Overview of Examination Process Subjective History ...
79
2/5/2015 1 CLINICAL EXAMINATION OF THE KNEE Robert C. Manske PT, DPT, SCS, MEd, ATC, CSCS Professor and Chair Wichita State University Department of Physical Therapy Via Christi Health, Wichita Overview of Examination Process Vital to determine pathology allowing successful treatment of knee Importance of complete and thorough examination cannot be overemphasized Ensures accurate and differential diagnosis Identify all involved and contributing structures Clinician should exhibit knowledge of biomechanics and pathomechanics of the knee Components of Clinical Examination Subjective History Inspection/Observation Palpation Clearing tests L spine, Hip, Foot Range of motion Accessory joint motion Laxity assessment Muscle strength test Special tests Neurovascular assessment Imaging studies Functional assessment Subjective History Inspection/Observation Palpation Clearing Tests L spine, Hip, Foot Range of Motion Accessory Joint Motion Laxity Assessment Muscle Strength Test Special Tests Neurovascular Assessment Imaging Studies Functional Assessment Subjective History Most important part of exam Will direct entire approach and direction of exam History of symptoms General information Subjective History Mechanism of Injury (MOI)? Previous injury? “Pop” when injury occurred? Clicking or catching? Pain Where? Type? Isolated or diffuse? Positional affect on injury?
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Overview of Examination Process Subjective History ...

2/5/2015
1
CLINICAL EXAMINATION OF THE KNEE Robert C. Manske PT, DPT, SCS, MEd, ATC, CSCS Professor and Chair Wichita State University Department of Physical Therapy Via Christi Health, Wichita
Overview of Examination Process Vital to determine pathology allowing successful treatment of
knee Importance of complete and thorough examination cannot be
overemphasized Ensures accurate and differential diagnosis Identify all involved and contributing structures Clinician should exhibit knowledge of biomechanics and
pathomechanics of the knee
Importance of complete and thorough examination cannot be
Components of Clinical Examination Subjective History Inspection/Observation Palpation Clearing tests L spine, Hip, Foot Range of motion Accessory joint motion Laxity assessment Muscle strength test Special tests Neurovascular assessment Imaging studies Functional assessment
Subjective History Inspection/Observation Palpation Clearing Tests L spine, Hip, Foot Range of Motion Accessory Joint Motion Laxity Assessment Muscle Strength Test Special Tests Neurovascular Assessment Imaging Studies Functional Assessment
Subjective HistorySubjective HistorySubjective HistorySubjective HistorySubjective HistorySubjective HistorySubjective HistorySubjective History
Subjective History
Most important part of exam Will direct entire approach
and direction of exam History of symptoms General information
Subjective History Mechanism of Injury (MOI)? Previous injury? “Pop” when injury occurred? Clicking or catching? Pain
Where? Type? Isolated or diffuse?
Positional affect on injury?
2/5/2015
2
Subjective History
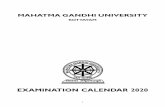
Does knee “give way”? Has knee “locked”? Swelling or feel “tight”?
Pain Scale
Visual Analog Pain Scale (VAS) Goal is < 3 on 0/10 VAS
Subjective History Inspection/Observation Palpation Clearing Tests L spine, Hip, Foot Range of Motion Accessory Joint Motion Laxity Assessment Muscle Strength Test Special Tests Neurovascular Assessment Imaging Studies Functional Assessment
Inspection/ObservationInspection/ObservationInspection/ObservationInspection/ObservationInspection/ObservationInspection/ObservationInspection/ObservationInspection/ObservationInspection/ObservationInspection/ObservationInspection/ObservationInspection/ObservationInspection/ObservationInspection/ObservationInspection/ObservationInspection/ObservationInspection/ObservationInspection/ObservationInspection/ObservationInspection/ObservationInspection/Observation Observation/Posture Anterior View Genu varum/valgum Normal
Observation/Posture Anterior View Miserable malalignment syndrome
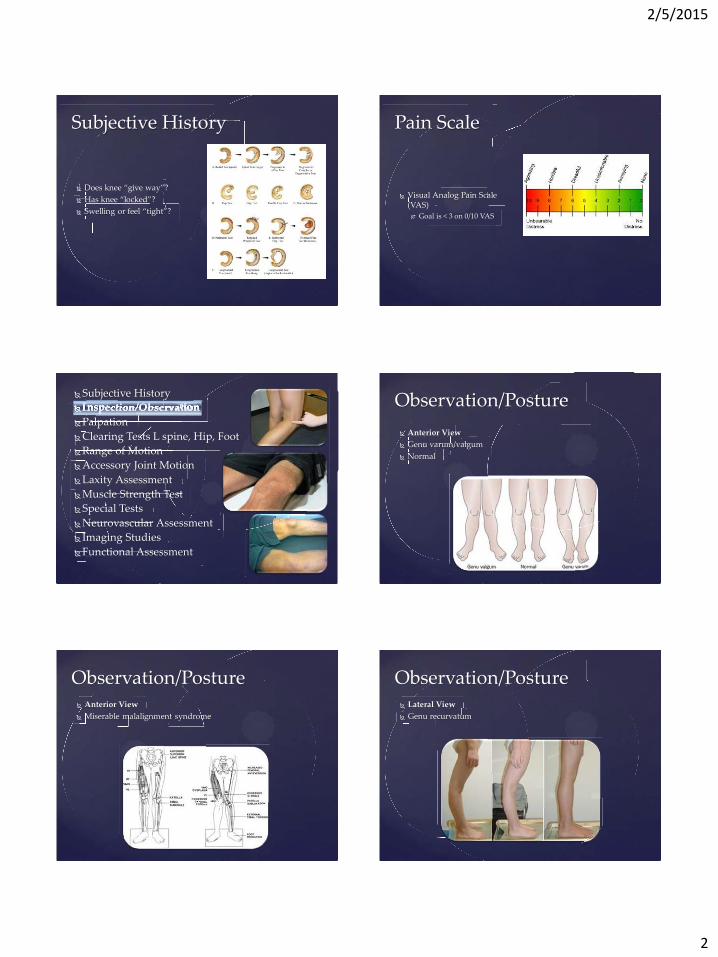
Observation/Posture Lateral View Genu recurvatum
2/5/2015
3
Observation/Posture Lateral View Genu recurvatum
Observation/Posture Lateral View Genu recurvatum
Observation/Posture Lateral View Patella alta/baja
Observation/Posture Lateral View Patella alta/baja
Observation/Posture Swelling
Anthropometric Measurements
Effusion 20 cm proximal 10 cm proximal Joint line 15 cm distal
Soderberg GL, Ballantyne BT, Kestel LL. Reliability of lower extremity girth measurements after anterior cruciate ligament reconstruction. Physiother Res Int. 19916;1:7-16.

2/5/2015
4
Observation/Posture
Effusion Patellar Ballotment Test Fluid Wave/Shift
Observation/Posture Observation/Posture Subjective History Inspection/Observation Palpation Clearing Tests L spine, Hip, Foot Range of Motion Accessory Joint Motion Laxity Assessment Muscle Strength Test Special Tests Neurovascular Assessment Imaging Studies Functional Assessment
PalpationPalpationPalpationPalpationPalpationPalpationPalpationPalpationPalpationPalpationPalpationPalpationPalpation
Palpation
Assess for: Tenderness Pain Swelling Abnormalities
Palpation Lateral Knee Assess for:
Lateral joint line Lateral meniscus LCL Lateral tibial plateau Head of fibula Iliotibial band Popliteus
http://pages.uoregon.edu/esorens1/hphy362.pbwiki.com/Knee+History,+Observation+and+Palpation.html
Palpation Anterior Knee
Assess for: Patella Patellar tendon Tibial tuberosity Quadriceps tendon Sartorius muscle
http://pages.uoregon.edu/esorens1/hphy362.pbwiki.com/Knee+History,+Observation+and+Palpation.html
Palpation Medial Knee Assess for:
Medial joint line Medial meniscus MCL Medial tibial plateau Medial femoral
condyle Pes anserine tendon Gracili muscle
http://pages.uoregon.edu/esorens1/hphy362.pbwiki.com/Knee+History,+Observation+and+Palpation.html

2/5/2015
5
Palpation Posterior Knee
Assess for: Popliteal fossa Biceps femoris Semimembranosus Semitendinosis Gastrocnemius
http://pages.uoregon.edu/esorens1/hphy362.pbwiki.com/Knee+History,+Observation+and+Palpation.html
Subjective History Inspection/Observation Palpation Clearing Tests L spine, Hip, Foot Range of Motion Accessory Joint Motion Laxity Assessment Muscle Strength Test Special Tests Neurovascular Assessment Imaging Studies Functional Assessment
Clearing Tests L spine, Hip, FootClearing Tests L spine, Hip, FootClearing Tests L spine, Hip, FootClearing Tests L spine, Hip, FootClearing Tests L spine, Hip, FootClearing Tests L spine, Hip, FootClearing Tests L spine, Hip, FootClearing Tests L spine, Hip, FootClearing Tests L spine, Hip, FootClearing Tests L spine, Hip, FootClearing Tests L spine, Hip, FootClearing Tests L spine, Hip, FootClearing Tests L spine, Hip, FootClearing Tests L spine, Hip, FootClearing Tests L spine, Hip, FootClearing Tests L spine, Hip, FootClearing Tests L spine, Hip, Foot
Clearing Tests
Assess for ROM/Strength: Spine Hip Ankle/Foot
Magee DJ. Orthopedic Physical Assessment, 5th ed. Saunders. 2008. St. Louis
Subjective History Inspection/Observation Palpation Clearing Tests L spine, Hip, Foot Range of Motion Accessory Joint Motion Laxity Assessment Muscle Strength Test Special Tests Neurovascular Assessment Imaging Studies Functional Assessment
Range of MotionRange of MotionRange of MotionRange of MotionRange of MotionRange of MotionRange of MotionRange of MotionRange of MotionRange of MotionRange of MotionRange of MotionRange of MotionRange of Motion
Range of Motion
Assess for: Knee flexion and extension
Magee DJ. Orthopedic Physical Assessment, 5th ed. Saunders. 2008. St. Louis
Range of Motion
AROM (Extensor Lag) PROM (Extensor Lag)
Magee DJ. Orthopedic Physical Assessment, 5th ed. Saunders. 2008. St. Louis

2/5/2015
6
Inability to Extend Knee
Factor Examples Decreased quad strength Dissuse
Lacerated femoral nerve Herniated disc L3-4 Severe pain Excessive swelling
Excessive resistance from connective tissue
Tight knee flexors Stiffness of collateral ligaments Tight posterior capsule Scarring posterior
Faulty arthrokinematics Excessive swelling Lack of “screw home” Lack of anterior glide Internal derangement Lack of superior patellar glide
Magee DJ. Orthopedic Physical Assessment, 5th ed. Saunders. 2008. St. Louis
Functional Testing
Before instituting Functional Testing
AROM/PROM (<10%)
Davies GJ, Zilmer DA. Functional progression of a patient through a rehabilitation program. Orthop Phys Ther Clin N Am. 2000;9:103-118.
Subjective History Inspection/Observation Palpation Clearing Tests L spine, Hip, Foot Range of motion Accessory Joint Motion Laxity Assessment Muscle Strength Test Special Tests Neurovascular Assessment Imaging Studies Functional Assessment
Range of motionRange of motionRange of motionRange of motion
Accessory Joint MotionAccessory Joint MotionAccessory Joint MotionAccessory Joint MotionAccessory Joint MotionAccessory Joint MotionAccessory Joint MotionAccessory Joint MotionAccessory Joint MotionAccessory Joint MotionAccessory Joint MotionAccessory Joint MotionAccessory Joint MotionAccessory Joint MotionAccessory Joint MotionAccessory Joint MotionAccessory Joint Motion
End Feels
Magee DJ. Orthopedic Physical Assessment, 5th ed. Saunders. 2008. St. Louis
Passive Movements of Knee and Normal End Feels Flexion (Tissue approximation) Extension (Tissue stretch) Medial rotation – tibia on femur (Tissue stretch) Lateral rotation – tibia on femur (Tissue stretch) Patellar movement (Tissue stretch all directions)
Subjective History Inspection/Observation Palpation Clearing Tests L spine, Hip, Foot Range of Motion Accessory Joint Motion Laxity Assessment Muscle Strength Test Special TestsNeurovascular Assessment Imaging Studies Functional Assessment
Laxity AssessmentLaxity AssessmentLaxity AssessmentLaxity AssessmentLaxity AssessmentLaxity AssessmentLaxity AssessmentLaxity AssessmentLaxity AssessmentLaxity AssessmentLaxity AssessmentLaxity AssessmentLaxity AssessmentLaxity AssessmentLaxity Assessment
Passive Patellar Mobility: Glides – M/L, S/I

2/5/2015
7
Passive Patellar Mobility: Tilts
KT 1000/2000 Ligament Arthrometer Goal < 3 mm difference
bilaterally
Don’t forget about the original “Arthrometer”
Subjective History Inspection/Observation Palpation Clearing Tests L spine, Hip, Foot Range of Motion Accessory Joint Motion Laxity Assessment Muscle Strength Test Special Tests Neurovascular Assessment Imaging Studies Functional Assessment
Muscle Strength TestMuscle Strength TestMuscle Strength TestMuscle Strength TestMuscle Strength TestMuscle Strength TestMuscle Strength TestMuscle Strength TestMuscle Strength TestMuscle Strength TestMuscle Strength TestMuscle Strength TestMuscle Strength TestMuscle Strength TestMuscle Strength TestMuscle Strength TestMuscle Strength Test
Strength Tests: Quads Strength Tests: Hamstrings

2/5/2015
8
Strength Tests: Isokinetic Strength Tests: Isokinetic
Strength Tests: Isokinetic
When safe to begin Functional Testing
CKC Device < 30% difference
OKC Device <25% difference
Subjective History Inspection/Observation Palpation Clearing Tests L spine, Hip, Foot Range of Motion Accessory Joint Motion Laxity Assessment Muscle Strength Test Special Tests Neurovascular Assessment Imaging Studies Functional Assessment
Special TestsSpecial TestsSpecial TestsSpecial TestsSpecial TestsSpecial TestsSpecial TestsSpecial TestsSpecial TestsSpecial TestsSpecial TestsSpecial Tests
Special Tests
70 different tests for knee pathology!
Cook CE, Hegedus EJ. Orthopedic Physical Examination Tests: An Evidence-Based Approach. 2nd ed, 2013 Pearson Education.
Special Tests
101 different tests for knee pathology!
Magee D. Orthopedic Physical Assessment, 5th ed, 2008, Saunders, Elsevier. St. Louis.

2/5/2015
9
Swelling/Effusion
Swelling/Effusion
Brush Test Stroke Test Bulge Test Indention Test Peripatellar Swelling Test Fluctuation Test Patellar Tap Test
Magee D. Orthopedic Physical Assessment, 5th ed, 2008, Saunders, Elsevier. St. Louis.
Medial – Lateral Instability
Medial Lateral Instability Varus Stress Test Valgus Stress Test
Magee D. Orthopedic Physical Assessment, 5th ed, 2008, Saunders, Elsevier. St. Louis.
Single-Plane Anterior Instability Single-Plane Anterior
Instability
Lachman Test Ritchie Test Trillat Test Lachman-Trillat Test
Stable Lachman Drop Leg Lachman Prone Lachman Active No-Touch Lachman Maximum Quadriceps Test Anterior Drawer Sign Sitting Anterior Drawer Active Drawer Test
Magee D. Orthopedic Physical Assessment, 5th ed, 2008, Saunders, Elsevier. St. Louis.
Single-Plane Posterior Instability Single-Plane Posterior
Instability Posterior Sag Sign Step-Off Test (Thumb
sign) Reverse Lachman Test Drawer Sign Active Drawer Godfey Test
Magee D. Orthopedic Physical Assessment, 5th ed, 2008, Saunders, Elsevier. St. Louis.
Anteromedial Rotary Instability
Anteromedial Rotary Instability
Slocum Test Lemaire’s T Drawer Test Dejour Test
Magee D. Orthopedic Physical Assessment, 5th ed, 2008, Saunders, Elsevier. St. Louis.
Anterolateral Rotary Instability Anterolateral Rotary
Instability
Slocum Test Lateral Pivot Shift
Maneuver Soft Pivot Shift Test Active Pivot Shift Test Loose Test Hughston Jerk Test Slocum ALRI Crossover Test of Arnold Noyes FRD Lemaire’s Jolt Test Flexion-Extension Valgus
Test Nakajima Test Martens Test
Magee D. Orthopedic Physical Assessment, 5th ed, 2008, Saunders, Elsevier. St. Louis.

