
Outpatient therapy with low molecular weight heparin for the treatment of venous thromboembolism: a...
11
REVIEWS Outpatient Therapy with Low Molecular Weight Heparin for the Treatment of Venous Thromboembolism: A Review of Efficacy, Safety, and Costs Jodi B. Segal, MD, MPH, Dennis T. Bolger, MD, MPH, Mollie W. Jenckes, MHSc, Jerry A. Krishnan, MD, Michael B. Streiff, MD, John Eng, MD, Leonardo J. Tamariz, MD, MPH, Eric B. Bass, MD, MPH PURPOSE: To summarize the evidence comparing the effi- cacy, safety, and costs of outpatient and inpatient treatment of venous thromboembolism. METHODS: We searched the literature through March 2002 for studies comparing outpatient and inpatient treatment of venous thromboembolism with low molecular weight heparin or unfractionated heparin, and for studies addressing the costs of low molecular weight heparin use in any setting. We included studies with comparison groups or decision analyses. RESULTS: Eight studies (three randomized trials and five cohort studies) compared outpatient use of low molecular weight heparin with inpatient use of unfractionated heparin in 3762 patients. The incidence of recurrent deep venous thrombosis was similar in the two groups (median, 4% [range, 0% to 7%] vs. 6% [range, 0% to 9%]), as was major bleeding (median, 0.5% [range, 0% to 2%] vs. 1% [range, 0% to 2%]). Use of low molecular weight heparin was associated with shorter hospitalization (median, 2.7 days [range, 0.03 to 5.1 days] vs. 6.5 days [range, 4 to 9.6 days]) and lower costs (median difference, $1600). Comparisons of outpatient and in- hospital use of low molecular weight heparin reported no differ- ence in outcomes, but there were savings in hospitalization costs. Low molecular weight heparin was also found to be more cost saving and cost-effective than unfractionated heparin, with savings of 0% to 64% (median, 57%). CONCLUSION: The evidence indicates that outpatient treat- ment of deep venous thrombosis with low molecular weight heparin is likely to be efficacious, safe, and cost-effective. Am J Med. 2003;115:298 –308. ©2003 by Excerpta Medica Inc. H igh-quality systematic reviews have concluded that low molecular weight heparin, adminis- tered subcutaneously, is as efficacious as intra- venous unfractionated heparin for the treatment of deep venous thrombosis and does not increase the likelihood of major hemorrhagic complications (1). However, most trials in these reviews compared the two agents in an in- patient setting (2–14). Because low molecular weight heparin does not re- quire intravenous administration, it is being used in- creasingly in an outpatient setting or at home. The safety and efficacy of this practice is not known, although the Food and Drug Administration approved enoxaparin for outpatient use in 1998. Furthermore, the costs associated with this practice need to be determined before it can be recommended widely. This situation calls for better understanding of the benefits and cost implications to be expected with use of low molecular weight heparin in an outpatient setting. Such information is important to clinicians choosing the best therapy for patient care, to insurers making decisions about reimbursement levels, to case managers appealing to insurers for coverage of outpatient therapy, to hospital and managed care administrators optimizing the use of hospital resources, and to researchers requiring evidence with which to design future studies. We therefore sought to review the evidence on the ef- ficacy and safety of treating deep venous thrombosis in an outpatient as compared with an inpatient setting, and on the cost-effectiveness of treatment with low molecular weight heparin or unfractionated heparin, regardless of the setting. From the Departments of Medicine (JBS, DTB, MWJ, JAK, MBS, LJT, EBB), and Radiology (JE), Johns Hopkins University School of Medi- cine, and the Bloomberg School of Public Health of the Johns Hopkins University (EBB), Baltimore, Maryland. This study was conducted by the Johns Hopkins Evidence-Based Practice Center under Contract No. 290-97-0006 to the Agency for Healthcare Research and Quality, Rockville, Maryland. The authors are responsible for the content of this article, including any treatment rec- ommendations. No statement in this article should be construed as an official position of the Agency for Healthcare Research and Quality or the U.S. Department of Health and Human Services. Requests for reprints should be addressed to Jodi B. Segal, MD, MPH, Department of Medicine, Johns Hopkins University School of Medi- cine, 720 Rutland Avenue, Ross Building #1025, Baltimore, Maryland 21205, or [email protected]. Manuscript submitted December 10, 2002, and accepted in revised form May 9, 2003. 298 © 2003 by Excerpta Medica Inc. 0002-9343/03/$–see front matter All rights reserved. doi:10.1016/S0002-9343(03)00326-7
Transcript of Outpatient therapy with low molecular weight heparin for the treatment of venous thromboembolism: a...
REVIEWS
Outpatient Therapy with Low Molecular WeightHeparin for the Treatment of Venous
Thromboembolism: A Review of Efficacy,Safety, and Costs
Jodi B. Segal, MD, MPH, Dennis T. Bolger, MD, MPH, Mollie W. Jenckes, MHSc,Jerry A. Krishnan, MD, Michael B. Streiff, MD, John Eng, MD, Leonardo J. Tamariz, MD, MPH,
Eric B. Bass, MD, MPH
PURPOSE: To summarize the evidence comparing the effi-cacy, safety, and costs of outpatient and inpatient treatment ofvenous thromboembolism.METHODS: We searched the literature through March 2002for studies comparing outpatient and inpatient treatment ofvenous thromboembolism with low molecular weight heparinor unfractionated heparin, and for studies addressing the costsof low molecular weight heparin use in any setting. We includedstudies with comparison groups or decision analyses.RESULTS: Eight studies (three randomized trials and five cohortstudies) compared outpatient use of low molecular weight heparinwith inpatient use of unfractionated heparin in 3762 patients. Theincidence of recurrent deep venous thrombosis was similar in thetwo groups (median, 4% [range, 0% to 7%] vs. 6% [range, 0% to
9%]), as was major bleeding (median, 0.5% [range, 0% to 2%] vs.1% [range, 0% to 2%]). Use of low molecular weight heparin wasassociated with shorter hospitalization (median, 2.7 days [range,0.03 to 5.1 days] vs. 6.5 days [range, 4 to 9.6 days]) and lower costs(median difference, $1600). Comparisons of outpatient and in-hospital use of low molecular weight heparin reported no differ-ence in outcomes, but there were savings in hospitalization costs.Low molecular weight heparin was also found to be more costsaving and cost-effective than unfractionated heparin, with savingsof 0% to 64% (median, 57%).CONCLUSION: The evidence indicates that outpatient treat-ment of deep venous thrombosis with low molecular weightheparin is likely to be efficacious, safe, and cost-effective. Am JMed. 2003;115:298 –308. ©2003 by Excerpta Medica Inc.
High-quality systematic reviews have concludedthat low molecular weight heparin, adminis-tered subcutaneously, is as efficacious as intra-
venous unfractionated heparin for the treatment of deepvenous thrombosis and does not increase the likelihoodof major hemorrhagic complications (1). However, mosttrials in these reviews compared the two agents in an in-patient setting (2–14).
Because low molecular weight heparin does not re-
quire intravenous administration, it is being used in-creasingly in an outpatient setting or at home. The safetyand efficacy of this practice is not known, although theFood and Drug Administration approved enoxaparin foroutpatient use in 1998. Furthermore, the costs associatedwith this practice need to be determined before it can berecommended widely.
This situation calls for better understanding of thebenefits and cost implications to be expected with use oflow molecular weight heparin in an outpatient setting.Such information is important to clinicians choosing thebest therapy for patient care, to insurers making decisionsabout reimbursement levels, to case managers appealingto insurers for coverage of outpatient therapy, to hospitaland managed care administrators optimizing the use ofhospital resources, and to researchers requiring evidencewith which to design future studies.
We therefore sought to review the evidence on the ef-ficacy and safety of treating deep venous thrombosis in anoutpatient as compared with an inpatient setting, and onthe cost-effectiveness of treatment with low molecularweight heparin or unfractionated heparin, regardless ofthe setting.
From the Departments of Medicine (JBS, DTB, MWJ, JAK, MBS, LJT,EBB), and Radiology (JE), Johns Hopkins University School of Medi-cine, and the Bloomberg School of Public Health of the Johns HopkinsUniversity (EBB), Baltimore, Maryland.
