
Selective inhibition of prostacyclin synthase activity by rofecoxib

Vascular Properties of Canine Lungs Perfused With Eurocollins Solution and Prostacyclin Helmut Unruh, MD, Mike Hoppensack, BSc, and Luis Oppenheimer, MD Respiratory Investigation Unit, Department of Surgery, Faculty of Medicine, University of Manitoba, Canada
Although Eurocollins solution (ECS) is commonly used for lung preservation, its vascular effects and their time course and response to pharmocological interventions are not well understood. The effect of 4°C ECS on the pulmonary circulation was assessed in excised canine left lower lobes. The roles of static oxygen inflation and prostacyclin infusion during ECS perfusion were also examined. The lobes were divided into five groups: time control (A), ECS with oxygen (B), ECS without oxygen (C), ECS with glycine buffer (D), and ECS with prosta- cyclin (E); group D was the control for E. Eurocollins solution had no effect on gas exchange but had a marked effect on the pulmonary circulation. Vascular conduc- tance decreased from 22.6 to 18.9 mL/min/cm H,O and
urrently, lung preservation methods for transplanta- C tion allow only four hours from the time of removal to implantation despite many efforts to extend this period [l-31. The most widely used approach is flushing with cold Eurocollins solution (ECS), followed by hypothermic storage. Eurocollins solution is a hyperosmolar electrolyte solution rich in potassium and phosphate. Its composition and hypothermia combine to decrease metabolism to a minimum, thereby preventing ischemic injury. Concerns about acute increases in pulmonary vascular resistance after lung transplantation (4, 51 have led to use of potent vasodilators such as prostaglandin El and prostacyclin (PGI,) [6, 71 as adjuvants to ECS.
The present report describes a method used to study systematically the pulmonary vascular effects of combined ECS perfusion and PGI, infusion and demonstrate its efficacy. Prostacyclin has two known effects on the pul- monary circulation that theoretically could prove benefi- cial in this setting. It is a very potent vasodilator of the pulmonary circulation and also strongly inhibits adeno- sine diphosphate-induced platelet aggregation. The role of static oxygen inflation during ECS perfusion was also examined. This could have important implications for lung preservation, as oxygen radicals have been impli- cated in lung injury; investigators have also shown that statically inflated lungs continue to consume oxygen at temperatures as low as 6°C and may therefore require oxygen [8].
Accepted for publication Oct 31, 1989.
Address reprint requests to Dr Unruh, RS 119-810 Sherbrook Ave, Winni- peg, Manitoba, Canada R3A 1R8.
from 21.3 to 14.1 mL/min/cm H,O with average vascular closure increasing by 1.2 and 2.1 cm H,O in groups B and C, respectively. The decreased vascular conductance and increased vascular closure was associated with a reduc- tion in vascular compliance from 1.63 to 1.25 mL/cm H,O. When prostacyclin was added to ECS, the reduc- tion in vascular closure was much less and was associ- ated with a decrease in vascular closure and no loss of vascular compliance. Eurocollins solution increases pres- sure cost for perfusion by causing both vascular obstruc- tion and increased tone, especially when oxygen is not provided. This is significantly overcome by addition of prostacyclin infusion during ECS perfusion.
(Ann Thorac Surg 1990;49:292-8)
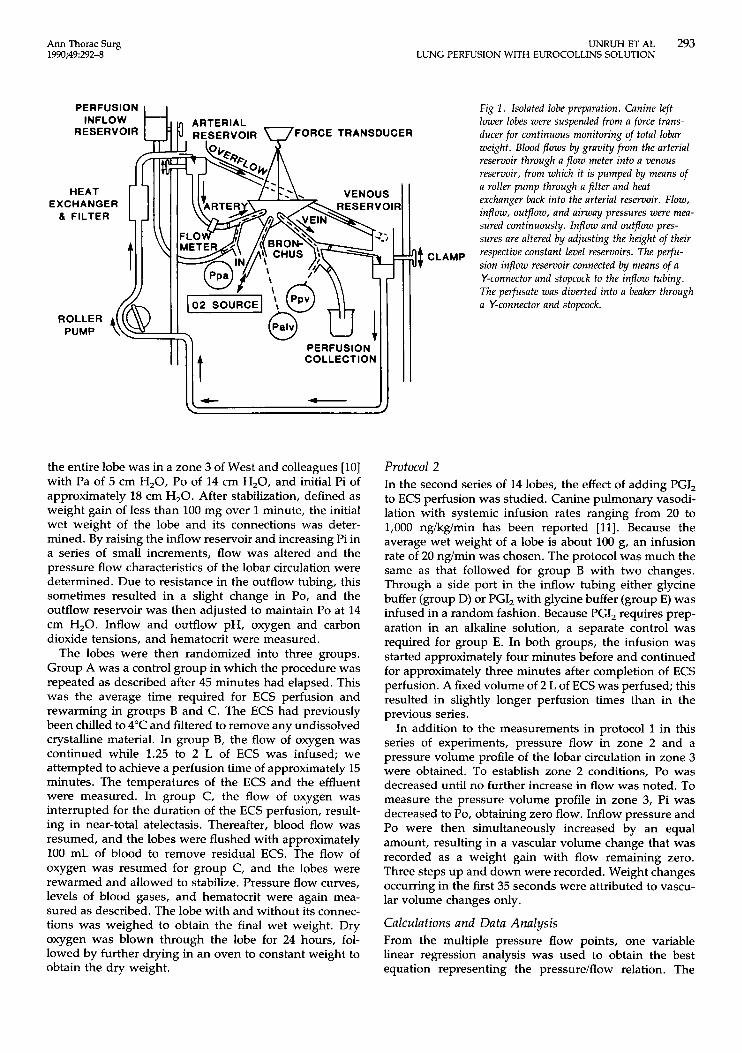
Material and Methods Animal and Lobar Preparation Thirty-three healthy mongrel dogs weighing between 16 and 32 kg were anesthetized with pentobarbital sodium (30 mg/kg), intubated, and ventilated with a small animal respirator. All animals received humane care in compli- ance with the “Guide for the Care and Use of Laboratory Animals” published by the National Institutes of Health (NIH publication No. 85-23, revised 1985). The basic preparation has been previously described in detail [9]. A left thoracotomy was performed, heparin was adminis- tered, and the left lower lobe artery, vein, and bronchus were cannulated. After the animals were exsanguinated, the lobe was excised and suspended from a force trans- ducer for continuous monitoring of lobar weight changes in the range of 100 mg. Arterial and venous cannulas were connected to constant level reservoirs of adjustable height, and inflow (Pi) and outflow (Po) pressures were continuously monitored using the hilum as the zero reference point. The bronchial cannula was connected to a 100% oxygen source and airway pressure (Pa) was con- tinuously measured. The blood was pumped by a roller pump from the outflow reservoir through a heat ex- changer, filter, inflow reservoir, and flow meter. A third reservoir was used for ECS perfusion and PGI, infusion, with additional tubing to divert the flow of ECS coming out of the lobe. The experimental preparation is shown in Figure 1.
