
Measuring ascending aortic stiffness in vivo in mice using ultrasound
Upload
independentCategory
view
2download
0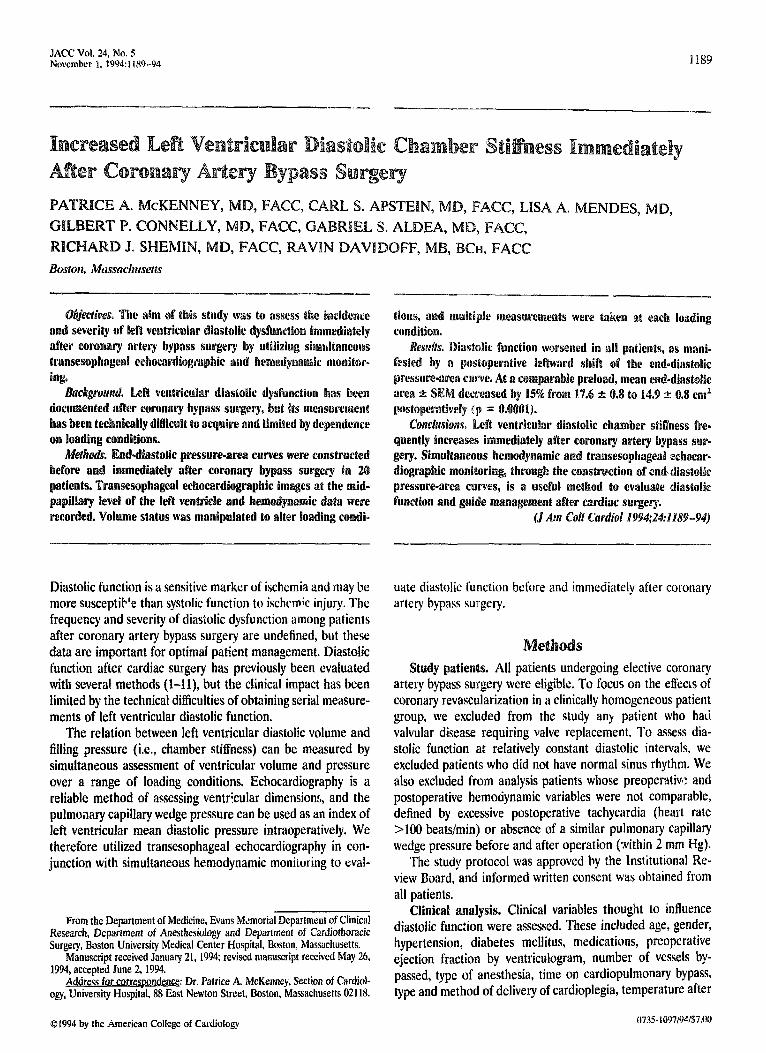
JACC Vol. 24. No. 5 Novcmbrr 1. 1994~1189-94
--._
M&t& En&diastailic pressure-area curves were c‘onstmcted before and inmediately after coronary bypass surgery in LX9 patients. ‘&ransesop~ageal echocardiographic images at the mid- papillary level of the lieft veatri~~e and ~e~~ody~amic data were recorded. V0lnme status was manipulated to alter loading roaadi-
Diastolic function is a sensitive marker of ischemia and may be more susceptib’e than systolic function to ischemic injury. The frequency and severity of diastolic dysfunction among patients after coronary artery bypass surgery are undefined, but these data are important for optimal patient management. Diastolic function after cardiac surgery has previously been evaluated with several. methods (l-11), but the clinical impact has been limited by the technical difficulties of obtaining serial measure- ments of left ventricular diastolic function.
The relation between left ventricular diastolic volume and filling pressure (i.e., chamber stiffness) can be measured by simultaneous assessment of ventricular volume and pressure over a range of loading conditions. Ecbocardiography is a reliable method of assessing ventricular dimensions, and the pulmo;lary capillary wedge pressure can be used as an index of left ventricular mean diastolic pressure intraoperatively. We therefore utilized transesophageal echocardiography in con- junction with simultaneous hemodynamic monitoring to evat-
From the Department of Medicine, Evans Memorial Department of Clinical Research, Department of Anesthesiology and Department of Cardiothoracic Surgery, Boston University Medical Center Hospital, Boston, Massachusetts.
Manuscript received January 21, 1994; revised manuscript received May 26, 1994, accepted June 2, 1994.
Address for correswndence: Dr. Patrice A. McKenney, Section of Cardiol- ogy, University Hospital, 88 East Newton Street, Boston, Massachusetts 02118.
01994 by the American College of Cdiliology
SCfWd in all patiewts, as nt&
ard shift off the e~d~diasto~i~
ft vcntricla!ar diastolic chamber stihess fre. r coronary artery bypass sir-
gery. Simultaneous hem0dynamic asld traamsesopleageangeall echecar- diographic rno~it~rj~g~ tRr0ugb the ~~~str~~ti0~ of end. ~~as~~~~E
presswre.area c es, is a usefkd method to evaluate diastolic functiona and p manragemerat after cardiac surgery.
