again, formany studies, unacceptably high losses in cell viabilitywere associated with the reported efficiencies of gene de-livery. These problems and the lack of experimental con-sensus also prevent appreciation of any underlying factorsrelated to exposure.
Miller and Quddus (2000) studied the effect of phys-ical parameters of a 3.5-MHz US field on delivering fluo-rescent dextran into cells, using an experimental set-updesigned to avoid the problems raised above. Sonoporationwas strongly dependent on sufficient microbubble contrastagent (Optison™); however, their restriction to the imagingmodes available on the diagnostic scanner used limited theranges of the parameters investigated, some of which couldalso not be varied independently. A more recent study byZarnitsyn and Prausnitz (2004), using 0.5-MHz US withOptison™, examined the importance of pressure and expo-sure time, but used very long (60-ms) pulses, which are notemployed in current diagnostic US machines. They con-cluded that the acoustic energy to which the cells wereexposed was the most significant influence on transfection,but cell viabilities were low and the experimental design(use of cells in suspension) did not allow an understandingto be gained of the relationship between transfection effi-ciency and position in the acoustic field. A detailed study ofthe acoustic field to which cells are exposed has not yetbeen carried out in the context of gene delivery. This paperproposes to fill this void.
In this work, we describe the design and use of asystem that allows high-resolution manipulation of thephysical parameters of the US beam to which the cells andbubbles are exposed. Cells were grown on the gas-perme-able membrane of a sealed, acoustically transparent cellculture unit to which vector and microbubbles were addedbefore US exposure. We have measured the acoustic pres-sures generated and determined the effect that each of thedifferent exposure parameters has on gene delivery effi-ciency and cell viability. This, in turn, led to a determinationof optimal parameters for transfection that are system-inde-pendent. The overarching hypothesis guiding this work wasthat varying the physical parameters of US-mediated genedelivery has an affect on both efficiency and cell viability.Our aim was to improve understanding of how to maximisegene delivery and minimise cell death.
MATERIAL AND METHODS
Cell cultureChinese hamster ovary (CHO) cells were cultured
in Dulbecco’s modified Eagle’s medium (DMEM, In-
vitrogen, Paisley, UK) supplemented with 3.7g/L sodium
Ultrasound/microbubble-mediated gene delivery ● A. RAHIM et al. 1271
bicarbonate and 10% (v/v) fetal bovine serum. The cellswere incubated at 37°C in a humidified environment of5% CO2/95% air. For US exposure, cells were grownusing the OptiCell™ culture system (BioCrystal Inc.,Westerville, OH, USA), in which the cells were adherentto one of the 50-cm2 100-�m-thick membranes enclosingthe 2-mm-deep chamber. The cells were detached usingtrypsin and introduced into the chamber using the man-ufacturer’s protocol: briefly, a syringe with an attachedtip was used to inject 10 mL of cell suspension into thechamber through one of the self-sealing access portsbefore inverting the OptiCell and withdrawing an equalvolume of air. The cells were left to grow until 80 to 90%confluent (4 � 106 – 5 � 106 cells) before US exposure.
PlasmidThe 7.5-kb pNGVL1-�-gal derived from pNGVL1
(Vector Core, University of Michigan, Ann Arbor, MI,USA) contains the �-galactosidase gene (LacZ) in framewith the SV40 large T-antigen nuclear localising se-quence (kindly provided by Dr. Richard Harbottle, Im-perial College, London, UK). pNGVL1-�-gal was usedto transform chemically competent DH5� Escherichiacoli (Invitrogen). Cultures of transformed bacteria weregrown in the presence of 20 �g/mL kanamycin, afterwhich plasmid DNA was extracted and purified using aQiaquick Midiprep Kit (Qiagen, Crawley, UK). Plasmidconcentration (typically 0.5 mg/mL) and purity (ratio ofoptical densities at 260 nm and 280 nm of 1.7 to 1.9)were evaluated using spectrophotometry.
Ultrasound apparatusAn arbitrary ultrasonic pulse generator system was
assembled to allow complete user-control over the expo-sure parameters. Software was written in the languageVEE™ to enable computer control of a function/arbitrarywaveform generator (model 33220A, Agilent Technolo-gies Inc., Loveland, CO, USA) feeding an RF poweramplifier (58-dB gain, model BT00500 BETA, TomcoTechnologies, Norwood, Australia), the output of whichwas connected to a 1-MHz US transducer (custom-madeby Imasonic, Besançon, France). In the experiments re-ported here, a sinusoidal pulse was generated with anamplifier input amplitude up to 100-mV; the pulse lengthwas varied up to 80 cycles, the pulse repetition frequencyup to 2.5-kHz and the overall duration of exposure up to60 s. The signal generator and amplifier outputs weresampled using a synchronised digital oscilloscope (Pico-scope, Pico Technology Ltd., St. Neots, UK). The trans-ducer was a single spherically focused piezoelectric el-ement of 20 mm diameter and 68% bandwidth, with aradius of curvature of 67 mm.
