
Dexamethasone-suppressible feminizing adrenal adenoma
6
rM 9 5 The Fellowship of Postgraduate Medicine, 1994 Dexamethasone-suppressible feminizing adrenal adenoma M. Paja, S. Diez, T. Lucas, A. Ojeda, L. Salto and J. Estrada Servicio de Endocrinologia, Clinica Puerta de Hierro, C/San Martin de Porres 4, 28035 Madrid, Spain Summary: A 39 year old man presented with gynaecomastia, loss of libido and high blood pressure. Hormone studies revealed elevated plasma levels of oestradiol and its precursors, which increased in response to adrenocorticotrophic hormone and were reduced to normal levels with dexamethasone. Computed tomography disclosed a left adrenal mass and surgery was performed. The removed tumour weighed 84 g and the histological diagnosis was of adenoma. Nine years after surgery, he is asymptomatic, without hypertension, and radiological and or hormonal evidence of recurrence. We discuss the hormone profile in this case and the dynamics of steroid production by the tumour which, in contrast to the classical concept of tumour autonomy, showed dependence of oestradiol secretion on endogenous adrenocortico- trophic hormone. Introduction Feminizing tumours of the adrenal cortex are rare and usually malignant neoplasms.' They are almost exclusively confined to middle-aged men and pro- duce symptoms that reflect the oestrogen excess and androgen deficiency-gynaecomastia, diminished libido and testicular atrophy.2 As in other adrenal tumours, there is no close relation- ship between the histopathology and the biological behaviour of the neoplasm.3 We present a patient with a feminizing adreno- cortical adenoma after a post-resection follow-up period of over 9 years. Hormone production by the tumour was unexpectedly suppressible with dexa- methasone. We present its hormone pattern and discuss the different parameters used to differentiate the biological behaviour of adrenocor- tical tumours. Case report A 39 year old man was evaluated for a 5 year history of progressive bilateral gynaecomastia and diminished libido without impotence. His right testicle was cryptorchid at birth and had never descended into the scrotum. Physical examination revealed no features of Cushing's syndrome. Blood pressure was 180/120 mmHg. Breasts were Tan- ner's stage IV, without tenderness or galactorrhea; no palpable abdominal masses were felt and sexual hair had a feminine distribution with absence of thoracic hair. The right testicle was not palpable and the left had a soft consistency and a volume of 20 cm.3 Correspondence: T. Lucas, M.D. Accepted: 13 December 1993 Blood count, urinalysis and blood biochemistry, as determined in the SMA-12 autoanalyser, and plain X-rays of the chest, abdomen and skull were normal. Serum levels of P-human chronic gonadot- rophin, a-fetoprotein and carcinoembryonic antigen were undetectable. Urinary vanillyl- mandelic acid and total metanephrine excretion were normal, as was urinary excretion of free cortisol. Other hormone studies are shown in Table I. Baseline serum levels of oestradiol (E2), pro- gesterone (P) and 17-hydroxyprogesterone (1 70H- P) were elevated but plasma testosterone levels were normal, as was urinary excretion of 17- ketosteroids (17KS). Intravenous infusion of P1-24 corticotrophin (ACTH; 0.25 mg) for 8 hours pro- duced substantial increases in the levels of E2, P, 1 70H-P and 17KS with no change in testosterone. Dexamethasone 0.5 mg/6 hours for 2 days decreased the levels of E2, P and 170H-P to normal values and suppressed the plasma cortisol value