
Internal Jugular Vein Valve Incompetence Is Highly Prevalent in Transient Global Amnesia
12
Internal Jugular Vein Valve Incompetence Is Highly Prevalent in Transient Global Amnesia Claudia Cejas, MD; Lucia Fernandez Cisneros, MD; Roberto Lagos, MD; Carlos Zuk, MD; Sebastia ´n F. Ameriso, MD Background and Purpose—Transient global amnesia (TGA) is the inability to retain new information and to recall past events during a period of minutes or hours. Its etiology is unclear, and flow disturbances in the mesial temporal lobes secondary to venous congestion have been proposed as a potential cause. Ultrasonographic evaluation of the internal jugular vein (IJV) has demonstrated valvular insufficiency in TGA. The prevalence of valvular insufficiency in the IJV in patients with TGA was assessed. Subjects without TGA of similar sex, age, and vascular risk factor profiles served as controls. Methods—A group of 142 patients with a clinical diagnosis of TGA within 7 days of the clinical event and 40 controls were prospectively evaluated. Venous Doppler examination of both IJVs was performed at baseline and after a manometer-controlled Valsalva maneuver. Valvular insufficiency was diagnosed when there was reflux for 0.8 seconds during the Valsalva maneuver. Results—Valve insufficiency was found in at least one jugular vein in 113 of 142 patients with TGA (79.5%) and in 10 of 40 controls (25.0%), P0.01. The right side was affected more often than the left side, P0.01, and 26.8% of the patients had bilateral incompetence. Conclusions—Patients with TGA have a high prevalence of IJV valve insufficiency. This finding may have pathophys- iologic implications. Doppler evaluation of the IJVs with dynamic maneuvers may help in the evaluation of this usually benign condition. (Stroke. 2010;41:67-71.) Key Words: internal jugular vein venous insufficiency transient global amnesia ultrasound T ransient global amnesia (TGA) is the transient inability to retain new information and to recall prior events. 1 It occasionally follows certain triggering events, such as sexual intercourse, exercise, and cold water immersion. 1 However, many patients do not refer to such prior events. The episode typically lasts a few hours, with complete recovery but persistence of partial amnesia of the events that occurred during the attack. Personal identity and consciousness are preserved, as well as the ability to perform a complex routine if required during the examination. 2–5 This is a common entity with an incidence between 23 and 32 episodes per 100 000 population per year in the United States. 1–3 It occurs more often in patients 50 years in good health and without any substantial heart or cerebrovascular disease. Recurrences are infrequent, and the episodes appear to be benign. How- ever, the vast majority of patients undergo several costly procedures to establish a diagnosis, usually with negative results. Patients and family members worry about the impli- cations of the amnesic episode, the risk of recurrences, and the absence of findings during the work-up. Because of this, it would be useful to develop a diagnostic method that can identify, in a noninvasive way, alterations associated with TGA that are not present in other conditions, thus allowing clinicians to confirm the diagnosis and to save resources and time. Despite the fact that TGA is a well-defined clinical entity, its etiology is still unclear. Logan and Sherman 4 postulated a relation with cardiovascular thromboembolic disease. Shupping et al 6 found a high incidence of cardiovascular risk factors in patients with TGA. However, Kushner and Hauser 7 did not confirm those findings. Studies with diffusion-weighted mag- netic resonance imaging (MRI) have found small, acute changes in the mesial temporal areas in a minority of patients with a clinical diagnosis of TGA. 8 Other authors have suggested an epileptic etiology 9,10 and association with brain tumors. 11,12 In recent years, the theory of brain venous congestion has been proposed. 5,13 The main brain venous drainage is attained through the sinuses that end in the internal jugular vein (IJV). This vessel starts off at the base of the skull, is the continu- ation of the lateral sinus, and drains into the subclavian vein at the end of its cervical portion. The mesial temporal area of the brain drains through the basal vein of Rosenthal, internal cerebral vein, vein of Galen, straight sinus, transverse sinus, Received August 21, 2009; accepted October 1, 2009. From the Institute for Neurological Research, FLENI, Ultrasound Laboratory (C.C., F.C., R.L., C.Z.) and the Neurology Department (S.F.A.), Buenos Aires, Argentina. Correspondence to Sebastia ´n F. Ameriso, MD, Institute for Neurological Research, FLENI, Neurology Department, Montan ˜eses 2325, C1428AQK, Buenos Aires, Argentina. [email protected] © 2009 American Heart Association, Inc. Stroke is available at http://stroke.ahajournals.org DOI: 10.1161/STROKEAHA.109.566315 67 by guest on September 6, 2016 http://stroke.ahajournals.org/ Downloaded from by guest on September 6, 2016 http://stroke.ahajournals.org/ Downloaded from by guest on September 6, 2016 http://stroke.ahajournals.org/ Downloaded from by guest on September 6, 2016 http://stroke.ahajournals.org/ Downloaded from by guest on September 6, 2016 http://stroke.ahajournals.org/ Downloaded from by guest on September 6, 2016 http://stroke.ahajournals.org/ Downloaded from by guest on September 6, 2016 http://stroke.ahajournals.org/ Downloaded from by guest on September 6, 2016 http://stroke.ahajournals.org/ Downloaded from
Transcript of Internal Jugular Vein Valve Incompetence Is Highly Prevalent in Transient Global Amnesia
Internal Jugular Vein Valve Incompetence Is HighlyPrevalent in Transient Global Amnesia
Claudia Cejas, MD; Lucia Fernandez Cisneros, MD; Roberto Lagos, MD;Carlos Zuk, MD; Sebastian F. Ameriso, MD
Background and Purpose—Transient global amnesia (TGA) is the inability to retain new information and to recall pastevents during a period of minutes or hours. Its etiology is unclear, and flow disturbances in the mesial temporal lobessecondary to venous congestion have been proposed as a potential cause. Ultrasonographic evaluation of the internaljugular vein (IJV) has demonstrated valvular insufficiency in TGA. The prevalence of valvular insufficiency in the IJVin patients with TGA was assessed. Subjects without TGA of similar sex, age, and vascular risk factor profiles servedas controls.
Methods—A group of 142 patients with a clinical diagnosis of TGA within 7 days of the clinical event and 40 controlswere prospectively evaluated. Venous Doppler examination of both IJVs was performed at baseline and after amanometer-controlled Valsalva maneuver. Valvular insufficiency was diagnosed when there was reflux for �0.8seconds during the Valsalva maneuver.
Results—Valve insufficiency was found in at least one jugular vein in 113 of 142 patients with TGA (79.5%) and in 10of 40 controls (25.0%), P�0.01. The right side was affected more often than the left side, P�0.01, and 26.8% of thepatients had bilateral incompetence.
Conclusions—Patients with TGA have a high prevalence of IJV valve insufficiency. This finding may have pathophys-iologic implications. Doppler evaluation of the IJVs with dynamic maneuvers may help in the evaluation of this usuallybenign condition. (Stroke. 2010;41:67-71.)
Key Words: internal jugular vein � venous insufficiency � transient global amnesia � ultrasound
Transient global amnesia (TGA) is the transient inabilityto retain new information and to recall prior events.1 It
occasionally follows certain triggering events, such as sexualintercourse, exercise, and cold water immersion.1 However,many patients do not refer to such prior events. The episodetypically lasts a few hours, with complete recovery butpersistence of partial amnesia of the events that occurredduring the attack. Personal identity and consciousness arepreserved, as well as the ability to perform a complex routineif required during the examination.2–5 This is a commonentity with an incidence between 23 and 32 episodes per100 000 population per year in the United States.1–3 It occursmore often in patients �50 years in good health and withoutany substantial heart or cerebrovascular disease. Recurrencesare infrequent, and the episodes appear to be benign. How-ever, the vast majority of patients undergo several costlyprocedures to establish a diagnosis, usually with negativeresults. Patients and family members worry about the impli-cations of the amnesic episode, the risk of recurrences, andthe absence of findings during the work-up. Because of this, itwould be useful to develop a diagnostic method that can
identify, in a noninvasive way, alterations associated with TGAthat are not present in other conditions, thus allowing cliniciansto confirm the diagnosis and to save resources and time.
