
Specific Issues After Extracardiac Fontan Operation: Ventricular Function, Growth Potential,...
10
2005;80:665-672 Ann Thorac Surg Patel and Panangipalli Venugopal Saxena, Rajvir Singh, Ganapathy K. Subramaniam, Kizakke K. Pradeep, Chetan D. Ujjwal K. Chowdhury, Balram Airan, Shyam Sundar Kothari, Sachin Talwar, Anita Growth Potential, Arrhythmia, and Thromboembolism Specific Issues After Extracardiac Fontan Operation: Ventricular Function, http://ats.ctsnetjournals.org/cgi/content/full/80/2/665 located on the World Wide Web at: The online version of this article, along with updated information and services, is Print ISSN: 0003-4975; eISSN: 1552-6259. Southern Thoracic Surgical Association. Copyright © 2005 by The Society of Thoracic Surgeons. is the official journal of The Society of Thoracic Surgeons and the The Annals of Thoracic Surgery by on June 4, 2013 ats.ctsnetjournals.org Downloaded from
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Specific Issues After Extracardiac Fontan Operation: Ventricular Function, Growth Potential,...

2005;80:665-672 Ann Thorac SurgPatel and Panangipalli Venugopal
Saxena, Rajvir Singh, Ganapathy K. Subramaniam, Kizakke K. Pradeep, Chetan D. Ujjwal K. Chowdhury, Balram Airan, Shyam Sundar Kothari, Sachin Talwar, Anita
Growth Potential, Arrhythmia, and ThromboembolismSpecific Issues After Extracardiac Fontan Operation: Ventricular Function,
http://ats.ctsnetjournals.org/cgi/content/full/80/2/665located on the World Wide Web at:
The online version of this article, along with updated information and services, is
Print ISSN: 0003-4975; eISSN: 1552-6259. Southern Thoracic Surgical Association. Copyright © 2005 by The Society of Thoracic Surgeons.
is the official journal of The Society of Thoracic Surgeons and theThe Annals of Thoracic Surgery
by on June 4, 2013 ats.ctsnetjournals.orgDownloaded from

SOAUSRCDC
tF
eFtttc“us
ofiramt
Ltsrlctetfloma
A
ArN
©P
CA
RD
IOV
AS
CU
LA
R
pecific Issues After Extracardiac Fontanperation: Ventricular Function, Growth Potential,rrhythmia, and Thromboembolism
jjwal K. Chowdhury, MCh, Diplomate NB, Balram Airan, MCh,hyam Sundar Kothari, DM, FACC, Sachin Talwar, MCh, Anita Saxena, DM,ajvir Singh, PhD, Ganapathy K. Subramaniam, MCh, Kizakke K. Pradeep, MS,hetan D. Patel, MD, and Panangipalli Venugopal, MCh
epartments of Cardiothoracic and Vascular Surgery, Cardiology, Biostatistics, and Cardiac-Nuclear Medicine, Cardiothoracic
entre, All India Institute of Medical Sciences, New Delhi, Indiaihaa(acvp
ctvtapap
Background. The purpose of this study was to definehe prevalence of specific sequelae after extracardiacontan operation.Methods. Sixty-five consecutive patients undergoing
xtracardiac Fontan operation were studied for mortality,ontan failure, systemic ventricular function, supraven-ricular arrhythmias, thromboembolism, and growth po-ential. Age was 3 to 31 years (mean � standard devia-ion, 9.4 � 1.8; median, 7 years). The conduits wereonstructed of polytetrafluoroethylene (n � 50), andviable” in situ pericardium (n � 15). The patientsnderwent serial echocardiogram, dynamic radionuclidetudies, and cardiac catheterization.
Results. Operative mortality was 3%, and the incidencef conduit thrombosis was 4.6%. There was paradoxiclling of the right lung after femoral injection of theadiotracer in all cases of conduit obstruction. Perioper-tive and late postoperative supraventricular arrhyth-ias were observed in 9.2% and 4.7% of patients, respec-
ively. Risk factors for supraventricular arrhythmias
(med
P
S
Pso
t0Fwptp
acic and Vascular Surgery, All India Institute of Medical Sciences, Ansariagar, New Delhi-110029, India; e-mail: [email protected].
2005 by The Society of Thoracic Surgeonsublished by Elsevier Inc
ats.ctsnetjournDownloaded from
ncluded systemic ventricular dysfunction (p � 0.000),eterotaxy syndrome (p � 0.008), systemic venous anom-lies (p � 0.015), and previous bidirectional Glenn oper-tion (p � 0.017). At a mean follow-up of 77 � 2 monthsrange, 8 to 79 months), there were no late deaths (actu-rial survival at 79 months, 96.9% � 0.02%). Serial echo-ardiograms demonstrated evidence of growth of theiable tunnels. Postoperatively, there was transient de-ression of ejection fraction in all patients (p � 0.000).Conclusions. Supraventricular arrhythmias after extra-
ardiac Fontan are more common in patients with hetero-axy syndrome, bilateral superior venae cavae, systemicentricular dysfunction, and those undergoing comple-ion Fontan operation. The viable tunnel may emerge asn optimal alternative by virtue of reduction of su-raventricular arrhythmias, elimination of the need fornticoagulation, and addressing the issue of growthotential in selected patients.
(Ann Thorac Surg 2005;80:665–72)
© 2005 by The Society of Thoracic Surgeonsate morbidity and mortality after the Fontan opera-tion are largely caused by systemic venous hyper-
ension, systemic and pulmonary venous obstruction,ystemic ventricular dysfunction, supraventricular ar-hythmias, and thrombus formation [1–3]. These prob-ems have been demonstrated for the atriopulmonaryonnections but remain to be defined for the lateralunnel and extracardiac Fontan operation [1–3]. The pres-nce of long intraatrial suture lines is thought to facilitatehe development of slow reentry circuits and hence atrialutter after the lateral tunnel Fontan operation [4]. Thebjectives of this retrospective study were (1) to deter-ine the frequency of early and late supraventricular
rrhythmias, (2) to identify the risk factors for the same,
ccepted for publication Feb 1, 2005.
ddress reprint requests to Dr Chowdhury, Department of Cardiotho-
3) to evaluate the effect on systemic ventricular perfor-ance, and (4) to determine the prevalence of thrombo-
mbolism and thrombotic obstruction after the extracar-iac Fontan operation.
