
Primary Thromboprophylaxis in Hospices: The Association Between Risk of Venous Thromboembolism and...
9
Original Article Primary Thromboprophylaxis in Hospices: The Association Between Risk of Venous Thromboembolism and Development of Symptoms Miriam J. Johnson, MD, FRCP, MBChB(Hons), Brian McMillan, PhD, BSSc, MBChB, Caroline Fairhurst, MMath, Rhian Gabe, PhD, MPhil, MSc, Jason Ward, MRCGP, MMEd, FHEA, MBBS, Jenny Wiseman, MRCGP, MBBS, Bruce Pollington, PDip Sup & Pall Care, MBChB, and Simon I.R. Noble, MD, FRCP, MBBS Palliative Medicine (M.J.J.), Hull York Medical School, University of Hull, Hull; Academic Unit of Primary Medical Care (B.M.), University of Sheffield, Sheffield; York Trials Unit (C.F.), Department of Health Sciences, University of York, York; Department of Health Sciences (R.G.), Hull York Medical School, University of York, York; Palliative Medicine (J.Wa.), St. Gemma’s Hospice Leeds and University of Leeds (J.Wa.), Leeds; Palliative Medicine (J.Wi.), Wrightington, Wigan and Leigh NHS Foundation Trust, Wigan; The Heart of Kent Hospice (B.P.), Maidstone; and Department of Palliative Medicine (S.I.R.N.), Cardiff University and Royal Gwent Hospital (S.I.R.N.), Newport, United Kingdom Abstract Context. Venous thromboembolism (VTE) risk assessment for adults admitted to hospital is commonplace, but the utility of assessment tools in patients admitted to hospices or palliative care units and prediction of symptomatic VTE is unknown. Objectives. To investigate the relationship between risk of VTE and development of symptoms. Methods. Retrospective consecutive admission, case-note data from seven U.K. hospices were collected during an evaluation of a VTE risk assessment protocol using the Pan Birmingham Cancer Network palliative-modified Thromboembolic Risk Factors (THRIFT) Consensus Group criteria and presence/absence of a temporary elevated risk (TER) of VTE. Symptoms/signs during admission consistent with possible VTE were documented. Results. A total of 1164 case-notes were analyzed (age range 23e99; men 627). THRIFT risk was high in 13%, medium in 83%, and low in 4%; a TER was identified in 24%. In the ‘‘clinically relevant group’’ (no contraindication, not anticoagulated), where primary thromboprophylaxis could have been prescribed (n ¼ 528), TER and symptoms were associated (21% symptoms with TER vs. 9% symptoms without TER: Chi-squared, P < 0.001). A high/moderate THRIFT score had a sensitivity of 98.4% (95% CI 91.3%e99.9%) and specificity of 5.8% (95% CI Address correspondence to: Miriam J. Johnson, MD, FRCP, MBChB(Hons), Hull York Medical School, Hertford Building, University of Hull, Cottingham Road, Hull HU6 7RX, United Kingdom. E-mail: [email protected] Accepted for publication: August 31, 2013. Ó 2014 U.S. Cancer Pain Relief Committee. Published by Elsevier Inc. All rights reserved. 0885-3924/$ - see front matter http://dx.doi.org/10.1016/j.jpainsymman.2013.08.016 56 Journal of Pain and Symptom Management Vol. 48 No. 1 July 2014
-
Upload
manchester -
Category
Documents
-
view
1 -
download
0
Transcript of Primary Thromboprophylaxis in Hospices: The Association Between Risk of Venous Thromboembolism and...

56 Journal of Pain and Symptom Management Vol. 48 No. 1 July 2014
Original Article
Primary Thromboprophylaxis in Hospices:The Association Between Risk of VenousThromboembolism and Developmentof SymptomsMiriam J. Johnson, MD, FRCP, MBChB(Hons),Brian McMillan, PhD, BSSc, MBChB, Caroline Fairhurst, MMath,Rhian Gabe, PhD, MPhil, MSc, Jason Ward, MRCGP, MMEd, FHEA, MBBS,Jenny Wiseman, MRCGP, MBBS, Bruce Pollington, PDip Sup & Pall Care, MBChB,and Simon I.R. Noble, MD, FRCP, MBBSPalliative Medicine (M.J.J.), Hull York Medical School, University of Hull, Hull; Academic Unit of
Primary Medical Care (B.M.), University of Sheffield, Sheffield; York Trials Unit (C.F.), Department of
Health Sciences, University of York, York; Department of Health Sciences (R.G.), Hull York Medical
School, University of York, York; Palliative Medicine (J.Wa.), St. Gemma’s Hospice Leeds and
University of Leeds (J.Wa.), Leeds; Palliative Medicine (J.Wi.), Wrightington, Wigan and Leigh NHS
Foundation Trust, Wigan; The Heart of Kent Hospice (B.P.), Maidstone; and Department of
Palliative Medicine (S.I.R.N.), Cardiff University and Royal Gwent Hospital (S.I.R.N.), Newport,
United Kingdom
Abstract
Context. Venous thromboembolism (VTE) risk assessment for adults admittedto hospital is commonplace, but the utility of assessment tools in patients admittedto hospices or palliative care units and prediction of symptomatic VTE is unknown.
Objectives. To investigate the relationship between risk of VTE anddevelopment of symptoms.
Methods. Retrospective consecutive admission, case-note data from seven U.K.hospices were collected during an evaluation of a VTE risk assessment protocolusing the Pan Birmingham Cancer Network palliative-modified ThromboembolicRisk Factors (THRIFT) Consensus Group criteria and presence/absence ofa temporary elevated risk (TER) of VTE. Symptoms/signs during admissionconsistent with possible VTE were documented.
