
Assessment of venous thromboembolism risk and the benefits of thromboprophylaxis in medical patients
10
Assessment of venous thromboembolism risk and the benefits of thromboprophylaxis in medical patients AlexanderT. Cohen 1 , Raza Alikhan 2 , Juan I. Arcelus 3 , Jean-François Bergmann 4 , Sylvia Haas 5 , Geno J. Merli 6 , Alex C. Spyropoulos 7 ,Victor F.Tapson 8 , Alexander G. G.Turpie 9 1 Guy’s, King’s and StThomas’ School of Medicine, London, UK; 2 John Radcliffe Hospital, Oxford, UK; 3 University of Granada Medical School and Hospital San Juan de Dios, Granada, Spain; 4 Hôpital Lariboisière, Paris, France; 5 Technical University of Munich, Munich, Germany; 6 Jefferson Medical College andThomas Jefferson University Hospital, Philadelphia, PA, USA; 7 Lovelace Medical Center, Albuquerque, NM, USA; 8 Duke University Medical Center, Durham, NC, USA; 9 Hamilton Health Sciences General Hospital, Hamilton, Ontario, Canada Summary Hospitalized patients with acute medical conditions are at sig- nificant risk of venous thromboembolism (VTE): approximately 10–30% of general medical patients may develop deep-vein thrombosis or pulmonary embolism, and the latter is a leading contributor to deaths in hospital. Despite consensus-group rec- ommendations that at-risk medical patients should receive thromboprophylaxis, there is currently no consensus as to which patients are at risk,and many patients may not receive ap- propriate thromboprophylaxis.This paper reviews evidence for the risk of VTE associated with different medical conditions and risk factors, and presents a risk-assessment model for risk strat- ification in medical patients. Medical conditions associated with Keywords Medical illness, risk-assessment model, thromboprophylaxis, venous thromboembolism a moderate to high risk of VTE include cardiac disease, cancer, respiratory disease, inflammatory bowel disease, and infectious diseases. Importantly, analyses of data from the MEDENOX study show that thromboprophylaxis significantly reduces the risk o f VTE in these patient subgroups. Risk factors in medical patients include a history of VTE, history of malignancy, increas- ing age, thrombophilia, prolonged immobility, and obesity.These medical conditions and risk factors are included in a risk-assess- ment model which is hoped will provide a simple means of assisting clinicians in deciding whether thromboprophylaxis should be used in an individual patient. Thromb Haemost 2005; 94: 750–9 Review Article Correspondence to: AlexanderT. Cohen Vascular Medicine Department of Surgery Guy’s, King’s and St.Thomas’ School of Medicine London, SE5 9PJ, UK Tel.: +44 20 7346 3015, Fax: +44 20 7346 3927 E-mail: [email protected] Received June 1, 2005 Accepted after revision July 29, 2005 Financial support: This initiative was funded by a grant from Aventis Pharmaceuticals, a member of The sanofi-aventis Group. Prepublished online September 10, 2005 DOI: 10.1160/TH05–06–0385 Introduction Venous thromboembolism (VTE) is a major cause of in-hospital mortality in medical (nonsurgical) patients. Postmortem studies indicate that pulmonary embolism (PE) is associated with up to 10% of deaths in hospitalized patients (1–3), and only about a quarter of these deaths occur following surgery (2, 4). This sug- gests that, although VTE is often regarded as a complication of surgery, about three quarters of hospitalized patients who suffer a fatal PE are in fact medical patients. Recent major clinical studies have shown that, in the absence of thromboprophylaxis, a significant proportion of acutely ill medical patients will develop VTE, with an incidence of VTE and proximal deep-vein thrombosis (DVT) of 10.9–14.9% and 4.1–4.9% in patients in placebo groups, respectively (5–7). In view of such findings, national and international consensus groups recommend that medical patients are assessed for their risk of VTE and given appropriate thromboprophylaxis when at moderate or high risk (8–11). There is, however, no current worldwide consensus on which medical patients should receive thromboprophylaxis, reflecting the heterogeneous nature of the patient population and uncertainty about appropriate risk strat- ification in these patients. Furthermore, underuse or misuse of thromboprophylaxis remains a problem, with estimates of 30–58% of general medical patients receiving appropriate thromboprophylaxis (12–16). An easy to use and reliable risk-assessment system that can be used to direct thromboprophylaxis to the most appropriate medical patients may improve the current situation (16). Pre- vious studies have identified a number of risk factors for VTE in medical patients, and risk-assessment models have been devel- oped based on these factors (17–20). However, many of these © 2005 Schattauer GmbH, Stuttgart 750
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Assessment of venous thromboembolism risk and the benefits of thromboprophylaxis in medical patients

Assessment of venous thromboembolism risk and the benefitsof thromboprophylaxis in medical patientsAlexander T. Cohen1, Raza Alikhan2, Juan I. Arcelus3, Jean-François Bergmann4, Sylvia Haas5, Geno J. Merli6,Alex C. Spyropoulos7, Victor F. Tapson8, Alexander G. G. Turpie9
1Guy’s, King’s and St Thomas’ School of Medicine, London, UK; 2John Radcliffe Hospital, Oxford, UK; 3University of Granada Medical Schooland Hospital San Juan de Dios, Granada, Spain; 4Hôpital Lariboisière, Paris, France; 5Technical University of Munich, Munich, Germany;6Jefferson Medical College and Thomas Jefferson University Hospital, Philadelphia, PA, USA; 7Lovelace Medical Center, Albuquerque, NM, USA;8Duke University Medical Center, Durham, NC, USA; 9Hamilton Health Sciences General Hospital, Hamilton, Ontario, Canada
SummaryHospitalized patients with acute medical conditions are at sig-nificant risk of venous thromboembolism (VTE): approximately10–30% of general medical patients may develop deep-veinthrombosis or pulmonary embolism, and the latter is a leadingcontributor to deaths in hospital.Despite consensus-group rec-ommendations that at-risk medical patients should receivethromboprophylaxis, there is currently no consensus as towhich patients are at risk,and many patients may not receive ap-propriate thromboprophylaxis.This paper reviews evidence forthe risk of VTE associated with different medical conditions andrisk factors,and presents a risk-assessment model for risk strat-ification in medical patients. Medical conditions associated with
KeywordsMedical illness, risk-assessment model, thromboprophylaxis,venous thromboembolism
a moderate to high risk of VTE include cardiac disease, cancer,respiratory disease, inflammatory bowel disease, and infectiousdiseases. Importantly, analyses of data from the MEDENOXstudy show that thromboprophylaxis significantly reduces therisk o f VTE in these patient subgroups. Risk factors in medicalpatients include a history of VTE,history of malignancy, increas-ing age, thrombophilia, prolonged immobility, and obesity.Thesemedical conditions and risk factors are included in a risk-assess-ment model which is hoped will provide a simple means ofassisting clinicians in deciding whether thromboprophylaxisshould be used in an individual patient.
Thromb Haemost 2005; 94: 750–9
Review Article
Correspondence to:Alexander T. CohenVascular MedicineDepartment of SurgeryGuy’s, King’s and St. Thomas’ School of MedicineLondon, SE5 9PJ, UKTel.: +44 20 7346 3015, Fax: +44 20 7346 3927E-mail: [email protected]
Received June 1, 2005Accepted after revision July 29, 2005
Financial support:This initiative was funded by a grant from Aventis Pharmaceuticals, a member of
The sanofi-aventis Group.
Prepublished online September 10, 2005 DOI: 10.1160/TH05–06–0385
IntroductionVenous thromboembolism (VTE) is a major cause of in-hospitalmortality in medical (nonsurgical) patients. Postmortem studiesindicate that pulmonary embolism (PE) is associated with up to10% of deaths in hospitalized patients (1–3), and only about aquarter of these deaths occur following surgery (2, 4). This sug-gests that, although VTE is often regarded as a complication ofsurgery, about three quarters of hospitalized patients who suffera fatal PE are in fact medical patients.
Recent major clinical studies have shown that, in the absenceof thromboprophylaxis, a significant proportion of acutely illmedical patients will develop VTE, with an incidence of VTEand proximal deep-vein thrombosis (DVT) of 10.9–14.9% and4.1–4.9% in patients in placebo groups, respectively (5–7). Inview of such findings, national and international consensus
groups recommend that medical patients are assessed for theirrisk of VTE and given appropriate thromboprophylaxis when atmoderate or high risk (8–11). There is, however, no currentworldwide consensus on which medical patients should receivethromboprophylaxis, reflecting the heterogeneous nature of thepatient population and uncertainty about appropriate risk strat-ification in these patients. Furthermore, underuse or misuse ofthromboprophylaxis remains a problem, with estimates of30–58% of general medical patients receiving appropriatethromboprophylaxis (12–16).
