
The chicken with four legs: A case of semantic amnesia and cryptogenic epilepsy
8
Case Report The chicken with four legs: A case of semantic amnesia and cryptogenic epilepsy Anna R. Giovagnoli a, * , Flavio Villani b , Brian Bell c , Alessandra Erbetta d , Giuliano Avanzini b a Neuropsychology Laboratory, ‘‘C. Besta” National Neurological Institute, Department of Clinical Neuroscience, Via Celoria 11, 20133 Milano, Lumbardy, Milan, Italy b Epilepsy Center, ‘‘C. Besta” National Neurological Institute, Milan, Italy c Charles G. Matthews Neuropsychology Laboratory, Department of Neurology, University of Wisconsin—Madison, Madison, WI, USA d Department of Neuroradiology, ‘‘C. Besta” National Neurological Institute, Milan, Italy article info Article history: Received 28 August 2008 Revised 18 September 2008 Accepted 19 September 2008 Available online 5 November 2008 Keywords: Semantic memory Object naming Amnesia Temporal lobe epilepsy Dementia Imaging abstract Here we describe the unusual condition of selective semantic amnesia related to cryptogenic temporal lobe epilepsy. XY, an adult male patient, presented with partial seizures and disabling dysnomia. Neuro- psychological tests revealed seriously impaired semantic memory. Electroencephalography documented ictal epileptic abnormalities in the left temporal lobe. Positron emission tomography showed reduced metabolism in the temporoparietal regions, but the results of magnetic resonance imaging and spectros- copy were normal. After 11 years, neuropsychological tests showed selective impairment of semantic memory and computed tomography provided normal results. This case shows that semantic memory may be selectively and lastingly altered, highlighting a distinction between semantic amnesia and global amnesia. Moreover, it is unique in that it occurred without evidence of gross temporal lobe pathology. The pathophysiological pattern of epileptic abnormalities in the left temporoparietal cortex supports the role played by dysfunctional neuronal networks (as provoked by focal epileptic discharges) in deter- mining selective semantic amnesia. Ó 2008 Elsevier Inc. All rights reserved. 1. Introduction In the framework of declarative memory, semantic memory is the complex of non-context-related knowledge acquired by means of education or other sources of information, whereas episodic memory comprehends spatial–temporal and autobiographical information, with each memory registered as a unique event [1]. Semantic amnesia is characterized by a selective cognitive profile, with deficits in naming, single-word comprehension, verbal flu- ency on semantic cues, cultural knowledge, and nonverbal concep- tual knowledge, but preservation of episodic memory, syntactic and phonological language components, perceptual abilities, and visual–spatial reasoning [2,3]. The distinction between episodic and semantic memory [1] has been demonstrated by reports of selectively impaired semantic memory [2–6] and selective deficits in episodic memory [7–11]. Different from such conditions, the amnesic syndrome is a permanent and global memory impairment that occurs in the absence of any other cognitive deficits and is characterized by severe anterograde amnesia, various degrees of retrograde amnesia, preserved immediate memory span, and nor- mal procedural memory [12]. The boundaries between global amnesia and semantic memory are not clear: some authors have claimed that semantic memory is preserved in global amnesia [12–15], but others have claimed that global amnesia usually in- volves semantic abilities [16–18]. The revised versions of Tulving’s model of declarative memory [19,20] suggest that episodic memory is dependent on semantic knowledge and only a simple dissociation is possible (i.e., impaired episodic memory and preserved semantic memory), which is in line with the finding of normal semantic learning in patients with global amnesia with onset in childhood [21] and adulthood [22]. The separation of chronic semantic amnesia from global mental decline [23] is also questionable because it has been described in the early stages of Alzheimer’s disease [24,25], Pick’s disease [26], bilateral temporal or widespread cortical atrophy without Alzheimer-type pathology [23], and dementia with ubiquitin-positive inclusion bodies [27]. Partial epilepsy may lead to various cognitive deficits depending on the location of cortical damage [28–30]. Left temporal lobe epi- lepsy (TLE) can cause semantic memory impairment reflected by deficits in naming and semantic judgment [31–35]. In patients with epilepsy, anterior left temporal lobectomy has also been reported to be a cause of semantic failures, including lexical-semantic deficits [36], altered semantic organization in word learning [37,38], and poor semantic encoding [39]. These deficits have usually been asso- ciated with primary or surgical brain lesions in the temporal lobes [31,33,35,36], whereas TLE may cause impaired verbal and nonver- bal episodic memory even in the absence of brain lesions [40–42]: this raises the question as to whether cryptogenic TLE may also cause the selective impairment of semantic memory. 1525-5050/$ - see front matter Ó 2008 Elsevier Inc. All rights reserved. doi:10.1016/j.yebeh.2008.09.015 * Corresponding author. Fax: +39 02 70638217. E-mail address: [email protected] (A.R. Giovagnoli). Epilepsy & Behavior 14 (2009) 261–268 Contents lists available at ScienceDirect Epilepsy & Behavior journal homepage: www.elsevier.com/locate/yebeh
-
Upload
istituto-besta -
Category
Documents
-
view
4 -
download
0
Transcript of The chicken with four legs: A case of semantic amnesia and cryptogenic epilepsy

Epilepsy & Behavior 14 (2009) 261–268
Contents lists available at ScienceDirect
Epilepsy & Behavior
journal homepage: www.elsevier .com/locate /yebeh
Case Report
The chicken with four legs: A case of semantic amnesia and cryptogenic epilepsy
Anna R. Giovagnoli a,*, Flavio Villani b, Brian Bell c, Alessandra Erbetta d, Giuliano Avanzini b
a Neuropsychology Laboratory, ‘‘C. Besta” National Neurological Institute, Department of Clinical Neuroscience, Via Celoria 11, 20133 Milano, Lumbardy, Milan, Italyb Epilepsy Center, ‘‘C. Besta” National Neurological Institute, Milan, Italyc Charles G. Matthews Neuropsychology Laboratory, Department of Neurology, University of Wisconsin—Madison, Madison, WI, USAd Department of Neuroradiology, ‘‘C. Besta” National Neurological Institute, Milan, Italy
a r t i c l e i n f o
Article history:Received 28 August 2008Revised 18 September 2008Accepted 19 September 2008Available online 5 November 2008
Keywords:Semantic memoryObject namingAmnesiaTemporal lobe epilepsyDementiaImaging
1525-5050/$ - see front matter � 2008 Elsevier Inc. Adoi:10.1016/j.yebeh.2008.09.015
* Corresponding author. Fax: +39 02 70638217.E-mail address: [email protected] (A.R.
a b s t r a c t
Here we describe the unusual condition of selective semantic amnesia related to cryptogenic temporallobe epilepsy. XY, an adult male patient, presented with partial seizures and disabling dysnomia. Neuro-psychological tests revealed seriously impaired semantic memory. Electroencephalography documentedictal epileptic abnormalities in the left temporal lobe. Positron emission tomography showed reducedmetabolism in the temporoparietal regions, but the results of magnetic resonance imaging and spectros-copy were normal. After 11 years, neuropsychological tests showed selective impairment of semanticmemory and computed tomography provided normal results. This case shows that semantic memorymay be selectively and lastingly altered, highlighting a distinction between semantic amnesia and globalamnesia. Moreover, it is unique in that it occurred without evidence of gross temporal lobe pathology.The pathophysiological pattern of epileptic abnormalities in the left temporoparietal cortex supportsthe role played by dysfunctional neuronal networks (as provoked by focal epileptic discharges) in deter-mining selective semantic amnesia.
