ChemInform Abstract: Recent Advances in the Treatment of Thromboembolic Diseases: Venous...
24
Recent Advances in theTreatment of Thromboembolic Diseases: VenousThromboembolism Y.K. Agrawal, 1 Hitesh Vaidya, 1 Hardik Bhatt, 1 Kuntal Manna, 1 Pathik Brahmkshatriya 2 1 Institute of Pharmacy, Nirma University of Science and Technology, Sarkhej-Gandhinagar Highway, Ahmedabad 382481, Gujarat, India 2 Department of Medicinal Chemistry, L.M. College of Pharmacy, Navrangpura, Ahmedabad 380009, Gujarat, India Published online 22 February 2007 in Wiley InterScience (www.interscience.wiley.com). DOI 10.1002/med.20100 ! Abstract: Venous thromboembolic diseases are the major concern of rising cost of healthcare and are commonest health problem across the globe. Both genetic and acquired risk factors are believed to be strongly linked with these diseases. Commonly encountered problems to the therapy include dose fixing and routine monitoring, yet some serious problems of bleeding also necessitate the immediate need to develop new agents. The review is primarily concerned with the new developments in the treatment of thromboembolic diseases. Therapeutic applications of anticoagulants, antiplatelets, and thrombolytics have been discussed in enough detail. ß 2007 Wiley Periodicals, Inc. Med Res Rev, 27, No. 6, 891 – 914, 2007 Key words: venous thromboembolic; antiplatelets; thrombolytics; pharmacoeconomics 1. INTRODUCTION Thromboembolic diseases, such as deep vein thrombosis (DVT), pulmonary embolism (PE), myocardial infraction (MI), and thromboembolic stroke are the leading causes of mortality and morbidity in many of developing and developed countries. 1 Venous thromboemolism (VTE) is potential fatal disorder and a significant national health problem worldwide. 2–4 VTE is manifested as deep vein thrombosis and pulmonary embolism. The treatment of VTE is fraught with substantial risk. 5 Antithrombotic drugs require precise dosing and meticulous monitoring. 6–9 In past decade, most of the research has been carried out focusing development of novel antithrombotic agents Correspondence to: Prof.Y.K. Agrawal, Institute of Pharmacy, Nirma University of Science and Technology, Sarkhej-Gandhinagar Highway, Ahmedabad 382481, Gujarat, India. E-mail: [email protected] Medicinal Research Reviews, Vol. 27, No. 6, 891^914, 2007 ß 2007 Wiley Periodicals, Inc.
-
Upload
tripurauniversity -
Category
Documents
-
view
0 -
download
0
Transcript of ChemInform Abstract: Recent Advances in the Treatment of Thromboembolic Diseases: Venous...

Recent Advances in theTreatmentof Thromboembolic Diseases:VenousThromboembolism
Y.K. Agrawal,1 Hitesh Vaidya,1 Hardik Bhatt,1 Kuntal Manna,1
Pathik Brahmkshatriya2
1Institute of Pharmacy, Nirma University of Science and Technology,
Sarkhej-Gandhinagar Highway, Ahmedabad 382481, Gujarat, India2Department of Medicinal Chemistry, L.M. College of Pharmacy,
Navrangpura, Ahmedabad 380009, Gujarat, India
Published online 22 February 2007 in Wiley InterScience (www.interscience.wiley.com).
DOI 10.1002/med.20100
!
Abstract: Venous thromboembolic diseases are the major concern of rising cost of healthcare and
are commonest health problem across the globe. Both genetic and acquired risk factors are believed
to be strongly linked with these diseases. Commonly encountered problems to the therapy include
dose fixing and routine monitoring, yet some serious problems of bleeding also necessitate the
immediate need to develop new agents. The review is primarily concerned with the new
developments in the treatment of thromboembolic diseases. Therapeutic applications of
anticoagulants, antiplatelets, and thrombolytics have been discussed in enough detail.
� 2007 Wiley Periodicals, Inc. Med Res Rev, 27, No. 6, 891–914, 2007
Key words: venous thromboembolic; antiplatelets; thrombolytics; pharmacoeconomics
1 . I N T R O D U C T I O N
Thromboembolic diseases, such as deep vein thrombosis (DVT), pulmonary embolism (PE),
myocardial infraction (MI), and thromboembolic stroke are the leading causes of mortality and
morbidity in many of developing and developed countries.1 Venous thromboemolism (VTE) is
potential fatal disorder and a significant national health problemworldwide.2–4 VTE ismanifested as
deep vein thrombosis and pulmonary embolism. The treatment of VTE is fraught with substantial
risk.5 Antithrombotic drugs require precise dosing and meticulous monitoring.6–9 In past decade,
most of the research has been carried out focusing development of novel antithrombotic agents
Correspondence to:Prof.Y.K. Agrawal, Instituteof Pharmacy,NirmaUniversityof ScienceandTechnology,Sarkhej-Gandhinagar
Highway, Ahmedabad 382481,Gujarat, India.E-mail: [email protected]
Medicinal Research Reviews, Vol. 27, No. 6, 891^914, 2007
� 2007 Wiley Periodicals, Inc.

among which thrombin inhibitors,10 inhibitors of factor Xa, fibrinogen receptor antagonists and GP
IIa/IIIb antagonists11 have drawn most of the attention.
Venous thrombosis is the thirdmost common cardiovascular disease after ischemic heart disease
and stroke. It is common in whites, affecting 1 in 1,000 individuals every year, and is strongly
associatedwith life-threatening pulmonary embolism. In addition to circumstantial predisposing risk
factors like surgery, pregnancy or immobilization; genetic abnormalities, molecular abnormalities of
components of the coagulation pathway leading to hypercoagulability, and in turn, to thrombophilia
have also been found in subjects who have had thromboembolic diseases.
2 . R I S K F A C T O R S F O R T H R O M B O E M B O L I C D I S E A S E S
The effect of risk factor in adults are additive, the greater the number of high-risk factors the greater
the risk of thromboembolic diseases. In the late 1800s, Dr Rudolf Virchow, a German pathologist,
recognized the role played by blood vessels, circulating elements in the blood, and the speed of the
blood flow in regulation of clot formation.12 Numerous risk factors for such alterations and thus, VTE
have been identified.Mechanisms that predispose individuals to thromboembolism aremany and can
be divided into two major categories: those because of a genetically inherited mutation of a gene(s)
involved in coagulation and those that are acquired as a direct or indirect result of trauma, systemic
illness (acute or chronic), or an altered physiologic state.
3 . G E N E T I C A L L Y I N H E R I T E D / H Y P E R C O A G U L A B L E S T A T E S
The earliest discoveries of genetic defects linked to venous thrombosis were the abnormalities of the
genes encoding for antithrombin III, protein C, and protein S.13–15
A. Factor V Leiden
This genetically inherited mutation was discovered in 1993 as a result of the studies done in Sweden
on patients with thromboembolic diseasewho characteristically had a poor anticoagulant response to
activated protein C. More recently, resistance to activated Protein C has been identified as the most
frequent risk factor for venous thrombosis, occurring in approximately 3%–5% of the general
population and in over 20% of patients with a history of venous thrombosis.16 This defect was first
recognized when activated Protein C failed to cleave the coagulation factors Va or VIIIa. Subsequent
genetic analysis demonstrated a unique single point mutation in the gene for factor V. This gene
mutation produces a factor Vmoleculewith glutamine instead of arginine at position 506 of its amino
acid sequence. Under normal conditions, this is the main point of factor Va cleavage by activated
Protein C. Glutamine makes this cleavage site inaccessible, leading to resistance to activated Protein
C. This mutation is commonly referred to as Factor V Leiden, named after the city in the Netherlands
where this mutation was first identified. Factor V leiden is currently recognized as the most common
genetic defect associated with thrombophilia.17 Its prevalence appears to be higher in Caucasians,
found in 4.4% in the general population of Northern Europe and 3% in North America, and is less
common in African Americans.18–20
B. Prothrombin Gene 20210G/A Mutation
In 1996, Poort et al. reported a gene mutation associated with elevated levels of plasma
prothrombin.21 The mutation occurs at the 20210 position in the 3 0 untranslated region of the
prothrombin gene where glutamine is substituted for arginine. This mutation is currently recognized
892 * AGRAWAL ET AL.

as the second most common genetic abnormality associated with an increased risk of
thromboembolism.21 Surprisingly, individuals having this mutation were also positive for factor V
leiden.21 The presence of both factor V leiden and prothrombin 20210G/Amutation further increases
the risk of thromboembolism.22,23
C. Hyperhomocysteinemia
Elevated levels of homocysteine in plasma (>15mmol/L) have been found to be an independent risk
factor for vascular disease and linked to early occurrence of atherosclerosis, and should be suspected
in patients with coronary artery disease, carotid atherosclerosis, and stroke occurring at a young age.
However, thrombosis can occur on the venous side of systemic circulation, as well as the arterial.
Hyperhomocysteinemia can be due to either a mutation of the gene that encodes for
methylenetetrahydrofolate reductase or acquired as a result of poor nutrition.24–26 Several
mechanisms have been proposed for the thrombophilic state induced by the elevated plasma levels
of homocysteine. Oxidative damage to the endothelium that results in inhibition of thrombomodulin
on the surface membrane which, in turn, decreases protein C activation and increases the activity of
factors Vand XII.27 Increasing folic acid intake alone, as well as combining folic acid with vitamin
B12 or vitamin B6, will promptly lower the plasma homocysteine level in both the genetically
inherited and the acquired forms of the deficiency.27
4 . A C Q U I R E D C A U S E S O F T H R O M B O E M B O L I S M
A. Lupus Anticoagulants and Antiphospholipid Antibody Syndrome (LA/APS)
Lupus anticoagulants and antiphosholipid antibody syndrome (LA/APS) has been associated with
both arterial and venous thrombosis. Patients, with positive LA/APS, are at higher risk of recurrent
VTE.28,29 It was found that among patients with LA/APS, approximately 20% of patients suffered
with recurrent VTE and 10% of patients had first ischemic stroke.30–32 LA/APS represents a plasma
inhibitor and its prevalence in the general population is not known. This inhibitor is usually an IgG
antibody that targets the phospholipid substrate of the prothrombin complex portion of the clotting
mechanism. It is difficult to evaluate increase of thromboembolismwith this prothrombin factor. LA/
APS can occur in patients of all ages.
B. Pregnancy
Pregnancy has been associated with fourfold increase in VTE; the majority occurring during the
second and third trimesters, and an even higher risk is reported during the immediate postpartum or
puerperal period.33–35 The increased venous stasis of pregnancy is the most constant predisposing
factor. Physiological changes associated with pregnancy result in an increase in venous distensibility
and capacity. These changes are evident from the first trimester.36,37 Several independent factors have
also been shown to be associated with an increased risk of thromboembolic diseases. These include
prolonged bed rest during pregnancy or the puerperium, instrument assisted or cesarean delivery,
hemorrhage, sepsis, multiparity, and advancematernal age.38 Pregnancy is also associated with mark
alteration in the protein of coagulation and fibrinolytic system. The level of coagulation factor II, VII,
and X increases substantially by the middle of pregnancy.39,40 Generation of fibrin also increases
markedly,41–43 level of protein S appear to decrease throughout pregnancy although level of proteinC
remains normal.42,44 The increased risk has long been attributed to the elevated levels of certain
procoagulants during the later stages of pregnancy, which results in heightened state of the clotting
system prone to activation by subtle triggering mechanisms often related to the altered physiologic
state.45,46
VENOUS THROMBOEMBOLISM * 893

