
Defining and measuring objective and subjective spinal stiffness
253
Defining and measuring objective and subjective spinal stiffness: A scoping review Joel Ranui Moses A 90-credit thesis submitted in partial fulfilment of the requirements for the degree of Master of Osteopathy, Unitec Institute of Technology, 2020
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of Defining and measuring objective and subjective spinal stiffness
Defining and measuring objective and subjective spinal stiffness:
A scoping review
Joel Ranui Moses
A 90-credit thesis submitted in partial fulfilment of the requirements
for the degree of Master of Osteopathy,
Unitec Institute of Technology, 2020

ii
Declaration
Name of candidate: Joel Moses
This thesis entitled “Defining and measuring objective and subjective spinal stiffness: A
scoping review” is submitted in partial fulfilment for the requirements for the Unitec degree of
Master of Osteopathy.
Principal Supervisor: Sylvia Hach
Associate Supervisor: Jesse Mason
Candidate’s declaration:
I confirm that:
• This thesis represents my work;
• The contribution of supervisors and others to this work was consistent with the Unitec
Regulations and Policies.
• Research for this work has been conducted in accordance with the Unitec Research
Ethics Committee Policy and Procedures and has fulfilled any requirements set for this
project by the Unitec Research Ethics Committee.
Candidate Signature: Date: 23/03/2020
Student number: 1458167

iii
Dedication/He mihi
Tihei mauri ora!
Te manu ka i te miro, nōna te ngahere, Te manu ka ii te mātauranga
Ko Tainui te Waka
Ko Hoturoa te Tangata
Ko Taupiri me Maungatautari te Māunga
Ko Waikato te Awa
Ko Waikato Tainui me Raukawa ngā Iwi
Ko Ngati Werokoko me Ngati Waenganui ngā Hapu
Ko Parawera te Marae
Ko Taneirangikapua te tupuna whare
Ko Sally rāua ko Rawhiti ōku mātua
Ko Joel Ranui Moses taku ingoa
Kua tau te mihi whakamana, ki a Waikato Tainui, mo te tautoko e pa ana ki taku kaupapa.
Tenei te mihinui mō tō rātou putea tautoko me tō rātou manaaki a Pai marire.
Waikato-taniwha-rau
He piko, he taniwha
He piko, he taniwha.
I also dedicate this thesis to my whanau who have shown endless support and encouragement
throughout this journey to completing my thesis.
I also dedicate this thesis to my best friend and partner, thank you for your endless love and
support.

iv
Acknowledgements
This thesis is the product of much collaboration. I would like to thank my supervisors, for
without their guidance, it would not have been possible to pull this thesis together. Sylvia, I
thank you for your persistence, dedication and assistance from the get-go. Your contributions
and research expertise have been invaluable. Jesse, I thank you for your great sense of humour
and for pulling me up at times on my discursive writing style. Your contributions and
perspectives have been an asset. It has been an absolute privilege and honour to work with you
both on this research project. I cannot thank you enough for the time you have put into the
preparation of this thesis.
I would like to make a special mention to Dipti Vora, Library Knowledge Specialist for her
expertise and guidance in the development of the search strategy.
To my lecturers and tutors, I thank you for providing me with a well-balanced perspective of
osteopathic principles, clinical expertise and evidence-based practice. These tools will be
invaluable as I begin my journey as a clinician.
To my classmates and now colleagues, what a privilege it has been to learn and develop
alongside you.

v
Preface
The notion of stiffness is a well-known entity within the clinical context. Despite this, there is
little agreement on the fundamental question – what the word ‘stiffness’ is specifically referring
to and how can it be assessed in the clinic. A diverse range of measures are used across different
research settings. However, these quantitative approaches appear to be poorly comparable to
the realities of patients and the pragmatics of clinical practice.
The purpose of this thesis is to examine the nature, range and extent of definitions and measures
of spinal stiffness in the existing literature. This is a critical first step, as it will provide a basis
for researchers to investigate how patients or clinicians understand stiffness, in a meaningful
and informed way. This thesis contributes to the understanding of what definitions and
measures are used in the literature. It will provide important future research directions and is
aimed at facilitating the development of a fuller understanding of how stiffness can be defined
and measured in the clinical context.
This thesis is presented in three sections. Section one contains the literature review. Here, the
consensus statement and standardised definition of pain is used as a reference point to allow
the reader to consider why stiffness might also benefit from a definition that provides a common
understanding for researchers, patients and clinicians. The historical evolutionary perspective
of stiffness and its subsequent adoption into the clinical context is described. This provides an
explanation of key concepts related to the origins and characterisation of stiffness.
Consideration is given to the role of primary care and rehabilitation professionals in the
assessment, evaluation and implementation of clinical interventions for patients that present
with stiffness. Following this, the quantitative and qualitative approaches to measuring stiffness
are explained and operational definitions employed in this thesis are described. This section
concludes by making the case that more clarity is needed regarding how stiffness is both
defined and measured.
Section two contains an outline of the methodology. This section begins by describing how the
philosophical perspective – positivism and the epistemological underpinnings of this review
are integrated into the chosen methodology – scoping review. The following will cite where
the chosen methodology is situated within the evidence hierarchy and establish why this
methodology was implemented to address the guiding research question. Subsequently, the key
characteristics of scoping reviews are compared to the more well-known systematic review.

vi
Finally, the methodological framework is outlined and described within the context of how this
scoping review was conducted
Section three contains a manuscript of the present project for submission to a peer-reviewed
journal for publication. Note, that a scoping review of this type required a broad scope, and
consequently yielded a large volume of data pertaining to the research question. For the purpose
of this thesis it was therefore determined that a detailed results section should be included,
irrespective of the word limitations of the target journal for the manuscript. This provides a
platform by which the reader may benefit from a more comprehensive coverage of the findings,
than could be achieved in a published manuscript. That is, a thorough and accurate
representation of the results could not have been achieved by adhering to the guidelines for the
purpose of a published manuscript. The intention is to abbreviate the manuscript following the
examination of the thesis in preparation for submission to the target journal.
Section four contains all appended resources including, for example, evidence of ethics
approval exemption and detailed data structure matrices. A scoping review protocol was
developed and registered prospectively on the open science framework which encourages
transparency during the review process and can also be found cross-referenced in the
appendices.

vii
Table of contents
Declaration............................................................................................................................................. ii
Dedication/He mihi ................................................................................................................................ iii
Acknowledgements ................................................................................................................................ iv
Preface .................................................................................................................................................... v
Table of Contents .................................................................................................................................. vii
List of Figures ........................................................................................................................................ ix
List of Tables ......................................................................................................................................... ix
Section 1: Literature review ................................................................................................................. 1
Definition of pain ............................................................................................................................... 2
Historical evolution of stiffness ........................................................................................................ 4
Considerations for primary care ..................................................................................................... 6
Considerations for rehabilitation .................................................................................................... 6
The importance of measuring stiffness ........................................................................................... 9
Objective measures of spinal stiffness ............................................................................................. 9
Subjective measures of spinal stiffness .......................................................................................... 11
Conclusion ............................................................................................................................................ 14
Section 2: Methodology ...................................................................................................................... 15
Philosophical perspective ............................................................................................................... 16
Comparison of key characteristics of scoping reviews and systematic reviews ......................... 18
Methodological approach ............................................................................................................... 20
Framework Stage 1: Identifying the research question ............................................................... 21
Framework Stage 2: Identifying the relevant studies .................................................................. 21
Grey literature .............................................................................................................................. 21
Clarification of terminology ........................................................................................................ 22
Framework Stage 3: Study selection ............................................................................................. 23
Framework Stage 4: Charting the data ........................................................................................ 23
Framework Stage 5: Collating, summarising and reporting the results .................................... 24
Framework Stage 6: (optional) Consultation ............................................................................... 24
References ............................................................................................................................................. 25
Section 3: Manuscript ......................................................................................................................... 39
Abstract ................................................................................................................................................ 41
Highlights ............................................................................................................................................. 42
List of abbreviations ........................................................................................................................... 43
Introduction ........................................................................................................................................... 44
Methods ................................................................................................................................................ 46

viii
Identification of the research question .......................................................................................... 46
Identification of the relevant studies ............................................................................................. 46
Study selection .............................................................................................................................. 47
Screening and Agreement ............................................................................................................ 48
Data charting process ..................................................................................................................... 48
Collating and summarising the findings of included studies ....................................................... 49
Analysing the data ........................................................................................................................ 49
Data validation ............................................................................................................................. 49
Reporting ...................................................................................................................................... 49
Results ................................................................................................................................................... 50
Overview of study characteristics .................................................................................................. 52
Characteristics of studies classified as biomechanical ............................................................. 55
Characteristics of studies classified as surgical ........................................................................ 58
Characteristics of studies classified as pathophysiological ...................................................... 60
Characteristics of studies classified as segmental assessment ................................................. 63
Discussion ......................................................................................................................................... 69
Study limitations ......................................................................................................................... 76
Conclusion ............................................................................................................................................ 77
References ......................................................................................................................................... 79
Section 4: Appendices ....................................................................................................................... 116
Appendix A; Ethics notification ..................................................................................................... 117
Appendix B: Search strategy ........................................................................................................... 118
Appendix C: Screening template .................................................................................................... 121
Appendix D: Interrater agreement .................................................................................................. 122
Appendix E: Data Items .................................................................................................................. 123
Appendix F: Data abstraction tables ............................................................................................... 124
Appendix G: Alternative descriptors .............................................................................................. 197
Appendix H: Surrogate measures ................................................................................................... 199
Refersences ......................................................................................................................................... 200

ix
List of figures
FIGURE 1. PRISMA-SCR (PREFERRED REPORTING ITEMS FOR SYSTEMATIC REVIEWS AND META-
ANALYSES EXTENSION FOR SCOPING REVIEWS) FLOW DIAGRAM OF THE SEARCH STRATEGY AND
STUDY SELECTION.15 ..................................................................................................................................................................................... 50
List of tables
TABLE 1. OVERVIEW OF INCLUDED STUDIES (N=333) ......................................................................... 51
TABLE 2. OVERVIEW OF THE INCLUSION OF DEFINITIONS, MEASURES, OR INDICATORS OF SPINAL
STIFFNESS AS PART OF THE STUDIES INCLUDED IN THE SCOPING REVIEW ............................................ 52
TABLE 3. BREAKDOWN OF STUDIES INCLUDED IN THE SCOPING REVIEW BY STUDY CATEGORY AND
THE INCLUSION OR OMISSION OF A DEFINITION OF STIFFNESS .................................................................. 53
TABLE 4. BREAKDOWN OF STUDIES INCLUDED IN THE SCOPING REVIEW BY STUDY CATEGORY AND
THE INCLUSION OR OMISSION OF OBJECTIVE OR SUBJECTIVE MEASURES OF STIFFNESS .................. 54
TABLE 5. OVERVIEW OF THE METHODS OF QUANTIFYING SPINAL STIFFNESS AS UTILISED BY STUDIES
INCLUDED IN THE BIOMECHANICAL THEME .................................................................................................... 55
TABLE 6. OVERVIEW OF THE METHODS OF QUANTIFYING SPINAL STIFFNESS AS UTILISED BY STUDIES
IN THE SURGICAL THEME ...................................................................................................................................... 58
TABLE 7. SUMMARY OF STIFFNESS INDICATORS REPORTED IN THE PATHOPHYSIOLOGICAL THEME ... 61
TABLE 8. KEY FEATURES OF QUALITATIVE DEFINITIONS REPORTED IN MANUAL SEGMENTAL
ASSESSMENT CATEGORY ....................................................................................................................................... 65
TABLE 9. OVERVIEW OF VARIOUS DESCRIPTORS USED TO DESCRIBE MANUAL SEGMENTAL
ASSESSMENT ............................................................................................................................................................. 65
TABLE 10. OVERVIEW OF HOW OBJECTIVE MEASURES WERE QUANTIFIED FOR MECHANICAL
STIFFNESS ASSESSMENT ........................................................................................................................................ 67
TABLE 11. KEY FEATURES OF QUANTITATIVE DEFINITIONS REPORTED IN MECHANICAL SEGMENTAL
ASSESSMENT CATEGORY ....................................................................................................................................... 68

1
Section 1: Literature review

2
Definition of pain
Pain is one of the most common reasons why patients consult a primary health care
professional (Tompkins et al., 2017). Therefore, the assessment of pain is an essential aspect
of clinical practice informing effective management options. The ability to effectively diagnose
and treat pain first requires an understanding of what constitutes pain. The International
Association for the Study of Pain (IASP), defines pain as “an unpleasant sensory and emotional
experience associated with actual or potential tissue damage, or described in terms of such
damage” (Merskey & Bogduk, 1994). This definition reflects the multidimensional nature of
pain by including both sensory and emotional features and avoids tying pain to the stimulus
(Merskey & Bogduk, 1994; Williams & Craig, 2016). Since the inception of the IASP
definition, there have been various criticisms of the definition in the literature. For example,
the use of certain terms such as ‘unpleasant’ has been argued to ‘trivialise’ severe chronic pain
(Aydede, 2019). Another example is the omission of cognitive and social dimensions of the
pain experience (Williams & Craig, 2016). Despite these criticisms, the IASP definition has
provided a common understanding and characterisation of the pain experience, that is both
relevant to clinicians and patient’s alike.
Spinal pain, and in particular low-back pain (LBP), are common musculoskeletal
problems that pose a significant social, psychologic, and economic burden (Rubin, 2007). It has
been estimated that approximately 15% to 20% of adults may be affected by LBP within a single
year, and approximately 50% to 80% of adults may experience one episode of LBP during their
lifetime (Rubin, 2007). LBP has been defined as “pain, muscular tension, or ‘stiffness’ that is
localized between the costal margins and the inferior gluteal folds, with or without radiating leg
pain” (Koes et al., 2006). It is apparent from the definition provided above, that the use of the
term ‘stiffness’ suggests that pain may co-exist with stiffness.
3
Further evidence towards this claim can be found in a contemporary theory that explains
the adaptation to pain, which was conceptualised by Hodges and Tucker (2011). The theory
for the ‘motor adaptation to pain’ hypothesises that the basis of adaptation to pain is to protect
the painful body part and to reduce pain (Hodges & Tucker, 2011). This is claimed to be, in
part, achieved through “changes in mechanical behaviour such as modified movement and
stiffness,” which is suggested to lead to protection from further pain or injury (Hodges &
Tucker, 2011). One limitation of the ‘motor adaptation to pain’ theory is that it emphasises the
role of ‘mechanical changes’ in augmenting ‘modified’ movement and ‘stiffness’. This is in
contrast to the growing body of literature suggesting that a disconnect may exist between the
mechanical (physiological) properties of joints and tissues, and subjective reports of stiffness
(Haigh et al., 2003; Helliwell et al., 1988; Karayannis et al., 2013; Stanton et al., 2017). For
example, Haigh et al. (2003) reported that patients with bilateral rheumatoid arthritis who have
had one limb amputated could still feel stiffness in the missing joint. This suggests that stiffness
may be neurally-driven, rather than being solely caused by ‘true’ physiological changes in the
joint itself.
Moreover, a recent study by Stanton et al. (2017) identified that pairing sound (e.g.
‘whooshing’ noise) with mobilisations applied to the back, modulated the participants’
perception of force. Interestingly, a ‘creaking’ sound heightened reports of back stiffness when
compared to mobilisations without noise. This emphasises the potential role of peripheral and
central neural mechanisms in protecting and guarding the spine from perceived harmful
movement (Moriarty et al., 2011; Wallwork et al., 2017). This is also in line with the current
understanding of how contextual variables may influence an individual’s pain experience
(Moseley & Arntz, 2007). According to Moseley and Butler (2015) pain represents a protective
mechanism rather than an indicator of tissue damage. It follows then, that stiffness,
4
just like pain is an unpredictable sensation that may cause an individual to protect and guard
the spine from further injury (Stanton et al., 2017).
Historical evolution of stiffness
Early work represented stiffness from a classical mechanics perspective in the field of
physics, where Robert Hooke, an English physicist, made a significant contribution to the
understanding of springing bodies. Hooke described that the force or power of an elastic body
“to restore itself to its natural position is always proportionate to the distance …” (Hooke, 1678,
p. 4). Subsequently, this came to be known as ‘Hooke’s law’ of elasticity and can be expressed
by; 𝐹𝑠 = −𝑘𝑥. Here, (𝐹𝑠) is the force applied to the spring, (𝑥) is the displacement of the spring,
and (𝑘) is the spring constant. This mathematical expression has been used to describe the
relationship between the force and displacement.
In engineering, stiffness is often used to characterise structural materials. Here, stiffness
has been defined as “a measure of a material’s resistance to elastic deformation” (Askeland &
Wright, 2015, p. 219). Because structural materials consist of an ‘area’ that must be accounted
for, the concepts of stress and strain were introduced. However, stress cannot be measured
directly, thus can only be inferred from the measure of strain and a constant known as Young’s
modulus (Askeland & Wright, 2015). The relationship between stress and strain has been
expressed by Heindl and Mong, (1936) as 𝑆𝑡𝑟𝑒𝑠𝑠 = 𝑙𝑜𝑎𝑑
. Here,
𝑆𝑡𝑟𝑎𝑖𝑛 𝑑𝑒𝑓𝑜𝑟𝑚𝑎𝑡𝑖𝑜𝑛 𝑝𝑒𝑟 𝑢𝑛𝑖𝑡 𝑜𝑓 𝑙𝑒𝑛𝑔𝑡ℎ 𝑋 𝑎𝑟𝑒𝑎
the deformation is a measure of the strain and relates to a change in the configuration of an
elastic structure, which is different from that of the original ‘unloaded’ configuration
(Baumgart & Cordey, 2000).
Although the concepts of stiffness related to structural material initially emerged in
physics and engineering, it has been extensively characterised in the field of biomechanics.
Here, stiffness has been used to describe the response of biological systems to mechanical

5
loading (Latash & Zatsiorsky, 2016). Stiffness appears to be synonymous with the relationship
between load and displacement and is expressed as 𝑆𝑡𝑖𝑓𝑓𝑛𝑒𝑠𝑠 = 𝐿𝑜𝑎𝑑
. Here, spinal 𝐷𝑖𝑠𝑝𝑙𝑎𝑐𝑒𝑚𝑒𝑛𝑡
stiffness can be calculated by dividing the load by the displacement.
Load is a vector quantity that is specified in terms of ‘magnitude’ and ‘direction,’ for
which Newton (N) is the unit of measurement. The load is described in terms of an applied
‘force’ or ‘moment’ (Ashton-Miller & Schultz, 1991). There are six possible orthogonal ‘load’
configurations related to the applied forces (i.e., anterior/posterior shear, left/right shear, and
axial compression/tension), moments, or torsions (i.e., flexion/extension, right/left lateral
bending, and clockwise/counter-clockwise axial torsion) (Ashton-Miller & Schultz, 1991;
Panjabi et al., 1986).
Displacement is a vector quantity specified in terms of the distance between the initial
position and the final position. The unit of measurement for displacement is millimetres (mm).
The displacement is described in terms of a ‘translation’ or ‘rotation’ (Ashton-Miller & Schultz,
1991; Panjabi et al., 1986). There are three possible points in the spinal motion segment, where
the displacement can be measured in terms of ‘translations’ (i.e., anterior, lateral, cranial) and
rotations (flexion, lateral bending and axial torsion) (Ashton-Miller & Schultz, 1991).
The term ‘stiffness’ and its related constructs are broadly recognised across the
biomechanical literature. Subsequently, the concept of stiffness has come into common usage
within the clinical context. In particular, it is evident that clinicians have adopted the term
‘stiffness’ to describe palpatory findings (e.g., the resistance of joints to movement) during the
physical examination (Latash & Zatsiorsky, 2016; Maher & Adams, 1995). In clinical practice,
stiffness is often used interchangeably with other alternative descriptors (i.e., synonyms and
antonyms) such as ‘resistance’ and ‘hypomobility’ during manual segmental assessment (see
Appendix G: Alternative descriptors). However, the adoption of biomechanical terminology to

6
describe findings during manual spinal assessment, appear to be ambiguous, inconsistent and
poorly defined, bringing their clinical utility into question (Lee et al., 2005; Maher, Latimer, et
al., 1998). This raises several issues. First, it is difficult for researchers to obtain valid and
reliable data when investigating manual spinal assessment. Second, the way stiffness is defined
has implications for how it is assessed in clinical practice. For example, it may make it difficult
to assess the impact of clinical interventions adequately. Third, it may impede clear
communication with the patient. For example, what clinicians describe as stiffness during
manual spinal assessment, may not reflect how stiffness is described or experienced by patients.
Finally, and most importantly, it may have therapeutic consequences and lead to ineffective
management of patients that present with stiffness in the clinic.
Considerations for primary care
Although a majority of patients present to primary care settings because of pain, some
patients may also consult their general practitioner because of pain and accompanying stiffness
(Almoallim et al., 2017). Spinal stiffness may be a symptom and potentially important clinical
indicator of disease (Amine et al., 2010; de Schepper et al., 2012). For example, morning
stiffness is characteristic of inflammatory conditions affecting the spine such as Ankylosing
Spondylitis and osteoarthritis (de Schepper et al., 2012; Sengupta & Stone, 2007), whereas a
stiff neck may be associated with Meningitis (Bachan et al., 2018). Although patients often
consult their general practitioner for spinal stiffness or pain, they may also seek the advice of
rehabilitative healthcare professionals, such as physiotherapists, osteopaths, and chiropractors
as they believe that clinical interventions may help alleviate stiffness or pain (Bishop et al.,
2013; Goodsell et al., 2000).
Considerations for rehabilitation
Stiffness is a common clinical feature associated with musculoskeletal conditions
affecting the spine, such as the neck, and lower back (Tomczyszyn et al., 2018; Yadla et al.,

7
2008). A key component of the consultation should be to precisely understand what patients
are referring to when describing stiffness in their presentation. Most importantly, clinicians
need to identify which aspects of the description and what features of the presentation are
relevant, when considering what stiffness means in the context of each individual patient.
Therefore, it is critical that clinical stiffness is clearly defined to assist clinical decision-making
processes. Failure to do so may lead to inappropriate interventions that do not alleviate
symptoms or improve functional impairment, negatively affecting patient outcomes.
Another important component of the consultation is the physical examination of the
spine. This may include both active and passive range of motion assessments (Maitland et al.,
2005; Wong & Kawchuk, 2017). Clinicians may use (static) manual assessment of the spine as
a part of the clinical examination to make a judgement about the patient’s stiffness (Maher et
al., 1999). This involves a clinician-applied force to a spinal landmark (i.e., spinous process or
articular pillar) at the spinal region(s) (e.g., lumbar or thoracic) of interest (Viner & Lee, 1995;
Wong & Kawchuk, 2017). The manual diagnosis of spinal stiffness may constitute the basis
for clinical decision making on where to apply manual therapy interventions (Koppenhaver et
al., 2014).
Manual therapy is a non-pharmacological management option for the treatment of
spinal related stiffness and is used by a wide range of rehabilitative healthcare professions
including, but not limited to physiotherapy, osteopathy, and chiropractic. Manual therapy has
been defined as “the use of hands in a curative and healing manner or a hands-on technique
with therapeutic intent” (Lederman, 2005). Manual therapy has also been defined as “the
application of therapist-applied manual forces in procedures intended to modify the quality
and range of motion of the target joint and soft tissue structures” (Abbott et al., 2009, p. 6).
Throughout this review, the term ‘clinician’ is used to describe any rehabilitation healthcare
professional who may or may not utilise manual therapy as a part of clinical interventions and
8
management of patients with spinal stiffness.
Manual therapy generally involves the application of passive movement/force to
joints (i.e., mobilisation and manipulation), muscles (i.e., soft tissue inhibition/sustained
stretching, muscle energy techniques), and neural tissues (i.e., neurodynamic interventions)
(Clar et al., 2014). Many different theories have been proposed to explain the physiological
and psychological mechanisms and clinical effects associated with manual therapy
interventions (Bialosky et al., 2011; Cook, 2011; Stamos-Papastamos et al., 2011). In a
recent study by Bialosky et al. (2018), the multifactorial mechanisms through which manual
therapy interventions exert their effectiveness are emphasised. This study highlighted the
importance of biomechanical and neurophysiological mechanisms that underpin the mode
of action of manual therapy techniques that are utilised in the clinical context.
There is a large volume of published studies describing the role of Spinal Manipulative
Therapy (SMT) and mobilisations in the management of patients with spinal stiffness
(Campbell & Snodgrass, 2010; Lascurain-Aguirrebena et al., 2016; Lee et al., 1993; Shum et
al., 2013; Stamos-Papastamos et al., 2011). It has been suggested that a relationship exists
between pain, reduced movement and abnormal spinal joint stiffness (Maher & Latimer, 1992).
Clinically, facet joints that are identified as stiff may be considered candidates for High-
Velocity Low Amplitude (HVLA) techniques (Fernández-de-las-Peñas et al., 2005). HVLA is
one type of SMT where a clinician-applied high-velocity low-magnitude force is exerted on a
spinal motion segment at the end of the joint range. The application of HVLA often creates
increased joint surface separation resulting in a fluid cavitation (audible ‘crack’) (Campbell &
Snodgrass, 2010). Therapeutic rationales that underpin the application of SMT relate to a
reduction in spinal stiffness, increase in segmental motion, and reduction in pain (hypoalgesia)
(Colloca & Keller, 2001; Fritz et al., 2011).
9
The importance of measuring stiffness
Objective and subjective measures comprise a diverse range of tools, instruments or
scales utilised in the assessment of clinical phenomena (variables) that are meaningful to
patients, assist clinical decision-making processes, and assist in the development of measures
for research purposes (Rothstein, 1989; Soobiah et al., 2019). To determine whether a measure
is objective, reliability may be assessed to see if a repeated measure provides consistent results
(Elasy & Gaddy, 1998). Reliability estimates may be used to indicate the degree of error
associated with a measure (Rothstein, 1989). To determine if an objective measure is useful for
making inferences about a specific variable, it is important to assess the extent to which an
instrument measures what it claims to measure; its validity (Elasy & Gaddy, 1998).
For this review, the term ‘objective’ will describe the data-driven (quantitative)
approaches used to quantify the biometric characteristics of spinal stiffness. The adjectives
objective and subjective have also been used to describe the quality of a measure rather than
the phenomena being measured (Rothstein, 1989). For example, stiffness is a subjective
phenomenon that could, in theory, be objectively measured if it has been demonstrated to be
reliable and valid. However, for this review, the term ‘subjective’ is used to indicate measures
based on an individual’s perception or experience of spinal stiffness.
Objective measures of spinal stiffness
Stiffness is a fundamental concept in biomechanics used to evaluate structural and
functional characteristics of the spine (Oxland, 2016). In general terms, stiffness is tested by
the application of a load and observing the displacement response (behaviour, relationships or
characteristics). Objective spinal stiffness measures may provide important biometrics relating
to stiffness of the spine and surrounding structures. Spinal stiffness has been extensively
characterised in the field of biomechanics. Biomechanical studies utilise mechanical
instruments to assess the in-vitro stiffness properties of cadaveric Functional Spinal Unit (FSU)
10
specimens. The motion segment or FSU is defined as two adjacent vertebrae, the intervertebral
disc, the facet joints, and the spinal ligaments (Oxland, 2016). The FSU has been defined as
“the smallest motion segment of the spine and exhibits biomechanical characteristics similar to
that of the entire spine” (Benzel, 2012, p. 45). The FSU exhibits 6 degrees of freedom; three
linear directions and three rotations (Panjabi et al., 1986). During biomechanical testing, a load
or force vector is applied, and the relative displacement between the vertebrae of the FSU is
measured. Various quantitative approaches can be used to generate load-displacement graphs
which represent visual interpretations of the load-displacement responses, where the Y-axis
represents the load application, and the X-axis represents the displacement response.
A wide range of mechanical instruments have been developed to assess spinal stiffness
in human subjects. Instrumented measurements were operationalised in an attempt to offer
better consistency and reliability of spinal measures of stiffness (Stanton & Kawchuk, 2009),
as opposed to manual measures of spinal stiffness which have been shown to be affected by
relatively poor reliability (Snodgrass et al., 2006; Stanton & Kawchuk, 2009; Wong &
Kawchuk, 2017). The two main types of instruments are mechanical and mechanically assisted
methods of indentation; which employ similar basic operations and mechanisms of assessment.
Objective measurements of stiffness are obtained by the application of an instrumented
posterior to anterior (P-A) load at the target motion segment resulting in a force and
displacement response data generated by various customised computer software programs. A
standard mechanical spinal stiffness- testing device generally consists of an indentor, which is
a cylindrical instrument that contacts the target spinous process. The indentor is driven by a
motor or a pulley system that controls the upward and downward movement of the indentor.
(Wong & Kawchuk, 2017). The load cell generally, consists of a strain gauge and transducer,
which converts compression and tension forces into electrical signals that can be measured and
standardised. Load cells quantify the indentation forces (N) that are pre-determined, and the
displacement sensor quantifies the indentor displacement (mm) (Wong & Kawchuk, 2017).

11
The test-retest reliability of mechanical spinal stiffness measurements in humans has been
reported to be high (Wong & Kawchuk, 2017), yet their invasiveness, size, complex operation,
and low ecological validity limits their clinical utility.
Subjective measures of spinal stiffness
Subjective measures of stiffness can be obtained from the clinician’s perspective during
the physical examination (e.g. palpation), often referred to as the objective examination with
reference to the acronym: SOAP – Subjective, Objective, Assessment, and Plan (Fruth, 2017).
For the purpose of this review, clinician-reported measures are referred to as ‘subjective
measure of spinal stiffness’. One of the most common forms of manual spinal assessment
reported in the literature is the P-A central pressure test. This involves the application of a P-A
oscillatory force to the spine of a prone patient to assess the perceived vertebral movement and
its resistance, (i.e., spinal stiffness) (Maitland et al., 2005). P-As are intended to localise and
assess the dysfunctional intervertebral movement, whereby the clinician forms a subjective
impression of the P-A movement response to load (Kiviniemi et al., 2001). The information
gained from the clinical examination may be used to determine the spinal levels that may benefit
from treatment and facilitate decisions of where to apply manual techniques.
An important consideration when assessing PA movement is the contribution of
stiffness from adjacent vertebral segments. The PA test is not a direct test of the stiffness of a
motion segment and has been interpreted as a passive test of the stiffness of the entire lumbar
spine in three-point bending (Lee & Evans, 1997). During the application of the PA force at

12
the target spinous process, (i) the pelvic reaction force can be assumed to be acting through the
anterior superior iliac spines, (ii) the vertebral segment above is subjected to an extension
moment, and posterior shear force, and (iii) the vertebral segment below is subjected to
extension moment and anterior shear force. Thus, the application of the PA force can be
considered as a three-point bending relationship between the target motion segment and
adjacent motion segments during PA segmental assessment (Lee & Evans, 1997).
The patient’s perspective may be obtained during the case history and by the use of
various self-report and Patient-Reported Outcome Measures (PROMS). The most common
self-reported outcome measure identified in the literature appears to be the adaption of pain
rating scales, such as the Visual Analogue Scale (VAS) and Numerical Rating Scale (NRS) for
the assessment of spinal stiffness intensity (severity) and duration. The VAS may be
represented as a 6, 11 or 101-point scale, which is generally anchored by a verbal description.
For example, The VAS has been used to obtain participants’ subjective symptoms of neck
stiffness on a 6-point scale (0–5), where 0 indicated that patients did not feel any neck stiffness
and 5 indicated that patients were acutely aware of neck stiffness (Akagi & Kusama, 2015).
The NRS has also been adapted by studies for the assessment of stiffness and required the
respondent to rate their stiffness on a scale accompanied by a verbal description. For example,
participants’ subjective measure of stiffness was established by asking participants to report
how they ‘felt’ ranging from “not stiff at all” to “most stiff imaginable’’, scored from 0 – 100
(Stanton et al., 2017).
In summary, self-report measures have been used to assess stiffness from the patient’s
perspective. The most common approach is the adaption of simple pain rating scales such as
the NRS and VAS, which allow for a self-assessment of stiffness intensity and duration.
However, these self-report measures may be argued to represent a unifocal understanding of
the patient’s experience of stiffness. There is evidence to suggest that the clinical concept of

13
spinal stiffness is multifactorial and is unlikely to be satisfactorily rated on a single scale
(Maher & Adams, 1995). A similar view is supported by Williamson and Hoggart, (2005) in
the context of pain rather than stiffness, but nonetheless points out the limitations of only
including unidimensional aspects of pain (e.g., intensity).
Patient-reported outcome measures (PROM) are tools or instruments that can be used
to measure the patients’ health outcomes. PROMs can be used to gather information about the
patients’ symptoms, function or overall wellbeing (Nelson et al., 2015). Disease-specific
PROMs are designed to identify specific symptoms, disease activity and assess their impact on
function (Weldring & Smith, 2013). For example, the Bath Ankylosing Spondylitis Disease
Activity Index (BASDAI) is a six-item self-administered questionnaire that includes a subset
of questions relating to symptoms of morning stiffness. Questions about the severity and
duration of stiffness are presented on a VAS accompanied by verbal descriptor “How would
you describe the overall level of […]” (Cardiel et al., 2003). Specific questions that relate to
stiffness are included in two items within the BASDAI which ask the patient about their
morning stiffness duration and severity (Sengupta & Stone, 2007).
Another PROM specific for assessing postoperative complications following lumbar
spinal fusion is the Lumbar Stiffness Disability Index (Hart, Gundle, et al., 2013). This tool
consists of 10 questions specifically designed to assess the impact of functional limitations
following surgery. This PROM adapted items from the Activities of Daily Living scale, which
is used to assess routine aspects of self-care tasks necessary for managing basic physical needs
such as getting out of bed, bathing and showering, personal hygiene and grooming, dressing,
and toilet hygiene (Hart, Pro, et al., 2013; Mlinac & Feng, 2016). One reason for including an
assessment of Activities of Daily Living, is because functional limitations and a loss of mobility,
independent of pain, can cause difficulties for patients to perform certain Activities of Daily
Living (Hart et al., 2014).

14
Conclusion
Primary healthcare professionals have an essential role to play in assessing and
managing patients presenting with spinal stiffness in the clinic. Despite this, it appears that the
term ‘stiffness’ is often used implicitly and without clear explication of its meaning (Latash &
Zatsiorsky, 2016; Maher, Latimer, et al., 1998). As a consequence, there may be considerable
confusion regarding the applicability of the term stiffness in the clinical context. Self-reported
subjective stiffness measures have often been used in conjunction with objective measures of
stiffness in clinical research. However, a growing body of literature suggests that subjective
measures may not correlate well with objective measures of stiffness (Haigh et al., 2003;
Karayannis et al., 2013; Stanton et al., 2017). This indicates a need for more clarity regarding
the use of definitions and what types of objective and subjective measures are being used in
research. Most importantly, an emphasis should be placed on how these definitions and
measures may inform clinical decision-making processes. At present, there appears to be no
clear definition, nor is there a “gold standard” measure of spinal stiffness that is representative
of the clinical context. Therefore, more research in this area is needed.

15
Section 2: Methodology
16
Philosophical perspective
The two main philosophical approaches employed in scientific research are
constructivism and positivism. Positivism emphasises objectivity, experimentation, and
generalisability, in contrast to constructivism, which emphasises constructed realities,
interaction with participants, and rich description (Mertens, 2019). Contained within these two
paradigms are theoretical and philosophical assumptions about the way knowledge is
constructed and understood. The constructivist paradigm proposes that reality is socially
constructed from subjective accounts and perceptions that explain how the world is experienced
by individuals (Mertens, 2019). By contrast, positivism is grounded in a rationalistic, empiricist
philosophy, which proposes that absolute truth can be uncovered and known with certainty by
scientists (Gordon, 2016; Mertens, 2019).
The underlying philosophy guiding this review is positivism; which calls for a scientific
approach to research based on verifiable data that can be observed and accounted for by
empirical evidence. Positivism is grounded in empiricism, and from an epistemological
perspective is one of several sources of knowledge that claims all knowledge is derived from
the senses (Gordon, 2016). Empirical research is determined through observation or
experimentation, whereby conclusions are logically drawn from empirical data rather than from
theoretical construction or belief (Allen, 2017; Gordon, 2016). The positivist paradigm aligns
with the empirical approach to research and is a suitable way to frame the theoretical-
methodological framework for the design of the present project.
The scoping review methodology is particularly appropriate to meet the purpose and
address the objective(s) of this study. In particular, this review seeks to understand
generalisable knowledge about spinal stiffness based on the objective data identified in
empirical literature, providing a comprehensive account of what forms the basis of clinical
knowledge regarding spinal stiffness. This is a critical first step in understanding what is

17
actually known, what is generally accepted, and the current state of thinking around defining
and measuring spinal stiffness in the literature. The following section will establish how the
chosen methodology – scoping review, is situated within the evidence hierarchy.
One major challenge that researchers are presented with when undertaking a review of
the literature is the difficulty in adopting a suitable study design and framework in which to
structure their review (Noble & Smith, 2018). An extensive range of different types of literature
reviews can be used to summarise the current state of the existing literature. Scoping reviews,
in particular, are a useful methodology for mapping the literature and clarifying key concepts
and definitions, as well as identifying outcome measures used in the broader context. For this
scoping review, providing clarity regarding how the term stiffness is defined and measured is
an important gap in the literature. This can be demonstrated by the fact that a search for a
definition of pain reveals important guiding documents, including consensus statements and
standardised definitions. However, a search for a definition of stiffness reveals neither a
consensus statement nor a standardised definition. Therefore, the question of ‘what’ needs to
be asked, before the questions of ‘how’ and ‘why’ can be addressed. To illustrate this,
Randomised Controlled Trials are generally conducted to evaluate the cause-effect relationship
that exists between a specified treatment and outcome (Spieth et al., 2016). However, in cases
whereby, the outcome variable (e.g., stiffness) has not having been clearly defined, it would be
difficult to meaningfully investigate the cause-effect relationship within this specific
population group.
Conducting a systematic review of the literature around a topic with no clear definition
is similarly less feasible. This is because systematic reviews require a highly focused clinical
question (Noble & Smith, 2018). Systematic reviews are often used to evaluate interventions
and combine the results of several empirical studies to give a more reliable estimation of an
intervention’s effectiveness (Centre for Reviews and Dissemination., 2009). The problem with

18
undertaking a systematic review at present is the lack of a clear definition of stiffness. Therefore,
leading to difficulties in combining results and interpreting findings in a meaningful way.
Comparison of key characteristics of scoping reviews and systematic reviews
According to Mays et al (2001, p. 194) “scoping reviews aim to map rapidly the key
concepts underpinning a research area and the main sources and types of evidence available”.
Arksey and O’Malley (2005) expanded on this definition, describing four reasons a scoping
review may be undertaken: (1) to examine the extent, range, and nature of research evidence;
(2) to determine the value of undertaking a full systematic review; (3) to summarise and
disseminate research findings, and (4) to identify research gaps in the existing literature.
Colquhoun et al. (2014, p. 1292) has recommended the following definition: “a scoping
review is a form of knowledge synthesis that addresses an exploratory research question aimed
at mapping key concepts, types of evidence, and gaps in research related to a defined area or
field by systematically searching, selecting, and synthesising existing knowledge”. This builds
on Mays et al., (2001) definition and the descriptions provided by Arksey and O’Malley (2005)
providing a more succinct definition that relates to the methodology, but also describes key
differences that make scoping reviews distinct from other forms of knowledge syntheses
(Colquhoun et al., 2014). Scoping reviews follow similar processes as systematic reviews, both
employing transparent and rigorous methods to identify and analyse the literature relating to a
research question (DiCenso et al., 2010).
Systematic and scoping reviews both aim to provide a summary of the existing literature
on a specific topic and share some methodological features such as they employ a systematic
approach to reviewing the literature. However, the nature and purpose of the research question
is distinctively different. Crucially, systematic reviews aim to provide an in-depth summary
and synthesis of high-quality evidence concerning a specific topic against a predefined research

19
question and selection criteria (Munn et al., 2018). By contrast, scoping reviews allow for more
general questions and exploration, aiming instead for breadth rather than depth of a topic
(Peterson et al., 2017; Pham et al., 2014). Scoping reviews allow for more flexibility and
encourage the researcher to be more reactive to what presents itself in the literature.
Additionally, the scoping review method involves the identification of all relevant literature by
enabling ongoing modifications to search terms or methods throughout the review process
(Arksey & O’Malley., 2005).
Scoping reviews may be used for ‘reconnaissance’ to clarify key concepts or definitions,
identify key characteristics or factors relating to a concept, identify trends or gaps, and inform
future research (Levac et al., 2010; Munn et al., 2018; Peters et al., 2015). Scoping reviews may
be used to address broad topics which include a variety of study designs and methodologies and
to explore a field of research that has not been comprehensively reviewed (Pham et al., 2014).
Arksey and O’Malley (2005) have proposed a methodological framework for the
conduct of scoping reviews. This has been further refined by the Joanna Briggs Institute (2015),
with the addition of more recent innovations and enhancements to the scoping review
methodology. Although no definitive method of scoping reviews exists, there have been
recommendations by several authors to develop a standard methodology for scoping reviews
(Colquhoun et al., 2014; Dwan et al., 2008; Tricco et al., 2016). In response to this, Tricco et
al (2018) developed a reporting checklist to assist researchers in conducting scoping reviews.
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for
Scoping Reviews (PRISMA-ScR) was developed by an expert panel of authors to guide the
reporting of scoping reviews. This checklist provides guidelines using explicit methods to
guide the reporting of scoping reviews.
20
Specifically, the original PRISMA statement was adapted with the following revisions:
five items from the original PRISMA were removed because they were deemed not relevant for
scoping reviews. For example, risk of bias across studies is not included as the scoping review
method is not intended to be used to critically appraise (or appraise the risk of bias of) a
cumulative body of evidence. Two items were deemed optional, (i.e., critical appraisal of
individual sources of evidence and critical appraisal within sources of evidence) and the
wording was modified for all items (Tricco et al., 2018). This reporting guideline is consistent
with the Joanna Briggs Institute (2015) Guidance for Scoping Reviews, which highlights the
importance of methodological rigour in the conduct of scoping reviews. Despite advances in the
scoping review methodology and the addition of frameworks, reporting guidelines and
checklists, several limitations still exist.
The lack of methodological quality appraisal of the evidence typical of scoping reviews
has been reported as a potential limitation (Peters et al., 2015). However, it has been suggested
by Arksey and O’Malley (2005) that critical appraisal is not an essential aspect of scoping
reviews. Additionally, current reporting guidelines include critical appraisal within sources of
evidence as an ‘optional’ component for the conduct of scoping reviews (Tricco et al., 2018).
This scoping review did not include a quality appraisal as it was intended to provide an
overview of the existing evidence regardless of the methodological quality or risk of bias
(Peters et al., 2015).
Methodological approach
Arksey and O’Malley (2005) have described a five-stage descriptive, analytical
framework which was followed in this scoping review. Specifically, framework stages one
(identifying the research question) through to framework stage five (charting the data) with the
option to include a sixth consultation stage. The five stages, as proposed by Arksey and
O’Malley, are as follows: (1) Identifying the research question, (2) Identifying the relevant
21
studies, (3) Study selection (4) Charting the data Stage, (5) Collating, summarising and
reporting the results, and (6) (optional): Consultation. The six stages, as recommended by
Arksey and O’Malley, are explained below in the context of this thesis.
Framework Stage 1: Identifying the research question
The first stage involves the identification of a research question. Arksey and O’Malley
(2005) acknowledge the need to maintain a broad scope, as the primary focus is to summarise
the breadth of evidence available on the selected topic (Levac et al., 2010). The present scoping
review broadly examined the extent, nature and range of ‘definitions and measures of objective
and subjective spinal stiffness reported in the literature’. This question facilitated the mapping
of ‘definitions’ and ‘measures’ of ‘subjective’ and ‘objective’ spinal stiffness in the literature.
Framework Stage 2: Identifying the relevant studies
The second stage involved the identification of all relevant studies that addressed the
research question. During this stage, decisions were made regarding the most appropriate
databases to use and consideration of the search terms used for the development of the search
strategy. Due to the need to execute a broad search strategy, consideration was given to the
limitations and resource constraints, such as, availability of supervisory team, resources
available to the researcher and the time frame available to complete this research. In line with
recommendations by Levac et al (2010), the supervisory research team of the present project
consisted of members with topic-specific, clinical and methodological knowledge.
Grey literature
It is often appropriate to include both published and unpublished grey literature in a
scoping review (Joanna Briggs Institute, 2015). However, this is irrelevant for the present
review due to only including peer-reviewed empirical literature. Furthermore, the lack of peer-
review typical of grey literature may have adversely affected the uptake and relevance of the
findings presented in this review (Levac et al., 2010).
22
Clarification of terminology
Arksey and O’Malley (2005) indicate the importance of defining terminology from the
outset of the scoping review due to the possibility that the search strategy may return a large
number of irrelevant studies that do not address the guiding research question. Despite this
recommendation, the current review did not include an operational definition of stiffness as the
review sought to identify what definitions are available. Additionally, it was determined that
the spine would not be operationally defined at the outset of the study. This was due to wanting
to begin with a broad search and encourage the researcher to be reactive to what presents itself
in the literature. As the researcher became more familiar with the available data, it became
apparent that it would be beneficial to define the spine in order to avoid including irrelevant
literature that did not contribute to the representativeness of the overall spine in the clinical
context.
After screening through the biomechanical literature, it was evident that most studies
agreed the FSU constituted the smallest motion segment unit of spine that exhibits similar
biomechanical characteristics to that of the overall spine (Panjabi et al., 1986). Therefore, an
informed decision was made to operationally define the spine in order to limit search results to
studies that described spinal stiffness in the context of the characteristics of the overall spine.
The spine was operationally defined as the vertebrae of the cervical, thoracic, lumbar, sacral
and the coccygeal regions along with the intervertebral discs, ligaments, rib cage, and spinal
musculature (Oxland, 2016). For the purpose of this review, The FSU was operationally
defined as “two adjacent vertebrae, the intervertebral disc, the facet joints, and the spinal
ligaments” (Oxland, 2016).

23
Framework Stage 3: Study selection
The third stage involved the selection of studies relevant to the research question.
According to Arksey and O’Malley (2005) arriving at search criteria is considered to be an
iterative process which enables a comprehensive coverage of the literature. For this review,
priori eligibility criteria were established before the commencement of the study selection
process. During the study selection, modifications were made to the eligibility criteria and are
explained in the methods section. A potential limitation during the screening of studies was the
inherent subjectivity associated with interpreting the eligibility criteria. A strategy employed
to minimise inconsistencies in the selection of studies in this review was the use of two
independent reviewers. Additionally, pilot-testing was conducted by two reviewers, and the
selection consistency and agreement score were calculated to assess the inter-rater reliability
between the two reviewers (see Appendix D: Interrater agreement).
Framework Stage 4: Charting the data
The abstraction of data for a scoping review is often referred to as ‘charting the results’.
Generally, the data charting includes a mixture of general information about the study and
specific information relating to, for instance, citation details, key definitions, and outcome
measures employed (Arksey & O’Malley, 2005). For this review, key data items were extracted
and documented according to their relevance to the guiding question and objectives of the
review (Levac et al., 2010; Peters et al., 2015) (see Appendix E: Data Items). A data table was
developed to chart the relevant data and was summarised according to the themes that were
identified (see Appendix F: Data abstraction tables). This enabled the identification of key
definitions and subjective and objective measures of spinal stiffness to be identified in the
literature. The data was abstracted based on the relevant study characteristics that related to
definitions and measures of spinal stiffness.
24
Framework Stage 5: Collating, summarising and reporting the results
Due to the potentially large volume, breadth, clinical and methodological diversity of
studies that may be included in a scoping review, Arksey and O’Malley (2005) recommend a
variety of numerical and narrative methods that can be employed during this stage. For this
review, the studies identified were analysed according to themes utilising an informative
summary approach (see Appendix F: Data abstraction tables). This aligned with the purpose
and objectives of this present review and allowed the reporting of informational contents of
definitions and measures of subjective and objective spinal stiffness for the data items included.
This method was further refined towards the end of this review when there was better awareness
of and familiarity with the contents of included studies, in line with recommendations from the
Joanna Briggs Institute (2015).
Framework Stage 6: (optional) Consultation
According to Arksey and O’Malley (2005) stage six is considered an optional
component of scoping reviews. In contrast, the Joanna Briggs Institute (2015) recommends
adopting consultation as a required component of the scoping review methodology. However,
there appears to be agreement that there should be a clearly established purpose for consultation
(Arksey and O’Malley, 2005; Levac et al., 2010).
This preceding section described the methodological approach, outlining the basic
tenets of the positivist perspective, describing how this scoping review is situated within the
evidence hierarchy, and providing a comprehensive outline of the framework proposed by
Arksey and O’Malley (2005) as it applies to the scoping review presented as part of this Masters
thesis.
25
References
Abbott, J. H., Clare, M. C., McKenzie, J. E., David, G. D., Theis, J. C., & Campbell, A. J.
(2009). Exercise therapy, manual therapy, or both, for osteoarthritis of the hip or knee: A
factorial randomised controlled trial protocol. BioMed Central, 10, 1–12.
https://doi.org/10.1186/1745-6215-10-11
Akagi, R., & Kusama, S. (2015). Comparison Between Neck and Shoulder Stiffness
Determined by Shear Wave Ultrasound Elastography and a Muscle Hardness Meter.
Ultrasound in Medicine and Biology, 41(8), 2266–2271.
https://doi.org/10.1016/j.ultrasmedbio.2015.04.001
Allen, M. (2017). The SAGE Encyclopedia of Communication Research Methods. SAGE
Publications, Inc. https://doi.org/10.4135/9781483381411
Almoallim, H., Janoudi, N., Attar, S. M., Garout, M., Algohary, S., Siddiqui, M. I., Alosaimi,
H., Ibrahim, A., Badokhon, A., & Algasemi, Z. (2017). Determining early referral
criteria for patients with suspected inflammatory arthritis presenting to primary care
physicians: A cross-sectional study. Open Access Rheumatology: Research and Reviews,
9, 81–90. https://doi.org/10.2147/OARRR.S134780
Amine, B., Abouqal, R., Ibn Yacoub, Y., Hajjaj-Hassouni, N., Ali Ou Alla, S., Rostom, S.,
Benbouaaza, K., & Bahiri, R. (2010). Psychometric evaluation of the Moroccan version
of the Bath Ankylosing Spondylitis Functional Index (BASFI) and Bath Ankylosing
Spondylitis Disease Activity Index (BASDAI) for use in patients with ankylosing
spondylitis. Clinical Rheumatology, 29(7), 781–788. https://doi.org/10.1007/s10067-
010-1431-5
Arksey, H., & O’Malley, L. (2005). Scoping studies: Towards a methodological framework.
International Journal of Social Research Methodology: Theory and Practice, 8(1), 19–

26
32. https://doi.org/10.1080/1364557032000119616
Ashton-Miller, J. A., & Schultz, A. B. (1991). Spine instability and segmental hypermobility
biomechanics: A call for the definition and standard use of terms. Seminars in Spine
Surgery, 3(2), 136–148.
Askeland, D. R., & Wright, W. J. (2015). The Science and Engineering of Materials (7th ed.).
Cengage Learning.
Aydede, M. (2019). Does the IASP definition of pain need updating? PAIN Reports, 4(5), 1–
7. https://doi.org/10.1097/pr9.0000000000000777
Bachan, E. G., Aikins, M., Kenu, E., Kye-Duodu, G., Nyarko, K. M., Issah, K., Ameme, D.
K., Kuffour, O. A., Opare, J., Asiedu, E., Afari, E., Aseidu-Bekoe, F., Kuma, G. K.,
Letsa, T., & Noora, C. L. (2018). Pneumococcal meningitis outbreak and associated
factors in six districts of Brong Ahafo region, Ghana, 2016. BMC Public Health, 18(1),
1–11. https://doi.org/10.1186/s12889-018-5529-z
Baumgart, F., & Cordey, J. (2000). Stiffness - An unknown world of mechanical science?
Injury, 32, 14–23. https://doi.org/10.1016/S0020-1383(01)00057-2
Benzel, E. C. (2012). The Cervical Spine (5th ed.). Lippincott Williams & Wilkins.
Bialosky, J. E., Beneciuk, J. M., Bishop, M. D., Coronado, R. A., Penza, C. W., Simon, C. B.,
& George, S. Z. (2018). Unraveling the Mechanisms of Manual Therapy: Modeling an
Approach. Journal of Orthopaedic & Sports Physical Therapy, 48(1), 8–18.
https://doi.org/10.2519/jospt.2018.7476
Bialosky, J. E., Bishop, M. D., George, S. Z., & Robinson, M. E. (2011). Placebo response to
manual therapy: Something out of nothing? Journal of Manual and Manipulative
Therapy, 19(1), 11–19. https://doi.org/10.1179/2042618610Y.0000000001

27
Bishop, M. D., Mintken, P., Bialosky, J. E., & Cleland, J. A. (2013). Patient expectations of
benefit from interventions for neck pain and resulting influence on outcomes. Journal of
Orthopaedic and Sports Physical Therapy, 43(7), 457–465.
https://doi.org/10.2519/jospt.2013.4492
Campbell, B. D., & Snodgrass, S. J. (2010). The effects of thoracic manipulation on
posteroanterior spinal stiffness. Journal of Orthopaedic and Sports Physical Therapy,
40(11), 685–693. https://doi.org/10.2519/jospt.2010.3271
Cardiel, M. H., Londoño, J. D., E, G., Pacheco-Tena, C., Vázquez-Mellado, J., & Burgos-
Vargas, R. (2003). Translation, cross-cultural adaptation, and validation of the Bath
Ankylosing Spondylitis Functional Index (BASFI), the Bath Ankylosing Spondylitis
Disease Activity Index (BASDAI) and the Dougados Functonal Index (DFI) in a
Spanish speaking population wit. Clinical and Experimental Rheumatology, 21(4), 451–
458.
http://www.embase.com/search/results?subaction=viewrecord&from=export&id=L3695
0313%0Ahttp://wx7cf7zp2h.search.serialssolutions.com?sid=EMBASE&issn=0392856
X&id=doi:&atitle=Translation%2C+cross-
cultural+adaptation%2C+and+validation+of+the+Bath+Ankylosing+Sp
Centre for Reviews and Dissemination. (2009). Guidance for undertaking reviews in
heathcare. (3rd ed.). CRD, University of York.
Clar, C., Tsertsvadze, A., Court, R., Hundt, G. L., Clarke, A., & Sutcliffe, P. (2014). Clinical
effectiveness of manual therapy for the management of musculoskeletal and non-
musculoskeletal conditions: Systematic review and update of UK evidence report.
Chiropractic and Manual Therapies, 22(1), 1–34. https://doi.org/10.1186/2045-709X-
22-12

28
Colloca, C. J., & Keller, T. S. (2001). Stiffness and neuromuscular reflex response of the
human spine to posteroanterior manipulative thrusts in patients with low back pain.
Journal of Manipulative and Physiological Therapeutics, 24(8), 489–500.
https://doi.org/10.1067/mmt.2001.118209
Colquhoun, H. L., Levac, D., O’Brien, K. K., Straus, S., Tricco, A. C., Perrier, L., Kastner,
M., & Moher, D. (2014). Scoping reviews: Time for clarity in definition, methods, and
reporting. In Journal of Clinical Epidemiology (Vol. 67, Issue 12, pp. 1291–1294).
https://doi.org/10.1016/j.jclinepi.2014.03.013
Cook, C. (2011). Immediate effects from manual therapy: Much ado about nothing? Journal
of Manual and Manipulative Therapy, 19(1), 3–4.
https://doi.org/10.1179/106698110X12804993427009
de Schepper, E. I. T., Luijsterburg, P. A. J., Koes, B. W., van Meurs, J. B. J., Scheele, J.,
Hofman, A., & Bierma-Zeinstra, S. M. A. (2012). Association between spinal morning
stiffness and lumbar disc degeneration: the Rotterdam Study. Osteoarthritis and
Cartilage, 20(9), 982–987. https://doi.org/10.1016/j.joca.2012.05.011
DiCenso, A., Martin-Misener, R., Bryant-Lukosius, D., Bourgeault, I., Kilpatrick, K.,
Donald, F., Kaasalainen, S., Harbman, P., Carter, N., Kioke, S., Abelson, J., McKinlay,
R. J., Pasic, D., Wasyluk, B., Vohra, J., & Charbonneau-Smith, R. (2010). Advanced
practice nursing in Canada: overview of a decision support synthesis. Nursing
Leadership (Toronto, Ont.), 23 Spec No, 15–34.
https://doi.org/10.12927/cjnl.2010.22267
Dwan, K., Altman, D. G., Arnaiz, J. A., Bloom, J., Chan, A., Cronin, E., Decullier, E.,
Easterbrook, P. J., Elm, E. Von, Gamble, C., Ghersi, D., John, P. A., Simes, J., &
Williamson, P. (2008). Systematic Review of the Empirical Evidence of Study

29
Publication Bias and Outcome Reporting Bias. PLoS ONE, 3(8).
https://doi.org/10.1371/journal.pone.0003081
Elasy, T. A., & Gaddy, G. (1998). Measuring subjective outcomes: Rethinking reliability and
validity. Journal of General Internal Medicine, 13(11), 757–761.
https://doi.org/10.1046/j.1525-1497.1998.00228.x
Fernández-de-las-Peñas, C., Downey, C., & Miangolarra-Page, J. C. (2005). Validity of the
lateral gliding test as tool for the diagnosis of intervertebral joint dysfunction in the
lower cervical spine. Journal of Manipulative and Physiological Therapeutics, 28(8),
610–616. https://doi.org/10.1016/j.jmpt.2005.08.014
Fritz, J. M., Koppenhaver, Shane Kawchuk, Gregory N. N.L.Teyhen, D. S., Hebert, J. J., &
Childs, J. D. (2011). Preliminary Investigation of the Mechanisms Underlying the
Effects of Manipulation. Spine, 36(21), 1772–1781.
https://doi.org/10.1097/brs.0b013e318216337d
Fruth, S. J. (2017). Fundamentals of the Physical Therapy Examination: Patient Interview
and Tests & Measures (2nd ed.). Jones & Bartlett Learning.
Goodsell, M., Lee, M., & Latimer, J. (2000). Short-term effects of lumbar posteroanterior
mobilization in individuals with low-back pain. Journal of Manipulative and
Physiological Therapeutics, 23(5), 332–342.
Gordon, M. (2016). Are we talking the same paradigm ? Considering methodological choices
in health education systematic review. Medical Teacher, 38(7), 746–750.
Haigh, R. C., McCabe, C. S., Halligan, P. W., & Blake, D. R. (2003). Joint stiffness in a
phantom limb: evidence of central nervous system involvement in rheumatoid arthritis.
Rheumatology (Oxford, England), 42(October 2002), 888–892.