Protocol 1 In the first series of 19 lobes, the pulmonary vascular effects of ECS with and without oxygen were studied. Inflow pressure, Po, and Pa were set in such a way that
0 1990 by The Society of Thoracic Surgeons 0003-4975/90/$3.50
Ann Thorac Surg 1990;49292-8
UNRUH ET AL 293 LUNG PERFUSION WITH EUROCOLLINS SOLUTION
PERFUSION I I
RESERVOIR FORCE TRANSDUCER
EXCHANGER
t PERFUSION COLLECTION
f J
the entire lobe was in a zone 3 of West and colleagues [lo] with Pa of 5 cm H,O, Po of 14 cm H,O, and initial Pi of approximately 18 cm H,O. After stabilization, defined as weight gain of less than 100 mg over 1 minute, the initial wet weight of the lobe and its connections was deter- mined. By raising the inflow reservoir and increasing Pi in a series of small increments, flow was altered and the pressure flow characteristics of the lobar circulation were determined. Due to resistance in the outflow tubing, this sometimes resulted in a slight change in Po, and the outflow reservoir was then adjusted to maintain Po at 14 cm H,O. Inflow and outflow pH, oxygen and carbon dioxide tensions, and hematocrit were measured.
The lobes were then randomized into three groups. Group A was a control group in which the procedure was repeated as described after 45 minutes had elapsed. This was the average time required for ECS perfusion and rewarming in groups B and C. The ECS had previously been chilled to 4°C and filtered to remove any undissolved crystalline material. In group B, the flow of oxygen was continued while 1.25 to 2 L of ECS was infused; we attempted to achieve a perfusion time of approximately 15 minutes. The temperatures of the ECS and the effluent were measured. In group C, the flow of oxygen was interrupted for the duration of the ECS perfusion, result- ing in near-total atelectasis. Thereafter, blood flow was resumed, and the lobes were flushed with approximately 100 mL of blood to remove residual ECS. The flow of oxygen was resumed for group C, and the lobes were rewarmed and allowed to stabilize. Pressure flow curves, levels of blood gases, and hematocrit were again mea- sured as described. The lobe with and without its connec- tions was weighed to obtain the final wet weight. Dry oxygen was blown through the lobe for 24 hours, fol- lowed by further drying in an oven to constant weight to obtain the dry weight.
]$ CLAMP
Fig 1 . Isolated lobe preparation. Canine left lower lobes were suspended from a force trans- ducer for continuous monitoring of total lobar weight. Blood flows by gravity from the arterial reservoir through a flow meter into a venous reservoir, from which it is pumped by means of a roller pump through a filter and heat exchanger back into the arterial reservoir. Flow, inflow, outflow, and airway pressures were mea- sured continuously. Inflow and outflow pres- sures are altered by adjusting the height o j their respective constant level reservoirs. The perfu- sion inflow reservoir connected by means of a Y-connector and stopcock to the inflow tubing. The perfusate was diverted into a beaker through a Y-connector and stopcock.
Protocol 2 In the second series of 14 lobes, the effect of adding PGI, to ECS perfusion was studied. Canine pulmonary vasodi- lation with systemic infusion rates ranging from 20 to 1,000 ng/kg/min has been reported [ l l ] . Because the average wet weight of a lobe is about 100 g, an infusion rate of 20 ng/min was chosen. The protocol was much the same as that followed for group B with two changes. Through a side port in the inflow tubing either glycine buffer (group D) or PGI, with glycine buffer (group E) was infused in a random fashion. Because PGI, requires prep- aration in an alkaline solution, a separate control was required for group E. In both groups, the infusion was started approximately four minutes before and continued for approximately three minutes after completion of ECS perfusion. A fixed volume of 2 L of ECS was perfused; this resulted in slightly longer perfusion times than in the previous series.
