
Genetic and Molecular Basis of Cardiac Arrhythmias: Impact on Clinical Management Parts I and II
Upload
independentCategory
view
0download
0
DOI: 10.1161/CIRCEP.114.001615
1
Ventricular Arrhythmias near the Distal Great Cardiac Vein:
A Challenging Arrhythmia for Ablation
Running title: Nagashima et al.; Ventricular arrhythmias near the GCV
Koichi Nagashima, MD, PhD; Eue-Keun Choi, MD, PhD; Kaity Y. Lin, MD; Saurabh Kumar,
MD, PhD; Usha B. Tedrow, MD, MSc; Bruce A. Koplan, MD, MPH; Gregory F. Michaud, MD;
Roy M. John, MD, PhD; Laurence M. Epstein, MD; Michifumi Tokuda, MD, PhD;
Keiichi Inada, MD, PhD; Gregory S. Couper, MD; William G. Stevenson, MD
Arrhythmia Unit, Cardiovascular Division, Brigham and Women’s Hospital, Boston, MA
Correspondence:
William G. Stevenson, MD
Cardiovascular Division
Brigham and Women’s Hospital
75 Francis St.
Boston, MA 02115
Tel: 1-857-307-1948
Fax: 1-857-307-1944
E-mail: [email protected]
Journal Subject Codes: [106] Electrophysiology, [22] Ablation/ICD/surgery
GrGrGrGregegegegorororory y y y F.F.F.F. MMMMicicicichahahahaudududud
i Tokkududududa,a,a,a, MMMMD,D,D,D, PPPPhDhDhDhD;
K
h M
Keeeeiiiiiichchchi Inaddddaa, MD, PhD; Greggggory yy S. Coupperr, MD;;;; Willllililiam G. Stevenson,, MD
hmiaaa UUUniniit,t,, CCCararardididiovovovasasascucuculalalalar r DiD vivvisisiooon,n,n,, BBBriiiighghghghamamam aaandndnd WWWomomomennen’sss HHHososospipipipitatatal,lll BBBososostotton,nn M
by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from

DOI: 10.1161/CIRCEP.114.001615
2
Abstract:
Background - Catheter ablation (CA) for ventricular arrhythmia (VA) near the distal great
cardiac vein (GCV) is often challenging and data are limited.
Methods and Results - Analysis was performed of 30 patients (19 male; age 52.8±15.5 years)
who underwent CA for focal VA (11 ventricular tachycardia, 19 premature contractions) with
early activation in the GCV (36.7±8.0 ms pre-QRS). Angiography in 27 patients showed earliest
GCV site within 5 mm of a coronary artery in 20 (74%). Ablation was performed in the GCV in
15 patients and abolished VA in 8. Ablation was attempted at adjacent non-GCV sites in 19
patients and abolished VA in 5 patients (4 from the left ventricular endocardium and 1 from the
the GCV (GCV-nonGCV interval). In 13 patients percutaneous epicardial mapping was
performed, but due to adjacent coronaries only 2 received radiofrequency application with VA
elimination in 1. Surgical cryoablation was performed in 3 patients and abolished VA in 2.
Overall acute success was achieved in 16 (53%) patients. After a median of 2.8 months, 13
patients remained free of VA. Major complications occurred in 4 patients including coronary
injury requiring stenting.
Conclusions - Ablation for this arrhythmia is challenging and often limited by the adjacent
coronary vessels. Success of anatomically guided endocardial ablation may be identified by a
short GCV-nonGCV interval and r wave in lead I.
Key words: ventricular arrhythmia, catheter ablation, great cardiac vein
rdial mamamamappppppppinininng g g g wawawawassss
but due to adjacent coronaries only 2 received radiofrequency application with
n in 1. Surgical cryoablation was performed in 3 patients and abolished VA in 2
u 3
mained free of VA. Major complications occurred in 4 patients including corona
u
n y g g y e adjacent
butututut ddddueuue ttttooo adddjajajacent coronaries only 2 recececeieived radiofreeequenenenency application with
n innnn 1. Surgicacacal crrryoyoyoyoabababa lalalaatitititionnnn wwwwaaas perrfooormmed innn n 3333 papapap tiiienenentts aaandnd aaaabobobobolilililishshshhedededed VVVA AAA ininini 2
uttteee sususuccessss wawaw s achihhievedededd iiiin 1616166 ((5333%)%)%)% pppatieientssss. AAAfA tter a medidiannnn ooof fff 2.8888 mommonnthsss, 13
maineneneed freeeeee of VAVAVA. Majjajjororoor complpp icatatattioii nsnsnns ooooccurrerered in 4 pppatatata ients inininincludududu ing gg corona
uiringgg stentinii g.g.g.
nnss - AbAblalatititit onon fffforor ttthihihih s ss ararrhrhhhyttythmhhmhmiaia iiiiss chchchhallallellel ngnginiini g g annnand dd d ofofffteten n lilililimiimiitettet d d dd bybbyb tttthhhhe e adadjajacecentnt
by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from

DOI: 10.1161/CIRCEP.114.001615
3
Introduction
Catheter ablation (CA) for ventricular arrhythmia (VA) is a widely accepted therapy for patients
without structural heart disease, but the approach and outcomes depend on the site of arrhythmia
origin.1 Most VAs originate from the right or left ventricular outflow regions, including
myocardium around the aortic cusps and the summit of the left ventricle (LV). Approaches to
ablation of VA from specific areas are being increasingly refined. Ablation of VA originating
from near the distal great cardiac vein (GCV) is often difficult due to proximity to coronary
arteries limited capability of radiofrequency (RF) energy application in the GCV itself.2-5 We
have targeted these arrhythmias from various approaches including the endocardial, epicardial
via the GCV and pericardial space, and also with open chest surgery. The aim of this study was
to evaluate the mapping features, outcomes and risks for ablation of these VAs.
Methods
Patient characteristics
Of 270 patients (133 male, 49.2±14.0 years) without structural heart disease who underwent CA
for focal VA from January 2006 to January 2014, 30 patients (19 male, age 52.8±15.5 years)
with VA [11 with ventricular tachycardia (VT) and 19 with premature ventricular contractions
(PVC)] for which the earliest activation site before pericardial mapping was in the GCV were
analyzed. In 25 patients there was no evidence of structural heart disease. One patient had a
history of anthracycline chemotherapy and later developed cardiomyopathy. The remaining 4
patients had a history of LV dysfunction felt to be PVC induced. Each patient gave written
informed consent. Studies and data collection were performed according to protocols approved
by the Human Research Committee of Brigham and Women’s Hospital.
n the GCV itself.2 55 W
e endododd cacardddrdiiiaiallll, eepipiipicacacacardrd
V y
a
V aaaandndndd pperererericicicicarrrdidididial space, and also with opopopenn chest surgeegery. TTTThe aim of this study
tttht eee e mapping feeatuuurees, ouououtcommesss aandd rrriskks forrr aablblbllatatationnn of theheseee VVVAs..
araracacteteriristststiciici ss
by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from