2/5/2015
10
Posteromedial Rotary Instability
Posteromedial Rotary Instability
Hughston’s Posteromedial/Posterolateral Drawer Sign
Posteromedial Pivot Shift Test
Magee D. Orthopedic Physical Assessment, 5th ed, 2008, Saunders, Elsevier. St. Louis.
Posterolateral Rotary Instability
Posterolateral Rotary Instability
Hughston’s Posteromedial and Posterolateral Drawer Sign
Jakob Test External Rotation Recurvatum
Test Loomer’s Posterolateral Rotary
Instability Test Bousquet External
Hypermobility Test Tibial Lateral Rotation Test Dial Test Dynamic Posterior Shift Test Active Posterolateral Drawer
Sign Standing Apprehension Test
Magee D. Orthopedic Physical Assessment, 5th ed, 2008, Saunders, Elsevier. St. Louis.
Patellofemoral
Patellofemoral Tests
VM Coordination Test Clarke’s Sign McConnell Test Active Patellar Grind Step Up Test Eccentric Step Test Waldron Test Passive Patellar Tilt Passive Patellar Glide Lateral Pull Test Zohler’s Sign Frund’s Sign
Magee D. Orthopedic Physical Assessment, 5th ed, 2008, Saunders, Elsevier. St. Louis.
Meniscus Meniscus Tests
Recurvatum Test McMurray Test Apley’s Test Bounce Home Test Thessaly Test O’Donohue’s Test Modified Helfet Test Test for Retracting Meniscus Steinman’s Tenderness Test Payr’s Test Bohler’s Sign Bragard’s Sign Kromer’s Sgin Childress’ Sign Anderson Medial-Lateral
Grind Passler Rotational Grind Test Cabot’s Popliteal Sign
Magee D. Orthopedic Physical Assessment, 5th ed, 2008, Saunders, Elsevier. St. Louis.
Plica Tests
Plica Tests
Mediopatellar Plica Test Plica “Stutter” Test Hughston’s Plica Test Patellar Bowsting Test
Magee D. Orthopedic Physical Assessment, 5th ed, 2008, Saunders, Elsevier. St. Louis.
Subjective History Inspection/Observation Palpation Clearing Tests L spine, Hip, Foot Range of Motion Accessory Joint Motion Laxity Assessment Muscle Strength Test Special TestsNeurovascular Assessment Imaging Studies Functional Assessment
Neurovascular AssessmentNeurovascular AssessmentNeurovascular AssessmentNeurovascular AssessmentNeurovascular AssessmentNeurovascular AssessmentNeurovascular AssessmentNeurovascular AssessmentNeurovascular AssessmentNeurovascular AssessmentNeurovascular AssessmentNeurovascular Assessment

2/5/2015
11
Reflexes and Cutaneous Distribution
Patellar tendon reflex (L3-L4) Medial hamstring reflex (L5-S1)
Reflexes and Cutaneous Distribution Cutaneous distribution
Kinesthetic Joint Angular Reproduction
Active angular joint reproduction Passive angular joint reproduction Threshold to detect motion OKC/CKC
Balance Testing
Timed Tests Reach Tests
Subjective History Inspection/Observation Palpation Clearing Tests L spine, Hip, Foot Range of Motion Accessory Joint Motion Laxity Assessment Muscle Strength Test Special TestsNeurovascular Assessment Imaging Studies Functional Assessment
Imaging StudiesImaging StudiesImaging StudiesImaging StudiesImaging StudiesImaging StudiesImaging StudiesImaging StudiesImaging StudiesImaging StudiesImaging StudiesImaging Studies
Imaging Studies
All radiographs Used as adjunct Not indiscriminately Used primarily to confirm a
diagnosis

2/5/2015
12
Imaging Studies
AP Lateral
Other Views - Imaging Studies
Intercondylar Notch (Tunnel View) Prone, knee flexed 45-90° Tibia and intercondylar notch Condyles Loose bodies
Other Views - Imaging Studies
Axial (Skyline View) Supine, knee flexed various
angles Type of patella Lateral patellar displacement Sulcus angle
Subjective History Inspection/Observation Palpation Clearing Tests L spine, Hip, Foot Range of Motion Accessory Joint Motion Laxity Assessment Muscle Strength Test Special Tests Neurovascular Assessment Imaging Studies Functional Assessment
Functional AssessmentFunctional AssessmentFunctional AssessmentFunctional AssessmentFunctional AssessmentFunctional AssessmentFunctional AssessmentFunctional AssessmentFunctional AssessmentFunctional AssessmentFunctional AssessmentFunctional AssessmentFunctional Assessment
Thank you! [email protected]

2/7/2014
1
Robert C. Manske, PT, DPT, MEd, SCS, ATC, CSCS Professor and Chair Department of Physical Therapy Wichita State University Via Christi Sports Wichita, KS
*Elsevier Science
Human Kinetics
*
*
*Summarize importance of thorough knowledge of biomechanical factors associated with rehabilitation
*Discuss tibiofemoral shear forces observed during OKC and CKC exercises
*Describe in-vivo forces on ACL and PCL during OKC, CKC, cycling and stair climbing
* Identify which exercises produce co-contraction of quadriceps and hamstring muscles
*Summarize stresses on PFJ during OKC, CKC exercises
*
*Cadaveric
*Electromyography
*Kinematics
*Kinetics
*Mathematical modeling
*In vivo strain gauge

2/7/2014
2
*
*Anterior cruciate ligament (ACL)
*Posterior cruciate ligament (PCL)
*Patellofemoral joint
*
*
*
**
* *
*ACL loaded during quadriceps contraction due to anterior directed force from attachment at proximal tibia
*ACL loaded most between 0-60°of flexion
*
Butler DL, Noyes FR, Grood ES. Ligamentous restraints to anterior-posterior drawer in the human knee. A biomechanical study. J Bone Joint Surg. 1980; 62A:259-270. Herzog W, Read LJ. Lines of action and moment arms of the major force-carrying structures crossing the human knee joint. J Anat. 1993;182:213-230.

2/7/2014
3
*
*Healthy adults
*Normal native ACL ultimate strength is ~ 2000N
*Post ACL reconstruction it is not known how much force to the graft’s fixation is
either too great or too little
*
Woo SL, et al. Tensile properties of the human femur-anterior cruciate ligament-tibia complex. The effects of specimen age and orientation. Am J Sports Med. 1991;19:217-225.
**In-Vivo
*Direct measurements
*No individuals with repairs
*Normal individuals intact ACLs
*Experimental models *Not measured directly
*
All results should be interpreted with caution
*
*Soft tissue autografts 8-12 weeks before proper incorporation
*Bone autograft 6-8 weeks before proper incorporation
*Allografts may take twice the time that it takes autografts
*
Jackson DW, Windler GE, Simon TM. Intraarticular reaction associated with the use of freeze-dried, ethylene oxide-sterilized bone-patellar tendon-bone allografts in the reconstruction of the anterior cruciate ligament. Am J Sports Med. 1990;18:1-10.
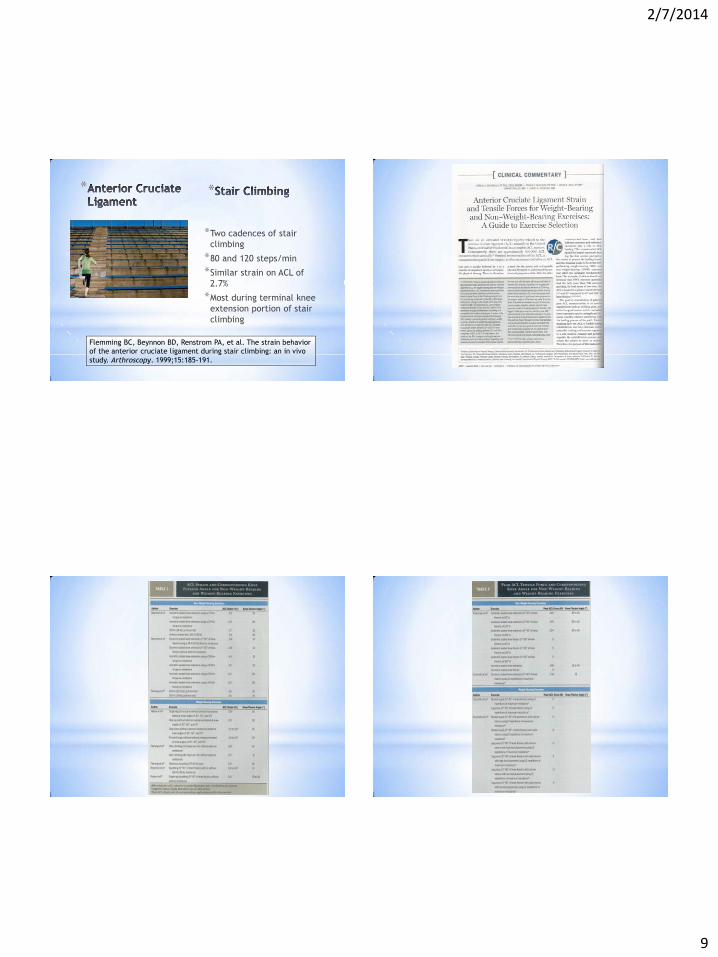
*Isometric quadriceps contraction 15° 4.4% Squatting with resistance 4.0% Active knee flexion with resistance 3.8% Lachman’s test (150N anterior shear at 30°) 3.7% Squatting without resistance 3.6% Active knee flexion without resistance 2.8% Quadriceps and hamstring co-contraction at 15° 2.7% Isometric quadriceps contraction at 30° 2.7% Stair climbing 2.7% Anterior drawer test (150 N anterior shear at 90°) 1.8% Stationary bicycle 1.7% Quadriceps and hamstrings co-contraction at 30° 0.4% Passive knee range of motion 0.1% Isometric quadriceps at 60° and 90° 0.0% Quad and hamstring co-contraction at 60 ° and 90 ° 0.0% Isometric hamstring contraction at 30°, 60°, 90° 0.0%
Fleming BC, Beynnon BD, Renstrom PA, et al. The strain behavior of the ACL during stair climbing. An in vivo study. Arthroscopy. 1999;15:185-191.

2/7/2014
4
*
*Compressive loads on cadaveric knees to stimulate WB
*Compared to OKC - compressive forces decreased strain on ACL
*
Markolf KL, Gorek JF, Kabo JM, Shapiro MS. Direct measurement of resultant forces in the anterior cruciate ligaments. An in vitro study performed with new experimental technique. J Bone Joint Surg 1990;72:557-567.
*
*Tested with in vivo strain gauge measurements on the ACL
*Direct measurement of strain on ACL during activities
*Strain increased from -2.0% during NWB to 2.1% in WB
*
Fleming BC, Renstrom PA, Beynnon BD, et al. The effect of weightbearing and external loading on anterior cruciate ligament strain. J Biomech 2001;34:163-170.
*
*Although strain increased in weight bearing it is unclear at what point strain becomes deleterious to graft
*
Fleming BC, Renstrom PA, Beynnon BD, et al. The effect of weightbearing and external loading on anterior cruciate ligament strain. J Biomech 2001;34:163-170.
*
*Mathematical modeling to determine shear forces at tibiofemoral joint during same exercises
*
Wilk KE, Escamilla RF, Fleisig GS, et al. A comparison of the tibiofemoral joint forces and electromyographic activity during open and closed kinetic chain exercises. Am J Sports Med. 1996;24:518-527.

2/7/2014
5
*
*Co-contraction of hamstring and quadriceps muscles
*EMG of quads during *Squat
*Leg press
*OKC knee extension
*
Wilk KE, Escamilla RF, Fleisig GS, et al. A comparison of the tibiofemoral joint forces and electromyographic activity during open and closed kinetic chain exercises. Am J Sports Med. 1996;24:518-527.
*
*Co-contraction occurred from 30-0° during ascent phase of squat
**When body is positioned directly over knees
*Did not occur at other ROM
*Did not occur with leg press or leg extension
*
Wilk KE, Escamilla RF, Fleisig GS, et al. A comparison of the tibiofemoral joint forces and electromyographic activity during open and closed kinetic chain exercises. Am J Sports Med. 1996;24:518-527.
*
*Multiple factors affect muscle activation patterns during CKC exercises *Knee flexion angle
*Body positioning * Relative to knee
*Direction of movement * Ascending
* Descending
*
Wilk KE, Escamilla RF, Fleisig GS, et al. A comparison of the tibiofemoral joint forces and electromyographic activity during open and closed kinetic chain exercises. Am J Sports Med. 1996;24:518-527.
*
*CKC squats in upright position with knees to 30° *Should be safe for ACL
*Squats
*Lateral lunges
*
Wilk KE, Escamilla RF, Fleisig GS, et al. A comparison of the tibiofemoral joint forces and electromyographic activity during open and closed kinetic chain exercises. Am J Sports Med. 1996;24:518-527.

2/7/2014
6
*
*Posterior shear forces predominated *Entire ROM squatting and
knee extension
*Deep angles of OKC knee extension (100-40°)
*Anterior shear forces predominant *OKC knee extension from
40-10°
*
Wilk KE, Escamilla RF, Fleisig GS, et al. A comparison of the tibiofemoral joint forces and electromyographic activity during open and closed kinetic chain exercises. Am J Sports Med. 1996;24:518-527.
*
*Ten healthy male subjects
*3 reps of 12R max *Squat
*Leg press
*Knee extension
*
Escamilla RF, Fleisig GS,Zheng N, et al. Biomechanics of the knee during closed kinetic chain and open kinetic chain exercises. Med Sci Sports Exerc. 1998;30(4):556-569.
*
*PCL tensile forces increased for all exercises as knee flexed and PCL tensile forces decreased with knee extension
*Only PCL tensioned in CKC
*ACL tension only near full extension in OKC (15-25°)
*
Escamilla RF, Fleisig GS,Zheng N, et al. Biomechanics of the knee during closed kinetic chain and open kinetic chain exercises. Med Sci Sports Exerc. 1998;30(4):556-569.
PCL Forces
PCL Forces
*
*In vivo strain gauge study *Greatest strain during OKC
extension from 40-0° *Increased in linear fashion
with application of 45N boot *Strain greatest at 3.8% *However – strain of 3.6%
during CKC squat
*
Beynnon BD, Johnson RJ, Flemming BC, et al. The strain behavior of the anterior cruciate ligament during squatting and active flexion-extension: A comparison of an open and closed kinetic chain exercise. Am J Sports Med. 1997;25:823-829.

2/7/2014
7
*
*Lunges
*Varying step lengths
*
Escamilla RF, Zheng N, Imamura R, et al. Cruciate ligament forces between short-step and long-step forward lunge. Med Sci Sports Exerc. 2010;42:1932-1942.
*
*Minimal strain during both long or short stride lunges
*Loading only occurred during short stride between 0-10°flexion
*Only 0-50N
*
Escamilla RF, Zheng N, Imamura R, et al. Cruciate ligament forces between short-step and long-step forward lunge. Med Sci Sports Exerc. 2010;42:1932-1942.
*
*Forward lunge long recruits more hamstring activity
*May be even safer during early rehabilitation
*
Escamilla RF, Zheng N, Imamura R, et al. Cruciate ligament forces between short-step and long-step forward lunge. Med Sci Sports Exerc. 2010;42:1932-1942.
*
*Anterior shear during wall squats and single leg squats
*Wall squats bilaterally close or farther from wall caused no increased strain on ACL
*
Escamilla RF, Zheng N, Imamura R, et al. Cruciate ligament forces during the wall squat and the one-leg squat. Med Sci Sports Exerc. 2009;41:408-417.

2/7/2014
8
*
*Anterior shear force did
increase in one-legged squats from 0-40° *Knee moved forward an
average 10.0+/- 2 cm beyond toes during one-legged squat
*Peak of 60N at 30° *A mild strain may enhance
healing process
*
Escamilla RF, Zheng N, Imamura R, et al. Cruciate ligament forces during the wall squat and the one-leg squat. Med Sci Sports Exerc. 2009;41:408-417.
*
*Squat with trunk tilted forward *Decreased ACL loading
* Increased hamstring activity
*Anterior tilted 30-40° from vertical
*
Kulas AS, Hortobagyi T, DeVita P. Trunk position modulates anterior cruciate ligament forces and strains during single-leg squat. Clin Biomech. 2012;27:16-21. Ohkoshi T, Yasuda K, Kaneda K, Wada T, Yamanaka M. Biomechanical analysis of rehabilitation in the standing position. Am J Sports Med. 1991;19:605-611.
*
*Six different cycling conditions
*Manipulated by speed and power
*No differences between conditions
*Minimal mean ACL strain of 1.7%
*
Flemming BC, Beynnon BD, Renstrom PA, et al. The strain behavior of the anterior cruciate ligament during bicycling: an in vivo study. Am J Sports Med. 1998;26:109-118.
*
*Greatest amount of strain seen when knee reached greatest amount of extension
*
Flemming BC, Beynnon BD, Renstrom PA, et al. The strain behavior of the anterior cruciate ligament during bicycling: an in vivo study. Am J Sports Med. 1998;26:109-118.
2/7/2014
9
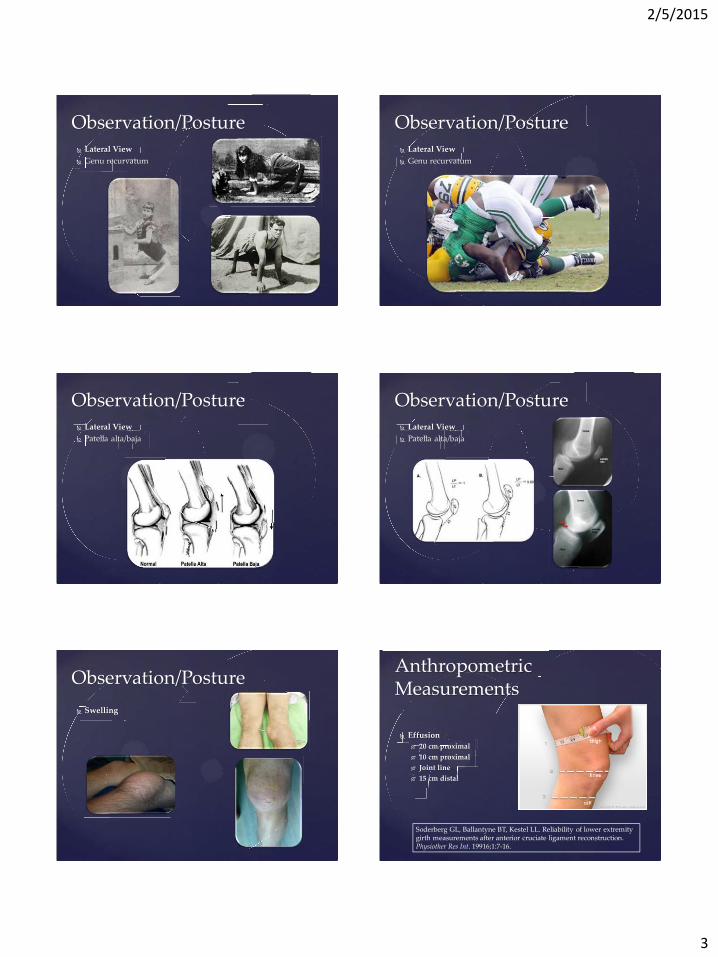
*
*Two cadences of stair climbing
*80 and 120 steps/min
*Similar strain on ACL of 2.7%
*Most during terminal knee extension portion of stair climbing
*
Flemming BC, Beynnon BD, Renstrom PA, et al. The strain behavior of the anterior cruciate ligament during stair climbing: an in vivo study. Arthroscopy. 1999;15:185-191.

