Improving Access to Psychological Services through Therapist-Assisted, Internet-Delivered Cognitive...
10
Improving Access to Psychological Services Through Therapist-Assisted, Internet-Delivered Cognitive Behaviour Therapy Heather D. Hadjistavropoulos, Nicole M. Alberts, Marcie Nugent, and Greg Marchildon University of Regina Depression and anxiety are prevalent yet undertreated conditions. Therapist-assisted Internet-delivered cognitive behaviour therapy (ICBT) is efficacious for these conditions and can serve to overcome barriers to accessing mental health care (e.g., distance, time). In therapist-assisted ICBT, patients review cognitive behavioural treatment materials over the Internet. In addition, providers offer support and direction most commonly through weekly emails or phone calls. Despite the evidence for and advantages of therapist-assisted ICBT, very few patients have access to this treatment in Canada. In this paper, we describe the Online Therapy Unit for Service, Education and Research that was developed at the University of Regina to improve patient access to ICBT in Saskatchewan. With the support of national and provincial funding, this unit created an ICBT web application for the treatment of depression and anxiety, established policies and procedures for delivery of ICBT, trained therapists to deliver the service, and has been coordinating the delivery of ICBT across multiple diverse settings in Saskatchewan. The current paper describes how the Unit is organized and collaborates with community mental health clinics, thus serving to improve access to ICBT. We provide information on the web application, and the process of ICBT from both the patient and provider perspective. We further describe patient and provider utilization of and feedback about ICBT along with recent and future directions for the Unit. Thus far, the Unit has had a positive impact expanding access to psychological services in Saskatchewan and has the potential to inform similar initiatives in other provinces. Keywords: Internet, therapist-assisted, cognitive behaviour therapy, depression, anxiety Depression and anxiety are highly prevalent in Canada (Pearson, Janz, & Ali, 2013), but many Canadians report that these condi- tions go untreated (Sunderland & Findlay, 2013). Multiple factors contribute to the undertreatment of mental health problems, in- cluding a shortage of mental health providers and access difficul- ties resulting from poor mobility, time constraints, rural and re- mote location, or patient concerns about being stigmatized (Collins, Westra, Dozois, & Burns, 2004; Sunderland & Findlay, 2013). Therapist-assisted, Internet-delivered cognitive behaviour therapy (ICBT) is a promising approach for overcoming these barriers and improving access to mental health care (Andersson, 2010). Therapist-assisted ICBT involves presenting patients with the same psychoeducation and cognitive and behavioural strategies as traditional face-to-face cognitive behaviour therapy (CBT), but information is presented through structured modules over the Internet. Between modules, patients work on assignments. In ad- dition, in this form of treatment, patients communicate with a provider by secure email or phone, with communication typically occurring once a week. Randomized controlled trials have consistently demonstrated that therapist-assisted ICBT results in large clinical effects (Andrews, Cuijpers, Craske, McEvoy, & Titov, 2010; Spek et al., 2007) that are comparable to best-practices, face-to-face CBT (Cuijpers, Donker, van Straten, Li, & Andersson, 2010; Wagner, Horn, & Maercker, 2013), even in terms of the devel- opment of a strong therapeutic relationship (e.g., Klein et al., 2009). It is recognised that this approach has limitations requir- ing management (e.g., requires computer access, language and computer skills, close monitoring of patient safety and privacy; Hadjistavropoulos et al., 2011). However, therapist-assisted ICBT also has many advantages over traditional face-to-face therapy. For example, it offers greater convenience and privacy for patients, often involves more active engagement of patients in their own care (Andersson, 2010), takes significantly less time to deliver than traditional face-to-face therapy (e.g., Klein This article was published Online First September 1, 2014. Heather D. Hadjistavropoulos, Nicole Alberts, and Marcie Nugent, Department of Psychology, University of Regina; Gregory Marchildon, Graduate School of Public Policy, University of Regina. This work was supported by funding awarded to Heather D. Hadjistav- ropoulos by the Canadian Institutes of Health Research (Grants 101526, 293379), the Saskatchewan Health Research Foundation, and Rx & D Health Research Foundation. Initial program materials used by the Online Therapy Unit for Service, Education, and Research at the University of Regina were licensed from Anxiety Online at Swinburne University of Technology in Melbourne, Australia through Drs. David Austin and Britt Klein. Recent program materials were obtained from Drs. Nick Titov and Blake Dear through a collaboration agreement with the eCentreClinic at Macquarie University. We would like to extend our thanks to the staff, students, and faculty associated with the University of Regina Online Therapy Unit. We also acknowledge the contributions of mental health providers and administrators from the Cypress, Five Hills, Regina Qu’Appelle, Saskatoon and Sun Country Health Regions and administra- tors from Saskatchewan Health. Correspondence concerning this article should be addressed to Heather D. Hadjistavropoulos, Department of Psychology, University of Regina, 3737 Wascana Parkway, Regina, SK, Canada S4S 0A2. E-mail: hadjista@ uregina.ca Canadian Psychology / Psychologie canadienne © 2014 Canadian Psychological Association 2014, Vol. 55, No. 4, 303–311 0708-5591/14/$12.00 http://dx.doi.org/10.1037/a0037716 303
Transcript of Improving Access to Psychological Services through Therapist-Assisted, Internet-Delivered Cognitive...

Improving Access to Psychological Services Through Therapist-Assisted,Internet-Delivered Cognitive Behaviour Therapy
Heather D. Hadjistavropoulos, Nicole M. Alberts, Marcie Nugent, and Greg MarchildonUniversity of Regina
Depression and anxiety are prevalent yet undertreated conditions. Therapist-assisted Internet-deliveredcognitive behaviour therapy (ICBT) is efficacious for these conditions and can serve to overcome barriersto accessing mental health care (e.g., distance, time). In therapist-assisted ICBT, patients reviewcognitive behavioural treatment materials over the Internet. In addition, providers offer support anddirection most commonly through weekly emails or phone calls. Despite the evidence for and advantagesof therapist-assisted ICBT, very few patients have access to this treatment in Canada. In this paper, wedescribe the Online Therapy Unit for Service, Education and Research that was developed at theUniversity of Regina to improve patient access to ICBT in Saskatchewan. With the support of nationaland provincial funding, this unit created an ICBT web application for the treatment of depression andanxiety, established policies and procedures for delivery of ICBT, trained therapists to deliver the service,and has been coordinating the delivery of ICBT across multiple diverse settings in Saskatchewan. Thecurrent paper describes how the Unit is organized and collaborates with community mental health clinics,thus serving to improve access to ICBT. We provide information on the web application, and the processof ICBT from both the patient and provider perspective. We further describe patient and providerutilization of and feedback about ICBT along with recent and future directions for the Unit. Thus far, theUnit has had a positive impact expanding access to psychological services in Saskatchewan and has thepotential to inform similar initiatives in other provinces.