to below 140 nmol/l. Intramuscular injection of human chorionic gonadotrophin (hCG) (5,000 IU daily for 3 days), performed 2 weeks after dex- amethasone administration, did not change any hormonal values. Plasma luteinizing hormone (LH) and follicle stimulating hormone (FSH) levels were low to normal, with response to luteiniz- ing hormone releasing hormone (LHRH) (100 lag IV, bolus) (Table II). The plasma aldosterone level was 0.92 nmol/l (normal upright value: 0.1 1-0.84) and upright plasma renin activity while on a low sodium diet was 2.35 ng/l/second (normal value: 1.1-2.25), both slightly increased. Chromosomal karyotype was 46XY. Computed tomography (CT) of the abdomen revealed a homogeneous mass in the left adrenal gland measuring 5-6 cm in diameter (Figure 1). The right testicle was not Postgrad Med J (I 994) 70, 584 588 group.bmj.com on July 14, 2011 - Published by pmj.bmj.com Downloaded from
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Dexamethasone-suppressible feminizing adrenal adenoma

rM 9 5 The Fellowship of Postgraduate Medicine, 1994
Dexamethasone-suppressible feminizing adrenal adenoma
M. Paja, S. Diez, T. Lucas, A. Ojeda, L. Salto and J. Estrada
Servicio de Endocrinologia, Clinica Puerta de Hierro, C/San Martin de Porres 4, 28035 Madrid, Spain
Summary: A 39 year old man presented with gynaecomastia, loss of libido and high blood pressure.Hormone studies revealed elevated plasma levels of oestradiol and its precursors, which increased inresponse to adrenocorticotrophic hormone and were reduced to normal levels with dexamethasone.Computed tomography disclosed a left adrenal mass and surgery was performed. The removed tumourweighed 84 g and the histological diagnosis was ofadenoma. Nine years after surgery, he is asymptomatic,without hypertension, and radiological and or hormonal evidence of recurrence. We discuss the hormoneprofile in this case and the dynamics ofsteroid production by the tumour which, in contrast to the classicalconcept of tumour autonomy, showed dependence of oestradiol secretion on endogenous adrenocortico-trophic hormone.
Introduction
Feminizing tumours of the adrenal cortex are rareand usually malignant neoplasms.' They are almostexclusively confined to middle-aged men and pro-duce symptoms that reflect the oestrogen excessand androgen deficiency-gynaecomastia,diminished libido and testicular atrophy.2 As inother adrenal tumours, there is no close relation-ship between the histopathology and the biologicalbehaviour of the neoplasm.3We present a patient with a feminizing adreno-
cortical adenoma after a post-resection follow-upperiod of over 9 years. Hormone production by thetumour was unexpectedly suppressible with dexa-methasone. We present its hormone pattern anddiscuss the different parameters used todifferentiate the biological behaviour ofadrenocor-tical tumours.
Case report
A 39 year old man was evaluated for a 5 yearhistory of progressive bilateral gynaecomastia anddiminished libido without impotence. His righttesticle was cryptorchid at birth and had neverdescended into the scrotum. Physical examinationrevealed no features ofCushing's syndrome. Bloodpressure was 180/120 mmHg. Breasts were Tan-ner's stage IV, without tenderness or galactorrhea;no palpable abdominal masses were felt and sexualhair had a feminine distribution with absence ofthoracic hair. The right testicle was not palpableand the left had a soft consistency and a volume of20 cm.3
Correspondence: T. Lucas, M.D.Accepted: 13 December 1993
