Physiotherapy management of joint hypermobility syndrome—patient and therapist perspectives

ORIGINAL PAPER
Therapist Feelings of Incompetence and Suboptimal Processesin Psychotherapy
Anne Theriault • Nicola Gazzola
Published online: 7 April 2010
� Springer Science+Business Media, LLC 2010
Abstract This study focused on novice therapists’ feel-
ings of incompetence (FOI). FOI are moments where
therapists’ beliefs in their abilities, judgment, and/or
effectiveness is diminished, reduced, or challenged inter-
nally. In order to get at the subtleties of this internal and
subjective process, ten novice therapists were interviewed
for approximately 90 min using a semi-structured inter-
view protocol. The interviews were analyzed by two
researchers using procedures adapted from grounded the-
ory methodology with the aim of developing thick
descriptions and a conceptual structure. Findings indicate
that novice therapists struggle with FOI, which vary in
nature and intensity, and that FOI are multiply determined
and complex. Implications for supervision and for psy-
chotherapy process are discussed.
Keywords Therapist self-doubt �Feelings of Incompetence � Professional issues
Therapists’ feelings of self-doubt, insecurity, and uncer-
tainty about their effectiveness are among the most fre-
quently reported hazards of the psychotherapeutic profession
regardless of the experience level of the practitioner. When
therapists are asked to describe what contributes to their
difficulties, stress, and burnout, they often report experi-
encing doubts about their competence. The nomenclature
utilized by researchers to report this experience is varied: (a)
perceptions that their efforts are inconsequential (Deutsch
1984), (b) self-perceived incompetence (Davis et al. 1987),
(c) low perceived mastery (Orlinsky et al. 1999), (d) pro-
fessional self-doubts (Daniels 1974; Farber and Heifetz
1981; Hellman et al. 1986), (e) a sense of failure (Howard
et al. 1969; Norcross and Guy 2007), (f) self-perceived
failure (Mearns 1990), (g) ‘‘doubts about their own thera-
peutic effectiveness’’ (Mahoney 1997, p. 15), (h) acute per-
formance anxiety and fear (Skovholt and Ronnestad 2003),
and (j) self-criticism about performance (Hill et al. 2007).
Although this phenomenon is labeled differently across
studies, the pervasiveness of this experience is underscored
in the psychotherapy literature; the number of therapists
reporting experiences of self-doubt regarding their thera-
peutic effectiveness is between 42% and 83.2% (Mahoney
1991; Orlinsky et al. 1999). In this paper we will refer to this
cluster of thematically related experiences as a therapist’s
feelings of incompetence (FOI).
A variety of negative consequences have been associ-
ated with FOI, such as stress (Farber and Heifetz 1981),
burnout (Hannigan et al. 2004), premature exit from the
field of psychotherapy (Theriault and Gazzola 2008a, b),
and experiencing personal problems (Mahoney 1997).
Very often the personal life of the therapist is compromised
because of FOI and related experiences (Guy 2000).
While an important aspect of FOI is their impact on the
therapists’ well being, a number of process disturbances have
also been associated with FOI. Hahn (2004) reports that
therapists’ FOI are associated with clients’ feelings of shame
which have a deleterious effect on the therapeutic alliance
(Watson and Greenberg 2000). Therapists concede that FOI
can lead to premature or delayed termination (Brady et al.
1996), alliance ruptures and untimely interpretations (Strean
1993) as well as disengagement and withdrawal (Theriault
and Gazzola 2006). Because therapists are often unequipped
to recognize and cope with FOI (Theriault and Gazzola
2008a, b), they may not be able to prevent these self-doubts
A. Theriault (&) � N. Gazzola
Faculty of Education, University of Ottawa, 145 Jean Jacques
Lussier, Ottawa, ON K1N 6N5, Canada
e-mail: [email protected]
123
J Contemp Psychother (2010) 40:233–243
DOI 10.1007/s10879-010-9147-z

from contributing to a distracting type of self-awareness at the
expense of productive levels of self-involvement in the
therapeutic relationship (Fauth and Williams 2005).
Although FOI are reported by therapists in all experi-
ence levels (Orlinsky et al. 1999; Theriault and Gazzola
2006, 2008a, b) they are particularly prevalent among
novice clinicians. A study by Orlinsky and his associates
(1999) examined the relationship between experience and
insecurity and they underscored the prevalence of self-
doubts about competence, especially among novice clini-
cians. The results indicated that self-perceived low mastery
was reported by 83.2% of novice therapists with
0–1.33 years of experience, 69.2% of therapists with 1.33–
3.15 years of experience, and just over half (52.3%) of
therapists with 3.15–5 years of experience. Indeed, acute
performance anxiety can seriously tax the novice therapist
(Skovholt and Ronnestad 2003).
Models of Therapist Development
Developmental models of therapist growth also propose an
intensity of anxiety about performance (more general than
FOI) that gradually declines as trainees accede to progressive
stages of professional development (Loganbill et al. 1981;
Skovholt and Ronnestad 2003; Stoltenberg 2005). This
struggle is alternately labeled insecurity, anxiety about per-
formance, professional confidence, and sense of competence
but the theme converges around professional self-doubts and
FOI. While weakened by semantic impreciseness, develop-
mental theorists generally seem to agree that therapists’
sense of their competence (or professional self-confidence)
is a key component of growth and maturation.
The notion that FOI decrease with experience has
intuitive appeal however, not all opinions are unequivocal.
Although some of the models of therapist development
have received at least partial support (Bernard and Good-
year 2004, 2009), the research in this area has generally
been criticized for its lack of methodological and concep-
tual rigor and for its exclusive focus on trainees (Ellis and
Ladany 1997; Holloway 1992). Empirical studies that track
and thicken the description of the FOI experience beyond
the training years are lacking.
