ELP4 in rolandic epilepsy and BRD2 in juvenile myoclonic epilepsy
Upload
independentCategory
view
2download
0
ORIGINAL ARTICLE
Genetic and forensic implications in epilepsy and cardiacarrhythmias: a case series
Sara Partemi & Monica Coll Vidal & Pasquale Striano & Oscar Campuzano &
Catarina Allegue &Marianna Pezzella &Maurizio Elia & Pasquale Parisi &Vincenzo Belcastro &
Susanna Casellato & Lucio Giordano & Massimo Mastrangelo & Nicola Pietrafusa &
Salvatore Striano & Federico Zara & Amedeo Bianchi & Daniela Buti & Angela La Neve &
Carlo Alberto Tassinari & Antonio Oliva & Ramon Brugada
Received: 20 May 2014 /Accepted: 5 August 2014# Springer-Verlag Berlin Heidelberg 2014
Abstract Epilepsy affects approximately 3 % of the world’spopulation, and sudden death is a significant cause of death inthis population. Sudden unexpected death in epilepsy(SUDEP) accounts for up to 17 % of all these cases, whichincreases the rate of sudden death by 24-fold as compared tothe general population. The underlying mechanisms are still
not elucidated, but recent studies suggest the possibility that acommon genetic channelopathy might contribute to both ep-ilepsy and cardiac disease to increase the incidence of deathvia a lethal cardiac arrhythmia. We performed genetic testingin a large cohort of individuals with epilepsy and cardiacconduction disorders in order to identify genetic mutations
Sara Partemi and Monica Coll Vidal equally contributed to this study.
Antonio Oliva and Ramon Brugada are co-senior authors
S. Partemi :M. C. Vidal :A. Oliva (*)Institute of LegalMedicine, School ofMedicine, Catholic University,Rome, Italye-mail: [email protected]
S. Partemi :M. C. Vidal :O. Campuzano :C. Allegue : R. BrugadaCardiovascular Genetics Center, Institut d’Investigació BiomèdicaGirona-IdIBGi, Universitat de Girona, Girona, Spain
P. Striano :M. PezzellaPediatric Neurology and Muscular Diseases Unit,DINOGMI-Department of Neurosciences, Rehabilitation,Ophthalmology, Genetics, Maternal and Child Health, University ofGenova, Genoa, Italy
M. EliaOasi Institute for Research on Mental Retardation and Brain Aging(IRCCS), Troina, EN, Italy
P. ParisiChild Neurology, Chair of Pediatrics, NESMOSDepartment, Facultyof Medicine and Psychology, Sapienza University, Rome, Italy
V. BelcastroNeurology Unit, Department of Medicine, S. Anna Hospital, Como,Italy
S. CasellatoDepartment of Child Neuropsychiatry, University of Sassari, Sassari,Italy
L. GiordanoPediatric Neuropsychiatric Division, Spedali Civili, Brescia, Italy
M. MastrangeloPediatric Neurology Unit, V. Buzzi Hospital, A.O. ICP, Milan, Italy
N. Pietrafusa :A. La NeveDepartment of Neurological and Psychiatric Sciences, Section of 1stNeurologic Clinic, University of Bari, Bari, Italy
S. StrianoEpilepsy Center, Department of Neuroscience, Reproductive Scienceand Odontostomatology, Federico II University, Naples, Italy
F. ZaraLaboratory of Neurogenetics, Department of Neuroscience, InstituteG. Gaslini, Genoa, Italy
A. BianchiDepartment of Neurology and Epilepsy Centre (A.B..), San DonatoHospital, Arezzo, Italy
D. ButiPediatric Neurology Unit and Laboratories, Children’s Hospital A.Meyer—University of Florence, Florence, Italy
C. A. TassinariDepartment of Neurological Sciences, University of Bologna,Bologna, Italy
Int J Legal MedDOI 10.1007/s00414-014-1063-4

that could play a role in the mechanism of sudden death.Putative pathogenic disease-causing mutations in genesencoding cardiac ion channel were detected in 24 % of unre-lated individuals with epilepsy. Segregation analysis throughgenetic screening of the available family members and func-tional studies are crucial tasks to understand and to prove thepossible pathogenicity of the variant, but in our cohort, onlytwo families were available. Despite further research shouldbe performed to clarify the mechanism of coexistence of bothclinical conditions, genetic analysis, applied also in post-mortem setting, could be very useful to identify genetic factorsthat predispose epileptic patients to sudden death, helping toprevent sudden death in patients with epilepsy.
Keywords Sudden unexplained death in epilepsy .
Channelopathy . LongQTsyndrome . Brugada syndrome .