2/7/2014
10
*
*Hamstring tendon autografts on cadaveric knees
*Immediate post operative mean maximum strength 352 N
*Sheep
*4 wks = 376 N
*8 wks = 415 N
*12 wks = 323 N
Goradia VK, Rochat MC, Grana WA, Engle DM. Strength of ACL reconstruction using semitendinosus tendon grafts. J Okla State Med Assoc. 1998;91(5):275-277.
**Intrinsic fibroblast necrosis was predominant
between 2-12 weeks
*Necrotic tissue in core of ACL at 12 weeks
*Mechanical properties deteriorated after surgery at 12 weeks
*Complete recovery at 52 weeks
Goradia VK, Rochat MC, Grana WA, Engle DM. Strength of ACL reconstruction using semitendinosus tendon grafts. J Okla State Med Assoc. 1998;91(5):275-277.
**Similar findings seen in:
*Goat – 31% at 1 year (PT Auto)
*Sheep – 45% at 1 year (AT Auto)
*Sheep - 41% at 1 year (SDFlex T Auto)
*Sheep - 47% at 1 year (ST Auto)
NG GY, et al. Biomechanics of patellar tendon autograft for reconstruction of the ACL in goat: three year study. J Orthop Res. 1995;13:602-608. Weiler A, et al. Tendon healing in a bone tunnel, part I: Biomechanical results after biodegradable interference fit fixation in model of ACL reconstruction in sheep. Arthroscopy. 2002;18:113-123. Hunt P, et al. A model of soft-tissue graft anterior cruciate ligament reconstruction in sheep. Arch Orthop Trauma Surg. 2005;125:238-248. Goradia VK, Rochat MC, Grana WA, Engle DM. Strength of ACL reconstruction using semitendinosus tendon grafts. J Okla State Med Assoc. 1998;91(5):275-277.
2/7/2014
11
*
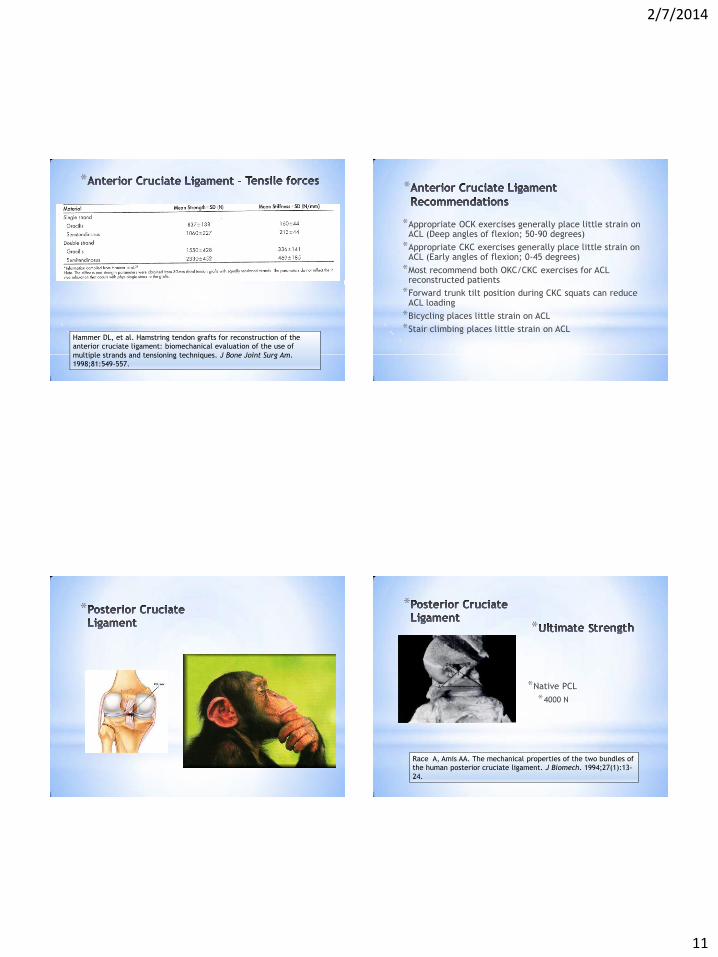
Hammer DL, et al. Hamstring tendon grafts for reconstruction of the anterior cruciate ligament: biomechanical evaluation of the use of multiple strands and tensioning techniques. J Bone Joint Surg Am. 1998;81:549-557.
*
*Appropriate OCK exercises generally place little strain on ACL (Deep angles of flexion; 50-90 degrees)
*Appropriate CKC exercises generally place little strain on ACL (Early angles of flexion; 0-45 degrees)
*Most recommend both OKC/CKC exercises for ACL reconstructed patients
*Forward trunk tilt position during CKC squats can reduce ACL loading
*Bicycling places little strain on ACL *Stair climbing places little strain on ACL
*
*
*Native PCL *4000 N
*
Race A, Amis AA. The mechanical properties of the two bundles of the human posterior cruciate ligament. J Biomech. 1994;27(1):13-24.

2/7/2014
12
*
*High activity of hamstrings
*Isometric activation
*Maximum force of: *1780 N at 90° flexion
*1526 N at 60° flexion
*939 N at 30° flexion
*
Lutz GE, Palmitier RA, An KN, Chao EY. Comparison of tibiofemoral joint forces during open and closed kinetic chain exercises. J Bone Joint Surg 1993;75A:732-735.
*
*High activity of hamstrings
*Isometric activation
*Maximum force of: *1.7 x BW @75°
*
Kaufman KR, An KN, Litchy WJ, et al. Dynamic joint forces during knee isokinetic exercise. Am J Sports Med. 1991;19:305-316.
*
*High forces between 100-40° resisted OKC knee extension
*
Wilk KE, Escamilla RF, Fleisig GS, et al. A comparison of the tibiofemoral joint forces and electromyographic activity during open and closed kinetic chain exercises. Am J Sports Med. 1996;24:518-527.
*
*Highest forces found between 85-95° resisted OKC knee flexion
*
Wilk KE, Escamilla RF, Fleisig GS, et al. A comparison of the tibiofemoral joint forces and electromyographic activity during open and closed kinetic chain exercises. Am J Sports Med. 1996;24:518-527.

2/7/2014
13
*
*Lowest forces found between 60-0° resisted OKC knee extension.
**
Wilk KE, Escamilla RF, Fleisig GS, et al. A comparison of the tibiofemoral joint forces and electromyographic activity during open and closed kinetic chain exercises. Am J Sports Med. 1996;24:518-527.
*
*Increase in correlation to angle of knee flexion.
*
Wilk KE, Escamilla RF, Fleisig GS, et al. A comparison of the tibiofemoral joint forces and electromyographic activity during open and closed kinetic chain exercises. Am J Sports Med. 1996;24:518-527.
*
*Linear increase shear force from 40-100°during front squat.
*
Meglan D, Lutz G, Stuart M. Effects of closed kinetic chain exercises for ACL rehabilitation up the load in the capsular and ligamentous structures of the knee. Presented at the Orthopedic Research Society Meeting. San Francisco, 1993.
*
*Ten healthy male subjects
*3 reps of 12R max *Squat
*Leg press
*Knee extension
*
Escamilla RF, Fleisig GS,Zheng N, et al. Biomechanics of the knee during closed kinetic chain and open kinetic chain exercises. Med Sci Sports Exerc. 1998;30(4):556-569.

2/7/2014
14
*
*PCL tensile forces increased for all exercises as knee flexed and PCL tensile forces decreased with knee extension
*Only PCL tensioned in CKC
*ACL tension only near full extension in OKC (15-25°)
*
Escamilla RF, Fleisig GS,Zheng N, et al. Biomechanics of the knee during closed kinetic chain and open kinetic chain exercises. Med Sci Sports Exerc. 1998;30(4):556-569.
PCL Forces
PCL Forces
*
*OCK PCL was tensioned when knee was in greater flexion (>25°)
*Peak PCL forces *CKC = 2000 N
*OKC = 1000 N
*
Escamilla RF, Fleisig GS,Zheng N, et al. Biomechanics of the knee during closed kinetic chain and open kinetic chain exercises. Med Sci Sports Exerc. 1998;30(4):556-569.
0200400600800
100012001400160018002000
CKC OKC
*
*Load during wall squat and single leg squat
*Wall squat with legs farther from wall created more posterior shear force
*Wall squat with legs closer to wall created less posterior shear force
*
Escamilla RF, Zheng N, Imamura R, et al. Cruciate ligament forces during the wall squat and the one-leg squat. Med Sci Sports Exerc. 2009;41:408-417.
*
*Wall squat with legs farther from wall produced higher posterior shear forces than single leg squat
*
Escamilla RF, Zheng N, Imamura R, et al. Cruciate ligament forces during the wall squat and the one-leg squat. Med Sci Sports Exerc. 2009;41:408-417.

2/7/2014
15
*
*To reduce PCL stress during CKC exercises.
*Leg presses and squats should be performed between 0-60°of knee flexion.
*Legs should be closer to wall.
*Wall squat with legs close to wall and single leg squat may be helpful during early PCL rehabilitation
*
Escamilla RF, Zheng N, Imamura R, et al. Cruciate ligament forces during the wall squat and the one-leg squat. Med Sci Sports Exerc. 2009;41:408-417.
*
*Low levels of hamstring activity during wall squat
*Wall squats done in erect posture – less hip extensor torque needed to overcome gravity
*Wall squats primarily target quadriceps
*
Escamilla RF, Zheng N, Imamura R, et al. Cruciate ligament forces during the wall squat and the one-leg squat. Med Sci Sports Exerc. 2009;41:408-417.
*
*During wall squat significant greater PCL force at angles of 60-90° during ascent
*PCL forces significantly greater during ascent between 20-70°
*
Escamilla RF, Zheng N, Imamura R, et al. Cruciate ligament forces during the wall squat and the one-leg squat. Med Sci Sports Exerc. 2009;41:408-417.
*
*Lunges
*Varying step lengths
*
Escamilla RF, Zheng N, Imamura R, et al. Cruciate ligament forces between short-step and long-step forward lunge. Med Sci Sports Exerc. 2010;42:1932-1942.
2/7/2014
16
*
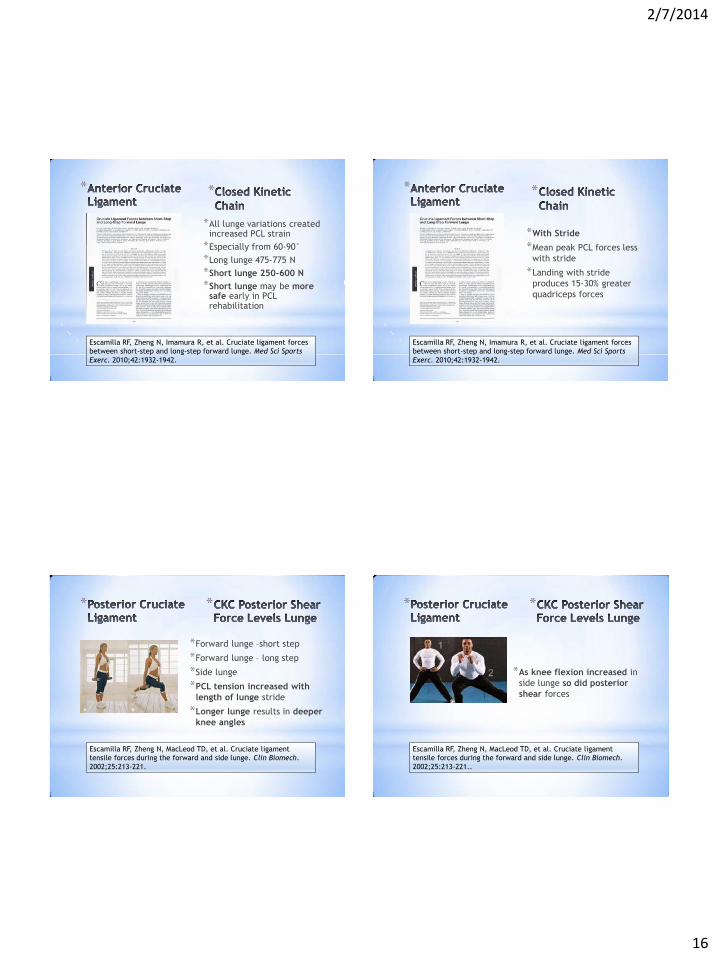
*All lunge variations created increased PCL strain
*Especially from 60-90° *Long lunge 475-775 N *Short lunge 250-600 N *Short lunge may be more
safe early in PCL rehabilitation
*
Escamilla RF, Zheng N, Imamura R, et al. Cruciate ligament forces between short-step and long-step forward lunge. Med Sci Sports Exerc. 2010;42:1932-1942.
*
*With Stride
*Mean peak PCL forces less with stride
*Landing with stride produces 15-30% greater quadriceps forces
*
Escamilla RF, Zheng N, Imamura R, et al. Cruciate ligament forces between short-step and long-step forward lunge. Med Sci Sports Exerc. 2010;42:1932-1942.
*
*Forward lunge –short step
*Forward lunge – long step
*Side lunge
*PCL tension increased with length of lunge stride
*Longer lunge results in deeper knee angles
*
Escamilla RF, Zheng N, MacLeod TD, et al. Cruciate ligament tensile forces during the forward and side lunge. Clin Biomech. 2002;25:213-221.
*
*As knee flexion increased in side lunge so did posterior shear forces
*
Escamilla RF, Zheng N, MacLeod TD, et al. Cruciate ligament tensile forces during the forward and side lunge. Clin Biomech. 2002;25:213-221..

2/7/2014
17
*
*Use caution when performing lunges forward and side during PCL rehabilitation
*This is especially true during early stages
*Closely monitor levels of knee flexion
*
Escamilla RF, Zheng N, MacLeod TD, et al. Cruciate ligament tensile forces during the forward and side lunge. Clin Biomech. 2002;25:213-221.
*
*Unsafe *Any OKC knee flexion activity produces very high posterior
tibiofemoral shear forces and should be limited early *OKC knee extension displays high posterior shear forces 40-
100° *CKC exercises in deeper ranges of knee flexion *Safer *OKC knee extension 0-40° or 0-60°minimize strain on PCL *CKC exercises safer in lower ranges of knee flexion. 0-30°– 0-
45°– 0-60°
*
*
*PF Biomechanics
*Articulation begins around approximately 10-20°of knee flexion
*Inferior patella and femur
*As knee flexion is increased contact articulation progressively moves superior on patella
Hungerford DS, Barry M. Biomechanics of the patellofemoral joint. Clin Orthop Rel Res. 1979;144:9-15.
2/7/2014
18
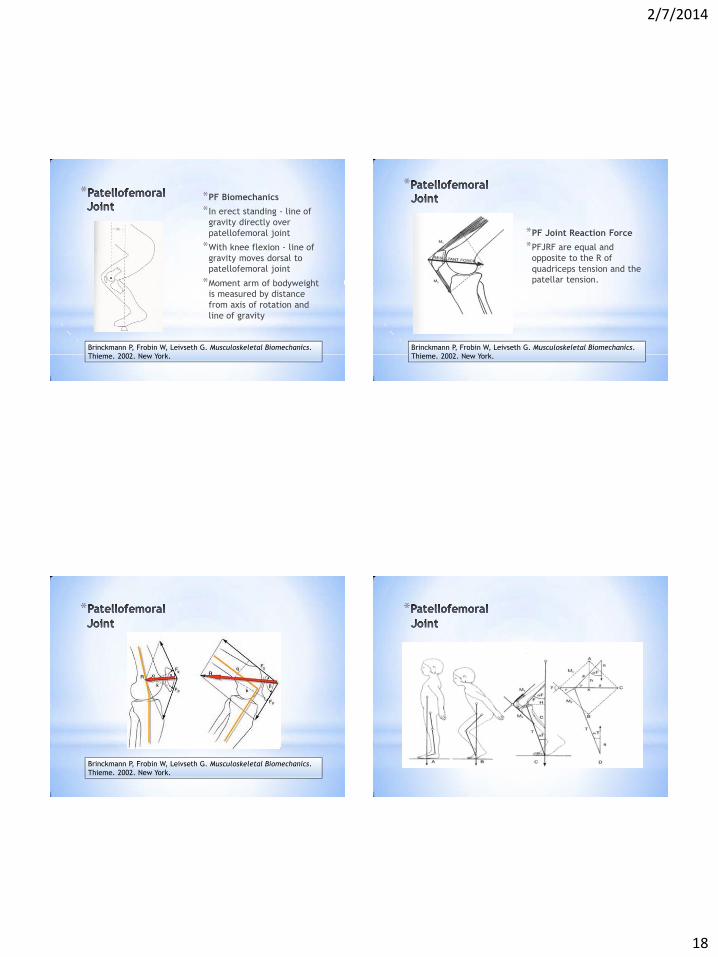
* *PF Biomechanics
*In erect standing - line of gravity directly over patellofemoral joint
*With knee flexion - line of gravity moves dorsal to patellofemoral joint
*Moment arm of bodyweight is measured by distance from axis of rotation and line of gravity
Brinckmann P, Frobin W, Leivseth G. Musculoskeletal Biomechanics. Thieme. 2002. New York.
*
*PF Joint Reaction Force
*PFJRF are equal and opposite to the R of quadriceps tension and the patellar tension.
Brinckmann P, Frobin W, Leivseth G. Musculoskeletal Biomechanics. Thieme. 2002. New York.
*
Brinckmann P, Frobin W, Leivseth G. Musculoskeletal Biomechanics. Thieme. 2002. New York.
*

2/7/2014
19
*
*Contact Stress
*At approximately 30°- contact area is ~ 2.0 cm
*At 90° contact area is increased to ~ 6.0 cm
Hungerford DS, Barry M. Biomechanics of the patellofemoral joint. Clin Orthop Rel Res. 1979;144:9-15.
**Alteration in Q-angle may
change contact area
*This may change joint reaction forces
*Maximum contact area at 90°of flexion
*Force of 6.5 x BW
*Increased Q-angle by 10°increased contact pressures and decreased contact area
Huberti HH, Hayes WC. Patellofemoral contact pressures. J Bone Joint Surg. 66A:715-724.
*
**Leg press and knee extension
exercises – isometric contractions *0°-30°-60°-90°
*From 0-46° JRF lower in CKC leg press
*From 50-90° JRF lower during OKC extension
*JRF minimal at 90° of knee flexion in OKC
Steinkamp LA, Dillingham MF, Markel MD, et al. Biomechanical considerations in patellofemoral joint rehabilitation. Am J Sports Med. 1993;21:438-444.
** *Similar findings as Steinkamp
*OKC knee extension
*CKC vertical squat
*CKC leg press
*OKC knee extension produced greater force than CKC at angles < 57°of knee flexion
*OCK knee extension forces decreased near full flexion
*Both CKC activities produced greater force at knee flexion angles > 85°
*Maximum compressive forces of 4000-5000 N
Escamilla RF, Fleisig GS, Zheng N et al. Biomechanics of the knee during closed kinetic chain and open kinetic chain exercises. Med Sci Sports Exerc. 1998;30:556-569.
*

