
Assessment of venous thromboembolism risk and the benefits of thromboprophylaxis in medical patients
Upload
vanderbiltCategory
view
0download
0
Hidden Barriers to Delivery of PharmacologicalVenous Thromboembolism Prophylaxis:The Role of Nursing Beliefs and PracticesStacy Elder, PharmD, Deborah B. Hobson, BSN, Cynthia S. Rand, PhD,Michael B. Streiff, MD, Elliott R. Haut, MD, Leigh E. Efird, PharmD,
Peggy S. Kraus, PharmD, Christoph U. Lehmann, MD, and Kenneth M. Shermock, PharmD, PhD
Background: Standardized electronic order sets for venous thrombo-embolism prophylaxis have increased the proportion of patients receivingvenous thromboembolism prophylaxis. However, ordering venous throm-boembolism prophylaxis does not ensure consistent administration.Objective: To explore causes of variability in the rate of administrationof ordered doses of pharmacological venous thromboembolism prophy-laxis among hospital units.Design: Mixed methods study, including qualitative observation andquantitative nursing survey administration.Subjects: Nurses included in observations were practicing on an in-patient unit, caring for patients with orders to receive venous thrombo-embolism prophylaxis consisting of low-dose unfractionated heparinor lowYmolecular weight heparin. Nurses on 12 inpatient units with dis-parate rates of administration were included in the survey.Measures: Qualitative observation data were collected until thematicsaturation was achieved. Survey was conducted to identify beliefs andpractices surrounding nursing administration of venous thromboembo-lism prophylaxis.Results: During observations, some nurses presented pharmacologicalvenous thromboembolism prophylaxis to their patients as an optionaltherapy. Nurses on low-performing units are more likely to believe thatpharmacological venous thromboembolism prophylaxis is ordered forpatients who do not require it. More often, they also acknowledge thatnurses use their clinical decision-making skills to determine when to omitunnecessary doses of prescribed venous thromboembolism prophylaxis.Conclusions: Nurses on units with low administration rates oftenbelieve they have the skills to determine which patients require phar-macological venous thromboembolism prophylaxis. They are also morelikely to believe that ordered doses are discretionary and offer themedication as optional to patients.
Key Words: venous thromboembolism, pharmacological venousthromboembolism prophylaxis, prophylaxis, nursing, mixed methods,heparin, lowYmolecular weight heparin
(J Patient Saf 2014;00: 00Y00)
Venous thromboembolism (VTE) is a significant cause ofmorbidity and mortality in hospitalized patients, represent-
ing a major cause of preventable harm and a patient safetyconcern.1Y3 Meta-analyses support the benefit of VTE pro-phylaxis in hospitalized patients.4,5 Because most hospitalizedpatients have at least one risk factor for VTE, guidelines recom-mend that all hospitals implement a strategy for risk-appropriateVTE prophylaxis.1,4,6 Since 1991, numerous national and
international surveys have documented that clinicians often fail toprescribe VTE prophylaxis for at-risk patients.7Y11 Consequently,health care reimbursement organizations, such as the Centersfor Medicare and Medicaid Services (CMS), have designatedhospital-acquired VTE as an event that should never occur insome patient populations because of the availability of prophy-lactic measures.12 In an attempt to comply with these objec-tives and maximize patient safety, the development ofcomputerized electronic alerts and standardized VTE prophy-laxis order sets have increased the proportion of patients re-ceiving VTE prophylaxis and decreased VTE events.13,14
However, ordering VTE prophylaxis does not necessarilyensure consistent administration. Nonadherence has been ob-served with mechanical prophylaxis and may contribute to pre-ventable, hospital-acquired VTE.15Y17 Fanikos et al. reviewed2047 doses and observed that 10% of prophylactic low doseunfractionated heparin (LDUH) and low molecular weight hepa-rin (LMWH) doses were not administered.18 The most commonreason for missed doses of prophylaxis was cited as patient re-fusal, accounting for 44% of omitted doses.18 We noted a simi-lar pattern at our institution where a review of 107,000 doses ofVTE prophylaxis suggested that 11.8% of doses were not ad-ministered, and 59% of those were documented as refused.17
Furthermore, we observed marked variation in the percent ofordered doses of VTE prophylaxis that were not administeredacross hospital units (range, 5%Y27%).17
To explore potential causes for variation in the rate of ad-ministration of pharmacological VTE prophylaxis, we initiateda mixed methods study of VTE prophylaxis delivery on selectedhigh and low performing nursing units at the Johns HopkinsHospital. We hypothesized that nursing attitudes, beliefs, andpractices surrounding VTE prophylaxis corresponded with pat-terns in administration rate of these medications.
