Long-term retrograde amnesia . . . the crucial role of the hippocampus
22
Neuropsychologia 39 (2001) 151 – 172 Long-term retrograde amnesia… the crucial role of the hippocampus Lisa Cipolotti a, *, Tim Shallice b,c , Dennis Chan d , Nick Fox d , Rachel Scahill d , Gail Harrison a , John Stevens e , Peter Rudge e a Department of Clinical Neuropsychology, National Hospital for Neurology and Neurosurgery, Queen Square, London WC1N 3BG, UK b Institute of Cogniti6e Neuroscience, Uni6ersity College London, London, UK c SISSA, Trieste, Italy d Dementia Research Group, National Hospital for Neurology and Neurosurgery, Queen Square, London, UK e National Hospital for Neurology and Neurosurgery, Queen Square, London, UK Received 27 October 1999; received in revised form 12 July 2000; accepted 17 July 2000 Abstract For patients with hippocampal pathology, disagreement exists in the literature over whether retrograde amnesia is temporally limited or very extensive depending on whether the anatomical damage is restricted to this structure or also involves additional temporal cortex. We report a comprehensive assessment of retrograde and anterograde memory functions of a severely global amnesic patient (VC). We found that he presented with a remarkably extensive and basically ungraded retrograde amnesia. This impairment profoundly affected four decades preceding the onset of his amnesia and encompassed both non personal and personal facts and events. VC also presented with a severe anterograde amnesia and a deficit in the acquisition of new semantic knowledge in the post-morbid period. Detailed MRI volumetric measurements revealed gross abnormalities in both hippocampi which were markedly shrunken. Of relevance to the debate on retrograde amnesia were the observations that the volumes of both entorhinal cortices and the remainder of both temporal lobes were normal. These data suggest that the hippocampus is critical not only for the efficient encoding and hence normal recall of new information but also for the recall of episodic information acquired before the onset of amnesia. Our results are compatible with the view that retrograde amnesia is both extensive and ungraded when the damage is limited to the hippocampus. © 2000 Elsevier Science Ltd. All rights reserved. Keywords: Hippocampal pathology; Retrograde amnesia; Memory functions www.elsevier.com/locate/neuropsychologia 1. Introduction Organic amnesia caused by non-progressive brain damage is a selective impairment of memory that usu- ally occurs in the absence of clear intellectual dysfunc- tion and/or loss of general knowledge [43]. The memory impairment in amnesia is usually global, being both anterograde and retrograde [55]. Occasionally patients may present with severe anterograde amnesia (AA) but minimal retrograde amnesia (RA) [90,91]. Even less commonly, patients may present with what Kapur [26] named ‘focal retrograde amnesia’, namely severe RA in the context of very mild or completely absent AA [16,34,73]. Both the anterograde and the retrograde memory impairments cover complex sets of phenomena whose extent, nature and anatomical bases are still relatively poorly understood. Thus, the precise relation- ship between RA, AA and additional ‘executive’ cogni- tive deficits remains unclear (see for discussion [58]). Also different, often contrasting, cognitive theories have been put forward to account for the pattern of retrograde and anterograde memory loss [8,10,11,30,57]. The present paper focuses on the controversial issue of the structures involved in RA. It is generally ac- cepted that severe amnesic states are only observed in patients with bilateral damage [42]. However, there is considerable debate over the role played in amnesia by * Corresponding author. Tel.: +44-207-8298793; fax: +44-207- 8132516. E-mail address: [email protected] (L. Cipolotti). 0028-3932/00/$ - see front matter © 2000 Elsevier Science Ltd. All rights reserved. PII:S0028-3932(00)00103-2
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Long-term retrograde amnesia . . . the crucial role of the hippocampus

Neuropsychologia 39 (2001) 151–172
Long-term retrograde amnesia… the crucial role of thehippocampus
Lisa Cipolotti a,*, Tim Shallice b,c, Dennis Chan d, Nick Fox d, Rachel Scahill d,Gail Harrison a, John Stevens e, Peter Rudge e
a Department of Clinical Neuropsychology, National Hospital for Neurology and Neurosurgery, Queen Square, London WC1N 3BG, UKb Institute of Cogniti6e Neuroscience, Uni6ersity College London, London, UK
c SISSA, Trieste, Italyd Dementia Research Group, National Hospital for Neurology and Neurosurgery, Queen Square, London, UK
e National Hospital for Neurology and Neurosurgery, Queen Square, London, UK
Received 27 October 1999; received in revised form 12 July 2000; accepted 17 July 2000
Abstract
For patients with hippocampal pathology, disagreement exists in the literature over whether retrograde amnesia is temporallylimited or very extensive depending on whether the anatomical damage is restricted to this structure or also involves additionaltemporal cortex. We report a comprehensive assessment of retrograde and anterograde memory functions of a severely globalamnesic patient (VC). We found that he presented with a remarkably extensive and basically ungraded retrograde amnesia. Thisimpairment profoundly affected four decades preceding the onset of his amnesia and encompassed both non personal andpersonal facts and events. VC also presented with a severe anterograde amnesia and a deficit in the acquisition of new semanticknowledge in the post-morbid period. Detailed MRI volumetric measurements revealed gross abnormalities in both hippocampiwhich were markedly shrunken. Of relevance to the debate on retrograde amnesia were the observations that the volumes of bothentorhinal cortices and the remainder of both temporal lobes were normal. These data suggest that the hippocampus is critical notonly for the efficient encoding and hence normal recall of new information but also for the recall of episodic information acquiredbefore the onset of amnesia. Our results are compatible with the view that retrograde amnesia is both extensive and ungradedwhen the damage is limited to the hippocampus. © 2000 Elsevier Science Ltd. All rights reserved.
Keywords: Hippocampal pathology; Retrograde amnesia; Memory functions
www.elsevier.com/locate/neuropsychologia
1. Introduction
Organic amnesia caused by non-progressive braindamage is a selective impairment of memory that usu-ally occurs in the absence of clear intellectual dysfunc-tion and/or loss of general knowledge [43]. The memoryimpairment in amnesia is usually global, being bothanterograde and retrograde [55]. Occasionally patientsmay present with severe anterograde amnesia (AA) butminimal retrograde amnesia (RA) [90,91]. Even lesscommonly, patients may present with what Kapur [26]named ‘focal retrograde amnesia’, namely severe RA in
the context of very mild or completely absent AA[16,34,73]. Both the anterograde and the retrogradememory impairments cover complex sets of phenomenawhose extent, nature and anatomical bases are stillrelatively poorly understood. Thus, the precise relation-ship between RA, AA and additional ‘executive’ cogni-tive deficits remains unclear (see for discussion [58]).Also different, often contrasting, cognitive theorieshave been put forward to account for the pattern ofretrograde and anterograde memory loss[8,10,11,30,57].
The present paper focuses on the controversial issueof the structures involved in RA. It is generally ac-cepted that severe amnesic states are only observed inpatients with bilateral damage [42]. However, there isconsiderable debate over the role played in amnesia by
* Corresponding author. Tel.: +44-207-8298793; fax: +44-207-8132516.
E-mail address: [email protected] (L. Cipolotti).
0028-3932/00/$ - see front matter © 2000 Elsevier Science Ltd. All rights reserved.PII: S 0 0 2 8 -3932 (00 )00103 -2

L. Cipolotti et al. / Neuropsychologia 39 (2001) 151–172152
several critical structures within the medial temporallobe (hippocampus, entorhinal, perirhinal andparahippocampal cortices) and the related diencephalicmidline structures (mammillary bodies, anterior thala-mic nuclei, medial dorsal thalamic nuclei, thalamicnucleus and mammillothalamic tract). We will be pri-marily concerned with the role of the hippocampus.The role of the hippocampus in memory has been atopic of much debate and speculation. Different theo-ries have been put forward regarding its function andits interaction with the neocortex. Those theories sug-gesting that only a particular kind of memory is depen-dent on the hippocampus will not be considered here[19,49,50].
Central to most of the theories focusing on the roleof the hippocampus in RA is the notion expressed byRibot [54] more than 100 years ago that the loss ofmemories from the past could be temporally graded.This phenomenon has influenced a number of accountswhich have accorded to the hippocampus a relativelyextended but nevertheless time limited role in memorytasks. Marr [36] was among the first to propose that thehippocampus acts as a temporary memory store for thestorage of new information whilst the neocortex acts asa permanent memory store. On this type of theory, thehippocampus is viewed as a ‘simple memory’ temporar-ily storing traces and playing them back to be consoli-dated in the neocortex for permanent storage possiblyduring dream sleep. The view that the hippocampusplays a role in memory consolidation and in providingextra learning opportunities for the neocortical perma-nent memory store is also present in the work of Squireand colleagues [65,69–72]. The authors proposed thatover a somewhat vaguely specified period of time,contents are assumed to become gradually independentof the hippocampus and dependent on neocortical stor-age sites. This is due to the action of the memoryconsolidation process.
Recently, a number of neuronal network modelshave also been based on this view ([39,40,45,76,77]; seefor a review [67]). For example, on the Treves and Rolls[76,77] model there is detailed discussion of how thehippocampus might store information rapidly and havea crucial role in directing memory consolidation. Inparticular, in this model, when a partial cue is presentedthe hippocampus can reconstruct memory in theneocortex by activating neocortical sites. Across timeand as a result of repeated reactivation, memories arefully established in the neocortex. Similar ideas arepresent in the model described by Murre [44,45] andAlvarez and Squire [2]. Murre’s TraceLink modelstressed the importance of hippocampus as a temporary‘scaffold’ for new memories, serving as an intermediate‘link system’ of connections, before they are well estab-lished at a neocortical level, the ‘trace system’. In theAlvarez and Squire’s neuronal network model of con-
solidation, information is first stored in a fast learning‘medial temporal lobe area’ which then graduallystrengthens slower-changing connections in a dis-tributed ‘neocortical’ network. In the computationalmodel proposed by McClelland and colleagues [40] ithas also been suggested that recently experienced eventsare first stored through fast-changing synapses in thehippocampus in a ‘condensed’ form. This computa-tional model offered a principled justification of whythe consolidation process would require complementarylearning systems in the hippocampus and neocortex.According to this view, rapid learning of new associa-tion would provoke fast changes in the cortical repre-sentations that would lead to so-called catastrophicinterference. Thus, it is crucial to have a system thatcan learn rapidly independently of neocortex, but ableto gradually modify it. So, on this model, repeatedreinstatement of the hippocampal memory results in theaccumulation of gradual and slow neocortical changes.This process allows the new memory to be integratedinto existing neocortical networks. Remote memory isbased on these accumulated neocortical changes.
All these theories would predict that if the pathologyis restricted to the hippocampus, the RA should betemporally graded such that recent memory is moreimpaired than remote memory. The existence of anextensive and ungraded RA would only occur if thepathology also involves the neocortex and is not re-stricted to the hippocampus. Furthermore, if the dam-age is limited to the neocortex and the hippocampus isspared then the RA should primarily affect remotememories with recent memories being preserved. Insupport of this, several empirical studies have docu-mented extensive and ungraded RA in patients whosepathology was NOT confined to the hippocampus butalso extends to the neocortex [9,14,37,78]. Furthermore,relative preservation of more recent memories has beenfound in patients with semantic dementia, a pathologythat is thought to mainly involve the temporal neocor-tex and much less so the hippocampus [21].
Even more compelling evidence for the view that thehippocampus has an important but temporally limitedrole in memory comes from studies reporting thathippocampal amnesics show selective memory deficitsonly for material acquired shortly before their lesion.Retrieval of more remote memories appears to be rela-tively preserved (see for review [66,67]). Among the bestknown examples, are four patients (RB, [92] and GD,WH and LM, [53]) who presented with RA limited to 1or 2 years (RB and GD) or �15 years (WH and LM).Neurohistological data indicated that RB and GD hada bilateral lesion limited to the CA1 region of thehippocampus. WH and LM presented with a bilaterallesion involving all the cell fields of the hippocampusand the dentate gyrus. However, LM also had cell lossin layers II and III of the midportion of the entorhinal