Results. A total of 1164 case-notes were analyzed (age range 23e99; men 627).THRIFT risk was high in 13%, medium in 83%, and low in 4%; a TER wasidentified in 24%. In the ‘‘clinically relevant group’’ (no contraindication, notanticoagulated), where primary thromboprophylaxis could have been prescribed(n ¼ 528), TER and symptoms were associated (21% symptoms with TER vs. 9%symptoms without TER: Chi-squared, P < 0.001). A high/moderate THRIFT scorehad a sensitivity of 98.4% (95% CI 91.3%e99.9%) and specificity of 5.8% (95% CI
Address correspondence to: Miriam J. Johnson, MD,FRCP, MBChB(Hons), Hull York Medical School,Hertford Building, University of Hull, Cottingham
Road, Hull HU6 7RX, United Kingdom. E-mail:[email protected]
Accepted for publication: August 31, 2013.
� 2014 U.S. Cancer Pain Relief Committee.Published by Elsevier Inc. All rights reserved.
0885-3924/$ - see front matterhttp://dx.doi.org/10.1016/j.jpainsymman.2013.08.016
UOS
Highlight
UOS
Sticky Note
Rejected set by UOS

Vol. 48 No. 1 July 2014 57Primary Thromboprophylaxis in Hospices
3.9%e8.3%). The TER assessment had a more evenly balanced sensitivity (41.9%;95% CI 29.5%e55.2%) and specificity (79%; 95% CI 75.0%e82.6%).
Conclusion. Hospice inpatients are at risk for VTE. TER alone is simpler to useand may be more useful in this population than the THRIFT but still haslimitations regarding ability to predict symptoms. J Pain Symptom Manage2014;48:56e64. � 2014 U.S. Cancer Pain Relief Committee. Published by Elsevier Inc. Allrights reserved.
Key Words
Palliative, venous thromboembolism, hospice, primary thromboprophylaxisIntroductionVenous thromboembolism (VTE) is the sec-
ond leading cause of death in cancer patients,yet preventable with appropriate risk assess-ment and prophylaxis.1 A systematic reviewby the Agency for Healthcare Research andQuality ranked thromboprophylaxis highestof 79 evaluated safety interventions.2 VTE pre-vention, therefore, is a health care priority formany countries, with some using financial in-centives and targets to drive implementation.3
The association between VTE and cancer isrecognized, but its clinical relevance in the pal-liative care setting has only recently gained cli-nician and researcher interest.4,5 In additionto the procoagulant effects of the cancer itself,the risk of VTE is increased in patients withadvanced disease, increasing age, immobility,and those receiving anticancer therapies suchas surgery or chemotherapy.6,7 Therefore, pal-liative care inpatients with cancer are at signif-icant risk for VTE. However, although VTErisk assessment for adults admitted to hospitalis now commonplace, the utility of risk as-sessment tools and thromboprophylaxis forthose admitted to palliative care units remainsunclear.
Several evidence-based VTE prevention clin-ical guidelines exist, including cancer specificguidance.7e9 They all identify cancer as a partic-ular risk factor and recommend that oncologypatients admitted to hospital should be consid-ered for low molecular weight heparin throm-boprophylaxis.8 This is supported by Level1A evidence and covers a variety of clinical pa-tient groups.10 However, there is controversysurrounding the appropriate management inadvanced cancer, and the extrapolation ofhospital-based recommendations to hospice
care has been challenged.11,12 Most clinicalstudies informing the guidance excludedpatients with poorer performance status, al-though these people may have much to gain,because of increased thrombotic stimulusfrom extensive disease.11,12 Outcome measuresmay not be the most relevant in the context ofadvanced disease where symptom control andquality of life may outweigh survival consider-ations with reluctance to administer an ‘‘inva-sive’’ injection of LMWH.13 Finally, an attitudepersists that a fatal pulmonary embolus mightbe a ‘‘nice way to go,’’ but this, and assumptionsthat patients would be unwilling to have injec-tions, are not supported by the literature.14,15
Thus, primary thromboprophylaxis (PTP) hasnot been rigorously applied in palliative careunits, although practice appears to be chang-ing as palliative care teams are now also in-volved in the care of people who, despiteadvanced disease, are not imminently dying.16
Clinical guidelines do not recommend PTPin dying patients, but some suggest it shouldbe considered where there is a temporary ele-vation of thrombotic risk because of reversiblepathology.8 A survey using prepared scenariosdemonstrated that the willingness to prescribePTP is directly related to Karnofsky Perfor-mance Status; most clinicians in the surveystated that they would be more likely to givePTP if performance status was >40%.17 How-ever, routine risk assessment for all patientsadmitted to a hospice is unusual and PTPmay be given solely in relation to their placeof admission rather than any clinical risk.The cost-effectiveness of PTP in terms of qual-ity of life for the patient or the treatment costsof a potentially preventable VTE in this patientgroup is questioned because there are no data

Table 1Specific Elements of the THRIFT and TER in thePan Birmingham Cancer Network Palliative Care
Modified Flowchart
THRIFT riskHigh� Acute illness þ previous VTE� Acute illness þ hypercoagulable state� Stroke� Acute MI� Acute respiratory failure� Acute cardiac failure� Lower limb paralysisMedium