Another notable limitation is the lack of clear distinction in
these models between objective and subjective perceptions of
competency. For example the Integrated Developmental
Model (IDM model) proposes to describe how competency
evolves yet it uses self-perceptions of one’s ability to be
effective interchangeably with actual competency and effec-
tiveness (Stoltenberg 1981; Stoltenberg et al. 1998).
A notable exception to the focus on the training years
are Ronnestad and Skovohlt (2003) who incorporate
purely subjective professional self-confidence as a central
progressive feature across the six phases of development in
their lifelong learning model. The evolution of perceived
competency is clearly self-referential and traced across the
professional life. The stages, however, have received little
empirical support, especially those that go beyond training
(Bernard and Goodyear 2009) and the construct of self-
confidence is somewhat sketchy. Developmental models in
general have been criticized as being too simplistic (Rus-
sell et al. 1984). Indeed, in-depth investigations of FOI
among seasoned clinicians reveal that the experience is
multiply determined and much more complex than the
obvious correlation of confidence and experience (Theria-
ult and Gazzola 2005, 2006).
Among seasoned clinicians, FOI vary in both degree and
type from mild concern about technique to deep concern
regarding therapist identity. They have identifiable sources
and a variety of possible consequences that range from
increased intentionality within sessions to complete
detachment from the client. There are dynamic intra- and
interpersonal processes that may contaminate the thera-
pist’s self-evaluation process as well as the therapeutic
process in general. While experience is a potent moderator
of FOI, it is but one of a large number of determinants
(Theriault and Gazzola 2008a, b). Seasoned therapists
decry the lack of preparation for this aspect of professional
practice and several wonder aloud whether early-career
anguish resulting from self-doubts might have been cur-
tailed had they been forewarned about FOI (Gazzola and
Theriault 2007). Retroactive accounts by seasoned clini-
cians suggest that while some forms of FOI may abate with
experience others forms may in fact be exacerbated. Fur-
thermore, a sense of competence is not a static milestone to
be achieved in phase bound increments but rather a
dynamic flowing process in experienced clinicians.
The empirical evidence cited above provides a compel-
ling backdrop for the purpose of this study. FOI and related
emotions (e.g., doubts about one’s effectiveness, insecurity)
are prominent and they persist throughout one’s psycho-
therapeutic career in different forms and intensities. They are
potentially quite destructive for the therapist and can disturb
the therapeutic process. The developmental models that we
as a profession rely onto understand the experience of
becoming a professional provide a compelling but vague and
unsubstantiated portrait of therapist self-doubt and feelings
of incompetence, especially beyond the training years. We
would like to build on the existing knowledge by focusing
exclusively on subjective FOI among novices and by pro-
viding an empirical footing for the discourse.
Particularly, we were interested in discovering the mul-
tiple dimensions of self-doubt and the experiential com-
plexity of the phenomenon of questioning one’s competence.
We suspected that FOI were not one-dimensional or solely a
result of inexperience, therefore we were compelled by the
234 J Contemp Psychother (2010) 40:233–243
123

following questions: (a) How do novice clinicians describe
self-doubts, insecurities, and FOI? (i.e., What is the nature of
their subjective experiences of FOI?); (b) What are the key
components and dimensions of this experience from their
perspective?; and (c) What are the sources of FOI?
We decided to proceed with procedures borrowed from
grounded theory methodology in order to ensure methodo-
logical rigor and systematic manipulation of empirical data,
qualities often decried as absent in critical reviews of research
supporting developmental models. We define FOI as ‘‘the
therapists’ belief in their ability, judgment, and/or effective-
ness in their role as therapists is diminished, reduced, or
challenged internally’’ (Theriault and Gazzola 2005). This
definition of FOI provided the parameters for a common
understanding among the researchers and operated as a
backdrop during research decisions such as when to prompt
and include interview material for analysis. However, this
definition was not provided to participants during interviews.
While the definition of FOI was deliberately left vague
for the participants to provide their phenomenological take
on the experience, several assumptions that were reflected
in the definition were held by the researchers and influ-
enced the interactions. The researchers’ working precepts
were that FOI are subjective cognitive-emotional experi-
ences that may or may not be reflective of objective per-
formance indicators. In other words, feeling inadequate
does not necessarily imply being inadequate. Secondly, the
experience of FOI is principally an intrapersonal experi-
ence; it is self-induced and is a product of reflexivity.
Method
Sampling
Purposive sampling was the method of choice: Participants
were selected because they had some characteristics
defined as central to the study. A pool of potential partic-
ipants were identified by the second author and contacted
by a research assistant (RA) to enlist their participation in
the study. Participants were therapists that had recently
(1–5 years prior to the study) graduated from a Master’s-
level training program where the first and second authors
worked (i.e., they were former students of the program). The
RA contacted them and interviewed them. He had previously
met only one of the participants when they had been peers in
a classroom. Code names were given to all participants by the
RA from the moment of informed consent. The students were
all complete strangers to the first author who was hired
subsequent to their graduation. The second author, who had
previous contact with the participants as their professor was
kept unaware of the true identity of the participants; he
neither knew who had agreed to participate nor did he have
access the participant—code key at any time during the study
or subsequently.
Participants
Ten participants were interviewed once. The interviews
ranged from 45 to 90 min and were recorded on audio-
cassettes and subsequently transcribed verbatim. This
resulted in approximately 300 pages of typed text. A basic
set of criteria for the selection of participants reflected the
ideology of the study. The participants (a) were novice
therapists who had between 1 and 5 years of clinical
experience (direct counseling/therapeutic involvement with
clients/patients), (b) were actively engaged in the practice
of psychotherapy at the time of the study (the focus of the
study was on ongoing struggles and a practicing therapist
would offer a contemporary/present day view into the
experience as opposed to a possibly diluted, retrospective
analysis of an experience removed in time), and (c) had a
minimum of a Master’s degree in either clinical or coun-
seling psychology (this criterion was established to offer
some uniformity to the sample base). We used the
parameters specified by Orlinsky et al. (1999) to define
‘‘novice therapists.’’ These were practicing clinicians with
experience levels ranging from 0 to 5 years because
5 years is the point beyond which less than 50% of ther-
apists report FOI in the study by Orlinsky et al. (1999).
