
Simulated amnesia (Wiggins)
23
The Detection of Simulated Amnesia Author(s): Elizabeth C. Wiggins and Jason Brandt Source: Law and Human Behavior, Vol. 12, No. 1 (Mar., 1988), pp. 57-78 Published by: Springer Stable URL: http://www.jstor.org/stable/1393908 Accessed: 07/08/2009 09:58 Your use of the JSTOR archive indicates your acceptance of JSTOR's Terms and Conditions of Use, available at http://www.jstor.org/page/info/about/policies/terms.jsp. JSTOR's Terms and Conditions of Use provides, in part, that unless you have obtained prior permission, you may not download an entire issue of a journal or multiple copies of articles, and you may use content in the JSTOR archive only for your personal, non-commercial use. Please contact the publisher regarding any further use of this work. Publisher contact information may be obtained at http://www.jstor.org/action/showPublisher?publisherCode=springer. Each copy of any part of a JSTOR transmission must contain the same copyright notice that appears on the screen or printed page of such transmission. JSTOR is a not-for-profit organization founded in 1995 to build trusted digital archives for scholarship. We work with the scholarly community to preserve their work and the materials they rely upon, and to build a common research platform that promotes the discovery and use of these resources. For more information about JSTOR, please contact [email protected]. Springer is collaborating with JSTOR to digitize, preserve and extend access to Law and Human Behavior. http://www.jstor.org
-
Upload
johnshopkins -
Category
Documents
-
view
0 -
download
0
Transcript of Simulated amnesia (Wiggins)
The Detection of Simulated AmnesiaAuthor(s): Elizabeth C. Wiggins and Jason BrandtSource: Law and Human Behavior, Vol. 12, No. 1 (Mar., 1988), pp. 57-78Published by: SpringerStable URL: http://www.jstor.org/stable/1393908Accessed: 07/08/2009 09:58
Your use of the JSTOR archive indicates your acceptance of JSTOR's Terms and Conditions of Use, available athttp://www.jstor.org/page/info/about/policies/terms.jsp. JSTOR's Terms and Conditions of Use provides, in part, that unlessyou have obtained prior permission, you may not download an entire issue of a journal or multiple copies of articles, and youmay use content in the JSTOR archive only for your personal, non-commercial use.
Please contact the publisher regarding any further use of this work. Publisher contact information may be obtained athttp://www.jstor.org/action/showPublisher?publisherCode=springer.
Each copy of any part of a JSTOR transmission must contain the same copyright notice that appears on the screen or printedpage of such transmission.
JSTOR is a not-for-profit organization founded in 1995 to build trusted digital archives for scholarship. We work with thescholarly community to preserve their work and the materials they rely upon, and to build a common research platform thatpromotes the discovery and use of these resources. For more information about JSTOR, please contact [email protected].
Springer is collaborating with JSTOR to digitize, preserve and extend access to Law and Human Behavior.
http://www.jstor.org
Law and Human Behavior, Vol. 12, No. 1, 1988
The Detection of Simulated Amnesia*
Elizabeth C. Wigginst and Jason Brandtt
Claims of amnesia are frequently raised in criminal and civil cases. There is a consensus in the legal community that amnesia is easily faked and practically impossible to disprove, and that many who claim to be amnesic are malingering. The present studies compared, on a variety of memory tasks, subjects instructed to simulate amnesia with subjects who had memory impairments due to brain damage. The simulators displayed patterns of performance different from those of memory-impaired subjects. These results suggest that lay-people have inaccurate beliefs about the cognitive features of amnesia, and do not distinguish among etiologically distinct amnestic disorders. Tasks that exploit lay-people's inaccurate beliefs about amnesia appear promising for the detection of malingering.
INTRODUCTION
Claims of amnesia arise in a variety of legal situations. Criminal defendants have often claimed to be amnesic in efforts to prove their incompetency to stand trial and to reduce legal responsibility for crimes (Gibbens & Williams, 1977; Ru- binsky & Brandt, 1986; Schacter, 1986a). Such claims are particularly prevalent in cases involving violent crime (Bradford & Smith, 1979; Guttmacher, 1955; Schacter, 1986a). It is also common for claims of amnesia to surface in disability and social security hearings, as well as in personal injury suits (Guthkelch, 1980). In such cases, the amount of compensation, if any, is dependent on the duration and severity of the disability. Proof of memory impairment may therefore entitle the plaintiff to sizable monetary awards (Deutsch & Raffa, 1986).
Judges tend to treat claims of amnesia with skepticism, especially when raised by criminal defendants. There appears to be consensus in the legal commu-
* The first author received support from a NIMH Law and Psychology Training Grant (No. MH16820). This research was also supported by grants Nos. AG05146, RR07041, MH38387, and NS16375 to the Johns Hopkins University. The authors thank Steven Breckler, Michael McCloskey, Hilly Rubinsky, and Molly Treadway for their helpful comments on the manuscript. The assistance of Pat Anders in collecting the data for Study 2 is gratefully acknowledged.
t Department of Psychology, Johns Hopkins University; now at the Department of Psychology, Ohio State University.
t Department of Psychiatry and Behavioral Sciences, Johns Hopkins University School of Medicine. 57
0147-7307/88/0300-0057$06.00/0 ? 1988 Plenum Publishing Corporation
WIGGINS AND BRANDT
nity that amnesia is easily faked and practically impossible to disprove, and that many criminal defendants may submit claims of amnesia simply to avoid punish- ment ("Comment, Capacity to Stand Trial," 1967; Rubinsky & Brandt, 1986). Similarly, plaintiffs in civil cases may be malingering or exaggerating their symptoms for financial gain.
Psychologists have long been aware of the legal and economic benefits that may accrue from malingered memory disorders (Gibbens & Williams, 1977; Lezak, 1983). Behavioral observations, as well as personality and cognitive test batteries, are typically used in attempts to uncover feigned disorders (Bash & Alpert, 1980). Professional judgment is therefore needed to discern behaviors and performances that are substantially different from those expected of genuine am- nesics (Bash & Alpert, 1980; Lezak, 1983; Price and Terhune, 1919). The few psychological techniques that have been developed specifically for the clinical assessment of suspected malingerers also require extensive clinical judgment for their interpretation (Lezak, 1983; Swiercinsky, 1985). However, highly trained clinicians are often no better than lay-persons in their detection of psychological abnormalities (Heaton et al., 1978; but cf. Bruhn & Reed, 1975). Therefore, there remains a substantial need for objective and empirically supported techniques to detect malingered amnesia.
Research on malingering is obviously hindered by the absence of a popula- tion of subjects willing to acknowledge their deceitfulness. Several investigators have therefore employed normal subjects instructed to mimic or simulate mental disorders. Whether this is an adequate approximation to the malingerer is dis- cussed later in this paper.
Suprisingly little research has specifically examined whether normal indi- viduals can successfully feign clinical memory disorders. However, studies that examine whether normal individuals are able to simulate the symptoms of other cognitive impairments may be relevant. Most simulation studies assume that people have inaccurate knowledge about important aspects of the disorder in question. Techniques that uncover these inaccurate beliefs can therefore be used to detect malingering.
Benton and Spreen (1961), for example, found that when normal individuals were instructed to simulate brain damage, they overestimated the range of def- icits of truly brain-damaged patients and made errors of a qualitatively different nature on the Benton Visual Retention Test. Similar results were found when the performances of moderately retarded persons were compared to those of normal subjects who were simulating retardation (Spreen & Benton, 1963).
Heaton et al. (1978) found that the overall level of "cognitive impairment" of normal individuals who had been instructed to simulate a cognitive disability re- sulting from head trauma was comparable to that of nonlitigating head trauma patients on the Halstead-Reitan Neuropsychological Test Battery. However, the pattern of deficits was quite different. The head trauma patients performed worse than the simulators on the Category Test, Part B of the Trail Making Test, and on the Tactual Performance Test. The simulators, on the other hand, performed worse than the patients on the Speech-Sounds Perception Test, the Finger Oscil- lation Test, finger agnosia, sensory suppression, hand dynamometer, and the
58
DETECTION OF SIMULATED AMNESIA
WAIS digit span. Goebel (1983) similarly found that the performance of simu- lators on the Halstead-Reitan Battery was qualitatively different from that of brain-damaged patients. It is also noteworthy that, although Goebel asked sub- jects to simulate one of four different types of brain damage, the four groups of simulators performed similarly. Thus, it appears that people are unaware of the performance characteristics of different types of brain-damaged individuals. It is not yet known whether the same would be true of a more circumscribed set of mental symptoms, such as those comprising amnesia.
The detection of malingered amnesia might be facilitated if tasks designed specifically for that purpose, rather than standard clinical test batteries, were used. Schacter (1986a) recently suggested a strategy based on principles of meta- memory to detect feigned memory loss. Metamemory refers to one's knowledge and beliefs about memory, including information storage and retrieval processes (Flavell & Wellman, 1977). In Schacter's studies, subjects viewed videotapes or listened to audiotapes describing complex events. They were then questioned about aspects of the events that were nearly impossible to recall. One subject group was given the correct answers and then instructed to simulate amnesia during the remainder of the experiment. A second group of subjects was not told the an- swers. All subjects were then asked to rate the likelihood that they would re- member the information under a variety of conditions (e.g., if given a hint). The simulators gave lower likelihood ratings than did the uninformed subjects.