30
https://doi.org/10.1093/rheumatology/keg243
Hart, R. A., Gundle, K. R., Pro, S. L., & Marshall, L. M. (2013). Lumbar Stiffness Disability
Index: Pilot testing of consistency, reliability, and validity. Spine Journal, 13(2), 157–
161. https://doi.org/10.1016/j.spinee.2012.12.001
Hart, R. A., Marshall, L. M., Hiratzka, S. L., Kane, M. S., Volpi, J., & Hiratzka, J. R. (2014).
Functional limitations due to stiffness as a collateral impact of instrumented arthrodesis
of the lumbar spine. Spine, 39(24), E1468–E1474.
https://doi.org/10.1097/BRS.0000000000000595
Hart, R. A., Pro, S. L., Gundle, K. R., & Marshall, L. M. (2013). Lumbar stiffness as a
collateral outcome of spinal arthrodesis: A preliminary clinical study. Spine Journal,
13(2), 150–156. https://doi.org/10.1016/j.spinee.2012.10.014
Heindl, R. A., & Mong, L. E. (1936). Young’s modulus of elasticity, strength, and
extensibility of refractories in tension. Journal of Research of the National Bureau of
Standards, 17(3), 464–481. https://doi.org/10.6028/jres.017.021
Helliwell, P. S., Howe, A., & Wright, V. (1988). Lack of objective evidence of stiffness in
rheumatoid arthritis. Annals of the Rheumatic Diseases, 47(9), 754–758.
https://doi.org/10.1136/ard.47.9.754
Hodges, P. W., & Tucker, K. (2011). Moving differently in pain: A new theory to explain the
adaptation to pain. Pain, 152(SUPPL.3), S90–S98.
https://doi.org/10.1016/j.pain.2010.10.020
Hooke, R. (1678). De Potentia Restitutiva, or of Spring. Explaining the Power of Springing
Bodies. Printed for John Martyn Printer to the Royal Society, London.
Joanna Briggs Institute. (2015). The Joanna Briggs Institute Reviewers’ Manual 2015:
31
Methodology for JBI scoping reviews. Joanne Briggs Institute, 1–24.
https://doi.org/10.1017/CBO9781107415324.004
Karayannis, N. V., Smeets, R. J. E. M., van den Hoorn, W., & Hodges, P. W. (2013). Fear of
Movement Is Related to Trunk Stiffness in Low Back Pain. PLoS ONE, 8(6).
https://doi.org/10.1371/journal.pone.0067779
Kiviniemi, K., Allison, G., Lanigan, H., Edmonston, S., Walcher, S., & Simonsen, A. V.
(2001). Influence of standardized mobilization on the posteroanterior stiffness of the
lumbar spine in asymptomatic subjects. Physiotherapy Research International, 6(3),
145–156. https://doi.org/10.1002/pri.223
Koes, B. W., Tulder, M. W., & Thomas, S. (2006). Diagnosis and treatment of low back pain.
BMJ, 332, 1430–1433. https://doi.org/10.1136/bmj.332.7555.1430
Koppenhaver, S. L., Hebert, J. J., Kawchuk, G. N., Childs, J. D., Teyhen, D. S., Croy, T., &
Fritz, J. M. (2014). Criterion validity of manual assessment of spinal stiffness. Manual
Therapy, 19(6), 589–594. https://doi.org/10.1016/j.math.2014.06.001
Lascurain-Aguirrebena, I., Newham, D., & Critchley, D. J. (2016). Mechanism of action of
spinal mobilizations a systematic review. Spine, 41(2), 159–172.
https://doi.org/10.1097/BRS.0000000000001151
Latash, M. L., & Zatsiorsky, V. M. (2016). Stiffness and Stiffness-like Measures. In
Biomechanics and Motor Control (pp. 25–47). https://doi.org/10.1016/B978-0-12-
800384-8.00002-8
Lederman, E. (2005). The Science and Practice of Manual Therapy (2nd ed.).
Lee, M., Latimer, J., & Maher, C. G. (1993). Manipulation: investigation of a proposed
mechanism. Clinical Biomechanics, 8(6), 302–306. https://doi.org/10.1016/0268-

32
0033(93)90004-2
Lee, R., & Evans, J. (1997). An in vivo study of the intervertebral movements produced by
posteroanterior mobilization. Clinical Biomechanics, 12(6), 400–408.
https://doi.org/10.1016/S0268-0033(97)00019-3
Lee, R., Tsung, B., Evans, J., & Tong, P. (2005). Analysis of the Bending Behavior of the
Lumbar Spine During Posteroanterior Mobilization. Journal of Mechanics in Medicine
and Biology, 05(01), 55–61. https://doi.org/10.1142/s0219519405001266
Levac, D., Colquhoun, H., & O’Brien, K. K. (2010). Scoping studies: Advancing the
methodology. Implementation Science, 5(1), 1–9. https://doi.org/10.1186/1748-5908-5-
69
Maher, C. G., & Adams, R. D. (1995). Is the clinical concept of spinal stiffness
multidimensional? Physical Therapy, 75(10), 854–860; discussion 861-4.
http://www.ncbi.nlm.nih.gov/pubmed/7568385
Maher, C. G., & Latimer, J. (1992). Pain or resistance - the manual therapists’ dilemma.
Australian Journal of Physiotherapy, 38(4), 257–260. https://doi.org/10.1016/S0004-
9514(14)60568-7
Maher, C. G., Latimer, J., & Adams, R. D. (1998). An investigation of the reliability and
validity of posteroanterior spinal stiffness judgments made using a reference-based
protocol. Physical Therapy, 78(8), 829–837. https://doi.org/10.1093/ptj/78.8.829
Maher, C. G., Latimer, J., & Mathew, H. J. (1999). Plinth padding confounds measures of
posteroanterior spinal stiffness. Manual Therapy, 4(3), 145–150.
https://doi.org/10.1054/math.1999.0197
Maitland, G., Hengeveld, E., Banks, K., & English, K. (2005). Maitland’s Vertebral

33
Manipulation. (Butterworth - Heinemann (ed.); 6th ed.).
Mays, N., Roberts, E., & Popay, J. (2001). Synthesising research evidence. In Studying the
organisation and delivery of health services: Research methods, 220.
Merskey, H., & Bogduk, N. (1994). Classification of chronic pain : descriptions of chronic
pain syndromes and definitions of pain terms / prepared by the International
Association for the Study of Pain, Task Force on Taxonomy (2nd ed.). ISAP press.
https://doi.org/10.1097/00002508-199506000-00024
Mertens, D. M. (2019). Research and evaluation in education and psychology: integrating
diversity with quantitative, qualitative, and mixed methods (5th ed.). SAGE
Publications, Inc.
Mlinac, M. E., & Feng, M. C. (2016). Assessment of Activities of Daily Living , Self-Care ,
and Independence. 31(July), 506–516. https://doi.org/10.1093/arclin/acw049
Moriarty, O., McGuire, B. E., & Finn, D. P. (2011). The effect of pain on cognitive function:
A review of clinical and preclinical research. Progress in Neurobiology, 93(3), 385–404.
https://doi.org/10.1016/j.pneurobio.2011.01.002
Moseley, G. L., & Butler, D. S. (2015). Fifteen Years of Explaining Pain: The Past, Present,
and Future. The Journal of Pain, 16(9), 807–813.
https://doi.org/10.1016/j.jpain.2015.05.005
Moseley, L. G., & Arntz, A. (2007). The context of a noxious stimulus affects the pain it
evokes. Pain, 133(1–3), 64–71. https://doi.org/10.1016/j.pain.2007.03.002
Munn, Z., Peters, M. D. J., Stern, C., Tufanaru, C., McArthur, A., & Aromataris, E. (2018).
Systematic review or scoping review? Guidance for authors when choosing between a
systematic or scoping review approach. BMC Medical Research Methodology, 18(1), 1–
34
7. https://doi.org/10.1186/s12874-018-0611-x
Nelson, E. C., Eftimovska, E., Lind, C., Hager, A., Wasson, J. H., & Lindblad, S. (2015).
Patient reported outcome measures in practice. BMJ (Online), 350(February), 1–3.
https://doi.org/10.1136/bmj.g7818
Noble, H., & Smith, J. (2018). Reviewing the literature: Choosing a review design. Evidence-
Based Nursing, 21(2), 39–41. https://doi.org/10.1136/eb-2018-102895
Oxland, T. R. (2016). Fundamental biomechanics of the spine-What we have learned in the
past 25 years and future directions. In Journal of Biomechanics.
https://doi.org/10.1016/j.jbiomech.2015.10.035
Panjabi, M. M., Summers, D. J., Pelker, R. R., Videman, T., Friedlaender, G. E., &
Southwick, W. O. (1986). Three‐dimensional load‐displacement curves Due to Forces
on the Cervical Spine. Journal of Orthopaedic Research, 4(2), 152–161.
https://doi.org/10.1002/jor.1100040203
Peters, M. D. J., Godfrey, C. M., Khalil, H., McInerney, P., Parker, D., & Soares, C. B.
(2015). Guidance for conducting systematic scoping reviews. International Journal of
Evidence-Based Healthcare, 13(3), 141–146.
https://doi.org/10.1097/XEB.0000000000000050
Peterson, J., Pearce, P. F., Ferguson, L. A., & Langford, C. A. (2017). Understanding scoping
reviews: Definition, purpose, and process. Journal of the American Association of Nurse
Practitioners, 29(1), 12–16. https://doi.org/10.1002/2327-6924.12380
Pham, M. T., Rajić, A., Greig, J. D., Sargeant, J. M., Papadopoulos, A., & Mcewen, S. A.
(2014). A scoping review of scoping reviews: Advancing the approach and enhancing
the consistency. Research Synthesis Methods, 5(4), 371–385.

35
https://doi.org/10.1002/jrsm.1123
Rothstein, J. M. (1989). On defining subjective and objective measurements. Physical
Therapy, 69(7), 577–579. https://doi.org/10.1093/ptj/69.7.577
Rubin, D. (2007). Epidemiology and Risk Factors for Spine Pain. Neurologic Clinics, 25(2),
353–371. https://doi.org/10.1016/j.ncl.2007.01.004
Sengupta, R., & Stone, M. A. (2007). The assessment of ankylosing spondylitis in clinical
practice. Nature Clinical Practice Rheumatology, 3(9), 496–503.
https://doi.org/10.1038/ncprheum0591
Shum, G. L., Tsung, B. Y., & Lee, R. Y. (2013). The immediate effect of posteroanterior
mobilization on reducing back pain and the stiffness of the lumbar spine. Archives of
Physical Medicine and Rehabilitation, 94(4), 673–679.
https://doi.org/10.1016/j.apmr.2012.11.020
Snodgrass, S. J., Rivett, D. A., & Robertson, V. J. (2006). Manual Forces Applied During
Posterior-to-Anterior Spinal Mobilization: A Review of the Evidence. In Journal of
Manipulative and Physiological Therapeutics (Vol. 29, Issue 4, pp. 316–329).
https://doi.org/10.1016/j.jmpt.2006.03.006
Soobiah, C., Tadrous, M., Knowles, S., Blondal, E., Ashoor, H. M., Ghassemi, M., Khan, P.
A., Ho, J., Tricco, A. C., & Straus, S. E. (2019). Variability in the validity and reliability
of outcome measures identified in a systematic review to assess treatment efficacy of
cognitive enhancers for Alzheimer ’ s Dementia. PLoS ONE, 14(4), 1–15.
Spieth, P. M., Kubasch, A. S., Isabel Penzlin, A., Min-Woo Illigens, B., Barlinn, K.,
Siepmann, T., Carl, H., & Carus, G. (2016). Randomized controlled trials – a matter of
design. Dovepress, 12, 1341–1349. https://doi.org/10.2147/NDT.S101938

36
Stamos-Papastamos, N., Petty, N. J., & Williams, J. M. (2011). Changes in bending stiffness
and lumbar spine range of movement following lumbar mobilization and manipulation.
Journal of Manipulative and Physiological Therapeutics, 34(1), 46–53.
https://doi.org/10.1016/j.jmpt.2010.11.006
Stanton, T. R., & Kawchuk, G. N. (2009). Reliability of assisted indentation in measuring
lumbar spinal stiffness. Manual Therapy, 14(2), 197–205.
https://doi.org/10.1016/j.math.2008.01.011
Stanton, T. R., Moseley, L. G., Wong, A. Y. L., & Kawchuk, G. N. (2017). Feeling stiffness
in the back: A protective perceptual inference in chronic back pain. Scientific Reports,
7(1), 1–12. https://doi.org/10.1038/s41598-017-09429-1
Tomczyszyn, D., Solecki, L., & Pańczuk, A. (2018). Assessment of the type of farmers’ low
back pain. Medycyna Pracy, 69(4), 355–364. https://doi.org/10.13075/mp.5893.00690
Tompkins, A., Hobelmann, G., & Compton, P. (2017). Providing chronic pain management
in the “Fifth Vital Sign” Era: Historical and treatment perspectives on a modern-day
medical dilemma D. Physiology & Behavior, 176(1), 139–148.
https://doi.org/10.1016/j.physbeh.2017.03.040
Tricco, A. C., Lillie, E., Zarin, W., Brien, K. O., Colquhoun, H., Kastner, M., Levac, D., Ng,
C., Sharpe, J. P., Wilson, K., Kenny, M., Warren, R., Wilson, C., Stelfox, H. T., &
Straus, S. E. (2016). A scoping review on the conduct and reporting of scoping reviews.
BMC Medical Research Methodology, 16(15), 1–10. https://doi.org/10.1186/s12874-
016-0116-4
Tricco, A. C., Lillie, E., Zarin, W., O’Brien, K. K., Colquhoun, H., Levac, D., Moher, D.,
Peters, M. D. J., Horsley, T., Weeks, L., Hempel, S., Akl, E. A., Chang, C., McGowan,
J., Stewart, L., Hartling, L., Aldcroft, A., Wilson, M. G., Garritty, C., … Straus, S. E.

37
(2018). PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and
Explanation. Annals of Internal Medicine. https://doi.org/10.7326/M18-0850
Viner, A., & Lee, M. (1995). Direction of manual force applied during assessment of stiffness
in the lumbosacral spine. J Manipulative Physiol Ther, 18(7), 441–447.
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citat
ion&list_uids=8568425
Wallwork, S., Bellan, V., & Moseley, G. L. (2017). Applying Current Concepts in Pain-
Related Brain Science to Dance Rehabilitation. Journal of Dance Medicine & Science,
21(1), 13–23. https://doi.org/10.12678/1089-313X.21.1.13
Weldring, T., & Smith, S. M. S. (2013). Patient-Reported Outcomes (PROs) and Patient-
Reported Outcome Measures (PROMs). Health Services Insights, 6, 61–68.
https://doi.org/10.4137/hsi.s11093
Williams, A., & Craig, K. (2016). Updating the definition of pain. Pain, 157(11), 2420–2424.
http://ovidsp.tx.ovid.com.ezproxy.is.ed.ac.uk/sp-
3.27.1a/ovidweb.cgi?WebLinkFrameset=1&S=JCBNFPLDOPDDOOGMNCFKDEIBD
GOAAA00&returnUrl=ovidweb.cgi%3F%26Full%2BText%3DL%257cS.sh.27.28%25
7c0%257c00006396-201611000-
00006%26S%3DJCBNFPLDOPDDOOGMNCFKDEIBDGOAAA00&d
Williamson, A., & Hoggart, B. (2005). Pain: a review of three commonly used pain rating
scales. Journal of Clinical Nursing, 14, 798–804.
Wong, A. Y. L., & Kawchuk, G. N. (2017). The Clinical Value of Assessing Lumbar
Posteroanterior Segmental Stiffness: A Narrative Review of Manual and Instrumented
Methods. PM and R, 9(8), 816–830. https://doi.org/10.1016/j.pmrj.2016.12.001

38
Yadla, S., Ratliff, J. K., & Harrop, J. S. (2008). Whiplash: Diagnosis, treatment, and
associated injuries. Current Reviews in Musculoskeletal Medicine, 1(1), 65–68.
https://doi.org/10.1007/s12178-007-9008-x
39
Section 3: Manuscript
Note to the reader: This manuscript has been prepared according to the guidelines for
Archives of Physical Medicine and Rehabilitation, available here:
https://doi.org/10.1016/S0003-9993(09)00368-2

40
Defining and measuring objective and subjective spinal stiffness: A
scoping review
Joel R. Moses1, Sylvia Hach1, Jesse Mason1
1School of Community Studies, Unitec Institute of Technology, Auckland, New Zealand
Running Head: Defining and measuring objective and subjective spinal stiffness
Acknowledgements
We would like to thank Dipti Vora, Library Knowledge Specialist, for her guidance in the
development of the search strategy. “The authors declare no conflicts of interest”.
Corresponding Author:
Joel Moses, School of Community Studies,
Unitec Institute of Technology,
Auckland, New Zealand
[T] +64-274395635
41
Abstract
Objective: To examine and identify the breadth of definitions and measures of objective and
subjective spinal stiffness in the literature, with a focus on clinical implications and research
opportunities.
Data Sources: Eligible peer-reviewed studies were identified using PubMed, Ebsco health,
and Scopus electronic databases.
Study Selection: Inclusion criteria included human subjects, English language, no date
restrictions, studies that reported (a) definition(s) or included subjective or objective outcome
or experience measures or indicators of spinal stiffness (no date restrictions). Exclusion criteria
included grey literature, non-spinal stiffness and animal studies.
Data Extraction: Following the 6-step framework by Arksey and O’Malley1 and based on the
eligibility criteria, studies that reported definitions and measures of spinal stiffness were
collected using a data abstraction form and classified into four themes; biomechanical, surgical,
pathophysiological and segmental spinal assessment. Fifteen categories to identify similarities
and differences between studies were generated.
Data Synthesis: Among 2121 records that were identified, 333 met the eligibility criteria.
There were 299 subjective and objective measures (124 subjective;175 objective measures) and
60 indicators of spinal stiffness. The majority of studies (n = 72%) did not define stiffness and
there is no consensus regarding a standardised definition of stiffness in the reviewed literature.
Conclusion: This review highlights the breadth of objective and subjective measures that are
both clinically and methodologically diverse. There was marked variation in the definitions
reported in studies. There were no definitions of stiffness provided alongside self-reported or
patient-reported outcome measures. Stiffness is a clinically important symptom that may

42
indicate the presence of underlying pathophysiology/disease which has implications for
patients’ health outcomes. An important distinction should be made between the patient’s
subjective reports of stiffness and this may differ from objective clinical assessments.
Keywords: Spinal; Stiffness; Musculoskeletal; Rehabilitation; Biomechanics.
Highlights
► Only 36% of the studies reported a more or less explicit definition of stiffness.
► There is no consensus regarding a standardised definition of stiffness in the reviewed
literature.
► There are no definitions of stiffness provided alongside self-reported or patient-reported
outcome measures.
► The relationship between subjective and objective measures of stiffness is not well
established.
► Stiffness is a symptom that may indicate the presence of underlying pathophysiology.

43
List of abbreviations
FSU – Functional Spinal Unit
L-D – Load-displacement
F-D – Force-displacement
PROM – Patient-reported outcome measure
BASDAI – Bath Ankylosing Spondylitis Disease Activity Index
LSDI – Lumbar Spinal Disability Index
VAS – Visual Analogue Scale
P-A – Posterior to anterior

44
Introduction
Spinal stiffness has been extensively characterised in the biomechanical literature,
where it is most often synonymous with the relationship between load and displacement. This
broad description of stiffness has been applied to a wide range of different research contexts;
however, its clinical relevance remains unclear. Stiffness is a common clinical feature
encountered in rehabilitative settings and may indicate the presence of underlying
pathophysiology/disease.2–4 In routine clinical practice, stiffness may be assessed by clinicians
using a range of manual segmental assessment techniques.5 This generally involves a clinician-
applied posterior to anterior (P-A) force directed at the spine of a prone patient to assess the
perceived intervertebral movement.6
The clinical assessment of patients that report stiffness is an important aspect of the
consultation. However, communicating with patients about the stiffness they experience may
present a challenge to clinicians, given that the term is often used in a colloquial manner. This
is further complicated by the diverse range of biomechanical terminology used by clinicians
and researchers to describe stiffness, which may not correspond to how stiffness is described
by patients. The lack of conceptual clarity surrounding the use of the term stiffness not only
impedes communication between researchers, clinicians and patients, but has important
implications for clinical assessment and evaluation of patient outcomes.
A wide range of mechanical instruments have been employed for the assessment of
stiffness.7–9 These instruments appear to be highly dependent on experimental approaches,
methods, and operationalisations of stiffness used in these studies. A significant challenge has
been the inability to measure stiffness directly in patients.10–12 Although some attempts have
been made to compare (objective) instrumented measures with patient-reported subjective
measures (subjective), instrumented measures did not correlate well with patient-reported

45
measures of spinal stiffness.10,13 This may be further compounded by inconsistent definitions
provided alongside rating scales used to assess the patient's self-reported stiffness.5
At present, there is no clear definition of spinal stiffness, nor is there a definitive method
of assessment. Given the broad applications of definitions and measures of stiffness, this
scoping review sought to examine and identify what definitions and measures of objective and
subjective spinal stiffness have been reported in the existing literature.

46
Methods
A scoping review methodology according to the framework recommended by Arksey
and O’Malley1 and The Joanna Briggs Institute,14 in conjunction with the reporting checklist
developed by Tricco et al.,15 was used to gather and organise the relevant information that
addressed the broad research question and provided a comprehensive examination of existing
peer-reviewed literature. The objectives of the subsequent review were: (1) to examine the
nature, range and extent of peer-reviewed empirical research to identify definitions and
measures of subjective and objective spinal stiffness, (2) to clarify key concepts and definitions
of spinal stiffness, (3) to describe subjective and objective measures of spinal stiffness, and (4)
to provide an overview of the current literature and practical considerations for clinicians and
researchers. The local ethics committee (Unitec Research Ethics Committee) determined that
a specific ethics application was not required to undertake the present study (see Appendix A;
Ethics notification).
Identification of the research question
This scoping review was guided by the following broad research question: What
definitions and measures of objective and subjective spinal stiffness have been reported in the
literature?
Identification of the relevant studies
The search strategy (developed by the first author with input from a knowledge
specialist and revised by the remaining authors) was applied to PubMed, Scopus, and Ebsco
health database (final search: 20/12/2018). The search terms used were: “stiffness”, “spinal”,
“defin*”, and “measur*”. Two search syntaxes were constructed: [stiffness AND spinal AND
defin*] for definitions, and [stiffness AND spinal AND measur*] for measures of spinal
stiffness (Appendix B: Search strategy).

47
Study selection
Eligibility criteria were established before executing the search, and according to
instructions by Arksey and O’Malley,1 any necessary modifications were implemented as the
review progressed. The inclusion criteria were the following: (1) published peer-reviewed
empirical studies with no date restrictions, (2) studies included combinations of the initial
search terms within the title or abstract, (3) full-text studies available electronically, (4)
published in English, (5) studies that reported (a) definition(s) of spinal stiffness or included
subjective or objective measures or indicators of spinal stiffness, (6) studies that reported
patient/clinician/research outcome or experience measures. Exclusion criteria were as follows:
(1) published or unpublished grey literature, (2) studies investigating non-spinal (e.g., arterial,
hepatic or dermatological) stiffness, and (3) animal studies.
The review process consisted of two levels of screening: (1) a title/abstract/keyword
review and (2) full-text review. For the first level of screening, a title/abstract/keyword
screening template was developed by two of the authors (Appendix C: Screening template).
The first author independently screened titles and abstracts of all articles. All citations from
electronic bibliographic databases were imported into a Microsoft ® Excel (version 1907)
spreadsheet, reviewed against the eligibility criteria and either included, fenced or excluded.
During first level screening, it was noted that studies reported descriptive alternatives or
included surrogate measures that described the properties of stiffness. Thus, eligibility criteria
were modified to: (1) studies that used any term that (in)directly described stiffness, including
surrogate measures of stiffness identified in the initial search syntax. No additional
modifications were made to the initial search syntax as it was determined that the term ‘stiffness’
was sufficient to capture any associated terms or surrogate measures. The identification of these
terms was used to determine whether other terms were semantically linked or were being
conflated with other terminology which (in)directly described stiffness.
48
For the second level of screening, the full texts of studies were independently screened
by the first author to determine their eligibility. Reference lists of studies were manually
searched for other relevant studies. All studies identified during the full-text screen, which met
the inclusion criteria were uploaded to Mendeley Desktop (version 1.19). Two additional
exclusion criteria were implemented at this screening step due to the identification of studies
that were not relevant to the scope of this review: (1) studies that measured stiffness of
exogenous materials (e.g., rod, construct, screw), (2) studies that measured a component of
spinal stiffness, but not the stiffness of components that contributed to overall spinal stiffness.
Components of the spine included local anatomical structures of the Functional Spinal Unit
(FSU) (e.g., intervertebral disc, ligaments, facet joints) and other global contributions to spinal
stiffness (e.g., spinal musculature, intra-abdominal/thoracic pressure, rib cage support). The
reason for excluding components of the spine that do not contribute to overall spinal stiffness
was to improve the representativeness of the biomechanical characteristics of spinal stiffness
as it relates to the clinical utility of measures identified in the literature.
Screening and Agreement
During the first level of screening, studies screened by the first author were tested for
selection consistency. Eligibility criteria were reapplied to 150 studies from both search
strategies and across databases by the second author and demonstrated ‘substantial’ agreement,
according to Vera and Grant16 (Kappa = 0.77, see Appendix D: Interrater agreement).
Remaining discrepancies were resolved by the third author to arrive at a consensus.
Data charting process
Data was abstracted from the relevant studies using a standardised data charting form
(where applicable) on the following characteristics: (1) Citation details, (2) definitions of spinal

49
stiffness, (3) subjective measures of spinal stiffness, (4) objective measures of spinal stiffness,
and (5) indicators of spinal stiffness (Appendix E: Data Items).
Collating and summarising the findings of included studies
Analysing the data
The final 333 studies were assessed for commonalities and differences after gaining
familiarity with the data and were classified into the four themes as follows: (1) biomechanical,
(2) surgical, (3) pathophysiological, and (4) segmental assessment. Studies within each
respective theme were subsequently grouped into fifteen categories (for a summary of data
extracted for each theme and their respective categories, (Appendix F: Data abstraction tables)
Data validation
Validation of study selection into one of the four themes completed by the first author
was achieved through verification of 5% of the total number of articles (17 of total of 333) by
the remaining authors. Subsamples of each theme were selected according to proportional
sampling, whereby the proportion that each theme represented of the total sample were selected
at random for validation. Any discrepancies identified during the audit were discussed by
reviewers until a consensus was reached.
Reporting
Data were analysed by examining and summarising the informational contents of the
abstracted data in relation to the guiding research question and objectives of this review. The
results are presented according to the four themes and their respective categories, using a
descriptive summary of the main findings, condensed and presented in table format.

50
Results
Overall, the search yielded 2,121 studies, of which 1,096 were screened after the
removal of duplicates (see Figure 1). First level (title and abstract) screening excluded 649
studies, and a further 139 studies were excluded following second level (full text) screening. A
further 25 studies were identified during manual searching, which resulted in a total number of
333 studies included for review. Included studies were classified into four themes,
biomechanical, surgical, pathophysiological and segmental assessment, and within each theme,
studies were allocated to a particular category (see Table 1).
Figure 1. PRISMA-scR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses
extension for Scoping Reviews) flow diagram of the search strategy and study selection.15
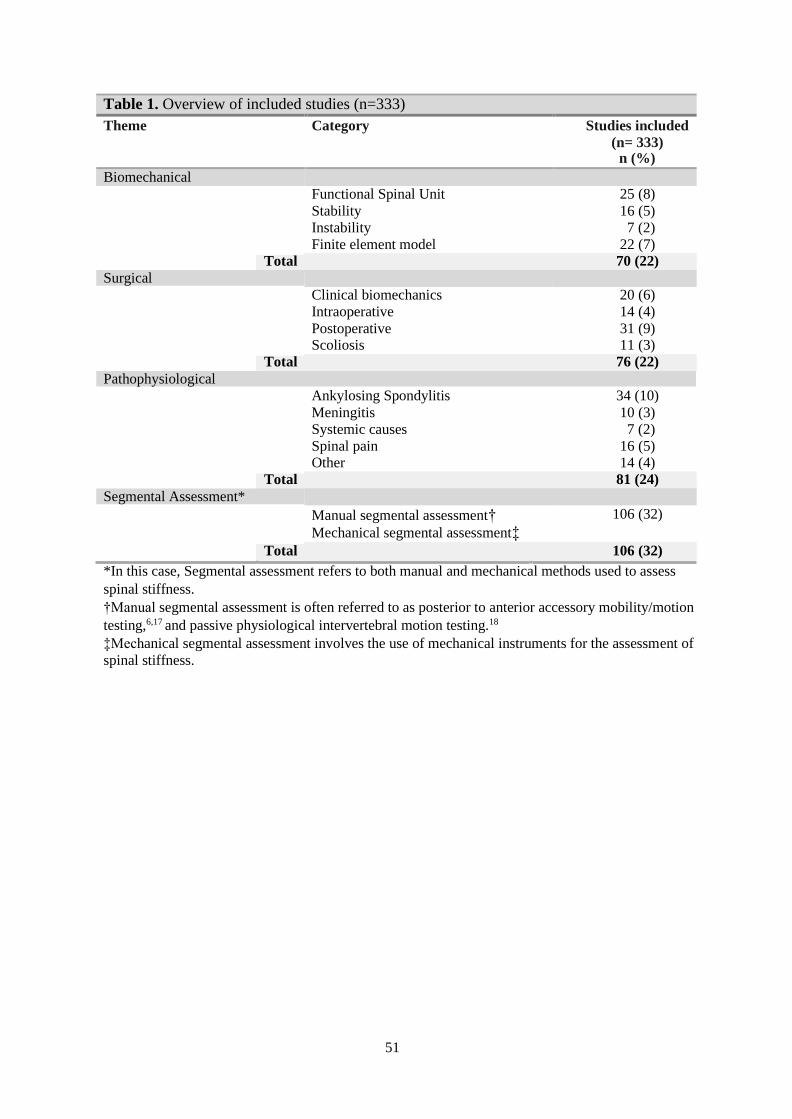
51
Table 1. Overview of included studies (n=333)
Theme Category Studies included
(n= 333) n (%)
Biomechanical
Functional Spinal Unit 25 (8) Stability 16 (5) Instability 7 (2) Finite element model 22 (7)
Total 70 (22)
Surgical
Clinical biomechanics 20 (6) Intraoperative 14 (4) Postoperative 31 (9) Scoliosis 11 (3)
Total 76 (22)
Pathophysiological Ankylosing Spondylitis 34 (10) Meningitis 10 (3) Systemic causes 7 (2) Spinal pain 16 (5) Other 14 (4)
Total 81 (24)
Segmental Assessment*
Manual segmental assessment† Mechanical segmental assessment‡
106 (32)
Total 106 (32)
*In this case, Segmental assessment refers to both manual and mechanical methods used to assess
spinal stiffness.
†Manual segmental assessment is often referred to as posterior to anterior accessory mobility/motion
testing,6,17 and passive physiological intervertebral motion testing.18
‡Mechanical segmental assessment involves the use of mechanical instruments for the assessment of
spinal stiffness.

52
Overview of study characteristics
In total, 122 (37%) of studies reported (a) definition(s), whereas, 240 (72%) did not
report (a) definition(s) of spinal stiffness. A total of 175 (52.5%) objective and 124 (37%)
subjective measures of spinal stiffness were included in this review. A subset of 60 (18%)
studies included indicators of spinal stiffness. The highest number of indicators (70%) were
included in the pathophysiological theme (see Table 2).
Table 2. Overview of the inclusion of definitions, measures, or indicators of spinal
stiffness as part of the studies included in the scoping review
Theme Defined Not
Defined
Objective
Measures
Subjective
Measures
Indicators
Biomechanical 24 46 63 0 4
Surgical 23 53 39 23 14†
Pathophysiological* 0 81 0 39 42
Segmental Assessment 75 60 73 62 0
Total 122 240 175 124 60
*In the case of the pathophysiological theme, 52% of the studies reported stiffness indicators
primarily related to clinically relevant symptoms.
†Fourteen studies reported symptom (indicators) of stiffness related to postoperative complications.
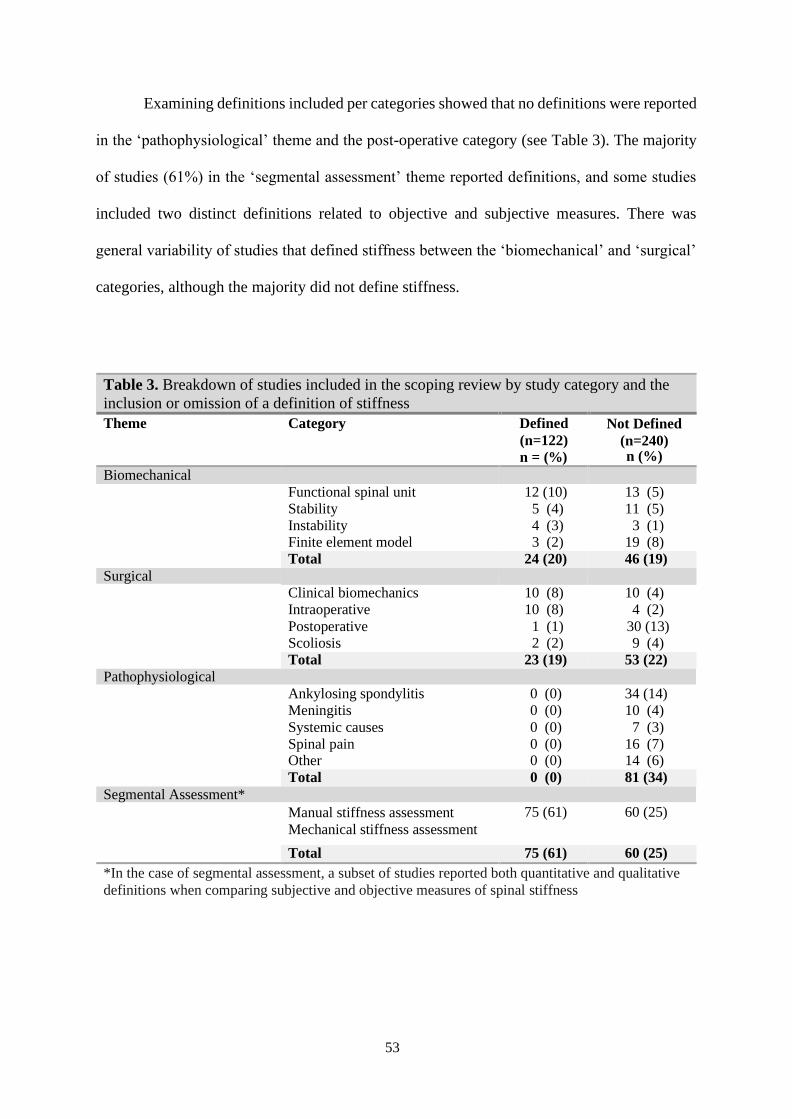
53
Examining definitions included per categories showed that no definitions were reported
in the ‘pathophysiological’ theme and the post-operative category (see Table 3). The majority
of studies (61%) in the ‘segmental assessment’ theme reported definitions, and some studies
included two distinct definitions related to objective and subjective measures. There was
general variability of studies that defined stiffness between the ‘biomechanical’ and ‘surgical’
categories, although the majority did not define stiffness.
Table 3. Breakdown of studies included in the scoping review by study category and the
inclusion or omission of a definition of stiffness
Theme Category Defined
(n=122)
n = (%)
Not Defined
(n=240) n (%)
Biomechanical
Functional spinal unit 12 (10) 13 (5) Stability 5 (4) 11 (5) Instability 4 (3) 3 (1) Finite element model 3 (2) 19 (8) Total 24 (20) 46 (19)
Surgical
Clinical biomechanics 10 (8) 10 (4) Intraoperative 10 (8) 4 (2) Postoperative 1 (1) 30 (13) Scoliosis 2 (2) 9 (4) Total 23 (19) 53 (22)
Pathophysiological Ankylosing spondylitis 0 (0) 34 (14) Meningitis 0 (0) 10 (4) Systemic causes 0 (0) 7 (3) Spinal pain 0 (0) 16 (7) Other 0 (0) 14 (6) Total 0 (0) 81 (34)
Segmental Assessment*
Manual stiffness assessment
Mechanical stiffness assessment
75 (61) 60 (25)
Total 75 (61) 60 (25)
*In the case of segmental assessment, a subset of studies reported both quantitative and qualitative
definitions when comparing subjective and objective measures of spinal stiffness

54
Examining stiffness measures included per categories showed that only objective
measures were included in the ‘biomechanical’ theme categories. However, the ‘segmental
assessment’ has the highest number of objective measures when compared to other categories.
Only subjective measures were included in the ‘pathophysiological’ theme categories and the
postoperative category. However, the ‘segmental assessment’ theme included the highest
number of subjective measures overall (see Table 4).
Table 4. Breakdown of studies included in the scoping review by study category and the
inclusion or omission of objective or subjective measures of stiffness
Theme Category Objective
Measures
(n=175) n (%)
Subjective
Measures
(n=124) n (%)
Biomechanical
Functional spinal unit 25 (14) 0 (0) Stability 12 (7) 0 (0) Instability 4 (2) 0 (0) Finite element model 22 (13) 0 (0) Total 63 (36) 0 (0)
Surgical
Clinical biomechanics 20 (11) 0 (0) Intraoperative 14 (8) 0 (0) Postoperative 0 (0) 23 (19) Scoliosis 5 (3) 0 (0) Total 39 (22) 23 (19)
Pathophysiological* Ankylosing spondylitis 0 (0) 25 (20) Meningitis 0 (0) 0 (0) Systemic causes 0 (0) 0 (0) Spinal pain 0 (0) 10 (8) Other 0 (0) 4 (3) Total 0 (0) 39 (31)
Segmental Assessment*
Manual stiffness assessment
Mechanical stiffness assessment
73 (42) 62 (50)
Total 73 (42) 62 (50)
*In the case of segmental assessment, a subset of studies included multiple measures; in total, 135
measures from 106 individual studies were included.

55
Characteristics of studies classified as biomechanical
The ‘biomechanical’ theme included studies that reported definitions and measures
related to structural and functional biometric properties of the spine. The load-displacement
(L-D) behaviour was generally used to quantify the stiffness of Functional Spinal Units (FSU)
in biomechanical studies (see Table 5).
Table 5. Overview of the methods of quantifying spinal stiffness as utilised by studies
included in the biomechanical theme
Quantification Frequency Relative frequency Reference
Load – displacement 16 39% 19,20,29–34,21–28
Force – displacement 8 20% 35–42
Torque – displacement 4 10% 43–46
Moment-displacement 4 10% 47–50
Load – deflection 3 7% 51–53
Force – torque 2 5% 54,55
Load – deformation 2 5% 56,57
The ‘FSU’ category comprised of studies that utilised a wide range of mechanical
instruments, experimental protocols, and set criteria to evaluate (in-vitro) biomechanics of
cervical, thoracic and lumbar spine stiffness. The majority of studies utilised FSUs,19,20,52,55,58–
61,22,23,25,35,37,44,45,49 whereas less studies utilised multi-segmental specimens during
experimental testing.36,47,54,62 Definitions in this category were described in terms of
mathematical laws, by the L-D relationship. (e.g., “applied load divided by the
displacement”23), and various characteristics on L-D graphs such as the ‘inverse slope’,22,47,61
and ‘linear’ region of the L-D curve”.35,36 Some studies reported less precise definitions, such
as “… hardening response”51 and the “… ability to withstand external force”.58 Twenty-five
studies included objective measures that utilised a diverse range of mechanical instruments for
the assessment of in-vitro spinal motion segment stiffness. Various types of mechanical
instruments were employed such as adapted or novel robotic machines,25 various custom

56
adaptations and jigs,19,54 Hexapod (Stewart platforms),41 and 3D coordinate systems.20 The
mechanical instruments were most commonly quantified by using data-driven approaches to
derive the L-D characteristics of FSUs.
The ‘stability’ category encompassed studies that investigated the passive, active and
neural components of stiffness that contributed to overall stability and stiffness of the spine.
Formal descriptions of concepts related to stiffness were often included in definitions of
stability.27,63 For example, segmental stability was defined as “the correlation of an applied
moment to the resultant deformation as shown in the L-D curves”,56 and the “force constant of
a spring calculated as change in force divided by displacement”.64 Spinal stability was generally
assessed by applying a perturbation to a system (i.e., a human subject) and observing the ability
of the body to resist displacement. Perturbation was the most commonly reported objective
measure of spinal stiffness identified in the stability category.42,64–68 Mechanical perturbations
were evaluated in terms of trunk muscle activity,42,65 kinetic and kinematic trunk responses,67,69
estimated mechanical properties of the trunk,70 and the contribution of trunk muscle activity to
overall spinal loading.
The ‘instability’ category was comprised of studies that investigated instability in terms
of its association with low back pain.50,71 The first attempts to define stiffness in the literature
as a whole were found in early studies investigating spinal instability, e.g.26,53. Here, spinal
instability was defined “as a loss of stiffness in the spine”,53 where ‘stiffness’ referred to “the
amount of motion within a system relative to a load applied to the structure”.53 A definition that
was suggested to be more workable was instability being “synonymous with a loss of motion
segment stiffness”, such that force applied to the motion segment produces greater
displacement than would be seen in a normal structure”.71 The term ‘stiffness’ has been used
to describe “the ratio of the applied load divided by displacement”.26 Here, ‘load’ and
‘displacement’ are described in four overlapping senses. Firstly, ‘loads’ and ‘motions’ are used

57
to define stiffness. Secondly, ‘load’ is defined as an applied ‘force’ or ‘moment’ that is
specified in terms of magnitude and direction. Thirdly, ‘motion’ is dependent on the applied
‘loads’ (forces and moments). Lastly, ‘displacement’ is defined as a ‘translation’ or ‘rotation’.
Flexibility was used to describe the inverse relationship to stiffness and has been defined as
“the ratio of displacement divided by the applied load”.26
The ‘finite element model’ category comprised of studies that utilised various
numerical simulation techniques in conjunction with experimental studies and provided insight
into the in-vivo loading conditions of the FSU.30,72 Finite element models were developed to
predict spinal motion or displacement responses to loading, where the vertebrae are described
as simple rigid bodies and other connective tissues representing beam or spring elements of an
FSU.73,74 The 6x6 stiffness matrices were used to define the L-D relationships,34 whereby, the
forces at the vertebral body centres are assumed to be related to the displacements by a 6x6
stiffness matrix with 36 terms (21 independent stiffness matrix terms due to the consideration
of matrix symmetry).30 However, Gardner-Morse and Stokes30 noted that a limitation of the 6x6
stiffness matrix approach was that the motion segment stiffness matrix required the assumption
of linear L-D behaviour. These authors proposed that in order to account for a motion segment
consisting of two vertebrae, each having six degrees of freedom would require a 12x12 stiffness
matrix.

58
Characteristics of studies classified as surgical
The ‘surgical’ theme encompassed studies that reported definitions and included
measures of spinal stiffness that related primarily to intraoperative measurement, pre- and
postoperative surgical interventions. The L-D behaviour was most commonly used to quantify
stiffness (see Table 6) and employed similar stiffness assessment protocols and methods to the
biomechanical theme.
Table 6. Overview of the methods of quantifying spinal stiffness as utilised by studies in
the surgical theme
Quantification Frequency Relative frequency Reference
Load – displacement 20 67% 75,76,85–94,77–84
Force – displacement 6 20% 95–100
Load – deformation 4 13% 83,101–103
The ‘clinical biomechanics’ category comprised of studies that utilised a wide range of
instruments to assess the structural and functional biomechanics of the spine, in the context of
surgical experimental interventions and procedures. One of the mechanical properties,
commonly used to characterise the stiffness of the spine, was the L-D relationship of the
FSU.100 Studies included in this category most commonly described stiffness in terms of the
slope of the L-D curve.76,77,79 The term ‘stiffness’ appeared to be used interchangeably with the
term ‘resistance’. For example, Dickman77 described the slope of the loading curve as “the
measurement of the relative resistance to the motion (stiffness)”. Twenty studies included
objective measures that utilised various mechanical instruments, e.g.,22,36,37 to investigate the
effects of surgical procedures and interventions of stiffness, e.g.81,83,95

59
The ‘intraoperative’ category encompassed studies that investigated spinal instability
by conducting in-vivo quantitative measurement of spinal stiffness.85 Data obtained from these
methods were primarily used to assess the operative level and provided a basis for treatment
recommendations and decisions regarding surgical intervention. In the year 1996, Frank85 was
the first to define the term stiffness as “the force needed to distract adjacent vertebrae within a
motion segment”. A mathematical definition is given by Krenn et al.104 who describes the
stiffness formula, “(S) of a body that deflects a distance (d) under an applied force (F); S=F/d”.
Other quantitative descriptions of stiffness include calculations used to quantify segmental
stiffness. For example, “the peak applied distraction force divided by the displacement between
the screws,”86 and the slope of the L-D curve.90,92,94 Several mechanical instruments have been
developed for the intraoperative (in-vivo) measurement of spinal motion segment stiffness. The
first documented use of intraoperative stiffness assessment was by Frank,85 who used a
vertebral retractor system to measure cervical spine stiffness. The vertebral retractor system
consisted of a spinal spreader equipped with force and distance sensors which measured the
distraction stiffness between two adjacent vertebrae. This provided surgeons with the ability to
quantify the intraoperative L-D responses exhibited by patients.85 Similar intra-operative in
vivo stiffness quantitative assessment techniques have been described by Hashimoto et al.86 and
Krenn et al.89 The ‘distraction’ stiffness was most commonly quantified by the slope of the L-
D response.84,85,94,86–93
The ‘scoliosis’ category encompassed studies that assessed the flexibility of the scoliotic
spine. Flexibility and stiffness were common biomechanical parameters for the planning of
surgical correction in subjects with scoliosis.105 F-D and L-D characteristics were often used to
describe the vertebral displacement observed in bending X-rays.98,99,105 The terms ‘stiffness’ and
‘flexibility’ appear to be used interchangeably to describe experimental measurements and
parameters in the characterisation of the scoliotic spine.98,105,106 For example,thoracic curves
were described as being stiffer than lumbar curve”.107 Inversely, “the flexibility of the spine was

60
decreased in the thoracic regions while the stiffness of the lumbar spine is increased”.98
Radiography was used to identify the degree of scoliosis curvature (5 studies). Plain film X-ray
was used to measure the spinal flexibility of subjects with scoliosis. During the preoperative
assessment of flexibility, radiographs were evaluated to assess the cobb angle measurements
and reducibility of the spinal curves. There were several methods employed to assess curve
flexibility, including fulcrum bending,107 anteroposterior and lateral standing, traction and
bending radiographs in the supine position,108 and the spinal suspension test.99
The ‘postoperative’ category encompassed studies that utilised patient-reported
outcome measures (PROMs). One study described spinal stiffness to contextualise how
stiffness applied to the Lumbar Spinal Disability Index (LSDI). In this study, ‘potential
stiffness’ was expressed in terms of “a loss of flexibility”.109 The LSDI109,110,119,111–118 was the
most commonly included PROM, followed by the Visual Analogue Scale (VAS).120–128 Several
postoperative stiffness indicators were included in studies investigating outcome measures and
complications after surgical intervention (see Table 2). For example, stiffness was reported as
a symptom of myelopathy,129,130 prolotherapy,131 cervical dorsal rhizotomy,132 and
postoperative complication of disc arthroplasty.133
Characteristics of studies classified as pathophysiological
The ‘pathophysiological’ theme included studies that reported stiffness as being
characteristic or indicative of pathophysiological processes. The majority of studies (42)
included stiffness indicators (seeTable 7.). The most common indicators were the presence of
symptom-reported stiffness related to various clinically relevant pathophysiological processes.

61
Table 1. Summary of stiffness indicators reported in the pathophysiological theme
Disease/condition Stiffness
indicator
Description of indicator Reference
Ankylosing Spondylitis Symptom Morning stiffness 134–139
Pain and stiffness
Inflammatory Low Back Pain Symptom Stiffness after resting 140–142
Meningitis Symptom
(triad)
Neck stiffness, fever, and altered
mental status
3,143–150
Spinal Tumour Symptom Spinal stiffness 151,152
Diffuse Idiopathic Skeletal
Hyperostosis
Symptom Stiffness and non-radicular pain 153,154
Whiplash associated disorders Symptom Pain and stiffness
4,155
Traumatic Atlanto-axial
subluxation
Symptom Spontaneous neck stiffness 156
Congenital osseous anomalies
of the upper cervical spine
Symptom Neck pain and stiffness 157
Fibromyalgia Symptom Early morning stiffness 158
Japanese Viral Encephalitis Symptom Neck stiffness 159
Lyme Neuroborreliosis Symptom Neck stiffness 160
Non-paralytic Poliomyelitis Symptom Painful stiffness of the neck and back
with an objective finding of limited
neck flexion
161
Subarachnoid Haemorrhage Clinical
prediction
rule
Neck pain or stiffness 162
The ‘ankylosing spondylitis’ category encompassed studies that investigated the
clinical assessment, diagnostic criteria, and PROMs related to ankylosing spondylitis. The Bath
Ankylosing Spondylitis Disease Activity Index (BASDAI) was the most utilised PROM (10
studies) among available studies. The BASDAI was comprised of a six-item self-administered
questionnaire that measured symptoms such as fatigue, spinal pain, localised tenderness, and
morning stiffness.163 The BASDAI uses the VAS, which included specific items for assessing
stiffness include morning stiffness severity and duration.163–168Although no definitions of
stiffness were reported alongside the BASDAI, Mengshoel and Robinson169 attempted to
modify original stiffness items on the BASDAI and asked patients to indicate how they
62
perceived stiffness in the spine. This qualitative work provided insight into the patient
experience of ankylosing spondylitis and three new themes were developed: ‘stiffness’ and
‘well-being,’ ‘stiffness and bodily awareness,’ and ‘stiffness and hope’.
The ‘meningitis’ category encompassed studies that included neck stiffness as a
symptom indicator of meningitis. Stiffness was identified in this category as a characteristic
symptom included in the triad hallmark features of fever, neck stiffness and altered mental
status3,146 Neck stiffness was considered to be an important clinical feature of meningitis3,143,145
and postoperative complications following surgical procedures.146,150
The ‘systemic causes’ category consisted of studies that reported spinal stiffness arising
from systemic diseases. Seven indicators were reported in 7 studies related to symptoms of
neck stiffness: Retropharyngeal Ganglioneuroma,170 Lyme neuroborreliosis,160 Subarachnoid
Haemorrhage,162 and Retroclival Haematoma due to odontoid fracture,171 Neck and back
stiffness was also reported as a symptom of non-paralytic poliomyelitis,161 Vertebral
abnormalities associated with synthetic retinoid use,172 and Fibromyalgia.158
The ‘spinal pain’ category encompassed studies investigating pain in the lumbar region
(lower back), thoracic (mid-back), and cervical region (neck) which was associated with
stiffness. This category consisted of studies that included PROMs, symptoms, and clinical signs
that may be indicative of mechanical or inflammatory spinal pain and whiplash-associated
disorders. The VAS was the most utilised PROMs (4 studies) which assessed neck and back
stiffness. For example, three studies utilised various PROMs in an attempt to discriminate
between inflammatory and mechanical low back pain.140–142 One single discriminating factor
to emerge from these studies is that morning stiffness appears to be an important indicator of
inflammatory low back pain.140–142 Two studies that investigated clinical signs, symptoms, and
prognostic factors related to whiplash associated disorders,4,155 and reported that neck
symptoms (i.e., pain and stiffness) with or without objective clinical findings are common in

63
whiplash injuries.4
The ‘other’ category encompassed investigating clinical features, symptoms, adverse
events and rare occurrences due to various pathophysiological processes. Ten studies included
indicators of neck and back stiffness. Symptoms of stiffness were identified in the following:
Diffuse Idiopathic Skeletal Hyperostosis,154 Congenital Osseous Anomalies of the upper
cervical spine,157 Osteoarthritis of the cervical and lumbar spine,173 Lumbar Degenerative Disc
Disease,174,175 Post Lumbar Puncture Headache,150 and Primary Diffuse Leptomeningeal
Gliomatosis.176
Characteristics of studies classified as segmental assessment
The ‘segmental assessment’ theme encompassed studies that investigated manual
(qualitative) or mechanical (quantitative) segmental assessment of spinal stiffness in human
subjects. It was observed that a vast majority of studies used mechanical instrumentation to
assess the reliability and validity of manual segmental assessment (see Table 2). Of these, 75
definitions were reported, whereas 60 of the 135 measures included did not report a definition
of stiffness.
Manual segmental assessment was the most commonly employed measure in reliability
and validity studies assessing spinal stiffness. Typically, manual assessment involved a
clinician-applied manual force to a spinal landmark (i.e., spinous process or articular pillar) in
evaluating stiffness as well as other aspects of motion segment characteristics such as range of
motion, mobility and pain provocation.177–179 The P-A intervertebral motion test was the most
commonly employed subjective measure (30 studies) for the (static) assessment of manual
segmental stiffness, and is described elsewhere.180 A similar variation to the P-A intervertebral
motion test was the ‘Passive Physiological Intervertebral Motion’ test, which was a dynamic
assessment of stiffness, cf.181 Similar manual segmental assessment techniques have been
described with the subject sitting or in the side-lying position.182 Other types of manual

64
segmental assessment methods included: the lateral gliding test,183 joint end-play
Assessment,184 springing, and overpressure testing.185
In an attempt to investigate the reliability and validity of PA stiffness, a stiffness
reference-based protocol was used by Maher and Adams186 to compare a mechanical reference
stimulus with a mechanical instrumented device.180 Clinician-applied PA pressures were rated
on an 11-point scale assisted by a stiffness reference device anchored to discrete stiffness
stimuli. The -5 point on the scale was described as corresponding to “markedly reduced
stiffness”, and the +5 point on the scale was described as “markedly increased stiffness”.180,186
Raters were often advised to concentrate on the loading portion of the F-D curve when trying
to match the stiffness. 187,188
Stiffness has been most commonly defined from the clinician’s perspective. For
example, ‘quality’ of,18,189 ‘impression’ of,190,191 and ‘perceived’ by.192,193 The most common
feature included in definitions was ‘resistance’ (see Table 8). It appears that stiffness is used
synonymously with the term ‘resistance’ in the manual segmental assessment category. For
example, stiffness is described as the “perceived resistance through intervertebral joint range
of movement”.194 Other examples include; the “quality of resistance,”18 “range and resistance
to movement,”195 “increased tissue resistance to the displacement,”196 and “the resistance to
motion on force application”.197 The second most common feature included in definitions was
the F-D relationship, For example, stiffness is expressed in terms of ‘the ratio of change in
applied force to change in displacement,”8 the “amount of force applied to the displacement
produced,”187 and the “slope of the F-D curve”.196 Another feature of definitions was the
classification of spinal segment stiffness in terms of ‘increased’ or ‘decreased’ ‘mobility,’ for
example, ‘hypomobile,’ ‘normal,’ or ‘hypermobile’.17,191,198
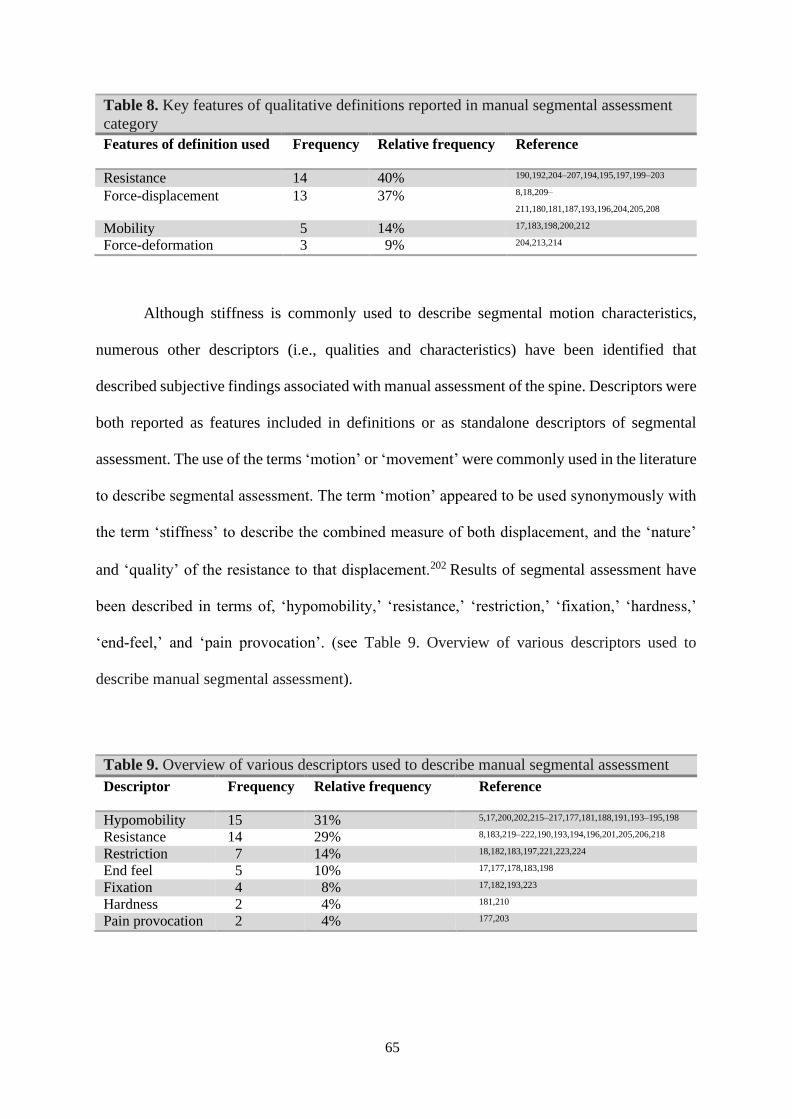
65
Table 8. Key features of qualitative definitions reported in manual segmental assessment
category
Features of definition used Frequency Relative frequency Reference
Resistance 14 40% 190,192,204–207,194,195,197,199–203
Force-displacement 13 37% 8,18,209–
211,180,181,187,193,196,204,205,208
Mobility 5 14% 17,183,198,200,212
Force-deformation 3 9% 204,213,214
Although stiffness is commonly used to describe segmental motion characteristics,
numerous other descriptors (i.e., qualities and characteristics) have been identified that
described subjective findings associated with manual assessment of the spine. Descriptors were
both reported as features included in definitions or as standalone descriptors of segmental
assessment. The use of the terms ‘motion’ or ‘movement’ were commonly used in the literature
to describe segmental assessment. The term ‘motion’ appeared to be used synonymously with
the term ‘stiffness’ to describe the combined measure of both displacement, and the ‘nature’
and ‘quality’ of the resistance to that displacement.202 Results of segmental assessment have
been described in terms of, ‘hypomobility,’ ‘resistance,’ ‘restriction,’ ‘fixation,’ ‘hardness,’
‘end-feel,’ and ‘pain provocation’. (see Table 9. Overview of various descriptors used to
describe manual segmental assessment).
Table 9. Overview of various descriptors used to describe manual segmental assessment
Descriptor Frequency Relative frequency Reference
Hypomobility 15 31% 5,17,200,202,215–217,177,181,188,191,193–195,198
Resistance 14 29% 8,183,219–222,190,193,194,196,201,205,206,218
Restriction 7 14% 18,182,183,197,221,223,224
End feel 5 10% 17,177,178,183,198
Fixation 4 8% 17,182,193,223
Hardness 2 4% 181,210
Pain provocation 2 4% 177,203
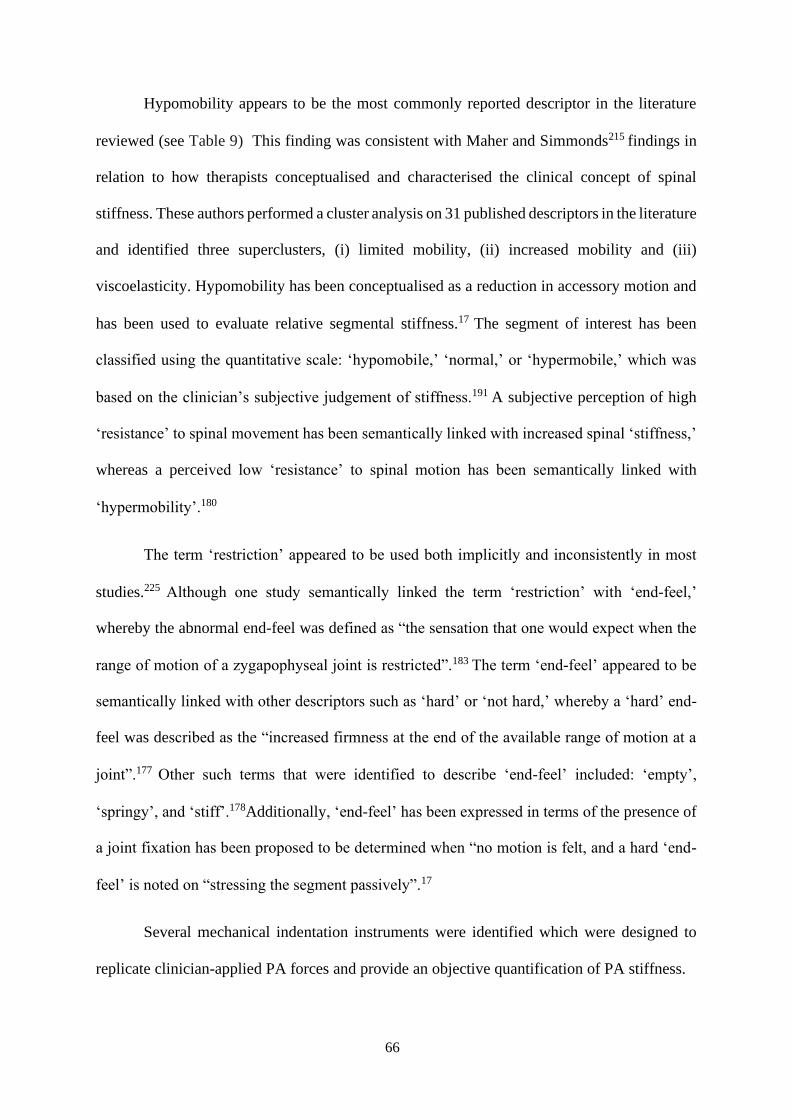
66
Hypomobility appears to be the most commonly reported descriptor in the literature
reviewed (see Table 9) This finding was consistent with Maher and Simmonds215 findings in
relation to how therapists conceptualised and characterised the clinical concept of spinal
stiffness. These authors performed a cluster analysis on 31 published descriptors in the literature
and identified three superclusters, (i) limited mobility, (ii) increased mobility and (iii)
viscoelasticity. Hypomobility has been conceptualised as a reduction in accessory motion and
has been used to evaluate relative segmental stiffness.17 The segment of interest has been
classified using the quantitative scale: ‘hypomobile,’ ‘normal,’ or ‘hypermobile,’ which was
based on the clinician’s subjective judgement of stiffness.191 A subjective perception of high
‘resistance’ to spinal movement has been semantically linked with increased spinal ‘stiffness,’
whereas a perceived low ‘resistance’ to spinal motion has been semantically linked with
‘hypermobility’.180
The term ‘restriction’ appeared to be used both implicitly and inconsistently in most
studies.225 Although one study semantically linked the term ‘restriction’ with ‘end-feel,’
whereby the abnormal end-feel was defined as “the sensation that one would expect when the
range of motion of a zygapophyseal joint is restricted”.183 The term ‘end-feel’ appeared to be
semantically linked with other descriptors such as ‘hard’ or ‘not hard,’ whereby a ‘hard’ end-
feel was described as the “increased firmness at the end of the available range of motion at a
joint”.177 Other such terms that were identified to describe ‘end-feel’ included: ‘empty’,
‘springy’, and ‘stiff’.178Additionally, ‘end-feel’ has been expressed in terms of the presence of
a joint fixation has been proposed to be determined when “no motion is felt, and a hard ‘end-
feel’ is noted on “stressing the segment passively”.17
Several mechanical indentation instruments were identified which were designed to
replicate clinician-applied PA forces and provide an objective quantification of PA stiffness.