DOI: 10.1161/CIRCEP.114.001615
4
Electrophysiological study and mapping
Procedures were performed either under conscious sedation or general anesthesia. Using
femoral venous and/or arterial access multipolar electrode catheters were positioned in the
coronary sinus to GCV, the right ventricular (RV) apex and the His bundle region. For the
patients with a history of sustained VT, programmed ventricular stimulation was performed with
up to 3 extrastimuli scanned to a minimum coupling interval of 180 ms following basic drives of
600 ms and 400 ms from 2 RV sites and burst pacing. If sustained VT was not reliably
inducible, non-sustained VT or PVCs felt likely to be originating from the same site, were
targeted. Intravenous infusion of isoproterenol and/or epinephrine was administered as needed
for arrhythmia induction.
Mapping and ablation was performed using a 3.5-mm-tip catheter (NaviStar ThermoCool
or ThermoCool SF; Biosense Webster, Diamond Bar, CA, USA) in 25 patients. In 5 patients a
4-mm-tip non-irrigated catheter (NaviStar, Biosense Webster) was used initially for mapping (5
patients) and attempted ablation (3 patients) before switching to an irrigated tip catheter.
Activation mapping of VT or PVCs utilized an electroanatomic mapping system (CARTO 3 or
XP, Biosense Webster) with bipolar electrograms high pass filtered at 20 to 30 Hz and low pass
filtered at 400 Hz. Bipolar electrograms were also band pass filtered from 30 to 500 Hz and
digitally recorded along with a 12-lead surface electrocardiogram (Cardiolab EP system, General
Electric Healthcare, Buckinghamshire, UK). Pace mapping utilized unipolar stimuli at 10 mA
and pulse width of 2 ms.6
Epicardial mapping was considered if a subepicardial VT origin was suspected based on
endocardial and GCV mapping, either at the same or a subsequent session. Percutaneous
subxiphoid epicardial access was obtained as previously described either before administration
m the same site, wwerererereeee
s admmininii isiiisttetet reredddd asas nnnneeee
m
p
Cool SF; Biosense Webster, Diamond Bar, CA, USA) in 25 patients. In 5 patien
n n
nd attempted ablation (3 patients) before s itching to an irrigated tip catheter
miaiaia iiiindndndnducucucctitititionnn. .. .
pppppiiiing and ablatationnn wwas pppep rforormedd ussinnng aa 3.5-555 mmmmmmmm--tippp cccathhetterrr (NNaN viviiiSStS arar TTheeermrmm
Coolll l SFSFSF;;;; BBBiosense WWWWebstttererere , Diammmmononono dddd BBaBB r,r, CCCCA,AAA UUUUSASASASA) ))) inininin 2222555 patiienenenentstststs. In 555 patititien
non-iiri iirigagg tedd d cacacaathhhheter (((NaNN viiiSStS ar, BiBiBiosense WWWW bbeb tster) ) ) waasss s usedededd iiinitiiialllllylyly fffforrrr mmmmapapapa pipp n
dd tattte ttedd babllatiti ((33 titi tts)) bbeffo iittchihi tt ii iig tat ded ttiip tathhette
by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from

DOI: 10.1161/CIRCEP.114.001615
5
of systemic anticoagulation or after anticoagulation was reversed.7
Ablation
Coronary angiography was performed prior to initial ablation at sites with the possibility of an
adjacent artery. If the distance of the catheter tip to a major coronary artery was < 4-5 mm, RF
delivery was avoided. RF application was also not attempted if there was diaphragmatic capture
during pacing from the ablation catheter. Irrigated RF energy was delivered at 25 to 50 Watts
targeting an impedance drop of 10 to 20 ohms. At endocardial sites below the aortic valve
applications were usually repeated until unipolar pacing at 10 mA at 2 ms stimulus strength
failed to capture.6 At target areas in the sinuses of Valsalva and GCV power exceeding 35 Watts
was avoided. At some sites where RF ablation was limited or coronary artery proximity was of
concern, ablation with a 6-mm-tip cryocatheter (Cryocath Technologies, Montreal, Canada) was
attempted.
At the end of the procedure, the same induction protocol was repeated. Acute success
was defined as the absence of any target arrhythmia.
Data collection and follow-up
Data were collected from a centralized system containing records of all patients treated and
followed at Brigham and Women’s Hospital and all associated Partners Healthcare sites. These
records include emergency department visits, outpatient clinic visits, data recorded during
inpatient care as well as follow-up progress notes from referring physicians monitoring out-of-
area patients. Referring physicians were contacted for clinical follow-up if necessary. Procedure
success was defined as more than an 80% reduction in VA on 24-hour Holter monitoring or
resolution of symptoms with no VA in all electrocardiograms during follow-up.
ms stimulus strengngngngttht
powwerer eexcxceeeedidididingng 33335555
ed. At some sites where RF ablation was limited or coronary artery proximity wa
b a
the end of the procedure, the same induction protocol was repeated. Acute succe
d as the absence of an target arrh thmia
ed. AtAtAtAt ssomomommee siiitetetetes where RF ablation was ss lilililimmited or corrronarararryy yy artery proximity wa
blllal tttit on with a 6---mmmm-tip p p cccryocac thhheeter (CCCryoyocathththth TTTeceece hnnnooologiies, MMMMontrrrreaaal, CCannnaddda
the endd d offf thehehe pppprocedudd re, thhthhe same iii dndduc iition ppprotot collll wawww s reeepepepep tat ddedd. AAAcuuuutetetete ssssuuucu ce
dd tthhe bbs ff tta tet hh thth imi
by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from

DOI: 10.1161/CIRCEP.114.001615
6
Statistical Analysis
Continuous variables were expressed as mean±SD values or median and interquartile ranges
(IQR) are shown in parentheses, as appropriate. Student’s t-test or Mann-Whitney’s U test was
used to compare continuous variables, depending on whether the values were normally
distributed, and the chi-square test was used to compare dichotomous variables unless the
expected values in any cells were <5, in which case Fisher exact test was used. P<0.05 was
considered to be statistically significant. Statistical analyses were performed with JMP 9
software (SAS Institute, Cary, NC, USA).
Results
Electrophysiological characteristics
Patient and arrhythmia characteristics are shown in Tables 1. Examples of VA morphology are
shown in Supplemental figure 1. Sustained VT was inducible in 10 of 11 patients who had a
history of sustained VT. The lead V1 morphology was right bundle branch block-like in 21
(70%), and left bundle branch block morphology with precordial transition before V3 in 8 (27%)
and after V3 in 1 (3%). All VAs had an inferior axis (98.6±10.0°). QRS duration was
161.9±18.8 ms (Table 1). The maximum deflection index (MDI) defined as the interval from the
earliest QRS onset to the earliest R-wave peak in the precordial leads divided by the QRS
duration8 was greater than 0.55, suggesting epicardial origin, in 10 (33%) patients, with a mean
of 0.52±0.06. Prior ablation attempts had failed in 16 patients, 5 of whom had received RF
applications at the earliest RV sites at our institution.
Mapping and ablation in the GCV
Activation mapping revealed the earliest ventricular activation in the GCV preceded the QRS
onset by 36.7±8.0 ms (Figures 1B and 2B, and supplemental figure 2B). At this site a perfect
y
d arrhythmia characteristics are shown in Tables 1. Examples of VA morphology
Supplemental figure 1. Sustained VT was inducible in 10 of 11 patients who had
sustained VT. The lead V1 morphology was right bundle branch block-like in 21
yyyysiooolo ogical ccchhah raraaccctc ererererisisistititiiccsc
d arrrrhrhrhrhytytytythmhmhmmiaiaiia cccchahahararararactcctc ererere istititiicscscs aaaarerr ssshohohoh wnwnwnwn iiin n n n TaTaTaablblblblesesese 111.. EEEExaxaxax mpmpmpmplelelesss s ofofof VVVVA A A A momomomorprprphohohoholololoogyggg
Supplplplplemememenenentatatalll fifififiguguguurerere 111... SSSusussustatatainnnnededed VVVTT T T waaaas ss ininindudududuciciciciblblblbleee inininin 11110 000 ofofof 1111111 papapap tititiienenene tstsss wwwhohoho hhhhad
ssusustataineded VVVVT.T.TT ThThThThe e leleel adaddd VVV1111 mooorpphohohh lololol gygy wwasas rigiigi hthththt bbbbunu dldldldle e brbrbb ana chchhh bbbblollol ckkckk-l-likee in 21
by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from

