
Pulmonary Vein Stenosis Complicating Catheter Ablation of Focal Atrial Fibrillation

Original Study
Comparison of themodified Seldinger and through-the-needle jugular catheter placement techniquesin the dogErin Portillo, MS, DVM, Andrew Mackin, BVMS, DVSc, DACVIM, P. K. Hendrix, DVM, PhD,
DACVA, Carolyn Boyle, PhD and Lisa Chrestman, CVT
Abstract
Objectives:
� To compare the ease of placement of central intravenous catheters in the dog using 2 techniques: themodified Seldinger jugular catheter placement technique and the through-the-needle jugular catheterplacement technique.
� To evaluate the ease and effectivness of teaching the 2 jugular catheter placement techniques.
� To determine the utility of a synthetic vascular access model for teaching the 2 techniques to veterinarystudents.
Design: Students were taught 2 jugular catheter placement techniques using a synthetic jugular venipuncturemodel and were then observed placing catheters using each technique in live dogs enrolled in a terminalsurgery laboratory. Time taken for catheter placement, success or failure of catheter insertion, indicators ofcatheter viability (time required for blood to be collected through the catheter and for fluid to flow through thecatheter), and complications associated with catheter insertion (hematoma presence/size post-mortem) wereobjectively evaluated by the authors, and ease of catheter placement was subjectively evaluated by thestudents.
Setting: Surgical techniques laboratory in a veterinary teaching hospital.
Animals: Dogs destined for a terminal student surgery laboratory (n 5 35).
Intervention: Jugular catheterization.
Measurements and main results: Catheter placement was successful for 27/35 (77.1%) first attempts on a livedog with the modified Seldinger technique, and for 26/35 (74.3%) first attempts on a live dog with thethrough-the-needle technique. The modified Seldinger technique took significantly longer (mean 452 seconds)than the through-the-needle technique (mean 273 seconds). There was no significant difference in time takento aspirate 5 mL of blood through catheters placed by either technique. Time required to flow 25 mL of fluidthrough the catheter was slightly longer for the modified Seldinger technique (mean 133 seconds) than for thethrough-the-needle technique (mean 113 seconds). Post-mortem hematomas were detected at 26/26 (100%)of through-the-needle insertion sites and at 24/27 (89%) of modified Seldinger insertion sites. Hematomadiameter at the through-the-needle insertion site (mean 2.2 cm) was significantly greater than at the modifiedSeldinger insertion site (mean 1.1 cm). Student assessments of the comparable difficulties of the 2 jugularcatheter placement techniques were not significantly different, and both techniques were assessed to be onlyslightly more difficult than placement of a cephalic catheter.
Conclusions: Jugular catheter placement by either the modified Seldinger or through-the-needle techniquecan be relatively easily mastered by entry-level veterinarians. Hematoma formation is common with bothtechniques. The teaching of jugular catheter placement is facilitated by the use of a synthetic jugularvenipuncture model.
(J Vet Emerg Crit Care 2006; 16(2): 88–95) doi: 10.1111/j.1476-4431.2005.00147.x
Keywords: central line, complications, jugular catheter, j-wire, vascular access model
& Veterinary Emergency and Critical Care Society 200588
Address correspondence and reprint requests to:Dr. Erin Portillo, MS DVM, Iowa State University, College of VeterinaryMedicine, Veterinary Teaching Hospital, Ames, IA 50011.E-mail: [email protected]
From the College of Veterinary Medicine, Iowa State University, Ames, IA(Portillo), and Mississippi State University, Mississippi State, MS (Mackin,Hendrix, Boyle, Chrestman).