67
The most commonly reported objective quantification of mechanical instrumented stiffness
was the F-D characteristics (see Table 10). These characteristics have been routinely used to
characterise the response of the spine to mechanically applied P-A forces. Three broad
categories of instruments have been described; (i) mechanical, (ii) mechanically assisted, and
(iii) dynamic.
Quantification Frequency Relative frequency Reference
Load-displacement 3 5% 197,253,254
Force-deformation 3 5% 9,255,256
Force-time 2 3% 257,258
Torque-angular
displacement
2 3% 259,260
Force-acceleration 1 2% 261
Force-velocity 1 2% 223
Load-deformation 1 2% 262
A wide range of mechanical instruments have been employed by researchers for the
assessment of spinal stiffness in human subjects. However, the basic construction and
mechanism of assessment was similar across all instruments. The experimental set-up involves
the subject lying in the prone position on a plinth with the indentor probe positioned over the
target spinous process. A vertical penetration load is delivered by the indentor extending along
a linear path, and the resultant displacement responses were recorded using various computer
software programs.5,188,191 For example, the Stiffness Assessment machine was one type of
mechanical instrument used to quantify stiffness, described elsewhere.180 Mechanically
assisted indentation methods utilised smaller, less automated techniques to measure
stiffness.191 Assisted indentation utilised a manual load application with the addition of
instrumentation, which was designed to give the operator improved reliability and accuracy.191
Table 10. Overview of how objective measures were quantified for mechanical stiffness
assessment
5,7,194,195,199,200,204,207,209,217,220,222,8,2
25–234,13,235–244,180,245–
252,182,184,188,191,192
79% 48 Force-displacement

68
Assisted indentation methods differ from previously used mechanical instruments, as the spinal
indentation force was produced by a human operator rather than a motor-driven device.242 More
recently, a dynamic continuous stiffness testing system has been designed to measure the
lumbar P-A stiffness and is described elsewhere.7,250
The most characteristic feature of the definitions reported in this category was the F-D
characteristics obtained from data-driven approaches that utilised various customised software
programs (see Table 11). Different features of definitions included descriptions of the slope of
the F-D curve such as the ‘linear portion’ (region) of the F-D curve,194,199,237,238,244 ‘slope’ or
‘first derivative’ of the F-D curve,191,225,249 ‘slope’ of the linear region of the F-D
curve,’187,199,233,241 and ‘gradient’ of the regression line’.8,192,231,263 Other features included in
definitions were the relationship between force and displacement (e.g., “the change in force per
unit change in displacement”).225 Stiffness has also been defined in terms of resistance to
movement or motion; for example, Xia et al222 operationally defined stiffness as the quantitative
measure of the resistance to motion.
Table 11. Key features of quantitative definitions reported in mechanical segmental
assessment category
Definition used Frequency Relative frequency Reference
Force – displacement 14 64% 187,191,241,249,250,264,194,199,200,209,225,233,237,238
Resistance 4 18% 13,203,222,245,256
Load – deformation 2 9% 9,255
Load – displacement 1 5% 265
Torque – angle 1 5% 260

69
Discussion
The overall aim of the present review was to identify what definitions and measures of
objective and subjective spinal stiffness have been reported in the existent literature, with a
focus on research implications and how this may inform clinical practice. These results show
that approximately one-third of the studies reported definitions of stiffness. For studies that did
include definitions, many different features were included. Most commonly, studies reported
definitions from a research perspective using quantitative descriptions to describe objective
measures used to quantify the biometric properties of spinal stiffness. Quantitative definitions
primarily related to mathematical laws, which referred to more or less explicitly stated
relationships between load and displacement,26,31 descriptions of L-D curve data,22,36 and
descriptions of formula.46,104 There was marked diversity in definitions that reported
quantitative descriptions of stiffness. This diversity could be attributed to the instruments
(techniques) used, the methods of measurement used, and the numerous operationalisations of
stiffness. Despite the use of data-driven approaches for measuring and defining stiffness, the
marked variation of definitions presented makes it difficult to compare findings between
studies.
Other quantitative descriptions (i.e., synonyms and antonyms) were also used to
describe different features of stiffness. For example, the term ‘resistance’ was typically used
synonymously with stiffness to describe load and displacement in terms of the resistance of
spinal movement. Another less frequently used term was ‘flexibility’, which represented the
inverse relationship to stiffness,26 although the term ‘flexibility’ was frequently used
implicitly.98,105 The use of alternative descriptors has the capacity to provide clarification of
concepts related to stiffness. However, these terms need to be described appropriately, and
sufficient context should be provided so that it is not possible for the reader to refer to any other
entity other than the alternative descriptive term being used. Moreover, formal descriptions

70
representing semantic links to stiffness related concepts were often included in definitions of
stability and instability. Stiffness was semantically linked with concepts related to stability (e.g.,
“… stiffening of the motion segment which results in greater stability” 64), and instability (e.g.,
“… loss of stiffness”71). Although the conflation of stability and instability with concepts of
stiffness may be facilitative in applied biomechanics, it may also lead to a certain degree of
ambiguity in the analysis of relationships and distinguishing features between these terms in the
clinical setting. The concepts of stability and instability would benefit from better clarification
for clinical purposes.
Stiffness has been commonly defined from a clinician perspective (how a clinician
perceives spinal stiffness) in studies that investigated manual segmental assessment. Most
definitions described characteristics of stiffness (e.g., “impression of …”190,191 or “quality of
…”18,189) from the clinicians’ perspective. Furthermore, clinician-based descriptions were often
accompanied by quantitative descriptions (e.g., “… force and displacement”205). The
integration of quantitative descriptions into manual segmental assessment of spinal stiffness
could be problematic for several reasons. First, qualitative and quantitative descriptions confer
fundamentally different approaches. Second, quantitative descriptions may not reflect
clinicians’ subjective judgements based on the realities of assessment in clinical practice. For
example, the clinician may concentrate on the “resistance through intervertebral joint range of
movement”,194 the “‘hard’ end-feel quality”,177 or some other entity not otherwise defined.
Third, the inherent subjectivity of manual palpation, means that the incorporation of
quantitative descriptions into stiffness judgements will inevitably result in variability in how
stiffness is perceived and interpreted in studies. Finally, and most importantly, this may
adversely affect the validity and reliability of future studies that assess stiffness in relation to
manual segmental assessment from the clinician’s perspective.

71
Another important finding was the marked variation of research-reported qualitative
descriptors used by clinicians to describe findings during manual segmental assessment. For
example, qualitative descriptors such as ‘hypomobility,’5,17,200,202,215–217,177,181,188,191,193–195,198
‘resistance,’8,183,219–222,190,193,194,196,201,205,206,218 ‘restriction,’ 18,182,183,197,221,223,224 and ‘end-
feel’17,177,178,183,198 may be integrated into clinician-judgements about stiffness. At first sight,
the diversity of descriptors appears to facilitate the paradigmatic perspective of clinicians who
use manual segmental assessment. However, the lack of explicit operational definitions of
descriptors, and the inconsistencies in the use of terminology, means that the exact meaning of
descriptors and their relationship with stiffness is not well delineated. In order to improve
reporting of qualitative descriptors of stiffness, operational definitions should be provided.
Further, consideration should be given to how these descriptors might influence the variability
of results. Most importantly, the variability of descriptors identified means that it would be
difficult to compare findings in a meaningful way in studies.
Self-report measures such as the VAS and PROMs such as the BASDAI and the LSDI,
did not provide explicit definitions of stiffness. However, in the case of the LSDI, the authors
provided a narrative explication of potential stiffness (i.e., loss of flexibility) which was
considered from the patient’s perspective, cf.109 In the case of the BASDAI, one study made
modifications to the original stiffness items, making them more specific to a patient’s
experience of Ankylosing Spondylitis, cf.169 In sum, the absence of explicit definitions of
stiffness concerning self-report measures and PROMs identified in this study has important
implications for future research. Most importantly, without operational (i.e., respondent)
definitions of stiffness on self-report scales, interpretations of stiffness may differ between
respondents (or patients), clinicians and authors of the scale. Furthermore, the lack of verbal
descriptors and the implicit use of the term ‘stiffness’ means that their clinical utility remains
unclear. A critical first step for the development of self-report measures and PROMs is to

72
ensure authors provide a respondent definition of stiffness at the outset of the study. This would
facilitate improved reporting and allow for more meaningful interpretations of stiffness-items
in future studies
The majority of studies used the term stiffness implicitly, without clear explication of
its meaning, which could be argued to raise several issues. First, there is no consensus statement
or standardised definition of stiffness. Second, it leaves the term stiffness open to interpretation
by the reader. Third, it hinders the reproducibility of results in subsequent studies. Fourth, it
could affect transparency across different research contexts. Finally, and most importantly, it
could represent a barrier for adopting evidence-based practice in clinical decision-making
processes. Unfortunately, this could represent a loss of clarity and impact clinical outcomes.
The current review identified over three hundred measures of spinal stiffness and found
that most studies used objective measure and methods for the assessment of stiffness, whereas
subjective measurements were less frequent. In relation to objective measures, the most
prevalent methods of quantifying stiffness were by studies that utilised various mechanical
instruments to quantify the load (or force)-displacement characteristics, using data-driven
approaches. The utilisation of mechanical instruments differed in whether they assessed
stiffness in human subjects (in-vivo and ex-vivo), or cadaveric specimens, (in-vitro).
Studies classified into the ‘biomechanical’ theme were particularly distinct, in that they
did not include any subjective measures of spinal stiffness. The absence of subjective measures
may be explained by the emphasis on the application of mechanical instruments to quantify the
behaviour of stiffness experimentally, and for this reason, could not assess subjective elements
of stiffness. Studies classified into the ‘surgical’ theme also employed similar mechanical
instruments to quantify stiffness, but in the context of surgical intervention. However, the
‘intraoperative’ category was unique, in that a subset of studies utilised intraoperative

73
techniques (e.g., spinal stiffness gauge), for the assessment of the stability of motion segments
at the operative level. Intraoperative techniques were used to quantify the behaviour of motion
segments and added to the objectivity of treatment recommendations and decisions regarding
surgical procedures.
Studies classified into the ‘segmental assessment’ theme emerged as particularly
distinct, as studies often compared clinician-perceived manual segmental assessment to
mechanical instruments or stiffness reference-based devices to investigate the reliability and
validity of manual segmental assessment. The differentiation of stiffness into subjective and
objective measures allowed for the application of methodological triangulation (i.e., using
quantitative and qualitative methods to investigate the stiffness phenomenon) to identify
similarities and differences across methods.266 In the case of spinal stiffness, triangulation
appears to be impractical for assessing segmental stiffness from a subjective (sensory) and
objective (biomechanical) perspective. In general, it appears that judgements of spinal stiffness
obtained from manual segmental assessment do not appear to correlate well with instrumented
measurement.198,200
In relation to subjective measures, the most prevalent were self-reported measures,
followed by PROMs. The VAS represented a simple self-reported measure that reflected
unidimensional characteristics (i.e., severity and duration) of stiffness. PROMs represented a
wide range of measurable outcomes related to stiffness, which included disease activity, quality
of life and functional status. At present, the LSDI was the only PROM that addressed the impact
of stiffness on Activities of Daily Living, cf.109 In contrast, other PROMs were generally
restricted to severity (sensory) and duration (time-dependent) characteristics, cf.2,267
The reliance on sensory and time-dependent characteristics for the assessment of self-
reported and PROMs meant that the patients (respondents) own self-conceptualisation of
74
stiffness was not considered. Although these measures may be practical from a research
perspective, failure to consider stiffness from a multidimensional perspective means that their
clinical utility as a measure remains unclear. More work is needed to develop self-reported
measures and PROMs that assess responses (behavioural and psychological) and impacts
across different life domains relevant to patients. Furthermore, PROMs should reflect the
multidimensional factors associated with the patient’s perceptions of stiffness, providing
clinicians with a more comprehensive understanding of the issues faced by patients with spinal
stiffness. This would improve clinical decision-making processes by facilitating the
implementation of outcome measures that matter to patients and thereby enhancing treatment
efficacy.
Studies classified into the ‘pathophysiological’ theme had two distinguishable features.
First, none of the studies included objective measures of spinal stiffness. The absence of
objective measures may be explained by the fact that studies were mainly interested in self-
reported, PROs and other indicators relevant to the clinical presentation of spinal stiffness.
Second, approximately half of the studies included stiffness as an indicator; often included as
part of a set of indicators, symptom triad, or clinical prediction rule. The most prevalent
indicators were symptoms and characteristics, describing patient-specific features of various
clinically relevant pathophysiological processes. Patient-reported symptoms appeared
particularly relevant to patients and may provide clinicians with an indication of the patient’s
current health status, thereby informing clinical decision-making processes.
Important clinical implications of findings
Stiffness is a clinically relevant symptom reported by patients and has implications for
patient-relevant health outcomes in the rehabilitation setting. In the initial evaluation of patients
presenting with spinal stiffness, consideration should be given to the possibility of serious

75
causes such as inflammatory disease,2,141 degenerative conditions,173,175 infection (bacterial or
viral),160,268 cancer,152 trauma,4,155,156 intracranial pathology,162,171 and postoperative
complications.129–133 The symptom of stiffness and its relationship to other clinical
manifestations is essential to differentiate between a benign condition and pathophysiology.
For instance, neck stiffness accompanied by fever and altered mental status may suggest
meningitis,3 while morning stiffness and back pain may suggest Ankylosing Spondylitis2 or
Osteoarthritis.175 The recognition of these symptoms is critical to prompt further clinical
investigations to confirm or deny pathophysiological aetiology of the patient presenting with
spinal stiffness.
The clinical assessment may rely on the presence of subjective stiffness in the absence
of objective clinical findings. It appears that disparities exist between objective measures and
subjective reports of spinal stiffness in the literature,4,13,118 This highlights several clinical
implications. First, an important distinction should be made between the patient’s subjective
reports of stiffness, which may be different from objective clinical assessments.13,118 Second,
the mismatch between subjective and objective measures of stiffness may be further
compounded by the absence of definitions from patients’ perspectives. Third, clinical outcomes
may be better assessed by improving patients’ self-reported assessments. Finally, the
relationship between subjective and objective measurements of spinal stiffness does not appear
to be well established in the literature. An emergent theory that has been identified in the
literature is the notion that stiffness may serve a ‘protective’ or ‘guarding’ function.13,269,270
This is thought to be related to the patient’s state of consciousness and various psychological
factors, such as fear, anxiety and pain.13,161
Protective stiffness may be neurally-driven in an attempt to protect the spine for
different reasons.13 This is in line with recent research suggesting the experience of feeling stiff
may not reflect biomechanical stiffness.13,271 Similar research also suggests an association

76
between spinal stiffness and the muscle guarding phenomenon as well as possible
proprioceptive deficits.270 Pain and anxiety may increase spinal stiffness due to co-contraction
of spinal muscles,272,273 emphasising the role of psychological processes influencing stiffness
on a physiological level. Stiffness is also reported as a postoperative complication and may
serve a protective function during recovery following surgical procedures.269 There is clinical
diversity in studies that report stiffness as serving a ‘protective’ or ‘guarding’ function in both
acute and chronic patient populations. Therefore, more work is required to characterise further
the relationship between the ‘protective’ and ‘guarding’ phenomenon concerning spinal
stiffness. This may have important implications for assessment and treatment of patients with
spinal stiffness. It further emphasises the need to understand how patients explain and
understand their symptoms in relation to spinal stiffness.
Study limitations
Only peer-reviewed literature was included in this scoping review, which represents the
evidence base of what informs clinical knowledge. Therefore, secondary sources of evidence
such as grey literature, books and manuals were not included. The purpose of this scoping
review was to be exploratory in addressing the question of ‘what’ rather than ‘how’; therefore,
the methodological quality of the included studies was not assessed. The ‘optional’ consultation
exercise was not conducted as a part of the present review, although future studies may use this
study as a basis in which to engage with key stakeholders in a more meaningful and informed
consultation process. Although the scoping review framework14 recommends the involvement
of multiple reviewers for the second level of screening, following pilot-testing, agreement
scores suggested that the screening template was sufficient for determining the eligibility of
studies. Therefore, it was determined that the first author would conduct the second level
screening independently.15

77
Conclusion
The findings of this scoping review highlight the marked diversity in the reporting of
definitions both within and across different research contexts. At present, there are several
limitations of using the term stiffness in clinical practice. Stiffness has evolved semantically
following the development of concepts originating in physics and engineering, as well as
following the extensive characterisation of stiffness in biomechanical literature. Given the
historical evolution of the term ‘stiffness’ and its various conceptualisations, new ad hoc
(operational) definitions, and other descriptors of stiffness frequently appear in the literature.
Unfortunately, this may lead to a variety of issues; most importantly, it impedes clear
communication between clinicians and patients. At this point, it is important to stress that the
literature appears not to address definitions of stiffness from the patient’s perspective, which
includes the absence of definitions alongside self-reported, PRO measures. Further,
symptomatic stiffness is still less well characterised and understood in the current literature.
Adopting a patient-centred approach to defining stiffness and evaluating the strengths and
weaknesses of current definitions/descriptors and measures of spinal stiffness may provide the
clinician with better insight into how to effectively assess and manage stiffness in rehabilitative
settings.
The breadth of outcomes measures reflects the multifactorial nature of spinal stiffness.
Subjective and objective measures of stiffness are widely used in research and clinical settings,
to evaluate motion segment behaviour, to evaluate the effect of an intervention, for clinical
assessment and evaluate patient outcomes. Objective measures of stiffness have been
extensively characterised utilising mechanical instruments to quantify the behaviour of spinal
stiffness experimentally across different methodological and clinical contexts. Attempts to
employ methodological triangulation to investigate subjective and objective spinal stiffness to
assess the reliability and validity of manual segmental assessment appear impractical. Thus,
78
the relationship between objective and subjective measures of stiffness remains elusive.
Moreover, the tendency to rely on sensory and time-dependent characteristics in both self-
report and PRO measures fails to capture the multifactorial nature of spinal stiffness. Therefore,
the development of multidimensional indices and scales is necessary to reflect outcomes that
matter to patients.

79
References
1. Arksey H, O’Malley L. Scoping studies: Towards a methodological framework. Int. J.
Soc. Res. Methodol. Theory Pract. 2005;8:19–32.
2. Sengupta R, Stone MA. The assessment of ankylosing spondylitis in clinical practice.
Nat. Clin. Pract. Rheumatol. 2007;3:496–503.
3. Brouwer M, van de Beek D, Sebastiaan H, Spanjaard L, Gans J de G. Community-
Acquired Listeria monocytogenes Meningitis in Adults. J. Nerv. Ment. Dis.
2006;60:195.
4. Rydevik B, Szpalski M, Aebi M, Gunzburg R. Whiplash injuries and associated
disorders: New insights into an old problem. Eur. Spine J. 2008;17.
5. Wong A, Kawchuk G. The Clinical Value of Assessing Lumbar Posteroanterior
Segmental Stiffness: A Narrative Review of Manual and Instrumented Methods. PM R
[Internet]. 2017 [cited 2018 Jun 25];9:816–30. Available from:
http://dx.doi.org/10.1016/j.pmrj.2016.12.001
6. Maitland G, Hengeveld E, Banks K, English K. Maitland’s Vertebral Manipulation.
6th ed. London: 2005.
7. Hadizadeh M, Kawchuk GN, Parent E. Reliability of a new loaded rolling wheel
system for measuring spinal stiffness in asymptomatic participants. BMC
Musculoskelet. Disord. [Internet]. 2019 [cited 2019 Apr 29];20:176. Available from:
https://doi.org/10.1186/s12891-019-2543-y
8. Lee M, Svensson N. Measurement of stiffness during simulated spinal physiotherapy.
Clin. Phys. Physiol. Meas. 1990;11:201–7.
9. Kumar S, Stoll S. Device, protocol and measurement of regional spinal stiffness. J.

80
Electromyogr. Kinesiol. [Internet]. 2011;21:458–65. Available from:
http://dx.doi.org/10.1016/j.jelekin.2011.01.001
10. Akagi R, Kusama S. Comparison Between Neck and Shoulder Stiffness Determined
by Shear Wave Ultrasound Elastography and a Muscle Hardness Meter. Ultrasound
Med. Biol. 2015;41:2266–71.
11. Stanton TR, Lorimer Moseley G, Wong AYLL, Kawchuk GN, Moseley GL, Wong
AYLL, et al. Feeling stiffness in the back: A protective perceptual inference in chronic
back pain. Sci. Rep. [Internet]. 2017 [cited 2018 Apr 28];7:1–12. Available from:
http://dx.doi.org/10.1038/s41598-017-09429-1
12. Maher C, Adams R. Is the clinical concept of spinal stiffness multidimensional? Phys.
Ther. [Internet]. 1995;75:854–60; discussion 861-4. Available from:
http://www.ncbi.nlm.nih.gov/pubmed/7568385
13. Stanton TR, Moseley LG, Wong AYL, Kawchuk GN. Feeling stiffness in the back: A
protective perceptual inference in chronic back pain. Sci. Rep. [Internet]. 2017;7:1–12.
Available from: http://dx.doi.org/10.1038/s41598-017-09429-1
14. Joanna Briggs Institute. The Joanna Briggs Institute Reviewers’ Manual 2015:
Methodology for JBI scoping reviews. Joanne Briggs Inst. [Internet]. 2015;1–24.
Available from: http://joannabriggs.org/assets/docs/sumari/ReviewersManual_Mixed-
Methods-Review-Methods-2014-ch1.pdf
15. Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, et al. PRISMA
Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann.
Intern. Med. [Internet]. 2018;Available from:
http://annals.org/article.aspx?doi=10.7326/M18-0850
81
16. Viera A, Garret J. Understanding Interobserver Agreement: The Kappa Statistic
Anthony. Fam. Med. 2005;37:360–3.
17. Binkley J, Stratford PW, Gill C. Interrater Reliability of Lumbar Accessory Motion
Mobility Testing. Phys. Ther. 1995;75:786–92.
18. Abbott JH, Flynn TW, Fritz JM, Hing WA, Reid D, Whitman JM. Manual physical
assessment of spinal segmental motion: Intent and validity. Man. Ther. 2009;14:36–44.
19. Panjabi MM, Summers DJ, Pelker RR, Videman T, Friedlaender GE, Southwick WO.
Three‐dimensional load‐displacement curves Due to Forces on the Cervical Spine. J.
Orthop. Res. 1986;4:152–61.
20. Wen N, Lavaste F, Santin JJ, Lassau JP. Three-dimensional biomechanical properties
of the human cervical spine in vitro - I. Analysis of normal motion. Eur. Spine J.
1993;2:2–11.
21. Kayanja M, Evans K, Milks R, Lieberman I. Adjacent level load transfer following
vertebral augmentation in the cadaveric spine. Spine (Phila. Pa. 1976). 2006;31:790–7.
22. Busscher I, Van Dieën JH, Kingma I, Van Der Veen AJ, Verkerke GJ, Veldhuizen
AG. Biomechanical characteristics of different regions of the human spine: An in vitro
study on multilevel spinal segments. Spine (Phila. Pa. 1976). 2009;34:2858–64.
23. Neumann P, Osvalder AL, Nordwall A, Lövsund P, Hansson T. The ultimate flexural
strength of the lumbar spine and vertebral bone mineral content. J. Spinal Disord.
1993;6:314–23.
24. Edwards WT, Mann RW, Posner I, White AA, Hayes WC. Variation of Lumbar Spine
Stiffness With Load. J. Biomech. Eng. 2009;109:35.
25. Amin DB, Lawless IM, Sommerfeld D, Stanley RM, Ding B, Costi JJ. The effect of

82
six degree of freedom loading sequence on the in-vitro compressive properties of
human lumbar spine segments. J. Biomech. [Internet]. 2016;49:3407–14. Available
from: http://dx.doi.org/10.1016/j.jbiomech.2016.09.009
26. Ashton-Miller JA, Schultz AB. Spine instability and segmental hypermobility
biomechanics: A call for the definition and standard use of terms. Semin. Spine Surg.
1991;3:136–48.
27. Szust A. Experimental investigation of the lumbar spine - Influence of destabilization
on the stiffness characteristic. Acta Bioeng. Biomech. 2006;8:127–33.
28. Fry RW, Alamin TF, Voronov LI, Fielding LC, Ghanayem AJ, Parikh A, et al.
Compressive preload reduces segmental flexion instability after progressive
destabilization of the lumbar spine. Spine (Phila. Pa. 1976). 2014;39:74–81.
29. Panjabi MM, Kato Y, Hoffman H, Cholewicki J, Krag M. A study of stiffness protocol
as exemplified by testing of a burst fracture model in sagittal plane. Spine (Phila. Pa.
1976). 2000;25:2748–54.
30. Gardner-Morse MG, Stokes IAF. Structural behavior of human lumbar spinal motion
segments. J. Biomech. 2004;37:205–12.
31. Kleinberger M. Application of Finite Element Techniques to the Study of Cervical
Spine Mechanics. SAE Tech. Pap. Ser. 2010;1.
32. Schmidt H, Bashkuev M, Dreischarf M, Rohlmann A, Duda G, Wilke HJ, et al.
Computational biomechanics of a lumbar motion segment in pure and combined shear
loads. J. Biomech. [Internet]. 2013;46:2513–21. Available from:
http://dx.doi.org/10.1016/j.jbiomech.2013.06.038
33. Holewijn RM, Faraj SSA, Kingma I, van Royen BJ, de Kleuver M, van der Veen AJ.
83
Spinal biomechanical properties are significantly altered with a novel embalming
method. J. Biomech. [Internet]. 2017;55:144–6. Available from:
http://dx.doi.org/10.1016/j.jbiomech.2017.02.012
34. Malakoutian M, Street J, Wilke HJ, Stavness I, Fels S, Oxland T. A musculoskeletal
model of the lumbar spine using ArtiSynth–development and validation. Comput.
Methods Biomech. Biomed. Eng. Imaging Vis. 2018;6:483–90.
35. Wolfla C, Stemper B, Board D, Yoganandan N. Biomechanical properties of human
thoracic spine disc segments. J. Craniovertebr. Junction Spine. 2010;1:18.
36. Wagnac E, Aubin CÉ, Chaumoître K, Mac-Thiong JM, Ménard AL, Petit Y, et al.
Substantial vertebral body osteophytes protect against severe vertebral fractures in
compression. PLoS One. 2017;12.
37. Gay RE, Ilharreborde B, Zhao K, Boumediene E, An K-N. The effect of loading rate
and degeneration on neutral region motion in human cadaveric lumbar motion
segments. Clin. Biomech. 2007;23:1–7.
38. Ng H-W, Teo E-C. Nonlinear finite-element analysis of the lower cervical spine (C4-
C6) under axial loading. J. Spinal Disord. 2001;14:201–10.
39. Ng HW, Teo EC, Lee KK, Qiu TX. Finite element analysis of cervical spinal
instability under physiologic loading. J. Spinal Disord. Tech. 2003;16:55–65.
40. Hans N, Jan H, Thelonius H, Julia S. Non-linearity of flexion – extension
characteristics in spinal segments. Acta Bioeng. Biomech. 2009;11.
41. Stokes IAF, Gardner-Morse M. A database of lumbar spinal mechanical behavior for
validation of spinal analytical models. J. Biomech. [Internet]. 2016;49:780–5.
Available from: http://dx.doi.org/10.1016/j.jbiomech.2016.01.035

84
42. Vera-Garcia FJ, Brown SHM, Gray JR, McGill SM. Effects of different levels of torso
coactivation on trunk muscular and kinematic responses to posteriorly applied sudden
loads. Clin. Biomech. 2006;21:443–55.
43. Dugailly PM, Decuyper A, Salem W, De Boe A, Espí-López GV, Lepers Y. Analysis
of the upper cervical spine stiffness during axial rotation: A comparative study among
patients with tension-type headache or migraine and asymptomatic subjects. Clin.
Biomech. [Internet]. 2017 [cited 2018 Nov 13];42:128–33. Available from:
https://linkinghub.elsevier.com/retrieve/pii/S026800331730030X
44. Schmidt TA, An HS, Lim TH, Nowicki BH, Haughton VM. The stiffness of lumbar
spinal motion segments with a high-intensity zone in the anulus fibrosus. Spine (Phila.
Pa. 1976). 1998;23:2167–73.
45. Stolworthy DK, Zirbel SA, Howell LL, Samuels M, Bowden AE. Characterization and
prediction of rate-dependent flexibility in lumbar spine biomechanics at room and
body temperature. Spine J. [Internet]. 2014;14:789–98. Available from:
http://dx.doi.org/10.1016/j.spinee.2013.08.043
46. McGill S, Seguin J, Bennett G. Passive stiffness of the lumbar torso in flexion,
extension, lateral bending, and axial rotation. Effect of belt wearing and breath
holding. Spine (Phila. Pa. 1976). 1994;19:696–704.
47. Verkerke GJ, Meijer GJM, Kingma I, Busscher I, van der Veen AJ, van Dieën JH, et
al. The effects of creep and recovery on the in vitro biomechanical characteristics of
human multi-level thoracolumbar spinal segments. Clin. Biomech. [Internet].
2011;26:438–44. Available from: http://dx.doi.org/10.1016/j.clinbiomech.2010.12.012
48. Parkinson RJ, Beach TAC, Callaghan JP. The time-varying response of the in vivo
lumbar spine to dynamic repetitive flexion. Clin. Biomech. 2004;19:330–6.
85
49. Borkowski SL, Ebramzadeh E, Sangiorgio SN, Masri SF. Application of the Restoring
Force Method for Identification of Lumbar Spine Flexion-Extension Motion Under
Flexion-Extension Moment. J. Biomech. Eng. 2014;136:044501.
50. Dolan P, Hole BD, Pollintine P, Adams MA, Zhao F. Discogenic Origins of Spinal
Instability. Spine (Phila. Pa. 1976). 2005;30:2621–30.
51. McElhaney JH, Brian J, Paver JG, Myers BS, Gray L. Combined Bending and Axial
Loading Responses of the Human Cervical Spine. SAE Trans. 1988;97:1090–7.
52. van Engelen SJPM, Ellenbroek MHM, van Royen BJ, de Boer A, van Dieën JH.
Validation of vibration testing for the assessment of the mechanical properties of
human lumbar motion segments. J. Biomech. 2012;45:1753–8.
53. Pope MH, Panjabi M. Biomechanical definitions of spinal instability. Spine (Phila. Pa.
1976). 1985;10:255–6.
54. Tawackoli W, Marco R, Liebschner MAK. The Effect of Compressive Axial Preload
on the Flexibility of the Thoracolumbar Spine. Spine (Phila. Pa. 1976). 2004;29:988–
93.
55. Caride M, Zysset PK, Mordasini P, Orr TE, Charriere EA, Beutler T. Compliance of
the L5-S1 spinal unit: a comparative study between an unconstrained and a partially
constrained system. Eur. Spine J. 2005;15:74–81.
56. Quint U, Wilke H-J. Importance of the Intersegmental Trunk Muscles for the Stability
of the Lumbar Spine. Spine J. 1998;23:1937–45.
57. Haigh RC, McCabe CS, Halligan PW, Blake DR. Joint stiffness in a phantom limb:
evidence of central nervous system involvement in rheumatoid arthritis. Rheumatology
(Oxford). [Internet]. 2003;42:888–92. Available from:
86
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?db=pubmed&cmd=Retrieve&
;dopt=AbstractPlus&list_uids=12730550%5Cnhttp://opus.bath.ac.uk/6741/
58. Myklebust JB, Sances A, Pintar FA, Yoganandan N, Ray G. Stiffness and strain
energy criteria to evaluate the threshold of injury to an intervertebral joint. J. Biomech.
2004;22:135–42.
59. Edwards WT, Hayes WC, Posner I, White AA, Mann RW. Variation of lumbar spine
stiffness with load. J. Biomech. Eng. 1987;109:35–42.
60. Bisschop A, Kingma I, Bleys RLAW, Paul CPL, van der Veen AJ, van Royen BJ, et
al. Effects of repetitive movement on range of motion and stiffness around the neutral
orientation of the human lumbar spine. J. Biomech. 2013;46:187–91.
61. Zirbel SA, Stolworthy DK, Howell LL, Bowden AE. Intervertebral disc degeneration
alters lumbar spine segmental stiffness in all modes of loading under a compressive
follower load. Spine J. [Internet]. 2013;13:1134–47. Available from:
http://dx.doi.org/10.1016/j.spinee.2013.02.010
62. Kayanja MM, Ferrara LA, Lieberman IH. Distribution of anterior cortical shear strain
after a thoracic wedge compression fracture. Spine J. 2004;4:76–87.
63. Chad MJ, Stephen HM, Stuart M. Comparison of Different Rowing Exercises : Trunk
Muscle Activation and ... J. Strength Cond. Res. 2009;23:1408–17.
64. Bull Andersen T, Essendrop M, Schibye B. Movement of the upper body and muscle
activity patterns following a rapidly applied load: The influence of pre-load alterations.
Eur. J. Appl. Physiol. 2004;91:488–92.
65. Essendrop M, Andersen TB, Schibye B. Increase in spinal stability obtained at levels
of intra-abdominal pressure and back muscle activity realistic to work situations. Appl.

87
Ergon. 2002;33:471–6.
66. Lee P, Granata K, Moorhouse K. Active Trunk Stiffness During Voluntary Isometric
Flexion and Extension Exertions. Hum. Factors J. Hum. Factors Ergon. Soc.
2007;49:100–9.
67. Shojaei I, Suri C, van Dieën JH, Bazrgari B. Alterations in trunk bending stiffness
following changes in stability and equilibrium demands of a load holding task. J.
Biomech. [Internet]. 2018;77:163–70. Available from:
https://doi.org/10.1016/j.jbiomech.2018.07.005
68. Talebian S, Maroufi N, Olyaei GR, Toosizadeh N, Mousavi-Khatir R. The effect of
static neck flexion on mechanical and neuromuscular behaviors of the cervical spine. J.
Biomech. [Internet]. 2018;72:152–8. Available from:
https://doi.org/10.1016/j.jbiomech.2018.03.004
69. Petra V der B, Kingma I, Van Dieen J. Effects of unexpected lateral mass placement
on trunk loading in lifting. Spine (Phila. Pa. 1976). [Internet]. 2003;28:764–70.
Available from:
http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=emed6&NEWS=N&
AN=2003164676
70. Moorhouse KM, Granata KP. Role of reflex dynamics in spinal stability: Intrinsic
muscle stiffness alone is insufficient for stability. J. Biomech. 2007;40:1058–65.
71. Pope MH, Frymoyer JW, Krag MH. Diagnosing Instability. Clin. Orthop. Relat. Res.
2006;60–7.
72. Lafon Y, Lafage V, Steib JP, Dubousset J, Skalli W. In Vivo distribution of spinal
intervertebral stiffness based on clinical flexibility tests. Spine (Phila. Pa. 1976).

88
2010;35:186–93.
73. van Deursen DL, Lengsfeld M, Snijders CJ, Evers JJM, Goossens RHM. Mechanical
effects of continuous passive motion on the lumbar spine in seating. J. Biomech.
2000;33:695–9.
74. Roberts SB, Ward CC, Nahum AM. Head trauma - A parametric dynamic study. J.
Biomech. 1969;2:397–415.
75. Ferguson RL, Tencer AF, Woodard PPE, Allen BL. Biomechanical Comparisons of
Spinal Fracture Models and the Stabilizing Effects of Posterior Instrumentations. Spine
(Phila. Pa. 1976). 1988;13:453–60.
76. Wang X-Y, Dai L-Y, Xu H-Z, Chi Y-L. Biomechanical effect of the extent of vertebral
body fracture on the thoracolumbar spine with pedicle screw fixation: An in vitro
study. J. Clin. Neurosci. 2008;15:286–90.
77. Dickman CA, Crawford NR, Paramore CG. Biomechanical characteristics of C1–2
cable fixations. J. Neurosurg. 2009;85:316–22.
78. Bisschop A, Van Dieën JH, Kingma I, Van Der Veen AJ, Jiya TU, Mullender MG, et
al. Torsion biomechanics of the spine following lumbar laminectomy: A human
cadaver study. Eur. Spine J. 2013;22:1785–93.
79. Bisschop A, Van Royen BJ, Mullender MG, Paul CPL, Kingma I, Jiya TU, et al.
Which factors prognosticate spinal instability following lumbar laminectomy? Eur.
Spine J. 2012;21:2640–8.
80. Kingma I, Paul CPL, Bisschop A, van Dieën JH, Bleys RLAW, van der Veen AJ, et al.
Which factors prognosticate rotational instability following lumbar laminectomy? Eur.
Spine J. 2013;22:2897–903.

89
81. van Royen BJ, van Engelen SJPM, van Dieën JH, Smit TH, Bisschop A. The effect of
neighboring segments on the measurement of segmental stiffness in the intact lumbar
spine. Spine J. 2013;15:1302–9.
82. Kingma I, Stadhouder A, Holewijn RM, van Royen BJ, van der Veen AJ, Bisschop A,
et al. The Effects of Single-Level Instrumented Lumbar Laminectomy on Adjacent
Spinal Biomechanics. Glob. Spine J. 2014;5:39–47.
83. Drazin D, Hussain M, Harris J, Hao J, Phillips M, Kim TT, et al. The role of sacral
slope in lumbosacral fusion: A biomechanical study. J. Neurosurg. Spine [Internet].
2015;23:754–62. Available from: https://www.scopus.com/inward/record.uri?eid=2-
s2.0-
84974728175&doi=10.3171%2F2015.3.SPINE14557&partnerID=40&md5=3b517e2f
4404afd795157de7fa004cb1
84. Frank E, Chamberland D, Ragel B. Instrumentation for intraoperative measurement of
cervical spine stiffness. Neurol. Res. 1996;18:217–9.
85. Frank E, Chamberland D, Ragel B. A proposed technique for intraoperative
measurement of cervical spine stiffness. Neurosurgery. 1996;39:147–50.
86. Hashimoto T, Yamane S, Kanayama M, Shigenobu K, Ishida T, Oha F. Intraoperative
Biomechanical Assessment of Lumbar Spinal Instability: Validation of Radiographic
Parameters Indicating Anterior Column Support in Lumbar Spinal Fusion. Spine
(Phila. Pa. 1976). 2003;28:2368–72.
87. Karami M, Sadat MM, Zehtab MJ, Habibollah-Zadeh P, Akrami K, Zareei MR.
Intraoperative spinal stiffness measurement in management of spinal canal stenosis.
Acta Med. Iran. 2005;43:365–8.

90
88. Tanaka M, Morimoto Y, Harada T, Inoue M, Hosono N, Ono K, et al. Intraoperative
Measurement of Lumbar Spinal Instability. Spine (Phila. Pa. 1976). 2006;17:44–50.
89. Ambrosetti-Giudici S, Pfenniger A, Krenn MH, Piotrowski WP, Ferguson SJ, Burger
J. Surgical instrumentation for the in vivo determination of human lumbar spinal
segment stiffness and viscoelasticity. Med. Eng. Phys. 2009;31:1063–8.
90. Kitahara K, Oribe K, Hasegawa K, Hara T. A new intraoperative measurement system
for rotational motion properties of the spine. IFMBE Proc. 2009;23:1781–4.
91. Hasegawa K, Kitahara K, Shimoda H, Hara T. Facet joint opening in lumbar
degenerative diseases indicating segmental instability. J. Neurosurg. Spine.
2010;12:687–93.
92. Hasegewa K, Kitahara K, Hara T, Takano K, Shimoda H. Biomechanical evaluation of
segmental instability in degenerative lumbar spondylolisthesis. Eur. Spine J.
2009;18:465–70.
93. Li C De, Sun HL, Lu HZ. Comparison of the effect of posterior lumbar interbody
fusion with pedicle screw fixation and interspinous fixation on the stiffness of adjacent
segments. Chin. Med. J. (Engl). 2013;126:1732–7.
94. Hasegawa K, Kitahara K, Shimoda H, Ishii K, Ono M, Homma T, et al. Lumbar
degenerative spondylolisthesis is not always unstable: Clinicobiomechanical evidence.
Spine (Phila. Pa. 1976). 2014;39:2127–35.
95. Dahl MC, Nuckley DJ, Papadopoulos S, Rouleau JP, Ching RP. Dynamic
Characteristics of the Intact, Fused, and Prosthetic-Replaced Cervical Disk. J.
Biomech. Eng. 2006;128:809.
96. Clin J, Aubin CÉ, Parent S, Labelle H. Biomechanical modeling of brace treatment of

91
scoliosis: Effects of gravitational loads. Med. Biol. Eng. Comput. 2011;49:743–53.
97. Brown M, Holmes D, Heiner A, Wehman K. Measurement of cadaver lumbar spine
motion segment stiffness. Spine (Phila. Pa. 1976). 2002;27:918–22.
98. Duke K, Aubin CE, Dansereau J, Labelle H. Biomechanical simulations of scoliotic
spine correction due to prone position and anaesthesia prior to surgical
instrumentation. Clin. Biomech. 2005;20:923–31.
99. de Oliveria ME, Büchler P, Schneider J, Hasler CC, Studer D, Zheng G, et al. Axial
suspension test to assess pre-operative spinal flexibility in patients with adolescent
idiopathic scoliosis. Eur. Spine J. 2014;23:2619–25.
100. Jalalian A, Tay FEH, Arastehfar S, Liu G. A new method to approximate load–
displacement relationships of spinal motion segments for patient-specific multi-body
models of scoliotic spine. Med. Biol. Eng. Comput. 2017;55:1039–50.
101. Luo J, Bertram W, Sangar D, Adams MA, Annesley-Williams DJ, Dolan P. Is
kyphoplasty better than vertebroplasty in restoring normal mechanical function to an
injured spine? Bone [Internet]. 2010;46:1050–7. Available from:
http://dx.doi.org/10.1016/j.bone.2009.11.036
102. Perrin G, Barrey C, Mosnier T, Jund J, Skalli W. In vitro evaluation of a ball-and-
socket cervical disc prosthesis with cranial geometric center. J. Neurosurg. Spine.
2011;11:538–46.
103. van Royen BJ, Holewijn RM, van Dieën JH, Kingma I, Bisschop A, Stadhouder A, et
al. Single level lumbar laminectomy alters segmental biomechanical behavior without
affecting adjacent segments. Clin. Biomech. [Internet]. 2014;29:912–7. Available
from: http://dx.doi.org/10.1016/j.clinbiomech.2014.06.016

92
104. Krenn MH, Ambrosetti-Giudici S, Pfenniger A, Burger J, Piotrowski WP. Minimally
invasive intraoperative stiffness measurement of lumbar spinal motion segments.
Neurosurgery. 2008;63:309–14.
105. Salmingo RA, Tadano S, Fujisaki K, Abe Y, Ito M. Relationship of forces acting on
implant rods and degree of scoliosis correction. Clin. Biomech. [Internet].
2013;28:122–8. Available from: http://dx.doi.org/10.1016/j.clinbiomech.2012.12.001
106. Stokes IAF, Laible JP. Three-Dimensional Osseo-Ligamentous Model of the Thorax
Representin Initiation of Scoliosis by Asymmetric Growth. J. Biomech. 1990;23:589–
95.
107. Clamp JA, Andrews JR, Grevitt MP. A Study of the Radiologic Predictors of Curve
Flexibility in Adolescent Idiopathic Scoliosis. J Spinal Disord Tech. 2008;21:213–5.
108. Mahaudens P, Detrembleur C, Mousny M, Banse X. Gait in thoracolumbar/lumbar
adolescent idiopathic scoliosis: Effect of surgery on gait mechanisms. Eur. Spine J.
2010;19:1179–88.
109. Hart RA, Pro SL, Gundle KR, Marshall LM. Lumbar stiffness as a collateral outcome
of spinal arthrodesis: A preliminary clinical study. Spine J. [Internet]. 2013;13:150–6.
Available from: http://dx.doi.org/10.1016/j.spinee.2012.10.014
110. Hart RA, Gundle KR, Pro SL, Marshall LM. Lumbar Stiffness Disability Index: Pilot
testing of consistency, reliability, and validity. Spine J. 2013;13:157–61.
111. Hart RA, Marshall LM, Hiratzka SL, Kane MS, Volpi J, Hiratzka JR. Functional
limitations due to stiffness as a collateral impact of instrumented arthrodesis of the
lumbar spine. Spine (Phila. Pa. 1976). 2014;39:E1468–74.
112. Kim HJ, Protopsaltis TS, Scheer JK, Ames CP, Koski T, Mundis GM, et al. Which

93
Daily Functions Are Most Affected by Stiffness Following Total Lumbar Fusion.
Spine (Phila. Pa. 1976). 2015;40:1338–44.
113. Kimura H, Fujibayashi S, Otsuki B, Takahashi Y, Nakayama T, Matsuda S. Effects of
Lumbar Stiffness after Lumbar Fusion Surgery on Activities of Daily Living. Spine
(Phila. Pa. 1976). 2016;41:719–27.
114. Zhang H-C, Zhang Z-F, Wang Z-H, Cheng J-Y, Wu Y-C, Fan Y-M, et al. Optimal
Pelvic Incidence Minus Lumbar Lordosis Mismatch after Long Posterior
Instrumentation and Fusion for Adult Degenerative Scoliosis. Orthop. Surg. [Internet].
2017;9:304–10. Available from: http://www.ncbi.nlm.nih.gov/pubmed/28960816
115. Choi J-H, Jang J-S, Yoo K-S, Shin J-M, Jang I-T. Functional Limitations Due to
Stiffness after Long Level Spinal Instrumented Fusion Surgery to Correct Lumbar
Degenerative Flat Back. Spine (Phila. Pa. 1976). [Internet]. 2018;43:1044–51.
Available from: http://insights.ovid.com/crossref?an=00007632-900000000-95272
116. Daniels AH, Smith JS, Hiratzka J, Ames CP, Bess S, Shaffrey CI, et al. Functional
limitations due to lumbar stiffness in adults with and without spinal deformity. Spine
(Phila. Pa. 1976). 2015;40:1599–604.
117. Daniels AH, Koller H, Hiratzka SL, Mayer M, Meier O, Contag AG, et al. Selecting
caudal fusion levels: 2 year functional and stiffness outcomes with matched pairs
analysis in multilevel fusion to L5 versus S1. Eur. Spine J. 2017;26:1645–51.
118. Hart RA, Hiratzka J, Kane MS, Lafage V, Klineberg E, Ames CP, et al. Stiffness after
Pan-Lumbar Arthrodesis for Adult Spinal Deformity Does Not Significantly Impact
Patient Functional Status or Satisfaction Irrespective of Proximal Endpoint. Spine
(Phila. Pa. 1976). 2017;42:1151–7.

94
119. Ailon T, Hamilton DK, Klineberg E, Daniels AH, Lafage V, Bess S, et al.
Radiographic Fusion Grade Does Not Impact Health-Related Quality of Life in the
Absence of Instrumentation Failure for Patients Undergoing Posterior Instrumented
Fusion for Adult Spinal Deformity. World Neurosurg. [Internet]. 2018;117:e1–7.
Available from: https://doi.org/10.1016/j.wneu.2018.04.127
120. Million R, Haavik Nilsen K, Jayson MIV, Baker RD. Evaluation of low back pain and
assessment of lumbar corsets with and without back supports. Ann. Rheum. Dis.
1981;40:449–54.
121. Mori E, Maeda T, Itaru Y, Kawano O, Ueta T, Shiba K, et al. Spinous process-splitting
open pedicle screw fusion provides favorable results in patients with low back
discomfort and pain compared to conventional open pedicle screw fixation over 1 year
after surgery. Eur. Spine J. 2012;21:745–53.
122. Larson AN, Fletcher ND, Daniel C, Richards BS. Lumbar curve is stable after
selective thoracic fusion for adolescent idiopathic scoliosis: A 20-year follow-up.
Spine (Phila. Pa. 1976). 2012;37:833–9.
123. Rizvi SAM, Fredø HL, Lied B, Nakstad PH, Rønning P, Helseth E. Surgical
management of acute odontoid fractures: Surgery-related complications and long-term
outcomes in a consecutive series of 97 patients. J. Trauma Acute Care Surg.
2012;72:682–90.
124. Wang L, Lu X, Guo X, Ni B, Guo Q. Posterior Temporary Fixation Versus
Nonoperative Treatment for Anderson–D’Alonzo Type III Odontoid Fractures:
Functional Computed Tomography Evaluation of C1–C2 Rotation. World Neurosurg.
[Internet]. 2016;100:675–80. Available from:
http://dx.doi.org/10.1016/j.wneu.2016.01.004

95
125. Guo Q, Zhang M, Wang L, Lu X, Guo X, Ni B. Comparison of Atlantoaxial Rotation
and Functional Outcomes of Two Nonfusion Techniques in the Treatment of
Anderson-D’Alonzo Type II Odontoid Fractures. Spine (Phila. Pa. 1976).
2016;41:E751–8.
126. Zhu C, Wang L, Liu H, Song Y, Liu L, Li T, et al. Treatment of type II odontoid
fracture with a novel technique: Titanium cable-dragged reduction and cantilever-
beam internal fixation. Medicine (Baltimore). 2017;96:e8521.
127. Iizuka H, Iizuka Y, Mieda T, Tsunoda D, Kobayashi R, Sorimachi Y. The clinical
outcomes of atlanto-axial arthrodesis in patients with rheumatoid arthritis –
Assessment according to the Japanese Orthopaedic Association Cervical Myelopathy
Evaluation Questionnaire (JOACMEQ). J. Orthop. Sci. [Internet]. 2017;22:401–4.
Available from: http://dx.doi.org/10.1016/j.jos.2017.01.016
128. Guo Q, Chen F, Lu X, Ni B, Wu L, Guo X. Posterior Open Reduction and
Interlaminae Compression Fusion for Os Odontoideum with Atlantoaxial Dislocation.
World Neurosurg. [Internet]. 2016;91:326–31. Available from:
http://dx.doi.org/10.1016/j.wneu.2016.04.014
129. Sherief T., White J., Bommireddy R., Klezl Z. b. Cervical spondylotic myelopathy:
The outcome and potential complications of surgical treatment. Acta Chir. Orthop.
Traumatol. Cech. [Internet]. 2013;80:328–34. Available from:
http://www.scopus.com/inward/record.url?eid=2-s2.0-
84886695146&partnerID=40&md5=4d69b83baf0dfd68c2d0923939e5be6b
130. Ohnari H, Sasai K, Akagi S, Iida H, Takanori S, Kato I. Investigation of axial
symptoms after cervical laminoplasty, using questionnaire survey. Spine J.
2006;6:221–7.

