
Venous Thromboembolism Risk and Prophylaxis in the Acute Care Hospital Setting (ENDORSE Survey)
22
www.medscape.com Abstract and Introduction Abstract Objective: To evaluate venous thromboembolism (VTE) risk in patients who underwent a major operation, including the use of, and factors influencing, American College of Chest Physicians-recommended types of VTE prophylaxis. Summary background data: The Epidemiologic International Day for the Evaluation of Patients at Risk for Venous Thromboembolism in the Acute Hospital Care Setting (ENDORSE) survey, conducted in 358 hospitals in 32 countries, reported that globally, more than 40% of at-risk patients do not receive VTE prophylaxis. Limited data are available regarding VTE prophylaxis practices according to surgery type and patient characteristics. Methods: Patients aged ≥18 years undergoing major surgery were included in this prespecified subanalysis. VTE risk and use of prophylaxis were determined from hospital medical records according to the 2004 American College of Chest Physicians guidelines. Multivariable analyses were performed to identify factors associated with VTE prophylaxis use. Results: Of the 18,461 patients in ENDORSE who had undergone major surgery, 17,084 (92.5%) were at-risk for VTE and 10,638 (62.3%) received prophylaxis. Use of prophylaxis varied according to major surgery type from 86.0% for orthopedic surgery to 53.8% in urologic/gynecologic and 53.6% in other procedures. Major orthopedic surgery was most strongly associated with prophylaxis use (hip replacement: odds ratio 6.2, 95% confidence interval [CI] 5.0–7.6; knee replacement: odds ratio 5.9, 95% CI 4.6–7.8). Conclusions: The majority of surgical patients are at high-risk for VTE. Despite long-standing recognition of the high-risk for VTE in surgical patients, thromboprophylaxis remains underutilized. Introduction Venous thromboembolism (VTE) remains an important clinical problem in surgical practice despite the benefits of pharmacological thromboprophylaxis for the prevention of deep vein thrombosis (DVT) and fatal pulmonary embolism (PE) having been established more than 30 years ago. [1–3] Furthermore, as many as one-third of these thrombi could lead to PE, which is recognized as the most common preventable cause of inpatient mortality. [4] VTE prophylaxis reduces the relative risk of postoperative DVT by up to 75%, and reduces the relative risk for nonfatal PE and fatal PE in surgical patients by 40% and 64%, respectively. [5] Prophylaxis also reduces all- cause mortality in this patient population. [5] Evidence-based guidelines from the American College of Chest Physicians (ACCP) categorize VTE risk and recommend prophylaxis regimens according to type of operation and known patient risk factors. [6] General surgery is associated with moderate risk for VTE; operations for cancer are associated with higher risk; and major orthopedic surgery is considered to put patients at the highest risk with up to an 80% chance of developing postoperative DVT. [6,7] Despite the solid body of evidence that validates both the risk for VTE and benefits of thromboprophylaxis in surgical patients, the recent Epidemiologic International Day for the Evaluation of Patients at Risk for Venous Thromboembolism in the Acute Hospital Care Setting (ENDORSE) survey reported that only 59% of patients admitted to surgical wards and considered at-risk for VTE received thromboprophylaxis. [6,8] From Annals of Surgery Venous Thromboembolism Risk and Prophylaxis in the Acute Care Hospital Setting (ENDORSE Survey): Findings in Surgical Patients Ajay K. Kakkar, MD, PhD; Alexander T. Cohen, MD; Victor F. Tapson, MD; Jean-Francois Bergmann, MD; Samuel Z. Goldhaber, MD; Bruno Deslandes; Wei Huang, MS; Frederick A. Anderson, Jr., PhD Posted: 04/02/2010; Annals of Surgery. 2010;251(2):330-338. © 2010 Lippincott Williams & Wilkins Page 1 of 22 Venous Thromboembolism Risk and Prophylaxis in the Acute Care Hospital Setting (... 4/18/2010 http://www.medscape.com/viewarticle/718702_print
Transcript of Venous Thromboembolism Risk and Prophylaxis in the Acute Care Hospital Setting (ENDORSE Survey)

www.medscape.com
Abstract and Introduction
Abstract
Objective: To evaluate venous thromboembolism (VTE) risk in patients who underwent a major operation,
including the use of, and factors influencing, American College of Chest Physicians-recommended types of VTE
prophylaxis.
Summary background data: The Epidemiologic International Day for the Evaluation of Patients at Risk for
Venous Thromboembolism in the Acute Hospital Care Setting (ENDORSE) survey, conducted in 358 hospitals
in 32 countries, reported that globally, more than 40% of at-risk patients do not receive VTE prophylaxis. Limited
data are available regarding VTE prophylaxis practices according to surgery type and patient characteristics.
Methods: Patients aged ≥18 years undergoing major surgery were included in this prespecified subanalysis.
VTE risk and use of prophylaxis were determined from hospital medical records according to the 2004 American
College of Chest Physicians guidelines. Multivariable analyses were performed to identify factors associated
with VTE prophylaxis use.
Results: Of the 18,461 patients in ENDORSE who had undergone major surgery, 17,084 (92.5%) were at-risk
for VTE and 10,638 (62.3%) received prophylaxis. Use of prophylaxis varied according to major surgery type
from 86.0% for orthopedic surgery to 53.8% in urologic/gynecologic and 53.6% in other procedures. Major
orthopedic surgery was most strongly associated with prophylaxis use (hip replacement: odds ratio 6.2, 95%
confidence interval [CI] 5.0–7.6; knee replacement: odds ratio 5.9, 95% CI 4.6–7.8).
Conclusions: The majority of surgical patients are at high-risk for VTE. Despite long-standing recognition of the
high-risk for VTE in surgical patients, thromboprophylaxis remains underutilized.
Introduction
Venous thromboembolism (VTE) remains an important clinical problem in surgical practice despite the benefits
of pharmacological thromboprophylaxis for the prevention of deep vein thrombosis (DVT) and fatal pulmonary
embolism (PE) having been established more than 30 years ago.[1–3] Furthermore, as many as one-third of
these thrombi could lead to PE, which is recognized as the most common preventable cause of inpatient
mortality.[4]
VTE prophylaxis reduces the relative risk of postoperative DVT by up to 75%, and reduces the relative risk for
nonfatal PE and fatal PE in surgical patients by 40% and 64%, respectively.[5] Prophylaxis also reduces all-
cause mortality in this patient population.[5]
Evidence-based guidelines from the American College of Chest Physicians (ACCP) categorize VTE risk and
recommend prophylaxis regimens according to type of operation and known patient risk factors.[6] General
surgery is associated with moderate risk for VTE; operations for cancer are associated with higher risk; and
major orthopedic surgery is considered to put patients at the highest risk with up to an 80% chance of
developing postoperative DVT.[6,7] Despite the solid body of evidence that validates both the risk for VTE and
benefits of thromboprophylaxis in surgical patients, the recent Epidemiologic International Day for the Evaluation
of Patients at Risk for Venous Thromboembolism in the Acute Hospital Care Setting (ENDORSE) survey
reported that only 59% of patients admitted to surgical wards and considered at-risk for VTE received
thromboprophylaxis.[6,8]
From Annals of Surgery
Venous Thromboembolism Risk and Prophylaxis in the Acute Care Hospital Setting (ENDORSE Survey): Findings in Surgical PatientsAjay K. Kakkar, MD, PhD; Alexander T. Cohen, MD; Victor F. Tapson, MD; Jean-Francois Bergmann, MD; Samuel Z. Goldhaber, MD; Bruno Deslandes; Wei Huang, MS; Frederick A. Anderson, Jr., PhD
Posted: 04/02/2010; Annals of Surgery. 2010;251(2):330-338. © 2010 Lippincott Williams & Wilkins
Page 1 of 22Venous Thromboembolism Risk and Prophylaxis in the Acute Care Hospital Setting (...
4/18/2010http://www.medscape.com/viewarticle/718702_print

