
Thyroid, Parathyroid, and Adrenal Gland Imaging
26
13 Thyroid, Parathyroid, and Adrenal Gland Imaging William H. Martin, Martin P. Sandler, and Milton D. Gross 13.1 The Thyroid 13.1.1 Anatomy The thyroid is a bilobed structure evolving from the fourth and fifth branchial pouches. It is ini- tially attached to the ventral floor of the pharynx by the thyroglossal duct. Thyroid tissue may be found anywhere between the base of the tongue and the retrosternal anterior mediastinum (Fig- ure 13.1). The fetal thyroid gland begins to con- centrate iodine and synthesize thyroid hormones by approximately 10.5 weeks, which is pertinent when the administration of 131 I to fertile women is contemplated. The two ellipsoid lobes of the adult thyroid are joined by a thin isthmus. Each lobe is approximately 2 cm in thickness and width and averages 4–4.5 cm in length. The thy- roid gland, averaging approximately 20 grams in weight, resides in the neck at the level of the cricoid cartilage. A pyramidal lobe is present in approxi- mately 30–50%, arising from either the isthmus or the superomedial aspect of either lobe; it under- goes progressive atrophy in adulthood but may be prominent in patients with Graves’ disease. Although the right lobe tends to be somewhat larger than the left lobe, there is a great deal of variability in both size and shape of the normal gland. 13.1.2 Physiology An appreciation of thyroid physiology and patho- physiology is essential for the optimal manage- ment of thyroid disorders. The function of the thyroid gland includes the concentration of io- dine, synthesis of thyroid hormones, storage of these hormones as part of the thyroglobulin (Tg) molecule in the colloid, and their secretion into the circulation as required. Over 99% of circu- lating thyroid hormones are bound to plasma proteins, primarily thyroxine-binding globulin (TBG). Only the unbound fraction of thyroid hor- mone is metabolically active and, for this reason, accurate assays of free thyroid hormone, “free T 4 ” and “free T 3 ”, have been developed. Dietary sources of iodine include seafood, milk, eggs, and iodized products such as salt and bread. Approximately one-third of the absorbed dietary iodide is trapped by the thyroid, the remainder being excreted in the urine. Although gastric mu- cosa, salivary glands, and the lactating breast may also trap iodide, none of these organify it. The con- centration of iodide by the thyroid gland, synthe- sis, and release of thyroid hormones are under the regulatory control of the hypothalamic-pituitary- thyroid axis. Thyroid stimulating hormone (TSH) from the pituitary plays the major role in reg- ulating thyroid function and this, in turn, is 247
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Thyroid, Parathyroid, and Adrenal Gland Imaging
13Thyroid, Parathyroid, and AdrenalGland ImagingWilliam H. Martin, Martin P. Sandler,and Milton D. Gross
13.1 The Thyroid13.1.1 Anatomy
The thyroid is a bilobed structure evolving fromthe fourth and fifth branchial pouches. It is ini-tially attached to the ventral floor of the pharynxby the thyroglossal duct. Thyroid tissue may befound anywhere between the base of the tongueand the retrosternal anterior mediastinum (Fig-ure 13.1). The fetal thyroid gland begins to con-centrate iodine and synthesize thyroid hormonesby approximately 10.5 weeks, which is pertinentwhen the administration of 131I to fertile womenis contemplated. The two ellipsoid lobes of theadult thyroid are joined by a thin isthmus. Eachlobe is approximately 2 cm in thickness andwidth and averages 4–4.5 cm in length. The thy-roid gland, averaging approximately 20 grams inweight, resides in the neck at the level of the cricoidcartilage. A pyramidal lobe is present in approxi-mately 30–50%, arising from either the isthmus orthe superomedial aspect of either lobe; it under-goes progressive atrophy in adulthood but maybe prominent in patients with Graves’ disease.Although the right lobe tends to be somewhatlarger than the left lobe, there is a great deal ofvariability in both size and shape of the normalgland.
13.1.2 Physiology
An appreciation of thyroid physiology and patho-physiology is essential for the optimal manage-ment of thyroid disorders. The function of thethyroid gland includes the concentration of io-dine, synthesis of thyroid hormones, storage ofthese hormones as part of the thyroglobulin (Tg)molecule in the colloid, and their secretion intothe circulation as required. Over 99% of circu-lating thyroid hormones are bound to plasmaproteins, primarily thyroxine-binding globulin(TBG). Only the unbound fraction of thyroid hor-mone is metabolically active and, for this reason,accurate assays of free thyroid hormone, “free T4”and “free T3”, have been developed.
Dietary sources of iodine include seafood, milk,eggs, and iodized products such as salt and bread.Approximately one-third of the absorbed dietaryiodide is trapped by the thyroid, the remainderbeing excreted in the urine. Although gastric mu-cosa, salivary glands, and the lactating breast mayalso trap iodide, none of these organify it. The con-centration of iodide by the thyroid gland, synthe-sis, and release of thyroid hormones are under theregulatory control of the hypothalamic-pituitary-thyroid axis. Thyroid stimulating hormone (TSH)from the pituitary plays the major role in reg-ulating thyroid function and this, in turn, is
247
248
PRACTICAL NUCLEAR MEDICINE
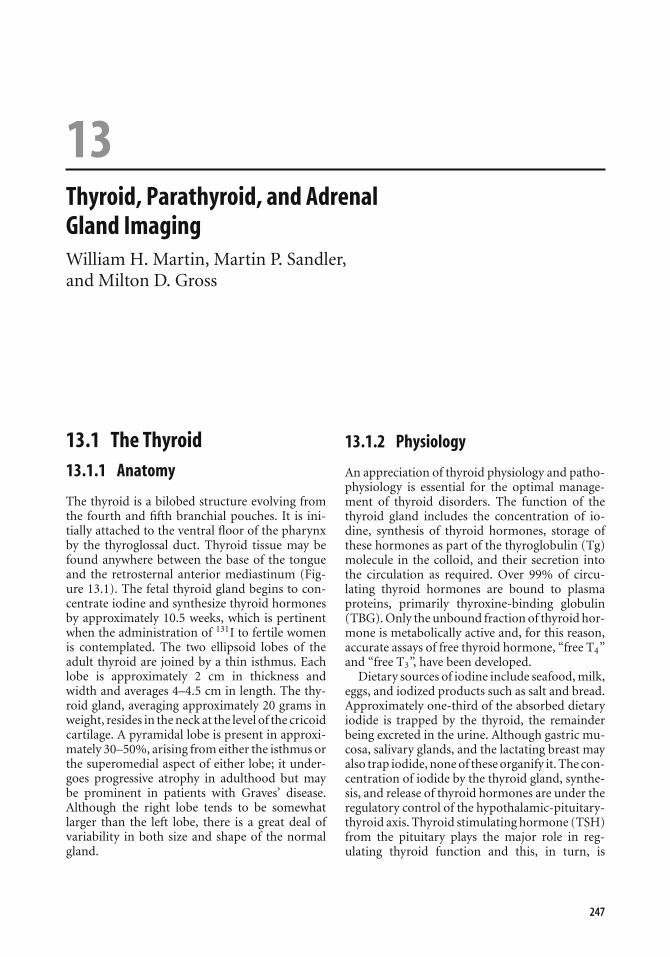
Figure 13.1. Normal and aberrant locations of thyroid tissue.
under the control of hypothalamic thyrotropin-releasing hormone (TRH) secretion. The presentthird generation assay for circulating TSH is highlysensitive and represents the most sensitive bio-chemical indicator of both hypothyroidism andhyperthyroidism; the serum TSH is elevated toabove 5 mIU/l with even subclinical primary hy-pothyroidism and is suppressed usually to un-detectable levels with hyperthyroidism. Numer-ous exogenous factors such as systemic illness,nutritional status, thionamides, beta blockers,steroids, iodide, lithium, amiodarone, and anti-convulsants, may affect thyroid hormone secre-tion and metabolism.
13.1.3 Clinical Applications
Radionuclide imaging and the measurement ofthyroid radioactive iodine uptake (RAIU) both
play an important role in the investigation ofpatients with thyroid disorders, especially thosewith thyroid nodules. RAIU is discussed in Sec-tion 4.12.
Thyroid Scintigraphy
With the development of fine needle aspirationbiopsy (FNA) for evaluation of nodular diseasecombined with the exquisite anatomic detail pro-vided by sonography, CT, and MRI, the use ofthyroid scintigraphy has decreased appropriately.However, it will continue to play an important rolein the functional evaluation of a variety of thyroiddisorders as well as the detection of metastatic thy-roid cancer. Technetium-99m pertechnetate is themost readily available radionuclide employed forthyroid imaging. Pertechnetate ions (TcO−
4 ) aretrapped by the thyroid in the same manner as
249
THYROID, PARATHYROID, AND ADRENAL GLAND IMAGING
Table 13.1. Thyroid scintigraphy
Radiopharmaceutical [99mTc]pertechnetate [123I]sodium iodide
Activity administered 80–370 MBq (2–10 mCi) 20 MBq (500 µCi)Intravenous Oral or intravenous
Effective dose equivalent 1–5 mSv (200–400 mrem) 4 mSv (400 mrem)Patient preparation Withdrawal of thyroid medication, avoidance
of foodstuffs with high iodine contentWithdrawal of thyroid medication, avoidance of
foodstuffs with high iodine contentCollimator Pinhole; low-energy, high-resolution
parallel-hole; low energy convergingPinhole; low-energy, high-resolution
parallel-hole; low energy convergingImages acquired Imaging started 15 min post-injection Imaging started 1–2 h post-injection if
intravenous or 24 h if oralAnterior, right and left anterior oblique
views, 600 second exposure per image or200 kcounts/image
Anterior, right and left anterior oblique views
iodine through an active iodine transporter, butpertechnetate ions are not organified. 123Iodine isboth trapped and organified by the thyroid gland,allowing overall assessment of thyroid function.Since 123I is cyclotron-produced and has a rel-atively short half-life of 13.6 hours, it is moreexpensive and advance notice is necessary forimaging. Because of its inferior image quality andthe high thyroid and total body radiation dosefrom its β-emission, 131I is not used for routinethyroid imaging other than for metastatic thyroidcancer assessment. Due primarily to less back-ground activity, 123I imaging provides somewhathigher quality images than 99mTc, but the diag-nostic information provided by each is roughly
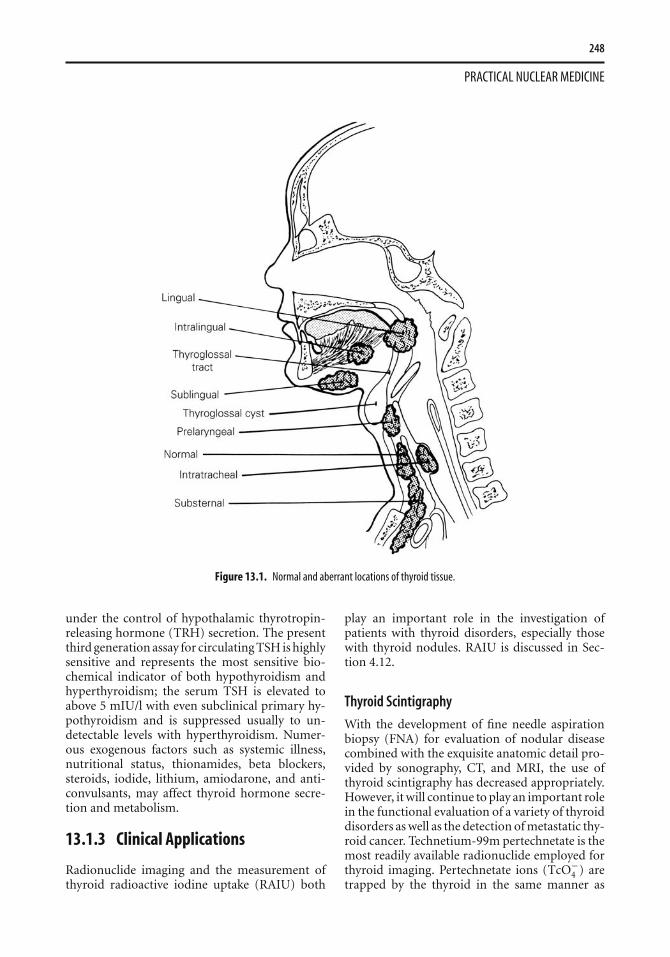
Figure 13.2. Normal 99mTc thyroid scan. Symmetric, homogeneous uptake with less intense salivary gland uptake and only mild back-ground uptake. The inferior activity is due to a 57Co marker at the suprasternal notch.
equivalent [1]. 123I imaging is used in specificsituations, such as retrosternal goiter. The protocolfor thyroid imaging is given in Table 13.1.
The normal thyroid scintigram is shown inFigure 13.2. High-resolution images are obtainedby using a pinhole collimator, thus permitting thedetection of nodules as small as 5 mm in diameter.The oblique views permit detection of small nod-ules obscured by overlying or underlying physio-logical activity. Pinhole SPECT has been used tobetter detect subtle abnormalities. The radionu-clide is distributed homogeneously throughoutthe gland with some increase seen centrally dueto physiological thickness of the gland there; ac-tivity within the isthmus is variable and must
250
PRACTICAL NUCLEAR MEDICINE
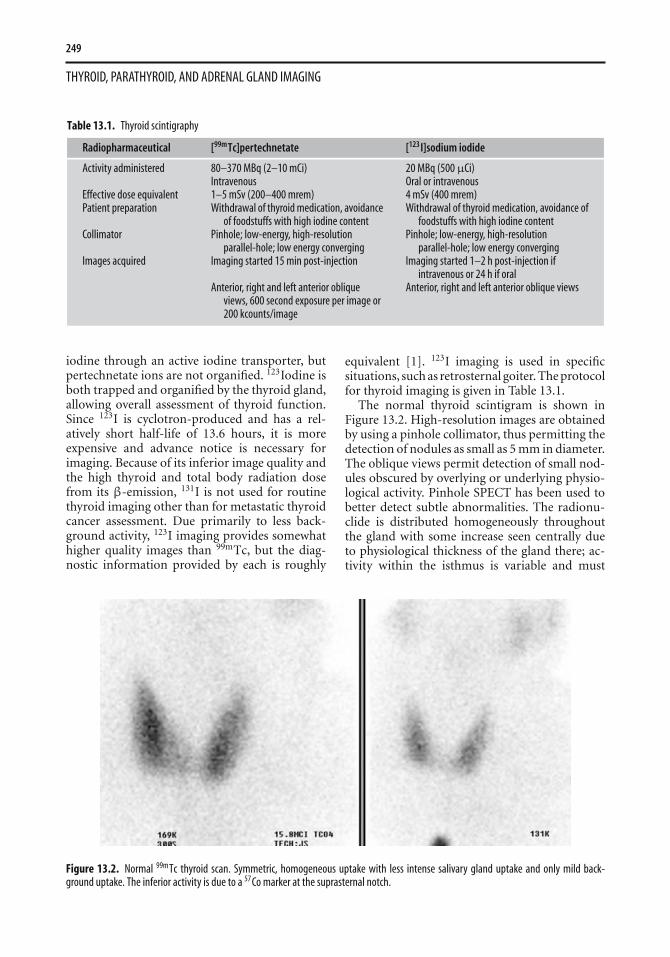
Figure 13.3. Subtle cold nodule. 99mTc pertechnetate anterior view a demonstrates a subtle hypofunctioning left lower pole nodule extendinginto the isthmus, confirmed on a subsequent contrast-enhanced CT b to be a thyroid cyst.