Journal of Veterinary Emergencyand Critical Care 16(2) 2006, pp 88–95
doi:10.1111/j.1476-4431.2005.00147.x

Introduction
The central intravenous (IV) catheter is a valuable tool
that is increasingly utilized in referral and emergency
veterinary practice. Central lines are extremely useful
for collection of multiple blood samples, measurement
of central venous pressures, rapid fluid delivery, andadministration of hyperosmolar fluids such as total
parenteral nutrition solutions. Central lines, by defini-
tion, must terminate within a body cavity (either the
thoracic or abdominal cavity), typically within the cra-
nial or caudal vena cava.1
There are many different techniques available for
placement of central venous catheters. Two commonly
used percutaneous insertion techniques are the through-the-needle technique and the modified Seldinger tech-
nique.2 The through-the-needle technique involves
placement of a large bore needle into a jugular or sap-
henous vein, with the catheter then threaded through
the needle to terminate in a body cavity. The modified
Seldinger technique involves placement of an intro-
ducer needle or catheter into an accessible vein.
A guide wire used as a place-holder is then threadedthrough the introducer and subsequently a catheter
is passed over the guide wire to terminate in a body
cavity.
In the authors’ experience, central lines tend to be
under-utilized by many veterinary practitioners. Po-
tential impediments to the routine use of central lines
include a lack of familiarity with catheter placement
techniques, the perception that central catheter place-ment is a difficult or advanced procedure, and discom-
fort with the perceived risks associated with catheter
placement. Under-utilization of central lines leads to
the neglect of diagnostically and therapeutically im-
portant procedures such as the measurement of central
venous pressure and the administration of total paren-
teral nutrition. Practitioner utilization of central lines
may be enhanced by a greater awareness of catheterinsertion techniques and familiarity with the risks and
benefits associated with catheter placement.
The immediate objective of this study was to evaluate
the ability to teach 2 standard central catheter place-
ment techniques in dogs, and to objectively compare
the ease of placement of central IV catheters using the
two techniques. This study was designed to teach jun-
ior and senior veterinary students, as models for naiveveterinarians, the through-the-needle and modified Sel-
dinger catheter placement techniques on a synthetic
jugular venipuncture model, and to then observe the
students placing catheters using each technique in live
dogs enrolled in a terminal surgery lab. Time taken for
catheter placement, success or failure of catheter inser-
tion, indicators of catheter viability and complications
associated with catheter insertion were objectively eval-
uated by the authors, and ease of catheter placement
was subjectively evaluated by the students. The overall
goal of the project was to demonstrate, in as clear and
practical a fashion as possible, whether the adoption of
one or both central catheter placement procedures was
feasible for practitioners with limited or no experiencewith either technique.
Materials and Methods
Junior and senior veterinary students at Mississippi
State University, College of Veterinary Medicine were
recruited to participate in the study. Students were first
taught the through-the-needle and modified Seldinger
catheter placement techniques on a synthetic jugularvenipuncture modela (Figure 1) in a 1 or 2 hour teach-
ing laboratory. Each student was given written instruc-
tions describing the steps of both procedures, and both
techniques were then demonstrated to the students.
The students were allowed to practice catheter place-
ment using both techniques on the synthetic model
until they were comfortable with the procedures. Then,
in the main study, scheduled days to weeks after theteaching laboratory, the students were evaluated using
both techniques in live anesthetized dogs. The students
were taught and then evaluated by 2 of the authors,
(E.P. and L.C.), both of whom have had several years
experience placing and teaching both catheter place-
ment techniques in the university setting.
Instructions for catheter placement techniques
The through-the-needle catheter placement technique
utilizes a single lumen 16 gauge, 8 inch Intravets
cath-
Figure 1: Vascular access training model used to teach students
jugular catheter placement techniques.
& Veterinary Emergency and Critical Care Society 2005, doi: 10.1111/j.1476-4431.2005.00147.x 89
Comparison of seldinger and catheter placement techniques in dog

Figure 2: (a) Through-the-needle technique basic equipment: 14-gauge 2 in. introducer needle, 16-gauge 8 inch catheter with
protective sleeve, and adjacent plastic needle guard. (b) Through-the-needle technique demonstrated on vascular access training
model. A 14-gauge introducer needle is advanced through the skin into the vein until a fluid flashback is seen. (c) A 16-gauge 8 in.
catheter is then advanced through the needle to the needle hub. (d) The outer plastic sleeve is then removed from the needle hub. (e)
The stylet is removed from the center of the catheter. (f) A T-port is attached to the catheter and needle is backed out of the vein (in the
anesthetized dogs utilized in the study, a luer-lock injection cap was used rather than a T-port). (g) A needle guard is secured around
the needle to prevent shearing. (h) Once the needle guard is secure, it is glued to the skin with tissue adhesive.