Participant Demographic Data
The participants included nine women and one man with an
average of 2 years and 2 months of psychotherapy expe-
rience. Five participants were between 20 and 30 years old,
two were between 30 and 40, three were between 40 and
50, and one was between 50 and 60 years old. The par-
ticipants’ self-identified primary theoretical orientations
were cognitive behavioral (3), humanistic/existential (3),
solution–focused (2), eclectic (1), and art/play therapy (1).
Four of the participants worked for non-profit community
counselling agencies, three participants worked in institu-
tions of higher education (university and college), two were
in private practice, and one worked in a hospital. Half of
our participants did not engage in supervision whereas the
other half received ongoing supervision. While three par-
ticipants received approximately 8–10 h of individual
supervision per month, the other two received 1 h per
month. Only one candidate also engaged in group super-
vision and this occurred for 3 h every 2 weeks.
Data Collection
A structured questionnaire was used to gather basic
demographic data about the therapists who participated in
J Contemp Psychother (2010) 40:233–243 235
123

the study. A semi-structured interview protocol was adap-
ted from previous research studies on FOI originally con-
ducted by Theriault and Gazzola (2003). It included a pool
of potential questions and prompts addressing the research
question to be implemented at the interviewer’s discretion
in accordance with the principles of semi-structured inter-
viewing delineated by Gorden (1992). A typical opening
question was as follows: ‘‘The literature suggests that many
therapists experience moments where they feel uncertain
about what they are doing in therapy, feelings of being
incompetent. Does this sound familiar/have you had these
types of feelings? If the answer is yes, prompt for exam-
ple.’’ The interview schedule evolved across interviews to
reflect queries into emergent categories, relationships, and
insights as is the usual practice in grounded theory whereby
data collection is guided by prior data analysis (Strauss and
Corbin 1998). All interviews were conducted by the
research assistant, a 25-year-old male who was himself a
novice clinician in his first year of counselling practice.
Data Analysis
Adaptation of Grounded Theory Methodology
Select procedures proposed by Strauss and Corbin’s (1998)
grounded theory method guided the discovery process. A
grounded theory approach was selected because it affords a
level of rigor from the standpoint of constructivist criteria. The
approach also permits a level of interpretation that fits with the
objectives of conceptual ordering established a priori.
Also, because the researchers conducted this study
within a larger research program consisting of multiple
studies using grounded theory, methodological uniformity
across studies was also a concern in terms of secondary use
of data to contribute to a more formal theory to be elabo-
rated at a future point in time.
Coding
The transcribed exchange was analyzed for thematic con-
tent using procedures inspired from grounded theory
methodology. Because the aim of the analysis was
description and conceptual ordering, we sought to organize
the data into discrete categories according to their dimen-
sions and properties. In light of Strauss and Corbin’s
(1998) concession that ‘the researcher can use some, but
not all, of the procedures to satisfy his or her research
purposes’ (Strauss and Corbin 1998, p. 288), we elected to
employ procedures called open coding and axial coding.
These systematic procedures position increasingly abstract
understandings of participant’s thoughts in relation to each
other through thematic coding of verbal content. The pro-
cedures were selected because they are both rigorous and
interpretive. Throughout the coding and categorizing pro-
cess, the constant comparative process was applied. In
order to refine themes and categories, instances of a phe-
nomenon were compared to each other to tease out subtle
differences and exceptions, or to further identify levels
within a category.
Open Coding
The most basic exercise in the process of open coding is to
label or name an idea, event, incident, or act using a descrip-
tive ‘‘code’’ that represents the data as faithfully as possible.
This exercise generally elicits a number of elementary labels
that can be synthesized along common elements into cate-
gories that are more abstract and comprehensive. As the
coding continues, some new categories are generated, others
eliminated, and still others relocated within the scheme under
different labels. They serve as basis from which to engage in
the next level of analysis, axial coding.
Axial Coding
Axial coding uncovers relationships between categories,
such as, for example, causal, cyclical, or interactional
patterns. Comparing instances of observed phenomena
allows for the specification of conditions that gave rise to a
category and the context in which it appears.
Coding and Auditing
The coding was conduct by the first author, a female
assistant professor who had been in private practice for
over 15 years prior to joining the faculty of the midsized
university where the study was conducted. Coding was also
done simultaneously by a novice clinician. Codes gener-
ated by both coders were amalgamated within one coding
scheme through a process of consensus that was held across
four meetings and numerous electronic exchanges of data
sets. While most themes identified by the two coders were
the same, several themes were identified solely by one or
the other. When this occurred the themes were incorporated
into the scheme when both agreed that they were relevant.
While this is not the usual procedure in grounded theory,
this modification was employed in order to guard against
potential bias by the first coder who had conducted similar
studies with experienced clinicians.
Enhancing Methodological Rigor
In addition to the protection against contamination by
previous analysis of similar data, the use of the second
coder served as an in vivo member check. This triangula-
tion ensured the viability of the data as the coder could
236 J Contemp Psychother (2010) 40:233–243
123

check the evolving category scheme against his own
experience of FOI as a novice clinician. Other credibility
checks were naturally built into the interview process and
data analytic methods.
Participant Reflection and In Vivo Member Check
The interviewer systematically invited a period of reflex-
ivity at the end of each interview by asking for feedback
regarding the content and the process of the interview. A
typical set of questions to open the topic were: ‘‘How does
it feel to talk about this experience with me? Does talking
about feelings of inadequacy change your perception of
that experience in any way? Is there anything you would
like to add that you feel might be important in under-
standing feelings of incompetence?’’