(J Am Cdl Cardid l994;.24:1189-94)
uate diastolic function before and immediately after coronary artery bypass surgery.
Study patients. All patients undergoing elective coronary artery bypass surgery were eligible. To focus on the effects of coronary revascularization in a clinically homogeneous patient group, we excluded from the study any patient who hair valvular disease requiring valve replacement. To assess dia- stolic function at relatively constant diastolic intervals, we excluded patients who did not have normal sinus rhythm. We also excluded from analysis patients whose preoperativ: and postoperative hemodynamic variables were not comparable, defined by excessive postoperative tachycardia (heart rate >lOO beatsfmin) or absence of a similar pulmonary capillary wedge pressure before and after operation (within 2 mm Hg).
The study protocol was approved by the institutional Re- view Board, and informed written consent was obtained from all patients.
Clinical analysis. Clinical variables thought to influence diastolic function were assessed. These included age, gender, hypertension, diabetes mellitus, medications, preoperative ejection fraction by ventriculogram, number of vessels by passed, type of anesthesia, time on cardiopulmonary bypass, type and method of delivery of cardioplegia, temperature after
0735 1~97/94/$7.~lU
1190 MCKENNEY ET AL. DLGTOLIC FUNCTION AFTER BYPASS SURGERY
JACC Vol. 24. No. 5 November I. 1994~1189-94
cardiopulmonary bypass and use of postoperative hOtrOpiC agents.
wphic analysis. For the purpose of this study, d&o]k chamber stifiess is defined as the increase in left vent&& diastolic pressure per unit of left ventricular dia- stoljc volume. -use of limitations in obtaining reproducible ]oag_axis views by tmnsesophageal echocardiography, volume assessment may be problematic. lhereforc two-dimensional cros~_s&iona1 left ventricular diastolic area was measured as an index of volume, To minimize geometric distortion, we measured the kft ventricular area at the midpapillary level in all studies. Diastolic function was evaluated by analyzing left ventricular diastolic pressure-area curves at this fixed standard- ized level of the left ventricle.
F&h patient was continuously monitored for arterial pres- sure, heart rate, central venous pressure, pulmonary artery pressure and pulmonary capillary wedge pressure. The pulmo- nary capillorry wedge pressure reflects the mean left atrial pressure; therefore, in the absence of mitral valve disease, it closely approximates left ventricular mean diastolic pressure. The mc~ wedge pressure at end-expiration was measured at each loading condition before and after operation. Represen- tative tracings of the pulmonary artery and wedge pressures were recorded and inspected for a decrease in pressure from mean pulmonary artery to mean wedge and for a definit; left atrial pressure waveform in the wedge tracing 10 ensure that an accurate wedge measurement had been made.
After induction of anesthesia, the transesophagcai probe was placed and images of the short axis of the left ventricle at the midpapiilary level were obtained.
HemdyMmic and echocutdiqmphic measctnmenrs were obtained 15 min after anesthesia induction once the patient was in stable condition. If filling pressures were low, volume loading with 1 to 2 liters of normal saline solution was performed. Baseline hemodynamic and echocardiographic measurements were obtained before volume loading, and multipk subsequent measurements were made with varying loading conditions. Immediately after coronary bypass surgery, the patient again undement hemodynamic and echocardio- graphic measurements with volume manipulation to generate a second left ventricular diastolic pressure-area curve, End-
diastolic areas ma determined as the average of three consccutivc hand-traced images at each loading condition, utilizing off-line analysis on the Freeland GTI Cinc View Plus system.