& Veterinary Emergency and Critical Care Society 2005, doi: 10.1111/j.1476-4431.2005.00147.x90
E. Portillo et al.
eterb (Figures 2a–h). The desired length of the catheter
is predetermined by measuring from the approximate
jugular insertion site to the first intercostal space. The
through-the-needle catheter is maintained within its
sterile protective sheath, although the attachment of the
sheath to the needle hub is loosened in order to facil-
itate later removal. Once the jugular vein is identified,the skin is nicked over the vein with a #15 scalpel blade
to allow easy placement of the catheter. An introducer
needle (14 g, 200) is inserted aborally into the jugular
vein. Once blood is observed in the catheter lumen (a
flashback), the catheter is advanced aborally through
the introducer needle into the vein to its predetermined
location. The protective sleeve is removed exposing the
hub of the catheter and the central stylet, and the cen-
tral stylet is removed and discarded. The introducerneedle is then removed from the skin by backing the
needle out of the vein while still over the catheter. An
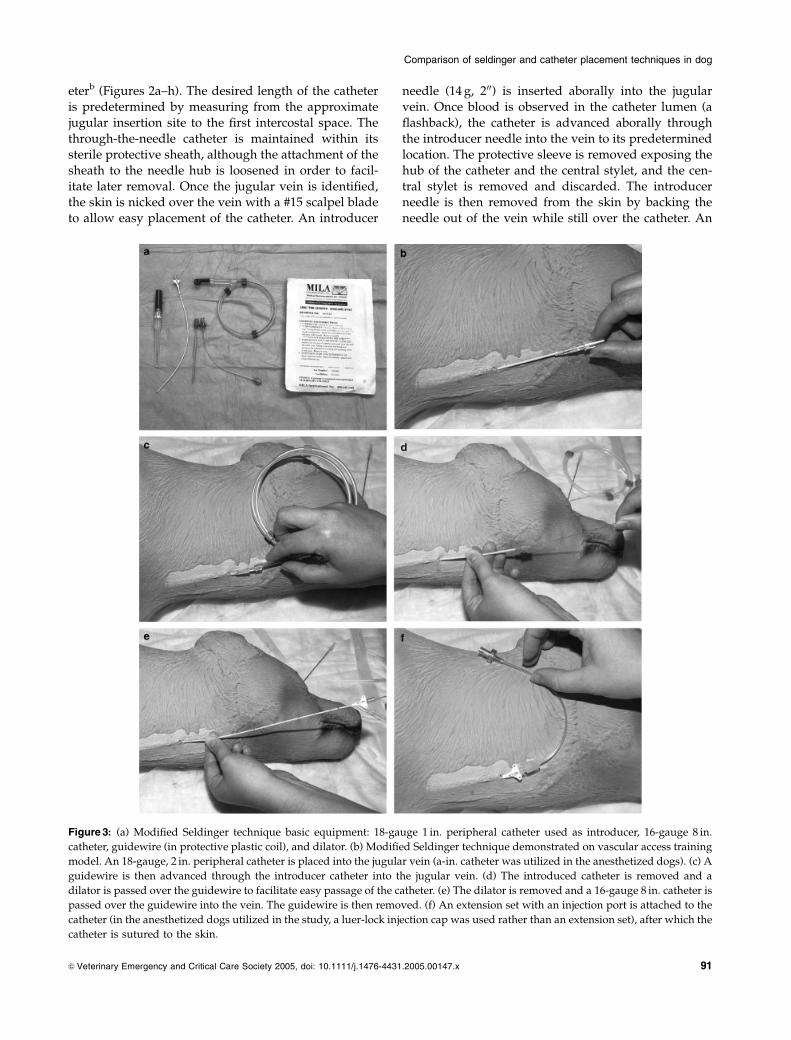
Figure 3: (a) Modified Seldinger technique basic equipment: 18-gauge 1 in. peripheral catheter used as introducer, 16-gauge 8 in.