C. Oral Contraceptive and Hormone Replacement Therapy
It was reported as early as in 1967 and recently in 1990, that oral contraceptive users had three- to
sixfold increased risk of venous thromboembolism compared to nonusers.47–51 The use of
postmenopausal hormone substitution has become widespread in recent decades.52 Besides
relief from menopausal complaints, hormone replacement is prescribed to reduce the progression
of osteoporosis and the development of cardiovascular disease. In an early study of adverse effects of
estrogen replacement therapy, an increase risk of venous thrombosis was observed.53 This was not
confirmed in subsequent studies,54–56 and the idea that estrogen replacement could cause venous
thrombosis was dismissed as ‘‘medical superstition.’’57 However, from 1996 onward, a series of
studies has demonstrated that hormone replacement users have a two- to fourfold increased risk of
venous thrombosis.58–66
Estrogens increase the risk of venous thrombosis when used as oral contraceptives or as
postmenopausal hormone replacement.67–69 A similar effect was observed in men when estrogens
were used as a treatment of coronary disease70 or in sex-change treatment.71 Recently, it has been
demonstrated that the progestin in combination with oral contraceptives also increased the risk of
thrombosis.72–74
Estrogens havemanydifferent effects on the coagulation system.75–79 These include increases in
the levels of procoagulant factors VII, X, XII, and XIII and reductions in the anticoagulant factors
protein S and antithrombin. These changes predict a change toward amore procoagulant state (which
is confirmed in studies examining global tests, such as APC resistance or thrombin generation),80–84
which is not counter balanced by an increased fibrinolytic activity.85
D. Malignancy
It has been well established that malignancies are associated with an increased incidence of VTE and
are a common complication of advanced stage cancers, perhaps because of the procoagulant
substances elaborated by the tumor.86,87 Although the risks vary with the different types of cancer,
higher risks have been found in a variety of adenocarcinomas, for example, pancreatic, ovarian and
breast, as well as tumors of the brain.86–88 Hematologic malignancies, especially myeloproliferative
diseases, are frequently complicated by VTEs occurring in the large visceral vessels like mesenteric,
portal, and hepatic veins, as well as the deep veins of the lower extremities.
E. Infectious and Inflammatory Diseases
The clinical setting of acute and chronic infection, as well as chronic inflammatory diseases, have
been associated with some degree of endothelial cell damage resulting from a complex network of
inflammatory mediator substances and cytokines such as interleukins, C-reactive protein, tumor
necrosis factor-a, and endotoxins capable of activating the clotting mechanism, inducing a
hypercoagulable state.89–91 In addition, levels of certain clotting factors such as factor VIII and
fibrinogen are believed to increase the risk of DVT, as well as auto-antibodies, are reported to be
elevated in rheumatoid arthritis, inflammatory bowel disease, Kawasaki disease.92–94
F. Surgery
Surgical intervention, whether elective or emergent, has been associated with an increased risk of
VTE. This risk is especially high during the first 2 weeks following surgery, but has been reported as
late as 5weeks postsurgery.95,96 Orthopedic and neurosurgical procedures have the highest incidence
of VTE and pulmonary emboli, and although these risks have been mitigated to a significant degree
by the routine use of prophylactic anticoagulants, the risk remains high, with a DVT incidence of
20%–30% in patients undergoing hip or knee replacement surgery.97–100 Additionally, reports of
894 * AGRAWAL ET AL.

fatal pulmonary emboli have been reported in 3%–6% of patients following hip replacement surgery
and 13% of those with traumatic hip fractures.101 The risk of VTE in neurosurgical patients remains
high and has been reported as occurring in 20%–50% of patients not receiving prophylactic
anticoagulant therapy and 1.5%–5% incidence of fatal pulmonary emboli, providing a compelling
need for thromboprophylaxis.102–105 The risk will be even higher in these patients with a concurrent
illness, malignancy, or predisposing geneticmutation in the patient. Another high-risk group forVTE
are those patients who have sustained major trauma, with an incidence of 50%–60% being reported
with traumatic fractures and head injuries.106,107 In the UK, the reports of the Thromboembolic Risk
Factors (THRIFT) Consensus Group108 and the Scottish Intercollegiate Guidelines Network Group
(SIGN)109 have recommended that pharmacological prophylactic regimens be used routinely after
major orthopedic procedures in the lower limb because surgical procedures, particularly on the lower
limb, predispose to both venous thromboembolism and wound complications.
G. Heparin-Induced Thrombocytopenia (HIT)
Heparin-induced thrombocytopenia (HIT) is an adverse drug reaction mediated by the immune
system with clinical manifestations triggered by antibodies directed against platelet factor IV. This
becomes an antigenic target when bound to heparin. This antibody-platelet factor IV–heparin
complex is able to activate platelets and may cause venous and arterial thrombosis. Although the
immediate discontinuation of heparin ismandatory in this condition, the strategy is insufficient, given
the high-cumulative risk of thrombosis during 30-day administration of the drug up to 53% without
antithrombotic treatment.91 Thus, for patients with suspected or confirmedHIT, the use of alternative
anticoagulants is recommended.91 The use of direct thrombin inhibitors (DTIs) for this condition is
theoretically supported by the intense thrombin activity observed in these patients.110–113
5 . T R E A T M E N T G O A L S
Therapy is directed toward management of concomitant congestive heart failure (CHF) or serious
arrhythmias when present; general patient support, including nutritional supplementation, and
correction of hypothermia; adjunctive therapies to limit thrombus growth or formation; close patient
monitoring for limb viability, heart rate and rhythm, progression or regression of CHF, creatinine and
electrolyte levels and appetite; and prevention of repeated events.
6 . T R E A T M E N T O F T H R O M B O E M B O L I S M
The treatment of venous thromboembolism has rapidly changed over the last decades. The standard
therapy, intravenous anticoagulation with unfractionated heparin, was first introduced as primary
treatment of pulmonary embolism in 1960.10 Most commonly used drug classes include:
Anticoagulan/Antithrombin therapy, Antiplatelet therapy, Thrombolytic therapy.
7 . A N T I C O A G U L A N T S / A N T I T H R O M B I N T H E R A P Y
Anticoagulants/antithrombin therapy can be either direct or indirect thrombin inhibitors. Direct
thrombin inhibitors are those inhibiting thrombin itself, while indirect inhibitors inhibit formation of
thrombin (Fig. 1). Both classes of drugs are very potent and specific to the target.
VENOUS THROMBOEMBOLISM * 895

A. Unfractionated Heparin
Since 1930s, clinicians have used unfractionated heparin (UFH) (1) for the prevention and treatment
of thrombosis.8,113 McLean discovered UFH in 1916, when he found that extract of dog liver was an
inhibitor of heparin co-factor to produce anti-coagulant effect.114While it has been known since 1939
that UFH requires a ‘heparin cofactor’ to produce an anticoagulant effect, it was not until 1968 that
antithrombin (previously known as antithrombin-III) was identified and isolated.10 Soon thereafter, it
was recognize that UFH greatly accelerates the activity of antithrombin.
Figure 1. Sites ofactionofanticoagulants.
896 * AGRAWAL ET AL.

The anticoagulant effect of UFH is mediated through a specific pentasaccharide sequence of the
heparin molecule that binds to antithrombin, provoking conformational changes.8,113 The UFH-
antithrombin complex is 100–1,000 timesmore potent as an anticoagulant compared to antithrombin
alone.10 Antithrombin inhibits factor IXa, Xa, XIIa, and thrombin(IIa). The UFH–antithrombin
complex also inhibits thrombin-induced activation of factorVandVIII. Factor IIa andXa are themost
sensitive to inhibition by the UFH–antithrombin complex. To inactivate thrombin, heparin molecule
must form a ternary complex as a bridge between antithrombin and thrombin,8 which requires
minimum 18 saccharide units and thus smaller heparin molecules cannot facilitate the interaction
between antithrombin and thrombin.
Major drawbacks of UFH involve bleeding115,116 and poor absorption of UFH because of its
large molecular size and anionic structure.8 Hirsh et al.117 described the hemorrhagic risk of heparin
therapy in 100 consecutive patients treated with continuous IV heparin, which was adjusted
according to the results of the whole blood clotting time. Four patients had major hemorrhagic
episodes, and in three, the results ofwhole blood clotting timewere prolonged considerably above the
upper limit of the targeted therapeutic range (three times control). Recently, a lipophilic vehicle
sodiumN-(8-(2-hydroxy benzoyl)) amino caprylate has been developedwhich facilitated absorption
of UFH.112
Propensity of UHF to bind with plasma proteins, platelets factor-IV, macrophages, and
endothelial cells limits the bioavailability and biologic activity.8,113,118 Patients with active
thrombosis have rapid changes in the circulating levels of heparin-binding proteins and often appear
to have heparin resistance and hence require high dose of UHF to achieve therapeutic response.8,119
Thrombocytopenia, defined as platelets count lesser than 150,000, is common with UFH
therapy.120–123 Heparin use commonly leads to mild reductions in the level of circulating
antithrombin III and rarely has been reported to induce disseminated thrombosis.124 Long-term high-
dose (4 months at 15,000 U or more) heparin administration can lead to severe osteopenia.125–129
In the rare patient with hypoaldosteronism, heparin may induce hyperkalemia.130
B. Low-Molecular-Weight Heparin (LMWH)
In recent years, low-molecular-weight fractions of commercial heparin have been prepared by either
enzymatic or chemical depolymerization. They are believed to be fragments of UFH,8,118,131 that
have a mean molecular weight of 4,000–5,000 d in contrast to unfractionated heparin, which has a
mean molecular weight of 15,000 d.132,133 Low-molecular-weight heparin (LMWHs) are
heterogeneousmixtures of sulfated glycosaminoglycans. LMWHs are resembled in their mechanism
of action with UFH, and they have excellent bioavailabity, together with a longer plasma half-
life.134–139 These agents have advantages over UFHwhich includes: predictable anticoagulant dose:
improved subcutaneous bioavailability; dose-independence clearance; longer biological half life;
lower incidence of thrombocytopenia; and a reduced need for routine laboratory monitoring.131
Currently, there are three LMWH products available in the US market: dalteparin, enoxaprin,
and tinzaprin. They prevent the growth and propagation of formed thombi.8,131,140,141 Like UFH, the
LMWHs enhance and accelerate the activity of antithrombin by binding to a specific pentasaccharide
sequence. The principle difference in pharmacological activity of LMWHs and UFH is their relative
inhibition of factor Xa and thrombin (IIa). LMWHs have requisite chain length to simultaneously
VENOUS THROMBOEMBOLISM * 897