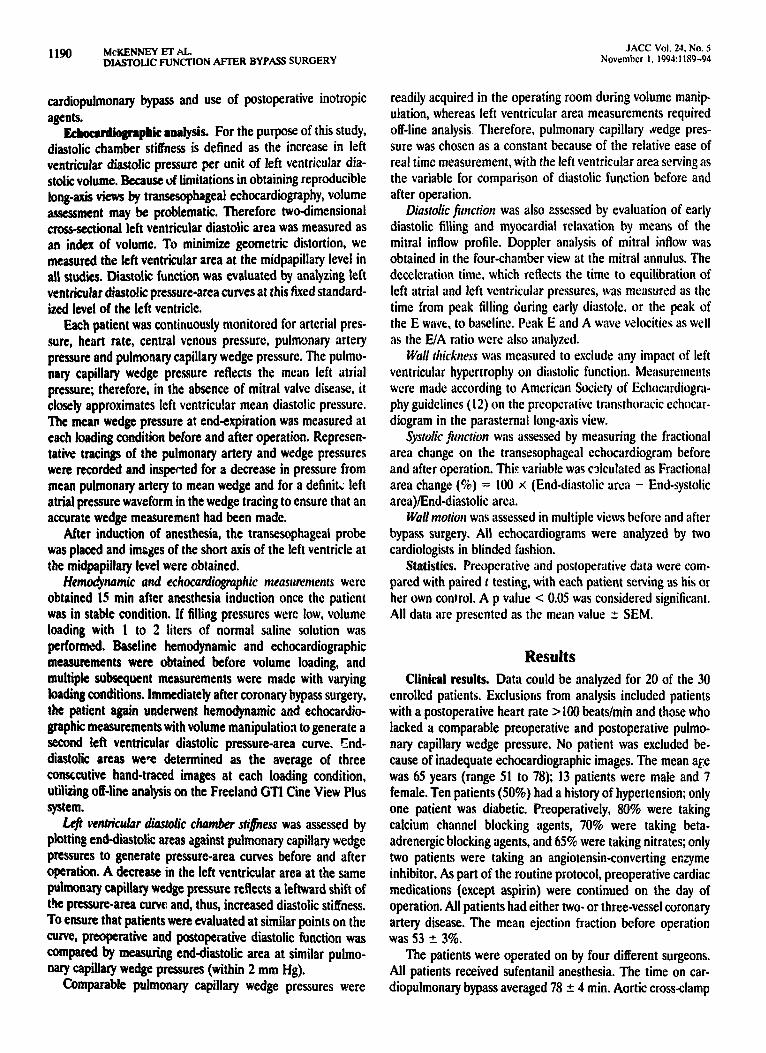
I.@ W&U&W diaudic chamber stifiess was assessed by plotting end-diastolic areas against pulmonary capillary wedge pmures to generate pressure-area curves before and after operation. A decrease in the left ventricular area at the same Pu]mOn;uy capillary wedge pressure reflects a leftward shift of the pressure-area curve and, thus, increased diastolic stiffness. To ensure that patients were evaluated at similar points on the me, preoperative aad postoperative diastolic function was Compared by measuring end-diastolic area at similar puhno- narY capillary wedge pressures (within 2 mm Hg),
Comparable pulmonary capillary wedge pressures were
readily acquired in the operating room during volume manip- ulation, whereas left ventricular area measurements required off-line analysis. Therefore, pulmonary capillary #edge pres- sure was chosen as a constant because of the relative ease of real time measurement, with the left ventricular area serving as the variable for comparison of diastolic function before and after operation.
Diastolic firnction was also assessed by evaluation of early diastolic filling and myocardia] relaxation by means of the mitral inflow profile. Doppler analysis of mitral inflow was obtained in the four-chamber view at the mitral annulus. The deceleration time. which reflects the time to equilibration of left atrial and left ventricular pressures. was measured as the time from peak filling during early diastole, or the peak of the E wave, to baseline. Peak E and A wave velocities as well as the EIA ratio were also analyzed.
Wall tltickrrcss Was measured 10 exclude any impact of left ventricular hypertrophy on diastolic function. Measurements were made according lo American Society of Echocardiogra- phy guidelines (12) on the preoperative transthoracic cchocar- diogram in the parastemat long-axis view.
Systdic ,htction WBS assessed by measuring the fractional area change on the transesophagcal echocardiogram before and after operation. Thi.(: variable was calculated as Fractional area change (%) = 100 x (End-diastolic arca - End-systolic area)/Enddiastolic area.
Wall ntotiort was assessed in multiple views before and after bypass surgery. Ail echocardiograms were analyzed by two cardiologists in blinded fashion.
Statistics. Preoperative and postoperative data were com- pared with paired t testing, with each patient serving as his or her own control. A p value < 0.05 was considered significant. Ail data are presented as the mean value t SEM.
Results Clinkal results. Data could be analyzed for 20 of the 30
enrolled patients. Exclusions from analysis included patients with a postoperative heart rate > 100 beats/min and those who lacked a comparable preoperative and postoperative pulmo- nary capillary wedge pressure. No patient was excluded be- cause of inadequate echocardiographic images. The mean age was 65 years (range 51 to 78); 13 patients were male and 7 female. Ten patients (50%) had a history of hypertension; only one patient was diabetic. Preoperatively, 80% were taking calcium channel blocking agents, 70% were taking beta- adrenergic blocking agents, and 65% were taking nitrates; only two patients were taking an angiotcnsinconverting er,yme inhibitor. As part of the routine protocol, preoperative cardiac medications (except aspirin) were continued on the day of operation. All patients had either two- or three-vessel coronary artery disease. The mean ejection fraction before operation was 53 t 3%.
