
Effectiveness of Management Strategies for Renal Artery Stenosis: A Systematic Review
Upload
independentCategory
view
0download
0
677
Pulmonary Vein Stenosis Complicating Catheter Ablation ofFocal Atrial Fibrillation
MAURICIO I. SCANAVACCA, M.D., LUIZ J. KAJITA. M.D.,MARCELO VIEIRA, M.D., and EDUARDO A. SOSA, M.D.
From the Heart Institute (InCor), University of SSo Paulo Medical Schotil, Sao Paulo, Brazil
P u l m o n a r y Vein Stenosis . Introduction: A recently described focal origin of atri»l hhrillution,mainly inside pulmonary veins., Is creating new perspectives for radiofrequency catheter ablation.However, pulmonary venous stenosis may occur witb uncertain clinical consequences. Tbis reportdescribes a veno-occlusive syndrome secondary to left pulmonary vein stenosis after radiofrequencycatbeter ablation.
Methods and Resi4Us: A 36-year-old man who experienced daily episodes of atrial fibrillation tbatwas refractory to antiarrbytbmic medication, including amiodarone, was enrolled in our focal atrialfibrillation radiofrequency catbeter ablation protocol. The left superior pulmonary vein was theearliest site mapped, and radiofrequency ablation was performed. Atrial fibrillation was interruptedand sinus rbythm rest<»red after one radiofrequency pulse Inside the left superior pulmonary vein.Atrial fibrillation recurred and a new procedure was performed in an attempt to isolate (26radiofreqtiency pulses around tbe ostium) tbe left superior pulmonary vein. Ten days later, tbepatient developed cbest pain and bentoptysis related to severe left superior and inferior pulmonaryveins stenosis. Balloon angioplasty of botb veins was followed by complete relief of symptoms after2 montbs of recurrent pulmonary symptoms. Tbe patient has been asymptomatic for 12 months,without antiarrhythmic drugs.
Conclusion: Multiple radiofrequency pulses applied inside tbe pulmonary veins ostia can inducesevere pulmonary venous stenosis and veno-occlusive pulmonary syndrome. (7 Cardiovasc Electro-physiol, Vol. II, pp. 677-6HI. Jtme 2000)
atrial fibriiiation, radiofrequency catheter ablation, pulmonary veno-occlusive syndrome
Introduction
Airial fibriUaiion originating fnim ectopic f(K'i situ-ated inside the pulmonary' veins was described recently,and a relatively simple focal ablative radiofrequencyprocedure can prevent it.s recurrence.' ' Allhtiugh theseresulls have opened new perspectives for managctnent ofatrial tibtillation. the .safety of radiofrequency abiation inthe pulmonary veins is unknown.'-^ This report deseribe.sa veno-Dcclusive pulmonary syndrome that was observedin a patient who underwent radiofrequency catheter ab-lation to treat focal atrial tibrillation situated in the leftsuperior pulmonary vein.
Case Report
A 36-year-old man with no structural heart disease,who had presented with occasional episodes of paroxy.s-
Address for correspondence: Mauricio I. Scanavacca, M.I>., Av. DrEndas de Carvalho Aguiar. 44-Cep: O.'S4O3.(HK), Sao Paulo. SP Brazil.Fax: 55-1 l-3069.'i3l2; E-mail: arrscanfe'incor.usp.br
Manuscript received 23 August 1999; Accepted for publication 10January 2000.
mal atrial fibrillalit)n during the past 10 years and dailyrecurrences in the past 2 years, was enrolled in the atrialfibrillation radiofrequency ablation protocol in our insti-tution.
The procedure was performed in June 1998. Thepatient was sedated with propofol, midazolam, andfentanyl. Sustained atrial librillation, tUicumented 12hours before the study, persisted during the entireprocedure. Three catheters were inserted into the rightfemoral vein. A decapolar catheter was positioned atthe lateral wall of the right atrium, an dctapolar cath-eter was inserted in the coronary sinus, and a 4-mtii tipquadripolar catheter was inserted in the left atrium viaa transseptal approach. An intravenous bolus of hep-arin .*>.{)()() IU was given, followed by continuousinfusion at a rale of 1.000 fU/hour.