DOI: 10.1161/CIRCEP.114.001615
7
pace-map, matching the VA in 12 of 12 ECG leads was present in 21 of 24 (88%) patients
(Figures 1A and 2A, and supplemental figure 2A). In the remaining 3 (12%) patients an 11 of 12
lead pace-map match was observed. In 3 patients pacing at the earliest GCV site failed to
capture the ventricular myocardium even with the strength of 10 mA and pulse width of 9 ms.
A flow chart indicating procedure details is shown in Supplemental figure 3. In 3
patients an ablation catheter could not be advanced to the distal GCV. Coronary venography and
angiography was performed in the remaining 27 patients. In 7 patients (23%) the target site in
successfully abolishing the VA in 5 patients (Figures 1C-E). In 8 of remaining 20 patients in
whom the target site in the distal GCV was <5mm from the coronary artery (Supplemental
figures 2C-D), ablation was attempted at a region 2-3 mm proximal to the target site with
elimination of VA in 3 patients. For all GCV RF ablation applications the average RF power
was 23 (IQR 15, 27) Watts and duration 30 (IQR 23, 39) seconds, limited by an impedance rise
that typically began after 15 to 20 seconds starting from a relatively high initial impedance of
244 (IQR 186, 266) ohms. In 4 patients cryoablation in GCV was attempted due to low power
and high impedance with failure of RF ablation in 3 patients and for reinforcement of an acutely
successful RF ablation in 1. Cryoapplication of -80 °C freezes was performed for 4-8 minutes
successfully abolishing the VA in 2 patients.
Characteristics of patients for whom radiofrequency energy was delivered in the GCV are
shown in Supplemental table. The surface ECG of the VA morphology including R-S in lead I,
R ratio in lead III/II and Q ratio in aVL/aVR suggested that the VA origin was more leftwards in
the patients with successful ablation in the GCV compared with patients in whom ablation in the
GCV failed. The MDI was greater in those with successful ablation. However, there were no
emainini inini gg 20202020 ppatatieieeentntntntss
t
-
n of VA in 3 patients. For all GCV RF ablation applications the average RF pow
QR 15, 27) Watts and duration 30 (IQR 23, 39) seconds, limited by an impedance
ll began after 15 to 20 seconds starting from a relati el high initial impedance
tarrgegegegetttt sisisis tetetee iiiinn thhhee ee distal GCV was <5mm frfrfrfroom the coronnnary ararara tery (Supplemental
-D)D)D)D), ablation wwaas aaatttttemptptptpted aattt t a reegiononn 2---3 mmmm pppprorror ximamm l too ttheeee tttargeeeet siss tte wittthhh
n off VVVVAAAA inininin 3 p ttatieiii ttnts. For r allalalllll GCCCCVVV V RFRFRFRF ablblbl tttatioii nnnn apapplplplpliicatatattiiions ttthehhh aaveveveverage RRRRF FFF pow
QQQR 1515151 , 272727))) WaWaWatttttttts andd d dudd ratiitiion 3333000 (I(I(IQRQRQRQ 2222333, 3339)9)9)9 secondddsd , llil mimimiteteteed ddd bybyby an impepepepedadadadance
llll bb ftft 1155 tto 2200 dnd tst titi ff llatiti ll hhiighh iinititiiall iim dda
by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from

DOI: 10.1161/CIRCEP.114.001615
8
differences in the RF power and duration, and initial impedance between the 2 groups.
Endocardial Ablation Outside the GCV
In all patients additional non-GCV mapping was performed before successful GCV ablation or
after GCV ablation failed; in the RV in all, and in the LV cavity and the aortic sinus in 26
patients respectively. RF was applied at the earliest RV site in 4 patients and failed to abolish
VA in all. In the LV and the aortic sinus the earliest ventricular activation preceded the surface
QRS onset by 20.9±6.6 ms and none had a perfect pace-map. (Figures 2A-B and supplemental
figures 2A-B). In 4 of 12 (33%) patients who had RF application below the aortic-mitral
continuity (AMC) and 1 of 5 (20%) patients who had RF application in left coronary cusp
(LCC), VA was successfully abolished despite later activation at these sites that in the GCV
(Figures 2C-D). Ablation failed at endocardial LV sites or the aortic sinus in 10 patients.
As shown in table 2, all patients with successful LV endocardial or LCC ablation had a
VA morphology with an initial r wave in lead I compared to 33% of patients with ablation failure
at these sites (P=0.01). Furthermore, patients with successful LV endocardial or LCC ablation
tended to have later activation times at the GCV (31.0±5.0 vs. 38.1±8.7 ms preceding surface
QRS, P=0.09) and the activation times at the earliest LV endocardial or LCC sites tended to be
earlier (25.8±4.0 vs. 19.6±6.6 ms preceding surface QRS, P=0.06) compared to patients with
ablation failure at these sites. Thus, the interval between the GCV site and earliest LV
endocardial or LCC site activation during the VA (GCV-nonGCV interval) was shorter for those
with successful endocardial ablation compared to those in whom ablation failed (5.8±1.6 vs.
18.9±8.5 ms, P=0.003; Table 2) and was -map
morphology for those with successful versus unsuccessful endocardial ablation.
Percutaneous Epicardial Ablation
ow the aortic-mitrralalalal
n lefffft ttt cocororonanaryryyy ccususususppp p
A V
C
shown in table 2, all patients with successful LV endocardial or LCC ablation ha
o
es (P 0 01) F rthermore patients ith s ccessf l LV endocardial or LCC ablat
A wawawawassss sussuccccccccesee sfffuuully abolished despite lateeer rr aactivation at thtt esssee e e sites that in the GCV
CCCC-DDD). Ablatioon faiiileed atttt eeendoco arrrddial LLLV ssittes ororrr tttthehheh aaaorrrtic siinunuus in 10 000 papap tiientttst ...
showwwwnnn ininnin tabbbblelll 2222, alllllll patiiienenenntsttsts withhh h sususucccces ffsful LLLLVVV V enenenendddod cacacaca ddrddiiiallll or LLLLCCCCCCCC ablblblb tttatioi n hhahh
ologggy yy wiiith hh annn iiiiniiiitiiialll r wave in llleaddd III I compppar dded to 333333%%% % fofof pppatatattiiiei tnts iwii hththh ablblblblatatatatiiioi n
((PP 00 0101)) FF trthhe tatiie tnt iithth ff ll LVLV dnd didi lal LCLCCC babllatt
by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from

DOI: 10.1161/CIRCEP.114.001615
9
Percutaneous epicardial mapping from the pericardial space was performed in 13 patients and
revealed sites where the earliest ventricular activation preceded onset of surface QRS by
29.1±6.3 ms (Supplemental figure 2B); and 2 patients had sites that were slightly earlier than that
of the GCV (by approximately 2 ms in both). At the earliest epicardial site, a perfect pace-map
was acquired in 2 of 10 patients despite slightly later activation (by approximately 2 ms) than the
GCV (Supplemental figure 2A). Coronary angiography was repeated during epicardial mapping
in 10 patients; no ablation was performed due to the proximity to a coronary artery in 8 (80%)
patients (Supplemental figure 2D). RF ablation was performed in 2 patients (20%) with
elimination of VA in 1 (10%). No cryoablation was performed.
Complications of catheter ablation
Major complication occurred in 3 patients. Coronary artery occlusion requiring stenting of a
marginal branch of the circumflex artery occurred in 2 who received average RF energies of 23
and 27 Watts at ablation sites felt to be 2 mm and 5-7 mm distant from the vessel, respectively.
GCV perforation without tamponade occurred in 1 patient.
Open-chest surgical epicardial ablation
In 3 patients who failed percutaneous catheter ablation, open-chest cryothermal surgical
epicardial ablation with direct vision through a median sternotomy was subsequently performed.
After dissection to reach the GCV area freezes performed under direct visualization successfully
abolished the VA in 2 patients. In the remaining patient ablation was limited due to the
vasospasm of the left anterior descendant (LAD) and difficulty fully dissecting the LAD.
Furthermore, angina developed several months after the procedure, angina and angiography
revealed a stenosis in the LAD at the site of cryoablation that was treated with a drug-eluting
stent.9
atients (2( 0%)) withhhh
t
m f
ranch of the circumflex artery occurred in 2 who received average RF energies o
t v
oration itho t tamponade occ rred in 1 patient
tionnnnssss ofofof ccccatatatheheeteteteter ablation
mppplp iccation occuurrreddd inn 3 pappp tienntttst . CCorroonarry artetetteryryryry occlululusionn rreqqquuiu ringggg sssteenntinggg of
ranchhh h ofofofof tttthhhe ciiircumfffflelll x arrrrtetetetery occcccuururu rerereddd d iniii 2222 whohohoho rrececececeiiiiveveveveddd d averaggeeee RFRFRRF energieiii s o
tts at babblatiiionnn ssssittes fff llelt to bbbbe 2 22 mm and 555-77 7 mm dddiiisi tantnt ffffrom mm ththththe vess llel, reeeespspspspeeece tiv
tatiio iithth tt tta dad ded ii 11 titi tt
by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from