L. Cipolotti et al. / Neuropsychologia 39 (2001) 151–172 153
cortex. WH had more substantial cell loss in the en-torhinal cortex.
Recently four new patients (LJ, AB, EP and GT)have been reported whose RA has been investigatedextensively [52]. In two patients (LJ and AB), the RAwas limited to the decade preceding the onset of amne-sia whilst in the other two (EP and GT) the RA wassevere and extensive. MRI examinations revealed thatLJ presented with a roughly 36% bilateral volumetricreduction of the hippocampus. In contrast EP and GTpresented with severe bilateral temporal damage involv-ing the hippocampus. For AB the authors presumed acircumscribed hippocampal lesion on the basis of theaetiology of his amnesia, a cardiac arrest. Thus, accord-ing to the authors, this study provides further com-pelling support for the position that damage to thehippocampus produces only limited RA and that addi-tional temporal cortical damage is needed to producesevere and extensive RA. Moreover, the authors referspecifically in their discussion to the two patients (WHand LH; see [53]) who presented with an extensive RAof 15 and 25 years, respectively, in whom the additionaltemporal damage was located in the entorhinal cortex.
However, there are also on record a few patients inwhom it is unclear what role any impairment in tempo-ral cortical areas is playing in their extensive and un-graded RA. One example is patient NT. This patientwas first reported in 1964 as presenting a severe mem-ory impairment following a right temporal lobectomyfor the treatment of epilepsy [15]. Formal investigationof her remote memories indicated an extensive andungraded RA [56]. The neuropathological investigationrevealed an old sclerotic lesion of the left hippocampus.Examination of the previously removed right temporallobe revealed no clear abnormalities [84]. Thus, it istempting to conclude that the RA in this patient was aconsequence of the bilateral damage to the hippocam-pus, given that the left temporal lobe was pathologi-cally intact. Patient HJ with a Korsakoff’s psychosispresented with a severe amnesia in the absence of anyother focal cognitive impairment [33]. His retrogradeamnesia was of very long duration and not temporallygraded on formal testing. The only abnormalitiespresent at the neuropathological investigation involvedthe mammillary bodies and the medial dorsal nucleus ofthe thalamus. All other regions, including the neocor-tex, were normal.
In the context of these findings it is useful to considerthe patient described by Kartsounis et al. [29]. TheMRI findings on this patient showed a circumscribedabnormal signal in the CA1 and CA2 fields. An initialneuropsychological investigation suggested a severe am-nesic syndrome. In particular, the patient was describedas having an extensive retrograde memory loss, al-though no formal documentation of the extent of theRA was reported This study, therefore provided some
preliminary clinical evidence of severe RA due to dam-age limited to the hippocampus.
Thus, attempts to identify the role of the hippocam-pus on RA have produced conflicting and controversialresults, which have led to extensive debate in the litera-ture. For example, suggestions have been made that thepatients reported above with extensive and ungradedRA without clear cortical involvement must have hadcortical ‘hidden pathology’ (see for further discussion[1,28,52,67]). One possible problem which is often men-tioned is that the neuronal dysfunction caused by is-chaemia may be more extensive than the region of grosspathology [3,20]. In line with this position, a recentPET study [35] has been held to highlight the limitationof relying on MRI to uncover functional damage, espe-cially in cases of anoxia (for example see [1]). It should,however, be noted that the patient described byMarkowitsch and colleagues to demonstrate this pointperformed poorly on non-verbal tests of general intelli-gence and had an MRI scan indicating subcortical andcortical atrophy with widening of the ventricles.
The problems of hidden cortical pathology, for ex-ample, apply to Kartsounis et al.’s [29] patient. How-ever, they apply equally to the hippocampal patient LJdescribed by Reed and Squire [52]. Reed and Squire[52] also described patient AB as an hippocampal pa-tient. However, this was based on an highly speculativeinference based on the aetiology. No neuroradiologicalor post-mortem evidence was available. It should alsobe noted that the argument for hypothetical but unde-tected cortical pathology is one which allows theoriststo select findings as they please. For instance, Reed andSquire [52] in the same paper quote the Kartsounis etal.’s patient as supporting their position that thehippocampus is central for learning new factual knowl-edge but reject the evidence from him on the role of thehippocampus in retrograde amnesia. On the basis of aninadequate argument from his neurological history,they conclude ‘…it seems unlikely that his damagecould be limited to the CA fields of thehippocampus…’.
In addition, concerns have been expressed about thepatients presenting with temporally limited RA whereremote memories are spared. Often in these cases theseverity of the amnesia [89] and the methodology em-ployed for testing remote memories [60] have beencriticised. For instance, consider the two hippocampalpatients (AB and LJ) with temporally limited RA re-cently reported by Reed and Squire [52]. For the onlypatient (LJ) who we can be relatively sure had circum-scribed hippocampus damage, there is a serious ques-tion over the severity of the amnesia. This patient’sWMS-R verbal score was only one standard deviationbelow her IQ, although her WMS-R visual score wastwo standard deviations below her IQ. More critically,her performance on recall tests of public events and
L. Cipolotti et al. / Neuropsychologia 39 (2001) 151–172154
famous faces was within the control range for all threetime periods considered (1–10 years before amnesia;11–20 years before amnesia; and 21–30 years beforeamnesia). Given these indications of only limited amne-sia, the significance of her apparent temporal gradientin autobiographical memory is questionable.
Even more critically, the methodology used to testretrograde memory was inadequate. Tests were used inwhich the level of performance was equated acrossdifferent retention intervals. However, it was shownmathematically by Shallice [60] that if one differentiatessemantic from episodic memory processes, for whichnow there is strong neurological evidence, then this ismethodologically inappropriate (see also [86]). One iscomparing the retention of predominantly semantic, orpersonal semantic [9] information for longer time inter-vals with retention of predominantly episodic informa-tion over shorter time periods. No justification isprovided by Reed and Squire [52] for the methodologyused. It should be noted that a similar problem alsoapplies to the investigation of the retrograde amnesia ofpatient RB reported by Zola-Morgan et al. [91].
An alternative methodology is not subject to thiscriticism. This involves matching information retainedover different time intervals by how well it was initiallylaid down, rather than by how well it is remembered.This was the procedure adopted in the initial investiga-tion of retrograde memory by Warrington and Sanders[87]. The authors carried out an internal test of theirassumption. They confirmed that the material used intheir tests was not part of the general knowledge (se-mantic memory) of anyone in the culture by showingthat intelligent teenagers could only retrieve the mostrecent events.
In this Introduction we have concentrated on thecontroversial issue related to the role of the hippocam-pus in retrograde memory. It seems likely that for thisissue, detailed investigations of a large number of indi-vidual case studies are needed in order to determine thecritical anatomical structures. Without such studies wewill be unable to identify the roles not only of thehippocampus but also of a number of structures in themedial temporal lobe and diencephalic midline whichmay be of potential relevance for the processes involvedin retrograde memory. For this purpose two types ofpatients are important: (1) those who show surprisingsparing in memory skills given the relevant anatomicalstructures damaged; (2) those who despite restrictedlesions show severe deficits in retrograde memory tasks.
In this study we report a further examination of apatient of the second type, namely the profoundlyamnesic patient (VC) previously described by Kartsou-nis et al. [29]. Detailed MRI volumetric examinationswere undertaken and revealed the presence of veryrestricted and quantifiable areas of neuronal damage.Comprehensive assessment of his amnesia revealed a
remarkably extensive and ungraded RA affecting bothpersonal and non-personal memories. These results as-sist in the understanding of the anatomical structureswhich are necessary for effective storing and retrieval ofthe mnestic traces.
2. Case report
The patient (VC) is a 73-year-old (born 1926) retiredchief engineer in large ships such as liners who wasreported by his wife as having an excellent memory. InMay 1992 he developed an apparent severe migraineattack which was followed by a seizure. He was foundto have a tachyrhythmia when admitted to hospital andrecovered. In September 1993 he had two furtherseizures four days apart with a tachyrhythmia requiringcardioversion. Following these episodes, at the age of67, he was profoundly amnesic. Since then he had nofurther epileptic episodes. His past history was unre-markable apart from mild reversible chronic obstructiveairways disease. Whilst working at sea he had con-sumed considerable amounts of alcohol but this hadnever impaired his ability to function at a high level inhis highly responsible position. Moreover, his memoryfunctions were reportedly excellent during this period.For at least 15 years prior to his presentation he hadnever consumed more than 20 units per week, and oftenmuch less according to his wife. Neurological examina-tion revealed a profound amnesia and a minor butvariable impairment of pain assessed by pin prick overthe left hand and foot. The remainder of the neurolog-ical examination was normal.
Extensive investigations were undertaken. Apartfrom the neuroradiological abnormalities (see below),the only abnormality was a mild impairment of leftventricular function of echocardiography. In particular,VDRL, liver function tests, full blood count, serum B12and thyroid function were all negative or normal. An-giography of the extra-cranial vessels was normal.
3. Neuroradiological studies
3.1. Qualitati6e studies
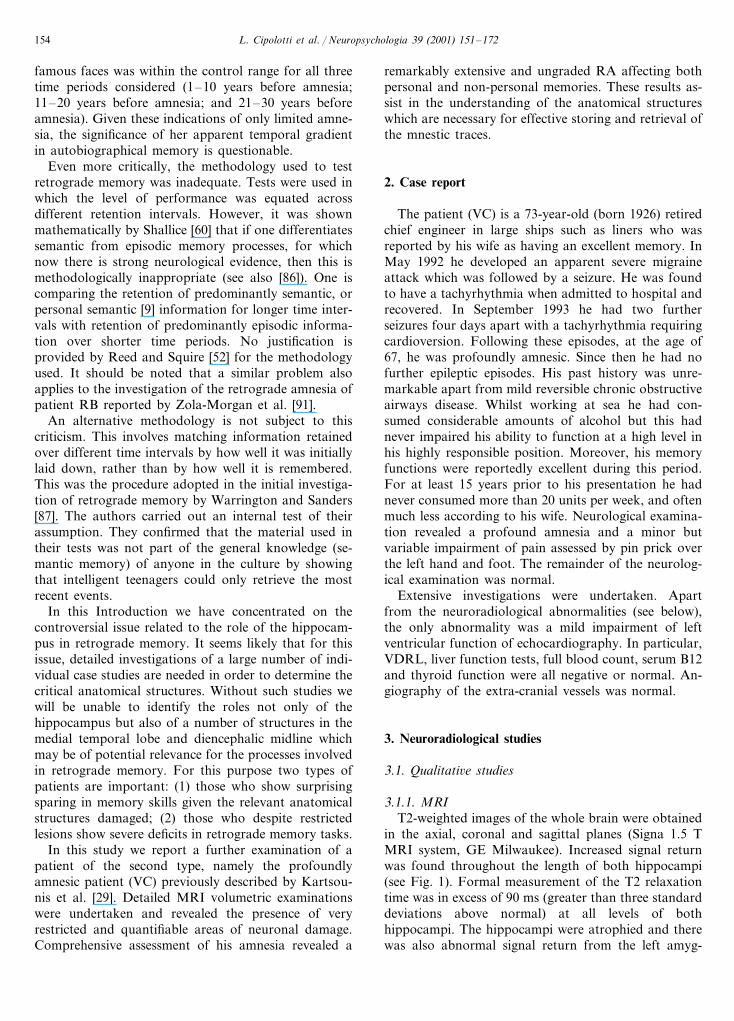
3.1.1. MRIT2-weighted images of the whole brain were obtained
in the axial, coronal and sagittal planes (Signa 1.5 TMRI system, GE Milwaukee). Increased signal returnwas found throughout the length of both hippocampi(see Fig. 1). Formal measurement of the T2 relaxationtime was in excess of 90 ms (greater than three standarddeviations above normal) at all levels of bothhippocampi. The hippocampi were atrophied and therewas also abnormal signal return from the left amyg-