Three transthoracic shocks (200 J) were delivered inan attempt to restore sintis rhythm, which otily persistedfora few seconds. With ihe catheter positioned in the leftsuperior pulmonary vein ostium, an electrogram occur-ring I(K) msec before the peripheral P wave could beobserved during the ectopie beat that reinitiated atrialfibrillation. A radiofrequency pulse at 60°C was deliv-

678 Journal of Cardiova.scular Electrophysiology Vol. 11. No. 6. June 2000
BWSclBCtcd: tl ColScIeettd 0 10 1Z51 BW Selected:"
Co<6S% hhp3WF MedPRF8000 H IFlofr Opt FR
10/21/199B 101241 BWSalvcird OCotSeivcira a
Figure 1. Transesophageal echocardiofiraphy showing seven' left superiur pubnoiujry vein (LSPV) steiio.si.s. A: Bidimensional echocardiographyshowing anatomic aspect of LSPV stenosis. B: Color Doppler showing high-velocity flow at the site of .stenosis. Pulsed-wave Doppler displayspreMem>tic blood flow velocities of 26.5 cm/s (C) and poststenoiic blood flow velocities (D) reaching 220 cin/s.
ered to that site, and sinus rhythm was restored after 20seconds. Contrast media was injected into the pulmonaryveins, suggesting a common ostium for superior and
Figure 2. Kiuliomtclide veiuilation-peijiisiim lung sain showing re-duced pattern in both ventilation and perjiision lo the left lung. Rightlung presents a normal aspect.
inferior left pulmonary veins. Twenty-four hours afterthe procedure, the patient had a new episode of atriultibrillation. He was discharged with propafenone 600nig/day. atenolol 50 mg/day. and aspirin 100 mg/day. Hewas free of symptoms for about 40 days, when dailyepisodes of atrial tibrillation recurred.
He was readmitted to the hospital for a new proce-dure, which was performed in October 1998. Sustainedatrial tibtillation was converted to sinus rhythm duringpositioning of the quadtipolar catheter inside the leftsuperior pultnonary vein ostium. No atrial ectopic beatswere observed, and sinus rhythm persisted after admin-istration of isoproterenol and adenosine. and pro-grammed atrial stimulation. A pulmonary venogram per-formed before the ablation did not show left superior[iiilinonary vein stenosis. Although the atrial tibrillationfocus was known to be situated in the left superiorpulmonary vein, there was no ectopic beat to allowmapping. Accordingly, we decided to isolate the leftsuperior pulmonary vein ostium. Electrophysiologicevaluation was based on atrial capture during pacinginside the left superior pulmonary vein. Despite deliveryof several radiofrequency pulses (26 applications, range54° to 64°C, for 17 to 60 sec) around und inside theeotnmon ostium of left pulmonary veins, atrial capture

Scanavacca et at. Pulmonarv Vein Stenosis 679
persisted and the procedure was interrupted. The patientwas discharged the next day with atenolol 50 mg/day andaspirin 100 mg/day.
Ten days later, he was readmitted to the hospitalbecause of ehest pain and hemoptysis. Physical exami-nation. ECG. and plain chest radiography revealed nor-mal findings. Fiberoptic bioncboscopic e.xaminationshowed bleeding within the bronchus related to the lin-gula. Ultrasound of the lower extremities disclosed noabnormalities. Spiral computer totnography showed nor-mal arterial Mow to the lungs, with no evidence of pul-monary thrt)nihoemboiism, but opacity in the area ofthe left lobe. Transesophageal echoeardiography (TEE)showed severe stenosis of the left superior pulmonaryvein. Doppler How veltKities proximal to the stenosiswere 26.5 cm/sec, with flow velocities reaching up to220 em/see distal to the stenosis (Fig. I).
Systemic anticoagulation was initiated with intrave-nous heparin. tbllowed by sodium warfarin. Chest painceased in 24 hours, but the hemoptysis lasted I weekafter anticoagulation. TEE repeated after 10 days showedthe same pattern of Doppler How veliKrities und pulmo-nary artery pressures estimated at 15/8 mmHg. Ambula-tory Holter analysis showed isolated atrJul preinaturebeats but no episodes of atrial tachycardia or tibrillation.The patient remained a.symptomatic for I month with
taking oral antieoagulatton (international normalized ra-tio between 2.0 and 3.0). when he again complained ofchest pain and hemoptysis. Chest X-ray showed a pul-monary infiltrate involving the left lung. Radionuclideventilation-perfusion lung sean detnonstrated a ditiiin-ished pattern uf ventilation and perfusion to the left lung(Fig. 2). The patient underwent pulmonary venous an-giography. which confirmed severe left superior pulmo-nary vein and left inferior pulmonary vein stenosis (Fig.3. left). Systolic, diastolic. and mean pulmonary arterialpressures were 25. 12. and 16 mmHg. respectively. Meanpulmonary capillary wedge pressure was 12 mmHg, andmean transstenotic gradient in the left superior pulmo-nary vein was 7 mmHg. Successful dilation of the ste-notic pulmonary veins was performed using 9-mnt andI2-mm balloons (Fig. 3. middle and right). The patienthas been asymptomatic for 12 months. He currently isnot taking antiarrhythmic drugs, und atriul librillation hasnot recurred. Control chest X-ray and tomographyshowed mild retraction of the left lung with librosismainly related to the lingula (Fig. 4).