2/7/2014
20
*
*OCK knee extension forces decreased near full extension
*During knee extension from full flexion, stress increased up to 60° and then progressively decreased as knee continued to extend
*May be differences between isometric and isotonic force/stress data
Escamilla RF, Fleisig GS, Zheng N et al. Biomechanics of the knee during closed kinetic chain and open kinetic chain exercises. Med Sci Sports Exerc. 1998;30:556-569.
**
*During lunge as knee flexion increased PF JRF increased linearly
*PF JRF decreased as knee flexion decreased
*PF compression forced greater in lunge with stride than without
*Side lunge produced more compressive force than forward lunge
Escamilla RF, Zheng N, MacLeod TD, et al. Patellofemoral joint compressive force and stress during the forward and side lunges with and without a stride. Clin Biomech. 2008;23:1026-1037.
*
*
*Quadriceps force is greatest near full knee extension OKC
*Increased with external loading
*Small PF contact area observed near full extension
* *Near extension
*Decreased contact area
*Increased quadriceps force
*Larger force applied to smaller area of contact
*In deeper flexion contact area is increased as is contact stress
*Leads to wider dissipation of contact stress over larger surface area
Grood ES, Suntay WH, Noyes FR, Butler DL. Biomechanics of the knee-extension exercise. Effect of cutting the anterior cruciate ligament. J Bone Joint Surg. 66A:725-734.
*
2/7/2014
21
*
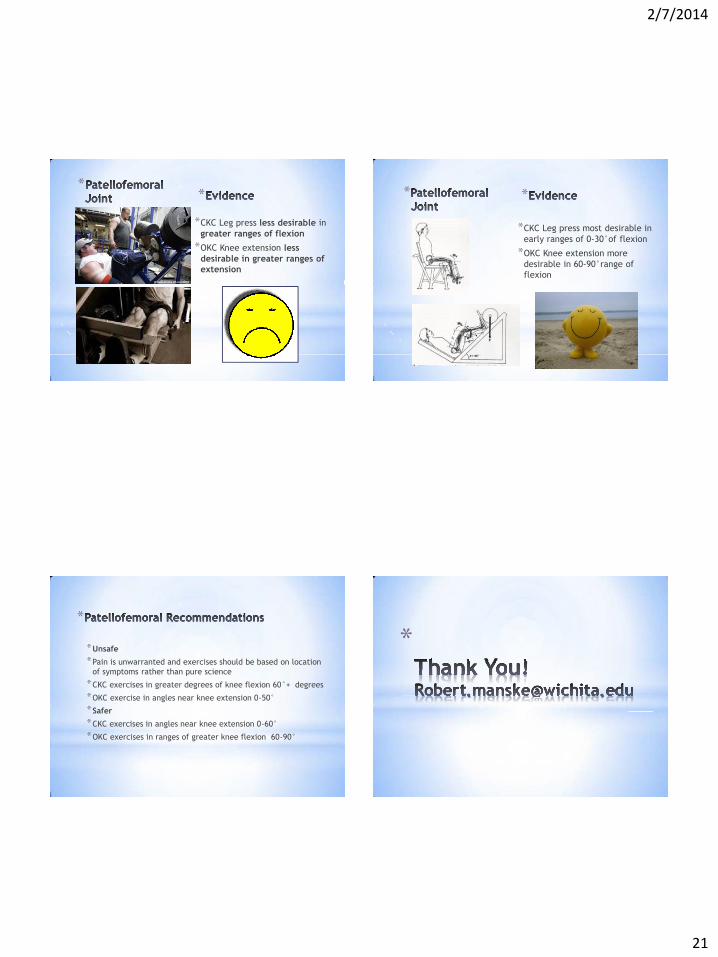
*CKC Leg press less desirable in greater ranges of flexion
*OKC Knee extension less desirable in greater ranges of extension
* *
*CKC Leg press most desirable in early ranges of 0-30°of flexion
*OKC Knee extension more desirable in 60-90°range of flexion
*
*
*Unsafe
*Pain is unwarranted and exercises should be based on location of symptoms rather than pure science
*CKC exercises in greater degrees of knee flexion 60°+ degrees
*OKC exercise in angles near knee extension 0-50°
*Safer
*CKC exercises in angles near knee extension 0-60°
*OKC exercises in ranges of greater knee flexion 60-90°
*

2/22/2016
1
Robert C. ManskePT, DPT, MEd, SCS, ATC, CSCS
Professor and ChairWichita State University Department of Physical
TherapyVia Christi Health Outpatient Orthopedic and
Sports Physical Therapy - Wichita
Injury of young activeBoth sexesRecurrence rate higher in
females
Fithian DC, Paxton EW, Stone ML, et al. Epidemiology and natural history of acute patellar dislocation. Am J Sports Med. 2004;32:1114-1121.Hinton RY, Sharma KM. Acute and recurrent patellar instability in the young athlete. Orthop Clin North Am. 2003;34:385-396.Sillanpaa P, et al. Incidence and risk factors of acute traumatic primary patellar dislocation. Med Sci Sports Exerc. 2008;40:606-611.
Acute dislocations 2-3% of knee injuries
2nd most common cause of traumatic hemarthrosis in knee
Stefancin JJ, Parker RD. First-time traumatic patellar dislocation: a systematic review. Clin Orthop Rel Res. 2007;455:93-101.
2/22/2016
2
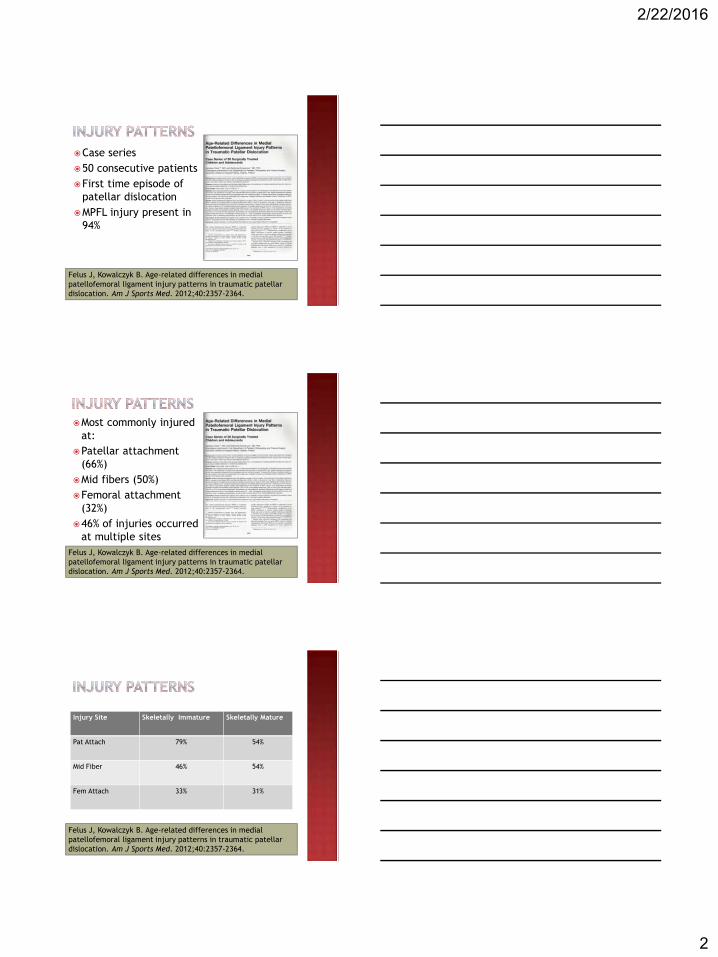
Case series50 consecutive patientsFirst time episode of
patellar dislocationMPFL injury present in
94%
Felus J, Kowalczyk B. Age-related differences in medial patellofemoral ligament injury patterns in traumatic patellar dislocation. Am J Sports Med. 2012;40:2357-2364.
Most commonly injured at:
Patellar attachment (66%)
Mid fibers (50%)Femoral attachment
(32%)46% of injuries occurred
at multiple sites Felus J, Kowalczyk B. Age-related differences in medial patellofemoral ligament injury patterns in traumatic patellar dislocation. Am J Sports Med. 2012;40:2357-2364.
Injury Site Skeletally Immature Skeletally Mature
Pat Attach 79% 54%
Mid Fiber 46% 54%
Fem Attach 33% 31%
Felus J, Kowalczyk B. Age-related differences in medial patellofemoral ligament injury patterns in traumatic patellar dislocation. Am J Sports Med. 2012;40:2357-2364.

2/22/2016
3
Trochlear DysplasiaPatella AltaMPFL Insufficiency
Reider B, et al. The anterior aspect of the knee joint. J Bone Joint Surg Am. 1981; 63:351-356.
Overall = 40%Primary = 17%Repeat = 49%
Maenpaa H, Huhtala H, Lehto MU. Recurrence after patellar dislocation. Redislocation in 37/57 patients followed for 6-24 years. Acta Orthop Scand. 1997;68:424-426.
Once thought to be present in only 29-88% of all knees
Conlan T, Garth WP, Lemons JE. Evaluation of the medial soft-tissue restraints of the extensor mechanism of the knee. J Bone Joint Surg Am. 1993;75:682-693.Reider B, et al. The anterior aspect of the knee joint. J Bone Joint Surg Am. 1981; 63:351-356.
2/22/2016
4
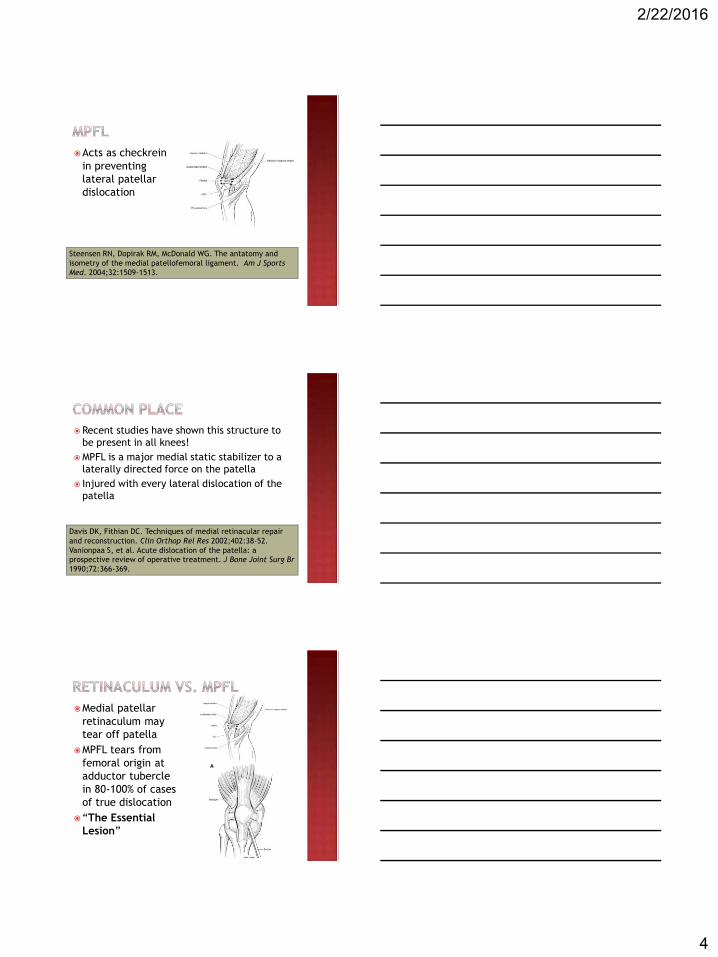
Acts as checkrein in preventing lateral patellar dislocation
Steensen RN, Dopirak RM, McDonald WG. The antatomy and isometry of the medial patellofemoral ligament. Am J Sports Med. 2004;32:1509-1513.
Recent studies have shown this structure to be present in all knees!
MPFL is a major medial static stabilizer to a laterally directed force on the patella
Injured with every lateral dislocation of the patella
Davis DK, Fithian DC. Techniques of medial retinacular repair and reconstruction. Clin Orthop Rel Res 2002;402:38-52.Vanionpaa S, et al. Acute dislocation of the patella: a prospective review of operative treatment. J Bone Joint Surg Br 1990;72:366-369.
Medial patellar retinaculum may tear off patella
MPFL tears from femoral origin at adductor tubercle in 80-100% of cases of true dislocation
“The Essential Lesion”

2/22/2016
5
Primary static restraint to lateral patellar displacement at 20° of knee flexion, contributing 60% of total restraining force.
Medial retinaculum and patellotibial ligaments minimal contributions at 11% and 5% respectively
Desio SM, Burks RT, Bachus KN. Soft tissue restraints to lateral patellar translation in the human knee. Am J Sports Med1998;26:59-65.
55% of passive soft tissue restraint to lateral patellar subluxation
Amis AA. Current concepts on anatomy and biomechanics of patellar stability. Sports Med Arthrosc. 2007;15:48-56.
Primary soft tissue restraint to lateral patellar displacement during low degrees of flexion, when patella has not yet engaged the femoral trochlea
Conlan T, Garth WP Jr, Lemons JE. Evaluation of the medial soft-tissue restraints of the extensor mechanism of the knee. J Bone Joint Surg. 1993;75A(5):682-693.
Desio SM, Burks RT, Bachus KN. Soft tissue restraints to lateral patellar translation in the human knee. Am J Sports Med1998;26:59-65.
Warren LF, Marshall JL, Girgis F. The prime static stabilizer of the medial side of the knee. J Bone Joint Surg. 1974;56(4):665-674.

2/22/2016
6
Numerous biomechanical studies note importance of anatomical placement.
Femoral side importantMinimize graft length changes throughout full
knee range of motion
Steensen RN, Dopirak RM, McDonald WG. The anatomy and isometry of the medial patellofemoral ligament. Implications for reconstruction. Am J Sports Med. 2004;32(6):1509-1513.
Yoo YS, et al. Changes in length of the medial patellofemoralligament. An in vivo analysis using 3-D computed tomography. Am J Sports Med. 2012;40(9):2142-2148.
Elias JJ, Cosgarea AJ. Technical errors during medial patellofemoralligament reconstruction could overload medial patellofemoralcartilage – a computational analysis. Am J Sports Med. 2006;34:1478-1485.
Stephen JM, Lumpaopong P, Deehan DJ, Kader D, Amis AA. The medial patellofemoral ligament-location of femoral attachment and length change patterns resulting from anatomic And nonanatomicattachments. Am J Sports Med. 2012;40:1871-1879.
Bollier M, Fulkerson J, Cosgarea A, Tanaka M. Case report: technical failure of medial patellofemoral ligament reconstruction. Arthroscopy. 2011;27:1153-1159.
MPFL experiences maximal loads at full knee extension or early flexion
Quadriceps femoris neuromuscular activation pulls patella toward femoral trochlea
Bicos J, Fulkerson JP, Amis A. Current concepts review: The medial patellofemoral ligament. Am J Sports Med. 2007;35:484-492.
Desio SM, Burks RT, Bachus KN. Soft tissue restraints to lateral patellar translation in the human knee. Am J Sports Med 1998;26:59-65.
Saveavangse W, Amis AA. The effects of articular, retinacular, or muscular deficiencies on patellofemoral joint stabillity. A biomechanical study in vitro. J Bone Joint Surg Br. 2005;87:577-582.

2/22/2016
7
20 limbs from 17 cadavers
MPFL identified in 66.7%
More commonly found than LPFL
Waligora AC, Johanson NA, Hirsch BE. Clinical anatomy of the quadriceps femoris and extensor apparatus of the knee. ClinOrthop Rel Res 2009;467:3297-3306.
Average width of MPFL 17 mm (range 14-20 mm)
Average width of femoral origin 15.4 mm (range 11-20 mm)
Vertical distance from superior pole of patella to superior portion of MPFL 6.1 mm (range 0-13 mm)
Vertical distance from superior pole of patella to inferior edge of MPFL 23.1 mm (range 15-29 mm)
Waligora AC, Johanson NA, Hirsch BE. Clinical anatomy of the quadriceps femoris and extensor apparatus of the knee. ClinOrthop Rel Res 2009;467:3297-3306.
Main insertion site superior medial aspect of patella
Undersurface of the VMO Aponeurosis of the vastus intermediusMedial undersurface of patella
Conlan T, Garth WP, Lemons JE. Evaluation of the medial soft tissue restraints of the knee. J Bone Joint Surg. 1993;75A:682-693.
Desio SM, Burks RT, Bachus KN. Soft tissue restraints to lateral patellar translation in the human knee. Am J Sports Med. 1998;26:59-65.
Feller JA, Feagin JA, Garrett WE. The medial patellofemoralligament revisited: an anatomical study. Knee Surg Sports Traumatol Arthrosc. 1993;1:184-186.