This study was conducted by the Johns Hopkins Evidence-BasedPractice Center under Contract No. 290-97-0006 to the Agency forHealthcare Research and Quality, Rockville, Maryland. The authors areresponsible for the content of this article, including any treatment rec-ommendations. No statement in this article should be construed as anofficial position of the Agency for Healthcare Research and Quality orthe U.S. Department of Health and Human Services.
Requests for reprints should be addressed to Jodi B. Segal, MD, MPH,Department of Medicine, Johns Hopkins University School of Medi-cine, 720 Rutland Avenue, Ross Building #1025, Baltimore, Maryland21205, or [email protected].
Manuscript submitted December 10, 2002, and accepted in revisedform May 9, 2003.
298 © 2003 by Excerpta Medica Inc. 0002-9343/03/$–see front matterAll rights reserved. doi:10.1016/S0002-9343(03)00326-7

METHODS
Literature SearchWe identified studies through March 2002 usingMEDLINE (which includes articles since 1966) as wellas the Cochrane Database of Systematic Reviews and theCochrane Controlled Trials Register (15). We then exam-ined reference lists from retrieved articles and referenceliterature, queried experts in the field, and reviewed thetables of contents (October 2001 through March 2002)from journals cited most frequently in the literaturesearches.
Abstract ReviewTwo researchers independently reviewed abstracts to ex-clude those that were not relevant to the research ques-tions, reported on prevention but not treatment of ve-nous thromboembolism, were not written in English, didnot include human data, or were published only as anabstract. Articles that did not include a comparison groupfor the evaluation of outpatient versus inpatient therapywere also excluded. We included analyses that modeledthe costs associated with use of the two heparins, as well ascost-effectiveness (i.e., reported results as costs associatedwith some unit of benefit) and cost-minimization (i.e.,reported overall benefits in monetary terms) studies.
Data AbstractionWe developed and pilot tested article review forms, whichincluded a quality assessment and a content abstractionform. The quality assessment forms for the treatmentstudies included items in the following categories: de-scription and representativeness of the study sample,likelihood of bias and confounding, adequacy of descrip-tion of therapy, completeness of outcomes reporting, andquality of the statistical analyses. These items were de-rived from study quality forms used in previous projects(16,17) and are available for review (15). Each item wasscored as 0 (criteria not met), 1 (criteria partially met), or2 (criteria fully met). The score for each category was thepercentage of the total points available in each category(0% to 100%). The overall quality score was the averageof the five categorical scores.
We created a separate quality assessment form for thecost-effectiveness studies using information suggested bythe Evidence-Based Medicine Working Group (18). Thiscomprised nine items (scored from 0 to 2) particular tomodeled analyses, including the perspective taken, sourceof parameter estimates, use of sensitivity analyses, andappropriate reporting of results (19). The overall qualityscore was the average of the scores from these nine items.
The content abstraction form included items describ-ing the type of study; geographical location; definition ofstudy groups; specific aims; inclusion and exclusion cri-teria; demographic, social, and clinical characteristics of
subjects; sources of data for the decision analyses; andoutcomes or results relevant to each question.
Article Review ProcessTwo investigators reviewed each article and came to con-sensus by discussion. They were not blinded to author orjournal names because previous work has shown thatblinding is unlikely to affect the results of the data ab-straction (20).
We developed a database for the quality assessmentand content abstraction data. The evidence tables werebuilt using Microsoft Access 2000 (Microsoft Corpora-tion, Redmond, Washington), with a data-entry frontend developed with Delphi (Borland Delphi, Scotts Val-ley, California).
Summary of EvidenceAbstracted information was put into evidence tables. Thequalitative heterogeneity among the outpatient versus in-patient studies (including differences in enrolled popula-tion, study design, duration of therapy) precluded aquantitative pooling of the results. No standard method-ology exists for pooling the results of decision analyses,and the qualitative heterogeneity in these studies alsomade pooling the results unsuitable. For trials that re-ported monetary outcomes, we converted all costs to2001 U.S. dollars by using year-specific conversion ratesand inflating the estimates to 2001 dollars.
Evidence GradesFive investigators independently graded the strength ofthe evidence on the two questions addressed in this re-view. If there was disagreement, the final grade was basedon the majority decision. The grading system was as fol-lows (16,21): A (strong)—appropriate data are available,including one well-designed randomized controlled trial;study sample is sufficiently large; adequate controls; dataare consistent across studies; one intervention is clearlysuperior, equivalent, or inferior to another strategy; B(moderate)—appropriate data are available; study sam-ple is sufficiently large; adequate controls; data are rea-sonably consistent across studies; one intervention islikely to be superior, equivalent, or inferior to another,but not enough evidence to conclude definitively; C(weak)—some data are available; study sample is reason-ably large; data indicate a trend supporting benefit (orequivalence) of one intervention compared with another,but not enough evidence to conclude that intervention islikely to be superior, equivalent, or inferior to another;and I (insufficient)—appropriate data are not availableor insufficient number of patients studied.