� 2008 Elsevier Inc. All rights reserved.
1. Introduction
In the framework of declarative memory, semantic memory isthe complex of non-context-related knowledge acquired by meansof education or other sources of information, whereas episodicmemory comprehends spatial–temporal and autobiographicalinformation, with each memory registered as a unique event [1].Semantic amnesia is characterized by a selective cognitive profile,with deficits in naming, single-word comprehension, verbal flu-ency on semantic cues, cultural knowledge, and nonverbal concep-tual knowledge, but preservation of episodic memory, syntacticand phonological language components, perceptual abilities, andvisual–spatial reasoning [2,3]. The distinction between episodicand semantic memory [1] has been demonstrated by reports ofselectively impaired semantic memory [2–6] and selective deficitsin episodic memory [7–11]. Different from such conditions, theamnesic syndrome is a permanent and global memory impairmentthat occurs in the absence of any other cognitive deficits and ischaracterized by severe anterograde amnesia, various degrees ofretrograde amnesia, preserved immediate memory span, and nor-mal procedural memory [12]. The boundaries between globalamnesia and semantic memory are not clear: some authors haveclaimed that semantic memory is preserved in global amnesia
ll rights reserved.
Giovagnoli).
[12–15], but others have claimed that global amnesia usually in-volves semantic abilities [16–18]. The revised versions of Tulving’smodel of declarative memory [19,20] suggest that episodicmemory is dependent on semantic knowledge and only a simpledissociation is possible (i.e., impaired episodic memory andpreserved semantic memory), which is in line with the finding ofnormal semantic learning in patients with global amnesia withonset in childhood [21] and adulthood [22]. The separation ofchronic semantic amnesia from global mental decline [23] is alsoquestionable because it has been described in the early stagesof Alzheimer’s disease [24,25], Pick’s disease [26], bilateraltemporal or widespread cortical atrophy without Alzheimer-typepathology [23], and dementia with ubiquitin-positive inclusionbodies [27].
Partial epilepsy may lead to various cognitive deficits dependingon the location of cortical damage [28–30]. Left temporal lobe epi-lepsy (TLE) can cause semantic memory impairment reflected bydeficits in naming and semantic judgment [31–35]. In patients withepilepsy, anterior left temporal lobectomy has also been reported tobe a cause of semantic failures, including lexical-semantic deficits[36], altered semantic organization in word learning [37,38], andpoor semantic encoding [39]. These deficits have usually been asso-ciated with primary or surgical brain lesions in the temporal lobes[31,33,35,36], whereas TLE may cause impaired verbal and nonver-bal episodic memory even in the absence of brain lesions [40–42]:this raises the question as to whether cryptogenic TLE may also causethe selective impairment of semantic memory.

262 A.R. Giovagnoli et al. / Epilepsy & Behavior 14 (2009) 261–268
Therefore, semantic amnesia has to be distinguished from glo-bal amnesia and progressive cognitive decline, and partial epilepsymay make it possible to investigate the role of focal dysfunctionsunrelated to detectable brain lesions. In relation to this hypothesis,we describe a case of selective semantic impairment associatedwith cryptogenic epilepsy with the aim of documenting: (1) thedissociation between semantic and episodic memory; (2) the dis-tinction between chronic semantic amnesia and progressive cogni-tive disorders; and (3) the relationship between semantic amnesiaand cortical dysfunction caused by focal epileptic discharges.
2. Methods
2.1. Case report
At the time of our first evaluation, XY was a 24-year-old man inthe fifth year of his university philosophy course. His family historywas negative for epilepsy and febrile convulsions; his birth andpsychomotor development were reported as normal, and his med-ical history was unremarkable. At the age of 14, he experienced hisfirst generalized tonic–clonic seizures preceded by psychophysicaldiscomfort, which suggested a focal origin with secondary general-ization. At that time, the results of a computed tomography (CT)scan were normal. Despite the introduction of phenobarbital treat-ment by his family physician, he began to experience complex par-tial seizures characterized by an early alteration of consciousness,followed by staring, facial pallor, and simple vocalizations (hum-ming and moaning) or automatic verbalizations. The altered con-sciousness was occasionally preceded by a visual illusion ofmovement and shivering with a feeling of coldness, but he morefrequently reported an inaugural intrusive repetitive thought or asubjective experience of ‘‘time flowing.” Secondary generalizationwas also observed. His postictal behavior was characterized by se-vere depression with crying and suicidal thoughts. During thepostictal period, he also had serious naming difficulties, but his oralcomprehension was well retained. The complex partial seizureswere never controlled by any of a number of different antiepilepticdrug regimens (phenobarbital, carbamazepine, clobazam, valpro-ate, phenytoin, vigabatrin, lamotrigine), despite high plasma druglevels. The naming difficulties observed during the previous 3 yearsby the patient and his family were always present during the inter-ictal periods, not just only postictally, but the results of the neuro-logical examination were otherwise normal. In addition, XYreported obsessive and meticulous behaviors, often related to hisfear of unexpected events, but his parents had previously notedsuch personality traits and introverted attitudes. The diagnosiswas cryptogenic TLE.
Six years after diagnosis, at age 30, XY’s symptoms were un-changed, with persistent complex partial seizures and dysnomia,but otherwise his cognitive functioning, as expressed by activitiesthat required reasoning, comprehension, perception, attention, ini-tiative, and planning, was maintained. XY was completely autono-mous in everyday life, achieved the degree in philosophy, and wasaccepted for different jobs (e.g., as a librarian). However, his per-sonality continued to be characterized by obsessive, meticulous,touchy, and introverted attitudes, which caused difficulties inmaintaining consistent interpersonal relationships and job-relatedfunctions. On clinical examination, he showed naming difficultiesand impaired definition of word meanings, associated with pre-served awareness of the disease and self-awareness, secondaryanxiety and pessimism, and adequate inhibitory behavior controland social conduct.
At age 32, owing to ongoing drug-resistant seizures with thepresence of bilateral temporal epileptic discharges on the electro-encephalogram (EEG) recordings, vagal nerve stimulation wasinstituted. At age 35, the frequency of the seizures was reduced
and partial seizures only occurred; in particular, XY reported ictalthoughts relating to time perception during which his mind wasprojected to the future and he could experience future events. Hestill presented with frequent anomias, while his behavior wascharacterized by obsessive–compulsive aspects (e.g., he performedbrief motor exercises many times a day) and ideational distur-bances (e.g., he felt constrained to check if someone was tryingto swindle his family).