Despite the fact that TGA is a well-defined clinical entity, itsetiology is still unclear. Logan and Sherman4 postulated arelation with cardiovascular thromboembolic disease. Shuppinget al6 found a high incidence of cardiovascular risk factors inpatients with TGA. However, Kushner and Hauser7 did notconfirm those findings. Studies with diffusion-weighted mag-netic resonance imaging (MRI) have found small, acute changesin the mesial temporal areas in a minority of patients with aclinical diagnosis of TGA.8 Other authors have suggested anepileptic etiology9,10 and association with brain tumors.11,12
In recent years, the theory of brain venous congestion hasbeen proposed.5,13 The main brain venous drainage is attainedthrough the sinuses that end in the internal jugular vein (IJV).This vessel starts off at the base of the skull, is the continu-ation of the lateral sinus, and drains into the subclavian veinat the end of its cervical portion. The mesial temporal area ofthe brain drains through the basal vein of Rosenthal, internalcerebral vein, vein of Galen, straight sinus, transverse sinus,
Received August 21, 2009; accepted October 1, 2009.From the Institute for Neurological Research, FLENI, Ultrasound Laboratory (C.C., F.C., R.L., C.Z.) and the Neurology Department (S.F.A.), Buenos
Aires, Argentina.Correspondence to Sebastian F. Ameriso, MD, Institute for Neurological Research, FLENI, Neurology Department, Montaneses 2325, C1428AQK,
Buenos Aires, Argentina. [email protected]© 2009 American Heart Association, Inc.
Stroke is available at http://stroke.ahajournals.org DOI: 10.1161/STROKEAHA.109.566315
67
by guest on September 6, 2016
http://stroke.ahajournals.org/D
ownloaded from
by guest on Septem
ber 6, 2016http://stroke.ahajournals.org/
Dow
nloaded from
by guest on September 6, 2016
http://stroke.ahajournals.org/D
ownloaded from
by guest on Septem
ber 6, 2016http://stroke.ahajournals.org/
Dow
nloaded from
by guest on September 6, 2016
http://stroke.ahajournals.org/D
ownloaded from
by guest on Septem
ber 6, 2016http://stroke.ahajournals.org/
Dow
nloaded from
by guest on September 6, 2016
http://stroke.ahajournals.org/D
ownloaded from
by guest on Septem
ber 6, 2016http://stroke.ahajournals.org/
Dow
nloaded from
and lateral sinus. The IJV has a single valve just proximal toits end in the subclavian vein.14,15
Lewis16 proposed that insufficiency of the IJV valve cancause venous congestion in the mesial temporal lobe area,thereby inducing the episodes of amnesia. Diencephalic struc-tures involving the hippocampus may play a substantial role inthe pathophysiology of TGA. Using time-of-flight magneticresonance angiography, Chung et al17 found intracranial venousreflux in a group of patients with TGA. This finding supports thehypothesis that retrograde venous hypertension causing transientcerebral venous ischemia is important in the pathogenesis ofTGA. Preliminary studies with ultrasound have shown anelevated prevalence of IJV valve insufficiency during the Val-salva maneuver in patients with TGA.18–22
The objective of the present study was to determinewhether subjects with a clinical diagnosis of TGA have ahigher prevalence of IJV valve insufficiency in comparisonwith subjects of similar age, sex, and risk factor profile butwithout a prior episode of TGA. We used a standardizedmethodology and compared TGA subjects with controls.
Subjects and MethodsThe present study was approved by the institutional ethics committee,and every subject gave informed consent. Between December 2005 andAugust 2008, patients with recent (ie, �7 days) episodes of TGA wereprospectively evaluated. As controls, a group of patients without ahistory of TGA of similar age range, sex distribution, and vascular riskfactors profiles who were referred to the ultrasound laboratory forexamination of their neck vessels was studied as the control group.
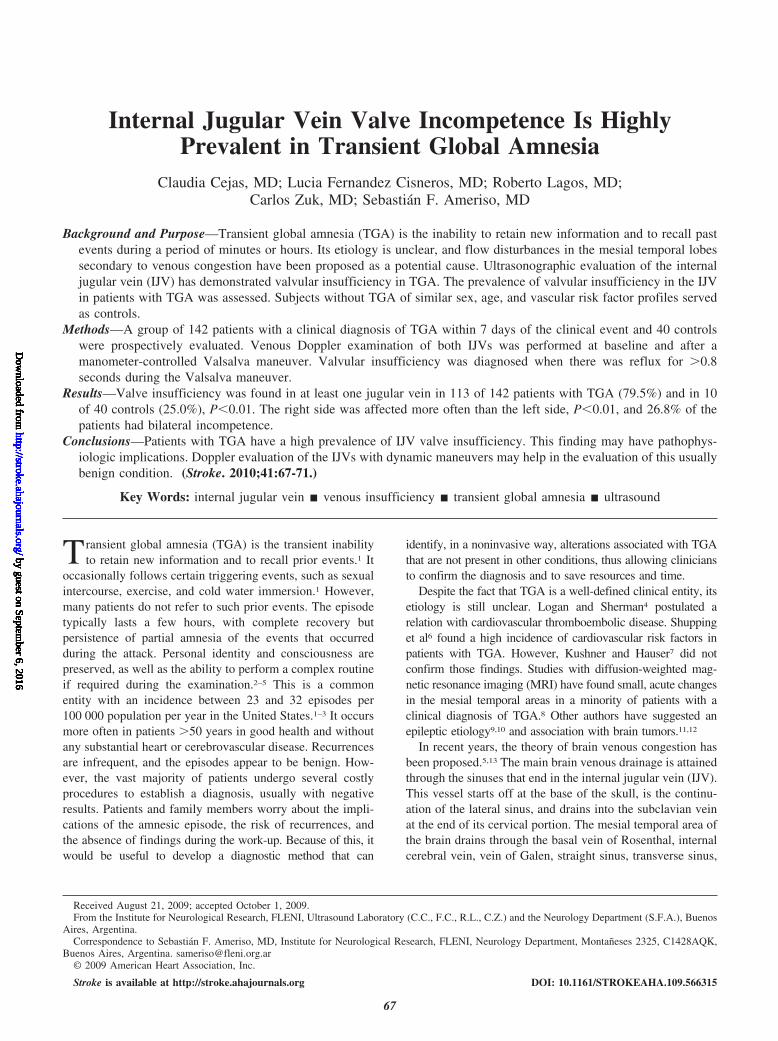
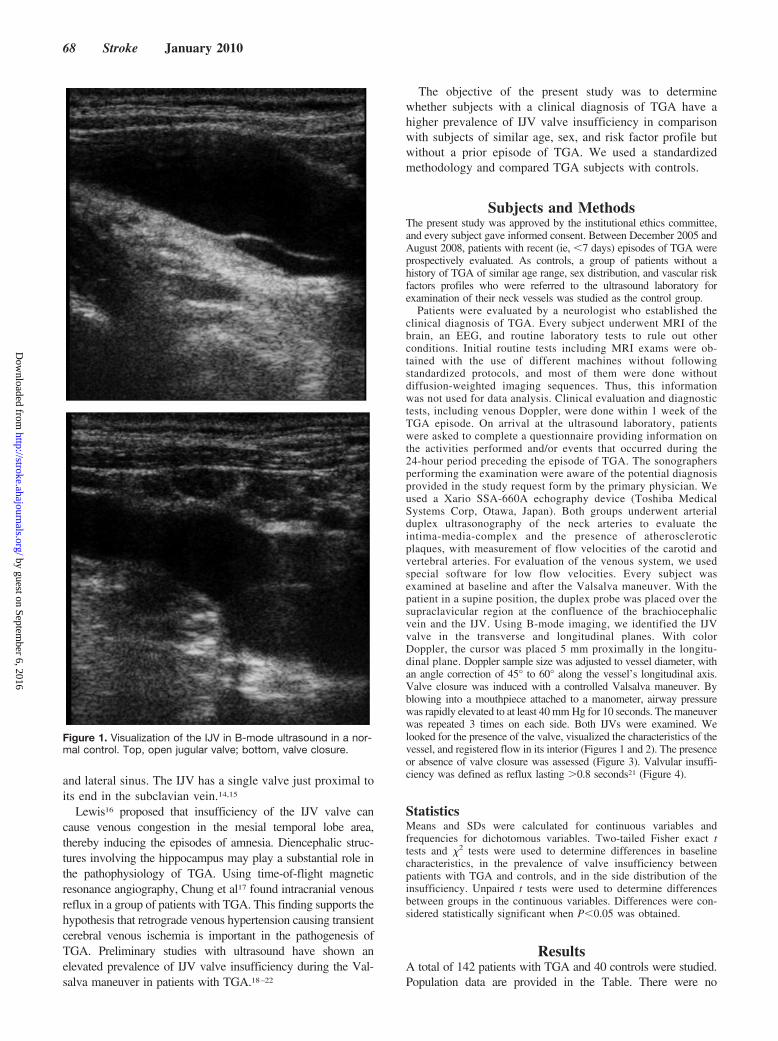
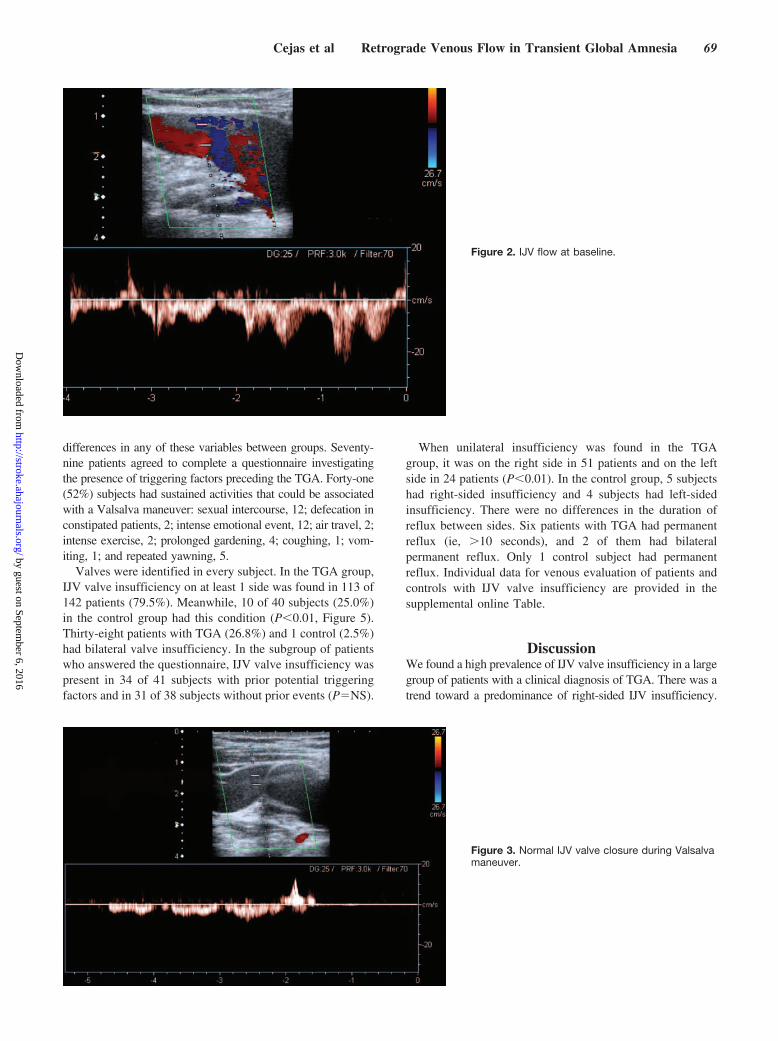
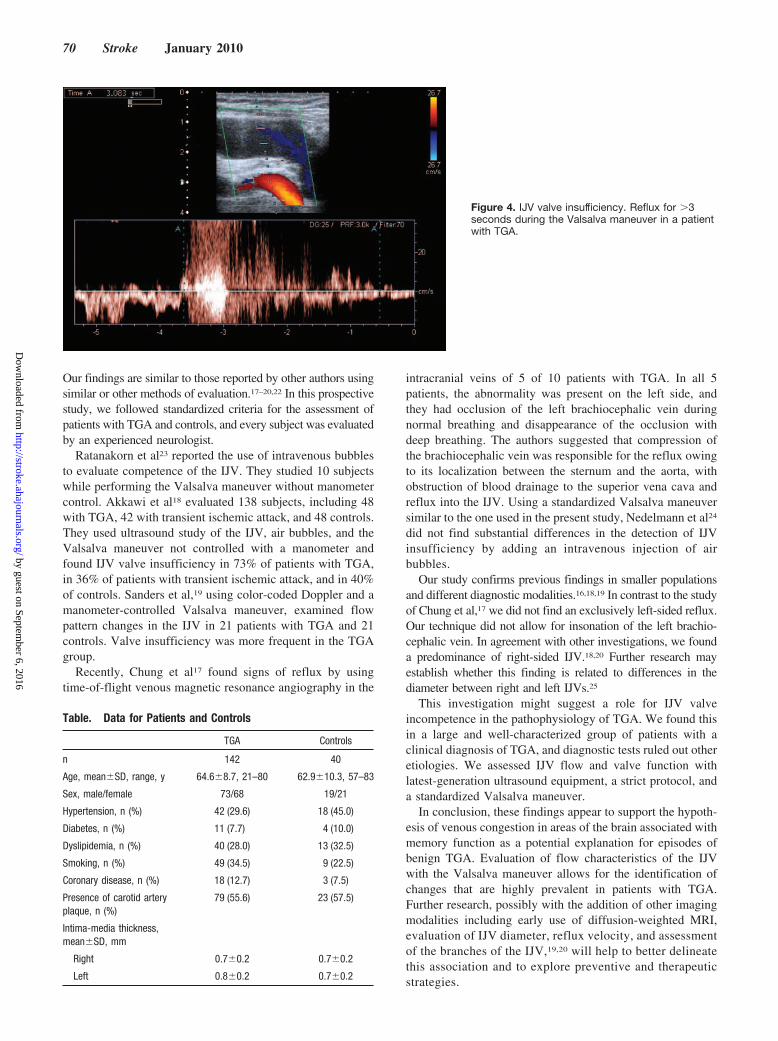