bind antithrombin and thrombin. For these reasons, LMWHs have proportionally greater anti-factor
Xa activity. Studies in experimental animal models of venous thrombosis have shown that some low-
molecular-weight fractions have equal (or greater) antithrombotic efficacy, but less hemorrhagic
effects, in comparison to heparin (UFH).132,133,142–145 Currently a clinical study have been carried
out between heparin (UFH) and LMWHs and with venographically proven proximal deep vein
thrombosis; group of 85 patients received standard heparin (to achieve an activated partial
thromboplastin time of 1.5–2.0 times the pretreatment value) and 85 patients received LMWH
(adjusted only for body weight) for 10 days. Oral coumarin therapy was started on day 7 and
continued for at least 3 months. The frequency of recurrent venous thromboembolism diagnosed
objectively did not differ significantly between the standard heparin and LMWH groups. Clinically
important bleeding was infrequent in both groups.146
C. Heparinoids
Currently, danaparoid sodium is themost frequently prescribe heparinoid. Chemically, it is amixture
of three sulfated glycosaminoglycans: heparan (84%), dermatan (12%), and chondroitin (4%). It is
derived from the porcine gut mucosa. Danaparoid binds to antithrombin and heparin cofactor II and
greatly accelerates their activity.97 It inhibits factor Xa and to a lesser extent thrombin. Randomized
trials have demonstrated that danaparoid sodium is effective and safe for prevention of postoperative
venous thromboembolism in patients undergoing general or orthopaedic surgery.147 and 148 However,
because it is substantially more expensive than other LMWheparin preparations, danaparoid sodium
is rarely used for this indication. Currently, danaparoid sodium is used mainly to treat immune
heparin-induced thrombocytopenia and for prevention and treatment of venous thromboembolism or
arterial thrombosis in patients with a past history of immune heparin-induced thrombocytopenia149
Bleeding is the most common side effect associated with its use.150,151
D. Factor Xa Inhibitors
Anumber of direct and indirect factor Xa inhibitors are currently under development.152Direct factor
Xa inhibitors thwart thrombin generation by binding directly to circulating or clot-bound factor Xa.
They are not dependent on antithrombin to produce their antithrombic effects. Some natural direct
factor Xa inhibitors such as tick anticoagulation peptide (TAP), antistasin, and lefaxin from leeches
are also under investigation.
Similar to UFH and LMWHs, the indirect factor Xa inhibitors bind to antithrombin, greatly
accelerating their activity.152,153 UFH and LMWHs possess varying proportions of factor Xa and
factor IIa inhibitory activity. Understanding of the structure activity relationship of heparin resulted
in the development of the synthetic pentasaccharide with only anti-Xa activity.154–156 A recently
developed synthetic analogue of UFH and LMWHs like Fondaparinux and idraparinux have high
affinity for antithrombin.156
Factor Xa inhibitors may be separated into three broad classes: (a) proteins derived from natural
sources which include TAP, antistasin, soya trypsin inhibitor, yagin, and tissue factor pathway
inhibitor and its variants; (b) synthetic peptides, peptidomimetics, and other organicmolecules (non-
heparinomimetics), which are low-molecular-weight (<1,000 Da) agents; and (c) synthetic
heparinomimetics (see Table I). The relative specificity and the mode of the inhibitory actions of
each of these agents vary.157
DX-9065a (2) [Ki ¼ 41 nM] is an inhibitor of factor Xa. Currently it is in Phase-II clinical
trials in Japan and US for the treatment of general thrombosis and unstable angina. Razaxaban (3)
DPC-906, BMS-561389 is factor Xa inhibitor in development by Bristol-Myers Sqibb for
venousthrombosis and is in phase-II trials. It is a potent, selective non-covalent inhibitor of factor Xa
898 * AGRAWAL ET AL.

(Ki, factor Xa 0.19 nM, thrombin 540 nM), with IC50 values>2 mM against all other enzymes in the
coagulation cascade.
Compared with antithrombin agents such as the recombinant hirudin, factor Xa-inhibiting agents
aremore safer andmaynot inducebleeding and a fibrinolytic deficit. In preclinical studies, the efficacy-
safety ratios with these agents were better than those of heparin and antithrombin agents.157
E. Direct Thrombin Inhibitors
Direct thrombin inhibitors stand out as a relatively new class of very potent anticoagulant agents,
include lepirudin, bivalirudine, argatroban (4), and ximelagatran (5) BIBR 953 (6). These agents are
directly interacting with the thrombin molecule and they do not require antithrombin or heparin
cofactor II to have antithrombotic activity. Moreover, they are capable of inhibiting both circulating
and clot-bonded thrombin, which distinguishes them fromUFHand the LMWHs.158Also they do not
induce immune mediated thrombocytopenia.
Table I. Classification of Factor Xa Inhibitors
VENOUS THROMBOEMBOLISM * 899
Hirudin, the prototype of this class, was isolated from salivary secretion of medicinal leech.155
Bivalirudin, formally known as hirulog, is a semisynthetic polypeptide and a reversible inhibitor of
thrombin.152,159
Argatroban is a small synthetic molecule derived from arginine that reversibly binds to the
catalytic site of thrombin.160 Ximelagetran is a prodrug which gets converted by hydrolysis and
reduction in the liver to melagatran, the active moiety.152,159 Contraindication for the use of direct
thrombin inhibitors are similar to those for the other antithrombic drugs. Hemorrhage is the most
common and dreadful side effect associated with all thrombin inhibitors.120,159
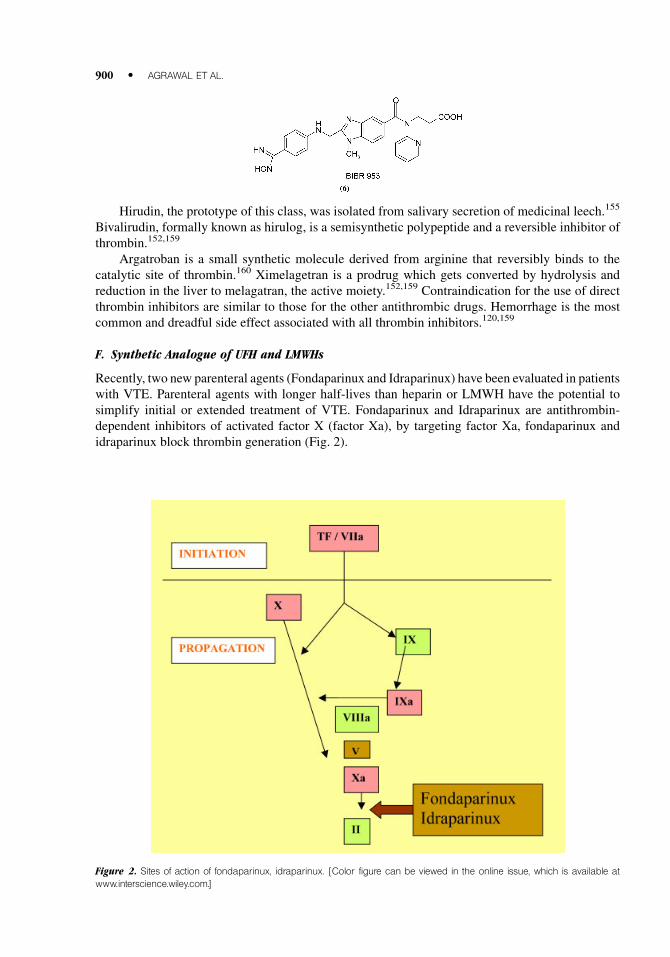
F. Synthetic Analogue of UFH and LMWHs
Recently, two new parenteral agents (Fondaparinux and Idraparinux) have been evaluated in patients
with VTE. Parenteral agents with longer half-lives than heparin or LMWH have the potential to
simplify initial or extended treatment of VTE. Fondaparinux and Idraparinux are antithrombin-
dependent inhibitors of activated factor X (factor Xa), by targeting factor Xa, fondaparinux and
idraparinux block thrombin generation (Fig. 2).
Figure 2. Sites of action of fondaparinux, idraparinux. [Color figure can be viewed in the online issue, which is available at
www.interscience.wiley.com.]
900 * AGRAWAL ET AL.

G. Fondaparinux and Idraparinux
A synthetic analog of the antithrombin-binding pentasaccharide sequence found on heparin or
LMWH, fondaparinux (7) binds antithrombin with high affinity. Once bound, fondaparinux evokes
conformational changes in the reactive center loop of antithrombin that enhance its reactivity with
factor Xa.161,162 Fondaparinux is a catalytic inhibitor; thus, after promoting the formation of the
factor Xa/antithrombin complex, fondaparinux dissociates from antithrombin and is available
to activate additional antithrombin molecules. A second-generation synthetic pentasaccharide,
idraparinux (8) is more negatively charged than fondaparinux. Consequently, idraparinux binds to
antithrombin with an affinity higher than that of fondaparinux.156 Because it binds antithrombin so
tightly, idraparinux has a plasma half-life similar to that of antithrombin, 80 hr.
Fondaparinux and Idraparinux have potential advantages like Table II.
1. Rapid onset of action.
2. Fondaparinux and idraparinux exhibit almost complete bioavailability and has half life of 17 H
and 80 H, respectively, after subcutaneous administration.161–163
3. Subcutaneous fixed doses, of fondaparinux produces a predictable anticoagulant response.
4. Fondaparinux has no effect on routine tests of coagulation, such as the activated partial
thromboplastin time (APTT) or activated clotting time.164 Fondaparinux and idraparinux do not
cause HIT because they do not bind to platelets or platelet factor 4 (PF4). Thus, HIT is triggered
Table II. Comparison of Fondaparinux and Idraparinux with LMWH
LMWHindicates low-molecular-weightheparin; SC, subcutaneous; HIT,heparin-inducedthrombocytopenia.
VENOUS THROMBOEMBOLISM * 901

