
Off-Pump Epicardial Tissue Sealing—A Novel Method for Atrioventricular Disruption Complicating...
7
2004;78:569-573 Ann Thorac Surg Albert Schuetz, Costas Schulze and Stephen M. Wildhirt complicating mitral valve procedures Off-pump epicardial tissue sealing—a novel method for atrioventricular disruption http://ats.ctsnetjournals.org/cgi/content/full/78/2/569 located on the World Wide Web at: The online version of this article, along with updated information and services, is Print ISSN: 0003-4975; eISSN: 1552-6259. Southern Thoracic Surgical Association. Copyright © 2004 by The Society of Thoracic Surgeons. is the official journal of The Society of Thoracic Surgeons and the The Annals of Thoracic Surgery by on June 8, 2013 ats.ctsnetjournals.org Downloaded from
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Off-Pump Epicardial Tissue Sealing—A Novel Method for Atrioventricular Disruption Complicating...

2004;78:569-573 Ann Thorac SurgAlbert Schuetz, Costas Schulze and Stephen M. Wildhirt
complicating mitral valve proceduresOff-pump epicardial tissue sealing—a novel method for atrioventricular disruption
http://ats.ctsnetjournals.org/cgi/content/full/78/2/569located on the World Wide Web at:
The online version of this article, along with updated information and services, is
Print ISSN: 0003-4975; eISSN: 1552-6259. Southern Thoracic Surgical Association. Copyright © 2004 by The Society of Thoracic Surgeons.
is the official journal of The Society of Thoracic Surgeons and theThe Annals of Thoracic Surgery
by on June 8, 2013 ats.ctsnetjournals.orgDownloaded from
OMCAD
rpdswto
9Tobtbwfw
Adt
dvsatlai
itwabctd
A
ATe
©P
IOV
AS
CU
LA
R
ff-Pump Epicardial Tissue Sealing—A Novelethod for Atrioventricular Disruption
omplicating Mitral Valve Procedureslbert Schuetz, MD, PhD, Costas Schulze, MD, and Stephen M. Wildhirt, MD, PhD
epartment of Cardiac Surgery, Heart Center Augustinum, University of Munich, Munich, Germany
tbOowmm
iictcd
CA
RD
Background. Atrioventricular disruption (AVD) is aare (1%–2%) but fatal complication after mitral valverocedures; the intraoperative mortality is more than 50%espite the current standard procedure of surgical clo-ure of the defect. We compared the outcome of 9 patientsith intraoperative AV disruption, 4 being surgically
reated on-pump and 5 receiving epicardial tissue sealingff-pump.Methods. Between March 1998 and May 2002 a total ofpatients presented with AV disruption intraoperative.he first 4 patients were treated with surgical repairn-pump by reconstruction of the defects with patch oruttressed suture. The second series of 5 patients were
reated with a biodegradable collagen system with fi-rinogen-based coating off-pump. Three to six layersere placed over the bleeding site with manual pressure
or 30–60 minutes on the beating heart until bleeding
as stopped. Cell saved blood was retransfused.svb
ppvmrts
rasis
M
PBpcti-mail: [email protected].
2004 by The Society of Thoracic Surgeonsublished by Elsevier Inc
ats.ctsnetjournDownloaded from
Results. In the on-pump surgical repair group 3 pa-ients (75%) died within the first day after repair eitherecause of persistent bleeding or cardiac tamponade.ne patient survived at 30 days and 1 year. In the
ff-pump tissue sealing group 30 days and 1 year survivalas 100%. Postoperative echocardiography showed nor-al left ventricular (LV) function with no regional wallotion abnormalities.Conclusions. Our data show that epicardial tissue seal-
ng off-pump results in successful termination of bleed-ng from AVD and considerably improves survival whenompared with the standard procedure. Because of thisremendous improvement in patient survival we nowonsider this technique as standard therapy for AVisruption in our center.
(Ann Thorac Surg 2004;78:569–74)
© 2004 by The Society of Thoracic Surgeonstrioventricular disruption (AVD) is a rare but oftenfatal complication following mitral valve proce-
ures. It occurs in approximately 1%–2% of patients andhe mortality associated with it is beyond 50% [1, 2].