2/22/2016
8
Attachment to VMO may add active component to ligamentous function
Feller JA, Feagin JA, Garrett WE. The medial patellofemoralligament revisited. An anatomical study. Knee Surg Sports Traumatol Arthrosc. 1993;1:184-186.
Ligament avulsed of medial femoral epicondyle
Healing capacity inconsistent
Salley PI, Poggi J, Speer KP, Garrett WE. Acute dislocation of the patella: a correlative pathoanatomic study. Am J Sports Med. 1996; 24:52-60.
Portion of MPFL extending from inferior aspect patellar attachment to superior aspect of its femoral attachment
Most isometricKnee flexion 0-90 Total change in length 1.1 mm

2/22/2016
9
More than 100 surgical procedures Lateral release Imbrication Distal realignment Anteromedialization of tibial tubercle
Recurrent lateral instability
Excessive lateral translation
Patellar malalignment
PFP not related to instability
PF arthritis

2/22/2016
10
Anywhere from 4-11x as strong as native MPFL
Hammer DL, et al. Hamstring tendon grafts for reconstruction of the anterior cruciate ligament: biomechanical evaluation of the use of multiple strands and tensioning techniques. J Bone Joint Surg Am. 1998;81:549-557.
Load to failure of intact MPFL = 208N
Farr J, Schepsis AA. Reconstruction of the medial patellofemoralligament for recurrent patellar instability. J Knee Surg. 2006;19:307-316.
Mountney J, Senavongse W, Amis AA, Thomas NP. Tensile strength of the medial patellofemoral ligament before and after repair or reconstruction. J Bone Joint Surg Br. 2005;87:36-40.
Almqvist KF, Jan H, Vercruysse C, Berbeeck R, Verdonk R. The tibialis tendon as a valuable anterior cruciate ligament allograft substitute: biomechanical properties. Knee Surg Sports Traumatol Arthrosc. 2007;15:1326-1330.
Sherman SL, et al. Graft tensioning during knee ligament reconstruction: principles and practice. J Am Acad Orthop Surg. 2012;20:633-645.
Quadriceps tendonLoad to failure
strength of QT = 205N
Native MPFL 190N
Herbort M, et al. MPFL reconstruction using quadriceps tendon graft. Part 1: Biomechanical properties of QT MPFL reconstruction in comparison to intact MPFL. Cadaveric study. Knee, 2014.
2/22/2016
11
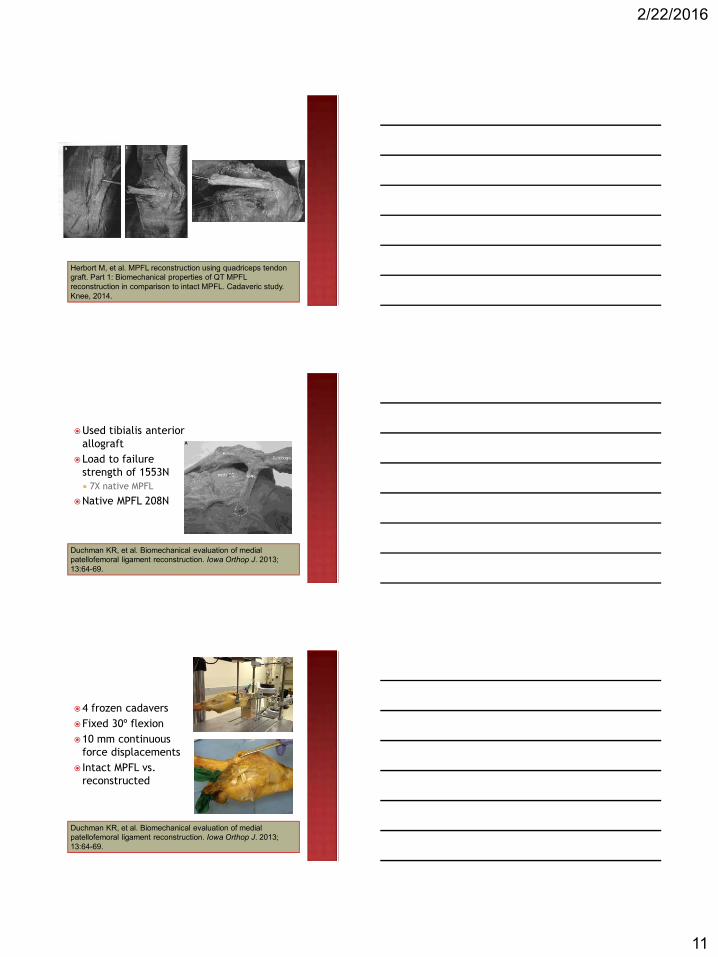
Herbort M, et al. MPFL reconstruction using quadriceps tendon graft. Part 1: Biomechanical properties of QT MPFL reconstruction in comparison to intact MPFL. Cadaveric study. Knee, 2014.
Used tibialis anterior allograft
Load to failure strength of 1553N 7X native MPFL
Native MPFL 208N
Duchman KR, et al. Biomechanical evaluation of medial patellofemoral ligament reconstruction. Iowa Orthop J. 2013; 13:64-69.
4 frozen cadaversFixed 30º flexion10 mm continuous
force displacements Intact MPFL vs.
reconstructed
Duchman KR, et al. Biomechanical evaluation of medial patellofemoral ligament reconstruction. Iowa Orthop J. 2013; 13:64-69.

2/22/2016
12
Duchman KR, et al. Biomechanical evaluation of medial patellofemoral ligament reconstruction. Iowa Orthop J. 2013; 13:64-69.
Based upon Available science Type of graft Patellofemoral biomechanics Ligament biomechanics Soft tissue healing constraints Clinical experience Evolving

2/22/2016
13
Protect repairDecrease pain/inflammationPrevent (-) effects of immobilizationRestore normal arthrokinematicsPrevent hypomobilityPromote dynamic stabilityPrevent reflex inhibitionDevelop neuromuscular control
EMG data based on studies of surrounding hip musculature
Hierarchy based on MVIC data of normal individuals
Bolgla LA, Uhl TL. Electromyographic analysis of hip rehabilitation exercises in a group of healthy subjects. J OrthopSports Phys Ther. 2005;35(8):487-494.
Ayotte NW, Stetts DM, Keenan G, Greenway EH. Electromyographical analysis of selected lower extremity muscles during 5 unilateral weight bearing exercises. J OrthopSports Phys Ther. 2007;37(2):48-55.

2/22/2016
14
Ekstrom RA, Donatelli RA, Carp KC. Electromyographic analysis of core, trunk, hip and thigh muscles during 9 rehabilitation exercises. J Orthop Sports Phys Ther. 2007;37(12):754-762.
Distefano L, Blackburn JT, Marshall SW, Padu DA. Gluteal muscle activation during common therapeutic exercises. J Orthop Sports Phys Ther. 2009;39(7):532-540.

2/22/2016
15
Kendall FP, et al: Muscle Testing and Function with Posture and Pain. 5th ed. Lippincott Williams and Wilkins, 2005.
Kendall FP, et al: Muscle Testing and Function with Posture and Pain. 5th ed. Lippincott Williams and Wilkins, 2005.
Kendall FP, et al: Muscle Testing and Function with Posture and Pain. 5th ed. Lippincott Williams and Wilkins, 2005.
2/22/2016
16
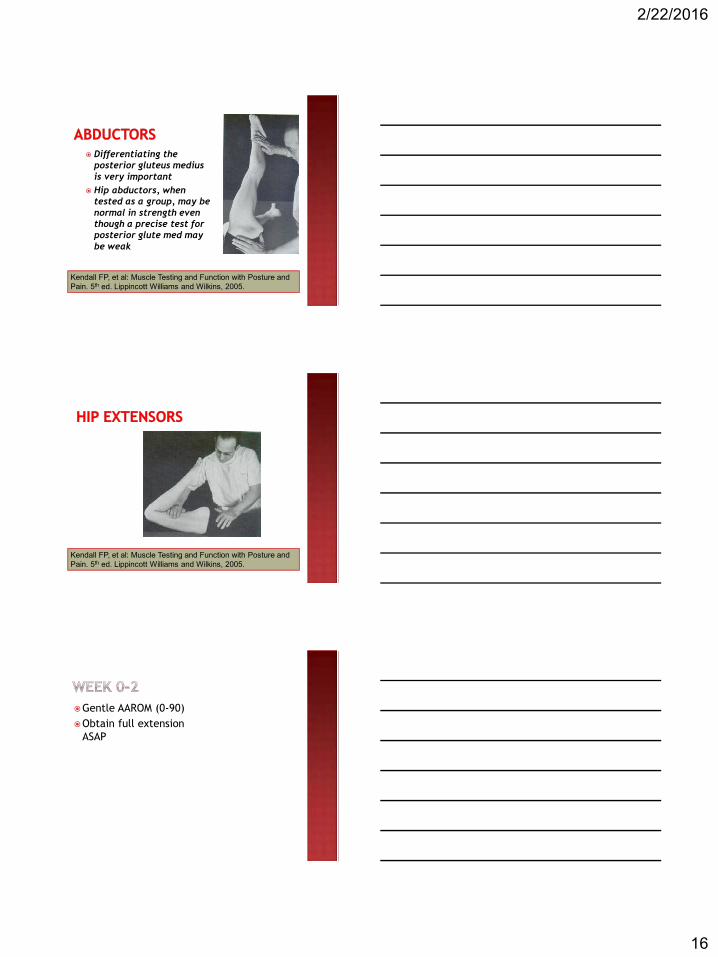
Differentiating the posterior gluteus medius is very important
Hip abductors, when tested as a group, may be normal in strength even though a precise test for posterior glute med may be weak
Kendall FP, et al: Muscle Testing and Function with Posture and Pain. 5th ed. Lippincott Williams and Wilkins, 2005.
Kendall FP, et al: Muscle Testing and Function with Posture and Pain. 5th ed. Lippincott Williams and Wilkins, 2005.
Gentle AAROM (0-90)Obtain full extension
ASAP
2/22/2016
17
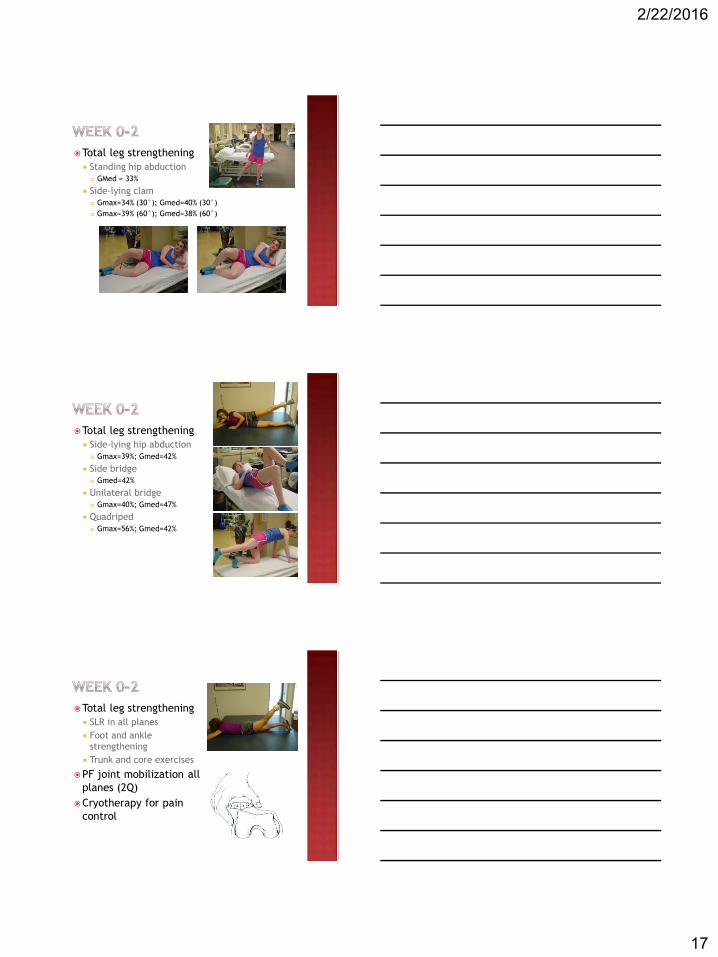
Total leg strengthening Standing hip abduction
GMed = 33%
Side-lying clam Gmax=34% (30°); Gmed=40% (30°) Gmax=39% (60°); Gmed=38% (60°)
Total leg strengthening Side-lying hip abduction
Gmax=39%; Gmed=42%
Side bridge Gmed=42%
Unilateral bridge Gmax=40%; Gmed=47%
Quadriped Gmax=56%; Gmed=42%
Total leg strengthening SLR in all planes Foot and ankle
strengthening Trunk and core exercises
PF joint mobilization all planes (2Q)
Cryotherapy for pain control

2/22/2016
18
Progress knee motion to 0-120 degrees
Continue cryotherapy prn
Begin CKC exercises Kinesthetic awareness
trainer Single leg balance
exercises Limited arc leg press Limited arc Total Gym
Begin CKC exercises Retro step up
Gmax=59% Gmed 37%
Lateral step up Gmax=56% Gmed=43%

2/22/2016
19
Begin CKC exercises Forward lunge
Gmax=44% Gmed=42%
Forward step up Gmax=74% Gmed=44%
Begin CKC exercises Sideways lunge
Gmax=41% Gmed 39%
Transverse lunge Gmax=49% Gmed=48%
Begin CKC exercises Pelvic drop
Gmax=NA Gmed=57%
Single-leg deadlift Gmax=59% Gmed=58%
Lateral band walks Gmax=27% Gmed=61%
Single leg wall squats Gmax=86% Gmed 52%

2/22/2016
20
Return to light work activities
Continue to improve ROM to full after 5-6 weeks
Full ROM should be achieved by week 10-12
Week 1-2 0-45 flexion
Week 3-4 0-90 flexion
Week 5-6 0-120 flexion
Xie G, et al. Medial patellofemoral ligament reconstruction using semitendinosus tendons. Am J Sports Med. 2012;40:1365-1374.
Advance exercises to: Mini squats Mini lunge Hamstring curls Single leg squats
Gmax=59% Gmed=64%

2/22/2016
21
Progressively store ROM*Full by week 12Maintain repairProgressively restore motion, strength and balance
Continue to progress motion
Exercise progression Submaximal to maximal Double leg to single leg Eyes open to eyes closed Slow speeds to fast speeds
Advanced exercises BOSU/ Dynadisc lunges BOSU/ Dynadisc step-overs

2/22/2016
22
Full non painful AROM/PROM
Restoration of strength, power and endurance
No pain or tendernessFull
balance/proprioceptionGradual initiation into
functional activities
Progress intensity and decrease repetitions of exercises
Advance to: Double-leg jump in place Double-leg jumping multiple planes Single-leg hopping in place Light functional plyometric activities
Advance Exercises Forward hop
Gmax=35% Gmed=45%
Sideways hop Gmax=30% Gmed=57%
Transverse hop Gmax=35% Gmed=58%

2/22/2016
23
Full strength, power, and endurance
Maintain knee motionMaintain balance and
proprioceptionProgress functional
activitiesReturn to unrestricted
sports activities
Continue previous exercise
Advance to: Single-leg plyo’s
Sports specific training Interval sports programs Jogging Swimming Basketball Baseball
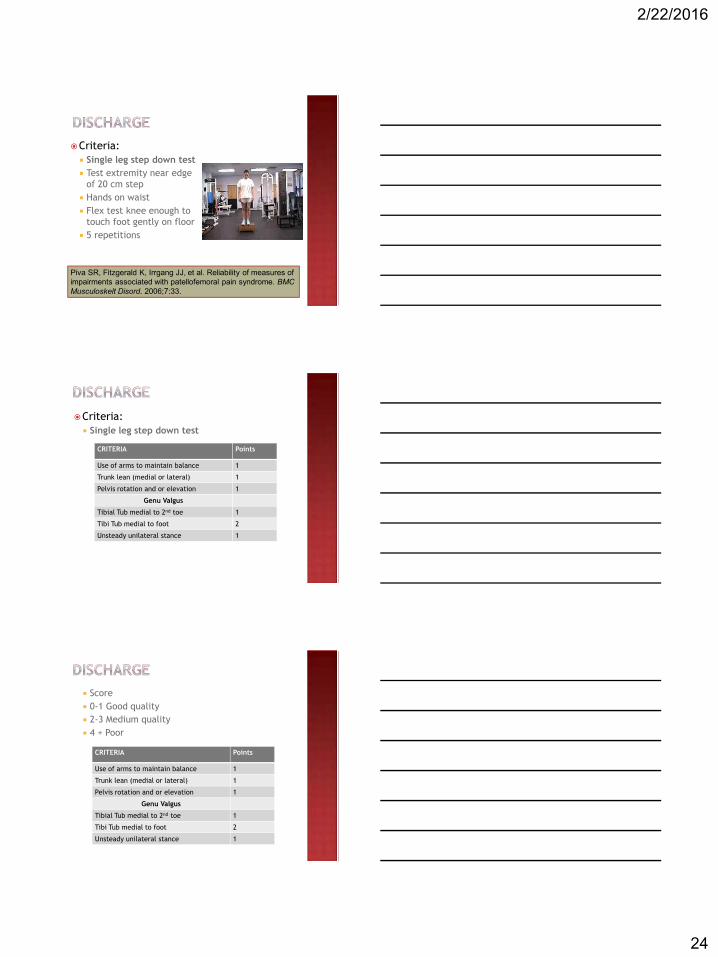
Criteria: Full LE strength Full ROM Functional tests
Single leg step down
Piva SR, Fitzgerald K, Irrgang JJ, et al. Reliability of measures of impairments associated with patellofemoral pain syndrome. BMCMusculoskelt Disord. 2006;7:33.
2/22/2016
24
Criteria: Single leg step down test Test extremity near edge
of 20 cm step Hands on waist Flex test knee enough to
touch foot gently on floor 5 repetitions
Piva SR, Fitzgerald K, Irrgang JJ, et al. Reliability of measures of impairments associated with patellofemoral pain syndrome. BMCMusculoskelt Disord. 2006;7:33.
Criteria: Single leg step down test
CRITERIA Points
Use of arms to maintain balance 1
Trunk lean (medial or lateral) 1
Pelvis rotation and or elevation 1
Genu Valgus
Tibial Tub medial to 2nd toe 1
Tibi Tub medial to foot 2
Unsteady unilateral stance 1
Score 0-1 Good quality 2-3 Medium quality 4 + Poor
CRITERIA Points
Use of arms to maintain balance 1
Trunk lean (medial or lateral) 1
Pelvis rotation and or elevation 1
Genu Valgus
Tibial Tub medial to 2nd toe 1
Tibi Tub medial to foot 2
Unsteady unilateral stance 1
2/22/2016
25
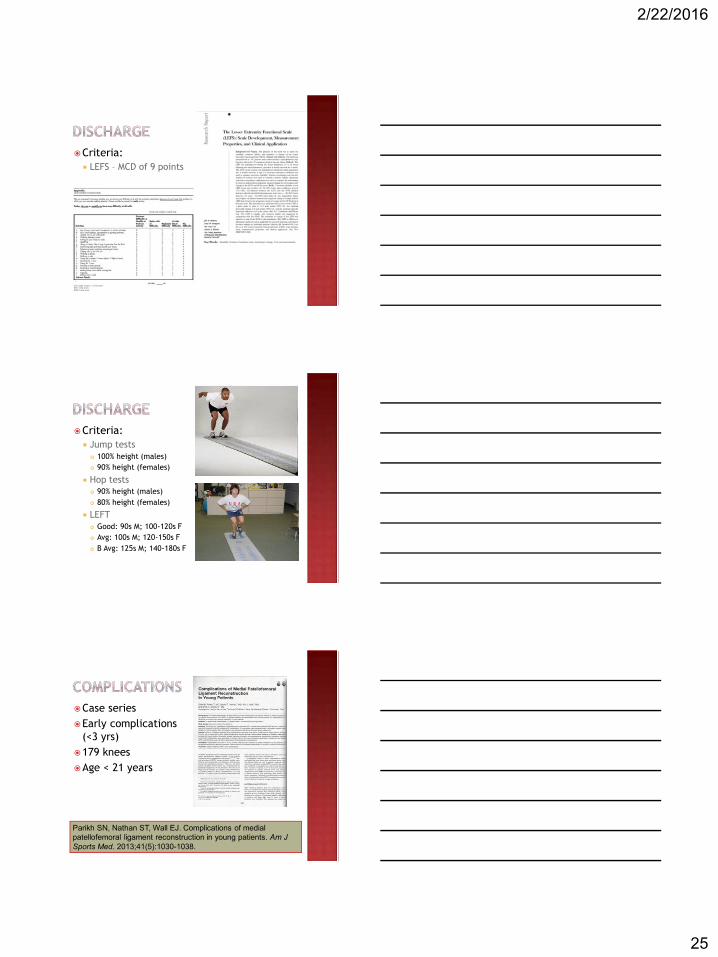
Criteria: LEFS – MCD of 9 points
Criteria: Jump tests
100% height (males) 90% height (females)
Hop tests 90% height (males) 80% height (females)
LEFT Good: 90s M; 100-120s F Avg: 100s M; 120-150s F B Avg: 125s M; 140-180s F
Case seriesEarly complications
(<3 yrs)179 kneesAge < 21 years
Parikh SN, Nathan ST, Wall EJ. Complications of medial patellofemoral ligament reconstruction in young patients. Am J Sports Med. 2013;41(5):1030-1038.