RESULTS
Our search identified 1786 potential citations. Weexcluded citations of articles that did not address the
LMWH for Treatment of Venous Thromboembolism/Segal et al
September 2003 THE AMERICAN JOURNAL OF MEDICINE� Volume 115 299
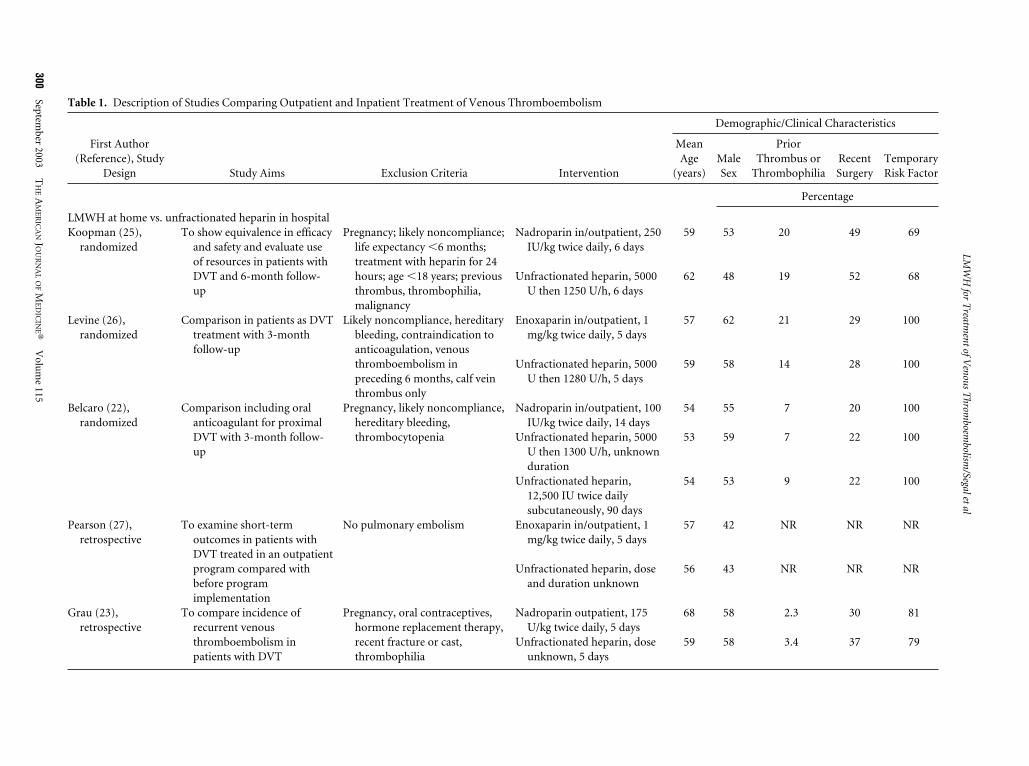
Table 1. Description of Studies Comparing Outpatient and Inpatient Treatment of Venous Thromboembolism
First Author(Reference), Study
Design Study Aims Exclusion Criteria Intervention
Demographic/Clinical Characteristics
MeanAge
(years)MaleSex
PriorThrombus or
ThrombophiliaRecentSurgery
TemporaryRisk Factor
Percentage
LMWH at home vs. unfractionated heparin in hospitalKoopman (25),
randomizedTo show equivalence in efficacy
and safety and evaluate useof resources in patients withDVT and 6-month follow-up
Pregnancy; likely noncompliance;life expectancy �6 months;treatment with heparin for 24hours; age �18 years; previousthrombus, thrombophilia,malignancy
Nadroparin in/outpatient, 250IU/kg twice daily, 6 days
59 53 20 49 69
Unfractionated heparin, 5000U then 1250 U/h, 6 days
62 48 19 52 68
Levine (26),randomized
Comparison in patients as DVTtreatment with 3-monthfollow-up
Likely noncompliance, hereditarybleeding, contraindication toanticoagulation, venousthromboembolism inpreceding 6 months, calf veinthrombus only
Enoxaparin in/outpatient, 1mg/kg twice daily, 5 days
57 62 21 29 100
Unfractionated heparin, 5000U then 1280 U/h, 5 days
59 58 14 28 100
Belcaro (22),randomized
Comparison including oralanticoagulant for proximalDVT with 3-month follow-up
Pregnancy, likely noncompliance,hereditary bleeding,thrombocytopenia
Nadroparin in/outpatient, 100IU/kg twice daily, 14 days
54 55 7 20 100
Unfractionated heparin, 5000U then 1300 U/h, unknownduration
53 59 7 22 100
Unfractionated heparin,12,500 IU twice dailysubcutaneously, 90 days
54 53 9 22 100
Pearson (27),retrospective
To examine short-termoutcomes in patients withDVT treated in an outpatientprogram compared withbefore programimplementation
No pulmonary embolism Enoxaparin in/outpatient, 1mg/kg twice daily, 5 days
57 42 NR NR NR
Unfractionated heparin, doseand duration unknown
56 43 NR NR NR
Grau (23),retrospective
To compare incidence ofrecurrent venousthromboembolism inpatients with DVT
Pregnancy, oral contraceptives,hormone replacement therapy,recent fracture or cast,thrombophilia
Nadroparin outpatient, 175U/kg twice daily, 5 days
68 58 2.3 30 81
Unfractionated heparin, doseunknown, 5 days
59 58 3.4 37 79
LMW
Hfor
Treatm
entofVenous
Throm
boembolism
/Segaletal
300Septem
ber2003
TH
EA
ME
RIC
AN
JOU
RN
AL
OF
ME
DIC
INE�
Volu
me
115
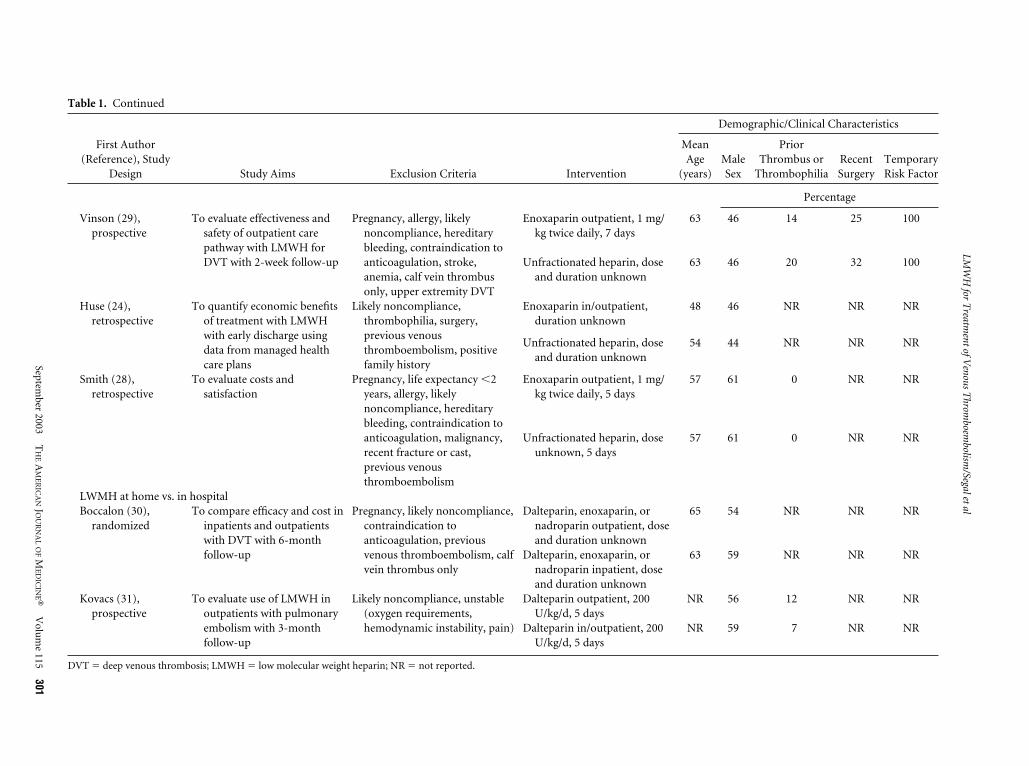
Table 1. Continued
First Author(Reference), Study
Design Study Aims Exclusion Criteria Intervention
Demographic/Clinical Characteristics
MeanAge
(years)MaleSex
PriorThrombus or
ThrombophiliaRecentSurgery
TemporaryRisk Factor
Percentage
Vinson (29),prospective
To evaluate effectiveness andsafety of outpatient carepathway with LMWH forDVT with 2-week follow-up
Pregnancy, allergy, likelynoncompliance, hereditarybleeding, contraindication toanticoagulation, stroke,anemia, calf vein thrombusonly, upper extremity DVT
Enoxaparin outpatient, 1 mg/kg twice daily, 7 days
63 46 14 25 100
Unfractionated heparin, doseand duration unknown
63 46 20 32 100
Huse (24),retrospective
To quantify economic benefitsof treatment with LMWHwith early discharge usingdata from managed healthcare plans
Likely noncompliance,thrombophilia, surgery,previous venousthromboembolism, positivefamily history
Enoxaparin in/outpatient,duration unknown
48 46 NR NR NR
Unfractionated heparin, doseand duration unknown
54 44 NR NR NR
Smith (28),retrospective
To evaluate costs andsatisfaction
Pregnancy, life expectancy �2years, allergy, likelynoncompliance, hereditarybleeding, contraindication toanticoagulation, malignancy,recent fracture or cast,previous venousthromboembolism
Enoxaparin outpatient, 1 mg/kg twice daily, 5 days
57 61 0 NR NR
Unfractionated heparin, doseunknown, 5 days
57 61 0 NR NR
LWMH at home vs. in hospitalBoccalon (30),
randomizedTo compare efficacy and cost in
inpatients and outpatientswith DVT with 6-monthfollow-up
Pregnancy, likely noncompliance,contraindication toanticoagulation, previousvenous thromboembolism, calfvein thrombus only
Dalteparin, enoxaparin, ornadroparin outpatient, doseand duration unknown
65 54 NR NR NR
Dalteparin, enoxaparin, ornadroparin inpatient, doseand duration unknown
63 59 NR NR NR
Kovacs (31),prospective
To evaluate use of LMWH inoutpatients with pulmonaryembolism with 3-monthfollow-up
Likely noncompliance, unstable(oxygen requirements,hemodynamic instability, pain)
Dalteparin outpatient, 200U/kg/d, 5 days
NR 56 12 NR NR
Dalteparin in/outpatient, 200U/kg/d, 5 days
NR 59 7 NR NR
DVT � deep venous thrombosis; LMWH � low molecular weight heparin; NR � not reported.
LMW
Hfor
Treatm
entofVenous
Throm
boembolism
/Segaletal
September
2003T
HE
AM
ER
ICA
NJO
UR
NA
LO
FM
ED
ICIN
E�V
olum
e115
301
study questions (n � 1122 studies), contained nooriginal data or analyses (n � 354), were not in English(n � 99), had no human data (n � 18), were limited toprevention of venous thromboembolism (n � 126),were case reports (n � 29), or presented data reportedin other publications (n � 2), as well as excluded ab-stracts that had no accompanying published article(n � 3). Another 14 articles were excluded during thearticle review process for not containing original data,lacking a comparison group, involving only outpatients,or lacking relevance. Thus, 19 studies remained eligiblefor review.