In addition to the measurements in protocol 1 in this series of experiments, pressure flow in zone 2 and a pressure volume profile of the lobar circulation in zone 3 were obtained. To establish zone 2 conditions, Po was decreased until no further increase in flow was noted. To measure the pressure volume profile in zone 3, Pi was decreased to Po, obtaining zero flow. Inflow pressure and Po were then simultaneously increased by an equal amount, resulting in a vascular volume change that was recorded as a weight gain with flow remaining zero. Three steps up and down were recorded. Weight changes occurring in the first 35 seconds were attributed to vascu- lar volume changes only.
Calculations and Data Analysis From the multiple pressure flow points, one variable linear regression analysis was used to obtain the best equation representing the pressure/flow relation. The
294 UNRUH ET AL LUNG PERFUSION WITH EUROCOLLINS SOLUTION
Ann Thorac Surg 1990:49:292-8
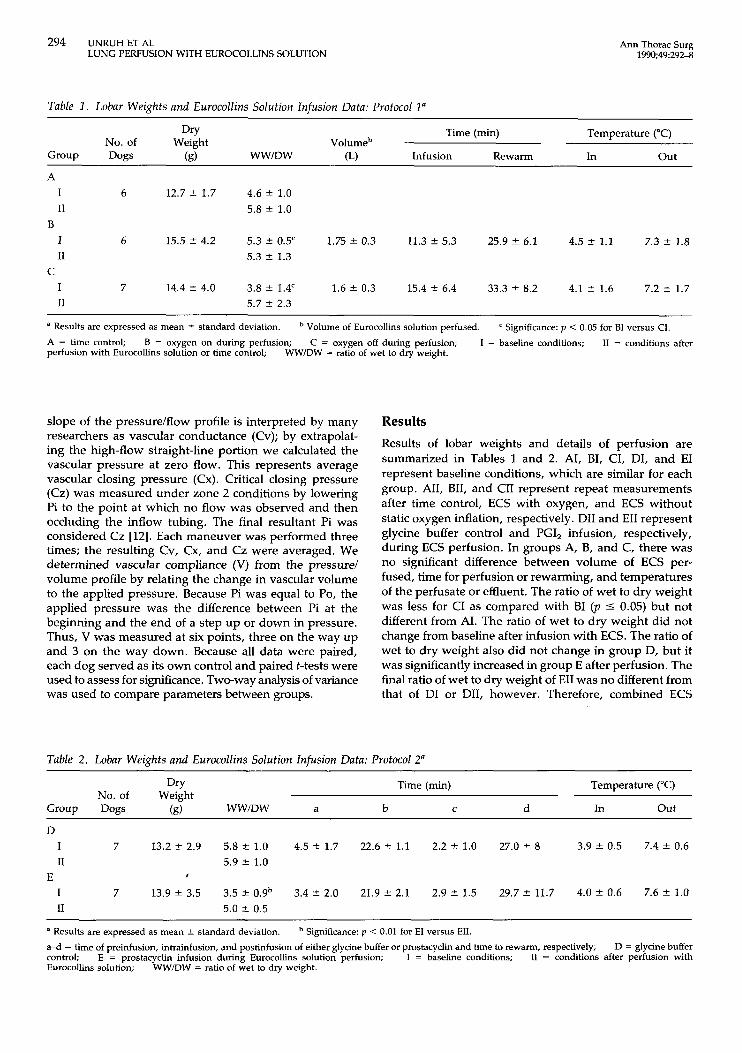
Table 1 . Lobar Weights and Eurocollins Solution Infusion Data: Protocol 1"
Dry Time (min) Temperature ("C) No. of Weight Volumeb
Group Dogs (g) WW/DW (L) Infusion Rewarm In o u t
A I 6 12.7 ? 1.7 4.6 t 1.0 I1
B 5.8 t 1.0
I 6 15.5 * 4.2 5.3 ? 0.5' 1.75 * 0.3 11.3 f 5.3 25.9 * 6.1 4.5 ? 1.1 7.3 5 1.8 I1
C 5.3 2 1.3
I 7 14.4 f 4.0 3.8 ? 1.4' 1.6 ? 0.3 15.4 t 6.4 33.3 ? 8.2 4.1 t 1.6 7.2 f 1.7 I1 5.7 f 2.3
a Results are expressed as mean * standard deviation. A = time control; perfusion with Eurocollins solution or time control;
Volume of Eurocollins solution perfused. Significance: p < 0.05 for BI versus CI. B = oxygen on during perfusion; C = oxygen off during perfusion; 1 = baseline conditions; I1 = conditions after
WW/DW = ratio of wet to dry weight.
slope of the pressurelflow profile is interpreted by many researchers as vascular conductance (Cv); by extrapolat- ing the high-flow straight-line portion we calculated the vascular pressure at zero flow. This represents average vascular closing pressure (Cx). Critical closing pressure (Cz) was measured under zone 2 conditions by lowering Pi to the point at which no flow was observed and then occluding the inflow tubing. The final resultant Pi was considered Cz [12]. Each maneuver was performed three times; the resulting Cv, Cx, and Cz were averaged. We determined vascular compliance (V) from the pressure1 volume profile by relating the change in vascular volume to the applied pressure. Because Pi was equal to Po, the applied pressure was the difference between Pi at the beginning and the end of a step up or down in pressure. Thus, V was measured at six points, three on the way up and 3 on the way down. Because all data were paired, each dog served as its own control and paired t-tests were used to assess for significance. Two-way analysis of variance was used to compare parameters between groups.