catheter, guidewire (in protective plastic coil), and dilator. (b) Modified Seldinger technique demonstrated on vascular access training
model. An 18-gauge, 2 in. peripheral catheter is placed into the jugular vein (a-in. catheter was utilized in the anesthetized dogs). (c) A
guidewire is then advanced through the introducer catheter into the jugular vein. (d) The introduced catheter is removed and a
dilator is passed over the guidewire to facilitate easy passage of the catheter. (e) The dilator is removed and a 16-gauge 8 in. catheter is
passed over the guidewire into the vein. The guidewire is then removed. (f) An extension set with an injection port is attached to the
catheter (in the anesthetized dogs utilized in the study, a luer-lock injection cap was used rather than an extension set), after which the
catheter is sutured to the skin.
& Veterinary Emergency and Critical Care Society 2005, doi: 10.1111/j.1476-4431.2005.00147.x 91
Comparison of seldinger and catheter placement techniques in dog

Intravets
needle guard is applied to cover the needle
and protect the skin. Skin adhesivec is then used to
secure the catheter hub to the needle hub and the nee-
dle to the needle guard to prevent rotational movement
or accidental disconnection. A luer-lock injection cap is
secured to the hub of the Intravets
catheter, and the
catheter is flushed with heparinized saline. The Intra-vet
s
catheter and needle guard are secured to the skin
using skin adhesive.c
The modified Seldinger catheter placement technique
utilizes a single lumen 16 gauge, 8 inch Milas
catheterd
(Figures 3a–f). The desired length of the catheter is
predetermined by measuring from the approximate
jugular insertion site to the first intercostal space, and
the skin is nicked over the jugular vein with a #15scalpel blade. An 18 g, 100 over-the-needle peripheral
cathetere is advanced aborally into the jugular vein as
the introducer, and the stylet is removed. A 20 g J-wiref
is passed aborally through the peripheral catheter. The
peripheral introducer catheter is removed, so that only
the guide wire remains in the vein as a place-holder. A
dilatorg is passed over the J-wire to ensure sufficient
dilation to enable easy passage of the Milas
jugularcatheter. The dilator is then removed, and the Mila
s
catheter is passed over the J-wire to its predetermined
location. The J-wire is then removed. A luer-lock injec-
tion cap is secured to the hub of the Milas
catheter, and
the catheter is flushed with heparinized saline. The
Milas
catheter is then sutured to the skin via suture
anchors built into the catheter hub.
Once the students were comfortable using both cath-eter placement techniques in the synthetic model, they
were asked to place a jugular catheter by each tech-
nique in anesthetized dogs (weight range from 10 to
23 kg) immediately prior to a Mississippi State Univer-
sity Institutional Animal Care and Use Committee ap-
proved terminal surgery laboratory. After anesthetic
induction, intubation, and connection to inhalant an-
esthesia, the dogs were placed in lateral recumbency.The dogs’ necks were clipped and surgically prepared
using Operands
scrub and solution.h An assistant dig-
itally occluded the jugular vein at the level of the tho-
racic inlet. The students, while wearing latex gloves,
attempted to place a jugular catheter by one technique
in one jugular vein. The dog was then turned on its
other side, and the students attempted to place a sec-
ond jugular catheter via the second technique in theother jugular vein. The side (left versus right) and the
order (through-the-needle versus modified Seldinger
technique) in which the catheters were placed were
randomized.
Following catheter placement, the students were
asked to score the jugular catheters for ease of place-
ment based on a 1–8 scale comparing jugular catheter
placement to peripheral (cephalic) catheter placement
(Appendix 1). The students also subjectively reported
which catheter technique seemed the least difficult.
During the live dog catheter placement laboratory,
the authors timed all catheter placements starting from
the time the skin was nicked until the time the last
suture was tied or the catheter was glued to the skin.Students were aware that they were being timed. Place-
ment was considered to be a failure if the catheter could
not be placed during the original venipuncture attempt.