The complication often results from overly aggressiveebridement and decalcification of the posterior mitralalve annulus and subvalvular apparatus or from over-izing the prosthesis [3]. The clinical picture varies fromhematoma of the posterior AV groove to cardiac rup-
ure with massive bleeding. Quite frequently it is fol-owed by compromised blood flow to the circumflexrtery with signs of posterolateral wall motion abnormal-ties or left ventricular pump failure.
To date, the standard procedure for this complications to go back on-pump with cardioplegic arrest, reopenhe left atrium, remove the prosthesis, and close the tearith patch or buttress suture. However, even with the
ttempt of surgical repair the mortality rate remains highecause of persistent bleeding as well as prolongedardiopulmonary bypass (CPB) and aortic cross-clampime associated with pump-related complications. Theevelopment of biological tools (hemostyptics, sealants)
ccepted for publication Feb 6, 2004.
ddress reprint requests to Dr Wildhirt, German Heart Center Munich,echnical University of Munich, Lazarettstr. 36, 80636 Munich, Germany;
uch as biodegradable scaffolds has been shown to pro-ide excellent hemostasis even in augmented form inoth experimental and clinical settings [4, 5].The devastating results in patients with AVD
rompted us to investigate the outcome in a series of 9atients with documented AVD complicating mitralalve procedures with regard to 1-year morbidity andortality. The first 4 patients were treated with surgical
epair on-pump. The second series of 5 patients werereated off-pump with a method of epicardial tissueealing in layers.
Our data show that off-pump epicardial tissue sealingesults in successful termination of bleeding from AVDnd considerably improves survival when compared withurgical repair. Because of this tremendous improvementn patient survival we now consider this technique astandard therapy for AV disruption in our center.
aterial and Methods
atientsetween March 1998 and October 2002 a total of 723atients received single our combined mitral valve pro-edures in our center. In 9 patients (1.2%) the complica-ion of atrioventricular disruption (AVD) was diagnosed
ntraoperative.0003-4975/04/$30.00doi:10.1016/j.athoracsur.2004.02.029
by on June 8, 2013 als.org

ecpa
cdmpmaaa
tPpdahpc
RTtvdmddtab
oLe(mwsbTtuopc
T
P
AHWSMP
I
P
Ctcb
Fbsptatc
570 SCHUETZ ET AL Ann Thorac SurgEPICARDIAL TISSUE SEALING FOR ATRIOVENTRICULAR DISRUPTION 2004;78:569–74
CA
RD
IOV
AS
CU
LA
R
The first 4 patients (group: surgical repair) receivedlective surgery for single mitral valve repair (n � 3) andombined aortic and mitral valve replacement (n � 1) forostrheumatic disease. Relevant patient demographicsre given in Table 1.Surgical repair was performed on-pump with aortic
ross clamping, cardioplegic arrest (Bredtschneider’s car-ioplegic solution) under moderate systemic hypother-ia (30°–32°C). The left atrium was reopened and the
reviously implanted prosthesis (valve or ring) was re-oved. A tear in the posterior aspect of the mitral valve
nnulus was found and repaired with prosthetic patchnd buttressed suture (n � 3). The left atrium was closed
able 1. Patient Demographics
atient Demographics
SurgicalClosure(n � 4)
TissueSealing(n � 5) p Value
ge (years) 68 � 4 69 � 7 0.79eight (cm) 174 � 12 166 � 10 0.35eight (kg) 76 � 5 67 � 12 0.25
ex (% male) 25 40 0.46ean CV risk factors 2.2 � 1.1 2.3 � 0.8 0.34
reoperative dataLeft ventricular function (EF%) 55 � 5 56 � 19 0.92NYHA 3.3 3.2 0.72Serum creatinine (mg/dl) 1.2 � 0.2 1.13 � 0.1 0.54Hemoglobin (g/l) 11.3 � 2.5 9.6 � 1.7 0.22Hematocrit (%) 31.1 � 7.2 26.7 � 4.2 0.34WBCs (G/l) 6.9 � 0.1 10.6 � 6 0.35Platelets (G/l) 199 � 41 234 � 62 0.43
ntraoperative dataLowest temperature (°C) 32 32.3 � 0.5 0.54Pump time (min) 135 � 9 125 � 37 0.84Aortic cross clamp time (min) 76 � 19 73 � 20 0.79Re CPB, pump time (min) 56 � 15 n.a.Re CPB, clamp time (min) 38 � 11 n.a.Cell saved blood (ml) 1300 � 900 n.a.