Cardiac arrhythmias . Epilepsy
Introduction
Epilepsy is one of the most common serious neurologicaldisorders seen in 3 % of the world’s population [1]. Mortalityrates are considerably higher in patients with epilepsy incomparison with general population, and it accounts for amean of 17 % of deaths in this population [2–7]. The leadingepilepsy-related cause of death is believed to be sudden un-expected death in epilepsy (SUDEP), especially in patientswith chronic, uncontrolled disease. Concretely, it is defined asa sudden, unexplained, non-traumatic, witnessed orunwitnessed death in patients with epilepsy, excluding docu-mented status epilepticus, in which post-mortem examinationdoes not reveal a toxicological or anatomic cause of death [8].The mechanisms of SUDEP is presumed to be multifactorial,autonomic dysfunction, heart rate variability (HRV), catechol-amine surge, antiepileptic medications, and underlying cardi-ac arrhythmias during and between seizures all result in dys-regulation of cerebral and cardiac blood flow contributing tosudden death [9]. Several studies have focused the research onthe possibility that a common channelopathy might contributeto both epilepsy and cardiac disease [10]. Hence, genetically,ion channels co-expressed in brain and heart are logical can-didates for SUDEP because defects in intrinsic membraneexcitability could underlie both epilepsy and cardiac arrhyth-mias that precipitate death [11–15]. In addition, a recent studyhas analyzed for the first time a SUDEP case using NGStechnology. This report shows a complex combination ofseveral genetic variations of unknown clinical significance(GVUS) in cardiac and brain genes supporting the crucial roleof comprehensive genetic analysis in the assessment ofSUDEP [16]. Despite recent reports focused on this connec-tion between both clinical entities, several key points remainto clarify in order to translate the information into clinical
practice. The aim of our study is to characterize a cohort ofepileptic individuals also diagnosed with heart rhythm disor-ders performing genetic screening of ion channels co-expressed in brain and heart. We have selected this subgroupof epilepsy patients in order to investigate the genetic predis-position in developing arrhythmias responsible in increasingthe risk or leading to SUDEP.
Material and methods
In this prospective study, we recruited—from January 2009 toDecember 2012—a total of 41 consecutive individuals withnon-lesional/metabolic focal or generalized epilepsy showinga personal history of heart rhythm disturbances and/or a first-degree family history of cardiac arrhythmias/sudden death.We have included also one case enrolled in this series after acomprehensive autopsy investigation classified as SUDEPwhere autopsy examination and toxicological analysis werecompletely negative. All patients received at least one surfaceelectrocardiogram (ECG) and were evaluated by an expertcardiologist who classified the cardiac phenotype of the pro-bands and/or of the relatives. Vague histories of heart rhythmdisturbances in family members not clearly known by theproband or with any available clinical/instrumental data wereexcluded. All individuals or their family members signed awritten informed consent to participate in the study. Informedconsent of all patients was obtained in accordance with inter-national review board guidelines of Catholic University. Thestudy was approved by the ethics committee of CatholicUniversity (Rome, Italy) and conforms to the principlesoutlined in the Declaration of Helsinki.
Genetic testing
Blood samples were collected, and DNAwas extracted by theautomatic extractor Chemagic MSM I from whole blood(Chemagic human blood). Sanger sequencing was performedfor 10 potassium and sodium ion channel genes (Table 1),including the most common genes associated with Brugadasyndrome (BrS) and long QT syndrome (LQTS) (SCN5A,KCNQ1, KCNH2, KCNE1, KCNE2, and KCNE3), and genescoding for the beta subunits of sodium channel (SCN1B,SCN2B, SCN3B, and SCN4B), also associated with heartrhythm disturbances. Genetic analysis included all exonicand flanking intronic regions (−7 to +10) corresponding tothe 3′ and 5′ extremes of the exons, as potentially related toerroneous splicing processes (Splice Site Tools. A compara-tive analysis report. Beth Hellen). Briefly, samples were am-plified by polymerase chain reaction (PCR) using intronicprimers for each exon; PCR product was purified byExoSAP-IT and directly sequenced by dideoxy chain-
Int J Legal Med

termination method in ABI Prism Big Dye® Terminator v3.1Cycle Sequencing Kit (Applied Biosystems, USA). Sequenc-ing process was processed in a 3130xl Genetic Analyzer(Applied Biosystems) and analyzed by means of SeqScapeSoftware v2.5 (Life Technologies) comparing obtained resultswith the reference sequence from hg19. Several free-accessinternational databases and locus-specific database werechecked to contrast the detected variants: Ensembl genomebrowser [17]; 1000 Genomes Browser [18]; NHLBI GOExome Sequencing Project (ESP) or Exome Server Variant(ESV), Seattle, WA; Human Gene Mutation Database(HGMD) [19], and dbSNP, NCBI [20]. In non-synonymousand not previously described variants, the following criteriawere applied to assess their potential pathogenicity: rare var-iants were considered when the minor allele frequency (MAF)was <0.01 and variants with “probably damaging” status afterin silico analysis in CONsensus DELeteriousness score ofmissense single nucleotide variants (SNV) (CONDEL) [21],PROVEAN (http://provean.jcvi.org/index.php), and MutationTaster [22]. All possible pathogenic variants were denotedusing the accepted Human Genome Variation Society’sguidelines for nomenclature [23]: “c.” was used to indicate acoding DNA sequence and “p.” for a protein sequence.Nucleotide numbering reflects cDNA numbering with +1corresponding to the A of the ATG translation initiationcodon in the reference sequence; the initiation codon iscodon 1. Protein numbering reflects the translation initiatormethionine numbered as +1. Sequence variant descriptionswere checked using the Mutalyzer program (http://www.LOVD.nl/mutalyzer).
Results
We have recruited 42 epilepsy cases (41 patients+one casefrom post-mortem setting) fulfilling the inclusion clinicalcriteria. Ten (23.8 %) individuals had clinical and ECG
evidence of heart rhythm disturbances (BrS or LQTS), where-as a first-degree family history of cardiac arrhythmias/suddendeath was recorded in the other 32 patients (76.2 %).
Genetic study identified 40 single nucleotide variants(SNV) classified as common variants either because they weresynonymous or because had a MAF>0.01 in CEU population(Table 2). We identified 13 in the SCN5A gene, eight inKCNQ1, nine in KCNH2, two in KCNE1, one in KCNE3,two in SCN1B, three in SCN3B, and two in the SCN4B gene.