DOI: 10.1161/CIRCEP.114.001615
10
Acute success and long term success during follow-up
Overall acute success was achieved in 16 (53%); 8 in GCV, 4 at AMC, 1 in LCC, 1 in
pericardium space and 2 with surgical ablation. In these patients 1 patient who had had incessant
VT before ablation procedure resumed low-dose amiodarone for 2 months.
After a median follow-up of 2.8 (0.9, 26.5) months in these 16 patients, procedure
success was evaluated by 24-hour Holter in 7 patients (2 with VT and 5 with PVCs), and clinical
symptom and electrocardiography in 9 (7 with symptomatic VTs and 2 with symptomatic
recurrent PVCs) patients. Thirteen patients (81%) were free of VA; VA recurred in 3 patients
(19%) which had been ablated in the GCV in 1, from the endocardium at the AMC in 1, and
from the pericardial space in 1.
Discussion
Catheter ablation of VA originating from near the GCV is often challenging. However, in 5 of 7
patients (71%), in whom RF application was effectively delivered in the GCV, VA was
successfully eliminated. During follow-up 88% of patients in whom VA was successfully
ablated in the GCV were free from VA recurrence. Therefore, acute and long-term success can
be favorable, if RF application can successfully be performed.2-5
Unfortunately, ablation is often not possible. In some cases it is not possible to advance
an ablation catheter to the distal GCV. Probably the most important risk when delivering RF
energy in the GCV is coronary artery injury. Coronary artery damage may be evident acutely or
may not become manifest until several weeks after the procedure.10, 11 The minimal safe distance
between ablation sites and coronary arteries is not clear. It is likely that tissue contact, power,
duration, and coronary blood flow all influence the risk. During angiography cardiac motion can
make the distance and time spent between the ablation catheter and coronary arteries difficult to
VA recurred in 3 ppatatatatieieii
m at thhhhe e AMAMAMAMCC CC iiinin 1111, aaanan
e
n
blation of VA originating from near the GCV is often challenging. However, in
1%), in whom RF application was effectively delivered in the GCV, VA was
ericacacacardrdrdrdiaiaiai llll spsspaccccee e e in 1.
n
blatioioioionn n ofofof VVVA AA ororoorigigigiginininatatatinining gg frfrfrfromomomm nnneaeaear rr thththt e GCGCGCG V V VV isisisi oooftftftf enenen ccchahahah llllllenenenngigigigingnngng. HHHHowowowweveveverererer,,, , in
1%)%),, in wwhohohoh m RFRFRFRF aappppplilililicacatitititiono wwwasas eeffffffffecectititit vevelyllyl ddddellelivivivivere eddedd iiin ththththee GCGCGCGCV,V,VV VVVVA AA A wawass
by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from

DOI: 10.1161/CIRCEP.114.001615
11
assess. Distances of 5 to 12 mm between the catheter tip and the coronary artery may be needed
to avoid any risk of injury.7
Inability to deliver sufficient RF energy due to high impedance and/or limited cooling
from surrounding blood flow likely contributes to limit the effectiveness of ablation in the GCV.
Cooling the saline infusion has been suggested,12 but was not assessed in this study. In the GCV,
impedance was typically high and began increasing further within 25 seconds of RF delivery. In
our experience attempted additional RF applications at the same site after an initial impedance
rise typically produce an even more rapid impedance rise. Occasionally the GCV is of sufficient
size to allow longer RF applications. More leftward VA origin in the patients with successful
ablation in the GCV might indicate that the origin in the GCV was relatively proximal where the
vessel size was sufficiently large to allow greater power. RF power was not, however,
statistically different between the patients with and without successful ablation in the GCV in
this small study. Cryoablation can be considered, as it is not limited by high impedance, and is
likely facilitated by low blood flow. Freezing also appears less likely to damage adjacent
coronary arteries.13 However, the cryocatheter can be difficult to maneuver in the coronary
venous system.
When ablation in the GCV was not feasible or failed, we attempted to ablate at the best
identifiable endocardial sites. In 20% of patients who underwent additional non-GCV mapping
including endocardial LV and the aortic sinus, RF application at the site closest to the early GCV
site successfully eliminated the VA despite later activation at these sites. Interestingly, in those
patients the GCV-nonGCV interval was shorter for successful endocardial LV or LCC ablation
sites compared to unsuccessful ablation at these sites. In all patients with successful endocardial
ablation the GCV-
ly y the GCV is of susususufff
patienenttsts wwitititithhh h susucccccesesesesss
e
y different between the patients with and without successful ablation in the GCV
study. Cryoablation can be considered, as it is not limited by high impedance, an
itated b lo blood flo Free ing also appears less likel to damage adjacent
the e ee GCGCGCG V VVV mimmm ghghghhtt t indicate that the origin iiiinn n tht e GCV waaas relalalal titt vely proximal whe
wawawawas sufficienttlyy laaargge ttto o o alloooww grggreateerrr poowwer. RFRFRFF ppowwwer wwaas nnnoot, hoooowwew vever,
y diffffffferereerennenenttt t betttween thhththe paatitititieenents witititithhhh anaa d ddd wiiiiththtt ououououttt t susususuccesesess ffsffulll ablbbb attttioioioionnn n in ttthhhe GGGGCVVCVCV
studydydyd . CCCryyyoablblbllattiiioi n can bbeb con iisidded red, as iiti iiis nott llil mimiteteeed dd bybybyy hhhhigigigi hhh iimii pepp dadadaancncncn eee,e an
itit tat ded bb llo blbl dd flfl FF iin lal ll lilikkell tt dda djdj tt
by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from