An easy to use and reliable risk-assessment system that canbe used to direct thromboprophylaxis to the most appropriatemedical patients may improve the current situation (16). Pre-vious studies have identified a number of risk factors for VTE inmedical patients, and risk-assessment models have been devel-oped based on these factors (17–20). However, many of these
© 2005 Schattauer GmbH, Stuttgart
750

Risk factors Risk
Heit et al., 2001 (22) OR (95% CI)
Independent risk factors Institutionalization without recent surgery 27.98 (4.49–14.18)
Institutionalization with recent surgery 21.72 (9.44–49.93)
Trauma 12.69 (4.06–39.66)
Malignancy without chemotherapy 24.05 (1.93–8.52)
Malignancy with chemotherapy 26.53 (2.11–20.23)
Prior CVC or transvenous pacemaker 25.55 (1.57–19.58)
Prior superficial-vein thrombosis 24.32 (1.76–10.61)
Neurological disease with extremity paresis 23.04 (1.25–7.38)
Heit et al., 2002 (23) AR (95% CI)
Immobilization (total confinement to bed orto bed and armchair)
25.61 (2.30–13.67)
Long-distance travel (not defined) 22.35 (1.45–3.80)
Infectious disease 21.95 (1.31–2.92)
AR, attributable risk; CI, confidence interval; CVC, central venous catheter; DVT, deep-veinthrombosis; OR, odds ratio; PE, pulmonary embolism;VTE, venous thromboembolism.*Odds ratios for risk factors should be interpreted with caution because at the time of the study itwas not usual practice in France to treat patients with severe conditions as outpatients.
Independent risk factors Hospitalization with surgery 23.8 (20.3–27.3)
Hospitalization without surgery 21.5 (17.3–25.6)
Malignant neoplasm 18.0 (13.4–22.6)
Trauma 12.0 (9.0–14.9)
Congestive heart failure 29.5 (3.3–15.8)
CVC or pacemaker placement 29.1 (5.7–12.6)
Neurological disease with extremity paresis 26.9 (3.5–10.2)
Superficial-vein thrombosis 25.4 (3.0–7.7)
Samama, 2000* (24) OR (95% CI)
Intrinsic factors History of VTE 15.6 (6.77–35.89)
Venous insufficiency 24.45 (3.10–6.38)
Chronic heart failure 22.93 (1.55–5.56)
Obesity 22.39 (1.48–3.87)
Immobile standing position (>6 hours/day) 21.85 (1.12–3.06)
History of >3 pregnancies 21.74 (1.06–2.87)
Triggering factors Pregnancy 11.41 (1.40–93.29)
Violent effort or muscular trauma 27.59 (2.95–19.53)
Deterioration of general condition 25.75 (2.20–15.01)
risk-assessment models have been subject to limitations such ascomplexity and lack of generalizability to medical patients.
In this paper, we review evidence in the literature for medicalconditions or factors that increase the risk of VTE in medical pa-tients and for the benefits of thromboprophylaxis in patients withthese conditions or factors. We also present a risk-assessmentmodel that takes into account both the underlying medical con-dition and risk factors and is intended to give clinicians a simple‘yes’ or ‘no’ answer when deciding whether a medical patientshould receive thromboprophylaxis. The model is based on evi-dence from the literature and the consensus views of the authors.
Risk of venous thromboembolism and thebenefits of thromboprophylaxis
Evidence of risk from epidemiological studiesLarge epidemiological studies have contributed to the identifica-tion of risk factors for VTE. For example, in a US study, 80% ofpatients with a first diagnosis of VTE had ≥3 risk factors, includ-ing age ≥40 years, cancer, congestive heart failure, chronic ob-structive pulmonary disease (COPD), obesity, stroke, and myo-cardial infarction (MI) (21). In another US population-basedstudy, independent risk factors for VTE included increasing age,institutionalization (hospitalization or residence in a nursinghome), malignancy, neurological disorders with extremity pare-sis, and the presence of central venous catheters (CVCs) or trans-venous pacemakers (Table 1) (22). A subsequent study fromthe same group found that 59% of cases of VTE in the commu-nity could be attributed to institutionalization; hospitalizationfor surgery or medical conditions accounted for 24% and 22%of VTE cases, respectively (23). Almost 75% of all cases ofVTE could be accounted for by a cluster of 8 risk factors shownin Table 1.
A multicenter case-control study of medical outpatientstreated for DVT by general practitioners in France also identified‘intrinsic’or ‘triggering’risk factors for VTE (Table 1) (24). Fur-thermore, a prospective registry in Spain showed that in 4011 pa-tients with confirmedVTE, of whom 90% were outpatients at thetime of VTE diagnosis, only 14.6% had undergone surgery in thepast 2 months, and the main VTE risk factors were immobili-zation, cancer, varicose veins and a history of VTE (25).
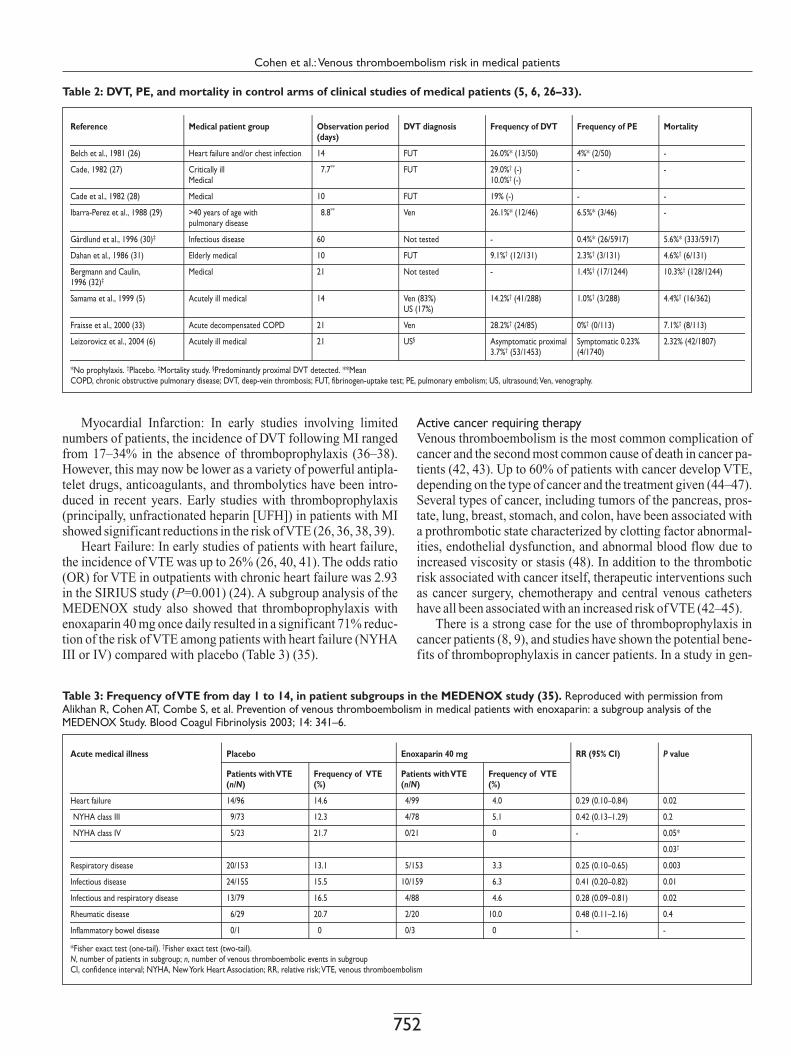
Evidence from thromboprophylaxis studiesInsights into the risk of VTE in medical patients can also be ob-tained from placebo- or no-prophylaxis-controlled thrombopro-phylaxis studies. The incidence of DVT in the control groups ofsuch studies ranges from approximately 9–29%, and that of PE0–6.5% (Table 2) (5, 6, 26–33). In the absence of thrombopro-phylaxis, mortality in these studies was approximately 4–10%(Table 2). It should be noted, however, that in many studies DVTwas diagnosed by ultrasonography or the fibrinogen-uptake test.These techniques are less sensitive than venography, which is re-garded as the ‘gold standard’, and may result in an underesti-mation of the incidence of VTE.
Analyses of clinical-trial data have also contributed to clar-ifying which factors lead to an increased risk of VTE. A recentrisk-factor analysis of the Prophylaxis in Medical Patients with
Enoxaparin (MEDENOX) study identified a number of indepen-dent risk factors for VTE in acutely ill medical patients (34). Anadditional subgroup analysis from the same study also showedthe benefits of thromboprophylaxis in defined groups of acutelyill medical patients (35). Evidence from these analyses for VTErisk and the benefits of thromboprophylaxis, along with otherevidence from the literature, is reviewed below.
Acute medical illnesses
Cardiac diseaseBoth MI and congestive heart failure increase the risk of VTE,and thromboprophylaxis reduces the risk of VTE in patients withheart disease, hence it is routinely recommended in this patientgroup (8, 9).
Table 1: Risk factors for DVT or PE.