METHODSWe conducted a mixed methods study at a large academic
medical center, between October 2010 and October 2011. Be-fore study initiation, we obtained approval from the JohnsHopkins Medical Institutions (JHMI) institutional review board(IRB), as well as from hospital and nursing administration. Nursesalso gave individual consent for participation. In the absence ofcontraindications, most patients at our institution are prescribedprophylaxis, typically with LDUH or LMWH, in accordancewitha VTE risk-assessment tool that is embedded in the PhysicianOrder Entry system.18
The study consisted of two parts. The first part includeddirect observation of the administration of pharmacological VTEprophylaxis (preparing, offering, and administering the injec-tion to the patient). The study concept was explained to nurses atthe beginning of their shift during a focus group discussion.
ORIGINAL ARTICLE
J Patient Saf & Volume 00, Number 00, Month 2014 www.journalpatientsafety.com 1
From the Department of Pharmacotherapy, Johns Hopkins Hospital, Baltimore,Maryland.Correspondence: Stacy Elder, PharmD, Philadelphia College of Pharmacy,
University of the Sciences, 600 S. 43rd Street, Philadelphia, PA 19104(email: [email protected]).
The authors disclose no conflict of interest.
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

The second part of this study involved the administra-tion of a survey to nurses on high (averaged 8.5% doses notadministered) and low (averaged 18.2% doses not administered)performing units in order to assess attitudes and beliefs regardingVTE prophylaxis. Nurses practicing on inpatient units were in-cluded in direct observations if they were caring for a patient witha current order for VTE prophylaxis with LDUH or LMWH.Observations were conducted by one investigator, with the con-sent of both the nurse and the patient. All actions and statementsfrom the time of dose preparation to the end of the nurse’s inter-action with the patient regarding the administration of their VTEprophylaxis were recorded. All qualitative data were read thor-oughly, and prevailing themes and information were extracted andrefined.19 Data collection for the qualitative portion of the studycontinued until thematic/information saturation was achieved, andno new themes or ideas were recognized.19
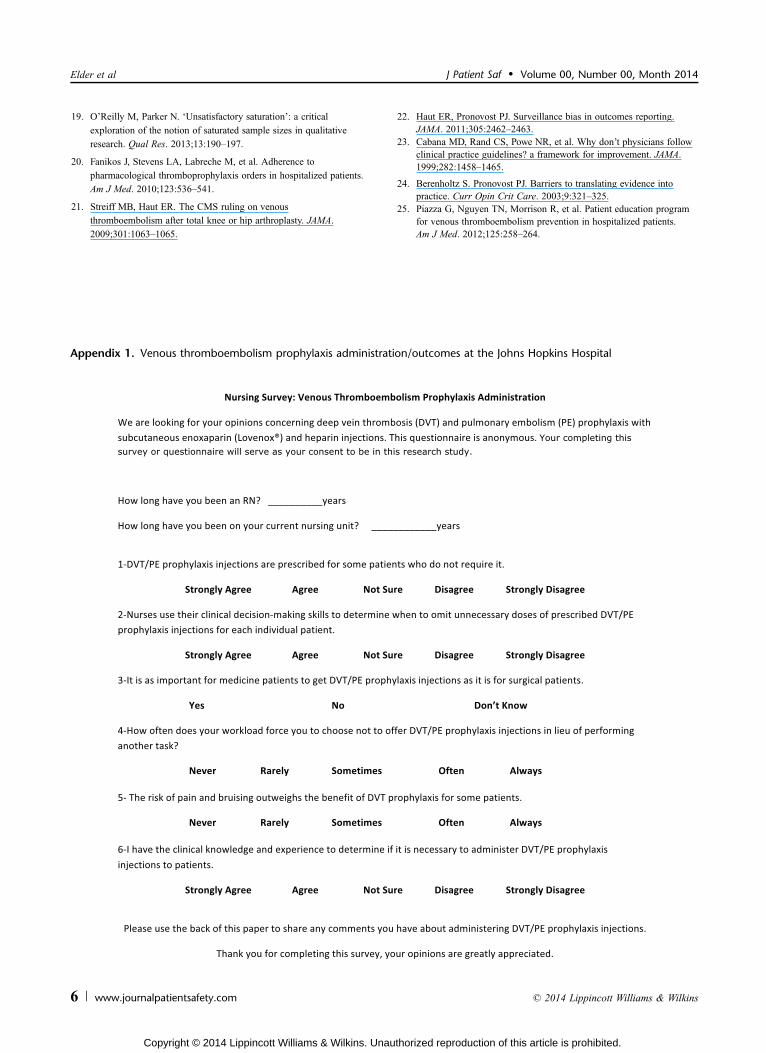