atients and Methods
election Criteria for One-Stage Univentricular Repair
atients with a functionally univentricular heart andatisfying the standard prescribed criteria underwentne-stage univentricular repair [1, 3, 5].Preoperatively, these patients were grouped according
o Texas Heart Institute Fontan risk score [6]. Those withto 3 risk points were considered to be at low risk for
ontan operation (n � 56). Patients with 4 to 5 pointsere at moderate risk (n � 9). Patients with 6 or more riskoints, or 3 points in any single category, were subjected
o bidirectional Glenn operation (BDG) as an interim
alliation.0003-4975/05/$30.00doi:10.1016/j.athoracsur.2005.02.024
by on June 4, 2013 als.org

SOcwtvFm
PAocNcutaHcic
m3p4whnvaiFo(vgdmwrcar
ansHsH
STwcg“
onti2pasT2w12maispsa(
ottp
ssamtr
AC
wiwAO
uiwepentdE
plttcA
H
666 CHOWDHURY ET AL Ann Thorac SurgEXTRACARDIAC FONTAN 2005;80:665–72
CA
RD
IOV
AS
CU
LA
R
election Criteria for Extracardiac Fontann the basis of our early experience, extracardiac total
avopulmonary connection was performed in patientsith (1) age older than 3 years, (2) body weight greater
han 10 kg, (3) anomalies of systemic and pulmonaryenous return, (4) auricular juxtaposition, (5) completionontan circuit after a previous BDG, and (6) no require-ent of additional intracardiac procedures [3, 7].
atient Characteristicstotal of 215 patients underwent various modifications
f univentricular repair between January 1998 and De-ember 2003 at All India Institute of Medical Sciences,ew Delhi, India, and 65 patients met the selection
riteria for extracardiac Fontan. In addition, 182 childrennderwent BDG during this study period. The records of
hese patients were reviewed for demographic, operative,nd perioperative features, follow-up echocardiographic,olter electrocardiographic, radionuclide angiographic,
atheterization, and clinical data. Descriptive character-stics, underlying cardiac diagnoses, and the relevantardiac catheterization data are summarized in Table 1.
Age ranged from 3 to 31 years (mean, 9.4 � 1.8 years;edian, 7 years). Body weight ranged between 10.5 and
4 kg (mean, 20.5 � 6.5 kg; median, 19 kg). Eighteenatients (27.7%) had tricuspid atresia, and the remaining7 patients (72.3%) had complex cyanotic heart diseasesith a functionally univentricular heart. Five patientsad associated total anomalous pulmonary venous con-ection, and 3 patients had partial anomalous pulmonaryenous connection. Forty-one patients (63%) had righttrial isomerism, and 6 patients (9.2%) had left atrialsomerism. Ten patients (15.3%) underwent completionontan operation after a BDG. Thirty patients had vari-us palliative procedures before univentricular repairTable 1). Twenty-eight patients had bilateral superiorenae cavae. Atrioventricular valve regurgitation wasraded as none, mild, moderate, or severe by echocar-iographic or cineangiographic evaluation. Patients withoderate or severe atrioventricular valve regurgitationere repaired surgically at the time of univentricular
epair, and these patients underwent lateral tunnel totalavopulmonary connection. Seven patients had only mildtrioventricular valve regurgitation, which was notepaired.
Hemoglobin ranged from 15 to 22 g/dL, and systemicrterial oxygen saturation was 65% to 88%. Mean pulmo-ary artery pressure or pulmonary capillary wedge pres-ure ranged between 9 and 20 mm Hg (median, 16 mmg), and mean systemic ventricular end-diastolic pres-
ure ranged between 8 and 16 mm Hg (median, 14 mmg).
urgical Techniquewo modifications of the extracardiac Fontan operationere used on surgeon preference: (1) extracardiac lateral
onduit (n � 50) made of polytetrafluoroethylene (PTFE)raft (W.L. Gore and Associates, Flagstaff, AZ), and (2)
viable” in situ pericardial lateral tunnel (n � 15). All uats.ctsnetjournDownloaded from
perations were performed without clamping the aorta atormothermia on a perfused beating heart. The ligamen-
um arteriosum or patent ductus arteriosus was dividedn all cases, the Blalock-Taussig’s shunt was ligated (n �0). A unilateral (n � 37) or bilateral (n � 28) BDG waserformed. Total extracardiac right heart bypass wasccomplished using either a PTFE conduit or a viable initu pedicled pericardium as described by us earlier [7].he conduit size ranged between 18 and 22 mm (mean,0.4 � 1.3 mm; median, 20 mm). Size of the conduit andeight distribution of the patients were as follows: (PTFE
8 mm: 7 patients, 10.5 to 14 kg; 20 mm: 27 patients, 12 to0 kg; 22 mm: 16 patients, 21 to 34 kg). Fenestration wasade using a 4-mm coronary punch in the PTFE conduit
nd on the thicker portion of the atrial wall close to thenteratrial groove. Fenestration was used only in theetting of suboptimal anatomy or hemodynamics. Specialrecaution was taken to avoid injury to the coronaryinus, sinus node, and sinoatrial nodal artery, and tovoid mechanical compression of nearby structuresright superior pulmonary vein and right atrium).
In situ pericardial lateral tunnel was the preferredption in patients with levocardia, l-malposition or l-ransposition of the aorta and dextrocardia, d-ransposition, d-malposition of the aorta, or posteriorlylaced main pulmonary artery.To retain the maximal amount of atriopulmonary tis-
ue as part of the viable tunnel and to avoid injury to theinoatrial nodal artery the technique of Gundry andssociates [8] was further modified by transecting theain pulmonary artery (MPA) at the sinotubular junc-
ion, and the posterior wall was sutured to the anterioright atrial wall as low as possible [7, 8].