Patients were evaluated by a neurologist who established theclinical diagnosis of TGA. Every subject underwent MRI of thebrain, an EEG, and routine laboratory tests to rule out otherconditions. Initial routine tests including MRI exams were ob-tained with the use of different machines without followingstandardized protocols, and most of them were done withoutdiffusion-weighted imaging sequences. Thus, this informationwas not used for data analysis. Clinical evaluation and diagnostictests, including venous Doppler, were done within 1 week of theTGA episode. On arrival at the ultrasound laboratory, patientswere asked to complete a questionnaire providing information onthe activities performed and/or events that occurred during the24-hour period preceding the episode of TGA. The sonographersperforming the examination were aware of the potential diagnosisprovided in the study request form by the primary physician. Weused a Xario SSA-660A echography device (Toshiba MedicalSystems Corp, Otawa, Japan). Both groups underwent arterialduplex ultrasonography of the neck arteries to evaluate theintima-media-complex and the presence of atheroscleroticplaques, with measurement of flow velocities of the carotid andvertebral arteries. For evaluation of the venous system, we usedspecial software for low flow velocities. Every subject wasexamined at baseline and after the Valsalva maneuver. With thepatient in a supine position, the duplex probe was placed over thesupraclavicular region at the confluence of the brachiocephalicvein and the IJV. Using B-mode imaging, we identified the IJVvalve in the transverse and longitudinal planes. With colorDoppler, the cursor was placed 5 mm proximally in the longitu-dinal plane. Doppler sample size was adjusted to vessel diameter, withan angle correction of 45° to 60° along the vessel’s longitudinal axis.Valve closure was induced with a controlled Valsalva maneuver. Byblowing into a mouthpiece attached to a manometer, airway pressurewas rapidly elevated to at least 40 mm Hg for 10 seconds. The maneuverwas repeated 3 times on each side. Both IJVs were examined. Welooked for the presence of the valve, visualized the characteristics of thevessel, and registered flow in its interior (Figures 1 and 2). The presenceor absence of valve closure was assessed (Figure 3). Valvular insuffi-ciency was defined as reflux lasting �0.8 seconds21 (Figure 4).
StatisticsMeans and SDs were calculated for continuous variables andfrequencies for dichotomous variables. Two-tailed Fisher exact ttests and �2 tests were used to determine differences in baselinecharacteristics, in the prevalence of valve insufficiency betweenpatients with TGA and controls, and in the side distribution of theinsufficiency. Unpaired t tests were used to determine differencesbetween groups in the continuous variables. Differences were con-sidered statistically significant when P�0.05 was obtained.
ResultsA total of 142 patients with TGA and 40 controls were studied.Population data are provided in the Table. There were no
Figure 1. Visualization of the IJV in B-mode ultrasound in a nor-mal control. Top, open jugular valve; bottom, valve closure.
68 Stroke January 2010
by guest on September 6, 2016
http://stroke.ahajournals.org/D
ownloaded from
differences in any of these variables between groups. Seventy-nine patients agreed to complete a questionnaire investigatingthe presence of triggering factors preceding the TGA. Forty-one(52%) subjects had sustained activities that could be associatedwith a Valsalva maneuver: sexual intercourse, 12; defecation inconstipated patients, 2; intense emotional event, 12; air travel, 2;intense exercise, 2; prolonged gardening, 4; coughing, 1; vom-iting, 1; and repeated yawning, 5.
Valves were identified in every subject. In the TGA group,IJV valve insufficiency on at least 1 side was found in 113 of142 patients (79.5%). Meanwhile, 10 of 40 subjects (25.0%)in the control group had this condition (P�0.01, Figure 5).Thirty-eight patients with TGA (26.8%) and 1 control (2.5%)had bilateral valve insufficiency. In the subgroup of patientswho answered the questionnaire, IJV valve insufficiency waspresent in 34 of 41 subjects with prior potential triggeringfactors and in 31 of 38 subjects without prior events (P�NS).