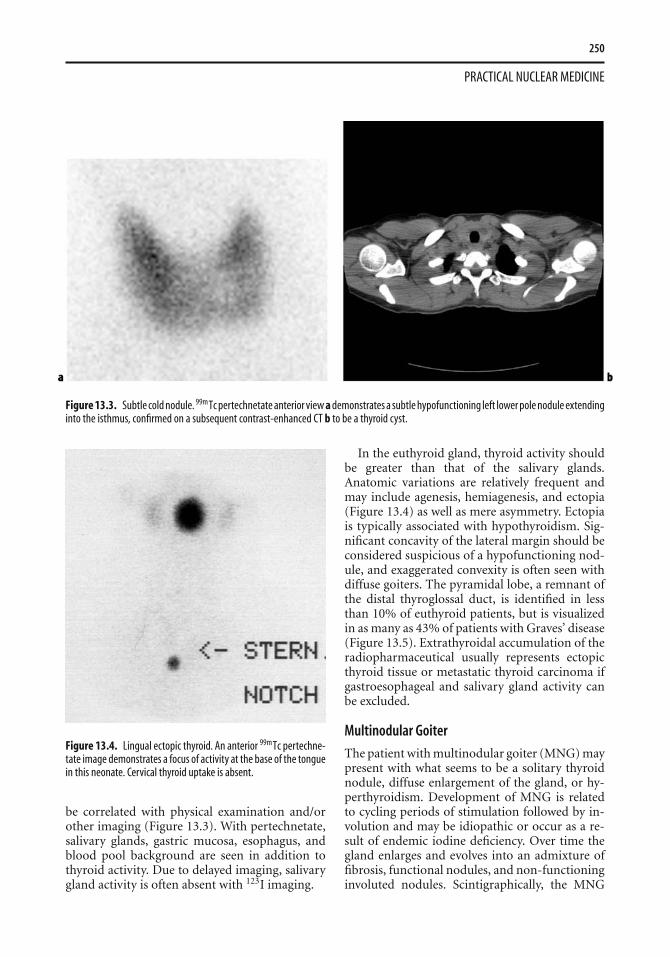
Figure 13.4. Lingual ectopic thyroid. An anterior 99mTc pertechne-tate image demonstrates a focus of activity at the base of the tonguein this neonate. Cervical thyroid uptake is absent.
be correlated with physical examination and/orother imaging (Figure 13.3). With pertechnetate,salivary glands, gastric mucosa, esophagus, andblood pool background are seen in addition tothyroid activity. Due to delayed imaging, salivarygland activity is often absent with 123I imaging.
In the euthyroid gland, thyroid activity shouldbe greater than that of the salivary glands.Anatomic variations are relatively frequent andmay include agenesis, hemiagenesis, and ectopia(Figure 13.4) as well as mere asymmetry. Ectopiais typically associated with hypothyroidism. Sig-nificant concavity of the lateral margin should beconsidered suspicious of a hypofunctioning nod-ule, and exaggerated convexity is often seen withdiffuse goiters. The pyramidal lobe, a remnant ofthe distal thyroglossal duct, is identified in lessthan 10% of euthyroid patients, but is visualizedin as many as 43% of patients with Graves’ disease(Figure 13.5). Extrathyroidal accumulation of theradiopharmaceutical usually represents ectopicthyroid tissue or metastatic thyroid carcinoma ifgastroesophageal and salivary gland activity canbe excluded.
Multinodular Goiter
The patient with multinodular goiter (MNG) maypresent with what seems to be a solitary thyroidnodule, diffuse enlargement of the gland, or hy-perthyroidism. Development of MNG is relatedto cycling periods of stimulation followed by in-volution and may be idiopathic or occur as a re-sult of endemic iodine deficiency. Over time thegland enlarges and evolves into an admixture offibrosis, functional nodules, and non-functioninginvoluted nodules. Scintigraphically, the MNG
251
THYROID, PARATHYROID, AND ADRENAL GLAND IMAGING
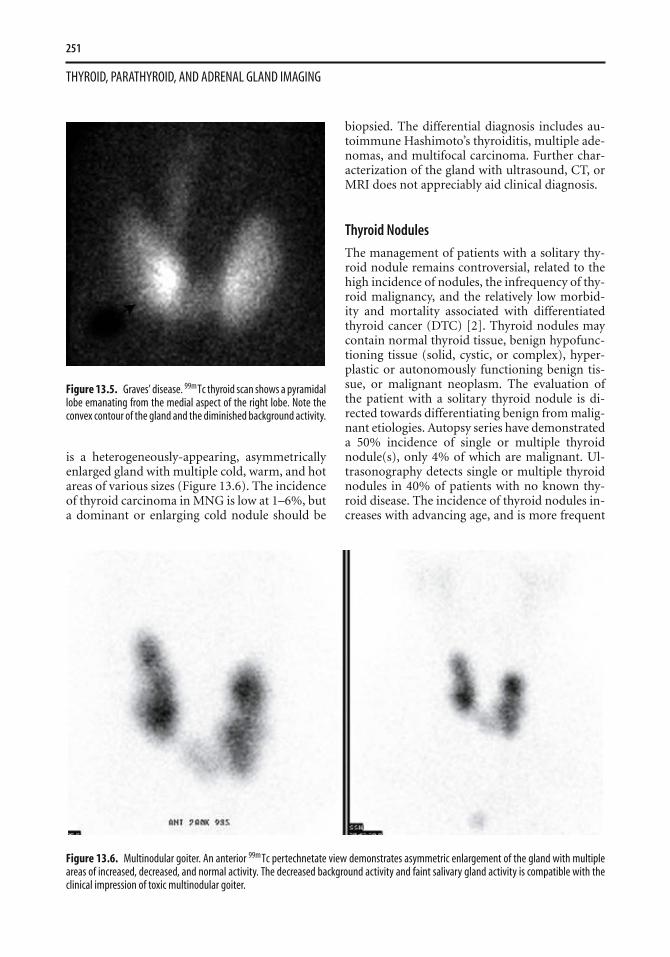
Figure 13.5. Graves’ disease. 99mTc thyroid scan shows a pyramidallobe emanating from the medial aspect of the right lobe. Note theconvex contour of the gland and the diminished background activity.
is a heterogeneously-appearing, asymmetricallyenlarged gland with multiple cold, warm, and hotareas of various sizes (Figure 13.6). The incidenceof thyroid carcinoma in MNG is low at 1–6%, buta dominant or enlarging cold nodule should be
biopsied. The differential diagnosis includes au-toimmune Hashimoto’s thyroiditis, multiple ade-nomas, and multifocal carcinoma. Further char-acterization of the gland with ultrasound, CT, orMRI does not appreciably aid clinical diagnosis.
Thyroid Nodules
The management of patients with a solitary thy-roid nodule remains controversial, related to thehigh incidence of nodules, the infrequency of thy-roid malignancy, and the relatively low morbid-ity and mortality associated with differentiatedthyroid cancer (DTC) [2]. Thyroid nodules maycontain normal thyroid tissue, benign hypofunc-tioning tissue (solid, cystic, or complex), hyper-plastic or autonomously functioning benign tis-sue, or malignant neoplasm. The evaluation ofthe patient with a solitary thyroid nodule is di-rected towards differentiating benign from malig-nant etiologies. Autopsy series have demonstrateda 50% incidence of single or multiple thyroidnodule(s), only 4% of which are malignant. Ul-trasonography detects single or multiple thyroidnodules in 40% of patients with no known thy-roid disease. The incidence of thyroid nodules in-creases with advancing age, and is more frequent
Figure 13.6. Multinodular goiter. An anterior 99mTc pertechnetate view demonstrates asymmetric enlargement of the gland with multipleareas of increased, decreased, and normal activity. The decreased background activity and faint salivary gland activity is compatible with theclinical impression of toxic multinodular goiter.
252
PRACTICAL NUCLEAR MEDICINE
in females and in patients with a prior history ofneck or facial irradiation.
Hypofunctioning (“cold”) nodules concentrateless radioisotope relative to the remainder of thethyroid gland (see Figure 13.3). Eighty-five toninety percent of thyroid nodules are hypofunc-tioning, but only 10–20% of cold nodules aremalignant [2]. The remaining hypofunctioningnodules consist of degenerative nodules, nodularhemorrhage, cysts, thyroiditis, infiltrative disor-ders such as amyloid, and non-thyroid neoplasms.Clinical features that suggest thyroid cancer in-clude male gender, a prior history of radiationexposure up to 15 Gy (1500 rad), a family his-tory of medullary or papillary thyroid carcinoma,and relative youth. Local fixation of the noduleor palpable adenopathy is also suggestive. Recentrapid enlargement of a nodule is more often re-lated to hemorrhage into a cyst or nodule ratherthan carcinoma.
Although ultrasound and MRI are sensitive forthe detection of thyroid nodules, specificity formalignancy is poor. Similarly, sensitivity for de-tection of thyroid cancer is approximately 90%with scintigraphy, but specificity is poor at 15–20%. If extrathyroidal activity is seen in the neckon thyroid scintigraphy in a patient with a solitarythyroid nodule, metastatic thyroid carcinoma islikely. Some investigators have recommended theuse of serum thyroglobulin and calcitonin deter-minations to improve the accuracy of clinical as-sessment and scintigraphy.
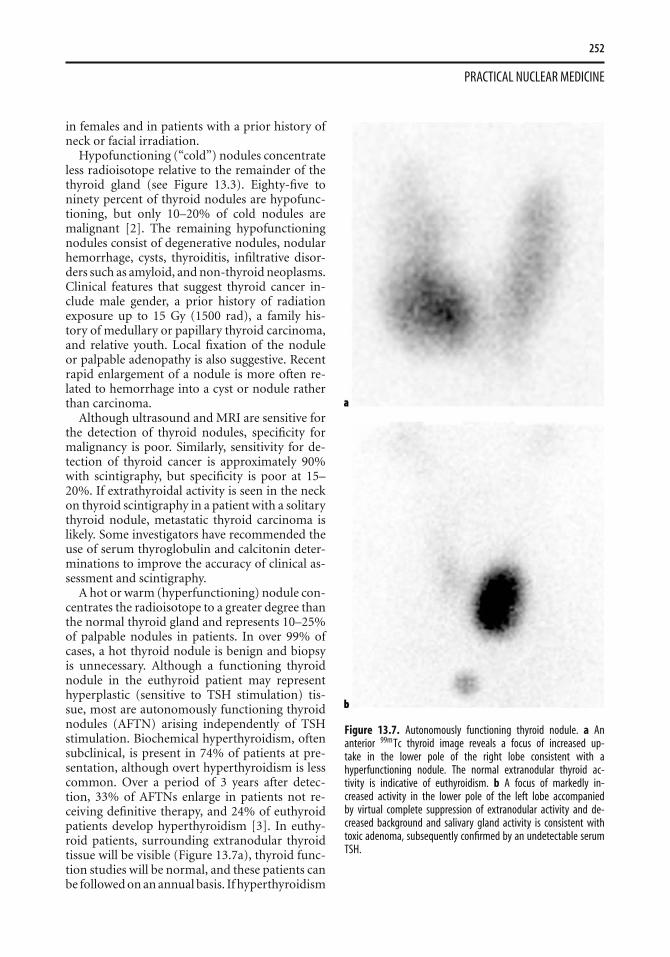
A hot or warm (hyperfunctioning) nodule con-centrates the radioisotope to a greater degree thanthe normal thyroid gland and represents 10–25%of palpable nodules in patients. In over 99% ofcases, a hot thyroid nodule is benign and biopsyis unnecessary. Although a functioning thyroidnodule in the euthyroid patient may representhyperplastic (sensitive to TSH stimulation) tis-sue, most are autonomously functioning thyroidnodules (AFTN) arising independently of TSHstimulation. Biochemical hyperthyroidism, oftensubclinical, is present in 74% of patients at pre-sentation, although overt hyperthyroidism is lesscommon. Over a period of 3 years after detec-tion, 33% of AFTNs enlarge in patients not re-ceiving definitive therapy, and 24% of euthyroidpatients develop hyperthyroidism [3]. In euthy-roid patients, surrounding extranodular thyroidtissue will be visible (Figure 13.7a), thyroid func-tion studies will be normal, and these patients canbe followed on an annual basis. If hyperthyroidism
Figure 13.7. Autonomously functioning thyroid nodule. a Ananterior 99mTc thyroid image reveals a focus of increased up-take in the lower pole of the right lobe consistent with ahyperfunctioning nodule. The normal extranodular thyroid ac-tivity is indicative of euthyroidism. b A focus of markedly in-creased activity in the lower pole of the left lobe accompaniedby virtual complete suppression of extranodular activity and de-creased background and salivary gland activity is consistent withtoxic adenoma, subsequently confirmed by an undetectable serumTSH.

253
THYROID, PARATHYROID, AND ADRENAL GLAND IMAGING
exists, the surrounding normal thyroid tissuewill be suppressed, and the TSH level will beundetectable (Figure 13.7b). Spontaneous cysticdegeneration occurs in 27%, manifested by centralphotopenia; there is little concern for malignancy.