Although such likelihood ratings are potentially useful in detecting malin- gered amnesia, there are several shortcomings to Schacter's approach. The labo- ratory analogue of amnesia may not parallel genuine amnesia because the same cognitive mechanisms may not underlie the memory failings of normal individuals and amnesics alike (cf. Meudell & Mayes, 1982). Furthermore, even assuming a close parallel between normal forgetting and amnesia, Schacter's subjects may have never encoded the critical information, and thus cannot be said to have "forgotten" it. In addition, Schacter's simulators are different from real-life ma- lingerers in important ways. The simulators do not remember the critical informa- tion from their first exposure to it. Instead, they remember the information be- cause the experimenter reviewed it with them. Most importantly, the simulators are not instructed to simulate a syndrome of amnesia, but rather are instructed to simulate the forgetting of a few items of information.
An advantage of the simulation studies described earlier (e.g., Benton & Spreen, 1961; Heaton et al., 1978) is that simulators' behavior can be compared to that of genuinely impaired persons. A disadvantage is that the experimental tasks typically used are often not well grounded in psychological theory, and therefore are often relatively ineffective in detecting malingering. Some research (e.g., Schacter, 1986a) has had a firmer basis in psychological theory, but has not directly compared simulators with genuinely impaired persons. The present ap- proach to the detection of malingered amnesia combines the methodological and theoretical advantages of previous studies.
The present studies assume that naive malingerers are unaware of recent neuropsychological research that describes the performance characteristics of amnesia due to different etiologies (Butters, Milotis, Albert, and Sax, 1985;
59
WIGGINS AND BRANDT
Corkin et al., 1985; Rubinsky & Brandt, 1986; Squire & Butters, 1984). By capi- talizing on these misconceptions, it should be possible to develop a variety of tasks that can detect malingered amnesia.
The present studies were designed to (1) test the relative efficacy of several tasks in detecting simulated amnesia, (2) determine whether lay-persons distin- guish among varieties of amnesia, and (3) learn about their naive conceptions of these disorders.
STUDY 1
Global amnesia is a severe inability to acquire and retain new permanent memories (anterograde amnesia) and is typically coupled with some degree of impairment in the retrieval of previously acquired memories (retrograde amnesia; Squire & Butters, 1984). However, when appropriately tested, even global am- nesics can learn and display the effects of exposure to new information (Mosco- vitch, 1984; Schacter, 1985).
Learning and memory for new information can be measured in several ways (Moscovitch, 1984; Schacter, 1985). Explicit memory tests require people to re- member, in the colloquial sense of recollecting or "calling to mind," information to which they have been exposed. In contrast, implicit memory tests instruct people to engage in tasks seemingly unrelated to memory, but for which recent experience with the stimulus material facilitates performance. By definition, am- nesics exhibit little evidence of memory if questioned explicitly about information to which they have been exposed. However, their performance on implicit memory tests often shows that the information was, in fact, registered and main- tained in some form.
Schacter (1985) described two sets of phenomena that illustrate the pre- served mnemonic abilities of amnesics. First, amnesics are able to acquire a va- riety of motor, perceptual, and cognitive skills even when they cannot remember details of the learning episode itself and are unaware of having learned something new (Corkin, 1965, 1968; Moscovitch, 1982, 1984; Warrington & Weiskrantz, 1968). Amnesics of several etiologies, for example, can learn and retain the skill of reading mirror-reversed words without explicitly remembering the words themselves (cf. Martone et al., 1984). Second, prior exposure to test stimuli facili- tates performance on a variety of retention tasks that do not require explicit memory of the learning episode (Graf, Squire & Mandler, 1984; Warrington and Weiskrantz, 1968, 1970, 1974). This latter phenomenon can be described as a mental activation or priming of target information through prior exposure (Dia- mond & Rozin, 1984).
Graf et al. (1984) illustrated priming in amnesia by assessing memory for a list of words with three explicit memory tests (free recall, yes/no recognition, cued recall) and one implicit memory test (wordstem completion). In both the cued recall and the wordstem completion tests, the first three letters of the target words were shown to the subject. In the cued recall test, subjects were instructed
60
DETECTION OF SIMULATED AMNESIA
to use these wordstems as recall cues. In the wordstem completion test, subjects were instructed to complete each wordstem with the first English word that came to mind. Although the amnesics performed poorly on the recall, recognition, and cued recall tasks (explicit memory tests), they performed normally on the word- stem completion task (implicit memory test).
In another study involving priming of target information, a list of words was presented to a group of hypnotized subjects, a group of subjects who were simu- lating a hypnotic state, and a nonhypnotized, nonsimulating control group (Wil- liamsen, Johnson, and Erikson, 1965). The subjects in the first two groups were told that they would not remember the words after the hypnotic session. When all the subjects were in a nonhypnotic or posthypnotic state, their memory for the word list was tested with two explicit memory tests (free recall and yes/no recog- nition of target items) and two implicit memory tests (free associations to cues that elicited target words as primary associates and identification of perceptually degraded fragments of study words). The performance of the hypnotically am- nesic subjects was similar to that of brain-damaged amnesics reported in other studies (Shimamura & Squire, 1984; Warrington & Weiskrantz, 1968; 1970). Al- though the hypnotic subjects performed poorly on the recall and recognition tests relative to the controls, they gave the target words as responses in the association test as frequently as did the controls. They also identified the words presented in fragmented form as accurately as did the control subjects. The simulators, how- ever, overplayed the amnesic role, performing poorly on the associative and word fragment (i.e., implicit memory) tasks as well as on the recall and recognition (explicit memory) tasks.
One approach to the detection of malingered amnesia, then, is to exploit the fact that many amnesics can learn new information and display their knowledge when appropriately tested. Naive malingerers presumably do not know about the retained memory skills of amnesics, and thus should overplay their role. Study 1 addressed whether normal individuals simulating amnesia would distinguish be- tween explicit and implicit demands on memory. More specifically, it examined whether simulators would exhibit intact priming of new information. Two experi- mental tasks were used: a wordstem completion task patterned after that of Graf et al. (1984) and a word association task similar to that of Williamsen et al. (1965). It was predicted that the simulators would perform poorly on both the explicit (free recall) and implicit (wordstem completion or word association) portions of these tasks, and would not exhibit a priming effect, as would genuine amnesics.
One other qualitative feature of memory performance was examined in Study 1. In normal individuals, the probability of recalling the first few items and the final few items of a word list is higher than the probability of recalling the middle items (Klatzky, 1980). That is, the serial position curve illustrates both primacy and recency effects. Amnesics often exhibit a recency effect but not a primacy effect in free recall (Baddeley and Warrington, 1970; Milner, 1978), presumably because of an inability to transfer information in immediate consciousness to more long-term storage. Because most nonpsychologists presumably do not know about this characteristic of amnesia, it was predicted that simulators' serial
61
WIGGINS AND BRANDT
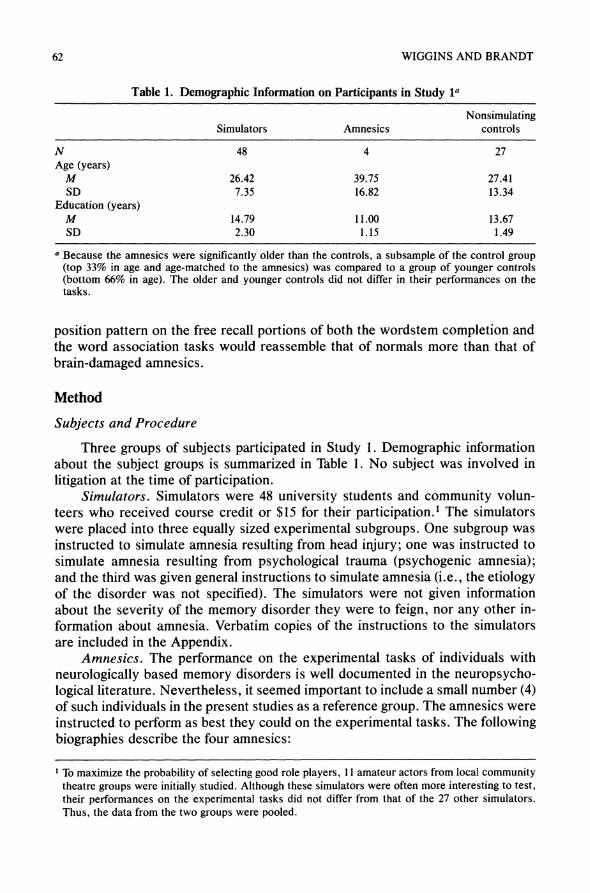
Table 1. Demographic Information on Participants in Study la
Nonsimulating Simulators Amnesics controls
N 48 4 27 Age (years)
M 26.42 39.75 27.41 SD 7.35 16.82 13.34
Education (years) M 14.79 11.00 13.67 SD 2.30 1.15 1.49
a Because the amnesics were significantly older than the controls, a subsample of the control group (top 33% in age and age-matched to the amnesics) was compared to a group of younger controls (bottom 66% in age). The older and younger controls did not differ in their performances on the tasks.
position pattern on the free recall portions of both the wordstem completion and the word association tasks would reassemble that of normals more than that of brain-damaged amnesics.