A cylindrical Perspex water tank was built for US
exposure of cells growing in an OptiCell™ (Fig. 1). Thelatter chamber was held horizontally in a plate holder�10 cm above the bottom of the tank; it was supportedby the external edges so that the holder did not interferewith the US field. The US transducer face was placed ontop of the OptiCell™ upper membrane. To prevent un-
Fig. 1. The US exposure apparatus used in this study. (a) The1-MHz transducer is shown on top of the OptiCell™ unit forexposure of cells underlying the uppermost window; and (b)schematic diagram of the transducer and OptiCell™ as posi-tioned in the apparatus illustrated in (a). The microbubbles are
shown rising to lie beneath the cell layer.
wanted reflections, a 14-mm-thick polyurethane rubber-

1272 Ultrasound in Medicine and Biology Volume 32, Number 8, 2006
based anechoic absorber (Zeqiri and Bickley 2000) (Na-tional Physical Laboratory, Teddington, UK) was held�5 cm below the OptiCell™, at an angle of 6°. Theeffectiveness of this material was verified by monitoringthe magnitude of internally reflected pulses received atthe transducer; these were completely eradicated with theabsorber in position.
US dosimetryFor characterisation of the US field close to the
transducer face, as would be experienced by cellsduring US exposure, the transducer was held in apositioning device at the base of the tank, in contactwith a Mylar window and coupled through acousticgel (Clear Image LV, Diagnostic Sonar, UK). The fieldwas characterised by measurement of the local pres-sure detected with a 0.2-mm needle hydrophone (Pre-cision Acoustics Ltd., Dorchester, UK), and applyingthe manufacturer-supplied calibration to the digitaloscilloscope readout (PicoScope). The transducer andhydrophone were vertically aligned, both geometri-cally and by maximising the received signal when thehydrophone was placed at the focus. The hydrophonewas lowered so that the tip was 1 mm away from thetransducer face and tracked in increments of 0.25 mmacross the transducer surface using a robotic workcell(model RW-9b, Arrick Robotics, Hurst, TX, USA).The relationship of acoustic pressure to amplifier inputvoltage amplitude was determined with the hydro-phone positioned at the centre of the transducer. Theequipment was also used in this orientation to measurethe attenuation of the acoustic signal by the Opti-Cell™ membrane; this was found to be �1%.
Exposure protocolA volume of OptiMEM I (Invitrogen), heated to
37°C and containing 50 �g of plasmid DNA (unlessotherwise stated), was used to replace the DMEM in anOptiCell™ in which CHO cells had reached 80 to 90%confluence. SonoVue® microbubble contrast agent(Bracco, High Wycombe, UK) was reconstituted in sa-line solution according to the manufacturer’s protocoland the required volume was injected to bring the totalvolume in the OptiCell™ to 10 mL. The microbubbleswere evenly distributed by inversion/agitation of the unit.SonoVue® reconstitution using the manufacturer-sup-plied saline solution resulted in a preparation that con-tained 2 � 108 � 5 � 108 microbubbles/mL. Therefore,a concentration of 0.5% SonoVue® (the lowest used inthis study) would result in an average microbubble-to-cell ratio of approximately 4:1. The microbubble shell iscomposed of phospholipid and encapsulates sulfurhexafluoride gas. Bubble diameter is typically 1 to
10 �m.Water at a temperature of 37°C was used to fill theexposure tank until the level reached 3 cm above theplate holder. The OptiCell™ was then submerged in thewater and placed on the plate holder with the cellsuppermost (Fig. 1). The OptiCell™ was left in thisposition for 1 min for the temperature of the medium toreach 37°C and for the microbubbles to rise toward thecells. The number of cycles per pulse, the pulse ampli-tude, the pulse repetition frequency and the length ofexposure were set using the software. Each of these wasvaried as required. The OptiCell™ had previously beenmarked with a pen into six sections of equal area (the sizeof the 25-mm diameter transducer housing) in whichdifferent exposure conditions could be used; the trans-ducer was placed on top of the OptiCell™ within amarked area, ensuring that no air bubbles were trappedbetween the transducer face and the membrane, and thecells were exposed to the US . On completion of the sixthexposure, the OptiCell™ was removed from the tank,wiped dry and returned to the incubator for 24 h to allowfor LacZ gene expression.
Analysis of gene delivery efficiency24 h after US exposure, the cells were washed using
phosphate-buffered saline (PBS) and then fixed for 20min with cold 0.8% formaldehyde/1.8% glutaraldehydesolution in PBS. After they were washed twice with PBS,the cells were stained overnight in the dark at roomtemperature in 1 mg/mL X-Gal (5-bromo-4-chloro-3-indolyl-�-D-galactopyranoside), 2 mM MgCl2, 0.01%sodium deoxycholate, 0.02% NP-40, 5 mM potassiumferricyanide, 5 mM potassium ferrocyanide. The stainwas replaced with PBS and the sections of theOptiCell™ exposed to US were examined microscopi-cally using �100 magnification: for 10 random fields ofview within each exposure region, the number of bluecells and the total number of cells within a 7 � 7 grid inthe microscope eyepiece were counted. An average ofthe number of blue cells and total number of cells wastaken over the 10 fields counted and used to calculate thegene delivery efficiency.