2.2. Neurophysiological and neuroradiological aspects
At age 24, interictal EEG recordings showed slowed backgroundactivity (7–8 Hz) and frequent spikes and sharp and slow waves lo-cated in the left temporoparietal regions (Fig. 1), and rare spikes inthe right temporal areas. Five seizures were recorded by video/EEGmonitoring: the inaugural symptoms were characterized by a sub-jective experience of ‘‘time flowing,” followed by speech arrest andloss of contact. The ictal EEG was characterized by low-voltage fastactivity in the middle and posterior left temporal areas, followedby a spike-and-wave discharge involving the same area with latediffusion to the right temporal lobe.
A magnetic resonance imaging (MRI) study was performedusing a 1.5-T scanner. The examination included spin–echo (SE)T1, proton density, and T2 weighted images in the sagittal, axial,and coronal planes; a three-dimensional fast field echo (FFE) T1weighted image in the coronal plane (2-mm adjacent slices) wasalso obtained. The study, examined by one neuroradiologist for siteand extent of cerebral cortical atrophy, size and shape of the ven-tricles, abnormal signal intensity in gray and white matter, andvolume and signal abnormalities of the hippocampi, revealed onlya slightly enlarged right temporal horn.
Multivoxel proton magnetic resonance spectroscopy (MRS) datasets were acquired with the same 1.5-T scanner using a point-re-solved spectroscopy sequence (PRESS TR/TE 1500/136) and a trans-verse field of view (160 * 160, matrix 16 * 16). A 20-mm-thickvolume of interest was located at the level of the temporal lobes.MRS of the mesial temporal regions showed a normal N-acetyl-aspartate peak. Positron emission tomography (PET) revealedslightly reduced metabolic capture in the cortical and subcorticaltemporoparietal areas, mainly on the left side.
From age 30 to age 35, EEG recordings maintained previous fea-tures and, at age 35, the CT scan of the brain excluded atrophy.
2.3. Neuropsychological evaluation
Three neuropsychological evaluations were carried out in Janu-ary 1998, March 1999, and March 2008. At the time of the first andsecond evaluations, XY experienced two to six seizures a week, anda few overt seizures occurred 6–12 hours before the tests. At thetime of the third evaluation, XY reported one to three seizures aday; a partial seizure occurred 2 hours before the examinationand another occurred during the evaluation, just before the verballearning test.
3. Results
3.1. First and second assessments
XY uses both hands in everyday life, but he is left-handedaccording to the Edinburgh Handedness Inventory [43] as he useshis right hand only to cut and write. During the three evaluations,he was alert, cooperative, and oriented in space and time. Nobehavioral alterations were observed, although he said he was feel-ing nervous and irritable. His awareness of cognitive impairmentwas fully preserved: he complained of naming difficulties, rareparaphasias, and a poor understanding of oral and written texts

Fig. 1. Interictal EEG showing epileptic abnormalities in the left temporo-parietal regions.
A.R. Giovagnoli et al. / Epilepsy & Behavior 14 (2009) 261–268 263
that did not fluctuate significantly from hour to hour or day to dayand interfered with his activities.
3.1.1. Self-evaluations and general neuropsychological aspectsOn the basis of self-report questionnaires, his general cognitive
function [44] was poor, and his levels of anxiety [45] and depres-sion [46] were high; quality of life was reported as being unsatis-factory [47] (Table 1).
Results from the neuropsychological tests [48–54] showed nor-mal abstract reasoning; selective attention; divided attention; setshifting; orofacial, ideomotor, and constructive praxis; and visualrecognition (Table 1).
Table 1First assessment: Self-evaluation and general neuropsychological evaluation
Self-evaluation scale Score
Multiple ability self-report questionnaire 124/140 (frequently perceiveddifficulties)
Beck Depression Inventory 12/39 (mild depression)State–Trait Anxiety InventoryForm 1 54/80 (severe anxiety)Form 2 61/80 (severe anxiety)Quality of Life in Epilepsy Inventory—89 47/100 (poor quality of life)
Neuropsychological testsa Raw score Equivalent score
Raven Coloured Progressive Matrices 33/36 3Attentive Matrices 54/60 2Trail Making TestPart B 98” 2Part A 37” 3Wisconsin Card Sorting Test 6 criteria —
0 perseverations —Street Completion Test 9/14 3Rey Complex Figure Copying 36/36 4Imitating gestures 20/20 4Imitating facial expressions 20/20 4
a Except for the Wisconsin Card Sorting Test, test scores were compared withsingle cutoff scores after transformation into age- and education-adjusted scores;such scores could be assessed with respect to performance ranges named equiva-lent scores (five categories from 0 to 4 corresponding to healthy control ranges,where 0 indicates a deficit and 1–4 indicate low to high performance), allowingspecification of the performance levels.
3.1.2. LanguageSpontaneous speech was correct in articulation and intonation,
but characterized by frequent word-finding difficulties (anomia forliving and nonliving things, tip-of-the-tongue phenomena, wordsubstitutions, and circumlocutions). The phonemic structure wascorrect. Use of grammar-syntactic rules was well preserved, asXY could produce complex sentences with well-articulated propo-sitions and could change the structure of sentences when needed.His comprehension of sentences was good, and communicativeefficiency was well retained.
His language was formally assessed using the Italian version ofthe Aachener Aphasia Test (AAT) [55]. His comprehension of spo-ken commands and all syntactic changes, repetition, written lan-guage, and naming of line drawings and colors were wellpreserved, whereas the production of compound object nameswas impaired (e.g., ‘‘tennis racket” instead of ‘‘carpet beater,” ‘‘foodfor cats” instead of ‘‘can opener,” ‘‘to crush” instead of ‘‘nut-cracker,” and ‘‘dish drying” instead of ‘‘dish washing”). Descriptionof complex figures was impaired due to anomias and paraphasias(e.g., ‘‘the woman is washing spaghetti” instead of ‘‘the woman isstraining spaghetti”; ‘‘the child is giving food to the dog” insteadof ‘‘the child is playing with the dog”), and his oral and writtencomprehension was poor due to an altered comprehension of indi-vidual words (e.g., he pointed at a sheep instead of a goat, stairs in-stead of an escalator, an arrow instead of a bow, a skate instead of ascooter, a padlock instead of a key, a rose instead of a thorn, and agirl instead of a boy) (Table 2). The Standard Language Examination[56] revealed that his oral and written naming of pictures was nor-mal when using semantically unrelated words, but severely im-paired when using related words; his written comprehension andnaming were similarly poor when using semantically relatedwords. Description Naming [57] and Word Fluency [57] were verypoor (Table 2) (Appendix).