58 Vol. 48 No. 1 July 2014Johnson et al.
to inform this debate.11 The need for researchto identify new subclasses of risk for VTE inpalliative care has been highlighted.5
An attempt to delineate the group at tem-porary higher risk (e.g., acute medical illness,recent surgery, spinal cord compression for re-habilitation, reduced mobility with expecta-tion of recovery) led to the development ofpalliative care focused guidelines by the PanBirmingham Cancer Network (PBCN) fromthe U.K. and the PBCN palliative-modifiedThromboembolic Risk Factors (THRIFT) Con-sensus Group criteria.18
There are few published data from palliativecare patients regarding PTP. A prospective sur-vey of 21 units in Austria described experiencewith 134 patients from 18 responding units,and there is a single unit survey of 127 consecu-tive admissions.19 We have previously reportedour initial evaluation of the effect of institu-tional implementation of a routine VTE risk as-sessment on PTP prescribing on consecutiveadmissions from three U.K. hospices (300 firstcycle; 350 second cycle).20 These reports givesome indication of the PTPpractice in hospices,the numbers of patients who have contraindica-tions to LMWH, and the impact of systematicrisk assessment on PTP prescribing. The levelof PTP prescription remained low (1% in-creased to 3.7%) even with regular VTE risk as-sessment, and nearly half of all admissions hada contraindication to PTP with LMWH.20 How-ever, such data provide little by way of clinicaloutcomes.
Subsequent to our previous report, we con-tinued to collect data from seven U.K. hospicesuntil the last hospice unit had completed bothaudit cycles. This article presents the findingsfrom this larger dataset.
� Major medical illness� Malignancy/myeloproliferative disorder� Inflammatory disease� Nephritic syndrome� Hormone treatment� Major trauma/burns� Fracture/orthopedic surgeryLow� Minor trauma or medical illnessTERdrecent event with the expectation of recovery fromthat event such as:
� Recent major surgery� Acute medical illness� New diagnosis of spinal cord compression and expectedto recover
� Pathological fracture and expected to recover mobility
THRIFT¼ ThromboembolicRiskFactors;TER¼ temporary elevatedrisk; VTE¼ venous thromboembolism; MI ¼ myocardial infarction.
MethodsData Collection
SevenU.K. hospices participated in this study.All case-note documentation relating to judg-ments about VTE risk and contraindications toPTP was carried out by the usual admitting clin-ical team as part of usual daily practice. NationalHealth Service Research Ethics Committee ap-proval was not required for this secondary useof anonymized data collected as part of a servicedevelopment in accordance to National Re-search Ethics Service guidance.21
Retrospective case-note audit data from con-secutive admissions were collected using a stan-dard data extraction proforma by clinical staffor research nurses attached to the unit as partof an evaluation of VTE risk assessment andPTP prescribing. The first hospice (St. Cather-ine’s Hospice, Scarborough) began data col-lection in May 2009 and the database wascapped for analysis in April 2011.The PBCN palliative-modified THRIFT flow-
chart VTE risk assessment tool was used, whichprovides two descriptions of risk: 1) THRIFTrisk (risk classified as low, moderate, or high)and 2) presence or absence of a temporary ele-vated risk (TER) of VTE in the judgment of theclinician (Table 1). The PBCN palliative-modified THRIFT was used as this was the onlyavailablepalliative-modified risk assessment tool.
Data ExtractionThe following information was recorded for
all admissions: patient demographics, THRIFTand TER assessment, prescription of PTP, do-cumentation relating to decisions regardingPTP, and contraindications to PTP. PTP was con-sidered to be inappropriate in patients: witha contraindication to anticoagulation (bleeding,

Vol. 48 No. 1 July 2014 59Primary Thromboprophylaxis in Hospices
thrombocytopenia [platelet count<50� 10�9]),deemed to be dying, and already on therapeuticanticoagulation for a confirmed VTE.
Note also wasmade of documented symptomsand signs during the admission consistent witha possible VTE as a ‘‘proxy’’ measure of VTEevents, recognizing that only a percentage ofthesewouldbecausedbyaVTE.These symptomswere new onset pleuritic chest pain, new onsetleg swelling, or new onset or worsening breath-lessness. Confirmation of VTE by appropriateinvestigation was not required for this dataset.
Statistical AnalysisData from individual anonymizeddata extrac-
tion sheets were collected by the co-ordinatingcenter (St. Catherine’s Hospice) and enteredinto a customized Microsoft Excel (2007)spreadsheet. Data were analyzed using STATAv. 12 (StataCorp LP, College Station, TX). Forpatient baseline characteristics, categoricaldata were summarized as frequency (n, %),and continuous measures were summarized us-ing descriptive statistics (n, mean, SD, median,interquartile range,minimum, andmaximum).We investigated whether the VTE risk assess-ment tools (THRIFT, TER) were associatedwith PTP prescription, and whether patientcharacteristics, PTP prescription, THRIFT,TER, or length of hospital stay were associatedwith symptoms. Relationships between categor-ical data were analyzed using Chi-squared andFisher’s exact tests as appropriate, whereas theMann-Whitney U test was used to investigatethe continuous data (age, length of hospitalstay) not normally distributed. The potentialuse of the VTE risk assessment tools in termsof decisionmaking for PTP prescription was ex-plored through estimation of the sensitivity,specificity, predictive value (positive predictivevalue and negative predictive value), likelihoodratios (LR (þ/�)), and odds ratios (ORs) ofTHRIFT and TER in identifying patients at riskof developing symptomatic VTE. Tests weretwo sided, using a significance level of 5%;ORs and accuracy measures such as sensitivityare presented with 95% CIs.
ResultsData from the case-notes of 1164 patients
were extracted. The baseline characteristics
of the patients comprising the total populationare given in Table 2. The age distribution of allpatients was negatively skewed, with a medianage of 72 (range 23e99) years. The proportionof males to females was fairly balanced, with54% male. Characteristics of all patients bycenter are presented in Table 3.
Anticoagulation and Prescription of PTPOn admission, 139 patients were receiving
therapeutic anticoagulation for an establishedVTE, and 68 patients were receiving PTP. Ofthe latter, only 13 patients were continued onPTP by the admitting team, but PTP was com-menced for a further 32 (Table 2).