Di.scussion
Following the observations suggesting a foeal mech-anism for atrial fibrillation involving pulmonary veins,'-^
PRE ANGIOPLASTY POST
Figure 3. Left pulmonary vein .ttenosis and angioplasty. Left columns (PRE) .show left superior pulmonaiy rein (LSPV) and left inferior pulmonaryvein lUPV) venography before angiopla.sty. Note enlargemeni of the vessels. Middle columns (ANGIOPIASTY) .\how pulmonary vein dilation. Rightcolumns (POST) .show normal venous flow and significant reduction of pulmonary vein diameter after angioplasty.
6S0 Journal of Cardiova-scular Electrophysiology Vol. 11. No. 6. June 2000
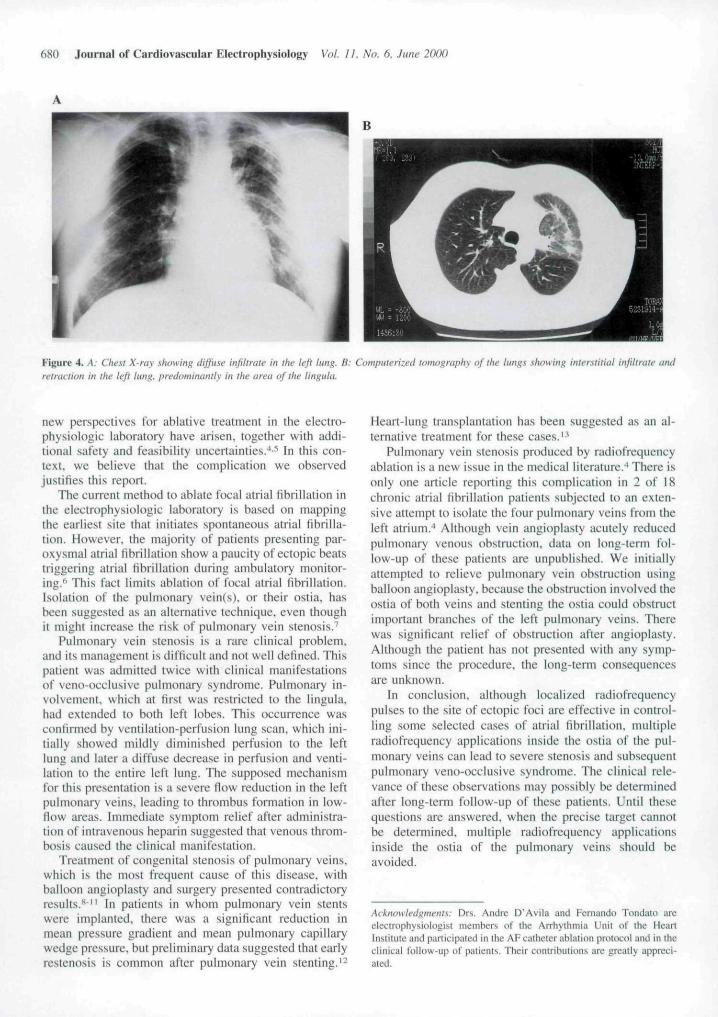
Figure 4. A: Che.-{t X-ray showing diffuse infiltrate in the left Itmg. B: Computerized tomography of the lungs .showing interstitial iiifiltraic andretraction in the left lung, predominantly in the area of the lingula.
new perspectives for ablative treatment in the electro-phy.siologic laboratory have arisen, together with addi-tional safety and feasibility uncertainties.' '• In thi.s con-text, we believe that the complication we observedjustifies this report.
The curreni method to ablate focal atrial fibrillation inthe electrophysiologic laboratory is based on mappingthe earliest site that initiates spontaneous atrial fibrilla-tion. However, the majority of patients presenting par-oxysmal atrial librillation show a paucity of ectopic beatstriggering atrial tibrillation during ambulatory monitor-ing.'' This fact limits ablation of focal atriai fibrillation.Isolation of the pulmonary vein(s). or their ostia. hasbeen suggested as an alternative technique, even thoughit mighl increase the risk of pulmonary vein stenosis.^
Pulmonary vein stenosis is a rare clinical problem,and its management is difficult and not well defined. Thispatient was admitted twice with clinical manifestationsof veno-occlusive pulmonary syndrome. Pulmonary in-volvement, which al (irsl was restricted lo the lingula,had extended to both left lobes. This occurrence wasconfirmed by ventilation-perfusion lung scan, which ini-tially showed mildly diminished perfusion to the leftlung and later a diffuse decrease in perfusion and venti-lation to the entire left lung. The supposed mechanismfor this presentation is a severe flow reduction in the leftpulmonary veins, leading to thrombus formation in low-flow areas. Immediate symptom relief after administra-tion of intravenous heparin suggested that venous throm-bosis caused the clinical manifestation.