3.1.3. Semantic memorySemantic memory was evaluated using tests that require verbal
(naming, judgment) or nonverbal (pointing, drawing, association)responses to visual and verbal stimuli. Picture Naming [58]assessed the same 80 items used in Picture Pointing and the
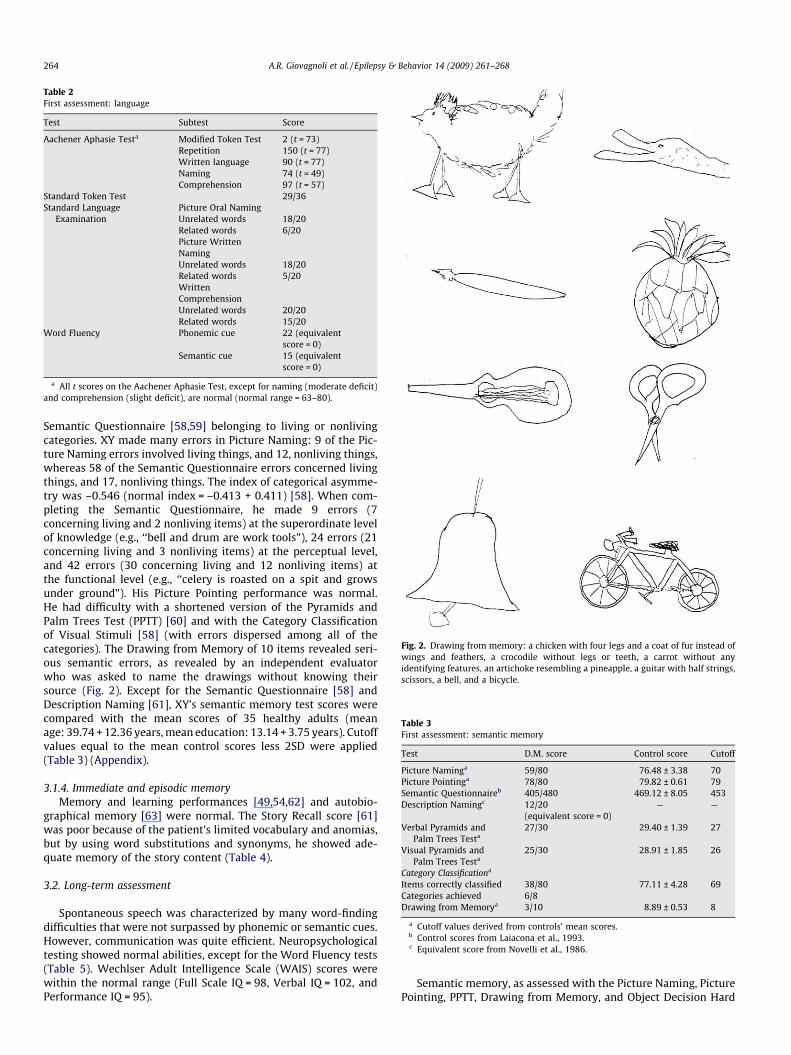
Fig. 2. Drawing from memory: a chicken with four legs and a coat of fur instead ofwings and feathers, a crocodile without legs or teeth, a carrot without anyidentifying features, an artichoke resembling a pineapple, a guitar with half strings,scissors, a bell, and a bicycle.
Table 2First assessment: language
Test Subtest Score
Aachener Aphasie Testa Modified Token Test 2 (t = 73)Repetition 150 (t = 77)Written language 90 (t = 77)Naming 74 (t = 49)Comprehension 97 (t = 57)
Standard Token Test 29/36Standard Language
ExaminationPicture Oral NamingUnrelated words 18/20Related words 6/20Picture WrittenNamingUnrelated words 18/20Related words 5/20WrittenComprehensionUnrelated words 20/20Related words 15/20
Word Fluency Phonemic cue 22 (equivalentscore = 0)
Semantic cue 15 (equivalentscore = 0)
a All t scores on the Aachener Aphasie Test, except for naming (moderate deficit)and comprehension (slight deficit), are normal (normal range = 63–80).
Table 3First assessment: semantic memory
Test D.M. score Control score Cutoff
Picture Naminga 59/80 76.48 ± 3.38 70Picture Pointinga 78/80 79.82 ± 0.61 79Semantic Questionnaireb 405/480 469.12 ± 8.05 453Description Namingc 12/20
(equivalent score = 0)— —
Verbal Pyramids andPalm Trees Testa
27/30 29.40 ± 1.39 27
Visual Pyramids andPalm Trees Testa
25/30 28.91 ± 1.85 26
Category Classificationa
Items correctly classified 38/80 77.11 ± 4.28 69Categories achieved 6/8Drawing from Memorya 3/10 8.89 ± 0.53 8
a Cutoff values derived from controls’ mean scores.b Control scores from Laiacona et al., 1993.c Equivalent score from Novelli et al., 1986.
264 A.R. Giovagnoli et al. / Epilepsy & Behavior 14 (2009) 261–268
Semantic Questionnaire [58,59] belonging to living or nonlivingcategories. XY made many errors in Picture Naming: 9 of the Pic-ture Naming errors involved living things, and 12, nonliving things,whereas 58 of the Semantic Questionnaire errors concerned livingthings, and 17, nonliving things. The index of categorical asymme-try was –0.546 (normal index = –0.413 + 0.411) [58]. When com-pleting the Semantic Questionnaire, he made 9 errors (7concerning living and 2 nonliving items) at the superordinate levelof knowledge (e.g., ‘‘bell and drum are work tools”), 24 errors (21concerning living and 3 nonliving items) at the perceptual level,and 42 errors (30 concerning living and 12 nonliving items) atthe functional level (e.g., ‘‘celery is roasted on a spit and growsunder ground”). His Picture Pointing performance was normal.He had difficulty with a shortened version of the Pyramids andPalm Trees Test (PPTT) [60] and with the Category Classificationof Visual Stimuli [58] (with errors dispersed among all of thecategories). The Drawing from Memory of 10 items revealed seri-ous semantic errors, as revealed by an independent evaluatorwho was asked to name the drawings without knowing theirsource (Fig. 2). Except for the Semantic Questionnaire [58] andDescription Naming [61], XY’s semantic memory test scores werecompared with the mean scores of 35 healthy adults (meanage: 39.74 + 12.36 years, mean education: 13.14 + 3.75 years). Cutoffvalues equal to the mean control scores less 2SD were applied(Table 3) (Appendix).
3.1.4. Immediate and episodic memoryMemory and learning performances [49,54,62] and autobio-
graphical memory [63] were normal. The Story Recall score [61]was poor because of the patient’s limited vocabulary and anomias,but by using word substitutions and synonyms, he showed ade-quate memory of the story content (Table 4).
3.2. Long-term assessment
Spontaneous speech was characterized by many word-findingdifficulties that were not surpassed by phonemic or semantic cues.However, communication was quite efficient. Neuropsychologicaltesting showed normal abilities, except for the Word Fluency tests(Table 5). Wechlser Adult Intelligence Scale (WAIS) scores werewithin the normal range (Full Scale IQ = 98, Verbal IQ = 102, andPerformance IQ = 95).