DOI: 10.1161/CIRCEP.114.001615
12
than at failed sites. A possible mechanism of the shorter GCV-nonGCV interval in the
successful endocardial ablation group is shown in Supplemental figure 4. Furthermore, all VA
successfully ablated from endocardial LV or LCC had an initial r wave in lead I. Hence, those 2
features suggest that VA origin might be located relatively closer to the endocardium and might
be predictors for the successful ablation from those sites. Pace-mapping at the LV endocardium
was not a reliable marker for successful ablation. These observations are similar to those of
Abularach and colleagues, who reported successful ablation from the LV endocardium from the
left sinus of Valsalva, LV endocardium, or both sites in 9 of 16 in a similar group of patients14.
Epicardial mapping was also limited in this patient population. Sedation and anesthesia
as is generally used for epicardial procedures can suppress arrhythmias, although we did not
encounter this as a significant issue in the present small series. The GCV area is often covered
by fat and the overlying left atrial appendage and coronary arteries are present. Further right-
ward from the GCV, the LV myocardium is beneath the RV outflow.5 In only 1 patient (8%) in
whom RF energy was delivered from the pericardial space, the VA was acutely abolished, but
later recurred during follow-up.
Open-chest surgical epicardial ablation successfully eliminated VA in 2 of 3 patients
(67%). A direct cardiac surgical approach can offer a potential solution for these VAs; deep
lesions can be achieved with surgical application of cryoablation, which achieves temperatures
-160°C) than those that can be achieved with present catheter
cryoablation, and coronary arteries can be avoided under direct vision or occasionally mobilized
for ablation of tissue beneath the vessel.15, 16 However, surgical morbidity is a concern.
Coronary injury is also possible. Mapping to identify the ablation target can be difficult in the
operating room andanesthesia can suppresses the arrhythmia.17
milar grg oupp of ppatatttieieieienn
Seddddatattioioii nn anandddd anannesesesesttthth
a o
this as a significant issue in the present small series. The GCV area is often cove
the overlying left atrial appendage and coronary arteries are present. Further righ
%
energ as deli ered from the pericardial space the VA as ac tel abolished b
ally y yy usuusu edededed fffforoo eeepipipicardial procedures can sususuppppress arrhythhmiasasasas, although we did no
thhhhissss as a signifficcanttt iiissuuue e in ttttheheheh ppprreseenttt smamall sssererrrieieieess. ThThThe GCGCV VV V aarea iiiis offteen cococove
the ovevevverlrllrlyiyingng lll ffefftt tt ttat iiirial apppppppeeendagegegee aa dndndnd coronararryyyy arrrteteteteriiiiesesess are preseeeentntntnt. Furthththher riiiigh
the GGGCVCVCV, thhhe ee LVLVLVLV myoyy ca drdddiiui m iiis bbbenea hhth thehhh RRRRVVV V ou ftftfflolooow.555 InInInIn onlly yy 111 papp tititit enenenenttt t (8(( %
dd lelii ded ff thth iri drdiiall tthhe VVAA tt lel bab loliishhedd bb
by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from
DOI: 10.1161/CIRCEP.114.001615
13
Limitations
This is a retrospective descriptive case series, with a relatively small number of patients.
Patients were referred for ablation and 16 had failed prior ablation attempts.
Conclusions
Catheter ablation for arrhythmias originating in the region of the distal great cardiac vein is
challenging with a favorable ablation outcome in only 53% in this referral population and likely
a greater risk of complications than expected for idiopathic VA. Although epicardial ablation is
often limited by the proximity of coronary vessels, anatomically guided endocardial ablation can
be successful and predicted by a relatively short GCV-nonGCV interval and r wave in lead I.
Surgical ablation can also be effective. Future studies to identify optimal strategies are
warranted.
Acknowledgments: Dr. Nagashima was supported in part by a Medtronic Japan Fellowship.
Conflict of Interest Disclosures: William Stevenson is co-holder of a patent for needle ablation
that is consigned to Brigham and Women’s Hospital.
References:
1. Sacher F, Tedrow UB, Field ME, Raymond JM, Koplan BA, Epstein LM, Stevenson WG. Ventricular tachycardia ablation: Evolution of patients and procedures over 8 years. Circ Arrhythm Electrophysiol. 2008;1:153-161.
2. Baman TS, Ilg KJ, Gupta SK, Good E, Chugh A, Jongnarangsin K, Pelosi F, Jr., Ebinger M, Crawford T, Oral H, Morady F, Bogun F. Mapping and ablation of epicardial idiopathic ventricular arrhythmias from within the coronary venous system. Circ Arrhythm Electrophysiol.2010;3:274-279.
3. Obel OA, d'Avila A, Neuzil P, Saad EB, Ruskin JN, Reddy VY. Ablation of left ventricular epicardial outflow tract tachycardia from the distal great cardiac vein. J Am Coll Cardiol.2006;48:1813-1817.
g p
ed d ennnndodododocacacacardrdrdrdiaiaiaial l l l abababablalalalatitiiioooo
ful and predicted by a relatively short GCV-nonGCV interval and r wave in lead
b
d i
ful annnddd prprpredidd cttttedeee by a relatively short GCVCVCV-nonGCV intervvvvalaaa and r wave in lead
bllllattttiiioi n can allllsososo be ee fefefeffefefef ctctctctivivivive. FuFuFuFututut re ssttuudiiess tooo o ididididenenene tifyfyfyf optptptimiimal sssstrtrtrattategegeggieeeesss arararare ee
dgments:::: DDDDr.r.r.r NNNNagagagagasasasashiihihimamamam wwwasasasas sssupupupuppopopoportrtrttedededed iiiin n nn papapapartrtrt bbby y y y a aa a MeeMeMedtdtdtdtrorororonininnic cc c JaJaJaJapapapapan nnn FeFFF llowshi
by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from

DOI: 10.1161/CIRCEP.114.001615
14
4. Steven D, Pott C, Bittner A, Sultan A, Wasmer K, Hoffmann BA, Kobe J, Drewitz I, Milberg P, Lueker J, Monnig G, Servatius H, Willems S, Eckardt L. Idiopathic ventricular outflow tract arrhythmias from the great cardiac vein: Challenges and risks of catheter ablation. Int J Cardiol.2013;169:366-370.
5. Yamada T, McElderry HT, Doppalapudi H, Okada T, Murakami Y, Yoshida Y, Yoshida N, Inden Y, Murohara T, Plumb VJ, Kay GN. Idiopathic ventricular arrhythmias originating from the left ventricular summit: Anatomic concepts relevant to ablation. Circ Arrhythm Electrophysiol. 2010;3:616-623.
6. Soejima K, Stevenson WG, Maisel WH, Sapp JL, Epstein LM. Electrically unexcitable scar mapping based on pacing threshold for identification of the reentry circuit isthmus: Feasibility for guiding ventricular tachycardia ablation. Circulation. 2002;106:1678-1683.
7. Sosa E, Scanavacca M, d'Avila A. Transthoracic epicardial catheter ablation to treat recurrent ventricular tachycardia. Curr Cardiol Rep. 2001;3:451-458.
8. Daniels DV, Lu YY, Morton JB, Santucci PA, Akar JG, Green A, Wilber DJ. Idiopathic epicardial left ventricular tachycardia originating remote from the sinus of valsalva: Electrophysiological characteristics, catheter ablation, and identification from the 12-lead electrocardiogram. Circulation. 2006;113:1659-1666.
9. Lampert SM, Michaud GF, Couper GS, Muehlschlegel JD. Epicardial cryoablation resulting in precipitous left ventricular dysfunction. J Thorac Cardiovasc Surg. 2013;145:e41-42.
10. Roberts-Thomson KC, Steven D, Seiler J, Inada K, Koplan BA, Tedrow UB, Epstein LM, Stevenson WG. Coronary artery injury due to catheter ablation in adults: Presentations and outcomes. Circulation. 2009;120:1465-1473.
11. Castano A, Crawford T, Yamazaki M, Avula UM, Kalifa J. Coronary artery pathophysiology after radiofrequency catheter ablation: Review and perspectives. Heart Rhythm. 2011;8:1975-1980.
12. Sternick EB, Gerken LM, Scarpelli RB, Soares FC. Cooling with near-freezing saline improves efficacy of cool-tip radiofrequency catheter ablation. Heart Rhythm. 2010;7:983-986.
13. Stavrakis S, Jackman WM, Nakagawa H, Sun Y, Xu Q, Beckman KJ, Lockwood D, Scherlag BJ, Lazzara R, Po SS. Risk of coronary artery injury with radiofrequency ablation and cryoablation of epicardial posteroseptal accessory pathways within the coronary venous system. Circ Arrhythm Electrophysiol. 2014;7:113-119.
14. Jauregui Abularach ME, Campos B, Park KM, Tschabrunn CM, Frankel DS, Park RE, Gerstenfeld EP, Mountantonakis S, Garcia FC, Dixit S, Tzou WS, Hutchinson MD, Lin D, Riley MP, Cooper JM, Bala R, Callans DJ, Marchlinski FE. Ablation of ventricular arrhythmias arising
abababablalalalatitititionononon tttto ooo trtrtrtreaeaeaeatttt rereeecucuuu
Dl
yd
t SM, Michaud GF, Couper GS, Muehlschlegel JD. Epicardial cryoablation resulo
s Thomson KC Ste en D Seiler J Inada K Koplan BA Tedro UB Epstein L
DV,V,V,V LLLLuuu YYYYYYY , MoMMM rton JB, Santucci PA, AkAkAkAkaar JG, Green A, WiWWW lber DJ. Idiopathic leeeeftftft ventriculululu ararar tttacchyhyhyycacacaardrdiaaaia oooorir gigiginananatiiingngng remmote e e frfrfrfromomomom tthehehehe sssininusususu of vavavavalslslslsalaa vavava:::
ysssis ooolo ogical chaaraactereeriiisticscscs, caththththettterr abblaaatioonn, andndndn iiidedded ntifififiiicatioion fffrf oom tttheheheh 1122-leadadad diogogogrraram. CiCiiircrrr uulaatiooonn. 200006060606;1131313:11116656 99-9 111666..
t SM,M,M,, MMMicicicchahahaudududud GGGF,F,F,F CCCCououououpepepeer r rr GSSSS,,, MuMuMuMueheehe lssschchchc leleleegegegegelll JDJDJDJ . EpEpEpEpiciccicararardidididialalall ccccryryryoaoaoaoablblblatatatatioioioonn n rerereresulous llleffft ventririricuccc lalll r dydydy ffsfun tction. J JJ ThThThhorac CCCardididiiovasc SuSuuurggg. 202020201313131 11;14545454 :e41414141-4-4-442.222
ThTh KCKC StSt DD SSeilil JJ IIn dad KK KK lla BABA TTeddr UUBB EE tteiin LL
by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from