ostoperative dataIntubation time (hours) 240 (n � 1) 93 � 22 n.a.ICU stay (days) 14 (n � 1) 8.4 � 4.7 n.a.Blood loss (ml/24h) 3930 � 233 1539 � 121 �0.001Postoperative EF (%) 25 (n � 1) 58 � 9Need for IABP n, (%) 2, (50) 0, (0) 0.16Peak inotropic support
Epinephrine (mg/h)0.4 � 04 0.27 � 0.25 0.62
Norepinephrine (mg/h) 1.4 � 0.4 09 � 0.1 0.06Milrinone (mg/h) 10 � 2 2.5 � 0.5 0.05
Survival (n; %) 30 days 1; 25 5; 100 �0.01Cause of death
Acute cardiac tamponade 1 n.a.Massive bleeding 2 n.a.
NYHA class at 1 year follow-up 2 (n � 1) 2.2 n.a.EF (%) at 1 year follow-up 55 (n � 1) 61 � 13 n.a.
PB � cardiopulmonary bypass; CV � cardiovascular; EF � ejec-ion fraction; IABP � intraaortic balloon pump; n.a. � not appli-able; NYHA � New York Heart Association; WBCs � whitelood cells.
nd the patients weaned from bypass. In 1 patient addi- r
ats.ctsnetjournDownloaded from
ional surgical repair was attempted on-pump using 4-0rolene sutures (Ethicon, Somerville, NJ) with pledgeslaced from the epicardial side. In all patients moderateoses of inotropic agents, phosphodiesterase inhibitors,nd vasopressors were required to maintain acceptableemodynamics. In addition, intraaortic balloon counter-ulsation (IABP) was used in 2 patients to maintain stableardiovascular hemodynamics (Table 1).
epair Off-Pump With Epicardial Tissue Sealinghe other 5 patients (group: tissue sealing) were referred
o our hospital for mitral valve surgery because of mitralalve endocarditis (2 patients), mitral valve regurgitationue to chorda rupture (2 patients), and postrheumaticitral valve stenosis in combination with coronary artery
isease (1 patient), (group B; Table 1). When AVD wasiagnosed and other bleedings sites had been excluded,
hese patients were left off-pump and protamine wasdministered. A cell saver was initiated and cell savedlood was washed and retransfused.Layers of a biodegradable collagen-system with fibrin-
gen-based coating (Tacho Comb, Nycomed Pharma,inz, Austria) were carefully placed on the posterolateralpicardium starting from the center of the bleeding siteFig 1). Manual pressure with a moist gauze for 10–15
inutes on the posterolateral aspect of the beating heartas applied. This procedure was repeated until hemo-
tasis was achieved. In all patients we observed recurrentleeding from the edge of each collagen fleece applied.herefore, it was of utmost importance to spend enough
ime for the manual pressure procedure of each layerntil the collagen-system exerted the best gluing effectn the epicardium. In addition, the manual pressure waserformed using moisturized gauze that prevented theollagen system from sticking to the surgeon’s glove
ig 1. Placement in layers of the collagen system with fibrinogenased coating (Tacho Comb, Nycomed Pharma, Linz, Austria) ishown on the posterolateral aspect of the heart. Each layer is ap-lied by manual compression for 10–15 minutes starting in the cen-er of the bleeding sit. Between 3–6 layers may be necessary tochieve hemostasis. The layers are placed in overlapping fashionhereby creating a large area of mechanical resistance against intra-ardiac bleeding.