ssessment of Operative OutcomeOHORT OF SURVIVORS. Of the 65 original patients, thereere 2 perioperative and no late deaths. Risk factors for
n-hospital deaths were analyzed. All survivors (n � 63)ere examined and studied between December 2003 andugust 2004, which was the closing interval for the study.UTCOME VARIABLES. Outcome variables were Fontan fail-re and postoperative pleural effusion. Fontan failure
ncluded all deaths within 30 days of operation and thoseho required Fontan takedown. Postoperative pleural
ffusion of more than 14 days duration or recurrentleural effusion after removal of chest tubes was consid-red significant. The patients’ clinical course (survival,eed for cardiac medications, New York Heart Associa-
ion class, occurrence of late complications) after hospitalischarge was monitored.CHOCARDIOGRAMS. Echocardiographic variables com-ared before and after the operation were atrioventricu-
ar valve regurgitation, presence or absence of flowhrough the fenestration, and systemic ventricular func-ion. Transesophageal echocardiogram was performed toonfirm a thrombus in case of doubt.NALYSIS OF RHYTHM CHANGES. All 63 survivors underwentolter monitoring in the closing interval of the study
sing a Mortara H-12 Holter unit (Mortara Instrumentsby on June 4, 2013 als.org
T
V
A
M
D
H
T
A
F
P
P
P
M
P
A
S
667Ann Thorac Surg CHOWDHURY ET AL2005;80:665–72 EXTRACARDIAC FONTAN
CA
RD
IOV
AS
CU
LA
R
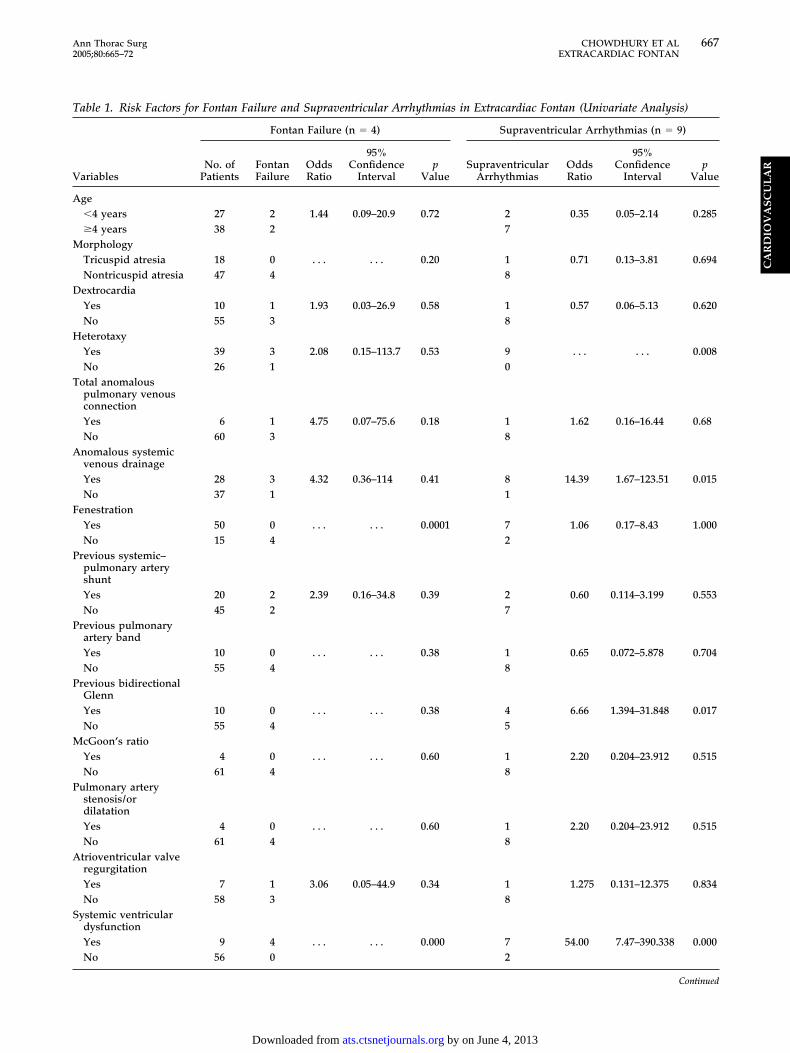
able 1. Risk Factors for Fontan Failure and Supraventricular Arrhythmias in Extracardiac Fontan (Univariate Analysis)
ariables
Fontan Failure (n � 4) Supraventricular Arrhythmias (n � 9)
No. ofPatients
FontanFailure
OddsRatio
95%Confidence
Intervalp
ValueSupraventricular
ArrhythmiasOddsRatio
95%Confidence
Intervalp
Value
ge�4 years 27 2 1.44 0.09–20.9 0.72 2 0.35 0.05–2.14 0.285�4 years 38 2 7orphologyTricuspid atresia 18 0 . . . . . . 0.20 1 0.71 0.13–3.81 0.694Nontricuspid atresia 47 4 8extrocardiaYes 10 1 1.93 0.03–26.9 0.58 1 0.57 0.06–5.13 0.620No 55 3 8eterotaxyYes 39 3 2.08 0.15–113.7 0.53 9 . . . . . . 0.008No 26 1 0
otal anomalouspulmonary venousconnectionYes 6 1 4.75 0.07–75.6 0.18 1 1.62 0.16–16.44 0.68No 60 3 8nomalous systemicvenous drainageYes 28 3 4.32 0.36–114 0.41 8 14.39 1.67–123.51 0.015No 37 1 1
enestrationYes 50 0 . . . . . . 0.0001 7 1.06 0.17–8.43 1.000No 15 4 2
revious systemic–pulmonary arteryshuntYes 20 2 2.39 0.16–34.8 0.39 2 0.60 0.114–3.199 0.553No 45 2 7
revious pulmonaryartery bandYes 10 0 . . . . . . 0.38 1 0.65 0.072–5.878 0.704No 55 4 8
revious bidirectionalGlennYes 10 0 . . . . . . 0.38 4 6.66 1.394–31.848 0.017No 55 4 5cGoon’s ratioYes 4 0 . . . . . . 0.60 1 2.20 0.204–23.912 0.515No 61 4 8
ulmonary arterystenosis/ordilatationYes 4 0 . . . . . . 0.60 1 2.20 0.204–23.912 0.515No 61 4 8trioventricular valveregurgitationYes 7 1 3.06 0.05–44.9 0.34 1 1.275 0.131–12.375 0.834No 58 3 8
ystemic ventriculardysfunctionYes 9 4 . . . . . . 0.000 7 54.00 7.47–390.338 0.000No 56 0 2
Continued
by on June 4, 2013 ats.ctsnetjournals.orgDownloaded from
Ifdsi[R
dbamf�fiP
t4ptodu
SDSBCmaftaus
uFt
fycatw
R
SOwsmaF
raealt
urvadopflrOBtkt
T
V
S
M
C
668 CHOWDHURY ET AL Ann Thorac SurgEXTRACARDIAC FONTAN 2005;80:665–72
CA
RD
IOV
AS
CU
LA
R
nc, Milwaukee, WI). However, Holter studies were per-ormed earlier if patients had symptoms with electrocar-iographic evidence of dysrhythmias. The diagnosis ofinus nodal dysfunction and arrhythmias was made us-ng the electrocardiographic criteria as defined by Kugler9] and Balaji and colleagues [10].ADIONUCLIDE STUDIES. In a prior publication, we haveetailed the standard protocol for this study [5]. A com-ination of both first-pass and equilibrium radionuclidengiocardiography were used to assess systemic or pul-onary venous pathway obstruction and ventricular
unction. Patients with supraventricular arrhythmias (n9) were digitalized, and the method of online postbeat
ltration was used.OSTOPERATIVE CARDIAC CATHETERIZATION. Only 19 of 65 pa-ients consented for cardiac catheterization. This includespatients with Fontan failure and 15 patients with in situericardial lateral tunnel. Correlation between the sys-
emic venous pressures and arrhythmias was possiblenly in the early postoperative phase when the pressureata were available by invasive catheters and in patientsndergoing cardiac catheterization.
tatistical Analysisata were analyzed with Biomedical Data Processingtatistical Software (University of California Press,erkeley, CA) and SPSS 7.5 statistical package (SPSS Inc,hicago, IL). Interval-related data were expressed asean � standard deviation. Categorical variables were
ssessed individually for their relationship to Fontanailure and supraventricular arrhythmias by determininghe odds ratio, and �2 analysis was attained to assess theirssociation to each other. Interval data were analyzedsing unpaired Student’s t test. Analysis of time-relatedurvival was performed using the Kaplan-Meier method.