L. Cipolotti et al. / Neuropsychologia 39 (2001) 151–172 155
dala. There was no evidence of abnormal signal returnfrom any other part of the brain. In particular boththalami were normal. In view of the report by Kapur etal. [25] of focal retrograde amnesia and bilateral tempo-ral lobe pathology particular attention was paid to theappearance of the anterior temporal lobes. In this in-stance the temporal poles, anterior middle temporalgyri and anterior parahippocampal gyri of both sideswere observed to be entirely normal.
3.1.2. PETResting PET scans (Siemens ECAT 951 scanner)
were obtained; 250 Mbq of 18FDG were administered.The field of view was 10 cm and the resolution 7 mmFWHM. Decreased tracer uptake was seen throughoutthe right thalamus and possibly the right parietal regioncompared to the left (see for further details [28]).
3.2. Quantitati6e studies
In order to measure more precisely the anatomicalstructures involved detailed MRI volumetric analysiswas undertaken.
3.2.1. Volumetric MRI: methodology and regions ofinterest
The patient VC and six age-matched healthy controlmales (see Table 1) underwent high resolution volumet-ric T1-weighted MRI scanning. All images were ob-tained using a 1.5 T Signa scanner. Volumetric imagingwas performed in the coronal plane using a spoiledgradient echo technique with a 24 cm field of viewyielding 124 1.5 mm thick contiguous coronal slicesthrough the head on a 256×128 image matrix withacquisition parameters (35/5/1/35–TR/TE/NEX/FLIP),which have been used previously in studies ofhippocampal volumetric and morphometric studies [12].This allowed regions of interest to be outlined with
comparable landmarks and orientation in such way asto improve reproducibility. The MIDAS image analysistools were used for regional segmentation [17]. Theseinclude semi-automated morphological operators whichallow brain volumes to be extracted reliably from thevolume data set. The editing tools allow simultaneousmultiplanar display and editing, which permits viewingof sagittal sections through a region while the region isoutlined in the coronal plane. Editing appears in realtime on all planes and this improves the reproducibilityof volumetric analysis. In order to compensate fordifferent brain sizes between individuals all measure-ments were normalised to the total brain volume. Allmeasurements were performed blind to the subject andto the left/right orientation of the measured region.
3.2.1.1. The hippocampus. Segmentation of thehippocampus was undertaken using the followingguidelines. Rostrally, measurements commenced at itsjunction with the caudalmost portion of the amygdala.The caudalmost hippocampal measurement was takenat the point of the longest length of the fornix (thecrus). Superiorly, medially and laterally the hippocam-pus was bounded by the cerebrospinal fluid (CSF) inthe choroid fissure and the ambient cistern and inferi-orly the hippocampus was bounded by the white matterseparating it from the parahippocampal gyrus. Thismethod excludes the tail of the hippocampus in orderto achieve satisfactory reproducibility of segmentation,and has been documented elsewhere [62]. Mean intra-rater (RS) variability for segmentation of this regionwas 3%.
3.2.1.2. The entorhinal cortex. Segmentation of the en-torhinal cortex (EC) was undertaken using a protocolsimilar to that of Insausti et al. [23,24], which wasbased on cytoarchitectonic guidelines observed in thenormal adult human brain. White matter was not in-
Fig. 1. Coronal sections through temporal lobe at the level of the body of the hippocampus. High signal return seen in each hippocampus(TR2000/TE30 ms and 5 mm thick).

L. Cipolotti et al. / Neuropsychologia 39 (2001) 151–172156
Tab
le1
Vol
umet
ric
MR
Ida
taon
VC
and
six
cont
rol
subj
ects
a
LP
HG
RP
HG
LT
LR
TL
LST
GR
STG
LM
ITG
RM
ITG
LF
GB
rain
vol.
(mm
3)
RF
GL
HP
CR
HP
CL
EN
TR
EN
T
0.26
30.
292
5.47
85.
928
1.82
62.
000
2.03
40.
041
1.93
50.
047
0.43
40.
568
0.13
40.
124
105
652
8V
CN
o.of
S.D
.BC
TR
X−
2.90
−0.
96−
0.96
−0.
29−
0.38
0.87
1.45
−0.
21−
0.98
0.30
1.60
−5.
89−
4.16
−1.
45−
0.18
Con
trol
s(C
TR
)0.
414
0.32
66.
232
6.35
31.
594
1.51
80.
235
2.43
50.
226
2.26
40.
452
0.49
10.
069
124
814
8C
10.
063
0.05
10.
054
0.34
10.
495
4.97
06.
233
1.36
21.
696
1.80
52.
296
0.27
20.
418
0.24
4C
20.
273
105
407
0C
30.
444
101
472
80.
334
5.68
26.
203
1.73
71.
804
1.99
62.
488
0.55
70.
529
0.23
20.
241
0.06
60.
049
0.33
80.
339
5.72
06.
045
1.64
61.
701
2.23
80.
030
2.43
70.
257
0.37
90.
500
0.03
8C
41
198
406
0.26
30.
053
115
294
00.
367
0.33
85.
344
5.61
01.
774
1.96
22.
025
1.72
30.
280
0.54
80.
237
0.23
10.
058
C5
0.36
70.
317
5.64
95.
782
1.89
11.
908
1.98
82.
056
0.46
10.
491
C6
127
518
60.
204
0.20
00.
062
0.04
5
0.37
90.
358
5.59
96.
038
1.66
71.
765
2.08
10.
057
2.21
10.
238
0.40
00.
496
0.04
9M
ean
(X)
115
724
60.
236
S.D
.0.
040
104
730
0.06
90.
421
0.28
70.
182
0.16
20.
221
0.28
30.
112
0.04
50.
019
0.02
50.
011
0.01
1
aL
,lef
t;R
,rig
ht;H
PC
,hip
poca
mpu
s;E
NT
,ent
orhi
nalc
orte
x;P
HG
,par
ahip
poca
mpa
lgyr
us;T
L,t
empo
rall
obe;
STG
,sup
erio
rte
mpo
ralg
yrus
;MIT
G,m
iddl
ean
din
feri
orte
mpo
ralg
yri;
FG
,fus
ifor
mgy
rus.
All
volu
mes
for
the
abov
ere
gion
sar
eex
pres
sed
aspe
rcen
tage
sof
the
tota
lbr
ain
volu
me.

L. Cipolotti et al. / Neuropsychologia 39 (2001) 151–172 157
cluded within this measurement. Rostrally, the EC ex-tended as far as the rostral extreme of the sulcussemiannularis and caudally the EC is found to endapproximately 1mm beyond the end of the gyrus in-tralimbicus. However, for the purposes of reproduci-bility in this study the EC was not measured beyondthe end of the gyrus intralimbicus. Superiorly, the ECwas bounded by the white matter separating it fromthe amygdala (rostrally) and the hippocampus (cau-dally). Inferomedially, the EC was bounded by theCSF of the ambient cistern and laterally the EC ex-tended as far as the collateral sulcus. As with Insaustiet al. [24], the termination of the EC along the collat-eral sulcus was determined by the depth of the sulcus:if the sulcus depth was less than 1cm then the cytoar-chitectonic border of the entorhinal and perirhinalcortices was located at the fundus; if the sulcus depthwas between 1 and 1.5 cm then this border wasfound approximately halfway along the medial bankof the collateral sulcus; and if the sulcus depth wasgreater than 1.5cm then the border was located at themedial edge of the sulcus. Mean intra-rater (DC)variability for segmentation of this region was 4%.
3.2.1.3. The parahippocampal gyrus. A measurementwas made of the parahippocampal gyrus correspond-ing to the rostrocaudal length of the hippocampus.This extended from the coronal section containing themost rostral part of the head of the hippocampus tothe longest length of the fornix caudally. The whitematter layer was included in the measurements. Thesuperomedial border was the interface between theinferior boundary of the hippocampus and the whitematter layer, and superolaterally the border wastaken as the junction of the white matter layer withthe inferior edge of the choroid fissure. Inferomediallythe gyrus was bounded by the CSF of the ambientcistern and inferolaterally by the collateral sulcus.Mean intra-rater (RS) variability for segmentation ofthis region was 6%.
3.2.1.4. The temporal lobe. Segmentation of the wholetemporal lobe was achieved by using the difference insignal intensity between the grey matter of the tempo-ral lobe and the surrounding CSF. Satisfactory out-lining of this region was produced by setting aminimum threshold of 60% of the mean brain inten-sity. At this setting it was ensured that no parts ofthe temporal lobe were incorrectly excluded. Theboundary between the temporal lobe and the remain-der of the brain was defined by drawing a straightline across the temporal stem. The lateral extreme ofthis line was taken as the junction of the superome-dial base of the superior temporal gyrus and the in-feromedial extreme of the sylvian fissure. A line wasdrawn from this point to the most superior point of
the temporal lobe on the medial side of the stem.This point corresponded to the juxtaposition of thestem to the superomedial portion of the amygdalarostrally, and to the superomedial extreme of thehippocampus at more caudal levels. Mean intra-rater(RS) variability for segmentation of this region was3%.
4. Results
Summary of the results are reported in Table 1.
4.1. The hippocampus
The longest length of the hippocampus in midsagit-tal section, from the rostralmost extent of the head tothe body of the hippocampus caudally at the level ofthe crus of the fornix, measured 32.4 mm for the lefthippocampus and 31.4 mm for the right hippocam-pus. Both measures were well below the controlsrange (normal controls: left mean 39.3 mm, range36.2–41.2 mm; right mean 37.6 mm, range 33.6–40.6mm) Striking loss of hippocampal volume was notedthroughout the length (see Fig. 2a, VC; and Fig. 2b,healthy control). The morphology of the head wasstrikingly abnormal, with a sharp demarcation fromthe caudomedial amygdala and near total loss of thedigitationes hippocampi. At this level the cross-sec-tional area is markedly reduced, suggesting damage tothe CA1 field. Both the uncal sulcus and the tempo-ral horn are particularly prominent (see Fig. 3a andb). More caudally, the portion of the hippocampussuperior to the uncal sulcus is reduced in cross-sec-tional area, reflecting damage not only to CA1 butalso to the CA3 and CA2 fields (and possibly alsothe dentate gyrus). Beyond the caudal end of the un-cus, the morphology of the hippocampal body wasless distorted but still reduced in cross-sectional area(see Fig. 4a and b). At this level the left fimbria wasso reduced it was virtually absent and the width ofthe right fimbria was severely reduced. At the level ofthe crus of the fornix the hippocampal body was stillof small cross-sectional area, but it was not possibleto relate this reduction in area to specific damagewithin the different hippocampal subfields. Both leftand right fornices are also noted to be reduced insize, which again represents the loss of efferent fibresfrom the hippocampal formation, although it must benoted that the fornix also contains afferent fibresfrom the medial septum to the hippocampus.
The reduction in volume across the rostrocaudallength of the hippocampus is illustrated in Fig. 5aand b. Of particular interest is the observation thatthe volume loss in cross-sectional area is seen alongthe entire length of both hippocampi.