Clinical Outcomes of Outpatient and InpatientTherapyDescription of studies. Eight studies compared the clin-ical outcomes of patients with deep venous thrombosiswho were treated with either low molecular weight hep-arin at home or unfractionated heparin in the hospital(Table 1) (22–29). Three were randomized trials(22,25,26) and five were cohort studies. Two other stud-ies (30,31) compared the clinical outcomes of and costsfor patients who received low molecular weight heparinat home or in the hospital (Table 1).
The smallest of these 10 studies enrolled 28 patients ineach arm (28), whereas the largest comprised 1850 pa-tients (164 of whom had received low molecular weightheparin and the remainder had received unfractionatedheparin) (24). All of the studies used enoxaparin, na-droparin, or dalteparin, administered subcutaneously,during the intervention, and an oral anticoagulant duringthe follow-up (Table 1). Enoxaparin was always given at adosage of 1 mg/kg two times daily; the dosages of theother low molecular weight heparins varied. Unfraction-
ated heparin was always given intravenously in the hos-pital, except for one trial in which a group of patientstreated at home received unfractionated heparin subcu-taneously (22). Six studies allowed a brief inpatient ad-mission before completion of therapy at home for thepatients who had been randomly assigned to the outpa-tient therapy group (22,24 –27,31).
All but one study (31) excluded patients with pul-monary embolism. This study, however, excluded pa-tients who required oxygen, had severe pain, or werehemodynamically unstable, leaving only patients withgood cardiopulmonary reserve or small clot burden. Theexclusion criteria in the other studies were moderatelyrestrictive; most excluded patients with known throm-bophilic conditions, including prior venous thrombo-embolism. More than half of the studies excluded pa-tients who were considered likely to be noncompliantwith outpatient therapy. Only three studies used sched-uled radiological surveillance to detect recurrences(22,26,30).
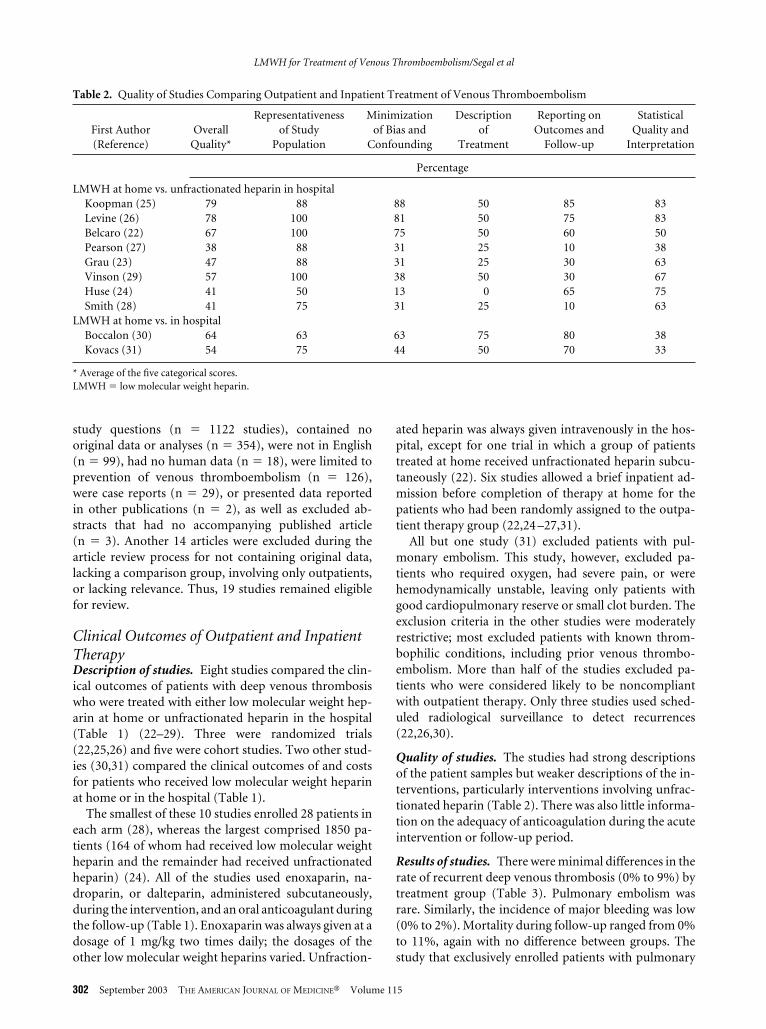
Quality of studies. The studies had strong descriptionsof the patient samples but weaker descriptions of the in-terventions, particularly interventions involving unfrac-tionated heparin (Table 2). There was also little informa-tion on the adequacy of anticoagulation during the acuteintervention or follow-up period.
Results of studies. There were minimal differences in therate of recurrent deep venous thrombosis (0% to 9%) bytreatment group (Table 3). Pulmonary embolism wasrare. Similarly, the incidence of major bleeding was low(0% to 2%). Mortality during follow-up ranged from 0%to 11%, again with no difference between groups. Thestudy that exclusively enrolled patients with pulmonary
Table 2. Quality of Studies Comparing Outpatient and Inpatient Treatment of Venous Thromboembolism
First Author(Reference)
OverallQuality*
Representativenessof Study
Population
Minimizationof Bias and
Confounding
Descriptionof
Treatment
Reporting onOutcomes and
Follow-up
StatisticalQuality and
Interpretation
Percentage
LMWH at home vs. unfractionated heparin in hospitalKoopman (25) 79 88 88 50 85 83Levine (26) 78 100 81 50 75 83Belcaro (22) 67 100 75 50 60 50Pearson (27) 38 88 31 25 10 38Grau (23) 47 88 31 25 30 63Vinson (29) 57 100 38 50 30 67Huse (24) 41 50 13 0 65 75Smith (28) 41 75 31 25 10 63
LMWH at home vs. in hospitalBoccalon (30) 64 63 63 75 80 38Kovacs (31) 54 75 44 50 70 33
* Average of the five categorical scores.LMWH � low molecular weight heparin.