Discordant thyroid imaging is a dissociation be-tween trapping and organification, measured re-spectively with 99mTc pertechnetate and 123I. Itoccurs in only 2–8% of thyroid nodules and isnot specific for malignant disease. A nodule thattraps 99mTc (hot) but is unable to organify iodine(cold) is much more likely to be benign than ma-lignant. If it is assumed that 8% of hot nodules with99mTc are cold with 123I, and if 10% of those aremalignant, then less than 1% of hot nodules seenwith 99mTc imaging are malignant. Additional ra-dioiodine imaging of hot nodules identified on a99mTc scan should probably be reserved for pa-tients deemed at higher risk for malignancy.
Hyperthyroidism
Hyperthyroidism is a clinical syndrome of tachy-cardia, weight loss, and hypermetabolism re-sulting from supraphysiological circulating lev-els of thyroid hormones, leading to suppressionof TSH secretion. Most cases of hyperthyroidismare due to increased endogenous synthesis andsecretion of thyroid hormones from the thyroid.Other less common etiologies are shown in Table13.2. Clinical assessment combined with circulat-ing hormone and thyroid autoantibody measure-ments, thyroid scintigraphy, and RAIU usually al-
Table 13.2. Classification of hyperthyroidism
RadioiodineEtiology uptake
A. Thyroid gland (95%)Diffuse toxic goiter (Graves’ disease) ↑Toxic nodule goiter:
multinodular (Plummer’s disease) ↑solitary nodule ↑
Thyroiditis (subacute/chronic) ↓B. Exogenous thyroid hormone/iodine (4%)Iatrogenic ↓Factitious ↓Iodine-induced (Jod–Basedow) ↓C. Rarely encountered causes (1%)Hypothalamic-pituitary neoplasms ↑Struma ovarii ↓Excessive HCG production by trophoblastic ↑
tissueMetastatic thyroid carcinoma ↓
low identification of the various disease processesthat may be responsible.
Graves’ disease (autoimmune diffuse toxic goi-ter) is due to the presence of thyroid-stimulatingimmunoglobulins and is associated with autoim-mune exophthalmos and pretibial myxedema. Al-though it occurs primarily in young women, itmay also occur in children and in the elderly.Radioiodine uptake will usually be elevated at 4hours and/or 24 hours, and the gland will re-veal diffuse enlargement in most cases with in-creased thyroid activity and minimal backgroundand salivary gland activity (Figure 13.5). Hyper-plasia of the pyramidal remnant is seen as in-creased paramedial activity in as many as 43% ofGraves’ patients. Occasionally, the gland will ap-pear normal size. The low RAIU (usually ≤5%)of hyperthyroid patients with subacute thyroidi-tis, postpartum thyroiditis, silent thyroiditis, andsurreptitious thyroid hormone administration iseasily differentiated from the normal RAIU seenin the occasional patient with Graves’ disease(Table 13.2). Although ultrasound demonstratesan enlarged homogeneously hypoechoic glandwith prominent vascularity on color-flow Dopplerimaging (“thyroid inferno”), it is usually unnec-essary for diagnosis clinically. The thyroid scanshould easily be able to distinguish toxic nodu-lar goiters from Graves’ disease. The clinical im-portance of this is that many patients with toxicnodular goiter will require a higher dose of 131I fortherapy than will Graves’ disease patients.
Radioiodine Therapy of Hyperthyroidism
Graves’ disease and toxic nodular goiter may betreated successfully with 131I therapy. Radioio-dine was first used for the treatment of hyper-thyroidism in 1941 and has since evolved to thetreatment modality of choice for the majority ofadult patients, particularly in the USA. Antithy-roid drug therapy achieves a permanent remis-sion in only 10–40% of patients, but is used ini-tially in many patients, particularly in Europe andAsia. Although subtotal thyroidectomy is effectiveand complications are infrequent, thyroidectomyis used only occasionally at present. It is normallylimited to patients in whom radioiodine is un-suitable, such as women who may be pregnant, orwho have extremely large goiters with compressivesymptoms. Radioiodine therapy is effective, prac-tical, inexpensive, and available on an outpatientbasis.

254
PRACTICAL NUCLEAR MEDICINE
Prior to initiation of therapy, the diagnosis ofhyperthyroidism must be confirmed by elevationof thyroid hormone levels and suppression of cir-culating TSH. An elevated RAIU confirms that en-dogenous thyroidal secretion is the source of thehyperthyroidism and aids in excluding other eti-ologies of hyperthyroidism, such as silent thyroidi-tis, subacute thyroiditis, postpartum thyroiditis,iodine-induced hyperthyroidism, and factitioushyperthyroidism, all of which are associated witha low RAIU (Table 13.2). Rarely, clinical hyper-thyroidism with diffuse goiter and elevated RAIUmay be related to excessive secretion of humanchorionic gonadotropin (HCG) by a trophoblas-tic tumor or by inappropriate secretion of TSHby a functioning pituitary adenoma. The presenceof exophthalmos, pretibial myxedema, and diffusegoiter on physical examination confirms Graves’disease as the etiology. Otherwise, thyroid scintig-raphy is useful to differentiate diffuse involvementdue to Graves’ disease from localized disease dueto AFTN.
The patient must be counseled prior to therapyregarding the advantages and disadvantages of al-ternative therapies. Because iodide readily crossesthe placenta, 131I may not be administered duringpregnancy so a pregnancy test is mandatory priorto administration. Exposure of the fetus to 131I af-ter the 10th week of gestation may result in severefetal hypothyroidism.
The effectiveness of radioiodine treatment forhyperthyroidism is due to radiation-induced cel-lular damage resulting from high-energy betaemission, the magnitude of which is directly pro-portional to the radiation dose received by thethyroid gland. The major effect of radiation is im-pairment of the reproductive capacity of follicularcells. The radiation dose to the thyroid is relatedto (1) the amount of radioiodine administered,(2) the fraction deposited in the gland (uptake),(3) the duration of retention by the thyroid (bio-logic half-life), and (4) the radiosensitivity of theirradiated tissue. Administered dose is usually cal-culated with the goal of administering approxi-mately 70–120 Gy (7000–12 000 rad) to the thy-roid gland [4]. Some practitioners have adopted afixed dose administration, usually approximately370 MBq (10 mCi) with perhaps 300 MBq (8 mCi)for a small gland and 440–520 MBq (12 to 14 mCi)for a large gland. In the UK, a relatively larger fixeddose of 550 MBq (15 mCi) is given to the major-ity of adult patients [5]. Other practitioners willcalculate a dose of 3–4.4 MBq (80 to 120 µCi)
per gram of thyroid tissue for the usual patientwith Graves’ disease. Even higher dosages of upto 7.4 MBq (200 µCi) per gram will be used toproduce a more rapid response in patients withsevere hyperthyroidism. The calculation is madeas follows: administered microcuries = µCi/g de-sired × gland weight (g) × 100 ÷ percent uptake(24 hours). A higher dose may also be requiredfor patients with toxic nodular goiter, in patientspreviously treated with antithyroid medications,patients with extremely large glands, patients withrapid iodine turnover (a 4 h/24 h RAIU ratio >1),and in patients with renal insufficiency. Althoughestimation of thyroid size is relatively accurate forglands weighing less than 60 grams, the degree ofinaccuracy increases in larger glands. Ultrasoundmay provide an accurate estimation of size, butthe increase in accuracy of thyroid radiation dosedetermination is limited.
The complications of radioiodine therapy in-clude rare exacerbation of hyperthyroidism, pos-sible exacerbation of existing Graves’ orbitopathy,and post-therapeutic hypothyroidism. It is esti-mated that less than 10% of patients require re-treatment, and this is rarely undertaken before3–4 months following therapy. Most practition-ers will give at least 20–30% more radioiodine ona second treatment. Pretreatment with antithyroidmedications is advisable in elderly patients, in pa-tients with known cardiac disease, and in patientswith large thyroid glands, particularly multinodu-lar goiters. These medications should be discon-tinued 48–72 hours prior to administration of131I, and it is preferable to wait several days be-fore reinitiation of therapy. The administration ofbeta blockers before or after therapy serves onlyto ameliorate peripheral manifestations of hyper-thyroidism and will not affect therapeutic efficacyof radioiodine.
The incidence of early post-131I hypothyroidismvaries from 10% to 50% according to the dose ad-ministered. Subsequently, there is an additionalincidence of hypothyroidism at a relatively con-stant rate of 2–3% per year. A similar incidence ofhypothyroidism occurs following surgery. Somedegree of hypothyroidism may be a natural conse-quence of the autoimmune process of Graves’ dis-ease, since a small percentage of patients treatedonly with antithyroid medications will becomehypothyroid during long-term follow-up after re-mission.
Although radiation exposure of more than500 mGy (50 rad) is reported to increase the
255
THYROID, PARATHYROID, AND ADRENAL GLAND IMAGING
occurrence of leukemia, with a peak incidence atapproximately 6 years after exposure, a single 131Itreatment delivers only 80–160 mGy (8–16 rad)to the blood and has not been associated with anyincreased incidence of leukemia, thyroid cancer,infertility, or congenital malformations. Althoughthe desire for subsequent pregnancy is not a con-traindication to radioiodine therapy for hyper-thyroidism, patients are usually advised to avoidconception for 6 months in case retreatment isrequired.
Following radioiodine therapy, the patientshould be advised to have serum thyroid hormoneand TSH levels checked within 2 to 3 months. Pa-tients may be symptomatically improved within4 to 6 weeks, but clinically significant hypothy-roidism rarely occurs before 2 to 3 months. Hy-pothyroidism is only a problem if not adequatelytreated, and many practitioners will initiate thy-roxine replacement therapy at the earliest indica-tion of post-therapy hypothyroidism.
Thyroiditis
Thyroiditis may be classified as acute, subacute,chronic/autoimmune, and other miscellaneoustypes; these different types of thyroiditis are un-related to each other (see Further Reading). Acutesuppurative thyroiditis is rare and is caused byhematogenous spread of infectious organisms.This is usually defined clinically and evaluated by
CT and/or sonography; scintigraphy is only rarelyperformed.
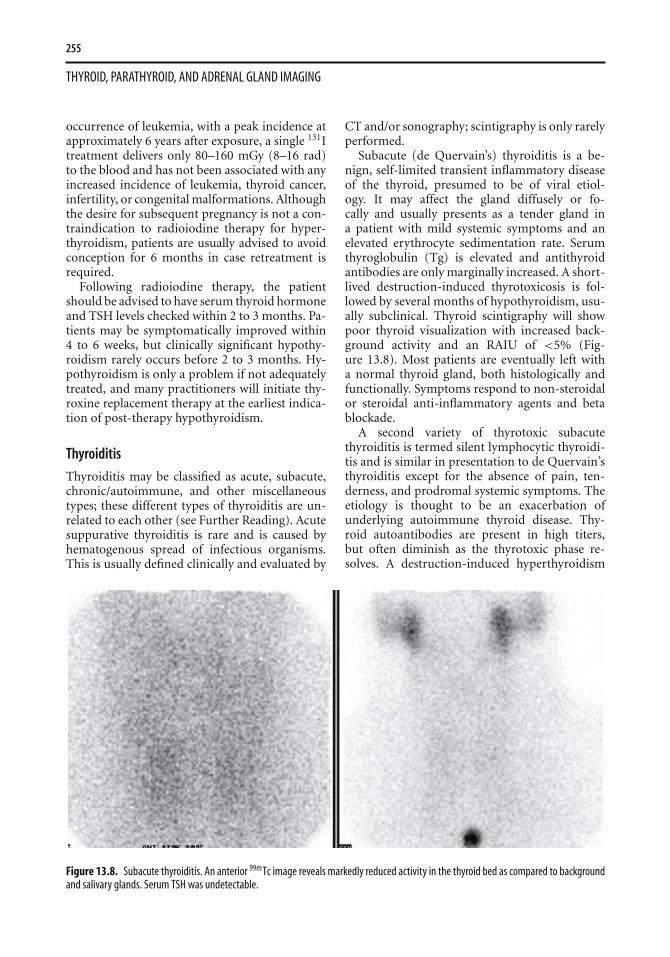
Subacute (de Quervain’s) thyroiditis is a be-nign, self-limited transient inflammatory diseaseof the thyroid, presumed to be of viral etiol-ogy. It may affect the gland diffusely or fo-cally and usually presents as a tender gland ina patient with mild systemic symptoms and anelevated erythrocyte sedimentation rate. Serumthyroglobulin (Tg) is elevated and antithyroidantibodies are only marginally increased. A short-lived destruction-induced thyrotoxicosis is fol-lowed by several months of hypothyroidism, usu-ally subclinical. Thyroid scintigraphy will showpoor thyroid visualization with increased back-ground activity and an RAIU of <5% (Fig-ure 13.8). Most patients are eventually left witha normal thyroid gland, both histologically andfunctionally. Symptoms respond to non-steroidalor steroidal anti-inflammatory agents and betablockade.
A second variety of thyrotoxic subacutethyroiditis is termed silent lymphocytic thyroidi-tis and is similar in presentation to de Quervain’sthyroiditis except for the absence of pain, ten-derness, and prodromal systemic symptoms. Theetiology is thought to be an exacerbation ofunderlying autoimmune thyroid disease. Thy-roid autoantibodies are present in high titers,but often diminish as the thyrotoxic phase re-solves. A destruction-induced hyperthyroidism
Figure 13.8. Subacute thyroiditis. An anterior 99mTc image reveals markedly reduced activity in the thyroid bed as compared to backgroundand salivary glands. Serum TSH was undetectable.

256
PRACTICAL NUCLEAR MEDICINE
is accompanied by markedly suppressed RAIUand mild thyromegaly, all of which resolve overmonths. This entity presents more frequentlyin postpartum women (termed postpartum thy-roiditis) and tends to recur with subsequent preg-nancies. Many of these women will eventually de-velop permanent hypothyroidism.
