
Sweat gland differentiation in mammary adenoid cystic carcinoma
9
SWEAT GLAND DIFFERENTIATION IN MAMMARY ADENOID CYSTIC CARCINOMA PHILIP G. PRIOLEAU, MD, DANIEL J. SANTA CRUZ, hlD, JOHN B. BUETTNER, MD,* AND WALTER C. BAUER, MD A breast tumor is described which presented as an exophytic mass, and which by both light and electron microscopic examination had a biphasic histologic composition. In the superficial area adjacent to the epidermis, it showed tubular differentiation similar to a cutaneous tubular apocrine adenoma and salivary basal cell adenoma, and, in the deeper portion, it had the characteristic features of adenoid cystic carcinoma. Their possible interrelationships are discussed, and mammary adenoid cystic carcinoma is briefly reviewed. Cancer 43:1752- 1760, 1979. LTHOUCH THE SUBJECT OF numerous A recent reports, adenoid cystic car- cinoma of the breast is a rare tumor char- acterized by definite histologic criteria and a low malignant potential. Diagnosis generally poses little difficulty. Recently, we encountered a large breast tumor which had many features of adenoid cystic carcinoma. However, it presented as a fungating mass, appeared to arise from areolar epithelium, and in large areas was composed of densely cellular islands sug- gestive of both tumors of skin adnexal glands, notably the tubular apocrine adenoma, and salivary basal cell adenomas. The juxtaposi- tion of the malignant tumor to the relatively benign appearing epithelial islands is rem- iniscent of the two reported cases of com- bined adenoid cystic carcinoma and basal cell adenoma in salivary g la~d~.~ and supports the theory of a common cellular rigi in.^ We are not aware of a report of a mammary tumor with similar gross and microscopic features. CASE REPORT A 64-year-old black woman presented with a right breast mass discovered six months pre- viously when she fell on ice sustaining blunt trauma to her breast. Following the injury, her From the Division of Surgical Pathology and *Depart- ment of Surgery, Washington University School of Medicine and Barnes Hospital, St. Louis, Missouri. Supported in part by USPHS 5 7'01 CA05201-08. Address for reprints: Philip G. Prioleau. MD. Division of Surgical Pathology, Barnes Hospital, Barnes Hospital Plaza. St. Louis, MO 63 I 10. Accepted for publication June 12, 1978. breast became swollen and discolored. and three to four weeks later drained spontaneously pus and blood. In the ensuing weeks, there was a significant increase in hreast size with associated skin erosion. Finally. she sought medical attention and was re- terred forevaluation. The patient, who was gravida three, para one, abortus two, had undergone meno- pause ten years earlier. She was otherwise asymp- tomatic, and had a negative family history for breast cancer. On physical examination, the patient had a bosselated, reddish, weeping exophytic breast mass involving the upper areola (Fig. 1, left). Beneath, there was extensive involvement of the breast hy tumor although it was not fixer1 to the underlying pectoral fascia. Neither nipple dis- charge nor palpable axillary lymphadenopathy was noted. The remainder of the physical exam- ination was unreinarkable. Arlmission chest radiograph, routine blood studies and livet- scan were within normal limits. A biopsy taken trom the superficial portion of the Inass was interpreted as most likely a low grade malignant tumor of sweat gland origin. As there was no evidence that this tumor had metastasized or was one of the common breast carcinomas, a total mastectomy with lower axillary dissection was performed six days later. MATERIALS AND METHODS Immediately following mastectomy, the specimen was sectioned vertically into slices at approximately 2 cm intervals and placed in 10% buffered formalin. Tissue was sub- sequently embedded in paraffin for hema- toxylin and eosin, Alcian blue, inucicarmine and periodic acid-Schiff staining. Following initial sectioning, portions of the superficial part of the tumor adjacent to the 0008-543X/79/0500/1752 $0.95 0 American Cancer Society 1752
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Sweat gland differentiation in mammary adenoid cystic carcinoma

SWEAT GLAND DIFFERENTIATION I N MAMMARY ADENOID CYSTIC CARCINOMA
PHILIP G. PRIOLEAU, MD, DANIEL J. SANTA CRUZ, hlD, J O H N B. BUETTNER, MD,* A N D WALTER C. BAUER, M D
A breast tumor is described which presented as an exophytic mass, and which by both light and electron microscopic examination had a biphasic histologic composition. In the superficial area adjacent to the epidermis, it showed tubular differentiation similar to a cutaneous tubular apocrine adenoma and salivary basal cell adenoma, and, in the deeper portion, it had the characteristic features of adenoid cystic carcinoma. Their possible interrelationships are discussed, and mammary adenoid cystic carcinoma is briefly reviewed.