Logistic regression was used to represent Fontan fail-re and supraventricular arrhythmias in extracardiacontan operation using 17 risk factors through the “En-
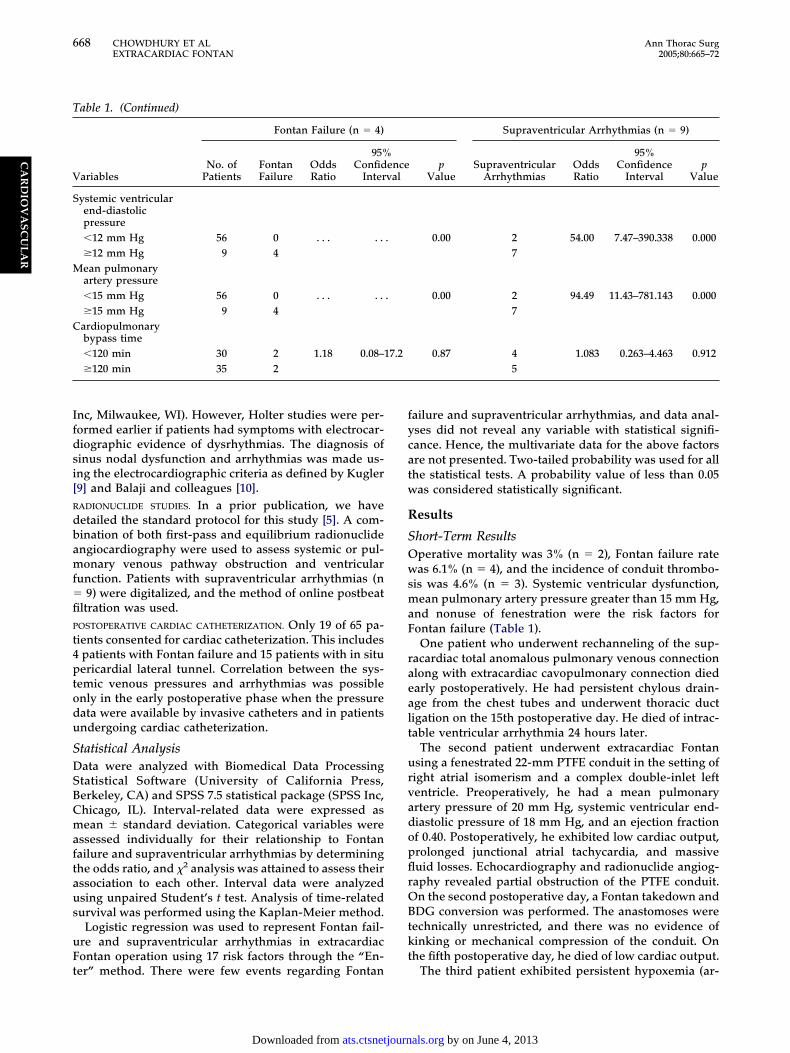
able 1. (Continued)
ariables
Fontan Failure (n � 4)
No. ofPatients
FontanFailure
OddsRatio
95%Confid
Inter
ystemic ventricularend-diastolicpressure�12 mm Hg 56 0 . . . . .�12 mm Hg 9 4ean pulmonaryartery pressure�15 mm Hg 56 0 . . . . .�15 mm Hg 9 4
ardiopulmonarybypass time�120 min 30 2 1.18 0.08–1�120 min 35 2
er” method. There were few events regarding Fontan
ats.ctsnetjournDownloaded from
ailure and supraventricular arrhythmias, and data anal-ses did not reveal any variable with statistical signifi-ance. Hence, the multivariate data for the above factorsre not presented. Two-tailed probability was used for allhe statistical tests. A probability value of less than 0.05as considered statistically significant.
esults
hort-Term Resultsperative mortality was 3% (n � 2), Fontan failure rateas 6.1% (n � 4), and the incidence of conduit thrombo-
is was 4.6% (n � 3). Systemic ventricular dysfunction,ean pulmonary artery pressure greater than 15 mm Hg,
nd nonuse of fenestration were the risk factors forontan failure (Table 1).One patient who underwent rechanneling of the sup-
acardiac total anomalous pulmonary venous connectionlong with extracardiac cavopulmonary connection diedarly postoperatively. He had persistent chylous drain-ge from the chest tubes and underwent thoracic ductigation on the 15th postoperative day. He died of intrac-able ventricular arrhythmia 24 hours later.
The second patient underwent extracardiac Fontansing a fenestrated 22-mm PTFE conduit in the setting ofight atrial isomerism and a complex double-inlet leftentricle. Preoperatively, he had a mean pulmonaryrtery pressure of 20 mm Hg, systemic ventricular end-iastolic pressure of 18 mm Hg, and an ejection fractionf 0.40. Postoperatively, he exhibited low cardiac output,rolonged junctional atrial tachycardia, and massiveuid losses. Echocardiography and radionuclide angiog-aphy revealed partial obstruction of the PTFE conduit.n the second postoperative day, a Fontan takedown andDG conversion was performed. The anastomoses were
echnically unrestricted, and there was no evidence ofinking or mechanical compression of the conduit. Onhe fifth postoperative day, he died of low cardiac output.
Supraventricular Arrhythmias (n � 9)
pValue
SupraventricularArrhythmias
OddsRatio
95%Confidence
Intervalp
Value
0.00 2 54.00 7.47–390.338 0.0007
0.00 2 94.49 11.43–781.143 0.0007
0.87 4 1.083 0.263–4.463 0.9125
enceval
.
.
7.2
The third patient exhibited persistent hypoxemia (ar-
by on June 4, 2013 als.org
tmopcbpctTUepApf
tdwoff
pwo
obdiwfttw
LM
d0(Ye(cA
rdp6rtatBbrs
vtE
S
Tnt0sS
avvpaw
wpetpnHrth1ali
r(AFhi�d
F
669Ann Thorac Surg CHOWDHURY ET AL2005;80:665–72 EXTRACARDIAC FONTAN
CA
RD
IOV
AS
CU
LA
R
erial oxygen saturation � 60%) and progressive hepato-egaly on the fourth postoperative day without evidence
f low cardiac output. The lungs were adequately ex-anded, and there was no evidence of superior venaaval obstruction. Echocardiography revealed sluggishlood flow through the conduit. Reoperation on the fifthostoperative day revealed graft thrombosis with techni-ally unrestricted anastomoses. There was extensivehrombosis of the inferior vena cava and hepatic veins.he pulmonary arteries were free from any blood clots.nder cardiopulmonary bypass on a beating heart, the
ntire graft was removed with thrombectomy of theulmonary arteries, inferior vena cava, and hepatic veins.