Keywords: Internet, therapist-assisted, cognitive behaviour therapy, depression, anxiety
Depression and anxiety are highly prevalent in Canada (Pearson,Janz, & Ali, 2013), but many Canadians report that these condi-tions go untreated (Sunderland & Findlay, 2013). Multiple factorscontribute to the undertreatment of mental health problems, in-cluding a shortage of mental health providers and access difficul-ties resulting from poor mobility, time constraints, rural and re-
mote location, or patient concerns about being stigmatized(Collins, Westra, Dozois, & Burns, 2004; Sunderland & Findlay,2013). Therapist-assisted, Internet-delivered cognitive behaviourtherapy (ICBT) is a promising approach for overcoming thesebarriers and improving access to mental health care (Andersson,2010). Therapist-assisted ICBT involves presenting patients withthe same psychoeducation and cognitive and behavioural strategiesas traditional face-to-face cognitive behaviour therapy (CBT), butinformation is presented through structured modules over theInternet. Between modules, patients work on assignments. In ad-dition, in this form of treatment, patients communicate with aprovider by secure email or phone, with communication typicallyoccurring once a week.
Randomized controlled trials have consistently demonstratedthat therapist-assisted ICBT results in large clinical effects(Andrews, Cuijpers, Craske, McEvoy, & Titov, 2010; Spek etal., 2007) that are comparable to best-practices, face-to-faceCBT (Cuijpers, Donker, van Straten, Li, & Andersson, 2010;Wagner, Horn, & Maercker, 2013), even in terms of the devel-opment of a strong therapeutic relationship (e.g., Klein et al.,2009). It is recognised that this approach has limitations requir-ing management (e.g., requires computer access, language andcomputer skills, close monitoring of patient safety and privacy;Hadjistavropoulos et al., 2011). However, therapist-assistedICBT also has many advantages over traditional face-to-facetherapy. For example, it offers greater convenience and privacyfor patients, often involves more active engagement of patientsin their own care (Andersson, 2010), takes significantly lesstime to deliver than traditional face-to-face therapy (e.g., Klein
This article was published Online First September 1, 2014.Heather D. Hadjistavropoulos, Nicole Alberts, and Marcie Nugent,
Department of Psychology, University of Regina; Gregory Marchildon,Graduate School of Public Policy, University of Regina.
This work was supported by funding awarded to Heather D. Hadjistav-ropoulos by the Canadian Institutes of Health Research (Grants 101526,293379), the Saskatchewan Health Research Foundation, and Rx & DHealth Research Foundation. Initial program materials used by the OnlineTherapy Unit for Service, Education, and Research at the University ofRegina were licensed from Anxiety Online at Swinburne University ofTechnology in Melbourne, Australia through Drs. David Austin and BrittKlein. Recent program materials were obtained from Drs. Nick Titov andBlake Dear through a collaboration agreement with the eCentreClinic atMacquarie University. We would like to extend our thanks to the staff,students, and faculty associated with the University of Regina OnlineTherapy Unit. We also acknowledge the contributions of mental healthproviders and administrators from the Cypress, Five Hills, ReginaQu’Appelle, Saskatoon and Sun Country Health Regions and administra-tors from Saskatchewan Health.
Correspondence concerning this article should be addressed to HeatherD. Hadjistavropoulos, Department of Psychology, University of Regina,3737 Wascana Parkway, Regina, SK, Canada S4S 0A2. E-mail: [email protected]
Canadian Psychology / Psychologie canadienne © 2014 Canadian Psychological Association2014, Vol. 55, No. 4, 303–311 0708-5591/14/$12.00 http://dx.doi.org/10.1037/a0037716
303

et al., 2009), and can be offered as an initial step in stepped-careprograms (Green & Iverson, 2009).
Given the multiple benefits of, and the research evidence sup-porting ICBT, the Online Therapy Unit for Service Education andResearch (henceforth, the Online Therapy Unit, or simply the Unit;www.onlinetherapyuser.ca) was created at the University of Re-gina. The primary goal of the Unit is to improve patient access toevidenced-based care for depression and anxiety in Saskatchewan.As suggested by its title, the Unit supports service delivery, edu-cation of providers, and research related to ICBT. In this paper, wedescribe (a) how the unit is organized, funded and situated withinthe mental health system in Saskatchewan; (b) the web applicationthat was developed to support the delivery of ICBT in Saskatch-ewan; (c) the patient experience of ICBT from screening throughtreatment; (d) the provider experience of ICBT from training todelivery; (e) utilization of the service to date, as well as patient andprovider feedback on ICBT; and (f) recent and future directions forthe Unit stemming from our initial experiences of offering ICBT.Given the absence of similar units in Canada, information pertain-ing to the organisation and management of the Unit in Saskatch-ewan is of likely value to those who have a similar interest in usingthe Internet to improve access to psychological services.
Organisation
The Online Therapy Unit is based out of the Department ofPsychology at the University of Regina and led by first author.Several researchers from psychology, social work, computer sci-ence, and public policy at the University of Regina have alsocontributed to the development and operation of the Unit. Inaddition, several administrators involved in overseeing mentalhealth services within Saskatchewan have been involved in thedevelopment and operation of the Unit. Specifically, these re-searchers and administrators have worked together to secure ex-ternal funding for the Unit (further details provided below) andhave met regularly (ranging from biannual to quarterly) to discussthe ongoing operation of the Unit. The mission of the Unit, as setby the group, is to develop, manage, and research a web applica-tion that mental health providers and students working in varioussettings in Saskatchewan can use to deliver therapist-assistedICBT to individuals with depression and anxiety. The initial aim ofthe Unit was to provide services to individuals in four regionalhealth authorities covering most of southern Saskatchewan (i.e.,Cypress, Five Hills, Regina Qu’Appelle, and Sun Country HealthRegions), but this has gradually expanded to all residents ofSaskatchewan. The Unit is staffed by a full-time coordinator,part-time web developer, and part-time student assistants who areall central to the day-to-day operations of the Unit.
A previously published paper by our group outlines the processesinvolved in establishing the Online Therapy Unit (Hadjistavropouloset al., 2011). In brief, we began by developing the necessary ICBTweb application (see below for more information pertaining to theapplication). Following a review of the existing literature, we thenconcurrently developed policies and procedures for how to deliverICBT (e.g., screening, informed consent, provider credentials,training, supervision, record keeping). Community mental healthproviders (psychologists and social workers) and graduate studentswere subsequently trained in ICBT. Once these components werein place, we began to advertise the Unit, screen patients to deter-
mine their eligibility for ICBT, and assign them to be treated bytrained community mental health providers or graduate studentsunder supervision.
Funding for the Unit was initially provided by a Partnerships forHealth Systems Improvement grant awarded by the CanadianInstitutes of Health Research and the Saskatchewan Health Re-search Foundation; this particular grant competition is designed tosupport teams of researchers and decision makers undertakinghealth research that will strengthen the Canadian health system.This grant provided $500,000 in funding and supported the oper-ation of the Unit from approximately January 2010 until Septem-ber 2013. The majority of funding went toward salaries for thecoordinator, web developer, and student assistants (!$354,000).Additional funding was needed for computers and local serversupport (!$63,000); a 3-year license for three ICBT programs fordepression, anxiety, and panic ($45,000 " $5,000 # 3 programs #3 years); day-to-day operational expenses (!$8,000 for officeexpenses); as well as meeting and travel expenses related to thecollaborative nature of the project ($30,000).