Results Results of lobar weights and details of perfusion are summarized in Tables 1 and 2. AI, BI, CI, DI, and EI represent baseline conditions, which are similar for each group. AII, BII, and CII represent repeat measurements after time control, ECS with oxygen, and ECS without static oxygen inflation, respectively. DII and EII represent glycine buffer control and PGI, infusion, respectively, during ECS perfusion. In groups A, B, and C, there was no significant difference between volume of ECS per- fused, time for perfusion or rewarming, and temperatures of the perfusate or effluent. The ratio of wet to dry weight was less for CI as compared with BI ( p 5 0.05) but not different from AI. The ratio of wet to dry weight did not change from baseline after infusion with ECS. The ratio of wet to dry weight also did not change in group D, but it was significantly increased in group E after perfusion. The final ratio of wet to dry weight of EII was no different from that of DI or DII, however. Therefore, combined ECS
Table 2. Lobar Weights and Eurocollins Solution Infusion Data: Protocol 2"
Dry Time (min) Temperature ("C)
Group Dogs (R) WWIDW a b C d In Out No. of Weight
D I 7 13.2 2 2.9 5.8 2 1.0 4.5 t 1.7 22.6 t 1.1 2.2 t l . 0 27.0 t 8 3.9 * 0.5 7.4 t 0.6 I1 5.9 2 1.0
I 7 13.9 f 3.5 3.5 * 0.9b 3.4 t 2.0 21.9 t 2.1 2.9 f 1.5 29.7 * 11.7 4.0 * 0.6 7.6 f 1.0 I1 5.0 2 0.5
E I
a Results are expressed as mean & standard deviation.
a 4 = time of preinfusion, intrainfusion, and postinfusion of either glycine buffer or prostacyclin and time to rewarm, respectively; control; Eurocollins solution;
Significance: p < 0.01 for EI versus EII D = glycine buffer
I1 = conditions after perfusion with E = prostacyclin infusion during Eurocollins solution perfusion; I = baseline conditions; WWDW = ratio of wet to dry weight.
Ann Thorac Surg 1990;49292-8
UNRUH ET AL 295 LUNG PERFUSION WITH EUROCOLLINS SOLUTION
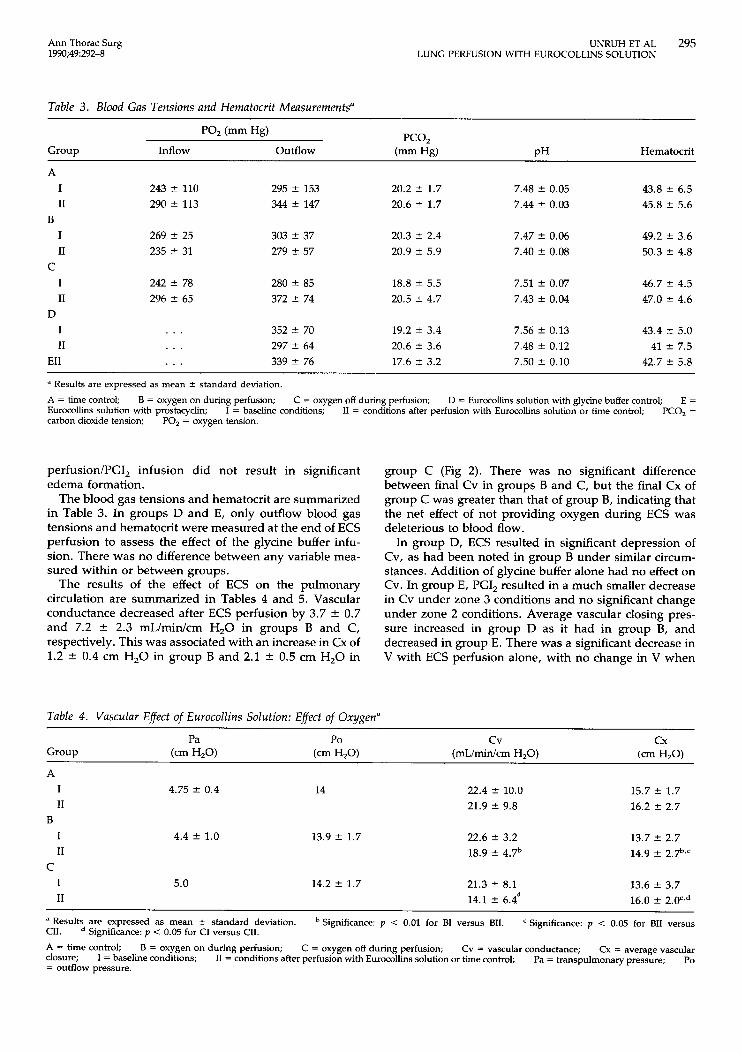
Table 3. Blood Gas Tensions and Hernatocrit Measurements'
PCO, PO2 (mm Hg)
Group Inflow outflow (mm Hg) PH Hematocrit
A I I1
B I I1
C I I1
D I I1
EII
243 f 110 290 f 113
269 2 25 235 t 31
242 f 78 296 f 65
. . .