The patients were operated on by four different surgeons. All patients received sufentanil anesthesia. The time on car- diopulmonary bypass averaged 78 + 4 min. Aortic cross-clamp
JACC’ Vol. 24. No. 5 November 1. 1994:1189-94
MrKENNEY ET AL. DIASTOLIC FUNCTBON AFTER BYPASS SURGERY
time averaged 37 5 3 min. The type and method of delivery of cardioplegia varied. Ten patients undenvent crystalloid and 10 underwent blood cardioplegia; cardioplegia was only antero- grade in 14 patients but both anterograde and retrograde in 6. At the time of echocardiographic and hemodynamic measure- ments, the bladder temperature averaged 36.7 + O.W. Four patients received pheny~epbrine hydroc loride transiently be- cause of vasodilation during rewarming, but all were hemo- dynamically stable at the time of echocardiographic measure- ments. Seven patients received low dose dopamine (5 pg/kg
eight per min) in the immediate postoperative period. c~rd~o~~~~~i~ molts. Diastolic functiott. After oper-
ation, diastolic function worsened in all patients, as evidenced by a ieftwarcl shift of the left ventricular diastolic pressure-area curve for each patient (Fig. 1, Table 1). The mean end-diastolic area was 17.6 + 0.8 cm2 preoperatively but decreased after coronary artery bypass surgery to a mean of 14.9 + 0.8 cm2 at a comparable pulmonary capillary wedge pressure. Tiiis CiiiTer-
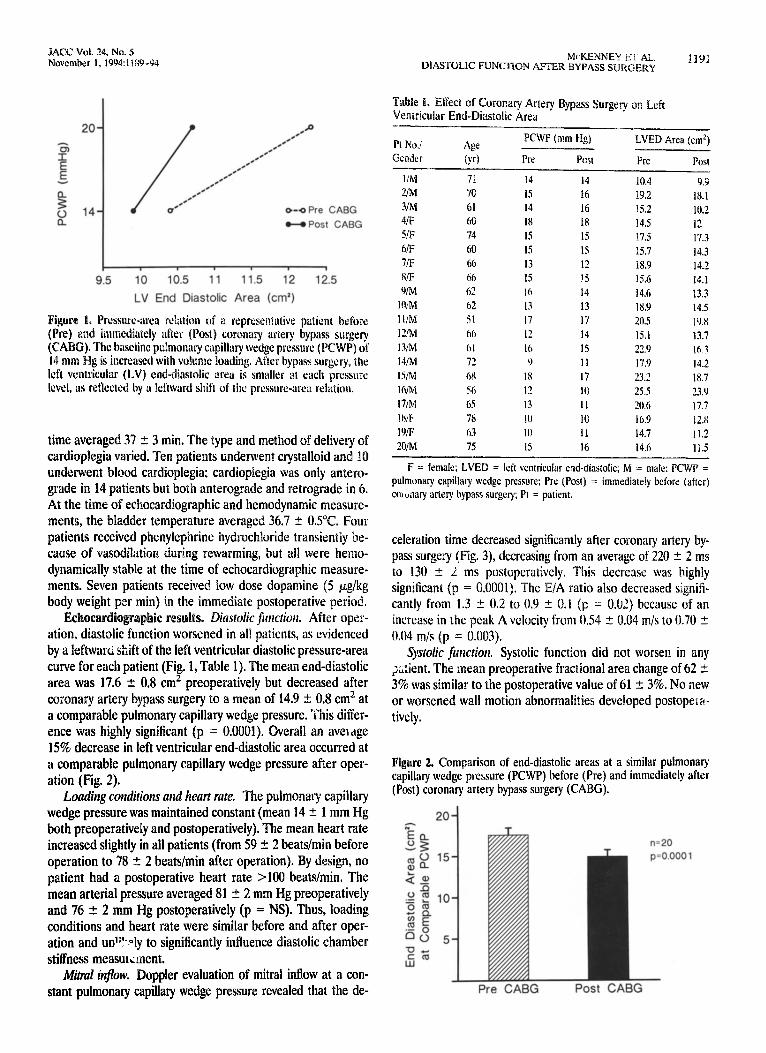
ence was highly significant (p = 0.0001). Overall an aveldge 15% decrease in left ventricular end-diastolic area occurred at a comparable pulmonary capillary wedge pressure after oper- ation (Fig. 2).
Lou&q conditions attd heart me. The pulmonary capillary wedge pressure was maintained constant (mean 14 +_ 1 mm Hg both preoperatively and postoperatively). The mean heart rate increased slightly in all patients (from 59 ? 2 beatslmin before operation to 78 t 2 beatslmin after operation). By design, no patient had a postoperative heart rate >lOO beats/min. The mean arterial pressure averaged 81 2 2 mm Hg preoperatively and 76 5 2 mm Hg postoperatively (p = NS). Thus, loading conditions and heart rate were similar before and after oper- ation and un’Vy to significantly influence diastolic chamber stiffness measmcinent.
M&al inflow. Doppler evaluation of mitral inflow at a con- stant pulmonary capillary wedge pressure revealed that the de-
Tabk 1. ~tkct of Corona9 Artery Bypass Surge9 on Left Ventricular End-Diastolic Area
LVED Area (cm?)
l/M 7i
mt 70
3/M 61
4/F 60
5/F 74
6/F 60
7/F 66
8iF 66
9/M 62
l%M 62
I I/M 51
12/M 66
13/M 61
14/M 72
wvl 6K
I h/M 56
17/M 65
111/k 7x
19iF 63
‘O/M 75
14
15
I4
18
IS
15
13
15
I6
I3
17
I?