StatisticsEach exposure condition was evaluated in three
separate experiments. Statistical significance of observedeffects was determined by analysis of variance(ANOVA) followed by groupwise comparison byTukey’s honestly significant differences post hoc test orDunnett’s test using Analyse-It software for Excel. Al-pha levels of 0.01 and 0.05, where indicated, were used
to assess statistical significance.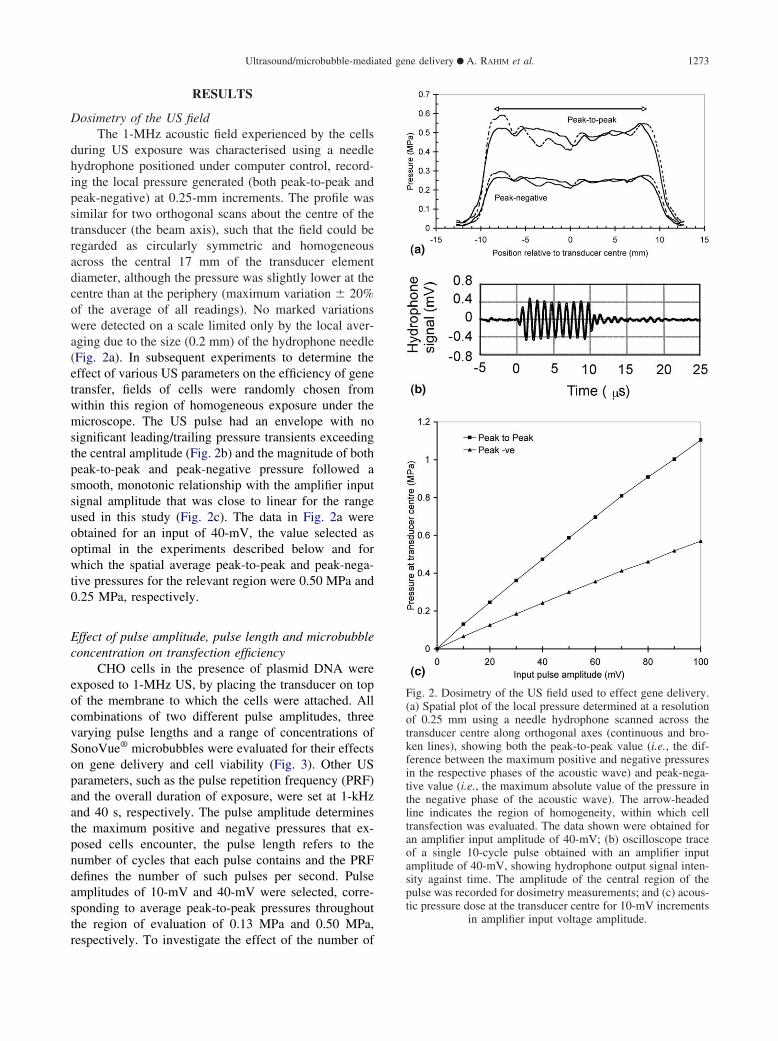
in amplifier input voltage amplitude.
Ultrasound/microbubble-mediated gene delivery ● A. RAHIM et al. 1273
RESULTS
Dosimetry of the US fieldThe 1-MHz acoustic field experienced by the cells
during US exposure was characterised using a needlehydrophone positioned under computer control, record-ing the local pressure generated (both peak-to-peak andpeak-negative) at 0.25-mm increments. The profile wassimilar for two orthogonal scans about the centre of thetransducer (the beam axis), such that the field could beregarded as circularly symmetric and homogeneousacross the central 17 mm of the transducer elementdiameter, although the pressure was slightly lower at thecentre than at the periphery (maximum variation � 20%of the average of all readings). No marked variationswere detected on a scale limited only by the local aver-aging due to the size (0.2 mm) of the hydrophone needle(Fig. 2a). In subsequent experiments to determine theeffect of various US parameters on the efficiency of genetransfer, fields of cells were randomly chosen fromwithin this region of homogeneous exposure under themicroscope. The US pulse had an envelope with nosignificant leading/trailing pressure transients exceedingthe central amplitude (Fig. 2b) and the magnitude of bothpeak-to-peak and peak-negative pressure followed asmooth, monotonic relationship with the amplifier inputsignal amplitude that was close to linear for the rangeused in this study (Fig. 2c). The data in Fig. 2a wereobtained for an input of 40-mV, the value selected asoptimal in the experiments described below and forwhich the spatial average peak-to-peak and peak-nega-tive pressures for the relevant region were 0.50 MPa and0.25 MPa, respectively.