DOI: 10.1161/CIRCEP.114.001615
15
near the anterior epicardial veins from the left sinus of valsalva region: Ecg features, anatomic distance, and outcome. Heart Rhythm. 2012;9:865-873.
15. Mulpuru SK, Feld GK, Madani M, Sawhney NS. A novel, minimally-invasive surgical approach for ablation of ventricular tachycardia originating near the proximal left anterior descending coronary artery. Circ Arrhythm Electrophysiol. 2012;5:e95-97.
16. Stevenson WG, Couper GS. A surgical option for ventricular tachycardia caused by nonischemic cardiomyopathy. Circ Arrhythm Electrophysiol. 2011;4:429-431.
17. Bhavani SS, Tchou P, Chung M, Fahmy T, Gillinov AM. Intraoperative electro-anatomical mapping and beating heart ablation of ventricular tachycardia. Ann Thorac Surg. 2006;82:1091-1093.
by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from

DOI: 10.1161/CIRCEP.114.001615
16
Table 1. Patient characteristics with VA close to the GCV
Values are the mean±SD, median (25th, 75th interquartile range) or n (%). VA, ventricular arrhythmia; GCV, great cardiac vein; LVEF, left ventricular ejection fraction; VT, ventricular tachycardia; RBBB, right bundle branch block; LBBB, left bundle branch block; MDI, maximum deflection index; RFA, radiofrequency ablation.
Patients(n=30)
Age (y) 52.8±15.5Male 19 (63)LVEF (%) 52.0±12.9History of prior ablation 16 (53)Clinical ArrhythmiasSustained VT 11 (37)Nonsustained VT or PVCs 19 (63)
VA morphology during EPSVT sustained 10 (33)Cycle length of VTs (ms) 396.2±81.8QRS width (ms) 161.9±18.8MDI 0.52±0.06QRS axis (°) 98.6±10.0Limb leadsQS pattern in lead I 16 (53)R-S in lead I (mV) -0.23±0.35R in lead II (mV) 1.78±0.59
R in lead III (mV) 1.97±0.61Ratio in III/II 1.12±0.16
R in aVF (mV) 1.87±0.59Q in aVL (mV) 1.12±0.38Q in aVR (mV) 0.85±0.36Ratio in aVL/aVR 1.46±0.60
Precordial leadsRBBB pattern 21 (70)LBBB with R- 8 (27)
MappingActivation time at GCV (ms) 36.7±8.0
12/12 pace map at GCV 21/24 (88)Ablation in GCVAverage power (Watts) 23 (15, 27)Average duration (seconds) 30 (23, 39)Initial impedance (ohms) 244 (186, 266)RFA + cryoablation 4 (13%)
sndI
I(mV) 1 87±0 59
°) 9989 ..6±10.0sn iin lead I 16 (53))))d I II (m(m(m( V)V)V) -00.0 2232 ±0±0±0±0.3.3.3.35555II (mVVVV) 1.1.1.78777 ±0.5999(mV)V)V)V) 1.1.1.97979797±0±0±0±0.6.6.661111
IIIIII/I/I/IIII 111.121212±0±0±0.1.1.1666(((mVmVmV))) 111.878787±0±0±0 55.5999
by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from

DOI: 10.1161/CIRCEP.114.001615
17
Table 2: Characteristics of patients who had ablation attempted at the left ventricular endocardium or aortic sinus according to acute outcome
Successful(n=5)
Failure(n=21) P value
Age (y) 59.0±8.1 53.8±15.9 0.50Male 4 (80) 13 (62) 0.63Successful siteAMC 4 (80) -LCC 1 (20) -
VA morphology during EPSVT sustained 2 (40) 7 (33) 1.00Cycle length of VTs (ms) 334.5±36.1 392.7±46.8 0.15QRS width (ms) 159.8±17.0 162.7±20.6 0.78MDI 0.51±0.06 0.51±0.06 0.92QRS axis (°) 94.2±12.8 98.8±9.4 0.36Limb leadsInitial r wave in lead I 5 (100) 7 (33) 0.01R-S in lead I (mV) -0.05±0.27 -0.23±0.36 0.30R in lead II (mV) 2.01±0.93 1.69±0.52 0.31
R in lead III (mV) 2.07±1.00 1.88±0.51 0.54Ratio in III/II 1.02±0.06 1.13±0.17 0.18R in aVF (mV) 1.98±1.02 1.80±0.50 0.56Q in aVL (mV) 1.01±0.52 1.10±0.37 0.67Q in aVR (mV) 0.96±0.46 0.83±0.35 0.47Ratio in aVL/aVR 1.07±0.22 1.47±0.57 0.14
Precordial leadsRBBB pattern 4 (80) 13 (62) 0.63LBBB with R-wave transition V3 5 (100) 20 (95) 1.00
MappingActivation time at GCV (ms) 31.0±5.0 38.1±8.7 0.09Activation time at the earliest endocardial site (ms) 25.8±4.0 19.6±6.6 0.06Interval between these 2 sites (ms) 5.8±1.6 18.9±8.5 0.00312/12 pace-map at GCV 3/3 (100) 17/19 (89) 1.00
12/12 pace-map at the earliest endocardial site 0/5 (0%) 0/13 (0%) 1.00
Values are the mean±SD or n (%). AMC, aortic-mitral continuity; LCC, left coronary cusp; other abbreviations are as in Table 1
92.7±46.8 0.15555666622.22 7777±±±±20202020.6.6.66 00.0.0 78787878.51±0.0.00 0606 0.0.0.0.9292929
) 94 2±12 8 98 8±9 4 0 36
adI
ImV) 1.98 1.02 1.80 0.50 0.56
) 94.2±12.8 9898998.8±9.4 0.36
avvve in lead I 5 (1(1(1( 000000)))) 77 7 (33)3)3)3 00.00 01111d I II (m(m(mV) -0...0500 ±±±0.2777 --000.23333±±±±0.36666 000.3000I (mVVVV))) 222.01001±0.0 9993 11.669±0.00 525252 00.3131(mV)V)V)V) 2.2.2.2 0707070 ±±±1.11 00000000 1.1.1.1 8888888 ±±±±0.0.0.5151515 0.00.0 5454544
IIII/I/III 11.0202±±00.0606 11.1313±±00.1717 00.1818mVmVmV))) 1.11 989898±±±1.11 020202 111.808080±±±00.0 505050 000.565656
by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from
DOI: 10.1161/CIRCEP.114.001615
18
Figure Legends:
Figure 1: An example of one patient with successful ablation of ventricular arrhythmia (VA) in
the great cardiac vein (GCV). (A) Twelve-lead electrocardiogram morphologies of sinus rhythm,
VA and pace-map morphologies recorded during electrophysiological study. A perfect pace-
map (12/12 leads) is acquired in the GCV. (B) The local electrogram of successful ablation site
in the GCV. (C) Corresponding fluoroscopic view of catheter positions during coronary
venography from contrast injection thorough the irrigated ablation catheter.2 The ablation
catheter tip is at the distal GCV. (D) Corresponding fluoroscopic view of catheter positions
distant from any coronary artery. (E) The surface electrocardiogram (top) and ablation catheter
electrogram (bottom) during radiofrequency delivery. Cessation of the target VA is observed
shortly after radiofrequency initiation.
SR, sinus rhythm; PVC, premature ventricular contraction; PM, pace-map; GCV, great cardiac
vein; V-QRS, the interval between ventricular electrogram and surface QRS; ABL-d, ablation
catheter distal; ABL-p, ablation catheter proximal; EA, the earliest activation; LAD, left anterior
descendant; AIV, anterior interventricular vein; LCX, left circumflex; RAO, right anterior
oblique; LAO, left anterior oblique; RF, radiofrequency.
Figure 2: Data from a patient in whom ventricular arrhythmia (VA) was successfully ablated
from the endocardium below the aortomitral continuity (AMC) region despite later activation at
that site than in the GCV. (A) Twelve-lead electrocardiogram morphologies of sinus rhythm, VA
and pace-map morphologies recorded during electrophysiological study. A perfect pace-map
heter.2 The ablattioioioion nnn
w of cacathththh tetetterer pposositittioioioionnnns
m h
m (bottom) during radiofrequency delivery. Cessation of the target VA is observ
e
rh thm; PVC premat re entric lar contraction; PM pace map; GCV great card
mmmm aaaanyn coronarry arttterry. (E(E(EE) Thhhhe sussurfacceee elecectrocoocararara diddid ogograraram ((toop)))) aand ababaa lall ttioon cccaaath
m (bbbotototottototom)m)m)m dduriiing g radiddd offreeeeququququencyyy ddddeleleliiivi ery.y CeCeCCesssssatatatioioioion ofofofo tttthehh ttttargegeeettt VAVVV iiis obbbbserv
er radididi foffrequqq enenenncyyy iiiniii iitiatioii n.
hrh tthhm PVPVCC tt ttriic ll ttr titi PMPM GGCVCV tt drd
by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from