The VTE prophylaxis beliefs and attitudes survey was ad-ministered to nurses on 12 inpatient units, which were identifiedduring our previous study as having disparate rates of VTE pro-phylaxis refusal. We targeted 6 high performing and 6 low per-forming units. Surveys were either administered during nursingshift change meetings or placed in the mailboxes of registerednurses with a central collection location for return of the surveys.In addition to 6 Likert scale questions, the survey (Appendix 1)assessed the nurse’s experience in practice and, specifically, ontheir current unit. The survey provided an optional section forthe respondent to record any additional thoughts concerning VTEprophylaxis. Completed surveys were collated by unit so that spe-cific units could be compared during data analysis.
The quantitative data from the surveys were compiled andanalyzed using STATA 11.0 statistical software (Stata Corp.,College Station, TX). The distribution of survey responses be-tween high and low performing units was compared using chi-squared analysis. A P G 0.05 was considered to be statisticallysignificant.
RESULTS
Quantitative Survey ResultsWe distributed surveys to nurses on 12 inpatient units
(Table 1). Overall, 248 (83%) of the 299 surveys distributedwere completed. Response rates were not significantly differentbetween units. On low performing units, 118 (87%) of 136 sur-veys were returned, whereas 130 (80%) of 162 surveys were re-ceived from high performing units. The time in practice wassimilar among nurses on high and low performing units, butnurses on the high performing units typically had a shorter timeon their current unit than nurses on the low performing units(5.5 years vs 7.6 years, P = 0.006).
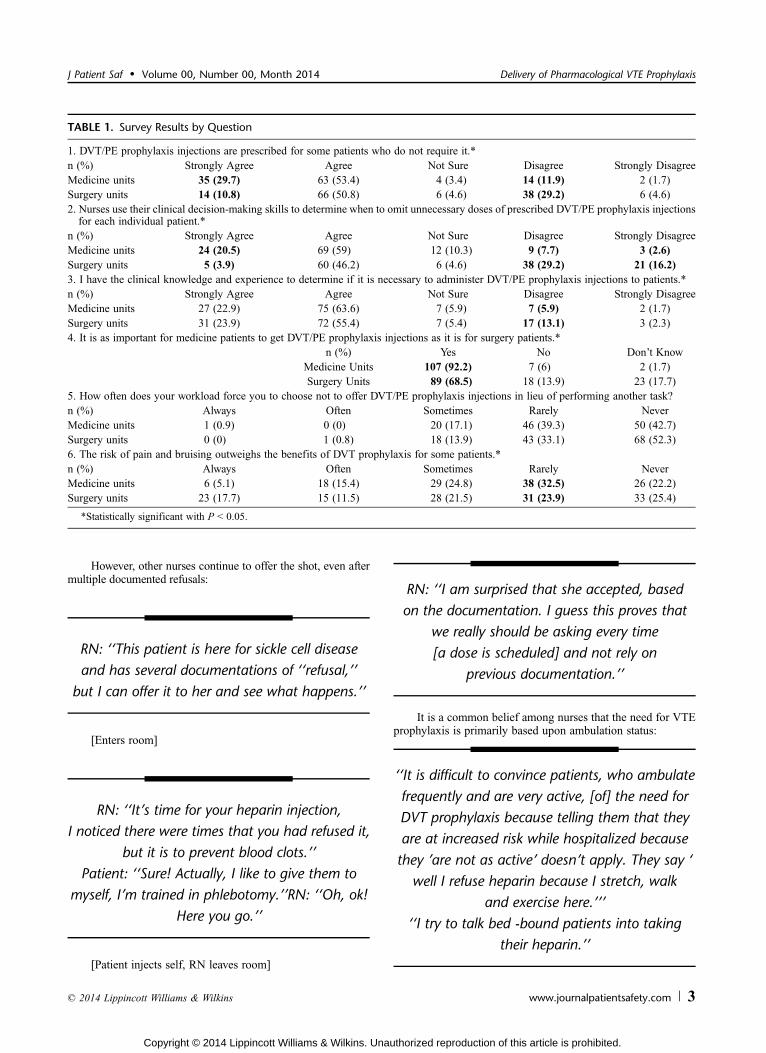
A majority of nurses (83%) responded that they agree orstrongly agree that they have the clinical knowledge and expe-rience to determine if administration of VTE prophylaxis is nec-essary. However, nurses on low performing units are more likelyto say that VTE prophylaxis is prescribed for patients who do notrequire it (83% vs 62%, P G 0.0001). Nurses on low performingunits are much more likely to acknowledge that nurses use theirclinical decision-making skills to determine when to omit unnec-essary doses of prescribed VTE prophylaxis injections for in-dividual patients (80% vs 50%, P G 0.0001). Whereas 92% ofnurses on low performing units believe that VTE prophylaxis isas important for medicine patients as it is for surgery patients,only 68% of nurses on high performing units believe that it isequally important for both patient populations (P G 0.0001).Nursing workload was not found to be a major reason for
omitting doses of VTE prophylaxis. Patient pain and bruisingwas identified as a possible reason for failure to administer VTEprophylaxis, as 30% of nurses on high performing units and 20%of nurses on low performing units (P = 0.025) feel that avoidingpain and bruising often or always outweighs the potential benefitof pharmacological VTE prophylaxis.