LMWH for Treatment of Venous Thromboembolism/Segal et al
302 September 2003 THE AMERICAN JOURNAL OF MEDICINE� Volume 115
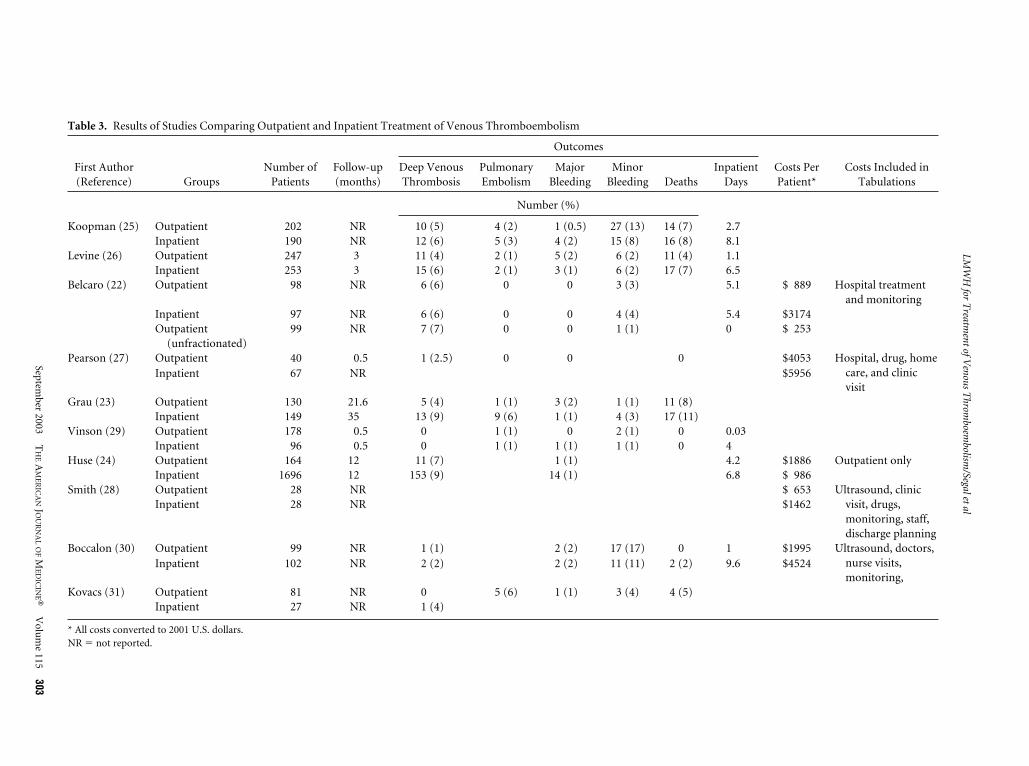
Table 3. Results of Studies Comparing Outpatient and Inpatient Treatment of Venous Thromboembolism
First Author(Reference) Groups
Number ofPatients
Follow-up(months)
Outcomes
Costs PerPatient*
Costs Included inTabulations
Deep VenousThrombosis
PulmonaryEmbolism
MajorBleeding
MinorBleeding Deaths
InpatientDays
Number (%)
Koopman (25) Outpatient 202 NR 10 (5) 4 (2) 1 (0.5) 27 (13) 14 (7) 2.7Inpatient 190 NR 12 (6) 5 (3) 4 (2) 15 (8) 16 (8) 8.1
Levine (26) Outpatient 247 3 11 (4) 2 (1) 5 (2) 6 (2) 11 (4) 1.1Inpatient 253 3 15 (6) 2 (1) 3 (1) 6 (2) 17 (7) 6.5
Belcaro (22) Outpatient 98 NR 6 (6) 0 0 3 (3) 5.1 $ 889 Hospital treatmentand monitoring
Inpatient 97 NR 6 (6) 0 0 4 (4) 5.4 $3174Outpatient
(unfractionated)99 NR 7 (7) 0 0 1 (1) 0 $ 253
Pearson (27) Outpatient 40 0.5 1 (2.5) 0 0 0 $4053 Hospital, drug, homecare, and clinicvisit
Inpatient 67 NR $5956
Grau (23) Outpatient 130 21.6 5 (4) 1 (1) 3 (2) 1 (1) 11 (8)Inpatient 149 35 13 (9) 9 (6) 1 (1) 4 (3) 17 (11)
Vinson (29) Outpatient 178 0.5 0 1 (1) 0 2 (1) 0 0.03Inpatient 96 0.5 0 1 (1) 1 (1) 1 (1) 0 4
Huse (24) Outpatient 164 12 11 (7) 1 (1) 4.2 $1886 Outpatient onlyInpatient 1696 12 153 (9) 14 (1) 6.8 $ 986
Smith (28) Outpatient 28 NR $ 653 Ultrasound, clinicvisit, drugs,monitoring, staff,discharge planning
Inpatient 28 NR $1462
Boccalon (30) Outpatient 99 NR 1 (1) 2 (2) 17 (17) 0 1 $1995 Ultrasound, doctors,nurse visits,monitoring,
Inpatient 102 NR 2 (2) 2 (2) 11 (11) 2 (2) 9.6 $4524
Kovacs (31) Outpatient 81 NR 0 5 (6) 1 (1) 3 (4) 4 (5)Inpatient 27 NR 1 (4)
* All costs converted to 2001 U.S. dollars.NR � not reported.
LMW
Hfor
Treatm
entofVenous
Throm
boembolism
/Segaletal
September
2003T
HE
AM
ER
ICA
NJO
UR
NA
LO
FM
ED
ICIN
E�V
olum
e115
303
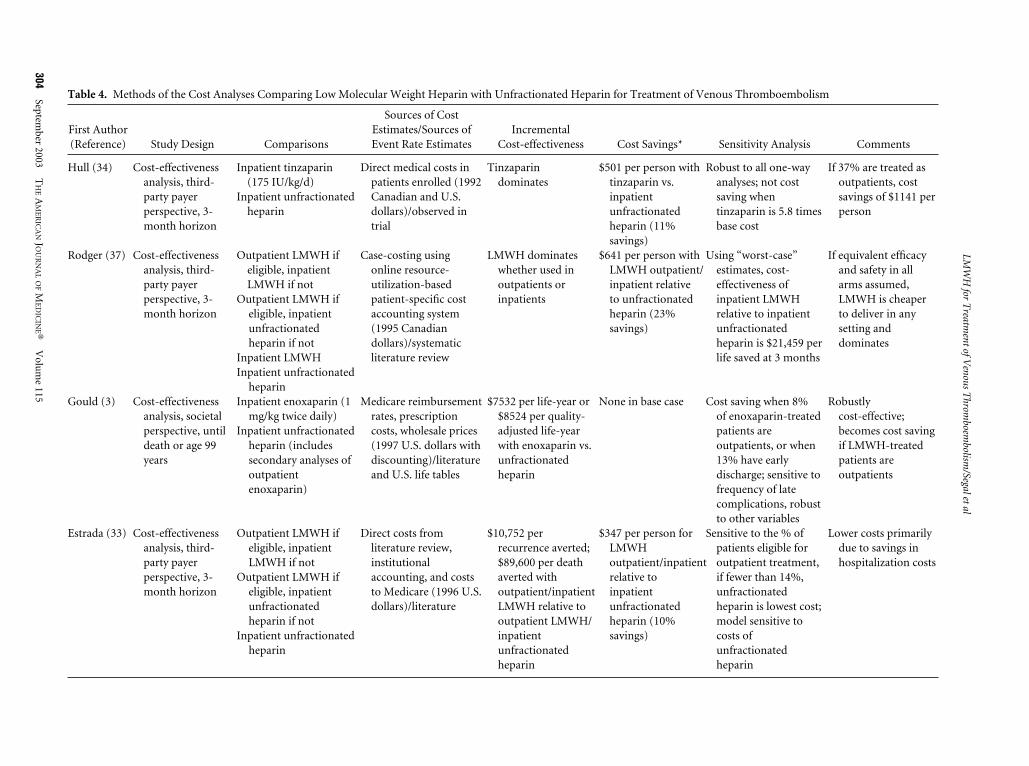
Table 4. Methods of the Cost Analyses Comparing Low Molecular Weight Heparin with Unfractionated Heparin for Treatment of Venous Thromboembolism
First Author(Reference) Study Design Comparisons
Sources of CostEstimates/Sources ofEvent Rate Estimates
IncrementalCost-effectiveness Cost Savings* Sensitivity Analysis Comments
Hull (34) Cost-effectivenessanalysis, third-party payerperspective, 3-month horizon
Inpatient tinzaparin(175 IU/kg/d)
Inpatient unfractionatedheparin
Direct medical costs inpatients enrolled (1992Canadian and U.S.dollars)/observed intrial
Tinzaparindominates
$501 per person withtinzaparin vs.inpatientunfractionatedheparin (11%savings)
Robust to all one-wayanalyses; not costsaving whentinzaparin is 5.8 timesbase cost
If 37% are treated asoutpatients, costsavings of $1141 perperson
Rodger (37) Cost-effectivenessanalysis, third-party payerperspective, 3-month horizon
Outpatient LMWH ifeligible, inpatientLMWH if not
Outpatient LMWH ifeligible, inpatientunfractionatedheparin if not
Inpatient LMWH
Case-costing usingonline resource-utilization-basedpatient-specific costaccounting system(1995 Canadiandollars)/systematicliterature review
LMWH dominateswhether used inoutpatients orinpatients
$641 per person withLMWH outpatient/inpatient relativeto unfractionatedheparin (23%savings)
Using “worst-case”estimates, cost-effectiveness ofinpatient LMWHrelative to inpatientunfractionatedheparin is $21,459 perlife saved at 3 months
If equivalent efficacyand safety in allarms assumed,LMWH is cheaperto deliver in anysetting anddominates
Inpatient unfractionatedheparin
Gould (3) Cost-effectivenessanalysis, societalperspective, untildeath or age 99years
Inpatient enoxaparin (1mg/kg twice daily)
Inpatient unfractionatedheparin (includessecondary analyses ofoutpatientenoxaparin)
Medicare reimbursementrates, prescriptioncosts, wholesale prices(1997 U.S. dollars withdiscounting)/literatureand U.S. life tables
$7532 per life-year or$8524 per quality-adjusted life-yearwith enoxaparin vs.unfractionatedheparin
None in base case Cost saving when 8%of enoxaparin-treatedpatients areoutpatients, or when13% have earlydischarge; sensitive tofrequency of latecomplications, robustto other variables
Robustlycost-effective;becomes cost savingif LMWH-treatedpatients areoutpatients
Estrada (33) Cost-effectivenessanalysis, third-party payerperspective, 3-month horizon
Outpatient LMWH ifeligible, inpatientLMWH if not
Outpatient LMWH ifeligible, inpatientunfractionatedheparin if not
Inpatient unfractionatedheparin
Direct costs fromliterature review,institutionalaccounting, and coststo Medicare (1996 U.S.dollars)/literature
$10,752 perrecurrence averted;$89,600 per deathaverted withoutpatient/inpatientLMWH relative tooutpatient LMWH/inpatientunfractionatedheparin