In terms of ongoing funding, we have secured further funding(!$708,000) from the Canadian Institutes of Health Research, theSaskatchewan Health Research Foundation and the Rx & D HealthResearch Foundation to support the Unit for an additional threeyears (June 2013 until June 2016). The majority of funding will beused for personnel ($626,000 for the coordinator, web developer,student assistants). The remaining funds will be used for day-to-day operational expenses ($12,000 for office expenses, advertis-ing), knowledge exchange ($75,000 for travel, meetings, dissem-ination costs), and technology ($7,000 for software, server costs,computers). It should be noted that community mental healthproviders who deliver ICBT are paid by community mental healthclinics and not by the Unit.
Web Application
The development of the web application that would allow forthe delivery of ICBT was an expectedly crucial component toestablishing the Unit. The web application was designed and ismanaged by students and staff at the University of Regina; it ishosted on a dedicated virtual server in a secure environment at theUniversity of Regina. Patients and providers require usernamesand passwords to access the server that hosts the web application.Once patients and providers are logged onto the server, they canaccess ICBT program materials. Once logged on, patients andproviders can also communicate using an internal messaging sys-tem on the server. This messaging system increases security byensuring that emails are not exchanged over the Internet. Whenproviders are logged on, the web application also allows them totrack patient use of the ICBT programs, examine outcome mea-sures completed by patients, make contact notes related to care(e.g., phone calls), and review documents that support the deliveryof ICBT (e.g., the policy and procedures manual). All informationstored on the secure server located at the University of Regina isencrypted using a strong industry-standard encryption algorithm(AES-256).
In terms of ICBT program content, during the first phase offunding, the Online Therapy Unit offered patients ICBT for de-pression, generalised anxiety, or panic. All three ICBT programswere licensed from Swinburne University of Technology in Mel-
304 HADJISTAVROPOULOS, ALBERTS, NUGENT, AND MARCHILDON
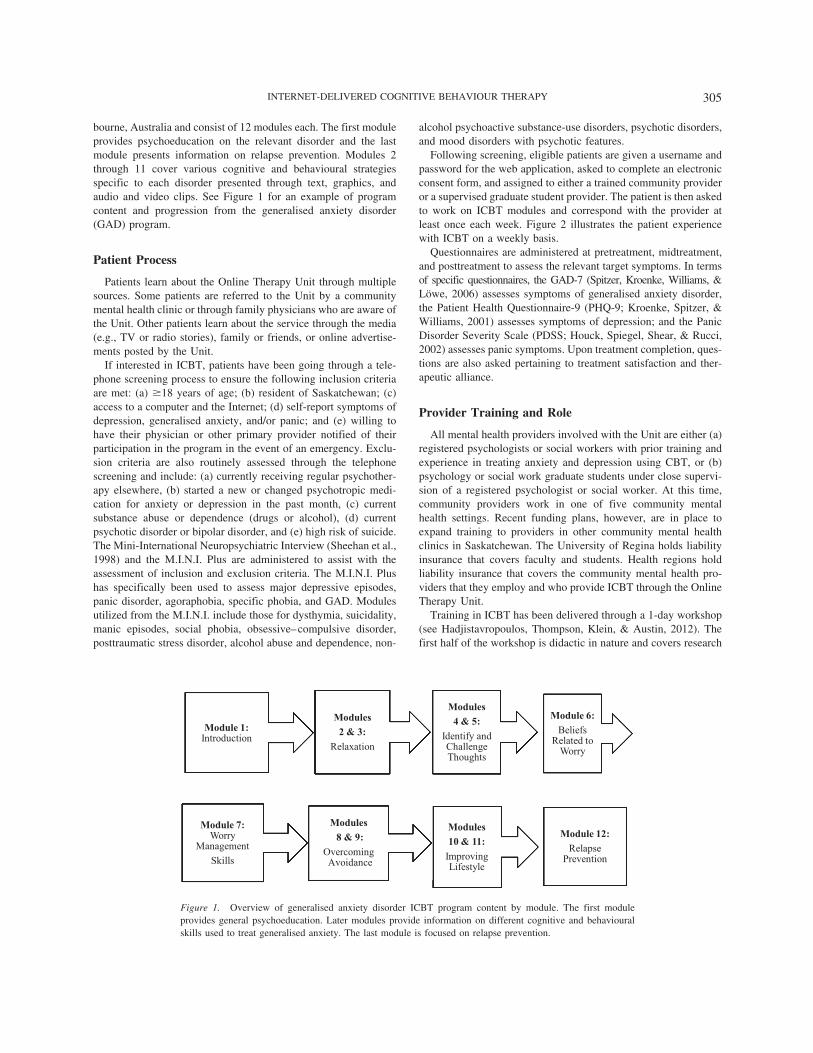
bourne, Australia and consist of 12 modules each. The first moduleprovides psychoeducation on the relevant disorder and the lastmodule presents information on relapse prevention. Modules 2through 11 cover various cognitive and behavioural strategiesspecific to each disorder presented through text, graphics, andaudio and video clips. See Figure 1 for an example of programcontent and progression from the generalised anxiety disorder(GAD) program.
Patient Process
Patients learn about the Online Therapy Unit through multiplesources. Some patients are referred to the Unit by a communitymental health clinic or through family physicians who are aware ofthe Unit. Other patients learn about the service through the media(e.g., TV or radio stories), family or friends, or online advertise-ments posted by the Unit.
If interested in ICBT, patients have been going through a tele-phone screening process to ensure the following inclusion criteriaare met: (a) !18 years of age; (b) resident of Saskatchewan; (c)access to a computer and the Internet; (d) self-report symptoms ofdepression, generalised anxiety, and/or panic; and (e) willing tohave their physician or other primary provider notified of theirparticipation in the program in the event of an emergency. Exclu-sion criteria are also routinely assessed through the telephonescreening and include: (a) currently receiving regular psychother-apy elsewhere, (b) started a new or changed psychotropic medi-cation for anxiety or depression in the past month, (c) currentsubstance abuse or dependence (drugs or alcohol), (d) currentpsychotic disorder or bipolar disorder, and (e) high risk of suicide.The Mini-International Neuropsychiatric Interview (Sheehan et al.,1998) and the M.I.N.I. Plus are administered to assist with theassessment of inclusion and exclusion criteria. The M.I.N.I. Plushas specifically been used to assess major depressive episodes,panic disorder, agoraphobia, specific phobia, and GAD. Modulesutilized from the M.I.N.I. include those for dysthymia, suicidality,manic episodes, social phobia, obsessive–compulsive disorder,posttraumatic stress disorder, alcohol abuse and dependence, non-
alcohol psychoactive substance-use disorders, psychotic disorders,and mood disorders with psychotic features.
Following screening, eligible patients are given a username andpassword for the web application, asked to complete an electronicconsent form, and assigned to either a trained community provideror a supervised graduate student provider. The patient is then askedto work on ICBT modules and correspond with the provider atleast once each week. Figure 2 illustrates the patient experiencewith ICBT on a weekly basis.