ather than the epicardium. We used 3–6 single layers
by on June 8, 2013 als.org

pocTHmc
raswtl
pvcdilwp
SDDtvvs
R
EI3p2spsw
cfitpao
(
fmwta
PBAgptpwWgHon
PMTVlftdebwbgcf
Ftc
571Ann Thorac Surg SCHUETZ ET AL2004;78:569–74 EPICARDIAL TISSUE SEALING FOR ATRIOVENTRICULAR DISRUPTION
CA
RD
IOV
AS
CU
LA
R
er patient to achieve complete hemostasis. With eachverlapping layer the epicardial area covered with theollagen fleece increased resulting in decreased bleeding.he total time for the procedure was 45–90 minutes.owever, the method was applied off-pump under nor-othermic conditions avoiding the risk of pump-related
omplications.Once hemostasis was achieved, manual pressure was
eleased and the heart was left in its regular position forn additional 15–20 minutes to ensure sufficient hemo-tasis. Thereafter the chest was closed in routine fashionith stainless steel wires and patients were brought to
he intensive care unit (ICU) in stable condition withow-to-moderate amounts of inotropic agents.
During the early postoperative course echocardiogra-hy was used for the evaluation of cardiac function, leftentricular (LV) wall motion, and the presence of intra-ardiac hematoma or pericardial effusion. The techniqueescribed here was adopted from our centers experience
n treating other bleeding sites (i.e. smaller epicardialacerations or injuries to the lungs in redo operations)ith this technique in combination with what has beenublished in the literature [5]
tatisticsata are presented as mean � standard deviation (SD).ichotomous variables were analyzed by the �2 test and
he Fisher exact test. The Student t test for unpairedariables was used to compare clinical parameters. A Palue of less than 0.05 was considered statisticallyignificant.
esults