Clinically Relevant PopulationIn addition to the 139 patients recorded on
admission as receiving a therapeutic dose of an-ticoagulation, a further 496 patients had othercontraindications to PTP. Removing all patientswhere PTP would not have been consideredgave us our primary population of interest(Table 2). This group might gain clinical bene-fit from PTP prescription; the ‘‘clinicallyrelevant population’’ (n¼ 528). Patient charac-teristics were similar for all patients and theclinically relevant population, except that inthe clinically relevant population there wasa slightly lower proportion of cancer patients(still the majority) and higher proportion ofneurological patients. Analyses were conductedon the clinically relevant group and repeatedon the entire set of patients.
We investigated the relationship betweenTHRIFT and TER assessment and PTP pre-scription in our clinically relevant population.The vast majority of these patients were as-sessed as having moderate THRIFT risk(87%), followed by high risk (8%) then lowrisk (5%). There were no patients in the lowTHRIFT risk group started on PTP on admis-sion, 21 patients (5%) in the moderate riskgroup, and 12 patients (30%) in the high-riskgroup. Of patients reported as having a TER,19 (15%) were prescribed PTP, as opposed to3% of the patients without a TER. A strong sta-tistical association was found between prescrip-tion of PTP and both THRIFT (Fisher’s exacttest, P < 0.001) and TER risk assessment(Chi-squared, P < 0.001).
Overall, 12% in the clinically relevant po-pulation developed symptoms. A summary of

Table 2Patient Characteristics
Variable
Clinically Relevant Populationa (n¼ 528) Total Population (N¼ 1164)
n (%) n (%)
Number on TA on admission 139 (12)Missing 1
Number on PTP on admission 68 (6)Number of patients where PTP considered
inappropriate635 (54)
Number started or continued on PTP onadmission
45 (4)
Age (yrs)Mean (SD) 68.9 (13.5) 70.1 (13.1)Median (IQR) 71 (61e78) 72 (62e80)Range 23e96 23e99Missing 2 (0) 2 (0)
SexMale 273 (52) 627 (54)
Diagnostic categoryCancer 402 (76) 949 (82)Heart failure 17 (3) 48 (4)Neurological 72 (14) 80 (7)Other 37 (7) 87 (7)
THRIFT risk scoreLow 28 (5) 48 (4)Moderate 460 (87) 968 (83)High 40 (8) 148 (13)
TER risk scoreNo 404 (77) 880 (76)Yes 124 (23) 279 (24)Missing 0 (0) 5 (0)
TA¼ therapeutic anticoagulation; PTP¼ primary thromboprophylaxis; IQR¼ interquartile range; THRIFT¼ Thromboembolic Risk Factors;TER¼ temporary elevation of risk.aNo venous thromboembolism treatment and no other contraindications to PTP.
60 Vol. 48 No. 1 July 2014Johnson et al.
symptom occurrence is presented in Table 4;some patients developed multiple symptoms.Patients who were not prescribed PTP on ad-mission (n ¼ 495) had a higher estimatedrisk of developing symptoms than those whowere (n ¼ 33) (OR 1.74; 95% CI 0.69e4.4;P ¼ 0.241), although this difference was notstatistically significant.
The overwhelming majority of patients hadcancer, despite many hospices now extendingservices to those with nonmalignant disease(Table 2). More patients with cancer devel-oped symptoms (13%) than patients withheart failure (12%) or neurological disease(4%), although this difference was not statisti-cally significant (Fisher’s exact test, P ¼ 0.141).There was no evidence of a difference in sex(Chi-squared, P ¼ 0.578) or age (Mann-Whit-ney, P ¼ 0.198) by symptom development.
The relationship between THRIFT score andsymptom development was investigated; 4% ofthe low-risk patients, 12% of the moderate-riskpatients, and 10% of the high-risk patients de-veloped symptoms (Table 5). No association