$347 per person forLMWHoutpatient/inpatientrelative toinpatientunfractionatedheparin (10%savings)
Sensitive to the % ofpatients eligible foroutpatient treatment,if fewer than 14%,unfractionatedheparin is lowest cost;model sensitive tocosts ofunfractionatedheparin
Lower costs primarilydue to savings inhospitalization costs
LMW
Hfor
Treatm
entofVenous
Throm
boembolism
/Segaletal
304Septem
ber2003
TH
EA
ME
RIC
AN
JOU
RN
AL
OF
ME
DIC
INE�
Volu
me
115
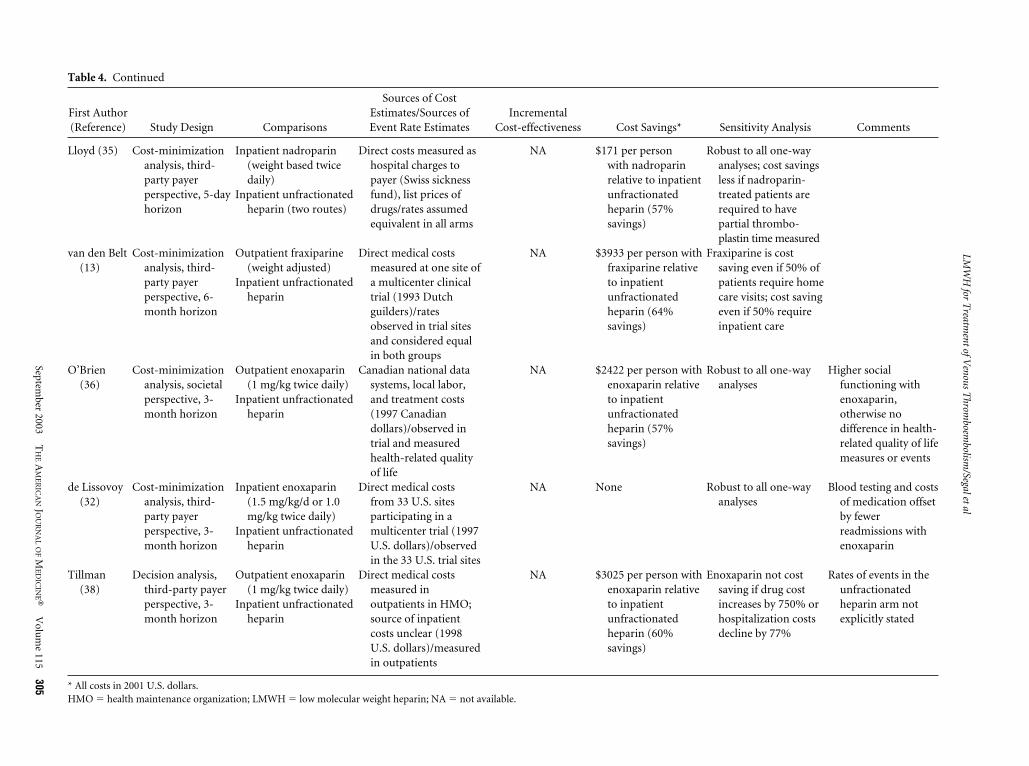
Table 4. Continued
First Author(Reference) Study Design Comparisons
Sources of CostEstimates/Sources ofEvent Rate Estimates
IncrementalCost-effectiveness Cost Savings* Sensitivity Analysis Comments
Lloyd (35) Cost-minimizationanalysis, third-party payerperspective, 5-dayhorizon
Inpatient nadroparin(weight based twicedaily)
Inpatient unfractionatedheparin (two routes)
Direct costs measured ashospital charges topayer (Swiss sicknessfund), list prices ofdrugs/rates assumedequivalent in all arms
NA $171 per personwith nadroparinrelative to inpatientunfractionatedheparin (57%savings)
Robust to all one-wayanalyses; cost savingsless if nadroparin-treated patients arerequired to havepartial thrombo-plastin time measured
van den Belt(13)
Cost-minimizationanalysis, third-party payerperspective, 6-month horizon
Outpatient fraxiparine(weight adjusted)
Inpatient unfractionatedheparin
Direct medical costsmeasured at one site ofa multicenter clinicaltrial (1993 Dutchguilders)/ratesobserved in trial sitesand considered equalin both groups
NA $3933 per person withfraxiparine relativeto inpatientunfractionatedheparin (64%savings)
Fraxiparine is costsaving even if 50% ofpatients require homecare visits; cost savingeven if 50% requireinpatient care
O’Brien(36)
Cost-minimizationanalysis, societalperspective, 3-month horizon
Outpatient enoxaparin(1 mg/kg twice daily)
Inpatient unfractionatedheparin
Canadian national datasystems, local labor,and treatment costs(1997 Canadiandollars)/observed intrial and measuredhealth-related qualityof life
NA $2422 per person withenoxaparin relativeto inpatientunfractionatedheparin (57%savings)
Robust to all one-wayanalyses
Higher socialfunctioning withenoxaparin,otherwise nodifference in health-related quality of lifemeasures or events
de Lissovoy(32)
Cost-minimizationanalysis, third-party payerperspective, 3-month horizon
Inpatient enoxaparin(1.5 mg/kg/d or 1.0mg/kg twice daily)
Inpatient unfractionatedheparin
Direct medical costsfrom 33 U.S. sitesparticipating in amulticenter trial (1997U.S. dollars)/observedin the 33 U.S. trial sites
NA None Robust to all one-wayanalyses
Blood testing and costsof medication offsetby fewerreadmissions withenoxaparin
Tillman(38)
Decision analysis,third-party payerperspective, 3-month horizon
Outpatient enoxaparin(1 mg/kg twice daily)
Inpatient unfractionatedheparin
Direct medical costsmeasured inoutpatients in HMO;source of inpatientcosts unclear (1998U.S. dollars)/measuredin outpatients
NA $3025 per person withenoxaparin relativeto inpatientunfractionatedheparin (60%savings)
Enoxaparin not costsaving if drug costincreases by 750% orhospitalization costsdecline by 77%
Rates of events in theunfractionatedheparin arm notexplicitly stated
* All costs in 2001 U.S. dollars.HMO � health maintenance organization; LMWH � low molecular weight heparin; NA � not available.
LMW
Hfor
Treatm
entofVenous
Throm
boembolism
/Segaletal
September
2003T
HE
AM
ER
ICA
NJO
UR
NA
LO
FM
ED
ICIN
E�V
olum
e115
305

embolism also reported no significant difference in eventrates (31).
There were fewer inpatient days in the treatment armsthat used low molecular weight heparin either entirely athome or after a brief inpatient stay than in the arms thatused unfractionated heparin in the hospital. Few studiesreported the statistical significance of these differences.The duration of hospitalization depended strongly on thestudy design.
Four (22,27,28,30) of the five cost studies suggestedcost savings with outpatient therapy. The study (24) thatreported higher costs with low molecular weight heparin,however, included only outpatient costs in the estimates.The authors did state that if 2.5 hospital days were elim-inated per patient treated as an outpatient, a savings of$1911 per patient might be seen. Only two studies (27,30)reported a statistically significant difference in costs be-tween the study arms, although cost differences also ap-peared to be substantial in other studies. As each studyincluded different items in the tabulations of costs, thecost savings between studies cannot be compared easily.
