PJB
110
Pemicu 5 Bayiku Sesak & Tidak Kuat Menyusu Pitri Erlina Lay 405110177
-
Upload
cuncunalandra -
Category
Documents
-
view
3 -
download
1
description
text
Transcript of PJB

Pemicu 5Bayiku Sesak & Tidak Kuat Menyusu
Pitri Erlina Lay405110177

LO mm PJB
1. PDA2. ASD3. VSD4. PS5. TGA6. PPAVR7. TOF8. COA9. ECD10. Anomali Ebstein




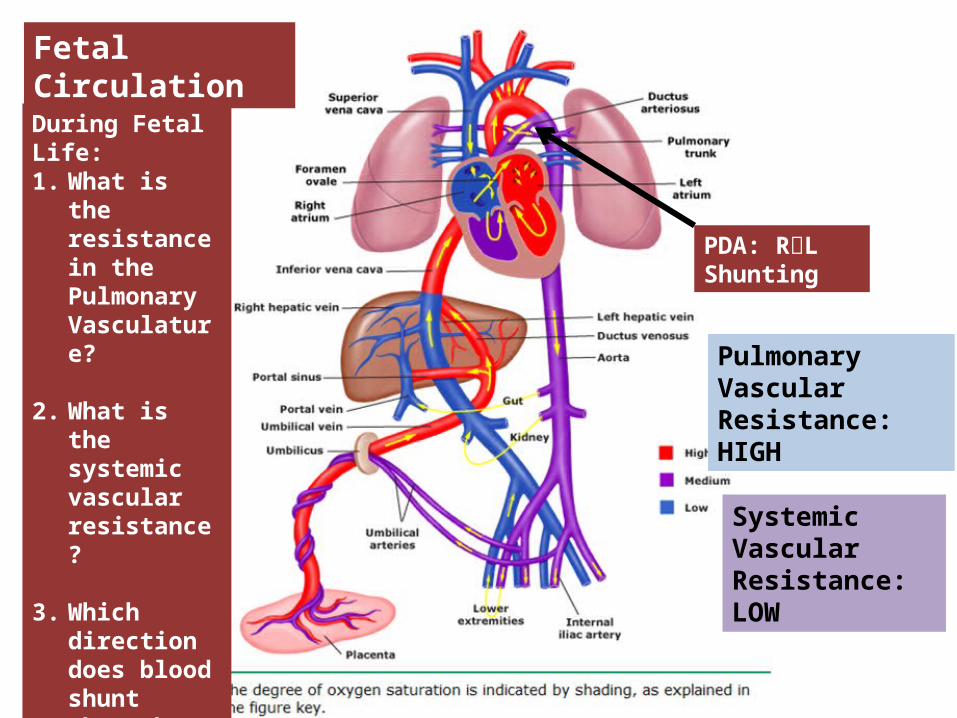
Fetal Circulation
PDA: RL Shunting
Pulmonary Vascular Resistance: HIGH
Systemic Vascular Resistance: LOW
During Fetal Life:1. What is the
resistance in the Pulmonary Vasculature?
2. What is the systemic vascular resistance?
3. Which direction does blood shunt through the Ductus Arteriosus?



Embriologi PDA

Epidemiologi

Patofisiologi
• Lungs: – Lungs expand– PaO2↑’s Pulmonary vasodilatation – Drop in pulmonary vascular resistance.
• Systemic Circulation:– Resistance ↑’s with placental removal
• PDA: – flow reverses to L R shunting– Begins to functionally close due to ↑ PaO2, and decreased
PGE2 levels

Patofisiologi



DD dari PDA
• Respiratory:– Pneumothorax– Pulmonary Hemorrhage
• Cardiac– Ductal Dependent Heart
Lesion
• ID– Sepsis– Pneumonia
• GI– NEC (Necrotising Entero Colitis)
• Neuro:– IVH (Intra Ventricular
Haemorrage)– Seizures / kejang

Sign & symptom


Physical Exam
• Vitals: 160, RR 68, BP 45/20, SaO2 85%• Weight: 980 grams (up 80 grams from 1 day prior)• HEENT: unremarkable• Pulm: tachypneic, decreased lung sounds at bases, crackles
heard bilaterally posterior lung fields• CV: 3/6 systolic murmur loudest at LUSB, bounding palmar
pulses, active precordium, 2+femoral pulses, CR <2 seconds
• Abdomen: soft, active bowel sounds• Skin: warm, dry

What Physical Exam findings are consistent with PDA?
Murmur: systolic at LUSB/Left Infraclavicular, may progress to continuous (machinery)
Cardiac: Active Precordium, Widened Pulse Pressure, Bounding Pulses
Respiratory Ex: Tachypnea, Apnea, CO2, increased vent settings