was found between THRIFT risk assessmentand whether the patients developed symptomsor not (Fisher’s exact test, P ¼ 0.437). How-ever, 21% of those with a TER developed symp-toms compared with 9% of patients withouta TER (Chi-squared, P < 0.001).To calculate accuracy measures for the
THRIFTscore,we investigatedtwocombinations:high plus moderate vs. low score (THRIFT 1),and high vs. moderate plus low score (THRIFT2). The sensitivity, specificity, predictive values,likelihood ratios, and odds ratios of these two dif-ferent THRIFT score combinations and of TERassessment were estimated with respect to devel-opment of symptoms (Table 6).In anticipating patients who develop symp-
toms in the clinically relevant patient popula-tion, a high or moderate THRIFT score hada sensitivity of 98.4% (95% CI 91.3%e99.9%)and specificity of 5.8% (95% CI 3.9%e8.3%).A high THRIFT score had a sensitivity of6.5% (95% CI 1.8%e15.7%) and specificityof 92.3% (95% CI 89.5%e94.5%). Assessmentof having a TER was more evenly balanced
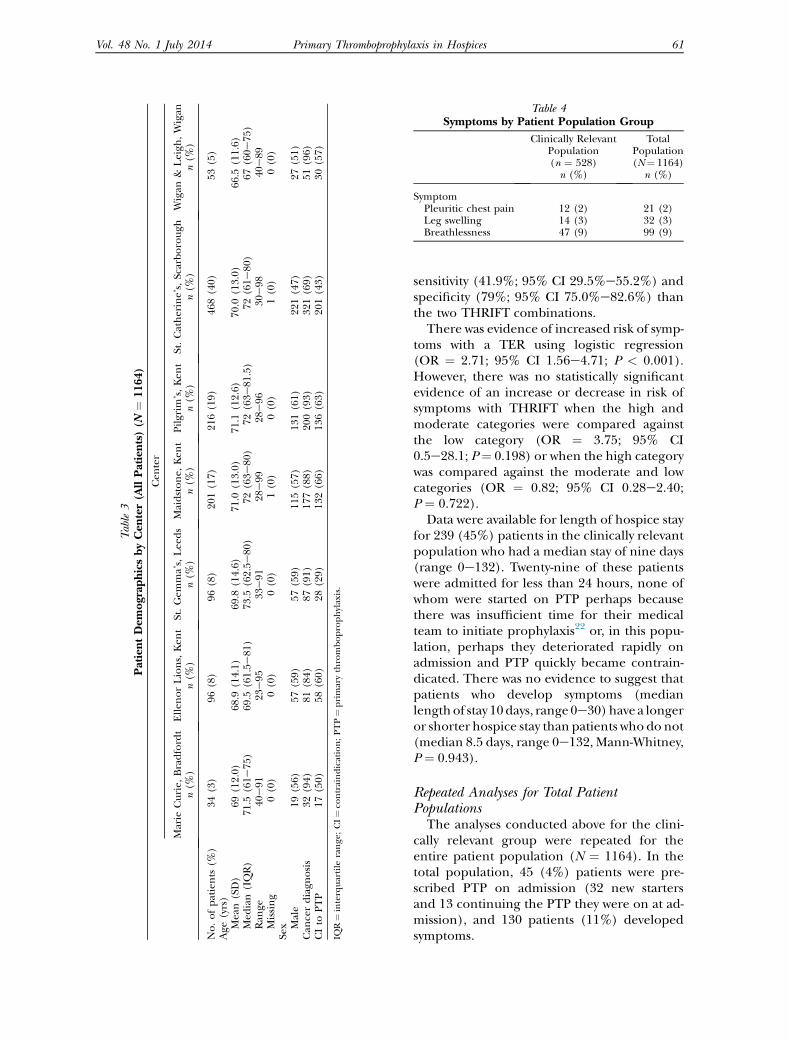
Table3
PatientDem
ograp
hicsbyCen
ter(A
llPatients)(N
¼1164)
Cen
ter
Marie
Curie,
Bradfordt
n(%
)Ellen
orLions,Ken
tn(%
)St.Gem
ma’s,Lee
ds
n(%
)Maidstone,
Ken
tn(%
)Pilgrim
’s,Ken
tn(%
)St.Catherine’s,Scarborough
n(%
)Wigan
&Leigh
,Wigan
n(%
)
No.ofpatients
(%)
34(3)
96(8)
96(8)
201(17)
216(19)
468(40)
53(5)
Age
(yrs)
Mean(SD)
69(12.0)
68.9
(14.1)
69.8
(14.6)
71.0
(13.0)
71.1
(12.6)
70.0
(13.0)
66.5
(11.6)
Med
ian(IQR)
71.5
(61e
75)
69.5
(61.5e
81)
73.5
(62.5e
80)
72(63e
80)
72(63e
81.5)
72(61e
80)
67(60e
75)
Ran
ge40
e91
23e95
33e91
28e99
28e96
30e98
40e89
Missing
0(0)
0(0)
0(0)
1(0)
0(0)
1(0)
0(0)
Sex Male
19(56)
57(59)
57(59)
115(57)
131(61)
221(47)
27(51)
Can
cerdiagn
osis
32(94)
81(84)
87(91)
177(88)
200(93)
321(69)
51(96)
CIto
PTP
17(50)
58(60)
28(29)
132(66)
136(63)
201(43)
30(57)
IQR¼interquartile
range
;CI¼co
ntraindication;PTP¼primarythromboprophylaxis.
Table 4Symptoms by Patient Population Group
Clinically RelevantPopulation(n ¼ 528)n (%)
TotalPopulation(N¼ 1164)
n (%)
SymptomPleuritic chest pain 12 (2) 21 (2)Leg swelling 14 (3) 32 (3)Breathlessness 47 (9) 99 (9)
Vol. 48 No. 1 July 2014 61Primary Thromboprophylaxis in Hospices
sensitivity (41.9%; 95% CI 29.5%e55.2%) andspecificity (79%; 95% CI 75.0%e82.6%) thanthe two THRIFT combinations.
There was evidence of increased risk of symp-toms with a TER using logistic regression(OR ¼ 2.71; 95% CI 1.56e4.71; P < 0.001).However, there was no statistically significantevidence of an increase or decrease in risk ofsymptoms with THRIFT when the high andmoderate categories were compared againstthe low category (OR ¼ 3.75; 95% CI0.5e28.1; P¼ 0.198) or when the high categorywas compared against the moderate and lowcategories (OR ¼ 0.82; 95% CI 0.28e2.40;P ¼ 0.722).
Data were available for length of hospice stayfor 239 (45%) patients in the clinically relevantpopulation who had a median stay of nine days(range 0e132). Twenty-nine of these patientswere admitted for less than 24 hours, none ofwhom were started on PTP perhaps becausethere was insufficient time for their medicalteam to initiate prophylaxis22 or, in this popu-lation, perhaps they deteriorated rapidly onadmission and PTP quickly became contrain-dicated. There was no evidence to suggest thatpatients who develop symptoms (medianlengthof stay 10days, range0e30)have a longeror shorter hospice stay than patients who do not(median 8.5 days, range 0e132, Mann-Whitney,P ¼ 0.943).