. . .
. . .
295 f 153 344 f 147
303 f 37 279 f. 57
280 f 85 372 f 74
352 f 70 297 f 64 339 f 76
20.2 f 1.7 20.6 f 1.7
20.3 f 2.4 20.9 f 5.9
18.8 f 5.5 20.5 f 4.7
19.2 f 3.4 20.6 2 3.6 17.6 2 3.2
7.48 2 0.05 7.44 f 0.03
7.47 t 0.06 7.40 f 0.08
7.51 f 0.07 7.43 f 0.04
7.56 f 0.13 7.48 f 0.12 7.50 f 0.10
43.8 f 6.5 45.8 f 5.6
49.2 2 3.6 50.3 f 4.8
46.7 f 4.5 47.0 f 4.6
43.4 f. 5.0 41 f 7.5
42.7 t 5.8
a Results are expressed as mean 2 standard deviation.
A = time control; Eurocollins solution with prostacyclin; carbon dioxide tension;
B = oxygen on during perfusion; C = oxygen off during perfusion; D = Eurocollins solution with glycine buffer control; E = PCO, = I = baseline conditions; I1 = conditions after perfusion with Eurocollins solution or time control;
PO, = oxygen tension.
perfusion/PGI, infusion did not result in significant edema formation.
The blood gas tensions and hematocrit are summarized in Table 3. In groups D and E, only outflow blood gas tensions and hematocrit were measured at the end of ECS perfusion to assess the effect of the glycine buffer infu- sion. There was no difference between any variable mea- sured within or between groups.
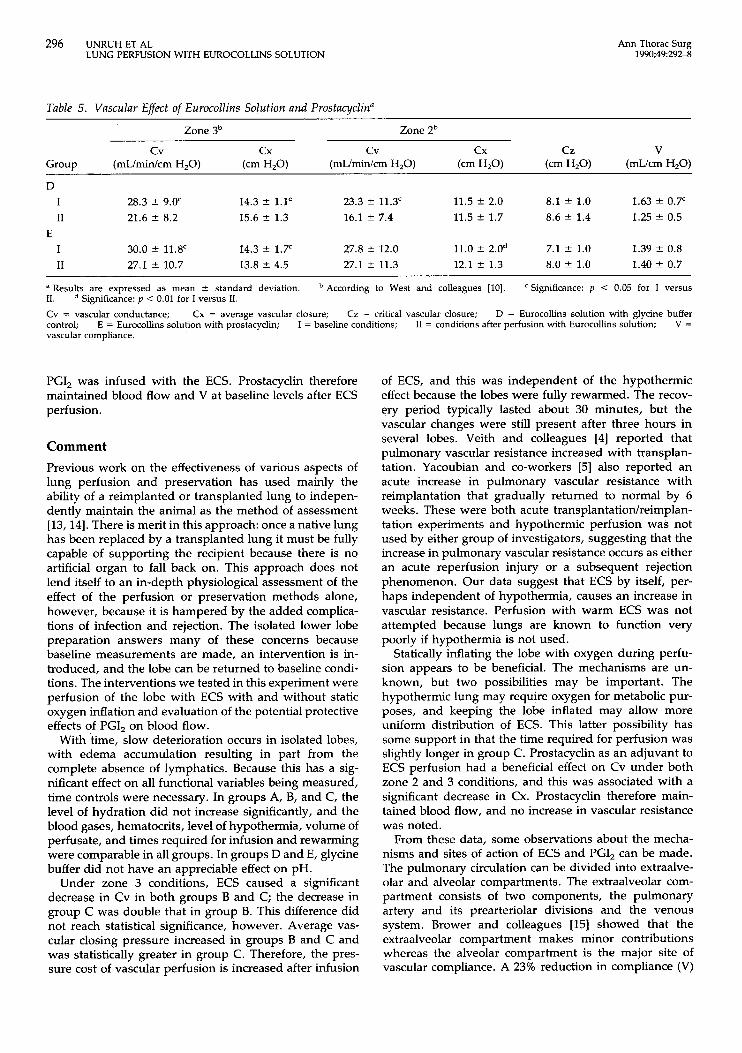
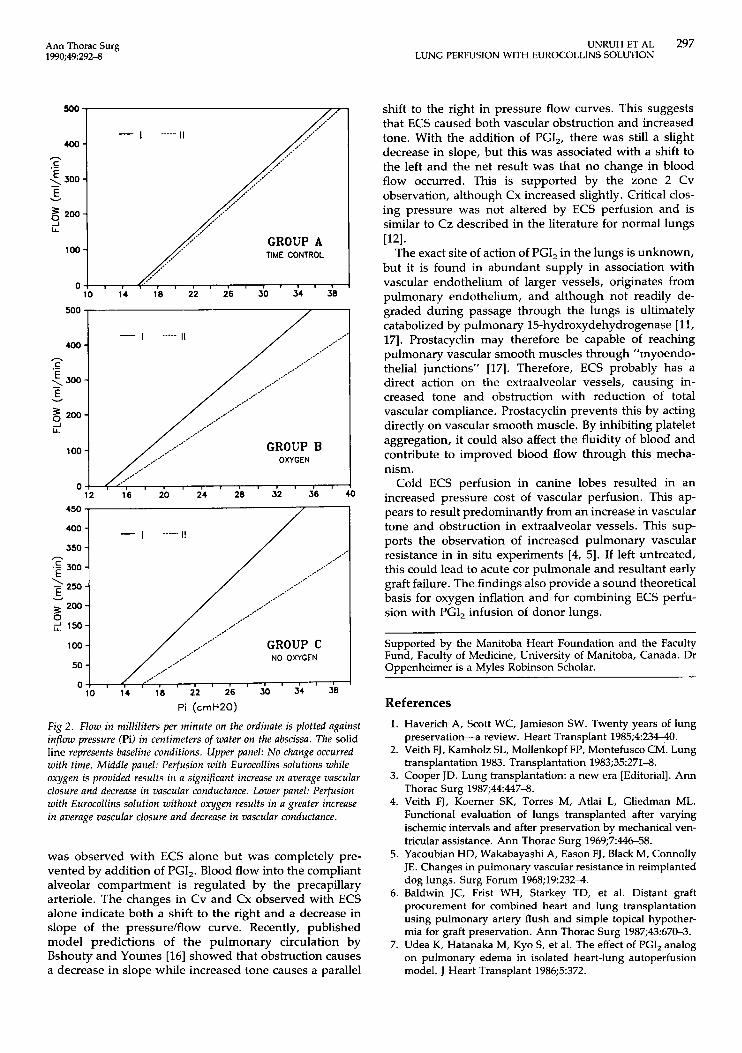
The results of the effect of ECS on the pulmonary circulation are summarized in Tables 4 and 5. Vascular conductance decreased after ECS perfusion by 3.7 * 0.7 and 7.2 * 2.3 mL/min/cm H,O in groups B and C, respectively. This was associated with an increase in Cx of 1.2 * 0.4 cm H,O in group B and 2.1 * 0.5 cm H,O in
Table 4. Vascular Effect of Eurocollins Solution: Effect of Oxygen"
group C (Fig 2). There was no significant difference between final Cv in groups B and C, but the final Cx of group C was greater than that of group B, indicating that the net effect of not providing oxygen during ECS was deleterious to blood flow.