IO
9
I8
I2
I3
IO
IO
I5
I4
16
16
18
IS
IS
12
15
14
13
I7
I4
I5
11
I7
10
II
IO
II
I6
10.3 9.9
19.2 18.1
15.2 10.2
14.5 1’ b
17.5 17.3
15.1 14.3
18.Y 14.2
15.6 14.1
14.6 13.3
18.Y 14.5
20.5 19.8
15.1 13.7
22.9 !rr 3
17.0 14.2
23.2 18.7
25.5 23.Y
20.6 17.7
16.9 12.N
14.7 11.2
14.6 11.5
F = female; LVED = left ventricular end-diastolic; M = mate; PCWP =
pulmonary capillary wedge pressure: Pre (Post) = immediately before (after)
cownary artery bypass surgery; PI = patient.
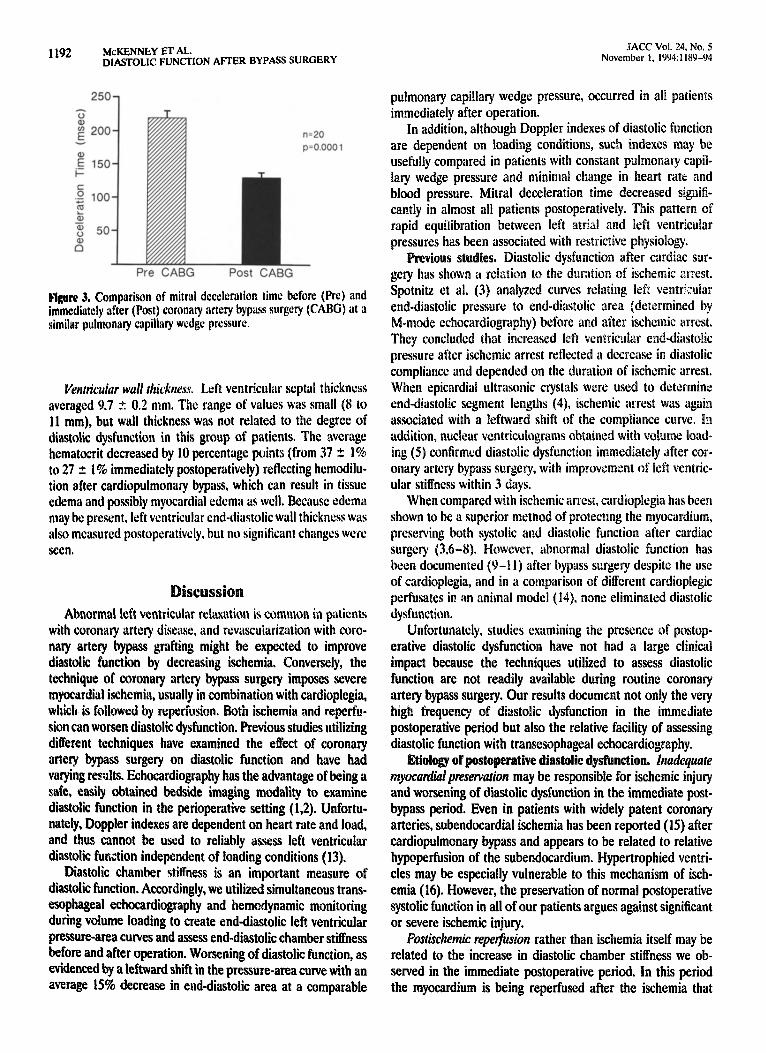
celeration time decreased significantly after coronary artery by- pass surgery (Fig. 3), decreasing from an average of 220 5 2 ms to 130 2 L ms postoperatively. This decrease was highly
significant (p = 0.0001). The E/A ratio also decreased signifi-
cantly from 1.3 -C 0.2 to 0.9 2 0.1 (p = O.U?) because of an increase in the peak A velocity from 0.54 2 0.04 m/s to 0.70 -C 0.04 m/s (p = 0.003).
Systolic function. Systolic function did not worsen in any +:ient. The mean preoperative fractional area change of 62 + 3% was similar to the postoperative value of 61 -C 3%. No new or worsened wall motion abnormalities developed postopera- tively.
Figure 2. Comparison of end-diastolic areas at a similar pulmonary capillary wedge pressure (PCWP) before (Pre) and immediately after (Post) corona9 artery bypass surge9 (CABG).
1192 McKENNLY ET AL. DIASTOLIC FUNCDON AFTER BYPASS SURGERY
JACC Vol. 24, No. 5 November 1, 1994:1189-94
25k
n=20 p=o.ooo 1
Prs CABG Post CAFG
ix 3. Comparison of mitrui deceleration time before (Prc) and immediatdy sftcr (Post) coronary artcry bypuss surgery (CABS) iIt iI similwr pulmonary capillary wcdgc prcsurc.