Effect of pulse amplitude, pulse length and microbubbleconcentration on transfection efficiency
CHO cells in the presence of plasmid DNA wereexposed to 1-MHz US, by placing the transducer on topof the membrane to which the cells were attached. Allcombinations of two different pulse amplitudes, threevarying pulse lengths and a range of concentrations ofSonoVue® microbubbles were evaluated for their effectson gene delivery and cell viability (Fig. 3). Other USparameters, such as the pulse repetition frequency (PRF)and the overall duration of exposure, were set at 1-kHzand 40 s, respectively. The pulse amplitude determinesthe maximum positive and negative pressures that ex-posed cells encounter, the pulse length refers to thenumber of cycles that each pulse contains and the PRFdefines the number of such pulses per second. Pulseamplitudes of 10-mV and 40-mV were selected, corre-sponding to average peak-to-peak pressures throughoutthe region of evaluation of 0.13 MPa and 0.50 MPa,
respectively. To investigate the effect of the number ofFig. 2. Dosimetry of the US field used to effect gene delivery.(a) Spatial plot of the local pressure determined at a resolutionof 0.25 mm using a needle hydrophone scanned across thetransducer centre along orthogonal axes (continuous and bro-ken lines), showing both the peak-to-peak value (i.e., the dif-ference between the maximum positive and negative pressuresin the respective phases of the acoustic wave) and peak-nega-tive value (i.e., the maximum absolute value of the pressure inthe negative phase of the acoustic wave). The arrow-headedline indicates the region of homogeneity, within which celltransfection was evaluated. The data shown were obtained foran amplifier input amplitude of 40-mV; (b) oscilloscope traceof a single 10-cycle pulse obtained with an amplifier inputamplitude of 40-mV, showing hydrophone output signal inten-sity against time. The amplitude of the central region of thepulse was recorded for dosimetry measurements; and (c) acous-tic pressure dose at the transducer centre for 10-mV increments

1274 Ultrasound in Medicine and Biology Volume 32, Number 8, 2006
cycles in each pulse, 10-, 40- and 80-cycle pulses wereused for each amplitude value. In addition, concentra-tions of SonoVue® ranging from 0 to 16% (v/v) wereevaluated (i.e., up to an average 5.6 � 107 microbubbles/mL). These parameters were evaluated in combinationbecause they were considered unlikely to be indepen-
Fig. 3. Effect of pulse amplitude, pulse length and concentra-tion of SonoVue® on gene delivery efficiency and cell viability.CHO cells were exposed to 1-MHz US in the presence of5-�g/mL pNGVL1. Amplifier input amplitudes of 10-mV and40-mV—corresponding to spatial average peak-to-peak acous-tic pressures at the position of the cells of 0.13 MPa and 0.5MPa, respectively—were used for pulse lengths of 10, 40 and80 cycles, in the presence of 0 to 16% SonoVue® micro-bubbles. Exposure was for 40-s with a PRF of 1-kHz. (a)Transfection efficiency was scored 24 h later by histochemicalstaining and cell counting. At each concentration of SonoVue®
there was a statistically significant difference in gene deliveryefficiency when using 0.5 MPa compared with 0.13 MPa(ANOVA and Tukey’s HSD test, p � 0.01); and (b) cellviability relative to an unexposed control was determined for apulse length of 40 cycles. The asterisks highlight statisticalsignificant difference in cell viability compared with that mea-sured using 0% SonoVue® (ANOVA and Dunnett’s test, p �0.01). Data are the mean � standard deviation (SD) for three
independent experiments.
dent.
No gene delivery was observed for exposures with-out SonoVue®, indicating that US alone has no effect; inaddition, in the absence of US, no gene delivery tookplace under any of the conditions, confirming that mi-crobubbles alone have no effect. For US exposure in thepresence of microbubbles, clearance of the microbubbles(as observed by loss of opacity immediately followingexposure) and transfection were confined to the area ofinsonation determined by the dosimetry detailed above.Statistical analysis of the data showed that there was nosignificant difference in gene delivery efficiency whenusing 10, 40 or 80 cycles/pulse regardless of micro-bubble concentration or pressure used (Fig. 3a). Therewas also no significant difference made by the concen-tration of microbubbles used to gene delivery efficiencywhen using either 0.13 MPa or 0.5 MPa with varyingpulse length. Because no significant difference wasfound between exposures using 10, 40 or 80 cycles/pulse, the data for pulse lengths were pooled into twogroups for 0.13 MPa and 0.50 MPa exposures at eachmicrobubble concentration to address whether pulse am-plitude affected gene delivery efficiency. There was sig-nificantly greater gene delivery for 0.50 MPa pulse am-plitude compared with 0.13 MPa, regardless of the mi-crobubble concentration. The cells scored fortransfection efficiency were also scored for viabilitycompared with that for control cells not exposed to US:there was no significant effect for 0.13-MPa exposuresbut there was microbubble-dependent loss of viability for0.50 MPa (Fig. 3b).
To address whether the position in which the trans-ducer was placed affected gene delivery, cells were ex-posed to the same conditions in each of the sixOptiCell™ sections (0.50 MPa pulse amplitude, 40 cy-cles/pulse, 4% SonoVue®). After fixing and staining,blue cell counts in each section showed no significantdifferences (data not shown). Similarly, to ensure that no“cross talk” occurred, a single section was exposed: noblue cells were found in neighbouring sections. Finally,to eliminate possible effects due to exposure of the cellsto sound waves reflected from the bottom of the tank, anacoustic absorber was inserted beneath the OptiCell™:gene delivery efficiency was identical in the presenceand absence of the absorber. Together with the experi-ments above that showed no effects outside the trans-ducer diameter, these controls validate the experimentalset-up.