Evolving Nature of Interview Protocol and Interviewer
Style
As is the nature of semi-structured interviewing in groun-
ded theory approaches, neither the exact wording nor the
order of questions was predetermined (Gorden 1992).
Rather the interview questions evolved to reflect and dee-
pen the ongoing analysis in an iterative process which
moves from data generation and data analysis to category
verification and elaboration. Emergent categories were
incorporated into subsequent queries and participants gui-
ded the interviewer to the salient aspects providing for the
ongoing refinement of the category scheme across inter-
views. Also, the interviewer paraphrased and offered ten-
tative interpretations that participants freely verified and
corrected throughout the interview. This interview process
and style offered the participants an ongoing opportunity to
correct, enrich, and add subtlety to the inductive process
thereby reinforcing the trustworthiness of the analysis.
Credibility Through Methodological Procedure
The set of procedures utilized to gather and analyze data is
clearly defined and systematic and they guard against
whimsical and idiosyncratic approaches to the data. For
example, the constant comparative method ensures that
categories that are not truly reflective of the lived experi-
ence shared by participants will be modified and rendered
accurate. Likewise, the fact that the interviews are recorded
and transcribed verbatim guards against retrospective dis-
tortion of data and selective memory.
Investigator Triangulation
When the analysis was complete, the second author, a male
associate professor who had accumulated 14 years of
clinical experience, conducted a thorough audit of all the
transcripts and resulting category scheme to ensure via-
bility and fit. This investigator triangulation (Denzin 1994)
was direct test of the credibility and viability of the con-
ceptual structure.
Verisimilitude
A final maneuver to enhance rigor invites the reader to
verify whether the interpretations and themes are faithful to
the disclosures they represent; Is the text telling the truth?
By providing ample and intact transcriptions, the writer
draws the audience ‘so closely into the subject’s world that
it can be palpably felt’ (Adler and Adler 1994, p. 381). The
inclusion of numerous and extensive verbatims and para-
phrases in Table 1 allows the reader to bear witness to the
fidelity of the analysis.
Results
Participants readily recognized the experience of FOI as
ongoing aspects of their professional and personal lives. As
such they were relieved to offer candid examples and to detail
rich descriptions of their struggles with self-doubt. The anal-
ysis of the data yielded three principal categories; phenome-
nological hues, depth and nature of FOI, and sources of FOI.
Phenomenological Hues of FOI
Within the main category of phenomenological experience
of FOI, three salient subcategories emerged; familiarity and
pervasiveness of FOI, nuances of the subjective experience
of FOI, and emotionality.
Familiarity and Pervasiveness
Nine of the ten novice clinicians interviewed expressed a
high level of familiarity with FOI. They admitted that the
struggle with self-doubts and feelings of being incompetent
was a common experience of counseling from their per-
spective. FOI occupied an important part of their reflec-
tions about counselling. One of the participants declared
‘‘I can’t think of a day when I don’t experience that.’’ The
dissenting therapist experienced FOI as ‘‘lurking right
beneath the surface’’ and ‘‘likely to pop up at any time’’ but
she did not put FOI at the forefront of her conscious
deliberations as the others had.
Nuances of the Subjective Experience of FOI
Therapists described experiencing FOI as transitory and
pervasive. That is, they experienced them both as ‘‘split
J Contemp Psychother (2010) 40:233–243 237
123

second moments between their interactions’’ and across
time in global level self-evaluations. FOI were described
both as fleeting, moment-bound experiences and more
widespread and free floating. For example:
‘‘Maybe I’m completely incompetent and that’s why I
don’t see any movement in what’s happening.’’ So
there’s that kind of lack of movement in general and
then there’s just like moments within a session where
I think ‘‘I don’t know where to go, I have no idea
what to do, oh, my god maybe I’m just not there
(laugh) somehow.’’
Participants used a variety of terms to define their
understanding of FOI such as ‘‘unsure,’’ ‘‘uncertain,’’
‘‘lost,’’ ‘‘not going anywhere,’’ ‘‘not able to find something
that works,’’ ‘‘running out of things to try,’’ ‘‘cannot make
a shift,’’ and ‘‘fear that it’s not working.’’
Emotionality
Self-doubts and feelings of incompetence pulled for a wide
range of emotions, some quite intense. For example,
participants disclosed helplessness, anger, anxiety, dis-
couragement, feeling burdened, feeling ‘‘shaken-up,’’
frustrated, and powerless. While participants struggled to
contain and manage these feelings, the work/home
boundary became more porous in the presence of FOI.
Therapists’ after-hour ruminations were replete with FOI-
related themes. The depth and intensity of the emotions
were related to the nature of the self-doubt.
Depth and Nature of FOI
FOI subsume self-doubting processes that vary along a
continuum in terms of the intensity experienced by the
clinician and the level of anguish generated. The self-
doubting processes also contained a number of themes that
we regrouped under four distinct subcategories: (a) pro-
cedural uncertainty, (b) micro-outcomes, (c) professional
insecurity, and (d) self and identity doubts. Disclosures
from transcripts coupled with extrapolation from our own
experience allowed us to position the themes within levels
that represent increasing levels of depth, from one to four,
respectively.
Table 1 Category one: Depth
and nature of self-doubting
processes among novice
therapists
Depth of
FOI;Thematic label Nature of self-doubt Paraphrased examples
Level 1 Procedural and
technical
uncertainty
Self-doubts about
‘the mechanics’
of therapy
• Am I not saying this right?
• Where to go from here?
• What do I say next? Is that a
useful question?
• I am afraid to do the wrong thing.
Should I try this technique?
• Was it something I said?
Level 2 Being bound to
micro-outcomes
Self-doubts about the
immediate impact
of therapy
• Did this work?
• How did the client respond when
I said that?
• Is what the client saying related
to what I just said?
• Why is he not engaged with what
I said?