Questionnaires are administered at pretreatment, midtreatment,and posttreatment to assess the relevant target symptoms. In termsof specific questionnaires, the GAD-7 (Spitzer, Kroenke, Williams, &Löwe, 2006) assesses symptoms of generalised anxiety disorder,the Patient Health Questionnaire-9 (PHQ-9; Kroenke, Spitzer, &Williams, 2001) assesses symptoms of depression; and the PanicDisorder Severity Scale (PDSS; Houck, Spiegel, Shear, & Rucci,2002) assesses panic symptoms. Upon treatment completion, ques-tions are also asked pertaining to treatment satisfaction and ther-apeutic alliance.
Provider Training and Role
All mental health providers involved with the Unit are either (a)registered psychologists or social workers with prior training andexperience in treating anxiety and depression using CBT, or (b)psychology or social work graduate students under close supervi-sion of a registered psychologist or social worker. At this time,community providers work in one of five community mentalhealth settings. Recent funding plans, however, are in place toexpand training to providers in other community mental healthclinics in Saskatchewan. The University of Regina holds liabilityinsurance that covers faculty and students. Health regions holdliability insurance that covers the community mental health pro-viders that they employ and who provide ICBT through the OnlineTherapy Unit.
Training in ICBT has been delivered through a 1-day workshop(see Hadjistavropoulos, Thompson, Klein, & Austin, 2012). Thefirst half of the workshop is didactic in nature and covers research
Module 1: Introduction
Modules 2 & 3:
Relaxation
Modules 4 & 5:
Identify and Challenge Thoughts
Module 6:Beliefs
Related to Worry
Module 7: Worry
ManagementSkills
Modules 8 & 9:
Overcoming Avoidance
Modules 10 & 11:
Improving Lifestyle
Module 12: Relapse
Prevention
Figure 1. Overview of generalised anxiety disorder ICBT program content by module. The first moduleprovides general psychoeducation. Later modules provide information on different cognitive and behaviouralskills used to treat generalised anxiety. The last module is focused on relapse prevention.
305INTERNET-DELIVERED COGNITIVE BEHAVIOUR THERAPY

on the efficacy of ICBT as well as ethical and professional issuesrelated to its delivery. Attention, for instance, is given to theguidelines for psychologists providing psychological services viaelectronic media that have been produced by the Canadian Psy-chological Association (CPA, 2013). The second half of the work-shop is experiential in nature and involves reviewing the use of theweb application as well as practicing responding to patient emails.Within these emails, providers are given the following generalguidelines: (a) provide support and encourage patients to workthrough the program, (b) answer questions, (c) offer assistance inapplying cognitive and behavioural treatment strategies, and (d)highlight self-efficacy.
A key component of training is supporting providers in how toaddress high-risk situations when delivering ICBT, such as in-
creased risk for suicide. Providers are reminded that, as withface-to-face therapy, patients receiving ICBT services can becomeat risk of suicide even if risk at the time of screening was assessedas low. If this occurs, providers are instructed to (a) consult withthe Unit coordinator, (b) call the patient by telephone immediatelyupon learning of the threat to assess the level of risk, (c) take actionconsistent with the level of threat assessed (e.g., immediate highthreat requires call to emergency services), and (d) document theirassessments and the actions taken.
Following training, providers are required to sign an agreementwith the Unit indicating that they will (a) seek supervision whenthey have questions or difficulties arise (e.g., patient crisis, lack ofprogress, nonresponsiveness, therapeutic impasse); (b) providepatients with information on their credentials; (c) maintain confi-
Patient Weekly Role
CompleteCheck-In
ReviewModule Content
CompleteHomework
Email Therapist
Therapist Weekly Role
Review Patient
Progress
Review Emails from
Patient
Email Answering Questions,
Encouraging Patient and
Assisting with Application of
Strategies
Telephone Call if
Patient Not Using or Having
Difficulties with
Program
Document Service
ESTIMATED TIME : 15-30 MINUTES
Figure 2. Patient and provider weekly roles in ICBT. The figure illustrates the tasks that patients and providersengage in on a weekly basis when receiving/providing ICBT.
306 HADJISTAVROPOULOS, ALBERTS, NUGENT, AND MARCHILDON
dentiality of information and professional boundaries with pa-tients; and (d) monitor, provide guidance (e.g., email or phone),and document patient progress on a weekly basis. Graduate stu-dents sign a similar agreement, but supervision is more involved,with all emails reviewed before being sent to patients. As students’skills advance, supervision is gradually reduced to periodic emailreview and requests for assistance as needed. With both mentalhealth providers and graduate students, the Unit coordinator reg-ularly monitors the delivery of ICBT to ensure that emails are sentand recommendations for ICBT are followed.
In terms of documentation, a health record is created for eachpatient who is screened and offered ICBT. This health recordconsists of the consent form, summary of screening, patient andprovider weekly emails, letters to physicians or other providers,and contact notes made by the provider. Figure 2 summarizes theprovider’s role in the delivery of ICBT.
Utilization and Feedback
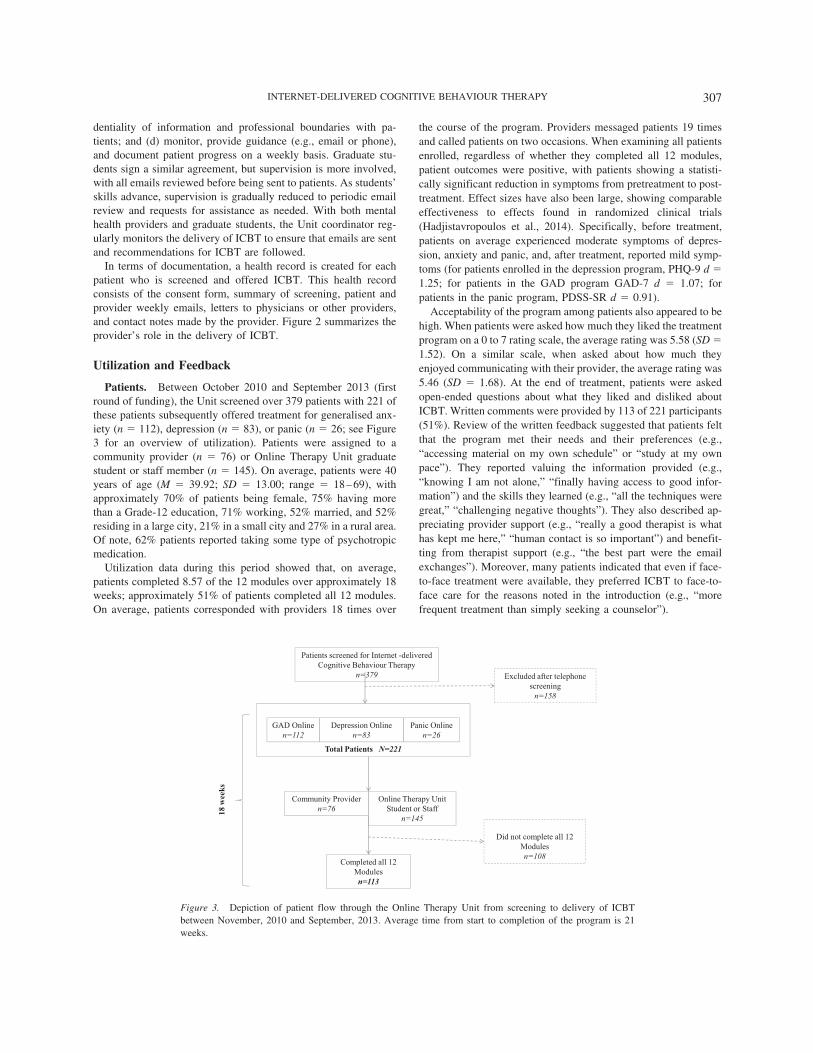
Patients. Between October 2010 and September 2013 (firstround of funding), the Unit screened over 379 patients with 221 ofthese patients subsequently offered treatment for generalised anx-iety (n ! 112), depression (n ! 83), or panic (n ! 26; see Figure3 for an overview of utilization). Patients were assigned to acommunity provider (n ! 76) or Online Therapy Unit graduatestudent or staff member (n ! 145). On average, patients were 40years of age (M ! 39.92; SD ! 13.00; range ! 18–69), withapproximately 70% of patients being female, 75% having morethan a Grade-12 education, 71% working, 52% married, and 52%residing in a large city, 21% in a small city and 27% in a rural area.Of note, 62% patients reported taking some type of psychotropicmedication.
