Hepatobilier Pemicu 4

of 42
-
Upload
kartikasari-pratiwi -
Category
Documents
-
view
239 -
download
0
Transcript of Hepatobilier Pemicu 4
-
8/13/2019 Hepatobilier Pemicu 4
1/42
Hepatobilier
Pemicu 4
Ryan Putra
405080212
-
8/13/2019 Hepatobilier Pemicu 4
2/42
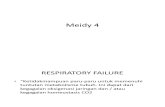
Computed tomography (CT) scan findings of liver abscess are shown. A large, septated
abscess of the right hepatic lobe is revealed. Abscess was successfully treated with
percutaneous drainage and antimicrobial therapy.
-
8/13/2019 Hepatobilier Pemicu 4
3/42
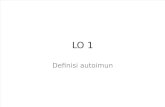
Computed tomography (CT) scan findings of liver abscess are shown. A large anterior
abscess involving the left hepatic lobe is revealed. Abscess was successfully treated with
percutaneous drainage and antimicrobial therapy.
-
8/13/2019 Hepatobilier Pemicu 4
4/42
The 3 major forms of liver abscess, classifiedby etiology, are as follows:
Pyogenic abscess, which is most often
polymicrobial, accounts for 80% of hepaticabscess cases in the United States.
Amebic abscess due to Entamoeba histolytica
accounts for 10% of cases. Fungal abscess, most often due to Candida
species, accounts for less than 10% of cases.
-
8/13/2019 Hepatobilier Pemicu 4
5/42
Pathophysiology
The liver receives blood from both systemicand portal circulations. Increasedsusceptibility to infections would be expected
given the increased exposure to bacteria.However, Kupffer cells lining the hepaticsinusoids clear bacteria so efficiently thatinfection rarely occurs. Multiple processes
have been associated with the developmentof hepatic abscesses
-
8/13/2019 Hepatobilier Pemicu 4
6/42
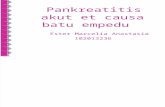
Underlying etiology of 1086 cases of liver abscess compiled from the literature.
-
8/13/2019 Hepatobilier Pemicu 4
7/42
Appendicitis was traditionally the major cause of liver abscess.
As diagnosis and treatment of this condition has advanced, itsfrequency as a cause for liver abscess has decreased to 10%.
Biliary tract disease is now the most common source of pyogenicliver abscess (PLA). Obstruction of bile flow allows for bacterial
proliferation. Biliary stone disease, obstructive malignancy affecting the biliary
tree, stricture, and congenital diseases are common incitingconditions.
With a biliary source, abscesses usually are multiple, unless they are
associated with surgical interventions or indwelling biliary stents. Inthese instances, solitary lesions can be seen.
-
8/13/2019 Hepatobilier Pemicu 4
8/42
Infections in organs in the portal bed canresult in a localized septic thrombophlebitis,which can lead to liver abscess.
Septic emboli are released into the portalcirculation, trapped by the hepatic sinusoids,and become the nidus for microabscessformation.
These microabscesses initially are multiple butusually coalesce into a solitary lesion.
-
8/13/2019 Hepatobilier Pemicu 4
9/42
Microabscess formation can also be due tohematogenous dissemination of organisms inassociation with systemic bacteremia, such as
endocarditis and pyelonephritis. Cases also are reported in children with
underlying defects in immunity, such as chronicgranulomatous disease and leukemia.
Approximately 4% of liver abscesses result fromfistula formation between local intra-abdominalinfections.
-
8/13/2019 Hepatobilier Pemicu 4
10/42
Despite advances in diagnostic imaging, cryptogenic causesaccount for a significant proportion of cases; surgicalexploration has impacted this minimally. These lesionsusually are solitary in nature.
Penetrating hepatic trauma can inoculate organismsdirectly into the liver parenchyma, resulting in pyogenicliver abscess.
Nonpenetrating trauma can also be the precursor topyogenic liver abscess by causing localized hepatic necrosis,intrahepatic hemorrhage, and bile leakage.