Cohen et al.: Venous thromboembolism risk in medical patients
751
Reference Medical patient group Observation period(days)
Mortality
Belch et al., 1981 (26) Heart failure and/or chest infection 14 -
Cade, 1982 (27) Critically illMedical
07.7** -
Cade et al., 1982 (28) Medical 10 -
Ibarra-Perez et al., 1988 (29) >40 years of age withpulmonary disease
08.8** -
Gårdlund et al., 1996 (30)‡ Infectious disease 60 5.6%* (333/5917)
Dahan et al., 1986 (31) Elderly medical 10 4.6%† (6/131)
Bergmann and Caulin,1996 (32)‡
Medical 21 10.3%† (128/1244)
Samama et al., 1999 (5) Acutely ill medical 14 4.4%† (16/362)
Fraisse et al., 2000 (33) Acute decompensated COPD 21 7.1%† (8/113)
Leizorovicz et al., 2004 (6) Acutely ill medical 21 2.32% (42/1807)
*No prophylaxis. †Placebo. ‡Mortality study. §Predominantly proximal DVT detected. **MeanCOPD, chronic obstructive pulmonary disease; DVT, deep-vein thrombosis; FUT, fibrinogen-uptake test; PE, pulmonary embolism; US, ultrasound;Ven, venography.
DVT diagnosis
FUT
FUT
FUT
Ven
Not tested
FUT
Not tested
Ven (83%)US (17%)
Ven
US§
Frequency of DVT
26.0%* (13/50)
29.0%† (-)10.0%† (-)
19% (-)
26.1%* (12/46)
-
9.1%† (12/131)
-
14.2%† (41/288)
28.2%† (24/85)
Asymptomatic proximal3.7%† (53/1453)
Frequency of PE
4%* (2/50)
-
-
6.5%* (3/46)
0.4%* (26/5917)
2.3%† (3/131)
1.4%† (17/1244)
1.0%† (3/288)
0%† (0/113)
Symptomatic 0.23%(4/1740)
Acute medical illness Placebo Enoxaparin 40 mg RR (95% CI) P value
Patients withVTE(n/N)
Frequency of VTE(%)
Patients withVTE(n/N)
Frequency of VTE(%)
Heart failure 14/96 14.6 04/99 04.0 0.29 (0.10–0.84) 0.02
NYHA class III 09/73 12.3 04/78 05.1 0.42 (0.13–1.29) 0.2
NYHA class IV 05/23 21.7 00/21 00 - 0.05*
Respiratory disease 20/153 13.1 05/153 03.3 0.25 (0.10–0.65) 0.003
Infectious disease 24/155 15.5 10/159 06.3 0.41 (0.20–0.82) 0.01
Infectious and respiratory disease 13/79 16.5 04/88 04.6 0.28 (0.09–0.81) 0.02
Rheumatic disease 06/29 20.7 02/20 10.0 0.48 (0.11–2.16) 0.4
Inflammatory bowel disease 00/1 00 00/3 00 - -
*Fisher exact test (one-tail). †Fisher exact test (two-tail).N, number of patients in subgroup; n, number of venous thromboembolic events in subgroupCI, confidence interval; NYHA, NewYork Heart Association; RR, relative risk;VTE, venous thromboembolism
0.03†
Myocardial Infarction: In early studies involving limitednumbers of patients, the incidence of DVT following MI rangedfrom 17–34% in the absence of thromboprophylaxis (36–38).However, this may now be lower as a variety of powerful antipla-telet drugs, anticoagulants, and thrombolytics have been intro-duced in recent years. Early studies with thromboprophylaxis(principally, unfractionated heparin [UFH]) in patients with MIshowed significant reductions in the risk ofVTE (26, 36, 38, 39).
Heart Failure: In early studies of patients with heart failure,the incidence of VTE was up to 26% (26, 40, 41). The odds ratio(OR) for VTE in outpatients with chronic heart failure was 2.93in the SIRIUS study (P=0.001) (24). A subgroup analysis of theMEDENOX study also showed that thromboprophylaxis withenoxaparin 40 mg once daily resulted in a significant 71% reduc-tion of the risk of VTE among patients with heart failure (NYHAIII or IV) compared with placebo (Table 3) (35).
Active cancer requiring therapyVenous thromboembolism is the most common complication ofcancer and the second most common cause of death in cancer pa-tients (42, 43). Up to 60% of patients with cancer develop VTE,depending on the type of cancer and the treatment given (44–47).Several types of cancer, including tumors of the pancreas, pros-tate, lung, breast, stomach, and colon, have been associated witha prothrombotic state characterized by clotting factor abnormal-ities, endothelial dysfunction, and abnormal blood flow due toincreased viscosity or stasis (48). In addition to the thromboticrisk associated with cancer itself, therapeutic interventions suchas cancer surgery, chemotherapy and central venous cathetershave all been associated with an increased risk ofVTE (42–45).
There is a strong case for the use of thromboprophylaxis incancer patients (8, 9), and studies have shown the potential bene-fits of thromboprophylaxis in cancer patients. In a study in gen-
Table 2: DVT, PE, and mortality in control arms of clinical studies of medical patients (5, 6, 26–33).
Table 3: Frequency ofVTE from day 1 to 14, in patient subgroups in the MEDENOX study (35). Reproduced with permission fromAlikhan R, Cohen AT, Combe S, et al. Prevention of venous thromboembolism in medical patients with enoxaparin: a subgroup analysis of theMEDENOX Study. Blood Coagul Fibrinolysis 2003; 14: 341–6.
Cohen et al.:Venous thromboembolism risk in medical patients
752

eral medical inpatients, thromboprophylaxis with UFH reducedmortality in the subgroup with cancer from 32% to 19% (49).
Chemotherapy is a recognized risk factor for VTE in cancerpatients. In patients with stage II breast cancer undergoingchemotherapy, the risk of VTE is approximately 7–11% and de-creases when chemotherapy is discontinued (50, 51). This riskcan be reduced by appropriate thromboprophylaxis (52).
The use of CVCs also increases the risk of VTE in cancer pa-tients. In one study, the incidence of thrombosis in cancer pa-tients with CVCs not receiving thromboprophylaxis was 37.5%,compared with 9.5% in those receiving warfarin (P<0.001) (53).The risk of VTE associated with CVCs was also illustrated in astudy with the low-molecular-weight heparin (LMWH) daltepa-rin, which was discontinued prematurely when an interim analy-sis showed that the incidence of confirmed DVT in the LMWHgroup was 6% (1/16 patients), compared with 62% (8/13) in pa-tients who were not receiving thromboprophylaxis (relative risk[RR] 6.75, 95% confidence interval [CI] 1.05–43.58) (54). Fur-thermore, a meta-analysis of data from 14 randomized trialsshowed that thromboprophylaxis with heparin reduces the inci-dence of catheter-related VTE by over half (RR 0.43, 95% CI0.23–0.78), compared with patients not receiving thrombopro-phylaxis (55). The use of femoral vein catheters to provide cen-tral venous access is also associated with an increased risk ofVTE (56, 57).
Respiratory diseaseThe prevalence of VTE in patients hospitalized with respiratorydiseases has been estimated to be 8–25% (33), while postmortemstudies have shown that PE is present in 28–51% of patients withCOPD (58). In the MEDENOX study, the incidence of VTE was13.1% in patients with respiratory disease receiving placebo (5),and subgroup analyses (35) showed that thromboprophylaxiswith enoxaparin 40 mg once daily reduced the incidence of VTEin these patients (Table 3). Similarly, a study of patients hospital-ized with COPD and requiring mechanical ventilation showedthat thromboprophylaxis with nadroparin reduced the incidenceof DVT from 28.2% in the placebo group to 15.5% (P=0.045)(33). These findings are supported by the results of other trials ingeneral medical patients that have included substantial numbersof patients with respiratory disease (59–61).
Inflammatory bowel diseaseThe relationship between VTE and inflammatory bowel disease(IBD) is not fully understood. A study by Motykie et al. (62) didnot show a significant relationship between the two conditions.However, the SIRIUS study showed a trend towards a significantassociation between IBD and DVT (OR 1.89, P=0.09) (24), anda recent case-control study showed that IBD is associated with a4-fold increase in the risk of VTE (OR 3.6, P<0.001) (63). In apopulation-based cohort study, the risk of VTE was approxi-mately 3 times higher in patients with IBD than in the controlgroup (64). In patients with ulcerative colitis, the incidence rateratios (IRRs) for DVT and PE were 2.8 (95% CI 2.1–3.7) and 3.6(95% CI 2.5–5.2), respectively; the corresponding figures forpatients with Crohn’s disease were 4.7 (95% CI 3.5–6.3) and 2.9(95% CI 1.8–4.7), respectively. Furthermore, VTE is associatedwith high mortality and morbidity in patients with IBD (65).
No large controlled trials of thromboprophylaxis have beenconducted in patients with IBD. However, open studies in smallnumbers of patients have reported beneficial results in terms ofremittance of ulcerative colitis with UFH or LMWH (66, 67).Al-though there is currently a lack of strong evidence from clinicalstudies, our consensus view is that thromboprophylaxis isbeneficial in patients with IBD.
Rheumatic diseaseIn the MEDENOX study, the incidence of VTE in patients withacute rheumatoid arthritis of the lower extremities or acute backdisorders (including sciatica and vertebral compression) and atleast 1 other risk factor for VTE was 20.7% (35). Epidemiologi-cal data indicate that the incidence of VTE is approximately 50%higher in patients with rheumatoid arthritis than in nonarthriticindividuals, and that cardiovascular mortality in patients withrheumatoid arthritis is about twice as high as in age- and sex-matched controls (68).