In this analysis of the ENDORSE surgical population, we report VTE risk, rates of prophylaxis, and the influence
of site of operation, age, bleeding risk, and presence of malignancy on prophylaxis practices in patients who
underwent surgery in acute care hospitals. In addition, we evaluate the key factors associated with the decision
to provide VTE prophylaxis to this patient population.
Methods
Study Design
The ENDORSE survey was a cross-sectional, global survey of VTE risk and prophylaxis provision in the acute
care hospital setting. The study design has been published in detail elsewhere.[8] In this prespecified, surgical
population analysis, we evaluated VTE risk and use of recommended prophylaxis in patients who had
undergone a major surgical procedure by the day of survey according to the 2004 ACCP guidelines.[6]
Study Population
Eligible patients were enrolled between August 2006 and January 2007 from 358 participating hospitals across
32 countries in 6 continents.[8] Participating hospitals contained at least 50 acute care beds, routinely performed
major surgical procedures, and admitted patients for the treatment of acute medical illnesses. Ethics committee
approval for the survey was obtained according to national and local regulations.
Patients aged ≥18 years admitted to a surgical ward and undergoing elective or emergency major surgery,
defined as an operation which required general or epidural anesthesia and lasting ≥45 minutes, were eligible for
inclusion in this surgical population analysis.
Data Collection
Data including patient demographics, admission and postadmission diagnoses, surgery type, surgical indication,
VTE risk factors (as defined in the 2004 ACCP guidelines),[6] bleeding risk factors, duration of stay, and VTE
prophylaxis type were collected from a review of hospital charts by trained data abstractors.[8]
Assessment of VTE Risk and Prophylaxis
VTE risk and use of recommended prophylaxis were evaluated according to the 2004 ACCP guideline criteria
for surgical patients.[6]
Patients were considered to be at sufficient VTE risk to warrant prophylaxis if they: had multiple risk factors for
VTE at the time of surgery, underwent hip or knee arthroplasty, or were admitted for major trauma or spinal cord
injury; underwent surgery aged >60 years with no additional risk factors for VTE, or were aged 40 to 60 years
with risk factors; or underwent surgery and were aged 40 to 60 years or underwent minor surgery and had
additional risk factors for VTE.[6]
Recommended types of VTE prophylaxis included pharmacological agents (low molecular weight heparin,
unfractionated heparin, or vitamin K antagonists), mechanical prophylaxis (graduated compression stockings or
intermittent pneumatic compression), or a combination of both. Only the type of prophylaxis (not dose or
duration) was considered.
Analysis of Factors Influencing VTE Risk and Prophylaxis Use
Surgical procedures were grouped into the following categories: major orthopedic (hip replacement, knee
replacement, hip fracture repair), abdominal/thoracic (colon/small bowel, rectosigmoid, gastric, hepatobiliary,
thoracic), vascular, urologic/gynecologic, and other (curative arthroscopy, other orthopedic trauma, and other
surgeries).
Patient medical histories were used to determine the number of VTE risk factors present before and during
hospitalization. Defined risk factors (in addition to surgical procedure performed) include: previous VTE,
admission with major trauma, significant medical comorbidity, and immobilization.[6]
Page 2 of 22Venous Thromboembolism Risk and Prophylaxis in the Acute Care Hospital Setting (...
4/18/2010http://www.medscape.com/viewarticle/718702_print

Use of Prophylaxis According to Bleeding Risk and the Presence of Active Malignancy
Patients were considered to have a high bleeding risk, sufficient to be a contraindication to pharmacological
prophylaxis, if they presented with or developed: intracranial hemorrhage, hepatic impairment, bleeding at
hospital admission, active gastroduodenal ulcer, or a known bleeding disorder.[9] Moderate bleeding risk was
defined as patients who did not have high bleeding risk who had any of the following at current admission:
significant renal impairment, low platelet count (<100,000/µL), use of aspirin or NSAID (continued during current
admission). Patients who presented none of the above at current admission were considered at low risk for
bleeding.
Use of VTE prophylaxis in patients with cancer was assessed in those who underwent abdominal or
urologic/gynecologic surgery. Patients were subdivided according to surgical indication: for the cancer itself
(surgery for cancer), unrelated to the cancer (surgery with cancer), or without a cancer diagnosis (no/unknown
cancer).
Statistical Analysis
Quantitative data were summarized as median values with interquartile range. Categorical data were
summarized as the number and proportion of the population. Summary data are reported globally, by country,
and by type of surgical procedure. For the main outcomes, 95% confidence intervals (CI) were calculated.
Two multivariable logistic regression analyses were performed to assess the key factors associated with the use
of recommended types of prophylaxis. The first analysis included the following candidate variables: baseline
characteristics, type of surgery, VTE risk factors, and bleeding risk factors. To further investigate the potential
role of nonsurgery type-related risk factors in the association between prophylaxis use and comorbidities a
second multivariable analysis was performed, using the above candidate variables, excluding surgery type.
Criteria for entry and removal of candidate variables in the stepwise analysis were assigned a significance level
of P < 0.05. Adjusted odds ratios and 95% CI were reported.
SAS version 9.1 was used for all statistical analyses.
Results
Of the total 68,183 evaluable patients enrolled in the ENDORSE study, 30,827 (45.2%) were classified as
evaluable surgical patients (Fig. 1).[8] On the day of the survey, 18,461 evaluable surgical patients had
undergone major surgery. Of these, 17,084 (92.5%) were considered at risk for VTE and of these 10,638
(62.3%) received ACCP-recommended types of VTE prophylaxis.
Page 3 of 22Venous Thromboembolism Risk and Prophylaxis in the Acute Care Hospital Setting (...
4/18/2010http://www.medscape.com/viewarticle/718702_print

Figure 1. Study population included in the ENDORSE survey.*VTE risk defined according to 2004 ACCP
guidelines.6
Patient Baseline Characteristics
Baseline characteristics of patients who underwent surgery and were at-risk of VTE are shown in Table 1. The
most common preadmission risk factors for VTE were obesity, chronic heart failure, and chronic pulmonary
disease. After hospital admission, the most common VTE risk factors, in addition to major operation, were
complete immobilization, reduced mobility (with bathroom privileges), and admission to an intensive care unit
(Table 1).
Table 1. Baseline Characteristics of Patients Who Have Undergone Surgery and Are At-Risk
for VTE
Total
n (%)
Surgery Type, n (%)
Major
Orthopedic Abdominal/Thoracic Urologic/Gynecologic Vascular Other
Page 4 of 22Venous Thromboembolism Risk and Prophylaxis in the Acute Care Hospital Setting (...
4/18/2010http://www.medscape.com/viewarticle/718702_print

Patient
Characteristics*
N =
17,084 n = 2300 n = 4527 n = 2344 n = 1012
n =
6901
No. females, (%)8120
(48.3)
1,456
(64.4)2069 (46.5) 1236 (53.6)
407
(41.0)
2952
(43.4)
Median age,
years (range)
61.0
(48.0–
73.0)
72.0 (62.0–
80.0)62.0 (50.0–73.0) 60.0 (47.0–71.0)
66.0
(55.5–
74.0)
55.0
(43.0
–
69.0)
Median length of
hospitalization up
to survey date,
days (range)
7.0
(3.0–
14.0)
6.0 (3.0–
12.0)7.0 (3.0–15.0) 5.0 (2.0–9.0)
8.0 (3.0–
16.0)
7.0
(3.0–
14.0)
Median body
mass index, kg/m2
(range)
26.3
(23.4–
30.3)
27.7 (24.5–
31.7)25.8 (23.0–29.9) 26.0 (23.5–29.4)
26.4
(23.6–
29.5)
26.1
(23.1
–
30.0)
Preadmission
risk factors for
VTE*, n (%)
N =
16,143 n = 2202 n = 4345 n = 2231 n = 994
n =
6371
Previous VTE425
(2.6)77 (3.5) 130 (3.0) 45 (2.0) 32 (3.2)
141
(2.2)
Thrombophilia41
(0.3)5 (0.2) 8 (0.2) 7 (0.3) 2 (0.2)
19
(0.3)
Varicose veins or
venous
insufficiency
1213
(7.5)199 (9.0) 265 (6.1) 173 (7.8)
195
(19.6)
381
(6.0)
Postmenopausal
hormone
replacement
therapy
134
(0.8)25 (1.1) 31 (0.7) 34 (1.5) 3 (0.3)
41
(0.6)
Chronic
pulmonary disease
1387
(8.6)210 (9.5) 449 (10.3) 157 (7.0)
116
(11.7)
455
(7.1)
Long-term
immobility
386
(2.4)58 (2.6) 73 (1.7) 26 (1.2) 35 (3.5)
194
(3.0)
Pregnancy
(within 3 months)
56
(0.3)0 8 (0.2) 33 (1.5) 1 (0.1)
14
(0.2)
Obesity1758
(10.9)326 (14.8) 486 (11.2) 225 (10.1)
121
(12.2)
600
(9.4)
Contraceptives151
(0.9)2 (0.1) 37 (0.9) 63 (2.8) 6 (0.6)
43
(0.7)
Chronic heart
failure
1390
(8.6)210 (9.5) 339 (7.8) 155 (6.9)
191
(19.2)
495
(7.8)
VTE risk during
hospitalization
N =
17,084 n = 2300 n = 4527 n = 2344 n = 1012
n =
6901
Page 5 of 22Venous Thromboembolism Risk and Prophylaxis in the Acute Care Hospital Setting (...
4/18/2010http://www.medscape.com/viewarticle/718702_print