Repeated Analyses for Total PatientPopulations
The analyses conducted above for the clini-cally relevant group were repeated for theentire patient population (N ¼ 1164). In thetotal population, 45 (4%) patients were pre-scribed PTP on admission (32 new startersand 13 continuing the PTP they were on at ad-mission), and 130 patients (11%) developedsymptoms.
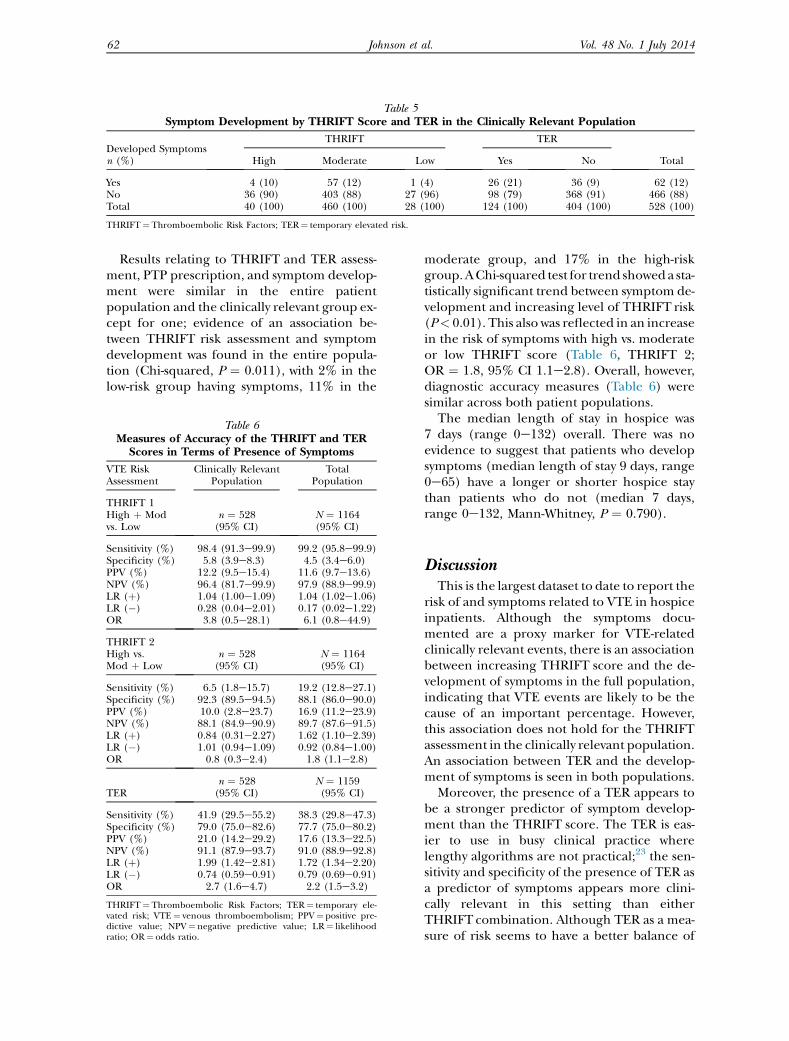
Table 5Symptom Development by THRIFT Score and TER in the Clinically Relevant Population
Developed Symptomsn (%)
THRIFT TER
TotalHigh Moderate Low Yes No
Yes 4 (10) 57 (12) 1 (4) 26 (21) 36 (9) 62 (12)No 36 (90) 403 (88) 27 (96) 98 (79) 368 (91) 466 (88)Total 40 (100) 460 (100) 28 (100) 124 (100) 404 (100) 528 (100)
THRIFT¼ Thromboembolic Risk Factors; TER¼ temporary elevated risk.
62 Vol. 48 No. 1 July 2014Johnson et al.
Results relating to THRIFT and TER assess-ment, PTP prescription, and symptom develop-ment were similar in the entire patientpopulation and the clinically relevant group ex-cept for one; evidence of an association be-tween THRIFT risk assessment and symptomdevelopment was found in the entire popula-tion (Chi-squared, P ¼ 0.011), with 2% in thelow-risk group having symptoms, 11% in the
Table 6Measures of Accuracy of the THRIFT and TER
Scores in Terms of Presence of Symptoms
VTE RiskAssessment
Clinically RelevantPopulation
TotalPopulation
THRIFT 1High þ Modvs. Low
n ¼ 528(95% CI)
N ¼ 1164(95% CI)
Sensitivity (%) 98.4 (91.3e99.9) 99.2 (95.8e99.9)Specificity (%) 5.8 (3.9e8.3) 4.5 (3.4e6.0)PPV (%) 12.2 (9.5e15.4) 11.6 (9.7e13.6)NPV (%) 96.4 (81.7e99.9) 97.9 (88.9e99.9)LR (þ) 1.04 (1.00e1.09) 1.04 (1.02e1.06)LR (�) 0.28 (0.04e2.01) 0.17 (0.02e1.22)OR 3.8 (0.5e28.1) 6.1 (0.8e44.9)
THRIFT 2High vs.Mod þ Low
n ¼ 528(95% CI)
N ¼ 1164(95% CI)
Sensitivity (%) 6.5 (1.8e15.7) 19.2 (12.8e27.1)Specificity (%) 92.3 (89.5e94.5) 88.1 (86.0e90.0)PPV (%) 10.0 (2.8e23.7) 16.9 (11.2e23.9)NPV (%) 88.1 (84.9e90.9) 89.7 (87.6e91.5)LR (þ) 0.84 (0.31e2.27) 1.62 (1.10e2.39)LR (�) 1.01 (0.94e1.09) 0.92 (0.84e1.00)OR 0.8 (0.3e2.4) 1.8 (1.1e2.8)
TERn ¼ 528(95% CI)
N ¼ 1159(95% CI)
Sensitivity (%) 41.9 (29.5e55.2) 38.3 (29.8e47.3)Specificity (%) 79.0 (75.0e82.6) 77.7 (75.0e80.2)PPV (%) 21.0 (14.2e29.2) 17.6 (13.3e22.5)NPV (%) 91.1 (87.9e93.7) 91.0 (88.9e92.8)LR (þ) 1.99 (1.42e2.81) 1.72 (1.34e2.20)LR (�) 0.74 (0.59e0.91) 0.79 (0.69e0.91)OR 2.7 (1.6e4.7) 2.2 (1.5e3.2)
THRIFT¼ Thromboembolic Risk Factors; TER¼ temporary ele-vated risk; VTE¼ venous thromboembolism; PPV¼ positive pre-dictive value; NPV¼ negative predictive value; LR¼ likelihoodratio; OR¼ odds ratio.