2/22/2016
26
38 complications (16.2%)34 major; 4 minorRecurrent lateral instability Knee motion stiffness and flexion
deficitsPatellar fractures Patellar arthrosis and pain
Parikh SN, Nathan ST, Wall EJ. Complications of medial patellofemoral ligament reconstruction in young patients. Am J Sports Med. 2013;41(5):1030-1038.
Surgery and understanding of pathology continues to evolve.
Rehabilitation respect healing constraints
But…. Not at
expense of stiffness
2-4 weeks Off assistive device Good quadriceps tone
10-12 weeks Full knee ROM
16 weeks Functional activities
20+ weeks Discharge with full
return of activities

2/22/2016
27
Compared MPFL vs non operative treatment
39 patients/41 kneesAcute dislocations Randomized into 2 groupsMin follow-up 2 yearsNon op 7 redislocationsMPFL 0 redislocationsKujala score significantly
lower in non op group
Bitar AC, et al. Traumatic patellar dislocation. Nonoperativetreatment compared with MPFL reconstruction using patellar tendon. Am J Sports Med. 2012;40:114-122.

1
Knee Osteoarthritis
Robert C. Manske PT,DPT, MEd, SCS, ATC, CSCSRobert C. Manske PT,DPT, MEd, SCS, ATC, CSCSProfessor and Chair Professor and Chair
Wichita State Department of Physical TherapyWichita State Department of Physical TherapyVia Christi Health Sports and Orthopedic Physical TherapyVia Christi Health Sports and Orthopedic Physical Therapy
Wichita, KS
OSTEOARTHRITISThe most prevalent form of arthritis, The most prevalent form of arthritis, with an associated risk of mobility with an associated risk of mobility disability (defined as needing help disability (defined as needing help
walking or climbing stairs) for those walking or climbing stairs) for those with affected knees.
Greater than that due to any other Greater than that due to any other medical condition in people age > 65
Insertion of coronary artery stents:
Insertion of coronary artery stents: 454,000
454,000 Coronary artery bypass graft:
Coronary artery bypass graft:395,000
395,000 Total knee replacement:
Total knee replacement: 719,000
719,000 Total hip replacement:
Total hip replacement:332,000
Source: CDC NCHS Fast Statistics 2015 Datahttp://www.cdc.gov/nchs/fastats/insurg.htm
Knee OA one of most Knee OA one of most Knee OA one of most common joint disorders common joint disorders and causes considerable and causes considerable pain and immobility.
pain and immobility. Most knee OA is in the Most knee OA is in the Most knee OA is in the
medial compartment
Felson DT, Zhang Y. An update on the epidemiology of knee and hip osteoarthritis with a view to prevention. Arthritis Rheum. 1998;41:1343-1355.Cooke TD, et al. Analysis of limb alignment in the pathogenesis of osteoarthritis: a comparison of Saudi Arabian and Canadian cases. Rheumatol Int. 2002;22:160-164.
Knee OA Symptoms Pain Muscle weakness Swelling
SwellingSwelling Stiffness Limited ROM Joint deformity
Wei IP, Hsu WC, Chien HL, et al. Leg and joint stiffness in patients with bilateral medial knee osteoarthritis during level walking. J Mech. 2009;25(3):279-287.

2
Knee OA Effective nonEffective non-Effective non-pharmacological & Effective nonEffective nonEffective nonEffective non pharmacological & pharmacological & pharmacological &
pharmacological treatments available for pharmacological treatments available for OA
Conservative Pharmacological Surgery
Knee OA Current thought holds that OA involves Current thought holds that OA involves Current thought holds that OA involves
entire joint organ, including:
entire joint organ, including:Subchondral
entire joint organ, including:entire joint organ, including:SubchondralSubchondral bone
Meniscus Ligaments
LigamentsLigamentsMuscleCapsule
CapsuleCapsuleSynovium
Felson D. N Engl J Med 2006;354:841-848
Osteoarthritis of the Medial Side of the Knee
Felson D. N Engl J Med 2006;354:841-848
Radiograph Showing Osteoarthritis of the Medial Side of the Knee
Knee OA Systematic Factors
Systematic Factors Increasing age
Increasing ageIncreasing ageFemale sexNutritional deficiencies
Knee OA Local mechanical factors put people at risk
Local mechanical factors put people at riskMalalignment
MalalignmentMalalignmentMuscle weaknessAlteration of structural integrity
3
Knee OA Joint loading can be affected by obesity and Joint loading can be affected by obesity and Joint loading can be affected by obesity and
joint injury
Risk Factors Multifactorial
Age
AgeAge Family history
Family historyFamily history Certain work Obesity
ObesityObesity Muscle weakness Previous trauma
Arden N, Vevitt MC. Osteoarthritis: epidemiology. Best Pract Res ClinRheumatol. 2006;20:3-25.
Elite Athletes Prevalence of hip and Prevalence of hip and Prevalence of hip and
knee OA or knee OA or arthroplasty
arthroplasty709 former male elite 709 former male elite
athletes Median age 70 years
Median age 70 yearsMedian age 70 years 1368 age matched 1368 age matched
controls.
Tveit M, et al. Former male elite athletes have a higher prevalence of osteoarthritis and arthroplasty in the hip and knee than expected. Am J Sports Med. 2012;40:527-533.
Elite Athletes Risk of OA or Risk of OA or arthroplastyarthroplasty higher.
arthroplastyarthroplastyarthroplasty Risk of hip OA doubled.
Risk of hip OA doubled.Risk of hip OA doubled. Risk of hip
Risk of hip OA doubled.Risk of hip OA doubled.Risk of hip Risk of hip arthroplastyRisk of hip OA doubled.
arthroplastyarthroplasty 2.5x higher.
Risk of hip Risk of hip Risk of hip arthroplastyarthroplasty Risk of knee OA or
arthroplastyarthroplasty 2.5x higher.2.5x higher.arthroplastyRisk of knee OA or Risk of knee OA or arthroplasty
2.5x higher.2.5x higher.arthroplastyarthroplasty 1.5x Risk of knee OA or Risk of knee OA or
higher .
Tveit M, et al. Former male elite athletes have a higher prevalence of osteoarthritis and arthroplasty in the hip and knee than expected. Am J Sports Med. 2012;40:527-533.
Recommended Treatment Algorithm
Osteoarthritis: Knee Criteria*Clinical and Lab Clinical and Imaging Clinical
Knee Pain and Knee Pain and Knee Pain and5 or more of these: One or more of these: 3 or more of these:Age > 50 Age > 50 Age > 50Stiffness < 30 min Stiffness < 30 min Stiffness < 30 minCrepitus Crepitus CrepitusBony tenderness Plus osteophytes on
imagingBony tenderness
Bony enlargement Bony enlargementNo palpable warmth No palpable warmthESR < 40 mm/hourRF < 1:40Synovial signs OA
Altman et al. The ACR criteria for the classification and reporting of osteoarthritis of the knee. Arthritis and Rheumatism, 1986;29:1039-49.

4
Osteoarthritis: Knee Criteria Knee ACR criteria
Clinical and Lab Sensitivity 92%
Sensitivity 92%Sensitivity 92%Specificity 75%
• Knee ACR criteria– Clinical and Imaging
• Sensitivity 91%• Specificity 86%
• Knee ACR criteria– Clinical
• Sensitivity 95%• Specificity 69%
Non Surgical Treatment
Rehabilitation Dilemma Importance of cartilage undisputed
Importance of cartilage undisputedImportance of cartilage undisputed Avascular
Importance of cartilage undisputedImportance of cartilage undisputedAvascularAvascular nature complicates pathology*
nature complicates pathology*nature complicates pathology* No real hemorrhage or fibrin clot formation No real hemorrhage or fibrin clot formation – No real hemorrhage or fibrin clot formation No real hemorrhage or fibrin clot formation
no inflammatory response
no inflammatory response Minimal potential for regeneration
Minimal potential for regenerationMinimal potential for regeneration PROMOTE HEALING: DO NOT PROMOTE HEALING: DO NOT PROMOTE HEALING: DO NOT
OVERLOAD TISSUE
Alford SW, Cole BJ. Cartilage restoration, Part 1. Basic science, historical perspective, patient evaluation, and treatment options. Am J Sports Med 2005;33(2):295-306.
Rehabilitation Rest Analgesics
AnalgesicsAnalgesics PT
AnalgesicsPT PT –AnalgesicsAnalgesicsAnalgesics
– useful for strengthening and increasing ROM
useful for strengthening and increasing ROMuseful for strengthening and increasing ROM No evidence that PT heals
useful for strengthening and increasing ROMuseful for strengthening and increasing ROMNo evidence that PT heals No evidence that PT heals articular
useful for strengthening and increasing ROMuseful for strengthening and increasing ROMarticulararticular cartilage in No evidence that PT heals No evidence that PT heals
humans
Angel MJ, Sgaglione NA, Latterman C. Articular cartilage lesions/osteoarthritis. Orthopedic Knowledge Update: Sports Medicine 4. AAOS, 2009.
Rehabilitation Exercise Animal studies Exercised horses and dogs
Exercised horses and dogsExercised horses and dogs Cartilage stiffer, thicker, and greater concentration Cartilage stiffer, thicker, and greater concentration Cartilage stiffer, thicker, and greater concentration
of Cartilage stiffer, thicker, and greater concentration Cartilage stiffer, thicker, and greater concentration of of proteoglycanCartilage stiffer, thicker, and greater concentration Cartilage stiffer, thicker, and greater concentration
proteoglycanproteoglycan than nonCartilage stiffer, thicker, and greater concentration
than nonthan non-Cartilage stiffer, thicker, and greater concentration Cartilage stiffer, thicker, and greater concentration Cartilage stiffer, thicker, and greater concentration
than nonthan non-exercised animals French DA, Barber SM, Leach DH, Doige CE. The effect of exercise on healing of articular cartilage defects in the equine carpus. Vet Surg. 1989;18:312-321.
Jurvelin J, et al. Effect of physical exercise in indention stiffness of articular cartilage in the canine knee. Int J Sports Med. 1986;7:106-110.
Kiviranta I, et al. Moderate running exercise augments glycosaminoglycans and thickness of articular cartilage in the knee joint of young beagle dogs. J Orthop Res. 1988;6:188-195.
Oettmeier R, et al. Quantitative study of articular cartilage and subchondral bone remodeling in the knee joint of dogs after strenuous running training. J Bone Miner Res. 1992;7(Suppl):419-424.
Controversial Steroid injections
Steroid injectionsSteroid injections Hyaluronic
Steroid injectionsSteroid injectionsHyaluronicHyaluronic acid
HyaluronicHyaluronicHyaluronic Glucosamine ChondroitinChondroitinChondroitin Sulfate
May provide temporary pain relief!
May provide temporary pain relief!May provide temporary pain relief! No evidence that support application for focal No evidence that support application for focal No evidence that support application for focal
defectsAngel MJ, Sgaglione NA, Latterman C. Articular cartilage lesions/osteoarthritis. Orthopedic Knowledge Update: Sports Medicine 4. AAOS, 2009.

5
Glucosamine Chondroitin
2003-2006 GAIT NIH Study Glucosamine / Glucosamine / ChondroitinChondroitin Arthritis MultiArthritis Multi-Arthritis Multi-Center Glucosamine / Glucosamine / ChondroitinChondroitin
Intervention Trial Compared 5 groups ( approx. N=300 each)
Compared 5 groups ( approx. N=300 each) Placebo Celebrex® (Celebrex® (celecoxibcelecoxib)
Celebrex® (Celebrex® (Celebrex® ( ) 1500 mg of glucosamine hydrochloride daily
1500 mg of glucosamine hydrochloride daily 1200 mg of
1500 mg of glucosamine hydrochloride daily1500 mg of glucosamine hydrochloride daily1200 mg of 1200 mg of chondroitin1500 mg of glucosamine hydrochloride daily1500 mg of glucosamine hydrochloride daily
chondroitinchondroitin sulfate daily
1200 mg of 1200 mg of sulfate dailysulfate daily The above two in combination
Clegg DO, et al. Glucosamine, chondroitin sulfate, and the two in combination for painful knee arthritis. NEJM. 2006;354:795-808.
The GAIT NIH Study Glucosamine and Glucosamine and chondroitinchondroitin sulfate were not Glucosamine and Glucosamine and Glucosamine and chondroitinchondroitinchondroitin sulfate were not sulfate were not
significantly better than placebo in reducing significantly better than placebo in reducing knee pain by 20 percent
knee pain by 20 percent Response to placebo (60%)
Response to placebo (60%) Rate of response to glucosamine was 3.9% higher than Rate of response to glucosamine was 3.9% higher than
placebo
placebo Rate of response to Rate of response to chondroitinchondroitin sulfate was 5.3% higher
Rate of response to Rate of response to sulfate was 5.3% highersulfate was 5.3% higher Rate of response to combined treatment was 6.5% Rate of response to combined treatment was 6.5%
higher
higher Rate of response to Celebrex was 10% higher
Clegg DO, et al. Glucosamine, chondroitin sulfate, and the two in combination for painful knee arthritis. NEJM. 2006;354:795-808.
Clegg et al, NEJM, 2006
9/29/08 NICAM Headline
Dietary Supplements Glucosamine and/or Dietary Supplements Glucosamine and/or Dietary Supplements Glucosamine and/or ChondroitinDietary Supplements Glucosamine and/or Dietary Supplements Glucosamine and/or ChondroitinChondroitin Fare No Better than Placebo in ChondroitinChondroitin Fare No Better than Placebo in Fare No Better than Placebo in Slowing Structural Damage of Knee Slowing Structural Damage of Knee Osteoarthritis
Extension of Original GAIT study

6
The GAIT NIH Study
“On the basis of the results from GAIT, “On the basis of the results from GAIT, “On the basis of the results from GAIT,
it seems prudent to tell our patients with it seems prudent to tell our patients with symptomatic osteoarthritis of the knee symptomatic osteoarthritis of the knee that neither glucosamine hydrochloride that neither glucosamine hydrochloride nor that neither glucosamine hydrochloride that neither glucosamine hydrochloride nor nor chondroitinthat neither glucosamine hydrochloride that neither glucosamine hydrochloride
chondroitinchondroitin sulfate alone has been nor nor chondroitinchondroitinchondroitin sulfate alone has been sulfate alone has been shown to be more efficacious than shown to be more efficacious than
placebo for the treatment of knee pain.”
The GAIT NIH Study
“If patients choose to take dietary “If patients choose to take dietary “If patients choose to take dietary
supplements to control their symptoms, supplements to control their symptoms, they should be advised to take they should be advised to take glucosamine sulfate rather than glucosamine sulfate rather than glucosamine hydrochloride and, for glucosamine hydrochloride and, for those with severe pain, that taking those with severe pain, that taking chondroitinthose with severe pain, that taking those with severe pain, that taking chondroitinchondroitin sulfate with glucosamine chondroitinchondroitin sulfate with glucosamine sulfate with glucosamine sulfate may have an additive effect.”
The GAIT NIH Study
“Three months of treatment is a “Three months of treatment is a
sufficient period for the sufficient period for the evaluation of efficacy; if there is evaluation of efficacy; if there is
no clinically significant no clinically significant decrease in symptoms by this decrease in symptoms by this
time, the supplements should be time, the supplements should be discontinued”
“Most positive studies regarding “Most positive studies regarding “Most positive studies regarding
viscosupplementation“Most positive studies regarding “Most positive studies regarding
viscosupplementationviscosupplementation may be viscosupplementationviscosupplementation may be may be the result of a robust placebo the result of a robust placebo
effect”
Chen AL, Mears SC, Hawkins RJ. Orthopaedic care of the aging athlete. J Am Aca Orthop Surg 2005;13(6):407-416.
HochberbM, et al. Combined chondroitin sulfate and glucosamine for painful knee osteoarthritis; a multicenter, randomized, double-blind, non-inferiority trial versus celecoxib. Ann Rheum Dis. 2016;75:37-44.
HochberbM, et al. Combined chondroitin sulfate and glucosamine for painful knee osteoarthritis; a multicenter, randomized, double-blind, non-inferiority trial versus celecoxib. Ann Rheum Dis. 2016;75:37-44.