Chronic Hashimoto’s autoimmune lympho-cytic thyroiditis is the most common cause of hy-pothyroidism in the Western world and usuallypresents in women with a small to moderately-enlarged firm goiter, elevated antithyroglobulinand/or antimicrosomal (antiperoxidase) antibod-ies, and rarely any tenderness. Patients may beeuthyroid or hypothyroid and rarely hyperthy-roid. Scintigraphy reveals inhomogeneous activitythroughout the gland in 50%, though a patternof multinodular goiter, solitary hot nodule, orsolitary cold nodule as well as a normal scanmay occur. RAIU may be normal, low, or ele-vated. Biopsy is rarely necessary for diagnosis, andmost patients are treated with thyroid hormonesupplementation.
Iodine-induced thyrotoxicosis occurs most fre-quently in patients with pre-existing thyroiddisease via the Jod–Basedow phenomenon. Pa-tients with autonomously functioning thyroidadenoma(s), previously treated Graves’ disease,and colloid goiter are most susceptible. Scintigra-phy usually reveals a pattern of MNG, and RAIU isdiminished. On the other hand, the patient withiatrogenic or factitious hyperthyroidism will ex-hibit only background activity on thyroid scintig-raphy and may not have a palpable goiter. RAIUwill be very low.
Mediastinal Goiter
The most common neoplasms of the anterior me-diastinum are thymomas, lymphomas, and germcell tumors. Although retrosternal thyroid ac-counts for only 7–10% of all mediastinal masses,the non-invasive demonstration of radioiodineuptake within a mediastinal mass is useful as itavoids more invasive tissue diagnosis. Retroster-nal thyroid tissue is usually the result of inferiorextension of a cervical goiter, but may be related toenlargement of ectopic mediastinal thyroid tissue.Continuity between the cervical and intrathoraciccomponents of a mediastinal goiter may consistof only a narrow fibrous band and may not bedemonstrable by CT or ultrasound. If goiter isconsidered, thyroid scintigraphy should be per-formed prior to CT imaging to avoid interference
Figure 13.9. Mediastinal goiter. An anterior 123I image demon-strates a relatively normal appearing cervical thyroid accompaniedby heterogeneous irregular uptake within the superior mediastinum.
by administration of iodinated contrast media, themost common cause of false negatives.
Due to high background activity related to sur-rounding blood pool activity, 99mTc images aresuboptimal and difficult to interpret. Iodine-123is the radionuclide of choice for imaging ret-rosternal thyroid masses. 123I scintigraphy yieldshigh-quality images of thoracic goiters, even whenuptake is relatively decreased (Figure 13.9). De-spite the fact that clinically significant thyroid can-cer occurs in only 4% of mediastinal goiters, themajority of patients with significant mediastinalgoiters eventually undergo surgical resection [6].However, 131I treatment, sometimes augmentedby administration of recombinant human TSH(rhTSH), can be used to reduce the size of the massand alleviate tracheal compression in appropriatepatients.
Neonatal Hypothyroidism
Congenital hypothyroidism (CHT) has an in-cidence of 1 per 2500–5000 births, and mostinfants do not exhibit signs or symptoms ofhypothyroidism at birth. A delay in the institution

257
THYROID, PARATHYROID, AND ADRENAL GLAND IMAGING
of thyroxine replacement therapy beyond 6–8weeks of life is likely to be associated with mea-surable impairment of intellectual function (cre-tinism). Since the institution of newborn screen-ing programs for CHT by measuring serum TSHand/or T4 levels, the intellectual impairment ofCHT has been eradicated in developed countries.
Thyroid dysgenesis (agenesis, hypoplasia, ec-topia) is the most common cause of neonatalhypothyroidism in the industrialized world andUSA. 99mTc pertechnetate thyroid scintigraphy isperformed immediately after CHT is confirmed.It can easily detect eutopic and ectopic thyroidtissue as well as assess degree of thyroidal uptake[7]. Using a pinhole collimator, a close-up and amore distant view (to include the face and chest)in the anterior projection as well as a lateral vieware acquired 20–30 minutes after intravenous in-jection of 18 MBq (0.5 mCi). A normal image isseen in cases of false positive screening results. Asmall focus of relatively faint uptake cephalad tothe thyroid cartilage is consistent with ectopia andindicates the need for lifelong thyroxine therapy(see Figure 13.4). A eutopic enlarged gland withincreased uptake, usually marked, is most consis-tent with dyshormonogenesis; a small proportionof these are due to transient immaturity of the io-dine organification process and will be normal atreassessment after age 3 years. Non-visualizationof the thyroid on scintigraphy is due to agene-sis in over 90% of cases, the remainder being dueto the presence of maternal transmission of TSH-receptor blocking antibodies; these latter patientswill be euthyroid at reassessment when these ma-ternal antibodies have cleared. Patients with a non-visualized gland or patients with images suggest-ing dyshormonogenesis are all re-evaluated at age3–4 years to exclude transient CHT; patients withectopia are not reassessed.
Therefore, thyroid scintigraphy in the neonateis indispensable in the proper diagnostic work-upof congenital hypothyroidism, because it (1) pro-vides a more specific diagnosis, (2) is cost-effectivefor selecting patients for subsequent reassessmentto uncover transient CHT and allow discontinua-tion of thyroid hormone replacement therapy, and(3) defines dyshormonogenesis, which is familialand requires genetic counseling [7].
Detection of Thyroid Carcinoma and MetastaticThyroid Carcinoma
Thyroid carcinoma accounts for 90% of all en-docrine malignancies and 1.5% of all malignan-
cies, with approximately 19 000 new cases oc-curring annually in the USA; but it constitutesonly 1200 cancer deaths per year, resulting ina relatively high prevalence of disease with al-most 200 000 patients living in the USA hav-ing undergone thyroidectomy for thyroid can-cer and requiring regular assessment. Although80% of thyroid malignancies are DTCs (papil-lary and follicular), medullary carcinomas (7%),lymphomas (5%), and undifferentiated anaplasticcarcinomas (<5%) present specific challenges inimaging.
Differentiated Thyroid Carcinoma
Differentiated thyroid cancers (DTC), which con-stitute 80% of thyroid carcinomas, grow slowly,occur in young people, and are frequently respon-sive to therapy (90% 15-year survival). Eightypercent of DTCs are of the papillary or mixedpapillary/follicular histology and the remainingare follicular. The behavior of the two tumortypes differs, with papillary typically metasta-sizing to locoregional nodes and the lungs andfollicular disseminating hematogenously to thebones. DTC usually maintains the capacity to trapand organify iodine and to synthesize and re-lease Tg. These characteristics of DTC allow post-thyroidectomy treatment of iodine-avid diseasewith high-dose 131I and the monitoring of ther-apy using (1) radioiodine scintigraphy and (2)serum Tg. However, dedifferentiation occurs toa variable extent with both types of DTC withloss of the iodide symporter and/or loss of Tg ex-pression, thus presenting challenges for imagingand monitoring these patients. Other less differ-entiated thyroid malignancies have characteristics(such as calcitonin expression or increased glu-cose metabolism) that permit specific imaging andpost-therapy monitoring.
The traditional methods of follow-up for pa-tients with DTC are whole body radioiodinescintigraphy (RIS) and serum Tg monitoring. Op-timal 131I uptake by neoplastic tissue is TSH-dependent, so RIS is performed under conditionsof TSH stimulation, either endogenous via thyroidhormone withdrawal or by exogenous administra-tion of rhTSH. Adequate endogenous TSH levelsof greater than 30 mIU/l can be attained 10–14days after the discontinuance of exogenous tri-iodothyronine (T3) (liothyronine) or 1–4 weeksafter the discontinuance of thyroxine (T4) therapy[8]. Recombinant human TSH (rhTSH) adminis-tration as a method of stimulating RAIU (and Tg

258
PRACTICAL NUCLEAR MEDICINE
release) is now available for use in patients main-tained on thyroid hormone therapy.
Thyroglobulin is a complex iodinated glyco-protein synthesized and released by both benignand malignant thyroid cells but no other tissues.Circulating Tg, normally 1–25 ng/ml, should beundetectable in the absence of functioning thy-roid tissue. An elevated serum Tg determination(>2 ng/ml) in post-thyroidectomy patients withDTC after 131I ablation of the normal remnant is ahighly sensitive and specific indicator of residualor metastatic thyroid carcinoma. TSH-stimulatedTg determinations are more sensitive for the de-tection of metastases than are levels done in pa-tients on suppressive therapy. Traditionally, RISin combination with TSH-stimulated serum Tgmeasurements are performed due to reports of re-current disease occurring in the absence of TSH-stimulated Tg elevation.
Whole body RIS is first performed several weeksafter thyroidectomy. Due to its potentially ad-verse effects on a fetus, exclusion of pregnancy ismandatory prior to administering scanning dosesof 131I. Following the oral administration of 2–5mCi of 131I, static whole body images are acquiredat 48 to 72 hours. A low iodine diet may signifi-cantly increase RAIU into metastatic lesions. Al-though the specificity of 131I scanning is 95%, onemust not confuse the normal physiological activ-ity in the salivary glands, nose, gastric mucosa,urinary bladder, bowel, and lactating breast withmetastatic disease. Due to hepatic catabolism ofiodothyronines, diffuse liver uptake is seen physi-ologically if there is benign or malignant function-ing thyroid tissue present. Typically, 131I uptake isnot seen in Hurthle cell, medullary, or anaplastictumors.
The sensitivity of 131I scintigraphy for the detec-tion of persistent or metastatic thyroid carcinomais 50–70%, dependent in part on the dose admin-istered. Imaging 3–7 days after a therapeutic doseof 3.7–5.4 GBq (100–200 mCi) of 131I may increasethe detection of metastatic lesions by up to 45%[9]. The combination of RIS and serum Tg de-termination augments the detection of metastaticdisease to 85–100% [10, 11].
A schedule of follow-up examinations at 6–12 month intervals is recommended until theserum Tg is undetectable and RIS demonstratesno pathologic uptake. Scanning at 2–3 year inter-vals can then be instituted, remembering that 50%of DTC recurrences occur more than 5 years afterinitial treatment.
Stunning is the phenomenon in which the initialdiagnostic dose of 131I, 75–185 MBq (2–5 mCi),reduces trapping of the subsequently administeredtreatment dose. The frequency of this effect and itsclinical significance is controversial, but quantita-tive uptake studies seem to confirm a 30–50% re-duction of therapeutic radioiodine uptake as com-pared to the diagnostic dose. Many investigatorsnow advocate utilizing 123I scintigraphy with 37–185 MBq (1–5 mCi) partly to avoid 131I-inducedstunning but also because of the superior imagequality. In most reports, there is little if any differ-ence in the sensitivity for detection of thyroid rem-nant and metastases using 123I versus post-therapyhigh-dose 131I imaging, and SPECT acquisitionswith or without CT fusion can be performed withdiagnostic 123I imaging when deemed appropriate[12].
Other DTC-avid radiopharmaceuticals suchas 201Tl, 99mTc-MIBI, and 18FDG (18F-fluoro-deoxyglucose) are most importantly used in thecohort that is 131I scan-negative but serum Tg-positive, which constitutes about 10–15% of pa-tients with negative diagnostic RIS. These alter-native radiopharmaceuticals should not be usedinstead of RIS unless the patient is known fromearlier studies to be 131I-negative. Although skele-tal metastases of DTC are mostly osteolytic, 99mTcdiphosphonate scintigraphy is often positive in pa-tients with bone metastases (64–85%) but may notaccurately demonstrate the extent of disease.
Thallium-201 whole body scintigraphy hasa sensitivity of 60–90% for the detection ofmetastatic DTC, including 131I-negative, Tg-positive metastases, and SPECT may increase thesensitivity for the detection of small metastaticfoci. False positive findings may be seen with non-thyroidal tumors, vascular structures, and sali-vary glands. 99mTc-MIBI is highly sensitive forthe detection of cervical and mediastinal lym-phadenopathy, but is less useful for detection ofpulmonary metastases. In a large multicenter trialcomprising 222 patients, sensitivity of 18FDG PETwas 85% for the patients with negative RIS and wassignificantly higher for 18FDG than for 201Tl or99mTc-MIBI [13]. In a review of 14 studies, 18FDGPET exhibited a consistently high sensitivity fordetection of recurrent tumor in patients with ele-vated serum Tg and negative RIS [14]. The higherthe serum Tg, the higher the sensitivity for de-tection of tumor (50% for Tg 10–20 ng/ml and93% for Tg >100 ng/ml), but 18FDG PET re-portedly detects 70% of cervical nodes less than

259
THYROID, PARATHYROID, AND ADRENAL GLAND IMAGING
1 cm in diameter. Furthermore, there is prelim-inary evidence that 18FDG PET may have prog-nostic importance with 3-year survival of only18% in patients with a high volume of 18FDG-avid disease versus 96% survival in those withless bulky disease [15]. Patients whose metastasesare 18FDG-negative have a good prognosis, and18FDG-positive lesions tend to be resistant to 131Itherapy. There is accumulating evidence that TSHstimulation may increase sensitivity for 18FDGPET detection of metastatic disease by up to 30%,with a 63% increase in tumor-to-background ra-tio. Many institutions now perform 18FDG PETfor thyroid cancer utilizing rhTSH administrationor exogenous hormone withdrawal.
Seventy-five percent of patients with recurrentDTC will have positive 131I scans. When treatedwith high-dose 131I therapy, many of the remain-ing RIS-negative patients demonstrate positivepost-therapy scans, indicating that their DTC is tosome degree iodine-avid. Although the long-termsuccess of 131I therapy in RIS-negative/Tg-positivepatients is controversial in regard to outcome,many do demonstrate a post-therapy reductionin serum Tg. Interestingly, 89% of patients withnegative diagnostic RIS and elevated serum Tgbut no radiographic evidence of tumor experi-ence a significant reduction in serum Tg overprolonged follow-up, 68% down to undetectablelevels, without 131I or any other treatment [16].Therefore, the extent of disease and advisabilityfor surgical management in some of these patientswith positive post-therapy scans and elevatedserum Tg may better be demonstrated by 18FDGPET combined with conventional cross-sectionalimaging. Those patients with elevated serumTg and negative RIS after 131I therapy are bestevaluated with 18FDG PET, resulting in a changein management in over 50%. In fact, the possi-bility of the coexistence of iodine-negative andiodine-positive lesions and the discordance in lo-calization of iodine-positive and 18FDG-positivelesions are clinical challenges that may furtherincrease the clinical utility of 18FDG PET even inthe presence of iodine-positive disease.