Cancer 43:1752- 1760, 1979.
LTHOUCH THE SUBJECT OF numerous A recent reports, adenoid cystic car- cinoma of the breast is a rare tumor char- acterized by definite histologic criteria and a low malignant potential. Diagnosis generally poses little difficulty.
Recently, we encountered a large breast tumor which had many features of adenoid cystic carcinoma. However, it presented as a fungating mass, appeared to arise from areolar epithelium, and in large areas was composed of densely cellular islands sug- gestive of both tumors of skin adnexal glands, notably the tubular apocrine adenoma, and salivary basal cell adenomas. T h e juxtaposi- tion of the malignant tumor to the relatively benign appearing epithelial islands is rem- iniscent of the two reported cases of com- bined adenoid cystic carcinoma and basal cell adenoma in salivary g l a ~ d ~ . ~ and supports the theory of a common cellular rigi in.^ We are not aware of a report of a mammary tumor with similar gross and microscopic features.
CASE REPORT A 64-year-old black woman presented with a
right breast mass discovered six months pre- viously when she fell on ice sustaining blunt trauma to her breast. Following the injury, her
From the Division of Surgical Pathology and *Depart- ment of Surgery, Washington University School of Medicine and Barnes Hospital, St. Louis, Missouri.
Supported in part by USPHS 5 7'01 CA05201-08. Address for reprints: Philip G . Prioleau. MD. Division
of Surgical Pathology, Barnes Hospital, Barnes Hospital Plaza. St. Louis, MO 63 I 10.
Accepted for publication June 12, 1978.
breast became swollen and discolored. a n d three t o four weeks later drained spontaneously pus and blood. In the ensuing weeks, there was a significant increase in hreast size with associated skin erosion. Finally. she sought medical attention and was re- terred forevaluation. T h e patient, who was gravida three, para one, abortus two, had undergone meno- pause ten years earlier. She was otherwise asymp- tomatic, and had a negative family history for breast cancer.
On physical examination, the patient had a bosselated, reddish, weeping exophytic breast mass involving the upper areola (Fig. 1 , left). Beneath, there was extensive involvement of the breast hy tumor although it was not fixer1 to the underlying pectoral fascia. Neither nipple dis- charge nor palpable axillary lymphadenopathy was noted. T h e remainder of the physical exam- ination was unreinarkable.
Arlmission chest radiograph, routine blood studies and livet- scan were within normal limits. A biopsy taken t rom the superficial portion of the Inass was interpreted as most likely a low grade malignant tumor of sweat gland origin. As there was no evidence that this tumor had metastasized o r was one of the common breast carcinomas, a total mastectomy with lower axillary dissection was performed six days later.
MATERIALS A N D METHODS
Immediately following mastectomy, the specimen was sectioned vertically into slices at approximately 2 cm intervals and placed in 10% buffered formalin. Tissue was sub- sequently embedded in paraffin for hema- toxylin and eosin, Alcian blue, inucicarmine and periodic acid-Schiff staining.
Following initial sectioning, portions of the superficial part of the tumor adjacent to the
0008-543X/79/0500/1752 $0.95 0 American Cancer Society
1752

No. 5 MAMMARY ADENOID CYSTIC CA Priolvau et (11. 1753
FIG. 1. (left) Lateral view of patient’s right breast showing pro- t r u d i 11 g i m 111 ed ia t el y above the nipple. (right) Sagittal section of inastectoiny speciinen.
t u m o r
areola were placed in 2.5% glutaraldehyde and processed by standard techniques for electron microscopy. When it was recognized that the tumor had a biphasic histologic com- position, tissue from the deeper areas of tumor was retrieved from formalin and processed for electron microscopic examination; the fixation of this material was poor, and exam- ination was suboptimal.