Blood count, urinalysis and blood biochemistry,as determined in the SMA-12 autoanalyser, andplain X-rays of the chest, abdomen and skull werenormal. Serum levels ofP-human chronic gonadot-rophin, a-fetoprotein and carcinoembryonicantigen were undetectable. Urinary vanillyl-mandelic acid and total metanephrine excretionwere normal, as was urinary excretion of freecortisol. Other hormone studies are shown in TableI. Baseline serum levels of oestradiol (E2), pro-gesterone (P) and 17-hydroxyprogesterone (1 70H-P) were elevated but plasma testosterone levelswere normal, as was urinary excretion of 17-ketosteroids (17KS). Intravenous infusion of P1-24corticotrophin (ACTH; 0.25 mg) for 8 hours pro-duced substantial increases in the levels of E2, P,1 70H-P and 17KS with no change in testosterone.Dexamethasone 0.5 mg/6 hours for 2 daysdecreased the levels ofE2, P and 170H-P to normalvalues and suppressed the plasma cortisol value tobelow 140 nmol/l. Intramuscular injection ofhuman chorionic gonadotrophin (hCG) (5,000 IUdaily for 3 days), performed 2 weeks after dex-amethasone administration, did not change anyhormonal values. Plasma luteinizing hormone(LH) and follicle stimulating hormone (FSH) levelswere low to normal, with response to luteiniz-ing hormone releasing hormone (LHRH) (100 lagIV, bolus) (Table II). The plasma aldosterone levelwas 0.92 nmol/l (normal upright value: 0.11-0.84)and upright plasma renin activity while on a lowsodium diet was 2.35 ng/l/second (normal value:1.1-2.25), both slightly increased. Chromosomalkaryotype was 46XY. Computed tomography(CT) of the abdomen revealed a homogeneousmass in the left adrenal gland measuring 5-6 cm indiameter (Figure 1). The right testicle was not
Postgrad Med J (I 994) 70, 584 588
group.bmj.com on July 14, 2011 - Published by pmj.bmj.comDownloaded from
CLINICAL REPORTS 585
Table I Hormone studies performed prior to surgery
Oestradiol Progesterone Testosterone Cortisol 170H-P 17-KSMedication Time (pmol/l) (nmol/l) (nmol/l) (nmol/l) (nmol/l) (pmol/day)
None 8 hours 1,193 5.5 26.0 356 34 40ACTH 8 hours 1,267 7.3 23.6 552 69 43
16 hours 2,037 >127 25.0 1,062 314 194Dexamethasone Day 2 371 1.0 21.5 - - -
Day 3 220 0.9 26.7 80 4 33HCG Post 496 3.5 33.6 232 34 43Normal basal values <220 <3.2 10-35 220-660 1.5-7.5 31.5-77
Table II Luteinizing hormone (LH) and folliclestimulating hormone (FSH) before and after surgery.
Values are expressed in IU/I
LH* LHi FSH* FSHt
Before surgery 5.5 29.3 3.9 7.7Immediate post- 13.9 - 13.6 -
operative periodThree months after 3.5 43.5 4.8 17.1surgery
*Basal value; tpeak value after LHRH (100 jig i.v.).
Figure 1 Abdominal CT scan showing the presence ofahomogeneous isointense mass in the external branch ofthe left adrenal gland, corresponding to the adenoma(indicated by a white square in its interior).
observed either in CT or abdominal ultrasonog-raphy. The 9Tc bone scan and hepatic scintigraphywere normal. In the ejaculate, 5.7 ml of seminalfluid were collected, with 8.4 million sperm/ml,20% of which had spontaneous motility.The patient underwent laparotomy, with
removal of an encapsulated left adrenal mass andthe surrounding left adrenal gland. No glucocor-ticoid replacement was required during or aftersurgery. The tumour, oval-shaped, was well encap-
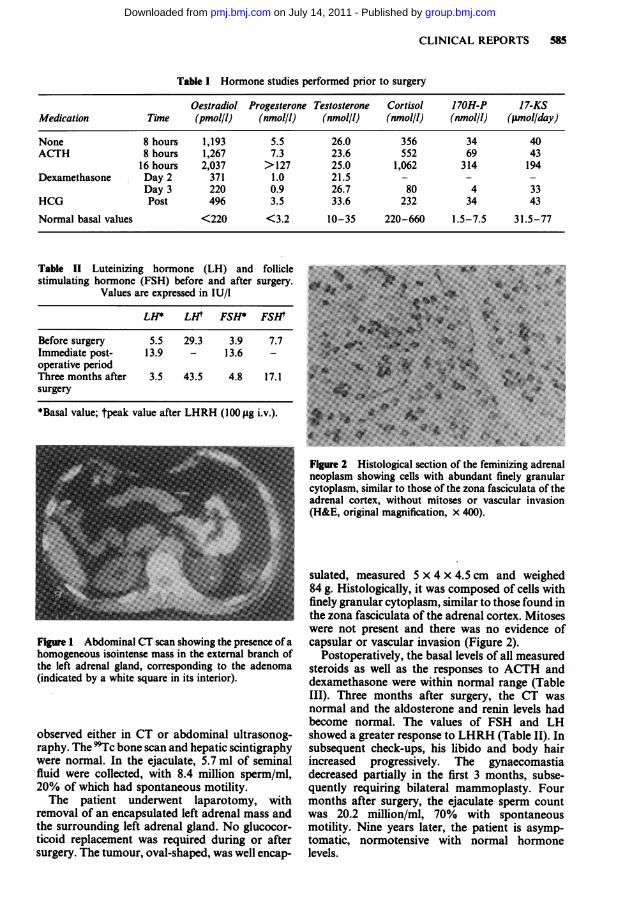
Figure 2 Histological section of the feminizing adrenalneoplasm showing cells with abundant finely granularcytoplasm, similar to those of the zona fasciculata of theadrenal cortex, without mitoses or vascular invasion(H&E, original magnification, x 400).