Utilization data during this period showed that, on average,patients completed 8.57 of the 12 modules over approximately 18weeks; approximately 51% of patients completed all 12 modules.On average, patients corresponded with providers 18 times over
the course of the program. Providers messaged patients 19 timesand called patients on two occasions. When examining all patientsenrolled, regardless of whether they completed all 12 modules,patient outcomes were positive, with patients showing a statisti-cally significant reduction in symptoms from pretreatment to post-treatment. Effect sizes have also been large, showing comparableeffectiveness to effects found in randomized clinical trials(Hadjistavropoulos et al., 2014). Specifically, before treatment,patients on average experienced moderate symptoms of depres-sion, anxiety and panic, and, after treatment, reported mild symp-toms (for patients enrolled in the depression program, PHQ-9 d !1.25; for patients in the GAD program GAD-7 d ! 1.07; forpatients in the panic program, PDSS-SR d ! 0.91).
Acceptability of the program among patients also appeared to behigh. When patients were asked how much they liked the treatmentprogram on a 0 to 7 rating scale, the average rating was 5.58 (SD !1.52). On a similar scale, when asked about how much theyenjoyed communicating with their provider, the average rating was5.46 (SD ! 1.68). At the end of treatment, patients were askedopen-ended questions about what they liked and disliked aboutICBT. Written comments were provided by 113 of 221 participants(51%). Review of the written feedback suggested that patients feltthat the program met their needs and their preferences (e.g.,“accessing material on my own schedule” or “study at my ownpace”). They reported valuing the information provided (e.g.,“knowing I am not alone,” “finally having access to good infor-mation”) and the skills they learned (e.g., “all the techniques weregreat,” “challenging negative thoughts”). They also described ap-preciating provider support (e.g., “really a good therapist is whathas kept me here,” “human contact is so important”) and benefit-ting from therapist support (e.g., “the best part were the emailexchanges”). Moreover, many patients indicated that even if face-to-face treatment were available, they preferred ICBT to face-to-face care for the reasons noted in the introduction (e.g., “morefrequent treatment than simply seeking a counselor”).
Patients screened for Internet -deliveredCognitive Behaviour Therapy
n=379 Excluded after telephone screeningn=158
GAD Onlinen=112
Depression Onlinen=83
Total Patients N=221
Panic Onlinen=26
Community Providern=76
Online Therapy UnitStudent or Staff
n=145
Did not complete all 12 Modulesn=108
Completed all 12 Modulesn=113
18 w
eeks
Figure 3. Depiction of patient flow through the Online Therapy Unit from screening to delivery of ICBTbetween November, 2010 and September, 2013. Average time from start to completion of the program is 21weeks.
307INTERNET-DELIVERED COGNITIVE BEHAVIOUR THERAPY

In terms of negative feedback the most common feedbackrelated to aspects of CBT itself more than ICBT, such as complet-ing recommended homework (e.g., “the exercises after each mod-ule”) and not liking some of the strategies presented (e.g., “worryexposure,” “producing panic sensations”). In terms of negativefeedback about ICBT, some patients felt that the treatment re-quired significant motivation (e.g.,“ trying to find motivation to doprogram weekly”), and, that it was difficult to open up and writeabout concerns to the therapist (e.g., “having to put everything intowords”). Other times, patients reported wanting more contact (e.g.,“communication only being weekly” or “not having immediatefeedback”) or face-to-face contact (e.g., “no face-to-face interac-tion”) with therapists. Some patients also provided negative feed-back about the generality of information (e.g., “the fact that it wasgeneralised”). Of relevance, many patients could not identify lim-itations to share (e.g., “can’t really think of a worst part!”).
It should be noted that approximately 4% of patients whoscreened as eligible for ICBT and were offered treatment, did notstart treatment. In addition, 47% of patients who started ICBT didnot complete all 12 modules. What is interesting about thesepatients, however, is that they remained engaged for a substantialperiod of time prior to termination. On average, these patientscompleted 5 modules, and logged into the website 26 times overthe course of 15 weeks. They messaged or checked-in with thetherapist, on average, 12 times and received 16 messages and twophone calls from the therapist. In 33% of cases, the patient did notprovide an explanation for their dropout; other times, however,patients specified that their symptoms had improved (32%), theyhad gained access to other services (10%), or had other problemsthat were not appropriate for ICBT (e.g., alcohol; 14%). It was rarefor patients to directly report that they did not find the servicehelpful (4%) or their availability to participate had changed (6%).
Providers. During the first phase of the project, we offeredtraining in ICBT to 44 students who were under supervision and 49registered community mental health providers. Of these providers,28 students and 27 community providers delivered ICBT to thepatients described above. Not all those who were trained were ableto or appropriate to deliver ICBT (e.g., insufficient training inCBT, health regions allocated certain providers to deliver ICBT).To ensure quality and reduce risk, we have restricted the deliveryof ICBT to registered mental health providers employed by healthauthorities and graduate students supervised by registered provid-ers working in the Unit. However, there is some literature tosuggest that this level of education may not be necessary, astechnician-assisted treatment has been shown to result in clinicallysignificant improvements that appear to be similar to those foundwith therapist-assisted ICBT (Robinson et al., 2010; Titov et al.,2010).
Semistructured interviews were conducted with 11 of the 27community providers (provider interviews were discontinued oncethere was saturation of information provided) to explore theirperceptions of ICBT after delivering ICBT to at least one patient.Analysis of the transcripts revealed mental health providers, eventhose who were initially skeptical of ICBT, reported positiveattitudes toward ICBT. Providers reported feeling surprised bytheir ability to help patients attain skills to improve depression andanxiety and to develop a relationship with patients over the Inter-net. They described finding it particularly helpful to have outcomemeasures available to assess patient progress. Additional benefits
reported by providers included that the program content improvedtheir knowledge of CBT, they enjoyed having variety in theirpractice, and that they often referred to the content when workingwith patients attending face-to-face CBT. Reflecting the positiveattitudes toward ICBT, providers highlighted how they would liketo see ICBT used for other populations (e.g., chronic pain, addic-tions) and expressed a desire to continue to deliver ICBT.