PATHOLOGY
Gross
T h e resected tissue consisted of a right total mastectomy specimen with attached lower axillary contents. Lying immediately above and adjacent to the nipple and partially in- volving the areola was a red fungating ir- regular mass which measured 8 cm in diameter and which protruded 2.5 cm from the areola. O n cut section, the tumor had a yellow-gray coloration and gritty consistency, and ex- tended to a depth of 6.5 cm. Most of the tumor was solid; however, several cysts con- taining bloody fluid were present, the largest measuring 4.5 cm in diameter (Fig. 1, right). Thirty-one axillary lymph nodes were identified.
Light Microscopy
There were two rather distinct histologic patterns. In the exophytic portion adjacent to the areola, the tumor was composed of
small nests of cells which were contiguous with the epidermis and gave the impression of havingarisen from it (Figs. 2, left and right). In some sections, these islands had a ribbon- like configuration and contained small central ducts. Most of the cells were relatively uni- form and had basophilic nuclei, sparce eosinophilic cytoplasm and palasading bor- ders. In the central portion of each island there was frequently a single row of smaller cells with a paler nucleus and cytoplasm. Many of these showed cuticular differentiation and the ducts which they surrounded often contained debris. Mitoses in these cells were rare.
In the deeper areas of breast, the histologic picture differed markedly. Here, the tumor was composed of larger islands with a cribri- form pattern typical of adenoid cystic car- cinoma (Fig. 3). T h e several larger cystic structures seen grossly had walls of dense fibrous tissue containing hemosiderin and an epithelial lining of a single cuboidal cell laver. Neither cytologic pleomorphism nor peri- neural invasion by tumor was noted in the 35 sections examined, and the adjacent un- involved breast tissue was unremarkable. None of the 31 axillary lymph nodes con- tained a metastasis.
T h e extracellular material in the lakes in the deeper portion of the tumor as well as occasional tiny foci in the middle of the super- ficial nests stained with the periodic acid- Schiff reagent after diastase digestion as well as with Alcian blue, the larger the

1754 CANCER May 1979 VOl. 43
FIG. 2. (left) Breast tumor adjacent to the areola showing contiguity of ductal structures with overlying epidermis (H & E, X38). (right) A higher magnification of epidermal junction ( H & E. x472).
lake, the more intense the staining. These same areas were faintly positive with muci- carmine stain.
Electron Microscopy
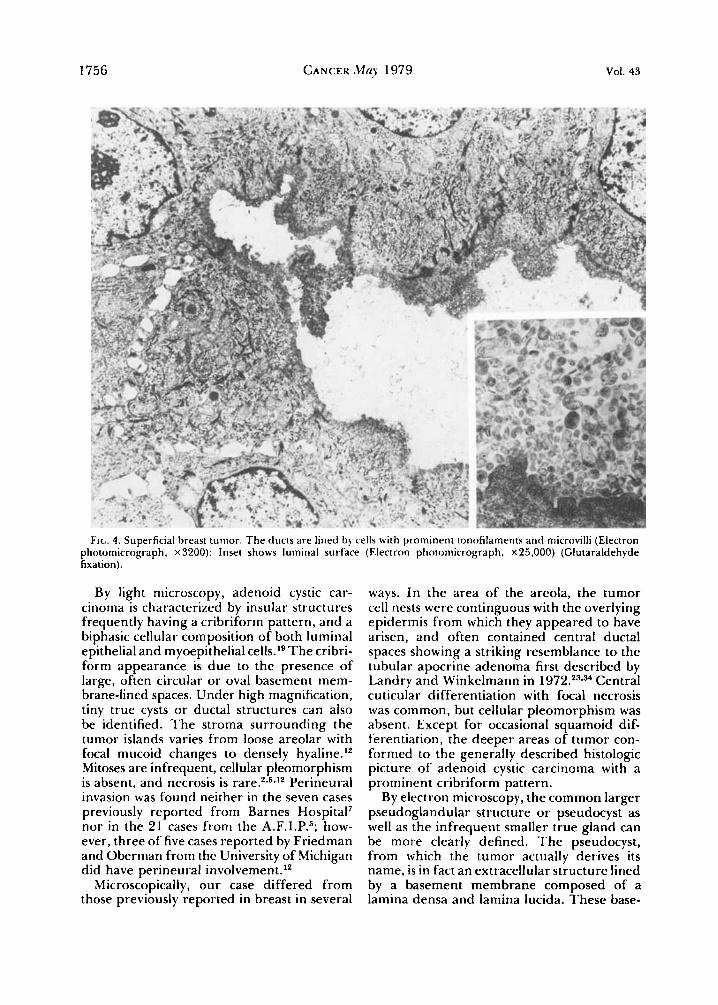
The tumor adjacent to the areola was com- posed of cells arranged in islands often with a central lumen or cystic space. The cells bordering the lumen were relatively close to- gether, and on the luminal side had short microvilli, and contained prominent tonofila- ments, glycogen and occasional dense bodies (Fig. 4). In the cystic spaces were fragmented villi and membrane bound material similar to lysosomes. The cells situated more peripherally contained less cytoplasm and fewer tonofila- ments, and were more widely separated. N o myoepithelial cells were seen.