Immediately after successful placement, the catheters
were first evaluated for ease of blood sample collection
by timing how long it took to aspirate 5 mL of blood
through the catheter, and then for ease of fluid flow by
timing 25 mL of fluid (0.9% salinei) running into thecatheter through a measured fluid administration
chamberj and 10 drops/mL IV line.k The fluid admin-
istration chamber was positioned at a standard height
above the animal (3600), and contained a standard vol-
ume of fluid (25 mL). The dogs were then moved onto a
student terminal surgery teaching laboratory for a va-
riety of surgical procedures, after which they were eu-
thanized. After the terminal surgery laboratory wasconcluded (approximately 4 hours after catheter inser-
tion), a limited necropsy was performed to determine
the degree of trauma at the insertion site.
After completion of the project, an additional survey
of the students was taken to obtain more information
about past catheter placement experience. Students
were asked to estimate the number of cephalic and
jugular catheters that they had successfully placed priorto enrolment in this study. Students were also asked
whether they were right handed or left handed.
The effect of catheter placement technique on ease of
use and on effectiveness variables was analyzed using
the paired t-test. The residuals from this model were
examined using frequency histograms and normal
probability plots to validate the normality assumption.
The clinical importance of observed differences wasassessed using confidence intervals.3 All calculations
were performed using SASs
Version 8.2;l all statistical
tests used the 0.05 level of significance.
Results
Results of the study are summarized in Table 1. In the
introductory catheter placement teaching laboratory,
most students were comfortable placing the cathetersvia both techniques after practicing once or twice on the
model. Jugular catheter placement was attempted in 35
anesthetized dogs by 35 junior and senior veterinary
students, leading to 35 attempts at the through-
the-needle technique and 35 attempts at the modified
Seldinger technique. Catheter placement was unsuc-
& Veterinary Emergency and Critical Care Society 2005, doi: 10.1111/j.1476-4431.2005.00147.x92
E. Portillo et al.

cessful for 9/35 (25.7%) attempts with the through-the-needle technique, and for 8/35 (22.3%) with the mod-
ified Seldinger technique. Two students were unsuc-
cessful at both techniques. Failure of accurate
venipuncture because of inability to enter the vein af-
ter skin puncture was subjectively assessed by the stu-
dents and authors to be the cause of failure in all failed
catheterization attempts.
Catheter placement by the modified Seldinger tech-nique took significantly longer (mean 452 seconds, me-
dian 455 seconds, range 267–690 seconds) than catheter
placement by the through-the-needle technique (mean
273 seconds, median 188 seconds, range 103–858 sec-
onds). The mean insertion time using the through-
the-needle technique was about 210 seconds less, with a
95% confidence interval of 144–275 seconds less, than
the insertion time using the modified Seldinger tech-nique. There was no significant difference in time taken
to aspirate 5 mL of blood through catheters placed by
the through-the-needle technique (mean 8 seconds, me-
dian 5 seconds, range 2–44 seconds) and catheters
placed by the modified Seldinger technique (mean 13
seconds, median 8 seconds, range 3–64 seconds). The
mean time taken to aspirate 5 mL of blood through
catheters placed by the through-the-needle techniquewas about 4 seconds less, with a 95% confidence inter-
val of 10 seconds less to 2 seconds greater, than through
catheters placed by the modified Seldinger technique.
Time to flow 25 mL of fluid through the catheter was
significantly longer for the modified Seldinger tech-
nique (mean 133 seconds, median 131, range 69–186
seconds) than for the through-the-needle technique
(mean 114 seconds, median 116 seconds, range 43–194
seconds). The mean time to flow 25 mL of fluid throughthe catheter using the through-the-needle technique
was about 20 seconds less, with a 95% confidence in-
terval of 3–36 seconds less, than using the modified
Seldinger technique.
The mean subjective score for ease of placement for
the Seldinger technique was 4.39, and for the through-
the-needle technique was 4.74, where a score of 4 in-
dicated a level of difficulty comparable with that asso-ciated with the placement of a cephalic catheter, and a
score of higher than 4 indicated a procedure that was
more difficult than the placement of a cephalic catheter.