DOI: 10.1161/CIRCEP.114.001615
19
(12/12 leads) is acquired in the GCV compared to poor pace-map at AMC. (B) The local
electrograms in the GCV and AMC. The earliest ventricular activation is obtained in the GCV.
(C) Activation map and the successful ablation site at the AMC. (D) The surface
electrocardiogram (top) and ablation catheter electrogram (bottom) during radiofrequency
delivery. Cessation of the target VA is observed shortly after radiofrequency initiation.
AMC, aortic-mitral continuity; LV, left ventricle; AV, aortic valve; CS, coronary sinus; other
abbreviations are as in Figure 1.
by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from

I
III
II
aVR
aVL
aVF
V1
V2
V3
V4
V5
V6
PM at GCV
SR
PVC
I
IIIII
ABL-d
ABL-p
V1
V5
(A) (B)
100 ms1 mV
V-QRS: 35ms
SR 100 ms
1 mV
VVVV-QQQQRRRRABL-dddd
AAAABBBBLLL-pppp
by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from

(D)
RAO LAO
LAD
LCX
EA site EA site
LCX
LAD
(C)
RAO LAO
AIV
AIV
GCV
GCV
EA site
EA site
5mm
5mm
A i
A
A i
AAAAOOOO LLLLAAAAOOOO
by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from

(E) 1 s
RF
by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from

I
III
II
aVR
aVL
aVF
V1
V2
V3
V4
V5
V6
PM at GCVPVC PM at AMC
(A)
SR 100 ms
1 mV
by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from

I
IIIII
ABL-d
ABL-p
V1
V5
GCV
AMC
I
IIIII
ABL-d
ABL-p
V1
V5
(B)
100 ms1 mV
V-QRS: 35ms
V-QRS: 28ms
I
GGGCCCCVVVV
III
by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from

(D)
(C)
1 s
RF
LAO
LV
CS
GCV
AV
LAOLLLAAAOOO
LLLVVV
by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from

Gregory S. Couper and William G. StevensonKoplan, Gregory F. Michaud, Roy M. John, Laurence M. Epstein, Michifumi Tokuda, Keiichi Inada,
Koichi Nagashima, Eue-Keun Choi, Kaity Y. Lin, Saurabh Kumar, Usha B. Tedrow, Bruce A.Ablation
Ventricular Arrhythmias near the Distal Great Cardiac Vein: A Challenging Arrhythmia for
Print ISSN: 1941-3149. Online ISSN: 1941-3084 Copyright © 2014 American Heart Association, Inc. All rights reserved.
Dallas, TX 75231is published by the American Heart Association, 7272 Greenville Avenue,Circulation: Arrhythmia and Electrophysiology
published online August 10, 2014;Circ Arrhythm Electrophysiol.
http://circep.ahajournals.org/content/early/2014/08/10/CIRCEP.114.001615World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circep.ahajournals.org/content/suppl/2014/08/10/CIRCEP.114.001615.DC1.htmlData Supplement (unedited) at:
http://circep.ahajournals.org//subscriptions/
is online at: Circulation: Arrhythmia and Electrophysiology Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answerinformation about this process is available in the
requested is located, click Request Permissions in the middle column of the Web page under Services. FurtherCenter, not the Editorial Office. Once the online version of the published article for which permission is being
can be obtained via RightsLink, a service of the Copyright ClearanceCirculation: Arrhythmia and Electrophysiology Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on June 21, 2016http://circep.ahajournals.org/Downloaded from

1
SUPPLEMENT MATERIAL Supplemental Table. Characteristics of patients for whom radiofrequency energy was delivered at the distal of great cardiac vein according to acute outcome
Successful
(n=8) Failure (n=7)
P value
Age (y) 44.4±18.6 54.3±10.2 0.23 Male 4 (50) 3 (43) 1.0 VA morphology during EPS VT sustained 6 (75) 2 (29) 0.13 Cycle length of VTs (ms) 423.2±102.8 349.5±57.2 0.39 QRS width (ms) 162.0±19.8 159.0±15.3 0.76 MDI 0.56±0.06 0.49±0.03 0.02 QRS axis (°) 102.7±6.1 94.5±12.1 0.14 Limb leads Initial r wave in lead I 4 (50) 4 (57) 1.00 R-S in lead I (mV) -0.35±0.22 0.02±0.39 0.08 R in lead II (mV) 1.60±0.60 1.85±0.64 0.46
R in lead III (mV) 1.87±0.72 1.84±0.53 0.92 Ratio in III/II 1.16±0.13 1.01±0.13 0.05 R in aVF (mV) 1.74±0.62 1.83±0.63 0.79 Q in aVL (mV) 1.07±0.43 0.93±0.26 0.49 Q in aVR (mV) 0.73±0.26 0.92±0.28 0.20 Ratio in aVL/aVR 1.49±0.47 1.03±0.21 0.04 Precordial leads RBBB pattern 7 (88) 3 (43) 0.12 LBBB with R-wave transition ≤ V3 7 (88) 7 (100) 1.00 Mapping Activation time at GCV (ms) 37.5±11.0 36.0±7.33 0.76
12/12 pace map at GCV 7/7 (86) 7/7 (86) 1.00 Ablation
Irrigated catheter 7 (88) 5 (71) 0.57 Average power (Watts) 24 (21, 31) 17 (9, 27) 0.41 Average duration (seconds) 30 (25, 56) 30 (18, 51) 0.78 Initial impedance (ohms) 240 (181, 414) 248 (190, 279) 1.00 RFA + cryoablation 3 (38) 1 (14) 0.57

2
Values are the mean±SD or n (%). VA, ventricular arrhythmia; GCV, great cardiac vein; LVEF, left ventricular ejection fraction; VT, ventricular tachycardia; RBBB, right bundle branch block; LBBB, left bundle branch block; MDI, maximum deflection index; RFA, radiofrequency ablation.