Method
Subjects and Procedure
Three groups of subjects participated in Study 1. Demographic information about the subject groups is summarized in Table 1. No subject was involved in
litigation at the time of participation. Simulators. Simulators were 48 university students and community volun-
teers who received course credit or $15 for their participation.' The simulators were placed into three equally sized experimental subgroups. One subgroup was instructed to simulate amnesia resulting from head injury; one was instructed to simulate amnesia resulting from psychological trauma (psychogenic amnesia); and the third was given general instructions to simulate amnesia (i.e., the etiology of the disorder was not specified). The simulators were not given information about the severity of the memory disorder they were to feign, nor any other in- formation about amnesia. Verbatim copies of the instructions to the simulators are included in the Appendix.
Amnesics. The performance on the experimental tasks of individuals with
neurologically based memory disorders is well documented in the neuropsycho- logical literature. Nevertheless, it seemed important to include a small number (4) of such individuals in the present studies as a reference group. The amnesics were instructed to perform as best they could on the experimental tasks. The following biographies describe the four amnesics:
To maximize the probability of selecting good role players, 11 amateur actors from local community theatre groups were initially studied. Although these simulators were often more interesting to test, their performances on the experimental tasks did not differ from that of the 27 other simulators. Thus, the data from the two groups were pooled.
62
DETECTION OF SIMULATED AMNESIA
FR. is a 40-year-old female with a high school education. She scored be- tween the 53rd and 60th percentile on Raven's Standard Progressive Matrices, indicating that she is of roughly average nonverbal intelligence. Her Memory Quotient of 53 on the Weschler Memory Scale, however, indicates a severe memory impairment. Her amnesia is most likely related to a life-long history of poorly controlled epilepsy and an episode of status epilepticus in 1981. Aside from her severe amnesia, F.R. displays a speech articulation disorder, which pre- dates her amnesia.
K.L., a 32-year-old female with a tenth grade education, suffered a pulmo- nary embolism and cardiopulmonary arrest with subsequent hypoxia in 1984. Based on her demographic characteristics and academic and work histories, K.L.'s premorbid Full-Scale IQ was estimated to be 94 (Barona, Reynolds, & Chastain, 1984). On evaluation, she received a Full-Scale IQ of 74 on the WAIS- R, but profound apathy coupled with a great many "I don't know" responses may have artificially lowered her scores. On a multiple-choice vocabulary and abstraction test (Shipley Institute of Living Scale), she received an IQ equivalent of 100. Clinically, she displays both retrograde and anterograde amnesia, and earned an M.Q. of 73 on the Weschler Memory Scale.
M.T., is a 24-year-old female with a high school education. In 1982, she un- derwent surgery for the removal of a left intraventricular tumor. Her resulting neurological impairments include poor verbal (and to a lesser degree nonverbal) memory, loss of vision in the right visual field, and a mild language disorder (dys- nomia). Intelligence testing with a short form of the WAIS-R yielded an estimated full-scale I.Q. within the low normal range (80). This I.Q. probably represents a significant drop from her premorbid level, as her estimated premorbid full-scale I.Q. based on her age, education, and occupational level is 106. On the Weschler Memory Scale, M.T. earned an M.Q. of 72, reflecting a moderately severe memory disorder.
A.W. is a 63-year-old female with a tenth grade education who had worked as a psychiatric aide. She has a long history of severe alcohol abuse and was ad- mitted to the hospital confused and disoriented in June 1965. She now displays the profound memory disorder of alcoholic Korsakoff's syndrome. Although psychometric scores were not available, clinical examination revealed that A.W. is grossly unable to remember any new events.
Nonsimulating Controls. Controls were 27 university students and commu- nity volunteers who received course credit or $15 for their participation. The controls were instructed to perform their best on the experimental tasks.
Experimental Tasks
Subjects participated in two experimental sessions held on consecutive days. Table 2 outlines the tasks completed by subjects during each session.
Autobiographical Interview. Subjects were queried about their personal his- tories and recent daily activities. The interview questions are listed in Table 3. Because subjects' accuracy could not be verified, answers were scored as either
63
WIGGINS AND BRANDT
Table 2. Experimental Tasks in Study 1
Session 1 Autobiographical Interview (Questions 1-12 from Table 3)a Wordstem Completion Task
Free Recall Testa Completion Testb
Word Associations Task Free Recall Testa Word Associations Testb
Session 2 Autobiographical Interview (Questions 13 and 14 from Table 3)a Wordstem Completion Task
Completion Testb
a Explicit memory test. b Implicit memory test.
plausible or incorrect. Answers were scored as incorrect when the subject gave unambiguously wrong answers or when the subject claimed no knowledge or memory of the answer.
Wordstem Completion Task. Forty words, selected according to the criteria of Graf et al. (1982), were used in the wordstem completion task. Each five- or six-letter word had a different "stem" (the first three letters), and for each, Web- ster's Dictionary (Allee, 1981) listed at least four additional words of the same length beginning with the same stem. The stimulus words were never the most frequently occurring word beginning with a wordstem. The 40 words were di- vided into two 20-word lists, matched for frequency and word length (mean fre- quency was 32.27 occurrences per million; Carroll, Davies, and Richman, 1971).
Each subject read one of the word lists with instructions to remember the 20 words. Presentation of the two lists was counterbalanced across subjects. Imme- diately thereafter, a free recall test was administered. The wordstem completion test was then administered. In this test, the subject was given all 40 wordstems and instructed to complete each stem to form any English word, except a proper noun. The follow day, the subject returned to the laboratory and the completion test was readministered. Subjects did not read the word list or take the free recall test on the second day.
Word Association Task. Forty stimulus words and their first associations were drawn from the Connecticut Word Association Norms (Bousfield et al., 1961). Simulus words were selected according to the following criteria: (1) The first association accounted for at least 45% of the associative responses to the stimulus word; and (2) the first, second, and third associations collectively ac- counted for at least 70% of all associative responses to the word. The 40 stimulus words along with their first associations were divided into two lists, matched for percentage of associative responses accounted for by the first association (List 1: 65%; List 2: 65%).
The subject read the first associations from one of the lists. Presentation of the two lists was counterbalanced across subjects. Immediately thereafter, a free
64
DETECTION OF SIMULATED AMNESIA
recall test was administered. Then, all 40 stimulus words were read to the subject, who was asked to respond to each stimulus word as quickly as possible with the first word that came to mind. (The stimulus words were read in the same order to each subject.) A priming effect is indicated when more previously presented first associations are used in response to the stimulus words than nonpresented asso- ciations.
Results
Prior to conducting the main data analyses, the three simulator subgroups were compared on all tasks. These preliminary analyses revealed similar perfor- mances. Therefore, except where noted, the simulator subgroups were pooled for comparison with the nonsimulating control group. The amnesics' data are pre- sented descriptively because the sample was too small for statistical comparison to the other two groups.
Autobiographical Interview
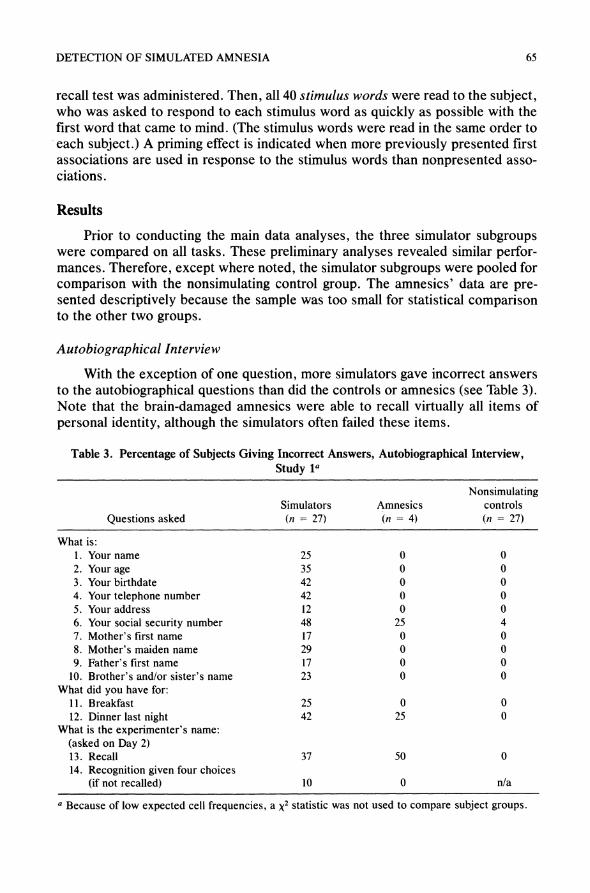
With the exception of one question, more simulators gave incorrect answers to the autobiographical questions than did the controls or amnesics (see Table 3). Note that the brain-damaged amnesics were able to recall virtually all items of personal identity, although the simulators often failed these items.