Pemeriksaan Penunjang

Pemeriksaan foto Ro
Increased Pulmonary vascular makings
Cardiomegaly
Uptodate.com

Echocardiogram
• Gold standard for diagnosing PDA
Taken from Neo Reviews


Faktor resiko tjd PDA• The Youngest/premature: risk increases with
decreasing gestational age• The Smallest (BBLR): 80% of ELBW infants
(BW <1000g) with a murmur progress to large persistent PDAs

Komplikasi PDA

What makes a PDA Hemodynamically Significant?
Systemic Hypoperfusion (↓ Qs)
Pulmonary Overcirculation (↑ Qp)
Systemic HypotensionEnd-Organ HypoperfusionRenal InsufficiencyNECIVHAcidosis (metabolic, lactic)
Oxygenation failureIncreased Vent RequirementsPulmonary Edema Cardiomegaly

2. Pharmacotherapy
1. Conservative/Supportive Management
Surgery


contraindications indomethacin :
Proven/ suspected infection Active bleeding
e.g. IVH, NEC Thrombocytopenia and/or coagulation defects Necrotizing enterocolitis Severe Renal Impairment Congenital heart disease with ductal dependent lesion

ADR of Indomethacin
• What are you going to instruct the RN to notify you about in this patient?– Decreased Urine Output
• Indocin should be held if UOP < 1 ml/kg/h– Abdominal Changes– Signs/Sx of bleeding
• Are there any labs you would like to check before/after starting indomethacin?– CBC: to check platelets– BMP: to check BUN and Creatinine

After two trials of indocin your patient still has a symptomatic PDA what next steps might
you take?
• Continue supportive therapy through ventilator and fluid management
• If infant continues to require high ventilator support and echo demonstrates a large PDA consider surgical ligation

What Supportive Measures can you take in an infant with a symptomatic PDA?
• Ventilator Strategies:– Adequate Oxygenation– Permissive Hypercapnea– Use of PEEP (Positive End Expiratory Pressure)
• Mild Fluid restriction: 110-130 ml/kg/day• Heme: Maintenance of HCT 35-40%


Surgical Ligation• Indications? – Persistent Symptomatic PDA after 1-2 trials of
Indomethacin or Motrin– Contraindication to Indomethacin or Motrin
• Complications?– recurrent laryngeal nerve paralysis– blood pressure fluctuations– respiratory compromise– infection– intraventricular hemorrhage– chylothorax– BPD (Broncho Pulmonary Displasia)– death

Surgical Ligation• Long Term Outcomes
– Current studies do not demonstrate that ligation decreases incidence of BPD
– Some data to suggest infants that have surgical ligation are at greater risk for neurocognitive delays
• Surgery should only be used for infants that have failed medical management and are symptomatic


ATRIAL SEPTAL DEFECT

• Normally, oxygen-poor (blue) blood returns to the right atrium from the body, travels to the right ventricle, then is pumped into the lungs where it receives oxygen. Oxygen-rich (red) blood returns to the left atrium from the lungs, passes into the left ventricle, and then is pumped out to the body through the aorta.



GROSS SPECIMENS

EMBRYOLOGY
• The heart is forming during the first 8 weeks of fetal development. It begins as a hollow tube, then partitions within the tube develop that eventually become the septa (or walls) dividing the right side of the heart from the left. Atrial septal defects occur when the partitioning process does not occur completely, leaving an opening in the atrial septum.

HEMODYNAMICS
• PULM. VALVE CLOSES LATE & P2 IS DELAYED• RV IS FULLY LOADED,SO FURTHER RISE IN RV
VOLUME CANNOT OCCUR
• WIDELY SPLIT S2
• FIXED SPLIT S2
• ACCENTUATED S2

Sign & symptom
• recurrent chest infections • fatigue • sweating • rapid breathing • shortness of breath • poor growth


ON EXAMINATION
• INSPECTION• PARASTRNL IMPULSE• PALPATION• SYSTOLIC THRILL AT 2ND LT SPACE

AUSCULTATION
• WIDE FIXED SPLIT S2• ACCENTUATED P2• ESM AT LT 2nd & 3rd INTERSPACES• DELAYED DIASTOLIC MURMUR AT LOW LT
INTERSPACE

CXR FINDINGS
• MOD. CARDIOMEGALY• RA ENLARGEMENT • RV ENLARGEMENT• PROMINENT MAIN
PULM ARTERY• PLETHORIC LUNG
FIELDS

ECG CHANGES
• RT AXIS DEVIATION• RT VENT HYPERTROPHY• rsR’ PATTERN IN V1

ECHO PICTURES

SEVERITY ASSESMENT
• INTENSITY OF THE TWO MURMURS• THE HEART SIZE

COMPLICATION
• PULMONARY HYPERTENSION(ABOVE 20 YEARS)
• DISAPPEARANCE OF DIASTOLIC MURMUR• APPEARANCE OF PULM EJECN CLICK• LOUD PALPABLE P2• P2_STILL WIDELY SPLIT