sulated, measured 5 x 4 x 4.5 cm and weighed84 g. Histologically, it was composed of cells withfinely granular cytoplasm, similar to those found inthe zona fasciculata of the adrenal cortex. Mitoseswere not present and there was no evidence ofcapsular or vascular invasion (Figure 2).
Postoperatively, the basal levels of all measuredsteroids as well as the responses to ACTH anddexamethasone were within normal range (TableIII). Three months after surgery, the CT wasnormal and the aldosterone and renin levels hadbecome normal. The values of FSH and LHshowed a greater response to LHRH (Table II). Insubsequent check-ups, his libido and body hairincreased progressively. The gynaecomastiadecreased partially in the first 3 months, subse-quently requiring bilateral mammoplasty. Fourmonths after surgery, the ejaculate sperm countwas 20.2 million/ml, 70% with spontaneousmotility. Nine years later, the patient is asymp-tomatic, normotensive with normal hormonelevels.
group.bmj.com on July 14, 2011 - Published by pmj.bmj.comDownloaded from

586 CLINICAL REPORTS
Table III Hormone studies performed 2 weeks and 3 months after surgery. For reference values see Table I
Oestradiol Progesterone Testosterone Cortisol 1 70H-P 17-KSMedication Time (pmol/l) (nmol/l) (nmol/l) (nmol/l) (nmol/l) (pmol/day)
None* 8 hours 37 1.1 30.2 356 7.8 -
Nonet 8 hours 95 1.1 29.4 353 3.9 51ACTHt 8 hours 169 0.8 21.2 229 3.9 -
16 hours 140 7.9 17.7 527 7.9 54Dexamethasone Day 2 121 1.1 14.6 <27 - -
Day 3 125 0.9 20.4 <27 1.2 50
a*Studies 2 weeks after surgery; btstudies 3 months after surgery.
Discussion
Most feminizing adrenal tumours occur in malesbetween 25 and 45 years of age, although somehave also been reported in females,4'5 and beforepuberty in both sexes.6'0 Since Gabrilove's reviewin 1965,' updated 5 years later by the same author,"only isolated cases have been reported. In thisreview, 61 cases were studied, six of which wereadenomas and the remainder carcinomas. As in ourpatient, the most common presenting complaintwas gynaecomastia accompanied by varyingdegrees ofhypogonadism. Testicular dysfunction isprobably due to the inhibitory effect of the oestro-gen excess on the secretion of gonadotrophins. Itappears that endogenous hyperoestrogenism supp-resses the secretion of biologically active LH ascompared with immunologically active LH.2 Thiswould explain a certain degree ofresponse ofLH toLHRH, as in the case presented, in which thisresponse increased after removal of the tumour.Moreover, the sustained oestrogen excess couldimpair testicular steroidogenesis by inhibiting theenzymes dependent on the cytochrome P450,172"2.This latter mechanism would explain the absence ofresponses of testosterone to hCG in our patient,despite it being testosterone of testicular origin; asshown by its lack of increase after the infusion ofACTH. At the same time, the increase in thehepatic synthesis of sex hormone-binding globulininduced by hyperoestrogenism would explain thetotal testosterone determinations being within thenormal range.