Table 3. Percentage of Subjects Giving Incorrect Answers, Autobiographical Interview, Study 1a
Nonsimulating Simulators Amnesics controls
Questions asked (n = 27) (n = 4) (n = 27)
What is: 1. Your name 25 0 0 2. Your age 35 0 0 3. Your birthdate 42 0 0 4. Your telephone number 42 0 0 5. Your address 12 0 0 6. Your social security number 48 25 4 7. Mother's first name 17 0 0 8. Mother's maiden name 29 0 0 9. Father's first name 17 0 0
10. Brother's and/or sister's name 23 0 0 What did you have for:
11. Breakfast 25 0 0 12. Dinner last night 42 25 0
What is the experimenter's name: (asked on Day 2) 13. Recall 37 50 0 14. Recognition given four choices
(if not recalled) 10 0 n/a
a Because of low expected cell frequencies, a X2 statistic was not used to compare subject groups.
65
WIGGINS AND BRANDT
Wordstem Completion Task
Free Recall. The subject groups differed significantly in the number of words freely recalled (F3,71 = 7.86, p < .01). The controls (M = 7.9) recalled more words than did any other group except that psychogenic simulators (Tukey's HSD, p < .05). The psychogenic simulators (M = 7.2) recalled more words than did the general simulators (M = 4.8; Tukey's HSD, p < .01). The recall perfor- mance of the head injury simulators (M = 5.8) did not differ significantly from either of the other simulating groups. The amnesics (M = 2.5) recalled fewer words than the other groups, but this difference was not tested statistically, be- cause of the small sample size.
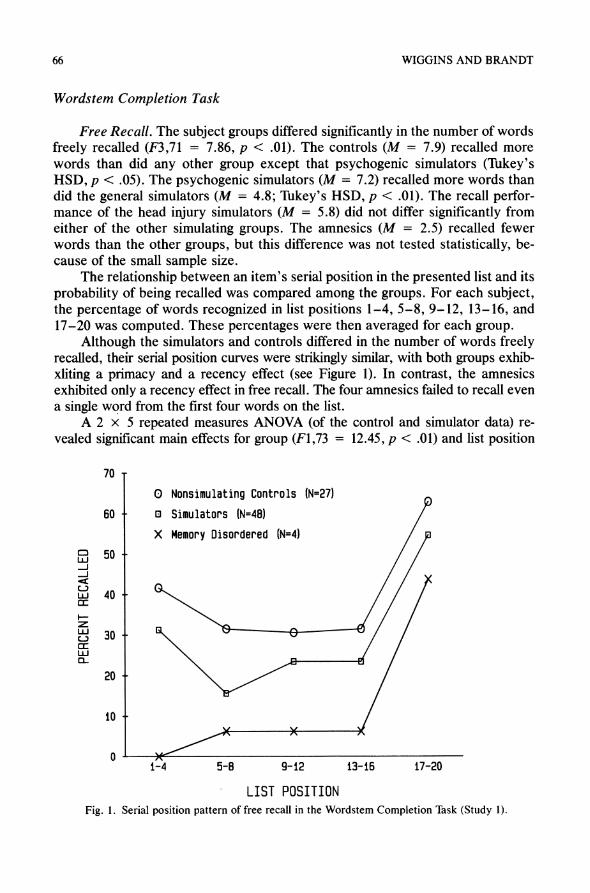
The relationship between an item's serial position in the presented list and its probability of being recalled was compared among the groups. For each subject, the percentage of words recognized in list positions 1-4, 5-8, 9-12, 13-16, and 17-20 was computed. These percentages were then averaged for each group.
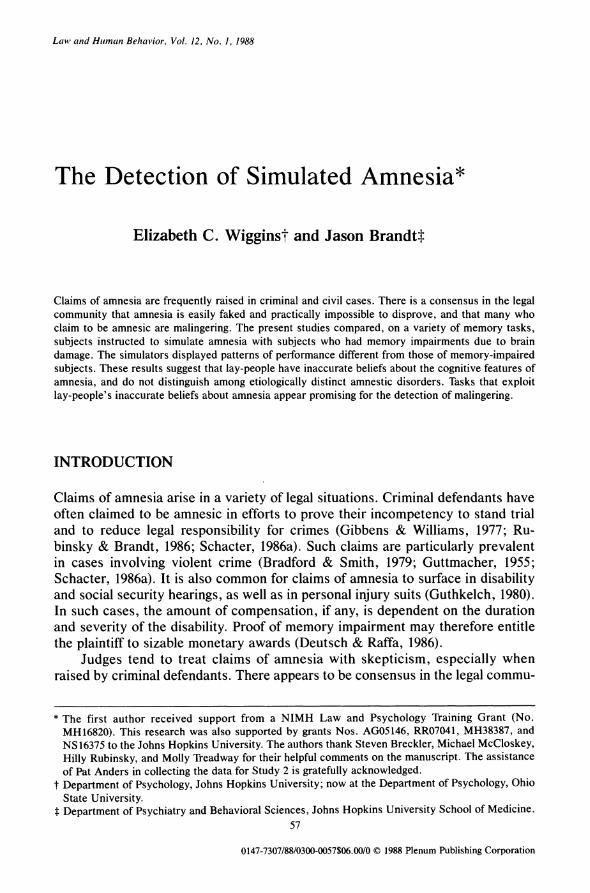
Although the simulators and controls differed in the number of words freely recalled, their serial position curves were strikingly similar, with both groups exhib- xliting a primacy and a recency effect (see Figure 1). In contrast, the amnesics exhibited only a recency effect in free recall. The four amnesics failed to recall even a single word from the first four words on the list.
A 2 x 5 repeated measures ANOVA (of the control and simulator data) re- vealed significant main effects for group (F1,73 = 12.45, p < .01) and list position
70 -
0 Nonsimulating Controls (N=27)
60 - e Simulators (N=48)
X Memory Disordered (N=4)
? 50 -
UJ 40/ /
X 30 - /
20 -
10 -
0 X 1-4 5-8 9-12 13-16 17-20
LIST POSITION Fig. 1. Serial position pattern of free recall in the Wordstem Completion Task (Study 1).
66
DETECTION OF SIMULATED AMNESIA
(F1,292 = 25.81, p < .01). An orthogonal component analysis of list position revealed a strong quadratic trend (F1,73 = 65.07, p < .01), as well as a signifi- cant linear trend (F1,73 = 21.98, p < .01). As expected, the quadratic trend ac- counted for the greatest portion of the sums of squares for list position (SSquratic/ SSwithin = .64; SSSina/SS,ith = .29). Thus, the expected serial position effect, with both primacy and recency components, was found in both the simulators and the controls.
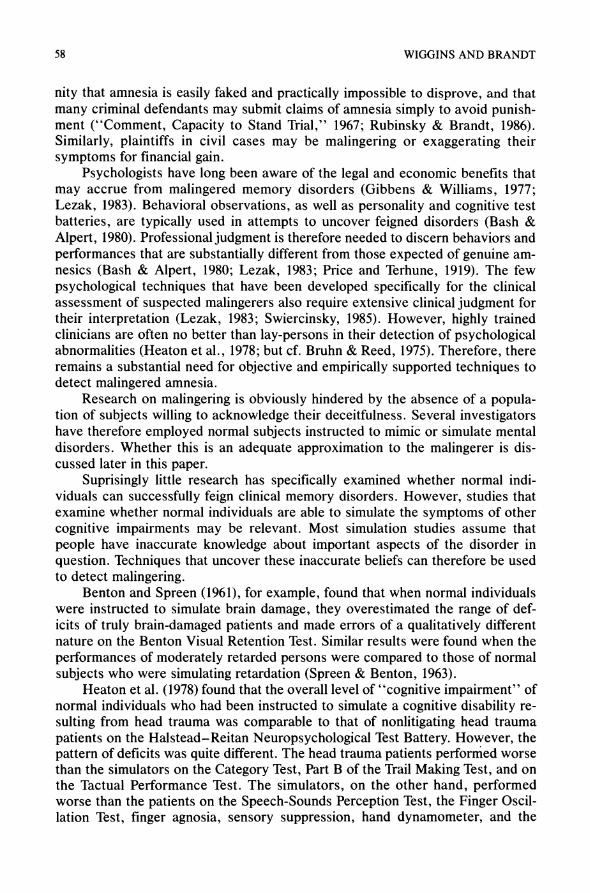
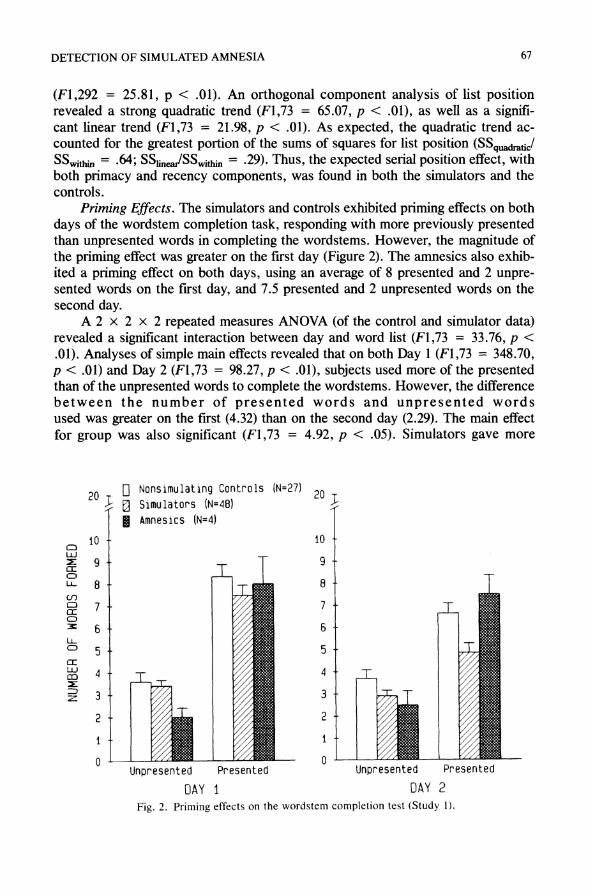
Priming Effects. The simulators and controls exhibited priming effects on both days of the wordstem completion task, responding with more previously presented than unpresented words in completing the wordstems. However, the magnitude of the priming effect was greater on the first day (Figure 2). The amnesics also exhib- ited a priming effect on both days, using an average of 8 presented and 2 unpre- sented words on the first day, and 7.5 presented and 2 unpresented words on the second day.