arly and 1-Year Morbidity and Mortalityn the surgical repair group, 1 patient (25%) survived at0 days and 1 year follow-up (Table 1, Fig 2). In thisatient the endocardial injury was in the posterior region(p2) of the mitral valve annulus due to rupture of a
uture of the implanted device. It was successfully re-aired with two single sutures with pledges. The patienturvived at 30 days. At 1 year follow-up she presentedith NYHA class II and an ejection fraction (EF) of 55%.The remaining 3 patients in this group died because of
ontinued bleeding and cardiac tamponade within therst 24 hours after the initial mitral valve procedure. In
hese patients the sites of bleeding were at the region of2–p3 due to a tear adjacent to the sewing ring (n � 2)nd in a decalcified area (n � 1) which were repairedn-pump with patch and buttressed sutures.In the off-pump “tissue sealing” group all 5 patients
100%) survived 30 days and 1 year follow-up (Fig 2).Echocardiographic evaluation at 30 days and 1 year
ollow-up did not reveal any signs for regional wallotion abnormalities. The average EF was 61% � 13%ith an average NYHA class of 2.2. It is important to note
hat the epicardial bleeding sites with regard to location
nd severity did not differ among both groups. eats.ctsnetjournDownloaded from
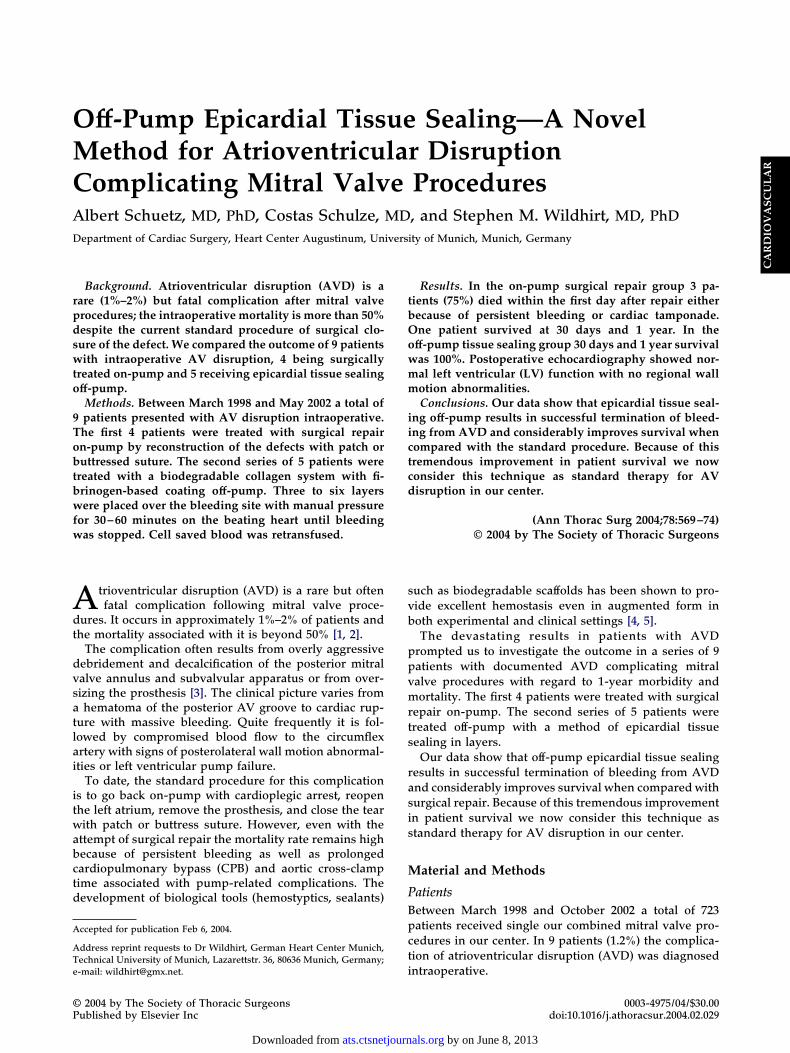
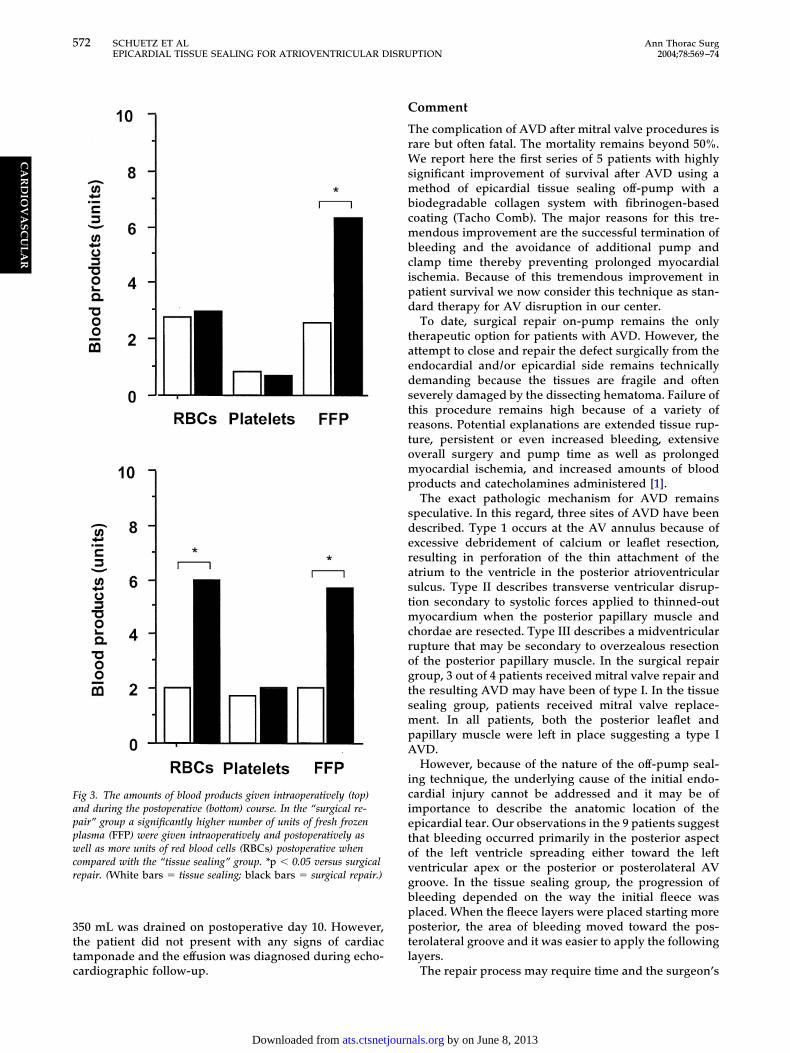
ostoperative Inotropic Support and Requirement forlood Productss shown in Figure 3, patients in the surgical repairroup received significantly more units of fresh frozenlasma (FFP) and red blood cells during the intraopera-
ive and postoperative course. In addition, this groupresented with a significant increased chest tube losshen compared with the tissue sealing group (Table 1).ith regard to cardiovascular hemodynamics, the “sur-
ical repair” group required higher doses of milrinone.owever, during the postoperative course the peak doses
f epinephrine and norepinephrine administered wereot statistically significant (Table 1).