L. Cipolotti et al. / Neuropsychologia 39 (2001) 151–172158
Fig. 2. Mid-sagittal sections through the left hippocampus of VC (a)and control subject (b) (T1-weighted MRI). In VC the uncal sulcus isprominent and there is a reduction in size along the entire length ofthe hippocampus.
subjects), as did the length of the entorhinal cortexfrom its junction with the pre- and parasubiculum at itssuperomedial border to its inferolateral border with theperirhinal cortex. The volume of the left entorhinalcortex was less than 2 S.D. below the control mean andthe volume of the right entorhinal cortex was less than1 S.D. below the control mean. These measurementsare provided in Table 1.
Fig. 3. Coronal sections through the head of the left hippocampus ofVC (a) and the control subject (b) (T1-weighted MRI). In VC thereis a near total destruction of the hippocampus (consisting primarily ofthe CA1 field) superior to the uncal sulcus.
4.2. The entorhinal cortex
There were no gross morphological abnormalities. Inthe case of VC, the greatest depth of the collateralsulcus was less than 1 cm and the border of theentorhinal cortex with the perirhinal cortex was there-fore considered to be situated at the fundus of thecollateral sulcus (see above). Of note is the fact thatthere was no widening of the collateral sulcus, and thethickness of the grey matter in this region appearedwithin normal limits (when compared with the control

L. Cipolotti et al. / Neuropsychologia 39 (2001) 151–172 159
Fig. 4. Coronal section through the body of the left hippocampus ofVC (a) and the control subject (b) (T1-weighted MRI). In VC thereis a general reduction of cross-sectional area.
control mean while the volume of the leftparahippocampal gyrus was slightly reduced (betweentwo-three SD below the control mean; see Table 1).This mild degree of volume loss was clearly much lessthan that noted for the hippocampi.
4.4. The temporal lobe
There were no gross morphological abnormalities. Inparticular, there was no thinning of the temporal stem,no flattening of the gyri, and no widening of the sulci.The absence of obvious structural abnormalities wasreflected in the volumetric analyses of the temporallobe. The volumes of both left and right lobes werewithin normal limits as were the volumes of the gyriwhen measured individually (see Table 1).
4.5. Neuropsychological assessment
The patient was first referred to the NeuropsychologyDepartment of the National Hospital for Neurologyand Neurosurgery in September 1993 for evaluation ofhis memory difficulties. The results of this first assess-ment, together with an experimental investigation fo-cusing on his amnesia, are reported elsewhere [28]. Hehas subsequently been reassessed on three differentoccasions. The experimental investigation that will bedescribed here took place around the time of his fourthand last neuropsychological assessment (April 1998).The results of his four formal neuropsychological as-sessments are reported in Table 2.
When first assessed on the Wechsler Adult Intelli-gence Scale-Revised (WAIS-R) in September 1993 heobtained an average verbal IQ and a high averageperformance IQ. This reflected only a very mild under-functioning of his verbal skills with respect to hisestimated high average pre-morbid optimum on theNational Adult Reading Test [48]. His nominal skills,as assessed by the Graded Difficulty Naming test forboth objects were intact (GNT [41]). Similarly, hisvisuoperceptual and visuo spatial skills were well withinnormal limits (incomplete letters and cube analysisfrom the visual object and space perception battery(VOSP) [85]). He also performed within normal limitson two tests sensitive to frontal lobe dysfunction (Weiglsorting test [88], and the cognitive estimates test [61]).By contrast, his memory functions were severely im-paired, with deficits both in anterograde memory, af-fecting both verbal and visual material, and inretrograde memory, affecting both personal and non-personal memories.
In the second and third assessments, his cognitiveprofile remained static, except for a steady improve-ment of his performance on the non-verbal part of theWAIS-R. However, it seems likely that this improvedperformance was due to well-known ‘practice effect’
4.3. The parahippocampal gyrus
There were no obvious morphological abnormalitiesof the grey matter of the parahippocampal gyrus butthe white matter layer was noted to be reduced in size,particularly at the rostral end of the gyrus, between thehead of the hippocampus superiorly and the entorhinalcortex inferiorly. The depth of the collateral sulcus waswithin normal limits, as was the mediolateral length ofthe gyrus, from the white matter medial to the pre- andparasubiculum to the lateral border of the gyrus at thefundus of the collateral sulcus. The volume of the rightparahippocampal gyrus was less than one SD below the

L. Cipolotti et al. / Neuropsychologia 39 (2001) 151–172160
artefacts. The most notable feature remained his severememory impairment (see Table 3). By the time of hisfourth neuropsychological assessment (April 1998) hisverbal IQ continued to remain static in the upper endof the average range while his performance IQ hadfurther improved and was at a very superior level. Hisperformance on the GNT remained at a high averagelevel and his performance on the object decision test ofvisuoperception remained at a normal level. On twotests of frontal ‘executive’ skills (Wisconsin card sorting
[47]; Hayling test [6]) his performance was entirelysatisfactory. In particular on the Wisconsin card sortingtest he obtained the 6 categories rapidly and made noperseverative errors. His attention and concentrationabilities were clearly completely intact. The most nota-ble feature at this time remained his global amnesia.
In summary, VC presented with an intact perfor-mance on general intelligence, focal language, percep-tion and frontal ‘executive’ tasks which remained staticover a 5-year period. This indicated that there was no
Fig. 5. Cross-sectional areas along the rostrocaudal length of left (a) and right (b) hippocampi.

L. Cipolotti et al. / Neuropsychologia 39 (2001) 151–172 161
Table 2Cognitive test scoresa
March 96 Febuary 97 April 98March 93
105Verbal IQ 10299 105Performance IQ 111 120 136 141GNT (O) 20/30 (25–50%ile) 17/30 (10–25%ile) 23/30 (75%ile) 23/30 (75%ile)
n.t. n.t. 20/30 (75%ile)GNT (P)20/20Incomplete letters 20/20 n.t. n.t.10/10Cube analysis 10/10 n.t. n.t.
18/20 17/20n.t. 17/20Object decisionWeigl PP P n.t.
P PP n.t.Cognitive estimatesn.t.Wisconsin card sorting n.t. P Pn.t.Hayling test n.t. n.t. 17 (average)
a GNT (O), graded difficulty naming test — objects; GNT (P), graded difficulty naming test — proper nouns; %ile, percentile; n.t., not tested;P, passed.
Table 3Anterograde memory test scoresa
March 96 Febuary 97 April 98March 93
35/50 (5%ile)RMW 35/50 (5%ile)33/50 (B5%ile) 36/50 (B10%ile)RMF 32/50 (B5%ile) 34/50 (B5%ile) 41/50 (25–50%ile) 39/50 (B25%ile)TM n.t.13/30 (B5%ile) 14/30 (B5%ile) 13/30 (5%ile)
n.t. 3/12 (B5%ile) 3/12 (B5%ile)3/12 (B5%ile)Famous faces
Story recall5 (B5%ile)Immediate n.t. n.t. 7.5 (B5%ile)
n.t n.t.0 0Delay
List learning 18/95 (B5%ile)Paired associates n.t.n.t n.t T1=4/24 (5%ile)
T2=8/24 (5%ile)
Rey–Osterrieth figure10/36 (B10%ile)Immediate n.t. n.t. 35/36 (90%ile)
n.t. n.t0/36 5/36 (B5%ile)Delay
Door and peoples testNames testImmediate verbal recall 6/36 (B1%ile)
3/12Delayed verbal recallVerbal recognition test A 5/12 (B1%ile)
2/12 (B1%ile)Verbal recognition test B
Doors visual recognition test7/12 (B1%ile)Test A
Test B 1/12 (B1%ile)
Shapes testImmediate visual recall 13/36 (B1%ile)Delayed visual recall 4/12
a RMW, recognition memory test for words; RMF, recognition memory test for faces; TM, topographical memory test; %ile, percentile; n.t.,not tested.
progressive cognitive decline. An in depth assessment ofhis severe memory impairment is documented below.
4.6. Anterograde memory assessment: recognition andrecall tests
Throughout the four neuropsychological investiga-tions, VC was assessed on a variety of anterograde
memory tests involving both recognition and recallparadigms (see Table 3). Verbal and visual recognitionmemory was assessed using alternative versions of therecognition memory test (RMT) [82] and on the topo-graphical memory test of outdoor scenes recognition[83]. Verbal recall memory was assessed on the storyrecall and the list learning subtests of the adult memoryand information processing battery [13] and on the

L. Cipolotti et al. / Neuropsychologia 39 (2001) 151–172162
paired associates learning test [83]. Visual recall memorywas assessed on the Rey–Osterreith complex figure [51]and on the current famous faces test. In addition, thedoors and people test [4], which includes parallel recog-nition and recall based tests of verbal and non-verbalmemory was administered at the time of his fourthneuropsychological assessment.
At the initial assessment (March 1993), his perfor-mance was globally impaired on recognition and recallmemory tests. Through the second (March 1996) andthird (February 1997) assessments only his verbal, visualrecognition and visual recall memory were re-assessed.His verbal recognition memory, as assessed by theRMT, remained severely impaired whilst his perfor-mance had somewhat improved for visual recognitionmemory for unfamiliar faces. However, his visual recog-nition memory functions remained gravely impaired foroutdoor scenes. Similarly, his visual recall memory forcurrent famous faces remained profoundly impaired.
At the time of his fourth neuropsychological investi-gation (April 1998) it was clear that he remainedseverely amnesic. For example, he was never able torecognise the experimenters although he saw two ofthem (LC and PR) on several occasions for prolongedperiods of time over a period of several years. It wasnoted, on one occasion, that when the experimenters lefthim alone for a few minutes, they were not recognisedon their return. His amnesia was so severe that he wasnot able to recall even extremely poignant personalevents. For example, the experimenters went to visit himat his home, very shortly after the funeral of his wife,with whom he had been happily married for 40 years.He had no recollection of her death nor of the funeral.Indeed, he asked on several occasions why she was notaround the house.
A further formal reassessment of his memory func-tions was undertaken. His verbal and visual recognitionmemory skills remained severely impaired. He obtaineda borderline defective score on the verbal version of theRMT and a low average score on the visual version. Hissomewhat improved performance on the RMT couldhave arisen through practice effects (Cipolotti et al., inpreparation). On a further and more stringent visualrecognition memory test (the topographical memorytest) his performance remained gravely impaired. On thefamous current faces test his score remained as gravelyimpaired as at the time of his first assessment. Interest-ing paramnesic errors were noted in this test. Forexample he named Clinton as ‘Nixon… no… he fol-lowed Nixon… I think he is Kennedy’ and he namedTerry Wogan, an Irish TV personality, as ‘EamonAndrews’, an Irish TV personality famous in the 60s.When asked to recall the Coughlan and Hollows’ Storyand the Rey–Osterreith figure, following a 30-min de-lay, he was unable to remember even being exposed tothem. Similarly, his performance was very impaired on
the list learning and the paired associated learning test.On the doors and people test [4], he did not achieve thecut-off for an overall age-scaled score of 1. Analysis ofhis performance on the various subtests revealed that hepresented with a marked verbal and visual memoryimpairment. Interestingly, this grave impairment equallyaffected recognition and recall processes.
In summary, the results of the anterograde memoryassessment indicate the presence of a severe globalmemory impairment affecting both recognition and re-call which remained static over a 5-year period.
5. Experimental investigation
In the following experimental investigation we investi-gated VC’s memory functions further. We assessedsystematically the severity and the temporal extent ofVC’s retrograde memory using four different tests: thedead or alive test, the famous public events question-naire test, the famous faces test, and the famous peoplenames familiarity test. The status of VC’s autobiograph-ical memory and semantic knowledge in both theanterograde and the retrograde domains was alsoexplored.
For the novel tests, groups of normal control subjectsmatched to VC on the basis of age and educational levelwere used. Different groups of control subjects arereported for the different tests. Their biographical de-tails and performance will be reported below.
5.1. Retrograde memory
5.1.1. Experiment 1: dead or ali6e testThis test of retrograde memory [27] assesses memory
for personalities who have been famous over the last 30years. In this test the patient is required to indicatewhether a famous personality was dead or alive,whether he/she had been killed or had died of naturalcauses and to indicate when the person died by choosingbetween eight time periods, sampling 4 years between1950 and 1989. VC’s performance was compared withthat of the control subjects reported in the Kapur et al.,[27] study. These controls were comparable to VC interms of age and optimal level of pre-morbid function-ing. VC performed extremely poorly on this test. Hispercentage of overall correct answers was only 47%,which is severely impaired relative to the controls. Thus,this result provides the first formal evidence that VCshowed a marked memory loss for public events.
5.1.2. Experiment 2: famous public e6ents questionnairetest (recall and three alternati6e forced choice)
Following the procedure used by Sanders and War-rington [56] a questionnaire test of famous public