Treatment of congenital stenosis of pulmonary veins,which is the most frequent cause of this disease, withballoon angioplasty and surgery presented contradictoryresults.""" In patients in whom pulmonary vein stentswere implanted, there was a significant reduction inmean pressure gradient and mean pulmonary capillarywedge pressure, but preliminary data suggested that earlyrestenosis is common after pulmonary vein stenting.'-
Heart-lung transplantation has been suggested as an al-ternative treatment for these cases."
Pulmonary vein stenosis produced by radiofrequencyablation is a new issue in the medical literature.^ There isonly one article reporting this complicalion in 2 of 18chronic atrial fibrillation patients subjected to an exten-sive attempt to isolate the four pulmonary veins from theleft atrium."* Although vein angioplasly acutely reducedpulmonary venous obstruction, data on long-term fol-low-up of these patients are unpublished. We initiallyattempted to relieve pulmonary vein obstruction usingballoon angioplasty, because the obstruction involved theostia of both veins and stenting the ostia could obstructimportant branches of the left pulmonary veins. Therewas signilicant relief of obstruction after angioplasty.Although the patient has not presented with any symp-toms since the procedure, the long-term consequencesare unknown.
In conclusion, although localized radiofrequeneypulses to the site of ectopic foci are effective in control-ling some selected cases of atrial librillation. multipleradiofrequency applications inside the ostia of the pul-monary veins can lead to severe stenosis and subsequentpulmonary veno-occlusive syndrome. The clinical rele-vance of these observations may possibly be determinedafter long-term follow-up of these patients. Until thesequestions are answered, when the precise tiyget cannotbe determined, multiple radiofrequency applicationsinside the ostia of the pulmonary veins should beavoided.
Acknowledgments: Drs. Andre D'Avila and Fernando Tondato areelectrophysiologist members of the Arrhythmia Unit nf ihe HeartInstitute and participated in the AF catheter ablation pRit(K:o! and in theclinical Ibllow-up ol" patients. Their contributions are greatly appreci-ated.

Scanavacca et al. Pulmonary Vein Stenosis 681
References
1. Haissaguerre M. Marcus R. Fisher B, Clementy J: Radiofrequencycatheler ablation in unu.sual mechanisms of atrial tibrillation: Re-port of three cases. J Cardiovasc Electrophysiol 1994:5:743-751.
2. Jai.s P. Haissaguerre M. Shah DC. el al: A focal source of atrialfibrillation Ireated by discrete radiofrequeney ablation. Circulation1997:95:572-576.
3. Haissaguerre M, Jais P. Shah DC, et al; Spontaneous initiation ofatrial fibrillation hy ectopic beats originating in the pulmonaryveins. N Engl J Med 1998:339:659-666.
4. Robbins IM. Colvin EV, Doyle TP. et al: Pulmonary vein stenosisafter catheter ablation nf atrial libHllation. Circulation 1998;98;1769-1775.
5. Yu W-C. Hsu T-L. Cheng H-C. et al; Focal stenosis of pulmonaryvein after application of radiofrequency energy in patients withparoxysmal atrial Hbrillation. (Abstract) PACE 1999:22:712.
6. Areniz T. Ott P. Slockinger J. et al: Radiofrequency catheterablation of focal atrial fibrillation. (Abstract) PACE 1998;2I:963.
7. Sehwart7man D: Circumferential radiofrequency ablation of pul-monary vein orifices: Feasibility of a new technique. (Abstract)PACE 1999:22:711.
8. Driscoil DJ. Hesslein PS. Mullins CE: Congenital stenosis ofindividual pulmonary veins: Clinical spectrum and unsuccessfultreatmeni by transvenous balloon dilation. Am J Cardiol 1982:49:1767-1772.
9. Lock JE, Bass JL, Castaneda-Zuniga W, et al: Dilation angioplastyof congenital or operative narrowing of venous channels. Circula-tion 1984:70:457-464.
10. Binotto MA. Atik E. Kajita L, et ai: Transluminal angioplasly intotal anomalous drainage of obstructed pulmonary veins. Arq BrasCardiol 19S9-.53:339-341.
11. Hyde JA, Stumper O. Barth MJ. el al: Toial anomalous pulmonaryvenous connection: Outcome of surgical correction and manage-ment of recurrent venous obstruction. Eur J Cardiothorae Surg1999:15:735-740.
!2. Mendelsohn AM. Bove EL. Lupinetti FM, et ai: Intraoperative andpercutaneous stenting of congenital pulmonary anery and veinstenosis. Circulation 1993;8S:II-2IO-n-217.
13. Mendeloff EN, Huddleston CB: Lung transplantation and repairof eomplex congenital heart lesions in patienis wilh pulmonaryhypertension. Semin Thorac Cardiovasc Surg I99X:IO:I44-151.

Copyright © 2022 FDOKUMEN




