Level 3 Professional
insecurity
Self-doubts about my
capacity to be
effective as a clinician
• Do I have enough training?
• Am I capable of doing what
needs to be done?
• Can I reach the objectives?
• Am I a competent practitioner?
Level 4 Self and identity
doubts
Preoccupations about my
adequacy as a person,
character flaws, and personal
shortcomings
• Is it me? What if there something
fundamental missing in my
personality?
• Who am I that I should be doing
this?
• Doubting own intention, like a
fraud-imposter phenomenon
• Do I have it in me give?
238 J Contemp Psychother (2010) 40:233–243
123

In level 1 self-doubt, procedural uncertainty dominated.
The therapist’s main preoccupation was regarding techni-
cal maneuvers and the adequacy of specific interventions
chosen. For example, one participant said: ‘‘What the hell
was I thinking when I said this?’’
In level two, the therapist was concerned with the
immediate result of an intervention, the micro outcome.
‘‘Did it work?’’ reflects this level of preoccupation. At the
third level, professional insecurity, the self-doubts moved
beyond the immediate level of intervention and began to
include the therapist’s professional self. One participant
said: ‘‘How come I can’t figure out what it is they need?’’
The preoccupation was about the capacity to be effective
globally as a clinician. In level 4, self-and identity doubts,
the personhood of the therapist was called into question.
The therapists feared that some profound character flaw or
personal shortcoming may prevent them from becoming
the therapists they would like to be. This deeper more
pervasive level was more difficult to disclose and haunted
these therapists. For example:
It’s much more threatening…. It has a moral quality
to it…. It’s that I’m not in touch with some feelings,
not willing to be in touch with some feelings…. I
don’t have this in me to give.
Many of the participants spontaneously alluded to an
experiential gradient of emotionality that depended on the
nature of thematic content of the self-doubting process.
Using the participant disclosures and our own experiences
as guides we established a relational trend between nature
of self-doubt and depth of experiencing of FOI. At the
lighter end of the continuum FOI were experienced as
minor aggravations, more fleeting and context-bound. They
were easier to classify and cope with. For example:
Participant: Um, well, when it comes to, you know,
questions like, you know ‘‘why did I ask
that open, or, close ended question? I should
have asked this.
Interviewer: ’’Right.
Participant: O.K., that’s, I sort of see that as a surface
level thing, yeah, it bothers me but it
doesn’t really hit my core.
Um, well, when it comes to, you know, questions like, you
know ‘‘why did I ask that open, or, close ended question? I
should have asked this.’’Interviewer:Right.Partici-
pant:O.K., that’s, I sort of see that as a surface level thing,
yeah, it bothers me but it doesn’t really hit my core.
At the deeper ends are FOI that were tied into personal
identity issues, they contaminated self-image and were
more likely to immobilize the therapist. The therapist’s
level of experiential distress was related to the nature of the
self-doubts (see Table 1).
Sources of FOI
Participants in the study reported that their FOI had a
variety of origins. They provided detailed information
about where the FOI stemmed by direct identification of
causes as well as through multiple examples. These were
grouped under 5 subcategories: (a) permissible fallibility,
(b) professional, (c) process issues, (d) pressure, and (e)
personal sources.
Permissible Fallibility
Therapists realized the limits of their influence on clients
and also invoked human limitations as bases for their FOI.
They usually were able to absolve themselves from guilt or
torment when FOI were related to this source by internal
prompts such as ‘‘it’s ok to be still learning,’’ ‘‘I’m only
human,’’ ‘‘I can’t be all things to all people.’’ Several
therapists went so far as to value FOI stemming from this
source because they ‘‘provided a humbling experience,’’
kept them on their toes, and fuelled their intentionality.
Thus FOI were considered by some to be conditionally
positive, that is, they could be used to bolster mindfulness
and used as a motivator for professional and personal
growth.
Professional Sources
A majority of the participants focused on professional
issues as the main source of FOI. Principally they attributed
FOI to lack of knowledge, experience, and training. Lack
of knowledge was cited by all participants and was the
most popular source of FOI. They described a chronic
unsatisfied need for ever more tools, a state we labeled the
‘‘empty toolbox syndrome.’’ Therapists with this incessant
need to acquire more skills and techniques seem to hang on
the notion that when a sufficient number of techniques
were acquired, the feeling of FOI would abate once and for
all. As such they frequently criticized their training pro-
grams for falling short of this ideal and many displayed a
type of yearning what we labeled ‘‘one workshop away
from being good-enough.’’
Process Issues
Noxious elements in the dynamic exchange between ther-
apist and client and specific elements of the process could
induce FOI. Therapists reported experiencing FOI when
there were serious impediments to the therapeutic rela-
tionship, when they were blinded to the person by the
problem, and also when there were unclear boundaries
around responsibility for change. For example, many
therapists described having assumed full responsibility for
J Contemp Psychother (2010) 40:233–243 239
123

therapeutic progress and movement and having felt that if
they saw no progress they were at fault. They also
described shifts in their FOI when they started to question
their role in the change process. Likewise, they decried the
increased intensity of FOI that accompanied playing the
‘‘expert role.’’ For example:
And I know that I have a bit of a tendency to want to
just fix them and do all the right stuff for them, but
sometimes that’s not possible, I guess that’s part
of…. I guess that’s controlling on my behalf
(laugh)…thinking I’m a little more important than I
really am.
When they adopted stances that were decentralizing of
their own power and empowered the client to assume some
responsibility for therapeutic movement, FOI decreased.
These shifts were not permanent and therapists had not
consolidated their role or permanently fixed the boundaries
around who is responsible for change. There were ongoing
internal struggles and dynamic debates regarding these two
process issues.