by antibodies directed against the heparin/PF4 complex.165 Fondaparinux and idraparinux do
not bind to platelets. Therefore, they do not cause platelet activation and subsequent PF4 release.
Likewise, because these agents do not bind to PF4, they do not induce the conformational
changes in PF4 that render it antigenic. These properties endow fondaparinux and idraparinux
with a safety advantage over heparin and LMWH and may render these new agents useful for
HIT treatment.
Fondaparinuxwas developed to replace heparin or LMWH for initial treatment of VTE, whereas
idraparinux were designed to compete with vitamin K antagonists. Because of its rapid onset of
action, however, idraparinux may be useful for initial treatment of VTE, as well as for extended
therapy. Osteoporosis can occur after long-term treatment with heparin or LMWH166,167 and the risk
of this complication should be lower with fondaparinux and idraparinux because shorter heparin
chains cause less bone loss than longer chains in cell culture systems and in laboratory animal
models.168,169 Like all anticoagulants, the major side effect of these new drugs is bleeding. To
counteract this problem, a safe rapidly acting antidote is desirable. Unfortunately, none of these new
agents has an antidote.
8 . T H R O M B O L Y T I C T H E R A P Y
Thrombosis is a pathologic event that results in the obstruction of coronary, cerebral, or peripheral
blood flow.170 Thrombolytic agents dissolve thrombi by activating a zymogen, plasminogen, to the
active agent, plasmin. Plasmin, when in proximity to a thrombus or a hemostatic plug, degrades fibrin
to soluble peptides (Fig. 3).171 Circulating plasmin also degrades soluble fibrinogen and, to some
extent, several other plasma proteins. The advantages of this type of therapy include potentially rapid
resolution of acute disease and shorter recovery times. The disadvantages, which are extensive,
include risk of hemorrhage, little to no clinical data regarding efficacy or safety in domestic animals,
and potentially prohibitive costs. The two main thrombolytic drugs available are streptokinase/
urokinase and recombinant tissue plasminogen activator (see Table III).
Streptokinase is a plasminogen activator derived from b-hemolytic Streptococcus spp. It
catalyzes the conversion of plasminogen to plasmin, which is the primary protein responsible for
Figure 3. Common mechanism of thrombolytic agents. [Color figure can be viewed in the online issue, which is available at
www.interscience.wiley.com.]
902 * AGRAWAL ET AL.

fibrinolysis. Unfortunately, streptokinase is active in vivo against all circulating plasminogen, and
causes fibrinolysis systemically. This creates a risk of hemorrhage. Because it is of bacterial origin,
anaphylactic reactions are also a risk.Unlike streptokinase, urokinase directly activates conversion of
plasminogen to plasmin.10Urokinase is a protein produced endogenously by the kidney and exists in
high- and low-molecular-weight forms, both with similar clinical effects.172 Both Streptokinase and
Urokinase have similar thrombolytic effects as judged by large clinical trials in pulmonary
embolism.173,174 Using paired angiographic comparisons in each patient, resolution of thromboem-
bolus, seen with 12 or 24 hr of UK or with 24 hr of SK, was comparable at 24 hr and was
approximately three times that seen with heparin alone.173
A recombinant form of endogenous tissue plasminogen activator (TPA) was created for human
medicine to address some of the disadvantages of streptokinase, most notably its lack of clot
specificity. TPA’s mechanism of action is the same as streptokinase; it is released from vascular
endothelial cells and acts to balance coagulation with fibrinolysis in vivo. In circulation, however,
TPA is bound to an inhibitory protein, plasminogen activator inhibitor (PA-i), until it comes in contact
with a fibrin clot, at which point TPA is cleaved, becoming active. This relative fibrin specificity
allows use of TPA therapy with a significantly reduced risk of systemic hemorrhage. The extremely
short half-life of TPA in vivo (2–3 min) also reduces the risk of unintended hemorrhage. However,
this risk is still present because of residual anticoagulant effects, and may increase with higher
doses, such as those needed to break up large thrombi175 In humans, TPA is used often for cerebral,
cardiac, and pulmonary embolisms, which are typically smaller than those seen in aortic
thromboembolism. This raises the possibility of decreased clot specificity at clinically useful doses
for canine peripheral thromboembolism. Finally, TPA is extremely expensive; the cost of the drug
alone for a large-breed dog exceeds $1,000.
Beside the lack of a provenmortality effect, thrombolytic therapy ofVTE differs from therapy of
myocardial infarction in another way. In myocardial infarction, thrombolytic therapy appears to
dissolve the coronary thrombus in most cases, but in VTE, particularly PE, complete dissolution of
thrombus is the exception.176–179 Partial dissolution is the rule because venous thromboemboli are
older, larger, and more organized than coronary thrombi. Since no currently available agent or
regimen usually dissolves the VTE completely, interest has turned to smaller doses and shorter
duration of therapy in an effort to achieve the desired clinical effect with less bleeding. It is not yet
clear that these regimens will cause less bleeding, but they appear to effect comparable thrombus
resolution to regimens of longer duration.180,181 Contraindications of thrombolytic therapy are
absolute and relative (see Table IV).
9 . A N T I P L A T E L E T T H E R A P Y
Antiplatelet therapy consists of aspirin, ticlopidine hydrochloride (9), clopidogrel bisulfate (10), and
Glycoprotein (Gp) IIb/IIIa inhibitors. Figure 4 shows the sites of action of these platelet inhibitors.185
Table III. Thrombolytic Agents Approved by the Food and Drug Administration
*Recentlyapproved,PifarreandScanlon.182
VENOUS THROMBOEMBOLISM * 903
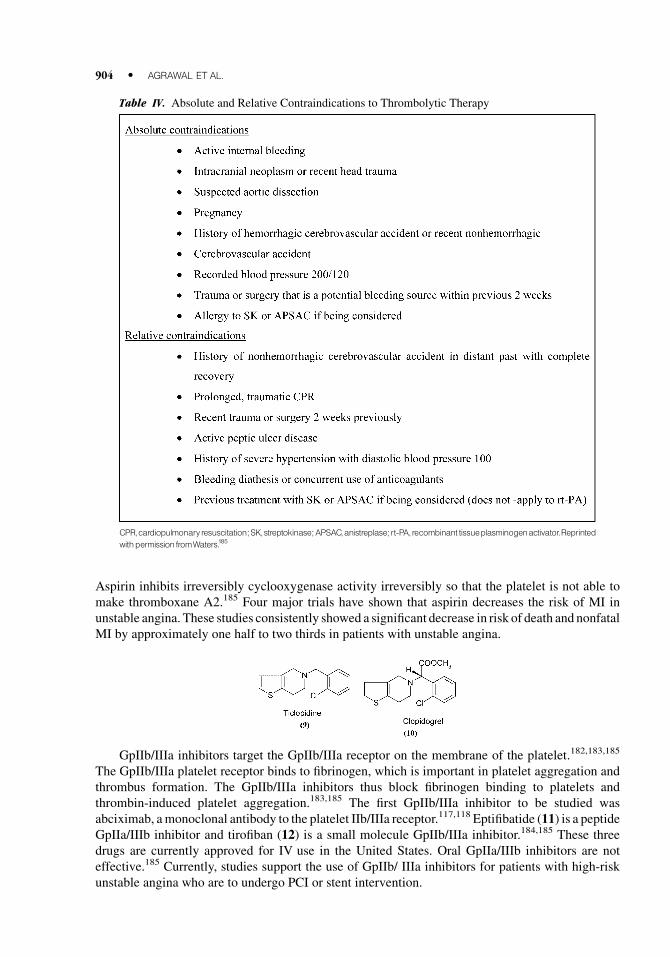
Aspirin inhibits irreversibly cyclooxygenase activity irreversibly so that the platelet is not able to
make thromboxane A2.185 Four major trials have shown that aspirin decreases the risk of MI in
unstable angina. These studies consistently showed a significant decrease in risk of death and nonfatal
MI by approximately one half to two thirds in patients with unstable angina.
GpIIb/IIIa inhibitors target the GpIIb/IIIa receptor on the membrane of the platelet.182,183,185
The GpIIb/IIIa platelet receptor binds to fibrinogen, which is important in platelet aggregation and
thrombus formation. The GpIIb/IIIa inhibitors thus block fibrinogen binding to platelets and
thrombin-induced platelet aggregation.183,185 The first GpIIb/IIIa inhibitor to be studied was
abciximab, amonoclonal antibody to the platelet IIb/IIIa receptor.117,118 Eptifibatide (11) is a peptide
GpIIa/IIIb inhibitor and tirofiban (12) is a small molecule GpIIb/IIIa inhibitor.184,185 These three
drugs are currently approved for IV use in the United States. Oral GpIIa/IIIb inhibitors are not
effective.185 Currently, studies support the use of GpIIb/ IIIa inhibitors for patients with high-risk
unstable angina who are to undergo PCI or stent intervention.
Table IV. Absolute and Relative Contraindications to Thrombolytic Therapy
CPR,cardiopulmonaryresuscitation; SK,streptokinase; APSAC,anistreplase; rt-PA, recombinant tissueplasminogenactivator.Reprinted
withpermissionfromWaters.185
904 * AGRAWAL ET AL.