Admitted to
critical care unit
4207
(24.6)286 (12.4) 1635 (36.1) 318 (13.6)
383
(37.8)
1585
(23.0)
Central venous
catheter
2909
(17.0)158 (6.9) 1229 (27.1) 191 (8.1)
308
(30.4)
1023
(14.8)
Mechanical
ventilation
2244
(13.1)121 (5.3) 916 (20.2) 126 (5.4)
227
(22.4)
854
(12.4)
Immobile with
bathroom
privileges
4056
(23.7)565 (24.6) 1066 (23.5) 533 (22.7)
207
(20.5)
1685
(24.4)
Complete
immobilization
6646
(38.9)
1162
(50.5)1755 (38.8) 704 (30.0)
427
(42.2)
2598
(37.6)
Surgery for
cancer
2631
(15.4)10 (0.4) 1253 (27.7) 676 (28.8) 4 (0.4)
688
(10.0)
Cancer (active)212
(1.2)24 (1.0) 66 (1.5) 45 (1.9) 9 (0.9)
68
(1.0)
No/unknown
cancer
14,241
(83.4)
2266
(98.5)3208 (70.9) 1623 (69.2)
999
(98.7)
6145
(89.0)
*Data on some patient characteristics and prehospital admission risk factors for VTE were
unavailable for some surgical patients.
Table 1. Baseline Characteristics of Patients Who Have Undergone Surgery and Are At-Risk
for VTE
Total
n (%)
Surgery Type, n (%)
Major
Orthopedic Abdominal/Thoracic Urologic/Gynecologic Vascular Other
Patient
Characteristics*
N =
17,084 n = 2300 n = 4527 n = 2344 n = 1012
n =
6901
No. females, (%)8120
(48.3)
1,456
(64.4)2069 (46.5) 1236 (53.6)
407
(41.0)
2952
(43.4)
Median age,
years (range)
61.0
(48.0–
73.0)
72.0 (62.0–
80.0)62.0 (50.0–73.0) 60.0 (47.0–71.0)
66.0
(55.5–
74.0)
55.0
(43.0
–
69.0)
Median length of
hospitalization up
to survey date,
days (range)
7.0
(3.0–
14.0)
6.0 (3.0–
12.0)7.0 (3.0–15.0) 5.0 (2.0–9.0)
8.0 (3.0–
16.0)
7.0
(3.0–
14.0)
Median body
mass index, kg/m2
(range)
26.3
(23.4–
30.3)
27.7 (24.5–
31.7)25.8 (23.0–29.9) 26.0 (23.5–29.4)
26.4
(23.6–
29.5)
26.1
(23.1
–
30.0)
Preadmission
risk factors for
VTE*, n (%)
N =
16,143 n = 2202 n = 4345 n = 2231 n = 994
n =
6371
Page 6 of 22Venous Thromboembolism Risk and Prophylaxis in the Acute Care Hospital Setting (...
4/18/2010http://www.medscape.com/viewarticle/718702_print

Previous VTE425
(2.6)77 (3.5) 130 (3.0) 45 (2.0) 32 (3.2)
141
(2.2)
Thrombophilia41
(0.3)5 (0.2) 8 (0.2) 7 (0.3) 2 (0.2)
19
(0.3)
Varicose veins or
venous
insufficiency
1213
(7.5)199 (9.0) 265 (6.1) 173 (7.8)
195
(19.6)
381
(6.0)
Postmenopausal
hormone
replacement
therapy
134
(0.8)25 (1.1) 31 (0.7) 34 (1.5) 3 (0.3)
41
(0.6)
Chronic
pulmonary disease
1387
(8.6)210 (9.5) 449 (10.3) 157 (7.0)
116
(11.7)
455
(7.1)
Long-term
immobility
386
(2.4)58 (2.6) 73 (1.7) 26 (1.2) 35 (3.5)
194
(3.0)
Pregnancy
(within 3 months)
56
(0.3)0 8 (0.2) 33 (1.5) 1 (0.1)
14
(0.2)
Obesity1758
(10.9)326 (14.8) 486 (11.2) 225 (10.1)
121
(12.2)
600
(9.4)
Contraceptives151
(0.9)2 (0.1) 37 (0.9) 63 (2.8) 6 (0.6)
43
(0.7)
Chronic heart
failure
1390
(8.6)210 (9.5) 339 (7.8) 155 (6.9)
191
(19.2)
495
(7.8)
VTE risk during
hospitalization
N =
17,084 n = 2300 n = 4527 n = 2344 n = 1012
n =
6901
Admitted to
critical care unit
4207
(24.6)286 (12.4) 1635 (36.1) 318 (13.6)
383
(37.8)
1585
(23.0)
Central venous
catheter
2909
(17.0)158 (6.9) 1229 (27.1) 191 (8.1)
308
(30.4)
1023
(14.8)
Mechanical
ventilation
2244
(13.1)121 (5.3) 916 (20.2) 126 (5.4)
227
(22.4)
854
(12.4)
Immobile with
bathroom
privileges
4056
(23.7)565 (24.6) 1066 (23.5) 533 (22.7)
207
(20.5)
1685
(24.4)
Complete
immobilization
6646
(38.9)
1162
(50.5)1755 (38.8) 704 (30.0)
427
(42.2)
2598
(37.6)
Surgery for
cancer
2631
(15.4)10 (0.4) 1253 (27.7) 676 (28.8) 4 (0.4)
688
(10.0)
Cancer (active)212
(1.2)24 (1.0) 66 (1.5) 45 (1.9) 9 (0.9)
68
(1.0)
No/unknown
cancer
14,241
(83.4)
2266
(98.5)3208 (70.9) 1623 (69.2)
999
(98.7)
6145
(89.0)
Page 7 of 22Venous Thromboembolism Risk and Prophylaxis in the Acute Care Hospital Setting (...
4/18/2010http://www.medscape.com/viewarticle/718702_print

The frequency of contraindications to pharmacological prophylaxis in surgical patients is shown in Table 2.[9]
Overall, 9.2% of surgical patients at-risk of VTE presented with potential contraindications to anticoagulation.
The most common contraindication was bleeding at the time of hospital admission.
VTE Risk and Prophylaxis According to Surgery Type
The proportion of patients at risk for VTE who received recommended prophylaxis ranged from 86.0% in
patients undergoing major orthopedic surgery to 53.8% in urologic/gynecologic and 53.6% in other procedures
(Table 3).
*Data on some patient characteristics and prehospital admission risk factors for VTE were
unavailable for some surgical patients.
Table 2. Contraindications to Anticoagulation in Patients Who Have Undergone Surgery and
Are at Risk for Venous Thromboembolism
Total, n
(%)(N =
17,084)
Surgery Type, n (%)
Major
Orthopedic
(n = 2300)
Abdominal/Thoracic
(n = 4527)
Urologic/Gynecologic
(n = 2344)
Vascular
(n =
1012)
Other
(n =
6901)
Contraindications to anticoagulant prophylaxis*
Intracranial
hemorrhage
312
(1.8)6 (0.3) 12 (0.3) 0 20 (2.0)
274
(4.0)
Known
bleeding
disorder
(congenital or
acquired)
77 (0.5) 8 (0.3) 27 (0.6) 7 (0.3) 2 (0.2)33
(0.5)
Clinically
relevant hepatic
impairment
305
(1.8)18 (0.8) 192 (4.2) 15 (0.6) 8 (0.8)
72
(1.0)
Bleeding at
hospital
admission
836
(4.9)51 (2.2) 230 (5.1) 165 (7.0) 44 (4.3)
346
(5.0)
Active
gastroduodenal
Ulcer
206
(1.2)14 (0.6) 150 (3.3) 6 (0.3) 8 (0.8)
28
(0.4)
Additional bleeding risk factors
Significant
renal
impairment
811
(4.7)63 (2.7) 188 (4.2) 194 (8.3)
104
(10.3)
262
(3.8)
Low platelet
count
(<100,000/µL)
259
(1.5)28 (1.2) 91 (2.0) 17 (0.7) 21 (2.1)
102
(1.5)
*Defined in accordance with reference 9.
Page 8 of 22Venous Thromboembolism Risk and Prophylaxis in the Acute Care Hospital Setting (...
4/18/2010http://www.medscape.com/viewarticle/718702_print