In summary, most patients who are RIS neg-ative but serum Tg positive will have RIS per-formed after a therapeutic dose of 131I. If no metas-tases are identified with the post-therapy RIS, thepatient will be followed using a combination ofconventional imaging including chest X-ray, neckultrasound, and cross-sectional imaging with orwithout the use of alternative radiopharmaceuti-
cals. 18FDG PET seems to be the radiopharmaceu-tical of choice and would be expected to be moresensitive than 99mTc-MIBI or 201Tl for small vol-ume disease.
Medullary Thyroid Carcinoma
Medullary thyroid carcinoma (MTC), represent-ing approximately 3–5% of all thyroid cancers, isan intermediate grade malignancy occurring inboth a sporadic (80%) and a familial (20%) form.Nearly 50% of patients have metastatic cervicaladenopathy at presentation. Five-year survival is94% in patients with metastatic lymphadenopa-thy but only 41% in those with extranodal dis-ease. Typically, MTC does not concentrate iodine,so RIS is not useful and 131I treatment results inno improvement in survival or recurrence rate.
Although numerous scintigraphic modali-ties including 123I/131I-MIBG, 99mTc-(V)-DMSA,111In octreotide, 201Tl and 99mTc-MIBI imaginghave been successfully utilized to a varying degree,18FDG PET is evolving into the primary modalityfor detection of MTC with a sensitivity of 73–94%in patients with MTC and elevated calcitonin lev-els [17].
Somatostatin receptors are present on the cellsurface of medullary carcinomas, and many MTCmetastases can be visualized using 111In-labeledsomatostatin receptor scintigraphy (SRS). In pa-tients with recurrent MTC, 111In octreotide imag-ing detects 44–65% of metastatic lesions, but it isnot sensitive for detection of hepatic involvementdue to its physiological liver uptake.
In summary, the early detection of recurrentMTC and the localization of the metastases is im-portant because microdissection offers the chancefor long-term remission for up to 40% of patients,improvement in symptomatology, reduction inthe occurrence of distant metastases, and possiblythe prolongation of survival. No single diagnosticmodality is able to reliably demonstrate the fullextent of disease in these patients, but the com-bination of cross-sectional radiography (US, CT,MR) with scintigraphy using 18FDG PET or 111Inoctreotide is recommended.
Thyroid Lymphoma and Anaplastic Carcinoma
Primary lymphoma of the thyroid, which ac-counts for less than 5% of all thyroid malignancies,presents as a rapidly enlarging goiter usually in anelderly patient with preexisting autoimmune lym-phocytic thyroiditis. 99mTc and 131I scintigraphy as
260
PRACTICAL NUCLEAR MEDICINE
well as 18FDG, 201Tl, and 99mTc-MIBI imaging areof little utility in differentiating thyroid lymphomafrom thyroiditis. 18FDG, 201Tl, and 99mTc-MIBIactivity is increased in lymphoma, so these modal-ities may be useful in the detection of extrathy-roidal lymphoma and its response to therapy.
The rare undifferentiated or anaplastic carci-noma of the thyroid presents as a rapidly en-larging goiter in an elderly individual; survival isextremely poor. 99mTc and 123I scintigraphy willdemonstrate non-specific areas of diminished ac-tivity. Preliminary reports indicate that 18FDGPET, 201Tl, or 99mTc-MIBI imaging may be use-ful in evaluating recurrent anaplastic carcinoma,especially if CT/US findings are equivocal.
13.2 The Parathyroid Glands13.2.1 Introduction
The diagnosis of hyperparathyroidism is madebiochemically by the presence of both hypercal-cemia and elevated parathyroid hormone (PTH)levels in the serum. The major contribution ofimaging techniques is the localization of thesource of abnormal PTH production in patientswith hyperparathyroidism. Whereas the use ofimaging techniques for localization in individuals
undergoing re-exploration for persistent or recur-rent hyperparathyroidism is well accepted, sub-stantial controversy surrounds the efficacy andcost effectiveness of localization procedures usedprior to initial surgery.
13.2.2 Anatomy
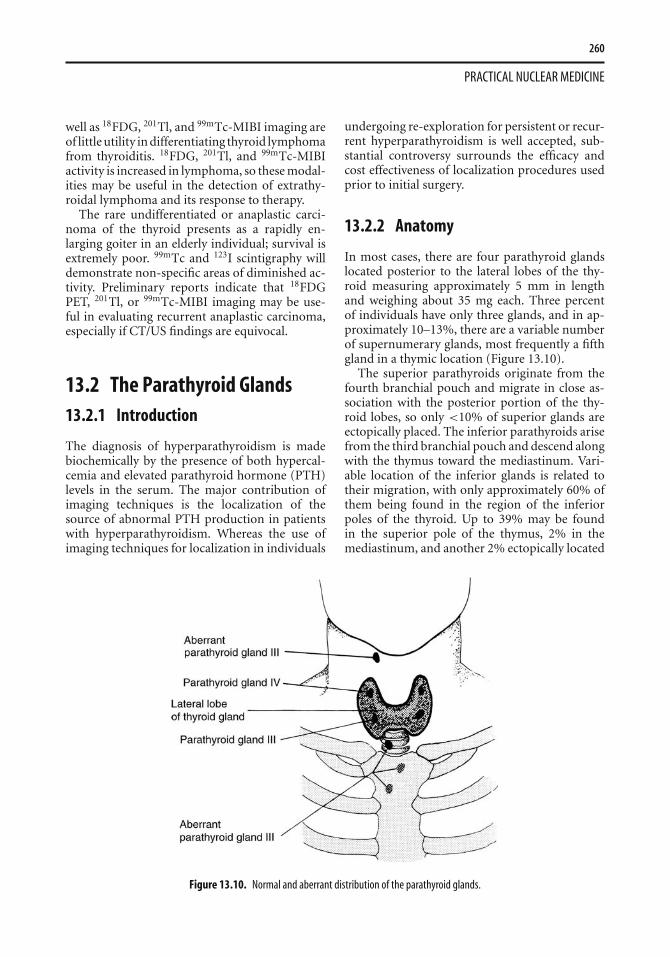
In most cases, there are four parathyroid glandslocated posterior to the lateral lobes of the thy-roid measuring approximately 5 mm in lengthand weighing about 35 mg each. Three percentof individuals have only three glands, and in ap-proximately 10–13%, there are a variable numberof supernumerary glands, most frequently a fifthgland in a thymic location (Figure 13.10).
The superior parathyroids originate from thefourth branchial pouch and migrate in close as-sociation with the posterior portion of the thy-roid lobes, so only <10% of superior glands areectopically placed. The inferior parathyroids arisefrom the third branchial pouch and descend alongwith the thymus toward the mediastinum. Vari-able location of the inferior glands is related totheir migration, with only approximately 60% ofthem being found in the region of the inferiorpoles of the thyroid. Up to 39% may be foundin the superior pole of the thymus, 2% in themediastinum, and another 2% ectopically located
Figure 13.10. Normal and aberrant distribution of the parathyroid glands.

261
THYROID, PARATHYROID, AND ADRENAL GLAND IMAGING
anywhere from the angle of the jaw to the level ofthe aortic arch. Intrathyroidal parathyroid adeno-mas may be found in 2–5% of cases. The arterialand venous anatomy supplying the parathyroidglands are variable depending upon the locationof the gland, the presence of vascular variance, andprevious neck surgery. Knowledge of the venousdrainage is a prerequisite for successful diagnosticvenous sampling for PTH.
13.2.3 Pathophysiology
Routine automated screening of the general pop-ulation for serum calcium has resulted in earlierdetection of patients with hyperparathyroidism.More than 80% of patients now are asymptomaticor have non-specific symptoms with less than 15%of patients presenting with renal stones. Primaryhyperparathyroidism results from a solitary ade-noma in over 80% of cases with multiple ade-nomas, diffuse hyperplasia, or rarely carcinomaaccounting for the rest (Table 13.3). Treatmentis usually surgical with a success rate of 90–95% without preoperative localizing procedures.Recurrent and persistent hyperparathyroidism isusually related to aberrant or ectopically locatedglands or recurrent hyperplasia. Re-explorationis technically difficult with a higher morbidityand poorer success rate than initial surgery. Pre-operative non-invasive localization improves thecure rate of second surgery from 50–60% up to90%. Diffuse hyperplasia accounts for approxi-mately 15% of the cases of primary hyperparathy-roidism, and a substantial proportion of these mayoccur in association with the multiple endocrineneoplasias. Secondary hyperparathyroidism inassociation with chronic renal failure is alsorelated to diffuse hyperplasia, and may require sur-gical therapy due to progressive bone disease. To-tal parathyroidectomy plus autotransplantation ofremnant tissue into upper extremity musculatureis the conventional therapy for this group of pa-tients.
Table 13.3. Pathologic classification of parathyroid lesions inpatients with primary hyperparathyroidism
Class Type Percentage
Adenomas Single 80Hyperplasia Chief cell 15
Clear cell 1Carcinoma 4
13.2.4 Parathyroid Scintigraphy
Both thyroid and parathyroid tissue take up201Tl, whereas only thyroid tissue will trap 99mTcpertechnetate. Beginning in 1983, this principlewas exploited for the localization of parathyroidadenomas in patients with primary hyperparathy-roidism using combined 99mTc/201Tl subtractionimaging. (Table 13.4). Although this technique hasa relatively high sensitivity and specificity for thedetection of parathyroid adenomas, it is not sensi-tive for the detection of hyperplasia or for smalleradenomas. Patient motion during the acquisitionof the two sets of images may cause misregistra-tion of data, resulting in both false positive andfalse negative interpretations [18].
99mTc-MIBI has been found to accumulate in awide variety of neoplasms including parathyroidadenomas. 99mTc-MIBI is distributed in propor-tion to blood flow and is sequestered intracellu-larly within the mitochondria. The large numberof mitochondria present in the cells of mostparathyroid adenomas, especially oxyphil cells,may be responsible for the avid uptake and slow re-lease of 99mTc-MIBI seen in parathyroid adenomascompared to surrounding thyroid tissue. Phys-iological thyroid 99mTc-MIBI activity graduallywashes out with a half-life of 60 minutes, whereasparathyroid activity is stable over 2 hours, thusexplaining the better visualization of parathyroidadenomas at 2–3 hours post-injection. Due to itssimplicity and the better imaging characteristics of99mTc, the detection and localization of parathy-roid adenomas with 99mTc-MIBI is now the uni-versally preferred nuclear medicine technique.
Typically 99mTc-MIBI parathyroid scintigraphyis performed as a double-phase study. Follow-ing injection with 740 MBq (20 mCi) 99mTc-MIBI, two sets of planar images of the neck andmediastinum are obtained using a low-energyhigh-resolution collimator (Table 13.4). The ini-tial set of images acquired at 10–15 minutespost-injection corresponds to the thyroid phaseand a second set acquired at 2–3 hours post-injection to the parathyroid phase. A focus ofactivity in the neck or mediastinum that ei-ther progressively increases over the durationof the study or persists on delayed imaging incontrast to the decreased thyroidal activity onthe delayed imaging is interpreted as differen-tial washout consistent with parathyroid adenoma(Figure 13.11).

262
PRACTICAL NUCLEAR MEDICINE
Table 13.4. Parathyroid imaging
Radiopharmaceutical 99mTc pertechnetate and 201Tl 99mTc sestamibi
Activity administered 80 MBq (2 mCi) 201Tl;370 MBq (10 mCi) 99mTc
925 MBq (25 mCi)
Effective dose equivalent 4.6 mSv (460 mrem) 5 mSv (500 mrem)Patient preparation As for thyroid scanning NoneCollimator Converging or low-energy, high-resolution,
parallel-holeLow-energy, parallel-hole,
high-resolutionImages acquired Inject Tl first and acquire 15-min 100 000 count view of
neck and mediastinum. Then acquire similar Tcimages without moving patient. Subtract Tc datafrom Tl after normalization to equal count densities
Anterior (and oblique) views at 15 minand at 2–3 h; SPECT as needed
This double-phase technique for the detectionof abnormal parathyroid glands was reported tobe successful in 671 of 803 (84%) patients whohad adenomas and was successful in 59 of 93(63%) patients with multiglandular disease orhyperplasia [19]. Because of the lower sensitiv-ity for detection of very small adenomas andhyperplasia, a “normal” 99mTc-MIBI scan, in thecontext of hyperparathyroidism, should be inter-preted with due caution. The mean sensitivityand specificity of preoperative 99mTc-MIBI imag-ing for the detection of a solitary adenoma is re-ported to be 91% and 99% respectively [20]. Al-though the parathyroid pathology is usually bestvisualized on the delayed images, an adenomais occasionally best seen on the initial imagesdue to rapid washout from the adenoma (Fig-ure 13.12). As with 201Tl imaging, thyroid pathol-ogy and lymphadenopathy may contribute to falsepositive findings with 99mTc-MIBI imaging, al-though specificity is generally reported to be in therange of 95%. In the patient with known thyroidpathology, a dual radioisotope technique may bepreferable; 99mTc pertechnetate or 123I subtractionhas been used with reported sensitivities of 80–100% and improved specificity. SPECT may some-times detect abnormalities not seen on the planarviews, and SPECT/CT fusion imaging is promis-ing for improved localization. Both 201Tl subtrac-tion imaging and positron emission tomographyusing 18FDG may sometimes detect a parathyroidadenoma not identified using 99mTc-MIBI scintig-raphy.
There is universal agreement on the need foraccurate preoperative imaging for localization inpatients undergoing reoperative parathyroid ex-ploration and in patients undergoing parathy-roid surgery after previous thyroidectomy. With
accurate preoperative localization, reoperation issuccessful in over 90% of patients probably dueto the fact that ectopia is 3–5 times higher andmultiglandular disease is twice as high as in pa-tients undergoing initial surgery. In the eval-uation of patients with recurrent or persistenthyperparathyroidism, most surgeons prefer cor-relative imaging with at least two and sometimesthree modalities, scintigraphy and at least onecross-sectional technique. Using high-frequencytransducers, sonography can reliably detect eu-topic enlarged parathyroid glands. Although CTscanning has been used successfully, its use is com-promised by artifacts from metallic clips and theanatomic distortion related to post-surgical scar-ring. Magnetic resonance imaging (MRI) witha variety of echo sequences is highly accuratein the detection of aberrant glands in the neck,thoracic inlet, and mediastinum. Recent reportsindicate that MRI is approximately 82–88% sen-sitive and 99mTc-MIBI scintigraphy is approx-imately 79–85% sensitive for the accurate lo-calization of parathyroid pathology in patientswith recurrent or persistent hyperparathyroidism[21]. The combination of these two modali-ties has provided a substantial improvement inthe sensitivity and positive predictive value inthe range of 89–94% for localizing the offend-ing gland(s) in patients with recurrent/persistenthyperparathyroidism.