When unilateral insufficiency was found in the TGAgroup, it was on the right side in 51 patients and on the leftside in 24 patients (P�0.01). In the control group, 5 subjectshad right-sided insufficiency and 4 subjects had left-sidedinsufficiency. There were no differences in the duration ofreflux between sides. Six patients with TGA had permanentreflux (ie, �10 seconds), and 2 of them had bilateralpermanent reflux. Only 1 control subject had permanentreflux. Individual data for venous evaluation of patients andcontrols with IJV valve insufficiency are provided in thesupplemental online Table.
DiscussionWe found a high prevalence of IJV valve insufficiency in a largegroup of patients with a clinical diagnosis of TGA. There was atrend toward a predominance of right-sided IJV insufficiency.
Figure 2. IJV flow at baseline.
Figure 3. Normal IJV valve closure during Valsalvamaneuver.
Cejas et al Retrograde Venous Flow in Transient Global Amnesia 69
by guest on September 6, 2016
http://stroke.ahajournals.org/D
ownloaded from
Our findings are similar to those reported by other authors usingsimilar or other methods of evaluation.17–20,22 In this prospectivestudy, we followed standardized criteria for the assessment ofpatients with TGA and controls, and every subject was evaluatedby an experienced neurologist.
Ratanakorn et al23 reported the use of intravenous bubblesto evaluate competence of the IJV. They studied 10 subjectswhile performing the Valsalva maneuver without manometercontrol. Akkawi et al18 evaluated 138 subjects, including 48with TGA, 42 with transient ischemic attack, and 48 controls.They used ultrasound study of the IJV, air bubbles, and theValsalva maneuver not controlled with a manometer andfound IJV valve insufficiency in 73% of patients with TGA,in 36% of patients with transient ischemic attack, and in 40%of controls. Sanders et al,19 using color-coded Doppler and amanometer-controlled Valsalva maneuver, examined flowpattern changes in the IJV in 21 patients with TGA and 21controls. Valve insufficiency was more frequent in the TGAgroup.
Recently, Chung et al17 found signs of reflux by usingtime-of-flight venous magnetic resonance angiography in the
intracranial veins of 5 of 10 patients with TGA. In all 5patients, the abnormality was present on the left side, andthey had occlusion of the left brachiocephalic vein duringnormal breathing and disappearance of the occlusion withdeep breathing. The authors suggested that compression ofthe brachiocephalic vein was responsible for the reflux owingto its localization between the sternum and the aorta, withobstruction of blood drainage to the superior vena cava andreflux into the IJV. Using a standardized Valsalva maneuversimilar to the one used in the present study, Nedelmann et al24
did not find substantial differences in the detection of IJVinsufficiency by adding an intravenous injection of airbubbles.
Our study confirms previous findings in smaller populationsand different diagnostic modalities.16,18,19 In contrast to the studyof Chung et al,17 we did not find an exclusively left-sided reflux.Our technique did not allow for insonation of the left brachio-cephalic vein. In agreement with other investigations, we founda predominance of right-sided IJV.18,20 Further research mayestablish whether this finding is related to differences in thediameter between right and left IJVs.25
This investigation might suggest a role for IJV valveincompetence in the pathophysiology of TGA. We found thisin a large and well-characterized group of patients with aclinical diagnosis of TGA, and diagnostic tests ruled out otheretiologies. We assessed IJV flow and valve function withlatest-generation ultrasound equipment, a strict protocol, anda standardized Valsalva maneuver.
In conclusion, these findings appear to support the hypoth-esis of venous congestion in areas of the brain associated withmemory function as a potential explanation for episodes ofbenign TGA. Evaluation of flow characteristics of the IJVwith the Valsalva maneuver allows for the identification ofchanges that are highly prevalent in patients with TGA.Further research, possibly with the addition of other imagingmodalities including early use of diffusion-weighted MRI,evaluation of IJV diameter, reflux velocity, and assessmentof the branches of the IJV,19,20 will help to better delineatethis association and to explore preventive and therapeuticstrategies.
Figure 4. IJV valve insufficiency. Reflux for �3seconds during the Valsalva maneuver in a patientwith TGA.
Table. Data for Patients and Controls
TGA Controls
n 142 40
Age, mean�SD, range, y 64.6�8.7, 21–80 62.9�10.3, 57–83
Sex, male/female 73/68 19/21
Hypertension, n (%) 42 (29.6) 18 (45.0)
Diabetes, n (%) 11 (7.7) 4 (10.0)
Dyslipidemia, n (%) 40 (28.0) 13 (32.5)
Smoking, n (%) 49 (34.5) 9 (22.5)
Coronary disease, n (%) 18 (12.7) 3 (7.5)
Presence of carotid arteryplaque, n (%)
79 (55.6) 23 (57.5)
Intima-media thickness,mean�SD, mm
Right 0.7�0.2 0.7�0.2
Left 0.8�0.2 0.7�0.2
70 Stroke January 2010
by guest on September 6, 2016
http://stroke.ahajournals.org/D
ownloaded from

DisclosuresNone.
References1. Miller JW, Petersen RC, Metter EJ, Millikan CH, Yanagihara T. Transient
global amnesia: clinical characteristics and prognosis. Neurology. 1987;37:733–737.
2. Zorzon M, Antonutti L, Mase G, Biasutti E, Vitrani B, Cazzato G.Transient global amnesia and transient ischemic attack. Stroke. 1995;26:1536–1542.
3. Hodges JR, Warlow CP. The aetiology of transient global amnesia: a casecontrol study of 114 cases with prospective follow-up. Brain. 1990;113:639–657.
4. Logan W, Sherman DG. Transient global amnesia. Stroke. 1983;14:1005–1007.
5. Hodges J. Unraveling the enigma of transient global amnesia. AnnNeurol. 1998;43:151–153.
6. Shuping J, Rollinson R, Toole J. Transient global amnesia. Ann Neurol.1980;7:281–285.
7. Kushner M, Hauser W. Transient global amnesia: a case-control study.Ann Neurol. 1985;18:684–691.
8. Enzinger C, Thimary F, Kapeller P, Ropele S, Schmidt R, Ebner F,Fazekas F. Transient global amnesia: diffusion-weighted imaging lesionsand cerebrovascular disease. Stroke. 2008;39:2219–2225.
9. Fisher C. Transient global amnesia: precipitating activities and otherobservations. Arch Neurol. 1982;39:605–608.
10. Gilbert G. Transient global amnesia: manifestation of medial temporallobe epilepsy. Clin Electroencephalogr. 1978;9:147–152.
11. Lizak R, Zimmerman R. Transient global amnesia due to a dominanthemisphere tumor. Arch Neurol. 1977;34:317–318.
12. Miador K, Adams R, Flanigin H. Transient global amnesia andmeningioma. Neurology. 1985;35:769–771.
13. Strupp M, Bruning R, Wu R, Deimling M, Reiser M, Brandt T. Diffusion-weighted MRI in transient global amnesia: elevated signal intensity in the
left mesial temporal lobe in 7 of 10 patients. Ann Neurol. 1998;43:164–170.
14. Testut L, Latarjet A. Circulacion cerebral. In: Testut L, y Latarjet A, eds.Tratado de Anatomía Humana. Barcelona: Salvat; 1979:1195–1237.
15. Dresser LP, Mc Kinney WM. Anatomic and pathophysiologic studies ofthe human internal jugular valve. Am J Surg. 1987;154:220–224.
16. Lewis SL. Aetiology of transient global amnesia. Lancet. 1998;352:397–399.
17. Chung C, Hsu H, Chao A, Chang F, Sheng W, Hu H. Detection ofintracranial venous reflux in patients with transient global amnesia. Neu-rology. 2006;66:1873–1877.
18. Maalikjy Akkawi N, Agosti C, Anzola GP, Borroni B, Magoni M, PezziniA, Rozzini L, Vignolo LA, Padovani A. Transient global amnesia: aclinical and sonographic study. Eur Neurol. 2003;49:67–71.
19. Sander D, Winbeck K, Etgen T, Knapp R, Kingelhofer J, Conrad B.Disturbance of venous flow patterns in patients with transient globalamnesia. Lancet. 2000;356:1982–1984.
20. Schreiber SJ, Doepp F, Klingebiel R, Valdueza JM. Internal jugular veinvalve incompetence and intracranial venous anatomy in transient globalamnesia. J Neurol Neurosurg Psychiatry. 2005;76:509–513.
21. Nedelmann M, Eicke B, Dieterich M. Functional and morphologicalcriteria of internal jugular valve insufficiency as assessed by ultrasound.J Neuroimaging. 2005;15:70–75.