Other process issues that were fingered as responsible
for FOI were discrepancies between process and outcome
and between theoretical and applied counseling. In the
former, therapists described poor results despite what
appeared to them as a productive and positive process. In
the latter, a revered strategy failed; therapists became dis-
illusioned when a prized intervention failed to deliver the
promised results. One therapist described it as the
‘‘moment when you realize that the client is more complex
than the theory.’’ In other examples provided, therapists
exposed the struggles created when outcomes are unpre-
dictable or ambiguous.
Finally, therapists identified certain client characteristics
that could induce FOI: unmotivated, perceived fragility,
high stakes clients, critical clients, aggressive clients with
intense affect, and high levels of anguish among others.
Also, therapists provided several labels and diagnostic
categories that could elicit FOI from them, such as bor-
derline, violent, deeply depressed, suicidal, and psychotic.
Throughout our analysis of the data we repeatedly
encountered a second order phenomenon that we labeled
‘‘FOI feeds unto itself.’’ This subcategory regroups
instances where FOI were a by-product of attempts to cope
with and manage FOI. For example, one therapist descri-
bed a process where she became more vigilant as a result of
FOI. This hyperawareness magnified all elements of the
process including her own insecurities and self-doubts thus
feeding into the FOI. In another example, the therapist
described becoming more intentional and self-reflecting
with a new client in response to what she labeled ‘‘stranger
danger.’’ The increased self-scrutiny invited FOI. Rigid
over-adherence to a theoretical model used to counter FOI
provoked more FOI in a third participant. This therapist
described an uncharacteristic reliance on her theoretical
model and prescriptions to fend off FOI.
Pressure
A fourth source of FOI for novice therapists was pressure.
This pressure could be self-induced or external. Internal
pressure was the result of numerous self-imposed and
perceived imperatives. Therapists declared the following,
among others: primo non nocere! Be great! Fix it! Hurry
up! You’re it—the client’s last chance! It’s now or never!
Give them a bang for their Buck! Internal pressure also
resulted when therapists attempted to respect an artificial
agenda. That is, when they insisted on following a plan that
did not match the client’s agenda, internal pressure ensued.
For example, therapists described being invested in keep-
ing things positive or sticking to their therapeutic goals
when clients strayed into other topics.
External forms of pressure were also identified as FOI
producing. Third party payers, referral sources, and
supervisors were all identified as potential sources of
external pressure conducive to FOI. These players were
viewed as critical witnesses with an evaluative function.
Several therapists mentioned their reputation and risks of
damage thereof as sources of pressure.
Personal
A number of the sources of FOI identified by therapists
were personal. Several participants admitted that their
personality traits left them vulnerable to FOI. They rec-
ognized that they emphasized weakness and had perfec-
tionist tendencies. Others declared being overly sensitive to
criticism in general and having a deep need to be liked.
Therapists also attributed some of their FOI moments to
their state at the time (e.g., feeling tired, hungry, or ill,
etc.).
Therapists personal values often interfered with their
usual ways of practice, leaving the door open to FOI. For
example when a client’s behavior violated a therapist’s
value, they were not as able to be objective and were
unable to maintain a therapeutic distance. As a result, their
self-doubt increased. Other situations exposed conflicts
between the therapist’s values and the therapeutic contract.
Finally, therapists’ personal wounds and unfinished busi-
ness from their histories fuelled FOI. When client problems
too closely paralleled those of the therapist, boundaries
became more easily blurred and therapists felt more
uncertain. When therapist wounds were exposed, a com-
mon response was to take some distance. Being too
removed, however, jeopardized the relationship and the
therapists’ FOI surged. Also, clients who were critical and
240 J Contemp Psychother (2010) 40:233–243
123

distant, at times, reminded therapists of similar experiences
from their upbringing and stimulated profound self-esteem
dilemmas.
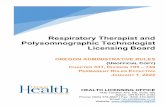
Relational Trends Between Sources of FOI and Their
Depth/Nature
Several of the participants indicated that the depth of FOI
experienced depended on the source of the FOI. For
example novice 3 makes a link between a process source
(sub-category = serious impediment to therapeutic rela-
tionship) and a ‘deeper’ feeling of FOI. For example:
But it’s usually when a client gets really, really upset
to a point where you’ve got to end the visit, either
because they need you to or because for your safety
you need to. So, those are moments when I have felt
that deeper feeling that I talked about…like, that sits
with you a little longer.
Levels of depth of FOI generally progressed across the
source from permissible infallibility, professional, pres-
sure, process, to personal, respectively. (See Fig. 1)
We must stipulate that while the links made were
compelling, they were made tentatively and sporadically.
Direct questioning of subsequent participants hailed sket-
chy associations as well. As a result, this glimpse into the
relational trends between categories is informed by our
own preconceptions as well as participant disclosure.
Discussion
The ten participants in our study reported that they fre-
quently experience FOI. They were able to provide rich,
contextual insights into how their feelings of inadequacy
and incompetence were stimulated and experienced. These
specifications into the nature of FOI in this particular
subset of practicing novice clinicians shed light on the
nagging questions of what happens to this element of
therapist difficulty after the training years described by
most developmental theories. Our findings also lend
empirical support for Ronnestad and Skovholt’s (2003)
assertions that novice therapists struggle with issues of
insecurity, lack of confidence, and doubts about their
competency.
Implications for Supervision and Training
Beyond providing some support for theoretical claims
regarding FOI, our study provides a more detailed
description of this element in the development of the
therapist’s professional-self. It exposes some of the previ-
ously unexamined complexity of this internal experience.
Increased self-knowledge regarding FOI can help therapists
prevent erosion of their professional self-confidence as well
as increase mindfulness regarding how their FOI are being
played out in the therapeutic process; ‘‘Praemonitus, pra-
emunita -forewarned-forearmed’’ (Skovholt and Ronnestad
2003, p. 56). Thus, normalizing the FOI experience among
novice therapists is a worthy implication of our findings.
More detailed and contextualized knowledge of this phe-
nomenon can also be used to address the specifics of novice
struggles and avoid cookie cutter type of interventions that
are often decried as a major weakness of supervisory
interventions within developmental models (Ladany 2004).