L. Cipolotti et al. / Neuropsychologia 39 (2001) 151–172 163
Fig. 6. Results on the famous public events questionnaire test.
tempt was made to avoid events subject to repeatedreview in the media, movies and books. For example,events such as the Watergate scandal were excluded.These types of event, being regularly re-discussed in themedia, have effectively become part of generalknowledge.
The test was first administered in a recall format (e.g.Where in India was the chemical leak which killed 2000and affected a further 200 000?), and then immediatelyafterwards in a three-alternative multiple choice format.This consisted of the correct answers and two plausiblealternative answers (e.g. Bhopal, Kanpur or Bombay?).Alternatives which were phonologically similar or re-lated to another similar event were, for the most part,avoided. The patient was asked to choose the correctone, guessing if necessary. The questions were presentedin a random order, with contemporary events mixed inwith more remote events.
A normal control sample of 24 subjects, age (meanage=67.31 years; S.D.=4.56) and matched education-ally (mean age left full time education=17.2 years;S.D.=3.3) were also given this test. The results for VCand the control subjects are shown in Fig. 6. Thisshows mean percentage correct for each 5-year periodsampled.
VC’s performance on the recall version of the testwas at floor. He was virtually unable to recall any eventfrom all the time periods sampled. On three alternativeforced choice version of the test his performance wasalso markedly impaired. Indeed, his performance was atchance for two time periods (1980–84 and 1975–79)and only marginally above chance level for the remain-ing time periods.
For the purposes of statistical analyses the eight timeperiods were collapsed into four decades (1960s, 1970s,1980s and 1990s). For the recall condition, raw scoreswere first converted using a square root transformation,because the distribution was skewed upwards with along tail. As shown in Table 4(a) there was a significantdifference between VC and the normal control groupfor recalling all four time periods.
events was constructed with the aim of matching themeasurability of events at the time of their occurrence(for discussion of the importance of this procedure, see[38,60]). The test consisted of 120 questions aboutpublic events which were deemed to be of major impor-tance. The Chronicle of the 20th Century 1995 andwidely distributed British newspapers (Times, DailyTelegraph, Independent and the Guardian) were usedas source of items. There were eight sets of 15 questionssampling events for each 5-year period between 1960and 1998. The questions required a mixture of placenames (e.g. Where in India was the chemical leak whichkilled 2000 and affected a further 200 000?), people’snames (e.g. Which female tennis player was stabbed inthe back by a rival’s fan?) and a description of an eventas the response (e.g. What caused the fire at YorkMinster?). The questions were matched as far as possi-ble across the eight different time periods. For eachtime period an effort was made to choose questionsjudged to be most striking at the time of the event, thiswas subject to the constraint that in the case of themore remote events only those which were no longerdiscussed in public life were included. Thus, every at-
Table 4Famous public events questionnaire test: (a) recall and (b) multiple choice recognition
Controls mean percentage score (%)VC percentage score (%) Z P
(a) Comparison of square root transform of raw scores ( /30) for VC and controls3.31960s 42 2.61 B0.005
281970s B0.0251.973.31980s 470 4.37 B0.001
533.31990s B0.0013.31
(b) Comparison of arcsin transform of raw scores ( /30) for VC and controls1960s 50 67 1.03 B0.2
B0.081.4154301970s81 2.981980s B0.00243841990s 2.156 B0.02

L. Cipolotti et al. / Neuropsychologia 39 (2001) 151–172164
For the three alternative forced choice condition,prior to analysis raw scores were converted using arcsintransform, as scores were distributed binomially. Asshown in Table 4(b), there were significant differencesbetween VC and the control group on the performancefor the 1980s and 1990s. However, no statistical signifi-cance was found for the 1960s and 1970s. This mayhave been simply due to decreasing power of the testsfor the later time periods. The controls were performingless well and thus the probability of finding a significantdifference with VC was reduced. In this context, itshould be noted that if one collapse together the 60sand 70s decades his performance did not significantlydiffer from chance. VC’s performance was less than twostandard deviations above chance for those twodecades. In contrast, the performance of the controlsfor both decades was well above two standard devia-tions from chance.
The performance of the control subjects showed theexpected superiority of the three alternative forcedchoice condition over the recall condition. Further-more, there was a clear decline both on the threealternative forced choice and the recall versions of thetest, as the questions referred to events that were moreremote in time (see for similar results [87]). This wasconfirmed by a page test for ordered alternatives. Thistest was carried out on both recall and three alternativeforced choice conditions for the normal controls scores.For both conditions significant trends were found,(N=24, K=4, recall−ZL=4.24, PB0.001, recogni-tion−ZL=5.44, PB0.001), indicating that more re-cent events were more likely to be answered correctlythan more remote events. This suggests that our selec-tion criteria for the construction of the test weremethodologically sound and the questions for the dif-ferent time periods were balanced.
In summary, the performance of VC on the famousevents questionnaire provides no evidence that moreremote memories were spared or less impaired thanmore recent memories. The time span covered by thistest antedates the onset of VC’s amnesia by more than30 years and post-dates the onset of VC’s amnesia by�5 years. Nonetheless, VC was grossly impaired in themore sensitive version of the test, i.e. the recalling ofboth very remote and very recent events. Thus, VCexhibited an equally severe anterograde and retrogradememory loss. The severe retrograde memory loss ap-pears to cover a period of more than 30 years.
5.1.3. Experiment 3: famous faces test (recall and threealternati6e forced choice)
Using principles and techniques similar to thoseutilised for the public events questionnaire test, a retro-grade memory test for famous faces was constructed.This test included 145 monochrome photographs ofpublic figures, judged to be the most striking at a
particular period of time. There were four sets ofphotographs sampling famous faces of four decades,between 1960 and 1998. In each decade there were thefollowing number of photographs: 1960s=31, 1970s=32, 1980s=43 and 1990s=39. It would be inappropri-ate to attempt to limit faces to a 5-year period as ispossible for events. The famous public figures where amixture of British and American politicians (e.g. Clin-ton), actors, singers and TV personalities (e.g. OprahWinfrey), sportsmen (e.g. the footballer Paul Gas-coigne), and people associated with a famous event (e.g.Louise Woodward, recently involved in the death of achild). An effort was made to ensure that the differenttypes of professions were as matched as possible acrossthe four different time periods. As in the case of the‘remote’ events only those famous personalities whosepublic life was no longer much discussed in the media,were included. Thus, for example photographs of some-one like Jacqueline Kennedy–Onassis who rose to famein the sixties but continued to remain so until thenineties were excluded. A pilot study on seven youngpeople (mean age=19.9 years; S.D.=3.5) revealed thatthe chosen personalities of the 60s and 70s were un-known to them (0 for both decades). This confirmedthat our chosen personalities were indeed famous onlywithin that period.
As with the famous public events questionnaire test,there were two versions of the famous faces test: recalland three alternative forced choice. On the recall ver-sion VC was presented with each photograph andrequested to orally name the famous person (e.g.William Hague, current leader of the UK ConservativeParty). On the three alternative forced choice versioneach unrecalled famous face photograph was presentedtogether with three multiple choice names (e.g. Whichof the following is the name of the person? MichaelPortillo, William Hague or Chris Patten?; all are well-known UK Conservative politicians). The alternativeswere other names of famous people. The patient wasasked to choose the correct one, guessing if necessary.The recall condition was tested first, followed immedi-ately by the recognition condition, which was givenwhile the patient was inspecting the photograph. Thefamous faces photographs belonging to different timeperiods were presented in a random order.
VC’s performance was compared with that of 20control subjects, age (mean age=68.6 years; S.D.=10.8) and educationally matched (mean age left fulltime education=16.8 years; S.D.=2.4). The results forVC and the control subjects are shown in Fig. 7. Thisshows the percentage correct for each decade sampled.
Similar results were obtained on the famous faces testas with the famous events questionnaire test. Thus,VC’s performance was at floor in the recall version. Hewas virtually unable to recall any famous personalityfor all the time periods sampled. On the three alterna-

L. Cipolotti et al. / Neuropsychologia 39 (2001) 151–172 165
Fig. 7. Results on the famous faces test.
native forced choice conditions (n=4, k=20, recall−ZL=6.66, PB0.001, recognition−ZL=5.42,PB0.001).
In summary, these results replicated and extendedthose obtained in the previous task. VC has a profoundmemory impairment for recent and remote famousfaces. In particular in the recall condition he was gravelyimpaired for items from his period of anterogradeamnesia as well as for items from the three decadespreceding his stroke. Thus, in the recall condition therewas again a lack of evidence for the preservation ofremote memories. This indicated that VC suffered froman extensive and ungraded retrograde amnesia. Thethree alternative forced choice condition will be consid-ered further in the discussion.
5.1.4. Experiment 4: famous people names familiaritytest
In experiments 1, 2, and 3 we demonstrated that whenassessed with recall and alternative forced choice tech-niques VC had an extensive loss of retrograde memoriesinvolving both events and famous people. The aim ofthis experiment was to investigate whether VC mighthave implicitly retained retrograde memories by using afamiliarity judgement test. Familiarity judgement testshave been shown to be performed within normal limitsby some densely amnesic patients who presented withpreserved implicit knowledge of public figures [89].
Four sets of 15 names of famous people were assem-bled; one set was of personalities who were prominent inthe 60s; one set was of personalities who were promi-nent in the seventies; one set was of personalities whowere prominent in the 80s and; one set was of personal-ities who were prominent in the 90s. As in the case ofthe ‘remote’ famous faces test only those names offamous people whose public life was no longer muchdiscussed in the media were included. Each famousname was paired with two unknown distractors (e.g.Boris Chronnell, Paul Chenier, Konstantin Chernenko).In the list of three names (the target and the twodistractors) the target name occurred equally often ineach position. The triplets of names were presented in a
tive forced choice version of the test his performancewas superior to his performance on the recall version.However, his performance in this condition, althoughabove chance, was also impaired.
For the recall condition, raw scores were first con-verted using a square root transformation, as the con-trol distribution was skewed upwards with a long tail.As shown in Table 5(a) there was a significant differencebetween VC and the normal control group for the recallof famous faces for all the four decades tested.
For the three alternative forced choice condition priorto analysis raw scores were first transformed using anarcsin transform, as scores were distributed binomially.As shown in Table 5(b) there was a significant differencebetween VC and the control group for the recognitionperformance in the 1990s and a strong trend in the1980s result. However, no statistical difference wasfound for the other two decades.
Control subjects showed the expected decline in per-formance as the photographs were of people that werefamous at an earlier period in time, both on the recalland on the three alternative forced choice version of thetest. This was confirmed by a page test for orderedalternatives which demonstrated the expected decrementin performance with more remote faces. A significanttrend was indeed found both for recall and three alter-
Table 5Famous faces test: (a) recall and (b) multiple choice recognition
VC percentage score (%) Controls mean percentage score (%) Z P
(a) Comparison of square root transform of proportional scores for VC and controls6 271960s 1.98 B0.02
1970s 2.200 18 B0.011980s B0.0014.19400
5 50 3.781990s B0.001
(b) Comparison of arcsin transform of proportional scores for VC and controls70 B0.151.101960s 54
B0.40.46641970s 56B0.081980s 65 82 1.41B0.0021990s 46 85 2.91