Pulse repetition frequency and duration of exposureIn consideration of the need to maximise transfec-
tion efficiency and minimise cell damage, exposure pa-rameters of 0.50 MPa pulse amplitude, 40-cycle pulselength and 4% SonoVue® were selected while optimising
further factors. In keeping with reducing unnecessary
Ultrasound/microbubble-mediated gene delivery ● A. RAHIM et al. 1275
exposure, subsequent experiments included the acousticabsorber. To investigate whether PRF affected gene de-livery, cells were exposed using values of 0.5, 1, 1.5, 2and 2.5-kHz, maintaining the duration of exposure(which included the periods between pulses) at 40 s. In aseparate experiment, the PRF was fixed at 1-kHz and theexposure duration varied from 10 to 60 s. Significantlyless gene delivery occurred for 0.5-kHz PRF and 40-sexposure compared with 1 to 2-kHz (Fig. 4a), whereas at1-kHz PRF there was no significant effect of varyingduration on microbubble clearance (i.e., reduced opacityimmediately following exposure) or transfection effi-ciency (Fig. 5a). Increasing PRF had no statisticallysignificant effect on cell viability (Fig. 4b), althoughincreasing the exposure duration resulted in significantlylower cell viability following 40-s, 50-s and 60-s expo-sures when compared with 10-s exposures (Fig. 5b).When considering achieving transfection compatiblewith minimum US exposure, these data indicate that1-kHz PRF (the default for the experiments described
Fig. 4. Effect of PRF on gene delivery efficiency and cellviability. CHO cells were exposed to 1-MHz US in the pres-ence of 5-�g/mL pNGVL1 for 40 s, using an amplifier inputamplitude of 40-mV (0.5 MPa peak-to-peak pressure ampli-tude), pulse length of 40 cycles, 4% SonoVue® and variablePRF. Transfection efficiency (a) and cell viability relative to anunexposed control (b) were scored 24 h later by histochemicalstaining and cell counting. Data are the mean � SD for threeindependent experiments. The asterisks highlight statisticallysignificant differences in gene delivery efficiency comparedwith that measured using 0.5-kHz (ANOVA and Tukey’s HSD
test, p � 0.05).
above) and 10-s overall exposure duration are optimal.
Plasmid concentrationAll the experiments reported above were with a
plasmid concentration of 5 �g/mL. To address whetherthis was a limitation on gene delivery efficiency, cellswere exposed to US in the presence of 2.5, 5 and 10�g/mL plasmid DNA; exposure conditions were 0.50-MPa pulse amplitude, 40-cycle pulse length, 1-kHz PRFwith 4% SonoVue® for 40 s. While there was a signifi-cant increase in gene delivery efficiency for each in-crease in plasmid concentration (Fig. 6), this was notproportional; within the range of concentrations studied,the trend was logarithmic and at concentrations lowerthan those studied, the relationship must go through theorigin. This indicates that gene delivery in the precedingexperiments was saturating with respect to DNA concen-tration. Plasmid availability was therefore not a limita-tion on the efficiency obtained in these experiments, andso would not have influenced the identification of thresh-old values for the US exposure parameters consideredabove.
Fig. 5. Effect of duration of exposure on gene delivery effi-ciency and cell viability. CHO cells were exposed to 1-MHzUS in the presence of 5-�g/mL pNGVL1, using an amplifierinput amplitude of 40-mV (0.5 MPa peak-to-peak pressureamplitude), pulse length of 40 cycles, 1-kHz PRF, 4%SonoVue® and variable exposure times. Transfection efficiency(a) and cell viability relative to an unexposed control (b) werescored 24 h later by histochemical staining and cell counting.Data are the mean � SD for three independent experiments.The asterisks highlight statistically significant differences incell viability compared with that measured following exposure
for 10-s (ANOVA and Tukey’s HSD test (p � 0.05).

1276 Ultrasound in Medicine and Biology Volume 32, Number 8, 2006
DISCUSSION
While a growing body of literature provides proof-of-principle for using US for plasmid-based gene deliv-ery in both in vitro and in vivo models, there is noconsensus regarding methodology, and existing data pro-vide no insights into the fundamental US parametersaffecting or effecting gene delivery. There are unsatis-factory aspects to many of these studies: the difficultiesin determining dosimetry and potential heating effects ofusing cells attached to plastic in vitro, working withundefined acoustic fields and the establishment of stand-ing waves due to an air/medium interface complicatetheir interpretation and extrapolation to clinical applica-tion. Two issues need to be addressed to improve both invitro and in vivo gene delivery efficiency: a better un-derstanding of the mechanism of plasmid entry and amore detailed grasp of the physical side of the technol-ogy. A few studies have investigated how the character-istics of the US beam affect gene delivery efficiency(Liang et al. 2004; Miller and Quddus 2000; Zarnitsynand Prausnitz 2004), but these have addressed only arestricted number of the parameters due, in part, to thelimited flexibility of the US sources used.
In this study we tested the hypothesis that varyingthe physical parameters of US-mediated gene deliveryhas an affect on both efficiency and cell viability. Weevaluated US/microbubble-mediated gene delivery underclinically relevant conditions, using an arbitrary pulsed
Fig. 6. Effect of plasmid concentration on gene delivery effi-ciency. CHO cells were exposed to 1-MHz US for 40 s, usingan amplifier input amplitude of 40-mV (0.5 MPa peak-to-peakpressure amplitude), pulse length of 40 cycles, 1-kHz PRF, 4%SonoVue® and variable concentration of pNGVL1. Transfec-tion efficiency was scored 24 h later by histochemical stainingand cell counting. Data are the mean � SD for three indepen-dent experiments. One asterisk highlights a statistically signif-icant difference in gene delivery efficiency when comparedwith that measured using 2.5-�g/mL plasmid DNA. Two as-terisks highlight a statistically significant difference in genedelivery efficiency when compared with that measured whenusing both 2.5 and 5.0 �g/mL of plasmid DNA (ANOVA and
Tukey’s HSD test, p � 0.05).