Electron microscopic examination of the deeper portion of tumor was suboptimal due
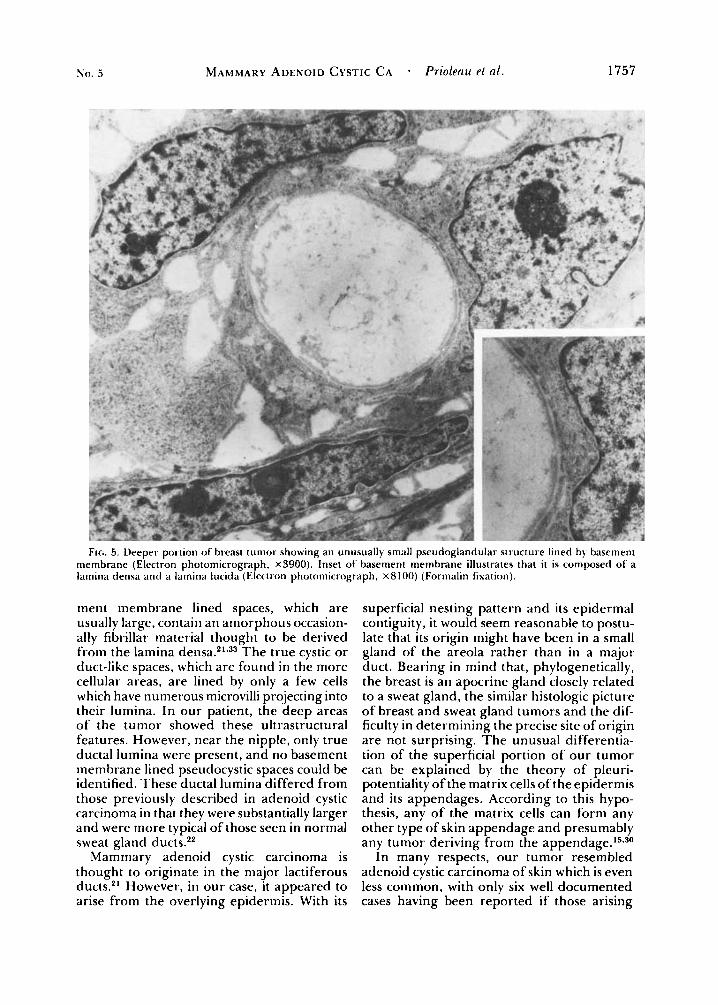
to the initial formalin fixation; however, the two distinctly different cyst-like structures characteristic of adenoid cystic carcinoma were readily identified. T h e larger, which formed the cribriform pattern and was not a true gland, was lined by a uniformly flat basal lamina composed of two layers, a lamina densa and lamina lucida. Lakes of amorphous material were present within these cyst-like spaces, and no villi were seen (Fig. 5 ) . Oc- casional much smaller true cystic structures were present, each being bordered by only a few cells and lined by microvilli (Fig. 6); these did not contribute to the cribriform pattern seen by light microscopy. Myoepi- thelial cells, described in adenoid cystic car- cinoma,Ig could not be identified possibly due to poor tissue preservation.
This tumor was interpreted as an adenoid cystic carcinoma with features suggestive of skin adnexal gland origin.

No. 5 MAMMARY ADENOID CYSTIC CA * Prioleau et al. 1755
FIG. 3. Deeper portion of breast tumor showing cribriform pattern characteristic of adenoid cystic carcinoma (left) and ductal structures typical of the superficial portion o f the tumor (right) ( H & E, x350).