13.2.5 Conclusions
In summary, parathyroid imaging may not benecessary in the initial preoperative evalua-tion of patients with primary hyperparathy-roidism. Exceptions to this may be patients
263
THYROID, PARATHYROID, AND ADRENAL GLAND IMAGING
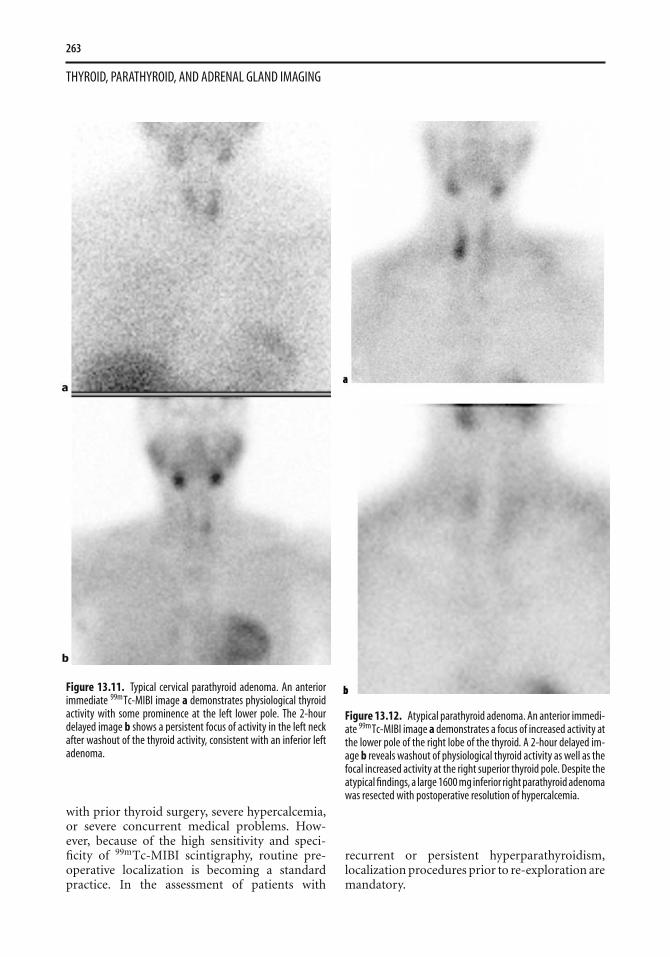
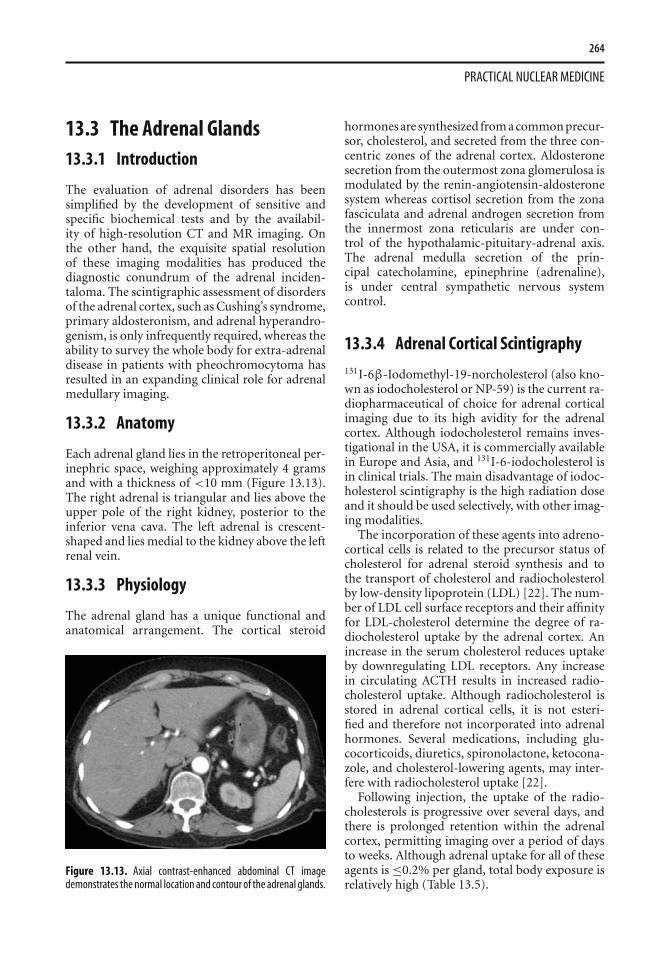
Figure 13.11. Typical cervical parathyroid adenoma. An anteriorimmediate 99mTc-MIBI image a demonstrates physiological thyroidactivity with some prominence at the left lower pole. The 2-hourdelayed image b shows a persistent focus of activity in the left neckafter washout of the thyroid activity, consistent with an inferior leftadenoma.
with prior thyroid surgery, severe hypercalcemia,or severe concurrent medical problems. How-ever, because of the high sensitivity and speci-ficity of 99mTc-MIBI scintigraphy, routine pre-operative localization is becoming a standardpractice. In the assessment of patients with
Figure 13.12. Atypical parathyroid adenoma. An anterior immedi-ate 99mTc-MIBI image a demonstrates a focus of increased activity atthe lower pole of the right lobe of the thyroid. A 2-hour delayed im-age b reveals washout of physiological thyroid activity as well as thefocal increased activity at the right superior thyroid pole. Despite theatypical findings, a large 1600 mg inferior right parathyroid adenomawas resected with postoperative resolution of hypercalcemia.
recurrent or persistent hyperparathyroidism,localization procedures prior to re-exploration aremandatory.
264
PRACTICAL NUCLEAR MEDICINE
13.3 The Adrenal Glands13.3.1 Introduction
The evaluation of adrenal disorders has beensimplified by the development of sensitive andspecific biochemical tests and by the availabil-ity of high-resolution CT and MR imaging. Onthe other hand, the exquisite spatial resolutionof these imaging modalities has produced thediagnostic conundrum of the adrenal inciden-taloma. The scintigraphic assessment of disordersof the adrenal cortex, such as Cushing’s syndrome,primary aldosteronism, and adrenal hyperandro-genism, is only infrequently required, whereas theability to survey the whole body for extra-adrenaldisease in patients with pheochromocytoma hasresulted in an expanding clinical role for adrenalmedullary imaging.
13.3.2 Anatomy
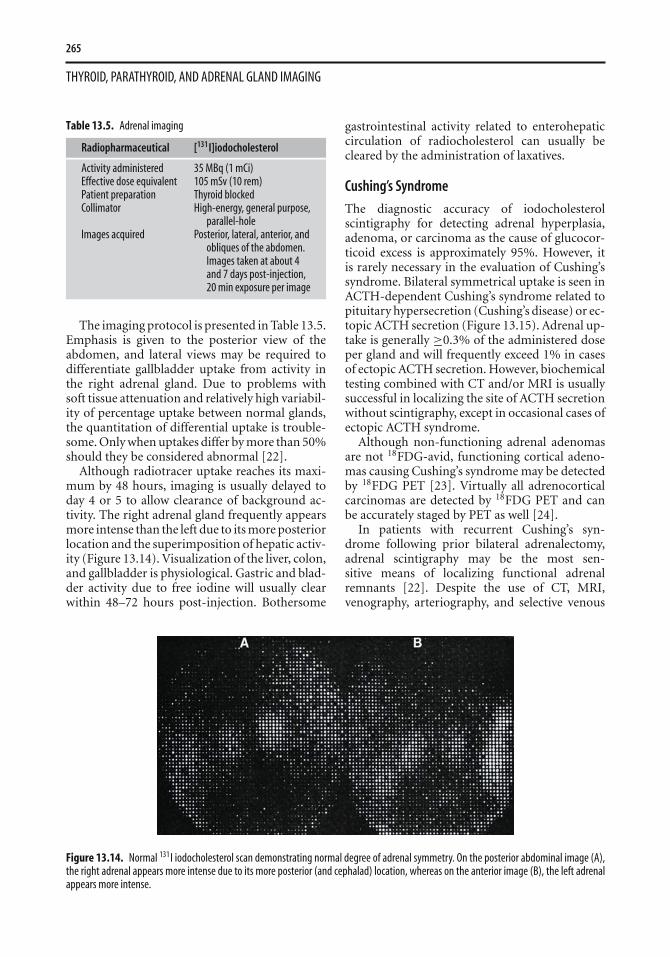
Each adrenal gland lies in the retroperitoneal per-inephric space, weighing approximately 4 gramsand with a thickness of <10 mm (Figure 13.13).The right adrenal is triangular and lies above theupper pole of the right kidney, posterior to theinferior vena cava. The left adrenal is crescent-shaped and lies medial to the kidney above the leftrenal vein.
13.3.3 Physiology
The adrenal gland has a unique functional andanatomical arrangement. The cortical steroid
Figure 13.13. Axial contrast-enhanced abdominal CT imagedemonstrates the normal location and contour of the adrenal glands.
hormones are synthesized from a common precur-sor, cholesterol, and secreted from the three con-centric zones of the adrenal cortex. Aldosteronesecretion from the outermost zona glomerulosa ismodulated by the renin-angiotensin-aldosteronesystem whereas cortisol secretion from the zonafasciculata and adrenal androgen secretion fromthe innermost zona reticularis are under con-trol of the hypothalamic-pituitary-adrenal axis.The adrenal medulla secretion of the prin-cipal catecholamine, epinephrine (adrenaline),is under central sympathetic nervous systemcontrol.
13.3.4 Adrenal Cortical Scintigraphy131I-6β-Iodomethyl-19-norcholesterol (also kno-wn as iodocholesterol or NP-59) is the current ra-diopharmaceutical of choice for adrenal corticalimaging due to its high avidity for the adrenalcortex. Although iodocholesterol remains inves-tigational in the USA, it is commercially availablein Europe and Asia, and 131I-6-iodocholesterol isin clinical trials. The main disadvantage of iodoc-holesterol scintigraphy is the high radiation doseand it should be used selectively, with other imag-ing modalities.
The incorporation of these agents into adreno-cortical cells is related to the precursor status ofcholesterol for adrenal steroid synthesis and tothe transport of cholesterol and radiocholesterolby low-density lipoprotein (LDL) [22]. The num-ber of LDL cell surface receptors and their affinityfor LDL-cholesterol determine the degree of ra-diocholesterol uptake by the adrenal cortex. Anincrease in the serum cholesterol reduces uptakeby downregulating LDL receptors. Any increasein circulating ACTH results in increased radio-cholesterol uptake. Although radiocholesterol isstored in adrenal cortical cells, it is not esteri-fied and therefore not incorporated into adrenalhormones. Several medications, including glu-cocorticoids, diuretics, spironolactone, ketocona-zole, and cholesterol-lowering agents, may inter-fere with radiocholesterol uptake [22].
Following injection, the uptake of the radio-cholesterols is progressive over several days, andthere is prolonged retention within the adrenalcortex, permitting imaging over a period of daysto weeks. Although adrenal uptake for all of theseagents is ≤0.2% per gland, total body exposure isrelatively high (Table 13.5).
265
THYROID, PARATHYROID, AND ADRENAL GLAND IMAGING
Table 13.5. Adrenal imaging
Radiopharmaceutical [131I]iodocholesterol
Activity administered 35 MBq (1 mCi)Effective dose equivalent 105 mSv (10 rem)Patient preparation Thyroid blockedCollimator High-energy, general purpose,
parallel-holeImages acquired Posterior, lateral, anterior, and
obliques of the abdomen.Images taken at about 4and 7 days post-injection,20 min exposure per image
The imaging protocol is presented in Table 13.5.Emphasis is given to the posterior view of theabdomen, and lateral views may be required todifferentiate gallbladder uptake from activity inthe right adrenal gland. Due to problems withsoft tissue attenuation and relatively high variabil-ity of percentage uptake between normal glands,the quantitation of differential uptake is trouble-some. Only when uptakes differ by more than 50%should they be considered abnormal [22].
Although radiotracer uptake reaches its maxi-mum by 48 hours, imaging is usually delayed today 4 or 5 to allow clearance of background ac-tivity. The right adrenal gland frequently appearsmore intense than the left due to its more posteriorlocation and the superimposition of hepatic activ-ity (Figure 13.14). Visualization of the liver, colon,and gallbladder is physiological. Gastric and blad-der activity due to free iodine will usually clearwithin 48–72 hours post-injection. Bothersome
gastrointestinal activity related to enterohepaticcirculation of radiocholesterol can usually becleared by the administration of laxatives.