7
HochberbM, et al. Combined chondroitin sulfate and glucosamine for painful knee osteoarthritis; a multicenter, randomized, double-blind, non-inferiority trial versus celecoxib. Ann Rheum Dis. 2016;75:37-44.
HochberbM, et al. Combined chondroitin sulfate and glucosamine for painful knee osteoarthritis; a multicenter, randomized, double-blind, non-inferiority trial versus celecoxib. Ann Rheum Dis. 2016;75:37-44.
HochberbM, et al. Combined chondroitin sulfate and glucosamine for painful knee osteoarthritis; a multicenter, randomized, double-blind, non-inferiority trial versus celecoxib. Ann Rheum Dis. 2016;75:37-44.
ChondrotinChondrotin + ChondrotinChondrotinChondrotin + + Glucosamine has a Glucosamine has a compableGlucosamine has a Glucosamine has a compablecompable efficacy to compablecompable efficacy to efficacy to Celebrex in reducing Celebrex in reducing pain, stiffness, functional pain, stiffness, functional limitation and joint limitation and joint swelling/effusion after 6 swelling/effusion after 6 months in patients with months in patients with painful knee OA.
Knee Unloading Braces
Valgus Bracing for Knee DJD
Medial compartment Medial compartment Medial compartment most frequently affected
most frequently affected PF joint second most PF joint second most PF joint second most
common
common Medial compartment Medial compartment Medial compartment
narrowing seen as bownarrowing seen as bownarrowing seen as bow-narrowing seen as bownarrowing seen as bowlegged or narrowing seen as bownarrowing seen as bownarrowing seen as bownarrowing seen as bowlegged or varuslegged or legged or legged or legged or varusvarusvarusvarusdeformity
Valgus Bracing for Knee DJD Pros:
Decreased pain
Decreased painDecreased pain Improved symmetry
Improved symmetryImproved symmetry Improved
Improved symmetryImproved symmetryImproved Improved proprioception
Improved Improved Cons:
Cons: Works better in patients Works better in patients Works better in patients
with a lower BMI
with a lower BMI Compliance
ComplianceCompliance Transfer of brace force may Transfer of brace force may Transfer of brace force may
cause pain
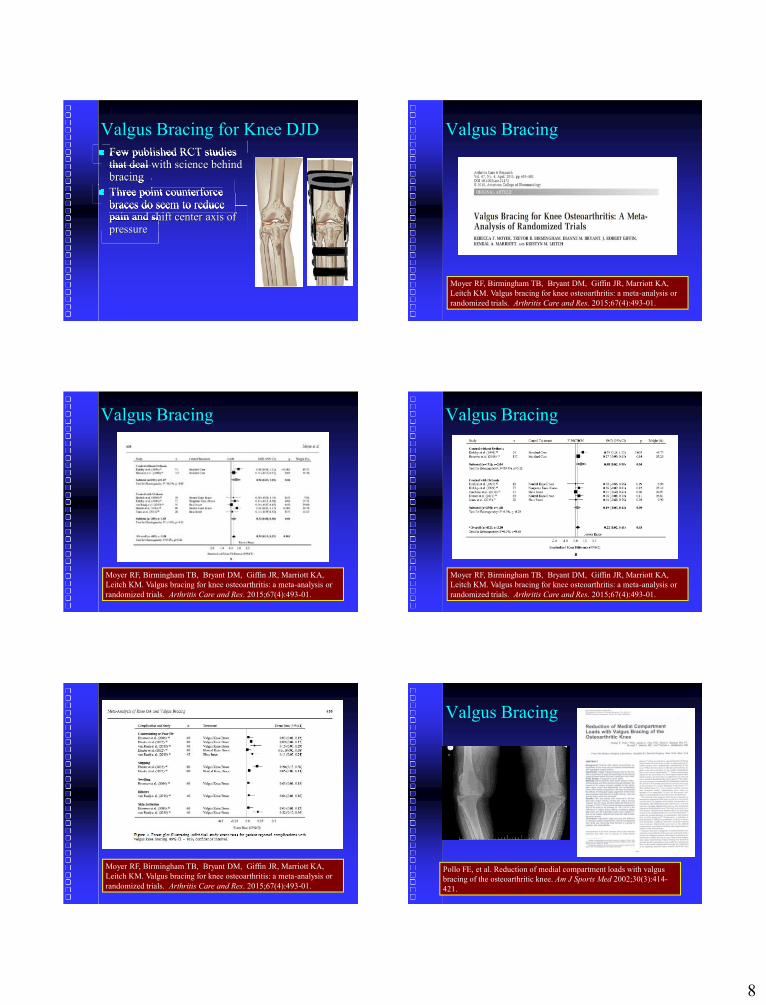
8
Valgus Bracing for Knee DJD Few published RCT studies Few published RCT studies Few published RCT studies
that deal with science behind that deal with science behind that deal with science behind bracing
bracing Three point counterforce Three point counterforce Three point counterforce
braces do seem to reduce braces do seem to reduce braces do seem to reduce pain and shift center axis of pain and shift center axis of pain and shift center axis of pressure
Valgus Bracing
Moyer RF, Birmingham TB, Bryant DM, Giffin JR, Marriott KA, Leitch KM. Valgus bracing for knee osteoarthritis: a meta-analysis or randomized trials. Arthritis Care and Res. 2015;67(4):493-01.
Valgus Bracing
Moyer RF, Birmingham TB, Bryant DM, Giffin JR, Marriott KA, Leitch KM. Valgus bracing for knee osteoarthritis: a meta-analysis or randomized trials. Arthritis Care and Res. 2015;67(4):493-01.
Valgus Bracing
Moyer RF, Birmingham TB, Bryant DM, Giffin JR, Marriott KA, Leitch KM. Valgus bracing for knee osteoarthritis: a meta-analysis or randomized trials. Arthritis Care and Res. 2015;67(4):493-01.
Moyer RF, Birmingham TB, Bryant DM, Giffin JR, Marriott KA, Leitch KM. Valgus bracing for knee osteoarthritis: a meta-analysis or randomized trials. Arthritis Care and Res. 2015;67(4):493-01.
Valgus Bracing
Pollo FE, et al. Reduction of medial compartment loads with valgus bracing of the osteoarthritic knee. Am J Sports Med 2002;30(3):414-421.
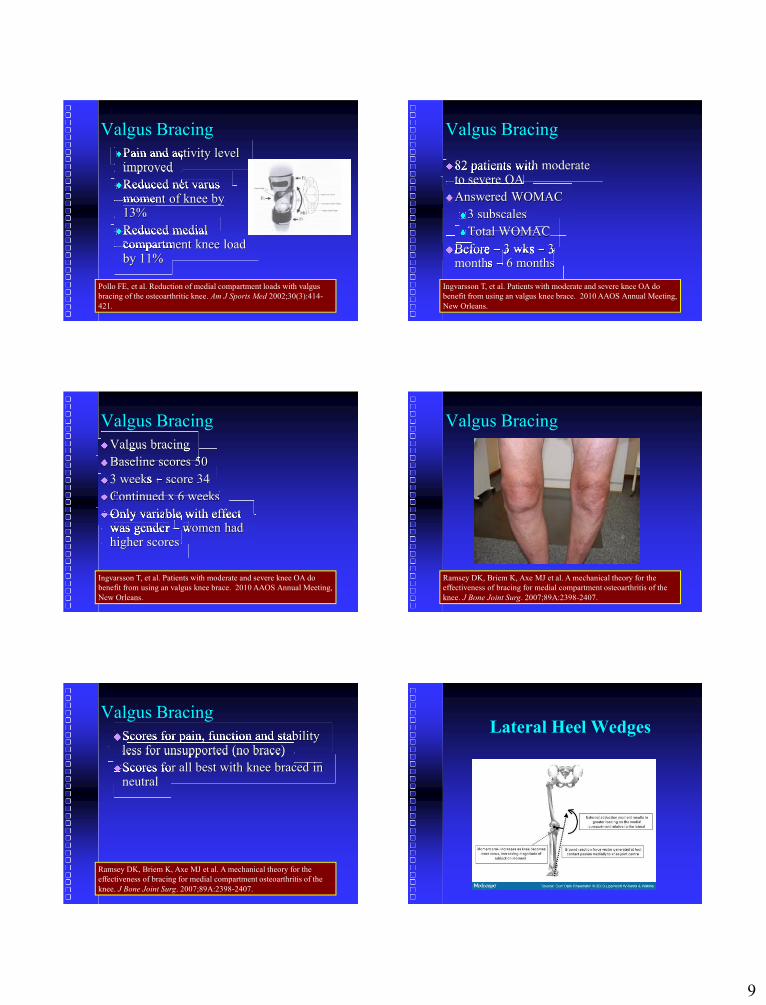
9
Valgus BracingPain and activity level Pain and activity level Pain and activity level
improved
improvedReduced net varus Reduced net varus Reduced net varus
moment of knee by moment of knee by moment of knee by 13%
Reduced medial Reduced medial Reduced medial compartment knee load compartment knee load compartment knee load by 11%
Pollo FE, et al. Reduction of medial compartment loads with valgus bracing of the osteoarthritic knee. Am J Sports Med 2002;30(3):414-421.
Valgus Bracing
82 patients with moderate 82 patients with moderate 82 patients with moderate to severe OA
to severe OAAnswered WOMAC
3 subscales
Total WOMAC
Before Before Before –– 3 wks 3 wks 3 wks –– 3 Before Before Before months Before months months –
3 wks 3 wks 3 3 3 wks 3 wks 3 wks –– 6 months
Ingvarsson T, et al. Patients with moderate and severe knee OA do benefit from using an valgus knee brace. 2010 AAOS Annual Meeting, New Orleans.
Valgus BracingValgus bracing
Valgus bracingValgus bracingBaseline scores 50
3 weeks 3 weeks 3 weeks –– score 34
Continued x 6 weeks
Only variable with effect Only variable with effect Only variable with effect was gender Only variable with effect was gender –Only variable with effect Only variable with effect Only variable with effect
– women had was gender was gender was gender was gender women had women had women had women had higher scores
Ingvarsson T, et al. Patients with moderate and severe knee OA do benefit from using an valgus knee brace. 2010 AAOS Annual Meeting, New Orleans.
Valgus Bracing
Ramsey DK, Briem K, Axe MJ et al. A mechanical theory for the effectiveness of bracing for medial compartment osteoarthritis of the knee. J Bone Joint Surg. 2007;89A:2398-2407.
Valgus BracingScores for pain, function and stability Scores for pain, function and stability Scores for pain, function and stability
less for unsupported (no brace)
less for unsupported (no brace)Scores for all best with knee braced in Scores for all best with knee braced in Scores for all best with knee braced in
neutral
Ramsey DK, Briem K, Axe MJ et al. A mechanical theory for the effectiveness of bracing for medial compartment osteoarthritis of the knee. J Bone Joint Surg. 2007;89A:2398-2407.
Lateral Heel Wedges

10
Lateral Heel Wedges Pros:
Safe Easy to dispense
Easy to dispenseEasy to dispenseCost effective
Cons:Adherence
Doesn’t work if individual Doesn’t work if individual Doesn’t work if individual has ankle instability
Lateral Heel Wedges Use of lateral wedge Use of lateral wedge Use of lateral wedge
shifts distribution of shifts distribution of shifts distribution of load in the foot load in the foot load in the foot laterally
laterally Causes lateral shift of Causes lateral shift of Causes lateral shift of
load across knee joint
load across knee joint Unloads medial Unloads medial Unloads medial
compartment
Yasuda K, Sasaki T. The mechanics of treatment of osteoarthritic knees with a wedged insole. Clin Orthop Relat Res. 1987;221:181-187.
Lateral Heel Wedges - RCT
Pham et al. Laterally elevated wedged insoles in the treatment of medial knee osteoarthritis. A two year RCT study. Osteoarthritis Cartilage 2004;12:46-55.
Lateral Heel Wedges - RCT At 2 years
At 2 yearsAt 2 years More compliance in laterally wedged More compliance in laterally wedged More compliance in laterally wedged
versus neutral No SSD between 2 groups
No SSD between 2 groups WOMAC
WOMACWOMACJoint space narrowing
Pham et al. Laterally elevated wedged insoles in the treatment of medial knee osteoarthritis. A two year RCT study. Osteoarthritis Cartilage 2004;12:46-55.
Lateral Heel Wedges Full length lateral wedge beneficial
Crenshaw S, et al. Effects of lateral-wedged insoles on kinetics of the knee. Clin Orthop Relat Res 2000;375;185-192.
Hinman RS, et al. Effect of length on laterally-wedged insoles in knee osteoarthritis. Arthritis Care Res 2008;59:144-147.
Kahikhana W, et al. Changes of joint moments in the gait of normal subjects wearing laterally wedged insoles. Am J Phys Med Rehabil 2004;83;273-278.
Kakihana W, et al. Effects of laterally wedged insoles on knees and subtalar joint moments. Arch Phys Med Rehabil 2005;86:1465-1471.
Kerrigan DC, et al. Effectiveness of a lateral-wedge insole on knee varus torque in patients with knee osteoarthritis. Arch Phys Med Rehabil. 2002;83:889-893.
Lateral Heel Wedges May not be as effective if only in rear foot
Maly M, et al. Static and dynamic biomechanics of foot orthoses in people with medial compartment knee osteoarthritis. Clin Biomech. 2002;17:603-610.
Nester C, et al. Effect of foot orthoses on the kinematics and kinetics of normal walking gait. Gait Posture 2003;17:180-187.
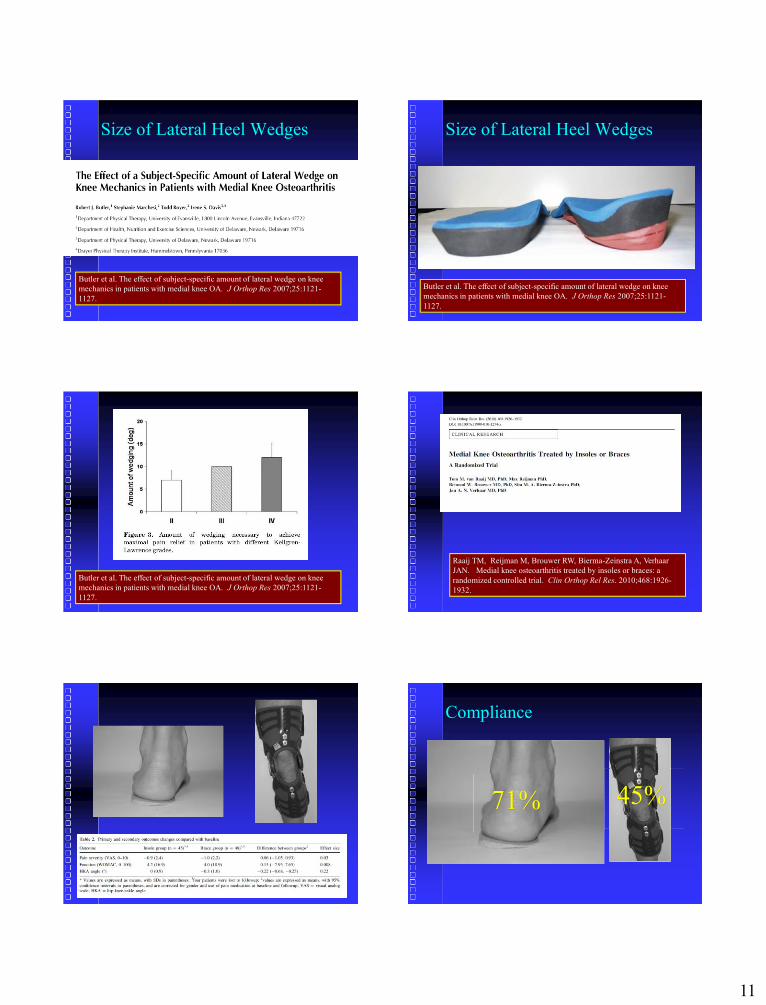
11
Size of Lateral Heel Wedges
Butler et al. The effect of subject-specific amount of lateral wedge on knee mechanics in patients with medial knee OA. J Orthop Res 2007;25:1121-1127.
Size of Lateral Heel Wedges
Butler et al. The effect of subject-specific amount of lateral wedge on knee mechanics in patients with medial knee OA. J Orthop Res 2007;25:1121-1127.
Butler et al. The effect of subject-specific amount of lateral wedge on knee mechanics in patients with medial knee OA. J Orthop Res 2007;25:1121-1127.
Raaij TM, Reijman M, Brouwer RW, Bierma-Zeinstra A, Verhaar JAN. Medial knee osteoarthritis treated by insoles or braces: a randomized controlled trial. Clin Orthop Rel Res. 2010;468:1926-1932.
Compliance
45%71%

12
Hsu WC, Jhong YC, Chen HL, et al. Immediate and long-term efficacy on laterally-wedged insoles on persons with bilateral medial knee osteoarthritis during walking. BioMed Eng OnLine. 2015;14:43. DOI 10.1186/s12938-015-0040-6.
KAMs with insoles significantly reduced KAMs with insoles significantly reduced KAMs with insoles significantly reduced when compared to barefoot
when compared to barefoot Insoles effective in reducing loadings Insoles effective in reducing loadings Insoles effective in reducing loadings
on medial knee
Hsu WC, Jhong YC, Chen HL, et al. Immediate and long-term efficacy on laterally-wedged insoles on persons with bilateral medial knee osteoarthritis during walking. BioMed Eng OnLine. 2015;14:43. DOI 10.1186/s12938-015-0040-6.
After 6 weeks no new significant findings After 6 weeks no new significant findings After 6 weeks no new significant findings compared to baseline
compared to baselineA gait adaption was seen after 6 weeks A gait adaption was seen after 6 weeks A gait adaption was seen after 6 weeks
without insoles
without insolesResult of lateral shift of COP combined Result of lateral shift of COP combined Result of lateral shift of COP combined
with reduced frontal plane GRF lever with reduced frontal plane GRF lever with reduced frontal plane GRF lever arm while with reduced frontal plane GRF lever with reduced frontal plane GRF lever with reduced frontal plane GRF lever with reduced frontal plane GRF lever arm while arm while wearing insoles
Hsu WC, Jhong YC, Chen HL, et al. Immediate and long-term efficacy on laterally-wedged insoles on persons with bilateral medial knee osteoarthritis during walking. BioMed Eng OnLine. 2015;14:43. DOI 10.1186/s12938-015-0040-6.
Adaptive strategy was Adaptive strategy was Adaptive strategy was to reduce external to reduce external to reduce external rotation at hip at heel rotation at hip at heel rotation at hip at heel strike and increased strike and increased strike and increased ankle eversion during ankle eversion during ankle eversion during stance which leads to stance which leads to stance which leads to significantly reduced significantly reduced significantly reduced lever arm length on lever arm length on lever arm length on the frontal GRF the frontal GRF the frontal GRF available at the knee.Hsu WC, Jhong YC, Chen HL, et al. Immediate and long-term efficacy on laterally-wedged insoles on persons with bilateral medial knee osteoarthritis during walking. BioMed Eng OnLine. 2015;14:43. DOI 10.1186/s12938-015-0040-6.
Exercise
Aerobic Exercise Prospective RCT
Prospective RCTProspective RCT 102 patients
102 patients102 patients 8 week supervised fitness walking program
8 week supervised fitness walking program8 week supervised fitness walking program Patient education Results
Results Increased walking distance and Increased walking distance and Increased walking distance and
decreased pain
Kovar PA, et al. Supervised fitness walking in patients with osteoarthritis of the knee. Ann Int Med 1992;116:529-534.