ostoperative Evaluation of Cardiac Function, LV Wallotion, and Intracardiac Hematoma After Epicardial
issue Sealingarious echocardiographic evaluations during early fol-
ow-up were performed. We focused on global cardiacunction, LV wall motion abnormalities (particularly inhe posterolateral region), development of LV intracar-iac hematoma, and the development of pericardialffusion. Postoperative cardiac function was normal inoth groups (Table 1). In addition, no specific regionalall abnormality suggestive of compromised coronarylood flow was found in the epicardial tissue sealingroup. Moreover, we did not find specific signs of intra-ardiac hematoma indicative for prolonged bleedingrom the site of AVD. In 1 out of 5 patients in the
ig 2. Survival at 1-year follow-up is shown. No deaths occurred inhe “tissue sealing” group compared with 25% survival in the surgi-al repair group. *p � 0.05 versus surgical repair.
picardial tissue sealing group a pericardial effusion of
by on June 8, 2013 als.org
3ttc
C
TrWsmbcmbcipd
taedstrtomp
sderastmcrogtsmpA
icietovgbpptl
Fappwcr
572 SCHUETZ ET AL Ann Thorac SurgEPICARDIAL TISSUE SEALING FOR ATRIOVENTRICULAR DISRUPTION 2004;78:569–74
CA
RD
IOV
AS
CU
LA
R
50 mL was drained on postoperative day 10. However,he patient did not present with any signs of cardiacamponade and the effusion was diagnosed during echo-
ig 3. The amounts of blood products given intraoperatively (top)nd during the postoperative (bottom) course. In the “surgical re-air” group a significantly higher number of units of fresh frozenlasma (FFP) were given intraoperatively and postoperatively asell as more units of red blood cells (RBCs) postoperative when
ompared with the “tissue sealing” group. *p � 0.05 versus surgicalepair. (White bars � tissue sealing; black bars � surgical repair.)
ardiographic follow-up.
ats.ctsnetjournDownloaded from
omment
he complication of AVD after mitral valve procedures isare but often fatal. The mortality remains beyond 50%.
e report here the first series of 5 patients with highlyignificant improvement of survival after AVD using aethod of epicardial tissue sealing off-pump with a
iodegradable collagen system with fibrinogen-basedoating (Tacho Comb). The major reasons for this tre-endous improvement are the successful termination of
leeding and the avoidance of additional pump andlamp time thereby preventing prolonged myocardialschemia. Because of this tremendous improvement inatient survival we now consider this technique as stan-ard therapy for AV disruption in our center.To date, surgical repair on-pump remains the only
herapeutic option for patients with AVD. However, thettempt to close and repair the defect surgically from thendocardial and/or epicardial side remains technicallyemanding because the tissues are fragile and ofteneverely damaged by the dissecting hematoma. Failure ofhis procedure remains high because of a variety ofeasons. Potential explanations are extended tissue rup-ure, persistent or even increased bleeding, extensiveverall surgery and pump time as well as prolongedyocardial ischemia, and increased amounts of blood
roducts and catecholamines administered [1].The exact pathologic mechanism for AVD remains
peculative. In this regard, three sites of AVD have beenescribed. Type 1 occurs at the AV annulus because ofxcessive debridement of calcium or leaflet resection,esulting in perforation of the thin attachment of thetrium to the ventricle in the posterior atrioventricularulcus. Type II describes transverse ventricular disrup-ion secondary to systolic forces applied to thinned-out
yocardium when the posterior papillary muscle andhordae are resected. Type III describes a midventricularupture that may be secondary to overzealous resectionf the posterior papillary muscle. In the surgical repairroup, 3 out of 4 patients received mitral valve repair andhe resulting AVD may have been of type I. In the tissueealing group, patients received mitral valve replace-ent. In all patients, both the posterior leaflet and
apillary muscle were left in place suggesting a type IVD.However, because of the nature of the off-pump seal-
ng technique, the underlying cause of the initial endo-ardial injury cannot be addressed and it may be ofmportance to describe the anatomic location of thepicardial tear. Our observations in the 9 patients suggesthat bleeding occurred primarily in the posterior aspectf the left ventricle spreading either toward the leftentricular apex or the posterior or posterolateral AVroove. In the tissue sealing group, the progression ofleeding depended on the way the initial fleece waslaced. When the fleece layers were placed starting moreosterior, the area of bleeding moved toward the pos-
erolateral groove and it was easier to apply the followingayers.