3
Supplemental figure legends
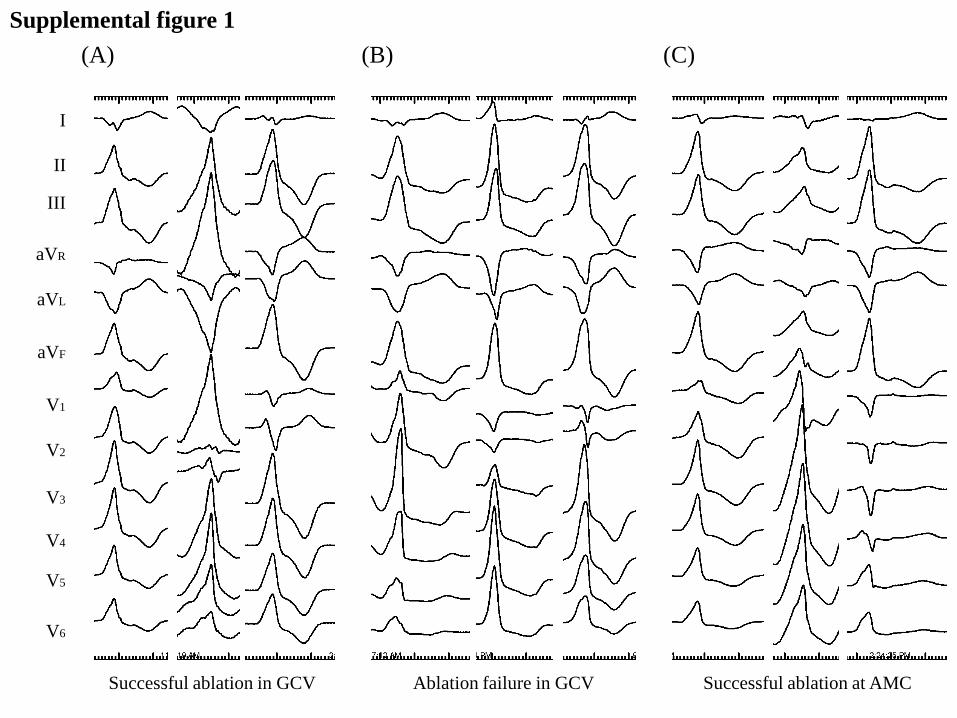
Supplemental Figure 1.
Examples of 12-lead electrocardiogram morphologies of VA. (A) Patients who had
successful ablation in the great cardiac vein (GCV). (B) Patients who failed ablation
in the GCV. (C) Patients who had successful ablation at the aortic-mitral continuity
(AMC).
Supplemental Figure 2.
An example from a patient in whom ablation of ventricular arrhythmia (VA) close to the
great cardiac vein (GCV) failed.
(A) Twelve-lead electrocardiogram morphologies of sinus rhythm, VA and pace-map
morphologies recorded during electrophysiological study. A perfect pace-map (12/12
leads) is acquired in the GCV and pericardium compared to poor pace-map at
aortic-mitral continuity (AMC)
(B) The local electrograms in the GCV, AMC and pericardium. Earliest ventricular
activation is obtained in the GCV.
(C) Corresponding fluoroscopic view of catheter positions during coronary venography
from contrast injection thorough the irrigated ablation catheter. The ablation catheter
tip is at the distal GCV.
(D) Corresponding fluoroscopic view of catheter positions during coronary angiography
of the left coronary artery. The earliest site in the GCV is 2mm distant from the left
anterior descending coronary artery, and the earliest site in the pericardium is adjacent
to the diagonal branch of the left anterior descendant.
AMC, aortic-mitral continuity; other abbreviations are as in Figure 1.

4
Supplemental Figure 3.
A flow chart indicating the procedure details and follow-up data in patients with
ventricular arrhythmias close to the distal great cardiac vein.
GCV, great cardiac vein; LCA, left coronary artery; RF, radiofreuency; RV, right
ventricle; Ao, aorta; LV, left ventricle; AMC, aortic-mitral continuity; LCC, left
coronary cusp.
Supplemental Figure 4.
A schematic diagram (A) and the ladder diagrams (B and C) explaining possible
mechanism of the GCV-nonGCV interval is shown. The GCV-nonGCV interval is
shorter in the successful endocardial ablation group (B) than the endocardial ablation
failure group (C). In the successful endocardial ablation group, VA origin might locate
relatively closer to the endocardium compared to failure group as the endocardial RF
lesion reached the origin. Therefore, that location might result in a shorter activation
time interval between the GCV and the earliest LV endocardial or LCC sites.
VA, ventricular arrhythmia; other abbreviations are as in Supplemental figure 3.
I
III
II
aVR
aVL
aVF
V1
V2
V3
V4
V5
V6
Supplemental figure 1
(A) (B) (C)
Successful ablation at AMC Ablation failure in GCV Successful ablation in GCV

I
III
II
aVR
aVL
aVF
V1
V2
V3
V4
V5
V6
PM at GCV PVC PM in pericardial space PM at AMC
(A)
SR 100 ms
1 mV
Supplemental figure 2

I
III
II
ABL-d
ABL-p
V1
V5
GCV
AMC
Pericardial space
I
III
II
ABL-d
ABL-p
V1
V5
I
III
II
ABL-d
ABL-p
V1
V5
(B)
100 ms 1 mV
V-QRS: 33ms
V-QRS: 15ms
V-QRS: 31ms

(C)
RAO LAO
EA site at pericardium
EA site in GCV
LAD
LCX
EA site at pericardium
(adjacent to Diagonal)
LAD
LCX
EA site in GCV (2mm to LAD)
Diagonal
Diagonal
(D)
AIV
AIV
GCV GCV EA site
EA site
RAO LAO

< 5mm to LCA
n=20
≥ 5mm to LCA
n=7
Ablation catheter could not
be advanced to the distal GCV.
n=3 GCV ablation
n=7
GCV mapping
n=30
Ao cusp or LV mapping
n=26
Epicardial mapping
n=13
RV mapping
n=30
AMC ablation
n=12
No coronary angiography
n=3
≥ 5mm to LCA
n=2
< 5mm to LCA
n=8
RV ablation
n=4
LCC ablation
n=5
Pericardial ablation
n=2
Non-GCV
mapping
No coronary angiography
n=3
Proximal GCV ablation
n=8
Acute success
n=3
Procedure success
n=3
Procedure success
n=1
Procedure success
n=0
Acute success
n=5
Acute success
n=0
Acute success
n=4
Acute success
n=1
Acute success
n=1
Open-chest
Surgical ablation
n=3
Procedure success
n=2
Acute success
n=2
Procedure success
n=4
Procedure success
n=3
Supplemental figure 3

(B) (C)
*
LV myocardium
Epicardium
Endocardium
GCV-nonGCV interval ≤ 7ms
*
GCV-nonGCV interval > 7ms
RF lesion
VA origin
VA origin
GCV
(A)
LV cavity
Successful endocardial ablation Endocardial ablation failure
Supplemental figure 4
Copyright © 2022 FDOKUMEN




