Table 3. VTE Risk and Prophylaxis According to Type of Surgery and by Country
Country
Surgery Types, n (%)
Major Orthopedic Abdominal/Thoracic Urologic/Gynecologic Vascular Other
At-
Risk
for
VTE
At-Risk
Receiving
Px
At-
Risk
for
VTE
At-Risk
Receiving
Px
At-Risk
for VTE
At-Risk
Receiving
Px
At-
Risk
for
VTE
At-Risk
Receiving
Px
At-
Risk
for
VTE
Receiving
Algeria (n =
252)
23
(100.0)
23
(100.0)
55
(93.2)31 (56.4)
39
(90.7)33 (84.6)
2
(100)1 (50)
110
(88)73
Australia (n
= 371)
73
(100.0)69 (94.5)
86
(98.9)72 (83.7)
33
(97.1)19 (57.6)
16
(100)9 (56.3)
157
(97.5)
Bangladesh
(n = 491)
4
(100.0)0
114
(58.2)0
77
(57.0)0
2
(100)0
131
(85.1)
Brazil (n =
417)
19
(100.0)13 (68.4)
100
(93.5)53 (53.0)
62
(84.9)16 (25.8)
54
(98.2)30 (55.6)
149
(91.4)
Bulgaria (n
= 867)
113
(100.0)
109
(96.5)
215
(92.3)164 (76.3)
140
(90.9)77 (55.0)
26
(100)21 (80.8)
318
(93.3)
Colombia
(n = 151)
12
(100.0)6 (50.0)
41
(85.4)17 (41.5)
34
(94.4)10 (29.4)
10
(90.9)9 (90)
42
(95.5)16 (38.1)
Czech
Republic (n
= 548)
110
(100.0)
101
(91.8)
105
(92.9)81 (77.1)
90
(95.7)67 (74.4)
22
(95.7)14 (63.6)
194
(93.3)
Egypt (n =
266)
8
(100.0)6 (75.0)
68
(81.9)24 (35.3)
29
(70.7)10 (34.5)
11
(91.7)6 (54.5)
102
(83.6)31 (30.4)
France (n =
614)
85
(100.0)73 (85.9)
196
(94.7)156 (79.6)
49
(94.2)32 (65.3)
21
(100)9 (42.9)
235
(94.4)
Germany (n
= 826)
206
(100.0)
198
(96.1)
134
(92.4)129 (96.3)
105
(91.3)105 (100.0)
87
(98.9)67 (77.0)
254
(93.4)
Greece (n
= 478)
78
(100.0)77 (98.7)
114
(92.7)86 (75.4)
83
(95.4)49 (59.0)
34
(94.4)23 (67.6)
135
(87.7)97 (71.9)
Hungary (n
= 249)
28
(100.0)
28
(100.0)
77
(85.6)74 (96.1)
29
(96.7)25 (86.2)
31
(100)31 (100)
67
(95.7)49 (73.1)
India (n =
584)
30
(100.0)8 (26.7)
117
(84.8)39 (33.3)
76
(84.4)5 (6.6)
29
(93.5)14 (48.3)
274
(92.9)38 (13.9)
Ireland (n =
163)
22
(100.0)18 (81.8)
38
(84.4)34 (89.5)
15
(93.8)10 (66.7)
12
(100)4 (33.3)
65
(95.6)34 (52.3)
Kuwait (n =
76)NA NA
22
(62.9)13 (59.1) 1 (50.0) 0 3 (75) 1 (33.3)
28
(80)15
Mexico (n =
312)
11
(100.0)9 (81.8)
84
(78.5)36 (42.9)
38
(82.6)10 (26.3)
17
(100)13 (76.5)
121
(92.4)54 (44.6)
Pakistan (n
= 342)
3
(100.0)1 (33.3)
70
(67.3)8 (11.4)
57
(58.2)3 (5.3) 6 (75) 2 (33.3)
116
(89.9)14
Page 9 of 22Venous Thromboembolism Risk and Prophylaxis in the Acute Care Hospital Setting (...
4/18/2010http://www.medscape.com/viewarticle/718702_print