96
131. Dagenais S, Haldeman S, Wooley JR. Intraligamentous injection of sclerosing
solutions (prolotherapy) for spinal pain: A critical review of the literature. Spine J.
2005;5:310–28.
132. Chivukula S, Moossy JJ, Agarwal V, Rothfus W, Gande A V., Gardner PA, et al.
Long-term outcomes of intradural cervical dorsal root rhizotomy for refractory
occipital neuralgia. J. Neurosurg. 2015;102–10.
133. O’Shaughnessy J, Drolet M, Roy J-F, Descarreaux M. Chiropractic management of
patients post-disc arthroplasty: Eight case reports. Chiropr. Osteopat. [Internet].
2010;18:1–7. Available from:
http://www.embase.com/search/results?subaction=viewrecord&from=export&id=L508
84646%0Ahttp://www.chiroandosteo.com/content/18/1/7%0Ahttp://dx.doi.org/10.118
6/1746-1340-18-
7%0Ahttp://sfx.aub.aau.dk/sfxaub?sid=EMBASE&issn=17461340&id=doi:10.1186%
2F1746-1340-
134. Hill H, Hill A, Bodmer J. Clinical diagnosis of ankylosing spondylitis in women and
relation to presence of HLA B27. Ann. Rheum. Dis. 1976;35:267–70.
135. Hanly JG, Russell ML, Gladman DD. Psoriatic spondyloarthropathy: A long term
prospective study. Ann. Rheum. Dis. 1988;47:386–93.
136. Rodriguez VR, Poddubnyy D. Old and new treatment targets in axial spondyloarthritis.
RMD Open. 2015;1.
137. Hegde D, Ballal A, Vinay Kumar C, Ravindranath Rai H. Type III Cawley Andersson
lesion in a case of ankylosing spondylitis. Nitte Univ. J. Heal. Sci. [Internet].
2014;4:136–9. Available from:
http://www.embase.com/search/results?subaction=viewrecord&from=export&id=L373

97
546546%0Ahttp://sfx.library.uu.nl/utrecht?sid=EMBASE&issn=22497110&id=doi:&a
title=Type+III+Cawley+Andersson+lesion+in+a+case+of+ankylosing+spondylitis&sti
tle=Nitte+Univ.+J.+Healt
138. Eroğlu E, Tosun A, Fidan F, Alemdar A, Erten Ş, Alkan BM, et al. Fatigue and
correlation with disease-specific variables, spinal mobility measures, and health-
related quality of life in ankylosing spondylitis. Mod. Rheumatol. 2014;23:1101–7.
139. Bal S, Bal K, Turan Y, Deniz G, Gürgan A, Berkit IK, et al. Sexual functions in
ankylosing spondylitis. Rheumatol. Int. 2011;31:889–94.
140. Keeling SO, Majumdar SR, Conner-Spady B, Battié MC, Carroll LJ, Maksymowych
WP. Preliminary validation of a self-reported screening questionnaire for inflammatory
back pain. J. Rheumatol. 2012;39:822–9.
141. Arnbak B, Jurik AG, Jensen TS, Manniche C. Association Between Inflammatory
Back Pain Characteristics and Magnetic Resonance Imaging Findings in the Spine and
Sacroiliac Joints. Arthritis Care Res. 2018;70:244–51.
142. Walker BF, Williamson OD. Mechanical or inflammatory low back pain. What are the
potential signs and symptoms? Man. Ther. [Internet]. 2009;14:314–20. Available
from: http://dx.doi.org/10.1016/j.math.2008.04.003
143. Anga G, Kaminiel O, Vince J, Riddell M, Tefuarani N, Ripa P, et al. The aetiology,
clinical presentations and outcome of febrile encephalopathy in children in Papua New
Guinea. Ann. Trop. Paediatr. 2010;30:109–18.
144. Bachan EG, Aikins M, Kenu E, Kye-Duodu G, Nyarko KM, Issah K, et al.
Pneumococcal meningitis outbreak and associated factors in six districts of Brong
Ahafo region, Ghana, 2016. BMC Public Health. 2018;18:1–11.

98
145. Bang ND, Caws M, Truc TT, Duong TN, Dung NH, Ha DTM, et al. Clinical
presentations, diagnosis, mortality and prognostic markers of tuberculous meningitis in
Vietnamese children: a prospective descriptive study. BMC Infect. Dis. 2016;16:1–10.
146. Lin T-Y, Chen W-J, Hsieh M-K, Lu M-L, Tsai T-T, Lai P-L, et al. Postoperative
meningitis after spinal surgery: a review of 21 cases from 20,178 patients. BMC Infect.
Dis. 2014;14:2–6.
147. Menaker J, Martin IBK, Hirshon JM. Marked elevation of cerebrospinal fluid white
blood cell count: An unusual case of Streptococcus pneumoniae meningitis,
differential diagnosis, and a brief review of current epidemiology and treatment
recommendations. J. Emerg. Med. 2005;29:37–41.
148. Nicholson AG, Wilson R, Shirodaria CC, Wells AU, Hansell DM. Lesson of the
month. Histopathology. 2004;44:91–3.
149. Pagliano P, Fusco U, Attanasio V, Rossi M, Pantosti A, Conte M, et al. Pneumococcal
meningitis in childhood: A longitudinal prospective study. FEMS Immunol. Med.
Microbiol. 2007;51:488–95.
150. Shin W, Kim M-K, Kim J, Woo M, Cho D, Lim KS. Post lumbar puncture headache:
Case report of a serious adverse event in first-in-human study. Transl. Clin. Pharmacol.
2017;25:162.
151. Alaya Z, Osman W. Lumbosciatica revealing intramedullary ependymoma Zeineb. Pan
Afr. Med. J. 2017;26:2–3.
152. Gilbert MR, Cleeland C, Vera-Bolanos E, Mendoza TR, Weinberg JS, Burton AW, et
al. Reliability and validity of the M. D. Anderson Symptom Inventory–Spine Tumor
Module. J. Neurosurg. Spine. 2011;12:421–30.

99
153. Kuperus JS, Samsour L, Buckens CF, Oner FC, de Jong PA, Verlaan JJ. Bone mineral
density changes over time in diffuse idiopathic skeletal hyperostosis of the thoracic
spine. Bone [Internet]. 2018;112:90–6. Available from:
https://doi.org/10.1016/j.bone.2018.04.005
154. Mata S, Fortin PR, Fitzcharles MA, Starr MR, Joseph L, Watts CS, et al. A controlled
study of diffuse idiopathic skeletal hyperostosis: Clinical features and functional
status. Medicine (Baltimore). 1997;76:104–17.
155. Richter M, Ferrari R, Otte D, Kuensebeck HW, Blauth M, Krettek C. Correlation of
clinical findings, collision parameters, and psychological factors in the outcome of
whiplash associated disorders. J. Neurol. Neurosurg. Psychiatry. 2004;75:758–64.
156. Lemus MC, Uribe EV, Avila JMJ. Traumatic atlantoaxial subluxation, posterior
transfacet fixation: a case report. Coluna/Columna. 2015;14:53–5.
157. Hosalkar HS, Sankar WN, Wills BPD, Goebel J, Dormans JP, Drummond DS.
Congenital osseous anomalies of the upper cervical spine. J. Bone Jt. Surg. - Ser. A.
2008;90:337–48.
158. Fitzcharles MA, Boulos P. Inaccuracy in the diagnosis of fibromyalgia syndrome:
Analysis of referrals. Rheumatology. 2003;42:263–7.
159. Solomon T, Thi TT, Lewthwaite P, Mong HO, Kneen R, Nguyen MD, et al. A cohort
study to assess the new WHO Japanese encephalitis surveillance standards. Bull.
World Health Organ. 2008;86:178–86.
160. Djukic M, Schmidt-Samoa C, Lange P, Spreer A, Neubieser K, Eiffert H, et al.
Cerebrospinal fluid findings in adults with acute Lyme neuroborreliosis. J. Neurol.
2012;259:630–6.

100
161. Huston AF, Morwood JB, Christofinis GJ, Wood W. Poliomyelitis in Suburban
Surrey. Br. Med. J. 1956;2:629–34.
162. Perry JJ, Stiell IG, Sivilotti MLA, Bullard MJ, Hohl CM, Sutherland J, et al. Clinical
decision rules to rule out subarachnoid hemorrhage for acute headache. JAMA - J. Am.
Med. Assoc. 2013;310:1248–55.
163. Cardiel MH, Londoño JD, E G, Pacheco-Tena C, Vázquez-Mellado J, Burgos-Vargas
R. Translation, cross-cultural adaptation, and validation of the Bath Ankylosing
Spondylitis Functional Index (BASFI), the Bath Ankylosing Spondylitis Disease
Activity Index (BASDAI) and the Dougados Functonal Index (DFI) in a Spanish
speaking population wit. Clin. Exp. Rheumatol. [Internet]. 2003;21:451–8. Available
from:
http://www.embase.com/search/results?subaction=viewrecord&from=export&id=L369
50313%0Ahttp://wx7cf7zp2h.search.serialssolutions.com?sid=EMBASE&issn=03928
56X&id=doi:&atitle=Translation%2C+cross-
cultural+adaptation%2C+and+validation+of+the+Bath+Ankylosing+Sp
164. Brandt J, Listing J, Sieper J, Rudwaleit M, Van Der Heijde D, Braun J. Development
and preselection of criteria for short term improvement after anti-TNFα treatment in
ankylosing spondylitis. Ann. Rheum. Dis. 2004;63:1438–44.
165. Madsen OR, Hansen LB, Rytter A, Suetta C, Egsmose C. The Bath metrology index as
assessed by a trained and an untrained rater in patients with spondylarthropathy: A
study of intra- and inter-rater agreements. Clin. Rheumatol. 2009;28:35–40.
166. Jenks K, Stebbings S, Burton J, Schultz M, Herbison P, Highton J. Probiotic therapy
for the treatment of spondyloarthritis: A randomized controlled trial. J. Rheumatol.
2010;37:2118–25.

101
167. Amine B, Abouqal R, Ibn Yacoub Y, Hajjaj-Hassouni N, Ali Ou Alla S, Rostom S, et
al. Psychometric evaluation of the Moroccan version of the Bath Ankylosing
Spondylitis Functional Index (BASFI) and Bath Ankylosing Spondylitis Disease
Activity Index (BASDAI) for use in patients with ankylosing spondylitis. Clin.
Rheumatol. 2010;29:781–8.
168. Ibn Yacoub Y, Amine B, Laatiris A, Hajjaj-Hassouni N. Gender and disease features
in Moroccan patients with ankylosing spondylitis. Clin. Rheumatol. 2012;31:293–7.
169. Mengshoel AM, Robinson HS. Clinical significance of specific spinal mobilization for
patients with ankylosing spondylitis evaluated by quantitative assessments and patient
interviews. Disabil. Rehabil. 2008;30:355–64.
170. Gary C, Robertson H, Ruiz B, Zuzukin V, Walvekar RR. Retropharyngeal
Ganglioneuroma Presenting with Neck Stiffness : Report of a Case and Review of
Literature. 2010.
171. Datar S, Daniels D, Wijdicks EFM. A major pitfall to avoid: Retroclival hematoma
due to odontoid fracture. Neurocrit. Care. 2013;19:206–9.
172. Gerber LH, Helfgott RK, Gross EG, Hicks JE, Ellenberg SS, Peck GL. Vertebral
abnormalities associated with synthetic retinoid use. J. Am. Acad. Dermatol.
1984;10:817–23.
173. Wassenaar MJE, Biermasz NR, van Duinen N, van der Klaauw AA, Pereira AM,
Roelfsena F, et al. High prevalence of arthropathy, according to the definitions of
radiological and clinical osteoarthritis, in patients with long-term cure of acromegaly:
A case-control study. Eur. J. Endocrinol. 2009;160:357–65.
174. Deane JA, McGregor AH. Current and future perspectives on lumbar degenerative disc

102
disease: A UK survey exploring specialist multidisciplinary clinical opinion. BMJ
Open. 2016;6:1–12.
175. de Schepper EIT, Luijsterburg PAJ, Koes BW, van Meurs JBJ, Scheele J, Hofman A,
et al. Association between spinal morning stiffness and lumbar disc degeneration: the
Rotterdam Study. Osteoarthr. Cartil. [Internet]. 2012;20:982–7. Available from:
http://dx.doi.org/10.1016/j.joca.2012.05.011
176. Baborie A, Dunn EM, Bridges LR, Bamford JM. Primary diffuse leptomeningeal
gliomatosis predominantly affecting the spinal cord: Case report and review of the
literature. J. Neurol. Neurosurg. Psychiatry. 2001;70:256–8.
177. Manning DM, Dedrick GS, Sizer PS, Brismée J-M. Reliability of a seated three-
dimensional passive intervertebral motion test for mobility, end-feel, and pain
provocation in patients with cervicalgia. J. Man. Manip. Ther. [Internet]. 2012;20:135–
41. Available from:
http://www.tandfonline.com/doi/full/10.1179/2042618611Y.0000000023
178. van Trijffel E, Oostendorp RAB, Lindeboom R, Bossuyt PMM, Lucas C. Perceptions
and use of passive intervertebral motion assessment of the spine: a survey among
physiotherapists specializing in manual therapy. Man. Ther. [Internet]. 2009;14:243–
51. Available from: http://www.ncbi.nlm.nih.gov/pubmed/18387332
179. Jull G, Bullock M. A motion profile of the lumbar spine in an ageing population
assessed by manual examination. Physiother. Theory Pract. 1987;
180. Maher CG, Latimer J, Adams RD. An investigation of the reliability and validity of
posteroanterior spinal stiffness judgments made using a reference-based protocol.
Phys. Ther. 1998;78:829–37.

103
181. Abbott JH, McCane B, Herbison P, Moginie G, Chapple C, Hogarty T. Lumbar
segmental instability: A criterion-related validity study of manual therapy assessment.
BMC Musculoskelet. Disord. 2005;6:1–10.
182. Owens EF, DeVocht JW, Wilder DG, Gudavalli MR, Meeker WC. The Reliability of a
Posterior-to-Anterior Spinal Stiffness Measuring System in a Population of Patients
With Low Back Pain. J. Manipulative Physiol. Ther. 2007;30:116–23.
183. Fernández-de-las-Peñas C, Downey C, Miangolarra-Page JC. Validity of the lateral
gliding test as tool for the diagnosis of intervertebral joint dysfunction in the lower
cervical spine. J. Manipulative Physiol. Ther. 2005;28:610–6.
184. Wilder DG, Owens EF, Meeker WC, DeVocht JW, Gudavalli MR. Comparison of
Posteroanterior Spinal Stiffness Measures to Clinical and Demographic Findings at
Baseline in Patients Enrolled in a Clinical Study of Spinal Manipulation for Low Back
Pain. J. Manipulative Physiol. Ther. 2007;30:493–500.
185. Triano JJ, Budgell B, Bagnulo A, Roffey B, Bergmann T, Cooperstein R, et al. Review
of methods used by chiropractors to determine the site for applying manipulation.
Chiropr. Man. Ther. 2013;21:1–29.
186. Maher CG, Adams RD. A psychophysical evaluation of manual stiffness
discrimination. Aust. J. Physiother. [Internet]. 1995;41:161–7. Available from:
http://dx.doi.org/10.1016/S0004-9514(14)60426-8
187. Chiradejnant A, Maher CG, Latimer J. Objective Manual Assessment of Lumbar
Posteroanterior Stiffness Is Now Possible. J. Manipulative Physiol. Ther. 2003;34–9.
188. Ferreira ML, Ferreira PH, Latimer J, Herbert RD, Maher C, Refshauge K. Relationship
between spinal stiffness and outcome in patients with chronic low back pain. Man.
104
Ther. [Internet]. 2009;14:61–7. Available from:
http://dx.doi.org/10.1016/j.math.2007.09.013
189. Maher CG, Adams RD. Stiffness judgments are affected by visual occlusion. J.
Manipulative Physiol. Ther. [Internet]. 1996;19:250–6. Available from:
http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=emed4&NEWS=N&
AN=1996161941
190. Kiviniemi K, Allison G, Lanigan H, Edmonston S, Walcher S, Simonsen AV.
Influence of standardized mobilization on the posteroanterior stiffness of the lumbar
spine in asymptomatic subjects. Physiother. Res. Int. 2001;6:145–56.
191. Stanton TR, Kawchuk GN. Reliability of assisted indentation in measuring lumbar
spinal stiffness. Man. Ther. [Internet]. 2009;14:197–205. Available from:
http://dx.doi.org/10.1016/j.math.2008.01.011
192. Lee M, Latimer J, Maher CG. Manipulation: investigation of a proposed mechanism.
Clin. Biomech. 1993;8:302–6.
193. Holt K, Russell D, Cooperstein R, Young M, Sherson M, Haavik H. Interexaminer
Reliability of Seated Motion Palpation for the Stiffest Spinal Site. J. Manipulative
Physiol. Ther. [Internet]. 2018 [cited 2018 Nov 13];Available from:
https://linkinghub.elsevier.com/retrieve/pii/S0161475417300684
194. Campbell BD, Snodgrass SJ. The effects of thoracic manipulation on posteroanterior
spinal stiffness. J. Orthop. Sports Phys. Ther. [Internet]. 2010 [cited 2018 Nov
13];40:685–93. Available from: www.jospt.org
195. Edmondston SJ, Allison GT, Althorpe BM, McConnell DR, Samuel KK. Comparison
of ribcage and posteroanterior thoracic spine stiffness: An investigation of the normal

105
response. Man. Ther. 1999;4:157–62.
196. Jull G. Examination of the articular system. Grime’s Mo. Edinburgh, Scotland:
Churchill Livingstone; 1995.
197. Kumar S. Posteroanterior Spinal Stiffness at T5, T10, and L3 Levels in Normal
Subjects. PM R [Internet]. 2012;4:342–8. Available from:
http://dx.doi.org/10.1016/j.pmrj.2011.12.009
198. Koppenhaver SL, Hebert JJ, Kawchuk GN, Childs JD, Teyhen DS, Croy T, et al.
Criterion validity of manual assessment of spinal stiffness. Man. Ther. [Internet].
2014;19:589–94. Available from: http://dx.doi.org/10.1016/j.math.2014.06.001
199. Snodgrass SJ, Rivett DA, Robertson VJ, Stojanovski E. Forces Applied to the Cervical
Spine During Posteroanterior Mobilization. J. Manipulative Physiol. Ther. [Internet].
2009;32:72–83. Available from: http://dx.doi.org/10.1016/j.jmpt.2008.09.012
200. Snodgrass SJ, Haskins R, Rivett DA. A structured review of spinal stiffness as a
kinesiological outcome of manipulation: Its measurement and utility in diagnosis,
prognosis and treatment decision-making [Internet]. J. Electromyogr. Kinesiol. 2012
[cited 2018 Nov 13];22:708–23. Available from:
http://dx.doi.org/10.1016/j.jelekin.2012.04.015
201. Gudavalli MR, DeVocht JW, Xia T, Vining RD, Wilder DG, Meeker WC, et al. Forces
applied during manual assessments of Low Back Pain patients. In: Proceedings of the
ASME 2014 International mechanical engineering congress and exposition. 2014. p. 2.
202. Jull G, Bullock M. A motion profile of the lumbar spine in an ageing population
assessed by manual examination. Physiother. Theory Pract. 1987;
203. Jull G, Treleaven J, Versace G. Manual examination: is pain provocation a major cue
106
for spinal dysfunction. Aust. J. Physiother. [Internet]. 1994;40:159–65. Available
from: http://dx.doi.org/10.1016/S0004-9514(14)60574-2
204. Latimer J, Lee M, Adams RD. The effects of high and low loading forces on
measured. J. Manip. Physiol. Ther. 1998;21:157–63.
205. Snodgrass SJ, Rivett DA, Robertson VJ. Manual Forces Applied During Posterior-to-
Anterior Spinal Mobilization: A Review of the Evidence. J. Manipulative Physiol.
Ther. 2006;29:316–29.
206. Abbott JH, Clare MC, McKenzie JE, David GD, Theis JC, Campbell AJ. Exercise
therapy, manual therapy, or both, for osteoarthritis of the hip or knee: A factorial
randomised controlled trial protocol. BioMed Cent. 2009;10:1–12.
207. Xia T, Wilder DG, Gudavalli MR, DeVocht JW, Vining RD, Pohlman KA, et al. Study
protocol for patient response to spinal manipulation – a prospective observational
clinical trial on physiological and patient-centered outcomes in patients with chronic
low back pain. BMC Complement. Altern. Med. [Internet]. 2014 [cited 2018 Nov
13];14:292. Available from:
http://bmccomplementalternmed.biomedcentral.com/articles/10.1186/1472-6882-14-
292
208. Viner A, Lee M. Direction of manual force applied during assessment of stiffness in
the lumbosacral spine. J Manip. Physiol Ther [Internet]. 1995;18:441–7. Available
from:
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Cit
ation&list_uids=8568425
209. Latimer J, Goodsell MM, Lee M, Maher CG, Wilkinson BN, Moran CC. Evaluation of
a New Device for Measuring Responses to Posteroanterior Forces in a Patient

107
Population, Part 1: Reliability Testing. Phys. Ther. 1996;76:158–65.
210. Nicholson LL, Adams RD, Maher CG. Magnitutde estimation of manually assessed
elastic stifness: stability of the exponent. Percept. Mot. Skills. 2000;581–92.
211. Snodgrass SJ, Cleland JA, Haskins R, Rivett DA. The clinical utility of cervical range
of motion in diagnosis, prognosis, and evaluating the effects of manipulation: a
systematic review. Physiotherapy [Internet]. 2014 [cited 2018 Nov 13];100:290–304.
Available from: https://linkinghub.elsevier.com/retrieve/pii/S0031940614000558
212. Keller TS, Colloca CJ, Fuhr AW. In vivo transient vibration assessment of the normal
human thoracolumbar spine. J. Manipulative Physiol. Ther. 2000;23:521–30.
213. Maher CG, Adams RD. Is the clinical concept of spinal stiffness multidimensional?
Phys. Ther. [Internet]. 1995;75:854–60; discussion 861-4. Available from:
http://www.ncbi.nlm.nih.gov/pubmed/7568385
214. Sran MM, Khan KM, Zhu Q, Oxland TR. Posteroanterior stiffness predicts sagittal
plane midthoracic range of motion and three-dimensional flexibility in cadaveric spine
segments. Clin. Biomech. 2005;20:806–12.
215. Maher CG, Simmonds M, Adams RD. Therapists’ conceptualization and
characterization of the clinical concept of spinal stiffness. Phys. Ther. 1998;78:289–
300.
216. Rey-Eiriz G, Alburquerque-Sendín F, Barrera-Mellado I, Martín-Vallejo FJ,
Fernández-de-las-Peñas C. Validity of the Posterior-Anterior Middle Cervical Spine
Gliding Test for the Examination of Intervertebral Joint Hypomobility in Mechanical
Neck Pain. J. Manipulative Physiol. Ther. 2010;33:279–85.
217. Tuttle N, Barrett R, Laakso L. Relation between changes in posteroanterior stiffness
108
and active range of movement of the cervical spine following manual therapy
treatment. Spine (Phila. Pa. 1976). 2008;33:673–9.
218. Hofstetter L, Häusler M, Wirth B, Swanenburg J. Instrumented Measurement of Spinal
Stiffness: A Systematic Literature Review of Reliability. J. Manipulative Physiol.
Ther. [Internet]. 2019;41:704–11. Available from:
https://doi.org/10.1016/j.jmpt.2018.03.002
219. Jull G, Bullock M. The influence of segmental level and direction of movement on age
changes in lumbar motion as assessed by manual examination. Physiother. Theory
Pract. 1987;3:107–16.
220. Lee M, Svensson NL. Effect of muscle activation on response to lumbar
posteroanterior forces. J. Manipulative Physiol. Ther. [Internet]. 1993;16:439–46.
Available from:
http://search.ebscohost.com/login.aspx?direct=true&db=cmedm&AN=8228646&site=
ehost-live
221. Maher CG, Latimer J. Pain or resistance - the manual therapists’ dilemma. Aust. J.
Physiother. [Internet]. 1992;38:257–60. Available from:
http://dx.doi.org/10.1016/S0004-9514(14)60568-7
222. Xia T, Long CR, Vining RD, Gudavalli MR, DeVocht JW, Kawchuk GN, et al.
Association of lumbar spine stiffness and flexion-relaxation phenomenon with patient-
reported outcomes in adults with chronic low back pain – a single-arm clinical trial
investigating the effects of thrust spinal manipulation. BMC Complement. Altern.
Med. [Internet]. 2017 [cited 2018 Nov 13];17:303. Available from:
http://bmccomplementalternmed.biomedcentral.com/articles/10.1186/s12906-017-
1821-1
109
223. Colloca CJ, Keller TS, Peterson TK, Seltzer DE. Comparison of dynamic
posteroanterior spinal stiffness to plain film radiographic images of lumbar dise height.
J. Manipulative Physiol. Ther. 2003;26:233–41.
224. Haas M, Panzer D, Aickin M, Groupp E, Partna L, Lumsden S. Efficacy of Cervical
Endplay Assessment as an Indicator for Spinal Manipulation. Spine (Phila. Pa. 1976).
2011;28:1091–6.
225. Tuttle N, Hazle C. Spinal PA movements behave ‘as if’ there are limitations of local
segmental mobility and are large enough to be perceivable by manual palpation: A
synthesis of the literature. Musculoskelet. Sci. Pract. [Internet]. 2018;36:25–31.
Available from: https://doi.org/10.1016/j.msksp.2018.04.005
226. Lee M, Latimer J, Maher CG. Normal response to large posteroanterior lumbar loads--
a case study approach. J Manip. Physiol Ther. 1997;20:369–71.
227. Lee M, Steven GP, Crosbie J, Higgs RJED. Variations in posteroanterior stiffness in
the thoracolumbar spine: Preliminary observations and proposed mechanisms. Phys.
Ther. 1998;78:1277–87.
228. Edmondston SJ, Allison GT, Gregg CD, Purden SM, Svansson GR, Watson AE.
Effect of position on PA stiffness of Lumbar spine. Man. Ther. 1998;3:21–6.
229. Maher CG, Latimer J, Mathew HJ. Plinth padding confounds measures of
posteroanterior spinal stiffness. Man. Ther. 1999;4:145–50.
230. Brodeur RR, DelRe L. Stiffness of the thoracolumbar spine for subjects with and
without low back pain. Jnms-Journal Neuromusculoskel. Syst. 1999;7:127–33.
231. Goodsell M, Lee M, Latimer J. Short-term effects of lumbar posteroanterior
mobilization in individuals with low-back pain. J. Manipulative Physiol. Ther.
110
2000;23:332–42.
232. Hodges PW, Eriksson AEM, Shirley D, Gandevia SC. Intra-abdominal pressure
increases stiffness of the lumbar spine. J. Biomech. 2005;38:1873–80.
233. Snodgrass SJ, Rivett DA, Robertson VJ. Measuring the posteroanterior stiffness of the
cervical spine. Man. Ther. [Internet]. 2008 [cited 2018 Nov 13];13:520–8. Available
from: https://www-sciencedirect-
com.libproxy.unitec.ac.nz/science/article/pii/S1356689X07001245
234. Tuttle N, Barrett R, Laakso L. Postero-anterior movements of the cervical spine:
Repeatability of force displacement curves. Man. Ther. 2008;13:341–8.
235. Stanton TR, Kawchuk GN. The effect of abdominal stabilization contractions on
posteroanterior spinal stiffness. Spine (Phila. Pa. 1976). 2008;33:694–701.
236. Tuttle N, Barrett R, Laakso L. Posteroanterior movements in tender and less tender
locations of the cervical spine. Man. Ther. [Internet]. 2009;14:28–35. Available from:
http://dx.doi.org/10.1016/j.math.2007.09.003
237. Snodgrass SJ, Rivett DA, Robertson VJ, Stojanovski E. A Comparison of Cervical
Spine Mobilization Forces Applied by Experienced and Novice Physiotherapists. J.
Orthop. Sport. Phys. Ther. 2010;40:392–401.
238. Snodgrass SJ, Rivett DA, Robertson VJ, Stojanovski E. Cervical spine mobilisation
forces applied by physiotherapy students. Physiotherapy [Internet]. 2010;96:120–9.
Available from: http://dx.doi.org/10.1016/j.physio.2009.08.008
239. Vaillant M, Pickar JG, Kawchuk GN. Performance and reliability of a variable rate,
force/displacement application system. J. Manipulative Physiol. Ther. [Internet].
2010;33:585–93. Available from: http://dx.doi.org/10.1016/j.jmpt.2010.08.020

111
240. Fritz JM, Koppenhaver, Shane Kawchuk, Gregory N.L.Teyhen DS, Hebert JJ, Childs
JD. Preliminary Investigation of the Mechanisms Underlying the Effects of
Manipulation. Spine (Phila. Pa. 1976). 2011;36:1772–81.
241. Snodgrass SJ, Rhodes HR. Cervical spine posteroanterior stiffness differs with neck
position. J. Electromyogr. Kinesiol. [Internet]. 2012 [cited 2018 Nov 13];22:829–34.
Available from: http://dx.doi.org/10.1016/j.jelekin.2012.04.014
242. Tiantian W, Jian H, Yongji W, Xiaolin H, Jinghui Z. Development of the
Measurement System of the Postero-to-Anterior Movements of the Cervical Spine. In:
Proceedings of 2012 International Conference on Modelling, Identification and
Control, Wuhan, China, June 24-26, 2012. IEEE; 2012. p. 24–6.
243. Wong AYL, Kawchuk G, Parent E, Prasad N. Within- and between-day reliability of
spinal stiffness measurements obtained using a computer controlled mechanical
indenter in individuals with and without low back pain. Man. Ther. [Internet].
2013;18:395–402. Available from: http://dx.doi.org/10.1016/j.math.2013.02.003
244. Snodgrass SJ, Rivett DA, Sterling M, Vicenzino B. Dose Optimization for Spinal
Treatment Effectiveness: A Randomized Controlled Trial Investigating the Effects of
High and Low Mobilization Forces in Patients With Neck Pain. J. Orthop. Sport. Phys.
Ther. [Internet]. 2014 [cited 2018 Nov 13];44:141–52. Available from:
http://www.jospt.org/doi/10.2519/jospt.2014.4778
245. Ingram LA, Snodgrass SJ, Rivett DA. Comparison of Cervical Spine Stiffness in
Individuals With Chronic Nonspecific Neck Pain and Asymptomatic Individuals. J.
Orthop. Sport. Phys. Ther. [Internet]. 2015 [cited 2018 Nov 13];45:162–9. Available
from: http://www.jospt.org/doi/10.2519/jospt.2015.5711
246. Wong AYL, Parent EC, Dhillon SS, Prasad N, Kawchuk GN. Do Participants With

112
Low Back Pain Who Respond to Spinal Manipulative Therapy Differ Biomechanically
From Nonresponders, Untreated Controls or Asymptomatic Controls? Spine (Phila. Pa.
1976). 2015;40:1329–37.
247. Kawchuk GN, Edgecombe TL, Wong AYL, Cojocaru A, Prasad N. A non-randomized
clinical trial to assess the impact of nonrigid, inelastic corsets on spine function in low
back pain participants and asymptomatic controls. Spine J. [Internet]. 2015;15:2222–7.
Available from: http://dx.doi.org/10.1016/j.spinee.2015.06.047
248. Wong AYL, Parent EC, Prasad N, Huang C, Chan KM, Kawchuk GN. Does
experimental low back pain change posteroanterior lumbar spinal stiffness and trunk
muscle activity? A randomized crossover study. Clin. Biomech. [Internet].
2016;34:45–52. Available from: http://dx.doi.org/10.1016/j.clinbiomech.2016.03.006
249. Björnsdóttir SV, Gudmundsson G, Audunsson GA, Matthíasson J, Ragnarsdóttir M.
Posterior-anterior(PA) pressure Puffin for measuring and treating spinal stiffness:
Mechanism and repeatability. Man. Ther. 2016;22:72–9.
250. Brown B, Blacke A, Carroll V, Graham P, Kawchuk G, Downie A, et al. The comfort
and safety of a novel rolling mechanical indentation device for the measurement of
lumbar trunk stiffness in young adults. Chiropr. Man. Ther. 2017;25:1–10.
251. Pagé I, Nougarou F, Lardon A, Descarreaux M. Changes in spinal stiffness with
chronic thoracic pain: Correlation with pain and muscle activity. PLoS One [Internet].
2018 [cited 2018 Nov 13];13:1–15. Available from:
https://doi.org/10.1371/journal.pone.0208790
252. Kawchuk GN, Miazga S, Pagé I, Swain M, De Carvalho D, Funabashi M, et al.
Clinicians’ Ability to Detect a Palpable Difference in Spinal Stiffness Compared With
a Mechanical Device. J. Manipulative Physiol. Ther. [Internet]. 2019;Available from:

113
https://doi.org/10.1016/j.jmpt.2019.02.002
253. Reiman MP. Trunk stabilization training: An evidence basis for the current state of
affairs. J. Back Musculoskelet. Rehabil. 2009;22:131–42.
254. Kumar S. Spinal stiffness in asymptomatic subjects. J. Electromyogr. Kinesiol.
[Internet]. 2011;21:762–6. Available from:
http://dx.doi.org/10.1016/j.jelekin.2011.07.008
255. Stamos-Papastamos N, Petty NJ, Williams JM. Changes in bending stiffness and
lumbar spine range of movement following lumbar mobilization and manipulation. J.
Manipulative Physiol. Ther. [Internet]. 2011;34:46–53. Available from:
http://dx.doi.org/10.1016/j.jmpt.2010.11.006
256. Shum GL, Tsung BY, Lee RY. The immediate effect of posteroanterior mobilization
on reducing back pain and the stiffness of the lumbar spine. Arch. Phys. Med. Rehabil.
[Internet]. 2013;94:673–9. Available from:
http://dx.doi.org/10.1016/j.apmr.2012.11.020
257. Keller TS, Colloca CJ. Mechanical force spinal manipulation increases trunk muscle
strength assessed by electromyography: A comparative clinical trial. J. Manipulative
Physiol. Ther. 2000;23:585–95.
258. Descarreaux M, Nougarou F, Dugas C. Standardization of spinal manipulation therapy
in humans: Development of a novel device designed to measure dose-response. J.
Manipulative Physiol. Ther. 2013;36:78–83.
259. Dugailly PM, Coucke A, Salem W, Feipel V. Assessment of cervical stiffness in axial
rotation among chronic neck pain patients: A trial in the framework of a non-
manipulative osteopathic management. Clin. Biomech. [Internet]. 2018;53:65–71.

114
Available from: https://doi.org/10.1016/j.clinbiomech.2018.02.005
260. Gombatto SP, Klaesner JW, Norton BJ, Minor SD, Van Dillen LR. Validity and
reliability of a system to measure passive tissue characteristics of the lumbar region
during trunk lateral bending in people with and people without low back pain. J.
Rehabil. Res. Dev. [Internet]. 2008;45:1415. Available from:
http://www.rehab.research.va.gov/jour/08/45/9/gombatto.html
261. Colloca CJ, Keller TS. Active trunk extensor contributions to dynamic posteroanterior
lumbar spinal stiffness. J. Manipulative Physiol. Ther. 2004;27:229–37.
262. Tsung BYS, Evans J, Tong P, Lee RYW. Measurement of lumbar spine loads and
motions during rotational mobilization. J. Manipulative Physiol. Ther. 2005;28:238–
44.
263. Squires MC, Latimer J, Adams RD, Maher CG. Indenter head area and testing
frequency effects on posteroanterior lumbar stiffness and subjects’ rated comfort. Man.
Ther. 2001;6:40–7.
264. Snodgrass SJ, Rivett DA, Sterling M, Vicenzino B. Dose optimization for spinal
treatment effectiveness: A randomized controlled trial investigating the effects of high
and low mobilization forces in patients with neck pain. J. Orthop. Sports Phys. Ther.
[Internet]. 2014 [cited 2018 Nov 13];44:141–52. Available from:
http://www.jospt.org/doi/10.2519/jospt.2014.4778
265. Pagé I, Nougarou F, Lardon A, Descarreaux M, Pagé Id I, Ois Nougarou F, et al.
Changes in spinal stiffness with chronic thoracic pain: Correlation with pain and
muscle activity. PLoS One [Internet]. 2018 [cited 2018 Nov 13];13:1–15. Available
from: https://doi.org/10.1371/journal.pone.0208790

115
266. Bekhet AK, Zauszniewski JA. Methodological triangulation: an approach to
understanding data. Nurse Res. 2012;20:40–3.
267. Farasyn A, Meeusen R. Validity of the new Backache Index (BAI) in patients with low
back pain. Spine J. 2006;6:565–71.
268. Lee J, Kwon H, Lee JS, Kim HD, Kang HC. Applying the bacterial meningitis score in
children with cerebrospinal fluid pleocytosis: A single center’s experience. Korean J.
Pediatr. 2015;58:251–5.
269. Kaminsky SB, Clark CR, Traynelis VC. Operative treatment of cervical spondylotic
myelopathy and radiculopathy. A comparison of laminectomy and laminoplasty at five
year average follow-up. Iowa Orthop. J. [Internet]. 2004;24:95–105. Available from:
http://www.ncbi.nlm.nih.gov/pubmed/15296214%0Ahttp://www.pubmedcentral.nih.g
ov/articlerender.fcgi?artid=PMC1888413
270. Cheng C-H, Wang S-F, Chen CP-C, Liu W-Y, Hsu W-L, Chuang Y-F, et al. Altered
Co-contraction of Cervical Muscles in Young Adults with Chronic Neck Pain during
Voluntary Neck Motions. J. Phys. Ther. Sci. 2014;26:587–90.
271. Karayannis N V., Smeets RJEM, van den Hoorn W, Hodges PW. Fear of Movement Is
Related to Trunk Stiffness in Low Back Pain. PLoS One. 2013;8.
272. Cheng C-H, Lin K-H, Wang J-L. Co-contraction of cervical muscles during sagittal
and coronal neck motions at different movement speeds. Eur. J. Appl. Physiol.
2008;103:647–54.
273. Graham RB, Oikawa LY, Ross GB. Comparing the local dynamic stability of trunk
movements between varsity athletes with and without non-specific low back pain. J.
Biomech. 2014;

116
Section 4: Appendices
The scoping review protocol was registered prospectively with the open science framework
on 7 of March 2019. Reference: Moses, J. (2019, March 7). Scoping review protocol:
Defining and measuring objective and subjective spinal stiffness. Available here;
https://doi.org/10.17605/OSF.IO/SWKU6
117
Appendix A; Ethics notification

118
Appendix B: Search strategy
Keyword search
• Stiffness
• Definition
• Measure
• Objective
• Subjective
• Spinal
Initial search terms and key phrases
Initial searches were undertaken in order to survey the available literature and to arrive at a
search syntax for the present project that would maximally capture the available literature and
be feasible for a research project of 90 credits. The following search terms were gathered
from the listed key words of relevant journal articles and relevant terms in the MeSH
database.
Title and/or abstract must include any combination of:
stiffness, stiffness AND pain
AND
definition, meaning, concept, construct,
AND
measure, outcome, assessment, utility.
AND
objective, static OR passive, active, dynamic, perturbation.
AND
subjective, symptom, experience, perception, sensation, psychosomatic.
AND
spinal, back, low back pain, lumbar spine, thoracic spine, cervical spine.

119
Table showing the initial electronic search strategy executed in PubMed (04/09/2018)
for preliminary syntax check
Sample search syntax Database Yield
Stiffness AND defin* PubMed 4003
Stiffness AND Body AND measur* PubMed 3077
Stiffness AND musculoskeletal AND measur*
(note includes arterial and visceral stiffness)
PubMed 1431
Stiffness AND back AND measur* PubMed 531
Stiffness AND musculoskeletal AND measur* AND defin* PubMed 512
Stiffness AND perception AND measur* PubMed 42
Stiffness AND subjective AND measur*: PubMed 66
Stiffness AND Body AND measur* AND defin* PubMed 271
Stiffness AND pain AND spinal PubMed 749
Stiffness AND pain AND back AND subjective PubMed 28
Stiffness AND spinal AND measur* PubMed 891
Stiffness AND spinal AND defin* PubMed 175
Rationale for search strategy selection
The initial search strategy was broad and included any type of musculoskeletal OR body
stiffness. However, for reasons of clinical relevance regarding the manual therapy profession,
the preliminary searches were constrained to focus on the spinal region. The final search
syntax that was used for the present study included: “stiffness AND spinal AND defin*” and
“stiffness AND spinal AND measur*”.

120
Final search strategy
Database: PUBMED
Date: 01/11/2018
#Search (stiffness AND spinal AND defin*).
#Search (stiffness AND spinal AND measur*)
Sort by: Relevance Filters: Humans; English
The search strategy was adapted to Scopus and Ebsco health database (Academic Search
Complete, The Allied and Complementary Medicine Database, CINAHL with Full Text,
Health Business Elite, Health Source: Nursing/Academic Edition, LGBT Life with Full Text,
MasterFILE Premier, MEDLINE with Full Text, Psychology and Behavioural Sciences
Collection, SocINDEX with Full Text, SPORTDiscus with Full Text).
Table showing an overview of the final search strategy
Date of retrieval Search syntax Database Yield
01/11/2018 stiffness AND spinal
AND defin*
PubMed 119
01/11/2018 stiffness AND spinal
AND measur*
PubMed 652
12/11/2018 stiffness AND spinal
AND defin*
Ebsco 94
12/11/2018 stiffness AND spinal
AND measur*
Ebsco 417
20/12/2018 stiffness AND spinal
AND defin*
Scopus 157
20/12/2018 stiffness AND spinal
AND measur*
Scopus 682
TOTAL: 2121

121
Appendix C: Screening template
Screening Questions and Inclusion Criteria were the following:
Does the title/abstract/keywords include any combination of search terms?
AND
Does the study report (a) definition(s) of spinal stiffness or include subjective or objective
measures or indicators of spinal stiffness?
AND
Does the study investigate patient/clinician/research-reported outcome or experience
measures of spinal stiffness?
Exclusion criteria were as follows:
Studies published in the grey literature
Studies investigating animal stiffness
Studies investigating non-spinal stiffness
Studies not published in English

122
Appendix D: Interrater agreement
Definitions for level of agreement
Kappa
Range Definition
< 0 Less than chance
0.01-0.20 Slight
0.21-0.40 Moderate 0.61-0.80 Substantial
0.81-0.99 Near perfect
Example data of 2x2 table format showing data distribution with balanced marginal
distribution
Rater 2 Total Yes No
Rater 1 Yes 83 4 87 0.87% No 12 51 63 0.63% Total 95 55 150
0.95% 0.55%
𝑃𝑜 = 51 + 83
= 0.89 150
87 𝑃𝑒 =
150 ×
95 +
150
55 ×
150
63 = 0.52
150
𝐾𝑎𝑝𝑝𝑎, 𝐾 = 0.89 − 0.52
1 − 0.52
= 0.77

123
Appendix E: Data Items
These data items were used to gather the relevant full-text data:
1. Citation details
2. Objective measures of spinal stiffness
- Measure/indicator
- Definition/description
3. Subjective measures of spinal stiffness
- Measure/indicator
- Definition/description
4. Surrogate definitions or measures of spinal stiffness
- Alternative descriptor
▪ Synonym
▪ Antonym
- Characteristic

124
Appendix F: Data abstraction tables
Data abstraction: Biomechanical theme
Functional spinal unit Cervical spine (n=4)
Reference Objective measure Measure/Indicator Definition/Description
(Panjabi et al., Two customised spine testing jigs Load – displacement No definition of stiffness reported
1986)
(McElhaney et Minneapolis Test Systems – servo-controlled Load – deflection Increasing stiffness explained in terms of
al., 1988) hydraulic testing machine (Hardening response)
(Wen et al., 3D coordinate systems Load – displacement The secant stiffness is the slope of the
1993) straight line calculated by a simple linear
regression of the loading part of a load-
displacement curve in the elastic zone
between the first point after the greatest
variation in the curve gradient and the
point with maximum loading.
(Dugailly et al.,
2017) A customized spine testing device Torque – angular displacement. 𝑆𝑡𝑖𝑓𝑓𝑛𝑒𝑠𝑠 (𝑁𝑚⁄⸰) =
∆ 𝑇𝑜𝑟𝑞𝑢𝑒𝐸𝑍
∆𝑅𝑂𝑀𝐸𝑍

125
Functional spinal unit: Thoracic spine (n=7)
Reference Objective measure Measure/Indicator Definition/Description
(Tawackoli et
al., 2004) Custom designed spine testing machine Force – torque No definition of stiffness reported
(Myklebust et
al., 2004)
Axial compressive load experiments were Force – deflection Stiffness is defined as a measure of the
ability to withstand an external force
(Kayanja et al.,
2006)
Material Testing System Load – displacement No definition of stiffness reported
(Busscher et al.,
2009)
Custom designed four-point bending device Load – displacement The stiffness of a spinal segment is
generally calculated as the inverse slope
of a part of the load-displacement curve.
(Wolfla et al.,
2010)
Custom designed electro-hydraulic testing
device
Force – displacement Stiffness was defined as the slope in the
linear region of the force-displacement
response.
(Verkerke et al.,
2011)
Custom designed four-point bending device Moment – angular displacement Stiffness in the Neutral Zone was
calculated as the inverse of the slope in
the complete range of the Neutral Zone,
since this part of the curve showed linear
characteristics (Fig.
(Wagnac et al.,
2017)
Material Testing System Force – displacement Stiffness was defined as the slope of the
most linear portion of the curve, prior to
failure. Failure energy was defined as the
area under the force-displacement curve,
up to failure.
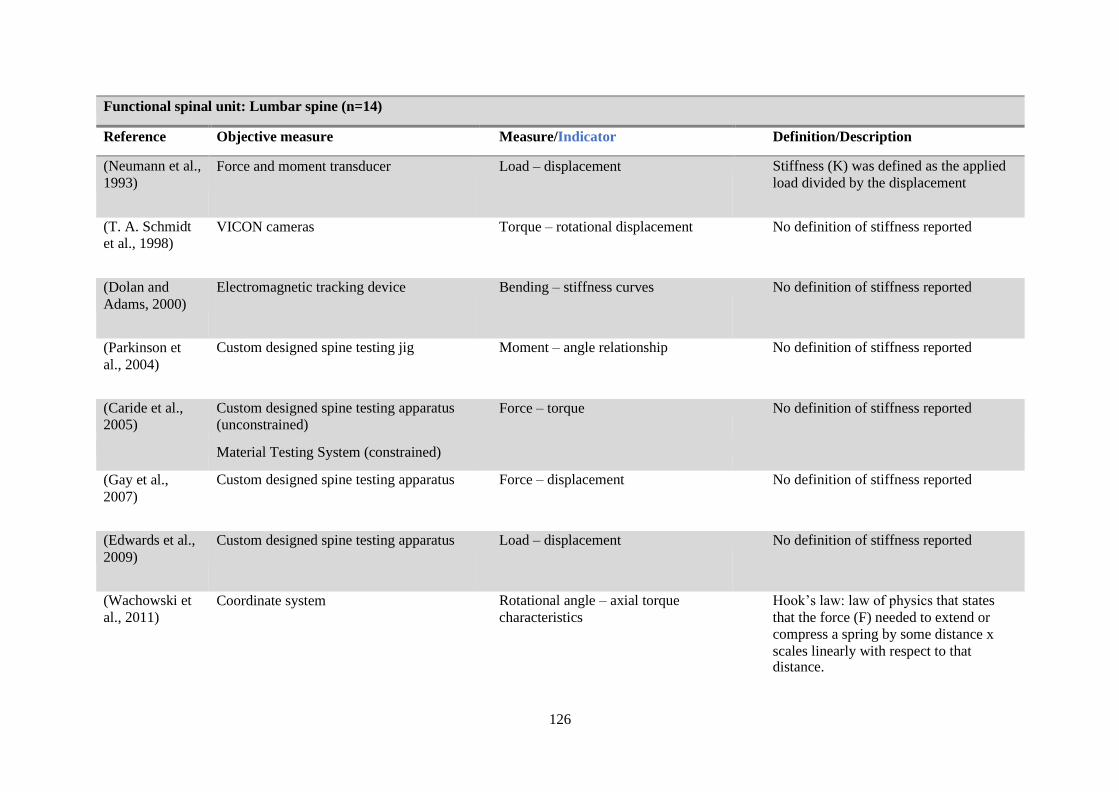
126
Functional spinal unit: Lumbar spine (n=14)
Reference Objective measure Measure/Indicator Definition/Description
(Neumann et al.,
1993) Force and moment transducer Load – displacement Stiffness (K) was defined as the applied
load divided by the displacement
(T. A. Schmidt
et al., 1998) VICON cameras Torque – rotational displacement No definition of stiffness reported
(Dolan and
Adams, 2000)
Electromagnetic tracking device Bending – stiffness curves No definition of stiffness reported
(Parkinson et
al., 2004)
Custom designed spine testing jig Moment – angle relationship No definition of stiffness reported
(Caride et al.,
2005)
Custom designed spine testing apparatus
(unconstrained) Force – torque No definition of stiffness reported
Material Testing System (constrained)
(Gay et al.,
2007)
Custom designed spine testing apparatus Force – displacement No definition of stiffness reported
(Edwards et al.,
2009)
Custom designed spine testing apparatus Load – displacement No definition of stiffness reported
(Wachowski et
al., 2011)
Coordinate system Rotational angle – axial torque
characteristics
Hook’s law: law of physics that states
that the force (F) needed to extend or
compress a spring by some distance x
scales linearly with respect to that distance.

127
(van Engelen et
al., 2012)
Custom designed device – hydraulic material
testing system
Load – deflection No definition of stiffness reported
(Bisschop, Custom designed four-point bending device Load – displacement No definition of stiffness reported
Kingma, et al.,
2013)
(Stolworthy et Custom designed spine simulator Torque – rotational displacement (Nm/1⸰) Operational definition of Neutral zone
al., 2014) stiffness (Nm/1⸰) as the amount of torque required to cause 1⸰ of rotation within the
near constant-slope neutral- zone region.
(Borkowski et The restoring force method Moment – displacement No definition of stiffness reported
al., 2014)
(Amin et al., Six degree of freedom hexapod robotic Load – displacement No definition of stiffness reported
2016) testing system.
(Zirbel et al., DIP-Boltzmann presents several potential Torque – rotational displacement (Nm/1⸰) This stiffness represents the inverse of
2013) advantages in terms of standardizing the the slope of the line in the Neutral Zone. calculation of flexibility parameters (i.e.,
ROM, stiffness, and hysteresis).

128
Reference Objective measure Measure/Indicator Definition/Description
(Quint and
Wilke, 1998) Custom designed spine testing device Load – angular deformation
Reduced mobility is considered to be a
stiffening of the motion segment, which
results in greater stability.
The segmental stability was defined by
the correlation of an applied moment to
the resultant deformation, as shown in
the load-displacement curves.
(Essendrop et
al., 2002)
Sudden Mechanical Perturbation
Co-measure-Electromyography
The stiffness of the spine was calculated
from the equation of motion of the system
after the release.
No definition of stiffness reported
(Petra et al.,
2003) Electromyography The summed muscle force relative to the
resultant net moment was calculated at the
instant of peak resultant net moment to
obtain an indication of the stiffness of the
spine.
No definition of stiffness reported
(Bull Andersen
et al., 2004)
Sudden Mechanical Perturbation Stiffness is described as the force that
tends to restore the static equilibrium
(e.g. force constant of a spring calculated
as change in force divided by
displacement)
(Vera-Garcia et
al., 2006)
Sudden posterior loading
Co-measure-Electromyography
Force – displacement No definition of stiffness reported
Stability (active, passive, neural contribution to spinal stiffness) (n=16)
𝑑𝑇/𝑑𝑎 = 𝑠𝑡𝑖𝑓𝑓𝑛𝑒𝑠𝑠 (𝑁𝑚/𝑑𝑒𝑔𝑟𝑒𝑒) Torque – rotational displacement 3-SPACE isotrak system (McGill et al.,
1994)

129
(Moorhouse and
Granata, 2007)
Pseudorandom binary sequence of position
perturbations
Force – time No definition of stiffness reported
(Lee et al., Pseudorandom force perturbations The parameters were described as effective No definition of stiffness reported
2007) stiffness, effective damping, and effective
mass because the stiffness represented
combined behaviours from intrinsic and
reflexive stiffness, and the damping
represented combined behaviours from
intrinsic and reflexive damping.
(Bazrgari and A three-camera Optotrak system Loads on the human spine are influenced No definition of stiffness reported
Shirazi-Adl, not only by the gravity, inertia and external
2007) loads but also by the stiffness of the
ligamentous spine and forces in trunk
muscles.
(Cheng et al., Co-contraction of antagonistic muscles is Insufficient co-contraction and No definition of stiffness reported
2008) important to augment the stiffness of the neuromuscular control could decrease
spine. stiffness in the cervical spine.
(Chad et al., Spine Load and Stiffness Estimation: Force – time Stiffness is the closest quantifiable
2009) Electromyography surrogate of spine stability. With reference to the spine, stability can be thought of as ensuring sufficient stiffness by optimally coordinated muscle contraction and therefore stiffness around
the spine
(Howarth et al., Trunk muscle activity during wheelchair Trunk muscles are important for generating No definition of stiffness reported
2010) ramp accent active stiffness surrounding the spinal
column.
(Cheng et al., Co-contraction of antagonistic muscles is This indicated that the spinal stiffness of the No definition of stiffness reported
2014) important to augment the stiffness of the patients is predominantly taken up from the
spine.

130
(Lamberg and
Hagins, 2014)
(Shojaei et al.,
2018)
Intra-abdominal pressure increases the ability
for the lumbar and thoracic segmental control
by facilitating spinal stiffness.
Six trunk stiffness tests in upright posture
under (to estimate contribution to spine
stability)
Breath control is linked in predictable ways
to potentially improve lumbar spine
stiffness when presented with mechanical
challenges during functional tasks and
should be incorporated into physical
therapy interventions.
Changes in the moment and the lumbar
flexion angle
No definition of stiffness reported
Spinal stability, in a biomechanical
sense, is defined as the capacity of the
system that provides spinal equilibrium
to sustain the equilibrium in the presence
of mechanical perturbations. Therefore,
spinal stability can partially be assessed
through measures of trunk bending
stiffness.
(Talebian et al.,
2018) Sudden perturbation Neck Stiffness calculated based on the
kinematic responses to the sudden
perturbation. The head and neck were
modelled as a linear second-order system,
with scalar coefficients of stiffness,
damping, and inertia.
No definition of stiffness reported
muscle guarding phenomenon as well as
possible proprioceptive deficits.

131
Instability (n=7)
Reference Objective measure Measure/Indicator Definition/Description
(Pope and
Panjabi, 1985) No objective measure of stiffness reported Load – deflection Stiffness was defined as the amount of motion
within a system relative to a load applied to the
structure.
Instability is defined from a biomechanical
perspective, as a loss of stiffness in the spine.
(Ashton-Miller
and Schultz,
1991)
No objective measure of stiffness reported Load – displacement Stiffness is generally defined as the ratio of the
applied load divided by displacement.
(Dolan et al.,
2005)
Mechanical Testing Apparatus Moment – angular rotation Bending Stiffness was defined as the gradient of the
tangent to the linear region of the graph at 20 Nm.
Biomechanical reviews agree that segmental
instability is best defined in terms of reduced
stiffness (reduced resistance to movement)
(Szust, 2006) Material Testing System – Bionix testing
machine
Load – displacement No definition of stiffness reported
(Pope et al.,
2006)
No objective measure of stiffness reported No objective measure of stiffness
reported
Instability is synonymous with a loss of motion
segment stiffness, such that force applied to that
motion segment produces greater displacement than
would be seen in a normal structure.
(Fry et al.,
2014)
Opto-electronic motion measurement
system.
Load – displacement No definition of stiffness reported
(Sayson and
Lotz, 2015)
Spinal Kinematics with the KineGraph
Vertebral Motion Analyzer Measure in vivo spinal kinematics
to assess segmental stiffness and
biomechanical instability
No definition of stiffness reported

132
Finite element model (n=22)
Reference Objective measure Measure/Indicator Definition/Description
(Roberts et al.,
1969) Stiffness matrix Motion and deformation in the head-neck region. No definition of stiffness reported
(Yang and King, Materials testing machine Force – deformation No definition of stiffness reported
1984) Force – deflection
(Gardner-Morse
et al., 1990)
6 X 6 stiffness matrix The reported linear stiffnesses is either from 1) the
stiffness at a point on the curve (tangent stiffness),
or 2) a line between two points on the curve
(secant stiffness), or 3) the stiffness from a
relatively linear portion of the curve.
No definition of stiffness reported
(Pitzen et al.,
2000)
Finite element model Values are given in N/mm for testing in axial
compression. Range of motion was used to
calculate the stiffness of the model.
No definition of stiffness reported
(Panjabi et al.,
2000)
Center of rotation apparatus Load – displacement The stiffness test protocol, by
definition, requires the application
of one motion component and
measurement of the loads
generated.
The flexibility protocol is the
reverse, i.e., apply one
displacement component and
measure the resulting motions.