Qualitative ObservationsWe observed and recorded the interactions between 19 dif-
ferent patients and their nurses during the administration of VTEprophylaxis doses. Focus groups encompassing approximately50 nurses at shift change meetings were also noted for thematicanalysis, in addition to the qualitative data provided by nurseson the survey. All qualitative data were analyzed and collatedby theme (see the 6 themes identified below) utilizing key wordsand phrases consistent with these domains. The main theme thatemerged during these interactions was that some nurses con-sider prescribed VTE prophylaxis doses to be optional or dis-cretionary and present the therapy to the patients in a way thatreflects that belief:
‘‘Hey Ms. R, it’s time for your heparin dose,but as long as I see you up, high-fiving me in the
hallways, we can hold off for now.’’‘‘We make the clinical decision all the time as towhether a patient needs VTE prophylaxis every day,based on how much the patient is ambulating.’’‘‘I push harder for my patients to accept heparin[prophylaxis] if they have, like, sickle cell disease,as opposed to say pneumonia or something where
they are just here for [IV] antibiotics.’’‘‘Sometimes, if it is the middle of the night and[LDUH] is the only medication I have to givea patient, I won’t wake them up just to give
VTE prophylaxis.’’’’
If documentation indicates that patients have previouslyrefused doses of VTE prophylaxis, we observed that somenurses continue to document refusal without actually offeringVTE prophylaxis:
‘‘I’ve had Mr. F all weekend and he has beenrefusing. I’m not even going to ask him.’’
‘‘This patient has been here four months andhe literally yells at us when we ask him about
heparin because he says we should know by nowthat he doesn’t want it. So we try to avoid that[situation] and we don’t ask him anymore.’’
Elder et al J Patient Saf & Volume 00, Number 00, Month 2014
2 www.journalpatientsafety.com * 2014 Lippincott Williams & Wilkins
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
However, other nurses continue to offer the shot, even aftermultiple documented refusals:
RN: ‘‘This patient is here for sickle cell diseaseand has several documentations of ‘‘refusal,’’
but I can offer it to her and see what happens.’’
[Enters room]
RN: ‘‘It’s time for your heparin injection,I noticed there were times that you had refused it,
but it is to prevent blood clots.’’Patient: ‘‘Sure! Actually, I like to give them to
myself, I’m trained in phlebotomy.’’RN: ‘‘Oh, ok!Here you go.’’