The resulting tissue environment permits bacterial growth,which may lead to pyogenic liver abscess. These lesions aretypically solitary.
-
8/13/2019 Hepatobilier Pemicu 4
11/42
Pyogenic liver abscess has been reported as asecondary infection of amebic abscess, hydatid cysticcavities, and metastatic and primary hepatic tumors.
It is also a known complication of liver transplantation,hepatic artery embolization in the treatment ofhepatocellular carcinoma, and the ingestion of foreignbodies, which penetrate the liver parenchyma.
Trauma and secondarily infected liver pathology
account for a small percentage of liver abscess cases.
-
8/13/2019 Hepatobilier Pemicu 4
12/42
The right hepatic lobe is affected more often than theleft hepatic lobe by a factor of 2:1.
Bilateral involvement is seen in 5% of cases.
The predilection for the right hepatic lobe can be
attributed to anatomic considerations. The right hepatic lobe receives blood from both the
superior mesenteric and portal veins, whereas the lefthepatic lobe receives inferior mesenteric and splenicdrainage. It also contains a denser network of biliarycanaliculi and, overall, accounts for more hepatic mass.
Studies have suggested that a streaming effect in theportal circulation is causative.
-
8/13/2019 Hepatobilier Pemicu 4
13/42
Epidemiology
United States
The incidence of pyogenic liver abscess hasessentially remained unchanged by both hospital
and autopsy data. Liver abscess was diagnosed in0.7%, 0.45%, and 0.57% of autopsies during theperiods of 1896-1933, 1934-1958, and 1959-1968, respectively. The frequency in hospitalized
patients ranges from 8-16 cases per 100,000persons. Studies suggest a small, but significant,increase in the frequency of liver abscess.
-
8/13/2019 Hepatobilier Pemicu 4
14/42
Mortality/Morbidity
Untreated, pyogenic liver abscess remains
uniformly fatal. With timely administration of
antibiotics and drainage procedures, mortality
currently occurs in 5-30% of cases. The mostcommon causes of death include sepsis,
multiorgan failure, and hepatic failur
-
8/13/2019 Hepatobilier Pemicu 4
15/42
Sex
While abscesses once showed a predilection
for males in earlier decades, no sexual
predilection currently exists. Males have a
poorer prognosis from hepatic abscess thanfemales.
-
8/13/2019 Hepatobilier Pemicu 4
16/42
Age
Prior to the antibiotic era, liver abscess was most commonin the fourth and fifth decades of life, primarily due tocomplications of appendicitis. With the development ofbetter diagnostic techniques, early antibioticadministration, and the improved survival of the general
population, the demographic has shifted toward the sixthand seventh decades of life. Frequency curves display asmall peak in the neonatal period followed by a gradual risebeginning at the sixth decade of life.
Cases of liver abscesses in infants have been associated
with umbilical vein catheterization and sepsis. When abscesses are seen in children and adolescents,
underlying immune deficiency, severe malnutrition, ortrauma frequently exists.
-
8/13/2019 Hepatobilier Pemicu 4
17/42
-
8/13/2019 Hepatobilier Pemicu 4
18/42
Signs and Symptoms
The most frequent symptoms of hepatic
abscess include the following:
Fever (either continuous or spiking)
Chills
Right upper quadrant pain
Anorexia Malaise
-
8/13/2019 Hepatobilier Pemicu 4
19/42
Signs and Symptoms
Cough or hiccoughs due to diaphragmatic irritation may bereported.Referred pain to the right shoulder may bepresent.
Individuals with solitary lesions usually have a moreinsidious course with weight loss and anemia of chronicdisease. With such symptoms, malignancy often is theinitial consideration.
Fever of unknown origin (FUO) frequently can be an initialdiagnosis in indolent cases.
Multiple abscesses usually result in more acutepresentations, with symptoms and signs of systemictoxicity.
Afebrile presentations have been documented.
-
8/13/2019 Hepatobilier Pemicu 4
20/42
Physical Examination
Fever and tender hepatomegaly are the most commonsigns.
A palpable mass need not be present.