133
(van Deursen et
al., 2000)
Biomechanical computer model Vertical displacement and axial torsion. No definition of stiffness reported
(Ng and Teo,
2001)
Nonlinear Finite-Element Analysis Force – displacement No definition of stiffness reported
(Buford et al.,
2002)
Model Study (Spinal kinematics) Torsional stiffness No definition of stiffness reported
(Ng et al., 2003) Model study – 3D cervical spine finite
element model
Force – displacement No definition of stiffness reported
(Gardner-Morse
and Stokes,
2004)
12 X 12 stiffness matrix. Load – displacement No definition of stiffness reported
(Hans et al.,
2009)
Custom-made 6D apparatus Force – displacement No definition of stiffness reported
(Iyer et al.,
2010)
Quasi-static stiffness-based biomechanical
model Force and moments No definition of stiffness reported
(Lafon et al.,
2010)
Virtual model (spine and pelvis) – 3D
stiffness distribution along scoliotic spine.
Vertebral displacements between standing and
bending positions were computed No definition of stiffness reported
(Kleinberger,
2010)
3D finite element model. Load – displacement The large strain axial stiffness of
the column was defined by the
peak load divided by the maximum displacement.
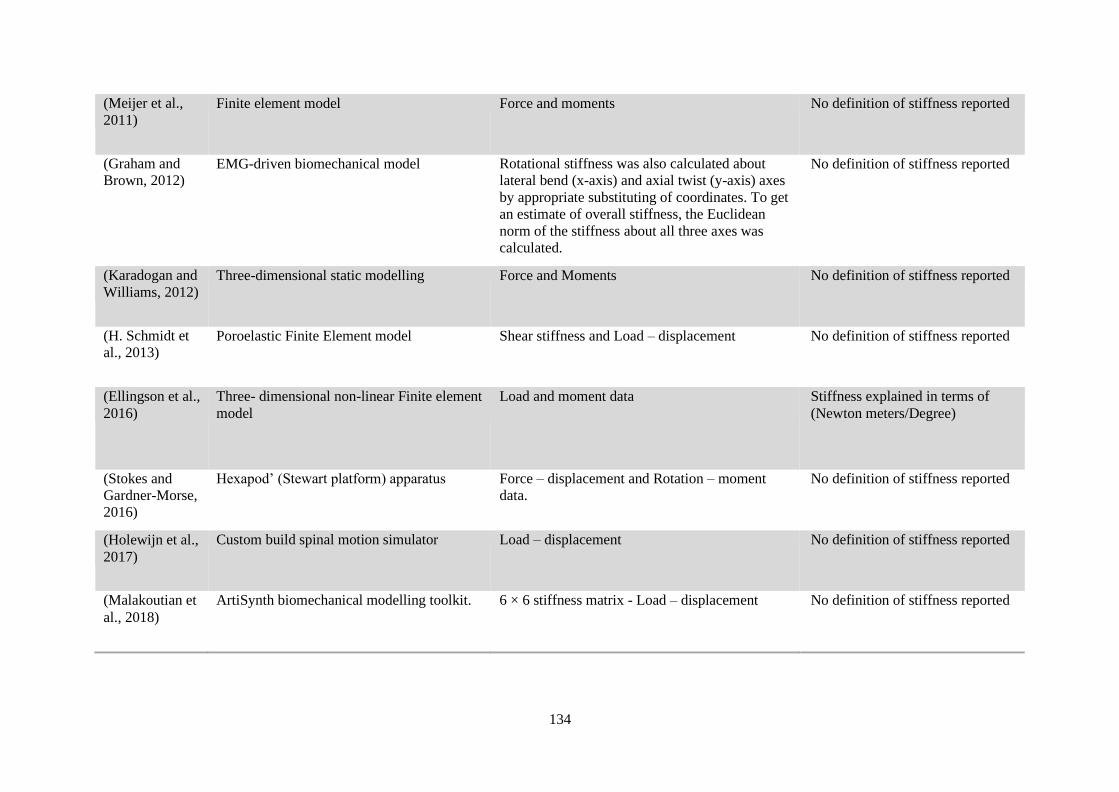
134
(Meijer et al.,
2011)
Finite element model Force and moments No definition of stiffness reported
(Graham and
Brown, 2012) EMG-driven biomechanical model Rotational stiffness was also calculated about
lateral bend (x-axis) and axial twist (y-axis) axes
by appropriate substituting of coordinates. To get
an estimate of overall stiffness, the Euclidean
norm of the stiffness about all three axes was
calculated.
No definition of stiffness reported
(Karadogan and
Williams, 2012)
Three-dimensional static modelling Force and Moments No definition of stiffness reported
(H. Schmidt et
al., 2013) Poroelastic Finite Element model Shear stiffness and Load – displacement No definition of stiffness reported
(Ellingson et al.,
2016)
Three- dimensional non-linear Finite element
model
Load and moment data Stiffness explained in terms of
(Newton meters/Degree)
(Stokes and
Gardner-Morse,
2016)
Hexapod’ (Stewart platform) apparatus Force – displacement and Rotation – moment
data.
No definition of stiffness reported
(Holewijn et al.,
2017)
Custom build spinal motion simulator Load – displacement No definition of stiffness reported
(Malakoutian et
al., 2018)
ArtiSynth biomechanical modelling toolkit. 6 × 6 stiffness matrix - Load – displacement No definition of stiffness reported

135
Total
biomechanical
studies (n = 70)
Total objective measures = 63
No objective measures = 3
Total subjective measure = 0
Total indicators = 4 Yes definition =24/70
No definition = 46/70

136
Data abstraction: Surgical theme
Biomechanics (n=20)
Reference Objective stiffness measure Measure/Indicator Definition/Description
(Ferguson et Minneapolis Test Systems Load – displacement Stiffness values are described in terms of
al., 1988) the moment (N-m) required to produce a unit shear (mm) or angular (degree)
displacement.
(Patwardhan Three-dimensional Finite element model of the Moment – angular displacement No definition of stiffness reported
et al., 1990) spine
(Stokes and Model study - Finite element model Hook distraction from the changes in the No definition of stiffness reported
Gardner- distance between the hook sites
Morse, 1993)
(Dahl et al., Material testing system Force – displacement Dynamic stiffness described in terms of
2006) force load per unit of displacement under
dynamic or high rate loading.
(X.-Y. Wang Shenzhen SANS Testing Machine Load – displacement The stiffness was defined as the linear
et al., 2008) slope of the curve. (load-displacement)
(Dickman et Minneapolis test systems – Bionix frame Load – displacement Dynamic stiffness described in terms of
al., 2009) force load per unit of displacement under dynamic or high rate loading

137
The slope of the loading curve provided
the measurement of the relative resistance
to motion (stiffness)
(Buttermann VICON motion measurement system Axis of applied motion derived from the Stiffness expressed in terms of (Nm/deg)
et al., 2009) flexibility curves of each specimen.
(Luo et al., Computer-controlled, hydraulic materials testing Load – deformation No definition of stiffness reported
2010) machine.
(Perrin et al., 3D measurement system Load – deformation The stiffness was defined as the quotient of
2011) the loading to the deformation and was
calculated for the elastic zone.
(Clin et al., Radiographic self-calibration technique Force – displacement No definition of stiffness reported
2011)
(Bisschop et Hydraulic materials testing machine Load – displacement Shear yield force (SYF) was defined as the
al., 2012) point at which shear load caused a decrease in stiffness, i.e. a decrease in the
slope of the load-displacement curve.
(Bisschop, Hydraulic materials testing machine Load – displacement No definition of stiffness reported
Van Dieën,
et al., 2013)
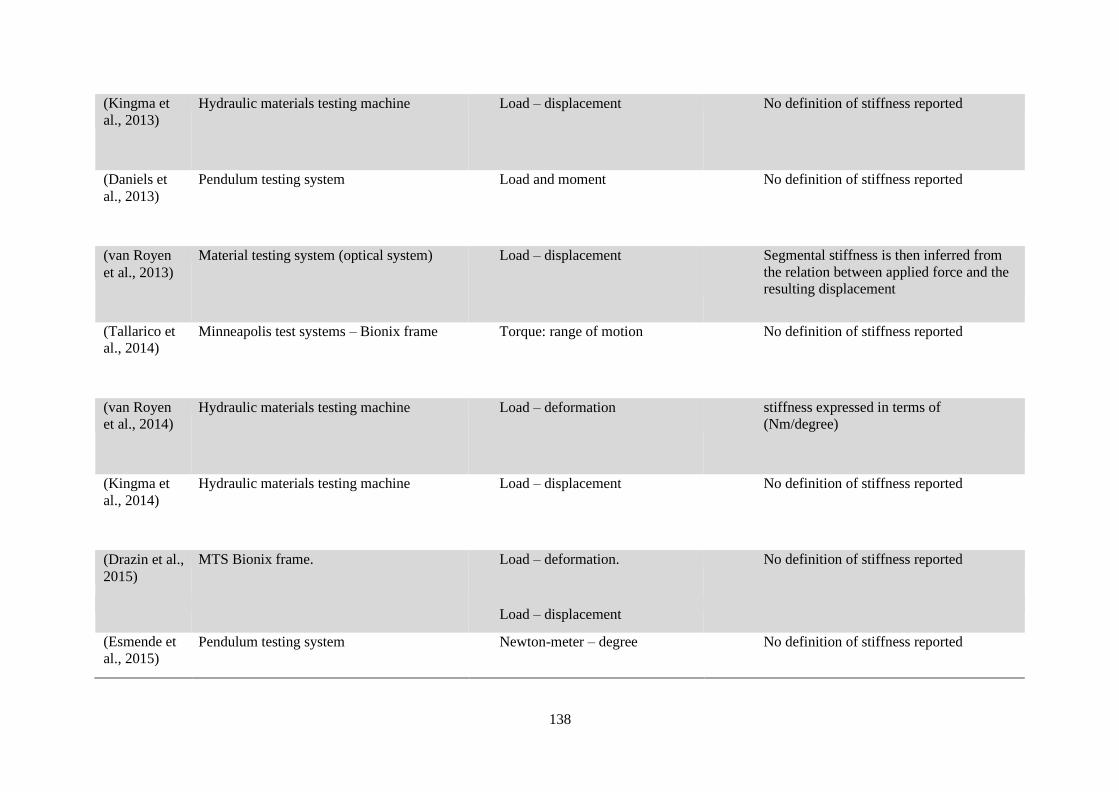
138
(Kingma et
al., 2013)
Hydraulic materials testing machine Load – displacement No definition of stiffness reported
(Daniels et
al., 2013)
Pendulum testing system Load and moment No definition of stiffness reported
(van Royen
et al., 2013)
Material testing system (optical system) Load – displacement Segmental stiffness is then inferred from
the relation between applied force and the
resulting displacement
(Tallarico et
al., 2014) Minneapolis test systems – Bionix frame Torque: range of motion No definition of stiffness reported
(van Royen
et al., 2014) Hydraulic materials testing machine Load – deformation stiffness expressed in terms of
(Nm/degree)
(Kingma et
al., 2014)
Hydraulic materials testing machine Load – displacement No definition of stiffness reported
(Drazin et al.,
2015)
MTS Bionix frame. Load – deformation. No definition of stiffness reported
Load – displacement
(Esmende et
al., 2015)
Pendulum testing system Newton-meter – degree No definition of stiffness reported

139
Intraoperative (n=14)
Reference Objective Stiffness measure Measure/Indicator Definition/Description
(Frank et al., Vertebral retractor Load – displacement Stiffness defined as the force needed to
1996a) distract adjacent vertebrae within a motion
segment.
(Frank et al., Sensor-equipped vertebral retractor system Load – displacement The stiffness (S) of a body that deflects a
1996b) distance (d) under an applied force (F) is
given by S=F/d
(M. Brown, Spinal Stiffness Gauge No quantification of objective measure No definition of stiffness reported
Wehman, et
al., 2002)
(M. Brown, Spinal Stiffness Gauge Force – displacement No definition of stiffness reported
Holmes, et
al., 2002)
(Hashimoto Spinal Distractor Load – displacement Distraction stiffness of the operative
et al., 2003) segment (N/mm) was calculated as the peak applied distraction force (N) divided by the displacement between the screws
(mm).
(Karami et Spinal Stiffness Gauge Load – displacement No definition of stiffness reported al., 2005)

140
(Tanaka et
al., 2006)
Spinal Distractor Load – displacement Stiffness was defined as the curve
produced during cyclic loading from 0-100
(N). More precisely, stiffness was defined
as the tangent stiffness at the middle range
of loading.
(Krenn et al.,
2008) Spinal Spreader Force – deflection The stiffness (S) of a body that deflects a
distance (d) under an applied force (F) is
given by S=F/d
(Ambrosetti-
Giudici et al.,
2009)
Computer-assisted spinal distractor includes Load – displacement No definition of stiffness reported
(Kitahara et
al., 2009)
Intraoperative measurement system Load – displacement Stiffness described as the relationship
between the load and displacement of the
spinal segment while rotation is applied.
The stiffness is operationally defined as the
slope of the line fitting the load-
displacement curve from 1 to 2mm on right
rotation and from 1 to 2 mm on left
rotation
(Hasegewa et
al., 2009)
Intraoperative measurement system Load – displacement Stiffness (N/mm) was defined as the slope
of the line fitting the load-displacement
curve from -15 mm to -10 mm on flexion
motion.
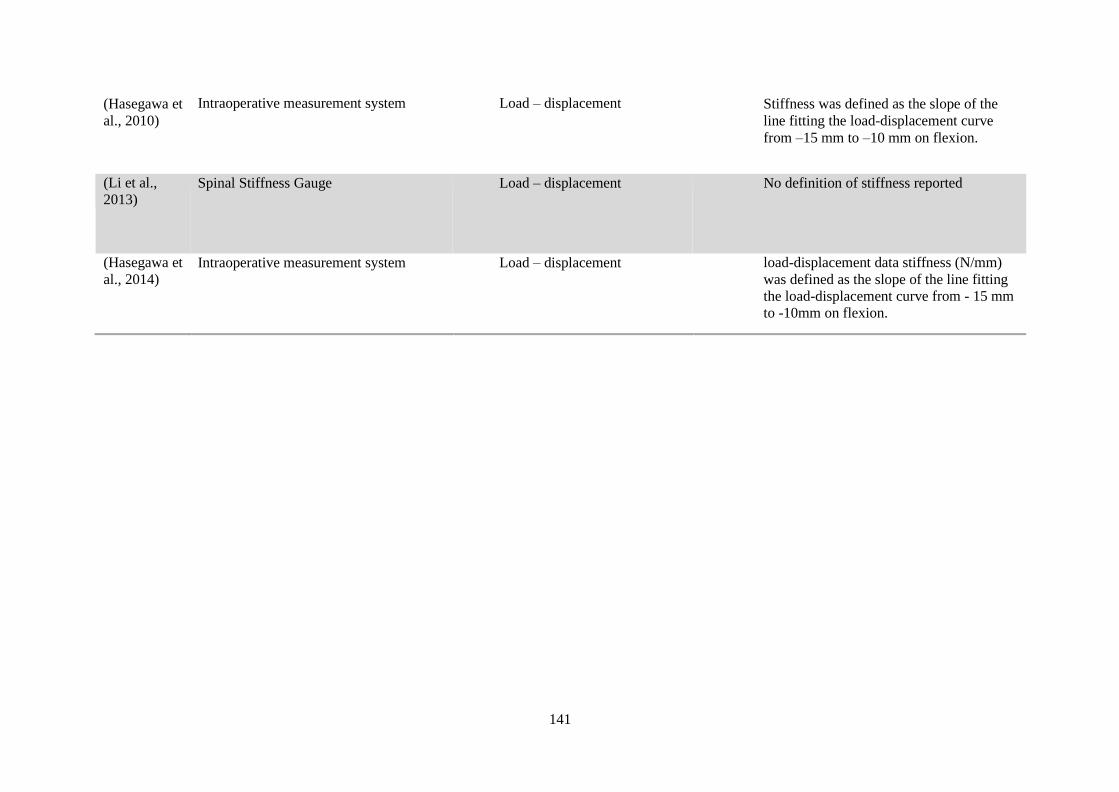
141
(Hasegawa et
al., 2010)
Intraoperative measurement system Load – displacement Stiffness was defined as the slope of the
line fitting the load-displacement curve
from –15 mm to –10 mm on flexion.
(Li et al.,
2013) Spinal Stiffness Gauge Load – displacement No definition of stiffness reported
(Hasegawa et
al., 2014)
Intraoperative measurement system Load – displacement load-displacement data stiffness (N/mm)
was defined as the slope of the line fitting
the load-displacement curve from - 15 mm
to -10mm on flexion.

142
Postoperative (n=31)
Lumbar Spinal Disability Index
Reference Subjective stiffness measure Measure/Indicator Definition/Description
(Hart, Gundle, et al., 2013) Lumbar spinal disability index
(LSDI)
Activities of daily living (ADLs) No definition of stiffness reported on LSDI
(Hart, Pro, et al., 2013) LSDI ADLs Stiffness operationally defined: Potential stiffness
expressed in terms of (loss of flexibility)
(Hart et al., 2014) LSDI ADLs No definition of stiffness reported on LSDI
(Kim et al., 2015) LSDI ADLs No definition of stiffness reported on LSDI
(Kimura et al., 2016a) LSDI ADLs No definition of stiffness reported on LSDI
(Zhang et al., 2017) LSDI ADLs No definition of stiffness reported on LSDI
(Choi et al., 2018) Korean (modified) – LSDI ADLs No definition of stiffness reported on LSDI
(Daniels et al., 2015) LSDI ADLs No definition of stiffness reported on LSDI
(Daniels et al., 2017) LSDI ADLs No definition of stiffness reported on LSDI
(Hart et al., 2017) LSDI ADLs No definition of stiffness reported on LSDI
(Ailon et al., 2018) LSDI ADLs No definition of stiffness reported on LSDI

143
Postoperative
Additional outcome measures
Reference Subjective Stiffness measure Measure/Indicator Definition/Description
(Million et VAS(VAS) – Back stiffness Verbal descriptor: Do you have any stiffness No definition of stiffness reported on
al., 1981) in the back? (No stiffness- intolerable VAS scale
stiffness)
(T.-C. Lee, Low back pain The authors found that a variable degree of No definition of stiffness reported
1996) stiffness of the low back was a very common,
although acceptable, complaint in the follow-
up interviews.
(Kaminsky et Neck stiffness was subjectively graded on a 1. No or occasional neck stiffness. No definition of stiffness reported for this
al., 2004) three-point scale 2. Intermittent or frequent neck scale. stiffness, but no difficulties with
activities of daily living.
3. Neck stiffness causing difficulty or
interfering with activities of daily
living (ADL’s).
(Dagenais et Prolotherapy Symptom Stiffness reported as a symptom of No definition of stiffness reported
al., 2005) prolotherapy injection
(Ohnari et Myelopathy Symptom Stiffness reported axial symptom of cervical No definition of stiffness reported
al., 2006) myelopathy

144
(O’Shaughne
ssy et al.,
2010)
Post-disc arthroplasty Soreness and stiffness of the lumbopelvic
region are frequently reported by patients
after this surgery
The second most frequently reported side-
effect was light to moderate stiffness of short
duration (12 to 24 hours).
The most frequent side-effects reported were
a slight increase in pain as well as minor to
moderate lower back stiffness.
No definition of stiffness reported
(Lykomitros
et al., 2010)
Removal of cervical collar Resolution of stiffness after cervical collars
were removed
No definition of stiffness reported
(Mori et al.,
2012)
VAS – Back stiffness low back discomfort as surrogate for heavy
feeling or stiffness
No definition of stiffness reported on
VAS scale
(Larson et
al., 2012)
VAS – Back stiffness No verbal descriptors No definition of stiffness reported on
VAS scale
(Rizvi et al., 2012)
VAS – Neck stiffness verbal descriptors: None/mild/severe No definition of stiffness reported on VAS scale

145
(Kawaguchi
et al., 2013)
The axial symptoms, such as the feeling of
limited neck motion and neck stiffness, were
assessed by a questionnaire.
Verbal description ‘‘Do you have any
problems with neck rotation when driving or
when someone calls out to you from behind
you?’’ When the symptoms were positive for
more than several months, and the patients
answered that the symptoms disturbed their
activities of daily living, the axial symptoms
were judged to be ‘‘present’’.
No definition of stiffness reported
(Sherief et
al., 2013)
Myelopathy Symptom Stiffness reported symptom of cervical
myelopathy
No definition of stiffness reported
(Mori et al.,
2015)
Stiffness classified as a type of pain Surrogate measure: Axial neck pain was
classified as 1 of 5 types as follows: pain,
stiffness, tension, tightness,
No definition of stiffness reported
(Chivukula
et al., 2015)
Cervical dorsal rhizotomy Neck stiffness and a complication of
intradural cervical dorsal root rhizotomy
No definition of stiffness reported
(L. Wang et
al., 2016)
VAS – Neck stiffness verbal descriptors: None/mild/severe No definition of stiffness reported on
VAS scale
(Guo, Chen,
et al., 2016)
VAS – Neck stiffness verbal descriptors: None/mild/severe No definition of stiffness reported on
VAS scale
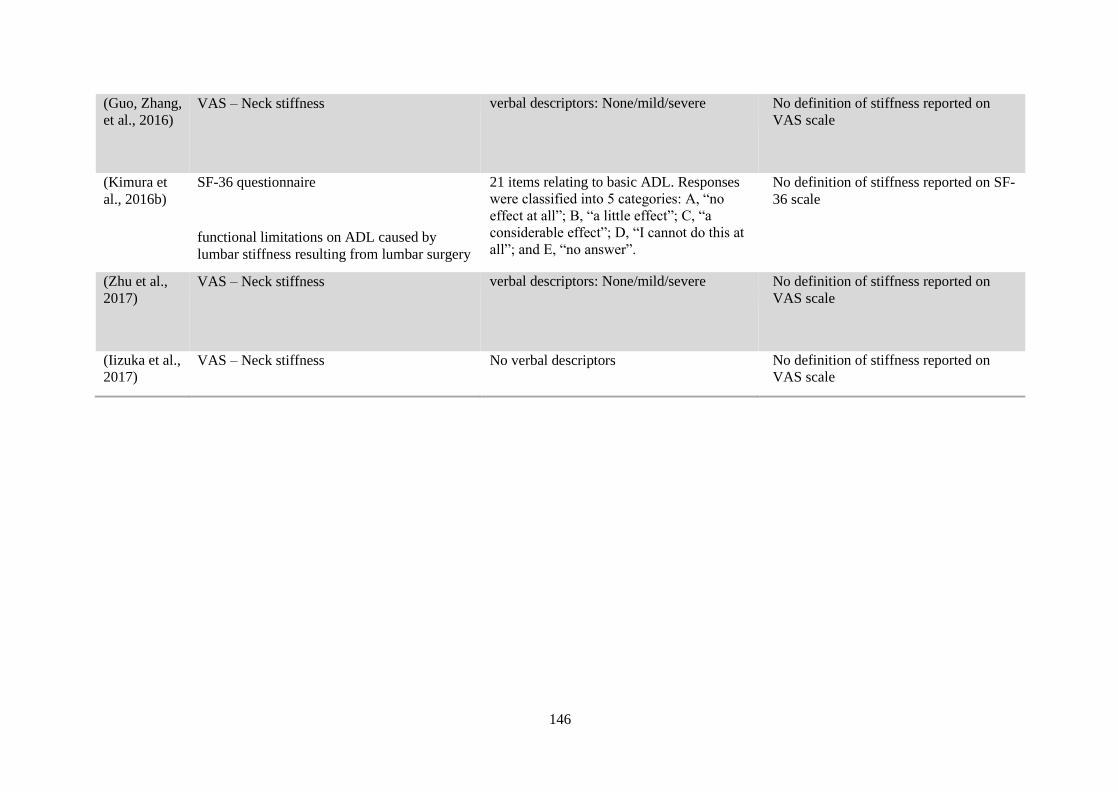
146
(Guo, Zhang,
et al., 2016)
VAS – Neck stiffness verbal descriptors: None/mild/severe No definition of stiffness reported on
VAS scale
(Kimura et
al., 2016b)
SF-36 questionnaire
functional limitations on ADL caused by
lumbar stiffness resulting from lumbar surgery
21 items relating to basic ADL. Responses
were classified into 5 categories: A, “no
effect at all”; B, “a little effect”; C, “a
considerable effect”; D, “I cannot do this at
all”; and E, “no answer”.
No definition of stiffness reported on SF-
36 scale
(Zhu et al.,
2017)
VAS – Neck stiffness verbal descriptors: None/mild/severe No definition of stiffness reported on
VAS scale
(Iizuka et al.,
2017) VAS – Neck stiffness No verbal descriptors No definition of stiffness reported on
VAS scale

147
Scoliosis (n=11)
Reference Objective Stiffness measure Measure/Indicator Definition/Description
(Stokes and
Laible, 1990)
12 X 12 Stiffness Matrix (Finite element
model)
The stiffness matrices representing the
intervertebral motion segments were taken
from published data for the thoracic spine
No definition of stiffness reported
(Duke et al., Finite element model Force – displacement No definition of stiffness reported
2005) Supine bending test
(Radiograph) Flexibility of the spine was decreased in the
upper thoracic and thoracic regions while the
stiffness of the lumbar spine was increased.
(Clamp et al., Fulcrum bending test The bending Cobb angle was measured from No definition of stiffness reported
2008) (Radiograph)
the fulcrum bending radiographs. Statistical analysis was used to relate the parameters to
the flexibility index.
(de Oliveria
et al., 2014)
Spinal suspension test (SST)
(Radiograph)
Force – displacement
The flexibility of the spine was calculated
based on the change of curvature induced by
the loading force.
No definition of stiffness reported

148
The stiffness matrices have been mainly
defined according to Hooke’s law, which
is a linear approximation to the responses
of motion segments to loads. One of the
Force – displacement 6 × 6 stiffness matrix
(finite element model)
(Jalalian et
al., 2017)

149
mechanical properties, crucial for
characterizing the spine stiffness, is the
load-displacement relationships of the
spinal motion segments.
(Mahaudens
et al., 2010)
Antero-posterior (AP) and lateral standing
spinal digital radiographs.
After surgery, the spine becomes stiffer with
the decrease of the spinal range of motion
No definition of stiffness reported
Traction and bending radiographs in supine
position
(Janssen et
al., 2013)
Radiographic analysis of the sagittal profile of
the spine and spinopelvic alignment
The human spine shows less rotatory
stiffness compared with other spines in
nature due to the occurrence of posteriorly
directed shear loads that act uniquely on
certain areas of the human spine
No definition of stiffness reported
(Salmingo et
al., 2013)
Assessed the impact of implant rods on
scoliotic correction
Parameters such as flexibility or stiffness of
the scoliotic spine need to be considered. As
it is one of the major factors that influence
the outcome of the clinical operation.
No definition of stiffness reported
(Rousseau et
al., 2014) Implications of hip surgery of spine stiffness Hip surgery must be carefully planned in the
case of stiff lumbar spine. No definition of stiffness reported
(H. Chen et Investigated body morphology (slender and Posterior shear loads were shown to play a No definition of stiffness reported
al., 2017) tall) adolescents on mechanical stiffness role in the rotational stiffness of the human
spine due to its unique biomechanical
loading.
Implicit use of mechanical stiffness
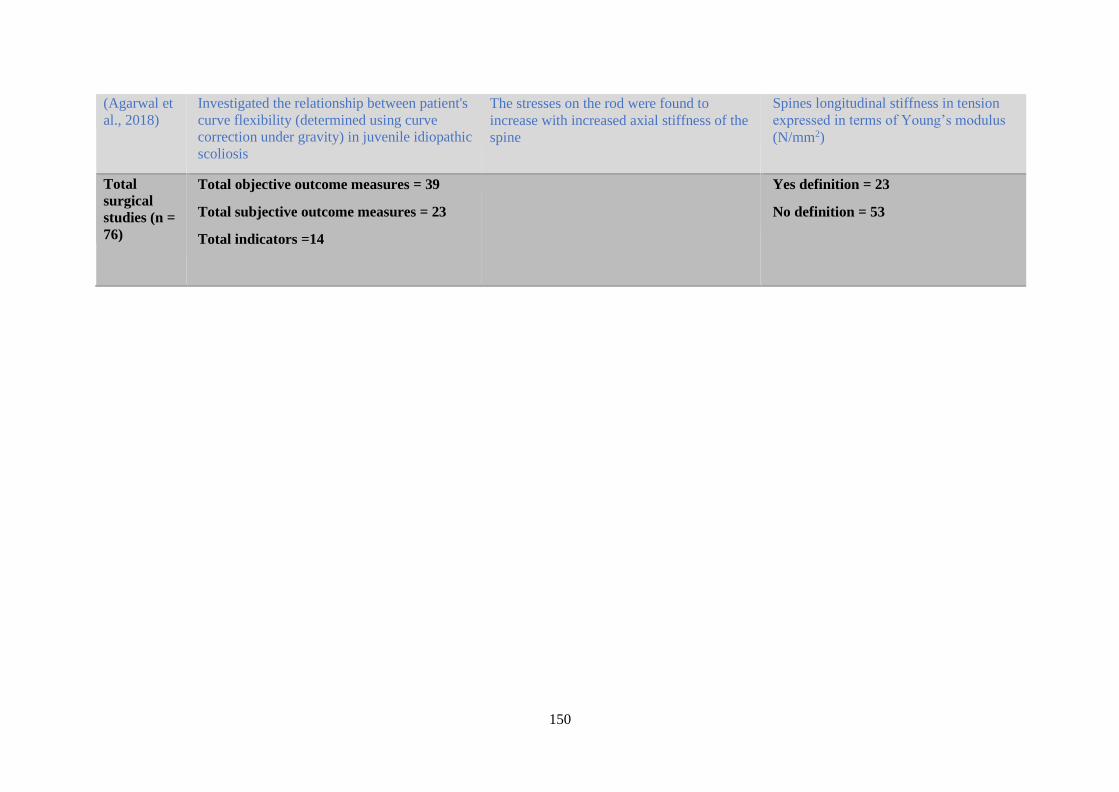
150
(Agarwal et
al., 2018)
Investigated the relationship between patient's
curve flexibility (determined using curve
correction under gravity) in juvenile idiopathic
scoliosis
The stresses on the rod were found to
increase with increased axial stiffness of the
spine
Spines longitudinal stiffness in tension
expressed in terms of Young’s modulus
(N/mm2)
Total
surgical
studies (n =
76)
Total objective outcome measures = 39
Total subjective outcome measures = 23
Total indicators =14
Yes definition = 23
No definition = 53

151
Data abstraction: Pathophysiological theme
Ankylosing Spondylitis (n=34)
Reference Subjective measure Measure/Indicator Definition/Description
(Kinsella et Subjective response of morning stiffness, The subjective evaluation was based on No definition of stiffness reported
al., 1967) duration and severity of morning stiffness patients' opinions, which were graded as
following showed “no change”, were
“worse” or “improved”.
(Hill et al., Clinical diagnosis of ankylosing spondylitis The term immobility stiffness or pain has No definition of stiffness reported
1976) been used to cover discomfort which starts
while the patient is at rest
(Hanly et al., Psoriatic spondyloarthropathy Presence of spinal pain and stiffness No definition of stiffness reported
1988)
(Hidding and VAS – stiffness Pain and stiffness were each assessed by No definition of stiffness reported on VAS
Van der asking the patient to describe his or her scale
Linden, perceived pain or stiffness on a 0 –10 cm
1995) horizontal VAS(0 = no pain or stiffness, 10
= worst pain or stiffness imaginable)
(Averns et VAS – stiffness No verbal descriptors No definition of stiffness reported on VAS
al., 1996) scale
(Ozgocmen Duration of morning stiffness (min) Duration of morning stiffness was No definition of stiffness reported
et al., 2000) indicated as time, in minutes, elapsed
between arising in the morning and the
development of noticeable improvement.

152
(Yaron et al.,
2002)
Clinical characteristics of patients with
psoriasis arthritis
Morning stiffness No definition of stiffness reported
(Gorman et
al., 2002)
Questionnaire Duration of morning stiffness (in minutes) No definition of stiffness reported
(Cardiel et
al., 2003)
Bath Ankylosing Spondylitis Functional
Index – VAS
Severity and duration of stiffness (0 hours
to 2 or more hours). 0 –100 mm with
“none” anchored at one extreme and “very
severe” at the other.
No definition of stiffness reported
(Brandt et
al., 2004)
Bath Ankylosing Spondylitis Disease
Activity Index – VAS
The severity and duration of morning
stiffness.
No definition of stiffness reported
(Dagfinrud et
al., 2004)
Ankylosing Spondylitis (AS) is a chronic inflammatory disease
characterised clinically by pain and
stiffness of the back
No definition of stiffness reported
(Riyazi et al.,
2005)
WOMAC (Osteoarthritis index) Stiffness (2 items): after first waking and
later in the day
No definition of stiffness reported o
(J. Chen et
al., 2006) What is Ankylosing Spondylitis Pain and stiffness occur and limits
movement in the back and in other joints
that are affected
No definition of stiffness reported

153
(Kaya et al.,
2007)
VAS – stiffness Morning stiffness No definition of stiffness reported on VAS
scale
(Sengupta
and Stone,
2007)
Bath Ankylosing Spondylitis Disease
Activity Index – VAS Severity and duration of morning stiffness
Morning-related stiffness (0 – 100), where
0 = no stiffness and 100 = very severe
stiffness).
No definition of stiffness reported on VAS
scale
(Mengshoel
and
Robinson,
2008)
Bath Ankylosing Spondylitis Disease
Activity Index – VAS Severity and duration of morning stiffness
The two extremes of the 0 – 100 mm line
were ‘no pain/ stiffness’ and ‘most severe
pain/stiffness’.
No definition of stiffness reported on scale
The stiffness items were modified to make
them more specific. Instead of asking about
general stiffness, we asked the patients to
indicate how they perceived stiffness in the
lumbar, thoracic and cervical spine.
The meaningful statements were coded, for
example under ‘stiffness’, and new
categories were developed, for example
‘stiffness and well-being’, ‘stiffness and
bodily awareness’, and ‘stiffness and hope’.
(Khoo et al.,
2008)
Bath Ankylosing Spondylitis Disease
Activity Index – VAS
Stiffness and duration of morning stiffness
0 – 10 cm, for overall level of morning
No definition of stiffness reported on VAS
scale
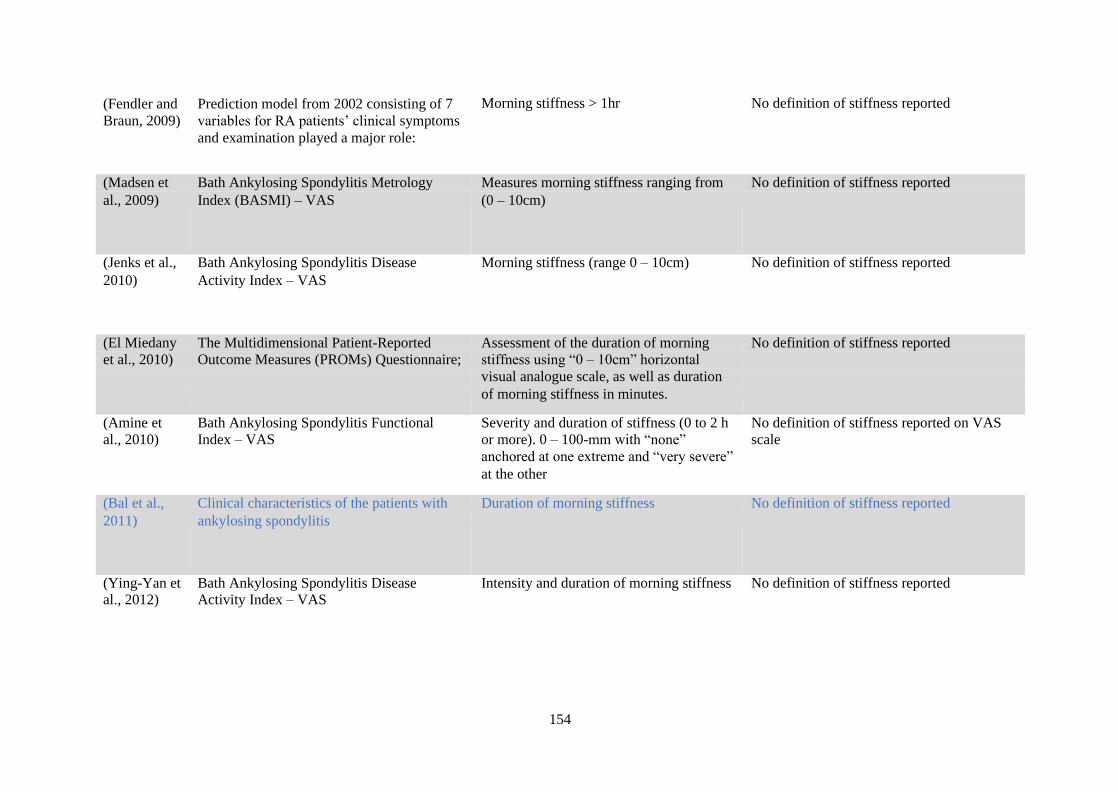
154
(Fendler and
Braun, 2009)
Prediction model from 2002 consisting of 7
variables for RA patients’ clinical symptoms
and examination played a major role:
Morning stiffness > 1hr No definition of stiffness reported
(Madsen et Bath Ankylosing Spondylitis Metrology Measures morning stiffness ranging from No definition of stiffness reported
al., 2009) Index (BASMI) – VAS (0 – 10cm)
(Jenks et al., Bath Ankylosing Spondylitis Disease Morning stiffness (range 0 – 10cm) No definition of stiffness reported
2010) Activity Index – VAS
(El Miedany The Multidimensional Patient-Reported Assessment of the duration of morning No definition of stiffness reported
et al., 2010) Outcome Measures (PROMs) Questionnaire; stiffness using “0 – 10cm” horizontal
visual analogue scale, as well as duration
of morning stiffness in minutes.
(Amine et Bath Ankylosing Spondylitis Functional Severity and duration of stiffness (0 to 2 h No definition of stiffness reported on VAS
al., 2010) Index – VAS or more). 0 – 100-mm with “none” scale anchored at one extreme and “very severe”
at the other
(Bal et al., Clinical characteristics of the patients with Duration of morning stiffness No definition of stiffness reported
2011) ankylosing spondylitis
(Ying-Yan et Bath Ankylosing Spondylitis Disease Intensity and duration of morning stiffness No definition of stiffness reported al., 2012) Activity Index – VAS

155
(Ibn Yacoub Gender and disease features in Moroccan Morning stiffness duration (minutes) No definition of stiffness reported
et al., 2012) patients with ankylosing spondylitis measured on a 0 – 100 VAS
(Hegde et al.,
2014) Ankylosing spondylitis The main clinical symptom is
inflammatory back pain typically occurring
at night and morning stiffness improving
after exercise. The pain, stiffness, and
limited mobility of the spine can cause
severe limitations in daily life activities.
No definition of stiffness reported
(Addimanda Bath Ankylosing Spondylitis Disease 0 – 100 mm – stiffness intensity No definition of stiffness reported
et al., 2014) Activity Index – VAS Duration of morning stiffness
(Eroğlu et
al., 2014)
Demographic and clinical data in patients
with ankylosing spondylitis
Morning stiffness as an indicator of
ankylosing spondylitis
No definition of stiffness reported
Duration of morning stiffness (minutes)
(Der Heijde
et al., 2014)
VAS 0–10- cm VAS – Morning stiffness No definition of stiffness reported on VAS
scale
Inflammation (morning stiffness)
(Boonen et
al., 2015)
Primary and secondary outcome measures
will be based on the DC-ART Ankylosing
Spondylitis Working Group Core Set.
Spinal stiffness (duration of morning
stiffness)
No definition of stiffness reported
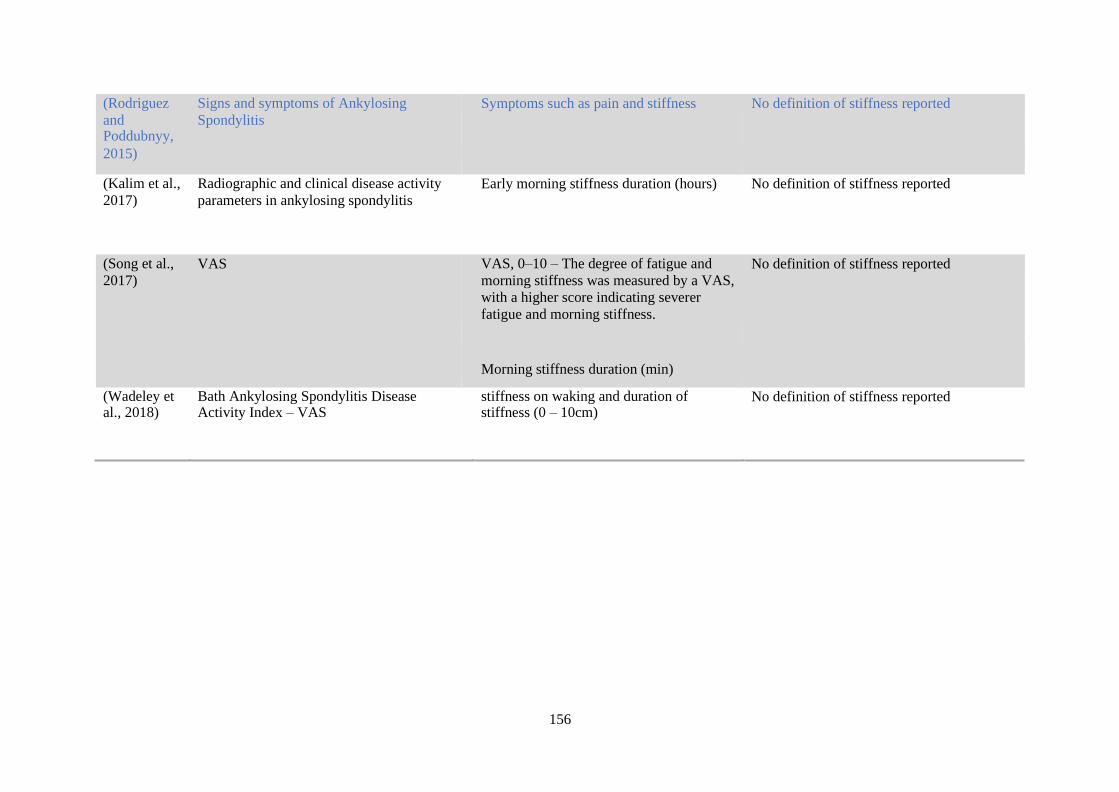
156
(Rodriguez
and Poddubnyy,
Signs and symptoms of Ankylosing
Spondylitis
Symptoms such as pain and stiffness No definition of stiffness reported
2015)
(Kalim et al.,
2017)
Radiographic and clinical disease activity
parameters in ankylosing spondylitis
Early morning stiffness duration (hours) No definition of stiffness reported
(Song et al.,
2017)
VAS VAS, 0–10 – The degree of fatigue and
morning stiffness was measured by a VAS,
with a higher score indicating severer
fatigue and morning stiffness.
No definition of stiffness reported
Morning stiffness duration (min)
(Wadeley et al., 2018)
Bath Ankylosing Spondylitis Disease Activity Index – VAS
stiffness on waking and duration of stiffness (0 – 10cm)
No definition of stiffness reported
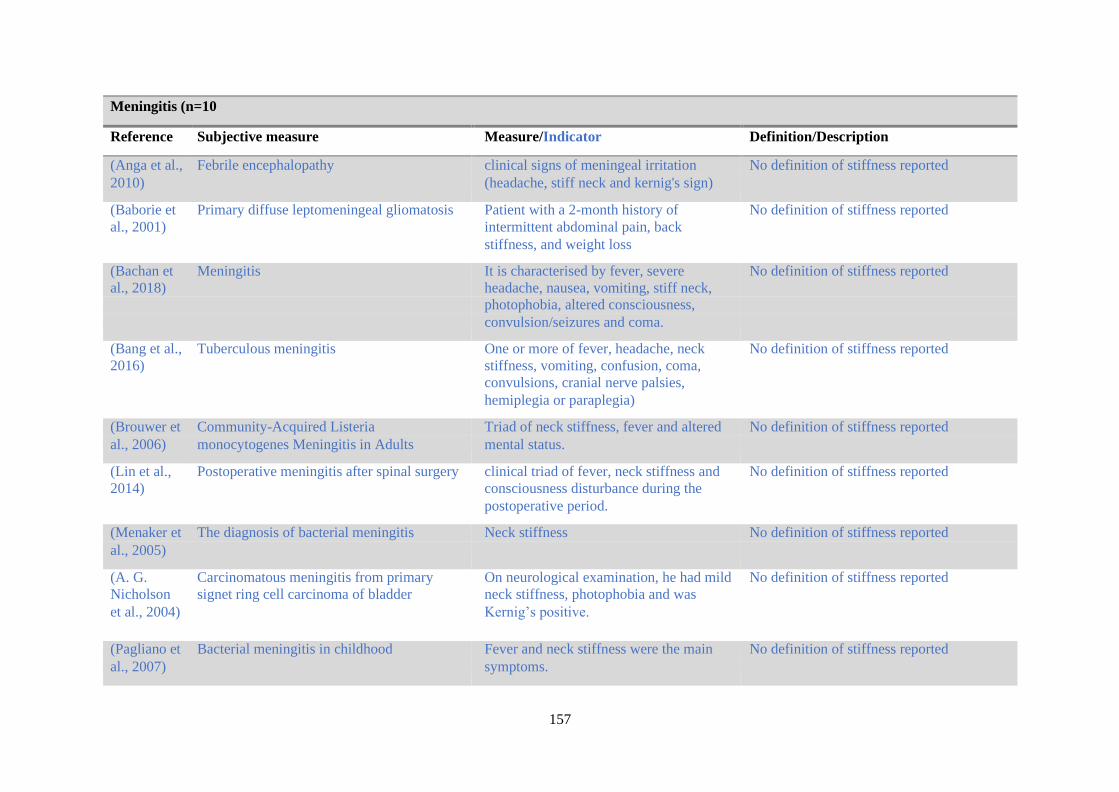
157
Meningitis (n=10
Reference Subjective measure Measure/Indicator Definition/Description
(Anga et al., Febrile encephalopathy clinical signs of meningeal irritation No definition of stiffness reported
2010) (headache, stiff neck and kernig's sign)
(Baborie et Primary diffuse leptomeningeal gliomatosis Patient with a 2-month history of No definition of stiffness reported
al., 2001) intermittent abdominal pain, back
stiffness, and weight loss
(Bachan et Meningitis It is characterised by fever, severe No definition of stiffness reported
al., 2018) headache, nausea, vomiting, stiff neck,
photophobia, altered consciousness,
convulsion/seizures and coma.
(Bang et al., Tuberculous meningitis One or more of fever, headache, neck No definition of stiffness reported
2016) stiffness, vomiting, confusion, coma,
convulsions, cranial nerve palsies,
hemiplegia or paraplegia)
(Brouwer et Community-Acquired Listeria Triad of neck stiffness, fever and altered No definition of stiffness reported
al., 2006) monocytogenes Meningitis in Adults mental status.
(Lin et al., Postoperative meningitis after spinal surgery clinical triad of fever, neck stiffness and No definition of stiffness reported
2014) consciousness disturbance during the
postoperative period.
(Menaker et The diagnosis of bacterial meningitis Neck stiffness No definition of stiffness reported
al., 2005)
(A. G. Carcinomatous meningitis from primary On neurological examination, he had mild No definition of stiffness reported
Nicholson signet ring cell carcinoma of bladder neck stiffness, photophobia and was
et al., 2004) Kernig’s positive.
(Pagliano et Bacterial meningitis in childhood Fever and neck stiffness were the main No definition of stiffness reported
al., 2007) symptoms.

158
(Shin et al.,
2017)
Post lumbar puncture headache Intracranial bleed - subarachnoid
Throbbing = Occipital headache with
sudden onset, severe, constant. Prodromal
pain in one eye, ptosis, blunting of
consciousness, vomiting, stiff neck.
Meningitis = Acute occipital headache,
neck stiffness, fever, photophobia.
No definition of stiffness reported

159
Spinal pathophysiology (n= 14)
Reference Subjective measure Measure/Indicator Definition/Description
(Alaya and Lumbosciatica revealing intramedullary lumbar spine stiffness No definition of stiffness reported
Osman, 2017) ependymoma
(Al-Herz et al., VAS- DISH How would you describe the overall level No definition of stiffness reported on VAS
2008) of morning stiffness you have had from scale the time you wake up? And, how long
does your morning stiffness last from the
time you wake up?). They were all scaled
from 0 to 100 mm, 0 being none and 100
being extreme, except for the duration of
stiffness VAS which was scaled from 0 to
120 min.
(An and Intervertebral disc degeneration (IDD) With disc degeneration, biomechanical No definition of stiffness reported
Masuda, 2006) changes in the intervertebral disc and the
motion segment follow. In the early stages
of disc degeneration, the involved motion
segment is less stiff than in the advanced
stages, particularly in flexion-extension
(Datar et al., Retroclival Hematoma due to Odontoid He presented to the hospital 6 weeks after No definition of stiffness reported
2013) Fracture falling from standing height, with
(case report) headache, neck pain, and stiffness.
Following that episode, he started
experiencing headache, neck pain, and
stiffness.
No definition of stiffness reported The interviewer also asked about the
presence, duration and location of
morning stiffness. If morning stiffness
was present, the interviewer asked what
its duration was (possible answers were:
Interview questions about pain and morning
stiffness
(de Schepper
et al., 2012)
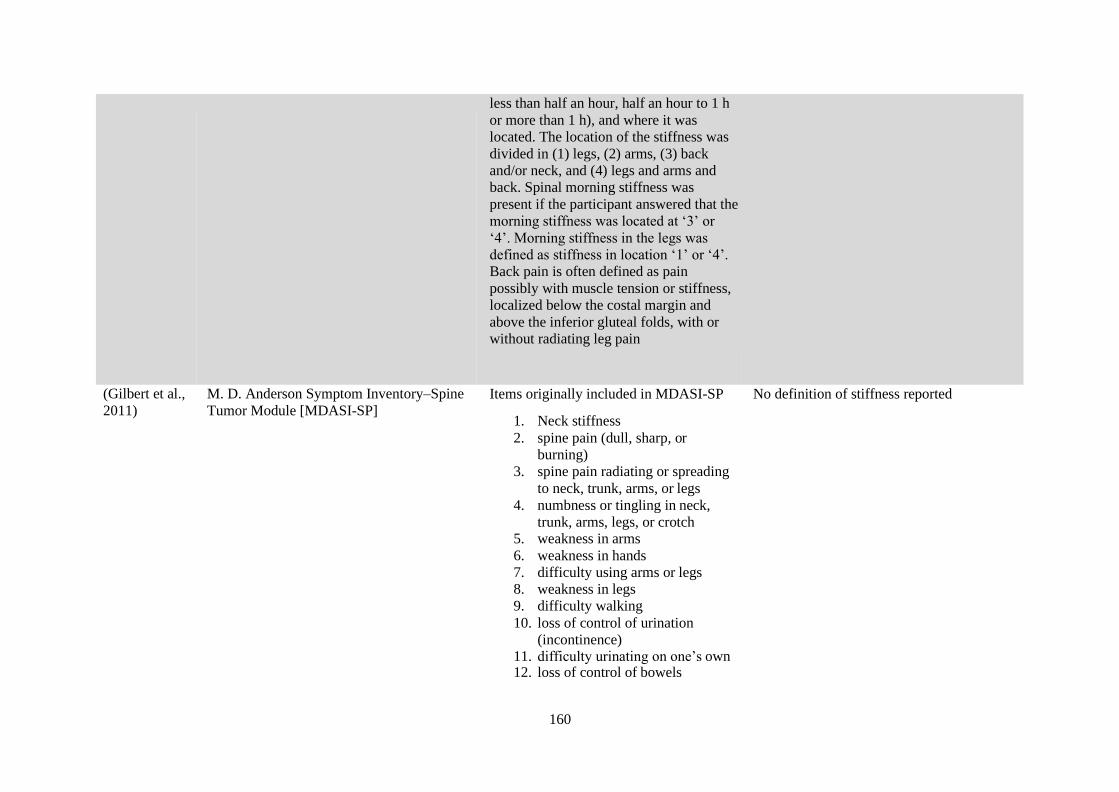
160
less than half an hour, half an hour to 1 h
or more than 1 h), and where it was
located. The location of the stiffness was
divided in (1) legs, (2) arms, (3) back
and/or neck, and (4) legs and arms and
back. Spinal morning stiffness was
present if the participant answered that the
morning stiffness was located at ‘3’ or
‘4’. Morning stiffness in the legs was
defined as stiffness in location ‘1’ or ‘4’.
Back pain is often defined as pain
possibly with muscle tension or stiffness,
localized below the costal margin and
above the inferior gluteal folds, with or
without radiating leg pain
(Gilbert et al.,
2011)
M. D. Anderson Symptom Inventory–Spine
Tumor Module [MDASI-SP]
Items originally included in MDASI-SP
1. Neck stiffness
2. spine pain (dull, sharp, or
burning)
3. spine pain radiating or spreading
to neck, trunk, arms, or legs
4. numbness or tingling in neck,
trunk, arms, legs, or crotch 5. weakness in arms
6. weakness in hands
7. difficulty using arms or legs
8. weakness in legs
9. difficulty walking
10. loss of control of urination
(incontinence) 11. difficulty urinating on one’s own 12. loss of control of bowels
No definition of stiffness reported

161
13. change in bowel pattern
(diarrhoea or constipation) 14. sexual function
15. trouble caring for oneself (eating,
grooming, toileting, or dressing)
16. difficulty completing tasks
(Hosalkar et
al., 2008)
Congenital Osseous Anomalies of the Upper
Cervical Spine
Neck pain and stiffness have been
reported to be a presenting complaint in
patients with upper cervical anomalies
No definition of stiffness reported
(Kuperus et
al., 2018)
Diffuse idiopathic skeletal hyperostosis
(DISH)
Increased spinal stiffness may play a more
important role in the increased fracture
risk of and the typical fracture patterns
observed in individuals with DISH.
The ankylotic effect of the bridging
ossifications in DISH is often not
significant enough to be perceived by a
patient (e.g., he/she experiences stiffness
in a portion of the spine), the
biomechanical effects should be large
enough to measure.
No definition of stiffness reported
(Lemus et al.,
2015)
Traumatic Atlanto-axial subluxation Spontaneous stiffness of the patient’s
neck
No definition of stiffness reported

162
(Mata et al.,
1997)
Diffuse idiopathic skeletal hyperostosis
(DISH)
The principal symptoms are stiffness and
non-radicular pain about the spine and the
enthesis
No definition of stiffness reported
(Nibu et al., Neck dissection questionnaire (NDQ) NDQ developed by Nibu et al., was used No definition of stiffness reported
2010) to assess quality of life after neck
dissection. These items were: (1) neck
stiffness, (2) neck constriction, (3) neck
pain, (4) neck numbness, (5) shoulder
drop, (6) reach above, and (7) neck
appearance
(Wassenaar et The diagnosis of osteoarthritis Osteoarthritis of the cervical and lumbar No definition of stiffness reported
al., 2009) spine was present when there was pain
and/or stiffness in the cervical or lumbar
spine region on most days
(Y. W. Wong Spinal epidural hematoma Possible risk factors for spinal epidural No definition of stiffness reported
and Luk, hematoma include stiffness along the
2008) fusion block
Systemic cause (n=7)
Reference Subjective measure Measure/Indicator Definition/Description
(Huston et al.,
1956)
Non-paralytic poliomyelitis Painful stiffness of the neck and Back were
common physical signs. An objective
observation of limited flexion was much
more common than a subjective complaint
of pain. Stiffness of the neck was as
common as spinal stiffness in patients
exhibiting paralysis or poliomyelitis virus
excretion. However, it was also found in
many patients in whom the clinical
diagnosis of poliomyelitis was not made.
The state of anxious alertness characteristic
No definition of stiffness reported

163
(Gerber et al.,
1984)
Vertebral abnormalities associated with
synthetic retinoid use
Symptoms of stiffness and tenderness upon
compression of the long bones were noted
In addition, a pattern of axial stiffness and
arthralgias has been noted.
No definition of stiffness reported
(Solomon et
al., 2008)
Japanese encephalitis virus Neck stiffness No definition of stiffness reported
of poliomyelitis was seen more often,
usually associated with stiffness of the
neck and spine.
Prolonged early morning stiffness, which is
considered an indicator of inflammatory
musculoskeletal disease,
No definition of stiffness reported Early morning stiffness, defined as
stiffness in the morning on rising, lasting
for at least 1 hr.
The diagnosis of fibromyalgia syndrome.
Clinical characteristics were reported as
symptom description and physical
examination findings
(Fitzcharles
and Boulos,
2003)

164
No definition of stiffness reported Presenting with an unusual symptom
complex that consisted primarily of neck
stiffness, neck pain, and dysphagia.
Retropharyngeal Ganglioneuroma
Presenting with Neck Stiffness
(Gary et al.,
2010)

165
(Djukic et al.,
2012)
Lyme neuroborreliosis Patients with headache and fever displayed
more often neck stiffness.
No definition of stiffness reported
(Perry et al.,
2013)
Decision Rules to Rule Out Subarachnoid
Hemorrhage
Patients with subarachnoid haemorrhage
were older and had more rapid peaking
headaches, onset during exertion, loss of
consciousness, neck pain or stiffness, and
vomiting.
No definition of stiffness reported
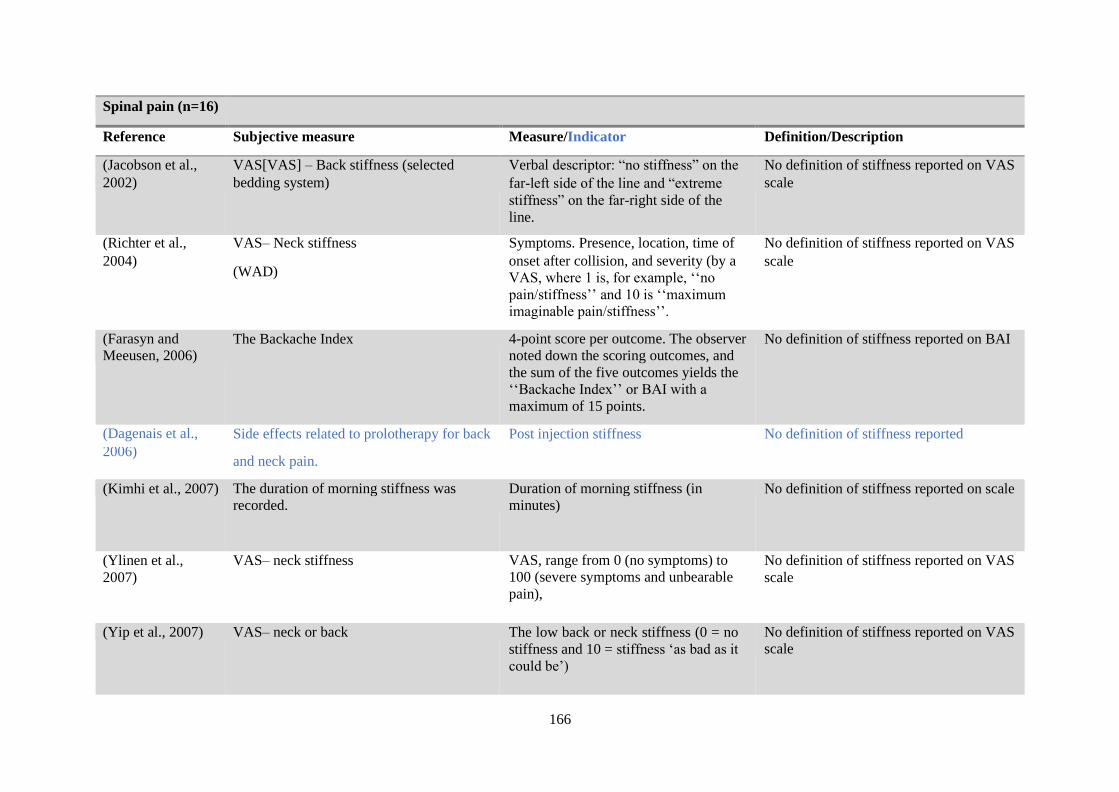
166
Spinal pain (n=16)
Reference Subjective measure Measure/Indicator Definition/Description
(Jacobson et al., VAS[VAS] – Back stiffness (selected Verbal descriptor: “no stiffness” on the No definition of stiffness reported on VAS
2002) bedding system) far-left side of the line and “extreme
stiffness” on the far-right side of the
line.
scale
(Richter et al., VAS– Neck stiffness Symptoms. Presence, location, time of No definition of stiffness reported on VAS
2004) (WAD)
onset after collision, and severity (by a
VAS, where 1 is, for example, ‘‘no
pain/stiffness’’ and 10 is ‘‘maximum
imaginable pain/stiffness’’.
scale
(Farasyn and
Meeusen, 2006) The Backache Index 4-point score per outcome. The observer
noted down the scoring outcomes, and
the sum of the five outcomes yields the
‘‘Backache Index’’ or BAI with a
maximum of 15 points.
No definition of stiffness reported on BAI
(Dagenais et al., Side effects related to prolotherapy for back Post injection stiffness No definition of stiffness reported
2006) and neck pain.
(Kimhi et al., 2007) The duration of morning stiffness was
recorded.
Duration of morning stiffness (in
minutes) No definition of stiffness reported on scale
(Ylinen et al.,
2007)
VAS– neck stiffness VAS, range from 0 (no symptoms) to
100 (severe symptoms and unbearable
pain),
No definition of stiffness reported on VAS
scale
(Yip et al., 2007) VAS– neck or back The low back or neck stiffness (0 = no
stiffness and 10 = stiffness ‘as bad as it
could be’)
No definition of stiffness reported on VAS
scale

167
(Rydevik et al.,
2008)
Whiplash injuries and associated disorders Neck symptoms in terms of pain and
stiffness with or without objective
clinical findings are the most important
and common symptoms associated with
whiplash injuries. Neck motion may be
considerably restricted because of pain
but also due to stiffness. Neck pain often
occurs soon after a whiplash trauma,
while stiffness can occur later.
No definition of stiffness reported
(Grenier and
McGill, 2008)
Low back pain and spine stability The passive stiffness was combined with
active stiffness generated by the muscles
and calculated using the moment
distribution.
No definition of stiffness reported
They appeared to stiffen the torso
muscles which stabilize the spine
partially via additional compression to
the column.
(Luca Vismara,
Francesco
Menegoni, Fabio
Zaina, Manuela
Galli, Stefano
Negrini, 2010)
Obesity-related thoracic stiffness Thoracic stiffness with normal lumbar
ROM appears to be a feature of obesity No definition of stiffness reported
(Keeling et al.,
2012)
The 6-item questionnaire to assess
Inflammatory low back pain.
Has the back been stiff, especially in the
morning [morning stiffness]?
No definition of stiffness reported
Do you experience stiffness in your back
and/or hips [YES]/[NO]?