L. Cipolotti et al. / Neuropsychologia 39 (2001) 151–172166
Table 6Famous people names familiarity test: comparison of arcsin trans-form of raw scores ( /15) for VC and controls
Controls mean rawVC raw score Z Pscore
10.77 0.821960s B0.21912.03 0.9810 B0.171970s
91980s 11.84 1.42 B0.081990s 6 10.42 1.61 B0.06
Table 8Pre-and post-morbid vocabulary scores
VC Controls mean(S.D.)
Vocabulary subtest score 12 (age-scaled(WAIS-R) score)
New vocabulary test (recall) 14.9 (2.08)4/2012/20New vocabulary test 18.0 (1.15)
(recognition)
5.2. Autobiographical memory
5.2.1. Autobiographical memory inter6iewThis test of autobiographical memory [32] requires
the patient to generate information concerning threeperiods of his life (childhood, early adult life and recentlife). For each time period, the patient is requested torecall both personal semantic knowledge (for example,‘What was your home address when attending highschool?’) as well as autobiographical episodes (for ex-ample, ‘Describe an incident which occurred in theperiod when you were attending elementary school’).VC’s scores are presented in Table 7.
Inspection of Table 7 demonstrates that VC wascompletely unable to recall autobiographical episodesfrom his recent life and almost completely unable torecall autobiographical episodes from childhood andearly adult life. Although he was able to produce a fewpieces of personal semantic knowledge (e.g. his addresswhen starting school but his address has remained thesame throughout his life), he scored in the abnormalrange for all three periods of life. This shows that hehad severe impairment of both autobiographical andpersonal semantic memory from his childhood, earlyadult life and recent life. Thus, in this task there was noindication of a temporal gradient in his recall of per-sonal memories just as for the retrograde non personalmemory tasks.
5.3. Retrograde and anterograde semantic memory
5.3.1. Pre-morbidly acquired 6ocabulary: WAIS-R6ocabulary subtest
Knowledge of vocabulary from the retrograde periodwas evaluated from the vocabulary subtest of theWAIS-R. His age-scaled scores are reported in Table 8.VC’s performance in this test was in the high averagerange. This indicates that VC’s knowledge of semanticinformation from the pre-morbid periods is clearlyintact. Thus, there is a remarkable contrast betweenVC’s intact ability to store and retrieve old lexical-se-mantic knowledge and his severe and pervasive impair-ment in retrieving remote personal and non personalmemories.
pseudorandom order with contemporary famous namesalternating with more remote names. VC was told thatin the list only one of the three names was famous. Hewas asked to indicate which was the most familiarname from the list of three names, guessing if necessary.After he chose the most familiar name he was requestedto provide information that would allow the identifica-tion of the public personality.
A normal control sample of 31 subjects, age (meanage=58.4 years; S.D.=7.88) and matched education-ally (mean age left full time education=17.69 years;S.D.=3.13) were also given this test. The results of VCand the control subjects for each decade sampled, areshown in Table 6.
For the purposes of the statistical analysis the rawscores were converted using an arcsin transform, asscores were distributed binomially. As shown in Table6, there was no significant difference between VC’sperformance and the control performance over the fourdecades period. VC’s scores were within normallimits in all four decades tested. Thus, these findingsindicated that VC had retained some implicit knowl-edge of public figures despite the severe loss of explicitknowledge.
Table 7Autobiographical memory performance
CommentAutobiographical memory No. correctinterview
AutobiographicalChildhood 1/9 Definitely
abnormalEarly adult life 2/9 Definitely
abnormalDefinitely0/9Recent lifeabnormal
SemanticChildhood 11/24 Definitely
abnormalProbably15/24Early adult lifeabnormal
3/24 DefinitelyRecent lifeabnormal

L. Cipolotti et al. / Neuropsychologia 39 (2001) 151–172 167
5.3.2. Post-morbidly acquired 6ocabulary: new6ocabulary test
In order to assess VC’s ability to acquire new vocab-ulary we selected 20 words (from the Oxford Dictionaryof New Words) which had entered the British lexiconsubsequent to his becoming amnesic. This dictionaryincludes the date of entry of words into the Britishlexicon. There were two conditions of testing: (a) recall— he was presented with a word and asked to define itand; (b) multiple-choice — the words that he wasunable to correctly define were re-presented using analternative multiple two-choice format. This consistedof the correct definition of the word and a plausiblefalse definition (e.g. BSE — ‘Is it an incurable braincondition in cattle that can cause neurological disordersand results in death?’ or ‘Does it stand for the BritishSociety for Epilepsy?’). VC was asked to choose thecorrect one, or guess if necessary. Ten control subjectswere also given this test (mean age=57.8 years, S.D.=10.42). VC’s and controls’ scores are given in Table 8.
VC performed extremely poorly both in the recalland in the multiple choice conditions by comparisonwith the performance of the control subjects. The goodperformance of the control subjects especially in therecognition version suggests that our new vocabularytest was relatively easy and therefore VC’s severelyimpaired performance (recall 5.2 S.D.s below the nor-mal mean; recognition 5.2 S.D.s below the normalmean) cannot be attributed to a task difficulty artefact.Thus, his inability to update his vocabulary reflects aremarkable degree of impairment in comparison withhis excellent lexical-semantic knowledge from the pre-morbid period. In summary, VC was unable to acquirenew semantic knowledge in the post-morbid period.
6. Discussion
The neuroanatomy of the different aspects of theamnesic syndrome is the subject of intense and exten-sive debate. In the Introduction we have argued thatdetailed analysis of neurological patients presentingwith restricted lesions and severe memory impairmentsare of great theoretical interest. In this series of experi-ments we have reported our investigation of the pro-foundly globally amnesic patient VC, whose intellectualand cognitive skills were otherwise entirely satisfactory.In particular, we have focused on the retrograde com-ponent of his global memory impairment and on thestatus of his semantic fact learning skills. Detailedanatomical measurements were undertaken in an at-tempt to clarify the functional role of the hippocampusand related anatomical structures in these mnesticprocesses.
As far as the extent of VC’s anatomical lesion isconcerned the high resolution volumetric MR scans
provided unequivocal evidence of damage to bothhippocampi, with significant bilateral loss of volumeand abnormal signal return. This volume loss wasnoted throughout the length of both hippocampi. Themagnitude and distribution of loss makes it inevitablethat the CA1 field sustained considerable damage. Thisis shown by the near-total loss of the digitationeshippocampi at the rostral end which contains only theCA1 field and also by the fact that the most severelyaffected portion of the hippocampus was the head inwhich CA1 is the predominant cell field. In addition,the outflow tracts of the CA1 fields to subcorticalregions — the fimbriae — were reduced markedly insize. Damage to the CA3 field is suggested by the globalreduction in the cross-sectional area of the hippocam-pus at more caudal levels, although the degree ofpathological involvement of each subfield is difficult toquantify. Similarly, the loss of grey matter in the regionbetween distal CA1 and the superomedial border of theentorhinal cortex strongly suggests damage to thesubiculum and to the pre- and parasubiculum. How-ever, at present methods for quantitative measurementsof these areas are relatively unreliable.
Could lesions external to the hippocampus be playinga causal role in VC’s amnesia? In this respect theentorhinal cortex is the most critical structure. Theentorhinal cortex is the major supply of cortical affer-ents to the hippocampus and damage to this area hasbeen associated with extensive RA [53]. Moreover,Reed and Squire [52] contrasted hippocampal patientswith and without damage to the entorhinal cortex withrespect to the length of their RA. However, in the caseof VC the volume of this anatomical structure was inthe normal range. The left parahippocampal gyrus wasslightly reduced in volume (between 2 and 3 S.D. belowthe control mean). The right parahippocampal gyruswas less than 1 S.D. below the control mean. Thedifference between the two sides was not significant.
At present there is no reliable technique for quantita-tive analysis of the subdivisions of the parahippocam-pal gyrus other than the entorhinal cortex. However, itis estimated that a significant proportion of the de-crease in parahippocampal gyrus volume in VC may beattributable to a reduction in the white matter, com-prising the efferent fibres from the hippocampus (par-ticularly CA1) to the cortical regions within theparahippocampal gyrus [5]. The efferents from CA1 tosubcortical and cortical sites consist of collaterals aris-ing from the primary axons that contribute to thefimbria [74,79]. Given the marked reduction in the sizeof the fimbriae in VC one would expect a concomitantdiminution in the number of cortically-directed efferentfibres from CA1 which comprise in part the whitematter layer of the parahippocampal gyrus. Qualitativeanalysis in this instance reveals that there is attenuationof the white matter bilaterally involving the portion of

L. Cipolotti et al. / Neuropsychologia 39 (2001) 151–172168
the anterior parahippocampal gyrus that is subjacent tothe head of the hippocampus and superior to theentorhinal cortex. In this context it is of note that theentorhinal cortex receives more inputs from CA1 thanfrom the subiculum in the rat [75] and in the primateCA1 is found to provide the majority of the directhippocampal projections to the parahippocampal gyrus,with a particularly strong projection to the anteriorportion [5]. Some comments on other parahippocampalregions are also possible. The small fraction of theperirhinal cortex contained within the parahippocampalgyrus, namely the portion located at the fundus of thecollateral sulcus, appeared qualitatively to be intact, asdoes the remainder of the perirhinal cortex. Finally, it isworth mentioning that areas TF and TH in the poste-rior parahippocampal gyrus are believed to representvisual association areas and there is little evidencelinking these regions directly to mnemonic function.
In addition to the hippocampal damage, there wasabnormal signal return from the left amygdala. Thisdamage is unlikely to be of importance for three rea-sons. First, isolated lesions of the amygdala do notimpair memory in lower primates [92]. Secondly, inman the resection for epilepsy of the amygdala, sparingthe hippocampus, does not cause amnesia [59]. Thirdly,Cahill and colleagues [7] have previously demonstratedin a patient with Urbach–Wiethe disease that amygdalalesions impair the encoding of emotionally salientepisodic memories (dealing with mutilation) but notthose involved with more emotionally neutral material.
Some students of amnesia have argued that func-tional imaging studies may show more extensive abnor-malities than anatomical sectional scans and thereforethey can be considered a more reliable indicator of theextent of the damage. In our patient the resting 18FDGPET scan showed less signal return from the rightthalamus and possibly right parietal region. By contrastthere was no sign of structural abnormality on thethalamus on the MRI. Functional imaging is not ananatomical parameter; it is, as the name implies, afunctional variable. Once an anatomical abnormalityhad occurred at one point in a functional pathwayareas downstream will also probably be abnormal. Thisdoes not mean that there are anatomical abnormalitiesdownstream. Indeed the functional imaging abnormal-ity is consistent with the variable superficial sensoryimpairment in his left limbs but does not indicate wherethe lesion is located. Moreover, even if the right thala-mic abnormality on PET were to reflect a hiddenstructural lesion this could hardly account for the ver-bal memory impairment of VC. VC’s impairment onthe verbal memory domain was if anything worse thanthe visual memory domain (see [63,64] for relevantunilateral thalamic patients).
Turning to the nature of VC’s memory impairment,our investigation on the retrograde component of VC’s
global amnesia revealed severe memory loss. On a testof retrograde memory [27] requiring him to indicatewhether personalities who had been famous at sometime over the last 30 years were dead or alive, heobtained a very poor score. However, not only wasVC’s retrograde amnesia severe it was also found to beextensive and ungraded. We have constructed two newretrograde memory tests which measured solelyepisodic memory retrieval at all time periods. On thequestionnaire designed to probe recall and multiplechoice recognition of famous public events, his scoreswere extremely poor. Of particular relevance is thefinding that his scores remained equally poor over thefour decades tested (1990s; 1980s; 1970s; and 1960s).On the recall version he was virtually unable to score atany decade. The multiple choice recognition version hasless power for the earliest decades but his poor scoresdid not indicate any sparing for the most remote events.Similarly, on a task requiring him to recall and recog-nise photographs of famous personalities, his perfor-mance was very severely impaired. On the recall versionof the test he was found again to be virtually unable toidentify the famous faces across four decades. In themultiple choice recognition version again we obtainedan extensive, ‘flat’ gradient of retrograde amnesia butproblems with statistical sensitivity were greater at ear-lier decades because of the poorer performance of thecontrols. Nonetheless, there may have been a marginalsaving of his face recognition performance for the 1960sand 1970s decades. However, his recall performancewith this material, which was equally bad to that ofReed and Squire’s [52] post-encephalitic patients, indi-cate that retrieval of face memory from the earlierdecades is profoundly abnormal. Together with hiseven poorer performance on multiple choice recogni-tion and recall of remote public events these resultssuggest that Ribot’s law of forgetting claiming ‘that thedissolution of memory is inversely related to the re-cency of the event’ is not confirmed in our amnesicpatient.
These findings have implications for those theoriessharing the idea that the hippocampus has only atemporary role in memory storage and that ultimatelythe neocortex is responsible for long-term memory stor-age (e.g. for a review [65]). These theories, althoughdifferent in detail, predict extensive and ungraded RAonly when the damage is not restricted to thehippocampus but also involves temporal neocortex.However, VC had lesions which were principallyconfined to the hippocampus and yet showed extensiveand ungraded RA. This suggests that the role of thehippocampus is not limited to the temporary consolida-tion of memory traces. On the position of Squire andcolleagues, one has to assume that the recall perfor-mance of no more than 10% of that of normal controlsand a public events recognition performance at chance