Cushing’s Syndrome
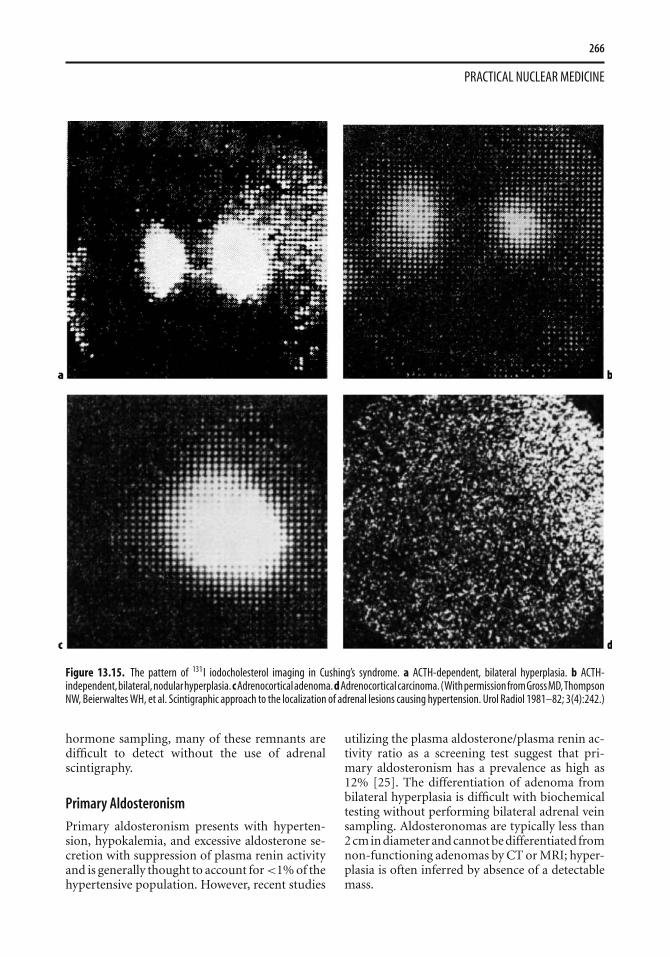
The diagnostic accuracy of iodocholesterolscintigraphy for detecting adrenal hyperplasia,adenoma, or carcinoma as the cause of glucocor-ticoid excess is approximately 95%. However, itis rarely necessary in the evaluation of Cushing’ssyndrome. Bilateral symmetrical uptake is seen inACTH-dependent Cushing’s syndrome related topituitary hypersecretion (Cushing’s disease) or ec-topic ACTH secretion (Figure 13.15). Adrenal up-take is generally ≥0.3% of the administered doseper gland and will frequently exceed 1% in casesof ectopic ACTH secretion. However, biochemicaltesting combined with CT and/or MRI is usuallysuccessful in localizing the site of ACTH secretionwithout scintigraphy, except in occasional cases ofectopic ACTH syndrome.
Although non-functioning adrenal adenomasare not 18FDG-avid, functioning cortical adeno-mas causing Cushing’s syndrome may be detectedby 18FDG PET [23]. Virtually all adrenocorticalcarcinomas are detected by 18FDG PET and canbe accurately staged by PET as well [24].
In patients with recurrent Cushing’s syn-drome following prior bilateral adrenalectomy,adrenal scintigraphy may be the most sen-sitive means of localizing functional adrenalremnants [22]. Despite the use of CT, MRI,venography, arteriography, and selective venous
Figure 13.14. Normal 131I iodocholesterol scan demonstrating normal degree of adrenal symmetry. On the posterior abdominal image (A),the right adrenal appears more intense due to its more posterior (and cephalad) location, whereas on the anterior image (B), the left adrenalappears more intense.
266
PRACTICAL NUCLEAR MEDICINE
Figure 13.15. The pattern of 131I iodocholesterol imaging in Cushing’s syndrome. a ACTH-dependent, bilateral hyperplasia. b ACTH-independent,bilateral,nodularhyperplasia.cAdrenocorticaladenoma.dAdrenocorticalcarcinoma.(WithpermissionfromGrossMD,ThompsonNW, Beierwaltes WH, et al. Scintigraphic approach to the localization of adrenal lesions causing hypertension. Urol Radiol 1981–82; 3(4):242.)
hormone sampling, many of these remnants aredifficult to detect without the use of adrenalscintigraphy.
Primary Aldosteronism
Primary aldosteronism presents with hyperten-sion, hypokalemia, and excessive aldosterone se-cretion with suppression of plasma renin activityand is generally thought to account for <1% of thehypertensive population. However, recent studies
utilizing the plasma aldosterone/plasma renin ac-tivity ratio as a screening test suggest that pri-mary aldosteronism has a prevalence as high as12% [25]. The differentiation of adenoma frombilateral hyperplasia is difficult with biochemicaltesting without performing bilateral adrenal veinsampling. Aldosteronomas are typically less than2 cm in diameter and cannot be differentiated fromnon-functioning adenomas by CT or MRI; hyper-plasia is often inferred by absence of a detectablemass.
267
THYROID, PARATHYROID, AND ADRENAL GLAND IMAGING
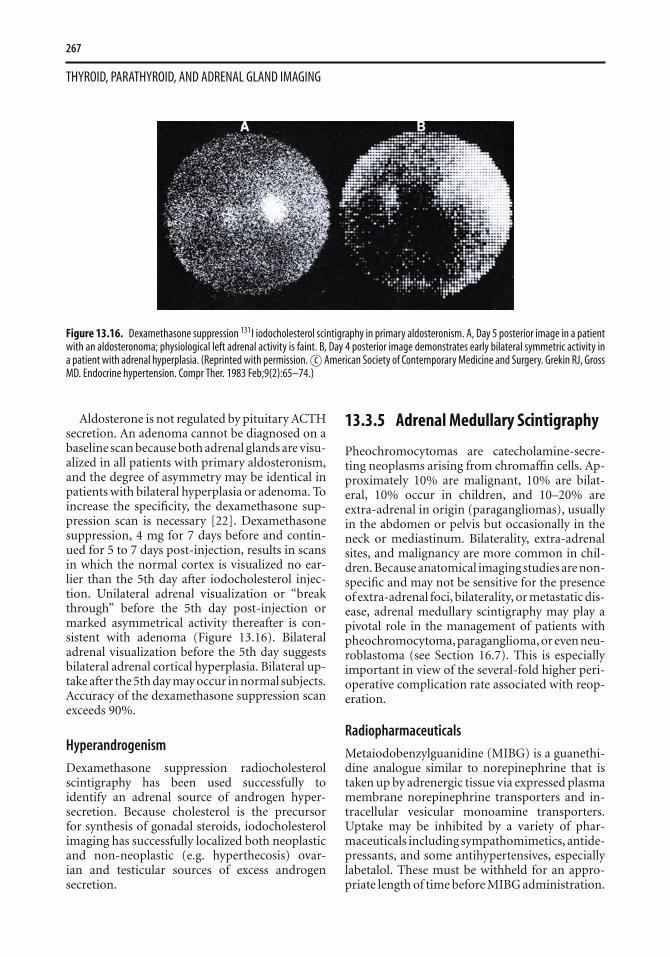
Figure 13.16. Dexamethasone suppression 131I iodocholesterol scintigraphy in primary aldosteronism. A, Day 5 posterior image in a patientwith an aldosteronoma; physiological left adrenal activity is faint. B, Day 4 posterior image demonstrates early bilateral symmetric activity ina patient with adrenal hyperplasia. (Reprinted with permission. c© American Society of Contemporary Medicine and Surgery. Grekin RJ, GrossMD. Endocrine hypertension. Compr Ther. 1983 Feb;9(2):65–74.)
Aldosterone is not regulated by pituitary ACTHsecretion. An adenoma cannot be diagnosed on abaseline scan because both adrenal glands are visu-alized in all patients with primary aldosteronism,and the degree of asymmetry may be identical inpatients with bilateral hyperplasia or adenoma. Toincrease the specificity, the dexamethasone sup-pression scan is necessary [22]. Dexamethasonesuppression, 4 mg for 7 days before and contin-ued for 5 to 7 days post-injection, results in scansin which the normal cortex is visualized no ear-lier than the 5th day after iodocholesterol injec-tion. Unilateral adrenal visualization or “breakthrough” before the 5th day post-injection ormarked asymmetrical activity thereafter is con-sistent with adenoma (Figure 13.16). Bilateraladrenal visualization before the 5th day suggestsbilateral adrenal cortical hyperplasia. Bilateral up-take after the 5th day may occur in normal subjects.Accuracy of the dexamethasone suppression scanexceeds 90%.
Hyperandrogenism
Dexamethasone suppression radiocholesterolscintigraphy has been used successfully toidentify an adrenal source of androgen hyper-secretion. Because cholesterol is the precursorfor synthesis of gonadal steroids, iodocholesterolimaging has successfully localized both neoplasticand non-neoplastic (e.g. hyperthecosis) ovar-ian and testicular sources of excess androgensecretion.
13.3.5 Adrenal Medullary Scintigraphy
Pheochromocytomas are catecholamine-secre-ting neoplasms arising from chromaffin cells. Ap-proximately 10% are malignant, 10% are bilat-eral, 10% occur in children, and 10–20% areextra-adrenal in origin (paragangliomas), usuallyin the abdomen or pelvis but occasionally in theneck or mediastinum. Bilaterality, extra-adrenalsites, and malignancy are more common in chil-dren. Because anatomical imaging studies are non-specific and may not be sensitive for the presenceof extra-adrenal foci, bilaterality, or metastatic dis-ease, adrenal medullary scintigraphy may play apivotal role in the management of patients withpheochromocytoma, paraganglioma, or even neu-roblastoma (see Section 16.7). This is especiallyimportant in view of the several-fold higher peri-operative complication rate associated with reop-eration.
Radiopharmaceuticals
Metaiodobenzylguanidine (MIBG) is a guanethi-dine analogue similar to norepinephrine that istaken up by adrenergic tissue via expressed plasmamembrane norepinephrine transporters and in-tracellular vesicular monoamine transporters.Uptake may be inhibited by a variety of phar-maceuticals including sympathomimetics, antide-pressants, and some antihypertensives, especiallylabetalol. These must be withheld for an appro-priate length of time before MIBG administration.
268
PRACTICAL NUCLEAR MEDICINE
Table 13.6. Pheochromocytoma and sympathomedullary imaging
Radiopharmaceutical 123I-MIBG 131I-MIBG
Activity administered 400 MBq (10 mCi) 20 MBq (0.5 mCi)Effective doseequivalent
6 mSv (600 mrem) 3 mSv (300 mrem)
Patient preparation Lugol’s solution or a saturated solution ofpotassium iodide (100 mg twice a day) begunthe day prior to administration of theradiopharmaceutical and continued for 4 daysafterwards
Lugol’s solution or a saturated solution of potassiumiodide (100 mg twice a day) begun the day prior toadministration of the radiopharmaceutical andcontinued for 7 days afterwards
Collimator Low-energy, high-resolution, parallel-hole High-energy, general purpose, parallel-holeImages acquired Whole body images, anterior and posterior, 10
minutes per step, at 24 h (and 48 h as needed).SPECT of abdomen
Whole body images, anterior and posterior, 20minutes per step, at 24 and 48 h (and 72 h asneeded)
Although both 131I and 123I have been used to labelMIBG, 123I is preferable because of its favorabledosimetry and imaging characteristics. Plasmaclearance of MIBG is rapid, with 50–70% of thedose excreted unchanged into the urine within 24hours. Due to the release of free radioiodine fromthe radiopharmaceutical, the co-administration ofstable iodine to block thyroid uptake is necessary.
Technique
The imaging protocol is presented in Table 13.6.Although posterior images of the abdomen aremost important, whole body imaging is recom-mended for detection of paragangliomas andmetastatic disease. When 123I-MIBG is utilized,
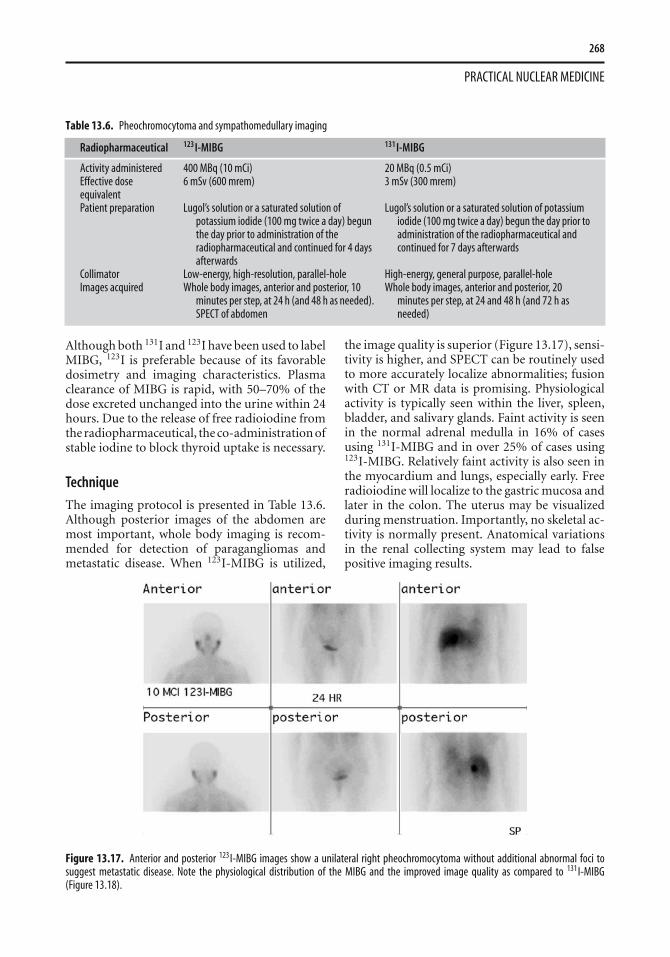
Figure 13.17. Anterior and posterior 123I-MIBG images show a unilateral right pheochromocytoma without additional abnormal foci tosuggest metastatic disease. Note the physiological distribution of the MIBG and the improved image quality as compared to 131I-MIBG(Figure 13.18).
the image quality is superior (Figure 13.17), sensi-tivity is higher, and SPECT can be routinely usedto more accurately localize abnormalities; fusionwith CT or MR data is promising. Physiologicalactivity is typically seen within the liver, spleen,bladder, and salivary glands. Faint activity is seenin the normal adrenal medulla in 16% of casesusing 131I-MIBG and in over 25% of cases using123I-MIBG. Relatively faint activity is also seen inthe myocardium and lungs, especially early. Freeradioiodine will localize to the gastric mucosa andlater in the colon. The uterus may be visualizedduring menstruation. Importantly, no skeletal ac-tivity is normally present. Anatomical variationsin the renal collecting system may lead to falsepositive imaging results.