Venrvirular wall r/zicknc~ Left ventricular scptal thickness
averaged 9.7 2 0.2 mm. The range of values was small (8 to 11 mm), but wall thickness was not related to the degree of diastolic dysfunction in this group of patients. The average hematoerit decreased by 10 percentage points (from 37 I 1% to 27 + 1% immediately postoperatively) reflecting hemodilu- tion after cardiopulmomuy bypass, which can result in tissue edema and possibly myocardial edema as well. Because edema may be present, left ventricular cud-diastolic wall thickness was also measured postoperatively. but uo significant changes were seen.
Abnormal bft ventricular relaxation is common in patients with coronary artety disease, and revascularization with coro- nary artery bypass grafting might be expected to improve diastolic function by decreasing ischemia. Conversely, the technique of coronary artcty bypass surgery imposes severe
m rdirl isehemia, usually in combination with cardioplgia, which is followed by reperfusion. Eoth i,schemia and rcperfu- sion ean worsen diastolic dysfunction. Previous studies utilizing dikrent techniques have examined the effect of coronary artery bypass surgery on diastolic function and have had varying results. bhocardiography has the advantage of being a safe, easily obtained bedside imaging modality to examine diastolic function in the p&operative setting (1.2). Unfortu- nately, Doppler indexes are dependent on heart rate and load, and thus cannot be used to reliably assess left ventricular diastolic fimction independent of loading conditions (13).
Diastolic chamber stiffness is an important measure of diastolic function. Accordingly, we utilized simultaneous trans-
esophageal echocardiography and hemodynamic monitoring during volume loading to create end-diastolic left ventricular pressure-area curves and assess end-diastolic chamber stiffness before and after operation. Worsening of diastolic function, as
evidenced by a leftward shift in the pressure-area curve with an average 15% decrease in end-diastolic area at a comparable
pulmonary capillary wedge pressure, occurred in all patients
immediately after operation. In addition, although Doppler indexes of
are dependent on loading conditions, such usefully compared in patients with constant p~lrno~a~ capil-
laty wedge pressure and minimal change in heart rate and blood pressure. Mitral deceleration time decreased signifi- cantly in almost all patients postoperatively. This pattern of rapid equilibration between left atria1 and left
pressures has been associated with restrictive physi ies. Diastolic dysfunctiQ~ after cardiac sur-
gery has shown a rciatics to the d~rat~~~ of is&e arrest.
Spotnitz et al. (3) anal ed curves relating left tr~~u~ar
end-diastolic pressure to end-diasto ic area ~determjned by
M-mode c hy) before and after isc~~e~ic arrest.
They cnru reased left v~t~tric~ia~ crud-dii~sto~ic pressure after ischemic arrest reflected a decrease in diastolic
compliance and depended on the ~ur~lti~n of ischemic arrest. When epicardial ultrasonic crystals were used to determine
end-diastolic segment lengths (4) ischemi associated with a leftward shift of the corn addition, ~ucle~~r ventric~~~~ran~s ~~~ti~~fled ing (5) con~rm~d diastolic dysfunction immediately after cor-
onary artery bypass surgery, with improvement of left ventric-
ular stiffness within 3 days. When compared with ischetnic arrest, cardi
shown to bc a superior method of protectmg preserving both systolic and diastolic function after cardiac surgery (3.6-g). However, abnormal diastolic function has been documented (9-11) after bypass surgery despite the use
of cardioplegia, and in a comparison of different cardioplegic perfusates in an animal model (14), none eliminated diastolic
dysfunction.
Unfortunately, studies examining the presence of postop- erative diastolic dysfunction have not had a large clinical
impact because the techniques utilized to assess diastolic function are not readily available during routine coronary artery bypass surgery. Our results document not only the very high frequency of diastolic dysfunction in the immediate
postoperative period but also the relative facility of assessing
diastolic function esophageal echocardiography.
Etiology of pas diastolic dys~nction. Inadequate myucudiuf preservation may be responsible for ischemic injury and worsening of diastolic dysfunction in the immediate post-
bypass period. Even in patients with widely patent coronary
arteries, subendocardial &hernia has been reported (15) after
cardiopulmonary bypass and appears to be related to relative
hypoperfusion of the subendocardium. Hypertrophied ventri-
cles may be especially vulnerable to this mechanism of isch-
emia (16). However, the preservation of normal postoperative
systolic function in all of our patients argues against significant or severe ischemic injury.
Postischemic repetjksion rather than ischemia itself may be related to the increase in diastolic chamber stiffness we ob-
served in the immediate postoperative period. In this period
the myocardium is being reperfused after the ischemia that

radicals (20). Lipid ~e~o~~dut~o~ can result in Loss of
overload and diastolic dysfunction. In u clinical trial in which allopurino8 was given ~reo~er~~t~vely to reduce the Of CytotoXic free r~~iC~~S~ ~~~~~~~tS hdd S~~~jfiCa~t~~
5yst~~ic cardiac fu~ct~Q~~ and lower mortality rates after surgery (24).
~~Q~~~d~al edema can ~otel~t~a~~y occur during cardiac surgery and lead to diastolic dysfunction. In this study- al- though the average hematocrit dec ,ased by 10 percentage points postoperatively as a result of bcmodilution after cardio- pulmonary bypass, we were unable to detect a change in left ventricular wall thickness postoperatively. It may be that small changes in wall thickness could not be detected echocardio- graphically.