moderate group, and 17% in the high-riskgroup.AChi-squared test for trend showeda sta-tistically significant trend between symptom de-velopment and increasing level of THRIFT risk(P< 0.01). This also was reflected in an increasein the risk of symptoms with high vs. moderateor low THRIFT score (Table 6, THRIFT 2;OR ¼ 1.8, 95% CI 1.1e2.8). Overall, however,diagnostic accuracy measures (Table 6) weresimilar across both patient populations.The median length of stay in hospice was
7 days (range 0e132) overall. There was noevidence to suggest that patients who developsymptoms (median length of stay 9 days, range0e65) have a longer or shorter hospice staythan patients who do not (median 7 days,range 0e132, Mann-Whitney, P ¼ 0.790).
DiscussionThis is the largest dataset to date to report the
risk of and symptoms related to VTE in hospiceinpatients. Although the symptoms docu-mented are a proxy marker for VTE-relatedclinically relevant events, there is an associationbetween increasing THRIFT score and the de-velopment of symptoms in the full population,indicating that VTE events are likely to be thecause of an important percentage. However,this association does not hold for the THRIFTassessment in the clinically relevant population.An association between TER and the develop-ment of symptoms is seen in both populations.Moreover, the presence of a TER appears to
be a stronger predictor of symptom develop-ment than the THRIFT score. The TER is eas-ier to use in busy clinical practice wherelengthy algorithms are not practical;23 the sen-sitivity and specificity of the presence of TER asa predictor of symptoms appears more clini-cally relevant in this setting than eitherTHRIFT combination. Although TER as a mea-sure of risk seems to have a better balance of

Vol. 48 No. 1 July 2014 63Primary Thromboprophylaxis in Hospices
sensitivity and specificity than the THRIFT, thesensitivity is still low at 42%, thus missing overhalf of those who would develop symptoms; itmay be that, depending on the risk of harm(again unknown) in this patient group, rou-tine administration of PTP in the absence ofa contraindication is appropriate.
Implications for ResearchWe found no evidence of an association be-
tween PTP and symptom development; how-ever, the percentage of patients prescribedPTP on admission was low (4%) in the wholepopulation, too small to draw any useful con-clusion about whether prescription of PTP pre-vents symptoms. There was an indication thatsymptoms may increase hospice length ofstay, but this was not significant. Further studyis clearly needed to answer whether PTP hasa net benefit compared with none in thosewithout a contraindication to anticoagulation.
Implications for Clinical PracticeSymptomatic VTE may be more common in
hospice patients than has been traditionally re-garded, where such symptoms are often attrib-uted to the underlying disease. Consistentclinical assessment, bearing in mind the pa-tient’s risk of VTE, should be embedded in dailycare. TER alonemay bemore useful in this pop-ulation than the currently used palliative careadapted THRIFT but still has limitations re-garding ability to predict symptoms. Our resultsshould be interpreted in the light of the meth-odological limitations inherent with analysisof retrospective clinical record data.
LimitationsThe main limitations are those inevitable with
the use of retrospective clinical record data. As-sessment of contraindications to PTP and thepresence or absence of TER all depend on theclinical judgment of and documentation by thedoctor responsible for clinical care who willhave had a variable expertise and training inthis regard. In addition, symptoms were not sys-tematically sought, graded, or documented aswould have been the case in a prospective obser-vation studyand thus theprevalenceof symptomsin our dataset are likely to be an underestimate.
We did not routinely investigate symptomswith imaging; thus, we do not know howmany were caused by VTE events, nor their
severitydexcept they were significant enoughfor the patient to report to the doctor who,in turn, thought them significant enough todocument.
We did not have enough data to answer im-portant clinical questions regarding effective-ness of PTP or the effect of symptoms ondays in hospice.
The PBCN palliative adapted THRIFT hasnot undergone any formal clinimetric testingin the palliative care or any other setting.There are cancer-specific risk assessment tools(such as that developed by Khorana24), whichmay be more useful than the generic THRIFT;however, they have not been developed withthe hospice population in mind and includebiomarkers that may not be immediately avail-able on hospice admission.
ConclusionOur data indicate that the binary assessment
of TER is better than the THRIFT in this pa-tient population. The vast majority of patientsadmitted to these hospices were at moderateto high risk of developing a VTE during theirstay. Those with a TER were over twice as likelyto develop symptoms as those without, irrespec-tive of baseline risk. Although there is no pub-lished evidence to suggest that PTP improvessurvival in advanced disease, and this is a ne-glected area in hospice practice, the associationbetween VTE risk and symptoms is concerning.Now that hospices are managing patients whoare not necessarily imminently dying, it is im-portant that we understand the effect of VTE-related events on quality of life and place ofcare and the best way to manage this risk.