22. Chung C, Hsu H, Chao A, Sheng W, Soong B, Hu H. Transient globalamnesia: cerebral venous outflow impairment: insight from the abnormalflow patterns of the internal jugular vein. Ultrasound Med Biol. 2007;33:1727–1735.
23. Ratanakorn D, Tesh P, Tegeler C. A new dynamic method for detectionof internal jugular valve incompetence using air contrast ultrasonography.J Neuroimaging. 1999;9:10–14.
24. Nedelmann M, Teschner D, Dieterich M. Analysis of internal jugular veininsufficiency: a comparison of two ultrasound methods. Ultrasound MedBiol. 2007;33:857–862.
25. Lichtenstein D, Saifi R, Augarde R, Prin S, Schmitt JM, Page B, Pipien I,Jardin F. The internal jugular veins are asymmetric: usefulness ofultrasound before catheterization. Intensive Care Med. 2001;27:301–305.
Figure 5. IJV reflux in patients and controls (seetext for details). *P�0.01 vs controls, 2-tailedFisher exact t test.
Cejas et al Retrograde Venous Flow in Transient Global Amnesia 71
by guest on September 6, 2016
http://stroke.ahajournals.org/D
ownloaded from
Claudia Cejas, Lucia Fernandez Cisneros, Roberto Lagos, Carlos Zuk and Sebastián F. AmerisoAmnesia
Internal Jugular Vein Valve Incompetence Is Highly Prevalent in Transient Global
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 2009 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/STROKEAHA.109.566315
2010;41:67-71; originally published online November 19, 2009;Stroke.
http://stroke.ahajournals.org/content/41/1/67World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org/content/suppl/2013/10/06/STROKEAHA.109.566315.DC1.htmlData Supplement (unedited) at:
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer process is available in the
Request Permissions in the middle column of the Web page under Services. Further information about thisOnce the online version of the published article for which permission is being requested is located, click
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Strokein Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on September 6, 2016
http://stroke.ahajournals.org/D
ownloaded from

2/3(16/17)’2010
73
Транзиторная глобальная амнезия (ТГА) характе-ризуется преходящей внезапной утратой способнос-ти запоминать новую информацию и выпадением из памяти некоторых недавних событий [1]. Иногда ТГА развивается после определенных инициирую-щих событий, таких как половой акт, физические упражнения или погружение в холодную воду [1]. Тем не менее у многих пациентов ТГА развивает-ся без провоцирующих факторов. Эпизод обычно длится несколько часов, затем происходит полное восстановление способности к запоминанию, одна-ко сохраняется частичная амнезия относительно событий, которые произошли во время эпизода ТГА. Ориентация в собственной личности и сознание, а также способность выполнять сложные задания, необходимые для проведения исследований при ТГА, не нарушаются [2–5]. ТГА является довольно распространенной нозологической формой, заболева-емость ТГА в Соединенных Штатах составляет от 23 до 32 случаев на 100 тыс. населения в год [1–3].
ТГА чаще всего развивается на фоне хорошего самочувствия и при отсутствии серьезной сердечно-сосудистой патологии у пациентов в возрасте старше 50 лет. Рецидивы возникают редко, а эпизоды носят доброкачественный характер. Однако подавляющему большинству пациентов для уточнения диагноза прово-дят дорогостоящее обследование, как правило, с отри-цательными результатами. Пациенты и члены их семей проявляют беспокойство в отношении последствий эпизода амнезии, риска развития рецидивов, а также
отсутствия результатов проведенных обследований. В связи с этим было бы целесообразно разработать неинвазивный диагностический метод для выявления нарушений, связанных с ТГА и не характерных для других состояний, позволяющий врачам подтвердить диагноз и сэкономить ресурсы и время.
Несмотря на то, что ТГА является четко выделен-ной нозологической формой, ее этиология до сих пор неизвестна. W. Logan и D.G. Sherman [4] предположили наличие взаимосвязи ТГА с тромбоэмболическими и сер-дечно-сосудистыми заболеваниями. J. Shuping и соавт. [6] обнаружили высокую распространенность факторов риска сердечно-сосудистых заболеваний у пациентов с ТГА. Несмотря на это, M. Kushner и W. Hauser [7] не подтвердили эти выводы. В исследованиях с исполь-зованием диффузионно-взвешенной магнитно-резо-нансной томографии (ДВ-МРТ) были обнаружены незначительные, остро возникшие изменения в меди-альных областях височных долей у небольшого числа пациентов с клиническим диагнозом ТГА [8]. Другие авторы предположили наличие связи ТГА с эпилепсией [9, 10] и опухолями головного мозга [11, 12].
В последние годы была предложена гипотеза о наличии венозного застоя в головном мозге [5, 13]. Основной отток венозной крови от головного мозга осуществляется через синусы твердой мозго-вой оболочки во внутреннюю яремную вену (ВЯВ). Этот сосуд начинается у основания черепа, является продолжением латерального синуса и сливается с под-ключичной веной в конце ее шейного отдела. Отток венозной крови от медиальных областей височной доли осуществляется через базальные вены Розенталя, внутреннюю мозговую вену, вену Галена, прямой, поперечный, а также латеральный синус. В ВЯВ есть
При транзиторной глобальной амнезии часто встречается недостаточность клапана внутренней яремной веныИсточник. C. Cejas, L.F. Cisneros, R. Lagos, C. Zuk, S.F. Ameriso. Internal jugular vein valve incompetence is highly prevalent in transient global amnesia. Stroke 2010;41:1:67–71
Institute for Neurological Research, FLENI, Ultrasound Laboratory and the Neurology Department, Buenos Aires, Argentina.
Предпосылки и цель исследования. Транзиторная глобальная амнезия (ТГА) – клинический синдром, характеризующийся внезапной утратой способности запоминать новую информацию и выпадением из памяти некоторых недавних событий в течение нескольких минут или часов. Этиология ТГА не ясна, но потенциальной причиной ее развития считают нарушение кровотока в медиальных отделах височ-ных долей на фоне венозного застоя. При ультрасонографическом исследовании внутренней яремной вены (ВЯВ) при ТГА обнаружили клапанную недостаточность. Распространенность клапанной недостаточности ВЯВ изучили у пациентов с ТГА. Пациентов без ТГА анало-гичного пола, возраста и с аналогичным профилем сосудистых факторов риска включили в контрольную группу. Методы. Провели про-спективное исследование с выборкой, состоящей из 142 пациентов с клиническим диагнозом ТГА в первые 7 дней после клинического эпизода ТГА, и сформировали контрольную группу из 40 пациентов. Допплерографическое исследование венозного кровотока в обеих ВЯВ проводили, в т. ч. после пробы Вальсальвы, контролируемой с помощью манометра. Критерием наличия клапанной недостаточности ВЯВ было выявление рефлюкса продолжительностью более 0,8 секунд во время проведения пробы Вальсальвы. Результаты. Клапанную недостаточность, по крайней мере одной яремной вены, обнаружили у 113 (79,5%) из 142 пациентов с ТГА и у 10 (25,0%) из 40 пациен-тов контрольной группы ( р<0,01). Чаще встречалась клапанная недостаточность правой ВЯВ, чем левой (р<0,01), а у 26,8% пациентов выявили наличие клапанной недостаточности обеих ВЯВ. Выводы. У пациентов с ТГА часто встречается клапанная недостаточность ВЯВ. Это открытие может уточнить патофизиологию ТГА. Допплерографическое исследование ВЯВ с динамическими пробами может помочь в изучении этого состояния, протекающего преимущественно доброкачественно.
Ключевые слова: внутренняя яремная вена (internal jugular vein), венозная недостаточность (venous insufficiency), транзиторная глобаль-ная амнезия (transient global amnesia), ультразвук (ultrasound)
© American Heart Association, Inc., 2010 Адрес для корреспонденции: Sebastián F. Ameriso, MD, Institute for Neurological Research, FLENI, Neurology Department, Montaňeses 2325, C1428AQK, Buenos Aires, Argentina. E-mail: [email protected]
2/3(16/17)’2010 ПАТОГЕНЕЗ И ДИАГНОСТИКА
74
только один клапан, расположенный проксимальнее места слияния с подключичной веной [14, 15].
S.L. Lewis [16] предположил, что недостаточность клапана ВЯВ может привести к венозному застою в меди-альных областях височной доли, тем самым стимулируя возникновение эпизодов амнезии. Диэнцефальные струк-туры и гиппокамп могут играть большую роль в пато-физиологии ТГА. При проведении время-пролетной магнитно-резонансной ангиографии С. Chung и соавт. [17] обнаружили наличие рефлюкса во внутричерепных венах в группе пациентов с ТГА. Этот результат подтверж-дает гипотезу, что ретроградная венозная гипертензия, приводящая к транзиторной церебральной ишемии,
является ключевым звеном патогенеза ТГА. Результаты предварительных исследований с использованием уль-трасонографии показали высокую распространенность недостаточности клапана ВЯВ при проведении пробы Вальсальвы у пациентов с ТГА [18–22].