Of the patients admitted for emergency surgery (n = 4269) and elective surgery (n = 14,192), 3854 (90.3%) and
13,230 (93.2%) were at risk for VTE, respectively. However, only 57.9% of emergency and 66.3% of elective
surgery patients received any prophylaxis.
Poland (n =
550)
74
(100.0)72 (97.3)
135
(93.1)96 (71.1)
77
(93.9)30 (39.0)
55
(96.5)43 (78.2)
164
(85.4)
Portugal (n
= 465)
57
(100.0)48 (84.2)
114
(92.7)82 (71.9)
73
(92.4)35 (47.9)
11
(100)6 (54.5)
187
(95.9)
Romania (n
= 1489)
124
(100.0)
117
(94.4)
385
(95.3)257 (66.8)
248
(95.8)176 (71.0)
43
(93.5)25 (58.1)
622
(94.8)
Russia (n =
1277)
61
(100.0)39 (63.9)
249
(85.3)93 (37.3)
155
(83.3)47 (30.3)
69
(94.5)49 (71)
591
(88.9)
Saudi
Arabia (n =
146)
13
(100.0)5 (38.5)
16
(53.3)7 (43.8) 7 (87.5) 3 (42.9)
3
(100)1 (33.3)
76
(82.6)28 (36.8)
Slovakia (n
= 548)
81
(100.0)78 (96.3)
111
(88.8)98 (88.3)
114
(93.4)70 (61.4)
23
(100)16 (69.6)
179
(90.9)
Spain (n =
657)
137
(100.0)
136
(99.3)
170
(98.8)148 (87.1)
108
(99.1)77 (71.3)
35
(97.2)23 (65.7)
193
(95.1)
Switzerland
(n = 752)
94
(100.0)84 (89.4)
207
(94.1)173 (83.6)
71
(95.9)64 (90.1)
41
(95.3)29 (70.7)
294
(91.6)238 (81)
Thailand (n
= 543)
27
(100.0)0
132
(95.7)1 (0.8)
68
(86.1)0
15
(100)0
275
(96.8)
Tunisia (n =
103)NA NA
51
(87.9)46 (90.2)
10
(83.3)9 (90.0)
5
(100)0
23
(82.1)15 (65.2)
Turkey (n =
299)
40
(100.0)24 (60.0)
85
(95.5)37 (43.5)
30
(90.9)4 (13.3) 8 (80) 5 (62.5)
124
(97.6)
United Arab
Emirates (n
= 125)
13
(100.0)8 (61.5)
16
(59.3)6 (37.5)
11
(64.7)5 (45.5) NA NA
64
(94.1)29
United
Kingdom (n
= 1272)
281
(100.0)
218
(77.6)
340
(92.9)290 (85.3)
143
(94.7)105 (73.4)
66
(100)52 (78.8)
385
(94.4)
United
States (n =
3044)
471
(100.0)
409
(86.8)
825
(95.8)668 (81.0)
248
(91.9)164 (66.1)
250
(100)
171
(68.4)
1135
(95.2)
Venezuela
(n = 184)
2
(100.0)2 (100.0)
55
(94.8)4 (7.3)
24
(92.3)1 (4.2)
5
(100)2 (40)
91
(97.8)19 (20.9)
Total (N =
18,461)
2300
(100.0)
1979
(86.0)
4527
(90.0)3023 (66.8)
2344
(88.4)1261 (53.8)
1012
(97.5)
676
(66.8)
6901
(92.7)
NA indicates not applicable; Px, prophylaxis; VTE, venous thromboembolism.
Page 10 of 22Venous Thromboembolism Risk and Prophylaxis in the Acute Care Hospital Settin...
4/18/2010http://www.medscape.com/viewarticle/718702_print
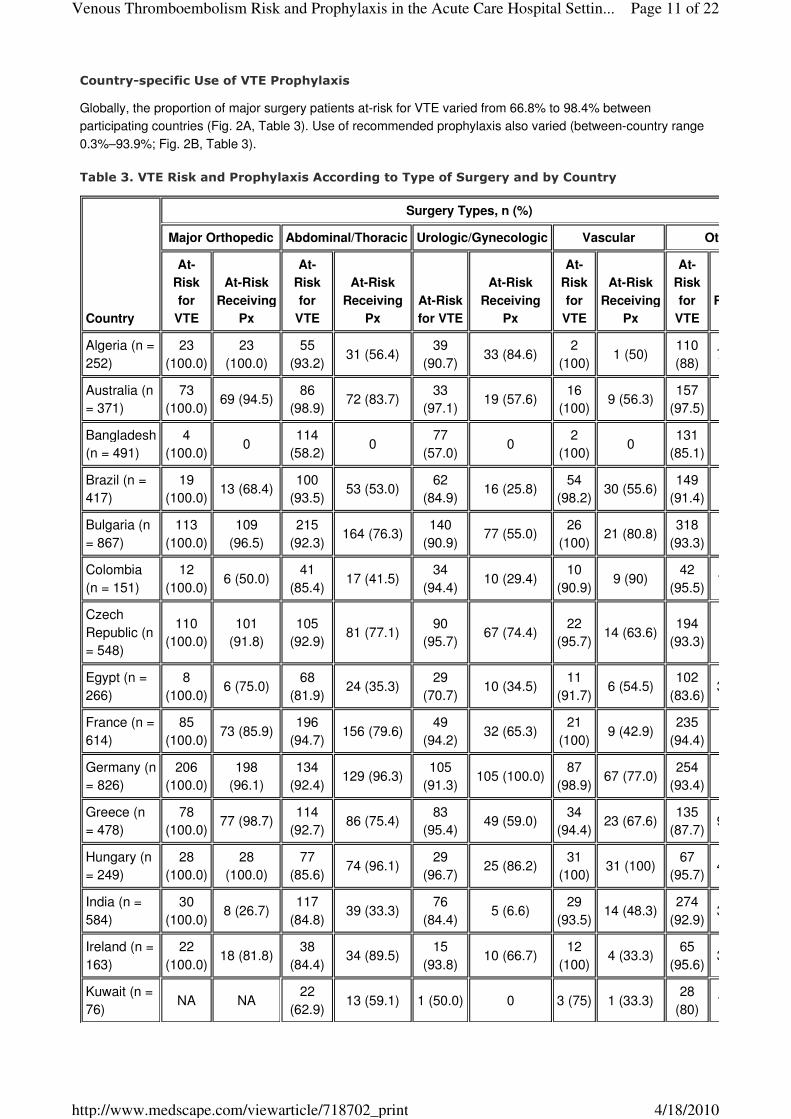
Country-specific Use of VTE Prophylaxis
Globally, the proportion of major surgery patients at-risk for VTE varied from 66.8% to 98.4% between
participating countries (Fig. 2A, Table 3). Use of recommended prophylaxis also varied (between-country range
0.3%–93.9%; Fig. 2B, Table 3).
Table 3. VTE Risk and Prophylaxis According to Type of Surgery and by Country
Country
Surgery Types, n (%)
Major Orthopedic Abdominal/Thoracic Urologic/Gynecologic Vascular Other
At-
Risk
for
VTE
At-Risk
Receiving
Px
At-
Risk
for
VTE
At-Risk
Receiving
Px
At-Risk
for VTE
At-Risk
Receiving
Px
At-
Risk
for
VTE
At-Risk
Receiving
Px
At-
Risk
for
VTE
Receiving
Algeria (n =
252)
23
(100.0)
23
(100.0)
55
(93.2)31 (56.4)
39
(90.7)33 (84.6)
2
(100)1 (50)
110
(88)73
Australia (n
= 371)
73
(100.0)69 (94.5)
86
(98.9)72 (83.7)
33
(97.1)19 (57.6)
16
(100)9 (56.3)
157
(97.5)
Bangladesh
(n = 491)
4
(100.0)0
114
(58.2)0
77
(57.0)0
2
(100)0
131
(85.1)
Brazil (n =
417)
19
(100.0)13 (68.4)
100
(93.5)53 (53.0)
62
(84.9)16 (25.8)
54
(98.2)30 (55.6)
149
(91.4)
Bulgaria (n
= 867)
113
(100.0)
109
(96.5)
215
(92.3)164 (76.3)
140
(90.9)77 (55.0)
26
(100)21 (80.8)
318
(93.3)
Colombia
(n = 151)
12
(100.0)6 (50.0)
41
(85.4)17 (41.5)
34
(94.4)10 (29.4)
10
(90.9)9 (90)
42
(95.5)16 (38.1)
Czech
Republic (n
= 548)
110
(100.0)
101
(91.8)
105
(92.9)81 (77.1)
90
(95.7)67 (74.4)
22
(95.7)14 (63.6)
194
(93.3)
Egypt (n =
266)
8
(100.0)6 (75.0)
68
(81.9)24 (35.3)
29
(70.7)10 (34.5)
11
(91.7)6 (54.5)
102
(83.6)31 (30.4)
France (n =
614)
85
(100.0)73 (85.9)
196
(94.7)156 (79.6)
49
(94.2)32 (65.3)
21
(100)9 (42.9)
235
(94.4)
Germany (n
= 826)
206
(100.0)
198
(96.1)
134
(92.4)129 (96.3)
105
(91.3)105 (100.0)
87
(98.9)67 (77.0)
254
(93.4)
Greece (n
= 478)
78
(100.0)77 (98.7)
114
(92.7)86 (75.4)
83
(95.4)49 (59.0)
34
(94.4)23 (67.6)
135
(87.7)97 (71.9)
Hungary (n
= 249)
28
(100.0)
28
(100.0)
77
(85.6)74 (96.1)
29
(96.7)25 (86.2)
31
(100)31 (100)
67
(95.7)49 (73.1)
India (n =
584)
30
(100.0)8 (26.7)
117
(84.8)39 (33.3)
76
(84.4)5 (6.6)
29
(93.5)14 (48.3)
274
(92.9)38 (13.9)
Ireland (n =
163)
22
(100.0)18 (81.8)
38
(84.4)34 (89.5)
15
(93.8)10 (66.7)
12
(100)4 (33.3)
65
(95.6)34 (52.3)
Kuwait (n =
76)NA NA
22
(62.9)13 (59.1) 1 (50.0) 0 3 (75) 1 (33.3)
28
(80)15
Page 11 of 22Venous Thromboembolism Risk and Prophylaxis in the Acute Care Hospital Settin...
4/18/2010http://www.medscape.com/viewarticle/718702_print