Based on these studies (Evidence grade B), we con-cluded that outpatient treatment of deep venous throm-bosis with low molecular weight heparin is likely to beefficacious, safe, and economically favorable.
Analyses of Costs and Cost-effectivenessDescription of studies. Nine studies used decision anal-ysis to address the costs of treatment with low molecularweight heparin or unfractionated heparin, regardless ofinpatient or outpatient setting (Table 4). Four were cost-effectiveness analyses (3,33,34,37), four were cost-mini-mization studies (13,32,35,36), and one used a decisionmodel that could not be classified as either (38). A societalperspective was used in quantifying costs in two studies(3,36), whereas the other seven took the perspective of athird-party payer.
The comparisons fell into two categories: the use of lowmolecular weight heparin compared with unfractionatedheparin, with all drugs administered in the hospital(3,32,34,35); and the use of low molecular weight heparinat home compared with unfractionated heparin in thehospital (13,33,36 –38). Two of these latter studies(33,37) modeled the use of low molecular weight heparinin patients at home if they were considered medically el-igible to be treated as outpatients, and in the hospital ifthey were not. The estimates for the costs in the modelsvaried; half used actual costs measured in the setting of aclinical trial and others used costs obtained from data-bases maintained by the government or a payer, or costsabstracted from literature review. Similarly, the rates ofevents included in the models came from actual data ob-served in trials or from the literature. Two studies (13,35)assumed on the basis of earlier work that the rates ofrecurrent thrombosis and adverse events were similar for
low molecular weight heparin and unfractionatedheparin.
Quality of studies. The quality scores for studies oncost-effectiveness or cost minimization were high (67%to 100%; median, 89%), with the studies by Hull et al (34)and Gould et al (3) ranking the highest. Studies wereweakest in their descriptions of the sensitivity analysesand of the samples to which the results were expected toapply.
Results of studies. Of the four studies that compared lowmolecular weight heparin with unfractionated heparin ininpatients, two were cost-minimization studies (32,35).One projected a cost savings of 57% with nadroparin in-stead of with unfractionated heparin (35) (Table 4),whereas the other found no difference in costs betweentreatment with enoxaparin and unfractionated heparin(32). The authors concluded that because these costs wereaccrued in the setting of a clinical trial, some of the labo-ratory tests were protocol driven, thus raising the costsabove what would be seen in usual practice, particularlyin the enoxaparin arm (32). One (34) of the two cost-effectiveness studies comparing inpatient treatment ofthe two heparins found that tinzaparin was both lesscostly and more efficacious than unfractionated heparin.This study predicted a cost savings of 11% with the use oftinzaparin in the hospital in place of unfractionated hep-arin. Gould et al (3) found that although inpatient enox-aparin treatment was more expensive, it was more cost-effective than inpatient unfractionated heparin becauseof the increase in quality-adjusted life-years. Further-more, if 8% of the patients taking enoxaparin weretreated as outpatients, treatment with low molecularweight heparin would be both cost-effective and costsaving.
Outpatient treatment with low molecular weight hep-arin was less costly than hospitalization for treatmentwith unfractionated heparin (Table 4). One cost-effec-tiveness study (33) found that use of low molecularweight heparin, at home for clinically stable patients andin the hospital for unstable patients, yielded a cost savingsof 10% as compared with use of unfractionated heparinin the hospital for all patients, largely due to savings oninpatient costs. Another study (37) found a cost savingsof 23% in a similar comparison. The two cost-minimiza-tion studies found outpatient low molecular weight hep-arin to be associated with a cost savings of 57% (36) and64% (13) as compared with inpatient unfractionatedheparin. The study by Tillman et al (38) provided littledata on event rates in the unfractionated heparin arm;however, the authors reported a cost savings of 60% withenoxaparin at home as compared with unfractionatedheparin in the hospital, and suggested that this treatmentwould be cost saving even if hospitalization costs were77% lower.
LMWH for Treatment of Venous Thromboembolism/Segal et al
306 September 2003 THE AMERICAN JOURNAL OF MEDICINE� Volume 115

The cost-effectiveness studies were consistent in sug-gesting that low molecular weight heparin is either costsaving or cost-effective as compared with unfractionatedheparin (Evidence grade A).
DISCUSSION
The randomized trials that compared treatment with lowmolecular weight heparin in outpatients (or in patientswith early discharge) with unfractionated heparin in in-patients demonstrated no difference in adverse outcomesbetween groups (including recurrent deep venousthrombosis, pulmonary embolism, major bleeding, ordeath), but showed that use of low molecular weight hep-arin reduced the duration of hospitalization and associ-ated costs substantially. Similarly, comparisons of use oflow molecular weight heparin in the hospital or at homerevealed no difference in outcomes but demonstrated amajor savings in hospitalization costs.
No study was adequately powered to detect small dif-ferences in the rates of adverse events between groups.Thus, although a difference in outcomes between groupswas not demonstrated, equivalency cannot be definitivelyclaimed. Nonetheless, the direction of the results wasconsistent and suggested that it is very unlikely that at-home use of low molecular weight heparin will be less safethan unfractionated heparin in appropriately selected pa-tients.
Cost studies were consistent in showing that low mo-lecular weight heparin was either cost saving or cost-ef-fective as compared with unfractionated heparin, regard-less of whether it was administered in the hospital or athome, although the cost savings would be greater if hos-pitalization were avoided. A retrospective analysis pub-lished after completion of our literature search reportedcost savings with enoxaparin that was similar to thoseseen in the trials we reviewed (39).
This review has several limitations. Most of the studieswere small with infrequent adverse events and thus wereunderpowered to look at the designated outcomes. Coststudies often did not include all relevant costs (e.g., timelost from work, cost of outpatient visits). The trials hadstrict criteria for patients considered for outpatient ther-apy; consequently, the results may not apply to all pa-tients seen in usual clinical practice. In particular, moststudies excluded patients who were thought to be un-likely to comply with therapy. Furthermore, some pa-tients in the outpatient groups were initially treated in thehospital before early discharge, raising the possibility thatinitial inpatient treatment contributed to the safety dem-onstrated in these studies. Additionally, the use of onlyEnglish-language literature, the possible exclusion ofsome primary literature by our search strategy, and the
use of quality assessment instruments that have not beenvalidated in other settings may have affected results.
In conclusion, the evidence suggests that outpatienttreatment of deep venous thrombosis with low molecularweight heparin is likely to be efficacious, safe, and costbeneficial. Still, additional studies are needed to evaluatethe use of outpatient treatment among a less restrictedgroup of patients or in patients at high risk of adverseevents, such as those with pulmonary embolism, malig-nancies, or hereditary thrombophilias. High-qualityequivalency studies are needed to confirm that the use oflow molecular weight heparin in outpatients is as effica-cious and safe as unfractionated heparin in the hospital inless select patients. Studies are also needed to evaluate theshort-term and long-term efficacy of low molecularweight heparin as outpatient therapy for symptomaticcalf vein thrombosis.
REFERENCES1. Brewer D. Should low-molecular-weight heparins replace unfrac-
tionated heparin as the agent of choice for adults with deep venousthrombosis? J Fam Pract. 1998;47:185–192.
2. Dolovich LR, Ginsberg JS, Douketis JD, et al. A meta-analysis com-paring low-molecular-weight heparins with unfractionated hepa-rin in the treatment of venous thromboembolism: examining someunanswered questions regarding location of treatment, producttype, and dosing frequency. Arch Intern Med. 2000;160:181–188.
3. Gould MK, Dembitzer AD, Sanders GD, et al. Low-molecular-weight heparins compared with unfractionated heparin for treat-ment of acute deep venous thrombosis. A cost-effectiveness analy-sis. Ann Intern Med. 1999;130:789 –799.
4. Green D, Hirsh J, Heit J, et al. Low molecular weight heparin: acritical analysis of clinical trials. Pharmacol Rev. 1994;46:89 –109.
5. Hettiarachchi RJ, Prins MH, Lensing AW, et al. Low molecularweight heparin versus unfractionated heparin in the initial treat-ment of venous thromboembolism. Curr Opin Pulm Med. 1998;4:220 –225.