168
A: When you get out of bed
B: Afternoon
C: Evening
D: No consistent time
(Walker and
Williamson, 2009)
Potential signs and symptoms of ILBP or
MLBP
Stiffness after resting (includes sitting) No definition of stiffness reported
(Farasyn et al.,
2013)
The Backache Disability Index. Morning back stiffness score (MBS)
with a maximum of 5 points.
No definition of stiffness reported
(Ferreira and de
Luca, 2017)
Low back pain The pathoanatomical changes at the
spinal segment result in stiffness
No definition of stiffness reported
(Tomczyszyn et al.,
2018)
Interview question Have you experienced low back pain,
i.e., long-lasting pain or stiffness within
the last 12 months? Yes/No
No definition of stiffness reported
(Arnbak et al.,
2018) The Calin Criteria At least 4 of 5 of Back pain >3 months
Age at onset <40 years Insidious onset
Morning stiffness Improvement with
exercise
No definition of stiffness reported
Mandatory: Back pain >3 months
At least 2 of 4 of:
Morning stiffness >30 minutes
Improvement with exercise but not with
rest. Waking in the second half of the
night because of back pain Alternating
buttock pain
No definition of stiffness reported
“ “ The Berlin criteria

169
Total studies in
Pathophysiological
theme (n = 81)
Total subjective outcome measures =
39
Total indicators = 42 Yes definition = 0
No definition = 81

170
Data abstraction: Segmental assessment
Segmental Stiffness Assessment (n=106)
Reference Manual and/or Mechanical stiffness
measure
Measure/Indicator Definition/Description
(Howe et al., 1983)
Mechanical
Goniometer The angle between the two positions of the
pointer was measured and divided by 2 to
give the average.
No definition of stiffness reported
(Maitland,
1986)
Manual
Posterior to anterior spinal mobilisation
(P/A) force, or ‘springing’, applied to the
spinous process.
Evaluation of segmental hypomobility
based in part on tests of passive
intervertebral movement
No definition of stiffness reported
(Jull and
Bullock, 1987)
Manual
P/A spinal stiffness assessment Thoracic and lumbar: palpation of
intersegmental motion and manual PA
pressures L1–L5, rated on a 5-point scale.
The stiffness properties of the materials
comprising the joint are perceived manually
as a consistently increasing resistance which
then limits movement. Any change in the
stiffness properties of the joint are perceived
as changes in the nature and quality of
resistance.
Manual
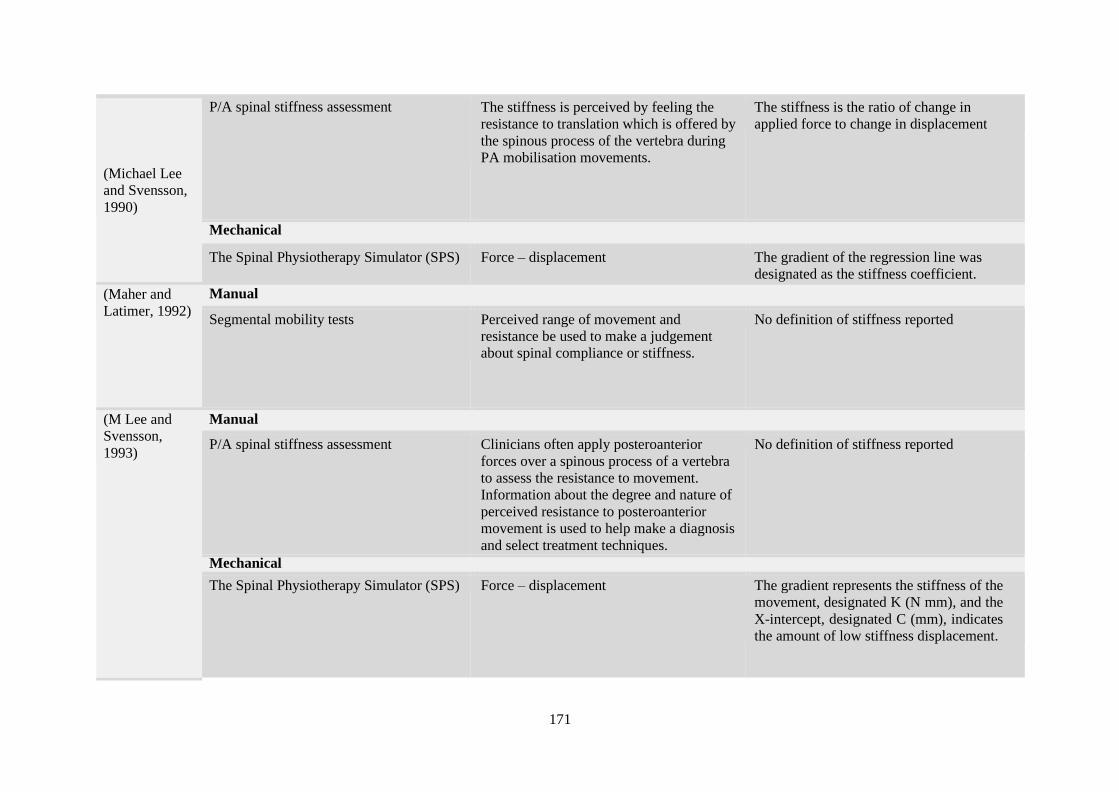
171
(Michael Lee
and Svensson,
1990)
P/A spinal stiffness assessment The stiffness is perceived by feeling the
resistance to translation which is offered by
the spinous process of the vertebra during
PA mobilisation movements.
The stiffness is the ratio of change in
applied force to change in displacement
Mechanical
The Spinal Physiotherapy Simulator (SPS) Force – displacement The gradient of the regression line was
designated as the stiffness coefficient.
(Maher and
Latimer, 1992)
Manual
Segmental mobility tests Perceived range of movement and
resistance be used to make a judgement
about spinal compliance or stiffness.
No definition of stiffness reported
(M Lee and
Svensson,
1993)
Manual
P/A spinal stiffness assessment Clinicians often apply posteroanterior
forces over a spinous process of a vertebra
to assess the resistance to movement.
Information about the degree and nature of
perceived resistance to posteroanterior
movement is used to help make a diagnosis
and select treatment techniques.
No definition of stiffness reported
Mechanical
The Spinal Physiotherapy Simulator (SPS) Force – displacement The gradient represents the stiffness of the
movement, designated K (N mm), and the
X-intercept, designated C (mm), indicates
the amount of low stiffness displacement.

172
(Michael Lee et al., 1993)
Manual
P/A spinal stiffness assessment Clinician judged: P/A stiffness testing at the
T4 and T5 spinal levels.
‘Spinal’ stiffness is perceived by feeling the
resistance provided by the patient
Mechanical
The Spinal Physiotherapy Simulator (SPS) Force – displacement The stiffness coefficient ‘K’, the gradient of
the regression line.
(Maher and
Adams, 1994)
Manual
P/A spinal stiffness assessment Clinician judged: P/A pressures to L1-L5
rated on an 11-point scale
The scale ranged from - 5 (markedly
decreased stiffness) to 5 (markedly
increased stiffness), with 0 representing normal stiffness.
No definition of stiffness reported
(Jull et al.,
1994)
Manual
Passive accessory and physiological
intersegmental movements from CO-l to
C6-7
Cervical; Manual PAIVM assessment of
segmental tissue stiffness and the presence
or absence of symptomatic joint dysfunction.
The relationship between displacement and
the nature of tissue resistance to
displacement
(Binkley et al.,
1995)
Manual
P/A spinal stiffness assessment Clinician judged P/A accessory mobility at
L1 – L5-S1
Stiffness was recorded on an 11-point scale,
from -5 (markedly reduced stiffness) to 5
(markedly increased stiffness), with 0 being
normal stiffness.
Segmental stiffness described in terms of
increased or decreased mobility (i.e.,
(hypermobility and hypomobility).
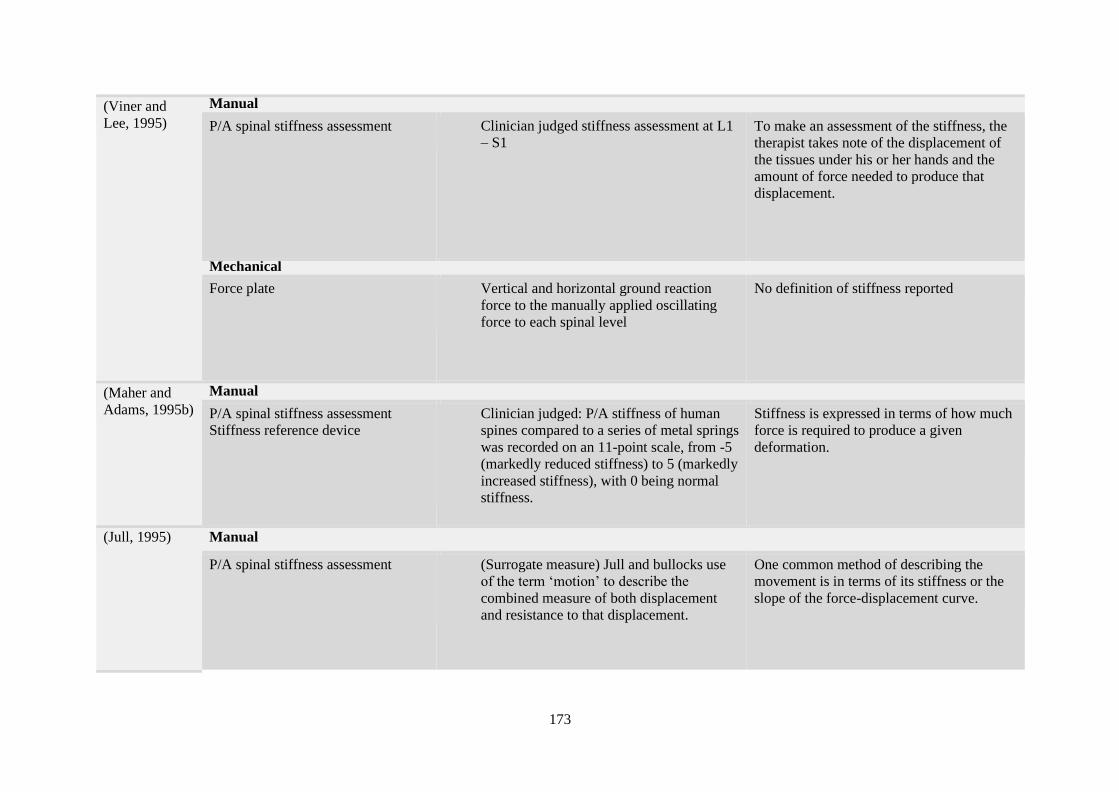
173
(Viner and
Lee, 1995)
Manual
P/A spinal stiffness assessment Clinician judged stiffness assessment at L1
– S1 To make an assessment of the stiffness, the
therapist takes note of the displacement of
the tissues under his or her hands and the
amount of force needed to produce that
displacement.
Mechanical
Force plate Vertical and horizontal ground reaction
force to the manually applied oscillating
force to each spinal level
No definition of stiffness reported
(Maher and
Adams, 1995b)
Manual
P/A spinal stiffness assessment
Stiffness reference device
Clinician judged: P/A stiffness of human
spines compared to a series of metal springs
was recorded on an 11-point scale, from -5
(markedly reduced stiffness) to 5 (markedly
increased stiffness), with 0 being normal
stiffness.
Stiffness is expressed in terms of how much
force is required to produce a given
deformation.
(Jull, 1995) Manual
P/A spinal stiffness assessment (Surrogate measure) Jull and bullocks use
of the term ‘motion’ to describe the
combined measure of both displacement
and resistance to that displacement.
One common method of describing the
movement is in terms of its stiffness or the
slope of the force-displacement curve.

174
(Simmonds et
al., 1995)
Manual
Passive motion testing The degree to which the spinal model
simulated normal motion was assessed
using two 11-point numerical rating scales.
(least stiff, medium stiff, most stiff) For
each level of stiffness, the therapists were
asked to grade the spinal model according
to how well it simulated normal physiologic
motion.
Intervertebral ''fixations'' (i.e., a stiff or
locked motion segement.
(Maher and
Adams, 1995a)
Manual
Mechanical device incorporating metal
springs was used to generate the stiffness
stimuli.
Clinician judged: whether the second
stimulus was "greater" or "less" in stiffness
than the first stimulus
No definition of stiffness reported
(Maher and
Adams, 1996)
Manual
Mechanical device that generates purely
elastic stiffness stimuli similar to the PA
stiffness of the human spine was used to
provide the stiffness stimuli.
Clinician judged: by pushing on the
stimulus once or twice with either vision
occluded or not occluded and to rate the
stiffness on a 1 to 5 scale.
There are a number of terms used to
describe the quality of the movement. The
most common describes the movement in
terms of its stiffness, i.e. the load/
displacement relationship.
(Latimer et al.,
1996)
Manual
P/A spinal stiffness assessment Clinician applied P/A force to the Lumbar
spine.
Stiffness is perceived by estimating the
amount of force applied and the amount of
displacement that results.
Mechanical
The Portable Stiffness Device Force – displacement Stiffness is equal to the slope of the linear
portion of the force-displacement curve.
Mechanical

175
(Raymond and
Evans, 1997)
P/A mobilisation Specifically, designed loading frame
applied P/A mobilisation to L4 spinous
process
No definition of stiffness reported
(Michael Lee
et al., 1997)
Mechanical
Portable Stiffness Measuring Device. Force – displacement In the region from 30 to 100 N, the response
has been characterized by describing the
gradient of this linear region (that is, the
stiffness coefficient, K)
(L. L.
Nicholson et
al., 1998)
Manual
Mechanical device incorporating metal
springs was used to generate the stiffness
stimuli.
Clinician judged: both samples of the
stimuli and then to judge whether the
second stimulus was 'stiffer' or 'less stiff'
than the first.
No definition of stiffness reported
(Michael Lee
et al., 1998)
Mechanical
The Spinal Physiotherapy Simulator (SPS) Force – displacement No definition of stiffness reported
(Edmondston
et al., 1998)
Mechanical
Spinal Posteroanterior Mobilization
Apparatus (SPAM)
Force – displacement No definition of stiffness reported
Manual

176
(Maher,
Latimer, et al.,
1998)
P/A spinal stiffness assessment Lumbar: manual PA pressures to L3 rated
on an 11-point scale assisted by a stiffness
reference device and compared to
instrumented oscillating PA pressures
One common method of describing the
movement is in terms of its stiffness or the
slope of the force-displacement curve. These
authors cited (Jull, 1995, p. 522)
Mechanical
The Stiffness Assessment Machine Force – displacement Stiffness is obtained by calculating the slope
of the linear portion of the force-
displacement curve above 30 N. The second
measure (D30) characterizes the toe, region
of the force-displacement curve and is
obtained by measuring the displacement to
30 N.
(Maher,
Simmonds, et
al., 1998)
Manual
P/A spinal stiffness assessment The relationship among P/A pressure
descriptors were examined using cluster
analysis.
Stiffness descriptors described in terms of
three superclusters (limited mobility,
increased mobility, and viscoelasticity)
(Latimer et al.,
1998)
Manual
P/A spinal stiffness assessment The P/A pressure test is used to provoke the
patient's pain and to identify areas of
increased stiffness, manual therapists
perform the central posteroanterior (PA)
pressure test, which involves the therapist
applying an anteriorly directed force over
the spinous process of the prone patient.
Increased tissue resistance to displacement
(i.e., increased stiffness) Stiffness being the
relationship between load and deformation
Mechanical
Mechanical spinal indentation Force – displacement The slope of the regression line is defined as
the stiffness coefficient
Mechanical

177
(Maher et al.,
1999)
The Stiffness Assessment Machine (SAM) Force – displacement No definition of stiffness reported
(Edmondston
et al., 1999)
Manual
P/A spinal stiffness assessment The diagnosis of symptomatic segmental
hypomobility is based in part on tests of
passive intervertebral movement, which
include testing the response to
posteroanterior (PA) pressure applied to the
spinous process.
Stiffness expressed in terms of the
therapist's perception of the range and
resistance to movement (stiffness), and the
associated symptom response.
Mechanical
Spinal Posteroanterior Mobilisation
Apparatus
Force – displacement Stiffness coefficient (in N/mm) was
calculated from the slope of the line of best
fit using linear regression analysis.
(Brodeur and
DelRe, 1999)
Mechanical
The Portable Stiffness Device Force – displacement No definition of stiffness reported
(Keller et al.,
2000)
Manual
P/A spinal manipulation The clinician takes note of the stiffness felt
during mobilization palpation procedures.
The displacement of the vertebra and the
resistance to the displacement.
Spinal stiffness or the load/displacement
response
Stiffness is expressed in terms of (mobility)
Manual (objective)

178
(L. L.
Nicholson et
al., 2000)
Mechanical device incorporating metal
springs was used to generate the stiffness
stimuli.
Clinician judged spring stiffness comparing
sample baseline stiffness stimuli to a
second stiffness stimuli
The relationship between the force applied
to the spine by the hand of the therapist and
the displacement that occurs at the point of
force application determines "spinal elastic
stiffness" and is described by the equation
𝑆𝑡𝑖𝑓𝑓𝑛𝑒𝑠𝑠 = 𝐹𝑜𝑟𝑐𝑒 𝑎𝑝𝑝𝑙𝑖𝑒𝑑/ 𝑑𝑖𝑠𝑝𝑙𝑎𝑐𝑒𝑚𝑒𝑛𝑡
(Goodsell et
al., 2000)
Mechanical
A stiffness measurement device was
custom-made to quantify central P/A force
Force – displacement The stiffness coefficient (K) is the gradient
of the regression line fitted to the data between 30 and 90 N
(Keller and
Colloca, 2000)
Mechanical
Activator Methods Chiropractic Technique
(AMCT) assessment protocol; Dynamic
stiffness assessment protocol
Force – time No definition of stiffness reported
(Colloca and
Keller, 2001)
Mechanical
Activator Methods Chiropractic Technique
(AMCT) assessment protocol; Dynamic
stiffness assessment protocol
Force – time No definition of stiffness reported
(L. L.
Nicholson et
al., 2001)
Mechanical
The stiffness Assessment Machine (SAM) Force – displacement The stiffness coefficient K is the slope of the
regression line between 30 and 90 N of
applied force.
(Kiviniemi et
al., 2001)
Manual
Posteroanterior (PA) force, or ‘springing’,
applied to the spinous process.
Clinician applied P/A mobilisation at L1-3
and L5
Through this technique, the physiotherapist
gains an impression of the movement
response to load, or stiffness.
Mechanical
The Spinal Posteroanterior Mobilization Force – displacement No definition of stiffness reported
Mechanical

179
(Gregory N.
Kawchuk and
Fauvel, 2001)
Spinal indentation equipment with subject
restraint system.
Force – displacement The most accurate method of stiffness
determination of curvilinear data is to
determine the slope of tangent lines fit to
small sections of the curve.
(Squires et al.,
2001)
Mechanical
Stiffness Assessment Machine (SAM) Force – displacement The stiffness coefficient (K) is the gradient
of the regression line between 30–90N of
the stiffness curve, with units of Newtons
per millimetre
(Gregory N.
Kawchuk and
Fauvel, 2001)
Mechanical
Spinal indentation equipment with subject
restraint system.
Force – displacement The most accurate method of stiffness
determination of curvilinear data is to
determine the slope of tangent lines fit to
small sections of the curve.
tissue stiffness or the slope of the Force –
displacement curve
(Petty et al.,
2002)
Mechanical
The Stiffness Assessment Machine (SAM) Force – displacement No definition of stiffness reported
(Keller and
Colloca, 2002)
Mechanical
5-degree-of-freedom (DOF) mass,
massless-spring, and damper model of P/A
motion response of the lumbar spine.
The spring element of each FJS is assumed
to have a linear force-deflection
relationship, following Hooke’s law, F ⫽ kx,
where k is the stiffness coefficient (N/m)
and x is the deflection (m

180
(L. L.
Nicholson et
al., 2003)
Manual (Objective)
Mechanical device for stiffness testing was
a hydraulic device incorporating a spring-
return plunger in a water-filled cylinder
Clinician judged: whether the second
stiffness stimulus was more or less stiff
than the first
Elastic stiffness, defined as the force (in
Newtons) required to displace a stiffness
stimulus by 1 mm.
(Chiradejnant
et al., 2003)
Manual
P/A spinal stiffness assessment
Reference-based protocol
A stiffness reference device was used to
anchor judgements of stiffness based on an
11-point scale. Raters were also told to
concentrate on the loading portion of the
force-displacement curve when trying to
match the stiffness.
Stiffness expressed in terms of the amount
of force applied to the displacement
produced (i.e., stiffness)
(Shirley et al.,
2003)
Mechanical
The Stiffness Assessment Machine Force – displacement Stiffness is defined as the average slope of
the linear region of the force-displacement
curves for oscillation cycles 2 through 5
(Colloca et al.,
2003)
Manual
P/A spinal stiffness assessment Lumbar: PA manipulative thrusts with
modified Activator Adjusting Instrument at
L4 and L5
Biomechanical assessments of the spine
using motion palpation procedures for the
presence of “fixation” (increased stiffness or
restricted mobility)
Mechanical
A motorized vertical/horizontal table. An
Activator Adjusting Instrument (AAI)
equipped with a preload control frame and
impedance head (load cell and
accelerometer) was then used to deliver PA
manipulative thrusts
Force – velocity No definition of stiffness reported
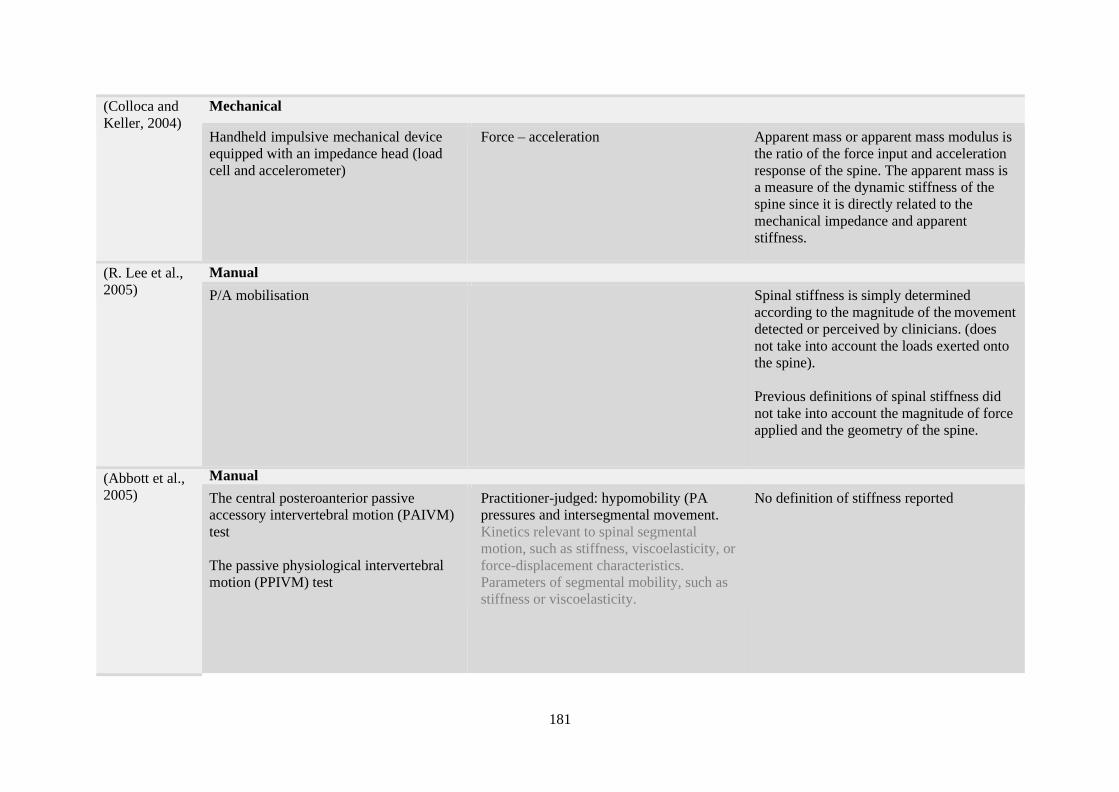
181
(Colloca and
Keller, 2004)
Mechanical
Handheld impulsive mechanical device
equipped with an impedance head (load
cell and accelerometer)
Force – acceleration Apparent mass or apparent mass modulus is
the ratio of the force input and acceleration
response of the spine. The apparent mass is
a measure of the dynamic stiffness of the
spine since it is directly related to the
mechanical impedance and apparent
stiffness.
(R. Lee et al.,
2005)
Manual
P/A mobilisation Spinal stiffness is simply determined
according to the magnitude of the movement
detected or perceived by clinicians. (does
not take into account the loads exerted onto
the spine).
Previous definitions of spinal stiffness did
not take into account the magnitude of force
applied and the geometry of the spine.
(Abbott et al.,
2005)
Manual
The central posteroanterior passive
accessory intervertebral motion (PAIVM)
test
The passive physiological intervertebral
motion (PPIVM) test
Practitioner-judged: hypomobility (PA
pressures and intersegmental movement.
Kinetics relevant to spinal segmental
motion, such as stiffness, viscoelasticity, or
force-displacement characteristics.
Parameters of segmental mobility, such as
stiffness or viscoelasticity.
No definition of stiffness reported

182
(Sran et al.,
2005)
Manual
P/A mobilisation It can be applied at an individual spinous
process to assess stiffness at a specific
segmental level.
Stiffness is a term used to describe the force
needed to achieve a certain deformation of a
structure.\
Mechanical
Precision optoelectronic camera system and
a custom spine testing machine
Moment – angular rotation Stiffness during PA mobilization was
determined as the slope of the PA force
versus T6–T7 rotation angle curve for the
loading portion of the curve between the two force limits (50–200 N)
(Tsung et al.,
2005)
Manual
Clinician applied mobilisation to the
lumbar spine by which the 3-dimensional
movements of the lumbar spine were
measured by an electromagnetic motion
tracking system
Load – deformation The load-deformation characteristics would
allow one to assess the stiffness of the spine
that could be altered by clinical pathologies.
Axial rotation stiffness of the lumbar spine,
which was defined as the ratio of the
amplitude of the twisting moment to the
amplitude of the axial rotation of the spine.
The bending stiffness of the spine was
derived from the relationship between the
mobilisation force and the change in spinal curvature.
(Hodges et al.,
2005)
Mechanical
The Spinal Physiotherapy Simulator (SPS) Force – displacement No definition of stiffness reported
Manual
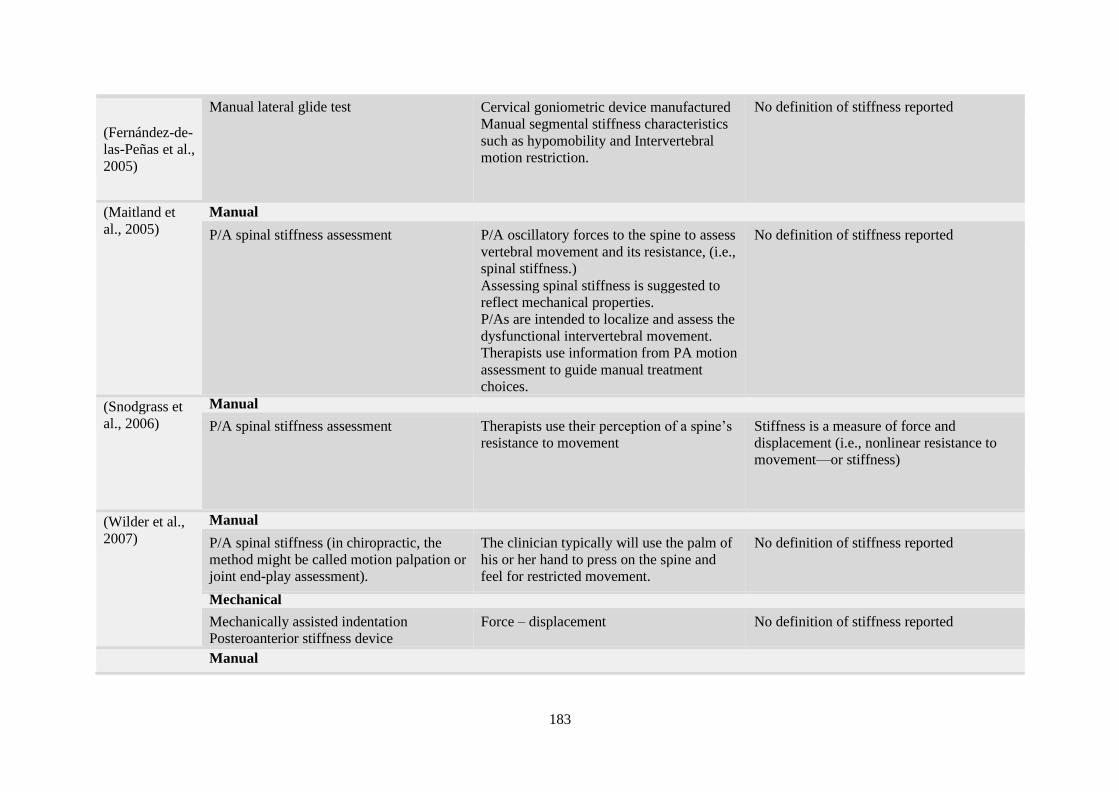
183
(Fernández-de-
las-Peñas et al.,
2005)
Manual lateral glide test Cervical goniometric device manufactured
Manual segmental stiffness characteristics
such as hypomobility and Intervertebral
motion restriction.
No definition of stiffness reported
(Maitland et
al., 2005)
Manual
P/A spinal stiffness assessment P/A oscillatory forces to the spine to assess
vertebral movement and its resistance, (i.e.,
spinal stiffness.)
Assessing spinal stiffness is suggested to
reflect mechanical properties.
P/As are intended to localize and assess the
dysfunctional intervertebral movement.
Therapists use information from PA motion
assessment to guide manual treatment
choices.
No definition of stiffness reported
(Snodgrass et
al., 2006)
Manual
P/A spinal stiffness assessment Therapists use their perception of a spine’s
resistance to movement
Stiffness is a measure of force and
displacement (i.e., nonlinear resistance to
movement—or stiffness)
(Wilder et al.,
2007)
Manual
P/A spinal stiffness (in chiropractic, the
method might be called motion palpation or
joint end-play assessment).
The clinician typically will use the palm of
his or her hand to press on the spine and
feel for restricted movement.
No definition of stiffness reported
Mechanical
Mechanically assisted indentation
Posteroanterior stiffness device
Force – displacement No definition of stiffness reported
Manual

184
(Owens et al.,
2007)
P/A spinal stiffness assessment Practitioner-judged: Stiff or not stiff on a 2-
level scale to assess spinal joint stiffness
(yes or no).
Co-measure: Range of motion and
tenderness
No definition of stiffness reported
Mechanically assisted
Mechanically assisted indentation
Posteroanterior stiffness device
Force – displacement No definition of stiffness reported
(Snodgrass et
al., 2008)
Mechanical
The cervical spine stiffness assessment
device
Force – displacement Stiffness was defined as the slope of the
linear region of the force-displacement
curve (coefficient K).
(Stanton and
Kawchuk,
2008)
Mechanical
Assisted indentation Force – displacement P/A stiffness is a combined response of soft
tissue deformation and rigid body displacement.
(Gombatto et
al., 2008)
Mechanical
Passive movement device and a six-
camera, three-dimensional motion capture
system consisting of a table, platform,
moveable cradle, two force transducers,
and a guide
Torque – angular displacement In the biomechanics literature, stiffness is
often defined as the slope of the torque-
angle curve
(Tuttle et al.,
2008a)
Mechanically assisted
Passive movement assessment device
(PMAD)
Force – displacement No definition of stiffness reported
Use of displacement/stiffness
interchangeably
Manual

185
(Tuttle et al.,
2008b)
P/A spinal stiffness assessment Practitioner-judged unilateral P/A to
segment selected by physiotherapist as
being hypomobile and most likely to be
contributing to symptoms.
No definition of stiffness reported
Mechanically assisted
Posteroanterior Movement Assessment
Device (PMAD)
Force – displacement No definition of stiffness reported
(Ferreira et al.,
2009)
Manual
P/A spinal stiffness assessment Practitioner-judged: stiffness (PA
pressures) on an 11-point scale, assisted by
a stiffness reference device. Raters were
also told to concentrate on the loading
portion of the force-displacement curve
when trying to match the stiffness.
No definition of stiffness reported
Mechanical
The Stiffness Assessment Machine (SAM) Force – displacement No definition of stiffness reported
(van Trijffel et
al., 2009)
Manual
Passive intervertebral motion (PIVM) Practitioner-judged; Maitland’s movement
diagram for grading mobility and a three-
point scale (hypomobile, normal,
hypermobile)
For classifying end-feel, scales were used
with terms like ‘hard’, ‘empty’, ‘springy’,
and ‘stiff’ reported most often.
No definition of stiffness reported
Manual (survey instrument)

186
(Abbott et al.,
2009)
The central posteroanterior passive
accessory intervertebral motion (PAIVM)
test
The passive physiological intervertebral
motion (PPIVM) test
Survey instrument distributed to New
Zealand Manipulative Physiotherapists. In
the first question, participants were asked to
choose (on a Likert scale) how accurate
they believe each of the physical
assessment procedures (PAIVMs and
PPIVMs) are for estimating the quantity of
movement present at a lumbar segment. In
the second question, participants were
asked the quantity of movement present at a
lumbar segment. In the second question,
participants were asked if they believe that
it is possible, from the clinical examination,
to recognise restricted or excessive lumbar
segmental motion.
Quality of resistance (e.g. greater or lesser
stiffness, force-displacement relationship)
(Stanton and
Kawchuk,
2009)
Manual
P/A spinal stiffness assessment Practitioner judged; The resulting
impression formed by the clinician during
the pressure test is then used to judge if the
spine is too compliant (hypermobility), too
stiff (hypomobility), or within normal
limits.
No definition of stiffness reported
Mechanical
Assisted indentation device Force – displacement Global Stiffness expressed as the slope of
the force-displacement data
Mean Maximal Stiffness expressed in terms
of the peak force/peak displacement
Manual

187
(Snodgrass et
al., 2009)
P/A mobilisation 1 of 4 grades as defined by (Maitland et al.,
2005) their choice of grade determined by
their interpretation of a patient's spinal
stiffness and the treatment aims
The level of resistance or stiffness of the
mobilized subjects' tissues would likely
affect the level of force applied for
particular mobilization grades.
Mechanical
Cervical spine stiffness was measured
using a Customised device that applied 5
consecutive mechanical force oscillations
with a steel probe at a speed of 1 Hz to the
spinous processes of C2 and C7.
Force – displacement Stiffness was defined as the mean slope of
the linear portions of the force-displacement
curves for oscillations 2 through 5.
(Tuttle et al.,
2009)
Mechanically assisted
Passive Movement Assessment Device
(PMAD)
Force – displacement No definition of stiffness reported
(Reiman,
2009)
Mechanical
Spinal Indentation to determine posterior-
anterior spinal stiffness, asymptomatic
subjects who used bracing demonstrated a
significantly larger increase in spinal
stiffness than those who used hollowing.
Load – displacement No definition of stiffness reported
(Vaillant et al.,
2010)
Mechanically assisted
Variable rate force/displacement (VRFD)
device.
Force – displacement No definition of stiffness reported
Manual
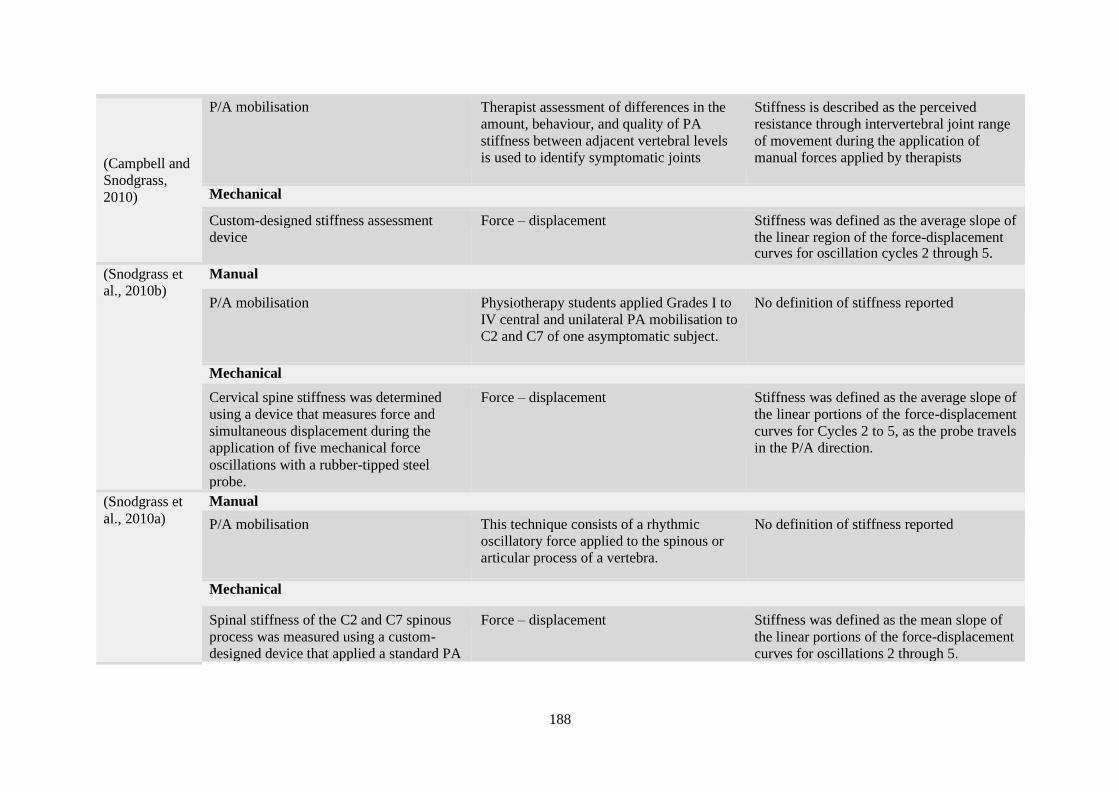
188
(Campbell and
Snodgrass,
2010)
P/A mobilisation Therapist assessment of differences in the
amount, behaviour, and quality of PA
stiffness between adjacent vertebral levels
is used to identify symptomatic joints
Stiffness is described as the perceived
resistance through intervertebral joint range
of movement during the application of
manual forces applied by therapists
Mechanical
Custom-designed stiffness assessment
device
Force – displacement Stiffness was defined as the average slope of
the linear region of the force-displacement curves for oscillation cycles 2 through 5.
(Snodgrass et
al., 2010b)
Manual
P/A mobilisation Physiotherapy students applied Grades I to
IV central and unilateral PA mobilisation to
C2 and C7 of one asymptomatic subject.
No definition of stiffness reported
Mechanical
Cervical spine stiffness was determined
using a device that measures force and
simultaneous displacement during the
application of five mechanical force
oscillations with a rubber-tipped steel
probe.
Force – displacement Stiffness was defined as the average slope of
the linear portions of the force-displacement
curves for Cycles 2 to 5, as the probe travels
in the P/A direction.
(Snodgrass et
al., 2010a)
Manual
P/A mobilisation This technique consists of a rhythmic
oscillatory force applied to the spinous or
articular process of a vertebra.
No definition of stiffness reported
Mechanical
Spinal stiffness of the C2 and C7 spinous
process was measured using a custom-
designed device that applied a standard PA
Force – displacement Stiffness was defined as the mean slope of
the linear portions of the force-displacement
curves for oscillations 2 through 5.

189
mobilisation force oscillating at 1 Hz for 5
cycles.
(Rey-Eiriz et al., 2010)
Manual
P/A spinal stiffness assessment
Cervical spine gliding test
Practitioner judged; Posterior-anterior
cervical spine gliding to determine the
presence of joint hypomobility over the C3-
C4, C4-C5, and C5-C6 levels.
No definition of stiffness reported
(Stamos-
Papastamos et
al., 2011)
Mechanical
A custom-made wooden and padded
treatment plinth securely screwed on a
nonconductive force platform. An
electromagnetic tracking system recording
at 100 Hz, was used to measure spinal
angular displacement during force
application for the calculation of bending
stiffness and to measure lumbar flexion and
extension ROM.
Load – deformation Bending stiffness as applied in this study as
the relationship between load and
deformation modelling the spine during 3 –
point bending
(Fritz et al.,
2011)
Mechanical
Spinal stiffness was assessed using a
mechanized indentation
Force – displacement No definition of stiffness reported
(Kumar and
Stoll, 2011)
Mechanical
The Therapeutic Spinal Mobiliser Load – deformation Stiffness was defined as the relationship
between load and deformation
(Kumar, 2011) Mechanical
The Therapeutic Spinal Mobiliser Load – displacement No definition of stiffness reported

190
(Haas et al.,
2011)
Subjective – self-report measure
VAS – Secondary outcomes included
immediate post-treatment stiffness.
No verbal descriptors provided No definition of stiffness reported on VAS
(Snodgrass et
al., 2012)
Manual
Manual assessment of spinal stiffness Stiffness is usually assessed manually using
practitioner judgment to determine whether
a joint is hypo- or hypermobile.
From the practitioner’s perspective, spinal
stiffness can be described as the perceived
resistance of the spine during the application
of a manually applied force
Stiffness expressed in terms of hypo- or
hypermobility.
Mechanical
Structured review of spinal stiffness
measurement
Force – displacement Spinal stiffness operationally defined as the
relationship between force and
displacement.
(Manning et
al., 2012)
Manual
Passive intervertebral motion-cervical
segmental side bending test
Practitioner judged; Side-bending motion
performed at each cervical joint from C2–
C3 to C6–C7, allowing segmental
synkinetic rotation and extension to occur.
Each joint was assessed for hypomobility, hard end- feel, and pain provocation.
No definition of stiffness reported
(Tiantian et al.,
2012)
Mechanical
Mechanically assisted P/A spinal stiffness Force – displacement No definition of stiffness reported
(Snodgrass and
Rhodes, 2012)
Mechanical
Mechanical spinal indentation Force – displacement Stiffness defined as the slope of the linear
portion of the force-displacement curve

191
(Kumar, 2012) Manual
P/A spinal stiffness assessment No subjective measure of spinal stiffness The resistance to motion on force
application, that is, the stiffness
Mechanical
The Therapeutic Spinal Mobilizer Load – displacement No definition of stiffness reported
(Triano et al.,
2013)
Manual
Palpatory assessment (motion palpation)
I. Passive physiologic/accessory
motion. II. Joint springing
III. Overpressure testing
Motion palpation uses examiner guided
motions to manually monitor the relative
displacement of bony landmarks through
the skin surface. Motions are categorized as
being limited/restricted; excessive/unstable
or aberrant, suggesting a deviation in path
at some point within the range of motion.
During the process of tissue palpation, the
examiner attempts to assess the relative
stiffness (conversely, compliance) to
postural or applied load to a segment.
(Shum et al.,
2013)
Manual
Grade III central P/A mobilisation Curvature, bending stiffness
(force/displacement) of the lumbar spine
and onset of pain on application of PA to
L4 at forces between 50N and 250N at 50N
intervals.
Stiffness is defined as the resistance of this
beam to the bending deformation caused by
PA mobilization.
Mechanical
Force plate Load – deformation Stiffness is defined as the resistance of this
beam to the bending deformation caused by
PA mobilization. This definition is
consistent with that used in the conventional
engineering method
Mechanical
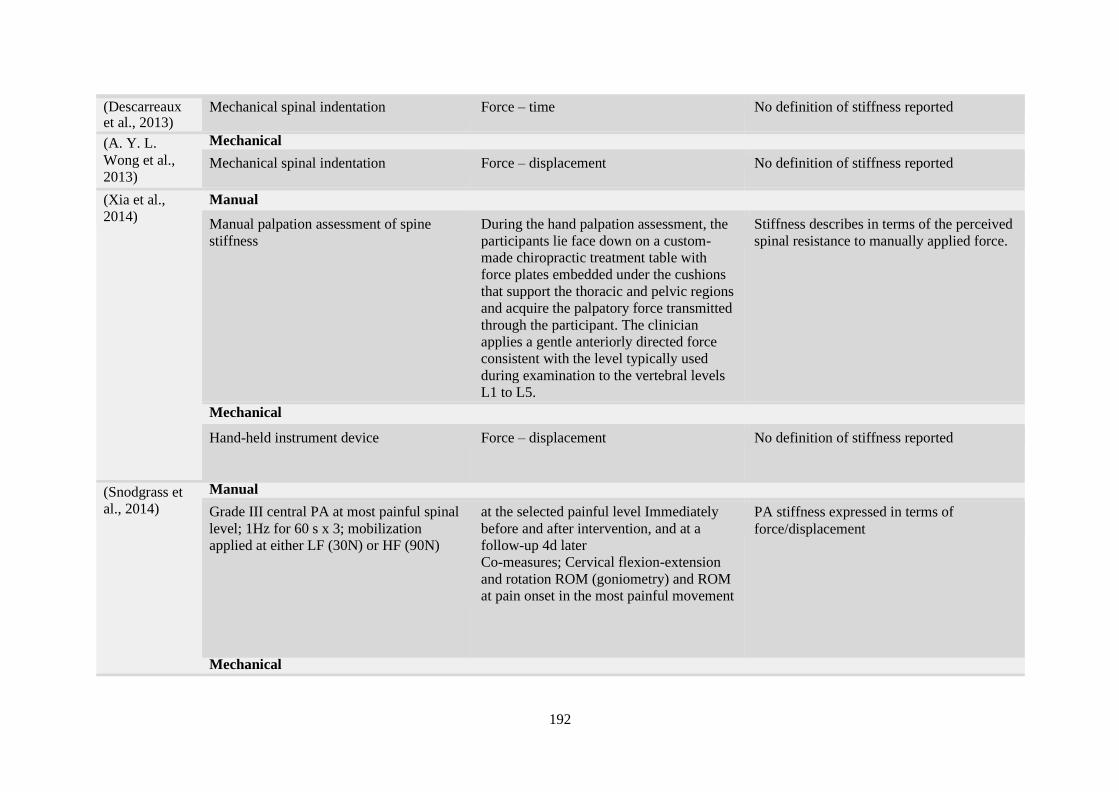
192
(Descarreaux et al., 2013)
Mechanical spinal indentation Force – time No definition of stiffness reported
(A. Y. L.
Wong et al.,
2013)
Mechanical
Mechanical spinal indentation Force – displacement No definition of stiffness reported
(Xia et al.,
2014)
Manual
Manual palpation assessment of spine
stiffness
During the hand palpation assessment, the
participants lie face down on a custom-
made chiropractic treatment table with
force plates embedded under the cushions
that support the thoracic and pelvic regions
and acquire the palpatory force transmitted
through the participant. The clinician
applies a gentle anteriorly directed force
consistent with the level typically used
during examination to the vertebral levels
L1 to L5.
Stiffness describes in terms of the perceived
spinal resistance to manually applied force.
Mechanical
Hand-held instrument device Force – displacement No definition of stiffness reported
(Snodgrass et
al., 2014)
Manual
Grade III central PA at most painful spinal
level; 1Hz for 60 s x 3; mobilization
applied at either LF (30N) or HF (90N)
at the selected painful level Immediately
before and after intervention, and at a
follow-up 4d later
Co-measures; Cervical flexion-extension
and rotation ROM (goniometry) and ROM
at pain onset in the most painful movement
PA stiffness expressed in terms of
force/displacement
Mechanical
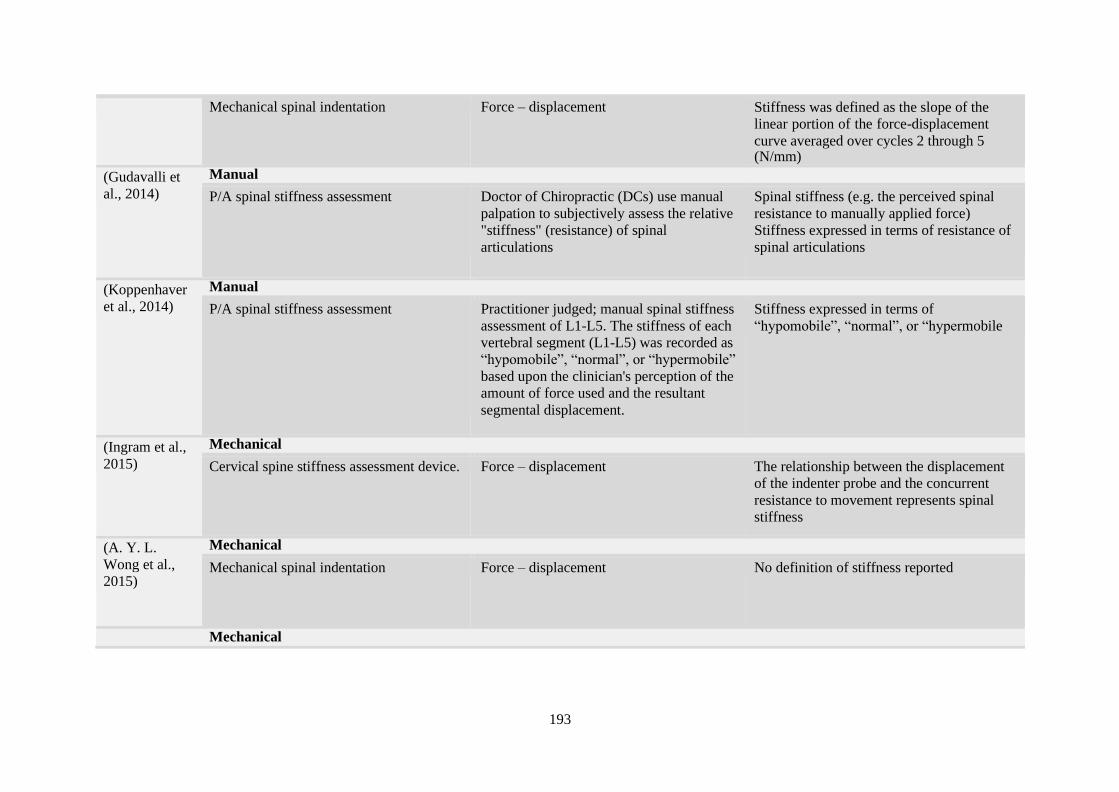
193
Mechanical spinal indentation Force – displacement Stiffness was defined as the slope of the
linear portion of the force-displacement
curve averaged over cycles 2 through 5 (N/mm)
(Gudavalli et
al., 2014)
Manual
P/A spinal stiffness assessment Doctor of Chiropractic (DCs) use manual
palpation to subjectively assess the relative
"stiffness" (resistance) of spinal
articulations
Spinal stiffness (e.g. the perceived spinal
resistance to manually applied force)
Stiffness expressed in terms of resistance of
spinal articulations
(Koppenhaver
et al., 2014)
Manual
P/A spinal stiffness assessment Practitioner judged; manual spinal stiffness
assessment of L1-L5. The stiffness of each
vertebral segment (L1-L5) was recorded as
“hypomobile”, “normal”, or “hypermobile”
based upon the clinician's perception of the
amount of force used and the resultant
segmental displacement.
Stiffness expressed in terms of
“hypomobile”, “normal”, or “hypermobile
(Ingram et al.,
2015)
Mechanical
Cervical spine stiffness assessment device. Force – displacement The relationship between the displacement
of the indenter probe and the concurrent
resistance to movement represents spinal
stiffness
(A. Y. L.
Wong et al.,
2015)
Mechanical
Mechanical spinal indentation Force – displacement No definition of stiffness reported
Mechanical

194
(Buzzatti et al.,
2015)
Zebris CMS20 ultrasound-based motion
tracking system
Thrust – displacement No definition of stiffness reported
(Gregory Neil
Kawchuk et
al., 2015)
Mechanical
Mechanical spinal indentation Force – displacement No definition of stiffness reported
(A. Y. L.
Wong et al.,
2016)
Mechanical
Mechanical spinal indentation Force – displacement No definition of stiffness reported
(Björnsdóttir et
al., 2016)
Mechanical
P/A Pressure Puffin Force – displacement Stiffness expressed in terms of the
(derivatives of displacement on force)
(Xia et al.,
2017)
Manual
Posterior-anterior spinal stiffness over the
spinous processes of the lumbar spine
Practitioner Judged; anteriorly directed
force over each lumbar segment
sequentially from L5 to L1.
Stiffness operationally defined in this study
as the quantitative measure of the resistance
to motion.
Mechanical
Hand-held instrument device consists of a
force transducer and infrared smart markers
for accurate force and displacement
measurement.
Automated device method, a
programmable indenter applied force
anteriorly up to 60 N with a force feedback
control.
Force – displacement Stiffness operationally defined in this study
as the quantitative measure of the resistance
to motion.
Manual
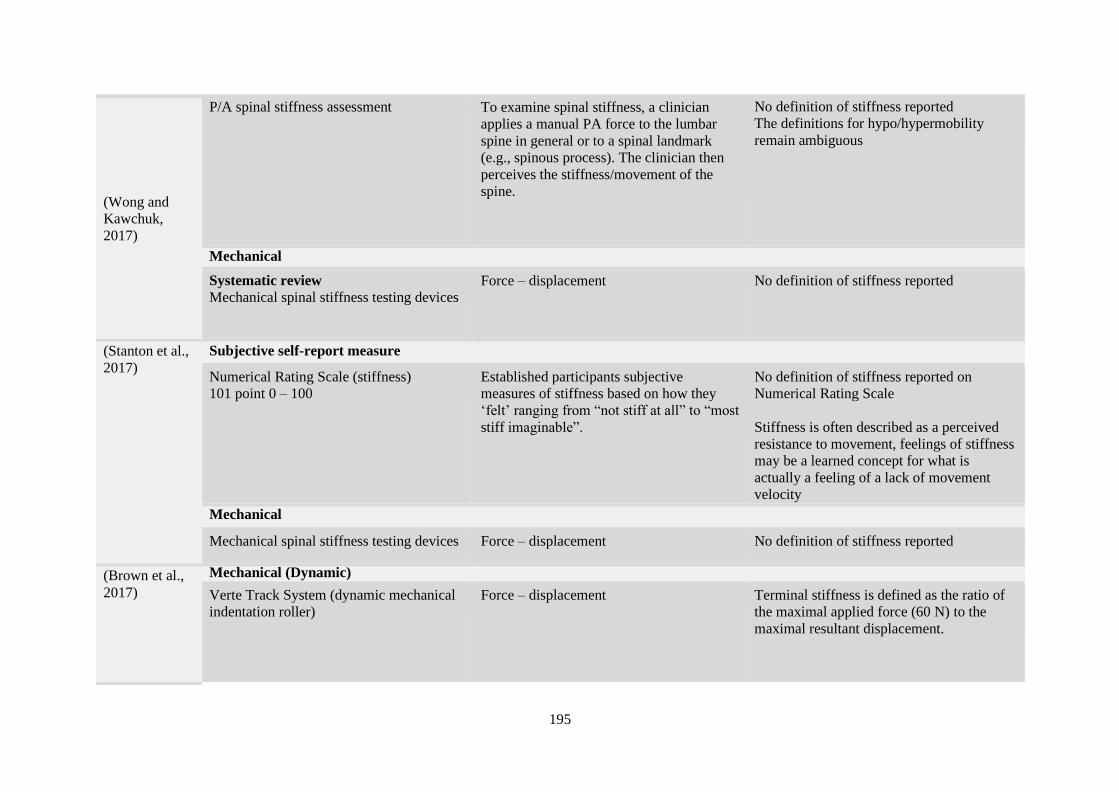
195
(Wong and
Kawchuk,
2017)
P/A spinal stiffness assessment To examine spinal stiffness, a clinician
applies a manual PA force to the lumbar
spine in general or to a spinal landmark
(e.g., spinous process). The clinician then
perceives the stiffness/movement of the
spine.
No definition of stiffness reported
The definitions for hypo/hypermobility
remain ambiguous
Mechanical
Systematic review
Mechanical spinal stiffness testing devices Force – displacement No definition of stiffness reported
(Stanton et al.,
2017)
Subjective self-report measure
Numerical Rating Scale (stiffness)
101 point 0 – 100
Established participants subjective
measures of stiffness based on how they
‘felt’ ranging from “not stiff at all” to “most
stiff imaginable”.
No definition of stiffness reported on
Numerical Rating Scale
Stiffness is often described as a perceived
resistance to movement, feelings of stiffness
may be a learned concept for what is
actually a feeling of a lack of movement
velocity
Mechanical
Mechanical spinal stiffness testing devices Force – displacement No definition of stiffness reported
(Brown et al.,
2017)
Mechanical (Dynamic)
Verte Track System (dynamic mechanical
indentation roller)
Force – displacement Terminal stiffness is defined as the ratio of
the maximal applied force (60 N) to the
maximal resultant displacement.