DISCUSSION
Although most frequently found in salivary glands, adenoid cystic carcinoma also occurs in the breast, tracheobronchial tree, naso- pharynx, external auditory canal, maxillary sinus, prostate, uterine cervix, esophagus, Bartholin’s gland and kin.'*^-^^^'**^ In spite of marked differences in biologic behavior, the histologic pattern of these tumors arising at different sites is the same.
For this tumor to involve the breast is rare, the total number of reported cases being almost Of 2686 patients with breast cancer studied in a ten-year period by Anthony and James at the Middlesex Hospital in London, only three had adenoid cystic car- cinoma.? Over a 40-year period at the Mayo Clinic, nine cases were found,I3 and at Barnes Hospital from 1952- 1968, seven cases were de~cribed.~ The largest single series comprised
21 cases reported from the Armed Forces Institute of Pathology by Cavanzo and T a y l ~ r . ~ The ages of their patients ranged from 31 to 69 years (median 49.9), and the main pre- senting symptom was a breast mass which was sometimes tender and which had been recognized for a period varying from a few weeks to many years. T w o of the seven pa- tients reported from Barnes Hospital had noted a tumor for as long as 12 years.’Six cases have been in men.9*10*18*35*3s*38
When adenoid cystic carcinoma occurs in breast, it usually presents beneath the nipple. The overlying epithelium is uninvolved. In Cavanzo and Taylor’s series, the median tumor diameter was 2.4 cm. with a range of 1 to 5 ~ m . ~ Our patient also had a lesion situated in the areolar area. However, it pre- sented as a fungating mass protruding 2.5 cm above the skin, and measured 8 cm in great- est dimension.
1756 CANCER M q 1979 VOl. 43
FIL. 4. Superficial breast tumor. T h e ducts are lined by cells with prominent tonofilaments and microvilli (Electron photomicrograph, x 3200): lnser shows luininal surface (Electron photomirrograph, ~ 2 5 , 0 0 0 ) (Glutaraldehyde fixation)
By light microscopy, adenoid cystic car- cinoma is characterized by insular structures frequently having a cribriform pattern, and a biphasic cellular composition of both luminal epithelial and myoepithelial cells.19 T h e cribri- form appearance is due to the presence of large, often circular or oval basement mem- brane-lined spaces. Under high magnification, tiny true cysts or ductal structures can also be identified. T h e stroma surrounding the tumor islands varies from loose areolar with focal mucoid changes to densely hyaline.I2 Mitoses are infrequent, cellular pleomorphism is absent, and necrosis is rare.2*5*12 Perineural invasion was found neither in the seven cases previously reported from Barnes Hospital' nor in the 21 cases frotn the A.F.I.P.5; how- ever, three of five cases reported by Friedman and Oberman from the University of Michigan did have perineural involvement.'2
Microscopically, our case differed from those previously reported in breast in several
ways. In the area of the areola, the tumor cell nests were continguous with the overlying epidermis from which they appeared to have arisen, and often contained central ductal spaces showing a striking resemblance to the tubular apocrine adenoma first described by Landry and Winkelmann in 1 972.23934 Central cuticular differentiation with focal necrosis was common, but cellular pleomorphism was absent. Except for occasional squamoid dif- ferentiation, the deeper areas of tumor con- formed to the generally described histologic picture of adenoid cystic carcinoma with a prominent cribriform pattern.
By electron microscopy, the common larger pseudoglandular structure or pseudocyst as well as the infrequent smaller true gland can be more clearly defined. T h e pseudocyst, from which the tumor actually derives its name, is in fact an extracellular structure lined by a basement membrane composed of a lamina densa and lamina lucida. These base-
N o . 5 MAMMARY ADENOID CYSTIC CA . Priole(m el (11. 1757
Fir;. 5. Deeper poi-tion of breast tumor showing an unusually small pseudoglandular structure lined by basement membrane (Elcctron photomicrograph, x3900). Inset of basement membrane illustrates that it is composed of a lamina densa and a lainina lucida ( Electron photomicrograph, X 8 100) (Formalin fixation).