A 2 x 2 x 2 repeated measures ANOVA (of the control and simulator data) revealed a significant interaction between day and word list (F1,73 = 33.76, p < .01). Analyses of simple main effects revealed that on both Day 1 (F1,73 = 348.70, p < .01) and Day 2 (F1,73 = 98.27, p < .01), subjects used more of the presented than of the unpresented words to complete the wordstems. However, the difference between the number of presented words and unpresented words used was greater on the first (4.32) than on the second day (2.29). The main effect for group was also significant (F1,73 = 4.92, p < .05). Simulators gave more
20 0D Nonsimulating Controls (N=27) 2 u Simulators (N=48)
* Amnesics (N=4)
10 - 10 -
i 9- 9- ao T LL 8- , 8-
z2 3 7- 7- - 1:
6- 6- o 5- 5-
U- 44- T
Fig. 2. Priming effects on the wordstem completion test (Study 1).
z 3- ~ ;i~idki 3-.
Unpresented Presented Unpresented Presented DAY I DAY 2
Fig. 2. Priming effects on the wordstem completion test (Study 1).
67
WIGGINS AND BRANDT
idiosyncratic responses, using fewer of both the presented and the unpresented target words than the controls.
The consistency of a subject's response on the two days was used as another measure of implicit memory. The percentage of words used to complete the wordstems on Day 1 that were also used as responses on Day 2 was computed. As seen in Table 4, the simulators were less likely to give the same responses on the two days than were the controls (F1,73 = 7.42, p < .01) or the amnesics.
Word Association Task
Free Recall. The simulators (M = 6.4) recalled significantly fewer target words from the word association task than did the controls (M = 9.6; F1,73 = 20.46, p < .01). However, the simulators recalled more words than did the am- nesics (M = 4.5).
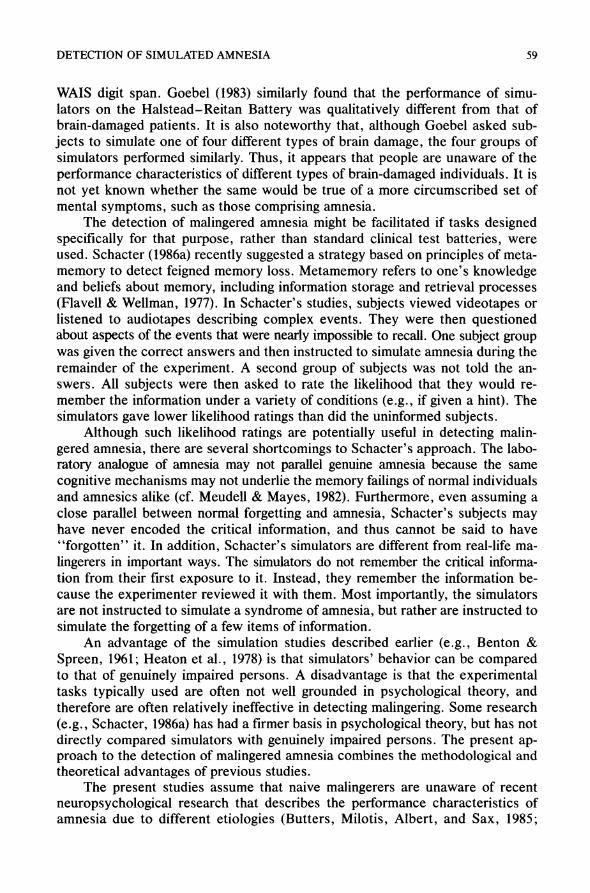
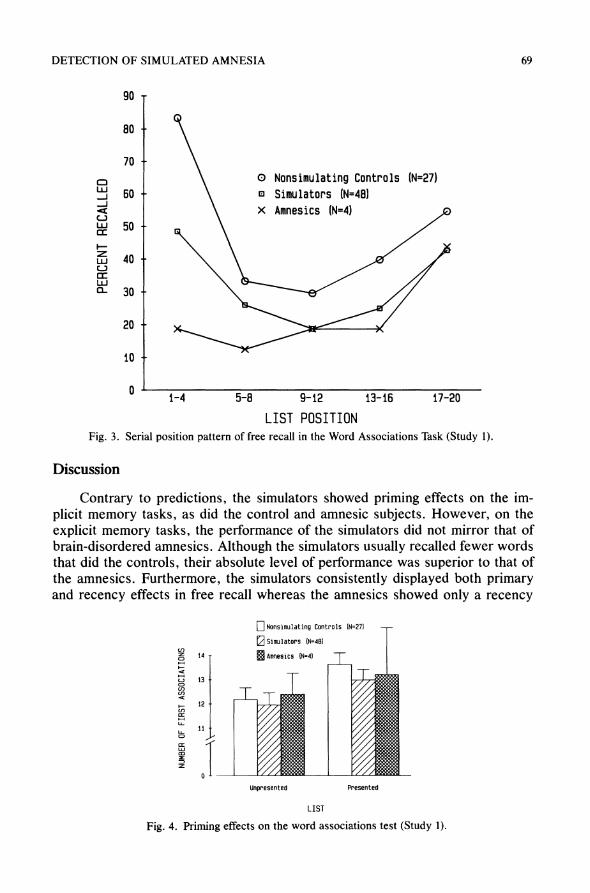
Despite slight differences in the shapes of their serial position curves, both the simulators and the controls exhibited primacy and recency effects in free re- call (Figure 3). The simulators and controls differed only in the magnitude of the primacy effect, with that of the controls being more pronounced. In contrast, the amnesics exhibited only a recency effect.
A 2 x 5 repeated measures ANOVA (of the control and simulator data) re- vealed a significant group by list position interaction (F4,292 = 3.29, p < .01). An orthogonal component analysis of list position showed this interaction due to a significant quadratic trend by group interaction (F1,73 = 6.05, p < .01). Although the primacy effect of the controls was larger, both groups exhibited a primacy and a recency effect. To confirm this result, each group was analyzed separately. Within each group, the quadratic trend accounted for the greatest portion of the sums of squares for list position (controls: SSquadratic/SSposition = 64; simulators:
SSquadratic/SSposition = 97). First Associations Test. As seen in Figure 4, both the simulators and the
controls exhibited a priming effect, giving a greater number of first associations to the stimulus words from the presented list than to those from the unpresented list (F1,73 = 13.08, p < .01). However, the magnitude of the priming effect was quite small and was equivalent across the control and simulating groups (average dif- ference = 1.3 words). The memory-disordered subjects also exhibited a slight priming effect, giving 13.25 presented and 12.5 unpresented words as their first associations.
Table 4. Percentage of Form 1 Responses Used as Responses on Form 2, Wordstem Completion Task, Study 1a
Memory Nonsimulating Simulators disordered controls
M 44.74 54.98 55.98 SD 17.87 15.55 15.80
a The simulators differ significantly from the controls (p < .01).
68
DETECTION OF SIMULATED AMNESIA
90 -
80 -
70
60 - O Nonsimulating Controls (N=27) o Simulators (N=48) x Amnesics (N=4)
50 -
40-
30 -
20 -
10 -
n 1-4 5-8 9-12 13-16 17-20
LIST POSITION Fig. 3. Serial position pattern of free recall in the Word Associations Task (Study 1).
Discussion
Contrary to predictions, the simulators showed priming effects on the im- plicit memory tasks, as did the control and amnesic subjects. However, on the explicit memory tasks, the performance of the simulators did not mirror that of brain-disordered amnesics. Although the simulators usually recalled fewer words that did the controls, their absolute level of performance was superior to that of the amnesics. Furthermore, the simulators consistently displayed both primary and recency effects in free recall whereas the amnesics showed only a recency
14
13
12
11
Unpresented Presented
LIST
Fig. 4. Priming effects on the word associations test (Study 1).
CJ
c:, LU
LLI C- I-r
LU c0
69
z o H
C _
o L-
cr
WIGGINS AND BRANDT
effect. Finally, the simulators more often gave implausible responses to the auto- biographical questions than did the amnesics.