Figure 4. Site of action of platelet inhibitors. [Color figure can be viewed in the online issue, which is available at www.
interscience.wiley.com.]
VENOUS THROMBOEMBOLISM * 905

1 0 . P H A R M A C O E C O N O M I C S
Ahealth economics analysis is the evaluation of the consequences (outcomes) and/or costs (inputs) of
health care therapies and services with the goal of obtaing the highest possible value of health care
expenditures. In economics terms, thee analysis are used to try to improve the efficiency bywhich we
produce health outcomes.186,187 Pharmacoeconomics is the branch of health economics specifically
focused upon the evaluation of pharmaceutical consequences and/or cost. A well-constructed
pharmacoeconomic (PE) study identifies, measures, and compares the benefits and cost of various
treatment alternatives; it looks beyond the direct acquisition cost by including the impact of drug on
total health resources utilization and cost.186,188 John E. Murphy, PharmD, Professor and Head,
Department of Pharmacy Practice and Science, The University of Arizona College of Pharmacy,
Tucson, discussed pharmacoeconomic issues regarding the LMWH, enoxaparin versus unfractio-
nated heparin in venous thromboembolism. DrMurphy described a cost-effectiveness comparison of
enoxaparin to unfractionated heparin,189 They looked at probabilities for clinical outcomes from a
meta-analysis they had conducted; costs were determined from Medicare reimbursements. The
population was a hypothetical cohort of 60-year-olds, and the interventionwas fixed dose enoxaparin
compared to adjusted dose unfractionated heparin. The perspective was societal. The total costs for
inpatient treatmentwere $26,516 for enoxaparin and $26,361 for unfractionated heparin, a difference
of $155 in favor of unfractionated heparin. However, patients treated with enoxaparin had a reduced
risk for early major bleeding complications, recurrent DVT, and death.
Gould and colleagues also performed a sensitivity analysis. The sensitivity analysis varied costs
and probabilities in the model along a range of conservative to liberal estimates of variation. They
used the following ranges: a 6-day hospitalization costs $2,100–3,500; unfractionated heparin costs
$9–15 plus $33–55 for supplies and ancillary resources; enoxaparin costs $63–105 plus $8–14 for
supplies and ancillary resources. There was a cost saving with enoxaparin when as few as 8% of
patients were treated at home.
A study by Witter and colleagues compared enoxaparin to unfractionated heparin for DVT in a
long-term care facility versus a hospital190 Enoxaparin was more cost effective. The authors found
that the pharmacoeconomic analysis was robust in favor of LMWH, with a large degree of change
necessary before unfractionated heparin would become beneficial. A study by Devlin et al.191
examined enoxaparin versus low-dose heparin for prophylaxis after major trauma. Although
enoxaparin increased overall health care costs, it was associated with an incremental cost per
additional life-year saved of only $2,300, which is lower than the convention for ‘‘a good use of
resources’’ of $30,000 for each life year saved.
1 1 . C O N C L U S I O N
Multiple risk factors (most of which are beyond control) associated with venous thromboembolic
diseases have triggered medicinal chemists to develop new chemical entities in this category. The
usual problems of dose fixing and tedious routine monitoring are also best overcome by these newer
anticoagulants. Novel thrombolytics and antiplatelets are rapidly emerging as an attractive
therapeutic tool for intervention of thromboembolic diseases. Besides these newer approaches, the
future research will also focus on mechanical thrombectomy and surgical intervention.
R E F E R E N C E S
1. Murry CJL, lopaz AD. Mortality by causes for eight regions of the world: Globle burden of diseasesstudies. Lancet 1997;349:1269–1276.
2. Lesing AW, Prandoni P, Prins MH, Buller HR. Deep-vein thrombosis. Lancet 1999;353:479–485.3. Weinmann EE, Salzman EW. Deep-vein thrombosis. N Engl J Med 1994;331:479–485.4. Goldharber SZ. Pulmonary Embolism. N Engl J Med 1998;339:93–104.
906 * AGRAWAL ET AL.

5. LevineM, Raskob GE, Landefeld S, Kearon C. Heamorrhagic complication of anticoagulation treatment.Chest 2001;119:108S–121S.
6. Hirsh J, Dalen JE, Anderson DR, et al. Oral Anticoagulant; mechanism of action, clinical effectiveness,and optimal therapeutic range. Chest 2001;119:8S–21S.
7. Ansell J, Hirsh J, Dalen JE, et al. Managing oral anticoagulant therapy. Chest 2001;119:22S–38S.8. Hirsh J, Warkentin TE, Shaughnessy SG, et al. Heparin and lowmolecular-weight heparin: Mechanism of
action, pharmacokineics, dosing, monitering, efficacy, and safety. Chest 2001;119:64S–94S.9. Chiquette E, Amato MG, Bussey HI. comparison of an anticoagulation clinic with usual medical care:
Anticoagulation control, patient outcomes and health care cost. Arch Intern Med 1998;158:1641–1647.10. Haines ST, Racine E, Zeolla M. Venous Thromboembolism. In: Dipiro JT, Talbert RL, Yee GC, Malzke
GR,Wells BG, Posey LM, editors. Pharmacotherapy. 6th Edition NewYork:McGraw-Hill, 2005. 337–373.11. Hirsh J, Heparin N. Engl J Med 1991;324:1565–1574.12. Virchow RLK. Thrombosis and emboli (1846–1856). Science history publicationinternational 1998.13. Egeberg O. On the natural blood coagulation inhibitor system. Investigations of inhibitor factors based on
antithrombin deficient blood. Thromb Diath Haemorrh 1965;14:473–489.14. Griffin JH, Evatt B, Zimmerman TS, Kleiss AJ, Wideman C. Deficiency of protein C in congenital
thrombotic disease. J Clin Invest 1981;68:1370–1373.15. Schwarz HP, Fischer M, Hopmeier P, Batard MA, Griffin JH. Plasma protein S deficiency in familial
thrombotic disease. Blood 1984;64:1297–1300.16. TheReader, Volume-7, Number 6, December 1997, Published byREAADSMedical Products, Inc., 12061
Tejon Street, Westminster, Colorado 8023.17. Dahlback B, Carlsson M, Svensson PJ. Familial thrombophilia due to a previously unrecognized
mechanism characterized by poor anticoagulant response to activated protein C: Prediction of a cofactor toactivated protein C. Proc Natl Acad Sci USA 1993;90:1004–1008.
18. Ridker PM, Miletich JP, Stampfer MJ, Goldhaber SZ, Lindpaintner K, Hennekens CH. Factor V Leidenand risks of recurrent idiopathic venous thromboembolism. Circulation 1995;92:2800–2802.
19. De Stefano V, Chiusolo P, Paciaroni K, Leone G. Epidemiology of factor V Leiden: Clinical implications.Semin Thromb Hemost 1998;24:367–379.
20. Eichinger S, Pabinger I, StumpflenA, et al. The risk of recurrent venous thromboembolism in patients withand without factor V Leiden. Thromb Haemost 1997;77:624–628.
21. Poort SR, Rosendaal FR, Reitsma PH, Bertina RM. A common geneticvariation in the 3 0-untranslatedregion of the prothrombin gene is associated with elevated plasma prothrombin levels and an increase invenous thrombosis. Blood 1996;88:3698–3703.
22. Ehrenforth S, LudwigG, Klinke S, KrauseM, Scharrer I, Nowak-Gottl U. The prothrombin 20210A alleleis frequently coinherited in young carriers of the factor V Arg 506 to Gln mutation with venousthrombophilia. Blood 1998;91:2209–2210.
23. De Stefano V, Martinelli I, Mannucci PM, et al. The risk of recurrent deep venous thrombosis amongheterozygous carriers of both factor V Leiden and the G20210A prothrombin mutation. N Engl J Med,1999;341:801–806.
24. Fermo I, Vigano’ D’Angelo S, Paroni R, Mazzola G, Calori G, D’Angelo A. Prevalence of moderatehyperhomocysteinemia in patients with early-onset venous and arterial occlusive disease. Ann InternMed1995;123:747–753.
25. Den Heijer M, Koster T, BlomHJ, et al. Hyperhomocysteinemia as a risk factor for deep-vein thrombosis.N Engl J Med 1996;334:759–762.
26. Simioni P, Prandoni P, Burlina A, et al. Hyperhomocysteinemia and deep-vein thrombosis. A case-controlstudy. Thromb Haemost 1996;76:883–886.
27. Welch GN, Loscalzo J. Homocysteine and atherothrombosis. N Engl J Med 1998;338:1042–1050.28. Rosove MH, Brewer PM. Antiphospholipid thrombosis: Clinical course after the first thrombotic event in
70 patients. Ann Intern Med 1992;117:303–308.29. Crowther MA, Ginsberg JS. Antiphospholipid antibody syndrome. In: Goldhaber SZ, Ridker PM, editors.
Thrombosis and thromboembolism, Vol. 44 of fundamental and clinical cardiology. New York: MarcelDekker; 2002. 49–66.
30. Ginsberg JS,Wells PS, Brill-Edwards P, et al. Antiphospholipid antibodies and venous thromboembolism.Blood 1995;86:3685–3691.
31. Doig RG, O’Malley CJ, Dauer R, McGrath KM. An evaluation of 200 consecutive patients withspontaneous or recurrent thrombosis for primary hypercoagulable states. Am J Clin Pathol 1994;102:797–801.
32. The Antiphospholipid Antibodies in Stroke Study (APASS) Group. Anticardiolipin antibodies are anindependent risk factor for first ischemic stroke. Neurology 1993;43:2069–2073.
VENOUS THROMBOEMBOLISM * 907