ment membrane lined spaces, which are usually large, contain an amorphous occasion- ally fibrillar material thought to be derived from the lamina d e n s a . * l ~ ~ ~ T h e true cystic or duct-like spaces, which are found in the more cellular areas, are lined by only a few cells which have numerous microvilli projecting into their lumina. In ou r patient, the deep areas of the tumor showed these ultrastructural features. However, near the nipple, only true ductal lumina were present, and no basement membrane lined pseudocystic spaces could be identified. These ductal lumina differed from those previously described in adenoid cystic carcinoma in that they were substantially larger and were more typical of those seen in normal sweat gland ducts.22
Mammary adenoid cystic carcinoma is thought to originate in the major lactiferous ducts.*' However, in our case, it appeared to arise from the overlying epidermis. With its
superficial nesting pattern and its epidermal contiguity, it would seem reasonable to postu- late that its origin might have been in a small gland of the areola rather than in a major duct. Bearing in mind that, phylogenetically, the breast is an apocrine gland closely related to a sweat gland, the similar histologic picture of breast and sweat gland tumors and the dif- ficulty in determining the precise site of origin are not surprising. T h e unusual differentia- tion of the superficial portion of our tumor can be explained by the theory of pleuri- potentiality of the matrix cells of the epidermis and its appendages. According to this hypo- thesis, any of the matrix cells can form any other type of skin appendage and presumably any tumor deriving from the appendage.15*30
In many respects, our tumor resembled adenoid cystic carcinoma of skin which is even less common, with only six well documented cases having been reported if those arising

1758 CANCER May 1979 VOl. 43
FIG. 6. Deeper area of breasl tumor showing irue glandular or cystic structure. T h e lumen is never surrounded by more than a few cells (Electron photomicrograph, ~ 4 5 5 0 ) (Formalin fixation).
in the external auditory canal a re ex- ~ l ~ d e d . ~ . ~ ~ * ~ ~ * ~ ~ * ~ ~ Like their counterpart in the breast, these tumors have often followed a protracted, indolent course over many years prior to the patients’ seeking medical atten- tion. As adenoid cystic carcinoma has oc- curred in the external auditory canal possibly arising from modified apocrine (ceruminous) glands, Headington et a l . have suggested that by implication apocrine glands in other cutaneous areas may be the site of origin, although they do not preclude the possibility of an eccrine ductal contribution.”
Bernacki et al. have stated that the basal cell adenoina of salivary gland is the benign homologue of adenoid cystic ~ a r c i n o m a , ~ and there have been t w o case reports in which a combination of these two tumors was pres- ent.3*8 In the superficial portion of our pa- tient’s tumor, there was an inner row of ductal cells with palisading peripheral cells
quite similar to salivary monomorphic ade- nomas,6*20 and the resemblance of these tumors to dermal cylindroma of the scalp has recently been described.I6 Crumpler et al. note that the presence of an inner row of ductal o r secretory cells with peripheral cel- lular palisading can be a valuable indicator of a benign salivary gland tumor.6 With its biphasic histologic composition, our case is illustrative of the complex interrelationship of tumors derived from dermal appendages and the possible difficulty in determining their biologic behavior.
Unlike their salivary gland counterpart, adenoid cystic carcinoma of breast or skin is neither aggressive nor highly malignant. None from the skin has been reported to have metastasized, and in the breast only two cases of regional metastases have been reported: one occurred in a man seven years following “extensive local excision,”38 and the other was

No. 5 MAMMARY ADENOID CYSTIC CA . Prioleau et uL. 1759
in a 63-year-old woman who underwent radical mastectomy and was found to have tumor in 11 of 22 axillary lymph nodes and yet was symptom-free for 14 years before metastatic tumor was found in her mediasti- num and right lung.36 Following mastectomy, only four patients reported have had local re- currence of their t u r n ~ ~ - ~ * ~ ~ , ~ ~ and six have had distant m e t a s t a s e ~ . ' * ~ ~ * ~ ~ * ~ ~ . ~ ~ T h e time for dis- tant metastatic disease to manifest itself ranged from 6 months to 15 years (mean 7.75 years). T h e case occurring at 6 months was not docu- mented h is to l~gica l ly~~ and if this case is omitted, the mean period for the appearance of metastatic disease is 9.2 years. Only four deaths in patients with mammary adenoid cystic carcinoma have ben and one of these was not proven his t~logical ly .~~ N o deaths have been noted when the tumor arose primarily in the skin.