Although there are no studies of thromboprophylaxis specifi-cally in patients with rheumatoid arthritis, the MEDENOX studyrecruited patients with acute rheumatic disorders and at least 1other risk factor for VTE, and also included a small number ofpatients with acute back disorders (5). Subgroup analysisshowed that thromboprophylaxis with enoxaparin 40 mg oncedaily reduced the risk of VTE by 52% in these patients (Table 3),although the effect did not reach statistical significance, prob-ably because of the relatively small number of patients (35).
Neurological disordersStroke Patients: Stroke patients are at high risk of VTE with aprevalence of objectively confirmed DVT between 20–50% inthe absence of thromboprophylaxis (8). Numerous studies(69–74), but not all (75), have shown that thromboprophylaxissignificantly reduces the risk of VTE in stroke patients.
Thromboprophylaxis with UFH or LMWH in patients withacute ischemic stroke was evaluated in a meta-analysis of datafrom 10 randomized trials involving 1047 patients (76). Overall,the risk of DVT was reduced by 81% in patients receiving UFHor LMWH compared with control groups (2P<0.00001). Therisk of PE was reduced by 58%, compared with controls, but thiseffect did not reach statistical significance (2P>0.1).
Such findings underline the importance of thromboprophy-laxis in patients with acute ischemic stroke. In contrast, in pa-tients with suspected or proven hemorrhagic stroke, the potentialbenefits of thromboprophylaxis are outweighed by the risk ofbleeding complications; hence, the possibility of intracranialhemorrhage should be excluded before thromboprophylaxis isstarted (9, 76, 77). Furthermore, there may be a dose-dependentincrease in the risk of hemorrhagic transformation of a cerebralinfarct in patients receiving heparin thromboprophylaxis (76).
Although the benefits of pharmacological thromboprophyla-xis in acute ischemic stroke patients have been clearly demon-strated, there is less evidence to support the use of mechanicalforms of thromboprophylaxis. A recent Cochrane review evalu-ated results from 2 trials, involving a total of 123 patients, andconcluded that there was insufficient evidence from randomizedtrials to support the routine use of physical methods for prevent-ing DVT in acute stroke (78).
Cohen et al.:Venous thromboembolism risk in medical patients
753
Spinal Cord Injury: Patients with spinal cord injuries havethe highest incidence of VTE of any medical patient group, withstudies reporting confirmed DVT in 60–100% of patients (8). Anumber of small studies have shown that thromboprophylaxis isbeneficial in patients with spinal cord injuries. For example, 2studies involving a total of 99 patients showed that adjusted-doseUFH was more effective at preventing DVT than low-dose UFH(incidence 7% vs. 31%, respectively; P<0.05), and that low-doseLMWH was significantly more effective than low-dose UFH(incidence 0% vs. 26%, respectively; P=0.02) (79, 80).
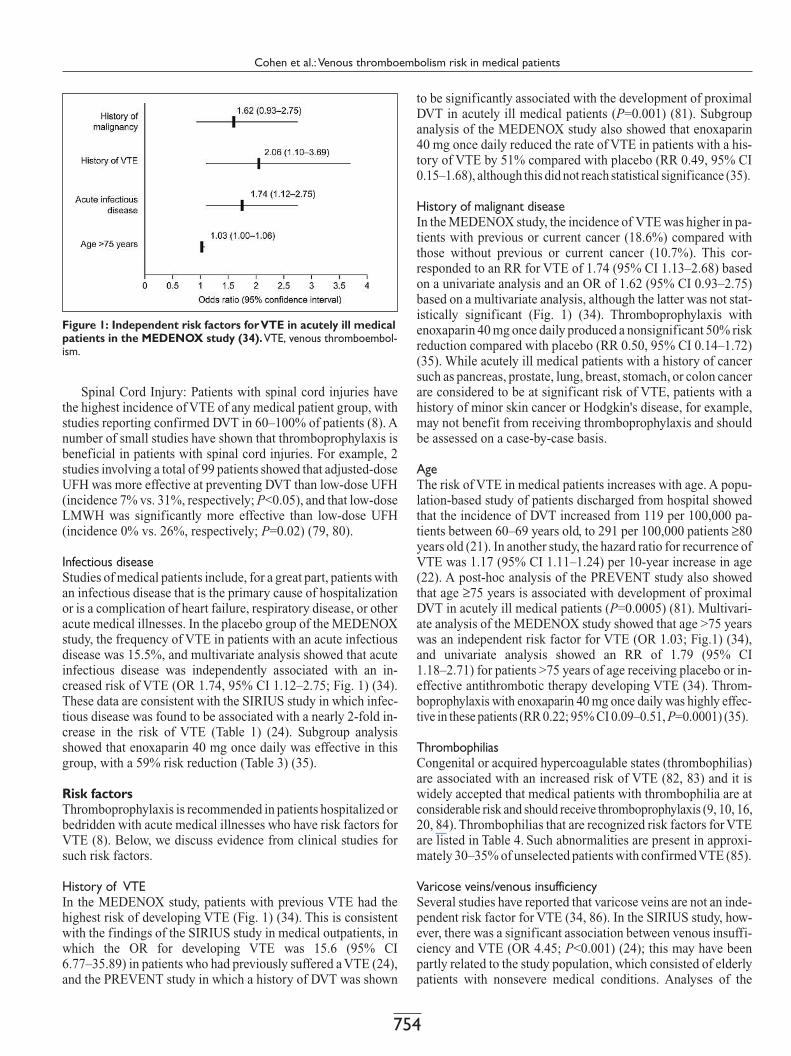
Infectious diseaseStudies of medical patients include, for a great part, patients withan infectious disease that is the primary cause of hospitalizationor is a complication of heart failure, respiratory disease, or otheracute medical illnesses. In the placebo group of the MEDENOXstudy, the frequency of VTE in patients with an acute infectiousdisease was 15.5%, and multivariate analysis showed that acuteinfectious disease was independently associated with an in-creased risk of VTE (OR 1.74, 95% CI 1.12–2.75; Fig. 1) (34).These data are consistent with the SIRIUS study in which infec-tious disease was found to be associated with a nearly 2-fold in-crease in the risk of VTE (Table 1) (24). Subgroup analysisshowed that enoxaparin 40 mg once daily was effective in thisgroup, with a 59% risk reduction (Table 3) (35).
Risk factorsThromboprophylaxis is recommended in patients hospitalized orbedridden with acute medical illnesses who have risk factors forVTE (8). Below, we discuss evidence from clinical studies forsuch risk factors.
History of VTEIn the MEDENOX study, patients with previous VTE had thehighest risk of developing VTE (Fig. 1) (34). This is consistentwith the findings of the SIRIUS study in medical outpatients, inwhich the OR for developing VTE was 15.6 (95% CI6.77–35.89) in patients who had previously suffered a VTE (24),and the PREVENT study in which a history of DVT was shown
to be significantly associated with the development of proximalDVT in acutely ill medical patients (P=0.001) (81). Subgroupanalysis of the MEDENOX study also showed that enoxaparin40 mg once daily reduced the rate of VTE in patients with a his-tory of VTE by 51% compared with placebo (RR 0.49, 95% CI0.15–1.68), although this did not reach statistical significance (35).
History of malignant diseaseIn the MEDENOX study, the incidence of VTE was higher in pa-tients with previous or current cancer (18.6%) compared withthose without previous or current cancer (10.7%). This cor-responded to an RR for VTE of 1.74 (95% CI 1.13–2.68) basedon a univariate analysis and an OR of 1.62 (95% CI 0.93–2.75)based on a multivariate analysis, although the latter was not stat-istically significant (Fig. 1) (34). Thromboprophylaxis withenoxaparin 40 mg once daily produced a nonsignificant 50% riskreduction compared with placebo (RR 0.50, 95% CI 0.14–1.72)(35). While acutely ill medical patients with a history of cancersuch as pancreas, prostate, lung, breast, stomach, or colon cancerare considered to be at significant risk of VTE, patients with ahistory of minor skin cancer or Hodgkin's disease, for example,may not benefit from receiving thromboprophylaxis and shouldbe assessed on a case-by-case basis.
AgeThe risk of VTE in medical patients increases with age. A popu-lation-based study of patients discharged from hospital showedthat the incidence of DVT increased from 119 per 100,000 pa-tients between 60–69 years old, to 291 per 100,000 patients ≥80years old (21). In another study, the hazard ratio for recurrence ofVTE was 1.17 (95% CI 1.11–1.24) per 10-year increase in age(22). A post-hoc analysis of the PREVENT study also showedthat age ≥75 years is associated with development of proximalDVT in acutely ill medical patients (P=0.0005) (81). Multivari-ate analysis of the MEDENOX study showed that age >75 yearswas an independent risk factor for VTE (OR 1.03; Fig.1) (34),and univariate analysis showed an RR of 1.79 (95% CI1.18–2.71) for patients >75 years of age receiving placebo or in-effective antithrombotic therapy developing VTE (34). Throm-boprophylaxis with enoxaparin 40 mg once daily was highly effec-tive in these patients (RR 0.22; 95% CI 0.09–0.51, P=0.0001) (35).