Mexico (n =
312)
11
(100.0)9 (81.8)
84
(78.5)36 (42.9)
38
(82.6)10 (26.3)
17
(100)13 (76.5)
121
(92.4)54 (44.6)
Pakistan (n
= 342)
3
(100.0)1 (33.3)
70
(67.3)8 (11.4)
57
(58.2)3 (5.3) 6 (75) 2 (33.3)
116
(89.9)14
Poland (n =
550)
74
(100.0)72 (97.3)
135
(93.1)96 (71.1)
77
(93.9)30 (39.0)
55
(96.5)43 (78.2)
164
(85.4)
Portugal (n
= 465)
57
(100.0)48 (84.2)
114
(92.7)82 (71.9)
73
(92.4)35 (47.9)
11
(100)6 (54.5)
187
(95.9)
Romania (n
= 1489)
124
(100.0)
117
(94.4)
385
(95.3)257 (66.8)
248
(95.8)176 (71.0)
43
(93.5)25 (58.1)
622
(94.8)
Russia (n =
1277)
61
(100.0)39 (63.9)
249
(85.3)93 (37.3)
155
(83.3)47 (30.3)
69
(94.5)49 (71)
591
(88.9)
Saudi
Arabia (n =
146)
13
(100.0)5 (38.5)
16
(53.3)7 (43.8) 7 (87.5) 3 (42.9)
3
(100)1 (33.3)
76
(82.6)28 (36.8)
Slovakia (n
= 548)
81
(100.0)78 (96.3)
111
(88.8)98 (88.3)
114
(93.4)70 (61.4)
23
(100)16 (69.6)
179
(90.9)
Spain (n =
657)
137
(100.0)
136
(99.3)
170
(98.8)148 (87.1)
108
(99.1)77 (71.3)
35
(97.2)23 (65.7)
193
(95.1)
Switzerland
(n = 752)
94
(100.0)84 (89.4)
207
(94.1)173 (83.6)
71
(95.9)64 (90.1)
41
(95.3)29 (70.7)
294
(91.6)238 (81)
Thailand (n
= 543)
27
(100.0)0
132
(95.7)1 (0.8)
68
(86.1)0
15
(100)0
275
(96.8)
Tunisia (n =
103)NA NA
51
(87.9)46 (90.2)
10
(83.3)9 (90.0)
5
(100)0
23
(82.1)15 (65.2)
Turkey (n =
299)
40
(100.0)24 (60.0)
85
(95.5)37 (43.5)
30
(90.9)4 (13.3) 8 (80) 5 (62.5)
124
(97.6)
United Arab
Emirates (n
= 125)
13
(100.0)8 (61.5)
16
(59.3)6 (37.5)
11
(64.7)5 (45.5) NA NA
64
(94.1)29
United
Kingdom (n
= 1272)
281
(100.0)
218
(77.6)
340
(92.9)290 (85.3)
143
(94.7)105 (73.4)
66
(100)52 (78.8)
385
(94.4)
United
States (n =
3044)
471
(100.0)
409
(86.8)
825
(95.8)668 (81.0)
248
(91.9)164 (66.1)
250
(100)
171
(68.4)
1135
(95.2)
Venezuela
(n = 184)
2
(100.0)2 (100.0)
55
(94.8)4 (7.3)
24
(92.3)1 (4.2)
5
(100)2 (40)
91
(97.8)19 (20.9)
Total (N =
18,461)
2300
(100.0)
1979
(86.0)
4527
(90.0)3023 (66.8)
2344
(88.4)1261 (53.8)
1012
(97.5)
676
(66.8)
6901
(92.7)
NA indicates not applicable; Px, prophylaxis; VTE, venous thromboembolism.
Page 12 of 22Venous Thromboembolism Risk and Prophylaxis in the Acute Care Hospital Settin...
4/18/2010http://www.medscape.com/viewarticle/718702_print

Table 3. VTE Risk and Prophylaxis According to Type of Surgery and by Country
Country
Surgery Types, n (%)
Major Orthopedic Abdominal/Thoracic Urologic/Gynecologic Vascular Other
At-
Risk
for
VTE
At-Risk
Receiving
Px
At-
Risk
for
VTE
At-Risk
Receiving
Px
At-Risk
for VTE
At-Risk
Receiving
Px
At-
Risk
for
VTE
At-Risk
Receiving
Px
At-
Risk
for
VTE
Receiving
Algeria (n =
252)
23
(100.0)
23
(100.0)
55
(93.2)31 (56.4)
39
(90.7)33 (84.6)
2
(100)1 (50)
110
(88)73
Australia (n
= 371)
73
(100.0)69 (94.5)
86
(98.9)72 (83.7)
33
(97.1)19 (57.6)
16
(100)9 (56.3)
157
(97.5)
Bangladesh
(n = 491)
4
(100.0)0
114
(58.2)0
77
(57.0)0
2
(100)0
131
(85.1)
Brazil (n =
417)
19
(100.0)13 (68.4)
100
(93.5)53 (53.0)
62
(84.9)16 (25.8)
54
(98.2)30 (55.6)
149
(91.4)
Bulgaria (n
= 867)
113
(100.0)
109
(96.5)
215
(92.3)164 (76.3)
140
(90.9)77 (55.0)
26
(100)21 (80.8)
318
(93.3)
Colombia
(n = 151)
12
(100.0)6 (50.0)
41
(85.4)17 (41.5)
34
(94.4)10 (29.4)
10
(90.9)9 (90)
42
(95.5)16 (38.1)
Czech
Republic (n
= 548)
110
(100.0)
101
(91.8)
105
(92.9)81 (77.1)
90
(95.7)67 (74.4)
22
(95.7)14 (63.6)
194
(93.3)
Egypt (n =
266)
8
(100.0)6 (75.0)
68
(81.9)24 (35.3)
29
(70.7)10 (34.5)
11
(91.7)6 (54.5)
102
(83.6)31 (30.4)
France (n =
614)
85
(100.0)73 (85.9)
196
(94.7)156 (79.6)
49
(94.2)32 (65.3)
21
(100)9 (42.9)
235
(94.4)
Germany (n
= 826)
206
(100.0)
198
(96.1)
134
(92.4)129 (96.3)
105
(91.3)105 (100.0)
87
(98.9)67 (77.0)
254
(93.4)
Greece (n
= 478)
78
(100.0)77 (98.7)
114
(92.7)86 (75.4)
83
(95.4)49 (59.0)
34
(94.4)23 (67.6)
135
(87.7)97 (71.9)
Hungary (n
= 249)
28
(100.0)
28
(100.0)
77
(85.6)74 (96.1)
29
(96.7)25 (86.2)
31
(100)31 (100)
67
(95.7)49 (73.1)
India (n =
584)
30
(100.0)8 (26.7)
117
(84.8)39 (33.3)
76
(84.4)5 (6.6)
29
(93.5)14 (48.3)
274
(92.9)38 (13.9)
Ireland (n =
163)
22
(100.0)18 (81.8)
38
(84.4)34 (89.5)
15
(93.8)10 (66.7)
12
(100)4 (33.3)
65
(95.6)34 (52.3)
Kuwait (n =
76)NA NA
22
(62.9)13 (59.1) 1 (50.0) 0 3 (75) 1 (33.3)
28
(80)15
Mexico (n =
312)
11
(100.0)9 (81.8)
84
(78.5)36 (42.9)
38
(82.6)10 (26.3)
17
(100)13 (76.5)
121
(92.4)54 (44.6)
Pakistan (n
= 342)
3
(100.0)1 (33.3)
70
(67.3)8 (11.4)
57
(58.2)3 (5.3) 6 (75) 2 (33.3)
116
(89.9)14
Page 13 of 22Venous Thromboembolism Risk and Prophylaxis in the Acute Care Hospital Settin...
4/18/2010http://www.medscape.com/viewarticle/718702_print

Poland (n =
550)
74
(100.0)72 (97.3)
135
(93.1)96 (71.1)
77
(93.9)30 (39.0)
55
(96.5)43 (78.2)
164
(85.4)
Portugal (n
= 465)
57
(100.0)48 (84.2)
114
(92.7)82 (71.9)
73
(92.4)35 (47.9)
11
(100)6 (54.5)
187
(95.9)
Romania (n
= 1489)
124
(100.0)
117
(94.4)
385
(95.3)257 (66.8)
248
(95.8)176 (71.0)
43
(93.5)25 (58.1)
622
(94.8)
Russia (n =
1277)
61
(100.0)39 (63.9)
249
(85.3)93 (37.3)
155
(83.3)47 (30.3)
69
(94.5)49 (71)
591
(88.9)
Saudi
Arabia (n =
146)
13
(100.0)5 (38.5)
16
(53.3)7 (43.8) 7 (87.5) 3 (42.9)
3
(100)1 (33.3)
76
(82.6)28 (36.8)
Slovakia (n
= 548)
81
(100.0)78 (96.3)
111
(88.8)98 (88.3)
114
(93.4)70 (61.4)
23
(100)16 (69.6)
179
(90.9)
Spain (n =
657)
137
(100.0)
136
(99.3)
170
(98.8)148 (87.1)
108
(99.1)77 (71.3)
35
(97.2)23 (65.7)
193
(95.1)
Switzerland
(n = 752)
94
(100.0)84 (89.4)
207
(94.1)173 (83.6)
71
(95.9)64 (90.1)
41
(95.3)29 (70.7)
294
(91.6)238 (81)
Thailand (n
= 543)
27
(100.0)0
132
(95.7)1 (0.8)
68
(86.1)0
15
(100)0
275
(96.8)
Tunisia (n =
103)NA NA
51
(87.9)46 (90.2)
10
(83.3)9 (90.0)
5
(100)0
23
(82.1)15 (65.2)
Turkey (n =
299)
40
(100.0)24 (60.0)
85
(95.5)37 (43.5)
30
(90.9)4 (13.3) 8 (80) 5 (62.5)
124
(97.6)
United Arab
Emirates (n
= 125)
13
(100.0)8 (61.5)
16
(59.3)6 (37.5)
11
(64.7)5 (45.5) NA NA
64
(94.1)29
United
Kingdom (n
= 1272)
281
(100.0)
218
(77.6)
340
(92.9)290 (85.3)
143
(94.7)105 (73.4)
66
(100)52 (78.8)
385
(94.4)
United
States (n =
3044)
471
(100.0)
409
(86.8)
825
(95.8)668 (81.0)
248
(91.9)164 (66.1)
250
(100)
171
(68.4)
1135
(95.2)
Venezuela
(n = 184)
2
(100.0)2 (100.0)
55
(94.8)4 (7.3)
24
(92.3)1 (4.2)
5
(100)2 (40)
91
(97.8)19 (20.9)
Total (N =
18,461)
2300
(100.0)
1979
(86.0)
4527
(90.0)3023 (66.8)
2344
(88.4)1261 (53.8)
1012
(97.5)
676
(66.8)
6901
(92.7)
NA indicates not applicable; Px, prophylaxis; VTE, venous thromboembolism.
Page 14 of 22Venous Thromboembolism Risk and Prophylaxis in the Acute Care Hospital Settin...
4/18/2010http://www.medscape.com/viewarticle/718702_print