Mid epigastric tenderness, with or without a palpable mass,
is suggestive of left hepatic lobe involvement. Decreased breath sounds in the right basilar lung zones,
with signs of atelectasis and effusion on examination orradiologically, may be present.
A pleural or hepatic friction rub can be associated with
diaphragmatic irritation or inflammation of Glisson capsule. Jaundice may be present in as many as 25% of cases and
usually is associated with biliary tract disease or thepresence of multiple abscesses.
-
8/13/2019 Hepatobilier Pemicu 4
21/42
Cause
Polymicrobial involvement is common, with
Escherichia coliand Klebsiella pneumoniae
being the 2 most frequently isolated
pathogens.
Reports suggest that K pneumoniaeis an
increasingly prominent cause.
-
8/13/2019 Hepatobilier Pemicu 4
22/42
-
8/13/2019 Hepatobilier Pemicu 4
23/42
Enterobacteriaceae are especially prominent when theinfection is of biliary origin. Abscesses involving Kpneumoniaehave been associated with multiple cases ofendophthalmitis.
The pathogenic role of anaerobes was underappreciateduntil the isolation of anaerobes from 45% of cases ofpyogenic liver abscess was reported in 1974. Since thattime, increasing rates of anaerobic involvement have beenreported, likely because of increased awareness andimproved culturing techniques. The most frequently
encountered anaerobes are Bacteroidesspecies,Fusobacteriumspecies, and microaerophilic and anaerobicstreptococci. A colonic source is usually the initial source ofinfection.
-
8/13/2019 Hepatobilier Pemicu 4
24/42
Staphylococcus aureusabscesses usually resultfrom hematogenous spread of organismsinvolved with distant infections, such asendocarditis. S milleriis neither anaerobic nor
microaerophilic. It has been associated with bothmonomicrobial and polymicrobial abscesses inpatients with Crohn disease, as well as with otherpatients with pyogenic liver abscess.
Amebic liver abscess is most often due to Ehistolytica. Liver abscess is the most commonextraintestinal manifestation of this infection.
-
8/13/2019 Hepatobilier Pemicu 4
25/42
Fungal abscesses primarily are due to Candidaalbicansand occur in individuals with prolongedexposure to antimicrobials, hematologic
malignancies, solid-organ transplants, andcongenital and acquired immunodeficiency. CasesinvolvingAspergillusspecies have been reported.
Other organisms reported in the literature
includeActinomycesspecies, Eikenella corrodens,Yersinia enterocolitica, Salmonella typhi,andBrucella melitensis.
-
8/13/2019 Hepatobilier Pemicu 4
26/42
Workup
Laboratory Studies
CBC count with differential
Anemia of chronic disease
Neutrophilic leukocytosis
Liver function studies
Hypoalbuminemia and elevation of alkaline phosphatase (mostcommon abnormalities)
Elevations of transaminase and bilirubin levels (variable)
Blood cultures are positive in roughly 50% of cases.
Culture of abscess fluid should be the goal in establishing
microbiologic diagnosis. Enzyme immunoassay should be performed to detect E histolytica
in patients either from endemic areas or who have traveled toendemic areas.
-
8/13/2019 Hepatobilier Pemicu 4
27/42
-
8/13/2019 Hepatobilier Pemicu 4
28/42
Treatment
Medical Care
Surgical Care
Consultations
-
8/13/2019 Hepatobilier Pemicu 4
29/42
Medical Care
An untreated hepatic abscess is nearly uniformly fatal due tocomplications that include sepsis, empyema, or peritonitis fromrupture into the pleural or peritoneal spaces, and retroperitonealextension. Treatment should include drainage, either percutaneousor surgical.
Antibiotic therapy as a sole treatment modality is not routinelyadvocated, though it has been successful in a few reported cases.
It may be the only alternative in patients too ill to undergo invasiveprocedures or in those with multiple abscesses not amenable topercutaneous or surgical drainage.
In these instances, patients are likely to require many months of
antimicrobial therapy with serial imaging and close monitoring forassociated complications.
Antimicrobial treatment is a common adjunct to percutaneous orsurgical drainage.