MANAGEMENT
• MEDICAL• ANTIBIOTICS FOR CHEST INFECTIONS • DIGOXIN TO INCREASE WORK OF HEART• DIURETICS TO REDUCE PRELOAD
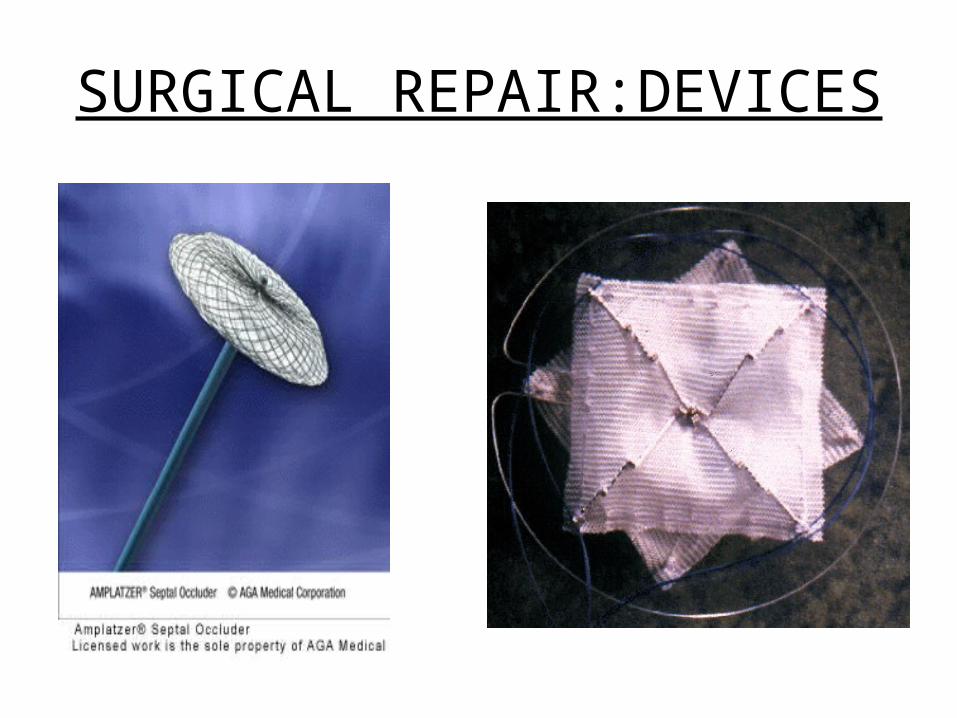
SURGICAL REPAIR:DEVICES

REPAIR

ROBO REPAIR





ECD (Endocarditis Cushing Syndrome)









Stenosis pulmonalis

Manifestasi klinik


Scimitar Syndrome
1-3 per 1,oo,ooo births Hypogenetic lung syndrome /
Congenital pulmonary venolobar syndrome
FELSON – coined the term CPVS WOODRING et al – extended the term CPVS to
cover a range of anomalies including pulmonary hypoplasia & pulmonary sequestration

• An anomalous vein connects between the pulmonary venous circulation and systemic venous circulation. This anomalous pulmonary venous return can be either partial (PAPVR) or total (TAPVR). The syndrome associated with PAPVR is more commonly known as "Scimitar syndrome"

Components : Total or partial anomalous connection of the pulmonary
veins in one lung to the inferior vena cava. This connection can be above or below the level of the diaphragm. Right lung is commonly involved
Variable degree of hypoplasia (small-size) and malformation
of the pulmonary arteries and lung in the same side.
Often presence of aortic-pulmonary artery collateral arteries to the lung that is small. Pulmonary hypertension is present if these arteries are large
• Bronchial tree on involved side is stunted & arterial supply to lungs derive in greater proportion than normal from SYSTEMIC ARTERIES.
• Syndrome derives its name from anomalous pulmonary vein that descends vertically in lung before curving medially to enter inf.vena cava above / below diaphragm

• The vein broadens as it curves downward, resulting in configuration resembling TURKISH SWORD, SCIMITAR

• Occasionally, there are 2 or more veins• Anomalous venous drainage may involve
entire / part of lung.• The anomalous vein can also drain into right
atrium, portal vein.