Figure 2. Proportion of patients in participating countries who have undergone surgery and who are (A) at
-risk for VTE and (B) at-risk for VTE and receiving ACCP-recommended prophylaxis. ACCP indicates
American College of Chest Physicians; VTE, venous thromboembolism.
Additional Factors Influencing VTE Risk and Prophylaxis Use
Overall, 61% and 60% of major surgery patients aged 18 to 29 and 30 to 39 years, respectively, were
considered at-risk for VTE. All patients aged ≥40 years who underwent a major surgical procedure were
considered at-risk for VTE. The proportion of patients with high bleeding risk (sufficient to present a
contraindication to anticoagulant use) decreased with age, from 11% in patients aged 18 to 29 years to 6% of
patients aged ≥90 years.
Page 15 of 22Venous Thromboembolism Risk and Prophylaxis in the Acute Care Hospital Settin...
4/18/2010http://www.medscape.com/viewarticle/718702_print

Use of recommended prophylaxis in patients with 1 to 3 VTE risk factors was 58.0% (5911/10,188), compared
with 68.6% (4727/6896) in major surgery patients with >3 risk factors.
Use of Recommended Types of VTE Prophylaxis in Special Populations
Our data suggest that use of pharmacological agents alone was the most frequently used form of VTE
prophylaxis across all the patient subgroups assessed (Figs. 3A, B).
Page 16 of 22Venous Thromboembolism Risk and Prophylaxis in the Acute Care Hospital Settin...
4/18/2010http://www.medscape.com/viewarticle/718702_print

Figure 3. Types of VTE prophylaxis used according to (A) bleeding risk levels and the number of VTE risk
factors present and (B) an active malignancy diagnosis in patients undergoing abdominal, urologic or
gynecologic surgery. VTE risk factors in addition to surgery type were defined according to the 2004 ACCP
guidelines.6 VTE indicates venous thromboembolism.
The relative proportions of patients receiving pharmacological-only, mechanical-only, or combined
pharmacological and mechanical prophylaxis appears to vary according to both the number of risk factors for
VTE (1–3 vs >3 risk factors) and bleeding risk (low/moderate vs high) (Fig. 3A). Due to reduced use of
combined pharmacological and mechanical prophylaxis in patients with a high bleeding risk, we observed a
smaller difference in rates of use for mechanical alone versus combined pharmacological and mechanical
prophylaxis in these patients, compared with those with a low/moderate bleeding risk (Fig. 3A).
All patients with cancer who underwent abdominal, urologic, or gynecologic surgery were considered at-risk for
VTE (Table 4), as almost a third of these procedures were related to a cancer diagnosis. Patients undergoing
surgery for cancer more commonly received recommended prophylaxis, compared with those undergoing
surgical procedures unrelated to cancer (Table 4). A greater proportion of patients with cancer who underwent
surgical procedures unrelated to their cancer had a high bleeding risk compared with other subgroups (Table 4).
In addition, we observed a trend toward lower rates of pharmacological prophylaxis use in these patients (Fig.
3B). Use of pharmacological-only, mechanical-only, or a combination of the 2 appeared to be similar in
noncancer patients and in patients who underwent surgery for cancer.
Table 4. Risk for VTE and Bleeding in Patients Who Have Undergone Abdominal, Urologic, or
Gynecologic Surgery According to the Presence of an Active Malignancy Diagnosis
Active
Malignancy
Status*
At Risk for
VTE, n (%)
At Risk and Receiving ACCP-
Recommended Prophylaxis, n (%)
Bleeding Risk in At Risk
Patients, n (%)
High Moderate Low
Cancer
diagnosis 1868 (30.3) 1350 (72.3)
200
(10.7)291 (15.6)
1377
(73.7)
Surgery for
cancer1767 1295 (73.3)
183
(10.4)267 (15.1)
1317
(74.5)
Surgery with
cancer101 55 (54.5)
17
(16.8)24 (23.8) 60 (59.4)
No cancer
diagnosis 4304 (69.7) 2495 (58.0)
470
(10.9)837 (19.4)
2997
(69.6)
*Active malignancy status defined according to whether a patient had a cancer diagnosis at the time
of surgery, and whether patients diagnosed with cancer underwent major surgery related to their
active malignancy "surgery for cancer," or unrelated "surgery with cancer."
Table 4. Risk for VTE and Bleeding in Patients Who Have Undergone Abdominal, Urologic, or
Gynecologic Surgery According to the Presence of an Active Malignancy Diagnosis
Active
Malignancy
Status*
At Risk for
VTE, n (%)
At Risk and Receiving ACCP-
Recommended Prophylaxis, n (%)
Bleeding Risk in At Risk
Patients, n (%)
High Moderate Low
Cancer
diagnosis 1868 (30.3) 1350 (72.3)
200
(10.7)291 (15.6)
1377
(73.7)
Surgery for
cancer1767 1295 (73.3)
183
(10.4)267 (15.1)
1317
(74.5)
Page 17 of 22Venous Thromboembolism Risk and Prophylaxis in the Acute Care Hospital Settin...
4/18/2010http://www.medscape.com/viewarticle/718702_print

Factors Associated with the Use of ACCP-recommended VTE Prophylaxis
Operation type was the factor most strongly associated with prophylaxis provision in major surgery patients at
risk for VTE (Fig. 4). When type of surgery was excluded from the multivariable analysis, the comorbidities
commonly associated with the use of prophylaxis were preadmission obesity, in-hospital rheumatologic or
inflammatory disease, preadmission VTE, and presence of a central venous catheter (Fig. 5).
Surgery with
cancer101 55 (54.5)
17
(16.8)24 (23.8) 60 (59.4)
No cancer
diagnosis 4304 (69.7) 2495 (58.0)
470
(10.9)837 (19.4)
2997
(69.6)
*Active malignancy status defined according to whether a patient had a cancer diagnosis at the time
of surgery, and whether patients diagnosed with cancer underwent major surgery related to their
active malignancy "surgery for cancer," or unrelated "surgery with cancer."
Table 4. Risk for VTE and Bleeding in Patients Who Have Undergone Abdominal, Urologic, or
Gynecologic Surgery According to the Presence of an Active Malignancy Diagnosis
Active
Malignancy
Status*
At Risk for
VTE, n (%)
At Risk and Receiving ACCP-
Recommended Prophylaxis, n (%)
Bleeding Risk in At Risk
Patients, n (%)
High Moderate Low
Cancer
diagnosis 1868 (30.3) 1350 (72.3)
200
(10.7)291 (15.6)
1377
(73.7)
Surgery for
cancer1767 1295 (73.3)
183
(10.4)267 (15.1)
1317
(74.5)
Surgery with
cancer101 55 (54.5)
17
(16.8)24 (23.8) 60 (59.4)
No cancer
diagnosis 4304 (69.7) 2495 (58.0)
470
(10.9)837 (19.4)
2997
(69.6)
*Active malignancy status defined according to whether a patient had a cancer diagnosis at the time
of surgery, and whether patients diagnosed with cancer underwent major surgery related to their
active malignancy "surgery for cancer," or unrelated "surgery with cancer."
Page 18 of 22Venous Thromboembolism Risk and Prophylaxis in the Acute Care Hospital Settin...
4/18/2010http://www.medscape.com/viewarticle/718702_print