In group D, ECS resulted in significant depression of Cv, as had been noted in group B under similar circum- stances. Addition of glycine buffer alone had no effect on Cv. In group E, PGI, resulted in a much smaller decrease in Cv under zone 3 conditions and no significant change under zone 2 conditions. Average vascular closing pres- sure increased in group D as it had in group B, and decreased in group E. There was a significant decrease in V with ECS perfusion alone, with no change in V when
I I1
B
4.75 f 0.4 14 22.4 f 10.0 21.9 f 9.8
15.7 k 1.7 16.2 f 2.7
13.7 f 2.7 I 4.4 t 1.0 13.9 f 1.7 22.6 f 3.2 I1
C 18.9 f 4.7b 14.9 f 2.7b*c
I 5.0 14.2 f 1.7 21.3 f 8.1 13.6 f 3.7 I1 14.1 2 6.4d 16.0 f 2 . 0 ' ~ ~
a Results are expressed as mean 2 standard deviation. CII. Significance: p < 0.05 for CI versus CII.
A = time control; closure; = outflow pressure.
Significance: p < 0.01 for BI versus BII. Significance: p < 0.05 for BII versus
Cx = average vascular Po
B = oxygen on during perfusion; C = oxygen off during perfusion; Cv = vascular conductance; I = baseline conditions; I1 = conditions after perfusion with Eurocollins solution or time control; Pa = transpulmonary pressure;
296 UNRUH ET AL LUNG PERFUSION WITH EUROCOLLINS SOLUTION
Ann Thorac Surg 1990;49292-8
Table 5 . Vascular Effect of Eurocollins Solution and Prostacyclin"
Zone 3b Zone zb c v cx c v cx C Z V
Group (mL/min/cm H,O) (cm H,O) (mL/min/cm H20) (cm H20) (cm H2O) (mL/cm H,O)
D I 28.3 f 9.0' 14.3 ? 1.1' 23.3 f 11.3' 11.5 ? 2.0 8.1 f 1.0 1.63 f 0.7' I1 21.6 2 8.2 15.6 f 1.3 16.1 ? 7.4 11.5 f 1.7 8.6 f 1.4 1.25 * 0.5
I 30.0 2 11.8' 14.3 f 1.7' 27.8 ? 12.0 11.0 f 2.Od 7.1 * 1.0 1.39 -C 0.8 I1 27.1 2 10.7 13.8 f 4.5 27.1 ? 11.3 12.1 ? 1.3 8.0 f 1.0 1.40 * 0.7
E
a Results are expressed as mean * standard deviation. 11. Cv = vascular conductance; control; vascular compliance.
According to West and colleagues [lo]. Significance: p < 0.05 for I versus
D = Eurocollins solution with glycine buffer V =
Significance: p < 0.01 for I versus 11.