L. Cipolotti et al. / Neuropsychologia 39 (2001) 151–172 169
for the 1960s and 1970s decades results from hiddenpathology in the temporal lobe.
The hidden pathology argument is of course a verypopular [1]. The claim that cortical deficit resultingfrom hidden pathology would not show up on MRI orcomprehensive cognitive testing is often based on thestudy of Markowitsch [35]. The authors reported anamnesic patient whose PET investigation revealed wide-spread regions of hypoactivity that, according to him,could not be predicted from the MRI scans. However,the MRI report on this patient refer to non specificcortical/subcortical atrophy, with widening of the lat-eral ventricle. Moreover, the patient, an office clerk,who had been in coma for 14 days, had a FIQ of 85and showed other deficits on cognitive testing, forexample performing very poorly on attention and con-centration tests. By contrast, VC’s MRI showed noatrophy compared with intact control subjects of hisage, has not been in a coma and apart from theepisodic memory abnormality his performance on aseries of cognitive tests was in the expected average/high average range.
Instead our findings are much more easily explainedon the view that the hippocampus provides a form ofrepresentation (or learning or processing) which is notavailable to the neocortex and that is critical for effec-tive retrieval of both recent and remote episodic memo-ries. According to this view and in keeping with ourfindings retrograde amnesia is not temporally gradedfollowing a hippocampal lesion, given appropriate test-ing for retrograde amnesia.
It is noteworthy that our patient was also incapableof autobiographical recollections. His performance onthe AMI was very poor both for personal semanticmemory and autobiographical memory. His very poorperformance equally affected all the periods of his lifespanning from very recent times to his childhood. Thesefindings count against an idea suggested by Verfaellieand colleagues [81] and recently favoured by Reed andSquire [52] that ‘…learning of any kind, whether it beepisodic or semantic, may be more impaired in amnesiawhen information was acquired recently rather thanremotely…’ (p. 451). Instead, our data implicates thatthe hippocampus is needed to retrieve autobiographicalmemories throughout life [46]. Thus, overall our find-ings indicate that retrieval of event memory requires theprocessing provided by the hippocampus.
It is also worth noting that despite VC’s exception-ally severe retrograde deficit, there was evidence thathis performance did not differ from that of the controlgroup on a test designed to assess simple familiarity forfamous people names. Using a variant of a multiplechoice recognition memory test in which the names offamous people were paired with two unknown distrac-tor items his performance was within normal limits forthree decades (1960; 1970; 1980). Only for the 90s was
his performance slightly worse than the controls. In thisrespect, his performance was similar to the post-en-cephalitic patient described by Warrington and Mc-Carthy [86] who exhibited no deficit on this type oftask. However, it should be noted that 4 further post-encephalitic patients, although presenting a somewhatimproved performance in the familiarity for famousnames test, were distinctively impaired [52,68]. War-rington and McCarthy [83] suggest that this type offamiliarity judgement depends on lexical-semantic pro-cesses. In this case this would fit with these processesnot involving the hippocampus.
Finally this study provides interesting results on thestatus of post-morbid semantic learning. VC’s semanticknowledge from the post-morbid period is clearly ab-normal. He demonstrated no post-morbid semantic ac-quisition on our tests of public knowledge both forfamous events as well as for famous personalities. Hewas also unable to acquire new terms and novel con-cepts, despite having maintained excellent pre-morbidword knowledge. Evidence of no new vocabulary acqui-sition has been previously reported in long-standingamnesia [18,79]. However, our patient together withpatient LJ reported by Reed and Squire [52], appear tobe the only instances in which impaired vocabularyacquisition has been established following damage re-stricted to the hippocampal structure. This evidencesuggests that new fact learning is impaired byhippocampal pathology. Recently Vargha-Kadhem etal. [80], in order to explain the relatively normal acqui-sition of semantic knowledge by three teenage amnesicpatients who had suffered early hippocampal damage,stressed the role of the perirhinal and entorhinal cor-tices in the acquisition of new context-free semanticmemories. It remains possible that the age at whichdamage to these systems occurs is a critical feature andthus, important factors such as developmental reorgan-isation must be considered.
Alternatively other authors have implicated sparingof the left and right inferolateral temporal cortices toaccount for the acquisition and storage of post-morbidsemantic knowledge in amnesic patients [22,31]. In par-ticular, the patient (RS) recently described by Kitcheneret al. [31] was found to have acquired new informationof rather limited amount about famous people, publicevents and new vocabulary during the 13-year periodsince he became amnesic. VC, despite normal left andright inferolateral temporal cortices, was unable tolearn new semantic material. A critical difference maybe that the patient of Kitchener et al. [31] suffered amuch more asymmetrical lesion. The MRI showedmultifocal limbic damage on the left involving thehippocampal complex, posterior thalamus and medialfrontal lobe. In contrast the lesion in the right hemi-sphere was much more circumscribed. In particularonly the posterior part of the right hippocampus was

L. Cipolotti et al. / Neuropsychologia 39 (2001) 151–172170
involved. Perhaps the relative sparing of the remainderof the right hippocampus may be sufficient to allow thevery limited semantic acquisition shown by their pa-tient. Alternatively, the computational model of Mc-Clelland et al. [40] explicitly postulates that in theabsence of a functioning hippocampal system theneocortex can learn (albeit slowly), in isolation, throughrepeated exposure to the information. Given the unspe-cified ‘slow’ interval of time necessary for such anisolated neocortex to learn it is possible that VC’s6-year post-morbid period was not of sufficient length.In contrast, the 13 year post-morbid period of theKitchener et al. [30] patient might have allowed theslow learning of vocabulary and semantic facts. Onlyfurther re-assessment of our patient could serve toresolve this issue. Nevertheless, our findings emphasisethe point that learning of new semantic factual knowl-edge does not accrue to normal levels in the face ofhippocampal pathology.
In summary, our patient represents one of the firstinstances in the amnesia literature where the involve-ment of key anatomical structures was quantitativelyverified and extensive and theoretically motivated cog-nitive tests have been carried out. We are aware thatquantitative analysis of structural lesions cannot ir-refutably eliminate the possibility of hidden corticalpathology. Nevertheless the best quantitative analysisso far available has failed to detect further anatomicallesions. Our findings suggest that retrograde amnesiaboth for personal and non-personal events can be bothextensive and ungraded when the damage is limited tothe hippocampus. Thus, these findings are not consis-tent with those theories claiming that the hippocampusplays a critical role only for the retention of eventswhich have occurred relatively recently.
Acknowledgements
We thank Dr Sally Barrington of the Clinical PETUnit of St. Thomas’s Hospital for the PET images andhelpful discussion. We are also grateful to ProfessorM.N. Rossor for his advice and support.
References
[1] Aggleton JP, Brown MW. Episodic memory, amnesia and thehippocampal-anterior thalamic axis. Behavioral and Brain Sci-ences 1999;22:425–90
[2] Alvarez P, Squire LR. Memory consolidation and the medialtemporal lobe: a simple network model. Proceedings of theNational Academy of Sciences of the USA 1994;91:7041–5.
[3] Bachevalier J, Meunier M. Cerebral ischemia: are the memorydeficits associated with hippocampal cell loss? Hippocampus1996;6:553–60.
[4] Baddeley AD, Emslie H, Nimmo-Smith I. Doors and People.Bury St. Edmunds, UK: Thames Valley Test Company, 1994.
[5] Blatt GJ, Rosene DL. Organization of direct hippocampal effer-ent projections to the cerebral cortex of the Rhesus monkey:projections from CA1, prosubiculum, and subiculum to thetemporal lobe. Journal of Comparative Neurology 1998;392:92–114.
[6] Burgess P, Shallice T. The Hayling sentence completion test.Neuropsychologia 1996;34:263–73.
[7] Cahill L, Babinsky R, Markowitsch H, McGaugh JL. Theamygdala and emotional memory [letter]. Nature 1995;377:295–6.
[8] Cermak LS. The episodic-semantic distinction in amnesia. In:Squire LR, Butters N, editors. Neuropsychology of Memory.New York: Guilford, 1984.
[9] Cermak LS, O’Connor M. The anterograde and retrograderetrieval ability of a patient with amnesia due to encephalitis.Neuropsychologia 1983;21:213–34.
[10] Cohen NJ. Preserved learning capacity in amnesia: evidence formultiple memory systems. In: Butters NL, Squire L, editors. TheNeuropsychology of Memory. New York: Guilford, 1984.
[11] Cohen NJ, Squire LR. Preserved learning and retention ofpattern analyzing skill in amnesia: dissociation of knowing howand ‘knowing that’. Science 1980;210:207–9.
[12] Cook MJ, Fish DR, Shorvon SD, Straughan K, Stevens JM.Hippocampal volumetric and morphometric studies in frontaland temporal lobe epilepsy. Brain 1992;115:1001–15.
[13] Coughlan AK, Hollows SE. The Adult Memory and Informa-tion Processing Battery. Leeds, UK: St. James’s University Hos-pital, 1985.
[14] Damasio AR, Eslinger PJ, Damasio H, Van Hoesen GW. Multi-modal amnesic syndrome following bilateral temporal and basalforebrain damage. Archives of Neurology 1985;42:252–9.
[15] Dimsdale H, Logue V, Piercy M. A case of persisting impair-ment of recent memory following right temporal lobectomy.Neuropsychologia 1964;1:287–98.
[16] Evans JJ, Breen EK, Antoun N, Hodges JR. Focal retrogradeamnesia for autobiographical events following cerebral vasculi-tis: a connectionist account. Neurocase 1996;2:1–11.
[17] Freeborough PA, Woods RP, Fox NC. Accurate registration ofserial 3D MR brain images and its application to visualizingchange in neurodegenerative disorders. Journal of ComputerAssisted Tomography 1996;20:1012–22.
[18] Gabrieli JDE, Cohen NJ, Corkin S. The impaired learning ofsemantic knowledge following bilateral medial temporal-loberesection. Brain and Cognition 1988;7:157–77.
[19] Gaffan D. Recognition impaired and association intact in thememory of monkeys after transection of the fornix. Journal ofComparative and Physiological Psychology 1974;86:1100–9.
[20] Gaffan D, Lim C. Hippocampus and blood supply to TE:parahippocampal pial section impairs visual discriminationlearning in monkeys. Experimental Brain Research 1991;87:227–31.
[21] Graham KS, Hodges JR. Differentiating the roles of thehippocampal complex and the neocortex in long term memorystorage: evidence from the study of semantic dementia andAlzheimer’s disease. Neuropsychology 1997;11:77–89.
[22] Hodges JR, Graham KS. A reversal of the temporal gradient forperson knowledge: Implications for the neural organisation oflong-term memory. Neuropsychologia 1998;36:803–25.
[23] Insausti R, Runon T, Sobreviela T, Insausti AM, Gonzalo LM.The human entorhinal cortex: a cytoarchitectonic analysis. Jour-nal of Comparative Neurology 1995;355:171–98.
[24] Insausti R, Juottonen K, Soininen H. MR volumetric MRIanalysis of the human entorhinal, perirhinal, and temporopolarcortices. American Journal of Neuroradiology 1998;19:659–71.