For example, a common supervisor response and pre-
scription for supervisee angst is to become more structured
and directive. Our findings suggest that while this style
may attenuate FOI in certain circumstances, it may
aggravate it in others and may also lead to a narrowing of
supervisee experience in supervision (Gazzola and The-
riault 2007). While supervisors may want to be attuned to
supervisees’ need for instruction, this approach will not
provide reassurance for every manifestation of professional
self-doubt. For instance, FOI that stem from personal
sources may require another type of corrective. FOI are
normal and follow a developmental trend but they are also
complex and ever present. Preventative and corrective
strategies need to be tailored to reflect the nature, depth,
and provenance of the FOI. It behooves the supervisor to
respect the multiple dimensions of this experience and to
be mindful of the very individual phenomenology of this
internal challenge. To do otherwise is to risk coming across
as coercive and insisting on irrelevant structure and
ProfoundModerateMild Intensity
Note: Arrows represent the tendency towards increased intensity from left to right.
Permissible Professional Pressure Process Personal Sources
Level 1 Procedural and
technical uncertainty
Level 2 Being bound to micro outcomes
Level 3 Professional uncertainty
Level 4 Self and identity
doubts
Depth and Nature of Self-Doubts
Fig. 1 Axial representation of
relational trends between the
sources and depth and nature
categories. Note: Arrows
represent the tendency towards
increased intensity from left to
right
J Contemp Psychother (2010) 40:233–243 241
123

instructions (cf. Gazzola and Theriault 2007). Also, while
FOI may decrease and/or take different forms with expe-
rience (see Theriault and Gazzola 2008a, b), a lackadaisical
reliance on experience to counter the damaging effects of
FOI is potentially neglectful. Forewarned counselors are
better equipped to cope with FOI (Theriault and Gazzola
2005) and educating them about this aspect of the profes-
sion is imperative in proactive self-care training. Our
results could be useful for preventative and precautionary
work at the graduate level.
Implications for Research
This study contributes nuance and context to the FOI of
novices described in theories of therapist development.
Similar studies have begun to buttress such knowledge for
seasoned clinicians as well (Theriault and Gazzola 2005,
2006, 2008a, b). Further inquiry with therapists -in-training
and at different stages of career development will continue
to fortify and enrich our understanding of how therapists
struggle with FOI across levels of development. These
understandings can then be consolidated through compar-
ative studies and through studies that use a quantitative
approach.
Limitations
Because the authors had previously conducted FOI
research with seasoned clinicians, the risk of preconfigur-
ing the categories during data analysis was a concern.
Three measures were taken to minimize this potential
contamination. The first author and coder bracketed pre-
conceived themes and coded the data with a fresh slate.
Secondly, a second coder was used to ensure that catego-
ries reflected the data at hand. He was privy to bracketed
themes and was sensitized to the possibility of cross-over
from previous research. The second coder was a novice
clinician who had the added benefit of viability; he was
able to ascertain the level of fit between the evolving cat-
egory scheme and his own experience of the phenomenon.
Thirdly, a thorough audit of each transcript and category
scheme was performed by an experienced researcher.
Another limitation of the study is the added pull for
impression management that the topic may generate. While
nine of the ten participants and interviewer were strangers
to each other (the tenth participant was a remote acquain-
tance), disclosing doubts about competence is very sensi-
tive and there is always the possibility that participants
filtered some aspects of their experience to avoid uncom-
fortable levels of vulnerability. Also, as in all grounded
studies, the category scheme is an abstract representation of
responses that were provided by a limited subset of the
population of novice therapists. The extent conceptual
structure may not apply to all novice therapists and appli-
cations of the findings from the study to other groups ought
to be considered tentatively. The results depict the con-
ceptual ordering and reveal a thick description of the
experience of FOI among these particular novices but we
do not claim to have elaborated a formal theory with uni-
versal merit. Rather, in the spirit of discovery-oriented
research, the category scheme ought to be used to generate
ideas and hypotheses about FOI experiences among novice
clinicians.
References
Adler, P., & Adler, P. (1994). Observational techniques. In N. Denzin
& Y. Lincoln (Eds.), Handbook of qualitative research (pp. 377–
392). Thousand Oakes, CA: Sage.
Bernard, J., & Goodyear, R. (2004). Fundamentals of clinicalsupervision (3rd ed.). Boston: Pearson.
Bernard, J. M., & Goodyear, R. K. (2009). Fundamentals of clinicalsupervision (4th ed.). Upper Saddle River, NJ: Pearson
Education.
Brady, J. L., Guy, J. D., Poelstra, P., & Brown, C. K. (1996). Difficult
goodbyes: A national survey of therapists’ hindrances to
successful terminations. Psychotherapy in Private Practice,14(4), 65–76.
Daniels, A. K. (1974). What troubles the trouble shooters? In P. M.
Roman & H. M. Trice (Eds.), The sociology of psychotherapy.
New York: Aronson.
Davis, J. D., Elliott, R., Davis, M. L., Binns, M., Francis, V. M.,
Kelman, J. E., et al. (1987). Development of a taxonomy of
therapist difficulties: Initial report. British Journal of MedicalPsychology, 60, 109–119.
Denzin, N. (1994). The art and politics of interpretation. In N. Denzin
& Y. Lincoln (Eds.), Handbook of qualitative research (pp. 500–
515). Thousand Oakes, CA: Sage.
Deutsch, C. (1984). Self reported sources of stress among psycho-
therapists. Professional Psychology: Research and Practice, 15,
833–845.
Ellis, M. V., & Ladany, N. (1997). Inferences concerning supervisees
and clients in clinical supervision. An integrative review. In E.
C. Watkins Jr. (Ed.), Handbook of psychotherapy supervision(pp. 447–507). New York: Wiley.
Farber, B. A., & Heifetz, L. J. (1981). The satisfactions and stresses of
psychotherapeutic work: A factor analytic study. ProfessionalPsychology, 12, 621–630.