Figure 4. Independent factors associated with the use of ACCP-recommended VTE prophylaxis in
surgical patients at risk for VTE. ACCP indicates American College of Chest Physicians; CCU, critical care
unit; CI, confidence interval; GI, gastrointestinal; ICU, intensive care unit; VTE, venous thromboembolism.
Page 19 of 22Venous Thromboembolism Risk and Prophylaxis in the Acute Care Hospital Settin...
4/18/2010http://www.medscape.com/viewarticle/718702_print

Figure 5. Independent factors, excluding surgery type, associated with the use of ACCP-recommended
VTE prophylaxis in surgical patients at-risk for VTE. ACCP indicates American College of Chest
Physicians; CCU, critical care unit; CI, confidence interval; GI, gastrointestinal; ICU, intensive care unit;
VTE, venous thromboembolism.
Discussion
We found that 93% of patients who underwent a major surgical procedure were at-risk for VTE, with only 62%
receiving ACCP-recommended prophylaxis. Rates of prophylaxis use varied across the participating countries
according to surgery type, and the presence of comorbidities including active malignancy. Major surgery was the
most important factor associated with the use of VTE prophylaxis.
The highest rates of prophylaxis were seen in orthopedic patients. Those undergoing urologic/gynecologic or
other procedures were least likely to receive prophylaxis; approximately half of these patients received no
prophylaxis despite being considered at-risk for VTE.
The proportion of patients undergoing vascular surgery who were considered at-risk for VTE (97.5%) was higher
than published estimates of around 21%.[7] This may result from higher rates of comorbidity in these patients
and the failure to recognize comorbidities which heighten VTE risk.
Our finding that type of operation is the factor most strongly associated with VTE prophylaxis use is consistent
with previous reports.[10,11] Excluding major surgery, obesity was the comorbidity most strongly associated with
the use of prophylaxis. The number of additional risk factors for VTE did not appear to correlate strongly with an
increased use of ACCP-recommended prophylaxis. This apparent lack of an increase in prophylaxis use with
increasing numbers of risk factors may lead to the underuse of prophylaxis in certain patient subgroups, for
example, vascular surgery patients.
Current American Society of Clinical Oncology guidelines on the prevention of VTE in patients with cancer
recommend that all patients with cancer undergoing laparotomy should be considered for pharmacological VTE
Page 20 of 22Venous Thromboembolism Risk and Prophylaxis in the Acute Care Hospital Settin...
4/18/2010http://www.medscape.com/viewarticle/718702_print

prophylaxis in the absence of bleeding or other contraindications.[12] Our findings support the conclusion that
VTE prophylaxis in patients with malignant disease needs to be improved.[12,13]
Due to the cross-sectional study design, duration of prophylaxis could not be recorded. Also, physicians may
have become aware of the study and altered their use of VTE prophylaxis. A further potential limitation is that
data were not collected on the subtype and stage of malignant disease in patients who were diagnosed with
cancer before surgery.
A major strength of this study is that it incorporates data gathered from 32 countries in 6 continents to provide a
truly global view of current VTE prophylaxis practices in surgical inpatients. Unlike previous clinical research
studies or trials which enrolled patients according to the type of surgery performed, this survey included a broad
and real-world sample of patients undergoing a variety of surgical operations.
Conclusions
The ENDORSE surgical population survey highlights the continuing gap between the prevalence of VTE risk in
patients who undergo major surgical procedures and the use of ACCP-recommended prophylaxis. Our
systematic evaluation of the risk for VTE in surgical patients provides improved estimates for both the current
disease burden of VTE and the potential clinical benefits of VTE prophylaxis. These data can also be used to
help guide clinical practice and assist the targeting of guideline dissemination, to improve adherence to existing
recommendations.
References
Kakkar VV, Corrigan T, Spindler J, et al. Efficacy of low doses of heparin in prevention of deep-vein
thrombosis after major surgery. A double-blind, randomized trial. Lancet. 1972;2:101–106.
1.
Prevention of fatal postoperative pulmonary embolism by low doses of heparin. An international
multicentre trial. Lancet. 1975;2:45–51.
2.
Sagar S, Massey J, Sanderson JM. Low-dose heparin prophylaxis against fatal pulmonary embolism. Br
Med J. 1975;4:257–259.
3.
Geerts WH, Bergqvist D, Pineo GF, et al. Prevention of venous thromboembolism: American College of
Chest Physicians Evidence-Based Clinical Practice Guidelines (8th edition). Chest. 2008;133(6
suppl):381S–453S.
4.
Collins R, Scrimgeour A, Yusuf S, et al. Reduction in fatal pulmonary embolism and venous thrombosis
by perioperative administration of subcutaneous heparin. Overview of results of randomized trials in
general, orthopedic, and urologic surgery. N Engl J Med. 1988;318:1162–1173.
5.
Geerts WH, Pineo GF, Heit JA, et al. Prevention of venous thromboembolism: the Seventh ACCP
Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004;126(3 suppl):338S–400S.
6.
Agnelli G. Prevention of venous thromboembolism in surgical patients. Circulation. 2004;110(24 suppl
1):IV4–IV12.
7.
Cohen AT, Tapson VF, Bergmann JF, et al. Venous thromboembolism risk and prophylaxis in the acute
hospital care setting (ENDORSE study): a multinational cross-sectional study. Lancet. 2008;371:387–
394.
8.
Baglin T, Barrowcliffe TW, Cohen A, et al. Guidelines on the use and monitoring of heparin. Br J
Haematol. 2006;133:19–34.
9.
Stratton MA, Anderson FA, Bussey HI, et al. Prevention of venous thromboembolism: adherence to the
1995 American College of Chest Physicians consensus guidelines for surgical patients. Arch Intern Med.
2000;160:334–340.
10.
Mommertz G, Sigala F, Glowka TR, et al. Differences of venous thromboembolic risks in vascular
general and trauma surgery patients. J Cardiovasc Surg (Torino). 2007;48:727–733.
11.
Lyman GH, Khorana AA, Falanga A, et al. American Society of Clinical Oncology guideline:
recommendations for venous thromboembolism prophylaxis and treatment in patients with cancer. J Clin
Oncol. 2007;25:5490–5505.
12.
Page 21 of 22Venous Thromboembolism Risk and Prophylaxis in the Acute Care Hospital Settin...
4/18/2010http://www.medscape.com/viewarticle/718702_print

Acknowledgments The authors thank the physicians and study coordinators participating in ENDORSE, the staff at the Center for Outcomes Research, and Olivia Wu, PhD, Division of Developmental Medicine, University of Glasgow, United Kingdom. ENDORSE is overseen by a medical advisory board of clinicians. A full list of the investigators who participated in ENDORSE, and further information about the registry can be found at http://www.outcomes.org/endorse.
Annals of Surgery. 2010;251(2):330-338. © 2010 Lippincott Williams & Wilkins
Seddighzadeh A, Zurawska U, Shetty R, et al. Venous thromboembolism in patients undergoing surgery:
low rates of prophylaxis and high rates of filter insertion. Thromb Haemost. 2007;98:1220–1225.
13.
Authors and Disclosures
Ajay K. Kakkar, MD, PhD,*† Alexander T. Cohen, MD,‡ Victor F. Tapson, MD,§ Jean-Francois Bergmann,
MD,¶ Samuel Z. Goldhaber, MD,|| Bruno Deslandes,** Wei Huang, MS,†† and Frederick A. Anderson, Jr.,
PhD,†† for the ENDORSE Investigators
*Barts and The London School of Medicine and Dentistry, London, United Kingdom; †Thrombosis Research
Institute, London, United Kingdom; ‡King's College Hospital, London, United Kingdom; §Duke University
Medical Center, Durham, NC; ¶Hôpital Lariboisière, University Paris 7, Paris, France; ||Brigham and Women's
Hospital, Harvard Medical School, Boston, MA; **sanofi-aventis, Paris, France; and ††Department of Surgery,
Center for Outcomes Research, University of Massachusetts Medical School, Worcester, MA.
Reprints
Ajay K. Kakkar, MD, PhD, Barts and the London School of Medicine and Dentistry, and Thrombosis Research
Institute, London, SW3 6LR, United Kingdom. E-mail: [email protected].
Page 22 of 22Venous Thromboembolism Risk and Prophylaxis in the Acute Care Hospital Settin...
4/18/2010http://www.medscape.com/viewarticle/718702_print




