Semantic memory, as assessed with the Picture Naming, PicturePointing, PPTT, Drawing from Memory, and Object Decision Hard
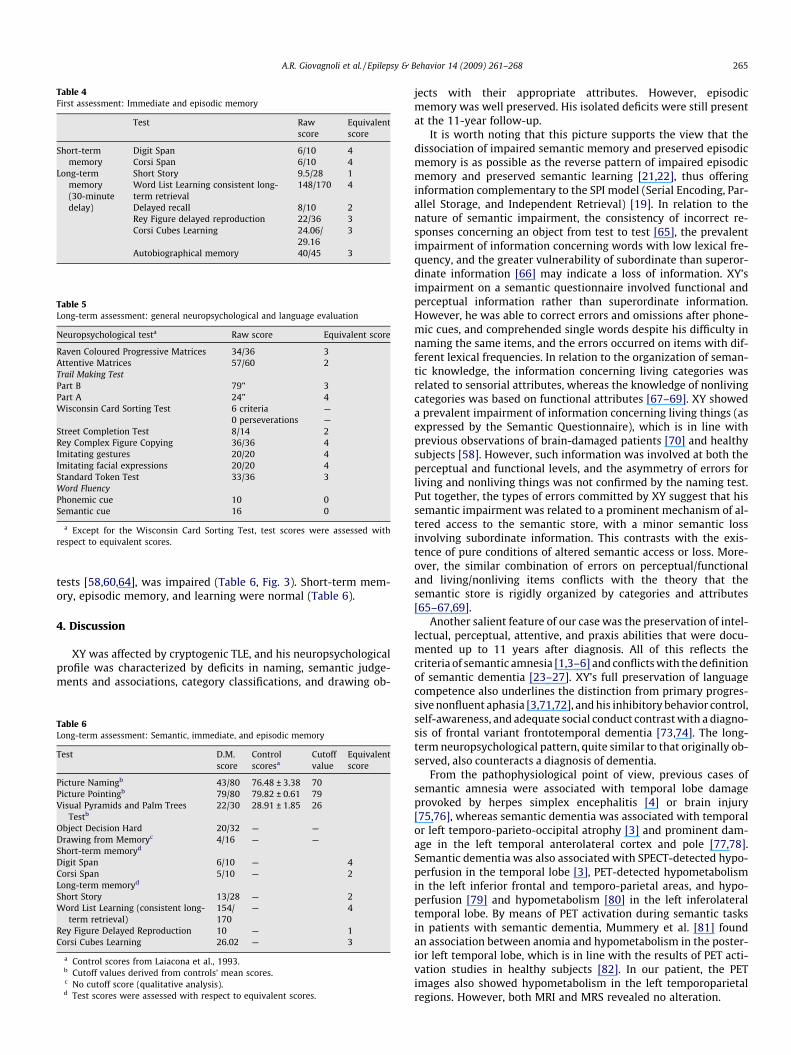
Table 4First assessment: Immediate and episodic memory
Test Rawscore
Equivalentscore
Short-termmemory
Digit Span 6/10 4Corsi Span 6/10 4
Long-termmemory(30-minutedelay)
Short Story 9.5/28 1Word List Learning consistent long-term retrieval
148/170 4
Delayed recall 8/10 2Rey Figure delayed reproduction 22/36 3Corsi Cubes Learning 24.06/
29.163
Autobiographical memory 40/45 3
Table 5Long-term assessment: general neuropsychological and language evaluation
Neuropsychological testa Raw score Equivalent score
Raven Coloured Progressive Matrices 34/36 3Attentive Matrices 57/60 2Trail Making TestPart B 79” 3Part A 24” 4Wisconsin Card Sorting Test 6 criteria —
0 perseverations —Street Completion Test 8/14 2Rey Complex Figure Copying 36/36 4Imitating gestures 20/20 4Imitating facial expressions 20/20 4Standard Token Test 33/36 3Word FluencyPhonemic cue 10 0Semantic cue 16 0
a Except for the Wisconsin Card Sorting Test, test scores were assessed withrespect to equivalent scores.
A.R. Giovagnoli et al. / Epilepsy & Behavior 14 (2009) 261–268 265
tests [58,60,64], was impaired (Table 6, Fig. 3). Short-term mem-ory, episodic memory, and learning were normal (Table 6).
4. Discussion
XY was affected by cryptogenic TLE, and his neuropsychologicalprofile was characterized by deficits in naming, semantic judge-ments and associations, category classifications, and drawing ob-
Table 6Long-term assessment: Semantic, immediate, and episodic memory
Test D.M.score
Controlscoresa
Cutoffvalue
Equivalentscore
Picture Namingb 43/80 76.48 ± 3.38 70Picture Pointingb 79/80 79.82 ± 0.61 79Visual Pyramids and Palm Trees
Testb22/30 28.91 ± 1.85 26
Object Decision Hard 20/32 — —Drawing from Memoryc 4/16 — —Short-term memoryd
Digit Span 6/10 — 4Corsi Span 5/10 — 2Long-term memoryd
Short Story 13/28 — 2Word List Learning (consistent long-
term retrieval)154/170
— 4
Rey Figure Delayed Reproduction 10 — 1Corsi Cubes Learning 26.02 — 3
a Control scores from Laiacona et al., 1993.b Cutoff values derived from controls’ mean scores.c No cutoff score (qualitative analysis).d Test scores were assessed with respect to equivalent scores.
jects with their appropriate attributes. However, episodicmemory was well preserved. His isolated deficits were still presentat the 11-year follow-up.
It is worth noting that this picture supports the view that thedissociation of impaired semantic memory and preserved episodicmemory is as possible as the reverse pattern of impaired episodicmemory and preserved semantic learning [21,22], thus offeringinformation complementary to the SPI model (Serial Encoding, Par-allel Storage, and Independent Retrieval) [19]. In relation to thenature of semantic impairment, the consistency of incorrect re-sponses concerning an object from test to test [65], the prevalentimpairment of information concerning words with low lexical fre-quency, and the greater vulnerability of subordinate than superor-dinate information [66] may indicate a loss of information. XY’simpairment on a semantic questionnaire involved functional andperceptual information rather than superordinate information.However, he was able to correct errors and omissions after phone-mic cues, and comprehended single words despite his difficulty innaming the same items, and the errors occurred on items with dif-ferent lexical frequencies. In relation to the organization of seman-tic knowledge, the information concerning living categories wasrelated to sensorial attributes, whereas the knowledge of nonlivingcategories was based on functional attributes [67–69]. XY showeda prevalent impairment of information concerning living things (asexpressed by the Semantic Questionnaire), which is in line withprevious observations of brain-damaged patients [70] and healthysubjects [58]. However, such information was involved at both theperceptual and functional levels, and the asymmetry of errors forliving and nonliving things was not confirmed by the naming test.Put together, the types of errors committed by XY suggest that hissemantic impairment was related to a prominent mechanism of al-tered access to the semantic store, with a minor semantic lossinvolving subordinate information. This contrasts with the exis-tence of pure conditions of altered semantic access or loss. More-over, the similar combination of errors on perceptual/functionaland living/nonliving items conflicts with the theory that thesemantic store is rigidly organized by categories and attributes[65–67,69].
Another salient feature of our case was the preservation of intel-lectual, perceptual, attentive, and praxis abilities that were docu-mented up to 11 years after diagnosis. All of this reflects thecriteria of semantic amnesia [1,3–6] and conflicts with the definitionof semantic dementia [23–27]. XY’s full preservation of languagecompetence also underlines the distinction from primary progres-sive nonfluent aphasia [3,71,72], and his inhibitory behavior control,self-awareness, and adequate social conduct contrast with a diagno-sis of frontal variant frontotemporal dementia [73,74]. The long-term neuropsychological pattern, quite similar to that originally ob-served, also counteracts a diagnosis of dementia.