Целью исследования было определение распростра-ненности недостаточности клапана ВЯВ у пациентов с клиническим диагнозом ТГА по сравнению с лицами аналогичного возраста, пола и с аналогичным профи-лем факторов риска развития сосудистых заболеваний без эпизодов ТГА в анамнезе. Были использованы стандартизированные методики исследования и про-ведено сравнение данных пациентов с ТГА и данных лиц контрольной группы.
■ПАЦИЕНТЫ И МЕТОДЫ
Исследование было одобрено этическим комитетом, все участники исследования дали письменное информи-рованное согласие. В период с декабря 2005 г. по август 2008 г. проводили проспективное исследование с участи-ем пациентов, недавно (т. е. менее 7 дней назад) пере-несших эпизод ТГА. В контрольную группу включили пациентов без ТГА в анамнезе, аналогичного возраста, пола и с аналогичным профилем сосудистых факторов риска, которым выполняли исследование сосудов шеи в отделении ультразвуковой диагностики.
Пациенты проходили обследование у невроло-га, поставившего клинический диагноз ТГА. Всем пациентам выполнили МРТ головного мозга, элект- роэнцефалографию и стандартные лабораторные исследования для исключения других заболеваний. Первоначальные рутинные исследования, включая МРТ, выполняли с использованием различных аппара-тов без соблюдения стандартизированных протоколов, и в большинстве случаев диффузионно-взвешенные изображения не получали, поэтому эти данные для анализа не использовали.
Клиническое обследование и диагностические про-цедуры, в т. ч. ультразвуковое допплеровское скани-рование вен, проводили в течение 1-й недели после эпизода ТГА. По прибытии в отделение ультразвуко-вой диагностики пациентам предлагали заполнить анкету, предусматривающую получение информации о видах деятельности и/или событиях, произошедших в течение 24 часов перед эпизодом ТГА. Специалисты по ультразвуковой диагностике, проводящие обследо-вание, были осведомлены о предполагаемом диагнозе, поскольку его указывал врач на бланке направления на исследование. Исследование выполняли на аппарате ультразвуковой диагностики Xario SSA-660a (Toshiba Medical Systems Corp, Otawa, Япония). Пациентам обеих групп выполнили дуплексное сканирование артерий шеи для оценки толщины комплекса интима-медиа, выявления атеросклеротических бляшек и измерения скорости кровотока в сонных и позвоночных артериях. Для изучения венозной системы было использовано специализированное программное обеспечение для регистрации низких скоростей кровотока. Каждому пациенту исследование выполняли до и после про-
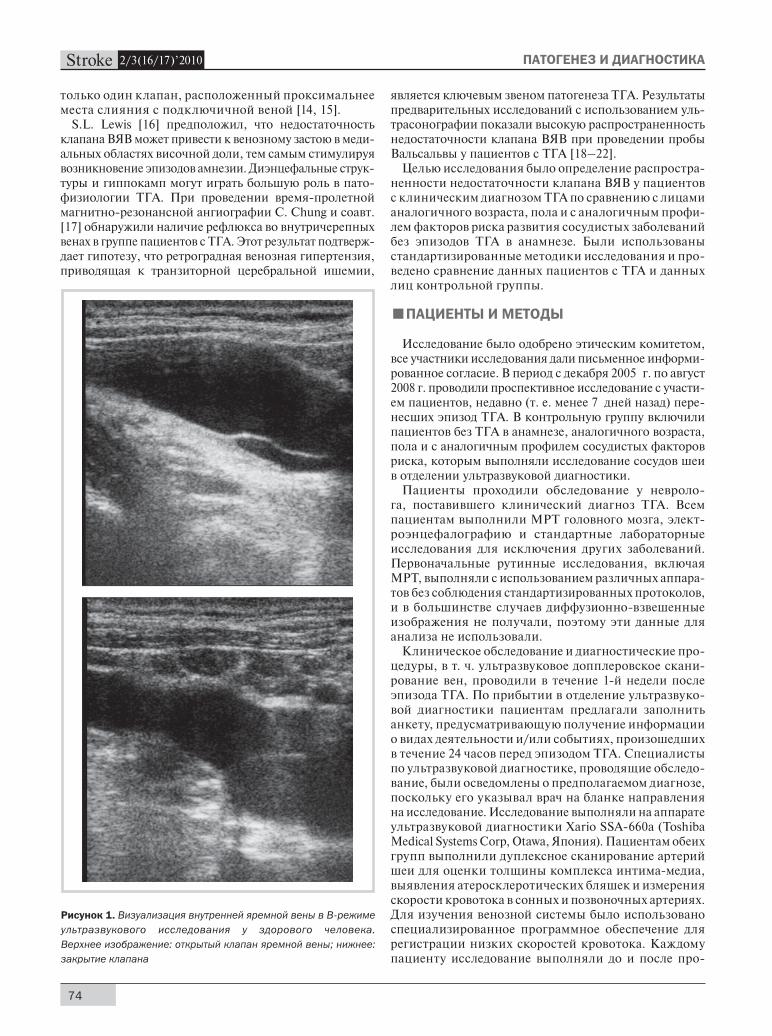
Рисунок 1. Визуализация внутренней яремной вены в B-режиме
ультразвукового исследования у здорового человека.
Верхнее изображение: открытый клапан яремной вены; нижнее:
закрытие клапана
2/3(16/17)’2010
75
ведения пробы Вальсальвы. В положении пациента лежа на спине ультразвуковой датчик располагали над надключичными ямками в проекции слияния плече-головной вены и ВЯВ. В B-режиме визуализировали клапан ВЯВ в продольной и поперечной плоскостях. При проведении допплерографии с цветовым карти-рованием курсор располагали на 5 мм проксимальнее клапана ВЯВ в продольной плоскости. Размер выбор-ки был скорректирован по данным допплерографии в зависимости от диаметра сосуда с угловой коррекцией от 45° до 60° вдоль продольной оси сосуда. Закрытие клапана провоцировали с помощью контролируемой пробы Вальсальвы. При выдыхании в мундштук, соединенный с манометром, давление в дыхательных путях быстро повышалось не менее чем на 40 мм рт. ст. в течение 10 секунд. Пробу повторяли 3 раза с каждой стороны. Провели оценку следующих данных: наличие клапана, характеристики сосуда, а также регистриро-вали показатели кровотока в нижней его части (рис. 1, рис. 2, см. цветную вклейку). Оценивали наличие или отсутствие закрытия клапана (рис. 3, см. цветную вклейку). Критерием недостаточности клапана было выявление рефлюкса длительностью более 0,8 секунд [21] (рис. 4, см. цветную вклейку).
СТАТИСТИчЕСКИЕ ДАННЫЕДля непрерывных переменных были рассчитаны
средние значения и стандартные отклонения (СО), для дихотомических переменных рассчитывали частоты. Двухсторонние точные t-критерии Фишера и критерий хи-квадрат использовали для определения различий в исходных характеристиках, оценки распространенности недостаточности клапана в двух группах наблюдения, а также при оценке недостаточности клапана. Непарный t-критерий использовали для определения различий между группами по непрерывным переменным. Различия считались статистически значимыми при р<0,05.
■РЕЗулЬТАТЫ
В общей сложности в исследовании приняли участие 142 пациента с ТГА и 40 человек составили контроль-ную группу. Демографические данные приведены в таблице. Различия по любой из указанных пере-менных между группами отсутствовали. Семьдесят девять пациентов согласились заполнить анкету, оценивающую наличие провоцирующего фактора для ТГА. У 41 (52%) пациента выявили существенные факторы, которые по своим патофизиологическим следствиям в отношении венозного кровотока в ВЯВ могли быть сходными с пробой Вальсальвы: половой акт – 12 случаев; дефекация – 2 пациента, страдаю-щих запором; яркие эмоциональные события – 12; путешествия воздушным транспортом – 2; интенсив-ные физические упражнения – 2; продолжительное занятие садоводством – 4; кашель – 1; рвота — 1 и приступы зевоты – 5 случаев.