Although provider experiences were positive, challenges wereidentified that offer the opportunity for future development of theUnit. Providers noted that many patients do not need or want tocomplete all modules and that many patients have both anxiety anddepression, thus suggesting that a transdiagnostic program de-signed to treat depression and anxiety would be helpful. Providersnoted that it often took patients a substantial period of time tocomplete all 12 modules. They also noted that although the weeklyamount of time they spent working with patients was shorter thanif patients were attending face-to-face therapy (e.g., 15–30 mincompared with 1 hr), the duration of the service over time in weekswas greater than the time spent with many patients in face-to-facetherapy. Providers highlighted that it would be ideal if fewermodules were provided and if the modules focused on core skillswith the potential to offer additional resources only if patientsrequired these resources. Several providers also indicated that itwould be preferable if ICBT could not only be offered as analternative form of care, but also as an adjunct to care or a stepdown from care for patients following initial stabilization. Provid-ers shared that they generally had no difficulties working withpatients, but noted that they would benefit from learning additionalstrategies for working with patients who are less expressivethrough email. They reported a desire to have a mixed approach inworking with some patients (e.g., phone, email and in person).While some providers found it straightforward to integrate ICBTinto their workloads (e.g., they would email their patients when-ever they had time during the day), other providers noted that theyneeded further guidance around how to incorporate ICBT withintheir workload (e.g., they felt they needed a specific time duringthe day to send emails). All providers noted that as they gainedexperience, they required less time to email their patients. Theyalso noted, however, that there was significant variability in timeto respond to patients, with some emails taking little time tocompose (e.g., 15 min) and other emails taking considerablylonger (e.g., 30 min–1 hr).
In terms of a learning experience, providers noted that it takestime to learn to deliver ICBT. They highlighted that learning wasfacilitated by having: (a) an initial training workshop; (b) Unit staffavailable to answer questions and provide ongoing support; (c)clear policies and procedures for delivery; (d) strong ICBT pro-gram content; and (e) support from regional health authority man-agers, who were eager for the providers to learn and deliver ICBTas part of their workload.
Recent and Future Directions
As we have gained experience in the delivery of ICBT, we haveidentified several important directions for the Online TherapyUnit. Recent developments funded by a second Partnership forHealth Systems Improvement grant are described below.
Patient education. Given that ICBT is novel to patients, wehave found that substantial time is needed to educate patients about
308 HADJISTAVROPOULOS, ALBERTS, NUGENT, AND MARCHILDON

this form of treatment. This education occurs over the telephone,requires considerable time (20 to 30 min per patient), is inconve-nient for patients, and runs the risk of patients having an incom-plete understanding of ICBT. We are currently exploring whetheran ICBT presentation posted on the Internet can engage patients inICBT. We are currently inviting individuals who phone the OnlineTherapy Unit to review and evaluate an ICBT audio visual pre-sentation (incorporating text, images). This presentation includesinformation about the (a) the Online Therapy Unit, (b) the natureof ICBT, (c) treatment inclusion/exclusion criteria as assessedthrough screening, (d) benefits and limitations of ICBT, (e) pace oftreatment and frequency of communication, (f) provider qualifica-tions, (g) outcome assessment and ethics approval, (h) security ofinformation and limits to confidentiality, and (i) steps to be takenin the event of an emergency.
Online screening. Our experience in offering ICBT suggeststhat it is critical to screen patients to ensure those who need moreintensive face-to-face services are not inappropriately offeredICBT. This screening is necessary, but it is also a significantbarrier/bottleneck to ICBT when conducted exclusively over thetelephone, as the patient and screener must identify a 1-hr periodduring business hours when the patient is comfortable answeringpersonal questions. It has often taken several weeks to arrange thisscreening appointment. The need to collect extensive diagnosticinformation prior to delivery of low intensity service such as ICBThas also been questioned in the literature (Andersson & Hedman,2013).
At the present time, although we continue to use the sameinclusion and exclusion criteria as described above, we have re-cently developed and are evaluating a standardized online screen-ing process that allows patients to more efficiently complete as-pects of the screening. More specifically, prior to conducting thetelephone screening, patients complete brief background questionsonline (e.g., age, comfort with writing and computers, brief self-reported symptoms, mental health history). This online screeningis then followed by a telephone interview to clarify any responsesand determine eligibility for treatment. During the telephone in-terview, we assess risk for suicide with the Suicide BehaviourQuestionnaire Revised (Osman et al., 2001) and questions of amore sensitive nature are also asked at this time (e.g., questionsabout drug and alcohol abuse). Use of this new streamlined screen-ing process is underway and will be evaluated in terms of bothpatient and provider satisfaction with the process as well as anydifficulties that arise in assessing the appropriateness of patientsfor ICBT using this process.
Transdiagnostic ICBT. Review of patient feedback duringour first phase of funding suggested that, though patients arebenefitting significantly from ICBT, only 50% of them completedall 12 modules. Many patients also desired a shorter program inwhich they could select materials specific to their needs. Providerfeedback also indicated that providers felt a shorter program wouldbe preferable given that it took considerably more time to deliverICBT than providers had available due to competing demands ontheir time. Given this feedback from patients and providers, wehave recently been offering a 5-module transdiagnostic ICBTprogram developed by the eCentreClinic at Macquarie University(available at no cost through a research agreement). The transdi-agnostic ICBT program takes patients approximately 8 weeks tocomplete and treats both anxiety and depression in the same
protocol through the provision of core CBT skills that are relevantto both target disorders. Transdiagnostic ICBT covers education,cognitive, behavioural, and physical strategies, as well as relapseprevention over the course of 5 modules. Past research has shownthat, compared with a waiting-list condition, those receiving trans-diagnostic ICBT improve on measures of anxiety, depression, anddisability, with medium to large effect sizes identified and out-comes maintained at follow-up (Dear et al., 2011; Titov et al.,2011). Similar to our past programs, patients review modules andcomplete assigned exercises during the week. To supplement the 5modules, this particular program also offers extra resources (down-loadable PDFs) about various topics (e.g., problem solving, im-proving sleep). In addition, patients receive automated emailsreminding them to complete modules and notifying them when anew module is available thus reducing some burden on providersand increasing patient engagement. This program also offers con-siderable direction to providers in terms of content to include inweekly emails.
Our interest is to explore whether we will obtain similar out-comes when offering transdiagnostic ICBT in Saskatchewan. Weare also interested in better understanding factors that predictpatient outcomes, as this will provide information on how trans-diagnostic ICBT can be improved. Potential predictors includepatient background (e.g., age, sex, education, urban vs. rural res-idence, use of psychotropic medications), provider background(e.g., professional background, community provider vs. student),and patient–provider engagement (e.g., amount, frequency, andnature of contact).