In addition, 11 SNV with potential pathogenic significancewere identified in nine out of the 42 subjects analyzed(21.4 %). The demographic and genotype data of the patientswhere a mutation was found are summarized in Table 3. A45.45 % of the global cases carried a SNV in the SCN5A gene,followed by KCNQ1 (27.27 %), KCNH2 (18.18 %), andKCNE2 (9.1 %). Among the SNV carriers, seven patientshad only one SNV, whereas two patients carried doubleSNV. As showed in Table 3, patient no. 3 carried a compoundSNV in the SCN5A gene (p.I102Vand p.R1193Q), patient no.4 carried a digenic SNV (p.R34C in SCN5A and p.V207M inKCNQ1).
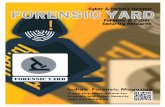
All SNV were in heterozygous state, inducingmissense changes except one nonsense variant(p.W1095X_SCN5A in patient no. 1). Most of the iden-tified SNV were localized in the extremes of theencoded protein (4 in C-terminus and 4 in N-terminusr e g i o n s ) e x c e p t t h r e e ( p .W1 0 9 5X_ SCN5A ,p.R1193Q_SCN5A, and p.V207M_KCNQ1) (Fig. 1).
Only one variation was novel (p.I102V_SCN5A) and pre-dicted in silico as potentially pathogenic. In addition to thisnovel SNV, in silico prediction also classifies as potentiallypathogenic two more SNV (p.R34C_SCN5A andp.D837G_KCNH2). All other SNV were previously reportedin HGMD database except three (p.I102V_SCN5A,p.R34C_SCN5A, and p.V648I_KCNQ1). Of all previouslyreported SNV in HGMD, four has been recently reclassifiedas GVUS due to identification in ESV (Table 3).
Table 1 The 10 potassium and sodium ion channel genes including the most common genes associated with heart rhythm disturbances used for thesequencing
Gene Ensembl database isoform RefSeq code Protein name
SCN5A ENST00000333535 NM_198056 Sodium channel, voltage-gated, type V, alpha subunit
SCN1B ENST00000262631 NM_001037 Sodium channel, voltage-gated, type I, beta subunit
SCN2B ENST00000278947 NM_004588 Sodium channel, voltage-gated, type II, beta subunit
SCN3B ENST00000392770 NM_018400 Sodium channel, voltage-gated, type III, beta subunit
SCN4B ENST00000324727 NM_001142348 Sodium channel, voltage-gated, type IV, beta subunit
KCNQ1 ENST00000155840 NM_000218 Potassium voltage-gated channel, KQT-like subfamily, member 1
KCNH2 ENST00000262186 NM_000238 Potassium voltage-gated channel, subfamily H (eag-related), member 2
KCNE1 ENST00000399289 NM_000219 Potassium voltage-gated channel, Isk-related family, member 1
KCNE2 ENST00000290310 NM_172201 Potassium voltage-gated channel, Isk-related family, member 2
KCNE3 ENST00000310128 NM_005472 Potassium voltage-gated channel, Isk-related family, member 3
Int J Legal Med

Two families (case no. 1 and case no. 7) were availableindividuals for the segregation analysis. In both cases theresults confirmed the inheritance pattern of the disease as wewill discuss in more detail later.
Discussion
Sudden unexpected death in epilepsy (SUDEP) is a tragiccomplication of human epilepsy, causing nearly 20 % of
Table 2 Common variants identified in all the 42 cases of the cohort
Gene Variant Exonic/intronic Ancestral allele (A1) Alternative allele (A2) Allelic frequency (A1) Allelic frequency (A2)
SCN5A rs6599230 Exonic T C 0.316 0.684
rs45533640 Exonic G A 0.986 0.014
rs7428779 Intronic T C 0.985 0.015
rs41312433a Intronic G T 0.974 0.026
rs1805124 Exonic C T 0.770 0.230
rs45624133 Exonic A G 0.986 0.014
rs7430407 Exonic C T 0.159 0.841
rs6799868 Intronic C T 0.962 0.038
rs41312393 Intronic A G 0.962 0.038
rs41312391 Intronic C T 0.962 0.038
rs41315507 Intronic C T 0.975 0.025
rs1805126 Exonic A G 0.647 0.353
rs13324293 Exonic G A 0.986 0.014
KCNQ1 rs1057128 Exonic G A 0.885 0.115
rs4151646 Exonic G A 0.962 0.038
rs163150 Intronic G A 0.987 0.013
rs760419 Intronic G A 0.987 0.013
rs81204 Intronic T C 0.974 0.026
rs41282928 Intronic G T 0.974 0.026
rs184844767 Exonic C A 0.974 0.026
rs11601907 Exonic C T 0.789 0.211
KCNH2 rs740952 Exonic G A 0.804 0.196
rs33959111 Exonic C T 0.981 0.019
rs1805120 Exonic G A 0.696 0.304
rs1805121 Exonic C T 0.648 0.352
rs1137617 Exonic G A 0.364 0.636
rs4725983 Intronic C T 0.984 0.016
rs2968860 Intronic A G 0.984 0.016
rs3815459 Intronic C T 0.971 0.029
rs72549420 Intronic G T 0.971 0.029
KCNE1 rs17846179 Exonic C T 0.605 0.395
rs1805127 Exonic C T 0.750 0.250
KCNE3 rs2270676 Exonic A G 0.865 0.135
SCN1B rs16969930 Exonic T C 0.933 0.067
rs77244433 Exonic T C 0.983 0.017
SCN3B rs1275085 Exonic G A 0.850 0.150
rs3851102 Intronic A G 0.984 0.016
rs1148110 Intronic G C 0.984 0.016
SCN4B rs45539032 Exonic G A 0.938 0.063
rs12804550 Intronic G A 0.984 0.016
a The common variant rs41312433 (CS057601) present in two patients was a common intronic variation with a MAF of 0.15 (T) but this substitutionaffects the position 3 nucleotides upstream of the 3′ acceptor splice site of intron 10 and is associated with longer QT interval (L. Gouas et al. Associationof KCNQ1, KCNE1, KCNH2 and SCN5A polymorphisms with QTc interval length in a healthy population. Eur J HumGenet. 2005 Nov;13(11):1213-22;Nishio Y et al. D85N, a KCNE1 polymorphism, is a disease-causing gene variant in long QT syndrome. J Am Coll Cardiol. 2009 Aug 25;54(9):812-9.)