Otherrjhctors during cardiac surgery may aEect left ventricu- on. These include temperature changes, uences, type and method of delivery of
cardioplegia, interaction with the right ventricle and alter- ations in left ventricular geometry once the pericardium has been opened (1 l&28).
Abnomzal diasrolic fiElirg, regardless of mechanism, may contribute to morbidity and mortality in these patients. De- creased cardiac output in the postoperative setting may reflect diastolic rather than systolic dysfunction, and the increased diastolic chamber stiffness diminishes the value of the pulmo- nary capillary wedge pressure as a guide to adequacy of preload in terms of myocardial fiber diastolic stretch. Although an early increase in diastolic chamber stiffness is frequent immediately after operation, this increase does not necessarily imply persistent dysfunction or irrevccsible cellular injury. A state of postoperative “diastolic stunnind’ may be Tresent.. The natural history and prognostic implications of such early diastolic stunning need to assessed in future studies.
Limitations of the s Heart rate and end-diastohc di- mensions. Elevated heart rates were present postoperatively, averaging 59 beatslmin before and 78 beatslmin after opera- tion. Harrison et al. (29) studied the effect of atrial pacing on left ventricular end-diastolic dimension in normal subjects and found no change in this dimension when heart rate was
increase in heart rate of EO beats/min. e in end-diastolic area that we documented
is more than would be expec alone. In addition, we found percent decrease in end-diast
essure than was the
function in the intr~o~erat~ve and ~erioperat~ve periods and left atrial lines are not routinely placed during bypass SIN 1~ three patients in whom a left atrial line was placed postop- eratively to measure kft at 1 pressure directly, the left atria! pressure was within 1 mm of the wedge pressure.
LeJ ventricuiar urea volume ~eas~~e:ncil~. e u:i- lized the left ventricular end-diastolic area measureme~~t rather than a volume measurement. Because some patients may have segmental wall motion abnormalities not visible at the mid~~illa~ level, pressure-voiume curves of the entire left ventricle obtained through biplane or omniplane imaging may be a better method ofaisessment. In our patient group, no patient developed new wall motion abnormalities, and thus the short-axis cut at the ~~~dpapilla~ level was considered repre- sentative of the behavior of the entire ventricle.
~u~c~us~~~s~ We demonstrated that diastolic dysfunction as assessed by end-diastolic left ventricular chamber stiffness and mitral valve deceicration time is very common immedi- ately after coronary bypass surgery, Because of this increased left ventricular stiffness, the pulmonary capillary wedge pres- sure does not accurately reflect left ventricular volume. Simul- taneous monitoring of the pulmonary capillary wedge pressure and transesophageal echocsrdiographic images, through the construction of pressure-area curves, is a clinically useful method for assessing diastolic function and guiding therapy immediately after coronary artery bypass surgery.
1. Lawson WE, Seifert F, Anagnostopoulos C, Hills D, Swinford RD, Cohn P. Effect of coronary artery bypass grafting on left ventricular didstOk function. Am J Cardioi 19888;61:283-7.
2. Wehlage DR, Bohrer H, Ruffmann K. Impairment of left ventricular diastolic function during coronary artery bypass grafting. Anaesthesia 1990; 45:549-51.
3. Spotnitz HM, Bregman D, Bowman FO, et al. Effects of open heart surgery on end-diastolic pressure-diameter relations of the human left ventricle. Circulation 1979;5$:662-71.
4. Chitwood WR, Hill RC, Sink JD, Wechsler AS. Diastolic ventricular
1194 McWNNEY ET AL. JACC Vol. 21, No. 5 DIASTOLIC FUNCTION AFTER BYPASS SURGERY November 1. 1994:1189-94
properties in patients during coronary revascularization: intermittent isch- emit arrest versus cardioplegia. J Thorac Cardiovasc Surg 1983;85:595-605.
5. Gray MD, Maddahi J, Berman D, et al. Scintigraphic and hemodynamic demonstration of transient left ventricular dysfunction immediately after uncomplicated coronary artery bypass grafting. J Thorac Cardiovasc Surg 197a,n:504-10.
6. Ellis RJ, hfangano MD, Van Dyke DC, Ebert PA. Hypothermic potassium cardioplegia preserves myocardial compliance. Surgery 1979$6:810-7.
7. Slack JD, Zcok I, Cole JS, Hanley HG, Comish AL, McKean HE. influence of potassium cardioplegia versus ischemic arrest on regional left ventricular diastolic compliance in humans. Ann Thorac Surg 1981;31:214-23.
8. Weisel RD, Bums RJ, Baird RI, et al. Optimal postoperative volume loading. J Thorac Cardiovasc Surg 1983;85:552-63.
9. Kawasuji M, Sawa S, Sakakibara N, fwa T. Taki J, Bunko J. Serial assessment of left ventricular function following coronary artery bypass surgcry by radionuclide angiocardiography, Jpn Circ J 198&52:1149-55.