20-mm aortic homograft was interposed between theulmonary artery and the inferior vena cava without
enestration. He made an uneventful recovery.The fourth patient exhibited thrombosis of the PTFE
ube on the fourth postoperative day diagnosed echocar-iographically and by radionuclide angiography. Thereas no technical error and no evidence of low cardiacutput early postoperatively. Fontan revision was per-ormed using viable in situ pericardium with a 5-mmenestration. Subsequent recovery was uneventful.
The remaining patients were extubated on the firstostoperative day. Mean duration of chest tube drainageas 7 days. Prolonged chest tube drainage (�14 days)ccurred in 2 patients with pericardial lateral tunnel.All patients were administered oral captopril on day
ne postoperatively (0.5 to 1.0 mg/kg, every 8 hours)efore discontinuing inotropic support. Postoperatively,igoxin, diuretics, and angiotensin-converting enzyme
nhibitors were discontinued from the third month on-ard. All patients with a PTFE conduit received warfarin
or 6 months for anticoagulation to maintain an interna-ional normalized ratio between 2.5 and 3.0. In addition,hey were administered aspirin (5 mg/kg per day), whichas continued indefinitely.
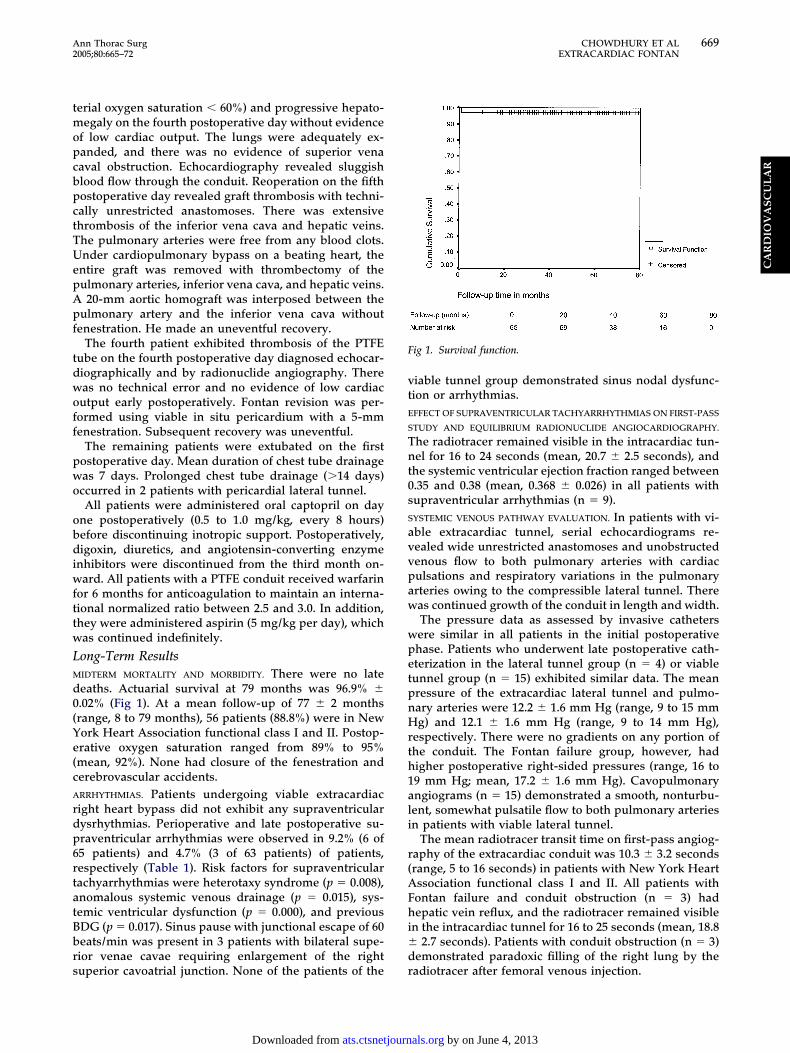
ong-Term ResultsIDTERM MORTALITY AND MORBIDITY. There were no lateeaths. Actuarial survival at 79 months was 96.9% �.02% (Fig 1). At a mean follow-up of 77 � 2 monthsrange, 8 to 79 months), 56 patients (88.8%) were in Nework Heart Association functional class I and II. Postop-rative oxygen saturation ranged from 89% to 95%mean, 92%). None had closure of the fenestration anderebrovascular accidents.RRHYTHMIAS. Patients undergoing viable extracardiacight heart bypass did not exhibit any supraventricularysrhythmias. Perioperative and late postoperative su-raventricular arrhythmias were observed in 9.2% (6 of5 patients) and 4.7% (3 of 63 patients) of patients,espectively (Table 1). Risk factors for supraventricularachyarrhythmias were heterotaxy syndrome (p � 0.008),nomalous systemic venous drainage (p � 0.015), sys-emic ventricular dysfunction (p � 0.000), and previousDG (p � 0.017). Sinus pause with junctional escape of 60eats/min was present in 3 patients with bilateral supe-ior venae cavae requiring enlargement of the right
uperior cavoatrial junction. None of the patients of the rats.ctsnetjournDownloaded from
iable tunnel group demonstrated sinus nodal dysfunc-ion or arrhythmias.FFECT OF SUPRAVENTRICULAR TACHYARRHYTHMIAS ON FIRST-PASS
TUDY AND EQUILIBRIUM RADIONUCLIDE ANGIOCARDIOGRAPHY.
he radiotracer remained visible in the intracardiac tun-el for 16 to 24 seconds (mean, 20.7 � 2.5 seconds), and
he systemic ventricular ejection fraction ranged between.35 and 0.38 (mean, 0.368 � 0.026) in all patients withupraventricular arrhythmias (n � 9).YSTEMIC VENOUS PATHWAY EVALUATION. In patients with vi-ble extracardiac tunnel, serial echocardiograms re-ealed wide unrestricted anastomoses and unobstructedenous flow to both pulmonary arteries with cardiaculsations and respiratory variations in the pulmonaryrteries owing to the compressible lateral tunnel. Thereas continued growth of the conduit in length and width.The pressure data as assessed by invasive cathetersere similar in all patients in the initial postoperativehase. Patients who underwent late postoperative cath-terization in the lateral tunnel group (n � 4) or viableunnel group (n � 15) exhibited similar data. The meanressure of the extracardiac lateral tunnel and pulmo-ary arteries were 12.2 � 1.6 mm Hg (range, 9 to 15 mmg) and 12.1 � 1.6 mm Hg (range, 9 to 14 mm Hg),
espectively. There were no gradients on any portion ofhe conduit. The Fontan failure group, however, hadigher postoperative right-sided pressures (range, 16 to9 mm Hg; mean, 17.2 � 1.6 mm Hg). Cavopulmonaryngiograms (n � 15) demonstrated a smooth, nonturbu-ent, somewhat pulsatile flow to both pulmonary arteriesn patients with viable lateral tunnel.