[Patient injects self, RN leaves room]
RN: ‘‘I am surprised that she accepted, basedon the documentation. I guess this proves that
we really should be asking every time[a dose is scheduled] and not rely on
previous documentation.’’
It is a common belief among nurses that the need for VTEprophylaxis is primarily based upon ambulation status:
‘‘It is difficult to convince patients, who ambulatefrequently and are very active, [of] the need forDVT prophylaxis because telling them that theyare at increased risk while hospitalized becausethey ’are not as active’ doesn’t apply. They say ‘
well I refuse heparin because I stretch, walkand exercise here.’’’
‘‘I try to talk bed -bound patients into takingtheir heparin.’’
TABLE 1. Survey Results by Question
1. DVT/PE prophylaxis injections are prescribed for some patients who do not require it.*n (%) Strongly Agree Agree Not Sure Disagree Strongly DisagreeMedicine units 35 (29.7) 63 (53.4) 4 (3.4) 14 (11.9) 2 (1.7)Surgery units 14 (10.8) 66 (50.8) 6 (4.6) 38 (29.2) 6 (4.6)2. Nurses use their clinical decision-making skills to determine when to omit unnecessary doses of prescribed DVT/PE prophylaxis injectionsfor each individual patient.*
n (%) Strongly Agree Agree Not Sure Disagree Strongly DisagreeMedicine units 24 (20.5) 69 (59) 12 (10.3) 9 (7.7) 3 (2.6)Surgery units 5 (3.9) 60 (46.2) 6 (4.6) 38 (29.2) 21 (16.2)3. I have the clinical knowledge and experience to determine if it is necessary to administer DVT/PE prophylaxis injections to patients.*n (%) Strongly Agree Agree Not Sure Disagree Strongly DisagreeMedicine units 27 (22.9) 75 (63.6) 7 (5.9) 7 (5.9) 2 (1.7)Surgery units 31 (23.9) 72 (55.4) 7 (5.4) 17 (13.1) 3 (2.3)4. It is as important for medicine patients to get DVT/PE prophylaxis injections as it is for surgery patients.*
n (%) Yes No Don’t KnowMedicine Units 107 (92.2) 7 (6) 2 (1.7)Surgery Units 89 (68.5) 18 (13.9) 23 (17.7)
5. How often does your workload force you to choose not to offer DVT/PE prophylaxis injections in lieu of performing another task?n (%) Always Often Sometimes Rarely NeverMedicine units 1 (0.9) 0 (0) 20 (17.1) 46 (39.3) 50 (42.7)Surgery units 0 (0) 1 (0.8) 18 (13.9) 43 (33.1) 68 (52.3)6. The risk of pain and bruising outweighs the benefits of DVT prophylaxis for some patients.*n (%) Always Often Sometimes Rarely NeverMedicine units 6 (5.1) 18 (15.4) 29 (24.8) 38 (32.5) 26 (22.2)Surgery units 23 (17.7) 15 (11.5) 28 (21.5) 31 (23.9) 33 (25.4)
*Statistically significant with P G 0.05.
J Patient Saf & Volume 00, Number 00, Month 2014 Delivery of Pharmacological VTE Prophylaxis
* 2014 Lippincott Williams & Wilkins www.journalpatientsafety.com 3
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

On a few occasions, nurses expressed that they communi-cate openly with physicians regarding the appropriateness oftheir patient’s ordered VTE prophylaxis:
‘‘[It’s] Not for me to determine if they needit but the physician. I can question the physician
if I feel the patient does not need it.’’‘‘If you walk up and down the entire floor three
times today, I will talk to the doctor aboutstopping the heparin.’’
‘‘Just so you know, often I forget to tell thephysician to discontinue the heparin shots
if a patient is ambulating, so I just documentit as ‘patient condition inappropriate.’
You may see a lot of that.’’
The primary feedback that nurses offer regarding im-provement of compliance with VTE prophylaxis is that furthereducation is needed for nurses and physicians:
‘‘Nurses don’t know what the screening criteria arefor giving or not giving the subcutaneous heparinshot. Nurses believe if the pt is ambulating thenthey do not need the subcutaneous injection.