From the pathophysiological point of view, previous cases ofsemantic amnesia were associated with temporal lobe damageprovoked by herpes simplex encephalitis [4] or brain injury[75,76], whereas semantic dementia was associated with temporalor left temporo-parieto-occipital atrophy [3] and prominent dam-age in the left temporal anterolateral cortex and pole [77,78].Semantic dementia was also associated with SPECT-detected hypo-perfusion in the temporal lobe [3], PET-detected hypometabolismin the left inferior frontal and temporo-parietal areas, and hypo-perfusion [79] and hypometabolism [80] in the left inferolateraltemporal lobe. By means of PET activation during semantic tasksin patients with semantic dementia, Mummery et al. [81] foundan association between anomia and hypometabolism in the poster-ior left temporal lobe, which is in line with the results of PET acti-vation studies in healthy subjects [82]. In our patient, the PETimages also showed hypometabolism in the left temporoparietalregions. However, both MRI and MRS revealed no alteration.
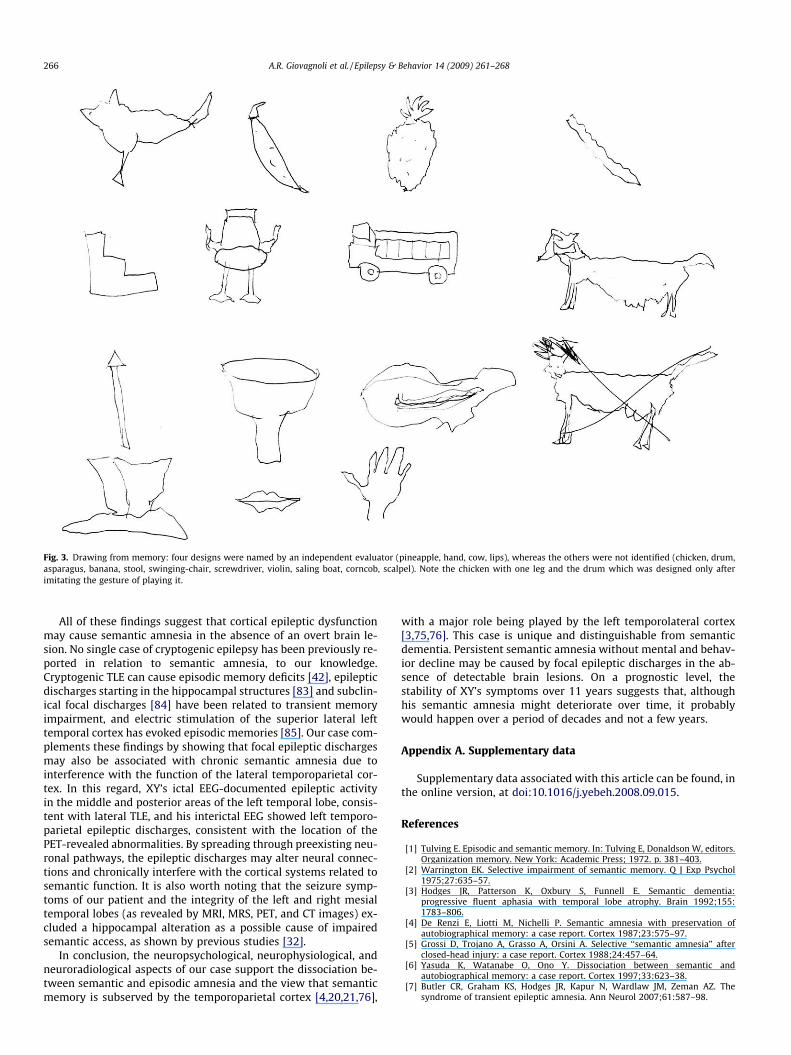
Fig. 3. Drawing from memory: four designs were named by an independent evaluator (pineapple, hand, cow, lips), whereas the others were not identified (chicken, drum,asparagus, banana, stool, swinging-chair, screwdriver, violin, saling boat, corncob, scalpel). Note the chicken with one leg and the drum which was designed only afterimitating the gesture of playing it.
266 A.R. Giovagnoli et al. / Epilepsy & Behavior 14 (2009) 261–268
All of these findings suggest that cortical epileptic dysfunctionmay cause semantic amnesia in the absence of an overt brain le-sion. No single case of cryptogenic epilepsy has been previously re-ported in relation to semantic amnesia, to our knowledge.Cryptogenic TLE can cause episodic memory deficits [42], epilepticdischarges starting in the hippocampal structures [83] and subclin-ical focal discharges [84] have been related to transient memoryimpairment, and electric stimulation of the superior lateral lefttemporal cortex has evoked episodic memories [85]. Our case com-plements these findings by showing that focal epileptic dischargesmay also be associated with chronic semantic amnesia due tointerference with the function of the lateral temporoparietal cor-tex. In this regard, XY’s ictal EEG-documented epileptic activityin the middle and posterior areas of the left temporal lobe, consis-tent with lateral TLE, and his interictal EEG showed left temporo-parietal epileptic discharges, consistent with the location of thePET-revealed abnormalities. By spreading through preexisting neu-ronal pathways, the epileptic discharges may alter neural connec-tions and chronically interfere with the cortical systems related tosemantic function. It is also worth noting that the seizure symp-toms of our patient and the integrity of the left and right mesialtemporal lobes (as revealed by MRI, MRS, PET, and CT images) ex-cluded a hippocampal alteration as a possible cause of impairedsemantic access, as shown by previous studies [32].
In conclusion, the neuropsychological, neurophysiological, andneuroradiological aspects of our case support the dissociation be-tween semantic and episodic amnesia and the view that semanticmemory is subserved by the temporoparietal cortex [4,20,21,76],
with a major role being played by the left temporolateral cortex[3,75,76]. This case is unique and distinguishable from semanticdementia. Persistent semantic amnesia without mental and behav-ior decline may be caused by focal epileptic discharges in the ab-sence of detectable brain lesions. On a prognostic level, thestability of XY’s symptoms over 11 years suggests that, althoughhis semantic amnesia might deteriorate over time, it probablywould happen over a period of decades and not a few years.
Appendix A. Supplementary data
Supplementary data associated with this article can be found, inthe online version, at doi:10.1016/j.yebeh.2008.09.015.
References
[1] Tulving E. Episodic and semantic memory. In: Tulving E, Donaldson W, editors.Organization memory. New York: Academic Press; 1972. p. 381–403.
[2] Warrington EK. Selective impairment of semantic memory. Q J Exp Psychol1975;27:635–57.
[3] Hodges JR, Patterson K, Oxbury S, Funnell E. Semantic dementia:progressive fluent aphasia with temporal lobe atrophy. Brain 1992;155:1783–806.
[4] De Renzi E, Liotti M, Nichelli P. Semantic amnesia with preservation ofautobiographical memory: a case report. Cortex 1987;23:575–97.
[5] Grossi D, Trojano A, Grasso A, Orsini A. Selective ‘‘semantic amnesia” afterclosed-head injury: a case report. Cortex 1988;24:457–64.