US system with complete flexibility for manipulating
exposure parameters. This system allowed us to producedata that support this hypothesis and has contributed toimproving understanding of how to maximise gene de-livery and minimise cell death.
The OptiCell™ system was used for exposure ofcells because of its potential to avoid problems associ-ated with use of conventional culture vessels; in valida-tion of this choice, there was negligible (�1%) attenua-tion of transmitted pressure amplitude by the 100-�m-thick membrane in contrast to reduction by �10% whenusing tissue culture plastic (1-mm-thick polystyrene).Use of immersible OptiCell™ chambers also avoided thepresence of a medium/air interface and thus the genera-tion of confounding reflections or standing waves. Bioef-fects such as transfection efficiency and loss of cellviability can thus be attributed to the chosen US param-eters.
The presence of microbubbles was critical for genedelivery for the parameter ranges studied, after which thegreatest single factor was the pulse amplitude. Our datashow a progressive decrease in cell viability with in-creasing microbubble concentration, probably due to in-creased membrane damage with larger microbubble tocell ratios. Although transfection was maximal for 4%SonoVue®, there was no significant difference in genedelivery efficiency over the wide concentration range ofmicrobubbles used (0.5 to 16%), i.e., while the micro-bubble dependence of gene delivery was absolute, theirconcentration was not critical. Similarly, there was aweak dependence on plasmid DNA concentration in therange studied, relative to the absolute requirement for itspresence.
We investigated the effect of pulse amplitude ongene delivery, first characterising the acoustic fieldthroughout the region of exposure. By increasing thepeak-to-peak pressure amplitude from 0.13 MPa to 0.50MPa, we were able to demonstrate a significant increasein gene delivery, with a concomitant decrease in cellviability. An explanation for both these observations liesin the cavitation phenomenon: an increase in pulse am-plitude causes larger oscillations of the microbubbles andthus generates greater shear forces, increasing the like-lihood of pore formation in cell membranes. Althoughthis allows for greater passage of plasmid into cells viatransient pore opening, the increased energy also causesirreparable damage. It was a general observation, regard-less of the parameter under investigation, that increasedUS energy resulted in reduced cell viability.
The US sources for many studies have been diag-nostic scanners, typically producing pulses containingfew cycles, often no more than 10. Pulse length is avariable that has not been previously addressed becauseof the limitations of such machines, but which our US
apparatus allows. Although maximal gene delivery was
Ultrasound/microbubble-mediated gene delivery ● A. RAHIM et al. 1277
achieved using 40 cycles/pulse, the data showed thatthere was no significant difference in mean gene deliveryefficiency regardless of the number of cycles/pulse used.This suggests that cavitation occurs within the first 10cycles so that additional cycles are superfluous. Theinefficacy of 0.13-MPa pressure amplitude regardless ofpulse length suggests that this value lies below a thresh-old needed to achieve cavitation within 80 cycles. Theissue of the cycles/pulse has relevance to other studiesthat have used very long pulses (e.g., tens of thousands ofcycles). The use of such pulses by Zarnitsyn andPrausnitz (2004) explains their attribution of gene deliv-ery using Optison™ (maximum efficiency �2%) to theoverall energy, rather than pressure amplitude, becausethe rapid microbubble-dependent component to gene de-livery would have been masked by the longer-term mi-crobubble-independent component (also responsible forsignificant viability loss). Consistent with this, a study byLiang et al. (2004), using a therapeutic US machine with2-ms pulses, similarly correlated transfection (maximumefficiency �5%) with acoustic power and duration, withno benefit from adding microbubbles.
An exposure duration of 10 s, the minimum used,was above the threshold for maximum transfection; theinefficacy of longer exposures was consistent with clear-ance of the microbubbles from the area of insonationwithin this period. The lack of reduction in efficiency forshorter duration of exposure indicates that the fall for0.5-kHz PRF and 40-s was unrelated to the lower overallexposure time (i.e., PRF � duration); rather, it implies adependence on the frequency of repetition of micro-bubble excitation, in addition to the magnitude of exci-tation. Importantly, our results indicate that optimal ef-ficiency can be achieved with pulsing modes not mark-edly different from those, such as for spectral Doppler, inroutine clinical use.
Our placement of the transducer close to the targetcells in these experiments is consistent with the practicecommon to many of the published studies. The trans-ducer “near-field” is associated with spatially heteroge-neous pressure amplitudes, varying markedly in threedimensions, owing to interference between sound wavesgenerated from different positions across the transducerface. The use in several published studies of an equip-ment set-up in which there is a gap between the trans-ducer face and the cells, but for which the latter are notplaced at a homogeneous region of the acoustic field,greatly complicates any assessment of the pressures ef-fecting gene delivery. In contrast, we determined that thefield to which the cells were exposed in our experiments,less than one wavelength away from the transducer face,could be regarded as homogeneous; we were unable toidentify significant departure from homogeneity, pre-
sumably due to the proximity to the source. The utility ofthis region of the acoustic field was that its homogeneityfacilitated measurement of the US parameters necessaryfor gene delivery. The importance of our study lies inhaving established the ranges and thresholds of suchparameters within which to work while developing thistechnology toward clinical application. These same pa-rameters will be applicable to exposure of cells at thetransducer focus because they are relevant to the behav-iour of microbubbles in the field.