Student scores for difficulty for the through-the-needle
and modified Seldinger techniques were not signifi-
cantly different. The mean difficulty score for the
through-the-needle technique was about 0.4 greater,
with a 95% confidence interval of 0.5 less to 1.2 greater,than the mean difficulty score for the modified Se-
ldinger technique. Of the 35 students participating in
the project, 19 (54%) of the students thought the mod-
ified Seldinger technique was easier to place and 16
(46%) thought the through-the-needle technique was
easier.
Post-mortem dissection of successful catheter inser-
tion sites revealed local hematoma formation at 26/26(100%) of through-the-needle insertion sites and at 24/
27 (89%) of modified Seldinger insertion sites. Hemat-
oma diameter at the through-the-needle insertion site
(mean 2.2 cm, range 0.5–5.5 cm) was significantly great-
er than at the modified Seldinger insertion site (mean
1.1 cm, range 0–2.0 cm). The mean hematoma diameter
with the through-the-needle technique was 1.4 cm larg-
er, with a 95% confidence interval of 0.9–2.0 cm larger,
Table 1: Results of catheter placement study
Variable
Modified Seldinger technique Through-the-needle technique Difference
P-valuen
Mean
(1SD) Median n
Mean
(1SD) Median n Mean
95% CI
(lower limit,
upper limit)
Successful catheter
placement
27/35
(77.7%)
26/35 (74.3%)
Time for catheter
placement (seconds)
27 452.4 � 96.1 455 26 273.2 � 179.1 188 20 209.4 (144.0, 274.8) o.0001n
Time to flow 25 mL
of fluid (seconds)
27 133.3 � 23.6 131 26 113.6 � 32.0 116 20 19.5 (3.1, 35.8) 0.0222n
Time to aspirate 5 mL
of blood (seconds)
27 12.8 � 13.1 8 26 8.5 � 9.2 5 20 4.2 (� 1.9, 10.2) 0.1705
Scores for difficulty of
placement
35 4.4 � 1.8 35 4.7 � 1.8 35 �0.4 (� 1.2, 0.5) 0.3872
Easiest technique 19/35 (54%) 16/35 (46%)
Hematoma present 23/26 (88.5%) 25/25 (100%)
Hematoma diameter (cm) 26 1.1 � 0.6 25 2.2 � 1.3 19 �1.4 (� 2.0, � 0.9) o.0001n
Note: SD, standard deviation; CI, confidence interval.nSignificant difference between the two groups (0.05 level of significance).
& Veterinary Emergency and Critical Care Society 2005, doi: 10.1111/j.1476-4431.2005.00147.x 93
Comparison of seldinger and catheter placement techniques in dog

than the hematoma diameter formed with the modified
Seldinger technique. No other gross evidence of signif-
icant vascular or tissue trauma was detected.
All 32 students that responded to the post-study sur-
vey reported that they had successfully placed cephalic
catheters on multiple occasions prior to this study. The
estimated number of successful placements rangedfrom 5 to 600, with a median of 42.5 placements. Only 1
student, however, had previously attempted to place a
jugular catheter, and this attempt was unsuccessful. The
majority of the students were right handed (28/32 stu-
dents). Interestingly, of the 4 left-handed students, 3
(75%) thought the through-the-needle catheter was eas-
ier to place, whereas 17 (61%) of the right-handed stu-
dents thought the modified Seldinger was easier toplace. This observation, however, was not statistically
significant.