Hypertension is occasionally present in feminiz-ing adrenal tumours,' and is usually secondary tothe tumour secretion ofmineralocorticoids, mainlydesoxycorticosterone'3 and sometimes aldo-sterone.'4 In our case, the non-suppressed reninvalue excludes the possibility of an autonomousproduction of mineralocorticoids. We believe thatthe arterial hypertension, which disappeared fol-lowing excision of the tumour, could be a conse-quence of the oestrogen excess. These hormonesincrease the hepatic synthesis of renin substrate,
which leads to an increase in plasma angiotensin IIand aldosterone'5 levels.Some authors have suggested excessive extra-
glandular aromatization of precursors to explainthe increased oestrogen levels in thesetumours.8' 6 7 The return of oestradiol to normallevels and the disappearance of its increase inresponse to ACTH after surgery is in agreementwith tumour production in our case.
Adrenal tumours may be relatively or absolutelydeficient in one or more enzymes involved innormal steroidogenesis, such as 21 -hydroxylase,1 lp-hydroxylase or 3p-hydroxysteroid dehydro-genase.'8 The lack of cortisol hypersecretion or anautonomous production of mineralocorticoids, inspite of the increased availability of precursors inour patient, suggests a 21-hydroxylase deficit.The secretion of oestrogens and their precursors
in response to ACTH has been reported previouslyin feminizing adrenal tumours in vivo"9 and invitro.20 Similarly, about half of adrenal adenomasproducing Cushing's syndrome2' respond toexogenous ACTH with an increase in 17-hydroxy-corticosteroids. Saez et al.22 demonstrated theexistence of binding sites for the ACTH moleculeon adrenal tumour membranes.
In spite of their capacity to respond to exogenousACTH, most tumours derived from steroidogenictissue function independently of trophic hormonecontrol. The patient reported here is unusualbecause the administration of dexamethasonereduced oestradiol and its previously elevatedprecursors to normal levels. This suggests that thetumour hormone production was at least partiallydependent on pituitary ACTH.
In the literature reviewed, there is only onereport of an oestrogen-producing adrenal tumourwhose levels were partially reduced with dexa-methasone.5 These authors suggested that thearomatase activity of the tumour was either depen-dent on ACTH or directly inhibited by dexa-methasone, as in other tissues under experimentalconditions.23 This latter mechanism cannot beapplied in our case because dexamethasone
group.bmj.com on July 14, 2011 - Published by pmj.bmj.comDownloaded from

CLINICAL REPORTS 587
reduced not only oestradiol, but progesterone andhydroxy-progesterone as well, which is notexplained by changes in the aromatase activityalone. Perhaps some cases of adrenocorticalfeminizing syndrome, initially described as non-tumoural,24 were adenomas susceptible to suppres-sion by dexamethasone and invisible to theradiological techniques available at the time.
Differentiation between benign and malignanttumours of the adrenal glands still remains themain problem and only the existence of metastasesis a reliable indicator of malignancy. The regulardensity ofCT (with no necrosis or calcification),25 atumour weight of less than 30 g,26 the absence ofmitoses, cellular pleomorphism and vascular orcapsular invasion on microscopic examination,27 aswell as urinary 17 ketosteroid levels below 20 mg/day21'28 and, in some series, the response toACTH,2' are characteristic of benign tumours. Ourpatient demonstrated all these features with theexception of the tumour weight (84 g). However,
the long follow-up period without recurrence sup-ports the benign nature in this case. Finally, theapplication of modern chromatographic techni-ques in the analysis of the urinary steroidprofile,29'30 flow cytometry analysis of the tumourtissue'6 and the study of the steroid profile of thealdosterone synthesis pathway3' provide new app-roaches for the differential diagnosis.