Cx = average vascular closure; Cz = critical vascular closure; E = Eurocollins solution with prostacyclin; I = baseline conditions; I1 = conditions after perfusion with Eurocollins solution;
PGI, was infused with the ECS. Prostacyclin therefore maintained blood flow and V at baseline levels after ECS perfusion.
Comment Previous work on the effectiveness of various aspects of lung perfusion and preservation has used mainly the ability of a reimplanted or transplanted lung to indepen- dently maintain the animal as the method of assessment [13,14]. There is merit in this approach: once a native lung has been replaced by a transplanted lung it must be fully capable of supporting the recipient because there is no artificial organ to fall back on. This approach does not lend itself to an in-depth physiological assessment of the effect of the perfusion or preservation methods alone, however, because it is hampered by the added complica- tions of infection and rejection. The isolated lower lobe preparation answers many of these concerns because baseline measurements are made, an intervention is in- troduced, and the lobe can be returned to baseline condi- tions. The interventions we tested in this experiment were perfusion of the lobe with ECS with and without static oxygen inflation and evaluation of the potential protective effects of PGI, on blood flow.
With time, slow deterioration occurs in isolated lobes, with edema accumulation resulting in part from the complete absence of lymphatics. Because this has a sig- nificant effect on all functional variables being measured, time controls were necessary. In groups A, B, and C, the level of hydration did not increase significantly, and the blood gases, hematocrits, level of hypothermia, volume of perfusate, and times required for infusion and rewarming were comparable in all groups. In groups D and E, glycine buffer did not have an appreciable effect on pH.
Under zone 3 conditions, ECS caused a significant decrease in Cv in both groups B and C; the decrease in group C was double that in group B. This difference did not reach statistical significance, however. Average vas- cular closing pressure increased in groups B and C and was statistically greater in group C. Therefore, the pres- sure cost of vascular perfusion is increased after infusion
of ECS, and this was independent of the hypothermic effect because the lobes were fully rewarmed. The recov- ery period typically lasted about 30 minutes, but the vascular changes were still present after three hours in several lobes. Veith and colleagues [4] reported that pulmonary vascular resistance increased with transplan- tation. Yacoubian and co-workers [5] also reported an acute increase in pulmonary vascular resistance with reimplantation that gradually returned to normal by 6 weeks. These were both acute transplantatiodreimplan- tation experiments and hypothermic perfusion was not used by either group of investigators, suggesting that the increase in pulmonary vascular resistance occurs as either an acute reperfusion injury or a subsequent rejection phenomenon. Our data suggest that ECS by itself, per- haps independent of hypothermia, causes an increase in vascular resistance. Perfusion with warm ECS was not attempted because lungs are known to function very poorly if hypothermia is not used.
Statically inflating the lobe with oxygen during perfu- sion appears to be beneficial. The mechanisms are un- known, but two possibilities may be important. The hypothermic lung may require oxygen for metabolic pur- poses, and keeping the lobe inflated may allow more uniform distribution of ECS. This latter possibility has some support in that the time required for perfusion was slightly longer in group C. Prostacyclin as an adjuvant to ECS perfusion had a beneficial effect on Cv under both zone 2 and 3 conditions, and this was associated with a significant decrease in Cx. Prostacyclin therefore main- tained blood flow, and no increase in vascular resistance was noted.
From these data, some observations about the mecha- nisms and sites of action of ECS and PGI, can be made. The pulmonary circulation can be divided into extraalve- olar and alveolar compartments. The extraalveolar com- partment consists of two components, the pulmonary artery and its prearteriolar divisions and the venous system. Brower and colleagues [15] showed that the extraalveolar compartment makes minor contributions whereas the alveolar compartment is the major site of vascular compliance. A 23% reduction in compliance (V)
Ann Thorac Surg 1990;49:292-8
UNRUH ET AL 297 LUNG PERFUSION WITH EUROCOLLINS SOLUTION
500 -
- I I I 400 -
GROUP A lool / TIME CONTROL
,c' ,'. o ! , , 4 , , , I 1 1 I 1 I 1 1 I
10 14 18 22 26 30 34 38
*,+' ,.,' - I I I 400 - ,.*'
*,-'
C _,/." h
.- 5 500 - - E v
3 200- s LL
GROUP B OXYGEN
100 -
12 16 20 24 28 32 36 40 450 /
/
100 4 / /.-- GROUP C NO OXYGEN
/- 0 ' I ./ ,*'
lb 14 ' 18 22 26 30 34 38 Pi (cmH20)
Fig 2. Flow in milliliters per minute on the ordinate is plotted against inflow pressure (Pi) in centimeters of water on the abscissa. The solid line represents baseline conditions. Upper panel: No change occurred with time. Middle panel: Perfusion with Eurocollins solutions while oxygen is provided results in a significant increase in average vascular closure and decrease in vascular conductance. Lower panel: Perfusion with Eurocollins solution without oxygen results in a greater increase in average vascular closure and decrease in vascular conductance.