Discussion
In addition to performing similar functions as periph-
eral lines, central lines are valuable tools for rapid fluid
resuscitation, evaluating central venous pressure in pa-
tients receiving fluid therapy (particularly in patientssubject to volume overload, including those with con-
ditions such as renal failure or congestive heart failure),
for obtaining multiple blood samples from patients re-
quiring regular monitoring of blood samples (i.e., dur-
ing the performance of a glucose curve in diabetic
patients), and for delivering IV hyperosmolar fluids
such as total parenteral nutrition solutions. Catheter
research in human medicine also suggests that, com-pared with peripheral lines, central lines can be left in
for a longer time period with limited risk.4 Many fac-
tors contribute to the need for a long-term vascular ac-
cess method, including a limited number of IV injection
sites, difficulties handling some animals, personnel
time, patient trauma associated with the placement
of multiple catheters, and complications associated
with the perivascular administration of some drugs be-cause of inadvertent dislodgement of the peripheral
catheter.5
The 2 different techniques for catheter placement de-
scribed in this paper come with some inherent advan-
tages and disadvantages. Compared with the modified
Seldinger technique, the through-the-needle technique
is faster and involves fewer steps, and the catheters
themselves are less expensive (Intravets
through-the-needle catheter cost is about $12, compared with $20 for
the Milas
single lumen catheter set used for the mod-
ified Seldinger technique). However, through-the-nee-
dle catheters are more difficult to secure to the animal
because of the cumbersome needle guard, and they are
only available with a single lumen. Catheters placed by
the modified Seldinger technique are easier to secure to
the animal via suture because, unlike in the through-
the-needle technique, there is no needle guard (which
can be difficult to secure). Furthermore, when using the
modified Seldinger technique, clinicians can potentially,
at a later date, re-insert the guide wire and exchange
catheters without the need for a second venipuncture inanother vein. In order to facilitate direct comparison
between techniques, our study used single lumen
catheters of comparable dimensions for each catheter
placement method. However, one significant clinical
advantage conferred by the use of the modified Se-
ldinger technique compared with the through-the-
needle technique is that multiple lumen (double, tri-
ple, or quadruple lumen) catheters can be inserted us-ing an identical technique. The ability to use multiple
lumen catheters can significantly improve the quality of
patient care in those patients that require the use of a
single dedicated line (i.e., for administering parenteral
nutrition) while simultaneously requiring IV fluid ther-
apy, IV medications, through-the-catheter blood sample
collection, or measurement of central venous pressure.
Disadvantages of the modified Seldinger technique in-clude increased catheter cost, and a longer placement
time requiring more steps and equipment (such as ster-
ile gloves, sterile drapes, and sutures). In this study, it
took students on average more than 3 minutes longer to
place catheters using the modified Seldinger technique
compared with the through-the-needle technique. Stu-
dents commented on the difficulty associated with han-
dling the long guide wire used in the modified Seldingertechnique. Many reported that the guide wire was cum-
bersome and found it difficult to maintain sterility.
This study revealed a significant difference in the
time it took to run fluid through the line for catheters
placed by the 2 different techniques. The time differ-
ence can be explained by the design of the catheters
used for the modified Seldinger technique. Although
the catheters used for both techniques were the samelength and gauge, there was decreased length of the
through-the-needle catheter in the animal because 200 of
the catheter remained in the introducer needle which
was backed out of the skin. Additionally, the Milas
catheters used in the modified Seldinger technique are
tapered slightly at the distal end of the catheter. The
slightly slower fluid flow observed through the cathe-
ters placed by the modified Seldinger technique, how-ever, is unlikely to be of clinical importance.
A significant finding in this study was the difference
in the size of hematomas formed at the catheter inser-
tion site for the 2 techniques. The through-the-needle
technique was associated with the formation of larger
hematomas than the modified Seldinger technique.
Hematoma formation may have been exacerbated by
& Veterinary Emergency and Critical Care Society 2005, doi: 10.1111/j.1476-4431.2005.00147.x94
E. Portillo et al.

the larger introducer needle used with the through-the-
needle technique.1 Once the introducer was removed in
the through-the-needle technique, a smaller gauge cath-
eter remains in the vein, possibly allowing for some
leakage of blood out of the vein at the catheter entry
site. Hematoma formation may also reflect the veni-
puncture skill of the students. Many students com-mented that it was easier to place the 100 18 g over-the-
needle catheter used for the modified Seldinger tech-
nique, and that the over-the-needle catheter seemed to
cause less trauma than the 200 14 g needle used for the
through-the-needle technique. The smaller introducer
needle used in the modified Seldinger technique may
be beneficial in reducing insertion-related hemorrhage,
especially in patients with abnormal hemostasis.Although the students involved in this study report-
ed some difficulties associated with learning to use the
2 jugular catheter placement techniques, most students
(approximately 75%) were able to competently place
the catheters on their first attempt in a live dog. None of
the junior and senior students enrolled in this study
had previously successfully placed a jugular catheter.