33. Pabinger I, Grafenhofer H, Kyrle PA, et al. Temporary increase in the risk for recurrence during pregnancyin women with a history of venous thromboembolism. Blood 2002;100:1060–1062.
34. Ginsberg JS, Greer I, Hirsh J. Use of antithrombotic agents during pregnancy. Chest 2001;119:122S–131S.
35. Brill-Edwards P, Ginsberg JS, Gent M, et al. Safety of withholding heparin in pregnant women with ahistory of venous thromboembolism. Recurrence of clot in this pregnancy study group. N Engl J Med2000;343:1439–1444.
36. Goodrich SM, Wood JE. Peripheral venous distensibility and velocity of venous blood flow duringpregnancy or during oral contraceptive therapy. Am J Obstet Gynecol 1964;90:740–744.
37. Clarke-pearson DL, Jelovsek FR. Alteration of occlusive cuff impendence plethysmogrphy results in theobstetric patient. Surgery 1981;89:594–598.
38. Report on confidential inquiries into maternal deaths in England and Wales, 1976-1978. London:Department of Health and Social Security, 1982.
39. Bonnar J. Haemostasis and coagulation Disorder in pregnancy. In: Bloom AL, Thomas DP, editors.Haemostasis and thrombosis, 2nd edition. Edinburgh, Scotland: Churchill Livingstone; 1987. 570–584.
40. Woodhams BJ, Candotti G, Shaw R, Kernnoff PB. Change in coagulation and fibrinolysis duringpregnancy: Evidencce of activation of coagulation proceeding spontaneous abortion. Thromb Res1989;55:99–107.
41. Weiner CP, Kwaan H, Hauck WW, Duboe FJ, Paul M, Walemark CB. Fibrin generation in pregnancy42. Bremme K, Ostund E, Almquvist I, Henomen K, Blomeback M. Enhanced Thrombin generation and
fibrinolytic activity in normal pregnancy in the puerperium. Obstet gynecol43. Gerbasi FR, Bottoms S, Farag A, Mammen E. Increased intravascular coagulation associated with
pregnancy. Obstet Gynecol 1990;75:385–389.44. Faught W, Garner P, Jones G, Ivey B. Change in protein C and Protein S level in normal pregnancy. Am J
Obstet Gynecol 1995;172:147–150.45. Schafer AI. The hypercoagulable states. Ann Intern Med 1985;102:814–828.46. Rutherford SE, Phelan JP. Thromboembolic disease in pregnancy. Clin Perinatol 1986;13:719–739.47. Records Unit and Research Advisory Service of the Royal College of General Practitioners. Oral
contraception and thrombo-embolic disease. J R Coll Gen Pract 1967;13:267–279.48. Vandenbroucke JP, Koster T, Briet E, Reitsma PH, Bertina RM, Rosendaal FR. Increased risk of venous
thrombosis in oral-contraceptive users who are carriers of factor V Leiden mutation. Lancet 1994;344:1453–1457.
49. Thorogood M, Mann J, Murphy M, Vessey M. Risk factors for fatal venous thromboembolism in youngwomen: A case-control study. Int J Epidemiol 1992;21:48–52.
50. WorldHealthOrganization. Venous thromboembolic disease and combined oral contraceptives: Results ofinternational multicentre casecontrol study: World Health Organization Collaborative Study ofCardiovascular Disease and Steroid Hormone Contraception. Lancet 1995;346:1575–1582.
51. Farmer RDT, Preston TD. The risk of venous thromboembolism associated with low-oestrogen oralcontraceptives. J Obstet Gynecol 1995;15:195–200.
52. Grady D, Rubin SM, Petitti DB, Fox CS, Black D, Ettinger B, Ernster VL, Cummings SR. Hormonetherapy to prevent disease and prolong life in postmenopausal women. Ann Intern Med 1992;117:1016–1037.
53. Boston Collaborative Drug Surveillance program. Surgically confirmed gallbladder disease, venousthromboembolism and breast tumors in relation to postmenopausal estrogen therapy. N Engl J Med1974;290:15–19.
54. Nachtigall LE, Nachtigall RH, Nachtigall RD, Beckman EM. Estrogen replacement therapy II: Aprospective study in the relationship to carcinoma and cardiovascular and metabolic problems. ObstetGynecol 1979;54:74–79.
55. Devor M, Barrett-Connor E, Renvall M, Feigal D, Jr., Ramsdell J. Estrogen replacement therapy and therisk of venous thrombosis. Am J Med 1992;92:275–282.
56. Petitti DB, Wingerd J, Pellegrin F, Ramcharan S. Risk of vascular disease in women: Smoking, oralcontraceptives, noncontraceptive estrogens, and other factors. JAMA 1979;242:1150–1154.
57. Young RL, Goepfert AR, Goldzieher HW. Estrogen replacement therapy is not conducive of venousthromboembolism. Maturitas 1991;13:189–192.
58. Daly E, Vessey MP, Hawkins MM, Carson JL, Gough P, Marsh S. Risk of venous thromboembolism inusers of hormone replacement therapy. Lancet 1996;348:977–980.
59. Jick H, Derby LE, Wald Myers M, Vasilakis C, Newton KM. Risk of hospital admission for idiopathicvenous thromboembolism among users of postmenopausal oestrogens. Lancet 1996;348:981–983.
908 * AGRAWAL ET AL.

60. Grodstein F, Stampfer MJ, Goldhaber SZ, Manson JE, Colditz GA, Speizer FE, Willett WC, HennekensCH. Prospective study of exogenous hormones and risk of pulmonary embolism in women. Lancet 1996;348:983–987.
61. Daly E, VesseyMP, Painter R, HawkinsMM.Case-control study of venous thromboembolism risk in usersof hormone replacement therapy. Lancet 1996;348:1027.
62. Varas Lorenzo C, Garcia Rodriguez LA, Cattaruzzi C, Troncon MG, Agostinis L, Perez Gutthann S.Hormone replacement therapy and the risk of hospitalization for venous thromboembolism: A population-based study in southern Europe. Am J Epidemiol 1998;147:387–390.
63. Perez Gutthann S, Garcia Rodriguez LA, Castellsague J, Duque Oliart A. Hormone replacementtherapy and risk of venous thromboembolism: Population based case-control study. BMJ 1997;314:796–800.
64. Grady D, Furberg C. Venous thromboembolic events associated with hormone replacement therapy.JAMA 1997;278:477.
65. Grady D, Wenger NK, Herrington D, Khan S, Furberg C, Hunninghoke D, Vittinghoff E, Hulley S.Postmenopausal hormone therapy increases.risk for venous thromboembolic disease. Ann Intern Med2000;132:689–696.
66. Hoibraaten E, AbdelnoorM, Sandset PM. Hormone replacement therapy with estradiol and risk of venousthromboembolism: A population-based case-control study. Thromb Haemost 1999;82:1218–1221.
67. Daly E, Vessey MP, Hawkins MM, Carson JL, Gough P, Marsh S. Risk of venous thromboembolism inusers of hormone replacement therapy. Lancet 1996;348:977–980.
68. Jick H, Derby LE, Wald Myers M, Vasilakis C, Newton KM. Risk of hospital admission for idiopathicvenous thromboembolism among users of postmenopausal oestrogens. Lancet 1996;348:981–983.
69. Grodstein F, Stampfer MJ, Goldhaber SZ, Manson JE, Colditz GA, Speizer FE, Willett WC, HennekensCH. Prospective study of exogenous hormones and risk of pulmonary embolism in women. Lancet1996;348:983–987.
70. The Coronary Drug Project Research Group. The Coronary Drug Project: Findings leading todiscontinuation of the 2.5-mg day estrogen group. JAMA 1973;226:652–657.
71. Van Kesteren PJ, Asscheman H, Megens JA, Gooren LJ. Mortality and morbidity in transsexual subjectstreated with cross-sex hormones. Clin Endocrinol (Oxf) 1997;47:337–342.
72. Bloemenkamp KWM, Rosendaal FR, Helmerhorst FM, Buller HR, Vandenbroucke JP. Enhancement byfactor V Leiden mutation of risk of deep-vein thrombosis associated with oral contraceptives containing athird-generation progestagen. Lancet 1995;346:1593–1596.
73. World Health Organization. Effect of different progestagens in low oestrogen oral contraceptives onvenous thromboembolic disease. World Health Organization Collaborative Study of CardiovascularDisease and Steroid Hormone Contraception. Lancet 1995;346:1582–1588.
74. Jick H, Jick SS, Gurewich V,MyersMW,Vasilakis C. Risk of idiopathic cardiovascular death and nonfatalvenous thromboembolism in women using oral contraceptives with differing progestagen components.Lancet 1995;346:1589–1593.
75. Olivieri O, Friso S, Manzato F, Guella A, Bernardi F, Lunghi B, Girelli D, Azzini M, Brocco G, Russo C.Resistance to activated protein C in healthy women taking oral contraceptives. Br J Haematol 1995;91:465–470.
76. Scarabin PY, Plu-Bureau G, Zitoun D, Bara L, Guize L, Samama MM. Changes in haemostatic variablesinduced by oral contraceptives containing 50 micrograms or 30 micrograms oestrogen: Absence ofdosedependent effect on PAI-1 activity. Thromb Haemost 1995;74:928–932.
77. Quehenberger P, Loner U, Kapiotis S, Handler S, Schneider B, Huber J, Speiser W. Increased levels ofactivated factor VII and decreased plasma protein S activity and circulating thrombomodulin during use oforal contraceptives. Thromb Haemost 1996;76:729–734.
78. A multicentre study of coagulation and haemostatic variables during oral contraception: Variations withfour formulations: Task force on oral contraceptives:WHOSpecial Programme ofResearch, Developmentand Research Training in Human Reproduction, World Health Organization, Geneva, Switzerland. Br JObstet Gynaecol 1991;98:1117–1128.
79. Meade TW, Haines AP, NorthWR, Chakrabarti R, Howarth DJ, Stirling Y. Haemostatic, lipid, and blood-pressure profiles of women on oral contraceptives containing 50 microgram or 30 microgram oestrogen.Lancet 1977;2:948–951.
80. Henkens CM, Bom VJ, Seinen AJ, van der MJ. Sensitivity to activated protein C; influence of oralcontraceptives and sex. Thromb Haemost 1995;73:402–404.
81. Olivieri O, Friso S, Manzato F, Guella A, Bernardi F, Lunghi B, Girelli D, Azzini M, Brocco G, Russo C.Resistance to activated protein C in healthy women taking oral contraceptives. Br J Haematol 1995;91:465–470.
VENOUS THROMBOEMBOLISM * 909

82. Rosing J, Middeldorp S, Curvers J, Christella M, Thomassen LG, Nicolaes GA, Meijers JC, Bouma BN,Buller HR, PrinsMH, et al. Low-dose oral contraceptives and acquired resistance to activated protein C: Arandomised cross-over study. Lancet 1999;354:2036–2040.
83. Middeldorp S,Meijers JCM, van den EndeAE, vanEnkA,BoumaBN, TansG, Rosing J, PrinsMH,BullerHR. Effects on coagulation of levonorgestrel- and desogestrel-containing low dose oral contraceptives:A cross-over study. Thromb Haemost 2000;84:4–8.
84. Tans G, Curvers J, Middeldorp S, Thomassen MCLGD, Meijers JCM, Prins MH, Bouma BN, Buller HR,Rosing J. A randomized cross-over study on the effects of levonorgestrel- and desogestrel-containing oralcontraceptives on the anticoagulant pathways. Thromb Haemost 2000;84:15–21.
85. Meijers JCM, Middeldorp S, Tekelenburg W, van den Ende AE, Tans G, Prins MH, Rosing J, Buller HR,BoumaBN. Increased fibrinolytic activity during use of oral contraceptives is counteracted by an enhancedfactorXI-independent downregulation offibrinolysis: A randomized cross-over study of two low-dose oralcontraceptives. Thromb Haemost 2000;84:9–14.
86. Bick RL. Coagulation abnormalities in malignancy: A review. Semin Thromb Hemost 1992;18:353–372. 52.
87. Baron JA, Gridley G, Weiderpass E, Nyren O, Linet M. Venous thromboembolism and cancer. Lancet1998;351:1077–1080.
88. Zurborn KH, Duscha H, Gram J, Bruhn HD. Investigations of coagulation system and fibrinolysisin patients with disseminated adenocarcinomas and non-Hodgkin’s lymphomas. Oncology 1990;47:376–380.
89. Kerr R, Stirling D, Ludlam CA. Interleukin 6 and haemostasis. Br J Haematol 2001;115:3–12.90. Beilke MA. Vascular endothelium in immunology and infectious disease. Rev Infect Dis 1989;11:273–
283.91. Jutila MA. Role of changes in the vascular endothelium in chronic inflammation. Clin Transplant
1994;8:304–307.92. Grau GE, Roux-Lombard P, Gysler C, et al. Serum cytokine changes in systemic vasculitis. Immunology
1989;68:196–198.93. Introna M, Colotta F, Sozzani S, Dejana E, Mantovani A. Pro- and anti-inflammatory cytokines:
Interactions with vascular endothelium. Clin Exp Rheumatol 1994;12:S19–S23.94. O’Donnell J, Mumford AD,Manning RA, LaffanM. Elevation of FVIII: C in venous thromboembolism is
persistent and independent of the acute phase response. Thromb Haemost 2000;83:10–13.95. Johnson R, Green JR, Charnley J. Pulmonary embolism and its prophylaxis following the Charnley total
hip replacement. Clin Orthop 1977;127:123–132.96. Huber O, BounameauxH, Borst F, Rohner A. Postoperative pulmonary embolism after hospital discharge.
An underestimated risk. Arch Surg 1992;127:310–313.97. Hull R, Raskob G, Pineo G, et al. A comparison of subcutaneous low-molecular-weight heparin with
warfarin sodium for prophylaxis against deep-vein thrombosis after hip or knee implantation. N Engl JMed 1993;329:1370–1376.
98. Francis CW, Pellegrini VD, Jr., Totterman S, et al. Prevention of deep-vein thrombosis after total hiparthroplasty. Comparison of warfarin and dalteparin. J Bone Joint Surg Am 1997;79:1365–1372.
99. Bergqvist D. Prolonged prophylaxis in postoperative medicine. Semin Thromb Hemost 1997;23:149–154.
100. Eriksson BI, Kalebo P, Ekman S, Lindbratt S, Kerry R, Close P. Direct thrombin inhibition with Rec-hirudin CGP 39393 as prophylaxis of thromboembolic complications after total hip replacement. ThrombHaemost 1994;72:227–231.
101. Clagett GP, Anderson FA, Jr., Heit J, Levine MN, Wheeler HB. Prevention of venous thromboembolism.Chest 1995;108:312S–334S.
102. Hamilton MG, Hull RD, Pineo GF. Venous thromboembolism in neurosurgery and neurology patients: Areview. Neurosurgery 1994;34:280–296; discussion 296.
103. Melon E, Keravel Y, Gaston A, Huet Y, Combes S, and the Neuronox group. Deep venous thrombosisprophylaxis by low molecular weight heparin in neurosurgical patients. Anesthesiology 1991;75:A214(abstract).
104. Sigel B, Ipsen J, Felix WR, Jr. The epidemiology of lower extremity deep venous thrombosis in surgicalpatients. Ann Surg 1974;179:278–290.
105. Turpie AG. Low-molecular-weight heparins and heparinoids for prevention of VTE. In: Bounameaux H,editor. Low-molecular-weight heparins in prophylaxis and therapy of thromboembolic diseases. NewYork: Marcel Dekker; 1994. 213.
106. Geerts WH, Code KI, Jay RM, Chen E, Szalai JP. A prospective study of venous thromboembolism aftermajor trauma. N Engl J Med 1994;331:1601–1606.
910 * AGRAWAL ET AL.