In summary, we present a further case offeminiz-ing adrenal adenoma where hormone synthesisdepended, at least in part, on the endogenousACTH. This is exceptional and illustrates a failurein the dexamethasone suppression test to determinethe tumoural nature of an oestrogen excess ofadrenal origin.
Acknowledgement
The authors wish to thank Ms M. Messman for herexcellent editorial assistance.
References
1. Gabrilove, J.L., Sharma, D.C., Wotiz, H.H. & Dorfman, R.I.Feminizing adrenocortical tumors in the male. Medicine1965, 44: 37-79.
2. Veldhuis, J.D., Sowers, J.R., Rogol, A.D., Klein, F.A.,Miller, N. & Dufan, M.L. Pathophysiology of malehypogonadism associated with endogenous hyperestro-genism. N Engl J Med 1985, 312: 1371-1375.
3. Freeman, D.A. Steroid hormone-producing tumors in man.Endocrinol Rev 1986, 7: 204-220.
4. Barcel6, B., Abascal, J., Ardaiz, J. et al. Feminizingadrenocortical carcinoma in a postmenopausal woman.Postgrad Med J 1979, 55: 406-408.
5. McKenna, T.J., O'Connell, Y., Cunninghan, S., McCabe, M.& Culliton, M. Steroidogenesis in an estrogen-producingadrenal tumor in a young woman: comparison with steroidprofiles associated with cortisol- and androgen-producingtumors. J Clin Endocrinol Metab 1990, 70: 28-34.
6. Howard, C.P., Takahashi, H. & Hayles, A.B. Feminizingadrenocortical adenoma in a boy. Mayo Clin Proc 1977, 52:354-357.
7. Itami, R.M., Admundson, G.M., Kaplan, S.A. & Lipple,B.M. Prepubertal gynecomastia caused by an adrenal tumor.Am J Dis Child 1982, 136: 584-586.
8. Desai, M.B. & Kapadia, S.N. Feminizing adrenocorticaltumors in male patients: adenoma versus carcinoma. J Urol1988, 139: 101-103.
9. Bhettay, E. & Bonnici, F. Pure oestrogen-secreting feminizingadrenocortical adenoma. Arch Dis Child 1977, 52: 241-243.
10. Bacon, G.E. & Lowrey, G.H. Feminizing adrenal tumor in asix year old boy. J Clin Endocrinol 1965, 25: 1403-1406.
11. Gabrilove, J.L., Nicholis, G.L., Hausknecht, R.U. & Wotiz,H.H. Feminizing adrenocortical carcinoma in a man. Cancer1970, 25: 153-160.
12. Valensi, P., Coussieu, C., Kemeny, J.L., Attali, J.R.,Amouroux, J. & Sebaoun, J. Endocrine investigations in twocases of feminizing Leydig cell tumour. Acta Endocrinol(Copenh) 1987, 115: 365-372.
13. Solomon, S.S., Swersie, S.P., Paulsen, C.A. & Biglieri, E.G.Feminizing adrenocortical carcinoma with hypertension. J.Clin Endocrinol 1968, 28: 608-612.
14. Cathelineau, G. & Poizat, R. Feminizing adrenal tumor withprimary hyperaldosteronism. Report of a case. Ann Endoc-rinol (Paris) 1976, 37: 59-60.
15. McAreavey, D., Cumming, A.M.M., Boddy, K. et al. Therenin-angiotensin system and total body sodium and potas-sium in hypertensive women taking oestrogen-progestagencontraceptives. Clin Endocrinol 1983, 18: 111-118.
16. Klein, F.A., Miller, N.L. & Hackler, R.H. Flow cytometry infeminizing adrenocortical carcinoma. J Urol 1985, 134:933-935.
17. Comite, F., Schiebinger, R.J., Albertson, B.D. et al. Isosexualprecocious pseudopuberty secondary to a feminizing adrenaltumor. J. Clin Endocrinol Metab 1984, 58: 435-440.