Int J Legal Med

Tab
le3
Dem
ographicandgenotype
dataof
ourseries
Case
Epilepsy
phenotype
Cardiac
phenotype
Gene
Nucleotide/am
ino
acid
change
HGMD
variantclass
rscode
(dbS
NP/1000
Genom
es)
MAF
CONDELscore/
pathogenicity
predictio
n
PROVEANscore/
pathogenicity
predictio
n
MutationTaster
Protein
locatio
n
1Focalepilepsy
Brugada
syndrome
SCN5A
c.3284G>A/p.W
1095X
CM132761
pathogenic
––
––
–DII-D
III
2Focalepilepsy
None
SCN5A
c.5494C>G/p.Q1832E
HM050016
aGVUS
rs199473320
<0.01
(C)
0.009/neutral
−0.870/neutral
Disease
causing
C-terminus
3Generalized
epilepsy
LongQT
syndrome
SCN5A
c.304A
>G/p.I102V
––
–0.742/deleterious
−0.950/neutral
Disease
causing
N-terminus
SCN5A
c.3578G>A/p.R1193Q
CM020303
aGVUS
rs41261344
<0.01
(T)
0.011/neutral
−0.461/neutral
Disease
causing
DII-D
III
4Focalepilepsy
None
SCN5A
c.100C
>T/p.R34C
–rs6791924
<0.01
(A)
0.990/deleterious
−3.699/deleterious
Disease
causing
N-terminus
KCNQ1
c.619G
>A/p.V207M
CM093413
aGVUS
rs75813654
–0.272/neutral
−1.959/neutral
Disease
causing
S-IIIdomain
5Focal(frontal)
epilepsy
None
KCNQ1
c.1942G>A/p.V648I
–rs34150427
<0.01
(A)
0.001/neutral
0.004/neutral
Polymorphism
C-terminus
6Focalepilepsy
None
KCNQ1
c.136G
>A/p.A46T
CM057176
pathogenic
rs199473671
–0.001/neutral
−0.203/neutral
Polymorphism
N-terminus
7Generalized
epilepsy
LongQT
syndrome
KCNH2
c.245T>C/p.I82T
CM136999
pathogenic
––
0.005/neutral
−2.247/neutral
Disease
causing
N-terminus
8Focalepilepsy
LongQT
syndrome
KCNH2
c.2510A>G/p.D837G
CM045294
pathogenic
rs199473004
–0.883/deleterious
−6.312/deleterious
Disease
causing
C-terminus
9Focalepilepsy
LongQT
syndrome
KCNE1
c.253G
>A/p.D85N
CM040436
aGVUS
rs1805128
<0.01
(T)
0.055/neutral
−2.899/deleterious
Polymorphism
C-terminus
aIdentifiedin
ExomeSequencing
Project
MAFistheminor
allelefrequencyin
CEUpopulatio
nconsultedon
ExomeServerVariant
(ESV
)
GVUSgenetic
varianto
funknow
nsignificance
Int J Legal Med

patient deaths [24]. However, mechanisms and methods toprevent it are still largely unknown. A leading hypothesissuggests a dysfunction of excitability that could underlineboth epilepsy and cardiac arrhythmias, leading to death [24].Autosomal dominant idiopathic epilepsies are due largely topathogenic SNV in ion channel subunit genes, as well asautosomal dominant cardiac arrhythmias [25]. Likewise, thein vitro physiologic changes of mutant channels causing sei-zures or cardiac arrhythmias are similar [26]. However, cardi-ac conduction abnormalities are poorly recognized in patientswith epilepsy channelopathies and vice versa [27]. This sep-aration of phenotypes, despite similar molecular pathophysi-ology, may be due to organ-specific gene expression [28].There has been increased interest in the possible associationbetween epilepsy and cardiac channelopathies, such as longQT and Brugada syndromes [26]. A “seizure phenotype” wasrecorded in about 30 % unrelated patients from two indepen-dent cohorts with genetically confirmed LQT2 (pathogenicSNV in the KCNH2 gene encoding the potassium channelhuman ether-à-go-go-related gene-1 (hERG-1) [27]. A recentpost-mortem study identified mutations in the KCNH2 and
SCN5A genes, all previously associated with LQTS, in six outof 68 (13 %) SUDEP patients [29]. Moreover, mutations inKCNH2 that generates the rapid component of cardiac delayedrectifier potassium current have been recently reported inpatients with recurrent seizures and prolonged QTc interval[12, 30, 31]. In addition, mouse lines bearing dominant mu-tations in the Kv1.1 Shaker-like potassium channel, associatedto long QT syndrome type 1 in humans, exhibit severe epilep-sy and premature death [32].