Disclosures and AcknowledgmentsThis research received no specific grant
from any funding agency in the public, com-mercial, or not-for-profit sectors. Drs. Johnsonand Noble are co-directors of the TRAD Alli-ance, which is supported by an unrestricted ed-ucational grant from Pfizer. Dr. Noble hasreceived research funding and honoraria forconsultancy work and lectures on behalf ofPfizer and Leo Pharma. All honoraria are do-nated directly to charity. There are no conflictsof interests declared by any other author.

64 Vol. 48 No. 1 July 2014Johnson et al.
The authors thank the staff at all participat-ing centers, and Ms. Tracey Hawkes and Mrs.Anne Nunn for data entry.
References1. Lyman GH, Khorana AA. Cancer, clots and con-sensus: new understanding of an old problem. J ClinOncol 2009;27:4821e4826.
2. Shojania KG, Duncan BW, McDonald KM,Wachter RM, Markowitz AJ. Making health caresafer: a critical analysis of patient safety practices.Evid Rep Technol Assess (Summ) 2001;43:iex.1e668.
3. Department of Health (U.K.). Prevention ofvenous thromboembolism (VTE) in hospitalisedpatients. London: Department of Health, 2010.
4. Noble S. The challenges of managing cancer re-lated venous thromboembolism in the palliativecare setting. Postgrad Med J 2007;83:671e674.
5. Noble S, Johnson M. Finding the evidence forthromboprophylaxis in palliative care: first let usagree on the question. Palliat Med 2010;24:359e361.
6. Johnson MJ, Walker ID, Sproule MW, Conkie J.Abnormal coagulation and deep venous thrombosisin patients with advanced cancer. Clin Lab Haema-tol 1999;21:51e54.
7. Noble S, Pasi J. Epidemiology and pathophysiol-ogy of cancer-associated thrombosis. Br J Cancer2010;102(Suppl 1):S2eS9.
8. National Institute for Health and Care Excel-lence (NICE). Clinical guideline 92: reducing therisk of venous thromboembolism (deep vein throm-bosis and pulmonary embolism) in patients admit-ted to hospital. London: NICE, 2010.
9. Farge D, Debourdeau P, Beckers M, et al. Inter-national clinical practice guidelines for the treat-ment and prophylaxis of venous thromboembolismin patients with cancer. J Thromb Haemost 2013;11:56e70.
10. Lyman GH, Khorana AA, Falanga A, et al.American Society of Clinical Oncology guideline:recommendations for venous thromboembolismprophylaxis and treatment in patients with cancer.J Clin Oncol 2007;25:5490e5505.
11. Tassinari D, Santelmo C, Scarpi E, Tombesi P,Sartori S. Controversial issues in thromboprophy-laxis with low-molecular weight heparins in pallia-tive care. [Letter]. J Pain Symptom Manage 2008;36:e3ee4.
12. Legault S, Tierney S, Senecal I, Pereira J. Evalu-ation of a thromboprophylaxis quality improvementproject in a palliative care unit. J Pain SymptomManage 2011;41:503e510.
13. McLean S, Ryan K, O’Donnell JS. Primarythromboprophylaxis in the palliative care setting:a qualitative systematic review. Palliat Med 2010;24:386e395.
14. Havig O. Deep venous thrombosis and pulmo-nary embolism: an autopsy study with multiple re-gression analysis of possible risk factors. Acta ChirScand Suppl 1977;478:1e120.
15. Noble SI, Nelson A, Turner C, Finlay IG. Accept-ability of low molecular weight heparin thrombo-prophylaxis for inpatients receiving palliative care:qualitative study. BMJ 2006;332:577e580.
16. Noble SI, Finlay IG. Have palliative care teams’attitudes toward venous thromboembolismchanged? A survey of thromboprophylaxis practiceacross British specialist palliative care units in theyears 2000 and 2005. J Pain Symptom Manage2006;32:38e43.
17. Kierner KA, Gartner V, Schwarz M, Watzke HH.Use of thromboprophylaxis in palliative care pa-tients: a survey among experts in palliative care, on-cology, intensive care, and anticoagulation. Am JHosp Palliat Care 2008;25:127e131.
18. Aslett M, Lock A. Guidelines and evidence: pri-mary prophylaxis for venous thromboembolism(VTE) in palliative patients with malignancy. 2008.Available from http://www.birminghamcancer.nhs.uk/uploads/document_file/document/4d67a429358e982b8c000789/network_primary_thromboprophylaxis_guidance__version_2c pdf. AccessedMarch12, 2013.
19. Gartner V, Kierner KA, Namjesky A, et al.Thromboprophylaxis in patients receiving inpatientpalliative care: a survey of present practice in Aus-tria. Support Care Cancer 2012;20:2183e2187.
20. Gillon S, Noble S, Ward J, et al. Primary throm-boprophylaxis for hospice inpatients: who needs it?Palliat Med 2011;25:701e705.
21. National Health Service Health Research Author-ity. Requirements for ethical review under the policyof the UK Health Departments. 2013. Available fromhttp://www.nres.nhs.uk/applications/approval-requirements/ethical-review-requirements/requirements-for-ethical-review-under-the-policy-of-the-uk-health-departments/. Accessed March 12, 2013.
22. Rashid ST, Thursz MR, Razvi NA, et al. Venousthromboprophylaxis in UK medical inpatients. J RSoc Med 2005;98:507e512.
23. Sherlock R, Rawlinson F. Simplifying the reviewof thromboprophylaxis decisions in a palliative careinpatient unit. Palliat Med 2012;26:959e960.
24. Connolly GC, Khorana AA. Emerging risk strat-ification approaches to cancer-associated thrombo-sis: risk factors, biomarkers and a risk score.Thromb Res 2010;125(Suppl 2):S1eS7.




