-
8/13/2019 Hepatobilier Pemicu 4
30/42
Surgical Care
Surgical drainage was the standard of care until the introduction ofpercutaneous drainage techniques in the mid 1970s. With therefinement of image-guided techniques, percutaneous drainageand aspiration have become the standard of care.
Current indications for the surgical treatment of pyogenic liverabscess are for the treatment of underlying intra-abdominalprocesses, including signs of peritonitis; existence of a knownabdominal surgical pathology (eg, diverticular abscess); failure ofprevious drainage attempts; and the presence of a complicated,multiloculated, thick-walled abscess with viscous pus.
Shock with multisystem organ failure is a contraindication tosurgery.
O b f d b 2 h
-
8/13/2019 Hepatobilier Pemicu 4
31/42
Open surgery can be performed by 2 approaches. A transperitoneal approach allows for abscess drainage and abdominal
exploration to identify previously undetected abscesses and the location ofan etiologic source.
For high posterior lesions, a posterior transpleural approach can be used.
Although this allows easier access to the abscess, the identification ofmultiple lesions or a concurrent intra-abdominal pathology is lost.
A laparoscopic approach is also commonly used in select cases. Thisminimally invasive approach affords the opportunity to explore theentire abdomen and to significantly reduce patient morbidity. A growingliterature is defining the optimal population for this mode of
intervention. A retrospective chart review compared surgery versus percutaneous
drainage for liver abscesses greater than 5 cm. The morbidity wascomparable for the 2 procedures, but those treated with surgery hadfewer secondary procedures and fewer treatment failures.
Postoperative complications are not uncommon and include recurrentpyogenic liver abscess, intra-abdominal abscess, hepatic or renal failure,and wound infection.
-
8/13/2019 Hepatobilier Pemicu 4
32/42
Consultations
Interventional radiology: Obtain a consultation as soon as the diagnosis isconsidered to allow rapid collection of cavity fluid and the potential forearly therapeutic drainage of abscess.
General surgery Immediately seek a consultation with a general surgeon if the source of the
abscess is a known underlying abdominal pathology or in cases with
peritonitis. In cases undergoing percutaneous drainage, seek the involvement of a general
surgeon if drainage of the abscess cavity is unsuccessful.
Gastroenterology involvement may be useful after successful drainage toevaluate for underlying gastrointestinal disease using colonoscopy orendoscopic retrograde cholangiopancreatography (ERCP).
Infectious disease consultation should be considered in complicated casesand when the involved pathogens are unusual or difficult to treat, such asin fungal abscesses.
-
8/13/2019 Hepatobilier Pemicu 4
33/42
Antibiotics
Meropenem (Merrem) Adult
1.0 g IV q8h
Pediatric 40 mg/kg IV q8h
Interaksi: Probenecid may inhibit renal excretion of meropenem, increasing meropenem
levels
Bactericidal broad-spectrum carbapenem antibiotic that inhibits cell-wallsynthesis.
Effective against most gram-positive and gram-negative bacteria.
Has slightly increased activity against gram negatives and slightlydecreased activity against staphylococci and streptococci speciescompared to imipenem.
-
8/13/2019 Hepatobilier Pemicu 4
34/42
Imipenem and cilastatin (Primaxin) Adult
Base initial dose on severity of infection, and administer in equallydivided doses; dose may range from 250-500 mg IV q6h for maximumof 3-4 g/dAlternatively, 500-750 mg IM q12h or intra-abdominally
Pediatric
3 monthsFully susceptible organisms: Not to exceed 2 g/d IVInfections with moderately susceptible organisms: Not to exceed 4 g/d
For treatment of multiple organism infections in whichother agents do not have wide-spectrum coverage or arecontraindicated due to potential for toxicity.
-
8/13/2019 Hepatobilier Pemicu 4
35/42
Cefuroxime (Ceftin) Adult
500 mg PO bid for 20 d
Pediatric Children: 250 mg PO bid for 20 d
Adolescents: Administer as in adults
Second-generation cephalosporin maintains gram-positiveactivity that first-generation cephalosporins have; addsactivity against Proteus mirabilis, Haemophilus influenzae,
Escherichia coli, Klebsiella pneumoniae, and Moraxellacatarrhalis. Condition of patient, severity of infection, andsusceptibility of microorganism determine proper dose androute of administration.