The repair process may require time and the surgeon’s
by on June 8, 2013 als.org

pbttlfofttmc
TDTdisimtb
aamaptsoclChpoUaMpmtck
t(dpdd
hdihtdrT
beewopo
R
1
2
3
4
5
6
I
Pnsaopasor
573Ann Thorac Surg SCHUETZ ET AL2004;78:569–74 EPICARDIAL TISSUE SEALING FOR ATRIOVENTRICULAR DISRUPTION
©P
CA
RD
IOV
AS
CU
LA
R
atience. In 3 out of 5 patients we observed massiveleeding from the posterior aspect of the AV groove. A
otal of 1300 � 900 ml of blood was cell saved throughouthe repair procedures. In these patients a total of 3–6arge Tacho Comb layers were placed in overlappingashion to cover a large area of myocardium with theriginal bleeding site in its center. Manual compressionor up to 10–15 minutes for each layer may be necessaryo achieve hemostasis. The method of off-pump sealing ofhe epicardial tissue in up to 6 layers provides sufficient
echanical resistance to stabilize the injured transmyo-ardial tissue over a large area of the heart.
he Concept of Biological Repair of Larger Areaefectshe surgical approach for AVD repair remains veryifficult or may even be impossible because the dissect-
ng tissue defect is usually quite large. Single or multipleutures with pledges from the epicardial side are oftennsufficient to achieve hemostasis. Repair of the thin
yocardium from the endocardial side requires addi-ional pump and ischemic time and is often complicatedy the massive tissue damage and hematoma.Tissue sealing with biological and synthetic biodegrad-
ble scaffolds is especially suitable for managing larger-rea defects. With particular focus on the heart as aoving organ, one major aspect in tissue sealing is the
dhesive strength of the material (as a suture wouldrovide) necessary to achieve hemostasis but at the same
ime remaining flexible enough to adapt to the heart’shape change during every beat. Our results support thebservation published in a recent study by Carbon andolleagues; they demonstrated that the ready-to-use col-agen system with fibrinogen-based coating (Tachoomb) provides powerful gluing capacity and withstandsigh-pressure conditions in patients with recurringneumothorax [4]. The same group tested various formsf biomaterials with regard to their adhesive strength.sing a biosimulator, it was found that liquid sealants
chieve only low (fibrin glue: 4.1 hPa) adhesive strength.oreover, independent of the fleece material employed,
repare-to-use techniques (fleece � fibrin glue) achieveoderate adhesive strength (22.3–25.3 hPa). In contrast,
he ready-to use systems (Tacho Comb) provide biome-hanically relevant adhesive strength (50.2 hPa). The
nowledge of the adhesive strength may be of impor-upture is based on the anatomic site. Ruptures in the
apsIbcrmoo
2004 by The Society of Thoracic Surgeonsublished by Elsevier Inc
ats.ctsnetjournDownloaded from
ance in the clinical setting because different tissuesdynamic: heart, lung; static: liver, spleen, kidney) andefects may be treated with different sealants. For exam-le, fibrin glue may be more suitable to seal small tissueefects rather than to provide large area hemostasis onissected and fragile tissues [6]As shown in our series, sealing large area defects of the
uman myocardium is successfully achieved by the bio-egradable collagen system with fibrinogen-based coat-
ng (Tacho Comb) even when applied on the beatingeart and under systemic blood pressure conditions. This
echnique may also be applicable for other large areaefects on the heart such as postinfarction ventricularupture, where ischemic tissues are difficult to suture.his needs to be further evaluated.In summary, the present report shows that off-pump
iological tissue repair of the left ventricle is possibleven in the presence of large area defects. Because of thexcellent long-term outcome in 5 consecutive patientsith AVD we have changed the policy for the treatmentf AVD at our center. We strongly recommend thisrocedure for the treatment of patients with AVD orther large area defects on the heart.