The mean radiotracer transit time on first-pass angiog-aphy of the extracardiac conduit was 10.3 � 3.2 secondsrange, 5 to 16 seconds) in patients with New York Heartssociation functional class I and II. All patients withontan failure and conduit obstruction (n � 3) hadepatic vein reflux, and the radiotracer remained visible
n the intracardiac tunnel for 16 to 25 seconds (mean, 18.82.7 seconds). Patients with conduit obstruction (n � 3)
emonstrated paradoxic filling of the right lung by the
ig 1. Survival function.
adiotracer after femoral venous injection.
by on June 4, 2013 als.org

E
C
uA(pepf0r(st
C
TttsaptpcCtdp
GDwesti
smlwotps2a
ipdn[limdbp
pwSsaofloafwamiu
TT2cct
vawtnciascci
tvoucaierlpia
Fifirvnsua
670 CHOWDHURY ET AL Ann Thorac SurgEXTRACARDIAC FONTAN 2005;80:665–72
CA
RD
IOV
AS
CU
LA
R
VALUATION OF SYSTEMIC VENTRICULAR FUNCTION BY RADIONU-
LIDE ANGIOCARDIOGRAPHY. Postoperative systemic ventric-lar ejection fraction of patients with New York Heartssociation class I and II (n � 56) ranged from 0.45 to 0.60
mean, 0.517 � 0.048). Preoperatively, this subset ofatients had ejection fraction between 0.45 and 0.60 onchocardiography (mean, 0.547 � 0.048; p � 0.000). Allatients with Fontan failure (n � 2) had low ejection
raction ranging between 0.35 and 0.38 (mean, 0.368 �.026). Preoperatively, this subgroup was at moderateisk, and their ejection fraction ranged from 0.40 to 0.45mean, 0.411 � 0.049; p � 0.000). Serial evaluation ofurvivors did not demonstrate any deterioration of sys-emic ventricular ejection fraction.
omment
wo currently favored approaches to the modified Fon-an circuit include the extracardiac or lateral tunnelechniques [1–3, 6–8, 11]. The extracardiac techniqueeparates the high-pressure conduit from the atrial wallnd systemic venous atrial cavity, avoids intraatriallacement of prosthetic material, theoretically minimizes
he risk of supraventricular arrhythmias, and possiblyreserves ventricular and pulmonary function because itan be performed without aortic cross-clamp [1–4, 6–8].oncerns include lack of growth potential of the syn-
hetic conduit, late supraventricular dysrhythmias, con-uit narrowing or obstruction, and thromboembolic com-lications [1–12].
rowth Potentialirect connection of both cavae to the pulmonary arteryould be the ideal right heart bypass by virtue of
limination of prosthetic material and extensive atrialuture lines [13]. When direct connection is impossible,his may be accomplished by a prosthetic graft or a viablen situ pedicled pericardium [2, 7, 8, 13].
The prosthetic tube lacks growth potential. An adult-ized conduit (20 to 22 mm) may avoid reoperations, anday accommodate flow rates necessary for exercise. This
imits the operation to patients of a minimum age,eight, and size. We selected patients older than 3 yearsf age and weighing more than 10 kg to avoid reopera-ions and achieve adequate exercise tolerance. Minimumatient weight for an extracardiac Fontan candidatehould be approximately 10 to 15 kg because a 20- to2-mm conduit in a smaller child is relatively oversizednd risks the formation of thromboses [2].To address the problem of growth potential, some
ncluding us have used viable in situ pericardial tunnel,edicled on its lateral blood supply [7, 8]. The technicaletails, postoperative clinical course, and the hemody-amics have been addressed in our earlier publication
7]. It appears that patients with situs solitus, levocardia,-malposition or l-transposition of the aorta or situsnversus, dextrocardia, and d-transposition or d-
alposition of the aorta or those with anteroposteriorisposition of the aorta and main pulmonary artery maye the ideal candidates for this operation. Because the
ericardial tube is vascularized, it is viable and also wats.ctsnetjournDownloaded from
liable, thus capable of absorbing cardiac pulsations asell as being affected by respiratory bellow mechanisms.erial echocardiograms postoperatively have demon-trated continued growth of the tube. Cavopulmonaryngiograms in the late postoperative period have dem-nstrated smooth, nonturbulent, and somewhat pulsatileow without gradients. Because of nonthrombogenicityf the native pericardium, anticoagulation could bevoided in all patients and there was no peel or thrombusormation. Owing to reduction in right atrial distension,all stress, absence of extensive suture lines, and avoid-
nce of damage to the sinoatrial node, atrial dysrhyth-ias could be eliminated in all patients. The pericardium
s known to follow Laplace’s law, and does not dilatenless there is distal obstruction.
hromboembolism and Thrombotic Obstructionhromboembolic complications have ranged from 3% to0% and are unrelated to the modifications of the Fontanirculation [1–3, 10, 12]. There is no consensus aboutandidate selection and type or duration of anticoagula-ion [1–3, 10].
Although used worldwide, prosthetic conduits in theenous circulation carry the inherent risks of thrombosisnd obstruction [2, 12]. Thrombosis of the Fontan path-ay is often silent and may remain undetected until
here is significant elevation of venous pressures. Radio-uclide studies may be useful for early detection of thisomplication [1–3, 5, 12]. In this study, we observed threenstances of conduit thrombosis despite adequate oralnticoagulation. The anastomoses were technically unre-trictive, and there was no evidence of kinking or me-hanical compression of the conduit in any patient. Lowardiac output was the possible cause of graft thrombosisn 1 patient.
Radionuclide angiography detected conduit obstruc-ion in all patients, in particular, by paradoxic intenseisualization of both lungs after femoral injection. Thesebstructions allowed inferior vena caval blood to flowpward into the superior vena cava–pulmonary arteryonnection through the paravertebral and epidural veinsnd azygos system. These may have reduced blood flown the conduit and favored its thrombosis. There was novidence of low cardiac output in 2 patients. Four similareports of paradoxic filling of the right lung after lowerimb injection of microspheres have been described inatients with conduit obstruction [14]. The above find-
ngs were confirmed by Doppler echocardiography andngiocardiography before revision surgery.Routine anticoagulation for all patients undergoing the
ontan operation has been recommended [1–3, 12]. Ournstitutional policy is to use warfarin and aspirin for therst 6 months and then switch to aspirin alone withegular echocardiographic or radionuclide follow-up. Aiable pericardial extracardiac tunnel may eliminate theeed for anticoagulation. Although the observed in-tances of PTFE conduit obstruction would make theirse questionable, we have continued to use them as theyre easily available in all sizes and their use has been
idespread [2, 3, 5, 12]. However, with our growingby on June 4, 2013 als.org

ebo
STpb4dfmsnsal
Hmpirsae
fHvpucai
eptagm
fdvd
teptdf
stPrj
rthc
SIstu
mspapcpo
tccedsip
STomtpflmcetlHcbc
wcmc
CSotdtmv
671Ann Thorac Surg CHOWDHURY ET AL2005;80:665–72 EXTRACARDIAC FONTAN
CA
RD
IOV
AS
CU
LA
R
xperience with the viable tunnel procedure, we woulde inclined to consider the viable tunnel as the firstption whenever possible.