About 25 % of patients have associated congenital heart disease
Mostly Atrial septal defect When isolated, is compatible with normal life,
the consequent LT to RT shunt being small Associated with Bronchiectasis Tracheal Diverticula Eventeration RT diaphragm Horse- shoe lung


Radiographic features
• Enlarged curved vascular structure coursing medially toward the rt diaphragm; this structure enlarges in diameter as it approaches diaphragm
• Dextroposition of the heart• Hypoplasia of right lung

Differential diagnosis
• Scimitar sign is simulated radiographically by hypoplasia of Rt lung with aplasia of pulmonary artery
• Abnormal artery / arteries can simulate scimitar vein
• Abnormal meandering vein draining a hypoplastic Rt lung to Lt atrium can simulate scimitar vein.

• CT – also has advantage that tracheobronchial anomalies are better delineated
• MRI – estimate the degree of Lt to Rt shunt by means of velocity encoded cine MR.

TREATMENT There is a wide clinical spectrum for patients with scimitar
syndrome. The decision to intervene medically depends on the hemodynamic burden.
If the amount of blood flowing to the inferior vena cava from the anomalous pulmonary veins is small, no therapy is required.
If the anomalous pulmonary venous drainage is associated with a significant left-ro-right shunt, surgical correction is warranted.
Aortopulmonary collateral arteries can be closed either in the cardiac catheterization laboratory by placement of occluding coils or other devices, or surgically.

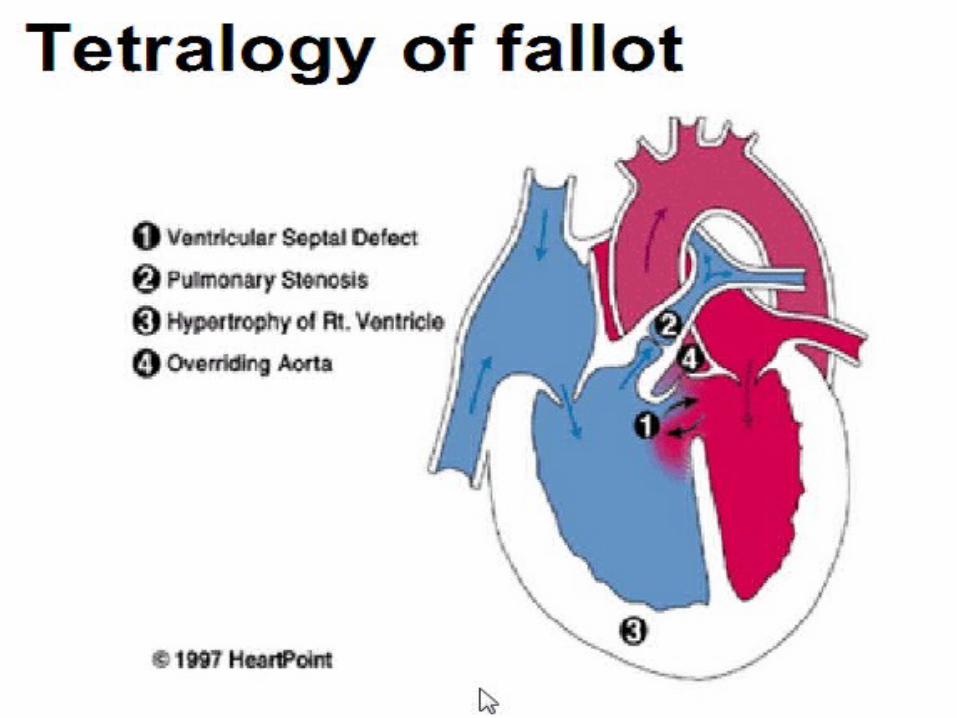
PJB yang sianosis :

• Kekuatan kontraksi jantung

TGA ( Transposisi of the Great Artery)


kelahiran


Tekanan sistolik ventrikel kanan

b. Transposisi dengan defek septum sebagian






map )



Kanan meningkat, foramen ovale tetap terbuka



Sianosis tsb.



References:• Chorne N, Leonard C, Piecuch R, Clyman RI. Patent ductus
arteriosus and its treatment as risk factors for neonatal and neurodevelopmental morbidity. Pediatrics. 2007;119(6):1165.
• Gien, J. Controversied in the Management of Patent Ductus Arteriosus. Neoreviews 2008: 9, 477-482
• Masalli, R. Optimal Fluid Management in Premature Infants with PDA. Neoreviews 2010; 11: 495-502
• Philips , Joseph B. Management of patent ductus arteriosus in premature infants. UptoDate (www.uptodate.com)
• Phillips, J. Pathophysiology, clinical manifestations, and diagnosis of patent ductus arteriosus in premature infants. UptoDate (www.uptodate.com)
• Nelson Text Book of Pediatrics