This study has provided an invaluable insight intothe way that physical parameters of US can affect genedelivery. We have been able to select the followingoptimised parameters based on the criteria of providinghigh levels of gene delivery and cell viability using1-MHz US: a pulse-pressure amplitude of 0.25 MPa(peak-negative), a PRF of 1-kHz, 40-cycles pulse length,10-s exposure and use of 4% SonoVue®. Maximal de-livery to CHO cells using 5 �g/mL plasmid DNA was�4%, retaining �90% viability. Because the minimumeffective exposure duration was not determined, it islikely that shorter periods, further minimising cell dam-age, will suffice. These conditions correspond to a spatialpeak pulse average intensity (ISPPA) of 2.1 W/cm2, timeaveraged (ISATA) to 0.083 W/cm2. Units of exposuresuch as these have been reported for other studies but donot in themselves disclose the characteristics of the USfield; however, with exposures as short as 10 s, it isapparent that we have achieved transfection at substan-tially lower energy per unit area levels (0.83 J/cm2)compared with other studies using exposures of 10 to 30J/cm2 (Liang et al. 2004; Zarnitsyn and Prausnitz 2004).Other studies have used much higher peak-negative pres-sures (1 to 2 MPa) and exposure conditions resulting ineven greater energy exposures of 140 to 460 J/cm2 (Law-rie et al. 2000). In contrast, our parameters and genedelivery efficiency are in close agreement with the sono-poration study by Miller and Quddus (2000), who re-ported 3% dextran uptake at the transducer focus in thepresence of Optison™, using a very similar experimentalexposure system, apart from the centre frequency of theacoustic pulse: Doppler mode 3.5-MHz US (providing17.5 cycles/pulse), 2.2% duty cycle and 0.23 MPa peaknegative pressure, corresponding to 1.5 W/cm2 (ISPPA).These authors reported pressure-dependent uptake withweak dependence on exposure duration up to 60 s, butPRF and amplitude could not be varied independently; atwo-dimensional scan mode, using very short pulses butgreater pressure amplitude, was similarly effective. Ourdata also parallel some aspects of a study using contin-uous wave 1-MHz US with Albunex® (although using anexperimental set-up in the near-field with cells on plasticand standing waves in the overlying medium), in whichthere was a linear relationship of transfection efficiency
with peak pressure above a threshold of 0.12 MPa and
1278 Ultrasound in Medicine and Biology Volume 32, Number 8, 2006
for which 1-s exposures were effective (Greenleaf et al.1998).
Higher efficiencies of gene delivery than those re-ported here will be required for many applications. Toachieve this, different routes of investigation are avail-able. The pressure amplitudes used in this study wererelatively low because we were conscious of the need toavoid unacceptably high levels of cell death; however,given that exposure as short as 10-s (probably less) aresufficient using our optimised parameters, it is likely thatshort-duration US of greater amplitude will increasegene delivery while maintaining adequate viability. Re-plenishment of microbubbles between multiple short-duration exposures (Greenleaf et al. 1998), or continuousinfusion of microbubbles/vector (comparable to the clin-ical situation of microbubble perfusion of the targettissue), will also enhance gene delivery. A number ofstudies have shown that microbubble agents that differ inthe structure of the shell or the internal gas mediatedifferent levels of gene delivery (Li et al. 2003; Pislaru etal. 2003). Increasing the concentration of plasmid DNAdoes increase gene delivery, but the enhancement isminimal. Further study of the mechanism by which plas-mid DNA enters cells may offer useful insights, while itsassociation with a nuclear localising signal is likely to bebeneficial because the passage of plasmid from the cy-toplasm to the nucleus is highly inefficient (Pollard et al.1998). A significant improvement over the use of nakedDNA is anticipated for the inclusion of DNA condensa-tion agents because a smaller vector is more likely toenter through a short-lived membrane opening. Associ-ation of plasmid with the microbubbles during synthesis(Frenkel et al. 2002), or by using cationic microbubbles(Christiansen et al. 2003), is also likely to improveefficiency. Finally, the full potential of this technologywill be recognised with the additional implementation ofmicrobubble targeting, such that cavitation and vectoravailability occur in close proximity to the target cellmembrane.
In terms of progressing on to an in vivo model, weenvision using the most effective conditions identified inthis study, but with the pulse amplitude increased tocompensate for attenuation of US by tissue. An in vivosystem offers the advantage of being able to perfuse thetarget tissue and provide a continuous supply of micro-bubbles for a short period of time. Because of the lowtoxicity of microbubble contrast agents and plasmidDNA, repeat administration is also a potential approach.However, possible constraints on microbubble oscilla-tion in vivo due to small intravascular or intercellularspace compared with an in vitro environment will needto be studied. In conclusion, the importance of this studylies in defining parameters associated with US exposure,
not greatly dissimilar from those employed by clinicaldiagnostic systems, that are translatable to eventual ther-apeutic gene delivery incorporating the microbubble/vector improvements discussed above.