Due to the rarity of axillary nodal metastasis associated with mammary adenoid cystic car- cinoma, it would seem reasonable to recom- mend that only a simple mastectomy be per- formed in the absence of clinically suspicious lymph nodes. One obvious problem which will be encountered is the occasional diffi- culty in distinguishing by frozen section ex- amination adenoid cystic carcinoma from an
invasive ductal carcinoma with a cribriform pattern. I4
The majority of cases of adenoid cystic car- cinoma of breast have been described since 1968. We know from experience with its counterpart in the salivary gland that this tumor frequently has a slow but relentless course, and that a 10-year survival does not adequately reflect its biologic behavior. Many of the case reports involving the breast con- tain little or no follow-up data, and those cases with documented recurrences manifested them on an average of 9.2 years later. It has been suggeted by Hoshino and Yamamoto that postirradiation recurrences of this type of cancer result from a proliferation of the relatively radiation resistant myoepithelial cell.'g Certainly adenoid cystic carcinoma is less malignant in breast than in salivary gland. Whether its prognosis is due to a dif- ference in biologic behavior or to the large margin of uninvolved tissue to which a total mastectomy lends itself can only be a subject of speculation. However, the biphasic pattern of our tumor and the close similarities to dermal tubular apocrine adenomas and sali- vary basal cell adenomas would suggest that at least in some cases a difference in biologic behavior may indeed be present.
ADDENDUM On examination of the patient 16 months postoperatively. there was no evidence of
tumor recurrence.
REFERENCES
1. Althaus, S. R., and Ross, J. A. T.: Cerumen gland neoplasia. At-rh. Ofolaryngol. 92:40-42, 1970.
2. Anthony. P. P., and James, P. D.: Adenoid cystic carcinoma of the breast; prevalence, diagnostic criteria. and histogenesis. J. Clin. Pnfhol. 28:647-655. 1975.
3. Bernacki, E. G., Batsakis, J. G., and Johns, M. E.: Basal cell adenoma. Arch. Ofolaryngol. 99:84-87, 1974.
4. Boggio. R.: Adenoid cystic carcinoma of scalp.
5. Cavanzo, F. J. . and Taylor. H. B.: Adenoid cystic carcinoma of the breast. Concrr 24:740-745, 1969.
6. Crumpler, C., Scharfenberg, J. C., and Reed, R. J.: Monoinorphic adenomas of salivaIy glands. Cutirvr 38:
7. Elsner. B.: Adenoid cystic carcinoma of the breast.
8. Evans, R. W.. and Cruickshank, A. H.: Epithelial Tumors of the Salivary Glands. Philadelphia, W. B. Saunders. 1970; pp. 58-76.
9. Ferlito. A,: Sul carcinoma adenoide-cistico della inammella maschile. Rwi.\fu Airut. Pnrhol. Oncol. 35:44 1 - 454, 1969.
10. Ferlito. A , , and Di Bonito, L.: Adenoid cystic car- cinoma of the male breast. Ani. Surg. 40:72-75, 1974.
Arch. D P T ~ I ~ ~ o ~ . 1 1 1 :793-794. 1975.
193-200, 1976.
P<iIhol. Eut-. 5:357-364. 1970.
1 1 . Frankel. K.. and Craig. J . R.: Adenoid cystic car- cinoma of the prostate. AIII. /. Clin. Pathol. 62539-645, 1974.
12. Friedinan. B. A,, and Oberman. H. A,: Adenoid cystic carcinoma of the bredsl. Am. , I . Chi. Pafhol. 54: 1-14. 1950.
13. Galloway, J. R., Woolner, L. B., and Clagett, 0. l'.: Adenoid cystic carcinoma of the breast. Surg. G ~ n r c o l . Obstef. 122: 1289- 1294, 1966.
14. Harris, M.: Pseudoadenoid cystic carcinoma of the breast. Arch. Pafhol. Lnb. Med. 101:307-309. 1977.
15. Hashimoto, K., and Lever, W. F.: Appendage Tumors 0 1 the Skin. Springfield, Charles C: l 'homas,
16. Headington, J. T., Batsakis, J. C . , Beak 'r. F.. Campbell, T. E.. Sinimons, J. L., and Stone, W. D.: Membranous basal cell adenoma of parotid gland, dermal cylindrornas. and trichoepitheliomas. Cunrrr 3932460- 2469, 1977.