107. Gando S. Disseminated intravascular coagulation in trauma patients. Semin Thromb Hemost 2001;27:585–592.
108. Thromboembolic Risk Factors (THRIFT) Consensus Group. Risk of and prophylaxis for venousthromboembolism in hospital patients. Br Med J 1992;305:567–574.
109. Prophylaxis of venous thromboembolism. Edinburgh. Scottish Intercollegiate Guidelines Network, 1995.110. Warkentin TE,GreinacherA.Heparininduced thrombocytopenia: Recognition, treatment, and prevention:
The Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest 2004;126:311S–337S. [Erratum, Chest 2005; 127:416.]
111. BoshkovLK,Warkentin TE,HaywardCP,AndrewM,Kelton JG. Heparin-induced thrombocytopenia andthrombosis: Clinical and laboratory studies. Br J Haematol 1993;84:322–328.
112. LubenowN,Eichler P, Lietz T, FarnerB,GreinacherA. Lepirudin for prophylaxis of thrombosis in patientswith acute isolated heparin-induced thrombocytopenia: An analysis of 3 prospective studies. Blood2004;104:3072–3077.
113. Hirsh J. Heparin. N Engl J Med 1991;324:1565–1574.114. Zacharski LR, Ornestein DL. Heparin and cancer. Thromb Heamost 1998;80:10–23.115. Ibrahim SA, Leandefeld CS. Bleeding and unfractinated heparin. In: Ginsberg JS, Kearon C, Hirsh J,
editors. Clinical decision in thrombosis and hemastasis. Hamilton, Ontario, Canada: B.C.Decker; 1998.154–160.
116. Levine M, Raskob GE, landefeld S, Kearon C. Hemmorrhagic complication of anticoagulant treatment.Chest 2001;119:108S–121S.
117. Hirsh J, McCarthy RA, DeGruchy GC. Heparin in the treatment of venous thromboembolic disease:Administration, control, and results. Med J Aust 1968;2:153–159.
118. Hirsh J, Levin MN. Low molecular weight heparin. Blood 1992;79:1–17.119. Brill-Edwards P. heparin resistnce. In: Ginsberg JS, Kearnon C, Hirsh J, editors. Clinical decisions in
thrombosis and hematosis. Hamilton, Ontario, Canada: B C Decker; 1998. 117–122.120. Greinacher A. Treatment of heparin-induced thrombocytopenia. Thromb Haemost 1999;82:457–467.121. Warkentin TE, Kelton JG. A 14 year study of heparin induced thrombocytopenia. Am J Med
1996;101:502–507.122. Warkentin TE, Chong BH, Greinacher A. heparin induced thrombocytopenia: Toward consensus. Thromb
Haemost 1998;79:1–7.123. Warkentin TE. Heparin induced thrombocytopenia: A clinicopathologic syndrome. Thromb Haemost
1999;82:439–447.124. White PW, Sadd JR, Nensel RE. Thrombotic complications of heparin therapy. Ann Surg 1979;190:595–
608.125. Griffith GC, Nichols G, Asher J, et al. Heparin osteoporosis. JAMA 1965;193:91–94.126. Jaffe MD, Willis PW III. Multiple fracture associated with long-term heparin therapy. JAMA
1965;193:158–160.127. Sackler JP, Liu L. Heparin-induced osteoporosis. Br J Radiol 1973;46:458–460.128. Squires JW, Pinch LW. Heparin-induced spinal fractures. JAMA 1979;241:2417–2418.129. Wise PW, Hall AJ. Heparin-induced osteopenia in pregnancy. BMJ 1980;2:110–111.130. Edes TE, Sunderrajan EV. Heparin-induced hyperkalemia. Arch Intern Med 1985;145:1070–1072.131. Weitz JI. Low molecular weight heparins. N Engl J Med 1997;337:688–698.132. Salzman EW. Low molecular weight heparin: Is small beautiful? N Engl J Med 1986;315:957–959.133. Verstraete M. Pharmacotherapeutic aspects of unfractionated and low molecular weight heparin. Drugs
1990;40:498–530.134. AiachM,Michaud A, Balian JL, et al. A new lowmolecular weight heparin derivative, in vitro and in vivo
studies. Thromb Res 1983;31:611–621.135. BaraL,BillandE,GramondG, et al. Comparative pharmacokinetics of a lowmolecularweight heparin and
unfractionated heparin after intravenous and subcutaneous administration. Thromb Res 1985;39:631–636.
136. Bergqvist D, Hedner U, Sjorin E, et al. Anticoagulant effects of two types of lowmolecular weight heparinadministered subcutaneously. Thromb Res 1983;32:381–391.
137. Bratt G, Tornebohm E, Widlund L, et al. Low molecular weight heparin (Kabi 2165; Fragmin):Pharmacokinetics after intravenous and subcutaneous administration in human volunteers. Thromb Res1986;42:613–620.
138. Matzsch T, Bergqvist D, Hedner U, et al. Effects of an enzymatically depolymerized heparin as comparedwith conventional heparin in healthy volunteers. Thromb Haemost 1987;57:97–101.
139. Harenberg J, Wurzner B, Zimmermann R, et al. Bioavailability and antagonization of the low molecularweight heparin CY216 in man. Thromb Res 1986;44:549–554.
VENOUS THROMBOEMBOLISM * 911

140. Turpie AG. Pharmacology of the low molecular weight heparins. Am heart J 1998;135:S329–S335.
141. Hirsh J. Low-molecular-weight heparin for the treatment of venous thromboembolism. Am Heart J1998;135:S336–S342.
142. Cade JF, BuchanonMR, Boneau B, et al. A comparison of the antithrombotic and haemorrhagic effects oflow molecular weight heparin fractions: The influence of the method of preparation. Thromb Res1984;35:613–625.
143. Carter CJ, Kelton JR, Hirsh J, et al. Relationship between the antithrombotic and anticoagulant effects oflow molecular weight heparin. Thromb Res 1981;21:169–174.
144. Carter CJ, Kelton JG, Hirsh J, et al. The relationship between the hemorrhagic and antithromboticproperties of low molecular weight heparin in rabbits. Blood 1982;59:1239–1245.
145. Holmer E, Mattsson C, Nilsson S. Anticoagulant and antithrombotic effects of heparin and lowmolecularweight heparin fragments in rabbits. Thromb Res 1982;25:475–485.
146. Hull RD, Raskob GE, Pineo GF, et al. Subcutaneous low-molecular-weight heparin compared withcontinuous intravenous heparin in the initial treatment of proximal-vein thrombosis. N Engl J Med1992;326:975–982.
147. Gallus A, Cade J, Ockelford P, et al. Orgaran (Org 10172) or heparin for preventing venous thrombosisafter elective surgery formalignant disease?Adouble-blind, randomisedmulticentre comparison. ThrombHaemost 1993;70:562–567.
148. Hoek JA, Nurmohamed MT, Hamelynk KJ, et al. Prevention of deep vein thrombosis following total hipreplacement by low molecular weight heparinoid. Thromb Haemost 1992;67:28–32.
149. Farner B, Eichler P, Kroll H, et al. A comparison of danaparoid and lepirudin in heparin-inducedthrombocytopenia. Thromb Haemost 2001;85:950–957.
150. Wilde MI, Markham A. Danaparoid: A review of its pharmacology and clinical use in the management ofheparin-induced thrombocytopenia. Drugs 1997;54:903–924.
151. Tardy-poncet B, Tandy B, Reynaud J, et al. Efficacy and safety of danapoid sodium (ORG 10172) incritically ill patient with heparin associated thrombocytopenia. Chest 1999;115:1616–1620.
152. Weitz JI, Hirsh J. New anticoagulant drugs. Chest 2001;119:95S–109S.153. Turpie AG, Gallus AS, Hoek JA. A synthetic pentasaccharide for the prevention of deep vein thrombosis
after total hip replacement. N Engl J Med 2001: 334:619–625.154. Choay J, Petitou M. Lormeau JC, Sinay P, Casu B, Gatti G. Structure-activity relationship in heparin: A
synthetic pentasaccharide with high affinity for antithrombin III and eliciting high anti-factor Xa activity.Biochim Biophys Acta 1983;116:492–499.
155. Walenga JM, PetitouM,Lormeau JC, SamamaM,Fareed J, Choay J.Antithrombotic activity of a syntheticheparin pentasaccharide in a rabbit stasis thrombosis model using different thrombogenic challenges.Thromb Res 1987;46:187–198.
156. Herbert JM, Heravlet JP, Bernat A, et al. Biochemical and pharmacologic properties of Sanorg 34006, apotent and long-acting synthetic pentasaccharide. Blood 1998;91:4197–4205.
157. Fareed J. 1999. Cited online: Factor Xa inhibitors: Impact on the development of anti thromibotic agents.Available from http://www.Medscape.com/viewarticle/426359 [accessed 15 July 2006].
158. Haker LA. Therapeutic inhibition of thrombin activities, receptors and production. Hematol Oncol ClinNorth Am 1998;12:1211–1230.
159. Agnelli G, Sonaglia F. Clinical Status of direct thrombin inhibitors. Crit Rev Oncol Hematol 1999;31:97–117.
160. Swan SK, HurstingMJ. The pharmacokinetic and pharmacodynamic of argatrobsn effect of age gender orhepatic or renal dysfunction. Pharmacotherapy 2006;20:318–329.
161. Bauer KA. New pentasaccharides for prophylaxis of deep vein thrombosis: Pharmacology. Chest 2003;124:364S–370S.
162. Samama MM, Gerotziafas GT. Evaluation of the pharmacological properties and clinical results of thesynthetic pentasaccharide (fondaparinux). Thromb Res 2003;109:1–11.
163. Donat F, Duret JP, Santoni A, et al. The pharmacokinetics of fondaparinux sodium in healthy volunteers.Clin Pharmacokinet 2002;42:1–9.
164. Linkins LA, Julian JA, Rischke J, et al. In vitro comparison of the effect of heparin, enoxaparin andfondaparinux on tests of coagulation. Thromb Res 2002;107:241–244.
165. Januzzi JL, Jr., Jang IK. Fundamental concepts in the pathobiology of heparin-induced thrombocytopenia.J Thromb Thrombolysis 2000;10:7–11.
166. Wawrzynska L, Tomkowski WZ, Przedlacki J, et al. Changes in bone density during long-termadministration of low-molecular-weight heparins or acenocoumarol for secondary prophylaxis of venousthromboembolism. Pathophysiol Haemost Thromb 2003;33:64–67.
912 * AGRAWAL ET AL.