10. Natsuwki M, ltoh T, Ohteki H, Minato N. Ishii K Suda H. Evaluation of left ventricular early diastolic function after coronary artery bypass grafting relrling to myocardial damage. Jpn Circ J 19QS.5: 117-24.
Il. lvanov J, Wiesel RD, Micklcborough LL, Hilton JD, McLaughlin PR. Rewarming hypovotemia after aortocoronary hypas surgery. Crit Care Med 19R4;12:1049J4,
12. Sahn DJ, DeMaria A, Kisslo J, Wcyman A. The Committee on M-mode Standardixntion of the American Society of Echocardiography. Recommcn- dations regarding quantitation in Memode echocardiography: result of a sutvcy of cchocardiographic measurements. Circulation 1978;58:1072-83.
13. Ch CY, Herrmann WC, Weyman AE, Fifer MA. Preload dependence of Doppler&rived indexes of left ventricular diastolic function in humans. J Am Coil Cardiol 1987;10:800-8.
14. Weng 2, Nicolosi AC, Detwiler PW, et al. Effects of crystalloid, blood, and University of Wisconsin p&sates on weight, water content, and left venlricular compliance in an edema-prone, isolated porcine heart model. J Thorac Cardiovasc Surg 1992;103:504-13.
15. Buckberg GD, Towers 8, Paalia DE, Mulder DG. Maloncv JV. Suhcndo- cardial &hernia after cardiopulmonary bypass. J Thorac Cardiovasc Surg 1972364z669-80.
16. Menasche P. Gmusset C. Apstein CS. Marotte F. Mouas C. Piwnica A. Increased injury of hypertrophicd myocardium with ischemic arrest: preser- vation with hypothermia and cardioplegiu. Am Heart J 198~;11O:l?O&Y.
17.
18.
19.
20.
21.
Apstein CS, Lore11 BH. The physiologic basis of left ventricular diastolic dysfunction. J Card Surg 1988;3:475-85.
Bolli R. Oxygen-delived free radicals and postischemic myocardial dysfunc- tion (LLstunned myocardium”). J Am Coil Cardiol 1988;11:139-49.
Feniera R, Llesuy S, Milei J, et al. Assessment of myocardial oxidative stress in patients after myocardial revascularization. Am Heart J 1988;115:367-11.
Prasad K, Kalra J, Bharadwaj B, Chaudhaty AK. Increased oxygen free radical activity in patients on cardiopulmonary bypass undergoing aortocoro- nary bypass surgery. Am Heart J 1992;123:37-45.
Prasad 6, Kalra J, Chan WP, Chaudhary AK. Effect of oxygen free radicals on cardiovascular functions at organ and cellular level. Am Heart J 198~11731196-202.
22. Rowe CT, Mattson NH, &plan M. Hess ML. Hydrogen peroxide and hydroxyl radical mediation of activated leukocyte depression of cardiac sarcoplasmic reticulum: participation of the cycle-oxygenasc pathway. Circ Rcs lY83$3:58&9l.
23. Schcrer NM, Dcamcr DW. Gaidativc stress impairs the function Jf sarco- plasmic reticulum by oxidation of sulphydtyl groups in the Ca * * -ATPasc. Arch Biochcm Eiophys 198S;246:589-601.
24. Johnson WD, Kuysor KL. Brcnowitz JB, Sacdi SF. A randomized controlled trial of allopurinol in coronary bypass suqcry. Am Heart 9 1991;121:20-4.
25. Moorcs WY, Weiskopf RB. B;lysinger M, Utlcy JR. Effects of hlothane and morphine sulfate on myocardial compliance following total cardiopulmonary bypass. J Thorac Cardiovasc Surg 1981:81:163-70.
26. Diehl JT, Eichhorn EJ, Konstam MA. et al. Efficacy of retrograde coronary sinus cardioplegir in patients undergoing myocardial rev~l~u~a~izatio~: a prospective randomized trial. Ann Thorac Sug I9813;45:5Y5-602.
27. Kelly DT, Spotnitz HM, Beiscr GD, Pierce JE. Epstein SE. Effects ofchronic right ventricular volume and pressure loading on left ventricular perfor- mance. Circulation 1971;44:403-12.
28. Spotnitz HM. Kaiser GA. The effect of the pericardium on pressure-volume relalions in the canine left ventricle. J Surg Res ~~71;~~:375-8~~.
19. Harrison MR. Clifton GD, Penncll AT, DcMaria AN. Effect of heart ram on left ventricular diastolic transmitrat flow velocity patterns asscsscd by Doppler cchocardiography in normal subjects. Am J Cardiol 1991;67:6?2-7.
30. Erber R, Schweizer P. Krebs W. Langen H, Meyer J, Efert S. Effects of heart rate changes on left ventricular volume and ejwtion fraction: LI ?-dimen- sioual cchocardiographic study. Am J Cardiol 1984:53:590-7.
Copyright © 2022 FDOKUMEN




