Состояние клапанов ВЯВ оценили у каждого пациента. В группе ТГА недостаточность клапана ВЯВ, по крайней мере с одной стороны, обнаружили
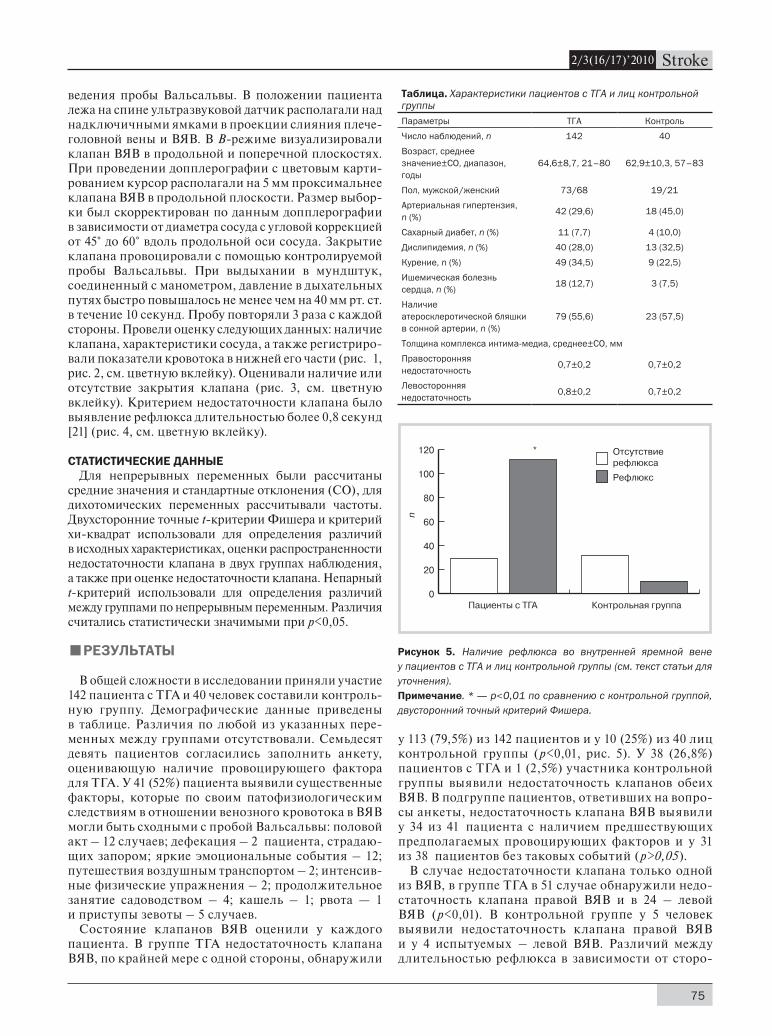
у 113 (79,5%) из 142 пациентов и у 10 (25%) из 40 лиц контрольной группы (р<0,01, рис. 5). У 38 (26,8%) пациентов с ТГА и 1 (2,5%) участника контрольной группы выявили недостаточность клапанов обеих ВЯВ. В подгруппе пациентов, ответивших на вопро-сы анкеты, недостаточность клапана ВЯВ выявили у 34 из 41 пациента с наличием предшествующих предполагаемых провоцирующих факторов и у 31 из 38 пациентов без таковых событий (р>0,05).
В случае недостаточности клапана только одной из ВЯВ, в группе ТГА в 51 случае обнаружили недо-статочность клапана правой ВЯВ и в 24 – левой ВЯВ (p<0,01). В контрольной группе у 5 человек выявили недостаточность клапана правой ВЯВ и у 4 испытуемых – левой ВЯВ. Различий между длительностью рефлюкса в зависимости от сторо-
Таблица. Характеристики пациентов с ТГА и лиц контрольной группы
Параметры ТГА Контроль
Число наблюдений, n 142 40
Возраст, среднее значение±СО, диапазон, годы
64,6±8,7, 21–80 62,9±10,3, 57–83
Пол, мужской/женский 73/68 19/21
Артериальная гипертензия, n (%)
42 (29,6) 18 (45,0)
Сахарный диабет, n (%) 11 (7,7) 4 (10,0)
Дислипидемия, n (%) 40 (28,0) 13 (32,5)
Курение, n (%) 49 (34,5) 9 (22,5)
Ишемическая болезнь сердца, n (%)
18 (12,7) 3 (7,5)
Наличие атеросклеротической бляшки в сонной артерии, n (%)
79 (55,6) 23 (57,5)
Толщина комплекса интима-медиа, среднее±СО, мм
Правосторонняя недостаточность
0,7±0,2 0,7±0,2
Левосторонняя недостаточность
0,8±0,2 0,7±0,2
Рисунок 5. Наличие рефлюкса во внутренней яремной вене
у пациентов с ТГА и лиц контрольной группы (см. текст статьи для
уточнения).
Примечание. * — р<0,01 по сравнению с контрольной группой,
двусторонний точный критерий Фишера.

2/3(16/17)’2010 ПАТОГЕНЕЗ И ДИАГНОСТИКА
76
ны клапанной недостаточности не обнаружили. У 6 пациентов с ТГА выявили постоянный рефлюкс (продолжительностью более 10 секунд) и у 2 из них он был двусторонним. Только у 1 представителя контрольной группы выявили постоянный рефлюкс. Данные пациентов с ТГА и лиц контрольной группы с недостаточностью клапана ВЯВ, выявленной при изучении венозной системы, приведены в дополни-тельной таблице on-line.
■ОбСужДЕНИЕ
Обнаружена высокая распространенность недоста-точности клапана ВЯВ в большой группе пациентов, перенесших ТГА. Отмечена тенденция к преобладанию недостаточности клапана правой ВЯВ. Наши выводы совпадают с заключениями других авторов, использо-вавших аналогичные или другие методы исследования [17–20, 22]. В настоящем проспективном исследова-нии мы руководствовались стандартизированными критериями исследования пациентов с ТГА и лиц контрольной группы, каждого пациента обследовал квалифицированный невролог.
D. Ratanakorn и соавт. [23] в своем исследовании, посвященном изучению состояния клапанов ВЯВ, использовали внутривенное введение пузырьков воз-духа. Они обследовали 10 пациентов, которым также выполняли пробу Вальсальвы без контроля с помо-щью манометра. N. Akkawi и соавт. [18] обследовали 138 пациентов, в т. ч. 48 с ТГА, 42 – с транзиторными ишемическими атаками и 48 человек составили груп-пу контроля. Было проведено ультразвуковое иссле-дование ВЯВ с внутривенным введением пузырьков воздуха и проба Вальсальвы без контроля с помощью манометра. Обнаружили недостаточность клапана ВЯВ у 73% пациентов с ТГА, 36% пациентов с ТИА и у 40% лиц контрольной группы. D. Sander и соавт. [19] изучали динамику изменений кровотока во ВЯВ у 21 пациента с ТГА и у 21 пациента группы конт-роля с использованием цветового допплеровского сканирования и пробы Вальсальвы, контролируемой с помощью манометра. Недостаточность клапана чаще выявляли в группе больных ТГА.
Недавно С. Chung и соавт. [17] при проведении время-пролетной магнитно-резонансной венозной ангиографии обнаружили наличие рефлюкса во внут-ричерепных венах у 5 из 10 пациентов с ТГА. У всех 5 пациентов аномалия была расположена слева, при этом при нормальном дыхании у них выявили окклюзию левой плечеголовной вены, а при глубоком
дыхании – исчезновение окклюзии. Авторы предпо-ложили, что причиной рефлюкса является компрессия плечеголовной вены в связи с ее локализацией между грудиной и аортой, что затрудняет отток крови в верх- нюю полую вену и обусловливает рефлюкс во ВЯВ. Используя стандартизированную методику проведе-ния пробы Вальсальвы, аналогичную применяемой в настоящем исследовании, M. Nedelmann и соавт. [24] не обнаружили существенных различий в отно-шении выявляемости недостаточности клапана ВЯВ при внутривенном введении пузырьков воздуха.
Наше исследование подтверждает результаты ранее проведенных исследований с небольшими выборками и с использованием различных методов диагностики [16, 18, 19]. В отличие от исследования C. Chung и соавт. [17] мы не обнаружили преобладания левостороннего рефлюкса. Наша методика не позволяет проводить инсонацию левой плечеголовной вены. В полном соответствии с результатами других исследований мы обнаружили преобладание недостаточности клапана правой ВЯВ [18, 20]. В дальнейших исследованиях необходимо установить, связаны ли эти результаты с различиями в диаметрах правой и левой ВЯВ [25].
Результаты настоящего исследования позволяют предположить, что недостаточность клапана ВЯВ играет определенную роль в патофизиологии ТГА. Мы сделали этот вывод после обследования боль-шой и хорошо изученной группы пациентов с кли-ническим диагнозом ТГА и получения результатов диагностических процедур, исключающих другие причины. Мы оценивали характеристики кровотока и функцию клапана ВЯВ с использованием ультра- звукового оборудования последнего поколения, со строгим соблюдением протокола и проведением стандартизированной пробы Вальсальвы.