ThrombophiliasCongenital or acquired hypercoagulable states (thrombophilias)are associated with an increased risk of VTE (82, 83) and it iswidely accepted that medical patients with thrombophilia are atconsiderable risk and should receive thromboprophylaxis (9, 10, 16,20, 84). Thrombophilias that are recognized risk factors for VTEare listed in Table 4. Such abnormalities are present in approxi-mately 30–35% of unselected patients with confirmedVTE (85).
Varicose veins/venous insufficiencySeveral studies have reported that varicose veins are not an inde-pendent risk factor for VTE (34, 86). In the SIRIUS study, how-ever, there was a significant association between venous insuffi-ciency and VTE (OR 4.45; P<0.001) (24); this may have beenpartly related to the study population, which consisted of elderlypatients with nonsevere medical conditions. Analyses of the
Figure 1: Independent risk factors forVTE in acutely ill medicalpatients in the MEDENOX study (34).VTE, venous thromboembol-ism.
Cohen et al.:Venous thromboembolism risk in medical patients
754

● Antithrombin deficiency*
● Protein C deficiency*
● Protein S deficiency*
● Hyperhomocysteinemia
● Raised prothrombin levels
● FactorV Leiden
● Raised factorVIII levels
● Hyperfibrinogenemia
*VTE risk is higher for homozygous compared with heterozygous mutations
PREVENT study also showed that varicose veins are signifi-cantly associated with the development of proximal DVT inacutely ill medical patients (P=0.04) (81).
Subgroup analysis of the MEDENOX study showed thatenoxaparin 40 mg once daily was effective in acutely ill medicalpatients with varicose veins (RR 0.24, 95% CI 0.08–0.68;P=0.05) (35). In view of these findings, there was consensusamong the authors that acutely ill medical patients with varicoseveins have an additional risk factor for thrombosis and shouldbenefit from thromboprophylaxis.
Prolonged immobilityProlonged immobility is a recognized risk factor for VTE (10,24). In the MEDENOX study, enoxaparin 40 mg once daily re-duced the incidence of VTE in patients with prolonged immobi-lization (defined as an inability to walk 10 m for 7–14 days afteradmission) from 20% to 9% (RR 0.44, 95% CI 0.22–0.88;P=0.02) (35).
ObesityAlthough analyses of the MEDENOX study did not show obes-ity to be a significant risk factor for VTE (34), other studies havedemonstrated a relationship between obesity and VTE. In theSIRIUS study, obesity (defined as a body mass index [BMI]>30 kg/m2) was associated with an OR for DVT of 2.39 (95% CI1.55–5.56) (24). Similarly, in the Nurses’ Health Study, the riskof primary PE was increased 3-fold in women with a BMI ≥29kg/m2 (RR 2.9, 95% CI 1.5–5.4) (87), while in a study in middle-aged men, a waist circumference of ≥100 cm was associated witha 4-fold increase in the risk ofVTE (RR 3.92, 95% CI 2.10–7.29)(88). A recent case-control study of patients with a first episodeof objectively diagnosed thrombosis showed that the risk of DVT(adjusted for age and gender) increases 2-fold in patients with aBMI ≥30 kg/m2 (OR 2.26, 95% CI 1.49–3.41) (89). Fur-thermore, the risk is 10 times higher in women aged 15–45 yearswith a BMI ≥25 kg/m2 who use oral contraceptives comparedwith women aged 15–45 years with a BMI <25 kg/m2 who do notuse oral contraceptives (89).
Other risk factorsA number of other risk factors for VTE have been identified, in-cluding myeloproliferative disease (90), hormone therapy (in-cluding hormone replacement therapy and oral contraception)(91–95), nephrotic syndrome (96), and dehydration (15). Todate, however, there is only limited evidence concerning the im-pact of these risk factors on the overall level of risk in medical pa-tients. It has also been recommended that thromboprophylaxisshould be considered during pregnancy or postpartum in womenwith other known risk factors, such as a history ofVTE or throm-bophilia (97).
Several studies have reported that VTE occurs in approxima-tely 30% of patients in medical intensive care units (27, 98). Thereis no evidence, however, that treatment in an intensive care unitper se confers an increased risk of VTE. By definition, patientsin medical intensive care units are very ill, with acute medicalconditions, and as such often require thromboprophylaxis.
Our consensus was that medical outpatients with an acutemedical illness that is not discussed above should still be con-
sidered for thromboprophylaxis on a case-by-case basis depend-ing on the severity of their acute medical illness and also on riskfactors for VTE that may be present.
Risk assessment in medical patientsThe use of risk-assessment models and implementation of evi-dence-based thromboprophylaxis strategies have been widelysupported by consensus groups. Well-designed risk-assessmentmodels can help physicians to identify at-risk medical patients,and to prescribe appropriate thromboprophylaxis.The process ofusing a risk-assessment model may also increase physicianawareness of, and vigilance for, risk factors (99).
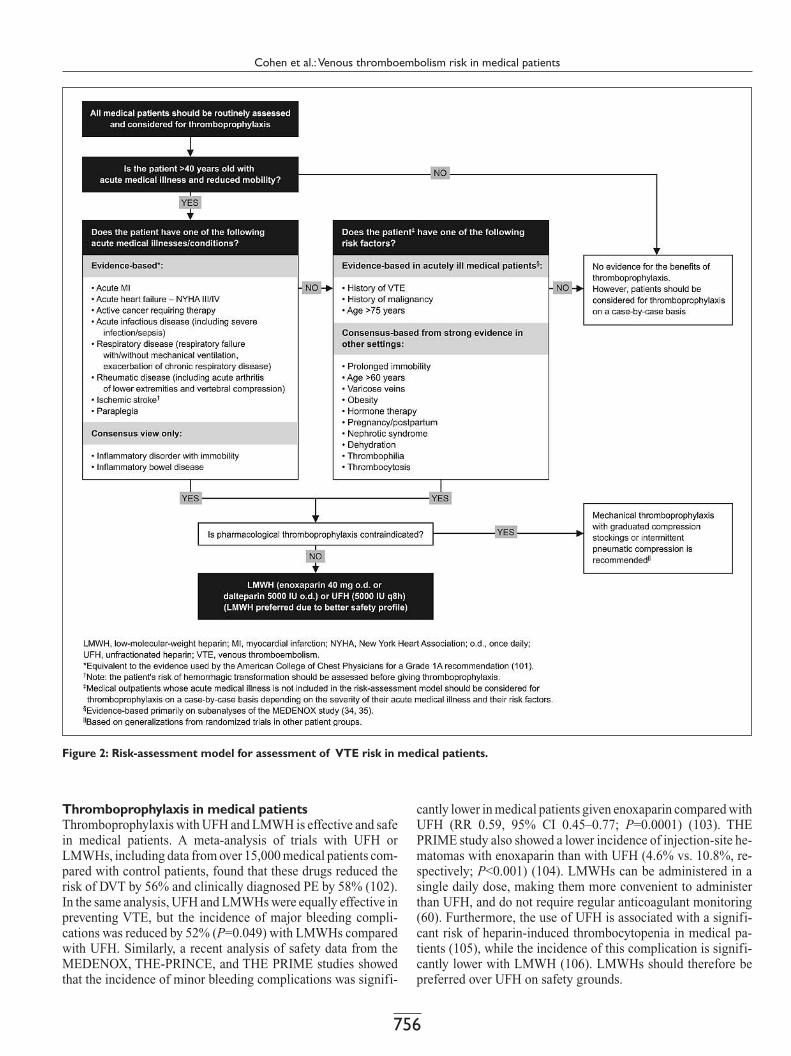
Existing risk-assessment models in medical patients (10,16–20, 85, 100), however, are subject to some limitations includ-ing complexity, lack of thromboprophylaxis recommendations,limited definitions of at-risk patients, and limited justificationfor inclusion of risk factors (i.e. inclusion on the basis of evi-dence or consensus). In light of these limitations, we developeda novel risk-assessment model for use in medical patients (Fig.2). The model is intended to assist physicians with determiningwhether thromboprophylaxis is warranted in an individual pa-tient, and to provide recommendations for appropriate thrombo-prophylaxis. It can also be used as an educational tool to promoteawareness of VTE risk in medical patients, and could form thebasis of clinical decision-making tools, such as quick-referenceguides for physicians.
In the risk-assessment model shown in Figure 2, physiciansare first encouraged to assess all medical patients for their riskfor VTE before progressing through simple steps, answering yesor no to each question in order to move to the next relevant step.Acute medical illnesses/conditions and risk factors for VTEwere included in the model on the basis of evidence from pros-pective studies in medical patients (reviewed above), or theconsensus views of the authors. If there is evidence or author-consensus for a patient being at risk for VTE or for the benefitsof thromboprophylaxis, then a recommendation for thrombopro-phylaxis is provided. The recommendation also takes intoaccount possible contraindications for pharmacological throm-boprophylaxis. Benefits of this model are its flexibility to theinclusion of further data that accumulate and its transparency injustifying inclusion of risk factors.
Table 4:Thrombophilic states resulting in a significant risk ofVTE (82–85).