The results of Study 1 suggest that people generally do not distinguish among amnesias of different etiologies and do not exhibit an awareness of the symptom- atic differences between neurologic and psychogenic amnesia. Although the three groups of subsimulators were given different instructions, they performed simi- larly on most of the experimental tasks.
The simulating subgroup did differ on one of the experimental measures. In the free recall test of the wordstem completion task, the psychogenic simulators recalled the same number of words as the control subjects, but fewer than the other simulating groups. Individuals with psychogenic or functional amnesia typi- cally have relatively mild anterograde memory disturbances (Pratt, 1977; Schacter et al., 1982). Therefore, as reflected by this particular task, the simu- lators were accurate in their differential portrayal of psychogenic amnesia. The generality of this result may be limited given that the three simulating groups recalled the same number of words on the other recall test (word associations task).
All three simulating groups feigned mild impairments on the anterograde memory tasks, but more severe impairments on the retrograde memory task (au- tobiographical interview). In fact, their performance on the autobiographical in- terview was far worse than that typical of brain-damaged amnesics, who rarely lose information about their personal identities (Pratt, 1977). Thus, it would ap- pear that simulators' feigned impairments are most like the impairments asso- ciated with psychogenic amnesia, which is characterized by a sudden inability to remember important personal information (Abeles & Schilder, 1935; Pratt, 1977).
These results reveal important information about lay-persons' beliefs con- cerning memory and amnesia. Evidently, memory is thought of as a process re- quiring attention and effort (i.e., recollecting), and does not include the "im- plicit" memory processes that cognitive psychologists have included under the rubric of "memory." These commonly held beliefs may prove useful in the de- tection of malingered amnesia.
STUDY 2
Amnesics of several neurological etiologies (e.g., alcoholic Korsakoff's syn- drome, rupture or repair of anterior communicating artery aneurysms, and herpes encephalitis) typically recognize previously presented material at much higher than chance rates, and often as well as normals (Huppert & Piercy, 1976, 1977; Volpe & Hirst, 1983; Starr & Phillips, 1970). This occurs even when recall perfor- mance is strikingly below normal. In the second study, free recall and forced- choice recognition tests were used to discover whether simulators would display this pattern of recall and recognition performance.
In addition to allowing a direct comparison of group performances, the two- alternative, forced-choice recognition procedure (Pankratz, 1983) allows another
70
DETECTION OF SIMULATED AMNESIA
potential way of distinguishing simulators from amnesics. Given that the baseline probability of success by guessing is 50%, simulated amnesia can be detected if an individual errs so consistently that accuracy is significantly worse than chance. A confidence level for chance performance can be determined by refer- ence to the binomial distribution (Meredith, 1967).
In a previous pilot experiment and case study, we suggested that simulated amnesia is characterized by forced-choice recognition performance worse than that found in organic amnesia (Brandt, Rubinsky, & Lassen, 1985). The present study replicates and extends the previous study, with different stimulus materials and a larger subject sample.
Method
Subjects
All of the subjects who participated in Study 1 participated in Study 2. An additional 53 subjects also participated in this second study.
Simulators. The composition of the three simulating groups was the same as in Study 1.
Memory disordered. An additional 21 patients with memory disorders re- sulting from brain damage were studied. The etiologies are listed in Table 5.
Nonsimulating Controls. An additional 32 subjects were recruited from the community and were paid for their participation. This increased the number of controls to 59.
Demographic information about the three subject groups is summarized in Table 6.
Experimental Task
Two 20-item lists of concrete nouns were used in this experiment. The lists were matched for word length, number of syllables, and frequency (mean fre- quency was 65.72 occurrences per million; Carroll, Davies, & Richman, 1971).
One of the word lists was read aloud by the subject. Presentation of the two lists was counterbalanced across subjects. Immediately after reading all 20 words, the subject was asked to recall as many words as possible. A two-alterna- tive, forced-choice recognition test was then administered. Choice cards, each containing a word from the presented list and a distractor (the matched word
Table 5. Etiology of Memory Disorders, Study 2
Number of Etiology subjects
"Fully resolved" closed head injury 15 Huntington's disease 3 Alzheimer's disease (early) 1 Frontal lobe infarct 1 Basal ganglia infarct 1
71
WIGGINS AND BRANDT
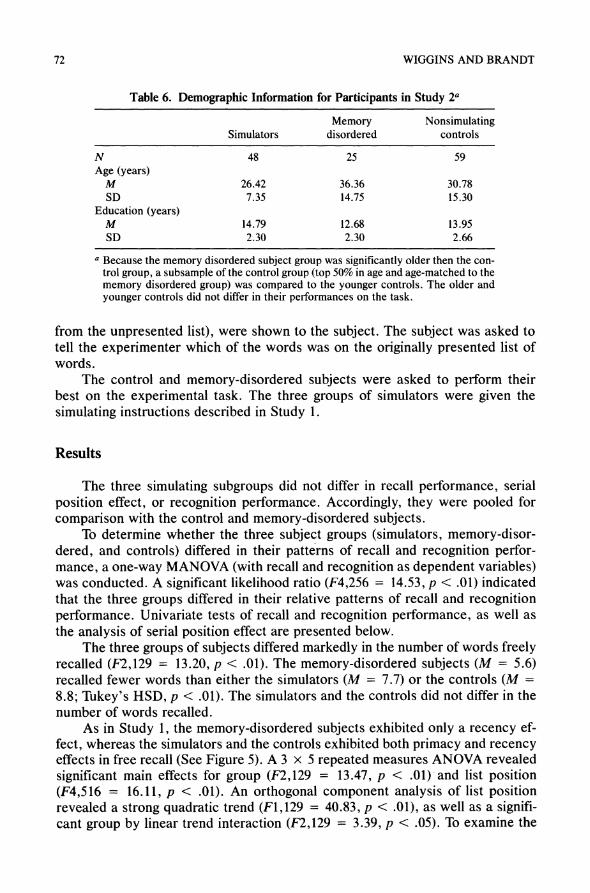
Table 6. Demographic Information for Participants in Study 2a
Memory Nonsimulating Simulators disordered controls
N 48 25 59 Age (years)
M 26.42 36.36 30.78 SD 7.35 14.75 15.30
Education (years) M 14.79 12.68 13.95 SD 2.30 2.30 2.66
a Because the memory disordered subject group was significantly older then the con- trol group, a subsample of the control group (top 50% in age and age-matched to the memory disordered group) was compared to the younger controls. The older and younger controls did not differ in their performances on the task.
from the unpresented list), were shown to the subject. The subject was asked to tell the experimenter which of the words was on the originally presented list of words.
The control and memory-disordered subjects were asked to perform their best on the experimental task. The three groups of simulators were given the simulating instructions described in Study 1.
Results
The three simulating subgroups did not differ in recall performance, serial position effect, or recognition performance. Accordingly, they were pooled for comparison with the control and memory-disordered subjects.
To determine whether the three subject groups (simulators, memory-disor- dered, and controls) differed in their patterns of recall and recognition perfor- mance, a one-way MANOVA (with recall and recognition as dependent variables) was conducted. A significant likelihood ratio (F4,256 = 14.53, p < .01) indicated that the three groups differed in their relative patterns of recall and recognition performance. Univariate tests of recall and recognition performance, as well as the analysis of serial position effect are presented below.
The three groups of subjects differed markedly in the number of words freely recalled (F2,129 = 13.20, p < .01). The memory-disordered subjects (M = 5.6) recalled fewer words than either the simulators (M = 7.7) or the controls (M =
8.8; Tukey's HSD, p < .01). The simulators and the controls did not differ in the number of words recalled.
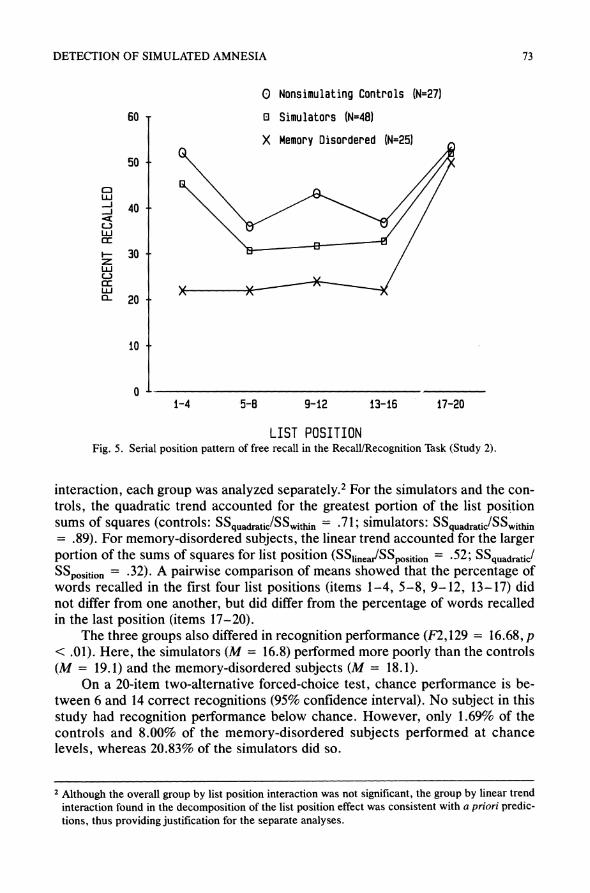
As in Study 1, the memory-disordered subjects exhibited only a recency ef- fect, whereas the simulators and the controls exhibited both primacy and recency effects in free recall (See Figure 5). A 3 x 5 repeated measures ANOVA revealed significant main effects for group (F2,129 = 13.47, p < .01) and list position (F4,516 = 16.11, p < .01). An orthogonal component analysis of list position revealed a strong quadratic trend (F1,129 = 40.83, p < .01), as well as a signifi- cant group by linear trend interaction (F2,129 = 3.39, p < .05). To examine the
72
DETECTION OF SIMULATED AMNESIA
0 Nonsimulating Controls (N=27)
60 - E Simulators (N=48)
X Memory Disordered (N=25)
50 -
Li. J 40 -
CLJ uJ a:
- 30-
Li
u- X X ?- 20 -
10 -
0- 1-4 5-8 9-12 13-16 17-20
LIST POSITION Fig. 5. Serial position pattern of free recall in the Recall/Recognition Task (Study 2).