[6] Yasuda K, Watanabe O, Ono Y. Dissociation between semantic andautobiographical memory: a case report. Cortex 1997;33:623–38.
[7] Butler CR, Graham KS, Hodges JR, Kapur N, Wardlaw JM, Zeman AZ. Thesyndrome of transient epileptic amnesia. Ann Neurol 2007;61:587–98.
A.R. Giovagnoli et al. / Epilepsy & Behavior 14 (2009) 261–268 267
[8] Dalla Barba G, Cipollotti E, Denes G. Autobiographical memory loss andconfabulations in Korsakoff’s syndrome: a case report. Cortex1990;26:525–34.
[9] Damasio AR, Enlinger PG, Damasio H, Van Hoesen GW, Cornell S. Multimodalamnesic syndrome following bilateral temporal and basal forebrain damage.Arch Neurol 1985;42:252–9.
[10] Hodges JR. Semantic memory and frontal executive function during transientglobal amnesia. J Neurol Neurosurg Psychiatry 1994;57:605–8.
[11] Tulving E, Schacter DL, McLachlan DR, Moscovitch M. Priming of semanticautobiographical knowledge: a case study of retrograde amnesia. Brain Cogn1988;8:3–20.
[12] Parkin AJ, Leng NRC. Neuropsychology of the amnesic syndrome. Hove/Hillsdale, NJ: Lawrence Erlbaum; 1993.
[13] Schacter DL, Tulving E. Memory, amnesia, and the episodic/semanticdistinction. In: Isaacson RL, Spear NE, editors. Expression of knowledge. NewYork: Plenum; 1982. p. 33–65.
[14] Teng E, Squire LR. Memory for places learned long ago is intact afterhippocampal damage. Nature 1999;400:675–7.
[15] Tulving E. Elements of episodic memory. Oxford: Clarendon Press; 1983.[16] Cohen NJ, Poldrack RA, Eichenbaum H. Memory for items and memory for
relations in the procedural/declarative memory framework. Memory1997;5:131–78.
[17] Squire LR, Zola SM. Structure and function of declarative and non declarativememory systems. Proc Natl Acad Sci USA 1996;93:13515–22.
[18] Squire LR, Zola SM. Episodic memory, semantic memory, and amnesia.Hippocampus 1998;8:205–11.
[19] Tulving E. Organization of memory: quo vadis? In: Gazzaniga MS, editor. Thecognitive neurosciences. Cambridge, MA: MIT Press; 1995.
[20] Tulving E, Markowitsch HJ. Episodic and declarative memory: role of thehippocampus. Hippocampus 1998;8:198–204.
[21] Varga-Khadem E, Gadian DG, Watkins KE, Connelly A, Van Paesschen W,Mishkin M. Differential effects of early hippocampal pathology on episodic andsemantic memory. Science 1997;277:376–80.
[22] Verfaellie M, Koseff P, Alexander MP. Acquisition of novel semanticinformation in amnesia: effects of lesion location. Neuropsychologia2000;38:484–92.
[23] Snowden JS, Goulding PJ, Neary D. Semantic dementia: a form ofcircumscribed cerebral atrophy. Behav Neurol 1989;2:167–82.
[24] Chertkow H, Bub D. Semantic memory loss in dementia of Alzheimer type.Brain 1990;113:397–417.
[25] Lambon Ralph MA, Patterson K, Hodges JR. The relationship between namingand semantic knowledge for different categories in dementia of Alzheimertype. Neuropsychologia 1997;35:1251–60.
[26] Hodges JR, Gurd JM. Remote memory and lexical retrieval in a case of frontalPick’s disease. Arch Neurol 1994;51:821–7.
[27] Rossor MN, Revesz T, Lantos PL, Warrington EK. Semantic dementia withubiquitin-positive tau-negative inclusion bodies. Brain 2000;123:267–76.
[28] Devinsky O. Cognitive and behavioral effects of antiepileptic drugs. Epilepsia1995;36:46–65.
[29] Dodrill CB, Matthews CG. The role of neuropsychology in the assessment andtreatment of persons with epilepsy. Am J Psychol 1992;47:1139–42.
[30] Jones-Gotman M. Commentary: psychological evaluation: testinghippocampal function. In: Engel Jr J, editor. Surgical treatment of theepilepsies. New York: Raven Press; 1987. p. 203–11.
[31] Bell DB, Hermann BP, Woodard AR, et al. Object naming and semanticknowledge in temporal lobe epilepsy. Neuropsychology 2001;15:434–43.
[32] Davies KG, Bell BD, Bush AJ, Hermann BP, Dohan FC, Jaap AS. Naming declineafter left anterior temporal lobectomy correlates with pathological status ofresected hippocampus. Epilepsia 1998;39:407–19.
[33] Giovagnoli AR. Verbal semantic memory in temporal lobe epilepsy. ActaNeurol Scand 1999;99:334–9.
[34] Giovagnoli AR. Characteristics of verbal semantic impairment in lefthemisphere epilepsy. Neuropsychology 2005;19:501–8.
[35] Giovagnoli AR, Erbetta A, Villani F, Avanzini G. Semantic memory in partialepilepsy: verbal and non-verbal deficits and neuroanatomical relationships.Neuropsychologia 2005;43:1482–92.
[36] Wilkins A, Moscovitch M. Selective impairment of semantic memory aftertemporal lobectomy. Neuropsychologia 1978;16:73–9.
[37] Hermann BP, Wyler AR, Richey ET, Rea JM. Memory function and verballearning ability in patients with complex partial seizures of temporal lobeorigin. Epilepsia 1987;28:547–54.
[38] Ribbler A, Rausch R. Performance of patients with unilateral temporallobectomy on selective reminding procedures using ether related orunrelated words. Cortex 1990;26:575–84.
[39] Helmstaedter C, Gleibner U, Di Perna M, Elger CE. Relational verbalmemory processing in patients with temporal lobe epilepsy. Cortex1997;33:667–78.
[40] Bell B, Fine J, Dow C, Seidenberg M, Hermann B. Temporal lobe epilepsy andthe selective reminding test: the conventional 30-minute delay suffices.Psychol Assess 2005;17:103–9.
[41] Bell B. WMS-III logical memory performance after a two-week delay intemporal lobe epilepsy and control groups. J Clin Exp Neuropsychol2006;28:1435–43.
[42] Giovagnoli AR, Avanzini G. Learning and memory impairment in patients withtemporal lobe epilepsy: relation to the presence, type, and location of brainlesion. Epilepsia 1999;40:904–11.
[43] Oldfield RC. The assessment and analysis of handedness: the EdinburghInventory. Neuropsychologia 1971;9:97–113.
[44] Seidenberg M, Haltiner A, Taylor AM, Hermann BP, Wyler A. Development andvalidation of a multiple ability self-report questionnaire. J Clin ExpNeuropsychol 1994;16:93–104.
[45] Spielberger CD. Inventario per l’ansia di ‘‘stato” e di ‘‘tratto”: nuovaversione italiana dello S.T.A.I.: Forma Y. Florence: Organizzazioni Speciali;1989.