This is FALSE and represents a knowledge deficitin nurses. Nurses need to know the screening
criteria and why they are giving thesubcutaneous injection.’’
‘‘I think MDs should review the overall conditionof the patient before ordering DVT prophylaxis.’’
‘‘Nurses need to be educated on the propersize of needle to use during [subcutaneous]
heparin administration.’’‘‘Need for more education and increasingawareness for the reason for administering
DVT/PE prophylaxis injection’’‘‘Physicians should not prescribe heparinSQ to every patient that is admitted.’’
CONCLUSIONSUsing a mixed methods approach, we were able to assess
nursing attitudes, beliefs, and practices surrounding administration
of pharmacological VTE prophylaxis. Our study revealed anursing belief regarding perception of a responsibility to assessindividual patient risks and benefits of pharmacological VTE pro-phylaxis before offering the medication to the patient. The nurse’sattitude concerning clinical decision-making capacity varied be-tween high and low performing units and may play a role in theprocess of assessing, offering and administering doses to thepatient. We believe these results shed new light on an importantbarrier to administration of prescribed doses of pharmacologicalVTE prophylaxis. Consequently, patient safety and health-carereimbursement organizations have made prevention of hospital-acquired VTE a priority.12 However, ordered prophylaxis can onlyprevent thromboembolic events if it is administered.21,20 Pre-vious studies established that the assumption that administrationof ordered VTE prophylaxis occurs consistently may be incor-rect.17,20 We found that caregiver beliefs significantly influencethe process and rate of administration.
A previous study at our institution also noted that practicewas varied, particularly between low and high performing units.17
Low performing units had significantly lower rates of pharmacol-ogical VTE prophylaxis administration and higher documentedrates of refusal.17 Our study revealed that differences in nursingattitudes and beliefs regarding pharmacological VTE prophylaxismay account for disparity among units. The observation that nurseson high performing units had spent less time on their current unitthan low performing nurses deserves further investigation butcould suggest that the attitudes with respect to administration ofVTE prophylaxis evolve over time. Notably, all of the low per-forming units were medicine units, and conversely, all of the highperforming units were surgical units, potentially revealing a dif-ference in nursing attitudes and beliefs between units based uponthe patient population served. Patients on surgery units also havean obvious major risk factor for VTE (i.e., recent surgery), sonurses may be more attuned to the need for VTE prophylaxis ad-ministration in these patients, contributing to a higher rate ofadministration on these units. However, our survey results indi-cated that medicine nurses felt that VTE prophylaxis was as im-portant for medicine patients as it was for surgery patients. Anotherpotential factor that may contribute to decreased administrationrates on medicine units is the higher patient-to-nurse ratio, onaverage, compared with surgery units. Nevertheless, the nursessurveyed did not feel that workload was a significant cause ofdecreased VTE prophylaxis administration rates.
Venous thromboembolism risk assessment is an automatedpart of all admission and transfer order sets at our institution,which results in prescribers ordering VTE prophylaxis for a vastmajority of patients at that time. However, our results suggestthat nurses believe that VTE prophylaxis is ordered for patientswho do not require it. A relationship was noted between this be-lief and the rate of administration of ordered doses as signifi-cantly more surgery nurses disagreed that orders are written forpatients who do not require them. Some nurses stated a belief thatVTE prophylaxis is automatically ordered for all patients uponadmission. This highlights an unintended consequence of an auto-mated quality improvement process, whereby nursing perceptionregarding prescriber ordering patterns is not a true reflection ofprescribing practice. If nursing perception of the clinical value ofVTE prophylaxis is low, development of a culture where adminis-tration decisions are made autonomously by nurses could result.23
Regardless of nursing unit, a recurrent theme of the qualita-tive data was that ambulation status was a primary factor influenc-ing decision making regarding the necessity of VTE prophylaxis.It is not as clear if other VTE risk factors are given equal atten-tion by nurses. A potentially successful intervention to reduce thefrequency of nonadministered doses of VTE prophylaxis would
Elder et al J Patient Saf & Volume 00, Number 00, Month 2014
4 www.journalpatientsafety.com * 2014 Lippincott Williams & Wilkins
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

be to develop a program to review VTE risk factors, their fre-quency among hospitalized patients, and the risks and benefits ofpharmacological and mechanical VTE prophylaxis. Althougheducation for providers and nurses may be helpful, interdisci-plinary clinical decision making may be a better method forimplementing patient safety initiatives.24 Therefore, another cor-rective action could be to improve communication among pro-viders by initiating daily interdisciplinary rounds includingnurses, pharmacists, and physicians.24 This would provide a fo-rum to discuss any concerns regarding VTE risk factors, the needfor prophylaxis, and the rationale in individual patients. Addi-tionally, interdisciplinary meetings could lead to open communi-cation among providers concerning other aspects of patient care.