18. Freeman, D.A. Steroid hormone-producing tumors of theadrenal, ovary and testes. Endrocinol Metab Clin North Am1991, 20: 751-766.
19. Mersey, J.H., Ceballos, L., Levin, P. & Busky, S. Estrogen-secreting adrenal tumor responsive to ACTH: localization byadrenal venous sampling. South Med J 1988, 81: 275-278.
20. Golder, M.P., Millington, D.S. & Cowley, T.H. Hormonalcontrol ofsteroid synthesis by a feminizing adrenal tumour. JEndocrinol 1975, 67: 17P.
21. Bertagna, C. & Orth, D.N. Clinical and laboratory findingsand results of therapy in 58 patients with adrenocorticaltumors admitted to a single medical center. Am J Med 1981,71, 855-875.
22. Saez, J.M., Dazord, A. & Gallet, D. ACTH and prostaglan-din receptors in human adrenocortical tumors. J Clin Invest1975, 56: 536-547.
23. Hsueh, J.W. & Erickson, G.F. Glucocorticoid inhibition ofFSH-induced estrogen production in cultured rat granulosacells. Steroids 1978, 32: 639-648.
24. Gabrilove, J.L., Nicolis, G.L. & Sohval, A.R. Non-tumorousfeminizing adrenogenital syndrome in the male subject. JUrol 1973, 110: 710-713.
25. Hussain, S., Belldegrun, A., Seltzer, S.E., Richie, J.P., Gittes,R.F. & Abrams, H.L. Differentiation of malignant frombenign adrenal masses: predictive indices on computedtomography. AJR 1985, 144: 61-65.
26. Schteingart, D.E., Obermen, H.A., Friedmen, B.D. & Conn,J.W. Adrenal cortical neoplasms producing Cushing's synd-rome. Cancer 1968, 22: 1005-1013.
27. King, D.R., & Lack, E.E. Adrenal cortical carcinoma. Aclinical and pathologic study of 49 cases. Cancer 1979, 44:239-244.
group.bmj.com on July 14, 2011 - Published by pmj.bmj.comDownloaded from

588 CLINICAL REPORTS
28. Lipsett, M.B., Hertz, R. & Ross, G.T. Clinical andpathophysiologic aspects of adrenocortical carcinoma. Am JMed 1965, 35: 374-382.
29. Minowada, S., Kinoshita, K., Hara, M., Isurugi, K.,Uchikawa, T. & Niiijima, T. Measurement of urinary steroidprofile in patients with adrenal tumor as a screening methodfor carcinoma. Endocrinol Jpn 1985, 32: 29-37.
30. Grondal, S., Eriksson, B., Hagenas, L., Werner, S. &Curstedt, T. Steroid profile in urine: a useful tool in thediagnosis and follow up of adrenocortical carcinoma. ActaEndocrinol (Copenh) 1990, 134: 653-663.
31. Aupetit-Faisant, B., Battaglia, C., Zenatti, M., Emeric-Blanchouin, N. & Legrand, J.C. Hypoaldosteronism accom-panied by normal or elevated mineralocorticosteroid path-way steroid: a marker of adrenal carcinoma. J Clin Endo-crinol Metab 1993, 76: 38-43.
group.bmj.com on July 14, 2011 - Published by pmj.bmj.comDownloaded from

doi: 10.1136/pgmj.70.826.584 1994 70: 584-588Postgrad Med J
M. Paja, S. Díez, T. Lucas, et al. adenoma.ble feminizing adrenalDexamethasone-suppressi
http://pmj.bmj.com/content/70/826/584found at: Updated information and services can be
These include:
References http://pmj.bmj.com/content/70/826/584#related-urls
Article cited in:
serviceEmail alerting
right corner of the online article.topcite this article. Sign up in the box at the
Receive free email alerts when new articles
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on July 14, 2011 - Published by pmj.bmj.comDownloaded from




