Acknowledgements—This work was funded by the Biotechnology andBiologic Sciences Research Council.
REFERENCES
Akowuah EF, Gray C, Lawrie A, et al. Ultrasound-mediated delivery ofTIMP-3 plasmid DNA into saphenous vein leads to increasedlumen size in a porcine interposition graft model. Gene Ther2005;12:1154–1157.
Bekeredjian R, Chen S, Frenkel PA, Grayburn PA, Shohet RV. Ultra-sound-targeted microbubble destruction can repeatedly directhighly specific plasmid expression to the heart. Circulation 2003;108:1022–1026.
Blomley MJ, Cooke JC, Unger EC, Monaghan MJ, Cosgrove DO.Microbubble contrast agents: A new era in ultrasound. BMJ 2001;322:1222–1225.
Christiansen JP, French BA, Klibanov AL, Kaul S, Lindner JR. Targetedtissue transfection with ultrasound destruction of plasmid-bearing cat-ionic microbubbles. Ultrasound Med Biol 2003;29:1759–1767.
Frenkel PA, Chen S, Thai T, Shohet RV, Grayburn PA. DNA-loadedalbumin microbubbles enhance ultrasound-mediated transfection invitro. Ultrasound Med Biol 2002;28:817–822.
Greenleaf WJ, Bolander ME, Sarkar G, Goldring MB, Greenleaf JF.Artificial cavitation nuclei significantly enhance acoustically in-duced cell transfection. Ultrasound Med Biol 1998;24:587–595.
Guo DP, Li XY, Sun P, et al. Ultrasound/microbubble enhances foreigngene expression in ECV304 cells and murine myocardium. ActaBiochim Biophys Sin (Shanghai) 2004;36:824–831.
Kim HJ, Greenleaf JF, Kinnick RR, Bronk JT, Bolander ME. Ultra-sound-mediated transfection of mammalian cells. Hum Gene Ther1996;7:1339–1346.
Lawrie A, Brisken AF, Francis SE, et al. Ultrasound enhances reportergene expression after transfection of vascular cells in vitro. Circu-lation 1999;99:2617–2620.
Lawrie A, Brisken AF, Francis SE, et al. Microbubble-enhanced ultra-sound for vascular gene delivery. Gene Ther 2000;7:2023–2027.
Lawrie A, Brisken AF, Francis SE, et al. Ultrasound-enhanced trans-gene expression in vascular cells is not dependent upon cavitation-induced free radicals. Ultrasound Med Biol 2003;29:1453–1461.
Li T, Tachibana K, Kuroki M. Gene transfer with echo-enhancedcontrast agents: Comparison between Albunex, Optison, and Levo-vist in mice—initial results. Radiology 2003;229:423–428.
Liang HD, Lu QL, Xue SA, et al. Optimisation of ultrasound-mediatedgene transfer (sonoporation) in skeletal muscle cells. UltrasoundMed Biol 2004;30:1523–1529.
Lindner JR. Microbubbles in medical imaging: Current applicationsand future directions. Nat Rev Drug Discov 2004;3:527–532.
Lu QL, Liang HD, Partridge T, Blomley MJ. Microbubble ultrasoundimproves the efficiency of gene transduction in skeletal muscle invivo with reduced tissue damage. Gene Ther 2003;10:396–405.
Miao CH, Brayman AA, Loeb KR, et al. Ultrasound enhances genedelivery of human factor IX plasmid. Hum Gene Ther 2005;16:893–905.
Miller DL, Quddus J. Sonoporation of monolayer cells by diagnosticultrasound activation of contrast-agent gas bodies. Ultrasound MedBiol 2000;26:661–667.
Miller DL, Dou C, Song J. DNA transfer and cell killing in epidermoidcells by diagnostic ultrasound activation of contrast agent gasbodies in vitro. Ultrasound Med Biol 2003;29:601–607.
Newman CM, Lawrie A, Brisken AF, Cumberland DC. Ultrasoundgene therapy: On the road from concept to reality. Echocardiogra-phy 2001;18:339–347.
Pislaru SV, Pislaru C, Kinnick RR, et al. Optimization of ultrasound-
mediated gene transfer: Comparison of contrast agents and ultra-sound modalities. Eur Heart J 2003;24:1690–1698.
Ultrasound/microbubble-mediated gene delivery ● A. RAHIM et al. 1279
Pollard H, Remy JS, Loussouarn G, et al. Polyethylenimine but notcationic lipids promotes transgene delivery to the nucleus in mam-malian cells. J Biol Chem 1998;273:7507–7511.
ter Haar GR. High intensity focused ultrasound for the treatment oftumors. Echocardiography 2001;18:317–22.
Unger EC, Hersh E, Vannan M, McCreery T. Gene delivery using
ultrasound contrast agents. Echocardiography 2001;18:355–361.Wells DJ. Gene therapy progress and prospects: Electroporation andother physical methods. Gene Ther 2004;11:1363–1369.
Zarnitsyn VG, Prausnitz MR. Physical parameters influencing optimi-zation of ultrasound-mediated DNA transfection. Ultrasound MedBiol 2004;30:527–538.
Zeqiri B, Bickley CJ. A new anechoic material for medical ultrasonic
applications. Ultrasound Med Biol 2000;26:481–485.