269
THYROID, PARATHYROID, AND ADRENAL GLAND IMAGING
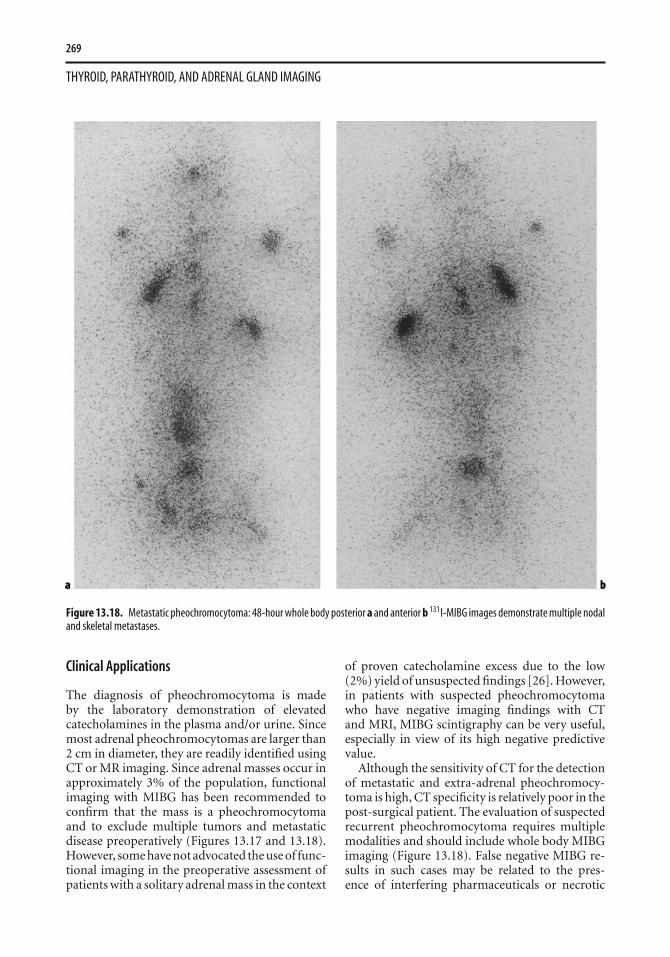
Figure 13.18. Metastatic pheochromocytoma: 48-hour whole body posterior a and anterior b 131I-MIBG images demonstrate multiple nodaland skeletal metastases.
Clinical Applications
The diagnosis of pheochromocytoma is madeby the laboratory demonstration of elevatedcatecholamines in the plasma and/or urine. Sincemost adrenal pheochromocytomas are larger than2 cm in diameter, they are readily identified usingCT or MR imaging. Since adrenal masses occur inapproximately 3% of the population, functionalimaging with MIBG has been recommended toconfirm that the mass is a pheochromocytomaand to exclude multiple tumors and metastaticdisease preoperatively (Figures 13.17 and 13.18).However, some have not advocated the use of func-tional imaging in the preoperative assessment ofpatients with a solitary adrenal mass in the context
of proven catecholamine excess due to the low(2%) yield of unsuspected findings [26]. However,in patients with suspected pheochromocytomawho have negative imaging findings with CTand MRI, MIBG scintigraphy can be very useful,especially in view of its high negative predictivevalue.
Although the sensitivity of CT for the detectionof metastatic and extra-adrenal pheochromocy-toma is high, CT specificity is relatively poor in thepost-surgical patient. The evaluation of suspectedrecurrent pheochromocytoma requires multiplemodalities and should include whole body MIBGimaging (Figure 13.18). False negative MIBG re-sults in such cases may be related to the pres-ence of interfering pharmaceuticals or necrotic

270
PRACTICAL NUCLEAR MEDICINE
tumor. However, malignant pheochromocytomamay dedifferentiate and thus no longer accumu-late MIBG. In these instances, 18FDG PET imag-ing or 111In octreotide scintigraphy may betterdemonstrate the extent of metastatic disease (Fig-ure 13.19). Benign pheochromocytoma is also of-ten 18FDG positive although 18FDG is more of-ten taken up by malignant pheochromocytoma[27]. Dopamine is a better substrate for the nore-pinephrine transporter than other amines, and theuse of 18F-fluorodopamine (DA) PET is promisingfor the determination of metastatic disease extent,especially in patients whose tumor is not MIBG-avid [27].
Most neuroendocrine tumors express so-matostatin receptors, and somatostatin receptorscintigraphy (SRS) using 111In octreotide has beenreported to be highly sensitive (>90%) for the de-tection of head and neck paragangliomas. How-ever, SRS has been reported to have a sensitivity aslow as 25% for the detection of primary adrenalpheochromocytoma [28]. SRS is at least as sensi-tive as MIBG imaging for detection of metastaticpheochromocytoma (87% versus 57% of lesions)[28]. Therefore, SRS is not recommended as a first-line modality for detection of suspected primarypheochromocytoma.
123I-MIBG imaging may be especially usefulin children who more frequently have heredi-tary syndromes (multiple endocrine neoplasia,von Hippel–Lindau, neurofibromatosis, familialpheochromocytoma, and Carney’s triad) and areat higher risk for multifocality, extra-adrenal dis-ease and malignant disease. Bilateral uptake dueto medullary hyperplasia may be demonstrated byMIBG scintigraphy, but sensitivity is insufficientto exclude contralateral disease [28]. It must be re-membered that MIBG imaging, SRS, and 18FDGPET may detect other neuroendocrine tumorssuch as medullary thyroid carcinoma, carcinoid,and islet cell tumors as well as neuroblastoma andsmall cell lung carcinoma (see Section 16.7). Thisis especially important in patients with hereditarysyndromes. Functional imaging with MIBG is es-pecially useful in differentiating pheochromocy-toma from neurofibromas in affected individuals.
13.3.6 Conclusions
In summary, radiocholesterol imaging of theadrenal cortex is most useful in (1) the differ-entiation of hyperplasia from adenoma in pri-
Figure 13.19. Metastatic pheochromocytoma. A 18FDG PET im-age demonstrates widespread nodal and parenchymal metastasesin this 39-year-old man who presented with labile hypertension.Biopsy of a hypermetabolic cervical node revealed pheochromo-cytoma. (With permission from Scanga DR, Martin WH, DelbekeD. Value of FDG PET imaging in the management of patients withthyroid, neuroendocrine, and neural crest tumors. Clin Nucl Med 2004;29(2):86–90.)
mary aldosteronism when CT and MR imagingare equivocal, (2) in the detection of functioningadrenal remnant in the patient with recur-rent/persistent Cushing’s syndrome despite priorbilateral adrenalectomy, and (3) in the charac-terization of ACTH-independent adrenal corticalnodular hyperplasia.
Pheochromocytoma and paragangliomasare diagnosed by demonstrating circulatingcatecholamine excess and are virtually always

271
THYROID, PARATHYROID, AND ADRENAL GLAND IMAGING
localized accurately by CT or MR imaging. MIBGimaging is complementary to CT/MR and canbe utilized before initial surgery to confirm thatthe detected mass is a pheochromocytoma and todetect multifocal, extra-adrenal, and metastaticdisease. 123I-MIBG is preferable to 131I-MIBG be-cause of better dosimetry, higher quality images,the ability to use SPECT, and probably highersensitivity. MIBG uptake is higher in sporadic,benign, unilateral, and adrenal pheochromo-cytoma than in familial, malignant, bilateral,and extra-adrenal pheochromocytoma. In theevaluation of patients with recurrent malignantpheochromocytoma, functional imaging playsa key role. MIBG imaging is useful for detec-tion of MIBG-avid metastatic disease that cansubsequently be resected, debulked, or treatedwith high-dose 131I-MIBG (Chapter 16). Fordedifferentiated pheochromocytoma that is notMIBG-avid, SRS using 111In octreotide or PETutilizing 18FDG or 18F-DA is useful.
References1. Kusic Z, Becker DV, Saenger EL, et al. Comparison of
technetium-99m and iodine123 imaging of thyroid nod-ules: correlation with pathologic findings. J Nucl Med1990; 31:393–399.
2. Mazzaferri EL. Management of a solitary thyroid nodule.N Engl J Med 1993; 328:553–559.
3. Shakir F, Fitzsimmons TR, Jaques DP, et al. Diagnosis andmanagement of the autonomously functioning thyroidnodule: the Walter Reed Army Medical Center experience,1975–1996. Thyroid 1998; 8:871–880.
4. Graham GD, Burman KD. Radioiodine treatment ofGraves’ disease. An assessment of its potential risks. AnnIntern Med 1986; 105:900–905.
5. Hedley AJ, Lazarus JH, McGhee SM, et al. Treatment ofhyperthyroidism by radioactive iodine. J R Coll PhysiciansLond 1992; 26:348–351.
6. Humphrey ML, Burman KD. Retrosternal and intratho-racic goiter. Endocrinologist 1992; 2:195–201.
7. Sfakianakis GN, Ezuddin SH, Sanchez JE, et al. Pertechne-tate scintigraphy in primary congenital hypothyroidism. JNucl Med 1999; 40:799–804.
8. Grigsby PW, Siegel BA, Bekker S, et al. Preparation of pa-tients with thyroid cancer for 131I scintigraphy or therapyby 1–3 weeks of thyroxine discontinuation. J Nucl Med2004; 45:567–570.
9. Spies WG, Wojtowizc CH, Spies SM, et al. Value of post-therapy whole-body I-131 imaging in the evaluation ofpatients with thyroid carcinoma having undergone high-dose I-131 therapy. Clin Nucl Med 1989; 14:793–800.
10. Haugen BR, Pacini F, Reiners C, et al. A comparison ofrecombinant human thyrotropin and thyroid hormonewithdrawal for the detection of thyroid remnant or cancer.J Clin Endocrinol Metab 1999; 84:3877–3885.
11. Lupin E, Mechlis-Frish S, Zatz S. Serum thyroglobulin andiodine-131 whole-body scan in the diagnosis and assess-ment of treatment for metastatic differentiated thyroid car-cinoma. J Nucl Med 1994; 35:257–262.
12. Alzahrani AS, Bakheet S, Mandil MA, et al. 123I isotope asa diagnostic agent in the follow-up of patients with differ-entiated thyroid cancer: Comparison with post 131I ther-apy whole body scanning. J Clin Endocrinol Metab 2001;86:5294–5300.
13. Grunwald F, Kalicke T, Feine U, et al. Fluorine-18 fluo-rodeoxyglucose positron emission tomography in thyroidcancer: results of a multicentre study. Eur J Nucl Med 1999;26:1547–1552.
14. Hooft L, Hoekstra OS, Deville W, et al. Diagnostic accuracyof 18F-fluorodeoxyglucose positron emission tomographyin the follow-up of papillary or follicular thyroid cancer. JClin Endocrinol Metab 2001; 86:3779–3786.
15. Wang W, Larson SM, Fazzari M, et al. Prognostic value of[18F]fluorodeoxyglucose positron emission tomographicscanning in patients with thyroid cancer. J Clin EndocrinolMetab 2000; 85:1107–1113.
16. Pacini F, Agate L, Elisei R, et al. Outcome of differ-entiated thyroid cancer with detectable serum Tg andnegative diagnostic 131I whole body scan: comparisonof patients treated with high 131I activities versus un-treated patients. J Clin Endocrinol Metab 2001; 86:4092–7097.
17. Szakall S Jr, Esik O, Bajzik G, et al. 18F-FDG PET detectionof lymph node metastases in medullary thyroid carcinoma.J Nucl Med 2002; 43:66–71.
18. Hauty M, Swartz K, McClung M, et al. Technetium 210Tlscintiscanning for localization of parathyroid adenomasand hyperplasia: a reappraisal. Am J Surg 1987; 153:479–486.
19. Taillefer R. Parathyroid scintigraphy. In: Khalkhali J,Maublant JC, Goldsmith SJ, eds. Nuclear Oncology: Di-agnosis and Therapy. Philadelphia: Lippincott; 2001: 221–244.
20. Denham DW, Norman J. Cost-effectiveness of preop-erative 99mTc MIBI scan for primary hyperparathy-roidism is dependent solely upon the surgeon’s choiceof operative procedure. J Am Coll Surg 1998; 186:293–304.
21. Gotway MB, Reddy GP, Webb WR, et al. Comparison be-tween MR imaging and 99mMIBI scintigraphy in the evalu-ation of recurrent or persistent hyperparathyroidism. Ra-diology 2001; 218:783–790.
22. Gross MD, Shapiro B, Bui C, et al. Adrenal scintigraphyand metaiodobenzylguanidine therapy of neuroendocrinetumors. In: Sandler MP, Coleman RE, Patton JA, WackersFJT, Gottschalk A, eds. Diagnostic Nuclear Medicine, 4thedn. Philadelphia: Lippincott Williams & Wilkins; 2003:6715–6733.
23. Shimizu A, Oriuchi N, Tsushima Y, et al. High [18F] 2-fluoro-2-deoxy-D-glucose (FDG) uptake of adrenocor-tical adenoma showing subclinical Cushing’s syndrome.Ann Nucl Med 2003; 17:403–406.
24. Bechereo A, Vierhapper H, Potzi C, et al. FDG-PET inadrenocortical carcinoma. Cancer Biother Radiopharm2001; 16:289–295.
25. Mulatero P, Stowasser M, Loh K-C, et al. Increased diag-nosis of primary aldosteronism, including surgically cor-rectable forms, in centers from five continents. J Clin En-docrinol Metab 2004; 89:1045–1050.

272
PRACTICAL NUCLEAR MEDICINE
26. Miskulin J, Shulkin BL, Doherty GM, et al. Is preoperativeiodine 123 meta-iodobenzylguanidine scintigraphyroutinely necessary before initial adrenalectomyfor pheochromocytoma? Surgery 2003; 134:918–923.
27. Ilias I, Yu J, Carrasquillo JA, et al. Superiority of 6-[18F]-fluorodopamine positron emission tomography versus[131I]-metaiodobenzylguanidine scintigraphy in the lo-calization of metastatic pheochromocytoma. J Clin En-docrinol Metab 2003; 88:4083–4087.
28. vander Harst E. de Herder WW, Bruining HA, et al. J ClinEndocrinol Metab 2001; 86:685–693.
Further Reading
Braverman LE, Utiger RD, eds. Werner & Ingbar’s The Thyroid:A Fundamental and Clinical Text, 8th edn. Philadelphia:Lippincott Williams & Wilkins; 2000.
Sandler MP, Coleman RE, Patton JA, Wackers FJT, GottschalkA, eds. Diagnostic Nuclear Medicine, 4th edn. Philadelphia:Lippincott Williams & Wilkins; 2003.
Ilias I, Pacak, K. Current approaches and recommended algo-rithm for the diagnostic localization of pheochromocytoma.J Clin Endocrinol Metab 2004; 89: 479–491.




