Cohen et al.: Venous thromboembolism risk in medical patients
755
Thromboprophylaxis in medical patientsThromboprophylaxis with UFH and LMWH is effective and safein medical patients. A meta-analysis of trials with UFH orLMWHs, including data from over 15,000 medical patients com-pared with control patients, found that these drugs reduced therisk of DVT by 56% and clinically diagnosed PE by 58% (102).In the same analysis, UFH and LMWHs were equally effective inpreventing VTE, but the incidence of major bleeding compli-cations was reduced by 52% (P=0.049) with LMWHs comparedwith UFH. Similarly, a recent analysis of safety data from theMEDENOX, THE-PRINCE, and THE PRIME studies showedthat the incidence of minor bleeding complications was signifi-
cantly lower in medical patients given enoxaparin compared withUFH (RR 0.59, 95% CI 0.45–0.77; P=0.0001) (103). THEPRIME study also showed a lower incidence of injection-site he-matomas with enoxaparin than with UFH (4.6% vs. 10.8%, re-spectively; P<0.001) (104). LMWHs can be administered in asingle daily dose, making them more convenient to administerthan UFH, and do not require regular anticoagulant monitoring(60). Furthermore, the use of UFH is associated with a signifi-cant risk of heparin-induced thrombocytopenia in medical pa-tients (105), while the incidence of this complication is signifi-cantly lower with LMWH (106). LMWHs should therefore bepreferred over UFH on safety grounds.
Figure 2: Risk-assessment model for assessment of VTE risk in medical patients.
Cohen et al.: Venous thromboembolism risk in medical patients
756

● Hypersensitivity to UFH or LMWH
● Heparin-induced thrombocytopenia
● Coagulopathy
● Spinal tap or epidural anesthesia within 12 hours
● Hemorrhagic stroke
● Other relative or absolute exclusion criteria for pharmacological thromboprophylaxis whichplace a patient at high risk for bleeding, including uncontrolled hypertension, some surgical pro-cedures, and significant renal insufficiency (creatinine clearance <30ml/min)*
*Patients should be assessed on a case by case basis in terms of benefit versus risk and withreference to product labeling.LMWH, low-molecular-weight heparin; UFH, unfractionated heparin.
● Bleeding (active and uncontrollable)
The optimal dose of LMWH was investigated in theMEDENOX study, in which patients received enoxaparin 20 mgor 40 mg once daily, or placebo (5). Compared with placebo,the RRs of VTE and DVT in patients receiving enoxaparin20 mg once daily were 1.02 (95% CI 0.70–1.51; P=0.9) and1.05 (0.71–1.57; P=0.81), respectively. By contrast, enoxaparin40 mg once daily produced significant reductions in the riskof VTE (RR 0.37, 95% CI 0.22–0.63; P<0.001) and DVT (RR0.40, 95% CI 0.23–0.69; P<0.001), compared with placebo.There were no significant differences in terms of safety out-comes between patients receiving enoxaparin 40 mg once dailyand placebo. The PREVENT study (6) also showed that daltepa-rin 5000 IU once daily reduced the incidence of the primarycomposite end point of objectively verified symptomatic DVT,symptomatic PE, sudden death, and asymptomatic proximalDVT detected by compression ultrasound in acutely ill medicalpatients compared with placebo (2.77% vs. 4.96%; P=0.0015)(6).
Use of LMWH (once-daily dosing) has been shown to be aseffective as UFH three times daily for prevention of VTE inmedical patients (59, 61, 104, 107). However, UFH twice dailyhas not, so far, been compared with effective doses of LMWH inclinical studies. We therefore recommend that either LMWH(enoxaparin 40 mg or dalteparin 5000 IU) once daily or UFHthree times daily (q8h) is used for thromboprophylaxis in acutelyill medical patients (Fig. 2).
The optimal duration of thromboprophylaxis in medical pa-tients remains to be determined. This question is currently beinginvestigated in the EXCLAIM Study, in which patients aretreated with enoxaparin 40 mg once daily for approximately 10days, after which they are randomized to receive enoxaparin orplacebo for a further 28 days (108).
If contraindications to anticoagulants are present (Table 5),mechanical thromboprophylaxis with graduated compressionstockings or intermittent pneumatic compression should be con-sidered (8). However, there is only limited evidence to supportthe use of such approaches, and the American College of ChestPhysicians (ACCP) consensus guidelines give these methods aGrade 1C+ level recommendation (a strong recommendation
based on secure generalizations from randomized trials in otherpatient groups [109]) (8).
ConclusionsMedical patients are at significant risk of VTE. Incidences of14.2% total DVT and 4.9% proximal DVT observed in medicalpatients in the placebo arm of the MEDENOX study mean thatthese patients are at moderate or high risk which warrantsproviding thromboprophylaxis (8, 10). Although the incidenceof symptomatic VTE seems to be low in medical patients, it issimilar to that observed in high-risk surgical patients, and clini-cal VTE or fatal PE remain important concerns in this setting.Moreover, despite consensus-group recommendations thatmedical patients should be assessed for their risk of VTE andgiven appropriate thromboprophylaxis, a significant proportionof patients do not routinely receive thromboprophylaxis. Therisk-assessment model presented in this paper is designed toassist clinicians in deciding whether an individual medical pa-tient should receive thromboprophylaxis, and should help to im-prove the currently suboptimal protection of this patient group.
Table 5: Common contraindications to pharmacologicalthromboprophylaxis in acutely ill medical patients. Modified withpermission of Thomson American Health Consultants, PO Box 740056Atlanta, GA 30374.
7. Cohen AT, Davidson BL, Gallus AS et al. Fonda-parinux for the prevention of VTE in acutely ill medi-cal patients. Blood 2003; 102: 42 (Abstract).8. Geerts WH, Pineo GF, Heit JA et al. Prevention ofvenous thromboembolism: the Seventh ACCP Confer-ence on Antithrombotic and Thrombolytic Therapy.Chest 2004; 126 (3 Suppl): 338S–400S.9. Nicolaides AN, Breddin HK, Fareed J et al;Cardiovascular Disease Educational and ResearchTrust and the International Union of Angiology.Prevention of venous thromboembolism. InternationalConsensus Statement. Guidelines compiled in accord-ance with the scientific evidence. Int Angiol 2001; 20:1–37.10. Second Thromboembolic Risk Factors (THRIFTII) Consensus Group. Risk of and prophylaxis for ve-nous thromboembolism in hospital patients. Phlebol-ogy 1998; 13: 87–97.11. Scottish Intercollegiate Guidelines Network(SIGN). Prophylaxis of Venous Thromboembolism.
2002; SIGN Publication No. 62: http://www.sign.ac.uk/pdf/sign62.pdf (accessed May 2005).12. Anderson FA Jr, Wheeler HB, Goldberg RJet al. Physician practices in the prevention ofvenous thromboembolism. Ann Intern Med 1991; 115:581–5.13. Ageno W, Squizzata A, Ambrosini F et al. Throm-bosis prophylaxis in medical patients: a retrospectivereview of clinical practice patterns. Haematologica2002; 87: 746–50.14. Ahmad HA, Geissler A, Maclellan DG. Deep ve-nous thrombosis prophylaxis: are guidelines being fol-lowed? ANZ J Surg 2002; 72: 331–4.15. Bergmann J-F, Mouly S. Thromboprophylaxis inmedical patients: focus on France. Semin Thromb He-most 2002; 28 (Suppl 3): 51–5.16. Arcelus JI, Candocia S, Traverso CI et al. Venousthromboembolism prophylaxis and risk assessment inmedical patients. Semin Thromb Hemost 1991; 17(Suppl. 3): 313–8.
References1. Lindblad B, Sternby NH, Bergqvist D. Incidence ofvenous thromboembolism verified by necropsy over 30years. BMJ 1991; 302: 709–11.2. Sandler DA, Martin JF. Autopsy proven pulmonaryembolism in hospital patients: are we detecting enoughdeep vein thrombosis? J R Soc Med 1989; 82: 203–5.3. Cohen AT, Edmondson RA, Phillips MJ et al. Thechanging pattern of venous thromboembolic disease.Haemostasis 1996; 26: 65–71.4. Sperry KL, Key CR, Anderson RE. Toward a popu-lation-based assessment of death due to pulmonary em-bolism in New Mexico. Hum Pathol 1990; 21: 159–65.5. Samama MM, CohenAT, Darmon J-Y et al.A com-parison of enoxaparin with placebo for the preventionof venous thromboembolism in acutely ill medical pa-tients. N Engl J Med 1999; 341: 793–800.6. Leizorovicz A, Cohen AT, Turpie AGG et al. Rando-mized, placebo-controlled trial of dalteparin for the pre-vention of venous thromboembolism in acutely ill medi-cal patients. Circulation 2004; 110: 874–9.