17. Headington, J. T.. Teedrs, R.. Niederhuber, J. E.. and Slinger. R. P.: Primary adenoid cystic carcinoma of skin. Arch. L)rrnintol. 114:421-424, 1978.
18. Hjorth, S.. Magnusson, P. H.. and Blomquist. P.:
1968; pp. 3, 55.
1760 CANCER Map 1979 VOl. 43
Adenoid cystic carcinoma of the breast. Acta Chir. Sca7d.
19. Hoshino, M., and Yamamoto. I.: Ultrastructure of adenoid cystic carcinoma. Cancer 25: 186- 198, 1970.
20. Jao, W., Keh, P. C., and Swerdlow. M. A.: Ultrastructure of the basal cell adenoma of parotid gland. Cancer 37: 1322- 1333, 1976.
21. Koss, L. G., Brannan, C. D., and Ashikari. R.: Histologic and ultrastructural features of adenoid cystic carcinoma of the breast. Cancer 26: 127 1- 1279, 1970.
22. Kurosumi, K.: Fine structure of the human sweat ducts of eccrine and apocrine types. Arch. Histol. Jpn .
23. Landry. M., and Winkelmann, R. K.: An unusual tubular apocrine adenoma. Arch. Dertatol. 105:869-879, 1972.
24. Lennox, B., Pearse, A. G . E., and Richards, H. G . H.: Mucinsecreting turnours of the skin: With special reference to the so-called mixed-salivary tuinour of the skin and its relation to hidradenoma. J. Pathol. Bacterial. 64 : 865- 880, 1952.
25. Lusted, D.: Structural and growth patterns of adenoid cystic carcinoma of breast. Am. J . Clin . Pathol.
26. Miller, W. L.: Sweat-gland carcinoma. Am. J. C h .
27. Nayer, H. R.: Cylindroma of the breast with
28. Nelms, D. C., and Luna, M. A.: Primary adenocys-
143:155-158. 1977.
40:203-224, 1977.
54:4 19-425, 1970.
Pathol. 47:767-780, 1967.
pulmonary metastases, Di.s. Chest 3 1:324-327, 1957.
tic carcinoma (cylindromatous carcinoma) of the esophagus. CancPr 29:440-443, 1972.
29. O K e l l , R. T.: Adenoid cystic carcinoma of the breast. Mksouri Med. 61:855-858, 1964.
30. Pinkus. H., and Mehregan, A. H.: A guide to Dermatohistopathology, 2nd ed. New York, Appleton- Century-Crofts, 1976; pp. 560-561.
31. Quizilbash, A. H., Patterson, M. C.. and Oliveira, K. F.: Adenoid cystic carcinoma of the breast. Arch. Pathol. Lab. Med. 101:302-306, 1977.
32. Stout, A. P., and Cooley, S. G. E.: Carcinoma of sweat glands. Cancer 4:521-536, 1951.
33. Tandler, B.: Ultrastructure of adenoid cystic carcinoma of salivary gland origin. Lab. Itwest. 24:504- 512, 1971.
34. Umbert. P., and Winkelmann, R. K.: Tubular apocrine adenoma. J. Cutan. Pathol. 3:75-87, 1976.
35. Van Bogaert, L.-J.. Maldague, P., Pham-Maldague, H.. and Staquet, J.-P.: Le cylindrome mammaire. Virchouls Arch. Palhol. Anal 368: 157- 165, 1975.
36. Verani, R. R., and Van Der Bel-Kahn, J.: Mam- mary adenoid cystic carcinoma with unusual features. Am. J. Clin. Pathol. 593653-658, 1973.
37. Wilson, W. B.. and Spell, J. P.: Adenoid cystic carcinoma of breast: a case with recurrence and regional metastasis. Ann. Surg. 166:861-864, 1967.
38. Woyke, S., Damagala, W., and Olszewski. W.: Fine structure of mammary adenoid cystic carcinoma. Polich Med. J. 9: 1140- 1148, 1970.




