196
(Holt et al.,
2018)
Manual
P/A spinal stiffness assessment Manual posteroanterior force to a specific
body landmark (e.g., spinous process) or to
a spinal region in general (e.g., lumbar) by
a clinician, and then the clinician perceives
the corresponding spinal movement or
stiffness.
The operational definition of the Stiffest
Spinal Site for this study was the spinal
location of maximal resistance to palpatory
pressure, as perceived by the clinician,
which is a force-displacement relationship
(Pagé et al.,
2018)
Mechanical
Mechanical spinal indentation Force – displacement The global stiffness was defined as the slope
of the straight line (represented by the dotted
line) best fitting the data between 10 and 45
N
The terminal stiffness as the ratio of the
variation of the load and the variation of the
displacement between 10 and 45 N ([L1-
L2]/[D1-D2]
(Dugailly et
al., 2018)
Mechanical
Cervical stiffness measurements were
achieved in axial rotation using a
customized device
Torque – angular displacement. No definition of stiffness reported
Mechanical

197
(Tuttle and
Hazle, 2018)
Multiple modelling studies and in vivo
measurements of PA movements.
Force – displacement Stiffness is the change in force per unit
change in displacement. In other words,
stiffness is the slope or first derivative of
force-displacement curves. Compliance,
which is the inverse of stiffness, is
sometimes used to indicate a comparable
perception.
(Swanenburg
et al., 2018)
Mechanical
Computer-assisted analytical device – P/A
stiffness
The instrument measured tissue compliance
according to the concept of impulse
response
No definition of stiffness reported
(Hadizadeh et
al., 2019)
Mechanical (Dynamic)
Verte Track System (dynamic mechanical
indentation roller)
Force – displacement No definition of stiffness reported
(Kawchuk et Mechanical (Dynamic)
al., 2019) Manual posteroanterior force in
conjunction with a computer-controlled
indentation probe.
Force – displacement No definition of stiffness reported
Total
segmental
stiffness
assessment (n = 106)
Total objective (Mechanical) outcome
measures = 73
Total subjective (Manual) outcome
measures = 62 Total Measures = 135
Yes definition = 75
No definition = 60
Total = 135

198
Total studies
(n= 333)
Total subjective measures = 124
Total objective measures = 175
No Measures = 3
Total indicators = 60
Total = 362
Yes definition = 122
No definition = 240
Total = 362

199
Appendix G: Alternative descriptors
Table showing segmental assessment descriptors
Synonyms
(Maher, Simmonds, et al., 1998) ► toe compliance
► friction
► resistance
► hypomobile
► restricted
► noncompliant
► limited Hypomobile
► tight
► firm
► inelastic
► thick
► non-springy
► blocked
► active recoil
► reactive
► rubbery
► boggy
(Binkley et al., 1995; Triano et al., 2013) ► hypomobility
(Keller et al., 2000) ► Less mobility
(Abbott et al., 2005; Nicholson et al., 2000) ► hardness
(Owens et al., 2007; Colloca et al., 2003) ► fixation
(Campbell & Snodgrass, 2010; Gudavalli et al., 2014; Lee et al., 1993;
Snodgrass et al., 2009, 2010b) ► resistance
(Maher and Adams, 1995b) ► range of motion

200
► end-feel
► spasm
► viscosity
(Haas et al., 2011; Maher and Adams, 1995a) ► end play restriction
(Manning et al., 2012) ► Hard end-feel
(Fernández-de-las-Peñas et al., 2005; Rey-Eiriz et al., 2010) ► Gliding, end-feel and resistance of zygapophyseal joints
(Simmonds et al., 1995) ► ‘Feel’ and extent of movement
Antonyms
(Maher, Simmonds, et al., 1998) ► elastic
► springy
► hypermobile
► loose
► yielding
► friction-free
► undue give
► compliant
► spasm-free
► smooth
► free running
► resistance-free
► soft
► well-oiled
► spongy
► squashy
► separately
(Binkley et al., 1995) ► hypermobility
(Kumar, 2011, 2012; Stanton and Kawchuk, 2009; Triano et al., 2013) ► Compliance

201
Appendix H: Surrogate measures
Table showing surrogate measures of segmental spinal stiffness
► Spinal stiffness is a measurement of spinal translation, defined as the displacement of spinal and paraspinal tissues due to the application of a posterior
to anterior (P-A) load at a spinal segment. (Snodgrass et al., 2012)
► Jull and bullocks use of the term "motion" to describe the combined measure of both displacement and resistance to that displacement (Jull and
Bullock, 1987) ► Jull and Bullock seem to be using the word "motion" as a synonym for stiffness (Jull and Bullock, 1987).
► According to Maitland, movement is synonymous with the term motion (Maitland et al., 2005)
► Accessory motion is defined as movement at a joint that cannot be performed voluntarily but can be performed passively by an external force.
► Accessory motion evaluation is performed to establish relative segmental stiffness (hypermobility and hypomobility) (Binkley et al., 1995)
► The segment of interest is classified as hypomobile, normal, or hypermobile, based on the clinician’s perception of stiffness (Stanton and Kawchuk,
2009) ► Too compliant (hypermobility), too stiff (hypomobility), or within normal limits (Maitland et al., 2001).
► In clinical practice, stiffness is usually assessed manually using practitioner judgment to determine whether a joint is hypo- or hypermobile (Snodgrass
et al., 2012). ► Clinicians measure both motion and resistance to motion, or spinal stiffness. (Koppenhaver et al., 2014)
► P/A Spinal stiffness is defined in the studies as at least one level (L1 - L5) being rated as “hypomobile” or “hypermobile” on a 3-point scale
(hypomobile, normal, hypermobile). (Koppenhaver et al., 2014) ► Anecdotal evidence suggests that spinal stiffness restricts motion (Kumar, 2012)
► Maitland"' uses the words "resistance" and "stiffness" interchangeably (Maitland et al., 2005)
► Absence of “fixations”, ‘’resistance or compliance’’ (Nicholson et al., 2003)
► Viscoelasticity (force application and the corresponding displacement velocity) (Wong and Kawchuk, 2017)
► Stabilise (Colloca and Keller, 2004)
► Stability (Ferreira et al., 2009; Shirley et al., 2003)
► Stiffness or movement (Snodgrass et al., 2010b; Viner and Lee, 1995;)
► Displacement (Tiantian et al., 2012; Tuttle et al., 2009)
► Movement response to load (Kiviniemi et al., 2001)
► Joint range perceived (Snodgrass et al., 2010b)
► Flexibility impairment (Dugailly et al., 2018)
► The association of low back pain and spinal stiffness and consequent impact on the spinal motion (Kumar, 2011).

200
References
Abbott, J. H., Flynn, T. W., Fritz, J. M., Hing, W. A., Reid, D., & Whitman, J. M. (2009).
Manual physical assessment of spinal segmental motion: Intent and validity. Manual
Therapy, 14(1), 36–44. https://doi.org/10.1016/j.math.2007.09.011
Abbott, J. H., McCane, B., Herbison, P., Moginie, G., Chapple, C., & Hogarty, T. (2005).
Lumbar segmental instability: A criterion-related validity study of manual therapy
assessment. BMC Musculoskeletal Disorders, 6, 1–10. https://doi.org/10.1186/1471-
2474-6-56
Addimanda, O., Perrotta, F. M., Olivieri, I., Ramonda, R., Salvarani, C., D’Angelo, S.,
Marchesoni, A., Lubrano, E., Spadaro, A., & Punzi, L. (2014). Predictive factors for
partial remission according to the Ankylosing Spondylitis Assessment Study working
group in patients with ankylosing spondylitis treated with anti-TNFα drugs.
Reumatismo, 66(3), 208. https://doi.org/10.4081/reumatismo.2014.756
Agarwal, A., Jayaswal, A., Goel, V. K., & Agarwal, A. K. (2018). Patient-specific
Distraction Regimen to Avoid Growth-rod Failure. Spine, 43(4), E221–E226.
https://doi.org/10.1097/BRS.0000000000002286
Ailon, T., Hamilton, D. K., Klineberg, E., Daniels, A. H., Lafage, V., Bess, S., Burton, D. C.,
Gupta, M., Schwab, F., Ames, C. P., Smith, J. S., Shaffrey, C. I., & Hart, R. A. (2018).
Radiographic Fusion Grade Does Not Impact Health-Related Quality of Life in the
Absence of Instrumentation Failure for Patients Undergoing Posterior Instrumented
Fusion for Adult Spinal Deformity. World Neurosurgery, 117, e1–e7.
https://doi.org/10.1016/j.wneu.2018.04.127
Al-Herz, A., Snip, J. P., Clark, B., & Esdaile, J. M. (2008). Exercise therapy for patients with
diffuse idiopathic skeletal hyperostosis. Clinical Rheumatology, 27(2), 207–210.
https://doi.org/10.1007/s10067-007-0693-z
Alaya, Z., & Osman, W. (2017). Lumbosciatica revealing intramedullary ependymoma
Zeineb. Pan African Medical Journal, 26, 2–3.
https://doi.org/10.11604/pamj.2017.26.171.11633
Ambrosetti-Giudici, S., Pfenniger, A., Krenn, M. H., Piotrowski, W. P., Ferguson, S. J., &
201
Burger, J. (2009). Surgical instrumentation for the in vivo determination of human
lumbar spinal segment stiffness and viscoelasticity. Medical Engineering and Physics,
31(9), 1063–1068. https://doi.org/10.1016/j.medengphy.2009.07.002
Amin, D. B., Lawless, I. M., Sommerfeld, D., Stanley, R. M., Ding, B., & Costi, J. J. (2016).
The effect of six degree of freedom loading sequence on the in-vitro compressive
properties of human lumbar spine segments. Journal of Biomechanics, 49(14), 3407–
3414. https://doi.org/10.1016/j.jbiomech.2016.09.009
Amine, B., Abouqal, R., Ibn Yacoub, Y., Hajjaj-Hassouni, N., Ali Ou Alla, S., Rostom, S.,
Benbouaaza, K., & Bahiri, R. (2010). Psychometric evaluation of the Moroccan version
of the Bath Ankylosing Spondylitis Functional Index (BASFI) and Bath Ankylosing
Spondylitis Disease Activity Index (BASDAI) for use in patients with ankylosing
spondylitis. Clinical Rheumatology, 29(7), 781–788. https://doi.org/10.1007/s10067-
010-1431-5
An, H., & Masuda, K. (2006). Relevance of in vitro and in vivo models for intervertebral disc
degeneration. Journal of Bone and Joint Surgery - Series A, 88-A(SUPPL. 2), 88–94.
https://doi.org/10.2106/JBJS.E.01272
Anga, G., Kaminiel, O., Vince, J., Riddell, M., Tefuarani, N., Ripa, P., Barnabas, R., & Duke,
T. (2010). The aetiology, clinical presentations and outcome of febrile encephalopathy
in children in Papua New Guinea. Annals of Tropical Paediatrics, 30(2), 109–118.
https://doi.org/10.1179/146532810x12703902243818
Arnbak, B., Jurik, A. G., Jensen, T. S., & Manniche, C. (2018). Association Between
Inflammatory Back Pain Characteristics and Magnetic Resonance Imaging Findings in
the Spine and Sacroiliac Joints. Arthritis Care and Research, 70(2), 244–251.
https://doi.org/10.1002/acr.23259
Ashton-Miller, J. A., & Schultz, A. B. (1991). Spine instability and segmental hypermobility
biomechanics: A call for the definition and standard use of terms. Seminars in Spine
Surgery, 3(2), 136–148.
Averns, H. L., Oxtoby, J., Taylor, H. G., Jones, P. W., Dziedzic, K., & Dawes, P. T. (1996).
Smoking and outcome in ankylosing spondylitis. Scandinavian Journal of
Rheumatology, 25(3), 138–142.
http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=med4&NEWS=N&A

202
N=8668955%5Cnhttp://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=eme
d4&NEWS=N&AN=1996181421
Baborie, A., Dunn, E. M., Bridges, L. R., & Bamford, J. M. (2001). Primary diffuse
leptomeningeal gliomatosis predominantly affecting the spinal cord: Case report and
review of the literature. Journal of Neurology Neurosurgery and Psychiatry, 70(2), 256–
258. https://doi.org/10.1136/jnnp.70.2.256
Bachan, E. G., Aikins, M., Kenu, E., Kye-Duodu, G., Nyarko, K. M., Issah, K., Ameme, D.
K., Kuffour, O. A., Opare, J., Asiedu, E., Afari, E., Aseidu-Bekoe, F., Kuma, G. K.,
Letsa, T., & Noora, C. L. (2018). Pneumococcal meningitis outbreak and associated
factors in six districts of Brong Ahafo region, Ghana, 2016. BMC Public Health, 18(1),
1–11. https://doi.org/10.1186/s12889-018-5529-z
Bal, S., Bal, K., Turan, Y., Deniz, G., Gürgan, A., Berkit, I. K., & Şendur, Ö. F. (2011).
Sexual functions in ankylosing spondylitis. Rheumatology International, 31(7), 889–
894. https://doi.org/10.1007/s00296-010-1406-5
Bang, N. D., Caws, M., Truc, T. T., Duong, T. N., Dung, N. H., Ha, D. T. M., Thwaites, G.
E., Heemskerk, D., Tarning, J., Merson, L., Van Toi, P., Farrar, J. J., Pouplin, T.,
Wolbers, M., & Day, J. N. (2016). Clinical presentations, diagnosis, mortality and
prognostic markers of tuberculous meningitis in Vietnamese children: a prospective
descriptive study. BMC Infectious Diseases, 16(1), 1–10.
https://doi.org/10.1186/s12879-016-1923-2
Bazrgari, B., & Shirazi-Adl, A. (2007). Spinal stability and role of passive stiffness in
dynamic squat and stoop lifts. Computer Methods in Biomechanics and Biomedical
Engineering, 10(5), 351–360. https://doi.org/10.1080/10255840701436974
Binkley, J., Stratford, P. W., & Gill, C. (1995). Interrater Reliability of Lumbar Accessory
Motion Mobility Testing. Physical Therapy, 75(9), 786–792.
https://doi.org/10.1093/ptj/75.9.786
Bisschop, A., Kingma, I., Bleys, R. L. A. W., Paul, C. P. L., van der Veen, A. J., van Royen,
B. J., & van Dieën, J. H. (2013). Effects of repetitive movement on range of motion and
stiffness around the neutral orientation of the human lumbar spine. Journal of
Biomechanics, 46(1), 187–191. https://doi.org/10.1016/j.jbiomech.2012.10.014
203
Bisschop, A., Van Dieën, J. H., Kingma, I., Van Der Veen, A. J., Jiya, T. U., Mullender, M.
G., Paul, C. P. L., De Kleuver, M., & Van Royen, B. J. (2013). Torsion biomechanics of
the spine following lumbar laminectomy: A human cadaver study. European Spine
Journal, 22(8), 1785–1793. https://doi.org/10.1007/s00586-013-2699-3
Bisschop, A., Van Royen, B. J., Mullender, M. G., Paul, C. P. L., Kingma, I., Jiya, T. U., Van
Der Veen, A. J., & Van Dieën, J. H. (2012). Which factors prognosticate spinal
instability following lumbar laminectomy? European Spine Journal, 21(12), 2640–2648.
https://doi.org/10.1007/s00586-012-2250-y
Björnsdóttir, S. V., Gudmundsson, G., Audunsson, G. A., Matthíasson, J., & Ragnarsdóttir,
M. (2016). Posterior-anterior(PA) pressure Puffin for measuring and treating spinal
stiffness: Mechanism and repeatability. Manual Therapy, 22, 72–79.
https://doi.org/10.1016/j.math.2015.10.005
Boonen, A., Wells, G. A., Tugwell, P., Maxwell, L. J., Veras, M. M., Zochling, J., Benkhalti
Jandu, M., Singh, J. A., & Tanjong Ghogomu, E. (2015). TNF-alpha inhibitors for
ankylosing spondylitis. Cochrane Database of Systematic Reviews, 3.
https://doi.org/10.1002/14651858.cd005468.pub2
Borkowski, S. L., Ebramzadeh, E., Sangiorgio, S. N., & Masri, S. F. (2014). Application of
the Restoring Force Method for Identification of Lumbar Spine Flexion-Extension
Motion Under Flexion-Extension Moment. Journal of Biomechanical Engineering,
136(4), 044501. https://doi.org/10.1115/1.4026893
Brandt, J., Listing, J., Sieper, J., Rudwaleit, M., Van Der Heijde, D., & Braun, J. (2004).
Development and preselection of criteria for short term improvement after anti-TNFα
treatment in ankylosing spondylitis. Annals of the Rheumatic Diseases, 63(11), 1438–
1444. https://doi.org/10.1136/ard.2003.016717
Brodeur, R. R., & DelRe, L. (1999). Stiffness of the thoracolumbar spine for subjects with
and without low back pain. Jnms-Journal of the Neuromusculoskeletal System, 7(4),
127–133.
Brouwer, M., van de Beek, D., Sebastiaan, H., Spanjaard, L., & Gans, J. de G. (2006).
Community-Acquired Listeria monocytogenes Meningitis in Adults. The Journal of
Nervous and Mental Disease, 60(2), 195. https://doi.org/10.1097/00005053-192408000-
00018

204
Brown, B., Blacke, A., Carroll, V., Graham, P., Kawchuk, G., Downie, A., & Swain, M.
(2017). The comfort and safety of a novel rolling mechanical indentation device for the
measurement of lumbar trunk stiffness in young adults. Chiropractic and Manual
Therapies, 25(1), 1–10. https://doi.org/10.1186/s12998-017-0153-z
Brown, M., Holmes, D., Heiner, A., & Wehman, K. (2002). Measurement of cadaver lumbar
spine motion segment stiffness. Spine, 27(9), 918–922.
https://doi.org/10.1097/00007632-200205010-00006
Brown, M., Wehman, K. F., & Heiner, A. D. (2002). The clinical usefulness of intraoperative
spinal stiffness measurements. Spine, 27(9), 959–961. https://doi.org/10.1097/00007632-
200205010-00015
Buford, W. L., Andersen, C. E., Garges, K. J., Muffoletto, A. J., & Simmons, J. W. (2002).
Simulation of the spine-extrapolation of function from the 3D form of structures derived
from the Visible Human CT data base. Proceedings of the Second Joint EMBS/BMES
Conference, 2507–2508. https://doi.org/10.1109/iembs.2002.1053398
Bull Andersen, T., Essendrop, M., & Schibye, B. (2004). Movement of the upper body and
muscle activity patterns following a rapidly applied load: The influence of pre-load
alterations. European Journal of Applied Physiology, 91(4), 488–492.
https://doi.org/10.1007/s00421-004-1040-6
Busscher, I., Van Dieën, J. H., Kingma, I., Van Der Veen, A. J., Verkerke, G. J., &
Veldhuizen, A. G. (2009). Biomechanical characteristics of different regions of the
human spine: An in vitro study on multilevel spinal segments. Spine, 34(26), 2858–
2864. https://doi.org/10.1097/BRS.0b013e3181b4c75d
Buttermann, G. R., Beaubien, B. P., Freeman, A. L., Stoll, J. E., & Chappuis, J. L. (2009).
Interbody device endplate engagement effects on motion segment biomechanics. Spine
Journal, 9(7), 564–573. https://doi.org/10.1016/j.spinee.2009.03.014
Buzzatti, L., Provyn, S., Van Roy, P., & Cattrysse, E. (2015). Atlanto-axial facet
displacement during rotational high-velocity low-amplitude thrust: An in vitro 3D
kinematic analysis. Manual Therapy, 20(6), 783–789.
https://doi.org/10.1016/j.math.2015.03.006
Campbell, B. D., & Snodgrass, S. J. (2010). The effects of thoracic manipulation on

205
posteroanterior spinal stiffness. Journal of Orthopaedic and Sports Physical Therapy,
40(11), 685–693. https://doi.org/10.2519/jospt.2010.3271
Cardiel, M. H., Londoño, J. D., E, G., Pacheco-Tena, C., Vázquez-Mellado, J., & Burgos-
Vargas, R. (2003). Translation, cross-cultural adaptation, and validation of the Bath
Ankylosing Spondylitis Functional Index (BASFI), the Bath Ankylosing Spondylitis
Disease Activity Index (BASDAI) and the Dougados Functonal Index (DFI) in a
Spanish speaking population wit. Clinical and Experimental Rheumatology, 21(4), 451–
458.
http://www.embase.com/search/results?subaction=viewrecord&from=export&id=L3695
0313%0Ahttp://wx7cf7zp2h.search.serialssolutions.com?sid=EMBASE&issn=0392856
X&id=doi:&atitle=Translation%2C+cross-
cultural+adaptation%2C+and+validation+of+the+Bath+Ankylosing+Sp
Caride, M., Zysset, P. K., Mordasini, P., Orr, T. E., Charriere, E. A., & Beutler, T. (2005).
Compliance of the L5-S1 spinal unit: a comparative study between an unconstrained and
a partially constrained system. European Spine Journal, 15(1), 74–81.
https://doi.org/10.1007/s00586-004-0807-0
Chad, M. J., Stephen, H. M., & Stuart, M. (2009). Comparison of Different Rowing
Exercises : Trunk Muscle Activation and ... Journal of Strength and Conditioning
Research, 23(5), 1408–1417.
Chen, H., Schlösser, T. P. C., Brink, R. C., Colo, Di., Van Stralen, M., Shi, L., Chu, W. C.
W., Heng, P. A., Castelein, R. M., & Cheng, J. C. Y. (2017). The Height-Width-Depth
Ratios of the Intervertebral Discs and Vertebral Bodies in Adolescent Idiopathic
Scoliosis vs Controls in a Chinese Population. Scientific Reports, 7(May 2016), 1–7.
https://doi.org/10.1038/srep46448
Chen, J., Liu, C., & Lin, J. (2006). Methotrexate for ankylosing spondylitis. Cochrane
Database of Systematic Reviews, 2, 2–4.
https://doi.org/10.1002/14651858.cd004524.pub3
Cheng, C.-H., Lin, K.-H., & Wang, J.-L. (2008). Co-contraction of cervical muscles during
sagittal and coronal neck motions at different movement speeds. European Journal of
Applied Physiology, 103(6), 647–654. https://doi.org/10.1007/s00421-008-0760-4
Cheng, C.-H., Wang, S.-F., Chen, C. P.-C., Liu, W.-Y., Hsu, W.-L., Chuang, Y.-F., Cheng,

206
H.-Y. K., & Lin, K.-H. (2014). Altered Co-contraction of Cervical Muscles in Young
Adults with Chronic Neck Pain during Voluntary Neck Motions. Journal of Physical
Therapy Science, 26(4), 587–590. https://doi.org/10.1589/jpts.26.587
Chiradejnant, A., Maher, C. G., & Latimer, J. (2003). Objective Manual Assessment of
Lumbar Posteroanterior Stiffness Is Now Possible. Journal of Manipulative and
Physiological Therapeutics, 34–39.
Chivukula, S., Moossy, J. J., Agarwal, V., Rothfus, W., Gande, A. V., Gardner, P. A., &
Horowitz, M. B. (2015). Long-term outcomes of intradural cervical dorsal root
rhizotomy for refractory occipital neuralgia. Journal of Neurosurgery, 102–110.
https://doi.org/10.3171/2015.6.jns142772
Choi, J.-H., Jang, J.-S., Yoo, K.-S., Shin, J.-M., & Jang, I.-T. (2018). Functional Limitations
Due to Stiffness after Long Level Spinal Instrumented Fusion Surgery to Correct
Lumbar Degenerative Flat Back. Spine, 43(15), 1044–1051.
https://doi.org/10.1097/BRS.0000000000002514
Clamp, J. A., Andrews, J. R., & Grevitt, M. P. (2008). A Study of the Radiologic Predictors
of Curve Flexibility in Adolescent Idiopathic Scoliosis. J Spinal Disord Tech, 21, 213–
215.
Clin, J., Aubin, C. É., Parent, S., & Labelle, H. (2011). Biomechanical modeling of brace
treatment of scoliosis: Effects of gravitational loads. Medical and Biological
Engineering and Computing, 49(7), 743–753. https://doi.org/10.1007/s11517-011-0737-
z
Colloca, C. J., & Keller, T. S. (2001). Stiffness and neuromuscular reflex response of the
human spine to posteroanterior manipulative thrusts in patients with low back pain.
Journal of Manipulative and Physiological Therapeutics, 24(8), 489–500.
https://doi.org/10.1067/mmt.2001.118209
Colloca, C. J., & Keller, T. S. (2004). Active trunk extensor contributions to dynamic
posteroanterior lumbar spinal stiffness. Journal of Manipulative and Physiological
Therapeutics, 27(4), 229–237. https://doi.org/10.1016/j.jmpt.2003.11.001
Colloca, C. J., Keller, T. S., Peterson, T. K., & Seltzer, D. E. (2003). Comparison of dynamic
posteroanterior spinal stiffness to plain film radiographic images of lumbar dise height.

207
Journal of Manipulative and Physiological Therapeutics, 26(4), 233–241.
https://doi.org/10.1016/S0161-4754(03)00005-8
Dagenais, S., Haldeman, S., & Wooley, J. R. (2005). Intraligamentous injection of sclerosing
solutions (prolotherapy) for spinal pain: A critical review of the literature. Spine
Journal, 5(3), 310–328. https://doi.org/10.1016/j.spinee.2004.09.011
Dagenais, S., Ogunseitan, O., Haldeman, S., Wooley, J. R., & Newcomb, R. L. (2006). Side
Effects and Adverse Events Related to Intraligamentous Injection of Sclerosing
Solutions (Prolotherapy) for Back and Neck Pain: A Survey of Practitioners. Archives of
Physical Medicine and Rehabilitation, 87(7), 909–913.
https://doi.org/10.1016/j.apmr.2006.03.017
Dagfinrud, H., Hagen, K., & Kvien, T. (2004). Physiotherapy interventions for ankylosing
spondylitis. Cochrane Database of Systematic Reviews, 3.
https://doi.org/10.1002/14651858.cd002822.pub2
Dahl, M. C., Nuckley, D. J., Papadopoulos, S., Rouleau, J. P., & Ching, R. P. (2006).
Dynamic Characteristics of the Intact, Fused, and Prosthetic-Replaced Cervical Disk.
Journal of Biomechanical Engineering, 128(6), 809. https://doi.org/10.1115/1.2354207
Daniels, A. H., Koller, H., Hiratzka, S. L., Mayer, M., Meier, O., Contag, A. G., Eltorai, A.
E. M., Hiratzka, J., Kojo Hamilton, D., Shaffrey, C. I., Smith, J. S., Bess, S., Klineberg,
E. O., Ames, C. P., Lafage, V., Line, B., Schwab, F. J., & Hart, R. A. (2017). Selecting
caudal fusion levels: 2 year functional and stiffness outcomes with matched pairs
analysis in multilevel fusion to L5 versus S1. European Spine Journal, 26(6), 1645–
1651. https://doi.org/10.1007/s00586-016-4790-z
Daniels, A. H., Paller, D. J., Koruprolu, S., Palumbo, M. A., & Crisco, J. J. (2013). Dynamic
Biomechanical Examination of the Lumbar Spine with Implanted Total Spinal Segment
Replacement (TSSR) Utilizing a Pendulum Testing System. PLoS ONE, 8(2).
https://doi.org/10.1371/journal.pone.0057412
Daniels, A. H., Smith, J. S., Hiratzka, J., Ames, C. P., Bess, S., Shaffrey, C. I., Schwab, F. J.,
Lafage, V., Klineberg, E. O., Burton, D., Mundis, G. M., Line, B., & Hart, R. A. (2015).
Functional limitations due to lumbar stiffness in adults with and without spinal
deformity. Spine, 40(20), 1599–1604. https://doi.org/10.1097/BRS.0000000000001090

208
Datar, S., Daniels, D., & Wijdicks, E. F. M. (2013). A major pitfall to avoid: Retroclival
hematoma due to odontoid fracture. Neurocritical Care, 19(2), 206–209.
https://doi.org/10.1007/s12028-013-9831-4
de Oliveria, M. E., Büchler, P., Schneider, J., Hasler, C. C., Studer, D., Zheng, G., &
Schumann, S. (2014). Axial suspension test to assess pre-operative spinal flexibility in
patients with adolescent idiopathic scoliosis. European Spine Journal, 23(12), 2619–
2625. https://doi.org/10.1007/s00586-014-3386-8
de Schepper, E. I. T., Luijsterburg, P. A. J., Koes, B. W., van Meurs, J. B. J., Scheele, J.,
Hofman, A., & Bierma-Zeinstra, S. M. A. (2012). Association between spinal morning
stiffness and lumbar disc degeneration: the Rotterdam Study. Osteoarthritis and
Cartilage, 20(9), 982–987. https://doi.org/10.1016/j.joca.2012.05.011
Der Heijde, D. Van, Sieper, J., Maksymowych, W. P., Brown, M. A., Lambert, R. G. W.,
Rathmann, S. S., & Pangan, A. L. (2014). Spinal inflammation in the absence of
sacroiliac joint inflammation on magnetic resonance imaging in patients with active
nonradiographic axial spondyloarthritis. Arthritis and Rheumatology, 66(3), 667–673.
https://doi.org/10.1002/art.38283
Descarreaux, M., Nougarou, F., & Dugas, C. (2013). Standardization of spinal manipulation
therapy in humans: Development of a novel device designed to measure dose-response.
Journal of Manipulative and Physiological Therapeutics, 36(2), 78–83.
https://doi.org/10.1016/j.jmpt.2012.12.007
Dickman, C. A., Crawford, N. R., & Paramore, C. G. (2009). Biomechanical characteristics
of C1–2 cable fixations. Journal of Neurosurgery, 85, 316–322.
https://doi.org/10.3171/jns.1996.85.2.0316
Djukic, M., Schmidt-Samoa, C., Lange, P., Spreer, A., Neubieser, K., Eiffert, H., Nau, R., &
Schmidt, H. (2012). Cerebrospinal fluid findings in adults with acute Lyme
neuroborreliosis. Journal of Neurology, 259(4), 630–636.
https://doi.org/10.1007/s00415-011-6221-8
Dolan, P., & Adams, M. A. (2000). When do Bending Stresses on the Spine Rise to
Damaging Levels? Proceedings of the Human Factors and Ergonomics Society Annual
Meeting, 4–635. https://doi.org/10.1177/154193120004402862
209
Dolan, P., Hole, B. D., Pollintine, P., Adams, M. A., & Zhao, F. (2005). Discogenic Origins
of Spinal Instability. Spine, 30(23), 2621–2630.
https://doi.org/10.1097/01.brs.0000188203.71182.c0
Drazin, D., Hussain, M., Harris, J., Hao, J., Phillips, M., Kim, T. T., Johnson, J. P., &
Bucklen, B. (2015). The role of sacral slope in lumbosacral fusion: A biomechanical
study. Journal of Neurosurgery: Spine, 23(6), 754–762.
https://doi.org/10.3171/2015.3.SPINE14557
Dugailly, P. M., Coucke, A., Salem, W., & Feipel, V. (2018). Assessment of cervical
stiffness in axial rotation among chronic neck pain patients: A trial in the framework of
a non-manipulative osteopathic management. Clinical Biomechanics, 53(January 2017),
65–71. https://doi.org/10.1016/j.clinbiomech.2018.02.005
Dugailly, P. M., Decuyper, A., Salem, W., De Boe, A., Espí-López, G. V., & Lepers, Y.
(2017). Analysis of the upper cervical spine stiffness during axial rotation: A
comparative study among patients with tension-type headache or migraine and
asymptomatic subjects. Clinical Biomechanics, 42, 128–133.
https://doi.org/10.1016/j.clinbiomech.2017.01.019
Duke, K., Aubin, C. E., Dansereau, J., & Labelle, H. (2005). Biomechanical simulations of
scoliotic spine correction due to prone position and anaesthesia prior to surgical
instrumentation. Clinical Biomechanics, 20(9), 923–931.
https://doi.org/10.1016/j.clinbiomech.2005.05.006
Edmondston, S. J., Allison, G. T., Althorpe, B. M., McConnell, D. R., & Samuel, K. K.
(1999). Comparison of ribcage and posteroanterior thoracic spine stiffness: An
investigation of the normal response. Manual Therapy, 4(3), 157–162.
https://doi.org/10.1054/math.1999.0202
Edmondston, S. J., Allison, G. T., Gregg, C. D., Purden, S. M., Svansson, G. R., & Watson,
A. E. (1998). Effect of position on PA stiffness of Lumbar spine. In Manual Therapy
(Vol. 3, Issue 1, pp. 21–26).
Edwards, W. T., Mann, R. W., Posner, I., White, A. A., & Hayes, W. C. (2009). Variation of
Lumbar Spine Stiffness With Load. Journal of Biomechanical Engineering, 109(1), 35.
https://doi.org/10.1115/1.3138639

210
El Miedany, Y., El Gaafary, M., Youssef, S., & Palmer, D. (2010). Towards a
multidimensional patient reported outcome measures assessment: Development and
validation of a questionnaire for patients with ankylosing spondylitis/spondyloarthritis.
Joint Bone Spine, 77(6), 575–581. https://doi.org/10.1016/j.jbspin.2010.02.017
Ellingson, A. M., Shaw, M. N., Giambini, H., An, K., Clinic, M., & States, U. (2016).
Comparative Role of Disc Degeneration and Ligament Failure on Functional Mechanics
of the Lumbar Spine. Computer Methods in Biomechanics and Biomedical Engineering,
19(9), 1–22. https://doi.org/10.1080/10255842.2015.1088524.Comparative
Eroğlu, E., Tosun, A., Fidan, F., Alemdar, A., Erten, Ş., Alkan, B. M., Aksekili, H., &
Ardıçoğlu, Ö. (2014). Fatigue and correlation with disease-specific variables, spinal
mobility measures, and health-related quality of life in ankylosing spondylitis. Modern
Rheumatology, 23(6), 1101–1107. https://doi.org/10.3109/s10165-012-0800-0
Esmende, S. M., Daniels, A. H., Paller, D. J., Koruprolu, S., Palumbo, M. A., & Crisco, J. J.
(2015). Cervical total disc replacement exhibits similar stiffness to intact cervical
functional spinal units tested on a dynamic pendulum testing system. Spine Journal,
15(1), 162–167. https://doi.org/10.1016/j.spinee.2014.08.442
Essendrop, M., Andersen, T. B., & Schibye, B. (2002). Increase in spinal stability obtained at
levels of intra-abdominal pressure and back muscle activity realistic to work situations.
Applied Ergonomics, 33(5), 471–476. https://doi.org/10.1016/S0003-6870(02)00028-5
Farasyn, A., & Meeusen, R. (2006). Validity of the new Backache Index (BAI) in patients
with low back pain. Spine Journal, 6(5), 565–571.
https://doi.org/10.1016/j.spinee.2006.01.021
Farasyn, A., Meeusen, R., Nijs, J., & Cuesta-Vargas, A. (2013). Exploration of the validity
and reliability of the “backache disability index” (BADIX) in patients with non-specific
low back pain. Journal of Back and Musculoskeletal Rehabilitation, 26(4), 451–459.
https://doi.org/10.3233/BMR-130405
Fendler, C., & Braun, J. (2009). Clinical measures in rheumatoid arthritis and ankylosing
spondylitis. Clinical and Experimental Rheumatology, 27(4 SUPPL. 55), 80–82.
Ferguson, R. L., Tencer, A. F., Woodard, P. P. E., & Allen, B. L. (1988). Biomechanical
Comparisons of Spinal Fracture Models and the Stabilizing Effects of Posterior
211
Instrumentations. Spine, 13(5), 453–460. https://doi.org/10.1097/00007632-198805000-
00003
Fernández-de-las-Peñas, C., Downey, C., & Miangolarra-Page, J. C. (2005). Validity of the
lateral gliding test as tool for the diagnosis of intervertebral joint dysfunction in the
lower cervical spine. Journal of Manipulative and Physiological Therapeutics, 28(8),
610–616. https://doi.org/10.1016/j.jmpt.2005.08.014
Ferreira, M. L., & de Luca, K. (2017). Spinal pain and its impact on older people. Best
Practice and Research: Clinical Rheumatology, 31(2), 192–202.
https://doi.org/10.1016/j.berh.2017.08.006
Ferreira, M. L., Ferreira, P. H., Latimer, J., Herbert, R. D., Maher, C., & Refshauge, K.
(2009). Relationship between spinal stiffness and outcome in patients with chronic low
back pain. Manual Therapy, 14(1), 61–67. https://doi.org/10.1016/j.math.2007.09.013
Fitzcharles, M. A., & Boulos, P. (2003). Inaccuracy in the diagnosis of fibromyalgia
syndrome: Analysis of referrals. Rheumatology, 42(2), 263–267.
https://doi.org/10.1093/rheumatology/keg075
Frank, E., Chamberland, D., & Ragel, B. (1996a). A proposed technique for intraoperative
measurement of cervical spine stiffness. Neurosurgery, 39(1), 147–150.
https://doi.org/10.1097/00006123-199607000-00030
Frank, E., Chamberland, D., & Ragel, B. (1996b). Instrumentation for intraoperative
measurement of cervical spine stiffness. Neurological Research, 18(3), 217–219.
https://doi.org/10.1080/01616412.1996.11740407
Fritz, J. M., Koppenhaver, Shane Kawchuk, Gregory N.L.Teyhen, D. S., Hebert, J. J., &
Childs, J. D. (2011). Preliminary Investigation of the Mechanisms Underlying the
Effects of Manipulation. Spine, 36(21), 1772–1781.
https://doi.org/10.1097/brs.0b013e318216337d
Fry, R. W., Alamin, T. F., Voronov, L. I., Fielding, L. C., Ghanayem, A. J., Parikh, A.,
Carandang, G., McIntosh, B. W., Havey, R. M., & Patwardhan, A. G. (2014).
Compressive preload reduces segmental flexion instability after progressive
destabilization of the lumbar spine. Spine, 39(2), 74–81.
https://doi.org/10.1097/BRS.0000000000000093

212
Gardner-Morse, M. G., Laible, J. P., & Stokes, I. A. F. (1990). Incorporation of Spinal
Flexibility Measurements Into Finite Element Analysis. Journal of Biomechanical
Engineering, 104(May 2009), 481–483.
Gardner-Morse, M. G., & Stokes, I. A. F. (2004). Structural behavior of human lumbar spinal
motion segments. Journal of Biomechanics, 37(2), 205–212.
https://doi.org/10.1016/j.jbiomech.2003.10.003
Gary, C., Robertson, H., Ruiz, B., Zuzukin, V., & Walvekar, R. R. (2010). Retropharyngeal
Ganglioneuroma Presenting with Neck Stiffness : Report of a Case and Review of
Literature (Issue 20). https://doi.org/http://dx.doi.org/10.1055/s-0030-1253580.
Gay, R. E., Ilharreborde, B., Zhao, K., Boumediene, E., & An, K.-N. (2007). The effect of
loading rate and degeneration on neutral region motion in human cadaveric lumbar
motion segments. Clinical Biomechanics, 23(1), 1–7.
https://doi.org/10.1016/j.clinbiomech.2007.08.006
Gerber, L. H., Helfgott, R. K., Gross, E. G., Hicks, J. E., Ellenberg, S. S., & Peck, G. L.
(1984). Vertebral abnormalities associated with synthetic retinoid use. Journal of the
American Academy of Dermatology, 10(5), 817–823. https://doi.org/10.1016/s0190-
9622(84)70097-1
Gilbert, M. R., Cleeland, C., Vera-Bolanos, E., Mendoza, T. R., Weinberg, J. S., Burton, A.
W., Sanchez-Williams, G., Armstrong, T. S., Levin, V., Rhines, L. D., & Gning, I.
(2011). Reliability and validity of the M. D. Anderson Symptom Inventory–Spine
Tumor Module. Journal of Neurosurgery: Spine, 12(April), 421–430.
https://doi.org/10.3171/2009.10.spine0943
Gombatto, S. P., Klaesner, J. W., Norton, B. J., Minor, S. D., & Van Dillen, L. R. (2008).
Validity and reliability of a system to measure passive tissue characteristics of the
lumbar region during trunk lateral bending in people with and people without low back
pain. The Journal of Rehabilitation Research and Development, 45(9), 1415.
https://doi.org/10.1682/JRRD.2008.02.0027
Goodsell, M., Lee, M., & Latimer, J. (2000). Short-term effects of lumbar posteroanterior
mobilization in individuals with low-back pain. Journal of Manipulative and
Physiological Therapeutics, 23(5), 332–342.

213
Gorman, J. D., Sack, K. E., & Davis, J. C. (2002). Treatment of Ankylosing Spondylitis by
Inhibition of Tumor Necrosis Factor α. New England Journal of Medicine, 346(18),
1349–1356. https://doi.org/10.1056/nejmoa012664
Graham, R. B., & Brown, S. H. M. (2012). A direct comparison of spine rotational stiffness
and dynamic spine stability during repetitive lifting tasks. Journal of Biomechanics,
45(9), 1593–1600. https://doi.org/10.1016/j.jbiomech.2012.04.007
Grenier, S. G., & McGill, S. M. (2008). When exposed to challenged ventilation, those with a
history of LBP increase spine stability relatively more than healthy individuals. Clinical
Biomechanics, 23(9), 1105–1111. https://doi.org/10.1016/j.clinbiomech.2008.06.010
Gudavalli, M. R., DeVocht, J. W., Xia, T., Vining, R. D., Wilder, D. G., Meeker, W. C., &
Goertz, C. M. (2014). Forces applied during manual assessments of Low Back Pain
patients. Proceedings of the ASME 2014 International Mechanical Engineering
Congress and Exposition, 2.
Guo, Q., Chen, F., Lu, X., Ni, B., Wu, L., & Guo, X. (2016). Posterior Open Reduction and
Interlaminae Compression Fusion for Os Odontoideum with Atlantoaxial Dislocation.
World Neurosurgery, 91, 326–331. https://doi.org/10.1016/j.wneu.2016.04.014
Guo, Q., Zhang, M., Wang, L., Lu, X., Guo, X., & Ni, B. (2016). Comparison of Atlantoaxial
Rotation and Functional Outcomes of Two Nonfusion Techniques in the Treatment of
Anderson-D’Alonzo Type II Odontoid Fractures. Spine, 41(12), E751–E758.
https://doi.org/10.1097/BRS.0000000000001370
Haas, M., Panzer, D., Aickin, M., Groupp, E., Partna, L., & Lumsden, S. (2011). Efficacy of
Cervical Endplay Assessment as an Indicator for Spinal Manipulation. Spine, 28(11),
1091–1096. https://doi.org/10.1097/01.brs.0000067276.16209.db
Hadizadeh, M., Kawchuk, G. N., & Parent, E. (2019). Reliability of a new loaded rolling
wheel system for measuring spinal stiffness in asymptomatic participants. BMC
Musculoskeletal Disorders, 20(1), 176. https://doi.org/10.1186/s12891-019-2543-y
Hanly, J. G., Russell, M. L., & Gladman, D. D. (1988). Psoriatic spondyloarthropathy: A long
term prospective study. Annals of the Rheumatic Diseases, 47(5), 386–393.
https://doi.org/10.1136/ard.47.5.386
Hans, N., Jan, H., Thelonius, H., & Julia, S. (2009). Non-linearity of flexion – extension

214
characteristics in spinal segments. Acta of Bioengineering and Biomechanics, 11(4).
Hart, R. A., Gundle, K. R., Pro, S. L., & Marshall, L. M. (2013). Lumbar Stiffness Disability
Index: Pilot testing of consistency, reliability, and validity. Spine Journal, 13(2), 157–
161. https://doi.org/10.1016/j.spinee.2012.12.001
Hart, R. A., Hiratzka, J., Kane, M. S., Lafage, V., Klineberg, E., Ames, C. P., Line, B. G.,
Schwab, F., Scheer, J. K., Bess, S., Hamilton, D. K., Shaffrey, C. I., Mundis, G., Smith,
J. S., Burton, D. C., Sciubba, D. M., Deviren, V., & Boachie-Adjei, O. (2017). Stiffness
after Pan-Lumbar Arthrodesis for Adult Spinal Deformity Does Not Significantly
Impact Patient Functional Status or Satisfaction Irrespective of Proximal Endpoint.
Spine, 42(15), 1151–1157. https://doi.org/10.1097/BRS.0000000000002006
Hart, R. A., Marshall, L. M., Hiratzka, S. L., Kane, M. S., Volpi, J., & Hiratzka, J. R. (2014).
Functional limitations due to stiffness as a collateral impact of instrumented arthrodesis
of the lumbar spine. Spine, 39(24), E1468–E1474.
https://doi.org/10.1097/BRS.0000000000000595
Hart, R. A., Pro, S. L., Gundle, K. R., & Marshall, L. M. (2013). Lumbar stiffness as a
collateral outcome of spinal arthrodesis: A preliminary clinical study. Spine Journal,
13(2), 150–156. https://doi.org/10.1016/j.spinee.2012.10.014
Hasegawa, K., Kitahara, K., Shimoda, H., & Hara, T. (2010). Facet joint opening in lumbar
degenerative diseases indicating segmental instability. Journal of Neurosurgery: Spine,
12(June), 687–693. https://doi.org/10.3171/2009.12.spine09623
Hasegawa, K., Kitahara, K., Shimoda, H., Ishii, K., Ono, M., Homma, T., & Watanabe, K.
(2014). Lumbar degenerative spondylolisthesis is not always unstable:
Clinicobiomechanical evidence. Spine, 39(26), 2127–2135.
https://doi.org/10.1097/BRS.0000000000000621
Hasegewa, K., Kitahara, K., Hara, T., Takano, K., & Shimoda, H. (2009). Biomechanical
evaluation of segmental instability in degenerative lumbar spondylolisthesis. European
Spine Journal, 18(4), 465–470. https://doi.org/10.1007/s00586-008-0842-3
Hashimoto, T., Yamane, S., Kanayama, M., Shigenobu, K., Ishida, T., & Oha, F. (2003).
Intraoperative Biomechanical Assessment of Lumbar Spinal Instability: Validation of
Radiographic Parameters Indicating Anterior Column Support in Lumbar Spinal Fusion.
215
Spine, 28(20), 2368–2372. https://doi.org/10.1097/01.brs.0000085357.24025.27
Hegde, D., Ballal, A., Vinay Kumar, C., & Ravindranath Rai, H. (2014). Type III Cawley
Andersson lesion in a case of ankylosing spondylitis. Nitte University Journal of Health
Science, 4(2), 136–139.
http://www.embase.com/search/results?subaction=viewrecord&from=export&id=L3735
46546%0Ahttp://sfx.library.uu.nl/utrecht?sid=EMBASE&issn=22497110&id=doi:&atitl
e=Type+III+Cawley+Andersson+lesion+in+a+case+of+ankylosing+spondylitis&stitle=
Nitte+Univ.+J.+Healt
Hidding, A., & Van der Linden, S. (1995). Factors related to change in global health after
group physical therapy in ankylosing spondylitis. Clinical Rheumatology, 14(3), 347–
351. https://doi.org/10.1007/BF02208352
Hill, H., Hill, A., & Bodmer, J. (1976). Clinical diagnosis of ankylosing spondylitis in
women and relation to presence of HLA B27. Annals of the Rheumatic Diseases, 35(3),
267–270. https://doi.org/10.1136/ard.35.3.267
Hodges, P. W., Eriksson, A. E. M., Shirley, D., & Gandevia, S. C. (2005). Intra-abdominal
pressure increases stiffness of the lumbar spine. Journal of Biomechanics, 38(9), 1873–
1880. https://doi.org/10.1016/j.jbiomech.2004.08.016
Holewijn, R. M., Faraj, S. S. A., Kingma, I., van Royen, B. J., de Kleuver, M., & van der
Veen, A. J. (2017). Spinal biomechanical properties are significantly altered with a
novel embalming method. Journal of Biomechanics, 55, 144–146.
https://doi.org/10.1016/j.jbiomech.2017.02.012
Holt, K., Russell, D., Cooperstein, R., Young, M., Sherson, M., & Haavik, H. (2018).
Interexaminer Reliability of Seated Motion Palpation for the Stiffest Spinal Site. Journal
of Manipulative and Physiological Therapeutics.
https://doi.org/10.1016/j.jmpt.2017.08.009
Hosalkar, H. S., Sankar, W. N., Wills, B. P. D., Goebel, J., Dormans, J. P., & Drummond, D.
S. (2008). Congenital osseous anomalies of the upper cervical spine. Journal of Bone
and Joint Surgery - Series A, 90(2), 337–348. https://doi.org/10.2106/JBJS.G.00014
Howarth, S. J., Polgar, J. M., Dickerson, C. R., & Callaghan, J. P. (2010). Trunk Muscle
Activity During Wheelchair Ramp Ascent and the Influence of a Geared Wheel on the
216
Demands of Postural Control. Archives of Physical Medicine and Rehabilitation, 91(3),
436–442. https://doi.org/10.1016/j.apmr.2009.10.016
Howe, D., Newcombe, R., & Wade, M. (1983). Manipulation of the cervical spine: a pilot
study. The Journal of the Royal College of General Practitioners, 33(254), 574–579.
http://www.ncbi.nlm.nih.gov/pubmed/8492064
Huston, A. F., Morwood, J. B., Christofinis, G. J., & Wood, W. (1956). Poliomyelitis in
Suburban Surrey. British Medical Journal, 2(4993), 629–634.
https://doi.org/10.1136/bmj.2.4993.629
Ibn Yacoub, Y., Amine, B., Laatiris, A., & Hajjaj-Hassouni, N. (2012). Gender and disease
features in Moroccan patients with ankylosing spondylitis. Clinical Rheumatology,
31(2), 293–297. https://doi.org/10.1007/s10067-011-1819-x
Iizuka, H., Iizuka, Y., Mieda, T., Tsunoda, D., Kobayashi, R., & Sorimachi, Y. (2017). The
clinical outcomes of atlanto-axial arthrodesis in patients with rheumatoid arthritis –
Assessment according to the Japanese Orthopaedic Association Cervical Myelopathy
Evaluation Questionnaire (JOACMEQ). Journal of Orthopaedic Science, 22(3), 401–
404. https://doi.org/10.1016/j.jos.2017.01.016
Ingram, L. A., Snodgrass, S. J., & Rivett, D. A. (2015). Comparison of Cervical Spine
Stiffness in Individuals With Chronic Nonspecific Neck Pain and Asymptomatic
Individuals. Journal of Orthopaedic & Sports Physical Therapy, 45(3), 162–169.
https://doi.org/10.2519/jospt.2015.5711
Iyer, S., Christiansen, B. A., Roberts, B. J., Valentine, M. J., Manoharan, R. K., & Bouxsein,
M. L. (2010). A biomechanical model for estimating loads on thoracic and lumbar
vertebrae. Clinical Biomechanics, 25(9), 853–858.
https://doi.org/10.1016/j.clinbiomech.2010.06.010
Jacobson, B. H., Gemmell, H. A., Hayes, B. M., & Altena, T. S. (2002). Effectivness of a
selected bedding system on quality of sleep, low back pain, shoulder pain, and spine
stiffness. J Manipulative Physiol Ther. https://doi.org/10.1067/mmt.2002.121410
Jalalian, A., Tay, F. E. H., Arastehfar, S., & Liu, G. (2017). A new method to approximate
load–displacement relationships of spinal motion segments for patient-specific multi-
body models of scoliotic spine. Medical and Biological Engineering and Computing,
217
55(6), 1039–1050. https://doi.org/10.1007/s11517-016-1576-8
Janssen, M. M. A., Vincken, K. L., Van Raak, S. M., Vrtovec, T., Kemp, B., Viergever, M.
A., Bartels, L. W., & Castelein, R. M. (2013). Sagittal spinal profile and spinopelvic
balance in parents of scoliotic children. Spine Journal, 13(12), 1789–1800.
https://doi.org/10.1016/j.spinee.2013.05.030
Jenks, K., Stebbings, S., Burton, J., Schultz, M., Herbison, P., & Highton, J. (2010). Probiotic
therapy for the treatment of spondyloarthritis: A randomized controlled trial. Journal of
Rheumatology, 37(10), 2118–2125. https://doi.org/10.3899/jrheum.100193
Jull, G. (1995). Examination of the articular system. (P. N. Boyling J (ed.); Grime’s Mo).
Churchill Livingstone.
Jull, G., & Bullock, M. (1987). A motion profile of the lumbar spine in an ageing population
assessed by manual examination. Physiotherapy Theory and Practice.
https://doi.org/10.3109/09593988709087743
Jull, G., Treleaven, J., & Versace, G. (1994). Manual examination: is pain provocation a
major cue for spinal dysfunction. Australian Journal of Physiotherapy, 40(3), 159–165.
https://doi.org/10.1016/S0004-9514(14)60574-2
Kalim, H., Handono, K., Khalasha, T., Pratama, M. Z., Dantara, T. W. I., Wulandari, A. P.,
Albinsaid, F., Fitria, S. N., & Mahardika, M. V. (2017). Poor Quality of Life in Indian
Ankylosing Spondylitis Patients Latika. Indian Journal of Rheumatology, 12(2), 86–93.
https://doi.org/10.4103/injr.injr
Kaminsky, S. B., Clark, C. R., & Traynelis, V. C. (2004). Operative treatment of cervical
spondylotic myelopathy and radiculopathy. A comparison of laminectomy and
laminoplasty at five year average follow-up. The Iowa Orthopaedic Journal, 24, 95–
105.
http://www.ncbi.nlm.nih.gov/pubmed/15296214%0Ahttp://www.pubmedcentral.nih.gov
/articlerender.fcgi?artid=PMC1888413
Karadogan, E., & Williams, R. L. (2012). Three-Dimensional Static Modeling of the Lumbar
Spine. Journal of Biomechanical Engineering, 134(8), 084504.
https://doi.org/10.1115/1.4007172
Karami, M., Sadat, M. M., Zehtab, M. J., Habibollah-Zadeh, P., Akrami, K., & Zareei, M. R.
218
(2005). Intraoperative spinal stiffness measurement in management of spinal canal
stenosis. Acta Medica Iranica, 43(5), 365–368.
Kawaguchi, Y., Nagami, S., Nakano, M., Yasuda, T., Seki, S., Hori, T., & Kimura, T. (2013).
Relationship between postoperative axial symptoms and the rotational angle of the
cervical spine after laminoplasty. European Journal of Orthopaedic Surgery and
Traumatology, 23(SUPPL. 1), 53–58. https://doi.org/10.1007/s00590-013-1219-9
Kawchuk, Gregory N., & Fauvel, O. R. (2001). Sources of variation in spinal indentation
testing: Indentation site relocation, intraabdominal pressure, subject movement,
muscular response, and stiffness estimation. Journal of Manipulative and Physiological
Therapeutics, 24(2), 84–91. https://doi.org/10.1067/mmt.2001.112566
Kawchuk, Gregory N., Miazga, S., Pagé, I., Swain, M., De Carvalho, D., Funabashi, M.,
Breen, A., & Wong, A. (2019). Clinicians’ Ability to Detect a Palpable Difference in
Spinal Stiffness Compared With a Mechanical Device. Journal of Manipulative and
Physiological Therapeutics. https://doi.org/10.1016/j.jmpt.2019.02.002
Kawchuk, Gregory Neil, Edgecombe, T. L., Wong, A. Y. L., Cojocaru, A., & Prasad, N.
(2015). A non-randomized clinical trial to assess the impact of nonrigid, inelastic corsets
on spine function in low back pain participants and asymptomatic controls. Spine
Journal, 15(10), 2222–2227. https://doi.org/10.1016/j.spinee.2015.06.047
Kaya, T., Bal, S., & Gunaydin, R. (2007). Relationship between the severity of enthesitis and
clinical and laboratory parameters in patients with ankylosing spondylitis. Rheumatology
International, 27(4), 323–327. https://doi.org/10.1007/s00296-006-0218-0
Kayanja, M., Evans, K., Milks, R., & Lieberman, I. (2006). Adjacent level load transfer
following vertebral augmentation in the cadaveric spine. Spine, 31(21), 790–797.
https://doi.org/10.1097/01.brs.0000238690.09903.4c
Keeling, S. O., Majumdar, S. R., Conner-Spady, B., Battié, M. C., Carroll, L. J., &
Maksymowych, W. P. (2012). Preliminary validation of a self-reported screening
questionnaire for inflammatory back pain. Journal of Rheumatology, 39(4), 822–829.
https://doi.org/10.3899/jrheum.110537
Keller, T. S., & Colloca, C. J. (2000). Mechanical force spinal manipulation increases trunk
muscle strength assessed by electromyography: A comparative clinical trial. Journal of