Cohen et al.:Venous thromboembolism risk in medical patients
757

17. Cohen AT, Alikhan R. Prophylaxis of venousthromboembolism in medical patients. Curr Opin PulmMed 2001; 7: 332–7.18. Thromboembolic Risk Factors (THRIFT) Consen-sus Group. Risk of and prophylaxis for venous throm-boembolism in hospital patients. BMJ 1992; 305:567–74.19. Caprini JA, Arcelus JA, Reyna JJ. Effective riskstratification of surgical and nonsurgical patients forvenous thromboembolic disease. Semin Hematol2001; 38 (Suppl 5): 12–9.20. Haas SK. Venous thromboembolic risk and its pre-vention in hospitalized medical patients. SeminThromb Hemost 2002; 28: 577–84.21. Anderson FA Jr, Wheeler HB, Goldberg RJ et al. Apopulation-based perspective of the hospital incidenceand case-fatality rates of deep vein thrombosis and pul-monary embolism. The Worcester DVT Study. Arch In-tern Med 1991; 151: 933–8.22. Heit JA, Silverstein MD, Mohr DN et al. The epi-demiology of venous thromboembolism in the commu-nity. Thromb Haemost 2001; 86: 452–63.23. Heit JA, O’Fallon WM, PettersonTM et al. Relativeimpact of risk factors for deep vein thrombosis and pul-monary embolism. A population-based study. Arch In-tern Med 2002; 162: 1245–8.24. Samama MM. An epidemiologic study of riskfactors for deep vein thrombosis in medical outpatients:the SIRIUS study. Arch Intern Med 2000; 160:3415–20.25. Arcelus JI, Caprini JA, Monreal M et al. The man-agement and outcome of acute venous thromboembol-ism: a prospective registry including 4011 patients. JVasc Surg 2003; 38: 916–22.26. Belch JJ, Lowe GD, Ward AG et al. Prevention ofdeep vein thrombosis in medical patients by low-doseheparin. Scott Med J 1981; 26: 115–17.27. Cade JF. High risk of the critically ill for venousthromboembolism. Crit Care Med 1982; 10: 448–50.28. Cade JF, Andrews JT, Stubbs AE. Comparison ofsodium and calcium heparin in prevention of venousthromboembolism. Aust N Z J Med 1982; 12: 501–4.29. Ibarra-Pérez C, Lau-Cortés E, Colmenero-ZubiateS et al. Prevalence and prevention of deep vein throm-bosis of the lower extremities in high-risk pulmonarypatients. Angiology 1988; 39: 505–13.30. Gårdlund B. Randomised, controlled trial of low-dose heparin for prevention of fatal pulmonary embol-ism in patients with infectious diseases. Lancet 1996;347: 1357–61.31. Dahan R, Houlbert D, Caulin C et al. Prevention ofdeep vein thrombosis in elderly medical in-patients bya low molecular weight heparin: a randomized double-blind trial. Haemostasis 1986; 16: 159–64.32. Bergmann JF, Caulin C. Heparin prophylaxis inbedridden patients. Lancet 1996; 348: 205–6.33. Fraisse F, Holzapfel L, Coulaud JM et al. Nadropa-rin in the prevention of deep vein thrombosis in acutedecompensated COPD. Am J Respir Crit Care Med2000; 161: 1109–14.34. Alikhan R, Cohen AT, Combe S et al; MEDENOXStudy. Risk factors for venous thromboembolism inhospitalized patients with acute medical illness: analy-sis of the MEDENOX Study. Arch Intern Med 2004;164: 963–8.35. Alikhan R, Cohen AT, Combe S et al. Prevention ofvenous thromboembolism in medical patients with en-oxaparin: a subgroup analysis of the MEDENOXStudy. Blood Coagul Fibrinolysis 2003; 14: 341–6.36. Emerson PA, Marks P. Preventing thromboembol-ism after myocardial infarction: effect of low-dose he-parin or smoking. BMJ 1977; 1: 18–20.37. Handley AJ. Low-dose heparin after myocardial in-farction. Lancet 1972; 2: 623–4.
38. Warlow C, Terry G, Kenmure AC et al. A double-blind trial of low doses of subcutaneous heparin in theprevention of deep-vein thrombosis after myocardialinfarction. Lancet 1973; 2: 934–6.39. Wray R, Maurer B, Shillingford J. Prophylacticanticoagulant therapy in the prevention of calf-veinthrombosis after myocardial infarction. N Engl J Med1973; 288: 815–7.40. Anderson GM, Hull E. The effect of dicumarolupon the mortality and incidence of thromboemboliccomplications in congestive heart failure. Am Heart J1950; 39: 697–702.41. Kierkegaard A, Norgren L, Olsson CG et al. Inci-dence of deep vein thrombosis in bedridden non-surgi-cal patients. Acta Med Scand 1987; 222: 409–14.42. Donati MB. Cancer and thrombosis. Haemostasis1994; 24: 128–31.43. Falanga A, Donati MB. Pathogenesis of thrombosisin patients with malignancy. Int J Hematol 2001; 73:137–44.44. Sutherland DE, Weitz IC, Liebman HA. Throm-boembolic complications of cancer: epidemiology, pa-thogenesis, diagnosis, and treatment. Am J Hematol2003; 72: 43–52.45. Otten HM, Prins MH, Smorenburg SM et al. Riskassessment and prophylaxis of venous thromboembol-ism in non-surgical patients: cancer as a risk factor.Haemostasis 2000; 30 (Suppl 2): 72–6.46. Clarke-Pearson DL, Synan IS, Colemen RE et al.The natural history of postoperative venous throm-boemboli in gynaecologic oncology: a prospectivestudy of 382 patients. Am J Obstet Gynecol 1984; 148:1051–4.47. Marras LC, Geerts WH, Perry JR. The risk of ve-nous thromboembolism is increased throughout thecourse of malignant glioma.An evidence-based review.Cancer 2000; 89: 640–6.48. Lip GY, Chin BS, Blann AD. Cancer and the pro-thrombotic state. Lancet Oncol 2002; 3: 27–34.49. Halkin H, Goldberg J, Modan M et al. Reduction ofmortality in general medical in-patients by low-doseheparin prophylaxis.Ann Intern Med 1982; 96: 561–5.50. Levine MN, Gent M, Hirsh J et al. The thrombo-genic effect of anticancer drug therapy in women withstage II breast cancer. N Engl J Med 1988; 318: 404–7.51. Saphner T, Tormey DC, Gray R. Venous and arterialthrombosis in patients who received adjuvant therapyfor breast cancer. J Clin Oncol 1991; 9: 286–94.52. Levine M, Hirsh J, Gent M et al. Double-blind ran-domised trial of very-low-dose warfarin for preventionof thromboembolism in stage IV breast cancer. Lancet1994; 343: 886–9.53. Bern MM, Lokich JJ, Wallach SR et al. Very lowdoses of warfarin can prevent thrombosis in central ve-nous catheters. A randomized prospective trial. Ann In-tern Med 1990; 112: 423–8.54. Monreal M,AlastrueA, Rull M et al. Upper extrem-ity deep venous thrombosis in cancer patients with ve-nous access devices – prophylaxis with a low molecularweight heparin (Fragmin). Thromb Haemost 1996; 75:251–3.55. Randolph AG, Cook DJ, Gonzales CA et al. Bene-fit of heparin in central venous and pulmonary arterycatheters. A meta-analysis of randomized controlledtrials. Chest 1998; 113: 165–71.56. Joynt GM, Kew J, Gomersall CD et al. Deep venousthrombosis caused by femoral venous catheters in criti-cally ill adult patients. Chest 2000; 117: 178–83.57. Mian NZ, Bayly R, Schreck DM et al. Incidence ofdeep venous thrombosis associated with femoral ve-nous catheterization. Acad Emerg Med 1997; 4:1118–21.58. Prescott SM, Richards KL, Tikoff G et al. Venousthromboembolism in decompensated chronic obstruc-
tive pulmonary disease. A prospective study. Am RevRespir Dis 1981; 123: 32–6.59. Harenberg J, Kallenbach B, Martin U et al.Randomized controlled study of heparin and lowmolecular weight heparin for prevention of deep-veinthrombosis in medical patients. Thromb Res 1990; 59:639–50.60. Bergmann JF, Neuhart E. A multicenter rando-mized double-blind study of enoxaparin compared withUFH in the prevention of venous thromboembolic dis-ease in elderly in-patients bedridden for an acute medi-cal illness. The Enoxaparin in Medicine Study Group.Thromb Haemost 1996; 76: 529–34.61. Kleber F-X, Witt C, Vogel G et al, for THE-PRINCE study group.A randomized comparison of en-oxaparin with unfractionated heparin for the preventionof venous thromboembolism in medical patients withheart failure or severe respiratory disease. Am Heart J2003; 145: 614–21.62. Motykie GD, Caprini JA, Arcelus JI et al. Risk fac-tor assessment in the management of patients with sus-pected deep vein thrombosis. Int Angiol 2000; 19:47–51.63. Miehsler W, Reinisch W, Valic E et al. Is inflamma-tory bowel disease an independent and disease specificrisk factor for thromboembolism? Gut 2004; 53:542–8.64. Bernstein CN, Blanchard