All students had, however, as part of their standardpreclinical and clinical training, previously placed ce-
phalic catheters in dogs. It is interesting to note that,
even on a first attempt, most students in this study
reported jugular catheter placement to be only slightly
more difficult than cephalic catheter placement. Both
jugular catheter placement techniques were subjective-
ly scored between 4 and 5, with 4 indicating the same
level of difficulty as cephalic catheter placement, and 5indicating slightly more difficulty.
This study also describes the use of a synthetic jug-
ular venipuncture model as a teaching aid. Prior train-
ing with the synthetic model enabled most students to
insert jugular catheters on their first attempt in a live
dog. The synthetic model may have potential as a
teaching tool that could serve to reduce the use of live
dogs for venipuncture training purposes, and furtherstudies that specifically evaluate the utility of this mod-
el are warranted.
Central venous catheters are an underutilized diag-
nostic and therapeutic tool in veterinary medicine. Our
study indicates that catheters inserted by either the
through-the-needle or the modified Seldinger tech-
niques are relatively easy to place. Furthermore, the
techniques can be readily learned by entry-level clini-
cians with limited clinical experience. Our study did
not compare the advantages and disadvantages associ-
ated with the long-term use of catheters placed by the 2
methods. A second phase of this study, currently underway, is evaluating the utility and complication rates
between the 2 techniques in clinic patients in the in-
tensive care setting.
Grant Support
This study was supported by the Mississippi State Uni-
versity, College of Veterinary Medicine Intern GrantFund and the Dr. Hugh G. Ward Memorial Chair Fund.
Footnotesa Vascular Access Training Model, UC Davis School of Veterinary
Medicine, Davis, CA.b Intracath, Becton Dickinson Vascular Access, Sandy, UT.c Mainstays
s
projects Superglue, Bentonville, AR.d MILA International Inc., Florence, KY.e Terumo Surflo
s
, Terumo Corporation, Tokyo, Japan.f J wire, MILA International Inc., Florence, KY.g Dilator, MILA International Inc., Florence, KY.h Operand, Aplicare Inc., Branford, CT.i 0.09% Saline, Abbott Laboratories, North Chicago, IL.j Baxter
s
Healthcare Corporation, Deerfield, IL.k Primary I.V. Set, Abbot Laboratories, North Chicago, IL.l SAS
s
is a registered trademark of the SAS Institute Inc., Cary, NC.
References
1. Beal MW, Hughes D. Vascular access: theory and techniques in thesmall animal emergency patient. Clin Tech Small Anim Pract 2000;15:101–109.
2. Valk WJC, Liem KD, Geven WB. Seldinger technique as an alter-native approach for percutaneous insertion of hydrophilic poly-urethane central venous catheters in newborns. J Parent Ent Nutr1995; 19:151–155.
3. Braitman LE. Confidence intervals assess both clinical significanceand statistical significance. Ann Intern Med 1991; 114(6):515–517.
4. Bregenzer T, Conen D, Sakmann P, et al. Is routine replacement ofperipheral intravenous catheters necessary? Arch Intern Med 1998;158:151–156.
5. Blaiset MA, Couto CG, Evans LK. Complications of indwelling,silastic central venous access catheters in dogs and cats. J Am AnimHosp Assoc 1995; 31:379–384.
Appendix 1
Subjective scoring system used by students toevaluate difficulty associated with jugular cathetertechniques
1 Extremely easy to place, much easier than a pe-
ripheral catheter
2 Moderately easier than a peripheral catheter
3 Slightly easier than a peripheral catheter
4 Same difficulty as a peripheral catheter5 Slightly more difficult than a peripheral catheter
6 Moderately more difficult than a peripheral cath-
eter
7 Extremely difficult to place, much more difficult
than a peripheral catheter
8 Impossible to place
& Veterinary Emergency and Critical Care Society 2005, doi: 10.1111/j.1476-4431.2005.00147.x 95
Comparison of seldinger and catheter placement techniques in dog
Copyright © 2022 FDOKUMEN




