[46] Beck AT, Weissman MM. An inventory for measuring depression. Arch GenPsychiatry 1987;4:561–71.
[47] Devinsky O, Vickrey BG, Cramer J, et al. Development of the quality of life inepilepsy inventory. Epilepsia 1995;36:1089–104.
[48] Basso A, Capitani E, Laiacona M. Raven’s Coloured Progressive Matrices:normative values on 305 adult controls. Funct Neurol 1987;2:189–94.
[49] Spinnler H, Tognoni G. Standardizzazione e taratura italiana di testneuropsicologici. It J Neurol Sci 1987;6(Suppl. 8).
[50] Giovagnoli AR, Del Pesce M, Mascheroni S, Simoncelli M, Laiacona M, CapitaniE. Trail Making Test: normative values from 287 normal adult controls. It JNeurol Sci 1996;17:305–9.
[51] Nelson HE. A modified card sorting test sensitive to frontal lobe defects. Cortex1976;12:313–24.
[52] De Renzi E, Pieczuro E, Vignolo LA. Oral apraxia and aphasia. Cortex1966;2:50–73.
[53] De Renzi E, Motti F, Nichelli P. Imitating gestures. A quantitative approach toideomotor apraxia. Arch Neurol 1980;37:6–10.
[54] Lezak M. Neuropsychological assessment. New York: Oxford Univ. Press; 1995.[55] Luzzati C, Willmes K, De Bleser R. Aachener Aphasie Test: Versione
Italiana. Florence: Organizzazioni Speciali; 1991.[56] Basso A, Capitani E, Vignolo LA. Influence of rehabilitation on language skills in
aphasic patients: a controlled study. Arch Neurol 1979;36:190–6.[57] Novelli G, Papagno C, Capitani E, Laiacona M, Vallar G, Cappa SF. Tre test clinici
di ricerca e produzione lessicale: taratura su soggetti normali. Arch PsicolNeurol Psichiatr 1986;47:447–506.
[58] Laiacona M, Barbarotto R, Trivelli C, Capitani E. Dissociazioni semanticheintercategoriali: descrizione di una batteria standardizzata e dati normativi.Arch Psicol Neurol Psichiat 1993;54:209–48.
[59] Snodgrass JG, Wandervart M. A standardized set of 260 pictures: norms forname agreement, image agreement, familiarity, and visual complexity. J ExpPsychol 1980;6:174–215.
[60] Howard D, Patterson K. Pyramids and Palm Trees: a test of semantic accessfrom pictures and words. Bury St. Edmunds, Suffolk: Thames Valley Test Co.;1992.
[61] Novelli G, Papagno C, Capitani E, Laiacona M, Cappa SF, Vallar G. Tre test clinicidi memoria verbale a lungo termine: Taratura su soggetti normali. Arch PsicolNeurol Psichiatr 1986;47:278–96.
[62] Buschke H, Fuld PA. Evaluating storage, retention, and retrieval in disorderedmemory and learning. Neurology 1974;24:1019–25.
[63] Borrini G, Dall’Ora P, Della Sala S, Marinelli L, Spinnler H. Autobiographicalmemory: sensitivity to age and education of a standardised enquiry. PsycholMed 1989;19:215–24.
[64] Riddoch MJ, Humphreys GW. BORB: Birmingham Object RecognitionBattery. Hove (UK): Lawrence Erlbaum; 1993.
[65] Coughlan AK, Warrington EK. The impairment of verbal semantic memory: asingle case study. J Neurol Neurosurg Psychiatry 1981;44:1079–83.
[66] Shallice T. Specialisation within the semantic system. Cogn Neuropsychol1988;5:133–42.
[67] Warrington EK, McCarthy RA. Category-specific access dysphasia. Brain1983;106:859–78.
[68] Warrington EK, McCarthy RA. Categories of knowledge: further fractionationand an attempted integration. Brain 1987;110:1273–96.
[69] Warrington EK, Shallice T. Category specific semantic impairments. Brain1984;197:829–54.
[70] Basso A, Capitani E, Laiacona M. Progressive language impairment withoutdementia: a case with isolated category specific semantic defect. J NeurolNeurosurg Psychiatry 1988;5:1201–7.
[71] Caselli RJ, Jack Jr CR. Asymmetric cortical degeneration syndromes: a proposedclinical classification. Arch Neurol 1992;49:770–80.
[72] Kertesz A, Davidson W, McCabe P. Primary progressive semantic amnesia: acase study. JINS 1998;4:388–98.
[73] The Lund and Manchester Groups. Consensus statement: clinical andneuropathological criteria for fronto-temporal dementia. J Neurol NeurosurgPsychiatry 1994;4:416–8.
[74] Neary D, Snowden JS, Northen B, Goulding PJ. Dementia of frontal lobe type. JNeurol Neurosurg Psychiatry 1998;51:353–61.
[75] Behrman M, Bub D. Surface dyslexia and dysgraphia: dual routes, singlelexicon. Cogn Neuropsychol 1992;9:209–51.
[76] Patterson K, Hodges JR. Disorders of semantic memory. In: Baddeley AD,Wilson BA, Watts FN, editors. Handbook of memorydisorders. Chichester: Wiley; 1995. p. 167–86.
[77] Hodges JR, Patterson K. Non fluent progressive aphasia and semanticdementia: a comparative neuropsychological study. JINS 1996;2:511–24.
[78] Snowden JS, Neary D, Mann DM. Fronto-temporal lobar degeneration. NewYork: Churchill Livingstone; 1996.
[79] Cardebat D, Demonet JF, Celsis P, Puel M. Living/non-living dissociation in acase of semantic dementia: a SPECT activation study. Neuropsychologia1996;34:1175–9.

268 A.R. Giovagnoli et al. / Epilepsy & Behavior 14 (2009) 261–268
[80] Patterson K, Croot K, Hodges JR. Speech production: insights from a study ofprogressive aphasia. In: Proceedings of International Conference on SpokenLanguage Processing. Tokyo: Acoustical Soc. of Japan; 1994. p. 755–8.
[81] Mummery CJ, Patterson K, Wise RJS, Vandenbergh R, Price CJ, Hodges JR.Disrupted temporal lobe connections in semantic dementia. Brain1999;122:61–73.
[82] Price CJ, Moore CJ, Humphreys GW, Wise RJS. Segregating semantic fromphonological processing during reading. J Cogn Neurosci 1997;9:727–33.
[83] Bridgman PA, Malamut BL, Sperling MR, Saykin AJ, O’Connor MJ. Memoryduring subclinical hippocampal seizures. Neurology 1989;39:953–6.
[84] Aarts JHP, Binnie CD, Smith AM, Wilkins AJ. Selective cognitive impairmentduring focal and generalised epileptiform EEG activity. Brain1984;107:293–308.
[85] Moriarity JL, Boatman D, Krauss GL, Storm PB, Lenz FA. Human ‘‘memories” canbe evoked by stimulation of the lateral temporal cortex after ipsilateral medialtemporal lobe resection. J Neurol Neurosurg Psychiatry 2001;71:549–51.




