JF, Houston DS et al. Theincidence of deep venous thrombosis and pulmonaryembolism among patients with inflammatory boweldisease: a population-based cohort study. Thromb Hae-most 2001; 85: 430–4.65. Talbot RW, Heppell J, Dozois RR et al. Vascularcomplications of inflammatory bowel disease. MayoClin Proc 1986; 61: 140–5.66. Gaffney PR, Doyle CT, GaffneyA et al. Paradoxicalresponse to heparin in 10 patients with ulcerative coli-tis. Am J Gastroenterol 1995; 90: 220–3.67. Vrij AA, Jansen JM, Schoon EJ et al. Low molecu-lar weight heparin treatment in steroid refractory ulce-rative colitis: clinical outcome and influence on muco-sal capillary thrombi. Scand J Gastroenterol 2001; 36(Suppl 234): 41–7.68. DeMariaAN. Relative risk of cardiovascular eventsin patients with rheumatoid arthritis. Am J Cardiol2002; 89: 33D–8D.69. McCarthy ST, Turner JJ, Robertson D et al. Low-dose heparin as a prophylaxis against deep-vein throm-bosis after acute stroke. Lancet 1977; 2: 800–1.70. McCarthy ST,Turner J. Low-dose subcutaneous he-parin in the prevention of deep-vein thrombosis andpulmonary emboli after acute stroke. Age Ageing1986; 15: 84–8.71. Prins MH, Gelsema R, Sing AK et al. Prophylaxisof deep venous thrombosis with a low-molecular-weight heparin (Kabi 2165/Fragmin®) in stroke pa-tients. Haemostasis 1989; 19: 245–50.72. Turpie AGG, Levine MN, Hirsh J et al. Double-blind randomised trial of ORG 10172 low-molecular-weight heparinoid in prevention of deep-vein thrombo-sis in thrombotic stroke. Lancet 1987; 1: 523–6.73. Hillbom M, Erilä T, Sotaniemi K et al. Enoxaparinvs heparin for prevention of deep vein thrombosis inacute ischaemic stroke: a randomized, double-blindstudy. Acta Neurol Scand 2002; 106: 84–92.74. Dumas R, Woitinas F, Kutnowski M et al. A multi-centre, double-blind, randomized study to compare thesafety and efficacy of once-daily ORG 10172 andtwice-daily low-dose heparin in preventing deep-veinthrombosis in patients with acute ischaemic stroke.Age Ageing 1994; 23: 512–6.75. Sandset PM, Dahl T, Stiris M et al. A double-blindand randomized placebo-controlled trial of low mol-ecular weight heparin once daily to prevent deep-vein
Cohen et al.: Venous thromboembolism risk in medical patients
758

thrombosis in acute ischemic stroke. Semin ThrombHemost 1990; 16 (Suppl): 25–33.76. Sandercock PA, van den Belt AG, Lindley RI et al.Antithrombotic therapy in acute ischaemic stroke: anoverview of the completed randomised trials. J NeurolNeurosurg Psychiatry 1993; 56: 17–25.77. Levine MN, Raskob G, Landefeld S et al. Hem-orrhagic complications of anticoagulant treatment.Chest 2001; 119 (1 Suppl): 108S–21S.78. Mazzone C, Chiodo Grandi F, Sandercock P et al.Physical methods for preventing deep vein thrombosisin stroke (Cochrane Review). In: The Cochrane Li-brary, Issue 1, 2003. Oxford: Update Software.79. Green D, Lee MY, Ito VY et al. Fixed- vs adjusted-dose heparin in the prophylaxis of thromboembolism inspinal cord injury. JAMA 1988; 260: 1255–8.80. Green D, Lee MY, Lim AC et al. Prevention ofthromboembolism after spinal cord injury using low-molecular-weight heparin. Ann Intern Med 1990; 113:571–4.81. Vaitkus PT, Leizorovicz A, Cohen AT et al; PRE-VENT Medical Thromboprophylaxis Study Group.Mortality rates and risk factors for asymptomatic deepvein thrombosis in medical patients. Thromb Haemost2005; 93: 76–9.82. Bauer KA. The thrombophilias: well-defined riskfactors with uncertain therapeutic implications. AnnIntern Med 2001; 135: 367–73.83. Laffan M, Tuddenham E. Science, medicine, andthe future: assessing thrombotic risk. BMJ 1998; 317:520–3.84. Bouthier J. The venous thrombotic risk in nonsur-gical patients. Drugs 1996; 52 (Suppl 7): 16–29.85. Gensini GF, Prisco D, Falciani M et al. Identifica-tion of candidates for prevention of venous throm-boembolism. SeminThromb Hemost 1997; 23: 55–67.86. Goldhaber SZ, Savage DD, Garrison RJ et al. Riskfactors for pulmonary embolism. The FraminghamStudy. Am J Med 1983; 74: 1023–8.87. Goldhaber SZ, Grodstein F, Stampfer MJ et al. Aprospective study of risk factors for pulmonary embo-lism in women. JAMA 1997; 277: 642–5.
88. Hansson PO, Eriksson H, Welin L et al. Smokingand abdominal obesity. Risk factors for venous throm-boembolism among middle-aged men: “the study ofmen born in 1913”. Arch Intern Med 1999; 159:1886–90.89. Abdollahi M, Cushman M, Rosendaal FR. Obesity:risk of venous thrombosis and the interaction with co-agulation factor levels and oral contraceptive use.Thromb Haemost 2003; 89: 493–8.90. Leone G, Sica S, Chiusolo P et al. Blood cell dis-eases and thrombosis. Haematologica 2001; 86:1236–44.91. Daly E, Vessey MP, Hawkins MM et al. Risk of ve-nous thromboembolism in users of hormone replace-ment therapy. Lancet 1996; 348: 977–80.92. Daly E, Vessey MP, Painter R et al. Case-controlstudy of venous thromboembolism in users of hormonereplacement therapy. Lancet 1996; 348: 1027.93. Grady D, Wenger NK, Herrington D et al. Post-menopausal hormone therapy increases risk for venousthromboembolic disease. The Heart and Estrogen/pro-gestin Replacement Study. Ann Intern Med 2000; 132:689–96.94. Hulley S, Furberg C, Barrett-Connor E et al; HERSResearch Group. Noncardiovascular disease outcomesduring 6.8 years of hormone therapy. Heart and Es-trogen/progestin Replacement Study follow-up (HERSII). JAMA 2002; 288: 58–66.95. Vandenbroucke JP, Rosing J, Bloemenkamp KW etal. Oral contraceptives and the risk of venous thrombo-sis. N Engl J Med 2001; 344: 1527–35.96. Orth SR, Ritz E. The nephrotic syndrome. N Engl JMed 1998; 338: 1202–11.97. Bates SM. Treatment and prophylaxis of venousthromboembolism during pregnancy. Thromb Res2003; 108: 97–106.98. Hirsch DR, Ingenito EP, Goldhaber SZ. Prevalenceof deep venous thrombosis among patients in medicalintensive care. JAMA 1995; 274: 335–7.99. Lassen MR, Borris LC, Backs S et al. Clinical limi-tations of risk assessment models. Blood Coagul Fibri-nolysis 1999; 10 (Suppl 2): S45–51.
100. Salzman EW, Hirsh J. Prevention of venousthromboembolism. In: Coleman RW, Hirsh J, MarderVJ, Salzman EW, Eds. Hemostasis and Thrombosis:Basic Principles and Clinical Practice. Lippincott1982; 986.101. Hirsh J, Guyatt G, Albers GW et al. The SeventhACCP Conference on Antithrombotic and Thrombo-lytic Therapy: evidence-based guidelines. Chest 2004;126: 172S–173S.102. Mismetti P, Laporte-Simitsidis S, Tardy B et al.Prevention of venous thromboembolism in internalmedicine with unfractionated heparin or low-molecu-lar-weight heparins: a meta-analysis of randomisedclinical trials. Thromb Haemost 2000; 83: 14–9.103. Alikhan R, Cohen AT. A safety analysis of throm-boprophylaxis in acute medical illness. Thromb Hae-most 2003; 89: 590–1.104. Lechler E, Schramm W, Flosbach CW.The venousthrombotic risk in non-surgical patients: epidemiologi-cal data and efficacy/safety profile of a low-molecular-weight heparin (enoxaparin). The PRIME StudyGroup. Haemostasis 1996; 26 (Suppl 2): 49–56.105. Girolami B, Prandoni P, Stefani PM et al.The inci-dence of heparin-induced thrombocytopenia in hospi-talized medical patients treated with subcutaneous un-fractionated heparin: a prospective cohort study. Blood2003; 101: 2955–9.106. Warkentin TE, Levine MN, Hirsh J et al. Heparin-induced thrombocytopenia in patients treated with low-molecular-weight heparin or unfractionated heparin.N Engl J Med 1995; 332: 1330–5.107. Harenberg J, Roebruck P, Heene DL. Subcu-taneous low-molecular-weight heparin versus standardheparin and the prevention of thromboembolism inmedical inpatients. The Heparin Study in InternalMedicine Group. Haemostasis 1996; 26: 127–39.108. Hull R, Schellong S, Tapson V et al. Extendedthromboprophylaxis with enoxaparin in acutely illmedical patients with prolonged periods of immobili-sation: the EXCLAIM study. J Thromb Haemost 2003;1 (Suppl. 1): OC397 (Abstract).
Cohen et al.:Venous thromboembolism risk in medical patients
759




