Полученные данные поддерживают гипотезу о наличии венозного застоя в областях мозга, свя-занных с функцией памяти, в качестве возможного объяснения возникновения эпизодов доброкачест- венной ТГА. Изучение характеристик кровотока во ВЯВ при проведении пробы Вальсальвы позво-ляет выявить изменения, широко распространенные среди пациентов с ТГА. Дальнейшие исследования в этом направлении, возможно, с применением других способов визуализации, включая раннее проведение ДВ-МРТ, оценку диаметра ВЯВ и ско-рость рефлюкса, а также изучение состояния ветвей ВЯВ [19, 20], помогут лучше описать выявленную взаимосвязь и разработать профилактические и терапевтические стратегии.
лИТЕРАТуРА
Miller J.W., Petersen R.C., Metter E.J., Millikan C.H., Yanagihara T. 1.
Transient global amnesia: clinical characteristics and prognosis.
Neurology. 1987;37:733–737.
Zorzon M., Antonutti L., Mas2. é G., Biasutti E., Vitrani B.,
Cazzato G. Transient global amnesia and transient ischemic
attack. Stroke. 1995;26:1536–1542.
Hodges J.R., Warlow C.P. The aetiology of transient global amnesia: 3.
a case control study of 114 cases with prospective follow-up. Brain.
1990;113:639–657.
Logan W., Sherman D.G. Transient global amnesia. 4.
2/3(16/17)’2010
77
Stroke. 1983;14:1005–1007.
Hodges J. Unraveling the enigma of transient global amnesia. Ann 5.
Neurol. 1998;43:151–153.
Shuping J., Rollinson R., Toole J. Transient global amnesia. Ann 6.
Neurol. 1980;7:281–285.
Kushner M, Hauser W. Transient global amnesia: a case-control 7.
study. Ann Neurol. 1985;18:684–691.
Enzinger C., Thimary F., Kapeller P., Ropele S., Schmidt R., 8.
Ebner F., Fazekas F. Transient global amnesia: diffusion-
weighted imaging lesions and cerebrovascular disease. Stroke.
2008;39:2219–2225.
Fisher C. Transient global amnesia: precipitating activities and 9.
other observations. Arch Neurol. 1982;39:605–608.
Gilbert G. Transient global amnesia: manifestation of medial 10.
temporal lobe epilepsy. Clin Electroencephalogr. 1978;9:147–152.
Lizak R., Zimmerman R. Transient global amnesia due to a dominant 11.
hemisphere tumor. Arch Neurol. 1977;34:317–318.
Miador K., Adams R., Flanigin H. Transient global amnesia and 12.
meningioma. Neurology. 1985;35:769–771.
Strupp M., Bruning R., Wu R., Deimling M., Reiser M., Brandt T. 13.
Diffusionweighted MRI in transient global amnesia: elevated signal
intensity in the left mesial temporal lobe in 7 of 10 patients. Ann
Neurol. 1998;43:164–170.
Testut L., Latarjet A. Circulaci14. ón cerebral. In: Testut L, y
Latarjet A, eds. Tratado de Anatomía Humana. Barcelona:
Salvat; 1979:1195–1237.
Dresser L.P., Mc Kinney W.M. Anatomic and pathophysiologic 15.
studies of the human internal jugular valve. Am J Surg.
1987;154:220–224.
Lewis S.L. Aetiology of transient global amnesia. Lancet. 16.
1998;352:397–399.
Chung C., Hsu H., Chao A., Chang F., Sheng W., Hu H. Detection of 17.
intracranial venous reflux in patients with transient global amnesia.
Neurology. 2006;66:1873–1877.
Maalikjy Akkawi N., Agosti C., Anzola G.P., Borroni B., Magoni M., 18.
Pezzini A., Rozzini L., Vignolo L.A., Padovani A. Transient
global amnesia: a clinical and sonographic study. Eur Neurol.
2003;49:67–71.
Sander D., Winbeck K., Etgen T., Knapp R., Kingelhofer J., Conrad B. 19.
Disturbance of venous flow patterns in patients with transient
global amnesia. Lancet. 2000;356:1982–1984.
Schreiber S.J., Doepp F., Klingebiel R., Valdueza J.M. Internal 20.
jugular vein valve incompetence and intracranial venous anatomy
in transient global amnesia. J Neurol Neurosurg Psychiatry.
2005;76:509–513.
Nedelmann M., Eicke B., Dieterich M. Functional and morphological 21.
criteria of internal jugular valve insufficiency as assessed by
ultrasound. J Neuroimaging. 2005;15:70–75.
Chung C., Hsu H., Chao A., Sheng W., Soong B., Hu H. Transient 22.
global amnesia: cerebral venous outflow impairment: insight from
the abnormal flow patterns of the internal jugular vein. Ultrasound
Med Biol. 2007;33:1727–1735.
Ratanakorn D., Tesh P., Tegeler C. A new dynamic method for 23.
detection of internal jugular valve incompetence using air contrast
ultrasonography. J Neuroimaging. 1999;9:10–14.
Nedelmann M., Teschner D., Dieterich M. Analysis of internal 24.
jugular vein insufficiency: a comparison of two ultrasound methods.
Ultrasound Med Biol. 2007;33:857–862.
Lichtenstein D., Saifi R., Augarde R., Prin S., Schmitt J.M., Page B., 25.
Pipien I., Jardin F. The internal jugular veins are asymmetric:
usefulness of ultrasound before catheterization. Intensive Care
Med. 2001;27:301–305.
КОММЕНТАРИй
В середине 50-х гг. ХХ столетия Morris Bender [Journal of the Hillside Hospital, 1956] впервые описал своеобраз-ные преходящие нарушения памяти, характеризующи-еся внезапным развитием мнестических расстройств с утратой возможности запоминания, ретроградной амнезией и отсутствием памяти на только что проис-шедшие события при полной сохранности сознания и высших познавательных процессов продолжитель-ностью от нескольких минут до нескольких часов, которые стали называть транзиторной глобальной амнезией (ТГА). Распространенность ТГА составляет 3,5±1,8% среди всех нарушений памяти. Однако есть основание полагать, что ТГА встречается чаще, чем описывается, т. к. из-за преходящего характера этого синдрома врачи наблюдают его достаточно редко.
Клиническая картина ТГА достаточно хорошо изу-чена, в то время как ее причины и механизмы разви-тия требуют дальнейшего анализа. В Международной классификации болезней 10-го пересмотра (МКБ-10) ТГА относится к преходящим транзиторным церебральным атакам и родственным синдромам. ТГА описана в дебюте субарахноидальных кровоиз-
лияний и после операций удаления аневризм сосу-дов мозга, кровоизлияниях в вещество мозга; при опухолях головного мозга различной локализации; кардиальной патологии (брадиаритмии, вызванной передозировкой препаратов дигиталиса; нарушени-ях атриовентрикулярной проводимости, остановке сердечной деятельности; пролапсе митрального клапана), при приеме антиаритмического препарата пропранолола; тяжелых формах сахарного диабета; склеродермии; после операции аортокоронарного шунтирования; во время проведения церебральной и коронарной ангиографии. Их развитие связыва-ют с мигренью и эпилепсией. В то же время боль-шинство исследователей связывают развитие ТГА с цереброваскулярными нарушениями в различных сосудистых бассейнах, развивающимися в результате вазоспазма или микроэмболии. При этом обнару-живали дисциркуляцию в различных сосудистых бассейнах, стенозы тех или иных мозговых сосудов различной степени выраженности, увеличение пер-фузии в левой средней височной извилине, включая гиппокамп, нарушение перфузии обеих затылочных

2/3(16/17)’2010 ПАТОГЕНЕЗ И ДИАГНОСТИКА
78
Л.В. Стаховская,руководитель отдела эпидемиологии и
профилактики НИИ инсультаГОУ ВПО РГМУ Росздрава,
доктор медицинских наук, профессор
долей, мозжечка, т. е. нарушение мозгового кро-вотока у больных с одним и тем же клиническим синдромом (ТГА) наблюдали в различных областях мозга (височных отделах справа, нижневисочной и лобной области слева, зрительном бугре, скорлупе или мозжечке). Полученные данные дали основа-ние авторам сделать вывод о разнонаправленности гемодинамических нарушений при ТГА, требующих дальнейшего исследования. В этом плане представ-
ляет несомненный интерес обнаруженная авторами настоящей статьи у большинства пациентов с ТГА недостаточность клапана внутренней яремной вены, что может быть рассмотрено в качестве значимого фактора в патофизиологии указанного синдрома. Однако вряд ли именно эти нарушения являются основополагающими, учитывая разнообразие забо-леваний и патологических состояний, при которых развивается ТГА.




