Our study represents an extended genetic analyses of thecardiac ion channels in a large cohort of epilepsy patientsapplied also in post-mortem setting; we have included onecase of sudden death in epilepsy classifying this case asSUDEP. Missense mutations are the most frequent (91 % ofthe total) form of SNV. In order to make an appropriatediagnosis also in forensic field, careful interpretation of iden-tified genetic variants is critical, because a missense SNVmayor may not cause an altered/distorted protein and a diseasephenotype; the failure to reveal a plausible molecular diagno-sis is showed by Klassen because of inherited non-synonymous single nucleotide polymorphisms (nsSNP) of
Fig. 1 Summary of topological depiction of all protein-altering muta-tions identified in the nine index cases. All 11 SNVwere in heterozygousstate, inducing missense changes except one nonsense variant(p.W1095X_SCN5A in patient no. 1 pointed out by a red indicator).
Most of the identified SNVwere localized in the extremes of the encodedprotein (four in C-terminus and four in N-terminus regions) except three(p.W1095X_SCN5A, p.R1193Q_SCN5A, and p.V207M_KCNQ1)
Int J Legal Med

unknown clinical significance in KCNH2 (LQT2), SCN5A(LQT3), and KCNE1 (LQT5) and in the context of the LQTgenotype [16]. We may summarize the genetic interpretationof the results for each case as follows:
Case 1
This patient, affected by Brugada syndrome and epilepsy,carried a nonsense mutation (p.W1095X) in the SCN5A gene.It induces that the protein predicted will be 921 amino acidsshorter than the wild-type protein. This mutation has beenrecently reported by our group, supporting its pathogenic role[33]. Although rare cases of stop mutations are reported asneutral because of allelic imbalance by Campuzano et al. [34],usually STOP mutations are classified as pathogenic. In ourcase, available family members allowed the segregation studyin this family concluding the pathogenic role in BrS patients.However, this family does not necessarily provide the definiteevidence for a link between BrS and epilepsy due to SCN5A_-p.W1095X. Nevertheless, the possibility that the two condi-tions may coexist deserves attention, especially if we cannotfully exclude the possibility that the arrhythmia can increasethe risk or lead to SUDEP and further support the concept ofcardiocerebral channelopathy [26, 35].
Case 2
This individual carried the missense variant p.Q1832E in theSCN5A gene, previously described by Arbustini et al. [36] andassociated with Brugada syndrome phenotype. Despite path-ogenic role is described, our patient did not show BrS pheno-type may due to variable penetrance, a hallmark of channelop-athies. Recently, the mentioned SNV has been reclassified asGVUS due to identification in EVS by Risgaard [37]reassessing the clinical interpretation. This case shows focalepilepsy may be due to SCN5A_p.Q1832E, but no familymembers were available for the segregation study. Therefore,we cannot conclude evidence for a clinical link between BrSand epilepsy, at least due to SCN5A_p.Q1832E.
Case 3
This proband carried a compound missense SNV potentiallypathogenic; one of them is a novel. The novel variant(p.I102V_SCN5A) was predicted in silico as deleterious. Theother variant p.R1193Q_SCN5A has been previously de-scribed in patients affected with Brugada syndrome [38, 39],long QT syndrome [40, 41], and other cardiac conductiondisorder [41]. However, in 2004 was classified as a commonpolymorphisms in Chinese population [42], and it has been
recently identified in ESV population [43] and classified asGVUS. Accordingly, in silico analysis classified the SNV asneutral. These studies suggest that p.R1193Q is a functionalsubstitution that can reduce the stability of the inactivatingstate of Nav1.5 channels, allowing brief returns frominactivated to open states in the plateau phase of action poten-tial and generates a persistent late inward current [44]. Nofurther relatives were available to establish segregation in thefamily in order to clarify the role of each genetic variant.Therefore, we cannot discard that the combined phenotypeof our case could be due to association of both genetic variantsdespite the p.I102V_SCN5A variation seem to be the mostplausible cause of the disease.
Case 4
This patient showed double potentially pathogenic SNV intwo different genes. Both of them were described by previousreports. The first one (p.R34C_SCN5A) despite predicted insilico as pathogenic, electrophysiological studies showed nofunctional differences and the polymorphic channel was phe-notypically indistinguishable from the WT channel [45]. Inaddition, it was detected among Hispanics [46]. Other SNV(p.V207M) was identified in the KCNQ1 gene. Previouslystudies demonstrated a significant prolongation of QT inter-vals in KCNQ1p.V207M-/p.V207M- mice [47], consistent with theclinical phenotype. Despite this fact, this SNV has been re-cently reclassified as GVUS [48] and in silico predictionshowed a neutral effect. Unfortunately, no family memberswere available in order to clarify the role of these both geneticvariations in our case.
Case 5
This patient carried p.V648I_KCNQ1 reported as likely path-ogenic in 2003 by Ackerman et al. [49] However, in silicoprediction showed a neutral effect, suggesting its no-pathogenic role. No previous studies and family memberswere available to conclude any clinical decision.
Case 6
This patient carried a previously described variant p.A46T(CM057176) in the KCNQ1 gene. In 2009, Yang et al. [50]demonstrated an activated more rapid current without aninitial delay at the very beginning phase of the IKs. Althoughthis apparent biophysical modification supports its pathogenicrole, in silico analysis predicted the SNVas neutral. Hence, thepathogenicity remains uncertain because the cosegregationwas inconclusive due to resistance to wider family screening.