was observed with ECS alone but was completely pre- vented by addition of PGI,. Blood flow into the compliant alveolar compartment is regulated by the precapillary arteriole. The changes in Cv and Cx observed with ECS alone indicate both a shift to the right and a decrease in slope of the pressure/flow curve. Recently, published model predictions of the pulmonary circulation by Bshouty and Younes [16] showed that obstruction causes a decrease in slope while increased tone causes a parallel
shift to the right in pressure flow curves. This suggests that ECS caused both vascular obstruction and increased tone. With the addition of PGI,, there was still a slight decrease in slope, but this was associated with a shift to the left and the net result was that no change in blood flow occurred. This is supported by the zone 2 Cv observation, although Cx increased slightly. Critical clos- ing pressure was not altered by ECS perfusion and is similar to Cz described in the literature for normal lungs
The exact site of action of PGI, in the lungs is unknown, but it is found in abundant supply in association with vascular endothelium of larger vessels, originates from pulmonary endothelium, and although not readily de- graded during passage through the lungs is ultimately catabolized by pulmonary 15-hydroxydehydrogenase [ 11, 171. Prostacyclin may therefore be capable of reaching pulmonary vascular smooth muscles through "myoendo- thelial junctions" [17]. Therefore, ECS probably has a direct action on the extraalveolar vessels, causing in- creased tone and obstruction with reduction of total vascular compliance. Prostacyclin prevents this by acting directly on vascular smooth muscle. By inhibiting platelet aggregation, it could also affect the fluidity of blood and contribute to improved blood flow through this mecha- nism.
Cold ECS perfusion in canine lobes resulted in an increased pressure cost of vascular perfusion. This ap- pears to result predominantly from an increase in vascular tone and obstruction in extraalveolar vessels. This sup- ports the observation of increased pulmonary vascular resistance in in situ experiments [4, 51. If left untreated, this could lead to acute cor pulmonale and resultant early graft failure. The findings also provide a sound theoretical basis for oxygen inflation and for combining ECS perfu- sion with PGI, infusion of donor lungs.
1121.
Supported by the Manitoba Heart Foundation and the Faculty Fund, Faculty of Medicine, University of Manitoba, Canada. Dr Oppenheimer is a Myles Robinson Scholar.
References 1. Haverich A, Scott WC, Jamieson SW. Twenty years of lung
preservation-a review. Heart Transplant 1985;4:234-40. 2. Veith FJ, Kamholz SL, Mollenkopf FP, Montefusco CM. Lung
transplantation 1983. Transplantation 1983;35:271-8. 3. Cooper JD. Lung transplantation: a new era [Editorial]. Ann
Thorac Surg 1987;44:447-8. 4. Veith FJ, Koerner SK, Torres M, Atlai L, Gliedman ML.
Functional evaluation of lungs transplanted after varying ischemic intervals and after preservation by mechanical ven- tricular assistance. Ann Thorac Surg 1969;744&58.
5. Yacoubian HD, Wakabayashi A, Eason FJ, Black M, Connolly JE. Changes in pulmonary vascular resistance in reimplanted dog lungs. Surg Forum 1968;19:2324.
6. Baldwin JC, Frist WH, Starkey TD, et al. Distant graft procurement for combined heart and lung transplantation using pulmonary artery flush and simple topical hypother- mia for graft preservation. Ann Thorac Surg 1987;43:670-3.
7. Udea K, Hatanaka M, Kyo S, et al. The effect of PGI, analog on pulmonary edema in isolated heart-lung autoperfusion model. J Heart Transplant 1986;5:372.

298 UNRUH ET AL LUNG PERFUSION WITH EUROCOLLINS SOLUTION
8. Faridy EE, Naimark A. The effect of distension on metabo- lism of excised dog lung. J Appl Physiol 1971;31:31-7.
9. Oppenheimer L, Unruh HW, Skoog C, Goldberg H. Trans- vascular fluid flux measured from intravascular water con- centration changes. J Appl Physiol 1983;54:64-72.
10. West JB, Dollery CT, Naimark A. Distribution of blood flow in isolated lung: relation to vascular and alveolar pressures. J Appl Physiol 1964;19:71>24.
11. Pace-Asaak C, Gryglewski R. Prostaglandins and related sub- stances. New York: Elsevier Science Publishers, 1983:95126.
12. Graham RC, Skoog C, Oppenheimer L, Rabson J, Goldberg H. Critical closure in the canine pulmonary vasculature. Circ Res 1982;50:556-72.
13. Pinsker KL, Montefusco C, Yipintsoi T, Kamholz SL, Norin
Ann Thorac Surg 1990;49292-8
A, Veith FJ. Total in vivo adequacy of canine lung autografts after 24-hour preservation. Transplant Proc 1979;11:97-105.
14. Pinsker KL, Kamholz SL, Montefusco C, Veith FJ. Long-term adequacy of canine lung autografts after 24-hour preserva- tion. Transplant Proc 1981;13:7157.
15. Brower RG, Wise RA, Hassapoyannes C, Hausknecht M, Permutt S. Longitudinal distribution of vascular compliance in the canine lung. J Appl Physiol 1986;61:240-7.
16. Bshouty Z, Younes M. Distensibility and dynamic behavior of the pulmonary circulation: model predictions. J Appl Physiol (in press).
17. Ryan US. Handbook of physiology, section 3: the respiratory system; vol 1: Circulation and nonrespiratory functions. Bethesda, MD: American Physiologic Society, 1985:3514.
Copyright © 2022 FDOKUMEN



