eferences
. Bjork V, Henze A, Rodriguez L. Left ventricular rupture as acomplication of mitral valve replacement. J Thorac Cardio-vasc Surg 1977;73:14–22.
. Karlson K, Ashraf M, Berger R. Rupture of left ventriclefollowing mitral valve replacement. Ann Thorac Surg 1988;46:590–7.
. Savage D, Garrison R, Brand F, Anderson S, Castelli W,Kannel W, et al. Prevalence and correlates of posterior extraechocardiographic spaces in a free-living population basedsample (the Framingham study). Am J Cardiol 1983;51:1207–12.
. Carbon R, Baar S, Gusinde J, Huemmer H, Baer K. Tissuesealing concept in minimally invasive surgery in children.Pediatr Endosurg Innovat Tech 2001;5:5–12.
. Schelling G, Block T, Gokel M, Blanke E, Hammer C, BrendelW. Application of a fibrinogen-thrombin-collagen based he-mostyptic agent in experimental injuries of the liver andspleen. J Trauma 1988;28:472–5.
. Carbon R, Baar S, Kriegelstein S, Huemmer H, Baar K, SimonS. Evaluating the in vitro adhesive strength of biomaterials.Biosimulator for selective leak closure. Biomaterials 2003;24:
1469–75.NVITED COMMENTARY
osterior rupture of the left ventricle has been a recog-ized complication since the origins of mitral valveurgery, and ironically, despite advances in virtually allspects of the treatment of valvular disease, the outcomef left ventricular rupture has remained exceptionallyoor. What is understood about left ventricular rupturefter mitral valve surgery can be gained from the manyporadic reports that have been published over the spanf more than 30 years. Classification of the ventricular
trioventricular groove (type I) or at the base of theapillary muscles (type II) are thought to be secondary tourgical trauma. The transverse midventricular tear (typeII), which occurs midway between the first two, iselieved to be the result of dividing the anatomic loopreated by the papillary muscle, mitral valve, and poste-ior ventricular wall. Modification of the technique ofitral valve surgery primarily based on the preservation
f the posterior leaflet has been reported to lower the risk
f ventricular rupture.0003-4975/04/$30.00doi:10.1016/j.athoracsur.2004.03.054
by on June 8, 2013 als.org

2004;78:569-573 Ann Thorac SurgAlbert Schuetz, Costas Schulze and Stephen M. Wildhirt
complicating mitral valve proceduresOff-pump epicardial tissue sealing—a novel method for atrioventricular disruption
& ServicesUpdated Information
http://ats.ctsnetjournals.org/cgi/content/full/78/2/569including high-resolution figures, can be found at:
References http://ats.ctsnetjournals.org/cgi/content/full/78/2/569#BIBL
This article cites 6 articles, 2 of which you can access for free at:
Citations http://ats.ctsnetjournals.org/cgi/content/full/78/2/569#otherarticles
This article has been cited by 5 HighWire-hosted articles:
Subspecialty Collections
http://ats.ctsnetjournals.org/cgi/collection/cardiac_other Cardiac - other
following collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
[email protected]: orhttp://www.us.elsevierhealth.com/Licensing/permissions.jsp
in its entirety should be submitted to: Requests about reproducing this article in parts (figures, tables) or
Reprints [email protected]
For information about ordering reprints, please email:
by on June 8, 2013 ats.ctsnetjournals.orgDownloaded from




