Int J Legal Med

Case 7
This case was studied after a comprehensive autopsy investi-gation classified as SUDEP by post-mortem genetic analysisthat showed the SNV p.I82T in the KCNH2 gene, classified aspathogenic. This variant was also found in her twin sisteraffected as well as by long QT syndrome and idiopathicgeneralized epilepsy as described by previous report [31].The striking reduction in current K+ density was the mainfunctional effect of the mutation well consistent with LQTSphenotype.
Case 8
This patient showed a previously described variant (p.D837G)in theKCNH2 gene. Khositseth et al. [51] associated this SNVwith the congenital long QT syndrome. In silico analysissupports the pathogenic role. Despite this fact explains theLQT phenotype in our case, no family members were avail-able in order to clarify the link between p.D837G_KCNH2and epilepsy.
Case 9
The last case showed the p.D85N (CM040436) SNV in theKCNE1 gene. It was a highly frequent variant in LQTs pro-bands and was found to cause loss-of-function effects on bothIKr and IKs and work as a disease-causing mutation [52]. Theallele frequency for D85N carriers was 0.81 % in healthypeople. In contrast, among LQTS probands, there were onehomozygous and 23 heterozygous carriers (allele frequency3.9 %). Seven of 23 heterozygous carriers had additionalmutations in LQTS-related genes, and three female subjectshad documented factors predisposing to the symptom, thep.D85N prevalence was significantly higher compared withcontrol subjects (allele frequency 2.1 %, p<0.05). In aheterologous expression study with Chinese hamsterovarian cells, KCNE1-D85N was found to exert signif-icant loss-of-function effects on both KCNQ1- andKCNH2-encoded channel currents. The functional vari-ant is a disease-causing gene variant of LQTS pheno-type that functions by interacting with KCNH2 andKCNQ1. Since its allele frequency was approximately1 % among control individuals, KCNE1-p.D85N, it hasbeen classified as GVUS [53] but may be clinically importantas phenotype modifier [54]. Despite all, no family memberswere available in order to clarify the role of this geneticvariation in our case, concluding a definite link betweenKCNE1-p.D85N and epilepsy.
Conclusions
Recently, great interest has been raised regarding the researchconcerning the molecular mechanisms underlying the coexis-tence of epilepsy and cardiac rhythm disorders. In forensicfield, few data are available on this issue [55]. A significantnumber of individuals (41), including one case (1) of suddendeath classified as SUDEP after autopsy examination, wasinvestigated in this study in order to verify the hypothesis of apossible link between heart rhythm disorders and epilepsy.Although the post-mortem cases are really very limited in ourseries, we do think that it could be helpful to perform a geneticinvestigation in the post-mortem setting where epilepsy andcardiac arrhythmias are suspected by anamnestic history eval-uation, especially in those cases where autopsy examinationdoes not reveal a toxicological or anatomic cause of death.These studies are important for the identification of geneticcarriers in familymembers who could benefit from thoroughlyclinical evaluation and eventually for cardiology and neurol-ogy assessments and preventive measures. We do believe thatmore investigations in large cohorts should be performed inorder to establish a robust evidence of connection betweenboth clinical entities. In fact, the possibility and the hypothesisthat these two conditions may coexist deserves further re-search, especially if we cannot fully exclude the possibilitythat the arrhythmia can increase the risk or lead to SUDEPsupporting the well-known concept of cardiocerebral chan-nelopathy. Moreover, although in silico prediction can beuseful to support pathogenicity, the results of this study shouldbe cautiously interpreted. Further investigation as functionalstudies or familiar segregation assessment should be per-formed to ascertain the malignancy of SNV classified asGVUS.
Limitations
Segregation studies and therefore available family membersare a crucial point to understand the possible pathogenicity ofthe SNV classified as GVUS. In our study, only two familieswere available. We did not evaluate in vitro the functional roleof each new SNV identified in our cohort. Biophysical ionchannel studies should be performed in order to clarify thepossible biophysical dysfunction due to each one, becauseseveral studies found that in silico predictors programs weresometimes disagree on their predictions [50]. A more com-prehensive genomic interrogation of ion channel candidategene pathways is essential for elucidate through the genemodels, but also the compound effect of SNV together withthe transmitted nsSNPs and Copy Number Variation (CNVs)of the cardiac arrhythmia, the accurate assessment of SUDEPrisk. Considering that it is increasingly hypothesized a possi-ble link between cardiac and neuronal channelopathies, post-
Int J Legal Med

mortem mRNA expression analysis on tissue from pathologicand non-pathologic hearts and brain could be a very usefulsource to investigate also the expression levels of ion channels[55, 56].
Acknowledgments This work was supported by the CardiovascularGenetics Center, University of Girona, Spain, and by Telethon Founda-tion Italy, Grant GGP10186A. We wish also to thank the CollaborativeGroup on SUDEP of Italian League Against Epilepsy (LICE) for thesupport in sample collections.
Authors’ contribution The study concept or design was made by SP,MCV, PS, AO, and RB. All authors draft/revise the manuscript. All theauthors made the analysis of interpretation.
Conflict of interests The authors declare that they have no competinginterests.
Disclosure All authors report no disclosure.