interaction, each group was analyzed separately.2 For the simulators and the con- trols, the quadratic trend accounted for the greatest portion of the list position sums of squares (controls: SSquadratic/SSwithin = -71; simulators: SSquadraticSSwithin = .89). For memory-disordered subjects, the linear trend accounted for the larger portion of the sums of squares for list position (SSineaSSposition = 52; SSquadrtiJ SSpoition = .32). A pairwise comparison of means showed that the percentage of words recalled in the first four list positions (items 1-4, 5-8, 9-12, 13-17) did not differ from one another, but did differ from the percentage of words recalled in the last position (items 17-20).
The three groups also differed in recognition performance (F2,129 = 16.68, p < .01). Here, the simulators (M = 16.8) performed more poorly than the controls (M = 19.1) and the memory-disordered subjects (M = 18.1).
On a 20-item two-alternative forced-choice test, chance performance is be- tween 6 and 14 correct recognitions (95% confidence interval). No subject in this study had recognition performance below chance. However, only 1.69% of the controls and 8.00% of the memory-disordered subjects performed at chance levels, whereas 20.83% of the simulators did so.
2 Although the overall group by list position interaction was not significant, the group by linear trend interaction found in the decomposition of the list position effect was consistent with a priori predic- tions, thus providing justification for the separate analyses.
73
WIGGINS AND BRANDT
Discussion
The differences in the recall and recognition patterns of the three subject groups suggest a method for the differential diagnosis of neurologically-based memory deficits and malingering. The simulators portrayed amnesia, regardless of its etiology, as characterized by recall performance better than, and recogni- tion performance worse than, that of brain-damaged memory-disordered sub- jects. In addition, the simulators' serial position pattern resembled that of normals rather than that of amnesics.
Study 2, in combination with other recent reports (Brandt, Rubinsky, & Lassen, 1985; Pankratz, 1985), demonstrates how the forced-choice procedure may be used in the assessment of memory deficits. Below-chance recognition performance can occur only with knowledge of the target information. If one assumes that this knowledge is conscious, below-chance recognition performance can be used to distinguish malingering from genuine amnesia. Although Brandt et al. (1985) reported that 3 out of 10 simulators performed below chance, no simu- lator in the present study had a below-chance recognition performance. There- fore, although below-chance performance may indicate the presence of malin- gering, chance or above-chance performance does not rule out the possibility of malingering.
The simulators in the present study performed at chance levels much more frequently than did the subjects with neurologically based memory disorders. Thus, chance performance may also be useful in distinguishing malingering from amnesia due to brain damage. However, because there is no empirical evidence of how psychogenic amnesics would perform on the forced-choice task, chance recognition performance is not useful in distinguishing malingering from psycho- genic amnesia.
The following case study reported by Brandt, Rubinsky, and Lassen (1985) illustrates how the recall and forced-choice recognition tasks might be used in legal settings, once their reliability and validity have been established by addi- tional research. A 64-year-old man (L.G.) was charged with the murder of his wife. Although there were several witnesses to the murder, L.G. claimed total amnesia for the event. A standard neuropsychological assessment (the Halstead- Reitan Battery) revealed global cognitive impairment (Impairment Index = 1.0). L.G. was given a free recall and two-alternative forced-choice recognition tests for a list of 20 words. L.G. recalled four of the 20 target words, a performance comparable to memory-disordered patients. However, on the forced-choice rec- ognition test, he correctly selected only three target words. This performance is worse than chance, indicating that at some level, L.G. knew most of the 20 words. Because L.G.'s performance suggests that he was feigning his anterograde memory deficit, it may be reasonable to assume that his retrograde memory def- icit was similarly malingered. However, as Schacter (1986b) has commented, it is also possible that L.G.'s amnesia for the crime is genuine, and that he believed that performing poorly on other memory tasks would substantiate his claim. To determine which of the two interpretations is most plausible, further studies should investigate whether people simulating amnesia for a specific event will exhibit cognitive deficits on memory tasks unrelated to that event.
74
DETECTION OF SIMULATED AMNESIA
GENERAL DISCUSSION
Both of the studies reported here reveal that people have inaccurate beliefs about the cognitive features of amnesia, and that they do not distinguish among etiologically distinct amnestic disorders. Thus, it appears that the use of diag- nostic tasks based on knowledge about amnesia in general is a fruitful approach to the detection of malingering.
However, the existence of a wide variety of clinical memory disorders makes our approach to the detection of malingering difficult to implement. Highly dis- criminative diagnostic tasks can be developed only with substantial knowledge about the genuine amnestic disorders. Although neurologically-based amnesias have been well studied, most information about psychogenic amnesia derives from clinical descriptions of patients rather than from carefully designed experi- mental research. Experimental tasks that reliably distinguish between psycho- genic amnesia and malingering cannot be developed until the cognitive features of psychogenic amnesia are better documented. The recent quantitative case report of Schacter et al. (1982) is a significant step in the right direction.
Litigants in civil cases usually claim to have a neurologically based amnestic disorder (Schacter, 1986a). However, many criminal defendants claim to have a psychogenic amnesia ("Comment, Capacity to Stand Trial," 1967). Given the prevailing knowledge about amnesia, the present approach to the detection of malingering may be more useful in civil than in criminal cases.
Several other factors limit the generalization of these research findings to legal settings. First, although there were significant group differences on the ex- perimental tasks, the distribution of scores for simulators, controls, and memory- disordered subjects overlapped considerably. Because of the overlapping distri- butions, distinguishing between genuine and feigned amnesia is problematic for individual cases.
Second, people can easily obtain scientific information about their alleged memory disorder. People who have such information are likely to simulate cogni- tive disorders more accurately than people who do not have such information. However, if a large number of experimental tasks were used, it would be more difficult for a person to assimilate all the information that is necessary to consis- tently and accurately portray a memory disorder. Also, if many trials of forced- choice tasks were administered, it is unlikely that people could keep an accurate count of their correct/incorrect responses (Pankratz, 1983). Such a count would be necessary to perform consistently at a predetermined level of accuracy.
Finally, the laboratory atmosphere is very different from that encountered in a legal situation. In the present studies, it may be presumed that it was relatively unimportant to the research subjects whether they portrayed an amnesic patient accurately. However, being a convincing feigner has important consequences to a person involved in a legal matter. The present studies address the logically prior question of what lay-persons believe about amnesia. Future research should ad- dress how the enhanced motivation of real-world malingerers will affect their per- formance on the experimental tasks. Subsequent laboratory research could be designed to provide meaningful incentives for successfully deceiving the experi- menter.
75
WIGGINS AND BRANDT
APPENDIX: SIMULATION INSTRUCTIONS
Amnesia Resulting from a Head Injury
"During the experimental sessions, please answer any questions that you are asked and perform any tests that you are given the way you think the person described below would do it.
One afternoon as you were driving home from work, a car ran a stop sign and hit you. During the accident, you hit your head on the windshield of your car and were rendered unconscious for 24 hours. When you regained consciousness, you did not remember the accident and had developed other memory problems. Your physician referred you to a psychologist for testing."
Psychogenic Amnesia
"During the experimental sessions, please answer any questions that you are asked and perform any tests that you are given the way you think the person described below would do it.
There is only a one-year age difference between you and your brother. As children and as you grew older, the two of you were very close friends. You both chose to attend the same college and were involved in many of the same activi- ties.
One night you and he decided to attend a party in a neighboring town. At the party he became intoxicated and wanted to leave around 11:00 to go home. You knew your brother should not drive. Nevertheless, you decided to stay at the party and spend the night with friends. Your brother decided to drive the car home that night and return for you the next day.
On his way home, your brother was involved in an automobile accident and was killed. Since his death, you have not been able to remember what happened (as described above) the night he died. Friends, however, have told you what happened. Your physician referred you to a psychologist for testing because of your memory problems."
General Simulation Instructions
"During the experimental sessions, please answer any questions that you are asked and perform any tests that you are given the way you think a person with amnesia would do it."