6. Howard PA. Dalteparin: a low-molecular-weight heparin. AnnPharmacother. 1997;31:192–203.
7. Hunt D. Low-molecular-weight heparins in clinical practice. SouthMed J. 1998;91:2–10.
8. Leizorovicz A. Comparison of the efficacy and safety of low molec-ular weight heparins and unfractionated heparin in the initial treat-ment of deep venous thrombosis. An updated meta-analysis. Drugs.1996;52(suppl 7):30 –37.
9. Lensing AW, Prins MH, Davidson BL, et al. Treatment of deepvenous thrombosis with low-molecular-weight heparins. A meta-analysis. Arch Intern Med. 1995;155:601–607.
10. Martineau P, Tawil N. Low-molecular-weight heparins in the treat-ment of deep-vein thrombosis. Ann Pharmacother. 1998;32:588 –598.
11. Rocha E, Martinez-Gonzalez MA, Montes R, et al. Do the low mo-lecular weight heparins improve efficacy and safety of the treatmentof deep venous thrombosis? A meta-analysis. Haematologica. 2000;85:935–942.
12. Siragusa S, Cosmi B, Piovella F, et al. Low-molecular-weight hepa-rins and unfractionated heparin in the treatment of patients withacute venous thromboembolism: results of a meta-analysis. Am JMed. 1996;100:269 –277.
13. van den Belt AG, Bossuyt PM, Prins MH, et al. Replacing inpatientcare by outpatient care in the treatment of deep venous thrombo-
LMWH for Treatment of Venous Thromboembolism/Segal et al
September 2003 THE AMERICAN JOURNAL OF MEDICINE� Volume 115 307
sis—an economic evaluation. TASMAN Study Group. ThrombHaemost. 1998;79:259 –263.
14. van der Heijden JF, Prins MH, Buller HR. For the initial treatmentof venous thromboembolism: are all low-molecular-weight hepa-rin compounds the same? Thromb Res. 2000;100:V121–V130.
15. Segal JB, Eng J, Jenckes MW, et al. Diagnosis and Treatment of DeepVenous Thrombosis and Pulmonary Embolism. Evidence Report/Technology Assessment [prepared by the Johns Hopkins Evidence-based Practice Center under Contract No. 290-097-006]. Rockville,MD: Agency for Healthcare Research and Quality; 2003.
16. Gebo KA, Jenckes MW, Chander G, et al: Evidence Report on Man-agement of Chronic Hepatitis C [prepared by the Johns HopkinsUniversity Evidence-based Practice Center under Contract No.290-097-006]. Rockville, MD: Agency for Healthcare Research andQuality; 2002.
17. Schein OD, Friedman DS, Fleisher LA, et al. Anesthesia Manage-ment During Cataract Surgery [prepared by the Johns HopkinsUniversity Evidence-based Practice Center under Contract No.290-097-006]. Rockville, MD: Agency for Healthcare Research andQuality; 2001. AHRQ Publication No. 01-E017.
18. Richardson WS, Detsky AS. Users’ guides to the medical literature.VII. How to use a clinical decision analysis. B. What are the resultsand will they help me in caring for my patients? Evidence-BasedMedicine Working Group. JAMA. 1995;273:1610 –1613.
19. Richardson WS, Detsky AS. Users’ guides to the medical literature.VII. How to use a clinical decision analysis. A. Are the results of thestudy valid? Evidence-Based Medicine Working Group. JAMA.1995;273:1292–1295.
20. Berlin JA. Does blinding of readers affect the results of meta-anal-yses? University of Pennsylvania Meta-analysis Blinding StudyGroup. Lancet. 1997;350:185–186.
21. Garbutt JC, West SL, Carey TS, et al. Pharmacological treatment ofalcohol dependence: a review of the evidence. JAMA. 1999;281:1318 –1325.
22. Belcaro G, Nicolaides AN, Cesarone MR, et al. Comparison of low-molecular-weight heparin, administered primarily at home, withunfractionated heparin, administered in hospital, and subcutane-ous heparin, administered at home for deep-vein thrombosis. An-giology. 1999;50:781–787.
23. Grau E, Tenias JM, Real E, et al. Home treatment of deep venousthrombosis with low molecular weight heparin: long-term inci-dence of recurrent venous thromboembolism. Am J Hematol. 2001;67:10 –14.
24. Huse DM, Cummins G, Taylor DC, et al. Outpatient treatment ofvenous thromboembolism with low-molecular-weight heparin: aneconomic evaluation. Am J Manag Care. 2002;8(suppl):S10 –S16.
25. Koopman MM, Prandoni P, Piovella F, et al. Treatment of venousthrombosis with intravenous unfractionated heparin administeredin the hospital as compared with subcutaneous low-molecular-
weight heparin administered at home. The TASMAN Study Group.N Engl J Med. 1996;334:682–687.
26. Levine M, Gent M, Hirsh J, et al. A comparison of low-molecular-weight heparin administered primarily at home with unfraction-ated heparin administered in the hospital for proximal deep-veinthrombosis. N Engl J Med. 1996;334:677–681.
27. Pearson SD, Blair R, Halpert A, et al. An outpatient program to treatdeep venous thrombosis with low-molecular-weight heparin. EffClin Pract. 1999;2:210 –217.
28. Smith BJ, Weekley JS, Pilotto L, et al. Cost comparison of at-hometreatment of deep venous thrombosis with low molecular weightheparin to inpatient treatment with unfractionated heparin. InternMed J. 2002;32:29 –34.
29. Vinson DR, Berman DA. Outpatient treatment of deep venousthrombosis: a clinical care pathway managed by the emergency de-partment. Ann Emerg Med. 2001;37:251–258.
30. Boccalon H, Elias A, Chale JJ, et al. Clinical outcome and cost ofhospital vs home treatment of proximal deep vein thrombosis witha low-molecular-weight heparin: the Vascular Midi-Pyreneesstudy. Arch Intern Med. 2000;160:1769 –1773.
31. Kovacs MJ, Anderson D, Morrow B, et al. Outpatient treatment ofpulmonary embolism with dalteparin. Thromb Haemost. 2000;83:209 –211.
32. de Lissovoy G, Yusen RD, Spiro TE, et al. Cost for inpatient care ofvenous thrombosis: a trial of enoxaparin vs standard heparin. ArchIntern Med. 2000;160:3160 –3165.
33. Estrada CA, Mansfield CJ, Heudebert GR. Cost-effectiveness oflow-molecular-weight heparin in the treatment of proximal deepvein thrombosis. J Gen Intern Med. 2000;15:108 –115.
34. Hull RD, Raskob GE, Rosenbloom D, et al. Treatment of proximalvein thrombosis with subcutaneous low-molecular-weight heparinvs intravenous heparin. An economic perspective. Arch Intern Med.1997;157:289 –294.
35. Lloyd AC, Aitken JA, Hoffmeyer UK, et al. Economic evaluation ofthe use of nadroparin in the treatment of deep-vein thrombosis inSwitzerland. Ann Pharmacother. 1997;31:842–846.
36. O’Brien B, Levine M, Willan A, et al. Economic evaluation of out-patient treatment with low-molecular-weight heparin for proximalvein thrombosis. Arch Intern Med. 1999;159:2298 –2304.
37. Rodger M, Bredeson C, Wells PS, et al. Cost-effectiveness of low-molecular-weight heparin and unfractionated heparin in treatmentof deep vein thrombosis. CMAJ. 1998;159:931–938.
38. Tillman DJ, Charland SL, Witt DM. Effectiveness and economicimpact associated with a program for outpatient management ofacute deep vein thrombosis in a group model health maintenanceorganization. Arch Intern Med. 2000;160:2926 –2932.
39. Spyropoulos AC, Hurley JS, Ciesla GN, et al. Management of acuteproximal deep vein thrombosis: pharmacoeconomic evaluation ofoutpatient treatment with enoxaparin vs inpatient treatment withunfractionated heparin. Chest. 2002;122:108 –114.
LMWH for Treatment of Venous Thromboembolism/Segal et al
308 September 2003 THE AMERICAN JOURNAL OF MEDICINE� Volume 115




