References
1. Annegers JF (2001) The epidemiology of epilepsy. In: Wyllie E (ed)The treatment of epilepsy: principles and practice, 3rd edn. LippincottWilliams & Wilkins, Philadelphia, pp 131–138
2. Shorvon S, Tomson T (2011) Sudden unexpected death in epilepsy.Lancet 378(9808):2028–38
3. Hughes JR (2009) A review of sudden unexpected death in epilepsy:prediction of patients at risk. Epilepsy Behav 14:280–287
4. Lhatoo SD, Johnson AL, Goodridge DM et al (2001) Mortality inepilepsy in the first 11 to 14 years after diagnosis: multivariateanalysis of a long-term, prospective, population-based cohort. AnnNeurol 49:336–344
5. Walczak TS, Leppik IE, D’Amelio M et al (2001) Incidence and riskfactors in sudden unexpected death in epilepsy: a prospective cohortstudy. Neurology 56:519–525
6. Johnston A, Smith P (2007) Sudden unexpected death in epilepsy.Expert Rev Neurother 7:1751–1761
7. Lee BI, Heo K (2014) Epilepsy: new genes, new technologies, newinsights. Lancet Neurol 13(1):7–9
8. Nashef L et al (2007) Risk factors in sudden death in epilepsy(SUDEP): the quest for mechanisms. Epilepsia 48(5):859–871
9. Jansen K, Lagae L (2010) Cardiac changes in epilepsy. Seizure 19:455–460
10. Kim JB (2014) Channelopathies. Korean J Pediatr 57(1):1–1811. Nashef L, HindochaN,Makoff A (2007) Risk factors in sudden death
in epilepsy (SUDEP): the quest for mechanisms. Epilepsia 48:859–871
12. Glasscock E, Yoo JW, Chen TTet al (2010) Kv1.1 potassium channeldeficiency reveals brain-driven cardiac dysfunction as a candidatemechanism for sudden unexplained death in epilepsy. J Neurosci30(15):5167–75
13. Haugaa KH, Vestervik TT, Andersson S, Amlie JP, Jørum E, GjerstadL, Taubøll E. Abnormal electroencephalograms in patients with longQT syndrome. Heart Rhythm. 2013 Sep 27. pii: S1547-5271(13)01081-3
14. Sandorfi G, Clemens B, Csanadi Z (2013) Electrical storm in thebrain and in the heart: epilepsy and Brugada syndrome. Mayo ClinProc 88(10):1167–1173
15. Jeppesen J, Fuglsang-Frederiksen A, Brugada R, Pedersen B,Rubboli G, Johansen P, Beniczky S (2014) Heart rate variability
analysis indicates preictal parasympathetic overdrive precedingseizure-induced cardiac dysrhythmias leading to sudden unexpecteddeath in a patient with epilepsy. Epilepsia
16. Klassen TL, Bomben VC, Patel A et al (2014) High-resolutionmolecular genomic autopsy reveals complex sudden unexpecteddeath in epilepsy risk profile. Epilepsia 55(2):e6–12
17. Kersey PJ et al (2012) Ensembl Genomes: an integrative resource forgenome-scale data from non-vertebrate species. Nucleic Acids Res40:D91
18. A map of human genome variation from population-scale sequenc-ing. Nature 467, 1061 (Oct 28, 2010)
19. Stenson PD et al (2003) Human Gene Mutation Database (HGMD):2003 update. Hum Mutat 21:577
20. S. T. Sherry et al., dbSNP: the NCBI database of genetic variation.Nucleic acids research 29, 308 (Jan 1, 2001).
21. Gonzalez-Perez A, Lopez-Bigas N (2011) Improving the assessmentof the outcome of nonsynonymous SNVs with a consensus deleteri-ousness score, Condel. Am J Hum Genet 88:440
22. Schwarz JM, Rödelsperger C, Schuelke M et al (2010) MutationTasterevaluates disease-causing potential of sequence alterations. NatMethods 7(8):575–6
23. den Dunnen JT, Antonarakis SE (2001) Nomenclature for thedescription of human sequence variations. HumGenet 109(1):121–4
24. Surges R, Thijs RD, Tan HL (2009) Sander JW Sudden unexpecteddeath in epilepsy: risk factors and potential pathomechanisms. NatRev Neurol 5:492–504
25. Campuzano O, Beltrán-Alvarez P, Iglesias A et al (2010) Geneticsand cardiac channelopathies. Genet Med 12(5):260–7
26. Heron SE, Hernandez M, Edwards C et al (2010) Neonatal seizuresand longQTsyndrome: a cardiocerebral channelopathy. Epilepsia 51:293–296
27. Johnson JN, Hofman N, Haglund CM et al (2009) Identification of apossible pathogenic link between congenital long QT syndrome andepilepsy. Neurology 72:224–231
28. Catalano O, Antonaci S, Moro G et al (2009) Magnetic resonanceinvestigations in Brugada syndrome reveal unexpectedly high rate ofstructural abnormalities. Eur Heart J 30(18):2241–2248
29. Tu E, Bagnall RD, Duflou J et al (2011) Post-mortem review andgenetic analysis of sudden unexpected death in epilepsy (SUDEP)cases. Brain Pathol 21:201–208
30. Anderson JH, Bos JM, Meyer FB et al (2012) Concealed long QTsyndrome and intractable partial epilepsy: a case report. Mayo ClinProc 87:1128–1131
31. Partemi S, Cestèle S, Pezzella M et al (2013) Loss-of-functionKCNH2 mutation in a family with long QT syndrome, epilepsy,and sudden death. Epilepsia 54(8):e112–6