Other conditions. Since developing the Unit, several studentsassociated with the Unit have initiated research to explore theeffectiveness of ICBT with specific high-needs populations, suchas older adults with generalised anxiety, women reporting post-partum depression, and patients experiencing depression and anx-iety following cancer treatment. Given the success we have dem-onstrated in treating depression and anxiety with ICBT, managersof the community mental health clinics involved with the Unithave expressed interest in expanding the scope of the Unit to otherdisorders, for which evidence suggests ICBT can be effective, suchas posttraumatic stress disorder (e.g., Klein et al., 2010), healthanxiety (e.g., Hedman et al., 2013), obsessive–compulsive disor-der (e.g., Wootton, Titov, Dear, Spence, & Kemp, 2011), addic-tions (Gainsbury & Blaszczynski, 2011), and chronic pain (e.g.,Dear et al., 2013).
Web-application development. Our current web applicationwas developed in 2010. Already, we see the need to update theweb application to include some additional features to facilitate thedelivery of ICBT. Recently, we began to include automated emailsto patients to remind them to work on the program on a weeklybasis, thus reducing burden on providers and increasing patientengagement. Ideally, in the future, we will incorporate emailtemplates for providers to work from, which could increase con-sistency in emails sent to patients within each module or whencertain issues arise (e.g., failure to log on). In turn, these featureswould likely increase provider efficiency, and allow for largerpatient caseloads. A further desirable addition would be the inte-gration of other methods of communication within the service tothe extent that these are requested by patients (e.g., texting, videoconferencing).
309INTERNET-DELIVERED COGNITIVE BEHAVIOUR THERAPY

Permanent funding. Following the completion of our currentgrant funding in 2016, it will be necessary to secure additionalfunding to support the Unit either through future grants, directprovincial funding, or indirect provincial funding from regionalhealth authorities or community partnerships. To scale up ICBTwithin Saskatchewan, ICBT will ultimately need to become part ofthe permanent basket of health-care services provided to residentsof Saskatchewan. The data on effectiveness already presenteddemonstrate the extent to which ICBT has the potential to reduceat least some Medicare and other health-care expenditures by theprovincial government. An increasing interest in offering patient-centered care (e.g., care is offered to patients in a way that takesinto account their preferences) in Saskatchewan provides incentivefor the government to fund ICBT. Future study of the cost effec-tiveness of ICBT in Saskatchewan, similar to studies that havebeen conducted on ICBT in other countries (Hedman, Ljotsson, &Lindefors, 2012), could provide additional information that wouldaid in the future development of ICBT in Saskatchewan.
Beyond a provincial Unit, it is possible that a national collab-orative ICBT unit could be formed to increase access to ICBT. Anational unit could include a common web application that wouldbe accessible to trained providers across the country. A collabor-ative such as this, although more challenging from an organisa-tional perspective, would increase access to ICBT across Canadaand also allow for cost sharing across provinces. With recentattention to eMental health by the Mental Health Commission ofCanada (Mental Health Commission of Canada, 2013), a nationalcollaborative Unit seems increasingly feasible.
Conclusion
In conclusion, services provided through the Online TherapyUnit are proving to significantly improve access to CBT amongindividuals in Saskatchewan who have depression and anxiety.The Unit has become essential to offering ICBT within Saskatch-ewan. It not only provides access to a web application, but alsotrains providers and students in best practices and coordinates thiscare provincially. Moreover, it monitors service quality, ensuringthe safe delivery of ICBT. Given increasing interest in Internet-based assessment and treatment, the Unit serves as a valuablemodel for mental health providers and administrators who aim toimprove access to evidence-based psychological services.
Résumé
La dépression et l’anxiété sont des troubles courants, mais les gensqui en souffrent restent souvent sans traitement. La thérapiecognitivo-comportementale offerte en ligne (TCCL) par desthérapeutes s’est révélée efficace pour ces conditions et peut aidera aplanir les obstacles a l’obtention de soins de santé mentale (parex., en raison de la distance ou du manque de temps). Dans le cadrede ce type de thérapie, les patients obtiennent en ligne des docu-ments sur la thérapie comportementale. De plus, les thérapeutesleur offrent un soutien et une orientation, le plus souvent au moyende courriels ou par téléphone une fois par semaine. En dépit despreuves et des avantages en faveur de la TCCL, très peu de patientsau Canada y ont accès. Dans cet article, nous décrivons la OnlineTherapy Unit for Service, Education and Research qui a été établiea l’Université de Regina dans le but d’améliorer l’accès a la TCCL.
Grâce a des fonds provenant de sources nationales et provinciales,l’unité a créé une application Web pour les services de TCCL pourle traitement de la dépression et de l’anxiété, a établi des politiqueset des procédures pour la prestation du traitement, et a formédes thérapeutes a cette fin. Elle coordonne la prestation de cesservices au sein de divers environnements en Saskatchewan.L’article décrit l’organisation de l’unité ainsi que sa façon detravailler en collaboration avec des cliniques communautaires desanté mentale afin d’améliorer l’accès a la TCCL. Il décrit aussil’application Web et le procédé thérapeutique, a la fois du point devue du patient et du thérapeute. Il précise l’utilisation des servicespar le patient et le fournisseur, et présente les commentairesobtenus sur la TCCL et les prochaines étapes pour l’unité. À cejour, l’unité a eu des répercussions positives en élargissant l’accèsa des services psychologiques en Saskatchewan et elle a le poten-tiel de contribuer, a titre de source d’information, a des initiativesdans d’autres provinces.
Mots-clés : en ligne, thérapeute, thérapie cognitivo-comportementale,anxiété.
References
Andersson, G. (2010). The promise and pitfalls of the internet for cognitivebehavioral therapy. BMC Medicine, 8, 82. doi:10.1186/1741-7015-8-82
Andersson, G., & Hedman, E. (2013). Effectiveness of guided Internet-based cognitive behavior therapy in regular clinical settings. Verhalten-stherapie, 23, 140–148. doi:10.1159/000354779
Andrews, G., Cuijpers, P., Craske, M. G., McEvoy, P., & Titov, N. (2010).Computer therapy for the anxiety and depressive disorders is effective,acceptable and practical health care: A meta-analysis. PLoS One, 5,e13196. doi:10.1371/journal.pone.0013196
Canadian Psychological Association. (2013). Ethical guidelines for psy-chologists providing psychological services via electronic media.Retrieved from http://www.cpa.ca/aboutcpa/committees/ethics/psychserviceselectronically/
Collins, K. A., Westra, H. A., Dozois, D. J., & Burns, D. D. (2004). Gapsin accessing treatment for anxiety and depression: Challenges for thedelivery of care. Clinical Psychology Review, 24, 583–616. doi:10.1016/j.cpr.2004.06.001
Cuijpers, P., Donker, T., van Straten, A., Li, J., & Andersson, G. (2010).Is guided self-help as effective as face-to-face psychotherapy for depres-sion and anxiety disorders? A systematic review and meta-analysis ofcomparative outcome studies. Psychological Medicine, 40, 1943–1957.doi:10.1017/S0033291710000772
Dear, B. F., Titov, N., Perry, K. N., Johnston, L., Wootton, B. M., Terides,M. D., . . . Hudson, J. L. (2013). The Pain Course: A randomisedcontrolled trial of a clinician-guided Internet-delivered cognitive behav-iour therapy program for managing chronic pain and emotional well-being. Pain, 154, 942–950.