13
Aerobic Exercise 365 patients
365 patients365 patients Aerobics vs. strengthening vs. Education
Aerobics vs. strengthening vs. EducationAerobics vs. strengthening vs. Education Aerobic and Strengthening
Aerobic and Strengthening8
Aerobic and Strengthening88-
Aerobic and StrengtheningAerobic and StrengtheningAerobic and Strengthening8888-10% lower disability scores
888-10% lower disability scores10% lower disability scores10% lower disability scores
8888-12% lower pain scores
12% lower pain scores12% lower pain scores12% lower pain scores Improved 6 min walk score
Ettigar WH., et al. A randomized trial comparing aerobic exercise and resistance exercise with a health education program in older adults with knee osteoarthritis. The Fitness Arthritis and Seniors Trial (FAST). JAMA 1997;277:25-31.
Aerobic Exercise 435 participants
435 participants435 participants Health Education Aerobic Exercise Weight Training
Mangani et al. Exercise and co-morbidity. Results of fitness and arthritis in seniors trial (FAST). Aging Clin Exp Res. 2006;18:374.
Aerobic Exercise 18 month protocol
18 month protocol18 month protocol 60 minute walking sessions
60 minute walking sessions3 month facility
60 minute walking sessions3 month facility3 month facility-
60 minute walking sessions60 minute walking sessions60 minute walking sessions3 month facility3 month facility-based
3 month facility3 month facility15 month home
3 month facility3 month facility15 month home15 month home15 month home-3 month facility3 month facility15 month home15 month home15 month home-based
Phone calls every 3 weeks during home Phone calls every 3 weeks during home Phone calls every 3 weeks during home based program
Mangani et al. Exercise and co-morbidity. Results of fitness and arthritis in seniors trial (FAST). Aging Clin Exp Res. 2006;18:374.
Aerobic Exercise Weight training
Weight trainingWeight training 18 month program
18 month program9 exercises
3 times/week, 2 sets x 12 reps
3 times/week, 2 sets x 12 reps3 times/week, 2 sets x 12 reps Increased in stepwise fashion to Increased in stepwise fashion to Increased in stepwise fashion to tol
Mangani et al. Exercise and co-morbidity. Results of fitness and arthritis in seniors trial (FAST). Aging Clin Exp Res. 2006;18:374.
Aerobic Exercise Aerobic exercise improved physical Aerobic exercise improved physical Aerobic exercise improved physical
function (walking speed) better than WT or function (walking speed) better than WT or function (walking speed) better than WT or HE
Aerobic exercise and weight training Aerobic exercise and weight training Aerobic exercise and weight training improved physical function (disability improved physical function (disability improved physical function (disability score) better than HE
Mangani et al. Exercise and co-morbidity. Results of fitness and arthritis in seniors trial (FAST). Aging Clin Exp Res. 2006;18:374.
Aerobic Exercise Aerobic exercise improved physical Aerobic exercise improved physical Aerobic exercise improved physical
function (walking speed) better than WT or function (walking speed) better than WT or function (walking speed) better than WT or HE
Aerobic exercise and weight training Aerobic exercise and weight training Aerobic exercise and weight training improved physical function (disability improved physical function (disability improved physical function (disability score) better than HE
Mangani et al. Exercise and co-morbidity. Results of fitness and arthritis in seniors trial (FAST). Aging Clin Exp Res. 2006;18:374.
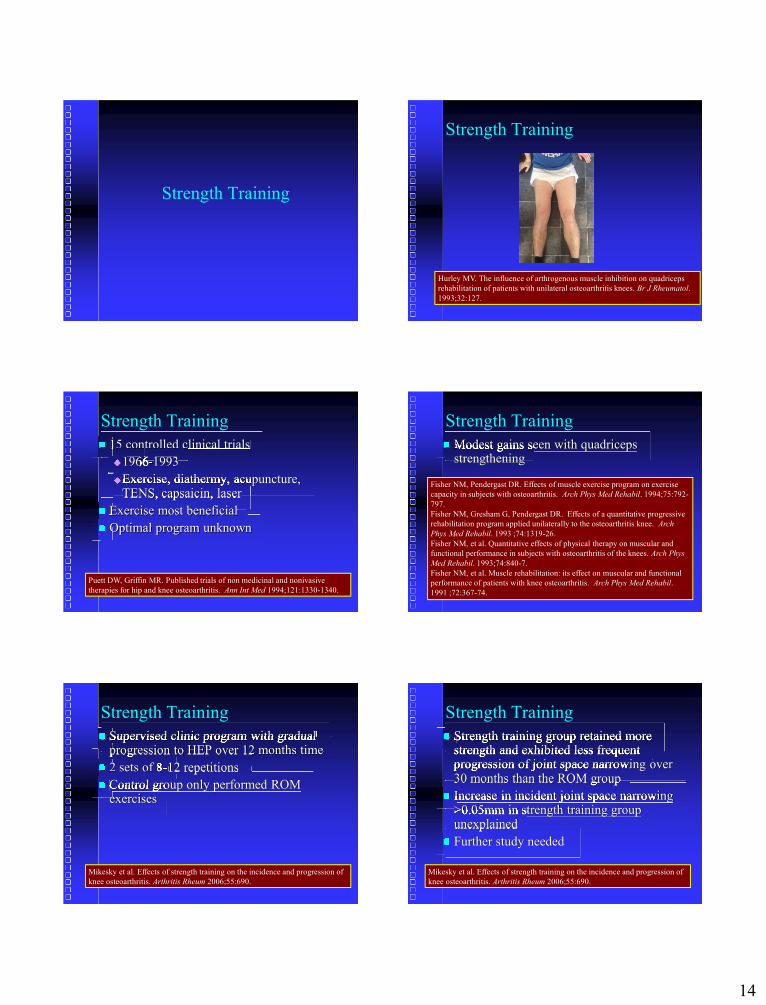
14
Strength Training
Strength Training
Hurley MV. The influence of arthrogenous muscle inhibition on quadriceps rehabilitation of patients with unilateral osteoarthritis knees. Br J Rheumatol. 1993;32:127.
Strength Training 15 controlled clinical trials
196619661966-19661966-1993
Exercise, diathermy, acupuncture, Exercise, diathermy, acupuncture, Exercise, diathermy, acupuncture, TENS, capsaicin, laser
TENS, capsaicin, laser Exercise most beneficial
Exercise most beneficialExercise most beneficial Optimal program unknown
Puett DW, Griffin MR. Published trials of non medicinal and nonivasive therapies for hip and knee osteoarthritis. Ann Int Med 1994;121:1330-1340.
Strength Training Modest gains seen with quadriceps Modest gains seen with quadriceps Modest gains seen with quadriceps
strengthening
Fisher NM, Pendergast DR. Effects of muscle exercise program on exercise capacity in subjects with osteoarthritis. Arch Phys Med Rehabil. 1994;75:792-797.Fisher NM, Gresham G, Pendergast DR. Effects of a quantitative progressive rehabilitation program applied unilaterally to the osteoarthritis knee. Arch Phys Med Rehabil. 1993 ;74:1319-26.Fisher NM, et al. Quantitative effects of physical therapy on muscular and functional performance in subjects with osteoarthritis of the knees. Arch Phys Med Rehabil. 1993;74:840-7.Fisher NM, et al. Muscle rehabilitation: its effect on muscular and functional performance of patients with knee osteoarthritis. Arch Phys Med Rehabil. 1991 ;72:367-74.
Strength Training Supervised clinic program with gradual Supervised clinic program with gradual Supervised clinic program with gradual
progression to HEP over 12 months time
progression to HEP over 12 months time 2 sets of 8
progression to HEP over 12 months time2 sets of 82 sets of 8-progression to HEP over 12 months timeprogression to HEP over 12 months timeprogression to HEP over 12 months time2 sets of 82 sets of 8-12 repetitions
2 sets of 82 sets of 82 sets of 82 sets of 8 12 repetitions 12 repetitions 12 repetitions Control group only performed ROM Control group only performed ROM Control group only performed ROM
exercises
Mikesky et al. Effects of strength training on the incidence and progression of knee osteoarthritis. Arthritis Rheum 2006;55:690.
Strength Training Strength training group retained more Strength training group retained more Strength training group retained more
strength and exhibited less frequent strength and exhibited less frequent strength and exhibited less frequent progression of joint space narrowing over progression of joint space narrowing over progression of joint space narrowing over 30 months than the ROM group
30 months than the ROM group Increase in incident joint space narrowing Increase in incident joint space narrowing Increase in incident joint space narrowing
>0.05mm in strength training group >0.05mm in strength training group >0.05mm in strength training group unexplained
unexplained Further study needed
Mikesky et al. Effects of strength training on the incidence and progression of knee osteoarthritis. Arthritis Rheum 2006;55:690.

15
Manual Therapy
Manual Therapy
Deyle GD et al. Effectiveness of manual physical therapy and exercise in osteoarthritis of the knee. A randomized controlled trial. Ann Int Med 2000;132:173-181.
Manual Therapy Manual Therapy
Manual TherapyManual Therapy Knee, Lumbar spine, hip, and ankle
Knee, Lumbar spine, hip, and anklePassive physiologic and accessory joint Passive physiologic and accessory joint Passive physiologic and accessory joint
movementsPassive stretching
Passive stretchingPassive stretchingSoft tissue mobilization
Deyle GD et al. Effectiveness of manual physical therapy and exercise in osteoarthritis of the knee. A randomized controlled trial. Ann Int Med 2000;132:173-181.
Manual Therapy Outcomes
OutcomesWOMAC
Distance walked in 6 minutes
Tester blinded to group assignments
Tester blinded to group assignmentsTester blinded to group assignmentsGroup comparisons time:
Group comparisons time:0, 4 weeks, 8 weeks, 1 year
Deyle GD et al. Effectiveness of manual physical therapy and exercise in osteoarthritis of the knee. A randomized controlled trial. Ann Int Med 2000;132:173-181.
Deyle GD et al. Effectiveness of manual physical therapy and exercise in osteoarthritis of the knee. A randomized controlled trial. Ann Int Med 2000;132:173-181.
Deyle GD et al. Effectiveness of manual physical therapy and exercise in osteoarthritis of the knee. A randomized controlled trial. Ann Int Med 2000;132:173-181.

16
Manual Therapy Treatment group (4 weeks)
Treatment group (4 weeks)Supervised PT
Supervised PTSupervised PTManual therapy
Manual therapyManual therapy HEP (4 weeks)
HEP (4 weeks)HEP
1 visit 2 weeks later for reinforcement
Deyle GD et al. Physical therapy treatment effectiveness for OA of the knee: A randomized comparison of supervised clinical exercise and manual therapy procedures versus a home exercise program. Phys Ther 2005;85:1301-1317.
Manual Therapy Both groups improved significantly with Both groups improved significantly with Both groups improved significantly with
walking distance and WOMAC by 4 and 8 walking distance and WOMAC by 4 and 8 walking distance and WOMAC by 4 and 8 weeks
WOMAC improved 52% in treatment WOMAC improved 52% in treatment WOMAC improved 52% in treatment group and only 26% in HEP group at 4 group and only 26% in HEP group at 4 group and only 26% in HEP group at 4 weeks
At 1 year both improved
Deyle GD et al. Physical therapy treatment effectiveness for OA of the knee: A randomized comparison of supervised clinical exercise and manual therapy procedures versus a home exercise program. Phys Ther 2005;85:1301-1317.
Manual Therapy HEP important benefit for those with knee HEP important benefit for those with knee HEP important benefit for those with knee
OA Adding small number of visits for manual Adding small number of visits for manual Adding small number of visits for manual
therapy adds greater relief
Deyle GD et al. Physical therapy treatment effectiveness for OA of the knee: A randomized comparison of supervised clinical exercise and manual therapy procedures versus a home exercise program. Phys Ther 2005;85:1301-1317.
Currier LL, et al. Development of CPR to identify patients with knee pain and clinical evidence of knee osteoarthritis who demonstrate a favorable short-term response to hip mobilization. Phys Ther 2007;87:1106-1119.
Manual Therapy
Currier LL, et al. Development of CPR to identify patients with knee pain and clinical evidence of knee osteoarthritis who demonstrate a favorable short-term response to hip mobilization. Phys Ther 2007;87:1106-1119.

17
Manual Therapy (4) Outcome Measures at 48 Hours
(4) Outcome Measures at 48 Hours(4) Outcome Measures at 48 Hours WOMAC PSFS: Patient specific functional scale
PSFS: Patient specific functional scalePSFS: Patient specific functional scale NPRS: Numeric pain rating scale
NPRS: Numeric pain rating scaleNPRS: Numeric pain rating scale GROC: Global rating of change
Currier LL, et al. Development of CPR to identify patients with knee pain and clinical evidence of knee osteoarthritis who demonstrate a favorable short-term response to hip mobilization. Phys Ther 2007;87:1106-1119.
Manual Therapy Criteria for Success
Criteria for SuccessCriteria for Success GROC score of at least 3 Decrease of at least 30% on the composite Decrease of at least 30% on the composite Decrease of at least 30% on the composite
NPRS score obtained during two NPRS score obtained during two NPRS score obtained during two functional activitiesSquat test
Squat testSquat testSit to stand test
Currier LL, et al. Development of CPR to identify patients with knee pain and clinical evidence of knee osteoarthritis who demonstrate a favorable short-term response to hip mobilization. Phys Ther 2007;87:1106-1119.
Manual Therapy If one variable had a positive likelihood If one variable had a positive likelihood If one variable had a positive likelihood
ratio of 5.1 it increased the probability of a ratio of 5.1 it increased the probability of a ratio of 5.1 it increased the probability of a successful response to 92% at 48 hours successful response to 92% at 48 hours successful response to 92% at 48 hours post treatment
post treatment If 2 variables were present, the positive If 2 variables were present, the positive If 2 variables were present, the positive
likelihood ratio was 12.9 and the likelihood ratio was 12.9 and the likelihood ratio was 12.9 and the probability of success increased to 97%
Currier LL, et al. Development of CPR to identify patients with knee pain and clinical evidence of knee osteoarthritis who demonstrate a favorable short-term response to hip mobilization. Phys Ther 2007;87:1106-1119.
Haxby Abbott J, et al. The incremental effects of manual therapy or booster sessions in addition to exercise therapy for knee osteoarthritis: A randomized clinical trial. J Orthop Sports Phys Ther. 2015; 45(12):975-983.
4 groups
4 groupsExercise in consecutive sessions
Exercise session over year with Exercise session over year with Exercise session over year with “booster” sessions
Exercise therapy + manual therapy
Exercise therapy + manual therapyExercise therapy + manual therapyExercise therapy + manual with Exercise therapy + manual with Exercise therapy + manual with
“booster”
Haxby Abbott J, et al. The incremental effects of manual therapy or booster sessions in addition to exercise therapy for knee osteoarthritis: A randomized clinical trial. J Orthop Sports Phys Ther. 2015; 45(12):975-983.
Outcomes
OutcomesWOMAC
NPRS
NPRSNPRSPerformance tests
Haxby Abbott J, et al. The incremental effects of manual therapy or booster sessions in addition to exercise therapy for knee osteoarthritis: A randomized clinical trial. J Orthop Sports Phys Ther. 2015; 45(12):975-983.

18
Courtney CA, et al. Joint mobilization enhances mechanisms of conditioned pain modulation in individuals with OA of the knee. J Orthop Sports Phys Ther. 2016; 46(3):168-176.
Courtney CA, et al. Joint mobilization enhances mechanisms of conditioned pain modulation in individuals with OA of the knee. J Orthop Sports Phys Ther. 2016; 46(3):168-176.
29 patients
29 patients 29 patients RCT Knee joint mobilization vs sham Knee joint mobilization vs sham Knee joint mobilization vs sham
mobilization
Courtney CA, et al. Joint mobilization enhances mechanisms of conditioned pain modulation in individuals with OA of the knee. J Orthop Sports Phys Ther. 2016; 46(3):168-176.
Courtney CA, et al. Joint mobilization enhances mechanisms of conditioned pain modulation in individuals with OA of the knee. J Orthop Sports Phys Ther. 2016; 46(3):168-176.

19
Courtney CA, et al. Joint mobilization enhances mechanisms of conditioned pain modulation in individuals with OA of the knee. J Orthop Sports Phys Ther. 2016; 46(3):168-176.
THANK YOU!Robert C. Manske, PT, DPT, SCS, ATC, CSCS
Associate ProfessorDepartment of Physical Therapy
Wichita State UniversityVia Christi Outpatient Sports and Orthopedic Rehab
Wichita, Kansas [email protected]




