32. Zamorano-León JJ, Yañez R, Jaime G et al (2012) KCNH2 genemutation: a potential link between epilepsy and long QT-2 syndrome.J Neurogenet 26(3–4):382–6
33. Parisi P, Oliva A, Coll Vidal M et al (2013) Coexistence of epilepsyand Brugada syndrome in a family with SCN5A mutation. EpilepsyRes 105(3):415–8
34. Campuzano O, Berne P, Selga E, Allegue C, Iglesias A, Brugada J,Brugada R, Brugada syndrome and p.E61X_ RANGRF. Cardiol J.2014 Mar 27
35. Omichi C, Momose Y, Kitahara S (2010) Congenital long QT syn-drome presenting with a history of epilepsy: misdiagnosis or rela-tionship between channelopathies of the heart and brain? Epilepsia51(2):289–92
36. Arbustini E, Scaffino MF, Diegoli M et al (2005) Genesymbol: SCN5A. Disease: Brugada syndrome. Hum Genet 118(3-4):536
37. Risgaard B, Jabbari R, Refsgaard L et al (2013) High prevalence ofgenetic variants previously associated with Brugada syndrome innew exome data. Clin Genet 84(5):489–95
Int J Legal Med

38. Vatta M, Dumaine R, Varghese G et al (2002) Genetic and biophys-ical basis of sudden unexplained nocturnal death syndrome(SUNDS), a disease allelic to Brugada syndrome. Hum Mol Genet11(3):337–45
39. Nakajima T, KanekoY, Saito A et al (2011) Identification of six novelSCN5A mutations in Japanese patients with Brugada syndrome. IntHeart J 52(1):27–31
40. WangQ, Chen S, Chen Q et al (2004) The common SCN5AmutationR1193Q causes LQTS-type electrophysiological alterations of thecardiac sodium channel. J Med Genet 41(5):e66
41. Sun A, Xu L, Wang S et al (2008) SCN5A R1193Q polymorphismassociated with progressive cardiac conduction defects and long QTsyndrome in a Chinese family. J Med Genet 45:127–128
42. Hwang HW, Chen JJ, Lin YJ et al (2005) R1193Q of SCN5A, aBrugada and long QT mutation, is a common polymorphism in HanChinese. J Med Genet 42(2):e7
43. Refsgaard L, Holst AG, Sadjadieh G et al (2012) High prevalence ofgenetic variants previously associated with LQT syndrome in newexome data. Eur J Hum Genet 20(8):905–8
44. Wang Q, Chen S, Chen Q, Wan X, Shen J, Hoeltge GA, Timur AA,et al. The common SCN5A mutation R1193Q causes LQTS-typeelectrophysiological alterations of the cardiac sodium channel. J MedGenet 2004
45. Tan BH, Valdivia CR, Rok BA et al (2005) Common human SCN5Apolymorphisms have altered electrophysiology when expressed inQ1077 splice variants. Heart Rhythm 2(7):741–7
46. Ackerman MJ, Splawski I, Makielski JC et al (2004) Spectrum andprevalence of cardiac sodium channel variants among black, white,Asian, and Hispanic individuals: implications for arrhythmogenicsusceptibility and Brugada/long QT syndrome genetic testing. HeartRhythm 1(5):600–7
47. Nishio H, Kuwahara M, Tsubone H et al (2009) Identification of anethnic-specific variant (V207M) of the KCNQ1 cardiac potassium
channel gene in sudden unexplained death and implications from aknock-in mouse model. Int J Legal Med 123(3):253–7
48. Giudicessi JR, Kapplinger JD, Tester DJ et al (2012) Phylogeneticand physicochemical analyses enhance the classification of rare non-synonymous single nucleotide variants in type 1 and 2 long-QTsyndrome. Circ Cardiovasc Genet 5:519–528
49. Ethnic differences in cardiac potassium channel variants: implica-tions for genetic susceptibility to sudden cardiac death and genetictesting for congenital long QT syndrome. Ackerman MJ, Tester DJ,Jones GS, Will ML, Burrow CR, Curran ME. Mayo Clin Proc. 2003Dec;78(12):1479-87
50. Yang T, Chung SK, ZhangWet al (2009) Biophysical properties of 9KCNQ1 mutations associated with long-QT syndrome. CircArrhythm Electrophysiol 2(4):417–26
51. Khositseth A, Tester DJ, Will ML et al (2004) Identification of acommon genetic substrate underlying postpartum cardiac events incongenital long QT syndrome. Heart Rhythm 1(1):60–4
52. Nishio Y, Makiyama T, Itoh H et al (2009) D85N, a KCNE1 poly-morphism, is a disease-causing gene variant in long QT syndrome. JAm Coll Cardiol 54(9):812–9
53. Lieve KV, Williams L, Daly A et al (2013) Results of genetictesting in 855 consecutive unrelated patients referred for longQTsyndrome in a clinical laboratory. Genet Test Mol Biomark 17(7):553–61
54. Yoshikane Y, Yoshinaga M, Hamamoto K et al (2013) A case of longQT syndrome with triple gene abnormalities: digenic mutations inKCNH2 and SCN5A and gene variant in KCNE1. Heart Rhythm10(4):600–3
55. Madea B, Saukko P, Oliva A et al (2010) Molecular pathology inforensic medicine—introduction. Forensic Sci Int 203(1–3):3–14
56. Partemi S, Berne PM, Batlle M et al (2010) Analysis of mRNA fromhuman heart tissue and putative applications in forensic molecularpathology. Forensic Sci Int 203(1–3):99–105
Int J Legal Med
Copyright © 2022 FDOKUMEN