Dear, B. F., Titov, N., Schwencke, G., Andrews, G., Johnston, L., Craske,M. G., . . . McEvoy, P. (2011). An open trial of a brief transdiagnosticinternet treatment for anxiety and depression. Behaviour Research andTherapy, 49, 830–837. doi:10.1016/j.brat.2011.09.007
Gainsbury, S., & Blaszczynski, A. (2011). A systematic review of Internet-based therapy for the treatment of addictions. Clinical Psychology Re-view, 31, 490–498. doi:10.1016/j.cpr.2010.11.007
Green, K. E., & Iverson, K. M. (2009). Computerized cognitive-behavioraltherapy in a stepped care model of treatment. Professional Psychology:Research and Practice, 40, 96–103. doi:10.1037/a0012847
Hadjistavropoulos, H. D., Pugh, N. E., Nugent, M., Hesser, H., Andersson,G., Ivanov, M., . . . Austin, D. W. (2014). Therapist-assisted internet-delivered cognitive behaviour therapy for depression and anxiety: Trans-
310 HADJISTAVROPOULOS, ALBERTS, NUGENT, AND MARCHILDON

lating evidence into clinical practice. Manuscript submitted for publica-tion.
Hadjistavropoulos, H. D., Thompson, M., Ivanov, M., Drost, C., Butz,C. J., Klein, B., . . . Austin, D. W. (2011). Considerations in thedevelopment of a therapist-assisted Internet cognitive behavior therapyservice. Professional Psychology: Research and Practice, 42, 463–471.doi:10.1037/a0026176
Hadjistavropoulos, H. D., Thompson, M. J., Klein, B., & Austin, D. W.(2012). Dissemination of therapist-assisted internet cognitive behaviourtherapy: Development and open pilot study of a workshop. CognitiveBehaviour Therapy, 41, 230–240. doi:10.1080/16506073.2011.645550
Hedman, E., Andersson, E., Lindefors, N., Andersson, G., Ruck, C., &Ljotsson, B. (2013). Cost-effectiveness and long-term effectiveness ofInternet-based cognitive behaviour therapy for severe health anxiety.Psychological Medicine, 43, 363–374. doi:10.1017/S0033291712001079
Hedman, E., Ljotsson, B., & Lindefors, N. (2012). Cognitive behaviortherapy via the Internet: A systematic review of applications, clinicalefficacy and cost-effectiveness. Expert Review of Pharmacoeconomics& Outcomes Research, 12, 745–764. doi:10.1586/erp.12.67
Houck, P. R., Spiegel, D. A., Shear, M. K., & Rucci, P. (2002). Reliabilityof the self-report version of the Panic Disorder Severity Scale. Depres-sion and Anxiety, 15(4), 183–185. doi:10.1002/da.10049
Klein, B., Austin, D., Pier, C., Kiropoulos, L., Shandley, K., Mitchell, J.,. . . Ciechomski, K. (2009). Internet-based treatment for panic disorder:Does frequency of therapist contact make a difference? Cognitive Be-haviour Therapy, 38, 100–113. doi:10.1080/16506070802561132
Kroenke, K., Spitzer, R. L., & Williams, J. B. (2001). The PHQ-9: Validityof a brief depression severity measure. Journal of General InternalMedicine, 16(9), 606–613.
Mental Health Commission of Canada. (2014). E-mental health in Canada:Transforming the mental health system using technology. Retrieved fromMental Health Commission website: http://www.mentalhealthcommission.ca/English/system/files/private/document/MHCC_E-Mental_Health-Briefing_Document_ENG.pdf
Osman, A., Bagge, C. L., Gutierrez, P. M., Konick, L. C., Kopper, B. A.,& Barrios, F. X. (2001). The Suicidal Behaviors Questionnaire–Revised(SBQ-R): Validation with clinical and nonclinical samples. Assessment,8, 443–454.
Pearson, C., Janz, T., & Ali, J. (2013). Health at a glance: Mental andsubstance-use disorders in Canada (Catologue No. 82–624-X). Re-trieved from http://www.statcan.gc.ca/pub/82-624-x/2013001/article/11855-eng.htm
Robinson, E., Titov, N., Andrews, G., McIntyre, K., Schwencke, G., &Solley, K. (2010). Internet treatment for generalized anxiety disorder: Arandomized controlled trial comparing clinician vs. technician assis-tance. PLoS One, 5, e10942. doi:10.1371/journal.pone.0010942
Sheehan, D., Lecrubier, Y., Sheehan, K. H., Amorim, P., Janavas, J.,Weiller, E., . . . Dunbar, G. C. (1998). The Mini-International Neuro-psychiatric Interview (M.I.N.I): the development and validation of astructured diagnostic interview for DSM-IV and ICD-10. Journal ofClinical Psychiatry, 59, 22–33.
Spek, V., Cuijpers, P., Nyklicek, I., Riper, H., Keyzer, J., & Pop, V. (2007).Internet-based cognitive behaviour therapy for symptoms of depressionand anxiety: A meta-analysis. Psychological Medicine, 37, 319–328.doi:10.1017/S0033291706008944
Spitzer, R. L., Kroenke, K., Williams, J. B., & Lowe, B. (2006). A briefmeasure for assessing generalized anxiety disorder: The GAD-7. Ar-chives of Internal Medicine, 166(10), 1092–1097. doi:10.1001/archinte.166.10.1092
Sunderland, A., & Findlay, L. C. (2013). Perceived need for mental healthcare in Canada: Results from the 2012 Canadian Community HealthSurvey–Mental Health. (Catalogue No. 82–003-X). Retrieved from http://www.statcan.gc.ca/pub/82-003-x/2013009/article/11863-eng.htm
Titov, N., Andrews, G., Davies, M., McIntyre, K., Robinson, E., & Solley,K. (2010). Internet treatment for depression: A randomized controlledtrial comparing clinician vs. technician assistance. PLoS One, 5, e10939.doi:10.1371/journal.pone.0010939
Titov, N., Dear, B. F., Schwencke, G., Andrews, G., Johnston, L., Craske,M. G., & McEvoy, P. (2011). Transdiagnostic internet treatment foranxiety and depression: A randomised controlled trial. Behaviour Re-search and Therapy, 49, 441–452. doi:10.1016/j.brat.2011.03.007
Wagner, B., Horn, A. B., & Maercker, A. (2013). Internet-based versusface-to-face cognitive-behavioral intervention for depression: A ran-domized controlled non-inferiority trial. Journal of Affective Disorders.Advance online publication. doi:10.1016/j.jad.2013.06.032
Wootton, B. M., Titov, N., Dear, B. F., Spence, J., & Kemp, A. (2011). Theacceptability of Internet-based treatment and characteristics of an adultsample with obsessive–compulsive disorder: An Internet survey. PLoSOne, 6, e20548. doi:10.1371/journal.pone.0020548
Received October 26, 2013Revision received May 21, 2014
Accepted May 22, 2014 !
311INTERNET-DELIVERED COGNITIVE BEHAVIOUR THERAPY

Copyright of Canadian Psychology is the property of Canadian Psychological Association andits content may not be copied or emailed to multiple sites or posted to a listserv without thecopyright holder's express written permission. However, users may print, download, or emailarticles for individual use.