upraventricular Arrhythmiaso date, the optimal surgical approach for avoidance ofostoperative arrhythmias after Fontan repair has noteen determined. Their incidence varies widely (12% to8%), reflecting difference in definitions, methods ofetection, changes in patients treated, and long-term
ollow-up [1–5, 10, 12]. Extracardiac Fontan may mini-ize the atrial arrhythmias by so-called atrial no-touch
urgery, avoiding manipulation or injury to the sinoatrialode, avoiding exposure of the right atrium to elevatedystemic venous pressure, and limiting the extensivetrial suture lines and scarring commonly seen with theateral tunnel Fontan operation [1–4, 7, 8].
Sinoatrial node function is best evaluated by 24-hourolter monitoring, which was done only once in the greatajority during the period of this study. Although this is a
otential source of error in this retrospective study, the biass more likely toward the underdetection of arrhythmiasather than an overestimation. In this series, patients withystemic ventricular dysfunction, heterotaxy syndrome,nomalous systemic venous drainage, and previous BDGxhibited a higher incidence of arrhythmia (Table 1).
Patients with preoperative systemic ventricular dys-unction (n � 9) were at moderate risk according to Texas
eart Institute Fontan risk score and had mean systemicenous pressure ranging between 16 and 19 mm Hgostoperatively. The increased incidence of supraventric-lar arrhythmias in this subset of patients was statisti-ally significant (Table 1). It manifested in the perioper-tive period and continued in the late follow-up,ndicating the effects of ongoing hemodynamic factors.
Abnormalities of the conduction system are known toxist in patients with heterotaxy syndrome, which mayrovoke tachyarrhythmia and bradyarrhythmia irrespec-
ive of the type of Fontan connection [1, 2, 10, 15]. Cohennd colleagues [16] demonstrated that avoidance of sur-ery near the sinus node had no effect on the develop-ent of sinus nodal dysfunction.Our study suggests that despite the best surgical ef-
orts, we must accept a certain incidence of sinus nodalysfunction in this patient population. Continued sur-eillance is necessary to determine which patients willevelop clinically significant arrhythmia.Staged surgical correction of the functionally univen-
ricular heart with the addition of an intermediate BDGxposes the sinoatrial nodal area to dissection twice, thusotentially risking dysfunction caused by direct injury to
he sinoatrial node or sinoatrial nodal artery [17]. Ourata suggest an additive risk of abnormal sinoatrial nodal
unction with a staged Fontan connection (Table 1).In patients with bilateral superior venae cavae, the
uperior vena cava–right atrial junction may be too smallo accommodate the entire inferior vena caval return.atients in this series with bilateral superior venae cavaeequiring enlargement of the right superior cavoatrial
unction exhibited sinus nodal dysfunction probably as a iats.ctsnetjournDownloaded from
esult of damage to the sinoatrial nodal artery. Theechnique of viable extracardiac lateral tunnel presentederein provides an alternative method of cavopulmonaryonnection that attempts to avoid this complication.
ystemic Ventricular Functionntact systolic and diastolic performance is critical for theuccessful establishment of an atrial-dependent circula-ion. The literature documents variable systemic ventric-lar performance after the Fontan operation [1–3, 10].In spite of performing the operation on a normother-ic, beating heart, there was transient significant depres-
ion of ejection fraction in all patients in the immediateostoperative period (p � 0.000). This could be related todecrease in left ventricular end-diastolic volume from
reoperative to postoperative measurements, mostly be-ause of elimination of systemic–pulmonary shunts orulmonary artery band and improvement in myocardialxygen supply.Varying ventricular morphologies (right, left, inde-
erminate, or biventricular) in the Fontan cohort makealculation of ejection fraction by conventional angio-ardiograms unreliable [18]. Radionuclide-derivedjection fraction is probably more accurate as it isevoid of geometric assumptions. The ability to obtainerial measurement of ejection fraction after a singlesotope injection makes this modality particularly ap-ealing [5, 18].
tudy Limitationshis study is retrospective and nonrandomized. Becausef the transient and intermittent nature of some arrhyth-ias, their incidence may be underestimated. Long su-
ure lines in the atrial wall of the viable tunnel mayredispose to late atrial arrhythmias [7, 8]. Second, theoor of the extracardiac lateral tunnel contains the pul-onary veins. There are isolated reports of anterior
ompression of the pulmonary veins by a markedlynlarged right atrium [8]. The issue of energy losses inhe extracardiac Fontan circuit as compared with theateral tunnel Fontan has been discussed recently [11].
owever, we did not measure this and are unable toomment on this aspect. Finally, the incidence of throm-oembolic complications is probably underestimated be-ause only clinically suspected cases were investigated.
Further investigations on a larger number of patientsith prospective longitudinal evaluation are needed to
onfirm the midterm results, especially atrial dysrhyth-ias, pulmonary venous obstruction, thromboembolic
omplications, and growth.
onclusionsupraventricular arrhythmias after extracardiac Fontanperation are probably multifactorial and mandate con-inuous surveillance. Patients with systemic ventricularysfunction, bilateral superior venae cavae, and hetero-
axy syndrome and those undergoing completion Fontanay exhibit a high incidence of these arrhythmias. The
iable extracardiac Fontan may be the operation of choice
n a selected subset of patients. Serial dynamic radionu-by on June 4, 2013 als.org

ca
Tr
R
1
1
1
1
1
1
1
1
1
I
Fubodntuatpcgpgc
Fhtcgmcd
672 CHOWDHURY ET AL Ann Thorac SurgEXTRACARDIAC FONTAN 2005;80:665–72
©P
CA
RD
IOV
AS
CU
LA
R
lide studies may be useful for evaluation of anatomicnd functional flaws of the Fontan circuit.
he authors are grateful to Mr Shankar Sharma for the prepa-ation of the manuscript.
eferences
1. Stamm C, Friehs I, Mayer JE, et al. Long-term results of thelateral tunnel Fontan operation. J Thorac Cardiovasc Surg2001;121:28–41.
2. Azakie A, McCrindle BW, Arsdell GV, et al. Extracardiacversus lateral tunnel cavopulmonary connections at a singleinstitution: impact on outcomes. J Thorac Cardiovasc Surg2001;122:1219–28.
3. Airan B, Sharma R, Chowdhury UK, et al. Univentricularrepair: is routine fenestration justified? Ann Thorac Surg2000;69:1900–6.