Fauth, J., & Williams, E. N. (2005). The in-session self-awareness of
therapist-trainees: Hindering or helpful? Journal of CounsellingPsychology, 52, 443–447.
Gazzola, N., & Theriault, A. (2007). Super- (and not-so-super-) vision
of counsellors-in-training: Supervisee perspectives on broaden-
ing and narrowing processes. British Journal of Guidance andCounselling, 35(2), 189–204.
Gorden, R. (1992). Basic interviewing skills. Ithasca, IL: Peacock.
Guy, J. (2000). Holding the holding environment together: Self
psychology and psychotherapist care. Professional Psychology:Research and Practice, 31, 351–352.
Hahn, W. K. (2004). The role of shame in negative therapeutic
reactions. Psychotherapy Theory, Research, Practice, Training,41, 3–12.
242 J Contemp Psychother (2010) 40:233–243
123

Hannigan, B., Edwards, D., & Burnard, P. (2004). Stress and stress
management in clinical psychology: Findings from a systematic
review. Journal of Mental Health, 13, 235–245.
Hellman, I. D., Morrison, T., & Abramowitz, S. (1986). The stresses
of psychotherapeutic work: A replication and extension. Journalof Clinical Psychology, 42, 197–205.
Hill, C., Sullivan, C., Knox, S., & Schlosser, L. (2007). Becoming
psychotherapists: Experiences of novice trainees in a beginning
graduate class. Psychotherapy: Theory, Research, Practice,Training., 44, 434–449.
Holloway, E. L. (1992). Supervision: A way of teaching and learning.
In S. D. Brown & R. W. Lent (Eds.), Handbook of counselingpsychology (2nd ed., pp. 177–214). New York: Wiley.
Howard, K. I., Orlinsky, D. E., & Hill, J. A. (1969). The therapist’s
feelings in the therapeutic process. Journal of Clinical Psychol-ogy, 25, 83–93.
Ladany, N. (2004). Psychotherapy supervision: What lies beneath.
Psychotherapy Research, 14, 1–19.
Loganbill, C., Hardy, E., & Delworth, U. (1981). Supervision: A
conceptual model. The Counseling Psychologist, 10, 3–42.
Mahoney, M. J. (1991). Human change processes: The Scientificfoundations of psychotherapy. New York: Basic.
Mahoney, M. J. (1997). Psychotherapists’ personal problems and self-
care patterns. Professional Psychology: Research and Practice,28, 14–16.
Mearns, D. (1990). Therapists experience of failure. In D. Mearns &
W. Dryden (Eds.), Experiences of counseling in action (pp. 80–
143). Thousand Oaks, CA: Sage.
Norcross, J., & Guy, J. (2007). Leaving it at the office: A guide topsychotherapist self-care. New York: Guilford.
Orlinsky, D., Ronnestad, M. H., Ambuhl, H., Willuttzki, U.,
Botermans, J. F., Cierpka, M., et al. (1999). Psychotherapists’
assessments of their development at different career levels.
Psychotherapy: Theory, Research, Practice, Training, 36(3),
203–215.
Ronnestad, M. H., & Skovholt, T. M. (2003). The journey of therapist
and therapist: Research findings and perspectives on professional
development. Journal of Career Development, 30, 5–44.
Russell, R. K., Crimmings, A. M., & Lent, R. W. (1984). Therapist
training and supervision: Theory and research. In S. D. Brown &
R. W. Lent (Eds.), Handbook of counseling psychology(pp. 625–681). New York: Wiley.
Skovholt, T. M., & Ronnestad, M. H. (2003). Struggles of the novice
counselor-therapist. Journal of Career Development, 30(1),
45–58.
Stoltenberg, C. D. (1981). Approaching supervision from a develop-
mental perspective: The counselor complexity model. Journal ofCounseling Psychologists, 28, 59–65.
Stoltenberg, C. D. (2005). Enhancing professional competence
through developmental approaches to supervision. AmericanPsychologist, 60, 857–864.
Stoltenberg, C. D., McNeill, B. W., & Delworth, U. (1998). IDM: Anintegrated developmental model for supervising counselors andtherapists. San Francisco: Jossey-Bass.
Strauss, A., & Corbin, J. (1998). Basics of qualitative research:Techniques and procedures for developing grounded theory (2nd
ed.). Thousand Oaks, CA: Sage.
Strean, H. S. (1993). Resolving counterresistances in psychotherapy.
New York: Brunner/Mazel.
Theriault, A. T. (2003). Therapists’ feelings of incompetence: A
grounded theory analysis of experienced clinicians. Unpublished
doctoral dissertation.
Theriault, A., & Gazzola, N. (2005). Feelings of inadequacy,
insecurity, and incompetence among experienced therapists.
Counselling and Psychotherapy Research, 5(1), 11–18.
Theriault, A., & Gazzola, N. (2006). What are the sources of feelings
of incompetence in experienced therapists? Counselling Psy-chology Quarterly, 19(4), 313–330.
Theriault, A., & Gazzola, N. (2008a). Feelings of incompetence
among experienced therapists: A substantive theory. EuropeanJournal of Qualitative Research in Psychotherapy, 3, 19–29.
Theriault, A., & Gazzola, N. (2008b). Feelings of incompetence in
novice and experienced clinicians: Causes, consequences, and
coping/correctives. In A. Reeves (Ed.), Key issues for counsel-ling in action (2nd ed., pp. 228–243). Thousand Oaks, CA: Sage.
Watson, J. C., & Greenberg, L. S. (2000). Alliance ruptures and
repairs in experiential therapy. In Session: Psychotherapy inPractice, 56, 175–186.
J Contemp Psychother (2010) 40:233–243 243
123
Copyright © 2022 FDOKUMEN