167. Bernardi E, Prandoni P. Safety of low molecular weight heparins in the treatment of venousthromboembolism. Expert Opin Drug Saf 2003;2:87–94.
168. Bhandari M, Hirsh J, Weitz JI. The effects of low molecular weight heparin on bone nodule formationin vitro. Thromb Haemost 1998;80:413–417.
169. Muir JM, Hirsh J,Weitz JI. A histomorphometric comparison of the effects of heparin and low-molecular-weight heparin on cancellous bone in rats. Blood 1997;89:3236–3242.
170. Bizjak ED, Mauro VF. Thrombolytic therapy: A review of its use in acute myocardial infarction. AnnPharmacother 1998;32:769–784.
171. Marder VJ, Sherry S. Thrombolytic therapy: Current status. N Engl J Med 1988;318:1512–1520; 1585–1594.
172. Gulba DC, Bode C, Runge MS, Huber K. Thrombolytic agents—An overview. Ann Hematol 1996:73:S9–S27.
173. The Urokinase Pulmonary Embolism Trial. A national cooperative study. Circulation 1973;47:1–100.174. Urokinase Pulmonary Embolism Trial. Phase I results. JAMA 1970: 214:2163–2172.175. Clare AC, et al. Use of recombinant tissue-plasminogen activator for aortic thrombolysis in a
hypoproteinemic dog. JAVMA 1998: 212:539.176. Urokinase Pulmonary Embolism Trial. Phase I results. JAMA 1970;214:2163–2172.177. Urokinase Streptokinase Pulmonary Embolism Trial. Phase II results. JAMA 1974;229:1606–1613.178. Marder VJ. The use of thrombolytic agents: Choice of patient, drug administration, laboratorymonitoring.
Ann Intern Med 1979. 90:802–808.179. Goldhaber SZ, Kessler CM, Heit J, et al. Randomized controlled trial of recombinant tissue plasminogen
activator versus urokinase in the treatment of acute pulmonary embolism. Lancet 1988;2:293–298.180. LevineM,Hirsh J,Weitz J, et al. A randomized trial of a single bolus dosage regimen of recombinant tissue
plasminogen activator in acute pulmonary embolism. Chest 1990: 98:1473–1479.181. TebbeU,GrafA,KamkeW, et al. Hemodynamic effects of double bolus reteplase versus alteplase infusion
in massive pulmonary embolism. Am Heart J 1999;138:39–44.182. Pifarre R, Scanlon P, editors. Evidence-based management of the acute coronary syndrome. Philadelphia:
Hanley & Belfus, Inc; 2001.183. Becker R. Fibrinolytic and antithrombotic therapy. New York: Oxford University Press 2000. 1-716.184. Braunwald E, Antman E, Beasley J, et al. ACC/AHA guidelines for the management of patients with
unstable angina and non-ST-segment elevation myocardial infarction. J Am Coll Cardiol 2000;36:970–1062.
185. Waters D. Diagnosis and management of patients with unstable angina. In: Fuster V, Alexander RW,O’Rourke RA, et al, editors. Hurst’s the heart (10th ed) New York: McGraw-Hill; 2001. 2129–2142.
186. ReederCE.Overviewof pharmacoeconomics and pharmaceutical outcomes evaluations.Am Jhealth-SystPharm 1995;52:S5–8.
187. Yee GC. Cost Utility analysis of taxane therapy. Am J of Health-Sys Pharm, 1997;54:S11–15.188. Brixner DI. Outcome research, pharmacoeconomics and the pharmaceutical industry. JMCP 1996;2:48–
52.189. Gould MK, Dembitzer AD, Sanders GD, Garber AM. Low-molecular-weight heparins compared with
unfractionated heparin for treatment of acute deep venous thrombosis Ann Intern Med 1999;130:789–799.
190. Witter MD. Gupchup GV, Dole EL, Singhal P, Black A. Pharmacoeconomic assessment of enoxaparin inthe skilled ward of a long-term care facility versus unfractionated heparin in the hospital for treatment ofproximal deep vein thrombosis. Consult Pharm 2000;15:151–154 , 157–159.
191. Devlin JW, Petitta A, ShepardAD, FarouckNO.Cost-effectiveness of enoxaparinversus low-dose heparinfor prophylaxis against venous thrombosis after major trauma. Pharmacotherapy 1998;18:1335–1342.
Prof. Y.K. Agrawal, M.Sc. Ph.D., D.Sc. (USA) in Pharmaceutical Science, D.Sc. (India), F.R.S.C., C.Chem.
(U.K.) is working as a Director in Institute of Pharmacy, Nirma University of Science & Technology. Formerly, he
worked as the Director in School of Sciences, Gujarat University, Ahmedabad and Professor and Head in
Pharmacy Department, Faculty of Technology Engineering, The M.S. University of Baroda. Prior to this he
served at various prestigious institutions of the country like IIT, Bombay, Bhabha Atomic Research Centre,
Trombay, etc. in various capacities. He has visited various countries, viz. USA, Australia, Spain, and Germany.
He is a fellow and member of several Chemical Societies of the country and also abroad. He has 38 years of
teaching and research experience and published 400 research papers in International Journals, 5 patents,
guided 90 Ph.D. students (Pharmacy, Chemistry, Engineering and Bio-sciences), 15 M.Pharm., 5 M.Phil and
VENOUS THROMBOEMBOLISM * 913

ME students. Recipient of ‘‘Russian Academy Award 1985’’, Hari Om Ashram Award 1989, Hari Om Ashram
Award 1991, Royal Society of Chemistry, London Research Award in 1997, 1998 (on Supramolecules), H.K. Sen
Memorial Award in Pharmaceutical Science, 1998, Dr. A.K. Ganguli Oration Award 2000, P.K. Bose Memorial
Award 2001, IDMA Eminent Analyst Award 2003, CSIR Bronze Medal for research contribution in Chemistry
2004. Member of Editorial Board, Indian Journal of Pharmaceutical Sciences, Indian Drugs, Indian Journal of
Chemistry, Chemical Research, etc. Member of the UGC, DST, CSIR, DSIR, etc.
Mr. Hitesh B. Vaidya, M.Pharm., has more than 2 years of Teaching and Research experience. He has worked
on Quantitative Structure Activity Relationship (QSAR) Models and on Molecular Modeling. He has published
two review articles in reputed international journals also has participated in various International & National
Conferences, Seminars, Symposiums and Workshop conducted by AICTE, DST, and various agencies. His main
areas of research are synthetic chemistry, microwave synthesis, and computer added drug design. He is a life
member of association of Pharmacy Teachers of India (APTI).
Mr. Hardik G Bhatt, M.Pharm., has 2 years of teaching and research experience. He is the recipient of the
GOLD MEDAL for standing FIRST in M.Pharm. (Department of Pharmaceutical Chemistry) from Gujarat
University. He is an author of ‘‘Practicals in Organic and Medicinal Chemistry’’ book for B.Pharm. students. He
has published two Research articles and three Review articles in reputed International and National journals. He
has attended and presented two research articles in various international and national level seminars and
conferences conducted by DST, AICTE, CSIR, UGC, and various universities. His areas of research are
Molecular Modeling, Drug Design, QSAR, Synthetic Heterocyclic Ring Systems. He is life member of Indian
Pharmaceutical Association (IPA) and Association of Pharmacy Teachers of India (APTI).
Mr. Kuntal Manna, Lecturer in Pharmaceutical Chemistry, has more than 3 years Teaching and Research
experiences. He has published three scientific research and two review articles in various reputed International
and National journals. He has presented two research articles and has participated in more then five
international & National Conferences, Seminars, Symposiums, and Workshop conducted by DST, AICTE, CSIR,
UGC, and various universities. His areas of research are synthetic chemistry (heterocyclic, asymmetric, and
supramolecular compounds), microwave synthesis, computer added molecular modeling & drug design.
Mr.PathikBrahmkshatriya, M.Pharm., has worked more than 2 year as a lecturer, and currently he is doing his
Ph.D. He has published three international publications in reputed journals. He has presented one research
article and has participated in more then five International and National Conferences, Seminars, Symposiums
and Workshops conducted by DST, AICTE, CSIR, UGC, and various universities.
914 * AGRAWAL ET AL.