REFERENCES
Abeles, M., & Schilder, P. (1935). Psychogenic loss of personal identity. Archives of Neurology and Psychiatry, 34, 587-604.
Allee, J. G. (1981). Webster's Dictionary. Baltimore: Ottenheimer Publishers. Baddley, A. D., & Warrington, E. K. (1970). Amnesia and the distinction between long and short-
term memory. Journal of Verbal Learning and Verbal Behavior, 9, 176-189.
76
DETECTION OF SIMULATED AMNESIA
Barona, A., Reynolds, C. R., & Chastain, R. (1984). A demographically based index of premorbid intelligence for the WAIS-R. Journal of Consulting and Clinical Psychology, 52, 885-887.
Bash, I. Y., & Alpert, M. (1980). The determination of malingering. Annals of the New York Academy of Sciences, 347, 86-99.
Benton, A., & Spreen, 0. (1961). Visual memory test: The simulation of mental imcompetence. Ar- chives of General Psychiatry, 4, 79-83.
Bousfield, W. A., Cohen, B. H., Whitmarsh, G. A., & Kincaid, W. D. (1961). The Connecticut free associational norms (Technical Report No. 35). University of Connecticut, Department of Psy- chology.
Bradford, J. W., & Smith, S. M. (1979). Amnesia and homicide: The Padola case and a study of thirty cases. Bulletin of the American Academy of Psychiatry and Law, 7, 219-231.
Brandt, J., Rubinsky, E. W. (Wiggins), & Lassen, G. (1985). Uncovering malingered amnesia. Annals of the New York Academy of Sciences, 44, 502-503.
Bruhn, A. R., & Reed, M. R. (1975). Simulation of brain damage on the Bender-Gestalt test by col- lege students. Journal of Personality Assessment, 39, 244-255.
Butters, N., Milotis, P., Albert, M. S., & Sax, D. S. (1985). Memory assessment: The evidence of the heterogeneity of amnesic symptoms. In G. Goldstein (Ed.), Advances in clinical neuropsy- chology. New York: Plenum Press.
Carroll, J. B., Davies, P., and Richman, B. (1971). Wordfrequency book. New York: American Heri- tage Publishing.
Comment, Capacity to stand trial: The amnesic criminal defendant. (1967). Maryland Law Review, 27, 182-193.
Corkin, S. (1965). Tactually-guided maze learning in man: Effects of unilateral cortical excision and bilateral hippocampal resions. Neuropsychologia, 3, 339-351.
Corkin, S. (1968). Acquisition of motor skill after bilateral hippocampal lesions. Neuropsychologia, 19, 337-356.
Corkin, S., Cohen, N. J., Sullivan, E. V., Clegg, R. A., Rosen, T. J., & Ackerman, R. H. (1985). Analyses of global memory impairments of different etiologies. Annals of the New York Academy of Sciences, 44, 10-40.
Diamond, R., & Rozin, P. (1984). Activation of existing memories in the amnesic syndrome. Journal of Abnormal Psychology, 93, 98-105.
Deutsch, P. M., & Raffa, F A. (1986). Damages in tort actions (Vol. 9). New York: Matthew Bender & Company.
Flavell, J., & Wellman, H. (1977). Metamemory. In R. V. Kail & J. W. Hagen (Eds.), Perspectives on the development of memory and cognition. Hillsdale, New Jersey: Erlbaum.
Gibbens, T. C. N., & Williams, J. E. H. (1977). Medicolegal aspects of amnesia. In C. W. M. Whitty & O. L. Zangwill (Eds.), Amnesia (2nd ed.) London: Butterworth.
Goebel, R. A. (1983). Detection of faking on the Halstead-Reitan neuropsychological test battery. Journal of Clinical Psychology, 39, 731-742.
Graf, P., Mandler, G., & Haden, P. E. (1982). Simulating amnesic symptoms in normals. Science, 218, 1243-1244.
Graf, P., Squire, L. R., & Mandler, G. (1984). The information that amnesics do not forget. Journal of Experimental Psychology: Learning, Memory, and Cognition, 10, 164-178.
Guthkelch, A. N. (1980). Posttraumatic amnesia, post-concussional symptoms and accident neurosis. European Neurology, 19, 91-102.
Guttmacher, M. S. (1955). Psychiatry and the law. New York: Grune & Stratton. Heaton, R. K., Smith, H. H., Lehman, R. A. W., & Vogt, A. T. (1978). Prospects for faking believ-
able deficits on neuropsychological testing. Journal of Consulting and Clinical Psychology, 46, 892-900.
Huppert, F. A., & Piercy, M. (1976). Recognition memory in amnesic patients: Effects of temporal context and familiarity of material. Cortex, 12, 3-20.
Huppert, F. A., & Piercy, M. (1977). Recognition memory in amnesiac patients: A defect of acquisi- tion? Neuropsychologia, 15, 643-652.
Kaushall, P., Zetin, M., & Squire, L. R. (1981). A psychosocial study of chronic circumscribed am- nesia. Journal of Nervous and Mental Disease, 169, 383-389.
77
WIGGINS AND BRANDT
Klatzky, R. L. (1980). Human memory. San Francisco: W. H. Freeman. Lezak, M. D. (1983). Neuropsychological assessment (2nd ed.). New York: Oxford University Press. Martone, M., Butters, N., Payne, M., Becker, J. T., and Sax, D. S. (1984). Dissociations between
skill learning and verbal recognition in amnesia and dementia. Archives of Neurology, 41, 965-970.
Meredith, W. M. (1967). Basic mathematical and statistical tables for psychology and education. New York: McGraw-Hill.
Meudell, P., & Mayes, A. (1982). Normal and abnormal forgetting: Some comments on the human amnesic syndrome. In A. W. Ellis (Ed.), Normality and pathology in cognitive functions (pp. 203-237). London: Academic Press.
Milner, B. (1978). Clues to the cerebral organization of memory. In P. A. Buser & A. Rougeul-Buser (Eds.), Cerebral correlates of conscious experience. Amsterdam: Elsevier.
Moscovitch, M. (1982). Multiple dissociations of function in amnesia. In L. S. Cermak (Ed.), Human memory and amnesia. Hillsdale, New Jersey: Erlbaum.
Moscovitch, M. (1984). The sufficient conditions for demonstrating preserved memory in amnesia: A task analysis. In L. R. Squire & N. Butters (Eds.), The neuropsychology of memory. New York: Guilford Press.
Pankratz, L. (1983). A new technique for the assessment and modification of feigned memory deficit. Perceptual and Motor Skills, 57, 367-372.
Pratt, R. T. C. (1977). Psychogenic loss of memory. In C. W. M. Whitty and 0. L. Zangwill (Eds.), Amnesia. London: Butterworth.
Price, G. E., & Terhune, W. B. (1919). Feigned amnesia as a defense reaction. Journal of the Amer- ican Medical Association, 72, 565-567.
Rubinsky, E. W. (Wiggins), & Brandt, J. (1986). Amnesia and criminal law: A clinical overview. Be- havioral Sciences and the Law, 4, 27-46.
Schacter, D. L. (1985). Priming of old and new knowledge in amnesic patients and normal subjects. Annals of the New York Academy of Sciences, 44, 41-53.
Schacter, D. L. (1986a). Amnesia and crime: How much do we really know? American Psychologist, 41, 286-295.
Schacter, D. L. (1986b). On the relationship between genuine and simulated amnesia. Behavioral Sciences and the Law, 4, 1-26.
Schacter, D. L., Wang, P. L., Tulving, E., & Freedman, M. (1982). Functional retrograde amnesia: A quantitative case study. Neuropsychologia, 20, 523-532.
Shimamura, A. P., & Squire, L. R. (1984). Paired-associate learning and priming effects in amnesia: A neuropsychological study. Journal of Experimental Psychology, 113, 556-570.
Spreen, O., & Benton, A. (1963). Simulation of mental deficiency on a visual memory test. American Journal of Mental Deficiency, 67, 909-913.
Squire, L. R., & Butters, N. (Eds.). (1984). The neuropsychology of memory. New York: Guilford Press.
Starr, A. & Phillips, L. (1970). Verbal and motor memory in the amnesic syndrome. Neuropsycho- logia, 8, 75-88.
Swiercinsky, D. P. (Ed.) (1985). Testing adults. Kansas City: Test Corporation of America. Volpe, B. T., & Hirst, W. (1983). Amnesia following the rupture and repair of an anterior communi-
cating artery aneurysm. Journal of Neurology, Neurosurgery, and Psychiatry, 46, 704-709. Warrington, E. K., & Weiskrantz, L. (1968). A new method of testing long-term retention with special
reference to amnesic patients. Nature, 217, 972-974. Warrington, E. K., & Weiskrantz, L. (1970). Amnesic syndrome: Consolidation or retrieval? Nature,
228, 628-630. Warrington, E. K., & Weiskrantz, L. (1974). The effect of prior learning on subsequent retention in
amnesic patients. Neuropsychologia, 16, 169-177. Williamsen, J. A., Johnson, H. J., & Eriksen, C. W. (1965). Some characteristics of post-hypnotic
amnesia. Journal of Abnormal Psychology, 70, 123-131.
78




