In the event that a patient refuses doses of medications, in-terdisciplinary rounds could provide a structured time when thecare team could engage patients and educate them on the benefitsand risks of VTE prophylaxis. From a patient safety standpoint,educating those who refuse medications could help them to un-derstand their treatment options and increase awareness of thelikely outcomes of their decisions.25 However, the evidence pre-sented in the current study suggests that the issue of nonadmin-istration of ordered doses is multidimensional. Furthermore, ourprevious work suggests that the patient-centered approach mayby highly inefficient; 60% of patients on the floor with the lowestadministration rate received at least 90% of their doses.17 We in-terpret these findings to suggest that increasing communicationwith our nursing staff is part of the most efficient and successfulintervention.
Venous thromboembolism prophylaxis remains an im-portant item in publicly reported quality data (i.e., http://www.hospitalcompare.hhs.gov) and is used by the newly de-fined ‘‘meaningful use criteria’’ for health-care information tech-nology per CMS. However, these definitions often categorizeevents as ‘‘present’’ or ‘‘not present,’’ based on ordering prophy-laxis.22 To date, no organizations are considering the issue ofmissed doses of VTE prophylaxis, which may be an importantmarker of quality and, potentially, result in higher event rates.
This study is limited in that it was conducted at a singleinstitution; however, we suspect that similar nursing attitudes,beliefs, and practices surrounding administration of pharma-cological VTE prophylaxis occur at other hospitals. Qualitativeobservations were relatively few but reached saturation and al-lowed for detection of important themes, in conjunction withqualitative data collected from the surveys and focus groups.The results of the observational portion of this study may havebeen limited by the Hawthorne effect; however, we postulate thatthere would only be more doses documented as refused duringperiods when staff were unobserved.
In conclusion, our mixed methods analysis demonstratedthat provider factors may contribute to the documented rates ofnonadministration and refusal of pharmacological VTE prophy-laxis. Initiatives at the local and national level have targeted thefailure of physicians to prescribe VTE prophylaxis.12,21 This studyindicates that interventions to improve administration rates ofVTE prophylaxis must focus not only on physicians but also onthe health-care providers administering the medications and theculture of care on individual units. We believe that a multidiscip-linary approach to patient care could optimize patient outcomesby decreasing inappropriate orders for VTE prophylaxis whileincreasing compliance with existing, appropriate orders.
REFERENCES
1. Geerts WH, Bergqvist D, Pineo GF, et al. Prevention of venousthromboembolism: American College of Chest Physicians
Evidence-Based Clinical Practice Guidelines (8th Edition). Chest.2008;133(Suppl 6):381SY453S.
2. Galson SK. The Surgeon General’s Call to Action to Prevent Deep
Vein Thrombosis and Pulmonary Embolism. U.S. Departmentof Health and Human Services; 2008.
3. Goldhaber SZ. Outpatient venous thromboembolism: a commonbut often preventable public health threat. Arch Intern Med.2007;167:1451Y1452.
4. Dentali F, Douketis JD, Gianni M, et al. Meta-analysis:anticoagulant prophylaxis to prevent symptomatic venousthromboembolism in hospitalized medical patients. Ann Intern Med.2007;146:278Y288.
5. Mismetti P, Laporte S, Darmon JY, et al. Meta-analysis of lowmolecular weight heparin in the prevention of venousthromboembolism in general surgery. Br J Surg. 2001;88:913Y930.
6. Anderson FA, Wheeler HB, Goldberg HB, et al. The prevalenceof risk factors for venous thromboembolism among hospital patients.Arch Int Med. 1992;152:1660Y1664.