4. Fishberger SB,Wernovsky G, Gentles TL, et al. Factors thatinfluence the development of atrial flutter after the Fontanoperation. J Thorac Cardiovasc Surg 1997;113:80–6.
5. Chowdhury UK, Sharma PK, Sharma R, et al. Postoperativeassessment of the univentricular repair by dynamic radio-nuclide studies. Ann Thorac Surg 2004;77:658–65.
6. Fisher DJ, Geva T, Feltes TF, et al. Life-long management ofpatients with a single functional ventricle: a protocol. TexHeart Inst J 1995;22:284–95.
7. Chowdhury UK, Kothari SS, Saxena A, et al. Viable extra-cardiac total right heart bypass: technical considerations andmid-term results. Heart Lung Circ 2004;13:56–63.
8. Gundry SR, Razzouk AJ, delRio MJ, et al. The optimal Fontanconnection: a growing extracardiac lateral tunnel with pedi-
cled pericardium. J Thorac Cardiovasc Surg 1997;114:552–9.espite administration of warfarin, and the surgical find-
i2cse(Fcgaegecap
M
SSEPe
2005 by The Society of Thoracic Surgeonsublished by Elsevier Inc
ats.ctsnetjournDownloaded from
9. Kugler JD. Sinus node dysfunction. In: Gillette PC, GarsonA, eds. Pediatric arrhythmias: electrophysiology and pacing,1st ed. Philadelphia: WB Saunders, 1990:250–300.
0. Balaji S, GeWillig M, Bull C, deLeval M, Deanfield E.Arrhythmias after the Fontan procedure. Circulation 1991;84(Suppl 3):162–7.
1. Bove EL, deLeval MR, Migliavacca F, Guadagni G, Dubini G.Computational fluid dynamics in the evaluation of hemody-namic performance of cavopulmonary connections after theNorwood procedure for hypoplastic left heart syndrome.J Thorac Cardiovasc Surg 2003;126:1040–7.
2. Shirai LK, Rosenthal DN, Reitz BA, et al. Arrhythmias andthromboembolic complications after the extracardiac Fontanoperations. J Thorac Cardiovasc Surg 1998;115:499–505.
3. Van Son JAM, Reddy VM, Hanley FL. Extracardiac modifi-cation of the Fontan operation without the use of prostheticmaterial. J Thorac Cardiovasc Surg 1995;110:1766–8.
4. Covitz W, Moore HV, Gray B, et al. Assessment of Fontangraft patency by radionuclide perfusion pulmonary scan intricuspid atresia with previous Glenn shunt. Am Heart J1982;103:1072–3.
5. Michelion G, Gharagozllo F, Julsrud PR, Danielson GK, PugaFJ. Modified Fontan operation in the presence of anomaliesof systemic and pulmonary venous connection. Circulation1993;88(Suppl 2):141–8.
6. Cohen MI, Bridges ND, Gaynor JW, et al. Modification of thecavopulmonary anastomosis do not eliminate early sinus nodedysfunction. J Thorac Cardiovasc Surg 2000;120:891–900.
7. Laschinger JC, Ringel RE, Brenner JI, McLaughlin JS. Theextra-cardiac total cavopulmonary connection for definitiveconversion to the Fontan circulation: summary of earlyexperience and results. J Card Surg 1993;8:524–33.
8. Akagi T, Benson LN, Green M, et al. Ventricular perfor-mance before and after Fontan repair for univentricularatrioventricular connection: angiographic and radionuclide
assessment. J Am Coll Cardiol 1992;20:920–6.NVITED COMMENTARY
rom their experience with more than 200 patients whonderwent various modifications of univentricular repairetween 1998 and 2003, the authors have chosen to focusn the group of 65 patients who underwent an extracar-iac conduit-type of modified Fontan procedure. Forearly one-half of the patients, the Fontan procedure was
he first operative intervention, and only 10 patients hadndergone a previous superior vena cava to pulmonaryrtery anastomosis. No patients in the group had morehan mild atrioventricular valve regurgitation, as suchatients all underwent intracardiac lateral tunnel totalavopulmonary connections. Of this highly selectedroup of 65 patients, 50 of them received conduits ofolytetrafluoroethylene (PTFE). A more highly selectedroup of 15 patients underwent construction of an extra-ardiac lateral tunnel of “viable” in situ pericardium.
What do we learn from this retrospective review? Theontan failure rate of 6.1% (N � 4) is similar to or slightlyigher than in other contemporary series. At least two of
he failures were associated with one-stage Fontan pro-edures on patients who most likely would have under-one prior superior cavopulmonary anastomoses atany institutions. Thrombotic obstruction of the PTFE
onduit played a role in three of the four Fontan failures,
ng of “technically unrestricted anastomoses.” Salvage ofpatients was achieved by replacement of the PTFE
onduit with an aortic homograft in 1 patient, and with initu pericardium in the other. The observation of periop-rative supraventricular arrhythmias in 9.2% of patients6 of 65) is certainly not lower than that observed in otherontan series, without regard to the type of Fontanonnection created. And the maximum follow-up of justreater than 7 years is too short to draw conclusionsbout late postoperative arrhythmias or other late-phasevents. Other than the very good results in the very smallroup with the pericardial lateral tunnel, there is notnough encouraging data in this report to suggest anyomparative advantage of the extracardiac Fontan oper-tion relative to other types of modified Fontanrocedures.
arshall Jacobs, MD
ection of Cardiothoracic Surgeryt. Christopher’s Hospital for Childrenrie Ave at Front Sthiladelphia, PA 19134-1095
-mail: [email protected]0003-4975/05/$30.00doi:10.1016/j.athoracsur.2005.03.085
by on June 4, 2013 als.org

2005;80:665-672 Ann Thorac SurgPatel and Panangipalli Venugopal
Saxena, Rajvir Singh, Ganapathy K. Subramaniam, Kizakke K. Pradeep, Chetan D. Ujjwal K. Chowdhury, Balram Airan, Shyam Sundar Kothari, Sachin Talwar, Anita
Growth Potential, Arrhythmia, and ThromboembolismSpecific Issues After Extracardiac Fontan Operation: Ventricular Function,
& ServicesUpdated Information
http://ats.ctsnetjournals.org/cgi/content/full/80/2/665including high-resolution figures, can be found at:
References http://ats.ctsnetjournals.org/cgi/content/full/80/2/665#BIBL
This article cites 17 articles, 9 of which you can access for free at:
Citations http://ats.ctsnetjournals.org/cgi/content/full/80/2/665#otherarticles
This article has been cited by 12 HighWire-hosted articles:
Permissions & Licensing
[email protected]: orhttp://www.us.elsevierhealth.com/Licensing/permissions.jsp
in its entirety should be submitted to: Requests about reproducing this article in parts (figures, tables) or
Reprints [email protected]
For information about ordering reprints, please email:
by on June 4, 2013 ats.ctsnetjournals.orgDownloaded from




