219
Manipulative and Physiological Therapeutics, 23(9), 585–595.
https://doi.org/10.1067/mmt.2000.110947
Keller, T. S., & Colloca, C. J. (2002). A rigid body model of the dynamic posteroanterior
motion response of the human lumbar spine. Journal of Manipulative and Physiological
Therapeutics, 25(8), 485–496. https://doi.org/10.1067/mmt.2002.127079
Keller, T. S., Colloca, C. J., & Fuhr, A. W. (2000). In vivo transient vibration assessment of
the normal human thoracolumbar spine. Journal of Manipulative and Physiological
Therapeutics, 23(8), 521–530. https://doi.org/10.1067/mmt.2000.109680
Khoo, K. B. K., Shadbolt, B., Cheung, P. P. M., Dorai Raj, A. K., Tymms, K. E., Brook, A.
S., & Wilson, B. J. (2008). Infliximab in severe active ankylosing spondylitis with spinal
ankylosis. Internal Medicine Journal, 38(6a), 396–401. https://doi.org/10.1111/j.1445-
5994.2007.01599.x
Kim, H. J., Protopsaltis, T. S., Scheer, J. K., Ames, C. P., Koski, T., Mundis, G. M.,
Klineberg, E., Lafage, V., Hiratzka, J. R., Shaffrey, C. I., Gupta, M., Smith, J. S.,
Sciubba, D. M., Hart, R. A., & Bess, S. (2015). Which Daily Functions Are Most
Affected by Stiffness Following Total Lumbar Fusion. Spine, 40(17), 1338–1344.
https://doi.org/10.1097/brs.0000000000000968
Kimhi, O., Caspi, D., Bornstein, N. M., Maharshak, N., Gur, A., Arbel, Y., Comaneshter, D.,
Paran, D., Wigler, I., Levartovsky, D., Berliner, S., & Elkayam, O. (2007). Prevalence
and Risk Factors of Atherosclerosis in Patients with Psoriatic Arthritis. Seminars in
Arthritis and Rheumatism, 36(4), 203–209.
https://doi.org/10.1016/j.semarthrit.2006.09.001
Kimura, H., Fujibayashi, S., Otsuki, B., Takahashi, Y., Nakayama, T., & Matsuda, S.
(2016a). Effects of Lumbar Stiffness after Lumbar Fusion Surgery on Activities of Daily
Living. Spine, 41(8), 719–727. https://doi.org/10.1097/BRS.0000000000001300
Kimura, H., Fujibayashi, S., Otsuki, B., Takahashi, Y., Nakayama, T., & Matsuda, S.
(2016b). Effects of Lumbar Stiffness after Lumbar Fusion Surgery on Activities of Daily
Living. Spine, 41(8), 719–727. https://doi.org/10.1016/S0004-9514(14)61093-X
Kingma, I., Paul, C. P. L., Bisschop, A., van Dieën, J. H., Bleys, R. L. A. W., van der Veen,
A. J., & van Royen, B. J. (2013). Which factors prognosticate rotational instability

220
following lumbar laminectomy? European Spine Journal, 22(12), 2897–2903.
https://doi.org/10.1007/s00586-013-3002-3
Kingma, I., Stadhouder, A., Holewijn, R. M., van Royen, B. J., van der Veen, A. J., Bisschop,
A., van Dieën, J. H., & Vergroesen, P.-P. A. (2014). The Effects of Single-Level
Instrumented Lumbar Laminectomy on Adjacent Spinal Biomechanics. Global Spine
Journal, 5(1), 39–47. https://doi.org/10.1055/s-0034-1395783
Kinsella, T. D., MacKenzie, K. R., Kim, S. O., & Johnson, L. G. (1967). Evaluation of
indomethacin by a controlled, cross-over technique in 30 patients with ankylosing
spondylitis. Canadian Medical Association Journal, 96(22), 1454–1459.
http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=med1&NEWS=N&A
N=4164930
Kitahara, K., Oribe, K., Hasegawa, K., & Hara, T. (2009). A new intraoperative measurement
system for rotational motion properties of the spine. IFMBE Proceedings, 23, 1781–
1784. https://doi.org/10.1007/978-3-540-92841-6_442
Kiviniemi, K., Allison, G., Lanigan, H., Edmonston, S., Walcher, S., & Simonsen, A. V.
(2001). Influence of standardized mobilization on the posteroanterior stiffness of the
lumbar spine in asymptomatic subjects. Physiotherapy Research International, 6(3),
145–156. https://doi.org/10.1002/pri.223
Kleinberger, M. (2010). Application of Finite Element Techniques to the Study of Cervical
Spine Mechanics. SAE Technical Paper Series, 1. https://doi.org/10.4271/933131
Koppenhaver, S. L., Hebert, J. J., Kawchuk, G. N., Childs, J. D., Teyhen, D. S., Croy, T., &
Fritz, J. M. (2014). Criterion validity of manual assessment of spinal stiffness. Manual
Therapy, 19(6), 589–594. https://doi.org/10.1016/j.math.2014.06.001
Krenn, M. H., Ambrosetti-Giudici, S., Pfenniger, A., Burger, J., & Piotrowski, W. P. (2008).
Minimally invasive intraoperative stiffness measurement of lumbar spinal motion
segments. Neurosurgery, 63(4 SUPPL.), 309–314.
https://doi.org/10.1227/01.NEU.0000335144.87931.A1
Kumar, S. (2011). Spinal stiffness in asymptomatic subjects. Journal of Electromyography
and Kinesiology, 21(5), 762–766. https://doi.org/10.1016/j.jelekin.2011.07.008
Kumar, S. (2012). Posteroanterior Spinal Stiffness at T5, T10, and L3 Levels in Normal

221
Subjects. PM and R, 4(5), 342–348. https://doi.org/10.1016/j.pmrj.2011.12.009
Kumar, S., & Stoll, S. (2011). Device, protocol and measurement of regional spinal stiffness.
Journal of Electromyography and Kinesiology, 21(3), 458–465.
https://doi.org/10.1016/j.jelekin.2011.01.001
Kuperus, J. S., Samsour, L., Buckens, C. F., Oner, F. C., de Jong, P. A., & Verlaan, J. J.
(2018). Bone mineral density changes over time in diffuse idiopathic skeletal
hyperostosis of the thoracic spine. Bone, 112(February), 90–96.
https://doi.org/10.1016/j.bone.2018.04.005
Lafon, Y., Lafage, V., Steib, J. P., Dubousset, J., & Skalli, W. (2010). In Vivo distribution of
spinal intervertebral stiffness based on clinical flexibility tests. Spine, 35(2), 186–193.
https://doi.org/10.1097/BRS.0b013e3181b664b1
Lamberg, E. M., & Hagins, M. (2014). Breath control during a tiptoe task. Physiotherapy
Theory and Practice, 30(3), 178–182. https://doi.org/10.3109/09593985.2013.834527
Larson, A. N., Fletcher, N. D., Daniel, C., & Richards, B. S. (2012). Lumbar curve is stable
after selective thoracic fusion for adolescent idiopathic scoliosis: A 20-year follow-up.
Spine, 37(10), 833–839. https://doi.org/10.1097/BRS.0b013e318236a59f
Latimer, J., Goodsell, M. M., Lee, M., Maher, C. G., Wilkinson, B. N., & Moran, C. C.
(1996). Evaluation of a New Device for Measuring Responses to Posteroanterior Forces
in a Patient Population, Part 1: Reliability Testing. Physical Therapy, 76(2), 158–165.
https://doi.org/10.1093/ptj/76.2.158
Latimer, J., Lee, M., & Adams, R. D. (1998). The effects of high and low loading forces on
measured. Journal of Manipulative & Physiological Therapeutics, 21(3), 157–163.
Lee, M, & Svensson, N. L. (1993). Effect of muscle activation on response to lumbar
posteroanterior forces. Journal Of Manipulative And Physiological Therapeutics, 16(7),
439–446.
http://search.ebscohost.com/login.aspx?direct=true&db=cmedm&AN=8228646&site=e
host-live
Lee, Michael, Latimer, J., & Maher, C. G. (1993). Manipulation: investigation of a proposed
mechanism. Clinical Biomechanics, 8(6), 302–306. https://doi.org/10.1016/0268-
0033(93)90004-2

222
Lee, Michael, Latimer, J., & Maher, C. G. (1997). Normal response to large posteroanterior
lumbar loads--a case study approach. J Manipulative Physiol Ther, 20(6), 369–371.
Lee, Michael, Steven, G. P., Crosbie, J., & Higgs, R. J. E. D. (1998). Variations in
posteroanterior stiffness in the thoracolumbar spine: Preliminary observations and
proposed mechanisms. Physical Therapy, 78(12), 1277–1287.
https://doi.org/10.1093/ptj/78.12.1277
Lee, Michael, & Svensson, N. (1990). Measurement of stiffness during simulated spinal
physiotherapy. Clinical Physics and Physiological Measurement, 11(3), 201–207.
https://doi.org/10.1088/0143-0815/11/3/002
Lee, P., Granata, K., & Moorhouse, K. (2007). Active Trunk Stiffness During Voluntary
Isometric Flexion and Extension Exertions. Human Factors: The Journal of the Human
Factors and Ergonomics Society, 49(1), 100–109.
https://doi.org/10.1518/001872007779597993
Lee, R., Tsung, B., Evans, J., & Tong, P. (2005). Analysis of the Bending Behavior of the
Lumbar Spine During Posteroanterior Mobilization. Journal of Mechanics in Medicine
and Biology, 05(01), 55–61. https://doi.org/10.1142/s0219519405001266
Lee, T.-C. (1996). Transpedicular reduction and stabilization for postlaminectomy lumbar
instability. Acta Neurochirurgica, 138(2), 139–145.
https://doi.org/10.1007/BF01411352 LK -
http://lh.cineca.it/Ccube/openclink.do?sid=EMBASE&sid=EMBASE&issn=00016268&
id=doi:10.1007%2FBF01411352&atitle=Transpedicular+reduction+and+stabilization+f
or+postlaminectomy+lumbar+instability&stitle=ACTA+NEUROCHIR.&title=Acta+Ne
urochirurgica&volume=138&issue=2&spage=139&epage=145&aulast=Lee&aufirst=T.
C.&auinit=T.C.&aufull=Lee+T.C.&coden=ACNUA&isbn=&pages=139-
145&date=1996&auinit1=T&auinitm=C
Lemus, M. C., Uribe, E. V., & Avila, J. M. J. (2015). Traumatic atlantoaxial subluxation,
posterior transfacet fixation: a case report. Coluna/Columna, 14(1), 53–55.
https://doi.org/10.1590/s1808-1851201514010r129
Li, C. De, Sun, H. L., & Lu, H. Z. (2013). Comparison of the effect of posterior lumbar
interbody fusion with pedicle screw fixation and interspinous fixation on the stiffness of
adjacent segments. Chinese Medical Journal, 126(9), 1732–1737.

223
https://doi.org/10.3760/cma.j.issn.0366-6999.20112393
Lin, T.-Y., Chen, W.-J., Hsieh, M.-K., Lu, M.-L., Tsai, T.-T., Lai, P.-L., Fu, T.-S., Niu, C.-
C., & Chen, L.-H. (2014). Postoperative meningitis after spinal surgery: a review of 21
cases from 20,178 patients. BMC Infectious Diseases, 14(1), 2–6.
https://doi.org/10.1186/1471-2334-14-220
Luca Vismara, Francesco Menegoni, Fabio Zaina, Manuela Galli, Stefano Negrini, P. C.
(2010). Effect of obesity and low back pain on spinalmobility: a cross sectional study in
woman. Journal of NeuroEngineering and Rehabilitation, 3(7), 1–8.
Luo, J., Bertram, W., Sangar, D., Adams, M. A., Annesley-Williams, D. J., & Dolan, P.
(2010). Is kyphoplasty better than vertebroplasty in restoring normal mechanical
function to an injured spine? Bone, 46(4), 1050–1057.
https://doi.org/10.1016/j.bone.2009.11.036
Lykomitros, V., Anagnostidis, K. S., Alzeer, Z., & Kapetanos, G. A. (2010). Percutaneous
anterolateral balloon kyphoplasty for metastatic lytic lesions of the cervical spine.
European Spine Journal, 19(11), 1948–1952. https://doi.org/10.1007/s00586-010-1465-
z
Madsen, O. R., Hansen, L. B., Rytter, A., Suetta, C., & Egsmose, C. (2009). The Bath
metrology index as assessed by a trained and an untrained rater in patients with
spondylarthropathy: A study of intra- and inter-rater agreements. Clinical
Rheumatology, 28(1), 35–40. https://doi.org/10.1007/s10067-008-0978-x
Mahaudens, P., Detrembleur, C., Mousny, M., & Banse, X. (2010). Gait in
thoracolumbar/lumbar adolescent idiopathic scoliosis: Effect of surgery on gait
mechanisms. European Spine Journal, 19(7), 1179–1188.
https://doi.org/10.1007/s00586-010-1292-2
Maher, C. G., & Adams, R. D. (1994). Reliability of Pain and Stiffness Assessments in
Clinical Manual Lumbar Spine Examination. Physical Therapy, 74(9), 801–809.
https://pdfs.semanticscholar.org/3299/18b54de6d207377e458e8e60b6f35d660613.pdf
Maher, C. G., & Adams, R. D. (1995a). A psychophysical evaluation of manual stiffness
discrimination. Australian Journal of Physiotherapy, 41(3), 161–167.
https://doi.org/10.1016/S0004-9514(14)60426-8

224
Maher, C. G., & Adams, R. D. (1995b). Is the clinical concept of spinal stiffness
multidimensional? Physical Therapy, 75(10), 854–860; discussion 861-4.
http://www.ncbi.nlm.nih.gov/pubmed/7568385
Maher, C. G., & Adams, R. D. (1996). Stiffness judgments are affected by visual occlusion.
Journal of Manipulative and Physiological Therapeutics, 19(4), 250–256.
http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=emed4&NEWS=N&
AN=1996161941
Maher, C. G., & Latimer, J. (1992). Pain or resistance - the manual therapists’ dilemma.
Australian Journal of Physiotherapy, 38(4), 257–260. https://doi.org/10.1016/S0004-
9514(14)60568-7
Maher, C. G., Latimer, J., & Adams, R. D. (1998). An investigation of the reliability and
validity of posteroanterior spinal stiffness judgments made using a reference-based
protocol. Physical Therapy, 78(8), 829–837. https://doi.org/10.1093/ptj/78.8.829
Maher, C. G., Latimer, J., & Mathew, H. J. (1999). Plinth padding confounds measures of
posteroanterior spinal stiffness. Manual Therapy, 4(3), 145–150.
https://doi.org/10.1054/math.1999.0197
Maher, C. G., Simmonds, M., & Adams, R. D. (1998). Therapists’ conceptualization and
characterization of the clinical concept of spinal stiffness. Physical Therapy, 78(3), 289–
300. https://doi.org/10.1093/ptj/78.3.289
Maitland, G. (1986). Vertebral Manipulation. London: Butterworths.
Maitland, G., Hengeveld, E., Banks, K., & English, K. (2005). Maitland’s Vertebral
Manipulation. (Butterworth - Heinemann (ed.); 6th ed.).
Malakoutian, M., Street, J., Wilke, H. J., Stavness, I., Fels, S., & Oxland, T. (2018). A
musculoskeletal model of the lumbar spine using ArtiSynth–development and
validation. Computer Methods in Biomechanics and Biomedical Engineering: Imaging
and Visualization, 6(5), 483–490. https://doi.org/10.1080/21681163.2016.1187087
Manning, D. M., Dedrick, G. S., Sizer, P. S., & Brismée, J.-M. (2012). Reliability of a seated
three-dimensional passive intervertebral motion test for mobility, end-feel, and pain
provocation in patients with cervicalgia. Journal of Manual & Manipulative Therapy,
20(3), 135–141. https://doi.org/10.1179/2042618611Y.0000000023

225
Mata, S., Fortin, P. R., Fitzcharles, M. A., Starr, M. R., Joseph, L., Watts, C. S., Gore, B.,
Rosenberg, E., Chhem, R. K., & Esdaile, J. M. (1997). A controlled study of diffuse
idiopathic skeletal hyperostosis: Clinical features and functional status. In Medicine
(Vol. 76, Issue 2, pp. 104–117). https://doi.org/10.1097/00005792-199703000-00003
McElhaney, J. H., Brian, J., Paver, J. G., Myers, B. S., & Gray, L. (1988). Combined Bending
and Axial Loading Responses of the Human Cervical Spine. SAE Transactions, 97,
1090–1097. https://doi.org/https://doi.org/10.4271/881709
McGill, S., Seguin, J., & Bennett, G. (1994). Passive stiffness of the lumbar torso in flexion,
extension, lateral bending, and axial rotation. Effect of belt wearing and breath holding.
Spine.
Meijer, G. J. M., Homminga, J., Veldhuizen, A. G., & Verkerke, G. J. (2011). Influence of
interpersonal geometrical variation on spinal motion segment stiffness. Spine, 36(14),
929–935. https://doi.org/10.1097/BRS.0b013e3181fd7f7f
Menaker, J., Martin, I. B. K., & Hirshon, J. M. (2005). Marked elevation of cerebrospinal
fluid white blood cell count: An unusual case of Streptococcus pneumoniae meningitis,
differential diagnosis, and a brief review of current epidemiology and treatment
recommendations. Journal of Emergency Medicine, 29(1), 37–41.
https://doi.org/10.1016/j.jemermed.2004.12.017
Mengshoel, A. M., & Robinson, H. S. (2008). Clinical significance of specific spinal
mobilization for patients with ankylosing spondylitis evaluated by quantitative
assessments and patient interviews. Disability and Rehabilitation, 30(5), 355–364.
https://doi.org/10.1080/09638280701270711
Million, R., Haavik Nilsen, K., Jayson, M. I. V., & Baker, R. D. (1981). Evaluation of low
back pain and assessment of lumbar corsets with and without back supports. Annals of
the Rheumatic Diseases, 40(5), 449–454. https://doi.org/10.1136/ard.40.5.449
Moorhouse, K. M., & Granata, K. P. (2007). Role of reflex dynamics in spinal stability:
Intrinsic muscle stiffness alone is insufficient for stability. Journal of Biomechanics,
40(5), 1058–1065. https://doi.org/10.1016/j.jbiomech.2006.04.018
Mori, E., Maeda, T., Itaru, Y., Kawano, O., Ueta, T., Shiba, K., & Okada, S. (2012). Spinous
process-splitting open pedicle screw fusion provides favorable results in patients with

226
low back discomfort and pain compared to conventional open pedicle screw fixation
over 1 year after surgery. European Spine Journal, 21(4), 745–753.
https://doi.org/10.1007/s00586-011-2146-2
Mori, E., Ueta, T., Maeda, T., Yugué, I., Kawano, O., & Shiba, K. (2015). Effect of
preservation of the C-6 spinous process and its paraspinal muscular attachment on the
prevention of postoperative axial neck pain in C3–6 laminoplasty. Journal of
Neurosurgery: Spine, 22(3), 221–229. https://doi.org/10.3171/2014.11.SPINE131153
Myklebust, J. B., Sances, A., Pintar, F. A., Yoganandan, N., & Ray, G. (2004). Stiffness and
strain energy criteria to evaluate the threshold of injury to an intervertebral joint. Journal
of Biomechanics, 22(2), 135–142. https://doi.org/10.1016/0021-9290(89)90036-5
Neumann, P., Osvalder, A. L., Nordwall, A., Lövsund, P., & Hansson, T. (1993). The
ultimate flexural strength of the lumbar spine and vertebral bone mineral content.
Journal of Spinal Disorders, 6(4), 314–323. https://doi.org/10.1097/00002517-
199306040-00005
Ng, H.-W., & Teo, E.-C. (2001). Nonlinear finite-element analysis of the lower cervical spine
(C4-C6) under axial loading. Journal of Spinal Disorders, 14(3), 201–210.
https://doi.org/10.1097/00002517-200106000-00003
Ng, H. W., Teo, E. C., Lee, K. K., & Qiu, T. X. (2003). Finite element analysis of cervical
spinal instability under physiologic loading. Journal of Spinal Disorders and
Techniques, 16(1), 55–65. https://doi.org/10.1097/00024720-200302000-00010
Nibu, K., Kawabata, K., Onitsuka, T., Fujii, T., Ebihara, Y., Ebihara, M., & Saikawa, M.
(2010). Quality of life after neck dissection: a multicenter longitudinal study by the
Japanese Clinical Study Group on Standardization of Treatment for Lymph Node
Metastasis of Head and Neck Cancer. International Journal of Clinical Oncology, 15(1),
33–38. https://doi.org/10.1007/s10147-009-0020-6
Nicholson, A. G., Wilson, R., Shirodaria, C. C., Wells, A. U., & Hansell, D. M. (2004).
Lesson of the month. Histopathology, 44(1), 91–93. https://doi.org/10.1046/j.1365-
2559.2003.01632.x
Nicholson, L. L., Adams, R. D., & Maher, C. G. (2000). Magnitutde estimation of manually
assessed elastic stifness: stability of the exponent. Perceptual and Motor Skills, 91, 581–

227
592.
Nicholson, L. L., Adams, R. D., & Maher, C. G. (2003). Manual discrimination capability
when only viscosity is varied in viscoelastic stiffness stimuli. Journal of Manipulative
and Physiological Therapeutics, 26(6), 365–373. https://doi.org/10.1016/S0161-
4754(03)00070-8
Nicholson, L. L., Maher, C. G., & Adams, R. D. (1998). Hand contact area, force applied and
early non-linear stiffness (toe) in a manual stiffness discrimination task. Manual
Therapy, 3(4), 212–219. https://doi.org/10.1016/S1356-689X(98)80050-7
Nicholson, L. L., Maher, C. G., Adams, R. D., & Phan-Thien, N. (2001). Stiffness properties
of the human lumbar spine: A lumped parameter model. Clinical Biomechanics, 16(4),
285–292. https://doi.org/10.1016/S0268-0033(00)00117-0
O’Shaughnessy, J., Drolet, M., Roy, J.-F., & Descarreaux, M. (2010). Chiropractic
management of patients post-disc arthroplasty: Eight case reports. Chiropractic and
Osteopathy, 18(7), 1–7. https://doi.org/10.1186/1746-1340-18-7
Ohnari, H., Sasai, K., Akagi, S., Iida, H., Takanori, S., & Kato, I. (2006). Investigation of
axial symptoms after cervical laminoplasty, using questionnaire survey. Spine Journal,
6(3), 221–227. https://doi.org/10.1016/j.spinee.2005.10.014
Owens, E. F., DeVocht, J. W., Wilder, D. G., Gudavalli, M. R., & Meeker, W. C. (2007). The
Reliability of a Posterior-to-Anterior Spinal Stiffness Measuring System in a Population
of Patients With Low Back Pain. Journal of Manipulative and Physiological
Therapeutics, 30(2), 116–123. https://doi.org/10.1016/j.jmpt.2006.12.006
Ozgocmen, S., Ardicoglu, O., & Kaya, A. (2000). The relationship of clinical and laboratory
measurements to two different radiological scoring methods in ankylosing spondylitis.
Journal of Back and Musculoskeletal Rehabilitation, 15(1), 37–40.
http://www.embase.com/search/results?subaction=viewrecord&from=export&id=L3306
1752%0Ahttp://resolver.ebscohost.com/openurl?sid=EMBASE&issn=10538127&id=do
i:&atitle=The+relationship+of+clinical+and+laboratory+measurements+to+two+differe
nt+radiological+scori
Pagé, I., Nougarou, F., Lardon, A., & Descarreaux, M. (2018). Changes in spinal stiffness
with chronic thoracic pain: Correlation with pain and muscle activity. PLoS ONE,

228
13(12), 1–15. https://doi.org/10.1371/journal.pone.0208790
Pagliano, P., Fusco, U., Attanasio, V., Rossi, M., Pantosti, A., Conte, M., & Faella, F. S.
(2007). Pneumococcal meningitis in childhood: A longitudinal prospective study. FEMS
Immunology and Medical Microbiology, 51(3), 488–495. https://doi.org/10.1111/j.1574-
695X.2007.00324.x
Panjabi, M. M., Kato, Y., Hoffman, H., Cholewicki, J., & Krag, M. (2000). A study of
stiffness protocol as exemplified by testing of a burst fracture model in sagittal plane.
Spine, 25(21), 2748–2754. https://doi.org/10.1097/00007632-200011010-00006
Panjabi, M. M., Summers, D. J., Pelker, R. R., Videman, T., Friedlaender, G. E., &
Southwick, W. O. (1986). Three‐dimensional load‐displacement curves Due to Forces
on the Cervical Spine. Journal of Orthopaedic Research, 4(2), 152–161.
https://doi.org/10.1002/jor.1100040203
Parkinson, R. J., Beach, T. A. C., & Callaghan, J. P. (2004). The time-varying response of the
in vivo lumbar spine to dynamic repetitive flexion. Clinical Biomechanics, 19(4), 330–
336. https://doi.org/10.1016/j.clinbiomech.2004.01.002
Patwardhan, A. G., Siping, L., Thomas, G., Mark, L., Kevin, M., & Michael, Z. (1990).
Orthotic Stabilization of Thoracolumbar Injuries. Spine, 15(7), 654–661.
Perrin, G., Barrey, C., Mosnier, T., Jund, J., & Skalli, W. (2011). In vitro evaluation of a ball-
and-socket cervical disc prosthesis with cranial geometric center. Journal of
Neurosurgery: Spine, 11(November), 538–546.
https://doi.org/10.3171/2009.6.spine0949
Perry, J. J., Stiell, I. G., Sivilotti, M. L. A., Bullard, M. J., Hohl, C. M., Sutherland, J.,
Émond, M., Worster, A., Lee, J. S., Mackey, D., Pauls, M., Lesiuk, H., Symington, C.,
& Wells, G. A. (2013). Clinical decision rules to rule out subarachnoid hemorrhage for
acute headache. JAMA - Journal of the American Medical Association, 310(12), 1248–
1255. https://doi.org/10.1001/jama.2013.278018
Petra, V. der B., Kingma, I., & Van Dieen, J. (2003). Effects of unexpected lateral mass
placement on trunk loading in lifting. Spine, 28(8), 764–770.
http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=emed6&NEWS=N&
AN=2003164676

229
Petty, N. J., Maher, C. G., Latimer, J., & Lee, M. (2002). Manual examination of accessory
movements-seeking R1. Manual Therapy, 7(1), 39–43.
https://doi.org/10.1054/math.2001.0431
Pitzen, T., Geisler, F., Matthis, D., Müller-Storz, H., Caspar, W., Ritz, R., & Steudel, W.-I.
(2000). A Finite Element Model for Predicting the Biomechanical Behaviour of the
Human Lumbar Spine. IFAC Proceedings Volumes, 33(3), 19–22.
https://doi.org/10.1016/S1474-6670(17)35482-4
Pope, M. H., Frymoyer, J. W., & Krag, M. H. (2006). Diagnosing Instability. Clinical
Orthopaedics and Related Research, 279, 60–67. https://doi.org/10.1097/00003086-
199206000-00008
Pope, M. H., & Panjabi, M. (1985). Biomechanical definitions of spinal instability. In Spine
(Vol. 10, Issue 3, pp. 255–256). https://doi.org/10.1097/00007632-198504000-00013
Quint, U., & Wilke, H.-J. (1998). Importance of the Intersegmental Trunk Muscles for the
Stability of the Lumbar Spine. Spine Journal, 23(18), 1937–1945.
Raymond, L., & Evans, J. (1997). An in vivo study of the intervertebral movements produced
by posteroanterior mobilization. Clinical Biomechanics. https://doi.org/10.1016/S0268-
0033(97)00019-3
Reiman, M. P. (2009). Trunk stabilization training: An evidence basis for the current state of
affairs. Journal of Back and Musculoskeletal Rehabilitation, 22(3), 131–142.
https://doi.org/10.3233/BMR-2009-0226
Rey-Eiriz, G., Alburquerque-Sendín, F., Barrera-Mellado, I., Martín-Vallejo, F. J., &
Fernández-de-las-Peñas, C. (2010). Validity of the Posterior-Anterior Middle Cervical
Spine Gliding Test for the Examination of Intervertebral Joint Hypomobility in
Mechanical Neck Pain. Journal of Manipulative and Physiological Therapeutics, 33(4),
279–285. https://doi.org/10.1016/j.jmpt.2010.03.005
Richter, M., Ferrari, R., Otte, D., Kuensebeck, H. W., Blauth, M., & Krettek, C. (2004).
Correlation of clinical findings, collision parameters, and psychological factors in the
outcome of whiplash associated disorders. Journal of Neurology, Neurosurgery and
Psychiatry, 75(5), 758–764. https://doi.org/10.1136/jnnp.2003.026963
Riyazi, N., Meulenbelt, I., Kroon, H. M., Ronday, K. H., Hellio Le Graverand, M. P.,
230
Rosendaal, F. R., Breedveld, F. C., Slagboom, P. E., & Kloppenburg, M. (2005).
Evidence for familial aggregation of hand, hip, and spine but not knee osteoarthritis in
siblings with multiple joint involvement: The GARP study. Annals of the Rheumatic
Diseases, 64(3), 438–443. https://doi.org/10.1136/ard.2004.024661
Rizvi, S. A. M., Fredø, H. L., Lied, B., Nakstad, P. H., Rønning, P., & Helseth, E. (2012).
Surgical management of acute odontoid fractures: Surgery-related complications and
long-term outcomes in a consecutive series of 97 patients. Journal of Trauma and Acute
Care Surgery, 72(3), 682–690. https://doi.org/10.1097/TA.0b013e318236b675
Roberts, S. B., Ward, C. C., & Nahum, A. M. (1969). Head trauma - A parametric dynamic
study. Journal of Biomechanics, 2(4), 397–415. https://doi.org/10.1016/0021-
9290(69)90016-5
Rodriguez, V. R., & Poddubnyy, D. (2015). Old and new treatment targets in axial
spondyloarthritis. RMD Open, 1(Suppl 1). https://doi.org/10.1136/rmdopen-2015-
000054
Rousseau, M. A., Lazennec, J. Y., Tassin, J. L., & Fort, D. (2014). Sagittal rebalancing of the
pelvis and the thoracic spine after pedicle subtraction osteotomy at the lumbar level.
Journal of Spinal Disorders and Techniques, 27(3), 166–173.
http://www.embase.com/search/results?subaction=viewrecord&from=export&id=L3732
71340%5Cnhttp://dx.doi.org/10.1097/BSD.0b013e318272faaf%5Cnhttp://elvis.ubvu.vu.
nl:9003/vulink?sid=EMBASE&issn=15392465&id=doi:10.1097%2FBSD.0b013e31827
2faaf&atitle=Sagittal+reb
Rydevik, B., Szpalski, M., Aebi, M., & Gunzburg, R. (2008). Whiplash injuries and
associated disorders: New insights into an old problem. European Spine Journal,
17(SUPPL.3). https://doi.org/10.1007/s00586-007-0484-x
Salmingo, R. A., Tadano, S., Fujisaki, K., Abe, Y., & Ito, M. (2013). Relationship of forces
acting on implant rods and degree of scoliosis correction. Clinical Biomechanics, 28(2),
122–128. https://doi.org/10.1016/j.clinbiomech.2012.12.001
Sayson, J. V, & Lotz, J. (2015). Microgravity-Induced Back Pain and Intervertebral Disc
Herniation : International Space Station Results. International Astronautical Congress,
October.

231
Schmidt, H., Bashkuev, M., Dreischarf, M., Rohlmann, A., Duda, G., Wilke, H. J., & Shirazi-
Adl, A. (2013). Computational biomechanics of a lumbar motion segment in pure and
combined shear loads. Journal of Biomechanics, 46(14), 2513–2521.
https://doi.org/10.1016/j.jbiomech.2013.06.038
Schmidt, T. A., An, H. S., Lim, T. H., Nowicki, B. H., & Haughton, V. M. (1998). The
stiffness of lumbar spinal motion segments with a high-intensity zone in the anulus
fibrosus. In Spine (Vol. 23, Issue 20, pp. 2167–2173). https://doi.org/10.1097/00007632-
199810150-00005
Sengupta, R., & Stone, M. A. (2007). The assessment of ankylosing spondylitis in clinical
practice. Nature Clinical Practice Rheumatology, 3(9), 496–503.
https://doi.org/10.1038/ncprheum0591
Sherief, T. ., White, J. ., Bommireddy, R. ., & Klezl, Z. . b. (2013). Cervical spondylotic
myelopathy: The outcome and potential complications of surgical treatment. Acta
Chirurgiae Orthopaedicae et Traumatologiae Cechoslovaca, 80(5), 328–334.
http://www.scopus.com/inward/record.url?eid=2-s2.0-
84886695146&partnerID=40&md5=4d69b83baf0dfd68c2d0923939e5be6b
Shin, W., Kim, M.-K., Kim, J., Woo, M., Cho, D., & Lim, K. S. (2017). Post lumbar puncture
headache: Case report of a serious adverse event in first-in-human study. Translational
and Clinical Pharmacology, 25(4), 162. https://doi.org/10.12793/tcp.2017.25.4.162
Shirley, D., Hodges, P. W., Eriksson, A. E. M., & Gandevia, S. C. (2003). Spinal stiffness
changes throughout the respiratory cycle. J Appl Physiol, 95, 1467–1475.
https://doi.org/10.1152/japplphysiol.00939.2002.-Posteroanterior
Shojaei, I., Suri, C., van Dieën, J. H., & Bazrgari, B. (2018). Alterations in trunk bending
stiffness following changes in stability and equilibrium demands of a load holding task.
Journal of Biomechanics, 77, 163–170. https://doi.org/10.1016/j.jbiomech.2018.07.005
Shum, G. L., Tsung, B. Y., & Lee, R. Y. (2013). The immediate effect of posteroanterior
mobilization on reducing back pain and the stiffness of the lumbar spine. Archives of
Physical Medicine and Rehabilitation, 94(4), 673–679.
https://doi.org/10.1016/j.apmr.2012.11.020
Simmonds, M. J., Kumar, S., & Lechelt, E. (1995). Use of a spinal model to quantify the

232
forces and motion that occur during therapists’ tests of spinal motion. Physical Therapy,
75(3), 212–222. https://doi.org/10.1093/ptj/75.3.212
Snodgrass, S. J., Haskins, R., & Rivett, D. A. (2012). A structured review of spinal stiffness
as a kinesiological outcome of manipulation: Its measurement and utility in diagnosis,
prognosis and treatment decision-making. In Journal of Electromyography and
Kinesiology (Vol. 22, Issue 5, pp. 708–723).
https://doi.org/10.1016/j.jelekin.2012.04.015
Snodgrass, S. J., & Rhodes, H. R. (2012). Cervical spine posteroanterior stiffness differs with
neck position. Journal of Electromyography and Kinesiology, 22(6), 829–834.
https://doi.org/10.1016/j.jelekin.2012.04.014
Snodgrass, S. J., Rivett, D. A., & Robertson, V. J. (2006). Manual Forces Applied During
Posterior-to-Anterior Spinal Mobilization: A Review of the Evidence. In Journal of
Manipulative and Physiological Therapeutics (Vol. 29, Issue 4, pp. 316–329).
https://doi.org/10.1016/j.jmpt.2006.03.006
Snodgrass, S. J., Rivett, D. A., & Robertson, V. J. (2008). Measuring the posteroanterior
stiffness of the cervical spine. Manual Therapy, 13(6), 520–528. https://www-
sciencedirect-com.libproxy.unitec.ac.nz/science/article/pii/S1356689X07001245
Snodgrass, S. J., Rivett, D. A., Robertson, V. J., & Stojanovski, E. (2009). Forces Applied to
the Cervical Spine During Posteroanterior Mobilization. Journal of Manipulative and
Physiological Therapeutics, 32(1), 72–83. https://doi.org/10.1016/j.jmpt.2008.09.012
Snodgrass, S. J., Rivett, D. A., Robertson, V. J., & Stojanovski, E. (2010a). A Comparison of
Cervical Spine Mobilization Forces Applied by Experienced and Novice
Physiotherapists. Journal of Orthopaedic & Sports Physical Therapy, 40(7), 392–401.
https://doi.org/10.2519/jospt.2010.3274
Snodgrass, S. J., Rivett, D. A., Robertson, V. J., & Stojanovski, E. (2010b). Cervical spine
mobilisation forces applied by physiotherapy students. Physiotherapy, 96(2), 120–129.
https://doi.org/10.1016/j.physio.2009.08.008
Snodgrass, S. J., Rivett, D. A., Sterling, M., & Vicenzino, B. (2014). Dose Optimization for
Spinal Treatment Effectiveness: A Randomized Controlled Trial Investigating the
Effects of High and Low Mobilization Forces in Patients With Neck Pain. Journal of
233
Orthopaedic & Sports Physical Therapy, 44(3), 141–152.
https://doi.org/10.2519/jospt.2014.4778
Solomon, T., Thi, T. T., Lewthwaite, P., Mong, H. O., Kneen, R., Nguyen, M. D., & White,
N. (2008). A cohort study to assess the new WHO Japanese encephalitis surveillance
standards. Bulletin of the World Health Organization, 86(3), 178–186.
https://doi.org/10.2471/BLT.07.043307
Song, Y., Wang, C., & Chen, H. (2017). Functional limitation and associated factors in
outpatients with ankylosing spondylitis in Southwest China. Clinical Rheumatology,
36(4), 871–877. https://doi.org/10.1007/s10067-017-3563-3
Squires, M. C., Latimer, J., Adams, R. D., & Maher, C. G. (2001). Indenter head area and
testing frequency effects on posteroanterior lumbar stiffness and subjects’ rated comfort.
Manual Therapy, 6(1), 40–47. https://doi.org/10.1054/math.2000.0379
Sran, M. M., Khan, K. M., Zhu, Q., & Oxland, T. R. (2005). Posteroanterior stiffness predicts
sagittal plane midthoracic range of motion and three-dimensional flexibility in cadaveric
spine segments. Clinical Biomechanics, 20(8), 806–812.
https://doi.org/10.1016/j.clinbiomech.2005.04.009
Stamos-Papastamos, N., Petty, N. J., & Williams, J. M. (2011). Changes in bending stiffness
and lumbar spine range of movement following lumbar mobilization and manipulation.
Journal of Manipulative and Physiological Therapeutics, 34(1), 46–53.
https://doi.org/10.1016/j.jmpt.2010.11.006
Stanton, T. R., & Kawchuk, G. N. (2008). The effect of abdominal stabilization contractions
on posteroanterior spinal stiffness. Spine, 33(6), 694–701.
https://doi.org/10.1097/BRS.0b013e318166e034
Stanton, T. R., & Kawchuk, G. N. (2009). Reliability of assisted indentation in measuring
lumbar spinal stiffness. Manual Therapy, 14(2), 197–205.
https://doi.org/10.1016/j.math.2008.01.011
Stanton, T. R., Moseley, L. G., Wong, A. Y. L., & Kawchuk, G. N. (2017). Feeling stiffness
in the back: A protective perceptual inference in chronic back pain. Scientific Reports,
7(1), 1–12. https://doi.org/10.1038/s41598-017-09429-1
Stokes, I. A. F., & Gardner-Morse, M. (2016). A database of lumbar spinal mechanical
234
behavior for validation of spinal analytical models. Journal of Biomechanics, 49(5),
780–785. https://doi.org/10.1016/j.jbiomech.2016.01.035
Stokes, I. A. F., & Gardner-Morse, M. G. (1993). Three-Dimensional Simulation of
Harrington Distraction Instrumentation for Surgical Correction of Scoliosis. Spine
Journal, 18(16), 2457–2464. https://doi.org/10.1097/00007632-199312000-00015
Stokes, I. A. F., & Laible, J. P. (1990). Three-Dimensional Osseo-Ligamentous Model of the
Thorax Representin Initiation of Scoliosis by Asymmetric Growth. J. Biomechanics,
23(6), 589–595. https://doi.org/10.1016/0021-9290(90)90051-4
Stolworthy, D. K., Zirbel, S. A., Howell, L. L., Samuels, M., & Bowden, A. E. (2014).
Characterization and prediction of rate-dependent flexibility in lumbar spine
biomechanics at room and body temperature. Spine Journal, 14(5), 789–798.
https://doi.org/10.1016/j.spinee.2013.08.043
Swanenburg, J., Meier, M. L., Langenfeld, A., Schweinhardt, P., & Humphreys, B. K. (2018).
Spinal Stiffness in Prone and Upright Postures During 0–1.8 g Induced by Parabolic
Flight. Aerospace Medicine and Human Performance, 89(6), 563–567.
https://doi.org/10.3357/AMHP.5031.2018
Szust, A. (2006). Experimental investigation of the lumbar spine - Influence of
destabilization on the stiffness characteristic. Acta of Bioengineering and Biomechanics,
8(2), 127–133.
Talebian, S., Maroufi, N., Olyaei, G. R., Toosizadeh, N., & Mousavi-Khatir, R. (2018). The
effect of static neck flexion on mechanical and neuromuscular behaviors of the cervical
spine. Journal of Biomechanics, 72, 152–158.
https://doi.org/10.1016/j.jbiomech.2018.03.004
Tallarico, R. A., Lavelle, W. F., J. Bianco, A., Taormina, J. L., & Ordway, N. R. (2014).
Positional effects of transforaminal interbody spacer placement at the L5-S1
intervertebral disc space: A biomechanical study. Spine Journal, 14(12), 3018–3024.
https://doi.org/10.1016/j.spinee.2014.06.023
Tanaka, M., Morimoto, Y., Harada, T., Inoue, M., Hosono, N., Ono, K., & Ebara, S. (2006).
Intraoperative Measurement of Lumbar Spinal Instability. In Spine (Vol. 17, pp. 44–50).
https://doi.org/10.1097/00007632-199203001-00010

235
Tawackoli, W., Marco, R., & Liebschner, M. A. K. (2004). The Effect of Compressive Axial
Preload on the Flexibility of the Thoracolumbar Spine. Spine, 29(9), 988–993.
https://doi.org/10.1097/00007632-200405010-00007
Tiantian, W., Jian, H., Yongji, W., Xiaolin, H., & Jinghui, Z. (2012). Development of the
Measurement System of the Postero-to-Anterior Movements of the Cervical Spine.
Proceedings of 2012 International Conference on Modelling, Identification and Control,
Wuhan, China, June 24-26, 2012, 24–26. https://doi.org/10.1016/S0004-9514(14)61093-
X
Tomczyszyn, D., Solecki, L., & Pańczuk, A. (2018). Assessment of the type of farmers’ low
back pain. Medycyna Pracy, 69(4), 355–364. https://doi.org/10.13075/mp.5893.00690
Triano, J. J., Budgell, B., Bagnulo, A., Roffey, B., Bergmann, T., Cooperstein, R., Gleberzon,
B., Good, C., Perron, J., & Tepe, R. (2013). Review of methods used by chiropractors to
determine the site for applying manipulation. Chiropractic and Manual Therapies,
21(1), 1–29. https://doi.org/10.1186/2045-709X-21-36
Tsung, B. Y. S., Evans, J., Tong, P., & Lee, R. Y. W. (2005). Measurement of lumbar spine
loads and motions during rotational mobilization. Journal of Manipulative and
Physiological Therapeutics, 28(4), 238–244. https://doi.org/10.1016/j.jmpt.2005.03.014
Tuttle, N., Barrett, R., & Laakso, L. (2008a). Postero-anterior movements of the cervical
spine: Repeatability of force displacement curves. Manual Therapy, 13(4), 341–348.
https://doi.org/10.1016/j.math.2007.03.005
Tuttle, N., Barrett, R., & Laakso, L. (2008b). Relation between changes in posteroanterior
stiffness and active range of movement of the cervical spine following manual therapy
treatment. Spine, 33(19), 673–679. https://doi.org/10.1097/BRS.0b013e31817f93f9
Tuttle, N., Barrett, R., & Laakso, L. (2009). Posteroanterior movements in tender and less
tender locations of the cervical spine. Manual Therapy, 14(1), 28–35.
https://doi.org/10.1016/j.math.2007.09.003
Tuttle, N., & Hazle, C. (2018). Spinal PA movements behave ‘as if’ there are limitations of
local segmental mobility and are large enough to be perceivable by manual palpation: A
synthesis of the literature. Musculoskeletal Science and Practice, 36(April), 25–31.
https://doi.org/10.1016/j.msksp.2018.04.005

236
Vaillant, M., Pickar, J. G., & Kawchuk, G. N. (2010). Performance and reliability of a
variable rate, force/displacement application system. Journal of Manipulative and
Physiological Therapeutics, 33(8), 585–593. https://doi.org/10.1016/j.jmpt.2010.08.020
van Deursen, D. L., Lengsfeld, M., Snijders, C. J., Evers, J. J. M., & Goossens, R. H. M.
(2000). Mechanical effects of continuous passive motion on the lumbar spine in seating.
Journal of Biomechanics, 33(6), 695–699. https://doi.org/10.1016/S0021-
9290(99)00231-6
van Engelen, S. J. P. M., Ellenbroek, M. H. M., van Royen, B. J., de Boer, A., & van Dieën,
J. H. (2012). Validation of vibration testing for the assessment of the mechanical
properties of human lumbar motion segments. Journal of Biomechanics, 45(10), 1753–
1758. https://doi.org/10.1016/j.jbiomech.2012.05.009
van Royen, B. J., Holewijn, R. M., van Dieën, J. H., Kingma, I., Bisschop, A., Stadhouder,
A., van Engelen, S. J. P. M., & van der Veen, A. J. (2014). Single level lumbar
laminectomy alters segmental biomechanical behavior without affecting adjacent
segments. Clinical Biomechanics, 29(8), 912–917.
https://doi.org/10.1016/j.clinbiomech.2014.06.016
van Royen, B. J., van Engelen, S. J. P. M., van Dieën, J. H., Smit, T. H., & Bisschop, A.
(2013). The effect of neighboring segments on the measurement of segmental stiffness
in the intact lumbar spine. The Spine Journal, 15(6), 1302–1309.
https://doi.org/10.1016/j.spinee.2013.08.020
van Trijffel, E., Oostendorp, R. A. B., Lindeboom, R., Bossuyt, P. M. M., & Lucas, C.
(2009). Perceptions and use of passive intervertebral motion assessment of the spine: a
survey among physiotherapists specializing in manual therapy. Manual Therapy, 14(3),
243–251. https://doi.org/10.1016/j.math.2008.02.005
Vera-Garcia, F. J., Brown, S. H. M., Gray, J. R., & McGill, S. M. (2006). Effects of different
levels of torso coactivation on trunk muscular and kinematic responses to posteriorly
applied sudden loads. Clinical Biomechanics, 21(5), 443–455.
https://doi.org/10.1016/j.clinbiomech.2005.12.006
Verkerke, G. J., Meijer, G. J. M., Kingma, I., Busscher, I., van der Veen, A. J., van Dieën, J.
H., & Veldhuizen, A. G. (2011). The effects of creep and recovery on the in vitro
biomechanical characteristics of human multi-level thoracolumbar spinal segments.

237
Clinical Biomechanics, 26(5), 438–444.
https://doi.org/10.1016/j.clinbiomech.2010.12.012
Viner, A., & Lee, M. (1995). Direction of manual force applied during assessment of stiffness
in the lumbosacral spine. J Manipulative Physiol Ther, 18(7), 441–447.
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citat
ion&list_uids=8568425
Wachowski, M. M., Mansour, M., Hawallek, T., Kubein-Meesenburg, D., Hubert, J., &
Nägerl, H. (2011). Parametric control of the stiffness of lumbar segments. Strain, 47(3),
281–287. https://doi.org/10.1111/j.1475-1305.2009.00686.x
Wadeley, A., Clarke, E., Leverment, S., & Sengupta, R. (2018). Sleep in ankylosing
spondylitis and non-radiographic axial spondyloarthritis: associations with disease
activity, gender and mood. Clinical Rheumatology, 37(4), 1045–1052.
https://doi.org/10.1007/s10067-018-3984-7
Wagnac, E., Aubin, C. É., Chaumoître, K., Mac-Thiong, J. M., Ménard, A. L., Petit, Y.,
Garo, A., & Arnoux, P. J. (2017). Substantial vertebral body osteophytes protect against
severe vertebral fractures in compression. PLoS ONE, 12(10).
https://doi.org/10.1371/journal.pone.0186779
Walker, B. F., & Williamson, O. D. (2009). Mechanical or inflammatory low back pain.
What are the potential signs and symptoms? Manual Therapy, 14(3), 314–320.
https://doi.org/10.1016/j.math.2008.04.003
Wang, L., Lu, X., Guo, X., Ni, B., & Guo, Q. (2016). Posterior Temporary Fixation Versus
Nonoperative Treatment for Anderson–D’Alonzo Type III Odontoid Fractures:
Functional Computed Tomography Evaluation of C1–C2 Rotation. World Neurosurgery,
100, 675–680. https://doi.org/10.1016/j.wneu.2016.01.004
Wang, X.-Y., Dai, L.-Y., Xu, H.-Z., & Chi, Y.-L. (2008). Biomechanical effect of the extent
of vertebral body fracture on the thoracolumbar spine with pedicle screw fixation: An in
vitro study. Journal of Clinical Neuroscience, 15(3), 286–290.
https://doi.org/10.1016/j.jocn.2006.12.007
Wassenaar, M. J. E., Biermasz, N. R., van Duinen, N., van der Klaauw, A. A., Pereira, A. M.,
Roelfsena, F., Smit, J. W. A., Kroon, H. M., Kloppenburg, M., & Romijn, J. A. (2009).
238
High prevalence of arthropathy, according to the definitions of radiological and clinical
osteoarthritis, in patients with long-term cure of acromegaly: A case-control study.
European Journal of Endocrinology, 160(3), 357–365. https://doi.org/10.1530/EJE-08-
0845
Wen, N., Lavaste, F., Santin, J. J., & Lassau, J. P. (1993). Three-dimensional biomechanical
properties of the human cervical spine in vitro - I. Analysis of normal motion. European
Spine Journal, 2(1), 2–11. https://doi.org/10.1007/BF00301048
Wilder, D. G., Owens, E. F., Meeker, W. C., DeVocht, J. W., & Gudavalli, M. R. (2007).
Comparison of Posteroanterior Spinal Stiffness Measures to Clinical and Demographic
Findings at Baseline in Patients Enrolled in a Clinical Study of Spinal Manipulation for
Low Back Pain. Journal of Manipulative and Physiological Therapeutics, 30(7), 493–
500. https://doi.org/10.1016/j.jmpt.2007.07.009
Wolfla, C., Stemper, B., Board, D., & Yoganandan, N. (2010). Biomechanical properties of
human thoracic spine disc segments. Journal of Craniovertebral Junction and Spine,
1(1), 18. https://doi.org/10.4103/0974-8237.65477
Wong, A., & Kawchuk, G. (2017). The Clinical Value of Assessing Lumbar Posteroanterior
Segmental Stiffness: A Narrative Review of Manual and Instrumented Methods. PM and
R, 9(8), 816–830. https://doi.org/10.1016/j.pmrj.2016.12.001
Wong, A. Y. L., Kawchuk, G., Parent, E., & Prasad, N. (2013). Within- and between-day
reliability of spinal stiffness measurements obtained using a computer controlled
mechanical indenter in individuals with and without low back pain. Manual Therapy,
18(5), 395–402. https://doi.org/10.1016/j.math.2013.02.003
Wong, A. Y. L., Parent, E. C., Dhillon, S. S., Prasad, N., & Kawchuk, G. N. (2015). Do
Participants With Low Back Pain Who Respond to Spinal Manipulative Therapy Differ
Biomechanically From Nonresponders, Untreated Controls or Asymptomatic Controls?
Spine, 40(17), 1329–1337. https://doi.org/10.1097/brs.0000000000000981
Wong, A. Y. L., Parent, E. C., Prasad, N., Huang, C., Chan, K. M., & Kawchuk, G. N.
(2016). Does experimental low back pain change posteroanterior lumbar spinal stiffness
and trunk muscle activity? A randomized crossover study. Clinical Biomechanics, 34,
45–52. https://doi.org/10.1016/j.clinbiomech.2016.03.006

239
Wong, Y. W., & Luk, K. D. K. (2008). Spinal epidural hematoma in a scoliotic patient with
long fusion: a case report. Spine Journal, 8(3), 538–543.
https://doi.org/10.1016/j.spinee.2007.03.011
Xia, T., Long, C. R., Vining, R. D., Gudavalli, M. R., DeVocht, J. W., Kawchuk, G. N.,
Wilder, D. G., & Goertz, C. M. (2017). Association of lumbar spine stiffness and
flexion-relaxation phenomenon with patient-reported outcomes in adults with chronic
low back pain – a single-arm clinical trial investigating the effects of thrust spinal
manipulation. BMC Complementary and Alternative Medicine, 17(1), 303.
https://doi.org/10.1186/s12906-017-1821-1
Xia, T., Wilder, D. G., Gudavalli, M. R., DeVocht, J. W., Vining, R. D., Pohlman, K. A.,
Kawchuk, G. N., Long, C. R., & Goertz, C. M. (2014). Study protocol for patient
response to spinal manipulation – a prospective observational clinical trial on
physiological and patient-centered outcomes in patients with chronic low back pain.
BMC Complementary and Alternative Medicine, 14(1), 292.
https://doi.org/10.1186/1472-6882-14-292
Yang, K. H., & King, A. I. (1984). Mechanism of Facet Load Transmission as a Hypothesis
for Low-Back Pain. Spine, 9(6), 557–565. https://doi.org/10.1097/00007632-
198409000-00005
Yaron, M., Shirazi, I., Elkayam, O., Caspi, D., & Yaron, I. (2002). Serum levels of IL-10, IL-
6, IL-1ra, and sIL-2R in patients with psoriatic arthritis. Rheumatology International,
19(3), 101–105. https://doi.org/10.1007/s002960050111
Ying-Yan, Z., Jie-Hua, L., Run-Yue, H., & Yi-Ting, H. (2012). Treatment of Ankylosing
With a Bushen-Qiangdu-Zhilv Decoction: A Case Report With a 3-year Follow-up.
Alternative Therapies, 22(S1), 35–40. https://doi.org/10.2174/187152310790711674
Yip, Y. B., Sonny Tse, H. M., & Wu, K. K. (2007). An experimental study comparing the
effects of combined transcutaneous acupoint electrical stimulation and electromagnetic
millimeter waves for spinal pain in Hong Kong. Complementary Therapies in Clinical
Practice, 13(1), 4–14. https://doi.org/10.1016/j.ctcp.2006.08.002
Ylinen, J., Kautiainen, H., Wirén, K., & Häkkinen, A. (2007). Stretching exercises vs manual
therapy in treatment of chronic neck pain: A randomized, controlled cross-over trial.
Journal of Rehabilitation Medicine, 39(2), 126–132. https://doi.org/10.2340/16501977-

240
0015
Zhang, H.-C., Zhang, Z.-F., Wang, Z.-H., Cheng, J.-Y., Wu, Y.-C., Fan, Y.-M., Wang, T.-H.,
& Wang, Z. (2017). Optimal Pelvic Incidence Minus Lumbar Lordosis Mismatch after
Long Posterior Instrumentation and Fusion for Adult Degenerative Scoliosis.
Orthopaedic Surgery, 9(3), 304–310. https://doi.org/10.1111/os.12343
Zhu, C., Wang, L., Liu, H., Song, Y., Liu, L., Li, T., & Gong, Q. (2017). Treatment of type II
odontoid fracture with a novel technique: Titanium cable-dragged reduction and
cantilever-beam internal fixation. Medicine, 96(44), e8521.
https://doi.org/10.1097/MD.0000000000008521
Zirbel, S. A., Stolworthy, D. K., Howell, L. L., & Bowden, A. E. (2013). Intervertebral disc
degeneration alters lumbar spine segmental stiffness in all modes of loading under a
compressive follower load. Spine Journal, 13(9), 1134–1147.
https://doi.org/10.1016/j.spinee.2013.02.010
Declaration Name of candidate: Joel Moses
This Thesis/Dissertation/Research Project entitled: Defining and measuring objective
and subjective spinal stiffness: A scoping review, is submitted in partial fulfillment for
the requirements for the Unitec degree of
Principal Supervisor: Sylvia Hach Associate Supervisor/s: Jesse Mason CANDIDATE’S DECLARATION I confirm that:
• This Thesis/Dissertation/Research Project represents my own work;
• The contribution of supervisors and others to this work was consistent with the
Unitec Regulations and Policies.
• Research for this work has been conducted in accordance with the Unitec
Research Ethics Committee Policy and Procedures, and has fulfilled any
requirements set for this project by the Unitec Research Ethics Committee.
Research Ethics Committee Approval Number: .................................................
Candidate Signature: ……….……………………………………. Date: 23/03/2020
Student number: 1458167

Unitec Institute of Technology TE WHARE WANANGA 0 WAIRAKA
Full name of author: Joel Ranui Moses
ORCID number (Optional): …………………………………………
Full title of thesis/dissertation/research project (‘the work’): Defining and measuring objective and subjective spinal stiffness: A scoping review.
School: School of Community studies.
Degree: MOst
Year of presentation: 2020
Principal Supervisor: Sylvia Hach
Associate Supervisor: Jesse Mason
Permission to make open access I agree to a digital copy of my final thesis/work being uploaded to the Unitec institutional repository and being made viewable worldwide.
Copyright Rights: Unless otherwise stated this work is protected by copyright with all rights reserved. I provide this copy in the expectation that due acknowledgement of its use is made.
AND
Copyright Compliance: I confirm that I either used no substantial portions of third party copyright material, including charts, diagrams, graphs, photographs or maps in my thesis/work or I have obtained permission for such material to be made accessible worldwide via the Internet.
Signature of author: ………………………………………...
Date: 23/03/2020




