-
8/13/2019 Hepatobilier Pemicu 4
36/42
Cefotetan (Cefotan) Adult
1-2 g IV/IM q12h for 5-10 d
Pediatric
20-40 mg/kg/dose IV/IM q12h for 5-10 d
Second-generation cephalosporin indicated forinfections caused by susceptible gram-positive cocciand gram-negative rods.
Dosage and route of administration depends oncondition of patient, severity of infection, andsusceptibility of causative organism.
-
8/13/2019 Hepatobilier Pemicu 4
37/42
Cefoxitin (Mefoxin) Adult
1-2 g IV q6-8h
Pediatric
Infants and children: 80-160 mg/kg/d IV divided q4-6h; higherdoses for severe or serious infections; not to exceed 12 g/d
Second-generation cephalosporin indicated for gram-positive cocci and gram-negative rod infections.
Infections caused by cephalosporin-resistant orpenicillin-resistant gram-negative bacteria mayrespond to cefoxitin.
-
8/13/2019 Hepatobilier Pemicu 4
38/42
Cefaclor (Ceclor) Adult
250-500 mg PO q8h
Pediatric
20-40 mg/kg/d PO divided q8-12h; not to exceed 2 g/d
Second-generation cephalosporin indicated forinfections caused by susceptible gram-positive cocciand gram-negative rods.
Determine proper dosage and route based oncondition of patient, severity of infection, andsusceptibility of causative organism.
-
8/13/2019 Hepatobilier Pemicu 4
39/42
Clindamycin (Cleocin) Adult
150-450 mg/dose PO q6-8h; not to exceed 1.8 g/d600-1200 mg/d IV/IM divided q6-8h, depending on degree of infection
Pediatric 8-20 mg/kg/d PO as hydrochloride and 8-25 mg/kg/d as palmitate divided
tid/qid20-40 mg/kg/d IV/IM divided tid/qid
Lincosamide for treatment of serious skin and soft tissuestaphylococcal infections. Also effective against aerobic andanaerobic streptococci (except enterococci). Inhibits bacterial
growth, possibly by blocking dissociation of peptidyl t-RNA fromribosomes causing RNA-dependent protein synthesis to arrest.
-
8/13/2019 Hepatobilier Pemicu 4
40/42
Metronidazole (Flagyl) Adult
Loading dose: 15 mg/kg or 1 g for 70-kg adult IV over 1 hMaintenance dose: 6 h following loading dose; infuse 7.5 mg/kg or500 mg IV for 70-kg adult over 1 h q6-8h; not to exceed 4 g/d
Pediatric 15-30 mg/kg/d PO divided bid/tid for 7 d, or 40 mg/kg once; do not
exceed 2 g/d
Imidazole ring-based antibiotic active against various
anaerobic bacteria and protozoa. Used in combinationwith other antimicrobial agents (except for Clostridiumdifficileenterocolitis).
-
8/13/2019 Hepatobilier Pemicu 4
41/42
Antifungal agents
Amphotericin B (AmBisome) Adult
3-5 mg/kg/d IV of liposomal amphotericin B over approximately120 min
Pediatric Administer as in adults
Produced by a strain of Streptomyces nodosus; can befungistatic or fungicidal. Binds to sterols, such as
ergosterol, in the fungal-cell membrane, causingintracellular components to leak with subsequentfungal-cell death.
-
8/13/2019 Hepatobilier Pemicu 4
42/42
Fluconazole (Diflucan) Adult
150 mg PO once or 400 mg/d, depending on severity ofinfection
Pediatric 3-6 mg/kg/d PO for 14-28 d or 6-12 mg/kg/d, depending on
severity of infection
Synthetic oral antifungal (broad-spectrumbistriazole) that selectively inhibits fungalcytochrome P-450 and sterol C-14 alpha-demethylation.