L. Cipolotti et al. / Neuropsychologia 39 (2001) 151–172 171
[25] Kapur N, Ellison D, Snith MP, McLellan DL, Burrows EH.Focal retrograde amnesia following bilateral temporal lobepathology. Brain 1992;115:73–85.
[26] Kapur N. Focal retrograde amnesia in neurological disease: acritical review. Cortex 1993;29:217–34.
[27] Kapur N, Young A, Bateman D, Kennedy P. Focal retrogradeamnesia: a long term clinical and neuropsychological follow-up.Cortex 1989;25:387–402.
[28] Kapur N, Thompson P, Kartsounis LD, Abbott P. Retrogradeamnesia: clinical and methodological caveats. Neuropsychologia1999;37:27–30.
[29] Kartsounis LD, Rudge P, Stevens JM. Bilateral lesions of CA1and CA2 fields of the hippocampus are sufficient to cause asevere amnesic syndrome in humans. Journal of Neurology,Neurosurgery and Psychiatry 1995;59:95–8.
[30] Kinsbourne M, Wood F. Short-term memory processes and theamnesic syndrome. In: Deutsch D, Deutsch JA, editors. Short-term Memory. New York: Academic Press, 1975.
[31] Kitchener EG, Hodges JR, McCarthy RA. Acquisition of post-morbid vocabulary and semantic facts in the absence of episodicmemory. Brain 1998;121:1313–27.
[32] Kopelman MD, Wilson BA, Baddeley AD. The autobiographi-cal memory interview: a new assessment of autobiographical andpersonal semantic memory in amnesic patients. Journal of Clini-cal and Experimental Neuropsychology 1989;11:724–44.
[33] Mair WGP, Warrington EK, Weiskrantz L. Neuropathologicaland psychological examination of two patients with Korsakoff’spsychosis. Brain 1979;102:749–83.
[34] Markowitsch HJ, Calabrese P, Haupts M, Durwen HF, Liess J,Gehlen W. Searching for the anatomical basis of retrogradeamnesia. Journal of Clinical and Experimental Neuropsychology1993;15:947–76.
[35] Markowitsch HJ, Weber-Luxemburger G, Ewald K, Kessler J,Heiss W-D. Patients with heart attacks are not valid models formedial temporal lobe amnesia. A neuropsychological and FDG-PET study with consequences for memory research. EuropeanJournal of Neurology 1997;4:178–84.
[36] Marr D. Simple memory: a theory for archicortex. PhilosopichalTransactions of the Royal Society of London, Series B1971;262:23–81.
[37] McCarthy RA, Warrington EK. Evidence for modality-specificmeaning systems in the brain. Nature 1988;334:428–30.
[38] McCarthy RA, Warrington EK. Cognitive Neuropsychology.New York: Academic Press, 1990.
[39] McClelland JL, McNaughton BL, O’Reilly RC, Nadel L. Com-plementary roles of hippocampus and neocortex in learning andmemory. Society for Neuroscience Abstracts 1992;18:1216.
[40] McClelland JL, McNaughton BL, O’Reilly RC. Why there arecomplementary learning systems in the hippocampus andneocortex: Insights from the successes and failures of connec-tionist models of learning and memory. Psychological Review1995;102:419–57.
[41] McKenna P, Warrington EK. Testing for nominal dysphasia.Journal of Neurology, Neurosurgery and Psychiatry1980;43:781–8.
[42] Milner B. Amnesia following operation on the temporal lobe. In:Whitty CWM, Zangwill OL, editors. Amnesia. Cambridge, MA:MIT Press, 1966.
[43] Milner B. Disorders of learning and memory after temporal lobelesions in man. Clinical Neurosurgery 1972;19:421–46.
[44] Murre JMJ. Categorization and Learning in Modular NeuralNetworks. Hillsdale, NJ: Lawrence Erlbaum, 1992.
[45] Murre JMJ. TraceLink: a model of amnesia and consolidationmemory. Hippocampus 1996;6:675–84.
[46] Nadel L, Moscovitch M. Memory consolidation, retrogradeamnesia and the hippocampal complex [review]. Current Opinionin Neurobiology 1997;7:217–27.
[47] Nelson HE. A modified card sorting test sensitive to frontal lobedefects. Cortex 1976;12:313–24.
[48] Nelson HE. National Adult Reading Test, 2nd edn. Windsor,UK: NFER-Nelson Publishing Co. Ltd., 1991.
[49] O’Keefe J, Nadel L. The Hippocampus as a Cognitive Map.Oxford, UK: Clarendon Press, 1978.
[50] Olton D, Becker J, Handelmann GE. Hippocampus, space, andmemory. Behavioural and Brain Sciences 1979;2:313–65.
[51] Osterreith PA. Le test de copie d’une figure complexe. Archivesde Psychologie 1944;30:206–356.
[52] Reed JM, Squire LR. Retrograde amnesia for facts and events:findings from four new cases. Journal of Neuroscience1998;18:3943–54.
[53] Rempel-Clower NL, Zola S, Squire LR, Amaral DG. Threecases of enduring memory impairment after bilateral damagelimited to the hippocampal formation. Journal of Neuroscience1996;16:5233–55.
[54] Ribot TA. Les Maladies de la Memoire. Paris: Germer Baillere,1881.
[55] Russell WR, Nathan PW. Traumatic amnesia. Brain1946;69:280–300.
[56] Sanders HI, Warrington EK. Memory for remote events inamnesic patients. Brain 1971;94:661–8.
[57] Schacter DL, Tulving E. Amnesia and memory research. In:Cermak LS, editor. Human Memory and Amnesia. Hillsdale,NJ: Lawrence Erlbaum, 1982.
[58] Schmidtke K, Vollmer H. Retrograde amnesia: a study of itsrelation to anterograde amnesia and semantic memory deficits.Neuropsychologia 1997;35:505–18.
[59] Scoville WB, Milner B. Loss of recent memory after bilateralhippocampal lesions. Journal of Neurology, Neurosurgery andPsychiatry 1957;20:11–21.
[60] Shallice T. From Neuropsychology to Mental Structure. NewYork: Cambridge University Press, 1988.
[61] Shallice T, Evans ME. The involvement of the frontal lobes incognitive estimation. Cortex 1978;14:294–303.
[62] Soininen H, Partanen K, Pitkanen A. Volumetric MRI analysisof the amygdala and the hippocampus in subjects with age-asso-ciated memory impairment: correlation to visual and verbalmemory. Neurology 1994;44:1660–8.
[63] Speedie LJ, Heilman KM. Amnesic disturbance following infarc-tion of the left dorsomedial nucleus of the thalamus. Neuropsy-chologia 1982;20:597–604.
[64] Speedie LJ, Heilman KM. Anterograde memory deficits forvisuospatial material after infarction of the right thalamus.Archives of Neurology, Chicago 1983;40:183–6.
[65] Squire LR. Memory and Brain. New York: Oxford UniversityPress, 1987.
[66] Squire LR. Memory and the hippocampus: a synthesis fromfindings with rats, monkeys, and humans. Psychological Review1992;99:195–231.
[67] Squire LR, Alvarez P. Retrograde amnesia and memory consol-idation: a neurobiological perspective. Current Opinion in Neu-robiology 1995;5:169–77.
[68] Squire LR, Cohen NJ. Memory and amnesia: resistance todisruption develops for years after learning. Behavioral andNeural Biology 1975;25:115–25.
[69] Squire LR, Cohen NJ, Nadel L. The medial temporal region andmemory consolidation: a new hypothesis. In: Weingartner H,Parker E, editors. Memory Consolidation. Hillsdale, NJ:Lawrence Erlbaum, 1984:185–210.
[70] Squire LR, Haist F, Shimamura AP. The neurology of memory:quantitative assessment of retrograde amnesia in two groups ofamnesic patients. Journal of Neuroscience 1989;9:828–39.
[71] Squire LR, Amaral DG, Press GA. Magnetic resonance mea-surements of hippocampal formation and mammillary nucleidistinguish medial temporal lobe and diencephalic amnesia.Journal of Neuroscience 1990;10:3106–17.

L. Cipolotti et al. / Neuropsychologia 39 (2001) 151–172172
[72] Squire LR, Ojemann JG, Miezin FM, Petersen SE, Videen TO,Raichle ME. Activation of the hippocampus in normal humans:a functional anatomical study of memory. Proceeding of theNational Academy of Sciences of the USA 1992;89:1837–41.
[73] Stracciari A, Ghidoni E, Guarino M, Poletti M, Pazzaglia P.Post-traumatic retrograde amnesia with selective impairment ofautobiographical memory. Cortex 1994;30:459–68.
[74] Swanson LW, Sawchencko PE, Cowan WM. Evidence for collat-eral projections by neurons in Ammon’s horn, the dentate gyrus,and the subiculum: a multiple retrograde labelling study in therat. Journal of Neuroscience 1981;1:548–59.
[75] Tamamaki N, Nojyo Y. Preservation of topography in theconnections between the subiculum, field CA1, and the entorhi-nal cortex. Journal of Comparative Neurology 1995;353:379–90.
[76] Treves A, Rolls ET. Computational constraints suggest the needfor two distinct input systems to the hippocampal CA3 network.Hippocampus 1992;2:189–99.
[77] Treves A, Rolls ET. Computational analysis of the role of thehippocampus in memory. Hippocampus 1994;4:374–91.
[78] Tulving E, Schacter DL, McLachlan DR, Moscovitch M. Prim-ing of semantic autobiographical knowledge: a case study ofretrograde amnesia. Brain 1988;8:3–20.
[79] Van Groen T, Wyss JM. Extrinsic projections from area CA1 ofthe rat hippocampus: olfactory, cortical, subcortical, and bilat-eral hippocampal formation projections. Journal of ComparativeNeurology 1990;302:515–28.
[80] Vargha-Kadhem F, Gadian DG, Watkins KE, Connelly A, VanPaesschen W, Mishkin M. Differential effects of early hippocam-pal pathology on episodic and semantic memory. Science1997;277:376–80.
[81] Verfaellie M, Reiss L, Roth HL. Knowledge of New Englishvocabulary in amnesia: an examination of premorbidly acquired
semantic memory. Journal of International NeuropsychologicalSociety 1995;1:443–53.
[82] Warrington EK. Recognition Memory Test. Windsor, UK:NFER Nelson Publishing Co. Ltd., 1984.
[83] Warrington EK. Studies of retrograde memory: a long-termview. Proceedings of the National Academy of Sciences of theUSA 1996;93:13523–6.
[84] Warrington EK, Duchen LW. A re-appraisal of a case ofpersistent global amnesia following right temporal lobectomy: aclinico-pathological study. Neuropsychologia 1992;30:437–50.
[85] Warrington EK, James M. The Visual Object and Space Percep-tion Battery. Bury St. Edmunds, UK: Thames Valley Test Com-pany, 1991.
[86] Warrington EK, McCarthy RA. The fractionation of retrogradeamnesia. Brain and Cognition 1988;7:184–200.
[87] Warrington EK, Sanders HI. The fate of old memories. Quar-terly Journal of Experimental Psychology 1971;23:432–42.
[88] Weigl E. On the psychology of so-called processes of abstraction.Journal of Abnormal and Social Psychology 1941;36:3–33.
[89] Weiskrantz L. On issues and theories of the human amnesicsyndrome. In: Weinberger NM, McGaugh JL, Lynch G, editors.Memory Systems of the Brain. New York: Guilford Press, 1985.
[90] Whitty CWM, Zangwill OL. Amnesia: Clinical, Psychologicaland Medicolegal Aspects, 2nd edn. London: Butterworth, 1977.
[91] Zola-Morgan S, Squire LR, Amaral DG. Human amnesia andthe medial temporal region: enduring memory impairment fol-lowing a bilateral lesion limited to field CAI of the hippocampus.Journal of Neuroscience 1986;6:2950–67.
[92] Zola-Morgan S, Squire LR, Amaral DG, Suzuki WA. Lesions ofperirhinal and parahippocampal cortex that spare the amygdalaand hippocampal formation produce severe memory impairment.Journal of Neuroscience 1989;9:4355–70.
.