7. Anderson FA Jr, Wheeler HB, Goldberg RJ, et al. Apopulation-based perspective of the hospital incidence andcase-fatality rates of deep vein thrombosis and pulmonary embolism.the Worcester DVT Study. Arch Intern Med. 1991;151:933Y938.
8. Bratzler DW, Raskob GE, Murray CK, et al. Underuse of venousthromboembolism prophylaxis for general surgery patients: physicianpractices in the community hospital setting. Arch Intern Med.1998;158:1909Y1912.
9. Goldhaber SZ, Tapson VF, DVT FREE Steering Committee.A prospective registry of 5,451 patients with ultrasound-confirmeddeep vein thrombosis. Am J Cardiol. 2004;93:259Y262.
10. Tapson VF, Decousus H, Pini M, et al. Venous thromboembolismprophylaxis in acutely ill hospitalized medical patients: findings fromthe International Medical Prevention Registry on VenousThromboembolism. Chest. 2007;132:936Y045.
11. Cohen AT, Tapson VF, Bergmann JF, et al. Venous thromboembolismrisk and prophylaxis in the acute hospital care setting(ENDORSE Study): a multinational cross-sectional study. Lancet.2008;371:387Y394.
12. Department of Health and Human Services Centers for Medicareand Medicaid Services. Federal Register. 2008;73:48433Y49084.
13. Kucher N, Koo S, Quiroz R, et al. Electronic alerts to preventvenous thromboembolism among hospitalized patients. N Engl J Med.2005;352:969Y977.
14. Manyard GA, Morris TA, Jenkins IH, et al. Optimizing preventionof hospital-acquired venous thromboembolism (VTE): prospectivevalidation of a VTE risk assessment model. J Hosp Med.2010;5:10Y18.
15. Comerota AJ, Katz ML, White JV. Why does prophylaxiswith external pneumatic compression for deep vein thrombosis fail?Am J Surg. 1992;164:265Y268.
16. Cornwell EE 3rd, Chang D, Velmahos G, et al. Compliance withsequential compression device prophylaxis in at-risk trauma patients:a prospective analysis. Am Surg. 2002;68:470Y473.
17. Shermock KM, Lau BD, Haut ER, et al. Patterns ofnon-administration of ordered doses of venous thromboembolismprophylaxis: implications for novel intervention strategies. PLoS ONE.2013;8:e66311.
18. Haut ER and Streiff MB. Mandatory Computer-Based DecisionSupport. April 9, 2010. Available at: http://natfonline.org/docs/Hopkins_HospStrategies_Summary_NATF.pdf. Accessed onFebruary 21, 2012.
J Patient Saf & Volume 00, Number 00, Month 2014 Delivery of Pharmacological VTE Prophylaxis
* 2014 Lippincott Williams & Wilkins www.journalpatientsafety.com 5
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
19. O’Reilly M, Parker N. ‘Unsatisfactory saturation’: a critical
exploration of the notion of saturated sample sizes in qualitative
research. Qual Res. 2013;13:190Y197.
20. Fanikos J, Stevens LA, Labreche M, et al. Adherence to
pharmacological thromboprophylaxis orders in hospitalized patients.
Am J Med. 2010;123:536Y541.
21. Streiff MB, Haut ER. The CMS ruling on venous
thromboembolism after total knee or hip arthroplasty. JAMA.
2009;301:1063Y1065.
22. Haut ER, Pronovost PJ. Surveillance bias in outcomes reporting.JAMA. 2011;305:2462Y2463.
23. Cabana MD, Rand CS, Powe NR, et al. Why don’t physicians followclinical practice guidelines? a framework for improvement. JAMA.1999;282:1458Y1465.
24. Berenholtz S. Pronovost PJ. Barriers to translating evidence intopractice. Curr Opin Crit Care. 2003;9:321Y325.
25. Piazza G, Nguyen TN, Morrison R, et al. Patient education programfor venous thromboembolism prevention in hospitalized patients.Am J Med. 2012;125:258Y264.
Appendix 1. Venous thromboembolism prophylaxis administration/outcomes at the Johns Hopkins Hospital
Elder et al J Patient Saf & Volume 00, Number 00, Month 2014
6 www.journalpatientsafety.com * 2014 Lippincott Williams & Wilkins
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
Copyright © 2022 FDOKUMEN




















